Phlebitis assessment scales: So many scales, so little value?
14
Phlebitis Assessment Scales: So many scales, so little value? Gillian Ray-Barruel Senior Research Assistant Griffith Health Institute, Griffith University ICN 25 th Quadrennial Congress Melbourne, May 2013
Transcript of Phlebitis assessment scales: So many scales, so little value?

Phlebitis Assessment Scales: So many scales, so little value?
Gillian Ray-Barruel Senior Research Assistant Griffith Health Institute, Griffith University
ICN 25th Quadrennial Congress Melbourne, May 2013

Background

Methods
Cochrane Library Medline CINAHL
COSMIN guidelines (COnsensus-based Standards for the selection of health Measurement Instruments) • Reliability (inter-rater, intra-rater, test-retest) • Validity (content, face, criterion, construct) • Responsiveness (the ability of a scale to detect
a true change in symptoms) • Feasibility (time to complete, ease of
completion, clarity of items, etc.)
Results
v 233 studies reported infusion phlebitis as the primary outcome measure
v Of these, 53 provided no actual definition of phlebitis, despite the study measuring phlebitis
v 180 studies reported measuring phlebitis incidence or severity and gave a definition
v Of these, 101 used an assessment scale v 79 used a definition only

Results continued
• Pain • Tenderness • Erythema or redness • Oedema or swelling • Palpable venous cord • Induration or hardness • Frank thrombosis • Streak formation or red line
• Purulence or exudate • Inflammation not specified • Local warmth • Local coolness • Infusion slowed or stopped • Fever or pyrexia • Tissue damage • Impaired function
We found 71 different phlebitis assessment scales in use! 16 symptoms were assessed by the various scales or tools:


Results
Reported phlebitis prevalence § 0-91% for studies using a scale § 0-100% for studies using a definition alone § Reporting measures varied widely
(per PIVC, per patient, per catheter day)

Results
Reported psychometric assessment § Many phlebitis scales and tools exist, but
none has been properly validated for use in the clinical setting.
§ Studies that reported testing the psychometric properties of scales (VIP, INS, PVC ASSESS, etc.) all had several major limitations.

Limitations?
Name of scale Limitations INS scale Groll et al, 2010
Inter-rater reliability kappa .45 (moderate) Criterion (concurrent) validity was assessed by comparing assessment to documentation (? ‘gold standard’). Correlation between observation and documentation 0.39. Did not assess intra-rater and test-retest reliability, or responsiveness. Sample size was only 6 nurses.
Documentation in the patient’s chart cannot be considered the gold standard!

Limitations continued
The psychometric properties of Baxter, Maddox, Lipman, Dinley and many other scales have never been reported.
Name of scale Limitations VIP score Gallant & Schultz, 2006
Reported to have good inter-rater reliability (0.85) & content validity. Inter-rater reliability was assessed by comparing each nurse’s assessment to an expert’s opinion (gold standard). Did not compute inter-rater reliability between nurses. No report of intra-rater reliability, test-retest reliability, responsiveness, feasibility, or construct validity.
Conclusions
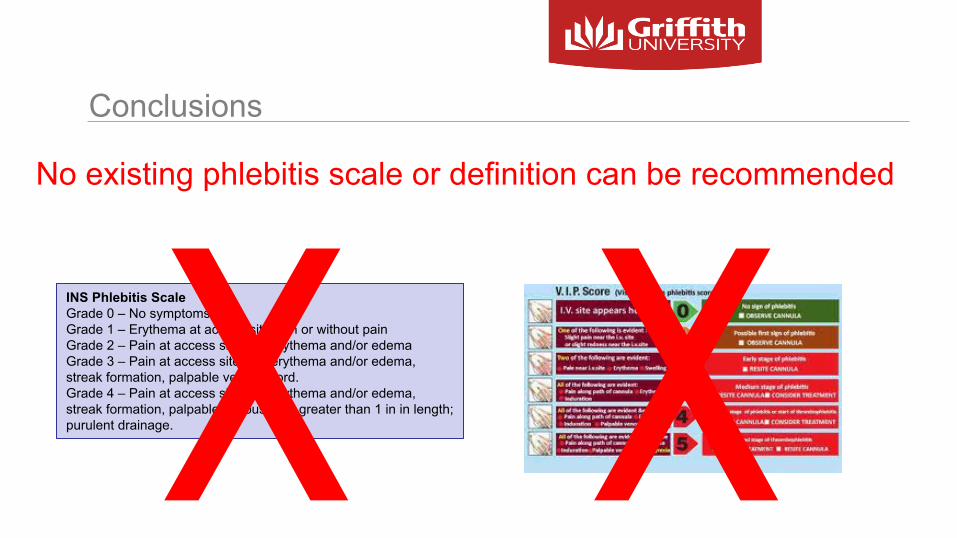
No existing phlebitis scale or definition can be recommended
XINS Phlebitis Scale Grade 0 – No symptoms Grade 1 – Erythema at access site with or without pain Grade 2 – Pain at access site with erythema and/or edema Grade 3 – Pain at access site with erythema and/or edema, streak formation, palpable venous cord. Grade 4 – Pain at access site with erythema and/or edema, streak formation, palpable venous cord greater than 1 in in length; purulent drainage. X

Final thoughts for assessing an IV cannula
Use clinical judgement! • Is it needed?
Ø If not, remove it. Don’t leave it there, just in case. • Is it working?
Ø If not, remove it. Resite IV or insert PICC. • Is it tolerated by the patient?
Ø If not, remove it. Consider other access (e.g. oral, PICC) • Is there any evidence of infection from an unknown source?
Ø If so, remove the cannula.
Thanks for listening!
Infusion phlebitis assessment techniques: A systematic review of their use and psychometric adequacy Gillian Ray-Barruel, Denise F. Polit, Jenny E. Murfield, Claire M. Rickard

If you want to be part of this ground-breaking study, please take a flyer!
Email: [email protected] Twitter @OMGstudy1