Platelet-5HT uptake and gastrointestinal symptoms in patients suffering from major depression
11
Platelet-5HT uptake and gastrointestinal symptoms in patients suffering from major depression Leonora Franke a, * , Hans-Ju ¨rgen Schewe a , Ralf Uebelhack a , Anne Bergho ¨fer b , Bruno Mu ¨ller-Oerlinghausen b a Department of Psychiatry, Laboratory of Clinical Neurobiolgy, Humboldt University (Charite ´), Schumannstr. 20-21, D-10117 Berlin, Germany b Former Clinical Psychopharmacology Research Group, Free University, 1405 Berlin, Germany Received 23 December 2002; accepted 9 July 2003 Abstract The objective of this study was to determine whether the presence of gastrointestinal symptoms, as defined by item 12 of Hamilton – Rating-Scale for Depression, is related to kinetic characteristics of platelet-5HT uptake in patients with major depression. The clinical picture of depression in patients with severe form of appetite loss with difficulties of eating (item 12 = 2) and weight loss was characterized by the combination of depressed mood with somatic symptoms of anxiety, sleep disturbances, decreased activity and the presence of nausea. The high frequency of relatively low Vmax and Km of 5HT uptake in this group (n = 12), all in the lower range of controls, resulted in significantly lower mean values compared with patients without gastrointestinal symptoms (n = 16; item 12 = 0) or 57 healthy subjects (Vmax = 1.36 F 0.27 vs. 2.14 F 0.85 vs. 2.05 F 0.74 nMol 5HT/10 9 plat.x min; Km = 382 F 68 vs. 467 F 94 vs. 492 F 123 nM respectively). Although our finding needs confirmation, it seems that in the research for serotonergic mechanisms in major depression, it makes sense to look at depressed patients with or without somatic symptoms separately. Based on findings in 5HT transporter knock-out mice (J. Neurosci. 15 (2001) 6348), we assume that the low apparent Vmax of platelet-5HT uptake reflects the low expression of 5HT transporter not only in platelets, but also in the gut 0024-3205/$ - see front matter D 2003 Elsevier Inc. All rights reserved. doi:10.1016/j.lfs.2003.07.004 * Corresponding author. Tel.: +49-030-450-51-70-75; fax: +49-030-450-51-79-02. E-mail address: [email protected] (L. Franke). www.elsevier.com/locate/lifescie Life Sciences 74 (2003) 521 – 531
-
Upload
charite-de -
Category
Documents
-
view
11 -
download
0
Transcript of Platelet-5HT uptake and gastrointestinal symptoms in patients suffering from major depression

www.elsevier.com/locate/lifescie
Life Sciences 74 (2003) 521–531
Platelet-5HT uptake and gastrointestinal symptoms in patients
suffering from major depression
Leonora Frankea,*, Hans-Jurgen Schewea, Ralf Uebelhacka,Anne Berghoferb, Bruno Muller-Oerlinghausenb
aDepartment of Psychiatry, Laboratory of Clinical Neurobiolgy, Humboldt University (Charite), Schumannstr. 20-21,
D-10117 Berlin, GermanybFormer Clinical Psychopharmacology Research Group, Free University, 1405 Berlin, Germany
Received 23 December 2002; accepted 9 July 2003
Abstract
The objective of this study was to determine whether the presence of gastrointestinal symptoms, as defined by
item 12 of Hamilton–Rating-Scale for Depression, is related to kinetic characteristics of platelet-5HT uptake in
patients with major depression.
The clinical picture of depression in patients with severe form of appetite loss with difficulties of eating (item 12
= 2) and weight loss was characterized by the combination of depressed mood with somatic symptoms of anxiety,
sleep disturbances, decreased activity and the presence of nausea. The high frequency of relatively low Vmax and
Km of 5HT uptake in this group (n = 12), all in the lower range of controls, resulted in significantly lower mean
values compared with patients without gastrointestinal symptoms (n = 16; item 12 = 0) or 57 healthy subjects
(Vmax = 1.36 F 0.27 vs. 2.14 F 0.85 vs. 2.05 F 0.74 nMol 5HT/109plat.x min; Km = 382 F 68 vs. 467 F 94
vs. 492 F 123 nM respectively).
Although our finding needs confirmation, it seems that in the research for serotonergic mechanisms in major
depression, it makes sense to look at depressed patients with or without somatic symptoms separately. Based on
findings in 5HT transporter knock-out mice (J. Neurosci. 15 (2001) 6348), we assume that the low apparent Vmax
of platelet-5HT uptake reflects the low expression of 5HT transporter not only in platelets, but also in the gut
0024-3205/$ - see front matter D 2003 Elsevier Inc. All rights reserved.
doi:10.1016/j.lfs.2003.07.004
* Corresponding author. Tel.: +49-030-450-51-70-75; fax: +49-030-450-51-79-02.
E-mail address: [email protected] (L. Franke).

L. Franke et al. / Life Sciences 74 (2003) 521–531522
mucosa and enteric serotonergic neurons, which probably increases the risk of typical gastrointestinal symptoms
such as appetite loss and nausea occurring in some depressed patients.
D 2003 Elsevier Inc. All rights reserved.
Keywords: Depression; Platelet; Serotonin; Serotonin uptake; Appetite
Introduction
The literature on platelet-5HT uptake activity and major depression is widespread and in part
contradictory (Meltzer and Arora, 1991 for review). Attention of the authors focused on simple
relationships between diagnostic subcategories of major depression and apparent kinetic parameters
of platelet-5HT uptake. About 70% of the previous reports associated decreased mean values of
maximum velocity (Vmax) of 5HT uptake in platelets with unipolar, bipolar or nonpsychotic
depression.
In view of the possible significance of 5HT transport disturbances for major depression, it is
surprising that only a few studies attempted to correlate apparent kinetic parameters of 5HT uptake
with the severity of depression or defined psychopathological symptoms. The absence of a
significant correlation between kinetic parameters of platelet-5HT uptake and HAMD total score
was reported in three studies (Kaplan and Mann, 1982; Faludi et al., 1988; Hrdina et al., 1997). On
the other hand, in 1991, Meltzer and Aurora described a significant, negative correlation between
Vmax, after adjustment for Km, and some aspects of psychopathology in a large group of 94
depressed patients. However, this finding must be interpreted with caution since the statistical
significance of the low correlation coefficients in the range � 0.21 and � 0.37 was only due to the
large sample size.
To our knowledge, no published studies have examined platelet-5HT uptake in relation to somatic
symptoms of depression, especially gastrointestinal (GI). This question seems to be of relevance
because 5HT is involved in the physiological control of GI motility and mucosal 5HT has been shown
to be inactivated by uptake into epithelial cells mediated by the same 5HT transporter (5HTT) that is
utilised in the brain and platelets (Read and Gwee, 1994; Wade et al., 1996; Chen et al., 1998;
Gershon, 1999). Furthermore, some previous studies in humans imply that the mucosal 5HT system
may be disturbed in patients with abnormal colonic motility (Bearcroft et al., 1998; Miwa et al.,
2001).
The fact that a single gene encodes the 5HTT in both the CNS and in non-neuronal tissues means that
genetic variations reported in the 5HTT promotor (5HTTLPR) (Heils et al., 1996) could be responsible
for the modulation of 5HTT transcription in not only the nervous systems but also in different peripheral
organs. 5HTT knock-out mice, completely lacking 5HTT in both the brain and periphery, are useful
models for investigating the functional consequences and compensatory mechanisms. Recently, Chen et
al. (2001) reported that 5HTT knock-out mice exhibit altered GI function. Stool water and colon motility
were increased in 75% of homozygous 5HTT (� /� ) mutants compared with their 5HTT (+/+)
littermates.
The aim of the study was to test the hypothesis that platelet serotonergic parameters are affected by
some somatic symptoms of major depression. Platelet-5HT concentration and apparent kinetic param-

L. Franke et al. / Life Sciences 74 (2003) 521–531 523
eters of 5HT uptake were compared in untreated, depressed patients with or without GI symptoms
according to item 12 of the HAMD scale.
During the preparation of this paper, Pata et al. (2002) reported that the short-short genotype of
5HTTLPR occurred with significantly greater frequency in the constipation-predominant group of
patients with irritable bowel syndrome (IBS) than in the diarrhoea-predominant group or alternating
diarrhoea and constipation group.
Material and methods
Patients and healthy subjects
Data of 28 patients with a diagnosis of major depression according to ICD-10 criteria were analysed.
The patients were selected from a large group of patients (n = 90) who were investigated for platelet
serotonergic parameters. The patients gave written informed consent to participate in our research
program, and the local ethical committees of both universities approved the study protocol. The severity
of depression was rated using the 21-item Hamilton–Rating-Scale for Depression (HAMD) and the
Bech-Rafaelsen–Depression-Scale.
To test the hypothesis that platelet serotonergic parameters are affected by some somatic
symptoms of major depression, item 12 of HAMD was used to form defined subgroups of
patients. 12 of the 90 patients were classified by severe gastrointestinal symptoms, indicated by
scores of 2 on HAMD item 12. Scores of 0 and a lack of weight loss were found in 16 of the 90
patients.
At the time of hospitalisation, 14 of the 28 patients were drug-naive, and the other 14 patients had
received psychotropic drugs (maprotiline n = 3, amitriptyline n = 4, trimipramine n = 1, doxepin n = 1,
paroxetine n = 1, clomipramine n = 1, benzodiazepines n = 2) or aspirin ( n = 1) with a wash-out period
of 14 days (n = 7) or 8 days (n = 8) before the blood collection and rating. These patients did not show
residual effects of previous drug treatments on serotonergic variables such as increased Km of 5HT
uptake combined with reduced 5HT concentration in platelets.
Data of 57 healthy subjects from a recent study (Franke et al., 2000) represented the reference values.
Demographic and clinical data of patients and controls are summarised in Table 1.
Blood collection and assay of serotonergic parameters
Venous blood was drawn between 8:00–8:30 a.m. in EDTA vacutainer tubes (1.6 mg EDTA/ml
blood), after overnight fasting. Preparation of platelet-rich plasma (PRP) or washed platelets, suspended
in Krebs phosphate buffer (pH = 7.4), and assays of 5HT uptake and 5HT concentration were
performed according to methodologies described elsewhere (Franke et al., 2000; Uebelhack et al.,
1998).
In brief, 5HT uptake kinetics were examined by incubation of 50 Al PRP or washed platelets in Krebs-
phosphate-buffer (pH = 7.4) at five different concentrations of [3H]-5HT/5HT ranging from 0.1 to 1.6
AM at 37 jC for 5 minutes (finale volume 200 Al). Platelets were collected by filtration on Whatman GF-
B filters. 5HT uptake kinetics were characterised by apparent Vmax, Km and uptake efficiency, which
was defined as the ratio of Vmax/Km (Franke et al., 2000).

Table 1
Demographic and clinical data of patients and controls
Appetite loss + weight loss + Appetite loss � weight loss � Healthy controls
gender (male/female) 6/6 5/11 27/30
age
median 48.5 54 42
range 29–56 32–59 23–75
diagnosis
F31 2 2
F32 5 6
F33 5 8
drug-naiv 5 9 57
drug-free 7 7
HAMD total score
mean F SD (range) 30.2 F 7.3 (16–41)* 19.6 F 3.4 (15–27)
Item 12 (GI symptoms) 2 0
Item 16 (weight loss) 2 0
Item 3 (suicidality) 1.6 F 1.2 0.88 F 1.0
life time suicide attempts 4 m/0 f 0 m/1 f –
L. Franke et al. / Life Sciences 74 (2003) 521–531524
Statistical analysis
In a recent study, we reported that there were no significant effects of age or gender on platelet
5HT measures in depressed patients; however, in healthy subjects, there was a trend towards higher
platelet-5HT concentration and lower apparent Km values in females (Franke et al., 2000). In this
study, we abstained from matching for age and gender because the ages and the ratio of male to
female subjects in the control and severe appetite loss groups were very similar (Table 1).
Statistics were performed with SPSS, V 10.0. Due to the small sizes of our samples, only
nonparametric tests for data analysis were used: Mann–Whitney U test and Spearman’s rank-order
correlation coefficients. Data is presented as mean F SD and the range is given in parenthesis.
*p < 0.01 vs. patients without GI symptoms.
Results
Clinical characteristic of patient subgroups
Severe appetite loss and nausea occurred in all 12 of the patients who had difficulty eating
without staff encouragement (scores of 2 on HAMD item 12). Constipation was reported by one
patient and diarrhoea/loose stools by two patients. All patients recorded notable weight loss in the
range of 4–12 kg during a period of 1–5 months. All 12 patients had normal blood pressure (116
F 10/78 F 7 mm Hg).
Patients with a score of 0 on the HAMD item 12 and a lack of weight loss had normal
appetites, and their HAMD total scores were, on average, significantly lower than in the appetite
disturbed group (Table 1). Untreated, elevated blood pressure was observed in 4 of the 15 patients
(>145/85 mm Hg).
L. Franke et al. / Life Sciences 74 (2003) 521–531 525
To determine if other differences existed in the clinical picture of depression in the subgroups, we
investigated which symptoms were the main factors determining the HAMD total score by a
correlation analysis (Table 2). This analysis was possible because in both groups there was a large
variability in the severity of depression, expressed by the HAMD total scores (Table 1). Strong
correlations between HAMD total score and some of the items of the scale indicated that the clinical
picture for the appetite-disturbed group was characterized by depressed mood (item 1), somatic
anxiety (item 11), and sleep disturbances (item 4–6). Depressed mood was significantly and
positively related to retardation (item 8), general somatic symptoms (item 13), somatic anxiety (item
11) and work and activities (item 7). On the other hand, the group of patients with item 12 = 0 and
no weight loss displayed low homogeneity with respect to clinical symptoms and their interrelations.
The Spearman correlation coefficients were moderate or low, and significant only for items 5
(insomnia -middle) and 18 (severity of diurnal variation) (Table 2). Similarities to the appetite
disturbed group existed only in the positive relationship between depressed mood (item 1) and
retardation (item 8).
While there was a higher frequency of lifetime suicide attempts in the appetite disturbed group, the
mean scores of item 3 (suicidality) were not significantly different in both groups of patients (Table 1).
Scores of item 3 were not significantly related to the severity of depression or its duration.
Comparison of apparent kinetic parameters of 5HT uptake
The appetite-disturbed group showed significantly lower mean Vmax and Km values than controls or
patients without GI symptoms (Table 3) and was characterized by a high homogeneity of Vmax values
(Fig. 1), because the variability was remarkably low in comparison with patients without GI symptoms
and controls (CVVmax: 19.6%–39.7%–29.5%, respectively ). The differences were statistically signif-
icant ( Levene test: F = 9.36 p < 0.01 vs. controls and F = 14.54 p = 0.001 vs. patients without GI
symptoms).
Table 2
Spearman correlation coefficients between HAMD total score and subcategories of the scale
HAMD total score vs. Appetite loss + weight loss + Appetite loss – weight loss –
Item 1(depressed mood) 0.762***
Item 4 (insomnia-early) 0.580*
Item 5 (insomnia-middle) 0.661* 0.577*
Item 6 (insomnia-late) 0.608*
Item 7 (work and activity) 0.611*
Item 11 (anxiety somatic) 0.873***
Item 18 (severity of diurnal variation) 0.550*
Item 1 vs. item 8 (retardation) 0.714** 0.647**
Item 1 vs. item 13 (general somatic symptoms) 0.761**
Item 1 vs. item 11 (somatic anxiety) 0.683*
Item 1 vs. item 7 (work and activity) 0.673*
Only correlation coefficients >0.5 were included in the table.
*p < 0.05.
**p < 0.01.
***p < 0.001.
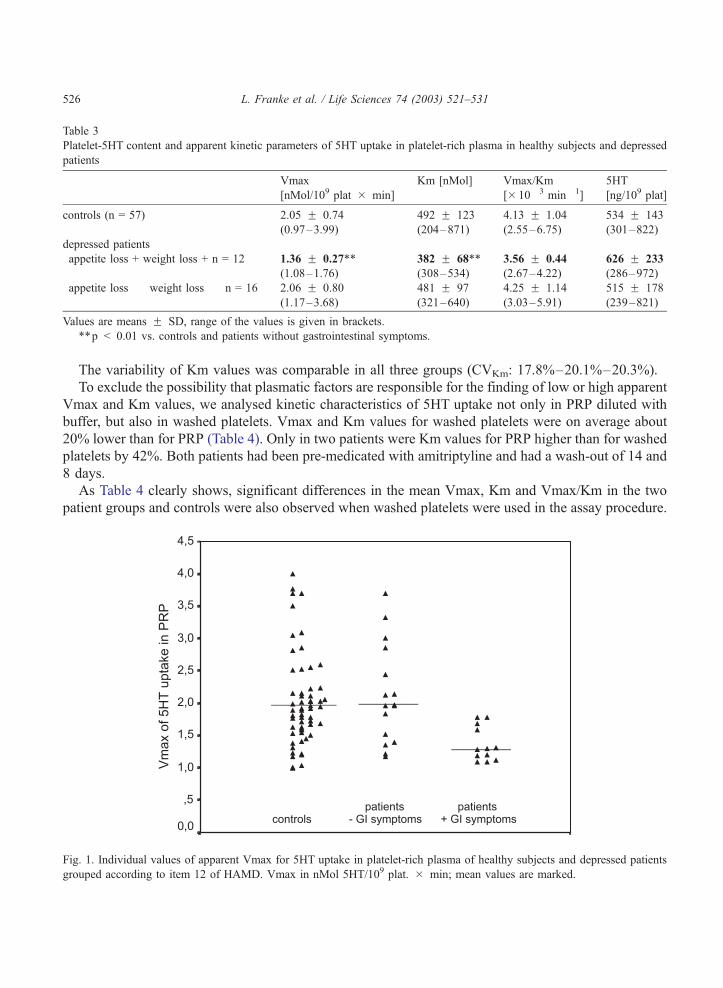
Table 3
Platelet-5HT content and apparent kinetic parameters of 5HT uptake in platelet-rich plasma in healthy subjects and depressed
patients
Vmax
[nMol/109 plat � min]
Km [nMol] Vmax/Km
[� 10� 3 min� 1]
5HT
[ng/109 plat]
controls (n = 57) 2.05 F 0.74
(0.97–3.99)
492 F 123
(204–871)
4.13 F 1.04
(2.55–6.75)
534 F 143
(301–822)
depressed patients
appetite loss + weight loss + n = 12 1.36 F 0.27**
(1.08–1.76)
382 F 68**
(308–534)
3.56 F 0.44
(2.67–4.22)
626 F 233
(286–972)
appetite loss � weight loss � n = 16 2.06 F 0.80
(1.17–3.68)
481 F 97
(321–640)
4.25 F 1.14
(3.03–5.91)
515 F 178
(239–821)
Values are means F SD, range of the values is given in brackets.
**p < 0.01 vs. controls and patients without gastrointestinal symptoms.
L. Franke et al. / Life Sciences 74 (2003) 521–531526
The variability of Km values was comparable in all three groups (CVKm: 17.8%–20.1%–20.3%).
To exclude the possibility that plasmatic factors are responsible for the finding of low or high apparent
Vmax and Km values, we analysed kinetic characteristics of 5HT uptake not only in PRP diluted with
buffer, but also in washed platelets. Vmax and Km values for washed platelets were on average about
20% lower than for PRP (Table 4). Only in two patients were Km values for PRP higher than for washed
platelets by 42%. Both patients had been pre-medicated with amitriptyline and had a wash-out of 14 and
8 days.
As Table 4 clearly shows, significant differences in the mean Vmax, Km and Vmax/Km in the two
patient groups and controls were also observed when washed platelets were used in the assay procedure.
Fig. 1. Individual values of apparent Vmax for 5HT uptake in platelet-rich plasma of healthy subjects and depressed patients
grouped according to item 12 of HAMD. Vmax in nMol 5HT/109 plat. � min; mean values are marked.
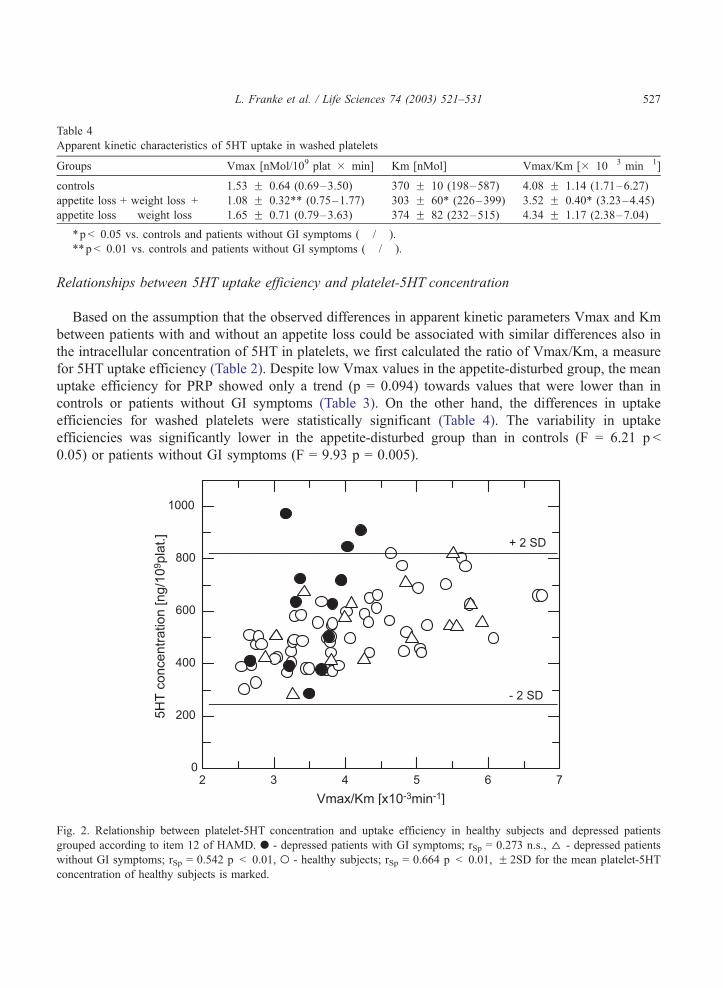
Table 4
Apparent kinetic characteristics of 5HT uptake in washed platelets
Groups Vmax [nMol/109 plat � min] Km [nMol] Vmax/Km [� 10� 3 min� 1]
controls 1.53 F 0.64 (0.69–3.50) 370 F 10 (198–587) 4.08 F 1.14 (1.71–6.27)
appetite loss + weight loss + 1.08 F 0.32** (0.75–1.77) 303 F 60* (226–399) 3.52 F 0.40* (3.23–4.45)
appetite loss � weight loss � 1.65 F 0.71 (0.79–3.63) 374 F 82 (232–515) 4.34 F 1.17 (2.38–7.04)
*p < 0.05 vs. controls and patients without GI symptoms (� /� ).
L. Franke et al. / Life Sciences 74 (2003) 521–531 527
Relationships between 5HT uptake efficiency and platelet-5HT concentration
Based on the assumption that the observed differences in apparent kinetic parameters Vmax and Km
between patients with and without an appetite loss could be associated with similar differences also in
the intracellular concentration of 5HT in platelets, we first calculated the ratio of Vmax/Km, a measure
for 5HT uptake efficiency (Table 2). Despite low Vmax values in the appetite-disturbed group, the mean
uptake efficiency for PRP showed only a trend (p = 0.094) towards values that were lower than in
controls or patients without GI symptoms (Table 3). On the other hand, the differences in uptake
efficiencies for washed platelets were statistically significant (Table 4). The variability in uptake
efficiencies was significantly lower in the appetite-disturbed group than in controls (F = 6.21 p <
0.05) or patients without GI symptoms (F = 9.93 p = 0.005).
**p < 0.01 vs. controls and patients without GI symptoms (� /� ).
Fig. 2. Relationship between platelet-5HT concentration and uptake efficiency in healthy subjects and depressed patients
grouped according to item 12 of HAMD. . - depressed patients with GI symptoms; rSp = 0.273 n.s., D - depressed patients
without GI symptoms; rSp = 0.542 p < 0.01, o - healthy subjects; rSp = 0.664 p < 0.01, F 2SD for the mean platelet-5HT
concentration of healthy subjects is marked.

L. Franke et al. / Life Sciences 74 (2003) 521–531528
The highest mean 5HT content was observed in the appetite-disturbed group, with a strong tendency
towards higher variability than in controls (CV = 37.2% vs. 18.8%; F = 4.07 p = 0.057).
We have previously reported (Franke et al., 2000) that in healthy subjects the platelet-5HT content and
uptake efficiency are significantly correlated (r = 0.627 p < 0.001). Therefore, we analysed the
discrepancy between low uptake efficiency and high mean 5HT content in platelets of patients with
severe appetite loss in more detail. As indicated in Fig. 2, the higher mean 5HT concentration in the
severe appetite loss group can be explained by uncommonly high 5HT concentrations in the platelets of
some patients. 3 of the 12 patients showed 5HT concentrations above + 2SD of the mean for controls. In
contrast to patients without GI symptoms and controls no significant relationship between 5HT
concentration and 5HT uptake efficiency in platelets of patients with severe appetite loss was found
(Fig. 2).
Discussion
Even though the mean Vmax of 5HT uptake in platelets of depressed patients has been found to be
reduced in many studies, it has not been previously demonstrated to be associated with GI symptoms.
This question could be important for further studies on peripheral serotonergic parameters because 5HT
in the gut seems to be a mucosal transmitter that stimulates sensory nerves and initiates peristaltic and
secretory reflexes (Grundy et al., 1994; Wade et al., 1996; Chen et al., 1998). It has been speculated that
the mechanism for terminating the action of 5HT in the mucosa could be the transporter-mediated uptake
of 5HT by enterocytes (Wade et al., 1996; Gershon, 1999).
Item 12 of HAMD records appetite disturbances unspecifically and considers different gastrointestinal
symptoms, such as constipation, diarrhoea or heavy feelings in the abdomen, as a whole. Despite this,
our simple selection of patients according to this item lead to a subgroup of patients having considerable
reduced variability of Vmax and Vmax/Km in comparison with controls and patients without GI
symptoms. With respect to the variability of Vmax values in healthy subjects or depressed patients as a
whole, our data are comparable with those reported in studies by Halbreich et al. (1991) on 87 healthy
subjects (CV = 33.4%) and Hrdina et al., 1997 on 40 controls (CV = 21.4%) and 60 depressed patients
(CV = 45.4%).
The use of item 12 as a criteria for subdivision also resulted in a clinically well-defined picture of
depression (Table 2). This picture was associated with a considerable high difference in the mean Vmax
compared with controls (� 41.4%) and patients without appetite and weight loss (� 36.4%). However, a
lower mean Vmax does not imply that patients with severe appetite loss are characterised in general by
decreased Vmax of 5HT in platelets, since all individual values of these patients were still in the lower
range of healthy subjects (Fig. 1).
The finding of a reduced mean Km value in comparison with healthy subjects opposes the general
view that the Michaelis constant is not changed in major depression. Significantly lower Km values
in major depression, however, have been described in two previous studies (Raisman et al., 1982;
Faludi et al., 1988;). This finding is not surprising, because we previously reported that the Vmax and
Km of 5HT uptake in platelets are significantly intercorrelated (Franke et al., 2000). Earlier
investigations used patients with short washout periods, and, therefore, it cannot be ruled out that
in highly diluted PRP, residual effects of drugs can simulate Km values in the range of healthy
subjects.

L. Franke et al. / Life Sciences 74 (2003) 521–531 529
Usually, PRP diluted with buffer is employed in assay procedures for 5HT uptake activity. The degree
of dilution varies between 1:40 and 1:3 (Tuomisto et al., 1979; Meltzer et al., 1981). Both the kind of
buffer and dilution influence the calculated values of apparent Vmax and Km. Earlier studies in which
the platelet-5HT uptake in PRP was compared with those of washed platelets in buffer, in both the
presence and absence of albumine and fatty acids, revealed that Vmax values were significantly higher
when PRP was used (Breyer-Pfaff et al., 1989). Our finding of about 20% higher mean Vmax values for
assays in diluted PRP compared to washed platelets is in accordance with this report. The finding of
lower Vmax and Km values in patients with severe appetite loss in comparison with controls or patients
without GI symptoms remained significant when washed platelets were used in the assay procedure.
Therefore, it seems that the effects of plasmatic factors are not of great significance, especially in diluted
samples. On the other hand, the comparison of apparent kinetic parameters for diluted PRP and washed
platelets could be very helpful for the assessment of measures in patients with withdrawal from
antidepressants.
It was expected that patients with severe appetite loss have relatively low platelet-5HT concentration
since they showed lower 5HT uptake efficiency in PRP and washed platelets (Tables 3 and 4).
Surprisingly, the mean platelet-5HT concentration was higher than in controls and of a high variability.
The frequently cited study of Mann et al. (1992) reported significantly higher variability of the
platelet-5HT concentration in 29 depressed patients compared with 25 healthy subjects (CV = 56.2% vs.
CV = 31.7%), but no significant differences in the mean values. Unfortunately, the high variability
remained and in some cases even increased when separating the same patients according to the presence
or absence of melancholia, comorbid borderline personality disorder or suicide attempts within 2 months
(Mann et al., 1992). It seems that either a low or a high platelet-5HT concentration by itself is not an
indicator for biological and/or clinical homogeneity.
In our study, the finding of higher mean 5HT concentration in the group with severe appetite loss can
be explained by considerable increased values in 25% of patients (Fig. 2). Two of the 3 patients with
5HT concentrations above + 2SD of the mean for controls had diarrhoea/loose stools.
For the understanding of our findings, it is interesting that 5HTT knock-out mice show an increase in
intestinal motility (diarrhoea) irregularly alternated with decreased motility (constipation) (Chen et al.,
2001). Inhibition of mucosal 5HTT (or lack of this transporter) potentates responses of intrinsic neurones
to the 5HT released by enterochromaffin cells and causes a desensitisation of neuronal 5HT receptors
(Chen et al., 1998). Chen et al. (2001) assume that an inadequate inactivation of 5HT, as is found in
5HTT (� /� ) mice might contribute to the pathogenesis of IBS.
The finding of a prokinetic action of paroxetin in the human small intestinum suggests that 5HT
and 5HTTs participate in the control of migrating motor complex in humans (Gorard et al., 1994). It is
well known that diarrhoea is a side effect of selective serotonin reuptake inhibitors in 10% to 15% of
patients.
Despite the limitation that the calculated Vmax and Km of 5HT uptake in intact platelets are not true
kinetic characteristics of the 5HT transporter, we postulate that the noticeable frequency of relatively low
apparent Vmax and Km values of platelet 5HT uptake in depressed patients with severe appetite loss
could be an indicator for a functional variation in 5HT transport, which could be based on a low
expression of 5HTTs in neuronal as well non-neuronal tissues.
Since clinical samples of patients with fuctional GI symtoms have been shown to have a high
prevalence of depression and anxiety (Creed, 1999), research efforts aiming at further elucidating the
impact of 5HTT on the association between major depression and GI symptoms are warranted.

L. Franke et al. / Life Sciences 74 (2003) 521–531530
Acknowledgements
Supported by German Research Foundation (DFG Ue38/2-1 and Mu477/9-1).
References
Bearcroft, C.P., Perrett, D., Farthing, M.J., 1998. Postprandial plasma 5-hydroxytryptamine in diarrhoea predominant irritable
bowel syndrome: a pilot study. Gut 42, 42–46.
Breyer-Pfaff, U., Fauss, Ch., Bohme, H.-P., 1989. Serum albumin stimulates serotonin uptake into human blood platelets. Life
Sciences 44, 1251–1258.
Chen, J.J., Li, Z., Pan, H., Murphy, D.L., Tamir, H., Koepsell, H., Gershon, M.D., 2001. Maintenance of serotonin in the
intestinal mucosa and ganglia of mice that lack the high-affinity serotonin transporter: Abnormal intestinal motility and the
expression of cation transporters. Journal of Neuroscience 15, 6348–6361.
Chen, J.-X., Pan, H., Rothman, T.P., Wade, P.R., Gershon, M.D., 1998. Guinea pig 5-HT transporter: cloning, expression,
distribution, and function in intestinal sensory reception. American Journal of Physiology 275, G433–G448.
Creed, F., 1999. The relationship between psychosocial parameters and outcome in the irritable bowel syndrome. American
Journal of Medicine 107 (Suppl. 5A), 74–80.
Faludi, G., Magyar, I., Tekes, K., Tothfalusi, L., Magyar, L., 1988. Measurement of 3H-serotonin uptake in platelets of major
depression episodes. Biological Psychiatry 23, 833–836.
Franke, L., Schewe, H.-J., Muller, B., Campman, V., Kitzrow, W., Uebelhack, R., Berghofer, A., Muller-Oerlinghausenm, B.,
2000. Serotonergic platelet variables in unmedicated patients suffering from major depression and healthy subjects. Rela-
tionship between 5HT content and 5HT uptake. Life Sciences 67, 301–315.
Gershon, M.D., 1999. Review article: roles played by 5-hydroxytryptamine in the physiology of the bowel. Aliment Pharma-
cology and Therapeutics 13 (Suppl. 2), 15–30.
Gorard, D.A., Libby, G.W., Farthing, M.J., 1994. 5-Hydroxytryptamine and human small intestinal motility: effect of inhibiting
5-hydroxytryptamine reuptake. Gut 35, 496–500.
Grundy, D., Blackshaw, L.A., Hillsley, K., 1994. Role of 5-hydroxytryptamine in gastrointestinal chemosensitivity. Digestive
Diseases and Sciences 39 (Suppl. 12), 44S–47S.
Halbreich, U., Rojansky, N., Zander, K.J., Barkai, A., 1991. Influence of age, sex and diurnal variability on imipramine receptor
binding and serotonin uptake in platelets of normal subjects. Journal of Psychiatric Research 25, 7–18.
Heils, A., Teufel, A., Petri, S., Stober, G., Riederer, P., Bengel, D., Lesch, K.P., 1996. Allelic variation of human serotonin
transporter gene expression. Journal of Neurochemistry 66, 2621–2624.
Hrdina, P.D., Bakish, D., Ravindran, A., Chudzil, J., Cavazzoni, P., Lapierre, D., 1997. Platelet serotonergic indices in
major depression: up-regulation of 5-HT2A receptors unchanged by antidepressant treatment. Psychiatric Research 66,
73–85.
Kaplan, R.D., Mann, J.J., 1982. Altered platelet serotonin kinetics in schizophrenia and depression. Life Sciences 31,
583–588.
Mann, J.J., McBride, P.A., Anderson, G.M., MIieczkowski, T.A., 1992. Platelet and whole blood serotonin content in depressed
patients; correlation with acute and life-time psychopathology. Biological Psychiatry 32, 243–257.
Meltzer, H.Y., Arora, R.C., 1991. Platelet serotonin studies in affective disorders: evidence for a serotonergic abnormal-
ity? In: Sander, M., et al. (Eds.), 5-Hydroxytryptamine in psychiatry - a spectrum of ideas. Oxford University Press,
pp. 50–89.
Meltzer, H.Y., Arora, R.C., Baber, R., Tricou, B.J., 1981. Serotonin uptake in blood platelets of psychiatric patients. Archive of
General Psychiatry 38, 1322–1326.
Miwa, J., Echizen, C.H., Matsued, K., Umeda, N., 2001. Patients with constipation-predominant irritable bowel syndrome
(IBS) may have elevated serotonin concentrations in colonic mucosa as compared with diarrhoea-predominant patients and
subjects with normal bowel habits. Digestion 63, 188–194.
Pata, C., Erdal, E., Derici, E., Yazar, A., Kanik, A., Ulu, O., 2002. Serotonin transporter gene polymorphism in irritable bowel
syndrome. American Journal of Gastroenterology 97, 1780–1784.

L. Franke et al. / Life Sciences 74 (2003) 521–531 531
Raisman, R., Briley, M.S., Bouchami, F., Sechter, D., Zarifian, E., Langer, S.Z., 1982. 3H-imipramine binding and serotonin
uptake in platelets from untreated depressed patients and control volunteers. Psychopharmacology 77, 332–333.
Read, N.W., Gwee, K.A., 1994. The importance of 5-hydroxytryptamine receptors in the gut. Pharmacology and Therapeutics
62, 159–173.
Tuomisto, J., Tukiainen, E., Ahlfors, U.G., 1979. Decreased uptake of 5-hydroxytryptamine in blood platelets from patients
with endogenous depression. Psychopharmacology 65, 141–147.
Uebelhack, R., Franke, L., Schewe, H.-J., 1998. Inhibition of platelet MAO-B by kava-pyrone-enriched extract from Piper
Methysticum Forster (Kava–Kava). Pharmacopsychiatry 31, 187–192.
Wade, P.R., Chen, J., Jaffe, B., Kassem, I.S., Blakely, R.D., Gershon, M.D., 1996. Localisation and function of a 5-HT
transporter in crypt epithelia of the gastrointestinal tract. Journal of Neuroscience 16, 2352–2364.