
Salivary cortisol, APOE-ε4 allele and cognitive decline in a prospective study of older persons
Upload
independentCategory
view
3download
0
Predicting Decline in Mild Cognitive Impairment A Prospective Cognitive Study
Sylvie BellevilleInstitut Universitaire de Geacuteriatrie de Montreacuteal Montreacuteal
Queacutebec Canada and Universiteacute de Montreacuteal
Serge GauthierMcGill Centre for Studies in Aging Verdun Queacutebec Canada
Eacutemilie LepageInstitut Universitaire de Geacuteriatrie de Montreacuteal Montreacuteal
Queacutebec Canada
Marie-Jeanne KergoatInstitut Universitaire de Geacuteriatrie de Montreacuteal Montreacuteal
Queacutebec Canada and Universiteacute de Montreacuteal
Brigitte GilbertInstitut Universitaire de Geacuteriatrie de Montreacuteal Montreacuteal Queacutebec Canada
Objective The primary aim of this study was to identify cognitive tests that differentiate between persons withmild cognitive impairment (MCI) who later develop cognitive decline and those who remain stable MethodThis study used a prospective longitudinal design One hundred twenty-two older adults with single-domainor multiple-domain amnestic MCI were recruited from memory clinics They completed tests to measurebaseline episodic memory working memory executive functions perception and language They were thenfollowed annually to determine with criteria independent from those tests whether they had remained stableor had developed dementia or significant cognitive decline This was used as the reference standard to measurediagnostic test accuracy value Results ANOVAs indicated that participants with progressive MCI showedmore impaired performance than those with stable MCI at baseline on episodic memory (word and storyrecall) the Brown-Peterson working memory test object naming object decision and position of gap testLogistic regression derived a significant model with 878 overall predictive value The model includeddelayed text memory free recall naming orientation match object decision and alpha span Its sensitivitywas 862 and its specificity was 889 Positive predictive value was 833 and negative predictive valuewas particularly high at 909 Conclusions Identifying individuals with MCI who will progress to dementiaor more severe cognitive impairment is a challenge This study shows that cognitive measures providevaluable information regarding the predictive diagnosis of persons with MCI Predictive accuracy of acognitive battery might be optimized by selecting both memory and nonmemory measures
Keywords diagnostic accuracy mild cognitive impairment Alzheimerrsquos disease neuropsychologicaltests sensitivity and specificity
It is now recognized that the defining pathological changes ofAlzheimerrsquos disease (AD) occur many years before patients meetthe clinical criteria for dementia of the Alzheimerrsquos type (Gauthier
et al 2006) This has led to the identification of a subset ofpersons with mild measurable cognitive decline who might be in apreclinical phase of AD These persons most often meet criteria foramnestic mild cognitive impairment (MCI) in that they have acomplaint and exhibit objective memory impairment (with orwithout additional cognitive deficits) yet they fail to reach currentcriteria for dementia (Albert et al 2011 Petersen 2003) Whilemost MCI patients progress to dementia not all of them willDepending on follow-up length recruitment source and initialdefinition criteria studies report that between 135 and 44 ofcases remain stable or revert back to normal (Gauthier et al 2006Petersen amp Morris 2003 Ritchie Artero amp Touchon 2001) It isthus critical to separate stable MCI from those who will decline Inspite of the increasing interest in biomarkers of AD cognitiveassessment remains a critical component of diagnosis in clinicalpractice Therefore it is vital to determine the capacity of cogni-tive measures in predicting progression and which set of tests havethe greatest predictive accuracy
Studies that have investigated the capacity of neurobiologicalandor cognitive diagnostic measures to predict which participantswill show future progression from MCI to dementia follow these
This article was published Online First March 3 2014Sylvie Belleville Research Centre Institut Universitaire de Geacuteriatrie de
Montreacuteal Montreacuteal Queacutebec Canada and Psychology Department Uni-versiteacute de Montreacuteal Serge Gauthier McGill Centre for Studies in AgingVerdun Queacutebec Canada Eacutemilie Lepage Research Centre Institut Uni-versitaire de Geacuteriatrie de Montreacuteal Montreacuteal Queacutebec Canada Marie-Jeanne Kergoat Research Centre Institut Universitaire de Geacuteriatrie deMontreacuteal Montreacuteal Queacutebec Canada and Faculty of Medicine Universiteacutede Montreacuteal Brigitte Gilbert Psychology Service Institut Universitaire deGeacuteriatrie de Montreacuteal Montreacuteal Queacutebec Canada
This study was supported by a CIHR grant to SB and SG We thankFrancine Giroux for her support in data analysis Heacutelegravene Audrit for help inreviewing the literature and Amanda de Fillippo for linguistic revision
Correspondence concerning this article should be addressed to SylvieBelleville Research Centre Institut Universitaire de Geacuteriatrie de Montreacuteal4565 Queen Mary Montreacuteal QC CANADA H3W 1W5 E-mailsylviebellevilleumontrealca
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
Neuropsychology copy 2014 American Psychological Association2014 Vol 28 No 4 643ndash652 0894-410514$1200 DOI 101037neu0000063
643
persons over certain periods of time (most often between 12 and 36months) Some of these studies have compared performance atentry in groups of persons with progressive versus stable MCI(Belanger amp Belleville 2009 Belleville Chertkow amp Gauthier2007 Ivanoiu et al 2005) Typically however these studies focuson a single domain of cognition include relatively small samplesizes and do not investigate predictive diagnostic accuracy Inturn predictive studies that rely on regression models to identifypredictors of progression can provide diagnostic accuracy esti-mates Notably most of the previous studies that have measuredpredictive diagnostic accuracy report an imbalance between sen-sitivity and specificity in that when the tests identified from thesestudies have good sensitivity they show relatively low specificityand vice versa This might be due to the fact that some of thesestudies have relied on a relatively short follow-up period [eg oneyear (Ahmed Mitchell Arnold Nestor amp Hodges 2008 Geroldiet al 2006) or two years (Artero Tierney Touchon amp Ritchie2003 Irish Lawlor Coen amp OrsquoMara 2011 Landau et al 2010Lekeu et al 2010 Mitchell Arnold Dawson Nestor amp Hodges2009 Tierney et al 1996)] which might increase the number offalse negatives thereby artificially reducing sensitivity Further-more many of these studies have focused on episodic memorytests because it is one of the first domains impaired in early ADand as a result they often include relatively few or no nonmemorytests Memory is also impaired in healthy aging and as a resultthis strategy might have favored sensitivity over specificity Non-memory domains are impaired early in AD (for a review Bel-leville Meacutenard De Boysson amp Sylvain-Roy 2008) and measur-ing them might increase the specificity of the model as thesedomains reflect neurobiological defects different from those sub-tending episodic memory impairment
Studies interested in the predictive accuracy of standard neuro-psychological tests have typically relied on those routinely used inclinical practice The advantage is that these measures are of easyaccess to clinicians However such tests are often not up to datewith the most recent research findings in the field of cognitiveneuroscience and therefore may lack theoretical validity Herewe employed a more recent set of theoretically based measuresThe selection of these measures was based on a number of meth-odological and theoretical criteria We avoided tests that weremultidetermined and favored those constructed to reduce contri-bution from cognitive capabilities other than the ones that the testintended to measure As an example we selected a word-listmemory test which controls the encoding of orientation cues thatreduce the effects of attentional or semantic problems on episodicmemory We also included measures of different cognitive pro-cesses within each large domain For instance we used bothsemantic and phonological tests of language domains and wemeasured different attentional control processes within the exec-utive domain Based on these criteria 10 tests were selected tomeasure episodic memory working memory and executive func-tions language and perception Two tests were used for episodicmemory One was a text memory measure constructed to containan equivalent number of details (the microstructure of the text) andgeneral ideas (the macrostructure of the text) The other was aword-list memory test that provides semantic orientation at encod-ing and includes both a free- and a cued-recall procedure Thethree executive functioning and working memory tasks we usedreflected different attentional control functions that were shown to
be differentially impaired in MCI switching divided attentionand online manipulation of information The two language teststarget the phonological (rhyme judgment) or the semantic (objectnaming) dimensions of language Finally we used three subtests ofthe Birmingham Object Recognition Battery which measure spa-tial and configural low-level aspects of perception (orientationposition of gap) and perceptual knowledge of an objectrsquos visualform (object decision subtest)
Thus the goals of this study were to compare cognition in stableand progressive MCI to determine a set of cognitive tests thataccurately differentiate between MCI persons who will remainstable and those who will progress to dementia to estimate diag-nostic accuracy with sensitivity specificity and predictive mea-sures and to compare accuracy between tests This study has anumber of added or innovative components relative to previouslypublished studies The first important element is that our batterywas designed to optimize sensitivity and specificity by includingboth memory and nonmemory tasks Second only a few studieshave reported a range of predictive diagnostic indices for theirpredictors and it is therefore unclear whether tests that differ at thegroup level allow individual classification A third major strengthwas relying on a prospective design as the majority of previousstudies have been retrospective One consequence of retrospectivestudies is that they rely on the same neuropsychological battery fordiagnosis and prediction andor they use a very restricted set oftests to measure progression Using a prospective design where thereference standard is determined independently from the predictivetests is of paramount importance because one is likely to find arelation among test scores used at successive times which artifi-cially increases their predictive value (see Tierney et al 1996 fora discussion) The patients received follow-up over up to 8 yearsto identify those who have entered a state of dementia Finally themajority of studies relied on clinical tests that are multideterminedand weak in terms of theoretical validity This is a drawback asincreasingly sophisticated tests are being developed Therefore werelied on more recent theoretically based measures Cognitivetests were expected to have a high predictive diagnostic value andit was expected that combining episodic memory and nonmemorydomains would provide an optimal cognitive algorithm to predictprogression to AD because they reflect different components of theneurobiological defect
Method
Participants
One hundred twenty-two participants with MCI were recruitedfrom different university-affiliated memory clinics in the Montrealarea At study entry all participants fulfilled criteria for amnesticsingle-domain MCI or amnestic multiple-domain MCI (Petersen2003) based on clinical and neuropsychological information (seeTable 1) Compared to normative values participants performed15 SD below the average level on at least one memory test(single-domain amnestic MCI) or on at least one memory test plusother tests (multiple-domain amnestic MCI) Participants did notmeet the DSMndashIV clinical criteria for dementia of the Alzheimertype at entry and they scored above the age- and education-adjusted cutoffs for dementia on the MMSE and MDRS Theircognitive difficulties had no significant impact on their functional
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
644 BELLEVILLE GAUTHIER LEPAGE KERGOAT AND GILBERT
independence as assessed through clinical interviews with thepatients and spouses and with activity of daily living scales Allparticipants were Francophone with normal or corrected visionand audition and made no use of psychotropic medication knownto impair cognition No participants were on acetylcholinesteraseinhibitors or memory-enhancing medications We excluded partic-ipants who reported major medical conditions those with presenceor history of alcoholism substance abuse severe psychiatric dis-
orders significant cerebrovascular neurological or neurodegen-erative disorders stroke or large-vessel disease or general anes-thesia in the last 6 months The Hachinski scale was used todocument cerebrovascular health (see Table 2) but not as anexclusion tool As shown on Table 2 participants showed very lowHachinski scores Approval was obtained according to the decla-ration of Helsinki and approval from the Ethical Committee of theInstitution in which the study was carried on
Table 1Testquestionnaires Used As Clinical Measures
Test Reference
Mini Mental State Evaluation (MMSE) Folstein M F Folstein S E amp McHugh P R (1975) ldquoMini-mental staterdquo A practical method forgrading the cognitive state of patients for the clinician Journal of Psychiatric Research 12189ndash198
Mattis Dementia Rating Scale (MDRS) Mattis S (1976) Mental status examination for organic mental syndrome in the elderly patient In RBellak amp T B Karasu (Eds) Geriatric psychiatry New York NY Grune amp Stratton
Functional Independence scale (Systegraveme demesure de lrsquoautonomie fonctionnelleSMAF)
Desrosiers J Bravo G Hebert R amp Dubuc N (1995) Reliability of the revised functionalautonomy measurement system (SMAF) for epidemiological research Age and Ageing 24402ndash406
RLRI 16 Free and Cued Recall Task Van der Linden M Adam S Agniel A Baisset-Mouly C amp Members of GREMEM (2004)Lrsquoeacutevaluation de troubles de la meacutemoire preacutesentation de quatre tests de meacutemoire eacutepisodique (aveceacutetalonnage) Marseille France Solal
Text Memory of the BEM-144 Signoret J L (1991) Batterie drsquoefficience mneacutesique BEM 144 Paris France ElsevierRey Figure Rey A (1959) Test de copie drdquoune figure complexe Manuel Paris France Les Eacuteditions du Centre
de Psychologie AppliqueacuteeStroop-Victoria Regard M (1981) Cognitive rigidity and flexibility A neuropsychological study (Doctoral
dissertation) University of Victoria CanadaCode subtest of the WAIS-R Wechsler D (1997) Wechsler Adult Intelligence Scale (3rd ed) San Antonio TX PearsonJudgment of line orientation Benton A L Hamsher K Varney N R amp Spreen O (Eds) (1983) Contributions to
neuropsychological assessment New York NY Oxford University PressBoston Naming Test Kaplan E F Goodglass H amp Weintraub S (1983) The Boston Naming Test (2nd ed)
Philadelphia PA Lea amp FebigerGeriatric Depression scale (GDS) Yesavage J A (1988) Geriatric Depression Scale Psychopharmacology Bulletin 24 709ndash711Hachinski scale Hachinski V C Iliff L D Zilhka E Du Boulay G H McAllister V L Marshall J
Symon L (1975) Cerebral blood flow in dementia Archives of Neurology 32 632ndash637
Table 2Clinical and Demographic Characteristics of the Participants (Standard Deviation inParentheses)
Stable MCI(n 33)
Progressors(n 59)
Effect size(Partial eta2)
Sex 64 women 60 womenAge 664 (91) 705 (79) 0054Years of education 157 (36) 145 (44) 0020SMAF (functional impact) 08 (07) 09 (07) 0011MMSE (max 30) 288 (11) 274 (19) 0137MDRS (max 144) 1394 (32) 1339 (54) 0241RLRI (delayed recall) (max 16) 121 (21) 75 (38) 0317BEM (delayed recall) (max 12) 73 (18) 51 (25) 0179Rey Figurerecall (max 36) 137 (63) 96 (53) 0111Rey Figurecopy (max 36) 306 (36) 298 (47) 0008Coding 102 (23) 89 (25) 0056Stroop (seconds) 315 (95) 372 (128) 0051Boston Naming Test (max 15) 136 (13) 122 (17) 0169Judgment of line orientation (max 30) 234 (4) 223 (48) 0012Geriatric Depression scale (max 15) 34 (27) 39 (37) 0006Hachinski scale 22 (21) 2 (15) 0003
Note SMAF Functional independence scale (Systegraveme de mesure de lrsquoautonomie fonctionnelle) MMSE Mini Mental State Evaluation MDRS Mattis dementia rating scale RLRI 16 free and cued recall task(Rappel libreindiceacute) BEM Text Memory of the BEM-144 (Batterie drsquoeacutevaluation de la meacutemoire) p 05 p 01 p 001 for the group difference
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
645PREDICTING DECLINE IN MCI
Predictive Battery
Episodic memory In the MEMO-TEXT (Geacutely-NargeotCadilhac Touchon amp Nespoulous 1997) a short story with asmany details (microelements) as general ideas (macroelements)was visually presented for a 3-min study period This was followedby an immediate and 10-min delayed recall In the Free and CuedRecall Test (Chatelois et al 1993 Mottron Morasse amp Belleville2001) 15 words were presented in a 3 5 visual matrix Wordswere encoded by their semantic category (eg show me the veg-etable) Free and category-cued recall was asked following a 45-sbackward counting
Working memory (WM) and executive functions In theadapted Brown-Peterson (Belleville Peretz amp Malenfant 1996Bherer Belleville amp Peretz 2001 Chatelois et al 1993) partic-ipants recalled 12 series of auditory consonant trigrams followingdelays of 0 10 20 or 30 sec filled with an addition task Theswitching procedure (Belleville Bherer Lepage Chertkow ampGauthier 2008) involved switching from adding to subtracting twoseries of digit pairs There were two 30-trial nonswitch blocks (onefor addition and one for subtraction) and two 74-trial switchblocks In the alpha span procedure (Belleville Rouleau amp Caza1998) participants were presented with 20 span-adjusted series ofwords that they were instructed to either report in the order ofpresentation or to mentally rearrange the words and report them inalphabetical order
Language Naming was measured with 80 line-drawings ofobjects (DOndash80 Deloche amp Hannequin 1997) A visual rhymejudgment task was also used in which participants were asked tojudge whether two written disyllabic nonwords rhymed or not(Belleville Caza amp Isabelle 2003)
Visuospatial processing We used three subtests of the Bir-mingham Object Recognition Battery (BORB Riddoch amp Hum-phreys 1993) In the orientation match test participants deter-mined if pairs of lines were parallel In the position of gap matchtest participants determined if pairs of truncated circles had theirgap in the same position In the object decision subtest partici-pants determined if drawings of tools or animalsmdashhalf of whichwere constructed by combining parts of two different objects oranimalsmdashwere real
Design
At study entry persons with MCI completed the clinical testsquestionnaires the clinical neuropsychology battery and the pre-dictive battery (see Figure 1) Clinical and experimental tests weredone in separate sessions Participants were then invited for ayearly clinical assessment to determine whether they had pro-gressed from MCI to AD or in their symptom severity At eachfollow-up clinical information was used by clinicians (SG MJKBG) to determine whether participants were stable or had pro-gressed to dementia Clinical diagnosis was established indepen-dently of the results from the predictive battery and cliniciansinvolved in the diagnosis were unaware of the results from thepredictive battery at the time of diagnosis Patients were identifiedas having progressive MCI (pMCI) if they met the current clinicalDSMndashIV criteria for dementia of the Alzheimer type or if theyshowed a significant decline on tests from the clinical batteryParticipants showing a significant decline had a cognitive profileconsistent with that of MCI However they showed an annual
reduction in performance that was larger than one SD unit (SD wastaken from the performance of a group of approximately 100healthy older adults tested in our laboratory on the same task) onmore than one clinical test This criterion was used because itrepresents a large effect size (8) and is more than 10 timesgreater than the annual decline reported by healthy older adults(approximately 002 SD annual decline for memory and approxi-mately 008 SD for speed of processing Bennett et al 2002)Persons showing no progression to dementia and no decline wereidentified as having stable MCI (sMCI)
Statistical Analysis
ANOVAs or t tests were used to compare pMCI and sMCI atbaseline on demographic characteristics clinical questionnairesclinical neuropsychology tests and tests from the predictor batteryWe used backward logistic regression to determine which testfrom the predictive battery predicted progression As there weremany possible dependent variables for each test it was necessaryto select those that were to be included in the model The variableswere selected based on their theoretical value and only one vari-able was chosen to reflect each cognitive test (eg we avoidedusing both the RTs and correct responses for the same condition)We also used the correlation matrix to exclude variables thatreflected one cognitive domain and that were highly correlated(r 8) Group membership (pMCI vs sMCI) at follow-up wasused as the reference standard Sociodemographic variables thatdiffered across groups were used as covariates This is anexploratory analysis as we made no a priori assumptions re-garding the predictive strength of the tests The analysis pro-vides a number of diagnosis accuracy measures sensitivity
Figure 1 Design of the study
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
646 BELLEVILLE GAUTHIER LEPAGE KERGOAT AND GILBERT
which refers to the percentage of times that performance on thederived predictive tests was abnormal at baseline among pMCIpersons specificity which refers to the percentage of time thatperformance on the derived predictive tests was normal at baselineamong sMCI persons overall accuracy which refers to caseswhere performance on those tests matches clinical diagnosis pos-itive predictive value (PPV) which refers to the percentage oftimes that a clinical diagnosis of pMCI was given based onabnormal performance on predictive tests and negative predictivevalue (NPV) which refers to the percentage of times that theclinical diagnosis was sMCI based on normal performance onpredictive tests The final model was the one that optimizedsensitivity and specificity and gave the best overall diagnosticaccuracy The Kaplan-Meier method measured the probability ofcrossover at designated time intervals as a function of wherepatients stood in the score distribution Scores on measures iden-tified as predictors in the regression analysis were used to stratifypatients in tertiles with the Kaplan-Meier Log-rank was used toassess whether the survival curves of the three tertile groupsdiffered in terms of progression rate All analyses were performedwith the SPSS-20 package
Results
Sociodemographic and Clinical Characteristics
Ten persons were excluded based on the clinical assessment asthey did not meet inclusion criteria and five persons withdrewconsent prior to being tested with the predictive battery (see Figure1) Fifteen additional persons withdrew consent during the follow-up Causes of withdrawal included loss of interest in the researchmoving to another town and death Persons who withdrew consentdid not differ from those remaining in the study on sociodemo-graphic and measures of global cognition variables Fifty-ninepersons were identified as pMCI and 33 as sMCI pMCI partici-pants were identified as progressors on average 3081 months afterentry (SD 20) Follow-up was interrupted after pMCI convertedto dementia Mean follow-up for sMCI was 5673 months (SD 232) sMCI and pMCI groups were equivalent on clinical ques-tionnaires and on sociodemographic characteristics except for ageas pMCI participants were older than sMCI participants ThepMCI group showed worse performance than sMCI participants onmost clinical neuropsychology measures (see Table 2) AmongpMCI participants 40 (678) presented with single-domain am-
Table 3Performances on the Predictive Battery (Standard Deviation in Parentheses) and Cut-Off Valuesto Optimize Diagnostic Accuracy on the Individual Cognitive Tests Kept by theRegression Model
Stable MCI Progressors Cut-off value
Episodic memory tasksMEMO-TEXT (max 24)
Macro-elements immediate 179 (33) 144 (4)Micro-elements immediate 114 (37) 69 (48)Macro-elements delayed 168 (32) 128 (43) 13Micro-elements delayed 103 (41) 52 (41)
Free and Cued recall test (max 15)Free recall 83 (28) 52 (23) 6Free and category cued recall 125 (24) 94 (32)
Working memory and executivefunctions
Brown Peterson - Items recalled (max9 ndash max 36 for total)
0-sec delay 84 (1) 84 (11)10-sec delay 67 (19) 57 (24)20-sec delay 62 (23) 47 (27)30-sec delay 65 (25) 56 (24)Total items recalled 277 (6) 244 (65)
Alpha span - Items recalled (max 100)Items direct 79 (143) 744 (197)Items alpha 611 (175) 509 (174) 58Manipulation cost 221 (188) 302 (197)
Switching task cost on errorsGlobal Switch 001 (033) 004 (034)Local Switch 011 (225) 029 (398)
Language and Visuo-spatial tasksDO80 (max 80) 785 (18) 768 (4) 78Rhyme judgment (max 32) 288 (33) 29 (28)BORB
Line judgment test (max 30) 253 (18) 247 (22)Circle test (max 30) 351 (27) 334 (29) 25Object decision test (max 32) 299 (19) 287 (28) 29
Note MEMO-TEXT Text Memory DO80 Denomination Object 80 items BORB BirminghamObject Recognition Battery
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
647PREDICTING DECLINE IN MCI
nestic MCI at entry and 19 with multiple-domain amnestic MCI(322) Among sMCI participants 19 presented with single-domain amnestic MCI (576) and 14 with multiple-domainamnestic MCI (424)
Group Comparisons on Predictive Battery
Table 3 reports performances of sMCI and pMCI on the pre-dictive battery In some cases technical problems prevented test-ing or data collection for some of the participants The N on whichthe analysis was done is thus provided in parentheses for each test
Episodic memory A Group Delay Type of elementANOVA on the number of items recalled from the MEMO-TEXT(pMCI 53 sMCI 32) indicated significant effects of theDelay F(1 88) 49747 p 0001 2 361 Type of elementF(1 88) 351247 p 0001 2 800 and Group F(1 88) 30553 p 0001 2 258 Recall was lower for the delayedthan immediate recall for micro- than macroelements and forpMCI than sMCI The Group Recall Condition ANOVA on thenumber of words recalled from the Free and Cued-recall test(pMCI 53 sMCI 32) indicated significant effects of theGroup F(1 83) 30712 p 0001 2 270 and Recallcondition F(1 83) 322938 p 0001 2 796 There werefewer words recalled in the Free than Cued condition and in pMCIthan sMCI All effects remained significant when correcting formultiple comparisons
WM and executive functions The Group Delay ANOVAon the number of correct items of the Brown-Peterson procedure(pMCI 58 sMCI 33) indicated a main Group F(1 89) 5568 p 005 2 06 and Delay effect F(3 267) 47983p 00001 2 35 Fewer items were recalled by pMCI thansMCI and fewer in the trials with longer delays The group effectwas no longer significant when correcting for multiple compari-son The Group Recall type ANOVA on the of recalled itemsfrom the alpha span (pMCI 57 sMCI 33) indicated a maineffect of Recall F(1 88) 146720 p 0001 2 625 witha lower recall in the alphabetical than direct condition and a mainGroup effect F(1 88) 4527 p 05 2 049 with pMCIrecalling fewer items than sMCI The group effect was no longersignificant when correcting for multiple comparison A manipula-tion cost score the of loss incurred by alphabetical recall[(direct alpha)direct] revealed a significant Group dif-ference as pMCI showed a larger manipulation cost than sMCI
t(88) 1914 p 05 2 04 This remained significant whencorrecting for multiple comparison There was no significanteffect or interaction on global or local switch cost definedrespectively as the number of errors on switch minus nonswitchblock and errors on switch trials minus nonswitch trials F13in all cases (pMCI 57 sMCI 33)
Language No group differences were found on the number ofcorrect responses for the rhyme judgment test t(86) 0340 2 001 However pMCI showed a lower number of correct responsesthan sMCI on the DO-80 naming test t(90) 2327 p 052 057 (pMCI 59 and 55 respectively sMCI 33) and thisremained significant when correcting for multiple comparison
Visuospatial processing No group differences were foundon the orientation match t(85) 1175 2 016 HoweverpMCI obtained a lower score than sMCI on the position of gapt(85) 2637 p 01 2 076 and object decisiont(85) 2329 p 05 2 060 tests (pMCI 54 sMCI 33) The effect remained significant when correcting for mul-tiple comparisons on position gap but not on object decision
Regression Analysis
The age-adjusted logistic model with the best overall diag-nostic accuracy was obtained after five iterations and wascomposed of six variables The strongest predictors were de-layed recall of macro elements of the MEMO-TEXT and freerecall of words The model also retained object naming (DO-80) orientation match (BORB) object decision (BORB) andalpha span (see Table 4) Odd ratios range from 1033 (for thealpha span) to 1689 (for free recall of words) The overallclassification success was 877 The model yielded high sensi-tivity and specificity values (88 and 871 respectively Table5) and excellent positive predictive value (PPV 818) andnegative predictive value (NPV 917)
Survival analyses (see Figure 2) indicated that those perform-ing in the lowest and middle tertiles on the MEMO-TEXT freerecall and alpha span showed faster progression than those inthe highest tertile Furthermore those performing in the lowesttertile on the naming test showed a faster progression rate thanthose performing in the middle and highest tertiles The differ-ence in decline as a function of tertile indicates that the first twotasks are more sensitive to the disease than is naming Nodifferences were found across tertiles for the object decisionand orientation match tests suggesting that when used on their
Table 4Logistic Regression Models on the Predictive Battery
PREDICTORS SE Waldrsquos 2 df pe
(odds ratio)
Age 005 048 011 1 918 995MEMO-TEXT 236 113 4377 1 036 1266delayed macroFree recall 496 171 8386 1 004 1643DO 80 181 147 1501 1 221 1198BORBndashLine judgment 379 243 2439 1 118 1461BORBndashObject decision 251 174 2095 1 148 1286Alpha span 031 021 2097 1 148 1031Constant 9566 4023 5654 1 017 NA
Note MEMO-TEXT Text Memory DO80 Denomination Object80 items BORB Birmingham Object Recognition Battery
Table 5Observed and Predicted Frequencies for the PredictiveDiagnostic Accuracy Provided by the Logistic Regression ModelWith a 060 Cutoff
Predicted
Observed Yes No Correct
Yes 44 6 88No 4 27 871 correct 917 818 877
Note Sensitivity 44(44 6) 88 Specificity 27(27 4) 871 False positive 4(4 44) 83 False negative 6(6 27) 182
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
648 BELLEVILLE GAUTHIER LEPAGE KERGOAT AND GILBERT
own these two tasks lack sensitivity This analysis also showsdifferences across tasks in sensitivity to time of progression Bythe 40-month follow-up 80 of those in the lowest tertile ofMEMO-TEXT had converted to dementia This was found 60and 80 months after follow-up among those in the lowest tertileof free recall and alpha-span respectively
Discussion
Not all MCI cases progress to dementia and it is critical toidentify tests that accurately predict future progression In this
study we found that combining tests of episodic memory (text andword recall) perception (naming orientation and object decision)and working memory (alpha span) correctly identifies 878 ofparticipants who will progress on an average of 45 years inadvance The six-test model yielded very good to excellent sensi-tivity and specificity values as both of them were above 85 Thiswas also the case for PPN and NPV values and in particular it wasfound that 917 of those found unimpaired on the tests remainedstable in spite of the fact they met clinical criteria for MCI Thusthis combination of measures is not only sensitive but it is also
Figure 2 Survival analyses
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
649PREDICTING DECLINE IN MCI
specific and it helps to identify those who are unlikely to progressThis is highly important for clinical trials as it can help identify theMCI persons who are most likely to benefit from disease-modifying therapies Survival analyses indicate that 80 of thepatients performing in the lowest tertile of the MCI group on thetext memory test will have developed dementia 40 months later
This study suggests that relying only on episodic memory mea-sures might not be optimal and that measuring different domains ofcognition represents the most balanced approach Several studieshave investigated the capacity of biological and cognitive mea-sures to predict future progression from MCI to dementia A firstimportant conclusion from many of these studies is that the patternof cognitive deficit might be as accurate as biological measures inpredicting future decline in MCI (Albert et al 2011 Dubois et al2007) a conclusion coherent with our finding of a strong predic-tive accuracy for the cognitive battery used here Another impor-tant conclusion is that it is possible to identify an optimal set ofcognitive tasks Studies vary in their design statistical approachand follow-up length and there is great variability in the cognitivetests used Nevertheless a coherent pattern seems to emerge fromprevious studies which is supported by our findings First itappears that combining episodic memory tests with tasks that relyon executive functions or the attentional control of WM is partic-ularly powerful for predicting conversion from MCI to dementia(Aretouli Tsilidis amp Brandt 2013 Chapman et al 2011 Conde-Sala et al 2012 Gavett et al 2010 Rabin et al 2009 Summersamp Saunders 2012) Second studies that measured only one or twocognitive domains have much lower predictive accuracy than theone found here They report either lower specificity (eg Mitchellet al 2009) or lower sensitivity (Dierckx et al 2009 Tabert et al2006 Tierney et al 1996) than what is reported here This isconsistent with studies indicating that cases of multiple-domainMCI are more likely to progress to dementia than single-domainMCI (Forlenza et al 2009 Nordlund et al 2010 RasquinLodder Visser Lousberg amp Verhey 2005 Summers amp Saunders2012) Our study indicates that an optimal battery should includeperceptual tests in addition to tests of episodic memory executivefunction and working memory The particular cognitive domainsidentified here match well with findings indicating that in additionto episodic memory semantic knowledge and working memoryare impaired early in AD (for a review see Belleville et al 2008)
Few studies have included perceptual or semantic componentsin their models contrary to this study and those that did measureda relatively small number of components It is therefore possiblethat measures of the perceptual or semantic domains have im-proved predictive accuracy However these tasks may be morespecific than sensitive Indeed our survival analyses suggest thatnaming and perceptual tasks were not as sensitive to future declineas episodic memory and executive tasks when taken on their ownIncluding measures of the perceptual or semantic domain mightcontribute to reducing the number of false positives hence increas-ing specificity This is a potentially useful finding for cliniciansand researchers When optimizing testing time is a critical issueand tasks need to be selected one can base the decision on whetherthe need is to have a more sensitive or more specific battery
This study is among those showing the best combination ofsensitivity and specificity values Perhaps inclusion of morenonmemory tests might have increased specificity and use of a
relatively long follow-up period likely reduced the number offalse negatives hence increasing sensitivity Another differencebetween this study and the current literature is that we did notrely on clinical measures but on theoretically motivated onesThus if selected well a relatively short battery of tests canpredict future decline in MCI and can help identify persons thatare likely to progress to more severe symptoms
The study resulted in a number of additional findings whichdeserve discussion One is that at entry progressive MCIpatients already differ from stable MCI patients in terms of ageand cognitive performance on several clinical tests Becausepatients are likely to vary in their decline rate and in their stageat entry it is possible that progressors are in a more advancedstage of neuropathology than persons with stable MCI and thatthe latter would decline later Thus a portion of stable MCIpatients may still actually be predementia (thus false negative)It is important to note however that this study makes use of amuch longer follow-up than is typically used in similar studiesStable MCI patients were followed for an average of 567months which is much longer than the period after whichprogressors converted to dementia (on average 308 monthsafter entry) This long follow-up probably reduced the contri-bution of ldquofalse negativesrdquo to the group of those with stableMCI by increasing the chance of progression during the studyperiod Admittedly it remains possible that some of the stableMCI patients will progress to dementia in the future Howeverwe do not believe that this represents a substantial portion ofour participants with stable MCI It is interesting that thefinding that the two groups differ on clinical measures is in factgood news as it supports our contention that cognitive mea-sures are sensitive to prognosis and will prove critical in iden-tifying the patients more likely to progress to dementia
This study has limitations which should be recognized Firstto improve generalizability the findings should be reproducedon a different sample Second we did not include biomarkers orimaging parameters in this study Our goal was to identify theideal set of cognitive measures and for future studies it will beimportant to assess the value of combining them with biologicalmarkers Finally it is important to point out that there might bedifferences between this cohort of patients and patients encoun-tered in other clinical settings In particular our exclusioncriteria might have led to a cohort with relatively few cases ofcomorbidity
References
Ahmed S Mitchell J Arnold R Nestor P J amp Hodges J R (2008)Predicting rapid clinical progression in amnestic mild cognitive impair-ment Dementia and Geriatric Cognitive Disorders 25 170ndash177 doi101159000113014
Albert M S DeKosky S T Dickson D Dubois B Feldman H HFox N C Phelps C H (2011) The diagnosis of mild cognitiveimpairment due to Alzheimerrsquos disease Recommendations from theNational Institute on Aging-Alzheimerrsquos Association workgroups ondiagnostic guidelines for Alzheimerrsquos disease Alzheimers amp Dementia7 270ndash279 doi101016jjalz201103008
Aretouli E Tsilidis K K amp Brandt J (2013) Four-year outcome ofmild cognitive impairment The contribution of executive dysfunctionNeuropsychology 27 95ndash106 doi101037a0030481
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
650 BELLEVILLE GAUTHIER LEPAGE KERGOAT AND GILBERT
Artero S Tierney M C Touchon J amp Ritchie K (2003) Prediction oftransition from cognitive impairment to senile dementia A prospectivelongitudinal study Acta Psychiatrica Scandinavica 107 390ndash393
Beacutelanger S amp Belleville S (2009) Semantic inhibition impairment inmild cognitive impairment A distinctive feature of upcoming cognitivedecline Neuropsychology 23 592ndash606 doi101037a0016152
Belleville S Bherer L Lepage Eacute Chertkow H amp Gauthier S (2008)Task switching capacities in persons with Alzheimerrsquos disease and mildcognitive impairment Neuropsychologia 46 2225ndash2233 doi101016jneuropsychologia200802012
Belleville S Caza N amp Peretz I (2003) A neuropsychological argu-ment for a processing view of memory Journal of Memory and Lan-guage 48 686ndash703 doi101016S0749-596X(02)00532-6
Belleville S Chertkow H amp Gauthier S (2007) Working memory andcontrol of attention in persons with Alzheimerrsquos disease and mild cog-nitive impairment Neuropsychology 21 458ndash469 doi1010370894-4105214458
Belleville S Meacutenard M C De Boysson C amp Sylvain-Roy S (2008)Characterizing memory deficits in mild cognitive impairment In WSossin J C Lacaille V Castellucci amp S Belleville (Eds) The essenceof memory (pp 365ndash375) Amsterdam Netherlands Elsevier doi101016S0079-6123(07)00023-4
Belleville S Peretz I amp Malenfant D (1996) Examination of theworking memory components in normal aging and in dementia of theAlzheimer type Neuropsychologia 34 195ndash207 doi1010160028-3932(95)00097-6
Belleville S Rouleau N amp Caza N (1998) Effect of normal aging onthe manipulation of information in working memory Memory amp Cog-nition 26 572ndash583 doi103758BF03201163
Bennett D A Wilson R S Schneider J A Evans D A BeckettL A Aggarwal N T Bach J (2002) Natural history of mildcognitive impairment in older persons Neurology 59 198ndash205
Bherer L Belleville S amp Peretz I (2001) Education age and theBrown-Peterson technique Developmental Neuropsychology 19 237ndash251 doi101207S15326942DN1903_1
Chapman R M Mapstone M McCrary J W Gardner M N Por-steinsson A Sandoval T C Reilly L A (2011) Predictingconversion from mild cognitive impairment to Alzheimerrsquos diseaseusing neuropsychological tests and multivariate methods Journal ofClinical and Experimental Neuropsychology 33 187ndash199 doi101080138033952010499356
Chatelois J Pineau H Belleville S Peretz I Lussier I FontaineF-S amp Renaseau-Leclerc C (1993) Batterie informatiseacutee drsquoeacutevaluationde la meacutemoire inspireacutee de lrsquoapproche cognitive Canadian PsychologyPsychologie Canadienne 34 45ndash63 doi101037h0078803
Conde-Sala J L Garre-Olmo J Vilalta-Franch J Llinas-Regla JTurro-Garriga O Lozano-Gallego M Loacutepez-Pousa S (2012)Predictors of cognitive decline in Alzheimerrsquos disease and mild cogni-tive impairment using the CAMCOG A five-year follow-up Interna-tional Psychogeriatrics 24 948ndash958 doi101017S1041610211002158
Deloche G amp Hannequin D (1997) Test de deacutenomination oraledrsquoimages (DO-80) Paris France Centre de Psychologie Appliqueacutee
Dierckx E Engelborghs S De Raedt R Van Buggenhout M DeDeyn P P Verte D amp Ponjaert-Kristoffersen I (2009) Verbal cuedrecall as a predictor of conversion to Alzheimerrsquos disease in mildcognitive impairment International Journal of Geriatric Psychiatry 241094ndash1100 doi101002gps2228
Dubois B Feldman H H Jacova C Dekosky S T Barberger-Gateau P Cummings J Scheltens P (2007) Research criteriafor the diagnosis of Alzheimerrsquos disease Revising the NINCDS-ADRDA criteria Lancet Neurology 6 734 ndash746 doi101016S1474-4422(07)70178 ndash3
Forlenza O V Diniz B S Nunes P V Memoria C M YassudaM S amp Gattaz W F (2009) Diagnostic transitions in mild cognitive
impairment subtypes International Psychogeriatrics 21 1088ndash1095doi101017S1041610209990792
Gauthier S Reisberg B Zaudig M Petersen R C Ritchie K BroichK Winblad B (2006) Mild cognitive impairment The Lancet 3671262ndash1270 doi101016S0140-6736(06)68542-5
Gavett B E Ozonoff A Doktor V Palmisano J Nair A K GreenR C Stern R A (2010) Predicting cognitive decline and conver-sion to Alzheimerrsquos disease in older adults using the NAB List Learningtest Journal of the International Neuropsychological Society 16 651ndash660 doi101017S1355617710000421
Geacutely-Nargeot M-C Cadilhac C Touchon J amp Nespoulous J L(1997) La meacutemoire de textes chez les sujets sains et deacutements Appli-cation drsquoun nouvel outil drsquoeacutevaluation pour neuropsychologues Meacutemo-textes In J Lambert amp J L Nespoulous (Eds) Perception auditive etcompreacutehension du langage (pp 273ndash293) Marseille France Solal
Geroldi C Rossi R Calvagna C Testa C Bresciani L Binetti G Frisoni G B (2006) Medial temporal atrophy but not memorydeficit predicts progression to dementia in patients with mild cognitiveimpairment Journal of Neurology Neurosurgery amp Psychiatry 771219ndash1222 doi101136jnnp2005082651
Irish M Lawlor B A Coen R F amp OrsquoMara S M (2011) Everydayepisodic memory in amnestic mild cognitive impairment A preliminaryinvestigation BMC Neuroscience 12 80 doi1011861471-2202-12-80
Ivanoiu A Adam S Van der Linden M Salmon E Juillerat A CMulligan R amp Seron X (2005) Memory evaluation with a new cuedrecall test in patients with mild cognitive impairment and Alzheimerrsquosdisease Journal of Neurology 252 47ndash55 doi101007s00415-005-0597-2
Landau S M Harvey D Madison C M Reiman E M Foster N LAisen P S Jagust W J (2010) Comparing predictors of conver-sion and decline in mild cognitive impairment Neurology 75 230ndash238doi101212WNL0b013e3181e8e8b8
Lekeu F Magis D Marique P Delbeuck X Bechet S GuillaumeB Salmon E (2010) The California Verbal Learning Test andother standard clinical neuropsychological tests to predict conversionfrom mild memory impairment to dementia Journal of Clinical andExperimental Neuropsychology 32 164 ndash173 doi10108013803390902889606
Mitchell J Arnold R Dawson K Nestor P J amp Hodges J R (2009)Outcome in subgroups of mild cognitive impairment (MCI) is highlypredictable using a simple algorithm Journal of Neurology 256 1500ndash1509 doi101007s00415-009-5152-0[doi]
Mottron L Morasse K amp Belleville S (2001) A study of memoryfunctioning in individuals with autism Journal of Child Psychology andPsychiatry 42 253ndash260 doi1011111469-761000716
Nordlund A Rolstad S Klang O Edman A Hansen S amp Wallin A(2010) Two-year outcome of MCI subtypes and aetiologies in theGoteborg MCI study Journal of Neurology Neurosurgery amp Psychia-try 81 541ndash546 doi101136jnnp2008171066
Petersen R C (2003) Mild cognitive impairment Aging to Alzheimerrsquosdisease Oxford UK Oxford University Press
Petersen R C amp Morris J C (2003) Clinical features In R C Petersen(Ed) Mild cognitive impairment Aging to Alzheimerrsquos disease (pp15ndash39) Oxford UK Oxford University Press
Rabin L A Pare N Saykin A J Brown M J Wishart H AFlashman L A amp Santulli R B (2009) Differential memory testsensitivity for diagnosing amnestic mild cognitive impairment and pre-dicting conversion to Alzheimerrsquos disease Neuropsychology Develop-ment and Cognition Section B Aging Neuropsychology and Cognition16 357ndash376 doi10108013825580902825220
Rasquin S M Lodder J Visser P J Lousberg R amp Verhey F R(2005) Predictive accuracy of MCI subtypes for Alzheimerrsquos diseaseand vascular dementia in subjects with mild cognitive impairment A
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
651PREDICTING DECLINE IN MCI
2-year follow-up study Dementia and Geriatric Cognitive Disorders19 113ndash119 doi101159000082662
Riddoch J M amp Humphreys G W (1993) BORB Birmingham ObjectRecognition Battery Hove UK Erlbaum
Ritchie K Artero S amp Touchon J (2001) Classification criteria formild cognitive impairment A population-based validation study Neu-rology 56 37ndash42 doi101212WNL56137
Summers M J amp Saunders N L (2012) Neuropsychological measurespredict decline to Alzheimerrsquos dementia from mild cognitive impair-ment Neuropsychology 26 498ndash508 doi101037a0028576
Tabert M H Manly J J Liu X Pelton G H Rosenblum S JacobsM Devanand D P (2006) Neuropsychological prediction of
conversion to Alzheimer disease in patients with mild cognitive impair-ment Archives of General Psychiatry 63 916ndash924 doi101001archpsyc638916
Tierney M C Szalai J P Snow W G Fisher R H Nores A NadonG St George-Hyslop P H (1996) Prediction of probable Alz-heimerrsquos disease in memory-impaired patients A prospective longitu-dinal study Neurology 46 661ndash665 doi101212WNL463661
Received May 15 2013Revision received December 19 2013
Accepted December 22 2013
Members of Underrepresented GroupsReviewers for Journal Manuscripts Wanted
If you are interested in reviewing manuscripts for APA journals the APA Publications andCommunications Board would like to invite your participation Manuscript reviewers are vital to thepublications process As a reviewer you would gain valuable experience in publishing The PampCBoard is particularly interested in encouraging members of underrepresented groups to participatemore in this process
If you are interested in reviewing manuscripts please write APA Journals at ReviewersapaorgPlease note the following important points
bull To be selected as a reviewer you must have published articles in peer-reviewed journals Theexperience of publishing provides a reviewer with the basis for preparing a thorough objectivereview
bull To be selected it is critical to be a regular reader of the five to six empirical journals that are mostcentral to the area or journal for which you would like to review Current knowledge of recentlypublished research provides a reviewer with the knowledge base to evaluate a new submissionwithin the context of existing research
bull To select the appropriate reviewers for each manuscript the editor needs detailed informationPlease include with your letter your vita In the letter please identify which APA journal(s) youare interested in and describe your area of expertise Be as specific as possible For exampleldquosocial psychologyrdquo is not sufficientmdashyou would need to specify ldquosocial cognitionrdquo or ldquoattitudechangerdquo as well
bull Reviewing a manuscript takes time (1ndash4 hours per manuscript reviewed) If you are selected toreview a manuscript be prepared to invest the necessary time to evaluate the manuscriptthoroughly
APA now has an online video course that provides guidance in reviewing manuscripts To learnmore about the course and to access the video visit httpwwwapaorgpubsauthorsreview-manuscript-ce-videoaspx
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
652 BELLEVILLE GAUTHIER LEPAGE KERGOAT AND GILBERT

persons over certain periods of time (most often between 12 and 36months) Some of these studies have compared performance atentry in groups of persons with progressive versus stable MCI(Belanger amp Belleville 2009 Belleville Chertkow amp Gauthier2007 Ivanoiu et al 2005) Typically however these studies focuson a single domain of cognition include relatively small samplesizes and do not investigate predictive diagnostic accuracy Inturn predictive studies that rely on regression models to identifypredictors of progression can provide diagnostic accuracy esti-mates Notably most of the previous studies that have measuredpredictive diagnostic accuracy report an imbalance between sen-sitivity and specificity in that when the tests identified from thesestudies have good sensitivity they show relatively low specificityand vice versa This might be due to the fact that some of thesestudies have relied on a relatively short follow-up period [eg oneyear (Ahmed Mitchell Arnold Nestor amp Hodges 2008 Geroldiet al 2006) or two years (Artero Tierney Touchon amp Ritchie2003 Irish Lawlor Coen amp OrsquoMara 2011 Landau et al 2010Lekeu et al 2010 Mitchell Arnold Dawson Nestor amp Hodges2009 Tierney et al 1996)] which might increase the number offalse negatives thereby artificially reducing sensitivity Further-more many of these studies have focused on episodic memorytests because it is one of the first domains impaired in early ADand as a result they often include relatively few or no nonmemorytests Memory is also impaired in healthy aging and as a resultthis strategy might have favored sensitivity over specificity Non-memory domains are impaired early in AD (for a review Bel-leville Meacutenard De Boysson amp Sylvain-Roy 2008) and measur-ing them might increase the specificity of the model as thesedomains reflect neurobiological defects different from those sub-tending episodic memory impairment
Studies interested in the predictive accuracy of standard neuro-psychological tests have typically relied on those routinely used inclinical practice The advantage is that these measures are of easyaccess to clinicians However such tests are often not up to datewith the most recent research findings in the field of cognitiveneuroscience and therefore may lack theoretical validity Herewe employed a more recent set of theoretically based measuresThe selection of these measures was based on a number of meth-odological and theoretical criteria We avoided tests that weremultidetermined and favored those constructed to reduce contri-bution from cognitive capabilities other than the ones that the testintended to measure As an example we selected a word-listmemory test which controls the encoding of orientation cues thatreduce the effects of attentional or semantic problems on episodicmemory We also included measures of different cognitive pro-cesses within each large domain For instance we used bothsemantic and phonological tests of language domains and wemeasured different attentional control processes within the exec-utive domain Based on these criteria 10 tests were selected tomeasure episodic memory working memory and executive func-tions language and perception Two tests were used for episodicmemory One was a text memory measure constructed to containan equivalent number of details (the microstructure of the text) andgeneral ideas (the macrostructure of the text) The other was aword-list memory test that provides semantic orientation at encod-ing and includes both a free- and a cued-recall procedure Thethree executive functioning and working memory tasks we usedreflected different attentional control functions that were shown to
be differentially impaired in MCI switching divided attentionand online manipulation of information The two language teststarget the phonological (rhyme judgment) or the semantic (objectnaming) dimensions of language Finally we used three subtests ofthe Birmingham Object Recognition Battery which measure spa-tial and configural low-level aspects of perception (orientationposition of gap) and perceptual knowledge of an objectrsquos visualform (object decision subtest)
Thus the goals of this study were to compare cognition in stableand progressive MCI to determine a set of cognitive tests thataccurately differentiate between MCI persons who will remainstable and those who will progress to dementia to estimate diag-nostic accuracy with sensitivity specificity and predictive mea-sures and to compare accuracy between tests This study has anumber of added or innovative components relative to previouslypublished studies The first important element is that our batterywas designed to optimize sensitivity and specificity by includingboth memory and nonmemory tasks Second only a few studieshave reported a range of predictive diagnostic indices for theirpredictors and it is therefore unclear whether tests that differ at thegroup level allow individual classification A third major strengthwas relying on a prospective design as the majority of previousstudies have been retrospective One consequence of retrospectivestudies is that they rely on the same neuropsychological battery fordiagnosis and prediction andor they use a very restricted set oftests to measure progression Using a prospective design where thereference standard is determined independently from the predictivetests is of paramount importance because one is likely to find arelation among test scores used at successive times which artifi-cially increases their predictive value (see Tierney et al 1996 fora discussion) The patients received follow-up over up to 8 yearsto identify those who have entered a state of dementia Finally themajority of studies relied on clinical tests that are multideterminedand weak in terms of theoretical validity This is a drawback asincreasingly sophisticated tests are being developed Therefore werelied on more recent theoretically based measures Cognitivetests were expected to have a high predictive diagnostic value andit was expected that combining episodic memory and nonmemorydomains would provide an optimal cognitive algorithm to predictprogression to AD because they reflect different components of theneurobiological defect
Method
Participants
One hundred twenty-two participants with MCI were recruitedfrom different university-affiliated memory clinics in the Montrealarea At study entry all participants fulfilled criteria for amnesticsingle-domain MCI or amnestic multiple-domain MCI (Petersen2003) based on clinical and neuropsychological information (seeTable 1) Compared to normative values participants performed15 SD below the average level on at least one memory test(single-domain amnestic MCI) or on at least one memory test plusother tests (multiple-domain amnestic MCI) Participants did notmeet the DSMndashIV clinical criteria for dementia of the Alzheimertype at entry and they scored above the age- and education-adjusted cutoffs for dementia on the MMSE and MDRS Theircognitive difficulties had no significant impact on their functional
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
644 BELLEVILLE GAUTHIER LEPAGE KERGOAT AND GILBERT
independence as assessed through clinical interviews with thepatients and spouses and with activity of daily living scales Allparticipants were Francophone with normal or corrected visionand audition and made no use of psychotropic medication knownto impair cognition No participants were on acetylcholinesteraseinhibitors or memory-enhancing medications We excluded partic-ipants who reported major medical conditions those with presenceor history of alcoholism substance abuse severe psychiatric dis-
orders significant cerebrovascular neurological or neurodegen-erative disorders stroke or large-vessel disease or general anes-thesia in the last 6 months The Hachinski scale was used todocument cerebrovascular health (see Table 2) but not as anexclusion tool As shown on Table 2 participants showed very lowHachinski scores Approval was obtained according to the decla-ration of Helsinki and approval from the Ethical Committee of theInstitution in which the study was carried on
Table 1Testquestionnaires Used As Clinical Measures
Test Reference
Mini Mental State Evaluation (MMSE) Folstein M F Folstein S E amp McHugh P R (1975) ldquoMini-mental staterdquo A practical method forgrading the cognitive state of patients for the clinician Journal of Psychiatric Research 12189ndash198
Mattis Dementia Rating Scale (MDRS) Mattis S (1976) Mental status examination for organic mental syndrome in the elderly patient In RBellak amp T B Karasu (Eds) Geriatric psychiatry New York NY Grune amp Stratton
Functional Independence scale (Systegraveme demesure de lrsquoautonomie fonctionnelleSMAF)
Desrosiers J Bravo G Hebert R amp Dubuc N (1995) Reliability of the revised functionalautonomy measurement system (SMAF) for epidemiological research Age and Ageing 24402ndash406
RLRI 16 Free and Cued Recall Task Van der Linden M Adam S Agniel A Baisset-Mouly C amp Members of GREMEM (2004)Lrsquoeacutevaluation de troubles de la meacutemoire preacutesentation de quatre tests de meacutemoire eacutepisodique (aveceacutetalonnage) Marseille France Solal
Text Memory of the BEM-144 Signoret J L (1991) Batterie drsquoefficience mneacutesique BEM 144 Paris France ElsevierRey Figure Rey A (1959) Test de copie drdquoune figure complexe Manuel Paris France Les Eacuteditions du Centre
de Psychologie AppliqueacuteeStroop-Victoria Regard M (1981) Cognitive rigidity and flexibility A neuropsychological study (Doctoral
dissertation) University of Victoria CanadaCode subtest of the WAIS-R Wechsler D (1997) Wechsler Adult Intelligence Scale (3rd ed) San Antonio TX PearsonJudgment of line orientation Benton A L Hamsher K Varney N R amp Spreen O (Eds) (1983) Contributions to
neuropsychological assessment New York NY Oxford University PressBoston Naming Test Kaplan E F Goodglass H amp Weintraub S (1983) The Boston Naming Test (2nd ed)
Philadelphia PA Lea amp FebigerGeriatric Depression scale (GDS) Yesavage J A (1988) Geriatric Depression Scale Psychopharmacology Bulletin 24 709ndash711Hachinski scale Hachinski V C Iliff L D Zilhka E Du Boulay G H McAllister V L Marshall J
Symon L (1975) Cerebral blood flow in dementia Archives of Neurology 32 632ndash637
Table 2Clinical and Demographic Characteristics of the Participants (Standard Deviation inParentheses)
Stable MCI(n 33)
Progressors(n 59)
Effect size(Partial eta2)
Sex 64 women 60 womenAge 664 (91) 705 (79) 0054Years of education 157 (36) 145 (44) 0020SMAF (functional impact) 08 (07) 09 (07) 0011MMSE (max 30) 288 (11) 274 (19) 0137MDRS (max 144) 1394 (32) 1339 (54) 0241RLRI (delayed recall) (max 16) 121 (21) 75 (38) 0317BEM (delayed recall) (max 12) 73 (18) 51 (25) 0179Rey Figurerecall (max 36) 137 (63) 96 (53) 0111Rey Figurecopy (max 36) 306 (36) 298 (47) 0008Coding 102 (23) 89 (25) 0056Stroop (seconds) 315 (95) 372 (128) 0051Boston Naming Test (max 15) 136 (13) 122 (17) 0169Judgment of line orientation (max 30) 234 (4) 223 (48) 0012Geriatric Depression scale (max 15) 34 (27) 39 (37) 0006Hachinski scale 22 (21) 2 (15) 0003
Note SMAF Functional independence scale (Systegraveme de mesure de lrsquoautonomie fonctionnelle) MMSE Mini Mental State Evaluation MDRS Mattis dementia rating scale RLRI 16 free and cued recall task(Rappel libreindiceacute) BEM Text Memory of the BEM-144 (Batterie drsquoeacutevaluation de la meacutemoire) p 05 p 01 p 001 for the group difference
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
645PREDICTING DECLINE IN MCI
Predictive Battery
Episodic memory In the MEMO-TEXT (Geacutely-NargeotCadilhac Touchon amp Nespoulous 1997) a short story with asmany details (microelements) as general ideas (macroelements)was visually presented for a 3-min study period This was followedby an immediate and 10-min delayed recall In the Free and CuedRecall Test (Chatelois et al 1993 Mottron Morasse amp Belleville2001) 15 words were presented in a 3 5 visual matrix Wordswere encoded by their semantic category (eg show me the veg-etable) Free and category-cued recall was asked following a 45-sbackward counting
Working memory (WM) and executive functions In theadapted Brown-Peterson (Belleville Peretz amp Malenfant 1996Bherer Belleville amp Peretz 2001 Chatelois et al 1993) partic-ipants recalled 12 series of auditory consonant trigrams followingdelays of 0 10 20 or 30 sec filled with an addition task Theswitching procedure (Belleville Bherer Lepage Chertkow ampGauthier 2008) involved switching from adding to subtracting twoseries of digit pairs There were two 30-trial nonswitch blocks (onefor addition and one for subtraction) and two 74-trial switchblocks In the alpha span procedure (Belleville Rouleau amp Caza1998) participants were presented with 20 span-adjusted series ofwords that they were instructed to either report in the order ofpresentation or to mentally rearrange the words and report them inalphabetical order
Language Naming was measured with 80 line-drawings ofobjects (DOndash80 Deloche amp Hannequin 1997) A visual rhymejudgment task was also used in which participants were asked tojudge whether two written disyllabic nonwords rhymed or not(Belleville Caza amp Isabelle 2003)
Visuospatial processing We used three subtests of the Bir-mingham Object Recognition Battery (BORB Riddoch amp Hum-phreys 1993) In the orientation match test participants deter-mined if pairs of lines were parallel In the position of gap matchtest participants determined if pairs of truncated circles had theirgap in the same position In the object decision subtest partici-pants determined if drawings of tools or animalsmdashhalf of whichwere constructed by combining parts of two different objects oranimalsmdashwere real
Design
At study entry persons with MCI completed the clinical testsquestionnaires the clinical neuropsychology battery and the pre-dictive battery (see Figure 1) Clinical and experimental tests weredone in separate sessions Participants were then invited for ayearly clinical assessment to determine whether they had pro-gressed from MCI to AD or in their symptom severity At eachfollow-up clinical information was used by clinicians (SG MJKBG) to determine whether participants were stable or had pro-gressed to dementia Clinical diagnosis was established indepen-dently of the results from the predictive battery and cliniciansinvolved in the diagnosis were unaware of the results from thepredictive battery at the time of diagnosis Patients were identifiedas having progressive MCI (pMCI) if they met the current clinicalDSMndashIV criteria for dementia of the Alzheimer type or if theyshowed a significant decline on tests from the clinical batteryParticipants showing a significant decline had a cognitive profileconsistent with that of MCI However they showed an annual
reduction in performance that was larger than one SD unit (SD wastaken from the performance of a group of approximately 100healthy older adults tested in our laboratory on the same task) onmore than one clinical test This criterion was used because itrepresents a large effect size (8) and is more than 10 timesgreater than the annual decline reported by healthy older adults(approximately 002 SD annual decline for memory and approxi-mately 008 SD for speed of processing Bennett et al 2002)Persons showing no progression to dementia and no decline wereidentified as having stable MCI (sMCI)
Statistical Analysis
ANOVAs or t tests were used to compare pMCI and sMCI atbaseline on demographic characteristics clinical questionnairesclinical neuropsychology tests and tests from the predictor batteryWe used backward logistic regression to determine which testfrom the predictive battery predicted progression As there weremany possible dependent variables for each test it was necessaryto select those that were to be included in the model The variableswere selected based on their theoretical value and only one vari-able was chosen to reflect each cognitive test (eg we avoidedusing both the RTs and correct responses for the same condition)We also used the correlation matrix to exclude variables thatreflected one cognitive domain and that were highly correlated(r 8) Group membership (pMCI vs sMCI) at follow-up wasused as the reference standard Sociodemographic variables thatdiffered across groups were used as covariates This is anexploratory analysis as we made no a priori assumptions re-garding the predictive strength of the tests The analysis pro-vides a number of diagnosis accuracy measures sensitivity
Figure 1 Design of the study
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
646 BELLEVILLE GAUTHIER LEPAGE KERGOAT AND GILBERT
which refers to the percentage of times that performance on thederived predictive tests was abnormal at baseline among pMCIpersons specificity which refers to the percentage of time thatperformance on the derived predictive tests was normal at baselineamong sMCI persons overall accuracy which refers to caseswhere performance on those tests matches clinical diagnosis pos-itive predictive value (PPV) which refers to the percentage oftimes that a clinical diagnosis of pMCI was given based onabnormal performance on predictive tests and negative predictivevalue (NPV) which refers to the percentage of times that theclinical diagnosis was sMCI based on normal performance onpredictive tests The final model was the one that optimizedsensitivity and specificity and gave the best overall diagnosticaccuracy The Kaplan-Meier method measured the probability ofcrossover at designated time intervals as a function of wherepatients stood in the score distribution Scores on measures iden-tified as predictors in the regression analysis were used to stratifypatients in tertiles with the Kaplan-Meier Log-rank was used toassess whether the survival curves of the three tertile groupsdiffered in terms of progression rate All analyses were performedwith the SPSS-20 package
Results
Sociodemographic and Clinical Characteristics
Ten persons were excluded based on the clinical assessment asthey did not meet inclusion criteria and five persons withdrewconsent prior to being tested with the predictive battery (see Figure1) Fifteen additional persons withdrew consent during the follow-up Causes of withdrawal included loss of interest in the researchmoving to another town and death Persons who withdrew consentdid not differ from those remaining in the study on sociodemo-graphic and measures of global cognition variables Fifty-ninepersons were identified as pMCI and 33 as sMCI pMCI partici-pants were identified as progressors on average 3081 months afterentry (SD 20) Follow-up was interrupted after pMCI convertedto dementia Mean follow-up for sMCI was 5673 months (SD 232) sMCI and pMCI groups were equivalent on clinical ques-tionnaires and on sociodemographic characteristics except for ageas pMCI participants were older than sMCI participants ThepMCI group showed worse performance than sMCI participants onmost clinical neuropsychology measures (see Table 2) AmongpMCI participants 40 (678) presented with single-domain am-
Table 3Performances on the Predictive Battery (Standard Deviation in Parentheses) and Cut-Off Valuesto Optimize Diagnostic Accuracy on the Individual Cognitive Tests Kept by theRegression Model
Stable MCI Progressors Cut-off value
Episodic memory tasksMEMO-TEXT (max 24)
Macro-elements immediate 179 (33) 144 (4)Micro-elements immediate 114 (37) 69 (48)Macro-elements delayed 168 (32) 128 (43) 13Micro-elements delayed 103 (41) 52 (41)
Free and Cued recall test (max 15)Free recall 83 (28) 52 (23) 6Free and category cued recall 125 (24) 94 (32)
Working memory and executivefunctions
Brown Peterson - Items recalled (max9 ndash max 36 for total)
0-sec delay 84 (1) 84 (11)10-sec delay 67 (19) 57 (24)20-sec delay 62 (23) 47 (27)30-sec delay 65 (25) 56 (24)Total items recalled 277 (6) 244 (65)
Alpha span - Items recalled (max 100)Items direct 79 (143) 744 (197)Items alpha 611 (175) 509 (174) 58Manipulation cost 221 (188) 302 (197)
Switching task cost on errorsGlobal Switch 001 (033) 004 (034)Local Switch 011 (225) 029 (398)
Language and Visuo-spatial tasksDO80 (max 80) 785 (18) 768 (4) 78Rhyme judgment (max 32) 288 (33) 29 (28)BORB
Line judgment test (max 30) 253 (18) 247 (22)Circle test (max 30) 351 (27) 334 (29) 25Object decision test (max 32) 299 (19) 287 (28) 29
Note MEMO-TEXT Text Memory DO80 Denomination Object 80 items BORB BirminghamObject Recognition Battery
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
647PREDICTING DECLINE IN MCI
nestic MCI at entry and 19 with multiple-domain amnestic MCI(322) Among sMCI participants 19 presented with single-domain amnestic MCI (576) and 14 with multiple-domainamnestic MCI (424)
Group Comparisons on Predictive Battery
Table 3 reports performances of sMCI and pMCI on the pre-dictive battery In some cases technical problems prevented test-ing or data collection for some of the participants The N on whichthe analysis was done is thus provided in parentheses for each test
Episodic memory A Group Delay Type of elementANOVA on the number of items recalled from the MEMO-TEXT(pMCI 53 sMCI 32) indicated significant effects of theDelay F(1 88) 49747 p 0001 2 361 Type of elementF(1 88) 351247 p 0001 2 800 and Group F(1 88) 30553 p 0001 2 258 Recall was lower for the delayedthan immediate recall for micro- than macroelements and forpMCI than sMCI The Group Recall Condition ANOVA on thenumber of words recalled from the Free and Cued-recall test(pMCI 53 sMCI 32) indicated significant effects of theGroup F(1 83) 30712 p 0001 2 270 and Recallcondition F(1 83) 322938 p 0001 2 796 There werefewer words recalled in the Free than Cued condition and in pMCIthan sMCI All effects remained significant when correcting formultiple comparisons
WM and executive functions The Group Delay ANOVAon the number of correct items of the Brown-Peterson procedure(pMCI 58 sMCI 33) indicated a main Group F(1 89) 5568 p 005 2 06 and Delay effect F(3 267) 47983p 00001 2 35 Fewer items were recalled by pMCI thansMCI and fewer in the trials with longer delays The group effectwas no longer significant when correcting for multiple compari-son The Group Recall type ANOVA on the of recalled itemsfrom the alpha span (pMCI 57 sMCI 33) indicated a maineffect of Recall F(1 88) 146720 p 0001 2 625 witha lower recall in the alphabetical than direct condition and a mainGroup effect F(1 88) 4527 p 05 2 049 with pMCIrecalling fewer items than sMCI The group effect was no longersignificant when correcting for multiple comparison A manipula-tion cost score the of loss incurred by alphabetical recall[(direct alpha)direct] revealed a significant Group dif-ference as pMCI showed a larger manipulation cost than sMCI
t(88) 1914 p 05 2 04 This remained significant whencorrecting for multiple comparison There was no significanteffect or interaction on global or local switch cost definedrespectively as the number of errors on switch minus nonswitchblock and errors on switch trials minus nonswitch trials F13in all cases (pMCI 57 sMCI 33)
Language No group differences were found on the number ofcorrect responses for the rhyme judgment test t(86) 0340 2 001 However pMCI showed a lower number of correct responsesthan sMCI on the DO-80 naming test t(90) 2327 p 052 057 (pMCI 59 and 55 respectively sMCI 33) and thisremained significant when correcting for multiple comparison
Visuospatial processing No group differences were foundon the orientation match t(85) 1175 2 016 HoweverpMCI obtained a lower score than sMCI on the position of gapt(85) 2637 p 01 2 076 and object decisiont(85) 2329 p 05 2 060 tests (pMCI 54 sMCI 33) The effect remained significant when correcting for mul-tiple comparisons on position gap but not on object decision
Regression Analysis
The age-adjusted logistic model with the best overall diag-nostic accuracy was obtained after five iterations and wascomposed of six variables The strongest predictors were de-layed recall of macro elements of the MEMO-TEXT and freerecall of words The model also retained object naming (DO-80) orientation match (BORB) object decision (BORB) andalpha span (see Table 4) Odd ratios range from 1033 (for thealpha span) to 1689 (for free recall of words) The overallclassification success was 877 The model yielded high sensi-tivity and specificity values (88 and 871 respectively Table5) and excellent positive predictive value (PPV 818) andnegative predictive value (NPV 917)
Survival analyses (see Figure 2) indicated that those perform-ing in the lowest and middle tertiles on the MEMO-TEXT freerecall and alpha span showed faster progression than those inthe highest tertile Furthermore those performing in the lowesttertile on the naming test showed a faster progression rate thanthose performing in the middle and highest tertiles The differ-ence in decline as a function of tertile indicates that the first twotasks are more sensitive to the disease than is naming Nodifferences were found across tertiles for the object decisionand orientation match tests suggesting that when used on their
Table 4Logistic Regression Models on the Predictive Battery
PREDICTORS SE Waldrsquos 2 df pe
(odds ratio)
Age 005 048 011 1 918 995MEMO-TEXT 236 113 4377 1 036 1266delayed macroFree recall 496 171 8386 1 004 1643DO 80 181 147 1501 1 221 1198BORBndashLine judgment 379 243 2439 1 118 1461BORBndashObject decision 251 174 2095 1 148 1286Alpha span 031 021 2097 1 148 1031Constant 9566 4023 5654 1 017 NA
Note MEMO-TEXT Text Memory DO80 Denomination Object80 items BORB Birmingham Object Recognition Battery
Table 5Observed and Predicted Frequencies for the PredictiveDiagnostic Accuracy Provided by the Logistic Regression ModelWith a 060 Cutoff
Predicted
Observed Yes No Correct
Yes 44 6 88No 4 27 871 correct 917 818 877
Note Sensitivity 44(44 6) 88 Specificity 27(27 4) 871 False positive 4(4 44) 83 False negative 6(6 27) 182
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
648 BELLEVILLE GAUTHIER LEPAGE KERGOAT AND GILBERT
own these two tasks lack sensitivity This analysis also showsdifferences across tasks in sensitivity to time of progression Bythe 40-month follow-up 80 of those in the lowest tertile ofMEMO-TEXT had converted to dementia This was found 60and 80 months after follow-up among those in the lowest tertileof free recall and alpha-span respectively
Discussion
Not all MCI cases progress to dementia and it is critical toidentify tests that accurately predict future progression In this
study we found that combining tests of episodic memory (text andword recall) perception (naming orientation and object decision)and working memory (alpha span) correctly identifies 878 ofparticipants who will progress on an average of 45 years inadvance The six-test model yielded very good to excellent sensi-tivity and specificity values as both of them were above 85 Thiswas also the case for PPN and NPV values and in particular it wasfound that 917 of those found unimpaired on the tests remainedstable in spite of the fact they met clinical criteria for MCI Thusthis combination of measures is not only sensitive but it is also
Figure 2 Survival analyses
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
649PREDICTING DECLINE IN MCI
specific and it helps to identify those who are unlikely to progressThis is highly important for clinical trials as it can help identify theMCI persons who are most likely to benefit from disease-modifying therapies Survival analyses indicate that 80 of thepatients performing in the lowest tertile of the MCI group on thetext memory test will have developed dementia 40 months later
This study suggests that relying only on episodic memory mea-sures might not be optimal and that measuring different domains ofcognition represents the most balanced approach Several studieshave investigated the capacity of biological and cognitive mea-sures to predict future progression from MCI to dementia A firstimportant conclusion from many of these studies is that the patternof cognitive deficit might be as accurate as biological measures inpredicting future decline in MCI (Albert et al 2011 Dubois et al2007) a conclusion coherent with our finding of a strong predic-tive accuracy for the cognitive battery used here Another impor-tant conclusion is that it is possible to identify an optimal set ofcognitive tasks Studies vary in their design statistical approachand follow-up length and there is great variability in the cognitivetests used Nevertheless a coherent pattern seems to emerge fromprevious studies which is supported by our findings First itappears that combining episodic memory tests with tasks that relyon executive functions or the attentional control of WM is partic-ularly powerful for predicting conversion from MCI to dementia(Aretouli Tsilidis amp Brandt 2013 Chapman et al 2011 Conde-Sala et al 2012 Gavett et al 2010 Rabin et al 2009 Summersamp Saunders 2012) Second studies that measured only one or twocognitive domains have much lower predictive accuracy than theone found here They report either lower specificity (eg Mitchellet al 2009) or lower sensitivity (Dierckx et al 2009 Tabert et al2006 Tierney et al 1996) than what is reported here This isconsistent with studies indicating that cases of multiple-domainMCI are more likely to progress to dementia than single-domainMCI (Forlenza et al 2009 Nordlund et al 2010 RasquinLodder Visser Lousberg amp Verhey 2005 Summers amp Saunders2012) Our study indicates that an optimal battery should includeperceptual tests in addition to tests of episodic memory executivefunction and working memory The particular cognitive domainsidentified here match well with findings indicating that in additionto episodic memory semantic knowledge and working memoryare impaired early in AD (for a review see Belleville et al 2008)
Few studies have included perceptual or semantic componentsin their models contrary to this study and those that did measureda relatively small number of components It is therefore possiblethat measures of the perceptual or semantic domains have im-proved predictive accuracy However these tasks may be morespecific than sensitive Indeed our survival analyses suggest thatnaming and perceptual tasks were not as sensitive to future declineas episodic memory and executive tasks when taken on their ownIncluding measures of the perceptual or semantic domain mightcontribute to reducing the number of false positives hence increas-ing specificity This is a potentially useful finding for cliniciansand researchers When optimizing testing time is a critical issueand tasks need to be selected one can base the decision on whetherthe need is to have a more sensitive or more specific battery
This study is among those showing the best combination ofsensitivity and specificity values Perhaps inclusion of morenonmemory tests might have increased specificity and use of a
relatively long follow-up period likely reduced the number offalse negatives hence increasing sensitivity Another differencebetween this study and the current literature is that we did notrely on clinical measures but on theoretically motivated onesThus if selected well a relatively short battery of tests canpredict future decline in MCI and can help identify persons thatare likely to progress to more severe symptoms
The study resulted in a number of additional findings whichdeserve discussion One is that at entry progressive MCIpatients already differ from stable MCI patients in terms of ageand cognitive performance on several clinical tests Becausepatients are likely to vary in their decline rate and in their stageat entry it is possible that progressors are in a more advancedstage of neuropathology than persons with stable MCI and thatthe latter would decline later Thus a portion of stable MCIpatients may still actually be predementia (thus false negative)It is important to note however that this study makes use of amuch longer follow-up than is typically used in similar studiesStable MCI patients were followed for an average of 567months which is much longer than the period after whichprogressors converted to dementia (on average 308 monthsafter entry) This long follow-up probably reduced the contri-bution of ldquofalse negativesrdquo to the group of those with stableMCI by increasing the chance of progression during the studyperiod Admittedly it remains possible that some of the stableMCI patients will progress to dementia in the future Howeverwe do not believe that this represents a substantial portion ofour participants with stable MCI It is interesting that thefinding that the two groups differ on clinical measures is in factgood news as it supports our contention that cognitive mea-sures are sensitive to prognosis and will prove critical in iden-tifying the patients more likely to progress to dementia
This study has limitations which should be recognized Firstto improve generalizability the findings should be reproducedon a different sample Second we did not include biomarkers orimaging parameters in this study Our goal was to identify theideal set of cognitive measures and for future studies it will beimportant to assess the value of combining them with biologicalmarkers Finally it is important to point out that there might bedifferences between this cohort of patients and patients encoun-tered in other clinical settings In particular our exclusioncriteria might have led to a cohort with relatively few cases ofcomorbidity
References
Ahmed S Mitchell J Arnold R Nestor P J amp Hodges J R (2008)Predicting rapid clinical progression in amnestic mild cognitive impair-ment Dementia and Geriatric Cognitive Disorders 25 170ndash177 doi101159000113014
Albert M S DeKosky S T Dickson D Dubois B Feldman H HFox N C Phelps C H (2011) The diagnosis of mild cognitiveimpairment due to Alzheimerrsquos disease Recommendations from theNational Institute on Aging-Alzheimerrsquos Association workgroups ondiagnostic guidelines for Alzheimerrsquos disease Alzheimers amp Dementia7 270ndash279 doi101016jjalz201103008
Aretouli E Tsilidis K K amp Brandt J (2013) Four-year outcome ofmild cognitive impairment The contribution of executive dysfunctionNeuropsychology 27 95ndash106 doi101037a0030481
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
650 BELLEVILLE GAUTHIER LEPAGE KERGOAT AND GILBERT
Artero S Tierney M C Touchon J amp Ritchie K (2003) Prediction oftransition from cognitive impairment to senile dementia A prospectivelongitudinal study Acta Psychiatrica Scandinavica 107 390ndash393
Beacutelanger S amp Belleville S (2009) Semantic inhibition impairment inmild cognitive impairment A distinctive feature of upcoming cognitivedecline Neuropsychology 23 592ndash606 doi101037a0016152
Belleville S Bherer L Lepage Eacute Chertkow H amp Gauthier S (2008)Task switching capacities in persons with Alzheimerrsquos disease and mildcognitive impairment Neuropsychologia 46 2225ndash2233 doi101016jneuropsychologia200802012
Belleville S Caza N amp Peretz I (2003) A neuropsychological argu-ment for a processing view of memory Journal of Memory and Lan-guage 48 686ndash703 doi101016S0749-596X(02)00532-6
Belleville S Chertkow H amp Gauthier S (2007) Working memory andcontrol of attention in persons with Alzheimerrsquos disease and mild cog-nitive impairment Neuropsychology 21 458ndash469 doi1010370894-4105214458
Belleville S Meacutenard M C De Boysson C amp Sylvain-Roy S (2008)Characterizing memory deficits in mild cognitive impairment In WSossin J C Lacaille V Castellucci amp S Belleville (Eds) The essenceof memory (pp 365ndash375) Amsterdam Netherlands Elsevier doi101016S0079-6123(07)00023-4
Belleville S Peretz I amp Malenfant D (1996) Examination of theworking memory components in normal aging and in dementia of theAlzheimer type Neuropsychologia 34 195ndash207 doi1010160028-3932(95)00097-6
Belleville S Rouleau N amp Caza N (1998) Effect of normal aging onthe manipulation of information in working memory Memory amp Cog-nition 26 572ndash583 doi103758BF03201163
Bennett D A Wilson R S Schneider J A Evans D A BeckettL A Aggarwal N T Bach J (2002) Natural history of mildcognitive impairment in older persons Neurology 59 198ndash205
Bherer L Belleville S amp Peretz I (2001) Education age and theBrown-Peterson technique Developmental Neuropsychology 19 237ndash251 doi101207S15326942DN1903_1
Chapman R M Mapstone M McCrary J W Gardner M N Por-steinsson A Sandoval T C Reilly L A (2011) Predictingconversion from mild cognitive impairment to Alzheimerrsquos diseaseusing neuropsychological tests and multivariate methods Journal ofClinical and Experimental Neuropsychology 33 187ndash199 doi101080138033952010499356
Chatelois J Pineau H Belleville S Peretz I Lussier I FontaineF-S amp Renaseau-Leclerc C (1993) Batterie informatiseacutee drsquoeacutevaluationde la meacutemoire inspireacutee de lrsquoapproche cognitive Canadian PsychologyPsychologie Canadienne 34 45ndash63 doi101037h0078803
Conde-Sala J L Garre-Olmo J Vilalta-Franch J Llinas-Regla JTurro-Garriga O Lozano-Gallego M Loacutepez-Pousa S (2012)Predictors of cognitive decline in Alzheimerrsquos disease and mild cogni-tive impairment using the CAMCOG A five-year follow-up Interna-tional Psychogeriatrics 24 948ndash958 doi101017S1041610211002158
Deloche G amp Hannequin D (1997) Test de deacutenomination oraledrsquoimages (DO-80) Paris France Centre de Psychologie Appliqueacutee
Dierckx E Engelborghs S De Raedt R Van Buggenhout M DeDeyn P P Verte D amp Ponjaert-Kristoffersen I (2009) Verbal cuedrecall as a predictor of conversion to Alzheimerrsquos disease in mildcognitive impairment International Journal of Geriatric Psychiatry 241094ndash1100 doi101002gps2228
Dubois B Feldman H H Jacova C Dekosky S T Barberger-Gateau P Cummings J Scheltens P (2007) Research criteriafor the diagnosis of Alzheimerrsquos disease Revising the NINCDS-ADRDA criteria Lancet Neurology 6 734 ndash746 doi101016S1474-4422(07)70178 ndash3
Forlenza O V Diniz B S Nunes P V Memoria C M YassudaM S amp Gattaz W F (2009) Diagnostic transitions in mild cognitive
impairment subtypes International Psychogeriatrics 21 1088ndash1095doi101017S1041610209990792
Gauthier S Reisberg B Zaudig M Petersen R C Ritchie K BroichK Winblad B (2006) Mild cognitive impairment The Lancet 3671262ndash1270 doi101016S0140-6736(06)68542-5
Gavett B E Ozonoff A Doktor V Palmisano J Nair A K GreenR C Stern R A (2010) Predicting cognitive decline and conver-sion to Alzheimerrsquos disease in older adults using the NAB List Learningtest Journal of the International Neuropsychological Society 16 651ndash660 doi101017S1355617710000421
Geacutely-Nargeot M-C Cadilhac C Touchon J amp Nespoulous J L(1997) La meacutemoire de textes chez les sujets sains et deacutements Appli-cation drsquoun nouvel outil drsquoeacutevaluation pour neuropsychologues Meacutemo-textes In J Lambert amp J L Nespoulous (Eds) Perception auditive etcompreacutehension du langage (pp 273ndash293) Marseille France Solal
Geroldi C Rossi R Calvagna C Testa C Bresciani L Binetti G Frisoni G B (2006) Medial temporal atrophy but not memorydeficit predicts progression to dementia in patients with mild cognitiveimpairment Journal of Neurology Neurosurgery amp Psychiatry 771219ndash1222 doi101136jnnp2005082651
Irish M Lawlor B A Coen R F amp OrsquoMara S M (2011) Everydayepisodic memory in amnestic mild cognitive impairment A preliminaryinvestigation BMC Neuroscience 12 80 doi1011861471-2202-12-80
Ivanoiu A Adam S Van der Linden M Salmon E Juillerat A CMulligan R amp Seron X (2005) Memory evaluation with a new cuedrecall test in patients with mild cognitive impairment and Alzheimerrsquosdisease Journal of Neurology 252 47ndash55 doi101007s00415-005-0597-2
Landau S M Harvey D Madison C M Reiman E M Foster N LAisen P S Jagust W J (2010) Comparing predictors of conver-sion and decline in mild cognitive impairment Neurology 75 230ndash238doi101212WNL0b013e3181e8e8b8
Lekeu F Magis D Marique P Delbeuck X Bechet S GuillaumeB Salmon E (2010) The California Verbal Learning Test andother standard clinical neuropsychological tests to predict conversionfrom mild memory impairment to dementia Journal of Clinical andExperimental Neuropsychology 32 164 ndash173 doi10108013803390902889606
Mitchell J Arnold R Dawson K Nestor P J amp Hodges J R (2009)Outcome in subgroups of mild cognitive impairment (MCI) is highlypredictable using a simple algorithm Journal of Neurology 256 1500ndash1509 doi101007s00415-009-5152-0[doi]
Mottron L Morasse K amp Belleville S (2001) A study of memoryfunctioning in individuals with autism Journal of Child Psychology andPsychiatry 42 253ndash260 doi1011111469-761000716
Nordlund A Rolstad S Klang O Edman A Hansen S amp Wallin A(2010) Two-year outcome of MCI subtypes and aetiologies in theGoteborg MCI study Journal of Neurology Neurosurgery amp Psychia-try 81 541ndash546 doi101136jnnp2008171066
Petersen R C (2003) Mild cognitive impairment Aging to Alzheimerrsquosdisease Oxford UK Oxford University Press
Petersen R C amp Morris J C (2003) Clinical features In R C Petersen(Ed) Mild cognitive impairment Aging to Alzheimerrsquos disease (pp15ndash39) Oxford UK Oxford University Press
Rabin L A Pare N Saykin A J Brown M J Wishart H AFlashman L A amp Santulli R B (2009) Differential memory testsensitivity for diagnosing amnestic mild cognitive impairment and pre-dicting conversion to Alzheimerrsquos disease Neuropsychology Develop-ment and Cognition Section B Aging Neuropsychology and Cognition16 357ndash376 doi10108013825580902825220
Rasquin S M Lodder J Visser P J Lousberg R amp Verhey F R(2005) Predictive accuracy of MCI subtypes for Alzheimerrsquos diseaseand vascular dementia in subjects with mild cognitive impairment A
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
651PREDICTING DECLINE IN MCI
2-year follow-up study Dementia and Geriatric Cognitive Disorders19 113ndash119 doi101159000082662
Riddoch J M amp Humphreys G W (1993) BORB Birmingham ObjectRecognition Battery Hove UK Erlbaum
Ritchie K Artero S amp Touchon J (2001) Classification criteria formild cognitive impairment A population-based validation study Neu-rology 56 37ndash42 doi101212WNL56137
Summers M J amp Saunders N L (2012) Neuropsychological measurespredict decline to Alzheimerrsquos dementia from mild cognitive impair-ment Neuropsychology 26 498ndash508 doi101037a0028576
Tabert M H Manly J J Liu X Pelton G H Rosenblum S JacobsM Devanand D P (2006) Neuropsychological prediction of
conversion to Alzheimer disease in patients with mild cognitive impair-ment Archives of General Psychiatry 63 916ndash924 doi101001archpsyc638916
Tierney M C Szalai J P Snow W G Fisher R H Nores A NadonG St George-Hyslop P H (1996) Prediction of probable Alz-heimerrsquos disease in memory-impaired patients A prospective longitu-dinal study Neurology 46 661ndash665 doi101212WNL463661
Received May 15 2013Revision received December 19 2013
Accepted December 22 2013
Members of Underrepresented GroupsReviewers for Journal Manuscripts Wanted
If you are interested in reviewing manuscripts for APA journals the APA Publications andCommunications Board would like to invite your participation Manuscript reviewers are vital to thepublications process As a reviewer you would gain valuable experience in publishing The PampCBoard is particularly interested in encouraging members of underrepresented groups to participatemore in this process
If you are interested in reviewing manuscripts please write APA Journals at ReviewersapaorgPlease note the following important points
bull To be selected as a reviewer you must have published articles in peer-reviewed journals Theexperience of publishing provides a reviewer with the basis for preparing a thorough objectivereview
bull To be selected it is critical to be a regular reader of the five to six empirical journals that are mostcentral to the area or journal for which you would like to review Current knowledge of recentlypublished research provides a reviewer with the knowledge base to evaluate a new submissionwithin the context of existing research
bull To select the appropriate reviewers for each manuscript the editor needs detailed informationPlease include with your letter your vita In the letter please identify which APA journal(s) youare interested in and describe your area of expertise Be as specific as possible For exampleldquosocial psychologyrdquo is not sufficientmdashyou would need to specify ldquosocial cognitionrdquo or ldquoattitudechangerdquo as well
bull Reviewing a manuscript takes time (1ndash4 hours per manuscript reviewed) If you are selected toreview a manuscript be prepared to invest the necessary time to evaluate the manuscriptthoroughly
APA now has an online video course that provides guidance in reviewing manuscripts To learnmore about the course and to access the video visit httpwwwapaorgpubsauthorsreview-manuscript-ce-videoaspx
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
652 BELLEVILLE GAUTHIER LEPAGE KERGOAT AND GILBERT

independence as assessed through clinical interviews with thepatients and spouses and with activity of daily living scales Allparticipants were Francophone with normal or corrected visionand audition and made no use of psychotropic medication knownto impair cognition No participants were on acetylcholinesteraseinhibitors or memory-enhancing medications We excluded partic-ipants who reported major medical conditions those with presenceor history of alcoholism substance abuse severe psychiatric dis-
orders significant cerebrovascular neurological or neurodegen-erative disorders stroke or large-vessel disease or general anes-thesia in the last 6 months The Hachinski scale was used todocument cerebrovascular health (see Table 2) but not as anexclusion tool As shown on Table 2 participants showed very lowHachinski scores Approval was obtained according to the decla-ration of Helsinki and approval from the Ethical Committee of theInstitution in which the study was carried on
Table 1Testquestionnaires Used As Clinical Measures
Test Reference
Mini Mental State Evaluation (MMSE) Folstein M F Folstein S E amp McHugh P R (1975) ldquoMini-mental staterdquo A practical method forgrading the cognitive state of patients for the clinician Journal of Psychiatric Research 12189ndash198
Mattis Dementia Rating Scale (MDRS) Mattis S (1976) Mental status examination for organic mental syndrome in the elderly patient In RBellak amp T B Karasu (Eds) Geriatric psychiatry New York NY Grune amp Stratton
Functional Independence scale (Systegraveme demesure de lrsquoautonomie fonctionnelleSMAF)
Desrosiers J Bravo G Hebert R amp Dubuc N (1995) Reliability of the revised functionalautonomy measurement system (SMAF) for epidemiological research Age and Ageing 24402ndash406
RLRI 16 Free and Cued Recall Task Van der Linden M Adam S Agniel A Baisset-Mouly C amp Members of GREMEM (2004)Lrsquoeacutevaluation de troubles de la meacutemoire preacutesentation de quatre tests de meacutemoire eacutepisodique (aveceacutetalonnage) Marseille France Solal
Text Memory of the BEM-144 Signoret J L (1991) Batterie drsquoefficience mneacutesique BEM 144 Paris France ElsevierRey Figure Rey A (1959) Test de copie drdquoune figure complexe Manuel Paris France Les Eacuteditions du Centre
de Psychologie AppliqueacuteeStroop-Victoria Regard M (1981) Cognitive rigidity and flexibility A neuropsychological study (Doctoral
dissertation) University of Victoria CanadaCode subtest of the WAIS-R Wechsler D (1997) Wechsler Adult Intelligence Scale (3rd ed) San Antonio TX PearsonJudgment of line orientation Benton A L Hamsher K Varney N R amp Spreen O (Eds) (1983) Contributions to
neuropsychological assessment New York NY Oxford University PressBoston Naming Test Kaplan E F Goodglass H amp Weintraub S (1983) The Boston Naming Test (2nd ed)
Philadelphia PA Lea amp FebigerGeriatric Depression scale (GDS) Yesavage J A (1988) Geriatric Depression Scale Psychopharmacology Bulletin 24 709ndash711Hachinski scale Hachinski V C Iliff L D Zilhka E Du Boulay G H McAllister V L Marshall J
Symon L (1975) Cerebral blood flow in dementia Archives of Neurology 32 632ndash637
Table 2Clinical and Demographic Characteristics of the Participants (Standard Deviation inParentheses)
Stable MCI(n 33)
Progressors(n 59)
Effect size(Partial eta2)
Sex 64 women 60 womenAge 664 (91) 705 (79) 0054Years of education 157 (36) 145 (44) 0020SMAF (functional impact) 08 (07) 09 (07) 0011MMSE (max 30) 288 (11) 274 (19) 0137MDRS (max 144) 1394 (32) 1339 (54) 0241RLRI (delayed recall) (max 16) 121 (21) 75 (38) 0317BEM (delayed recall) (max 12) 73 (18) 51 (25) 0179Rey Figurerecall (max 36) 137 (63) 96 (53) 0111Rey Figurecopy (max 36) 306 (36) 298 (47) 0008Coding 102 (23) 89 (25) 0056Stroop (seconds) 315 (95) 372 (128) 0051Boston Naming Test (max 15) 136 (13) 122 (17) 0169Judgment of line orientation (max 30) 234 (4) 223 (48) 0012Geriatric Depression scale (max 15) 34 (27) 39 (37) 0006Hachinski scale 22 (21) 2 (15) 0003
Note SMAF Functional independence scale (Systegraveme de mesure de lrsquoautonomie fonctionnelle) MMSE Mini Mental State Evaluation MDRS Mattis dementia rating scale RLRI 16 free and cued recall task(Rappel libreindiceacute) BEM Text Memory of the BEM-144 (Batterie drsquoeacutevaluation de la meacutemoire) p 05 p 01 p 001 for the group difference
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
645PREDICTING DECLINE IN MCI
Predictive Battery
Episodic memory In the MEMO-TEXT (Geacutely-NargeotCadilhac Touchon amp Nespoulous 1997) a short story with asmany details (microelements) as general ideas (macroelements)was visually presented for a 3-min study period This was followedby an immediate and 10-min delayed recall In the Free and CuedRecall Test (Chatelois et al 1993 Mottron Morasse amp Belleville2001) 15 words were presented in a 3 5 visual matrix Wordswere encoded by their semantic category (eg show me the veg-etable) Free and category-cued recall was asked following a 45-sbackward counting
Working memory (WM) and executive functions In theadapted Brown-Peterson (Belleville Peretz amp Malenfant 1996Bherer Belleville amp Peretz 2001 Chatelois et al 1993) partic-ipants recalled 12 series of auditory consonant trigrams followingdelays of 0 10 20 or 30 sec filled with an addition task Theswitching procedure (Belleville Bherer Lepage Chertkow ampGauthier 2008) involved switching from adding to subtracting twoseries of digit pairs There were two 30-trial nonswitch blocks (onefor addition and one for subtraction) and two 74-trial switchblocks In the alpha span procedure (Belleville Rouleau amp Caza1998) participants were presented with 20 span-adjusted series ofwords that they were instructed to either report in the order ofpresentation or to mentally rearrange the words and report them inalphabetical order
Language Naming was measured with 80 line-drawings ofobjects (DOndash80 Deloche amp Hannequin 1997) A visual rhymejudgment task was also used in which participants were asked tojudge whether two written disyllabic nonwords rhymed or not(Belleville Caza amp Isabelle 2003)
Visuospatial processing We used three subtests of the Bir-mingham Object Recognition Battery (BORB Riddoch amp Hum-phreys 1993) In the orientation match test participants deter-mined if pairs of lines were parallel In the position of gap matchtest participants determined if pairs of truncated circles had theirgap in the same position In the object decision subtest partici-pants determined if drawings of tools or animalsmdashhalf of whichwere constructed by combining parts of two different objects oranimalsmdashwere real
Design
At study entry persons with MCI completed the clinical testsquestionnaires the clinical neuropsychology battery and the pre-dictive battery (see Figure 1) Clinical and experimental tests weredone in separate sessions Participants were then invited for ayearly clinical assessment to determine whether they had pro-gressed from MCI to AD or in their symptom severity At eachfollow-up clinical information was used by clinicians (SG MJKBG) to determine whether participants were stable or had pro-gressed to dementia Clinical diagnosis was established indepen-dently of the results from the predictive battery and cliniciansinvolved in the diagnosis were unaware of the results from thepredictive battery at the time of diagnosis Patients were identifiedas having progressive MCI (pMCI) if they met the current clinicalDSMndashIV criteria for dementia of the Alzheimer type or if theyshowed a significant decline on tests from the clinical batteryParticipants showing a significant decline had a cognitive profileconsistent with that of MCI However they showed an annual
reduction in performance that was larger than one SD unit (SD wastaken from the performance of a group of approximately 100healthy older adults tested in our laboratory on the same task) onmore than one clinical test This criterion was used because itrepresents a large effect size (8) and is more than 10 timesgreater than the annual decline reported by healthy older adults(approximately 002 SD annual decline for memory and approxi-mately 008 SD for speed of processing Bennett et al 2002)Persons showing no progression to dementia and no decline wereidentified as having stable MCI (sMCI)
Statistical Analysis
ANOVAs or t tests were used to compare pMCI and sMCI atbaseline on demographic characteristics clinical questionnairesclinical neuropsychology tests and tests from the predictor batteryWe used backward logistic regression to determine which testfrom the predictive battery predicted progression As there weremany possible dependent variables for each test it was necessaryto select those that were to be included in the model The variableswere selected based on their theoretical value and only one vari-able was chosen to reflect each cognitive test (eg we avoidedusing both the RTs and correct responses for the same condition)We also used the correlation matrix to exclude variables thatreflected one cognitive domain and that were highly correlated(r 8) Group membership (pMCI vs sMCI) at follow-up wasused as the reference standard Sociodemographic variables thatdiffered across groups were used as covariates This is anexploratory analysis as we made no a priori assumptions re-garding the predictive strength of the tests The analysis pro-vides a number of diagnosis accuracy measures sensitivity
Figure 1 Design of the study
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
646 BELLEVILLE GAUTHIER LEPAGE KERGOAT AND GILBERT
which refers to the percentage of times that performance on thederived predictive tests was abnormal at baseline among pMCIpersons specificity which refers to the percentage of time thatperformance on the derived predictive tests was normal at baselineamong sMCI persons overall accuracy which refers to caseswhere performance on those tests matches clinical diagnosis pos-itive predictive value (PPV) which refers to the percentage oftimes that a clinical diagnosis of pMCI was given based onabnormal performance on predictive tests and negative predictivevalue (NPV) which refers to the percentage of times that theclinical diagnosis was sMCI based on normal performance onpredictive tests The final model was the one that optimizedsensitivity and specificity and gave the best overall diagnosticaccuracy The Kaplan-Meier method measured the probability ofcrossover at designated time intervals as a function of wherepatients stood in the score distribution Scores on measures iden-tified as predictors in the regression analysis were used to stratifypatients in tertiles with the Kaplan-Meier Log-rank was used toassess whether the survival curves of the three tertile groupsdiffered in terms of progression rate All analyses were performedwith the SPSS-20 package
Results
Sociodemographic and Clinical Characteristics
Ten persons were excluded based on the clinical assessment asthey did not meet inclusion criteria and five persons withdrewconsent prior to being tested with the predictive battery (see Figure1) Fifteen additional persons withdrew consent during the follow-up Causes of withdrawal included loss of interest in the researchmoving to another town and death Persons who withdrew consentdid not differ from those remaining in the study on sociodemo-graphic and measures of global cognition variables Fifty-ninepersons were identified as pMCI and 33 as sMCI pMCI partici-pants were identified as progressors on average 3081 months afterentry (SD 20) Follow-up was interrupted after pMCI convertedto dementia Mean follow-up for sMCI was 5673 months (SD 232) sMCI and pMCI groups were equivalent on clinical ques-tionnaires and on sociodemographic characteristics except for ageas pMCI participants were older than sMCI participants ThepMCI group showed worse performance than sMCI participants onmost clinical neuropsychology measures (see Table 2) AmongpMCI participants 40 (678) presented with single-domain am-
Table 3Performances on the Predictive Battery (Standard Deviation in Parentheses) and Cut-Off Valuesto Optimize Diagnostic Accuracy on the Individual Cognitive Tests Kept by theRegression Model
Stable MCI Progressors Cut-off value
Episodic memory tasksMEMO-TEXT (max 24)
Macro-elements immediate 179 (33) 144 (4)Micro-elements immediate 114 (37) 69 (48)Macro-elements delayed 168 (32) 128 (43) 13Micro-elements delayed 103 (41) 52 (41)
Free and Cued recall test (max 15)Free recall 83 (28) 52 (23) 6Free and category cued recall 125 (24) 94 (32)
Working memory and executivefunctions
Brown Peterson - Items recalled (max9 ndash max 36 for total)
0-sec delay 84 (1) 84 (11)10-sec delay 67 (19) 57 (24)20-sec delay 62 (23) 47 (27)30-sec delay 65 (25) 56 (24)Total items recalled 277 (6) 244 (65)
Alpha span - Items recalled (max 100)Items direct 79 (143) 744 (197)Items alpha 611 (175) 509 (174) 58Manipulation cost 221 (188) 302 (197)
Switching task cost on errorsGlobal Switch 001 (033) 004 (034)Local Switch 011 (225) 029 (398)
Language and Visuo-spatial tasksDO80 (max 80) 785 (18) 768 (4) 78Rhyme judgment (max 32) 288 (33) 29 (28)BORB
Line judgment test (max 30) 253 (18) 247 (22)Circle test (max 30) 351 (27) 334 (29) 25Object decision test (max 32) 299 (19) 287 (28) 29
Note MEMO-TEXT Text Memory DO80 Denomination Object 80 items BORB BirminghamObject Recognition Battery
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
647PREDICTING DECLINE IN MCI
nestic MCI at entry and 19 with multiple-domain amnestic MCI(322) Among sMCI participants 19 presented with single-domain amnestic MCI (576) and 14 with multiple-domainamnestic MCI (424)
Group Comparisons on Predictive Battery
Table 3 reports performances of sMCI and pMCI on the pre-dictive battery In some cases technical problems prevented test-ing or data collection for some of the participants The N on whichthe analysis was done is thus provided in parentheses for each test
Episodic memory A Group Delay Type of elementANOVA on the number of items recalled from the MEMO-TEXT(pMCI 53 sMCI 32) indicated significant effects of theDelay F(1 88) 49747 p 0001 2 361 Type of elementF(1 88) 351247 p 0001 2 800 and Group F(1 88) 30553 p 0001 2 258 Recall was lower for the delayedthan immediate recall for micro- than macroelements and forpMCI than sMCI The Group Recall Condition ANOVA on thenumber of words recalled from the Free and Cued-recall test(pMCI 53 sMCI 32) indicated significant effects of theGroup F(1 83) 30712 p 0001 2 270 and Recallcondition F(1 83) 322938 p 0001 2 796 There werefewer words recalled in the Free than Cued condition and in pMCIthan sMCI All effects remained significant when correcting formultiple comparisons
WM and executive functions The Group Delay ANOVAon the number of correct items of the Brown-Peterson procedure(pMCI 58 sMCI 33) indicated a main Group F(1 89) 5568 p 005 2 06 and Delay effect F(3 267) 47983p 00001 2 35 Fewer items were recalled by pMCI thansMCI and fewer in the trials with longer delays The group effectwas no longer significant when correcting for multiple compari-son The Group Recall type ANOVA on the of recalled itemsfrom the alpha span (pMCI 57 sMCI 33) indicated a maineffect of Recall F(1 88) 146720 p 0001 2 625 witha lower recall in the alphabetical than direct condition and a mainGroup effect F(1 88) 4527 p 05 2 049 with pMCIrecalling fewer items than sMCI The group effect was no longersignificant when correcting for multiple comparison A manipula-tion cost score the of loss incurred by alphabetical recall[(direct alpha)direct] revealed a significant Group dif-ference as pMCI showed a larger manipulation cost than sMCI
t(88) 1914 p 05 2 04 This remained significant whencorrecting for multiple comparison There was no significanteffect or interaction on global or local switch cost definedrespectively as the number of errors on switch minus nonswitchblock and errors on switch trials minus nonswitch trials F13in all cases (pMCI 57 sMCI 33)
Language No group differences were found on the number ofcorrect responses for the rhyme judgment test t(86) 0340 2 001 However pMCI showed a lower number of correct responsesthan sMCI on the DO-80 naming test t(90) 2327 p 052 057 (pMCI 59 and 55 respectively sMCI 33) and thisremained significant when correcting for multiple comparison
Visuospatial processing No group differences were foundon the orientation match t(85) 1175 2 016 HoweverpMCI obtained a lower score than sMCI on the position of gapt(85) 2637 p 01 2 076 and object decisiont(85) 2329 p 05 2 060 tests (pMCI 54 sMCI 33) The effect remained significant when correcting for mul-tiple comparisons on position gap but not on object decision
Regression Analysis
The age-adjusted logistic model with the best overall diag-nostic accuracy was obtained after five iterations and wascomposed of six variables The strongest predictors were de-layed recall of macro elements of the MEMO-TEXT and freerecall of words The model also retained object naming (DO-80) orientation match (BORB) object decision (BORB) andalpha span (see Table 4) Odd ratios range from 1033 (for thealpha span) to 1689 (for free recall of words) The overallclassification success was 877 The model yielded high sensi-tivity and specificity values (88 and 871 respectively Table5) and excellent positive predictive value (PPV 818) andnegative predictive value (NPV 917)
Survival analyses (see Figure 2) indicated that those perform-ing in the lowest and middle tertiles on the MEMO-TEXT freerecall and alpha span showed faster progression than those inthe highest tertile Furthermore those performing in the lowesttertile on the naming test showed a faster progression rate thanthose performing in the middle and highest tertiles The differ-ence in decline as a function of tertile indicates that the first twotasks are more sensitive to the disease than is naming Nodifferences were found across tertiles for the object decisionand orientation match tests suggesting that when used on their
Table 4Logistic Regression Models on the Predictive Battery
PREDICTORS SE Waldrsquos 2 df pe
(odds ratio)
Age 005 048 011 1 918 995MEMO-TEXT 236 113 4377 1 036 1266delayed macroFree recall 496 171 8386 1 004 1643DO 80 181 147 1501 1 221 1198BORBndashLine judgment 379 243 2439 1 118 1461BORBndashObject decision 251 174 2095 1 148 1286Alpha span 031 021 2097 1 148 1031Constant 9566 4023 5654 1 017 NA
Note MEMO-TEXT Text Memory DO80 Denomination Object80 items BORB Birmingham Object Recognition Battery
Table 5Observed and Predicted Frequencies for the PredictiveDiagnostic Accuracy Provided by the Logistic Regression ModelWith a 060 Cutoff
Predicted
Observed Yes No Correct
Yes 44 6 88No 4 27 871 correct 917 818 877
Note Sensitivity 44(44 6) 88 Specificity 27(27 4) 871 False positive 4(4 44) 83 False negative 6(6 27) 182
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
648 BELLEVILLE GAUTHIER LEPAGE KERGOAT AND GILBERT
own these two tasks lack sensitivity This analysis also showsdifferences across tasks in sensitivity to time of progression Bythe 40-month follow-up 80 of those in the lowest tertile ofMEMO-TEXT had converted to dementia This was found 60and 80 months after follow-up among those in the lowest tertileof free recall and alpha-span respectively
Discussion
Not all MCI cases progress to dementia and it is critical toidentify tests that accurately predict future progression In this
study we found that combining tests of episodic memory (text andword recall) perception (naming orientation and object decision)and working memory (alpha span) correctly identifies 878 ofparticipants who will progress on an average of 45 years inadvance The six-test model yielded very good to excellent sensi-tivity and specificity values as both of them were above 85 Thiswas also the case for PPN and NPV values and in particular it wasfound that 917 of those found unimpaired on the tests remainedstable in spite of the fact they met clinical criteria for MCI Thusthis combination of measures is not only sensitive but it is also
Figure 2 Survival analyses
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
649PREDICTING DECLINE IN MCI
specific and it helps to identify those who are unlikely to progressThis is highly important for clinical trials as it can help identify theMCI persons who are most likely to benefit from disease-modifying therapies Survival analyses indicate that 80 of thepatients performing in the lowest tertile of the MCI group on thetext memory test will have developed dementia 40 months later
This study suggests that relying only on episodic memory mea-sures might not be optimal and that measuring different domains ofcognition represents the most balanced approach Several studieshave investigated the capacity of biological and cognitive mea-sures to predict future progression from MCI to dementia A firstimportant conclusion from many of these studies is that the patternof cognitive deficit might be as accurate as biological measures inpredicting future decline in MCI (Albert et al 2011 Dubois et al2007) a conclusion coherent with our finding of a strong predic-tive accuracy for the cognitive battery used here Another impor-tant conclusion is that it is possible to identify an optimal set ofcognitive tasks Studies vary in their design statistical approachand follow-up length and there is great variability in the cognitivetests used Nevertheless a coherent pattern seems to emerge fromprevious studies which is supported by our findings First itappears that combining episodic memory tests with tasks that relyon executive functions or the attentional control of WM is partic-ularly powerful for predicting conversion from MCI to dementia(Aretouli Tsilidis amp Brandt 2013 Chapman et al 2011 Conde-Sala et al 2012 Gavett et al 2010 Rabin et al 2009 Summersamp Saunders 2012) Second studies that measured only one or twocognitive domains have much lower predictive accuracy than theone found here They report either lower specificity (eg Mitchellet al 2009) or lower sensitivity (Dierckx et al 2009 Tabert et al2006 Tierney et al 1996) than what is reported here This isconsistent with studies indicating that cases of multiple-domainMCI are more likely to progress to dementia than single-domainMCI (Forlenza et al 2009 Nordlund et al 2010 RasquinLodder Visser Lousberg amp Verhey 2005 Summers amp Saunders2012) Our study indicates that an optimal battery should includeperceptual tests in addition to tests of episodic memory executivefunction and working memory The particular cognitive domainsidentified here match well with findings indicating that in additionto episodic memory semantic knowledge and working memoryare impaired early in AD (for a review see Belleville et al 2008)
Few studies have included perceptual or semantic componentsin their models contrary to this study and those that did measureda relatively small number of components It is therefore possiblethat measures of the perceptual or semantic domains have im-proved predictive accuracy However these tasks may be morespecific than sensitive Indeed our survival analyses suggest thatnaming and perceptual tasks were not as sensitive to future declineas episodic memory and executive tasks when taken on their ownIncluding measures of the perceptual or semantic domain mightcontribute to reducing the number of false positives hence increas-ing specificity This is a potentially useful finding for cliniciansand researchers When optimizing testing time is a critical issueand tasks need to be selected one can base the decision on whetherthe need is to have a more sensitive or more specific battery
This study is among those showing the best combination ofsensitivity and specificity values Perhaps inclusion of morenonmemory tests might have increased specificity and use of a
relatively long follow-up period likely reduced the number offalse negatives hence increasing sensitivity Another differencebetween this study and the current literature is that we did notrely on clinical measures but on theoretically motivated onesThus if selected well a relatively short battery of tests canpredict future decline in MCI and can help identify persons thatare likely to progress to more severe symptoms
The study resulted in a number of additional findings whichdeserve discussion One is that at entry progressive MCIpatients already differ from stable MCI patients in terms of ageand cognitive performance on several clinical tests Becausepatients are likely to vary in their decline rate and in their stageat entry it is possible that progressors are in a more advancedstage of neuropathology than persons with stable MCI and thatthe latter would decline later Thus a portion of stable MCIpatients may still actually be predementia (thus false negative)It is important to note however that this study makes use of amuch longer follow-up than is typically used in similar studiesStable MCI patients were followed for an average of 567months which is much longer than the period after whichprogressors converted to dementia (on average 308 monthsafter entry) This long follow-up probably reduced the contri-bution of ldquofalse negativesrdquo to the group of those with stableMCI by increasing the chance of progression during the studyperiod Admittedly it remains possible that some of the stableMCI patients will progress to dementia in the future Howeverwe do not believe that this represents a substantial portion ofour participants with stable MCI It is interesting that thefinding that the two groups differ on clinical measures is in factgood news as it supports our contention that cognitive mea-sures are sensitive to prognosis and will prove critical in iden-tifying the patients more likely to progress to dementia
This study has limitations which should be recognized Firstto improve generalizability the findings should be reproducedon a different sample Second we did not include biomarkers orimaging parameters in this study Our goal was to identify theideal set of cognitive measures and for future studies it will beimportant to assess the value of combining them with biologicalmarkers Finally it is important to point out that there might bedifferences between this cohort of patients and patients encoun-tered in other clinical settings In particular our exclusioncriteria might have led to a cohort with relatively few cases ofcomorbidity
References
Ahmed S Mitchell J Arnold R Nestor P J amp Hodges J R (2008)Predicting rapid clinical progression in amnestic mild cognitive impair-ment Dementia and Geriatric Cognitive Disorders 25 170ndash177 doi101159000113014
Albert M S DeKosky S T Dickson D Dubois B Feldman H HFox N C Phelps C H (2011) The diagnosis of mild cognitiveimpairment due to Alzheimerrsquos disease Recommendations from theNational Institute on Aging-Alzheimerrsquos Association workgroups ondiagnostic guidelines for Alzheimerrsquos disease Alzheimers amp Dementia7 270ndash279 doi101016jjalz201103008
Aretouli E Tsilidis K K amp Brandt J (2013) Four-year outcome ofmild cognitive impairment The contribution of executive dysfunctionNeuropsychology 27 95ndash106 doi101037a0030481
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
650 BELLEVILLE GAUTHIER LEPAGE KERGOAT AND GILBERT
Artero S Tierney M C Touchon J amp Ritchie K (2003) Prediction oftransition from cognitive impairment to senile dementia A prospectivelongitudinal study Acta Psychiatrica Scandinavica 107 390ndash393
Beacutelanger S amp Belleville S (2009) Semantic inhibition impairment inmild cognitive impairment A distinctive feature of upcoming cognitivedecline Neuropsychology 23 592ndash606 doi101037a0016152
Belleville S Bherer L Lepage Eacute Chertkow H amp Gauthier S (2008)Task switching capacities in persons with Alzheimerrsquos disease and mildcognitive impairment Neuropsychologia 46 2225ndash2233 doi101016jneuropsychologia200802012
Belleville S Caza N amp Peretz I (2003) A neuropsychological argu-ment for a processing view of memory Journal of Memory and Lan-guage 48 686ndash703 doi101016S0749-596X(02)00532-6
Belleville S Chertkow H amp Gauthier S (2007) Working memory andcontrol of attention in persons with Alzheimerrsquos disease and mild cog-nitive impairment Neuropsychology 21 458ndash469 doi1010370894-4105214458
Belleville S Meacutenard M C De Boysson C amp Sylvain-Roy S (2008)Characterizing memory deficits in mild cognitive impairment In WSossin J C Lacaille V Castellucci amp S Belleville (Eds) The essenceof memory (pp 365ndash375) Amsterdam Netherlands Elsevier doi101016S0079-6123(07)00023-4
Belleville S Peretz I amp Malenfant D (1996) Examination of theworking memory components in normal aging and in dementia of theAlzheimer type Neuropsychologia 34 195ndash207 doi1010160028-3932(95)00097-6
Belleville S Rouleau N amp Caza N (1998) Effect of normal aging onthe manipulation of information in working memory Memory amp Cog-nition 26 572ndash583 doi103758BF03201163
Bennett D A Wilson R S Schneider J A Evans D A BeckettL A Aggarwal N T Bach J (2002) Natural history of mildcognitive impairment in older persons Neurology 59 198ndash205
Bherer L Belleville S amp Peretz I (2001) Education age and theBrown-Peterson technique Developmental Neuropsychology 19 237ndash251 doi101207S15326942DN1903_1
Chapman R M Mapstone M McCrary J W Gardner M N Por-steinsson A Sandoval T C Reilly L A (2011) Predictingconversion from mild cognitive impairment to Alzheimerrsquos diseaseusing neuropsychological tests and multivariate methods Journal ofClinical and Experimental Neuropsychology 33 187ndash199 doi101080138033952010499356
Chatelois J Pineau H Belleville S Peretz I Lussier I FontaineF-S amp Renaseau-Leclerc C (1993) Batterie informatiseacutee drsquoeacutevaluationde la meacutemoire inspireacutee de lrsquoapproche cognitive Canadian PsychologyPsychologie Canadienne 34 45ndash63 doi101037h0078803
Conde-Sala J L Garre-Olmo J Vilalta-Franch J Llinas-Regla JTurro-Garriga O Lozano-Gallego M Loacutepez-Pousa S (2012)Predictors of cognitive decline in Alzheimerrsquos disease and mild cogni-tive impairment using the CAMCOG A five-year follow-up Interna-tional Psychogeriatrics 24 948ndash958 doi101017S1041610211002158
Deloche G amp Hannequin D (1997) Test de deacutenomination oraledrsquoimages (DO-80) Paris France Centre de Psychologie Appliqueacutee
Dierckx E Engelborghs S De Raedt R Van Buggenhout M DeDeyn P P Verte D amp Ponjaert-Kristoffersen I (2009) Verbal cuedrecall as a predictor of conversion to Alzheimerrsquos disease in mildcognitive impairment International Journal of Geriatric Psychiatry 241094ndash1100 doi101002gps2228
Dubois B Feldman H H Jacova C Dekosky S T Barberger-Gateau P Cummings J Scheltens P (2007) Research criteriafor the diagnosis of Alzheimerrsquos disease Revising the NINCDS-ADRDA criteria Lancet Neurology 6 734 ndash746 doi101016S1474-4422(07)70178 ndash3
Forlenza O V Diniz B S Nunes P V Memoria C M YassudaM S amp Gattaz W F (2009) Diagnostic transitions in mild cognitive
impairment subtypes International Psychogeriatrics 21 1088ndash1095doi101017S1041610209990792
Gauthier S Reisberg B Zaudig M Petersen R C Ritchie K BroichK Winblad B (2006) Mild cognitive impairment The Lancet 3671262ndash1270 doi101016S0140-6736(06)68542-5
Gavett B E Ozonoff A Doktor V Palmisano J Nair A K GreenR C Stern R A (2010) Predicting cognitive decline and conver-sion to Alzheimerrsquos disease in older adults using the NAB List Learningtest Journal of the International Neuropsychological Society 16 651ndash660 doi101017S1355617710000421
Geacutely-Nargeot M-C Cadilhac C Touchon J amp Nespoulous J L(1997) La meacutemoire de textes chez les sujets sains et deacutements Appli-cation drsquoun nouvel outil drsquoeacutevaluation pour neuropsychologues Meacutemo-textes In J Lambert amp J L Nespoulous (Eds) Perception auditive etcompreacutehension du langage (pp 273ndash293) Marseille France Solal
Geroldi C Rossi R Calvagna C Testa C Bresciani L Binetti G Frisoni G B (2006) Medial temporal atrophy but not memorydeficit predicts progression to dementia in patients with mild cognitiveimpairment Journal of Neurology Neurosurgery amp Psychiatry 771219ndash1222 doi101136jnnp2005082651
Irish M Lawlor B A Coen R F amp OrsquoMara S M (2011) Everydayepisodic memory in amnestic mild cognitive impairment A preliminaryinvestigation BMC Neuroscience 12 80 doi1011861471-2202-12-80
Ivanoiu A Adam S Van der Linden M Salmon E Juillerat A CMulligan R amp Seron X (2005) Memory evaluation with a new cuedrecall test in patients with mild cognitive impairment and Alzheimerrsquosdisease Journal of Neurology 252 47ndash55 doi101007s00415-005-0597-2
Landau S M Harvey D Madison C M Reiman E M Foster N LAisen P S Jagust W J (2010) Comparing predictors of conver-sion and decline in mild cognitive impairment Neurology 75 230ndash238doi101212WNL0b013e3181e8e8b8
Lekeu F Magis D Marique P Delbeuck X Bechet S GuillaumeB Salmon E (2010) The California Verbal Learning Test andother standard clinical neuropsychological tests to predict conversionfrom mild memory impairment to dementia Journal of Clinical andExperimental Neuropsychology 32 164 ndash173 doi10108013803390902889606
Mitchell J Arnold R Dawson K Nestor P J amp Hodges J R (2009)Outcome in subgroups of mild cognitive impairment (MCI) is highlypredictable using a simple algorithm Journal of Neurology 256 1500ndash1509 doi101007s00415-009-5152-0[doi]
Mottron L Morasse K amp Belleville S (2001) A study of memoryfunctioning in individuals with autism Journal of Child Psychology andPsychiatry 42 253ndash260 doi1011111469-761000716
Nordlund A Rolstad S Klang O Edman A Hansen S amp Wallin A(2010) Two-year outcome of MCI subtypes and aetiologies in theGoteborg MCI study Journal of Neurology Neurosurgery amp Psychia-try 81 541ndash546 doi101136jnnp2008171066
Petersen R C (2003) Mild cognitive impairment Aging to Alzheimerrsquosdisease Oxford UK Oxford University Press
Petersen R C amp Morris J C (2003) Clinical features In R C Petersen(Ed) Mild cognitive impairment Aging to Alzheimerrsquos disease (pp15ndash39) Oxford UK Oxford University Press
Rabin L A Pare N Saykin A J Brown M J Wishart H AFlashman L A amp Santulli R B (2009) Differential memory testsensitivity for diagnosing amnestic mild cognitive impairment and pre-dicting conversion to Alzheimerrsquos disease Neuropsychology Develop-ment and Cognition Section B Aging Neuropsychology and Cognition16 357ndash376 doi10108013825580902825220
Rasquin S M Lodder J Visser P J Lousberg R amp Verhey F R(2005) Predictive accuracy of MCI subtypes for Alzheimerrsquos diseaseand vascular dementia in subjects with mild cognitive impairment A
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
651PREDICTING DECLINE IN MCI
2-year follow-up study Dementia and Geriatric Cognitive Disorders19 113ndash119 doi101159000082662
Riddoch J M amp Humphreys G W (1993) BORB Birmingham ObjectRecognition Battery Hove UK Erlbaum
Ritchie K Artero S amp Touchon J (2001) Classification criteria formild cognitive impairment A population-based validation study Neu-rology 56 37ndash42 doi101212WNL56137
Summers M J amp Saunders N L (2012) Neuropsychological measurespredict decline to Alzheimerrsquos dementia from mild cognitive impair-ment Neuropsychology 26 498ndash508 doi101037a0028576
Tabert M H Manly J J Liu X Pelton G H Rosenblum S JacobsM Devanand D P (2006) Neuropsychological prediction of
conversion to Alzheimer disease in patients with mild cognitive impair-ment Archives of General Psychiatry 63 916ndash924 doi101001archpsyc638916
Tierney M C Szalai J P Snow W G Fisher R H Nores A NadonG St George-Hyslop P H (1996) Prediction of probable Alz-heimerrsquos disease in memory-impaired patients A prospective longitu-dinal study Neurology 46 661ndash665 doi101212WNL463661
Received May 15 2013Revision received December 19 2013
Accepted December 22 2013
Members of Underrepresented GroupsReviewers for Journal Manuscripts Wanted
If you are interested in reviewing manuscripts for APA journals the APA Publications andCommunications Board would like to invite your participation Manuscript reviewers are vital to thepublications process As a reviewer you would gain valuable experience in publishing The PampCBoard is particularly interested in encouraging members of underrepresented groups to participatemore in this process
If you are interested in reviewing manuscripts please write APA Journals at ReviewersapaorgPlease note the following important points
bull To be selected as a reviewer you must have published articles in peer-reviewed journals Theexperience of publishing provides a reviewer with the basis for preparing a thorough objectivereview
bull To be selected it is critical to be a regular reader of the five to six empirical journals that are mostcentral to the area or journal for which you would like to review Current knowledge of recentlypublished research provides a reviewer with the knowledge base to evaluate a new submissionwithin the context of existing research
bull To select the appropriate reviewers for each manuscript the editor needs detailed informationPlease include with your letter your vita In the letter please identify which APA journal(s) youare interested in and describe your area of expertise Be as specific as possible For exampleldquosocial psychologyrdquo is not sufficientmdashyou would need to specify ldquosocial cognitionrdquo or ldquoattitudechangerdquo as well
bull Reviewing a manuscript takes time (1ndash4 hours per manuscript reviewed) If you are selected toreview a manuscript be prepared to invest the necessary time to evaluate the manuscriptthoroughly
APA now has an online video course that provides guidance in reviewing manuscripts To learnmore about the course and to access the video visit httpwwwapaorgpubsauthorsreview-manuscript-ce-videoaspx
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
652 BELLEVILLE GAUTHIER LEPAGE KERGOAT AND GILBERT

Predictive Battery
Episodic memory In the MEMO-TEXT (Geacutely-NargeotCadilhac Touchon amp Nespoulous 1997) a short story with asmany details (microelements) as general ideas (macroelements)was visually presented for a 3-min study period This was followedby an immediate and 10-min delayed recall In the Free and CuedRecall Test (Chatelois et al 1993 Mottron Morasse amp Belleville2001) 15 words were presented in a 3 5 visual matrix Wordswere encoded by their semantic category (eg show me the veg-etable) Free and category-cued recall was asked following a 45-sbackward counting
Working memory (WM) and executive functions In theadapted Brown-Peterson (Belleville Peretz amp Malenfant 1996Bherer Belleville amp Peretz 2001 Chatelois et al 1993) partic-ipants recalled 12 series of auditory consonant trigrams followingdelays of 0 10 20 or 30 sec filled with an addition task Theswitching procedure (Belleville Bherer Lepage Chertkow ampGauthier 2008) involved switching from adding to subtracting twoseries of digit pairs There were two 30-trial nonswitch blocks (onefor addition and one for subtraction) and two 74-trial switchblocks In the alpha span procedure (Belleville Rouleau amp Caza1998) participants were presented with 20 span-adjusted series ofwords that they were instructed to either report in the order ofpresentation or to mentally rearrange the words and report them inalphabetical order
Language Naming was measured with 80 line-drawings ofobjects (DOndash80 Deloche amp Hannequin 1997) A visual rhymejudgment task was also used in which participants were asked tojudge whether two written disyllabic nonwords rhymed or not(Belleville Caza amp Isabelle 2003)
Visuospatial processing We used three subtests of the Bir-mingham Object Recognition Battery (BORB Riddoch amp Hum-phreys 1993) In the orientation match test participants deter-mined if pairs of lines were parallel In the position of gap matchtest participants determined if pairs of truncated circles had theirgap in the same position In the object decision subtest partici-pants determined if drawings of tools or animalsmdashhalf of whichwere constructed by combining parts of two different objects oranimalsmdashwere real
Design
At study entry persons with MCI completed the clinical testsquestionnaires the clinical neuropsychology battery and the pre-dictive battery (see Figure 1) Clinical and experimental tests weredone in separate sessions Participants were then invited for ayearly clinical assessment to determine whether they had pro-gressed from MCI to AD or in their symptom severity At eachfollow-up clinical information was used by clinicians (SG MJKBG) to determine whether participants were stable or had pro-gressed to dementia Clinical diagnosis was established indepen-dently of the results from the predictive battery and cliniciansinvolved in the diagnosis were unaware of the results from thepredictive battery at the time of diagnosis Patients were identifiedas having progressive MCI (pMCI) if they met the current clinicalDSMndashIV criteria for dementia of the Alzheimer type or if theyshowed a significant decline on tests from the clinical batteryParticipants showing a significant decline had a cognitive profileconsistent with that of MCI However they showed an annual
reduction in performance that was larger than one SD unit (SD wastaken from the performance of a group of approximately 100healthy older adults tested in our laboratory on the same task) onmore than one clinical test This criterion was used because itrepresents a large effect size (8) and is more than 10 timesgreater than the annual decline reported by healthy older adults(approximately 002 SD annual decline for memory and approxi-mately 008 SD for speed of processing Bennett et al 2002)Persons showing no progression to dementia and no decline wereidentified as having stable MCI (sMCI)
Statistical Analysis
ANOVAs or t tests were used to compare pMCI and sMCI atbaseline on demographic characteristics clinical questionnairesclinical neuropsychology tests and tests from the predictor batteryWe used backward logistic regression to determine which testfrom the predictive battery predicted progression As there weremany possible dependent variables for each test it was necessaryto select those that were to be included in the model The variableswere selected based on their theoretical value and only one vari-able was chosen to reflect each cognitive test (eg we avoidedusing both the RTs and correct responses for the same condition)We also used the correlation matrix to exclude variables thatreflected one cognitive domain and that were highly correlated(r 8) Group membership (pMCI vs sMCI) at follow-up wasused as the reference standard Sociodemographic variables thatdiffered across groups were used as covariates This is anexploratory analysis as we made no a priori assumptions re-garding the predictive strength of the tests The analysis pro-vides a number of diagnosis accuracy measures sensitivity
Figure 1 Design of the study
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
646 BELLEVILLE GAUTHIER LEPAGE KERGOAT AND GILBERT
which refers to the percentage of times that performance on thederived predictive tests was abnormal at baseline among pMCIpersons specificity which refers to the percentage of time thatperformance on the derived predictive tests was normal at baselineamong sMCI persons overall accuracy which refers to caseswhere performance on those tests matches clinical diagnosis pos-itive predictive value (PPV) which refers to the percentage oftimes that a clinical diagnosis of pMCI was given based onabnormal performance on predictive tests and negative predictivevalue (NPV) which refers to the percentage of times that theclinical diagnosis was sMCI based on normal performance onpredictive tests The final model was the one that optimizedsensitivity and specificity and gave the best overall diagnosticaccuracy The Kaplan-Meier method measured the probability ofcrossover at designated time intervals as a function of wherepatients stood in the score distribution Scores on measures iden-tified as predictors in the regression analysis were used to stratifypatients in tertiles with the Kaplan-Meier Log-rank was used toassess whether the survival curves of the three tertile groupsdiffered in terms of progression rate All analyses were performedwith the SPSS-20 package
Results
Sociodemographic and Clinical Characteristics
Ten persons were excluded based on the clinical assessment asthey did not meet inclusion criteria and five persons withdrewconsent prior to being tested with the predictive battery (see Figure1) Fifteen additional persons withdrew consent during the follow-up Causes of withdrawal included loss of interest in the researchmoving to another town and death Persons who withdrew consentdid not differ from those remaining in the study on sociodemo-graphic and measures of global cognition variables Fifty-ninepersons were identified as pMCI and 33 as sMCI pMCI partici-pants were identified as progressors on average 3081 months afterentry (SD 20) Follow-up was interrupted after pMCI convertedto dementia Mean follow-up for sMCI was 5673 months (SD 232) sMCI and pMCI groups were equivalent on clinical ques-tionnaires and on sociodemographic characteristics except for ageas pMCI participants were older than sMCI participants ThepMCI group showed worse performance than sMCI participants onmost clinical neuropsychology measures (see Table 2) AmongpMCI participants 40 (678) presented with single-domain am-
Table 3Performances on the Predictive Battery (Standard Deviation in Parentheses) and Cut-Off Valuesto Optimize Diagnostic Accuracy on the Individual Cognitive Tests Kept by theRegression Model
Stable MCI Progressors Cut-off value
Episodic memory tasksMEMO-TEXT (max 24)
Macro-elements immediate 179 (33) 144 (4)Micro-elements immediate 114 (37) 69 (48)Macro-elements delayed 168 (32) 128 (43) 13Micro-elements delayed 103 (41) 52 (41)
Free and Cued recall test (max 15)Free recall 83 (28) 52 (23) 6Free and category cued recall 125 (24) 94 (32)
Working memory and executivefunctions
Brown Peterson - Items recalled (max9 ndash max 36 for total)
0-sec delay 84 (1) 84 (11)10-sec delay 67 (19) 57 (24)20-sec delay 62 (23) 47 (27)30-sec delay 65 (25) 56 (24)Total items recalled 277 (6) 244 (65)
Alpha span - Items recalled (max 100)Items direct 79 (143) 744 (197)Items alpha 611 (175) 509 (174) 58Manipulation cost 221 (188) 302 (197)
Switching task cost on errorsGlobal Switch 001 (033) 004 (034)Local Switch 011 (225) 029 (398)
Language and Visuo-spatial tasksDO80 (max 80) 785 (18) 768 (4) 78Rhyme judgment (max 32) 288 (33) 29 (28)BORB
Line judgment test (max 30) 253 (18) 247 (22)Circle test (max 30) 351 (27) 334 (29) 25Object decision test (max 32) 299 (19) 287 (28) 29
Note MEMO-TEXT Text Memory DO80 Denomination Object 80 items BORB BirminghamObject Recognition Battery
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
647PREDICTING DECLINE IN MCI
nestic MCI at entry and 19 with multiple-domain amnestic MCI(322) Among sMCI participants 19 presented with single-domain amnestic MCI (576) and 14 with multiple-domainamnestic MCI (424)
Group Comparisons on Predictive Battery
Table 3 reports performances of sMCI and pMCI on the pre-dictive battery In some cases technical problems prevented test-ing or data collection for some of the participants The N on whichthe analysis was done is thus provided in parentheses for each test
Episodic memory A Group Delay Type of elementANOVA on the number of items recalled from the MEMO-TEXT(pMCI 53 sMCI 32) indicated significant effects of theDelay F(1 88) 49747 p 0001 2 361 Type of elementF(1 88) 351247 p 0001 2 800 and Group F(1 88) 30553 p 0001 2 258 Recall was lower for the delayedthan immediate recall for micro- than macroelements and forpMCI than sMCI The Group Recall Condition ANOVA on thenumber of words recalled from the Free and Cued-recall test(pMCI 53 sMCI 32) indicated significant effects of theGroup F(1 83) 30712 p 0001 2 270 and Recallcondition F(1 83) 322938 p 0001 2 796 There werefewer words recalled in the Free than Cued condition and in pMCIthan sMCI All effects remained significant when correcting formultiple comparisons
WM and executive functions The Group Delay ANOVAon the number of correct items of the Brown-Peterson procedure(pMCI 58 sMCI 33) indicated a main Group F(1 89) 5568 p 005 2 06 and Delay effect F(3 267) 47983p 00001 2 35 Fewer items were recalled by pMCI thansMCI and fewer in the trials with longer delays The group effectwas no longer significant when correcting for multiple compari-son The Group Recall type ANOVA on the of recalled itemsfrom the alpha span (pMCI 57 sMCI 33) indicated a maineffect of Recall F(1 88) 146720 p 0001 2 625 witha lower recall in the alphabetical than direct condition and a mainGroup effect F(1 88) 4527 p 05 2 049 with pMCIrecalling fewer items than sMCI The group effect was no longersignificant when correcting for multiple comparison A manipula-tion cost score the of loss incurred by alphabetical recall[(direct alpha)direct] revealed a significant Group dif-ference as pMCI showed a larger manipulation cost than sMCI
t(88) 1914 p 05 2 04 This remained significant whencorrecting for multiple comparison There was no significanteffect or interaction on global or local switch cost definedrespectively as the number of errors on switch minus nonswitchblock and errors on switch trials minus nonswitch trials F13in all cases (pMCI 57 sMCI 33)
Language No group differences were found on the number ofcorrect responses for the rhyme judgment test t(86) 0340 2 001 However pMCI showed a lower number of correct responsesthan sMCI on the DO-80 naming test t(90) 2327 p 052 057 (pMCI 59 and 55 respectively sMCI 33) and thisremained significant when correcting for multiple comparison
Visuospatial processing No group differences were foundon the orientation match t(85) 1175 2 016 HoweverpMCI obtained a lower score than sMCI on the position of gapt(85) 2637 p 01 2 076 and object decisiont(85) 2329 p 05 2 060 tests (pMCI 54 sMCI 33) The effect remained significant when correcting for mul-tiple comparisons on position gap but not on object decision
Regression Analysis
The age-adjusted logistic model with the best overall diag-nostic accuracy was obtained after five iterations and wascomposed of six variables The strongest predictors were de-layed recall of macro elements of the MEMO-TEXT and freerecall of words The model also retained object naming (DO-80) orientation match (BORB) object decision (BORB) andalpha span (see Table 4) Odd ratios range from 1033 (for thealpha span) to 1689 (for free recall of words) The overallclassification success was 877 The model yielded high sensi-tivity and specificity values (88 and 871 respectively Table5) and excellent positive predictive value (PPV 818) andnegative predictive value (NPV 917)
Survival analyses (see Figure 2) indicated that those perform-ing in the lowest and middle tertiles on the MEMO-TEXT freerecall and alpha span showed faster progression than those inthe highest tertile Furthermore those performing in the lowesttertile on the naming test showed a faster progression rate thanthose performing in the middle and highest tertiles The differ-ence in decline as a function of tertile indicates that the first twotasks are more sensitive to the disease than is naming Nodifferences were found across tertiles for the object decisionand orientation match tests suggesting that when used on their
Table 4Logistic Regression Models on the Predictive Battery
PREDICTORS SE Waldrsquos 2 df pe
(odds ratio)
Age 005 048 011 1 918 995MEMO-TEXT 236 113 4377 1 036 1266delayed macroFree recall 496 171 8386 1 004 1643DO 80 181 147 1501 1 221 1198BORBndashLine judgment 379 243 2439 1 118 1461BORBndashObject decision 251 174 2095 1 148 1286Alpha span 031 021 2097 1 148 1031Constant 9566 4023 5654 1 017 NA
Note MEMO-TEXT Text Memory DO80 Denomination Object80 items BORB Birmingham Object Recognition Battery
Table 5Observed and Predicted Frequencies for the PredictiveDiagnostic Accuracy Provided by the Logistic Regression ModelWith a 060 Cutoff
Predicted
Observed Yes No Correct
Yes 44 6 88No 4 27 871 correct 917 818 877
Note Sensitivity 44(44 6) 88 Specificity 27(27 4) 871 False positive 4(4 44) 83 False negative 6(6 27) 182
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
648 BELLEVILLE GAUTHIER LEPAGE KERGOAT AND GILBERT
own these two tasks lack sensitivity This analysis also showsdifferences across tasks in sensitivity to time of progression Bythe 40-month follow-up 80 of those in the lowest tertile ofMEMO-TEXT had converted to dementia This was found 60and 80 months after follow-up among those in the lowest tertileof free recall and alpha-span respectively
Discussion
Not all MCI cases progress to dementia and it is critical toidentify tests that accurately predict future progression In this
study we found that combining tests of episodic memory (text andword recall) perception (naming orientation and object decision)and working memory (alpha span) correctly identifies 878 ofparticipants who will progress on an average of 45 years inadvance The six-test model yielded very good to excellent sensi-tivity and specificity values as both of them were above 85 Thiswas also the case for PPN and NPV values and in particular it wasfound that 917 of those found unimpaired on the tests remainedstable in spite of the fact they met clinical criteria for MCI Thusthis combination of measures is not only sensitive but it is also
Figure 2 Survival analyses
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
649PREDICTING DECLINE IN MCI
specific and it helps to identify those who are unlikely to progressThis is highly important for clinical trials as it can help identify theMCI persons who are most likely to benefit from disease-modifying therapies Survival analyses indicate that 80 of thepatients performing in the lowest tertile of the MCI group on thetext memory test will have developed dementia 40 months later
This study suggests that relying only on episodic memory mea-sures might not be optimal and that measuring different domains ofcognition represents the most balanced approach Several studieshave investigated the capacity of biological and cognitive mea-sures to predict future progression from MCI to dementia A firstimportant conclusion from many of these studies is that the patternof cognitive deficit might be as accurate as biological measures inpredicting future decline in MCI (Albert et al 2011 Dubois et al2007) a conclusion coherent with our finding of a strong predic-tive accuracy for the cognitive battery used here Another impor-tant conclusion is that it is possible to identify an optimal set ofcognitive tasks Studies vary in their design statistical approachand follow-up length and there is great variability in the cognitivetests used Nevertheless a coherent pattern seems to emerge fromprevious studies which is supported by our findings First itappears that combining episodic memory tests with tasks that relyon executive functions or the attentional control of WM is partic-ularly powerful for predicting conversion from MCI to dementia(Aretouli Tsilidis amp Brandt 2013 Chapman et al 2011 Conde-Sala et al 2012 Gavett et al 2010 Rabin et al 2009 Summersamp Saunders 2012) Second studies that measured only one or twocognitive domains have much lower predictive accuracy than theone found here They report either lower specificity (eg Mitchellet al 2009) or lower sensitivity (Dierckx et al 2009 Tabert et al2006 Tierney et al 1996) than what is reported here This isconsistent with studies indicating that cases of multiple-domainMCI are more likely to progress to dementia than single-domainMCI (Forlenza et al 2009 Nordlund et al 2010 RasquinLodder Visser Lousberg amp Verhey 2005 Summers amp Saunders2012) Our study indicates that an optimal battery should includeperceptual tests in addition to tests of episodic memory executivefunction and working memory The particular cognitive domainsidentified here match well with findings indicating that in additionto episodic memory semantic knowledge and working memoryare impaired early in AD (for a review see Belleville et al 2008)
Few studies have included perceptual or semantic componentsin their models contrary to this study and those that did measureda relatively small number of components It is therefore possiblethat measures of the perceptual or semantic domains have im-proved predictive accuracy However these tasks may be morespecific than sensitive Indeed our survival analyses suggest thatnaming and perceptual tasks were not as sensitive to future declineas episodic memory and executive tasks when taken on their ownIncluding measures of the perceptual or semantic domain mightcontribute to reducing the number of false positives hence increas-ing specificity This is a potentially useful finding for cliniciansand researchers When optimizing testing time is a critical issueand tasks need to be selected one can base the decision on whetherthe need is to have a more sensitive or more specific battery
This study is among those showing the best combination ofsensitivity and specificity values Perhaps inclusion of morenonmemory tests might have increased specificity and use of a
relatively long follow-up period likely reduced the number offalse negatives hence increasing sensitivity Another differencebetween this study and the current literature is that we did notrely on clinical measures but on theoretically motivated onesThus if selected well a relatively short battery of tests canpredict future decline in MCI and can help identify persons thatare likely to progress to more severe symptoms
The study resulted in a number of additional findings whichdeserve discussion One is that at entry progressive MCIpatients already differ from stable MCI patients in terms of ageand cognitive performance on several clinical tests Becausepatients are likely to vary in their decline rate and in their stageat entry it is possible that progressors are in a more advancedstage of neuropathology than persons with stable MCI and thatthe latter would decline later Thus a portion of stable MCIpatients may still actually be predementia (thus false negative)It is important to note however that this study makes use of amuch longer follow-up than is typically used in similar studiesStable MCI patients were followed for an average of 567months which is much longer than the period after whichprogressors converted to dementia (on average 308 monthsafter entry) This long follow-up probably reduced the contri-bution of ldquofalse negativesrdquo to the group of those with stableMCI by increasing the chance of progression during the studyperiod Admittedly it remains possible that some of the stableMCI patients will progress to dementia in the future Howeverwe do not believe that this represents a substantial portion ofour participants with stable MCI It is interesting that thefinding that the two groups differ on clinical measures is in factgood news as it supports our contention that cognitive mea-sures are sensitive to prognosis and will prove critical in iden-tifying the patients more likely to progress to dementia
This study has limitations which should be recognized Firstto improve generalizability the findings should be reproducedon a different sample Second we did not include biomarkers orimaging parameters in this study Our goal was to identify theideal set of cognitive measures and for future studies it will beimportant to assess the value of combining them with biologicalmarkers Finally it is important to point out that there might bedifferences between this cohort of patients and patients encoun-tered in other clinical settings In particular our exclusioncriteria might have led to a cohort with relatively few cases ofcomorbidity
References
Ahmed S Mitchell J Arnold R Nestor P J amp Hodges J R (2008)Predicting rapid clinical progression in amnestic mild cognitive impair-ment Dementia and Geriatric Cognitive Disorders 25 170ndash177 doi101159000113014
Albert M S DeKosky S T Dickson D Dubois B Feldman H HFox N C Phelps C H (2011) The diagnosis of mild cognitiveimpairment due to Alzheimerrsquos disease Recommendations from theNational Institute on Aging-Alzheimerrsquos Association workgroups ondiagnostic guidelines for Alzheimerrsquos disease Alzheimers amp Dementia7 270ndash279 doi101016jjalz201103008
Aretouli E Tsilidis K K amp Brandt J (2013) Four-year outcome ofmild cognitive impairment The contribution of executive dysfunctionNeuropsychology 27 95ndash106 doi101037a0030481
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
650 BELLEVILLE GAUTHIER LEPAGE KERGOAT AND GILBERT
Artero S Tierney M C Touchon J amp Ritchie K (2003) Prediction oftransition from cognitive impairment to senile dementia A prospectivelongitudinal study Acta Psychiatrica Scandinavica 107 390ndash393
Beacutelanger S amp Belleville S (2009) Semantic inhibition impairment inmild cognitive impairment A distinctive feature of upcoming cognitivedecline Neuropsychology 23 592ndash606 doi101037a0016152
Belleville S Bherer L Lepage Eacute Chertkow H amp Gauthier S (2008)Task switching capacities in persons with Alzheimerrsquos disease and mildcognitive impairment Neuropsychologia 46 2225ndash2233 doi101016jneuropsychologia200802012
Belleville S Caza N amp Peretz I (2003) A neuropsychological argu-ment for a processing view of memory Journal of Memory and Lan-guage 48 686ndash703 doi101016S0749-596X(02)00532-6
Belleville S Chertkow H amp Gauthier S (2007) Working memory andcontrol of attention in persons with Alzheimerrsquos disease and mild cog-nitive impairment Neuropsychology 21 458ndash469 doi1010370894-4105214458
Belleville S Meacutenard M C De Boysson C amp Sylvain-Roy S (2008)Characterizing memory deficits in mild cognitive impairment In WSossin J C Lacaille V Castellucci amp S Belleville (Eds) The essenceof memory (pp 365ndash375) Amsterdam Netherlands Elsevier doi101016S0079-6123(07)00023-4
Belleville S Peretz I amp Malenfant D (1996) Examination of theworking memory components in normal aging and in dementia of theAlzheimer type Neuropsychologia 34 195ndash207 doi1010160028-3932(95)00097-6
Belleville S Rouleau N amp Caza N (1998) Effect of normal aging onthe manipulation of information in working memory Memory amp Cog-nition 26 572ndash583 doi103758BF03201163
Bennett D A Wilson R S Schneider J A Evans D A BeckettL A Aggarwal N T Bach J (2002) Natural history of mildcognitive impairment in older persons Neurology 59 198ndash205
Bherer L Belleville S amp Peretz I (2001) Education age and theBrown-Peterson technique Developmental Neuropsychology 19 237ndash251 doi101207S15326942DN1903_1
Chapman R M Mapstone M McCrary J W Gardner M N Por-steinsson A Sandoval T C Reilly L A (2011) Predictingconversion from mild cognitive impairment to Alzheimerrsquos diseaseusing neuropsychological tests and multivariate methods Journal ofClinical and Experimental Neuropsychology 33 187ndash199 doi101080138033952010499356
Chatelois J Pineau H Belleville S Peretz I Lussier I FontaineF-S amp Renaseau-Leclerc C (1993) Batterie informatiseacutee drsquoeacutevaluationde la meacutemoire inspireacutee de lrsquoapproche cognitive Canadian PsychologyPsychologie Canadienne 34 45ndash63 doi101037h0078803
Conde-Sala J L Garre-Olmo J Vilalta-Franch J Llinas-Regla JTurro-Garriga O Lozano-Gallego M Loacutepez-Pousa S (2012)Predictors of cognitive decline in Alzheimerrsquos disease and mild cogni-tive impairment using the CAMCOG A five-year follow-up Interna-tional Psychogeriatrics 24 948ndash958 doi101017S1041610211002158
Deloche G amp Hannequin D (1997) Test de deacutenomination oraledrsquoimages (DO-80) Paris France Centre de Psychologie Appliqueacutee
Dierckx E Engelborghs S De Raedt R Van Buggenhout M DeDeyn P P Verte D amp Ponjaert-Kristoffersen I (2009) Verbal cuedrecall as a predictor of conversion to Alzheimerrsquos disease in mildcognitive impairment International Journal of Geriatric Psychiatry 241094ndash1100 doi101002gps2228
Dubois B Feldman H H Jacova C Dekosky S T Barberger-Gateau P Cummings J Scheltens P (2007) Research criteriafor the diagnosis of Alzheimerrsquos disease Revising the NINCDS-ADRDA criteria Lancet Neurology 6 734 ndash746 doi101016S1474-4422(07)70178 ndash3
Forlenza O V Diniz B S Nunes P V Memoria C M YassudaM S amp Gattaz W F (2009) Diagnostic transitions in mild cognitive
impairment subtypes International Psychogeriatrics 21 1088ndash1095doi101017S1041610209990792
Gauthier S Reisberg B Zaudig M Petersen R C Ritchie K BroichK Winblad B (2006) Mild cognitive impairment The Lancet 3671262ndash1270 doi101016S0140-6736(06)68542-5
Gavett B E Ozonoff A Doktor V Palmisano J Nair A K GreenR C Stern R A (2010) Predicting cognitive decline and conver-sion to Alzheimerrsquos disease in older adults using the NAB List Learningtest Journal of the International Neuropsychological Society 16 651ndash660 doi101017S1355617710000421
Geacutely-Nargeot M-C Cadilhac C Touchon J amp Nespoulous J L(1997) La meacutemoire de textes chez les sujets sains et deacutements Appli-cation drsquoun nouvel outil drsquoeacutevaluation pour neuropsychologues Meacutemo-textes In J Lambert amp J L Nespoulous (Eds) Perception auditive etcompreacutehension du langage (pp 273ndash293) Marseille France Solal
Geroldi C Rossi R Calvagna C Testa C Bresciani L Binetti G Frisoni G B (2006) Medial temporal atrophy but not memorydeficit predicts progression to dementia in patients with mild cognitiveimpairment Journal of Neurology Neurosurgery amp Psychiatry 771219ndash1222 doi101136jnnp2005082651
Irish M Lawlor B A Coen R F amp OrsquoMara S M (2011) Everydayepisodic memory in amnestic mild cognitive impairment A preliminaryinvestigation BMC Neuroscience 12 80 doi1011861471-2202-12-80
Ivanoiu A Adam S Van der Linden M Salmon E Juillerat A CMulligan R amp Seron X (2005) Memory evaluation with a new cuedrecall test in patients with mild cognitive impairment and Alzheimerrsquosdisease Journal of Neurology 252 47ndash55 doi101007s00415-005-0597-2
Landau S M Harvey D Madison C M Reiman E M Foster N LAisen P S Jagust W J (2010) Comparing predictors of conver-sion and decline in mild cognitive impairment Neurology 75 230ndash238doi101212WNL0b013e3181e8e8b8
Lekeu F Magis D Marique P Delbeuck X Bechet S GuillaumeB Salmon E (2010) The California Verbal Learning Test andother standard clinical neuropsychological tests to predict conversionfrom mild memory impairment to dementia Journal of Clinical andExperimental Neuropsychology 32 164 ndash173 doi10108013803390902889606
Mitchell J Arnold R Dawson K Nestor P J amp Hodges J R (2009)Outcome in subgroups of mild cognitive impairment (MCI) is highlypredictable using a simple algorithm Journal of Neurology 256 1500ndash1509 doi101007s00415-009-5152-0[doi]
Mottron L Morasse K amp Belleville S (2001) A study of memoryfunctioning in individuals with autism Journal of Child Psychology andPsychiatry 42 253ndash260 doi1011111469-761000716
Nordlund A Rolstad S Klang O Edman A Hansen S amp Wallin A(2010) Two-year outcome of MCI subtypes and aetiologies in theGoteborg MCI study Journal of Neurology Neurosurgery amp Psychia-try 81 541ndash546 doi101136jnnp2008171066
Petersen R C (2003) Mild cognitive impairment Aging to Alzheimerrsquosdisease Oxford UK Oxford University Press
Petersen R C amp Morris J C (2003) Clinical features In R C Petersen(Ed) Mild cognitive impairment Aging to Alzheimerrsquos disease (pp15ndash39) Oxford UK Oxford University Press
Rabin L A Pare N Saykin A J Brown M J Wishart H AFlashman L A amp Santulli R B (2009) Differential memory testsensitivity for diagnosing amnestic mild cognitive impairment and pre-dicting conversion to Alzheimerrsquos disease Neuropsychology Develop-ment and Cognition Section B Aging Neuropsychology and Cognition16 357ndash376 doi10108013825580902825220
Rasquin S M Lodder J Visser P J Lousberg R amp Verhey F R(2005) Predictive accuracy of MCI subtypes for Alzheimerrsquos diseaseand vascular dementia in subjects with mild cognitive impairment A
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
651PREDICTING DECLINE IN MCI
2-year follow-up study Dementia and Geriatric Cognitive Disorders19 113ndash119 doi101159000082662
Riddoch J M amp Humphreys G W (1993) BORB Birmingham ObjectRecognition Battery Hove UK Erlbaum
Ritchie K Artero S amp Touchon J (2001) Classification criteria formild cognitive impairment A population-based validation study Neu-rology 56 37ndash42 doi101212WNL56137
Summers M J amp Saunders N L (2012) Neuropsychological measurespredict decline to Alzheimerrsquos dementia from mild cognitive impair-ment Neuropsychology 26 498ndash508 doi101037a0028576
Tabert M H Manly J J Liu X Pelton G H Rosenblum S JacobsM Devanand D P (2006) Neuropsychological prediction of
conversion to Alzheimer disease in patients with mild cognitive impair-ment Archives of General Psychiatry 63 916ndash924 doi101001archpsyc638916
Tierney M C Szalai J P Snow W G Fisher R H Nores A NadonG St George-Hyslop P H (1996) Prediction of probable Alz-heimerrsquos disease in memory-impaired patients A prospective longitu-dinal study Neurology 46 661ndash665 doi101212WNL463661
Received May 15 2013Revision received December 19 2013
Accepted December 22 2013
Members of Underrepresented GroupsReviewers for Journal Manuscripts Wanted
If you are interested in reviewing manuscripts for APA journals the APA Publications andCommunications Board would like to invite your participation Manuscript reviewers are vital to thepublications process As a reviewer you would gain valuable experience in publishing The PampCBoard is particularly interested in encouraging members of underrepresented groups to participatemore in this process
If you are interested in reviewing manuscripts please write APA Journals at ReviewersapaorgPlease note the following important points
bull To be selected as a reviewer you must have published articles in peer-reviewed journals Theexperience of publishing provides a reviewer with the basis for preparing a thorough objectivereview
bull To be selected it is critical to be a regular reader of the five to six empirical journals that are mostcentral to the area or journal for which you would like to review Current knowledge of recentlypublished research provides a reviewer with the knowledge base to evaluate a new submissionwithin the context of existing research
bull To select the appropriate reviewers for each manuscript the editor needs detailed informationPlease include with your letter your vita In the letter please identify which APA journal(s) youare interested in and describe your area of expertise Be as specific as possible For exampleldquosocial psychologyrdquo is not sufficientmdashyou would need to specify ldquosocial cognitionrdquo or ldquoattitudechangerdquo as well
bull Reviewing a manuscript takes time (1ndash4 hours per manuscript reviewed) If you are selected toreview a manuscript be prepared to invest the necessary time to evaluate the manuscriptthoroughly
APA now has an online video course that provides guidance in reviewing manuscripts To learnmore about the course and to access the video visit httpwwwapaorgpubsauthorsreview-manuscript-ce-videoaspx
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
652 BELLEVILLE GAUTHIER LEPAGE KERGOAT AND GILBERT
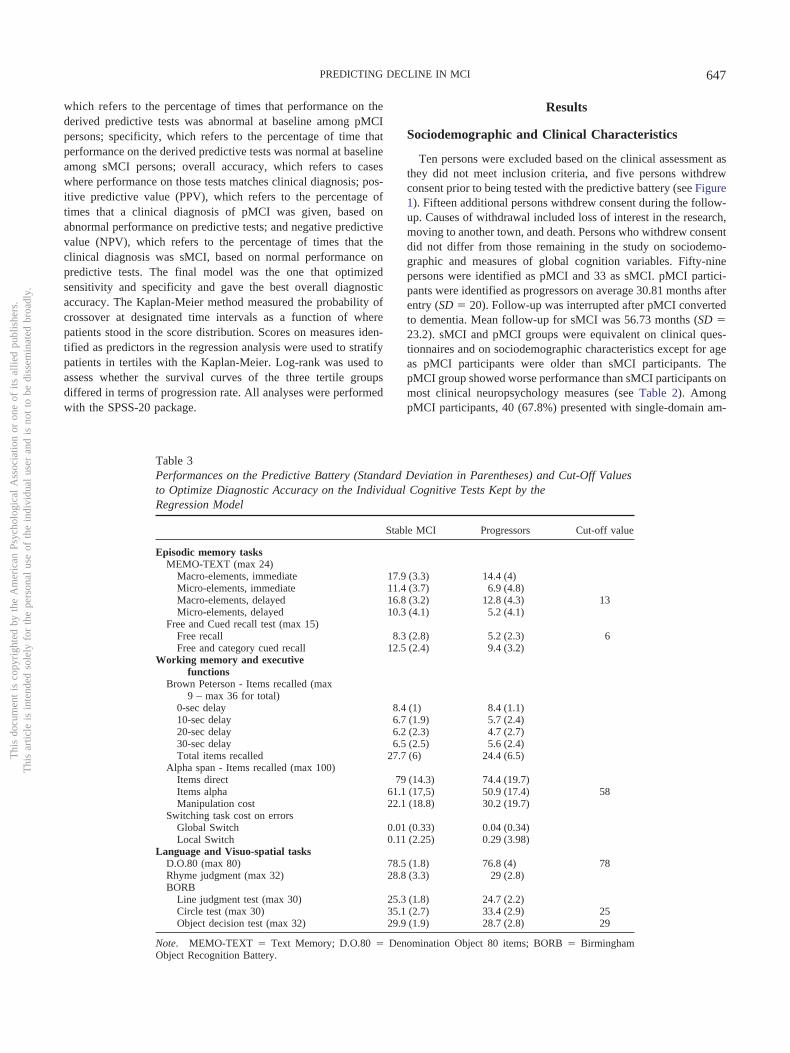
which refers to the percentage of times that performance on thederived predictive tests was abnormal at baseline among pMCIpersons specificity which refers to the percentage of time thatperformance on the derived predictive tests was normal at baselineamong sMCI persons overall accuracy which refers to caseswhere performance on those tests matches clinical diagnosis pos-itive predictive value (PPV) which refers to the percentage oftimes that a clinical diagnosis of pMCI was given based onabnormal performance on predictive tests and negative predictivevalue (NPV) which refers to the percentage of times that theclinical diagnosis was sMCI based on normal performance onpredictive tests The final model was the one that optimizedsensitivity and specificity and gave the best overall diagnosticaccuracy The Kaplan-Meier method measured the probability ofcrossover at designated time intervals as a function of wherepatients stood in the score distribution Scores on measures iden-tified as predictors in the regression analysis were used to stratifypatients in tertiles with the Kaplan-Meier Log-rank was used toassess whether the survival curves of the three tertile groupsdiffered in terms of progression rate All analyses were performedwith the SPSS-20 package
Results
Sociodemographic and Clinical Characteristics
Ten persons were excluded based on the clinical assessment asthey did not meet inclusion criteria and five persons withdrewconsent prior to being tested with the predictive battery (see Figure1) Fifteen additional persons withdrew consent during the follow-up Causes of withdrawal included loss of interest in the researchmoving to another town and death Persons who withdrew consentdid not differ from those remaining in the study on sociodemo-graphic and measures of global cognition variables Fifty-ninepersons were identified as pMCI and 33 as sMCI pMCI partici-pants were identified as progressors on average 3081 months afterentry (SD 20) Follow-up was interrupted after pMCI convertedto dementia Mean follow-up for sMCI was 5673 months (SD 232) sMCI and pMCI groups were equivalent on clinical ques-tionnaires and on sociodemographic characteristics except for ageas pMCI participants were older than sMCI participants ThepMCI group showed worse performance than sMCI participants onmost clinical neuropsychology measures (see Table 2) AmongpMCI participants 40 (678) presented with single-domain am-
Table 3Performances on the Predictive Battery (Standard Deviation in Parentheses) and Cut-Off Valuesto Optimize Diagnostic Accuracy on the Individual Cognitive Tests Kept by theRegression Model
Stable MCI Progressors Cut-off value
Episodic memory tasksMEMO-TEXT (max 24)
Macro-elements immediate 179 (33) 144 (4)Micro-elements immediate 114 (37) 69 (48)Macro-elements delayed 168 (32) 128 (43) 13Micro-elements delayed 103 (41) 52 (41)
Free and Cued recall test (max 15)Free recall 83 (28) 52 (23) 6Free and category cued recall 125 (24) 94 (32)
Working memory and executivefunctions
Brown Peterson - Items recalled (max9 ndash max 36 for total)
0-sec delay 84 (1) 84 (11)10-sec delay 67 (19) 57 (24)20-sec delay 62 (23) 47 (27)30-sec delay 65 (25) 56 (24)Total items recalled 277 (6) 244 (65)
Alpha span - Items recalled (max 100)Items direct 79 (143) 744 (197)Items alpha 611 (175) 509 (174) 58Manipulation cost 221 (188) 302 (197)
Switching task cost on errorsGlobal Switch 001 (033) 004 (034)Local Switch 011 (225) 029 (398)
Language and Visuo-spatial tasksDO80 (max 80) 785 (18) 768 (4) 78Rhyme judgment (max 32) 288 (33) 29 (28)BORB
Line judgment test (max 30) 253 (18) 247 (22)Circle test (max 30) 351 (27) 334 (29) 25Object decision test (max 32) 299 (19) 287 (28) 29
Note MEMO-TEXT Text Memory DO80 Denomination Object 80 items BORB BirminghamObject Recognition Battery
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
647PREDICTING DECLINE IN MCI
nestic MCI at entry and 19 with multiple-domain amnestic MCI(322) Among sMCI participants 19 presented with single-domain amnestic MCI (576) and 14 with multiple-domainamnestic MCI (424)
Group Comparisons on Predictive Battery
Table 3 reports performances of sMCI and pMCI on the pre-dictive battery In some cases technical problems prevented test-ing or data collection for some of the participants The N on whichthe analysis was done is thus provided in parentheses for each test
Episodic memory A Group Delay Type of elementANOVA on the number of items recalled from the MEMO-TEXT(pMCI 53 sMCI 32) indicated significant effects of theDelay F(1 88) 49747 p 0001 2 361 Type of elementF(1 88) 351247 p 0001 2 800 and Group F(1 88) 30553 p 0001 2 258 Recall was lower for the delayedthan immediate recall for micro- than macroelements and forpMCI than sMCI The Group Recall Condition ANOVA on thenumber of words recalled from the Free and Cued-recall test(pMCI 53 sMCI 32) indicated significant effects of theGroup F(1 83) 30712 p 0001 2 270 and Recallcondition F(1 83) 322938 p 0001 2 796 There werefewer words recalled in the Free than Cued condition and in pMCIthan sMCI All effects remained significant when correcting formultiple comparisons
WM and executive functions The Group Delay ANOVAon the number of correct items of the Brown-Peterson procedure(pMCI 58 sMCI 33) indicated a main Group F(1 89) 5568 p 005 2 06 and Delay effect F(3 267) 47983p 00001 2 35 Fewer items were recalled by pMCI thansMCI and fewer in the trials with longer delays The group effectwas no longer significant when correcting for multiple compari-son The Group Recall type ANOVA on the of recalled itemsfrom the alpha span (pMCI 57 sMCI 33) indicated a maineffect of Recall F(1 88) 146720 p 0001 2 625 witha lower recall in the alphabetical than direct condition and a mainGroup effect F(1 88) 4527 p 05 2 049 with pMCIrecalling fewer items than sMCI The group effect was no longersignificant when correcting for multiple comparison A manipula-tion cost score the of loss incurred by alphabetical recall[(direct alpha)direct] revealed a significant Group dif-ference as pMCI showed a larger manipulation cost than sMCI
t(88) 1914 p 05 2 04 This remained significant whencorrecting for multiple comparison There was no significanteffect or interaction on global or local switch cost definedrespectively as the number of errors on switch minus nonswitchblock and errors on switch trials minus nonswitch trials F13in all cases (pMCI 57 sMCI 33)
Language No group differences were found on the number ofcorrect responses for the rhyme judgment test t(86) 0340 2 001 However pMCI showed a lower number of correct responsesthan sMCI on the DO-80 naming test t(90) 2327 p 052 057 (pMCI 59 and 55 respectively sMCI 33) and thisremained significant when correcting for multiple comparison
Visuospatial processing No group differences were foundon the orientation match t(85) 1175 2 016 HoweverpMCI obtained a lower score than sMCI on the position of gapt(85) 2637 p 01 2 076 and object decisiont(85) 2329 p 05 2 060 tests (pMCI 54 sMCI 33) The effect remained significant when correcting for mul-tiple comparisons on position gap but not on object decision
Regression Analysis
The age-adjusted logistic model with the best overall diag-nostic accuracy was obtained after five iterations and wascomposed of six variables The strongest predictors were de-layed recall of macro elements of the MEMO-TEXT and freerecall of words The model also retained object naming (DO-80) orientation match (BORB) object decision (BORB) andalpha span (see Table 4) Odd ratios range from 1033 (for thealpha span) to 1689 (for free recall of words) The overallclassification success was 877 The model yielded high sensi-tivity and specificity values (88 and 871 respectively Table5) and excellent positive predictive value (PPV 818) andnegative predictive value (NPV 917)
Survival analyses (see Figure 2) indicated that those perform-ing in the lowest and middle tertiles on the MEMO-TEXT freerecall and alpha span showed faster progression than those inthe highest tertile Furthermore those performing in the lowesttertile on the naming test showed a faster progression rate thanthose performing in the middle and highest tertiles The differ-ence in decline as a function of tertile indicates that the first twotasks are more sensitive to the disease than is naming Nodifferences were found across tertiles for the object decisionand orientation match tests suggesting that when used on their
Table 4Logistic Regression Models on the Predictive Battery
PREDICTORS SE Waldrsquos 2 df pe
(odds ratio)
Age 005 048 011 1 918 995MEMO-TEXT 236 113 4377 1 036 1266delayed macroFree recall 496 171 8386 1 004 1643DO 80 181 147 1501 1 221 1198BORBndashLine judgment 379 243 2439 1 118 1461BORBndashObject decision 251 174 2095 1 148 1286Alpha span 031 021 2097 1 148 1031Constant 9566 4023 5654 1 017 NA
Note MEMO-TEXT Text Memory DO80 Denomination Object80 items BORB Birmingham Object Recognition Battery
Table 5Observed and Predicted Frequencies for the PredictiveDiagnostic Accuracy Provided by the Logistic Regression ModelWith a 060 Cutoff
Predicted
Observed Yes No Correct
Yes 44 6 88No 4 27 871 correct 917 818 877
Note Sensitivity 44(44 6) 88 Specificity 27(27 4) 871 False positive 4(4 44) 83 False negative 6(6 27) 182
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
648 BELLEVILLE GAUTHIER LEPAGE KERGOAT AND GILBERT
own these two tasks lack sensitivity This analysis also showsdifferences across tasks in sensitivity to time of progression Bythe 40-month follow-up 80 of those in the lowest tertile ofMEMO-TEXT had converted to dementia This was found 60and 80 months after follow-up among those in the lowest tertileof free recall and alpha-span respectively
Discussion
Not all MCI cases progress to dementia and it is critical toidentify tests that accurately predict future progression In this
study we found that combining tests of episodic memory (text andword recall) perception (naming orientation and object decision)and working memory (alpha span) correctly identifies 878 ofparticipants who will progress on an average of 45 years inadvance The six-test model yielded very good to excellent sensi-tivity and specificity values as both of them were above 85 Thiswas also the case for PPN and NPV values and in particular it wasfound that 917 of those found unimpaired on the tests remainedstable in spite of the fact they met clinical criteria for MCI Thusthis combination of measures is not only sensitive but it is also
Figure 2 Survival analyses
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
649PREDICTING DECLINE IN MCI
specific and it helps to identify those who are unlikely to progressThis is highly important for clinical trials as it can help identify theMCI persons who are most likely to benefit from disease-modifying therapies Survival analyses indicate that 80 of thepatients performing in the lowest tertile of the MCI group on thetext memory test will have developed dementia 40 months later
This study suggests that relying only on episodic memory mea-sures might not be optimal and that measuring different domains ofcognition represents the most balanced approach Several studieshave investigated the capacity of biological and cognitive mea-sures to predict future progression from MCI to dementia A firstimportant conclusion from many of these studies is that the patternof cognitive deficit might be as accurate as biological measures inpredicting future decline in MCI (Albert et al 2011 Dubois et al2007) a conclusion coherent with our finding of a strong predic-tive accuracy for the cognitive battery used here Another impor-tant conclusion is that it is possible to identify an optimal set ofcognitive tasks Studies vary in their design statistical approachand follow-up length and there is great variability in the cognitivetests used Nevertheless a coherent pattern seems to emerge fromprevious studies which is supported by our findings First itappears that combining episodic memory tests with tasks that relyon executive functions or the attentional control of WM is partic-ularly powerful for predicting conversion from MCI to dementia(Aretouli Tsilidis amp Brandt 2013 Chapman et al 2011 Conde-Sala et al 2012 Gavett et al 2010 Rabin et al 2009 Summersamp Saunders 2012) Second studies that measured only one or twocognitive domains have much lower predictive accuracy than theone found here They report either lower specificity (eg Mitchellet al 2009) or lower sensitivity (Dierckx et al 2009 Tabert et al2006 Tierney et al 1996) than what is reported here This isconsistent with studies indicating that cases of multiple-domainMCI are more likely to progress to dementia than single-domainMCI (Forlenza et al 2009 Nordlund et al 2010 RasquinLodder Visser Lousberg amp Verhey 2005 Summers amp Saunders2012) Our study indicates that an optimal battery should includeperceptual tests in addition to tests of episodic memory executivefunction and working memory The particular cognitive domainsidentified here match well with findings indicating that in additionto episodic memory semantic knowledge and working memoryare impaired early in AD (for a review see Belleville et al 2008)
Few studies have included perceptual or semantic componentsin their models contrary to this study and those that did measureda relatively small number of components It is therefore possiblethat measures of the perceptual or semantic domains have im-proved predictive accuracy However these tasks may be morespecific than sensitive Indeed our survival analyses suggest thatnaming and perceptual tasks were not as sensitive to future declineas episodic memory and executive tasks when taken on their ownIncluding measures of the perceptual or semantic domain mightcontribute to reducing the number of false positives hence increas-ing specificity This is a potentially useful finding for cliniciansand researchers When optimizing testing time is a critical issueand tasks need to be selected one can base the decision on whetherthe need is to have a more sensitive or more specific battery
This study is among those showing the best combination ofsensitivity and specificity values Perhaps inclusion of morenonmemory tests might have increased specificity and use of a
relatively long follow-up period likely reduced the number offalse negatives hence increasing sensitivity Another differencebetween this study and the current literature is that we did notrely on clinical measures but on theoretically motivated onesThus if selected well a relatively short battery of tests canpredict future decline in MCI and can help identify persons thatare likely to progress to more severe symptoms
The study resulted in a number of additional findings whichdeserve discussion One is that at entry progressive MCIpatients already differ from stable MCI patients in terms of ageand cognitive performance on several clinical tests Becausepatients are likely to vary in their decline rate and in their stageat entry it is possible that progressors are in a more advancedstage of neuropathology than persons with stable MCI and thatthe latter would decline later Thus a portion of stable MCIpatients may still actually be predementia (thus false negative)It is important to note however that this study makes use of amuch longer follow-up than is typically used in similar studiesStable MCI patients were followed for an average of 567months which is much longer than the period after whichprogressors converted to dementia (on average 308 monthsafter entry) This long follow-up probably reduced the contri-bution of ldquofalse negativesrdquo to the group of those with stableMCI by increasing the chance of progression during the studyperiod Admittedly it remains possible that some of the stableMCI patients will progress to dementia in the future Howeverwe do not believe that this represents a substantial portion ofour participants with stable MCI It is interesting that thefinding that the two groups differ on clinical measures is in factgood news as it supports our contention that cognitive mea-sures are sensitive to prognosis and will prove critical in iden-tifying the patients more likely to progress to dementia
This study has limitations which should be recognized Firstto improve generalizability the findings should be reproducedon a different sample Second we did not include biomarkers orimaging parameters in this study Our goal was to identify theideal set of cognitive measures and for future studies it will beimportant to assess the value of combining them with biologicalmarkers Finally it is important to point out that there might bedifferences between this cohort of patients and patients encoun-tered in other clinical settings In particular our exclusioncriteria might have led to a cohort with relatively few cases ofcomorbidity
References
Ahmed S Mitchell J Arnold R Nestor P J amp Hodges J R (2008)Predicting rapid clinical progression in amnestic mild cognitive impair-ment Dementia and Geriatric Cognitive Disorders 25 170ndash177 doi101159000113014
Albert M S DeKosky S T Dickson D Dubois B Feldman H HFox N C Phelps C H (2011) The diagnosis of mild cognitiveimpairment due to Alzheimerrsquos disease Recommendations from theNational Institute on Aging-Alzheimerrsquos Association workgroups ondiagnostic guidelines for Alzheimerrsquos disease Alzheimers amp Dementia7 270ndash279 doi101016jjalz201103008
Aretouli E Tsilidis K K amp Brandt J (2013) Four-year outcome ofmild cognitive impairment The contribution of executive dysfunctionNeuropsychology 27 95ndash106 doi101037a0030481
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
650 BELLEVILLE GAUTHIER LEPAGE KERGOAT AND GILBERT
Artero S Tierney M C Touchon J amp Ritchie K (2003) Prediction oftransition from cognitive impairment to senile dementia A prospectivelongitudinal study Acta Psychiatrica Scandinavica 107 390ndash393
Beacutelanger S amp Belleville S (2009) Semantic inhibition impairment inmild cognitive impairment A distinctive feature of upcoming cognitivedecline Neuropsychology 23 592ndash606 doi101037a0016152
Belleville S Bherer L Lepage Eacute Chertkow H amp Gauthier S (2008)Task switching capacities in persons with Alzheimerrsquos disease and mildcognitive impairment Neuropsychologia 46 2225ndash2233 doi101016jneuropsychologia200802012
Belleville S Caza N amp Peretz I (2003) A neuropsychological argu-ment for a processing view of memory Journal of Memory and Lan-guage 48 686ndash703 doi101016S0749-596X(02)00532-6
Belleville S Chertkow H amp Gauthier S (2007) Working memory andcontrol of attention in persons with Alzheimerrsquos disease and mild cog-nitive impairment Neuropsychology 21 458ndash469 doi1010370894-4105214458
Belleville S Meacutenard M C De Boysson C amp Sylvain-Roy S (2008)Characterizing memory deficits in mild cognitive impairment In WSossin J C Lacaille V Castellucci amp S Belleville (Eds) The essenceof memory (pp 365ndash375) Amsterdam Netherlands Elsevier doi101016S0079-6123(07)00023-4
Belleville S Peretz I amp Malenfant D (1996) Examination of theworking memory components in normal aging and in dementia of theAlzheimer type Neuropsychologia 34 195ndash207 doi1010160028-3932(95)00097-6
Belleville S Rouleau N amp Caza N (1998) Effect of normal aging onthe manipulation of information in working memory Memory amp Cog-nition 26 572ndash583 doi103758BF03201163
Bennett D A Wilson R S Schneider J A Evans D A BeckettL A Aggarwal N T Bach J (2002) Natural history of mildcognitive impairment in older persons Neurology 59 198ndash205
Bherer L Belleville S amp Peretz I (2001) Education age and theBrown-Peterson technique Developmental Neuropsychology 19 237ndash251 doi101207S15326942DN1903_1
Chapman R M Mapstone M McCrary J W Gardner M N Por-steinsson A Sandoval T C Reilly L A (2011) Predictingconversion from mild cognitive impairment to Alzheimerrsquos diseaseusing neuropsychological tests and multivariate methods Journal ofClinical and Experimental Neuropsychology 33 187ndash199 doi101080138033952010499356
Chatelois J Pineau H Belleville S Peretz I Lussier I FontaineF-S amp Renaseau-Leclerc C (1993) Batterie informatiseacutee drsquoeacutevaluationde la meacutemoire inspireacutee de lrsquoapproche cognitive Canadian PsychologyPsychologie Canadienne 34 45ndash63 doi101037h0078803
Conde-Sala J L Garre-Olmo J Vilalta-Franch J Llinas-Regla JTurro-Garriga O Lozano-Gallego M Loacutepez-Pousa S (2012)Predictors of cognitive decline in Alzheimerrsquos disease and mild cogni-tive impairment using the CAMCOG A five-year follow-up Interna-tional Psychogeriatrics 24 948ndash958 doi101017S1041610211002158
Deloche G amp Hannequin D (1997) Test de deacutenomination oraledrsquoimages (DO-80) Paris France Centre de Psychologie Appliqueacutee
Dierckx E Engelborghs S De Raedt R Van Buggenhout M DeDeyn P P Verte D amp Ponjaert-Kristoffersen I (2009) Verbal cuedrecall as a predictor of conversion to Alzheimerrsquos disease in mildcognitive impairment International Journal of Geriatric Psychiatry 241094ndash1100 doi101002gps2228
Dubois B Feldman H H Jacova C Dekosky S T Barberger-Gateau P Cummings J Scheltens P (2007) Research criteriafor the diagnosis of Alzheimerrsquos disease Revising the NINCDS-ADRDA criteria Lancet Neurology 6 734 ndash746 doi101016S1474-4422(07)70178 ndash3
Forlenza O V Diniz B S Nunes P V Memoria C M YassudaM S amp Gattaz W F (2009) Diagnostic transitions in mild cognitive
impairment subtypes International Psychogeriatrics 21 1088ndash1095doi101017S1041610209990792
Gauthier S Reisberg B Zaudig M Petersen R C Ritchie K BroichK Winblad B (2006) Mild cognitive impairment The Lancet 3671262ndash1270 doi101016S0140-6736(06)68542-5
Gavett B E Ozonoff A Doktor V Palmisano J Nair A K GreenR C Stern R A (2010) Predicting cognitive decline and conver-sion to Alzheimerrsquos disease in older adults using the NAB List Learningtest Journal of the International Neuropsychological Society 16 651ndash660 doi101017S1355617710000421
Geacutely-Nargeot M-C Cadilhac C Touchon J amp Nespoulous J L(1997) La meacutemoire de textes chez les sujets sains et deacutements Appli-cation drsquoun nouvel outil drsquoeacutevaluation pour neuropsychologues Meacutemo-textes In J Lambert amp J L Nespoulous (Eds) Perception auditive etcompreacutehension du langage (pp 273ndash293) Marseille France Solal
Geroldi C Rossi R Calvagna C Testa C Bresciani L Binetti G Frisoni G B (2006) Medial temporal atrophy but not memorydeficit predicts progression to dementia in patients with mild cognitiveimpairment Journal of Neurology Neurosurgery amp Psychiatry 771219ndash1222 doi101136jnnp2005082651
Irish M Lawlor B A Coen R F amp OrsquoMara S M (2011) Everydayepisodic memory in amnestic mild cognitive impairment A preliminaryinvestigation BMC Neuroscience 12 80 doi1011861471-2202-12-80
Ivanoiu A Adam S Van der Linden M Salmon E Juillerat A CMulligan R amp Seron X (2005) Memory evaluation with a new cuedrecall test in patients with mild cognitive impairment and Alzheimerrsquosdisease Journal of Neurology 252 47ndash55 doi101007s00415-005-0597-2
Landau S M Harvey D Madison C M Reiman E M Foster N LAisen P S Jagust W J (2010) Comparing predictors of conver-sion and decline in mild cognitive impairment Neurology 75 230ndash238doi101212WNL0b013e3181e8e8b8
Lekeu F Magis D Marique P Delbeuck X Bechet S GuillaumeB Salmon E (2010) The California Verbal Learning Test andother standard clinical neuropsychological tests to predict conversionfrom mild memory impairment to dementia Journal of Clinical andExperimental Neuropsychology 32 164 ndash173 doi10108013803390902889606
Mitchell J Arnold R Dawson K Nestor P J amp Hodges J R (2009)Outcome in subgroups of mild cognitive impairment (MCI) is highlypredictable using a simple algorithm Journal of Neurology 256 1500ndash1509 doi101007s00415-009-5152-0[doi]
Mottron L Morasse K amp Belleville S (2001) A study of memoryfunctioning in individuals with autism Journal of Child Psychology andPsychiatry 42 253ndash260 doi1011111469-761000716
Nordlund A Rolstad S Klang O Edman A Hansen S amp Wallin A(2010) Two-year outcome of MCI subtypes and aetiologies in theGoteborg MCI study Journal of Neurology Neurosurgery amp Psychia-try 81 541ndash546 doi101136jnnp2008171066
Petersen R C (2003) Mild cognitive impairment Aging to Alzheimerrsquosdisease Oxford UK Oxford University Press
Petersen R C amp Morris J C (2003) Clinical features In R C Petersen(Ed) Mild cognitive impairment Aging to Alzheimerrsquos disease (pp15ndash39) Oxford UK Oxford University Press
Rabin L A Pare N Saykin A J Brown M J Wishart H AFlashman L A amp Santulli R B (2009) Differential memory testsensitivity for diagnosing amnestic mild cognitive impairment and pre-dicting conversion to Alzheimerrsquos disease Neuropsychology Develop-ment and Cognition Section B Aging Neuropsychology and Cognition16 357ndash376 doi10108013825580902825220
Rasquin S M Lodder J Visser P J Lousberg R amp Verhey F R(2005) Predictive accuracy of MCI subtypes for Alzheimerrsquos diseaseand vascular dementia in subjects with mild cognitive impairment A
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
651PREDICTING DECLINE IN MCI
2-year follow-up study Dementia and Geriatric Cognitive Disorders19 113ndash119 doi101159000082662
Riddoch J M amp Humphreys G W (1993) BORB Birmingham ObjectRecognition Battery Hove UK Erlbaum
Ritchie K Artero S amp Touchon J (2001) Classification criteria formild cognitive impairment A population-based validation study Neu-rology 56 37ndash42 doi101212WNL56137
Summers M J amp Saunders N L (2012) Neuropsychological measurespredict decline to Alzheimerrsquos dementia from mild cognitive impair-ment Neuropsychology 26 498ndash508 doi101037a0028576
Tabert M H Manly J J Liu X Pelton G H Rosenblum S JacobsM Devanand D P (2006) Neuropsychological prediction of
conversion to Alzheimer disease in patients with mild cognitive impair-ment Archives of General Psychiatry 63 916ndash924 doi101001archpsyc638916
Tierney M C Szalai J P Snow W G Fisher R H Nores A NadonG St George-Hyslop P H (1996) Prediction of probable Alz-heimerrsquos disease in memory-impaired patients A prospective longitu-dinal study Neurology 46 661ndash665 doi101212WNL463661
Received May 15 2013Revision received December 19 2013
Accepted December 22 2013
Members of Underrepresented GroupsReviewers for Journal Manuscripts Wanted
If you are interested in reviewing manuscripts for APA journals the APA Publications andCommunications Board would like to invite your participation Manuscript reviewers are vital to thepublications process As a reviewer you would gain valuable experience in publishing The PampCBoard is particularly interested in encouraging members of underrepresented groups to participatemore in this process
If you are interested in reviewing manuscripts please write APA Journals at ReviewersapaorgPlease note the following important points
bull To be selected as a reviewer you must have published articles in peer-reviewed journals Theexperience of publishing provides a reviewer with the basis for preparing a thorough objectivereview
bull To be selected it is critical to be a regular reader of the five to six empirical journals that are mostcentral to the area or journal for which you would like to review Current knowledge of recentlypublished research provides a reviewer with the knowledge base to evaluate a new submissionwithin the context of existing research
bull To select the appropriate reviewers for each manuscript the editor needs detailed informationPlease include with your letter your vita In the letter please identify which APA journal(s) youare interested in and describe your area of expertise Be as specific as possible For exampleldquosocial psychologyrdquo is not sufficientmdashyou would need to specify ldquosocial cognitionrdquo or ldquoattitudechangerdquo as well
bull Reviewing a manuscript takes time (1ndash4 hours per manuscript reviewed) If you are selected toreview a manuscript be prepared to invest the necessary time to evaluate the manuscriptthoroughly
APA now has an online video course that provides guidance in reviewing manuscripts To learnmore about the course and to access the video visit httpwwwapaorgpubsauthorsreview-manuscript-ce-videoaspx
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
652 BELLEVILLE GAUTHIER LEPAGE KERGOAT AND GILBERT
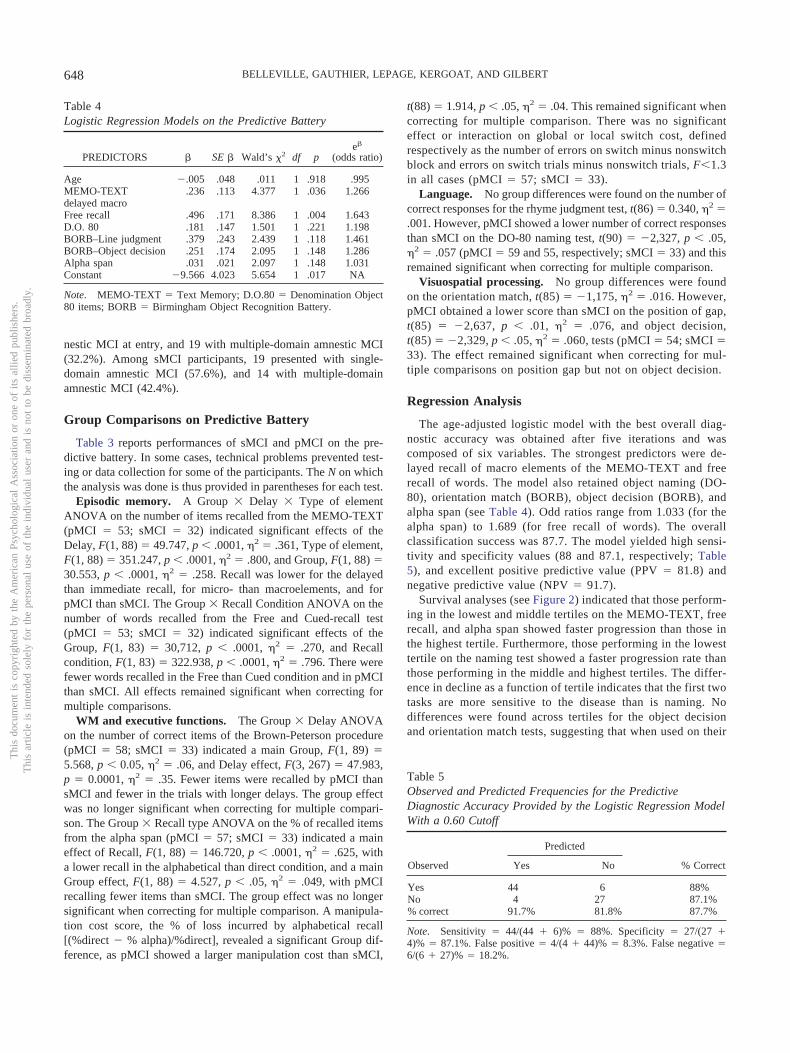
nestic MCI at entry and 19 with multiple-domain amnestic MCI(322) Among sMCI participants 19 presented with single-domain amnestic MCI (576) and 14 with multiple-domainamnestic MCI (424)
Group Comparisons on Predictive Battery
Table 3 reports performances of sMCI and pMCI on the pre-dictive battery In some cases technical problems prevented test-ing or data collection for some of the participants The N on whichthe analysis was done is thus provided in parentheses for each test
Episodic memory A Group Delay Type of elementANOVA on the number of items recalled from the MEMO-TEXT(pMCI 53 sMCI 32) indicated significant effects of theDelay F(1 88) 49747 p 0001 2 361 Type of elementF(1 88) 351247 p 0001 2 800 and Group F(1 88) 30553 p 0001 2 258 Recall was lower for the delayedthan immediate recall for micro- than macroelements and forpMCI than sMCI The Group Recall Condition ANOVA on thenumber of words recalled from the Free and Cued-recall test(pMCI 53 sMCI 32) indicated significant effects of theGroup F(1 83) 30712 p 0001 2 270 and Recallcondition F(1 83) 322938 p 0001 2 796 There werefewer words recalled in the Free than Cued condition and in pMCIthan sMCI All effects remained significant when correcting formultiple comparisons
WM and executive functions The Group Delay ANOVAon the number of correct items of the Brown-Peterson procedure(pMCI 58 sMCI 33) indicated a main Group F(1 89) 5568 p 005 2 06 and Delay effect F(3 267) 47983p 00001 2 35 Fewer items were recalled by pMCI thansMCI and fewer in the trials with longer delays The group effectwas no longer significant when correcting for multiple compari-son The Group Recall type ANOVA on the of recalled itemsfrom the alpha span (pMCI 57 sMCI 33) indicated a maineffect of Recall F(1 88) 146720 p 0001 2 625 witha lower recall in the alphabetical than direct condition and a mainGroup effect F(1 88) 4527 p 05 2 049 with pMCIrecalling fewer items than sMCI The group effect was no longersignificant when correcting for multiple comparison A manipula-tion cost score the of loss incurred by alphabetical recall[(direct alpha)direct] revealed a significant Group dif-ference as pMCI showed a larger manipulation cost than sMCI
t(88) 1914 p 05 2 04 This remained significant whencorrecting for multiple comparison There was no significanteffect or interaction on global or local switch cost definedrespectively as the number of errors on switch minus nonswitchblock and errors on switch trials minus nonswitch trials F13in all cases (pMCI 57 sMCI 33)
Language No group differences were found on the number ofcorrect responses for the rhyme judgment test t(86) 0340 2 001 However pMCI showed a lower number of correct responsesthan sMCI on the DO-80 naming test t(90) 2327 p 052 057 (pMCI 59 and 55 respectively sMCI 33) and thisremained significant when correcting for multiple comparison
Visuospatial processing No group differences were foundon the orientation match t(85) 1175 2 016 HoweverpMCI obtained a lower score than sMCI on the position of gapt(85) 2637 p 01 2 076 and object decisiont(85) 2329 p 05 2 060 tests (pMCI 54 sMCI 33) The effect remained significant when correcting for mul-tiple comparisons on position gap but not on object decision
Regression Analysis
The age-adjusted logistic model with the best overall diag-nostic accuracy was obtained after five iterations and wascomposed of six variables The strongest predictors were de-layed recall of macro elements of the MEMO-TEXT and freerecall of words The model also retained object naming (DO-80) orientation match (BORB) object decision (BORB) andalpha span (see Table 4) Odd ratios range from 1033 (for thealpha span) to 1689 (for free recall of words) The overallclassification success was 877 The model yielded high sensi-tivity and specificity values (88 and 871 respectively Table5) and excellent positive predictive value (PPV 818) andnegative predictive value (NPV 917)
Survival analyses (see Figure 2) indicated that those perform-ing in the lowest and middle tertiles on the MEMO-TEXT freerecall and alpha span showed faster progression than those inthe highest tertile Furthermore those performing in the lowesttertile on the naming test showed a faster progression rate thanthose performing in the middle and highest tertiles The differ-ence in decline as a function of tertile indicates that the first twotasks are more sensitive to the disease than is naming Nodifferences were found across tertiles for the object decisionand orientation match tests suggesting that when used on their
Table 4Logistic Regression Models on the Predictive Battery
PREDICTORS SE Waldrsquos 2 df pe
(odds ratio)
Age 005 048 011 1 918 995MEMO-TEXT 236 113 4377 1 036 1266delayed macroFree recall 496 171 8386 1 004 1643DO 80 181 147 1501 1 221 1198BORBndashLine judgment 379 243 2439 1 118 1461BORBndashObject decision 251 174 2095 1 148 1286Alpha span 031 021 2097 1 148 1031Constant 9566 4023 5654 1 017 NA
Note MEMO-TEXT Text Memory DO80 Denomination Object80 items BORB Birmingham Object Recognition Battery
Table 5Observed and Predicted Frequencies for the PredictiveDiagnostic Accuracy Provided by the Logistic Regression ModelWith a 060 Cutoff
Predicted
Observed Yes No Correct
Yes 44 6 88No 4 27 871 correct 917 818 877
Note Sensitivity 44(44 6) 88 Specificity 27(27 4) 871 False positive 4(4 44) 83 False negative 6(6 27) 182
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
648 BELLEVILLE GAUTHIER LEPAGE KERGOAT AND GILBERT
own these two tasks lack sensitivity This analysis also showsdifferences across tasks in sensitivity to time of progression Bythe 40-month follow-up 80 of those in the lowest tertile ofMEMO-TEXT had converted to dementia This was found 60and 80 months after follow-up among those in the lowest tertileof free recall and alpha-span respectively
Discussion
Not all MCI cases progress to dementia and it is critical toidentify tests that accurately predict future progression In this
study we found that combining tests of episodic memory (text andword recall) perception (naming orientation and object decision)and working memory (alpha span) correctly identifies 878 ofparticipants who will progress on an average of 45 years inadvance The six-test model yielded very good to excellent sensi-tivity and specificity values as both of them were above 85 Thiswas also the case for PPN and NPV values and in particular it wasfound that 917 of those found unimpaired on the tests remainedstable in spite of the fact they met clinical criteria for MCI Thusthis combination of measures is not only sensitive but it is also
Figure 2 Survival analyses
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
649PREDICTING DECLINE IN MCI
specific and it helps to identify those who are unlikely to progressThis is highly important for clinical trials as it can help identify theMCI persons who are most likely to benefit from disease-modifying therapies Survival analyses indicate that 80 of thepatients performing in the lowest tertile of the MCI group on thetext memory test will have developed dementia 40 months later
This study suggests that relying only on episodic memory mea-sures might not be optimal and that measuring different domains ofcognition represents the most balanced approach Several studieshave investigated the capacity of biological and cognitive mea-sures to predict future progression from MCI to dementia A firstimportant conclusion from many of these studies is that the patternof cognitive deficit might be as accurate as biological measures inpredicting future decline in MCI (Albert et al 2011 Dubois et al2007) a conclusion coherent with our finding of a strong predic-tive accuracy for the cognitive battery used here Another impor-tant conclusion is that it is possible to identify an optimal set ofcognitive tasks Studies vary in their design statistical approachand follow-up length and there is great variability in the cognitivetests used Nevertheless a coherent pattern seems to emerge fromprevious studies which is supported by our findings First itappears that combining episodic memory tests with tasks that relyon executive functions or the attentional control of WM is partic-ularly powerful for predicting conversion from MCI to dementia(Aretouli Tsilidis amp Brandt 2013 Chapman et al 2011 Conde-Sala et al 2012 Gavett et al 2010 Rabin et al 2009 Summersamp Saunders 2012) Second studies that measured only one or twocognitive domains have much lower predictive accuracy than theone found here They report either lower specificity (eg Mitchellet al 2009) or lower sensitivity (Dierckx et al 2009 Tabert et al2006 Tierney et al 1996) than what is reported here This isconsistent with studies indicating that cases of multiple-domainMCI are more likely to progress to dementia than single-domainMCI (Forlenza et al 2009 Nordlund et al 2010 RasquinLodder Visser Lousberg amp Verhey 2005 Summers amp Saunders2012) Our study indicates that an optimal battery should includeperceptual tests in addition to tests of episodic memory executivefunction and working memory The particular cognitive domainsidentified here match well with findings indicating that in additionto episodic memory semantic knowledge and working memoryare impaired early in AD (for a review see Belleville et al 2008)
Few studies have included perceptual or semantic componentsin their models contrary to this study and those that did measureda relatively small number of components It is therefore possiblethat measures of the perceptual or semantic domains have im-proved predictive accuracy However these tasks may be morespecific than sensitive Indeed our survival analyses suggest thatnaming and perceptual tasks were not as sensitive to future declineas episodic memory and executive tasks when taken on their ownIncluding measures of the perceptual or semantic domain mightcontribute to reducing the number of false positives hence increas-ing specificity This is a potentially useful finding for cliniciansand researchers When optimizing testing time is a critical issueand tasks need to be selected one can base the decision on whetherthe need is to have a more sensitive or more specific battery
This study is among those showing the best combination ofsensitivity and specificity values Perhaps inclusion of morenonmemory tests might have increased specificity and use of a
relatively long follow-up period likely reduced the number offalse negatives hence increasing sensitivity Another differencebetween this study and the current literature is that we did notrely on clinical measures but on theoretically motivated onesThus if selected well a relatively short battery of tests canpredict future decline in MCI and can help identify persons thatare likely to progress to more severe symptoms
The study resulted in a number of additional findings whichdeserve discussion One is that at entry progressive MCIpatients already differ from stable MCI patients in terms of ageand cognitive performance on several clinical tests Becausepatients are likely to vary in their decline rate and in their stageat entry it is possible that progressors are in a more advancedstage of neuropathology than persons with stable MCI and thatthe latter would decline later Thus a portion of stable MCIpatients may still actually be predementia (thus false negative)It is important to note however that this study makes use of amuch longer follow-up than is typically used in similar studiesStable MCI patients were followed for an average of 567months which is much longer than the period after whichprogressors converted to dementia (on average 308 monthsafter entry) This long follow-up probably reduced the contri-bution of ldquofalse negativesrdquo to the group of those with stableMCI by increasing the chance of progression during the studyperiod Admittedly it remains possible that some of the stableMCI patients will progress to dementia in the future Howeverwe do not believe that this represents a substantial portion ofour participants with stable MCI It is interesting that thefinding that the two groups differ on clinical measures is in factgood news as it supports our contention that cognitive mea-sures are sensitive to prognosis and will prove critical in iden-tifying the patients more likely to progress to dementia
This study has limitations which should be recognized Firstto improve generalizability the findings should be reproducedon a different sample Second we did not include biomarkers orimaging parameters in this study Our goal was to identify theideal set of cognitive measures and for future studies it will beimportant to assess the value of combining them with biologicalmarkers Finally it is important to point out that there might bedifferences between this cohort of patients and patients encoun-tered in other clinical settings In particular our exclusioncriteria might have led to a cohort with relatively few cases ofcomorbidity
References
Ahmed S Mitchell J Arnold R Nestor P J amp Hodges J R (2008)Predicting rapid clinical progression in amnestic mild cognitive impair-ment Dementia and Geriatric Cognitive Disorders 25 170ndash177 doi101159000113014
Albert M S DeKosky S T Dickson D Dubois B Feldman H HFox N C Phelps C H (2011) The diagnosis of mild cognitiveimpairment due to Alzheimerrsquos disease Recommendations from theNational Institute on Aging-Alzheimerrsquos Association workgroups ondiagnostic guidelines for Alzheimerrsquos disease Alzheimers amp Dementia7 270ndash279 doi101016jjalz201103008
Aretouli E Tsilidis K K amp Brandt J (2013) Four-year outcome ofmild cognitive impairment The contribution of executive dysfunctionNeuropsychology 27 95ndash106 doi101037a0030481
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
650 BELLEVILLE GAUTHIER LEPAGE KERGOAT AND GILBERT
Artero S Tierney M C Touchon J amp Ritchie K (2003) Prediction oftransition from cognitive impairment to senile dementia A prospectivelongitudinal study Acta Psychiatrica Scandinavica 107 390ndash393
Beacutelanger S amp Belleville S (2009) Semantic inhibition impairment inmild cognitive impairment A distinctive feature of upcoming cognitivedecline Neuropsychology 23 592ndash606 doi101037a0016152
Belleville S Bherer L Lepage Eacute Chertkow H amp Gauthier S (2008)Task switching capacities in persons with Alzheimerrsquos disease and mildcognitive impairment Neuropsychologia 46 2225ndash2233 doi101016jneuropsychologia200802012
Belleville S Caza N amp Peretz I (2003) A neuropsychological argu-ment for a processing view of memory Journal of Memory and Lan-guage 48 686ndash703 doi101016S0749-596X(02)00532-6
Belleville S Chertkow H amp Gauthier S (2007) Working memory andcontrol of attention in persons with Alzheimerrsquos disease and mild cog-nitive impairment Neuropsychology 21 458ndash469 doi1010370894-4105214458
Belleville S Meacutenard M C De Boysson C amp Sylvain-Roy S (2008)Characterizing memory deficits in mild cognitive impairment In WSossin J C Lacaille V Castellucci amp S Belleville (Eds) The essenceof memory (pp 365ndash375) Amsterdam Netherlands Elsevier doi101016S0079-6123(07)00023-4
Belleville S Peretz I amp Malenfant D (1996) Examination of theworking memory components in normal aging and in dementia of theAlzheimer type Neuropsychologia 34 195ndash207 doi1010160028-3932(95)00097-6
Belleville S Rouleau N amp Caza N (1998) Effect of normal aging onthe manipulation of information in working memory Memory amp Cog-nition 26 572ndash583 doi103758BF03201163
Bennett D A Wilson R S Schneider J A Evans D A BeckettL A Aggarwal N T Bach J (2002) Natural history of mildcognitive impairment in older persons Neurology 59 198ndash205
Bherer L Belleville S amp Peretz I (2001) Education age and theBrown-Peterson technique Developmental Neuropsychology 19 237ndash251 doi101207S15326942DN1903_1
Chapman R M Mapstone M McCrary J W Gardner M N Por-steinsson A Sandoval T C Reilly L A (2011) Predictingconversion from mild cognitive impairment to Alzheimerrsquos diseaseusing neuropsychological tests and multivariate methods Journal ofClinical and Experimental Neuropsychology 33 187ndash199 doi101080138033952010499356
Chatelois J Pineau H Belleville S Peretz I Lussier I FontaineF-S amp Renaseau-Leclerc C (1993) Batterie informatiseacutee drsquoeacutevaluationde la meacutemoire inspireacutee de lrsquoapproche cognitive Canadian PsychologyPsychologie Canadienne 34 45ndash63 doi101037h0078803
Conde-Sala J L Garre-Olmo J Vilalta-Franch J Llinas-Regla JTurro-Garriga O Lozano-Gallego M Loacutepez-Pousa S (2012)Predictors of cognitive decline in Alzheimerrsquos disease and mild cogni-tive impairment using the CAMCOG A five-year follow-up Interna-tional Psychogeriatrics 24 948ndash958 doi101017S1041610211002158
Deloche G amp Hannequin D (1997) Test de deacutenomination oraledrsquoimages (DO-80) Paris France Centre de Psychologie Appliqueacutee
Dierckx E Engelborghs S De Raedt R Van Buggenhout M DeDeyn P P Verte D amp Ponjaert-Kristoffersen I (2009) Verbal cuedrecall as a predictor of conversion to Alzheimerrsquos disease in mildcognitive impairment International Journal of Geriatric Psychiatry 241094ndash1100 doi101002gps2228
Dubois B Feldman H H Jacova C Dekosky S T Barberger-Gateau P Cummings J Scheltens P (2007) Research criteriafor the diagnosis of Alzheimerrsquos disease Revising the NINCDS-ADRDA criteria Lancet Neurology 6 734 ndash746 doi101016S1474-4422(07)70178 ndash3
Forlenza O V Diniz B S Nunes P V Memoria C M YassudaM S amp Gattaz W F (2009) Diagnostic transitions in mild cognitive
impairment subtypes International Psychogeriatrics 21 1088ndash1095doi101017S1041610209990792
Gauthier S Reisberg B Zaudig M Petersen R C Ritchie K BroichK Winblad B (2006) Mild cognitive impairment The Lancet 3671262ndash1270 doi101016S0140-6736(06)68542-5
Gavett B E Ozonoff A Doktor V Palmisano J Nair A K GreenR C Stern R A (2010) Predicting cognitive decline and conver-sion to Alzheimerrsquos disease in older adults using the NAB List Learningtest Journal of the International Neuropsychological Society 16 651ndash660 doi101017S1355617710000421
Geacutely-Nargeot M-C Cadilhac C Touchon J amp Nespoulous J L(1997) La meacutemoire de textes chez les sujets sains et deacutements Appli-cation drsquoun nouvel outil drsquoeacutevaluation pour neuropsychologues Meacutemo-textes In J Lambert amp J L Nespoulous (Eds) Perception auditive etcompreacutehension du langage (pp 273ndash293) Marseille France Solal
Geroldi C Rossi R Calvagna C Testa C Bresciani L Binetti G Frisoni G B (2006) Medial temporal atrophy but not memorydeficit predicts progression to dementia in patients with mild cognitiveimpairment Journal of Neurology Neurosurgery amp Psychiatry 771219ndash1222 doi101136jnnp2005082651
Irish M Lawlor B A Coen R F amp OrsquoMara S M (2011) Everydayepisodic memory in amnestic mild cognitive impairment A preliminaryinvestigation BMC Neuroscience 12 80 doi1011861471-2202-12-80
Ivanoiu A Adam S Van der Linden M Salmon E Juillerat A CMulligan R amp Seron X (2005) Memory evaluation with a new cuedrecall test in patients with mild cognitive impairment and Alzheimerrsquosdisease Journal of Neurology 252 47ndash55 doi101007s00415-005-0597-2
Landau S M Harvey D Madison C M Reiman E M Foster N LAisen P S Jagust W J (2010) Comparing predictors of conver-sion and decline in mild cognitive impairment Neurology 75 230ndash238doi101212WNL0b013e3181e8e8b8
Lekeu F Magis D Marique P Delbeuck X Bechet S GuillaumeB Salmon E (2010) The California Verbal Learning Test andother standard clinical neuropsychological tests to predict conversionfrom mild memory impairment to dementia Journal of Clinical andExperimental Neuropsychology 32 164 ndash173 doi10108013803390902889606
Mitchell J Arnold R Dawson K Nestor P J amp Hodges J R (2009)Outcome in subgroups of mild cognitive impairment (MCI) is highlypredictable using a simple algorithm Journal of Neurology 256 1500ndash1509 doi101007s00415-009-5152-0[doi]
Mottron L Morasse K amp Belleville S (2001) A study of memoryfunctioning in individuals with autism Journal of Child Psychology andPsychiatry 42 253ndash260 doi1011111469-761000716
Nordlund A Rolstad S Klang O Edman A Hansen S amp Wallin A(2010) Two-year outcome of MCI subtypes and aetiologies in theGoteborg MCI study Journal of Neurology Neurosurgery amp Psychia-try 81 541ndash546 doi101136jnnp2008171066
Petersen R C (2003) Mild cognitive impairment Aging to Alzheimerrsquosdisease Oxford UK Oxford University Press
Petersen R C amp Morris J C (2003) Clinical features In R C Petersen(Ed) Mild cognitive impairment Aging to Alzheimerrsquos disease (pp15ndash39) Oxford UK Oxford University Press
Rabin L A Pare N Saykin A J Brown M J Wishart H AFlashman L A amp Santulli R B (2009) Differential memory testsensitivity for diagnosing amnestic mild cognitive impairment and pre-dicting conversion to Alzheimerrsquos disease Neuropsychology Develop-ment and Cognition Section B Aging Neuropsychology and Cognition16 357ndash376 doi10108013825580902825220
Rasquin S M Lodder J Visser P J Lousberg R amp Verhey F R(2005) Predictive accuracy of MCI subtypes for Alzheimerrsquos diseaseand vascular dementia in subjects with mild cognitive impairment A
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
651PREDICTING DECLINE IN MCI
2-year follow-up study Dementia and Geriatric Cognitive Disorders19 113ndash119 doi101159000082662
Riddoch J M amp Humphreys G W (1993) BORB Birmingham ObjectRecognition Battery Hove UK Erlbaum
Ritchie K Artero S amp Touchon J (2001) Classification criteria formild cognitive impairment A population-based validation study Neu-rology 56 37ndash42 doi101212WNL56137
Summers M J amp Saunders N L (2012) Neuropsychological measurespredict decline to Alzheimerrsquos dementia from mild cognitive impair-ment Neuropsychology 26 498ndash508 doi101037a0028576
Tabert M H Manly J J Liu X Pelton G H Rosenblum S JacobsM Devanand D P (2006) Neuropsychological prediction of
conversion to Alzheimer disease in patients with mild cognitive impair-ment Archives of General Psychiatry 63 916ndash924 doi101001archpsyc638916
Tierney M C Szalai J P Snow W G Fisher R H Nores A NadonG St George-Hyslop P H (1996) Prediction of probable Alz-heimerrsquos disease in memory-impaired patients A prospective longitu-dinal study Neurology 46 661ndash665 doi101212WNL463661
Received May 15 2013Revision received December 19 2013
Accepted December 22 2013
Members of Underrepresented GroupsReviewers for Journal Manuscripts Wanted
If you are interested in reviewing manuscripts for APA journals the APA Publications andCommunications Board would like to invite your participation Manuscript reviewers are vital to thepublications process As a reviewer you would gain valuable experience in publishing The PampCBoard is particularly interested in encouraging members of underrepresented groups to participatemore in this process
If you are interested in reviewing manuscripts please write APA Journals at ReviewersapaorgPlease note the following important points
bull To be selected as a reviewer you must have published articles in peer-reviewed journals Theexperience of publishing provides a reviewer with the basis for preparing a thorough objectivereview
bull To be selected it is critical to be a regular reader of the five to six empirical journals that are mostcentral to the area or journal for which you would like to review Current knowledge of recentlypublished research provides a reviewer with the knowledge base to evaluate a new submissionwithin the context of existing research
bull To select the appropriate reviewers for each manuscript the editor needs detailed informationPlease include with your letter your vita In the letter please identify which APA journal(s) youare interested in and describe your area of expertise Be as specific as possible For exampleldquosocial psychologyrdquo is not sufficientmdashyou would need to specify ldquosocial cognitionrdquo or ldquoattitudechangerdquo as well
bull Reviewing a manuscript takes time (1ndash4 hours per manuscript reviewed) If you are selected toreview a manuscript be prepared to invest the necessary time to evaluate the manuscriptthoroughly
APA now has an online video course that provides guidance in reviewing manuscripts To learnmore about the course and to access the video visit httpwwwapaorgpubsauthorsreview-manuscript-ce-videoaspx
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
652 BELLEVILLE GAUTHIER LEPAGE KERGOAT AND GILBERT
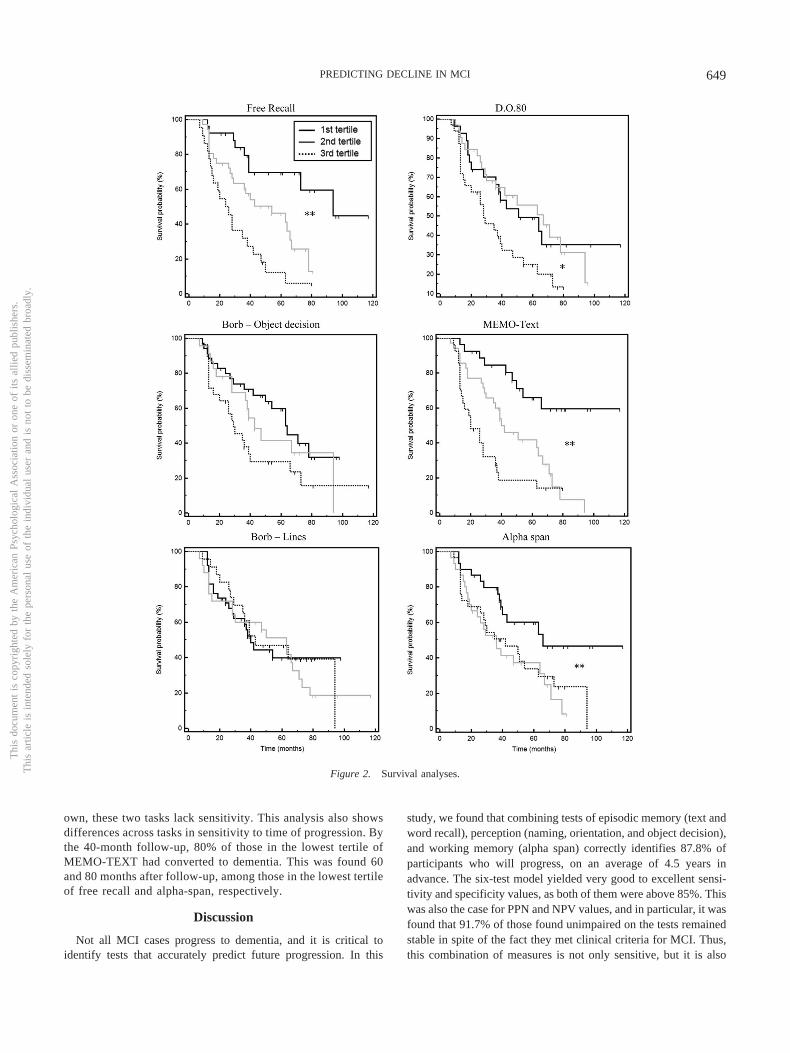
own these two tasks lack sensitivity This analysis also showsdifferences across tasks in sensitivity to time of progression Bythe 40-month follow-up 80 of those in the lowest tertile ofMEMO-TEXT had converted to dementia This was found 60and 80 months after follow-up among those in the lowest tertileof free recall and alpha-span respectively
Discussion
Not all MCI cases progress to dementia and it is critical toidentify tests that accurately predict future progression In this
study we found that combining tests of episodic memory (text andword recall) perception (naming orientation and object decision)and working memory (alpha span) correctly identifies 878 ofparticipants who will progress on an average of 45 years inadvance The six-test model yielded very good to excellent sensi-tivity and specificity values as both of them were above 85 Thiswas also the case for PPN and NPV values and in particular it wasfound that 917 of those found unimpaired on the tests remainedstable in spite of the fact they met clinical criteria for MCI Thusthis combination of measures is not only sensitive but it is also
Figure 2 Survival analyses
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
649PREDICTING DECLINE IN MCI
specific and it helps to identify those who are unlikely to progressThis is highly important for clinical trials as it can help identify theMCI persons who are most likely to benefit from disease-modifying therapies Survival analyses indicate that 80 of thepatients performing in the lowest tertile of the MCI group on thetext memory test will have developed dementia 40 months later
This study suggests that relying only on episodic memory mea-sures might not be optimal and that measuring different domains ofcognition represents the most balanced approach Several studieshave investigated the capacity of biological and cognitive mea-sures to predict future progression from MCI to dementia A firstimportant conclusion from many of these studies is that the patternof cognitive deficit might be as accurate as biological measures inpredicting future decline in MCI (Albert et al 2011 Dubois et al2007) a conclusion coherent with our finding of a strong predic-tive accuracy for the cognitive battery used here Another impor-tant conclusion is that it is possible to identify an optimal set ofcognitive tasks Studies vary in their design statistical approachand follow-up length and there is great variability in the cognitivetests used Nevertheless a coherent pattern seems to emerge fromprevious studies which is supported by our findings First itappears that combining episodic memory tests with tasks that relyon executive functions or the attentional control of WM is partic-ularly powerful for predicting conversion from MCI to dementia(Aretouli Tsilidis amp Brandt 2013 Chapman et al 2011 Conde-Sala et al 2012 Gavett et al 2010 Rabin et al 2009 Summersamp Saunders 2012) Second studies that measured only one or twocognitive domains have much lower predictive accuracy than theone found here They report either lower specificity (eg Mitchellet al 2009) or lower sensitivity (Dierckx et al 2009 Tabert et al2006 Tierney et al 1996) than what is reported here This isconsistent with studies indicating that cases of multiple-domainMCI are more likely to progress to dementia than single-domainMCI (Forlenza et al 2009 Nordlund et al 2010 RasquinLodder Visser Lousberg amp Verhey 2005 Summers amp Saunders2012) Our study indicates that an optimal battery should includeperceptual tests in addition to tests of episodic memory executivefunction and working memory The particular cognitive domainsidentified here match well with findings indicating that in additionto episodic memory semantic knowledge and working memoryare impaired early in AD (for a review see Belleville et al 2008)
Few studies have included perceptual or semantic componentsin their models contrary to this study and those that did measureda relatively small number of components It is therefore possiblethat measures of the perceptual or semantic domains have im-proved predictive accuracy However these tasks may be morespecific than sensitive Indeed our survival analyses suggest thatnaming and perceptual tasks were not as sensitive to future declineas episodic memory and executive tasks when taken on their ownIncluding measures of the perceptual or semantic domain mightcontribute to reducing the number of false positives hence increas-ing specificity This is a potentially useful finding for cliniciansand researchers When optimizing testing time is a critical issueand tasks need to be selected one can base the decision on whetherthe need is to have a more sensitive or more specific battery
This study is among those showing the best combination ofsensitivity and specificity values Perhaps inclusion of morenonmemory tests might have increased specificity and use of a
relatively long follow-up period likely reduced the number offalse negatives hence increasing sensitivity Another differencebetween this study and the current literature is that we did notrely on clinical measures but on theoretically motivated onesThus if selected well a relatively short battery of tests canpredict future decline in MCI and can help identify persons thatare likely to progress to more severe symptoms
The study resulted in a number of additional findings whichdeserve discussion One is that at entry progressive MCIpatients already differ from stable MCI patients in terms of ageand cognitive performance on several clinical tests Becausepatients are likely to vary in their decline rate and in their stageat entry it is possible that progressors are in a more advancedstage of neuropathology than persons with stable MCI and thatthe latter would decline later Thus a portion of stable MCIpatients may still actually be predementia (thus false negative)It is important to note however that this study makes use of amuch longer follow-up than is typically used in similar studiesStable MCI patients were followed for an average of 567months which is much longer than the period after whichprogressors converted to dementia (on average 308 monthsafter entry) This long follow-up probably reduced the contri-bution of ldquofalse negativesrdquo to the group of those with stableMCI by increasing the chance of progression during the studyperiod Admittedly it remains possible that some of the stableMCI patients will progress to dementia in the future Howeverwe do not believe that this represents a substantial portion ofour participants with stable MCI It is interesting that thefinding that the two groups differ on clinical measures is in factgood news as it supports our contention that cognitive mea-sures are sensitive to prognosis and will prove critical in iden-tifying the patients more likely to progress to dementia
This study has limitations which should be recognized Firstto improve generalizability the findings should be reproducedon a different sample Second we did not include biomarkers orimaging parameters in this study Our goal was to identify theideal set of cognitive measures and for future studies it will beimportant to assess the value of combining them with biologicalmarkers Finally it is important to point out that there might bedifferences between this cohort of patients and patients encoun-tered in other clinical settings In particular our exclusioncriteria might have led to a cohort with relatively few cases ofcomorbidity
References
Ahmed S Mitchell J Arnold R Nestor P J amp Hodges J R (2008)Predicting rapid clinical progression in amnestic mild cognitive impair-ment Dementia and Geriatric Cognitive Disorders 25 170ndash177 doi101159000113014
Albert M S DeKosky S T Dickson D Dubois B Feldman H HFox N C Phelps C H (2011) The diagnosis of mild cognitiveimpairment due to Alzheimerrsquos disease Recommendations from theNational Institute on Aging-Alzheimerrsquos Association workgroups ondiagnostic guidelines for Alzheimerrsquos disease Alzheimers amp Dementia7 270ndash279 doi101016jjalz201103008
Aretouli E Tsilidis K K amp Brandt J (2013) Four-year outcome ofmild cognitive impairment The contribution of executive dysfunctionNeuropsychology 27 95ndash106 doi101037a0030481
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
650 BELLEVILLE GAUTHIER LEPAGE KERGOAT AND GILBERT
Artero S Tierney M C Touchon J amp Ritchie K (2003) Prediction oftransition from cognitive impairment to senile dementia A prospectivelongitudinal study Acta Psychiatrica Scandinavica 107 390ndash393
Beacutelanger S amp Belleville S (2009) Semantic inhibition impairment inmild cognitive impairment A distinctive feature of upcoming cognitivedecline Neuropsychology 23 592ndash606 doi101037a0016152
Belleville S Bherer L Lepage Eacute Chertkow H amp Gauthier S (2008)Task switching capacities in persons with Alzheimerrsquos disease and mildcognitive impairment Neuropsychologia 46 2225ndash2233 doi101016jneuropsychologia200802012
Belleville S Caza N amp Peretz I (2003) A neuropsychological argu-ment for a processing view of memory Journal of Memory and Lan-guage 48 686ndash703 doi101016S0749-596X(02)00532-6
Belleville S Chertkow H amp Gauthier S (2007) Working memory andcontrol of attention in persons with Alzheimerrsquos disease and mild cog-nitive impairment Neuropsychology 21 458ndash469 doi1010370894-4105214458
Belleville S Meacutenard M C De Boysson C amp Sylvain-Roy S (2008)Characterizing memory deficits in mild cognitive impairment In WSossin J C Lacaille V Castellucci amp S Belleville (Eds) The essenceof memory (pp 365ndash375) Amsterdam Netherlands Elsevier doi101016S0079-6123(07)00023-4
Belleville S Peretz I amp Malenfant D (1996) Examination of theworking memory components in normal aging and in dementia of theAlzheimer type Neuropsychologia 34 195ndash207 doi1010160028-3932(95)00097-6
Belleville S Rouleau N amp Caza N (1998) Effect of normal aging onthe manipulation of information in working memory Memory amp Cog-nition 26 572ndash583 doi103758BF03201163
Bennett D A Wilson R S Schneider J A Evans D A BeckettL A Aggarwal N T Bach J (2002) Natural history of mildcognitive impairment in older persons Neurology 59 198ndash205
Bherer L Belleville S amp Peretz I (2001) Education age and theBrown-Peterson technique Developmental Neuropsychology 19 237ndash251 doi101207S15326942DN1903_1
Chapman R M Mapstone M McCrary J W Gardner M N Por-steinsson A Sandoval T C Reilly L A (2011) Predictingconversion from mild cognitive impairment to Alzheimerrsquos diseaseusing neuropsychological tests and multivariate methods Journal ofClinical and Experimental Neuropsychology 33 187ndash199 doi101080138033952010499356
Chatelois J Pineau H Belleville S Peretz I Lussier I FontaineF-S amp Renaseau-Leclerc C (1993) Batterie informatiseacutee drsquoeacutevaluationde la meacutemoire inspireacutee de lrsquoapproche cognitive Canadian PsychologyPsychologie Canadienne 34 45ndash63 doi101037h0078803
Conde-Sala J L Garre-Olmo J Vilalta-Franch J Llinas-Regla JTurro-Garriga O Lozano-Gallego M Loacutepez-Pousa S (2012)Predictors of cognitive decline in Alzheimerrsquos disease and mild cogni-tive impairment using the CAMCOG A five-year follow-up Interna-tional Psychogeriatrics 24 948ndash958 doi101017S1041610211002158
Deloche G amp Hannequin D (1997) Test de deacutenomination oraledrsquoimages (DO-80) Paris France Centre de Psychologie Appliqueacutee
Dierckx E Engelborghs S De Raedt R Van Buggenhout M DeDeyn P P Verte D amp Ponjaert-Kristoffersen I (2009) Verbal cuedrecall as a predictor of conversion to Alzheimerrsquos disease in mildcognitive impairment International Journal of Geriatric Psychiatry 241094ndash1100 doi101002gps2228
Dubois B Feldman H H Jacova C Dekosky S T Barberger-Gateau P Cummings J Scheltens P (2007) Research criteriafor the diagnosis of Alzheimerrsquos disease Revising the NINCDS-ADRDA criteria Lancet Neurology 6 734 ndash746 doi101016S1474-4422(07)70178 ndash3
Forlenza O V Diniz B S Nunes P V Memoria C M YassudaM S amp Gattaz W F (2009) Diagnostic transitions in mild cognitive
impairment subtypes International Psychogeriatrics 21 1088ndash1095doi101017S1041610209990792
Gauthier S Reisberg B Zaudig M Petersen R C Ritchie K BroichK Winblad B (2006) Mild cognitive impairment The Lancet 3671262ndash1270 doi101016S0140-6736(06)68542-5
Gavett B E Ozonoff A Doktor V Palmisano J Nair A K GreenR C Stern R A (2010) Predicting cognitive decline and conver-sion to Alzheimerrsquos disease in older adults using the NAB List Learningtest Journal of the International Neuropsychological Society 16 651ndash660 doi101017S1355617710000421
Geacutely-Nargeot M-C Cadilhac C Touchon J amp Nespoulous J L(1997) La meacutemoire de textes chez les sujets sains et deacutements Appli-cation drsquoun nouvel outil drsquoeacutevaluation pour neuropsychologues Meacutemo-textes In J Lambert amp J L Nespoulous (Eds) Perception auditive etcompreacutehension du langage (pp 273ndash293) Marseille France Solal
Geroldi C Rossi R Calvagna C Testa C Bresciani L Binetti G Frisoni G B (2006) Medial temporal atrophy but not memorydeficit predicts progression to dementia in patients with mild cognitiveimpairment Journal of Neurology Neurosurgery amp Psychiatry 771219ndash1222 doi101136jnnp2005082651
Irish M Lawlor B A Coen R F amp OrsquoMara S M (2011) Everydayepisodic memory in amnestic mild cognitive impairment A preliminaryinvestigation BMC Neuroscience 12 80 doi1011861471-2202-12-80
Ivanoiu A Adam S Van der Linden M Salmon E Juillerat A CMulligan R amp Seron X (2005) Memory evaluation with a new cuedrecall test in patients with mild cognitive impairment and Alzheimerrsquosdisease Journal of Neurology 252 47ndash55 doi101007s00415-005-0597-2
Landau S M Harvey D Madison C M Reiman E M Foster N LAisen P S Jagust W J (2010) Comparing predictors of conver-sion and decline in mild cognitive impairment Neurology 75 230ndash238doi101212WNL0b013e3181e8e8b8
Lekeu F Magis D Marique P Delbeuck X Bechet S GuillaumeB Salmon E (2010) The California Verbal Learning Test andother standard clinical neuropsychological tests to predict conversionfrom mild memory impairment to dementia Journal of Clinical andExperimental Neuropsychology 32 164 ndash173 doi10108013803390902889606
Mitchell J Arnold R Dawson K Nestor P J amp Hodges J R (2009)Outcome in subgroups of mild cognitive impairment (MCI) is highlypredictable using a simple algorithm Journal of Neurology 256 1500ndash1509 doi101007s00415-009-5152-0[doi]
Mottron L Morasse K amp Belleville S (2001) A study of memoryfunctioning in individuals with autism Journal of Child Psychology andPsychiatry 42 253ndash260 doi1011111469-761000716
Nordlund A Rolstad S Klang O Edman A Hansen S amp Wallin A(2010) Two-year outcome of MCI subtypes and aetiologies in theGoteborg MCI study Journal of Neurology Neurosurgery amp Psychia-try 81 541ndash546 doi101136jnnp2008171066
Petersen R C (2003) Mild cognitive impairment Aging to Alzheimerrsquosdisease Oxford UK Oxford University Press
Petersen R C amp Morris J C (2003) Clinical features In R C Petersen(Ed) Mild cognitive impairment Aging to Alzheimerrsquos disease (pp15ndash39) Oxford UK Oxford University Press
Rabin L A Pare N Saykin A J Brown M J Wishart H AFlashman L A amp Santulli R B (2009) Differential memory testsensitivity for diagnosing amnestic mild cognitive impairment and pre-dicting conversion to Alzheimerrsquos disease Neuropsychology Develop-ment and Cognition Section B Aging Neuropsychology and Cognition16 357ndash376 doi10108013825580902825220
Rasquin S M Lodder J Visser P J Lousberg R amp Verhey F R(2005) Predictive accuracy of MCI subtypes for Alzheimerrsquos diseaseand vascular dementia in subjects with mild cognitive impairment A
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
651PREDICTING DECLINE IN MCI
2-year follow-up study Dementia and Geriatric Cognitive Disorders19 113ndash119 doi101159000082662
Riddoch J M amp Humphreys G W (1993) BORB Birmingham ObjectRecognition Battery Hove UK Erlbaum
Ritchie K Artero S amp Touchon J (2001) Classification criteria formild cognitive impairment A population-based validation study Neu-rology 56 37ndash42 doi101212WNL56137
Summers M J amp Saunders N L (2012) Neuropsychological measurespredict decline to Alzheimerrsquos dementia from mild cognitive impair-ment Neuropsychology 26 498ndash508 doi101037a0028576
Tabert M H Manly J J Liu X Pelton G H Rosenblum S JacobsM Devanand D P (2006) Neuropsychological prediction of
conversion to Alzheimer disease in patients with mild cognitive impair-ment Archives of General Psychiatry 63 916ndash924 doi101001archpsyc638916
Tierney M C Szalai J P Snow W G Fisher R H Nores A NadonG St George-Hyslop P H (1996) Prediction of probable Alz-heimerrsquos disease in memory-impaired patients A prospective longitu-dinal study Neurology 46 661ndash665 doi101212WNL463661
Received May 15 2013Revision received December 19 2013
Accepted December 22 2013
Members of Underrepresented GroupsReviewers for Journal Manuscripts Wanted
If you are interested in reviewing manuscripts for APA journals the APA Publications andCommunications Board would like to invite your participation Manuscript reviewers are vital to thepublications process As a reviewer you would gain valuable experience in publishing The PampCBoard is particularly interested in encouraging members of underrepresented groups to participatemore in this process
If you are interested in reviewing manuscripts please write APA Journals at ReviewersapaorgPlease note the following important points
bull To be selected as a reviewer you must have published articles in peer-reviewed journals Theexperience of publishing provides a reviewer with the basis for preparing a thorough objectivereview
bull To be selected it is critical to be a regular reader of the five to six empirical journals that are mostcentral to the area or journal for which you would like to review Current knowledge of recentlypublished research provides a reviewer with the knowledge base to evaluate a new submissionwithin the context of existing research
bull To select the appropriate reviewers for each manuscript the editor needs detailed informationPlease include with your letter your vita In the letter please identify which APA journal(s) youare interested in and describe your area of expertise Be as specific as possible For exampleldquosocial psychologyrdquo is not sufficientmdashyou would need to specify ldquosocial cognitionrdquo or ldquoattitudechangerdquo as well
bull Reviewing a manuscript takes time (1ndash4 hours per manuscript reviewed) If you are selected toreview a manuscript be prepared to invest the necessary time to evaluate the manuscriptthoroughly
APA now has an online video course that provides guidance in reviewing manuscripts To learnmore about the course and to access the video visit httpwwwapaorgpubsauthorsreview-manuscript-ce-videoaspx
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
652 BELLEVILLE GAUTHIER LEPAGE KERGOAT AND GILBERT

specific and it helps to identify those who are unlikely to progressThis is highly important for clinical trials as it can help identify theMCI persons who are most likely to benefit from disease-modifying therapies Survival analyses indicate that 80 of thepatients performing in the lowest tertile of the MCI group on thetext memory test will have developed dementia 40 months later
This study suggests that relying only on episodic memory mea-sures might not be optimal and that measuring different domains ofcognition represents the most balanced approach Several studieshave investigated the capacity of biological and cognitive mea-sures to predict future progression from MCI to dementia A firstimportant conclusion from many of these studies is that the patternof cognitive deficit might be as accurate as biological measures inpredicting future decline in MCI (Albert et al 2011 Dubois et al2007) a conclusion coherent with our finding of a strong predic-tive accuracy for the cognitive battery used here Another impor-tant conclusion is that it is possible to identify an optimal set ofcognitive tasks Studies vary in their design statistical approachand follow-up length and there is great variability in the cognitivetests used Nevertheless a coherent pattern seems to emerge fromprevious studies which is supported by our findings First itappears that combining episodic memory tests with tasks that relyon executive functions or the attentional control of WM is partic-ularly powerful for predicting conversion from MCI to dementia(Aretouli Tsilidis amp Brandt 2013 Chapman et al 2011 Conde-Sala et al 2012 Gavett et al 2010 Rabin et al 2009 Summersamp Saunders 2012) Second studies that measured only one or twocognitive domains have much lower predictive accuracy than theone found here They report either lower specificity (eg Mitchellet al 2009) or lower sensitivity (Dierckx et al 2009 Tabert et al2006 Tierney et al 1996) than what is reported here This isconsistent with studies indicating that cases of multiple-domainMCI are more likely to progress to dementia than single-domainMCI (Forlenza et al 2009 Nordlund et al 2010 RasquinLodder Visser Lousberg amp Verhey 2005 Summers amp Saunders2012) Our study indicates that an optimal battery should includeperceptual tests in addition to tests of episodic memory executivefunction and working memory The particular cognitive domainsidentified here match well with findings indicating that in additionto episodic memory semantic knowledge and working memoryare impaired early in AD (for a review see Belleville et al 2008)
Few studies have included perceptual or semantic componentsin their models contrary to this study and those that did measureda relatively small number of components It is therefore possiblethat measures of the perceptual or semantic domains have im-proved predictive accuracy However these tasks may be morespecific than sensitive Indeed our survival analyses suggest thatnaming and perceptual tasks were not as sensitive to future declineas episodic memory and executive tasks when taken on their ownIncluding measures of the perceptual or semantic domain mightcontribute to reducing the number of false positives hence increas-ing specificity This is a potentially useful finding for cliniciansand researchers When optimizing testing time is a critical issueand tasks need to be selected one can base the decision on whetherthe need is to have a more sensitive or more specific battery
This study is among those showing the best combination ofsensitivity and specificity values Perhaps inclusion of morenonmemory tests might have increased specificity and use of a
relatively long follow-up period likely reduced the number offalse negatives hence increasing sensitivity Another differencebetween this study and the current literature is that we did notrely on clinical measures but on theoretically motivated onesThus if selected well a relatively short battery of tests canpredict future decline in MCI and can help identify persons thatare likely to progress to more severe symptoms
The study resulted in a number of additional findings whichdeserve discussion One is that at entry progressive MCIpatients already differ from stable MCI patients in terms of ageand cognitive performance on several clinical tests Becausepatients are likely to vary in their decline rate and in their stageat entry it is possible that progressors are in a more advancedstage of neuropathology than persons with stable MCI and thatthe latter would decline later Thus a portion of stable MCIpatients may still actually be predementia (thus false negative)It is important to note however that this study makes use of amuch longer follow-up than is typically used in similar studiesStable MCI patients were followed for an average of 567months which is much longer than the period after whichprogressors converted to dementia (on average 308 monthsafter entry) This long follow-up probably reduced the contri-bution of ldquofalse negativesrdquo to the group of those with stableMCI by increasing the chance of progression during the studyperiod Admittedly it remains possible that some of the stableMCI patients will progress to dementia in the future Howeverwe do not believe that this represents a substantial portion ofour participants with stable MCI It is interesting that thefinding that the two groups differ on clinical measures is in factgood news as it supports our contention that cognitive mea-sures are sensitive to prognosis and will prove critical in iden-tifying the patients more likely to progress to dementia
This study has limitations which should be recognized Firstto improve generalizability the findings should be reproducedon a different sample Second we did not include biomarkers orimaging parameters in this study Our goal was to identify theideal set of cognitive measures and for future studies it will beimportant to assess the value of combining them with biologicalmarkers Finally it is important to point out that there might bedifferences between this cohort of patients and patients encoun-tered in other clinical settings In particular our exclusioncriteria might have led to a cohort with relatively few cases ofcomorbidity
References
Ahmed S Mitchell J Arnold R Nestor P J amp Hodges J R (2008)Predicting rapid clinical progression in amnestic mild cognitive impair-ment Dementia and Geriatric Cognitive Disorders 25 170ndash177 doi101159000113014
Albert M S DeKosky S T Dickson D Dubois B Feldman H HFox N C Phelps C H (2011) The diagnosis of mild cognitiveimpairment due to Alzheimerrsquos disease Recommendations from theNational Institute on Aging-Alzheimerrsquos Association workgroups ondiagnostic guidelines for Alzheimerrsquos disease Alzheimers amp Dementia7 270ndash279 doi101016jjalz201103008
Aretouli E Tsilidis K K amp Brandt J (2013) Four-year outcome ofmild cognitive impairment The contribution of executive dysfunctionNeuropsychology 27 95ndash106 doi101037a0030481
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
650 BELLEVILLE GAUTHIER LEPAGE KERGOAT AND GILBERT
Artero S Tierney M C Touchon J amp Ritchie K (2003) Prediction oftransition from cognitive impairment to senile dementia A prospectivelongitudinal study Acta Psychiatrica Scandinavica 107 390ndash393
Beacutelanger S amp Belleville S (2009) Semantic inhibition impairment inmild cognitive impairment A distinctive feature of upcoming cognitivedecline Neuropsychology 23 592ndash606 doi101037a0016152
Belleville S Bherer L Lepage Eacute Chertkow H amp Gauthier S (2008)Task switching capacities in persons with Alzheimerrsquos disease and mildcognitive impairment Neuropsychologia 46 2225ndash2233 doi101016jneuropsychologia200802012
Belleville S Caza N amp Peretz I (2003) A neuropsychological argu-ment for a processing view of memory Journal of Memory and Lan-guage 48 686ndash703 doi101016S0749-596X(02)00532-6
Belleville S Chertkow H amp Gauthier S (2007) Working memory andcontrol of attention in persons with Alzheimerrsquos disease and mild cog-nitive impairment Neuropsychology 21 458ndash469 doi1010370894-4105214458
Belleville S Meacutenard M C De Boysson C amp Sylvain-Roy S (2008)Characterizing memory deficits in mild cognitive impairment In WSossin J C Lacaille V Castellucci amp S Belleville (Eds) The essenceof memory (pp 365ndash375) Amsterdam Netherlands Elsevier doi101016S0079-6123(07)00023-4
Belleville S Peretz I amp Malenfant D (1996) Examination of theworking memory components in normal aging and in dementia of theAlzheimer type Neuropsychologia 34 195ndash207 doi1010160028-3932(95)00097-6
Belleville S Rouleau N amp Caza N (1998) Effect of normal aging onthe manipulation of information in working memory Memory amp Cog-nition 26 572ndash583 doi103758BF03201163
Bennett D A Wilson R S Schneider J A Evans D A BeckettL A Aggarwal N T Bach J (2002) Natural history of mildcognitive impairment in older persons Neurology 59 198ndash205
Bherer L Belleville S amp Peretz I (2001) Education age and theBrown-Peterson technique Developmental Neuropsychology 19 237ndash251 doi101207S15326942DN1903_1
Chapman R M Mapstone M McCrary J W Gardner M N Por-steinsson A Sandoval T C Reilly L A (2011) Predictingconversion from mild cognitive impairment to Alzheimerrsquos diseaseusing neuropsychological tests and multivariate methods Journal ofClinical and Experimental Neuropsychology 33 187ndash199 doi101080138033952010499356
Chatelois J Pineau H Belleville S Peretz I Lussier I FontaineF-S amp Renaseau-Leclerc C (1993) Batterie informatiseacutee drsquoeacutevaluationde la meacutemoire inspireacutee de lrsquoapproche cognitive Canadian PsychologyPsychologie Canadienne 34 45ndash63 doi101037h0078803
Conde-Sala J L Garre-Olmo J Vilalta-Franch J Llinas-Regla JTurro-Garriga O Lozano-Gallego M Loacutepez-Pousa S (2012)Predictors of cognitive decline in Alzheimerrsquos disease and mild cogni-tive impairment using the CAMCOG A five-year follow-up Interna-tional Psychogeriatrics 24 948ndash958 doi101017S1041610211002158
Deloche G amp Hannequin D (1997) Test de deacutenomination oraledrsquoimages (DO-80) Paris France Centre de Psychologie Appliqueacutee
Dierckx E Engelborghs S De Raedt R Van Buggenhout M DeDeyn P P Verte D amp Ponjaert-Kristoffersen I (2009) Verbal cuedrecall as a predictor of conversion to Alzheimerrsquos disease in mildcognitive impairment International Journal of Geriatric Psychiatry 241094ndash1100 doi101002gps2228
Dubois B Feldman H H Jacova C Dekosky S T Barberger-Gateau P Cummings J Scheltens P (2007) Research criteriafor the diagnosis of Alzheimerrsquos disease Revising the NINCDS-ADRDA criteria Lancet Neurology 6 734 ndash746 doi101016S1474-4422(07)70178 ndash3
Forlenza O V Diniz B S Nunes P V Memoria C M YassudaM S amp Gattaz W F (2009) Diagnostic transitions in mild cognitive
impairment subtypes International Psychogeriatrics 21 1088ndash1095doi101017S1041610209990792
Gauthier S Reisberg B Zaudig M Petersen R C Ritchie K BroichK Winblad B (2006) Mild cognitive impairment The Lancet 3671262ndash1270 doi101016S0140-6736(06)68542-5
Gavett B E Ozonoff A Doktor V Palmisano J Nair A K GreenR C Stern R A (2010) Predicting cognitive decline and conver-sion to Alzheimerrsquos disease in older adults using the NAB List Learningtest Journal of the International Neuropsychological Society 16 651ndash660 doi101017S1355617710000421
Geacutely-Nargeot M-C Cadilhac C Touchon J amp Nespoulous J L(1997) La meacutemoire de textes chez les sujets sains et deacutements Appli-cation drsquoun nouvel outil drsquoeacutevaluation pour neuropsychologues Meacutemo-textes In J Lambert amp J L Nespoulous (Eds) Perception auditive etcompreacutehension du langage (pp 273ndash293) Marseille France Solal
Geroldi C Rossi R Calvagna C Testa C Bresciani L Binetti G Frisoni G B (2006) Medial temporal atrophy but not memorydeficit predicts progression to dementia in patients with mild cognitiveimpairment Journal of Neurology Neurosurgery amp Psychiatry 771219ndash1222 doi101136jnnp2005082651
Irish M Lawlor B A Coen R F amp OrsquoMara S M (2011) Everydayepisodic memory in amnestic mild cognitive impairment A preliminaryinvestigation BMC Neuroscience 12 80 doi1011861471-2202-12-80
Ivanoiu A Adam S Van der Linden M Salmon E Juillerat A CMulligan R amp Seron X (2005) Memory evaluation with a new cuedrecall test in patients with mild cognitive impairment and Alzheimerrsquosdisease Journal of Neurology 252 47ndash55 doi101007s00415-005-0597-2
Landau S M Harvey D Madison C M Reiman E M Foster N LAisen P S Jagust W J (2010) Comparing predictors of conver-sion and decline in mild cognitive impairment Neurology 75 230ndash238doi101212WNL0b013e3181e8e8b8
Lekeu F Magis D Marique P Delbeuck X Bechet S GuillaumeB Salmon E (2010) The California Verbal Learning Test andother standard clinical neuropsychological tests to predict conversionfrom mild memory impairment to dementia Journal of Clinical andExperimental Neuropsychology 32 164 ndash173 doi10108013803390902889606
Mitchell J Arnold R Dawson K Nestor P J amp Hodges J R (2009)Outcome in subgroups of mild cognitive impairment (MCI) is highlypredictable using a simple algorithm Journal of Neurology 256 1500ndash1509 doi101007s00415-009-5152-0[doi]
Mottron L Morasse K amp Belleville S (2001) A study of memoryfunctioning in individuals with autism Journal of Child Psychology andPsychiatry 42 253ndash260 doi1011111469-761000716
Nordlund A Rolstad S Klang O Edman A Hansen S amp Wallin A(2010) Two-year outcome of MCI subtypes and aetiologies in theGoteborg MCI study Journal of Neurology Neurosurgery amp Psychia-try 81 541ndash546 doi101136jnnp2008171066
Petersen R C (2003) Mild cognitive impairment Aging to Alzheimerrsquosdisease Oxford UK Oxford University Press
Petersen R C amp Morris J C (2003) Clinical features In R C Petersen(Ed) Mild cognitive impairment Aging to Alzheimerrsquos disease (pp15ndash39) Oxford UK Oxford University Press
Rabin L A Pare N Saykin A J Brown M J Wishart H AFlashman L A amp Santulli R B (2009) Differential memory testsensitivity for diagnosing amnestic mild cognitive impairment and pre-dicting conversion to Alzheimerrsquos disease Neuropsychology Develop-ment and Cognition Section B Aging Neuropsychology and Cognition16 357ndash376 doi10108013825580902825220
Rasquin S M Lodder J Visser P J Lousberg R amp Verhey F R(2005) Predictive accuracy of MCI subtypes for Alzheimerrsquos diseaseand vascular dementia in subjects with mild cognitive impairment A
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
651PREDICTING DECLINE IN MCI
2-year follow-up study Dementia and Geriatric Cognitive Disorders19 113ndash119 doi101159000082662
Riddoch J M amp Humphreys G W (1993) BORB Birmingham ObjectRecognition Battery Hove UK Erlbaum
Ritchie K Artero S amp Touchon J (2001) Classification criteria formild cognitive impairment A population-based validation study Neu-rology 56 37ndash42 doi101212WNL56137
Summers M J amp Saunders N L (2012) Neuropsychological measurespredict decline to Alzheimerrsquos dementia from mild cognitive impair-ment Neuropsychology 26 498ndash508 doi101037a0028576
Tabert M H Manly J J Liu X Pelton G H Rosenblum S JacobsM Devanand D P (2006) Neuropsychological prediction of
conversion to Alzheimer disease in patients with mild cognitive impair-ment Archives of General Psychiatry 63 916ndash924 doi101001archpsyc638916
Tierney M C Szalai J P Snow W G Fisher R H Nores A NadonG St George-Hyslop P H (1996) Prediction of probable Alz-heimerrsquos disease in memory-impaired patients A prospective longitu-dinal study Neurology 46 661ndash665 doi101212WNL463661
Received May 15 2013Revision received December 19 2013
Accepted December 22 2013
Members of Underrepresented GroupsReviewers for Journal Manuscripts Wanted
If you are interested in reviewing manuscripts for APA journals the APA Publications andCommunications Board would like to invite your participation Manuscript reviewers are vital to thepublications process As a reviewer you would gain valuable experience in publishing The PampCBoard is particularly interested in encouraging members of underrepresented groups to participatemore in this process
If you are interested in reviewing manuscripts please write APA Journals at ReviewersapaorgPlease note the following important points
bull To be selected as a reviewer you must have published articles in peer-reviewed journals Theexperience of publishing provides a reviewer with the basis for preparing a thorough objectivereview
bull To be selected it is critical to be a regular reader of the five to six empirical journals that are mostcentral to the area or journal for which you would like to review Current knowledge of recentlypublished research provides a reviewer with the knowledge base to evaluate a new submissionwithin the context of existing research
bull To select the appropriate reviewers for each manuscript the editor needs detailed informationPlease include with your letter your vita In the letter please identify which APA journal(s) youare interested in and describe your area of expertise Be as specific as possible For exampleldquosocial psychologyrdquo is not sufficientmdashyou would need to specify ldquosocial cognitionrdquo or ldquoattitudechangerdquo as well
bull Reviewing a manuscript takes time (1ndash4 hours per manuscript reviewed) If you are selected toreview a manuscript be prepared to invest the necessary time to evaluate the manuscriptthoroughly
APA now has an online video course that provides guidance in reviewing manuscripts To learnmore about the course and to access the video visit httpwwwapaorgpubsauthorsreview-manuscript-ce-videoaspx
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
652 BELLEVILLE GAUTHIER LEPAGE KERGOAT AND GILBERT

Artero S Tierney M C Touchon J amp Ritchie K (2003) Prediction oftransition from cognitive impairment to senile dementia A prospectivelongitudinal study Acta Psychiatrica Scandinavica 107 390ndash393
Beacutelanger S amp Belleville S (2009) Semantic inhibition impairment inmild cognitive impairment A distinctive feature of upcoming cognitivedecline Neuropsychology 23 592ndash606 doi101037a0016152
Belleville S Bherer L Lepage Eacute Chertkow H amp Gauthier S (2008)Task switching capacities in persons with Alzheimerrsquos disease and mildcognitive impairment Neuropsychologia 46 2225ndash2233 doi101016jneuropsychologia200802012
Belleville S Caza N amp Peretz I (2003) A neuropsychological argu-ment for a processing view of memory Journal of Memory and Lan-guage 48 686ndash703 doi101016S0749-596X(02)00532-6
Belleville S Chertkow H amp Gauthier S (2007) Working memory andcontrol of attention in persons with Alzheimerrsquos disease and mild cog-nitive impairment Neuropsychology 21 458ndash469 doi1010370894-4105214458
Belleville S Meacutenard M C De Boysson C amp Sylvain-Roy S (2008)Characterizing memory deficits in mild cognitive impairment In WSossin J C Lacaille V Castellucci amp S Belleville (Eds) The essenceof memory (pp 365ndash375) Amsterdam Netherlands Elsevier doi101016S0079-6123(07)00023-4
Belleville S Peretz I amp Malenfant D (1996) Examination of theworking memory components in normal aging and in dementia of theAlzheimer type Neuropsychologia 34 195ndash207 doi1010160028-3932(95)00097-6
Belleville S Rouleau N amp Caza N (1998) Effect of normal aging onthe manipulation of information in working memory Memory amp Cog-nition 26 572ndash583 doi103758BF03201163
Bennett D A Wilson R S Schneider J A Evans D A BeckettL A Aggarwal N T Bach J (2002) Natural history of mildcognitive impairment in older persons Neurology 59 198ndash205
Bherer L Belleville S amp Peretz I (2001) Education age and theBrown-Peterson technique Developmental Neuropsychology 19 237ndash251 doi101207S15326942DN1903_1
Chapman R M Mapstone M McCrary J W Gardner M N Por-steinsson A Sandoval T C Reilly L A (2011) Predictingconversion from mild cognitive impairment to Alzheimerrsquos diseaseusing neuropsychological tests and multivariate methods Journal ofClinical and Experimental Neuropsychology 33 187ndash199 doi101080138033952010499356
Chatelois J Pineau H Belleville S Peretz I Lussier I FontaineF-S amp Renaseau-Leclerc C (1993) Batterie informatiseacutee drsquoeacutevaluationde la meacutemoire inspireacutee de lrsquoapproche cognitive Canadian PsychologyPsychologie Canadienne 34 45ndash63 doi101037h0078803
Conde-Sala J L Garre-Olmo J Vilalta-Franch J Llinas-Regla JTurro-Garriga O Lozano-Gallego M Loacutepez-Pousa S (2012)Predictors of cognitive decline in Alzheimerrsquos disease and mild cogni-tive impairment using the CAMCOG A five-year follow-up Interna-tional Psychogeriatrics 24 948ndash958 doi101017S1041610211002158
Deloche G amp Hannequin D (1997) Test de deacutenomination oraledrsquoimages (DO-80) Paris France Centre de Psychologie Appliqueacutee
Dierckx E Engelborghs S De Raedt R Van Buggenhout M DeDeyn P P Verte D amp Ponjaert-Kristoffersen I (2009) Verbal cuedrecall as a predictor of conversion to Alzheimerrsquos disease in mildcognitive impairment International Journal of Geriatric Psychiatry 241094ndash1100 doi101002gps2228
Dubois B Feldman H H Jacova C Dekosky S T Barberger-Gateau P Cummings J Scheltens P (2007) Research criteriafor the diagnosis of Alzheimerrsquos disease Revising the NINCDS-ADRDA criteria Lancet Neurology 6 734 ndash746 doi101016S1474-4422(07)70178 ndash3
Forlenza O V Diniz B S Nunes P V Memoria C M YassudaM S amp Gattaz W F (2009) Diagnostic transitions in mild cognitive
impairment subtypes International Psychogeriatrics 21 1088ndash1095doi101017S1041610209990792
Gauthier S Reisberg B Zaudig M Petersen R C Ritchie K BroichK Winblad B (2006) Mild cognitive impairment The Lancet 3671262ndash1270 doi101016S0140-6736(06)68542-5
Gavett B E Ozonoff A Doktor V Palmisano J Nair A K GreenR C Stern R A (2010) Predicting cognitive decline and conver-sion to Alzheimerrsquos disease in older adults using the NAB List Learningtest Journal of the International Neuropsychological Society 16 651ndash660 doi101017S1355617710000421
Geacutely-Nargeot M-C Cadilhac C Touchon J amp Nespoulous J L(1997) La meacutemoire de textes chez les sujets sains et deacutements Appli-cation drsquoun nouvel outil drsquoeacutevaluation pour neuropsychologues Meacutemo-textes In J Lambert amp J L Nespoulous (Eds) Perception auditive etcompreacutehension du langage (pp 273ndash293) Marseille France Solal
Geroldi C Rossi R Calvagna C Testa C Bresciani L Binetti G Frisoni G B (2006) Medial temporal atrophy but not memorydeficit predicts progression to dementia in patients with mild cognitiveimpairment Journal of Neurology Neurosurgery amp Psychiatry 771219ndash1222 doi101136jnnp2005082651
Irish M Lawlor B A Coen R F amp OrsquoMara S M (2011) Everydayepisodic memory in amnestic mild cognitive impairment A preliminaryinvestigation BMC Neuroscience 12 80 doi1011861471-2202-12-80
Ivanoiu A Adam S Van der Linden M Salmon E Juillerat A CMulligan R amp Seron X (2005) Memory evaluation with a new cuedrecall test in patients with mild cognitive impairment and Alzheimerrsquosdisease Journal of Neurology 252 47ndash55 doi101007s00415-005-0597-2
Landau S M Harvey D Madison C M Reiman E M Foster N LAisen P S Jagust W J (2010) Comparing predictors of conver-sion and decline in mild cognitive impairment Neurology 75 230ndash238doi101212WNL0b013e3181e8e8b8
Lekeu F Magis D Marique P Delbeuck X Bechet S GuillaumeB Salmon E (2010) The California Verbal Learning Test andother standard clinical neuropsychological tests to predict conversionfrom mild memory impairment to dementia Journal of Clinical andExperimental Neuropsychology 32 164 ndash173 doi10108013803390902889606
Mitchell J Arnold R Dawson K Nestor P J amp Hodges J R (2009)Outcome in subgroups of mild cognitive impairment (MCI) is highlypredictable using a simple algorithm Journal of Neurology 256 1500ndash1509 doi101007s00415-009-5152-0[doi]
Mottron L Morasse K amp Belleville S (2001) A study of memoryfunctioning in individuals with autism Journal of Child Psychology andPsychiatry 42 253ndash260 doi1011111469-761000716
Nordlund A Rolstad S Klang O Edman A Hansen S amp Wallin A(2010) Two-year outcome of MCI subtypes and aetiologies in theGoteborg MCI study Journal of Neurology Neurosurgery amp Psychia-try 81 541ndash546 doi101136jnnp2008171066
Petersen R C (2003) Mild cognitive impairment Aging to Alzheimerrsquosdisease Oxford UK Oxford University Press
Petersen R C amp Morris J C (2003) Clinical features In R C Petersen(Ed) Mild cognitive impairment Aging to Alzheimerrsquos disease (pp15ndash39) Oxford UK Oxford University Press
Rabin L A Pare N Saykin A J Brown M J Wishart H AFlashman L A amp Santulli R B (2009) Differential memory testsensitivity for diagnosing amnestic mild cognitive impairment and pre-dicting conversion to Alzheimerrsquos disease Neuropsychology Develop-ment and Cognition Section B Aging Neuropsychology and Cognition16 357ndash376 doi10108013825580902825220
Rasquin S M Lodder J Visser P J Lousberg R amp Verhey F R(2005) Predictive accuracy of MCI subtypes for Alzheimerrsquos diseaseand vascular dementia in subjects with mild cognitive impairment A
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
651PREDICTING DECLINE IN MCI
2-year follow-up study Dementia and Geriatric Cognitive Disorders19 113ndash119 doi101159000082662
Riddoch J M amp Humphreys G W (1993) BORB Birmingham ObjectRecognition Battery Hove UK Erlbaum
Ritchie K Artero S amp Touchon J (2001) Classification criteria formild cognitive impairment A population-based validation study Neu-rology 56 37ndash42 doi101212WNL56137
Summers M J amp Saunders N L (2012) Neuropsychological measurespredict decline to Alzheimerrsquos dementia from mild cognitive impair-ment Neuropsychology 26 498ndash508 doi101037a0028576
Tabert M H Manly J J Liu X Pelton G H Rosenblum S JacobsM Devanand D P (2006) Neuropsychological prediction of
conversion to Alzheimer disease in patients with mild cognitive impair-ment Archives of General Psychiatry 63 916ndash924 doi101001archpsyc638916
Tierney M C Szalai J P Snow W G Fisher R H Nores A NadonG St George-Hyslop P H (1996) Prediction of probable Alz-heimerrsquos disease in memory-impaired patients A prospective longitu-dinal study Neurology 46 661ndash665 doi101212WNL463661
Received May 15 2013Revision received December 19 2013
Accepted December 22 2013
Members of Underrepresented GroupsReviewers for Journal Manuscripts Wanted
If you are interested in reviewing manuscripts for APA journals the APA Publications andCommunications Board would like to invite your participation Manuscript reviewers are vital to thepublications process As a reviewer you would gain valuable experience in publishing The PampCBoard is particularly interested in encouraging members of underrepresented groups to participatemore in this process
If you are interested in reviewing manuscripts please write APA Journals at ReviewersapaorgPlease note the following important points
bull To be selected as a reviewer you must have published articles in peer-reviewed journals Theexperience of publishing provides a reviewer with the basis for preparing a thorough objectivereview
bull To be selected it is critical to be a regular reader of the five to six empirical journals that are mostcentral to the area or journal for which you would like to review Current knowledge of recentlypublished research provides a reviewer with the knowledge base to evaluate a new submissionwithin the context of existing research
bull To select the appropriate reviewers for each manuscript the editor needs detailed informationPlease include with your letter your vita In the letter please identify which APA journal(s) youare interested in and describe your area of expertise Be as specific as possible For exampleldquosocial psychologyrdquo is not sufficientmdashyou would need to specify ldquosocial cognitionrdquo or ldquoattitudechangerdquo as well
bull Reviewing a manuscript takes time (1ndash4 hours per manuscript reviewed) If you are selected toreview a manuscript be prepared to invest the necessary time to evaluate the manuscriptthoroughly
APA now has an online video course that provides guidance in reviewing manuscripts To learnmore about the course and to access the video visit httpwwwapaorgpubsauthorsreview-manuscript-ce-videoaspx
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
652 BELLEVILLE GAUTHIER LEPAGE KERGOAT AND GILBERT

2-year follow-up study Dementia and Geriatric Cognitive Disorders19 113ndash119 doi101159000082662
Riddoch J M amp Humphreys G W (1993) BORB Birmingham ObjectRecognition Battery Hove UK Erlbaum
Ritchie K Artero S amp Touchon J (2001) Classification criteria formild cognitive impairment A population-based validation study Neu-rology 56 37ndash42 doi101212WNL56137
Summers M J amp Saunders N L (2012) Neuropsychological measurespredict decline to Alzheimerrsquos dementia from mild cognitive impair-ment Neuropsychology 26 498ndash508 doi101037a0028576
Tabert M H Manly J J Liu X Pelton G H Rosenblum S JacobsM Devanand D P (2006) Neuropsychological prediction of
conversion to Alzheimer disease in patients with mild cognitive impair-ment Archives of General Psychiatry 63 916ndash924 doi101001archpsyc638916
Tierney M C Szalai J P Snow W G Fisher R H Nores A NadonG St George-Hyslop P H (1996) Prediction of probable Alz-heimerrsquos disease in memory-impaired patients A prospective longitu-dinal study Neurology 46 661ndash665 doi101212WNL463661
Received May 15 2013Revision received December 19 2013
Accepted December 22 2013
Members of Underrepresented GroupsReviewers for Journal Manuscripts Wanted
If you are interested in reviewing manuscripts for APA journals the APA Publications andCommunications Board would like to invite your participation Manuscript reviewers are vital to thepublications process As a reviewer you would gain valuable experience in publishing The PampCBoard is particularly interested in encouraging members of underrepresented groups to participatemore in this process
If you are interested in reviewing manuscripts please write APA Journals at ReviewersapaorgPlease note the following important points
bull To be selected as a reviewer you must have published articles in peer-reviewed journals Theexperience of publishing provides a reviewer with the basis for preparing a thorough objectivereview
bull To be selected it is critical to be a regular reader of the five to six empirical journals that are mostcentral to the area or journal for which you would like to review Current knowledge of recentlypublished research provides a reviewer with the knowledge base to evaluate a new submissionwithin the context of existing research
bull To select the appropriate reviewers for each manuscript the editor needs detailed informationPlease include with your letter your vita In the letter please identify which APA journal(s) youare interested in and describe your area of expertise Be as specific as possible For exampleldquosocial psychologyrdquo is not sufficientmdashyou would need to specify ldquosocial cognitionrdquo or ldquoattitudechangerdquo as well
bull Reviewing a manuscript takes time (1ndash4 hours per manuscript reviewed) If you are selected toreview a manuscript be prepared to invest the necessary time to evaluate the manuscriptthoroughly
APA now has an online video course that provides guidance in reviewing manuscripts To learnmore about the course and to access the video visit httpwwwapaorgpubsauthorsreview-manuscript-ce-videoaspx
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y
652 BELLEVILLE GAUTHIER LEPAGE KERGOAT AND GILBERT
Copyright © 2022 FDOKUMEN




















