Ph.D. in physiotherapy - Al Neelain University
76
Al-Neelain University Graduate College Physiotherapy College Effects of Interferential Therapy versus Combination Therapy (Interferential Therapy +Ultrasound Therapy) in Patient's with Osteoarthritis knee in Khartoum state (2019) A thesis submitted in partial fulfilment for requirements of the Degree of Master in Physiotherapy (Orthopedic) Submitted by: SAGDA MOHAMED YOUSIF MAHAMOUD B.Sc. of Physiotherapy, Al-Neelain University 2014. Supervisor: DR: AHMED BANAGA AHMED ASSOCIATE PROFESSER OF PHYSIOTHERAPY Ph.D. in physiotherapy
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Ph.D. in physiotherapy - Al Neelain University

Al-Neelain University
Graduate College
Physiotherapy College
Effects of Interferential Therapy versus Combination Therapy (Interferential Therapy +Ultrasound Therapy) in Patient's with Osteoarthritis knee
in Khartoum state (2019)
A thesis submitted in partial fulfilment for requirements of the Degree
of Master in Physiotherapy (Orthopedic)
Submitted by:
SAGDA MOHAMED YOUSIF MAHAMOUD
B.Sc. of Physiotherapy, Al-Neelain University 2014.
Supervisor:
DR: AHMED BANAGA AHMED
ASSOCIATE PROFESSER OF PHYSIOTHERAPY Ph.D. in physiotherapy

بسم هللا الرمحن الرحمي
ق ال تعالي : )ال يكلف اهلل نفسا إال وسعها لها ما كسبت وعليها ما اكتسبت ربنا ال تؤاخذنا إن نسينا أو أخطأنا ربنا وال تحمل علينا إصرا كما حملتو علي الذين من قبلنا ربنا وال تحملنا
ن ( ماال طاقو لنا بو واعف عنا واغفر لنا وارحمنا أنت مولنا ف انصرنا علي القوم الكفري
( 682سورة البقره االيو )

TO My parents.
The reason of what I have become today .
Thank you for your great support and continuous care.
To my sisters and brothers .
I am really grateful to have both of you
To
All the people in my life who have touched my heart,
I dedicate this research
I

Acknowledgement Thanks to ALLAH for enabling me to accomplish my research on
such an essential issue in this field nowadays
I submit to my respected Supervisor
DR AHMED BANAGA AHMED for his sincere guidance and help
for me to complete this research .
I humbly extend my thanks to all the concerned persons who co-
operated with me in this research .
II

Abstract
Background: Osteoarthritis (OA) is the most common type of arthritis. And knee OA,
being highly prevalent, accounts for as much or more lower extremity disability (1).
Interferential Current stimulation is very useful in the treatment of circulatory and
muscular disorders, stiffness of joints, oedema, and inflammation. If the patients suffer
from health problems such as cumulative trauma disorders, body pain, joint injuries, or
pre and post orthopaedic surgery, interferential current therapy is an important option(2).
Objective: To study Effects of Interferential Therapy (IFT) versus Combination Therapy
(IFT+Ultrasound Therapy) on osteoarthritis knee patient.
Methodology: This is a randomized control trials a total of 30 patients with osteoarthritis
knee attended from June to September 2018 and they were identified according to the age
of group between (40-70) years. 30 Patients randomly assigned into two equal groups
(group A and group B) Each group received conventional therapy, GROUP(A):15
patients received Combination therapy (IFT+US). GROUP (B):15 patients received
Interferential therapy,12 sessions done to all patients . The two groups were assessed
before and after intervention The functional ability assessed by using WOMAC scale
,level of pain by using visual analog scale(VAS) and (ROM)by universal goniometer.
Data was collected by using structural questionnaire and scales, then analyzed by using
statistical package for social science (SPSS).
The Result: When comparing between groups was done, the study found statistical
significant difference between post treatment in the two groups there was reducing in
pain (p=0,002),but the combination therapy was more effective in reducing pain of
knee osteoarthritis .
Also there was statistical significant difference between post treatment in the two groups
as there was improving functional performance (p=0,003).
conclusion: the combination therapy was effective in improving functional performance
and reducing pain in osteoarthritis knee patient
III
.

ص اثحثسرخــ
خلفية:
.خشنو اروثو ن االراض انرشره وا انيا ذسيذ ن االعالو احرويو
االهداف:
خياز اىيرتاء اعالخي امارنح تينيا في لياش ذ فعايو خياز اخاخ فق اصذيو اعالخيو
.إغارعالج رظي خشنو اروثو
اذره اذيو اظطرتاخ اععالخ ذخشة افاص االرياتاخ ادياز اىيرتائي اعالخي ي في عالج
,ارا وند ذعاني ن شاو صحيو ث ا ادس خرذ افاص اعاده ارأىي لث تعذ عياخ خراحو
اعظا .
.منهجية البحث:
ريط ذ 03. اشررن فييا في اعيادج اخارخيح تىيح اعالج اطثيعي تداعح انيين ذ اخراء ذدرتح عشائيح
ىاا دعااحال ادعااح ا 51اخريااارى ذاازيعي عشااائيا إاا دااعرين رساااذيين اان حيااث اعااذد
خياااز اىيرتاااء اعالخاايا ض ذعرظااد رااارين اال اارمرار خياااز اخاااخ فااق اصااذيو اعالخيااو ذمااد
با ذماااد خياااز خيااااز اىيرتااااء اعالخااي ا ذااا ذمياااي األ ا اايح ععاااالخ ض ادعااح اثانيح ادعاااح
ادعرين لث تعذ خععيا الخيسه اسورهض فيا يرعك تااداء فعاياح وا نياا تا ارخذا الشار االداء
اظيف اه سار األا تا ارخذا ميااش ارثيا اثصار ض ذا ادخااي ذحيا اثيانااخ تا اطح ترنااح
االحصائيارحي
النتاتج:
ات دالله إحصائيه مختلفه بين المجموعتين رعندما أجريت المقارنه بين المجموعتين ,وجدت الدراسه أن هنالك فروق
.( p=0,002بعد العالج حيث كان هنالك انخفاض في االلم )
ات دالله إحصائيه رالم التهاب مفصل الركبه . ايضا كان هناك فرق ولكن العالج الثنائي كان اكثر فاعليه في الحد من
(. =0p,,0,كبيره بين المجموعتين بعد تلقي العالج حيث كان هنالك تحسين في االدء الحركي )
الخالصة:
.اعالج اسدج ذيو ذأثير اوثر في انخفاض اال زياده اعذي احروي في رظي خشنو اروثو
V

Table of content
Page Content No
I Dedication
II Acknowledgment
III Abstract
V اخالصح
VI Table of content
VII- VIII List of tables& figures
XI List of abbreviations
Chapter One
1-2 Introduction 1.1
Chapter Two
3-18 Literature Review 2-1
Chapter Three
19-24 Methodology 3-1
Chapter Four
25-41 Results. 4
Chapter Five
42-44 Discussion. 5
Chapter Six
45 Conclusion. 6-1
46 Recommendations. 2-6
47-51 References. 6-3
Annexes 6-4
VI

TABLE LIST OF
Content Page
Table 1 : Background characteristic of both groups . 25
Table 2: Pain assessment (VAS) Distribution of group A . 26
Table 3: Functional performance assessment (WOMAC) Distribution of group A 27
Table 4 : Statistical Analysis of flexion ROM in group A . 28
Table 5: Statistical Analysis of extension ROM in group A.
29
Table 6: Pain assessment (VAS) Distribution of group B 30
Table 7: Functional performance assessment (WOMAC) Distribution of group B 31
Table 8: Statistical Analysis of Flexion ROM in group B 32
Table 9: Statistical Analysis of extension ROM in group B 33
Table 10: pain assessment (VAS) between two groups (A-B) pre treatment 34
Table 11: fuctional performance assessment (womac) between two groups (A-B) Pre treatment. 35
Table 12: Statistical Analysis OF flexion ROM in both groups(A-B) .pre treatment 36
Table 13: Statistical Analysis OF extension ROM in both groups(A-B) .pre treatment . 37
Table 14: pain assessment (VAS) between two groups (A-B) post treatment 38
Table 15: fuctional performance assessment (womac) between two groups (A-B) post treatment. 39
Table 16: Statistical Analysis OF flexion ROM in both groups(A-B) post treatment . 40
Table 17: Statistical Analysis OF extension ROM in both groups(A-B) .post treatment . 41
VII

LIST OF FIGURES
Content Page
Figure 1: Avarge of pain measurement in group (A) combination therapy(IFT+US) by VAS. 26
Figure 2: Avarge of FUCTIONAL PERFORMANCE measurement in group (A) combination therapy
(IFT+US) by WOMAC.
27
Figure 3: Avarge of Flexion ROM in group (A) combination therapy(IFT+US) pre and post
treatment .
28
Figure 4: Avarge of Extention ROM in group (A) combination therapy(IFT+US) pre and post
treatment .
29
Figure 5: Avarge of pain measurement in group (B) (IFT) therapy by VAS. 30
Figure 6 :Avarge of FUCTIONAL PERFORMANCE measurement in group (B) (IFT) therapy by
WOMAC. 31
Figure 7: Avarge of Flexion ROM in group (B ) (IFT) therapy pre and post treatment.
Figure 8: Avarge of EXTENTION ROM in group (B ) (IFT) therapy pre and post treatment
Figure 9: Avarge of pain measurement in both group (A-B) pre treatment by VAS
Figure 10: Avarge of fuctional performance measurement in both group (A-B) pre treatment BY
WOMAC.
Figure 11: Avarge of Flexion ROM in both group (A-B) pre treatment.
Figure 12: Avarge of EXTENSON ROM in both group (A-B) pre treatment.
Figure 13: Avarge of pain measurement in both group (A-B) post treatment by VAS
Figure 14: Avarge of Fuctioinal performance both group (A-B) Post treatment by WOMAC.
Figure 15: Avarge of Flexion ROM both group (A-B) post treatment .
Figure 16:Avarge of Etension ROM both group (A-B) post treatment
VIII
32
33
34
35
36
37
38
39
40
41

LIST OF ABBREVIATION
XI
Active range of motion AROM
C –reactive protein (CRP) CRP
Erythrocyte Sedimentation Rate (ESR) ESR
Interferential currents IFC
Interferential Therapy IFT
Magnetic Resonance Imaging MRI
Neuromuscular Electrical Stimulation NMES
Osteoarthritis OK
Personal Computer PC
Passive Range of Motion PROM
Rheumatoid Arthritis RH
Stander Deviation SD
shortwave diathermy SWD
transcutaneous electrical nerve stimulation TENS
Ultrasound US
Visual Anlage Scale VAS
The Western Ontario and McMaster Universities Osteoarthritis Index WOMAC

Chapter one
Introduction, problem statement,
justification and objectives


1.Background :
Osteoarthritis (OA) is the most common type of arthritis, being highly prevalent, accounts for
as much or more lower extremity disability. Limited disease-modifying treatment exist and
still under investigations, and knee OA may progress from a dynamic process of injury and
repair to irreversible joint damage requiring joint replacement to treat the unrelenting pain
and/or significant disability. Nonsurgical management is an important first step to prevent
disability and maintain quality of life in the growing number of people with knee OA[1]
. In clinical practice, physiotherapists tailor multicomponent interventions to the needs of the
individual with knee OA in order to attain the goals of treatment. For example, physical
agents may be administered as adjunctive to exercise interventions. Efficacy of therapeutic
ultrasound (US) and interferential therapy (IFT) is of particular interest as this is the physical
agent most commonly used by physiotherapists for treatment of painful musculoskeletal
conditions and, therefore, widely available[1].
Electrotherapeutical modalities of rehabilitation are important resources in the treatment of
musculoskeletal pain[2].
osteoarthritis symptoms and signs include:
Knee joint pain
Knee joint swelling
Knee joint stiffness
knee joint creaking
loss of range of motion[3]
.
Problem Statement :
Dose interferential therapy have more effect in osteoarthritis patient than combination therapy?
1

justification:
osteoarthritis (OA) is one of the most prevalent condition resulting to disability particularly in
elderly population. OA is the most common articular disease of the developed world and a
leading cause of chronic disability, mostly as a consequence of the knee OA and/or hip OA (4).
Patients with OA are at a higher risk of death compared with the general population by
standardized mortality rate 1.54. History of diabetes, cancer, or cardiovascular disease and the
presence of walking disability are major risk factors. Excess mortality is observed for all diseases
with specific causes of death but is particularly pronounced for cardiovascular complications..(5)
A lot of studies have been done on osteoarthritis with the use of different modalities, but
unfortunately combination therapy is often missed which in turn is a new modality in
rehabilitation and there are a few studies done only for combination therapy At the present
time[6]
.Many unanswered questions still exist regarding the optimal treatment modality in
treating osteoarthritis of knee.
[2]Objectives of the study:
(2-1)General objective:
To study Effects of Interferential Therapy (IFT) versus Combination Therapy( IFT+Ultrasound
Therapy) on osteoarthritis knee patient.
(2-2) Spescifi objective:
1-To evaluate the alteration in functional performance by using interferential or combination.
2- To evaluate the effect of the interferential or combination modalities (IFT+Ultrasound
Therapy)in reducing pain for osteoarthritis knee patient
3- to study the change in range of motion after treatment with interferential or combination
(IFT+Ultrasound Therapy) .
2

Chapter two
Literature review

Literature Review
(2.1) Anatomy of knee joint:
The knee joint is the largest joint in the human body. It is designed to support the full weight of
the body, allowing us to stand, walk, run or dance with ease, grace and fluidity. The knee is also
a very common area for injury, Damage to any structure of the knee anatomy will impact normal
movement of the leg. It is important to understand the anatomy of knee joint to know how
different structures work together to ensure the normal functioning of the knee.(7) .
The knee joint is which connects the femur, our thigh bone and longest bone in the body, to the
tibia, our shinbone and second longest bone. There are two joints in the knee—the tibiofemoral
joint, which joins the tibia to the femur and the patellofemoral joint which joins the kneecap to
the femur. These two joints work together to form a modified hinge joint that allows the knee to
bend and straighten, but also to rotate slightly and from side to side.(8)
.
Anatomical Features of the Knee: The main features of the knee anatomy include bones,
cartilages, ligaments, tendons and muscles. In the knee joint, the femur articulates with the tibia
and the patella. The knee joint is a synovial joint this means it contains a fluid that lubricates it.
This fluid is known as the synovial fluid.(7).
The knee joint is the junction of three bones:
The femur, also known as the thigh bone or upper leg bone.
The tibia, also known as the shin bone or larger bone of the lower leg.
The patella or kneecap. The patella is 2 to 3 inches wide and 3 to 4 inches long. It sits over
the other bones at the front of the knee joint and slides when the knee moves. It protects the
knee and gives leverage to muscles.(9)
(2:1:1) Cartilages of the Knee:
Cartilages are white stiff flexible connective tissues that protect bony surfaces when they rub
against each other. They also act as shock absorbers and ensure smooth movement during
motion of the joint. In the knee anatomy, the surfaces of the bones inside the knee joint are
covered by two different types of cartilages.
The Menisci (the lateral and medial menisci cartilages) sit on top of the articular cartilage of
the tibial plateau. The structure of the menisci equalizes the pressure across the uneven
surface of the femur and this helps to even the weight distribution across the surface between
the femur and the tibia(7).
3

Articular cartilage, a tough elastic material that covers the ends of the three bones in the
knee joint. Articular cartilage helps absorb shock and allows the knee joint to move
smoothly.
Menisci, two crescent-shaped discs of connective tissue that separate the bones of the
knee. They are between the tibia and femur, on the outer and inner sides of each knee.
The two menisci in each knee act as shock absorbers, cushioning the lower part of the leg
from the weight of the rest of the body as well as enhancing stability.(9)
(2:1:2) Tendons of the Knee:
Tendons are tough fibrous connective tissues that attach muscles to bones. There are two
tendons in the anatomy of the knee.
Quadriceps tendon extends from the patella superiorly (up) to the quadriceps muscles. It
connects the quadriceps muscle to the patella. It continuous downwards and blend to the
patella tendon.
The patellar tendon (also known as the patellar ligament) is a downwards continuation of
the quadriceps tendon. It extends from the patella down inferiorly (down) to the tibia.(7)
Ligaments of the Knee:
The Anterior Cruciate Ligament (ACL) is located inside the knee joint, in front of the
Posterior Cruciate Ligament (PCL). It prevents the tibia from moving excessively
forward with respect to the femur. The Posterior Cruciate ligament (PCL) is located
inside the knee joint, posterior to the ACL. It prevents the tibia from moving excessively
backward with respect to the femur. The PCL extends from the anterior medial femur
down to the posterior lateral tibia.(7)
The Medial Collateral Ligament (MCL) extends from the medial side of the femur down
the tibia. The Lateral Collateral Ligament (LCL) extends from lateral side the femur
down to the lateral fibula. Together with the MCL it prevents excessive motions of the
knee joint by limiting joint mobility in the side-to-side direction.(7)
(2:1:3)The Joint Capsule:
The capsule is a thick, fibrous structure that wraps around the knee joint. Inside the
capsule is the synovial membrane which is lined by the synovium, a soft tissue that
secretes synovial fluid when it gets inflamed and provides lubrication for the knee.
(2:1:4) Bursae:
There are up to 13 bursa of various sizes in and around the knee. These fluid filled sacs
cushion the joint and reduce friction between muscles, bones, tendons and ligaments.
There are bursa located underneath the tendons and ligaments on both the lateral and
medial sides of the knee.(8)
4

(2:1:5) Plicae:
Plicae are folds in the synovium. Plicae rarely cause problems but sometimes they can get
caught between the femur and kneecap and cause pain.(8).
(2:1:6) Nerve supply and blood supply:
blood supply: main supply are the genicular branches of the popliteal artery .
nerve supply: branches from the femoral, tibial, common peroneal and obturator nerves (10).
(2:1:7) Muscles of the Knee: the hamstring muscles run down the posterior side of the femur.
They are involved in flexion of the knee (knee bends when the hamstring muscles contract). It is
composed mainly of 5 muscle groups: Sartorius, Gracilis, Semimembranosus, Semitendinosus
and Biceps Femoris(8).
(2:1:7:1)Quadriceps:
Location: front of the thigh from the hip to the knee , Action straighten the leg, Common
activities getting up from a chair, going upstairs, Common problems tightness, weakness, muscle
tear, tendonitis. The quadriceps are a group of four muscles found in the front of the thigh and
over the knee. Their primary role is to straighten the leg. These muscles (vastus medialis, vastus
intermedius, vastus lateralis and rectus femoris) all originate from the top of the femur (thigh
bone) and then join together near the knee to form the quadriceps tendon. The tendon flows
around the patella (kneecap) before finally attaching to the tibial tuberosity at the front of the
shin, .Rectus Femoris is the most superficial (closest to the surface), central muscle of thigh. (11)
(2:1:7:1:1) Function of Quadriceps muscle:
1) Straighten the leg
2) Work most frequently in closed chain activity (meaning when the foot is fixed on the floor)
e.g. getting up out of chair, walking upstairs
3) Work with the glutes (bottom muscles) and hamstrings to supply the thrusting forces of
walking, running and jumping.
4) Controls the movement of the patella (kneecap) (11)
(2:1:7:2)Hamstring:
Location: back of the thigh from the hip to the knee, Action bend the knee, Common activities
running, twisting the knee, Common problems tightness, weakness, muscle tear, tendonitis .(11)
5

(2:1:7:2:1)Function the Hamstrings muscle :
1/ Flex (bend) and rotate the knee
2/Help stabilize the knee by protecting the collateral and cruciate ligaments, especially
when the knee twists.
3/Lift the leg off the ground when walking .
4/Provides the strength for propulsion e.g. running and jumping(11)
(2:1:8)Normal Range of Motion:
Range of motion is typically measured using a tool called a goniometer. Normal ROM at the
(11knee is considered to be 0 degrees of extension (completely straight knee joint) to 135
degrees of flexion (fully bent knee joint).(12)
Flexion – 120-150 degrees
Internal rotation with knee flexed – 10 degrees
External rotation with knee flexed – 30-40 degrees(13)
(2:1:8:1) Flexion and Extension Movements of Knee in Detail:
This example considers foot fixed to the ground as in walking. When foot is fixed to the ground,
the last 30° of extension is associated with medial rotation of the femur (13).
the total range of
motion is dependent on several parameters such as soft-tissue restraints, active insufficiency, and
hamstring tightness. Flexion and extension are the chief movements. These take place in the
upper compartment of the joint, above the menisci.(13)
(2:1:8:2) Functional Motion:
Most functional activities require 0 to 117 degrees of motion at the knee. Walking requires
complete knee extension at heel strike and up to 60 degrees of flexion at the initiation of swing
phase.(12) .
(2:1:8:3) Impairments:
Common causes of decreased ROM include arthritis, knee surgery and knee injuries.(12)
6

(2:2) Arthritis:
A general term for conditions that cause inflammation (swelling) of the joints and surrounding
tissues. Some forms of arthritis may occur simultaneously with osteoporosis and Paget's disease.
Arthritis is a general term for conditions that affect the joints and surrounding tissues. Joints are
places in the body where bones come together, such as the knees, wrists, fingers, toes, and hips.
The two most common types of arthritis are osteoarthritis and rheumatoid arthritis.(14)
(2:2:1) Arthritis Symptoms:
Joint pain can be caused by injury affecting any of the ligaments, bursae, or tendons surrounding
the joint. Injury can also affect the ligaments, cartilage, and bones within the joint. Pain is also a
feature of joint inflammation (arthritis, such as rheumatoid arthritis and osteoarthritis), Arthritis
sufferers include men and women, children and adults.(15)
(2:2:2) Treatment of arthritis:
The treatment of arthritis is very dependent on the precise type of arthritis present. An accurate
diagnosis increases the chances for successful treatment. Treatments available include physical
therapy, home remedies, splinting, cold-pack application, paraffin wax dips, anti-inflammatory
drugs, pain medications (ranging from acetaminophen [Tylenol] and ibuprofen [Motrin, Advil]
to narcotics), immune-altering medications, biologic medications, and surgical operations.(15)
(2:2:3) Rheumatoid Arthritis (RA):
A disease in which the immune system attacks the linings of the joints. This results in joint pain,
stiffness, swelling, and destruction.
Rheumatoid arthritis (RA) is a disease that causes pain, swelling, and stiffness in the joints. In
some people, it can also cause the joints to become damaged and deformed. The cause of RA is
unknown, but researchers think the condition may be passed down in families.(16)
(2:3) Osteoarthritis (OA) :
is progressive joint disease characterized by joint inflammation and a reparative bone response
and is one of the top five most disabling conditions that affects more than one-third of persons >
65 years of age, with an average estimation of about 30 million Americans currently affected by
this disease(17).
7

Global estimates reveal more than 100 million people are affected by OA. The financial
expenditures for the care of persons with OA are estimated at a total annual national cost
estimate of $15.5-$28.6 billion per year. As the number of people >65 years increases,(18)
Osteoarthritis (OA) is one of the most prevalent condition resulting to disability particularly in
elderly population. OA is the most common articular disease of the developed world and a
leading cause of chronic disability, mostly as a consequence of the knee OA and/or hip OA (19).
The economic costs of OA are high, including those related to treatment, for those individuals
and their families who must adapt their lives and homes to the disease, and those due to lost
work productivity (20).
Patients with OA are at a higher risk of death compared with the general population by OR of
1.54. History of diabetes, cancer, or cardiovascular disease and the presence of walking disability
are major risk factors. Excess mortality is observed for all diseases with specific causes of death
but is particularly pronounced for cardiovascular complications. Knee OA is more important not
only for its high prevalence rate compared with other types of OA but also for its presentation at
earlier age groups particularly in younger age groups of obese women. The incidence of knee
OA increases by age and further increase with longer lifetime and higher average weight of the
population (21).
Pain and other symptoms of OA may have a profound effect on quality of life affecting both
physical function and psychological parameters. Knee OA is not a localized disease of cartilage
alone but is considered as a chronic disease of the whole joint, including articular cartilage,
meniscus, ligament, and peri-articular muscle that may result from multiple pathophysiological
mechanisms. It is painful and disabling disease that affects millions of patients (22).
Despite its severe consequences, however most patients with knee OA can be managed in the
community and primary care (23).
(2:3:1) Symptoms:
Osteoarthritis symptoms often develop slowly and worsen over time. Signs and symptoms of
osteoarthritis include:
Pain. Your joint may hurt during or after movement.
Tenderness. Your joint may feel tender when you apply light pressure to it.
Stiffness. Joint stiffness may be most noticeable when you wake up in the morning or
after a period of inactivity.
Loss of flexibility. You may not be able to move your joint through its full range of
motion.
8

Grating sensation. You may hear or feel a grating sensation when you use the joint.
Bone spurs. These extra bits of bone, which feel like hard lumps, may form around the
affected joint.(24)
(2:3:2) Risk factors:
Older age. The risk of osteoarthritis increases with age.
Sex. Women are more likely to develop osteoarthritis, though it isn't clear why.
Obesity. Carrying extra body weight contributes to osteoarthritis in several ways, and the
more you weigh, the greater your risk. Increased weight puts added stress on weight-
bearing joints, such as your hips and knees. In addition, fat tissue produces proteins that
may cause harmful inflammation in and around your joints.
Bone deformities. Some people are born with malformed joints or defective cartilage(24).
(2:3:3) Complications:
Osteoarthritis is a degenerative disease that worsens over time. Joint pain and stiffness may
become severe enough to make daily tasks difficult.
Some people are no longer able to work. When joint pain is this severe, doctors may suggest
joint replacement surgery.(25)
(2:3:4) Treatment:
The aims of management are:
To educate patients about the disease and its management
To control pain
To improve function(25)
(2:3:5) The non-pharmacological approach includes:
Education—Encourage patients to participate in self management programmers (such as those
conducted by the Arthritis Foundation in the United States and Arthritis Care in the United
Kingdom), and provide resources for social support and instruction on coping skills. Weight
loss—Exercise increases aerobic capacity, muscle strength, and endurance and also facilitates
weight loss.w4
Physical therapy consists of several strategies to facilitate resolution of symptoms
and improve functional deficits, including range of motion exercise, muscle strengthening,
muscle stretching, and soft tissue mobilization.(26).
9

(2:4) Osteoarthritis of knee:
It is Common in the knee joint. It happens when cartilage in the joint wears down. Cartilage is a
rubbery tissue at the end of bones that allows the joint to move easily. With osteoarthritis,
cartilage breaks down over time The knee can become painful, stiff, and swollen. The knee
contains a small amount of fluid that lubricates the cartilage. It also helps cushion the joint. With
osteoarthritis, this fluid does not work as well, so it can be hard to move your joint.(27)
(2:4:1) Prevalence:
About 13% of women and 10% of men aged 60 years and older have symptomatic knee OA. The
proportions of people affected with symptomatic knee OA is likely to increase due to the aging
of the population and the rate of obesity or overweight in the general population.(28).
Females,
particularly those ≥55 years, tended to have more severe OA in the knee but not in other sites.
The results of this study demonstrated sex differences incidence of knee OA particularly after
menopausal age (29).
(2:4:2) Etiology and Disease Diagnosis:
OA is characterized by a repetitive inflammatory response of the articular cartilage due to focal
loss or erosion of the articular cartilage and a hypertrophy of osteoblastic activity or a reparative
bone response known as osteophytosis.[30]
Both of these defining characteristics result in a joint space narrowing or subchondral sclerosis,
leading to pain, immobility, and often disability(31)
The symptoms of OA, such as pain and
stiffness of the joints and muscle weakness, are serious risk factors for mobility limitation and
lead to impaired quality of life for the affected population. (32)
To diagnose OA, the clinician might assess the nature and severity of the pain. It can also be
diagnosed to measure the amount of movement in the joint. An X-ray of the knee-narrowing of
the joint space is a good indicator of OA. Bony spurs can also be seen on an X-ray. In some
cases, for further clarity and better diagnosis, the magnetic resonance imaging (MRI) scan may
be necessary. This allows the clinician to see whether any damage to the soft tissue has taken
place within the joint. In certain cases, a blood sample may be necessary to rule out the presence
of other types of types of arthritis(33)
(2:4:2) Clinical features:
Persisted knee pain, limited morning stiffness, and reduced function are the three symptoms that
are recommended for the diagnosis of knee OA by the EULAR (34).
10

In addition crepitus, restriction of joint movement and bony enlargement are also very useful for
diagnosis of knee OA. Pain is the most common symptom in knee OA, a leading cause of
chronic disability, and a major source of the disability attributable to OA. Pain severity ranging
from barely perceptible to immobilizing. Pain, in knee OA typically exacerbates by activity and
relieves by rest, Tenderness to palpation of involved joints may be evident in physical
examination. Joint effusions may be present, .Crepitus during joint motion or walking is a
common .Limitation of range of motion are all common signs of OA of the knee. In advanced
cases malalignment may be apparent (genu varus or genu valgus). (35)
(2:4:3) Imaging:
Although the diagnosis of knee OA in the most cases can be made by the clinical findings and
physical examination ,however identification of joint damages are necessary for both diagnostic
confirmation as well as extent of joint involvement. Conventional plain radiographs is the first
diagnostic procedure as usually requested to demonstrate the structure-pain relationship in knee
OA. Radiographic examination has several limitations where as MRI has the capability to
visualize all the structures within the knee joint. There is a growing body of work using MRI to
examine the correlation between structural findings and symptoms (36).
(2:4:4) MRI imaging:
MRI is not necessary for most patients with suggestive symptoms of OA and/or typical plain
radiographic features. However, MRI of the knee has a diagnostic role in patients with joint pain
and symptoms such as locking, popping, or instability that suggest meniscal or ligamentous
damage. The presence of two MRI findings concomitantly correlates with painful OA of the
knee. (36)
(2:4:5) Laboratory findings:
Although mild synovitis may be seen in patients with knee OA but markers of inflammation such
as erythrocyte sedimentation rate (ESR) and C –reactive protein (CRP) levels are usually normal.
Synovial fluid in knee OA is of non-inflammatory type. Serum and synovial fluid levels of CRP
in OA are markedly lower than inflammatory arthritis. Synovial fluid anti-cyclic citrullinated
peptide antibody is negative in both serum and synovial fluid of patients with knee OA .(37)
(2:4:6) Treatment and Management: From the current studies available, no specific cure for
OA exists and the severity of condition varies from pharmacological and non pharmacological
treatment modalities Mostly, all exercise programs for knee OA should be practical, albeit
simple, but should be helpful in gradual and progressive cure of the condition. (38)
11

(2:5) Ultrasound:
Ultrasound (US)therapy it is used as a non-invasive modality reputed ability to relieve pain
reduce edema, increase the range of motion, and accelerate tissue repair via thermal and non-
thermal mechanisms (mechanical effects). (39)
US can be administered in either a continuous or a pulsed mode. Pulsed US produces non-
thermal effects and is beneficial for cartilage health
whereas continuous US aims to generate
thermal effects that could enhance fibrous tissue extensibility, increase tissue metabolism,
promote capillary permeability, and elevate the pain threshold (40)
A recent systematic review and meta-analysis suggested that pulsed US is the preferred
treatment mode both in terms of more effective pain relief and improved function without
significant adverse effects in clinical trials (41)
In addition, US can be administered in either an unfocused or a focused mode. The basic
differences between FLIPUS and traditional US are that the main biological effect of FLIPUS is
a mechanical effect and the targeted tissue is cartilage, while the biological effect of traditional
US is a thermal effect and the targeted tissues are periarticular soft tissue lesions.
The results of a number of studies have suggested that unfocused therapeutic US may be useful
for reducing the pain and disability associated with knee OA However, few studies of focused
low-intensity pulsed US have been published that describe knee OA rehabilitation.(42)
The vibrations (also called cavitation) cause a deep heating effect locally, with the patient
normally feeling no sensation of this heat. There are circumstances in which the heating effect is
not desired (such as a fresh injury with acute inflammation) and for these the ultrasound is pulsed
rather than continuously transmitted.(43)
(2:5:1) The Biophysical Bases for Therapeutic Ultrasound Applications:
Ultrasonic energy can be a potent modality for generating biological effects. Given sufficient
knowledge of the etiology and exposimeter, bioeffects can be planned for therapeutic purposes or
avoided in diagnostic applications. For therapy, ultrasound can induce effects not only through
heating, but also through non thermal mechanisms including ultrasonic cavitation, gas body
activation, mechanical stress or other undetermined non thermal processes .(44)
Starting from the diagnostic reference frame, ultrasound is usually produced from a piezoceramic
crystal in very short, i.e., 1- to 5-cycle, pulses. Diagnostic ultrasound is often characterized by
the center frequency of the pulses (typically in the 2–12 MHz range), which is usually the
12

frequency inherent to the thickness of the ceramic crystal, As the pressure amplitude, the
frequency, or the propagation length is increased, the ultrasound wave can distort, which could
ultimately lead to a discontinuity or shock in the waveform. In regard to bio effects, increasing
frequency, nonlinear acoustic distortion, or pulse length can increase heating and enhance some
non thermal mechanisms, e.g., radiation force. Decreasing frequency increases the likelihood of
cavitation and gas body activation. Increasing power or intensity tends to increase the likelihood
and magnitude of all bioeffects mechanisms. Therapeutic ultrasound devices may use short
bursts or continuous waves to deliver effective ultrasonic energy to tissues. Some devices operate
at higher amplitude and therefore tend to produce shocked or distorted waves.(44)
(2:5:2) Low Intensity Pulsed Ultrasound:
Low intensity pulsed ultrasound has therapeutic application to accelerate the healing of bone
fractures including cases of nonunion The characteristics of the pulsed ultrasound, for example,
1.5-MHz frequency with 30-mW/cm2 spatial average temporal average intensity, are in the range
of diagnostic ultrasound. The biophysical mechanisms for the therapeutic action are uncertain for
this application. Therapy involves multiple treatments of 20 min each day by applying the large
flat transducer to the site of injury and continuing treatment for periods of months. Although the
process appears to be safe and effective, the therapy is slow and its use is predominantly limited
to management of non-healing fractures.(45)
(2:5:3) Indication Of Therapeutic Ultrasound:
Ultrasound therapy is now primarily used in treating musculoskeletal injuries. Patients who will
benefit greatly from ultrasound technology as a form of musculoskeletal therapy are those who
are suffering from: Plantar fasciitis, Tennis elbow, Lower back pain, Temporomandibular
disorders, Ligament sprains, Muscle strains, Tendonitis, Joint inflammation, Metatarsalgia
Facet irritation, Impingement syndrome, Bursitis, Osteoarthritis, Scar tissue, Rheumatoid
arthritis(46).
also used in:
promoting bone fracture healing
phonophoresis – non-invasive topical delivery of medications to tissues below the skin,
where the ultrasonic energy forces the medication through the skin
lithotripsy, as focused high-energy pulses to break calculi (such as kidney stones, gallstones,
and stones in the bladder and ureter) into small enough bits that may be passed from the body
without undue difficulty(42)
.
13

(2:5:4) Contraindications of Ultrasound Therapy:
There are several situations in which the use of ultrasound therapy is not advised. These include
cases where the area being considered for treatment has metal implants, acute infection, active
growth plates (as in children), malignancy, or vascular abnormalities. Other areas to be avoided
are directly on the abdomen of pregnant women, as well as over the eyes, skull, and testes.
Included in the list of contraindications for ultrasound therapy is the region over the spinal cord
where there has been a laminectomy (removal of the back part of the vertebra that covers the
(pinal canal).(43)
(2:5:5) Side Effect of Ultrasound Physical Therapy:
Even though there are many health benefits of using ultrasound in physical therapy, but there are
some side effects. Using the ultrasound physical therapy will might cause the nausea, dizziness
and also the problems associated to breathing. Although the medical science studies stated that
using ultrasound is safe ,but there are some problems we should know before. The over exposure
of the ultrasound frequencies will cause the dangerous effects(.42)
14

(2:6) Interferential therapy:
The basic principle of Interferential Therapy (IFT) is to utilize the significant physiological
effects, it is an effective therapy option used by many physiotherapy clinics to relieve pain and
accelerate the self-healing process, getting your body back to a healthy, pain free state. The high
frequency signals of an IFC penetrate through the skin into deeper lying muscle tissues.(47)
Interferential current therapy has been in use for many years, and there have been numerous case
studies and research reports that have documented its versatility in treating diverse symptoms,
accelerating the healing process and restoring normal movement. Patients who chose to undergo
interferential current therapy have fewer post-op complications compared to people who rely
exclusively on medications for pain relief. It also helps in blood circulation and hastens the healing
process by stimulating endorphins.(48)
Of low frequency <250pps electrical stimulation of nerves without the associated painful and
Some what unpleasant side effects sometimes associated with low frequency stimulation.,
Numerous ‗portable‘ interferential devices have become easily available.
Despite their size, they are perfectly capable of delivering ‗proper‘ interferential therapy, though
some have limited functionality and ability for the practitioner to ‗set‘ all parameters. Most
multifunction stimulators include all interferential modes. (47)
(2:6:1) Techniques, contraindications and safety:
The area of skin to be treated is cleaned with soap and water to reduce linear electrical resistance
(reactance arising from capacitance is unchanged) and the electrodes are fixed to the skin with
tape. Some apparatus is supplied with electrodes that are held in place by suction cups evacuated
using a vacuum pump. This facility is useful when treating regions such as the trunk where it is
difficult to strap an electrode. The electrodes are orientated so that the two currents intersect
within the target structure. Alternatively, the therapist may wear one electrode of each pair as a
glove and vary the site of maximum interference during the treatment. Some units incorporate
four electrodes into a single small applicator, thus facilitating the effective treatment if
superficial and localized lesions. The intensity of the current is increased gradually until the
patient reports that a further rise would cause discomfort. Cutaneous nerves accommodate
rapidly to this stimulus and after a few seconds a larger current can be applied. (49)
Contraindications are few, although the prudent would not treat patients presenting with very
acute inflammation, fever, tumor, thrombosis, those who are pregnant, have a marked aversion to
this type of therapy, or persons wearing a cardiac pacemaker. Concern that interferential therapy
might promote the aggregation of platelets and induce thrombosis appears unfounded 1. This
apparatus should not be used within five meters of an operational short-wave diathermy unit
because the cables may act as antennae and conduct a dangerous quantity of RF energy to the
patient(50)
15

(2:6:2) Physiological and therapeutic effects of interferential currents:
The current flowing between each pair of electrodes is insufficient to stimulate nerve and musde
directly until amplitude is modulated by interference. Interferential therapy thus reduces the
stimulation of cutaneous sensory nerves near the electrodes whilst promoting the effect upon
deep tissues. The physiological effect of an amplitude modulated supra threshold current
depends upon frequency. Neurons exhibit a maximum rate at which action potentials are
conducted and this is a function of the degree of myelination and the diameter of the axon.
Repetitive stimulation at any frequency up to its maximum (1 kHz for a large motor neuron) will
cause action potentials to flow in the axon at the same rate. As the rate of stimulation increases
above this value, successive stimuli fall within the relative, and eventually the absolute
refractory period of the preceding action potential. A larger than normal flow of current is
necessary to stimulate a refractory neuronal membrane and thus the sensitivity of the nerve
decreases. This effect is termed Wedensky inhibition. Prolonged stimulation at a supra maximal
frequency will eventually cause the axon to cease conducting. Accommodation of the neuron is
responsible for this effect, caused by an increased threshold and synaptic fatigue(51)
(2:6:3)Stimulation of muscle:
A neurone showing the reduced sensitivity associated with Wedensky inhibition will also have a
rate of firing independent of the frequency of the applied stimulus. This rate is dictated instead
by the duration of the refractory period. Known as the Gildemeister effect, rapid stimulation of a
motor nerve with large although comfortable interferential currents will result in an
asynchronous depolarization of the individual motor units. This mimics the pattern observed
during a normal voluntary contraction. Traditional low-frequency neuromuscular stimulation
tends to recruit only the large axon motor neurons, which have a lower threshold than small
fibers, and innervate muscle fibers that fatigue readily. This pattern of discharge is synchronous
and unlike a normal contraction. Motor excitation using interferential currents is considered by
many to represent an advance over the other low-frequency methods of stimulation. The
optimum frequency of stimulation for most voluntary muscle appears to be 40-80Hz5 14, whilst
visceral muscle, supplied by the autonomic nervous system, is stimulated optimally at 10-50
Hz(51)
Interferential Current stimulation is very useful in the treatment of circulatory and muscular
disorders, stiffness of joints, edema, and inflammation. If you suffer from health problems such
as cumulative trauma disorders, body pain, joint injuries, or are pre or post orthopedic surgery,
interferential current therapy is and important option ,It has been in use for many years, and there
have been numerous case studies and research reports that have documented its versatility in
treating diverse symptoms, accelerating the healing process and restoring normal movement.
Patients who chose to undergo interferential current therapy have fewer post-op complications
compared to people who rely exclusively on medications for pain relief. It also helps in blood
circulation and hastens the healing process by stimulating endorphins.(52)
16

(2:6:4) Control of pain:
Electrical stimulation for pain relief has widespread clinical use, thought the direct research evidence for
the use of IFT in this role is limited. Logically one could use the higher frequencies (90-130Hz) to
stimulate the pain gate mechanisms & thereby mask the pain symptoms. Alternatively, stimulation with
lower frequencies (2-5Hz) can be used to activate the opioid mechanisms, again providing a degree of
relief. These two different modes of action can be explained physiologically & will have different latent
periods & varying duration of effect. It remains possible that relief of pain may be achieved by
stimulation of the reticular formation at frequencies of 10-25Hz or by blocking C fibre transmission at
>50Hz. Although both of these latter mechanisms have been proposed (theoretically) with IFT, neither
have been categorically demonstrated.(53)
The analgesic effect of interferential therapy can be explained in part by Wednesky inhibition of
Type C nociceptive fibers, although other mechanisms are certainly involved. 'Pain gate' theory,
proposed by Malzack and Wall'9 and much modified subsequently20 remains central to this
explanation. Briefly, this theory proposes that action potentials travelling in large-diameter
myelinated afferent nerves from cutaneous receptors compete for access to the central ascending
sensory tracts in the dorsal horn of the spinal cord with those of small-diameter unmyelinated
sensory fibers carrying pain information. Activity in the large fibers takes precedence over that
in small fibers, 'closing the gate' to pain information entering the central nervous system and
preventing it from reaching a conscious level. Pain is thus reduced. Large-diameter myelinated
fibers are stimulated optimally at 100 Hz5 2' and clinical experience indicates that interferential
therapy at this frequency reduces pain markedly, especially when applied to acupuncture
points.(54)
(2:6:5)Autonomic effects and the control of incontinence:
Type A6 and C fibers, and those of the autonomic nervous system, are generally small and
poorly myelinated. Clinical evidence suggests that these small neurons of the peripheral nervous
system fail to conduct when stimulated at frequencies exceeding 40 and 15Hz respectively2l.
When extrapolated to the autonomic nervous system, this behavior can be exploited
therapeutically5'26 by using the stimulus of an interferential current to reproduce by non-
invasive means the vasodilatation caused by chemical sympathectomy in peripheral vascular
disease and reflex sympathetic dystrophy, There is some disagreement regarding the precise
frequency at which this inhibitory response occurs Control of circulation and reducing
oedema.(53)
, IFT has been claimed to be effective as a treatment to promote the reabsorption of
oedema in the tissues. Again, the evidence is very limited in this respect and the physiological
mechanism by which is could be achieved as a direct effect of the IFT remains to be established.
The preferable clinical option in the light of the available evidence is to use the IFT to bring
about local muscle contraction(s) which combined with the local vascular changes that will result
(see above) could be effective in encouraging the reabsorption of tissue fluid. The use of suction
electrodes may be beneficial, but also remains unproven in this respect. (55)
17

(2:6:6) Reduce Oedema:
Several studies investigate changes in the rate of blood flow following transcutaneous electrical
nerve stimulation. Stimulation applied to the dorsal roots or spinal segment of origin of a
peripheral nerve causes peripheral vasodilatation in the structures innervated by it31. Sufferers
from Raynaud's syndrome treated for eight minutes at 90-10OHz in the region of the stellate
ganglion in the neck showed a doubling of pulse volume in the digital vessels. NikolovaTroeva3
demonstrated a similarly marked symptomatic improvement in patients with endarteritis
obliterans who failed to respond to chemical sympathectomy or medication. Supporting these
findings is a report that those with a peripheral vascular disease benefit from interferential
therapy at 0-10OHz for 10 minutes36, although recent investigations cast doubt on the
reproducibility of these effects (54).
IFT has been claimed to be effective as a treatment to promote the reabsorption of oedema in the
tissues. Again, the evidence is very limited in this respect and the physiological mechanism by
which is could be achieved as a direct effect of the IFT remains to be established. The preferable
clinical option in the light of the available evidence is to use the IFT to bring about local muscle
contraction(s) which combined with the local vascular changes that will result (see above) could
be effective in encouraging the reabsorption of tissue fluid. The use of suction electrodes may be
beneficial, but also remains unproven in this respect (56)
(2:6:7) Blood flow:
There is very little, if any quality evidence demonstrating a direct effect if IFT on local blood flow
changes. Most of the work that has been done involves laboratory experimentation on asymptomatic
subjects, and most blood flow measurements are superficial i.e. skin blood flow. Whether IFT is actually
capable of generating a change (increase) in blood flow at depth remains questionable. The elegant
experimentation by Noble et al (2000) demonstrated vascular changes at 10–20Hz, though was unable to
clearly identify the mechanism for this change. The stimulation was applied via suction electrodes, and
the outcome could therefore be as a result of the suction rather than the stimulation, though this is largely
negated by virtue of the fact that other stimulation frequencies were also delivered with the suction
electrodes without the blood flow changes.(56)
18

Chapter three
Methods & Materials

3. Materials and Methods
(3) material and method:
(3-1)study design:
it is randomized clinical trials.
(3-2)StudyArea:
this study was conducted in the outpatient clinic of the faculty of physical therapy- AL Neelain
University.
(3-3)study population:
the target populations of this study were the individuals who are diagnosed osteoarthritis of
knee.
Inclusion criteria:
Patients aging between 40-70 years with knee osteoarthritis.
Male and female.
Knee Osteoarthritis patient.
Exclusion criteria:
Neurological deficit.
Patient who has past history of physiotherapy treatment for their knee osteoarthritis .
Patient with knee surgery.
History of treatment with interferential or combination of (IFT+ Ultrasound Therapy).
Patient aged below 40 or above 70 years old.
Sever psychological disorders.
(3-4 )Sampling
(3-4-1) sampling technique:
Simple random sampling techniques used.
19

(3-4-2) sampling size:
30 Patients randomly assigned into two equal groups (group A and group B ) Each group
received conventional therapy.
Apart from the common conventional therapy of these groups received additional therapy:
GROUP A:15 patients received Combination therapy (IFT+US)
GROUP B:15 patients received Interferential therapy.
(3-5)Study instruments:
(3-5-1)instrumentations for evaluation:
Before conducting the actual treatment, the patients of osteoarthritis of knee evaluated by using
an evaluation format. Patients assessed on the first day before treatment and at end of 12 session
for following:
(A) Pain evaluation by visual analoge scale: (VAS) which is a one-dimensional measure of pain
intensity and widely used in diverse adult populations, or pain intensity, the scale is most
commonly anchored by ―no pain‖ (score of 0) and ―pain as bad as it could be‖ or ―worst
imaginable pain‖ (score of 100 [100-mm scale]) To avoid clustering of scores around a preferred
numeric value, numbers or verbal descriptors at intermediate points are not recommended[55]
(B) Knee range of motion.by goniometer A goniometer; is a device used in physical therapy to
measure the range of motion around a joint in the body. The word goniometer is derived from the
Greek terms gone and metro, which mean angle and measure, respectively.
A goniometer is usually made of plastic and is often transparent. Occasionally goniometers are
made of metal. There are two "arms" of the goniometer: the stationary arm and the moveable
arm. Each arm is positioned at specific points on the body and the center of the goniometer is
aligned at the joint to be measured. There are hash marks on the center of the goniometer that
your physical therapist uses to precisely measure joint range of motion.[57]
(C) Fuction of knee by WOMAC (western ontaria and Mcmaster universities osteoarthritis
index)is a propriety heath status questionnaire protect by copy right and treatment consist of 24
item divided into 3subscales.(58)
20

(3-5-2)Instrumentations for treatment:
GROUP A:
COMBINATION THERAPY (IFT+US):
Patient Position: Supine Lying.
Technique: Three Interferential pad electrodes placed around the affected knee joint.
US treatment head to be applied over the site of maximum pain of the affected knee joint.
The patient explained that he will feel a tingling sensation which should not be unpleasant
US dose: Frequency = 1 MHz
Intensity = 0.8 W/cm2,
Mode = Pulse (1:1)
Duration = 5 minutes
Interferential dose:
Frequency = 4000 Hz.
Base = 90Hz.
Sweep = 40Hz.
AMF / Beat Frequency = 90-130 Hz.
Quadripolar / Two channel.
Duration = 10 minutes.
First US will be turned on , followed by the IFT (parameters as above)
Starting with the US head over the maximum painful area of the joint, gradually the IFT output
intensity will be increased until the `normal' tingling is encountered by the patient[59].
GROUP B:
INTERFERENTIAL THERAPY
Patient Position. Technique: Four interferential pad electrodes placed around the affected knee joint.
The patient explained when he or she feel a tingling sensation which should not be unpleasant.
Interferential dose:
Frequency = 4000 Hz
Base = 90Hz
Sweep = 40Hz
AMF / Beat Frequency = 90-130 Hz
Quadripolar / Two channel
Duration = 10 minutes
21
IFT will be turned on (parameters as above)
Gradually the IFT output intensity increased until the `normal' tingling is encountered by the
patient(58)
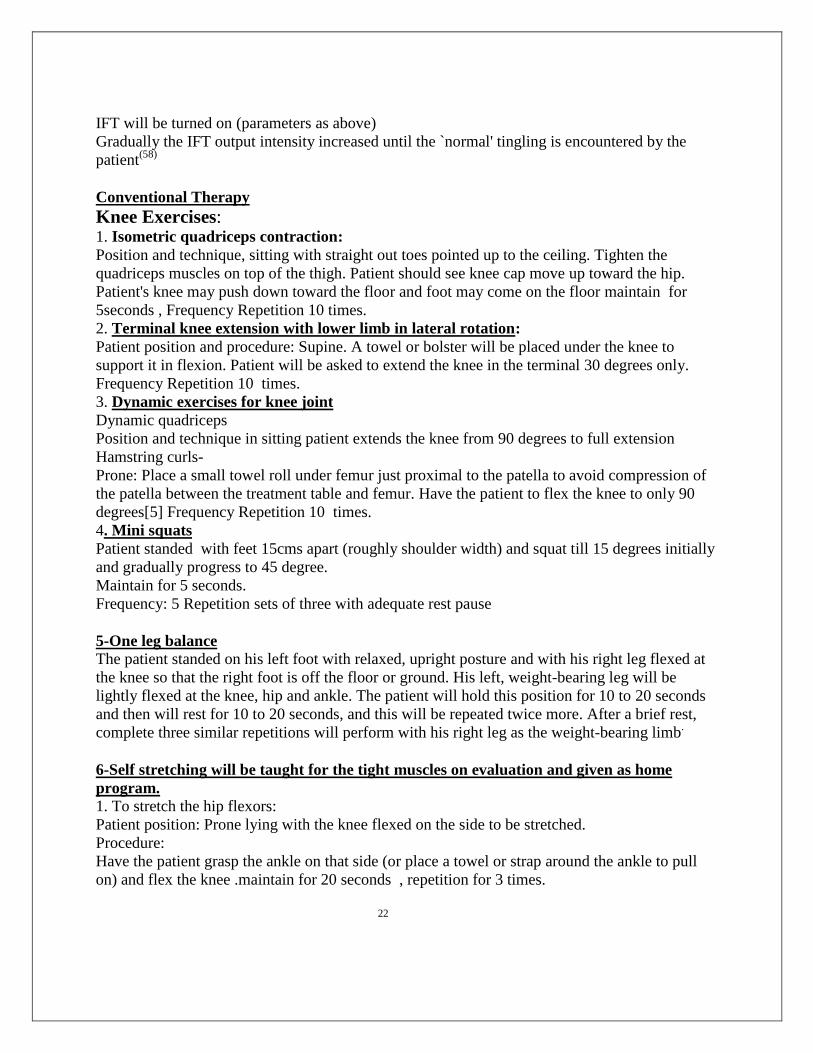
Conventional Therapy
Knee Exercises: 1. Isometric quadriceps contraction:
Position and technique, sitting with straight out toes pointed up to the ceiling. Tighten the
quadriceps muscles on top of the thigh. Patient should see knee cap move up toward the hip.
Patient's knee may push down toward the floor and foot may come on the floor maintain for
5seconds , Frequency Repetition 10 times.
2. Terminal knee extension with lower limb in lateral rotation:
Patient position and procedure: Supine. A towel or bolster will be placed under the knee to
support it in flexion. Patient will be asked to extend the knee in the terminal 30 degrees only.
Frequency Repetition 10 times.
3. Dynamic exercises for knee joint
Dynamic quadriceps
Position and technique in sitting patient extends the knee from 90 degrees to full extension
Hamstring curls-
Prone: Place a small towel roll under femur just proximal to the patella to avoid compression of
the patella between the treatment table and femur. Have the patient to flex the knee to only 90
degrees[5] Frequency Repetition 10 times.
4. Mini squats
Patient standed with feet 15cms apart (roughly shoulder width) and squat till 15 degrees initially
and gradually progress to 45 degree.
Maintain for 5 seconds.
Frequency: 5 Repetition sets of three with adequate rest pause
5-One leg balance The patient standed on his left foot with relaxed, upright posture and with his right leg flexed at
the knee so that the right foot is off the floor or ground. His left, weight-bearing leg will be
lightly flexed at the knee, hip and ankle. The patient will hold this position for 10 to 20 seconds
and then will rest for 10 to 20 seconds, and this will be repeated twice more. After a brief rest,
complete three similar repetitions will perform with his right leg as the weight-bearing limb.
6-Self stretching will be taught for the tight muscles on evaluation and given as home
program. 1. To stretch the hip flexors:
Patient position: Prone lying with the knee flexed on the side to be stretched.
Procedure:
Have the patient grasp the ankle on that side (or place a towel or strap around the ankle to pull
on) and flex the knee .maintain for 20 seconds , repetition for 3 times.
22

2. To stretch the hip extensors:
Patient position: Supine with a towel under the thigh.
Procedure:
Have the patient perform straight leg raising with one extremity and apply the stretch force by
pulling on the towel to move the hip into more flexion. Maintain for 20 seconds ,Repetition 3
times .
3. To stretch the hip abductors:
Patient position: Side-lying, with the leg to be stretched uppermost.
Procedure:
The bottom extremity is flexed for support and the pelvis tilted laterally so the waist is against
the mate or floor maintain for 20 seconds , repetition 3 times.
Abduct the top leg and align it in the plane of the body.
While maintaining this position, have the patient externally rotate the hip and then gradually
lower the thigh to the point of stretch. maintain for 20 seconds , repetition 3 times.
4. To stretch the hip adductors:
Patient position: Standing in a fencer's position but with the hind leg externally rotated.
Procedure:
Have the patient shift the weight onto the front leg until a stretch sensation is felt along the
medial thigh in the hind leg. maintain for 20 seconds , repetition 3 times.
5. To stretch the knee flexors:
Patient position: Place the patient in prone with a belt or sheet strapped around the ankle and the
other end placed over the shoulder and held in the hand.
Procedure:
Have the patient perform knee flexion with one extremity and apply the stretch force by pulling
on the belt or sheet to move the knee into more flexion. maintain for 20 seconds ,repetition 3
times.
6. To stretch the knee extensors:
Patient position: Standing with the foot of the involved knee on a step.
Procedure:
Have the patient rock forward over the stabilized foot, flexing the knee to the limit of its range,
then rock back and forth in a slow, rhythmic manner or hold the stretched position(59)
maintain for
20 seconds , repetition 3 times.
(3-6) Methods of data collection:
(3-6-1) Tools of data collection:
Structural questionnaire was involved for personal variable personal (age –gender)
about osteoarthritis patient and (VAS ,WMAC) scale.
23

(3-6-2 )study variables:
1-Age
2-gender
3-pain
4-knee Range of motion
5- knee and functional performance
(3-7)data management and analysis plain:
Statistical analysis was done by using statistical package of social science (SPSS). The test of
significance was calculated using the P value of 0.05.
data storage on personal computer( PC)and E-mail
(3-8)Ethical consideration:
1-Permission tacked before start the application There writted informed consent from each
participant and participation will be voluntary.
2- selected suitable time for data collection from patients.
3-Explanation of the method of application and using for assessment will be done.
4-Ethical approval tacked from research committee
24

Chapter four
Results

Table(4- 1): Background characteristic of both groups:
Group B Group A
Percentage Frequency Characteristic Percentage Frequency Characteristic
Gender Gender
20.0 6 Male 13.3 4 Male
30.0 9 Female 36.7 11 Female
Age Age
23.3 7 40-50 26.7 8 40-50
16.7 5 51-60 20.0 6 51-60
10.0 3 61-70 3.3 1 61-70
100 15 Total 100 15 Total
25

Comparisons within groups:
Table(4-2):Statistical Analysis of pain measurement in group(A).pre and post treatment with
Combination therapy (IFT+US) by VAS.
VAS Mean N
Std.
Deviation P-VALUE
SIG
Pain(A) pre 5.80 15 1.859 0,000 SIG
Pain(A)post 1.33 15 .900
P Value =probability value (significant<=0.o5)
There was a singnificant difference recorded pre and post (VAS)in group(A)P=(0,000).
VAS(A)
FIGER (4-1):Avarge of pain measurement in group (A) combination therapy(IFT+US) by VAS.
26
5.80
1.33
0.00
1.00
2.00
3.00
4.00
5.00
6.00
7.00
painApre painApost
Pair 1
vas

Table (4-3):Statistical analysis of fuctional performance in group (A) pre and post treatment
with combination therapy (IFT+US) by WOMAC .
Womac Mean N
Std.
Deviation P.value
Sig
Womac(A) Pre 60.07 15 16.303 0.000
Sig
Womac(A)post 30.67 15 15.814
P Value =probability value (significant<=0.o5)
There was a significant difference OF functional performance in group(A) per and post
treatment with combination therapy(IFT+US) by WOMAC .
P=(0,000).
WOMAC(A)
MEAN 60.07 30.67
FIGER (4-2):Avarge of FUCTIONAL PERFORMANCE measurement in group (A) combination
therapy(IFT+US) by WOMAC.
27
60.07
30.67
0.00
10.00
20.00
30.00
40.00
50.00
60.00
70.00
WomacApre womacApost
Pair 1
WO
MA
C

Table (4-4): Statistical Analysis of flextion ROM in group (A) pre and post treatment with
combination therapy(IFT+US) .
flexion Mean N
Std.
Deviation p.value
Sig
Flexion(A)pre 112.60 15 10.294 .000 Sig
Flexion(A)post 119.87 15 8.959
P Value =probability value (significant<=0.o5.
There was a significant difference OF flexion ROM in group(A) per and post treatment with
combination therapy(IFT+US)
P=(0,000).
MEAN 112.60 119.87
FIGER (4-3):Avarge of Flexion ROM in group (A) combination therapy(IFT+US) pre and post
treatment .
28
112.60
119.87
108.00
110.00
112.00
114.00
116.00
118.00
120.00
122.00
flextionApre flextionApost
Pair 1
FLEX
ION
FLEXION(A)

Table (4-5): Statistical Analysis of Extension ROM in group (A) pre and post treatment with
combination therapy(IFT+US) .
Extension Mean N
Std.
Deviation P.value
Sig
Extension(A)pre 2.33 15 2.498 0.000 Sig
Extension(A)post .60 15 1.404 .
P Value =probability value (significant<=0.o5)
There was a significant difference OF Extension ROM in group(A) per and post treatment with
combination therapy(IFT+US)
P=(0,000).
Extension(A)
Mean 2.33 ,60
FIGER (4-4):Avarge of Extension ROM in group (A) combination therapy(IFT+US) pre and post
treatment .
29
2.33
.60
0.00
0.50
1.00
1.50
2.00
2.50
extentionApre extentionApost
Pair 1
Exte
nti
on

Table (4-6): Statistical Analysis of pain measurement in group(B).pre and post treatment with
(IFT)Therapy by VAS.
VAS Mean N
Std.
Deviation P.value
Sig
Pain(B) pre 4.40 15 1.844 0.021 Sig
Pain(B) post 1.47 15 .915
P Value =probability value (significant<=0.o5)
There was a singnificant difference recorded pre and post (VAS)in group(B)P=(0,021).
MEAN 4.40 1.47
FIGER (4-5):Avarge of pain measurement in group (B) (IFT) therapy by VAS.
30
4.40
1.47
0.00
0.50
1.00
1.50
2.00
2.50
3.00
3.50
4.00
4.50
5.00
painBpre painBpost
Pair 1
vas
VAS (B)

Table (4-7): Statistical Analysis of functional performance in group(B).pre and post treatment
with (IFT)Therapy by WOMAC .
Womac Mean N
Std.
Deviation P.value
Sig
Womac Bpre 51.73 15 14.058 0.000 Sig
Womac Bpost 24.20 15 12.824
P Value =probability value (significant<=0.o5)
There was a singnificant difference OF functional performance in group(B) per and post
treatment with (IFT) therapy by WOMAC .
P=(0,000)
WOMAC(B)
MEAN 51.73 24.20
FIGER (4-6):Avarge of FUCTIONAL PERFORMANCE measurement in group (B) (IFT) therapy by
WOMAC.
31
51.73
24.20
0.00
10.00
20.00
30.00
40.00
50.00
60.00
WomacBpre WomacBpost
Pair 1
WO
MA
C

Table (4-8): Statistical Analysis of flexion ROM in group (B) pre and post treatment with (IFT)
therapy.
flexion Mean N
Std.
Deviation P.value
Sig
Flexion(B)pre 106.00 15 11.155 0.000 Sig
Flexion(B)post 117.87 15 6.621
P Value =probability value (significant<=0.o5)
There was a singnificant difference OF flexion ROM in group(B) per and post treatment with
(IFT) therapy.
P=(0,000).
MEAN 106.00 117.87
FIGER (4-7):Avarge of Flexion ROM in group (B ) (IFT) therapy pre and post treatment .
32
106.00
117.87
100.00
102.00
104.00
106.00
108.00
110.00
112.00
114.00
116.00
118.00
120.00
flextionBpre flextionBpost
Pair 1
FLEX
TIO
N
FLEXION(B)

Table (4-9): Statistical Analysis of EXTION ROM in group (B) pre and post treatment with (IFT)
therapy.
Extension Mean N
Std.
Deviation P.value
Sig
Extension(B)pre 4.47 15 9.141 0.000 Sig
Extension(B)post 1.27 15 2.890
P Value =probability value (significant<=0.o5)
There was a significant difference OF EXTENSION ROM in group(B) per and post treatment
with (IFT) therapy.
P=(0,000).
MEAN 4.47 1.27
FIGER (4-8):Avarge of EXTENSION ROM in group (B ) (IFT) therapy pre and post treatment .
33
4.47
1.27
0.00
0.50
1.00
1.50
2.00
2.50
3.00
3.50
4.00
4.50
5.00
extentionBpre extentionBpost
Pair 1
EXTE
NTI
ON
EXTENSION(B)
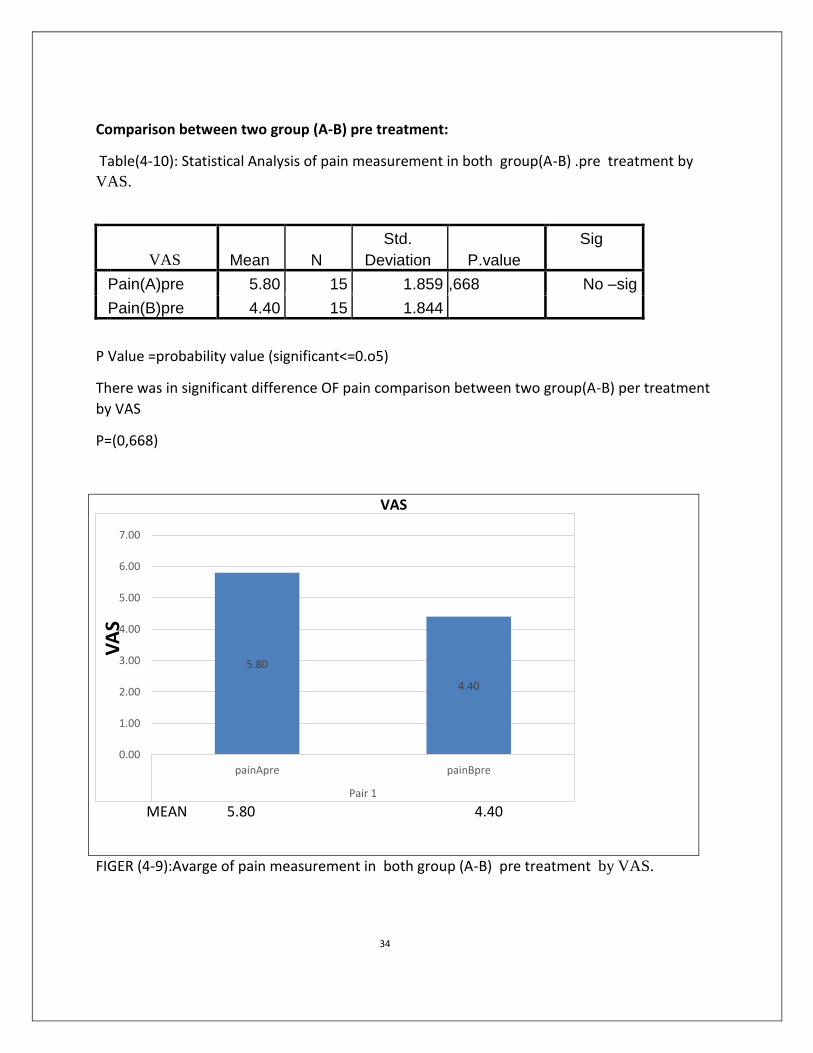
Comparison between two group (A-B) pre treatment:
Table(4-10): Statistical Analysis of pain measurement in both group(A-B) .pre treatment by
VAS.
VAS Mean N
Std.
Deviation P.value
Sig
Pain(A)pre 5.80 15 1.859 ,668 No –sig
Pain(B)pre 4.40 15 1.844
P Value =probability value (significant<=0.o5)
There was in significant difference OF pain comparison between two group(A-B) per treatment
by VAS
P=(0,668)
VAS
MEAN 5.80 4.40
FIGER (4-9):Avarge of pain measurement in both group (A-B) pre treatment by VAS.
34
5.80
4.40
0.00
1.00
2.00
3.00
4.00
5.00
6.00
7.00
painApre painBpre
Pair 1
VA
S

Table(4-11): Statistical Analysis of functional performance measurement in both group(A-B)
.pre treatment by WOMAC.
WOMAC Mean N
Std.
Deviation P.value
Sig
Womac(A)pre 60.07 15 16.303 0.000 sig
Womac( B)pre 51.73 15 14.058
P Value =probability value (significant<=0.o5)
There was significant difference OF functional performance comparison between two group(A-
B) per treatment BY WOMAC.
P=(0,000)
WOMAC
Mean 60.07 51.73
FIGER (4-10):Avarge of fuctional performance measurement in both group (A-B) pre treatment
BY WOMAC.
35
60.07
51.73
46.00
48.00
50.00
52.00
54.00
56.00
58.00
60.00
62.00
WomacApre WomacBpre
Pair 1
WO
MA
C

Table(4-12): Statistical Analysis OF Flexion ROM in both group(A-B) .pre treatment .
Flexion Mean N
Std.
Deviation P.VALUE
SIG
Flexion(A)pre 112.60 15 10.294 0.06 No –sig
Flexion(B)pre 106.00 15 11.155
P Value =probability value (significant<=0.o5)
There was in singnificant difference OF flexion ROM in both group(A-B) per treatment .
P=(0,060)
FLEXION
MEAN 112,60 106,60
FIGER (4-11):Avarge of Flexion ROM in both group (A-B) pre treatment .
36
112.60
106.00
102.00
104.00
106.00
108.00
110.00
112.00
114.00
flextionApre flextionBpre
Pair 1
flex
ion

Table(4-13): Statistical Analysis OF EXTENSION ROM in both group(A-B) .pre treatment
Extension Mean N
Std.
Deviation p.value
Sig
Extension(A)pre 2.33 15 2.498 0.668 No-sig
Extension(B)pre 4.47 15 9.141
P Value =probability value (significant<=0.o5)
There was in singnificant difference OF EXTENSION ROM in both group(A-B) per treatment .
P=(0,668).
MEAN 2.33 4.47
FIGER (4-12):Avarge of EXTENSION ROM in both group (A-B) pre treatment .
37
2.33
4.47
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
extentionApre extentionBpre
EXTE
NSI
ON

Comparison between two group (A-B) POST treatment:
Table(4-14): Statistical Analysis of pain measurement in both group(A-B) .post treatment by
VAS.
VAS Mean N
Std.
Deviation P-VALUE
SIG
Pain(A)post 1.33 15 .900 0,002 SIG
Pain(B)post 1.47 15 .915
P Value =probability value (significant<=0.o5)
There was singnificant difference OF pain in both group(A-B) post treatment .
P=(0,002).
MEAN 1,33 1,47
FIGER (4-13):Avarge of pain measurement in both group (A-B) post treatment by VAS.
38
1.33
1.47
1.25
1.30
1.35
1.40
1.45
1.50
painApost painBpost
Pair 1
VA
S
VAS

Table(4-15): Statistical Analysis of functional performance measurement in both group(A-B)
.post treatment by WOMAC.
WOMAC Mean N
Std.
Deviation P-VALUE
SIG
Womac(A)post 30.67 15 15.814 ,003 SIG
Womac(B)post 24.20 15 12.824
P Value =probability value (significant<=0.o5)
There was significant difference OF functional performance in both group(A-B) post treatment .
P=(0,003)
WOMAC
MEAN 30,67 24,20
FIGER (4-14):Avarge of Fuctioinal performance both group (A-B) post treatment by WOMAC.
39
30.67
24.20
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
womacApost WomacBpost
Pair 1
WO
MA
C

Table(4-16): Statistical Analysis of Flexion ROM in both group(A-B) .post treatment.
Flexion Mean N
Std.
Deviation P.VALUE
SIG
Flexion(A)post 119.87 15 8.959 .193 NO.SIG
Flexion(B)post 117.87 15 6.621
P Value =probability value (significant<=0.o5)
There was in significant difference OFF FLEXION in both group(A-B) post treatment .
FLEXION
MEAN 119,87 117,87
FIGER (4-15):Avarge of Flexion ROM both group (A-B) post treatment .
40
119.87
117.87
116.5
117
117.5
118
118.5
119
119.5
120
120.5
flextionApost flextionBpost
FLEX
ION

Table(4-17): Statistical Analysis of Extension ROM in both group(A-B) .post treatment.
Extension Mean N
Std.
Deviation p-value
Sig
Extension (A) post .60 15 1.404 ,864 No-sig
extension (B) post 1.27 15 2.890
P Value =probability value (significant<=0.o5)
There was in significant difference OFF Extension in both group(A-B) post treatment .
EXTENSION
MEAN ,60 1,27
FIGER (4-16):Avarge of EXTENSION ROM both group (A-B) post Treatment.
41
.60
1.27
.00
.20
.40
.60
.80
1.00
1.20
1.40
extentionApost extentionBpost
Pair 1
EXTE
NTI
ON

Chapter five
Discussion

DISCUSSION
This study is randomizing control trial study to determine whether ultrasound therapy or
combination therapy (ultrasound and interferential therapy) more effective treatment in
osteoarthritis knee patients . This study was done to measure their effect in decreasing pain ,
improving ROM , functional performance.
This study was conducted on peoples with knee osteoarthritis ,30 male and female their age
from 40-70 years they were divided into two groups each group had equal number of patients,
group (A) received combination therapy (IFT+US), group (B) received Interferential therapy,
each group received same therapeutic exercise .
Statistical analysis of the data was performed using SPSS software for medical
There was significant difference in pain between pre and post in group (A) and functional
performance of knee and Rom (p=.000) .
There was statisitical singnificant difference post treatment in reducing pain in group (A) and
functional performance knee and Range of motion .this finding has been supported by many
studies (Judith Flancor 2000) Effect of ultrasound on mobility in osteoarthritis of the knee. A
randomized clinical trial both groups significantly improved in active ROM, pain, and gait
velocity(61),
Erkan Kozanoglu et al. demonstrated that phonophoresis and ultrasound both
therapeutic modalities were found to be effective, Boyaci A et al. showed that in comparison of
phonophoresis ultrasound, and short-wave diathermy in patients with OA knee there was
significant difference efficacy (62)
There was significant difference between post and pre in reducing pain in group (B) and
functional performance knee and ROM(p=,021).
42

And also there was significant difference between pre and post range of motion in group (B)
(flexion, extension ,internal and external rotation )pre and post treatment (p=.000). this finding
has been support by( Am J Phys Med Rehabil2009). Interferential current therapy in patients
with knee osteoarthritis: comparison of the effectiveness of different amplitude-modulated
frequencies. Shown significant improvement of functional performance (WOMAC) and ROM in
knee osteoarthritis (63).
There was statisticaly significant difference in post treatment group (B) in pain , range of motion
and functional performance (p=,000) this finding has been supported by many studies (Bina
Eftekharsadat, Arash Babaei-Ghazani, Afshin Habibzadeh,2015 ) the efficacy of APS and IFT
as electrotherapeutic modalities in rehabilitating patients with knee OA, VAS and WOMAC
subscales were significantly improved after treatment in OA and IFT groups (p < 0.001 for
all).(64)
, Atamaz FC et al. studied that use of physical therapy agents like transcutaneous
electrical nerve stimulation (TENS), interferential currents (IFCs), and shortwave diathermy
(SWD) with exercise training and education provided additional benefits in improving pain as
compared to sham intervention with exercise training and education in knee OA(65).
IFT is an electrotherapy modality that is thought to decrease pain, increase range of motion, and
decrease oedema [Jarit et al. 2003; Jorge et al. 2006; Werners et al. 1999](66).
Similar to our
findings, other studies has shown significant improvement in VAS, and WOMAC subscales
including pain, stiffness and physical function in knee related pathologies [Burch et
al. 2008; Cheing and Hui-Chan, 2003; Gundog et al. 2012].(67)
Burch and colleagues [Burch et al. 2008] believed that IFT stimulation provides better pain
management and allows the underlying OA condition to be more comfortably treated with
patterned muscle stimulation.(67)
Atamaz and colleagues [Atamaz et al. 2012] showed that using
physical therapy including IFT can reduce pain more effectively than therapies without
electrostimulation, which was observed with lower paracetamol use during the study.(64)
The beneficiary effects of IFT in improving pain and disability have been evaluated in some
other disease and have shown a great improvement with its treatment [Lara-Palomo et
al. 2013; Montes-Molina et al. 2012a, 2012b].(68)
43

Comparison between two groups finding there was a difference between the application of each
method of treatment ,the combination therapy has a good effect in increase internal rotation
of knee ,reducing pain and improving functional performance . This finding has been supported
by (Archana Bodhale[1], Nilima Bedekar2015) Comparison of Effects of Interferential Therapy
(IFT) And Combination Therapy (IFT+Ultrasound Therapy) on Pain, Range of Motion and
Function in Patients With Osteoarthritis of Knee. Thus, the a combination therapy is more
effective as compared to IFT in pain, knee ROM and functional status in patients with OA
knee.(59)
also support by Tatiana F. Almeida et al showed that combination therapy with pulse
US and IFT can be an effective therapeutic approach for pain and sleep manifestations in OA(69).
44

Chapter six
Conclusion, recommendation

Conclusion
IFT and combination therapy both modalities of treatment can reduce pain, increase ROM and
improve functional performance but combination therapy can improve functional performance
and reduce pain better than IFT alone.
45

Recommendation
1 / physical therapy can be your first line of defense for managing knee osteoarthritis symptoms
and improve function.
2/ Electrotherapeutical modalities (ITF) therapy are important in the treatment of
musculoskeletal pain.
3/Therapeutic ultrasound beneficial for people with osteoarthritis of the knee.
4/A lot studies have been done on osteoarthritis with use of different modalities but unfortunately
combination therapy is often missed.
46

References
1/ Moretti FA, Marcondes FB, Provenza JR, Fukuda TY, The Scientific World
Journal,3th,2013; 10-9.
2/ Gillian A. Hawker Samra Mian, Tetyana Kendzerska Melissa French, Measures of adult pain:
Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain),2012; 2(2):
205–212.
3/ A.Loyola-SánchezJ.RichardsonaN.J.MacIntyre, September 2010; Osteoarthritis and Cartilage,
Efficacy of ultrasound therapy for the management of knee osteoarthritis: a systematic review
with meta-analysis, Pages 1117-1126, Volume 18, Issue 9.
4/ Grazio S, Balen D. Obesity: Risk factor and predictors of osteoarthritis. Lijec
Vjesn. 2009;131:22.
5/Bliddal H, Christensen R. The treatment and prevention of knee osteoarthritis: a tool for
clinical decision-making. Expert Opin Pharmacother. 2009;10:1793–804.
6/ Kisner C., Colby L. Stretching for impaired mobility. Therapeutic Exercise. Philadelphia:
F.A.Davis Company; 2012. p. 108-112. (3):665-72.
7/ Ciancle shamia , Anatomy of the Knee Joint , 2016; (3):888-43.
8/ Cindy Schmidler, . Knee Joint Anatomy, Function and Problems,2012; 121-211.
9/CHLISON WILSON, knee-pain-explained, 18th
,2019; 222.
10/ / Peat G, McCarney R, Croft P.re, Knee pain and osteoarthritis in older adults: a review of
community burden and current use of primary health care, 2001 Feb; 60(2): 91–97.
11/ WILIAM Morrison , How to prevent and treat knee injuries, 2017;65-87.
12/ Calmbach, W. L., & Hutchens, M. A. R. K. (2003). Evaluation of patients presenting with
knee pain: Part I. History, physical examination, radiographs, and laboratory tests. American
family physician, 68(5), 907-912 2/
13/ Dr Arun Pal Singh , Knee Range of Motion and Movements, 2005; 21
14/ Rockville Pike, Bethesda MD, Arthritis , 2011: 122-34.
15/ J Aging Res , Treatment and Prevention of Osteoarthritis through Exercise and Sports, 2011;
2011: 374653
16/ COMANF ADAM , Center for prevention , Rheumatoid Arthritis , 2019 ; 291-222;
47

17/ Hinman RS1, Hunt MA, Creaby MW, Wrigley TV, McManus FJ, Bennell KL, Hip muscle
weakness in individuals with medial knee osteoarthritis , 2010 ;(8):1190-3.
18/ Heiden TL1, Lloyd DG, Ackland TR , Knee extension and flexion weakness in people with
knee osteoarthritis: is antagonist contraction a factor , 2009;39(11):807-15.
19/ /Heidari B. Rheumatic diseases. . Indian Journal of R hematology . Relationship between
bone mineral density and duration of rheumatoid arthritis 2015; 10(1):
20/ / Altman RD. Am J Manag Care, Early management of osteoarthritis. , 200; 23-45.
21/ Bliddal H1, Christensen R , The treatment and prevention of knee osteoarthritis: a tool for
clinical decision-making, 2009;;10(11):1793-804
22/ Hayami T , Osteoarthritis of the knee joint as a cause of musculoskeletal ambulation
disability symptom complex (MADS), 2008 ;(11):1574-80.
23/ Peat G1, McCarney R, Croft P , Knee pain and osteoarthritis in older adults: a review of
community burden and current use of primary health care, 2001 Feb;60(2):91-7
24/ Mayo sandy, oundation for Medical Education and Research (MFMER,),
Osteoarthritis,2019; 12-22.
25/ Messier SP1, Loeser RF, Miller GD, Morgan TM, Rejeski WJ, Sevick MA, Ettinger WH
Jr, Pahor M, Exercise and dietary weight loss in overweight and obese older adults with knee
osteoarthritis: the Arthritis, Diet, and Activity Promotion Trial, 2004 ;50(5):1501-10.
26/David J Hunter, Osteoarthritis, 2006 Mar 18; 332(7542): 639–642.
27/Rockville, Rheumatoid Arthritis, 20118 ; 110-233
28/Zhang Y, Jordan JM, Epidemiology of ostearthritis,2011; 222-26.
29/ G Peat, R McCarney, P Croft, Knee pain and osteoarthritis in older adults: a review of
community burden and current use of primary health , 2001 - Volume 60 – 2.
30/ V andai K.SrikanthPh.D.(Research Fellow), Jayne L.FryerB.Math. Grad. Dip. Med. Stat.,
GuangjuZhaiM.Sc., Tania M.WinzenbergEL , Osteoarthritis and Cartilage, A meta-analysis of
sex differences prevalence, incidence and severity of osteoarthritis, September 2005; Volume
13, Issue 9 ,769-781.
31/ Sowers M, Karvonen-Gutierrez CA, Jacobson JA, Jiang Y, Yosef .Role of magnetic
resonance imaging in the evaluation of articular cartilage in painful knee joint. Medical Jornal
2014; 7(2).
48
https://www.ncbi.nlm.nih.gov/pubmed/?term=Wrigley%20TV%5BAuthor%5D&cauthor=true&cauthor_uid=20704005
https://www.ncbi.nlm.nih.gov/pubmed/?term=McManus%20FJ%5BAuthor%5D&cauthor=true&cauthor_uid=20704005
https://www.ncbi.nlm.nih.gov/pubmed/?term=Bennell%20KL%5BAuthor%5D&cauthor=true&cauthor_uid=20704005
https://www.ncbi.nlm.nih.gov/pubmed/?term=Ackland%20TR%5BAuthor%5D&cauthor=true&cauthor_uid=19881006
https://www.ncbi.nlm.nih.gov/pubmed/?term=McCarney%20R%5BAuthor%5D&cauthor=true&cauthor_uid=11156538
https://www.ncbi.nlm.nih.gov/pubmed/?term=Messier%20SP%5BAuthor%5D&cauthor=true&cauthor_uid=15146420

32/ Buckland-Wright C , Which radiographic techniques should we use for research and
clinical practice?, 2006 Feb;20(1):39-55.
33/ (44) Esser S1, Bailey A , Effects of exercise and physical activity on knee osteoarthritis, 2011
Dec;15(6):423-30
34/ Liikavainio T1, Lyytinen T, Tyrväinen E, Sipilä S, Arokoski JP, Physical function and
properties of quadriceps femoris muscle in men with knee osteoarthritis, 2008 Nov;89(11):2185-
94
35/ Carvalho NA1, Bittar ST, Pinto FR, Ferreira M, Sitta RR. Manual for guided home exercises
for osteoarthritis of the knee, 2010 Jun;65(8):775-80
36/ Zhang W1, Doherty M, Peat G, Bierma-Zeinstra MA, Arden NK, Bresnihan B, Herrero-
Beaumont G, Kirschne, EULAR evidence-based recommendations for the diagnosis of knee
osteoarthritis, 2010 Mar;69(3):483-9
37/ Behzad Heidari,, Knee osteoarthritis prevalence, risk factors, pathogenesis and features: Part
I, 2011 Spring; 2(2): 205–212
38/ Garnero P1, Peterfy C, Zaim S, Schoenharting M, Bone marrow abnormalities on magnetic
resonance imaging are associated with type II collagen degradation in knee osteoarthritis: a
three-month longitudinal study, 2005; Sep;52(9):2822-9
39/ Felson DT1, Anderson JJ, Naimark A, Kannel W, Meenan RF, The prevalence of
chondrocalcinosis in the elderly and its association with knee osteoarthritis: the Framingham
Study, 1989 Sep;16(9):1241-5
40/ Buckland-Wright C , Which radiographic techniques should we use for research and clinical
practice?, 2006;20(1):39-55.
41/ Sukenik S1, Henkin J, Zimlichman S, Skibin A, Neuman L, Pras M, Horowitz J, Shainkin-
Kestenbaum R, Serum and synovial fluid levels of serum amyloid A protein and C-reactive
protein in inflammatory and noninflammatory arthritis, 1988 Jun;15(6):942-5.
42/ Heidari B1, Abedi H, Firouzjahi A, Heidari P, Diagnostic value of synovial fluid anti-cyclic
citrullinated peptide antibody for rheumatoid arthritis, 2010 Sep;30(11):1465-70.
43/Jordan KM1, Arden NK, Doherty M, Bannwarth B, Bijlsma JW, Dieppe P, Gunther
K, Hauselmann H, Herrero-Beaumont G, Kaklamanis P, Lohmander S, Leeb B, Lequesne
M, Mazieres B, Martin-Mola E, Pavelka K, Pendleton A, Punzi L, Serni U, Swoboda
B, Verbruggen G, Zimmerman-Gorska I, Dougados M; Standing , EULAR Recommendations
2003: an evidence based approach to the management of knee osteoarthritis: Report of a Task
Force of the Standing Committee for International Clinical Studies Including Therapeutic Trials
(ESCISIT), 2003 Dec;62(12):1145-55.
49
https://www.ncbi.nlm.nih.gov/pubmed/?term=Lyytinen%20T%5BAuthor%5D&cauthor=true&cauthor_uid=18996249
https://www.ncbi.nlm.nih.gov/pubmed/?term=Ferreira%20M%5BAuthor%5D&cauthor=true&cauthor_uid=20835554
https://www.ncbi.nlm.nih.gov/pubmed/?term=Anderson%20JJ%5BAuthor%5D&cauthor=true&cauthor_uid=2810282
https://www.ncbi.nlm.nih.gov/pubmed/?term=Bijlsma%20JW%5BAuthor%5D&cauthor=true&cauthor_uid=14644851
https://www.ncbi.nlm.nih.gov/pubmed/?term=Lequesne%20M%5BAuthor%5D&cauthor=true&cauthor_uid=14644851
https://www.ncbi.nlm.nih.gov/pubmed/?term=Lequesne%20M%5BAuthor%5D&cauthor=true&cauthor_uid=14644851
https://www.ncbi.nlm.nih.gov/pubmed/?term=Mazieres%20B%5BAuthor%5D&cauthor=true&cauthor_uid=14644851

44/ Michelle J Lespasio, Knee Osteoarthritis: A Primer, 2017; 21: 16-183, permente journal
, 2017 Sep 13
45/ DR.Amal Alias, Massage Therapy Techniques, 2013;234-233
46/ Levent Özgönenel'Correspondence information about the author Levent ÖzgönenelEmail the
author Levent Özgönenel, Ebru Aytekin, ulis Durmu o lu. A Double-Blind Trial of Clinical
Effects of Therapeutic Ultrasound in Knee Osteoarthritis. ultrasound 2009; 35(1):
47/ DocDoc Pte, Ultrasound Therapy: Overview, Benefits, and Expected Results, 2008;28-45.
48/ . The journal Physical Therapy published a research summary in 2006 which talked about
interferential therapy used in various models of inflammatory pain.
49/Kloth, L. Interference current. In: Clinical Electrotherapy Nelson, R.M., Currier, D.P. (Ed.)
Ch 9, 183-49
50/Wadsworth, H. and Chanmugam, A.P.P. Electro physical Agents in Physiotherapy. 2nd Ed.
Science Press, 1983.
51/ Krnjevic, K. and Miledi, R. Failure of neuromuscular propagation in rats I Physiology 1958,
140, 440-461
52/ Laycock, J. and Green, R.J. Interferential therapy in the treatment of incontinence
Physiotherapy 1988, 74 (4), 161-168
53\ Alves-Guerreiro, J.et al. (2001). "The effect of three electrotherapeutic modalities upon peripheral
nerve conduction and mechanical pain threshold." Clinical Physiology 21(6): 704-711
54/ De Domenico, G. Pain relief with interferential therapy Aust I Physiother 1982, 28 (3), 14-
55/ Bergslien, O., Thoresen, M. and Odemark, H. The effects of three electrotherapeutic methods
on blood velocities in human peripheral arteries Scand J Rehabil Med 1988, 20,
56\ Nikolova, L. and Davidov, M. Influence of interferential current on enzyme activity of
traumatized nerve (experimental study) Vopr Kurortol Fizioter Lech Fiz Kult
57/ Gillian A. Hawker,Samra Mian , Tetyana Kendzerska, Measures of adult pain: Visual
Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain
Questionnaire ,2019;134-345
58/ Brett Sears , Goniometer for Measuring a Joint's Range of Motion, 2018;23-25
59/ WOMAC Osteoarthritis Index. http://www.womac.org/womac/index.htm. (accessed 12
July 2013).
60/Kisner C., Colby L. Stretching for impaired mobility. Therapeutic Exercise. Philadelphia:
F.A.Davis Company; 2012. p. 108-112.
50

61/ Archana Bodhale,Nilima Bedeka , Comparison of Effects of Interferential Therapy (IFT)
And Combination Therapy (IFT+Ultrasound Therapy) on Pain, Range of Motion and Function in
Patients With Osteoarthritis of Knee: A Hypothesis, 2015 | page:3-7
62/ Lang Jia,1,2
Yan Wang,2 Jinyun Chen,
a,2 and Wenzhi , Efficacy of focused low-intensity
pulsed ultrasound therapy for the management of knee osteoarthritis: a randomized, double blind,
placebo-controlled trial, 2016; 6: 35453.
63/Falconer J, Hayes KW, Chang RW., Effect of ultrasound on mobility in osteoarthritis of the
knee. A randomized clinical trial, 1992 Mar;5(1):29-35
64/Kozanoglu, Erkan, et al. "Short term efficacy of ibuprofen phonophoresis versus continuous
ultrasound therapy in knee osteoarthritis." Swiss medical weekly133.23-24 (2003): 333-338.
65/ Gundog M1, Atamaz F, Kanyilmaz S, Kirazli Y, Celepoglu G, Interferential current therapy
in patients with knee osteoarthritis: comparison of the effectiveness of different amplitude-
modulated frequencies, 2012 Feb;91(2):107-13.
66/ Bina Eftekharsadat, Arash Babaei-Ghazani, Afshin Habibzadeh, and Babak Kolahi,
Efficacy of action potential simulation and interferential therapy in the rehabilitation of patients
with knee osteoarthritis, 2015 Jun; 7(3): 67–75
67/Almeida TF, Roizenblatt S, Benedito-Silva AA, Tufik S. The effect of combined therapy
(ultrasound and interferential current) on pain and sleep in fibromyalgia. Pain. 2003 Aug; 104
(3):665-72.
68/ Jarit et, Jorge et al, Werners et al, the effect of ITF in knee osteoarthritis , 2006; 344-233.
69/ Gundog M, Atamaz F, Kanyilmaz S, Kirazli Y, Celepoglu G. Interferential current therapy in
patients with knee osteoarthritis: comparison of the effectiveness of different amplitude-
modulated frequencies. Am J Phys Med Rehabil (2012) Feb; 91(2):107-13
70/ Burch and colleagues , IFT stimulation provides better pain management and allows the
underlying OA condition to be more comfortably treated with patterned muscle stimulation ,
2008: 102-344.
71/Lara-Palomo , Montes-Molina , The beneficiary effects of IFT in improving pain and
disability have been evaluated in some other disease and have shown a great improvement with
its treatment,2013; 346-469.
72/ Almeida TF, Roizenblatt S, Benedito-Silva AA, Tufik S. The effect of combined therapy
(ultrasound and interferential current) on pain and sleep in fibromyalgia. Pain ,2003;104-72
51

Annexes

Annex 2: Structured questionnaire
Al-Neelain University
Graduate collage
Structural questionnaire
NAME :
Age:
Sex:
Occupation:
Telephone number :
Patient signature :
Physiotherapy signature :

Annex 2
The Western Ontario and McMaster Universities Osteoarthritis Index
WOMAC
Name:____________________________________________ Date:________________
Instructions: Please rate the activities in each category according to the following scale of
difficulty: 0 = None, 1 = Slight, 2 = Moderate, 3 = Very, 4 = Extremely
Circle one number for each activity
Pain 1. Walking 0 1 2 3 4
2. Stair Climbing 0 1 2 3 4
3. Nocturnal 0 1 2 3 4
4. Rest 0 1 2 3 4
5. Weight bearing 0 1 2 3 4
Stiffness 1. Morning stiffness 0 1 2 3 4
2. Stiffness occurring later in the day 0 1 2 3 4
Physical Function 1. Descending stairs 0 1 2 3 4
2. Ascending stairs 0 1 2 3 4
3. Rising from sitting 0 1 2 3 4
4. Standing 0 1 2 3 4
5. Bending to floor 0 1 2 3 4
6. Walking on flat surface 0 1 2 3 4
7. Getting in / out of car 0 1 2 3 4
8. Going shopping 0 1 2 3 4
9. Putting on socks 0 1 2 3 4
10. Lying in bed 0 1 2 3 4
11. Taking off socks 0 1 2 3 4

12. Rising from bed 0 1 2 3 4
13. Getting in/out of bath 0 1 2 3 4
14. Sitting 0 1 2 3 4
15. Getting on/off toilet 0 1 2 3 4
16. Heavy domestic duties 0 1 2 3 4
17. Light domestic duties 0 1 2 3 4
Total Score: ______ / 96 = _______% Comments / Interpretation (to be completed by therapist
only):

Annex 3
VAS
( VISUAL ANALOG SCAL)
Place a mark on the following line to show the intensity of pain that you are feeling
No pain ……………………………………………………………………………. Worst pain
VAS
0 1 2 3 4 5 6 7 8 9 10

Annex 4
Assessment of Range of motion :
Group A
Pre treatment Post treatment
flexion
extension

Annex 5
Al-Neelain University
Graduate College
Informed consent
Effects of Interferential Therapy verse Combination Therapy (Interferential Therapy
+Ultrasound Therapy) in Osteoarthritis knee Patient's:
The purpose of this study is to assess Effectiveness of Interferential Therapy (IFT) versus
Combination Therapy(interferential therapy +Ultrasound Therapy) on osteoarthritis knee
patient.
Duration of participation 4 weeks.
Patient in group(A) well receive combination therapy interferential therapy and ultrasound
therapy 3 times per 4 weeks, while group (B)well receive interferential therapy only.
All record identifying the subject will be confidential.
Participation is voluntary refuse to participation involve no penalty or loss of benefit.
Patient can discontinue participation at any time without penalty.
Signature:
Participant……………………………investigator……………………………
Date……………………………………..

جامعة النيلين
كلية الدراسات العليا
الموافقة المسبقة
خياز اىيرتاء اعالخي امارنح تينيا في لياش ذ فعايو خياز اخاخ فق اصذيو اعالخيو
إغارعالج رظي خشنو اروثو
خياز اىيرتاء فعايو خياز اخاخ فق اصذيو اعالخيوالغزض هي ىذه الدراست ى حمن
رظي خشنو اروثوإغارعالج اعالخي امارنح تينيا في
أسابع 4هدة الوشاركت
أ( العالج الثنائ )جياس الوجاث الفق صحو (خلمى الوزض ف هجوعت
العالجو جياسالكيزباء العالج ( فخزه العالج حسخوز اربعو اسابع ثالثو جلساث
.اسبعا بنوا الوجوعو )ب( حخلم جياس الكيزباء العالج فمط
السجالث الخ ححدد الوضع سخكى سزاكل
الوشاركت حطعت. حنطي الوشاركت على عدم فزض أي عمبت أ خسارة ف
الفائدة. وكي للوزض الخلف عي الوشاركت ف أي لج بدى عمبت.
:الخلع
هشارن....................هحمك......................
............حارخ.........