Predictors of Psychological Adjustment (Codori)
15
Health Psychology 1997, Vol. 16, No. 1,36-50 Copyright 1997 by the American Psychological Association, Inc. 0278-6133/97/$3.00 Predictors of Psychological Adjustment to Genetic Testing for Huntington's Disease Ann-Marie Codori, Phillip R. Slavney, Candace Young, Diana L. Miglioretti, and Jason Brandt Johns Hopkins University School of Medicine In the present study the authors assessed predictors of adjustment to genetic testing for Huntington's disease. Fifty-two genetically positive and 108 genetically negative persons were studied for 1 year following testing. Adjustment, defined by hopelessness and depressive symptoms, was measured at 3, 6, 9, and 12 months after disclosure and was within normal limits for both groups. Those less well adjusted had tested positive, were married, had no children, or were closer to their estimated ages of onset. The study delineated risk factors for psychological distress that should be considered by people contemplating testing for Huntington's disease. Key words: Huntington's disease, genetic testing, predictive testing, adjustment, psychological impact The discovery of a genetic marker for Hunting- ton's disease by Gusella et al. (1983) made it the first adult-onset genetic disorder for which at risk Ann-Marie Codori, Phillip R. Slavney, Candace Young, and Jason Brandt, Department of Psychiatry and Behavioral Sciences, Johns Hopkins University School of Medicine; Diana L. Miglioretti, Department of Neurology, Johns Hopkins University School of Medicine. This work was presented in part at the 44th annual meeting of the American Society of Human Genetics, 1994. This work was supported in part by the National Institutes of Mental Health Grant MH46034 and the National Institute of Neurological Disease and Stroke Grant NS16375. We acknowledge the contributions of Gary A. Chase, Susan Folstein, Haig H. Kazazian, Jr., Chris- topher Ross, Neal Ranen, and Deborah Meyers. We also acknowledge Laura Krafft, Laura Kasch, Mary Louise Franz, Rachel Gross, Margaret Abbott, and Michael Magdalinski. Correspondence concerning this article should be addressed to Ann-Marie Codori, Department of Psy- chiatry and Behavioral Sciences, Johns Hopkins University School of Medicine, Meyer 218, 600 North Wolfe Street, Baltimore, Maryland 21287- 4218. Electronic mail may be sent via Internet to acodori @welchlink.welch.jhu.edu. persons could be tested. Given the possibility that a presymptomatic diagnosis could produce years of unnecessary suffering, there has been concern that people testing positive for the mutation might become depressed and suicidal (Brandt, 1994; Farrer, 1987; Huggins et al., 1990; Kessler, 1987a, 1987b; Post, 1992; Wexler, 1992). Huntington's disease is a progressive and ulti- mately fatal neuropsychiatric disorder character- ized by emotional disturbance (including irritabil- ity, apathy, and depression), dementia, and abnormalities of movement (Folstein, 1989; Harper, 1991). The average age of onset is 40, with death in about 15 years. It is inherited as an autosomal dominant trait through a mutation on chromosome 4 in the gene IT-15 (Huntington's Disease Collaborative Research Group, 1993). The gene, that normally includes 15-30 repeats of the nucleotide sequence cytosine-adenine- guanine (CAG), shows 35 or more CAG repeats when it is mutated. Because Huntington's disease is currently incurable, the potential benefits of a positive genetic test primarily include relief from uncertainty, the chance to avoid passing on the mutation, and prudent future planning. The psychological impact of predictive testing for Huntington's disease has been evaluated through case reports (Bloch, Adam, Wiggins, 36
-
Upload
johnshopkins -
Category
Documents
-
view
3 -
download
0
Transcript of Predictors of Psychological Adjustment (Codori)

Health Psychology1997, Vol. 16, No. 1,36-50
Copyright 1997 by the American Psychological Association, Inc.0278-6133/97/$3.00
Predictors of Psychological Adjustment to Genetic Testingfor Huntington's Disease
Ann-Marie Codori, Phillip R. Slavney, Candace Young,Diana L. Miglioretti, and Jason Brandt
Johns Hopkins University School of Medicine
In the present study the authors assessed predictors of adjustment to genetictesting for Huntington's disease. Fifty-two genetically positive and 108genetically negative persons were studied for 1 year following testing.Adjustment, defined by hopelessness and depressive symptoms, wasmeasured at 3, 6, 9, and 12 months after disclosure and was within normallimits for both groups. Those less well adjusted had tested positive, weremarried, had no children, or were closer to their estimated ages of onset.The study delineated risk factors for psychological distress that should beconsidered by people contemplating testing for Huntington's disease.
Key words: Huntington's disease, genetic testing, predictive testing,adjustment, psychological impact
The discovery of a genetic marker for Hunting-
ton's disease by Gusella et al. (1983) made it thefirst adult-onset genetic disorder for which at risk
Ann-Marie Codori, Phillip R. Slavney, CandaceYoung, and Jason Brandt, Department of Psychiatryand Behavioral Sciences, Johns Hopkins UniversitySchool of Medicine; Diana L. Miglioretti, Departmentof Neurology, Johns Hopkins University School ofMedicine.
This work was presented in part at the 44th annualmeeting of the American Society of Human Genetics,1994.
This work was supported in part by the NationalInstitutes of Mental Health Grant MH46034 and theNational Institute of Neurological Disease and StrokeGrant NS16375.
We acknowledge the contributions of Gary A.Chase, Susan Folstein, Haig H. Kazazian, Jr., Chris-topher Ross, Neal Ranen, and Deborah Meyers. Wealso acknowledge Laura Krafft, Laura Kasch, MaryLouise Franz, Rachel Gross, Margaret Abbott, andMichael Magdalinski.
Correspondence concerning this article should beaddressed to Ann-Marie Codori, Department of Psy-chiatry and Behavioral Sciences, Johns HopkinsUniversity School of Medicine, Meyer 218, 600North Wolfe Street, Baltimore, Maryland 21287-4218. Electronic mail may be sent via Internet toacodori @ welchlink.welch.jhu.edu.
persons could be tested. Given the possibility that
a presymptomatic diagnosis could produce years
of unnecessary suffering, there has been concern
that people testing positive for the mutation
might become depressed and suicidal (Brandt,
1994; Farrer, 1987; Huggins et al., 1990; Kessler,
1987a, 1987b; Post, 1992; Wexler, 1992).
Huntington's disease is a progressive and ulti-
mately fatal neuropsychiatric disorder character-
ized by emotional disturbance (including irritabil-
ity, apathy, and depression), dementia, and
abnormalities of movement (Folstein, 1989;
Harper, 1991). The average age of onset is 40,
with death in about 15 years. It is inherited as an
autosomal dominant trait through a mutation on
chromosome 4 in the gene IT-15 (Huntington's
Disease Collaborative Research Group, 1993).
The gene, that normally includes 15-30 repeats
of the nucleotide sequence cytosine-adenine-
guanine (CAG), shows 35 or more CAG repeats
when it is mutated. Because Huntington's disease
is currently incurable, the potential benefits of a
positive genetic test primarily include relief from
uncertainty, the chance to avoid passing on the
mutation, and prudent future planning.
The psychological impact of predictive testing
for Huntington's disease has been evaluatedthrough case reports (Bloch, Adam, Wiggins,
36

SPECIAL ISSUE: PREDICTING PSYCHOLOGICAL ADJUSTMENT 37
Huggins, & Hayden, 1992; Muggins et al., 1992),group studies (Brandt et al., 1989; Tibben et al.,1994; Wiggins et al., 1992), and surveys (Codori& Brandt, 1994). In these outcome studies,reactions in people who test positive have variedfrom "severe depression" (Meissen et al., 1988),to mild distress (Brandt et al., 1989; Tibben,Duivenvoorden et al., 1993; Tibben, Frets et al.,1993), to actual improvements in psychologicalstate (Wiggins et al., 1992). Despite concernabout potentially dire consequences (e.g., Kessler,1987b), there have been no published reports ofcatastrophic reactions to testing positive amongasymptomatic gene carriers.
Still, adjustment in some tested individuals hasbeen less than optimal (Bloch et al., 1992; Codori& Brandt, 1994; Huggins et al., 1992; Lam et al.,1988; Meissen et al., 1988). Tibben, Duivenvoor-den et al. (1993) studied predictors of adjustmentafter Huntington's disease testing and found that,regardless of the genetic test result, the bestpredictors of postdisclosure hopelessness, intru-sive thoughts, and avoidance behaviors werebaseline levels of the same variables. As notedbelow, other predictors of adjustment have beenimplicated in outcome studies, but not systemati-cally examined. The predisclosure factors thatmight predict adverse outcomes are unknown.Delineation of the risk factors for maladjustmentmight reveal contraindications for genetic testing.At the very least, it would identify those in needof extra psychological preparation beforehandand support afterward.
In the present study we examined pretestpredictors of posttesting adjustment in healthypeople who test positive or negative for Hunting-ton's disease. Adjustment is conceptualized asemotional distress (hopelessness-pessimism anddepressive symptoms). We examined the follow-ing as predictors: genetic status, sex, maritalstatus, parenting status, perception of risk forHuntingdon's disease, and estimated years toonset of Huntmgton's disease in those testingpositive. Furthermore, we expected that reactionsto the genetic information would change overtime after disclosure.
After testing, depressive symptoms are morecommon among those who test positive (Brandtet al., 1989; Meissen et al., 1988; Tibben, Duiven-voorden et al., 1993), and we predicted the sameoutcome. In addition, however, we expected that
distress among the positives would vary overtime. Consistent with other studies of stressresponses (Andersen, Anderson, & DeProsse,1989; Blanchard et al., 1995; Martin & Dean,1993; McCain & Gramling, 1992; Solomon,1989; Steinglass & Gerrity, 1990; Surtees &Miller, 1994; Ursano, Fullerton, Rao, & Bhartiya,1995), positives could experience increased dis-tress immediately after disclosure with linearlydecreasing distress over time. Alternatively, dis-tress in positives may be minimal initially, in-crease as the person reacts to the full meaning ofthe news (Codori & Brandt, 1994; Moulton,Stempel, Bacchetti, Temoshok, & Moss, 1991),and then decrease as the stress reaction fades.Given these competing hypotheses, we examinedthe interactions of each predictor with both thelinear and quadratic time trends.
There is general consensus that women experi-ence greater psychological distress than do men(Gove, 1984). Although experts disagree on theexplanation of such findings (e.g., Gove, 1984;Verbrugge, 1985), previous research has shownthat women who experienced a particular stressor,for example, colon cancer (Baider, Perez, &De-Nour, 1989), HIV (Kennedy, Skurnick, Foley,& Louria, 1995), and natural disaster (Steinglass& Gerrity, 1990), were more distressed than menwho experienced the same stressor. Conse-quently, we predicted that women who testedpositive would report more hopelessness anddepressive symptoms than men.
Married persons are typically better adjustedand healthier than unmarried persons (Gove,Hughes, & Style, 1983; Joung, van der Meer, &Mackenbach, 1995; Mastekaasa, 1994; Rodrigue& Park, 1996). Presumably, married personsbenefit from greater material resources, de-creased stress, and greater social support (Wyke& Ford, 1992). Therefore, we predicted thatmarried persons would adjust more favorably totesting positive than unmarried persons but thatmarried positives would be less well adjustedthan married negatives because of the burden ofthe genetic information.
Parents of children with disabilities are apt tofeel guilty about their perceived role in "passingon" the condition (Eden-Pierey, Blacher, &Eyman, 1986; Gardner, 1969; Olsen, 1994; Ryan& Smith, 1989). Thus, we predicted that positiveswith children would experience greater distress

38 CODORI, SLAVNEY, YOUNG, MIGLIORETTI, AND BRANDT
than positives without children and negativeswith children.
Optimists predict that good things will happento them, are more psychologically and physicallyhealthy, and use more active coping strategies ascompared with pessimists (Norem & Cantor,1986; Scheier & Carver, 1992, 1993). However,Scheier and Carver (1993) hypothesized thatexcessive optimism may be maladaptive in situa-tions that are uncontrollable. Supporting thishypothesis, active coping and expectations oftesting negative suggested less favorable adjust-ment among persons tested for Huntington'sdisease (Bloch et al., 1992; Codori & Brandt,1994, 1995; Huggins et al., 1992). We hypoth-esized that, among persons who tested positive,those with low perceived risk for Huntington'sdisease would be more distressed than partici-pants with high perceived risk for Huntington'sdisease.
Comparison groups for the current sample donot exist because the genetic bases for othercertainly fatal diseases are not yet known. How-ever, on the basis of studies of reactions ofHIV-positive patients to HIV testing (Catania,Turner, Choi, & Coates, 1992), and other studiesof patients temporally close to death (Filipp,1992), we predicted that genetically positivepersons closer to their estimated ages of onset ofHuntington's disease would be less well adjustedthan those farther from onset.
Method
Participants
The study sample consisted of adults participat-ing in the Baltimore Huntington's Disease Pre-symptomatic Testing Program at the Johns Hop-kins University School of Medicine. Allneurologically healthy (described below) andpsychologically healthy people (no serious Axis Idisorder or mental retardation) 18 or over with anaffected parent were eligible to participate.
One hundred sixty participants who receivedtheir genetic test results as of January 1. 1996were studied. Ninety-six persons were tested bylinkage, and 64 by direct detection. For the sakeof brevity, those who tested positive by linkage(marker positive, n = 30) or direct detection(gene positive, n = 22) are referred to as positive(n = 52). Similarly, those negative by linkage
(marker negative, n = 66) or direct detection(gene negative, n = 42) are labeled negative(n= 108; Table 1).
The sample included 4 positive and 3 negativeparticipants who chose to discontinue participa-tion before completing 1 year of follow-up. Aswe describe, the data analytic strategy usedallows inclusion of these participants. Compari-sons of those retained and those who discontin-ued (« = 7) on all predictor variables revealed nosignificant differences. However, those who dis-continued before 1 year had significantly lowerestimated IQ scores (95.43 versus 106.71),f(157) = -2.57, p = .01. Aside from these "dropouts," the remaining participants were activelyinvolved in follow-up, but not all participants haddata at all time points (Table 2).
Materials and Measures
Selection variables. To determine eligibility,we assessed participants in the following do-mains. Psychometric intelligence was estimatedby using a two-subtest short form of the WechslerAdult Intelligence Scale—Revised (WAIS-R: Vo-cabulary and Block Design subscales; Silver-stein, 1982). Neurologic status was evaluatedwith the Quantified Neurologic Exam (QNE;Folstein, 1983) conducted by a nurse and re-viewed by a physician. The QNE is a standard-ized and highly reliable examination of, largely,motor functioning that was specifically designedto rate the severity of Huntington's disease.Scores range from 0 to 120, and lower scores areindicative of better neurologic functioning. Psy-chologic status was assessed with the Schedulefor Affective Disorders and Schizophrenia—Lifetime Version (Endkott & Spitzer, 1978,1979;Hesselbrock, Stabenau, Hesselbrock, Mirkin, &Meyer, 1982).
Predictor variables. Sex, marital status (mar-ried vs. unmarried), and parenting status (havechildren vs. no children) were extracted from apersonal history questionnaire. Risk perceptionwas measured with a visual analogue scale.Visual analogue scales are a valid and reliablemeans of quantifying psychological constructsand have been used in the measurement of pain(Carlsson, 1983; Melzack, 1987), mood (Davies,Burrows, Poynton, 1975), quality of life (Ahlsio,Britton, Murray, & Theorell, 1984), and reactions

SPECIAL ISSUE: PREDICTING PSYCHOLOGICAL ADJUSTMENT 39
Table 1Sample Characteristics, Predictor Mean Scores, and Standard Deviations
Positive (n = 52) Negative (n = 108)
Variable M SD % M SD %
Education (in years) 14.92 2.60 14.36 2.58Employment status (at baseline)
Employed 86.5 90.7Homemaker 3.8 3.7Student 2 3.7Unemployed' 7.7 1.8
Estimated IQ 106.65 11.63 106.01 11.58Quantified Neurologic Exam 3.21 3.07 2.69 2.63Age 32.08 6.57 35.54 9.23*Sex (% women)" 52 59
Marital status"Unmarried 44.2 45.4Married 55.8 54.6
Parenting status" 46.2 49.1Risk perception (% risk)" 50.71 24.84 43.25 24.03Estimated years to onset" 9.77 6.12
"Indicates temporarily unemployed, disabled, or retired.*p = .007.
to HTV testing (Perry et al., 1990). Our scale make a vertical mark across the horizontal line,consisted of a 20-cm line with the anchors indicating their perceived likelihood for havingranging from (/ am absolutely certain that I will the Huntington's disease mutation. Position alongnot develop HD) to (/ am absolutely certain that I this line was converted to a 0 to 100 scale.will develop HD). Participants were asked to Huntington's disease most often begins by age
Table 2Raw Mean (and Standard Deviations) Adjustment Scores
Positive
Measurement
Beck Depression Inventory
Baseline
3 months
6 months
9 months
12 months
Beck Hopelessness Scale
Baseline
3 months
6 months
9 months
12 months
M
3.15
2.68
2.61
2.63
2.67
2.17
3.12
3.07
3.44
3.22
SD
3.53
3.01
4.21
3.56
4.10
2.14
3.16
3.13
3.09
3.51
n
52
4141
36
33
5241
41
3632
Negative
M
3.37
2.28
2.30
1.83
2.05
2.51
1.44
1.66
1.66
1.65
SD
3.59
3.24
3.42
2.72
3.11
2.30
1.73
1.97
2.07
2.45
n
107"
92
94
7276
107"
92
927175
P
ns
ns
ns
ns
ns
ns
.0002
.0016
.0012
.0029
"One participant was missing baseline Beck Depression Inventory score and was excludedfrom these analyses; a different participant was missing baseline Beck Hopelessness Scalescore and was excluded from these analyses.

40 CODORI, SLAVNEY, YOUNG, MIGLIORETTI, AND BRANDT
40, but can start in childhood or in senescence.Because onset is insidious and symptoms heterog-enous, onset is difficult to verify. By convention,disease onset is declared when movement disor-der (usually chorea) occurs. It is possible toestimate age of onset in gene carriers fromparental age of onset, parental sex, and the at riskperson's Huntington's disease mutation (CAGrepeat size; Ranen et al., 1995). Therefore, wecalculated estimated age of onset for all geneti-cally positive participants and used this to com-pute estimated years to onset by subtracting theparticipant's age at baseline from the estimatedonset age. For participants who tested positive bylinkage, we verified that they had the mutation bydirect detection and used this information tocalculate their estimated ages of onset.
Outcome variables. The Beck DepressionInventory (BDI; Beck, Steer, & Garbin, 1988)served as the first measure of adjustment. TheBDI consists of 21 items pertaining to the cogni-tive, affective, and somatic symptoms of depres-sion. It is well researched and has substantialsupport for its reliability and validity (Beck et al.,1988). Scores 0-9 are considered normal; scoresof 10-16 suggest mild depression; higher scoressuggest moderate-to-severe depression.
The Beck Hopelessness Scale (BHS; Beck,1974) was the second measure of adjustment. TheBHS is a 20-item true-false measure of pessi-mism and hopelessness (e.g., "I look forward tothe future with hope and enthusiasm" and "Ihave enough time to accomplish the tilings I mostwant to do"). Scores nine or above have beenshown to identify eventual suicides among psychi-atric inpatients and outpatients (Beck, Brown,Berchick, Stewart, & Steer, 1990; Beck &Weishaar, 1990). In addition, the future orienta-tion of the items may distinguish between peoplecurrently depressed and those who are pessimis-tic about the future because of their geneticstatus.
Design and Procedure
The research protocol has been approved bythe Johns Hopkins Joint Committee on ClinicalInvestigation and is fully described elsewhere(Brandt et al., 1989). The protocol includes a6-month baseline phase of counseling and evalu-ation followed by in-person disclosure of results.
A minimum of four psychoeducational counsel-ing sessions are conducted by a psychologist.Two of these sessions involve the participant'sspouse, or other family member or close friend,.who participates in the counseling and providessocial support. At least one session focuses on thedisease, its mode of inheritance, symptomatictreatments, the quantifiable risk to participant andoffspring, associations between parental and off-spring ages of onset, and the genetic test. Theremaining sessions are devoted to exploration ofthe participant's motives and expectations forbeing tested and the potential favorable andadverse consequences for the participant and hisor her family. Reasons for extremely optimistic orpessimistic perceptions of risk are explored.Additional counseling sessions are always of-fered and sometimes required by program staffbefore test results are disclosed. The counselingpsychologist is unaware of the participant's ge-netic test result before disclosure. The test resultis disclosed in person to the participant and his orher support person, and there is telephone contactthe next day with those who test positive. Regard-less of test result, every participant is assigned toa member of the clinical research staff (psychiat-ric nurse or psychiatrist) who is available to offerpsychological support, referrals, or both as needed.
Follow-up consists of eight in-person reassess-ments over a 3-year period at 3, 6, 9, 12, 18, 24,30, and 36 months after disclosure. In the currentstudy we examined adjustment during the firstyear after disclosure.
Early on in this project, genetic linkage was theavailable test (Brandt et al., 1989). In brief, at riskpersons were tested for the presence or absenceof a DNA marker that was linked to the Hunting-ton's disease gene mutation in their families.Having the marker conferred a very high probabil-ity (greater than 50%, and usually greater than90%) for having inherited the mutation. Con-versely, the absence of the marker was indicativeof low risk (less than 50%, and usually less than10%). The information disclosed to participantstested by linkage was the percentage of likeli-hood for having inherited the Huntington's dis-ease mutation. About 1 year after the discovery ofthe mutation for Huntington's disease, the directdetection test was used. Persons tested by directdetection were told either that they had or had not

SPECIAL ISSUE: PREDICTING PSYCHOLOGICAL ADJUSTMENT 41
inherited the mutation for Huntington's disease
(CAG repeats > 35). This test was described asbeing at least 99% accurate. Because of thechange in technology, some of the current samplewere tested by linkage and others by directdetection.
A random effects data analytic strategy wasused (Laird & Ware, 1982), which allows theinclusion of a "participant" variable that istreated as a random effect and accounts for thedependence between the repeated observations(Laird & Ware, 1982). In addition, a randomeffects model accepts the kind of unbalanced datagenerated in a longitudinal study in which newlyrecruited participants have missing (i.e., yet to becollected) observations (Laird & Ware, 1982).Assuming no cohort effect, data missing for thisreason were ignorable because the pattern ofabsence was independent of the outcome vari-ables (Little & Rubin, 1987). Furthermore, be-cause the parameters of the random effects modelwere estimated by using restricted maximumlikelihood, a likelihood-based approach, this type
of missing data was ignorable for the purpose ofmaking inferences about outcomes (Diggle,Liang, & Zeger, 1995). To test whether ourmissing data were truly ignorable, we created acode identifying participants whose data had notyet been collected because of recent ascertain-ment. Including this variable in a preliminaryanalysis showed that it had no relation to adjust-ment. Missing observations due to participantsdropping out may not be ignorable, however.Given our low drop out rate (4%), these partici-pants would have to be extremely different fromthe retained participants to alter the analysis.Nonetheless, we compared the retained and lostgroups on predictor and baseline adjustmentvariables and found no differences. In addition,we performed all analyses with and without thedrop outs to ensure that inferences were indepen-dent of their inclusion.
Data analyses were an iterative, hierarchicalprocess. First, separate random effects analysesexamining the relation between each predictor(genetic status, sex, marital status, parentingstatus, risk perception, and estimated years toonset) and both multiple-time-point outcome vari-ables were performed (PROC MIXED, SAS/STAT Software, 1992). In each model, the effect
of years to onset was nested within genetic testresult, meaning that it was estimated only for thepositives (Cohen & Cohen, 1983; Keppel, 1982).Next, all predictors, regardless of significancetests from the previous analysis, were included ina random effects model, entering covariates (base-line adjustment score and a code for the genetictest taken [linkage or direct detection]), main
effects, and interactions (Predictor X Genetic Sta-tus and Predictor X Genetic Status X Time Trend[linear and quadratic]; PROC MIXED, SAS/
STAT Software, 1992) in two models (one foreach adjustment measure). All time points of therepeated measures outcome data were includedtogether in the same model, and the linear andquadratic time trends were each captured by asingle parameter (i.e., the slope of the line acrossthe whole follow-up period). Thus, a singledegree-of-freedom estimate was used for eachtime effect (linear and quadratic). All predictorswere included to determine whether a variable,nonsignificant by itself, might be significant afteradjusting for other variables. In a final step,nonsignificant interactions with time were elimi-nated from the analyses, allowing us to examinethe lower order interactions of genetic status withthe predictors. Significant predictors in the finalmodels account for unique variance after adjust-ing for all other variables in the equation. Thisstrategy offers the mpst rigorous test of theassociations between predictors and adjustmentbecause associations are independent of the orderof variables in the equation. For all F tests,denominator degrees of freedom were calculatedby using the Satterthwaite approximation(McLean & Sanders, 1988; SAS/STAT Software,1996). This method adjusts the degrees of free-dom to account for the dependence between
repeated observations. Post hoc tests were per-formed only when there was a significant omni-bus F in a final model for a given predictor.
Because the ranges of the BDI and BHS scoreswere positively skewed, log,, transformationswere performed. Associations between predictorsand baseline levels of adjustment were examined(t tests or Pearson correlation). In addition, thegenetically positive and genetically negativegroups were compared at baseline on all mea-sures (r tests or chi-squares) to identify baselinegroup differences.

42 CODORI, SLAVNEY, YOUNG, MIOLIORETTI, AND BRANDT
Results
Sample Characteristics, Predictor and
Adjustment Mean Scores
The sample was well educated, employed, andhad average-range estimated IQ (Table 1). Onepercent were African American, with the remain-der Caucasian. Among marker-positive persons,average risk for Huntington's disease was 97%and ranged from 94% to 99%, signifying ex-
tremely high likelihood for having inherited theHuntington's disease mutation. Risk for marker-negative persons ranged from 1% to 8%, with theexception of 1 person at 30% risk.
All participants were neurologically symptom
free at baseline. Average QNE scores (M - 2.83SD = 2.81) were well below that of even mildlyaffected persons, whose scores average 19. Re-analysis of Baseline QNE X Genetic Statusshowed no differences between groups, f(158) =
0.56, p = .58; Table 1. Estimated years to onsetamong positives averaged 9.77 (SD — 6.12) andranged from -6.37 years to 22.18 years. The 1person with a negative estimate was clearly
unaffected, showing a QNE score of 0. Estimated
years to onset was uncorrelated with QNE scores(r=-.22,p = .ll).
Sample characteristics and predictor meanscores are summarized in Table 1. The onlybaseline group difference was on age, such thatpositive persons were significantly younger. Thiswas probably due to selection for asymptomaticpeople: Older positive persons would likely have
already become affected and been excluded fromthe study. The same selection factors likelyaccount for the greater number of negatives thanpositives in the sample.
Baseline adjustment was within normal limits,and there were no associations between predic-tors and baseline adjustment for the whole sample,
except that women were more hopeless than men,F(l, 175) = 4.69, p = .03. There were nobaseline adjustment differences between posi-tives and negatives (Table 2). Estimated years toonset in positives was uncorrelated with baselineBDI and BHS, further verification of the fact thatHuntington's disease (specifically psychologicalsymptoms) had not begun in those estimated tobe closer to onset. Mean BDI and BHS scoreswere in the normal range at all follow-ups in bothgroups (Table 2).
Multivariate Analyses
All predictors that were significant in theseparate analyses remained significant in the finalmodels, indicating that they contributed uniquevariance to adjustment both alone and afteraccounting for the covariates, other variables, andinteractions.
BDI. The final model is delineated in Table3. Baseline depressive symptoms strongly pre-dicted follow-up depressive symptoms. Afteraccounting for baseline level, however, only thetype of genetic test taken predicted adjustment, arelation that was not hypothesized. Regardless ofgenetic status, those tested by direct detectionhad more depressive symptoms at all follow-upsthan those tested by linkage. However, the link-
age- and direct-detection-tested participants wereequally well adjusted at baseline, suggesting thatthe difference was in their reaction to the geneticinformation.
BHS. The final model is delineated in Table4. Baseline hopelessness was a strong predictorof follow-up hopelessness. After accounting forbaseline level, other significant predictors in-cluded a significant Genetic Status X MaritalStatus X Quadratic Time interaction, with hope-lessness highest at 6 and 9 months. Post hoc
Table 3
Final Model: Beck Depression Inventory
Variable
Intercept
Baseline Beck DepressionInventory
Linear time
Quadratic time
Genetic status (GS)
Test code (TC; linkage vs.direct)
GSXTC
Estimated years to onset
Sex (S)
GS X S
Marital status (MS)
GSXMS
Parenting status (PS)GSXPS
Risk perception (RP)GS X RP
P
0.79
0.38
-0.02
0.00
-0.63
-0.43
0.30
-0.03
-0.14
0.37
0.04
-0.39
-0.05
0.47
0.00
0.00
SE
0.234
0.057
0.0460.003
0.342
0.119
0.219
0.015
0.117
0.217
0.128
0.246
0.128
0.249
0.0020.004
P
.0008
.0001
.68
.79
.07
.0004
.17
.10
.24
.09
.78
.12
.71
.06
.79
.38

SPECIAL ISSUE: PREDICTING PSYCHOLOGICAL ADJUSTMENT 43
Table 4Final Model: Beck Hopelessness Scale
Variable
Intercept
Baseline Beck HopelessnessScale
Linear time (LT)
Quadratic time (QT)
Genetic status (GS)
GSXLT
GSXQTTest code (TC; linkage vs.
direct)
GSXTC
Estimated years to onset
Sex (S)
G S X S
Marital status (MS)
MSXLT
MSXQT
GSXMS
GS X MS X LTGS X MS X QT
Parenting status (PS)
GSXPS
Risk perception (RP)GSXRP
p SE
0.39 0.217
0.53 0.063-0.12 0.048
0.00 0.003
0.04 0.395
0.15 0.086
0.00 0.006
-0.04 0.099
0.00 0.181-0.03 0.013
-0.01 0.097
0.17 0.179-0.32 0.255
0.13 0.073
-0.01 0.004
0.72 0.474
-0.42 0.1350.03 0.009
0.19 0.1050.46 0.200
0.00 0.002
0.00 0.004
P
.07
.0001
.73
.82
.91
.08
.09
.72
1.00.01
.88
.34
.21
.09
.12
.13
.002
.003
.08
.02
.46
.63
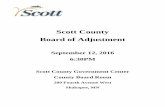
analyses showed that married positives weremote hopeless than unmarried positives at the 6-,9-, and 12-month follow-ups, f(194) = -3.73,p < .001; f(197) = -3.87, p < .001; andf(290) = -1.97, p= .05, respectively, and morehopeless than married negatives at all follow-ups,f(272) = 4.42, p < .001; f(214) = 6.19, p < .001;r(219) = 6.22, p < .001; and f(311) = 4.42, p <.001, for 3-12 months, respectively; see Figure 1.
Among the positives, there was a significanteffect for estimated years to onset, and no interac-tion with time (see Table 4). Positives closer toonset were more hopeless than those further fromonset throughout the follow-up period (see Fig-
ure 2). This effect remained even after eliminat-ing the 1 participant with a negative estimated
years-to-onset estimate.Finally, there was a significant Genetic Status X
Parenting Status interaction, and no interactionwith time. Post hoc tests showed that positiveswithout children were more hopeless than nega-
tives without children, f(235) = 4.77, p < .001;see Figure 3.
In summary, baseline hopelessness, geneticstatus, marital status, follow-up time, parentingstatus, and years to onset (among positives) weresignificant predictors of hopelessness after test-ing, with each effect contributing unique variancebeyond that accounted for by the others.
Discussion
In the present study, average distress measuresin both genetically positive and genetically nega-tive groups were below clinical cutoffs. It isstriking that mean levels of adjustment in bothgroups were good. Generally good adjustmentmay reflect self-selection for the perceived capac-ity to handle "bad news" (Codori, Hanson, &Brandt, 1994; Tyler, Ball, & Craufurd, 1992; vander Steenstraten, Tibben, Roos, van de Kamp, &Niermeijer, 1994). People who feel ill-equippedto know that they will develop this fatal diseasemay not ask for the test. In addition, it is possiblethat the drop outs could have been destined tobecome severely distressed during the first year.Baseline adjustment was the strongest predictorof both measures of follow-up adjustment, asfound by Tibben, Duivenvoorden, et al. (1993)and as would be predicted without additionalinformation on those tested.
Only the BHS showed the predicted adjust-ment difference between positives and negatives,suggesting that unfavorable genetic informationdoes not generally produce clinical depressivesyndromes. Rather, it leads to more pessimisticviews of the future, understandable in light of thefact that the genetic information is most relevantfor future, not current, health. As hypothesized,all other predictors of adjustment showed signifi-cant interactions with genetic status.
Several variables added to the prediction ofadjustment over and above baseline adjustment.One was unpredicted. People tested by directdetection had higher depression scores at fol-low-up than those tested by linkage. The lack ofbaseline differences between these two groupsimplies that something about the informationaccounts for the effect. A partial explanation ofthis testing method effect may be found in thegreater certainty of prediction in the direct detec-tion method. Among the positives, the marker

44 CODORI, SLAVNEY, YOUNG, MIGLIORETn, AND BRANDT
Unnwiwd PosRlvBs
Unn
6Monttu 9 Months 12 Month*
Figure 1. Adjusted hopelessness score (Beck Hopelessness Scale; Beck, 1974) as afunction of genetic status and marital status. Scores are adjusted for variables inTable 4 in the text. Means at each time point were estimated from the model and backtransformed to the original scale.
' 2
0-1
- 6 - 4 - 2 0 2 4 6 8 10 12 14
Estimated Years to Onset
16 IB 20 22
Figure 2. Association between adjusted hopelessness score (Beck HopelessnessScale; Beck, 1974) and estimated years to onset among positives. Scores are adjustedfor variables in Table 4 in the text.

SPECIAL ISSUE: PREDICTING PSYCHOLOGICAL ADJUSTMENT
4
NoCMUran
45
2 CMUran
3 Month* Month*
Figure 3. Adjusted hopelessness score (Beck Hopelessness Scale; Beck 1974) as afunction of genetic status and parenting status. Scores are adjusted for variables inTable 4 in the text. Means at each time point were estimated from the model and backtransformed to the original scale.
positives may have been consoled by knowingthat there existed at least a 1% chance that theyreally did not "have the gene." Among genepositives, there was virtually no such margin.Greater test accuracy does not account for thefact that the gene negatives were among thosewho were less well adjusted. In fact, given thisreasoning, gene negatives should have been morewell adjusted. One other possibility is a cohorteffect (Adam, Wiggins, Lawson, McKellin, &Hayden, 1995), whereby people who present forlinkage testing may be more well adjusted andhave greater social support than those who do nothave to orchestrate a family wide effort to collectblood samples. As previously noted, however,our linkage and direct detection groups did notdiffer at baseline. Exploration of this findingawaits future research.
Contrary to prediction, women were just aswell adjusted as men. Although this is inconsis-tent with research on the psychological reactionsof men and women to the same stressors, it mayreflect the fact that the studied sample asked forthe information that they received. Availableresearch on reactions to illness or crisis is focused
on an unexpected stressor, whereas predictivetesting for Huntington's disease is the epitome ofan "elective stressor." This finding may befurther evidence for the view that those who askto be tested are self-selected for the capacity tohandle the news.
We hypothesized that positives who had lowerperception of risk for Huntington's disease wouldbe less well adjusted. The prediction was unsup-ported. One explanation concerns the issue ofcontrollability. Although the test outcome wasuncontrollable, participants had control over thedecision to be tested. Perhaps control over thedecision to be tested mitigated the effects of lowrisk perception. Alternatively, it may not be riskperception, but rather coping style, more directly,that would have predicted adjustment The cur-rent data cannot address this possibility, butcoping and reactions to testing are a subject ofongoing research. Finally, dichotomizing riskperception scores as well-below or well-above50% may have more effectively categorized thesample into groups with extreme expectations ofthe test outcome.
Contrary to our prediction and previous re-

46 CODORI, SLAVNEY, YOUNG, MIGLIORETTI, AND BRANDT
search, married positive persons were less welladjusted than single positives at the 6-, 9-, and12-month follow-ups. Given that this effect isindependent of parenting status, it is not simplythat married persons were reacting to demandedchanges in their family planning or to guilt forhaving possibly passed on the mutation. Rather, itmay be that married positives were concernedabout becoming burdens to their spouses. Thisconcern has been reported by participants whotest positive for Huntington's disease (Codori &Brandt, 1994). Unlike single persons, marriedpositives have the added psychological stress ofknowing that they are "causing" distress insomeone close to them. Alternatively, positivesmay have been affected by their spouses' reac-tions to the news. With no measure of spousereactions, it is impossible to test this hypothesis.
Partially consistent with prediction, marriedpositives were less well adjusted than marriednegatives throughout the follow-up period. Giventhe preceding discussion, however, it is unlikelythat the genetic information, alone, accounts forthe differences between the two married groups.Additional research is needed to clarify thesefindings.
Closer proximity to estimated onset amongpositives was associated with poorer adjustmentat all time points. As suggested by research withterminally ill and asymptomatic HIV popula-tions, distress increased as positives moved closerto confronting their mortality. Such a meaningfulinterpretation of our finding is dependent onruling out the onset of Huntington's disease,which could also account for the observed changesin mood in positives. In the neurologic domain,the current sample is unequivocally asymptom-atic. Of course, it is possible that mood symptomscould precede neurological symptoms (Folstein,1989). If this were the case, however, estimatedyears to onset should have been correlated withbaseline BHS. One final possibility is that, de-spite the lack of symptoms correlated with prox-imity to onset, there may be underlying neuropa-thology that is correlated with mood changes(i.e., hopelessness; Aylward et al., 1994).
Our prediction that parents who tested positivewould be less well adjusted than positives with-out children was unsupported. Instead, positiveswithout children were more hopeless throughoutthe follow-up period than negatives without chil-
dren. If positives with children experienced guiltat the possibility of having passed on the gene, itwas not evident in their hopelessness scores. Aspecific guilt measure might have been moresensitive to such a reaction. The identified reac-tion suggests a different process. Many married,childless persons seek out predictive testing withthe intention of foregoing children if they testpositive. Consequently, the observed finding mayreflect disappointment at foregoing a family.Many of our positive participants have foregonehaving children, but not all. Among those whosubsequently had children hi spite of their testresult, there may have been trepidation aboutpassing on the mutation—not only for them-selves but for what any mutation-positive chil-dren may face in the future.
We hypothesized that adjustment after genetictesting would show one of two relations withtime. One possibility is that there could have beenlinearly decreasing distress after the 3-monthfollow-up, as shown in much research on stressreactions. Alternatively, we speculated that therecould have been a delayed reaction until theinformation, pertaining mostly to the future, wasassimilated. The latter reasoning predicts thatdistress after testing may fit a quadratic trend.Only for marital status did we find any interactionwith time, although there were other interactionswith time that approached significance (Table 4).Married positives were most distressed at 6 and 9months, and distress was on the downturn at 12months. This finding is perhaps most interest-ingly discussed in relation to the lack of timetrends for positives without children and posi-tives closer to estimated onset, in whom hopeless-ness remained elevated throughout follow-up.Enduring hopelessness in positives without chil-dren may reflect ongoing contemplation abouthow to use the genetic information in familyplanning. It is likely that family planning deci-sions would evolve over months, perhaps prolong-ing the resolution of the stress reaction. For thosecloser to estimated onset, the passage of timeonly brings them closer to onset, also prolongingexposure to the stressor. Whatever specific factorwas operative among married positives, theyappeared to be starting to "put it behind them" bythe 12-month follow-up (McCain & Gramling,1992).
We found no obvious contraindications to

SPECIAL ISSUE: PREDICTING PSYCHOLOGICAL ADJUSTMENT 47
predictive genetic testing for Huntington's dis-
ease. We have, however, identified risk factors forsuboptimal adjustment. Baseline level of distresswill certainly predict psychological reaction. Be-yond baseline adjustment, given a positive testresult, married persons, persons without children,and those closer to onset will fare less well. The
distress affecting married persons may declinetoward the end of the first follow-up year. Thedistress experienced by those closer to onset and
by those without children may persist throughoutthe first year. The present findings may be appliedto the preparation of at risk persons for predictivetesting, however, they raise more questions thanthey answer. For example, it is not yet clear whatabout being married, not having children, or
being closer to onset are the critical factors inadjustment. Future research will undoubtedlyhelp clarify these issues.
References
Adam, S., Wiggins, S., Lawson, K., McKellin, B., &.Hayden, M. (1995). Predictive testing for Hunting-ton disease (HD): Differences in uptake and charac-teristics of linked marker and direct test cohorts.American Journal of Human Genetics, 57 (Suppl.),A292.
Ahlsio, B., Britton. M., Murray, V., & Theorell, T.(1984). Disablement and quality of life after stroke.Stroke, 15, 886-890.
Andersen, B. L., Anderson, B., & DeProsse, C. (1989).Controlled prospective longitudinal study of womenwith cancer: II. Psychological outcomes. Journal ofConsulting and Clinical Psychology, 57, 692-697.
Aylward, E. H., Brandt, J., Codori, A. M., Mangus,R. S., Barta, P. E., & Harris, G. J. (1994). Reducedbasal ganglia volume associated with the gene forHuntington's disease in asymptomatic at-risk per-sons. Neurology, 44, 823-828.
Baider, L., Perez, T., & De-Nour, A. K. (1989). Genderand adjustment to chronic disease: A study ofcouples with colon cancer. General Hospital Psy-chiatry, II, 1-8.
Beck, A. T. (1974). The measurement of pessimism:The Hopelessness Scale. Journal of Consulting andClinical Psychology, 42, 861-865.
Beck, A. T., Brown, G., Beichick, R. J., Stewart, B. L.,& Steer, R. A. (1990). Relationship between hope-lessness and ultimate suicide: A replication with
psychiatric outpatients. American Journal of Psy-chiatry, 147, 190-195.
Beck, A. T., Steer, R. A., & Gatbin, M. (1988).Psychometric properties of the Beck DepressionInventory: Twenty-five years of evaluation. ClinicalPsychology Review, 8, 77-100.
Beck, A. T., & Weishaar, M. W. (1990). Suicide riskassessment and prediction. Crisis, 11, 22-30.
Blanchard, E. B., Hickling, E. J., Vollmer, A. J., Loos,W. R., Buckley, t. C., & Jaccard, J. (1995).Short-term follow-up of post-traumatic stress symp-toms in motor vehicle accident victims. BehaviourResearch and Therapy, 33, 369-377.
Bloch, M., Adam, S., Wiggins, S., Muggins, M., &Hayden, M. (1992). Predictive testing for Hunting-ton disease in Canada: The experience of thosereceiving an increased risk. American Journal ofMedical Genetics, 42, 499-507.
Brandt, J. (1994). Ethical considerations in genetictesting: An empirical study of presymptomaticdiagnosis of Huntington's disease. In K. W. M.Fulford (Ed.), Medicine and moral reasoning (pp.41-59). New York: Cambridge University Press.
Brandt, J., Quaid, K., Folstein, S., Garter, R, Maestri,N., Abbott, M., Slavney, P. R., Franz, M. L., Kasch,L., & Kazazian, H. H. (1989). Presymptomaticdiagnosis of delayed-onset disease with linkedDNA markers: The experience of Huntington'sdisease. Journal of the American Medical Associa-tion, 261', 3108-3114.
Carlsson, A. M. (1983). Assessment of chronic pain: I.Aspects of the reliability and validity of the visualanalogue scale. Pain, 16, 87-101.
Catania, J. A., Turner, H. A., Choi, K. H., & Coates,T. J. (1992). Coping with death anxiety: Help-seeking and social support among gay men withvarious HIV diagnoses. AIDS, 6, 999-1005.
Codori, A. M., & Brandt, J. (1994). Psychologicalcosts and benefits of predictive genetic testing forHuntington's disease. American Journal of MedicalGenetics (Neuropsychiatric Genetics), 54, 174-184.
Codori, A. M., & Brandt, J. (1995). Stress and copingin predictive genetic testing for Huntington's dis-ease. Annals of Behavioral Medicine, 17 (Suppl.),S139.
Codori, A. M., Hanson, R., & Brandt, J. (1994).Self-selection in predictive testing for Huntington'sdisease. American Journal of Medical Genetics(Neuropsychiatric Genetics), 54, 167-173.
Cohen, J., & Cohen, P. (1983). Applied multiple

48 CODORI, SLAVNEY, YOUNG, MIGLIORETTI, AND BRANDT
regression/correlation analysis for the behavioralsciences (2nd ed). Hfflsdale, NJ: Erlbaum.
Davies, B., Burrows, G., & Poynton, C. (1975). Acomparative study of four depression rating scales.Australian and New Zealand Journal of Psychiatry,9, 21-24.
Diggte, P. J., Liang, K. -Y., & Zeger, S. L. (1995).Analysis of longitudinal data. New York: OxfordUniversity Press.
Eden-Piercy, G. V., Blacher, J. B., & Eyman, R. K.(1986). Exploring parents' reactions to their youngchild with severe handicaps. Mental Retardation,24, 285-291.
Endicott, J., & Spitzer, R. L. (1978). A diagnosticinterview: The Schedule for Affective Disordersand Schizophrenia. Archives of General Psychiatry,35, 837-844.
Endicott, J., & Spitzer, R. L. (1979). Use of theResearch Diagnostic Criteria and the Schedule forAffective Disorders and Schizophrenia to studyaffective disorders. American Journal of Psychia-try, 136, 52-56.
Fairer, L. (1987). Suicide and presyDiplomatic testingin Huntington disease. American Journal of Medi-cal Genetics, 25,577-588.
Filipp, S. -H. (1992). Could it be worse? The diagnosisof cancer as a prototype of traumatic life events. InL. Montada, S. -H. Filipp, & M. J. Lerner (Eds.),Life crises and experiences of loss in adulthood (pp.23-56). Hillsdale, NJ: Erlbaum.
Folstein, S. E. (1983). The measurement of abnormalmovement: Methods developed for Huntington'sdisease. Neumbehavioral toxicology and teratol-ogy, 5, 605-609.
Folstein, S. E. (1989). Huntington's disease: A disor-der of families. Baltimore, MD: Johns HopkinsUniversity Press.
Gardner, R. A. (1969). The guilt reaction of parents ofchildren with severe physical disease. AmericanJournal of Psychiatry, 126, 636-644.
Gave, W. R. (1984). Gender differences in mental andphysical illness: The effects of fixed roles andnurturant roles. Social Science and Medicine, 19,77-91.
Gove, W. R., Hughes, M., & Style, C. B. (1983). Doesmarriage have positive effects on the psychologicalwell-being of the individual? Journal of Health andSocial Behavior, 24, 122-131.
Gusella, J. R, Wexler, N. S., Conneally, P. M., Naylor,S. L., Anderson, M. A., Tanzi, R. E., Watkins, P. C.,Ottina, K., Wallace, M. R., Sakaguchi, A. Y., Young,
A. B., Shoulson, I., Bonilla, E., & Martin, J. B.(1983). A polymorphic DNA marker genetically
linked to Huntington's disease. Nature, 306, 234-238.
Harper, P. (Ed.). (1991). Huntington's disease. Phila-delphia: W. B. Saunders.
Hesselbrock, V, Stabenau, J., Hesselbrock, M., Mir-kin, P., & Meyer, R. (1982). A comparison of twointerview schedules. The Schedule for Affective
Disorders and Schizophrenia—Lifetime and theNational Institute for Mental Health DiagnosticInterview Schedule. Archives of General Psychia-try, 39, 674-677.
Huggins, M., Bloch, M., Kanani, S., Quarrel], O. W. J.,Theilman, J., Hedrick, A., Dickens, B., Lynch, A., &Hayden, M. (1990). Ethical and legal dilemmas
arising during predictive testing for adult-onsetdisease: The experience of Huntington disease.American Journal of Human Genetics, 47, 4—12.
Huggins, M., Bloch, M., Wiggins, S., Adam, S.,Suchowersky, O., Trew, M., Klimek, M., Green-berg, C. R., Eleff, M., Thompson, L. P., Knight, J.,MacLeod. P., Girard, K., Theilmann, J., Hedrick, A.,& Hayden, M. (1992). Predictive testing for Hunting-ton disease in Canada: Adverse effects and unex-pected results hi those receiving a decreased risk.American Journal of Medical Genetics, 42, 508-515.
Huntington's Disease Collaborative Research Group.(1993). A novel gene containing a trinucleotide
repeat that is expanded and unstable on Hunting-ton's disease chromosomes. Cell, 72,971-983.
Joung, I. M., van der Meer, J. B., & Mackenbach, J. P.(1995). Marital status and health care utilization.International Journal of Epidemiology, 24, 569-575.
Kennedy, C. A., Skurnick, J. H., Foley, M., & Louria,D. B. (1995). Gender differences in HTV-reiatedpsychological distress in heterosexual couples. AIDSCare, 7 (Suppl.), S33-38.
Keppel, G. (1982). Design and analysis: A research-er's handbook (2nd ed.). Englewood Cliffs, NJ:Prentice Hall.
Kessler, S. (1987a). The dilemma of suicide andHuntington disease. American Journal of MedicalGenetics, 26, 315-317.
Kessler, S. (1987b). Psychiatric implications of pre-symptomatic testing for Huntington's disease. Ameri-can Journal of 'Orthopsychiatry, 57, 212-219.
Laird, N. M., & Ware, J. H. (1982). Random-effects

SPECIAL ISSUE: PREDICTING PSYCHOLOGICAL ADJUSTMENT 49
models for longitudinal data. Biometrics, 38, 963-974.
Lam, R. W., Bloch, M., Jones, B. D., Marcus, A. M.,Fox, S., Amman, W., & Hayden, M. (1988). Psychi-atric morbidity associated with early clinical diagno-sis of Huntington disease in a predictive testingprogram. Journal of Clinical Psychiatry, 49, 444-447.
Little, R. J. A., & Rubin, D. B. (1987). Statisticalanalysis with missing data. New York: Wiley.
Martin, J. L., & Dean, L. (1993). Effects of AIDS-related bereavement and HIV-related illness onpsychological distress among gay men: A 7-yearlongitudinal study, 1985-1991. Journal of Consult-ing and Clinical Psychology, 61,94-103.
Mastekaasa, A. (1994). Marital status, distress, andwell-being: An international comparison. Journal ofComparative Family Studies, 25, 183-205.
McCain, N. L., & Gramling, L. F. (1992). Living withdying: Coping with HIV disease. Issues in MentalHealth Nursing, 13, 271-284.
McLean, R. A., & Sanders, W. L. (1988). Approximat-ing degrees of freedom for standard errors in mixedlinear models. In Proceedings of the StatisticalComputing Section, American Statistical Associa-tion (pp. 50-69). Alexandria, VA: American Statisti-cal Association.
Meissen, G., Myers, R., Mastromauro, C., Koroshetz,W., Klinger, K., Farrer, L., Watkins, P., Gusella, J.,Bird, E., & Martin, J. (1988). Predictive testing forHuntington's disease with use of a linked DNAmarker. New England Journal of Medicine, 318,535-542.
Melzack, R. (1987). The short-form McGill PainQuestionnaire. Pain, 30, 191-197.
Moulton, J. M., Stempel, R. R., Bacchetti, P., Temo-shok, L., & Moss, A. R. (1991). Results of a oneyear longitudinal study of HIV antibody test notifi-cation from the San Francisco General Hospitalcohort. Journal of Acquired Immune DeficiencySyndromes, 4, 787-794.
Norem, J. K., & Cantor, N. (1986). Anticipatory andpost hoc cushioning strategies: Optimism and defen-sive pessimism in "risky" situations. CognitiveTherapy and Research, 10, 347-362.
Olsen, D. G. (1994). Parental adjustment to a childwith genetic disease: One parent's reflections. Jour-nal of Obstetric and Gynecological Neonatal Nurs-ing, 23, 516-518.
Perry, S. W., Jacobsberg, L. B., Fishman, B., Weiler,P. H., Gold, J. W., & Frances, A. J. (1990).
Psychological responses to serological testing fortOV.AIDS,4, 145-152.
Post, N. (1992). Ethical implications of screeningasymptomatic individuals. FASEB Journal, 6, 2813-2817.
Ranen, N. G., Stine, O. C., Abbott, M. H., Sherr, M.,Codori, A. M., Franz, M. L., Chao, N. I., Chung,A. S., Pleasant, N., Callahan, C., Kasch, L. M.,Ghaffari, M., Chase, G. A., Kazazian, H. H., Brandt,J., Folstein, S. E., & Ross, C. A. (1995). Anticipa-tion and instability of the IT-15 (CAG)n repeats inparent-offspring pairs with Huntington disease.American Journal of Human Genetics, 57, 593-602.
Rodrigue, J. R., & Park, T. L. (1996). General andillness-specific adjustment to cancer: Relationshipto marital status and marital quality. Journal ofPsychosomatic Research, 40, 29-36.
Ryan, A. S., & Smith, M. J. (1989). Parental reactionsto developmental disabilities in Chinese Americanfamilies: Families of children with developmentaldisabilities [Special issue}. Child and AdolescentSocial Work Journal, 6, 283-299.
SAS/STAT Software. (1992). Changes & enhance-ments (Release 6.07). SAS technical report P-229(p. 354). Gary, NC: SAS Institute.
SAS/STAT Software. (1996). SAS manual (p. 566).Gary, NC: SAS Institute.
Scheier, M. F., & Carver, C. S. (1992). Effects ofoptimism on psychological and physical well-being: Theoretical overview and empirical update.Cognitive Therapy and Research, 16, 201-228.
Scheier, M. F., & Carver, C. S. (1993). On the powerof positive thinking: The benefits of being optimis-tic. Current Directions in Psychological Science, 2,26-30.
Silverstein, A. B. (1982). Two- and four-subtest shortforms of the Wechsler Adult Intelligence Scale—Revised. Journal of Consulting and Clinical Psy-chology, 50, 415-«8.
Solomon, Z. (1989). Psychological sequelae of wan A3-year prospective study of Israeli combat stressreaction casualties. Journal of Nervous and MentalDisease, 177, 342-346.
Steinglass, P., & Gerrity, E. (1990). Natural disastersand post-traumatic stress disorder: Short-term ver-sus long-term recovery in two disaster-affectedcommunities. [Special issue]. Journal of AppliedSocial Psychology, 20, 1746-1765.
Surtees, P. G., & Miller, P. M. (1994). Partners inadversity: III. Mood status after the event. Euro-

50 CODORI, SLAVNEY, YOUNG, MIGLIORETTI, AND BRANDT
peon Archives of Psychiatry and Clinical Neurosci-
ence, 243, 311-318.
Tibben, A., Duivenvoorden, H., Niermeijer, M., Vegter-
van der Vlis, M., Roos, R., & Verhage, F. (1994).
Psychological effects of presymptomatic DNA test-
ing for Huntington's disease in the Dutch program.
Psychosomatic Medicine, 56, 526-532.
Tibben, A., Duivenvoorden, H., Vegter-van der Vlis,
M., Niermeijer, M., Frets, P., van de Kamp, J., Roos,
R., Rooijmans, H., & Verhage, F. (1993). Presymp-
tomatic DNA testing for Huntington disease: Identi-
fying the need for psychological intervention. Ameri-
can Journal of Medical Genetics (Neuropsychiatric
Genetics), 48, 137-144.
Tibben, A., Frets, P., van de Kamp, J., Niermeijer, M.,
Vegter-van der Vlis, M,, Roos, R., Rooymans, H.,
van Ommen, G. -J., & Verhage, F. (1993). On
attitudes and appreciation 6 months after predictive
DNA testing for Huntington disease in the Dutch
program. American Journal of Medical Genetics
(Neuropsychiatric Genetics), 48, 103-111.
Tyler, A., Ball, D., & Craufurd, D. (1992). Presymp-
tomatic testing for Huntington's disease in the
United Kingdom. British Medical Journal, 304,
1593-1596.
Ursano, S. J., Fulleiton, C. S., Kao, T. C., & Bhartiya,
V. R. (1995). Journal of Nervous and Mental
Disorders, 183, 36-42.
van der Steenstraten, I. M., Tibben, A., Roos, R., van
de Kamp, J., & Niermeijer, M. (1994). Predictive
testing for Huntington's disease: Nonparticipants
compared with participants in the Dutch program.
American Journal of Human Genetics, 55, 618—
625.
Verbrugge, L. M. (1985). Gender and health: An
update on hypotheses and evidence. Journal of
Health and Social Behavior, 26, 156-182.
Wexler, N. (1992). The Tiresias complex: Hunting-
ton's disease as a paradigm of testing for late-onset
disorders. FASEB Journal, 6, 2820-2825.
Wiggins, S., Whyte, P., Huggins, M., Adam, S.,
Theilmann, J., Bloch, M., Sheps, S., Schechter,
M. T., & Hayden, M. (1992). The psychological
consequences of predictive testing for Huntington's
disease. New England Journal of Medicine, 327,
1401-1405.
Wyke, S., & Ford, G. (1992). Competing explanations
for associations between marital status and health.
Social Science and Medicine, 34, 523-532.