Dopaminergic and clinical correlates of pathological gambling in Parkinson's disease: A case report
Upload
independentCategory
view
3download
0
Scandinavian Journal of Psychology, 2009, 50, 55–64 DOI: 10.1111/j.1467-9450.2008.00667.x
© 2008 The Authors. Journal compilation © 2008 The Scandinavian Psychological Associations. Published by Blackwell Publishing Ltd., 9600 Garsington Road, Oxford OX4 2DQ, UK and 350 Main Street, Malden, MA 02148, USA. ISSN 0036-5564.
Blackwell Publishing Ltd Personality and Social Sciences
Prevalence and correlates of gambling among 16 to 19-year-old
adolescents in Norway
HELGE MOLDE,1 STÅLE PALLESEN,1 PAUL BARTONE,2 SIGURD HYSTAD1 and BJØRN HELGE JOHNSEN1
1Department of Psychosocial Science, University of Bergen, Norway2National Defense University, Washington, DC, USA
Molde, H, Pallesen, S., Bartone, P., Hystad, S. & Johnsen, B. H. (2009). Prevalence and correlates of gambling among 16 to 19-year-old adolescentsin Norway. Scandinavian Journal of Psychology, 50, 55–64.
There is evidence that young people are at high risk of developing gambling disorders. The prevalence and correlates of gambling among youth thereforemerit closer study. During spring 2004, a sample of 1,351 boys and girls (aged 16–19 years) from 151 high-school classes (clusters) participated inan internet survey about gambling. The response rate was 69.8%. The instruments used in the survey were the Hospital Anxiety and Depression Scale,the Alcohol Use Disorders Identification Test and the Massachusetts Adolescent Gambling Screen, in addition to questions about demography.Controlling for the design effect, the estimated prevalence rate was 2.5% for pathological gambling and 1.9% for problem gambling. In all, 7.3% ofthe boys and 0.6% of the girls fulfilled the criteria for pathological or problem gambling. The results of item analysis of the DSM-IV subscale ofMAGS provide support for differential item functioning between boys and girls. A multiple logistic regression analysis revealed that gender(male: OR = 9.09), depression (OR = 9.23), alcohol abuse (OR = 3.62), and dissociation (OR = 1.96) were related to problem and pathological gambling.These results support the view that gambling disorders are best understood as part of an addictive behavior spectrum (Jacobs, 2000).
Key words: Gambling, youth, adolescence, prevalence, correlates, high school.
Helge Molde, Department of Psychosocial Science, University of Bergen, Christiesgate 12, Bergen, Norway, 5020. E-mail: [email protected]
INTRODUCTION
According to Dickerson and O’Connor (2006), no consensusexists regarding the formal definition of gambling. In Westernsocieties, it has an economic definition, referring to “wageringmoney or something of material value on an event with anuncertain outcome with the primary intent of winning additionalmoney and/or material goods”. Typically, the outcome of the wageris evident within a short period of time (Bolen and Boyd, 1968).
Today’s young generation is the first to be exposed to a largenumber of gambling opportunities, advertising for gamblingand general social approval of gaming (Jacobs, 2004; Stinch-field, 2004). Research shows that youth experience of gamblingin general occurs on a continuum of involvement, from non-participating to experimenting, and, for a minority, it developsinto an excessive problem with serious adverse consequences(Jacobs, 2000, 2004; Shaffer, LaBrie, LaPlante, Nelson & Stan-ton, 2004). Due to high rates of risk-taking among adolescents,their self-perceived invulnerability and their presumed lack ofrecognition that gambling may lead to serious problems, adoles-cents are assumed to constitute a particularly high risk group interms of developing gambling problems (Derevensky, Gupta &Winters, 2003).
The lifetime prevalence for problem and pathological gam-bling is between 4.6 and 7.5% in the adult population of NorthAmerica. The prevalence is even higher for adolescents, withproblem gambling rates two to four times that of adult popula-tions (Shaffer & Hall, 2001).
In most of the prevalence studies that have been carried out,the DSM-criteria for pathological gambling have been emphasized.When classifying different levels of gambling, problem gamblinghas often been operationalized as fulfilling three or four of the tenDSM-IV criteria, whereas the diagnosis of pathological gamblinginvolves meeting at least five of the criteria (Shaffer et al., 2004).
Several adolescent gambling instruments have been developed,adopting the adult criteria while modifying the questions tomake them more age appropriate, such as the South OaksGambling Screen – Revised for Adolescents (SOGS-RA; Winters,Stinchfield & Fulkerson, 1993), the Massachusetts AdolescentGambling Screen (MAGS; Shaffer, LaBrie, Scanlan & Cummings,1994) and the Diagnostic Statistical Manual-IV-Adapted-MultipleResponse format for Juveniles (DSM-IV-MR-J; Fisher, 2000).
Two international publications have reported data concerningthe prevalence of adolescent gambling in Norway. Using theDSM-IV criteria (American Psychiatric Association, 2000),Johansson and Gøtestam (2003) estimated the past-year problemgambling rate among 12 to 18-year-old adolescents to be1.76%. In a nationwide survey, Rossow and Molde (2006) esti-mated the problem rate among 13 to19-year-old students inNorway to be 2.5% using the SOGS-RA, and 3.5% using theLie/Bet questionnaire.
Due to changing gambling opportunities, such as those avail-able on the internet, and the massive increase in gamblingexpenditure among the general Norwegian population over thelast decade (Norwegian Gaming Board, 2004), it is necessary tostudy how these contextual changes affect the prevalence rates

56 H. Molde et al. Scand J Psychol 50 (2009)
© 2008 The Authors. Journal compilation © 2008 The Scandinavian Psychological Associations.
for pathological gambling among youths and which factorspredict problematic levels of adolescent gambling. This is inline with the “Action Plan” of the Norwegian Gaming Board,which states that “the knowledge base concerning gaming andgambling problems must be expanded” and that “data should becollected on a continuous basis from the gaming market”(Norwegian Gaming Board, 2004, p. 5). There is also a need inthe gambling field to check how well the DSM-IV criteria,considered by many to be “the gold standard” (Derevensky &Gupta, 2000), function as a valid measure for both adolescentboys and girls. Population-based studies have reported a threeto five times higher proportion of male gamblers than femalegamblers (Jacobs, 2000). However, there is evidence that,within the screening instruments, certain items are understooddifferently by males and females (Derevensky & Gupta, 2006).Thus, there is concern that the validity of the screening instru-ments may differ for boys and girls (Rossow & Molde, 2006).
Studies also indicate that problem gambling is more pervasiveamong ethnic minorities (Shaffer et al., 2004; Stinchfield &Winters, 1998). While earlier studies supported the notion thatolder youths gamble more often than younger ones and developmore gambling problems (Stinchfield & Winters, 1998), thismay have changed in recent years as a result of the sheer expo-sure to gambling and opportunities to gamble experiencedby the younger adolescents (Gupta & Derevensky, 1998a;Jacobs, 2000, 2004).
In addition, some researchers have reported higher rates ofgambling-related problems among individuals with lowersocioeconomic status (SES) than among those with highersocioeconomic status. Although the total amount of moneywagered is less than among people with higher SES, theirrelative spending is higher due to their income being lower(Shaffer et al., 2004). Other studies have not found a linkbetween SES and gambling. In a longitudinal study, Barnes,Welte, Hoffman and Dintcheff (2005) found no relationshipbetween low SES and gambling among male adolescents, andonly weak associations for females. In a Norwegian context,Rossow and Hansen (2003) reported that adolescents withgambling problems have a low SES ratio of 2:1 compared withnon-problem youths. From a public health perspective, oneconcern is that disordered gambling may not only be a prob-lem in itself, it may also be a gateway to substance abuse,depression, anxiety and other mental health disorders (Korn &Shaffer, 1999).
There have been extensive reviews of co-morbidity andgambling (e.g. Crockford & el-Guebaly, 1998; National ResearchCouncil, 1999; Petry & Armentano, 1999). The relationshipbetween depression and gambling among adolescents was notinvestigated until recently (Langhinrichsen-Rohling, 2004).Problem and pathological youth gamblers do report moredepressive symptoms than non-problem, occasional and regulargamblers (Gupta & Derevensky, 1998a; Langhinrichsen-Rohling,Rohde, Seeley & Rohling, 2004).
Several authors (Stinchfield, Cassuto, Winters & Latimer,1997; Shaffer et al., 2004; Winters, Arthur, Leitten & Botzet,
2004) suggest that high-frequency gambling may be part of awider constellation of deviant behavior with a male preponderance,such as frequent alcohol use and antisocial behavior. There mayalso be common risk factors between gambling and deviantbehavior (Clayton, 1992). Testing this hypothesis, Barnes et al.(2005) analyzed data from two longitudinal samples and con-cluded that problem behavior in adolescence has commonantecedent factors, although gambling did not correlate ashighly as would be expected on the basis of “deviant behavior(cluster) theory”.
Although there are mixed notions about gambling as part ofa deviance syndrome, adolescence is often considered a periodof heightened risk behavior, and retrospective studies from adultpathological gamblers indicated that gambling involvementpeaked in the late adolescence period and in early adulthood(Stinchfield & Winters, 1998).
Gambling is often considered to be part of an addictivebehavior spectrum due to its common correlates with otheraddictive behavior (Jacobs, 2000; Langewisch & Frisch, 1998).Pathological gambling is frequently co-morbid with substanceuse disorders among adults (Crockford & el-Guebaly, 1998).Winters and Anderson (2000) and Winters et al. (2004), concludedthat involvement in one of the behaviors probably increases therisk of involvement in the other. Others report that adolescentgamblers are more likely to drink alcohol, smoke tobacco anduse drugs than non-gamblers (Griffiths & Sutherland, 1998;Griffiths, Parke & Wood, 2002; Shaffer & Korn, 2002). Custerand Milt (1985) have suggested that gambling has many over-lapping commonalities with other addictions, but there are alsocharacteristics specific to gambling. These specific factors areimportant to understand, and several authors have pointed tocognitions specific to gambling (e.g. Toneatto, 1999). One suchcognition is “the illusion of control”, a belief that games inwhich the outcome is determined by chance can be skillfullymastered. According to Ladouceur, Sylvain, Boutin and Doucet(2002), this illusion of control is seen among a majority ofpathological gamblers. Regarding young pathological gamblers,they have been found to have greater belief in the role of skillin slot machine gaming, while at the same time also over-estimating the amount of money they can win during a gamecompared with non-problem gamblers (Carrol & Huxley, 1994;Griffiths, 1995). Ladouceur et al. (2002) claim that pathologicalgamblers always have positive outcome expectancies and that theprimary motive or reason for gambling is the opportunity to winmoney. A consistent finding among adult pathological gamblersis a history of an “early big win”, which may presumably resultin positive outcome expectancies about the chances of winning.
Gambling may also have the function of elevating mood andfunction as an escape from reality. Jacobs (2000) proposes therelieving of stress as a common attribute with other addictivedisorders, and that dissociation while gambling serves this func-tion. Gupta and Derevensky (1998b) reported empirical supportfor Jacobs’s “General theory of addiction”.
All in all, close monitoring of developments in the gamblingmarket appears to be warranted (Norwegian Gaming Board,

Scand J Psychol 50 (2009) Youth gambling in Norway 57
© 2008 The Authors. Journal compilation © 2008 The Scandinavian Psychological Associations.
2004, p. 5). Our first aim in this study was to determine theprevalence of problem and pathological gambling among 16 to19-year-old youths. Our second aim was to study how well theDSM-IV criteria (MAGS) functioned as a valid measure ofmale and female adolescent gambling problems. Using ItemResponse Theory (IRT), we tested for possible measurementvariance between boys and girls in the items measuring theDSM-IV criteria (MAGS). Our third aim was to investigatewhich risk factors (correlates), together with motivationalvariables, would predict gambling involvement in this sample.In light of earlier findings, we predicted that specific risk factorsrelating to gambling would include “being male”, “belonging toan ethnic minority”, “having a depressive disorder” and “alcoholand substance abuse”, and also a history of an “early big win”,“dissociation” and “gambling to earn money”.
METHOD
Participants
The survey was conducted in a county in Western Norway, in collabo-ration with Hordaland County school administration. The present studyincluded 2,542 high-school students (11th–13th grade) randomlyselected at the class level from a total population consisting of approxi-mately 16,000 youths.
Questionnaires
AUDIT. Alcohol use and potential abuse was measured using theAlcohol Use Disorders Identification Test (AUDIT; Saunders, Aasland,Babor, de la Fuente & Grant, 1993), a ten-item self-reporting question-naire developed for the screening of harmful or hazardous alcoholconsumption (Babor, de la Fuente, Saunders & Grant, 1989). The firsteight items are rated on a five-point scale (0–4) and items nine and tenare rated on a three-point scale (0–2–4). Hence, the total scores couldrange from zero to 40. Scores below 11 represent non-harmful drinking,and scores of 11 or above represent harmful drinking (Claussen &Aasland, 1993).
MAGS. In the present study, the DSM-IV subscale MAGS (Shafferet al., 1994) was used to measure the prevalence rate for pathologicaland problem gambling. The scale consists of 12 items which are dicho-tomized (yes or no). Four items are scored 0.5, the other eight items arescored zero or one. Thus, the range of scores varies from zero to ten.A score of 3 to 4.5 was deemed to represent problem gambling, and ascore of 5 or above was deemed to represent pathological gambling.
HADS. The Hospital Anxiety and Depression Scale (HADS; Zigmond& Snaith, 1983) was used to measure anxiety and depression. Thequestionnaire consists of one anxiety and one depression subscale, eachconsisting of seven items. The subscales are correlated in most patientgroups, but there is evidence that both subscales differ in a clinicallymeaningful way (Herrmann, 1997). The items are rated on a four-pointscale (0–3). Hence, the scores vary from zero to 21 on each scale. Ascore of 11 or above on either subscale was deemed to represent clinicaldepression or anxiety.
DEMOGRAPHICS. In addition, the questionnaire included items aimedat assessing demographic and background information (age, gender,parental education and ethnicity).
GAMBLING MOTIVES. We included 12 different items to test for gamblingmotives. The first was “Do you think someone could make a livingfrom money earned from gambling”, with dichotomized “yes” or“no” alternative answers. The second item was “Did you have an ‘earlybig win’ when you first started to gamble?”, with three responseoptions (“yes”, “no” and “do not remember”). The 10 remainingitems were as follows: “I gamble to earn money”, “I expect to win”,“When I gamble (play) the most important thing is to keep the gamegoing”, “I play because it is exciting”, “I gamble in order to have agood time”, “I gamble because it is fun”, “I forget myself whileplaying”, “Time stands still while I am playing”, “I believe I have agreater chance of winning than other people” and, finally, “Knowledgeand experience are important in order to win.” These items wererated from completely disagree (1) to completely agree (5) on aLikert scale.
Procedure
The study was reviewed and approved by the Regional Ethics Committeeof Western Norway (REK-Vest) and the Norwegian Social Data Service(NSD). Our sample was drawn randomly at the class level from 41schools across the region by the school authorities. Before data collec-tion started, information letters were sent to headmasters and principalsat the schools, class teachers, students and their parents, in which weexplained the purpose of and procedure for the study. The participationof students was voluntary and there was a passive consent procedure,by which is meant that the student did not have to sign a consent form.During a six-week period in spring 2004, schoolteachers and principalswere asked to set aside time to allow data to be collected in the indi-vidual schools and classes. In the region, every student had access tointernet at school and an individual e-mail address. E-mails were sentto every student included in our sample, in which the purpose of andprocedure for the study were again explained. As a data collectionprocedure, the students could log onto an internet address duringdesignated school time to answer the questionnaire. Every class wasassigned a unique six-number code sent randomly to the classes, whichmeans that every student in the same class had the same number, but adifferent one from the other classes (clusters). This procedure ensuredanonymous personal data collection and anonymous cluster identifica-tion. Only five students could not be reached by e-mail. A total of 1,351students responded. At the cluster level, we obtained responses from115 of 151 classes. In accordance with the requirements of the Norwe-gian Social Data Service, the sampling procedure had to ensure theabsolute anonymity of the responding students, classes and schools.Thus, the proportion of the final participating sampling units and thesize of the responding clusters had to be estimated, using the meancluster size of the drawn sample, which was known. Hence, our finalsample consisted of 115 school classes with an estimated total of 1,936students (using the mean cluster size of the original sample), of whom1,351 participated, yielding a response rate of 69.8%. A total of 66respondents were not teenagers, and they were subsequently excludedfrom the analyses. Thus, the final sample consisted of 1,285 subjects,668 boys and 610 girls. In addition, there were seven participants forwhom gender data was missing. The participants were either 16, 17, 18or 19 years old, and the mean age of the respondents was 17.3 years(SD = 0.8).
Several of the independent variables were transformed before thestatistical analyses: the different ethnic groups were recoded into“Western” (European and North American) or “non-Western” (Asian,African, South American and Oceanian). As previous research hasestablished that a strong delineation can be made in prevalence researchbetween “non-problem” gamblers and those who score either as“problem” or “pathological” (Volberg & Abbott, 1994; Jacobs, 2000), wechose one dependent variable where the combined problem and patho-logical gambling group comprised one level (“problem/pathological”).

58 H. Molde et al. Scand J Psychol 50 (2009)
© 2008 The Authors. Journal compilation © 2008 The Scandinavian Psychological Associations.
In the logistic regression analysis, this variable was coded zero (noproblems) and one (problem or pathological gambling).
Statistics
The data analyses were performed using STATA version 8.2 andMULTILOG version 7.03. Using classes as primary sampling units(clusters), the analyses were controlled for the cluster design effect(Kish, 1987). First, estimates of prevalence were computed for the problem,pathological and combined problem and pathological gambling groups,respectively. These estimates were also broken down by gender. There-after, logistic univariate regression was performed, testing the predictorvariables for the problem and pathological gambling group combined.The significant univariate variables were then entered in a multivariateregression model.
To test for possible differential item functioning (DIF) among theitems on the DSM-IV subscale (MAGS) between boys and girls, weadopted a model-testing approach (Thissen, Steinberg & Gerrard,1986). The specific model-testing approach that was chosen wasarticulated by Reise, Widaman and Pugh (1993). It involves comparing abaseline model with a series of constrained models. The baseline modelallows all item parameters to differ between groups, and it is comparedwith models where the target item’s parameters are constrained toequality. Using a G2 statistic, the difference between the baseline andconstrained models can be tested for statistical significance. The G2
statistic is the difference in “−2 Log-Likelihood function” of the base-line and constrained models. The “−2 Log-Likelihood function” isprovided by IRT modelling programs such as MULTILOG 7.03 for eachmodel (Thissen, 2003). The G2 statistic is distributed as a chi-squarewith degrees of freedom equal to the differences in the number ofparameters estimated in each model. If constraining an item parameteracross groups in this manner results in a significant increase in G2, thisitem is considered as exhibiting DIF. If constraining item parametersacross groups does not result in a significant increase in G2, the item isdeemed non-DIF.
The DIF analysis consisted of 653 boys and 580 girls who hadresponded to the 12 MAGS items. In practice, the data in this analysiswere treated as a 24-item measure/test, with responses from boys asitems 1–12, and responses from girls as items 13–24. Responses toitems 1–12 were coded as missing for the girl respondents, andresponses to items 13–24 were coded as missing for the boy respond-ents. The models were estimated using the IRT modeling programMULTILOG 7.03 (Thissen, 2003) using marginal maximum likelihooditem parameter estimation. We selected a two-parameter logistic model(2PL), which estimates two parameters for every single item, one itemdifficulty parameter and one item discrimination parameter. The 2PLmodel is appropriate for measures in which items are not assumed tobe equally related to the latent trait, or where the items are not assumedto be equally indicative of an individual’s standing in relation to thelatent trait.
RESULTS
The prevalence of problem gambling and pathological gambling
The estimated prevalence of problem gambling in the populationwas 1.9% (95% CI = 0.09−2.76); the estimated prevalence ofpathological gambling was 2.5% (95% CI = 1.54−3.46) and theestimated prevalence of problem and pathological gamblingcombined was 4.4% (95% CI = 3.04−5.68). Thus, the estimatedmean of non-problem gambling was 95.6%.
When the prevalence rate in the population was examined bygender, the estimated prevalence of problem gambling for males
was 3.1% (95% CI = 1.50−4.70), whereas the correspondingprevalence for females was 0.41% (95% CI = −0.14−0.96). Forpathological gambling, the estimated prevalence for males was4.20% (95% CI = 2.58−5.95) and 0.20% (CI = −0.20−0.60) forfemales. The estimated prevalence of problem and pathologicalgambling combined was 7.30% (95% CI = 5.08−9.60) formales, and 0.61% (95% CI = −00.7−1.20) for females. Thus,the estimate for non-problem gambling for males is 92.7% andfor females 99.39%.
Differential item functioning
First, the baseline model was compared with a fully constrainedmodel, in which all the item parameters between boys and girlswere constrained to equality. The resulting G2 value was signi-ficant (G2(24) = 184.8, p = 0.0001), indicating that constraining theitems across the groups resulted in a significantly poorer fit tothe data. This is evidence of measurement variance and DIFamong the items. Next, model comparisons were carried out onan item-by-item basis, constraining the parameters of one itemat a time to equality. The results of these model comparisonsare presented in Table 1. As can be seen from Table 1, everysingle model comparison resulted in a significant increase inG2, indicating that none of the items was invariant across thegroups. Table 1 also shows the item difficulty parameters forboys and girls estimated from the baseline model. The values ofthese parameters denote the value of the latent trait at which theprobability of agreement with the particular item is 0.5. Thelatent trait is further assumed to be measured on a scale with a
Table 1. Baseline parameter estimates and model comparisons in theDIF analysis
Item constrained
df change G² value
Item difficulty parametera
Boys Girls
All 24 184.8*1 2 151.4* 0 2.862 2 148.8* 0.17 3.133 2 143.8* 0.10 4.044 2 100.1* 0.36 2.585 2 95.2* 0.32 2.506 2 82.9* 0.53 4.127 2 184.8* −0.35 1.928 2 134.7* 0.19 2.479 2 86.8* 0.42 4.1010 2 56.9* 0.64 3.5511 2 131.6* 0.19 4.4512 2 84* 0.47 2.91
Notes: The model with no item parameters constrained to equality across groups is the baseline model.a Denotes item difficulty parameters estimated in the baseline model. The parameters indicate levels of the latent trait at which the probability of agreement with the items is 0.5. The latent trait is given an arbitrary mean point of 0.* p < 0.0001.

Scand J Psychol 50 (2009) Youth gambling in Norway 59
© 2008 The Authors. Journal compilation © 2008 The Scandinavian Psychological Associations.
midpoint of zero, a unit of measurement of one, and a rangefrom negative infinity to positive infinity. For example, if aperson with a latent score of −0.25 (0.25 SD below the mean)had a 50% probability of passing item X, then the item difficultyparameter for item X is −0.25. Similarly, if a person with alatent score of 0.50 (0.50 SD above the mean) had a 50% prob-ability of passing item Y, then the item difficulty parameter foritem Y is 0.50. As can be seen from Table 1, the item difficultyparameters are consistently lower for boys than for girls, whichmeans that boys have a higher probability of agreeing withevery item, given otherwise equal scores for the latent trait. Forexample, boys with a latent trait score of 0 (representing themean) have a 50% probability of agreeing with item 1, whereas,for girls, the latent trait score indicating a 50% probability isnearly 3 SD above the mean.
Results of the predictor analysis
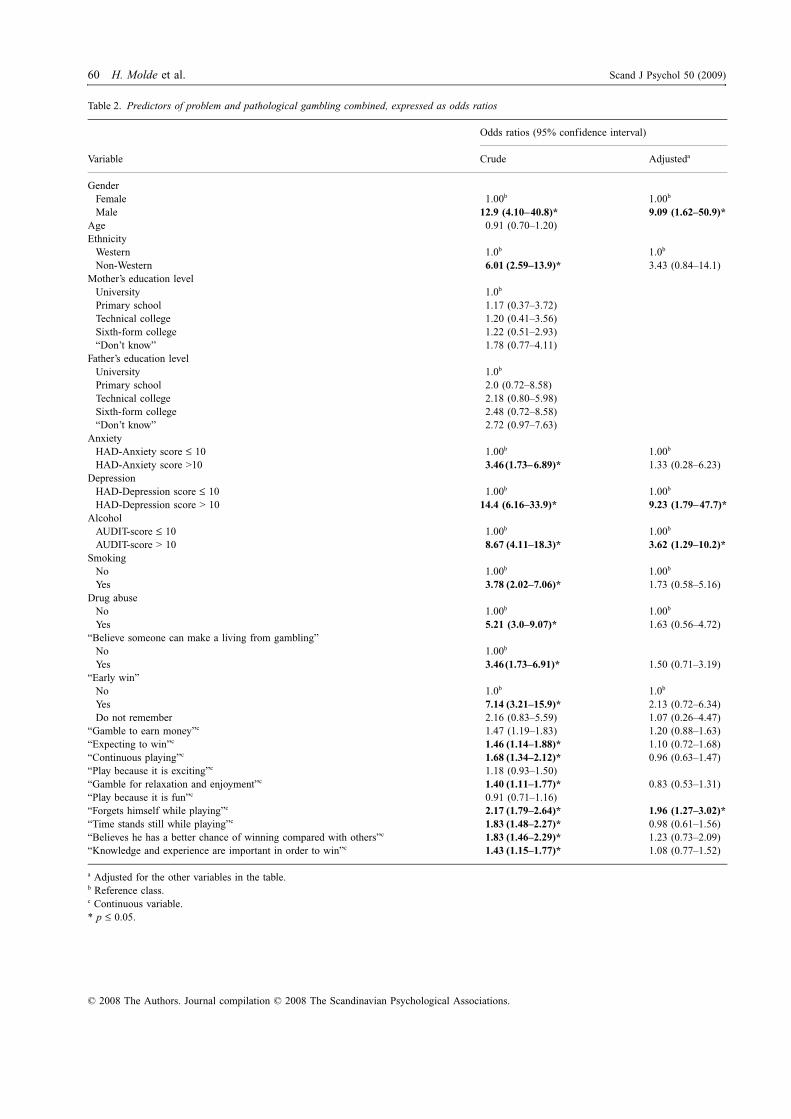
Table 2 presents predictors for all variables for problem andpathological gambling combined in one group. In a univariatelogistic regression analysis, gender (male; OR = 12.9), ethnicity(non-Western; OR = 6.01), anxiety (OR = 3.46), depression(OR = 14.4), alcohol use (OR = 8.67), smoking (OR = 3.78),drug abuse (OR = 5.21), “believing someone can make a livingfrom gambling” (OR = 3.46), “early win” (OR = 7.14), “expectingto win” (OR = 1.46), “continuous playing” (OR = 1.68), “gamblefor relaxation and enjoyment” (OR = 1.40), “forgets himselfwhile playing” (OR = 2.17), “time stands still while playing”(OR = 1.83), “believing he has a better chance of winningcompared with others” (OR = 1.83) and “knowledge andexperience are important in order to win” (OR = 1.43), were allsignificant. When the same variables were entered in a multi-variate logistic regression model, the significant predictors forproblem and pathological gambling (combined) were gender(male; OR = 9.09), depression (OR = 9.23), alcohol abuse (OR= 3.62) and “I forget myself while playing” (OR = 1.96).
DISCUSSION
The first aim of this study was to estimate the prevalence ofproblem and pathological gambling among high-school youth inwestern Norway. The results from our sample, which show that2.5% and 1.9% fulfilled the diagnostic criteria for pathologicaland problem gambling, respectively, are in line with otherrecent surveys in the field (Shaffer et al., 2004). The DSM-criterion with a cut-off of five used in our study is considereda conservative measure of pathological gambling. In the gam-bling field, however, the use of different measures with differentcut-offs makes it somewhat difficult to compare prevalencerates across studies. Some authors have argued that a cut-off offour for pathological gambling (Fisher, 1992, 2000) is morefeasible due to the need to screen adolescents “at risk” of devel-oping a serious gambling problem. It could therefore be arguedthat our estimates are conservative measures of prevalence ratesof pathological gambling problems in Norway.
Our results revealed that the male to female ratio was 12:1for problem and pathological gambling combined. A consistentfinding reported in the literature is that males are more likelyto gamble than females. It may be that gambling is part of malegender role risk-taking behavior to a greater degree than amongwomen (Chalmers & Willoughby, 2006). Social norms may alsoprotect (vulnerable) women more strongly against developinggambling problems or from developing a greater degree of gam-bling problems (Potenza, Steinberg, McLauglin, Wu, Rousaville& O’Malley, 2001). Previous studies have typically reported aratio three to five times higher for males than for females(Jacobs, 2000; Johansson & Gøtestam, 2004; Rossow & Hansen,2003). Hence, the ratio in this study is exceptionally high, evenhigher than the ratio found in the early studies from treatmentand Gamblers Anonymous settings (7:1 to 10:1; Custer & Milt,1985; Legarda, Babio & Abreau, 1992). One explanation for thelarge gender difference may be that gambling problems surfaceat a higher age among females than among males (Lesieur,Cross, Frank et al., 1991). Given that our sample was restrictedto youths aged 16 to19, a large gender difference should thereforebe expected. However, the gender differences could also be afunction of the properties of the diagnostic criteria, which couldhave a male bias.
Our second aim for the study was therefore to see how wellthe DSM-IV criteria measured by MAGS functioned as a validmeasure of male and female adolescent gambling problems,using item response theory. The results provide support formeasurement variance between boys and girls for every item onthe DSM-IV subscale of MAGS. Every item exhibited DIF, sothat boys were more likely to respond positively to the DSM-IVitems than girls, given otherwise equal scores for the latentvariable. This indicates that the DSM-IV criteria function as amore valid set of criteria for boys than for girls. Hence, thediagnostic criteria seem to be biased towards male preponderanceof problem and pathological gambling.
Our third aim was to investigate which identified risk factorswould predict involvement in problem/pathological gambling.Combining both levels of gambling revealed that being male,being depressed, abusing alcohol and dissociating while playingwere all significant predictors of having a gambling problem.These results are largely in line with our predictions and earlierresearch. For example, the finding that alcohol predictedproblem/pathological gambling involvement is well establishedin the research literature (e.g. National Research Council, 1999).Another finding in the present study was that depression was asignificant predictor of gambling problems after controlling forall the other predictors. Several studies have found that gamblingis associated to a greater extent with alcohol and drug abuse inmales than in females, while a gambling problem has been shownto be more strongly associated with mood disorders such asdepression among women than men (Desai, MaciejewskiPantalon & Potenza, 2005; Ibanez, Blanco, Moreyra & Sàiz-Ruiz, 2003). In the present study, alcohol abuse was a weakerpredictor of gambling than gender and depression. As such, ourresults indicate that mood disturbance, such as depression, is an
60 H. Molde et al. Scand J Psychol 50 (2009)
© 2008 The Authors. Journal compilation © 2008 The Scandinavian Psychological Associations.
Table 2. Predictors of problem and pathological gambling combined, expressed as odds ratios
Variable
Odds ratios (95% confidence interval)
Crude Adjusteda
GenderFemale 1.00b 1.00b
Male 12.9 (4.10–40.8)* 9.09 (1.62–50.9)*Age 0.91 (0.70–1.20)Ethnicity
Western 1.0b 1.0b
Non-Western 6.01 (2.59–13.9)* 3.43 (0.84–14.1)Mother’s education level
University 1.0b
Primary school 1.17 (0.37–3.72)Technical college 1.20 (0.41–3.56)Sixth-form college 1.22 (0.51–2.93)“Don’t know” 1.78 (0.77–4.11)
Father’s education levelUniversity 1.0b
Primary school 2.0 (0.72–8.58)Technical college 2.18 (0.80–5.98)Sixth-form college 2.48 (0.72–8.58)“Don’t know” 2.72 (0.97–7.63)
AnxietyHAD-Anxiety score ≤ 10 1.00b 1.00b
HAD-Anxiety score >10 3.46 (1.73–6.89)* 1.33 (0.28–6.23)Depression
HAD-Depression score ≤ 10 1.00b 1.00b
HAD-Depression score > 10 14.4 (6.16–33.9)* 9.23 (1.79–47.7)*Alcohol
AUDIT-score ≤ 10 1.00b 1.00b
AUDIT-score > 10 8.67 (4.11–18.3)* 3.62 (1.29–10.2)*Smoking
No 1.00b 1.00b
Yes 3.78 (2.02–7.06)* 1.73 (0.58–5.16)Drug abuse
No 1.00b 1.00b
Yes 5.21 (3.0–9.07)* 1.63 (0.56–4.72)“Believe someone can make a living from gambling”
No 1.00b
Yes 3.46 (1.73–6.91)* 1.50 (0.71–3.19)“Early win”
No 1.0b 1.0b
Yes 7.14 (3.21–15.9)* 2.13 (0.72–6.34)Do not remember 2.16 (0.83–5.59) 1.07 (0.26–4.47)
“Gamble to earn money”c 1.47 (1.19–1.83) 1.20 (0.88–1.63)“Expecting to win”c 1.46 (1.14–1.88)* 1.10 (0.72–1.68)“Continuous playing”c 1.68 (1.34–2.12)* 0.96 (0.63–1.47)“Play because it is exciting”c 1.18 (0.93–1.50)“Gamble for relaxation and enjoyment”c 1.40 (1.11–1.77)* 0.83 (0.53–1.31)“Play because it is fun”c 0.91 (0.71–1.16)“Forgets himself while playing”c 2.17 (1.79–2.64)* 1.96 (1.27–3.02)*“Time stands still while playing”c 1.83 (1.48–2.27)* 0.98 (0.61–1.56)“Believes he has a better chance of winning compared with others”c 1.83 (1.46–2.29)* 1.23 (0.73–2.09)“Knowledge and experience are important in order to win”c 1.43 (1.15–1.77)* 1.08 (0.77–1.52)
a Adjusted for the other variables in the table.b Reference class.c Continuous variable.* p ≤ 0.05.

Scand J Psychol 50 (2009) Youth gambling in Norway 61
© 2008 The Authors. Journal compilation © 2008 The Scandinavian Psychological Associations.
important gender-independent factor in the development ormaintenance of a gambling problem, for boys as well as forgirls. One obvious explanation is that gambling problems leadto a depressed mood (Langhinrichsen-Rohling, 2004). Anotherexplanation is that depression may function as an incitement togambling. This notion is in line with Jacobs (1986, 2000), whoargues that gambling behavior functions as a means of alleviat-ing stress and negative feelings, a characteristic shared withother addictions such as alcohol and substance abuse. Thisassumption was supported by our analyses, since dissociationwas found to be a significant predictor of problem/pathologicalgambling. Overall, this lends support to the notion that a gam-bling disorder is part of an addictive behavior spectrum. Tworecent studies reported that, in addition to the effects of stressfulcircumstances, gambling is predicted by emotion-focusedcoping, which has been found to promote involvement in high-riskbehavior such as gambling (Bergevin, Gupta, Derevensky &Kaufman, 2006; Gupta, Derevensky & Marget, 2005).
Contrary to our predictions, ethnicity was not a significantpredictor of problem/pathological gambling in the multivariatemodel. An explanation for this could be that the small sub-sample size of the non-Western group (n = 53) made it hard toreach statistical significance. As a risk factor, however, theassociation between ethnicity and gambling involvement is welldocumented by previous research (Burge, Pietrzak & Petry,2006; Jacobs, 2000; NRC, 1999; Welte, Barnes, Wieczorek,Tidwell & Parker, 2004).
The reason that no association was found between SES andproblem/pathological gambling in our sample may be the relativeequity that prevails in Norwegian society, where all adolescentsgenerally receive the same public education. The differencebetween our results and those of Rossow and Hansen (2003)may be due to the narrow age group of our sample, whichfocused exclusively on 16 to 19-year-old adolescents, whileRossow and Hansen had a youth sample ranging from 12 to19 years. In line with this reasoning, it is well documentedfrom research that older youth are more autonomous fromparental influence than younger adolescents (Siegel & Scovill,2000).
Contrary to our predictions, having a “big win” early in one’s“gambling career” was not a significant predictor of gamblingproblems. One reason that it did not reach significance in oursample may be the low statistical power. Tentative support forthis argument is found in the fact that this variable had an oddsratio in the magnitude of about seven in the crude analysis,which is quite high. Studies of clinical populations report thatmany pathological gamblers have histories of an early “big” winin their gambling careers (Ladouceur et al., 2002). The argu-ment is that such experiences “enrich” otherwise very intermittentearly schedules of reinforcement. Abrams and Kushner (2004)speculate that different early win-loss patterns early in a person’sgambling career may produce distinct bio-behavioral trajectories,in which only some pathways lead to pathological gambling. Theyspeculate that individual differences may regulate the responseto the operant contingencies inherent in gambling. Thus, for
some individuals, positive or negative reinforcement fromgambling may have a more powerful influence on futuregambling behavior than for others.
It is interesting that dissociation was the only item or variableconcerning the motives expressed for problem/pathologicalgambling (e.g. “gamble to win money”) that was significant inthe multivariable analysis. It thus seems that the mood alteringfunction of the developed (addictive) behavior is much moreimportant with respect to maintenance of the gambling disorderthan the other motives. It is also possible that there are otherimportant individual factors, such as impulsivity (Sharpe, 2002)or competitiveness (Parke, Griffiths & Irwing, 2004) that couldbetter explain the development and maintenance of problem/pathological gambling among more vulnerable adolescent groups.In that context, a recent study (Gupta, Derevensky & Ellenbogen,2006) reports that, based on their gambling behavior, therewere qualitative differences in personality and risk-taking stylesamong adolescents. Unfortunately, questions about such traitswere not included in the present study.
A common finding in the literature is that the age of adoles-cents shows a positive correlation with problem gambling. Inour sample, no such age-related difference was found. This isin line with the findings of Rossow and Hansen (2003), and theexplanation for this result may be the sheer exposure to andopportunities for gambling that the younger generation hasexperienced. This is somewhat disturbing, considering thatrecent studies indicate that more problematic forms of gamblingare predicted by earlier gambling involvement (e.g. Burge et al.,2006).
Study limitations
This study had an estimated response rate of 69.8% (the finalsample). The prevalence estimates must therefore be interpretedwith some caution. The use of the internet as a medium forcollecting responses (data) is a possible source of non-participation.However, results from web-based surveys have not beenfound to differ from paper-and-pencil-based surveys (e.g.Miller, Neal, Roberts, Baer, Cressler, Metrik & Marlatt, 2002;Pealer, Weiler, Pigg, Miller & Dorman, 2001). For some popu-lations, web-based data collection may actually prove to bemore appropriate than paper-and-pencil-based studies (Milleret al., 2002).
If dropping out from our final sample is systematic, forexample as a result of student characteristics (e.g. abstainers),this could affect the results. As non-response is often associatedwith different types of problems (Mattila, Parkkari & Rimpelä,2007), the estimates for problem and pathological gambling inthe present study could be underestimates.
Another possible bias in relation to the prevalence estimatesis the lack of adequate criterion validity for the screeninginstruments (Winters, 2001). Some authors have raised thequestion of whether prevalence rates may be inflated due toscreening tool bias (e.g. Ladouceur, 2001). Discussing thisissue, Derevensky et al. (2003) argue that, in spite of this

62 H. Molde et al. Scand J Psychol 50 (2009)
© 2008 The Authors. Journal compilation © 2008 The Scandinavian Psychological Associations.
limitation, it could still be the case that the estimates are actuallyconservative due to the above-mentioned problems relating tonon-responders.
The study was based upon a randomized sample of olderadolescents from the Hordaland county of Norway, hence theresults cannot be generalized to other populations without anyreservations. Still, studies concerning psychological healthamong Norwegian adolescents show that the differences acrosscounties are relatively small (Statistics Norway, 1999). Studieshave also shown that the prevalence of psychological problemsin Norway is comparable to the prevalence figures found inother European countries (Kringlen, Torgersen & Cramer, 2001).
CONCLUSION
Our results show that gambling may represent a considerableproblem for an alarmingly high proportion of students in highschool in Norway. The ratio of male to female youths with agambling problem was high and, overall, gender, depression,alcohol abuse and dissociation during gambling were predictorsof problem/pathological gambling involvement in our sample.Future studies should include item response theory in order tocompare different screening instruments with respect to howwell they function in relation to gender. Longitudinal designsshould also be used in future research in order to monitor ageof onset and gambling behavior over time (incidence rates), thusrevealing the stability of the behavior in question (Shaffer et al.,2004). With respect to risk factors, future research should alsoinclude personality trait questionnaires, measuring impulsivityand competitiveness, as well as questions about delinquentbehavior.
REFERENCES
American Psychiatric Association (2000). Diagnostic and statisticalmanual of mental disorders (rev. 4th edn). Washington DC: Author.
Abrams, K. & Kushner, M. G. (2004). Behavioral understanding. InG. J. Grant & M. N. Potenza (Eds.), Pathological gambling: A clinicalguide to treatment (pp. 113–126). London: American PsychiatricPublishing.
Babor, T. F., de la Fuente, J. R., Saunders, J. & Grant, M. (1989). TheAlcohol Use Disorders Identification Test: Guidelines for use inprimary health care. Geneva: World Health Organization.
Barnes, G. C., Welte, J. W., Hoffman, J. H. & Dintcheff, B. A. (2005).Shared predictors of youthful gambling, substance use, and delin-quency. Psychology of Addictive Behaviors, 19, 165–174.
Bergevin, T., Gupta, R., Derevensky, J. & Kaufman, F. (2006). Adolescentgambling: Understanding the role of stress and coping. Journal ofGambling Studies, 22, 195–208.
Bolen, D. W. & Boyd, W. H. (1968). Gambling and the gambler: Areview and preliminary findings. Archives of General Psychiatry,18, 617–629.
Burge, A. N., Pietrzak, R. H. & Petry, N. M. (2006). Pre/early adolescentonset of gambling and psychosocial problems in treatment-seekingpathological gamblers. Journal of Gambling Studies, 22, 263–274.
Carrol, D. & Huxley, J. A. A. (1994). Cognitive, dispositional, andpsychophysiological correlates of dependent slot machine gam-bling in young people. Journal of Applied Social Psychology, 24,1070–1083.
Chalmers, H. & Willoughby, T. (2006). Do predictors of gamblinginvolvement differ across male and female adolescents? Journal ofGambling Studies, 22, 373–392.
Clayton, R. (1992). Transitions in drug use: Risk and protective factors.In M. Glantz & R. Pickens (Eds.), Vulnerability to drug abuse(pp. 15–52). Washington, DC: American Psychological Association.
Claussen, B. & Aasland, O. G. (1993). The Alcohol Use Disorder Iden-tification Test (AUDIT) in a routine health examination of long-term unemployed. Addiction, 88, 363–368.
Crockford, D. N. & el-Guebaly, N. (1998). Psychiatric comorbidity inpathological gambling: A critical review. Canadian Journal ofPsychiatry, 89, 1369–1376.
Custer, R. L. & Milt, H. (1985). When luck runs out. New York: Factson File Publications.
Desai, R. A., Maciejewski, P. K., Pantalon, M. V. & Potenza, M. N.(2005). Gender differences in adolescent gambling. Annals ofClinical Psychiatry, 17, 249–258.
Derevensky, J. L. & Gupta, R. (2000). Prevalence estimates of adoles-cent gambling: A comparison of the SOGS-RA, DSM-IV-J, and theGA-20 questions. Journal of Gambling Studies, 16, 227–250.
Derevensky, J. L. & Gupta, R. (2006). Measuring gambling problemsamong adolescents: Current status and future directions, Interna-tional Gambling Studies, 6, 201–215.
Derevensky, J. L., Gupta, R. & Winters, K. (2003). Prevalence rates ofyouth gambling problems: Are the current rates inflated? Journal ofGambling Studies, 19, 405–425.
Derevensky, J. L., Gupta, R., Harpoon, K., Dickson, L. & Daguerre, A.-E.(2003). Youth gambling. Some social policy issues. In G. Reith (Ed.),Who wins? Who loses? New York: Prometheus Books.
Dickerson, M. & O’Connor, J. (2006). Gambling as an addictivebehaviour: Impaired control, harm minimisation, treatment andprevention. Cambridge: Cambridge University Press.
Farrell, A. D. (1991). Computers and behavioral assessment: Currentapplications, future possibilities, and obstacles to routine use.Behavioral Assessment, 13, 159–179.
Fisher, S. (1992). Measuring pathological gambling in children: Thecase of fruit machine gamblers in the U. K. Journal of GamblingStudies, 8, 263–285.
Fisher, S. (2000). Developing the DSM-IV-MR-J criteria to identifyadolescent problem gambling in non clinical populations. Journal ofGambling Studies, 16, 253–273.
Griffiths, M. (1995). Adolescent gambling. London: Routledge.Griffiths, M. & Sutherland, I. (1998). Adolescent gambling and drug
use. Journal of Community and Applied Social Psychology, 8,423–427.
Griffiths, M., Parke, J. & Wood, R. (2002). Excessive gambling andsubstance abuse: Is there a relationship? Journal of Substance Use,7, 187–190.
Gupta, R. & Derevensky, J. L. (1998a). Adolescent gambling behavior:A prevalence study and examination of the correlates associatedwith problem gambling. Journal of Gambling Studies, 14, 319–345.
Gupta, R. & Derevensky, J. L. (1998b). An empirical examination ofJacobs’ General Theory of Addictions: Do adolescent gamblers fitthe theory? Journal of Gambling Studies, 14, 17– 49.
Gupta, R., Derevensky, J. L. & Ellenbogen, S. (2006). Personality char-acteristics and risk-taking tendencies among adolescent gamblers.Canadian Journal of Behavioural Science, 38, 201–213.
Gupta, R., Derevensky, J. L. & Marget, N. (2005). Coping strategiesemployed by adolescents with gambling problems. Child andAdolescent Mental Health, 9, 115–120.
Herrmann, C. (1997). International experience with the HospitalAnxiety and Depression Scale – A review of validation and clinicalresults. Journal of Psychosomatic Research, 42, 17–41.
Ibanez, A., Blanco, C., Moreryra, P. & Sàiz-Ruiz, J. (2003). Genderdifferences in pathological gambling. Journal of Clinical Psychiatry,64, 295–301.
Scand J Psychol 50 (2009) Youth gambling in Norway 63
© 2008 The Authors. Journal compilation © 2008 The Scandinavian Psychological Associations.
Jacobs, D. F. (1986). A general theory of addictions: A new theoreticalmodel. Journal of Gambling Behavior, 2, 27–37.
Jacobs, D. F. (2000). Juvenile gambling in North America: An analysis oflong term trends and future prospects. Journal of Gambling Studies,16, 119–152.
Jacobs, D. F. (2004). Juvenile gambling in North America: Long termtrends and future prospects. In J. L. Derevensky & R. Gupta (Eds.),Gambling problems in youth: Theoretical and applied perspectives(pp. 1–26). New York: Kluwer Academic/Plenum Publishers.
Johansson, A. & Gøtestam, G. K. (2003). Gambling and problematicgambling with money among Norwegian youth (12–18 years).Nordic Journal of Psychiatry, 57, 317–321.
Kish, L. (1987). Statistical design for research. New York: Wiley.Korn, D. A. & Shaffer, H. J. (1999). Gambling and the health of the
public: Adopting a public health perspective. Journal of GamblingStudies, 15, 289–365.
Kringlen, E., Torgersen, S. & Cramer, V. (2001). A Norwegian psychi-atric epidemiological study. American Journal of Psychiatry, 158(7),1091–1098.
Ladouceur, R. (2001). Conceptual issues in screening and diagnosticinstruments: Implications for treatment and prevention of gamblingdisorders. Paper presented at the Toward Meaningful Diagnosis ofGambling Disorders: From Theory to Practice Conference, LasVegas, Nevada.
Ladouceur, R., Sylvain, C., Boutin, C. & Doucet, C. (2002). Under-standing and treating the pathological gambler. New York: Wiley.
Langewisch, M. W. J. & Frisch, G. R. (1998). Gambling behavior andpathology in relation to impulsivity, sensation seeking, and riskbehavior in male college students. Journal of Gambling Studies, 14,245–262.
Langhinrichsen-Rohling, J. (2004). Gambling, depression, and suicidal-ity in adolescents. In J. L. Derevensky & R. Gupta (Eds.), Gamblingproblems in youth: Theoretical and applied perspectives (pp. 41–56). New York: Kluwer Academic/Plenum Publishers.
Langhinrichsen-Rohling, J., Rohde, P., Seeley, J. R. & Rohling, M. L.(2004). Individual, family, and peer correlates of adolescent gambling.Journal of Gambling Studies, 20, 23–46.
Legarda, J. J., Babio, R. & Abreau, J. M. (1992). Prevalence estimatesof pathological gambling in Seville (Spain). British Journal ofAddiction, 87, 767–770.
Lesieur, H., Cross, J., Frank, M., Welch, M., White, C. M., Rubenstein, G.,Moseley, K. & Mark, M. (1991). Gambling and pathological gam-bling among university students. Addictive Behaviors, 16, 517–527.
Mattila, V. M., Parkkari, J. & Rimpelä, A. (2007). Adolescent surveynon-response and later risk of death. A prospective cohort study of78,609 persons with 11-year follow-up. BMC Public Health, 7, Artno. 87, 1–6.
Miller, E. T., Neal, D. J., Roberts, L. J., Baer, J., Cressler, S. O.,Metrik, J. & Marlatt, G. A. (2002). Test-Retest reliability of alco-hol measures: Is there a difference between internet-based assess-ment and traditional methods? Psychology of Addictive Behaviors,16, 56–63.
National Research Council (1999). Pathological gambling: A criticalreview. Washington, DC: National Academy Press.
Norwegian Gaming Board (2004). Proposal for an action plan to pre-vent problem gambling and reduce the harmful effects of excessivegambling.
Parke, J., Griffiths, M. & Irwing, P. (2004). Personality traits in patho-logical gambling: Sensation seeking, deferment of gratification andcompetitiveness as risk factors. Addiction Research and Theory, 12,201–212.
Pealer, L. N., Weiler, R. M., Pigg, R. M., Miller, D. & Dorman, S. M.(2001). The feasibility of a web-based surveillance system to collecthealth risk behavior data from college students. Health Educationand Behavior, 28, 547–559.
Petry, N. M. & Armentano, C. (1999). Prevalence, assessment, andtreatment of pathological gambling: A review. Psychiatric Services,50, 1021–1027.
Potenza, M. N., Steinberg, M. A., McLaughlin, S. D., Wu, R.,Rousaville, B. J. & O’Malley, S. S. (2001). Gender-related differ-ences in the characteristics of problem gamblers using a gamblinghelpline. American Journal of Psychiatry, 158, 1500–1505.
Reise, S. P., Widaman, K. F. & Pugh, R. H. (1993). Confirmatoryfactor analysis and item response theory: Two approaches forexploring measurement invariance. Psychological Bulletin, 114,552–566.
Rossow, I. & Hansen, M. (2003). Underholdning med bismak: Ungdomog pengespill. NOVA Rapport 1/2003.
Rossow, I. & Molde, H. (2006). Chasing the criteria. ComparingSOGS-RA and the Lie/Bet screen to assess prevalence of problemgambling and “at-risk” gambling among adolescents. Journal ofGambling Issues, 18, 57–71.
Saunders, J. B., Aasland, O. G., Babor, T. F., de la Fuente, J. R. & Grant,M. (1993). Development of the Alcohol Use Disorders Identifica-tion Test (AUDIT): WHO Collaborative Project on Early Detectionof Persons with Harmful Alcohol Consumption – II. Addiction 88,791–804.
Shaffer, H. J. & Hall, M. N. (2001). Updating and refining prevalenceestimates of disordered gambling behaviour the United States andCanada. Canadian Journal of Public Health, 92, 168–172.
Shaffer, H. J. & Korn, D. A. (2002). Epidemiology and biostatistics –Gambling and related mental disorders: A public health analysis.Annual Review of Public Health, 23, 171–212.
Shaffer, H. J., LaBrie, R. A., LaPlante, D. A., Nelson, S. E. & Stanton,M. V. (2004). The road less travelled: Moving from distributions todeterminants in the study of gambling epidemiology. CanadianJournal of Psychiatry, 49, 504–516.
Shaffer, H. J., LaBrie, R., Scanlan, K. M. & Cummings, T. H. (1994).Pathological gambling among adolescents: Massachusetts gamblingscreen (MAGS). Journal of Gambling Studies, 10, 339–362.
Sharpe, L. (2002). A reformulated cognitive–behavioral model of prob-lem gambling: A biopsychosocial perspective. Clinical PsychologyReview, 22, 1–25.
Siegel, A. W. & Scovill, L. C. (2000). Problem behaviour: The doublesymptom of adolescence. Development and Psychopathology, 12,763–793.
Statistics Norway. Health Survey 1995. Oslo: Statistics Norway; 1999.Stewart, D. G. & Brown, S. A. (1995). Withdrawal and dependency
symptoms among adolescent alcohol and drug abusers. Addiction,90, 627–635.
Stinchfield, R., Cassuto, N., Winters, K. C. & Latimer, W. (1997).Prevalence of gambling by Minnesota public school students in1992 and 1995. Journal of Gambling Studies, 13, 25–48.
Stinchfield, R. & Winters, K. C. (1998). Gambling and problem gam-bling among youths. In J. H. Frey (Ed.), Gambling: Socioeconomicimpact and public policy (pp. 172–185). The Annals of the AmericanAcademy of Political and Social Science.
Stinchfield, R. (2004). Demographic, psychosocial, and behavioralfactors associated with youth gambling and problem gambling. InJ. L. Derevensky & R. Gupta (Eds.), Gambling problems in youth:Theoretical and applied perspectives (pp. 27–40). New York:Kluwer Academic/Plenum Publishers.
Thissen, D. (2003). MULTILOG: multiple, categorical item analysis andtest scoring using Item response theory (Version 7.03) [computersoftware]. Chicago: Scientific Software.
Thissen, D., Steinberg, L. & Gerrard, M. (1986). Beyond group-meandifferences: The concept of item bias. Psychological Bulletin, 99,118–128.
Toneatto, T. (1999). Cognitive psychopathology of problem gambling.Substance Use and Misuse, 34, 1593–1604.
Volberg, R. A. & Abbott, M. W. (1994). Lifetime prevalence estimates

64 H. Molde et al. Scand J Psychol 50 (2009)
© 2008 The Authors. Journal compilation © 2008 The Scandinavian Psychological Associations.
of pathological gambling in New Zealand. International Journal ofEpidemiology, 23, 976–983.
Welte, J. H., Barnes, G. M., Wieczorek, W. F., Tidwell, M-C. O. & Parker,J. C. (2004). Risk factors for pathological gambling. Addictive Behav-iors, 29, 323–335.
Winters, K. C. (2001). Screening, assessment, and diagnosis of gam-bling disorders: Are adolescents different? Paper presented at theToward Meaningful Diagnosis of Gambling Disorders: FromTheory to Practice Conference, Las Vegas, December.
Winters, K. C. & Anderson, N. (2000). Gambling involvement anddrug use among adolescents. Journal of Gambling Studies, 16,175–198.
Winters, K. C., Stinchfield, R. D. & Fulkerson, J. (1993). Toward thedevelopment of an adolescent gambling problem severity scale.Journal of Gambling Studies, 9, 371–386.
Winters, K. C., Arthur, N., Leitten, W. & Botzet, A. (2004). Gamblingand drug abuse in adolescence. In J. L. Derevensky & R. Gupta(Eds.), Gambling problems in youth: Theoretical and appliedperspectives (pp. 57–80). New York: Kluwer Academic/PlenumPublishers.
Zigmond, A. B. & Snaith, R. P. (1983). The Hospital Anxiety andDepression Scale. Acta Psychiatrica Scandinavica, 67, 361–370.
Received 7 November 2007, accepted 15 February 2008
Copyright © 2022 FDOKUMEN