Preoperative Chlorhexidine Skin Preparation for Patients ...
Preoperative fasting for preventing perioperative
complications in children (Review)
Brady M, Kinn S, O’Rourke K, Randhawa N, Stuart P
This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library2005, Issue 4
http://www.thecochranelibrary.com
1Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

T A B L E O F C O N T E N T S
1ABSTRACT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2SYNOPSIS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2BACKGROUND . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3OBJECTIVES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
4CRITERIA FOR CONSIDERING STUDIES FOR THIS REVIEW . . . . . . . . . . . . . . . . . .
4SEARCH STRATEGY FOR IDENTIFICATION OF STUDIES . . . . . . . . . . . . . . . . . . . .
5METHODS OF THE REVIEW . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
6DESCRIPTION OF STUDIES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
7METHODOLOGICAL QUALITY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
9RESULTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
26DISCUSSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
28AUTHORS’ CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
29NOTES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
29POTENTIAL CONFLICT OF INTEREST . . . . . . . . . . . . . . . . . . . . . . . . . . .
29ACKNOWLEDGEMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
30SOURCES OF SUPPORT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
30REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
35TABLES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
35Characteristics of included studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
47Characteristics of excluded studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
47ADDITIONAL TABLES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
47Table 01. Guidelines for Paediatric Preoperative Fasting . . . . . . . . . . . . . . . . . . . . .
48Table 02. The ASA Physical Status Classification System . . . . . . . . . . . . . . . . . . . . .
49Table 03. Search strategy for electronic databases . . . . . . . . . . . . . . . . . . . . . . . .
54Table 04. Participants’ Age and Paediatric Age Groups . . . . . . . . . . . . . . . . . . . . . .
54Table 05. Details of Quality Evaluation by Trial . . . . . . . . . . . . . . . . . . . . . . . .
59Table 06. Summary Statistics - Gastric Volume (ml/kg) - Intervention Groups . . . . . . . . . . . . . .
61Table 07. Summary Statistics - Gastric Volume (ml/kg) - Control Group . . . . . . . . . . . . . . . .
63Table 08. Summary Statistics - Gastric pH - Intervention Groups . . . . . . . . . . . . . . . . . .
66Table 09. Summary Statistics - Gastric pH - Control Group . . . . . . . . . . . . . . . . . . . .
69Table 10. Key to Secondary Outcome Data Tables . . . . . . . . . . . . . . . . . . . . . . .
69Table 11. Details of Particles Observed in Gastric Aspirates . . . . . . . . . . . . . . . . . . . .
71Table 12. Duration of Fast - Aspiration/Regurgitation . . . . . . . . . . . . . . . . . . . . . .
73Table 13. Duration of Fast - Secondary Outcome Measures . . . . . . . . . . . . . . . . . . . .
74Table 14. Shortened Fluid Fast versus Standard Fast - Thirst . . . . . . . . . . . . . . . . . . . .
75Table 15. Shortened Fluid Fast versus Standard Fast - Hunger . . . . . . . . . . . . . . . . . . .
76Table 16. Shortened Fluid Fast versus Standard Fast - Behaviour . . . . . . . . . . . . . . . . . . .
76Table 17. Shortened Fluid Fast versus Standard Fast - Comfort . . . . . . . . . . . . . . . . . . .
77Table 18. Shortened Fluid Fast versus Standard Fast - Vomiting . . . . . . . . . . . . . . . . . . .
77Table 19. Shortened Solid + Fluid Fast versus Short Fluid Fast - Hunger . . . . . . . . . . . . . . . .
78Table 20. Short Fluid Fast 1 versus Short Fluid Fast 2 - Hunger . . . . . . . . . . . . . . . . . . .
78Table 21. Short Fluid Fast 1 versus Short Fluid Fast 2 - Behaviour . . . . . . . . . . . . . . . . . .
78Table 22. Short Fluid Fast 1 versus Short Fluid Fast 2 - Vomiting . . . . . . . . . . . . . . . . . .
78Table 23. Type of Intake - Aspiration/Regurgitation . . . . . . . . . . . . . . . . . . . . . . .
80Table 24. Type of Intake - Secondary Outcome Measures . . . . . . . . . . . . . . . . . . . . .
81Table 25. Type of Fluid versus Standard Fast - Thirst . . . . . . . . . . . . . . . . . . . . . .
82Table 26. Type of Fluid versus Standard Fast - Hunger . . . . . . . . . . . . . . . . . . . . . .
82Table 27. Type of Fluid versus Standard Fast - Behaviour . . . . . . . . . . . . . . . . . . . . .
83Table 28. Type of Fluid versus Standard Fast - Comfort . . . . . . . . . . . . . . . . . . . . . .
83Table 29. Type of Fluid versus Standard Fast - Vomiting . . . . . . . . . . . . . . . . . . . . .
84Table 30. Volume of Intake - Aspiration/Regurgitation . . . . . . . . . . . . . . . . . . . . . .
iPreoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

86Table 31. Volume of Intake - Secondary Outcome Measures . . . . . . . . . . . . . . . . . . . .
87Table 32. Volume of Fluid versus Standard Fast - Thirst . . . . . . . . . . . . . . . . . . . . .
87Table 33. Volume of Fluid versus Standard Fast - Hunger . . . . . . . . . . . . . . . . . . . . .
88Table 34. Volume of Fluid versus Standard Fast - Behaviour . . . . . . . . . . . . . . . . . . . .
89Table 35. Volume of Fluid versus Standard Fast - Comfort . . . . . . . . . . . . . . . . . . . . .
89Table 36. Volume of Fluid versus Standard Fast - Vomiting . . . . . . . . . . . . . . . . . . . .
90Table 37. Volume 1 [V1] versus Volume 2 [V2] - Thirst . . . . . . . . . . . . . . . . . . . . .
90Table 38. Volume 1 [V1] versus Volume 2 [V2] - Hunger . . . . . . . . . . . . . . . . . . . . .
91Table 39. Volume 1 [V1] versus Volume 2 [V2] - Behaviour . . . . . . . . . . . . . . . . . . . .
91Table 40. Sensitivitiy Analysis - excluding trials with inadequate randomisation . . . . . . . . . . . . .
91GRAPHS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
91Comparison 01. Duration - Short Fluid Fast versus Standard Fast . . . . . . . . . . . . . . . . . .
92Comparison 02. Duration - Short Solid + Fluid Fast versus Standard Fast . . . . . . . . . . . . . . .
92Comparison 03. Duration - Short Solid + Fluid Fast versus Short Fluid Fast . . . . . . . . . . . . . .
92Comparison 04. Duration - Short Fluid Fast 1 versus Short Fluid Fast 2 . . . . . . . . . . . . . . . .
92Comparison 05. Type of Intake - Fluid versus Standard Fast . . . . . . . . . . . . . . . . . . . .
92Comparison 06. Type of Intake - Fluid 1 versus Fluid 2 . . . . . . . . . . . . . . . . . . . . .
92Comparison 07. Volume of Intake - Volume of Fluid versus Standard Fast . . . . . . . . . . . . . . .
93Comparison 08. Volume of Intake - Volume 1 versus Volume 2 . . . . . . . . . . . . . . . . . . .
93INDEX TERMS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
93COVER SHEET . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
94GRAPHS AND OTHER TABLES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
94Fig. 1. Comparison 01. Duration - Short Fluid Fast versus Standard Fast. . . . . . . . . . . . . . . .
9402 Gastric contents - Volume (ml/kg) . . . . . . . . . . . . . . . . . . . . . . . . . .
96Fig. 2. Comparison 01. Duration - Short Fluid Fast versus Standard Fast. . . . . . . . . . . . . . . .
9603 Gastric contents - pH . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
97Fig. 3. Comparison 01. Duration - Short Fluid Fast versus Standard Fast. . . . . . . . . . . . . . . .
9704 Gastric contents - Phenol red based volume (ml) . . . . . . . . . . . . . . . . . . . . .
98Fig. 4. Comparison 02. Duration - Short Solid + Fluid Fast versus Standard Fast. . . . . . . . . . . . . .
9802 Gastric Contents - Volume (ml/kg) . . . . . . . . . . . . . . . . . . . . . . . . . .
98Fig. 5. Comparison 02. Duration - Short Solid + Fluid Fast versus Standard Fast. . . . . . . . . . . . . .
9803 Gastric Contents - pH . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
99Fig. 6. Comparison 03. Duration - Short Solid + Fluid Fast versus Short Fluid Fast. . . . . . . . . . . . .
9902 Gastric Contents - Volume (ml/kg) . . . . . . . . . . . . . . . . . . . . . . . . . .
100Fig. 7. Comparison 03. Duration - Short Solid + Fluid Fast versus Short Fluid Fast. . . . . . . . . . . . .
10003 Gastric Contents - pH . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
101Fig. 8. Comparison 04. Duration - Short Fluid Fast 1 versus Short Fluid Fast 2. . . . . . . . . . . . . .
10102 Gastric Contents - Volume (ml/kg) . . . . . . . . . . . . . . . . . . . . . . . . . .
102Fig. 9. Comparison 04. Duration - Short Fluid Fast 1 versus Short Fluid Fast 2. . . . . . . . . . . . . .
10203 Gastric Contents - pH . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
103Fig. 10. Comparison 05. Type of Intake - Fluid versus Standard Fast. . . . . . . . . . . . . . . . . .
10302 Gastric Contents - Volume (ml/kg) . . . . . . . . . . . . . . . . . . . . . . . . . .
105Fig. 11. Comparison 05. Type of Intake - Fluid versus Standard Fast. . . . . . . . . . . . . . . . . .
10503 Gastric contents - pH . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
107Fig. 12. Comparison 05. Type of Intake - Fluid versus Standard Fast. . . . . . . . . . . . . . . . . .
10704 Gastric contents - Phenol red based volume (ml) . . . . . . . . . . . . . . . . . . . . .
107Fig. 13. Comparison 06. Type of Intake - Fluid 1 versus Fluid 2. . . . . . . . . . . . . . . . . . .
10702 Gastric Contents - Volume (ml/kg) . . . . . . . . . . . . . . . . . . . . . . . . . .
108Fig. 14. Comparison 06. Type of Intake - Fluid 1 versus Fluid 2. . . . . . . . . . . . . . . . . . .
10803 Gastric Contents - pH . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
109Fig. 15. Comparison 07. Volume of Intake - Volume of Fluid versus Standard Fast. . . . . . . . . . . . .
10902 Gastric Contents - Volume (ml/kg) . . . . . . . . . . . . . . . . . . . . . . . . . .
110Fig. 16. Comparison 07. Volume of Intake - Volume of Fluid versus Standard Fast. . . . . . . . . . . . .
iiPreoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

11003 Gastric contents - pH values . . . . . . . . . . . . . . . . . . . . . . . . . . . .
112Fig. 17. Comparison 08. Volume of Intake - Volume 1 versus Volume 2. . . . . . . . . . . . . . . . .
11202 Gastric Contents - Volume (ml/kg) . . . . . . . . . . . . . . . . . . . . . . . . . .
112Fig. 18. Comparison 08. Volume of Intake - Volume 1 versus Volume 2. . . . . . . . . . . . . . . . .
11203 Gastric contents - pH . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
iiiPreoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Preoperative fasting for preventing perioperativecomplications in children (Review)
Brady M, Kinn S, O’Rourke K, Randhawa N, Stuart P
This record should be cited as:
Brady M, Kinn S, O’Rourke K, Randhawa N, Stuart P. Preoperative fasting for preventing perioperative complications in children. TheCochrane Database of Systematic Reviews 2005, Issue 2. Art. No.: CD005285. DOI: 10.1002/14651858.CD005285.
This version first published online: 20 April 2005 in Issue 2, 2005.
Date of most recent substantive amendment: 10 February 2005
A B S T R A C T
Background
Children, like adults, are required to fast before general anaesthesia with the aim of reducing the volume and acidity of their stomach
contents. It is thought that fasting reduces the risk of regurgitation and aspiration of gastric contents during surgery. Recent developments
have encouraged a shift from the standard ’nil-by-mouth-from-midnight’ fasting policy to more relaxed regimens. Practice has been
slow to change due to questions relating to the duration of a total fast, the type and amount of intake permitted.
Objectives
To systematically assess the effects of different fasting regimens (duration, type and volume of permitted intake) and the impact on
perioperative complications and patient wellbeing (aspiration, regurgitation, related morbidity, thirst, hunger, pain, comfort, behaviour,
nausea and vomiting) in children.
Search strategy
We searched Cochrane Wounds Group Specialised Register, the Cochrane Central Register of Controlled Trials, MEDLINE, CINAHL,
the National Research Register, relevant conference proceedings and article reference lists and contacted experts.
Selection criteria
Randomised and quasi randomised controlled trials of preoperative fasting regimens for children were identified.
Data collection and analysis
Data extraction and trial quality assessment was conducted independently by two authors. Trial authors were contacted for additional
information including adverse events.
Main results
Forty-three randomised controlled comparisons (from 23 trials) involving 2350 children considered to be at normal risk of regurgitation
or aspiration during anaesthesia. Only one incidence of aspiration and regurgitation was reported.
Children permitted fluids up to 120 minutes preoperatively were not found to experience higher gastric volumes or lower gastric pH
values than those who fasted. The children permitted fluids were also less thirsty and hungry, better behaved and more comfortable
than those who fasted.
Clear fluids preoperatively did not result in a clinically important difference in the children’s gastric volume or pH. Evidence relating
to the preoperative intake of milk was sparse. The volume of fluid permitted during the preoperative period did not appear to impact
on children’s intraoperative gastric volume or pH contents.
Authors’ conclusions
There is no evidence that children who are not permitted oral fluids for more than six hours preoperatively benefit in terms of
intraoperative gastric volume and pH over children permitted unlimited fluids up to two hours preoperatively. Children permitted
fluids have a more comfortable preoperative experience in terms of thirst and hunger. This evidence applies only to children who are
considered to be at normal risk of aspiration/regurgitation during anaesthesia.
1Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

S Y N O P S I S
Most children can safely drink clear liquids until two hours before surgery, although more research is needed for some groups of children
General anaesthetic inhibits the protective reflexes that stop the stomach contents reaching the lungs. In order to prevent the inadvertent
inhalation of stomach contents, children are often advised to have nothing to eat or drink from the midnight before surgery. However,
the review of trials found that drinking clear fluids up to a few hours before surgery did not increase the risk of regurgitation during
or after surgery. Indeed there is an added benefit of a more comfortable preoperative experience in terms of thirst and hunger. Some
children are considered more likely to regurgitate under anaesthetic, including those who are obese, diabetic or have stomach disorders.
More research is needed to determine whether these children can also safely drink up to a few hours before surgery.
B A C K G R O U N D
NEEDS OF CHILDREN FASTING PREOPERATIVELY
The amount and type of food and fluid that children need preop-
eratively varies with age. A neonate (a baby less than one month
old) needs to be fed often with milk (breast milk, non-human milk
or formula) to prevent hunger and thirst while the physiological
needs of the adolescent (child 12 to 18 years) are similar to those
of an adult (Aitkenhead 1996). Reflexes that normally protect the
airway and lungs are depressed or may even be absent during gen-
eral anaesthesia (Aitkenhead 1996, Litman 1999). Food or fluid
regurgitated from the stomach and entering the lungs (aspiration)
may lead to aspiration pneumonia (Mendelson 1946) and even
death. The aspiration of breast milk or infant formula in particular
results in severe damage to the lungs (O’Hare 1996). Children are
usually starved of food and fluid before their surgery to reduce the
risk of aspiration during anaesthesia.
CRITICAL GASTRIC CONTENT VALUES
Fasting aims to reduce the volume and acidity of children’s stom-
ach contents. Children and adults however are often fasted (nil-by-
mouth or NPO) from midnight before their surgery which may
result in a fast of 12 hours or more (MacLean 1993; Veall 1995;
While 1992). The incidence and severity of aspiration pneumo-
nia is thought to be dependent on the volume and acidity of the
stomach contents aspirated. No study has looked at the resulting
pneumonia following aspiration of various volumes and pHs of
gastric contents in humans but there are animal model studies as
listed below such as James 1984 and Raidoo 1990. The link be-
tween fasting, the content of children’s stomachs during surgery
and the risk of injury, should the contents be regurgitated and as-
pirated, is not clear. Many researchers have adopted the arbitrarily
defined critical values of acidity (a pH value of less than 2.5) and
volume (below 0.4 ml/kg) based on unpublished rhesus monkey
data (Roberts 1974). It is widely recognised that these measures
are flawed (Schreiner 1998) and recent research suggests that the
acidity of the contents maybe more relevant than volume (James
1984; Raidoo 1990). The evidence in relation to human breast
milk and formula however is equivocal (O’Hare 1996; O’Hare
1999).
Before stomach contents can be regurgitated and aspirated into
the lungs (leading to aspiration pneumonia) there must be a suf-
ficient volume of contents in the stomach. We do not know what
this critical volume is and it may never be possible to accurately
establish the exact values required to pose a threat to child safety.
As outcome measures, volume and pH value of stomach contents
can only be considered surrogate measures of risk while more re-
liable measures are not (and may never be) available. Children
rarely regurgitate and aspirate their stomach contents while anaes-
thetised and so aspiration pneumonia (and related death) is even
rarer (Engelhardt 2001; Kluger 1999; NCEPOD 2003; SASM
2002). Therefore large multicenter trials would be required to
demonstrate a difference in the effectiveness of a fasting regimen
based on such rare but clinically important outcome measures.
FASTING REGIMENS
Despite the uncertainty surrounding the critical values of gastric
contents older children and adults have traditionally followed a
nil-by-mouth (NPO) from midnight instruction before morning
surgery. For afternoon surgery, an early light breakfast is permitted
which in the UK is typically a cup of tea and slice of toast. The
traditional fast for younger children however appears to be less
globally defined. Fasting regimens shorter than NPO from mid-
night were in place at some centres (Hunt 1987). Typically this
more relaxed approach permitted clear fluids up to four hours pre-
operatively for infants (1 to 12 months), six hours for children (1
to 5 years) and eight hours for children older than 5 years. Other
centres continued to apply the nil-by-mouth-from-midnight pol-
icy.
GUIDELINES
The American Academy of Pediatrics (Committee on Drugs) was
the first to publish specific guidelines for children fasting preoper-
atively. They recommended that clear fluids could be taken up to
two hours prior to anaesthesia while milk or solids could be con-
sumed up to four hours preoperatively for neonates, six hours for
infants and eight hours for children. More recent guidelines pub-
lished by the American Society of Anesthesiologists (ASA) recom-
mended a six-hour fast from non-human milk or infant formula
for neonates and infants but a less conservative fast from breast
milk of four hours preoperatively (see Table 01 for details). Several
2Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

other national guidelines suggest that their members adhere to the
recommendations of the ASA (AAGBI 2001; NHSQIS 2003) and
guidelines continue to be developed (RCN).
PRACTICE
Despite the publication of guidelines, many hospitals have been
slow to adjust children’s fasts (Engelhardt 2001; Ferrari 1999; Haas
1998). In a recent survey many British and Irish paediatric anaes-
thetists* allowed children to drink clear fluids up to two hours pre-
operatively (guidelines recommendation) but as many as 25% did
not. Instructions relating to other intake, i.e. breast milk, formula,
non-human milk and solids demonstrated even more variation
(Emerson 1998). Similar variations in permitted milk intake have
also been found (Engelhardt 2001) and in some cases anaesthetists
are permitting milk intake closer to surgery time than is currently
supported by the guidelines (Hofer 2001). Milk, although a liquid,
behaves more like a solid within the stomach with curds forming.
Such inconsistencies in practice may reflect a degree of uncertainty
in evaluating the evidence relating to the preoperative intake of
milk. Local policies require the consensus of the whole preopera-
tive care multidisciplinary team (anaesthetists and nurses) as they
strive to achieve a balance between a child’s unnecessary starvation
and their safety, hydration and well being. Thus, some clinicians
may well be reluctant to alter an existing policy (or their own prac-
tice) that they believe ensures patients’ safety (though not perhaps
their comfort). The disparate nature of the evidence in relation to
fasting from milk and other food and fluid intake makes it difficult
for clinicians to independently evaluate the quality and relevance
of the evidence for themselves.
EVALUATING THE EVIDENCE
Researchers have investigated the duration of fasting, the volume
and the type of intake permitted during a restricted fasting pe-
riod using a variety of outcome measures. We have described the
complexities of using the objective (if surrogate) outcome mea-
sures of gastric content volume and pH above. In some cases non-
absorbable marker dyes were used to measure the volume of chil-
dren’s stomach contents. Phenolsulfonphthalein (phenol red) or
bromosulphthalein (BSP) were added to children’s stomach con-
tents (either before or during surgery) and the concentration of
the dyes in the stomach was expressed as a percentage of the orig-
inal dye ingested and thus provided an indication of gastric emp-
tying. In addition, children’s ratings of thirst, hunger and comfort
were also collected using visual analogue scales (VAS). Very young
children however were unable to complete the scale (or other for-
mal measure) and so, in some cases parents described their child’s
thirst, hunger, behaviour and comfort.
Following our systematic review of preoperative fasting for adults
(Brady 2004) we expected some complexity in evaluating the evi-
dence. Pharmacological co-interventions such as H2 receptor an-
tagonists (for example ranitidine) which function to inhibit the
production of gastric acid, antacids which raise gastric pH or anti-
emetic drugs which increase gastrointestinal motility (for exam-
ple metoclopramide, domperidone) were anticipated. We also ex-
pected the evidence to address a wide age range of children with
fasting policy varying according to the child’s age making compar-
isons difficult. In addition, some children are considered to be at
a high risk of regurgitation and aspiration. For example, children
who require emergency surgery or those who are obese may have
delayed rates of gastric emptying and thus require a specific fast to
ensure an empty stomach (Hofer 2001).
Results that are not statistically significant should be interpreted
with caution as they do not necessarily indicate no difference ex-
ists (Alderson 2004). Instead our interpretation should be clini-cally based on how certain we are that any important benefits or
harms have been excluded (Alderson 2004, Altman 2004, Man-
Son-Hing 2002). This judgement should be made on the basis
of predetermined thresholds or limits of equivalence (Man-Son-
Hing 2002). It is difficult to establish precise values especially in
relation to preoperative fasting and many of the issues have been
mentioned above. They include the low incidence (and reporting)
of the primary outcome of aspiration and regurgitation, the sur-
rogate nature of the alternative primary outcomes gastric pH and
volume, the lack of valid critical gastric values and differences be-
tween individual clinicians’ and patients’ interpretation of what is
considered clinically important (for example Smith 2004). Given
these complexities the picture in relation to the optimum preop-
erative fasting regimen for children is a complex one. We set out
to systematically gather and review the available evidence in rela-
tion to preoperative fasting for children and make it available to
clinicians so that they could independently evaluate the evidence.
*Where we have used the title anaesthetist it is inclusive of the
professional title anesthesiologist (as used in North America).
O B J E C T I V E S
Our objective was to systematically identify, appraise and synthe-
sise the evidence of the effects of different preoperative fasting reg-
imens (duration, type and volume of permitted intake) on periop-
erative complications and patient wellbeing (including aspiration,
regurgitation and related morbidity, thirst, hunger, pain, comfort,
behaviour, nausea, vomiting) in children. We examined the evi-
dence to establish:
1. The optimal duration of a preoperative fast from fluids/solids
for children (in terms of minimising perioperative complications)
During a preoperative fasting period that permits some restricted
intake:
2. What is the optimal type of intake permitted
3. What is the optimal volume of permitted intake in terms of
minimising perioperative complications?
Some children are considered to be at a high risk of aspiration and
related complications, for example those who are obese
4. To what extent does the evidence support different fasting reg-
imens for different high-risk patient populations?
3Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

C R I T E R I A F O R C O N S I D E R I N G
S T U D I E S F O R T H I S R E V I E W
Types of studies
All randomised controlled trials (RCTS) which evaluated different
fasting regimens in terms of duration or type/volume of intake
prior to general anaesthesia. Less robust methods of allocation
(for example quasi-randomised trials based on surgical lists) were
considered for inclusion.
Types of participants
Children and young people (18 years of age or less) undergoing
general anaesthesia.
Those considered to be at normal risk of regurgitation/aspiration
are those who are described as healthy (ASA I-II) and undergoing
elective surgery (see Table 02). Children considered to be at high
risk of regurgitation/aspiration include those who are:
(a) emergency cases (especially following trauma);
(b) obese;
(c) have gastric disorders or disease.
The results from the trials based on these subgroups have been
presented separately as specified in the protocol (see Objective 4).
Types of intervention
Within the parallel adult review we defined a standard fast as NPO
from midnight before morning surgery with a light breakfast per-
mitted early in the morning before afternoon surgery. However,
as described above many traditional fasting policies for children
recognise the varied in this population. Typically, these more le-
nient traditional NPO fasts are four hours for infants (1 to 12
months), six hours for children (1 to 5 years) and eight hours for
children older than 5 years. A small drink (up to 30 ml) to assist
the intake of oral medication was also permitted during the stan-
dard fasting period. Studies that evaluated the following fasting
regimens were considered for inclusion in the review. The order
they are presented in corresponds to the objectives of the review.
Types of interventions
1. Duration of fast
(a) Shortened Fluid Fast versus Standard Fast
(b) Shortened Solid and Fluid Fast versus Standard Fast
(c) Shortened Solid and Fluid Fast versus Short Fluid Fast
(d) Short Fluid Fast 1 versus Short Fluid Fast 2
2. Type of Permitted Intake (during a restricted fasting period)
(a) Fluid Intake Permitted (e.g. water, coffee, orange juice) versus
Standard Fast.
(b) Fluid 1 versus Fluid 2
3. Volume of Permitted Intake (during a restricted fasting period)
(a) Volume of Fluid Intake versus Standard Fast
(b) Volume of Fluid Intake 1 versus Volume 2
Investigations which also evaluated the administration of a proki-
netic, H2-receptor antagonist or antacid agent but in which the
control group did not receive a similar administration of the drug
were excluded from the review.
Types of outcome measures
Primary outcomes:
• rate of adverse events (aspiration/regurgitation) or those arising
as a result of aspiration including related morbidity (primarily
aspiration pneumonia) or case fatality;
• volume and/or pH of gastric contents (on induction of anaes-
thesia) with the quality of the aspirate (nature of any particles
observed) described narratively;
• concentration of marker dye (for example phenol red) as an
indicator of gastric emptying.
Secondary outcomes:
• thirst;
• hunger;
• pain;
• behaviour;
• comfort;
• nausea; and
• vomiting.
S E A R C H S T R A T E G Y F O R
I D E N T I F I C A T I O N O F S T U D I E S
See: Wounds Group search strategy
We identified relevant studies through the following sources.
Electronic databases
MEDLINE from 1966 to October 2004
CINAHL from 1982 to October 2004
Cochrane Central Register of Controlled Trials (CENTRAL)
Issue 3 2004
National Research Register (UK) as of October 2004
Cochrane Wounds Group Specialised Register September 2004
The Cochrane Wounds Group Specialised Register has been
complied through searching of the major health databases
including MEDLINE, CINAHL and EMBASE and is regularly
updated through searching of the Cochrane Central Register of
Controlled Trials, handsearching of wound care journals and
relevant conference proceedings.
We searched the above databases using the specific search
strategies detailed in Table 03. The search strategies were
constructed using controlled vocabulary (MeSH) and free text
terms following consultation with the Cochrane Wounds Group.
There were no language restrictions on the searches.
4Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Journal handsearch
We did not handsearch any journals.
Conference proceedings
We hand searched the following key conference proceedings to
identify any relevant studies unavailable in print.
American Society of Anaesthesiologists Annual Meeting 1979 to
2004
Anaesthetic Research Society Abstracts 1978 to April 2003
Canadian Anesthetist’s Society Annual Meeting 1983 to 2004
European Society of Anaesthesiologists Annual Congress
Abstracts 1993 to 2003
Scandinavian Society of Anaesthesiologists 1977 to 2003
Society for Obstetric Anaesthesia and Perinatology Annual
Meeting 1998 to 2002
We checked reference lists from relevant articles for further
sources of preoperative fasting studies.
Personal communication
We attempted to contact the main authors from all studies
included in the review to ask if they had been involved in any
further studies or articles or whether they were aware of any
recent or on going studies (published or unpublished) on the
topic of preoperative fasting. They were also asked if they were
aware of any other individuals prominent or active in the field
that the review authors should contact.
M E T H O D S O F T H E R E V I E W
IDENTIFICATION AND SELECTION OF TRIALS
We identified the relevant literature using the search strategies
detailed in Table 03. Procite, a bibliographic database package, was
used to manage the references. lnvestigative trials which addressed
preoperative fasting amongst children (in terms of duration of fast,
type/volume of intake permitted) were identified. References from
an early version of the search (MEDLINE 1966 to Nov 1999;
CINAHL 1982 to 1999) were screened by a second researcher.
We did not identify any additional trials relevant to the review in
this second screening.
Relevant trials were evaluated (based on the full texts) by three
independent authors. They confirmed the inclusion of the study in
the review. In some cases additional information was required from
the author(s) before a final decision could be made. We resolved
any conflicting decisions through discussion.
DATA EXTRACTION
Two authors (MB and PS) carried out data extraction using a
standardised data extraction sheet which detailed the following:
- children’s age, weight, ASA physical status (see Table 02),
inpatient/outpatient;
- participant inclusion/exclusion criteria;
- fast duration;
- premedication;
- intake permitted (amount, type, duration of fast);
- concurrent interventions;
- operation type (elective, emergency, region);
- type of anaesthesia;
- timing of data collection; and
- outcomes.
In addition, we extracted the following information from those
studies that used residual gastric content values as an outcome
measure:
- instrument and method of gastric content collection;
- method of pH measurement.
Where relevant information was unavailable from the text, we
contacted the trial authors and asked them to provide missing
details. Where trials were published more than once, we used
all the available sources of information to retrieve the maximum
amount of information possible. In the event of any inconsistency
we contacted the authors to resolve the issue. Where this was
not possible the most comprehensive trial report was used and all
publications referring to the results of the trials were recorded.
METHODOLOGICAL QUALITY
A system of coding the methodological quality of trials was adapted
from a report by the Centre for Reviews and Dissemination
(CRD Report Number 4) and piloted. Two authors (MB and SK)
independently evaluated quality and we resolved any disagreement
in coding through discussion. Aspects of methodological quality
considered included:
- listing of inclusion and exclusion criteria;
- evidence of an a priori sample size calculation;
- indication of the comparability of groups at baseline ;
- evidence of an intention-to-treat analysis (coded as yes/no);
- details of the method of generating the randomisation sequence
;
- evidence of concealment of allocation;
- evidence of blinding of assessors.
Details of the coding system can be found in CRD Report Number
4. Where relevant information was unavailable from the text, trial
authors were contacted. Details of whether trial quality evaluations
were based on published information or information provided by
authors can be found in Table 05 Details of Quality Evaluation
by Trial.
STATISTICAL ANALYSIS
Some of the outcome variables in this review (for example residual
gastric values of volume and pH) have skewed distributions. Except
for trials with very small sample sizes, treatment comparisons based
on mean and standard deviation (SD) summary data can be safely
assumed as being approximately normally distributed i.e. with the
mean and SD summary data the usual weighted mean difference
approach is robust to skewness. Unfortunately often authors only
report group medians and ranges (for example minimum and
5Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

maximum or 25th and 75th percentiles) for skewed data and
do not present means and SDs. While mean and SD summary
statistics were sought it was not always possible to get these from
the available data or directly from the authors. Where this was the
case, pseudo-values were calculated (O’Rourke 2002) so that the
usual weighted mean difference approach could be used. For the
purposes of this review, the term pseudo is used to indicate that
the values for the mean (pseudo-mean) and SD (pseudo-SD) are
not true mean and SD values. These pseudo-values are estimates
of what the true mean and SD values might be and allow for the
uncertainty entailed by not actually observing them directly, only
estimating them indirectly via other summary measures.
One of the authors (KO’R) has developed two approaches to the
calculation of these values (O’Rourke 2002). The first, which is
fairly mathematical, calculates and uses a likelihood based on the
summaries in hand and requires the use of numerical optimization
software (O’Rourke 2002). The second avoids the need for
numerical optimization software by drawing on statistical methods
for dealing with reported group medians and various ranges as
linear combinations of order statistics (Arnold 1992). This method
uses least squares to estimate the best linear estimates of the
unreported mean and SD along with an appropriate standard error
for the pseudo-mean, which again reflects uncertainty entailed by
not actually observing the mean. These pseudo-means and pseudo-
SDs are then entered into RevMan and treated as if they were
actually observed (again, the process above having made allowance
for them being estimated rather than actually observed). In general
the first approach was used and where this was not possible the
second approach was used. Except for highly skewed data, the
results tend to be very similar and for highly skewed data the
first approach is arguably more correct. Sensitivity analysis for the
amount of skew can be carried out for the second approach, and
this was done whenever the first approach was not available. With
the pseudo-means and pseudo-SDs in hand, the usual methods
for meta-analysis of means and SDs via weighted mean differences
can be carried out.
In some cases a trial which randomly allocated children to
two (or more) intervention groups but only one control group
were included within one meta-analysis (e.g. Splinter 1990a and
Splinter 1990b are included in Comparison 05: Type of Intake
- Fluid versus Standard Fast, Outcome: 03 Gastric Contents -
pH 04 Fruit Juice versus Standard Fast). Where this was the
case, we avoided counting the individuals in the control group
twice by ’splitting’ the numbers in the control group across
both interventions (Oxford 2001). This splitting ensures that
the pooled results are correct, but does understate the evidence
available for the various individual comparisons in that these
individual confidence intervals are wider than they ideally need to
be. Division of the number of children was as equal as possible
using whole numbers.
The primary continuous outcome variables in relation to
gastric content (volume, pH, marker dye concentration) were
summarised using weighted mean differences. Chi squared
calculations (significance level set at p < 0.1) were made using
RevMan 4.2.1. Trials which evaluated similar interventions
using similar outcome measures in the absence of clinical or
methodological heterogeneity were pooled. We used a random
effects model in the presence of statistical heterogeneity and to pool
summary data that included pseudo-value calculations. Details of
these aspects will be reported for each section.
Sensitivity analyses were planned based on the method of
randomisation and the presence of assessor blinding. The various
subjective approaches used to evaluate the secondary outcome
measures of thirst, hunger, behaviour, comfort, nausea and
vomiting could not be pooled in a quantitative fashion but were
summarised in a tabular format. Details of the measurement tool,
the timing of the measurement, the comparisons made and the
results of the comparison were profiled and discussed in a narrative
fashion within the results section.
INTERPRETING THE EVIDENCE
To enable us to interpret the evidence from the meta-analyses
where no significant difference between the groups was observed
ideally requires some definition of threshold values or limits of
equivalence. We mentioned above the lack of valid gastric content
volume and pH limits of equivalence. However, some degree of
interpretation is possible. Where the results of a meta-analysis
demonstrated very narrow confidence intervals it was possible to
state that the results provided little indication of an important
clinical difference between the two groups. Similarly, where the
confidence intervals were clearly wide and scattered, a statement
was made to indicate that based on this result, insufficient evidence
was available at present to state whether or not an important
difference exists. In some cases the decision as to whether or not
a clinically important difference existed was more subjective and
in such cases individual readers should interpret the results within
their own framework of clinical importance.
D E S C R I P T I O N O F S T U D I E S
Twenty three trials met the criteria for inclusion and included
children up to 18 years of age. Splinter 1991 had extended the
participant age range to include individuals up to the age of 19
and a decision was made to include this trial within this review of
preoperative fasting for children. Nicolson 1992 included children
described as ASA IV who were all undergoing cardiac surgery. We
included this work within the main body of the results section as
the classification of ASA IV reflects the risk of surgery rather than
a specific increase in the regurgitation/aspiration risk.
The 23 trials were conducted in a number of different coun-
tries. Ten were conducted in Canada (Crawford 1990; Goresky
1992; Sandhar 1989; Splinter 1989; Splinter 1990; Splinter 1991;
6Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Splinter Schaefer 1a; Splinter Schaefer 1b; Splinter Schaefer 2;
Splinter Schaefer 3), five in USA (Cook-Sather 2003; Miller
1990; Nicolson 1992; Schreiner 1990; Welborn 1993), two in
Japan (Kushikata 1996; Maekawa 1993) and one each in China
(Aun 1990), India (Gombar 1997), UK (Meakin 1985), Mexico
(Moyao-García 2001) Italy (Sarti 1991) and Australia (van der
Walt 1986). Given the wide range of geographical settings there
is remarkable methodological consistency across all 23 trials that
sampled gastric contents.
Gastric contents were generally collected using a syringe to aspirate
the stomach contents following insertion of a tube. Two trials used
a nasogastric tube (Aun 1990; Gombar 1997) while Moyao-García
2001 mention the collection of gastric contents during an endo-
scopic examination. The remaining 20 trials all used oro-gastric
tubing which was in some cases further described as multi orifice
(Cook Sather 2003; Crawford 1990; Sandhar 1989; Sarti 1991),
Salem sump (Goresky 1992; Kushikata 1996; Maekawa 1993;
Nicolson 1992; Schreiner 1990; Splinter 1989; Splinter 1990;
Splinter Schaefer 3; Splinter Schaefer 2), Ryles (Meakin 1985),
Levine (Spinter Schaefer 1a; Spinter Schaefer 1b) or a catheter
(Welborn 1993). Sizes of tubing ranged from 10 to 18 gauge and
all but seven trials (Cook-Sather 2003; Goresky 1992; Kushikata
1996; Meakin 1985; Miller 1990, Moyao-García 2001; Sandhar
1989) described tilting the children to ensure the maximum vol-
ume of gastric contents could be aspirated. In all cases the collec-
tion of gastric contents appears to have taken place within a similar
time frame just following induction and intubation. Nine of these
trials also described the quality of the aspirated gastric contents
in terms of any particles observed (Cook-Sather 2003; Kushikata
1996; Maekawa 1993; Meakin 1985; Moyao-García 2001; Splin-
ter 1990; Splinter 1991; Splinter Schaefer 2; Splinter Schaefer 3).
All but one trial (Gombar 1997) that collected gastric volume
as an outcome measure also measured gastric pH. A variety of
tools were used to measure pH values including pH radiometer
(Crawford 1990; Sarti 1991), pH meter (Goresky 1992; Maekawa
1993; Welborn 1993), electrode (Meakin 1985), digital Ionalyzer
pH meter (Nicolson 1992; Sandhar 1989; Scheriner 1990 ), and
pH paper (Aun 1990; Miller 1990; Moyao-García 2001; Splinter
1989; Splinter 1990; Splinter 1991; Splinter Schaefer 1a; Splinter
Schaefer 1b; Splinter Schaefer 2; Splinter Schaefer 3; van der Walt
1986). Some reports also described calibration of the pH mea-
surement tool (Crawford 1990; Goresky 1992; Nicolson 1992;
Sandhar 1989; Schreiner 1990; Welborn 1993). It is unclear how
Cook-Sather 2003 and Kushikata 1996 measured pH.
Eleven trials reported at least one of the secondary outcomes
addressed by this review; thirst (Gombar 1997; Nicolson 1992;
Splinter 1989; Splinter 1990; Splinter 1991), hunger (Cook-
Sather 2003; Kushikata 1996; Nicolson 1992; Splinter 1989;
Splinter 1990; Splinter 1991), behaviour (Cook-Sather 2003;
Gombar 1997; Schreiner 1990; Splinter 1990), comfort (Nicol-
son 1992; Schreiner 1990) and vomiting (Aun 1990; Cook-Sather
2003; Goresky 1992; Maekawa 1993; Schreiner 1990). No trial
reported children’s experience of nausea during the preoperative
period. Given the wide variety of methods used to evaluate these
secondary measures and the subjective nature of their report (in
most cases children’s self-report) a qualitative approach to between-
trial comparisons was adopted. Details of the secondary outcome
measures employed (detailing the method and timing of the data
collection) will be presented within the results section. Splinter
1989; Splinter 1990 and Splinter 1991 employed a linear analogue
scale to measure secondary outcomes, which will be referred to
here as a visual analogue scale.
No trial specifically recruited children considered to be at a high
risk of regurgitation/aspiration during anaesthesia, for example
obese children (calculated with reference to age, height, weight).
All the remaining trials recruited children undergoing elective
surgery with most described as ASA I-II (Table 02). Five trials
did not report the children’s ASA status (Kushikata 1996; Splinter
Schaefer 1a; Splinter Schaefer 1b; van der Walt 1986; Welborn
1993) but described the children as ’healthy’. One trial (Nicolson
1992), was based on children undergoing elective cardiac surgery
classed as ASA II-IV. Most trials took measures to exclude gastric
disease, disorders and/or drugs that affected gastric secretion or
motility with only three failing to indicate these as exclusion cri-
teria (Kushikata 1996; Sarti 1991; Welborn 1993).
In conducting this systematic review we had prespecified three
main age groups of children that we felt were of clinical relevance
- neonate (under 1 month), infant (1 to 12 months), and children
(over 12 months). While eighteen trials had limited recruitment
to children other trials had recruited across age ranges (see Table
04 for details). Three had recruited neonates (Cook Sather 2003;
Splinter Schaefer 3; van der Walt 1986), five had recruited infants
(Cook Sather 2003; Miller 1990; Nicolson 1992; Splinter Schaefer
3; van der Walt 1986) and five had recruited older children (over
12 years) that could be classified as adolescents (Crawford 1990;
Maekawa 1993; Meakin 1985; Sandhar 1989; Schreiner 1990;
Splinter 1991). There was a considerable degree of overlap within
and between trials and it was not always possible to extract the age-
group specific data. Given the degree of overlap all age group data
will initially be presented together which will then be followed
with a further exploration of age specific issues as permitted by the
available data.
M E T H O D O L O G I C A L Q U A L I T Y
This review describes the randomised allocation of 2350 children
across 59 control/intervention arms in 23 trials. Twenty-five chil-
dren in Gombar 1997 were not included in the review as the inter-
vention they were exposed to did not contribute to the evaluation
of a preoperative fasting regimen but evaluated the effectiveness of
a pharmacological intervention. The trials within the review were
small with all control and intervention groups consisting of fewer
7Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

than 100 children. Only three trials randomised more than 150
children; Goresky 1992 (n = 240); Splinter 1991 (n = 152); Wel-
born 1993 (n = 200). Nine trials randomised between 100 and 150
children (Crawford 1990; Maekawa 1993; Meakin 1985; Nicol-
son 1992; Schreiner 1990; Splinter Schaefer 1b; Splinter Schae-
fer 2; Splinter Schaefer 3; van der Walt 1986) and the remaining
eleven trials were based on fewer than 100 children (Aun 1990;
Cook-Sather 2003; Gombar 1997; Kushikata 1996; Miller 1990;
Moyao-García 2001; Sandhar 1989; Sarti 1991; Splinter 1989;
Splinter 1990; Splinter Schaefer 1a).
The quality of the investigative studies was independently exam-
ined by two of the authors (MB and SK). The method of gen-
erating the randomisation sequence was evaluated as adequate in
16 trials (Aun 1990; Cook-Sather 2003; Crawford 1990; Gombar
1997; Miller 1990; Moyao-García 2001; Sandhar 1989; Schreiner
1990; Splinter 1989; Splinter 1990; Splinter 1991; Splinter Schae-
fer 1a; Splinter Schaefer 1b; Splinter Schaefer 2; Spinter Schaefer
3; van der Walt 1986), inadequate in three trials (Kushikata 1996;
Meakin 1985; Welborn 1993) and unclear for the remaining four
trials (Goresky 1992; Maekawa 1993; Nicolson 1992; Sarti 1991).
Similarly methods of concealment of allocation varied. Conceal-
ment of allocation was classified as adequate in five trials (Aun
1990; Cook-Sather 2003; Moyao-García 2001; Nicolson 1992;
Schreiner 1990), inadequate in three (Kushikata 1996; Meakin
1985; Welborn 1993), and unclear in the remaining fifteen trials
(Crawford 1990; Gombar 1997; Goresky 1992; Maekawa 1993;
Miller 1990; Sandhar 1989; Sarti 1991; Splinter 1989; Splinter
1990; Splinter 1991; Splinter Schaefer 1a; Splinter Schaefer 1b;
Splinter Schaefer 2; Spinter Schaefer 3; van der Walt 1986) (see
Characteristics of Included Studies and Table 05).
Blinding of participants and assessors as to the intake of food/fluid
is difficult if not impossible to achieve in a trial evaluating a pre-
operative fasting regimen. However, blinding of the anaesthetist,
sample collector and assessor is possible for trials that aim to mea-
sure children’s gastric content values. Children cannot be blinded
as to whether or not they have had something to eat or drink, and
even blinding as to the volume of intake is difficult. Some compar-
isons do allow for such blinding. Two trials blinded children as to
the type of pharmacological co intervention by administering ei-
ther placebo or ranitidine (Goresky 1992; Sandhar 1989) but eval-
uation of such pharmacological interventions was not the focus of
this review. The difficulty of blinding children (and their parents)
as to whether they have had a drink or eaten is acknowledged and
the impact this might have on the collection of outcome measures
(e.g. ratings of thirst, hunger, comfort) is recognised and will be
returned to in the results and discussion sections.
For the purposes of evaluating the quality of the trials, blinding
ratings refer to the adequacy of blinding the assessors that collected
and measured the gastric content values only and not to the blind-
ing of participants or individuals involved in the collection of pa-
tient reported secondary outcome measures. Blinding details were
unavailable for five trials (Kushikata 1996; Miller 1990; Sandhar
1989; Sarti 1991; Welborn 1993) while for an additional three
trials there were some qualifications to the blinding observed. In
these three cases the blinding was restricted to either the raniti-
dine/placebo intervention (Goresky 1992), the assessor collecting
the thirst and behaviour reports (Gombar 1997), or the assessor
measuring gastric pH and food particles (Meakin 1989). The re-
maining 15 trials were found to have adequate blinding of the
assessors collecting gastric pH and volume measures.
Inclusion and exclusion criteria were available for most trials, al-
though the degree of reporting detail varied (see Characteristics
of Included Studies table). The exclusion criteria for three trials
were unavailable (Kushikata 1996; Welborn 1993; Sarti 1991).
We noted five trials described an a priori sample size calculation
(Cook-Sather 2003; Splinter 1990; Splinter Schaefer 1a; Splinter
Schaefer 1b; Splinter Schaefer 2) although one trial recalculated
this during the trial (Cook-Sather 2003). The remaining trials
made no reference to such a calculation.
Participant groups were demonstrated to be comparable at base-
line by most trials although the level of comparison varied. Three
trials found significant differences between the groups. Gombar
found the children who were fasted in the standard manner were
heavier, older and had more females than the intervention group
while the children given 10 ml/kg of fluid were lighter than the
children given 6ml/kg in the trial by Splinter 1990. Neither trial-
ists undertook an adjusted analysis to account for these differences.
The children permitted intake in the van der Walt 1986 study we
heavier than those that continued to fast. The comparability of
groups in Crawford 1990 was unclear from the text.
Intention to treat analysis was considered by Cook-Sather 2003
but following protocol deviations (n = 30) they only reported a
per protocol analysis. Twelve trials reported omission of some data
from analysis (see Characteristics of Included Studies) and these
usually referred to an absence of pH values as no aspirate was
available from the participant. The remaining 10 trials did not
report any withdrawals and in all trials except one it was clear that
all participants had been included in the data analysis (Moyao-
García 2001; Sarti 1991; Splinter 1989; Splinter 1990; Splinter
1991; Spinter Schaefer 1a; Spinter Schaefer 1b; Spinter Schaefer
2; Spinter Schaefer 3). Quality was not used to weight the trials
in the meta-analyses of this review but will be commented on, as
appropriate, within the results and discussion sections. Full details
of the trials’ quality evaluation are presented in Table 05 Details
of Quality Evaluation by Trials.
As observed in the systematic review relating to adults fasting
preoperatively (Brady 2004), it became clear from examining the
available mean and standard deviation (SD) summary data in this
review that there was also some indication of skewed distribution
(mean/SD < 1.64). Given the nature of the gastric volume and
pH continuous outcome measures, it was not unexpected to find
naturally positively skewed distributions. As described previously
8Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

(Brady 2004), some authors had as a result chosen to present the
skewed distributions using median and range values. In our pre-
vious work we developed a method of calculating pseudo-values
(described above) which allowed us to include within the meta-
analysis those trials that reported only median and range summary
statistics.
All 23 trials measured children’s intra-operative gastric contents
volume and pH. Methods of reporting the summary data for these
continuous outcome measures (volume and pH) varied across tri-
als. Mean and standard deviation gastric content values (volume
and pH) were available in either published or unpublished format
for 16 trials (details in Tables 06 to 09). Meakin 1985 reported the
mean and standard deviation values for the gastric volume mea-
sure only. Mean and range values were reported for both volume
and pH measures (Sandhar 1989; Welborn 1993) or for volume
alone (Aun 1990) while Meakin 1985 reported gastric pH using
median and range values and van der Walt 1986 only reported
range values for both gastric volume and pH. Four trials required
pseudo-values calculated for gastric volume summary data (Aun
1990; Sandhar 1989; van der Walt 1986; Welborn 1993) and for
pH summary data (Meakin 1985; Sandhar 1989; van der Walt
1986; Welborn 1993). Details of the summary statistics reported
by the authors and (when relevant) pseudo-values used within the
meta-analysis can be referred to in Table 06 - Table 09.
R E S U L T S
We addressed four main elements of a preoperative fast within this
review, namely:
(A) the duration of fast;
(B) the type of permitted intake;
(C) the volume of intake permitted during a fasting period and
(D) patient risk of aspiration/regurgitation during anaesthesia as
perceived by the peri-operative team.
The evidence in relation to these four elements of preoperative fast-
ing was evaluated within this review with reference to the primary
outcome measures of aspiration/regurgitation, and gastric content
values (volume, pH, marker dye concentration). The evidence re-
garding the secondary outcome measures of thirst, hunger, pain,
nausea, vomiting and anxiety was also considered and details are
presented in Table 13 - Table 39 with reference made within the
text to the relevant tables as appropriate. For a key to these tables
refer to Table 10.
There is a substantial body of evidence in relation to preoperative
fasting for children and the evidence presented within this review
is extensive. The presentation of the results is organised by the
four parameters of a preoperative fast (as listed above) and within
each of the parameters by outcome measure, which includes (01)
adverse events (02) gastric volume, (03) gastric pH (04) marker
dye and (05) secondary outcomes (as listed above). Whenever pos-
sible labels for each section correspond with the relevant meta-
analysis graph. The incidence of aspiration/regurgitation (and any
associated morbidity/mortality), one of the primary outcomes of
this review, was not consistently addressed by the included trials.
Whenever possible these details were directly sought from the au-
thors. Available results have been presented in Tables 12, 23 and
30.
Eight of the 23 trials included made comparisons between three
or more randomly allocated participant groups of relevance to this
review (Crawford 1990; Goresky 1992; Maekawa 1993; Meakin
1985; Sandhar 1989; Splinter 1990; Splinter Schafer 3; van der
Walt 1986). Thus, for these trials above, two or more comparisons
were made within each trial. For the purposes of this review a
distinction was made between these comparisons by using the
suffix a, b, c etc to the trial name as appropriate (e.g. Splinter
1990a; Splinter 1990b). Details of the randomised comparisons
are available in the Characteristics of Included Studies Table and
to reduce the complexity of the language used within the text, they
will be referred to as trials throughout the remainder of the review.
Following the adult preoperative fasting review (Brady 2004) there
was a clear indication that comparisons that included a H2 re-
ceptor antagonist co-intervention should be presented separately.
We adopted this approach a priori for this review and any meta-
analysis that is based on comparisons that included a H2 receptor
antagonist co-intervention are clearly marked as ’+ H2 receptor
antagonist’.
Given the complexity of the topic and the number of comparisons
and outcomes addressed within this review, readers can refer to an
overview of the results available at the end of the results section.
A. Duration of Fast
Trials that compared two different fasting regimens on the basis of
the duration of the preoperative nil-by-mouth fast are presented in
this section. Standard fasting regimens were compared to a short
fluid fast and a short solid fast, while shortened fluid fasts were
compared to a short solid fast or other short fluid fasts. Chil-
dren within these trials were all considered to be at normal risk
of regurgitation/aspiration during anaesthesia, undergoing elec-
tive surgery and generally ASA I-II. The evidence in relation to
each comparison is presented by outcome used to measure the ef-
fectiveness of the fasting regimens; (01) aspiration/regurgitation,
(02) the volume of gastric contents, (03) the pH of gastric con-
tents, (04) measures of gastric volume and emptying using marker
dye and the secondary outcomes. An overview is available at the
end of the results section.
Comparison 01: Duration - short fluid fast versus standard fast
Outcome 01: Aspiration/RegurgitationEleven trials reported the incidence of adverse events including
regurgitation and aspiration, though an additional eight authors
provided unpublished data on this outcome. Of the 19 trials that
specifically commented on the occurrence of aspiration/regurgita-
tion, only Goresky 1992a and Goresky 1992b reported any events
9Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

of note. Only one incidence of aspiration/regurgitation was ob-
served and occurred within the group that were permitted flu-
ids up to 120 minutes preoperatively. The authors felt this inci-
dence was related to airway management rather than as a result
of the study intervention (Goresky 1992a). The additional eight
events reported included a possible vaso-vagal response (flushing
and sweating post intervention) and children that vomited or spat
out the intervention fluid. These latter events occurred across the
two trials Goresky 1992a and Goresky 1992b but it is unclear to
which groups the children belonged. Details can be found in Table
12 Duration of Fast - Aspiration/Regurgitation.
Outcome 02: Gastric Contents - VolumeTwenty-four trials measured intra-operative gastric volume for a
standard preoperative fast versus a fast that permitted some fluid
intake. The trials within this section are grouped based on the tim-
ing of the experimental intake; fluids permitted up to 120 min-
utes, 150 minutes, 180 minutes and 240 minutes preoperatively.
The results were pooled within the meta-analysis using a random
effects model and can be referred to in Comparison: 01 Duration
- Shortened Fluid Fast versus Standard Fast; Outcome 02 Gastric
Contents - Volume (ml/kg).
(i) Fluids (up to 120 minutes preoperatively) versus Standard Fast
Eight trials compared the intake of fluids up to 120 minutes pre-
operatively (n = 248) with a standard fasting regimen (n = 261).
Pseudo-values were required for two trials (Sandhar 1989a; Wel-
born 1993). Goresky 1992a also compared the intake of fluids up
to 120 minutes preoperatively with a group that followed a tra-
ditional fast. The gastric volume data were reported as one cross-
group summary mean (0.42ml/kg) and standard deviation value
(0.04). As a result these data could not be included within this (or
any other relevant) meta-analysis. On pooling the available data
there was no evidence of a difference for gastric volume (weighted
mean difference (WMD) 0.03 ml/kg confidence interval (CI) 95%
-0.03 to 0.10).
(ii) Fluids (up to 120 minutes preoperatively) versus Standard Fast
(+ H2 Receptor Antagonist)
Two trials that compared the intake of fluid up to 120 minutes
preoperatively (n = 18) to a standard fasting regimen (n = 15)
also administered ranitidine, a H2 receptor antagonist, to all the
children (Goresky 1992b; Sandhar 1989b). Psuedo-standard de-
viation values were calculated for the Sandhar 1989b trial to allow
inclusion of the trial within the meta-analysis. There was no ev-
idence of a difference between the intra-operative gastric volume
of these groups that fasted and those that were permitted fluids
(WMD 0.01ml/kg 95% CI -0.12 to 0.14). Separate summary data
for the groups in the Goresky 1992b trial were not available and
so the data could not be pooled.
(iii) Fluids (up to 150 minutes preoperatively) versus Standard
Fast
The intra-operative gastric volume of 102 children permitted flu-
ids up to 150 minutes preoperatively was compared to the gastric
volume of 71 children that followed a standard fast across three
trials (Splinter 1989; Splinter 1990a; Splinter 1990b). There was
no evidence of a difference between the groups’ gastric content
volume (WMD 0.07 ml/kg 95% CI -0.25 to 0.39).
(iv) Fluids (up to 180 minutes preoperatively) versus Standard Fast
Eight trials asked children to take fluids up to 180 minutes pre-
operatively while a second group of children continued to fast in
the standard manner (Gombar 1997; Miller 1990; Moyao-García
2001; Splinter 1991; Splinter Schaefer 2; van der Walt 1986a; van
der Walt 1986b; van der Walt 1986c). Three of the comparisons
did not provide mean and standard deviation summary data and
so pseudo-values were calculated to permit inclusion of these tri-
als within the meta-analysis (van der Walt 1986a; van der Walt
1986b; van der Walt 1986c). On pooling the data the children
permitted fluids up to 180 minutes prior to surgery (n = 287) had
a significantly lower volume of gastric contents than those children
that fasted in the standard manner (n = 243) (WMD -0.12 ml/kg
95% CI -0.22 to -0.03) p = 0.01.
(v) Fluids (up to 240 minutes preoperatively) versus Standard Fast
Sixty children were randomised to drink fluids up to 240 minutes
preoperatively while 65 others followed a traditional fasting policy
across three trials (Aun 1990; Maekawa 1993b; Meakin 1985e).
Pseudo-standard deviation values were calculated for Aun 1990.
On pooling the data there was no evidence of a difference between
the two groups (WMD 0.03ml/kg 95% CI -0.10 to 0.17).
Outcome 03: Gastric Contents - pHTwenty-three trials compared the intra-operative gastric pH of
children after a shortened fluid fast compared with a standard fast.
This represents all but one of the trials (Aun 1990) that measured
gastric content volume (as detailed above). In many trials individ-
ual children’s gastric pH could not be measured as a gastric sam-
ple could not always be collected and so the numbers of children
included in this comparison differs from the numbers of children
observed in the gastric volume comparison above. A total of 695
children were permitted a shorter fluid fast while 632 continued
a standard preoperative fast. The results of this comparison are
presented in Comparison: 01 Duration - Short Fluid Fast versus
Standard Fast; Outcome 03 Gastric Contents - pH. As with the
gastric volume outcome measure presented above, the trials are
grouped based on the timing of intake (up to 120 minutes, 150
minutes, 180 minutes and 240 minutes preoperatively). The trial
results were pooled using a random effects model.
(i) Fluids (up to 120 minutes preoperatively) versus Standard Fast
Eight trials compared the intake of fluids up to 120 minutes
preoperatively (n = 246) and a standard fasting regimen (n =
238) (Goresky 1992a; Maekawa 1993a; Meakin 1985a; Nicol-
son 1992; Sandhar 1989a; Sarti 1991; Schreiner 1990; Welborn
1993). Psuedo-values were calculated for three of the trials (Meakin
1985a; Sandhar 1989a; Welborn 1993). On pooling the data there
was no evidence of a difference in gastric pH (WMD 0.04, 95%
10Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

CI -0.01 to 0.09) and the narrow confidence intervals indicate that
an important difference between the groups is highly unlikely.
(ii) Fluids (up to 120 minutes preoperatively) versus Standard Fast
(+ H2 Receptor Antagonist)
Two additional trials permitted some children fluids up to 120
minutes preoperatively (n = 68) and compared their gastric pH
with that of children that continued a standard fasting regimen (n =
61) (Sandhar 1989b; Goresky 1992b). The children in these trials
were all also administered ranitidine (an H2 receptor antagonist).
Pseudo-values were calculated for the Sandhar 1989b trial and on
pooling the data there was no statistically significant difference
in gastric pH (WMD 0.53, 95% CI -0.20 to 1.26) though this
comparison is underpowered with only 129 children.
(iii) Fluids (up to 150 minutes preoperatively) versus Standard
Fast
Children permitted fluids up to 150 minutes preoperatively (n =
102) were compared with those who remained fasting (n = 71) in
three trials (Splinter 1989; Splinter 1990a; Splinter 1990b). On
pooling the data there was no evidence of a difference in gastric pH
values between the groups (WMD 0.19, 95% CI -0.11 to 0.49).
(iv) Fluids (up to 180 minutes preoperatively) versus Standard Fast
Eight trials compared fluid intake up to 180 minutes preopera-
tively (n = 242) to a standard fast (n = 223) by evaluating children’s
intra-operative gastric pH (Gombar 1997; Miller 1990; Moyao-
García 2001; Splinter 1991; Splinter Schaefer 2; van der Walt
1986a; van der Walt 1986b; van der Walt 1986c). Pseudo-values
were required for three trials (van der Walt 1986a; van der Walt
1986b; van der Walt 1986c). After pooling the data, there was
no evidence of a difference in gastric pH (WMD 0.32, 95% CI
-0.14 to 0.78) though the high degree of heterogeneity (I2= 88%)
should be noted.
(v) Fluids (up to 240 minutes preoperatively) versus Standard Fast
Both Meakin 1985e and Maekawa 1993b permitted children flu-
ids up to 240 minutes preoperatively (n = 37) while a second group
continued to fast (n = 39). Although Aun 1990 also compared the
intake of fluids up to 240 minutes preoperatively to a standard fast
they did not report separate gastric content pH summary data for
the two groups. Instead, they reported that all children in the study
had a gastric pH of < 2.5. Pseudo-standard deviation values were
required for Meakin 1985e and on pooling these results with those
from Maekawa 1993b, there was no indication of a difference in
intra-operative gastric pH (WMD -0.02, 95% CI -0.23 to 0.18).
Whilst this comparison involved only 76 children the confidence
intervals are narrow and there is no evidence of heterogeneity.
Outcome 04: Gastric Contents - Marker DyesPhenol red
Three trials used phenolsulfonphthalein (also known as PSP or
phenol red) as a marker dye to measure gastric volume.
(i) Fluids (up to 120 minutes preoperatively) versus Standard Fast
Sandhar 1989a used the marker dye to compare gastric volume
after the intake of fluids up to 120 minutes preoperatively (n =
13) and with a standard fast (n = 19). One child who fasted for
an hour after the intervention was found to have a 33% percent
of dye retrieval. Dye retrieval for the remaining children was less
than five percent and for many children no dye was found. No
additional details were available.
(ii) Fluids (up to 120 minutes preoperatively) versus Standard Fast
(+ H2 receptor antagonist)
A second study compared the intake of fluids up to 120 minutes
preoperatively (n = 15) with the standard fast (n = 18) but included
a ranitidine co-intervention (Sandhar 1989b). Dye retrieval was
12% for one child that fasted for one hour following a juice and
ranitidine intervention while the remaining children had a dye
retrieval of less than five percent.
(iii) Fluids (up to 180 minutes preoperatively) versus Standard
Fast
Miller 1990 used phenol red to calculate the volume of intra-op-
erative gastric contents (expressed in ml). The marker dye based
measure of gastric volume of the children permitted fluids up to
180 minutes preoperatively (n = 19) and those that followed a
standard fast (n = 25) are presented in Comparison: 01 Duration -
Short Fluid Fast versus Standard Fast; Outcome: 04 Gastric Con-
tents - Phenol Red. There was no evidence of a between group
difference in gastric volume (WMD -3.10 ml, 95% CI -6.66 to
0.46) though with an increased sample size this result may have
achieved statistical significance.
Bromosulphthalein
Two trials used the marker dye bromosulphthalein (also known as
sulfobromophthalein or BSP).
(i) Fluids (up to 120 minutes preoperatively) versus Standard Fast
Two trials used the dye bromosulphthalein to measure the con-
tribution of the ingested fluids to the intra-operative gastric vol-
ume (Goresky 1992a; Goresky 1992b). Results were reported as a
percentage (%) of recovered dye. Both trials compared the intake
of fluids up to 120 minutes preoperatively to the standard fasting
regimen but one included a ranitidine (H2 receptor antagonist)
co-intervention. In reporting the results the two standard fasting
groups were combined and compared to the recovered marker dye
values from the combined group permitted fluids. The fluid in-
take was reported to have had an insignificant effect on the dye
recovery and the dye recovery represented less than 0.3% of the
volume of intake at the time of marker dye administration. More
dye was recovered from those children given ranitidine than the
children that did not receive this co-intervention (p < 0.001). No
other details were available.
Secondary OutcomesTwelve of the total 24 comparisons presented within this review
compared a shortened fluid fast to a standard fast by evaluating
children’s thirst, hunger, behaviour, comfort and vomiting. No
trial addressed nausea. Additional information on the methods of
11Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

measurement and the nature of the comparisons made is presented
in Table 13 Duration of Fast - Secondary Outcome Measures. The
key to this table is available in Table 10.
• Thirst
Six trials comparing a shortened fluid fast to a standard preopera-
tive fasting regimen considered children’s thirst. In all cases visual
analogue scales were completed immediately preoperatively (time
point f or g) (see Table 10 for key). The children (Splinter 1989;
Splinter 1990a; Splinter 1990b; Gombar 1997; Splinter 1991) or
their parents (Splinter 1989; Nicolson 1992) were asked to de-
scribe their perceptions of thirst by completing the VAS scale. De-
tails of the tools used and the timing of measures are presented
in Table 14 - Shortened Fluid Fast versus Standard Fast - Thirst.
Where differences were noted, the children (or the parents of chil-
dren) who took fluids up to 150 minutes and 180 minutes preop-
eratively described less preoperative thirst than those that followed
a standard fasting regimen. One trial reported no difference in
reported thirst between the children given apple juice 150 min-
utes preoperatively and those that continued fasting preoperatively
(Splinter 1990b).
• Hunger
Five trials compared a shortened fluid fasting regimen with a stan-
dard fasting regimen by measuring patients’ hunger. A visual ana-
logue scale was used to rate preoperative hunger by either a par-
ent (Nicolson 1992; Splinter 1989) or by the children themselves
(Splinter 1989; Splinter 1990a; Splinter 1990b; Splinter 1991).
Details can be referred to in Table 15 Shortened Fluid Fast versus
Standard Fast - Hunger. In three trials there was no difference be-
tween the children’s report of hunger regardless of whether they
had fasted in the traditional manner or received fluids up to 150
(Splinter 1990a; Splinter 1990b) or 180 minutes preoperatively
(Splinter 1991). In the remaining trials, children (and/or parents
of children) given fluids up to 120 (Nicolson 1992) or 150 min-
utes preoperatively (Splinter 1989) reported less hunger.
• Behaviour
The preoperative behaviour of children was evaluated by parents
using a VAS in four trials. Parents were asked to rate how irri-
table (Schreiner 1990; Gombar 1997) or irritable/upset (Splin-
ter 1990a; Splinter 1990b) their child was. Schreiner 1990 and
Splinter 1990a found the children permitted fluids 120 minutes
preoperatively were rated as statistically significantly less irritable
than those who fasted. Interestingly, Splinter 1990a (fluids up to
120 minutes) and Gombar 1997 (fluids up to 180 minutes) found
no difference. Details are presented in Table 16 Shortened Fluid
Fast versus Standard Fast - Behaviour.
• Comfort
Parents in two trials used a VAS to describe their child’s com-
fort during (Nicolson 1992) or tolerance of (Schreiner 1990) the
preoperative experience. Both trials found the children permitted
fluids up to 120 minutes preoperatively were described as statis-
tically significantly more comfortable (or as tolerating the pre-
operative experience better) than the children who fasted in the
standard way. See Table 17 Shortened Fluid Fast versus Standard
Fast - Comfort. Schreiner 1990 also asked parents of children who
had a prior experience of surgery and who were randomised to
receive fluids preoperatively in their trial to consider whether their
child’s preoperative experience was improved in comparison to
prior experiences. For 14 of the 18 children, their parents con-
sidered the preoperative experience that included fluid intake up
to 120 minutes before surgery better than previous preoperative
episodes while the remaining four parents had no opinion.
• Vomiting
Six trials noted the occurrence of vomiting over the preopera-
tive period (Goresky 1992a; Goresky 1992b), on induction (Aun
1990; Maekawa 1993a; Maekawa 1993b; Schreiner 1990), intra-
operatively and on recovery (Aun 1990). Only eight children were
reported as having vomited preoperatively following the intake of
the fluid or fluid and medication intervention across two related
comparisons (Goresky 1992a; Goresky 1992b). It is not clear to
which groups these children belonged. No other vomiting inci-
dent was reported by the remaining four trials. These details are
presented in Table 18 Shortened Fluid Fast versus Standard Fast -
Vomiting.
Comparison 02: Duration - short solid and fluid fast versus
standard fast
Two trials compared a fasting regimen that permitted a shorter fast
from solid food and fluids to a standard fasting regimen (Meakin
1985b; Meakin 1985f). These trials will be presented below in re-
lation to (01) the incidence of aspiration/regurgitation, (02) gastric
contents - volume, and (03) gastric contents - pH. The secondary
outcomes of children’s thirst, hunger, behaviour, comfort, nausea
or vomiting were not considered by these trials. An overview of
the results in relation to a shortened solid and fluid fast is available
at the end of the results section.
Outcome 01: Aspiration/RegurgitationMeakin 1985b and Meakin 1985f report no incidence of regur-
gitation, aspiration, related morbidity or mortality was observed
during these comparisons. This information is presented in Table
12 Duration of Fast - Aspiration/Regurgitation in the additional
tables section.
Outcome 02: Gastric Contents - Volume(i) Solids and Fluids up to 120 minutes preoperatively versus Stan-
dard Fast
Meakin 1985b used a quasi-randomised approach (randomisation
by operation list) to allocate children to either a standard fast (n =
20) or to a fasting regimen that permitted the intake of two plain
biscuits and a drink of orange squash [10 ml/kg max 200 ml] up
to two hours preoperatively (n = 32). Pseudo-standard deviation
values were calculated and included within Comparison 02 Du-
12Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

ration - Short Solid Fast and Fluids versus Standard Fast, 01 Gas-
tric Contents - Volume. The children permitted solids and fluids
up to 120 minutes preoperatively had a significantly higher mean
volume of intra-operative gastric contents than those children that
fasted in the usual manner (WMD 0.25 ml/kg 95% CI 0.07 to
0.43) (p = 0.006).
It is also of note that particles of the solid food intervention were
observed in the gastric aspirate of 13 children permitted solid and
fluid intake while no particles were observed in the aspirate of
the fasted group (see Table 11). This significant result however is
based on a small number of children in a single quasi-randomised
trial.
(ii) Solids and Fluids up to 240 minutes preoperatively versus
Standard Fast
Meakin 1985f asked some children to eat two plain biscuits and
drink orange squash [10 ml/kg max 200 mls] up to four hours
preoperatively (n = 14) while the second group continued to fast
(n = 20). The results of this quasi-randomised trial are presented
in Comparison 02 Duration - Short Solid and Fluid Fast versus
Standard Fast, 01 Gastric Contents - Volume and pseudo-sum-
mary statistics were calculated. There was no indication of a dif-
ference between the groups’ intra-operative volume of gastric con-
tents (WMD 0.09 ml/kg 95% CI -0.12 to 0.30). Particles of food
were observed in the aspirate of three of the group permitted solids
and fluids but none of the fasted group (Table 11).
Outcome 03: Gastric Contents - pH(i) Solids and Fluids up to 120 minutes preoperatively versus Stan-
dard Fast
One trial evaluated the intake of solids and fluids up to 120 min-
utes preoperatively (Meakin 1985b). Children either followed a
standard fasting regimen (n = 14) or were permitted two plain
biscuits and a drink of orange squash [10 ml/kg max 200 mls]
(n = 29). Pseudo-mean and pseudo-standard deviations were cal-
culated and the quasi-randomised trial is presented in Compari-
son 02 Duration - Short Solid Fluid Fast versus Standard Fast, 02
Gastric Contents - pH. There was no indication of a difference
between the groups’ intra-operative gastric pH (WMD 0.35 95%
CI -0.08 to 0.78) however this comparison is extremely under-
powered.
(ii) Solids and Fluids up to 240 minutes preoperatively versus
Standard Fast
Similarly, Meakin 1985f quasi-randomised some children to re-
ceive two biscuits and a drink of orange squash [10 ml/kg max
200 mls] (n = 10) up to 240 minutes preoperatively. The intra-
operative gastric pH values were then compared with those of a
standard preoperative fast group (n = 14). Again, pseudo-mean
and pseudo-standard deviation values were required. Details of
this trial can be referred to in Comparison 02 Duration - Short
Solid Fluid Fast versus Standard Fast, 02 Gastric Contents - pH.
There was no indication of a difference between the groups’ intra-
operative gastric pH (WMD 0.11 95% CI -0.13 to 0.35).
Comparison 03: Duration - short solid and fluid fast versus
short fluid fast
Three trials compared a short solid and fluid fast with a shortened
fluid fast (Kushikata 1996; Meakin 1985c; Meakin 1985d). The
outcomes of these trials will be presented below in relation to (01)
the incidence of aspiration/regurgitation (02) volume of gastric
contents, (03) pH of gastric contents and the secondary outcomes.
No trial that compared a short solid and fluid fast with a short fluid
fast measured gastric volume using a marker dye. An overview of
the results is available at the end of the results section.
Outcome 01: Aspiration/regurgitationInformation on the incidence of aspiration and regurgitation was
available from two trials (n = 95). In the Meakin 1985c trial all chil-
dren were permitted an orange drink preoperatively (10 ml/kg up
to a maximum of 200 ml) and some children were also given two
plain biscuits up to two hours preoperatively. In Meakin 1985d
children received similar interventions but up to 4 hours preop-
eratively. There was no reported occurrence of regurgitation, as-
piration or any related morbidity or mortality. See Table 12 for
details.
Outcome 02: Gastric Contents - VolumeThree small trials compared a short solid and fluid fast to a short
fluid fast by measuring children’s gastric content volume. See Com-
parison: 03 Duration - Short Solid and Fluid Fast versus Short
Fluid Fast; Outcome 02 Gastric Contents - Volume for details.
(i) Solids and Fluids versus Fluids up to 120 minutes preoperatively
Meakin 1985c asked the children to drink 10 ml/kg [max 200 ml]
of an orange drink (n = 35) while some children were, in addition,
quasi-randomised to eat two plain biscuits up to 120 minutes
preoperatively (n = 32). There was no indication of difference in
intra-operative gastric volume (WMD 0.09 ml/kg 95% CI -0.08
to 0.26). Particles of the food intervention were observed in the
gastric aspirate of 13 of the children that were given solids and
fluid and none were noted in the aspirate of those permitted fluids
(Table 11).
(ii) Solids and Fluids versus Fluids up to 240 minutes preopera-
tively
Similarly, Meakin 1985d permitted children 10 ml/kg [max 200
ml] of an orange drink while some of the individuals were also
quasi-randomised to solid intake of two plain biscuits up to 240
minutes preoperatively. Again, there was no evidence of a differ-
ence in gastric volume regardless of whether they had taken solids
and fluids (n = 14) or fluids alone (n = 15) (WMD 0.04 ml/kg
95% CI -0.18 to 0.26). The authors report evidence of food par-
ticles in three children’s gastric aspirate and all three children were
in the group permitted solid fluid intake (Table 11).
(iii) Solids and Fluids versus Fluids up to 330 minutes preopera-
tively
The children in a third quasi-randomised trial were permitted clear
fluids [less than 200 ml] up to 300 minutes preoperatively while
13Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

half the group were allocated to a regimen that also permitted the
intake of rice porridge [55g rice + 245 ml water + salt] up 330
minutes preoperatively (Kushikata 1996). There was no difference
in the gastric content volume (WMD 0.12 ml/kg 95% CI -0.30 to
0.54). No particles were observed in the children’s gastric samples
(Table 11).
Outcome 03: Gastric Contents - pHThe three trials that compared a short solid and fluid fast to a
short fluid fast by measuring gastric content volume also measured
intra-operative gastric pH. Details of these quasi-randomised trials
can be referred to in Comparison 03 Duration - Short Solid and
Fluid Fast versus Standard Fast, 03 Gastric Contents - pH.
(i) Solids and Fluids versus Fluids up to 120 minutes preoperatively
Meakin 1985c gave children 10 ml/kg [max 200 ml] of an orange
drink (n = 31) while approximately half the children were also
given two plain biscuits up to 120 minutes preoperatively (n = 29).
There was no indication of difference in intra-operative gastric
pH of the children permitted solids and fluids and those only
permitted fluids (WMD 0.06, 95% CI -0.57 to 0.69).
(ii) Solids and Fluids versus Fluids up to 240 minutes preopera-
tively
A second small quasi-randomised trial asked children to drink 10
ml/kg [max 200 ml] of an orange drink while some of the children,
in addition, ate two plain biscuits up to 240 min preoperatively
(Meakin 1985d). There was no evidence of a difference in gastric
pH regardless of whether they had taken solids and fluids (n = 10)
or fluids alone (n = 12) (WMD 0.18, 95% CI -0.13 to 0.49).
(iii) Solids and Fluids versus Fluids up to 330 minutes preopera-
tively
Children in the Kushikata 1996 trial were quasi-randomised either
to a fast that permitted the intake of rice porridge up to 330
minutes preoperatively (n = 10) or to continue a standard fasting
regimen (n = 10). The rice porridge consisted of 55 g rice + 245 ml
water + salt. There was no evidence of a difference in intraoperative
gastric pH (WMD 0.46, 95% CI -0.03 to 0.95).
Secondary OutcomesKushikata 1996 also compared a shortened solid fast to a standard
fast by considering the children’s hunger. Hunger was recorded
on a three point scale (satisfied, moderate, very hungry) after they
had either followed a standard fast or after they had eaten rice
porridge and drank clear fluids (less than 200 ml) up to 330 min-
utes preoperatively. It is unclear whether the children or the re-
searchers completed the evaluation. The children permitted solid
intake were found to be less hungry than the children permitted
fluids alone. Details can be referred to in Table 19 Short Solid and
Fluid Fast versus Short Fluid Fast - Hunger. The additional sec-
ondary outcomes of thirst, behaviour, comfort or vomiting were
not considered.
Comparison 04: Duration - short fluid fast 1 versus short fluid
fast 2
Seven trials compared two different shortened fluid fasting reg-
imens i.e. both fasting regimens permitted the intake of fluids
nearer to the time of surgery than a traditional standard fast
(Cook-Sather 2003; Maekawa 1993c; Splinter Schaefer 1a; Splin-
ter Schaefer 1b; Splinter Schaefer 3a; Splinter Schaefer 3b; Splin-
ter Schaefer 3c) The evidence is presented in relation to the (i)
incidence of aspiration/regurgitation (ii) children’s gastric content
volume, (iii) gastric content pH and (iv) the secondary outcomes
of hunger, behaviour and vomiting. Gastric marker dye was not
considered as an outcome measure, nor were the secondary out-
comes of thirst, comfort or nausea.
Outcome 01: Aspiration/regurgitationNo regurgitation or aspiration was observed during three trials that
compared a short fluid fast to an even shorter fluid fast (Cook-
Sather 2003; Splinter Schaefer 1a; Splinter Schaefer 1b). In addi-
tion, Maekawa 1993c reported there was no coughing or laryn-
gospasm during their trial. This information is presented in more
detail in Table 12 Duration of Fast - Aspiration/Regurgitation.
Outcome 02: Gastric Contents - VolumeSeven trials compared the effects of two short fluid fasts on gastric
content volume on induction of anaesthesia (Cook-Sather 2003;
Maekawa 1993c; Splinter Schaefer 1a; Splinter Schaefer 1b; Splin-
ter Schaefer 3a; Splinter Schaefer 3b; Splinter Schaefer 3c). The
results of these comparisons can be referred to in Comparison: 04
Duration - Short Fluid Fast 1 versus Short Fluid Fast 2; Outcome
02 Gastric Contents - Volume.
(i) Fluids up to 120 minutes versus 150 minutes preoperatively
Splinter Schaefer 3c randomly permitted children unlimited in-
take of clear fluids up to 120 minutes (n = 50) or 150 minutes (n
= 50) preoperatively. There was no evidence of a between group
difference in the volume of gastric contents collected (WMD 0.06
ml/kg, 95% CI -0.05 to 0.17).
(ii) Fluids up to 120 minutes versus 180 minutes preoperatively
Two trials compared the unlimited intake of clear fluids up to
120 minutes (n = 124) with 180 minutes (n = 124) preoperatively
(Splinter Schaefer 1b; Splinter Schaefer 3a). Again, there was no
evidence of a difference in volume of gastric contents (WMD 0.04
ml/kg, 95% CI -0.08 to 0.15).
(iii) Fluids up to 120 minutes versus up to 240 minutes preoper-
atively
Two short fluid fasts were compared by an additional two trials
(Cook-Sather 2003; Maekawa 1993c). Children were either per-
mitted fluids up to 120 minutes (n = 71) or 240 minutes preoper-
atively (n = 66). In Maekawa 1993c both groups of children were
required to drink apple juice [10 ml/kg] while in the Cook-Sather
trial children in the shorter fasting group (120 minutes preop-
eratively) were permitted clear fluids and the second group were
permitted formula up to 240 minutes preoperatively. There was
no difference in (WMD 0.00 ml/kg, 95% CI -0.13 to 0.13). The
gastric aspirate of nine of the children in Cook-Sather 2003 was
14Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

found to have evidence of formula (eight were tinged white and
one clear aspirate contained small particles). One of these children
had fasted (excluding the intervention) for a total of 10 hours (Ta-
ble 11 for details).
(iv) Fluids up to 150 minutes versus up to 180 minutes preoper-
atively
Splinter Schaefer 1a and Splinter Schaefer 3b compared the in-
take of unlimited clear fluids up to 150 (n = 90) and 240 minutes
preoperatively (n = 90). On pooling the data there was no statisti-
cally significant difference between the two groups’ gastric volume
(WMD -0.04 ml/kg 95% CI -0.16 to 0.09).
Outcome 03: Gastric Contents - pHThe intra-operative volume of children’s gastric pH was used to
compare two short fluid fasts in seven trials (Cook-Sather 2003;
Maekawa 1993c; Splinter Schaefer 1a; Splinter Schaefer 1b; Splin-
ter Schaefer 3a; Splinter Schaefer 3b; Splinter Schaefer 3c). The
results of these comparisons can be referred to in Comparison: 04
Duration - Short Fluid Fast 1 versus Short Fluid Fast 2; Outcome
03 Gastric Contents - pH.
(i) Fluids up to 120 minutes versus up to 150 minutes preopera-
tively
Splinter Schaefer 3c compared the unlimited intake of clear fluids
up to 120 minutes (n = 50) or 150 minutes (n = 50) preoperatively
by comparing gastric pH. There was no evidence of a between
group difference (WMD 0.10, 95% CI -0.41 to 0.61).
(ii) Fluids up to 120 minutes versus up to 180 minutes preopera-
tively
The two trials that compared the unlimited intake of clear fluids
up to 120 minutes (n = 124) and up to 180 minutes (n = 124)
preoperatively by measuring gastric volume also measured gastric
pH (Splinter Schaefer 1b; Splinter Schaefer 3a). On pooling the
data there was no evidence of a difference in intra-operative gastric
pH (WMD 0.12, 95% CI -0.36 to 0.61).
(iii) Fluids up to 120 minutes versus up to 240 minutes preoper-
atively
Maekawa 1993c and Cook-Sather 2003 compared two short fluid
fasts using the outcome measure gastric pH. Children drank apple
juice [10ml/kg] up to 120 minutes or 240 minutes preoperatively
in one trial (Maekawa 1993c) while the children in the other
trial (Cook-Sather 2003) were permitted clear fluids up to 120
minutes or formula up to 240 minutes preoperatively. There was
no difference in intra-operative gastric pH (WMD 0.13, 95% CI
-0.33 to 0.60).
(iv) Fluids up to 150 minutes versus up to 180 minutes preoper-
atively
Splinter Schaefer 1a and Splinter Schaefer 3b compared the intra-
operative gastric pH of children permitted unlimited intake of
clear fluids up to 150 minutes (n = 90) and up to 180 minutes (n
= 90) preoperatively. There was no evidence of a difference in pH
(WMD 0.19, 95% CI -0.12 to 0.50).
Secondary OutcomesTwo of the trials that compared a short fluid fast with a very short
fluid fast, also measured hunger, behaviour or vomiting (Cook-
Sather 2003; Maekawa 1993c). Cook-Sather 2003 asked parents
to rate their child’s hunger and behaviour (irritability) on a VAS
after the child had left for the operating room. The children had
either been permitted clear fluids up to 120 minutes preoperative
or formula up to 240 minutes preoperatively. There was no appar-
ent difference between the two group’s observed hunger (Table 20)
or behaviour (Table 21). Vomiting was not observed amongst the
children in either the Cook-Sather 2003 nor the Maekawa 1993c
trials (Table 22 for details).
B. Type of permitted intake
The type of intake permitted prior to a child’s surgery has been
a clinical consideration for many years. The variety of milk feeds
(breast milk, formula milk, cows’ milk) and other drinks available
and consumed by children raises the issue of what the evidence is
in relation to type of intake permitted during a restricted fasting
period. As outlined within the protocol, two subgroup analyses
were conducted which examined the Comparison 05 Fluid Intake
Permitted versus Standard Fast and Comparison 06 Fluid 1 versus
Fluid 2. Each analysis is presented in relation to the outcomes used
to measure the effectiveness of the experimental fasting regimens,
namely (01) aspiration/regurgitation (02) volume of gastric con-
tents, (03) pH of gastric contents, (04) marker dye measures of
gastric contents and secondary outcomes.
Comparison 05: Type of Intake - fluid versus standard fast
Outcome 01: Aspiration/RegurgitationInformation on the incidence of aspiration or regurgitation was
available in relation to 18 trials that compared a standard fasting
regimen to the intake of water, clear fluids, fruit juice, or other
fluids. Only one incidence of regurgitation and aspiration on in-
duction was reported. See Table 23 Type of Intake - Aspiration/
Regurgitation for details.
Outcome 02: Gastric Contents - VolumeTwenty-four trials compared a shortened fluid fast with a standard
fasting regimen and are grouped according to the type of intake
children were permitted prior to surgery. The categories include
water, clear fluids, fruit juice, milk, dextrose solutions and other
types of fluid intake. Pseudo-values were calculated for several trials
and these are detailed below. As a result, a conservative approach
to pooling these data was taken and a random effects model was
used. The results can be referred to in Comparison: 05 Type of
Intake - Fluid versus Standard Fast; Outcome 02 Gastric Contents
- Volume.
(i) Water versus Standard Fast
One trial (Gombar 1997) gave the children water (n = 25) during
a period of restricted intake and compared their gastric volume
with that of children after a standard fast (n = 25). There was no
evidence of a difference in gastric volume (WMD -0.04 ml/kg,
95% CI -0.16 to 0.08).
15Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

(ii) Other Clear Fluids versus Standard Fast
Five trials compared the effect of permitted intake of clear fluids
preoperatively (n = 257) and a standard fast (n = 284) on gas-
tric content volume (Nicolson 1992; Sarti 1991; Schreiner 1990;
Splinter 1991; Splinter Schaefer 2). There was little heterogene-
ity (I2 = 7%) and no evidence of a difference in volume of intra-
operative gastric contents (WMD -0.02 ml/kg, 95% CI -0.09 to
0.05).
(iii) Dextrose Solution (five percent) versus Standard Fast
Three trials administered a drink of five percent dextrose solution
to 58 children while an additional 52 children continued to fast
(Aun 1990; Miller 1990; van der Walt 1986b). Psuedo-values were
calculated for two of the trials (Aun 1990; van der Walt 1986b)
and wide confidence intervals were observed especially in relation
to the Aun data. On pooling the data there was no indication of
a difference in intra-operative volume of gastric contents (WMD
-0.14 ml/kg, 95% CI -0.43 to 0.15).
(iv) Fruit Juice versus Standard Fast
Children’s gastric volume following the intake of fruit juice (n =
226) and following a standard fast (n = 168) was compared in eight
trials (Goresky 1992a; Maekawa 1993a; Maekawa 1993b; Sand-
har 1989a; Splinter 1989; Splinter 1990a; Splinter 1990b; Wel-
born 1993). Pseudo-values were calculated for two trials (Sand-
har 1989a; Welborn 1993) and included within the meta-analysis
while the Goresky 1992a trial did not report the separate group
summary data and therefore could not be included within the
meta-analysis. On pooling the data there was no evidence of a dif-
ference in volume of intra-operative gastric contents (WMD 0.02
ml/kg, 95% CI -0.08 to 0.11).
(v) Fruit Juice versus Standard Fast (+ H2-receptor antagonist)
Sandhar 1989b and Goresky 1992b also measured gastric content
volume in order to compare children’s preoperative intake of fruit
juice to a standard fast. Ranitidine was also administered to all
children as a preoperative co-intervention. Goresky 1992b how-
ever, did not report separate group summary data and so could not
be included within the meta-analysis. Pseudo- mean and standard
deviation values were calculated for Sandhar 1989b data. There
was no evidence of a between group difference in gastric volume
(WMD 0.01 ml/kg, 95% CI -0.11 to 0.13).
(vi) Milk versus Standard Fast
Only one trial (van der Walt 1986c) compared the preoperative
intake of cow’s milk during a shortened fluid fast (n = 31) with
a standard fasting regimen (n = 33). Pseudo-values were required
to allow presentation of the trial in the graph though there was
no evidence of a between group difference in the children’s gastric
volume (WMD 0.08 ml/kg, 95% CI -0.29 to 0.45).
(vii) Other Fluids versus Standard Fast
Four trials compared the intake of a variety of other fluids during a
preoperative fast (n = 100) with a standard fasting regimen (n = 56)
by measuring the volume of children’s intra-operative gastric con-
tents. Fluids permitted included poly-joule (van der Walt 1986a),
orange squash (Meakin 1985a; Meakin 1985e) and an isosmolar
solution of electrolytes (Moyao-García 2001). Pseudo-values were
required for van der Walt 1986a. The confidence intervals noted,
however, are wide and scattered and there is evidence of hetero-
geneity (p = 0.002).
Outcome 03: Gastric Contents - pHA total of 24 trials measured the pH of children’s gastric contents
and compared preoperative fluids with a fast in the standard man-
ner. Trials permitted the intervention group to drink water (i),
other clear fluids (ii), dextrose solution (iii), fruit juice (iv and v),
cows’ milk (vi) and a variety of other fluids (vii). The data was
pooled using a random effects model and details can be referred
to in Comparison 05 Type of Intake - Fluid versus Standard Fast;
Outcome 03 Gastric Contents - pH.
(i) Water versus Standard Fast
Only Gombar 1997 compared the preoperative intake of water (n
= 24) with a standard fast (n = 25) by measuring the children’s
gastric pH. There was no indication of a difference in gastric pH
(WMD 0.27, 95% CI -0.12 to 0.66).
(ii) Other Clear Fluids versus Standard Fast
Five trials permitted some children to drink a variety of clear flu-
ids preoperatively (n = 220) while the remaining children were
fasted (n = 235). Pseudo-standard deviation values were required
for Schreiner 1990. With all five trials presenting relatively nar-
row confidence intervals the results provide little indication of an
important clinical difference between the two groups’ gastric pH
values (WMD 0.09, 95% CI -0.03 to 0.21).
(iii)Dextrose Solution (five percent) versus Standard Fast
Drinking a dextrose solution preoperatively (n = 34) was compared
to a standard fasting regimen (n = 31) by two trials (van der Walt
1986b; Miller 1990). An additional trial (Aun 1990) also made
this comparison but group specific data in relation to the children’s
gastric pH was unavailable. Pseudo-values were required for van
der Walt 1986b. There was no indication of a difference between
gastric pH of children given dextrose and those who fasted (WMD
-0.51, 95% CI -2.21 to 1.19).
(iv) Fruit Juice versus Standard Fast (no H2-receptor antagonist)
The eight trials that compared the effect on gastric volume of fruit
juice (n = 255) and a standard fast (n = 200) also measured the
children’s gastric pH. To permit inclusion within the meta-analy-
sis pseudo-standard deviation values were calculated for Sandhar
1989a and Welborn 1993. On pooling the data, there was no in-
dication of a difference between the group’s intra-operative gastric
pH (WMD 0.04, 95% CI -0.01 to 0.10).
(v) Fruit Juice versus Standard Fast (+ H2-receptor antagonist)
Two trials (Goresky 1992b; Sandhar 1989b) compared the pre
operative intake of fruit juice (n = 68) with a standard fasting
regimen (n = 61). Both trials also administered a H2-receptor
antagonist co-intervention. Pseudo-standard deviation values were
16Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

calculated for Sandhar 1989b and there was no indication of a
difference in gastric pH (WMD 0.53, 95% CI -0.19 to 1.26).
(vi) Milk versus Standard Fast
The gastric pH of children who were permitted cows’ milk pre-
operatively and those who fasted were compared in van der Walt
1986c. Pseudo-values were calculated to allow presentation within
the meta-analysis. There was no indication based on this small
trial that the intake of milk up to three hours preoperatively had
any impact on intra-operative gastric pH (WMD -0.01, 95% CI
-1.82 to 1.80).
(vii) Other Fluids versus Standard Fast
Four trials evaluated the intake of a range of other fluids during a
preoperative fast by measuring the children’s intra-operative gastric
pH. Fluids permitted included poly-joule (a mixture of glucose
polymers - maltodextrin) (van der Walt 1986a), orange squash
(Meakin 1985a; Meakin 1985e) and an isosmolar solution of elec-
trolytes (Moyoa-Garcia 2001). Pseudo-mean and standard devi-
ation values were calculated for three trials (van der Walt 1986a;
Meakin 1985a; Meakin 1985e). The trial results indicate widely
scattered confidence intervals (see in particular van der Walt 1986a
and Moyao-García 2001) which at present provide insufficient ev-
idence to state whether or not an important difference exists be-
tween the groups permitted fluids (n = 80) and those that fasted
(n = 41) (WMD 0.34 95% CI -0.62 to 1.31).
Outcome 04: Gastric Contents - Marker DyeThe marker dyes phenol red and bromosulphthalein were used by
five trials as a means of comparing a fasting regimen that permitted
fluid intake with a prolonged fast. The results will be presented
below in relation to the marker dye used and the type of fluid
permitted during the restricted fasting period.
Phenol red
(i) Fruit Juice versus Standard Fast
Sandhar 1989a and Sandhar 1989b used phenol red to compare
the intake of orange juice up to 120 minutes preoperatively with
a standard fast. Sandhar 1989b also administered a ranitidine co-
intervention to all children. One child in the Sandhar 1989a trial
who had fasted for an hour since the placebo intervention was
found to have a 33% percent dye retrieval. Dye retrieval for the
remaining children was less than five percent and for many children
no dye was found. In the Sandhar 1989b trial dye retrieval was
12% for one child (juice and ranitidine intervention) that fasted
for one hour while the remaining children had a dye retrieval of
less than five percent.
(ii) Dextrose Solution (five percent) versus Standard Fast
Miller 1990 used phenol red to compare the effect on gastric vol-
ume of a dextrose solution drink (n = 19) with no fluid intake (n
= 25). The results are reported as ml and details can be referred to
in Comparison 05 Type of Fluid Intake versus Standard Fast 04
Gastric contents - Phenol Red based volume (ml). There was no
evidence of a between group difference in the marker dye based
measure of intraoperative gastric volume (WMD -3.10 ml, 95%
CI -6.66 to 0.46).
Bromosulphthalein
(i) Fruit Juice versus Standard Fast
The dye bromosulphthalein was used by two trials to evaluate
the contribution fluids ingested during a restricted fasting period
made to children’s intra-operative gastric volume. Results were
reported as a percentage of recovered dye. Goresky 1992a and
Goresky 1992b compared the preoperative intake of orange juice
with a standard fast. Goresky 1992b also asked children to take
a ranitidine (H2 receptor antagonist) co-intervention. Separate
group data were not available. It was reported however, that the
dye recovered from those children who were permitted to drink
during the preoperative period represented less than 0.3% of the
volume of intake at the time of marker dye administration. The
researchers also noted that more dye was recovered from those
children given ranitidine than those that did not receive this drug
(p < 0.001). Additional details were unavailable.
Secondary OutcomesReports of thirst, hunger, behaviour, comfort and vomiting were
noted by thirteen trials that compared the intake of a variety of
fluids with a standard fast. No trial measured nausea. An overview
of these trials and the measures used can be referred to in Table
24 Type of Intake - Secondary Outcome Measures. These results
are presented below.
• Thirst
Thirst was measured in six different trials that compared the in-
take of a preoperative fluid to a standard fast. All trials used a VAS
(Splinter 1989 used two) and measures were taken either prein-
duction (time point f ) or after the child had left for surgery (time
point g - see Table 10). The children permitted water or clear
fluids preoperatively described significantly less thirst than those
who fasted (Gombar 1997; Nicolson 1992; Splinter 1991). Sim-
ilarly, the trials that evaluated pre operative apple juice found the
children (or parents of children) permitted apple juice recorded
significantly less thirst on the VAS than the children who fasted
(Splinter 1990a; Splinter 1989). Splinter 1989 and Splinter 1990b
found no difference between the children’s description of thirst.
Details can be seen in Table 25 Type of Fluid versus Standard Fast
- Thirst.
This indicates an interesting difference between the trials that eval-
uated the administration of apple juice preoperatively (Splinter
1989; Splinter 1990a; Splinter 1990b). All three recruited chil-
dren aged 5-10 years and randomly allocated them to receive ap-
ple juice up to 150 minutes preoperatively or to the standard fast-
ing regimen. The only obvious difference between these trials re-
lates to the volume of intake permitted which varied from 3ml/kg
(Splinter 1989), 6ml/kg (Splinter 1990a) and 10ml/kg (Splinter
1990b). The issue of volume of intake will be dealt with in more
detail below.
17Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

• Hunger
Five trials measured children’s hunger in a comparison of a fast
that permitted the intake of clear fluids (Nicolson 1992; Splin-
ter 1991) or apple juice (Splinter 1989; Splinter 1990a; Splinter
1990b) to a standard fasting regimen. Descriptions of hunger were
made by either the children themselves (Splinter 1989; Splinter
1990a; Splinter 1990b; Splinter 1991) and/or their parents (Nicol-
son 1992; Splinter 1989). All respondents used VAS to measure
children (or parent’s) ratings of preoperative hunger with measures
taken pre-induction or after the child had left for surgery. Parental
reports indicated that the children permitted clear fluids or apple
juice were less hungry than those that continued to fast (Nicolson
1992; Splinter 1989). Based on children’s report, only one of the
trials that permitted preoperative apple juice described less hunger
than those that fasted (Splinter 1989). In the remaining trials that
administered either preoperative clear fluids (Splinter 1991) or ap-
ple juice (Splinter 1990a; Splinter 1990b) while the control group
fasted, there was no difference between the children’s descriptions
of hunger. Details are presented in Table 26 Type of Fluid versus
Standard Fast - Hunger.
• Behaviour
Behaviour was measured by four trials that compared the preoper-
ative intake of water, clear fluids and apple juice to a standard fast-
ing regimen. In all cases parents rated their children’s behaviour in
terms of irritability on a VAS immediately prior to surgery or after
the child had left for surgery. In three of the four trials children
permitted water (Gombar 1997), clear fluids (Schreiner 1990) and
apple juice (Splinter 1990a) were rated by their parents as less ir-
ritable when compared to the ratings made by the parents of chil-
dren who fasted. Splinter 1990b however, found no difference in
the parents’ report of the behaviour amongst children permitted
apple juice preoperatively and those that fasted. See details in Ta-
ble 27 Type of Fluid versus Standard Fast - Behaviour.
• Comfort
Nicolson 1992 and Schreiner 1990 measured parents’ perceptions
of their child’s comfort using VAS. Both trials found that the
parents of children permitted clear fluids preoperatively described
their children as more comfortable (or as having tolerated the
experience better) than the children who followed a standard fast.
Details can be referred to in Table 28 Type of Fluid versus Standard
Fast - Comfort.
• Vomiting
The incidence of vomiting amongst children was reported in
six trials that evaluated the preoperative intake of clear fluids
(Schreiner 1990), apple juice (Goresky 1992a; Goresky 1992b;
Maekawa 1993a; Maekawa 1993b) and a dextrose solution (Aun
1990). Only Goresky 1992a and Goresky 1992b reported any
vomiting but these incidents appear to be linked to vomiting of
the preoperative intervention (apple juice [5 ml/kg] and placebo/
ranitidine [2 mg/kg]) rather than vomiting on immediately pre-
or post-induction. The report also does not report how many of
this group (n = 8) vomited, gagged or spat out the intervention,
nor is it clear to which group these children belonged. See Table
29 Type of Fluid versus Standard Fast - Vomiting for details.
Comparison 06: Type of intake - fluid 1 versus fluid 2
Three related trials directly compared the preoperative intake of
two different types of fluids during a shortened fluid fast. The
outcomes measured included (01) aspiration/regurgitation, (02)
the volume and (03) pH of children’s gastric contents. Marker
dye measures and secondary outcomes (thirst, hunger, behaviour,
comfort, nausea or vomiting) were not considered by any of these
trials.
Outcome 01: Aspiration/RegurgitationThe three trials that compared the intake of a dextrose solution
with Polyjoule (van der Walt 1986d), dextrose solution with cows’
milk (van der Walt 1986e) and Poly joule with cows’ milk (van
der Walt 1986f ) reported the incidence of aspiration and regur-
gitation observed within their trials. No significant aspiration or
other drink-related complications were observed. For details see
Table 23 Type of Intake - Aspiration/Regurgitation.
Outcome 02: Gastric Contents - VolumeTrials that compared the effects on intraoperative gastric volume
of two different types of preoperative fluid intake are presented
within this section. Pseudo-mean and standard deviation values
were calculated for all three trials. The trials are presented in Com-
parison: 06 Type of Intake - Fluid 1 [F1] versus Fluid 2 [F2]; Out-
come 02 Gastric Contents - Volume.
(i) Dextrose solution versus Polyjoule
van der Walt 1986d compared the preoperative intakes of five
percent dextrose solution (n = 29) with Polyjoule (maltodextrin)
(n = 30) by measuring children’s gastric volume during surgery.
There was no indication of a difference between the two groups’
gastric volume (WMD 0.03 ml/kg, 95% CI -0.15 to 0.21).
(ii) Dextrose solution versus Cows’ milk
The preoperative intake of five percent dextrose solution (n = 29)
was compared with the intake of cows’ milk (n = 31) in van der
Walt 1986e. A significantly lower volume of gastric contents was
recovered from the children who drank the dextrose solution than
those who were given cows’ milk (WMD -0.44 ml/kg, 95% CI
-0.75 to -0.13) (p = 0.005). This significant result however is based
on a small number of children within a single trial.
(iii) Poly joule versus Cows’ milk
In a third comparison, van der Walt 1986f compared the effect on
gastric volume of Polyjoule (n = 30) and cows’ milk (n = 31). There
was a significantly lower gastric volume in the children who drank
Polyjoule than those who drank cows’ milk (WMD -0.47ml/kg,
95% CI -0.78 to -0.16) (p = 0.005) but this result is based on a
very small number of children within a single trial.
Outcome 03: Gastric Contents - pH
18Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

All three trials that compared the effect on gastric volume of the
intake of two different fluids during the preoperative period also
measured the gastric pH. Pseudo-mean and standard deviation
values were calculated and a random effects model was used to
present the data which can be referred to in Comparison: 06 Type
of Intake - Fluid 1 versus Fluid 2; Outcome 03 Gastric Contents
- pH.
(i) Dextrose solution versus Polyjoule
The preoperative intake of five percent dextrose solution (n = 29)
and Polyjoule (n = 30) were compared by van der Walt 1986d.
There was no indication of a difference in intra-operative gastric
pH (WMD -0.75, 95% CI -1.62 to 0.12).
(ii) Dextrose solution versus Cows’ milk
Similarly, van der Walt 1986e measured gastric pH after preop-
erative intake of 5% dextrose (n = 29) and cows’ milk (n = 31).
The children who drank dextrose had significantly higher gastric
acidity than those who drank cows’ milk (WMD -1.74 95% CI
-3.09 to -0.39) (p = 0.01). This significant result is in contrast to
the result in relation to children’s gastric volume which was lower
after dextrose. However, both results should be considered in light
of the very small number of children this one trial was based on.
(iii) Poly joule versus Cows’ milk
Polyjoule (n = 30) and cows’ milk (n = 31) were compared in
relation to gastric pH and there was no evidence of a difference
between the two groups (WMD -1.01, 95% CI -2.49 to 0.47)(van
der Walt 1986f ).
For summary of Type of Permitted Intake Results - see end of
results section.
C. Volume of permitted intake
While very small volumes of fluids are usually permitted during
the preoperative period (for example up to 30 ml to allow the in-
take of medication) many clinicians question whether higher vol-
umes of fluids could be permitted during this period. A total of 25
trials are presented in this section in relation to the volume of in-
take permitted during a period of restricted intake. Comparisons
were either made between several different volumes of intake and
a standard fasting regimen, or between two different volumes of
intake. For analysis purposes the various volumes permitted pre-
operatively were categorised into three types of intake; low vol-
ume (less than or equal to 5 ml/kg), high volume (more than 5
ml/kg) and unlimited volumes (where no restriction was placed
on the volume of children’s preoperative fluid intake). As outlined
at the protocol stage, two subgroup analyses were conducted to
examine Comparison 07 Volume of Intake versus Standard Fast
and Comparison 08 Volume 1 versus Volume 2. For each analysis
the outcome measures (01) aspiration/regurgitation, (02) volume
of gastric contents, (03) pH of gastric contents, (04) marker dye
measures and secondary outcomes were considered.
Comparison 07 Volume of fluid versus standard fast
Outcome 01: Aspiration/Regurgitation
Eighteen trials made a specific report (either published or unpub-
lished) in relation to the incidence of aspiration and regurgitation
during an investigation which evaluated the intake of a volume
of fluid during a restricted fasting period. No aspiration or regur-
gitation was reported by any of the trials that compared the pre-
operative intake of unrestricted volumes of fluid (Nicolson 1992;
Schreiner 1990; Splinter Schaefer 2) or the intake of a high volume
of fluid (Aun 1990; Maekawa 1993a; Maekawa 1993b; Meakin
1985a; Meakin 1985b; Splinter 1990a; Splinter 1990b; van der
Walt 1986a; van der Walt 1986b; van der Walt 1986c) with a
standard fast. Of the five trials that compared the intake of a low
volume of fluids preoperatively with a standard fasting regimen
(Gombar 1997; Goresky 1992a; Goresky 1992b; Moyao-García
2001; Splinter 1989) only one incident of coughing and aspira-
tion on induction was observed by Goresky 1992a. The authors
of the trial suggest this event was related to airway management
rather than the intervention. Details can be referred to in Table
30 Volume of Intake - Aspiration/Regurgitation.
Outcome 02: Gastric Contents - VolumeA total of 23 trials compared the effect on gastric content volume
of different volumes of preoperative intake and a standard fasting
regimen. Wherever possible the data were pooled using a random
effects model and presented in Comparison: 08 Volume of Intake
- Volume of Fluid versus Standard Fast; Outcome 02 Gastric Con-
tents - Volume.
(i) Low Volume Fluid Intake versus Standard Fast
Four trials administered a volume of fluid less than or equal to 5
ml/kg to the children in the intervention group (n = 98) while
the other children continued to fast (n = 104) (Gombar 1997;
Moyao-García 2001; Sandhar 1989a; Splinter 1989). The volume
of fluids administered to the intervention groups included 3 ml/kg
of apple juice (Splinter 1989), 4 ml/kg of an isomolar solution of
electrolytes (Moyao-García 2001) and 5 ml/kg of water (Gombar
1997) and orange juice (Sandhar 1989a). Pseudo-standard devi-
ation values were required to allow the inclusion of the Sandhar
1989a trial within the meta-analysis. On pooling the data there
was no evidence of a difference in gastric content volumes between
the children who had a low volume of preoperative fluid intake
and those who fasted (WMD -0.12 ml/kg, 95% CI -0.29 to 0.05).
The pooled results are underpowered, there is high heterogeneity,
and do not exclude the possibility of a clinically important differ-
ence in favour of the intake of a low volume of fluids. The results
from Goresky 1992a could not be included in the meta-analysis
as no group specific data were available.
(ii) Low Volume Fluid Intake versus Standard Fast (+ H2-receptor
antagonist)
Two additional trials (Goresky 1992b; Sandhar 1989b) also com-
pared the effect on gastric volume of the intake of a low volume of
fruit juice (5ml/kg) and a standard fast. The children within these
trials also received ranitidine, a H2-receptor antagonist. Separate
group data for the Goresky 1992b trial however were unavailable
19Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

and so this trial could not be included within the meta-analysis.
Pseudo-standard deviation values were required to allow inclusion
of the Sandhar 1989b trial. There was no evidence of a difference
in gastric volume of children permitted a low volume of orange
juice (n = 18) and those who fasted in the usual manner (n = 15)
(WMD 0.01 ml/kg, 95% CI -0.11 to 0.13).
(iii) High Volume Fluid Intake versus Standard Fast
Eleven trials compared the effect on gastric volume of a high vol-
ume of fluids preoperatively (n = 323) and a standard fast (n = 172).
Children in the fluid group were permitted 6 ml/kg of apple juice
(Splinter 1990a), 10 ml/kg of dextrose solution (Aun 1990; van
der Walt 1986b), cows’ milk (van der Walt 1986c) Polyjoule (van
der Walt 1986a), orange squash (Meakin 1985a; Meakin 1985e)
or apple juice (Maekawa 1993a; Maekawa 1993b; Splinter 1990b;
Welborn 1993). Pseudo-mean and standard deviation values were
required for a number of trials (Aun 1990; Meakin 1985a; van der
Walt 1986a; van der Walt 1986b; van der Walt 1986c; Welborn
1993). The was no significant difference in gastric content volume
(WMD 0.04 ml/kg, 95% CI -0.05 to 0.13).
(iv) Unlimited Fluid Intake versus Standard Fast
Five trials permitted children in the experimental group to have
preoperative access to an unlimited volume of clear fluid (n = 257)
whilst the control groups underwent a standard fast (n = 284).
The duration of fast amongst the intervention groups ranged from
120 minutes (Nicolson 1992; Sarti 1991; Schreiner 1990) to 180
minutes (Splinter 1991; Splinter Schaefer 2). The fluid and fasted
groups’ volume of gastric contents were then compared. There
was no difference in intra-operative gastric volume (WMD -0.02
ml/kg, 95% CI -0.09 to 0.05).
Outcome 03: Gastric Contents - pHIntra-operative gastric pH was measured in 22 trials that compared
different volumes of preoperative intake with a standard fasting
regimen. Pseudo-values were calculated for some trials and a ran-
dom effects model was used to pool the data which can be referred
to in Comparison: 08 Volume of Intake - Volume of Fluid versus
Standard Fast; Outcome 03 Gastric Contents - pH.
(i) Low Volume Fluid Intake versus Standard Fast (no H2-receptor
antagonist)
Five trials compared the effect on gastric pH of a low volume of
fluid (n = 144) and a standard fasting regimen (n = 146). Hetero-
geneity was very high (I2 = 91%) and there is insufficient evidence
of an effect on gastric pH values (WMD 0.42, 95% CI -0.19 to
1.04).
(ii) Low Volume Fluid Intake versus Standard Fast (+ H2-receptor
antagonist)
Two trials compared the effect on gastric pH of a low volume of
preoperative fluid and a standard fast (Sandhar 1989b; Goresky
1992a). The children in these trials also received a H2 receptor an-
tagonist as a co-intervention. The data from Goresky 1992a could
not be included as the outcome measures were only reported as a
cross-group summary. Pseudo-mean and pseudo-standard devia-
tion values were calculated for Sandhar 1989b to allow inclusion
of the trial within the meta-analysis. There was no evidence of a
difference in gastric pH of those children given a low volume of
fluid (n = 68) and those who fasted (n = 61) (WMD 0.53, 95%
CI -0.19 to 1.26).
(iii) High Volume Fluid Intake versus Standard Fast
Children permitted a high volume of fluids (n = 244) and chil-
dren who were fasted in the standard manner (n = 126) were
compared by measuring the pH of their intra-operative gastric
contents. Ten trials gave children in the intervention group ei-
ther apple juice (Splinter 1990a; Splinter 1990b; Maekawa 1993a;
Maekawa 1993b; Welborn 1993), dextrose (Aun 1990; van der
Walt 1986b), cows’ milk (van der Walt 1986c), Poly joule (van der
Walt 1986a) or orange squash (Meakin 1985a; Meakin 1985e) at
volumes ranging from 6 ml/kg to 10 ml/kg. Pseudo-values were
required for five trials (Aun 1990; van der Walt 1986a; van der
Walt 1986b; van der Walt 1986c; Welborn 1993) to permit in-
clusion within the meta-analysis. The variance in the data from
the van der Walt study was large, although overall heterogeneity
was low (I2 - 0%) and using a random effects model, there was
insufficient evidence to indicate whether a difference between the
groups’ gastric pH existed (WMD 0.04, 95% CI -0.02 to 0.09).
(iv) Unlimited Fluid Intake versus Standard Fast
Children in the intervention groups of five trials (Nicolson 1992;
Sarti 1991; Schreiner 1990; Splinter 1991; Splinter Schaefer 2)
were permitted unlimited volumes of clear fluids or a choice be-
tween apple juice and water (Sarti 1991) during the preoperative
period (n = 220) while those in the study group continued to fast
(n = 235). There was little indication of an important clinical dif-
ference in gastric pH (WMD 0.09, 95% CI -0.03 to 0.21).
Outcome 04: Gastric Contents - Marker DyeFour trials compared the intake of a low volume of fluid with a
standard fasting regimen using the marker dyes phenol red and
bromosulphthalein.
Phenol red
Two trials used phenol red as a marker dye.
(i) Low Volume of Fluids versus Standard Fast
Sandhar 1989a and Sandhar 1989b used the marker dye to com-
pare low volume of orange juice preoperatively (n = 31) with a
standard fast (n = 34). Sandhar 1989b included a ranitidine co-
intervention. For many children in the Sandhar 1989a trial no dye
was found. One child who had fasted for an hour after the placebo
intervention, was found to have 33% percent dye retrieval. Sim-
ilarly, in the Sandhar 1989b trial, dye retrieval was 12% for one
child who had ingested a low volume of orange juice (plus raniti-
dine). The remaining children in both trials had a dye retrieval of
less than 5%.
Bromosulphthalein
Two trials used bromosulphthalein as a marker dye.
20Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

(i) Low Volume of Fluids versus Standard Fast
Goresky 1992a and Goresky 1992b used BSP to measure the con-
tribution of the ingested fluids to the intra-operative gastric vol-
ume. Results were reported as a percentage (%) of recovered dye.
Both trials compared the intake of a low volume of fluids (5 ml/kg)
with a standard fast but one included a ranitidine (H2receptor an-
tagonist) co-intervention (Goresky 1992b). Separate group sum-
mary data were unavailable and instead the results for the two
groups that followed a standard fast were combined and compared
to the recovered marker dye values from the combined group per-
mitted a low volume of fluids. Fluid intake was reported to have
had an insignificant effect on the dye recovery. The dye recovered
represented less than 0.3% of the volume of intake at the time of
marker dye administration. More dye was recovered from those
children given ranitidine than the children that did not receive
this co-intervention (p < 0.001). No other details were available.
Secondary Outcome MeasuresTwelve trials compared the preoperative intake of a low (less than
or equal to 5 ml/kg), high (over 5 ml/kg) or unlimited volume of
fluid preoperatively to a standard fasting regimen by measuring
children’s thirst, hunger, behaviour, comfort, or vomiting. No trial
attempted to measure children’s reports of nausea. Details of these
trials, the outcomes measured and the measurement tools used can
be referred to in Table 31 Volume of Intake - Secondary Outcome
Measures.
• Thirst
Children’s thirst was measured by six trials that compared a stan-
dard fasting regimen to one that permitted the preoperative intake
of a low, high or unlimited volume of fluid intake. In all cases, re-
ports of thirst were measured preoperatively using a VAS and were
completed by the child (Gombar 1997; Splinter 1989; Splinter
1990a; Splinter 1990b, Splinter 1991) or their parent (Nicolson
1992; Splinter 1989). Details can be referred to in Table 32 Vol-
ume of Fluid versus Standard Fast - Thirst. In all cases where a
statistically significant difference was noted, the children permit-
ted a low (Gombar 1997), high (Splinter 1990a) or unlimited vol-
ume of fluid (Splinter 1991) reported less thirst than the children
who fasted. Similarly, parents also described less thirst amongst
the children permitted a low (Splinter 1989) or unlimited fluid
intake (Nicolson 1992) than the parents of children who fasted.
Two trials found no difference in descriptions of thirst (Splinter
1989; Splinter 1990b).
• Hunger
Five trials compared the preoperative intake of a low (Splinter
1989), high (Splinter 1990a; Splinter 1990b) or unlimited vol-
ume of fluid (Nicolson 1992; Splinter 1991) with a standard
fast by measuring hunger. In most cases children were asked to
record their preoperative hunger on a VAS (Splinter 1989; Splin-
ter 1990a; Splinter 1990b; Splinter 1991) but two trials (Splinter
1989; Nicolson 1992) asked parents to rate their perceptions of
their child’s preoperative hunger. Details can be referred to in Ta-
ble 33 Volume of Fluid versus Standard Fast - Hunger.
Only two trials noted a statistically significant difference between
children’s hunger as rated by the children (Splinter 1989) or by
their parents (Splinter 1989; Nicolson 1992). In both cases the
children permitted a low or unlimited volume of fluids preoper-
atively reported less hunger than those children who fasted. No
differences in the reports of the children’ hunger was noted in the
remaining trials.
• Behaviour
Four trials asked parents to record their children’s preoperative be-
haviour using a VAS. Comparisons were made between those chil-
dren who followed a standard fast and those who were permitted
the preoperative intake of a low (Gombar 1997), high (Splinter
1990a; Splinter 1990b) or unlimited volume of fluids (Schreiner
1990). In three of the four trials parents of children permitted flu-
ids described their children as significantly less irritable and upset
than the parents of children who fasted in the standard manner.
Only Splinter 1990b found no difference between the two groups.
See Table 34 Volume of Fluid versus Standard Fast - Behaviour for
details.
• Comfort
Two trials compared the unlimited intake of clear fluids to a stan-
dard fasting regimen by asking parents to rate their children’s pre-
operative comfort on a VAS (Nicolson 1992; Schreiner 1990).
In both cases the parents of children permitted a drink described
their children as more comfortable than did the parents of children
who continued to fast preoperatively. Schreiner 1990 also asked
18 parents how the experimental fasting regimen had been experi-
enced by the children compared with previous experiences. Most
parents (14/18) said the unlimited intake of clear fluids preopera-
tively had improved the preoperative experience for their children.
Four parents had no opinion.
• Vomiting
The incidence of vomiting during the preoperative period was
available in relation to six trials as either published or unpublished
information. Trials compared groups of children who followed
either a standard fast or were permitted a low (Goresky 1992a;
Goresky 1992b), high (Aun 1990; Maekawa 1993a; Maekawa
1993b) or unlimited volumes (Schreiner 1990) of preoperative
fluids. No between group differences were observed in four of the
trials (Aun 1990; Maekawa 1993a; Maekawa 1993b; Schreiner
1990). Some reports of vomiting observed on introduction of the
intervention were made in Goresky 1992a and Goresky 1992b (n
= 8) but it is unclear to which group these individuals belonged.
The vomiting appears to have occurred in response to the taste
of the intervention and marker dye. Details can be referred to in
Table 36 Volume of Fluid versus Standard Fast - Vomiting.
Comparison 08: Volume of intake - volume 1 versus volume 2
21Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Only one trial (Splinter 1990c) directly compared two volumes of
fluid intake. The outcome measures of (01) aspiration/regurgita-
tion, (02) volume of gastric contents, (03) pH of gastric contents
and (04) the secondary outcome measures were considered and are
presented below in turn. Splinter 1990c did not use any marker
dye measures nor were children’s ratings of comfort, nausea or
vomiting recorded.
Outcome 01: Aspiration/RegurgitationSplinter 1990c directly compared the preoperative intake of 6
ml/kg (n = 30) and 10 ml/kg (n = 32) of apple juice by children
up to 2.5 hours preoperatively. No aspiration or regurgitation was
observed. See Table 30 Volume of Intake - Aspiration/Regurgita-
tion for details.
Outcome 02: Gastric Contents - VolumeSplinter 1990c compared the intake of the two different volumes
of apple juice by measuring the volume of gastric contents. There
was no indication of a difference between 6 ml/kg (n = 30) and
10 ml/kg (n = 32) of apple juice (WMD -0.05 ml/kg, 95% CI
-0.44 to 0.34) and the results can be referred to in Comparison:
08 Volume of Intake - Volume 1 [V1] versus Volume 2 [V2];
Outcome 02 Gastric Contents - Volume. Particles were observed
in the gastric aspirate of one child permitted 6 ml/kg and four
children permitted 10 ml/kg of apple juice. All five were noted to
have gastric volumes in excess of 1 ml/kg.
Outcome 03: Gastric Contents - pHThe intake of 6 ml/kg and 10 ml/kg of apple juice preoperatively
was also compared by measuring the pH of children’s gastric con-
tents (Splinter 1990c). There was no evidence of a difference be-
tween the children who had the lower volume of apple juice (n
= 30) and those who had the higher volume (n = 32) (WMD
-0.10, 95% CI -0.45 to 0.25). These results can be referred to in
Comparison: 08 Volume of Intake - Volume 1 versus Volume 2;
Outcome 03 Gastric Contents - pH.
Secondary OutcomesSplinter 1990c asked the children participating to report their
thirst and hunger and their parents were asked to rate their chil-
dren’s behaviour over the preoperative period on a VAS. Two chil-
dren aged less than five years were unable to complete the VAS.
There was no difference in reports of thirst and hunger between
children permitted 6 ml/kg and 10 ml/kg of apple juice during
the preoperative period, nor was there any difference in parents’
description of how irritable the children were over the preopera-
tive period. For details see Table 37 Volume 1 versus Volume 2 -
Thirst; Table 38 Volume 1 versus Volume 2 -Hunger and Table
39 Volume 1 versus Volume 2 - Behaviour.
For summary of Volume of Intake Results - see end of results
section.
D. Subgroups of ’high-risk’ patient populations
Patient groups with delayed gastric emptying are considered to
be at an increased risk of regurgitation/aspiration/related morbid-
ity during anaesthesia. Conservative approaches to preoperative
fasting are generally employed with these patient groups which
include those with systemic disease/disorders (for example dia-
betes) and the obese. It is of note that this review failed to identify
any randomised controlled trial that specifically recruited children
from these ’high-risk’ groups.
Summary of results - A. Duration of fast
(where H2RA = H2-receptor antagonist; NSD = no statistically
significant difference)
Comparison 01: Short Fluid Fast versus Standard Fast
Outcome 01: Aspiration/RegurgitationNineteen trials; 1274 children; One incident - regurgitation and
aspiration possibly related to airway management.
Outcome 02: Gastric VolumeUp to 120 minutes: 7 trials (- H2RA); 509 children; WMD 0.03
ml/kg, 95% CI -0.03 to 0.10; NSD.
Up to 120 minutes: 1 trial (+ H2RA); 33 children; WMD
0.01ml/kg 95% CI -0.12 to 0.14; NSD.
Up to 150 minutes: 3 trials; 173 children; WMD 0.07 ml/kg 95%
CI -0.25 to 0.39; NSD.
Up to 180 minutes: 8 trials; 530 children; WMD -0.12 ml/kg
95% CI -0.22 to -0.03; Favours Fluid Intake (p = 0.01).
Up to 240 minutes: 3 trials; 125 children; WMD 0.03 ml/kg 95%
CI -0.10 to 0.17; NSD.
Outcome 03: Gastric pHUp to 120 minutes: 8 trials (- H2RA); 484 children; WMD 0.04
95% CI -0.01 to 0.09; NSD.
Up to 120 minutes: 2 trials (+ H2RA); 129 children; WMD 0.53
95% CI -0.20 to 1.26; NSD.
Up to 150 minutes: 3 trials; 173 children; WMD 0.19 95% CI
-0.11 to 0.49; NSD.
Up to 180 minutes: 8 trials; 465 children; WMD 0.32 95% CI
-0.14 to 0.78; NSD.
Up to 240 minutes: 2 trials; 76 children; WMD -0.02 95% CI
-0.23 to 0.18; NSD.
Outcome 04: Gastric Contents measured by Marker DyePhenol RedUp to 120 minutes; 1 trial; (- H2RA); 32 children; NSD.
Up to 120 minutes; 1 trial; (+ H2RA); 33 children; NSD.
Up to 180 minutes; 1 trial; 44 children; WMD -3.10 ml 95% CI
-6.66 to 0.46; NSD.
BromosulphthaleinUp to 120 minutes; 2 trials; (- and + H2RA); 240 children; No
evidence of a difference (combined groups).
Secondary OutcomesTwelve trials. Where differences occurred, fasted children (or their
parents) rated thirst and hunger as worse than those who were
given fluids. Similarly, parents or children were asked to report
behaviour and comfort and those children who were permitted
22Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

fluids were described as less irritable and more comfortable than
those that fasted in the standard manner. Eight children across two
comparisons were reported as vomiting gagging or spitting out an
intervention but it is unclear to which intervention they belonged.
Comparison 02: Short Solid and Fluid Fast versus Standard
Fast
Outcome 01: Aspiration/RegurgitationTwo trials; 86 children; No aspiration/regurgitation.
Outcome 02: Gastric VolumeSolids and Fluids up to 120 minutes: 1 trial; 52 children; WMD
0.25 ml/kg 95% CI 0.07 to 0.43; Favours Standard Fast (p =
0.006).
Solids and Fluids up to 240 minutes: 1 trial; 34 children; WMD
0.09 ml/kg 95% CI -0.12 to 0.30; NSD.
Outcome 03: Gastric pHSolids and Fluids up to 120 minutes: 1 trial; 43 children; WMD
0.35 95% CI -0.08 to 0.78; NSD.
Solids and Fluids up to 240 minutes: 1 trial; 24 children; WMD
0.11 95% CI -0.13 to 0.35; NSD.
Outcome 04: Gastric Volume measured by Marker DyeNot addressed.
Secondary OutcomesNot addressed.
Comparison 03: Short Solid and Fluid Fast versus Short Fluid
Fast
Outcome 01: Aspiration/RegurgitationTwo trials; 96 children; No aspiration/regurgitation.
Outcome 02: Gastric VolumeUp to 120 minutes: 1 trial; 67 children; WMD 0.09 ml/kg 95%
CI -0.08 to 0.26; NSD.
Up to 240 minutes: 1 trial; 29 children; WMD 0.04 ml/kg 95%
CI -0.18 to 0.26; NSD.
Up to 330 minutes: 1 trial; 20 children; WMD 0.12 ml/kg 95%
CI -0.30 to 0.54; NSD.
Outcome 03: Gastric pHUp to 120 minutes: 1 trial; 60 children; WMD 0.06 95% CI -0.57
to 0.69; NSD.
Up to 240 minutes: 1 trial; 22 children; WMD 0.18 95% CI -0.13
to 0.49; NSD.
Up to 330 minutes: 1 trial; 20 children; WMD 0.46 95% CI -0.03
to 0.95; NSD, (p = 0.07).
Outcome 04: Gastric Volume measured by Marker DyeNot addressed.
Secondary OutcomesOne trial. Children permitted solids and fluids reported less
hunger that those permitted fluids alone. Thirst, behaviour, com-
fort, nausea, vomiting were not addressed.
Comparison 04: Short Fluid Fast 1 versus Short Fluid Fast 2
Outcome 01: Aspiration/RegurgitationFour trials; 365 children; No aspiration/regurgitation.
Outcome 02: Gastric VolumeUp to 120 versus 150 minutes: 1 trial; 100 children; WMD 0.06
ml/kg 95% CI -0.05 to 0.17; NSD.
Up to 120 versus 180 minutes: 2 trials; 248 children; WMD 0.04
ml/kg 95% CI -0.08 to 0.15; NSD.
Up to 120 versus 240 minutes: 2 trials; 137 children; WMD 0.00
ml/kg 95% CI -0.13 to 0.13; NSD.
Up to 150 versus 180 minutes: 2 trials; 180 children; WMD -0.04
ml/kg 95% CI -0.16 to 0.09; NSD.
Outcome 03: Gastric pHUp to 120 versus 150 minutes: 1 trial; 100 children; WMD 0.10
95% CI -0.41 to 0.61; NSD.
Up to 120 versus 180 minutes: 2 trials; 248 children; WMD 0.12
95% CI -0.36 to 0.61; NSD.
Up to 120 versus 240 minutes: 2 trials; 119 children; WMD 0.13
95% CI -0.33 to 0.60; NSD.
Up to 150 versus 180 minutes: 2 trials; 180 children; WMD 0.19
95% CI -0.12 to 0.50; NSD.
Outcome 04: Gastric Volume measured by Marker DyeNot addressed.
Secondary OutcomesTwo trials. No difference in parents’ ratings of children’s hunger
or behaviour across groups. No vomiting observed.
Summary of results - B. Type of permitted intake
Comparison 05: Type of Intake v Standard Fast
Water versus Standard Fast
Outcome 01: Aspiration/RegurgitationOne trial; 50 children; No aspiration/regurgitation.
Outcome 02: Gastric VolumeOne trial; 50 children; WMD -0.04 ml/kg 95% CI -0.16 to 0.08;
NSD.
Outcome 03: Gastric pHOne trial; 49 children; WMD 0.27 95% CI -0.12 to 0.66; NSD.
Outcome 04: Gastric Volume measured by Marker DyeNot addressed.
Secondary OutcomesOne trial. Children given water preoperatively reported less thirst
than the fasted group. Parents rated the children permitted water
as less irritable than those children who fasted.
Other Clear Fluids versus Standard Fast
Outcome 01: Aspiration/RegurgitationThree trials; 333 children; No aspiration/regurgitation.
Outcome 02: Gastric Volume
23Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Five trials; 541 children; WMD -0.02 ml/kg 95% CI -0.09 to
0.05; NSD.
Outcome 03: Gastric pHFour trials; 455 children; WMD 0.09 95% CI -0.03 to 0.21; NSD.
Outcome 04: Gastric Volume measured by Marker DyeNot addressed.
Secondary OutcomesFour trials. Children given clear fluids preoperatively reported less
thirst than the fasted groups. Children permitted clear fluids were
rated by parents as less hungry, less irritable and more comfortable
than the children who fasted. There was no difference in children’s
reports of hunger. No vomiting was noted.
Fruit Juice versus Standard Fast
Outcome 01: Aspiration/RegurgitationSeven trials; 518 children; One incident - regurgitation and aspi-
ration in group permitted fruit juice.
Outcome 02: Gastric VolumeSeven trials (- H2RA); 394 children; WMD 0.02 ml/kg 95% CI
-0.08 to 0.11; NSD.
One trial (+ H2RA); 33 children; WMD 0.01 ml/kg 95% CI -0.11
to 0.13; NSD.
Outcome 03: Gastric pHEight trials (- H2RA); 455 children; WMD 0.04 95% CI -0.01
to 0.10; NSD.
Two trials (+ H2RA); 129 children; WMD 0.53 95% CI -0.19 to
1.26; NSD.
Outcome 04: Gastric Volume measured by Marker DyePhenol RedOne trial; 44 children; WMD -3.10 ml 95% CI -6.66 to 0.46;
NSD.
Secondary OutcomesSeven trials. Where differences were noted, children permitted
apple juice preoperatively described less thirst and hunger than the
fasted group. Parents reported the children permitted apple juice
were less irritable than those that fasted. Some vomiting noted (n
= or < 8) but exact number unclear as number included children
who gagged or spat out intervention.
Milk versus Standard Fast
Outcome 01: Aspiration/RegurgitationOne trial; 64 children; No aspiration/regurgitation.
Outcome 02: Gastric VolumeOne trial; 64 children; WMD 0.08 ml/kg 95% CI -0.29 to 0.45;
NSD.
Outcome 03: Gastric pHOne trial; 27 children; WMD -0.01 95% CI -1.82 to 1.80; NSD.
Outcome 04: Gastric Volume measured by Marker Dye
Not addressed
Secondary OutcomesNot addressed.
Dextrose Solution versus Standard Fast
Outcome 01: Aspiration/RegurgitationTwo trials; 82 children; No aspiration/regurgitation.
Outcome 02: Gastric VolumeThree trials; 110 children; WMD -0.14 ml/kg 95% CI -0.43 to
0.15; NSD.
Outcome 03: Gastric pHTwo trials; 65 children; WMD -0.51 95% CI -2.21 to 1.19; NSD.
Outcome 04: Gastric Volume measured by Marker DyeNot addressed
Secondary OutcomesNot addressed.
Other Fluids versus Standard Fast
Outcome 01: Aspiration/RegurgitationFour trials; 193 children; No aspiration/regurgitation.
Outcome 02: Gastric VolumeFour trials; 156 children; WMD -0.13 ml/kg 95% CI -0.41 to
0.16; NSD.
Outcome 03: Gastric pHFour trials; 121 children; WMD 0.34 95% CI -0.62 to 1.31; NSD.
Outcome 04: Gastric Volume measured by Marker DyeNot addressed
Secondary OutcomesOne trial. No vomiting noted.
Comparison 06: Fluid 1 versus Fluid 2
Dextrose versus Polyjoule
Outcome 01: Aspiration/RegurgitationOne trial; 59 children; No aspiration/regurgitation.
Outcome 02: Gastric VolumeOne trial; 59 children; WMD 0.03 ml/kg 95% CI -0.15 to 0.21;
NSD.
Outcome 03: Gastric pHOne trial; 32 children; WMD -0.75 95% CI -1.62 to 0.12; NSD.
Outcome 04: Gastric Volume measured by Marker DyeNot addressed
Secondary OutcomesNot addressed
Dextrose versus Cows’ Milk
Outcome 01: Aspiration/Regurgitation
24Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

One trial; 60 children; No aspiration/regurgitation.
Outcome 02: Gastric VolumeOne trial; 60 children; WMD -0.44 ml/kg 95% CI -0.75 to -0.13;
Favours Dextrose (p = 0.005).
Outcome 03: Gastric pHOne trial; 29 children; WMD -1.74 95% CI -3.09 to -0.39;
Favours Cows’ milk (p = 0.01).
Outcome 04: Gastric Volume measured by Marker DyeNot addressed
Secondary OutcomesNot addressed
Polyjoule versus Cows’ Milk
Outcome 01: Aspiration/RegurgitationOne trial; 61 children; No aspiration/regurgitation.
Outcome 02: Gastric VolumeOne trial; 61 children; WMD -0.47 ml/kg 95% CI -0.78 to -0.16;
Favours Polyjoule (p = 0.003).
Outcome 03: Gastric pHOne trial; 31 children; WMD -1.01 95% CI -2.49 to 0.47; NSD.
Outcome 04: Gastric Volume measured by Marker DyeNot addressed
Secondary OutcomesNot addressed
Summary of results - C. Volume of permitted intake
Comparison 07: Volume of Fluid versus Standard Fast
Low Volume Fluid Intake versus Standard Fast
Outcome 01: Aspiration/RegurgitationFive trials; 410 children; one incident - regurgitation and aspira-
tion.
Outcome 02: Gastric VolumeFour trials (- H2RA); 202 children; WMD -0.12 ml/kg 95% CI
-0.29 to 0.05; NSD.
One trial (+ H2RA); 33 children; WMD 0.01 ml/kg 95% CI -0.11
to 0.13; NSD.
Outcome 03: Gastric pHFive trials (- H2RA); 290 children; WMD 0.42 95% CI -0.19 to
1.04; NSD.
Two trials(+ H2RA); 129 children; WMD 0.53 95% CI -0.19 to
1.26; NSD.
Outcome 04: Gastric Volume measured by Marker DyeNot addressed
Secondary OutcomesFour trials. Where there was a difference, children given a low
volume of fluids preoperatively (or their parents) reported less
thirst and hunger than those that fasted. Children who fasted were
reported by parents as more irritable than those in the low volume
fluid group. Some reports of vomiting made (two related trials)
but report includes children who gagged or spat out intervention
(n = 8).
High Volume Fluid Intake versus Standard Fast
Outcome 01: Aspiration/RegurgitationTen trials; 431 children; No aspiration/regurgitation.
Outcome 02: Gastric VolumeEleven trials; 495 children; WMD 0.04 ml/kg 95% CI -0.05 to
0.13; NSD.
Outcome 03: Gastric pHTen trials; 370 children; WMD 0.04 95% CI -0.02 to 0.09; NSD.
Outcome 04: Gastric Volume measured by Marker DyeNot addressed
Secondary OutcomesFive trials. Where a difference was noted, children permitted a
high volume of fluids preoperatively were less thirsty and irritable
than those in the fasted group. There was no difference between
the children’s hunger or the incidence of vomiting.
Unlimited Fluid Intake versus Standard Fast
Outcome 01: Aspiration/RegurgitationThree trials; 333 children; No aspiration/regurgitation.
Outcome 02: Gastric Volume5 trials; 541 children; WMD -0.02 ml/kg 95% CI -0.09 to 0.05;
NSD.
Outcome 03: Gastric pH5 trials; 455 children; WMD 0.09 95% CI -0.03 to 0.21; NSD.
Outcome 04: Gastric Volume measured by Marker DyeNot addressed
Secondary OutcomesThree trials. Where a difference was noted, children permitted
unlimited volumes of fluid preoperatively were reported to be less
thirsty and hungry than the children who were fasted. Parents also
rated them as less irritable but more comfortable than those that
fasted. There was no between group difference in the incidence of
vomiting.
Comparison 08: Volume 1 versus Volume 2
Outcome 01: Aspiration/RegurgitationOne trial; 62 children; No aspiration/regurgitation.
Outcome 02: Gastric VolumeOne trial; 62 children; WMD 0.05 ml/kg 95% CI -0.44 to 0.34;
NSD.
Outcome 03: Gastric pHOne trial; 62 children; WMD -0.10 95% CI -0.45 to 0.25; NSD.
25Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Outcome 04: Gastric Content measured by Marker DyeNot addressed
Secondary OutcomesOne trial. No difference in the two groups’ description of preop-
erative thirst or hunger. No difference in behaviour.
’High risk’ populations:
No children considered to be at an increased risk of regurgitation
and aspiration during anaesthesia were specifically addressed by
any trial within this review.
Sensitivity analysis
As planned at protocol stage, we conducted a sensitivity analysis
to evaluate the impact of including trials known to have employed
inadequate methods of randomisation. These methods included
randomisation by alternate cases (Kushikata 1996), operation list
(Meakin 1985a; Meakin 1985b; Meakin 1985c; Meakin 1985d;
Meakin 1985e; Meakin 1985f) and day of the week (Welborn
1993). The original results and the results excluding the above
trials can be found in Table 40. Only one result was noted to
alter. On pooling the remaining data within Comparison: 05 Type
of Intake - Fluid versus Standard Fast, 07 Other Fluids versus
Standard Fast the children administered Polyjoule or an isosmolar
solution of electrolytes solution were found to have significantly
lower gastric volume than those children who fasted (WMD -0.38
ml/kg, 95% CI -0.58 to -0.19 p = < 0.0001). This comparison
did not demonstrate a significant difference when all trials are
included.
The only available data in relation to the preoperative intake of
solids was provided by the Meakin 1985 and Kushikata 1996 trials
(see Comparison: 02 Duration - Short Solid Fluid Fast versus
Standard Fast and 03 Duration - Short Solid Fluid Fast versus Short
Fluid Fast) and so a sensitivity analysis was unnecessary for these
comparisons. Similarly, for Comparison Duration - Short Fluid
Fast versus Standard Fast 05 Fluids (up to 240 minutes preop)
only one trial Maekawa 1993b remains when Meakin 1985e is
excluded and so a sensitivity analysis was not conducted for this
comparison.
D I S C U S S I O N
In this review we aimed to systematically identify, appraise and
synthesise the reliable evidence from valid research in relation to
preoperative fasting for children. We appraised this evidence in re-
lation to children’s safety and comfort, directly or indirectly, using
a variety of outcome measures. The complexity of the preopera-
tive fasting intervention was addressed by looking at the evidence
relating to the three main parameters of a fasting regimen i.e. the
duration of fast and the type and volume of intake permitted dur-
ing a period of restricted intake. We also searched for evidence in
relation to specific ’high-risk’ patient groups. These complexities
were not unexpected and had already been addressed by the related
adult based review (Brady 2004).
We encountered some additional complexities, including the need
to consider specific age groups (e.g. neonates, infants, children).
Many trials were based on children whose ages spanned these sub-
group bandings and while the resulting evidence was of relevance
it was not specific to these groups. This was surprising given the
great clinical awareness of the different physiological and psycho-
logical needs of these subgroups of children.
We identified a need to define a ’traditional’ or ’standard’ fasting
regimen. The traditional approach to the care of children preoper-
atively often indicated a more lenient approach to fasting (which
also accounted for the age of the child) than the ’nil-by-mouth-
from-midnight’ fast observed in adult practice. As a result, the
review classified a ’typical’ traditional standard fast of NPO for 4
hours for infants 1-12 months, 6 hours for children 12 months-5
years and 8 hours for children over the age of 5 years.
The data in relation to the primary outcome measure of aspiration
and regurgitation (and associated morbidity) was sparse. Of 1208
children in the trials that reported this primary outcome only one
incident of aspiration and regurgitation was reported and this (ac-
cording to the trialists) appeared to have been related to airway
management rather than as a result of the intervention. Given the
rarity of the incidence of regurgitation and aspiration we must be
cautious in making any firm judgements based on this evidence.
While some trialists reported on the incidence of aspiration and
regurgitation as an outcome (or made this information available to
the authors), most relied on surrogate measures of risk - children’s
gastric volume and pH during surgery. Most surrogate outcome
measures are known to be poorly validated (for example DeMets
2002), and the validity of the link between regurgitation, aspira-
tion, associated morbidity and mortality and the surrogate mea-
sures of gastric volume and pH is no exception. Thus we can only
make some tentative extrapolations about the risk of aspiration on
the basis of the evidence from these surrogate outcomes. We can
however be more confident about the effect of the various fasting
regimens on children’s gastric pH and volume.
To permit inclusion within the review of trials that did not re-
port (and the data were unavailable) mean and SD data, we cal-
culated pseudo-means and pseudo-standard deviations (Arnold
1992; O’Rourke 2002) . The use of actual means and SDs would,
of course, be preferential and we would encourage researchers and
editors to report (or make available) such data for meta-analysis
purposes - in addition to the median and ranges that better de-
scribe the study population characteristics. In fact, it would be
preferable to report at least the mean, SD, median, minimum,
maximum, 25th and 75th percentile for each group reported on
and ideal to list the sorted outcome values for each group or the
mean and SD and every nth outcome value as space permits.
26Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

After collecting and presenting the evidence in relation to the in-
take of fluids during a period of restricted intake there is no evi-
dence to indicate that children permitted fluids up to 120 minutes
preoperatively experience higher gastric volumes or lower gastric
pH values than those children who fasted. Interestingly, the confi-
dence intervals observed also suggest there is little possibility that
a clinically important difference exists in relation to the children’s
gastric pH and volume. We found similar results in our review
based on adults (Brady 2004). Children permitted fluids up to 180
minutes preoperatively actually had a lower mean gastric volume
(WMD 0.12 ml/kg) than those who had experienced a prolonged
fast, though this difference is not considered to be clinically signif-
icant. Where differences were noted, the children permitted fluids
were also noted to be less thirsty and hungry and better behaved
and more comfortable than the children who fasted. These find-
ings are supported by the trials that made a direct comparison be-
tween the intake of fluids at two different time points. When com-
pared with children permitted fluids at 150, 180 and 240 min-
utes preoperatively there was no difference in the groups’ gastric
volume or pH nor in their descriptions of hunger, behaviour or
vomiting.
The outcome measures thirst, hunger and comfort were prob-
lematic. Not only are such outcomes based on subjective ratings
transferred to a VAS, but the ratings for some children were made
by proxy, with parents reporting on their child’s thirst, hunger or
other aspects of their child’s preoperative experience. In addition,
the difficulties of attempting to blind the raters as to whether they
(or their child) were given something to drink or eat have already
been mentioned. In some cases very young children (less than 5
years) were unable to complete a VAS and so their reports of the
experience were not included within the results.
The evidence in relation to the intake of solid food was less defini-
tive with only a handful of small pioneering trials conducted that
employed alternation (now known to be inadequate) methods of
randomisation. The type of solid intake varied between plain bis-
cuits (Meakin 1985) and rice porridge (Kushikata 1996), as did
the timing of the solid intake which ranged from up to 120 and
330 minutes preoperatively. No aspiration or regurgitation was re-
ported, although there was some indication (Meakin 1985b) that
the children permitted biscuits and a drink 120 minutes preop-
eratively had a higher mean gastric volume than the fasted group
(WMD 0.25 ml/kg). Particles of ingested food were observed in
the gastric aspirate of a quarter of children. At present, the avail-
able evidence does not support a shift in practice from the current
established guidelines which permit children solid food up to 6 (or
8 hours) preoperatively until additional evidence can be reviewed.
Additional large, high quality studies are required to extend the
evidence in this area.
We also evaluated the available evidence relating to the type of
fluid intake within the review. The range of fluids included water,
clear fluid, dextrose solution (all of which could be classed as clear
fluids) milk and other fluids (for example orange squash). The tri-
als that investigated the preoperative intake of clear fluids demon-
strated narrow confidence intervals and thus provide little support
for the existence of a clinically important difference between the
gastric volume or pH of children permitted clear fluids and those
that fasted. Where there was a difference between the groups, the
children given a drink were less thirsty and hungry, better behaved
and more comfortable than the children who fasted. This finding
again supports the finding of the adult review (Brady 2002) and
current preoperative fasting recommendations that indicate clear
fluids can be permitted up to two hours preoperatively. As for most
of the comparisons in this review, however, the trials were based
on fewer than 100 children and additional evidence from larger
studies would be welcome.
Other fluids administered preoperatively included orange juice,
apple juice and orange squash. Some fruit juice interventions also
included an H2-receptor antagonist co-intervention, so evalua-
tions of the type of fluid intake within the review were often the
result of a single trial conducted on a small number of children.
Where direct comparisons of two different types of intervention
were possible, some significant between group differences were
noted and indicate further avenues for targeting through more
rigorous investigations. For example, one small trial suggests that
children who drank dextrose or Polyjoule had a lower volume of
gastric contents than children that were given cows’ milk. Con-
versely, the children who drank dextrose had more acidic gastric
contents that those that drank cows’ milk. Additional investiga-
tion of these issues is warranted.
The evidence in relation to the preoperative intake of milk was sur-
prisingly lacking given the prominence this substance has amongst
the young children for nutritional intake. Only van der Walt 1989
(cows’ milk) and Cook-Sather 2003 (formula milk) addressed the
intake of milk in their investigations. There is insufficient evi-
dence on the basis of these two small trials to guide clinical prac-
tice though some additional non-randomised studies can also be
referred to (e.g. Litman 1994; Sethi 1999; van der Walt 1990).
For clinical purposes, guidance in relation to the intake of milk
by children during the preoperative period should be sought from
the available professional guidelines (e.g. ASA 1999; RCN). This
is a complex issue and will require detailed study given the variety
of milk types available to children but this should not dissuade
researchers from addressing the need for high quality evidence in
this area.
The volume of the fluid intake permitted preoperatively did not
did not appear to have an impact on children’s gastric volume or
pH when compared with a standard fast. The majority of trials
permitted children to drink what was classified for the purposes of
this review as a high volume [over 5 ml/kg] while others permitted
children an unlimited volume of fluid intake. There were some
reports of children refusing to drink the intervention or declin-
ing to drink the prescribed volume in full (for example Sandhar
27Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

1989a). Across the trials that addressed the low, high and unlim-
ited intake of fluid there was no significant difference in relation to
the intra-operative gastric volume or pH contents from those who
drank and those who fasted. Narrow confidence intervals amongst
the trials that addressed the intake of unlimited fluids were noted
in relation to gastric volume and pH supporting the assertion it
is unlikely that a clinically important difference exists. The one
small, high quality trial that directly compared two different vol-
umes of intake (6 ml/kg and 10 ml/kg of apple juice) did not find
a significant difference in volume of gastric contents or on any of
the secondary outcome measures. The results of the parallel re-
view based on adults (Brady 2004) also suggested the volume of
intake was unlikely to be of significance. Current national clinical
guidelines have taken a pragmatic approach and omit mention of
specific volumes in relation to preoperative fluid intake (AAGBI
2001; ASA 1999; NHSQIS 2003).
As noted in the Methodological Quality section most trials within
this review employed some of the procedures that minimise the
possibility of bias. For example detailed listing of inclusion and
exclusion criteria and using appropriate methods to generating the
randomisation sequence in a non-biased manner. However, as has
been previously discussed (Brady 2004; Søreide 1995) additional
steps towards methodological quality could have been taken in
many preoperative fasting trials by ensuring concealment of the
children’s
allocation to the control and intervention groups. Awareness of
the importance allocation concealment in preventing bias in a ran-
domised trial is a relatively new development (Schultz 2001) and
so it is not surprising that only some of the more recently con-
ducted trials adequately utilised this precaution. This is something
that future research in this area should strive to incorporate within
the study design.
This review failed to identify any RCT that specifically recruited
children considered to be at an increased risk of regurgitation
and aspiration. In most cases children were recruited from a very
specific surgical population group i.e. healthy, ASA I-II children
undergoing elective surgery. The findings are therefore applica-
ble only to those patient populations and do not extend to many
groups considered to be at high risk of regurgitation/aspiration, for
example obese children or emergency cases. The global rising epi-
demic of obesity amongst children has been widely acknowledged
(IASO 2004; WHO 2003) together with the realisation of the
concomitant problems this group of children will experience (for
example diabetes, hypertension). In England obesity has tripled in
the last twenty years and if childhood obesity continues unchecked
by 2020 half of all children will be obese (Health Comm 2004).
There is an urgent need to establish high quality evidence that
relates specifically to the preoperative intake and fasting needs of
this group. The only relevant evidence available at the moment
is based on a single high quality trial within which obese adults
permitted 300 ml of clear fluids two hours preoperatively had a
statistically and clinically significant higher mean gastric volume
than the group that fasted from midnight (Maltby Ptyka 2004).
Only one trial included within the review recruited children who
were classified as ASA III-IV undergoing cardiac surgical proce-
dures. This ASA rating refers to children who have a severe sys-
temic disease that is (at ASA IV) a constant threat to life. Only
two children within this trial were classified as ASA IV. As the
ASA classification system is an indicator of surgical risk and not
as an indicator for risk of regurgitation and aspiration, a decision
was made to include this trial within the main body of the re-
view. The results of this high quality trial (n = 91) taken in iso-
lation found no difference between the children permitted intake
of unlimited clear fluids up to 120 minutes preoperatively and
the control group that were permitted clear fluids. The children
who followed the less conservative fast were also described as less
thirsty, less hungry and more comfortable than the children who
fasted. Other ’high-risk’ preoperative groups also require closer
consideration including children undergoing urgent and emer-
gency surgery (NCEPOD 2002) or those with particular preop-
erative nutritional needs such as those with cancer (for example
Sala 2004). For other groups, for example children with gastroin-
testinal disease or disorders, there appears to be some debate as
to whether they are actually at increased risk of regurgitation and
aspiration (for example Schwartz et al 1998).
A U T H O R S ’ C O N C L U S I O N S
Implications for practice
Multidisciplinary teams responsible for the care of surgical patients
should be aware of the evidence in relation to preoperative fasting,
the relevant clinical guidelines and local fasting policies. When-
ever possible such policies should be prepared with the involve-
ment of the whole team and presented in a simple and easy-to-
follow format. Compliance with preoperative fasting instructions
has always been crucial, but will become increasingly important
with the growth and promotion of day surgery for elective surgi-
cal procedures (Audit Commission). Staff will need to ensure that
children and their parents are educated on the benefits of more
relaxed fasting policies than the traditional fast.
Following this systematic review we can conclude there is evi-
dence that children at normal risk of regurgitation and aspiration,
given unlimited clear fluids up to two hours preoperatively are
not at a clinically significant risk of increased gastric volume and
pH than children who follow a standard fast. Similar conclusions
with regard to risk of aspiration/regurgitation can only be reached
with some cautious judgement. The risks of aspiration/regurgita-
tion were very low in this group of patients (either 1 or 0 out of
1208). Given this, the size of relative effect would be unacceptable
and the possibility that it may not be picked up via the surrogate
outcomes needs to be carefully considered. Children permitted a
28Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

drink during the preoperative period were found to be less thirsty,
less hungry, better behaved and more comfortable that those who
fasted. Clinical guidelines on the fasting of children before surgery
have preceded the publication of this review and urge clinicians to
permit the children to drink clear fluids up to two hours preop-
eratively (ASA 1999, Committee on Drugs) as do more generalist
guidelines (NNCG 1993).
It should be remembered however that this evidence (and the
recommendations made by available guidelines) only applies to
healthy children who are not considered to be at an increased risk
of aspiration/regurgitation during anaesthesia. There is a paucity
of evidence in relation to high-risk groups and so clear preopera-
tive fasting recommendations for these groups cannot be made at
this time. Conducting studies with some high-risk children (such
as children requiring emergency surgery) may never be ethically
possible. Additional sources of evidence and opinion including ob-
servational studies and best practice statements should be sought
when considering the preoperative fasting preparations for these
children.
Preoperative carers have an obligation to ensure that their pa-
tients are fully informed (Smith 2004) about the preoperative
fasting procedure and that this information is based on the cur-
rent evidence. Not only has a recent survey demonstrated that
information given to many patients in the UK falls short of this
(Markham 2003) but we also know that many sites still demand
that healthy patients remain nil-by-mouth-from-midnight. This
practice should no longer be tolerated.
Implications for research
Well designed, methodologically sound randomised controlled tri-
als are still required to further examine the intake of solid food
and some fluid types preoperatively. The paucity of evidence in
relation to the intake of milk is especially surprising given the re-
liance of younger children on this form of nutritional intake. Some
interesting developments in clinical practice indicate possible av-
enues of investigation with some children reportedly permitted
breast milk and formula up to two hours prior to surgery (Hofer
2001). Such fasting regimens are more lenient than the evidence
reviewed here would support and further investigation, reporting
and monitoring of this development should be a matter of priority.
Researchers should ensure that the numbers of children recruited
to such investigations are based on upon a priori sample size calcu-
lations and that adequate concealment of children’s allocation to
the trial groups should be incorporated whenever possible. Given
the tendency for the gastric volume and pH data to be skewed,
we would also encourage researchers to report mean and standard
deviation data thus permitting accurate representation of the data
within meta-analyses when required.
In clinical settings there is a clear awareness of the different pre-
operative fasting requirements for neonates, infants, children and
adolescents. This distinction is not reflected within the available
evidence and further investigation of these boundaries and gener-
ation of additional age-group specific evidence should be pursued.
In addition, many children considered to be at ’high-risk’ of regur-
gitation and aspiration (e.g. the growing population of obese chil-
dren or those with gastrointestinal disorders) have been specifically
excluded from the evidence presented here. High quality trials that
specifically target and recruit children from these groups would
provide much needed evidence in this area. It remains crucial that
the incidence of aspiration/regurgitation continues to be reported.
For the moment, the surrogate measures of risk i.e. intra-opera-
tive gastric content volume and pH should continue to be used,
though reliance on the ’critical values’ (Roberts 1974) should be
discouraged. The possibility of developing a clinically meaningful
composite surrogate outcome measure based on the two outcomes
of gastric volume and pH as a statistically more powerful indicator
of risk should be explored (DeMets 2002), though it is acknowl-
edged the development and use of such an outcome would not be
without its challenges (e.g. Cannon 1997, Freemantle 2003).
Despite the availability of research evidence, through reviews of
the literature and widely available guideline recommendations,
kick starting an evolution in fasting policies remains a difficult
task. Researchers should consider how best to communicate the
evidence from this review (and others) to the preoperative multi-
disciplinary team so that it has a positive impact on clinical prac-
tice during the preoperative period. Exploration of this issue will
no doubt raise issues such as the quality of patient (and parent)
preoperative education, the information communicated regarding
the preoperative fasting regimen and patient compliance.
N O T E S
Readers of this review should also refer to the companion review
published in the Cochrane Library:
Preoperative fasting for adults to prevent perioperative complica-
tions. Brady M, Kinn S, Stuart P.
P O T E N T I A L C O N F L I C T O F
I N T E R E S T
None known.
A C K N O W L E D G E M E N T S
The authors would like to thank
• The trial authors for their extensive contribution; the time they
took to respond to queries and the provision of additional details
whenever possible.
• Sally Bell-Syer, Nicky Cullum and Andrea Nelson from the
Cochrane Wounds Group for their assistance.
29Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

• Seokyung Hahn from the Cochrane Wounds Group for statis-
tical advice.
• Linda Scott, Debbie Cattermole, Sarah Hinks for assistance
with handsearching, re-running searches or second screening of
retrieved references.
• Namiko Ikeda, Audrey Morrison and Elizabeth Stirrat for trans-
lations.
• Cochrane Wounds Group referees (Anne Marie Bagnall, Adrian
Barbul, Michelle Briggs, Anne Humphreys) and the Cochrane
Anaesthesia Group Editor John Carlisle for their comments to
improve the review.
• The Cochrane Child Health Field Third Bursary Scheme for
support in completion of this Cochrane review in child health.
S O U R C E S O F S U P P O R T
External sources of support
• Chief Scientist Office, Scottish Executive UK
• Cochrane Child Health Field Bursary 2004 CANADA
Internal sources of support
• Nursing, Midwifery and Allied Health Professions Research
Unit UK
R E F E R E N C E S
References to studies included in this review
Aun 1990 {published and unpublished data}∗ Aun CS, Panesar NS. Paediatric glucose homeostasis during anaes-
thesia. British Journal of Anaesthesia 1990;64(4):413–8.
Cook-Sather 2003 {published and unpublished data}∗ Cook-Sather SD, Harris KA, Rosetta Chiavacci R, Gallagher PR,
Schreiner MS. A liberalized fasting guideline for formula-fed infants
does not increase average gastric fluid volume before elective surgery.
Pediatric Anesthesia 2003;96:965–9.
Crawford 1990a {published and unpublished data}∗ Crawford M, Lerman J, Christensen S, Farrow-Gillespie A. Effects
of Duration of Fasting on Gastric Fluid pH and Volume in Healthy
Children. Anesthesia & Analgesia 1990;71(4):400–3.
Farrow-Gillespie A, Christensen S, Lerman J. Effect of the Fasting
Interval on Gastric pH and Volume in Children. Anesthesia & Anal-
gesia. 1988;67:S59.
Crawford 1990b {published and unpublished data}∗ Crawford M, Lerman J, Christensen S, Farrow-Gillespie A. Effects
of Duration of Fasting on Gastric Fluid pH and Volume in Healthy
Children. Anesthesia & Analgesia 1990;71:400–3.
Farrow-Gillespie A, Christensen S, Lerman J. Effect of the Fasting
Interval on Gastric pH and Volume in Children. Anesthesia & Anal-
gesia 1988;67:S59.
Crawford 1990c {published and unpublished data}∗ Crawford M, Lerman J, Christensen S, Farrow-Gillespie A. Effects
of Duration of Fasting on Gastric Fluid pH and Volume in Healthy
Children. Anesthesia & Analgesia 1990;71:400–3.
Farrow-Gillespie A, Christensen S, Lerman J. Effect of the Fasting
Interval on Gastric pH and Volume in Children. Anesthesia & Anal-
gesia 1988;67:S59.
Gombar 1997 {published and unpublished data}∗ Gombar S, Dureja J, Kiran S, Gombar K, Chhabra B. The effect
of pre-operative intake of oral water and ranitidine on gastric fluid
volume and pH in children undergoing elective surgery. Journal of
the Indian Medical Association 1997;95(6):166–8.
Goresky 1992a {published data only}
Finely GA, Bissonnette B, Goresky GV, Klassen K, Lerman J, Mc-
Diarmid C, et al. The effect of oral ranitidine and preoperative oral
fluids on gastric fluid pH and volume in children. Canadian Journal
of Anaesthesia. 1989;36:S95.
30Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

∗ Goresky GV, Finley GA, Bissonnette B, Shaffer EA. Efficacy, Dura-
tion and Absorption of a Paediatric Oral Liquid Preparation of Ran-
itidine Hydrochloride. Canadian Journal of Anaesthesia 1992;39(8):
791–8.
Goresky 1992b {published data only}
Finely GA, Bissonnette B, Goresky GV, Klassen K, Lerman J, Mc-
Diarmid C, et al. The effect of oral ranitidine and preoperative oral
fluids on gastric fluid pH and volume in children. Canadian Journal
of Anaesthesia. 1989;36:S95.
∗ Goresky GV, Finley GA, Bissonnette B, Shaffer EA. Efficacy, Dura-
tion and Absorption of a Paediatric Oral Liquid Preparation of Ran-
itidine Hydrochloride. Canadian Journal of Anaesthesia 1992;39(8):
791–8.
Kushikata 1996 {published and unpublished data}∗ Kushikata T, Matsuki A, Murakawa T, Sato K. Possibility of rice
porridge for preoperative feeding in children [[Japanese]]. Masui -
Japanese Journal of Anesthesiology 1996;45(8):943–7.
Maekawa 1993a {published data only}∗ Maekawa N, Mikawa K, Yaku H, Nishina K, Obara H. Effects of
2-, 4- and 12-hour fasting intervals on preoperative gastric fluid pH
and volume, and plasma glucose and lipid homeostasis in children.
Acta Anaesthesiologica Scandinavica 1993;37(8):783–7.
Mikawa K, Maekawa N, Nishina K, Obara H. A short fasting interval
does not increase preoperative plasma atrial natriuretic polypeptide
concentrations in children. Acta Anaesthesiologica Scandinavica 1993;
37:713–4.
Maekawa 1993b {published data only}∗ Maekawa N, Mikawa K, Yaku H, Nishina K, Obara H. Effects of
2-, 4- and 12-hour fasting intervals on preoperative gastric fluid pH
and volume, and plasma glucose and lipid homeostasis in children.
Acta Anaesthesiologica Scandinavica 1993;37(8):783–7.
Mikawa K, Maekawa N, Nishina K, Obara H. A short fasting interval
does not increase preoperative plasma atrial natriuretic polypeptide
concentrations in children. Acta Anaesthesiologica Scandinavica 1993;
37:713–4.
Maekawa 1993c {published data only}∗ Maekawa N, Mikawa K, Yaku H, Nishina K, Obara H. Effects of
2-, 4- and 12-hour fasting intervals on preoperative gastric fluid pH
and volume, and plasma glucose and lipid homeostasis in children.
Acta Anaesthesiologica Scandinavica 1993;37(8):783–7.
Mikawa K, Maekawa N, Nishina K, Obara H. A short fasting interval
does not increase preoperative plasma atrial natriuretic polypeptide
concentrations in children. Acta Anaesthesiologica Scandinavica 1993;
37:713–4.
Meakin 1985a {published and unpublished data}
Meakin G, Dingwall AE, Addison GM. Effects of fasting and oral
premedication on the pH and volume of gastric aspirate in children.
British Journal of Anaesthesia 1987;59(6):678–82.
∗ Meakin G, Dingwall AE, Addison GM. Effects of Preoperative
Feeding on Gastric pH and Volume in Children. British Journal of
Anaesthesia. 1985;57:832–3P.
Meakin 1985b {published and unpublished data}
Meakin G, Dingwall AE, Addison GM. Effects of fasting and oral
premedication on the pH and volume of gastric aspirate in children.
British Journal of Anaesthesia 1987;59(6):678–82.
∗ Meakin G, Dingwall AE, Addison GM. Effects of Preoperative
Feeding on Gastric pH and Volume in Children. British Journal of
Anaesthesia. 1985;57:832–3P.
Meakin 1985c {published and unpublished data}
Meakin G, Dingwall AE, Addison GM. Effects of fasting and oral
premedication on the pH and volume of gastric aspirate in children.
British Journal of Anaesthesia 1987;59(6):678–82.
∗ Meakin G, Dingwall AE, Addison GM. Effects of preoperative
feeding on gastric pH and volume in children. British Journal of
Anaesthesia. 1985;57:832–3P.
Meakin 1985d {published and unpublished data}∗ Meakin G, Dingwall AE, Addison GM. Effects of Preoperative
Feeding on Gastric pH and Volume in Children. British Journal of
Anaesthesia. 1985;57:832–3P.
Meakin 1985e {published and unpublished data}∗ Meakin G, Dingwall AE, Addison GM. Effects of Preoperative
Feeding on Gastric pH and Volume in Children. British Journal of
Anaesthesia. 1985;57:832–3P.
Meakin 1985f {published and unpublished data}∗ Meakin G, Dingwall AE, Addison GM. Effects of Preoperative
Feeding on Gastric pH and Volume in Children. British Journal of
Anaesthesia. 1985;57:832–3P.
Miller 1990 {published and unpublished data}∗ Miller BR, Tharp JA, Issacs WB. Gastric Residual Volume in In-
fants and Children following a Three Hour Fast. Journal of Clinical
Anesthesia 1990;2:301–5.
Moyao-García 2001 {published and unpublished data}∗ Moyao-García D, Corrales-Fernández MA, Blanco-Rodríguez G,
Sánchez-Hernández E, Nava-Ocampo A. Benefits of oral administra-
tion of an electrolyte solution interrupting a prolonged preoperatory
fasting period in pediatric patients. Journal of Pediatric Surgery 2001;
36(3):457–9.
Nicolson 1992 {published and unpublished data}∗ Nicolson SC, Dorsey AT, Schreiner MS. Shortened Preanesthetic
Fasting Interval in Pediatric Cardiac Surgical Patients. Anesthesia &
Analgesia 1992;74:694–7.
Sandhar 1989a {published data only}∗ Sandhar BK, Goresky GV, Maltby JR, Shaffer EA. Effect of oral
liquids and ranitidine on gastric fluid volume and pH in children un-
dergoing outpatient surgery. Journal of Anesthesiology 1989;71:327–
30.
Sandhar BK, Goresky GV, Shaffer L, Strunin L. Pre-operative fasting
in children: how long is enough?. Canadian Journal of Anaesthesia.
1988;35:S141–2.
Sandhar BK, Maltby JR, Goresky G, Strunin, L. Preoperative fluids
and ranitidine in children. British Journal of Anaesthesia. 1988;60
(3):324P–5P.
Sandhar 1989b {published data only}∗ Sandhar BK, Goresky GV, Maltby JR, Shaffer EA. Effect of oral
liquids and ranitidine on gastric fluid volume and pH in children un-
dergoing outpatient surgery. Journal of Anesthesiology 1989;71:327–
30.
31Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Sandhar BK, Goresky GV, Shaffer L, Strunin L. Pre-operative fasting
in children: how long is enough?. Canadian Journal of Anaesthesia.
1988;35:S141–2.
Sandhar BK, Maltby JR, Goresky G, Strunin L. Preoperative fluids
and ranitidine in children. British Journal of Anaesthesia. 1988;60
(3):324P–325P.
Sarti 1991 {published data only}∗ Sarti A, Calamandrei M, Messeri A, Busoni P. Preoperative Fasting
in Pediatrics [Il Digiuno Preoperatorio in Pediatria]. Minerva Aneste-
siologica 1991;57(11):1179–80.
Schreiner 1990 {published and unpublished data}∗ Schreiner MS, Triebwasser A, Keon TP. Ingestion of liquids com-
pared with preoperative fasting in pediatric outpatients. Anesthesiol-
ogy 1990;72:593–7.
Triebwasser A, Schreiner MS, Parness J, Keon TP. Effect of preop-
erative clear fluids gastric volume in children. Anesthesiology. 1989;
71:A1177.
Splinter 1989 {published and unpublished data}∗ Splinter WM, Stewart JA, Muir JG. The effect of preoperative apple
juice on gastric contents, thirst and hunger in children. Canadian
Journal of Anaesthesia 1989;36:55–8.
Splinter 1990a {published and unpublished data}∗ Splinter WM, Stewart JA, Muir JG. Large volumes of apple juice
preoperatively do not affect gastric pH and volume in children. Cana-
dian Journal of Anaesthesia 1990;37:36–9.
Splinter 1990b {published and unpublished data}∗ Splinter WM, Stewart JA, Muir JG. Large volumes of apple juice
preoperatively do not affect gastric pH and volume in children. Cana-
dian Journal of Anaesthesia 1990;37:36–9.
Splinter 1990c {published and unpublished data}∗ Splinter WM, Stewart JA, Muir JG. Large volumes of apple juice
preoperatively do not affect gastric pH and volume in children. Cana-
dian Journal of Anaesthesia 1990;37:36–9.
Splinter 1991 {published and unpublished data}∗ Splinter WM, Schaefer JD. Ingestion of clear fluids is safe for ado-
lescents up to 3 h before anaesthesia. British Journal of Anaesthesia
1991;66(1):48–52.
Splinter WM, Schneider ME, Schaefer JD. Unrestricted clear fluid
ingestion 3-hours before anesthesia is safe for adolescents. Anesthesia
& Analgesia. 1990;70:S387.
Splinter Schaefer 1a {published and unpublished data}
Splinter W, Schaefer JD, Zunder IH. A 2-hour clear fluid fast is safe
for children. Anesthesia & Analgesia. 1990;70:S386.
∗ Splinter WM, Schaefer JD. Unlimited clear fluid ingestion two
hours before surgery in children does not affect volume or pH of
stomach contents. Anaesthesia & Intensive Care 1990;18(4):522–6.
Splinter Schaefer 1b {published and unpublished data}
Splinter W, Schaefer JD, Zunder IH. A 2-hour clear fluid fast is safe
for children. Anesthesia & Analgesia. 1990;70:S386.
∗ Splinter WM, Schaefer JD. Unlimited clear fluid ingestion two
hours before surgery in children does not affect volume or pH of
stomach contents. Anaesthesia & Intensive Care 1990;18(4):522–6.
Splinter Schaefer 2 {published and unpublished data}∗ Splinter WM, Schaefer JD, Zunder IH. Clear fluids three hours
before surgery do not affect the gastric fluid contents of children.
Canadian Journal of Anaesthesia 1990;37(5):498–501.
Zunder IH, Splinter WM, Schaefer EA. Preoperative clear fluids do
not affect gastric pH and volume in children. Anesthesiology. 1989;
71:3A.
Splinter Schaefer 3a {published data only}∗ Splinter WM, Schaefer JD, Bonn GE. Unlimited clear fluid inges-
tion by infants up to 2 hours before surgery is safe. Canadian Journal
of Anaesthesia. 1990;37(4(ii)):S95.
Splinter Schaefer 3b {published data only}
Splinter WM, Schaefer JD, Bonn GE. Unlimited clear fluid ingestion
by infants up to 2 hours before surgery is safe. Canadian Journal of
Anaesthesia. 1990;37(4(ii)):S95.
Splinter Schaefer 3c {published data only}
Splinter WM, Schaefer JD, Bonn GE. Unlimited clear fluid ingestion
by infants up to 2 hours before surgery is safe. Canadian Journal of
Anaesthesia. 1990;37(4(ii)):S95.
van der Walt 1986a {published and unpublished data}
van der Walt JH, Carter J. Preoperative fasting in infancy. Anaesthesia
and Intensive Care. 1985;13(1):97.
∗ van der Walt JH, Carter JA. The effect of different pre-operative
feeding regimens on plasma glucose and gastric volume and pH in
infancy. Anaesthesia & Intensive Care 1986;14(4):352–9.
van der Walt 1986b {published and unpublished data}
van der Walt JH, Carter J. Preoperative fasting in infancy. Anaesthesia
and Intensive Care. 1985;13(1):97.
∗ van der Walt JH, Carter JA. The effect of different pre-operative
feeding regimens on plasma glucose and gastric volume and pH in
infancy. Anaesthesia & Intensive Care 1986;14(4):352–9.
van der Walt 1986c {published and unpublished data}
van der Walt JH, Carter J. Preoperative fasting in infancy. Anaesthesia
and Intensive Care. 1985;13(1):97.
∗ van der Walt JH, Carter JA. The effect of different pre-operative
feeding regimens on plasma glucose and gastric volume and pH in
infancy. Anaesthesia & Intensive Care 1986;14(4):352–9.
van der Walt 1986d {published and unpublished data}
van der Walt JH, Carter J. Preoperative fasting in infancy. Anaesthesia
and Intensive Care. 1985;13(1):97.
∗ van der Walt JH, Carter JA. The effect of different pre-operative
feeding regimens on plasma glucose and gastric volume and pH in
infancy. Anaesthesia & Intensive Care 1986;14(4):352–9.
van der Walt 1986e {published and unpublished data}
van der Walt JH, Carter J. Preoperative fasting in infancy. Anaesthesia
and Intensive Care. 1985;13(1):97.
∗ van der Walt JH, Carter JA. The effect of different pre-operative
feeding regimens on plasma glucose and gastric volume and pH in
infancy. Anaesthesia & Intensive Care 1986;14(4):352–9.
van der Walt 1986f {published and unpublished data}
van der Walt JH, Carter J. Preoperative fasting in infancy. Anaesthesia
and Intensive Care 1985;13(1):97.
32Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

∗ van der Walt JH, Carter JA. The effect of different pre-operative
feeding regimens on plasma glucose and gastric volume and pH in
infancy. Anaesthesia & Intensive Care 1986;14(4):352–9.
Welborn 1993 {published data only}
Welborn L, Norden J, Hannallah R, Broadman L, Seiden N. Apple
juice ingestion two hours before surgery does not increase blood
glucose concentrations in pediatric patients. Canadian Journal of
Anaesthesia. 1992;39:A97.
∗ Welborn LG, Norden JM, Seiden N, Hannallah, RS, Patel, RI,
Broadman, L, et al. Effect of minimizing preoperative fasting on pe-
rioperative blood glucose homeostatsis in children. Paediatric Anaes-
thesia 1993;3:167–71.
References to studies excluded from this reviewBevan & Burn 1973
∗ Bevan JC, Burn MC. Acid-base and blood glucose levels of pae-
diatric cases at induction of anaesthesia: the effects of preoperative
starvation and feeding. British Journal of Anaesthesia. 1973;45(1):
115.
Bevan & Burn 1973b∗ Bevan JC, Burn MC. Acid-base changes and anaesthesia. The in-
fluence of pre-operative starvation and feeding in paediatric surgical
patients. Anaesthesia 1973;28(4):415–22.
Fry 1976∗ Fry ENS, Ibrahim AA. Hypoglycaemia in paediatric anaesthesia: the
influence of metoclopramide and oral maltose in paediatric surgical
patients. Anaesthesia 1976;31(4):552–4.
Graham 1979∗ Graham IF. Preoperative starvation and plasma glucose concentra-
tions in children undergoing outpatient anaesthesia. British Journal
of Anaesthesia 1979;51:161.
Hotta 1967∗ Hotta K. Effect of Pre-operative fasting and feeding on the acid
base equilibrium in new born infants and young children. Nippon
Shonika Gakkai Zasshi 1967;71(10):1288–300.
Ingebo 1997∗ Ingebo KR, Rayhorn NJ, Hecht RM, Shelton MT, Silber GH, Shub
MD. Sedation in children: adequacy of two-hour fasting. Journal of
Pediatrics 1997;131(1 Pt 1):155–8.
Jensen 1982∗ Jensen BH, Wernberg M, Andersen M. Preoperative Starvation and
Blood Glucose Concentrations in Children Undergoing Inpatient
and Outpatient Anaesthesia. British Journal of Anaesthesia 1982;54:
1071–4.
Litman 1994∗ Litman RS, Wu CL, Quinlivan JK. Gastric volume and pH in
infants fed clear liquids and breast milk prior to surgery. Anesthesia
& Analgesia 1994;79:482–5.
Morrice 1974∗ Morrice JJ, Taylor KM, Blair JI, Young DG. Preoperative plasma
glucose level. Archives of Disease in Childhood 1974;49:898–900.
Niija 1999∗ Niija S, Nakamura T, Hara T, Miyako M, Fukusaki M. The effect of
calories of preoperative oral intake on the glucose metabolic response
in children. Japanese Journal of Anesthesiology 1999;48(4):362–7.
Nilsson 1984∗ Nilsson K, Larsson LE, Andréasson S, Ekström-Jodal B. Blood-
glucose concentrations during anaesthesia in children. Effects of star-
vation and perioperative fluid therapy. British Journal of Anaesthesia
1984;56:375–9.
O’Flynn 1989∗ O’Flynn PE, Milford CA. Fasting in children for day case surgery.
Annals of the Royal College of Surgeons of England 1989;71(4):218–9.
Sandstrom 1993∗ Sandström K, Nilsson K, Andréasson S, Niklasson A, Larsson, LE.
Metabolic consequences of different perioperative fluid therapies in
the neonatal period. Acta Anaesthesiologica Scandinavica 1993;37(2):
170–5.
Schneider 1982∗ Schneider BM, Nahrwold ML. Fasting Plasma Glucose in Children.
Anesthesiology. 1982;57(Supp):A430.
Schurizek 1986∗ Schurizek BA, Rybro L, Boggild-Madsen NB, Juhl B. Gastric vol-
ume and pH in children for emergency surgery. Acta Anaesthesiologica
Scandinavica 1986;30(5):404–8.
Sethi 1999∗ Sethi AK, Chatterji C, Bhargava SK, Narang P, Tyagi A. Safe pre-
operative fasting times after milk or clear fluid in children. A pre-
liminary study using real-time ultrasound. Anaesthesia 1999;54(1):
51–9.
Stanley 1989∗ Stanley TH, Leiman BC, Rawal N, Marcus MA, van der Nieuwen-
huyzen M, Walford A, et al. The effects of oral transmucosal fentanyl
citrate premedication on preoperative behavioral responses and gas-
tric volume and acidity in children. Anesthesia & Analgesia 1989;69:
328–35.
Thomas 1974∗ Thomas, DKM. Hypoglycaemia in children before operation: its
incidence and prevention. British Journal of Anaesthesia 1974;46:66–
8.
van der Walt 1990∗ van der Walt JH, Foate JA, Murrell D, Jacob R, Bentley M. A
study of preoperative fasting in infants aged less than three months.
Anaesthesia & Intensive Care 1990;18(4):527–31.
Watson 1972∗ Watson BG. Blood glucose levels in children during surgery. British
Journal of Anaesthesia 1972;44:712–5.
Additional referencesAAGBI 2001
. Pre-operative Assessment: The Role of the Anaesthetist. The Asso-
ciation of Anaesthetists of Great Britain and Ireland Nov 2001.
Aitkenhead 1996
Aitkenhead AR, Smith G editorseditors. Textbook of Anaesthesia. Ed-
inburgh: Churchill Livingston, 1996.
Alderson 2004
Alderson P. Absence of evidence is not evidence of absence. British
Medical Journal 2004;328:476–7.
Altman 2004
Altman D, Bland JM. Confidence intervals illuminate absence of
evidence. British Medical Journal 2004; 328 (7446) 1016-7.
33Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Arnold 1992
Arnold BC, Balakrihnan N, Nagaraja HN. A first course in order
statistics. New York: John Wiley and Sons, 1992.
ASA 1999
American Society of Anesthesiologist Task Force on Preoperative
Fasting. Practice guidelines for preoperative fasting and the use of
pharmacologic agents to reduce the risk of pulmonary aspiration: ap-
plication to healthy patients undergoing elective procedures: a report
by the American Society of Anesthesiologist Task Force on Preoper-
ative Fasting. Anesthesiology 1999;90(3):896–905.
Audit Commission
. Day Surgery. Acute Hospital Portfolio Review of National Findings.
Audit Commission 2001.
Brady 2004
Brady M, Kinn S, Stuart P. Preoperative fasting for adults to pre-
vent perioperative complications. In: The Cochrane Library, 4, 2004.
Chichester, UK: John Wiley & Sons.
Cannon 1997
Cannon CP. Clinical perspectives on the use of composite endpoints.
Controlled Clinical Trials 1997;18(6):517–29.
Committee on Drugs
Committee on Drugs. Guidelines for monitoring and management
of pediatric patients during and after sedation for diagnostic and
therapeutic procedures. Pediatrics 1992;889:1110–5.
CRD Report Number 4
NHS Centre for Reviews, Dissemination. Report Number 4. Under-
taking Systematic Reviews of Effectiveness. CRD’s Guidance for those
carrying out or commissioning reviews. Vol. 2nd Edition ed, University
of York, 2001 Mar.
DeMets 2002
DeMets DL, Califf, RM. Lessons Learned from Recent Cardiovas-
cular Clinical Trials: Part I. Circulation 2002;106:746–51.
Emerson 1998
Emerson BM, Wrigley SR, Newton M. Pre-operative fasting for pae-
diatric anaesthesia. A survey of current practice. Anaesthesia 1998;53
(4):326–30.
Engelhardt 2001
Engelhardt T, Strachan L, Johnston G. Aspiration and regurgitation
prophylaxis in paediatric anaesthesia. Paediatric Anaesthesia 2001;11:
147–50.
Ferrari 1999
Ferrari LR, Rooney FM, Rockoff MA. Preoperative fasting practices
in pediatrics. Anesthesiology 1999;90(4):978–80.
Freemantle 2003
Freemantle N, Calvert M, Wood J, Eastaugh J, Griffin C. Composite
Outcomes in Randomized Trials: Greater precision but with greater
uncertainty?. JAMA 2003;289(19):2554–59.
Haas 1998
Haas U, Motsch J, Schreckenberger R, Bardenheuer HJ, Martin E.
Premedication and preoperative fasting in pediatric anaesthesia - A
survey of current practice. Anaesthetist 1998;47(10):838–43.
Health Comm 2004
House of Commons Health Select Committee. Third Report Obe-
sity. http://www.publications.parliament.uk/pa/cm/cmhealth.htm.
Accessed on 2nd August 2004 May 2004.
Hofer 2001
Hofer C, Tucci M, van Gessel E, Alon E, Zollinger A. Is traditional
preoperative fasting policy changing? Results of a Swiss survey on cur-
rent practice. European Society of Anaesthetists Proceedings. 2001:
8-9 (A-30).
Hunt 1987
Hunt, M. The process of translating research findings into nursing
practice. Journal of Advanced Nursing 1987;12(1):101–10.
IASO 2004
Lobstein T, Baur L, Uauy R for the IASO International Obesity Task
Force. Obesity in children and young people: a crisis in public health.
Obesity Reviews 2004;Suppl 1:4 – 85.
James 1984
James CF, Modell JH, Gibbs CP, Kuck EJ, Ruiz BC. Pulmonary
aspiration - effects of volume and pH in the rat. Anesthesia & Analgesia
1984;63:665–8.
Kluger 1999
Kluger MT, Short TG. Aspiration during anaesthesia: a review of 133
cases from the Australian Anaesthetic Incident Monitoring Study
(AIMS). Anaesthesia 1999;54(1):19–26.
Litman 1999
Litman RS. Sedation and anesthesia outside the operating room:
answers to common questions. Seminars in Pediatric Surgery 1999;8
(1):34–9.
MacLean 1993
MacLean AR, Renwick C. Audit of Pre-Operative Starvation. Anaes-
thesia 1993;48:164–6.
Maltby Ptyka 2004
Maltby JR, Pytka S, Watson NC, McTaggart Cowan RA, Fick GH.
Drinking 300 mL of clear fluid two hours before surgery has no effect
on gastric fluid volume and pH in fasting and non-fasting obese
patients [[Le fait de boire 300 mL de liquide clair deux heures avant
d’être opéré n’a pas d’effet sur le volume de liquide ni sur le pH
gastriques chez des patients obèses à jeun ou non]]. Canadian Journal
of Anesthesia 2004;51:111–5.
Man-Son-Hing 2002
Man-Son-Hing, M, Laupacis, A, O’Rourke, K, Molnar, F, Mahon,
J, Chan, K, Wells, G. Determining the clinical importance of study
results: a review. Journal of General Internal Medicine 2002;17:469–
476.
Markham 2003
Markham R, Smith A. Limits to patient choice: example from anaes-
thesia. British Medical Journal 2003;326:863–4.
Mendelson 1946
Mendelson CL. Aspiration of stomach contents into lungs during
obstetric anesthesia. American Journal of Obstetric Gynecology 1946;
52:191–203.
NCEPOD 2002
. National Confidential Enquiry into Perioperative Deaths. www.
ncepod.org.uk 2002. Accessed 05 Apr 2003.
NCEPOD 2003
. National Confidential Enquiry into Perioperative Deaths. www.
ncepod.org.uk Accessed 05 Apr 2003.
34Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

NHSQIS 2003
NHS Quality Improvement Scotland 2003. Anaesthesia Care Before,
During and After Anaesthesia. Clinical Standards Board for Scotland,
July 2003.
NNCG 1993
Norwegian National Consensus Guidelines for preoperative fasting
in elective surgery (1993). Reported In: Fasting, S, Søreide, E, Ræder,
JC. Acta Anaesthesiologica Scandinavica 1998;42:1188–91.
O’Hare 1996
O’Hare B, Lerman J, Endo J, Culz E. Acute lung injury after instil-
lation of human breast milk or infant formula into rabbits’ lungs.
Anesthesiology 1996;84(1):1386–91.
O’Hare 1999
O’Hare B, Chin C, Lerman J, Endo J. Acute lung injury after in-
stillation of human breast milk of rabbits’ lungs: effects of pH and
gastric juice. Anesthesiology 1999;90(4):1112–8.
O’Rourke 2002
O’Rourke, K. Mixed means and medians: a unified approach for deal-
ing with disparate outcome summaries. 4th Symposium on System-
atic Reviews: Pushing the Boundaries. Oxford 2002;http://www.ihs.
ox.ac.uk/csm/pushingthe boundaries/poster/11_oruk.html: Poster
presentation.
Oxford 2001
Centre for Statistics in Medicine. Oxford Systematic Review Devel-
opment Programme. Finishing School Oxford May-June 2001.
Raidoo 1990
Raidoo DM, Rocke DA, Brok-Utne JG, Marszalek A, Engelbrecht
HE. Critical Volume for pulmonary acid aspiration reappraisal in
primate model. British Journal of Anaesthesia 1990;65:248–50.
RCN
Royal College of Nursing, United Kingdom. Perioperative Fasting
Guidelines. In preparation.
Roberts 1974
Roberts RB, Shirley MA. Reducing the risk of acid aspiration during
cesarean section. Anesthesia & Analgesia 1974;53(6):859–68.
Sala 2004
Sala A, Pencharz P, Barr RD. Children, cancer and nutrition - a
dynamic triangle in review. Cancer 2004;100(40):677–87.
SASM 2002
. Scottish Audit of Surgical Mortality, Annual Report 2002. www.
show.scot.nhs.uk/sasm Accessed 05 Apr 2003.
Schreiner 1998
Schreiner MS. Gastric fluid volume: is it really a risk factor for pul-
monary aspiration?. Anesthesia & Analgesia 1998;87(4):754–6.
Schultz 2001
Schultz KF. Assessing allocation concealment and blinding in ran-
domised controlled trials: why bother?. Evidence Based Nursing 2001;
4:4–6.
Smith 2004
Smith R. Abusing Patients by denying them choice. British Medical
Journal 2004;328:7436.
Søreide 1995
Søreide E, Stromskag KE, Steen PA. Statistical aspects in studies of
preoperative fluid intake and gastric content. Acta Anaesthesiologica
Scandinavica 1995;39:738–43.
Veall 1995
Veall GR, Floor K, Dorman T. Prolonged starvation in paediatric
surgery. Anaesthesia 1995;50(5):458–60.
While 1992
While AE, Crawford J. Paediatric Surgery. Nursing Times 1992;88
(39):43–5.
WHO 2003
World Health Organization. WHO Obesity and overweight fact
sheet. http://www.who.int/hpr/NPH/docs/gs_obesity.pdf Accessed
18th of July 2004 2003.
∗Indicates the major publication for the study
T A B L E S
Characteristics of included studies
Study Aun 1990
Methods RCT (drawing lots by person independent of trial)
Participants 20 children, 1-5 years, ASA I-II, inpatients, elective minor surgery (herniotomy, repair of hydrocele, circum-
cision) 8-9am.
Exclusions; ASA > II, difficult venous access, lack of parental consent.
Interventions 1. Standard Fast (n =10)
2. Dextrose solution (5%) [10ml/kg] 4 hrs preop (n =10)
Outcomes Gastric volume - post induction and intubation. Gastric pH - post induction and intubation.
35Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Plasma glucose concentrations; cortisol; growth hormone; glucagon; insulin concentration.
Notes Standard Fast = milk feed at midnight then NPO. Assessor blinding adequate. No gastric pH value for four
participants.
Premedication; trimeprazine (plus morphine & atropine 1 hr preop). IV fluids; none.
Allocation concealment A
Study Cook-Sather 2003
Methods RCT (computer generated sequence allocated by coded envelope)
Participants 97 children, 0-9 months at recruitment, ASA I-II, elective surgery requiring tracheal intubation (mainly cleft
lip and palate repair, hernia/hydrocele surgery, circumcisions. Exclusions: exclusively breast fed infants, those
with gastrointestinal disease that impede emptying or diminish motility or result in reflux.
Interventions 1. Clear fluids [unlimited] up to 2 hrs (n = 36)
2. Formula [unlimited] up to 4 hrs pre op (n = 31)
Outcomes Gastric volume - post induction. Gastric pH - post induction. Irritability, Hunger, Parental satisfaction.
Notes No solids or cows milk from 8 hrs preop. Assessor blinding adequate. Premedication - atropine.
Protocol deviation 22 from group 1, 8 from group 2.
Allocation concealment A
Study Crawford 1990a
Methods RCT (random numbers table)
Participants 100 children, 1-14 years, ASA I-II, inpatients, elective surgery.
Exclusions; gastrointestinal disease, obese (> 20% ideal body weight), those taking drugs known to affect
gastric fluid composition and emptying.
Interventions 1. Water [2 ml/kg] 2 hrs preop (n = ?)
2. Water [2 ml/kg] 6 hrs preop (n = ?)
Outcomes Gastric volume - post induction and intubation. Gastric pH - post induction and intubation. Marker dye
[Sulfobromophthalein sodium - BSP].
Notes Assessor blinding inadequate. Premedication- none. Not possible to extract group specific data from reports.
No gastric aspirate in at least one participant (abstract report).
Allocation concealment A
Study Crawford 1990b
Methods RCT (random numbers table)
Participants 100 children, 1-14 years, ASA I-II, inpatients, elective surgery.
Exclusions; gastrointestinal disease, obese (> 20% ideal body weight), those taking drugs known to affect
gastric fluid composition and emptying.
Interventions 1. Water [2 ml/kg] 2 hrs preop (n = ?)
2. Water [2 ml/kg] 4 hrs preop (n = ?)
Outcomes Gastric volume - post induction and intubation. Gastric pH - post induction and intubation. Marker dye
[Sulfobromophthalein sodium - BSP].
Notes Assessor blinding inadequate. Premedication- none. Not possible to extract group specific data from reports.
No gastric aspirate in at least one participant (abstract report).
Allocation concealment A
36Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Study Crawford 1990c
Methods RCT (random numbers table)
Participants 100 children, 1-14 years, ASA I-II, inpatients, elective surgery.
Exclusions; gastrointestinal disease, obese (> 20% ideal body weight), those taking drugs known to affect
gastric fluid composition and emptying.
Interventions 1. Water [2 ml/kg] 4 hrs preop (n = ?)
2. Water [2 ml/kg] 6 hrs preop (n = ?)
Outcomes Gastric volume - post induction and intubation. Gastric pH - post induction and intubation. Marker dye
[Sulfobromophthalein sodium - BSP].
Notes Assessor blinding inadequate. Premedication- none. Not possible to extract group specific data from reports.
No gastric aspirate in at least one participant (abstract report).
Allocation concealment A
Study Gombar 1997
Methods RCT (computer generated random numbers)
Participants 50 children, 2-12 years, ASA I-II, elective surgery (e.g. herniotomy, orchiopexy, tonsillectomy, myringoplasty,
hypospadias correction, circumcision, cystolithotomy, strabismus repair) (+ 25 children with pharmacological
co-intervention excluded from review). Exclusions; active gastrointestinal disease, taking medication affecting
gastric fluid volume, pH or motility.
Interventions 1. Standard Fast ( n = 25)
2. Water 5 ml/kg 3 hrs preop (n = 25)
(3. Water + Ranitidine n = 25 excluded from review)
Outcomes Gastric volume - post induction before surgical incision. Gastric pH - post induction before surgical incision.
Thirst, Behaviour.
Notes Standard Fast = NPO from midnight. Thirst/behaviour assessor blinded. No gastric pH value for one
participant. Premedication - none. IV fluids administered as required.
Allocation concealment B
Study Goresky 1992a
Methods RCT (method not reported)
Participants 120 children, 1-6 years, ASA I-II, elective minor surgery. Exclusions; known gastrointestinal disease, those
taking any medications including premedication (except benzodiazepines).
Interventions 1. Standard Fast + placebo (n = 60)
2. Apple juice [5ml/kg] + placebo 2hrs preop (n = 60)
Outcomes Gastric volume - post induction and intubation. Gastric pH - post induction and intubation. Marker dye
[Sulfobromophthalein sodium - BSP]. Adverse events.
Notes Standard Fast = 5 ml of water. Assessors blinded to ranitidine/placebo. Premedication - only benzodiazepines.
Study supported by Glaxo Canada.
Allocation concealment D
Study Goresky 1992b
Methods RCT (method not reported)
Participants 120 children, 1-6 years, ASA I-II, elective minor surgery. Exclusions; known gastrointestinal disease, those
taking any medications including premedication (except benzodiazepines).
Interventions 1. Standard Fast + Ranitidine [2 mg/kg] (n = 60)
37Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
2. Apple juice [5ml/kg] + Ranitidine [2mg/kg] 2hrs preop (n = 60)
Outcomes Gastric volume - post induction and intubation. Gastric pH - post induction and intubation. Marker dye
[Sulfobromophthalein sodium - BSP]. Adverse events.
Notes Standard Fast = 5 ml of water. Assessors blinded to ranitidine/placebo. Premedication - only benzodiazepines.
Study supported by Glaxo Canada.
Allocation concealment D
Study Kushikata 1996
Methods RCT (alternate cases)
Participants 20 children, 5-12 years, ’healthy’ inpatients, elective ENT surgery. Exclusions; not listed.
Interventions 1. Standard Fast (n = 10)
2. Rice porridge [55g rice + 245 ml water + some salt] 330 mins preop + clear fluids [< 200 ml] up to 5 hrs
preop (n = 10)
Outcomes Gastric volume - post induction. Gastric pH - post induction. Hunger (?child).
Notes Standard Fast = Clear fluids [< 200 ml] up to 5 hrs preop. Assessor blinding unclear. Premedication (0.3mg/kg
of diazepam syrup). IV fluids - Lactic Ringer solution with 2% glucose 4ml/kg/hr.
Allocation concealment C
Study Maekawa 1993a
Methods RCT (method not reported)
Participants 70 children, 1-14 years, ASA I, inpatients, elective surgery. Exclusions; those with metabolic disorder, gas-
trointestinal disease, obese (> 20% over ideal body weight), taking drugs affecting gastric fluid or emptying.
Interventions 1. Standard Fast (n = 35)
2. Apple Juice [10 ml/kg] 2 hrs preop (n = 35)
Outcomes Gastric volume - post induction. Gastric pH - post induction. Vomiting. Plasma glucose, lipid homeostasis,
ANP concentration. Adverse events.
Notes Standard Fast = Apple juice [10 ml/kg] 12 hrs preop then NPO. Assessor blinding adequate. Gastric pH (n)
unclear. Premedication - none.
Allocation concealment B
Study Maekawa 1993b
Methods RCT (method not reported)
Participants 70 children, 1-14 years, ASA I, inpatients, elective surgery. Exclusions; those with metabolic disorder, gas-
trointestinal disease, obese (> 20% over ideal body weight), taking drugs affecting gastric fluid or emptying.
Interventions 1. Standard Fast (n = 35)
2. Apple Juice [10 ml/kg] 4 hrs preop (n = 35)
Outcomes Gastric volume - post induction. Gastric pH - post induction. Vomiting. Plasma glucose, lipid homeostasis,
ANP concentration. Adverse events.
Notes Standard Fast = Apple juice [10 ml/kg] 12 hrs preop then NPO. Assessor blinding adequate. Gastric pH (n)
unclear. Premedication - none.
Allocation concealment B
Study Maekawa 1993c
Methods RCT (method not reported)
38Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd
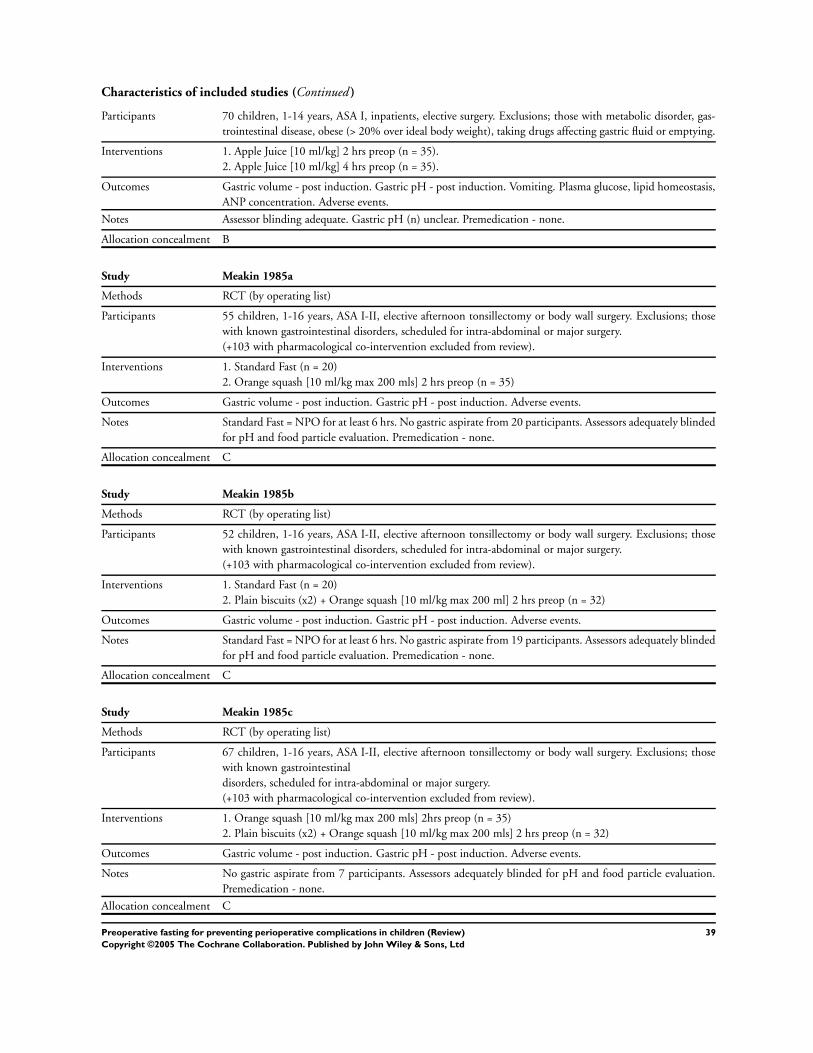
Characteristics of included studies (Continued )
Participants 70 children, 1-14 years, ASA I, inpatients, elective surgery. Exclusions; those with metabolic disorder, gas-
trointestinal disease, obese (> 20% over ideal body weight), taking drugs affecting gastric fluid or emptying.
Interventions 1. Apple Juice [10 ml/kg] 2 hrs preop (n = 35).
2. Apple Juice [10 ml/kg] 4 hrs preop (n = 35).
Outcomes Gastric volume - post induction. Gastric pH - post induction. Vomiting. Plasma glucose, lipid homeostasis,
ANP concentration. Adverse events.
Notes Assessor blinding adequate. Gastric pH (n) unclear. Premedication - none.
Allocation concealment B
Study Meakin 1985a
Methods RCT (by operating list)
Participants 55 children, 1-16 years, ASA I-II, elective afternoon tonsillectomy or body wall surgery. Exclusions; those
with known gastrointestinal disorders, scheduled for intra-abdominal or major surgery.
(+103 with pharmacological co-intervention excluded from review).
Interventions 1. Standard Fast (n = 20)
2. Orange squash [10 ml/kg max 200 mls] 2 hrs preop (n = 35)
Outcomes Gastric volume - post induction. Gastric pH - post induction. Adverse events.
Notes Standard Fast = NPO for at least 6 hrs. No gastric aspirate from 20 participants. Assessors adequately blinded
for pH and food particle evaluation. Premedication - none.
Allocation concealment C
Study Meakin 1985b
Methods RCT (by operating list)
Participants 52 children, 1-16 years, ASA I-II, elective afternoon tonsillectomy or body wall surgery. Exclusions; those
with known gastrointestinal disorders, scheduled for intra-abdominal or major surgery.
(+103 with pharmacological co-intervention excluded from review).
Interventions 1. Standard Fast (n = 20)
2. Plain biscuits (x2) + Orange squash [10 ml/kg max 200 ml] 2 hrs preop (n = 32)
Outcomes Gastric volume - post induction. Gastric pH - post induction. Adverse events.
Notes Standard Fast = NPO for at least 6 hrs. No gastric aspirate from 19 participants. Assessors adequately blinded
for pH and food particle evaluation. Premedication - none.
Allocation concealment C
Study Meakin 1985c
Methods RCT (by operating list)
Participants 67 children, 1-16 years, ASA I-II, elective afternoon tonsillectomy or body wall surgery. Exclusions; those
with known gastrointestinal
disorders, scheduled for intra-abdominal or major surgery.
(+103 with pharmacological co-intervention excluded from review).
Interventions 1. Orange squash [10 ml/kg max 200 mls] 2hrs preop (n = 35)
2. Plain biscuits (x2) + Orange squash [10 ml/kg max 200 mls] 2 hrs preop (n = 32)
Outcomes Gastric volume - post induction. Gastric pH - post induction. Adverse events.
Notes No gastric aspirate from 7 participants. Assessors adequately blinded for pH and food particle evaluation.
Premedication - none.
Allocation concealment C
39Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Study Meakin 1985d
Methods RCT (by operating list)
Participants 49 children, 1-16 years, ASA I-II, elective surgery. Exclusions; those with known gastrointestinal disorders,
scheduled for intra-abdominal or major surgery.
(+67 reported in more detail in Meakin 1987a-c)
Interventions 1. Orange squash [10 ml/kg max 200 mls] 4 hrs preop (n = 15)
2. Plain biscuits (x2) + Orange squash [10 ml/kg max 200 mls] 4 hrs preop (n = 14)
Outcomes Gastric volume - post induction. Gastric pH - post induction.
Notes Standard Fast = NPO for 6 hrs. Assessors adequately blinded for pH and food particle evaluation. Premedi-
cation - none.
Allocation concealment C
Study Meakin 1985e
Methods RCT (by operating list)
Participants 49 children, 1-16 years, ASA I-II, elective surgery. Exclusions; those with known gastrointestinal disorders,
scheduled for intra-abdominal or major surgery.
(+67 reported in more detail in Meakin 1987a-c)
Interventions 1. Standard Fast (n = 20)
2. Orange squash [10 ml/kg max 200 mls] 4 hrs preop (n = 15)
Outcomes Gastric volume - post induction. Gastric pH - post induction.
Notes Standard Fast = NPO for 6 hrs. Assessors adequately blinded for pH and food particle evaluation. Premedi-
cation - none.
Allocation concealment C
Study Meakin 1985f
Methods RCT (by operating list)
Participants 49 children, 1-16 years, ASA I-II, elective surgery. Exclusions; those with known gastrointestinal disorders,
scheduled for intra-abdominal or major surgery.
(+67 reported in more detail in Meakin 1987a-c)
Interventions 1. Standard Fast (n = 20)
2. Plain biscuits (x2) + Orange squash [10 ml/kg max 200 mls] 4 hrs preop (n = 14)
Outcomes Gastric volume - post induction. Gastric pH - post induction.
Notes Standard Fast = NPO for 6 hrs. Assessors adequately blinded for pH and food particle evaluation. Premedi-
cation - none.
Allocation concealment C
Study Miller 1990
Methods RCT (table of random numbers)
Participants 44 children, 1 month -5 years (greater than 44wks conceptual age), ASA I-II, elective surgery. Exclusions;
active cardiac, pulmonary, gastrointestinal disease.
Interventions 1. Standard Fast (n = 25)
2. Dextrose Solution (5%) [4 oz] 3 hrs preop (n = 19)
Outcomes Gastric volume - post induction. Gastric pH - post induction. Marker dye [ phenolsulfonphthalein - phenol
red].
40Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Notes Standard Fast = NPO for 10 hrs. 4US oz = 118 ml. Insufficient gastric aspirate to calculate volume and pH
for 23 participants. Assessor blinding unclear. Premedication - none.
Allocation concealment B
Study Moyao-García 2001
Methods RCT (table of random numbers)
Participants 40 children, 3-12 years, ASA I, elective surgery (ophthalmology, otorhinolaryngology, plastic surgery). Ex-
clusions: those taking drugs known to affect gastric motility or with any medical condition affecting gastric
or intestinal motility.
Interventions 1. Standard Fast (n = 20)
2. Isosmolar solution of electrolytes [4 ml/kg] 3 hrs preop (n = 20)
Outcomes Gastric volume - post induction. Gastric pH - post induction. Blood glucose level.
Notes Standard Fast = no solids, milk or formula overnight for at least 8 hours preop. Assessor blinding adequate.
Premedication - none.
Allocation concealment A
Study Nicolson 1992
Methods RCT (sealed envelopes)
Participants 100 children, ASA II-IV, (n II = 45; III = 44; IV = 2) inpatients, elective cardiac surgery. Exclusions; history
of gastrointestinal disease, taking medication known to affect gastric contents.
Interventions 1. Standard Fast (n = 44)
2. Clear fluids [unlimited] 2 hrs preop (n = 47)
Outcomes Gastric volume - post induction and intubation. Gastric pH - post induction and intubation. Thirst, Hunger,
Comfort.
Notes Standard Fast = after midnight clear fluids only [unlimited] up to 4 hrs (< 6 mths), 6 hrs (6 mths - 5 yrs)
or 8 hrs (> 5yrs) preop, NPO thereafter. Nine protocol deviations excluded. Assessor blinding adequate.
Premedication - < 6mth = atropine, 6-12mths = atropine + pentobarbital, > 1yr = meperidine.
Allocation concealment A
Study Sandhar 1989a
Methods RCT (table of random numbers)
Participants 44 children, 1-14 years, ASA I-II, outpatients, elective ENT, urology or minor general surgical procedures.
Exclusions; history of gastrointestinal disorder.
Interventions 1. Standard fast + placebo 2hrs preop (n = 19)
2. Orange juice [5ml/kg] + placebo 2hrs preop (n = 13)
Outcomes Gastric volume - post induction. Gastric pH - post induction. Marker dye [ phenolsulfonphthalein - PSP].
Notes Placebo = glucose water [0.2 ml/kg]. Max juice intake for patients > 30 kg was 150 ml. Assessor blinding
unclear. Twelve protocol deviations (ingestion-surgery interval < 90mins, refused orange juice/drank water
instead, did not complete drink). No gastric pH value for three participants. pH values for an additional 7
participants not reported. Premedication - none.
Allocation concealment B
Study Sandhar 1989b
Methods RCT (table of random numbers)
41Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Participants 44 children, 1-14 years, ASA I-II, outpatients, elective ENT, urology or minor general surgical procedures.
Exclusions: history of gastrointestinal disorder.
Interventions 1. Standard fast + Ranitidine [2 mg/kg] 2 hrs preop (n = 15)
2. Orange juice [5 ml/kg] + Ranitidine [2 mg/kg] 2 hrs preop (n = 18)
Outcomes Gastric volume - post induction. Gastric pH - post induction. Marker dye [ phenolsulfonphthalein - PSP].
Notes Assessor blinding unclear. Max juice intake for patients > 30 kg was 150 ml. Eleven protocol deviations
(ingestion-surgery interval < 90mins). No gastric pH value for four participants. Premedication - none.
Allocation concealment B
Study Sarti 1991
Methods RCT (method not reported)
Participants 62 children, 1-12 years, elective urological surgery. Exclusions: premedicated, prior surgery.
Interventions 1. Standard Fast (n = 30)
2. Water or apple juice [unlimited] up to 2hrs preop (n= 32)
Outcomes Gastric volume - post induction. Gastric pH - post induction.
Notes Standard Fast = NPO from midnight. Assessor blinding unclear. Premedication - none.
Allocation concealment B
Study Schreiner 1990
Methods RCT (shuffled opaque sealed envelopes)
Participants 121 children, 1-18 years, ASA I-II, outpatients (or admitted on day of ) elective surgery. Exclusions; medi-
cations or disease known to delay gastric emptying or increase acid production.
Interventions 1. Standard Fast (n = 68)
2. Clear fluids [unlimited] up to 2 hrs preop (n = 53)
Outcomes Gastric volume - post induction. Gastric pH - post induction. Compliance with fasting instructions, Irri-
tability, Tolerance of preop experience, comparison with other preoperative experiences (parent). Adverse
events.
Notes Standard Fast = after 8pm only clear fluids [unlimited] until 6hrs (< 5yrs) or 8hrs (> 5yrs). For intervention
group final clear fluid ingestion limited to < 8oz (approx 237 ml). One gastric sample unobtainable. Five
mishandled samples. No gastric pH values for thirty-two participants. Assessor blinding adequate. Premedi-
cation - (as required) meperidine, diazepam and atropine.
Allocation concealment A
Study Splinter 1989
Methods RCT (random numbers table)
Participants 80 children, 5-10 years, ASA I-II, elective surgery. Exclusions; history of gastrointestinal disease, taking
medication known to affect gastric contents.
Interventions 1. Standard Fast (n = 40)
2. Apple Juice [3ml/kg] 2.5hrs preop (n = 40)
Outcomes Gastric volume - post induction. Gastric pH - post induction. Thirst, Hunger. Adverse events.
Notes Standard Fast = NPO from midnight. Three children (< 5yrs) unable to answer questionnaire. Assessor
blinding adequate. Premedication- none.
Allocation concealment B
42Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Study Splinter 1990a
Methods RCT (random numbers table)
Participants 61 children, 5-10 years, ASA I-II, elective surgery. Exclusions; history of gastrointestinal disease or medication
known to affect gastric contents.
Interventions 1. Standard Fast (n = 31)
2. Apple Juice [6 ml/kg] 2.5 hrs preop (n = 30)
Outcomes Gastric volume - post induction. Gastric pH - post induction. Thirst, Hunger, Behaviour. Adverse events.
Notes Standard Fast = NPO from midnight. Assessor blinding adequate. Premedication - unclear.
Allocation concealment B
Study Splinter 1990b
Methods RCT (random numbers table)
Participants 63 children, 5-10 years, ASA I-II, elective surgery. Exclusions; history of gastrointestinal disease or medication
known to affect gastric contents.
Interventions 1. Standard Fast (n = 31)
2. Apple Juice [10 ml/kg] 2.5 hrs preop (n = 32)
Outcomes Gastric volume - post induction. Gastric pH - post induction. Thirst, Hunger, Behaviour. Adverse events.
Notes Standard Fast = NPO from midnight. Assessor blinding adequate. Premedication - unclear. Children in
group 1 were heavier than children in group 2.
Allocation concealment B
Study Splinter 1990c
Methods RCT (random numbers table)
Participants 62 children, 5-10 years, ASA I-II, elective surgery. Exclusions; history of gastrointestinal disease or medication
known to affect gastric contents.
Interventions 1. Apple Juice [6 ml/kg] 2.5 hrs preop (n = 30)
2. Apple Juice [10 ml/kg] 2.5 hrs preop (n = 32)
Outcomes Gastric volume - post induction. Gastric pH - post induction. Thirst, Hunger, Behaviour. Adverse events.
Notes Standard Fast = NPO from midnight. Assessor blinding adequate. Premedication - unclear. Children in
group 1 were heavier than those in group 2.
Allocation concealment B
Study Splinter 1991
Methods RCT (table of random numbers)
Participants 152 adolescents, 13-19 years, ASA I-II, elective. Exclusions: history of gastrointestinal disease, medication
affected gastric contents.
Interventions 1. Standard Fast (n = 76)
2. Clear fluids [unlimited] up to 3 hrs preop (n = 76)
Outcomes Gastric volume - post induction Gastric pH - post induction Thirst, Hunger.
Notes Standard Fast = NPO from midnight. Assessor blinding adequate. Premedication - unclear.
Allocation concealment B
Study Splinter Schaefer 1a
Methods RCT (random numbers table)
43Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd
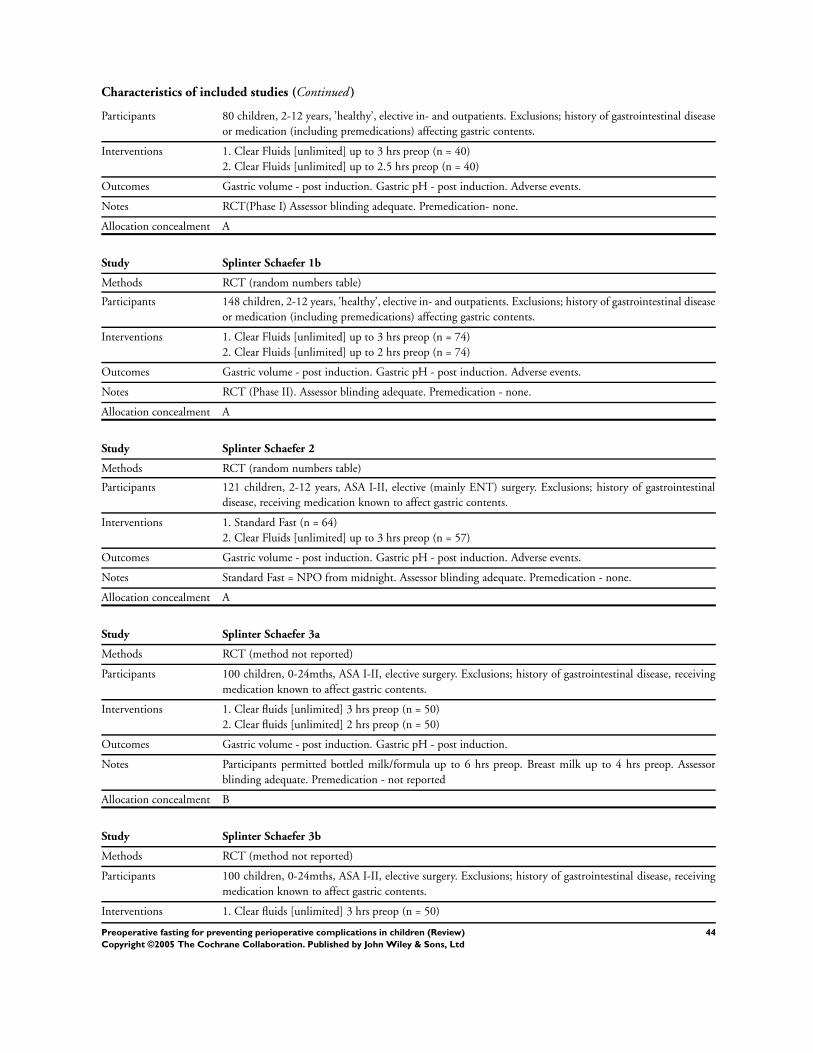
Characteristics of included studies (Continued )
Participants 80 children, 2-12 years, ’healthy’, elective in- and outpatients. Exclusions; history of gastrointestinal disease
or medication (including premedications) affecting gastric contents.
Interventions 1. Clear Fluids [unlimited] up to 3 hrs preop (n = 40)
2. Clear Fluids [unlimited] up to 2.5 hrs preop (n = 40)
Outcomes Gastric volume - post induction. Gastric pH - post induction. Adverse events.
Notes RCT(Phase I) Assessor blinding adequate. Premedication- none.
Allocation concealment A
Study Splinter Schaefer 1b
Methods RCT (random numbers table)
Participants 148 children, 2-12 years, ’healthy’, elective in- and outpatients. Exclusions; history of gastrointestinal disease
or medication (including premedications) affecting gastric contents.
Interventions 1. Clear Fluids [unlimited] up to 3 hrs preop (n = 74)
2. Clear Fluids [unlimited] up to 2 hrs preop (n = 74)
Outcomes Gastric volume - post induction. Gastric pH - post induction. Adverse events.
Notes RCT (Phase II). Assessor blinding adequate. Premedication - none.
Allocation concealment A
Study Splinter Schaefer 2
Methods RCT (random numbers table)
Participants 121 children, 2-12 years, ASA I-II, elective (mainly ENT) surgery. Exclusions; history of gastrointestinal
disease, receiving medication known to affect gastric contents.
Interventions 1. Standard Fast (n = 64)
2. Clear Fluids [unlimited] up to 3 hrs preop (n = 57)
Outcomes Gastric volume - post induction. Gastric pH - post induction. Adverse events.
Notes Standard Fast = NPO from midnight. Assessor blinding adequate. Premedication - none.
Allocation concealment A
Study Splinter Schaefer 3a
Methods RCT (method not reported)
Participants 100 children, 0-24mths, ASA I-II, elective surgery. Exclusions; history of gastrointestinal disease, receiving
medication known to affect gastric contents.
Interventions 1. Clear fluids [unlimited] 3 hrs preop (n = 50)
2. Clear fluids [unlimited] 2 hrs preop (n = 50)
Outcomes Gastric volume - post induction. Gastric pH - post induction.
Notes Participants permitted bottled milk/formula up to 6 hrs preop. Breast milk up to 4 hrs preop. Assessor
blinding adequate. Premedication - not reported
Allocation concealment B
Study Splinter Schaefer 3b
Methods RCT (method not reported)
Participants 100 children, 0-24mths, ASA I-II, elective surgery. Exclusions; history of gastrointestinal disease, receiving
medication known to affect gastric contents.
Interventions 1. Clear fluids [unlimited] 3 hrs preop (n = 50)
44Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
2. Clear fluids [unlimited] 2.5 hrs preop (n = 50)
Outcomes Gastric volume - post induction. Gastric pH - post induction.
Notes Participants permitted bottled milk/formula up to 6 hrs preop. Breast milk up to 4 hrs preop. Assessor
blinding adequate. Premedication - not reported
Allocation concealment B
Study Splinter Schaefer 3c
Methods RCT (method not reported)
Participants 100 children, 0-24mths, ASA I-II, elective surgery. Exclusions; history of gastrointestinal disease, receiving
medication known to affect gastric contents.
Interventions 1. Clear fluids [unlimited] 2.5 hrs preop (n = 50)
2. Clear fluids [unlimited] 2 hrs preop (n = 50)
Outcomes Gastric volume - post induction. Gastric pH - post induction.
Notes Participants permitted bottled milk/formula up to 6 hrs preop. Breast milk up to 4 hrs preop. Assessor
blinding adequate. Premedication - not reported
Allocation concealment B
Study Welborn 1993
Methods RCT (day of the week)
Participants 200 children, 1-10 years, outpatients, elective surgery (including hernia repair, circumcision, ochidopexy,
eye muscle). Exclusions; not listed.
Interventions 1. Standard Fast (n = 113)
2. Apple juice [10 ml/kg] 2 hrs preop (n = 87)
Outcomes Gastric volume - post induction. Gastric pH - post induction. Blood glucose.
Notes Standard Fast = clear fluids up to 6 hrs preop then NPO. Gastric aspirate only available for 84 participants.
Assessor blinding unclear. Premedication - none. IV fluids - all patients.
Allocation concealment C
Study van der Walt 1986a
Methods RCT (random numbers table)
Participants 63 children, 5 days -12 mths, ’healthy’, elective ’routine’ surgery. Exclusions; feeding problems, gastrointestinal
disorders, IV fluids.
Interventions 1. Standard Fast (n = 33)
2. Poly-joule (20%) [10 ml/kg] 3hrs preop (n = 30)
Outcomes Gastric volume - post induction. Gastric pH - post induction. Plasma glucose concentration, blood acid-
base value. Adverse events.
Notes Standard Fast = normal feeding up to four hours preop then NPO. Assessor blinding adequate. Premedication
- none.
Allocation concealment B
Study van der Walt 1986b
Methods RCT (random numbers table)
Participants 62 children, 5 days -12 mths, ’healthy’, elective ’routine’ surgery. Exclusions; feeding problems, gastrointestinal
disorders, IV fluids.
Interventions 1. Standard Fast (n = 33)
45Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
2. Dextrose Solution (5%) [10 ml/kg] 3 hrs preop (n = 29)
Outcomes Gastric volume - post induction. Gastric pH - post induction. Plasma glucose concentration, blood acid-
base value. Adverse events.
Notes Standard Fast = normal feeding up to four hours preop then NPO. Assessor blinding adequate. Premedication
- none.
Allocation concealment B
Study van der Walt 1986c
Methods RCT (random numbers table)
Participants 64 children, 5 days -12 mths, ’healthy’, elective ’routine’ surgery. Exclusions; feeding problems, gastrointestinal
disorders, IV fluids.
Interventions 1. Standard Fast (n = 33)
2. Cows’ milk [10 ml/kg] 3 hrs preop (n = 31)
Outcomes Gastric volume - post induction. Gastric pH - post induction. Plasma glucose concentration, blood acid-
base value. Adverse events.
Notes Standard Fast = normal feeding up to four hours preop then NPO. Assessor blinding adequate. Premedication
- none.
Allocation concealment B
Study van der Walt 1986d
Methods RCT (random numbers table)
Participants 59 children, 5 days -12 mths, ’healthy’, elective ’routine’ surgery. Exclusions; feeding problems, gastrointestinal
disorders, IV fluids.
Interventions 1. Dextrose (5%) [10 ml/kg] 3 hrs preop (n = 29)
2. Poly-joule (20%) [10 ml/kg] 3 hrs preop (n = 30)
Outcomes Gastric volume - post induction. Gastric pH - post induction. Plasma glucose concentration, blood acid-
base value. Adverse events.
Notes Assessor blinding adequate. Premedication - none.
Allocation concealment D
Study van der Walt 1986e
Methods RCT (random numbers table)
Participants 60 children, 5 days -12 mths, ’healthy’, elective ’routine’ surgery. Exclusions; feeding problems, gastrointestinal
disorders, IV fluids.
Interventions 1. Dextrose (5%) [10 ml/kg] 3 hrs preop (n = 29)
2. Cows’ milk [10 ml/kg] 3 hrs preop (n = 31)
Outcomes Gastric volume - post induction. Gastric pH - post induction. Plasma glucose concentration, blood acid-
base value. Adverse events.
Notes Assessor blinding adequate. Premedication - none.
Allocation concealment B
Study van der Walt 1986f
Methods RCT (random numbers table)
Participants 61 children, 5 days -12 mths, ’healthy’, elective ’routine’ surgery. Exclusions; feeding problems, gastrointestinal
disorders, IV fluids.
Interventions 1. Poly-joule (20%) [10 ml/kg] 3 hrs preop (n = 30)
46Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
2. Cows’ milk [10 ml/kg] 3 hrs preop (n = 31)
Outcomes Gastric volume - post induction. Gastric pH - post induction. Plasma glucose concentration, blood acid-
base value. Adverse events.
Notes Assessor blinding adequate. Premedication - none.
Allocation concealment B
Characteristics of excluded studies
Bevan & Burn 1973 Query random allocation. Outcome measures addressed - acid-base and blood glucose levels.
Bevan & Burn 1973b Query random allocation. Outcome measures addressed - acid-base and blood glucose levels.
Fry 1976 Outcome measures addressed - hypoglycaemia and blood glucose levels.
Graham 1979 Non-RCT. Plasma glucose concentration.
Hotta 1967 Data relevant to this review could not be extracted.
Ingebo 1997 Observational.
Jensen 1982 Outcome measures addressed - blood glucose concentrations.
Litman 1994 Non-random allocation.
Morrice 1974 Outcome measures addressed - blood glucose concentrations.
Niija 1999 Query random allocation. Outcome measures addressed - blood glucose, blood ketone body, plasma free fatty
acids (NEFA), insulin, glucagon and cortisol.
Nilsson 1984 Observational
O’Flynn 1989 Observational
Sandstrom 1993 Non-random allocation. (Also reported in part in Larsson, Nilsson, Niklasson, Andresson and Ekström-Jodal,
British Journal of Anaesthesia 1990; 64:419-424).
Schneider 1982 Outcome addressed - plasma glucose
Schurizek 1986 Observational. Based on emergency admissions.
Sethi 1999 Addresses gastric emptying times and the methodology of sampling the volume of intra-operative gastric
contents.
Stanley 1989 Lollipop based intervention not included in fluid/solid preoperative intake addressed by this review.
Thomas 1974 Hypoglycaemia
Watson 1972 Blood Glucose
NOTE - this table does not include those trials presented within the review Preoperative Fasting for adults to
prevent perioperative complications Brady et al 2004.
van der Walt 1990 Non-random allocation.
47Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

A D D I T I O N A L T A B L E S
Table 01. Guidelines for Paediatric Preoperative Fasting
Age Group Solids Clear Fluids Breast Milk Non-human Milk+form
Neonates < 6 mths N/A 2 hrs * † 4 hrs * (†milk type not
specified)
6 hrs *
4 hrs †(milk type not
specified)
Infants
6-36mths
6 hrs† 2 hrs * † 4 hrs *
6 hrs † (milk type not
specified)
6 hrs *(†milk type not
specified)
Children
>36mths
6 hrs *
8 hrs †
2 hrs * † 4 hrs *
8 hrs † (milk type not
specified)
6 hrs *
8 hrs †
KEY hrs = recommended
duration of preoperative
fasting measured in hours
* = American Society of
Anesthesiologists (1999)
† = American Academy of
Pediatricians (1992)
Table 02. The ASA Physical Status Classification System
Class I Class II Class III Class IV Class V Class VI
A normally healthy
patient
A patient with mild
systemic disease
A patient with
severe systemic
disease
A patient with
severe systemic
disease that is a
constant threat to
life
A moribund patient
who is not expected
to survive 24
hrs without the
operation
A declared brain-
dead patient whose
organs are being
removed (for)
donor purposes
48Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Tab
le03.
Sea
rch
stra
tegy
for
elec
tron
icd
atab
ases
Dat
abas
eSt
rate
gy
Med
lin
e19
66-
Au
gust
2003
1.(r
and
omiz
ed-c
ontr
olle
d-t
rial
orm
eta-
anal
ysis
orco
ntr
olle
dcl
inic
altr
ial)
.pt.
2.(R
and
om$
orm
eta-
anal
$or
met
aan
aly$
orm
eta
anal
y$).
tw.
3.((
dou
bl$
orsi
ngl
$)an
dbl
ind
$).t
w.
4.ex
pC
lin
ical
-Tri
als/
5.cr
osso
ver.
ti,a
b,tw
,mp.
6.1
or2
or3
or4
or5
7.ad
ult
$.m
p.
8.(A
nes
th$
orA
nae
sth
$).a
f.
9.an
esth
esia
/or
anes
thes
iolo
gy/
oran
aest
hes
ia/
oran
aest
hes
iolo
gy/
10.
An
esth
esia
,C
ond
uct
ion
/or
anes
thes
ia,
gen
eral
/or
anes
thet
ics
inh
alat
ion
/or
anes
thet
ics
dis
soci
ativ
e/or
anes
thes
ia
intr
atra
chea
l/or
anes
thes
iain
trav
enou
s/or
anes
thes
iacl
osed
circ
uit
/or
anes
thes
iaob
stet
rica
l/or
anes
thes
ia,
reco
very
per
iod
/
oran
esth
esia
,d
enta
l/or
anes
thes
iad
epar
tmen
t,h
osp
ital
/or
anes
thes
iain
hal
atio
n/
orad
juva
nts
,an
esth
esia
/or
intr
aop
erat
ive
com
pli
cati
ons.
mp.
11.
exp
An
esth
esia
,C
ond
uct
ion
/or
exp
anes
thes
ia,
gen
eral
/or
exp
anes
thet
ics
inh
alat
ion
/or
exp
anes
thet
ics
dis
soci
ativ
e/or
exp
anes
thes
iain
trat
rach
eal/
orex
pan
esth
esia
intr
aven
ous/
orex
pan
esth
esia
clos
edci
rcu
it/
orex
pan
esth
esia
obst
etri
cal/
or
exp
anes
thes
ia,r
ecov
ery
per
iod
/or
exp
anes
thes
ia,d
enta
l/or
exp
anes
thes
iad
epar
tmen
t,h
osp
ital
/or
exp
anes
thes
iain
hal
atio
n/
orex
pad
juva
nts
,an
esth
esia
/
12.
(pre
op$
orp
re-o
p$
orp
resu
rg$
orp
re-s
urg
$or
pre
anae
st$
orp
re-a
nae
st$
orp
rean
est$
orp
re-a
nes
t$).
af.
13.
8or
9or
10or
11or
12
14.
(fas
t$or
star
v$).
af.
15.
13an
d14
and
6
16.
15n
ot7
17.
lim
it16
toh
um
an
18.
(flu
id$
ord
rin
k$or
dig
est$
orin
take
orh
ydra
t$).
af.
19.
18an
d13
and
6
20.
19an
d7
21.
lim
it20
toh
um
an
22.
(foo
dor
eat$
orn
utr
itio
n).
mp.
23.
22an
d13
and
6
24.
23n
ot7
25.
lim
it24
toh
um
an
26.
(th
irst
$or
hu
ng$
).m
p.
27.
26an
d13
and
6
28.
27n
ot7
29.
lim
it28
toh
um
an
49Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Tab
le03.
Sea
rch
stra
tegy
for
elec
tron
icd
atab
ases
(Con
tinu
ed)
Dat
abas
eSt
rate
gy
30.
(pre
oper
ativ
efa
st$
orp
re-o
per
ativ
efa
st$)
.af.
31.
30n
ot7
32.
lim
it31
toh
um
an
33.
(Nil
bym
outh
orN
PO
orN
ull
ap
eros
orN
oth
ing
bym
outh
).af
.
34.
33n
ot7
35.
lim
it34
toh
um
an
36.
PN
EU
MO
NIA
/or
PN
EU
MO
NIA
,A
SPIR
AT
ION
/or
PN
EU
MO
NIA
,B
AC
TE
RIA
L/
orP
NE
UM
ON
IA,
LIP
ID/
or
PN
EU
MO
NIA
,MY
CO
PL
ASM
A.m
p.[m
p=t
itle
,ab
stra
ct,
cas
regi
stry
/ec
nu
mbe
rw
ord
,m
esh
subj
ect
hea
din
g]
37.
(pn
eum
onia
oras
pir
atio
n).
af.
38.
RIS
K/
orR
ISK
ASS
ESS
ME
NT
/or
RIS
KFA
CT
OR
S/or
RIS
KM
AN
AG
EM
EN
T/
39.
36or
37or
38
40.
39an
d13
and
6
41.
40n
ot7
42.
lim
it41
toh
um
an
43.
Hyd
roge
n-I
onC
once
ntr
atio
n/
44.
Stom
ach
/
45.
(gas
tric
orst
omac
hor
ph
orvo
lum
e).m
p.
46.
exp
intr
aop
erat
ive
com
pli
cati
ons/
orex
pp
osto
per
ativ
eco
mp
lica
tion
s/or
exp
pre
oper
ativ
eca
re/
47.
(pre
oper
ativ
eca
reor
pos
top
erat
ive
com
pli
cati
ons
orin
trao
per
ativ
eco
mp
lica
tion
s).a
f.
48.
43or
44or
45
49.
46or
47
50.
48an
d49
and
13an
d6
51.
50n
ot7
52.
lim
it51
toh
um
an
53.
17an
d21
and
25an
d19
and
32an
d35
and
42an
d52
CIN
AH
L19
82-t
oA
ugu
st20
031.
(ran
dom
ized
-con
trol
led
-tri
alor
met
a-an
alys
isor
con
trol
led
clin
ical
tria
l).p
t.
2.(R
and
om$
orm
eta-
anal
$or
met
aan
aly$
orm
eta
anal
y$).
tw.
3.((
dou
bl$
orsi
ngl
$)an
dbl
ind
$).t
w.
4.ex
pC
lin
ical
-Tri
als/
5.cr
osso
ver.
ti,a
b,tw
,mp.
6.1
or2
or3
or4
or5
7.(A
nes
th$
orA
nae
sth
$).a
f.
8.an
esth
esia
/or
anes
thes
iolo
gy/
oran
aest
hes
ia/
oran
aest
hes
iolo
gy/
9.A
nes
thes
ia,
Con
du
ctio
n/
oran
esth
esia
,ge
ner
al/
oran
esth
etic
sin
hal
atio
n/
oran
esth
etic
sd
isso
ciat
ive/
oran
esth
esia
intr
atra
chea
l/or
anes
thes
iain
trav
enou
s/or
anes
thes
iacl
osed
circ
uit
/or
anes
thes
iaob
stet
rica
l/or
anes
thes
ia,
reco
very
per
iod
/
50Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Tab
le03.
Sea
rch
stra
tegy
for
elec
tron
icd
atab
ases
(Con
tinu
ed)
Dat
abas
eSt
rate
gy
oran
esth
esia
,d
enta
l/or
anes
thes
iad
epar
tmen
t,h
osp
ital
/or
anes
thes
iain
hal
atio
n/
orad
juva
nts
,an
esth
esia
/or
intr
aop
erat
ive
com
pli
cati
ons.
mp.
10.
(pre
op$
orp
re-o
p$
orp
resu
rg$
orp
re-s
urg
$or
pre
anae
st$
orp
re-a
nae
st$
orp
rean
est$
orp
re-a
nes
t$).
af.
11.
7or
8or
9or
10
12.
(fas
t$or
star
v$).
af.
13.
11an
d12
14.
(flu
id$
ord
rin
k$or
dig
est$
orin
take
orh
ydra
t$).
af.
15.
14an
d11
16.
(foo
dor
eat$
orn
utr
itio
n).
mp.
17.
16an
d11
18.
(th
irst
$or
hu
ng$
).m
p.
19.
18an
d11
20.
(pre
oper
ativ
efa
st$
orp
re-o
per
ativ
efa
st$)
.af.
21.
(Nil
bym
outh
orN
PO
orN
ull
ap
eros
orN
oth
ing
bym
outh
).af
.
22.
pn
eum
onia
/or
pn
eum
onia
,as
pir
atio
n/
orp
neu
mon
ia,
bact
eria
l/or
pn
eum
onia
,li
pid
/or
pn
eum
onia
,m
ycop
lasm
a.m
p.
[mp
=tit
le,
cin
ahl
subj
ect
hea
din
gs,
abst
ract
,in
stru
men
tati
on]
23.
(pn
eum
onia
oras
pir
atio
n).
af.
24.
risk
/or
risk
asse
ssm
ent/
orri
skfa
ctor
s/or
risk
man
agem
ent/
25.
22or
23or
24
26.
25an
d11
and
6
27.
Hyd
roge
n-I
onC
once
ntr
atio
n/
28.
Stom
ach
/
29.
(gas
tric
orst
omac
hor
ph
orvo
lum
e).m
p.
30.
exp
intr
aop
erat
ive
com
pli
cati
ons/
orex
pp
osto
per
ativ
eco
mp
lica
tion
s/or
exp
pre
oper
ativ
eca
re/
31.
(pre
oper
ativ
eca
reor
pos
top
erat
ive
com
pli
cati
ons
orin
trao
per
ativ
eco
mp
lica
tion
s).a
f.
32.
27or
28or
29
33.
30or
31
34.
32an
d33
and
11
35.
13or
15or
17or
19or
20or
21or
26or
34
Coc
hra
ne
Cen
tral
Reg
iste
rof
Con
trol
led
Tri
als
1.FA
STIN
Gex
plo
de
allt
rees
(MeS
H)
2.F
LU
IDT
HE
RA
PY
sin
gle
term
(MeS
H)
3.fa
stin
g
4.st
arv*
5.(fl
uid
ord
rin
k*)
6.(o
ral
and
inta
ke*)
51Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Tab
le03.
Sea
rch
stra
tegy
for
elec
tron
icd
atab
ases
(Con
tinu
ed)
Dat
abas
eSt
rate
gy
7.h
ydra
t*
8.(f
ood
orea
t*or
nu
trit
ion
*)
9.((
nil
nex
tby
nex
tm
outh
)or
(not
hin
gn
ext
byn
ext
mou
th)
or(n
ull
an
ext
per
nex
tos
)or
np
o)
10.
(#1
or#2
or#3
or#4
or#5
or#6
or#7
or#8
or#9
)
11.
AN
EST
HE
SIA
exp
lod
etr
ee1
(MeS
H)
12.
PR
EO
PE
RA
TIV
EC
AR
Esi
ngl
ete
rm(M
eSH
)
13.
PE
RIO
PE
RA
TIV
EC
AR
Eex
plo
de
allt
rees
(MeS
H)
14.
(an
aest
hes
i*or
anes
thes
i*)
15.
(pre
anae
sth
esi*
orp
rean
esth
esi*
)
16.
((p
ren
ext
anae
sth
esi*
)or
(pre
nex
tan
esth
esi*
))
17.
((p
ren
ext
oper
at*)
orp
reop
erat
*)
18.
((p
ren
ext
surg
*)or
pre
surg
*)
19.
(#11
or#1
2or
#13
or#1
4or
#15
or#1
6or
#17
or#1
8)
20.
(#10
and
#19)
21.
PN
EU
MO
NIA
exp
lod
eal
ltre
es(M
eSH
)
22.
pn
eum
onia
23.
asp
irat
ion
24.
(((p
ost
nex
top
erat
ive)
orp
osto
per
ativ
e)an
dco
mp
lica
tion
*)
25.
(pos
tan
dop
erat
*an
din
fect
ion
*)
26.
(pos
top
erat
ive
and
infe
ctio
n*)
27.
PO
STO
PE
RA
TIV
EC
OM
PL
ICA
TIO
NS
exp
lod
eal
ltre
es(M
eSH
)
28.
(((p
erin
ext
oper
ativ
e)or
per
iop
erat
ive)
and
com
pli
cati
on*)
29.
(((i
ntr
an
ext
oper
ativ
e)or
intr
aop
erat
ive)
and
com
pli
cati
on*)
30.
(su
rg*
nea
rco
mp
lica
tion
*)
31.
(op
erat
ion
*n
ear
com
pli
cati
on*)
32.
(#21
or#2
2or
#23
or#2
4or
#25
or#2
6or
#27
or#2
8or
#29
or#3
0or
#31)
33.
(#20
and
#32)
34.
(ch
ild
orch
ild
ren
)
35.
CH
ILD
exp
lod
etr
ee1
(MeS
H)
36.
(ped
iatr
ics
orp
aed
iatr
ics)
37.
(#34
or#3
5or
#36)
38.
(#33
and
#37)
39.
fast
ing:
ti
40.
(#39
and
#19)
41.
(#39
and
#32)
42.
(#39
and
#37)
52Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Tab
le03.
Sea
rch
stra
tegy
for
elec
tron
icd
atab
ases
(Con
tinu
ed)
Dat
abas
eSt
rate
gy
43.
(#38
or#4
0or
#41
or#4
2)
53Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 04. Participants’ Age and Paediatric Age Groups
Trial Neonate (< 1mth) Infant (1-12 mth) Child (> 12 mths) Adolescent (12-18 y)
Cook-Sather 2003 0-9 months 0-9 months
Splinter Schafer 3 0-24 months 0-24 months 0-24 months
van der Walt 1986 5 days - 3 months 5 days - 3 months
Miller 1990 1 month - 5 years 1 month - 5 years
Nicolson 1992 * * *
Aun 1990 1-5 years
Gombar 1997 2-12 years
Goresky 1992 1-6 years
Kushikata 1996 5-12 years
Moyao-García 2001 3-12 years
Splinter 1989 5-10 years
Splinter 1990 5-10 years
Splinter Schafer 1a 2-12 years
Splinter Schafer 1b 2-12 years
Splinter Schafer 2 2-12 years
Welborn 1993 1-10 years
Sarti 1991 1-12 years
Crawford 1990 1-14 years 1-14 years
Maekawa 1993 1-14 years 1-14 years
Meakin 1985 1-16 years 1-16 years
Sandhar 1989 1-14 years 1-14 years
Schreiner 1990 1-18 years 1-18 years
Splinter 1991 13-19 years 13-19 years
* Participants exact age range unavailable though children < 6 months and > 5 years were included. Mean age ± SD for the two groups
was 3.1 ± 4.1 and 3.3 ± 3.9.
Table 05. Details of Quality Evaluation by Trial
Trial
Reference
Partici-
pants
Inclusion
criteria
Exclusion
criteria
A priori
sample
size
Random
Sequence
Con-
cealed
Allocation
Group
Compara-
bility Blinding
ITT
analysis
Aun 1990
(published
20
children in
Listed Listed Not
Reported
Adequate Adequate Yes (age,
weight)
Adequate Not
reported
54Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd
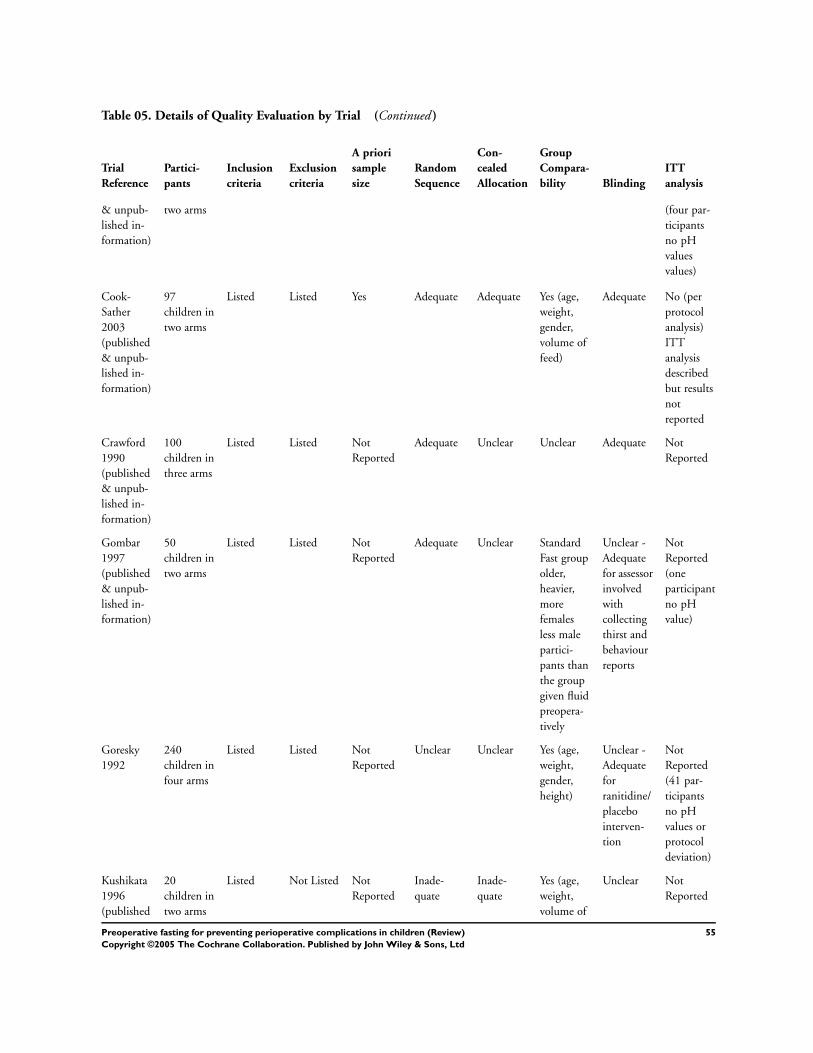
Table 05. Details of Quality Evaluation by Trial (Continued )
Trial
Reference
Partici-
pants
Inclusion
criteria
Exclusion
criteria
A priori
sample
size
Random
Sequence
Con-
cealed
Allocation
Group
Compara-
bility Blinding
ITT
analysis
& unpub-
lished in-
formation)
two arms (four par-
ticipants
no pH
values
values)
Cook-
Sather
2003
(published
& unpub-
lished in-
formation)
97
children in
two arms
Listed Listed Yes Adequate Adequate Yes (age,
weight,
gender,
volume of
feed)
Adequate No (per
protocol
analysis)
ITT
analysis
described
but results
not
reported
Crawford
1990
(published
& unpub-
lished in-
formation)
100
children in
three arms
Listed Listed Not
Reported
Adequate Unclear Unclear Adequate Not
Reported
Gombar
1997
(published
& unpub-
lished in-
formation)
50
children in
two arms
Listed Listed Not
Reported
Adequate Unclear Standard
Fast group
older,
heavier,
more
females
less male
partici-
pants than
the group
given fluid
preopera-
tively
Unclear -
Adequate
for assessor
involved
with
collecting
thirst and
behaviour
reports
Not
Reported
(one
participant
no pH
value)
Goresky
1992
240
children in
four arms
Listed Listed Not
Reported
Unclear Unclear Yes (age,
weight,
gender,
height)
Unclear -
Adequate
for
ranitidine/
placebo
interven-
tion
Not
Reported
(41 par-
ticipants
no pH
values or
protocol
deviation)
Kushikata
1996
(published
20
children in
two arms
Listed Not Listed Not
Reported
Inade-
quate
Inade-
quate
Yes (age,
weight,
volume of
Unclear Not
Reported
55Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 05. Details of Quality Evaluation by Trial (Continued )
Trial
Reference
Partici-
pants
Inclusion
criteria
Exclusion
criteria
A priori
sample
size
Random
Sequence
Con-
cealed
Allocation
Group
Compara-
bility Blinding
ITT
analysis
& unpub-
lished in-
formation)
ingested
fluids)
Maekawa
1993
(published
& unpub-
lished in-
formation)
105
children in
three arms
Listed Listed Not
Reported
Unclear Unclear Yes (age,
weight,
volume of
ingested
fluids)
Adequate Not
Reported
(28 partic-
ipants no
pH values)
Meakin
1987
(published
& unpub-
lished in-
formation)
116
children in
five arms
Listed Listed Not
Reported
Inade-
quate
Inade-
quate
Yes (age,
weight)
Unclear -
Adequate
for pH
and food
particle
measures
Not
Reported
(23 partic-
ipants no
pH values)
Miller
1990
44
children in
two arms
Listed Listed Not
Reported
Adequate Unclear Yes (age,
weight)
Unclear Not
Reported
(23 par-
ticipants
gastric
aspirate
unavail-
able)
Moyao-
García
2001
40
children in
two arms
Listed Listed Not
Reported
Adequate Adequate Yes (age,
weight,
gender)
Adequate Not
Reported
(no with-
drawals)
Nicolson
1992
100
children in
two arms
Listed Listed Not
Reported
Unclear Adequate Yes (age,
weight,
gender,
ASA
status,
type of
cardiac
procedure)
Adequate Not
Reported
(54 partic-
ipants no
pH values)
Sandhar
1989
88
children in
four arms
Listed Listed Not
Reported
Adequate Unclear Yes (age,
weight,
fast to
interven-
tion)
Unclear Not
Reported
(23
protocol
deviations,
seven no
gastric
aspirate)
Sarti 1991 62 Listed Not Listed Not Unclear Unclear Yes (age, Unclear Not
56Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 05. Details of Quality Evaluation by Trial (Continued )
Trial
Reference
Partici-
pants
Inclusion
criteria
Exclusion
criteria
A priori
sample
size
Random
Sequence
Con-
cealed
Allocation
Group
Compara-
bility Blinding
ITT
analysis
children in
two arms
Reported ASA
status)
Reported
(no with-
drawals)
Schreiner
1990
121
children in
two arms
Listed Listed Not
Reported
Adequate Adequate Yes (age,
weight,
gender)
Adequate Not
Reported
(32 partic-
ipants no
pH values,
six samples
mishan-
dled)
Splinter
1989
(published
& unpub-
lished in-
formation)
80
children in
two arms
Listed Listed Not
Reported
Adequate Unclear Yes (age,
gender,
ASA
status)
Adequate Not
Reported
(no with-
drawals)
Splinter
1990
(published
& unpub-
lished in-
formation)
93
children in
three arms
Listed Listed Yes Adequate Unclear 10 ml/kg
group
lighter
than 6
ml/kg and
control
groups.
Groups
compa-
rable in
terms
of age,
gender,
ASA
status.
Adequate Not
Reported
(no with-
drawals)
Splinter
1991
(published
& unpub-
lished in-
formation)
152 ado-
lescents in
two arms
Listed Listed Not
Reported
Adequate Unclear Yes (age,
weight,
gender,
ASA
status,
in/out
patient
status)
Adequate Not
reported
(no with-
drawals)
Splinter
Schaefer
1a
(published
80
children in
two arms
Listed Listed Yes Adequate Unclear Yes (age,
weight,
gender,
ASA
Adequate Not
reported
(no with-
drawals)
57Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd
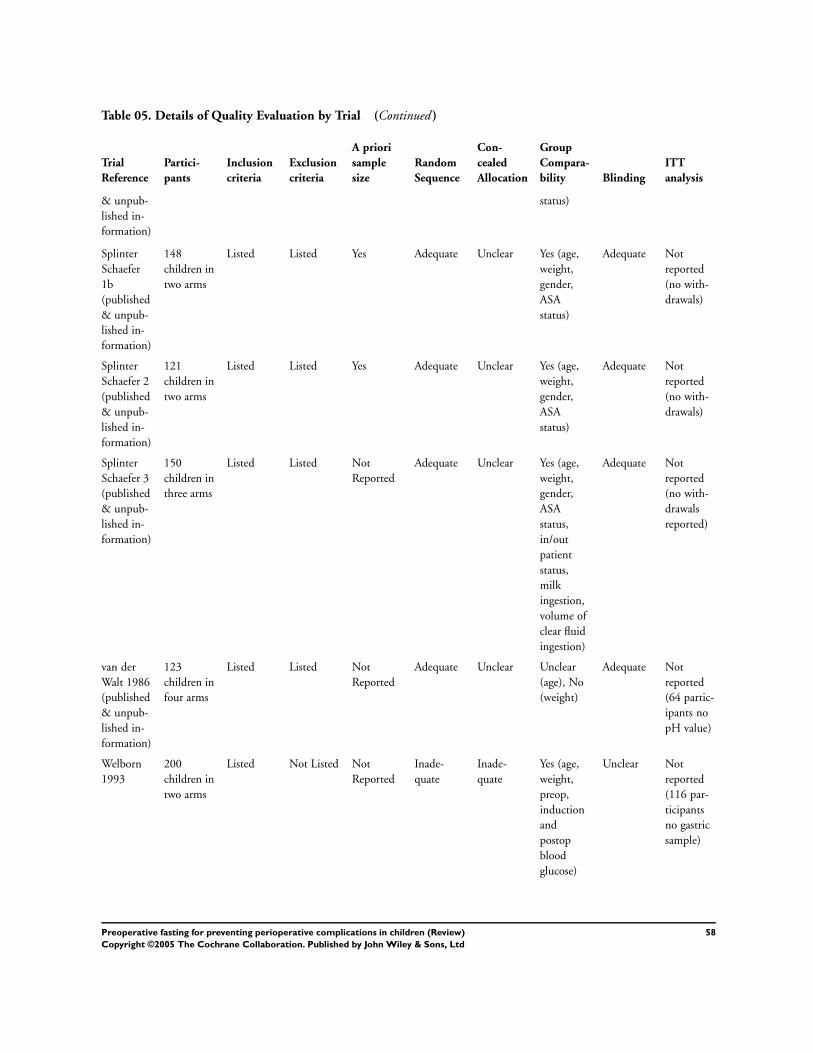
Table 05. Details of Quality Evaluation by Trial (Continued )
Trial
Reference
Partici-
pants
Inclusion
criteria
Exclusion
criteria
A priori
sample
size
Random
Sequence
Con-
cealed
Allocation
Group
Compara-
bility Blinding
ITT
analysis
& unpub-
lished in-
formation)
status)
Splinter
Schaefer
1b
(published
& unpub-
lished in-
formation)
148
children in
two arms
Listed Listed Yes Adequate Unclear Yes (age,
weight,
gender,
ASA
status)
Adequate Not
reported
(no with-
drawals)
Splinter
Schaefer 2
(published
& unpub-
lished in-
formation)
121
children in
two arms
Listed Listed Yes Adequate Unclear Yes (age,
weight,
gender,
ASA
status)
Adequate Not
reported
(no with-
drawals)
Splinter
Schaefer 3
(published
& unpub-
lished in-
formation)
150
children in
three arms
Listed Listed Not
Reported
Adequate Unclear Yes (age,
weight,
gender,
ASA
status,
in/out
patient
status,
milk
ingestion,
volume of
clear fluid
ingestion)
Adequate Not
reported
(no with-
drawals
reported)
van der
Walt 1986
(published
& unpub-
lished in-
formation)
123
children in
four arms
Listed Listed Not
Reported
Adequate Unclear Unclear
(age), No
(weight)
Adequate Not
reported
(64 partic-
ipants no
pH value)
Welborn
1993
200
children in
two arms
Listed Not Listed Not
Reported
Inade-
quate
Inade-
quate
Yes (age,
weight,
preop,
induction
and
postop
blood
glucose)
Unclear Not
reported
(116 par-
ticipants
no gastric
sample)
58Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 06. Summary Statistics - Gastric Volume (ml/kg) - Intervention Groups
Trial ref
No. of Par-
ticipants Mean
Standard
Deviation Median Minimum Maximum
Std. Error
of Mean
Pseudo-
Mean
Pseudo-Std
Dev
Splinter
1990a
30 0.66 0.79 0.37 0.01 4.08
Splinter
1990b
32 0.71 0.76 0.47 0.01 3.69
Splinter
1990c
32 0.71 0.76 0.76 0.01 3.69
Splinter
Schafer 2
57 0.34 0.28 0.27 0.03 1.53
Gombar
1997
25 0.34 0.18 0.0 0.88
Maekawa
1993a
35 0.39 0.46 0.0 1.63
Maekawa
1993b
35 0.35 0.36 0.0 1.30
Maekawa
1993c
35 0.39 0.46 0.0 1.63
Nicolson
1992
44 0.6 0.9 0.0 4.0
Schreiner
1990
48 0.44 0.51 0.0 2.23
Splinter
1989
40 0.24 0.31 0.01 1.39
Splinter
1991
76 0.46 0.39 0.02 1.47
Splinter
Schafer 1a
40 0.37 0.37 0.02 1.54
Splinter
Schafer 1b
74 0.33 0.49 0.02 2.81
Splinter
Schafer 3a
50 0.21 0.37 0.04 2.37
Splinter
Schafer 3b
50 0.15 0.14 0.03 0.52
Splinter
Schafer 3c
50 0.21 0.37 0.04 2.37
Cook-
Sather 2003
36 0.16 0.30
Meakin
1985a
35 0.37 0.35 0.06
Meakin
1985b
32 0.46 0.34 0.06
Meakin
1985c
32 0.46 0.34 0.06
59Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Meakin
1985d
14 0.30 0.30 0.08
Meakin
1985e
15 0.26 0.31 0.08
Meakin
1985f
14 0.30 0.30 0.08
Kushikata
1996
10 0.55 0.59
Miller 1990 19 0.23 0.21
Moyao-
García
2001
20 0.40 0.29
Sarti 1991 32 0.44 0.37
Aun 1990 10 0.53 0.0 2.9 1.00
Sandhar
1989a
13 0.34 0.0 1.0 0.30
Sandhar
1989b
18 0.17 0.0 0.7 0.20
Welborn
1993
41 0.08 0.0 0.80 0.18
van der
Walt 1986a
30 0.0 0.71 0.36 0.33
van der
Walt 1986b
29 0.0 0.77 0.38 0.37
van der
Walt 1986c
31 0.0 1.66 0.83 0.80
van der
Walt 1986d
[F1]
29 0.0 0.77 0.39 0.36
van der
Walt 1986e
[F1]
29 0.0 0.77 0.39 0.36
van der
Walt 1986f
[F1]
30 0.0 0.71 0.36 0.34
Crawford
1990a
group
specific data
unavailable
Crawford
1990b
group
specific data
unavailable
Crawford
1990c
group
specific data
unavailable
60Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 06. Summary Statistics - Gastric Volume (ml/kg) - Intervention Groups (Continued )
Trial ref
No. of Par-
ticipants Mean
Standard
Deviation Median Minimum Maximum
Std. Error
of Mean
Pseudo-
Mean
Pseudo-Std
Dev
Goresky
1992a
group
specific data
unavailable
Goresky
1992b
group
specific data
unavailable
Table 07. Summary Statistics - Gastric Volume (ml/kg) - Control Group
Trial ref
No. of Par-
ticipants Mean
Standard
Deviation Median Minimum Maximum
Std. Error
of Mean
Pseudo-
Mean
Pseudo-Std
Deviation
Splinter
1990a
31 0.45 0.31 0.45 0.02 1.15
Splinter
1990b
31 0.45 0.31 0.45 0.02 1.15
Splinter
1990c
32 1.8 0.8 1.6 1.2 6.0
Splinter
Schafer 2
64 0.39 0.37 0.29 0.04 1.97
Gombar
1997
25 0.38 0.25 0.07 1.35
Maekawa
1993a
35 0.36 0.42 0.0 1.64
Maekawa
1993b
35 0.36 0.42 0.0 1.64
Maekawa
1993c
35 0.35 0.36 0.0 1.30
Nicolson
1992
47 0.4 0.6 0.0 3.0
Scheiner
1990
67 0.57 0.51 0.0 2.09
Splinter
1989
40 0.43 0.46 0.01 1.65
Splinter
1991
76 0.48 0.40 0.02 2.11
Splinter
Schafer 1a
40 0.38 0.30 0.02 1.31
Splinter
Schafer 1b
74 0.27 0.30 0.02 1.81
Splinter
Schafer 3a
50 0.25 0.80 0.03 5.78
61Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd
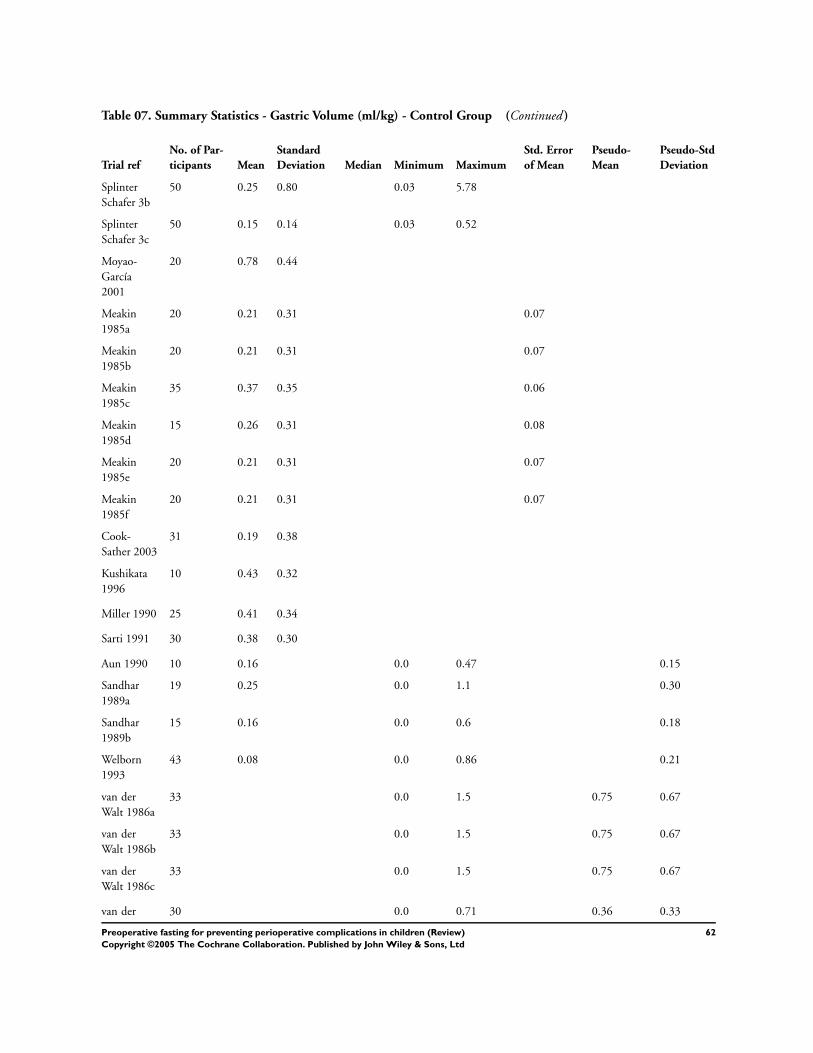
Table 07. Summary Statistics - Gastric Volume (ml/kg) - Control Group (Continued )
Trial ref
No. of Par-
ticipants Mean
Standard
Deviation Median Minimum Maximum
Std. Error
of Mean
Pseudo-
Mean
Pseudo-Std
Deviation
Splinter
Schafer 3b
50 0.25 0.80 0.03 5.78
Splinter
Schafer 3c
50 0.15 0.14 0.03 0.52
Moyao-
García
2001
20 0.78 0.44
Meakin
1985a
20 0.21 0.31 0.07
Meakin
1985b
20 0.21 0.31 0.07
Meakin
1985c
35 0.37 0.35 0.06
Meakin
1985d
15 0.26 0.31 0.08
Meakin
1985e
20 0.21 0.31 0.07
Meakin
1985f
20 0.21 0.31 0.07
Cook-
Sather 2003
31 0.19 0.38
Kushikata
1996
10 0.43 0.32
Miller 1990 25 0.41 0.34
Sarti 1991 30 0.38 0.30
Aun 1990 10 0.16 0.0 0.47 0.15
Sandhar
1989a
19 0.25 0.0 1.1 0.30
Sandhar
1989b
15 0.16 0.0 0.6 0.18
Welborn
1993
43 0.08 0.0 0.86 0.21
van der
Walt 1986a
33 0.0 1.5 0.75 0.67
van der
Walt 1986b
33 0.0 1.5 0.75 0.67
van der
Walt 1986c
33 0.0 1.5 0.75 0.67
van der 30 0.0 0.71 0.36 0.33
62Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 07. Summary Statistics - Gastric Volume (ml/kg) - Control Group (Continued )
Trial ref
No. of Par-
ticipants Mean
Standard
Deviation Median Minimum Maximum
Std. Error
of Mean
Pseudo-
Mean
Pseudo-Std
Deviation
Walt 1986d
[F2]
van der
Walt 1986e
[F2]
31 0.0 1.66 0.83 0.79
van der
Walt 1986f
[F2]
31 0.0 1.66 0.83 0.81
Crawford
1990a
group
specific data
unavailable
Crawford
1990b
group
specific data
unavailable
Crawford
1990c
group
specific data
unavailable
Goresky
1992a
group
specific data
unavailable
Goresky
1992b
group
specific data
unavailable
Table 08. Summary Statistics - Gastric pH - Intervention Groups
Trial ref
No. of
Partici-
pants Mean
Standard
Deviation Median Minimum Maximum
Std. Error
of Mean
Pseudo-
Mean
Pseudo-
Std
Deviation
Splinter
1990a
30 1.7 0.6 1.5 1.3 4.2
Splinter
1990b
32 1.8 0.8 1.6 1.2 6.0
Splinter
1990c
32 1.8 0.8 1.6 1.2 6.0
Splinter
Schafer 2
57 1.8 0.7 1.6 1.2 5.0
Gombar
1997
24 2.53 0.79 1.22 4.52
Maekawa
1993a
27 1.67 0.65 0.9 3.7
63Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 08. Summary Statistics - Gastric pH - Intervention Groups (Continued )
Trial ref
No. of
Partici-
pants Mean
Standard
Deviation Median Minimum Maximum
Std. Error
of Mean
Pseudo-
Mean
Pseudo-
Std
Deviation
Maekawa
1993b
25 1.75 0.61 1.1 3.4
Maekawa
1993c
27 1.67 0.65 0.9 0.65
Splinter
1989
40 2.2 1.2 1.1 7.0
Splinter
1991
76 1.80 1.00 1.20 6.50
Splinter
Schafer 1a
40 1.9 1.0 1.2 7.0
Splinter
Schafer 1b
74 1.8 1.0 1.3 7.0
Splinter
Schafer 3a
50 2.4 1.3 1.2 7.0
Splinter
Schafer 3b
50 2.3 1.3 1.2 6.0
Splinter
Schafer 3c
50 2.4 1.3 1.2 7.0
Goresky
1992a
48 1.96 1.18 0.17
Goresky
1992b
53 4.09 2.26 0.31
Cook-
Sather
2003
36 2.9 1.3
Kushikata
1996
10 1.89 0.75
Miller
1990
19 1.7 0.6
Moyao-
García
2001
20 3.18 0.61
Nicolson
1992
20 1.9 0.7
Sarti 1991 32 1.7 0.9
Schreiner
1990
35 1.81
(reported
as H ion
concentra-
tion 0.015
reported as
H ion con-
centration
0.008
64Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 08. Summary Statistics - Gastric pH - Intervention Groups (Continued )
Trial ref
No. of
Partici-
pants Mean
Standard
Deviation Median Minimum Maximum
Std. Error
of Mean
Pseudo-
Mean
Pseudo-
Std
Deviation
Sandhar
1989a
12 1.83 0.9 3.6 0.85
Sandhar
1989b
15 4.76 2.0 7.7 1.63
Welborn
1993
41 1.45 1.3 1.6 0.07
Meakin
1985a
31 1.7 1.3 6.0 2.14 1.31
Meakin
1985b
29 1.8 1.4 5.5 2.20 1.11
Meakin
1985c
29 1.8 1.4 5.5 2.20 1.16
Meakin
1985d
10 1.9 1.6 2.5 1.96 0.31
Meakin
1985e
12 1.8 1.1 2.4 1.78 0.42
Meakin
1985f
10 1.9 1.6 2.5 1.96 0.31
van der
Walt
1986a
17 1.5 5.0 3.25 1.57
van der
Walt
1986b
15 1.5 3.5 2.50 0.89
van der
Walt
1986c
14 1.5 7.0 4.26 2.42
van der
Walt
1986d
[F1]
15 1.5 3.5 2.50 0.88
van der
Walt
1986e [F1]
15 1.5 3.5 2.50 0.89
van der
Walt 1986f
[F1]
17 1.5 5.0 3.25 1.56
Aun 1990 10 group
specific
data
unavailable
65Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 08. Summary Statistics - Gastric pH - Intervention Groups (Continued )
Trial ref
No. of
Partici-
pants Mean
Standard
Deviation Median Minimum Maximum
Std. Error
of Mean
Pseudo-
Mean
Pseudo-
Std
Deviation
Crawford
1990b
group
specific
data
unavailable
Crawford
1990a
group
specific
data
unavailable
Crawford
1990c
group
specific
data
unavailable
Table 09. Summary Statistics - Gastric pH - Control Group
Trial ref
No. of
Partici-
pants Mean
Standard
Deviation Median Minimum Maximum
Std. Error
of Mean
Pseudo-
Mean
Pseudo-
Std
Deviation
Splinter
1990a
31 1.7 0.6 1.5 1.2 4.0
Splinter
1990b
31 1.7 0.6 1.5 1.2 4.0
Splinter
1990c
30 1.7 0.6 1.5 1.3 4.2
Splinter
Schafer 2
64 1.7 0.4 1.6 1.1 4.0
Gombar
1997
25 2.26 0.57 1.17 3.65
Maekawa
1993a
25 1.72 0.48 1.0 2.8
Maekawa
1993b
25 1.72 0.48 1.0 2.8
Maekawa
1993c
25 1.75 0.61 1.1 3.4
Splinter
1989
40 1.7 0.6 1.2 4.5
Splinter
1991
76 1.60 0.40 1.20 3.0
Splinter
Schafer 1a
40 1.8 0.9 1.20 7.0
Splinter 74 1.9 1.0 1.2 6.0
66Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 09. Summary Statistics - Gastric pH - Control Group (Continued )
Trial ref
No. of
Partici-
pants Mean
Standard
Deviation Median Minimum Maximum
Std. Error
of Mean
Pseudo-
Mean
Pseudo-
Std
Deviation
Schafer 1b
Splinter
Schafer 3a
50 2.0 1.0 1.3 6.0
Splinter
Schafer 3b
50 2.0 1.0 1.3 6.0
Splinter
Schafer 3c
50 2.3 1.3 1.2 6.0
Goresky
1992a
51 1.94 0.93 0.13
Goresky
1992b
47 3.70 2.33 0.34
Cook-
Sather
2003
31 2.5 0.5
Kushikata
1996
10 1.43 0.27
Miller
1990
25 1.6 0.7
Moyao-
García
2001
20 1.75 0.38
Nicolson
1992
17 2.0 0.4
Sarti 1991 30 1.6 1.0
Schreiner
1990
48 1.77
(reported
as H ion
concentra-
tion 0.017)
reported as
H ion con-
centration
0.01
Sandhar
1989a
17 2.1 1.2 4.1 0.96
Sandhar
1989b
14 3.97 1.3 7.3 1.79
Welborn
1993
43 1.41 0.93 1.65 0.17
Meakin
1985a
14 1.8 1.5 2.4 1.85 0.29
Meakin
1985b
14 1.8 1.5 2.4 1.85 0.28
67Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd
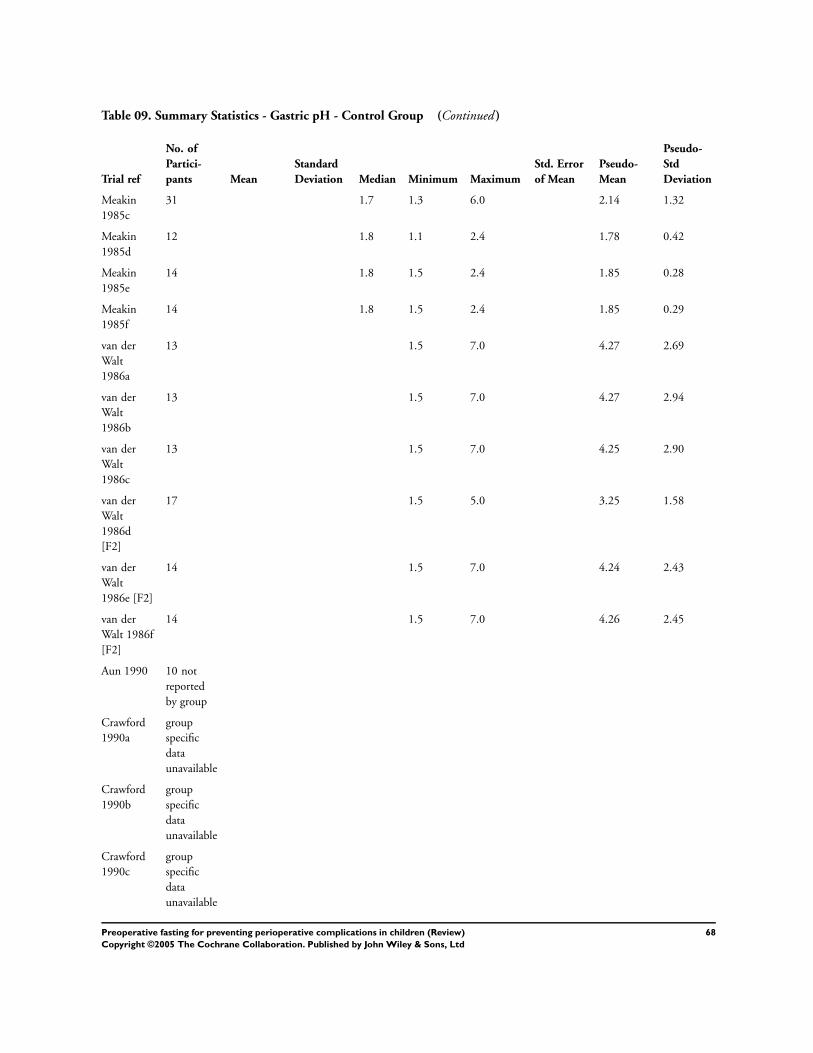
Table 09. Summary Statistics - Gastric pH - Control Group (Continued )
Trial ref
No. of
Partici-
pants Mean
Standard
Deviation Median Minimum Maximum
Std. Error
of Mean
Pseudo-
Mean
Pseudo-
Std
Deviation
Meakin
1985c
31 1.7 1.3 6.0 2.14 1.32
Meakin
1985d
12 1.8 1.1 2.4 1.78 0.42
Meakin
1985e
14 1.8 1.5 2.4 1.85 0.28
Meakin
1985f
14 1.8 1.5 2.4 1.85 0.29
van der
Walt
1986a
13 1.5 7.0 4.27 2.69
van der
Walt
1986b
13 1.5 7.0 4.27 2.94
van der
Walt
1986c
13 1.5 7.0 4.25 2.90
van der
Walt
1986d
[F2]
17 1.5 5.0 3.25 1.58
van der
Walt
1986e [F2]
14 1.5 7.0 4.24 2.43
van der
Walt 1986f
[F2]
14 1.5 7.0 4.26 2.45
Aun 1990 10 not
reported
by group
Crawford
1990a
group
specific
data
unavailable
Crawford
1990b
group
specific
data
unavailable
Crawford
1990c
group
specific
data
unavailable
68Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 09. Summary Statistics - Gastric pH - Control Group (Continued )
Trial ref
No. of
Partici-
pants Mean
Standard
Deviation Median Minimum Maximum
Std. Error
of Mean
Pseudo-
Mean
Pseudo-
Std
Deviation
Table 10. Key to Secondary Outcome Data Tables
Key Measure Key Time of Measure
VAS Visual Analogue Scale (a) > or = 1 day preoperatively
Y/N/O Yes/No/No Opinion (b) on admission
1-3 1 to 3 Scale (1. Satisfied; 2. moderately satisfied; 3. very hungry). (c) prerandomisation
noted note taken of any occurrence (d) > or = 120 mins preoperatively
reported participant report (e) < 120 mins preoperatively
˙ not measured (f ) preinduction/in operating room
[c]/[p] Completed by child/parent (g) after child has departed for operating room
Table 11. Details of Particles Observed in Gastric Aspirates
Trial Comparison Observed Results
Cook-Sather 2003 1. Clear fluids [unlimited] up to 2 hrs (n =
36)
2. Formula [unlimited] up to 4 hrs pre op (n
= 31)
Yes Gastric aspirate tinged white (evidence of
formula) for 9 infants (including one fasted
for 10 hrs). Several small particles in one
child’s (from clear fluid group) clear gastric
aspirate.
Kushikata 1996 1. Standard Fast (n = 10)
2. Rice porridge [55 g rice + 245 mls water +
some salt] 330 mins preop + clear fluids [<
200 ml] up to 5 hrs preop (n = 10)
Yes No solid particles observed.
Maekawa 1993a 1. Standard Fast (n = 35)
2. Apple Juice [10 ml/kg] 2 hrs preop (n = 35)
Yes No particles observed.
Maekawa 1993b 1. Standard Fast (n = 35)
2. Apple Juice [10 ml/kg] 4 hrs preop (n = 35)
Yes No particles observed.
Maekawa 1993c 1. Apple Juice [10 ml/kg] 2 hrs preop (n = 35)
2. Apple Juice [10 ml/kg] 4 hrs preop (n = 35)
Yes No particles observed.
Meakin 1985a 1. Standard Fast (n = 20)
2. Orange squash [10 ml/kg max 200 ml] 2
hrs preop (n = 35)
Yes No particles observed.
Meakin 1985b 1. Standard Fast (n = 20)
2. Plain biscuits (x2) + Orange squash [10
ml/kg max 200 ml] 2 hrs preop (n = 32)
Yes Particles observed in gastric aspirate of 0
participants in fast group and 13 participants
permitted food and fluids up to 2 hrs preop.
Meakin 1985c 1. Orange squash [10 ml/kg max 200 ml] 2
hrs preop (n = 35)
2. Plain biscuits (x2) + Orange squash [10
Yes Particles observed in gastric aspirate of 0
participants in fluid group and 13 participants
permitted food and fluids up to 2 hrs preop.
69Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 11. Details of Particles Observed in Gastric Aspirates (Continued )
Trial Comparison Observed Results
ml/kg max 200 ml] 2 hrs preop (n = 32)
Meakin 1985d 1. Orange squash [10 ml/kg max 200 ml] 4
hrs preop (n = 15)
2. Plain biscuits (x2) + Orange squash [10
ml/kg max 200 ml] 4 hrs preop (n = 14)
Yes Particles observed in gastric aspirate of 0
participants in fluid group and 3 participants
permitted food and fluids up to 4 hrs preop.
Meakin 1985e 1. Standard Fast (n = 20)
2. Orange squash [10 ml/kg max 200 ml] 4
hrs preop (n = 15)
Yes No particles observed.
Meakin 1985f 1. Standard Fast (n = 20)
2. Plain biscuits (x2) + Orange squash [10
ml/kg max 200 mls] 4 hrs preop (n = 14)
Yes Particles observed in gastric aspirate of
0 participants in fast group and and 3
participants permitted food and fluids up to 4
hrs preop.
Moyao-Garcia 2001 1. Standard Fast (n = 20)
2. Isosmolar solution of electrolytes [4 ml/kg]
3 hrs preop (n = 20)
Yes Results not reported
Splinter 1990a 1. Standard Fast (n = 31)
2. Apple Juice [6 ml/kg] 2.5 hrs preop (n =
30)
Yes Particles observed in gastric aspirate of 0
participants in fast group and 1 in fluid group.
This one participant had gastric volume of >
1 ml/kg.
Splinter 1990b 1. Standard Fast (n = 31)
2. Apple Juice [10 ml/kg] 2.5 hrs preop (n =
32)
Yes Particles observed in gastric aspirate of 0
participants in fast group and 4 in fluid group.
All four participants had gastric volume of >
1 ml/kg.
Splinter 1990c 1. Apple Juice [6 ml/kg] 2.5 hrs preop (n =
30)
2. Apple Juice [10 ml/kg] 2.5 hrs preop (n =
32)
Yes Particles observed in gastric aspirate of 1
participant in group permitted 6 ml/kg and 4
participants in group permitted 10 ml/kg. All
five had gastric volumes of > 1 ml/kg
Splinter 1991 1. Standard Fast (n=76)
2. Clear fluids [unlimited] up to 3 hrs preop
(n=76)
Yes Results not reported
Splinter Schaefer 2 1. Standard Fast (n = 64)
2. Clear Fluids [unlimited] up to 3 hrs preop
(n = 57)
Yes Particles observed in gastric aspirate of two
participants in fast and fluid groups.
Splinter Schaefer 3a/b/c 1. Clear fluids [unlimited] 3 hrs preop (n =
50)
2. Clear fluids [unlimited] 2.5 hrs preop (n =
50)
3. Clear fluids [unlimited] 2 hrs preop (n =
50)
Yes Milk curds observed in gastric aspirate of 5 of
36 participants who ingested bottled formula
milk (permitted up to 6 hrs preop) prior
to clear fluid interventions . No particles
observed in gastric aspirate of 8 participants
who ingested breast milk (permitted up to 4
hours preop).
70Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 12. Duration of Fast - Aspiration/Regurgitation
Trial Method Measure Comparison Result
SHORTENED FLUID FAST versus STANDARD FAST
Fluids up to 120 mins preoperatively
Goresky 1992a reported adverse event, coughing,
aspiration
1. Standard Fast + placebo (n =
60)
2. Apple juice [5 ml/kg] +
placebo 2 hrs preop (n = 60)
8 spat out or vomited treatment
agent (unclear which group).
1 experienced flushing and
sweating after intervention
(possibly vaso-vagal reponse).
1 coughing regurgitation and
aspiration on induction (65
ml apple juice, no H2RA
intervention, 190 mins preop).
Authors suggest related to
airway management.
Goresky 1992b reported adverse event, coughing,
aspiration
1. Standard Fast + Ranitidine
[2 mg/kg] (n = 60)
2. Apple juice [5 ml/kg] +
Ranitidine [2 mg/kg] 2 hrs
preop (n = 60)
8 spat out or vomited treatment
agent (unclear which group).
One experienced flushing and
sweating after intervention
(possibly vaso-vagal response).
Maekawa 1993a unclear coughing; laryngospasm. 1. Standard Fast (n = 35)
2. Apple Juice [10 ml/kg] 2 hrs
preop (n = 35)
All inductions uneventful. No
coughing or laryngospasm
noted.
Meakin 1987a noted regurgitation, aspiration,
related morbidity or mortality
1. Standard Fast (n = 20)
2. Orange squash [10 ml/kg
max 200 ml] 2 hrs preop (n =
35)
None observed
Nicolson 1992 unclear intra-operative anaesthetic
complications
1. Standard Fast (n = 44)
2. Clear fluids [unlimited] 2
hrs preop (n = 47)
None observed.
Schreiner 1990 noted present/absent 1. Standard Fast (n = 68)
2. Clear fluids [unlimited] up
to 2 hrs preop (n = 53)
No coughing or laryngospasm
or ’other complications’ noted.
Fluids up to 150 mins preoperatively
Splinter 1989 noted regurgitation or aspiration 1. Standard Fast (n = 40)
2. Apple Juice [3 ml/kg] 2.5 hrs
preop (n = 40)
None observed
Splinter 1990a noted regurgitation or aspiration 1. Standard Fast (n = 31)
2. Apple Juice [6 ml/kg] 2.5 hrs
preop (n = 30)
None observed
Splinter 1990b noted regurgitation or aspiration 1. Standard Fast (n = 31)
2. Apple Juice [10 ml/kg] 2.5
hrs preop (n = 32)
None observed
Fluids up to 180 mins preoperatively
Crawford 1990 noted aspiration pneumonitis 1. Water [2 ml/kg] 2 hrs preop None observed
71Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 12. Duration of Fast - Aspiration/Regurgitation (Continued )
Trial Method Measure Comparison Result
2. Water [2 ml/kg] 4 hrs preop
3. Water [2 ml/kg] 6 hrs preop
total n = 100
Gombar 1995 noted regurgitation, aspiration or
associated morbidity
1. Water (5 ml/kg) 3 hours
preop (n = 25)
2. Standard Fast (n = 25)
None observed
Moyao-Garcia noted complication or adverse event 1. Standard Fast (n = 20)
2. Isosmolar solution of
electrolytes [4 ml/kg] 3 hrs
preop (n = 20)
None observed
Splinter Schaefer 2 noted regurgitation or aspiration 1. Standard Fast (n = 64)
2. Clear Fluids [unlimited] up
to 3 hrs preop (n = 57)
None observed
van der Walt 1986a noted regurgitation, aspiration,
associated morbidity or
mortality
1. Standard Fast (n = 33)
2. Poly-joule (20%) [10 ml/kg]
3 hrs preop (n = 30)
No significant morbidity and
no mortality.
van der Walt 1986b noted regurgitation, aspiration,
associated morbidity or
mortality
1. Standard Fast (n = 33)
2. Dextrose Solution (5%) [10
ml/kg] 3 hrs preop (n = 29)
No significant morbidity and
no mortality.
van der Walt 1986c noted regurgitation, aspiration,
associated morbidity or
mortality
1. Standard Fast (n = 33)
2. Cows’ milk [10 ml/kg] 3 hrs
preop (n = 31)
No significant morbidity and
no mortality.
Up to 240 mins prep
Aun 1990 noted regurgitation at induction,
intraoperatively or during
recovery
1. Standard Fast (n = 10)
2. Dextrose solution (5%) [10
ml/kg] 4hrs preop (n = 10)
None observed
Maekawa 1993b unclear coughing; laryngospasm;
vomiting.
1. Standard Fast (n = 35)
2. Apple Juice [10 ml/kg] 4 hrs
preop (n = 35)
All inductions uneventful. No
coughing, laryngospasm or
vomiting noted.
Meakin 1987e noted regurgitation, aspiration,
related morbidity or mortality
1. Standard Fast (n = 20)
2. Orange squash [10 ml/kg
max 200 ml] 4 hrs preop (n =
15)
None observed
SHORT SOLID + FLUID FAST versus STANDARD FAST
Meakin 1987b noted regurgitation, aspiration,
related morbidity or mortality
1. Standard Fast (n = 55)
2. Plain biscuits (x2) + Orange
squash [10 ml/kg max 200 ml]
2hrs preop (n = 32)
None observed
Meakin 1987f noted regurgitation, aspiration,
related morbidity or mortality
1. Standard Fast (n = 20)
2. Plain biscuits (x2) + Orange
squash [10 ml/kg max 200 ml]
4 hrs preop (n = 14)
None observed
SHORT SOLID + FLUID FAST versus SHORT FLUID FAST
72Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Meakin 1987c noted regurgitation, aspiration,
related morbidity or mortality
1. Orange squash [10 ml/kg
max 200 ml] 2 hrs preop (n =
34)
2. Plain biscuits (x2) + Orange
squash [10 ml/kg max 200 ml]
2hrs preop (n = 32)
None observed
Meakin 1987d noted regurgitation, aspiration,
related morbidity or mortality
1. Orange squash [10 ml/kg
max 200 ml] 4 hrs preop (n =
15)
2. Plain biscuits (x2) + Orange
squash [10 ml/kg max 200 ml]
4 hrs preop (n = 14)
None observed
SHORT FLUID FAST 1 versus SHORT FLUID FAST 2
Cook-Sather 2003 unclear regurgitation, pulmonary
aspiration
1. Clear fluids [unlimited] up
to 2 hrs preop (n = 36)
2. Formula [unlimited] up to 4
hrs preop (n = 31)
None observed.
Maekawa 1993c unclear coughing, laryngospasm 1. Apple Juice [10 ml/kg] 2 hrs
preop (n = 35).
2. Apple Juice [10 ml/kg] 4 hrs
preop (n = 35).
All inductions uneventful. No
coughing or laryngospasm
noted.
Splinter Schaefer 1a noted regurgitation or aspiration 1. Clear Fluids [unlimited] up
to 3 hrs preop (n = 40) 2. Clear
Fluids [unlimited] up to 2.5
hrs preop (n = 40)
None observed.
Splinter Schaefer 1b noted regurgitation or aspiration 1. Clear Fluids [unlimited] up
to 3 hrs preop (n = 74)
2. Clear Fluids [unlimited] up
to 2 hrs preop (n = 74)
None observed.
Table 13. Duration of Fast - Secondary Outcome Measures
Comparison Thirst Hunger Behaviour Comfort Nausea Vomiting
SHORTENED FLUID FAST versus STANDARD FAST
Fluids up to 120 mins preoperatively
Goresky 1992a/b ˙ ˙ ˙ ˙ ˙ noted
Maekawa 1993a ˙ ˙ ˙ ˙ ˙ noted
Nicolson 1992 VAS VAS ˙ VAS ˙ ˙
Schreiner 1990 ˙ ˙ VAS VAS
Y/N/O (fluid group only)
˙ noted
Fluids up to 150 mins preoperatively
Splinter 1989 VAS x 2 VAS x 2 ˙ ˙ ˙ ˙
Splinter 1990a/b VAS VAS VAS ˙ ˙ ˙
Fluids up to 180 mins preoperatively
73Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd
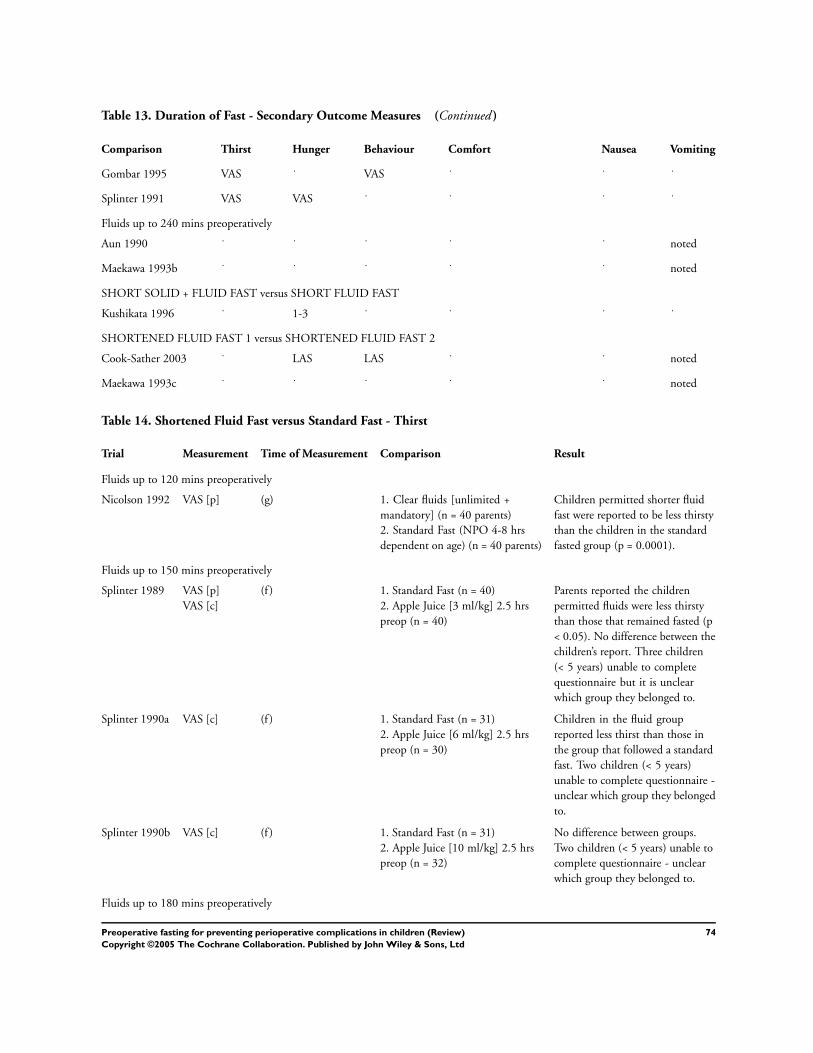
Table 13. Duration of Fast - Secondary Outcome Measures (Continued )
Comparison Thirst Hunger Behaviour Comfort Nausea Vomiting
Gombar 1995 VAS ˙ VAS ˙ ˙ ˙
Splinter 1991 VAS VAS ˙ ˙ ˙ ˙
Fluids up to 240 mins preoperatively
Aun 1990 ˙ ˙ ˙ ˙ ˙ noted
Maekawa 1993b ˙ ˙ ˙ ˙ ˙ noted
SHORT SOLID + FLUID FAST versus SHORT FLUID FAST
Kushikata 1996 ˙ 1-3 ˙ ˙ ˙ ˙
SHORTENED FLUID FAST 1 versus SHORTENED FLUID FAST 2
Cook-Sather 2003 ˙ LAS LAS ˙ ˙ noted
Maekawa 1993c ˙ ˙ ˙ ˙ ˙ noted
Table 14. Shortened Fluid Fast versus Standard Fast - Thirst
Trial Measurement Time of Measurement Comparison Result
Fluids up to 120 mins preoperatively
Nicolson 1992 VAS [p] (g) 1. Clear fluids [unlimited +
mandatory] (n = 40 parents)
2. Standard Fast (NPO 4-8 hrs
dependent on age) (n = 40 parents)
Children permitted shorter fluid
fast were reported to be less thirsty
than the children in the standard
fasted group (p = 0.0001).
Fluids up to 150 mins preoperatively
Splinter 1989 VAS [p]
VAS [c]
(f ) 1. Standard Fast (n = 40)
2. Apple Juice [3 ml/kg] 2.5 hrs
preop (n = 40)
Parents reported the children
permitted fluids were less thirsty
than those that remained fasted (p
< 0.05). No difference between the
children’s report. Three children
(< 5 years) unable to complete
questionnaire but it is unclear
which group they belonged to.
Splinter 1990a VAS [c] (f ) 1. Standard Fast (n = 31)
2. Apple Juice [6 ml/kg] 2.5 hrs
preop (n = 30)
Children in the fluid group
reported less thirst than those in
the group that followed a standard
fast. Two children (< 5 years)
unable to complete questionnaire -
unclear which group they belonged
to.
Splinter 1990b VAS [c] (f ) 1. Standard Fast (n = 31)
2. Apple Juice [10 ml/kg] 2.5 hrs
preop (n = 32)
No difference between groups.
Two children (< 5 years) unable to
complete questionnaire - unclear
which group they belonged to.
Fluids up to 180 mins preoperatively
74Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd
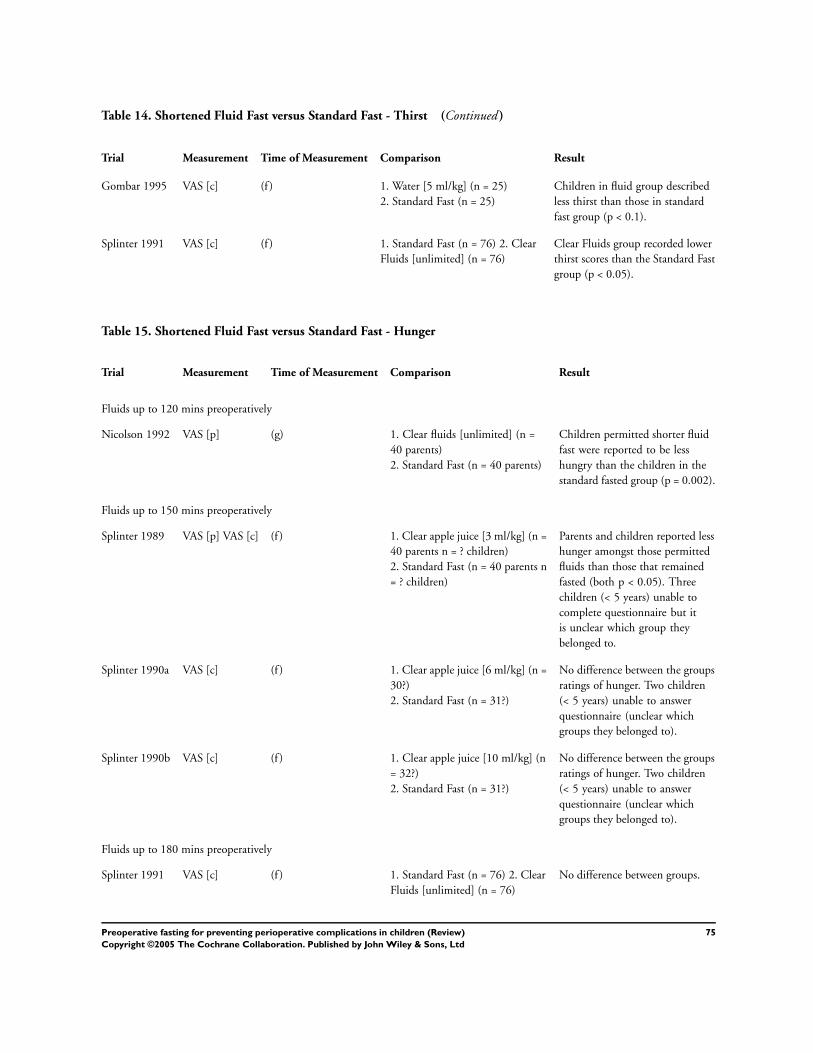
Table 14. Shortened Fluid Fast versus Standard Fast - Thirst (Continued )
Trial Measurement Time of Measurement Comparison Result
Gombar 1995 VAS [c] (f ) 1. Water [5 ml/kg] (n = 25)
2. Standard Fast (n = 25)
Children in fluid group described
less thirst than those in standard
fast group (p < 0.1).
Splinter 1991 VAS [c] (f ) 1. Standard Fast (n = 76) 2. Clear
Fluids [unlimited] (n = 76)
Clear Fluids group recorded lower
thirst scores than the Standard Fast
group (p < 0.05).
Table 15. Shortened Fluid Fast versus Standard Fast - Hunger
Trial Measurement Time of Measurement Comparison Result
Fluids up to 120 mins preoperatively
Nicolson 1992 VAS [p] (g) 1. Clear fluids [unlimited] (n =
40 parents)
2. Standard Fast (n = 40 parents)
Children permitted shorter fluid
fast were reported to be less
hungry than the children in the
standard fasted group (p = 0.002).
Fluids up to 150 mins preoperatively
Splinter 1989 VAS [p] VAS [c] (f ) 1. Clear apple juice [3 ml/kg] (n =
40 parents n = ? children)
2. Standard Fast (n = 40 parents n
= ? children)
Parents and children reported less
hunger amongst those permitted
fluids than those that remained
fasted (both p < 0.05). Three
children (< 5 years) unable to
complete questionnaire but it
is unclear which group they
belonged to.
Splinter 1990a VAS [c] (f ) 1. Clear apple juice [6 ml/kg] (n =
30?)
2. Standard Fast (n = 31?)
No difference between the groups
ratings of hunger. Two children
(< 5 years) unable to answer
questionnaire (unclear which
groups they belonged to).
Splinter 1990b VAS [c] (f ) 1. Clear apple juice [10 ml/kg] (n
= 32?)
2. Standard Fast (n = 31?)
No difference between the groups
ratings of hunger. Two children
(< 5 years) unable to answer
questionnaire (unclear which
groups they belonged to).
Fluids up to 180 mins preoperatively
Splinter 1991 VAS [c] (f ) 1. Standard Fast (n = 76) 2. Clear
Fluids [unlimited] (n = 76)
No difference between groups.
75Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 16. Shortened Fluid Fast versus Standard Fast - Behaviour
Trial Measurement Time of Measurement Comparison Result
Fluids up to 120 mins preoperatively
Schreiner 1990 VAS [p] Irritable (g) 1. Clear fluids [unlimited with
final ingestion up to 8 oz] (n =
45 parents)
2. Standard Fast (n = 50
parents)
Parents described children in
fluid group as less irritable
than those in the standard
fasting group (p < 0.001).
Splinter 1990a VAS [p] Upset/Irritable (f ) 1. Clear apple juice [6 ml/kg]
(n = 30 parents)
2. Standard Fast (n = 31
parents)
Children observed to be less
upset and irritable in fluid
group than in standard fasting
group (p < 0.05).
Splinter 1990b VAS [p] Upset/Irritable (f ) 1. Clear apple juice [10 ml/kg]
(n = 32 parents)
2. Standard Fast (n = 31
parents)
No difference between groups.
Fluids up to 180 mins preoperatively
Gombar 1997 VAS [p] Irritable (f ) 1. Water [5 ml/kg] (n = 25)
2. Standard Fast (n = 25)
Parents of children permitted
fluids reported their children
less irritable than those that
continued fasting (p > 0.01).
Table 17. Shortened Fluid Fast versus Standard Fast - Comfort
Trial Measurement Time of Measurement Comparison Result
Fluids up to 120 mins preoperatively
Nicolson 1992 VAS [p] Comfort (g) 1. Clear fluids [unlimited +
mandatory] (n = 40 parents)
2. Standard Fast (NPO 4-8
hrs dependent on age) (n =
40 parents)
Children permitted shorter
fluid fast were reported to
be more comfortable in the
hour before being taken to
the operating room, than
the children in the standard
fasted group (p = 0.004).
Schreiner 1990 VAS [p] Tolerance of preop
experience
Y/N/O [p fluid group]
Improved preop experience
(g) 1. Clear fluids [unlimited
with final ingestion up to 8
oz] (n = 45 parents)
2. Standard Fast (n = 50
parents)
Preoperative fasting
experience reported to be
tolerated better by the
children permitted fluids
than the children that
followed a standard fast (p <
0.01). Of the 18 children
who had prior experience
of the preoperative
procedures within the
hospital 14 parents reported
the shortened fluid fast
improved the experience for
their child, while the four
76Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 17. Shortened Fluid Fast versus Standard Fast - Comfort (Continued )
Trial Measurement Time of Measurement Comparison Result
remaining parents had no
opinion.
Table 18. Shortened Fluid Fast versus Standard Fast - Vomiting
Trial Method Measure Time of Measure Comparison Result
Fluids up to 120 mins preoperatively
Goresky 1992a noted vomiting preoperative period 1. Standard Fast + placebo
(n = 60)
2. Apple juice [5 ml/kg] +
placebo 2 hrs preop (n = 60)
Children who vomited were
not distinguished from
those that gagged or spat
out intervention. Children’s
allocation to groups across
Goresky 1992a and Goresky
1992b unclear.
Goresky 1992b noted vomiting preoperative period 1. Standard Fast + Ranitidine
[2 mg/kg] (n = 60)
2. Apple juice [5 ml/kg] +
Ranitidine [2 mg/kg] 2 hrs
preop (n = 60)
Children who vomited were
not distinguished from
those that gagged or spat
out intervention. Children’s
allocation to groups across
Goresky 1992a and Goresky
1992b unclear.
Maekawa 1993a noted vomiting on induction 1. Standard Fast (n = 35)
2. Apple Juice [10 ml/kg] 2
hrs preop (n = 35)
None noted
Schreiner 1990 noted vomiting on induction 1. Standard Fast (n = 68)
2. Clear fluids [unlimited]
up to 2 hrs preop (n = 53)
None noted
Fluids up to 240 mins preoperatively
Aun 1990 noted unclear on induction, intra-
operatively or recovery
1. Standard Fast (n = 10)
2. Dextrose solution (5%)
[10 ml/kg] 4 hrs preop (n =
10)
None noted
Maekawa 1993b unclear vomiting on induction 1. Standard Fast (n = 35)
2. Apple Juice [10 ml/kg] 4
hrs preop (n = 35)
None noted
Table 19. Shortened Solid + Fluid Fast versus Short Fluid Fast - Hunger
Trial Measurement Time of Measurement Comparison Result
Kushikata 1996 1-3 [c?] (e) 1. Standard Fast (n = 10)
2. Rice porridge [55 g rice + 245
ml water + some salt] 330 mins
preop + clear fluids [< 200 ml] up
Children in the group permitted
solid intake described less hunger
than those that fasted (p = 0.024).
It is unclear whether the hunger
77Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 19. Shortened Solid + Fluid Fast versus Short Fluid Fast - Hunger (Continued )
Trial Measurement Time of Measurement Comparison Result
to 5 hrs preop (n = 10) score was assigned by the child or
by the anaesthetist in response to
the child’s description.
Table 20. Short Fluid Fast 1 versus Short Fluid Fast 2 - Hunger
Trial Measure Time of Measurement Comparison Result
Cook-Sather 2003 VAS [p] (g) 1. Clear fluids [unlimited] up to 2
hrs (n = 36)
2. Formula [unlimited] up to 4 hrs
pre op (n = 31)
No difference between groups.
Table 21. Short Fluid Fast 1 versus Short Fluid Fast 2 - Behaviour
Trial Measure Time of Measurement Comparison Result
Cook-Sather 2003 VAS [p] Irritable (g) 1. Clear fluids [unlimited] up to
2 hrs (n = 36)
2. Formula [unlimited] up to 4
hrs pre op (n = 31)
No difference between groups.
Table 22. Short Fluid Fast 1 versus Short Fluid Fast 2 - Vomiting
Trial Method Measure Time of Measurement Comparison Result
Cook-Sather 2003 noted 1. Clear fluids [unlimited] up to 2
hrs (n = 36)
2. Formula [unlimited] up to 4 hrs
pre op (n = 31)
None reported
Maekawa 1993c noted vomiting on induction 1. Apple Juice [10 ml/kg] 2 hrs
preop (n = 35).
2. Apple Juice [10 ml/kg] 4 hrs
preop (n = 35).
None noted
Table 23. Type of Intake - Aspiration/Regurgitation
Trial Method Measure Comparison Result
WATER versus STANDARD FAST
Gombar 1995 noted regurgitation, aspiration or
associated morbidity
1. Water (5 ml/kg) 3 hours
preop (n = 25)
2. Standard Fast (n = 25)
None observed
CLEAR FLUIDS versus STANDARD FAST
Schreiner 1990 noted present/absent 1. Standard Fast (n = 68)
2. Clear fluids [unlimited] up
to 2 hrs preop (n = 53)
No coughing or laryngospasm
or ’other complications’ noted.
Nicolson 1992 unclear intra-operative anaesthetic
complications
1. Standard Fast (n = 44) 2.
Clear fluids [unlimited] 2 hrs
preop (n = 47)
None observed.
78Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Splinter Schaefer 2 noted regurgitation or aspiration 1. Standard Fast (n = 64)
2. Clear Fluids [unlimited] up
to 3 hrs preop (n = 57)
None observed
FRUIT JUICE versus STANDARD FAST
Goresky 1992a reported adverse event, coughing,
aspiration
1. Standard Fast + placebo (n =
60)
2. Apple juice [5 ml/kg] +
placebo 2 hrs preop (n = 60)
One experienced flushing and
sweating after intervention
(possibly vaso-vagal response).
1 coughing regurgitation and
aspiration on induction (65
ml apple juice, no H2RA
intervention, 190 mins preop).
Authors suggest related to
airway management.
Goresky 1992b reported adverse event, coughing,
aspiration
1. Standard Fast + Ranitidine
[2 mg/kg] (n = 60)
2. Apple juice [5 ml/kg] +
Ranitidine [2 mg/kg] 2 hrs
preop (n = 60)
One experienced flushing and
sweating after intervention
(possibly vaso-vagal response).
Maekawa 1993a unclear coughing; laryngospasm. 1. Standard Fast (n = 35)
2. Apple Juice [10 ml/kg] 2 hrs
preop (n = 35)
All inductions uneventful. No
coughing or laryngospasm
noted.
Maekawa 1993b unclear coughing; laryngospasm. 1. Standard Fast (n = 35)
2. Apple Juice [10 ml/kg] 4 hrs
preop (n = 35)
All inductions uneventful. No
coughing, laryngospasm or
vomiting noted.
Splinter 1989 noted regurgitation or aspiration 1. Standard Fast (n = 40)
2. Apple Juice [3 ml/kg] 2.5 hrs
preop (n = 40)
None observed
Splinter 1990a noted regurgitation or aspiration 1. Standard Fast (n = 31)
2. Apple Juice [6 ml/kg] 2.5 hrs
preop (n = 30)
None observed
Splinter 1990b noted regurgitation or aspiration 1. Standard Fast (n = 31)
2. Apple Juice [10 ml/kg] 2.5
hrs preop (n = 32)
None observed
MILK v STANDARD FAST
van der Walt 1986c noted regurgitation, aspiration,
associated morbidity or
mortality
1. Standard Fast (n = 33)
2. Cows’ milk [10 ml/kg] 3 hrs
preop (n = 31)
No significant morbidity and
no mortality.
DEXTROSE SOLUTION v STANDARD FAST
Aun 1990 noted regurgitation at induction,
intraoperatively or during
recovery
1. Standard Fast (n = 10)
2. Dextrose solution (5%) [10
ml/kg] 4 hrs preop (n=10)
None observed
van der Walt 1986b noted regurgitation, aspiration,
associated morbidity or
mortality
1. Standard Fast (n = 33)
2. Dextrose Solution (5%) [10
ml/kg] 3 hrs preop (n = 29)
No significant morbidity and
no mortality.
OTHER FLUIDS v STANDARD FAST
Meakin 1987a noted regurgitation, aspiration,
related morbidity or mortality
1. Standard Fast (n = 20)
2. Orange squash [10 ml/kg
None observed
79Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 23. Type of Intake - Aspiration/Regurgitation (Continued )
Trial Method Measure Comparison Result
max 200 ml] 2 hrs preop (n =
35)
Meakin 1987e noted regurgitation, aspiration,
related morbidity or mortality
1. Standard Fast (n = 20)
2. Orange squash [10 ml/kg
max 200 ml] 4 hrs preop (n =
15)
None observed
Moyao-Garcia noted complication or adverse event 1. Standard Fast (n = 20)
2. Isosmolar solution of
electrolytes [4 ml/kg] 3 hrs
preop (n = 20)
None observed
van der Walt 1986a noted regurgitation, aspiration,
associated morbidity or
mortality
1. Standard Fast (n = 33)
2. Poly-joule (20%) [10 ml/kg]
3 hrs preop (n = 30)
No significant morbidity and
no mortality.
FLUID 1 [F1] v FLUID 1 [F2]
van der Walt 1986d noted regurgitation, aspiration,
associated morbidity or
mortality
1. Dextrose (5%) [10ml/kg]
3hrs preop (n = 29)
2. Poly-joule (20%) [10ml/kg]
3hrs preop (n = 30)
No significant morbidity and
no mortality.
van der Walt 1986e noted regurgitation, aspiration,
associated morbidity or
mortality
1. Dextrose (5%) [10ml/kg]
3hrs preop (n = 29)
2. Cows’ milk [10ml/kg] 3hrs
preop (n = 31)
No significant morbidity and
no mortality.
van der Walt 1986f noted regurgitation, aspiration,
associated morbidity or
mortality
1. Poly-joule (20%) [10ml/kg]
3hrs preop (n = 30)
2. Cow’s milk [10ml/kg] 3hrs
preop (n = 31)
No significant morbidity and
no mortality.
Table 24. Type of Intake - Secondary Outcome Measures
Comparison Thirst Hunger Behaviour Comfort Nausea Vomiting
WATER versus STANDARD FAST
Gombar 1995 VAS ˙ VAS ˙ ˙ ˙
CLEAR FLUIDS versus STANDARD FAST
Nicolson 1992 VAS VAS ˙ VAS ˙ ˙
Schreiner 1990 ˙ ˙ VAS VAS Y/N/O (fluid group only) ˙ noted
Splinter Schaefer 2
Splinter 1991 VAS VAS ˙ ˙ ˙ ˙
FRUIT JUICE versus STANDARD FAST
Goresky 1992a/b ˙ ˙ ˙ ˙ ˙ noted
Maekawa 1993a/b ˙ ˙ ˙ ˙ ˙ noted
Splinter 1989 VAS x 2 VAS x 2 ˙ ˙ ˙ ˙
80Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Splinter 1990a/b VAS VAS VAS ˙ ˙ ˙
OTHER FLUIDS versus STANDARD FAST
Aun 1990 ˙ ˙ ˙ ˙ ˙ noted
Table 25. Type of Fluid versus Standard Fast - Thirst
Trial Measure Time of Measurement Comparison Result
Water versus Standard Fast
Gombar 1997 VAS [c] (f ) 1. Water [5 ml/kg] (n = 25)
2. Standard Fast (n = 25)
Children in water group described
less thirst than those in standard
fast group (p < 0.1).
Clear Fluids versus Standard Fast
Nicolson 1992 VAS [p] (g) 1. Clear fluids [unlimited +
mandatory] (n = 40 parents)
2. Standard Fast (NPO 4-8
hrs dependent on age) (n = 40
parents)
Children permitted clear fluids
were reported to be less thirsty
than the children in the standard
fasted group (p = 0.0001).
Splinter 1991 VAS [c] (f ) 1. Standard Fast (n = 76) 2. Clear
Fluids [unlimited] (n = 76)
Clear Fluids group recorded lower
thirst scores than the Standard
Fast group (p < 0.05).
Fruit Juice versus Standard Fast
Splinter 1989 VAS [p] VAS [c] (f ) 1. Clear apple juice [3 ml/kg] (n =
40?)
2. Standard Fast (n = 40?)
Parents reported the children
permitted apple juice were less
thirsty than those that remained
fasted (p < 0.05). No difference
between the children’s report.
Three children (< 5 years) unable
to complete questionnaire but
it is unclear which group they
belonged to.
Splinter 1990a VAS [c] (f ) 1. Clear apple juice [6 ml/kg] (n =
30?)
2. Standard Fast (n = 31?)
Children in the apple juice group
reported less thirst than those in
the group that followed a standard
fast. Two children (< 5 years)
unable to complete questionnaire
- unclear which group they
belonged to.
Splinter 1990b VAS [c] (f ) 1. Clear apple juice [10 ml/kg] (n
= 32?)
2. Standard Fast (n = 31?)
No difference between groups.
Two children (< 5 years) unable to
complete questionnaire - unclear
which group they belonged to.
81Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 26. Type of Fluid versus Standard Fast - Hunger
Trial Measure Time of Measurement Comparison Result
Clear Fluids versus Standard Fast
Nicolson 1992 VAS [p] (g) 1. Clear fluids [unlimited] (n =
40 parents)
2. Standard Fast (n = 40 parents)
Children permitted clear fluids
were reported to be less hungry
than the children in the standard
fasted group (p = 0.002).
Splinter 1991 VAS [c] (f ) 1. Standard Fast (n = 76) 2. Clear
Fluids [unlimited] (n = 76)
No difference between groups.
Fruit Juice versus Standard Fast
Splinter 1989 VAS [p] VAS [c] (f ) 1. Standard Fast (n = 40)
2. Apple Juice [3 ml/kg] 2.5hrs
preop (n = 40)
Parents and children reported less
hunger amongst those permitted
apple juice than those that
remained fasted (both p < 0.05).
Three children (< 5 years) unable
to complete questionnaire but
it is unclear which group they
belonged to.
Splinter 1990a VAS [c] (f ) 1. Standard Fast (n = 31)
2. Apple Juice [6 ml/kg] 2.5 hrs
preop (n = 30)
No difference between the groups
ratings of hunger. Two children
(< 5 years) unable to answer
questionnaire (unclear which
groups they belonged to).
Splinter 1990b VAS [c] (f ) 1. Standard Fast (n = 31)
2. Apple Juice [10 ml/kg] 2.5 hrs
preop (n = 32)
No difference between the groups
ratings of hunger. Two children
(< 5 years) unable to answer
questionnaire (unclear which
groups they belonged to).
Table 27. Type of Fluid versus Standard Fast - Behaviour
Trial Measure Time of Measurement Comparison Result
Water versus Standard Fast
Gombar 1995 VAS [p] Irritable (f ) 1. Water [5 ml/kg] (n = 25)
2. Standard Fast (n = 25)
Parents of children permitted
water reported their children
less irritable than those that
continued fasting (p > 0.01).
Clear Fluids versus Standard Fast
Schreiner 1990 VAS [p] Irritable (g) 1. Clear fluids [unlimited -
final ingestion up to 8 oz] (n =
45 parents)
2. Standard Fast (n = 50
parents)
Parents described children in
clear fluid group described as
less irritable than those in the
standard fasting group (p <
0.001).
Fruit Juice versus Standard Fast
Splinter 1990a VAS [p] Upset/Irritable (f ) 1. Clear apple juice [6 ml/kg] Children observed to be less
82Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 27. Type of Fluid versus Standard Fast - Behaviour (Continued )
Trial Measure Time of Measurement Comparison Result
(n = 30 parents)
2. Standard Fast (n = 31
parents)
upset and irritable in apple
juice group than in standard
fasting group (p < 0.05).
Splinter 1990b VAS [p] Upset/Irritable (f ) 1. Clear apple juice [10 ml/kg]
(n = 32 parents)
2. Standard Fast (n = 31
parents)
No difference between groups.
Table 28. Type of Fluid versus Standard Fast - Comfort
Trial Measure Time of Measurement Comparison Result
Clear Fluids versus Standard Fast
Nicolson 1992 VAS [p] (g) 1. Clear fluids [unlimited]
(n = 40 parents)
2. Standard Fast (n = 40
parents)
Children permitted clear
fluids were reported to be
more comfortable in the
hour before being taken to
the operating room, than
the children in the standard
fasted group (p = 0.004).
Schreiner 1990 VAS [p] Tolerance of
preoperative experience
Y/N/NoOpinion improved
overall experience as
reported by parents of
children in fluid group.
(g) 1. Clear fluids [unlimited
with final ingestion up to 8
oz] (n = 45 parents)
2. Standard Fast (n = 50
parents)
Preoperative fasting
experience reported to be
tolerated better by the
children permitted clear
fluids than the children that
followed a standard fast (p <
0.01). Of the 18 children
who had prior experience
of the preoperative
procedures within the
hospital 14 parents reported
the shortened fluid fast
improved the experience for
their child, while the four
remaining parents had no
opinion.
Table 29. Type of Fluid versus Standard Fast - Vomiting
Trial Method Measure Time of Measurement Comparison Result
CLEAR FLUIDS versus STANDARD FAST
Schreiner 1990 noted present/absent on induction 1. Standard Fast (n = 68)
2. Clear fluids [unlimited]
up to 2 hrs preop (n = 53)
None noted
FRUIT JUICE versus STANDARD FAST
83Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 29. Type of Fluid versus Standard Fast - Vomiting (Continued )
Trial Method Measure Time of Measurement Comparison Result
Goresky 1992a noted vomiting preoperative period 1. Standard Fast + placebo
(n = 60)
2. Apple juice [5 ml/kg] +
placebo 2 hrs preop (n =
60)
Children who vomited
were not distinguished
from those that gagged or
spat out intervention (n =
8). Children’s allocation
to groups across Goresky
1992a and Goresky 1992b
unclear.
Goresky 1992b noted vomiting preoperative period 1. Standard Fast +
Ranitidine [2 mg/kg] (n =
60)
2. Apple juice [5 ml/kg] +
Ranitidine [2 mg/kg] 2hrs
preop (n = 60)
Children who vomited
were not distinguished
from those that gagged or
spat out intervention (n =
8). Children’s allocation
to groups across Goresky
1992a and Goresky 1992b
unclear.
Maekawa 1993a noted vomiting on induction 1. Standard Fast (n = 35)
2. Apple Juice [10 ml/kg]
2 hrs preop (n = 35)
None noted
Maekawa 1993b unclear vomiting on induction 1. Standard Fast (n = 35)
2. Apple Juice [10 ml/kg]
4 hrs preop (n = 35)
None noted
OTHER FLUIDS versus STANDARD FAST
Aun 1990 noted unclear on induction, intra-
operatively or recovery
1. Standard Fast (n = 10)
2. Dextrose solution (5%)
[10 ml/kg] 4 hrs preop (n
= 10)
None noted
Table 30. Volume of Intake - Aspiration/Regurgitation
Trial Method Measure Comparison Results
LOW VOLUME FLUID INTAKE versus STANDARD FAST
Gombar 1995 noted regurgitation, aspiration or
associated morbidity
1. Water (5 ml/kg) 3 hours
preop (n = 25)
2. Standard Fast (n = 25)
None observed
Goresky 1992a reported adverse event, coughing,
aspiration
1. Standard Fast + placebo (n =
60)
2. Apple juice [5 ml/kg] +
placebo 2 hrs preop (n = 60)
One experienced flushing and
sweating after intervention
(possibly vaso-vagal response).
1 coughing regurgitation and
aspiration on induction (65
ml apple juice, no H2RA
intervention, 190 mins preop).
Authors suggest related to
airway management.
Goresky 1992b reported adverse event, coughing, 1. Standard Fast + Ranitidine One experienced flushing and
84Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 30. Volume of Intake - Aspiration/Regurgitation (Continued )
Trial Method Measure Comparison Results
aspiration [2 mg/kg] (n = 60)
2. Apple juice [5 ml/kg] +
Ranitidine [2 mg/kg] 2 hrs
preop (n = 60)
sweating after intervention
(possibly vaso-vagal response).
Moyao-García 2001 noted complication or adverse event 1. Standard Fast (n = 20)
2. Isosmolar solution of
electrolytes [4 ml/kg] 3 hrs
preop (n = 20)
None observed
Splinter 1989 noted regurgitation or aspiration 1. Standard Fast (n = 40)
2. Apple Juice [3 ml/kg] 2.5 hrs
preop (n = 40)
None observed
HIGH VOLUME FLUID INTAKE versus STANDARD FAST
Aun 1990 noted regurgitation at induction,
intraoperatively or during
recovery
1. Standard Fast (n = 10)
2. Dextrose solution (5%) [10
ml/kg] 4 hrs preop (n=10)
None observed
Maekawa 1993a unclear coughing, laryngospasm 1. Standard Fast (n = 35)
2. Apple Juice [10 ml/kg] 2 hrs
preop (n = 35)
All inductions uneventful. No
coughing or laryngospasm
noted.
Maekawa 1993b unclear coughing, laryngospasm 1. Standard Fast (n = 35)
2. Apple Juice [10 ml/kg] 4 hrs
preop (n = 35)
All inductions uneventful. No
coughing, laryngospasm or
vomiting noted.
Meakin 1987a noted regurgitation, aspiration,
related morbidity or mortality
1. Standard Fast (n = 20)
2. Orange squash [10 ml/kg
max 200 ml] 2 hrs preop (n =
35)
None observed
Meakin 1987e noted regurgitation, aspiration,
related morbidity or mortality
1. Standard Fast (n = 20)
2. Orange squash [10 ml/kg
max 200 ml] 4 hrs preop (n =
15)
None observed
Splinter 1990a noted regurgitation or aspiration 1. Standard Fast (n = 31)
2. Apple Juice [6 ml/kg] 2.5 hrs
preop (n = 30)
None observed
Splinter 1990b noted regurgitation or aspiration 1. Standard Fast (n = 31)
2. Apple Juice [10 ml/kg] 2.5
hrs preop (n = 32)
None observed
van der Walt 1986a noted regurgitation, aspiration,
associated morbidity or
mortality
1. Standard Fast (n = 33)
2. Poly-joule (20%) [10 ml/kg]
3 hrs preop (n = 30)
No significant morbidity and
no mortality.
van der Walt 1986b noted regurgitation, aspiration,
associated morbidity or
mortality
1. Standard Fast (n = 33)
2. Dextrose Solution (5%) [10
ml/kg] 3 hrs preop (n = 29)
No significant morbidity and
no mortality.
van der Walt 1986c noted regurgitation, aspiration,
associated morbidity or
1. Standard Fast (n = 33)
2. Cow’s milk [10 ml/kg] 3 hrs
No significant morbidity and
no mortality.
85Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 30. Volume of Intake - Aspiration/Regurgitation (Continued )
Trial Method Measure Comparison Results
mortality preop (n = 31)
UNLIMITED FLUID INTAKE versus STANDARD FAST
Nicolson 1992 unclear intra-operative anaesthetic
complications
1. Standard Fast (n = 44) 2.
Clear fluids [unlimited] 2 hrs
preop (n = 47)
None observed.
Schreiner 1990 noted present/absent 1. Standard Fast (n = 68)
2. Clear fluids [unlimited] up
to 2 hrs preop (n = 53)
No coughing or laryngospasm
or ’other complications’ noted.
Splinter Schaefer 2 noted regurgitation or aspiration 1. Standard Fast (n = 64)
2. Clear Fluids [unlimited] up
to 3 hrs preop (n = 57)
None observed
VOLUME 1 [V1] versus VOLUME 1 [V]2]
Splinter 1990c noted regurgitation or aspiration 1. Apple Juice [6 ml/kg] 2.5 hrs
preop (n = 30)
2. Apple Juice [10 ml/kg] 2.5
hrs preop (n = 32)
None observed
Table 31. Volume of Intake - Secondary Outcome Measures
Comparison Thirst Hunger Behaviour Comfort Nausea Vomiting
LOW VOLUME OF INTAKE versus STANDARD FAST
Gombar 1995 VAS ˙ VAS ˙ ˙ ˙
Goresky 1992a/b ˙ ˙ ˙ ˙ ˙ noted
Splinter 1989 VAS x 2 VAS x 2 ˙ ˙ ˙ ˙
HIGH VOLUME OF INTAKE versus STANDARD FAST
Aun 1990 ˙ ˙ ˙ ˙ ˙ noted
Maekawa 1993a/b ˙ ˙ ˙ ˙ ˙ noted
Splinter 1990a/b VAS VAS VAS ˙ ˙ ˙
UNLIMITED VOLUME OF INTAKE versus STANDARD FAST
Nicolson 1992 VAS VAS ˙ VAS ˙ ˙
Schreiner 1990 ˙ ˙ VAS VAS Y/N/O (fluid group only) ˙ noted
Splinter 1991 VAS VAS ˙ ˙ ˙ ˙
VOULME 1 [V1] versus VOLUME 2 [V2]
Splinter 1990c VAS VAS VAS ˙ ˙ ˙
86Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd
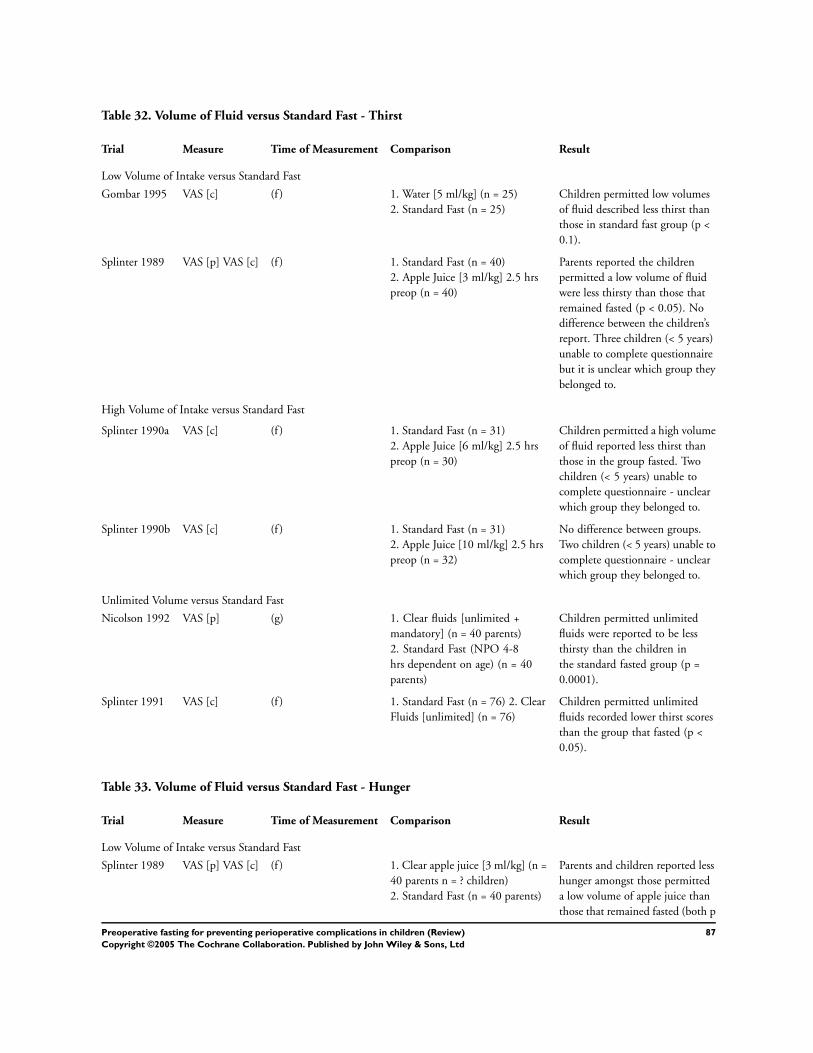
Table 32. Volume of Fluid versus Standard Fast - Thirst
Trial Measure Time of Measurement Comparison Result
Low Volume of Intake versus Standard Fast
Gombar 1995 VAS [c] (f ) 1. Water [5 ml/kg] (n = 25)
2. Standard Fast (n = 25)
Children permitted low volumes
of fluid described less thirst than
those in standard fast group (p <
0.1).
Splinter 1989 VAS [p] VAS [c] (f ) 1. Standard Fast (n = 40)
2. Apple Juice [3 ml/kg] 2.5 hrs
preop (n = 40)
Parents reported the children
permitted a low volume of fluid
were less thirsty than those that
remained fasted (p < 0.05). No
difference between the children’s
report. Three children (< 5 years)
unable to complete questionnaire
but it is unclear which group they
belonged to.
High Volume of Intake versus Standard Fast
Splinter 1990a VAS [c] (f ) 1. Standard Fast (n = 31)
2. Apple Juice [6 ml/kg] 2.5 hrs
preop (n = 30)
Children permitted a high volume
of fluid reported less thirst than
those in the group fasted. Two
children (< 5 years) unable to
complete questionnaire - unclear
which group they belonged to.
Splinter 1990b VAS [c] (f ) 1. Standard Fast (n = 31)
2. Apple Juice [10 ml/kg] 2.5 hrs
preop (n = 32)
No difference between groups.
Two children (< 5 years) unable to
complete questionnaire - unclear
which group they belonged to.
Unlimited Volume versus Standard Fast
Nicolson 1992 VAS [p] (g) 1. Clear fluids [unlimited +
mandatory] (n = 40 parents)
2. Standard Fast (NPO 4-8
hrs dependent on age) (n = 40
parents)
Children permitted unlimited
fluids were reported to be less
thirsty than the children in
the standard fasted group (p =
0.0001).
Splinter 1991 VAS [c] (f ) 1. Standard Fast (n = 76) 2. Clear
Fluids [unlimited] (n = 76)
Children permitted unlimited
fluids recorded lower thirst scores
than the group that fasted (p <
0.05).
Table 33. Volume of Fluid versus Standard Fast - Hunger
Trial Measure Time of Measurement Comparison Result
Low Volume of Intake versus Standard Fast
Splinter 1989 VAS [p] VAS [c] (f ) 1. Clear apple juice [3 ml/kg] (n =
40 parents n = ? children)
2. Standard Fast (n = 40 parents)
Parents and children reported less
hunger amongst those permitted
a low volume of apple juice than
those that remained fasted (both p
87Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 33. Volume of Fluid versus Standard Fast - Hunger (Continued )
Trial Measure Time of Measurement Comparison Result
< 0.05). Three children (< 5 years)
unable to complete questionnaire
but it is unclear which group they
belonged to.
High Volume of Intake versus Standard Fast
Splinter 1990a VAS [c] (f ) 1. Clear apple juice [6 ml/kg] (n =
30?)
2. Standard Fast (n = 31?)
No difference between the groups
ratings of hunger. Two children
(< 5 years) unable to answer
questionnaire (unclear which
groups they belonged to).
Splinter 1990b VAS [c] (f ) 1. Clear apple juice [10 ml/kg] (n
= 32?)
2. Standard Fast (n = 31?)
No difference between the groups
ratings of hunger. Two children
(< 5 years) unable to answer
questionnaire (unclear which
groups they belonged to).
Unlimited Volume versus Standard Fast
Nicolson 1992 VAS [p] (g) 1. Clear fluids [unlimited +
mandatory] (n = 40 parents)
2. Standard Fast (NPO 4-8
hrs dependent on age) (n = 40
parents)
Children permitted unlimited
volumes of fluid intake were
reported to be less hungry than
the children in the standard fasted
group (p = 0.002).
Splinter 1991 VAS [c] (f ) 1. Standard Fast (n = 76) 2. Clear
Fluids [unlimited] (n = 76)
No difference between groups.
Table 34. Volume of Fluid versus Standard Fast - Behaviour
Trial Measure Time of Measurement Comparison Result
Low Volume of Intake versus Standard Fast
Gombar 1995 VAS [p] Irritable (f ) 1. Water [5 ml/kg] (n = 25)
2. Standard Fast (n = 25)
Parents of children permitted
a low volume of fluid reported
their children less irritable
than those that continued
fasting (p > 0.01).
High Volume of Intake versus Standard Fast
Splinter 1990a VAS [p] Upset/Irritable (f ) 1. Clear apple juice [6 ml/kg]
(n = 30 parents)
2. Standard Fast (n = 31
parents)
Children observed to be less
upset and irritable in high
volume fluid group than in
standard fasting group (p <
0.05).
Splinter 1990b VAS [p] Upset/Irritable (f ) 1. Clear apple juice [10 ml/kg]
(n = 32 parents)
2. Standard Fast (n = 31
parents)
No difference between groups.
Unlimited Volume versus Standard Fast
88Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Schreiner 1990 VAS [p] Irritable (g) 1. Clear fluids [unlimited with
final ingestion up to 8 oz] (n =
45 parents)
2. Standard Fast (n = 50
parents)
Children in unlimited fluid
group described as less
irritable than those in the
standard fasting group (p <
0.001).
Table 35. Volume of Fluid versus Standard Fast - Comfort
Trial Measure Time of Measurement Comparison Result
Unlimited Volume versus Standard Fast
Nicolson 1992 VAS [p] (g) 1. Clear fluids [unlimited +
mandatory] (n = 40 parents)
2. Standard Fast (NPO 4-8
hrs dependent on age) (n =
40 parents)
Children permitted
unlimited fluid were
reported to be more
comfortable in the hour
before being taken to the
operating room, than the
children in the standard
fasted group (p = 0.004).
Schreiner 1990 VAS [p] Tolerance of
preoperative experience
Y/N/NoO improved overall
experience as reported by
parents of children in fluid
group.
(g) 1. Clear fluids [unlimited
with final ingestion up to 8
oz] (n = 45 parents)
2. Standard Fast (n = 50
parents)
Preoperative fasting
experience reported to be
tolerated better by the
children permitted fluids
than the children that
followed a standard fast (p <
0.01). Of the 18 children
who had prior experience
of the preoperative
procedures within the
hospital 14 parents reported
the shortened fluid fast
improved the experience for
their child, while the four
remaining parents had no
opinion.
Table 36. Volume of Fluid versus Standard Fast - Vomiting
Trial Method Measure Time of Measurement Comparison Result
Low Volume of Fluids versus Standard Fast
Goresky 1992a noted vomiting preoperative period 1. Standard Fast + placebo
(n = 60)
2. Apple juice [5 ml/kg] +
placebo 2 hrs preop (n =
60)
Children who vomited
were not distinguished
from those that gagged
or spat out intervention.
Children’s allocation to
groups across Goresky
1992a and Goresky 1992b
unclear.
Goresky 1992b noted vomiting preoperative period 1. Standard Fast +
Ranitidine [2mg/kg] (n =
Children who vomited
were not distinguished
89Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 36. Volume of Fluid versus Standard Fast - Vomiting (Continued )
Trial Method Measure Time of Measurement Comparison Result
60)
2. Apple juice [5 ml/kg]
+ Ranitidine [2 mg/kg] 2
hrs preop (n = 60)
from those that gagged
or spat out intervention.
Children’s allocation to
groups across Goresky
1992a and Goresky 1992b
unclear.
High Volume of Fluids versus Standard Fast
Aun 1990 noted unclear on induction, intra-
operatively or recovery
1. Standard Fast (n = 10)
2. Dextrose solution (5%)
[10 ml/kg] 4 hrs preop (n
= 10)
None noted
Maekawa 1993a noted vomiting on induction 1. Standard Fast (n = 35)
2. Apple Juice [10 ml/kg]
2 hrs preop (n = 35)
None noted
Maekawa 1993b unclear vomiting on induction 1. Standard Fast (n = 35)
2. Apple Juice [10 ml/kg]
4 hrs preop (n = 35)
None noted
Unlimited Volume of Fluids versus Standard Fast
Schreiner 1990 noted present/ absent on induction 1. Standard Fast (n = 68)
2. Clear fluids [unlimited]
up to 2 hrs preop (n = 53)
None noted
Table 37. Volume 1 [V1] versus Volume 2 [V2] - Thirst
Trial Method Measure Comparison Result
Splinter 1990c VAS [c] (f ) 1. Apple Juice [6 ml/kg] 2.5 hrs preop (n =
30)
2. Apple Juice [10 ml/kg] 2.5 hrs preop (n =
32)
No difference between groups. Two children
(< 5 years) unable to complete questionnaire
- unclear which group they belonged to.
Table 38. Volume 1 [V1] versus Volume 2 [V2] - Hunger
Trial Method Measure Comparison Result
Splinter 1990c VAS [c] (f ) 1. Apple Juice [6 ml/kg] 2.5 hrs preop (n =
30)
2. Apple Juice [10 ml/kg] 2.5 hrs preop (n =
32)
No difference between groups. Two children
(< 5 years) unable to complete questionnaire
- unclear which group they belonged to.
90Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Table 39. Volume 1 [V1] versus Volume 2 [V2] - Behaviour
Trial Method Measure Comparison Result
Splinter 1990c VAS [p] Upset/Irritable (f ) 1. Apple Juice [6 ml/kg] 2.5 hrs preop
(n = 30)
2. Apple Juice [10 ml/kg] 2.5 hrs
preop (n = 32)
No difference between groups.
Table 40. Sensitivitiy Analysis - excluding trials with inadequate randomisation
Comparison Outcome Subgroup Original WMD Exclusions WMD
01 Duration - Short
Fluid Fast versus
Standard Fast
02 Gastric Volume
(ml/kg)
01 Fluids (up to 120
minutes preop) versus
Standard Fast
WMD 0.03 95% CI
-0.03 to 0.10; NSD
WMD 0.03 95% CI
-0.07 to 0.12; NSD
05 Fluids (up to 240
minutes preop) versus
Standard Fast
WMD 0.03 95% CI
-0.10 to 0.17; NSD
WMD 0.06 95% CI
-0.23 to 0.34; NSD
03 Gastric pH 01 Fluids (up to 120
minutes preop) versus
Standard Fast
WMD 0.04 95% CI
-0.01 to 0.09; NSD
WMD -0.01 95% CI
-0.15 to 0.14; NSD
05 Type of Intake -
Fluid versus Standard
Fast
02 Gastric Volume
(ml/kg)
04 Fruit Juice versus
Standard Fast
WMD 0.02 95% CI
-0.08 to 0.11; NSD
WMD 0.04 95% CI
-0.10 to 0.17; NSD
07 Other Fluids versus
Standard Fast
WMD -0.13 95% CI
-0.41 to 0.16; NSD
WMD -0.38 95% CI
-0.58 to -0.19; (P <
0.0001)
03 Gastric pH 04 Fruit Juice versus
Standard Fast
WMD 0.04 95% CI
-0.01 to 0.10; NSD
WMD 0.07 95% CI
-0.08 to 0.22; NSD
07 Other Fluids versus
Standard Fast
WMD 0.34 95% CI
-0.62 to 1.31; NSD
WMD 0.42 95% CI
-1.92 to 2.77; NSD
07 Volume of Intake -
Volume of Fluid versus
Standard Fast
02 Gastric Volume
(ml/kg)
03 High Volume Fluid
Intake versus Standard
Fast
WMD 0.04 95% CI
-0.05 to 0.13; NSD
WMD 0.03 95% CI
-0.14 to 0.19; NSD
03 Gastric pH 03 High Volume Fluid
Intake versus Standard
Fast
WMD 0.04 95% CI
-0.02 to 0.09; NSD
WMD 0.00 95% CI
-0.18 to 0.19; NSD
WMD 0.00 95% CI
-0.18 to 0.19; NSD
G R A P H S
Comparison 01. Duration - Short Fluid Fast versus Standard Fast
Outcome titleNo. of
studies
No. of
participants Statistical method Effect size
02 Gastric contents - Volume
(ml/kg)
Weighted Mean Difference (Random) 95% CI Subtotals only
03 Gastric contents - pH Weighted Mean Difference (Random) 95% CI Subtotals only
91Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd
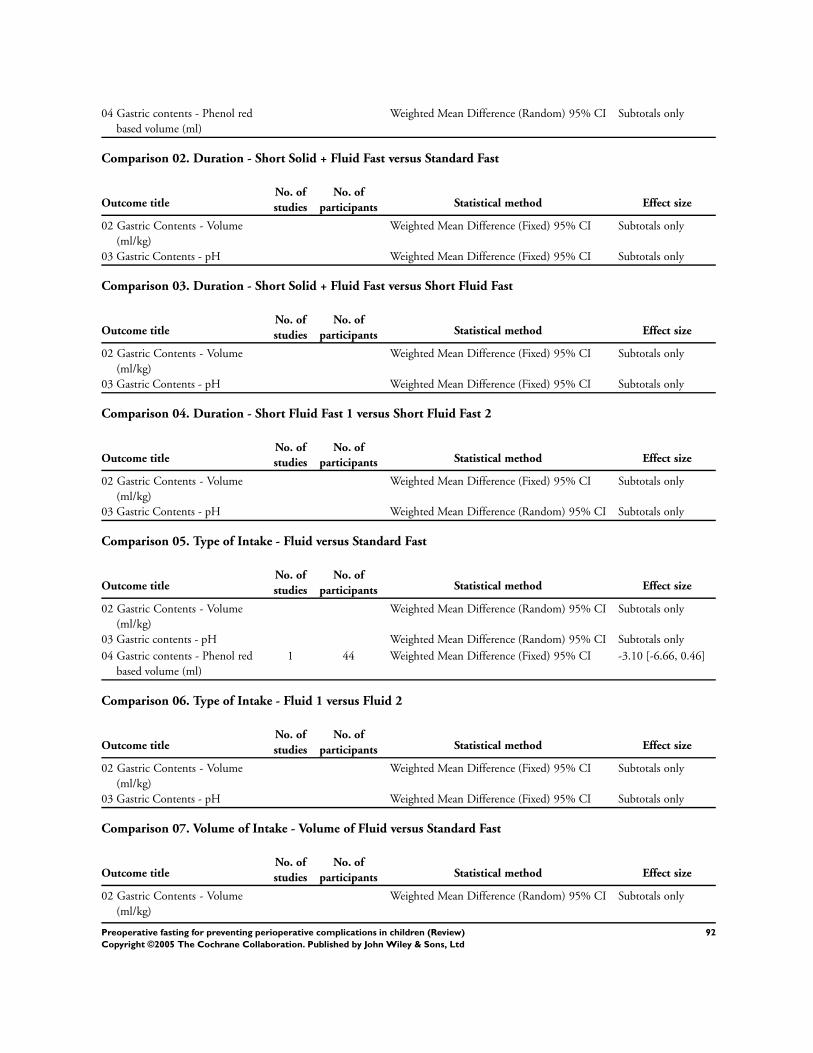
04 Gastric contents - Phenol red
based volume (ml)
Weighted Mean Difference (Random) 95% CI Subtotals only
Comparison 02. Duration - Short Solid + Fluid Fast versus Standard Fast
Outcome titleNo. of
studies
No. of
participants Statistical method Effect size
02 Gastric Contents - Volume
(ml/kg)
Weighted Mean Difference (Fixed) 95% CI Subtotals only
03 Gastric Contents - pH Weighted Mean Difference (Fixed) 95% CI Subtotals only
Comparison 03. Duration - Short Solid + Fluid Fast versus Short Fluid Fast
Outcome titleNo. of
studies
No. of
participants Statistical method Effect size
02 Gastric Contents - Volume
(ml/kg)
Weighted Mean Difference (Fixed) 95% CI Subtotals only
03 Gastric Contents - pH Weighted Mean Difference (Fixed) 95% CI Subtotals only
Comparison 04. Duration - Short Fluid Fast 1 versus Short Fluid Fast 2
Outcome titleNo. of
studies
No. of
participants Statistical method Effect size
02 Gastric Contents - Volume
(ml/kg)
Weighted Mean Difference (Fixed) 95% CI Subtotals only
03 Gastric Contents - pH Weighted Mean Difference (Random) 95% CI Subtotals only
Comparison 05. Type of Intake - Fluid versus Standard Fast
Outcome titleNo. of
studies
No. of
participants Statistical method Effect size
02 Gastric Contents - Volume
(ml/kg)
Weighted Mean Difference (Random) 95% CI Subtotals only
03 Gastric contents - pH Weighted Mean Difference (Random) 95% CI Subtotals only
04 Gastric contents - Phenol red
based volume (ml)
1 44 Weighted Mean Difference (Fixed) 95% CI -3.10 [-6.66, 0.46]
Comparison 06. Type of Intake - Fluid 1 versus Fluid 2
Outcome titleNo. of
studies
No. of
participants Statistical method Effect size
02 Gastric Contents - Volume
(ml/kg)
Weighted Mean Difference (Fixed) 95% CI Subtotals only
03 Gastric Contents - pH Weighted Mean Difference (Fixed) 95% CI Subtotals only
Comparison 07. Volume of Intake - Volume of Fluid versus Standard Fast
Outcome titleNo. of
studies
No. of
participants Statistical method Effect size
02 Gastric Contents - Volume
(ml/kg)
Weighted Mean Difference (Random) 95% CI Subtotals only
92Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

03 Gastric contents - pH values Weighted Mean Difference (Random) 95% CI Subtotals only
Comparison 08. Volume of Intake - Volume 1 versus Volume 2
Outcome titleNo. of
studies
No. of
participants Statistical method Effect size
02 Gastric Contents - Volume
(ml/kg)
Weighted Mean Difference (Fixed) 95% CI Subtotals only
03 Gastric contents - pH Weighted Mean Difference (Fixed) 95% CI Subtotals only
I N D E X T E R M S
Medical Subject Headings (MeSH)
Adolescent; Child; Drinking; Fasting; Gastrointestinal Contents; Pneumonia, Aspiration [prevention & control]; Practice Guidelines;
Preoperative Care [methods]; Randomized Controlled Trials; Thirst; Time Factors
Medical MeSH check words
Humans
C O V E R S H E E T
Title Preoperative fasting for preventing perioperative complications in children
Authors Brady M, Kinn S, O’Rourke K, Randhawa N, Stuart P
Contribution of author(s) MB conducted the search, screened retrieved references for inclusion/exclusion, extracted
the data from included trials, evaluated methodological quality, contacted trial authors,
entered data, conducted data analysis, wrote the review.
SK participated in an initial literature search which led to the registration of a review title
with the Cochrane Collaboration and participated in the evaluation of the methodological
quality of the trials.
KO’R Developed a method of calculating suitable pseudo-values as an estimate of the
means and standard deviation summary data unavailable from the original publications.
This permitted representation of these trials within the meta-analysis. He also commented
on review drafts.
NR Provided statistical support for data extraction and data analysis.
PS participated in extracting the data from included trials and commented on review drafts.
Issue protocol first published 2001/1
Review first published 2005/2
Date of most recent amendment 10 February 2005
Date of most recent
SUBSTANTIVE amendment
10 February 2005
What’s New Information not supplied by author
Date new studies sought but
none found
Information not supplied by author
Date new studies found but not
yet included/excluded
Information not supplied by author
Date new studies found and
included/excluded
Information not supplied by author
93Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Date authors’ conclusions
section amended
Information not supplied by author
Contact address Marian Brady
Programme Leader
Nursing, Midwifery and Allied Health Professions Research Unit
Glasgow Caledonian University
Cowcaddens Road
Glasgow
G4 0BA
UK
E-mail: [email protected]
Tel: 0141 331 8102
DOI 10.1002/14651858.CD005285
Cochrane Library number CD005285
Editorial group Cochrane Wounds Group
Editorial group code HM-WOUNDS
G R A P H S A N D O T H E R T A B L E S
Fig. 1. Comparison 01. Duration - Short Fluid Fast versus Standard Fast
01.02 Gastric contents - Volume (ml/kg)
Review: Preoperative fasting for preventing perioperative complications in children
Comparison: 01 Duration - Short Fluid Fast versus Standard Fast
Outcome: 02 Gastric contents - Volume (ml/kg)
Study Short Fluid Fast Standard Fast Weighted Mean Difference (Random) Weight Weighted Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
01 Fluids (up to 120 minutes preop) versus Standard Fast (no H2-receptor antagonists)
Maekawa 1993a 35 0.39 (0.46) 35 0.36 (0.42) 9.4 0.03 [ -0.18, 0.24 ]
Meakin 1985a 35 0.37 (0.35) 20 0.21 (0.31) 12.2 0.16 [ -0.02, 0.34 ]
Nicolson 1992 44 0.60 (0.90) 47 0.40 (0.60) 4.2 0.20 [ -0.12, 0.52 ]
Sandhar 1989a 13 0.34 (0.30) 19 0.25 (0.30) 9.0 0.09 [ -0.12, 0.30 ]
Sarti 1991 32 0.44 (0.37) 30 0.38 (0.30) 13.8 0.06 [ -0.11, 0.23 ]
Schreiner 1990 48 0.44 (0.51) 67 0.57 (0.51) 11.1 -0.13 [ -0.32, 0.06 ]
Welborn 1993 41 0.08 (0.18) 43 0.08 (0.21) 40.3 0.00 [ -0.08, 0.08 ]
Subtotal (95% CI) 248 261 100.0 0.03 [ -0.03, 0.10 ]
Test for heterogeneity chi-square=6.82 df=6 p=0.34 I² =12.0%
Test for overall effect z=0.97 p=0.3
-1.0 -0.5 0 0.5 1.0
Fav Short Fluid Fast Fav Standard Fast (Continued . . . )
94Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

(. . . Continued)
Study Short Fluid Fast Standard Fast Weighted Mean Difference (Random) Weight Weighted Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
02 Fluids (up to 120 minutes preop) versus Standard Fast (+ H2-receptor antagonists)
Sandhar 1989b 18 0.17 (0.20) 15 0.16 (0.18) 100.0 0.01 [ -0.12, 0.14 ]
Subtotal (95% CI) 18 15 100.0 0.01 [ -0.12, 0.14 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.15 p=0.9
03 Fluids (up to 150 minutes preop) versus Standard Fast
Splinter 1989 40 0.24 (0.31) 40 0.43 (0.46) 38.6 -0.19 [ -0.36, -0.02 ]
Splinter 1990a 30 0.66 (0.79) 16 0.45 (0.31) 30.3 0.21 [ -0.11, 0.53 ]
Splinter 1990b 32 0.71 (0.76) 15 0.45 (0.31) 31.1 0.26 [ -0.05, 0.57 ]
Subtotal (95% CI) 102 71 100.0 0.07 [ -0.25, 0.39 ]
Test for heterogeneity chi-square=8.92 df=2 p=0.01 I² =77.6%
Test for overall effect z=0.43 p=0.7
04 Fluids (up to 180 minutes preop) versus Standard Fast
Gombar 1997 25 0.34 (0.18) 25 0.38 (0.25) 20.2 -0.04 [ -0.16, 0.08 ]
Miller 1990 19 0.23 (0.21) 25 0.41 (0.34) 16.0 -0.18 [ -0.34, -0.02 ]
Moyao-García 2001 20 0.40 (0.29) 20 0.78 (0.44) 10.9 -0.38 [ -0.61, -0.15 ]
Splinter 1991 76 0.46 (0.39) 76 0.48 (0.40) 19.7 -0.02 [ -0.15, 0.11 ]
Splinter Schaefer 2 57 0.34 (0.28) 64 0.39 (0.37) 20.7 -0.05 [ -0.17, 0.07 ]
van der Walt 1986a 30 0.36 (0.33) 11 0.75 (0.67) 4.5 -0.39 [ -0.80, 0.02 ]
van der Walt 1986b 29 0.38 (0.37) 11 0.75 (0.67) 4.5 -0.37 [ -0.79, 0.05 ]
van der Walt 1986c 31 0.83 (0.80) 11 0.75 (0.67) 3.4 0.08 [ -0.41, 0.57 ]
Subtotal (95% CI) 287 243 100.0 -0.12 [ -0.22, -0.03 ]
Test for heterogeneity chi-square=13.74 df=7 p=0.06 I² =49.1%
Test for overall effect z=2.54 p=0.01
05 Fluids (up to 240 minutes preop) versus Standard Fast
Aun 1990 10 0.53 (1.00) 10 0.16 (0.15) 4.6 0.37 [ -0.26, 1.00 ]
Maekawa 1993b 35 0.35 (0.36) 35 0.36 (0.42) 53.6 -0.01 [ -0.19, 0.17 ]
Meakin 1985e 15 0.26 (0.31) 20 0.21 (0.31) 41.8 0.05 [ -0.16, 0.26 ]
Subtotal (95% CI) 60 65 100.0 0.03 [ -0.10, 0.17 ]
Test for heterogeneity chi-square=1.35 df=2 p=0.51 I² =0.0%
Test for overall effect z=0.47 p=0.6
-1.0 -0.5 0 0.5 1.0
Fav Short Fluid Fast Fav Standard Fast
95Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Fig. 2. Comparison 01. Duration - Short Fluid Fast versus Standard Fast
01.03 Gastric contents - pH
Review: Preoperative fasting for preventing perioperative complications in children
Comparison: 01 Duration - Short Fluid Fast versus Standard Fast
Outcome: 03 Gastric contents - pH
Study Short Fluid Fast Standard Fast Weighted Mean Difference (Random) Weight Weighted Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
01 Fluids (up to 120 minutes preop) versus Standard Fast (no H2-receptor antagonists)
Goresky 1992a 48 1.96 (1.18) 51 1.94 (0.93) 1.5 0.02 [ -0.40, 0.44 ]
Maekawa 1993a 27 1.67 (0.65) 25 1.72 (0.48) 2.8 -0.05 [ -0.36, 0.26 ]
Meakin 1985a 31 2.14 (1.31) 14 1.85 (0.29) 1.1 0.29 [ -0.20, 0.78 ]
Nicolson 1992 20 1.90 (0.70) 17 2.00 (0.40) 2.0 -0.10 [ -0.46, 0.26 ]
Sandhar 1989a 12 1.83 (0.85) 10 2.10 (0.96) 0.4 -0.27 [ -1.04, 0.50 ]
Sarti 1991 32 1.70 (0.90) 30 1.60 (1.00) 1.2 0.10 [ -0.37, 0.57 ]
Schreiner 1990 35 1.82 (0.53) 48 1.77 (0.59) 4.5 0.05 [ -0.19, 0.29 ]
Welborn 1993 41 1.45 (0.07) 43 1.41 (0.17) 86.5 0.04 [ -0.02, 0.10 ]
Subtotal (95% CI) 246 238 100.0 0.04 [ -0.01, 0.09 ]
Test for heterogeneity chi-square=2.62 df=7 p=0.92 I² =0.0%
Test for overall effect z=1.41 p=0.2
02 Fluids (up to 120 minutes preop) versus Standard Fast (+ H2-receptor antagonists)
Goresky 1992b 53 4.09 (2.26) 47 3.70 (2.33) 65.7 0.39 [ -0.51, 1.29 ]
Sandhar 1989b 15 4.76 (1.63) 14 3.97 (1.79) 34.3 0.79 [ -0.46, 2.04 ]
Subtotal (95% CI) 68 61 100.0 0.53 [ -0.20, 1.26 ]
Test for heterogeneity chi-square=0.26 df=1 p=0.61 I² =0.0%
Test for overall effect z=1.41 p=0.2
03 Fluids (up to 150 minutes preop) versus Standard Fast
Splinter 1989 40 2.20 (1.20) 40 1.70 (0.60) 31.4 0.50 [ 0.08, 0.92 ]
Splinter 1990a 30 1.70 (0.60) 16 1.70 (0.60) 36.7 0.00 [ -0.36, 0.36 ]
Splinter 1990b 32 1.80 (0.80) 15 1.70 (0.60) 31.9 0.10 [ -0.31, 0.51 ]
Subtotal (95% CI) 102 71 100.0 0.19 [ -0.11, 0.49 ]
Test for heterogeneity chi-square=3.36 df=2 p=0.19 I² =40.5%
Test for overall effect z=1.25 p=0.2
04 Fluids (up to 180 minutes preop) versus Standard Fast
Gombar 1997 24 2.53 (0.79) 25 2.26 (0.57) 17.8 0.27 [ -0.12, 0.66 ]
Miller 1990 19 1.70 (0.60) 25 1.60 (0.70) 17.8 0.10 [ -0.28, 0.48 ]
Moyao-García 2001 20 3.18 (0.61) 20 1.75 (0.38) 18.6 1.43 [ 1.12, 1.74 ]
-4.0 -2.0 0 2.0 4.0
Fav Standard Fast Fav Short Fluid Fast (Continued . . . )
96Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

(. . . Continued)
Study Short Fluid Fast Standard Fast Weighted Mean Difference (Random) Weight Weighted Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
Splinter 1991 76 1.80 (1.00) 76 1.60 (0.40) 19.2 0.20 [ -0.04, 0.44 ]
Splinter Schaefer 2 57 1.80 (0.70) 64 1.70 (0.40) 19.5 0.10 [ -0.11, 0.31 ]
van der Walt 1986a 17 3.25 (1.57) 5 4.27 (2.69) 3.0 -1.02 [ -3.49, 1.45 ]
van der Walt 1986b 15 2.50 (0.89) 4 4.27 (2.94) 2.2 -1.77 [ -4.69, 1.15 ]
van der Walt 1986c 14 4.26 (2.42) 4 4.25 (2.90) 2.0 0.01 [ -3.10, 3.12 ]
Subtotal (95% CI) 242 223 100.0 0.32 [ -0.14, 0.78 ]
Test for heterogeneity chi-square=57.31 df=7 p=<0.0001 I² =87.8%
Test for overall effect z=1.36 p=0.2
05 Fluids (up to 240 minutes preop) versus Standard Fast
Maekawa 1993b 25 1.75 (0.61) 25 1.72 (0.48) 45.7 0.03 [ -0.27, 0.33 ]
Meakin 1985e 12 1.78 (0.42) 14 1.85 (0.28) 54.3 -0.07 [ -0.35, 0.21 ]
Subtotal (95% CI) 37 39 100.0 -0.02 [ -0.23, 0.18 ]
Test for heterogeneity chi-square=0.23 df=1 p=0.64 I² =0.0%
Test for overall effect z=0.23 p=0.8
-4.0 -2.0 0 2.0 4.0
Fav Standard Fast Fav Short Fluid Fast
Fig. 3. Comparison 01. Duration - Short Fluid Fast versus Standard Fast
01.04 Gastric contents - Phenol red based volume (ml)
Review: Preoperative fasting for preventing perioperative complications in children
Comparison: 01 Duration - Short Fluid Fast versus Standard Fast
Outcome: 04 Gastric contents - Phenol red based volume (ml)
Study Short Fluid Fast Standard Fast Weighted Mean Difference (Random) Weight Weighted Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
01 Fluids (up to 180 minutes preop) versus Standard Fast
Miller 1990 19 6.30 (3.40) 25 9.40 (8.20) 100.0 -3.10 [ -6.66, 0.46 ]
Subtotal (95% CI) 19 25 100.0 -3.10 [ -6.66, 0.46 ]
Test for heterogeneity: not applicable
Test for overall effect z=1.71 p=0.09
-10.0 -5.0 0 5.0 10.0
Fav Short Fluid Fast Fav Standard Fast
97Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Fig. 4. Comparison 02. Duration - Short Solid + Fluid Fast versus Standard Fast
02.02 Gastric Contents - Volume (ml/kg)
Review: Preoperative fasting for preventing perioperative complications in children
Comparison: 02 Duration - Short Solid + Fluid Fast versus Standard Fast
Outcome: 02 Gastric Contents - Volume (ml/kg)
Study Short Solid Fast Standard Fast Weighted Mean Difference (Fixed) Weight Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
01 Solids + Fluids (up to 120 minutes preop) versus Standard Fast
Meakin 1985b 32 0.46 (0.34) 20 0.21 (0.31) 100.0 0.25 [ 0.07, 0.43 ]
Subtotal (95% CI) 32 20 100.0 0.25 [ 0.07, 0.43 ]
Test for heterogeneity: not applicable
Test for overall effect z=2.72 p=0.006
02 Solids + Fluids (up to 240 minutes preop) versus Standard Fast
Meakin 1985f 14 0.30 (0.30) 20 0.21 (0.31) 100.0 0.09 [ -0.12, 0.30 ]
Subtotal (95% CI) 14 20 100.0 0.09 [ -0.12, 0.30 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.85 p=0.4
-1.0 -0.5 0 0.5 1.0
Fav Short Solid Fast Fav Standard Fast
Fig. 5. Comparison 02. Duration - Short Solid + Fluid Fast versus Standard Fast
02.03 Gastric Contents - pH
Review: Preoperative fasting for preventing perioperative complications in children
Comparison: 02 Duration - Short Solid + Fluid Fast versus Standard Fast
Outcome: 03 Gastric Contents - pH
Study Short Solid Fast Standard Fast Weighted Mean Difference (Fixed) Weight Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
01 Solids + Fluids (up to 120 minutes preop) versus Standard Fast
Meakin 1985b 29 2.20 (1.11) 14 1.85 (0.28) 100.0 0.35 [ -0.08, 0.78 ]
Subtotal (95% CI) 29 14 100.0 0.35 [ -0.08, 0.78 ]
Test for heterogeneity: not applicable
Test for overall effect z=1.60 p=0.1
02 Solids + Fluids (up to 240 minutes preop) versus Standard Fast
Meakin 1985f 10 1.96 (0.31) 14 1.85 (0.29) 100.0 0.11 [ -0.13, 0.35 ]
Subtotal (95% CI) 10 14 100.0 0.11 [ -0.13, 0.35 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.88 p=0.4
-1.0 -0.5 0 0.5 1.0
Fav Standard Fast Fav Short Solid Fast
98Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Fig. 6. Comparison 03. Duration - Short Solid + Fluid Fast versus Short Fluid Fast
03.02 Gastric Contents - Volume (ml/kg)
Review: Preoperative fasting for preventing perioperative complications in children
Comparison: 03 Duration - Short Solid + Fluid Fast versus Short Fluid Fast
Outcome: 02 Gastric Contents - Volume (ml/kg)
Study Short Solid Fast Short Fluid Fast Weighted Mean Difference (Fixed) Weight Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
01 Solids + Fluids versus Fluids (up to 120 minutes preop)
Meakin 1985c 32 0.46 (0.34) 35 0.37 (0.35) 100.0 0.09 [ -0.08, 0.26 ]
Subtotal (95% CI) 32 35 100.0 0.09 [ -0.08, 0.26 ]
Test for heterogeneity: not applicable
Test for overall effect z=1.07 p=0.3
02 Solids + Fluids versus Fluids (up to 240 minutes preop)
Meakin 1985d 14 0.30 (0.30) 15 0.26 (0.31) 100.0 0.04 [ -0.18, 0.26 ]
Subtotal (95% CI) 14 15 100.0 0.04 [ -0.18, 0.26 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.35 p=0.7
03 Solids + Fluids versus Fluids (up to 330 minutes preop)
Kushikata 1996 10 0.55 (0.59) 10 0.43 (0.32) 100.0 0.12 [ -0.30, 0.54 ]
Subtotal (95% CI) 10 10 100.0 0.12 [ -0.30, 0.54 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.57 p=0.6
-1.0 -0.5 0 0.5 1.0
Fav Short Solid Fast Fav Standard Fast
99Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Fig. 7. Comparison 03. Duration - Short Solid + Fluid Fast versus Short Fluid Fast
03.03 Gastric Contents - pH
Review: Preoperative fasting for preventing perioperative complications in children
Comparison: 03 Duration - Short Solid + Fluid Fast versus Short Fluid Fast
Outcome: 03 Gastric Contents - pH
Study Short Solid Fast Standard Fast Weighted Mean Difference (Fixed) Weight Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
01 Solids + Fluids versus Fluids (up to 120 minutes preop)
Meakin 1985c 29 2.20 (1.16) 31 2.14 (1.32) 100.0 0.06 [ -0.57, 0.69 ]
Subtotal (95% CI) 29 31 100.0 0.06 [ -0.57, 0.69 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.19 p=0.9
02 Solids + Fluids versus Fluids (up to 240 minutes preop)
Meakin 1985d 10 1.96 (0.31) 12 1.78 (0.42) 100.0 0.18 [ -0.13, 0.49 ]
Subtotal (95% CI) 10 12 100.0 0.18 [ -0.13, 0.49 ]
Test for heterogeneity: not applicable
Test for overall effect z=1.15 p=0.2
03 Solids + Fluids versus Fluids (up to 330 minutes preop)
Kushikata 1996 10 1.89 (0.75) 10 1.43 (0.27) 100.0 0.46 [ -0.03, 0.95 ]
Subtotal (95% CI) 10 10 100.0 0.46 [ -0.03, 0.95 ]
Test for heterogeneity: not applicable
Test for overall effect z=1.82 p=0.07
-1.0 -0.5 0 0.5 1.0
Fav Standard Fast Fav Short Solid Fast
100Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd
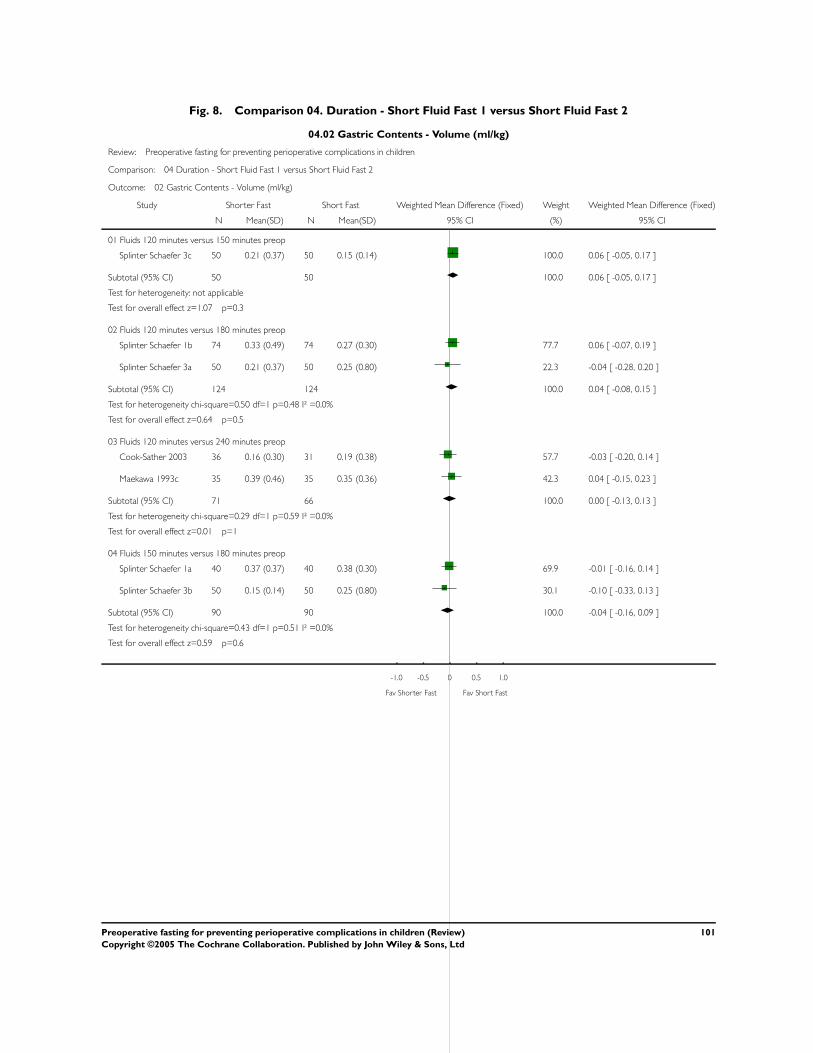
Fig. 8. Comparison 04. Duration - Short Fluid Fast 1 versus Short Fluid Fast 2
04.02 Gastric Contents - Volume (ml/kg)
Review: Preoperative fasting for preventing perioperative complications in children
Comparison: 04 Duration - Short Fluid Fast 1 versus Short Fluid Fast 2
Outcome: 02 Gastric Contents - Volume (ml/kg)
Study Shorter Fast Short Fast Weighted Mean Difference (Fixed) Weight Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
01 Fluids 120 minutes versus 150 minutes preop
Splinter Schaefer 3c 50 0.21 (0.37) 50 0.15 (0.14) 100.0 0.06 [ -0.05, 0.17 ]
Subtotal (95% CI) 50 50 100.0 0.06 [ -0.05, 0.17 ]
Test for heterogeneity: not applicable
Test for overall effect z=1.07 p=0.3
02 Fluids 120 minutes versus 180 minutes preop
Splinter Schaefer 1b 74 0.33 (0.49) 74 0.27 (0.30) 77.7 0.06 [ -0.07, 0.19 ]
Splinter Schaefer 3a 50 0.21 (0.37) 50 0.25 (0.80) 22.3 -0.04 [ -0.28, 0.20 ]
Subtotal (95% CI) 124 124 100.0 0.04 [ -0.08, 0.15 ]
Test for heterogeneity chi-square=0.50 df=1 p=0.48 I² =0.0%
Test for overall effect z=0.64 p=0.5
03 Fluids 120 minutes versus 240 minutes preop
Cook-Sather 2003 36 0.16 (0.30) 31 0.19 (0.38) 57.7 -0.03 [ -0.20, 0.14 ]
Maekawa 1993c 35 0.39 (0.46) 35 0.35 (0.36) 42.3 0.04 [ -0.15, 0.23 ]
Subtotal (95% CI) 71 66 100.0 0.00 [ -0.13, 0.13 ]
Test for heterogeneity chi-square=0.29 df=1 p=0.59 I² =0.0%
Test for overall effect z=0.01 p=1
04 Fluids 150 minutes versus 180 minutes preop
Splinter Schaefer 1a 40 0.37 (0.37) 40 0.38 (0.30) 69.9 -0.01 [ -0.16, 0.14 ]
Splinter Schaefer 3b 50 0.15 (0.14) 50 0.25 (0.80) 30.1 -0.10 [ -0.33, 0.13 ]
Subtotal (95% CI) 90 90 100.0 -0.04 [ -0.16, 0.09 ]
Test for heterogeneity chi-square=0.43 df=1 p=0.51 I² =0.0%
Test for overall effect z=0.59 p=0.6
-1.0 -0.5 0 0.5 1.0
Fav Shorter Fast Fav Short Fast
101Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd
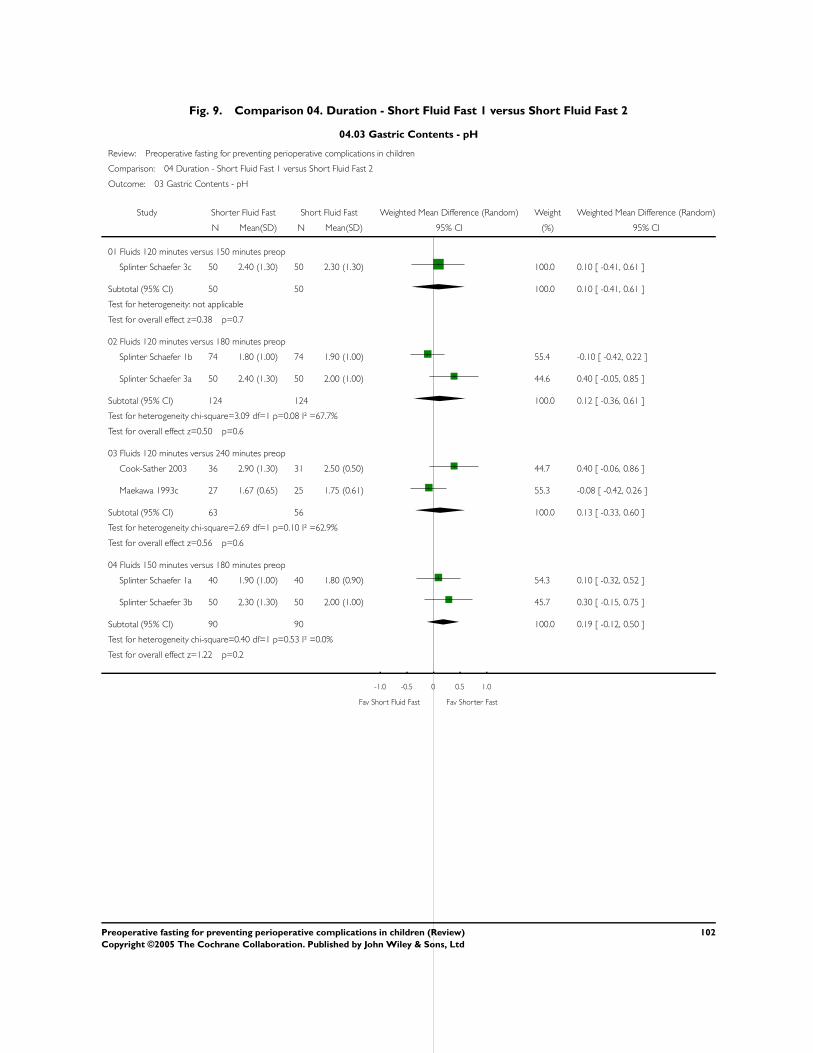
Fig. 9. Comparison 04. Duration - Short Fluid Fast 1 versus Short Fluid Fast 2
04.03 Gastric Contents - pH
Review: Preoperative fasting for preventing perioperative complications in children
Comparison: 04 Duration - Short Fluid Fast 1 versus Short Fluid Fast 2
Outcome: 03 Gastric Contents - pH
Study Shorter Fluid Fast Short Fluid Fast Weighted Mean Difference (Random) Weight Weighted Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
01 Fluids 120 minutes versus 150 minutes preop
Splinter Schaefer 3c 50 2.40 (1.30) 50 2.30 (1.30) 100.0 0.10 [ -0.41, 0.61 ]
Subtotal (95% CI) 50 50 100.0 0.10 [ -0.41, 0.61 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.38 p=0.7
02 Fluids 120 minutes versus 180 minutes preop
Splinter Schaefer 1b 74 1.80 (1.00) 74 1.90 (1.00) 55.4 -0.10 [ -0.42, 0.22 ]
Splinter Schaefer 3a 50 2.40 (1.30) 50 2.00 (1.00) 44.6 0.40 [ -0.05, 0.85 ]
Subtotal (95% CI) 124 124 100.0 0.12 [ -0.36, 0.61 ]
Test for heterogeneity chi-square=3.09 df=1 p=0.08 I² =67.7%
Test for overall effect z=0.50 p=0.6
03 Fluids 120 minutes versus 240 minutes preop
Cook-Sather 2003 36 2.90 (1.30) 31 2.50 (0.50) 44.7 0.40 [ -0.06, 0.86 ]
Maekawa 1993c 27 1.67 (0.65) 25 1.75 (0.61) 55.3 -0.08 [ -0.42, 0.26 ]
Subtotal (95% CI) 63 56 100.0 0.13 [ -0.33, 0.60 ]
Test for heterogeneity chi-square=2.69 df=1 p=0.10 I² =62.9%
Test for overall effect z=0.56 p=0.6
04 Fluids 150 minutes versus 180 minutes preop
Splinter Schaefer 1a 40 1.90 (1.00) 40 1.80 (0.90) 54.3 0.10 [ -0.32, 0.52 ]
Splinter Schaefer 3b 50 2.30 (1.30) 50 2.00 (1.00) 45.7 0.30 [ -0.15, 0.75 ]
Subtotal (95% CI) 90 90 100.0 0.19 [ -0.12, 0.50 ]
Test for heterogeneity chi-square=0.40 df=1 p=0.53 I² =0.0%
Test for overall effect z=1.22 p=0.2
-1.0 -0.5 0 0.5 1.0
Fav Short Fluid Fast Fav Shorter Fast
102Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd
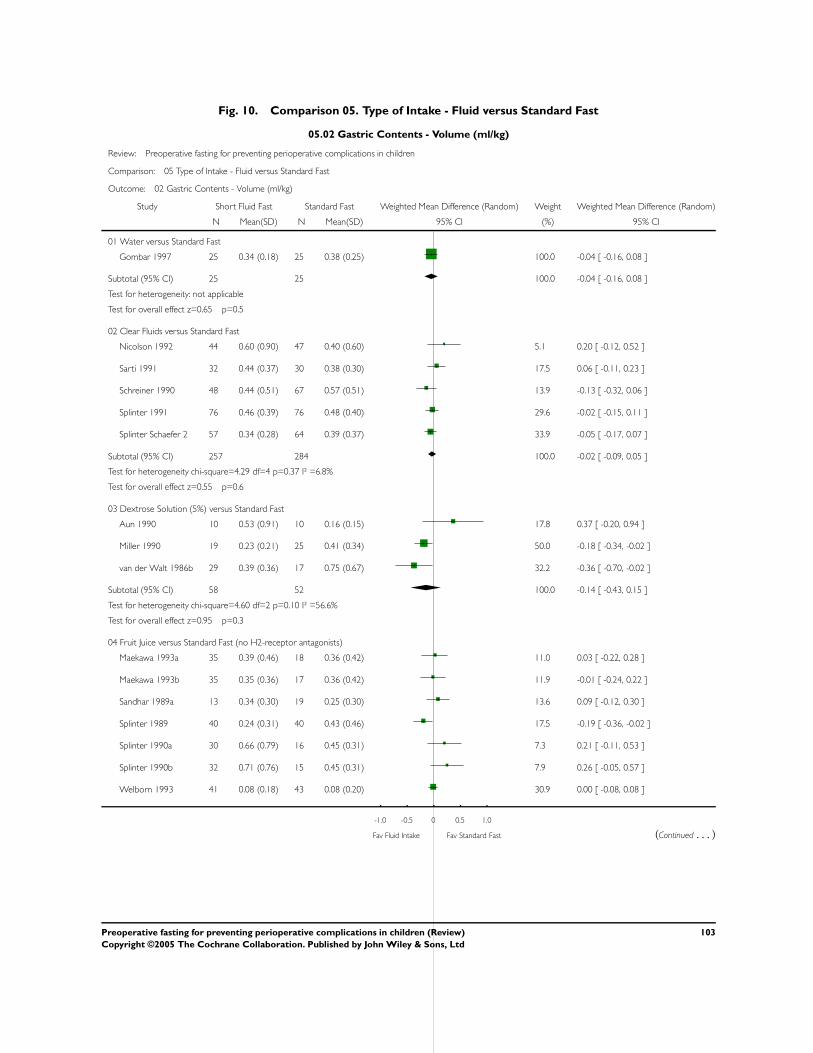
Fig. 10. Comparison 05. Type of Intake - Fluid versus Standard Fast
05.02 Gastric Contents - Volume (ml/kg)
Review: Preoperative fasting for preventing perioperative complications in children
Comparison: 05 Type of Intake - Fluid versus Standard Fast
Outcome: 02 Gastric Contents - Volume (ml/kg)
Study Short Fluid Fast Standard Fast Weighted Mean Difference (Random) Weight Weighted Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
01 Water versus Standard Fast
Gombar 1997 25 0.34 (0.18) 25 0.38 (0.25) 100.0 -0.04 [ -0.16, 0.08 ]
Subtotal (95% CI) 25 25 100.0 -0.04 [ -0.16, 0.08 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.65 p=0.5
02 Clear Fluids versus Standard Fast
Nicolson 1992 44 0.60 (0.90) 47 0.40 (0.60) 5.1 0.20 [ -0.12, 0.52 ]
Sarti 1991 32 0.44 (0.37) 30 0.38 (0.30) 17.5 0.06 [ -0.11, 0.23 ]
Schreiner 1990 48 0.44 (0.51) 67 0.57 (0.51) 13.9 -0.13 [ -0.32, 0.06 ]
Splinter 1991 76 0.46 (0.39) 76 0.48 (0.40) 29.6 -0.02 [ -0.15, 0.11 ]
Splinter Schaefer 2 57 0.34 (0.28) 64 0.39 (0.37) 33.9 -0.05 [ -0.17, 0.07 ]
Subtotal (95% CI) 257 284 100.0 -0.02 [ -0.09, 0.05 ]
Test for heterogeneity chi-square=4.29 df=4 p=0.37 I² =6.8%
Test for overall effect z=0.55 p=0.6
03 Dextrose Solution (5%) versus Standard Fast
Aun 1990 10 0.53 (0.91) 10 0.16 (0.15) 17.8 0.37 [ -0.20, 0.94 ]
Miller 1990 19 0.23 (0.21) 25 0.41 (0.34) 50.0 -0.18 [ -0.34, -0.02 ]
van der Walt 1986b 29 0.39 (0.36) 17 0.75 (0.67) 32.2 -0.36 [ -0.70, -0.02 ]
Subtotal (95% CI) 58 52 100.0 -0.14 [ -0.43, 0.15 ]
Test for heterogeneity chi-square=4.60 df=2 p=0.10 I² =56.6%
Test for overall effect z=0.95 p=0.3
04 Fruit Juice versus Standard Fast (no H2-receptor antagonists)
Maekawa 1993a 35 0.39 (0.46) 18 0.36 (0.42) 11.0 0.03 [ -0.22, 0.28 ]
Maekawa 1993b 35 0.35 (0.36) 17 0.36 (0.42) 11.9 -0.01 [ -0.24, 0.22 ]
Sandhar 1989a 13 0.34 (0.30) 19 0.25 (0.30) 13.6 0.09 [ -0.12, 0.30 ]
Splinter 1989 40 0.24 (0.31) 40 0.43 (0.46) 17.5 -0.19 [ -0.36, -0.02 ]
Splinter 1990a 30 0.66 (0.79) 16 0.45 (0.31) 7.3 0.21 [ -0.11, 0.53 ]
Splinter 1990b 32 0.71 (0.76) 15 0.45 (0.31) 7.9 0.26 [ -0.05, 0.57 ]
Welborn 1993 41 0.08 (0.18) 43 0.08 (0.20) 30.9 0.00 [ -0.08, 0.08 ]
-1.0 -0.5 0 0.5 1.0
Fav Fluid Intake Fav Standard Fast (Continued . . . )
103Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd
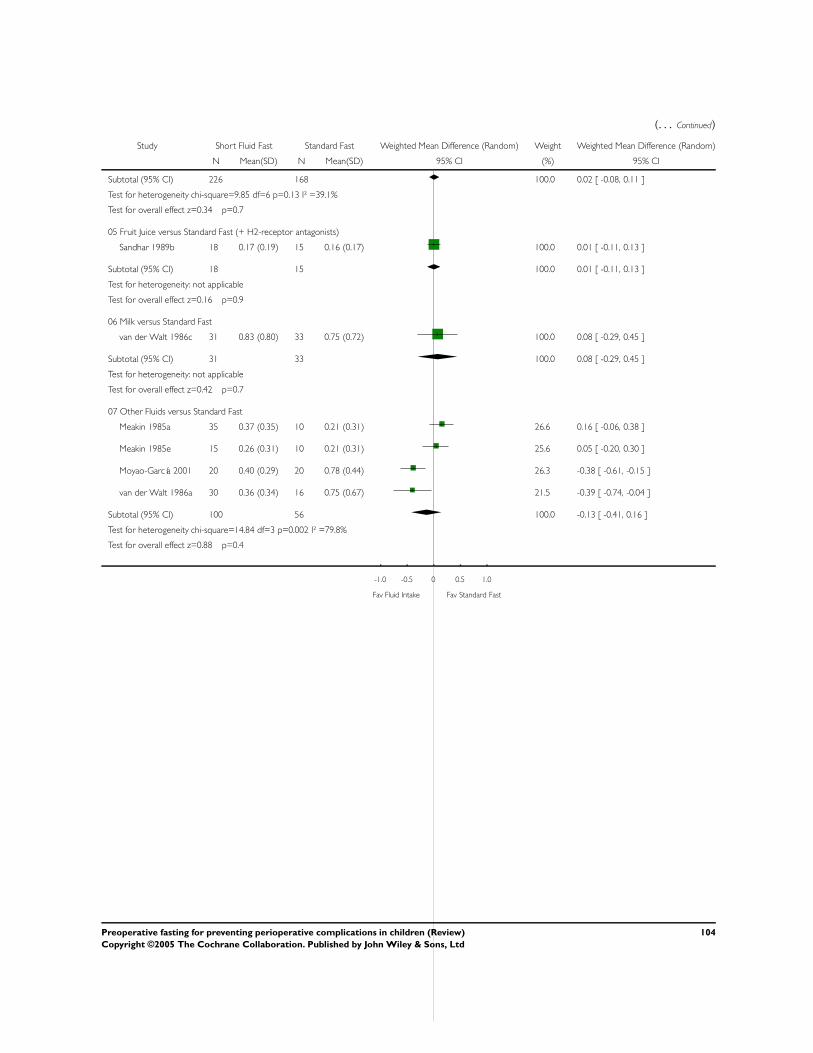
(. . . Continued)
Study Short Fluid Fast Standard Fast Weighted Mean Difference (Random) Weight Weighted Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
Subtotal (95% CI) 226 168 100.0 0.02 [ -0.08, 0.11 ]
Test for heterogeneity chi-square=9.85 df=6 p=0.13 I² =39.1%
Test for overall effect z=0.34 p=0.7
05 Fruit Juice versus Standard Fast (+ H2-receptor antagonists)
Sandhar 1989b 18 0.17 (0.19) 15 0.16 (0.17) 100.0 0.01 [ -0.11, 0.13 ]
Subtotal (95% CI) 18 15 100.0 0.01 [ -0.11, 0.13 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.16 p=0.9
06 Milk versus Standard Fast
van der Walt 1986c 31 0.83 (0.80) 33 0.75 (0.72) 100.0 0.08 [ -0.29, 0.45 ]
Subtotal (95% CI) 31 33 100.0 0.08 [ -0.29, 0.45 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.42 p=0.7
07 Other Fluids versus Standard Fast
Meakin 1985a 35 0.37 (0.35) 10 0.21 (0.31) 26.6 0.16 [ -0.06, 0.38 ]
Meakin 1985e 15 0.26 (0.31) 10 0.21 (0.31) 25.6 0.05 [ -0.20, 0.30 ]
Moyao-García 2001 20 0.40 (0.29) 20 0.78 (0.44) 26.3 -0.38 [ -0.61, -0.15 ]
van der Walt 1986a 30 0.36 (0.34) 16 0.75 (0.67) 21.5 -0.39 [ -0.74, -0.04 ]
Subtotal (95% CI) 100 56 100.0 -0.13 [ -0.41, 0.16 ]
Test for heterogeneity chi-square=14.84 df=3 p=0.002 I² =79.8%
Test for overall effect z=0.88 p=0.4
-1.0 -0.5 0 0.5 1.0
Fav Fluid Intake Fav Standard Fast
104Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Fig. 11. Comparison 05. Type of Intake - Fluid versus Standard Fast
05.03 Gastric contents - pH
Review: Preoperative fasting for preventing perioperative complications in children
Comparison: 05 Type of Intake - Fluid versus Standard Fast
Outcome: 03 Gastric contents - pH
Study Short Fluid Fast Standard Fast Weighted Mean Difference (Random) Weight Weighted Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
01 Water versus Standard Fast
Gombar 1997 24 2.53 (0.79) 25 2.26 (0.57) 100.0 0.27 [ -0.12, 0.66 ]
Subtotal (95% CI) 24 25 100.0 0.27 [ -0.12, 0.66 ]
Test for heterogeneity: not applicable
Test for overall effect z=1.37 p=0.2
02 Clear Fluids versus Standard Fast
Nicolson 1992 20 1.90 (0.70) 17 2.00 (0.40) 11.0 -0.10 [ -0.46, 0.26 ]
Sarti 1991 32 1.70 (0.90) 30 1.60 (1.00) 6.4 0.10 [ -0.37, 0.57 ]
Schreiner 1990 35 1.82 (0.53) 48 1.77 (0.59) 24.5 0.05 [ -0.19, 0.29 ]
Splinter 1991 76 1.80 (1.00) 76 1.60 (0.40) 24.5 0.20 [ -0.04, 0.44 ]
Splinter Schaefer 2 57 1.80 (0.70) 64 1.70 (0.40) 33.7 0.10 [ -0.11, 0.31 ]
Subtotal (95% CI) 220 235 100.0 0.09 [ -0.03, 0.21 ]
Test for heterogeneity chi-square=1.97 df=4 p=0.74 I² =0.0%
Test for overall effect z=1.48 p=0.1
03 Dextrose Solution (5%) versus Standard Fast
Miller 1990 19 1.70 (0.60) 25 1.60 (0.70) 66.8 0.10 [ -0.28, 0.48 ]
van der Walt 1986b 15 2.50 (0.88) 6 4.24 (2.60) 33.2 -1.74 [ -3.87, 0.39 ]
Subtotal (95% CI) 34 31 100.0 -0.51 [ -2.21, 1.19 ]
Test for heterogeneity chi-square=2.78 df=1 p=0.10 I² =64.1%
Test for overall effect z=0.59 p=0.6
04 Fruit Juice versus Standard Fast (no H2-receptor antagonist)
Goresky 1992a 48 1.96 (1.18) 51 1.94 (0.93) 1.5 0.02 [ -0.40, 0.44 ]
Maekawa 1993a 27 1.67 (0.65) 13 1.72 (0.48) 2.1 -0.05 [ -0.41, 0.31 ]
Maekawa 1993b 25 1.75 (0.61) 12 1.72 (0.48) 2.1 0.03 [ -0.33, 0.39 ]
Sandhar 1989a 12 1.83 (0.80) 10 2.10 (0.93) 0.5 -0.27 [ -1.00, 0.46 ]
Splinter 1989 40 2.20 (1.20) 40 1.70 (0.60) 1.6 0.50 [ 0.08, 0.92 ]
Splinter 1990a 30 1.70 (0.60) 15 1.70 (0.60) 1.9 0.00 [ -0.37, 0.37 ]
Splinter 1990b 32 1.80 (0.80) 16 1.70 (0.60) 1.7 0.10 [ -0.30, 0.50 ]
Welborn 1993 41 1.45 (0.07) 43 1.41 (0.17) 88.6 0.04 [ -0.02, 0.10 ]
-4.0 -2.0 0 2.0 4.0
Fav Standard Fast Fav Fluid Intake (Continued . . . )
105Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

(. . . Continued)
Study Short Fluid Fast Standard Fast Weighted Mean Difference (Random) Weight Weighted Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
Subtotal (95% CI) 255 200 100.0 0.04 [ -0.01, 0.10 ]
Test for heterogeneity chi-square=5.76 df=7 p=0.57 I² =0.0%
Test for overall effect z=1.64 p=0.1
05 Fruit Juice versus Standard Fast (+H2- receptor antagonist)
Goresky 1992b 53 4.09 (2.26) 47 3.70 (2.33) 64.7 0.39 [ -0.51, 1.29 ]
Sandhar 1989b 15 4.76 (1.64) 14 3.97 (1.71) 35.3 0.79 [ -0.43, 2.01 ]
Subtotal (95% CI) 68 61 100.0 0.53 [ -0.19, 1.26 ]
Test for heterogeneity chi-square=0.27 df=1 p=0.61 I² =0.0%
Test for overall effect z=1.43 p=0.2
06 Milk versus Standard Fast
van der Walt 1986c 14 4.24 (2.43) 13 4.25 (2.38) 100.0 -0.01 [ -1.82, 1.80 ]
Subtotal (95% CI) 14 13 100.0 -0.01 [ -1.82, 1.80 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.01 p=1
07 Other Fluids versus Standard Fast
Meakin 1985a 31 2.15 (1.33) 7 1.87 (0.35) 27.9 0.28 [ -0.26, 0.82 ]
Meakin 1985e 12 1.78 (0.42) 7 1.87 (0.35) 29.3 -0.09 [ -0.44, 0.26 ]
Moyao-García 2001 20 3.18 (0.61) 20 1.75 (0.38) 29.6 1.43 [ 1.12, 1.74 ]
van der Walt 1986a 17 3.25 (1.56) 7 4.25 (2.51) 13.2 -1.00 [ -3.00, 1.00 ]
Subtotal (95% CI) 80 41 100.0 0.34 [ -0.62, 1.31 ]
Test for heterogeneity chi-square=45.01 df=3 p=<0.0001 I² =93.3%
Test for overall effect z=0.69 p=0.5
-4.0 -2.0 0 2.0 4.0
Fav Standard Fast Fav Fluid Intake
106Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Fig. 12. Comparison 05. Type of Intake - Fluid versus Standard Fast
05.04 Gastric contents - Phenol red based volume (ml)
Review: Preoperative fasting for preventing perioperative complications in children
Comparison: 05 Type of Intake - Fluid versus Standard Fast
Outcome: 04 Gastric contents - Phenol red based volume (ml)
Study Treatment Control Weighted Mean Difference (Fixed) Weight Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
01 Dextrose Solution (5%) versus Standard Fast
Miller 1990 19 6.30 (3.40) 25 9.40 (8.20) 100.0 -3.10 [ -6.66, 0.46 ]
Total (95% CI) 19 25 100.0 -3.10 [ -6.66, 0.46 ]
Test for heterogeneity: not applicable
Test for overall effect z=1.71 p=0.09
-10.0 -5.0 0 5.0 10.0
Favours treatment Favours control
Fig. 13. Comparison 06. Type of Intake - Fluid 1 versus Fluid 2
06.02 Gastric Contents - Volume (ml/kg)
Review: Preoperative fasting for preventing perioperative complications in children
Comparison: 06 Type of Intake - Fluid 1 versus Fluid 2
Outcome: 02 Gastric Contents - Volume (ml/kg)
Study Fluid 1 Fluid 2 Weighted Mean Difference (Fixed) Weight Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
01 Dextrose versus Poly-joule
van der Walt 1986d 29 0.39 (0.36) 30 0.36 (0.33) 100.0 0.03 [ -0.15, 0.21 ]
Subtotal (95% CI) 29 30 100.0 0.03 [ -0.15, 0.21 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.33 p=0.7
02 Dextrose versus Cows’ milk
van der Walt 1986e 29 0.39 (0.36) 31 0.83 (0.79) 100.0 -0.44 [ -0.75, -0.13 ]
Subtotal (95% CI) 29 31 100.0 -0.44 [ -0.75, -0.13 ]
Test for heterogeneity: not applicable
Test for overall effect z=2.81 p=0.005
03 Poly-joule versus Cows’ Milk
van der Walt 1986f 30 0.36 (0.34) 31 0.83 (0.81) 100.0 -0.47 [ -0.78, -0.16 ]
Subtotal (95% CI) 30 31 100.0 -0.47 [ -0.78, -0.16 ]
Test for heterogeneity: not applicable
Test for overall effect z=2.97 p=0.003
-1.0 -0.5 0 0.5 1.0
Favours Fluid 1 Favours Fluid 2
107Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Fig. 14. Comparison 06. Type of Intake - Fluid 1 versus Fluid 2
06.03 Gastric Contents - pH
Review: Preoperative fasting for preventing perioperative complications in children
Comparison: 06 Type of Intake - Fluid 1 versus Fluid 2
Outcome: 03 Gastric Contents - pH
Study Fluid 1 Fluid 2 Weighted Mean Difference (Fixed) Weight Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
01 Dextrose versus Polyjoule
van der Walt 1986d 15 2.50 (0.88) 17 3.25 (1.58) 100.0 -0.75 [ -1.62, 0.12 ]
Subtotal (95% CI) 15 17 100.0 -0.75 [ -1.62, 0.12 ]
Test for heterogeneity: not applicable
Test for overall effect z=1.68 p=0.09
02 Dextrose versus Cows’ milk
van der Walt 1986e 15 2.50 (0.89) 14 4.24 (2.43) 100.0 -1.74 [ -3.09, -0.39 ]
Subtotal (95% CI) 15 14 100.0 -1.74 [ -3.09, -0.39 ]
Test for heterogeneity: not applicable
Test for overall effect z=2.53 p=0.01
03 Poly-Joule versus Cows’ Milk
van der Walt 1986f 17 3.25 (1.56) 14 4.26 (2.45) 100.0 -1.01 [ -2.49, 0.47 ]
Subtotal (95% CI) 17 14 100.0 -1.01 [ -2.49, 0.47 ]
Test for heterogeneity: not applicable
Test for overall effect z=1.34 p=0.2
-4.0 -2.0 0 2.0 4.0
Favours Fluid 2 Favours Fluid 1
108Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd
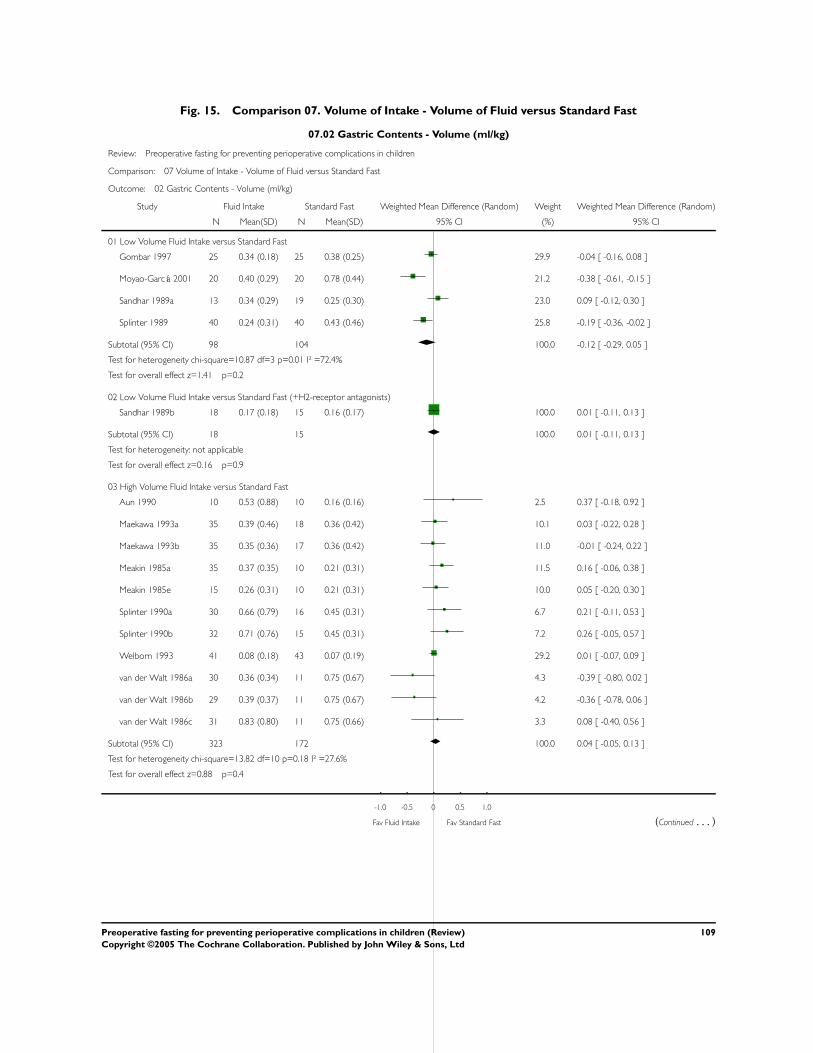
Fig. 15. Comparison 07. Volume of Intake - Volume of Fluid versus Standard Fast
07.02 Gastric Contents - Volume (ml/kg)
Review: Preoperative fasting for preventing perioperative complications in children
Comparison: 07 Volume of Intake - Volume of Fluid versus Standard Fast
Outcome: 02 Gastric Contents - Volume (ml/kg)
Study Fluid Intake Standard Fast Weighted Mean Difference (Random) Weight Weighted Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
01 Low Volume Fluid Intake versus Standard Fast
Gombar 1997 25 0.34 (0.18) 25 0.38 (0.25) 29.9 -0.04 [ -0.16, 0.08 ]
Moyao-García 2001 20 0.40 (0.29) 20 0.78 (0.44) 21.2 -0.38 [ -0.61, -0.15 ]
Sandhar 1989a 13 0.34 (0.29) 19 0.25 (0.30) 23.0 0.09 [ -0.12, 0.30 ]
Splinter 1989 40 0.24 (0.31) 40 0.43 (0.46) 25.8 -0.19 [ -0.36, -0.02 ]
Subtotal (95% CI) 98 104 100.0 -0.12 [ -0.29, 0.05 ]
Test for heterogeneity chi-square=10.87 df=3 p=0.01 I² =72.4%
Test for overall effect z=1.41 p=0.2
02 Low Volume Fluid Intake versus Standard Fast (+H2-receptor antagonists)
Sandhar 1989b 18 0.17 (0.18) 15 0.16 (0.17) 100.0 0.01 [ -0.11, 0.13 ]
Subtotal (95% CI) 18 15 100.0 0.01 [ -0.11, 0.13 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.16 p=0.9
03 High Volume Fluid Intake versus Standard Fast
Aun 1990 10 0.53 (0.88) 10 0.16 (0.16) 2.5 0.37 [ -0.18, 0.92 ]
Maekawa 1993a 35 0.39 (0.46) 18 0.36 (0.42) 10.1 0.03 [ -0.22, 0.28 ]
Maekawa 1993b 35 0.35 (0.36) 17 0.36 (0.42) 11.0 -0.01 [ -0.24, 0.22 ]
Meakin 1985a 35 0.37 (0.35) 10 0.21 (0.31) 11.5 0.16 [ -0.06, 0.38 ]
Meakin 1985e 15 0.26 (0.31) 10 0.21 (0.31) 10.0 0.05 [ -0.20, 0.30 ]
Splinter 1990a 30 0.66 (0.79) 16 0.45 (0.31) 6.7 0.21 [ -0.11, 0.53 ]
Splinter 1990b 32 0.71 (0.76) 15 0.45 (0.31) 7.2 0.26 [ -0.05, 0.57 ]
Welborn 1993 41 0.08 (0.18) 43 0.07 (0.19) 29.2 0.01 [ -0.07, 0.09 ]
van der Walt 1986a 30 0.36 (0.34) 11 0.75 (0.67) 4.3 -0.39 [ -0.80, 0.02 ]
van der Walt 1986b 29 0.39 (0.37) 11 0.75 (0.67) 4.2 -0.36 [ -0.78, 0.06 ]
van der Walt 1986c 31 0.83 (0.80) 11 0.75 (0.66) 3.3 0.08 [ -0.40, 0.56 ]
Subtotal (95% CI) 323 172 100.0 0.04 [ -0.05, 0.13 ]
Test for heterogeneity chi-square=13.82 df=10 p=0.18 I² =27.6%
Test for overall effect z=0.88 p=0.4
-1.0 -0.5 0 0.5 1.0
Fav Fluid Intake Fav Standard Fast (Continued . . . )
109Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

(. . . Continued)
Study Fluid Intake Standard Fast Weighted Mean Difference (Random) Weight Weighted Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
05 Unlimited Fluid Intake versus Standard Fast
Nicolson 1992 44 0.60 (0.90) 47 0.40 (0.60) 5.1 0.20 [ -0.12, 0.52 ]
Sarti 1991 32 0.44 (0.37) 30 0.38 (0.30) 17.5 0.06 [ -0.11, 0.23 ]
Schreiner 1990 48 0.44 (0.51) 67 0.57 (0.51) 13.9 -0.13 [ -0.32, 0.06 ]
Splinter 1991 76 0.46 (0.39) 76 0.48 (0.40) 29.6 -0.02 [ -0.15, 0.11 ]
Splinter Schaefer 2 57 0.34 (0.28) 64 0.39 (0.37) 33.9 -0.05 [ -0.17, 0.07 ]
Subtotal (95% CI) 257 284 100.0 -0.02 [ -0.09, 0.05 ]
Test for heterogeneity chi-square=4.29 df=4 p=0.37 I² =6.8%
Test for overall effect z=0.55 p=0.6
-1.0 -0.5 0 0.5 1.0
Fav Fluid Intake Fav Standard Fast
Fig. 16. Comparison 07. Volume of Intake - Volume of Fluid versus Standard Fast
07.03 Gastric contents - pH values
Review: Preoperative fasting for preventing perioperative complications in children
Comparison: 07 Volume of Intake - Volume of Fluid versus Standard Fast
Outcome: 03 Gastric contents - pH values
Study Fluid Intake Standard Fast Weighted Mean Difference (Random) Weight Weighted Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
01 Low Volume Fluid Intake versus Standard Fast
Gombar 1997 24 2.53 (0.79) 25 2.26 (0.57) 20.8 0.27 [ -0.12, 0.66 ]
Goresky 1992a 48 1.96 (1.18) 51 1.94 (0.93) 20.5 0.02 [ -0.40, 0.44 ]
Moyao-García 2001 20 3.18 (0.61) 20 1.75 (0.38) 21.4 1.43 [ 1.12, 1.74 ]
Sandhar 1989a 12 1.83 (0.84) 10 2.10 (0.96) 16.8 -0.27 [ -1.03, 0.49 ]
Splinter 1989 40 2.20 (1.20) 40 1.70 (0.60) 20.5 0.50 [ 0.08, 0.92 ]
Subtotal (95% CI) 144 146 100.0 0.42 [ -0.19, 1.04 ]
Test for heterogeneity chi-square=41.94 df=4 p=<0.0001 I² =90.5%
Test for overall effect z=1.35 p=0.2
02 Low Volume Fluid Intake versus Standard Fast (+H2-receptor antagonists)
Goresky 1992b 53 4.09 (2.26) 47 3.70 (2.33) 63.9 0.39 [ -0.51, 1.29 ]
Sandhar 1989b 15 4.76 (1.60) 14 3.97 (1.69) 36.1 0.79 [ -0.41, 1.99 ]
Subtotal (95% CI) 68 61 100.0 0.53 [ -0.19, 1.26 ]
Test for heterogeneity chi-square=0.27 df=1 p=0.60 I² =0.0%
-4.0 -2.0 0 2.0 4.0
Fav Standard Fast Fav Fluid Intake (Continued . . . )
110Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

(. . . Continued)
Study Fluid Intake Standard Fast Weighted Mean Difference (Random) Weight Weighted Mean Difference (Random)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
Test for overall effect z=1.45 p=0.1
03 High Volume Fluid Intake versus Standard Fast
Maekawa 1993a 27 1.67 (0.65) 13 1.72 (0.48) 2.1 -0.05 [ -0.41, 0.31 ]
Maekawa 1993b 25 1.75 (0.61) 12 1.72 (0.48) 2.1 0.03 [ -0.33, 0.39 ]
Meakin 1985a 31 2.15 (1.30) 7 1.87 (0.35) 1.0 0.28 [ -0.25, 0.81 ]
Meakin 1985e 12 1.78 (0.42) 7 1.88 (0.35) 2.2 -0.10 [ -0.45, 0.25 ]
Splinter 1990a 30 1.70 (0.60) 16 1.70 (0.60) 2.0 0.00 [ -0.36, 0.36 ]
Splinter 1990b 32 1.80 (0.80) 15 1.70 (0.60) 1.6 0.10 [ -0.31, 0.51 ]
Welborn 1993 41 1.45 (0.07) 43 1.41 (0.17) 88.9 0.04 [ -0.02, 0.10 ]
van der Walt 1986a 17 3.25 (1.57) 5 4.25 (2.71) 0.0 -1.00 [ -3.49, 1.49 ]
van der Walt 1986b 15 2.50 (0.89) 4 4.24 (2.90) 0.0 -1.74 [ -4.62, 1.14 ]
van der Walt 1986c 14 4.25 (2.44) 4 4.25 (2.92) 0.0 0.00 [ -3.13, 3.13 ]
Subtotal (95% CI) 244 126 100.0 0.04 [ -0.02, 0.09 ]
Test for heterogeneity chi-square=3.90 df=9 p=0.92 I² =0.0%
Test for overall effect z=1.37 p=0.2
05 Unlimited Fluid Intake versus Standard Fast
Nicolson 1992 20 1.90 (0.70) 17 2.00 (0.40) 11.0 -0.10 [ -0.46, 0.26 ]
Sarti 1991 32 1.70 (0.90) 30 1.60 (1.00) 6.4 0.10 [ -0.37, 0.57 ]
Schreiner 1990 35 1.82 (0.53) 48 1.77 (0.59) 24.5 0.05 [ -0.19, 0.29 ]
Splinter 1991 76 1.80 (1.00) 76 1.60 (0.40) 24.5 0.20 [ -0.04, 0.44 ]
Splinter Schaefer 2 57 1.80 (0.70) 64 1.70 (0.40) 33.7 0.10 [ -0.11, 0.31 ]
Subtotal (95% CI) 220 235 100.0 0.09 [ -0.03, 0.21 ]
Test for heterogeneity chi-square=1.97 df=4 p=0.74 I² =0.0%
Test for overall effect z=1.48 p=0.1
-4.0 -2.0 0 2.0 4.0
Fav Standard Fast Fav Fluid Intake
111Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Fig. 17. Comparison 08. Volume of Intake - Volume 1 versus Volume 2
08.02 Gastric Contents - Volume (ml/kg)
Review: Preoperative fasting for preventing perioperative complications in children
Comparison: 08 Volume of Intake - Volume 1 versus Volume 2
Outcome: 02 Gastric Contents - Volume (ml/kg)
Study Volume 1 Volume 2 Weighted Mean Difference (Fixed) Weight Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
01 6 ml/kg versus 10 ml/kg of apple juice 150 minutes preop
Splinter 1990c 30 0.66 (0.79) 32 0.71 (0.76) 100.0 -0.05 [ -0.44, 0.34 ]
Subtotal (95% CI) 30 32 100.0 -0.05 [ -0.44, 0.34 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.25 p=0.8
-1.0 -0.5 0 0.5 1.0
Favours Fluid 1 Favours Fluid 2
Fig. 18. Comparison 08. Volume of Intake - Volume 1 versus Volume 2
08.03 Gastric contents - pH
Review: Preoperative fasting for preventing perioperative complications in children
Comparison: 08 Volume of Intake - Volume 1 versus Volume 2
Outcome: 03 Gastric contents - pH
Study Volume 1 Volume 2 Weighted Mean Difference (Fixed) Weight Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
01 6 ml/kg versus 10 ml/kg of apple juice 150 minutes preop
Splinter 1990c 30 1.70 (0.60) 32 1.80 (0.80) 100.0 -0.10 [ -0.45, 0.25 ]
Subtotal (95% CI) 30 32 100.0 -0.10 [ -0.45, 0.25 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.56 p=0.6
-1.0 -0.5 0 0.5 1.0
Favours Fluid 2 Favours Fluid 1
112Preoperative fasting for preventing perioperative complications in children (Review)
Copyright ©2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd
Copyright © 2022 FDOKUMEN