Preclinical development of camptothecin derivatives and clinical trials in pediatric oncology
10
BhJ('himie (1998) 80, 271+ 280 © Soci6t6 ffan~'aise de biochimic cl bioh~gic mol6culaire / Elsevier, Paris Preclinica| development of camptothecin derivatives and clinical tria|s in pediatric onco|ogy G Vassal", !,, C PondarrG', I Boland", C CappellP, A Santos a, C Thomas a, E Lucchi b, K lmadalou b, F Pein b, J Morizet", A Gouyetle a 'tLaboratorv of Pharmacoto.~icology am/Pharmacogenetics ( URA CNRS 1471: b , l)( partmet~l o.f Pediatric Om'ology, rue Camille De.smoulins, lostilut Gu.slave-Rous.s.~; 94805 Vilh:ju(l: /-'ran('(, ( Received 15 Scplember 1997; accepted 20 November ! t197) Summary ~ Although the prognosis of childhood cancers has dramatically improved over the last three decades, new .'lctive drugs are needed. Camptothecins represent a very attractive new class of ant|cancer drugs to develop in paediatric ontology. The preclinical and clinical development of two of these DNA-topoisomerase i inhibitors, ie topotecan and irinotecan, is ongoing in paediatric malignancies. Here we review the currently available results of this evaluation. 'ropolecan proved to be active again.st several paediatric qunour xenografls. In paediatric phase I studies exploring several admi,fi.,,tratMn schedules, myeh)stq3rwes,,doll was dose-limiting. The prelimiaary results of topote- can evaluation in phase ii study showed antitumour activity in neuroblastoma (response rate: 15% at relapse and 37% in newly diagnosed patients with disseminated disease) and in metastatic rhabdomyosarcoma (40e/; in untreated patients). "Ibpotecan-containing drug combina- tions ate currently investigated. Irinotecan displayed a broad spectrum of ac|ivity in paedia*ric solid tumour xenografts, including rhabd,~- myosarcoma, neuroblastoma, peripheral primitive neuroectodennai tumour, medulloblastoma, ependymoma, malignant glioma and juvenile colon cancer. For several of these histology types, tumour-free survivors have been observed arnong animals bearing an advanced-stage tumour at time of tn'eatment. The clinical evaluation of irinotecan in) children is ongoing, Irinotecan undergoes a complex in vivo biotransfor- mat|on involving several enzyme systems, such as carboxylesterase, tlDPGT and cytochrome P450, in children as well as in adults. Preclinical studies of both drugs have shown that their activity was schedule-dependent. The optimal schedule of administration is an issue that needs to be addressed in children, in conclusionL the prelin'finary results of the paediatric evaluation of camptothecin derivatives show very encountging results in childhood ntalignancies. The potential place of Caml:~tothccins in the treatment of paediatric malignant tumours is discussed. ((O Soci6t6 Ii'an~'aise tie biochimie el biologic mol6culairc / Elsevier, Paris). irinotecan I topotecan / tol)oisomerase I / children / xenografls Introduction The prognosis ot' children with cancer has dramatically imo proved during the last three decades: 2 out of 3 children can be cured with the cun'ent multi°modality protocols. Chemotherapy plays a central role in the treatment of childhood malignant solid tumours and leukemias. Indeed, paediatric malignancies are particularly chemosensitive, as opposed to most adult cancers. Nevertheless, there are still cancers with a poor prognosis in children in which current protocols yield a 5-year survival rate of less than 50%. Among these are metastatic neuroblastomas, medulloblas- tomas and other malignant brain tumours, inert:static osteo- genie and Ewing's sarcomas, disseminated rhabdomyosarcomas and high risk acute leukaemias. New drugs are urgently needed to improve further the prognosis of children with these diseases. Topoisomerase i inhibitors, ie camptothecin derivatives, represent a very attractive new class of ant|cancer drugs to develop in paediatric oncoh)gy. They exhibit a novel mech- ;.ini~in of ;idion, .~illt:~ llOl|L' of the anlicanccr drug', currently u~cd iu the treatment of cam:or in children arc tar~dcd against topoisomentse I. Carnptothecin, the leading como pound of this class, and its water-soluble derivatives have demonstrated a broad spectrun~ of preclinical activity in murine models and adult tumour xenognffts, In addition, no major cross-resist,'mce has been so far observed with drugs involved in the multidrug resistance phenotypc or with alkylating agents. Finally, the camptothecin deriva- tives have shown clinical efficacy in several cancers, in adults. For these reasons, several teams have embarked on the preo clinical and clinical evaluation of canlptothecins in paedia* tric malignancies. A lot of knowledge has been accumulated about two of these new drugs, namely topote° can and irinotecan. Here, we review the current available results of this evaluation at the preclinical and clinical le- vels, and we address the issue of the future clinical devel- opment of topoisomerase 1 inhibitors for the treatment of children with cancer.
Transcript of Preclinical development of camptothecin derivatives and clinical trials in pediatric oncology

BhJ('himie (1998) 80, 271+ 280 © Soci6t6 ffan~'aise de biochimic cl bioh~gic mol6culaire / Elsevier, Paris
Preclinica| development of camptothecin derivatives and clinical tria|s in pediatric onco|ogy
G Vassal", !,, C PondarrG', I Boland", C Cappel lP , A Santos a, C T h o m a s a, E Lucchi b, K lmada lou b, F Pein b, J Morizet", A Gouye t l e a
'tLaboratorv of Pharmacoto.~icology am/Pharmacogenetics ( URA CNRS 1471: b , l)( partmet~l o.f Pediatric Om'ology, rue Camille De.smoulins, lostilut Gu.slave-Rous.s.~; 94805 Vilh:ju(l: /-'ran('(,
( Received 15 Scplember 1997; accepted 20 November ! t197)
Summary ~ Although the prognosis of childhood cancers has dramatically improved over the last three decades, new .'lctive drugs are needed. Camptothecins represent a very attractive new class of ant|cancer drugs to develop in paediatric ontology. The preclinical and clinical development of two of these DNA-topoisomerase i inhibitors, ie topotecan and irinotecan, is ongoing in paediatric malignancies. Here we review the currently available results of this evaluation. 'ropolecan proved to be active again.st several paediatric qunour xenografls. In paediatric phase I studies exploring several admi,fi.,,tratMn schedules, myeh)stq3rwes,,doll was dose-limiting. The prelimiaary results of topote- can evaluation in phase ii study showed antitumour activity in neuroblastoma (response rate: 15% at relapse and 37% in newly diagnosed patients with disseminated disease) and in metastatic rhabdomyosarcoma (40e/; in untreated patients). "Ibpotecan-containing drug combina- tions ate currently investigated. Irinotecan displayed a broad spectrum of ac|ivity in paedia*ric solid tumour xenografts, including rhabd,~- myosarcoma, neuroblastoma, peripheral primitive neuroectodennai tumour, medulloblastoma, ependymoma, malignant glioma and juvenile colon cancer. For several of these histology types, tumour-free survivors have been observed arnong animals bearing an advanced-stage tumour at time of tn'eatment. The clinical evaluation of irinotecan in) children is ongoing, Irinotecan undergoes a complex in vivo biotransfor- mat|on involving several enzyme systems, such as carboxylesterase, tlDPGT and cytochrome P450, in children as well as in adults. Preclinical studies of both drugs have shown that their activity was schedule-dependent. The optimal schedule of administration is an issue that needs to be addressed in children, in conclusionL the prelin'finary results of the paediatric evaluation of camptothecin derivatives show very encountging results in childhood ntalignancies. The potential place of Caml:~tothccins in the treatment of paediatric malignant tumours is discussed. ((O Soci6t6 Ii'an~'aise tie biochimie el biologic mol6culairc / Elsevier, Paris).
irinotecan I topotecan / tol)oisomerase I / children / xenografls
Introduction
The prognosis ot' children with cancer has dramatically imo proved during the last three decades: 2 out of 3 children c a n be cured with the cun'ent multi°modality protocols. Chemotherapy plays a central role in the treatment of childhood malignant solid tumours and leukemias. Indeed, paediatric malignancies are particularly chemosensitive, as opposed to most adult cancers. Nevertheless, there are still cancers with a poor prognosis in children in which current protocols yield a 5-year survival rate of less than 50%. Among these are metastatic neuroblastomas, medulloblas- tomas and other malignant brain tumours, inert:static osteo- genie and Ewing ' s sarcomas , d i s semina ted rhabdomyosarcomas and high risk acute leukaemias. New drugs are urgently needed to improve further the prognosis of children with these diseases.
Topoisomerase i inhibitors, ie camptothecin derivatives, represent a very attractive new class of ant|cancer drugs to develop in paediatric oncoh)gy. They exhibit a novel mech-
;.ini~in of ;idion, .~illt:~ llOl|L' of the anlicanccr drug', currently u~cd iu the treatment of cam:or in children arc tar~dcd against topoisomentse I. Carnptothecin, the leading como pound of this class, and its water-soluble derivatives have demonstrated a broad spectrun~ of preclinical activity in murine models and adult tumour xenognffts, In addition, no major cross-resist,'mce has been so far observed with drugs involved in the multidrug resistance phenotypc or with alkylating agents. Finally, the camptothecin deriva- tives have shown clinical efficacy in several cancers, in adults.
For these reasons, several teams have embarked on the preo clinical and clinical evaluation of canlptothecins in paedia* tric ma l ignanc i e s . A lot of knowledge has been accumulated about two of these new drugs, namely topote° can and irinotecan. Here, we review the current available results of this evaluation at the preclinical and clinical le- vels, and we address the issue of the future clinical devel- opment of topoisomerase 1 inhibitors for the treatment of children with cancer.

272
Topoisomerase ! as a target in paedlatric malignancies
The DNA-topoisomerase I is a nuclear enzyme which re- solves the topological problems that are generated during DNA ~plieafion, transcription, repair and recombination (for details ~ other articles of this issue). Topoisomerase ! is the nuclear target of eamptothecin and its derivati,,es I11. As op~sed to topoisomerase il, topoisomerase I activ- ity exhibits no significant changes throughout the different phases of the cell cycle. Meyer et al showed recently that in inte~hase, topoisomerase ! mainly has a homogeneous nuclear distribution and chromosomal staining Ibr topo- isomera~ 1 remained homogeneous in mitosis 121. Topo- isomerase I seems to be uniformly distributed in the cell cycle. However, topoisomerase ! inhibitors are cytotoxic fi~r cells in S-phase 131. Indeed, camptothecins induce cell ar- rest and specific cell death in S-phase. Duriag the S-phase, the collision between an advancing replication fork and the DNA-topoisomerase ! cleavable complex, stabilised by camptothecin, results in an arrest in fork progression, irre- versible DNA-damage characterised by double-strand breaks and apoptotic cell death 14, 51. Camptothecin and its derivatives are selectively more active against DNA-repli- caring cells. Thus, they are expected to be particularly active against tumours with a high fraction of cells in S-phase. For this reason, paediatric tumours which are rapidly dividing tumours may be sensitive to topoisomerase 1 inhibitiors.
Several studies have shown malignant tissues to contain higher levels of topoisomerase I, as measured by DNA.re. laxation activity or protein level, than their normal tissue counterpart~ or benign tumours, Tills was observed ill colon cancers 161, ovary carcinomas 17 I, and several other cancer types 18,91, To evaluale topoisomerasc I as It potent targel I'or tile tl~a|ll!e!!t of paediatric nlalignali~ies, we have Sill- died topoisomerase I aetivily in a panel of neuroblastomas and brain turnouts, A topoisonlerase I relaxation activity was present in all samples, 'l~poisomerase ! activity was five-lbld higher in immatu~ neuroblastomas than in gun- glioneuroblastomas and normal adrenal glands II01. Topo- isomerase I was five..l'old higher in medulloblastomas than in benign lt,~ strocytomas, ' l Ill , These differences in topo- isomerase I levels between malignant turnouts, normal tissues and benign turnouts have been thought to conl~r a certain level of specificity for the antiiumour activity of topoisomerase I interacting drugs. Indeed, the presence of topoisomerase I is required Ibr these drugs to be active I 12 l, and resistance to camptothecin or its analogs is associated with a deceased enzyme level and/or mutation in several cell lines 13, 131. However, further studies failed to find a significant ~lationship between topoisumerase ! level and sensitivity to camptothecins, the best celhilar parameters being the amount of stabilised cleavable complexes in the treated cells 1141.
Topotecan
Topotecan, mr 9-dimethylaminomethyl- ! O-hydroxycampto- thecin, (Hycamtin ®, Smith-Kiine Beecham) is a water-so- luble analog of camptothecin. Topotecan does not require biotransformation to be active. Topotecan exists as two forms in pH,dependent equilibrium, ie the lactone and car- boxylate forms: only the lactone form is able to stabilise the topoisomerase I-DNA cleavable complex.
Preclinicai evaluation of t~q~ote('an
Topotecan has demonstrated a high degree of activity in a broad spectrum of routine tumours such as colon carci- nomas 38 and 5 I, mammary adenocarcinoma, Lewis lung carcinoma, Bi6 nlelanonla and nlultidrug resistant P388 115. 161. These rliodels are relatively resistant to most anti- cancer drugs used in paediatric ontology.
Topotecan £].ficacy against paediatric tumour.wnografts The antitumour activity of topotecan has also been evalu- ated against several in vivo paediatric tumour xenografts of various histology types. Houghton et al showed complete tumour regressions in six rhabdomyosarcoma xenografts with topotccan given ip mr orally il71. Tumour-free survi- vors were observed in three of these six sensitive xeno- grafts. Topotecan displayed antitumour efficacy against three osteosarcorna xenografls, and induced a significant tumour growth inhibition in Ihrec juvenile colon cancer xenogral'ts, in addition, topotecan retained its efficacy in a mdrl-positive rhahdonlyosarcoma xenogral't selected for in z'ivo resistance to vincrisiine, but was cross-resistant with inelphalan.
The ill i,il,o i in! i ! i lni l inr aclivily of Iopolet'an iigainsl sub- culiilic'ous and inlriit:rlinilil pacdialrii: and adllll t:t+'nlral nerv- Oll,~ syslenl Itlnlour Xeliiigriifls has heen reporled by Fri~dnian lJl a l l l 8 I, hitrlt l)¢riloncal lopolecan illdueed ton i o plete tuulour regressions ill two el~lendynlotnlis, Olle nledtll. Ioblastoma and one nuilignant paediatric glial turnout xenolralt. We showed that topotecan, administered ip or iv was active against three neurohlastoma xenugrafts with sig- nificant tumour growth delays in all of them. In addition, complete regressions were observed in two of these ncuro- blastoma xenografts 1101.
Schethth,.dependeot acliviO' of topot('cau As an S-phase agent, topotecun activity is schedule-depend° ent. In vitro, short exposures result in typical phase-specific cell killing curves in which increasing concemrations kill progressively more cells and then reach a plateau wllen all susceptible cells, ie cells in S-phase during exposure to the drug, are killed. In contrast, prolonged exposures result in steep concentration-response curves with no plateau 119J, In vivo, topotecan plasma disposition shows a sho, ,;iimi- nation half-life (2-3 h) in animals as well as in humans 1201. Thus, prolonged administration of topolecan is likely to

provide prolonged exposure io aciive levels of ibis S+ph~sc specific agenl. /n i,il,o preclinical sllldies xhowcd lhal the anlitumour aclivily and toxicily of lopolecm~ is clearly schc- dule-dependenl during shori Irealmenls !15, !(~]. Pmlracled adnlini,~Iralion over 12 weeks proved to be highly acli,~c in rhabdonlyosai~onla and Io hlci¢ase iopoiecan alll i lunlour activiiy against juvenile colon cancer xenografts I17, 211.
clinic~d devehgmw~t q#" loPolecm~ i , children
Topotecan is registered for the Irealmenl of relapsed ovary cancer with a daily times x 5 schedule of administraiion al a dose o1" 1.5 mg/m2/day, in adults, Ihe clinical development has been seeking for lhe oplimal schedule of adnlinisiralhm of this schedule-del;lendeul drug. Pllas¢ I sludien have cx- ploi'ed various schedules fronl holus Io ]loday COlilintious iv inl%ision I/l" oral adnlinisiralion 1221. The clinical dcvel- opnlenl in paediairic onto logy is the nlosl advanced anlongsl all Ihe Iopoisomerase ! inhibilors. Aclually, the phase ! ! eval ualioil ot' iopolecan-conlai nil17 colnbi nal ions in ongoing.
Phtlse I ~uid l~haruulcologi,'ul st,dies o.f Ilqtoh'cOll ill chihlre, Five phase I sludies exphlring differenl schedules of adlnini- slralion kave been condu¢led and reporled in children wilh solid lUlUOtirs and acule leukaelnia,
]' l ie fii'sl paedialrh: phase I sltidy was reported by Blaney <,t . I 1231. Topolecali wa~ given as a 24-h COlllllltiolis ill- IravenotlS inl'tlsion every ;21 days wilh a dose ranging froln
to "7.$ lng/ni2/day, l)o,,e-rehih:d llet~lropenia aud Ihronlllo- eylorlenia were dose Ii luil i l lg. No olher nlln-haelualohl~ical Io,~iciiy was dose-Iiiniiing. The recoinnlended do,~e for phase II slullies was 5.5 lug/nl2/day. Nil difference wan oh- served in co,nl~a!'ison wilh Ihc ol)liuial dose ill heavily pl'c- Ii'ealed adtill piilicnln. The aulhors reconiliiendu'd Io illcleanc Ih_e dose Ult ill 7.$ lUg/lu2/day in 13ali¢lilS ~vllo wi l l lulcralc well Ihe 5.5 IIIg/lll2Ahiy. Oul l l f the 29 palienls enlel'¢d in the study, lie okieciive resl;ionse was obsei'vcd. "rile phisnla rihal'iUacokhletic sludy showed an eliluinalhln hall'-life of 2.9 ii wi lk a nlelln lolal iOl)Oleean pllisnlil clearance el ° t).~ L/hliu 2.
Prau ¢I a! ¢~phlred a 72-h continuous inlravenous infu- sion adn l i n i s l r a l i on in a dose range of 0.75 Io 1.9 nlg/m2/day l iven every 21 days 1241. Again, the dose Ihniihlg was myelosuppression, which involved all kaema- tological lineages. The recOlllnlended dose for phase !i studies was I nig/nl2/thiy. At this dosage, G-CSF ( I0 l.ig/kg) administration led to a shortened duration of neutropenia. without any substantial effect on throinbocylopenia. AI higher dosage, no other lmtior non-haenlatologieal Ioxiciiy was observed with lhis schedule. ()ill of 27 palienls wilh rel'raclory solid lUnlours, one complete remission was ob- served ai the 1.3 nlg/m2/day dose level in a paiieni with disseminaled neuroblastonla, and slable disease occurred in palienls with neuroblaslonla, rhahdonlyosarconla iilld lliela-
_ i . ~
ntalic i~Rct cmcinoma. In lhin ~ludy+ the climinatioll ha]f+~ih ~ of lopolccan ~a.n 2.~.~ h. arid lh¢ median k~tal lopoh~can ck'~r- imce wan 6.5 l_/h/m -+ Iranoe I.~-it).5 |./h/m-~L |)urin,, Ibis 72-h comintioln,, iv infusion adminislraiion schedule, lhc hiIcmillo]o~iciI] lox]c]ly wi~s corre]ii|ed v¢ilh ~,yslclllic expo- .nUlC at~d slcad), slate p]asnla coll~.'ClHriltioll 1o c]lhcr ]i~cl~nc or iolal topotecan [25 I.
Tubergen ¢I ul explored the schedule regisiered in adults, ie 30 rain infusion daily for Five consecutive days every 21 days, in a dose ranging from !.4 to 2.4 nnptnlZ/day wiih or withotn G-CSF (5 ~t~/kg) 1261. This topotecan schedule has been largely studied in phase |l in adult patien|s. Haemalo- logical toxicity occurred al all dose levels and was dose- l imiling, Over half of lhe paiienls received rod blood ceils and 19 oul of 40 plaielel Iransfushms, Febrile lleulropenia or doctlllleilled infeclions oCCtlrred ill 32 of !{~9 courses of Ireallnenl. Myehlsuppression was dose-liinilhlg. Mild-|o- nloderale 71i,~l i'oi nleslinal lox icily, incl tldlll 7 diarrhoea, v,, as ob~¢r;;¢d. The reCOllll l leilded dose's for phase 11 Cvitll.lilliOI1 wore !.4 inTtnv~/day wilhoui G-CSF and 2.0 ill~,lnl21day xvilh G-CSF. In Ihe 40 palienls irealcd, ol~jecii~e responses were ohserx, ed in netirobhisloiila tihree PR alid one SD oUl of nine palielitS). Slahle disease occurred in one anaphislic iislroc),lOllla, lille epelldylliOili~l alid oile Ewing's s~lrCOlllil. The phisnlli pharnlacokinelics were sludied usin 7 a lhlliiin~ salllp- ling slralegy and a Rayesian algoriihln. The plasnla clearailcex of lolal lopoiccan and ]aClOlle forni were siniilar io those re- porled in Ihe Iwo i)revious paedhitric phase ! sludy. However, a prolonged elinlinalion halflil 'e (4.5 h! was observed. In ad- dilion, a significanl pharnlacodynalnic relalionship was oh- served helween Ilk. ~ declease of peri='ellla~c" ill ilbsolulc nculrtll~lhil counl and IOlTlOlec~in hichlne A/J('.
Ili l:urlnan ¢I u/Sltldv, IopoleCiln ~'~i,~ adniilliM¢l'~)d ~i~ ~i 12iioh Clllililliioun inlra~i:li~lun ilifi inilln in i~illicni~ ~,iih tic'tilt' Ieuklielnia 1271. ~ynl¢llliC cxposllrc', its nieanUlCd h), nlu'iidy nlliic I~ilanlilli levels el' hll)l!h'¢all lliChillcL t'+~in c~C~l- lah'd I'rltlil I hi 5.3 n{2Jnil,. The rcqtlired tltl)lllc'c'an dll~;i~c ranged froni ().5 Io 3.3 Ilig/ln2/day. Mticosilis was expo.<,iJrl2 + l i iui l ing Ioxi¢iiy and the nlaximunl toleraled systenlic expoo Stile (MTSE) was 4 ng/tliL. Myc'losupllrcssion was observed hut nol COllsidered as dos¢+linliling. Oul of Ihe 18 palieni~ Irealed, one clinlplele response was ohs¢i°ved ill a palielll wilh a hone lnarrow and CNS I'ehips¢ of a Burkiu lynlphonla, and one parliai l'~Sl~onse in a refra¢lory B-cell ieukaenlia. The nlean Iolal Iopolecan I~lhisnla clearance was 8.9 IJhfnl ~ with an elimination halt-life o1"3 h. A significanl i~harnla¢odynamic rehilionship was observed helween loplilecall hicione syslenlic expostll°e and die severily of illUCOsilis.
Oral adnlinislralion ill' Iopolecan inliy he very helpftil Io develop prolracled IrealinelllS with Ihis scheduleodependenl drug. The preliminary replirl of a phase I sltldy of oral lll- polecan in chihlrcn wilh r¢lraclilry solid lunliiurs ~howed a good bioavaihihilily of 34-4lea 121~!. ()ral Iopolecari ~'ilS given in Iwo differenl schedules: daily for 21 conseculive days or five days on followed hy Iwo days ofl for il Iolal ill" 15 doses. Myelosuppresion was dose-liiniling.

274
Overall these paediatric phase I studies showed consist- ent results: myelosuppression that involved all three li- neages is dose-limiting and can be somewhat shortened by the administration of G-CSF; no major non-hematological toxicity was observed but mucositis, which happened to be the dose-limiting toxicity in acute leukaemia patients re-
ontinuous iv infusion (I 20-h). Other as nausea and vomiting, diarrhoea,
maculopapular rash or pruritus have been reported. The op- timal total dose in children seemed to depend on the admini- stration schedule {table I). When the continuous infusion is prolonged, the maximum tolerated dose is decreased.
In addition to these phase ! data, some pharmacological results arc important tbr the future development of topote- can in paediatric oncology, Earlier on, Blaney et al showed, using the NCI rhesus monkey model, that topotecan was distributed into the CSF alter intravenous administration with a CSF-to-plasma systemic exposure ratio of 0,32 1291, Intrathecal topotecan has been also evaluated in this non- human primate nlodel 1301. Later on, the CSF distribution of topotecan was studied in children with CNS tumours entered in phase I studios 13 ! I. The median CSF-to-plasma ratio of lactose topotecan during a 24-h and a 72-h infusion was 0.29 (range 0. I to 0.59) and 0.42 (range O. I ! to 0.86). This makes topotecan particularly attractive for the treat- ment of CNS malignal~cies in children. With this prospect, Stewart el al reported that phenytoin induced a 30% in- crease in topotecan clearance in a child with Inedulloblas. loma 1321.
Single,agent phuse II studies o1' loputecun in pm,diatri~' malignant'its Blaney et , I studied Ihe antitun~tmr activity of topt~tecau given as a 24,11 schedule every 21 days in 45 cllildret~ with a hraiu tumuur 1331. The i11itial tlo,~e of 5,5 IIIg/lll ~, a~ re o euntlnended by their phase I study, wan escalated to 7,5 I11~t111~ iu subseque111 ~our~e,,. in pallellts wh~J did ilol eXl~,~r:ience dosc-limitiug ~ ~' ,' t~ Xlclly, No COnlplele or partial ~s|~mses were observed in patients with medulloblastoma (~ ~ 9), malignant gliolua (n ~ 9) or brain stem glioma
(n = 14). One of two patients with a low grade glioma ex- perienced a partial response. This absence of activity, con- trasting with the encouraging preclinical data in childhood brain tumours [181, might be related to the administration schedule (24-h infusion) which might not be optimal, when 'all preclinical and clinical data so far available ~u'e considered.
The Paediatric Oncology Group has conducted a wide open phase II study in recurrent or progressive paediatric sol id t umour s , us ing the r e g i s t e r e d schedu le , ie 2 mg/m2/day x 5 every 21 days. The preliminary results were recently reported 1341. One-hundred-and-forty-six pa- tients received 535 courses of treatment. Partial remissions were achieved in six out of 40 patients with neuroblastoma (15%L in one out of 30 with Ewing's sarcoma and in a patient with retinoblastoma. Stable disease was observcd in neuroblastoma (12/4()), Ewing's sarcolna (6/30) and rb:d~- domyosarcoma (2t24). No objective efl~cts were observed in 19 patients with osteosarcoma, eight with hepatohlas- toma and three with nephroblastoma. The main toxicity was myelosuppressiou that lead to dose reduction in Ii% of courses and addition of G-CSF in 33%.
Up-front window phase !! sludies are designed to evalu- ate the antitumour activity of new drugs in chemotherapy naive I~atients with metastatic disease prior to the initiation td" their conventional treatment. The Paediatric Oncology Group has conducted such a phase I! study of topotecan in patients with disseminated neuroblastoma 1351. Topotecan was given at a daily dose o1" 2 mg/m 2 for five consecutive days with optional G-CSE Thirty-two palienls were evalu- ahle Ibr lUlnOt, r response: one complele and il partial re- missions (ie response rate, 37%) were observed, as described in 1he prclimilmry report o1' the results.
The Intergroup Rhabdo111yo~arcolua Study Group has ctqlducted all upqi'O!lt window phase II study in patien!s wilh newly diagnosed UlClastatic rhahdou!yt~sarcolna. The prcliulitlary restllls have beet1 recently rclmrted 1361, 'lb- p~tecan wa,,, adllfilliS!ercd at a daily th~se of 2 111g/|n~ for 5 ctmsecutive days. G-CSF wan added in case of neutropenia, and topolecan duse was escalated up to 2.4 inghna/day in patients who tolerated well the treatment. Out of 411 evalu-
Tabk I. Ptlase I and ~'d,arw.acological studies ,,1" toputccan in children. . . . .
Author (rel'erence) Schedule I)ismlsc Ntlm|~r uf paticntslcoul'sCs Daily dose range (lUgllu z) °R~lal dose range (mgllu2) Rc¢olUlUc1~dcd daily tlosc ~mglm- I R~¢t~mnlendcd Iolal dose (lughu o I l~seolindting toxicity 'Ik~lal Io|~Ie¢{m clearance l lolhlu~o, i ' T~lal tol~lecan eliluinatio1~ half.life ~hl I.a¢I~11c I~pnleca11 ¢learallCC ( IJhlln 2 )
. . . . . . . . . . . . . . . . . . . . .
1:31aney ! 23 ! Prau 1241 Tubergcu 1261 I:urman ~' 127 I 2441 civ 72-h civ 30 rain iv I~r day × 5 ! 20-h civ
Solid Iu111o1,1rs Solid tla111o1,11"s Solid Itlnluurx l.o, lkaenfias 29142 27153 40 18/23 27.5 (),1~ 1.9 1.4..-2.4 0.5~ 3.3 2~7.5 2. I-5.7 7~-! 2 2.54.3 5,5 1.0 i.4 a 5.5 3,11 7.11 ..... a
Myclo~ul~pl"C~,iol~ Myelosupprcsniou Myclusupi~rcsiou Mucositis t),S 'k 3, t) 6.5 7.54:2.7 8.7 2,9 :t I, I 2.9 ]: I 4,5 ± i,7 3.5
28,3 ]: 6,5 16,2 ± 5,2 16.7 _+ 1~.5 18,3
(~ !l~I this sttidy, the systenih: cxl~,,,urc as Izzea,,urcd by topolccan I'dastna Icvd at slcad~ state Was escalated, "rhc nzaxiln1.1nl tolerated svstctni¢

able patienls, two achieved a complete remission and 16 a partial remission m:sponse rate, 45%L
The results of the early clinical evaluation of topotecan in paediatric ontology are encouraging. Single-agent m- potecan displayed signil'icanl anthumour aclivity in patie|lts with neuroblastoma and rhabdomyosa~'oma. It is interes- ting to point out that most of turnout responses observed were partial. It remains to be evaluated whether protracted administrations, using for example the oral route, will in- crease the drug activity, an suggested by preclinical data. Clearly, the optimal schedule for topotecan treatment re- mains to be defined in children as well as in adults.
irinotecan
Irinotccan ( C H ' ! I ) or 7-elhyl-10-(411-piperidin~l I-pil~e- ridi no )-carbony lox y-campl othec in (Campto °!L R h6ne Pou- lent Rorer SA; Camptosar % Pharmacia and Upjohn Company) is a water-soluble analog of camptothecin, syn- thesised by Yakult Honnha. As opposed to topotecan, iri- notecan is intrinsically a poor topoisomerase ! inhibitor. The hydrolysis of the piperidino-piperidine side-chain by car- boxylesterase leads to the flmnation of an active metabolite SN-38. In vitro studies have demonstrated that SN-38 is the most potent active drug amongsl the Iopoisomcrane I inhibi- tors so lar available flw clinical development 137I. Like olher camptothecins, the aclive lactose forms of CPT-II and SN-38 undergo pH-dependenl reversible hydrolysis to yield inaclive carboxylate forlns.
Pr('('li,i(',l evalmttio, of irimm'('a,
CM \ I I has shown anlitumot, r aclivity againsl a broad spec- lrUlll of ~2xpel'illlC!llal ill vil'o lllurille lllllll)ur models folh~w- ing iv, ip lind oral adminislratim~ 13S 4()I. ()f il~U.,l'eS~, CPT-II wits aclive againsl some parlicuhlrly rcnislalll lu- IllOur models such as pancreatic dtlclal adellOt,'ilrcillOllia ()3 and BI6 inelanolna, and againsl mltllidrug-resislanl It1 o mours 13~J. 41 I. CPT-I I disphlyed also antilUlnOur activity in several adull hulilall ntalignanl lumour xel|ogral'ls 142l.
I{/.lic~r 3, o l'iri,otecon agai,st imediatric tumour .~e,ogrqfts During the htsl 5 years, irinotecan has been largely evalu- aled against several preclinical paediatric tumour xeno- grafts, including rhabdomyosarcoma, neuroblastoma. peripheral primitive neuroectodermal lumour, medulloblas- loma, ependymoma, malignant gliomas and .juvenile cohm cancel; In the history oI" paediatric ontology, this is the first time the clinical development of a new anticancer drug is started with such a large amount el" specific preclinical data obtained in paediatric tumour models.
In Houghton's first study, iv CPT I I wits highly active in 5 of 6 rhabdomyosarcoma xenografts, with a high proper- lion el' prolonged complete tumour regressions 143 I. CPT- I i wits shown to retain its anlitumour activity at dose levels
2v5
bcMw the maximmn toieraled dose. In addi~ioa, CPTo~ was a¢Iive against rhabdomyosan.-oma "~eno~rafl~ seh:vlcd ik~r |heir resis|anve to vmcristine, melphatan or topo~ecan.
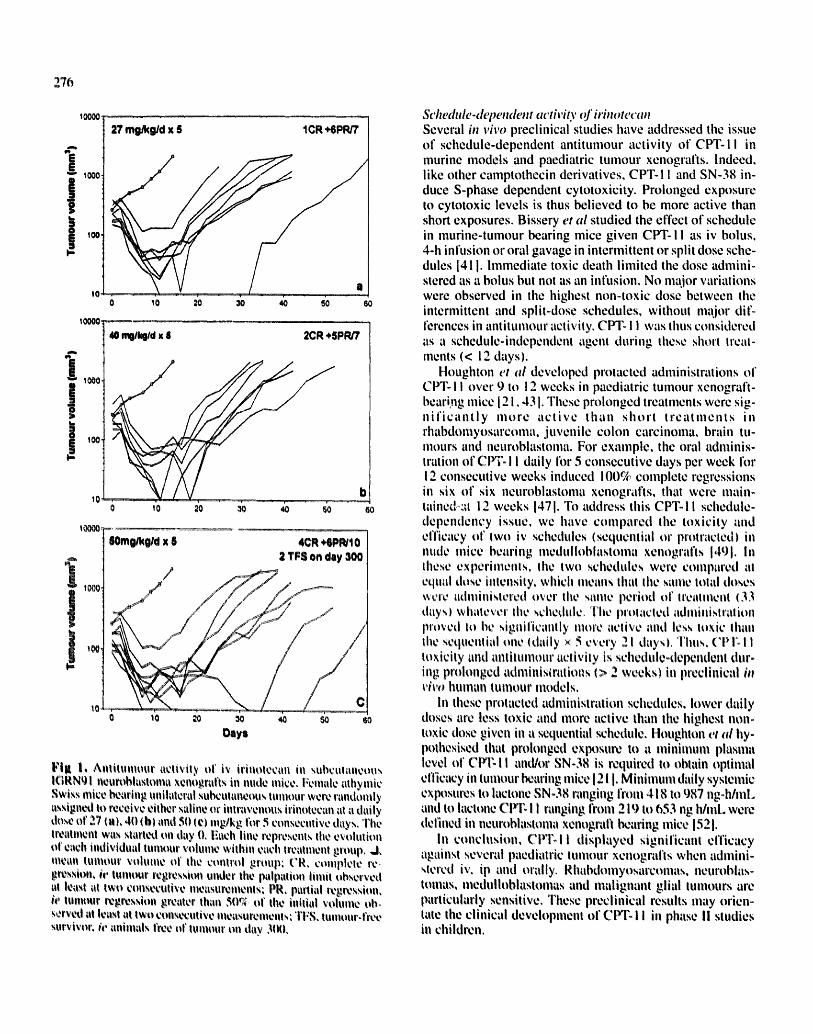
We have evahmted 1he h~ vivo efficacy of ix ¢'PI:B ~ m nude mice bearing neuroblastoma xenografls i10, 44j. These xenografls have been established from both untreated and previously treated tumours. They exhibit tile biological features of poor prognosis neuroblastomas, such as N-myc amplification, diploidy, chromosome l p deletion and over- expression of lhe mdrl gene. CPT-I ! induced complete re- gressions of advanced stage tumours in four neuroblastoma xenografls and tumour-free survivors in one of them (fig I :L This activity was comparable or even higher than that of conventional drugs used for the treatment of neuroblastoma in children, ie cyclophosphamide, cisplalin and thio|epa. Tumour growlh inhibition of a xenolransplanted neuroblas- loma cell line has been reposed by Komuro et ai 1451. The eMcacy of CPTI! against neuroblastoma xenografts was also observed by Thompson who showed at high proportion of mainlained complete regressions in six neuroblastoma xenogral'|s follm~ing oral and systemic administration of CPT-I l 146. 471.
Hare et al have evaluated the anlitumour activity of ip CPT-i I against a panel of paediatric and adult brain ttllllOtll"
xcnografts growing subcutaneously or inmtcranially in att- hymic mice 148 I. A significant eMcacy, evaluated as turnout growlh delays and turnout regressions, was observed in me- dulloblastoma, hi,,h~ grade glioma and ependymoma xeno- grafts. CH'-! ! retained its antitumour aclivil), in xenografts selected for resistance to cyciophosphamide, bunulfan or melphalan. We showed significant antitumour efficacy of iv CP'I:! I in five Otlt of five stibctllall¢Otls mcdulhflqas|oma xcnogralts eslahlislled fronl tllllrcaled or relapsed |UillOtlrs 1491. Ttlniotlr-fl¢e nvrvix~l's were ~fl~served ul lw~ illedtll.. hlhlaslOllla Xellogral'ln lllt)l'C than 4 III(HIIII,~ illlet" the treato nlenl slarl. 'I'he CPT-II activily wa,, cqui~:alcnl ~r c~.cn
CPToll i.,, clcally highly a~.'tiv~: in pacdiatri~: tuil1~m! xenografls. Can these pre¢linical resull.~ predict the efficacy of CPT- I I in children with solid lUlllOtlrs'~ ~ Actttally, CP%t I in bioli'anslk~rnled i , vice in its active melal~olile SNo38 by carboxyleslerase. Murine plasma Colltilhls carhoxylestcra~e while huillan plasma does nut. When plasma pharnlacoo kinetics are considered, the SN-38 to CPT-i i systemic ex. posure ratio ranges from 1 to 5~a in humans 150l. In mice, tile plmrmacokinetics of CPT I ! are nul linear, and the SNo 38 to plannla ratio ranges lroin 40 to 6(Jr;'; 1511. We have shown that Ihe anlitumour aclivily of Clri31 i againsl me o dulloblastoma xenografts was observed al systemic expo- sures Io t'P'l'- I I thal call be achieved in adults receiving the optimal dosage of CHLll I491. Conversely. the syslemic eXl~osure to SN-38 in mice wits i(I-I'old higher than thai observed in adulls given Ihc recommended d~sc. This sug- gests thai the i , vice preclinical aclivily of iv CPT~li in paediatric lulnour xenografls may overpredict, m a cerlain extent, its activity in children.
276
tOOCO
i ' ~ 1000 j
100,
10000,
2')' rng/kg/d x S lCR +6PR/7
0 10 2o 30 40 50 6o
i ~1000 j t~ ̧
t0
I t000
40 mlg/kg/d x 6 2CR +SPR/7
0 t 0 2o 3o 40 50 6O
Oays
Fig I, Anlilumour aclivily of i~' iritlolecan in subcutaneous IGRN~I neun~blastoma xenograt'ts in nude mice. Fclnale athymic Swiss mice ~aring unilaleral su~ulaneous turnout were randomly assigned |o receive either saline or intravenous irinolecan at a daily dose or 271,), 4t) {h) and 5111¢1 rngtkg for 5 consecutive days. The treatment was slatted on day O, Each line represents the evolulio, of eacll individual lumour volume wilhin each tlval,uenl group. ,J, recall turnout volume o1" Ihe conlrol group; CR. colnplcle rc, g~ssio11, ie lUlnour I'¢g~ssion under tile palpation limit observed at least at Iwo consecutive n|easul~inenls: PR, partial regression, ie turnout i~gr~ssion greater than 5tt~ or II~e initial volume oh, servt~tl at least at lwo COllSeculive IlleaSUl~lllenlM TFS, tumourffl~e survivor, h' animals free o1' turnout till day 3t~),
Schedule-dependent activity o[ irim~tecan Several ill vivo preclinical studies have addressed the issue of schedule-dependent antitumour activity of CPT-II in murine models and paediatric tumour xenografis, indeed, like other camptothecin derivatives, CPT-! ! and SN-38 in- duce S-phase dependent cytotoxicity. Prolonged exposure to cytotoxic levels is thus believed to be more active than short exposures. Bissery et al studied the effect of schedule in murine-tumour bearing mice given CPT-I! as iv bolus, 4-h infusion or oral gavage in intermittent or split dose sche- dules 1411. Immediate toxic death limited the dose admini- stered as a bolus but not as an infusion. No major variations were observed in the highest non-toxic dose between the intermittent and split-dose schedules, without major dif- ferences in antitumour activity. CPTII was thus considered as .'l schedule-independent agent during Ihese short treat- ments (< 12 days).
Houghton et al developed protacted administrations of CPT-! I over 9 to 12 weeks in paediatric tumour xenograft- beari.ng mice 12 I. 43 I. These prolonged treatments were sig- n i f ican t ly more act ive than short t rea tments in rhabdomyosarcoma, juvenile colon carcinoma, brain tu- mours and neuroblastoma. For example, the oral adminis- tration of CPT- I ! daily for 5 consecutive days per week for 12 consecutive weeks induced 100% complete regressions ill six of six neuroblastoma xenografts, that were main- rained-at 12 weeks 1471. To address this CPT-I I schedule- dependency issue, we have compared the toxicity and efficacy of two iv schedules {sequential or protracted) ill nude mice bearing medullohlastonla xenografts 1491. In these experiments. Ihe Iwo schedules were compared at equal dose illlensity, which nleans thal the same total tloses ~,cr¢ admilfistered over the Sallle period ol' Ire~lllnelll ( 3 3
days) whatever the .,,¢hedtllc. Tile I~rOlaclcd adll|il|istration proved hi be sigllifiealllly more active and less Ioxic ihall II!c sequential one (daily x 5 every 21 daysL Thtls, CPI:I I toxicity and antilumour activity is schedule-dependent dur- ing prolonged admilfiSm, tions (> 2 weeks) in p,~clinical in vivo human lumour models.
in these protacted administration schedules, lower daily doses are less toxic and more active than the highest non- toxic dose given in a sequential schedule. Houghton et al hy- pothesised that prolonged eXl~sure to a minimum plasma level ol' CFI'-I ! andh)r SN-38 in requited to obtain optimal eMcacy in turnout I~aring mice 121 I. Minimum daily systemic eXl'H3sui~s to lactone SN-38 ranging front 418 to 987 ng-hfmL and to lactone CPT- I ! ranging li'onl 219 to 653 lie h/inL were defined in neuroblastoma xenografl bearing mice 1521.
In conclusion, CPTI I displayed significant efficacy against several paediatric turnout xenognffts when admini- stered iv, ip and orally. Rhabdomyosarcomas, neuroblas- tomas, ntedulloblastomas and malignant glial turnouts are particularly sensitive, These preclinical results may orien- tate the clinical development of CPT-I I in phase !! studies in children.

Clin ical &'vchqmu'm o,/irim~w,,m i~ pacdiagH~ maligmmcie,~
Irinotecan phase ! slutlies haxe been conducicd in adults tlSlllg differeui schedules: OllCe c%el'\' 3 %%'ecks, three limes daily every 3 weeks and weekl 5 for 3 ~r 4 conscculi~c weeks repealed every 4 o r 6 weeks 1531. Diarrhoea proved to be tile dose-limiting toxicity, When this gastrointestinal toxici ty was control led with a high-dose loperamide mghnc, the irinotecan dose could be further escalated and neutropenia becanle dose-ihniting 154l. In phase ! sttidies, the toxicity of CPT-I! was considered as schedule-hide- pendent in hunmns. OIher observed side-effects ;ire: a cho- IJnergic syndrome during or i inmedialely after drug adnliilisiralion, nausea, von!iihlg, aslhenia and alopecia.
o's r irinolecall is re~l. Iv etl for Ihe li'ealnlenl of patients with nlelaslalic carcJiloilia of Ihe cololl or r¢clunl whose disease has recurred or progressed I]!ilowing 5-FU based Iherapy 155! The recolllnlended dosc is .'45{I nlg/lli 2, once e,,,ery 3 weeks, in Europe, and ! 25 nlg/m-' weekly for 4 conseculJve weeks repealed e~ery (~ weeks in Ihe I.!SA. The clinical developnlent of irinolecan hi children is less advallced Ihan lhal of topotecan: ph;ise I studies :ire Ollgoing.
Phase I and phto'mctt'ologfi'al sludie.s ~!l irinolec'an in ('hihhl'n In 199(-i, a phase I sludy of irinolecan in children wJlh re- hipsed or rel'raclory illalJgnanl solid lunlour was i llilJaled ill France 15~1. 'rile aJni of this sludy was Io define lhe recom- !nended dose of CH'-I I for phase Ii evahlalJOll, hi evaluale the dose-Iiiniling hlxicily in children, Io ailalyse Ihe dispo- sil i l l i l of { 'PT I I alld Jls illelaboliles in phisnla alld tlrinc, iilld hi dOCUliienl any anlill.lnlotlr activity. CH'- I I is gi~ren as a 121l-liiin Jnlravenous infusion every 21 days, with ;i fir,,I dose level ill 21111 qig/lii 7. I)ose-escalaiion is being per- I ' l lr l l led il l Iwl i s0p,,irale cllhi)l ' ln ill' palJelllS, dependJllg l l l l wh¢lher or nol Ihe), had I)rcviousl) , received high-dose cite= nlolherapy wilh aulologotlS henliilopitJ!21i¢ slcm cell Ii'ans- phinlillJoll and/or criillJo-spJniil jrriidialion. To dale, lilt dose,llnlJllng Ioxh:iiy was observed ill ililn-heavily pre- trollied patients up to Ihe dose o1' 351i l l lg/ili ~, which is the r e¢oinlnendetl dose ill aduils wiih the sanl¢ schedule. CP'I: I i and its iilellibolJles are assayed in pl;isnla and urine by HPLC, The prelhnhuu'y results in nine patients showed a Iolal plasnla clearance rate l'ronl 9.5 Io 26.~ L/h/ill-' 1571. Tile systemic expostlre Of SN-38 alld SN-38 glucuronide accounted for 0.5 to 4c, f, and I to 10% of Ihe syslemic ex- posure to CPT-I I, respectively. The recently identified cy o mchrome P450-dependent inactive metabolile RPRI21056 was present in all patients and its systemic exposure ac- counted for 9 Io 25c/b of the CPT- I ! AUC. Dose-escalation is being continued to define the nlaxilnunl toleraled dose of CPT-I I in children with solid tumours.
Tile Paediatric Ontology Group has initialed a phase I study o1' CPT-I I in children which explores another sche- dule ot' adminismliion, irinolecan is given daily for 5 con-
~7r
.,,ccuii\e days cxcr 3 21 da\n. ~'ith a pmpo~,cd starting dai~ dose of 30 mgtm -~ 15S I
Considering the preclinicai data about lhe schedule-de- pendent acliviD' of irinoiecan, other adm{nistrali~,:: .,cilc- dulcs will ha~c to bc explored in phase ! in cmldren Io seek tor the optimal one. In particu~,,, prolonged conlinuou.,, in- fusion or oral administration (when oral formulations are available) might be very interesting to evaluate. These new schedules are currenlly explored in adults. Herben reported recently a phase I study with a 14-day continuous iv infu- sion every 3 to 5 weeks 159l. Diarrhoea was dose-limiting. The maximum Iolerated dose was 175 mg/m e, ie much lower than tile recommended dose with a 90-nln infusion every 3 weeks, ie 350 mg/m 2, The SN38 to CP]: 11 systemic exposure ratio was higher, anti a cumulath:e efi~ct was ob- served during the second course. At llie reconunended total dose (14(l mg/m 2) wilh continuous iv infusion, the systemic exposure |o SN-38 was close lo lhal observed with a short i i lfiision of 350 nlgtnl 2,
Plmsc !! .~lmlic.~ of irinolc~'an i, Imcdiatrit' maligmmt'ic~ Since |he maximum toleralcd dose of ninotccan in children is sol yel defined, lhere is no ongoing phase II sludies in paedialric ontology. In the sex1 years, Ihe clinical cvalu- alR)n Of the efficacy of single-agent irinolecan will be con° duc|¢d in a broad speclrum of relapsed andA~r refractory pacdialric lumours and leukaemias. Tile design of lhese rue lure studies will have Io I;ike into accounl tile rcsulls of the preclinical evalualion of irinolecan in paediairic lumour models and lhc turnout responses, if any, in the different phase I sludies. In addilion, il wi!! be very inieresling to conduct up-fronl phase I! sltidies, especially in InelaMa|ic dis- eases such as netlroblasloilla, mcdtflloblasloma, rhabdomyo~ narconm ~, malignant glia! brain lum~ntrn, which showed a high sensilivily Io irinolecaii ill in I'ivo preclinical sludies.
A tlelailed amilysis of Ihe clinical pllarmacoh~gy ~d <.'lq'~ I I ;llld ils nlelabolJles ill chihlrell will have I~ I~c perlormcd Indeed, CPToll undergoes a complex m vivo biulran.~,tino malion in volving glucttrollidalion and ¢ymchmme P450 ox o
stlldlu, ill idalive nleiabttli.~nl Ifili:621. l~harnlacody imiilic L ' ,~ adulls have illready Stlggesled a rt.~'hllJollshi I) b¢lwe¢ll SNoJg glucuronidalion and ihe occurrence of dehiycd dhirrhoca. tile dose-iiiniling toxicity lft)l. The cxlended oxidative II10o labolisnl of il'Jnotecan raises the questioils of drtlg inlcrilc o l ions and I)harmacogeilelics, which wi l l have ltl be addressed during phase Ii sludJes.
Other Iopoisomerase I inhibilors
The clinical dcvehlpnlenl of o111¢t caniplolhccin analogs in ongoing in adults 1221.2(}-(S}-camplolhecin. 9oaminocanlp- Iolhecin (gAC), 9-nilrocmnpiolhccin (ON(') (which is con~ verted in vivo ill 9AC}, showed polcnl anlilunlour a¢iivily in preclinical models. The poor imlale aqueous solubility of these drugs, especially OAC, resulted ill difficulty devising

278
suitable lbrmulation, 9AC displayed antitulriour activity in paediatric brain turnout xenografts I631. The Gl147211C (or GG21 I) compound is a water-soluble canlptothecin analog, with antitumour efficacy in colon cancer xeno- grafts. To date. phase I studies :ff these camptothecin deri- valives havenot yet started in children,
W ~ t could be the place of topoi~merase i inhibi~ors In the treatment of ehild~n with cancer?
All the precliaical data with camptothecin derivatives in paediatric tumour models and the early results of the siilgle- agent topotecan clinical evaluation in children suggest that topoisomerase ! inhibitors represent an interesting new class of anticancer drugs I't~r the treatment of childhood cancers, If this efficacy of topoisoinerase I inhibitors as single-agents is conl'n'med, what can be the place of these new drugs in paediatric oilcology?
Several studies showed that camptopthecins sensitise cells to radiation therapy I64, 65I, This n'lay open an inter- esting field of clinical investigation in the treatment of pace diatfic brain turnouts, ie ihe combination of radiation thel~py and topoisomerase I inhibitors, Synergistic cytotoxi- city of topot¢can or irinotecan with classical anticancer drugs have been suggested or demonstrated at the preclinb gill level I I9, 66I, Several such combinations are being ex- plored in adults, In children, combinations with an alkylating agent su~:h as ~:yc!ophosphamide or with a plati- num compound may he worth to evaluate in relapsed and/or rel'ractory paediatric turnouts, Phase 1 alld I! studio,, o!' to- pote~:an in combination with eychlpht~l~h:m:id0 or ¢llrhoo phiihl al'e ill progress, These lieW conl!~illaliiuls liliiy ilion he pritl~ls~d its SeCiilld line Ihertipy ill' eveil in!:orl~orliled ill first
To d¢flil¢ lh~ Ol)titl~al sch~dul~ ibr th~ t l~ of topoisorne- r l t~ I inhibilor~ is cl~al'ly a challenge io he taken up, Indeed, if ch~t)ic lidiifiuisiral:iOll, l~)r ~,~anlple of an oral topoisome- rltse I inhibitor, is the optimal schedule in children with n~alignant solid tuinours, it Inay give birth tO now concepts ibr the treatment o1" ch i ldh t~ cancers, Prolonged mainten- illlC~ chemotherapy is a mltior part of the treatment of acute lyatphoblastic leukuernias in children, Conversely, these pixltrileted chemotherapies ate not used in the treatment of paediatri¢ solid turnouts, Most protocols are based on dose, intensity provided by sequential multi-agent chemotherapy courses given at the highest non,to×it doses, How can a drug which is active ill plxdonged chronic adminintration schedule ~ ustxl in pa~diatrit: ,~olid tuiilour,~? lu patient,~ with nieasurable disease lo achieve coillplele r~illis~hm? hi patienls wilh nfinimal ~sidual disease to inaintain colnplelo ~inission? As a singl~-agcni or in conibinaiion with oih~r aniicancer agents? These questions will have to I~, raised by paediatric on¢ologists in Ihe n¢,xt years,
Conclusion
Canlptothecins represeilt a very interesting new class of anticancer drugs to study in paediatric malignancies. The early results of their clinical evaluation in children are en- couraging. In the near future, prec!inical and clinical re- search wiil have to define whether or not topoisolnerase ! is a new important target for the treatment of childhood cancers, as presently expected.
Acknowledgments
This work was in parl siipporled by gralll~ IYolll Ihe I.iguc COlilri2 le Ciill¢t2r, the Asso¢ i l i l i o i l poi l r I;i l e d l c i ' d l e t:Oll lrc I0 C~1t1¢01 tl!|d the F~dt~raiiOll Na l ion l i l¢ d¢~ { '¢l i l ru's dc Lu l i e co1111~¢ Ic ( / l i l i l :o ' .
References
I I|siang YH, IAII !.1 ~ ( I~Jsl, I) Idl~nlifh:alioll of manunalian DNA lopoi- nOliiOi'iis~ I its itn ililt'il~'¢lhllar Itll'~¢! ill' Ihe anlieall¢¢r di'u~ Caniplo- ihechl, ( 'ancer Re,~ 48, 1722-1726
2 Meyer KN, Kjeldsen E, Slriltlb T, Klludsen BR, Ilickson IC, Kikilclii A, Krei W H, Boege F l lt}t)71 Cell cycle-coupled reh~ation l l f types I and !1 topoisonv2nises and modulation of catalytic eli~yillO activities, ,! Cell lliol 136. 77.q--TS8
3 Pominier Y, "l]lnizawa A, Kohn KW t 19t}4) Mct.iiiililSlilS ui topoi. SlllllTfilke I inhihi l ion by anlicancer drugs !n: advancv,~ ill Ptltlrlll~lco. hJ~v f l . i i i i.F, edi A¢iidcnlii: Press In¢, ~iill !)ieg~, 21JB, 7J- t ) ]
4 I lsi iui I ' i ' l l , I. ihou I.F, l.iu I.F I lltlll)¿ Artcsl uf DNA replicali~ln by drul-,, i l l ihil ized lilpllisllnierii~e I ,- ! )NA cleiivablo ~:Olllph:,xe~ il~i il nl0¢hllniSlU ill' ~'~11 ki l l ing by eaii l l l l l l l l iecin. Cmlccr Ri,,~ 411, .~1i77-.
,~ Itt l l i i t ( ', ('ove~, JM, K¢l~rigiin I), I~luiiiiiier Y I llit4!t! I) i [ fercl i l i i i l i i .- qii i lell iClil l l f I I 'NA rc, lll iealitil l I l ir l i l t • ¢yl~lo~,i~'il); el I )NA hllIOi~tllliC.r I ' i l '~P I illld II iilhihih~l~ ill (' l l l l l¢~c h~tlllo, l i ! / I ) ( '111 c~'ll~ t ' , . , c r Rl'~ ,.14!, li lllSt .,.h,lfl~
¢1 (i iovlt l i¢l l i l I t t ' , ~lt,'liliil ]~, fill;till Ml i , Walii M( ' , Nicllola~ AW, IAii !X, ~ilbt~'l' I'[, ltlllilic'nll M ! l ~1t4t! I I IN A luptunluiici list' I largeled l;lic' lllolho'~ll! ), of hlllliIin ¢llloli ¢iillCO ~ xenll~l'ii[Is, ,{'c,i¢lii'v ~4, 1ll4(i- 10414
1 Van tJ,~r ~ e A(I , Hifll~:nlil !-I, De ,!ring Sc l al I l~J~ll i P-gl~copl°lllcin cN~r¢~iou alltl I )NA hlpf~iSllliic'la,,,t~ ! ill ld II activity ill b¢llign lUliiors ot' Ih~ oviir), and ill nialignlinl illlilOrs ill" lhe OVal'), bcft~r¢ liiid ill'i~i" plalilitilil/¢ych+llht+sphalilidc ehenli+ihcrall)', ('~im'er Re<+ ~1..~ql.~- 5tJ20
14 I lusahl I, tvhllht~r l i . , Scigicr HV, el a l i i!}~Mi Eiet, alitm of t~ll~ison~eo i~li~ I illi~SSOl~r t N A , prolt:iu, aud catal),li¢ activity in ti i l l i l iul lu o illorx', di2111Oll~lrliliOll t l f lUlltlil~ol~ill: slx, cil~icii~ , t ind inlplii:liliOllS tor t2 i l l l l . ' l . ' l " cht:lllolh~rap),, Cmlcer/¢i,',~ .'14, ,~3q ~,.~46
U Mu~' t,¢~d iito. Dlmglas I:, Oaten M. Syll lollds RP, Priikanh [). Mil l dot ~t'e A(I , Ka)'t" ~It, Browli R. Keith WN i Ititt41 ltq~ilistullerll~e I and i l a~:tivity iu hunliin hl'~ii,4, t.'er'~ix, hilig alid ¢tlhlii ¢allCer~i, hi t 7 Calicer 5l), (l(t?:61 i
I(t Va~ai G, I~ondarr~ ('. CapwI l i ( ' , l~lTiei-Li lconlbe MI , l ioland I. Mori~cl J. I Io lard J. Volual AM, Arthmin I~ I larl l l ial in (), ( iou)et ie :\ I IqOTt I)NA4ttpoi~Olii~,ra.~e I, a li¢~x lar[2el I'tlr Ihe I I~al i i lo l i of ilcltrtil~!.i~illliia,/:'fir J C~mt'er .t3. 201 !,<, 2il 15
i l I-~tuitlai~-7 ( ' , Vassal (,i, llt3ilai-d l, Teri°icroloa¢olubc MI . I.¢ihlu~'h-Tu- hi'i l ia A, Fahl~ M, Morit~ei 1, Gtmyeue A i l!~t!$1 Tolalisolnenise I a¢li~'ily i!l 11~2Ul~l~blashllilli.~ iilld llletlilihibla,~loiiia~, li~ltw anl ils,~oc ( ' l l l l l ' i , r Rt,,~ .ll(ll, 450
12 Hsiaug ' i ' l l . loiti l l : , Wall ME, Wani M( ' , Nichola,~ AW, Manikunuir ( i . Kishehenhluiiit S, Sill ier R, Polu~e~il M I ItJl, i~li DNA lopoisiune-
IaS¢ l - i i ledia lcd I ) N . \ ~'~c:l\;17c and c) |o l t~\ l t ' l l~ i)l Caillt)h)lht, i-ln~ i l l l~ilog ( ' ,~n~ 't'r 4tJ, 4.tR5 43N i)
13 SagilUOhi Y, 'l '~ukahara N (Yt la0a l ' , g ~,,'i I~)~)I,~t I ) c t r c ; iwd C',l)~C~l,)u i l l [ ) N i \ htltoi~,t)lll¢l'~,c I ill c'~mlpht~ht't;iil i t '~i~l j l i l Ii~lil~l cell Iil!C~ a, d¢l t ' rni{ncd b% a IIl~)~lic']~t~li|l a~ll ibotlt, ("~t,~ ~'r I~'~ 5i!, Ihi)~5 (:1 {il
14 ( i t ) ld~ a~ct ' I:, B,Ic I, Valcnl i Hi. ' l\>r)c, K, POll lnl lc i ~ t I~)tl~! l t lp,) l ,,Olllt'r;l~.¢ I - i¢ lalcd p;ll; l l l lt, b,'l, .:.~d tTailiph)lhccHi ,iLlt~ I!) it! thc c't,li~'.) ¢~ircinonlli cell line~ fronl lhe Na{ioitcll ( 'a l icer l i l~ l i lu le ai l l icanccr
.... ~ ' 21 , ~ c r e e l i . ( ~l tt '~') ti{t'<~ 55, 16-2121 15 Johnsou RK ( I t ) ! ) l t i) i-cclinical prof i le o1 SKI : - I l l , iS64, ,i ~a ic l -~o-
hlb ic i 'anlp lo lhcci l l a|lah)g, ( '~lm'cr ln l 'c \ l i), 340- . t47 16 Mat ' ( ,abe FL, " : . . . . ,l~ iii lnitll R K 11')941 Col / ipdr l i lKc i ic l iVi l ) o l oril l ai~d
tlal'ei|lertil iopol¢c;in ill n l t i r ine lunlor nlod¢ln: elfie a c ) o f ~¢al Iopolc- i.';ill, ('(I/I('(T hll'c.%! ] 2, 3()N-313
17 H o u g h l o n IU. (Thenchirc P,I, M \ e r ~ !., Sic~\ari ( ' ! ' , S>no ld "I%%, t lough lo l i JA 119t)2) i{~,'ahialh)ii o i l )-di i l l¢ lh), ! ; l in inoni¢lh~ I III. h)- dlO~)+Caliil)hlihec'in iig;iii lnl ~Cll~!glall~ dcr i \¢d l io l l l adul i ~iiltl chi ld- hood :a)lid IiiIIiOlS, ('(llll'('#" ( 'h(' l l l() lh('r t) l t~tlnt, i<d 31, 22t) 2~q
IN I;l°iCdlilan l iS, i lo t lg l i lo i l 1',1, ,~chlihl S(', Kc i r £, lti):,ilcr ! ) t ) i Iq tM! : \c i iv i l ) ' ill l )d i i i i¢ lh~, la i l i ino inc lh \ I - l i l hvd l l )x )can ip i l l lhcc in ;l~,llll~l I lcdi l i l l ic illid aduh t%'llll;ll Ii¢l%tlll~. ~,\ ~.IcIII \Clltl,e_'l';lt!~ ("~1t1~ c ' l ( 'ht ' tnofh('r i)h~l#'ttlll('t~7.14, ! 7 I -. 174
I t) Chcng I%,11:, ( 'ha i ler ¢¢ ,%. I t¢ igcr N.,\ I It)l)-! i .~c'hcdl c-dcl)c lltl¢nl c, h)h)x ic i i ) ' o l h lp( l l¢can ah)n¢ and iii cl~)nbinalioi) ch¢i i iolhclap.~ l'¢gilll¢llS, f)ll('l)/ok, v Kl'~ fl. ~{~i} ~.Tt)
21) l l c lben V M M , Icii lJokkcl i t l l i i l l k \ \ ' \ \ ' . ltcl.i,icii .111 ( l l ) l ) h ) ( l i n i c , i I I )har l l iacokhlel ics of h)poi¢can. ( ' /HI l)hl~rllltll~.A/m,/ .{!, NS--11}2
21 Houghio l l IU, ( 'henchire P,I, I | i i lhn; i l i II ,11), I . i l l / !,, t:i i<:ll i i i; l l l i i It,~, I )anks M K , I loueh lon JA I l l) l)~! I{ f l icac~ o1 hlpt! i~olncla~c I iuhibi IOl'S, Iopol¢¢ali ;illd ii i l lOl?C;il i, ~idll i i i i iMt'rcd al Io~\ lhln¢ I¢~ci~ ill pil)- li',t~:lCd scl ledul¢~ Io illic'e I~¢;iliii 7 X¢liOgl~llls o1 hi inl ; i l i lUlii~)ln. ('~lll('('r ('l l('tll!)lll(' l" I)h¢lrlll¢i('l)l I('), tl) t.--4{)I
22 |)iU1¢¢~ ,I, I{ is¢llhauer I 'A I iqqOi ( 'urr¢l i l pcrsl)CCli~¢s ,in t:i l l l lplt l ihecins in c'iili¢0r l rcal i i lcnl , l i t .I ( ' l#l( ' t ,r 7d, 327o 3.t,R
23 III , l ; icy SM, lalali~ FM, ('o1¢ I/!'~. ( ' ra ig ( ' , Reid ,IM. :\lllCS M M , K la ih l I%+i, 14¢aluiul ( i . I la in inond !), I)ophick I ) ( i I l q q J i Pcdialr ic phase I l i ia l i|ild pharnlac'okin¢lit: Miidv ~1 Iol)l)l¢c';in '. idii i i i l iMcrt:d ;i~ ;i ,~4- hour u'l)iilii l i i l)u~ i l i lunh)n. ('~#ll'~'~ i{~'~ 5,t, I l l J2 II l , th
]-1 Prli l l i ' l l , ~ l¢~ i i l l ( ' , ,~;iiihiiiii V M , I l l i~ i l i i i i i I,, I i l r i i l an \\'. I )cl l~ }, Mi i r i i i l i IX1, Ki l l lCsdi Jl', I t l : idcni ; i l i l i R, N;inllhil ld .IT..'\<'<'iS I., Nl¢~ci W I I I li)li41 I)liiisc I siud)' o1 h!l lol t ' r ; ln I lu i )cl l ial i ic pal icni~ \~ill i lil;ili~!ililll sl)lid lil l l i l l i~, . I ( '!it,, f ) lh l )# I~, 5 ! q J4 1
75 ~h,,t~'iiil I'1:, li;ikt!l' ,~1), I I¢ ldCl l ian RI. , ]l)lil'~ I), ( ' r l ) i i i \lt 'R, I)rall i ' l l i Iql),l I ("l i l i~lal !~li~ii]li;ic()ll)llailii~ ~ i~l Clilil,,ililllii~ ilil ii~il)ll hl l~lh' l ,ili i i i ¢tiildii~*ii; ~)Mc'll i it ' q~ll! i~li i t ' liiCdi~'in lic i iih)lt)~!lcl l ! ) ~ i l i i ) ,/ ( ' / . i OIl( ' l i / 12, Ill,10-.., l l)54
26 Till~l:rgl;n I) [ i , ,qlt'Wiil*l ( ' ! ~, t)rii l l C l i , ~ainhl ln i W( ' , Wi i ik , k N, Nilii,, l i lnl i V M , I ) ruer ~ A . K i i r l / be lg ,I. Bell II, ( f r ier H, %,/k, l l i "1',1 I Iqi)f i i I)hiint, " I II'ilil, llhiii°iliii¢l)l~iiielic,~ aiid phl ir l i i l icodyi i i i l i l i t !n ,Mud)o l hi, pllli0~'iln liSilig it f ive-day ~'Olil'~t' hi cl i i ldix'n w i lh i¢l'l+achlr) ' ~olid I l l Iillll°S: ii I)edil i lr ic () l l¢l lh)~), ( i r i )up ,~llldV. ,I Pc,d th, l l lc l lo l f ire,t)/ I R. 35 2.3Sg
2=# I ;ur inl in WI. . l t l lker SI). l ) ial l i ' l l , Ri~ela ( IK . I::vans WI{ . S iewar i (3 : ( I ggf~ I [:,scallili l lg s VMelnic cxpt)sUl'¢ o1 uoiil inuous hi fusion ll)11111t, C;|li in d i i l d ren w i lh r0cui'reii l il~'uic Icukc in ia . . ! f ' /# l (Ji l t 'o/ 14. 1504,- 1511
}t~ Bi)\Vli lan !.( ' , ~lCWal'l (7,1", Ziillil~l)lli W ( ' . ( , l ' i )m W R , I . l i l l X. H¢idci i ia i i R, I loughio l i IU, Me) 'cr W I I , l l ia l l ( ' I t I li)!J(ll ' i bx i¢ i i y ii l id pharl l ia ¢l)tlyilii l i i ic,~ of l lrl l l hl l l l ) le¢iin ill pl,,diallit' i)alielll~ w i l h i'¢lapscd ~l)lhl Itlllllll'~. I ) l l l r AII I ,lt'c)(' ( ' / i l l ( ) t ! r t ) l 1 5 , 4 6 2
29 I,}hin¢~ .%M. ('o1¢ I)1']. I}al is FM. (h )dw in K, IMp!:u,k I ) ( ; I lql)3) I)lli,~lilll and i.'Lq'l.,hl'i)~pillill Huid pharlil~ll.'{ikill~ii~' ,Mild%, i l l Iol~,)K, m ili ll,)n hil l l lan plilllal¢.~. ( '~ lm{ ' r R('~ 5J. 725 727
3() l } lancy SM, [,o!¢ I ) IL G o d w i n K. ,%ung ( ' , I)ophick I } [ i . I};ll i~ 1.1%'1 ( I¢}t)~) IiiIr;illll~i.'{il ildlllilli.%lr;llh)ll o f IOl)l)k'C{lll ill l i l)llhllill l l l l I}rilll;llc~. ( ' l l l l ( 'er ( 'hcn lo lh l ' r Phclr lntwol 36. 1 2 1 12.)
31 Itlikel" S I ) . I|eitlu'llllilili R I . , Chi l l i WR, Kul lesch ,11:. ( i ; i i i ; i r ,%, SIt'~';irl ('1: I I() l}{) l ('¢i'¢brl),~i)ilial f lu id i)hl ir l i lacl lki l i t ' l i¢~ iii id i )¢ i icnal ion i)l
27U
~ Ndcv,:0~ ( ' t . (;a btU AJ. t |cit |cmatt RI . l|~ughhir) PJ. Zamb~,m ~,,g~."
,,,u P ( . Xllcn .R" S,dkm %!:. Ja~kacki RI. l.al~m: hi . ~'4c;mum (;t{. th)lox~ii: 1%1|'. Poplack DG. Bails FM (1996) Please 11[ e~.a[uathm oi lopoiecan f~)r pediatric celltral llervous s.'¢slem tumors. ( '~m:vr 7kt. 527-531
3.4 Nilschl,:c R. Park!lursl J. Sullivar~ J. Ham>, NI, Bernstam M, Prau C (l troT)Topoiezan in pediatric patients ~i th recurrent/progressive ,,olid l unlt~r,,: a Pediatric ()ncolog.~ Group (POG) phase l[ ,,tud~ t',;,( Am ,S~n ('fin i')m o/ 16. 511a
~5 Kl¢|nc.hlndr ('. KleI,,el M, Muria) K, Joshi V. Smilh E. Pao PV, ('a~- I lchcrrv R (IqK)S) t!pl'l'o)~l phase ill lhcl';ip> ' ~ilh la~.ol and Iopolccan in tmlicalt, d cluhhen (> 36q da}s) '~.ilh dixs¢llllllatcd (INNS sl~tec 4) IICIIItll~la~h)illa: a Pcdiall ' ic ()ilc*ohL, g)' ( i ro i lp { i ) ( ) ( ; ) ~ludy. 1I~,~/PtJ ¢)n(,d 7S, ~.-ll
t(~ Vict l i I , ( ' l i s l \V, Rtlh)' I!. R~ill¢) It, Ruvi i iann M, l , ink M. Gr i¢ , It. Mal l lCr I! ! IqqTi l(~polc%'lill \~ilit lo~t ill paiic~nis ~vilh rhabdt)lnX.osar ~.'tlllla I IINIS ): all IRS(; sl l td). #)l'i,(, xD#l ,~'ni' C/ in ( )m<d lh. 5 Il ia
17 [ , i n i : a \ t l i ,\, I t i l i i l io r i i \ , l : l l i i ! i l~ui Y. I)~)lillliicr Y ( l l iqJ )('Olilp~iris,~ll itl hlp~li~olliCla~C i inh ib i l i on , I) .N/\ dalnagc', alid c.%l l ) lo\ ic i l ) o1 ca! i i l lh l lhcci l l dcr i \d l ivc~ prcncllll% ill t t l l l ical Irhll~. / ,%:~lI/ ( ( i # i t ~ In~l NIi. £1li N-l]
.IN K imi i l l l ) lo "i. Ni lh l K, "|'~tlltika /', I,~¢hlil'ii N. l~aba tt. l akc i i ch i M. Yokliktl l-;t ']'..~ t\~;ltlll .%. Mi), l isaka T, Mi i la i M ( Iq<R7t Anf i lUlnOr ii~.. l i%i1\ i~f 7 c l h \ I ] t l (41 I I}ipcridin~)l.,, I -pq)ct id in l~i-ca~t~onyh,xy. . cal i l t )h) lh¢cl l l , a ill)vi.'l tvi i l¢r solubl¢ dc'l'iViili~'¢ of C;ll l lplltlhcc*ilL liTa|illsl Il lUtil l0 i l l l l l i l l~, [ ' ( l l l (cr #~'('~ 47, 51)44-5q47
l l ) ' l~ur i io I'. Mal~ i i /ak i ]*, Mi l lSi lshihi M. Sliil{) t l . YokOktll 'a ' [ II<JI~N) : \ l i l i lun io l * c11¢c1 o l ( ' l r r - i I. a m,\v dcrh~i l i~c ~)f c:all i lph)lhccil l. ; igai l lq p lc io l rnpi< dri ~ IC<,iqalll l l l l l l i) l~ n; t ' i lro and in vil'~) ('a#l~ ~'r { "hc'llll>lhi'r l i h , lm( l l 'o l 2 I, 7 I +7-I
4(i lx i~c l l¢ I;. tt issei)' M(' . / \ l ldro S. Rliqtl¢l 1:. Ril)u .ll: I Iqqh) l:q*eclmit al I,~/ihl~llRln ill' ( ' H ' - I I alld ilk aCli~C incqabolilc ,~NI .!lg, .%(,mill cJmol 2 l (suppl Jl, I I---2{1
41 lli~,cr~ ~I( ' , Vl ig l l l l i id P, I i l \c l l¢ I'. ( 'hl iblt l ( ; { ; I llJi)()t I ~pCNilienlal ; i l l l l l l l l l l l i r ;it ' l l\ II) ;ilid phatllli;icol~illCll~'~ t~l Ih¢ t ' i i l l iphi lh¢ci l l ainah)Q Hilililcc",lii l ( ' P l ' I1) ill ilih:C , ,Dll l !o~l( i 'r I)i'li,~'~ ?, 4.l? - lh l i
-l~ Kale\ ,ih) ~f, I'lll i ih i / . / \ l i l l t i l l l i l i M , ~i:;inilllkli M , Ylik(tl~lila "1". Miilninll~iht K I ICJiJll . , \ l l l i l i l l l i t) l iil 'li~ ii~' ot il l 'a l i iplulhci ili dcl i \dl l~C< ( ' l q l I, ,il.!,illlSl hil l l ldll IIIII l l i l \l ' l l i i}.!l,l l l,, ill Ill,dr' IIIi)'t' { (Itt~ ~'1 { ' / i i l l l~ /h l ' / l gn .m,~, , , I )S, li)) li),~
,13 I t t ) t lg l lh ln I',1. (ht '~i : l l l ic ' i)0t, th i lhnal l ,t(', I|ln~¢r)' M((, Mitthwu,,l tuuc- i \ , Ihm~hh) l i JA I Iq i i3 i Ti ier l ipeul ic acl iv i ly i l l l lw ltlplii~on/¢i~i~¢ 1 in l i ih i l tu ' 7,,elhyl, ill-, (4( i -p i t~¢r id in ! ) I - Iq~ ip¢r id ino! t:ar!~t)nylo~y- c:;i l l lphll l lct:i l i iiQ;iili~l Illl l!til l! l l l l l l! l l ' ~c'llllTl*iit'ln li!~:k i l l lo'fil~ ie~i~l- illlc't' Ill vil~) ill lllllit)l',~ %vilh ac:qtiiled i*t0~i~lliltc't~ li l l i lt ' hlpiti~l!l l lt 'ra~¢ I inh ib i lo f IJ d i l i l¢ ihy l i ln i in l )n lc lh) ' l - I l l h)*dl'li~)'l';itilit!liilhi:~lili, ( T t m T t il~('.~ ' 5 .1 . ~IR=il !R=!li
4d Vassal ( ; . T¢rricr-i. l i i : l i l l l l~e MJ. l l i~¢ l ' y M( ' , V01iII;I! ,,4tlttl, (iyel'~a)ity F, I l l 'nard J, M o i i / c l J, i l l )h ind I. Ardln i i l i I t I/rc~ii~'-d¢,,l)ail l¢i 'el~ It. ( hn i )e l l ¢ /% ( l l ) () f l l Thcrapeul ic al ' l iv i lv i)l ( ' H ' I I, il I )NAolop l ) i - Sl)lll¢l;ik¢ I i i l l i i l~ilor. ~i~li l lsl pcriph¢i*iil i~i'inlilivc Ilttllri)¢t:llidc°rlilill lUlliOlir ;inil ll¢ilrllblli,~lOlllll ~¢llllgl' i l l ln. l i t ,I ( 'atit el' ? 4 , 5 3 7 , 5 4 5
-l.q Ki ) l l i i l l l ) I I . I i I t ' l*~ildlid;i "1(, Yl lkt) l i i t i r i K. N;ikillilli.<i K0 Atly~lnla l . KiillCd~) M, K;iliCdli N I I()t)41 I';ll¢i'i~ i)l' ( 'P*I'.-I I I;i tlllitltlt! l )N/t l I t ) imis~,i l t ' i : i~c I in l i ib ih)r i nn ii h ig l i ly Illlililellalll ~C'lli)-ll'all~ilhtl!lt'd I1¢11 r l ibl i lMii l l la, M¢cl Pc,d ¢)n(*))l 2,11. ,1~R=/.=41)2
-if) *l 'hl)l l lp~lin J. Zall l l~l l l l i \~'( ' . ('h¢~dlil%, l)J. I , t l l / I,, i,tlO X, I,l Y. Ih)i lb'hh)l i ,IA..~l¢t~,'al'l ( 'F. I h)iil, hh)n !)01 i Iqq?) I { l l ' i ca t ') i l l ~)'.d¢liiic' ; idl i l i l l iMrl l l iOl l t) l irii;i)lt'c';ill ail~;illi~l liCilll)bla~l~tliia %l:lllqgrall~ ( ' l iH . ":, ,) , '( ,r R+',~ I . 4 2 I., 4 .1 I
47 Th lu l i I, )11 J. Zill l l l~Olii lili '('. ( ' h¢~d l i r¢ IU. I l i d l l n i l n t l I,. I ,uo X. I lo i igh lo i l .I/\. ,~lc~iii ' l ( '!-. I l l lu l2hhin PJ I Iql)71 I!t*l]c;ic'), o1' i)l'iil ~ill iIiiliiMlOilliOll i ) l ililil)l¢~'iili i i~ii i l ikl l iCii l i)bll iMimi;i %¢liOTl'at'ln, ,,lnft- i ' m . v r Rc~ 8, .I 13 .t22

280
48 Hare CB, Elimt GB, Houghton PJ, Houghton JA, Keir S, Mareelli SL, Bigner DD, Friedman HS ( 19971 Therapeutic efficacy of the topoi- ~omera~ I inhibittw 7.ethyb 10-141 ! -piperidinol- I -piperidino)- :arbo- nyloxy-camptothecin against pediatric aild adult central nervous system tumor xenografts, Cam'er Chemother Pharmaco139, ! 87- i 9 I
e ML otte A sche- • bt t J
(~mcer 73; 156--167 ~1 Chabot GG~ Abigerges D, Catin~l G, Culine S, de Forni M, Extnl JM,
Majhoubi M, H~rait P, Annand JP, Bugat R, CJavel M, Many ME (1~5) Pt~mlation phann~okinetics and pharmact~ynamics of iri- sol,can (CPT- I I ) and active melabolit¢ SN-38 during phase I trials. Ann Oncol 6, 1~151
51 Kaneda N, Nagata H, Furuta T, Yokokura T (P)9{I) Metabolism and pharmacokineti¢,~ of the camptoth¢cin analogue Clrr - I I in the mouse, Cancer Res 50, 1713~ 17211
$2 Stewart CF, Zamba)ni WC, Crom WR, Hought~)n lq ( 19971 Disposi- tion of irinotecan and SN-38 tifllowing oral and intravenous irinote- can &~ing in mice, Cancer Chemother l~harntacol 4(I, 259-265
5.~ Armand JP 11996)CPT-II; clinical exl~rie~ce in phase I. Scmin Otw.123 lsuppl 31, 27-33
54 Abigerg¢~ D, Chaba~t GG, Armand JP, Hdrait P, Gouyette A, Gandia D 11995)Phase I and pharmacologic studie~ of the camptothecin analog irinotecan administered every 3 ,,veek~ in cancer patients, ,/ C/in Om'ol 13, 210~221
55 Rougier P, Bugat R 11996)CPT-II in the treamlent of colorcctal cancer: clinical efficacy and safety, Semis Om'o123 (suppl 3h 34-41
56 Vassal G, Doe F, Lucchi E, Moretti S, Frappae D, Santos A, Mignard D, P¢in F 119t~71 Phase I trial of irinolecan (CPT-I !1 ill childhood re)lid tumors, Prm' Am ,S'oc Ottt Om,ol 16, 25.ta
57 Vassal G, Santos A, Pein F, Frappaz D, Mignard D, Doz F (It.~971 Pharluacokinetics of irinotecan ICPT- I I ) and its inetubtdites in child- ten. P~v,c, Am A.~,wc Cam'er Res 38, 75
58 Ste~,art CF, Zamboni WC, Crom WR, Gajjar A, Heideman RL, |:ur- man WL, Meyer WH, Houghton, PJ, Pratt, CB ( 19961Topoisomerase [ interactive drugs in children with cancer, hwest New Drugx [4, 37-47
59 Herben V, Schellens J, Swart M, Gruia G, Beynen J, ten Bokkel Hui- nink WW (1997) Phase ! and pharmacokinetic study of irinotecan (CPT- ! I ) with a prolonged ( 14 d) infusion schedule. Pt~w Am Soc Clin Oncol i 6, 201 a
61) Gupta E, Lestingi TM, Mick R, Ramirez J, Vokes t,~t~, Ratain MJ (1994) Metabolic late of irinotecan in humans: correlation of glucu- ronidation with diarrhea. Cancer Res 54, 3723-3725
61 Rivory LP, Riou JE Haaz MC, Sable S, Vuilhorgne M, Commeu'qon A, Pond SM, Robert J 11996) Identification and properties o1" a major plasma metabolite ol" irinotecan (CPT- i I ) isolated I'ron| tile plasma of patients. Cancer Rex 56, 3689-3694
t12 Lokiec E Monegier du Sorbicr II, Sanderink (;J 11q96) h'inotccau (CPT-II) inetaboliles in hunlan bile and urine, (Yin (' .m'cr R(,a ~ 1943-1949
63 Friedman HS, Houghton PJ (1996)Tt~atnlent of central uervous sys- te l l ) xenografts will) camptothecins. Ann NY A('ad S('i 803, 21 (1-212
64 Boothman DA. Kunkunaga N, Wang M t 19q41 I)own-regulation of topoiosonlenlse I in nlammalian cells tbllowing ionizing radiation. Canccr Rt',s 54, 4618-4626
t~5 l.atnond JP. Mefta MP, Boothman DA (19961 The potential of topoi- sonlerase I inhibittws in the treatment Of CNS rnalignancies: report of a synergistic effect between topotecan and radiation. J Neuro-Om'ol 311. I-6
66 ttoughton JA, Cheschire PJ, Halhuan ;! JD, Ltttz 1. Luo X, Li Y, Houghton PJ (1996) Evaluation of irinotecan in conlhinalion with 5qlutwouracil or etoposide in xenografl models of colou adenocarci- IlOllla i|lltl rhahdt~ll!yosarcollla, C/in Cant'or Rc,~' 2, 1117-1118