Predictors of Disease Onset and Progression in Early ...
66
UMEÅ UNIVERSITY MEDICAL DISSERTIONS New Series No 1001-ISSN 0346-6612-ISBN 91-7264-003-0 From the Department of Public Health and Clinical Medicine, Rheumatology, Umeå University, Umeå, Sweden Predictors of Disease Onset and Progression in Early Rheumatoid Arthritis A Clinical, Laboratory and Radiological Study Ewa Berglin Umeå 2006
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Predictors of Disease Onset and Progression in Early ...
UMEÅ UNIVERSITY MEDICAL DISSERTIONS New Series No 1001-ISSN 0346-6612-ISBN 91-7264-003-0
From the Department of Public Health and Clinical Medicine, Rheumatology,
Umeå University, Umeå, Sweden
Predictors of Disease Onset and Progression
in Early Rheumatoid Arthritis
A Clinical, Laboratory and Radiological Study
Ewa Berglin
Umeå 2006
Copyright © Ewa Berglin Department of Public Health and Clinical Medicine, Rheumatology University Hospital, Umeå, Sweden Printed in Sweden by Solfjädern Offset AB Umeå 2006

To Viking and Daniel

Contents _______________________________________________________________________________________
1
CONTENTS Abstract………………………………………………………………………………….... 2
Abbreviations……………………………………………………………………………... 3
Original papers……………………………………………………………………………. 4
Introduction……………………………………………………………………………….. 5 Rheumatoid arthritis……………………………………………………………………….. 5 History……………………………………………………………………………………… 5 Epidemiology………………………………………………………………………………. 5 Aethiology………………………………………………………………………………….. 5 Pathogenesis of synovial inflammation and joint destruction……………………………... 6 Autoantibodies in rheumatoid arthritis…………………………………………………….. 7 Disease onset, clinical presentation and diagnosis………………………………………… 8 Disease development………………………………………………………………………. 9 Assessment of disease activity and outcome……………………………………………... 10 Pharmacological treatment………………………………………………………………... 11 Prediction of radiological outcome in early RA………………………………………….. 13
Aims………………………………………………………………………………………. 15
Subjects and methods…………………………………………………………………… 16 The Medical Biobank, the Maternity cohort and identification of samples………………. 16 Patients, pre-patients and controls……………………………………………………….... 17 Methods………………………………………………………………………………….... 20
Results and discussions………………………………………………………………….. 25 CR/DXA-study (Paper I)…………………………………………………………………. 25 Discussion (Paper I)………………………………………………………………………. 28 Studies on autoantibodies and HLA SE alleles as predictors of RA onset (Papers II-III)... 29 Discussion (Papers II and III)…………………………………………………………….. 34 Study on autoantibodies and HLA SE alleles as predictors of RA severity and progression (Paper IV)……………………………………………………………………. 35 Discussion (Paper IV)…………………………………………………………………….. 39
Concluding remarks…………………………………………………………………….. 42
Conclusions………………………………………………………………………………. 44
Sammanfattning på svenska……………………………………………………………. 45
Acknowledgements………………………………………………………………………. 47
References……………………………………………………………………………….. 48
Papers I-IV

Abstract _______________________________________________________________________________________
2
Predictors of Disease Onset and Progression in Early Rheumatoid Arthritis A Clinical, Laboratory and Radiological Study Ewa Berglin, Department of Public Health and Clinical Medicine, Rheumatology, University Hospital, SE-901 87 Umeå, Sweden
To diagnose rheumatoid arthritis (RA) during the early stages of the disease is often difficult. The disease course shows great inter-individual variation from mild, self-limiting to very severe destruc-tive disease with extra-articular manifestations. Early aggressive treatment with potentially toxic drugs has been shown to improve the long-term outcome. Thus, it is desirable to make an early reliable di-agnosis and to identify those patients who would benefit from being treated most aggressively.
The aim of this thesis was to evaluate laboratory and clinically markers of inflammation as predic-tors of disease course, to compare dual-energy X-ray absorptiometry (DXA) and conventional radiog-raphy (CR) as measures of joint destruction and to investigate the significance of antibodies against cyclic citrullinated peptide (anti-CCP antibodies), rheumatoid factors (RFs) and HLA shared epitope (SE) alleles for the relative risk of future development of RA and as predictors of disease severity in patients with early RA.
Patients with RA of recent onset are included in the early RA programme at the Department of Rheumatology, University Hospital, Umeå and are followed longitudinally. The prediction of markers of inflammation for bone loss and radiological outcome was analyzed in the first 43 patients recruited. Radiographs of hands and feet (Larsen score) and bone mineral density (BMD) in hands (DXA), were assessed at baseline, after 1 and 2 years. The disease activity was evaluated clinically and by labora-tory tests. Radiological damage increased significantly during the study and was particularly corre-lated with Larsen score at baseline. BMD in hands decreased significantly in postmenopausal women and the decrease was greater than in healthy matched controls. Radiological progression and bone loss in hands was retarded by an early response to therapy.
In a case-control study within the Medical Biobank and the Maternity cohort of Northern Sweden, patients from the early RA programme were identified among blood donors from whom samples had been collected years before onset of symptoms. The prevalence of anti-CCP antibodies and RFs (IgA-RF, IgG-RF and IgM-RF) was investigated in samples from 83 individuals (pre-patients) and com-pared with matched controls. SE alleles were assessed in a sub-group of 59 individuals. Anti-CCP antibodies and RFs preceded onset of RA by several years and increased in prevalence closer to dis-ease onset. Anti-CCP antibodies and IgA-RF significantly predicted the onset of RA. The combination of anti-CCP antibodies and SE alleles was associated with a high relative risk for future development of RA.
In a later co-analysis between the register of patients in the early RA programme (n=138) and the Medical Biobank and the Maternity cohort, 93 pre-patient samples were identified. The significance of SE alleles and of the presence of anti-CCP antibodies and RFs before and at disease onset for disease activity and severity was studied. Radiographs of hands and feet were assessed at baseline and after 2 years (Larsen score). The presence of anti-CCP antibodies in pre-patient samples and at baseline was associated with radiological damage, as was presence of all RFs at baseline. A higher titre of anti-CCP antibodies was associated with greater radiological progression. The titre was lowered by a therapeutic response. In multiple logistic regression analyses anti-CCP antibodies, IgA-RF, ESR and swollen joint count predicted greater radiological progression, whilst a therapeutic response predicted a lesser pro-gression.
In conclusion, anti-CCP antibodies and IgA-RF are predictors for future onset of RA and for radio-logical destruction and progression. The combination of anti-CCP antibodies and SE alleles is associ-ated with a high relative risk for future RA. Therapeutic response decreases the radiological progres-sion and the bone loss in hands and lowers the titre of anti-CCP antibodies. Conventional radiography is a better measure of joint destruction than DXA.
Key-words: Early rheumatoid arthritis, anti-CCP antibodies, rheumatoid factors, radiological out-come, disease onset
Abbreviations _______________________________________________________________________________________
3
Abbreviations Abs Antibodies
ACR American College of Rheumatology
Anti-CCP anti-cyclic citrullinated peptide
APC(s) antigen presenting cell(s)
BMD bone mineral density
CI confidence interval
CR Conventional radiography
CRP C-reactive protein
DAS disease activity score
DAS28 disease activity score based on 28 joint count
DXA dual-energy X-ray absorptiometry
DMARD(s) disease modifying anti rheumatic drug(s)
EIA enzyme immunoassay
ELISA enzyme-linked immunosorbent assay
ESR erythrocyte sedimentation rate
EULAR European League Against Rheumatism
HAQ health assessment questionnaire
HLA human leukocyte antigen
Ig immunoglobulin
IQR interquartile range
MCP metacarpophalangeal
MRI magnetic resonance imaging
MTP metatarsophalangeal
NSHDS Northern Sweden Health and Disease Study
PIP proximal interphalangeal
RA rheumatoid arthritis
RF(s) rheumatoid factor(s)
SD standard deviation
SE shared epitope
SEM standard error of the mean
VAS visual analogue scale
Original papers _______________________________________________________________________________________
4
ORIGINAL PAPERS
I. Berglin E, Lorenzon R, Nordmark L, Nilsson-Sojka B and Rantapää Dahlqvist S. Pre-dictors of radiological progression and hand bone density in early rheumatoid arthritis. Rheumatology 2003;42:268-75.
II. Rantapää Dahlqvist S, de Jong BAW, Berglin E, Hallmans G, Wadell G, Stenlund H, Sundin U and van Venrooij WJ. Antibodies against cyclic citrullinated peptide and IgA rheumatoid factor predict the development of rheumatoid arthritis. Arthritis Rheum 2003;48:2741-49.
III. Berglin E, Padyukov L, Sundin U, Hallmans G, Stenlund H, van Venrooij WJ, Klare-skog L and Rantapää Dahlqvist S. A combination of autoantibodies to cyclic citrulli-nated peptide (CCP) and HLA-DRB1 locus antigens is strongly associated with future onset of rheumatoid arthritis. Arthritis Res Ther 2004, 6:R303-08 (DOI 10, 1186/ar1187).
IV. Berglin E, Johansson T, Sundin U, Jidell E, Wadell G, Hallmans G and Rantapää Dahlqvist S. Radiological outcome in rheumatoid arthritis is predicted by the presence of antibodies against cyclic citrullinated peptide before and at disease onset, and by IgA-rheumatoid factor at disease onset. Ann Rheum Dis published online 21 Sep 2005;doi:10.1136/ard.2005.041376.
Reprints were made with permission from the publishers.

Introduction _______________________________________________________________________________________
5
INTRODUCTION Rheumatoid arthritis Rheumatoid arthritis (RA) is a chronic systemic inflammatory disease characterized by persis-tent and progressive synovitis in joints and tendon sheaths. The disease course can vary widely from mild to aggressive forms, the latter leading to functional loss and increased mor-tality. Modern treatment strategy of RA is early aggressive anti-rheumatic therapy. Whilst the drugs utilized are potentially toxic, it is very important to make a diagnosis as early as possi-ble and to develop a prognosis in order to choose the treatment with respect to the expected disease severity. History The term rheuma was introduced about 2000 years ago, to describe a substance that flows. Lesions typical of RA in appearance and distribution have been found in skeletal remains of Archaic Indians, suggesting that RA may have existed in North America 3000 years ago (Rothschild and Woods 1990). Guillaume Baillou (Ballonius; 1558-1616) introduced the con-cept of rheumatism as a systemic musculoskeletal syndrome in a work published posthu-mously in 1642. In 1880 Landré-Beeauvais described in his thesis nine women having a joint disease that he designated “goutte asténique primitive”. Although that thesis is usually re-garded as the first clinical description of RA, the clinical picture and disease course were de-scribed more clearly by Brodie in 1819 and by Charcot in 1853. Garrod coined the term “rheumatoid arthritis” in 1858, but that name was not officially adopted before 1922 in the U.K and not until 1941 by the American Rheumatism Association (ARA). The discovery of rheumatoid factor (RF) (Waaler 1940; Rose 1949) made it possible to distinguish sero-positive arthritis. In 1958, Ropes et al. presented the ARA criteria for the classification of RA. Those classification criteria have been modified and the new set of criteria applied, was sub-sequently proposed by the American College of Rheumatology (ACR, formerly ARA) in 1987 (Arnett et al. 1988). Epidemiology Rheumatoid arthritis is a worldwide disease affecting adults with a peak incidence between the fourth and sixth decade. About two-thirds of patients with RA are women. The prevalence in Sweden and parts of the western world has been reported to be between 0.5 and 1% (Kvien et al. 1997; Simonsson et al.1999; Carmona et al. 2002; Silman and Pearson 2002). The inci-dence is higher in native American-Indian populations, e.g. about 5 % in the PIMA Indians (Jacobsson et al. 1994) and 7 % in the Chippewa Indians (Harvey et al. 1981) and lower in rural African populations (Brighton et al. 1988; Silman et al.1993) and in China and Japan (Lau et al. 1993; Shichikawa et al. 1999). The annual incidence of RA in Sweden was esti-mated by Söderlin et al. (2002) to be 24/100,000. There are studies suggesting that the inci-dence of RA is declining (Doran et al. 2002; Uhlig and Kvien 2005). Aethiology The aetiology of RA is still not elucidated. An association between RA and genetic compo-nents has been known for many years. Twin studies in Great Britain and Finland have sug-gested that between 50-60% of the occurrence of RA may be explained by shared genetic ef-fects (MacGregor et al. 2000). Approximately one-third of the genetic contribution is esti-mated to arise from genes in the human leukocyte antigen (HLA) region, and particularly the HLA-DRB1 alleles that share a similar amino acid sequence, i.e. the “shared epitope”(SE) (Gregersen et al. 1987; Seldin et al. 1999). The HLA region consists of a family of polymor-phic genes located on the short arm of chromosome 6 encoding transmembrane proteins that
Introduction _______________________________________________________________________________________
6
bind and present peptide antigens to T-lymphocytes. The HLA-DRB1 alleles encode HLA class II molecules on the surface of antigen presenting cells (APCs) that bind to extracellular antigens. Most theories concerning the role of the SE in RA focus on the possibility that SE may influence the strength of antigen or T-cell receptor binding and thereby influence the cellular immune response (Albani et al. 1992).
Recent studies have identified an association between RF-positive RA and a single-nucleotide polymorphism (SNP) of the PTPN22 (protein tyrosine phosphatase non-receptor 22) gene, i.e. a gene outside the HLA region (Begovich et al. 2004; Lee et al. 2005). How-ever, no association between PTPN22 and SE was found (Lee et al. 2005). Simkins et al. (2005) reported an association between PTPN22 and RA in both RF-positive and RF-negative patients. PTPN22 has also been reported to be associated with other autoimmune diseases such as type-1 diabetes, systemic lupus erythematosus (SLE), Grave´s disease, and Hashi-moto´s thyroiditis (Gregersen and Batliwalla 2005). The gene product of PTPN22 is a lym-phoid-specific phosphatase, tyrosine phosphatase, which is an important negative regulator of T-cell activation. It is suggested that this SNP yields a phenotype with dysregulated suppres-sion of T-cell activation, a suggestion supported by studies in PEP knockout mice, where PEP is the murine homologue of human PTPN22 (Hasegawa et al. 2004).
Great efforts have been made to identify an infectious agent responsible for triggering the disease; however, it has not been possible to isolate any micro-organism from RA-synovial tissue or fluid, and serological analyses have not revealed firm evidence for an underlying infection. There are reports that certain infections could induce an immune response leading to chronic arthropathy in man, e.g., Epstein-Barr virus (Kouri et al. 1990), rubella virus (Smith et al. 1987), Proteus (Ebringer et al.1985) and parvo B19 virus (Cohen et al. 1986, Harrison et al. 1998), but convincing evidence that these micro-organisms are significant ae-tiologic agents is lacking.
Several epidemiological studies have suggested smoking to be a risk factor for RA (Uhlig et al. 1999; Criswell et al. 2002) and rheumatoid factor sero-positivity (Uhlig et al.1999). Other environmental factors suggested to be risk factors for RA include occupational expo-sure to solvents (Lundberg et al.1994), asphalt (Reckner et al. 2000), asbestos (Reckner et al. 2000), silica (Klockars et al. 1987), and previous blood transfusion (Symmons et al. 1997).
The incidence of RA is 2-4 times higher in premenopausal women compared with men, whilst the incidence in postmenopausal women is more equal to that of men. This suggests that hormonal and pregnancy factors have a role in disease susceptibility. The postpartum period, particularly after the first pregnancy, has been reported as a strong risk period for de-veloping RA, whereas disease susceptibility is reduced during pregnancy (Silman et al. 1992; Nelson and Ostensen 1997). Further studies have indicated that the increased risk after the first pregnancy is associated with breastfeeding, suggesting a role of the pro-inflammatory hormone prolactin (Brennan et al. 1994). Several studies have reported that the use of oral contraceptives is associated with a reduced risk of developing RA or may postpone disease onset (Hannaford et al. 1990; Brennan et al. 1997; Symmons and Harrison 2000). Other autoimmune diseases (thyroid disease, Sjögren´s syndrome, insulin-dependent diabe-tes), previous blood transfusion, physical or psychological trauma and obesity have also been discussed as risk factors for RA (Symmons and Harrison 2000). Pathogenesis of synovial inflammation and joint destruction Rheumatoid arthritis is believed to start with the presentation of a still unidentified antigen by APCs, such as macrophages, fibroblast-like synoviocytes or dendritic cells in the synovial membrane, to T-lymphocytes (Harris 1990). This event initiates a cellular immune response in a genetically susceptible individual with T-and B-lymphocytes and macrophages infiltrat-ing the synovial tissue. In the sublining layer of the synovium neo-angiogenesis and tissue
Introduction _______________________________________________________________________________________
7
fibrosis occur. The synovial tissue proliferates forming a pannus, which invades and destroys adjacent cartilage, ligaments, and subchondral bone centripetally. Several studies have suggested that fibroblast-like synoviocytes may have a central role in the pathogenesis of RA. Fibroblast-like synoviocytes respond to cytokines, mainly those se-creted by macrophages, and to other stimulatory molecules by secretion of inflammatory cy-tokines, e.g. interleukin 1ß (IL-1ß), interleukin 6 (IL-6) and tumour necrosis factor α (TNF-α) and of tissue-degrading matrix metalloproteinases (MMP). Fibroblast-like synoviocytes have also been reported to secrete factors that attract macrophages, stimulate the differentiation of macrophages into osteoclasts and to activate osteoclasts at the bone surface, leading to bone erosions (reviewed by Mor et al. 2005). In recent years B-lymphocytes have been proposed to have a more important role in the pathogenesis of RA than was previously thought. B-lymphocytes can act as APCs, secrete pro-inflammatory cytokines, produce autoantibodies such as RF and antibodies against cyclic citrullinated peptides (CCP), and to activate T-lymphocytes (Schellekens 1998; Kim 2000; Takemura 2001).
There are studies suggesting that joint destruction can occur independently of clinical signs of synovial inflammation. For example, Moreland et al. (1989) found the presence of collagen type II fragments (markers for cartilage destruction) in synovial phagocytes did not correlate with the number of leukocytes in the synovial fluid. Continuing joint damage despite of im-provement of clinical and laboratory measures of inflammation has been reported, suggesting differential pathogenesis of synovial inflammation and articular erosions (Scott et al. 1984; Mulherin et al. 1996; Kirwan 1997). Autoantibodies in rheumatoid arthritis The occurrence of various autoantibodies is a hallmark of RA. The best known being RF, which are antibodies directed against the Fc-region of immunoglobulins of the IgG isotype. Their presence can be detected by agglutination assays, nephelometry and ELISA-tests. Low affinity RF are normal components of the B-cell repertoire. In RA high affinity RF develop by a process of somatic hypermutations from the inherited physiological repertoire of heavy or light chain RF-genes (Deftos et al. 1994). Rheumatoid factor has been suggested to have a pathogenic role in the inflammatory process of RA by forming immune complexes that trigger complement activation and cytokine release by leukocytes (Mannik 1992). About 70-80% of RA-patients are sero-positive for RF, but RF are also found in other conditions associated with either immune complex formation or with hypergammaglobulinaemia, such as chronic infections, lymphoproliferative and hepatic diseases and other rheumatic diseases. RF can also be detected in 1- 5 % of healthy individuals (Ball and Lawrence 1961; Thorsteinsson et al. 1975), and in nearly 20% elderly healthy individuals (Palosuo et al. 2003). The presence of IgM-RF may precede the onset of RA by several years (Aho et al. 1985). RF is the only sero-logical marker included in the ACR classification criteria for RA (Arnett et al. 1988).
Because RF has a limited specificity for RA, other more specific antibodies have been sought. Anti-perinuclear factor (APF) antibodies, i.e., antibodies against perinuclear kerato-hyalin granules of human buccal mucosal cells, and already described already in 1964, were found to be more specific for RA than RF, but with lower sensitivity (Nienhuis and Mandema 1964). Anti-keratin antibodies (AKA) were first described in 1979 and have also been shown to be more specific for RA than RF (Young et al. 1979). AKA are directed against epitopes of the stratum corneum in the rat oesophagus epithelium. It was subsequently shown that APF antibodies and AKA are reactive against the same antigen, namely filaggrin (Hoet et al. 1991; Simon et al. 1993; Sebbag et al. 1995). APF antibodies and AKA can be detected by indirect immunoflourocence (IIF). However, the test procedure is time-consuming and complicated, which explains why they are not routinely investigated. The antigen recognized by APF anti-
Introduction _______________________________________________________________________________________
8
bodies and AKA was later found to be citrulline-containing peptides generated post-translationally from arginine residues (Schellekens et al. 1998, Girbal-Neuhauser et al. 1999) by peptidylarginine deiminase (PAD) (Vossenaar et al. 2003). An ELISA using synthetic ci-trullinated peptides derived from filaggrin was developed (Schellekens et al. 1998). To in-crease the sensitivity of the test, the citrulline-containing peptides were modified to a structure in which the citrulline moiety is optimally exposed for antibody binding, the CCP1 test. With a single cyclic citrullinated peptide (CCP), antibodies could be detected in 68 % of sera from RA patients with a specificity of 98% (Schellekens et al. 2000). Since filaggrin is not ex-pressed in the synovium, it was not considered to be the natural antigen for anti-citrullinated antibodies. To further increase the sensitivity of the test, a second generation CCP test (CCP2) was developed, which uses cyclic peptides with no homology with filaggrin or other known proteins. This test has a sensitivity comparable to the IgM-RF test, and much higher specific-ity (van Venrooij et al. 2002; Vasishta 2002; Pinheiro et al. 2003). The CCP2 ELISA is commercially available (Euro-Diagnostica, Arnhem, The Netherlands; Axis-Shield, Dundee, Scotland; INOVA, San Diego, USA). The same type CCP2 peptides are used by all compa-nies.
Various citrullinated proteins have been described in the RA synovium, e.g., extravascular citrullinated fibrin (Masson-Bessière et al. 2001), intracellular citrullinated histones in granu-locytes (Nakashima et al. 2002) and vimentin in macrophages (Vossenaar et al. 2004a). The citrullination process requires the activity of the normally intracellular enzyme peptidyl argin-ine deiminase (PAD) which needs a threshold concentration of calcium ions for its activation. The intracellular concentration of calcium ions is too low for PAD to be activated. During cell death, for example as a result of oxidative stress in the inflamed synovium, PAD enzymes might leak out of the cells, become activated due to the much higher extra-cellular calcium ion concentration, and induce citrullination of extracellular proteins such as fibrin (Vossenaar et al. 2004a). The presence of citrullinated proteins in the inflamed synovium is not, how-ever, specific for RA, but can also be found in patients with other arthropathies. Vossenaar et al. (2004b) showed that it is the production of anti-citrullinated protein antibodies, not the presence of citrullinated proteins, which is highly specific for RA. They also presented evi-dence of local production of anti-CCP antibodies in the synovial fluid. Formation of immune complexes between anti-CCP antibodies produced in the synovium and citrullinated proteins, and thereby activation of inflammatory cells to produce pro-inflammatory cytokines, has been suggested as a possible role of anti-CCP antibodies in the pathophysiology of RA (Vossenaar et al. 2004a). The human stress protein BiP (immunoglobulin binding protein) has been found to be overexpressed in the rheumatoid synovium (Bläss et al. 2001) and to stimulate synovial T-cell proliferation (Bläss et al. 2001; Bodman-Smith et al. 2003). Anti-BiP antibodies can be de-tected with ELISA and have been shown to have a sensitivity and specificity of about 70% in established RA, and somewhat lower in early RA. Anti-BiP antibodies have also been de-tected in pre-disease sera of future RA patients (Bodman-Smith et al. 2004). Examples of other RA-associated antibodies are anti-RA33, anti-calpastatin, anti-neutrophil cytoplasmic antibody (ANCA) and anti-nuclear antibody (ANA), although present in a variety of autoimmune diseases and with limited specificity for RA. Disease onset, clinical presentation and diagnosis Rheumatoid arthritis is suggested to begin with the activation of a cellular immune response in a genetically susceptible individual. When the production and release of cytokines, such as TNF-α and IL-1, begins, the prodromal symptoms general fatigue and malaise may occur (Harris 1990). Joint symptoms, due to angiogenesis in and proliferation of synovial mem-brane, usually develop gradually over a period of several weeks. Disease presentation can also
Introduction _______________________________________________________________________________________
9
be acute or sub-acute. Synovitis in the joints of the hands is the typical early manifestation. RA can affect almost any joint, but involvement of metacarpophalangeal (MCP), proximal interphalangeal (PIP) and metatarsophalangeal (MTP) joints, wrists and knees are most com-mon. The distal interphalangeal (DIP) and the lumbar spine joints are rarely involved. Ten-donitis and bursitis are frequent and often dominant in early disease (Grassi et al. 1998). Morning stiffness, probably generated by an increase in extracellular fluid in and around the joint is common.
Laboratory findings may be an elevation of acute phase reactants including erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP). Biosynthesis of acute-phase reac-tants is induced by interleukin-6 (Guerne et al.1989). Haemoglobin levels can be slightly re-duced and thrombocytosis is common. RF and anti-CCP antibodies may be detectable and are the most RA-specific laboratory findings (Rantapää-Dahlqvist 2005). Positive RF is one of the seven classification criteria defined for RA (Arnett et al.1988). Early diagnosis of RA may be difficult. The most frequent differential diagnoses include other inflammatory joint diseases, such as SLE, and seronegative spondyloarthropathies, e.g., psoriatic arthritis. In elderly patients, RA can be clinically indistinguishable from polymyalgia rheumatica. The ACR criteria (Arnett et al. 1988) have low sensitivity in early RA (Saraux et al. 2001;Visser et al. 2002) and were developed to classify rather than to diagnose RA. The usefulness of the criteria to predict disease severity is also limited, in that they predict persis-tent rather than aggressive disease (Emery and Salmon 1995). Visser et al. (2002) have sug-gested a modification of the 1987 ACR criteria in order to make them more adapted to early disease. Consequently, they developed a model, based on their modified criteria, which showed excellent discrimination, at the first clinic visit, between self-limiting, persistent non-erosive and persistent erosive arthritis. The modified ACR criteria include a positive test for anti-CCP-antibodies. Disease development The disease course in RA is characterised by great inter-individual variation, ranging from mild, self-limiting to severe, erosive disease, sometimes with extra-articular manifestations, such as rheumatoid nodules, pleuritis, pericarditis, and vasculitis and secondary Sjögren syn-drome. Patients with RA have a reduced average life span, predominantly due to cardiovascu-lar mortality (Callahan and Pincus 1995; Wållberg Jonsson et al. 1997). Intra-individual fluc-tuations, whereby periods of lower disease activity are replaced by flare-ups are typical. As the disease proceeds, the daily activities and functional capacity of the patient are affected to a greater or lesser extent.
Early in disease patients with RA start to develop local and generalised bone loss, which can be quantified by dual energy x-ray absorptiometry (DXA) (Gough et al 1994; Deodhar et al. 1995). The direct effect of inflammatory mediators, decrease in physical activity and corti-costeroid treatment have been implicated as major aetiological factors for the bone loss during the disease course (Reid et al. 1982; Sambrook et al. 1987).
On conventional radiography (CR) of hands, wrists and forefeet at an early stage of dis-ease, soft tissue swelling symmetrically around the joints involved and juxtaarticular-articular osteopenia can be seen. Those changes are non-specific for RA, but are indicative of a local inflammatory process. The bone is often affected earlier than cartilage in RA (Fassbender et al. 1992) and the next radiographic changes are generally small erosions of the “bare” areas of bone (i.e. areas lacking articular cartilage) within the joint-space capsule, detected as a loss of continuity of the white cortical line. Those early changes merge into large subchondral ero-sions, and joint space loss arises due to cartilage breakdown. Subluxations, such as ulnar drift of the proximal phalanges of the MCP joints and swan-neck or boutonniére deformities of the
Introduction _______________________________________________________________________________________
10
PIP and DIP joints, can occur. In the last radiographic stage there is total destruction of the original bony outline of the joint, so-called mutilating changes.
Most patients develop erosions and joint space narrowing within the first two years of dis-ease and the joint destruction progresses over several decades (Fuchs et al. 1989). The pres-ence of erosions in the hands is one of the classification criteria of RA. In one study of pa-tients with early RA, 70% of the patients showed definite radiographic damage after 3 years; furthermore, those patients already had erosions after 1 year. The rate of radiological progres-sion was significantly higher during the first year compared with the second and third years (van der Heijde et al. 1995). In a 5 year study of early RA the rate of radiological progression was most prominent during the first 2 years after diagnosis (Fex et al. 1996). Fifty-three per-cent of the patients studied had non-erosive disease at start of the study, and only 11% after 5 years. Lindqvist and co-workers reported similar results (2003). In a cohort of 181 patients with early RA followed for 10 years, 49% had erosions at baseline, 90% after 5 and 96% after 10 years. Radiographic progression was most rapid during the first 2 years. Most patients in those three studies were treated with disease modifying anti-rheumatic drugs (DMARDs). Assessment of disease activity and outcome Clinical and laboratory markers of inflammation are used as measures of disease activity in RA. An often used measure is the European League Against Rheumatism (EULAR) “Disease Activity Score” (DAS), which was elaborated and validated for patients with early RA (van der Heijde et al. 1990, 1992a). DAS is a continuous composite measure including the Ritchie articular index (RAI ; based on 53 joints) (Ritchie et al. 1968), a swollen joint count (based on 44 joints), ESR, and the patients´s global assessment of her/his health measured by a visual analogue scale (VAS). A simplified, clinically more useful version using the 28-joint tender and swollen joint counts, DAS28, has been shown to be as valid as the original DAS (Prevoo et al.1995). DAS and DAS28 can also be calculated using CRP instead of ESR (http://www.DAS-score.nl DAS Score NL 2005). An even more simplified version called “Simplified Disease Activity Index” (SDAI) has been proposed for use in clinical practice (Smolen et al. 2003). The SDAI is the numerical sum of tender and swollen joint count based on 28-joints, patient and physician global assessment of disease activity assessed by a VAS, and the level of CRP. Using the activity scores, patients can be categorized as being in remis-sion, or having low, moderate or high disease activity (van Gestel et al. 1996, 1998; Smolen et al. 2003).
The clinical response to therapy can also be quantified using disease activity scores. EULAR response criteria reflect the change as well as the present level of DAS (van Gestel et al 1996) or DAS28 (van Gestel et al. 1998) from baseline (when the drug was introduced) to a given endpoint; the response is categorized as good, moderate or no response. Another method for defining response to therapy has been defined by the ACR (Felson et al.1995). The ACR response (ACR20) is defined as 20% improvement in tender and swollen joint counts and 20 % improvement in 3 of 5 of the following measures: patient’s assessments of pain and of physical function, patients and physician’s global assessment of disease activity and an acute-phase reactant. ACR50 and ACR70 reflect 50% and 70% improvement respec-tively. The ACR-N is a measure of the smallest degree of improvement from baseline in the following three criteria: tender joint count, swollen joint count and the medium of the five remaining measures of disease activity. (Felson et al.1998). Clinical remission was defined by the ARA- now ACR- (Pinals et al. 1981) and has been shown to correspond to the remission defined by EULAR using DAS (Prevoo et al. 1996) or DAS28 (Fransen et al. 2004). The degree of joint destruction is an important measure used for evaluating disease out-come in RA. Conventional radiography (CR) is still regarded as the gold standard for judging
Introduction _______________________________________________________________________________________
11
the degree of joint destructions, even though in recent years magnetic resonance imaging (MRI) has been shown to be more sensitive in demonstrating early pathological changes in the synovial tissue, cartilage and bone (Foley-Nolan et al. 1991; Forslind et al. 1997). One limitation of MRI is the high cost of the examination.
For CR, several validated scoring systems for assessing radiographic changes in hands and feet have been developed. In 1971, Sharp and co-workers presented a method for scoring both joint space narrowing and erosions in the hands and wrists. This method has been modified twice (Sharp et al. 1985; Fries et al. 1986) and by van der Heijde (1989) whose modification (HMS) also included assessment of the feet. According to the van der Heijde modification joints in hands and feet are assessed by scoring both the erosions and joint space narrowing separately. The maximum total score is 448. The Larsen score method was first presented in 1977 (Larsen et al. 1977) and has been modified several times (Larsen et al. 1984; Larsen and Thoen 1987; Larsen 1995). In the Larsen method joints in the hands, wrist and feet are as-sessed with respect to the joint destruction with a single score between 0 and 5, which is mainly determined by the erosive changes. The scoring is accomplished by comparison with standard reference films with and the maximal score according to the latest modification is 160 (Larsen 1995). Both the HMS and the Larsen score method have been used in many randomized clinical trials. The two scoring methods are highly significantly correlated (Pincus 1995). The HMS is more detailed and more sensitive in the detection of early changes, whilst the Larsen method is more specific and less time-consuming. Peri-articular osteoporosis in joints is an earlier sign of joint affection than erosions, but can not be quantified accurately using CR. With DXA the bone mineral density (BMD) and the bone mineral content (BMC) can be measured both in axial and in hand skeleton (Jergas and Genant 1993; Deodhar et al. 1994; Peel et al. 1994). Recent technological advances have made it possible to visualize inflammatory as well as destructive RA changes in hands and feet by ultrasonography (US) (Wakefield et al. 2000; Schmidt 2001). Ultrasonography has been reported to be more sensitive than CR and compa-rable to MRI for visualizing bone erosions in finger joints (Backhaus et al.1999; Wakefield et al. 2000) although dependency on a skilled operator and poor objective documentation of findings are disadvantages. Grading of the patient’s level of physical function is one commonly used measure for evaluation of disease outcome in RA. Fries (1980, 1983) developed the Stanford Health As-sessment Questionnaire Disability Index for evaluating the functional capacity of activities of daily living (ADL). The original questionnaire also included questions about drug toxicity, costs and social situation. More commonly used is a modified form, known as the Health As-sessment Questionnaire (HAQ), which includes only the disability part of the questionnaire. The HAQ has been shown to be a robust measure of the patient’s ADL status and has been validated in several countries. In 1988, Ekdahl et al. presented a validated Swedish version of the HAQ, which is used in clinical practice as well as in study settings. Pharmacological treatment The strategies for pharmacological treatment of RA have undergone substantial changes over the last 20 years. The earlier pyramidal approach starting with non-steroid-anti-inflammatory-drugs (NSAIDs) followed by the addition of a DMARD if the patient demonstrated high dis-ease activity and/or radiographic damage has been abandoned. It is now well documented that early DMARD therapy improves the long-term outcome for patients with RA and that treatment should be instituted as early as possible after disease onset, ideally before the patho-logical processes have become established and irreversible joint damage has arisen. Egsmose et al. (1995) and Tsakonas et al. (2000) demonstrated that a delay of 8-9 months in starting
Introduction _______________________________________________________________________________________
12
DMARD therapy has significant impact on disease parameters years later, even though the DMARDs employed were oral gold and hydroxychloroquine, which are regarded to be among the least effective of the DMARDs. Lard and co-workers (2000) showed significantly less radiological progression in a group of patients treated with chloroquine or sulphasalazine within 15 days of diagnosis, compared with another group who received therapy within 4 months of diagnosis. In another study, DMARD initiated in a group of “very early RA” (me-dian disease duration 3 months) patients was shown to have significantly better effect on ra-diological progression and disease activity during a 36 months follow-up than DMARD ther-apy in a group of “late early RA” (median disease duration 12 months) patients (Nell et al. 2004).
Although seldom reached, the main goal of treatment in RA treatment is to achieve remis-sion. There is still no international consensus as to which of the different strategies tried should be employed. The strategies are: Monotherapy: Methotrexate (MTX) has become the “anchor drug” for early and established RA treatment and its safety and efficacy for long-term treatment has been confirmed in a large number of studies (for a review, see Pincus et al. 2003). Methotrexate is the first choice for treatment of early RA for most rheumatologists for initial therapy when monotherapy is se-lected (Mikuls and O`Dell 2000) and has recently been shown to significantly prolong the survival of patients with RA, largely by reducing cardiovascular mortality (Wållberg-Jonsson et al. 1999; Choi et al. 2002). Combination DMARD therapy: Multiple trials have shown that combinations of DMARDs are more effective than monotherapy (Möttönen et al. 1999; O´Dell et al. 2002). The combi-nation therapy can be accomplished in a “step-up”, “parallel” or “step-down” mode. In the FIN-RACo trial in patients with early RA, initial combination therapy with sulphasalazine, methotrexate, hydrochloroquine and prednisolone was compared with monotherapy according to the “sawtooth” principle (Fries 1990) starting with sulphasalazine. In this trial a signifi-cantly higher proportion of patients reached remission at 1-year and at 2-year follow-up (Möt-tönen et al.1999). Patients in the combination-DMARD group had significantly less radio-logical damage at 2- and 5-year follow-up, even though the DMARD treatment after the ini-tial 2 years became unrestricted (Korpela et al. 2004). Also the working capacity was signifi-cantly higher after 5 years in the group receiving combination-DMARD treatment (Puolakka et al. 2005). Recently a meta-analysis of the efficacy and toxicity of combination DMARD therapy in early and established RA showed that combination DMARD therapy, both overall and in step-up, parallel and step-down studies, has reduced risk (75%) of withdrawals due to inefficacy compared with monotherapy, but has an increased risk of withdrawals due to side-effects (37%). Combination DMARD therapy was concluded to be effective in RA, with the strongest evidence in established RA for combinations of MTX with tumour necrosis factor inhibitors (anti-TNF) and MTX with sulphasalazine and/or hydroxychloroquine given to pa-tients with moderate response to DMARD monotherapy. The meta-analysis also suggested that combination DMARD therapy is superior to monotherapy in early RA and should be used in most patients early in disease process (Choy et al. 2005). Induction therapy: Conventional DMARDs commonly have a delayed action and do not reach maximal efficacy before 2-6 months of treatment. Two studies have investigated the advantage of prompt disease activity suppression over conventional DMARD therapy. The Early Rheumatoid Arthritis Trial (ERA) compared treatment with the anti-TNF product eta-nercept, with MTX treatment in 632 patients with early RA, with 1-year follow-up (Bathon et al. 2000). It was found that significantly more patients in the etanercept group had a treatment response as measured by the ACR-N after only 2 weeks, with a dramatic decrease in CRP (about 75%) and significantly more etanercept treated patients reached ACR20, ACR50 and ACR70 response after 6 months. The radiological progression was slower in the etanercept
Introduction _______________________________________________________________________________________
13
group compared with the MTX group during the first 6 months of the study, after which the progression in the two groups was similar. Significantly more patients in the etanercept group than in the MTX group had no increase in the erosion score during the study.
The COBRA study in which 155 early RA patients were randomized for treatment with ei-ther sulphazalazine alone or a step-down combination regime of prednisolone in high initial dose, methotrexate and sulphasalazine showed similar results. The combined therapy regime suppressed ESR by 75% following 2 weeks of treatment, whereas sulphasalazine alone took 6 months to cause similar suppression in ESR. The radiological progression in the combined-therapy group was significantly less than in the sulphazalazine group after 28, 56 and 80 weeks even though the clinical difference between the groups was no longer significant after prednisolone was stopped (Boers et al.1997). In a 5-year follow-up, patients from the step-down combination regime with high initial dose of prednisolone had significantly less radio-logical progression than patients in the sulphazalazine group, independent of subsequent anti-rheumatic therapy (Landewé et al. 2002). Prednisolone was a component of both the FIN-RACo (Möttönen et al. 1999) and the COBRA trial (Boers et al. 1997). Low dose prednisolone (7.5 mg/day) during the first 2 years of disease has been demonstrated to reduce the rate of radiological progression in RA when given in addition to other treatments (Kirwan 1995). The use of low dose glucocorticoids in early RA is however under discussion (Boers 1999; Morrison and Capell 1999; Strand and Simon 2003).
Thus, there is a body of evidence that early aggressive treatment improves the long-term outcome for patients with RA; although no international consensus yet exists as to which treatment strategy should be used. A step-up strategy, starting with methotrexate in monother-apy, is recommended by the Swedish Association of Rheumatologists (www.srfonline.org).
Treatment should be started as soon as possible, before irreversible damage has arisen. Early diagnosis is difficult, while incipient RA can be indistinguishable from self-limiting, mild joint affections; RA per se is a very heterogeneous disease. A relatively high proportion of patients experiences a good response to monotherapy and would not benefit by complex and expensive therapeutic regimes. Thus it is of great importance to find procedures to im-prove the possibility of making an early diagnosis and to find early reliable predictors for the disease course in a given individual patient. Prediction of radiological outcome in early RA
Predictors or radiological outcome are preferably evaluated in longitudinal studies on patients with early RA. Ideally a prognostic marker should be present at disease onset, reliable, easy to detect and valid. Many prognostic factors have been described including demographic, ge-netic, clinical and radiological factors. Some examples are: Early radiographic damage has repeatedly been demonstrated to predict severe radiological outcome (Kaarela 1985; Combe et al. 1995; Dixey et al. 2004) and also radiological progres-sion (Jansen et al. 2001; Goronzy et al. 2004; Forslind et al. 2004). Genetic factors: The prognostic value of HLA-DRB1 alleles that share a similar amino acid sequence, i.e., the SE alleles, has been investigated in many studies. Especially the alleles in the DR4 group, the HLA-DRB1*0401 and DRB1*0404 alleles have been consistently associ-ated with radiological erosions in different ethnic groups. A hierarchy of different SE alleles and genotypes in severity of RA has been proposed (Weyand et al. 1995). In that study HLA-DRB1*0401 particularly in double dose, DRB1*0401/0401 was associated to the most ag-gressive form of RA, with clinical manifestations such as vasculitis and bone erosions. This dose-dependent association between the presence of SE alleles and especially HLA-DRB1*0401 with erosions was confirmed in a recent meta-analysis of 29 studies and 3240 patients (Gorman et al. 2004). However, the association was dependent on the ethnic back

Introduction _______________________________________________________________________________________
14
ground and was particularly strong in Southern European Caucasians, but no association could be demonstrated in Greeks. Measures of inflammation such as ESR, CRP, especially high values at disease onset or dur-ing the first six months of early RA have been repeatedly correlated with radiological damage (Combe et al. 1995; Jansen et al. 2001; Lindqvist et al. 2003) as has the number of swollen joints in early disease (Feigenbaum et al. 1979; Möttönen 1988; van Zeben et al. 1993). Among immunological markers, RF is the most studied and has been associated with a more severe radiological outcome in early RA (van der Heide et al. 1995; Combe et al. 2001) and the titre of RF at baseline has also been reported to correlate with radiological damage after 3 years of follow-up (Paimela et al. 1995). In studies of various isotypes of RF, some studies have reported IgA-RF to be the best predictor of radiological damage (Teitsson et al. 1984; Scott 2000; Lindqvist et al. 2005), whilst others found no significant prediction of erosive disease with IgA-RF (Eberhardt et al. 1988; Visser et al. 1996). More recently the presence of anti-CCP antibodies has been demonstrated to be a good predictor of joint erosions in early RA with follow-up periods of 2-10 years (Kroot et al. 2000; Meyer et al. 2003; Forslind et al. 2004; Lindqvist et al. 2005).
Contradictory results have been obtained in studies on the influence of age on radiological outcome. Patients who were older at disease onset have been described to have more severe disease (Harrison and Symmons 2000) as well as milder disease (Young 1995). There are also studies reporting no difference between younger and older patients in radiological outcome (Pease et al. 1999). Differences in study design and patient selection might explain the differ-ent results. Sex and menopausal state have been suggested to influence the course of RA and to be part for the explanation of the difficulty of interpreting the effect of age. Postmeno-pausal women have been shown to have more erosive disease than premenopausal women and men (Kuiper et al. 2001). On the other hand, Tengstrand et al. (2004) reported no sex differ-ence in Larsen score in a prospective study of early RA patients with 2-year follow-up. How-ever, although women had higher DAS28 and HAQ scores, when stratified for age, women below 50 years of age at inclusion that had a milder disease than older women and close to that of men.
The aims of the thesis _______________________________________________________________________________________
15
THE AIMS OF THIS THESIS In this thesis I have analysed potential predictors for onset of RA, possibilities to earlier, reli-able diagnosis, and predictors of the disease course in RA. The aspects I have focused on are: • Evaluation of laboratory and clinical markers of inflammation as predictors of disease
course. Comparison of conventional radiography (CR) and dual-energy X-ray absorpti-ometry (DXA) as measures of joint destruction.
• To evaluate sensitivity and specificity of rheumatoid factors (RFs) of IgM, IgG and IgA
isotype and of antibodies against cyclic citrullinated peptides (anti-CCP antibodies) in in-dividuals who later develop RA
• The significance of the presence of HLA shared epitope (SE) alleles in relation to RFs and
anti-CCP antibodies for the relative risk of future development of RA • The significance of RFs and anti-CCP antibodies before and after onset of RA , in relation
to carriage of HLA SE alleles, for predicting disease activity and severity
Subjects and methods _______________________________________________________________________________________
16
SUBJECTS AND METHODS The Medical Biobank, the Maternity cohort and identification of samples The Medical Biobank of Northern Sweden is constituted of The Northern Sweden Health and Disease Study (NSHDS) cohort which contains three subcohorts: The Västerbotten In-tervention Project (VIP); the Northern Sweden part of the World Health Organization (WHO) study for Monitoring of Trends and Determinants in Cardiovascular Disease (MONICA), and the Mammary Screening Project.
The VIP is a long-term prospective cohort and intervention study intended for health pro-motion of the county of Västerbotten, Northern Sweden with approximately 254,000 inhabi-tants. Since 1985, VIP invites all individuals in the county aged 30, 40, 50 and 60 years for screening for primary prevention of cardiovascular disease and diabetes. The overall partici-pation rate is approximately 60%. Since 1994, a second blood sample and questionnaire is collected from individuals already in the cohort at 10 years intervals The MONICA study includes men and women from the counties of Västerbotten and Norr-botten, Northern Sweden with approximately 500,000 inhabitants. Participants were invited for cardiovascular screening in 1986, 1990, 1994 and 1999. The age range of recruited sub-jects ranged from 25 to 74 years. The overall participation rate was between 70 and 80%. Ap-proximately 20% of MONICA participants are also included in VIP. The Mammary Screening Project includes about 25,000 women from the county of Västerbot-ten who were recruited through a local mammographic screening project with a recruitment rate of about 7,000 subjects per year since 1995, and a participation rate of about 60%. Since 1997 blood samples were collected every second year from women aged 50-69. About half of the mammary project subjects also participate in the VIP. In total, the NSHDS cohort com-prised as of January 2002 122,800 blood samples from 79,940 individuals (34,375 men and 45,565 women) in the age of 25-74 years. The Maternity cohort comprises samples from pregnant women from the 4 northernmost counties of Sweden (900,000 inhabitants) who have undergone screening for rubella since 1975. As of January 2002 the Maternity cohort comprised 102,800 samples from 78,700 women.
Both the NSHDS cohort and the Maternity cohort are population-based and no one was excluded. Most participants are native Swedes with a small minority of Finnish descent. Sub-jects included in the NSHDS cohort completed a self-administrated questionnaire to collect demographic, medical, and lifestyle information, including smoking habits and diet. Their blood samples were collected into heparinized tubes and fractionated into plasma, buffy coat, and erythrocytes, and then stored at -80˚C. In the Maternity cohort blood samples were col-lected from all pregnant women according to routine procedures. Sera were collected and stored at -20˚C.The smoking habits of the included subjects were recorded from a question-naire.
The registers of patients fulfilling the 1987 ACR classification criteria for RA at the De-partment of Rheumatology, University Hospital, Umeå and with a known date of disease on-set were co-analysed with the registers of the NSHDS cohort and the Maternity cohort. Only patients with disease onset after 1985 (when the NSHDS started) and female patients of fertile age (≤ 45 years) and disease onset after 1975 (when the Maternity cohort started) were in-cluded in the co-analysis. The registers at the Department of Rheumatology also include the patients from an early RA programme, which began in 1996 and includes patients with recent onset (<12 months) RA. In total about 500 patients were screened for samples in the NSHDS
Subjects and methods _______________________________________________________________________________________
17
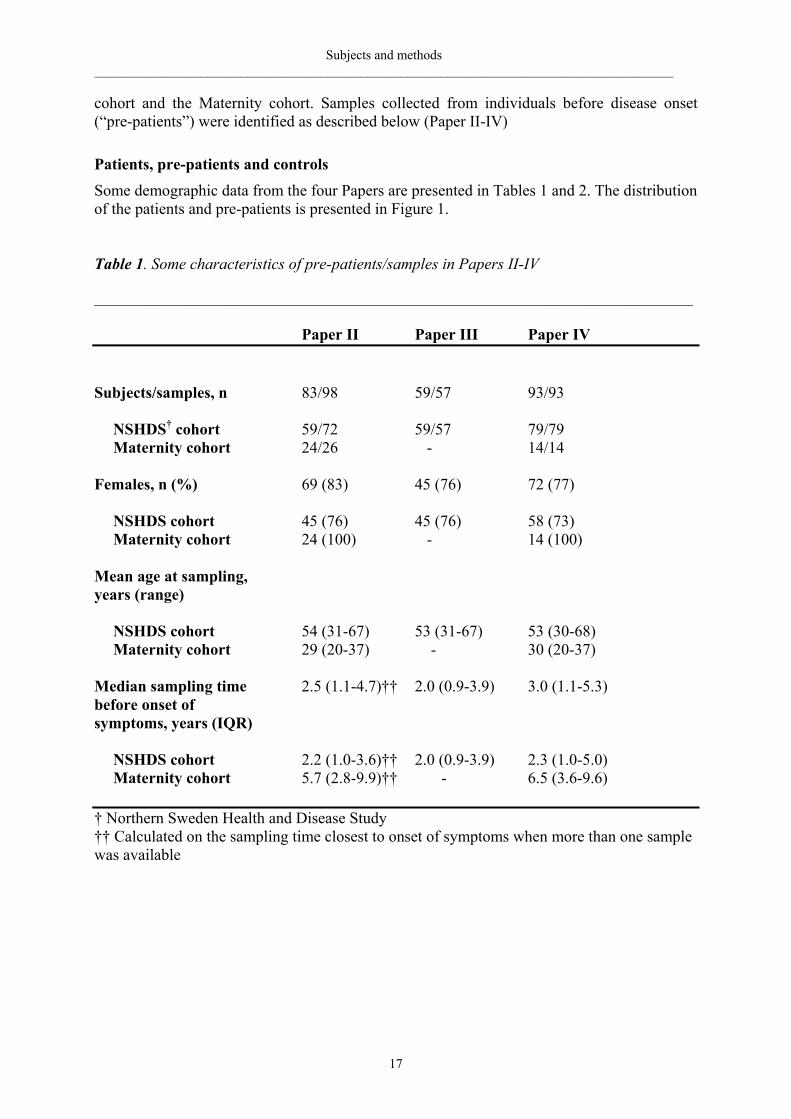
cohort and the Maternity cohort. Samples collected from individuals before disease onset (“pre-patients”) were identified as described below (Paper II-IV) Patients, pre-patients and controls Some demographic data from the four Papers are presented in Tables 1 and 2. The distribution of the patients and pre-patients is presented in Figure 1. Table 1. Some characteristics of pre-patients/samples in Papers II-IV ___________________________________________________________________________ Paper II Paper III Paper IV Subjects/samples, n 83/98 59/57 93/93 NSHDS† cohort 59/72 59/57 79/79 Maternity cohort 24/26 - 14/14 Females, n (%) 69 (83) 45 (76) 72 (77) NSHDS cohort 45 (76) 45 (76) 58 (73) Maternity cohort 24 (100) - 14 (100) Mean age at sampling, years (range) NSHDS cohort 54 (31-67) 53 (31-67) 53 (30-68) Maternity cohort 29 (20-37) - 30 (20-37) Median sampling time 2.5 (1.1-4.7)†† 2.0 (0.9-3.9) 3.0 (1.1-5.3) before onset of symptoms, years (IQR) NSHDS cohort 2.2 (1.0-3.6)†† 2.0 (0.9-3.9) 2.3 (1.0-5.0) Maternity cohort 5.7 (2.8-9.9)†† - 6.5 (3.6-9.6) † Northern Sweden Health and Disease Study †† Calculated on the sampling time closest to onset of symptoms when more than one sample was available
Subjects and methods _______________________________________________________________________________________
18
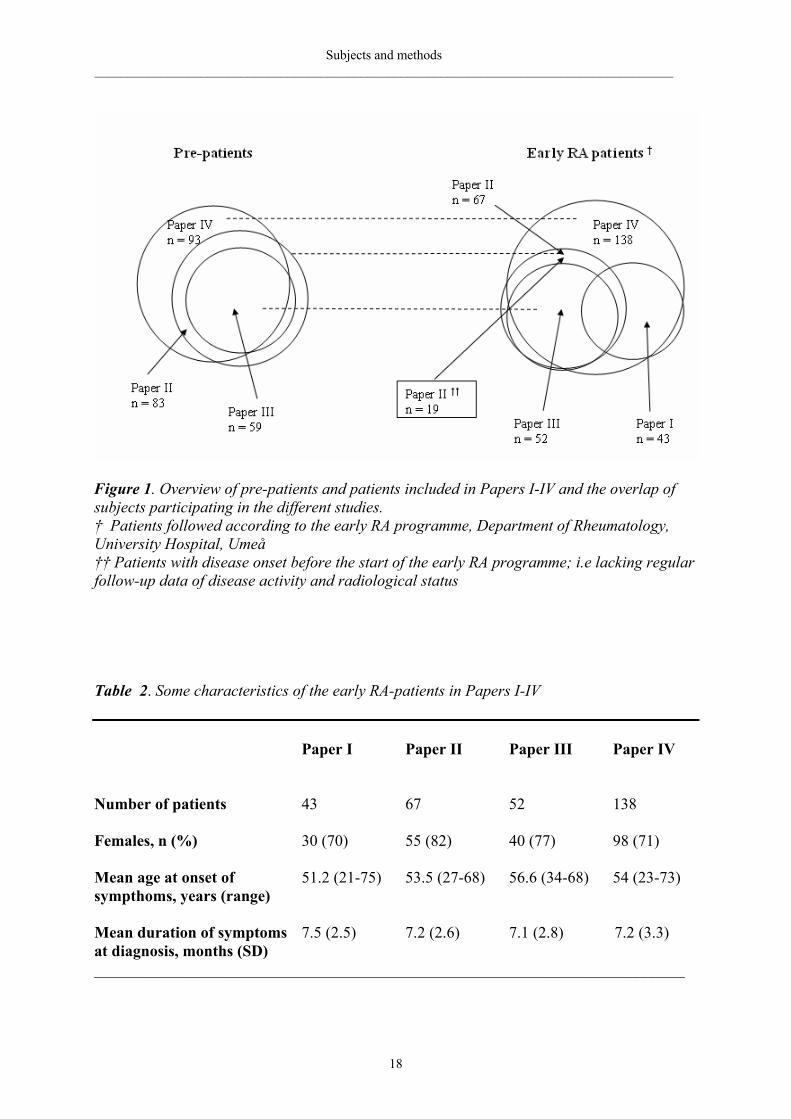
Figure 1. Overview of pre-patients and patients included in Papers I-IV and the overlap of subjects participating in the different studies. † Patients followed according to the early RA programme, Department of Rheumatology, University Hospital, Umeå †† Patients with disease onset before the start of the early RA programme; i.e lacking regular follow-up data of disease activity and radiological status Table 2. Some characteristics of the early RA-patients in Papers I-IV Paper I Paper II Paper III Paper IV Number of patients 43 67 52 138 Females, n (%) 30 (70) 55 (82) 40 (77) 98 (71) Mean age at onset of 51.2 (21-75) 53.5 (27-68) 56.6 (34-68) 54 (23-73) sympthoms, years (range) Mean duration of symptoms 7.5 (2.5) 7.2 (2.6) 7.1 (2.8) 7.2 (3.3) at diagnosis, months (SD) __________________________________________________________________________

Subjects and methods _______________________________________________________________________________________
19
Paper I: The first 43 patients from the early RA programme were consecutively included
into the study from January 1996 to October 1998 and followed for 2 years. All 43 patients completed the study. Thirty (70%) of the patients were women. Mean age at onset of disease was 49 years (range 21-75) for women and 56 years (39-74) for men. Mean duration of symp-toms at inclusion in the study was 7.5 months (range 3-12). Fifteen women were postmeno-pausal, six of whom were receiving hormone replacement therapy (HRT). Thirty-nine of the patients were RF positive according to the Waaler-Rose method. Sixteen healthy individuals (5 men and 11 women) were assessed as controls for DXA measurements of the hands; five of the women were postmenopausal.
Paper II: From a co-analysis undertaken during August 2001 between the registers of RA-
patients at the Department of Rheumatology, University Hospital, Umeå, and the registers of the NSHDS cohort and the Maternity cohort, given the date of onset of joint disease, 86 indi-viduals (pre-patients) were identified as having donated blood before onset of signs or symp-toms of joint disease. Median sampling time before the onset of symptoms was 2.5 years. Four control subjects for every pre-patient identified, matched for sex, age at the time of blood sampling, the time point of sampling, and area of residence (rural or urban) were ran-domly selected from the same cohort. Samples from 3 pre-patients and 16 controls (all from the Maternity cohort) were unavailable, and another 2 control tubes were empty. This resulted in 83 pre-patients (69 women, 14 men) and only 2 controls in 2 sets of case-control pairs and 3 controls in 6 sets of pairs. Blood had been collected from 15 of the 83 pre-patients on 2 oc-casions antedating the onset of symptoms, yielding a total of 98 pre-patient samples. For 67 (55 women, 12 men) of the 83 pre-patients samples collected at the first visit to the early RA clinic were available. The mean duration of symptoms at diagnosis was 7.2 months. Of the 83 pre-patients identified another 21, so-called “long-term samples” were also identified and evaluated independent of the other pre-patient samples. Those samples had been collected many years (a median of 10.9 years [IQR 8.7-18.4]) before the onset of symptoms of joint disease and were included in the study to verify a pre-patient sample potentially positive for anti-CCP antibodies or RFs collected closer to the disease onset. No control samples were identified for the long-term samples. Samples from pre-patients, controls and samples col-lected at early RA diagnosis were analysed for auto-antibody titres.
Paper III: Of the 83 pre-patients identified in the NSHDS cohort and the Maternity cohort
for Paper II, blood samples for DNA analyses were available from 59 individuals (45 women, 14 men) who constitute the pre-patient cohort in this part of study. Median blood sampling time before onset of symptoms was 2.0 years. Power calculations, based on pre-test probabil-ity of previous results of HLA-DR4 frequencies in patients and controls from this area (Ran-tapää- Dahlqvist 1985) showed that two controls per pre-patient would be sufficient. Hence, two controls from the four previously analysed for auto-antibody titres (Paper II) were ran-domly selected for genetic analysis. Samples from 52 (40 women, 12 men) of the 59 pre-patients, collected at the time-point of early RA diagnosis were available. The mean duration of symptoms at diagnosis was 7.1 months.
Paper IV: The register of all patients included in the early RA programme between January
1996 and December 2003 (n=138; 98 women, 40 men) at the Department of Rheumatology, University Hospital, Umeå was co-analysed with the register of the NSHDS cohort and the Maternity cohort. Ninety-three of the 138 early RA-patients (72 women, 21 men) were identi-fied as having donated blood before onset of symptoms of joint disease (referred to as

Subjects and methods _______________________________________________________________________________________
20
pre-patients). The median blood sampling time before onset of symptoms was 3.0 years and mean time of symptoms at the diagnosis of RA was 7.2 months.
The patients were treated with the aim of achieving remission, using disease-modifying-
anti-rheumatic drug(s) (DMARDs), corticosteroids, non-steroidal anti-inflammatory drug(s) (NSAIDs) and analgesics as regarded appropriate with respect to the clinical situation.
All individuals gave their written informed consent prior participation and the Ethics Committee of the University Hospital; Umeå approved the studies.
Methods
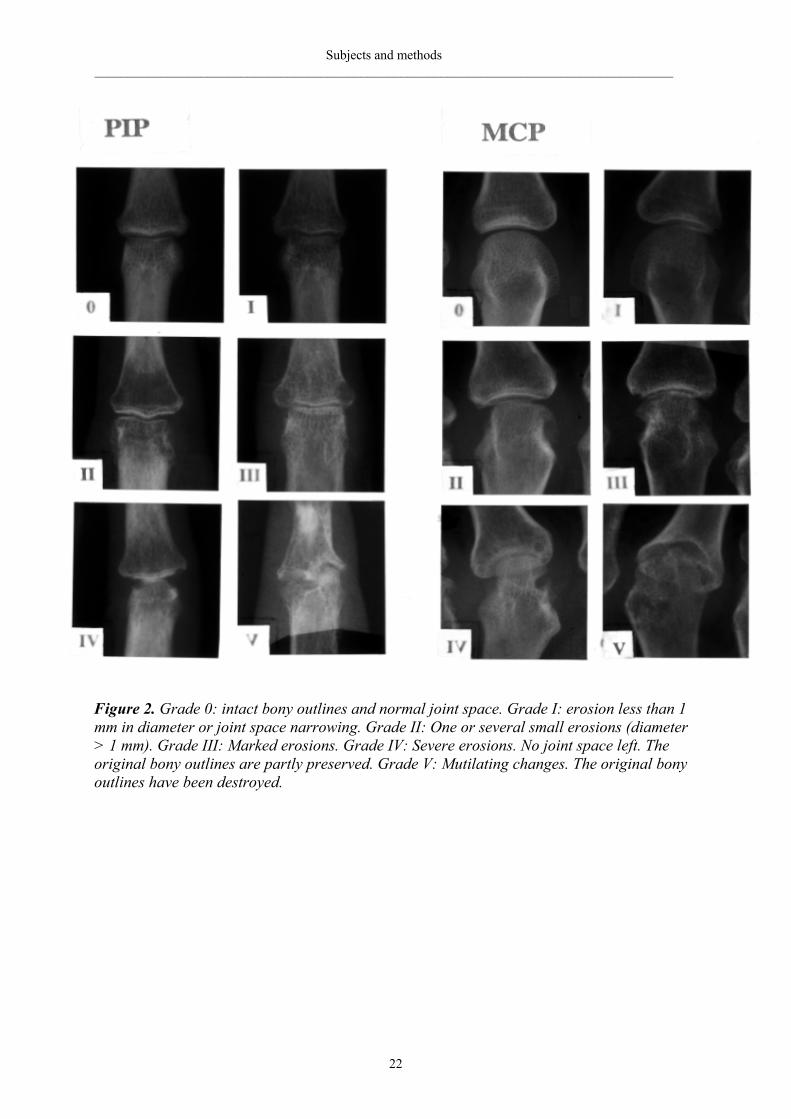
Radiological scoring of hands and feet (Papers I and IV) Radiological damage was used as an outcome variable. Radiographs of hands, wrists and fore-feet in frontal projection were obtained within 2 months of diagnosis and after 2 years. Paper I also included radiographs after 1 year. The radiographs were evaluated according to a modi-fied Larsen method (Larsen 1995) in which 32 joint areas are assessed: MCP II-V (n=8), PIP II-V (n=8), 4 areas in each wrist (n=8) and MTP II-V (n=8). Each area is graded from 0-V by comparison with standard reference films (Figure 2). Thus, using this grading system the maximal total score is 160. In Paper I all radiographs were assessed consecutively by one ra-diologist, Lars Nordmark (LN), without knowledge of the clinical or laboratory status of the patients. In Paper IV the radiographs were evaluated by two rheumatologists together, Ewa Berglin (EB) and Solbritt Rantapää Dahlqvist (SRD), who were specially trained by Arvi Lar-sen in evaluating radiological films according to Larsen score. At the time of the radiograph assessment neither EB nor SRD had knowledge of the clinical or laboratory status of the pa-tients. Forty-two of the 43 patients in Paper I were also included in Paper IV and their radio-graphs were consequently assessed both by LN and by EB &SRD. The scoring by LN was consistently higher than by EB & SRD, but there was a significant correlation between the different assessments (rs = 0.686, P<0.01 for baseline films; rs = 0.519, P<0.01 for films taken after two years). In Paper IV, 15 % of the baseline radiographs and 34 % of the 2 radiographs after 2 years were obtained using a digital technique and the remaining with conventional radiographic films. In 6 % of the patients both the baseline and 2 year radiographs were per-formed using digital technique. Dual-energy X-ray absorptiometry (DXA) of hands (Paper I) Bone mineral density (BMD) of hands, expressed as grams of bone mineral per square centi-metre (g/cm2), was estimated by DXA and used as an outcome variable. The patients were examined at baseline and after 1 and 2 years. In 14 patients (4 men, 5 premenopausal and 5 postmenopausal women) the first DXA examination was not performed until 6 months after diagnosis. There were no differences between the examination results at baseline and after 6 months for the other patients, consequently the 6-month values were used as baseline values for those 14 patients. The DXA examinations performed out by a single assessor using a Lu-nar densiometer (Lunar DPX-L; Lunar Corp; Madison;WI, USA). The proximal limit of the area examined was a line through the base of the metacarpal bones. The coefficient of varia-tion between 6 different BMD estimations in one healthy individual was 1.1 %.

Subjects and methods _______________________________________________________________________________________
21
Antibodies against cyclic citrullinated peptide (anti-CCP antibodies) (Papers II, III and IV) Anti-CCP antibodies were measured in serum or plasma samples from all pre-patients, all controls and all patients using the anti-CCP-2 enzyme immunoassay (EIA) from Euro-Diagnostica (Arnhem, The Netherlands) (Papers II and III). In Paper IV, the Diastat kit from Axis-Shield Diagnostics Limited (The Technology Park, Dundee, UK) was also used. The two methods are based on the same type of peptides (Vossenaar and van Venrooij 2004). All measurements were performed in duplicate and the mean values used. Titres above a cut-off value of 25units/mL (Euro-Diagnostica kit) or above 5 units/mL (Diastat kit), which were the 98th percentiles for controls, were considered positive as suggested by the manufacturers.
Subjects and methods _______________________________________________________________________________________
22
Figure 2. Grade 0: intact bony outlines and normal joint space. Grade I: erosion less than 1 mm in diameter or joint space narrowing. Grade II: One or several small erosions (diameter > 1 mm). Grade III: Marked erosions. Grade IV: Severe erosions. No joint space left. The original bony outlines are partly preserved. Grade V: Mutilating changes. The original bony outlines have been destroyed.
Subjects and methods _______________________________________________________________________________________
23
Rheumatoid factors (Papers II, III and IV) RF isotypes IgG-RF, IgA-RF and IgM-RF were measured in serum or plasma-samples from pre-patients, controls and in samples collected at baseline. All RF determinations were per-formed in duplicate using in-house enzyme-linked immunosorbent assays (ELISAs; Depart-ment of Immunology, Karolinska University Hospital, Huddinge, Sweden). The accepted variation for duplicates was set at <15%. If the variation exceeded this level, the samples were reassayed. The 95th percentile value of the controls from Paper II was used as cut-off point for all three RF classes. Shared epitope (Papers I, III and IV) HLA-DRB1 genotyping was performed using polymerase chain reaction sequence-specific primers (PCR-SSP) from a DR low-resolution kit and DRB1*04 subtyping kit from Dynal (Oslo, Norway) and from Olerup SSP AB, Saltsjöbaden, Sweden for Paper III. The HLA shared epitope (SE) alleles were defined as DRB1*0401 and DRB1*0404. Markers of bone turnover (Paper I) Markers of bone formation (osteocalcin and type 1 procollagen carboxyterminal propeptide [PICP]) and bone resorption (cross-linked carboxyterminal telopeptide of type I collagen [ICTP]) were measured. Osteocalcin level was determined using a commercially available immunoradiometric assay (Nichols Institute Diagnostics, San Juan Capistrano, CA, USA), whilst ICTP and PICP were measured using radioimmunoassay (RIA; Orion Diagnostica, Espoo, Finland). Standard laboratory analyses (Papers I and IV) The erythrocyte sedimentation rate (ESR, mm/h) and blood levels of C-reactive protein (CRP, mg/L) were determined at baseline and every six months up to 2 years using standard labora-tory methods. Clinical examinations (Papers I and IV) The disease activity was assessed by DAS28 (Prevoo et al. 1995) at baseline and every six months up to 2 years. DAS28 is calculated using a 28-joint count for tender and swollen joints, the ESR (mm/h) and patient’s global assessment of general health on a visual analogue scale (VAS). The therapy response at 6, 12 and 24 months were determined according to EULAR response criteria (van Gestel 1998). For Paper I the clinical examination also in-cluded assessment of grip strength (Grippit instrument; AB Detektor, Göteborg, Sweden) and the Health Assessment Questionnaire (HAQ; Ekdahl 1998). Statistical analyses For differences in continuous data for small samples and/or not normally distributed samples the Mann-Whitney U test was used, and comparisons between related samples were per-formed using Wilcoxon´s signed rank test or Friedman´s two way analysis by ranks. Other-wise continuous data were compared using Student´s t-test and related samples by paired t-test.
Variations over time in continuous data between and within groups were assessed by analysis of variance for repeated measurements using Statview statistical software in Paper IV and I. All other analyses were performed using the SPSS software. Categorical data were compared using Chi-square test or Fisher´s exact test. The Chi-square test for trends was used for comparing more than two categorical data. Correlation between continuous variables was analysed with Spearman´s rank correlation. Sensitivity, specificity, positive predictive value

Subjects and methods _______________________________________________________________________________________
24
(PPV) and negative predictive value (NPV) was analysed (Figure 3) and calculated using a computer program (Gahlinger and Abramson 1997). Multiple regression analyses were per-formed using the ANOVA general linear model, choosing included factors and covariates from results of simple regression analyses and/or clinical assumptions. In Paper IV multivari-ate logistic regression in backward stepwise approach was used to find predictors of and to calculate odds ratios for radiological progression. In Paper II and III conditional logistic re-gression analyses were used for matched pairs. All P-values were two-sided and P-values ≤0.05 were considered significant.
DISEASE
Present Absent
Positive
a b a + b →ba
aPPV+
=
TEST Negative
c d c + d →
dcdNPV+
=
a + c ↓
b + d ↓
ca
aSe+
= db
dSp+
=
dbb
caa
LR
+
+=
______________________________________________________________________ Figure 3. Diagnostic test characteristics and definitions PPV = Positive predictive value, NPV = Negative predictive value, Se = Sensitivity, Sp = Specificity, LR = likelihood ratio for a positive test
Results and discussions _______________________________________________________________________________________
25
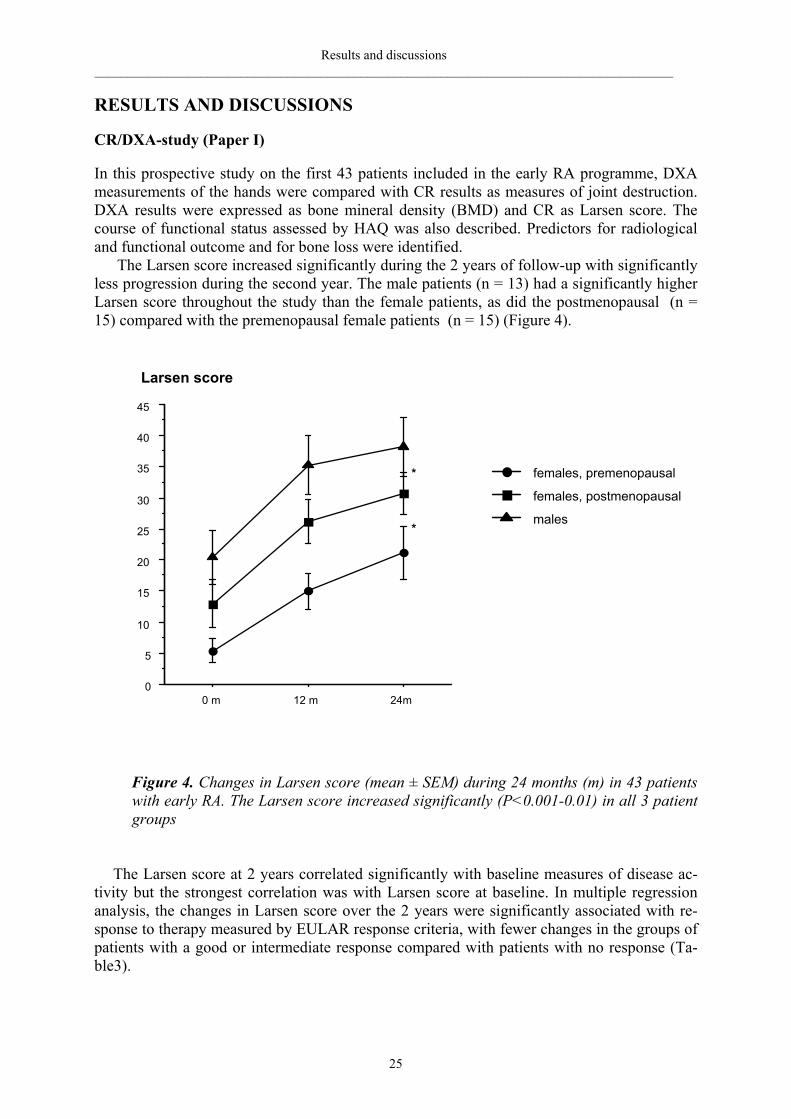
RESULTS AND DISCUSSIONS CR/DXA-study (Paper I) In this prospective study on the first 43 patients included in the early RA programme, DXA measurements of the hands were compared with CR results as measures of joint destruction. DXA results were expressed as bone mineral density (BMD) and CR as Larsen score. The course of functional status assessed by HAQ was also described. Predictors for radiological and functional outcome and for bone loss were identified.
The Larsen score increased significantly during the 2 years of follow-up with significantly less progression during the second year. The male patients (n = 13) had a significantly higher Larsen score throughout the study than the female patients, as did the postmenopausal (n = 15) compared with the premenopausal female patients (n = 15) (Figure 4).
Figure 4. Changes in Larsen score (mean ± SEM) during 24 months (m) in 43 patients with early RA. The Larsen score increased significantly (P<0.001-0.01) in all 3 patient groups
The Larsen score at 2 years correlated significantly with baseline measures of disease ac-tivity but the strongest correlation was with Larsen score at baseline. In multiple regression analysis, the changes in Larsen score over the 2 years were significantly associated with re-sponse to therapy measured by EULAR response criteria, with fewer changes in the groups of patients with a good or intermediate response compared with patients with no response (Ta-ble3).
0
5
10
15
20
25
30
35
40
45
0 m 12 m 24m
Larsen score
*
*males
females, postmenopausal
females, premenopausal
Results and discussions _______________________________________________________________________________________
26
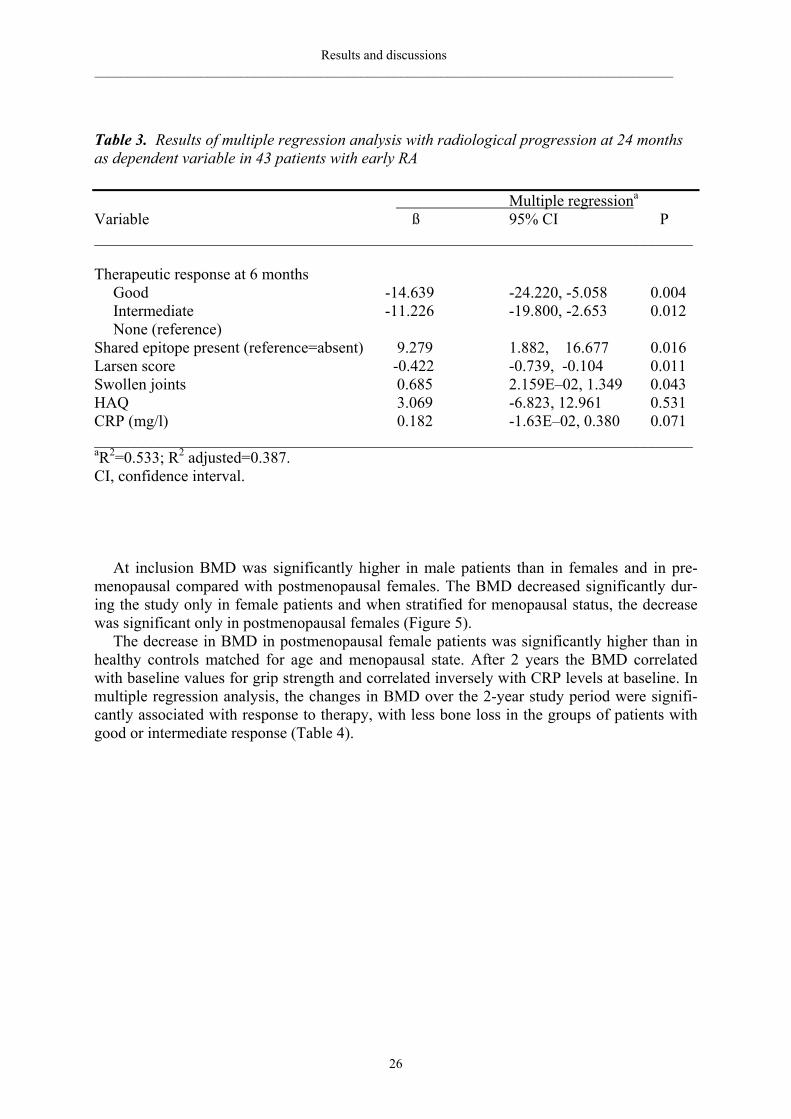
Table 3. Results of multiple regression analysis with radiological progression at 24 months as dependent variable in 43 patients with early RA Multiple regressiona Variable ß 95% CI P ___________________________________________________________________________ Therapeutic response at 6 months Good -14.639 -24.220, -5.058 0.004 Intermediate -11.226 -19.800, -2.653 0.012 None (reference) Shared epitope present (reference=absent) 9.279 1.882, 16.677 0.016 Larsen score -0.422 -0.739, -0.104 0.011 Swollen joints 0.685 2.159E–02, 1.349 0.043 HAQ 3.069 -6.823, 12.961 0.531 CRP (mg/l) 0.182 -1.63E–02, 0.380 0.071 ___________________________________________________________________________ aR2=0.533; R2 adjusted=0.387. CI, confidence interval.
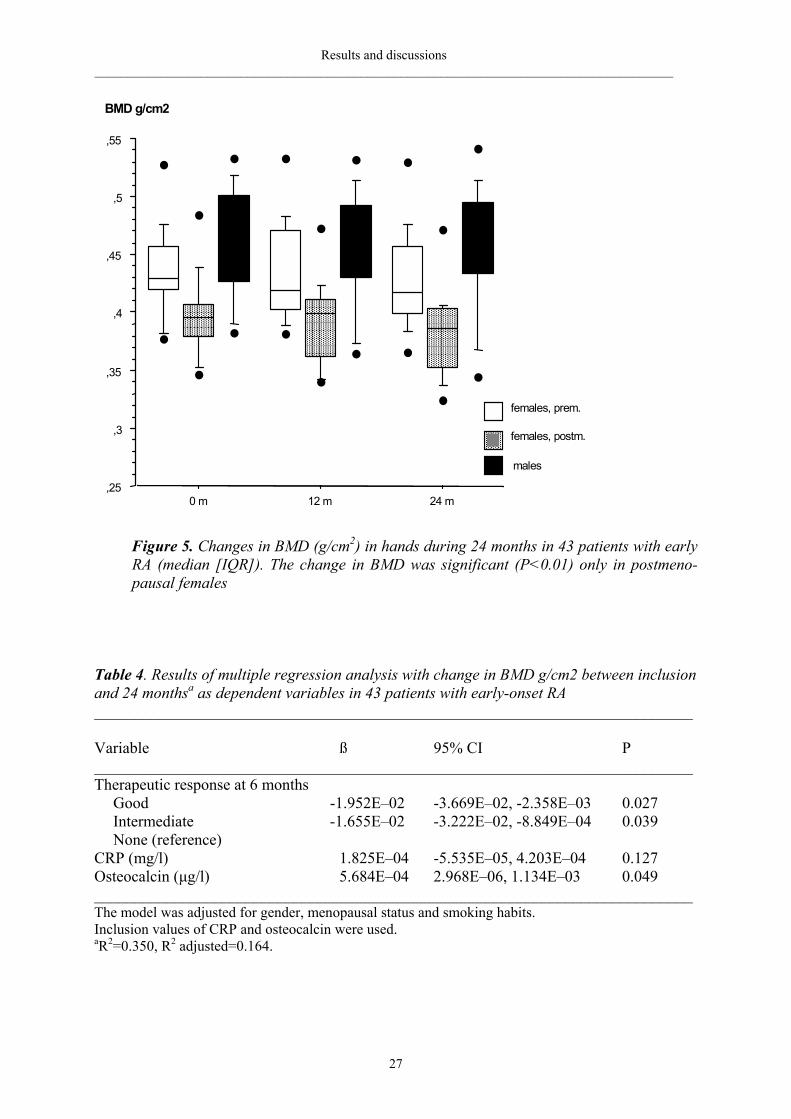
At inclusion BMD was significantly higher in male patients than in females and in pre-menopausal compared with postmenopausal females. The BMD decreased significantly dur-ing the study only in female patients and when stratified for menopausal status, the decrease was significant only in postmenopausal females (Figure 5).
The decrease in BMD in postmenopausal female patients was significantly higher than in healthy controls matched for age and menopausal state. After 2 years the BMD correlated with baseline values for grip strength and correlated inversely with CRP levels at baseline. In multiple regression analysis, the changes in BMD over the 2-year study period were signifi-cantly associated with response to therapy, with less bone loss in the groups of patients with good or intermediate response (Table 4).
Results and discussions _______________________________________________________________________________________
27
Figure 5. Changes in BMD (g/cm2) in hands during 24 months in 43 patients with early RA (median [IQR]). The change in BMD was significant (P<0.01) only in postmeno-pausal females
Table 4. Results of multiple regression analysis with change in BMD g/cm2 between inclusion and 24 monthsa as dependent variables in 43 patients with early-onset RA ___________________________________________________________________________ Variable ß 95% CI P ___________________________________________________________________________Therapeutic response at 6 months
Good -1.952E–02 -3.669E–02, -2.358E–03 0.027 Intermediate -1.655E–02 -3.222E–02, -8.849E–04 0.039 None (reference)
CRP (mg/l) 1.825E–04 -5.535E–05, 4.203E–04 0.127 Osteocalcin (µg/l) 5.684E–04 2.968E–06, 1.134E–03 0.049 ___________________________________________________________________________ The model was adjusted for gender, menopausal status and smoking habits. Inclusion values of CRP and osteocalcin were used. aR2=0.350, R2 adjusted=0.164.
,25
,3
,35
,4
,45
,5
,55
0 m 12 m 24 m
males
females, postm.
females, prem.
BMD g/cm2

Results and discussions _______________________________________________________________________________________
28
There was a significant inverse correlation between the percentage decrease in BMD and
the change in Larsen score during the study period (rs = -0.552, P<0.001). This correlation remained significant in analysis of the Larsen score for the hands only.
HAQ at 2 years was correlated with disease activity at baseline, but the strongest correla-tion was with baseline HAQ. In multiple regression analyses the change in HAQ over 2 years was significantly associated with global VAS, HAQ and Larsen score at baseline but not with therapeutic response. Discussion (Paper I) In this paper, a significant correlation between radiological progression in hands and feet and bone loss in hands during the follow-up period was demonstrated. Both the radiological pro-gression and the change in BMD were retarded by response to therapy. Peri-articular osteopo-rosis is an early radiological sign of RA and has been reported to be associated with disease activity (Deodhar et al. 1995; 2003). The presence of joint erosions has been reported to be associated with general osteoporosis (Forsblad et al. 2003) and with osteoporosis in metacar-pal bones (Jensen et al. 2005). A common mechanism for osteoporosis and erosions due to increased osteoclast activation has been proposed (Green and Deodhar 2001). There is a great body of evidence that response to DMARD treatment can decrease the radiological progres-sion in hand and foot skeleton. A sparing effect of DMARDs on osteoporosis in metacarpal bones (Kalla et al. 1991) as well as in spine and hip (Dolan et al. 2002) has also been re-ported. Consequently our results are in line with those reports. In our study several measures of inflammation at baseline correlated with the radiological outcome. This is in agreement with several other studies that have demonstrated the predictive value of a combination of initial factors, such as joint involvement (Feigenbaum et al. 1979; van Zeben et al. 1993), acute-phase response (Kaarela 1985; van der Heijde et al.1992b; van Leeuwen et al. 1995; Combe et al. 2001) and genetic predisposition for RA (van der Heijde et al. 1992b; van Leeuwen et al. 1995; Combe et al. 2001;). In our study presence of the HLA SE allele(s) did not contribute significantly to the radiological progression in a simple regression model. This could possibly be explained by the relative high frequency of HLA DR4 in the normal popula-tion of northern Sweden (35.1% among healthy blood donors; Rantapää Dahlqvist et al. 1985), resulting in a small contribution of the HLA SE allele(s) to the disease severity. How-ever, in a multiple regression model including therapeutic response at 6 months and baseline values of Larsen score, HAQ, swollen joint count and CRP, the HLA SE allele(s) significantly predicted the radiological progression. Grip strength and CRP were the only baseline variables tested that correlated with the bone mass in hands after 2 years. When analysing the sexes separately, the correlation with CRP was only significant for males. A significant, but rather weak correlation was found between the accumulated number of tender and swollen joints in the hands and the loss of BMD in the hands in postmenopausal females, suggesting some influence of inflammation in the hand region on changes in BMD. These measures of initial and accumulated inflammation did not, however, remain significant in multiple regression analysis. Hence, we could not find any convincing direct association between inflammatory activity and the loss of bone mass in hands. Rather the hand bone loss seemed to follow the same pattern as that found for general osteoporosis that has been recognised early in disease and has been reported to be associated with disease activity (Laan et al. 1993; Gough et al. 1994). In our study, reduced bone loss of the hands in patients with a response to therapy and the strong negative correlation with radio-logical progression indicate an indirect association with inflammation.
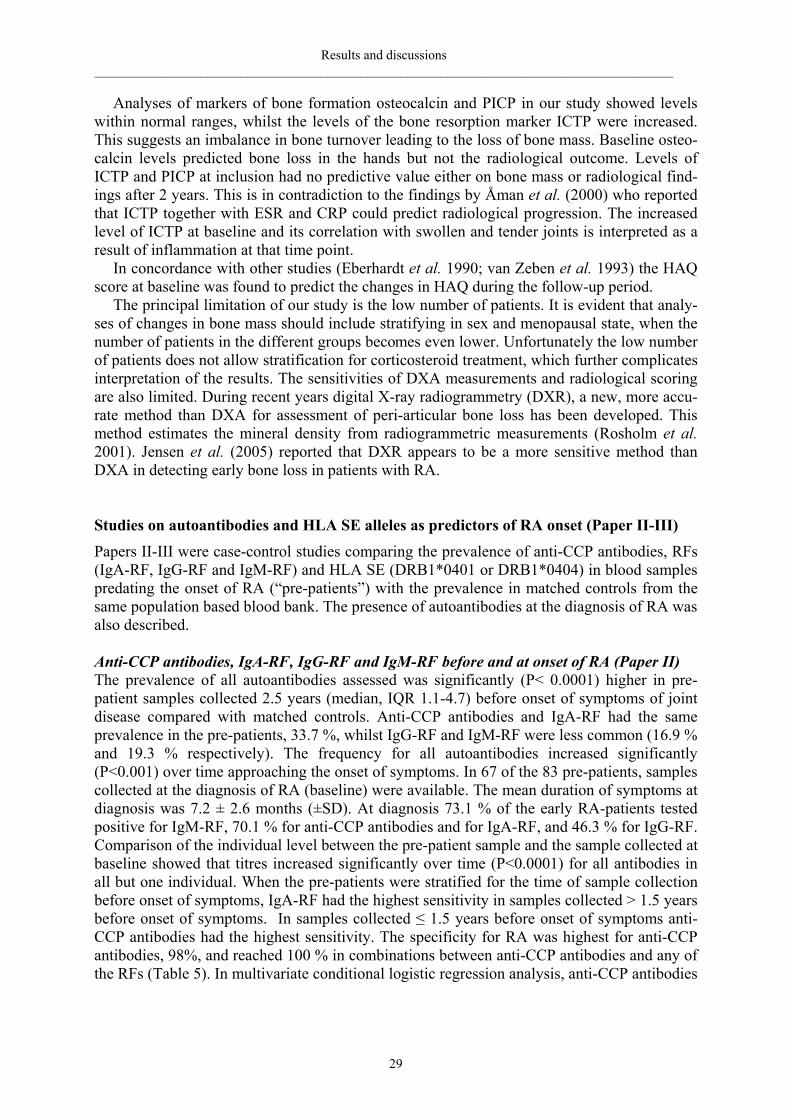
Results and discussions _______________________________________________________________________________________
29
Analyses of markers of bone formation osteocalcin and PICP in our study showed levels within normal ranges, whilst the levels of the bone resorption marker ICTP were increased. This suggests an imbalance in bone turnover leading to the loss of bone mass. Baseline osteo-calcin levels predicted bone loss in the hands but not the radiological outcome. Levels of ICTP and PICP at inclusion had no predictive value either on bone mass or radiological find-ings after 2 years. This is in contradiction to the findings by Åman et al. (2000) who reported that ICTP together with ESR and CRP could predict radiological progression. The increased level of ICTP at baseline and its correlation with swollen and tender joints is interpreted as a result of inflammation at that time point. In concordance with other studies (Eberhardt et al. 1990; van Zeben et al. 1993) the HAQ score at baseline was found to predict the changes in HAQ during the follow-up period. The principal limitation of our study is the low number of patients. It is evident that analy-ses of changes in bone mass should include stratifying in sex and menopausal state, when the number of patients in the different groups becomes even lower. Unfortunately the low number of patients does not allow stratification for corticosteroid treatment, which further complicates interpretation of the results. The sensitivities of DXA measurements and radiological scoring are also limited. During recent years digital X-ray radiogrammetry (DXR), a new, more accu-rate method than DXA for assessment of peri-articular bone loss has been developed. This method estimates the mineral density from radiogrammetric measurements (Rosholm et al. 2001). Jensen et al. (2005) reported that DXR appears to be a more sensitive method than DXA in detecting early bone loss in patients with RA. Studies on autoantibodies and HLA SE alleles as predictors of RA onset (Paper II-III) Papers II-III were case-control studies comparing the prevalence of anti-CCP antibodies, RFs (IgA-RF, IgG-RF and IgM-RF) and HLA SE (DRB1*0401 or DRB1*0404) in blood samples predating the onset of RA (“pre-patients”) with the prevalence in matched controls from the same population based blood bank. The presence of autoantibodies at the diagnosis of RA was also described. Anti-CCP antibodies, IgA-RF, IgG-RF and IgM-RF before and at onset of RA (Paper II) The prevalence of all autoantibodies assessed was significantly (P< 0.0001) higher in pre-patient samples collected 2.5 years (median, IQR 1.1-4.7) before onset of symptoms of joint disease compared with matched controls. Anti-CCP antibodies and IgA-RF had the same prevalence in the pre-patients, 33.7 %, whilst IgG-RF and IgM-RF were less common (16.9 % and 19.3 % respectively). The frequency for all autoantibodies increased significantly (P<0.001) over time approaching the onset of symptoms. In 67 of the 83 pre-patients, samples collected at the diagnosis of RA (baseline) were available. The mean duration of symptoms at diagnosis was 7.2 ± 2.6 months (±SD). At diagnosis 73.1 % of the early RA-patients tested positive for IgM-RF, 70.1 % for anti-CCP antibodies and for IgA-RF, and 46.3 % for IgG-RF. Comparison of the individual level between the pre-patient sample and the sample collected at baseline showed that titres increased significantly over time (P<0.0001) for all antibodies in all but one individual. When the pre-patients were stratified for the time of sample collection before onset of symptoms, IgA-RF had the highest sensitivity in samples collected > 1.5 years before onset of symptoms. In samples collected ≤ 1.5 years before onset of symptoms anti-CCP antibodies had the highest sensitivity. The specificity for RA was highest for anti-CCP antibodies, 98%, and reached 100 % in combinations between anti-CCP antibodies and any of the RFs (Table 5). In multivariate conditional logistic regression analysis, anti-CCP antibodies
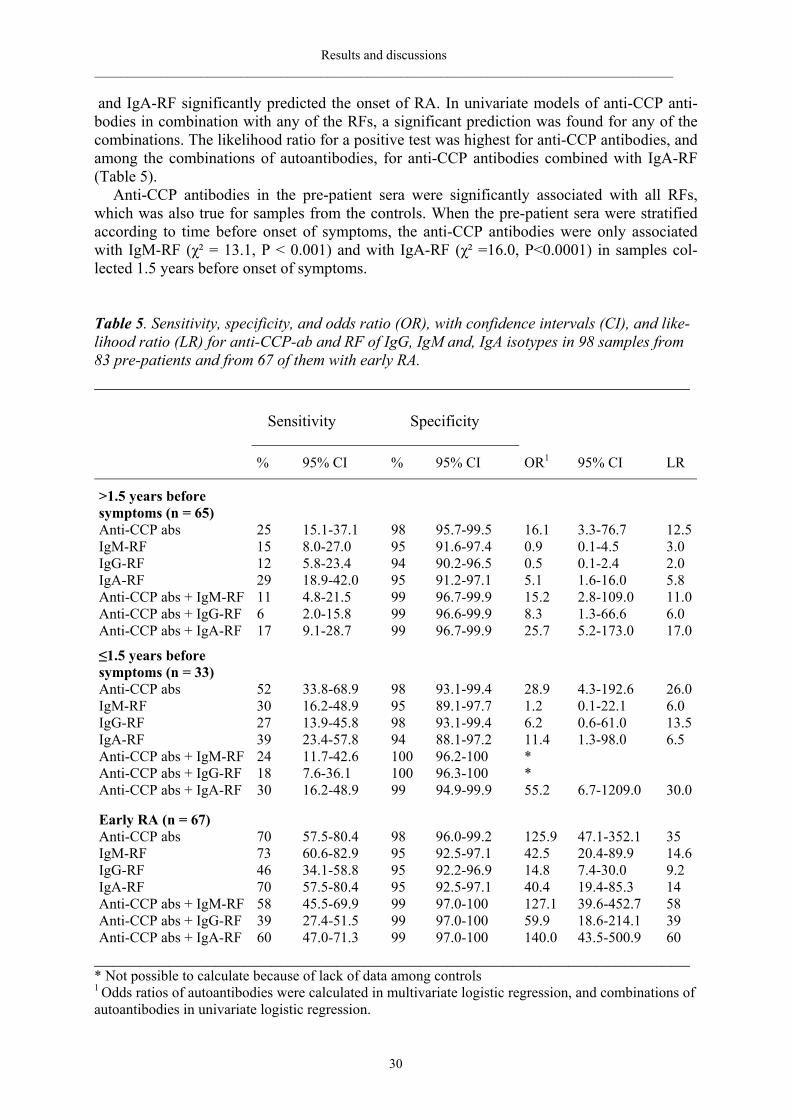
Results and discussions _______________________________________________________________________________________
30
and IgA-RF significantly predicted the onset of RA. In univariate models of anti-CCP anti-bodies in combination with any of the RFs, a significant prediction was found for any of the combinations. The likelihood ratio for a positive test was highest for anti-CCP antibodies, and among the combinations of autoantibodies, for anti-CCP antibodies combined with IgA-RF (Table 5). Anti-CCP antibodies in the pre-patient sera were significantly associated with all RFs, which was also true for samples from the controls. When the pre-patient sera were stratified according to time before onset of symptoms, the anti-CCP antibodies were only associated with IgM-RF (χ² = 13.1, P < 0.001) and with IgA-RF (χ² =16.0, P<0.0001) in samples col-lected 1.5 years before onset of symptoms. Table 5. Sensitivity, specificity, and odds ratio (OR), with confidence intervals (CI), and like-lihood ratio (LR) for anti-CCP-ab and RF of IgG, IgM and, IgA isotypes in 98 samples from 83 pre-patients and from 67 of them with early RA. ________________________________________________________________ Sensitivity Specificity
% 95% CI % 95% CI OR1 95% CI LR
>1.5 years before symptoms (n = 65)
Anti-CCP abs 25 15.1-37.1 98 95.7-99.5 16.1 3.3-76.7 12.5IgM-RF 15 8.0-27.0 95 91.6-97.4 0.9 0.1-4.5 3.0 IgG-RF 12 5.8-23.4 94 90.2-96.5 0.5 0.1-2.4 2.0 IgA-RF 29 18.9-42.0 95 91.2-97.1 5.1 1.6-16.0 5.8 Anti-CCP abs + IgM-RF 11 4.8-21.5 99 96.7-99.9 15.2 2.8-109.0 11.0Anti-CCP abs + IgG-RF 6 2.0-15.8 99 96.6-99.9 8.3 1.3-66.6 6.0 Anti-CCP abs + IgA-RF 17 9.1-28.7 99 96.7-99.9 25.7 5.2-173.0 17.0
≤1.5 years before symptoms (n = 33)
Anti-CCP abs 52 33.8-68.9 98 93.1-99.4 28.9 4.3-192.6 26.0IgM-RF 30 16.2-48.9 95 89.1-97.7 1.2 0.1-22.1 6.0 IgG-RF 27 13.9-45.8 98 93.1-99.4 6.2 0.6-61.0 13.5IgA-RF 39 23.4-57.8 94 88.1-97.2 11.4 1.3-98.0 6.5 Anti-CCP abs + IgM-RF 24 11.7-42.6 100 96.2-100 * Anti-CCP abs + IgG-RF 18 7.6-36.1 100 96.3-100 * Anti-CCP abs + IgA-RF 30 16.2-48.9 99 94.9-99.9 55.2 6.7-1209.0 30.0
Early RA (n = 67)
Anti-CCP abs 70 57.5-80.4 98 96.0-99.2 125.9 47.1-352.1 35 IgM-RF 73 60.6-82.9 95 92.5-97.1 42.5 20.4-89.9 14.6IgG-RF 46 34.1-58.8 95 92.2-96.9 14.8 7.4-30.0 9.2 IgA-RF 70 57.5-80.4 95 92.5-97.1 40.4 19.4-85.3 14 Anti-CCP abs + IgM-RF 58 45.5-69.9 99 97.0-100 127.1 39.6-452.7 58 Anti-CCP abs + IgG-RF 39 27.4-51.5 99 97.0-100 59.9 18.6-214.1 39 Anti-CCP abs + IgA-RF 60 47.0-71.3 99 97.0-100 140.0 43.5-500.9 60 ________________________________________________________________ * Not possible to calculate because of lack of data among controls 1 Odds ratios of autoantibodies were calculated in multivariate logistic regression, and combinations of autoantibodies in univariate logistic regression.
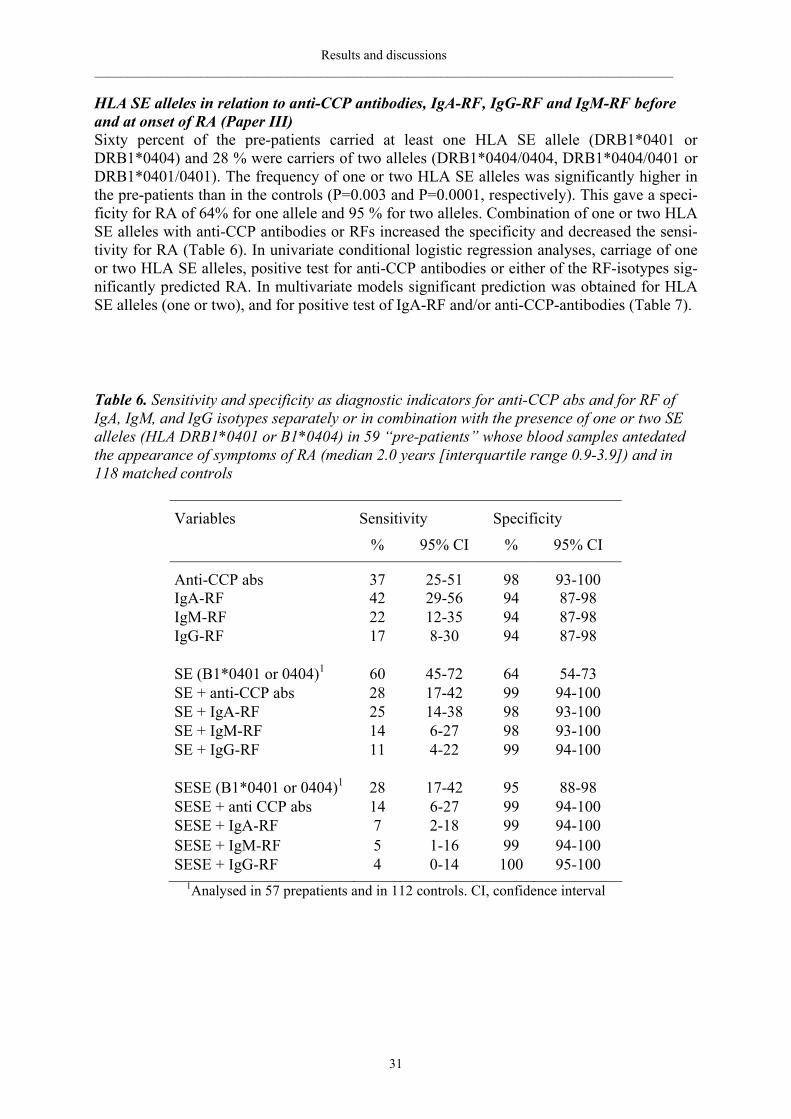
Results and discussions _______________________________________________________________________________________
31
HLA SE alleles in relation to anti-CCP antibodies, IgA-RF, IgG-RF and IgM-RF before and at onset of RA (Paper III) Sixty percent of the pre-patients carried at least one HLA SE allele (DRB1*0401 or DRB1*0404) and 28 % were carriers of two alleles (DRB1*0404/0404, DRB1*0404/0401 or DRB1*0401/0401). The frequency of one or two HLA SE alleles was significantly higher in the pre-patients than in the controls (P=0.003 and P=0.0001, respectively). This gave a speci-ficity for RA of 64% for one allele and 95 % for two alleles. Combination of one or two HLA SE alleles with anti-CCP antibodies or RFs increased the specificity and decreased the sensi-tivity for RA (Table 6). In univariate conditional logistic regression analyses, carriage of one or two HLA SE alleles, positive test for anti-CCP antibodies or either of the RF-isotypes sig-nificantly predicted RA. In multivariate models significant prediction was obtained for HLA SE alleles (one or two), and for positive test of IgA-RF and/or anti-CCP-antibodies (Table 7). Table 6. Sensitivity and specificity as diagnostic indicators for anti-CCP abs and for RF of IgA, IgM, and IgG isotypes separately or in combination with the presence of one or two SE alleles (HLA DRB1*0401 or B1*0404) in 59 “pre-patients” whose blood samples antedated the appearance of symptoms of RA (median 2.0 years [interquartile range 0.9-3.9]) and in 118 matched controls
Variables Sensitivity Specificity
% 95% CI % 95% CI
Anti-CCP abs 37 25-51 98 93-100 IgA-RF 42 29-56 94 87-98 IgM-RF 22 12-35 94 87-98 IgG-RF 17 8-30 94 87-98 SE (B1*0401 or 0404)1 60 45-72 64 54-73 SE + anti-CCP abs 28 17-42 99 94-100 SE + IgA-RF 25 14-38 98 93-100 SE + IgM-RF 14 6-27 98 93-100 SE + IgG-RF 11 4-22 99 94-100 SESE (B1*0401 or 0404)1 28 17-42 95 88-98 SESE + anti CCP abs 14 6-27 99 94-100 SESE + IgA-RF 7 2-18 99 94-100 SESE + IgM-RF 5 1-16 99 94-100 SESE + IgG-RF 4 0-14 100 95-100
1Analysed in 57 prepatients and in 112 controls. CI, confidence interval
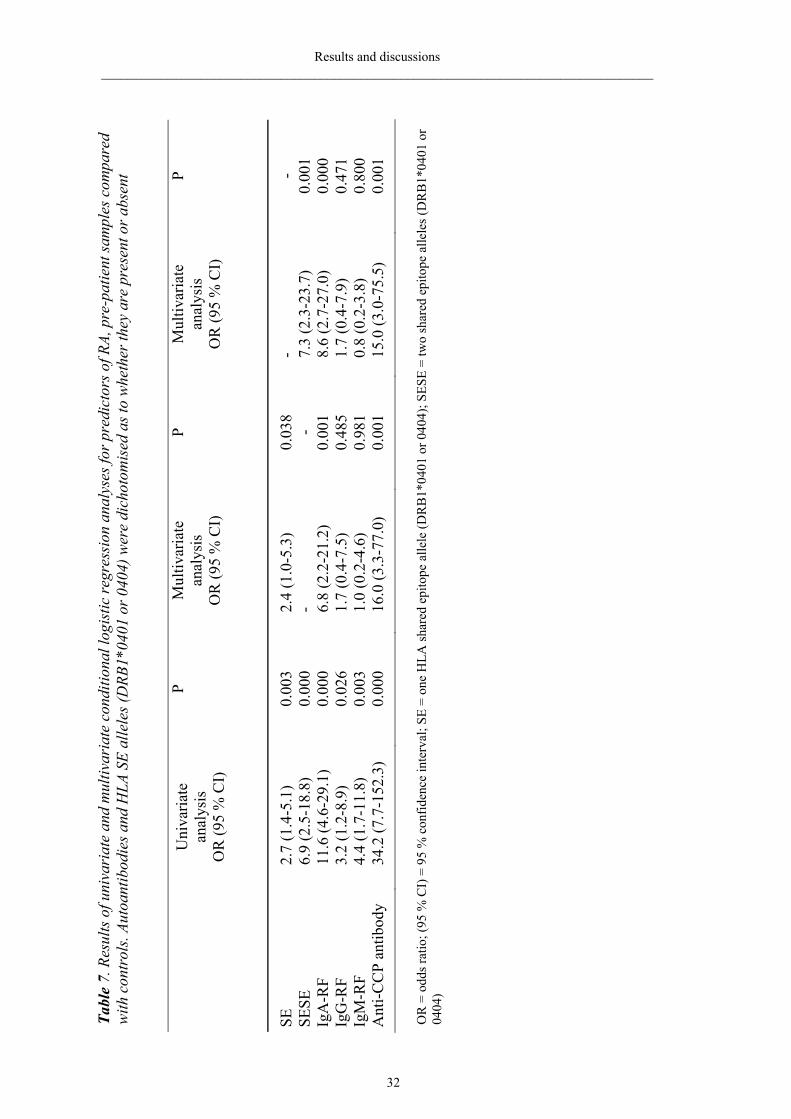
32
Tabl
e 7.
Res
ults
of u
niva
riat
e an
d m
ultiv
aria
te c
ondi
tiona
l log
istic
regr
essi
on a
naly
ses f
or p
redi
ctor
s of R
A, p
re-p
atie
nt sa
mpl
es c
ompa
red
with
con
trol
s. Au
toan
tibod
ies a
nd H
LA S
E al
lele
s (D
RB1*
0401
or 0
404)
wer
e di
chot
omis
ed a
s to
whe
ther
they
are
pre
sent
or a
bsen
t
U
niva
riate
an
alys
is
OR
(95
% C
I)
P M
ultiv
aria
te
anal
ysis
O
R (9
5 %
CI)
P M
ultiv
aria
te
anal
ysis
O
R (9
5 %
CI)
P
SE
2.7
(1.4
-5.1
) 0.
003
2.4
(1.0
-5.3
) 0.
038
- -
SESE
6.
9 (2
.5-1
8.8)
0.
000
- -
7.3
(2.3
-23.
7)
0.00
1 Ig
A-R
F 11
.6 (4
.6-2
9.1)
0.
000
6.8
(2.2
-21.
2)
0.00
1 8.
6 (2
.7-2
7.0)
0.
000
IgG
-RF
3.2
(1.2
-8.9
) 0.
026
1.7
(0.4
-7.5
) 0.
485
1.7
(0.4
-7.9
) 0.
471
IgM
-RF
4.4
(1.7
-11.
8)
0.00
3 1.
0 (0
.2-4
.6)
0.98
1 0.
8 (0
.2-3
.8)
0.80
0 A
nti-C
CP
antib
ody
34.2
(7.7
-152
.3)
0.00
0 16
.0 (3
.3-7
7.0)
0.
001
15.0
(3.0
-75.
5)
0.00
1
OR
= o
dds r
atio
; (95
% C
I) =
95
% c
onfid
ence
inte
rval
; SE
= on
e H
LA sh
ared
epi
tope
alle
le (D
RB
1*04
01 o
r 040
4); S
ESE
= tw
o sh
ared
epi
tope
alle
les (
DR
B1*
0401
or
0404
)
Results and discussions ___________________________________________________________________________________
32
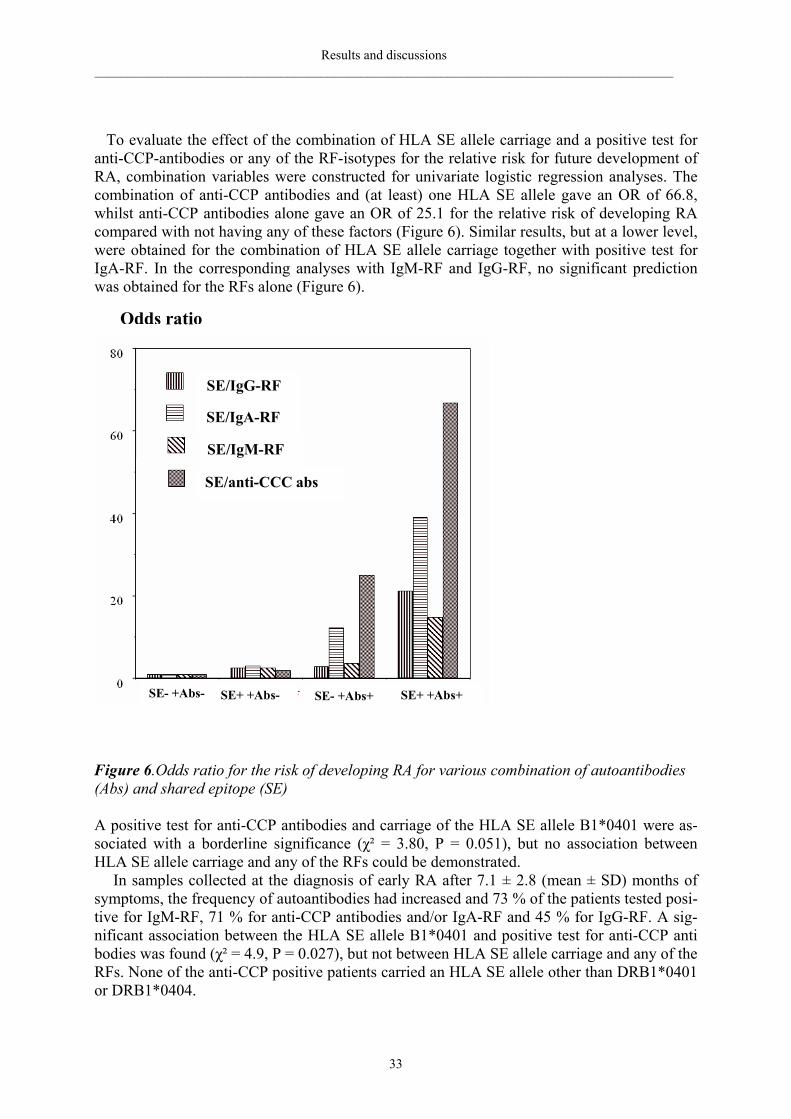
Results and discussions _______________________________________________________________________________________
33
To evaluate the effect of the combination of HLA SE allele carriage and a positive test for anti-CCP-antibodies or any of the RF-isotypes for the relative risk for future development of RA, combination variables were constructed for univariate logistic regression analyses. The combination of anti-CCP antibodies and (at least) one HLA SE allele gave an OR of 66.8, whilst anti-CCP antibodies alone gave an OR of 25.1 for the relative risk of developing RA compared with not having any of these factors (Figure 6). Similar results, but at a lower level, were obtained for the combination of HLA SE allele carriage together with positive test for IgA-RF. In the corresponding analyses with IgM-RF and IgG-RF, no significant prediction was obtained for the RFs alone (Figure 6).
Figure 6.Odds ratio for the risk of developing RA for various combination of autoantibodies (Abs) and shared epitope (SE) A positive test for anti-CCP antibodies and carriage of the HLA SE allele B1*0401 were as-sociated with a borderline significance (χ² = 3.80, P = 0.051), but no association between HLA SE allele carriage and any of the RFs could be demonstrated. In samples collected at the diagnosis of early RA after 7.1 ± 2.8 (mean ± SD) months of symptoms, the frequency of autoantibodies had increased and 73 % of the patients tested posi-tive for IgM-RF, 71 % for anti-CCP antibodies and/or IgA-RF and 45 % for IgG-RF. A sig-nificant association between the HLA SE allele B1*0401 and positive test for anti-CCP anti bodies was found (χ² = 4.9, P = 0.027), but not between HLA SE allele carriage and any of the RFs. None of the anti-CCP positive patients carried an HLA SE allele other than DRB1*0401 or DRB1*0404.
Odds ratio
SE/IgG-RF
SE/IgA-RF
SE/IgM-RF
SE/anti-CCC abs
SE- +Abs- SE+ +Abs- SE- +Abs+ SE+ +Abs+
Results and discussions _______________________________________________________________________________________
34
Discussion (Paper II and III) Anti-CCP antibodies and RFs predated the onset of RA symptoms by several years with in-creasing frequency and increasing titre the closer to disease onset that samples had been col-lected. The longest interval predating the onset of symptoms was 22 years for IgA-RF positiv-ity. When stratified for the time antedating disease onset, IgA-RF had the highest sensitivity in samples collected >1.5 years before disease onset, closely followed by anti-CCP antibod-ies. In samples collected ≤1.5 years before onset of RA symptoms anti-CCP antibodies had the highest sensitivity. At disease onset the frequency of anti-CCP antibodies, IgM-RF and IgA-RF were on the same level and corresponded to the frequencies reported by others (Eber-hardt et al. 1988; Kroot et al. 2000). Both anti-CCP antibodies and IgA-RF significantly pre-dicted the onset of RA in multivariate logistic regression analyses with the highest odds ratio for anti-CCP antibodies. A primary role of IgA-RF in the pathogenesis of RA has previously been suggested (Jonsson et al. 1992). This is consistent with our findings that IgA-RF was the earliest autoantibody detectable and the RF with the highest PPV among the individuals stud-ied and, in the pre-patient samples, the RF with the highest sensitivity. Anti-CCP antibodies were the autoantibodies with the highest specificity, likelihood ratio for a positive test and PPV for RA. The likelihood ratio for a positive test expresses how many times more likely a positive test will occur in disease, as compared with non-disease people, i.e., a composite ex-pression of sensitivity and specificity. Citrulline is a non-standard amino acid formed by posttranslational modification of argin-ine residues by peptidylarginine deiminase (PAD) enzymes (Vossenaar 2003). The production of citrullinated proteins has recently been demonstrated not to be specific for RA (Vossenaar 2004c). In that study immunohistochemical analysis of synovial tissue from RA patients and from patients with other arthropathies was performed using a variety of specific anti-CCP antibodies. Citrullinated proteins were found in the lining layer, the sublining layer, and in extravascular fibrin deposits in inflamed synovial tissue from RA as well as non-RA patients. In the same study local production of anti-CCP antibodies in the synovial fluid of RA patients was demonstrated by comparing the concentration of the antibodies, corrected for the total amount of IgG present, in paired samples of serum and synovial fluid from RA patients. The authors concluded that the high specificity for RA of the anti-CCP antibodies is probably the result of an abnormal humoral response to these proteins in RA patients. In our study RA was very strongly predicted by the combination of a positive test for anti-CCP antibodies and the carriage of the HLA SE alleles DRB1*0401 and/or DRB1*0404. The conversion of arginine to citrulline has in HLA-DRB1*0401 transgenic mice, been demonstrated to significantly increase the activation of CD4 +T-cells (Hill et al. 2003). In a previous study of patients with early RA, a significant association between anti-CCP antibodies and expression of HLA-DRB1*0401/0101 was reported (Goldbach-Mansky et al. 2000). This is in line with our find-ings in Paper III, where HLA DRB1*0401 was significantly associated with anti-CCP anti-bodies when the pre-patients were diagnosed after having developed RA. These findings sug-gest that individuals carrying the HLA SE alleles may have more sustained T-and B-cell re-sponses to citrullinated antigens than non-carriers. Taken together, these data suggest that, in individuals carrying one or two HLA SE alleles, a specific T-cell dependent response to citrullinated peptides may contribute to the development of RA.
However, consistent with the findings of other studies (Bas et al. 2003; Senkpiehl et al. 2005), not all individuals positive for anti-CCP antibodies carried HLA SE alleles. Thus, there is not an absolute requirement of HLA SE alleles to develop anti-CCP antibodies. The HLA-locus has been estimated to contribute to one-third of the genetic risk of developing RA (Deighton et al. 1989; Rigby et al. 1991). Recent studies have reported a strong association
Results and discussions _______________________________________________________________________________________
35
between several single-nucleotide polymorphisms in the gene encoding the PAD enzyme 4 and the development of RA. Carriers of the susceptibility haplotype were significantly more often positive for anti-CCP antibodies than non-carriers (Suzuki et al. 2003; Caponi et al. 2003). The studies by Suzuki and Caponi were performed using non-European patient cohorts and their results have not been confirmed by ourselves (unpublished data). Our studies do not answer the question as to why proteins are citrullinated in individuals’ years before they present with any clinical symptoms of joint disease. Nor do they explain why the production of RFs starts even earlier in the pre-clinical state of disease. The main limitation of Paper III is the lack of DNA from individuals from the Maternity cohort, resulting in relatively low number of individuals in each group when the data are stratified for individuals positive or negative for a given autoantibody. Furthermore, because it is a population-based case-control study, it is possible to establish associations between the outcome and the factors studied, but it is not possible to generalize the calculated probability of future development of RA in the general population. Study on autoantibodies and HLA SE alleles as predictors of RA severity and progres-sion (Paper IV) This was a prospective study on disease outcome and a retrospective study on the presence of autoantibodies in 138 patients with early RA. Samples donated to a population-based blood bank before the onset of symptoms of joint disease were identified for 93 of the patients. The significance of the presence of anti-CCP antibodies and RFs before onset of symptoms of joint disease and at the time of diagnosis of RA, for disease activity and severity, was evalu-ated. Patients with anti-CCP antibodies present before onset of symptoms of joint disease had significantly higher Larsen score at baseline and after 2 years, than patients without pre-disease anti-CCP antibodies. No significant difference in Larsen score at baseline or at 2 years of follow-up could be detected between patients with and without IgM-RF, IgA-RF or IgG-RF as pre-patients (Table 8).
In multiple regression analyses baseline values of anti-CCP antibodies or IgA-RF or IgG-RF or IgM-RF, together with baseline values of Larsen score and swollen joint count signifi-cantly predicted and explained about 50 % of the variation in Larsen score at 2 years (Table 9). Anti-CCP antibodies and RFs were not included in the same analysis model because they were significantly associated (χ2 = 38.0, P< 0.0001 for anti-CCP antibodies and IgA-RF; χ2 = 4.4, P< 0.05 for anti-CCP antibodies and IgG-RF; and χ2 = 22.9, P<0.0001 for anti-CCP anti-bodies and IgM-RF). The RFs were also correlated between themselves (χ2 = 20.6, P<0.0001 for IgG-RF and IgA-RF; χ2 = 5.8, P<0.05 for IgG-RF and IgM-RF; χ2 = 44.9, P<0.0001 for IgA-RF and IgM-RF).
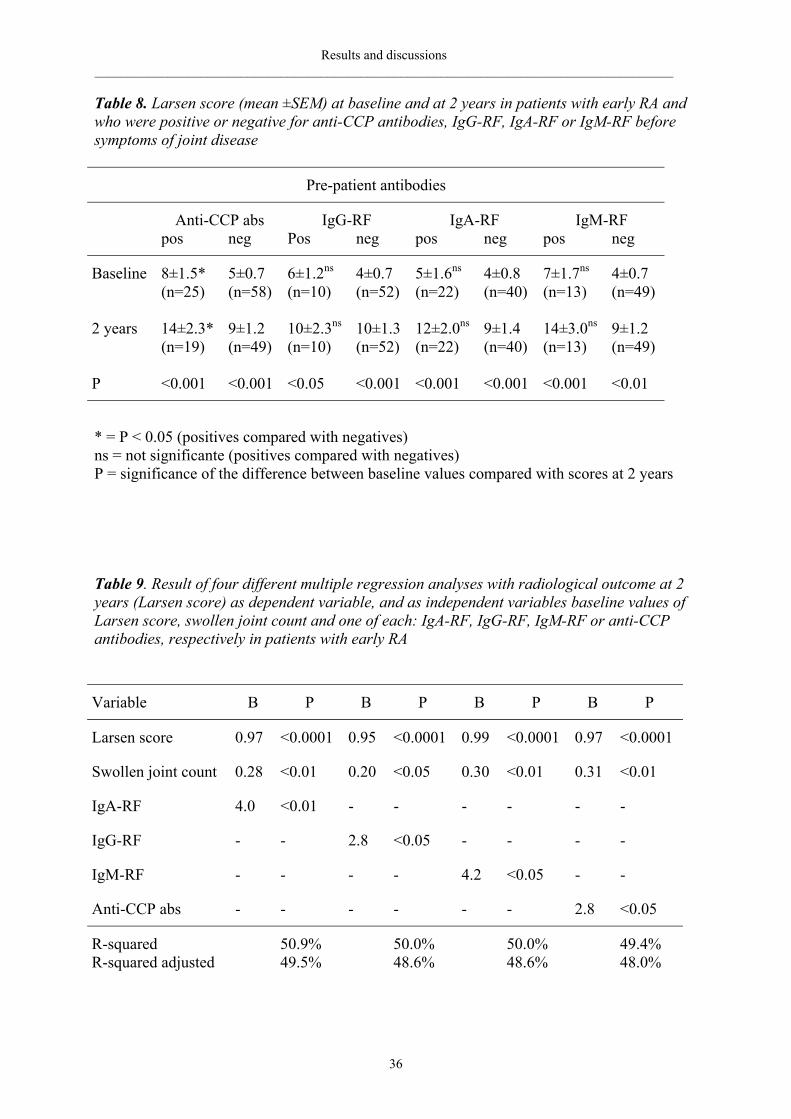
Results and discussions _______________________________________________________________________________________
36
Table 8. Larsen score (mean ±SEM) at baseline and at 2 years in patients with early RA and who were positive or negative for anti-CCP antibodies, IgG-RF, IgA-RF or IgM-RF before symptoms of joint disease
Pre-patient antibodies
Anti-CCP abs IgG-RF IgA-RF IgM-RF pos neg Pos neg pos neg pos neg
Baseline 8±1.5* 5±0.7 6±1.2ns 4±0.7 5±1.6ns 4±0.8 7±1.7ns 4±0.7 (n=25) (n=58) (n=10) (n=52) (n=22) (n=40) (n=13) (n=49) 2 years 14±2.3* 9±1.2 10±2.3ns 10±1.3 12±2.0ns 9±1.4 14±3.0ns 9±1.2 (n=19) (n=49) (n=10) (n=52) (n=22) (n=40) (n=13) (n=49) P <0.001 <0.001 <0.05 <0.001 <0.001 <0.001 <0.001 <0.01
* = P < 0.05 (positives compared with negatives) ns = not significante (positives compared with negatives) P = significance of the difference between baseline values compared with scores at 2 years Table 9. Result of four different multiple regression analyses with radiological outcome at 2 years (Larsen score) as dependent variable, and as independent variables baseline values of Larsen score, swollen joint count and one of each: IgA-RF, IgG-RF, IgM-RF or anti-CCP antibodies, respectively in patients with early RA
Variable Β P Β P Β P Β P
Larsen score 0.97 <0.0001 0.95 <0.0001 0.99 <0.0001 0.97 <0.0001
Swollen joint count 0.28 <0.01 0.20 <0.05 0.30 <0.01 0.31 <0.01
IgA-RF 4.0 <0.01 - - - - - -
IgG-RF - - 2.8 <0.05 - - - -
IgM-RF - - - - 4.2 <0.05 - -
Anti-CCP abs - - - - - - 2.8 <0.05
R-squared 50.9% 50.0% 50.0% 49.4% R-squared adjusted 49.5% 48.6% 48.6% 48.0%
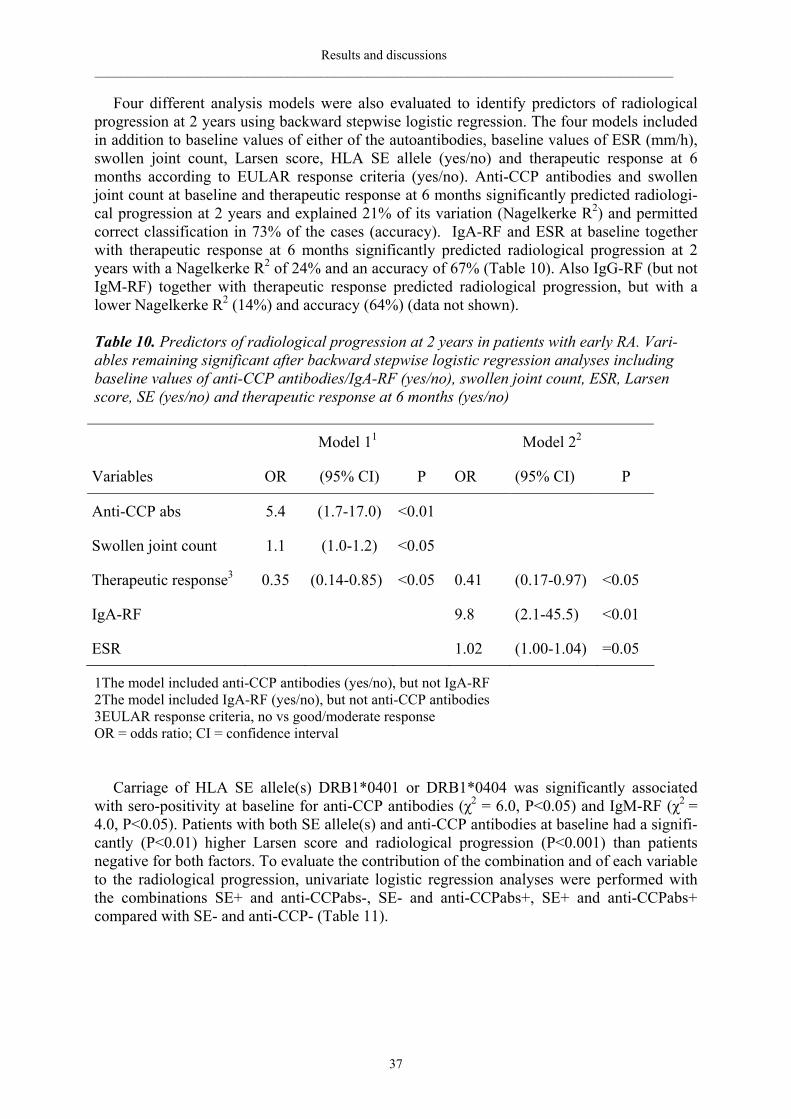
Results and discussions _______________________________________________________________________________________
37
Four different analysis models were also evaluated to identify predictors of radiological progression at 2 years using backward stepwise logistic regression. The four models included in addition to baseline values of either of the autoantibodies, baseline values of ESR (mm/h), swollen joint count, Larsen score, HLA SE allele (yes/no) and therapeutic response at 6 months according to EULAR response criteria (yes/no). Anti-CCP antibodies and swollen joint count at baseline and therapeutic response at 6 months significantly predicted radiologi-cal progression at 2 years and explained 21% of its variation (Nagelkerke R2) and permitted correct classification in 73% of the cases (accuracy). IgA-RF and ESR at baseline together with therapeutic response at 6 months significantly predicted radiological progression at 2 years with a Nagelkerke R2 of 24% and an accuracy of 67% (Table 10). Also IgG-RF (but not IgM-RF) together with therapeutic response predicted radiological progression, but with a lower Nagelkerke R2 (14%) and accuracy (64%) (data not shown). Table 10. Predictors of radiological progression at 2 years in patients with early RA. Vari-ables remaining significant after backward stepwise logistic regression analyses including baseline values of anti-CCP antibodies/IgA-RF (yes/no), swollen joint count, ESR, Larsen score, SE (yes/no) and therapeutic response at 6 months (yes/no)
Model 11 Model 22
Variables OR (95% CI) P OR (95% CI) P
Anti-CCP abs 5.4 (1.7-17.0) <0.01
Swollen joint count 1.1 (1.0-1.2) <0.05
Therapeutic response3 0.35 (0.14-0.85) <0.05 0.41 (0.17-0.97) <0.05
IgA-RF 9.8 (2.1-45.5) <0.01
ESR 1.02 (1.00-1.04) =0.05
1The model included anti-CCP antibodies (yes/no), but not IgA-RF 2The model included IgA-RF (yes/no), but not anti-CCP antibodies 3EULAR response criteria, no vs good/moderate response OR = odds ratio; CI = confidence interval
Carriage of HLA SE allele(s) DRB1*0401 or DRB1*0404 was significantly associated with sero-positivity at baseline for anti-CCP antibodies (χ2 = 6.0, P<0.05) and IgM-RF (χ2 = 4.0, P<0.05). Patients with both SE allele(s) and anti-CCP antibodies at baseline had a signifi-cantly (P<0.01) higher Larsen score and radiological progression (P<0.001) than patients negative for both factors. To evaluate the contribution of the combination and of each variable to the radiological progression, univariate logistic regression analyses were performed with the combinations SE+ and anti-CCPabs-, SE- and anti-CCPabs+, SE+ and anti-CCPabs+ compared with SE- and anti-CCP- (Table 11).
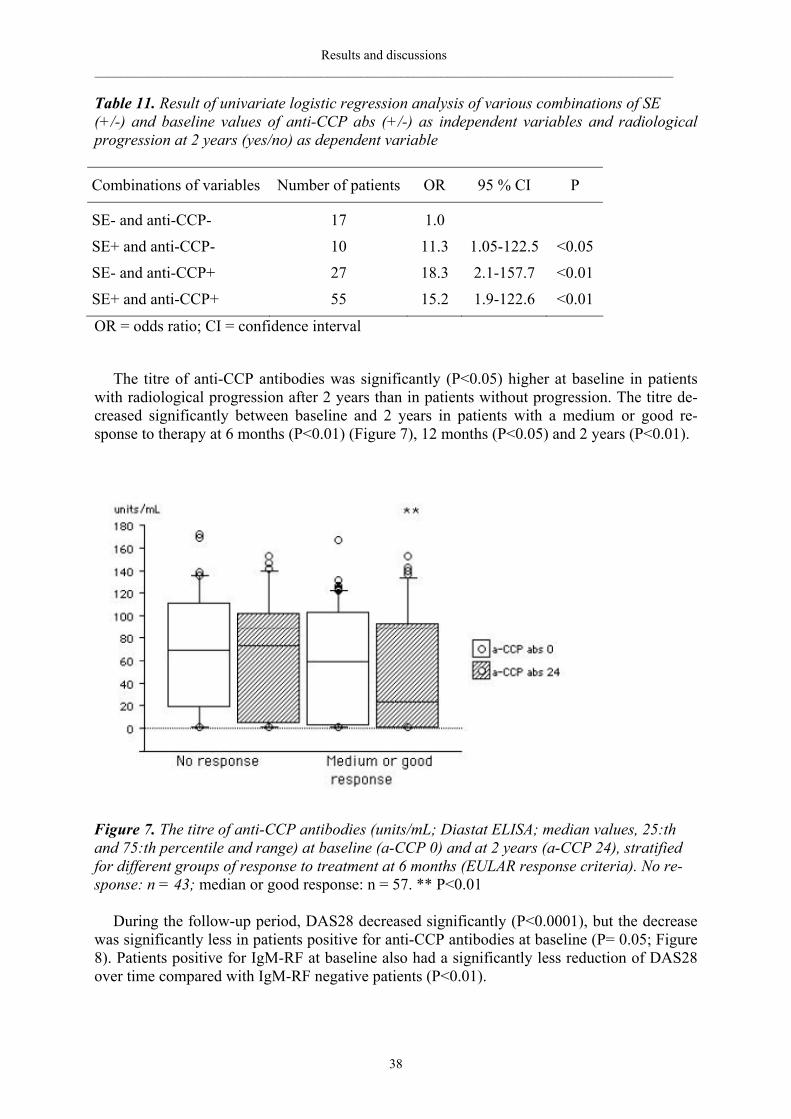
Results and discussions _______________________________________________________________________________________
38
Table 11. Result of univariate logistic regression analysis of various combinations of SE (+/-) and baseline values of anti-CCP abs (+/-) as independent variables and radiological progression at 2 years (yes/no) as dependent variable
Combinations of variables Number of patients OR 95 % CI P
SE- and anti-CCP- 17 1.0
SE+ and anti-CCP- 10 11.3 1.05-122.5 <0.05
SE- and anti-CCP+ 27 18.3 2.1-157.7 <0.01
SE+ and anti-CCP+ 55 15.2 1.9-122.6 <0.01
OR = odds ratio; CI = confidence interval
The titre of anti-CCP antibodies was significantly (P<0.05) higher at baseline in patients with radiological progression after 2 years than in patients without progression. The titre de-creased significantly between baseline and 2 years in patients with a medium or good re-sponse to therapy at 6 months (P<0.01) (Figure 7), 12 months (P<0.05) and 2 years (P<0.01).
Figure 7. The titre of anti-CCP antibodies (units/mL; Diastat ELISA; median values, 25:th and 75:th percentile and range) at baseline (a-CCP 0) and at 2 years (a-CCP 24), stratified for different groups of response to treatment at 6 months (EULAR response criteria). No re-sponse: n = 43; median or good response: n = 57. ** P<0.01 During the follow-up period, DAS28 decreased significantly (P<0.0001), but the decrease was significantly less in patients positive for anti-CCP antibodies at baseline (P= 0.05; Figure 8). Patients positive for IgM-RF at baseline also had a significantly less reduction of DAS28 over time compared with IgM-RF negative patients (P<0.01).
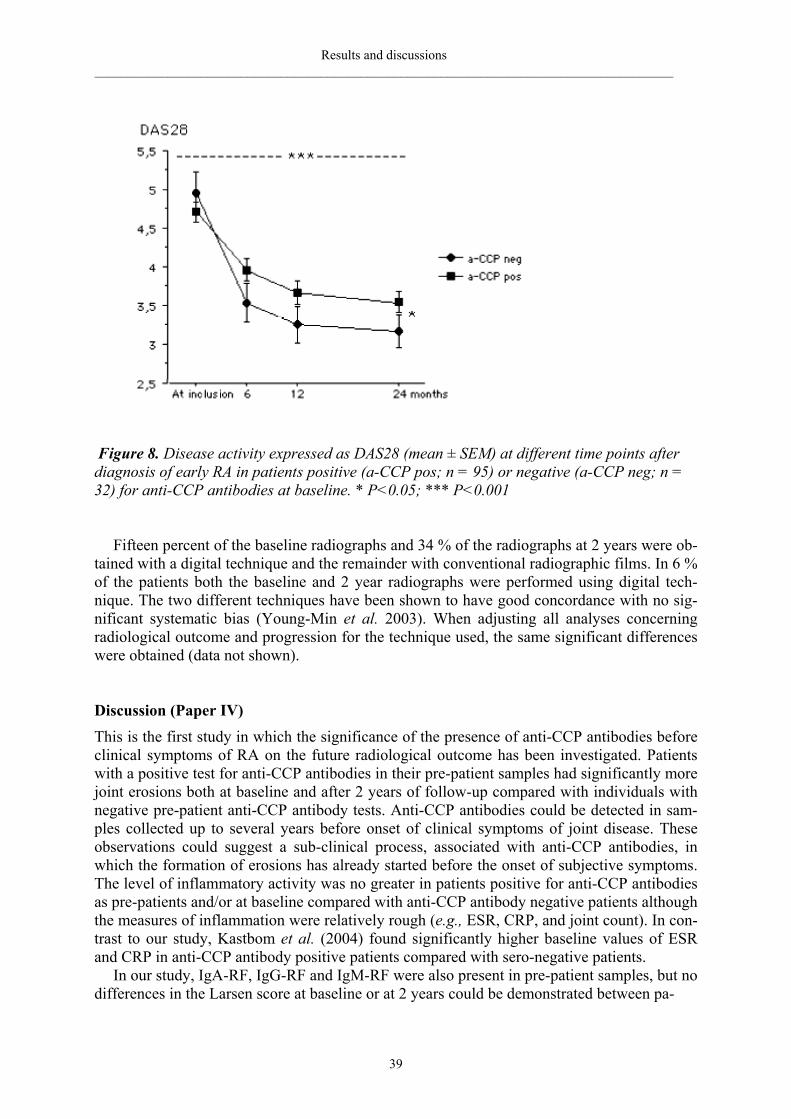
Results and discussions _______________________________________________________________________________________
39
Figure 8. Disease activity expressed as DAS28 (mean ± SEM) at different time points after diagnosis of early RA in patients positive (a-CCP pos; n = 95) or negative (a-CCP neg; n = 32) for anti-CCP antibodies at baseline. * P<0.05; *** P<0.001
Fifteen percent of the baseline radiographs and 34 % of the radiographs at 2 years were ob-
tained with a digital technique and the remainder with conventional radiographic films. In 6 % of the patients both the baseline and 2 year radiographs were performed using digital tech-nique. The two different techniques have been shown to have good concordance with no sig-nificant systematic bias (Young-Min et al. 2003). When adjusting all analyses concerning radiological outcome and progression for the technique used, the same significant differences were obtained (data not shown). Discussion (Paper IV)
This is the first study in which the significance of the presence of anti-CCP antibodies before clinical symptoms of RA on the future radiological outcome has been investigated. Patients with a positive test for anti-CCP antibodies in their pre-patient samples had significantly more joint erosions both at baseline and after 2 years of follow-up compared with individuals with negative pre-patient anti-CCP antibody tests. Anti-CCP antibodies could be detected in sam-ples collected up to several years before onset of clinical symptoms of joint disease. These observations could suggest a sub-clinical process, associated with anti-CCP antibodies, in which the formation of erosions has already started before the onset of subjective symptoms. The level of inflammatory activity was no greater in patients positive for anti-CCP antibodies as pre-patients and/or at baseline compared with anti-CCP antibody negative patients although the measures of inflammation were relatively rough (e.g., ESR, CRP, and joint count). In con-trast to our study, Kastbom et al. (2004) found significantly higher baseline values of ESR and CRP in anti-CCP antibody positive patients compared with sero-negative patients. In our study, IgA-RF, IgG-RF and IgM-RF were also present in pre-patient samples, but no differences in the Larsen score at baseline or at 2 years could be demonstrated between pa-

Results and discussions _______________________________________________________________________________________
40
tients with pre-dating RFs compared with those without. One interpretation of this finding is that pre-disease anti-CCP antibodies are predictors of a more aggressive form of RA. How-ever, the cut-off levels used for positive RFs were at the 95th percentile. For analyses of the disease severity higher cut-off levels with reduced sensitivity would possibly be more appro-priate. One should also consider that the lower number of individuals in the analyses of RFs decreases the possibility to obtain significant differences. We also found that the presence of anti-CCP antibodies at disease onset was associated with radiological progression. This is concordant with earlier reports (Forslind et al. 2004; Lindqvist et al. 2005). However, we could not confirm the finding (Forslind et al. 2004) that radiological progression was also predicted by baseline Larsen score. One possible explana-tion for this discrepancy is that the patients in our study had a better response to therapy, which slowed the damaging process. In Paper I, which includes a proportion of the patients in Paper IV, there was a negative association between baseline Larsen score and radiological progression. The low number of patients in that analysis, making the influence of ”outliers” greater probably explains this. In agreement with the reported results of Paper I, the present study also revealed a negative association between therapeutic response and radiological pro-gression, and a positive association between baseline swollen joint count and radiological progression. In multiple regression analyses in Paper IV, a positive test for either of the RFs or for anti-CCP antibodies at baseline predicted radiological outcome at 2 years. The correla-tion between anti-CCP antibodies and RFs and between the RFs themselves makes it difficult to conclude which of the autoantibodies has the strongest association to the radiological dam-age. However, the results of logistic regression analyses suggest anti-CCP antibodies and IgA-RF as the most important predictors, which is consistent with the results of Lindqvist et al. (2005). Patients with anti-CCP antibodies or IgM-RF at baseline had a significantly smaller reduc-tion in the DAS28 during the follow-up period compared with patients without these autoan-tibodies. This indicates a more persistent disease activity in patients with anti-CCP antibodies and IgM-RF, which is in line with other reports (Visser et al. 2002; Forslind et al. 2004; Kastbom et al. 2004). Although the strong correlation between the various autoantibodies studied makes com-parison between the effects of each of them difficult, our results suggest that anti-CCP anti-bodies and IgA-RF are associated with radiological progression, whilst IgM-RF and anti-CCP antibodies are associated with inflammatory activity and with HLA SE allele carriage. The association between a positive test for anti-CCP antibodies and HLA SE allele carriage is in concordance with results reported in Paper III and those of others (Goldbach-Mansky et al. 2000; Forslind et al. 2004;). Patients with both the SE allele(s) and anti-CCP antibodies at baseline showed a more severe radiological outcome and progression than patients lacking both. This concurs with the study by van Gaalen et al. (2004), who reported an association between HLA class II RA susceptibility alleles and the production of anti-CCP antibodies as well as an increased rate of joint destruction in patients with the combination of SE allele and anti-CCP antibodies. However, in logistic regression analysis of various combinations of SE and anti-CCP antibodies in our study, the combination of SE together with anti-CCP antibod-ies did not result in a higher odds ratio for radiological progression than anti-CCP antibodies without SE. This suggests that sero-positivity for anti-CCP antibodies is a more important predictor of radiological progression than SE allele carriage. Patients with radiological progression had significantly higher baseline titres of anti-CCP antibodies than patients without progression. The titres declined in patients with a therapeutic response. This is in agreement with the results of other studies reporting a significant decrease in anti-CCP antibody titres in patients with a decrease in disease activity (van Jaarsfeld et al. 1999; Visser et al. 2002; Kastbom et al. 2004).
Results and discussions _______________________________________________________________________________________
41
One limitations of this study is that not all individuals tested for anti-CCP antibodies in the
pre-patient samples were also tested for RFs, which could decrease the possibility to obtain significant differences in analyses with RF pre-patient samples. Another limitation is that the RFs were not analysed at 2 years, why comparisons with the course of anti-CCP antibody titres were not possible.
Concluding remarks _______________________________________________________________________________________
42
CONCLUDING REMARKS In Paper I, the first study of this thesis we found an association between initial swollen joint count and the radiological progression after 2 years. This was confirmed in the Paper IV, were swollen joint count and ESR were the initial markers of inflammation that were most useful as predictors of radiological progression. In both studies it was found that initial joint damage predicted joint damage also after 2 years. Several previous studies have reported similar re-sults (Feigenbaum et al. 1979; Kaarela 1985; Van Zeben et al. 1993; van der Heijde et al.1992 b). Early response to therapy was in both studies found to slow the radiological pro-gression and, in Paper I, also the bone loss in hands. This emphasizes the importance of insti-tuting effective treatment as early as possible in RA patients, with the goal of achieving re-mission. Bone loss in hands correlated with the radiological progression, but was not associ-ated with any initial marker of inflammation. Only postmenopausal female patients had a sig-nificantly larger bone loss than healthy matched controls during the 2-year follow-up. No change in hand bone mass was detectable during the first 6 months, why early bone loss could not be used as predictor of radiological damage. We concluded that measurements of hand bone density in patients with early RA did not add any information about joint destruction to that given by X-ray examination.
In Paper II it was demonstrated that anti-CCP antibodies and RF of IgG, IgM and IgA iso-types predated the onset of RA with several years with increasing prevalence closer to disease onset. IgA-RF was the earliest autoantibody to be detected and anti-CCP antibodies the one with the highest diagnostic specificity for RA. Both anti-CCP antibodies and IgA-RF signifi-cantly predicted the development of RA, suggesting that citrullination and production of anti-CCP antibodies as well as the production of RFs are early processes in the pathogenesis of RA.
Paper III showed greatly increased odds ratios for the development of RA in individuals with the combination of SE allele carriage and sero-positivity for anti-CCP antibodies or an RF of any isotype, in comparison with individuals not having any of the factors or having any one of them separately. In particular, the combination of anti-CCP antibody sero-positivity and carriage of HLA SE allele was associated with a very high relative risk for future devel-opment of RA. The conversion of arginine to citrulline in HLA DRB1*0401 transgenic mice has been reported to significantly increase activation of CD4+ T-cells (Hill et al. 2003). A significant association between anti-CCP antibodies and carriage of HLA DRB1*0401 has been reported in early RA patients (Goldbach-Mansky et al. 2000), which is in agreement with our findings in Paper III and IV. These data suggest that individuals carrying HLA SE alleles may have more sustained T-and B-cell responses to citrullinated antigens than noncar-riers, and that a specific T-cell dependent immune response to citrullinated peptides may con-tribute to the development of RA.
In Paper IV significantly more radiological joint damage was demonstrated at baseline and after 2 years in patients’ sero-positive for anti-CCP antibodies already as pre-patients com-pared with patients without predating anti-CCP antibodies. One explanation of this finding might be that, in pre-patients with anti-CCP antibodies, the joint disease and the formation of erosions already has started in a sub-clinical phase, without subjective symptoms.
Sero-positivity for anti-CCP antibodies and for either of the RFs at the time of diagnosis of RA significantly predicted higher radiological erosion score after 2 years. The best predictors for radiological progression after 2 years were baseline sero-positivity for anti-CCP antibodies and IgA-RF, which is consistent with an earlier report (Lindqvist et al. 2005). Patients with radiological progression had significantly higher titre of anti-CCP antibodies at baseline than patients without progression. The titre of anti-CCP antibodies declined significantly in pa-tients with response to therapy. This suggests that the titre of anti-CCP antibodies has an im-

Concluding remarks _______________________________________________________________________________________
43
pact on the disease process, and that repeated measurements of the anti-CCP antibody titre could be of clinical significance.
Patients carrying HLA SE alleles DRB1*0401 or DRB1*0404 and who were sero-positive for anti-CCP antibodies showed a more severe radiological outcome and progression, than patients negative for both factors. However, in logistic regression analysis, the combination of HLA SE allele and anti-CCP antibody sero-positivity did not result in a higher relative risk for radiological progression than anti-CCP antibody sero-positivity per se.
Conclusions _______________________________________________________________________________________
44
CONCLUSIONS Conclusions of this study of early RA patients in a population from northern Sweden, before and after disease onset are that:
• Initial swollen joint count and ESR predict radiological progression, while early re-sponse to therapy slows the progression rate
• Bone loss in hands measured by DXA is significantly correlated with radiological
progression measured by Larsen score, but adds no further information about joint de-struction to that given by X-ray examination
• Anti-CCP antibodies and RF of IgG, IgM and IgA isotypes predate the onset of RA by
several years with increasing prevalence and titre closer to disease onset
• The presence of each of anti-CCP antibodies and IgA-RF significantly predicts the de-velopment of RA, suggesting that citrullination and the production of anti-CCP anti-bodies and RF are early processes in the pathogenesis of RA
• The high specificity of anti-CCP antibodies as a diagnostic indicator of RA, especially
in combination with RFs of any isotype, could be used to establish an earlier, more re-liable diagnosis
• The combination of HLA SE alleles, DRB1*0401 or DRB1*0404, and anti-CCP anti-
bodies is associated with a very high relative risk of future development of RA
• The presence of anti-CCP antibodies before disease onset is associated with a higher radiological erosion score at baseline and after 2 years
• The presence of anti-CCP antibodies or RF of IgG, IgM or IgA isotypes at baseline
predicts higher radiological erosion score after 2 years, whilst radiological progression is mostly predicted by anti-CCP antibodies or IgA-RF in combination with clinical data
• Patients sero-positive for anti-CCP antibodies and IgM-RF at baseline have a more
persistent disease activity than patients without these autoantibodies
• Sero-positivity for anti-CCP antibody per se is associated with a higher relative risk of radiological progression than the combination of anti-CCP antibodies and HLA SE al-lele carriage
Sammanfattning på svenska _______________________________________________________________________________________
45
SAMMANFATTNING PÅ SVENSKA Sjukdomsförloppet vid kronisk ledgångsreumatism, reumatoid artrit (RA), kan variera mycket mellan olika individer, med ett panorama från diskreta, självbegränsande ledinflammationer till en mycket svår, leddestruerande sjukdom med extra-artikulära manifestationer. Kraftfull behandling med potentiellt toxiska läkemedel har visats förbättra långtidsprognosen vid RA. Denna behandling bör inledas så tidigt som möjligt, innan sjukdomen har etablerats och ir-reparabla vävnadsskador uppkommit. Det är därför önskvärt att kunna ställa en säker diagnos så tidigt som möjligt, samt att kunna identifiera de patienter som skulle ha nytta av den mest aggressiva behandlingen. Att diagnostisera RA i ett tidigt stadium av sjukdomen är dock ofta svårt.
Syftet med avhandlingen har varit att, för patienter med nydebuterad RA, utvärdera labora-tiva och kliniska inflammationsmarkörer som prediktorer för sjukdomsförlopp, att jämföra bentäthetsmätning (DXA) med konventionell röntgen som mått på leddestruktion, att un-dersöka betydelsen av antikroppar, som anti-CCP antikroppar och reumatoid faktorer (RFs) och av HLA shared epitope (SE) alleler för den relativa risken att utveckla RA och som prediktorer av sjukdomens svårighetsgrad. Avhandlingen består av fyra delarbeten.
I delstudie I inkluderades de första 43 patienterna i ett uppföljningsprogram för nydebute-rad RA, (Tidig Reumatoid Artrit Mottagningen [TRAM]), vid Reumatologkliniken, Norrlands Universitetssjukhus, Umeå. Patienterna följdes upp i två år med regelbundna ledstatusun-dersökningar, provtagning, samt konventionell röntgen (CR) av hand-och fotskelett och DXA-undersökningar av händer. Olika inflammationsmarkörers värde som prediktorer för benförlust och radiologiska förändringar analyserades. De radiologiska förändringarna, ana-lyserade med Larsen score, ökade signifikant under studien och var framförallt korrelerade till initialt Larsen score, men också till antal svullna leder och CRP vid inklusionen. Bentätheten i händer minskade signifikant endast hos postmenopausala kvinnor, vars minskning var signifi-kant även jämfört med matchade friska kontroller. Benförlusten i händer och den radiologiska progressionen i hand-och fotskelett var signifikant korrelerade och bromsades av tidig terapirespons.
I delstudie II-III analyserades blodprover (n = 98) från RA-patienter (n = 83) identifierade i Medicinska Biobanken och Maternitetskohorten i norra Sverige. I dessa prover (”pre-patienter”), som var samlade upp till flera år före sjukdomsdebuten, undersöktes prevalensen av anti-CCP antikroppar och RFs av IgA, IgG och IgM isotyp och jämfördes med prevalensen i matchade kontrollerprover. I delstudie III undersöktes även prevalensen av HLA SE alleler hos 59 pre-patienter. Anti-CCP antikroppar och RFs kunde påvisas flera år före sjukdomsde-buten och prevalensen ökade ju närmare insjuknandet som provet tagits. I logistiska regres-sionsanalyser utföll förekomst av positivt test för anti-CCP antikroppar och för IgA-RF som signifikanta prediktorer för utveckling av RA. Kombinationen av anti-CCP antikroppar och HLA SE allele var associerad med en särskilt hög relativ risk för framtida utveckling av RA.
I delstudie IV identifierades 93 av 138 patienter med tidig RA, vilka regelbundet kontrolle-rades vid TRAM, (se ovan) som pre-patienter i Medicinska Biobanken och Maternitetskohor-ten. Betydelsen av förekomst av anti-CCP antikroppar, RFs och HLA SE alleler före symp-tomdebut och vid diagnos, för insjuknande och sjukdomsförlopp studerades. Röntgen (CR) av hand-och fotskelett utfördes vid diagnos och efter 2 år och utvärderades med Larsen score. Förekomst av anti-CCP antikroppar före sjukdomsdebut och vid diagnos var associerat med utveckling av radiologiska destruktioner, vilket även gällde för förekomst av RFs vid diagnos. Högre titer av anti-CCP antikroppar var associerat med en mera uttalad röntgenprogress. Pati-enter med terapirespons sjönk signifikant i titern av anti-CCP antikroppar. I logistiska regres-

Sammanfattning på svenska _______________________________________________________________________________________
46
sionsanalyser predikterade anti-CCP antikroppar, IgA-RF, sänkningsreaktion och antal svull-na leder en högre radiologisk progress, medan terapirespons predikterade en lägre radiologisk progress. Sammanfattningsvis visade studierna i avhandlingen att anti-CCP antikroppar och IgA-RF är starka markörer för framtida utveckling av RA och för radiologisk leddestruktion och pro-gress. Kombinationen av anti-CCP antikroppar och SE alleler är associerad med en hög rela-tiv risk för framtida insjuknande i RA. Anti-CCP antikroppar har en mycket hög specificitet som diagnostisk indikator för RA, särskilt i kombination med RFs, varför dessa tester kan möjliggöra en tidigare, mera tillförlitlig diagnos. Terapirespons minskar den radiologiska pro-gressen i hand-och fotskelett och benförlusten i händer och sänker titern av anti-CCP an-tikroppar. Konventionell röntgen bedömdes vara ett bättre mått på leddestruktion än DXA.
Acknowledgements _______________________________________________________________________________________
47
ACKNOWLEDGEMENTS I would like to thank everyone who has helped and supported me in this project, and in par-ticular: Solbritt Rantapää Dahlqvist, my supervisor and friend, for introducing me into this work; for your enthusiasm, patience, pushing and encouragement; for interesting discussions; and for always being available when needed Solveig Wållberg Jonsson, Gerd-Marie Alenius, Lotta Ljung and Agneta Uddhammar, for interest, valuable feedback and discussions Marie Eriksson and Hans Stenlund for statistical guidance and advices All my co-authors, for fruitful collaboration All my colleagues and co-workers at the Department of Rheumatology, for friendliness and patience Arvi Larsen, for teaching me how to estimate the Larsen score The staff of the Medical Biobank, for invaluable help with identification of the “pre-patients” Torsten Sandström, for accomplishing all the DXA measurements Lisbet Ärlestig, Solveig Linghult, Inger Bucht and Inger Hamberg, for excellent technical assistance Aina Ågren Wilsson, for friendship, support and useful advices My parents Olle, in memoriam, and Märta for your support and for always having believed in my ability All nice horses and people at Södra Umeås Ryttarförening, for joy and excitement during the years Viking, my husband and dearest friend, for love and patience and for interesting discussions and computer assistance Daniel, my beloved son, for reminding me about what really matters in life All the patients who have participated in these studies
References _______________________________________________________________________________________
48
REFERENCES Aho K, Palosuo T, Raunio V, Puska P, Aromaa A, Salonen JT. When does rheumatoid dis-
ease start? Arthritis Rheum 1985;28:485-9. Albani S, Carson DA, Roudier J: Genetic and environmental factors in the immune patho-
genesis of rheumatoid arthritis. Rheum Dis Clin North Am 1992;18:729-40. Arnett FC, Edworthy SM, Bloch DA, McShane DJ, Fries JF, Cooper NS, et al. The American
Rheumatism Association 1987 revised criteria for the classification of rheumatoid ar-thritis. Arthritis Rheum 1988;31:315-24.
Backhaus M, Kamradt T, Sandrock D, Loreck D, Fritz J, Wolf KJ, et al. Arthritis of the finger
joints. A comprehensive approach comparing conventional radiography, scintigraphy, ultrasound, and contrast-enhanced magnetic resonance imaging. Arthritis Rheum 1999;42:1232-45.
Ball J, Lawrence JS. Epidemiology of the sheep cell agglutination test. Ann Rheum Dis
1961;20:235-43. Barrett JH, Brennan P, Fiddler M, Silman AJ. Does rheumatoid arthritis remit during preg-
nancy and relapse postpartum? Results from a nationwide study in the United Kingdom performed prospectively from late pregnancy. Arthritis Rheum 1999; 42:1219-27.
Bas S, Genevay S, Meyer O, Gabay C. Anti-cyclic citrullinated peptide antibodies, IgM and
IgA rheumatoid factors in the diagnosis and prognosis of rheumatoid arthritis. Rheuma-tology 2003;42:677-80.
Bathon JM, Martin RW, Fleischmann RM, Tesser JR, Schiff MH, Keystone EC, et al. A
comparison of etanercept and methotrexate in patients with early rheumatoid artritis. N Engl J Med 2000;343:1586-93.
Begovich AB,Carlton VE, Honigberg LA, Schrodi SJ, Chokkalingam AP, Alexander HC, et
al. A missense single-nucleotide polymorphism in a gene encoding a protein tyrosine phosphatase (PTPN22) is associated with rheumatoid arthritis. Am J Hum Genet 2004; 75:330-7.
Bläss S, Union A, Raymackers J, Schumann F, Ungethum U, Muller-Steinbach S, et al. The
stress protein BiP is overexpressed and is a major B and T cell target in rheumatoid ar-thritis. Arthritis Rheum 2001;44:761-71.
Bodman-Smith MD, Corrigall VM, Kemeny DM, Panayi GS. BiP, a putative autoantigen in
rheumatoid arthritis, stimulates IL-10-producing CD8-positive T cells from normal in-dividuals. Rheumatology 2003;42:637-44.
Bodman-Smith MD, Corrigall VM, Berglin E, Cornell HR, Tzioufas AG, Mavragani CP, et
al. Antibody response to the human stress protein BiP in rheumatoid arthritis. Rheuma-tology 2004;43:1283-7.
References _______________________________________________________________________________________
49
Boers M, Verhoeven AC, Markusse HM, van de Laar MA, Westhovens R, van Denderen JC et al. Randomised comparison of combined step-down prednisolone, methotrexate and sulphasalazine with sulphasalazine alone in early rheumatoid arthritis. Lancet 1997;350:309-18.
Boers M. The case for corticosteroids in the treatment of early rheumatoid arthritis (editorial).
Rheumatology 1999;38:95-97. Brennan P, Silman A: Breast-feeding and the onset of rheumatoid arthritis. Arthritis Rheum
1994, 37:808-13. Brennan P, Bankhead C, Silman A, Symmons D. Oral contraceptives and rheumatoid arthri-
tis: results from primary carebased incident case-control study. Semin Arthritis Rheum 1997;26:817-23.
Brighton SW, de la Harpe AL, van Staden DJ, Badenhorst JH, Myers OL. The prevalence of
rheumatoid arthritis in a rural African population. J Rheumatol 1988;15:405-8. Callahan LF, Pincus T. Mortality in the rheumatic disease. Arthritis Care Res 1995;8:229-41. Caponi L, Petit-Teixera E, Sebbag M, Bongiorni F, Moscato S, Pratesi F, et al. Analysis of
the peptidylarginine deaminase V gene in rheumatoid arthritis [abstract]. Arthritis Res 2003;Suppl 5:1.
Carmona L, Villaverde V, Hernández-García C, Ballina J, Gabriel R, Laffon A, EPISER
Study Group. The prevalence of rheumatoid arthritis in the general population of Spain. Rheumatology 2002;41:88-95.
Choi HK, Hernán MA, Seeger JD, Robins JM, Wolfe F. Methotrexate and mortality in pa-
tients with rheumatoid arthritis: a prospective study. Lancet 2002;359:1173-7. Choy EH, Smith C, Doré CJ, Scott DL. A meta-analysis of the efficacy and toxicity of com-
bining disease-modifying anti-rheumatic drugs in rheumatoid arthritis based on patient withdrawal. Rheumatology, Advance Access published July 19, 2005.
Cohen BJ, Buckley MM, Clewley JP, Jones VE, Puttick AH, Jacoby RK. Human parvovirus
infection in early rheumatoid and inflammatory arthritis. Ann Rheum Dis 1986;45:832-8.
Combe B, Dougados M, Goupille P, Cantagrel A, Eliaou JF, Sibilia J, et al. Prognostic factors
for radiographic damage in early rheumatoid arthritis. A multiparameter prospective study. Arthritis Rheum 2001;44:1736-43.
Combe B, Eliaou JF, Daures JP, Meyer O, Clot J, Sany J. Prognostic factors in rheumatoid
arthritis. Comparative study of two subsets of patients according to severity of articular damage. Br J Rheumatol 1995;34:529-34.
Criswell LA, Merlino LA, Cerhan JR, Mikuls TR, Mudano AS, Burma M, et al. Cigarette
smoking and the risk of of rheumatoid arthritis among postmenopausal women: results from the Iowa Women´s Health Study. Am J Med 2002;112:465-71.
References _______________________________________________________________________________________
50
DAS Score NL: Disease Activity Score in Rheumatoid Arthritis. http://www.das-score.nl]. Deftos M, Olee T, Carson DA, Chen PP. Defining the genetic origins of three rheumatoid
synovium-derived IgG rheumatoid factors. J. Clin Invest 1994;93:2545-53. Deighton CM, Walker DJ, Griffiths ID, Roberts DF. The contribution of HLA to rheumatoid
arthritis . Clin Genet 1989;36:178-82. Deodhar AA, Brabyn J, Jones PW, Davis MJ, Woolf A. Measurement of hand bone mineral
content by dual energy and its application in normal volunteers and in patients with rheumatoid arthritis. Ann Rheum Dis 1994;53:685-90.
Deodhar AA, Brabyn J, Jones PW, Davis MJ, Woolf AD. Longitudinal study of hand bone
densiometry in rheumatoid arthritis. Arthritis Rheum 1995;38:1204-10. Deodhar AA, Brabyn J, Pande I, Scott DL, Woolf AD. Hand bone densiometry in rheumatoid
arthritis, a five year longitudinal study: an outcome measure and a prognostic marker. Ann Rheum Dis 2003;62:767-70.
Dolan AL, Moniz C, Abraha H, Pitt P. Does active treatment of rheumatoid arthritis limit dis-
ease-associated bone loss? Rheumatology 2002;41:1047-51. Doran MF, Pond GR, Crowson CS, O´Fallon WM, Gabriel SE. Trends in incidence and mor-
tality in rheumatoid arthritis in Rochester, Minnesota, over a forty-year period. Arthritis Rheum. 2002;46:625-31.
Eberhardt KB, Svensson B, Truedsson L, Wollheim FA. The occurence of rheumatoid factor
isotypes in early definite rheumatoid arthritis-no relationship with erosions or disease activity. J Rheumatol 1988;15:1070-4.
Eberhardt KB, Rydgren LC, Pettersson H, Wollheim FA. Early rheumatoid arthritis-onset,
course, and outcome over 2 years. Rheumatol Int 1990;10:135-42. Ebringer A, Ptaszynska T, Corbett M, Wilson C, Macafee Y, Avakian H, et al. Antibodies to
proteus in rheumatoid arthritis. Lancet 1985;2:305-7. Egsmose C, Lund B, Borg G, Pettersson H, Berg E, Brodin U. Patients with rheumatoid ar-
thritis benefit from early 2nd line therapy: 5 year followup of a prospective double blind placebo controlled study. J Rheumatol 1995;22:2208-13.
Ekdahl C, Eberhardt K, Andersson SI, Svensson B. Assessing disability in patients with
rheumatoid arthritis. Use of Swedish version of Stanford Health assessment Question-naire. Scand J Rheumatol 1988;17:263-71.
Emery P, Salmon M. Early rheumatoid arthritis: time to aim for remission? Ann Rheum Dis
1995;54:944-7. Fassbender HG, Seibel M, Herbert T: Pathways of destruction in metacarpal and metatarsal
joints in patients with rheumatoid arthritis. Scand J Rheumatol 1992;21:10-6.
References _______________________________________________________________________________________
51
Feigenbaum SL, Masi AT, Kaplan SB. Prognosis in rheumatoid arthritis. A longitudinal study
of newly diagnosed younger adult patients. Am J Med 1979;66:377-84. Felson DT, Anderson JJ, Boers M, Bombardier C, Furst D, Goldsmith C, et al. American Col-
lege of Rheumatology preliminary definition of improvement in rheumatoid arthritis. Arthritis Rheum 1995;38:727-35.
Felson DT, Anderson JJ, Lange ML, Wells G, LaValley MP. Should improvement in rheuma-
toid arthritis clinical trials be defined as fifty percent or seventy percent improvement in core set measures, rather than twenty percent? Arthritis Rheum 1998;41:1564-70.
Fex E, Jonsson K, Johnson U, Eberhardt K. Development of radiographic damage during the
first 5-6 years of rheumatoid arthritis. A prospective follow-up study of a Swedish co-hort. Br J Rheumatol 1996;35:1106-15.
Foley-Nolan D, Stack JP, Ryan M, Redmond U, Barry C, Ennis J, et al. Magnetic resonance
imaging in assessment of rheumatoid arthritis-a comparison with plain film radiographs. Br J Rheumatol 1991;30:101-6.
Forsblad d´Elia H, Larsen A, Waltbrand E, Kvist G, Mellström D, Saxne T, et al. Radio-
graphic joint destruction in postmenopausal rheumatoid arthritis is strongly associated with generalised osteoporosis. Ann Rheum Dis 2003;62:617-23.
Forslind K, Almén M, Eberhardt K, Hafström I, Svensson B for the BARFOT study group.
Prediction of radiological outcome in early rheumatoid arthritis in clinical practice: role of antibodies to citrullinated peptides (anti-CCP). Ann Rheum Dis 2004;63:1090-5.
Forslind K, Larsson EM, Johansson Å, Svensson B. Detection of joint pathology by magnetic
resonance imaging in patients with early rheumatoid arthritis. Br J Rheumatol 1997;36:683-8.
Fransen J, Creemers MCW, van Riel PL. Remission in rheumatoid arthritis: agreement of the
disease activity score (DAS28) with the ARA preliminary remission criteria. Rheuma-tology 2004;43:1252-5.
Fries JF, Spitz P, Kraines RG, Holman HR. Measurement of patient outcome in arthritis. Ar-
thritis Rheum 1980;23:137-45. Fries JF. The assessment of disability: from first to future principles. Br J Rheumatol
1983;22(Suppl):48-58. Fries JF, Bloch DA, Sharp JT, McShane DJ, Spitz P, Bluhm GB, et al. Assessment of ra-
diologic progression in rheumatoid arthritis. Arthritis Rheum 1986;29:1-8. Fries JF. Re-evaluating the therapeutic approach to rheumatoid arthritis: the “sawtooth” strat-
egy. J Rheumatol Suppl 1990;22:12-5.
References _______________________________________________________________________________________
52
Fuchs HA, Kaye JJ, Callahan LF, Nance EP, Pincus T: Evidence of significant radiographic damage in rheumatoid arthritis within the first 2 years of disease. J Rheumatol 1989;16:585-91.
Gahlinger PM, Abramson JH, editors. Computer programs for epidemiologic analysis. Maka-
puu Medical Press: Honolulu;1997. Girbal-Neuhauser E, Durieux JJ, Arnaud M, Dalbon P, Sebbag M, Vincent C, et al. The epi-
topes targeted by the rheumatoid arthritis-associated antifilaggrin autoantibodies are posttranslationally generated on various sites of (pro)filaggrin by deamination of argin-ine residues. J Immunol 1999;162:585-94.
Goldbach-Mansky R, Lee J, McCoy A, Hoxworth J, Yarboro C, Smolen JS, et al. Rheuma-
toid arthritis associated autoantibodies in patients with synovitis of recent onset. Arthri-tis Res 2000; 2:236-43.
Gorman JD, Lum RF, Chen JJ, Suarez-Almazor ME, Thomson G, Criswell LA. Impact of
shared epitope genotype and ethnicity on erosive disease. Arthritis Rheum 2004;50:400-12.
Gough AK, Lilley J, Eyre S, Holder RL, Emery P. Generalised bone loss in patients with
early rheumatoid arthritis. Lancet 1994;344:23-7. Grassi W, De Angelis R, Lamanna G, Cervini C. The clinical features of rheumatoid arthritis.
Eur J Radiol. 1998;27 Suppl 1:S18-24. Green MJ, Deodhar AA. Bone changes in early rheumatoid arthritis. Best Prac Res Clin
Rheumatol 2001;15:105-23. Gregersen PK, Silver J, Winchester RJ. The shared epitope hypothesis. An approach to under-
standing the molecular genetics of susceptibility to rheumatoid arthritis. Arthritis Rheum 1987;30:1205-13.
Gregersen PK and Batliwalla F. PTPN22 and rheumatoid arthritis: gratifying replication. Ar-
thritis Rheum 2005;52:1952-5. Guerne PA, Zuraw BL, Vaughan JH, Carson DA, Lotz M. Synovium as a source of inter-
leukin 6 in vitro: contribution to local and systemic manifestations of arthritis. J Clin Invest 1989;83:585-92.
Hannaford PC, Kay CR, Hirsch S: Oral contraceptives and rheumatoid arthritis: new data
from the Royal College of General Practitioners´oral contraception study. Ann Rheum Dis 1990; 49:744-6.
Harris ED. Rheumatoid arthritis. Pathophysiologi and implications for therapy. Review arti-
cle, mechanisms of disease. N Engl J Med 1990;322:1277-89. Harrison B, Silman A, Barrett E, Symmons D. Low frequency of recent parvovirus infection
in a population-based cohort of patients with early inflammatory polyarthritis. Ann Rheum Dis 1998;57:375-7.
References _______________________________________________________________________________________
53
Harrison B and Symmons D.Early inflammatory polyarthritis: results from the Northfolk Ar-thritis register with a review of the literature.II. Outcome at three years. Rheumatology 2000;39:939-49.
Harvey J, Lotze M, Stevens MB, Lambert G, Jacobson D. Rheumatoid arthritis in a Chippewa
Band. I. Pilot screening study of disease prevalence. Arthritis Rheum 1981;24:717-21. Hasegawa K, Martin F, Huang G, Tumas D, Diehl L, Chan AC. PEST domain-enriched tyro-
sine phosphatase (PEP) regulation of effector/memory T cells. Science 2004;303:685-9. Hill JA, Southwood S, Sette A, Jevnikar AM, Bell DA, Cairns E. Cutting Edge: The conver-
sion of arginine to citrulline allows for a high-affinity peptide interaction with the rheumatoid arthritis-associated HLA-DRB1*0401 MHC class II molecule. J Immu-nol;2003;171:538-41.
Hoet RM, Boerbooms AM, Arends M, Ruiter DJ, van Venrooij WJ. Antiperinuclear factor, a
marker autoantibody for rheumatoid arthritis: colocalisation of the perinuclear factor and profilaggrin. Ann Rheum Dis 1991;50:611-8.
Jacobsson LT, Pillemer SR. What can we learn about rheumatoid diseases by studying Pima
Indians? J Rheumatol. 1994;21:1179-82. Jansen LM, van der Horst Bruinsma IE, van Schaardenburg D, Bezemer PD, Dijkmans B AC.
Predictors of radiographic damage in patients with early rheumatoid arthritis. Ann Rheum Dis 2001;60:924-7.
Jensen T, Hansen M, Jensen KE, Pødenphant J, Hansen TM, Hyldstrup L. Comparison of
dual X-ray absorptiometry (DXA), digital X-ray radiogrammetry (DXR), and conven-tional radiographs in the evaluation of osteoporosis and bone erosions in patients with rheumatoid arthritis. Scand J Rheumatol 2005;34:27-33.
Jergas M, Genant HK. Current methods and recent advances in the diagnosis of osteoporosis.
Arthritis Rheum 1993;36:1649-62. Jonsson T, Thorsteinsson J, Kolbeinsson A, Jonasdottir E, Sigfuson N, Valdimarsson H.
Population study of the importance of rheumatoid factor isotypes in adults. Ann Rheum Dis 1992;51:863-8.
Kaarela K. Prognostic factors and diagnostic criteria in early rheumatoid arthritis. Scand J
Rheumatol 1985;14 Suppl 57:1-54. Kalla AA, Meyers OL, Chalton D, Heath S, Brown GM, Smith PR, et al. Increased metacar-
pal bone mass following 18 months of slow-acting antirheumatic drugs for rheumatoid arthritis. Br J Rheumatol 1991;30:91-100.
Kastbom A, Strandberg G, Lindroos A, Skogh T. Anti-CCP antibody test predicts the disease
course during 3 years in early rheumatoid arthritis (the Swedish TIRA project). Ann Rheum Dis 2004;63:1085-9.
Kim HJ, Berek C. Review. B cells in rheumatoid arthritis. Arthritis Res 2000;2:126-31.
References _______________________________________________________________________________________
54
Kirwan JR. The relationship between synovitis and erosions in rheumatoid arthritis. Br J
Rheumatol 1997;36:225-8. Kirwan JR. The effect of glucocorticoids on joint destruction in rheumatoid arthritis. N Engl J
Med 1995;333:142-6. Klockars M, Koskela RS, Jarvinen E, Kolari PJ, Rossi A: Silica exposure and rheumatoid
arthritis: a follow up study of granite workers 1940-81. Br J Med J(Clin Res Ed) 1987;294:997-1000.
Korpela M, Laasonen L, Hannonen P, Kautiainen H, Leirisalo-Repo M, Hakala M, et al. Re-
tardation of joint damage in patients with early rheumatoid arthritis by initial aggressive treatment with disease-modifying antirheumatic drugs. Arthritis Rheum 2004;50:2072-81.
Kouri T, Petersen J, Rhodes G, Aho K, Palosuo T, Heliovaara M, et al. Antibodies to syn-
thetic peptides from Epstein-Barr nuclear antigen-1 sera of patients with early rheuma-toid arthritis and in preillness sera. J Rheumatol 1990;17:1442-9.
Kroot EJ, De Jong BA, Van Leeuwen MA, Swinkels H, Van den Hoogen FH, Van´t Hof M,et
al. The prognostic value of anti-cyclic citrullinated peptide antibody in patients with re-cent-onset rheumatoid arthritis. Arthritis Rheum 2000;43:1831-5.
Kuiper S, van Gestel AM, Swinkels HL, de Boo TM, da Silva JA, van Riel PL. Influence of
sex, age and menopausal state on the course of early rheumatoid arthritis. J Rheumatol 2001;28:1809-16.
Kvien TK, Glennås A, Knudsrød, Smedstad LM, Mowinckel P, Førre Ø. The prevalence and
severity of rheumatoid arthritis in Oslo. Scand J Rheumatol 1997;26:412-8. Laan RF, Buijs WC, Verbeek AL, Draad MP, Corstens FH, Van de Putte LB, et al. Bone
mineral density in patients with recent onset rheumatoid arthritis: influence of disease activity and functional capacity. Ann Rheum Dis 1993;52:21-6.
Landewé RB, Boers M, Verhoeven AC, Westhovens R, van der Laar MA, Markusse HM, et
al. COBRA combination therapy in patients with early rheumatoid arthritis. Long-term structural benefits of a brief intervention. Arthritis Rheum 2002;46:347-56.
Lard LR, Visser H, Speyer I, van der Horst-Bruinsma IE, Zwinderman AH, Breedveld FC, et
al. Early versus delayed treatment in patients with recent-onset rheumatoid arthritis: comparison of two cohorts who received different treatment strategies. Am J Med 2001;111:446-51.
Larsen A, Dale K, Eek M. Radiographic evaluation of rheumatoid arthritis and related condi-
tions by standard reference films. Acta Radiol Diagn 1977;18:481-91. Larsen A, Horton J, Howland C. The effect of auranofin and parenteral gold in the treatment
of rheumatoid arthritis: an X-ray analysis. Clin Rheumatol 1984;Suppl 1:97-104.
References _______________________________________________________________________________________
55
Larsen A, Thoen J. Hand radiography of 200 patients with rheumatoid arthritis after an inter-val of one year. Scand J Rheumatol 1987;16:395-401.
Larsen A. How to apply Larsen score in evaluating radiographs of rheumatoid arthritis in
longterm studies. J Rheumatol 1995;22:1974-5. Lau E, Symmons D, Bankhead C, MacGregor A, Donnan S, Silman A. Low prevalence of
rheumatoid arthritis in the urbanized Chinese of Hong Kong. J Rheumatol 1993;7:1133-7.
Lee AT, Li W, Liew A, Bombardier C, Weisman M, Massarotti EM, et al. The PTPN22
R620W polymorphism associates with RF positive rheumatoid arthritis in a dose-dependent manner but not with HLA-SE status. Genes Immun 2005;6:129-33.
Lindqvist E, Jonsson K, Saxne T, Eberhardt K. Course of radiographic damage over 10 years
in a cohort with early rheumatoid arthritis. Ann Rheum Dis 2003;62:611-6. Lindqvist E, Eberhardt K, Bendtzen K, Heinegård D, Saxne T. Prognostic laboratory markers
of radiographic outcome in rheumatoid arthritis. Ann Rheum Dis 2005;64:196-201. Lundberg I. Alfredsson L, Plato N, Sverdrup B, Klareskog L, Kleinau S. Occupation, occupa-
tional exposure to chemicals and rheumatological disease. Scand J Rheumatol 1994;23:305-10.
MacGregor AJ, Snieder H, Rigby AS, Koskenvuo M, Kaprio J, Aho K, et al. Characterizing
the quantitative genetic contribution to rheumatoid arthritis using data from twins. Ar-thritis Rheum 2000; 43:30-7.
Mannik M. Rheumatoid factors in the pathogenesis of rheumatoid arthritis. J Rheumatol
1992;(suppl 32)19:46-9. Masson-Bessière C, Sebbag M, Girbal-Neuhaser E, Nogueira L, Vincent C, Senshu T, et al.
The major synovial targets of the rheumatoid arthritis-specific antifilaggrin autoantibod-ies are deaminated forms of the alpha- and beta-chains of fibrin. J Immunol 2001;166:4177-84.
Mikuls TR, O´Dell J. The changing face of rheumatoid arthritis therapy: results of serial sur-
veys. Arthritis Rheum 2000;43:464-5. Mor A, Abramson SB, Pillinger MH. The fibroblast-like synovial cell in rheumatoid arthritis:
a key player in inflammation and joint destruction. Clin Immunol 2005;115:118-28. Moreland LW, Stewart T, Gay RE, Huang GQ, McGee N, Gay S. Immunohistologic demon-
stration of type II collagen in synovial fluid phagocytes of osteoarthritis and rheumatoid arthritis patients. Arthritis Rheum 1989;32:1458-64.
Morrison E, Capell HA. Corticosteroids in rheumatoid arthritis - the case against (editorial).
Rheumatology 1999;38:97-100.
References _______________________________________________________________________________________
56
Mulherin D, Fitzgerald O, Bresnihan B. Clinical improvement and radiological deterioration in rheumatoid arthritis: evidence that pathogenesis of synovial inflammation and articu-lar erosion may differ. Br J Rheumatol 1996;35:1263-8.
Möttönen T. Prediction of erosiveness and rate of development of new erosions in early
rheumatoid arthritis. Ann Rheum Dis 1988;47:648-53. Möttönen T, Hannonen P, Leirisalo-Repo M, Nissilä M, Kautiainen H, Korpela M, et al.
Comparison of the combination therapy with single-drug therapy in early arthritis: a randomised trial. Lancet 1999;353:1568-73.
Nakashima K, Hagiwara T, Yamada M. Nuclear localization of peptidylarginine deiminase V
and histone deimination in granulocytes. J Biol Chem 2002;277:49562-8. Nell VP, Machold KP, Eberl G, Stamm TA, Uffmann M, Smolen JS. Benefit of very early
referral and very early therapy with disease-modifying anti-rheumatic drugs in patients with early rheumatoid arthritis. Rheumatology 2004;43:906-14.
Nelson JL, Ostensen M: Pregnancy and rheumatoid arthritis. Rheum Dis Clin North Am
1997, 23:195-212. Nienhuis RL, Mandema E. A new serum factor in patients with rheumatoid arthritis. The an-
tiperinuclear factor. Ann Rheum Dis 1964;23:302-5. O'Dell JR, Leff R, Paulsen G, Haire C, Mallek J, Eckhoff PJ, et al. Treatment of rheumatoid
arthritis with methotrexate and hydroxychloroquine, methotrexate and sulfasalazine, or a combination of the three medications: results of a two-year, randomized, double-blind, placebo-controlled trial. Arthritis Rheum 2002;46:1164-70.
Palosuo T, Tilvis R, Strandberg T, Aho K. Filaggrin related antibodies among the aged. Ann
Rheum Dis 2003;62:261-3. Pease CT, Bhakta BB, Devlin J, Emery P. Does the age of onset of rheumatoid arthritis influ-
ence phenotype? A prospective study of outcome and prognostic factors. Rheumatology 1999;38:228-34.
Peel NF, Splittlehouse AJ, Bax DE, Eastell R. Bone mineral density of the hand in rheuma-
toid arthritis. Arthritis Rheum 1994;37:983-91. Pinals RS, Masi AT, Larsen RA. Preliminary criteria for clinical remission in rheumatoid ar-
thritis. Arthritis Rheum 1981;24:1308-15. Pincus T, Callahan LF, Fuchs HA, Larsen A, Kaye J. Quantitative analysis of hand radio-
graphs in rheumatoid arthritis: time course of radiographic changes, relation to joint ex-amination measures, and comparison of different scoring methods, J Rheumatol 1995;22:1983-9.
Pincus T, Yazici Y, Sokka T, Aletaha D, Smolen JS. Methotrexate as the “anchor drug” for
the treatment of early rheumatoid arthritis. Clin Exp Rheumatol 2003;21(Suppl 31):S179-85.
References _______________________________________________________________________________________
57
Pinheiro GC, Scheinberg MA, Aparecida DS, Maciel S. Anti-cyclic citrullinated peptide anti-
bodies in advanced rheumatoid arthritis. Ann Intern Med 2003;139:234-5. Puolakka K, Kautiainen H, Möttönen T, Hannonen P, Korpela M, Hakala M, et al. Early sup-
pression of disease activity is essential for maintenance of work capacity in patients with recent-onset rheumatoid arthritis. Five-year experience from the FIN-RACo trial. Arthritis Rheum 2005;52:36-41.
Prevoo ML, van´t Hof MA, Kuper HH, van Leeuwen MA, van de Putte LB, van Riel PL.
Modified disease activity scores that include twenty-eight-joint counts. Arthritis Rheum 1995;38:44-8.
Prevoo ML, van Gestel AM, van´t Hof MA, van Rijswijk MH, van de Putte LB, van Riel PL.
Remission in a prospective study of patients with rheumatoid arthritis. American Rheu-matology association preliminary remission criteria in relation to the Disease Activity Score. Br J Rheumatol 1996;35:1101-5.
Quinn MA, Conaghan PG, Emery P. The therapeutic approach of early intervention for rheu-
matoid arthritis: what is the evidence? Rheumatology 2001;40:1211-20. Rantapää Dahlqvist S, Ström H, Bjelle A, Möller E. HLA antigens in rheumatoid arthritis
patients with and without a family history of polyarthritis.Scand J Rheumatol 1985;14:375-380.
Rantapää-Dahlqvist S. Diagnostic and prognostic significance of autoantibodies in early
rheumatoid arthritis. Scand J Rheumatol 2005;34:83-96. Review. Reid DM, Kennedy NS, Smith MA, Tothill P, Nuki G. Total body calcium in rheumatoid ar-
thritis: effects of disease activity and corticosteroid treatment. Br Med J (Clin Res Ed):1982;285:330-2.
Reckner Olsson Å, Skogh T, Wingren G. Occupational determinants for rheumatoid arthritis.
Scand J Work Environ Health 2000;26:243-9. Rigby AS, Silman AJ, Voelm L, Gregory JC, Ollier WE, Khan MA, et al. Investigating the
HLA component in rheumatoid arthritis: an additative (dominant) mode of inheritance is rejected, a recessive mode is prefered. Genet Epidemiol 1991;8:153-75.
Ritchie DM, Boyle JA, McInnes JM, Jasani MK, Dalakos TG, Grieveson P, et al. Clinical
studies with an articular index for assessment of joint tenderness in patients with rheu-matoid arthritis. Q J Med 1968;37:393-406.
Ropes MW, Bennett GA, Cobbs S, Jacox R, Jessar RA. 1958 revision of the diagnostic crite-
ria for rheumatoid arthritis. Bull Rheum Dis 1958;9:175-6. Rose H, Ragan C, Pearce E, Lipman MO. Differential agglutination of normal and sentized
sheep erythrocytes by sera of patients with rheumatoid arthritis. Proc Soc Exp Biol Med 1949;68.
References _______________________________________________________________________________________
58
Rosholm A, HyldstrupL, Backsgaard L, Grunkin M, Thodberg HH. Estimation of bone min-eral density by digital X-ray radiogrammetry. Theoretical background and clinical test-ing. Osteoporosis Int 2001;12:961-9.
Rothschild BM, Woods RJ. Symmetrical erosive disease in Archaic Indians: the origin of
rheumatoid arthritis in the New World? Semin Arthritis Rheum 1990;19:278-84. Sambrook PN, Eisman JA, Champion GD, Yeates MG, Pocock NA, Eberl S. Determinants of
axial bone loss in rheumatoid arthritis. Arthritis Rheum 1987;39:721-8. Saraux A, Berthelot JM, Chalès G, Le Henaff C, Thorel JB, Hoang S, et al .Ability of the
American College of Rheumatology 1987 criteria to predict rheumatoid arthritis in pa-tients with early arthritis and classification of these patients two years later. Arthritis Rheum 2001;44:2485-91.
Schellekens GA, de Jong BA, van den Hogen FH, van de Putte LB, van Venrooij WJ. Citrul-
line is an essential constituent of antigenic determinants recognized by rheumatoid ar-thritis-specific autoantibodies. J. Clin Invest 1998;101:273-81.
Schellekens GA, Visser H, de Jong BA, van den Hoogen FH, Hazes JM, Breedveld FC et al.
The diagnostic propertiesof rheumatoid arthritis antibodies recognizing a cyclic citrulli-nated peptide. Arthritis Rheum 2000;43:155-63.
Schmidt W. Value of sonography in diagnosis of rheumatoid arthritis. Lancet 2001;357:1056-
7. Scott DL, Grindulis KA, Struthers GR, Coulton BL, Popert AJ, Bacon PA. Progression of
radiological changes in rheumatoid arthritis. Ann Rheum Dis 1984;43:8-17. Sebbag M, Simon M, Vincent C, Masson-Bessiere C, Girbal E, Durieux JJ, et al. The antiper-
inuclear factor and the so-called antikeratin antibodies are the same rheumatoid arthri-tis-specific autoantibodies. J Clin Invest 1995;95:2672-9.
Seldin MF, Amos CI, Ward R, Gregersen PK. The genetics revolution and the assault on
rheumatoid arthritis. Arthritis Rheum 1999;42:1071-9. Senkpiehl I, Marget M, Wedler M, Jenisch S, Georgi J, Kabelitz D, et al. HLA-DRB1 and
anti-cyclic citrullinated peptide antibody production in rheumatoid arthritis. Allergy Immunol 2005;137:315-8.
Sharp JT, Lidsky MD, Collins LC, Moreland J. Methods of scoring the progression of ra-
diologic changes in rheumatoid arthritis. Correlation of radiologic, clinical and labora-tory abnormalities. Arthritis Rheum 1971;14:706-20.
Sharp JT, Young DY, Bluhm GB, Brook A, Brower AC, Corbett M, et al. How many joints in
the hands and wrists should be included in a score of radiologic abnormalities used to assess rheumatoid arthritis? Arthritis Rheum 1985;28:1326-35.
References _______________________________________________________________________________________
59
Shichikawa K, Inoue K, Hirota S, Maeda A, Ota H, Kimura M, et al. Changes in the inci-dence and prevalence of rheumatoid arthritis in Kamitonda, Wakayama, Japan, 1965-1996. Ann Rheum Dis 1999;58:751-6.
Silman AJ, Pearson JE. Epidemiology and genetics of rheumatoid arthritis. Arthritis Res
2002; 4 Suppl 3:S265-72. Silman AJ, Ollier W, Holligan S, Birrell F, Adebajo A, Asuzu MC, et al. Absence of rheuma-
toid arthritis in a rural Nigerian population. J Rheumatol 1993;20:618-22. Silman AJ, Kay A, Brennan P: Timing of pregnancy in relation to the onset of rheumatoid
arthritis. Arthritis Rheum 1992;35:152-5. Simkins HM, Merriman ME, Chapman PT, O´Donnell JL, Jones PB, Gow PJ, et al. Associa-
tion of the PTPN22 locus with rheumatoid arthritis in a New Zealand Caucasian cohort. Arthritis Rheum 2005;52:2222-5.
Simon M, Girbal E, Sebbag M, Gomes-Daudrix V, Vincent C, Salama G. The cytokeratin
filameny-aggregating protein filaggrin is the target of the so-called “anti-keratin anti-bodies”, autoantibodies specific for rheumatoid arthritis. J Clin Invest 1993;92:1387-93.
Simonsson M, Bergman S, Jacobsson LT, Petesson IF, Svensson B. The prevalence of rheu-
matoid arthritis in Sweden. Scand J Rheumatol 1999;28:340-3. Smith CA, Petty RE, Tingle AJ. Rubella virus and arthritis. Rheum Dis Clin North Am.
1987;13:265-74. Smolen JS, Breedveld FC, Schiff MH, Kalden JR, Emery P, Eberl G, et al. A simplified dis-
ease activity index for rheumatoid arthritis for use in clinical practice. Rheumatology 2003;42:244-57.
Strand V and Simon LS. Low dose glucocorticoids in early rheumatoid arthritis. Clin Exp
Rheumatol 2003;21 (Suppl 31):S186-S190. Suzuki A, Yamada R, Chang X, Tokuhiro S, Sawada T, Suzuki M, et al . Functional haplo-
types of PADI4, encoding citrullinated enzyme peptidylarginine deiminase 4, are asso-ciated with rheumatoid arthritis. Nat Genet 2003;34:395-402.
Symmons D, Harrison B. Early inflammatory polyarthritis: results from the Norfolk arthritis
register with a review of the literature. I. Risk factors for the development of polyarthri-tis and rheumatoid arthritis. Rheumatology 2000;39:835-43.
Symmons DP, Bankhead CR, Harrison BJ, Brennan P, Barrett EM, Scott DG, et al. Blood
transfusion, smoking, and obesity as risk factors for the development of rheumatoid ar-thritis: results from a primary care-based incident case-control study in Norfolk, Eng-land. Arthritis Rheum 1997;40:1955-61.
Söderlin MK, Börjesson O, Kautiainen H, Skogh T, Leirisalo-Repo M. Annual incidence of
inflammatory joint diseases in a population based study in Southern Sweden. Ann Rheum Dis 2002;61:911-5.
References _______________________________________________________________________________________
60
Takemura S, Klimiuk PA, Braun A, Goronzy JJ, Weyand CM. T cell activation in rheumatoid
synovium is B cell dependent. J Immunol 2001;167:4710-18. Tengstrand B, Ahlmen M, Hafström I. The influence of sex on rheumatoid arthritis:a prospec-
tive study of onset and outcome after 2 years. J Rheumatol 2004;31:214-22. Thorsteinsson J, Björnsson OJ, Kolbeinsson A, Allander E, Sigfússon N, Ólafsson Ó. A popu-
lation study of rheumatoid factor in Iceland. Ann Clin Res 1975;7:183-94. Tsakonas E, Fitzgerald AA, Fitzcharles MA, Cividino A, Thorne JC, M´Seffar A, et al. Con-
sequences of delayed therapy with second-line agents in rheumatoid arthritis. A 3 year followup on the hydroxychloroquine in early rheumatoid arthritis (HERA) study. J Rheumatol 2000;27:623-9.
Uhlig T, Kvien TK. Is rheumatoid arthritis disappearing? Ann Rheum Dis 2005;64:7-10.doi:
10.1136/ard.2004.023044 Uhlig T, Hagen KB, Kvien TK. Current tobacco smoking, formal education and the risk of
rheumatoid arthritis. J Rheumatol 1999;26:47-54. van der Heijde DM, van`t Hof MA, van Riel PL, Theunisse LA, Lubberts EW, van Leeuwen
MA, et al. Judging disease activity in clinical practice in rheumatoid arthritis: first step in development of a disease activity score. Ann Rheum Dis 1990; 49:916-20.
van der Heijde DM, van`t Hof MA, van Riel PL, van Leeuwen MA, van Rijswijk MH, van de
Putte LB. Validity of single variables and composite indices for measuring disease ac-tivity in rheumatoid arthritis. Ann Rheum Dis 1992a;51;177-81.
van der Heijde DM, van Riel PL, van Leeuwen MA, van´t Hof MA, van Rijswijk MH, van de
Putte LB. Prognostic factors for radiographic damage and physical disability in early rheumatoid arthritis. A prospective follow-up study of 147 patients. Br J Rheumatol 1992b;31:519-25.
van der Heijde DM, van Leeuwen MA, van Riel PL, van de Putte LB. Radiographic progres-
sion of hands and feet during the first 3 years of rheumatoid arthritis measured accord-ing to Sharp´s method (van der Heijde modification). J Rheumatol 1995;22:1792-6.
van der Heijde DM, van Riel PL, Nuver-Zwart IH, Gribnau FW, van de Putte LB. Effects of
hydrochloroquine and sulphasalazine on progression of joint damage in rheumatoid ar-thritis, Lancet 1989;13:1036-8.
van Gaalen FA, van Aken J, Huizinga TW, Schreuder GM, Breedveld FC, Zanelli E, et al.
Association between HLA Class II genes and autoantibodies to cyclic citrullinated pep-tides (CCPs) influences the severity of rheumatoid arthritis. Arthritis Rheum 2004;50:2113-21.
van Gestel AM, Prevoo ML, van´t Hof MA, van Rijswijk MH, van de Putte LB, van Riel PL.
Development and validation of European League Against Rheumatism criteria for rheumatoid arthritis. Arthritis Rheum 1996;39:34-40.
References _______________________________________________________________________________________
61
van Gestel AM, Haagsma CJ, van Riel PL. Validation of rheumatoid arthritis improvement
criteria that include simplified joint counts. Arthritis Rheum 1998;41:1845-50. van Jaarsfeld CH, ter Borg EJ, Jacobs JW, Schellekens GA, Gmelig-Meyling FH, van Boo-
ma-Frankfort C, et al. The prognostic value of the antiperinuclear factor, anti-citrullinated peptide antibodies and rheumatoid factor in early rheumatoid arthritis. Clin Exp Rheumatol 1999;17:689-97.
van Leeuwen MA, Westra J, van Riel PL, Limburg PC, van Rijswijk MH. IgM, IgA, and IgG
rheumatoid factors in early rheumatoid arthritis predictive of radiological progression? Scand J Rheumatol 1995;24:136-53.
van Venrooij WJ, Hazes JM, Visser H. Anticitrullinated protein/peptide antibody and its role
in the diagnosis and prognosis of early rheumatoid arthritis. Neth J Med 2002;60:383-8. van Zeben D, Hazes JM, Zwinderman AH, Vandenbroucke JP, Breedveld FC. Factors pre-
dicting outcome of rheumatoid arthritis: results of a follow-up study. J Rheumatol 1993;20:1288-96.
Vasishta A. Diagnosing early-onset rheumatoid arthritis: the role of anti-CCP antibodies. Am
Clin Lab 2002;21:34-6. Visser H, le Cessie S, Vos K, Breedveld FC, Hazes JM. How to diagnose rheumatoid arthritis
early. A prediction model for persistent (erosive) arthritis. Arthritis Rheum 2002;46:357-65.
Vossenaar ER, Zendman AJ, van Venrooij WJ, Pruijn G. PAD, a growing family of citrulli-
nating enzymes: Genes, features and involvement in disease. Bioessays 2003;25:1106-18.
Vossenaar ER, van Venrooij WJ. Anti-CCP antibodies, a highly specific marker for (early)
rheumatoid arthritis. Clin Applied Immunol. 2004a:4;239-62. Vossenaar ER, Smeets TJ, Kraan MC, Raats JM, van Venrooij WJ, Tak PP. The presence of
citrullinated proteins is not specific for rheumatoid synovial tissue. Arthritis Rheum 2004b:50;3485-94.
Vossenaar ER, Radstake TR, van der Heijden A, van Mansum MA, Dieteren C, de Rooij DJ,
et al. Expression and activity of citrullinating peptidylarginine deiminase enzymes in monocytes and macrophages. Ann Rheum Dis 2004c;63:373-81.
Waaler E. On the occurrence of a factor in human serum activating the specific agglutination
of sheep blood corpuscles. Acta Pathologica Et Microbiologica Scandinavia 1940;17:172-88.
Wakefield RJ, Gibbon WW, Conaghan PG, O´Connor P, McGonagle D, Pease C, et al. The
value of sonography in the detection of bone erosions in patients with rheumatoid arthri-tis. Arthritis Rheum 2000;43:2762-70.
References _______________________________________________________________________________________
62
Weyand CM, McCarthy TG, Goronzy JJ. Correlation between disease phenotype and genetic heterogeneity in rheumatoid arthritis. J Clin Invest 1995;95:2120-6.
Wållberg-Jonsson S, Öhman ML, Dahlqvist SR. Cardiovascular morbidity and mortality in
patients with seropositive rheumatoid arthritis in Northern Sweden. J Rheumatol 1997;24:445-51.
Wållberg-Jonsson S, Johansson H, Öhman M-L, Rantapää-Dahlqvist S. Extent of inflamma-
tion predicts cardiovascular disease and overall mortality in seropositive rheumatoid ar-thritis. A retrospective cohort study from disease onset. J Rheumatol 1999;26:2562-71.
Young BJ, Mallya RK, Leslie RD, Clark CJ, Hamblin TJ. Anti-keratin antibodies in rheuma-
toid arthritis. Br Med J 1979; 2:97-9. Young A. Short-term outcomes in recent-onset rheumatoid arthritis. Br J Rheumatol 1995;34
Suppl 2:79-86. Åman S, Paimela L, Leirisalo-Repo M, Risteli J, Kautiainen H, Helve T, et al. Prediction of
disease progression in early rheumatoid arthritis by ICTP, RF and CRP. A comparative 3-year follow-up study. Rheumatology 2000;39:1009-13.