Post-Emergency Epidemiological Surveillance in Iraqi-Kurdish Refugee Camps in Iran
18
REPORTS AND COMMENTS Post-Emergency Epidemiological Surveillance in Iraqi-Kurdish Refugee Camps in Iran MARZIO BABILLE, PIERPAOLO DE COLOMBANI, RANIERI GUERRA, NEVI0 ZAGARIA and CHIARA ZANETTI In 1991 a computerized, comprehensive epidemiological surveillance sys tem was developed to monitor health trends in approximately 25,000 acutely displaced Kurds in Nowsood and Sa yas refugee camps, Bakhtaran region, Northwestern Iran. In addition, community-based surveys offered information unobtainable from health facilities. Weekly population movements, attack rates, point-prevalence estimates, and case fatality ratios were calculated, and the data were analysed and compared. The overall crude mortality rate (CMR) in the camps under study was still 9 times higher than the reported CMR for Iraq. Health problems with v e y low rates (less than 1.01 1,000 populationlweek) included the triad of measles, meningitis and tetanus. However, morbidity for the most common conditions (acute respirato y infections, diarrhoea, skin infections, eye diseases and, finally, typhoid fever) was shown to increase at the end of the intervention, highlighting that the pressure of repatriation on refugees made them progressively worse. This article concludes that epidemiological surveillance systems should be implemented during mass-migrations in developing countries also in post-emergency settings. Furthermore, surveillance appears to be indispensable in order for the international agencies to keep abreast of events and to safeguard human rights when international attention subsides. Epidemiological techniques have proved to be valuable for the assessment of health status and the evaluation of health services during emergencies. However, in times of disaster relief, surveillance data have seldom been used prospectively. Rapidity, accuracy and continuity represent the ideal components of the process. Furthermore, effective surveillance can predict what usually has been called ‘post- disaster lag’, that is, the late occurrence of outbreaks of communicable diseases. The role of surveillance during and after emergencies in the Least Developed Countries (LDCs) has been hampered by the difficulty in defining at-risk DISASTERS VOLUME 18 NUMBER 1 0 Basil Blackwell Ltd. 1994, 108 Cowley Road, Oxford OX4 lJF, UK and 238 Main Street, Cambridge, MA 02142, USA.
Transcript of Post-Emergency Epidemiological Surveillance in Iraqi-Kurdish Refugee Camps in Iran

REPORTS AND COMMENTS
Post-Emergency Epidemiological Surveillance in Iraqi-Kurdish Refugee Camps in Iran
MARZIO BABILLE, PIERPAOLO DE COLOMBANI, RANIERI GUERRA, NEVI0 ZAGARIA and CHIARA ZANETTI
In 1991 a computerized, comprehensive epidemiological surveillance sys tem was developed to monitor health trends in approximately 25,000 acutely displaced Kurds in Nowsood and Sa y a s refugee camps, Bakhtaran region, Northwestern Iran. In addition, community-based surveys offered information unobtainable from health facilities. Weekly population movements, attack rates, point-prevalence estimates, and case fatality ratios were calculated, and the data were analysed and compared. The overall crude mortality rate (CMR) in the camps under study was still 9 times higher than the reported CMR for Iraq. Health problems with v e y low rates (less than 1.01 1,000 populationlweek) included the triad of measles, meningitis and tetanus. However, morbidity for the most common conditions (acute respirato y infections, diarrhoea, skin infections, eye diseases and, finally, typhoid fever) was shown to increase at the end of the intervention, highlighting that the pressure of repatriation on refugees made them progressively worse. This article concludes that epidemiological surveillance systems should be implemented during mass-migrations in developing countries also in post-emergency settings. Furthermore, surveillance appears to be indispensable in order for the international agencies to keep abreast of events and to safeguard human rights when international attention subsides.
Epidemiological techniques have proved to be valuable for the assessment of health status and the evaluation of health services during emergencies. However, in times of disaster relief, surveillance data have seldom been used prospectively. Rapidity, accuracy and continuity represent the ideal components of the process.
Furthermore, effective surveillance can predict what usually has been called ‘post- disaster lag’, that is, the late occurrence of outbreaks of communicable diseases.
The role of surveillance during and after emergencies in the Least Developed Countries (LDCs) has been hampered by the difficulty in defining at-risk
DISASTERS VOLUME 18 NUMBER 1 0 Basil Blackwell Ltd. 1994, 108 Cowley Road, Oxford OX4 lJF, UK and 238 Main Street, Cambridge, MA 02142, USA.

Post-Emergency Epidemiological Surveillance 59
populations, limited health-reporting infrastructures and cost. Furthermore, surveillance has often been relegated to second place due to the mounting pressure to provide relief, and the diversion of media attention within days after the situation settles. This neglect has led to inefficient, ineffective or inappropriate use of limited health resources and, too often during emergencies, 'feedback loops' (Richards, 1989) have simply been left aside: that is, the processed information did not return to those who originally collected the data. These difficulties are still experienced by governmental and volunteer agencies, and international organizations in short- and long-term mass-displacements in these countries.
This paper describes the imple- mentation of a prospective disease surveillance system in Northwestern Iran. The system's main objectives were: (a) to provide quantitative estimates of morbidity and mortality during and after the acute phase of displacement; (b) to let local health personnel (Kurds of both nationalities, Iraqi and Iranian) become more familiar with the routine data collection network and health information system (HIS) in order to include in the system reliable data relevant for monitoring and action purposes; and (c) to respond to epidemic diseases by coordinating surveillance data with the implementation of appropriate control measures.
BACKGROUND AND RATIONALE
The Kurdish refugees who resided in Iran and Turkey in 1991 comprised one of the largest refugee populations in the world, following that of the Afghan population who fled to Pakistan. Before the major influx in February- March 1991, smaller movements of refugees had occurred across the Iraqi borders after armed struggles between Kurdish liberation
fronts and Iraqi government troops. The large exodus occurred after the unsuccessful attempt to overturn the Iraqi regime after the Gulf War.
In February and March 1991, around 1,200,000 refugees migrated over a very short period of time, using any means of transport to cross the mountains and both borders. After the peak of the influx in April 1991, around 720,000 refugees were accommodated in three different provinces of Western Iran (Ajerbajan, Kurdistan, Bakhtaran) under the authority and control of the local Ministry of the Interior (MOI). For political reasons and because of its geographical inaccessibility, few and inadequate attempts were made to channel aid and resources to Bakhtaran province, despite its higher concentration of refugees.
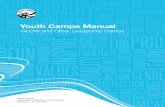
By the end of April 1991, 22 refugee camps had been established in Bakhtaran province, though they received different levels of relief. Appointees of the local MOI, Red Crescent (RC) and the Ministry of Health (MOH) were present in all camps. At that time, two camps had received foreign support and relief health teams. Local talks at the Regional Office of the MOH in Bakhtaran assigned to Centro Internazionale per la Cooperazione all0 Sviluppo (CICS), an Italian NGO, the task of implementing integrated public health activities in the Saryas and Nowsood camps, Paveh area (Figure 1). According to official estimates, the target population amounted to around 25,000 residents in both camps, which were located high in the mountains at an altitude of 1,500-1,900 m, at the end of a steep and muddy supply road from the regional capital town.
From July 1991, the majority of the displaced Kurdish population in Iran began to repatriate under the coordination of the Iranian MOI and the United Nations High Comissioner for Refugees (UNHCR) through the border checkpoints in areas
0 Basil Blackwell Ltd. 1994 DISASTERS VOLUME 18 NUMBER 1

60 Mania Babille et al.
Ajerbojan Provjnce
0 KIRKUK Kordestan province
BAGHDAD
Lores tan Province llam Province
7IGURE 1 The Iraq-Iran border area of intervention, Bakhtaran region, Iran, June- September 1992
controlled by the Peshmerga forces, such spontaneous vs. forced repatriation, as Nowsood, Sheikh Saleh and Bavisi. continued to occur. This represented the second move in the In October 1991, the Kurdish complex situation of the border area where population along the border of Iraq influxes and outfluxes, as well as amounted to around 200,000 individuals.
DISASTERS VOLUME 18 NUMBER 1 0 Basil Blackwell Ltd. 1994

Post-Emergency Epidemiological Surveillance 61
After registration, the majority of repatriates continued to live a scattered existence in either damaged villages or in temporary shelter camps, waiting for information about the negotiations between the Iraqi government and the Kurdish Front forces. This is why the population in some of those areas doubled rapidly over the last months of 1991 (Penjwin: 66,900; Halabja: 100,000). This situation forced the Kurds to become a permanently displaced group, since their movements across the Iranian border were continuous and reflected changes in their temporary sense of security. Though pertinent to the study population, these issues are not relevant to the present discussion.
METHODS
Both active and passive surveillance methods were adopted using computer- assisted epidemiological techniques. Passive data collection involves reports from fixed health facilities such as dispensaries, clinics, and hospitals. Although continuous, this source of information is biased by the health seeking behaviour of the community, the accessibility and geographical distribution of the fixed health structures, and the efficiency and motivation of peripheral health personnel. There is also a large body of evidence (Lagumir, 1963; Lucas, 1976; Henderson, 1987; Toole, 1992) that suggests that data from this system should be interpreted with care because of under- reporting, and several other constraints in the process of completing, processing, revising, collating, and submitting meaningful and timely information.
Active surveillance seems to be more reliable, providing community-based monitoring of conditions of interest by community health workers (CHWs). However, such activities are constrained by the lack of adequate training, time,
transport and supervision; cost is also assumed to be a major problem. Sample surveys and comprehensive searches constitute most of the active systems referred to in this paper.
During the first days of the intervention, a health committee was established in both camps with the participation of local authorities, RC appointees, Iraqi Kurdish doctors, and community representatives. Sentinel health service sites were thus reorganised in Nowsood and Saryas.
The logbooks of the admitting teams at sentinel sites were initially examined daily for five main diagnoses (fever of unknown origin; acute respiratory infections (ARI); diarrhoea; fever and allergy; and other conditions) in order to retrospectively assess the occurrence of health and illness prior to the adoption of any organised surveillance system and intervention. Cumulative data were extracted onto a preliminary standard form. Only verbal estimates of population size were available from both camps, despite requests to camp authorities for detailed population information. Because of the lack of precise population data to provide denominators for disease rates, proportionate morbidity was used to compare the relative importance of different disease groups over the period of time prior to the organised intervention. Proportionate morbidity is the proportion of all reported illness which is due to a specific disease or symptom complex (Woodruff, 1990).
The institutional recording and reporting system adopted by the Iranian government was based on symptom- complex conditions. Unreliable estimates, over-reporting and double entries did not allow for any efficiency in the preliminary assessment. At the end of May 1991, therefore, a simplified checklist was agreed upon by the permanent health committee and a form was finally produced. Case-definitions on health
0 Basil Blackwell Ltd. 1994 DISASTERS VOLUME 18 NUMBER 1

62 Marzio Babille et al.
conditions and events were established: ARI were broken down into upper and lower respiratory tract infections; bloody and watery diarrhoea were recorded separately, even though some authors suggest difficulties in distinguishing between the two categories (Woodruff, 1990). All items then underwent revision and handwritten translation in Kurdish; technical planning and revision sessions of surveillance data were held weekly.
The recording of outpatient consultations was reorganised in each of the established health facilities; patients were classified on the form as babies < 12 months, between 1-4 years, and > 5 years of age. The shelter surveillance system was established to monitor the daily number of cases seen in each shelter site. The form included: 20 reportable health conditions, the number of hospitalisations and evacuations, and new and repeated consultations; no relapses or treatment failures were considered. Addi- tionally, camp structure, current status of water supply and sanitation schemes, updated population figures and, finally, the rate of food subsidies distributed were recorded.
The health personnel in charge entered a case when it met specific case- definition criteria. In so doing, health problems with more than one symptom (for example, a febrile case of gastroenteritis) were prevented from causing duplication of reports. Shortlisted reportable health conditions are depicted in Table 1. The form also allowed for addition and deletion of cases from previous months and for the discussion of unusual and interesting topics. All the information underwent cross-checking procedures before being entered into the electronic register. Furthermore, these formats were continuously updated by computer-assisted entry and analysis.
As far as active surveillance was concerned, two health and nutrition
surveys that used questionnaires with pre- coded, closed questions and field anthrcrpometric measurements were conducted in both camps from 11 - 21 June 1991: a simple random sampling technique was used in Nowsood; cluster random sampling, with stratification before selection (Lemeshow, 1991), was applied in Saryas due to the different allocation of refugees in tents and concrete houses. As advocated by the WHO, the logic behind this method was to have a 95 per cent chance of being within 10 percentage points of the true value in the sample population. The survey tools were all pretested on a non-random sample of persons with characteristics similar to those of the study participants.
Raw numbers were then converted into attack rates as cases per 1,000 population per week over the three-month period of the project duration. Rates were computed by using the current weekly total population living in the camp as a denominator. Attack rates, point prevalence estimates, and case fatality rates (CFR) were calculated from data gained from cross-checking assessments at sentinel site services and retrospective mortality and morbidity information from survey data.
Study participants were the displaced Kurds living in both camps. Staff members . were selected among the available health personnel or lay people either because of previous medical experience or possession of special talents (linguists, teachers, engineers, students). In both camps, Iraqi Kurdish health personnel underwent training sessions on HIS, recording, and reporting. Delegation and a heavy reliance on volunteers (including certified Iraqi medical doctors) were an integral part of the system. Paying them a nominal salary for the hours they gave to the commu- nity insured team cohesiveness and motivation. A tent-to-tent search for patients requiring medical attention was
DISASTERS VOLUME 18 NUMBER 1 0 Basil Blackwell Ltd. 1994

Post-Emergency Epidemiological Surveillance 63
run by community health workers once they were specifically trained on the use of tally sheets. This allowed for the revision and updating of first-line surveillance data and was a major factor in the implementation of PHC in the camps.
RESULTS
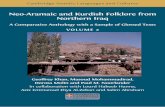
A progressive shift of Kurds towards more secure zones across the border in Iraq and the willingness of the Iranian authorities to declare the emergency relief over were assumed to have been the cause of the
consistent drop in population estimates during the project implementation (Figure 2). The denominators used well reflected these trends.
Retrospective data from one month prior to the organised intervention were available between 20 May and 16 June 1991. The average total weekly number of patients reported from the Saryas sentinel site was 1,997 (daily total: 307). Of them, 1,092 (1601day) were < 15 years of age and 904 (1391day) >15 years of age. From retrospective disease rates in the Saryas camp, symptom complexes such as
TABLE 1 Health conditions and diseases monitored by the surveillance system at sentinel
reporting sites, 6 June-1 September 1991, Bakhtaran region, Iran
Bloody diarrhoea Gastric pain Watery diarrhoea Rheumatic pain Severe Dehydrating Diarrhoea Enteroparasites Upper Respiratory Tract Infections Lower Respiratory Tract Infections
Cardiovascular diseases
Skin diseases: Allergic dermatitis Bacterial skin infections Fungal skin infections Scabies
Measles Meningitis Tetanus Typhoid fever
Eye infections Urinary Tract Infections
Obstetric and Gynaecological Problems Protein Energy Malnutrition
including: Genital herpes Animal bites Gonorrhoea Trauma and Burns Syphilis Sexually trans. dis. (other)
including: Motor vehicle related injuries Bullet injuries Burns by chemical weapons
Other conditions including: Assault
Dental problems Febrile illness (other causes) Counselling
Inappropriate referrals Hospitalizations
Note: Data, including proportionate morbidity, were collected weekly. Specified diseases (e.g. typhoid fever) required laboratory confirmation.
0 Basil Blackwell Ltd. 1994 DISASTERS VOLUME 18 NUMBER 1

64 Manio Babille et al.
Population Momments in Both Cmnps: 205-1 991
weeks
NOWSOOD
** Saryas camp hosted Rfugees also in 200 concrete houses
Clearing of Tents in &rfk Camps by fk OffiMt Authorities: 205 - 1997
Y B i
20.5-16.6 17.6-23.6 24.6-30.6 1.7.7.7 8.7-14.7 15.7-21.7 227-28.7 29.i4.8 5.8.11.8 iz.ai8.8 i 9 . a z . s z . a i . 9
W e e k
FIGURE 2 Population movements and tent clearing
diarrhoea + vomiting (22.5/1,000), fever + cough (14.5/1,000), fever > 38OC (10.51 1,000) were outnumbered by undiag- nosed, poorly specified ‘other’ conditions (more than 30 per cent of total con- sultations for both camps) prior to the implementation of the surveillance system in the Paveh area.
Data were available from both camps through the reorganised system between 16 June and 1 September 1991. The
average weekly total number of patients reported from the Saryas sentinel site was 52 in the group < 1 year of age; 162 in the group 1 - 4; and 687 in the group > 5 (daily total: 7.6; 23.8; and 101 respectively). In Nowsood the average weekly total of patients accounted for: 23 in the group < 1; 96 in the group 1-4; and 559 in the group >5 (daily total: 3.4; 14.1; and 82.2 respectively).
Diarrhoeal diseases, AH, skin infec-
DISASTERS VOLUME 18 NUMBER 1 0 Basil Blackwell Ltd. 1994

Post-Emergency Epidemiological Surveillance 65
tions, eye diseases and, finally, typhoid fever were the most common reported causes of non-fatal illness among both age groups from June to September 1991 (Table 2). Both upper and lower respira- tory infections accounted for 20 per cent of the total consultations. Thirty-three per cent of the total cases were children < 5 years old (both sexes) (Figure 3). The community-based surveys demonstrated a prevalence of ARI of 41.211,OOO and 69,411,000 in Nowsood and Saryas respec- tively. While no statistical difference occurred between the two camps related to
the age group >5, striking evidence suggested that children 0-5 years in Saryas were mostly at risk for ARI (OR =
2.41, 95% C.I. 1.38-4.24; p < 0.001, Chi- square with Yates correction). Local hospital referrals were 0.3 per cent of the total ARI patients. Attack rates per week, broken down by the two categories, are depicted in Figure 4.
Diarrhoea reported cases accounted for around 13 per cent of total consultations. Proportionate morbidity broken down by age group is shown in Figure 3. Cases of severe dehydrating
TABLE 2 Number of cases reported monthly from shelter sites broken down by age group,
6 June-1 September 1991, Bakhtaran region, Iran ~
June July August Total YO
<1 1-4 > 5 <1 1-4 >5 <1 1-4 > 5 _ _ _ _ _ ~
Bloody diarrhoea 1 13 12 5 36 43 2 13 41 Watery diarrhoea 117 212 220 172 412 481 50 114 194 SDD 1 4 1 3 8 4 2 1 1 URTI 36 163 416 87 331 814 46 241 606 LRTI 21 53 106 12 39 140 9 16 44 Gastric pain 0 3 173 0 8 417 0 2 203 Rheumatic pain 0 11 478 3 41 922 0 10 436 Enteroparasites 0 10 57 0 26 134 0 11 69 Cardiovascular dis. 0 1 2 8 0 3 161 0 1 97 Skin diseases 10 91 331 16 149 759 6 73 482 Eye infections 13 41 206 16 78 441 11 37 217 UTI 6 7 145 3 9 343 2 8 150 0B.GYN. 0 0 6 0 0 0 7 8 0 0 53 PEM 4 76 21 8 188 79 2 35 8 Measles 1 0 0 0 0 1 0 0 0 Meningitis 0 0 1 0 0 0 0 0 0 Tetanus 0 0 1 0 0 0 1 0 0 Typhoid fever 0 3 69 0 10 151 0 1 63 Animal bites 2 6 2 1 1 4 23 0 3 19 Trauma and Burns 0 15 69 0 23 150 0 25 104 Other conditions 23 37 522 16 53 638 9 33 398 Inappropriate referral 3 4 48 2 16 73 2 14 55
Total, all causes 238 750 2,985 344 1,434 5,852 142 638 3,240
166 1,972
25 2,740
440 806
1,901 307 291
1,917 1,060
673 191 421
2 1 2
297 79
386 1,729
217
15,623
1.06 12.62 0.16
17.54 2.82 5.16
12.17 1.97 1.86
12.27 6.78 4.31 1.22 2.69 0.01 0.01 0.01 1.90 0.51 2.47
11.07 1.39
100.00
0 Basil Blackwell Ltd. 1994 DISASTERS VOLUME 18 NUMBER 1

66 Manio Babille et al.
AGEG-UMONTHS N=726 AGE 5 YEARS N = 12,069
6%
36% 55% 28%
4%
AGE 1 - 4 YEARS N = 2,8U
BLOODYDIARRHOEA
WATERY DIARRHOEA
URTI
N LRn
SKIN CONDITIONS
0 EYEDISFASES
TYPHOIDEVER
FIGURE 3 Proportionate morbidity in sentinel reporting sites
diarrhoea represented <1 per cent of the total cases of diarrhoea and 0.16 per cent of the total consultations. None of those reported in this group were clinically suspected of having cholera. Rectal swab specimens from sentinel sites did not show positivity for Shigella pathogens or V. cholerae. It is worth mentioning that the latter (V. cholerae 01 El Tor, serotype Ogawa) was isolated from clinically suspected cases of cholera in Cukurca settlement camp in Turkey (P&coul, 1991). The shelter site temporary admissions for diarrhoea accounted for 2.4 per cent of the cases. Local hospital referrals were 0.6 per cent of the total diarrhoea patients. The trend of reported cases of diarrhoea at the shelter clinics before and during the
system implementation are depicted in Figure 5. Bloody diarrhoea cases were few; on the other hand, watery diarrhoea represented the first cause of the sentinel site consultations, due to the difficult situation concerning water supply and sanitation.
The community-based surveys demon- strated a diarrhoea prevalence of 92.71 1,000 and 127.411,OOO in Nowsood and Saryas respectively. Diarrhoea mor- bidity was significantly higher in Saryas and the female group < 5 years of age was shown to be the most affected, when stratifying by age and sex (p < 0.001, Chi-square with Yates correction). Attack rates per week fluctuated from 1111,000 up to 1911,000. From the reported
DISASTERS VOLUME 18 NUMBER 1 0 Basil Blackwell Ltd. 1994

Post-Emergency Epidemiological Surveillance 67
NOWSOOD 4 43 75 126 11 128 14.8
SARYAS 16.2 W.9 173 19.7 21.5 28.4 18.7
Upper Respiratory Tract Infections
122 10.4 17.4 165
25.7 31.3 37.7 36.1
40
35
30
P k20 @ 15
10
5
0
NOWSOOD 1.76 1.69 2.19 4.34 2.2 2.31
SARYAS 0 3 2.99 2.02 1.43 2.43
weeks
1.76 1.16 0.44 2.65 2.25
1.84 2.45 1.11 2.13 2.04
-6- SARYAS
Lower Respiratory Tract Infections
FIGURE 4 Attack rates of Upper and Lower Respiratory Tract infection over the eleven weeks of the intervention
0 Basil Blackwell Ltd. 1994 DISASTERS VOLUME 18 NUMBER 1

68 Marzio Babille et al.
NOWSOOD SARYAS 60 I - -'-
NOWSOOD 4833 28.54 10.59 6.93
S ARY AS 53.08 31.23 17.48 9.96 d
so 8 40 c4 I2 30 !j 20
10
0
U I I
I I
MAY JUNE JULY- AUGUST TIME
morbidity, Saryas camp was again shown to suffer more from diarrhoea1 morbidity. CFR for diarrhoea were: Nowsood = 3.8 per cent; Saryas = 2.1 per cent.
A typhoid epidemic hit the Bakhtaran camps at the beginning of May when 40 cases per day were reported. Surveillance of clinical typhoid cases began at the same time as the implementation of the system in Saryas and Nowsood. In the following months, around 2 per cent of the total consultations in the study area were typhoid cases, showing that the problem continued. Temporary admission in shelter clinics occurred in 13.4 per cent of cases, mainly due to the need to supervise i.v. treatment within the first few hours; all the cases or blood samples obtained from them were then referred to the local hospital. No deaths were reported. It should be mentioned that the point- prevalence of typhoid which emerged from the community survey was 18.41 1,000 in Nowsood and 14.311,OOO in
Saryas; no statistical significance was present when cross-tabulating the results.
Skin diseases ranked second in the reporting system with 12.3 per cent of cases: in fact, scabies and bacterial infections were rampant in both camps. The community-based surveys demon- strated a prevalence of skin diseases of 72.811,OOO and 93.711,OOO in Nowsood and Saryas respectively. While there were no differences in the disease occur- rence in children <5, relative risk of specific morbidity was shown to be significantly associated with the adult refugee population sheltered in Saryas (p = 0.002, Chi-square with Yates correc- tion). Eye infections accounted for 7 per cent of the consultations. No mis- classification of viral conjunctivitis as measles occurred, due to the specific training undergone by the local health personnel.
Prospective surveillance estimates with reference to vaccine-preventable
DISASTERS VOLUME 18 NUMBER 1 0 Basil Blackwell Ltd. 1994

Post-Emergency Epidemiological Surveillance 69
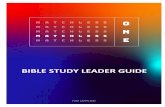
diseases such as measles, meningitis, and tetanus showed low rates in the system (less than 1.011,OOO populationlweek) and negligible figures in both surveys. Protein Energy Malnutrition including either wasting andfor stunting occurred in 2.7 per cent of total consultations. Adult malnutrition mainly hit the female population: 90 per cent of these cases also suffered from severe anaemia due to micronutrient deficiencies. The prevalence of acute malnutrition detected by weight- for-height measurements applying Z-score cut-off at < = -2 SD was 11.8 per cent in Saryas and 10 per cent in Nowsood (95% C.I. 7.4- 12). Height-for-age values applying the same criteria were 14.5 per cent and 16.2 per cent, respectively (95% C.I. 12.8-19.6). Figure 6 depicts the distribution of weight-for-height values of the index population plotted against the reference standard.
The overall crude mortality rate (CMR)
was 183110,000 for the study population when considering the total number of deaths recorded at household level since the departure from Iraq. This estimate was 123110,000 if deaths were clustered once refugees crossed the border; it decreased to 60110,000 when the retrospective estimate analysed in-camp deaths occurring one month prior to the survey. Children <5 accounted for 48 per cent of these deaths. Important differences between the two camps were detected by the survey estimates. First, converting the number of total deaths recorded since the flight of refugees from Iraq (February-March 1991) into CMR estimates, a striking statistical significance occurred. The overall mortality experienced by people who settled in Saryas was 242.6110,000, while for those hosted in Nowsood it was 103110,000 (p < 0.0001, Chi-square with Yates correction).
Second, the risk of dying in Iranian
N = 458 I -8- REFERENCE I
FIGURE 6 Weight-for-height distribution of index cases (Kurdish children 0- 5) against the reference
0 Basil Blackwell Ltd. 1994 DISASTERS VOLUME 18 NUMBER 1

70 Marzio Babille et al.
refugee camps, restricted by the elapsed time since their inital settlement in the host country was examined. CMR were 182110,000 in Saryas and 44.2110,OOO in Nowsood; a discrepancy between the time spent in Iran after arrival and that spent in the concerned settlement was detected in both camps under study, which prevented the expression of daily rates per 10,000 population. This was possibly caused by frequent population movements across the border and among different camps as well. In both former cases, these estimates approach those experienced in other refugee camps in Turkey in the same period (Morbidity and Mortality Weekly Report, 1991; Pkoul, 1991). No statistical differences were shown, however, when analysing mortality risks that were consistent with, and relative to, the actual stay in both camps and restricted to one month before the organised intervention: death rates declined to 2.02110,OOO per day and 1.96110,OOO per day respectively.
A threefold increase in mortality caused by the Gulf War, due to infectious diseases and to decreased quality and availability of medical care, food and water, was shown to affect selectively children under the age of five in Iraq (Ascherio, 1992). In addition, death rates 45 times higher than the expected CMR reported for Iraq were reported in the Cukurca camp in Turkey in April 1991 (Morbidity and Mortality Weekly Report, 1991). In the Iranian camps, taking the average of 1.99110,OOO per day during post- emergency, the rate was equivalent to an annual rate of 72/1,000 population, which is still nine times higher than the reported crude mortality rate for Iraq, 811,000 (UNICEF, 1991).
A weekly report was disseminated at district and regional level to keep those providing health services and assistance informed of the existing camp surveillance activities, important findings, and interventions in the Paveh area. The same
weekly reporting system by using pre- established formats provided data from the field to central structures: the electronic formats were sent back to donor and agency headquarters by telecommunication allowing for rapid update. Disease control measures channeled by surveillance data included the strengthening of water supply sources, the improvement of environmental health, the standardisation of medical care and referral, and a more efficient use of human resources, such as CHWs who provided primary care and health education as sector work.
DISCUSSION
Selected data from the period June - August 1991 demonstrate how surveillance information can affect public health practices in emergency and post- emergency settings. From the reported morbidity, Saryas camp was shown to have a higher trend in ARI, probably due to height, greater exposure to climate modification, overcrowding (an average of 7.5 persons per tent), and poorer camp management. Furthermore, globally increasing rates of ARI reflect the normal seasonal pattern of enhanced ARI transmission with the onset of wind at high altitudes. When examining CFR, however, no statistical difference was observed between the two camps (Nowsood = 1.75 per cent, Saryas = 1.57 per cent). Finally, the morbidity peak at the very end of the relief project might suggest that the pressure of repatriation on refugees made them progressively worse.
Water-borne diseases (Feachem, 1983) such as diarrhoea and eye and skin infections were rampant in Saryas, where overcrowding and poor water supply and sanitation management were the factors most responsible for higher specific morbidity. The trend of attack rates for skin and eye diseases showed that
DISASTERS VOLUME 18 NUMBER 1 0 Basil Blackwell Ltd. 1994

Post-Emergency Epidemiological Surveillance 71
increasing rates at the very end of the intervention were related to the lack of changes in overcrowding, and the progressive dismantling of camp infrastructures operated by the local authorities to enforce repatriation to Iraq.
Furthermore, water-borne outbreaks due to gross contamination are usually characterized by an explosive onset: the majority of cases develop over a period of a few days, and these may be followed by a secondary crop of contact cases. However, sometimes the outbreaks may occur as a series of scattered cases occurring over a considerable period of time, which may be due to a lower and intermittent contamination of the supply. This seems to have happened in both camps under study because of the role played by carriers. When studying the carrier state for Salmonellae among healthy adults in Baghdad, the prevalence rates were: 1.9 per cent of random persons, 2.9 per cent of buffalo owners, 3.2 per cent of hospital personnel, 4.2 per cent of slaughterhouse workers, 6.2 per cent of poultry processors, and 8.6 per cent of food handlers (Al-Ani, 1979). Al-Dulaimy (1979) reported a 1.2 per cent prevalence of Salmonella excretion in the Iraqi town of Mosul. Widal tests were available in limited quantity at Paveh hospital, but no culture confirmation was available. Around 35 per cent of the cases had a positive test. Although 0 and H antibodies were used in field epidemiology to determine typhoid seroprevalence, single positive titres did not necessarily indicate acute infection. Culture confirmation of typhoid is therefore still required (Baines, 1977; Gasser, 1991).
The lack of reported measles cases is self-explanatory. As other authors working with Iraqi refugees in the Turkish camps of Cukurca, Yekmal and Uzumlu have shown (Sandler, 1991; Morbidity and Mortality Weekly Report, 1991), measles did not represent the usual risk factor for
mortality and morbidity in this population, due to a relatively high immunization coverage. In Saryas and Nowsood, EPI was run under the auspices of the Iranian MOH; health problems with very low rates in the system (less than 1.01 1,000 populationlweek) included the triad of measles, meningitis and tetanus. Therefore, surveillance data in the post- emergency phase tends to substantiate this hypothesis.
Mortality levels experienced before settling in the camps were mainly due to a combination of those risk factors to which the migrating population had been exposed before crossing the border and to the critical situation faced before the relief implementation. In the stratified analysis, the female population of Saryas appeared to be the worst hit segment. However, when examining cause-specific death rates, it is interesting to note that the excess deaths in Saryas relative to the > 5 segment was represented by factors directly dependent on the war situation in the area of refugee provenance: Halabja, Sulaymaniyah, Kirkuk (p = 0.001, Chi- square with Yates correction).
Although the rates of some problems such as diarrhoea, ARI and skin conditions may appear high, substantially higher morbidity rates were observed in the same group who fled to Turkey in the same period (April- May- June) (PPcoul, 1991; Sandler, 1991). Comparison of data with other surveillance systems should be done with caution, but it may generate testable hypotheses for future well-controlled studies. The continual low rate of vaccine- preventable diseases observed in this case validates the practice of restarting or strengthening EPI local management during and after the initial relief effort, thus preventing the occurrence of any post-disaster lag.
In post-emergency settings, the surveillance system allows for the identification and control of public health
0 Basil Blackwell Ltd. 1994 DISASTERS VOLUME 18 NUMBER 1

72 Marzio Babille et al.
problems, which had proliferated in Bakhtaran despite local authority and media reports to the contrary. Diarrhoea mortality and morbidity is usually reported to rank first mainly during the early emergency; in this study, it was shown that refugee morbidity remained high and progressively worsened when resources were withdrawn.
The water supply and distribution systems in the area were affected by: camp altitude and layout; decreasing spring water outflow during the summer; insufficient water tanks; temporary breakdowns of pipes and lack of plumbing equipment; insufficient sewage drains; lack of availability of continuous tap water; and the impossibility of an appropriate rotation of water-trucks and vehicle scheduling. A considerable amount of resources were therefore locally allotted to overcome these constraints.
It should be noted that, in this case study, improvements in water quantity alone had little effect on diarrhoeal morbidity. Diarrhoea, in fact, continued to affect the population up until the provision of more water was coupled with the reconstruction of more culturally appropriate communal latrines and better excreta disposal practices. Improved sanitation practices were associated with a more than 20 per cent reduction in all episodes of diarrhoea that were reported to the clinics. However, the rapid rise in water-related diseases among refugees, who still remained in both camps at the end of the intervention, may reflect the limit of significant environmental benefits when local authorities do not back up the system effectively, and when vested interests are involved.
In many poor communities, the incidence of Salmonella infection is high, and many infections produce mild disease or no disease at all. The surveillance system did not distinguish between laboratory-confirmed typhoid fever and
presumptive clinical cases; therefore, changes in typhoid rates could not be accurately calculated. The slight decrease in typhoid rates should, therefore, be considered a result of the following factors: a possible overestimation of cases; the lack of early feedback from the laboratory; asymptomatic carriers that continued to excrete very high concentrations of agents; and, finally, the delayed restoration of safe drinking water supply and sewage disposal.
The surveillance system enables teams to monitor the effectiveness of the medical support available in the host country after the withdrawal of major relief efforts. Quality control checks can be made on the laboratory to determine whether a disease rate is real or laboratory-produced. Unfortunately, local authorities dis- couraged this practice, even though the specificity of the system could be improved.
The sensitivity of the system - that is, the proportion of cases of a disease or health condition detected by the system - was variable, but on the whole quite good. For example, it was possible to break down records in incident cases and re- examinations; inappropriate referrals were also detected, enabling both to screen out inconsistencies. The sensitivity of the system was also high for minor health conditions, such as parasitic diseases, cardiovascular diseases, maternal care- related conditions, and injuries.
The predictive positive value of the surveillance system - that is, the proportion of people identified as cases who actually have the condition - was high. For many illnesses, however, such as TB, intestinal parasites, typhoid fever and influenza-like syndrome, a laboratory confirmation seems necessary during the post-emergency phase. Results of the surveillance system were made available on time to the central governmental offices, UNHCR appointees, EEC donors,
DISASTERS VOLUME 18 NUMBER 1 0 Basil Blackwell Ltd. 1994

Post-Emergency Epidemiological Surveillance 73
and other medical agencies operating in the area. Unfortunately, this process, intended to enable further coordinated action, did not lead to major policy changes in the region, due to the adverse political climate. Pressures were applied, however, to obtain quicker delivery of aid and more equitable distribution of food rations.
There were several imperfections in this surveillance system, both in the design and implementation. First, in an effort to improve the efficiency of the system, the list of diseases and health conditions was kept to a minimum. The institutional recording and reporting system adopted by the Iranian government was, however, troublesome and unreliable, thus impairing the uniformity and standardization of reporting. Furthermore, since Iraqi health personnel were actively involved in routine data collection, they may have sometimes chosen not to follow guidelines in order to attract international attention and further donations.
Second, at the start of the epidemiological surveillance in Bakhtaran, the shelter clinics in the area provided a low level of service. In Nowsood, particularly, after the withdrawal of the ICRC personnel, only Iranian health personnel continued working on a forced roster basis and for less than a nominal salary under the regional MOH. Widespread dismay and lack of motivation caused conflicting reports on the availability of food, water and the current health status of refugees, which hampered technical judgements.
Third, the acceptance by the local authorities of western systems of refugee health care and prevention, including the epidemiological surveillance based on computerized equipment, was low. The enforcement of one line of authority, despite the establishment of camp health committees for better community
involvement, delayed the process of data collection and prevented immediate action.
Finally, from mid-July 1991, the Iranian authorities officially urged international agencies to accelerate the repatriation of Iraqi refugees; the collection of ration cards amongst refugees, the provision of free transport to Iraq - in some cases, physical force was used - and, finally, the mobilization of the army on the borders, did everything to encourage this process. The lack of 'safe havens' provided by allied military forces as implemented in the Turkey- Iraq border region certainly contributed to decreasing the potential impact of the surveillance system on public health measures.
CONCLUSIONS
A surveillance system is useful only if it includes the capacity to respond to the information collected and allay fears of negligence or cover-ups and good training and supervision. In terms of organization, a post-emergency surveillance system should have a well-defined at-risk population, some sort of centralized medical care, and excellent communi- cation facilities to follow up further population movements in border-crossing operations - advantages that other temporary projects may not have.
In this study the system was simple and flexible, and surveillance reports were able to be produced and disseminated by one person in 1-2 days. The case demonstrates that a comprehensive, computer-based, continuous monitoring of health conditions in a large displaced community in a post-emergency setting can be useful for detecting post- displacement risks, continuing to monitor changes, and for providing adequate feedback to communities, central bodies and donors, even though no major policy
0 Basil Blackwell Ltd. 1994 DISASTERS VOLUME 18 NUMBER 1

74 Marzio Babille et al.
adjustments took place in Bakhtaran. In addition, surveillance would appear to be an indispensable tool for both international and other concerned agencies in keeping abreast of rapidly changing events and safeguarding human rights. There is, in fact, a growing number of refugees, returnees, displaced and demobilized people (Somalia, Ethiopia, Sudan, Angola, Mozambique, Afghan- istan, Cambodia and ex-Yugoslavia).
With the advent of sophisticated international telecommunications and the availability of portable computers, international agencies and NGOs in the field should monitor health and disease amongst refugees, returnees and the permanently displaced, like Iraqi Kurds. These measures would provide epidemiological surveillance information necessary for a swifter response in back-up and assistance, for in-depth study and for disease control and prevention efforts.
The use of standby epidemiological teams for on-the-spot assessments, and the setting up of a system to establish a baseline for comparison with the post- disaster health status of the victims, would advance the potential for more rigorous case studies and longitudinal studies. Potential high-risk groups, those consisting of children, the elderly and, more generally, females who are the most economically disadvantaged persons, continue to deserve special attention, particularly when relief efforts decline.
This study, like most disaster research, used cross-sectional survey methods to estimate the strength of association between displacement and post-disaster exposures and health outcomes. It is acknowledged, however, that no information was obtained to estimate the magnitude of risk, it having been impossible under the circumstances to assess changing risks and the proportion of risk attributable to the disaster and post- disaster experience. Nonetheless, the
experience gained suggests that greater use should be made of existing information systems and complementary records to establish databases suitable for epidemiological research. Comparative data and data on trends from cross- sectional and prospective studies in post- emergency settings, still in the planning or further operational stages, can help to identify and solve specific health problems when the international donors begin to lose interest.
Note
We are indebted to the Iraqi-Kurdish people who participated in the study, and particularly to the health professionals who carried out the interviewing; to Dr Franco Piccinno and Mark Kanieff for computer assistance and editing; to Joanna Macrae and Anthony Zwi from the London School of Hygiene and Tropical Medicine; and to Dr Michel C. Thuriaux from the SES Division-WHO Geneva headquarters, who provided critical comments on earlier versions of the manuscript.
References
Ascherio, A., R. Chase, T. Cot6 et al. (1992) Effect of the Gulf War on infant and child mortality in Iraq. New England lournal of Medicine 327, 931 - 36.
Al-Ani, Z.I. and S. Saadallah (1979) Salmonella carriers in Baghdad. Journal of the Faculty of Medicine, Baghdad 21, 65 - 73.
Al-Dulaimy, S.B., G.A. Al-Allaf (1979) Salmonellae isolated from human carriers in Mosul. Annals of the College of Medicine, Mosul
Baines, W.B., J.J. Farmer 111, E.J. Gangarosa et al. (1977) Typhoid fever in the United States associated with the 1972- 73 epidemic in Mexico. Journal of Infectious Diseases 135,
Feachem, R.G., D.J. Bradley, H. Garelick and D.D. Mara (1983) Sanitation and Disease: Health Aspects of Excreta and Wastewater Management. John Wiley & Sons.
10, 5-11.
649-53.
DISASTERS VOLUME 18 NUMBER 1 0 Basil Blackwell Ltd. 1994

Post-Emergency Epidemiological Surveillance 75
Gasser, R.A. Jr, A.J. Magill, C.N. Oster and E.C. Tramont (1991) Medical aspects of the Persian Gulf War: Special Report. New England Journal of Medicine 324, 857-64.
Henderson, D . A . (1987) Principles and lessons from the smallpox eradication programme. Bulletin of the World Health Organization 65,
Lagumir, A.D. (1963) The surveillance of communicable diseases of national importance. New England Journal of Medicine 268, 182.
Levy, P.S. and S. Lemeshow (1991) Sampling of Populations: Mefhods and Applications. A Wiley - Interscience Publication, John Wiley & Sons, 1991.
Lucas, A.O. (1976) Surveillance of communicable diseases in tropical Africa. International Journal of Epidemiology 5, 39- 43.
Morbidity and Mortality Weekly Report (1991) Public health consequences of acute displacement of Iraqi citizens - March-May 1991. International Notes, Morbidity and Mortality Weekly Report 40,
PPcoul, 8. and P. Malfait (1991) Caring for Kurdish refugees (letter). The Lancet 338,190.
Richards, F. and D. Hopkins (1989) Surveillance: the foundation for control and elimination of dracunculiasis in Africa. lnternational Journal of Epidemiology 18, 934-43.
Sandler, R.H., P.R. Epstein, R.M. Cook-
535 - 46.
443-46.
Deegan et al. (1991) Initial medical assessment of Kurdish refugees in Turkey-Iraq border region. Journal of the American Medical Association 266, 638- 40.
Toole, M.J., T. Karsa, B. Fitzgibbon and K. Bussell (1992) Development of health surveillance in Togo, West Africa. Morbidity and Mortality Weekly Report 41, 19-26.
Woodruff, B.A., M.J. Toole, D.C. Rodrigue et al. (1990) Disease surveillance and control after a flood: Khartoum, Sudan, 1988. Disasters 15, 151-63.
Marzio Babille Ranieri Guena International Course for PHC Management in Developing Countries Istituto Superiore di Sanita Rome Italy
Pierpaolo de Colombani Nevio Zagaria Chiara Zanetti Centro Internazionale per la Cooperazione allo Sviluppo Rome Italy
0 Basil Blackwell Ltd. 1994 DISASTERS VOLUME 18 NUMBER 1