Positive psychology in rehabilitation medicine: a brief report
13
NeuroRehabilitation 34 (2014) 573–585 DOI:10.3233/NRE-141059 IOS Press 573 Positive psychology in rehabilitation medicine: A brief report Hilary Bertisch a,∗ , Joseph Rath a , Coralynn Long a , Teresa Ashman b and Tayyab Rashid c a Rusk Institute of Rehabilitation Medicine, NYU Langone Medical Center, Ambulatory Care Center, New York, NY, USA b Shepherd Center, NW Atlanta, GA, USA c Health & Wellness Centre, University of Toronto Scarborough Student Centre, SL, Toronto, ON, Canada Abstract. BACKGROUND: The field of positive psychology has grown exponentially within the last decade. To date, however, there have been few empirical initiatives to clarify the constructs within positive psychology as they relate to rehabilitation medicine. Character strengths, and in particular resilience, following neurological trauma are clinically observable within rehabilitation settings, and greater knowledge of the way in which these factors relate to treatment variables may allow for enhanced treatment conceptualization and planning. OBJECTIVE: The goal of this study was to explore the relationships between positive psychology constructs (character strengths, resilience, and positive mood) and rehabilitation-related variables (perceptions of functional ability post-injury and beliefs about treatment) within a baseline data set, a six-month follow-up data set, and longitudinally across time points. METHODS: Pearson correlations and supplementary multiple regression analyses were conducted within and across these time points from a starting sample of thirty-nine individuals with acquired brain injury (ABI) in an outpatient rehabilitation program. RESULTS: Positive psychology constructs were related to rehabilitation-related variables within the baseline data set, within the follow-up data set, and longitudinally between baseline positive psychology variables and follow-up rehabilitation-related data. CONCLUSIONS: These preliminary findings support relationships between character strengths, resilience, and positive mood states with perceptions of functional ability and expectations of treatment, respectively, which are primary factors in treatment success and quality of life outcomes in rehabilitation medicine settings. The results suggest the need for more research in this area, with an ultimate goal of incorporating positive psychology constructs into rehabilitation conceptualization and treatment planning. Keywords: Rehabilitation, brain injury, positive psychology, resilience, function, positive psychotherapy inventory 1. Introduction Over the past decade, interest in character strengths, as defined by traits such as well-being, optimism, engagement, and meaning, as well as positive mood states, has grown considerably under the rubric of “pos- itive psychology.” In January 2000, Martin Seligman, ∗ Address for correspondence: Hilary Bertisch, PhD, Rusk Insti- tute of Rehabilitation Medicine, NYU Langone Medical Center, Ambulatory Care Center, 240 East 38th Street, 17th floor, New York, NY 10016, USA. Tel.: +1 212 263 2282; Fax: +1 212 263 6807; E-mail: [email protected]. along with Mihaly Csikszentmihalyi, guest edited a special issue in the American Psychologist on positive psychology, and described the field in their introduction as such: “A science of positive subjective experience, pos- itive individual traits, and positive institutions promises to improve quality of life and prevent the pathologies that arise when life is barren and meaningless. The exclusive focus on pathology that has dominated so much of our discipline results in a model of the human being lacking the positive 1053-8135/14/$27.50 © 2014 – IOS Press and the authors. All rights reserved
Transcript of Positive psychology in rehabilitation medicine: a brief report
NeuroRehabilitation 34 (2014) 573–585DOI:10.3233/NRE-141059IOS Press
573
Positive psychology in rehabilitationmedicine: A brief report
Hilary Bertischa,∗, Joseph Ratha, Coralynn Longa, Teresa Ashmanb and Tayyab Rashidc
aRusk Institute of Rehabilitation Medicine, NYU Langone Medical Center, Ambulatory Care Center, New York,NY, USAbShepherd Center, NW Atlanta, GA, USAcHealth & Wellness Centre, University of Toronto Scarborough Student Centre, SL, Toronto, ON, Canada
Abstract.BACKGROUND: The field of positive psychology has grown exponentially within the last decade. To date, however, therehave been few empirical initiatives to clarify the constructs within positive psychology as they relate to rehabilitation medicine.Character strengths, and in particular resilience, following neurological trauma are clinically observable within rehabilitationsettings, and greater knowledge of the way in which these factors relate to treatment variables may allow for enhanced treatmentconceptualization and planning.OBJECTIVE: The goal of this study was to explore the relationships between positive psychology constructs (character strengths,resilience, and positive mood) and rehabilitation-related variables (perceptions of functional ability post-injury and beliefs abouttreatment) within a baseline data set, a six-month follow-up data set, and longitudinally across time points.METHODS: Pearson correlations and supplementary multiple regression analyses were conducted within and across these timepoints from a starting sample of thirty-nine individuals with acquired brain injury (ABI) in an outpatient rehabilitation program.RESULTS: Positive psychology constructs were related to rehabilitation-related variables within the baseline data set, within thefollow-up data set, and longitudinally between baseline positive psychology variables and follow-up rehabilitation-related data.CONCLUSIONS: These preliminary findings support relationships between character strengths, resilience, and positive moodstates with perceptions of functional ability and expectations of treatment, respectively, which are primary factors in treatmentsuccess and quality of life outcomes in rehabilitation medicine settings. The results suggest the need for more research in thisarea, with an ultimate goal of incorporating positive psychology constructs into rehabilitation conceptualization and treatmentplanning.
Keywords: Rehabilitation, brain injury, positive psychology, resilience, function, positive psychotherapy inventory
1. Introduction
Over the past decade, interest in character strengths,as defined by traits such as well-being, optimism,engagement, and meaning, as well as positive moodstates, has grown considerably under the rubric of “pos-itive psychology.” In January 2000, Martin Seligman,
∗Address for correspondence: Hilary Bertisch, PhD, Rusk Insti-tute of Rehabilitation Medicine, NYU Langone Medical Center,Ambulatory Care Center, 240 East 38th Street, 17th floor, New York,NY 10016, USA. Tel.: +1 212 263 2282; Fax: +1 212 263 6807;E-mail: [email protected].
along with Mihaly Csikszentmihalyi, guest edited aspecial issue in the American Psychologist on positivepsychology, and described the field in their introductionas such:
“A science of positive subjective experience, pos-itive individual traits, and positive institutionspromises to improve quality of life and preventthe pathologies that arise when life is barren andmeaningless. The exclusive focus on pathology thathas dominated so much of our discipline results ina model of the human being lacking the positive
1053-8135/14/$27.50 © 2014 – IOS Press and the authors. All rights reserved

574 H. Bertisch et al. / Positive psychology in rehabilitation medicine: A brief report
features that make life worth living. Hope, wisdom,creativity, future mindedness, courage, spiritual-ity, responsibility, and perseverance are ignoredor explained as transformations of more authenticnegative impulses.”
Positive psychology has made tremendous progressin the last decade. Between 2000 and 2010, morethan 1,000 articles on topics examining characterstrengths such as well-being, happiness, and opti-mism have been published in peer-reviewed journals(Azar, 2011). A classification system of characterstrengths that apply cross-culturally has been built(Peterson & Seligman, 2004), and initial instrumentsfor measurement have been developed. There isparticular enthusiasm regarding the study of interven-tions that increase character strengths in non-clinicalsamples, and outcome data supports the use of posi-tive psychology interventions in increasing happinessand reducing depression compared to standard ther-apeutic approaches and antidepressants in healthyvolunteers (Perlman et al., 2010; Seligman, Rashid,& Parks, 2006; Seligman, Steen, Park, & Peterson,2005).
While character strengths have been investigated innormal populations, the field is in its nascency andoperational definitions are still in development. White,Driver, and Warren (2008) stated that “a universaldefinition of resilience does not exist,” although it isknown clinically that some individuals are generallymore adaptable to traumatic events, including signifi-cant medical events, while others appear less so (Dunn,Uswatte, & Elliott, 2009). It has also only been withinthe past several years that the study of these conceptshas been applied to clinical samples, and particularlywithin rehabilitation medicine, where they may be high-lighted following the reductions in quality-of-life oftenresulting from medical trauma (Majini, 2011). Withinthe milieu of neurorehabilitation programs, individu-als present with sequelae of any number of devastatinginjuries or illnesses that affect the central nervoussystem, including traumatic brain injury, stroke, Mul-tiple Sclerosis, brain tumors, and spinal cord injury(SCI). In addition to the significant declines in phys-ical function these conditions can cause, there are alsodifficulties in cognition and emotional regulation thatdisrupt daily functioning (Dawson, Schwartz, Winocur,& Stuss, 2007; Silver, McAllister, & Arciniegas, 2009).It is within the framework of multidisciplinary reha-bilitation programs that individuals can evidence thecharacter strengths, in particular resilience, necessary
to challenge themselves and rebuild their lives. Becausethese strengths can now be better identified and nurturedthrough the developments in the field of positive psy-chology, rehabilitative potential and overall well-beingcan be increased (Majini, 2011).
As the field of positive psychology continues toexpand in a variety of settings, there have been sev-eral recent empirical initiatives to study characterstrengths and resilience within individuals with neuro-logical conditions, and to begin to expand these findingsinto treatment applications. White, Driver, and War-ren (2010) later defined resilience as “an individual’spersonal qualities and skills that enable that person toflourish in the face of adversity or a disruptive event (p.23).” In a sample of inpatients with spinal cord injury,they concluded that resilience was a stable character-istic that did not change from hospital admission todischarge. Resilience inversely correlated with symp-toms of depression, and positively with life satisfactionand spirituality. A second study (Quayle & Schanke,2010) defined resilience as “the ability of adults who arefacing a severe and potentially disabling physical injuryto maintain relatively stable, healthy levels of psycho-logical and social functioning and to maintain positiveemotions and a positive perception of self and the future(p. 13).” The authors reported that in a sample of inpa-tients with severe multiple trauma or SCI, indicators ofresilience were prevalent and contributed to increasedsatisfaction with social support at hospital admissionand discharge, less substance abuse, less fear of dying,and increased feelings of safety (Quale & Schanke,2010). There is also a growing body of literature thathas directly related similar traits such as optimismwith improved quality of life in individuals post-ABI(Ramanathan, Wardecker, Slocomb, & Hillary, 2011;Tøien, Bredal, Skogstad, Myhren, & Ekeberg, 2011).Further reports have extended these findings regardingthe roles of other strengths such as coping self-efficacy,in addition to optimism and resilience, in patients withdiagnoses ranging from traumatic brain injury, Parkin-son’s disease, post-polio syndrome, transplants, andsevere multiple trauma, within rehabilitation settings(deRoon-Cassini, Mancini, Rusch, & Bonanno, 2010;McCauley et al., 2012; Pierini & Stuifbergen, 2010;Robottom et al., 2012; Tallman, Shaw, Schultz, &Altmaier, 2010). There are even preliminary studiesattempting to clarify the neurobiology of characteristicssuch as resilience within the neuroimaging literature, asan innovative effort to improve pharmacological devel-opment for a range of conditions (Russo, Murrough,Han, Charney, & Nestler, 2012).
H. Bertisch et al. / Positive psychology in rehabilitation medicine: A brief report 575
An ultimate goal of understanding the constructsdefined as character strengths and resiliency in thecontext of rehabilitation is to identify methods ofincorporating these characteristics into treatment, witha model of “building positives,” to further improvequality-of-life as an essential part of recovery. Emerg-ing evidence has supported applications of this conceptin samples of children with acquired brain injury(ABI), and within the context of “resilience train-ing” for United States military personnel at increasedrisk for traumatic brain injury (Lester, Harms, Herian,Krasikova, & Beal, 2013; Tonks et al., 2011; Wells etal., 2011). One systematic approach to studying therelevance of character strengths and resilience withinrehabilitation settings is to clarify their relationshipsto factors already known to relate to treatment out-comes, such as use of coping strategies, appraisals orinterpretations of stressors, and perceptions of function,health and well-being (Bonanno, Kennedy, Galatzer-Levy, Lude, & Elfstrom, 2012; Catalano, Chan, Wilson,Chiu, & Muller, 2011; Chan, Lai, & Wong, 2007;Kortte, Stevenson, Hosey, Castillo, & Wegener, 2012).As these relationships are better understood within theframeworks of current standard-of-care models, furtherinitiatives may then be taken to expand them into indi-vidualized treatment conceptualization and planning(Tonks et al., 2011).
As there has been support for the impact of posi-tive psychology-related constructs on quality of life,the goal of this preliminary study is to augment theexisting literature on character strengths, and specif-ically resilience, in terms of rehabilitation for ABI,by clarifying their relationships to treatment-relatedfactors such as perceptions of functional status andbeliefs about treatment. While this study is intendedto be exploratory, the overall hypothesis is that (1)overall character strengths, (2) resilience, and (3) pos-itive mood states will correlate with perceptions offunctional ability and beliefs about treatment in a het-erogeneous ABI sample, both at treatment initiation andat longer-term follow-up.
2. Methods
2.1. Setting
Participants were continuously recruited from alarge, metropolitan, comprehensive outpatient neurore-habilitation program, specializing in the treatment ofadults with heterogeneous ABI diagnoses at various lev-
Table 1Demographics of starting sample
Characteristic n %
GenderMale 20 51.3Female 19 48.7
RaceWhite 31 79.5Black 4 10.2Asian 3 7.7Hispanic 1 2.6
EtiologyTBI 17 43.6Stroke 13 33.3Other 9 23.1
EmploymentEmployed 12 30.7Unemployed 11 28.2Retired 8 20.5SSD/Disability 4 10.3Other/Missing 4 10.3
Mean SDAge at baseline 52.62 18.62Months between onset and baseline 33.14 53.3Years of Education 16.54 2.33
els of function. The services provided in this programaddress both cognitive and emotional difficulties, withtreatment goals in these respective domains aimed atimproving the individual’s real-world functional ability,independence, and subsequent quality-of-life. Becauseof the diagnostic heterogeneity found in our pro-gram, patients are conceptualized by level of functionalimpairment at intake, rather than by type or severityof injury per se. In this classification system, patientsare assigned to treatments based upon a levels-of-residual-competence model, with sets of behaviorallyobservable criteria delineated for each level (Bertisch,Rath, Langenbahn, Sherr, & Diller, 2011; Langenbahn,Sherr, Simon, & Hanig, 1999; Sherr & Langenbahn,1992).
2.2. Participants
Participants were 39 individuals between 23–85years of age. While the gender ratios in the present studywere slightly more equivalent as compared to avail-able data from similar rehabilitation programs treatingindividuals with heterogeneous ABI diagnoses, otherdemographic characteristics were generally compara-ble (see Table 1; Bancroft Brain Injury Rehabilitation,2012; May Institute for Neurorehabilitation, 2013;Memorial Hermann Rehabilitation & Research, 2013).For inclusion in his study, all participants had to (1) havea diagnosis of any ABI, (2) have had fewer than five

576 H. Bertisch et al. / Positive psychology in rehabilitation medicine: A brief report
treatment sessions, and (3) have ability to comprehendthe measures included (including adequate command ofthe English language), as per performance on neuropsy-chological testing at intake. Participants were excludedif (1) they were not treated on the clinical service, (2) iftheir initial treatment plan was short-term (less than fourmonths), thereby making them unlikely to reach follow-up phase, (3) they were unable to read or complete theassessments, or (4) if they were not interested in par-ticipating in clinical research. Recruitment lasted fromDecember, 2010 until September, 2011. During thisperiod, a total of 110 participants were targeted for par-ticipation. Within this sample, 35.5% (n = 39) agreed toparticipate, 38% (n = 42) failed to meet the above inclu-sion/exclusion criteria, and 26% (n = 29) did not returnafter initial evaluation for clinical service. Twenty-fiveparticipants completed follow-up assessments, whilenine (23%) left treatment prior to the four-month-requirement for treatment-related reasons, and onlyfive (13%) participants refused to complete follow-upevaluations. This attrition rate was as expected for anoutpatient psychological service (Bados, Balaguer, &Saldana, 2007; Edlund et al., 2002; Sharf 2008). Themean follow-up period was 26.96 (SD = 4.02) weeksfrom baseline.
2.3. Procedures
During recruitment, all patients who met the inclu-sion criteria were queried about their interest inparticipation, and consented within their first four ses-sions of treatment. After consent, participants weregiven assessment packets to take home, so that theycould be completed at their own pace and at theirconvenience. Assistance with reading or writing wasprovided by study personnel for participants with dis-abilities that interfered with their ability to complete theforms (two patients requested assistance during base-line; only one of these patients requested assistanceduring follow-up). Approximately six months afterbaseline assessment was completed, participants werecontacted to complete the second time-point evaluation.The same procedures from baseline were repeated. Thisstudy has IRB approval by New York University Schoolof Medicine.
2.4. Assessment
For each participant, a general demographic formincluding age, gender, diagnosis, length of time sinceinjury, present medical status, level of education, and
types of rehabilitation services enrolled in was col-lected.
2.4.1. Positive psychology constructs1) The Positive Psychotherapy Inventory (PPTI;
Rashid, 2008; Appendix A). The PPTI is a gen-eral measure of character strength that is deeplyrooted in Seligman’s theories of positive psychol-ogy (2000). The self-report measure consists of21 Likert-type items from which a “Pleasant Life”score, an “Engaged Life” score, a “MeaningfulLife” score, and an “Overall Happiness” indexare derived. Individual items measure characterstrengths such as gratitude, connection with oth-ers, purpose, well-being, and positive mood asobserved by others. The PPTI has demonstratedgood internal consistency, test-retest reliability,factor analysis, and convergent validity for usecross-culturally in healthy and clinical (i.e., out-patient mental health) populations (Guney, 2011;Rashid, 2008). Within the present sample of indi-viduals with ABI, reliability analyses showed thatall four PPTI indices had high internal consistencyduring baseline data collection: Pleaseant Life(� = 0.84), Engaged Life (� = 0.69), MeaningfulLife (� = 0.76), and Overall Happiness (� =0.88).Further, all subscales were moderately and sig-nificantly correlated (r = 0.540 to 0.588), therebysuggesting adequate construct validity. To reducethe number of variables included in the presentanalyses, only the PPTI total “Overall Happiness”index was used as the primary index of characterstrength.
2) Connor-Davidson Resilience Scale (CD-RISC;Connor & Davidson, 2003). This measure definesresilience in terms of stress coping ability, andhas been normed in both healthy samples and pri-mary care outpatients. It consists of five factorswith 25 items rated on a 0–4 scale, with higherscores reflecting greater resilience. The CD-RISChas good psychometric properties and has been aprimary measure utilized in studies of resiliencein rehabilitation medicine (Shin, Goo, Yu, Kim,& Yoon, 2012; White et al., 2010). The total CD-RISC score was used in this study as a measure ofresilience.
3) Profile of Mood States (POMS; Lorr, McNair, &Droppleman, 2003). The POMS is a self-reportmeasure used to identify six fluctuating moodstates. It has 65 items and takes approximately 10minutes to complete. The POMS has been normed

H. Bertisch et al. / Positive psychology in rehabilitation medicine: A brief report 577
in both healthy and medical outpatient samples andhas been used in research, particularly in sampleswith neurological disorders and spinal cord injury(Arruda, Stern, & Sommerville, 1999; Affiliations;Davidson, 2002; Driver & Ede, 2009; Wijesuriya,Craig, Tran, & Middleton, 2011). As this study isdesigned to evaluate the effects of positive char-acteristics, only the POMS Vigor-Activity scale,which measures positive mood, was selected forthe present analyses.
2.4.2. Rehabilitation-related variables1) Head Injury Family Interview (HiFi; Kay, Cav-
allo, Ezrachi, & Vavagiakis, 1995). The HiFi is astructured interview designed for systematic datacollection from patients and/or family membersregarding symptomotology post-ABI. Within theHiFi, the Problem Checklist (PCL) is a 43-itemrating scale, in which specific symptoms in theemotional, cognitive, and physical domains arerated on a seven-point scale, ranging from 1 to7, in which “1” indicates that the symptom is “noproblem” in terms of impact on daily function-ing, “4” represents a “moderate problem,” and 7represents a “severe problem” in terms of dailyfunction. In contrast to other commonly-used func-tional measures that are either intended for usewith individuals with extreme impairment (e.g.,emergence from coma) or target fewer areas ofdeficit (e.g., Disability Rating Scale, Hall, Cope,& Rappaport, 1985; Glasgow Coma Scale, Hallet al., 1985; Mayo–Portland Inventory (4th Edi-tion), Malec & Thompson, 1994; Moss AttentionRating Scale, Hart, Whyte, Ellis, & Chervoneva,2009; Post-Acute Level of Consciousness Scale,Eilander et al., 2009), the HiFi PCL has a relativelybroad range of functional domains and severity ofimpairment, considerations that were crucial to itsselection as the functional outcome measure forthis study. The HiFi PCL has demonstrated goodclinical utility, excellent reliability, and demon-strates validity against comparable measures, suchas the Patient Competency Rating (Fourtassi et al.,2011; Kashluba, Paniak, & Casey, 2008; Kayet al., 1995; Nabors, Seacat, & Roenthal, 2002;Seel, Kreutzer, & Sanders, 1997). The HiFi PCLhas been used in prior ABI research (Bertischet al., 2013; Paniak et al., 2002; Rath et al., 2004;Struchen, Pappadis, Sander, Burrows, & Myszka,2011). For the purposes of this study, an abbrevi-ated version of the HiFi PCL was completed by
each participant as part of the assessment pack-ets, and used as an index of perception of functionpost-ABI.
2) Expectations of/Satisfaction with Treatment Scale:These Likert-type measures of expectations ofand satisfaction with treatment, respectively, aretypical of ratings used in psychotherapy out-come studies, and were adapted for our treatmentprogram (Heppner, Cooper, Mulholland, & Wei,2001). They each consist of 12 items that reflectexpectations of, and satisfaction with, variouscomponents of a rehabilitation program, withdirect application to cognitive rehabilitation forindividuals with ABI. Items include “I expect tobe/I am satisfied with therapy,” and “My needswill be/are being met by the program,” andare rated on a 1 to 6 point Likert scale. Themeasure reflecting expectations of treatment wasadministered at baseline, and the correspondingsatisfaction scale was administered at six-monthfollow-up.
2.5. Data analysis
Correlations between the positive psychology vari-ables (PPTI, CD-RISC, and POMS) were implementedas an initial analysis, in an effort to maximize efficiencyin variable selection while reducing the possibilityof Type I error, due to common variance betweenthese indices. Histograms for the rehabilitation-relatedvariables: (1) HiFi PCL pre-test, (2) Expectations ofTreatment (3) HiFi PCL post-test, and (4) Satisfactionwith Treatment were also reviewed, in order to assureappropriate variability in these measures for analysis.
Accounting for the small, albeit adequately pow-ered sample size (Cohen, 1992) and exploratorynature of the present study, Pearson correlations wereconducted as the primary analysis to examine therelationships between the positive psychology vari-ables (character strengths, resilience, and positivemood), and the rehabilitation-related variables (per-ceptions of function and expectations of/satisfactionwith treatment). The correlations of greatest interestwere: (1) PPTI, CD-RISC, and POMS in relation tothe HiFi PCL and Expectations of Treatment scaleswithin the baseline data, (2) PPTI, CD-RISC, andPOMS in relation to the HiFi PCL and Satisfac-tion with Treatment scales within the follow-up data,and (3) PPTI, CD-RISC, and POMS baseline datain relation to the HiFi PCL and Satisfaction withTreatment scales at follow-up, in an effort to better
578 H. Bertisch et al. / Positive psychology in rehabilitation medicine: A brief report
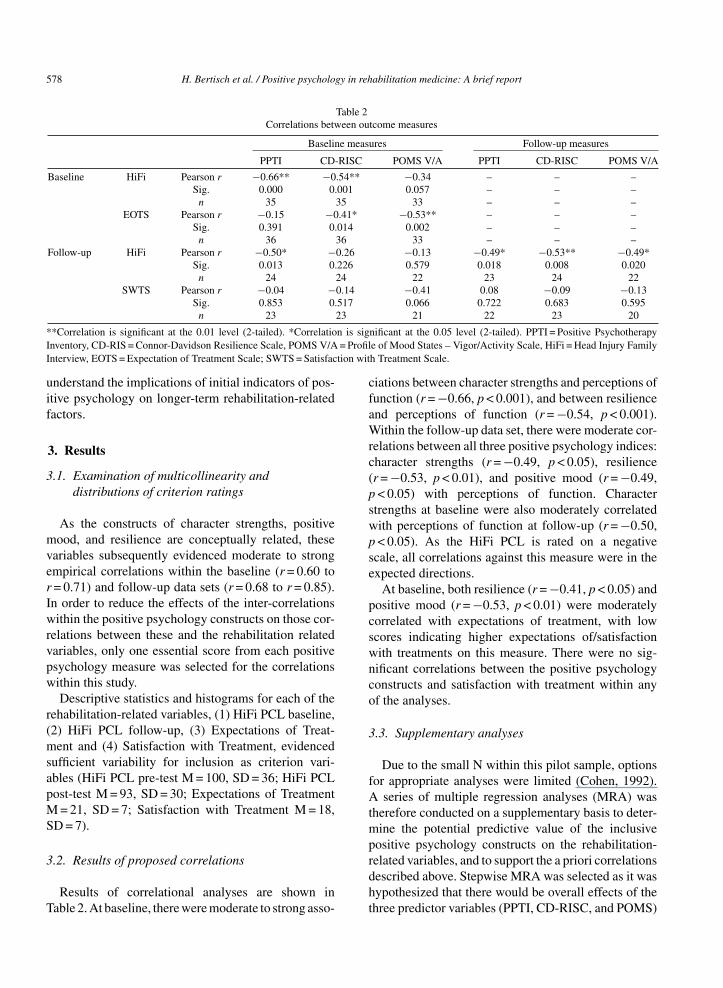
Table 2Correlations between outcome measures
Baseline measures Follow-up measures
PPTI CD-RISC POMS V/A PPTI CD-RISC POMS V/A
Baseline HiFi Pearson r −0.66** −0.54** −0.34 – – –Sig. 0.000 0.001 0.057 – – –
n 35 35 33 – – –EOTS Pearson r −0.15 −0.41* −0.53** – – –
Sig. 0.391 0.014 0.002 – – –n 36 36 33 – – –
Follow-up HiFi Pearson r −0.50* −0.26 −0.13 −0.49* −0.53** −0.49*Sig. 0.013 0.226 0.579 0.018 0.008 0.020
n 24 24 22 23 24 22SWTS Pearson r −0.04 −0.14 −0.41 0.08 −0.09 −0.13
Sig. 0.853 0.517 0.066 0.722 0.683 0.595n 23 23 21 22 23 20
**Correlation is significant at the 0.01 level (2-tailed). *Correlation is significant at the 0.05 level (2-tailed). PPTI = Positive PsychotherapyInventory, CD-RIS = Connor-Davidson Resilience Scale, POMS V/A = Profile of Mood States – Vigor/Activity Scale, HiFi = Head Injury FamilyInterview, EOTS = Expectation of Treatment Scale; SWTS = Satisfaction with Treatment Scale.
understand the implications of initial indicators of pos-itive psychology on longer-term rehabilitation-relatedfactors.
3. Results
3.1. Examination of multicollinearity anddistributions of criterion ratings
As the constructs of character strengths, positivemood, and resilience are conceptually related, thesevariables subsequently evidenced moderate to strongempirical correlations within the baseline (r = 0.60 tor = 0.71) and follow-up data sets (r = 0.68 to r = 0.85).In order to reduce the effects of the inter-correlationswithin the positive psychology constructs on those cor-relations between these and the rehabilitation relatedvariables, only one essential score from each positivepsychology measure was selected for the correlationswithin this study.
Descriptive statistics and histograms for each of therehabilitation-related variables, (1) HiFi PCL baseline,(2) HiFi PCL follow-up, (3) Expectations of Treat-ment and (4) Satisfaction with Treatment, evidencedsufficient variability for inclusion as criterion vari-ables (HiFi PCL pre-test M = 100, SD = 36; HiFi PCLpost-test M = 93, SD = 30; Expectations of TreatmentM = 21, SD = 7; Satisfaction with Treatment M = 18,SD = 7).
3.2. Results of proposed correlations
Results of correlational analyses are shown inTable 2. At baseline, there were moderate to strong asso-
ciations between character strengths and perceptions offunction (r = −0.66, p < 0.001), and between resilienceand perceptions of function (r = −0.54, p < 0.001).Within the follow-up data set, there were moderate cor-relations between all three positive psychology indices:character strengths (r = −0.49, p < 0.05), resilience(r = −0.53, p < 0.01), and positive mood (r = −0.49,p < 0.05) with perceptions of function. Characterstrengths at baseline were also moderately correlatedwith perceptions of function at follow-up (r = −0.50,p < 0.05). As the HiFi PCL is rated on a negativescale, all correlations against this measure were in theexpected directions.
At baseline, both resilience (r = −0.41, p < 0.05) andpositive mood (r = −0.53, p < 0.01) were moderatelycorrelated with expectations of treatment, with lowscores indicating higher expectations of/satisfactionwith treatments on this measure. There were no sig-nificant correlations between the positive psychologyconstructs and satisfaction with treatment within anyof the analyses.
3.3. Supplementary analyses
Due to the small N within this pilot sample, optionsfor appropriate analyses were limited (Cohen, 1992).A series of multiple regression analyses (MRA) wastherefore conducted on a supplementary basis to deter-mine the potential predictive value of the inclusivepositive psychology constructs on the rehabilitation-related variables, and to support the a priori correlationsdescribed above. Stepwise MRA was selected as it washypothesized that there would be overall effects of thethree predictor variables (PPTI, CD-RISC, and POMS)
H. Bertisch et al. / Positive psychology in rehabilitation medicine: A brief report 579
on the rehabilitation-related variables (HiFi PCL andExpectations of/Satisfaction with Treatment), but therewas no expected effect of their order of entry intothe equation. Three sets of MRA were conducted: 1)within the baseline data only, 2) within the follow-up data only, and finally, 3) with baseline predictorsand follow-up criterion data, in an effort to predictlonger term-treatment implications from baseline pos-itivity and resilience ratings. For each analysis, lengthof time since onset was entered into the first step of theequation, and the other predictor variables were enteredinto the second step of the equation.
As a complement to the proposed correlations, theseMRA indicated that the PPTI total scores significantlypredicted HiFi PCL total scores within the baseline dataset (F [2, 30] = 10.60, p < 0.001), within the follow-up data set (F [2, 19] = 6.54, p < 0.01) and withinthe longer-term predictions between baseline posi-tivity variables and HiFi PCL follow-up scores (F[2, 20] = 4.85, p < 0.05). Across these analyses, PPTIaccounted for 65.6%, 43.5%, and 59.2% of the vari-ance in HiFi PCL total scores, respectively. Length oftime since onset, the POMS Vigor-Activity scale, andthe CD-RISC had no significant effects on the criterionvariables in any of the analyses, and no variables signif-icantly predicted expectations of treatment at baseline,or satisfaction with treatment at follow-up. Limitationsin the MRA results may again be due to the small sam-ple that precluded implementation of these analyses asprimary in this pilot study.
4. Discussion
The results of this preliminary study provide initialevidence to support relationships between charac-ter strengths and perceptions of functional abilitypost-brain injury within the baseline and six-monthfollow-up data sets, and longitudinally from treatmentinitiation to six-month follow-up. Resilience and char-acter strengths were related to perceptions of functionalability within the baseline data and follow-up data sets,and positive mood correlated with perceptions of func-tional ability at follow-up. In addition, both resilienceand positive mood were related to positive expectationsof treatment within the baseline data set. Collec-tively, these findings suggest that character strengths,resilience, and positive mood may contribute to bothshort and longer-term perceptions of functional abilityand expectations of treatment, which have been shownto contribute to quality-of-life in studies of patients with
neurological conditions (Cicerone & Azulay, 2007;Hampton, 2000; Robinson-Smith, Johnston, & Allen,2000; Tsaousides et al., 2009). While relationshipsbetween depression, perceptions of functional ability,and quality-of-life are well-documented in the reha-bilitation literature (Breir et al., 1998; Hibbard et al.,2004; Hudak, Hynan, Harper, & Diaz-Arrastia, 2012;Mitchell, Benito-Leon, Gonzalez, & Rivera-Navarro,2005; Pagulayan, Hoffman, Temkin, Machamer, & Dik-men, 2008), there are few studies that have examinedthe role of positive functioning independent of negativesymptoms.
The most robust correlate and predictor of perceptionof function across time points was the PPTI, the primarymeasure of character strength in this study. Similarly,the CD-RISC, the main indicator of resilience, corre-lated with perception of function at both baseline andfollow-up. These results indicate that positive charactertraits, and specifically resilience, significantly impactthe way in which individuals may positively evaluatetheir strengths and functionality following a traumaticinjury or illness. Furthermore, resilience correlatedwith expectations of treatment at baseline, suggest-ing that individuals with stronger internal resourcesmay view treatment as a means of enhancing theirexisting resources, even prior to treatment commence-ment. As the available research suggests a relationshipbetween character strengths, resilience, coping self-efficacy, and quality of life in rehabilitation medicinesamples, our findings indicate that enhancement ofthese kinds of positive traits, for instance through train-ing on improved coping strategies, within rehabilitationmedicine would likely contribute to decreased experi-ence of symptoms, improved perceptions of function,and ultimately better treatment outcomes (deRoon-Cassini, Mancini, Rusch & Bonanno, 2010; McCauleyet al., 2012; Pierini & Stuifbergen, 2010; Robottomet al., 2012; Tallman, Shaw, Schultz, & Altmaier, 2010).
In addition to the potential role of stable characterstrengths in influencing perceptions of both functionand treatment, our findings also suggest a relationshipbetween positive mood and these rehabilitation-relatedvariables. The POMS, which was the primary indicatorof positive mood in this study, correlated significantlywith expectations of treatment at baseline and percep-tions of function at follow-up. It also demonstratedmoderate correlations and non-significant trends withperceptions of function at baseline and satisfaction withtherapy longitudinally, which may have reached sig-nificance in a larger sample. These findings suggestthat in addition to enhancement of inherent character
580 H. Bertisch et al. / Positive psychology in rehabilitation medicine: A brief report
strengths, improvement of state-dependent mood is animportant objective towards augmenting perceptions offunction and beliefs about treatment. In particular, aspositive mood correlates with treatment expectations,which is an important factor underlying success of psy-chological treatments (Tsai, Ogrodniczuk, Sochting, &Mirmiran, 2012; Vogel, Wester, Wei, & Boysen, 2005),enhancement of mood early in treatment may havelonger-term implications for both response to interven-tion and quality-of-life outcomes. As the applications ofpositive psychology continue to emerge within rehabili-tation medicine, our findings indicate that in addition toaddressing depression, supporting positive moods andcharacter strengths may be directly relevant to treat-ment success (Dunn & Dougherty, 2005; Evans, 2012;Majani, 2011; Tonks et al., 2011; Wells et al., 2011).
One important consideration unique to rehabilitationmedicine in the study of character strengths and percep-tions of functional ability post-injury is anosognosia, ororganically-based unawareness of deficits, secondary tobrain injury. Patients experiencing anosognosia reportless depression, and perhaps would subsequently reportgreater strengths, optimism, and well-being, that isclinically associated with decreased awareness of theirinjuries and subsequent functional limitations (Lucas &Fleming, 2005; Malec, Testa, Rush, Brown, & Moess-ner, 2007; Prigatano, 2009). While evaluation of theeffects of anosognosia was beyond the scope of thepresent study, it is necessary to consider the balancebetween awareness, self-report of positive traits, func-tional ability, and reactions to treatment, particularlywhen integrating these constructs into rehabilitationconceptualization and planning.
Other methodological limitations of the present studyinclude a small, albeit adequately-powered sample todetect a large effect size (Cohen, 1992), heterogene-ity of diagnoses, limited theoretical orientations withinthe field of positive psychology beyond Seligman’smodel on which to base methodology, limitations inavailable operational definitions and subsequent mea-sures of character strengths and positive mood statesthat are appropriate for a rehabilitation population,and inter-correlations between the positive psychol-ogy indices. While these factors were controlled to theextent possible in the present study design through care-ful selection of indices to include the analyses, theymay have obscured more subtle relationships betweenthe variables of interest.
This study is among the first of its kind to inves-tigate the relationships between character strengths,resilience, and positive mood states and rehabilitation-
related variables in an outpatient ABI sample withinand across time points in treatment. As the applica-tions of positive psychology to rehabilitation medicinecontinue to grow, there is an essential need for develop-ment of clearer operational definitions and appropriateinstruments to measure these constructs as they applyto individuals with ABI. In addition, interventionsalready exist to increase factors such as resilience andhappiness in healthy volunteers and in child and mili-tary samples (Perlman et al., 2010; Seligman, Rashid,& Parks, 2006; Seligman et al. 2005; Tonks et al.,2011; Wells et al., 2011), and there is a growingconsensus that in order to be maximally effective,neuropsychological rehabilitation must address bothobjective cognitive deficits and subjective attitudinal,motivational, and emotional factors (e.g., self-efficacy,confidence, self-esteem) in tandem. As such, build-ing empirically validated positive psychology treatmentmodels is crucial to maximizing rehabilitative poten-tial and research within adult civilian populations aswell (e.g., Ben–Yishay & Diller, 2011; Cicerone et al.,2005, 2011; Cicerone & Azulay, 2007; Gordon, Cantor,Ashman, & Brown, 2006; Mateer, Sira, & O’Connell,2005; Montgomery, 1995; Prigatano, 2003; Schutz &Trainor, 2007; Wilson, 2005). Once further progresshas been made in terms of these definitions, measure-ments, and systematic treatment methodologies, theseconstructs can be better evaluated, and new methods toincorporate the principles of positive psychology inter-ventions into rehabilitation treatment planning can takeplace.
Declaration of interest
The authors of this study have no financial or personalinterests to declare at this time.
References
Arruda, J. E., Stern, R. A., & Sommerville, J. A. (1999). Measurementof mood states in stroke patients: Validation of the Visual AnalogMood Scales. Archives of Physical Medicine and Rehabilitation,80, 676-680. doi: 10.1016/S0003-9993(99)90171-5
Azar, B. (2011). Positive Psychology advances, with growingpains. APA Monitor, 42, 32. Retrieved from www.apa.org/monitor/2011/04/positive-psychology.aspx
Bados, A., Balaguer, G., & Saldana, C. (2007). The efficacyof cognitive–behavioral therapy and the problem of drop-out. Journal of Clinical Psychology, 63(6), 585-592. doi:10.1002/jclp.20368
H. Bertisch et al. / Positive psychology in rehabilitation medicine: A brief report 581
Bancroft Brain Injury Rehabilitation. (2012). Bancroft BrainInjury Rehabilitation, 2012 Outcomes. Retrieved from:http://www.bancroft.org/brain-injury/
Ben–Yishay, Y., & Diller, L. (2011). Essentials of holistic neuropsy-chological rehabilitation. Oxford University Press, In Handbookof holistic neuropsychological rehabilitation, New York, NY, pp.7–16.
Bertisch, H., Long, C., Langenbahn, D. M., Rath, J. R., Diller, L.& Ashman, T., (in press). Anxiety as a primary predictor offunctional impairment after acquired brain injury: A brief report.Rehabilitation Psychology.
Bertisch, H., Rath, J. F., Langenbahn, D. M., Sherr, R. L., & Diller,L. (2011). Group treatment in acquired brain injury rehabilita-tion. Journal for Specialists in Group Work, 36, 264-277. doi:10.1080/01933922.2011.613901
Bonanno, G. A., Kennedy, P., Galatzer-Levy, I. R., Lude, P., & Elf-strom, M. L. (2012). Trajectories of resilience, depression, andanxiety following spinal cord injury. Rehabilitation Psychology,57, 236-47. doi: 10.1037/a0029256
Breier, J. I., Fuchs, K. L., Brookshire, B. L., Wheless, J., Thomas,A. B., Constantinou, J., & Willmore, L. J. (1998). Quality oflife perception in patients with intractable epilepsy or pseudo-seizures. Archives of Neurology, 55, 660-665. doi: 10-1001/pubs.Arch Neurol ISSN-0003-9942-55-5-noc7196
Catalano, D., Chan, F., Wilson, L., Chiu, C., & Muller, V. R. (2011).The buffering effect of resilience on depression among individualswith spinal cord injury: A structural equation model. Rehabilita-tion Psychology, 56, 2000-2011. doi: 10.1037/a0024571
Chan, I. W. S., Lai, J. C. L., & Wong, K. W. N. (2007). Resilienceis associated with better recovery in Chinese people diagnosedwith coronary heart disease. Psychology & Health, 21, 335-349.dx.doi.org/10.1080-14768320500215137.
Cicerone, K. D. & Azulay, J. (2007). Perceived self-efficacyand life satisfaction after traumatic brain injury. Jour-nal of Head Trauma Rehabilitation, 22, 257-266. doi:10.1097/01.HTR.0000290970.56130.81
Cicerone, K. D., Dahlberg, C., Malec, J. F., Langenbahn, D., Felicetti,T., Kneipp, S., Catanese, J., et al. (2005). Evidence-based cog-nitive rehabilitation: Updated review of the literature from 1998through 2002. Archives of Physical Medicine and Rehabilitation,86, 1681-1692. doi:10.1016/j.apmr.2005.03.024
Cicerone, K. D., Langenbahn, D., Braden, C., Malec, J. F., Kalmar,K., Frass, M., & Ashman, T. (2011). Evidence-based cognitiverehabilitation: Updated review of the literature from 2003 through2008. Archives of Physical Medicine and Rehabilitation, 92, 519-530. doi:10.1016/j.apmr.2010.11.015
Cohen, J. (1992). A power primer. Psychological Bulletin, 112, 155-159. doi. 10.1037/0033-2909.112.1.155
Connor, K. M. & Davidson, J. R. (2003). Development of a newresilience scale: The Connor-Davidson Resilience Scale (CD-RISC). Depression and Anxiety, 18, 76-82. doi: 10.1002/da.10113
Davidson, J. W. (2002). The effects of music therapy on mood statesin neurological patients: A pilot study. Journal of Music Therapy,1, 20-29.
Dawson, D. R., Schwartz, M. L., Winocur, G., & Stuss, D. T.(2007). Return to productivity following traumatic brain injury:Cognitive, psychological, physical, spiritual, and environmen-tal correlates. Disability and Rehabilitation, 29, 301-313. doi:10.1080/09638280600756687
deRoon-Cassini, T. A., Mancini, A. D., Rusch, M. D., & Bonanno, G.A. (2010). Psychopathology and resilience following traumatic
injury: A latent growth mixture model analysis. RehabilitationPsychology, 55, 1-11. doi:10.1037/a0018601
Driver, S. & Ede, A. (2009). Impact of physical activ-ity on mood after TBI. Brain Injury, 23, 203-212.doi:10.1080/02699050802695574
Dunn, D. S. & Dougherty, S. B. (2005). Prospects for a positivepsychology of rehabilitation. Rehabilitation Psychology, 50, 305-311. doi: 10.1037/0090-5550.50.3.305
Dunn, D., Uswatte, G., & Elliott, T. R. (2009). Happiness, resilience,and positive growth following physical disability: Issues forunderstanding, research, and therapeutic intervention. In: S. J.Lopez, & C. R. Snyder (Eds.), The Oxford handbook of positivepsychology, second edition. Oxford University Press, USA. pp.651-664.
Edlund, M. J., Wang, P. S., Berglund, P. A., Katz, S. J., Lin, E., &Kessler, R. C. (2002). Dropping out of mental health treatment:Patterns and predictors among epidemiological survey respon-dents in the United States and Ontario. American Journal ofPsychiatry, 159(5), 845-851. doi: 10.1176/appi.ajp.159.5.845
Eilander, H. J., van de Wiel, M., Wijers, M., van Heugten, C. M.,Buljevac, D., Lavrijsen J. C. M. Prevo, A. J., et al. (2009). Thereliability and validity of the PALOC-s: A post-acute level of con-sciousness scale for assessment of young patients with prolongeddisturbed consciousness after brain injury. NeuropsychologicalRehabilitation, 19, 1-27. doi:10.1080/09602010701694822
Evans, J. J. (2012). Positive psychology and brain injury rehabilita-tion. Brain Impairment, 12, 117-127. doi: 10.1375/brim.12.2.117
Fourtassi M., Hajjioui, A., Ouahabi, A. E., Benmassaoud, H.,Hajjaj-Hassouni, N., & Khamlichi, A. E. (2011). Long termoutcome following mild traumatic brain injury in Moroccanpatients. Clinical Neurology and Neurosurgery, 113, 716-720.doi: 10.1016/j.clineuro.2011.07.010
Gordon, W. A., Cantor, J., Ashman, T., & Brown, M. (2006). Treat-ment of post-TBI executive dysfunction: Application of theoryto clinical practice. Journal of Head Trauma Rehabilitation, 21,156-167. doi:10.1097/00001199-200603000-00008
Guney, S. (2011). The Positive Psychotherapy Inventory (PPTI): Reli-ability and validity study in Turkish population. Social and Behav-ioral Sciences, 29, 81-86. doi: 10.1016/j.sbspro.2011.11.209
Hall, K., Cope, N., & Rappaport, M. (1985). Glasgow Outcome Scaleand Disability Rating Scale: Comparative usefulness in followingrecovery in traumatic head injury. Archives of Physical Medicineand Rehabilitation, 66, 35-37.
Hampton, N. Z. (2000). Self-efficacy and quality of life in people withspinal cord injuries in China. Rehabilitation Counseling Bulletin,43, 66. doi: 10.1177/003435520004300202
Hart, T., Whyte J., Ellis, C., & Chervoneva, I. (2009). Constructvalidity of an attention rating scale for traumatic brain injury.Neuropsychology, 23, 729-735. doi: 10.1037/a0016153
Heppner, P. P., Cooper, C., Mulholland, A., & Wei, M. (2001).A brief, multidimensional, problem-solving psychotherapy out-come measure. Journal of Counseling Psychology, 48, 330-343.doi: 10.1037//0022-0167.48.3.330
Hibbard, M. R., Ashman, T. A., Spielman, L. A., Chun, D., Charatz,H. J., & Melvin, S. (2004). Relationship between depression andpsychosocial functioning after traumatic brain injury. Archives ofPhysical Medicine and Rehabilitation, 85(suppl 2), S43-S53. doi:10.1016/j.apmr.2003.08.116
Hudak, A. M., Hynan, L. S., Harper, C. R., & Diaz-Arrastia, R.(2012). Association of depressive symptoms with functionaloutcome after traumatic brain injury. Journal of Head Trauma
582 H. Bertisch et al. / Positive psychology in rehabilitation medicine: A brief report
Rehabilitation, 27, 87-98. doi: 10.1097/HTR.0b013e3182114efd
Kashluba, S., Paniak, C., & Casey, J. E. (2008). Persistent symptomsassociated with factors identified by the WHO task force on mildtraumatic brain injury. The Clinical Neuropsychologist, 22, 195-208. doi: 10.1080/13854040701263655
Kay, T., Cavallo, M. M., Ezrachi, O., & Vavagiakis, P. (1995).The head injury family interview: A clinical and researchtool. Journal of Head Trauma Rehabilitation, 10, 12-31. doi:10.1097/00001199-199504000-00004.
Kortte, K. B., Stevenson, J. E., Hosey, M. M., Castillo, R., & Wegener,S. T. (2012). Hope predicts positive functional role outcomes inacute rehabilitation populations. Rehabilitation Psychology, 57,248-255. doi: 10.1037/a0029004
Langenbahn, D. M., Sherr, R. L., Simon, D., & Hanig, B. (1999).Group psychotherapy. In K. G. Langer, L. Laatsch, & L. Lewis(Eds.), Psychotherapeutic interventions for adults with braininjury or stroke: A clinician’s treatment resource. Madison, CT:Psychosocial Press.
Lester, P. B., Harms, P. D., Herian, M. N., Krasikova, D.V.,& Beal, S. J. (2013). The Comprehensive Soldier FitnessProgram Evaluation. Report #3: Longitudinal Analysis ofthe Impact of Master Resilience Training on Self-ReportedResilience and Psychological Health Data. Available at:www.dma.wi.gov/dma/news/2012news/csf-tech-report.pdf
Lorr, M., McNair, D. M., & Droppleman, L. F. (2003). Profile ofMood States. Multi-Health Systems Inc., Canada.
Lucas, S. E. & Fleming, J. M. (2005). Interventions forimproving self-awareness following acquired brain injury. Aus-tralian Occupational Therapy Journal, 52, 160-170, doi:10.1111/j.1440-1630.2005.00485.x
Majani, G. (2011). Positive psychology in psychological interven-tions in rehabilitation medicine. Giornale Italiano di Medicinadel Lavoro ed Ergonomia, 33(suppl A), A64-A68.
Malec, J. F., Testa, J. A., Rush, B. K., Brown, A. W., & Moess-ner, A. M. (2007). Self-assessment of impairment, impairedself-awareness, and depression after traumatic brain injury.Journal of Head Trauma Rehabilitation, 22, 156-66. doi:10.1097/01.HTR.0000271116.12028.af
Malec, J. F., & Thompson, J. M. (1994). Relationship of theMay-Portland Adaptability Inventory to functional and cognitiveperformance measures. Journal of Head Trauma Rehabilitation,9, 1-15. doi: 10.1097/00001199-199412000-00003.
Mateer, C. A., Sira, C. S., & O’Connell, M. E. (2005). Putting HumptyDumpty together again: The importance of integrating cognitiveand emotional interventions. Journal of Head Trauma Rehabili-tation, 20, 62-75. doi:10.1097/00001199-200501000-00007.
May Institute for Neurorehabilitation. (2013). Enrollment,demographics, and student/teacher ratios for May Institutefor Neurorehabilitation in Brockton, M.A. Retrieved from:http://www.usaschoolinfo.com/school/may-institute-for-neurorehabilitation-brockton-massachusetts.117455/enrollment.
McCauley, S. R., Wilde, E. A., Miller, E. R., Firsby, M. L., Garza, H.M., Varghese, R., McCarthy, J., et al. (2012). Preinjury resilienceand mood as predictors of early outcome following mild traumaticbrain injury. Journal of Neurotrauma [Epub ahead of print]. doi:10.1089/neu.2012.2393.
Memorial Hermann Rehabilitation and Research. (2013). Programs& Specialties. Retrieved from: http://tirr.memorialhermann.org/programs-specialties/brain-injury-rehabilitation/.
Mitchell, A. J., Benito-Leon, J., Gonzalez, J. M., & Rivera-Navarro, J. (2005). Quality of life and its assessment inmultiple sclerosis: Integrating physical and psychological com-ponents of wellbeing. The Lancet Neurology, 4, 556-566. doi:10.1016/S1474-4422(05)70166-6
Nabors, N., Seacat, J., & Rosenthal, M. (2002). Predictors of caregiverburden following traumatic brain injury. Brain Injury, 16, 1039-1050. doi:10/1080/028990521010155285
Pagulayan, K. F., Hoffman, J. M., Temkin, N. R., Machamer, J. E., &Dikmen, S. S. (2008). Functional limitations and depression aftertraumatic brain injury: Examination of the temporal relationship.Archives of Physical Medicine and Rehabilitation, 87, 1887-1892.doi: 10.1016/j.apmr.2008.03.019
Paniak, C., Reynolds, S., Toller-Lobe, G., Melnyk, A., Nagy, J.,& Schmidt, D. (2002). A longitudinal study of the relation-ship between financial compensation and symptoms after treatedmild traumatic brain injury. Journal of Clinical and Experi-mental Neuropsychology, 24, 187-193. doi: 10.1076/jcen.24.2.187.999
Perlman, L. M., Cohen, J. L., Altiere, M. J., Brennan, J. A., Brown,S. R., Mainka, J. B., & Diroff, C. R. (2010). A multidimensionalwellness group therapy program for veterans with comorbidpsychiatric and medical conditions. Professional Psychology:Research and Practice, 41, 120-127. doi: 10.1037/a0018800
Peterson, C., & Seligman, M. (2004). Character Strengths andVirtues: A Handbook and Classification. USA: Oxford UniversityPress.
Pierini, D., & Stuifbergen, A. K. (2010). Psychological resilienceand depressive symptoms in older adults diagnosed with post-polio syndrome. Rehabilitation Nursing, 35, 167-175. doi:10.1002/j.2048-7940.2010.tb00043.x
Prigatano, G. P. (2003). Challenging dogma in neuropsychology andrelated disciplines. Archives of Clinical Neuropsychology, 18,811-825. doi:10.1016/S0887-6177(02)00205-6.
Prigatano, G. P. (2009). Anosognosia: Clinical and ethical con-siderations. Current Opinion in Neurology, 22, 606-611. doi:10.1097/WCO.0b013e328332a1e7
Quale, A. J., & Schanke, A. K. (2010). Resilience in the face ofcoping with a severe physical injury: A study of trajectories ofadjustment in a rehabilitation setting. Rehabilitation Psychology,55, 12-22. doi: 10.1037/a0018415
Ramanathan, D. M., Wardecker, B. M., Slocomb, J. E., & Hillary,F. G. (2011). Dispositional optimism and outcome follow-ing traumatic brain injury. Brain Injury, 25, 328-337. doi:10.3109/02699052.2011.554336
Rashid, T. (2008). Positive Psychotherapy. In Lopez, S. J. (Ed.) Pos-itive psychology: Exploring the best in people. Westport, CT:Greenwood Publishing Company.
Rashid, T. (2008). The positive psychotherapy inventory. In J.Magyar-Moe, Therapist’s Guide to Positive Psychological Inter-ventions (pp. 86-90). Oxford, UK: Academic Press in Elsevier.
Rath J. F., Langenbahn, D. M., Simon, D., Sherr, R. L., Fletcher,J., & Diller, L. (2004). The construct of problem solvingin higher level neuropsychological assessment and rehabilita-tion. Archives of Clinical Neuropsychology, 19, 613-635. doi:http://dx.doi.org/10.1016/j.acn.2003.08.006
Robinson-Smith, G., Johnston, M. V., & Allen, J. (2000). Self-care self-efficacy, quality of life, and depression after stroke.Archives of Physical Medicine and Rehabilitation, 81, 460-464.doi: dx.doi.org/10.1053/mr.2000.3863
H. Bertisch et al. / Positive psychology in rehabilitation medicine: A brief report 583
Robottom, B. J., Gruber-Baldini, A. L., Anderson, K. E., Reich, S.G., Fishman, P. S., Weiner, W. J., & Shulman, L. M. (2012).What determines resilience in patients with Parkinson’s dis-ease? Parkinsonism and Related Disorders, 18, 174-177. doi:http://dx.doi.org/10.1016/j.parkreldis.2011.09.021
Russo, S. J., Murrough, J. W., Han, M. H., Charney, D. S., & Nestler,E. J. (2012). Neurobiology of resilience. Nature Neuroscience,15, 1475-1484. doi:10.1038/nn.3234
Seel, R. T., Kreutzer, J. S., & Sanders, A. M. (1997). Con-cordance of patients and family members ratings ofneurobehavioral functioning after traumatic brain injury.Archives of Physical Medicine and Rehabilitation, 78,1254-1257. doi: http://dx.doi.org/10.1016/S0003-9993(97)90340-3.
Seligman, M., & Csikszentmihalyi, M. (2000). Positive psychol-ogy: An introduction. American Psychologist, 55, 5-14. doi:10.1037/0003-066X.55.1.5
Seligman, M. E. P., Rashid, T., & Parks, A. C. (2006). Positive psy-chotherapy. American Psychologist, 61, 774-788.
Seligman M. E. P, Steen T. A., Park, N., & Peterson, C.(2005). Positive psychology progress: Empirical validationof interventions. American Psychologist, 60, 410-421. doi:10.1037/0003-066X.60.5.410
Sharf, J. (2008). Psychotherapy dropout: A meta-analytic review ofpremature termination. Dissertation Abstracts International: Sec-tion B: The Sciences and Engineering, 68, 6336.
Schutz, L. E., & Trainor, K. (2007). Evaluation of cognitive reha-bilitation as a treatment paradigm. Brain Injury, 21, 545-557.doi:10.1080/02699050701426923
Sherr, R. L. & Langenbahn, D. M. (1992). An approach to large-scaleoutpatient neuropsychological rehabilitation. Neuropsychology,6, 417-426. doi:10.1037/0894-4105.6.4.417
Shin, J. C., Goo, H. R., Yu, S. J., Kim, D. H., & Yoon, S. Y. (2012).Depression and quality of life in patients within the first 6 monthsafter the spinal cord injury. Annals of Rehabilitation Medicine,36, 119-125, doi: 10.5535/arm.2012.36.1.119
Silver, J. M., McAllister, T. W., & Arciniegas, D. B. (2009). Depres-sion and cognitive complaints following mild traumatic braininjury. The American Journal of Psychiatry, 166, 653-661. doi:10.1176/appi.ajp.2009.08111676.
Struchen, M. A., Pappadis, M. R., Sander, A. M., Burrows, C.S., & Myszka, K. A. (2011). Examining the contribution ofsocial communication abilities and affective/behavioral function-ing to social integration outcomes for adults with traumatic braininjury. Journal of Head Trauma Rehabilitation, 26, 30-42. doi:10.1097/HTR.0b013e3182048f7c
Tallman, B., Shaw, K., Schultz, J., & Altmaier, E. (2010). Well-beingand posttraumatic growth in unrelated donor marrow transplantsurvivors: A nine-year longitudinal study. Rehabilitation Psychol-ogy, 55, 204-210. doi:10.1037/a0019541
Tøien, K., Bredal, I. S., Skogstad, L., Myhren, H., & Ekeberg, O.(2011). Health related quality of life in trauma patients. Data froma one-year follow up study compared with the general population.Scandinavian Journal of Trauma, Resuscitation, and EmergencyMedicine, 19-22. doi:10.1186/1757-7241-19-22
Tonks, J., Yates, P., Frampton, I., Williams, W. H., Harris, D.,& Slater, A. (2011). Resilience and the mediating effectsof executive dysfunction after childhood brain injury: Acomparison between children aged 9-15 years with braininjury and non-injured controls. Brain Injury, 25, 870-881.doi:10.3109/02699052.2011.581641
Tsai, M., Ogrodniczuk, J. S., Sochting, I., & Mirmiran J. (2012).Forecasting success: Patients’ expectations for improvement andtheir relations to baseline, process and outcome variables in groupcognitive-behavioural therapy for depression. Clinical Psychol-ogy & Psychotherapy, in press. doi: 10.1002/cpp.1831
Tsaousides, T., Warshowsky, A., Ashman, T. A., Cantor, J. B., Spiel-man, L., & Gordon, W. A. (2009). The relationship betweenemployment-related self-efficacy and quality of life followingtraumatic brain injury. Rehabilitation Psychology, 54, 399-405,doi: 10.1037/a0016807
Vogel, D. L., Wester, S. R., Wei, M., & Boysen, G. A. (2005). Therole of outcome expectations and attitudes on decisions to seekprofessional help. Journal of Counseling Psychology, 52, 459-470. doi: 10.1037/0022-0167.52.4.459
Wells T. S., Miller, S. C., Adler, A. B., Engel, C. C., Smith, T. C.,& Fairbank, J. A. (2011). Mental health impact of the Iraq andAfghanistan conflicts: A review of US research, service provision,and programmatic responses. International Review of Psychiatry,23, 144-152, doi:10.3109/09540261.2011.558833
White B., Driver S., & Warren, A. M. (2008). Considering resiliencein the rehabilitation of people with traumatic disabilities. Reha-bilitation Psychology, 53, 9-17. doi: 10.1037/0090-5550.53.1.9
White, B., Driver, S., & Warren, A. M. (2010). Resilience and indica-tors of adjustment during rehabilitation from a spinal cord injury.Rehabilitation Psychology, 55, 23-32, doi: 10.1037/a0018451.
Wijesuriya, N., Craig, A., Tran, Y., & Middleton, J. (2011). Catas-trophic injury and it’s association with negative mood states.Psychology Research, 5, 369-375.
Wilson, B. A. (2005). The clinical neuropsychologist’s dilemma.Journal of the International Neuropsychological Society, 11, 488-493. doi:10.1017/S1355617705050599
Appendix A
POSITIVE PSYCHOTHERAPY INVENTORY(PPTI)
Rashid, T. (2008). The positive psychotherapy inven-tory. In Magyar-Moe J, Therapist’s Guide to PositivePsychological Interventions (pp. 86-90). Oxford, UK:Academic Press in Elsevier.
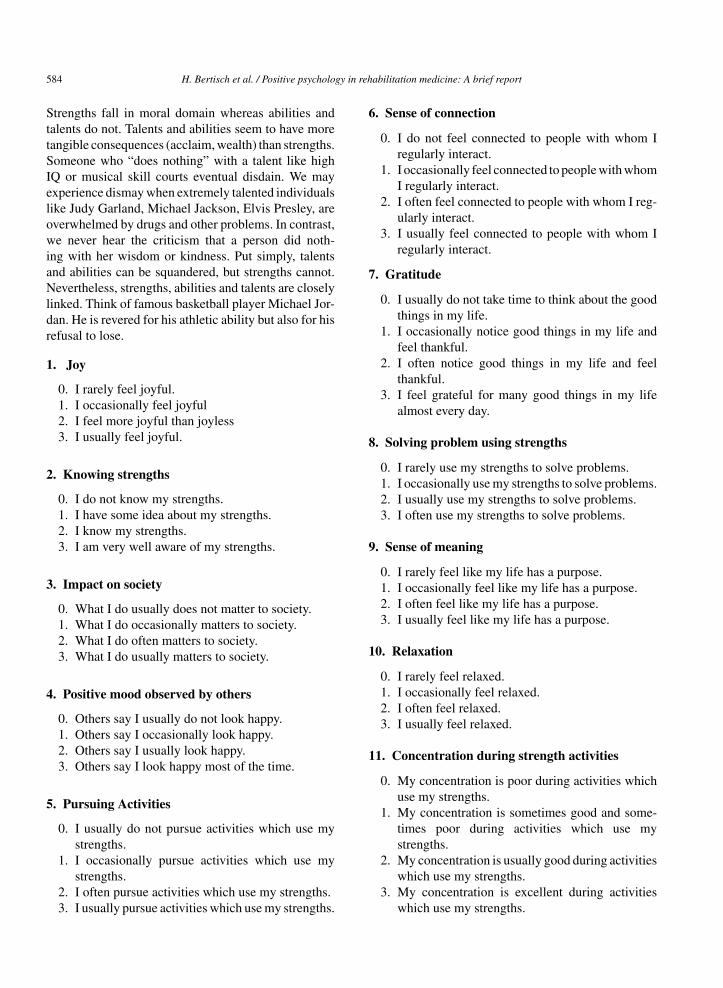
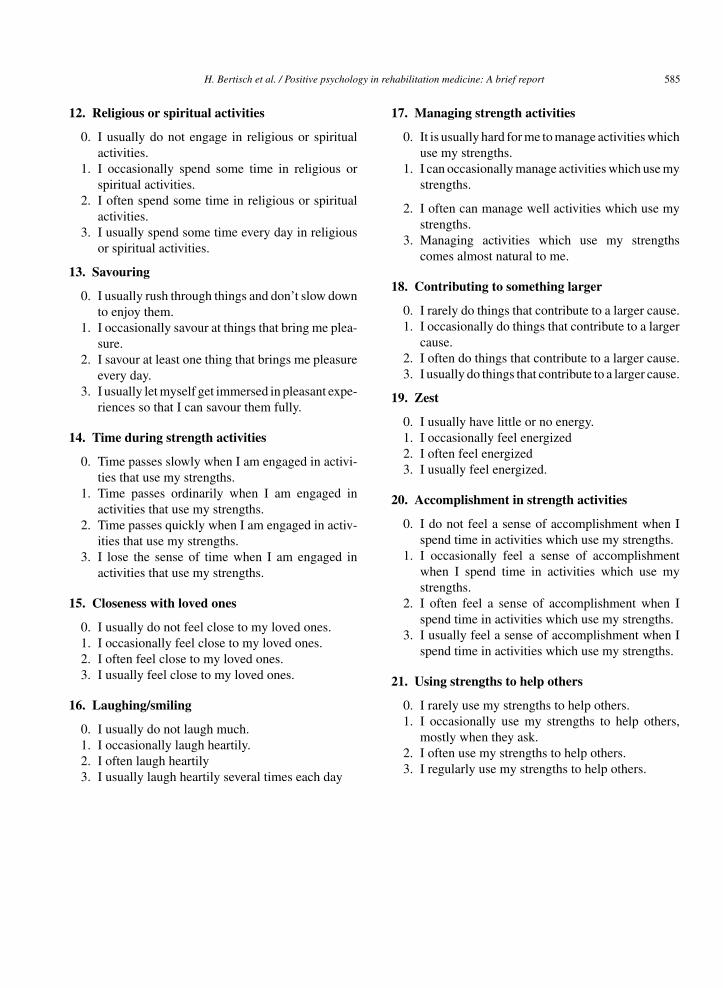
Please read each group of statements carefully. Then,pick the one statement in each group that best describesyou. Be sure to read all of the statements in each groupbefore making your choice.
Some questions are regarding strengths. Strengthrefers to a stable trait which manifests through thoughts,feelings and actions, is morally valued and is beneficialto self and others. Examples of strengths include but notlimited to optimism, zest, spirituality, fairness, modesty,social intelligence, perseverance, curiosity, creativity,teamwork... etc.
In responding to statements regarding strengths, itis important that you distinguish between strengths,abilities and talents. Abilities and talents are attributessuch as intelligence, perfect pitch, or athletic prowess.
584 H. Bertisch et al. / Positive psychology in rehabilitation medicine: A brief report
Strengths fall in moral domain whereas abilities andtalents do not. Talents and abilities seem to have moretangible consequences (acclaim, wealth) than strengths.Someone who “does nothing” with a talent like highIQ or musical skill courts eventual disdain. We mayexperience dismay when extremely talented individualslike Judy Garland, Michael Jackson, Elvis Presley, areoverwhelmed by drugs and other problems. In contrast,we never hear the criticism that a person did noth-ing with her wisdom or kindness. Put simply, talentsand abilities can be squandered, but strengths cannot.Nevertheless, strengths, abilities and talents are closelylinked. Think of famous basketball player Michael Jor-dan. He is revered for his athletic ability but also for hisrefusal to lose.
1. Joy
0. I rarely feel joyful.1. I occasionally feel joyful2. I feel more joyful than joyless3. I usually feel joyful.
2. Knowing strengths
0. I do not know my strengths.1. I have some idea about my strengths.2. I know my strengths.3. I am very well aware of my strengths.
3. Impact on society
0. What I do usually does not matter to society.1. What I do occasionally matters to society.2. What I do often matters to society.3. What I do usually matters to society.
4. Positive mood observed by others
0. Others say I usually do not look happy.1. Others say I occasionally look happy.2. Others say I usually look happy.3. Others say I look happy most of the time.
5. Pursuing Activities
0. I usually do not pursue activities which use mystrengths.
1. I occasionally pursue activities which use mystrengths.
2. I often pursue activities which use my strengths.3. I usually pursue activities which use my strengths.
6. Sense of connection
0. I do not feel connected to people with whom Iregularly interact.
1. I occasionally feel connected to people with whomI regularly interact.
2. I often feel connected to people with whom I reg-ularly interact.
3. I usually feel connected to people with whom Iregularly interact.
7. Gratitude
0. I usually do not take time to think about the goodthings in my life.
1. I occasionally notice good things in my life andfeel thankful.
2. I often notice good things in my life and feelthankful.
3. I feel grateful for many good things in my lifealmost every day.
8. Solving problem using strengths
0. I rarely use my strengths to solve problems.1. I occasionally use my strengths to solve problems.2. I usually use my strengths to solve problems.3. I often use my strengths to solve problems.
9. Sense of meaning
0. I rarely feel like my life has a purpose.1. I occasionally feel like my life has a purpose.2. I often feel like my life has a purpose.3. I usually feel like my life has a purpose.
10. Relaxation
0. I rarely feel relaxed.1. I occasionally feel relaxed.2. I often feel relaxed.3. I usually feel relaxed.
11. Concentration during strength activities
0. My concentration is poor during activities whichuse my strengths.
1. My concentration is sometimes good and some-times poor during activities which use mystrengths.
2. My concentration is usually good during activitieswhich use my strengths.
3. My concentration is excellent during activitieswhich use my strengths.
H. Bertisch et al. / Positive psychology in rehabilitation medicine: A brief report 585
12. Religious or spiritual activities
0. I usually do not engage in religious or spiritualactivities.
1. I occasionally spend some time in religious orspiritual activities.
2. I often spend some time in religious or spiritualactivities.
3. I usually spend some time every day in religiousor spiritual activities.
13. Savouring
0. I usually rush through things and don’t slow downto enjoy them.
1. I occasionally savour at things that bring me plea-sure.
2. I savour at least one thing that brings me pleasureevery day.
3. I usually let myself get immersed in pleasant expe-riences so that I can savour them fully.
14. Time during strength activities
0. Time passes slowly when I am engaged in activi-ties that use my strengths.
1. Time passes ordinarily when I am engaged inactivities that use my strengths.
2. Time passes quickly when I am engaged in activ-ities that use my strengths.
3. I lose the sense of time when I am engaged inactivities that use my strengths.
15. Closeness with loved ones
0. I usually do not feel close to my loved ones.1. I occasionally feel close to my loved ones.2. I often feel close to my loved ones.3. I usually feel close to my loved ones.
16. Laughing/smiling
0. I usually do not laugh much.1. I occasionally laugh heartily.2. I often laugh heartily3. I usually laugh heartily several times each day
17. Managing strength activities
0. It is usually hard for me to manage activities whichuse my strengths.
1. I can occasionally manage activities which use mystrengths.
2. I often can manage well activities which use mystrengths.
3. Managing activities which use my strengthscomes almost natural to me.
18. Contributing to something larger
0. I rarely do things that contribute to a larger cause.1. I occasionally do things that contribute to a larger
cause.2. I often do things that contribute to a larger cause.3. I usually do things that contribute to a larger cause.
19. Zest
0. I usually have little or no energy.1. I occasionally feel energized2. I often feel energized3. I usually feel energized.
20. Accomplishment in strength activities
0. I do not feel a sense of accomplishment when Ispend time in activities which use my strengths.
1. I occasionally feel a sense of accomplishmentwhen I spend time in activities which use mystrengths.
2. I often feel a sense of accomplishment when Ispend time in activities which use my strengths.
3. I usually feel a sense of accomplishment when Ispend time in activities which use my strengths.
21. Using strengths to help others
0. I rarely use my strengths to help others.1. I occasionally use my strengths to help others,
mostly when they ask.2. I often use my strengths to help others.3. I regularly use my strengths to help others.