PowerPoint 프레젠테이션 - SummitMD
13
Ultra Low Contrast Unprotected Left Main Percutaneous Coronary Intervention Using Intravascular Ultrasound And Sepal Technique Kristy Brillantes Garganera, MD 1 Bryan Rene F. Toledano, MD 1 Jose Paolo A. Prado, MD 2 , Michelangelo L. Sabas, MD 2 1. Fellow In Training – Interventional Cardiology 2. Consultant – Interventional Cardiology Cardiovascular Institute, The Medical City, Philippines
-
Upload
khangminh22 -
Category
Documents
-
view
6 -
download
0
Transcript of PowerPoint 프레젠테이션 - SummitMD

Ultra Low Contrast Unprotected Left Main
Percutaneous Coronary Intervention Using Intravascular Ultrasound
And Sepal Technique
Kristy Brillantes Garganera, MD1
Bryan Rene F. Toledano, MD1
Jose Paolo A. Prado, MD2, Michelangelo L. Sabas, MD2
1. Fellow In Training – Interventional Cardiology
2. Consultant – Interventional Cardiology
Cardiovascular Institute, The Medical City, Philippines

Disclosure
• All authors do not have financial interest or affiliations with one or more organizations that could be perceived as conflict of interest in context of this presentation

Clinical History and Physical Examination
• 60 year old male, hypertensive, diabetic, CKD stage 4
• Presenting with easy fatigability
• Managed as a case of Ischemic Cardiomyopathy and referred to this institution for coronary intervention
• At the ER: BP 110/70 mmHg, HR 71 bpm regular rhythm,
Respiratory rate 20 cpm not in distress
• Pink palpebral conjunctivae, non engorged neck veins, clear breath sounds, apex beat at the 5th intercostal space mid axillary line with no murmur on auscultation. There was note of grade 1 bipedal edema.

Pre-Procedural Tests
• Chest Xray AP view showed no significant chest findings
• Serum creatinine 251.40 umol/L, eGFR 23
• Uric acid 565.90 umol/L
• HbA1c 9.3
• ECG 12 leads showed sinus
bradycardia with poor R wave
progression

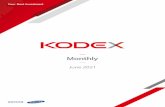
Coronary Angiography
BA C
Radial Access, 5F DxTerity catheter
LAD: 90-95% proximal to mid stenosis with myocardial bridging

Coronary Angiography
BA C
LM: 65% stenosis
LCx: 30-40% mid and 20% distal stenosis
RCA: 70-80% distal segment stenosis

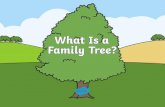
Pre-Intervention IVUS of the LAD to LMCA
2.08 mm2
3.85 mm2
Boston Scientific 3.0F OptiCross 40 MHz

PCI of the Left Anterior Descending Artery
1 2
3 4
Guide: 7F EBU 3.5
Guidewire: Asahi Sion Blue
Predilation: Emerge 2.50 x 15 mm
Synergy 3.0 x 38 mm Synergy 4.0 x 38 mm

Longitudinal stent deformation of Ostial stent struts
POT: NC Quantum Apex 5.0
A B
C D

Post PCI IVUS RUN of the Left Anterior Descending Artery to LMCA

Post PCI Angiography

Discussion Points
• Cost-effective method of Aorto-Ostial LM stenting done with the aid of a sepal technique
• Previous angiography shots used as roadmaps for wire placement, and IVUS in replacement for contrast injection proved useful and effective as alternative for PCI in patients with high risk for CIN

Conclusion
• With proper planning, IVUS-optimized ultra low contrast PCI of unprotected LM with crossover stenting to LAD is feasible and can be safely done especially in patients who are at high risk for having contrast induced nephropathy.
• IVUS was vital for assessment of vessel diameter, plaque morphology, adequacy of lesion preparation, stent sizing and length, and apposition of stent struts to vessel wall.
• Coronary wires were used as visual guides as to where we positioned our balloons and stents coupled with IVUS and strategies such as the sepal wire technique for aorto-ostial LMCA stenting to avoid geographic miss.