
Plasma Concentration of Amino-Terminal Pro-Brain Natriuretic Peptide in Chronic Heart Failure:...
12
doi:10.1016/j.jacc.2009.06.041 2009;54;1850-1859 J. Am. Coll. Cardiol. Wikstrand, on behalf of the CORONA Study Group Naresh Ranjith, Dirk J. van Veldhuisen, Finn Waagstein, Hans Wedel, John Lindberg, Dunselman, Cândida Fonseca, Åke Hjalmarson, Jerzy Korewicki, Magnus John G.F. Cleland, John J.V. McMurray, John Kjekshus, Jan H. Cornel, Peter Rosuvastatin Multinational Trial in Heart Failure) With the Effects of Rosuvastatin: A Report From CORONA (Controlled Chronic Heart Failure: Prediction of Cardiovascular Events and Interaction Plasma Concentration of Amino-Terminal Pro-Brain Natriuretic Peptide in This information is current as of May 18, 2011 http://content.onlinejacc.org/cgi/content/full/54/20/1850 located on the World Wide Web at: The online version of this article, along with updated information and services, is by on May 18, 2011 content.onlinejacc.org Downloaded from
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Plasma Concentration of Amino-Terminal Pro-Brain Natriuretic Peptide in Chronic Heart Failure:...

doi:10.1016/j.jacc.2009.06.041 2009;54;1850-1859 J. Am. Coll. Cardiol.
Wikstrand, on behalf of the CORONA Study Group Naresh Ranjith, Dirk J. van Veldhuisen, Finn Waagstein, Hans Wedel, John
Lindberg,Dunselman, Cândida Fonseca, Åke Hjalmarson, Jerzy Korewicki, Magnus John G.F. Cleland, John J.V. McMurray, John Kjekshus, Jan H. Cornel, Peter
Rosuvastatin Multinational Trial in Heart Failure)With the Effects of Rosuvastatin: A Report From CORONA (Controlled
Chronic Heart Failure: Prediction of Cardiovascular Events and Interaction Plasma Concentration of Amino-Terminal Pro-Brain Natriuretic Peptide in
This information is current as of May 18, 2011
http://content.onlinejacc.org/cgi/content/full/54/20/1850located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by on May 18, 2011 content.onlinejacc.orgDownloaded from

FKsCeLsonocC
Journal of the American College of Cardiology Vol. 54, No. 20, 2009© 2009 by the American College of Cardiology Foundation ISSN 0735-1097/09/$36.00P
Heart Failure
Plasma Concentration of Amino-TerminalPro-Brain Natriuretic Peptide in ChronicHeart Failure: Prediction of Cardiovascular Eventsand Interaction With the Effects of RosuvastatinA Report From CORONA (ControlledRosuvastatin Multinational Trial in Heart Failure)John G. F. Cleland, MD,* John J. V. McMurray, MD,† John Kjekshus, MD, PHD,‡Jan H. Cornel, MD,§ Peter Dunselman, MD, PHD,� Cândida Fonseca, MD,¶Åke Hjalmarson, MD, PHD,# Jerzy Korewicki, MD, PHD,** Magnus Lindberg, MSC,††Naresh Ranjith, MD,‡‡ Dirk J. van Veldhuisen, MD, PHD,§§ Finn Waagstein, MD, PHD,��Hans Wedel, PHD,¶¶ John Wikstrand, MD, PHD,## on behalf of the CORONA Study GroupKingston-upon-Hull and Glasgow, United Kingdom; Oslo, Norway; Alkmaar, Breda, and Groningen,the Netherlands; Lisbon, Portugal; Göteborg and Mölndal, Sweden; Warsaw, Poland; and Durban, South Africa
Objectives We investigated whether plasma amino-terminal pro-brain natriuretic peptide (NT-proBNP), a marker of cardiacdysfunction and prognosis measured in CORONA (Controlled Rosuvastatin Multinational Trial in Heart Failure),could be used to identify the severity of heart failure at which statins become ineffective.
Background Statins reduce cardiovascular morbidity and mortality in many patients with ischemic heart disease but not, overall,those with heart failure. There must be a transition point at which treatment with a statin becomes futile.
Methods In CORONA, patients with heart failure, reduced left ventricular ejection fraction, and ischemic heart diseasewere randomly assigned to 10 mg/day rosuvastatin or placebo. The primary composite outcome was cardiovas-cular death, nonfatal myocardial infarction, or stroke.
Results Of 5,011 patients enrolled, NT-proBNP was measured in 3,664 (73%). The midtertile included values between103 pmol/l (868 pg/ml) and 277 pmol/l (2,348 pg/ml). Log NT-proBNP was the strongest predictor (per logunit) of every outcome assessed but was strongest for death from worsening heart failure (hazard ratio [HR]:1.99; 95% confidence interval [CI]: 1.71 to 2.30), was weaker for sudden death (HR: 1.69; 95% CI: 1.52 to1.88), and was weakest for atherothrombotic events (HR: 1.24; 95% CI: 1.10 to 1.40). Patients in the lowesttertile of NT-proBNP had the best prognosis and, if assigned to rosuvastatin rather than placebo, had a greaterreduction in the primary end point (HR: 0.65; 95% CI: 0.47 to 0.88) than patients in the other tertiles (heteroge-neity test, p � 0.0192). This reflected fewer atherothrombotic events and sudden deaths with rosuvastatin.
Conclusions Patients with heart failure due to ischemic heart disease who have NT-proBNP values �103 pmol/l (868pg/ml) may benefit from rosuvastatin. (J Am Coll Cardiol 2009;54:1850–9) © 2009 by the AmericanCollege of Cardiology Foundation
ublished by Elsevier Inc. doi:10.1016/j.jacc.2009.06.041
WDrDRfhoAC
rom the *Department of Cardiology, University of Hull, Kingston-upon-Hull, Unitedingdom; †British Heart Foundation Glasgow Cardiovascular Research Centre, Univer-
ity of Glasgow, Glasgow, United Kingdom; ‡Rikshospitalet, Oslo, Norway; §Medischentrum Alkmaar, Alkmaar, the Netherlands; �Amphia Ziekenhuis, Breda, the Neth-
rlands; ¶Hospital de S. Francisco Xavier, Lisbon, Portugal; #Institute of Heart andung Diseases, Göteborg, Sweden; **Institute of Cardiology, Warsaw, Poland; ††Bio-
tatistics Department, AstraZeneca, Mölndal, Sweden; ‡‡Nelson R. Mandela Schoolf Medicine, Durban, South Africa; §§University Medical Center Groningen, Gro-ingen, the Netherlands; � �University of Göteborg, Göteborg, Sweden; ¶¶Nordic Schoolf Public Health, Göteborg, Sweden; and the ##Wallenberg Laboratory for Cardiovas-
ular Research, Göteborg, Sweden. This study was supported by AstraZeneca. Drs.leland, Hjalmarson, Kjekshus, Korewicki, McMurray, Ranjith, van Veldhuisen, acontent.onlinejDownloaded from
aagstein, and Fonseca have been paid lecture fees by AstraZeneca. Drs. Cornel,unselman, Hjalmarson, Kjekshus, McMurray, van Veldhuisen, Waagstein, Ko-
ewicki, and Wedel have received consulting or advisory board fees from AstraZeneca.r. Fonseca has received consulting or advisory board fees from AstraZeneca andoche. Drs. Hjalmarson, McMurray, and Wikstrand have received research grants
rom AstraZeneca. Mr. Lindberg is an employee of AstraZeneca. Dr. van Veldhuisenas received research grants from AstraZeneca and Roche. Dr. Waagstein reportswning shares in AstraZeneca. Dr. Wikstrand is a former Senior Medical Advisor atstraZeneca, now part time consultant. For disclosures for the other members of theORONA study group see Kjekshus et al. (11).
Manuscript received February 19, 2009; revised manuscript received June 15, 2009,ccepted June 29, 2009.
by on May 18, 2011 acc.org

Btwepov
ewte(pdosdPfneaisuSCboWNmtpp
M
Dcpodwoecoetp
hNt
eptcttlir
tuwituB
issAbtwm
rponaocMarmlaectppradd
1851JACC Vol. 54, No. 20, 2009 Cleland et al.November 10, 2009:1850–9 CORONA: NT-proBNP and Rosuvastatin
-type natriuretic peptide and amino-terminal pro-brain na-riuretic peptide (NT-proBNP) predict mortality in patientsith heart failure, whether (1–5) or not (6) left ventricular
jection fraction (LVEF) is reduced. Indeed, B-type natriureticeptide and NT-proBNP have usually proved superior to anyther variable in predicting outcome (7,8), and their prognosticalue may extend far beyond heart failure (8–10).
See page 1860
There is abundant evidence that statins reduce vascularvents and improve prognosis in a broad range of patientsith or at increased risk of atherosclerosis (10). However,
he prognosis of some patient groups at very high risk ofvents may not be amenable to modification with statins11–13). This may be because statins are ineffective in suchatients or because disease progression is not driven pre-ominantly by progression of atheroma. Most clinical trialsf statins have excluded patients with overt heart failure, buteveral suggested that they could reduce the risk of theevelopment of heart failure in a patient (14,15). The Heartrotection Study did not record which patients had heart
ailure at baseline but did measure NT-proBNP using aoncommercial assay (10,16). The risk of cardiovascularvents increased as NT-proBNP increased, and, therefore,lthough the relative benefits of simvastatin declined withncreasing plasma concentrations, the absolute benefits wereimilar regardless of the NT-proBNP level (10). However,nlike in CORONA, few patients in the Heart Protectiontudy had high plasma concentrations of NT-proBNP. InORONA, rosuvastatin reduced the rate of atherothrom-otic events and of cardiovascular hospitalizations, but noverall effect of rosuvastatin on mortality was demonstrated.
e investigated the possibility of a transition point forT-proBNP below which patients with heart failure had aore favorable outcome and greater benefit from rosuvas-
atin. We also investigated the ability of NT-proBNP toredict prognosis and mode of death in a large group ofatients with chronic heart failure.
ethods
etailed accounts of the design, enrollment, and patientharacteristics of CORONA have been reported. In brief,atients 60 years of age or older with, in the investigators’pinion, stable, symptomatic heart failure, ischemic heartisease, and a reduced LVEF were eligible, provided theyere not taking lipid-lowering drugs. Patients with a historyf intolerance to statins; those experiencing a recent vascularvent; those with severe uncorrected valve disease, a serumreatinine of �2.5 mg/dl (221 �mol/l), or any conditionther than heart failure that would substantially reduce lifexpectancy or limit compliance with the protocol; and thoseaking �80% of dispensed placebo tablets during the run-in
eriod were excluded. For most purposes, only patients who lcontent.onlinejDownloaded from
ad a baseline measurement ofT-proBNP were included in
his analysis.The trial was approved by the
thics committee at each of thearticipating hospitals, and pa-ients gave written informedonsent. Eligible patients werereated with single-blind placeboo demonstrate compliance for asong as 4 weeks before random-zation. Patients were randomly assigned, double-blind, toeceive 10-mg rosuvastatin or matching placebo once daily.
Baseline assessments including symptoms, medical his-ory, examination, and documentation of a low LVEF,sually by echocardiography, were recorded. Blood testsere done at the end of the run-in period before random-
zation. Patients were not required to rest or fast beforeesting. NT-proBNP was analyzed at a central laboratorysing a commercially available assay (Roche Diagnostics,asel, Switzerland).The steering committee designed the trial and supervised
ts conduct in collaboration with representatives of thetudy’s sponsor, AstraZeneca (Mölndal, Sweden). Theponsor collected the trial data.nalysis plan. Variables included in the analyses are showny tertile of NT-proBNP in Table 1. Continuous variableshat were not normally distributed, such as NT-proBNP,ere expressed as median and interquartile range, and forodeling purposes, a natural log transformation was used.The main objective was to investigate the effects of
osuvastatin according to the plasma concentration of NT-roBNP for various cardiovascular outcomes. The primaryutcome was the composite of cardiovascular mortality,onfatal myocardial infarction (MI), or nonfatal stroke,nalyzed as the time to the first event. The secondaryutcomes were (in listed order): all-cause mortality; anyoronary event (defined as sudden death, fatal or nonfatal
I, coronary revascularization, ventricular defibrillation byn implantable defibrillator, resuscitation from cardiac ar-est, or hospitalization for unstable angina); cardiovascularortality (cause-specific cardiovascular death was also ana-
yzed); and total number (episodes) of hospitalizations (forll causes, cardiovascular causes, unstable angina, and wors-ning heart failure). We also included 2 additional post hocomposite outcomes: death from any cause or hospitaliza-ion for worsening heart failure, which is commonly re-orted in heart failure trials, and an atherothrombotic endoint (fatal or nonfatal MI or fatal or nonfatal nonhemor-hagic stroke) constituting events likely to be related totherosclerothrombosis rather than myocardial disease. Theefinition and adjudication of all outcomes were previouslyescribed in detail (14).Cox proportional hazards models were used to calcu-
Abbreviationsand Acronyms
HR � hazard ratio
LVEF � left ventricularejection fraction
MI � myocardial infarction
NT-proBNP � amino-terminal pro-brainnatriuretic peptide
ate the hazard ratios (HRs) and 95 by on May 18, 2011 acc.org
% confidence intervals
(tCji
(tdF
B
Vm
eN ork Heac
1852 Cleland et al. JACC Vol. 54, No. 20, 2009CORONA: NT-proBNP and Rosuvastatin November 10, 2009:1850–9
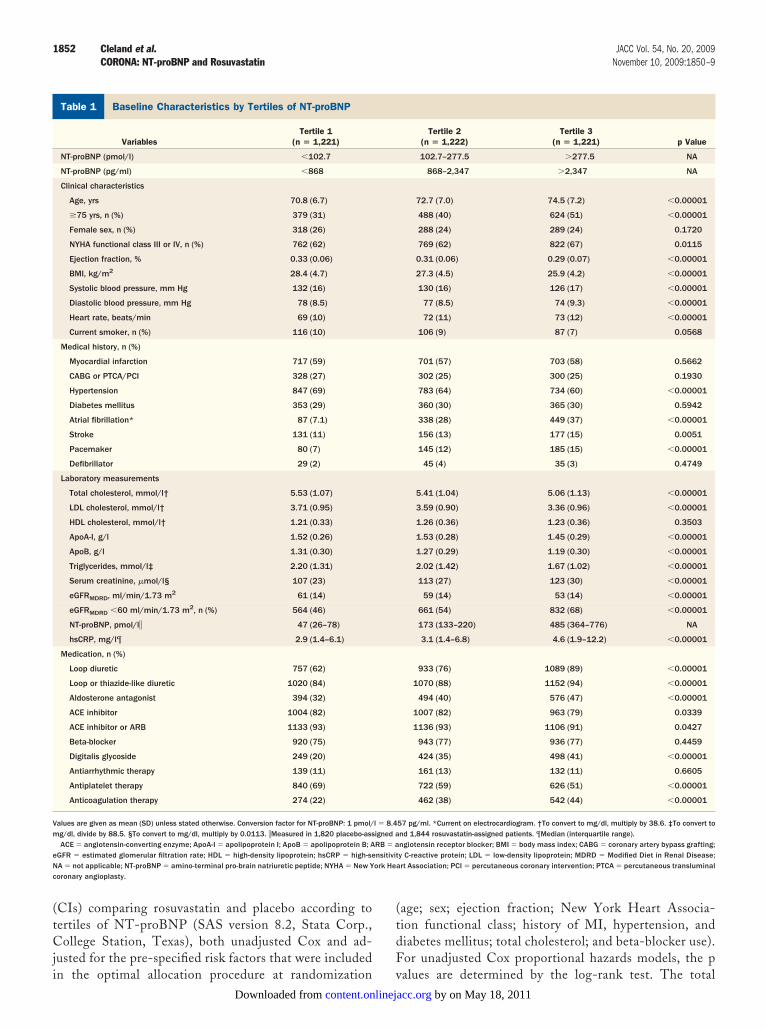
CIs) comparing rosuvastatin and placebo according toertiles of NT-proBNP (SAS version 8.2, Stata Corp.,ollege Station, Texas), both unadjusted Cox and ad-
usted for the pre-specified risk factors that were included
aseline Characteristics by Tertiles of NT-proBNPTable 1 Baseline Characteristics by Tertiles of NT-proBNP
VariablesTertile 1
(n � 1,221)
NT-proBNP (pmol/l) �102.7
NT-proBNP (pg/ml) �868
Clinical characteristics
Age, yrs 70.8 (6.7)
�75 yrs, n (%) 379 (31)
Female sex, n (%) 318 (26)
NYHA functional class III or IV, n (%) 762 (62)
Ejection fraction, % 0.33 (0.06)
BMI, kg/m2 28.4 (4.7)
Systolic blood pressure, mm Hg 132 (16)
Diastolic blood pressure, mm Hg 78 (8.5)
Heart rate, beats/min 69 (10)
Current smoker, n (%) 116 (10)
Medical history, n (%)
Myocardial infarction 717 (59)
CABG or PTCA/PCI 328 (27)
Hypertension 847 (69)
Diabetes mellitus 353 (29)
Atrial fibrillation* 87 (7.1)
Stroke 131 (11)
Pacemaker 80 (7)
Defibrillator 29 (2)
Laboratory measurements
Total cholesterol, mmol/l† 5.53 (1.07)
LDL cholesterol, mmol/l† 3.71 (0.95)
HDL cholesterol, mmol/l† 1.21 (0.33)
ApoA-I, g/l 1.52 (0.26)
ApoB, g/l 1.31 (0.30)
Triglycerides, mmol/l‡ 2.20 (1.31)
Serum creatinine, �mol/l§ 107 (23)
eGFRMDRD, ml/min/1.73 m2 61 (14)
eGFRMDRD �60 ml/min/1.73 m2, n (%) 564 (46)
NT-proBNP, pmol/l� 47 (26–78)
hsCRP, mg/l¶ 2.9 (1.4–6.1)
Medication, n (%)
Loop diuretic 757 (62)
Loop or thiazide-like diuretic 1020 (84)
Aldosterone antagonist 394 (32)
ACE inhibitor 1004 (82)
ACE inhibitor or ARB 1133 (93)
Beta-blocker 920 (75)
Digitalis glycoside 249 (20)
Antiarrhythmic therapy 139 (11)
Antiplatelet therapy 840 (69)
Anticoagulation therapy 274 (22)
alues are given as mean (SD) unless stated otherwise. Conversion factor for NT-proBNP: 1 pmol/g/dl, divide by 88.5. §To convert to mg/dl, multiply by 0.0113. �Measured in 1,820 placebo-assACE � angiotensin-converting enzyme; ApoA-I � apolipoprotein I; ApoB � apolipoprotein B; A
GFR � estimated glomerular filtration rate; HDL � high-density lipoprotein; hsCRP � high-seA � not applicable; NT-proBNP � amino-terminal pro-brain natriuretic peptide; NYHA � New Yoronary angioplasty.
n the optimal allocation procedure at randomization vcontent.onlinejDownloaded from
age; sex; ejection fraction; New York Heart Associa-ion functional class; history of MI, hypertension, andiabetes mellitus; total cholesterol; and beta-blocker use).or unadjusted Cox proportional hazards models, the p
Tertile 2(n � 1,222)
Tertile 3(n � 1,221) p Value
102.7–277.5 �277.5 NA
868–2,347 �2,347 NA
72.7 (7.0) 74.5 (7.2) �0.00001
488 (40) 624 (51) �0.00001
288 (24) 289 (24) 0.1720
769 (62) 822 (67) 0.0115
0.31 (0.06) 0.29 (0.07) �0.00001
27.3 (4.5) 25.9 (4.2) �0.00001
130 (16) 126 (17) �0.00001
77 (8.5) 74 (9.3) �0.00001
72 (11) 73 (12) �0.00001
106 (9) 87 (7) 0.0568
701 (57) 703 (58) 0.5662
302 (25) 300 (25) 0.1930
783 (64) 734 (60) �0.00001
360 (30) 365 (30) 0.5942
338 (28) 449 (37) �0.00001
156 (13) 177 (15) 0.0051
145 (12) 185 (15) �0.00001
45 (4) 35 (3) 0.4749
5.41 (1.04) 5.06 (1.13) �0.00001
3.59 (0.90) 3.36 (0.96) �0.00001
1.26 (0.36) 1.23 (0.36) 0.3503
1.53 (0.28) 1.45 (0.29) �0.00001
1.27 (0.29) 1.19 (0.30) �0.00001
2.02 (1.42) 1.67 (1.02) �0.00001
113 (27) 123 (30) �0.00001
59 (14) 53 (14) �0.00001
661 (54) 832 (68) �0.00001
173 (133–220) 485 (364–776) NA
3.1 (1.4–6.8) 4.6 (1.9–12.2) �0.00001
933 (76) 1089 (89) �0.00001
1070 (88) 1152 (94) �0.00001
494 (40) 576 (47) �0.00001
1007 (82) 963 (79) 0.0339
1136 (93) 1106 (91) 0.0427
943 (77) 936 (77) 0.4459
424 (35) 498 (41) �0.00001
161 (13) 132 (11) 0.6605
722 (59) 626 (51) �0.00001
462 (38) 542 (44) �0.00001
57 pg/ml. *Current on electrocardiogram. †To convert to mg/dl, multiply by 38.6. ‡To convert tond 1,844 rosuvastatin-assigned patients. ¶Median (interquartile range).ngiotensin receptor blocker; BMI � body mass index; CABG � coronary artery bypass grafting;y C-reactive protein; LDL � low-density lipoprotein; MDRD � Modified Diet in Renal Disease;rt Association; PCI � percutaneous coronary intervention; PTCA � percutaneous transluminal
l � 8.4igned aRB � ansitivit
alues are determined by the log-rank test. The total by on May 18, 2011 acc.org
nt
pmtpepfHchfm
R
ONhpwoaPNwmlildwb
csNipf�ipat
wtNwwaEcLrpmfCenl(am[2s[CNmb0Ip0iteabdotwr
1853JACC Vol. 54, No. 20, 2009 Cleland et al.November 10, 2009:1850–9 CORONA: NT-proBNP and Rosuvastatin
umbers of hospitalizations were analyzed with a permu-ation test.
The associations between [loge]NT-proBNP and thereviously cited outcomes were investigated in multivariableodels (17). Each analysis was conducted with and without
he exclusion of NT-proBNP and high-sensitivity C-reactiverotein to identify factors that they displaced or drew in whenntered into the model. The relationship between [loge]NT-roBNP and the number of events per 100 patient-years ofollow-up was also expressed using a cubic-spline function with
Rs adjusted for age, history of diabetes, coronary bypass orlaudication, New York Heart Association functional class,eart rate and rhythm, systolic blood pressure, and ejectionraction. The 95% CIs were estimated using the bootstrapethod with 1,000 resubstitutions.
esults
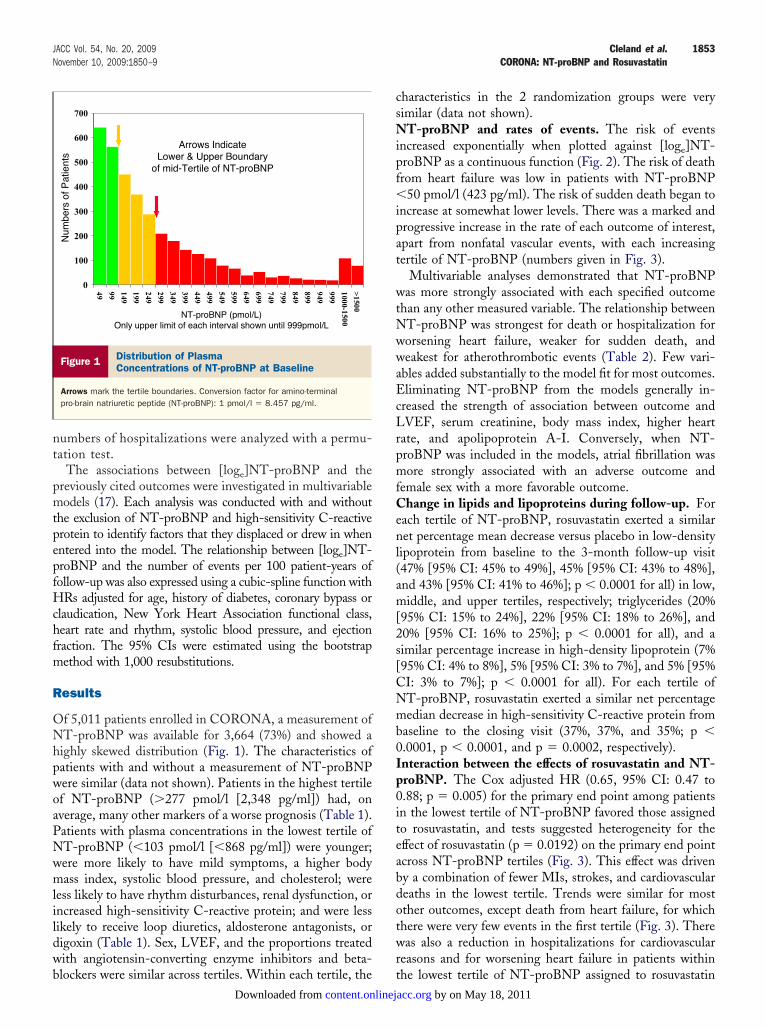
f 5,011 patients enrolled in CORONA, a measurement ofT-proBNP was available for 3,664 (73%) and showed a
ighly skewed distribution (Fig. 1). The characteristics ofatients with and without a measurement of NT-proBNPere similar (data not shown). Patients in the highest tertilef NT-proBNP (�277 pmol/l [2,348 pg/ml]) had, onverage, many other markers of a worse prognosis (Table 1).atients with plasma concentrations in the lowest tertile ofT-proBNP (�103 pmol/l [�868 pg/ml]) were younger;ere more likely to have mild symptoms, a higher bodyass index, systolic blood pressure, and cholesterol; were
ess likely to have rhythm disturbances, renal dysfunction, orncreased high-sensitivity C-reactive protein; and were lessikely to receive loop diuretics, aldosterone antagonists, origoxin (Table 1). Sex, LVEF, and the proportions treatedith angiotensin-converting enzyme inhibitors and beta-
0
100
200
300
400
500
600
700
49 99 149
199
249
2 99
34 9
399
449
499
5 49
59 9
649
699
749
7 99
84 9
899
949
999
1 000-1500
>1 500
Num
bers
of P
atie
nts
Arrows IndicateLower & Upper Boundary
of mid-Tertile of NT-proBNP
NT-proBNP (pmol/L)Only upper limit of each interval shown until 999pmol/L
Figure 1 Distribution of PlasmaConcentrations of NT-proBNP at Baseline
Arrows mark the tertile boundaries. Conversion factor for amino-terminalpro-brain natriuretic peptide (NT-proBNP): 1 pmol/l � 8.457 pg/ml.
lockers were similar across tertiles. Within each tertile, the tcontent.onlinejDownloaded from
haracteristics in the 2 randomization groups were veryimilar (data not shown).
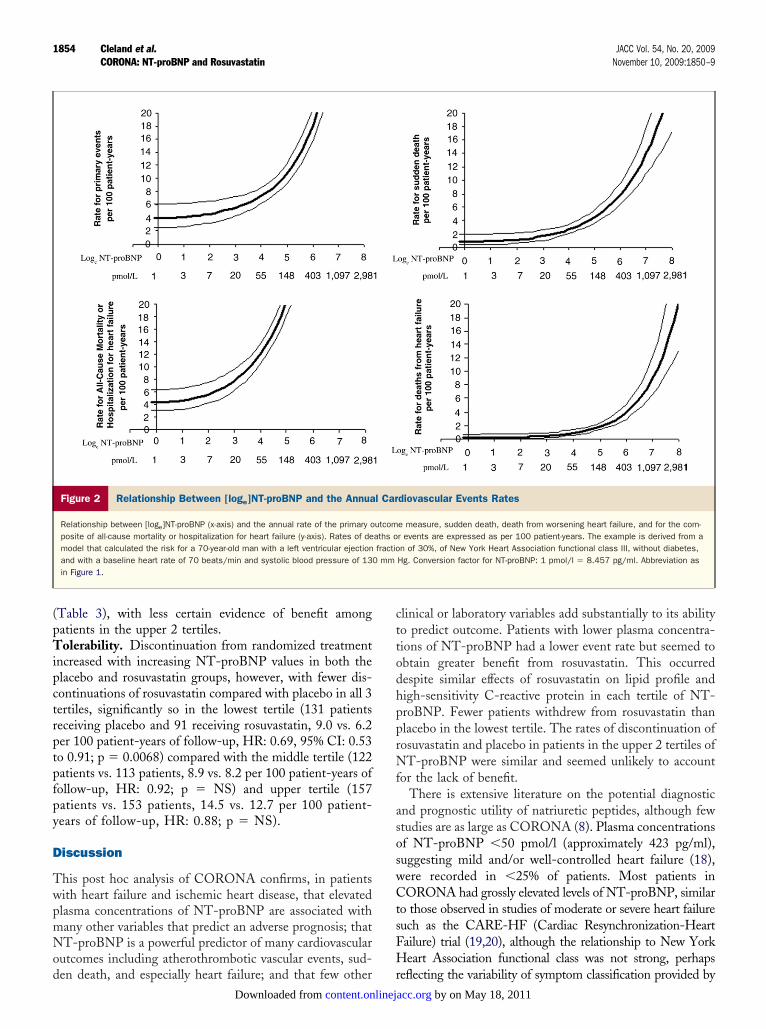
T-proBNP and rates of events. The risk of eventsncreased exponentially when plotted against [loge]NT-roBNP as a continuous function (Fig. 2). The risk of deathrom heart failure was low in patients with NT-proBNP
50 pmol/l (423 pg/ml). The risk of sudden death began toncrease at somewhat lower levels. There was a marked androgressive increase in the rate of each outcome of interest,part from nonfatal vascular events, with each increasingertile of NT-proBNP (numbers given in Fig. 3).
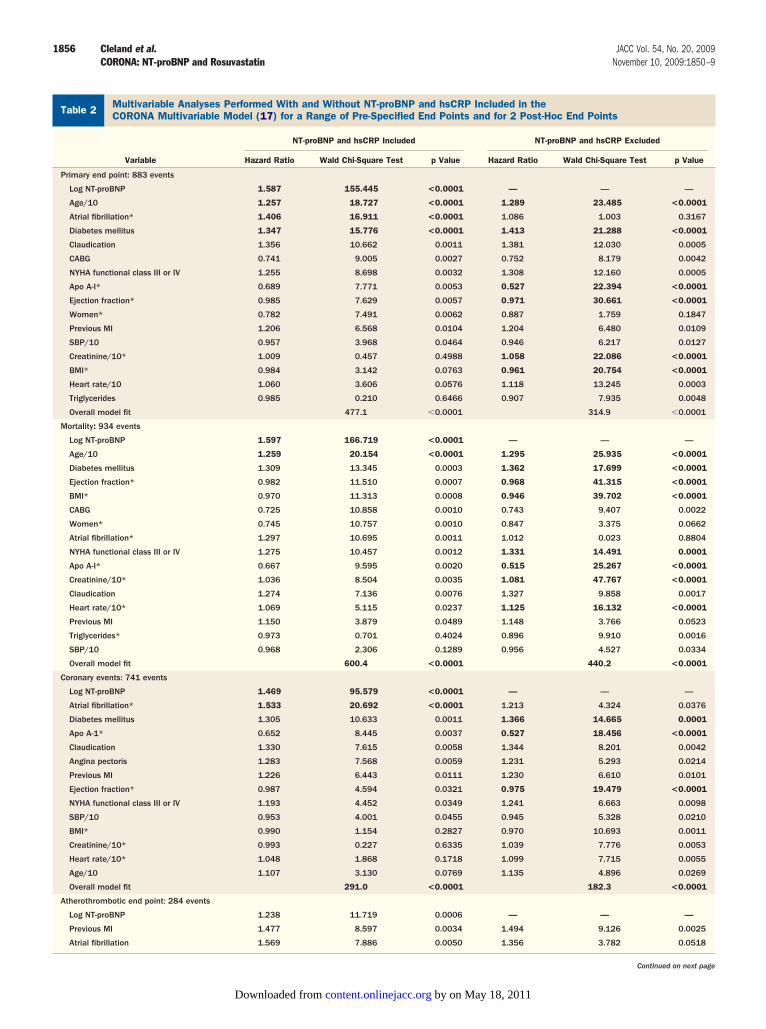
Multivariable analyses demonstrated that NT-proBNPas more strongly associated with each specified outcome
han any other measured variable. The relationship betweenT-proBNP was strongest for death or hospitalization fororsening heart failure, weaker for sudden death, andeakest for atherothrombotic events (Table 2). Few vari-
bles added substantially to the model fit for most outcomes.liminating NT-proBNP from the models generally in-
reased the strength of association between outcome andVEF, serum creatinine, body mass index, higher heart
ate, and apolipoprotein A-I. Conversely, when NT-roBNP was included in the models, atrial fibrillation wasore strongly associated with an adverse outcome and
emale sex with a more favorable outcome.hange in lipids and lipoproteins during follow-up. For
ach tertile of NT-proBNP, rosuvastatin exerted a similaret percentage mean decrease versus placebo in low-density
ipoprotein from baseline to the 3-month follow-up visit47% [95% CI: 45% to 49%], 45% [95% CI: 43% to 48%],nd 43% [95% CI: 41% to 46%]; p � 0.0001 for all) in low,iddle, and upper tertiles, respectively; triglycerides (20%
95% CI: 15% to 24%], 22% [95% CI: 18% to 26%], and0% [95% CI: 16% to 25%]; p � 0.0001 for all), and aimilar percentage increase in high-density lipoprotein (7%95% CI: 4% to 8%], 5% [95% CI: 3% to 7%], and 5% [95%I: 3% to 7%]; p � 0.0001 for all). For each tertile ofT-proBNP, rosuvastatin exerted a similar net percentageedian decrease in high-sensitivity C-reactive protein from
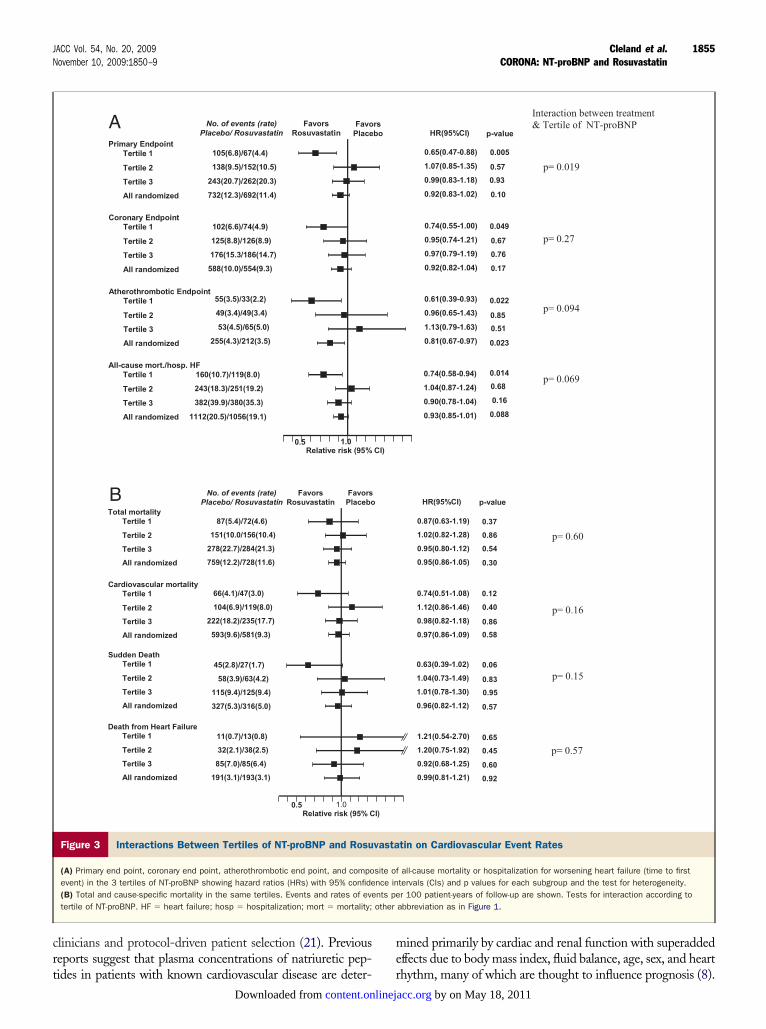
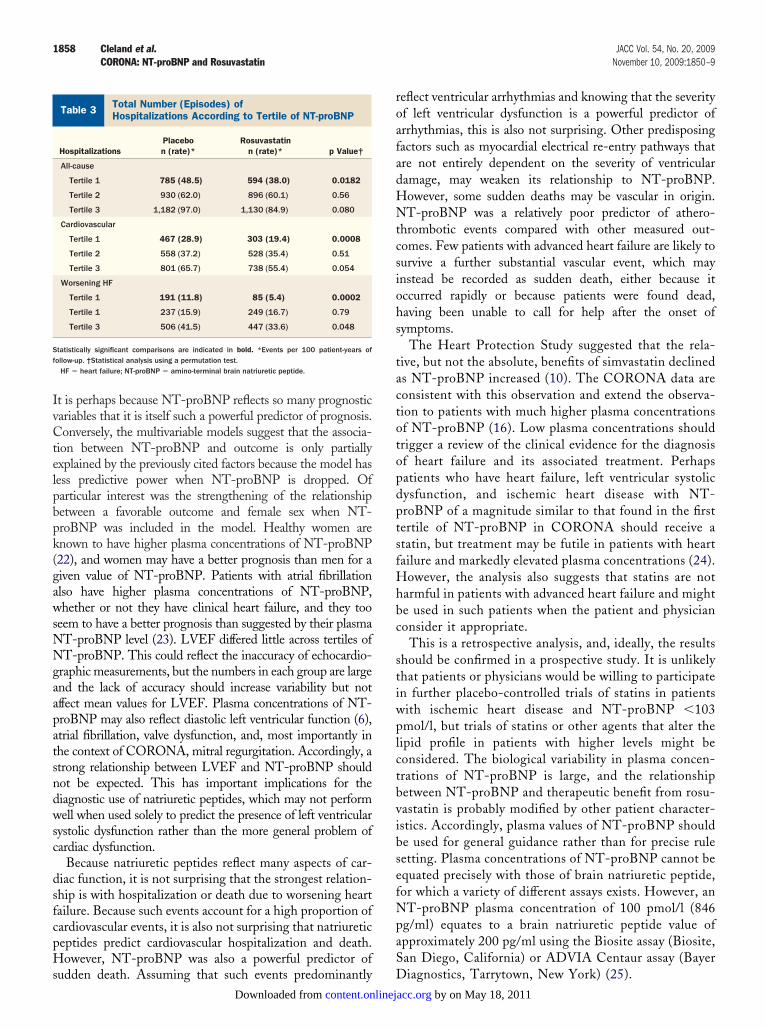
aseline to the closing visit (37%, 37%, and 35%; p �.0001, p � 0.0001, and p � 0.0002, respectively).nteraction between the effects of rosuvastatin and NT-roBNP. The Cox adjusted HR (0.65, 95% CI: 0.47 to.88; p � 0.005) for the primary end point among patientsn the lowest tertile of NT-proBNP favored those assignedo rosuvastatin, and tests suggested heterogeneity for theffect of rosuvastatin (p � 0.0192) on the primary end pointcross NT-proBNP tertiles (Fig. 3). This effect was driveny a combination of fewer MIs, strokes, and cardiovasculareaths in the lowest tertile. Trends were similar for mostther outcomes, except death from heart failure, for whichhere were very few events in the first tertile (Fig. 3). Thereas also a reduction in hospitalizations for cardiovascular
easons and for worsening heart failure in patients within
he lowest tertile of NT-proBNP assigned to rosuvastatinby on May 18, 2011 acc.org
(pTipctrptpfpy
D
TwpmNod
cttodhpprNf
asoswCtsFH
1854 Cleland et al. JACC Vol. 54, No. 20, 2009CORONA: NT-proBNP and Rosuvastatin November 10, 2009:1850–9
Table 3), with less certain evidence of benefit amongatients in the upper 2 tertiles.olerability. Discontinuation from randomized treatment
ncreased with increasing NT-proBNP values in both thelacebo and rosuvastatin groups, however, with fewer dis-ontinuations of rosuvastatin compared with placebo in all 3ertiles, significantly so in the lowest tertile (131 patientseceiving placebo and 91 receiving rosuvastatin, 9.0 vs. 6.2er 100 patient-years of follow-up, HR: 0.69, 95% CI: 0.53o 0.91; p � 0.0068) compared with the middle tertile (122atients vs. 113 patients, 8.9 vs. 8.2 per 100 patient-years ofollow-up, HR: 0.92; p � NS) and upper tertile (157atients vs. 153 patients, 14.5 vs. 12.7 per 100 patient-ears of follow-up, HR: 0.88; p � NS).
iscussion
his post hoc analysis of CORONA confirms, in patientsith heart failure and ischemic heart disease, that elevatedlasma concentrations of NT-proBNP are associated withany other variables that predict an adverse prognosis; thatT-proBNP is a powerful predictor of many cardiovascular
utcomes including atherothrombotic vascular events, sud-
Figure 2 Relationship Between [loge]NT-proBNP and the Annua
Relationship between [loge]NT-proBNP (x-axis) and the annual rate of the primary oposite of all-cause mortality or hospitalization for heart failure (y-axis). Rates of demodel that calculated the risk for a 70-year-old man with a left ventricular ejectionand with a baseline heart rate of 70 beats/min and systolic blood pressure of 13in Figure 1.
en death, and especially heart failure; and that few other rcontent.onlinejDownloaded from
linical or laboratory variables add substantially to its abilityo predict outcome. Patients with lower plasma concentra-ions of NT-proBNP had a lower event rate but seemed tobtain greater benefit from rosuvastatin. This occurredespite similar effects of rosuvastatin on lipid profile andigh-sensitivity C-reactive protein in each tertile of NT-roBNP. Fewer patients withdrew from rosuvastatin thanlacebo in the lowest tertile. The rates of discontinuation ofosuvastatin and placebo in patients in the upper 2 tertiles ofT-proBNP were similar and seemed unlikely to account
or the lack of benefit.There is extensive literature on the potential diagnostic
nd prognostic utility of natriuretic peptides, although fewtudies are as large as CORONA (8). Plasma concentrationsf NT-proBNP �50 pmol/l (approximately 423 pg/ml),uggesting mild and/or well-controlled heart failure (18),ere recorded in �25% of patients. Most patients inORONA had grossly elevated levels of NT-proBNP, similar
o those observed in studies of moderate or severe heart failureuch as the CARE-HF (Cardiac Resynchronization-Heartailure) trial (19,20), although the relationship to New Yorkeart Association functional class was not strong, perhaps
diovascular Events Rates
e measure, sudden death, death from worsening heart failure, and for the com-r events are expressed as per 100 patient-years. The example is derived from an of 30%, of New York Heart Association functional class III, without diabetes,Hg. Conversion factor for NT-proBNP: 1 pmol/l � 8.457 pg/ml. Abbreviation as
l Car
utcomaths ofractio
0 mm
eflecting the variability of symptom classification provided by by on May 18, 2011 acc.org
crt
me
1855JACC Vol. 54, No. 20, 2009 Cleland et al.November 10, 2009:1850–9 CORONA: NT-proBNP and Rosuvastatin
linicians and protocol-driven patient selection (21). Previouseports suggest that plasma concentrations of natriuretic pep-
FavorsRosuvastatin
FavoPlace
Primary EndpointTertile 1
Tertile 2
Tertile 3
All randomized
No. of events (rate)Placebo/ Rosuvastatin
105(6.8)/67(4.4)
138(9.5)/152(10.5)
243(20.7)/262(20.3)
732(12.3)/692(11.4)
Relative risk (95% 1.00.5
102(6.6)/74(4.9)
125(8.8)/126(8.9)
176(15.3/186(14.7)
588(10.0)/554(9.3)
Coronary EndpointTertile 1
Tertile 2
Tertile 3
All randomized
Atherothrombotic EndpointTertile 1
Tertile 2
Tertile 3
All randomized
All-cause mort./hosp. HFTertile 1
Tertile 2
Tertile 3
All randomized
160(10.7)/119(8.0)
243(18.3)/251(19.2)
382(39.9)/380(35.3)
1112(20.5)/1056(19.1)
55(3.5)/33(2.2)
49(3.4)/49(3.4)
53(4.5)/65(5.0)
255(4.3)/212(3.5)
FavorsRosuvastatin
FavorsPlacebo
No. of events (rate)Placebo/ Rosuvastatin
Relative risk (95% C1.00.5
87(5.4)/72(4.6)
151(10.0/156(10.4)
278(22.7)/284(21.3)
759(12.2)/728(11.6)
Total mortalityTertile 1
Tertile 2
Tertile 3
All randomized
Cardiovascular mortalityTertile 1
Tertile 2
Tertile 3
All randomized
Sudden DeathTertile 1
Tertile 2
Tertile 3
All randomized
45(2.8)/27(1.7)
58(3.9)/63(4.2)
115(9.4)/125(9.4)
327(5.3)/316(5.0)
Death from Heart FailureTertile 1
Tertile 2
Tertile 3
All randomized
11(0.7)/13(0.8)
32(2.1)/38(2.5)
85(7.0)/85(6.4)
191(3.1)/193(3.1)
66(4.1)/47(3.0)
104(6.9)/119(8.0)
222(18.2)/235(17.7)
593(9.6)/581(9.3)
A
B
Figure 3 Interactions Between Tertiles of NT-proBNP and Rosu
(A) Primary end point, coronary end point, atherothrombotic end point, and compoevent) in the 3 tertiles of NT-proBNP showing hazard ratios (HRs) with 95% confide(B) Total and cause-specific mortality in the same tertiles. Events and rates of evetertile of NT-proBNP. HF � heart failure; hosp � hospitalization; mort � mortality;
ides in patients with known cardiovascular disease are deter- rcontent.onlinejDownloaded from
ined primarily by cardiac and renal function with superaddedffects due to body mass index, fluid balance, age, sex, and heart
HR(95%CI)
0.65(0.47-0.88)
1.07(0.85-1.35)
0.99(0.83-1.18)
0.92(0.83-1.02)
0.74(0.55-1.00)
0.95(0.74-1.21)
0.97(0.79-1.19)
0.92(0.82-1.04)
0.74(0.58-0.94)
1.04(0.87-1.24)
0.90(0.78-1.04)
0.93(0.85-1.01)
0.61(0.39-0.93)
0.96(0.65-1.43)
1.13(0.79-1.63)
0.81(0.67-0.97)
p-value
0.005
0.57
0.93
0.10
0.049
0.67
0.76
0.17
0.022
0.85
0.51
0.023
0.014
0.68
0.16
0.088
HR(95%CI)
0.87(0.63-1.19)
1.02(0.82-1.28)
0.95(0.80-1.12)
0.95(0.86-1.05)
0.63(0.39-1.02)
1.04(0.73-1.49)
1.01(0.78-1.30)
0.96(0.82-1.12)
1.21(0.54-2.70)
1.20(0.75-1.92)
0.92(0.68-1.25)
0.99(0.81-1.21)
0.74(0.51-1.08)
1.12(0.86-1.46)
0.98(0.82-1.18)
0.97(0.86-1.09)
p-value
0.37
0.54
0.30
0.12
0.40
0.86
0.58
0.06
0.83
0.95
0.57
0.65
0.45
0.60
0.92
0.86
Interaction between treatment & Tertile of NT-proBNP
p= 0.019
p= 0.60
p= 0.27
p= 0.094
p= 0.069
p= 0.16
p= 0.15
p= 0.57
tin on Cardiovascular Event Rates
all-cause mortality or hospitalization for worsening heart failure (time to firsttervals (CIs) and p values for each subgroup and the test for heterogeneity.r 100 patient-years of follow-up are shown. Tests for interaction according to
abbreviation as in Figure 1.
rsbo
CI)
I)
vasta
site ofnce innts peother
hythm, many of which are thought to influence prognosis (8). by on May 18, 2011 acc.org
MC
1856 Cleland et al. JACC Vol. 54, No. 20, 2009CORONA: NT-proBNP and Rosuvastatin November 10, 2009:1850–9
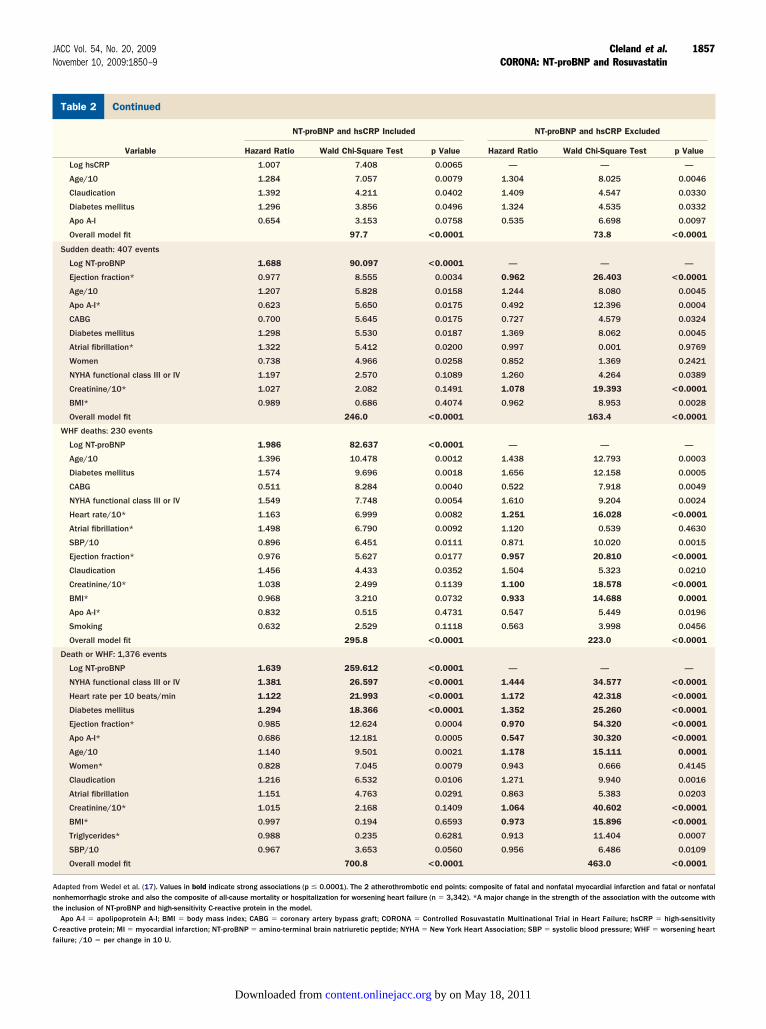
ultivariable Analyses Performed With and Without NT-proBNP and hsCRP Included in theORONA Multivariable Model (17) for a Range of Pre-Specified End Points and for 2 Post-Hoc End PointsTable 2 Multivariable Analyses Performed With and Without NT-proBNP and hsCRP Included in theCORONA Multivariable Model (17) for a Range of Pre-Specified End Points and for 2 Post-Hoc End Points
Variable
NT-proBNP and hsCRP Included NT-proBNP and hsCRP Excluded
Hazard Ratio Wald Chi-Square Test p Value Hazard Ratio Wald Chi-Square Test p Value
Primary end point: 883 events
Log NT-proBNP 1.587 155.445 <0.0001 — — —
Age/10 1.257 18.727 <0.0001 1.289 23.485 <0.0001
Atrial fibrillation* 1.406 16.911 <0.0001 1.086 1.003 0.3167
Diabetes mellitus 1.347 15.776 <0.0001 1.413 21.288 <0.0001
Claudication 1.356 10.662 0.0011 1.381 12.030 0.0005
CABG 0.741 9.005 0.0027 0.752 8.179 0.0042
NYHA functional class III or IV 1.255 8.698 0.0032 1.308 12.160 0.0005
Apo A-I* 0.689 7.771 0.0053 0.527 22.394 <0.0001
Ejection fraction* 0.985 7.629 0.0057 0.971 30.661 <0.0001
Women* 0.782 7.491 0.0062 0.887 1.759 0.1847
Previous MI 1.206 6.568 0.0104 1.204 6.480 0.0109
SBP/10 0.957 3.968 0.0464 0.946 6.217 0.0127
Creatinine/10* 1.009 0.457 0.4988 1.058 22.086 <0.0001
BMI* 0.984 3.142 0.0763 0.961 20.754 <0.0001
Heart rate/10 1.060 3.606 0.0576 1.118 13.245 0.0003
Triglycerides 0.985 0.210 0.6466 0.907 7.935 0.0048
Overall model fit 477.1 �0.0001 314.9 �0.0001
Mortality: 934 events
Log NT-proBNP 1.597 166.719 <0.0001 — — —
Age/10 1.259 20.154 <0.0001 1.295 25.935 <0.0001
Diabetes mellitus 1.309 13.345 0.0003 1.362 17.699 <0.0001
Ejection fraction* 0.982 11.510 0.0007 0.968 41.315 <0.0001
BMI* 0.970 11.313 0.0008 0.946 39.702 <0.0001
CABG 0.725 10.858 0.0010 0.743 9.407 0.0022
Women* 0.745 10.757 0.0010 0.847 3.375 0.0662
Atrial fibrillation* 1.297 10.695 0.0011 1.012 0.023 0.8804
NYHA functional class III or IV 1.275 10.457 0.0012 1.331 14.491 0.0001
Apo A-I* 0.667 9.595 0.0020 0.515 25.267 <0.0001
Creatinine/10* 1.036 8.504 0.0035 1.081 47.767 <0.0001
Claudication 1.274 7.136 0.0076 1.327 9.858 0.0017
Heart rate/10* 1.069 5.115 0.0237 1.125 16.132 <0.0001
Previous MI 1.150 3.879 0.0489 1.148 3.766 0.0523
Triglycerides* 0.973 0.701 0.4024 0.896 9.910 0.0016
SBP/10 0.968 2.306 0.1289 0.956 4.527 0.0334
Overall model fit 600.4 <0.0001 440.2 <0.0001
Coronary events: 741 events
Log NT-proBNP 1.469 95.579 <0.0001 — — —
Atrial fibrillation* 1.533 20.692 <0.0001 1.213 4.324 0.0376
Diabetes mellitus 1.305 10.633 0.0011 1.366 14.665 0.0001
Apo A-1* 0.652 8.445 0.0037 0.527 18.456 <0.0001
Claudication 1.330 7.615 0.0058 1.344 8.201 0.0042
Angina pectoris 1.283 7.568 0.0059 1.231 5.293 0.0214
Previous MI 1.226 6.443 0.0111 1.230 6.610 0.0101
Ejection fraction* 0.987 4.594 0.0321 0.975 19.479 <0.0001
NYHA functional class III or IV 1.193 4.452 0.0349 1.241 6.663 0.0098
SBP/10 0.953 4.001 0.0455 0.945 5.328 0.0210
BMI* 0.990 1.154 0.2827 0.970 10.693 0.0011
Creatinine/10* 0.993 0.227 0.6335 1.039 7.776 0.0053
Heart rate/10* 1.048 1.868 0.1718 1.099 7.715 0.0055
Age/10 1.107 3.130 0.0769 1.135 4.896 0.0269
Overall model fit 291.0 <0.0001 182.3 <0.0001
Atherothrombotic end point: 284 events
Log NT-proBNP 1.238 11.719 0.0006 — — —
Previous MI 1.477 8.597 0.0034 1.494 9.126 0.0025
Atrial fibrillation 1.569 7.886 0.0050 1.356 3.782 0.0518
Continued on next page
by on May 18, 2011 content.onlinejacc.orgDownloaded from
C
Ant
Cf
1857JACC Vol. 54, No. 20, 2009 Cleland et al.November 10, 2009:1850–9 CORONA: NT-proBNP and Rosuvastatin
ontinuedTable 2 Continued
Variable
NT-proBNP and hsCRP Included NT-proBNP and hsCRP Excluded
Hazard Ratio Wald Chi-Square Test p Value Hazard Ratio Wald Chi-Square Test p Value
Log hsCRP 1.007 7.408 0.0065 — — —
Age/10 1.284 7.057 0.0079 1.304 8.025 0.0046
Claudication 1.392 4.211 0.0402 1.409 4.547 0.0330
Diabetes mellitus 1.296 3.856 0.0496 1.324 4.535 0.0332
Apo A-I 0.654 3.153 0.0758 0.535 6.698 0.0097
Overall model fit 97.7 <0.0001 73.8 <0.0001
Sudden death: 407 events
Log NT-proBNP 1.688 90.097 <0.0001 — — —
Ejection fraction* 0.977 8.555 0.0034 0.962 26.403 <0.0001
Age/10 1.207 5.828 0.0158 1.244 8.080 0.0045
Apo A-I* 0.623 5.650 0.0175 0.492 12.396 0.0004
CABG 0.700 5.645 0.0175 0.727 4.579 0.0324
Diabetes mellitus 1.298 5.530 0.0187 1.369 8.062 0.0045
Atrial fibrillation* 1.322 5.412 0.0200 0.997 0.001 0.9769
Women 0.738 4.966 0.0258 0.852 1.369 0.2421
NYHA functional class III or IV 1.197 2.570 0.1089 1.260 4.264 0.0389
Creatinine/10* 1.027 2.082 0.1491 1.078 19.393 <0.0001
BMI* 0.989 0.686 0.4074 0.962 8.953 0.0028
Overall model fit 246.0 <0.0001 163.4 <0.0001
WHF deaths: 230 events
Log NT-proBNP 1.986 82.637 <0.0001 — — —
Age/10 1.396 10.478 0.0012 1.438 12.793 0.0003
Diabetes mellitus 1.574 9.696 0.0018 1.656 12.158 0.0005
CABG 0.511 8.284 0.0040 0.522 7.918 0.0049
NYHA functional class III or IV 1.549 7.748 0.0054 1.610 9.204 0.0024
Heart rate/10* 1.163 6.999 0.0082 1.251 16.028 <0.0001
Atrial fibrillation* 1.498 6.790 0.0092 1.120 0.539 0.4630
SBP/10 0.896 6.451 0.0111 0.871 10.020 0.0015
Ejection fraction* 0.976 5.627 0.0177 0.957 20.810 <0.0001
Claudication 1.456 4.433 0.0352 1.504 5.323 0.0210
Creatinine/10* 1.038 2.499 0.1139 1.100 18.578 <0.0001
BMI* 0.968 3.210 0.0732 0.933 14.688 0.0001
Apo A-I* 0.832 0.515 0.4731 0.547 5.449 0.0196
Smoking 0.632 2.529 0.1118 0.563 3.998 0.0456
Overall model fit 295.8 <0.0001 223.0 <0.0001
Death or WHF: 1,376 events
Log NT-proBNP 1.639 259.612 <0.0001 — — —
NYHA functional class III or IV 1.381 26.597 <0.0001 1.444 34.577 <0.0001
Heart rate per 10 beats/min 1.122 21.993 <0.0001 1.172 42.318 <0.0001
Diabetes mellitus 1.294 18.366 <0.0001 1.352 25.260 <0.0001
Ejection fraction* 0.985 12.624 0.0004 0.970 54.320 <0.0001
Apo A-I* 0.686 12.181 0.0005 0.547 30.320 <0.0001
Age/10 1.140 9.501 0.0021 1.178 15.111 0.0001
Women* 0.828 7.045 0.0079 0.943 0.666 0.4145
Claudication 1.216 6.532 0.0106 1.271 9.940 0.0016
Atrial fibrillation 1.151 4.763 0.0291 0.863 5.383 0.0203
Creatinine/10* 1.015 2.168 0.1409 1.064 40.602 <0.0001
BMI* 0.997 0.194 0.6593 0.973 15.896 <0.0001
Triglycerides* 0.988 0.235 0.6281 0.913 11.404 0.0007
SBP/10 0.967 3.653 0.0560 0.956 6.486 0.0109
Overall model fit 700.8 <0.0001 463.0 <0.0001
dapted from Wedel et al. (17). Values in bold indicate strong associations (p � 0.0001). The 2 atherothrombotic end points: composite of fatal and nonfatal myocardial infarction and fatal or nonfatalonhemorrhagic stroke and also the composite of all-cause mortality or hospitalization for worsening heart failure (n � 3,342). *A major change in the strength of the association with the outcome withhe inclusion of NT-proBNP and high-sensitivity C-reactive protein in the model.
Apo A-I � apolipoprotein A-I; BMI � body mass index; CABG � coronary artery bypass graft; CORONA � Controlled Rosuvastatin Multinational Trial in Heart Failure; hsCRP � high-sensitivity-reactive protein; MI � myocardial infarction; NT-proBNP � amino-terminal brain natriuretic peptide; NYHA � New York Heart Association; SBP � systolic blood pressure; WHF � worsening heartailure; /10 � per change in 10 U.
by on May 18, 2011 content.onlinejacc.orgDownloaded from
IvCtelpbpk(gawsNNgaapatsndwsc
dsfcpHs
roafadHNtcsiohs
tactotopdptsfHhbc
stiwplctbvibsefNpaS
TH
Sf
1858 Cleland et al. JACC Vol. 54, No. 20, 2009CORONA: NT-proBNP and Rosuvastatin November 10, 2009:1850–9
t is perhaps because NT-proBNP reflects so many prognosticariables that it is itself such a powerful predictor of prognosis.onversely, the multivariable models suggest that the associa-
ion between NT-proBNP and outcome is only partiallyxplained by the previously cited factors because the model hasess predictive power when NT-proBNP is dropped. Ofarticular interest was the strengthening of the relationshipetween a favorable outcome and female sex when NT-roBNP was included in the model. Healthy women arenown to have higher plasma concentrations of NT-proBNP22), and women may have a better prognosis than men for aiven value of NT-proBNP. Patients with atrial fibrillationlso have higher plasma concentrations of NT-proBNP,hether or not they have clinical heart failure, and they too
eem to have a better prognosis than suggested by their plasmaT-proBNP level (23). LVEF differed little across tertiles ofT-proBNP. This could reflect the inaccuracy of echocardio-
raphic measurements, but the numbers in each group are largend the lack of accuracy should increase variability but notffect mean values for LVEF. Plasma concentrations of NT-roBNP may also reflect diastolic left ventricular function (6),trial fibrillation, valve dysfunction, and, most importantly inhe context of CORONA, mitral regurgitation. Accordingly, atrong relationship between LVEF and NT-proBNP shouldot be expected. This has important implications for theiagnostic use of natriuretic peptides, which may not performell when used solely to predict the presence of left ventricular
ystolic dysfunction rather than the more general problem ofardiac dysfunction.
Because natriuretic peptides reflect many aspects of car-iac function, it is not surprising that the strongest relation-hip is with hospitalization or death due to worsening heartailure. Because such events account for a high proportion ofardiovascular events, it is also not surprising that natriureticeptides predict cardiovascular hospitalization and death.owever, NT-proBNP was also a powerful predictor of
otal Number (Episodes) ofospitalizations According to Tertile of NT-proBNPTable 3 Total Number (Episodes) ofHospitalizations According to Tertile of NT-proBNP
HospitalizationsPlacebon (rate)*
Rosuvastatinn (rate)* p Value†
All-cause
Tertile 1 785 (48.5) 594 (38.0) 0.0182
Tertile 2 930 (62.0) 896 (60.1) 0.56
Tertile 3 1,182 (97.0) 1,130 (84.9) 0.080
Cardiovascular
Tertile 1 467 (28.9) 303 (19.4) 0.0008
Tertile 2 558 (37.2) 528 (35.4) 0.51
Tertile 3 801 (65.7) 738 (55.4) 0.054
Worsening HF
Tertile 1 191 (11.8) 85 (5.4) 0.0002
Tertile 1 237 (15.9) 249 (16.7) 0.79
Tertile 3 506 (41.5) 447 (33.6) 0.048
tatistically significant comparisons are indicated in bold. *Events per 100 patient-years ofollow-up. †Statistical analysis using a permutation test.
HF � heart failure; NT-proBNP � amino-terminal brain natriuretic peptide.
udden death. Assuming that such events predominantly D
content.onlinejDownloaded from
eflect ventricular arrhythmias and knowing that the severityf left ventricular dysfunction is a powerful predictor ofrrhythmias, this is also not surprising. Other predisposingactors such as myocardial electrical re-entry pathways thatre not entirely dependent on the severity of ventricularamage, may weaken its relationship to NT-proBNP.owever, some sudden deaths may be vascular in origin.T-proBNP was a relatively poor predictor of athero-
hrombotic events compared with other measured out-omes. Few patients with advanced heart failure are likely tourvive a further substantial vascular event, which maynstead be recorded as sudden death, either because itccurred rapidly or because patients were found dead,aving been unable to call for help after the onset ofymptoms.
The Heart Protection Study suggested that the rela-ive, but not the absolute, benefits of simvastatin declineds NT-proBNP increased (10). The CORONA data areonsistent with this observation and extend the observa-ion to patients with much higher plasma concentrationsf NT-proBNP (16). Low plasma concentrations shouldrigger a review of the clinical evidence for the diagnosisf heart failure and its associated treatment. Perhapsatients who have heart failure, left ventricular systolicysfunction, and ischemic heart disease with NT-roBNP of a magnitude similar to that found in the firstertile of NT-proBNP in CORONA should receive atatin, but treatment may be futile in patients with heartailure and markedly elevated plasma concentrations (24).
owever, the analysis also suggests that statins are notarmful in patients with advanced heart failure and mighte used in such patients when the patient and physicianonsider it appropriate.
This is a retrospective analysis, and, ideally, the resultshould be confirmed in a prospective study. It is unlikelyhat patients or physicians would be willing to participaten further placebo-controlled trials of statins in patientsith ischemic heart disease and NT-proBNP �103mol/l, but trials of statins or other agents that alter the
ipid profile in patients with higher levels might beonsidered. The biological variability in plasma concen-rations of NT-proBNP is large, and the relationshipetween NT-proBNP and therapeutic benefit from rosu-astatin is probably modified by other patient character-stics. Accordingly, plasma values of NT-proBNP shoulde used for general guidance rather than for precise ruleetting. Plasma concentrations of NT-proBNP cannot bequated precisely with those of brain natriuretic peptide,or which a variety of different assays exists. However, anT-proBNP plasma concentration of 100 pmol/l (846
g/ml) equates to a brain natriuretic peptide value ofpproximately 200 pg/ml using the Biosite assay (Biosite,an Diego, California) or ADVIA Centaur assay (Bayer
iagnostics, Tarrytown, New York) (25).by on May 18, 2011 acc.org

C
Tadcata
RDUHU
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
1859JACC Vol. 54, No. 20, 2009 Cleland et al.November 10, 2009:1850–9 CORONA: NT-proBNP and Rosuvastatin
onclusions
he CORONA and the Heart Protection Study findingsre consistent and suggest that the relative benefits of statinsecline as the plasma concentration of NT-proBNP in-reases so that an effect is no longer apparent above values ofpproximately 103 pmol/l (868 pg/ml). These data supporthe use of statin therapy in patients with coronary diseasend less advanced heart failure.
eprint requests and correspondence: Prof. John G. F. Cleland,epartment of Cardiology, Hull York Medical School at theniversity of Hull, Medical Research Building, Gate 2, Castle Hillospital, Kingston-upon-Hull, East Yorkshire HU16 5JQ,nited Kingdom. E-mail: [email protected].
EFERENCES
1. Anand IS, Fisher LD, Chiang Y-T, et al. Changes in brain natriureticpeptide and norepinephrine over time and mortality and morbidity inthe Valsartan Heart Failure Trial (Val-HeFT). Circulation 2003;107:1278–83.
2. Masson S, Latini R, Anand IS, T et al., Val-HeFT Investigators.Prognostic value of changes in N-terminal pro-brain natriureticpeptide in Val-HeFT (Valsartan Heart Failure Trial). J Am CollCardiol 2008;52:1004–5.
3. Hartmann F, Packer M, Coats AJS, et al. Prognostic impact of plasmaN-terminal pro-brain natriuretic peptide in severe congestive heartfailure. Circulation 2004;110:1780–6.
4. Cleland JG, Freemantle N, Ghio S, et al. Predicting the long-term effectsof cardiac resynchronisation therapy on mortality from baseline variablesand the early response: a report from CARE-HF (Cardiac Resynchroni-zation in Heart Failure). J Am Coll Cardiol 2008;52:438–45.
5. Olsson LG, Swedberg K, Cleland JGF, et al. Prognostic importance ofplasma NT-pro BNP in chronic heart failure in patients treated witha beta-blocker: results from the Carvedilol Or Metroprolol EuropeanTrial (COMET) trial. Eur J Heart Fail 2007;9:795–801.
6. Cleland JGF, Tendera M, Taylor J. Prognosis in heart failure with anormal ejection fraction. N Engl J Med 2007;357:829–30.
7. Doust JA, Pietrzak E, Dobson A, Glasziou P. How well does B-typenatriuretic peptide predict death and cardiac events in patients withheart failure: systematic review. BMJ 2005;330:625–34.
8. Maisel A, Mueller C, Adams KF Jr., et al. State of the art: Usingnatriuretic peptide levels in clinical practice. Eur J Heart Fail 2008;10:824–39.
9. McDonagh TA, Cunningham AD, Morrison CE, et al. Left ventric-ular dysfunction, natriuretic peptides and mortality in an urbanpopulation. Heart 2001;86:21–6.
0. Heart Protection Study Collaborative Group. N-terminal pro-B-typenatriuretic peptide, vascular disease risk and cholesterol reductionamong 20,536 patients in the MRC/BHF Heart Protection Study.J Am Coll Cardiol 2007;49:311–9.
1. Kjekshus J, Apetrei E, Barrios V, et al. Rosuvastatin in older patientswith systolic heart failure. N Engl J Med 2007;357:2248–61.
Ky
content.onlinejDownloaded from
2. Wanner C, Krane V, Marz W, et al. Atorvastatin in patients with type2 diabetes mellitus undergoing hemodialysis. N Engl J Med 2005;353:238–48.
3. Gissi-HF I, Tavazzi L, Maggioni AP, et al. Effect of rosuvastatin inpatients with chronic heart failure (the GISSI-HF trial): a randomised,double-blind, placebo-controlled trial. Lancet 2008;372:1231–9.
4. Kjekshus J, Dunselman PH, Blideskog M, et al. A statin in thetreatment of heart failure? Controlled rosuvastatin multinational studyin heart failure (CORONA): study design and baseline characteristics.Eur J Heart Fail 2005;7:1059–69.
5. Khush KK, Waters DD, Bittner V, et al. Effect of high-doseatorvastatin on hospitalizations for heart failure: subgroup analysis ofthe Treating to New Targets (TNT) study. Circulation 2007;115:576–83.
6. Cleland JG, Squire I, Ng L. Interpretation of amino-terminal pro-brain natriuretic peptide levels in the HPS and the CORONA study.J Am Coll Cardiol 2008;52:1104–5.
7. Wedel H, McMurray JJ, Lindberg M, et al. Predictors of fatal andnon-fatal outcomes in the Controlled Rosuvastatin MultinationalTrial in Heart Failure (CORONA): incremental value of apolipopro-tein A-1, high-sensitivity C-reactive peptide and N-terminal proB-type natriuretic peptide. Eur J Heart Fail 2009;11:281–91.
8. Dickstein K, Cohen-Solal A, Filippatos G, et al. ESC guidelines forthe diagnosis and treatment of acute and chronic heart failure 2008:the Task Force for the Diagnosis and Treatment of Acute and ChronicHeart Failure 2008 of the European Society of Cardiology. Developedin collaboration with the Heart Failure Association of the ESC (HFA)and endorsed by the European Society of Intensive Care Medicine(ESICM). Eur Heart J 2008;29:2388–442.
9. Cleland JGF, Daubert J-C, Erdmann E, et al. The effect of cardiacresynchronization on morbidity and mortality in heart failure. N EnglJ Med 2005;352:1539–49.
0. Cleland JGF, Daubert J-C, Erdmann E, et al. Longer-term effects ofcardiac resynchronization therapy on mortality in heart failure {theCardiac Resynchronization-Heart Failure (CARE-HF) trial extensionphase}. Eur Heart J 2006;27:1928–32.
1. Goode KM, Nabb S, Cleland JGF, Clark AL. A comparison of patientand physician-rated New York Heart Association class in community-based heart failure clinic. J Card Fail 2008;14:379–87.
2. Maisel AS, Clopton P, Krishnaswamy P, et al. Impact of age, race, andsex on the ability of B-type natriuretic peptide to aid in the emergencydiagnosis of heart failure: results from the Breathing Not Properly(BNP) multinational study. Am Heart J 2004;147:1078–84.
3. Morello A, Lloyd-Jones DM, Chae CU, et al. Association of atrialfibrillation and amino-terminal pro-brain natriuretic peptide concen-trations in dyspneic patients with and without acute heart failure:results from the ProBNP Investigation of Dyspnea in the EmergencyDepartment (PRIDE) study. Am Heart J 2007;153:90–7.
4. Cleland JG, Tavazzi L, Daubert JC, Tageldien A, Freemantle N.Cardiac resynchronization therapy. Are modern myths preventingappropriate use? J Am Coll Cardiol 2009;53:608–11.
5. Austin WJ, Bhalla V, Hernandez-Arce I, et al. Correlation andprognostic utility of B-type natriuretic peptide and its amino-terminalfragment in patients with chronic kidney disease. Am J Clin Pathol2006;126:506–12.
ey Words: amino-terminal pro-brain natriuretic peptide y heart failuremortality y randomized controlled trial y rosuvastatin.
by on May 18, 2011 acc.org

doi:10.1016/j.jacc.2009.06.041 2009;54;1850-1859 J. Am. Coll. Cardiol.
Wikstrand, on behalf of the CORONA Study Group Naresh Ranjith, Dirk J. van Veldhuisen, Finn Waagstein, Hans Wedel, John
Lindberg,Dunselman, Cândida Fonseca, Åke Hjalmarson, Jerzy Korewicki, Magnus John G.F. Cleland, John J.V. McMurray, John Kjekshus, Jan H. Cornel, Peter
Rosuvastatin Multinational Trial in Heart Failure)With the Effects of Rosuvastatin: A Report From CORONA (Controlled
Chronic Heart Failure: Prediction of Cardiovascular Events and Interaction Plasma Concentration of Amino-Terminal Pro-Brain Natriuretic Peptide in
This information is current as of May 18, 2011
& ServicesUpdated Information
http://content.onlinejacc.org/cgi/content/full/54/20/1850including high-resolution figures, can be found at:
References
Lhttp://content.onlinejacc.org/cgi/content/full/54/20/1850#BIBfree at: This article cites 25 articles, 17 of which you can access for
Citations
articleshttp://content.onlinejacc.org/cgi/content/full/54/20/1850#otherThis article has been cited by 8 HighWire-hosted articles:
Rights & Permissions
http://content.onlinejacc.org/misc/permissions.dtltables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://content.onlinejacc.org/misc/reprints.dtl
Information about ordering reprints can be found online:
by on May 18, 2011 content.onlinejacc.orgDownloaded from








![Self-assembly of extended Schiff base amino acetate skeletons, 2-{[(2 Z)-(3-hydroxy-1-methyl-2-butenylidene)]amino}phenylpropionate and 2-{[( E)-1-(2-hydroxyaryl)alkylidene]amino}phenylpropionate](https://static.fdokumen.com/doc/165x107/631bb3c5665120b3330b7ec0/self-assembly-of-extended-schiff-base-amino-acetate-skeletons-2-2-z-3-hydroxy-1-methyl-2-butenylideneaminophenylpropionate.jpg)




![3-[(2-HYDROXYBENZYLIDENE) AMINO]PHENYL}IMINO)](https://static.fdokumen.com/doc/165x107/631c6e3f7051d371800f7901/3-2-hydroxybenzylidene-aminophenylimino.jpg)






