
Preoperative concurrent 5Fluorouracil infusion, Mitomycin C and pelvic radiation therapy in tethered...
9
Inr J Radrarm Oncoluny Blol Phys Vol. 25. PP. 791-799 Printed in the USA All rights reserved. 0360-3016/93 $6.00 + .I0 Copyright 0 1993 Pergamon Press Ltd. ??Clinical Original Contribution PREOPERATIVE CONCURRENT 5FLUOROURACIL INFUSION, MITOMYCIN C AND PELVIC RADIATION THERAPY IN TETHERED AND FIXED RECTAL CARCINOMA ALEXANDER CHAN, M.D.,’ ALFRED WONG, M.D.,2 JAMES LANGEVIN, M.D.3 AND ROBERT KHOO, M.D.3 ‘Departments of Radiation Oncology, ‘Medical Oncology, 3Surgery.Tom Baker Cancer Centre, Calgary, Alberta, Canada Purpose: This is a Phase I/II study of preoperative concurrent radiation and chemotherapy in tethered and fixed rectal carcinoma. This study examined the curative resectability, the acute toxicities during chemo-radiation and the surgical complications. Methods and Materials: Between 1986 and 1990,46 patients were treated with preoperative pelvic radiation (4000 cGy in 20 fractions in 4 weeks), 5Fluorouracil infusion (20 mg/m’, days l-4 and 15-18) and Mitomycin C (8 mg/ m’, day 1). This was followed by surgery 6 to 8 weeks later. 30 patients had tethered tumors and 16 patients had fixed tumors. Results: After preoperative chemo-radiation, 41 patients (89%) underwent curative resection. TWO patients (4%) had no residual tumor found (TONOMO). Seven patients (15%) had nodal metastases. Two patients developed grade 3 neutropenia (WBC = l-2 X 109/L) during chemo-radiation. Five patients had delay in perineal wound healing. One patient had an anastomotic leak. Four patients developed stoma1 stenosis which required surgical revision. The 2-year actuarial survival was 73%. The 2-year local relapse rate was 16%. Patients with fixed carcinoma had a higher incidence of local failure (38% vs. 10%) and the difference was statistically significant (p = 0.0036). The 2-year distant failure rate was 41%, and the rates were similar for both tethered and fixed carcinomas. Conclusion: Preoperative pelvic radiation, chemotherapy and surgery could achieve a curative resection rate of 89% in tethered and fixed rectal carcinomas. However, distant metastases remained the major cause of failure. Preoperative, Chemotherapy, Radiation therapy, Rectal Cancers, Resectability, Toxicity. INTRODUCTION In spite of advances made in surgical techniques in the management of rectal carcinoma, 20-40% of the tumors recur locally after potentially curative resection (5,24,25, 30,32, 36, 37). This has led to increasing employment of adjuvant radiation therapy, either preoperatively or post- operatively, to try to improve the outcome. Low dose preoperative radiation therapy of 500-2000 cGy had not shown significant benefit (8,9, 10, 38). More recent trials using a higher radiation dose of 2500-5000 cGy have demonstrated benefit in local disease control (14, 16, 17, 18, 21, 31, 41). Preoperative radiation therapy is particularly appealing for locally advanced rectal carcinoma. It can potentially shrink the primary tumor and improve resectability (7, 12, 15, 27, 34). In the clinico-pathological review of the British MRC trial, (10) Duncan et al. found that tumor mobility was the single most important pretreatment prognostic factor for survival and disease-free survival. Fixation significantly reduced the probability of achieving a curative resection. The curative resection rate for teth- ered cancers was 44%, and the 5-year local disease-free rate was only 37%. Therefore, this subgroup of patients with tethered and fixed tumors constitutes an appropriate population for study of the efficacy of preoperative therapy in rectal cancers. In 1986, we designed a protocol of pre- operative concurrent chemotherapy and pelvic radiation therapy for tethered or fixed rectal adenocarcinomas which were either unresectable or of doubtful curative resectability. Concurrent 5-Fluorouracil infusion and Mitomycin C were given for their potential radiation en- hancement effect (4, 39). The present report summarizes our initial experience with this preoperative chemo-ra- diation regimen, with emphasis on the curative resecta- bility, the acute toxicities during chemo-radiation, and the surgical complications in the perioperative and post- operative period. Reprint requests to: Alexander Chan, M.D., Department of Radiation Oncology, Tom Baker Cancer Centre, 1331 29 St. N.W., Calgary, Alberta, T2N 4N2 Canada. Accepted for publication 25 September 1992. 791
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Preoperative concurrent 5Fluorouracil infusion, Mitomycin C and pelvic radiation therapy in tethered...

Inr J Radrarm Oncoluny Blol Phys Vol. 25. PP. 791-799 Printed in the USA All rights reserved.
0360-3016/93 $6.00 + .I0
Copyright 0 1993 Pergamon Press Ltd.
??Clinical Original Contribution
PREOPERATIVE CONCURRENT 5FLUOROURACIL INFUSION, MITOMYCIN C AND PELVIC RADIATION THERAPY IN TETHERED
AND FIXED RECTAL CARCINOMA
ALEXANDER CHAN, M.D.,’ ALFRED WONG, M.D.,2 JAMES LANGEVIN, M.D.3 AND ROBERT KHOO, M.D.3
‘Departments of Radiation Oncology, ‘Medical Oncology, 3Surgery. Tom Baker Cancer Centre, Calgary, Alberta, Canada
Purpose: This is a Phase I/II study of preoperative concurrent radiation and chemotherapy in tethered and fixed rectal carcinoma. This study examined the curative resectability, the acute toxicities during chemo-radiation and the surgical complications. Methods and Materials: Between 1986 and 1990,46 patients were treated with preoperative pelvic radiation (4000 cGy in 20 fractions in 4 weeks), 5Fluorouracil infusion (20 mg/m’, days l-4 and 15-18) and Mitomycin C (8 mg/ m’, day 1). This was followed by surgery 6 to 8 weeks later. 30 patients had tethered tumors and 16 patients had fixed tumors. Results: After preoperative chemo-radiation, 41 patients (89%) underwent curative resection. TWO patients (4%) had no residual tumor found (TONOMO). Seven patients (15%) had nodal metastases. Two patients developed grade 3 neutropenia (WBC = l-2 X 109/L) during chemo-radiation. Five patients had delay in perineal wound healing. One patient had an anastomotic leak. Four patients developed stoma1 stenosis which required surgical revision. The 2-year actuarial survival was 73%. The 2-year local relapse rate was 16%. Patients with fixed carcinoma had a higher incidence of local failure (38% vs. 10%) and the difference was statistically significant (p = 0.0036). The 2-year distant failure rate was 41%, and the rates were similar for both tethered and fixed carcinomas. Conclusion: Preoperative pelvic radiation, chemotherapy and surgery could achieve a curative resection rate of 89% in tethered and fixed rectal carcinomas. However, distant metastases remained the major cause of failure.
Preoperative, Chemotherapy, Radiation therapy, Rectal Cancers, Resectability, Toxicity.
INTRODUCTION
In spite of advances made in surgical techniques in the management of rectal carcinoma, 20-40% of the tumors recur locally after potentially curative resection (5,24,25, 30,32, 36, 37). This has led to increasing employment of adjuvant radiation therapy, either preoperatively or post- operatively, to try to improve the outcome. Low dose preoperative radiation therapy of 500-2000 cGy had not shown significant benefit (8,9, 10, 38). More recent trials using a higher radiation dose of 2500-5000 cGy have demonstrated benefit in local disease control (14, 16, 17, 18, 21, 31, 41).
Preoperative radiation therapy is particularly appealing for locally advanced rectal carcinoma. It can potentially shrink the primary tumor and improve resectability (7, 12, 15, 27, 34). In the clinico-pathological review of the British MRC trial, (10) Duncan et al. found that tumor mobility was the single most important pretreatment
prognostic factor for survival and disease-free survival. Fixation significantly reduced the probability of achieving a curative resection. The curative resection rate for teth- ered cancers was 44%, and the 5-year local disease-free rate was only 37%. Therefore, this subgroup of patients with tethered and fixed tumors constitutes an appropriate population for study of the efficacy of preoperative therapy in rectal cancers. In 1986, we designed a protocol of pre- operative concurrent chemotherapy and pelvic radiation therapy for tethered or fixed rectal adenocarcinomas which were either unresectable or of doubtful curative resectability. Concurrent 5-Fluorouracil infusion and Mitomycin C were given for their potential radiation en- hancement effect (4, 39). The present report summarizes our initial experience with this preoperative chemo-ra- diation regimen, with emphasis on the curative resecta- bility, the acute toxicities during chemo-radiation, and the surgical complications in the perioperative and post- operative period.
Reprint requests to: Alexander Chan, M.D., Department of Radiation Oncology, Tom Baker Cancer Centre, 1331 29 St. N.W., Calgary, Alberta, T2N 4N2 Canada.
Accepted for publication 25 September 1992.
791

792 I. J. Radiation Oncology 0 Biology 0 Physics Volume 25, Number 5. 1993
METHODS AND MATERIALS
Patient population Between June 1986 and May 1990, 48 patients with
tethered or fixed rectal adenocarcinoma seen in the Tom Baker Cancer Center were considered for preoperative concurrent chemotherapy and pelvic radiation therapy. Of these 48 patients, 46 were enrolled in the protocol. Two patients were excluded because of hepatic metastases found during their staging assessment.
There were 37 males and 9 females. Their age ranged from 32 to 82 years, with a median age of 63 years. They all had biopsy-proven adenocarcinomas of the rectum which were judged to be unresectable or borderline-re- sectable by the referring surgeons. All tumors were located within 15 cm of the anal verge, and 63% were in the low rectum. (Table 1)
All tumors were adherent to adjacent structures by clinical assessment. Sites of adherence included vagina (6), prostate/bladder ( 19), sacrum ( 1 O), perirectal tissue/ pelvis (25), and gluteal musculature (1). Some tumors were adherent to multiple sites. Thirty patients had tethered tumors with some mobility in at least one direction. Six- teen patients had fixed tumors. In 39 patients, the tumor was palpable by digital examination. In the remaining seven patients, adherence or invasion of adjacent struc- tures was established by endoscopy, cystoscopy or lapa- rotomy.
Fifteen of the 46 patients had a pretreatment CT scan of the pelvis. Twelve patients had an endorectal ultrasound study which demonstrated tumor infiltration beyond the muscularis layer. Endorectal ultrasound studies were at- tempted in others, and were unsuccessful because of sig- nificant luminal obstruction by tumor. Forty-three pa- tients had a pretreatment CEA assay (Table 1). All 46
Table 1. Pretreatment natients characteristics
Characteristics No.
Sex Males Females
Age: Median: Range:
Tumor location (from the anus) I 5 cm 6-10 cm 11-13 cm
Degree of adherence Fixed Tethered
Pretreatment <5&L >5wg/L Not done
Grade of tumors Well-differentiated Moderately-differentiated Poorly-differentiated
31 9
63 years 32-82 years
29 14 3
16 30
33 10 3
11 30 5
patients had a normal pretreatment chest x-ray and liver ultrasonography or nucleotide scan. The mean pretreat- ment WBC count was 6.5 X 109/L (range: 2.6-12.7 X 109). The mean platelet count was 286 X 109/L (range: 168-861 X 109). The mean total bilirubin was 9 pmol/L (range: 3-20). The mean Alkaline phosphatase was 74 U/L (range: 61-135). The mean Lactic Dehydrogenase (LDH) was 148 U/L (range: 102-274) and the mean As- partate Transaminase was 18 U/L (range: 8-50).
Treatment schedule The preoperative chemotherapy and radiation schema
is outlined in Figure 1. All patients were treated with a megavoltage linear accelerator ( 10 or 15 MV). All patients were treated in a prone position using a 4-field box tech- nique (Posterior, Anterior and Right and Left Laterals). The superior border was the L5/Sl junction. The inferior border was at the level of the inferior edges of the obturator foramina, or 3 cm below the known tumor. For lesions lying within 5 cm of the anal verge, the anus was included in the irradiation field. The lateral borders were at least 1.5 cm laterai to the bony pelvis. The posterior border was the posterior sacral surface. The anterior border was 3 cm anterior to the tumor mass. For lesions adherent to the prostate, bladder, or vagina, this border was extended to the anterior edge of the symphysis pubis. Cerrobend blocks were employed whenever possible to reduce the amount of small bowel, bone marrow and soft tissue being irradiated. 4000 cGy was delivered in 20 fractions in 4 weeks. The radiation dose was prescribed to the 97% is- odose which encompassed the target volume.
Chemotherapy was given concurrently during the first and third week of pelvic radiation therapy. Two cycles of 96 hr of 5-Fluorouracil infusion were given on days l-4 and days 15- 18 respectively. The dose of 5-Fluorouracil was 20 mg/kg/24 hr. A single bolus injection of Mito- mycin C was given on day 1. The dose of Mitomycin C was 8 mg/m2.
Clinical assessment of tumor regression by physical ex- amination was undertaken at 4 to 6 weeks after concurrent chemotherapy and pelvic radiation. Follow-up studies were performed on those patients who had a pretreatment ultrasound or CT scan study. When patients had recovered from their acute side-effects of treatment, they proceeded to surgical resection. The mean interval between chemo- radiation therapy and surgery was 7 weeks. Forty-five pa- tients had no additional postoperative treatment. One pa- tient with macroscopic residual disease received additional pelvic radiation therapy.
Follow-up and toxicity assessment Acute toxicity was assessed weekly during chemo-ra-
diation therapy, and at 4-6 weeks post treatment. It was scored according to the RTOG toxicity scale. Perioperative and 30 days postoperative complications were obtained from the records of the hospitals where the patients had had their surgery.

Preop chemo-RT in rectal cancer 0 A. CHAN et al.
TREATMENT SCHEMA
Mi tomycin C 0 8 mg/sq. m. bolus
5 FU Inf us i on 20 mg/kg/24 hours
793
Day 1 8 15 22 29
Fig. I. Preoperative chemotherapy and radiation therapy in tethered/fixed rectal carcinoma, treatment schema.
All patients were seen for routine follow up every 3 months for the first 2 years, every 4 months for the next 2 years, and every 6 months thereafter. At each visit, a history was taken, physical examination performed, and serum CEA and liver function tests obtained. A chest x- ray was taken every year. Further investigations were un- dertaken whenever indicated by history, physical findings or a rising CEA. Sixteen patients were followed until death. For the remaining thirty patients, the median follow up was 26 months (range: 1 l-56 months).
All relapses were categorized into pelvic failure or dis- tant failure. The latter included both hematogenous me- tastases and abdominal failure. All relapses were docu- mented by clinical and/or radiological assessement. Most pelvic failures had histological confirmation by needle- aspiration or excisional biopsies.
Statistical analysis Survival was calculated from the first day of treatment
by the Kaplan-Meier method (20). The Log-rank test was used to test any difference between survival curves and actuarial relapse rates. All patients with incomplete re- section were scored as pelvic failure at day zero.
RESULTS
Resectability and pathology At the time of first assessment after preoperative che-
moradiation therapy, 24 patients had greater than 50% tumor regression by clinical assessment. Three patients had no palpable residual tumor. Of the 11 patients who had pre-treatment and post-treatment endorectal ultra- sound studies, 7 patients had radiological evidence of tu- mor regression.
All 46 patients underwent surgical resection. Forty- three patients had all visible tumors resected at the time of surgery. Three patients had palliative resection with a small amount of residual disease left. In the 43 patients who had complete resection, 2 had unclear radial resection
margins. The overall curative resection rate was 89% (4 l/ 46). Types of surgical resection included 31 abdomino- perineal resections, 2 abdominoperineal resections plus bilateral salpingoorphorectomies, 10 anterior resections, 1 anterior resection plus total cystectomy, 1 exenteration and 1 Hartmann’s resection. All 5 patients with incom- plete resection or positive resection margins belong to the fixed tumor group.
Pathological staging according to the AJCC-TNM (1988) system is listed in Table 2. Two patients (4%) had no tumor found in the resected specimens (TONOMO). Evidence of tumor necrosis and stromal fibrosis were present in all resected specimens. In 19 patients (4 1%) extensive fibrosis with scattered tumor islands were found throughout the bowel wall. In some instances, these tumor islands were present in the outer layer of the muscularis or in the perirectal tissue without any residual tumor being demonstrated in the inner aspect of the rectal wall. Lymph node metastases were present in 7 patients (15%). In all cases, only one or two lymph nodes were involved. One patient (2%) had a hepatic metastasis found at the time of surgery despite a negative preoperative nucleotide liver scan. There were 11 (24%) well-differentiated, 30 (65%) moderately-differentiated and 5 ( 11%) poorly-differen- tiated adenocarcinomas. Vascular and/or lymphatic in- vasion was present in 6 patients ( 13%).
Toxicity The main acute toxicities during chemo-radiation
therapy were diarrhea, skin reaction and neutropenia. The details are summarized in Table 3. Two patients (4%) had transient Grade 3 neutropenia with their WBC nadir dropping to the 1.0-2.0 X log/L range. Both patients completed the treatment as planned. Eight patients (17%) developed diarrhea that required loperamide for symp- tomatic control. None of the cases was severe enough to require interruption of their treatment. Three patients de- veloped patchy moist desquamation in the perineum. They all had low lying rectal tumor and the anus was

194 I. J. Radiation Oncology 0 Biology 0 Physics Volume 25, Number 5, 1993
Table 2. Pathological (post-RT) staging
All patients Tethered tumor
No. of patients 46 30 Stage*
TONOMO 2 1 TlNOMO 2 2 TZNOMO 16 12 T3NOMO 11 10 T4NOMO 7 1 T2N 1 MO 4 2 T3NlMO 3 2 T4NOM 1 1 0
Positive node 15% (7/46) 13% (4/30) Resectability* 89% (41/46) 100% (30/30)
* Stage according to the AJCC-TNM (1988) system. + Parentheses indicate number with incomplete resection or positive resection margins. * Complete resection with negative margins.
Fixed tumor
16
1 0 4 1 6 (4)+ 2 1 1 (I)+
19% (3/16) 69% (1 l/16)
included in the radiation portals. In all 46 patients, there obstruction at 4 months after surgery. At the time of lap- was no oral mucositis related to the Wluorouracil infu- arotomy, a pelvic recurrence was found responsible for sion. the small bowel obstruction.
There was no perioperative or postoperative death. Of the 33 abdominoperineal resections and one exenteration performed, 5 patients (15%) had delay in their perineal wound healing due to infection or dehiscence. All 5 pa- tients had complete wound closure in 4-6 weeks and they did not require any additional surgery or skin grafting. One patient had abdominal wound dehiscence. The per- ineal and abdominal wound problem occurred in patients treated in the first 2 years (1986-87). Since 1987, the problem has been minimized by delaying the removal of abdominal and perineal sutures till postoperative day 14 and 2 1, respectively. Four patients (12%, 4/34) developed colostomy stenosis which required revision. Of the 11 an- terior resections, 1 patient developed an anastomotic leak and required a colostomy. Two patients suffered myo- cardial infarction in the postoperative period. One patient with incomplete tumor resection developed a small bowel
Survival and failure analysis At the last review in 1991, 12 patients (26%) had died
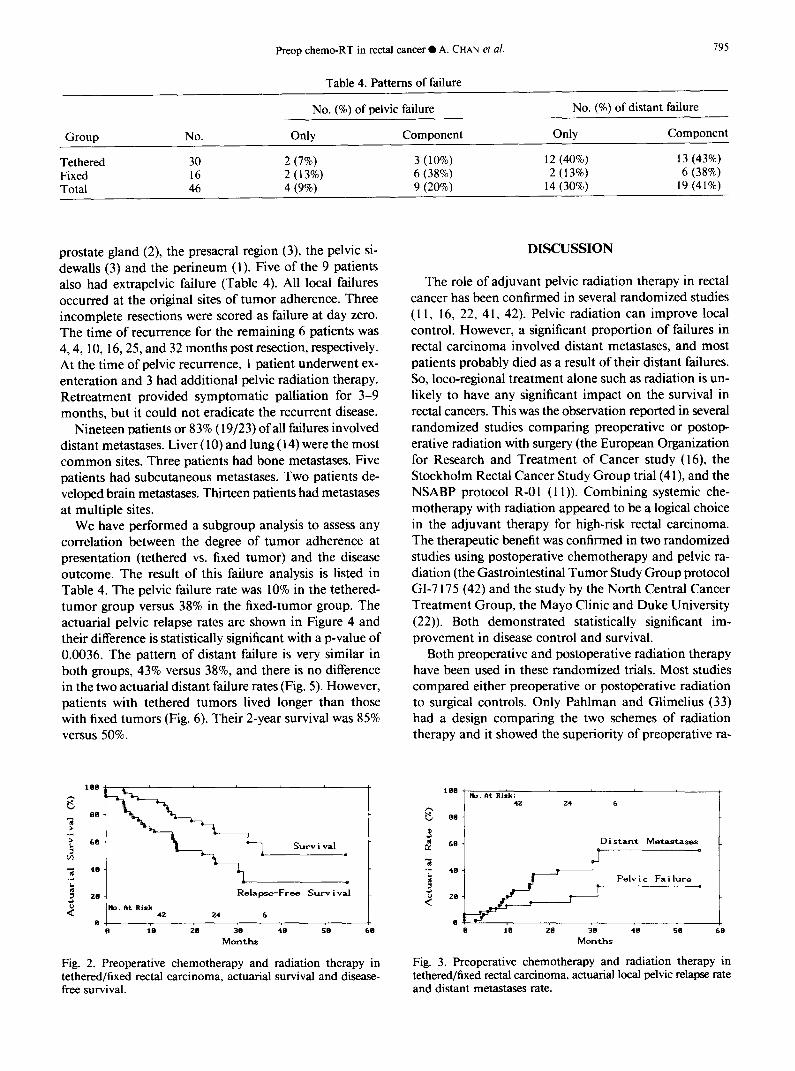
of their rectal cancer. One patient (2%) had died of a sec- ond primary cancer in the esophagus. Three patients (6.5%) had died of unrelated causes. Twenty patients (43.5%) are alive without disease, and 10 (22%) are alive with disease. Table 4 summarizes the overall failure pat- tern. The 2-year and 3-year actuarial survivals were 73% and 49%, respectively (Fig. 2). The 2-year and 3-year dis- ease-free survival were 5 1% and 3 1% (Fig. 2). At 2 years, the actuarial pelvic failure rate was 16%, and the distant failure rate was 4 1% (Fig. 3).
Of the 9 pelvic recurrences, 3 patients had tethered and 6 had fixed tumors at presentation. The latter group in- cluded all 5 patients with incomplete resection or unclear resection margins. The sites of recurrence included the
Table 3. Acute toxicity during chemo-radiation therapy
Grade Hemoglobin WBC Platelets Stomatitis Diarrhea Skin
0 46 16 46 46 20 36
: 0 0 11 17 0 0 0 0 18 8 7 3 3 0 2 0 0 0 0 4 0 0 0 0 0 0
Toxicity criteria: Hemoglobin (G/L): Grade 0 = > 110; Grade 1 = 95-110; Grade 2 = 75-95; Grade 3 = 50-75; Grade 4 = < 50. WBC (X 109/L): Grade 0 = > 4.5; Grade 1 = 3-4.5; Grade 2 = 2-3; Grade 3 = 1-2; Grade 4 = < . 1 .O. Platelets (X 109/L): Grade 0 = > 100; Grade 1 = 75-100; Grade 2 = 50-75; Grade 3 = 25-50; Grade 4 = < 25.
Stomatitis: Grade 0 = None; Grade 1 = Painless ulcers, erythema or mild soreness; Grade 2 = Painful erythema, edema or ulcers but can eat; Grade 3 = Painful erythema, edema or ulcers and cannot eat; Grade 4 = Requires parenteral or enteral support.
Diarrhea: Grade 0 = None; Grade 1 = Increase of stools, required no medication; Grade 2 = Increase of stools, required parasym- patholytic medication; Grade 3 = Increase of stools, required parenteral support; Grade 4 = Increase of stools, required treatment interruption.
Skin: Grade 0 = None; Grade 1 = Erythema/dry desquamation; Grade 2 = Patchy moist desquamation; Grade 3 = Confluent moist desquamation; Grade 4 = Ulcers.
Preop chemo-RT in rectal cancer 0 A. CHAN et a/. 195
Group No.
Tethered 30 Fixed 16 Total 46
Table 4. Patterns of failure
No. (%) of pelvic failure
Only Component
2 (7%) 3 (10%) 2 (13%) 6 (38%) 4 (9%) 9 (20%)
No. (%) of distant failure
Only Component
12 (40%) 13 (43%) 2 (13%) 6 (38%)
14 (30%) 19 (41%)
prostate gland (2), the presacral region (3), the pelvic si- dewalls (3) and the perineum ( 1). Five of the 9 patients also had extrapelvic failure (Table 4). All local failures occurred at the original sites of tumor adherence. Three incomplete resections were scored as failure at day zero. The time of recurrence for the remaining 6 patients was 4,4, 10, 16,25, and 32 months post resection, respectively. At the time of pelvic recurrence, 1 patient underwent ex- enteration and 3 had additional pelvic radiation therapy. Retreatment provided symptomatic palliation for 3-9 months, but it could not eradicate the recurrent disease.
Nineteen patients or 83% (19/23) of all failures involved distant metastases. Liver ( 10) and lung ( 14) were the most common sites. Three patients had bone metastases. Five patients had subcutaneous metastases. Two patients de- veloped brain me&stases. Thirteen patients had metastases at multiple sites.
We have performed a subgroup analysis to assess any correlation between the degree of tumor adherence at presentation (tethered vs. fixed tumor) and the disease outcome. The result of this failure analysis is listed in Table 4. The pelvic failure rate was 10% in the tethered- tumor group versus 38% in the fixed-tumor group. The actuarial pelvic relapse rates are shown in Figure 4 and their difference is statistically significant with a p-value of 0.0036. The pattern of distant failure is very similar in both groups, 43% versus 38%, and there is no difference in the two actuarial distant failure rates (Fig. 5). However, patients with tethered tumors lived longer than those with fixed tumors (Fig. 6). Their 2-year survival was 85% versus 50%.
Fig. 2. Preoperative chemotherapy and radiation therapy in tethered/fixed rectal carcinoma, actuarial survival and disease- free survival.
DISCUSSION
The role of adjuvant pelvic radiation therapy in rectal cancer has been confirmed in several randomized studies ( 11, 16, 22, 4 1, 42). Pelvic radiation can improve local control. However, a significant proportion of failures in rectal carcinoma involved distant metastases, and most patients probably died as a result of their distant failures. So, loco-regional treatment alone such as radiation is un- likely to have any significant impact on the survival in rectal cancers. This was the observation reported in several randomized studies comparing preoperative or postop- erative radiation with surgery (the European Organization for Research and Treatment of Cancer study (16) the Stockholm Rectal Cancer Study Group trial (4 l), and the NSABP protocol R-O 1 ( 11)). Combining systemic che- motherapy with radiation appeared to be a logical choice in the adjuvant therapy for high-risk rectal carcinoma. The therapeutic benefit was confirmed in two randomized studies using postoperative chemotherapy and pelvic ra- diation (the Gastrointestinal Tumor Study Group protocol GI-7 175 (42) and the study by the North Central Cancer Treatment Group, the Mayo Clinic and Duke University (22)). Both demonstrated statistically significant im- provement in disease control and survival.
Both preoperative and postoperative radiation therapy have been used in these randomized trials. Most studies compared either preoperative or postoperative radiation to surgical controls. Only Pahlman and Glimelius (33) had a design comparing the two schemes of radiation therapy and it showed the superiority of preoperative ra-
Fig. 3. Preoperative chemotherapy and radiation therapy in tethered/fixed rectal carcinoma, actuarial local pelvic relapse rate and distant metastases rate.

796 I. J. Radiation Oncology 0 Biology 0 Physics Volume 25, Number 5, 1993
P = a.0036
6 t I. 6 16 26
idtths 46 56 66
Fig. 4. Actuarial local pelvic relapse rate based on the degree of tumor adherence at presentation: Fixation (16) vs. Tethering (30).
diation over postoperative radiation. Preoperative radia- tion therapy is especially advantageous in unresectable or borderline-resectable tumors. It can sterilize the margin of the tumor and improve the curative resectability.
The main criticism about preoperative radiation ther- apy are the lack of a pretreatment clinical staging system for selecting the appropriate patients, and the potential over-treatment of early tumors which were cured by sur- gery alone. However, certain tumor characteristics like tumor adherence, tumor size, and tumor grade can iden- tify the high-risk subgroup which will benefit from pre- operative radiation. The prognostic significance of tumor mobility has been demonstrated in the clinico-patholog- ical review of 824 patients in the British MRC study ( 10). The curative resection rate was 44% for the tethered or fixed tumors, vs. 80% for the mobile tumors. The 5-year local disease-free rates were 37% and 70%, respectively (p < 0.001).
In the present study, we use tumor tethering or fixation as the selection criterion for preoperative concurrent che- motherapy and pelvic radiation. Some patients in our study had histological confirmation of tumor invasion of adjacent organs. Endorectal ultrasonography is a useful pretreatment assessment tool. It can determine the depth of rectal wall invasion and the length of the tumor. All eleven patients studied had ultrasound evidence of tumor invasion beyond the rectal wall. Endorectal ultrasound also provided post-treatment clinical reassessment. Seven
P = 0.91 I
6 16 26 36 46 56 66
Months
Fig. 5. Actuarial distant me&stases rate based on the degree of tumor adherence at presentation: Fixation (16) vs. Tethering (30).
Months
Fig. 6. Actuarial survival based on the degree of tumor adherence at presentation: Fixation ( 16) vs. Tethering (30).
of eleven post chemo-radiation ultrasound studies showed tumor regression at 4-6 weeks after preoperative therapy.
When we designed our protocol in 1986, we had two study objectives in mind. Was it feasible to give concurrent preoperative chemotherapy and moderate dose of pelvic radiation (4000 cGy) and then to perform radical resec- tion? Could preoperative chemotherapy and radiation therapy improve the resectability and local control in tethered and fixed rectal carcinoma? Adjuvant chemo- therapy was not routine practice in the management of rectal carcinoma in 1986, so the study did not incorporate any postoperative chemotherapy.
Our treatment regimen was well tolerated, even by the elderly patients. There was no major increase in acute toxicities such as diarrhea, skin desquamation, oral mu- cositis, and hematological toxicity (Table 3). Two patients developed transient Grade 3 neutropenia. All forty-six patients completed the planned course of chemotherapy and pelvic radiation and had surgery 6-8 weeks later.
Anterior resections with primary anastomosis in irra- diated bowel were performed in 11 patients. One of the 11 patients developed an anastomotic leak (9%). This anastomotic leak rate is comparable to the clinical leak rate of 3- 15% after anterior resection alone (2, 3, 6, 13, 26). Review of the operative report showed that technical fault, rather than preoperative therapy, was responsible for the leak in this patient. Fifteen percent of all abdom- inoperineal resection patients had delayed perineal wound healing from infection or dehiscence. This is slightly higher than the 8- 14% reported after abdominoperineal resection alone (1, 23, 35, 40). This problem can be reduced by leaving the perineal sutures in for 2 1 days. Four patients ( 12%) developed stoma1 stenosis and required colostomy revision. However, this happened only during the first 2 years of the study, and we suspect the problem was related to the surgical technique of colostomy formation. Since 1987, all colostomies were matured and carefully in- spected to insure their viability before the abdomen was closed. We have not observed any stomal stenosis since adopting this policy.
Of the 46 patients who underwent resection, 43 had complete resection at the time of surgery. Forty-one (89%) had curative resection with negative margins. This curative

Preop chemo-RT in rectal cancer 0 A. CHAN et a/. 791
resectability is better than the resectability rate (44%) re- Besides having a lower curative resectability, tethered ported in the MRC trial for tethered tumors. Using com- and fixed rectal cancers constitute a high-risk group for parable selection criteria: Tumor adherence or fixation to distant metastases. At a median follow up of 2 years, 4 1% an adjacent structure, Minsky et al. (28) reported a cu- ( 19 patients) of our patients developed distant failure (Ta- rative resectability rate of 90% with preoperative Wlu- ble 4). There was no difference between the two subgroups orouracil, leucovorin (200 mg/m*/day) and 5040 cGy of tethered and fixed cancer. The distant failure rates were pelvic radiation therapy in unresectable rectal carcinoma. 43% and 38%, respectively. They are similar to the result This curative resection rate was superior to their historical of the British MRC trial (9). Both treatment groups in the result of 64% with preoperative radiation alone (28). Sim- MRC trial had a 2-year distant metastases rate of ap- ilarly, Frykholm et al. (15) reported improvement from proximately 38%, and a 5-year rate of 50% after preop- 34% to 7 1% in tumor resectability when chemotherapy erative radiation. In another non-randomized study with was added to preoperative irradiation in the treatment of high-dose preoperative irradiation and surgery, Mohiud- non-resectable adenocarcinoma of rectum. For preoper- din et al. (3 1) reported a distant failure rate of 20-22% in ative radiation alone, Mendenhall et al. (27) reported a their partially fixed and fixed rectal cancers. It appeared complete resection rate of 48% after 3600-6000 cGy of that two cycles of preoperative 5Fluorouracil infusion radiation in unresectable carcinoma. Dosoretz et al. (7) and a single bolus of mitomycin C in the present study had a curative resection rate of 64% after 4000-4500 cGy. had not had any significant impact on the distant failure There appears to be improvement in curative resectability, pattern. In contrast, when comparing postoperative che- from 48-64% to 90%, when concurrent chemotherapy is motherapy (methyl-CCNU and 5-FU) and radiation to added to preoperative radiation therapy. However, cau- radiation alone, the North Central Cancer Treatment tion is advisable in drawing conclusions from these ob- Group-Mayo-Duke study showed a significant reduction servations because of the potential difference in patient in the distant metastases rate from 46% to 28.8% (31). selection and of the clinico-pathological factors which Thus the role of additional chemotherapy after surgery, might have contributed to the difference in curative re- such as WI_J/Leucovorin or 5FU/Levamisole, needs section rate. further investigation.
Two patients (4%) in our series had no residual tumor found in the resected specimen (TONOMO). Evidence of tumor shrinkage and necrosis were present in all resected specimens. In only seven patients (15%) were positive lymph nodes found. This incidence of node-positive can- cer was lower than anticipated. On the basis of the British MRC review of 824 patients, we had expected 40-45% of tethered rectal cancer to show lymph node involvement. This pathological down-staging phenomenon after pre- operative chemoradiation or radiation has also been re- ported by other authors: Minsky et al. (20% TONO, 30% node-positive) (28,29), Mohiuddin et al. (9% TONO, 27% node-positive) (3 l), Horn et al. (4.4% TONO, 18.4% node- positive) ( 19) Haghbin et al. ( 12.5% TONO, 26.5% node- positive) (17) and Kodnar et al. (22% node-positive) (21). However, in three randomized preoperative radiation trials: the British MRC trial (8, 9, lo), the European Or- ganization for Research and Treatment of Cancer (EORTC) trial (16) and the Stockholm trial (4 l), there was no evidence of pathological down-staging in the ir- radiated group when compared to the surgery control group.
Tumor fixation is indicative of a larger tumor mass and a greater depth of invasion of adjacent structures. There- fore, fixed rectal cancers were more difficult to eradicate than tethered ones. In our series, the curative resection rate was 69% for fixed cancers. The 2-year local disease- free rate was 60%. This was statistically inferior to the group with tethered cancers which had a 100% curative resection rate after preoperative chemotherapy and ra- diation therapy. Ninety percent of tethered rectal cancers were free of local recurrence at 2 years. All five patients with macroscopic or microscopic residual disease after surgery presented with fixed tumors. A higher dose of radiation therapy, 5000-5500 cGy, concurrent with in- fusional chemotherapy, may be needed to improve the resectability and local control in this subgroup with fixed rectal cancer.
Based on the experience of these 46 patients, we have started another Phase II study incorporating a higher dose of preoperative pelvic radiation, concurrent with Mito- mycin C, 5Fluorouracil infusion and Leucorvorin. This is followed by surgical resection and postoperative 5-Flu- orouracil/Leucovorin chemotherapy.
This discrepancy in the pathological downstaging can be explained on the basis of the radiation doses given, and the interval between radiation therapy and surgery. An interval of 4-6 weeks is needed for the tumor regres- sion to occur. In the MRC, EORTC and Stockholm trials, the preoperative radiation dose given ranged from 500 to 3450 cGy, and the interval between radiation and surgery was less than fourteen days. In contrast, all the series re- porting this down-staging phenomenon used radiation doses of 4000-7000 cGy, and surgical resection was per- formed 4-7 weeks after preoperative therapy.
CONCLUSION
Preoperative concurrent 5Fluorouracil infusion, Mi- tomycin C and 4000 cGy pelvic radiation could achieve an 89% curative resectability rate for tethered and fixed rectal carcinomas. There was a slight increase in the in- cidence of delayed perineal wound healing (15%) after preoperative therapy. Distant metastases remained the major cause of failure in this group of high-risk rectal carcinomas.

798 1. J. Radiation Oncology 0 Biology 0 Physics Volume 25, Number 5, 1993
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
Il.
12.
REFERENCES
Altemeier, W. A.; Culbertson, W. R.; Alexander, J. W.; Su- torius, D.; Bossert, J. Primary closure and healing of the perineal wound in abdominoperineal resection of the rectum for carcinoma. Am. J. Surg. 127:2 15-2 19; 1974. Antonsen, H. K.; Kronborg, 0. Early complications after low anterior resection for rectal cancer using the EEA sta- pling device, a prospective trial. Dis. Colon Rectum 30:579- 583;1987. Bear-t, R. W.; Kelly, K. A. Randomized prospective evalu- ation of the EEA stapler for colorectal anastomoses. Am. J. Surg. 141:143-147;1981. Byfield, J. E. Useful interactions between 5Fluorouracil and radiation in man: 5Fluorouracil as a radiosensitizer. In: Hill, B. T., Bellamy, A. S., eds. Antitumor drug-radiation interactions. Boca Raton, FL: CRC Press Inc.; 1990:87- 105. Carlsson, U.; Iasson, A.; Ekelund, G. Recurrence rates after curative surgery for rectal carcinoma, with special reference to their accuracy. Dis. Colon Rectum 30:43 l-434; 1987. Cunsolo, A.; Bragaglia, R. B.; Petrucci, C.; Poggioli, G.; Gozzetti, G. Survival and complications after radical surgery for carcinoma of the rectum. J. Surg. Oncol. 4 1:27-32;1989. Dosoretz, D. E.; Gunderson, L. L.; Hedberg, S.; Hoskins, B.; Blitzer, P. H.; Shipley, W.; Cohen, A. Preoperative ir- radiation for unresectable rectal and rectosigmoid carci- nomas. Cancer 52:8 14-8 18; 1983. Duncan, W.; Smith, A. N.; Freedman, L. F.; Alderson, M. R.; Amott, S. J.; Bleehen, N. M.; Bond, W. H.; Crowther, D.; Deeley, T. J.; Duthie, H. L.; Dykes, P. W.; Fielding, L. P.; Flatman, G. E.; Goligher, J. C.; Hawley, P. R.; Hughes, L. E.; Joslin, C. A. F.; Koriech, 0. M.; Morson B. C.; Oates, G. D.; Peckham, M. J.; Sandland, M. R.; Schofield, P. F.; Slack, W.; Slaney, G.; Smith, J. A. R.; Stewart Scott, J.; Whitehouse, J. M. A.; Wrigley, P. F. M.; York-Mason, A. First report of an MRC working party. A trial of preoperative radiotherapy in the management of operable rectal cancer. Br. J. Surg. 69:5 13-5 19; 1982. Duncan, W.; Smith, A. N.; Freedman, L. F.; Alderson, M. R.; Amott, S. J.; Bleehen, N. M.; Bond, W. H.; Crowther, D.; Deeley, T. J.; Duthie, H. L.; Dykes, P. W.; Fielding L. P.; Ratman, G. E.; Goligher, J. C.; Hawley, P. R.; Hughes, L. E.; Joslin, C. A. F.; Koriech, 0. M.; Morson, B. C.; Oates, G. D.; Peckham, M. J.; Sandland, M. R.; Schofield, P. F.; Slack, W.; Slaney, G.; Smith, J. A. R.; Stewart Scott, J.; Whitehouse, J. M. A.; Wrigley, P. F. M.; York-Mason, A. Second report of an MRC working party. The evaluation of low dose preoperative X-ray therapy in the management of operable rectal cancer; results of a randomly controlled trial. Br. J. Surg. 71:21-25;1984. Duncan, W.; Smith, A. N.; Freedman, L. F.; Alderson, M. R.; Amott, S. J.; Bleehen, N. M.; Bond, W. H.; Crowther, D.; Deeley, T. J.; Duthie, H. L.; Dykes, P. W.; Fielding L. P.; Flatman, G. E.; Goligher, J. C.; Hawley, P. R.; Hughes, L. E.; Joslin, C. A. F.; Koriech, 0. M.; Morson, B. C.; Oates, G. D.; Peckham, M. J.; Sandland, M. R.; Schofield, P. F.; Slack, W.; Slaney, G.; Smith, J. A. R.; Stewart Scott, J.; Whitehouse, J. M. A.; Wrigley, P. F. M.; York-Mason, A. Third report of an MRC working party. Clinico-pathological features of prognostic significance in operable rectal cancer in 17 centres in the U.K. Br. J. Cancer 50:435-442; 1984. Fisher, B.; Wolmark, N.; Rockette, H.; Redmond, C. Post- operative adjuvant chemotherapy or radiation therapy for rectal cancer: Results from NSABP protocol R-01. JNCI 80:21-29;1988. Fottier, G. A.; Constable, W. C.; Meyers, H.; Wanebo, H. J. Preoperative radiation therapy for rectal cancer: An
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
effective therapy in need of a clinical trial. Arch. Surg. 12 I : 1380-1385;1986. Friedmann, P.; Garg, J. L.; McCabe, D. P.; Chabot, J. R.; Park, W. C.; Stark, A.; Coe, N. P. W.; Page, D. W. Intestinal anastomosis after preoperative radiation therapy for carci- noma of the rectum. Surg. Gynecol. Obstet. 164:257- 260;1987. Friedmann, P.; Garb, J. L.; Park, W. C.; Stark, A.; DeConti, R. C.; Chabot, R.; Pace, 0. T. Survival following moderate- dose preoperative radiation therapy for carcinoma of the rectum. Cancer 55:967-973;1985. Frykholm, G.; Glimehus, B.; Pahlman, L. Preoperative ir- radiation with and without chemotherapy (MFL) in the treatment of primarily non-resectable adenocarcinoma of the rectum. Results from two consecutive studies. Eur. J. Cancer Clin. Oncol. 25:1535-1541;1989. Gerard, A.; Buyse, M.; Nordlinger, B.; Loygue, J.; Pene, F.; Kempf, P.; Bosset, J. F.; Gignoux, M.; Arnaud, J. P.; De- saive, C.; Duez, N. Preoperative radiotherapy as adjuvant treatment in rectal cancer. Final results of a randomized study of the European Organization for Research and Treatment of Cancer (EORTC). Ann. Surg. 208:606- 614;1988. Haghbin, M.; Sischy, B.; Hinson, J. Combined modality preoperative therapy in poor prognostic rectal adenocarci- noma. Radiother. Oncol. 13:75-8 1; 1988. Horn, A.; Halvorsen, J. F.; Dahl, 0. Preoperative radio- therapy in operable rectal cancer. Dis. Colon Rectum 33: 823-828; 1990. Horn, A.; Morild, 1.; Dahl, 0. Tumour shrinkage and down staging after preoperative radiation of rectal adenocarci- nomas. Radiother. Oncol. 18: 19-28; 1990. Kaplan, E. L.; Meier, P. Nonparametric estimation from incomplete observation. J. Am. Statist. Assoc. 53:457- 481;1958. Kodner. I. J.; Shemesh, E. I.; Fry, R. D.; Walz, B. J.; Myer- son, R.; Fleshman, J. W.; Schechtman, K. B. Preoperative irradiation for rectal cancer. Improved local control and long-term survival. Ann. Surg. 209: 194- 199; 1989. Krook, J. E.; Moertel, C. G.; Gunderson, L. L.; Wieand. H. S.; Collins, R. T.; Beart, R. W.; Kubista, T. P.; Poon. M. A.; Meyers, W. C.; Mailliard, J. A.; Twito, D. I.; Morton, R. F.; Veeder, M. H.; Witzig, T. E.; Cha, S.; Vidyarthi, S. C. Effective surgical adjuvant therapy for high-risk rectal carcinoma. N. Engl. J. Med. 324:709-7 15; 199 1. Liavag, 1.; Roland, M. Abdominoperineal excision of the rectum: A prospective study based on a standardized method. World J. Surg. I:24 l-246; 1983. Malcolm, A. W.; Perencevich, N. P.; Olson, R. M.; Hanley, J. A.; Chaffey, J. T.; Wilson, R. E. Analysis of recurrence patterns following curative resection for carcinoma of the colon and rectum. Surg. Gynecol. Obstet. 152:131- 136;1981. McDermott, F. T.; Hughes, E. S. R.; Pihl, E.; Johnson, W. R.; Price, A. B. Local recurrence after potentially curative resection for rectal cancer in a series of 1008 patients. Br. J. Surg. 72:34-37; 1985. McGinn, F. P.; Gartell, P. C.; Clifford, P. C.; Brunton, F. J. Staples or sutures for low colorectal anastomoses: a prospective randomized trial. Br. J. Sur. 72:603-605; 1985. Mendenhall, W. M.; Bland, K. I.; Pfaff, W. W.; Million, R. R.; Copeland III, E. M. Initially unresectable rectal ad- enocarcinoma treated with preoperative irradiation and surgery. Ann. Surg. 205:41-44;1987. Minsky, B. D.; Cohen, A. M.; Kemeny, N.; Enker, W. E.; Kelsen, D. P.; Reichman, B.; Saltz, L.; Sigurdson, E. R.;

Preop chemo-RT in rectal cancer 0 A. CHAN et al. 199
Frankel, J. Enhancement of radiation-induced downstaging of rectal cancer by Fluorouracil and high-dose Leucovorin chemotherapy. J. Clin. Oncol. 10:79-84;1992.
29. Minsky, B. D.; Kemeny, N.; Cohen, A. M.; Enker, W. E.; Kelsen, D. P.; Reichman, B.; Saltz, L.; Sigurdson, E. R.; Frankel, J. Preoperative high-dose Leucovorin/S-Fluoro- uracil and radiation therapy for unresectable rectal cancer. Cancer 67:2859-2866;1991.
30. Minsky, B. D.; Mies, C.; Recht, A.; Rich, T. A.; Chaffey, J. T. Resectable adenocarcinoma of the rectosigmoid and rectum, 1. Patterns of failure and survival. Cancer 6 1: 1408- 1416;1988.
3 1. Mohiuddin, M.; Marks, G. High dose preoperative irradia- tion for cancer of the rectum, 1976-1988. Int. J. Radiat. Oncol. Biol. Phys. 20:37-43;1991.
32. Neville, R.; Fielding, L. P.; Amendola, C. Local tumor re- currence after curative resection for rectal cancer-A ten- hospitals review. Dis. Colon Rectum 30: I2- 17; 1987.
33. Pahlman, L.; Glimelius, B. Pre- or postoperative radiother- apy in rectal and rectosigmoid carcinoma. Report from a randomized multicenter trial. Ann. Surg. 2 11: 187- 195; 1990.
34. Pahlman, L.; Glimelius, B.; Ginman, C.; Graffman, S.; Ad- alsteinsson, B. Preoperative irradiation of primary non-re- sectable adenocarcinoma of the rectum and rectosigmoid. Acta Radiol. Oncol. 24:35-39;1985.
35. Patek S. C.; Tovee, E. B.; Langer, B. Twenty-five years of experience with radical surgical treatment of carcinoma of the extraperitoneal rectum. Surgery 82:460-465;1977.
36. Pilipshen, S. J.; Heilweil, M.; Quan, S. H. Q.; Sternberg, S. S.; Enker, W. E. Patterns of pelvic recurrence following definitive resections of rectal cancer. Cancer 53:1354- 1362;1984.
37. Rich, T.; Gunderson, L. L.; Lew, R.; Galdibini, J. J.; Cohen, A. M.; Donaldson, G. Patterns of recurrence of rectal can- cer after potentially curative surgery. Cancer 52:1317- 1329; 1983.
38. Rider, W. D.: Palmer, J. A.; Mahoney, L. J.; Robertson, C. T. Preoperative irradiation of operable cancer of rectum: Report of the Toronto trial. Can. J. Surg. 20:335-338;1977.
39. Rockwell, S.; Sartorelli, A. C. Mitomycin C and radiation. In: Hill, B. T., Bellamy, A. S., eds. Antitumor drug-radiation interactions. Boca Raton, FL: CRC Press Inc.; 1990: I25- 139.
40. Rosen, L.; Veidenheimer, M. C.; Caller, J. A.; Corman, M. L. Mortality, morbidity, and patterns of recurrence after abdomino-perineal resection for cancer of the rectum. Dis. Colon Rectum 25:202-208;1982.
41. Stockholm Rectal Cancer Study Group. Short-term pre- operative radiotherapy for adenocarcinoma of the rectum. An interim analysis of a randomized multicenter trial. Am. J. Clin. Oncol. 10:369-375;1987.
42. Thomas, P. R. M.; Lindblad, A. S. Adjuvant postoperative radiotherapy and chemotherapy in rectal carcinoma: A re- view of the Gastrointestinal Tumor Study Group experience. Radiother. Oncol. 13:245-252: 1988.




















