
Potentials Evoked from the Abductor Digiti Minimi Muscle in ...
8
Potentials Evoked from the Abductor Digiti Minimi Muscle in the Normal and Neurologically Involved Hand NANCY URBSCHEIT, M.A., and BEVERLY BISHOP, Ph.D. Electrical stimulation of the ulnar nerve may evoke two possible second responses from the abductor digiti minimi muscle. One is the F-wave resulting from antidromic excitation of alpha motoneurons; the other is the H-response, an electrically elicited monosynaptic reflex. This study tests the diagnostic usefulness of these responses .by comparing their latencies, amplitudes, frequencies, arid probabilities of occurrence in normal subjects and in patients with hemiplegic paralysis. The F-wave and H-response evoked in normal subjects and patients were similar in most respects. Although the F-wave was more common in the patients, its probability of occurrence was less than that in the normal subjects. Based on these results, it seems unlikely that these responses will provide useful diagnostic clues to the clinician. An electrical shock to a nerve innervating an intrinsic muscle of the hand or foot may elicit two responses from the muscle. The first response is called the M-wave and results from peripherally conducted, i.e., orthodromically conducted, action potentials in the motor axons of the nerve. Action potentials are also propagated centrally, i.e., anti- dromically conducted, in the axons and will invade the cell soma of each excited axon. A small fraction of the alpha motoneurons com- prising the motoneuron pool of an intrinsic Miss Urbscheit is in the Department of Physiology, School of Medicine, State University of New York at Buffalo, Buffalo, New York 14214. Dr. Bishop is Associate Professor of Physiology, Department of Physiology, School of Medicine, State University of New York at Buffalo, Buffalo, New York 14214. Adapted from a paper presented at the forty-eighth annual conference of the American Physical Therapy Association, Boston, Massachusetts, June 2 8-July 2, 1971. muscle are excited by centrally conducted action potentials in their axons. 1 The periph- erally conducted action potentials thus gen- erated by this small fraction of excited alpha motoneurons will evoke a second muscle response, the F-wave, from the intrinsic muscle. 2 Figure 1 is a diagram of the conduc- tion pathway of this response, and Figure 2 is a series of electromyograms which illustrate F-waves evoked from the abductor digiti minimi muscle of a normal subject. An additional second response may be evoked from an intrinsic muscle other than the F-wave. The electrical shock to the mixed nerve excites sensory axons as well as motor axons. The large diameter la fibers arising from muscle spindles have a low threshold for electrical excitation. 3 Each la axon ends centrally in excitatory monosynaptic connections with alpha motoneurons innervating the homony- mous muscle. An alpha motoneuron will be discharged if spatial summation of the la excitatory impulses is sufficient to bring the 500 PHYSICAL THERAPY Downloaded from https://academic.oup.com/ptj/article/52/5/500/4589253 by guest on 21 January 2022
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Potentials Evoked from the Abductor Digiti Minimi Muscle in ...

Potentials Evoked from the Abductor Digiti
Minimi Muscle in the Normal and
Neurologically Involved Hand
NANCY URBSCHEIT, M.A., and BEVERLY BISHOP, Ph.D.
Electrical stimulation of the ulnar nerve may evoke two possible second responses from the abductor digiti minimi muscle. One is the F-wave resulting from antidromic excitation of alpha motoneurons; the other is the H-response, an electrically elicited monosynaptic reflex. This study tests the diagnostic usefulness of these responses .by comparing their latencies, amplitudes, frequencies, arid probabilities of occurrence in normal subjects and in patients with hemiplegic paralysis. The F-wave and H-response evoked in normal subjects and patients were similar in most respects. Although the F-wave was more common in the patients, its probability of occurrence was less than that in the normal subjects. Based on these results, it seems unlikely that these responses will provide useful diagnostic clues to the clinician.
An electrical shock to a
nerve innervating an intrinsic muscle of the hand or foot may elicit two responses from the
muscle. The first response is called the M-wave and results from peripherally conducted, i.e., orthodromically conducted, action potentials in the motor axons of the nerve. Action potentials are also propagated centrally, i.e., anti-dromically conducted, in the axons and will invade the cell soma of each excited axon. A small fraction of the alpha motoneurons comprising the motoneuron pool of an intrinsic
Miss Urbscheit is in the Department of Physiology, School of Medicine, State University of New York at Buffalo, Buffalo, New York 14214.
Dr. Bishop is Associate Professor of Physiology, Department of Physiology, School of Medicine, State University of New York at Buffalo, Buffalo, New York 14214.
Adapted from a paper presented at the forty-eighth annual conference of the American Physical Therapy Association, Boston, Massachusetts, June 2 8-July 2, 1971.
muscle are excited by centrally conducted action potentials in their axons.1 The peripherally conducted action potentials thus generated by this small fraction of excited alpha motoneurons will evoke a second muscle response, the F-wave, from the intrinsic muscle.2 Figure 1 is a diagram of the conduction pathway of this response, and Figure 2 is a series of electromyograms which illustrate F-waves evoked from the abductor digiti minimi muscle of a normal subject.
An additional second response may be evoked from an intrinsic muscle other than the F-wave. The electrical shock to the mixed nerve excites sensory axons as well as motor axons. The large diameter la fibers arising from muscle spindles have a low threshold for electrical excitation.3 Each la axon ends centrally in
excitatory monosynaptic connections with alpha motoneurons innervating the homony
mous muscle. An alpha motoneuron will be discharged if spatial summation of the la
excitatory impulses is sufficient to bring the
500 PHYSICAL THERAPY
Dow
nloaded from https://academ
ic.oup.com/ptj/article/52/5/500/4589253 by guest on 21 January 2022

motoneuron to its critical firing level. The
resulting reflex of the muscle is called an H-response.4 Figure 3 diagrams the reflex pathway of the H-response and Figure 4 is an electromyogram of an H-response evoked from
the abductor digiti minimi muscle of a normal subject.
The studies reported by Mayer and
Feldman,5 Magladery and McDougal,2 and Thorne6 demonstrated that normal individuals usually have an F-wave in the intrinsic muscles
Intrinsic Spinal Cord Muscle
Shock
Alpha Motoneuron
Alpha Motor Axon
Fig. 1. Schematic diagram of the conduction pathway of the F-wave. Arrows indicate the antidromic and orthodromic impulse in the motor axon.
of the hand with only an occasional individual having an H-response. In contrast, in individuals with central nervous system involvement, the H-response is the most commonly evoked second response from the intrinsic muscles of the hand.7,8 ,9 For example, Hodes and coworkers showed that during the active phase of Sydenham's chorea an ulnar-hypothenar H-response is consistently evoked and upon recovery the H-response disappears.7 Tyler found an exaggerated H-response in the hypo-thenar eminence during botulin toxin poisoning.8 He interpreted this to reveal a loss of inhibition of monosynaptic reflexes from the upper extremity caused by the poisoning. Also, Magladery and others found an ulnar-hypothenar H-response as the common second response in patients with upper brain stem or hemispheric damage.9
In view of these reports, it seems possible that the alterations of the second response in certain disorders could become useful in evaluating the severity of the disorder. The purpose of this study was to compare the amplitude, latency, frequency, and probability of occurrence of the ulnar-hypothenar F-wave and H-response in normal individuals and hemi-plegic patients to determine their diagnostic usefulness. It was hypothesized that normal subjects would predominantly have an F-wave as the second response, whereas patients would have an exaggerated H-response whose amplitude might correlate with the severity of each patient's dysfunction.
Spindle Fig. 2. Electromyograms evoked from the abductor digiti minimi muscle of a normal subject by successive shocks to the ulnar nerve at the elbow. Each trace was evoked with a single shock, the beam of the storage oscilloscope being moved downward after each stimulus. In each trace, the first and very large potential is the M-wave and the second, smaller potential is the F-wave. Note that in this subject the F-wave is present in every trace, which is very unusual. (Stimulus intensity =58 V, sensitivity = lmV/div., sweep speed = 10 msec/div.J
Muscle
Shock
I
Spinal Cord
Fig. 3. Schematic diagram of the conduction pathway of the H-response. Arrow directions indicate conduction of afferent and efferent impulses.
Intrinsic , x y
Muscle / ^ — Alpha Motor Axon
Motoneuron
Volume 52 / Number 5, May 1972 501
Dow
nloaded from https://academ
ic.oup.com/ptj/article/52/5/500/4589253 by guest on 21 January 2022

TABLE 1 Description of the Six Neurologically Involved Individuals Tested
Patient Age Disability Duration of Disability
G. K. 73 Right hemiparesis-cerebral thrombosis Two months
E. B. 76 Left hemiparesis-occlusion of right internal carotid artery Five weeks
L. W. 50 Right hemiparesis-cerebral hemorrhage Thirty-two months
J. B. 66 Right hemiparesis-thrombosis of left middle cerebral artery One year
B. H. 59 Right hemiparesis—thrombosis of left middle cerebral artery Seven weeks
J. H. 75 Left hemiparesis-cause undetermined Five weeks
METHOD ject pool. Six patients with hemiplegic paralysis formed the group of neurologically involved
Thirty-two individuals (average age of subjects (Tab. 1). twenty-five years) with no known history of The normal subjects were seated with the neurological disorders formed the normal sub- dorsal surface of the right forearm resting on a
TABLE 2 Criteria Used to Differentiate Between an F-wave and an H-response
F-wave H-response
1. The maximum amplitude is usually less than 0.5 mV
1. The maximum amplitude is usually greater than 1 mV
2. The latency ranges from 25 to 32 msec3
2. The latency ranges from 20 to 27 mseca
3. The duration ranges from 1 to 5 msec
3. The duration ranges from 5 to 9 msec
4. The threshold stimulus intensity is always higher than that for the M-wavea
4. The threshold stimulus intensity is usually less than that for the M-wavea
5. The amplitude will always be less than that of the M-wave
5. The amplitude can be greater than that of the M-wave at low stimulus intensities
6. There is no occlusion with stimulus intensities which evoke a maximum M-wavea
6. There is complete occlusion with stimulus intensities which evoke a maximum M-wavea
7. The F-wave when evoked will usually not be elicited by every shock above threshold
7. The H-response when evoked will usually be elicited by every shock above threshold
a Criteria proposed by Mayer and Feldman5
502 PHYSICAL THERAPY
Dow
nloaded from https://academ
ic.oup.com/ptj/article/52/5/500/4589253 by guest on 21 January 2022

level surface at the side. To prevent motion of the fingers, a plaster cast molded to the shape
of a hand was slipped on the subject's hand, the fifth digit being the only part of the hand outside the cast. The patients were allowed to remain in their wheelchairs. The arm to be studied was positioned comfortably on a pillow in the subject's lap.
The ulnar nerve was stimulated at the elbow
with a 0.5 millisecond square wave pulse delivered by a Grass S-8 stimulator.* The anode, a five- by ten-centimeter metal plate covered with saline-soaked felt, was strapped over the biceps.
The compound action potentials evoked from the abductor digiti minimi muscle were detected with metal disk surface electrodes filled with electrode paste and secured over the cleaned skin with tape. The active electrode was placed on the muscle belly, the indifferent on
the tendon of insertion. For a ground, a metal plate was secured on the subject's forearm. The action potentials were amplified by a 3A3 Tektronix differential amplifier and displayed on a Tektronix cathode ray storage oscilloscope (Model 564).f
The latency and the amplitude of the compound muscle action potential of the second response were measured. The latency of the action potential was measured as the time
delay between the moment of stimulation and
the start of the action potential. In these experiments, the shock triggered the beam of the oscilloscope; therefore, the latency of the second response was the time between the
beginning of the trace to the beginning of the upsweep of the action potential. The amplitude of the second response was measured as the peak of the rising phase of the response. In
addition, the frequency of occurrence of a response was measured by determining the number of subjects within the group from whom the response could be evoked. The probability of evoking a response at a constant stimulus intensity was the percentage of times the response was evoked in a given individual by ten or more shocks.
*Grass Medical Instruments, Quincy, MA 02169. fTektronix, Inc., S. W. Millikan Way, Beaverton,
OR 97005.
RESULTS
In previous studies by other investigators, any second response evoked from the intrinsic muscles of the hands of normal subjects was always called an F-wave.2,5 '6 Therefore, in the initial experiments with normal subjects, the authors expected most of the subjects to have readily identifiable F-waves. In approximately
30 percent of the subjects, however, the second
response had many of the characteristics of an H-response. Because of this, a list of standard criteria was established to judge whether the second response was an F-wave or an H-response. For example, the maximal amplitude,
latency, duration, threshold, relative amplitude with respect to the M-wave, evidence of occlusion, and probability of occurrence formed
the basis for the criteria which appear in Table
2. Some of these criteria are modifications of those first proposed by Mayer and Feldman.5
Others were derived from pilot experiments of
the authors on normal subjects. A response was judged an F-wave or an H-response if its properties fit the criteria of the respective wave.
To demonstrate the application of these criteria, the characteristics of the second response in Figures 2 and 4 will be reviewed. The maximum amplitude of the second response in
Fig. 4. An electromyogram evoked from the abductor digiti minimi muscle of a normal subject by a single shock to the ulnar nerve at the elbow. The earlier, fractionated compound action potential is the M-wave and the second, larger potential is the H-response. (Stimulus intensity = 50 V, sensitivity = 2 mV/div., sweep speed = 10 msec/div.)
Volume 52 / Number 5, May 1972 503
Dow
nloaded from https://academ
ic.oup.com/ptj/article/52/5/500/4589253 by guest on 21 January 2022
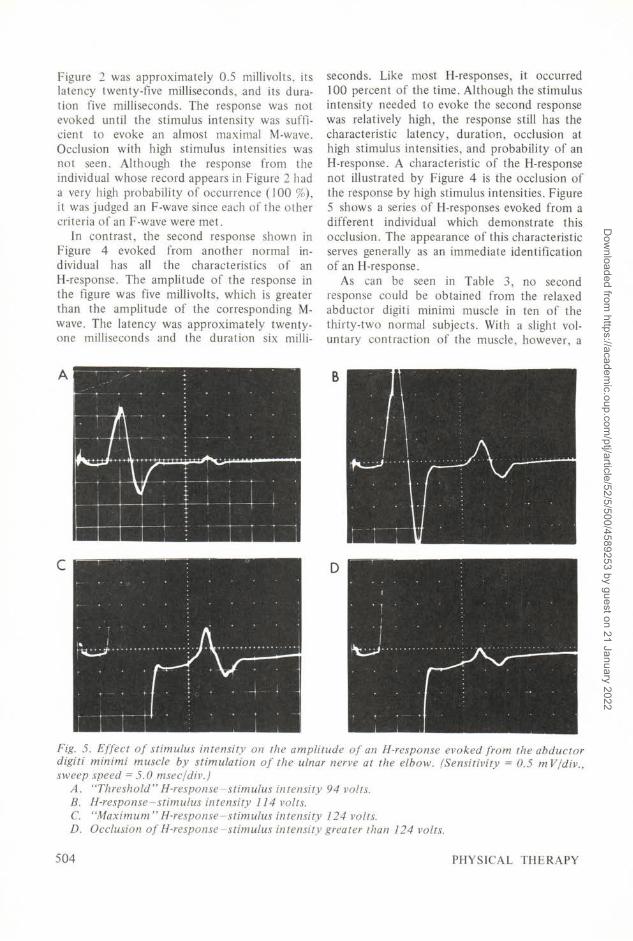
Figure 2 was approximately 0.5 millivolts, its latency twenty-five milliseconds, and its duration five milliseconds. The response was not evoked until the stimulus intensity was sufficient to evoke an almost maximal M-wave. Occlusion with high stimulus intensities was not seen. Although the response from the individual whose record appears in Figure 2 had a very high probability of occurrence (100 %), it was judged an F-wave since each of the other criteria of an F-wave were met.
In contrast, the second response shown in Figure 4 evoked from another normal individual has all the characteristics of an H-response. The amplitude of the response in the figure was five millivolts, which is greater than the amplitude of the corresponding M-
wave. The latency was approximately twenty-one milliseconds and the duration six milli
seconds. Like most H-responses, it occurred
100 percent of the time. Although the stimulus intensity needed to evoke the second response was relatively high, the response still has the characteristic latency, duration, occlusion at high stimulus intensities, and probability of an
H-response. A characteristic of the H-response not illustrated by Figure 4 is the occlusion of
the response by high stimulus intensities. Figure 5 shows a series of H-responses evoked from a different individual which demonstrate this occlusion. The appearance of this characteristic serves generally as an immediate identification of an H-response.
As can be seen in Table 3, no second response could be obtained from the relaxed abductor digiti minimi muscle in ten of the thirty-two normal subjects. With a slight voluntary contraction of the muscle, however, a
Fig. 5. Effect of stimulus intensity on the amplitude of an H-response evoked from the abductor digiti minimi muscle by stimulation of the ulnar nerve at the elbow. (Sensitivity = 0.5 mV/div., sweep speed =5.0 msec/div.)
A. "Threshold" H-response-stimulus intensity 94 volts. B. H-response-stimulus intensity 114 volts. C. "Maximum" H-response-stimulus intensity 124 volts. D. Occlusion of H-response-stimulus intensity greater than 124 volts.
504 PHYSICAL THERAPY
Dow
nloaded from https://academ
ic.oup.com/ptj/article/52/5/500/4589253 by guest on 21 January 2022

TABLE 3 Appearance of the Second Compound Muscle Action Potential from the Abductor Digiti Minimi Muscle in
Thirty-Two Normal Subjects
Number of Subjects
No Response H-response F-wave Unidentifiable
Relaxed Muscle 10 8 9 5 Contracted Muscle 3 10 14 5
second response was evoked from seven of these ten subjects. In those individuals who had a second response even in the relaxed muscle,
almost as many had an F-wave as an H-response. With voluntary contraction, however, the F-wave was seen in more individuals than was the H-response.
In contrast to the study by Magladery and his co-workers,9 the responses evoked from the intrinsic hand muscles in hemiplegic patients were not readily distinguishable from those of normal subjects; i.e., in examining the electro-myogram of a second response one would be unable to tell if it had been recorded from a normal subject or from a hemiplegic patient. Because the second response was similar in normal subjects and in the patients, the list of criteria in Table 2 was deemed applicable for the patients also.
The second response elicited from each hand
of the six patients appears in Table 4. Unexpectedly, the H-response appeared less frequently than the F-wave, and was evoked in
both uninvolved and involved hands. The F-wave appeared more commonly in the uninvolved hand. Only one patient showed symmetry of responses in his two hands, i.e., had the same
type of second response evoked in both of his
hands (see G.H.). Patient E.B.'s responses were most unusual in
that either an F-wave or an H-response could be evoked in his uninvolved hand. One shock elicited only one of the two types of responses. An H-response could not have been masking the F-wave because this patient's F-wave had a latency longer than the latency and duration of
his H-response. The mean probability of occurrence of the
F-wave in the patients and the normal subjects
is compared in Table 5. The mean probabilities of the F-wave were the same for the patients'
TABLE 4 The Second Responses Evoked from the Uninvolved (U)
and the Involved (I) Hands of the Hemiplegic Patients
Patient Side Response
B. H. U None I F
E. B. u F and H I None
J. B. u None I None
G. K. u F I H
L. W. u F I H
G. H. u F I F
TABLE 5 Percent Probability of Evoking an F-wave at Two
Strengths of Shocks
Normal Patients Subjects (U = I)
Stimulus Strength % %
Threshold voltage 70 33 Maximum tolerable
voltage 60 50
uninvolved and involved hands. With shocks of near threshold voltages, the F-wave had a higher mean probability of occurrence in normal subjects than in patients; however, with increases in the stimulus strength this difference between the means of the probabilities for the
two groups was abolished (Tab. 5).
Volume 52 / Number 5, May 1972 505
Dow
nloaded from https://academ
ic.oup.com/ptj/article/52/5/500/4589253 by guest on 21 January 2022

DISCUSSION AND CONCLUSIONS
The first intent of this study was to examine the second response evoked from the abductor digiti minimi muscle in normal subjects. From the reports of other investigators,2,5 ,6 it was anticipated that an F-wave would be readily elicited from most normal subjects, whereas an
H-response would be rarely seen. In contrast to these expectations, the F-wave was present in less than half of the normal subjects and the H-response was evoked in more than a quarter.
Apparently previous investigators called any second response evoked from an intrinsic muscle by stimulation of its motor nerve an F-wave. From this study it appears that a very careful examination of a second response is required before the response can be identified as an F-wave or an H-response.
Why can an F-wave be evoked from the abductor digiti minimi muscle in some normal subjects and an H-response from others? In
most newborn infants, a hypothenar H-response
is readily elicited by stimulation of the ulnar nerve.10 After one year of age the number of infants having an H-response decreases. With maturation of the nervous system, presumably a neural mechanism develops which suppresses the H-response in the intrinsic muscles. The exact neural mechanism for this suppression is unknown. Perhaps this suppression of the H-response is not equally developed in all individuals, thus accounting for the readily evoked H-response in about one-quarter of the normal subjects.
The majority of the hemiplegic patients were expected to have an H-response which would be exaggerated in amplitude. Instead, the types of responses evoked from the patients were not noticeably different in type or amplitude from those of the normal subjects. From this study, the unpredictability of the second response evoked in the abductor digiti minimi muscle of normal subjects and the hemiplegic patients and the lack of any distinguishing characteristics of the second response from the patients suggest the F-wave and the H-response of this intrinsic hand muscle are unlikely to provide helpful diagnostic information.
REFERENCES
1. Renshaw B: Influence of discharge of motoneurons upon excitation of neighboring moto
neurons. J Neurophysiol 4:167 — 183, 1941 2. Magladery JW, McDougal DB: Electrophysio
logical studies of nerve and reflex activity in normal man. I. Identification of certain reflexes in the electromyogram and the conduction velocity of peripheral nerve fibers. Bull Johns Hopkins Hosp 86:265-290, 1950
3. Erlanger J, Gasser HS: Electrical Signs of Nervous Activity. Philadelphia, University of Pennsylvania Press, 1 937
4. Hoffman P: Uber die bazeihungen der schnenre-flex zur willkurlichen bewung und zum tonus. Z Biol 68:351-370, 1918
5. Mayer RF, Feldman RG: Observations on the nature of the F-wave in man. Neurology 17:147-156, 1967
6. Thorne J: Central responses to electrical activation of the peripheral nerves supplying the intrinsic hand muscles. J Neurol Neurosurg Psychiatry 28:482-495, 1965
7. Hodes R, Gribetz I, Hodes HL: Abnormal occurrence of the ulnar nerve hypothenar muscle H-reflex in Sydenham's chorea. Pediatrics 30:49-56, 1962
8. Tyler RH: Botulinus toxin: Effect on the central nervous system of man. Science 139:847-848, 1963
9. Magladery JW, Teasdall RD, Park AM, et al: Electrophysiological studies of reflex activity in patients with lesions of the nervous system. I. A comparison of spinal motoneuron excitability following afferent nerve volleys in normal persons and patients with upper motoneuron lesions. Bull Johns Hopkins Hosp 91:219—244, 1952
10. Thomas JE, Lambert EH: Ulnar nerve conduction velocity and H-reflex in infants and children. J Appl Physiol 15:1-9, 1960
THE AUTHORS
Nancy Urbscheit received her B.S. in physical therapy and M.A. in physiology from the State University of New York at Buffalo. At present, she is a candidate for a Ph.D. degree in physiology at the same university. Upon completion of her graduate studies she plans to teach and to do research on neuropathologic conditions
treated by therapists.
Beverly Bishop, Ph.D., an associate professor at the State University of New York at Buffalo, teaches neurophysiology to undergraduate, graduate, and postdoctoral students. She encourages physical therapists to design objective methods for evaluating their therapeutic procedures. The objectives of her research efforts
are to define and analyze the neural mechanisms controlling respiration.
506 PHYSICAL THERAPY
Dow
nloaded from https://academ
ic.oup.com/ptj/article/52/5/500/4589253 by guest on 21 January 2022

COMMENTS OF DISCUSSANT
MARTHA ANNE CLENDENIN, Ph.D.
This is a valuable project in which the authors have studied two well-known and well-described electrical phenomena—the F-wave and the H-response. Both of these responses have potential value in clinical settings for evaluating the excitability threshold of the central nervous system. As the authors mentioned, the difference in the pathway of these reflex responses would appear to provide an index for differentiating excitability changes in the afferent, or sensory, and the efferent, or motor, components of the spinal cord neuronal pool. I concur, however, with the conclusions of this study that the F-wave and H-response cannot be used as a clear clinical index for comparisons of central excitatory states between patients with various neuromuscular disabilities and normal human subjects.
The authors report the difficulty of consistently recording either the F-wave or H-
response in the experimental subjects. We have experienced this in our laboratory in working with the H-reflex. This response is extremely variable and very sensitive to the slightest
Dr. Clendenin is a postdoctoral fellow, Medical College of Virginia, Health Sciences Center, Virginia Commonwealth University, Richmond, Virginia 23219.
postural change; therefore, it is difficult to evaluate this response for its presence or absence or alterations in its parameters may not always reflect accurately changes in the excitability state of the central nervous system. Repeated difficulty has been reported in the literature in eliciting an H-response from ulnar nerve stimulation in adults; therefore, I would suggest using the tibial nerve which has given a more consistent H-response with stimulation in most laboratories. The selection of the tibial nerve should not alter the antidromic response or F-wave and should ensure a more accurate interpretation of the H-response.
The criteria which were used to differentiate between the F-wave and the H-response are well documented. Since the size of the conducting nerve fibers is essentially the same for both responses, it would seem that the F-wave should have a shorter latency than the H-response based on the difference in the distance required for each response to occur.
I would like to compliment the authors on this relevant and timely study. Perhaps the use of needle electrodes rather than skin electrodes would facilitate determining whether the second response to electrical stimulation is an F-wave or an H-response. It would also be of value to repeat this study using the ulnar nerve in young children where the H-response is more consistently obtained.
Volume 52 / Number 5, May 1972 507
Dow
nloaded from https://academ
ic.oup.com/ptj/article/52/5/500/4589253 by guest on 21 January 2022




















