Plateau and Transpulmonary Pressure With Elevated Intra-Abdominal Pressure or Atelectasis
8
Plateau and Transpulmonary Pressure With Elevated Intra-Abdominal Pressure or Atelectasis Brian D. Kubiak, M.D.,* ,1 Louis A. Gatto, Ph.D.,† Edgar J. Jimenez, M.D.,‡ Hugo Silva-Parra, M.D., Ph.D.,‡ Kathleen P. Snyder,* Christopher J. Vieau, B.A.,* Jorge Barba, M.D.,‡ Niloofar Nasseri-Nik, M.D.,‡ Jay L. Falk, M.D.,‡ and Gary F. Nieman, B.A.* *Department of Surgery, Upstate Medical University, Syracuse, New York; †Department of Biological Sciences SUNY Cortland, Cortland, New York; and ‡Department of Critical Care Medicine, Orlando Regional Medical Center, Translational Critical Care Laboratory, Orlando Florida Submitted for publication June 1, 2009 Background. ARDSnet standards limit plateau pressure (Pplat) to reduce ventilator induced lung in- jury (VILI). Transpulmonary pressure (Ptp) [Pplat –pleural pressure (Ppl)], not Pplat, is the distending pressure of the lung. Lung distention can be affected by increased intra-abdominal pressure (IAP) and atel- ectasis. We hypothesized that the changes in disten- tion caused by increases in IAP and atelectasis would be reflected by Ptp but independent of Pplat. Methods. In Yorkshire pigs, esophageal pressure (Pes) was measured with a balloon catheter as a surro- gate for Ppl under two experimental conditions: (1) high IAP group (n [ 5), where IAP was elevated by CO 2 insufflation in 5mm Hg steps from 0 to 30mm Hg; and (2) Atelectasis group (n [ 5), where a double lumen endotracheal tube allowed clamping and degassing of either lung by O 2 absorption. Lung collapse was esti- mated by increases in pulmonary shunt fraction. Results. High IAP: Sequential increments in IAP caused a linear increase in Pplat (r 2 [ 0.754, P < 0.0001). Ptp did not increase (r 2 [ 0.014, P [ 0.404) with IAP due to the concomitant increase in Pes (r 2 [ 0.726, P < 0.0001). Partial Lung Collapse: There was no signifi- cant difference in Pplat between the atelectatic (21.83 ± 0.63cm H 2 O) and inflated lung (22.06 ± 0.61 cmH 2 O, P < 0.05). Partial lung collapse caused a signifi- cant decrease in Pes (11.32 ± 1.11mm Hg) compared with inflation (15.89 ± 0.72mm Hg, P < 0.05) resulting in a signif- icant increase in Ptp (inflated [ 5.97 ± 0.72mm Hg; collap- sed [ 10.55 ± 1.53mm Hg, P < 0.05). Conclusions. Use of Pplat to set ventilation may un- der-ventilate patients with intra-abdominal hyperten- sion and over-distend the lungs of patients with atelectasis. Thus, Ptp must be used to accurately set mechanical ventilation in the critically ill. Ó 2010 Elsevier Inc. All rights reserved. Key Words: transpulmonary pressure; intra-abdomi- nal pressure; atelectasis; ventilator induced lung injury. INTRODUCTION Severe trauma, hemorrhage, and sepsis in critically ill patients can result in systemic inflammation [1, 2] which, if untreated, can lead to multiple organ dysfunc- tion syndrome (MODS) [3–5]. One of the first organs to fail as a result of this inflammation is the lung, with the development of acute lung injury and, most severely, the acute respiratory distress syndrome (ARDS) [6]. Currently, the only treatment for ARDS is supportive mechanical ventilation [7]; however, improperly imple- mented mechanical ventilation can increase ARDS-in- duced morbidity and mortality in the form of ventilator induced lung injury (VILI) [8]. To avert this outcome, the landmark study by the ARDS Network (ARDSnet) demonstrated that low tidal volume (Vt) and limits on airway plateau pressures (Pplat) can sig- nificantly reduce VILI-induced mortality in ARDS patients [9]. One shortcoming of this paradigm, how- ever, is that the direct determinant of lung over-disten- sion and VILI is the transpulmonary pressure (Ptp), which is defined as the plateau pressure minus the pleural pressure (Pplat – Ppl) [10, 11]. It follows 1 To whom correspondence and reprint requests should be ad- dressed at Department of Surgery, Upstate Medical University, 750 East Adams Street, Syracuse, NY 13210. E-mail: kubiakb@upstate. edu. 0022-4804/09 $36.00 Ó 2010 Elsevier Inc. All rights reserved. e17 Journal of Surgical Research 159, e17–e24 (2010) doi:10.1016/j.jss.2009.08.002
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Plateau and Transpulmonary Pressure With Elevated Intra-Abdominal Pressure or Atelectasis

Journal of Surgical Research 159, e17–e24 (2010)doi:10.1016/j.jss.2009.08.002
Plateau and Transpulmonary Pressure With Elevated Intra-Abdominal
Pressure or Atelectasis
Brian D. Kubiak, M.D.,*,1 Louis A. Gatto, Ph.D.,† Edgar J. Jimenez, M.D.,‡ Hugo Silva-Parra, M.D., Ph.D.,‡Kathleen P. Snyder,* Christopher J. Vieau, B.A.,* Jorge Barba, M.D.,‡ Niloofar Nasseri-Nik, M.D.,‡
Jay L. Falk, M.D.,‡ and Gary F. Nieman, B.A.*
*Department of Surgery, Upstate Medical University, Syracuse, New York; †Department of Biological Sciences SUNY Cortland,Cortland, New York; and ‡Department of Critical Care Medicine, Orlando Regional Medical Center, Translational Critical Care
Laboratory, Orlando Florida
Submitted for publication June 1, 2009
Background. ARDSnet standards limit plateaupressure (Pplat) to reduce ventilator induced lung in-jury (VILI). Transpulmonary pressure (Ptp) [Pplat–pleural pressure (Ppl)], not Pplat, is the distendingpressure of the lung. Lung distention can be affectedby increased intra-abdominal pressure (IAP) and atel-ectasis. We hypothesized that the changes in disten-tion caused by increases in IAP and atelectasis wouldbe reflected by Ptp but independent of Pplat.
Methods. In Yorkshire pigs, esophageal pressure(Pes) was measured with a balloon catheter as a surro-gate for Ppl under two experimental conditions: (1)high IAP group (n [ 5), where IAP was elevated byCO2 insufflation in 5mm Hg steps from 0 to 30mm Hg;and (2) Atelectasis group (n [ 5), where a double lumenendotracheal tube allowed clamping and degassing ofeither lung by O2 absorption. Lung collapse was esti-mated by increases in pulmonary shunt fraction.
Results. High IAP: Sequential increments in IAPcaused a linear increase in Pplat (r2 [ 0.754, P < 0.0001).Ptp did not increase (r2 [ 0.014, P [ 0.404) with IAP dueto the concomitant increase in Pes (r2 [ 0.726,P < 0.0001). Partial Lung Collapse: There was no signifi-cant difference in Pplat between the atelectatic(21.83 ± 0.63cm H2O) and inflated lung (22.06 ± 0.61cmH2O, P < 0.05). Partial lung collapse caused a signifi-cant decrease in Pes (11.32 ± 1.11mm Hg) compared withinflation(15.89 ± 0.72mmHg,P < 0.05)resultinginasignif-icant increase in Ptp (inflated [ 5.97 ± 0.72mm Hg; collap-sed [ 10.55 ± 1.53mm Hg, P < 0.05).
1 To whom correspondence and reprint requests should be ad-dressed at Department of Surgery, Upstate Medical University, 750East Adams Street, Syracuse, NY 13210. E-mail: [email protected].
e17
Conclusions. Use of Pplat to set ventilation may un-der-ventilate patients with intra-abdominal hyperten-sion and over-distend the lungs of patients withatelectasis. Thus, Ptp must be used to accurately setmechanical ventilation in the critically ill. � 2010 Elsevier
Inc. All rights reserved.
Key Words: transpulmonary pressure; intra-abdomi-nal pressure; atelectasis; ventilator induced lunginjury.
INTRODUCTION
Severe trauma, hemorrhage, and sepsis in criticallyill patients can result in systemic inflammation [1, 2]which, if untreated, can lead to multiple organ dysfunc-tion syndrome (MODS) [3–5]. One of the first organs tofail as a result of this inflammation is the lung, with thedevelopment of acute lung injury and, most severely,the acute respiratory distress syndrome (ARDS) [6].Currently, the only treatment for ARDS is supportivemechanical ventilation [7]; however, improperly imple-mented mechanical ventilation can increase ARDS-in-duced morbidity and mortality in the form ofventilator induced lung injury (VILI) [8]. To avert thisoutcome, the landmark study by the ARDS Network(ARDSnet) demonstrated that low tidal volume (Vt)and limits on airway plateau pressures (Pplat) can sig-nificantly reduce VILI-induced mortality in ARDSpatients [9]. One shortcoming of this paradigm, how-ever, is that the direct determinant of lung over-disten-sion and VILI is the transpulmonary pressure (Ptp),which is defined as the plateau pressure minus thepleural pressure (Pplat – Ppl) [10, 11]. It follows
0022-4804/09 $36.00� 2010 Elsevier Inc. All rights reserved.

0
5
10
15
20
25
30
Stage One Stage Two
Increasing IAP (mmHg)
0 0
Vt PEEP
FIG. 1. Diagram of the experimental protocol. In Stage One, weincreased intra-abdominal pressure (IAP) in 5 mm Hg steps to a max-imum pressure of 30 mm Hg by CO2 insufflation. All lung pressureswere calculated at each IAP. In Stage Two, we degassed the abdomen,reducing the IAP to zero. We then increased tidal volume (Vt) suffi-ciently to elevate Pplat to a level similar to that at IAP¼ 30 mm Hg.All measurements were made at this Vt and Pplat and Vt was reducedto the baseline level. With the normal Vt positive end-expiratory pres-sure (PEEP) was elevated to a level sufficient to elevate Pplat to a levelsimilar to that at IAP¼ 30 mm Hg. All pressures were measured atthis PEEP and Pplat level and the experiment was terminated.
JOURNAL OF SURGICAL RESEARCH: VOL. 159, NO. 1, MARCH 2010e18
therefore that Ptp can show evidence of pronouncedlung distension not revealed by routine Vt and Pplatmonitoring.
It is well known that intra-abdominal hypertension(IAH) is a serious complication common in critically ill pa-tients [12, 13] that may significantly increase morbidityand mortality [14]. Abdominal compartment syndrome(ACS) is the pathologic consequence of IAH-inducedend-organ dysfunction [15]. The lung is subject to thenegative impact of IAH [16], as high intra-abdominalpressure compresses the thoracic cavity, significantly re-ducing chest wall compliance (Ccw) and increasing pleu-ral pressure. Due to this elevated pleural pressure, Ptpin patients with ACS may be much lower for any givenPplat and, consequently, the patient may be under-venti-lated. This poses a problem for the clinician because usingPtp values to guide mechanical ventilation could result ina Pplat considered unsafe by ARDSnet standards (> 30cmH2O) when the lung, in fact, was being ventilatedsafely.
Lung collapse secondary to surfactant deactivation isalso a common occurrence in the critically ill patientwith ARDS [17]. Lung collapse increases the negativeintrathoracic pressure causing a decrease in pleuralpressure [18], which may lead to an increase in Ptpfor a given Pplat. Under these circumstances, VILIcould occur at a Pplat considered to be safe by ARDSnetstandards (< 30 cm H2O) [9]. Without knowledge ofPtp, the patient with lung collapse cannot be optimallyventilated.
The goal of this study was to assess the use of a clini-cally available esophageal balloon catheter to deter-mine Ptp, using the esophageal pressure (Pes) asa surrogate for pleural pressure. We hypothesizedthat changes in Pes with increased intra-abdominalpressure (IAP) and atelectasis would result in distend-ing pressures that were not reflected by Pplat. Real-time awareness of Ptp alerts clinicians of the need toreduce or prevent VILI under circumstances that arenot included in the protective vigilance offered byARDSnet standards.
MATERIALS AND METHODS
Juvenile male Yorkshire pigs (n¼ 10) weighing 35–45 kg were pre-anesthetized with ketamine (20 mg/kg, IM) and xylazine (2 mg/kg, IM)10–15 min before intubation. Propofol (10 mg/mL at a rate of 25–90mL/h depending on need) was delivered intravenously (IV) via a Gem-ini Volumetric Infusion Pump (model PC-2TX; Imed Corp., San Diego,CA) for continuous anesthesia. The animals were ventilated with anAVEA ventilator (Viasys Health Care, Yorba Linda, CA) with 21%(Group 1) or 100% (Group 2) oxygen. Baseline ventilator settingswere tidal volume 8 mL/kg, PEEP 5 cmH2O, and respiratory rate 15breaths/min. Respiratory rate was adjusted to maintain arterial car-bon dioxide (PaCO2) between 35 and 45 cm H2O. Esophageal pressure(Pes) was measured with a Bicore monitor connected directly with theAVEA and a nasogastric esophageal balloon catheter (SmartCath Na-sogastric Pressure Monitoring Tug Set; Viasys Health Care, Palm
Springs, CA) positioned by pressure tracing (i.e., obvious cardiacinflections during expiration and a parallel rise and fall in Pes with air-way pressure) as described by Talmor et al. [11].
A left carotid arteriotomy was performed and a PiCCO Pulsiocath5 French catheter was inserted for blood gas measurements (GemPremier-3000; Instrumentation Laboratory Inc., Lexington, MA), sys-temic arterial blood pressure monitoring, and calculation of continu-ous cardiac output and extra vascular lung water (EVLW) (PulsionMedical Inc., East Brunswick, NJ). A double lumen catheter (MACtwo-lumen central venous access 7 or 8 French; Arrow International,Reading, PA) with Swan-Ganz inducer port was placed into the rightinternal jugular vein for fluid, anesthesia, and drug infusion. A sevenFrench flow-directed Swan-Ganz thermodilution catheter (EdwardsLife Science, LLC, Irvine CA) was passed through the inducer intothe pulmonary artery for mixed venous blood gas and O2 contentsampling along with continuous cardiac output (CO) determinations(Vigilance; Edwards Life Science, LLC, Irvine, CA). Blood pressureswere measured using transducers (open heart monitoring kit number46068-48; Hospira Inc, Lake Forest, IL) leveled with the rightatrium and recorded on a Hewlett-Packard monitor (model 56, PaloAlto, CA) with pressure (model M-1006BT), oxygen saturation (modelM-1029A), and ECG (model M-1002A) amplifiers.
An incision was made in the right groin and the bladder was ac-cessed in a retroperitoneal fashion to prevent leakage of CO2 duringinsufflation. A small incision was made in the bladder and a Foleycatheter with an inline pressure port (infection control 350 mL urinemeter Foley tray; Bardex I. C. Complete Care; C. R. Bard Inc., Coving-ton GA) was inserted and connected to a pressure transducer leveledto the mid-axillary line on the animal and to a Hewlett-Packard mon-itor (model 56) and amplifier (model M-1006BT) for measurement ofbladder pressure. A Veress needle (Stryker Endoscopy, Inc.) was in-serted midline in the abdomen (Group I only) and connected toa CO2 insufflator (16 L flow insufflator; Stryker Endoscopy, Inc.).The insufflator injected CO2 at a volume sufficient to maintain thepreset pressure (0–30 in 5 mm Hg increments) constant.
Protocol
Group I (High IAP, n¼ 5)
The animals were placed on the AVEA ventilator with 21% O2. Fol-lowing instrumentation, baseline hemodynamics [arterial (MAP),
TA
BL
E1
Resp
ira
tory
Pa
ra
mete
rs
IAP
Pp
lat
(cm
H20)
Pp
eak
(cm
H20)
Pm
ean
(cm
H20)
dP
aw
(cm
H20)
Pes
Pla
t(c
mH
20)
Pes
PE
EP
(cm
H20)
dP
es(c
mH
20)
Ptp
Pla
t(c
mH
20)
Ptp
PE
EP
(cm
H20)
Ccw
(mL
/cm
H20)
Cd
yn
(mL
/cm
H20)
Cst
at
(mL
/cm
H20)
019.2
60.6
20.6
60.5
8.4
60.2
15.4
60.6
16.3
61.9
9.2
61.6
7.4
60.7
4.2
62.4
-4.6
61.9
52.8
65.4
19.8
61.5
22.4
61.5
520.0
60.6
21.2
60.6
9.0
60.3
16.2
60.4
16.0
62.2
9.4
61.9
8.4
60.7
3.6
62.2
-4.8
61.9
44.8
64.1
18.5
61.4
21.4
61.5
10
24.0
60.7
25.4
60.9
10.8
60.7
20.2
60.7
20.9
61.5
9.3
61.6
12.4
61.3
3.8
62.2
-4.6
61.6
27.2
61.3
15.3
60.9
17.2
61.2
15
30.2
61.5
31.8
61.6
11.0
60.4
26.2
61.7
25.2
61.8
9.3
61.2
17.4
61.7
4.2
62.4
-4.8
61.5
20.2
61.0
12.0
60.8
12.8
60.6
20
35.0
61.0
36.6
61. 0
13.4
61.2
31.4
61.1
29.4
62.5
8.8
61.5
21.2
61.5
6.0
62.9
-4.0
61.5
15.4
60.7
9.8
60.6
10.8
60.5
25
41.2
62.3
41.8
62.4
12.6
60.5
36.8
62.4
31.4
62.8
8.6
60.6
25.6
62.9
6.8
62.9
-3.6
61.0
12.8
61.2
7.5
61.6
9.2
60.6
30
44.6
62.5
46.8
62.9
13.8
60.5
41.0
62.9
35.0
62.8
8.7
61.0
29.4
63.1
8.2
63.7
-3.6
61.1
11.6
60.9
8.0
60.4
8.2
60.4
IAP¼
intr
a-a
bd
omin
alp
ress
ure
;Pp
lat¼
pla
teau
pre
ssu
re;P
pea
k¼
pea
kp
ress
ure
;Pm
ean¼
mea
np
ress
ure
;dP
aw¼
chan
ge
inair
way
pre
ssu
rebet
wee
nen
d-i
nsp
irati
onan
den
d-
exp
irati
on;P
esP
lat¼
esop
hagea
lp
ress
ure
at
pla
teau
;Pes
PE
EP¼
esop
hagea
lp
ress
ure
at
PE
EP
;dP
es¼
chan
ge
ines
oph
agea
lp
ress
ure
bet
wee
nen
d-i
nsp
irati
onan
den
d-e
xp
irati
on;
Ptp
Pla
t¼
tran
spu
lmon
ary
pre
ssu
reat
pla
teau
;P
tpP
EE
P¼
tran
spu
lmon
ary
pre
ssu
reat
PE
EP
;C
cw¼
ches
tw
all
com
pli
an
ce;
Cd
yn¼
dyn
am
ics
com
pli
an
ce;
Cst
at¼
stati
cco
mp
lian
ce.
KUBIAK ET AL.: CHANGES IN TRANSPULMONARY PRESSURE e19
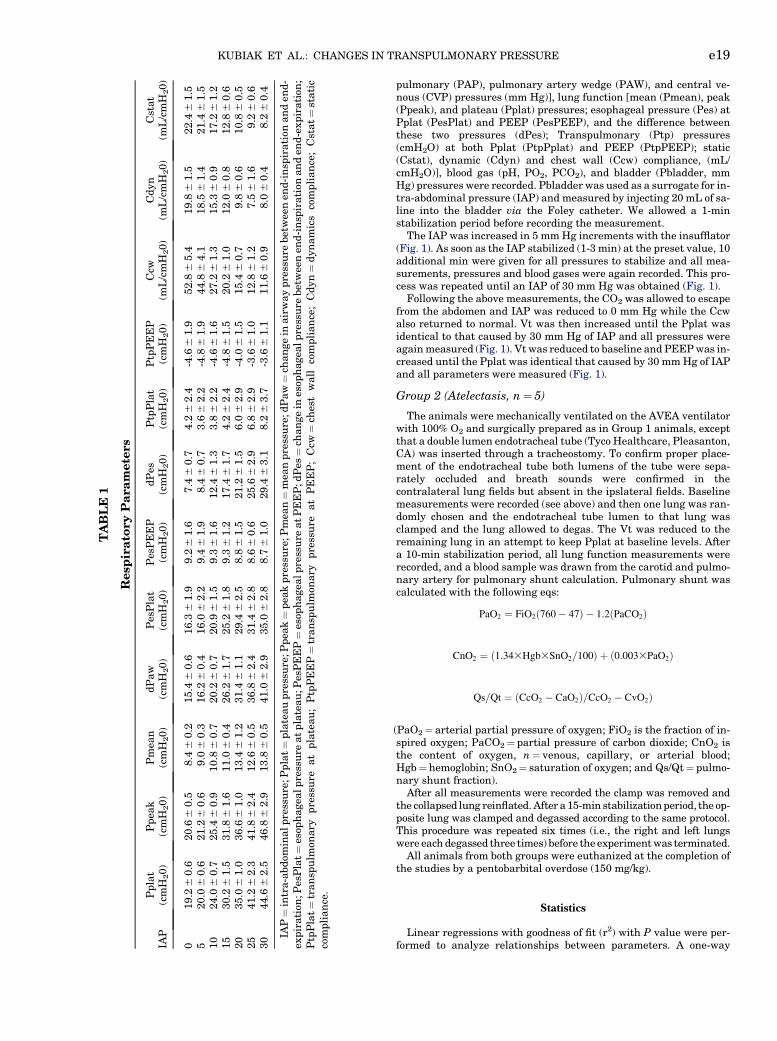
pulmonary (PAP), pulmonary artery wedge (PAW), and central ve-nous (CVP) pressures (mm Hg)], lung function [mean (Pmean), peak(Ppeak), and plateau (Pplat) pressures; esophageal pressure (Pes) atPplat (PesPlat) and PEEP (PesPEEP), and the difference betweenthese two pressures (dPes); Transpulmonary (Ptp) pressures(cmH2O) at both Pplat (PtpPplat) and PEEP (PtpPEEP); static(Cstat), dynamic (Cdyn) and chest wall (Ccw) compliance, (mL/cmH2O)], blood gas (pH, PO2, PCO2), and bladder (Pbladder, mmHg) pressures were recorded. Pbladder was used as a surrogate for in-tra-abdominal pressure (IAP) and measured by injecting 20 mL of sa-line into the bladder via the Foley catheter. We allowed a 1-minstabilization period before recording the measurement.
The IAP was increased in 5 mm Hg increments with the insufflator(Fig. 1). As soon as the IAP stabilized (1-3 min) at the preset value, 10additional min were given for all pressures to stabilize and all mea-surements, pressures and blood gases were again recorded. This pro-cess was repeated until an IAP of 30 mm Hg was obtained (Fig. 1).
Following the above measurements, the CO2 was allowed to escapefrom the abdomen and IAP was reduced to 0 mm Hg while the Ccwalso returned to normal. Vt was then increased until the Pplat wasidentical to that caused by 30 mm Hg of IAP and all pressures wereagain measured (Fig. 1). Vt was reduced to baseline and PEEP was in-creased until the Pplat was identical that caused by 30 mm Hg of IAPand all parameters were measured (Fig. 1).
Group 2 (Atelectasis, n¼ 5)
The animals were mechanically ventilated on the AVEA ventilatorwith 100% O2 and surgically prepared as in Group 1 animals, exceptthat a double lumen endotracheal tube (Tyco Healthcare, Pleasanton,CA) was inserted through a tracheostomy. To confirm proper place-ment of the endotracheal tube both lumens of the tube were sepa-rately occluded and breath sounds were confirmed in thecontralateral lung fields but absent in the ipslateral fields. Baselinemeasurements were recorded (see above) and then one lung was ran-domly chosen and the endotracheal tube lumen to that lung wasclamped and the lung allowed to degas. The Vt was reduced to theremaining lung in an attempt to keep Pplat at baseline levels. Aftera 10-min stabilization period, all lung function measurements wererecorded, and a blood sample was drawn from the carotid and pulmo-nary artery for pulmonary shunt calculation. Pulmonary shunt wascalculated with the following eqs:
PaO2 ¼ FiO2ð760� 47Þ � 1:2ðPaCO2Þ
CnO2 ¼ ð1:343Hgb3SnO2=100Þ þ ð0:0033PaO2Þ
Qs=Qt ¼ ðCcO2 � CaO2Þ=CcO2 � CvO2Þ
(PaO2¼ arterial partial pressure of oxygen; FiO2 is the fraction of in-spired oxygen; PaCO2¼ partial pressure of carbon dioxide; CnO2 isthe content of oxygen, n¼ venous, capillary, or arterial blood;Hgb¼ hemoglobin; SnO2¼ saturation of oxygen; and Qs/Qt¼ pulmo-nary shunt fraction).
After all measurements were recorded the clamp was removed andthe collapsed lung reinflated. After a 15-min stabilization period, the op-posite lung was clamped and degassed according to the same protocol.This procedure was repeated six times (i.e., the right and left lungswere each degassed three times) before the experiment was terminated.
All animals from both groups were euthanized at the completion ofthe studies by a pentobarbital overdose (150 mg/kg).
Statistics
Linear regressions with goodness of fit (r2) with P value were per-formed to analyze relationships between parameters. A one-way
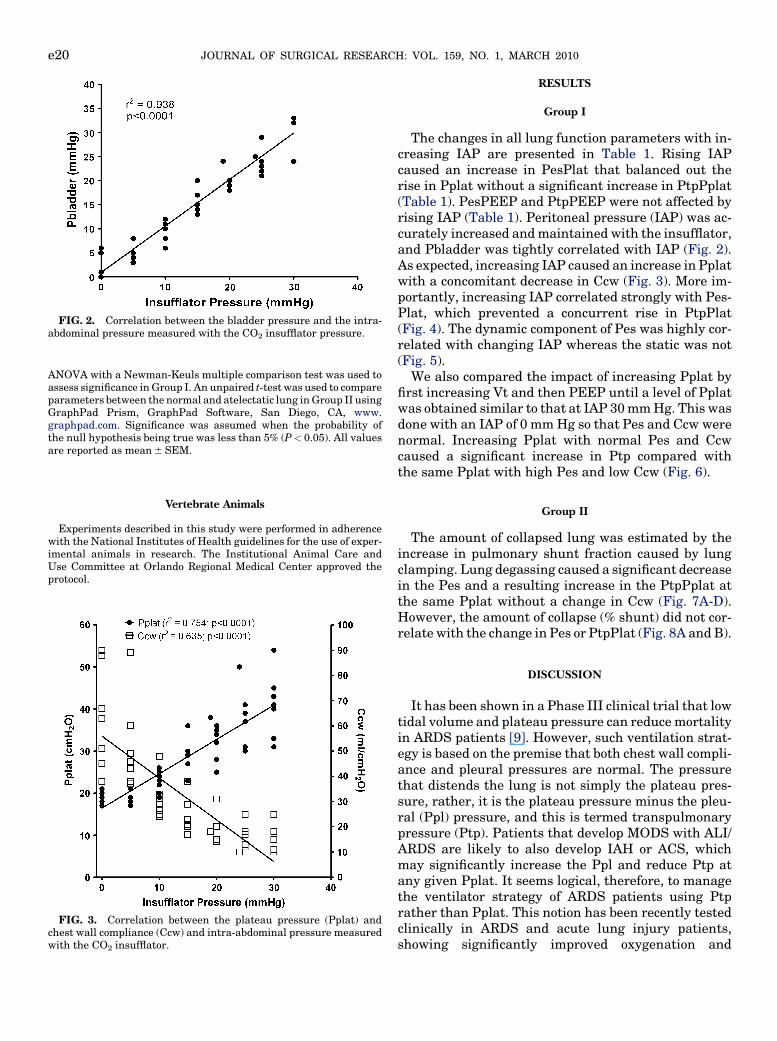
FIG. 2. Correlation between the bladder pressure and the intra-abdominal pressure measured with the CO2 insufflator pressure.
JOURNAL OF SURGICAL RESEARCH: VOL. 159, NO. 1, MARCH 2010e20
ANOVA with a Newman-Keuls multiple comparison test was used toassess significance in Group I. An unpaired t-test was used to compareparameters between the normal and atelectatic lung in Group II usingGraphPad Prism, GraphPad Software, San Diego, CA, www.graphpad.com. Significance was assumed when the probability ofthe null hypothesis being true was less than 5% (P< 0.05). All valuesare reported as mean 6 SEM.
Vertebrate Animals
Experiments described in this study were performed in adherencewith the National Institutes of Health guidelines for the use of exper-imental animals in research. The Institutional Animal Care andUse Committee at Orlando Regional Medical Center approved theprotocol.
FIG. 3. Correlation between the plateau pressure (Pplat) andchest wall compliance (Ccw) and intra-abdominal pressure measuredwith the CO2 insufflator.
RESULTS
Group I
The changes in all lung function parameters with in-creasing IAP are presented in Table 1. Rising IAPcaused an increase in PesPlat that balanced out therise in Pplat without a significant increase in PtpPplat(Table 1). PesPEEP and PtpPEEP were not affected byrising IAP (Table 1). Peritoneal pressure (IAP) was ac-curately increased and maintained with the insufflator,and Pbladder was tightly correlated with IAP (Fig. 2).As expected, increasing IAP caused an increase in Pplatwith a concomitant decrease in Ccw (Fig. 3). More im-portantly, increasing IAP correlated strongly with Pes-Plat, which prevented a concurrent rise in PtpPlat(Fig. 4). The dynamic component of Pes was highly cor-related with changing IAP whereas the static was not(Fig. 5).
We also compared the impact of increasing Pplat byfirst increasing Vt and then PEEP until a level of Pplatwas obtained similar to that at IAP 30 mm Hg. This wasdone with an IAP of 0 mm Hg so that Pes and Ccw werenormal. Increasing Pplat with normal Pes and Ccwcaused a significant increase in Ptp compared withthe same Pplat with high Pes and low Ccw (Fig. 6).
Group II
The amount of collapsed lung was estimated by theincrease in pulmonary shunt fraction caused by lungclamping. Lung degassing caused a significant decreasein the Pes and a resulting increase in the PtpPplat atthe same Pplat without a change in Ccw (Fig. 7A-D).However, the amount of collapse (% shunt) did not cor-relate with the change in Pes or PtpPlat (Fig. 8A and B).
DISCUSSION
It has been shown in a Phase III clinical trial that lowtidal volume and plateau pressure can reduce mortalityin ARDS patients [9]. However, such ventilation strat-egy is based on the premise that both chest wall compli-ance and pleural pressures are normal. The pressurethat distends the lung is not simply the plateau pres-sure, rather, it is the plateau pressure minus the pleu-ral (Ppl) pressure, and this is termed transpulmonarypressure (Ptp). Patients that develop MODS with ALI/ARDS are likely to also develop IAH or ACS, whichmay significantly increase the Ppl and reduce Ptp atany given Pplat. It seems logical, therefore, to managethe ventilator strategy of ARDS patients using Ptprather than Pplat. This notion has been recently testedclinically in ARDS and acute lung injury patients,showing significantly improved oxygenation and

FIG. 4. Correlation between esophageal and transpulmonarypressure with intra-abdominal pressure measured with the CO2
insufflator.
FIG. 6. Measurement of plateau pressure (Pplat), esophagealpressure at Pplat (PesPlat), transpulmonary pressure at Pplat(PtpPplat) and chest wall compliance (Ccw) at intra-abdominal pres-sure (IAP)¼ 30 mm Hg and at tidal volume (Vt) and positive end-ex-piratory pressure (PEEP) each raised to a level sufficient to elevatePplat to a level similar to IAP¼ 30 mm Hg. IAP remained at 0 mmHg as the Vt and PEEP were increased. The red horizontal line iden-tifies the Pplat at IAP¼ 30 mm Hg. Data Mean 6 SEM. *P< 0.05 ver-sus both other groups; yP< 0.05 between all groups.
KUBIAK ET AL.: CHANGES IN TRANSPULMONARY PRESSURE e21
compliance when Pes was used to estimate Ptp, com-pared with patients treated with the current standardof care (ARDSnet protocol) [11].
Our study demonstrated that the measurement ofesophageal pressure with clinically available equip-ment accurately determined Ptp and allowed the iden-tification of the known physiologic relationshipsbetween Pplat, Ccw, Ppl, and Ptp. Rising IAP causesthe push of abdominal contents against the diaphragm,manifested as a rise in Pplat and a fall in Ccw.
FIG. 5. Correlation between the esophageal pressure measuredat PEEP (PesPEEP) and the difference between the esophageal pres-sure measured at end-expiratory and end-inspiratory pressure (dPes)with intra-abdominal pressure measured with the CO2 insufflator.The dPes has been described as dynamic Pes and the PesPEEP asthe static Pes [19].
Increasing IAP also increased esophageal pressure(the surrogate measurement of Ppl), however, trans-pulmonary pressure did not correlate with increasingIAP. This is noteworthy because as Pplat rose, so didPpl and, thus, Ptp did not increase significantly.PtpPEEP was negative throughout the study, consis-tent with a recent clinical study [11] and representslung collapse secondary to insufficient PEEP. It is im-portant to note that several factors seen clinically canaugment the changes seen in this study. Abdominal as-cites is less distensible than the gas used, which maylead to larger elevations in IAP and, thus, Pplat andPtp. Body wall edema can decrease the compliance ofthe thorax and abdomen, also causing larger elevationsin pressure.
Another concept that was supported by esophagealpressure monitoring was the difference betweendynamic and static Pes [19]. It has recently been shownthat differentiating between static and dynamic compo-nents of esophageal pressure may be important to clin-ical assessment of patients with ACS [19]. Valenza et al.defined static Pes as Pes at PEEP (PesPEEP) anddynamic Pes as the difference between Pes at end-expi-ratory and end-inspiratory pressure (dPes) [19]. Theydemonstrated that the dynamic component of esopha-geal pressure (dPes) was highly correlated with IAP,
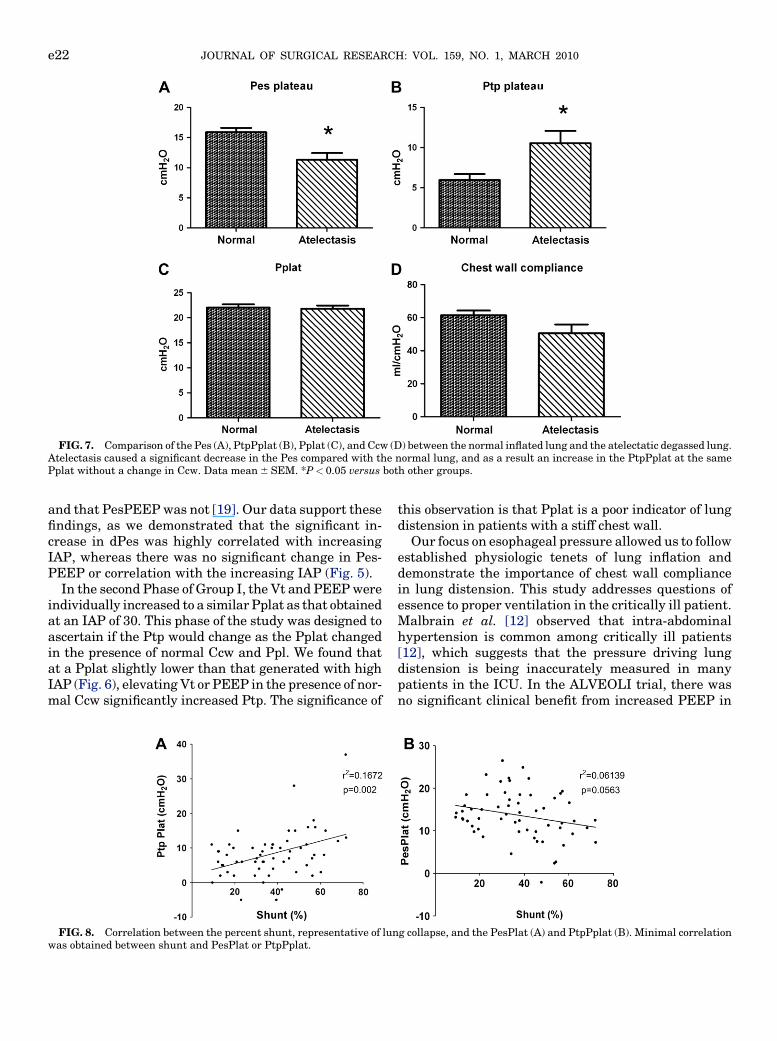
FIG. 7. Comparison of the Pes (A), PtpPplat (B), Pplat (C), and Ccw (D) between the normal inflated lung and the atelectatic degassed lung.Atelectasis caused a significant decrease in the Pes compared with the normal lung, and as a result an increase in the PtpPplat at the samePplat without a change in Ccw. Data mean 6 SEM. *P< 0.05 versus both other groups.
JOURNAL OF SURGICAL RESEARCH: VOL. 159, NO. 1, MARCH 2010e22
and that PesPEEP was not [19]. Our data support thesefindings, as we demonstrated that the significant in-crease in dPes was highly correlated with increasingIAP, whereas there was no significant change in Pes-PEEP or correlation with the increasing IAP (Fig. 5).
In the second Phase of Group I, the Vt and PEEP wereindividually increased to a similar Pplat as that obtainedat an IAP of 30. This phase of the study was designed toascertain if the Ptp would change as the Pplat changedin the presence of normal Ccw and Ppl. We found thatat a Pplat slightly lower than that generated with highIAP (Fig. 6), elevating Vt or PEEP in the presence of nor-mal Ccw significantly increased Ptp. The significance of
FIG. 8. Correlation between the percent shunt, representative of lunwas obtained between shunt and PesPlat or PtpPplat.
this observation is that Pplat is a poor indicator of lungdistension in patients with a stiff chest wall.
Our focus on esophageal pressure allowed us to followestablished physiologic tenets of lung inflation anddemonstrate the importance of chest wall compliancein lung distension. This study addresses questions ofessence to proper ventilation in the critically ill patient.Malbrain et al. [12] observed that intra-abdominalhypertension is common among critically ill patients[12], which suggests that the pressure driving lungdistension is being inaccurately measured in manypatients in the ICU. In the ALVEOLI trial, there wasno significant clinical benefit from increased PEEP in
g collapse, and the PesPlat (A) and PtpPplat (B). Minimal correlation

KUBIAK ET AL.: CHANGES IN TRANSPULMONARY PRESSURE e23
patients with ARDS [20], even though many other stud-ies have shown that PEEP is protective [21, 22]. It ispossible that the negative results from the ALVEOLIstudy were due to application of PEEP without regardto chest wall compliance and transpulmonary pressure.Knowledge of the patient’s pleural pressure allowsaccurate calculation of the transpulmonary pressure,which would avoid both over- and under-distension ofthe lung. Avoiding over-distension would reduce VILIcaused by volutrauma, and avoiding under-distensionwould lead to better oxygenation and ventilation ofthe patient.
Although the literature describing the impact of atel-ectasis on pleural pressure is scant, it seems intuitivethat lung collapse should cause a decrease in Ppl byincreasing the negative pressure in the chest, and inthis study we have demonstrated this to be true. Thereduction in Ppl effected an increase in PtpPplat atthe same Pplat, suggesting that PtpPplat values pro-vide an accurate measurement of the lung distendingpressure in the presence of significant atelectasis. Sur-factant deactivation resulting in atelectasis is a hall-mark of ARDS. Since patients with ARDS are at highrisk for secondary VILI, the possibility exists that pla-teau pressure may not be a good measure of the lungdistending pressure and, notably, that volutraumamay occur at lung pressures considered safe [9].
The amount of lung collapse did not closely correlatewith the PesPlat or the PtpPlat. This could be due to thelimitations of using % shunt as a parameter to repre-sent amount of collapse. Physiologic mechanisms existto prevent blood from flowing through atelectatic andnon-ventilated regions of the lung; alveolar hypoxiaresulting from atelectasis causes pulmonary vasocon-striction preventing ventilation-perfusion mismatch-ing and arterial hypoxia [23]. This vasoconstrictionoccurs to varying levels in individual animals, resultingin wide range of intrapulmonary shunting. The % shuntcould therefore inaccurately estimate the amount oflung collapse. It is known, though, that larger areas ofcollapse cause a less effective vascular response, result-ing in more intrapulmonary shunting [23].
In conclusion, we were able to successfully determinereal-time esophageal pressure during ventilatorymaneuvers in a large animal model using clinicallyavailable equipment. Our focus on physiologic relation-ships between IAP, Pplat, Ccw, Pes, and Ptp usingesophageal pressure catheters demonstrated theirvalue in assuring safe ventilation in the critical care pa-tient. This study also demonstrated that using Pplat toestimate the distending pressure of the lung is highlyinaccurate in the presence of a stiff chest wall or withatelectasis. From this we can infer that esophagealpressure should be routinely measured in critically illpatients at risk for IAH or atelectasis to prevent either
over- or under-distension of the lung while attemptingprotective mechanical ventilation.
ACKNOWLEDGMENTS
The authors thank Edward Sivak, M.D. for his comments and crit-icisms of this manuscript. This study was funded in part by a grantfrom Viasys Healthcare Inc.
REFERENCES
1. Matsuda N, Hattori Y. Systemic inflammatory response syn-drome (SIRS): Molecular pathophysiology and gene therapy.J Pharmacol Sci 2006;101:189.
2. Jaimes F, Garces J, Cuervo J, et al. The systemic inflammatoryresponse syndrome (SIRS) to identify infected patients in theemergency room. Intensive Care Med 2003;29:1368.
3. Baue AE. MOF, MODS, and Sirs: What is in a name or an acronym?Shock 2006;26:438.
4. Baue AE. Sepsis, systemic inflammatory response syndrome,multiple organ dysfunction syndrome, and multiple organ fail-ure: Are trauma surgeons lumpers or splitters? J Trauma2003;55:997.
5. Baue AE. Sepsis, multi-organ dysfunction syndrome (MODS)and multiple organ failure (MOF). Prevention is better thantreatment. Minerva Anestesiol 1999;65:477. discussion 481.
6. Fujishima S, Morisaki H, Ishizaka A, et al. Neutrophil elastaseand systemic inflammatory response syndrome in the initiationand development of acute lung injury among critically illpatients. Biomed Pharmacother 2008;62:333.
7. Gajic O, Frutos-Vivar F, Esteban A, et al. Ventilator settings asa risk factor for acute respiratory distress syndrome in mechan-ically ventilated patients. Intensive Care Med 2005;31:922.
8. Tremblay LN, Slutsky AS. Ventilator-induced lung injury: Fromthe bench to the bedside. Intensive Care Med 2006;32:24.
9. Network ARDS. Ventilation with lower tidal volumes as com-pared with traditional tidal volumes for acute lung injury andthe acute respiratory distress syndrome. N Engl J Med 2000;342:1301.
10. Hess DR, Bigatello LM. The chest wall in acute lung injury/acuterespiratory distress syndrome. Curr Opin Crit Care 2008;14:94.
11. Talmor D, Sarge T, Malhotra A, et al. Mechanical ventilationguided by esophageal pressure in acute lung injury. N Engl JMed 2008;359:2095.
12. Malbrain ML, Chiumello D, Pelosi P, et al. Prevalence of in-tra-abdominal hypertension in critically ill patients: A multi-center epidemiological study. Intensive Care Med 2004;30:822.
13. Kimball EJ, Rollins MD, Mone MC, et al. Survey of intensive carephysiciansontherecognitionandmanagementof intra-abdominalhypertension and abdominal compartment syndrome. Crit CareMed 2006;34:2340.
14. Peralta R, Hojman H. Abdominal compartment syndrome. IntAnesthesiol Clin 2001;39:75.
15. Malbrain ML, Cheatham ML, Kirkpatrick A, et al. Results fromthe International Conference of Experts on Intra-abdominalHypertension and Abdominal Compartment Syndrome. I.Definitions. Intensive Care Med 2006;32:1722.
16. Pelosi P, Quintel M, Malbrain ML. Effect of intra-abdominalpressure on respiratory mechanics. Acta Clin Belg 2007;1(Suppl 1):S78.
17. Cogo PE, Toffolo GM, Ori C, et al. Surfactant disaturated-phos-phatidylcholine kinetics in acute respiratory distress syndromeby stable isotopes and a two compartment model. Respir Res2007;8:13.

JOURNAL OF SURGICAL RESEARCH: VOL. 159, NO. 1, MARCH 2010e24
18. Ford GT, Bradley CA, Anthonisen NR. Forces involved in lobaratelectasis in intact dogs. J Appl Physiol 1980;48:29.
19. Valenza F, Chevallard G, Porro GA, et al. Static and dynamiccomponents of esophageal and central venous pressure dur-ing intra-abdominal hypertension. Crit Care Med 2007;35:1575.
20. Brower RG, Lanken PN, MacIntyre N, et al. Higher versus lowerpositive end-expiratory pressures in patients with the acuterespiratory distress syndrome. N Engl J Med 2004;351:327.
21. Amato MB, Barbas CS, Medeiros DM, et al. Effect of a protective-ventilation strategy on mortality in the acute respiratorydistress syndrome. N Engl J Med 1998;338:347.
22. Ranieri VM, Suter PM, Tortorella C, et al. Effect of mechanicalventilation on inflammatory mediators in patients with acute re-spiratory distress syndrome: A randomized controlled trial.JAMA 1999;282:54.
23. Peroni DG, Boner AL. Atelectasis: Mechanisms, diagnosis andmanagement. Paediatr Respir Rev 2000;1:274.