Photochemical internalization provides time- and space-controlled endolysosomal escape of...
12
This article appeared in a journal published by Elsevier. The attached copy is furnished to the author for internal non-commercial research and education use, including for instruction at the authors institution and sharing with colleagues. Other uses, including reproduction and distribution, or selling or licensing copies, or posting to personal, institutional or third party websites are prohibited. In most cases authors are permitted to post their version of the article (e.g. in Word or Tex form) to their personal website or institutional repository. Authors requiring further information regarding Elsevier’s archiving and manuscript policies are encouraged to visit: http://www.elsevier.com/copyright
-
Upload
rr-research -
Category
Documents
-
view
1 -
download
0
Transcript of Photochemical internalization provides time- and space-controlled endolysosomal escape of...
This article appeared in a journal published by Elsevier. The attachedcopy is furnished to the author for internal non-commercial researchand education use, including for instruction at the authors institution
and sharing with colleagues.
Other uses, including reproduction and distribution, or selling orlicensing copies, or posting to personal, institutional or third party
websites are prohibited.
In most cases authors are permitted to post their version of thearticle (e.g. in Word or Tex form) to their personal website orinstitutional repository. Authors requiring further information
regarding Elsevier’s archiving and manuscript policies areencouraged to visit:
http://www.elsevier.com/copyright

Author's personal copy
Review
Photochemical internalization provides time- and space-controlled endolysosomalescape of therapeutic molecules
Pål Kristian Selbo a,b,⁎, Anette Weyergang a, Anders Høgset b, Ole-Jacob Norum a,c, Maria Brandal Berstad a,Marie Vikdal a, Kristian Berg a
a Department of Radiation Biology, Institute for Cancer Research, Norwegian Radium Hospital, Oslo University Hospital, Norwayb PCI Biotech, Oslo, Norwayc Deparment of Surgical Oncology, Norwegian Radium Hospital, Oslo University Hospital, Norway
a b s t r a c ta r t i c l e i n f o
Article history:Received 5 April 2010Accepted 13 June 2010Available online 18 June 2010
Keywords:Drug deliveryPhotochemical internalizationPhotodynamic therapyGene deliveryTargeting
A successful cure of cancer by biopharmaceuticals with intracellular targets is dependent on both specificand sufficient delivery of the drug to the cytosol or nuclei of malignant cells. However, cytosolic delivery andefficacy of membrane-impermeable cancer therapeutics are often hampered by the sequestration anddegradation of the drugs in the endolysosomal compartments. Hence, we developed photochemicalinternalization (PCI) as a site-specific drug delivery technology, which bursts the membrane of endocyticvesicles inducing release of entrapped drugs to the cytosol of light exposed cells. The principle of PCI hasbeen demonstrated in N80 different cell lines and 10 different xenograft models of various cancers indifferent laboratories demonstrating its broad application potential. PCI-induced endosomal escape ofprotein- or nucleic acid-based therapeutics and some chemotherapeutics will be presented in this review.With a joint effort by life scientists the PCI technology is currently in a Phase I/II clinical trial with verypromising initial results in the treatment of solid tumors.
© 2010 Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32. Photochemical internalization (PCI) — a light-triggered drug delivery technology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
2.1. PCI is based upon the same principles as photodynamic therapy (PDT) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42.2. An optimal photosensitizer for PCI localizes to the membrane of endolysosomal vesicles . . . . . . . . . . . . . . . . . . . . . . . . 52.3. The viability of cancer cells treated with ribosomal inactivating protein toxins should be assessed at least 48 h after PCI . . . . . . . . 62.4. PCI improves delivery and efficacy of targeted macromolecular therapeutics without enhancing systemic toxicity . . . . . . . . . . . . 62.5. PCI enhances the efficacy of chemotherapeutics that accumulate in endocytic vesicles . . . . . . . . . . . . . . . . . . . . . . . . . 7
2.5.1. PCI enhances the cytotoxic effect of bleomycin in a synergistic manner . . . . . . . . . . . . . . . . . . . . . . . . . . . . 72.5.2. PCI-enhanced cytotoxicity of doxorubicin in multi-drug resistant (MDR) cancer cells is dependent on the partitioning effect . . 72.5.3. Surgery or ionizing radiation in combination with PCI . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
2.6. PCI enhance nucleic acid delivery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 72.7. PCI of nanomedicines . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 82.8. Photochemical rupture of endocytic vesicles before administration of molecular therapeutics: success of PCI is dependent on the type of
endocytosis of the drug . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 83. Targeting signalling effectors important for cell survival and proliferation by light-activation of PCI-photosensitizers . . . . . . . . . . . . . . 94. Limitations and advantages of the PCI technology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 95. Moving PCI from bench to bedside . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 96. Concluding remarks and future directions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
Journal of Controlled Release 148 (2010) 2–12
⁎ Corresponding author. Department of Radiation Biology, Institute for Cancer Research, Norwegian Radium Hospital, Oslo University Hospital, Montebello, N-0310 Oslo, Norway.Tel.: +47 22781469; fax: +47 22781495.
E-mail address: [email protected] (P.K. Selbo).
0168-3659/$ – see front matter © 2010 Elsevier B.V. All rights reserved.doi:10.1016/j.jconrel.2010.06.008
Contents lists available at ScienceDirect
Journal of Controlled Release
j ourna l homepage: www.e lsev ie r.com/ locate / jconre l
Author's personal copy
1. Introduction
Despite decades of efforts in drug design and development, amajor obstacle for cancer therapeutics is the lack of sufficient targeteddrug delivery. Low treatment selectivity is compensated with doseescalations, and patients are therefore subjected to repeated admin-istrations of high drug doses causing severe and often life-threateningadverse effects. Moreover, repeated exposure of cancer therapeuticsinevitably leads to development of drug resistance. To increase thespecificity and efficiency of cancer therapeutics, the anti-cancer
agents have been linked to targeted moieties. These are usuallymacromolecules such as proteins (i.e. antibody–drug conjugates) ornucleic acids (i.e. siRNA in targeting-polymers or adenoviruses/DNAlinked to antibodies). However, for such agents intracellular deliveryis often incomplete, since most therapeutic macromolecules arehydrophilic and thus unable to cross the plasma membrane. Evenwith a specific delivery to cancer cells these types of drugs are takenup by means of endocytosis and are sequestered in endolysosomalcompartments where they are subjected to enzymatic degradationresulting in lack of biological effect [1–3].
Another major barrier for macromolecular therapeutics is thesterical hindrance in the extracellular matrix and elevated interstitialfluid pressure of tumor tissues resulting in slow penetration,inhomogeneous distribution and low intracellular levels of thedrugs [4]. For this reason, cytotoxic cancer-targeting conjugatesrequire repeated administration, which may lead to the developmentof neutralizing antibodies and often inflammatory adverse effects, e.g.as shown in the therapy of malignant mesothelioma [5].
Hence, there is an urgent need for smart drug delivery systems(DDS) or technologies which enhance the endolysosomal release ofanti-cancer drugs [6]. There are currently several DDS underevaluation, where some are based on chemical manipulations forcytosolic release [7–9], while others are physically based [10,11].
2. Photochemical internalization (PCI) — a light-triggered drugdelivery technology
Photochemical internalization (PCI) was developed at the Norwe-gian RadiumHospital as amethod for light-enhanced cytosolic releaseof membrane-impermeable molecular therapeutics entrapped inendocytic vesicles (Fig. 1) [12–14].
Briefly, the drug or gene of interest colocalizes with a photosen-sitizer in endocytic vesicles. Light-activation of the photosensitizerresults in reactive oxygen species (ROS)-mediated damage of themembranes of these vesicles with the subsequent release of the drugor gene to cytosol. PCI has been demonstrated to be a feasible drugdelivery technology in more than 80 different cancer cell lines(Table 1) and different animal models (Table 2).
PCI has been shown to be a highly efficient technology for inducedendolysosomal escape for several cancer targeted therapeutics and toincrease the efficacy of some conventional anti-cancer agents. PCI canalso improve gene therapy by enhanced delivery of various forms ofRNA/DNA to the cytosol or nucleus of the targeted cells. In addition, ithas also been documented that PCI enhance the delivery ofnanoparticles (see references in Tables 1 and 2).
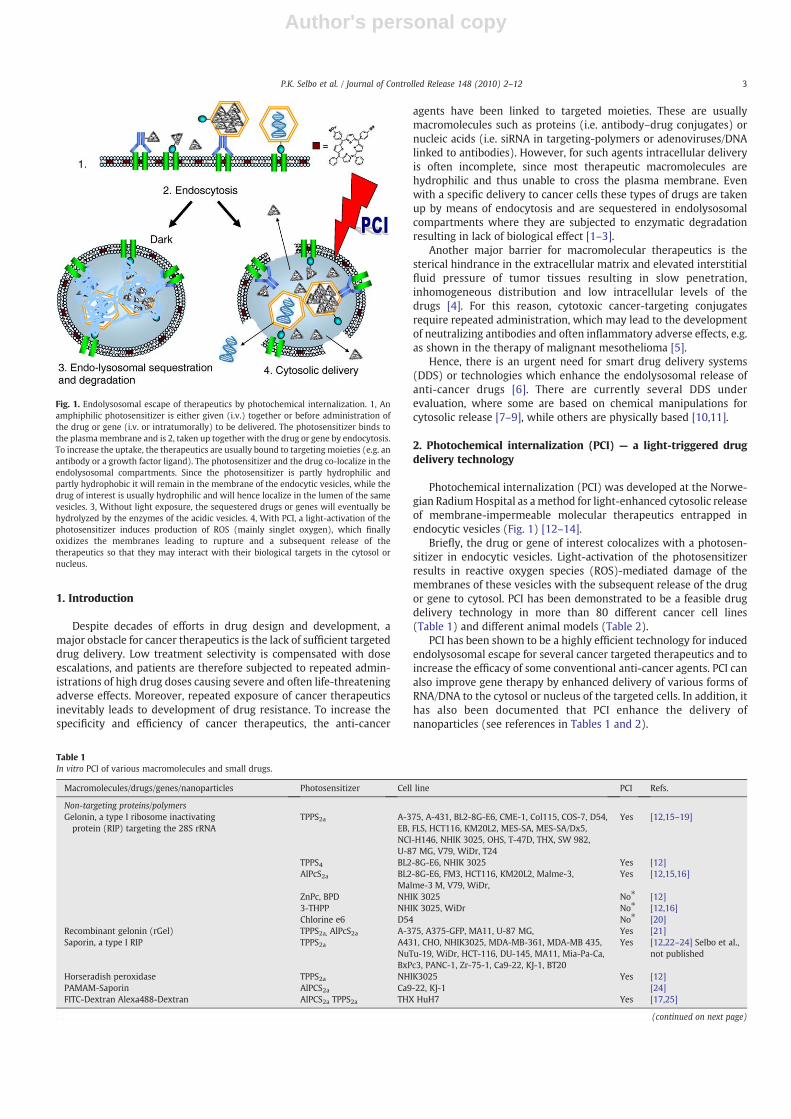
Fig. 1. Endolysosomal escape of therapeutics by photochemical internalization. 1, Anamphiphilic photosensitizer is either given (i.v.) together or before administration ofthe drug or gene (i.v. or intratumorally) to be delivered. The photosensitizer binds tothe plasmamembrane and is 2, taken up together with the drug or gene by endocytosis.To increase the uptake, the therapeutics are usually bound to targeting moieties (e.g. anantibody or a growth factor ligand). The photosensitizer and the drug co-localize in theendolysosomal compartments. Since the photosensitizer is partly hydrophilic andpartly hydrophobic it will remain in the membrane of the endocytic vesicles, while thedrug of interest is usually hydrophilic and will hence localize in the lumen of the samevesicles. 3, Without light exposure, the sequestered drugs or genes will eventually behydrolyzed by the enzymes of the acidic vesicles. 4, With PCI, a light-activation of thephotosensitizer induces production of ROS (mainly singlet oxygen), which finallyoxidizes the membranes leading to rupture and a subsequent release of thetherapeutics so that they may interact with their biological targets in the cytosol ornucleus.
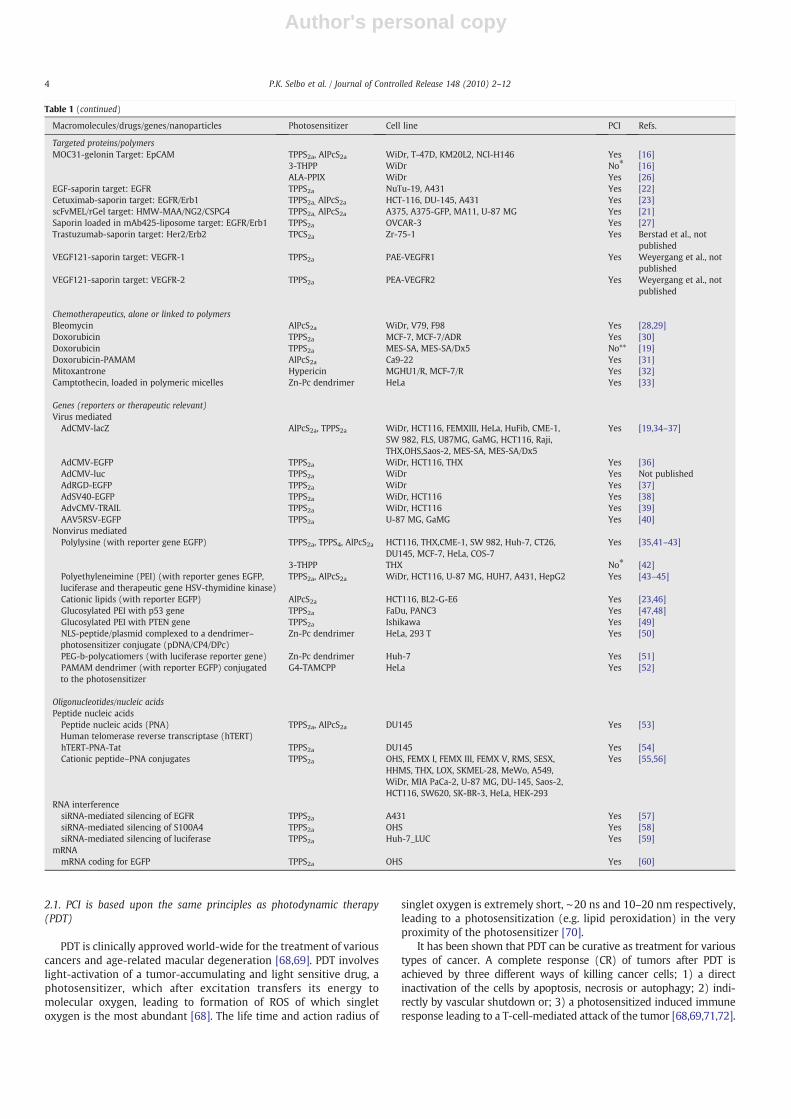
Table 1In vitro PCI of various macromolecules and small drugs.
Macromolecules/drugs/genes/nanoparticles Photosensitizer Cell line PCI Refs.
Non-targeting proteins/polymersGelonin, a type I ribosome inactivatingprotein (RIP) targeting the 28S rRNA
TPPS2a A-375, A-431, BL2-8G-E6, CME-1, Col115, COS-7, D54,EB, FLS, HCT116, KM20L2, MES-SA, MES-SA/Dx5,NCI-H146, NHIK 3025, OHS, T-47D, THX, SW 982,U-87 MG, V79, WiDr, T24
Yes [12,15–19]
TPPS4 BL2-8G-E6, NHIK 3025 Yes [12]AlPcS2a BL2-8G-E6, FM3, HCT116, KM20L2, Malme-3,
Malme-3 M, V79, WiDr,Yes [12,15,16]
ZnPc, BPD NHIK 3025 No⁎ [12]3-THPP NHIK 3025, WiDr No⁎ [12,16]Chlorine e6 D54 No⁎ [20]
Recombinant gelonin (rGel) TPPS2a, AlPcS2a A-375, A375-GFP, MA11, U-87 MG, Yes [21]Saporin, a type I RIP TPPS2a A431, CHO, NHIK3025, MDA-MB-361, MDA-MB 435,
NuTu-19, WiDr, HCT-116, DU-145, MA11, Mia-Pa-Ca,BxPc3, PANC-1, Zr-75-1, Ca9-22, KJ-1, BT20
Yes [12,22–24] Selbo et al.,not published
Horseradish peroxidase TPPS2a NHIK3025 Yes [12]PAMAM-Saporin AlPCS2a Ca9-22, KJ-1 [24]FITC-Dextran Alexa488-Dextran AlPCS2a TPPS2a THX HuH7 Yes [17,25]
(continued on next page)
3P.K. Selbo et al. / Journal of Controlled Release 148 (2010) 2–12
Author's personal copy
2.1. PCI is based upon the same principles as photodynamic therapy(PDT)
PDT is clinically approved world-wide for the treatment of variouscancers and age-related macular degeneration [68,69]. PDT involveslight-activation of a tumor-accumulating and light sensitive drug, aphotosensitizer, which after excitation transfers its energy tomolecular oxygen, leading to formation of ROS of which singletoxygen is the most abundant [68]. The life time and action radius of
singlet oxygen is extremely short, ∼20 ns and 10–20 nm respectively,leading to a photosensitization (e.g. lipid peroxidation) in the veryproximity of the photosensitizer [70].
It has been shown that PDT can be curative as treatment for varioustypes of cancer. A complete response (CR) of tumors after PDT isachieved by three different ways of killing cancer cells; 1) a directinactivation of the cells by apoptosis, necrosis or autophagy; 2) indi-rectly by vascular shutdown or; 3) a photosensitized induced immuneresponse leading to a T-cell-mediated attack of the tumor [68,69,71,72].
Table 1 (continued)
Macromolecules/drugs/genes/nanoparticles Photosensitizer Cell line PCI Refs.
Targeted proteins/polymersMOC31-gelonin Target: EpCAM TPPS2a, AlPcS2a WiDr, T-47D, KM20L2, NCI-H146 Yes [16]
3-THPP WiDr No⁎ [16]ALA-PPIX WiDr Yes [26]
EGF-saporin target: EGFR TPPS2a NuTu-19, A431 Yes [22]Cetuximab-saporin target: EGFR/Erb1 TPPS2a, AlPcS2a HCT-116, DU-145, A431 Yes [23]scFvMEL/rGel target: HMW-MAA/NG2/CSPG4 TPPS2a, AlPcS2a A375, A375-GFP, MA11, U-87 MG Yes [21]Saporin loaded in mAb425-liposome target: EGFR/Erb1 TPPS2a OVCAR-3 Yes [27]Trastuzumab-saporin target: Her2/Erb2 TPCS2a Zr-75-1 Yes Berstad et al., not
publishedVEGF121-saporin target: VEGFR-1 TPPS2a PAE-VEGFR1 Yes Weyergang et al., not
publishedVEGF121-saporin target: VEGFR-2 TPPS2a PEA-VEGFR2 Yes Weyergang et al., not
published
Chemotherapeutics, alone or linked to polymersBleomycin AlPcS2a WiDr, V79, F98 Yes [28,29]Doxorubicin TPPS2a MCF-7, MCF-7/ADR Yes [30]Doxorubicin TPPS2a MES-SA, MES-SA/Dx5 No** [19]Doxorubicin-PAMAM AlPcS2a Ca9-22 Yes [31]Mitoxantrone Hypericin MGHU1/R, MCF-7/R Yes [32]Camptothecin, loaded in polymeric micelles Zn-Pc dendrimer HeLa Yes [33]
Genes (reporters or therapeutic relevant)Virus mediated
AdCMV-lacZ AlPcS2a, TPPS2a WiDr, HCT116, FEMXIII, HeLa, HuFib, CME-1,SW 982, FLS, U87MG, GaMG, HCT116, Raji,THX,OHS,Saos-2, MES-SA, MES-SA/Dx5
Yes [19,34–37]
AdCMV-EGFP TPPS2a WiDr, HCT116, THX Yes [36]AdCMV-luc TPPS2a WiDr Yes Not publishedAdRGD-EGFP TPPS2a WiDr Yes [37]AdSV40-EGFP TPPS2a WiDr, HCT116 Yes [38]AdvCMV-TRAIL TPPS2a WiDr, HCT116 Yes [39]AAV5RSV-EGFP TPPS2a U-87 MG, GaMG Yes [40]
Nonvirus mediatedPolylysine (with reporter gene EGFP) TPPS2a, TPPS4, AlPcS2a HCT116, THX,CME-1, SW 982, Huh-7, CT26,
DU145, MCF-7, HeLa, COS-7Yes [35,41–43]
3-THPP THX No⁎ [42]Polyethyleneimine (PEI) (with reporter genes EGFP,luciferase and therapeutic gene HSV-thymidine kinase)
TPPS2a, AlPcS2a WiDr, HCT116, U-87 MG, HUH7, A431, HepG2 Yes [43–45]
Cationic lipids (with reporter EGFP) AlPcS2a HCT116, BL2-G-E6 Yes [23,46]Glucosylated PEI with p53 gene TPPS2a FaDu, PANC3 Yes [47,48]Glucosylated PEI with PTEN gene TPPS2a Ishikawa Yes [49]NLS-peptide/plasmid complexed to a dendrimer–photosensitizer conjugate (pDNA/CP4/DPc)
Zn-Pc dendrimer HeLa, 293 T Yes [50]
PEG-b-polycatiomers (with luciferase reporter gene) Zn-Pc dendrimer Huh-7 Yes [51]PAMAM dendrimer (with reporter EGFP) conjugatedto the photosensitizer
G4-TAMCPP HeLa Yes [52]
Oligonucleotides/nucleic acidsPeptide nucleic acids
Peptide nucleic acids (PNA)Human telomerase reverse transcriptase (hTERT)
TPPS2a, AlPcS2a DU145 Yes [53]
hTERT-PNA-Tat TPPS2a DU145 Yes [54]Cationic peptide–PNA conjugates TPPS2a OHS, FEMX I, FEMX III, FEMX V, RMS, SESX,
HHMS, THX, LOX, SKMEL-28, MeWo, A549,WiDr, MIA PaCa-2, U-87 MG, DU-145, Saos-2,HCT116, SW620, SK-BR-3, HeLa, HEK-293
Yes [55,56]
RNA interferencesiRNA-mediated silencing of EGFR TPPS2a A431 Yes [57]siRNA-mediated silencing of S100A4 TPPS2a OHS Yes [58]siRNA-mediated silencing of luciferase TPPS2a Huh-7_LUC Yes [59]
mRNAmRNA coding for EGFP TPPS2a OHS Yes [60]
4 P.K. Selbo et al. / Journal of Controlled Release 148 (2010) 2–12
Author's personal copy
2.2. An optimal photosensitizer for PCI localizes to the membrane ofendolysosomal vesicles
PCI-photosensitizers are amphiphilic compounds which bind tothe plasma membrane and localize to the membranes of endocytic
vesicles after endocytosis [12,14,15,42]. PCI is then performed by alocal and controlled light-activation of the photosensitizer thatcolocalizes with the drug of interest in endocytic vesicles of cancercells. The drug is usually hydrophilic and localizes to the endolyso-somal lumen while the photosensitizer mainly localizes to the vesicle
Table 2Macromolecules delivered by PCI in vivo in different tumor models and normal tissue.
Macromolecules Drug/gene Administration Xenograft/normal tissue model Photosensitizer PCI Refs.
Proteins/polymersGelonin scFvMEL/rGel, recombinant targeting toxin Intratumoral WiDr, THX AlPcS2a Yes [14,61]
Intratumoral Tax-1 AlPcS2a Yes [62]Intravenous Normal liver of Wistar rats AlPcS2a Yes [63]Intravenous A-375 AlPcS2a Yes [21]
Saporin, a type I RIP Intratumoral WiDr AlPcS2a Yes Selbo et al.,Not published
ChemotherapeuticsBleomycin, chemotherapeutic Intravenous WiDr, CT26, Tax-1 AlPcS2a Yes [28]
Intravenous Tax-1 AlPcS2a Yes [64]Intravenous HT1080 AlPcS2a Yes [65,66]Intravenous F98, AlPcS2a Yes [29]
Genes (reporters and therapeutic relevant)NLS-peptide/plasmid complexed to a dendrimer–photosensitizer conjugate (pDNA/CP4/DPc)
Subconjunctival injection Normal eye of Wistar rats Zn-Pc dendrimer Yes [50]
Glucosylated PEI with p53 gene Intratumoral HNSCC xenograft from ananonymous patient
AlPcS2a Yes [48]
Oligonucleotides/nucleic acidssiRNA-mediated silencing of EGFR Intratumoral A431 AlPcS2a Yes [67]
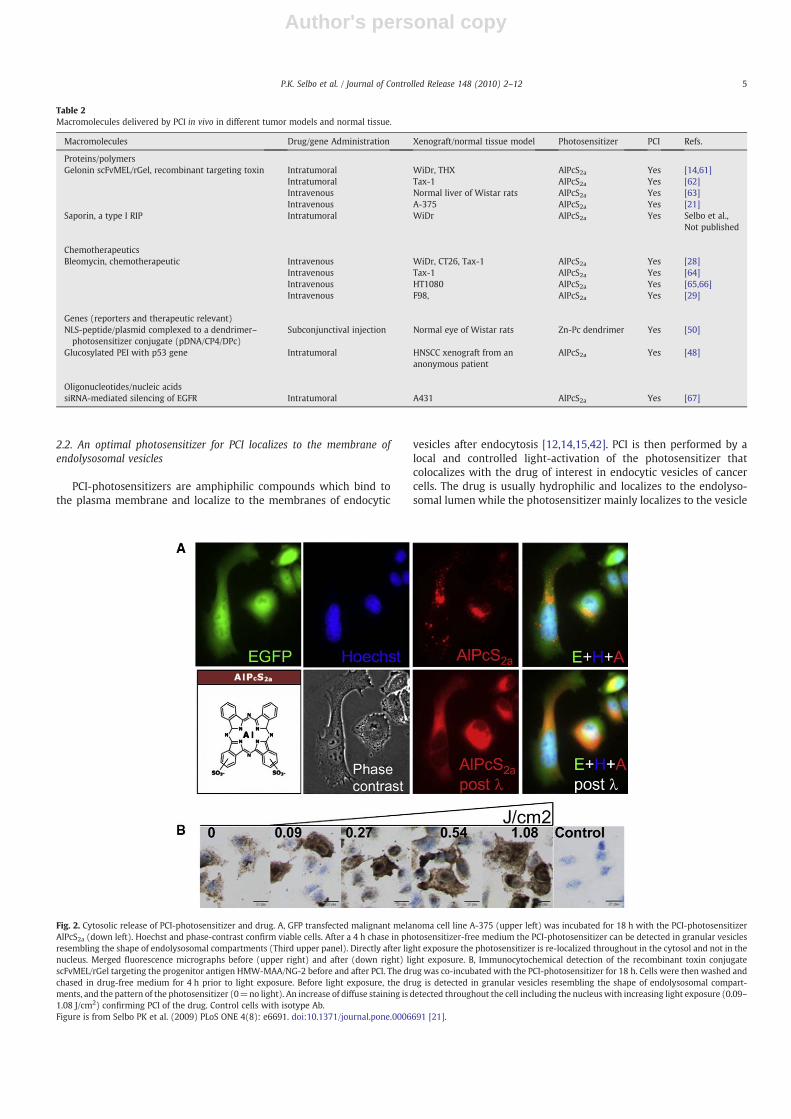
Fig. 2. Cytosolic release of PCI-photosensitizer and drug. A, GFP transfected malignant melanoma cell line A-375 (upper left) was incubated for 18 h with the PCI-photosensitizerAlPcS2a (down left). Hoechst and phase-contrast confirm viable cells. After a 4 h chase in photosensitizer-free medium the PCI-photosensitizer can be detected in granular vesiclesresembling the shape of endolysosomal compartments (Third upper panel). Directly after light exposure the photosensitizer is re-localized throughout in the cytosol and not in thenucleus. Merged fluorescence micrographs before (upper right) and after (down right) light exposure. B, Immunocytochemical detection of the recombinant toxin conjugatescFvMEL/rGel targeting the progenitor antigen HMW-MAA/NG-2 before and after PCI. The drug was co-incubated with the PCI-photosensitizer for 18 h. Cells were then washed andchased in drug-free medium for 4 h prior to light exposure. Before light exposure, the drug is detected in granular vesicles resembling the shape of endolysosomal compart-ments, and the pattern of the photosensitizer (0=no light). An increase of diffuse staining is detected throughout the cell including the nucleus with increasing light exposure (0.09–1.08 J/cm2) confirming PCI of the drug. Control cells with isotype Ab.Figure is from Selbo PK et al. (2009) PLoS ONE 4(8): e6691. doi:10.1371/journal.pone.0006691 [21].
5P.K. Selbo et al. / Journal of Controlled Release 148 (2010) 2–12
Author's personal copy
membrane. This ensures that the drug is kept on a distance from thephotosensitizer, thereby minimizing a potential photochemicaldestruction of the drug. The excitation of the PCI-photosensitizerinduces a photosensitized rupture of the lipid layer of the endolyso-somal membranes followed by the ultimate cytosolic release of thephotosensitizer and the drug (Fig. 2) [15].
By using subtoxic photochemical doses, it is possible to releaseapproximately 50% of the sequestered molecules from endocyticcompartments to the cytosol in the cell with no loss of biologicalactivity of the molecule [12]. A recent study demonstrated that the
PCI-induced release of macromolecules takes part within a range of0.01–4 s depending on the nature of the cargo [25].
2.3. The viability of cancer cells treated with ribosomal inactivatingprotein toxins should be assessed at least 48 h after PCI
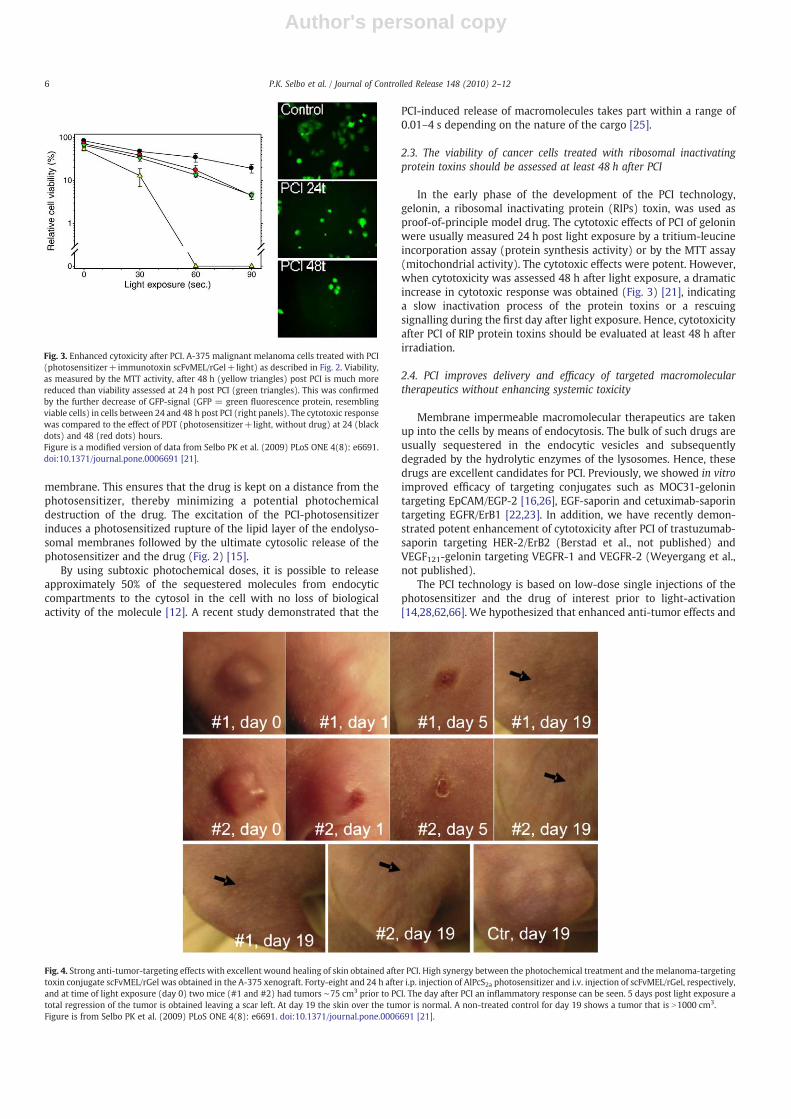
In the early phase of the development of the PCI technology,gelonin, a ribosomal inactivating protein (RIPs) toxin, was used asproof-of-principle model drug. The cytotoxic effects of PCI of geloninwere usually measured 24 h post light exposure by a tritium-leucineincorporation assay (protein synthesis activity) or by the MTT assay(mitochondrial activity). The cytotoxic effects were potent. However,when cytotoxicity was assessed 48 h after light exposure, a dramaticincrease in cytotoxic response was obtained (Fig. 3) [21], indicatinga slow inactivation process of the protein toxins or a rescuingsignalling during the first day after light exposure. Hence, cytotoxicityafter PCI of RIP protein toxins should be evaluated at least 48 h afterirradiation.
2.4. PCI improves delivery and efficacy of targeted macromoleculartherapeutics without enhancing systemic toxicity
Membrane impermeable macromolecular therapeutics are takenup into the cells by means of endocytosis. The bulk of such drugs areusually sequestered in the endocytic vesicles and subsequentlydegraded by the hydrolytic enzymes of the lysosomes. Hence, thesedrugs are excellent candidates for PCI. Previously, we showed in vitroimproved efficacy of targeting conjugates such as MOC31-gelonintargeting EpCAM/EGP-2 [16,26], EGF-saporin and cetuximab-saporintargeting EGFR/ErB1 [22,23]. In addition, we have recently demon-strated potent enhancement of cytotoxicity after PCI of trastuzumab-saporin targeting HER-2/ErB2 (Berstad et al., not published) andVEGF121-gelonin targeting VEGFR-1 and VEGFR-2 (Weyergang et al.,not published).
The PCI technology is based on low-dose single injections of thephotosensitizer and the drug of interest prior to light-activation[14,28,62,66]. We hypothesized that enhanced anti-tumor effects and
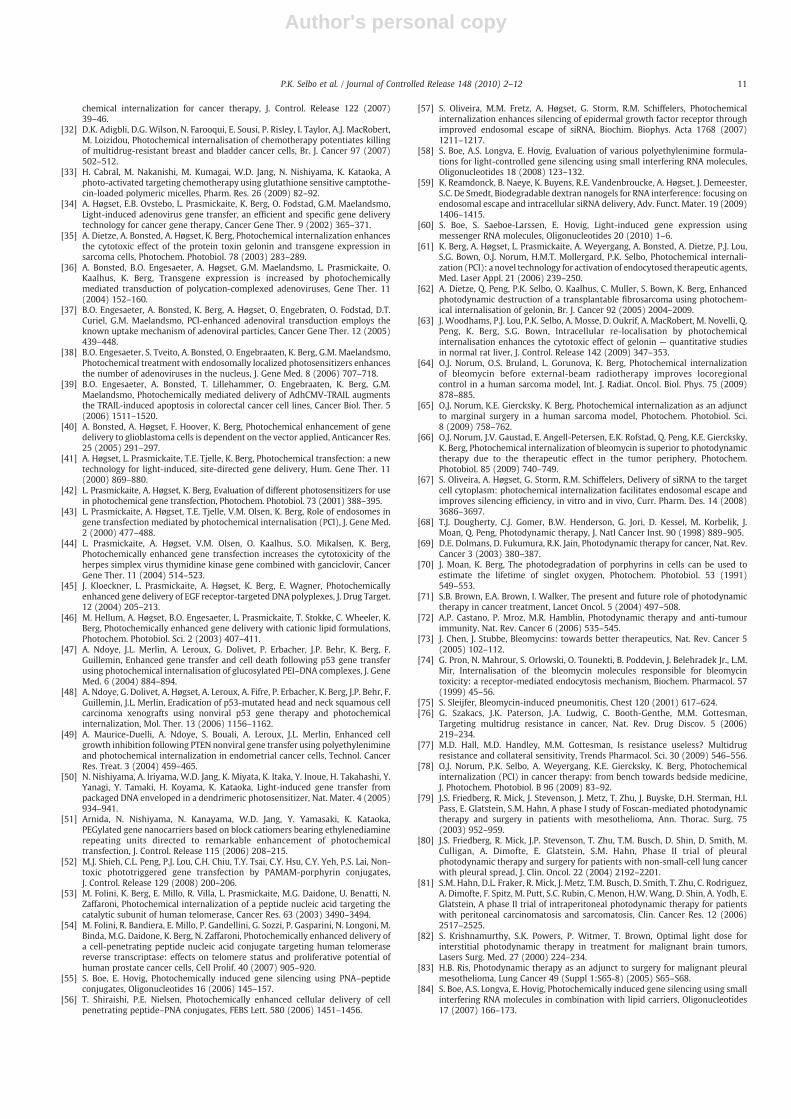
Fig. 4. Strong anti-tumor-targeting effects with excellent wound healing of skin obtained after PCI. High synergy between the photochemical treatment and the melanoma-targetingtoxin conjugate scFvMEL/rGel was obtained in the A-375 xenograft. Forty-eight and 24 h after i.p. injection of AlPcS2a photosensitizer and i.v. injection of scFvMEL/rGel, respectively,and at time of light exposure (day 0) two mice (#1 and #2) had tumors ∼75 cm3 prior to PCI. The day after PCI an inflammatory response can be seen. 5 days post light exposure atotal regression of the tumor is obtained leaving a scar left. At day 19 the skin over the tumor is normal. A non-treated control for day 19 shows a tumor that is N1000 cm3.Figure is from Selbo PK et al. (2009) PLoS ONE 4(8): e6691. doi:10.1371/journal.pone.0006691 [21].
Fig. 3. Enhanced cytoxicity after PCI. A-375 malignant melanoma cells treated with PCI(photosensitizer+immunotoxin scFvMEL/rGel+light) as described in Fig. 2. Viability,as measured by the MTT activity, after 48 h (yellow triangles) post PCI is much morereduced than viability assessed at 24 h post PCI (green triangles). This was confirmedby the further decrease of GFP-signal (GFP = green fluorescence protein, resemblingviable cells) in cells between 24 and 48 h post PCI (right panels). The cytotoxic responsewas compared to the effect of PDT (photosensitizer+light, without drug) at 24 (blackdots) and 48 (red dots) hours.Figure is a modified version of data from Selbo PK et al. (2009) PLoS ONE 4(8): e6691.doi:10.1371/journal.pone.0006691 [21].
6 P.K. Selbo et al. / Journal of Controlled Release 148 (2010) 2–12

Author's personal copy
lack of severe adverse systemic events after PCI of targeted toxinsshould provide significant improvement in anti-tumor specificity andefficacy, while at the same time sparing the normal tissue. Recently,this was confirmed in vivo by demonstrating no weight loss or otheradverse effects in animals after PCI of the fusion toxin scFvMEL/rGeltargeting the progenitor marker HMW-MAA (also known as NG2,MCSP, MCSPG, MSK16, MEL-CSPG, CSPG4 or gp240) [21]. This was thefirst study demonstrating that PCI is an efficient technology forenhancing the therapeutic efficacy of systemically (i.v.) deliveredtargeting drugs. Photosensitizer and drugs were administered onlyonce prior to laser light exposure (Figs. 2–4).
2.5. PCI enhances the efficacy of chemotherapeutics that accumulate inendocytic vesicles
A prerequisite to perform successful PCI is that the drug of interestis entrapped in endocytic vesicles and co-localize with the PCI-photosensitizer. Most chemotherapeutics are small molecules that areable to penetrate the plasma membrane and enter the cytosol.However, several weak-base chemotherapeutics tend to accumulatein endolysosomal compartments with low intraluminal pH, also calledthe partitioning effect. In addition, endosomal entrapment is alsocommon fate for chemotherapeutics that are packed in polymers/nanoparticles. Hence, such chemotherapeutics are promising drugs tobe released from endolysosomal entrapment by PCI (see Section 2.7).To date, four different chemotherapeutics have been delivered by PCI,including bleomycin [28,29,64–66], doxorubicin [30,31], mitoxan-trone [32] and camptothecin [33] (Table1). In the following twosections, PCI of Bleomycin and doxorubicin will be discussed.
2.5.1. PCI enhances the cytotoxic effect of bleomycin in a synergisticmanner
Bleomycin is a ∼1.4 kDa glycopeptide antibiotic with potent anti-tumor activity due to its ability to induce DNA strand breaks.Bleomycin is approved for several standard cancer chemotherapyregimens such as lymphoma, head and neck tumors and testicularcancer and has been used clinically for decades [73]. However, it has alimited ability to penetrate membrane structures causing accumula-tion of bleomycin in endolysosomal compartments leading to asignificant attenuation of its efficacy [74]. To compensate for this typeof resistance, relatively high doses of bleomycin are administeredleading to development of pneumonitis in near 50% of the patients,with a mortality rate of 3% due to severe lung fibrosis [75]. Hence,there is a need for strategies which can increase the efficacy ofbleomycin. Since bleomycin is taken up in cells by endocytosis it washypothesized that the drug was a potential candidate for PCI.
Thus, we have demonstrated in vivo synergistic effects after PCI ofbleomycin in four different xenografts in BALBc (nu/nu) mice [28,64–66]. Bleomycin was injected (i.v.) once prior to light exposure of thexenografts. In two of the xenograft models a curative response wasobserved in 60% of all mice that received PCI of bleomycin, while notumor control was observed in animals receiving bleomycin only.
The first clinical PCI study is ongoing at the University CollegeHospital, London, UK. This is a phase I/II clinical trial evaluating PCI ofbleomycin in patients with various cancer indications.
2.5.2. PCI-enhanced cytotoxicity of doxorubicin in multi-drug resistant(MDR) cancer cells is dependent on the partitioning effect
Many pre-clinical and clinical studies have demonstrated thatsingle agent chemotherapy provides only modest and short-livedresponses in several types of cancer. Even though tumor regression isinitially obtained, a substantial fraction of most types of cancers finallyrecur due to development of resistance to chemotherapeutical agents.MDR is one of the major limitations of effective cancer chemotherapy.Hence, one important criterion for improving efficacy of chemother-
apy is the development of novel drugs or delivery systems that bypassMDR [76].
PCI of doxorubicin has been shown to be efficient in breast cancerMCF-7/ADR cells that are resistant to doxorubicin [30]. These MDRcells have a lower pH of the endocytic vesicles than in normal cells andtherefore sequester the weak-base chemotherapeutic agent doxoru-bicin in the endolysosomal compartments. Doxorubicin was shown toco-localize with the PCI-photosensitizer TPPS2a, and after lightexposure doxorubicin was released from endocytic vesicles and re-localized to the cytosol and cell nuclei.
In another study, PCI did not improve the efficacy of doxorubicin inthe MDR uterine sarcoma cell line MES-SA/Dx5 [19]. This may beexplained by the fact that the MES-SA/Dx5 cells do not have adecreased pH in the endolysosomal compartments and hence thesecells will not have the same partitioning effects as described with theMCF-7/ADR cells described above. Surprisingly, the MES-SA/Dx5MDRcells were more sensitive to PCI of gelonin as compared to PCI ofgelonin in the maternal cell line MES-SA [19]. The mechanism of thisobservation is not known and should be elucidated. However, it isknown that MDR cells are hypersensitive to other drugs; aphenomenon named collateral sensitivity [77].
2.5.3. Surgery or ionizing radiation in combination with PCILocal treatment failure in cancer therapy is a major problem.
Extensive surgery may result in cosmetic or functional deficit, andtherapeutic doses of radiotherapy as well as chemotherapymay resultin short- and long-term normal tissue toxicity, limiting the treatmentdose given and hence the possibility to achieve local tumor control[78]. Thus, novel treatment strategies avoiding serious adverse effectsafter radiation therapy or mutilating surgery and improved locor-egional control, are warranted.
PDT for eradicating remaining tumor cells after debulking surgeryhas been the focus of several clinical trials [79–83]. The results havebeen promising, but not convincing in achieving local control. Ingeneral, the maximum tolerated dose in these clinical PDT trials islimited by treatment-related side effects on normal tissue [78]. In arecent publication, PCI of bleomycin was found superior to PDT ininhibiting growth of the HT1080 fibrosarcoma xenograft by moreefficiently targeting the peripheral zone of the tumor [66]. The PCI-induced cytotoxicity in the peripheral zone has been found due toboth targeting of the parenchyma cells as well as the vasculature(Vikdal et al., unpublished). This is similar to the effect of PDT in thetumor centre [66]. Moreover, PCI of bleomycin as an adjunct tosurgery has been shown to significantly delay tumor growth, incontrast to PDT in combination with surgery [65]. The results indicatethat PCI of bleomycin may be an efficient intra-operative technique toeradicate remaining cancer cells in the wound bed after surgery.
The first report on the treatment effect of PCI of bleomycin incombination with ionizing radiation in mice demonstrated that timeto progression increased when PCI of bleomycin was used as anadjunct to ionizing radiation in a human soft tissue sarcoma xenograft[64]. PCI treatment prior to ionizing radiation caused more than30 days delay in time to progression while ionizing radiation alonecaused only 17 days of reduced tumor growth and no reduction intumor volume. When PCI and ionizing radiation were separated intime, no adverse effects were observed.
Collectively, our pre-clinical data indicate that PCI of bleomycin incombination with surgery or external-beam radiotherapy is apromising treatment modality that may reduce the need formutilating surgery or toxic radiation effects, and thus improve localtumor control.
2.6. PCI enhance nucleic acid delivery
With most nucleic acid delivery systems the therapeutic nucleicacid is taken into the cell by endocytosis. For many of these systems,
7P.K. Selbo et al. / Journal of Controlled Release 148 (2010) 2–12

Author's personal copy
especially non-viral-based, translocation of the nucleic acid out of theendocytic vesicles constitutes a major hindrance for realization of itsfull therapeutic potential. PCI has been studied as a gene deliverytechnology (reviewed in [13]), both with several non-viral, as well aswith adenovirus and adeno-associated viral vectors, mainly byutilizing reporter genes such as genes encoding EGFP (enhancedgreen fluorescent protein) or ß-galactosidase. However, PCI has alsobeen shown to enhance the delivery of therapeutic genes, such as thegenes encoding HSV-tk (Herpes Simplex Virus thymidine kinase) [44],p53 [47] and [48], PTEN [49] and TRAIL [39] (see Table 2).
For non-viral vectors, PCI in general gives a strong enhancement oftransgene expression from plasmids delivered by polyplexes, whilethe PCI effect on lipoplexes is more dependent on the structure of thelipoplex on the transfection regimen and probably also on the cell line[46]. E.g. using 22 kDa linear polyethylenimine (PEI) for plasmiddelivery, expression of luciferase was enhanced by up to 600-fold, andexpression of an EGFP transgene more than 35-fold [44,45]. Similareffects have also been observed with other forms of PEI, but theoptimal conditions for PCI with PEI-based vectors are still to bedetermined. PCI has also been shown to be efficient in enhancingtransfection of poly-L-lysine polyplexes, which are highly inefficientalone since these polyplexes are not inducing any proton spongeeffect [13].
An in vivo study showed that treatment of p53-mutated head andneck squamous cell carcinomas with intratumoral injection of thephotosensitizer AlPcS2a and a plasmid encoding p53 complexed to aglycosylated PEI caused dramatic tumor regression in all thetransfected animals [48]. Since neither injecting the plasmid withoutPCI nor the photochemical treatment alone gave any delay in tumorgrowth this shows that the PCI-mediated enhancement of genedeliverywas essential to achieve the very good therapeutic effect seenin these experiments. In this study the tumors were relatively large atthe time of the first treatment (500 mm3) and the tumors weretreated once a week for up to 7 weeks. These results thus indicate thatPCI-enhanced repeated local gene therapymight be feasible to controlbulky tumors. However, the development of methods for systemicadministration of the polyplex for homogeneous and non-toxictransfection is a major goal for future gene therapy protocols. Tothis end, polyethylene glycol (PEG) is widely used for shieldingbiomolecular therapeutics and prolongs their circulating half-lives.However, PEGylation is also known to reduce transfection efficacy ofnon-viral vectors, probably due to decreased uptake of the transfec-tion complex into the target cells. PCI can significantly enhancetransfection with PEGylated vectors, and especially interesting in thisregard are the good effects seen when PEG is linked to a targetingligand, such as EGF [45], transferrin or amAb. Such vectors exert manyof the requirements needed for specific and efficient in vivo genedelivery, and the additional efficiency and specificity that can beobtained by combining such vectors with PCI should give a veryinteresting option for in vivo gene delivery.
Kataoka and coworkers have designed dendrimer-based nanopar-ticles that have shown great promise both in vitro and in vivo [50].Plasmids were complexed with a positively charged NLS (nuclear-localizing sequence) peptide at an N:P ratio of 2 and thereaftercovered by negatively charged dendrimers containing a centrallylocated phthalocyanine photosensitizer. In vitro PCI utilizing theseternary nanoparticles enhanced transgene expressionmore than 100-fold with low photocytotoxicity, and the nanoparticles also workedwell for gene delivery in vivo. Recently, Shieh and coworkers reportedsimilar results, i.e. high PCI-mediated gene delivery and low photo-cytotoxicity, by utilizing a photosensitizer linked to a cationic poly-amidoamine (PAMAM) dendrimer [52].
PCI has also been used successfully to deliver various types ofoligonucleotides. Thus, enhancement of in vitro delivery of both peptidenucleic acids [53,55,56] and siRNA [57–59] has been reported, andrecently it was reported that PCI could enhance siRNA delivery also in
vivo [67]. With oligonucleotides PCI can enhance delivery mediated bydifferent types of delivery vectors. Thus, PCI is efficient for delivery ofnaked peptide nucleic acids [53] and peptide nucleic acids conjugated tovarious types of cationic peptides [55,56]. As for gene delivery the effectof PCI seems to be most consistent for polycationic delivery vehiclessuch as PEI [58], polyarginine (Boe et al, unpublished), PAMAM den-drimers (Boe et al, unpublished) and dextran nanogels [59]. However,substantial enhancement has also been observedwith some lipid-basedvehicles such as Lipofectamine 2000 [57,67,84].
2.7. PCI of nanomedicines
An emerging field in drug delivery is the use of nanocarriers asdrug vehicles. Since such nanocarriers accumulate in endolysosomalcompartment after cellular uptake [85,86] they are excellentcandidates for PCI. Recently it was documented that PCI enhancethe therapeutic effect of nano-sized dendrimers linked to doxorubicin[31], camptothecin [33], saporin [24] and DNA [50,52,87]. It has alsobeen demonstrated that PCI can significantly enhance the biologicaleffect of a protein toxin delivered by means of a liposome, both withliposomes targeted by an antibody and with non-targeted liposomes[27]. Furthermore, as also described above PCI can enhance thedelivery of many different types of nucleic acid nanocarriers. A recentand very interesting example of this is the prolonged effect of siRNAthat can been achieved by inducing PCI-mediated endosomal releaseseveral days after the delivery of siRNA by nanogels [88]. Photo-sensitizers may also be incorporated into the dendrimers withoutsignificant photosensitization of the drug/gene to be delivered.Strikingly, these photosensitizer-loaded nanocarriers escape to thecytosol after light doses not inducing phototoxicity [50]. Thus, PCIwith such photosensitizers may be utilized for treatment of non-cancerous diseases where photocytotoxicity is not acceptable, such asin gene therapy for genetic diseases.
2.8. Photochemical rupture of endocytic vesicles before administrationof molecular therapeutics: success of PCI is dependent on the type ofendocytosis of the drug
A standard protocol for PCI of macromolecules in vitro involves aco-incubation of the PCI-photosensitizer and the drug of interestovernight, prior to wash and a few hours chase in drug-free mediumto remove the photosensitizer from the plasma membrane. Alterna-tively, after the overnight incubation of the photosensitizer, the drugor a gene of interest is incubated in the photosensitizer-free mediumup to 4 h prior to light exposure of the cells [12,13,15].
However, we discovered the option to incubate the drug or gene ofinterest post light exposure, also called the “light first procedure”.When gelonin, a ribosomal inactivating protein toxin that is taken upby fluid phase endocytosis, was administered to the cells directly afterlight exposure, even higher cytotoxicity was obtained than with thestandard protocol, also called the “light after procedure”. In addition,the efficiency of gene delivery was as high as with the standard PCIprotocol when the gene was delivered directly after light exposure,whilst introducing a chase period between illumination and the DNA-treatment decreased the transfection efficiency [17].
The PCI light first procedure was later confirmed in vivo where∼80% CR was obtained in BALBc nu/nu mice with subcutaneoushuman colorectal adenocarcinoma tumors. In this study gelonin wasadministered immediately after the light exposure [61].
A possible mechanism for the ‘light first’ effects could be a fusionbetween the newly endocytosed and intact vesicles carrying themacromolecules and the photochemically ruptured vesicles leading toa subsequent release of the molecules to the cytosol.
However, when the light first principle is combined with targetingcytotoxic conjugates that consist of an affinity ligand, e.g. EGF, or anantibody, e.g. cetuximab or scFv/MEL, successful PCI-effects are not
8 P.K. Selbo et al. / Journal of Controlled Release 148 (2010) 2–12

Author's personal copy
achievable [21–23]. A rationale for this could be photosensitization ofthe receptor or important mediators nearby the receptor, whichthereby loses its ability to perform efficient receptor-mediatedendocytosis.
3. Targeting signalling effectors important for cell survival andproliferation by light-activation of PCI-photosensitizers
PCI of targeted therapeutics in cancer cells results in synergisticeffects due to combination of two different modalities; first; thephotosensitization leading to rupture of the endolysosomal mem-branes and second; the administration of the drug which subse-quently is released into the cytosol and thereby reaches its target. Themechanisms of action after PCI treatment is therefore dependent onthe photochemical treatment as well as the drug which is delivered.The pharmacology of the drugs delivered by PCI, e.g. the RIPs gelonin[14] and saporin [22,23] or chemotherapeutics e.g. bleomycin [28],doxorubicin [30], mitoxantrone [32] and camptothecin [33] or nucleicacid based drugs [13] is relatively well known. However, knowledgeof PDT-mediated cytotoxicity and molecular effects using PCI-photosensitizers is sparse. Light-activation of PCI-photosensitizershas been shown to target several proteins associated with growth andsurvival such as the epidermal growth factor receptor (EGFR) [89,90],extracellular regulated kinase (ERKI/II) [91], mammalian target ofrapamycin (mTor) [92] and c-Jun N-terminal kinase/stress-activatedprotein kinase JNK/SAPK [91]. In addition, the photochemicaltreatment has been shown to activate pathways associated withboth apoptosis (caspase 3 and caspase 8 [39] and autophagy (LC3cleavage (not published)). Hence, the cytotoxic effect after photo-sensitization using PCI-photosensitizer may be due to inactivation ofmultiple cell survival effectors which takes place post light exposure.
Combination therapy has generally been recognized most effectivewhen the different treatment modalities have distinct mechanismsof action [93,94]. Mapping the cellular signalling involved in PDT-mediated cell death may therefore be important when selectingappropriate drugs for PCI delivery. On the other hand, we have recentlyreported on synergistic cytotoxicity when photochemical treatmentwith PCI relevant photosensitizers is combinedwith themTOR inhibitorrapamycin [92], as well as the EGFR inhibitor Tyrphostin AG1478 [90].Thus, a better understanding of the mechanisms of cell death andsurvival signalling after photochemical treatment using PCI-photosen-sitizers is important for optimizing the technology in the future.
4. Limitations and advantages of the PCI technology
Even though a significant fraction of sequestered molecules arereleased to the cytosol after PCI, some of the drugs may also be photo-oxidized due to localization near the membranes of the endocyticvesicles where singlet oxygen is formed. This seems to be a limitationin gene therapy when the carrier of the gene is lipophilic [43,46].However, with the use of more hydrophilic gene vectors this may becontrolled in a better manner. Likewise, significant fractions ofhydrophilic drugs are released and still maintain their biologicalactivity after PCI [12]. Also, if the PCI-photosensitizers used are morereadily photobleached (light-induced degradation), this will stopROS-formation ideally after rupture of the endocytic membrane.
One potential limitation of PCI, as for surgery, radiation therapy andPDT, is its restriction to ablate only local tumors and not metastases.However, this could also be considered as an advantage of thetechnology providing controlled cytosolic release or activation of thedrugs/genes confined to the tissue that is light exposed. Interestingly,it has been shown in pre-clinical models that PDT may have a cancer-vaccinating effect [95,96] and [72], including our lab (data notpublished). Recently, it was documented that a patient with reccurrentangiosarcoma that received PDT treatment achieved elimination of adistal tumor that was not exposed to light indicating an induction of
anti-tumor immunity [97]. The use of PCI and PDT is limited by thepenetration depth of the light in tissues due to scattering andabsorptionof the light. The volume of necrotic effects induced post PCI is stillsignificantly larger than that induced by PDT, since the cell killing effectinduced by the drugs delivered by PCI substantially exceeds what isachievable with the photochemical treatment alone [14,62,63,66].Hence, due to PCI, the cytotoxic drug will act in cells even when theyare exposed to illumination dose for which the pure photochemicaleffect is only subtoxic. Maximum penetration depth of near infraredlight (NIR) is considered to be 2 cm in low-pigmented tissues [98].However, with multiple fibres, as used in interstitial PDT (IPDT), whichalso should be feasible for use in PCI, there is a potential to treatrelatively large tumors [99].
PDT induces few adverse events which are predictable andtreatable [71]. Photosensitization of the skin and eyes is the mostpredictable systemic side-effect after PDT [100]. However, suchtoxicity is managed by avoiding direct sun exposure.
A major benefit of PCI is its curative potential using low doses oflight and drugs, while at the same time maintaining a high tumor tonormal tissue specificity, reflected in the lack of systemic side effectsas we reported recently [21]. As compared to chemotherapeutics,photosensitizers are non-toxic drugs and are only activated by lightwith specific wavelengths matching the absorption spectra of thephotosensitizer. Since most photosensitizers that are in clinical use donot localize to the nucleus of the cell, the possibility of achievingmutagenic effects of the treatment is very low [68]. After threedecades of clinical use world-wide there are no indications that PDTinduces secondary cancers, in contrast to radiation therapy andchemotherapy, suggesting that also PCI is non-carcinogenic. Anothermajor advantage of PCI is its potential to bypassmulti-drug resistance,as described in Section 2.2.
PCI is a minimally invasive treatment strategy and should therebylower the burden for the patient compared to surgery. This may beadvantageous e.g. for the treatment of subcutaneous and cutaneoustumors (e.g. sarcomas, head and neck cancers, and skin cancers),tumors in the mouth and body cavities, (e.g. oesophagus and bladder)and tumors in gastro-intestinal tract. Our pre-clinical results suggestthat patients will tolerate PCI-based cancer therapy better whencompared with radiotherapy and chemotherapy.
Compared to existing standard treatments of non-melanoma skinneoplasia, such as actinic keratoses, Bowen's disease, and basal cellcarcinoma (superficial and nodular), topical PDT has been documen-ted to be the best choice with respect to cosmesis at comparabletherapeutic effects [101]. PCI also appears to provide good cosmeticresults. After PCI of the HMW-MAA-targeting fusion toxin MEL/scFv-rGel achieved regrowth of the skin over the treated area with ex-cellent cosmetic outcome [21].
To establish PCI in the clinic, there is no need of significantinvestment in equipments, only a laser or filtered lamp is needed forthe activation of the drugs. New generation diode lasers areinexpensive, compact, portable, easy to use and reliable. In addition,there is no need of any specialized operating suite. Another importantfactor which may lower the cost per patient is the reduced drug dosesneeded. As observed pre-clinically, only one injection of the drugsfollowed by one light exposure is needed to obtain full ablation of thetumor [14,21,28,62,66]. This will certainly reduce the cost of drugsand possibly also reduce the length of hospitalization. As for PDT, itcould also be possible to perform the treatment on an out-patientbasis. However, this will depend on the drug of interest to bedelivered and phototoxicity.
5. Moving PCI from bench to bedside
The PCI technology is a promising strategy to improve theefficacy of many types of both small molecule and macromolecular
9P.K. Selbo et al. / Journal of Controlled Release 148 (2010) 2–12

Author's personal copy
therapeutics. PCI is widely documented in pre-clinical experimentsand has a potential to be used against many types of cancers as well asfor the treatment of several other types of diseases. Recently, PCIBiotech AS (Oslo, Norway) initiated the first PCI-based clinical trial(ClinicalTrials.gov identifier: NCT00993512) named “Phase I, Dose-escalating Study to Evaluate Safety and Tolerance of Amphinex BasedPhotochemical Internalisation (PCI) of Bleomycin in Patients WithLocal Recurrence or Advanced/Metastatic, Cutaneous or Sub-cutane-ous Malignancies”. This study is conducted at the University CollegeLondon Hospital with Colin Hopper, MD as principal investigator[102]. The primary goal of the study is to assess the safety andtolerance of the Amphinex photosensitizer and to determine themaximal tolerated dose (MTD) of Amphinex in a PCI therapy with thecytotoxic agent bleomycin. So far three dose levels of Amphinex havebeen tested in combination with a fixed dose of bleomycin, and nosevere treatment-related side effects have been observed. Veryinterestingly, preliminary data shows a fast and complete clinicalregression of all tumors that have been treated (n=11) with anapparently high tumor to normal tissue specificity.
In patients that at different time point after Amphinex adminis-tration were exposed to a controlled illumination simulating 5 min ofintense sun light non-significant skin photosensitivity was observed(oral communication with C. Hopper, and PCI Biotech press release 16March 2010).
PCI-induced therapeutic effects can be observed also for tumorswith a thickness of N3 cm, indicating that PCI can be used to treatrelatively large tumors, and constitute an interesting opportunity forlocal control (personal communication, and PCI Biotech press release16. March 2010), and constitute an interesting opportunity for localtumor control.
6. Concluding remarks and future directions
PCI is a feasible technology providing endosomal escape of manytypes of therapeutics including cytotoxic targeting conjugates,chemotherapeutics, siRNA, nanomedicines and gene-based therapeu-tics. The strong synergistic effects observed in PCI suggest a significantclinical potential.
Based on experimental pre-clinical data PCI may provide a tripletumor-targeting drug delivery strategy due to: 1) the targeting abilityof an antibody or ligand of a drug-conjugate having selectivity againstan antigen of interest expressed on the cancer cells; 2) a preferentialaccumulation and retention of PCI-photosensitizers in malignanttissues; and 3) confined light exposure of the cancerous tissue withwavelengths matching the absorption of light by the photosensitizer.In addition, photosensitizers are non-toxic in the absence of light andbecome activated only in the presence of light with wavelengthsmatching the absorption spectrum of the photosensitizer.
The therapeutic efficiency of several compounds that are alreadyapproved for cancer therapy can be improved by PCI, with bleomycinas our prime example. In addition, there is a vast number ofmembrane-impermeable compounds that show high efficacy wheninteracting with their target in cell-free systems. However, when itcomes to intracellular delivery, many of these compounds fail due toendocytic sequestration. These drugs are therefore not developedfurther for clinical applications. It will therefore be of high interest todo PCI of such compounds.
References
[1] Y. Lu, J. Yang, E. Sega, Issues related to targeted delivery of proteins and peptides,AAPS J. 8 (2006) E466–E478.
[2] J.B. Lloyd, Lysosome membrane permeability: implications for drug delivery,Adv. Drug Deliv. Rev. 41 (2000) 189–200.
[3] A.T. Jones, M. Gumbleton, R. Duncan, Understanding endocytic pathways andintracellular trafficking: a prerequisite for effective design of advanced drugdelivery systems, Adv. Drug Deliv. Rev. 55 (2003) 1353–1357.
[4] P.A. Netti, L.T. Baxter, Y. Boucher, R. Skalak, R.K. Jain, Time-dependent behavior ofinterstitial fluid pressure in solid tumors: implications for drug delivery, CancerRes. 55 (1995) 5451–5458.
[5] R. Hassan, S. Bullock, A. Premkumar, R.J. Kreitman, H. Kindler, M.C. Willingham, I.Pastan, Phase I study of SS1P, a recombinant anti-mesothelin immunotoxingiven as a bolus I.V. infusion to patients with mesothelin-expressing mesothe-lioma, ovarian, and pancreatic cancers, Clin. Cancer Res. 13 (2007) 5144–5149.
[6] L. Rajendran, H.J. Knolker, K. Simons, Subcellular targeting strategies for drugdesign and delivery, Nat. Rev. Drug Discov. 9 (2010) 29–42.
[7] A. Nori, J. Kopecek, Intracellular targeting of polymer-bound drugs for cancerchemotherapy, Adv. Drug Deliv. Rev. 57 (2005) 609–636.
[8] J.K. Vasir, V. Labhasetwar, Biodegradable nanoparticles for cytosolic delivery oftherapeutics, Adv. Drug Deliv. Rev. 59 (2007) 718–728.
[9] A. El-Sayed, S. Futaki, H. Harashima, Delivery of macromolecules using arginine-rich cell-penetrating peptides: ways to overcome endosomal entrapment, AAPSJ. 11 (2009) 13–22.
[10] S. Mehier-Humbert, R.H. Guy, Physical methods for gene transfer: improving thekinetics of gene delivery into cells, Adv. Drug Deliv. Rev. 57 (2005) 733–753.
[11] E. Wagner, Programmed drug delivery: nanosystems for tumor targeting, ExpertOpin. Biol. Ther. 7 (2007) 587–593.
[12] K. Berg, P.K. Selbo, L. Prasmickaite, T.E. Tjelle, K. Sandvig, J. Moan, G. Gaudernack,O. Fodstad, S. Kjølsrud, H. Anholt, G.H. Rodal, S.K. Rodal, A. Høgset,Photochemical internalization: a novel technology for delivery of macromole-cules into cytosol, Cancer Res. 59 (1999) 1180–1183.
[13] A. Høgset, L. Prasmickaite, P.K. Selbo, M. Hellum, B.O. Engesaeter, A. Bonsted, K.Berg, Photochemical internalisation in drug and gene delivery, Adv. Drug Deliv.Rev. 56 (2004) 95–115.
[14] P.K. Selbo, G. Sivam, O. Fodstad, K. Sandvig, K. Berg, In vivo documentation ofphotochemical internalization, a novel approach to site specific cancer therapy,Int. J. Cancer 92 (2001) 761–766.
[15] P.K. Selbo, K. Sandvig, V. Kirveliene, K. Berg, Release of gelonin from endosomesand lysosomes to cytosol by photochemical internalization, Biochim. Biophys.Acta 1475 (2000) 307–313.
[16] P.K. Selbo, G. Sivam, O. Fodstad, K. Sandvig, K. Berg, Photochemical internali-zation increases the cytotoxic effect of the immunotoxin MOC31-gelonin, Int. J.Cancer 87 (2000) 853–859.
[17] L. Prasmickaite, A. Høgset, P.K. Selbo, B.Ø. Engesæter, M. Hellum, K. Berg,Photochemical disruption of endocytic vesicles before delivery of drugs: a newstrategy for cancer therapy, Br. J. Cancer 86 (2002) 652–657.
[18] A. Dietze, B. Engesaeter, K. Berg, Transgene delivery and gelonin cytotoxicityenhanced by photochemical internalization in fibroblast-like synoviocytes(FLS) from rheumatoid arthritis patients, Photochem. Photobiol. Sci. 4 (2005)341–347.
[19] P.K. Selbo, A. Weyergang, A. Bonsted, S.G. Bown, K. Berg, Photochemicalinternalization of therapeutic macromolecular agents: a novel strategy to killmultidrug resistant cancer cells, J. Pharmacol. Exp. Ther. 319 (2006) 604–612.
[20] P.K. Selbo, A. Høgset, L. Prasmickaite, K. Berg, Photochemical internalisation(PCI) — a novel drug delivery system, Tumor Biol. 23 (2002) 103–112.
[21] P.K. Selbo, M.G. Rosenblum, L.H. Cheung, W. Zhang, K. Berg, Multi-modalitytherapeutics with potent anti-tumor effects: photochemical internalizationenhances delivery of the fusion toxin scFvMEL/rGel, PLoS ONE 4 (2009) e6691,doi:10.1371/journal.pone.0006691.
[22] A. Weyergang, P.K. Selbo, K. Berg, Photochemically stimulated drug deliveryincreases the cytotoxicity and specificity of EGF–saporin, J. Control. Release 111(2006) 165–173.
[23] W.L. Yip, A. Weyergang, K. Berg, H.H. Tonnesen, P.K. Selbo, Targeted delivery andenhanced cytotoxicity of cetuximab-saporin by photochemical internalization inEGFR-positive cancer cells, Mol. Pharm. 4 (2007) 241–251.
[24] P.S. Lai, C.L. Pai, C.L. Peng, M.J. Shieh, K. Berg, P.J. Lou, Enhanced cytotoxicity ofsaporin by polyamidoamine dendrimer conjugation and photochemical inter-nalization, J. Biomed. Mater. Res. A 87 (2008) 147–155.
[25] K.G. de Bruin, C. Fella, M. Ogris, E. Wagner, N. Ruthardt, C. Brauchle, Dynamics ofphotoinduced endosomal release of polyplexes, J. Control. Release 130 (2008)175–182.
[26] P.K. Selbo, O. Kaalhus, G. Sivam, K. Berg, 5-Aminolevulinic acid-basedphotochemical internalization of the immunotoxin MOC31-gelonin gen-erates synergistic cytotoxic effects in vitro, Photochem. Photobiol. 74 (2001)303–310.
[27] M.M. Fretz, A. Høgset, G.A. Koning, W. Jiskoot, G. Storm, Cytosolic delivery ofliposomally targeted proteins induced by photochemical internalization, Pharm.Res. 24 (2007) 2040–2047.
[28] K. Berg, A. Dietze, O. Kaalhus, A. Høgset, Site-specific drug delivery byphotochemical internalization enhances the antitumor effect of bleomycin,Clin. Cancer Res. 11 (2005) 8476–8485.
[29] H. Hirschberg, M.J. Zhang, H.M. Gach, F.A. Uzal, Q. Peng, C.H. Sun, D.Chighvinadze, S.J. Madsen, Targeted delivery of bleomycin to the brain usingphoto-chemical internalization of Clostridium perfringens epsilon prototoxin,J. Neurooncol. 95 (2009) 317–329.
[30] P.J. Lou, P.S. Lai, M.J. Shieh, A.J. MacRobert, K. Berg, S.G. Bown, Reversal ofdoxorubicin resistance in breast cancer cells by photochemical internalization,Int. J. Cancer 119 (2006) 2692–2698.
[31] P.S. Lai, P.J. Lou, C.L. Peng, C.L. Pai, W.N. Yen, M.Y. Huang, T.H. Young, M.J. Shieh,Doxorubicin delivery by polyamidoamine dendrimer conjugation and photo-
10 P.K. Selbo et al. / Journal of Controlled Release 148 (2010) 2–12
Author's personal copy
chemical internalization for cancer therapy, J. Control. Release 122 (2007)39–46.
[32] D.K. Adigbli, D.G. Wilson, N. Farooqui, E. Sousi, P. Risley, I. Taylor, A.J. MacRobert,M. Loizidou, Photochemical internalisation of chemotherapy potentiates killingof multidrug-resistant breast and bladder cancer cells, Br. J. Cancer 97 (2007)502–512.
[33] H. Cabral, M. Nakanishi, M. Kumagai, W.D. Jang, N. Nishiyama, K. Kataoka, Aphoto-activated targeting chemotherapy using glutathione sensitive camptothe-cin-loaded polymeric micelles, Pharm. Res. 26 (2009) 82–92.
[34] A. Høgset, E.B. Ovstebo, L. Prasmickaite, K. Berg, O. Fodstad, G.M. Maelandsmo,Light-induced adenovirus gene transfer, an efficient and specific gene deliverytechnology for cancer gene therapy, Cancer Gene Ther. 9 (2002) 365–371.
[35] A. Dietze, A. Bonsted, A. Høgset, K. Berg, Photochemical internalization enhancesthe cytotoxic effect of the protein toxin gelonin and transgene expression insarcoma cells, Photochem. Photobiol. 78 (2003) 283–289.
[36] A. Bonsted, B.O. Engesaeter, A. Høgset, G.M. Maelandsmo, L. Prasmickaite, O.Kaalhus, K. Berg, Transgene expression is increased by photochemicallymediated transduction of polycation-complexed adenoviruses, Gene Ther. 11(2004) 152–160.
[37] B.O. Engesaeter, A. Bonsted, K. Berg, A. Høgset, O. Engebraten, O. Fodstad, D.T.Curiel, G.M. Maelandsmo, PCI-enhanced adenoviral transduction employs theknown uptake mechanism of adenoviral particles, Cancer Gene Ther. 12 (2005)439–448.
[38] B.O. Engesaeter, S. Tveito, A. Bonsted, O. Engebraaten, K. Berg, G.M. Maelandsmo,Photochemical treatment with endosomally localized photosensitizers enhancesthe number of adenoviruses in the nucleus, J. Gene Med. 8 (2006) 707–718.
[39] B.O. Engesaeter, A. Bonsted, T. Lillehammer, O. Engebraaten, K. Berg, G.M.Maelandsmo, Photochemically mediated delivery of AdhCMV-TRAIL augmentsthe TRAIL-induced apoptosis in colorectal cancer cell lines, Cancer Biol. Ther. 5(2006) 1511–1520.
[40] A. Bonsted, A. Høgset, F. Hoover, K. Berg, Photochemical enhancement of genedelivery to glioblastoma cells is dependent on the vector applied, Anticancer Res.25 (2005) 291–297.
[41] A. Høgset, L. Prasmickaite, T.E. Tjelle, K. Berg, Photochemical transfection: a newtechnology for light-induced, site-directed gene delivery, Hum. Gene Ther. 11(2000) 869–880.
[42] L. Prasmickaite, A. Høgset, K. Berg, Evaluation of different photosensitizers for usein photochemical gene transfection, Photochem. Photobiol. 73 (2001) 388–395.
[43] L. Prasmickaite, A. Høgset, T.E. Tjelle, V.M. Olsen, K. Berg, Role of endosomes ingene transfection mediated by photochemical internalisation (PCI), J. Gene Med.2 (2000) 477–488.
[44] L. Prasmickaite, A. Høgset, V.M. Olsen, O. Kaalhus, S.O. Mikalsen, K. Berg,Photochemically enhanced gene transfection increases the cytotoxicity of theherpes simplex virus thymidine kinase gene combined with ganciclovir, CancerGene Ther. 11 (2004) 514–523.
[45] J. Kloeckner, L. Prasmickaite, A. Høgset, K. Berg, E. Wagner, Photochemicallyenhanced gene delivery of EGF receptor-targeted DNA polyplexes, J. Drug Target.12 (2004) 205–213.
[46] M. Hellum, A. Høgset, B.O. Engesaeter, L. Prasmickaite, T. Stokke, C. Wheeler, K.Berg, Photochemically enhanced gene delivery with cationic lipid formulations,Photochem. Photobiol. Sci. 2 (2003) 407–411.
[47] A. Ndoye, J.L. Merlin, A. Leroux, G. Dolivet, P. Erbacher, J.P. Behr, K. Berg, F.Guillemin, Enhanced gene transfer and cell death following p53 gene transferusing photochemical internalisation of glucosylated PEI–DNA complexes, J. GeneMed. 6 (2004) 884–894.
[48] A. Ndoye, G. Dolivet, A. Høgset, A. Leroux, A. Fifre, P. Erbacher, K. Berg, J.P. Behr, F.Guillemin, J.L. Merlin, Eradication of p53-mutated head and neck squamous cellcarcinoma xenografts using nonviral p53 gene therapy and photochemicalinternalization, Mol. Ther. 13 (2006) 1156–1162.
[49] A. Maurice-Duelli, A. Ndoye, S. Bouali, A. Leroux, J.L. Merlin, Enhanced cellgrowth inhibition following PTEN nonviral gene transfer using polyethylenimineand photochemical internalization in endometrial cancer cells, Technol. CancerRes. Treat. 3 (2004) 459–465.
[50] N. Nishiyama, A. Iriyama, W.D. Jang, K. Miyata, K. Itaka, Y. Inoue, H. Takahashi, Y.Yanagi, Y. Tamaki, H. Koyama, K. Kataoka, Light-induced gene transfer frompackaged DNA enveloped in a dendrimeric photosensitizer, Nat. Mater. 4 (2005)934–941.
[51] Arnida, N. Nishiyama, N. Kanayama, W.D. Jang, Y. Yamasaki, K. Kataoka,PEGylated gene nanocarriers based on block catiomers bearing ethylenediaminerepeating units directed to remarkable enhancement of photochemicaltransfection, J. Control. Release 115 (2006) 208–215.
[52] M.J. Shieh, C.L. Peng, P.J. Lou, C.H. Chiu, T.Y. Tsai, C.Y. Hsu, C.Y. Yeh, P.S. Lai, Non-toxic phototriggered gene transfection by PAMAM-porphyrin conjugates,J. Control. Release 129 (2008) 200–206.
[53] M. Folini, K. Berg, E. Millo, R. Villa, L. Prasmickaite, M.G. Daidone, U. Benatti, N.Zaffaroni, Photochemical internalization of a peptide nucleic acid targeting thecatalytic subunit of human telomerase, Cancer Res. 63 (2003) 3490–3494.
[54] M. Folini, R. Bandiera, E. Millo, P. Gandellini, G. Sozzi, P. Gasparini, N. Longoni, M.Binda, M.G. Daidone, K. Berg, N. Zaffaroni, Photochemically enhanced delivery ofa cell-penetrating peptide nucleic acid conjugate targeting human telomerasereverse transcriptase: effects on telomere status and proliferative potential ofhuman prostate cancer cells, Cell Prolif. 40 (2007) 905–920.
[55] S. Boe, E. Hovig, Photochemically induced gene silencing using PNA–peptideconjugates, Oligonucleotides 16 (2006) 145–157.
[56] T. Shiraishi, P.E. Nielsen, Photochemically enhanced cellular delivery of cellpenetrating peptide–PNA conjugates, FEBS Lett. 580 (2006) 1451–1456.
[57] S. Oliveira, M.M. Fretz, A. Høgset, G. Storm, R.M. Schiffelers, Photochemicalinternalization enhances silencing of epidermal growth factor receptor throughimproved endosomal escape of siRNA, Biochim. Biophys. Acta 1768 (2007)1211–1217.
[58] S. Boe, A.S. Longva, E. Hovig, Evaluation of various polyethylenimine formula-tions for light-controlled gene silencing using small interfering RNA molecules,Oligonucleotides 18 (2008) 123–132.
[59] K. Reamdonck, B. Naeye, K. Buyens, R.E. Vandenbroucke, A. Høgset, J. Demeester,S.C. De Smedt, Biodegradable dextran nanogels for RNA interference: focusing onendosomal escape and intracellular siRNA delivery, Adv. Funct. Mater. 19 (2009)1406–1415.
[60] S. Boe, S. Saeboe-Larssen, E. Hovig, Light-induced gene expression usingmessenger RNA molecules, Oligonucleotides 20 (2010) 1–6.
[61] K. Berg, A. Høgset, L. Prasmickaite, A. Weyergang, A. Bonsted, A. Dietze, P.J. Lou,S.G. Bown, O.J. Norum, H.M.T. Mollergard, P.K. Selbo, Photochemical internali-zation (PCI): a novel technology for activation of endocytosed therapeutic agents,Med. Laser Appl. 21 (2006) 239–250.
[62] A. Dietze, Q. Peng, P.K. Selbo, O. Kaalhus, C. Muller, S. Bown, K. Berg, Enhancedphotodynamic destruction of a transplantable fibrosarcoma using photochem-ical internalisation of gelonin, Br. J. Cancer 92 (2005) 2004–2009.
[63] J. Woodhams, P.J. Lou, P.K. Selbo, A. Mosse, D. Oukrif, A. MacRobert, M. Novelli, Q.Peng, K. Berg, S.G. Bown, Intracellular re-localisation by photochemicalinternalisation enhances the cytotoxic effect of gelonin — quantitative studiesin normal rat liver, J. Control. Release 142 (2009) 347–353.
[64] O.J. Norum, O.S. Bruland, L. Gorunova, K. Berg, Photochemical internalizationof bleomycin before external-beam radiotherapy improves locoregionalcontrol in a human sarcoma model, Int. J. Radiat. Oncol. Biol. Phys. 75 (2009)878–885.
[65] O.J. Norum, K.E. Giercksky, K. Berg, Photochemical internalization as an adjunctto marginal surgery in a human sarcoma model, Photochem. Photobiol. Sci.8 (2009) 758–762.
[66] O.J. Norum, J.V. Gaustad, E. Angell-Petersen, E.K. Rofstad, Q. Peng, K.E. Giercksky,K. Berg, Photochemical internalization of bleomycin is superior to photodynamictherapy due to the therapeutic effect in the tumor periphery, Photochem.Photobiol. 85 (2009) 740–749.
[67] S. Oliveira, A. Høgset, G. Storm, R.M. Schiffelers, Delivery of siRNA to the targetcell cytoplasm: photochemical internalization facilitates endosomal escape andimproves silencing efficiency, in vitro and in vivo, Curr. Pharm. Des. 14 (2008)3686–3697.
[68] T.J. Dougherty, C.J. Gomer, B.W. Henderson, G. Jori, D. Kessel, M. Korbelik, J.Moan, Q. Peng, Photodynamic therapy, J. Natl Cancer Inst. 90 (1998) 889–905.
[69] D.E. Dolmans, D. Fukumura, R.K. Jain, Photodynamic therapy for cancer, Nat. Rev.Cancer 3 (2003) 380–387.
[70] J. Moan, K. Berg, The photodegradation of porphyrins in cells can be used toestimate the lifetime of singlet oxygen, Photochem. Photobiol. 53 (1991)549–553.
[71] S.B. Brown, E.A. Brown, I. Walker, The present and future role of photodynamictherapy in cancer treatment, Lancet Oncol. 5 (2004) 497–508.
[72] A.P. Castano, P. Mroz, M.R. Hamblin, Photodynamic therapy and anti-tumourimmunity, Nat. Rev. Cancer 6 (2006) 535–545.
[73] J. Chen, J. Stubbe, Bleomycins: towards better therapeutics, Nat. Rev. Cancer 5(2005) 102–112.
[74] G. Pron, N. Mahrour, S. Orlowski, O. Tounekti, B. Poddevin, J. Belehradek Jr., L.M.Mir, Internalisation of the bleomycin molecules responsible for bleomycintoxicity: a receptor-mediated endocytosis mechanism, Biochem. Pharmacol. 57(1999) 45–56.
[75] S. Sleijfer, Bleomycin-induced pneumonitis, Chest 120 (2001) 617–624.[76] G. Szakacs, J.K. Paterson, J.A. Ludwig, C. Booth-Genthe, M.M. Gottesman,
Targeting multidrug resistance in cancer, Nat. Rev. Drug Discov. 5 (2006)219–234.
[77] M.D. Hall, M.D. Handley, M.M. Gottesman, Is resistance useless? Multidrugresistance and collateral sensitivity, Trends Pharmacol. Sci. 30 (2009) 546–556.
[78] O.J. Norum, P.K. Selbo, A. Weyergang, K.E. Giercksky, K. Berg, Photochemicalinternalization (PCI) in cancer therapy: from bench towards bedside medicine,J. Photochem. Photobiol. B 96 (2009) 83–92.
[79] J.S. Friedberg, R. Mick, J. Stevenson, J. Metz, T. Zhu, J. Buyske, D.H. Sterman, H.I.Pass, E. Glatstein, S.M. Hahn, A phase I study of Foscan-mediated photodynamictherapy and surgery in patients with mesothelioma, Ann. Thorac. Surg. 75(2003) 952–959.
[80] J.S. Friedberg, R. Mick, J.P. Stevenson, T. Zhu, T.M. Busch, D. Shin, D. Smith, M.Culligan, A. Dimofte, E. Glatstein, S.M. Hahn, Phase II trial of pleuralphotodynamic therapy and surgery for patients with non-small-cell lung cancerwith pleural spread, J. Clin. Oncol. 22 (2004) 2192–2201.
[81] S.M. Hahn, D.L. Fraker, R. Mick, J. Metz, T.M. Busch, D. Smith, T. Zhu, C. Rodriguez,A. Dimofte, F. Spitz, M. Putt, S.C. Rubin, C. Menon, H.W.Wang, D. Shin, A. Yodh, E.Glatstein, A phase II trial of intraperitoneal photodynamic therapy for patientswith peritoneal carcinomatosis and sarcomatosis, Clin. Cancer Res. 12 (2006)2517–2525.
[82] S. Krishnamurthy, S.K. Powers, P. Witmer, T. Brown, Optimal light dose forinterstitial photodynamic therapy in treatment for malignant brain tumors,Lasers Surg. Med. 27 (2000) 224–234.
[83] H.B. Ris, Photodynamic therapy as an adjunct to surgery for malignant pleuralmesothelioma, Lung Cancer 49 (Suppl 1:S65-8) (2005) S65–S68.
[84] S. Boe, A.S. Longva, E. Hovig, Photochemically induced gene silencing using smallinterfering RNA molecules in combination with lipid carriers, Oligonucleotides17 (2007) 166–173.
11P.K. Selbo et al. / Journal of Controlled Release 148 (2010) 2–12
Author's personal copy
[85] C. Tekle, B. Deurs, K. Sandvig, T.G. Iversen, Cellular trafficking of quantum dot–ligand bioconjugates and their induction of changes in normal routing ofunconjugated ligands, Nano Lett. 8 (2008) 1858–1865.
[86] G. Sahay, D.Y. Alakhova, and A.V. Kabanov. Endocytosis of nanomedicines,J. Control Release (2010) [Mar 10, Electronic publication ahead of print].doi:10.1016/j.jconrel.2010.01.036.
[87] N. Nishiyama, Arnida, W.D. Jang, K. Date, K. Miyata, K. Kataoka, Photochemicalenhancement of transgene expression by polymeric micelles incorporatingplasmid DNA and dendrimer-based photosensitizer, J. Drug Target. 14 (2006)413–424.
[88] K. Raemdonck, B. Naeye, A. Høgset, J. Demeester, S.C. De Smedt, Prolonged genesilencing by combining siRNA nanogels and photochemical internalization,J. Control Release. (2010).
[89] A. Weyergang, P.K. Selbo, K. Berg, Y1068 phosphorylation is the most sensitivetarget of disulfonated tetraphenylporphyrin-based photodynamic therapy onepidermal growth factor receptor, Biochem. Pharmacol. 74 (2007) 226–235.
[90] A. Weyergang, O. Kaalhus, K. Berg, Photodynamic targeting of EGFR does notpredict the treatment outcome in combination with the EGFR tyrosine kinaseinhibitor Tyrphostin AG1478, Photochem. Photobiol. Sci. 7 (2008) 1032–1040.
[91] A. Weyergang, O. Kaalhus, K. Berg, Photodynamic therapy with an endocyticallylocated photosensitizer cause a rapid activation of the mitogen-activated proteinkinases extracellular signal-regulated kinase, p38, and c-JunNH2 terminal kinasewith opposing effects on cell survival, Mol. Cancer Ther. 7 (2008) 1740–1750.
[92] A. Weyergang, K. Berg, O. Kaalhus, Q. Peng, P.K. Selbo, Photodynamic therapytargets the mTOR signaling network in vitro and in vivo, Mol. Pharm. 6 (2009)255–264.
[93] M.G. del Carmen, I. Rizvi, Y. Chang, A.C. Moor, E. Oliva, M. Sherwood, B. Pogue, T.Hasan, Synergism of epidermal growth factor receptor-targeted immunotherapywith photodynamic treatment of ovarian cancer in vivo, J. Natl Cancer Inst. 97(2005) 1516–1524.
[94] R. Soffietti, R. Ruda, E. Trevisan, New chemotherapy options for the treatment ofmalignant gliomas, Anticancer Drugs 18 (2007) 621–632.
[95] M. Korbelik, B. Stott, J. Sun, Photodynamic therapy-generated vaccines:relevance of tumour cell death expression, Br. J. Cancer 97 (2007) 1381–1387.
[96] S.O. Gollnick, C.M. Brackett, Enhancement of anti-tumor immunity by photody-namic therapy, Immunol. Res. 46 (2009) 216–226.
[97] P.S. Thong, K.W. Ong, N.S. Goh, K.W. Kho, V. Manivasager, R. Bhuvaneswari, M.Olivo, K.C. Soo, Photodynamic-therapy-activated immune response againstdistant untreated tumours in recurrent angiosarcoma, Lancet Oncol. 8 (2007)950–952.
[98] G. Jori, Far-red-absorbing photosensitizers: their use in the photodynamictherapy of tumours, Journal of Photochemistry and Photobiology A: Chemistry62 (1992) 371–378.
[99] W. Jerjes, T. Upile, Z. Hamdoon, F. Nhembe, R. Bhandari, S. Mackay, P. Shah, C.A.Mosse, J.A. Brookes, S. Morley, C. Hopper, Ultrasound-guided photodynamictherapy for deep seated pathologies: prospective study, Lasers Surg. Med. 41(2009) 612–621.
[100] M.M. Tsoukas, G.C. Lin, M.S. Lee, R.R. Anderson, N. Kollias, Predictive dosimetryfor threshold phototoxicity in photodynamic therapy on normal skin: redwavelengths produce more extensive damage than blue at equal thresholddoses, J. Invest Dermatol. 108 (1997) 501–505.
[101] L.R. Braathen, R.M. Szeimies, N. Basset-Seguin, R. Bissonnette, P. Foley, D. Pariser,R. Roelandts, A.M. Wennberg, C.A. Morton, Guidelines on the use of photody-namic therapy for nonmelanoma skin cancer: an international consensus, J. Am.Acad. Dermatol. 56 (2007) 125–143.
[102] C. Hopper, Phase I, dose-escalating study to evaluate safety and tolerance ofamphinex based photochemical internalisation (PCI) of bleomycin in patientswith local recurrence or advanced/metastatic, cutaneous or sub-cutaneousmalignancies, ClinicalTrials. gov NCT00993512 (2009).
12 P.K. Selbo et al. / Journal of Controlled Release 148 (2010) 2–12