Performing State Medicine During its ‘Frustrating’ Years: Epidemiology and Bacteriology at the...
26
Performing State Medicine During its ‘Frustrating’ Years: Epidemiology and Bacteriology at the Local Government Board, 1870–1900 Jacob Steere-Williams* Summary. This article is about the performance—referring to the projection and reception—of state medicine in late Victorian Britain. Moving away from the lens of the ideas and policies historians have previously explored, I focus on epidemiological and bacteriological investigations of typhoid fever as they were conducted through the Medical Department of the Local Government Board, during the period historian Roy MacLeod characterised as a ‘frustrating’ one in the history of state medicine. The article focuses on two late Victorian epidemiological investigations, Richard Thorne Thorne’s 1879 study of an outbreak of typhoid fever at Caterham, and H. Timbrell Bulstrode’s 1896 study of an outbreak of typhoid fever at Chichester, to demonstrate the complex ways that epidemiology was constructed and defended vis-à-vis the emergence of laboratory science during the so-called Bacterio- logical Revolution. Keywords: Victorian Britain; epidemiology; bacteriology; Medical Department; Local Government Board; performance Introduction In early February 1879 Richard Thorne Thorne descended into one of the wells of the Cater- ham Waterworks Company. Thorne is best known for representing the British Government at numerous International Sanitary Conferences from the mid 1880s, and for the time he spent as Chief Medical Officer of England and Wales, from 1892 to 1899. Throughout the 1870s though, in his formative years, Thorne was an ambitious epidemiologist with extensive fieldwork experience gained through his post as Medical Inspector to the Medical Department of the Local Government Board. When, in 1879, Thorne undertook the arduous task of inspecting the Caterham well, he was chasing after the source of a violent outbreak of enteric, or typhoid fever. 1 Caterham, a sparsely populated London suburb in the Rural Sanitary District of Godstone, and its more populous neighbour Red Hill [sic], in the Urban Sanitary District of Reigate, had been *College of Charleston, Department of History, 165 Calhoun Street, Maybank Hall 202, Charleston, SC 29424. Email: [email protected] Jacob Steere Williams is an Assistant Professor of History at the College of Charleston. He received his PhD at the Uni- versity of Minnesota’s Program in the History of Science, Technology, and Medicine in 2011. His research focuses on Victorian public health, and has recently appeared in The Journal of the History of Medicine and Allied Sciences, Ambix and Agricultural History. He is currently completing a book manuscript on typhoid fever and the practices of epidemi- ology in nineteenth-century Britain. © The Author 2014. Published by Oxford University Press on behalf of the Society for the Social History of Medicine. doi:10.1093/shm/hku064 1 There was a pattern to outbreak investigations: the Chief Medical Officer would receive information con- cerning a local outbreak; the local authority would be warned; and an inspector would be sent. Investigations could last days or several weeks, per the severity of the outbreak. Such investigations could be dangerous; Gwynne Harries, for example, a promising young epi- demiologist, died in 1873 after contracting scarlet fever while on investigation in the north of England. See, Obituary for Harries, BMJ, 1873, 2, 590. Social History of Medicine page 1 of 26 Social History of Medicine Advance Access published September 8, 2014 by guest on September 9, 2014 http://shm.oxfordjournals.org/ Downloaded from
Transcript of Performing State Medicine During its ‘Frustrating’ Years: Epidemiology and Bacteriology at the...

Performing State Medicine During its ‘Frustrating’Years: Epidemiology and Bacteriology at the Local
Government Board, 1870–1900
Jacob Steere-Williams*
Summary. This article is about the performance—referring to the projection and reception—of statemedicine in late Victorian Britain. Moving away from the lens of the ideas and policies historians havepreviously explored, I focus on epidemiological and bacteriological investigations of typhoid fever asthey were conducted through the Medical Department of the Local Government Board, during theperiod historian Roy MacLeod characterised as a ‘frustrating’ one in the history of state medicine. Thearticle focuses on two late Victorian epidemiological investigations, Richard Thorne Thorne’s 1879study of an outbreak of typhoid fever at Caterham, and H. Timbrell Bulstrode’s 1896 study of anoutbreak of typhoid fever at Chichester, to demonstrate the complex ways that epidemiology wasconstructed and defended vis-à-vis the emergence of laboratory science during the so-called Bacterio-logical Revolution.
Keywords: Victorian Britain; epidemiology; bacteriology; Medical Department; Local GovernmentBoard; performance
IntroductionIn early February 1879 Richard Thorne Thorne descended into one of thewells of the Cater-hamWaterworks Company. Thorne is best known for representing the British Governmentat numerous International Sanitary Conferences from the mid 1880s, and for the time hespent as Chief Medical Officer of England and Wales, from 1892 to 1899. Throughoutthe 1870s though, in his formative years, Thorne was an ambitious epidemiologist withextensive fieldwork experience gained through his post as Medical Inspector to theMedical Department of the Local Government Board.
When, in 1879, Thorne undertook the arduous task of inspecting the Caterhamwell, hewas chasing after the source of a violent outbreak of enteric, or typhoid fever.1 Caterham, asparsely populated London suburb in the Rural Sanitary District of Godstone, and its morepopulous neighbour Red Hill [sic], in the Urban Sanitary District of Reigate, had been
*CollegeofCharleston,Department ofHistory, 165Calhoun Street,MaybankHall 202,Charleston, SC29424. Email:[email protected]
Jacob SteereWilliams is an Assistant Professor of History at the College of Charleston. He received his PhD at the Uni-versity of Minnesota’s Program in the History of Science, Technology, andMedicine in 2011. His research focuses onVictorian public health, andhas recently appeared in The Journal of theHistory ofMedicine andAllied Sciences,AmbixandAgricultural History. He is currently completing a bookmanuscript on typhoid fever and the practices of epidemi-ology in nineteenth-century Britain.
© The Author 2014. Published by Oxford University Press on behalf of the Society for the Social History of Medicine.doi:10.1093/shm/hku064
1There was a pattern to outbreak investigations: theChief Medical Officer would receive information con-cerning a local outbreak; the local authority would bewarned; and an inspector would be sent. Investigationscould last days or several weeks, per the severity of the
outbreak. Such investigations could be dangerous;Gwynne Harries, for example, a promising young epi-demiologist, died in 1873 after contracting scarletfever while on investigation in the north of England.See, Obituary for Harries, BMJ, 1873, 2, 590.
Social History of Medicine page 1 of 26
Social History of Medicine Advance Access published September 8, 2014 by guest on Septem
ber 9, 2014http://shm
.oxfordjournals.org/D
ownloaded from

attacked by an explosive outbreak of typhoid fever; upwards of 350 individuals were struckwithin a six-week period.2 Caterham had largely been free of typhoid fever the twelvemonths preceding; it was faced with a public health crisis. Such sudden, or fulminatingoutbreaks, according to Thorne’s colleague and prolific public health writer, Edward CoxSeaton, ‘attracted so much notice that no wonder the impression they created inthis country has been deep and lasting’.3 Indeed, Thorne’s epidemiological fieldwork atCaterham served as a model of public health practice into the early twentieth century.
Thorne had descended the Caterhamwell because he believed it was there that the out-break had commenced. He was looking for what epidemiologists now call the index case,and what the Epidemiological Society of London, the hub of a complex network for con-structing, facilitating, and distributing epidemiological knowledge, described in 1863 as‘tracingwith scrupulousminuteness the history of the first cases’.4 It was by using basic stat-istical methods and case-tracing that Thorne had suspected the Caterham WaterworksCompany. Early in the outbreak, Thorne found that of the 47 persons attacked from 19January to 2 February, 45 received water from that source alone. He further interviewedDr James Adam, Medical Superintendent at the Caterham Asylum, and Dr James Magill,of the Caterham Barracks, and found that although there were 2,000 patients at theformer institution, and 500 soldiers at the latter—both of which were supplied by theirownwells—no cases of typhoid fever had arisen.Moreover, Thorne found that in the neigh-bouring town of Redhill, typhoid cases were exclusive to those houses supplied by waterfrom the Caterham Waterworks Company. With a ‘very strong presumption that it hadbeen caused by the use of the Caterham Company’s water’, Thorne narrowed theinvestigation.5
In late 1878 the Caterham Waterworks Company began constructing an adit from thewell in question to a new bore being sunk. A number of men were employed in thiswork, some on the surface and others below. Enquiring into the health of these workers,Thorne interviewed one, initialled J.K., aged 32, a ‘loading man’ who had been sufferingfrom a case of typhoid fever preceding the outbreak in early January 1879.6 While downin thewell, J.K. confessed, he regularly used the loadingbuckets,meant for raising the exca-vated chalk to the surface, for his frequent diarrhoeal dejections—at least twoor three timesper shift—much to the complaint of his fellow workmen on the surface. With this knowl-edge in hand, Thorne conducted a simple experiment in the well. He found that everytime a bucket was hoisted up the rope to be emptied, it oscillated to and fro, coming intoviolent contact with the walls of the well.7 About ten days after J.K.’s faecal mishaps in
2Thorne’s earlier report was published in full by theMedical Department, see, Dr. Thorne Thorne’s Reportto the Local Government Board on an Extensive Epi-demic of Enteric Fever, Affecting Especially Red Hill, inthe Urban Sanitary District of Reigate, and Caterhamin the Rural Sanitary District of Godstone (London:Eyre and Spottiswoode, 1879).
3EdwardC. Seaton, InfectiousDiseases and their Preven-tion (London, University of London Press, 1911), 96.
4Benjamin Guy Babington, ‘Objects of the Epidemio-logical Society’, Transactions of the EpidemiologicalSociety of London, 1863, 1, 6–8.
5Richard Thorne Thorne, ‘On an Extensive Epidemic ofEnteric Fever at RedHill, Caterham, andotherAdjoiningPlaces’, Ninth Annual Report of the Local GovernmentBoard, 1879–80. Supplement Containing the Reportof the Medical Officer for 1879, 78–92, 81.
6Ibid., 85–6. See also Transactions of the Epidemiologic-al Society of London (London: JohnW.Davies, 1863), 7.
7Edward Ballard, ‘Observations on Some of the Ways inWhich Drinking-Water May Become Polluted with theContagium of Enteric Fever’, BMJ, 1880, 1, 82–4.
Page 2 of 26 Jacob Steere-Williams
by guest on September 9, 2014
http://shm.oxfordjournals.org/
Dow
nloaded from

thewell, Thornededuced from the statistical distribution of the typhoid fever cases and con-temporary knowledge about the incubation period of the disease—about a fortnight—thatthe epidemic had becomewidespread across Caterhamand Redhill, both ofwhich receivedwater fromtheCaterhamWaterworksCompany.Typhoidcases, Thorne found,were largelylimited to those who received water from the faecally-polluted Caterham WaterworksCompany. Such was ‘one of the most striking instances’ Thorne later noted, showing‘howgreatwas the potency formischief of evenminute portions of the specifically diseasedevacuations of enteric fever patients’.8
Thorne’s public health practices at Caterhamwere emblematic of epidemiological inves-tigations in the late Victorian period conducted by inspectors at the Medical Department.9
Such practices were observational and experimental; when, on 5 February 1879, forexample, Thorne arrived in the Caterham and Redhill area—he left the day after theMedical Department received word of the outbreak from a local physician—he examinedthe localwater supply, themilk supply, the house drainage, and the sewerage.He consultedlocalmedical practitioners, especially E. L. Jacob,Medical Officer of Health for the combinedsanitarydistricts of Surrey, andeminentgeologistWilliamWhittaker, on the soil compositionof the area. Thorne tabulated the mortality statistics of the outbreak, and enquired fromhouse-to-house about the particulars of every case of suspected or confirmed typhoid,which led him to the above-mentioned index case of J.K.10 Thorne and the late Victorianpractitioners of epidemiology, as Anne Hardy has shown, championed careful casetracing, simple sanitary experimentation, and the marshalling of evidence predicated onstatistical inference.11 Thorne’s investigation spanned urban and rural physical environ-ments—and the administrative categories of Urban and Rural Sanitary Districts—it alsoincludedbasic experimentation, quantitative statistical analysis, andqualitative case-tracingand interviewing. Though it was population centred, individuals, especially the search forthe index case, were also the focus of Thorne’s study.
I begin with the example of Thorne’s 1879 Caterham investigation for two reasons. First,because it was characteristic—and later served as a model—of epidemiological practice atthe Medical Department in an age when epidemiology, rather than the incipient practicesand rhetoric of bacteriology, dominated British public health. Yet, in one critical wayThorne’s Caterham study diverged from the typical pattern of disease investigation con-ducted through the Medical Department; no bacteriologist or chemist was involved in theinvestigation. Thorne did not send a sample of Caterham water to be analysed by one ofthe Medical Department’s bacteriological or chemical analysts, a common, though incon-clusive practice for field epidemiologists from the 1870s.12 This illustrates the second
8Richard Thorne Thorne, On the Progressive of Prevent-ive Medicine During the Victorian Era (London; Shaw& Sons, 1888), 29.
9On methods at the Medical Department, see AnneHardy, ‘Methods of Outbreak Investigation in the Eraof Bacteriology, 1880–1920’, in A. Morabia, ed., AHistory of Epidemiologic Methods and Concepts(Berline: Birkhauser Verlag, 2004), 199–206.
10Both the rich and the poor had been struck by thedisease, and inhabitants in Lower Caterham had
been affected as had those living in Upper Caterham,which included the old village.
11Anne Hardy, ‘On the Cusp: Epidemiology and Bacteri-ology at the Local Government Board, 1890–1905’,Medical History, 1998, 42, 328–46.
12Thorne did refer in his 1879 report to the influence ofJohn Burdon Sanderson’s research on the ‘intimatepathologyof contagion’. See, JohnBurdonSanderson,‘Intimate Pathology of Contagion’, Twelfth AnnualReport of the Medical Officer of the Privy Council forthe Year 1870 (London: Spottiswoode, 1871).
The Local Government Board, 1870–1900 Page 3 of 26
by guest on September 9, 2014
http://shm.oxfordjournals.org/
Dow
nloaded from

reason tobeginwith Thorne’s study. By refusing to seek chemical or bacteriological confirm-ation of his aetiological hypothesis, Thorne was actively constructing the rhetorical claimthat epidemiological knowledge alone best-informed practical decisions in preventivepublic health.
Thorne’s 1879 investigation is a useful lens to begin a larger discussion—if at a veryfocused level—as to the practices of knowledge production in late Victorian epidemiology.MichaelWorboys has recently implored historians ofmedicine to explore ‘the complex rela-tions of different kinds of knowledge and practice… not just through programmatic state-ments, or generalisations about the successions of bedside, hospital, and laboratorymedicine, but through studies of performance in the clinic as well as in the laboratory andthe field’.13 As foremost a field-science, epidemiology, as itwas practised at theMedical De-partment, seems an ideal case to exploreWorboys’ call. Using performance as an analyticalframe necessitates that we ask new questions about late Victorian public health. It is usefulto reflect on both the actual methods of epidemiological enquiry during this period, whichHardy andothers, such as John Eyler have done, and to the performativeways inwhich suchpracticeswere communicatedby epidemiologists to larger political, professional, andpublicaudiences,whichhistorianshaveyet to fully examine.14Performance, as it applies to lateVic-torian public health, and as I employ the conceptual termhere,was about bothprojection—how epidemiologists displayed, pronounced, self-fashioned, and cajoled audiences intorecognising epidemiological authority—as well as reception—how audiences responded,identified and ultimately placed trust in epidemiological authority.15 ‘What practitionersdo to construct, maintain, and defend their practices’, as Iwan Rhys Morus has recentlyarticulated for historians of science, ‘should be understood as performative acts’.16
Recast as performative, as I do below, Thorne’s 1879 investigation reveals the way inwhich epidemiology, at perhaps its height in Britain, was, to borrow a phrase from VassilikiBetty Smocovitis, ‘part of a culturally embeddedbelief system’ thatVictorians used tounder-stand the spread of disease.17 That Thorne did not appropriate chemical or bacteriologicalscience, a practice others at the Medical Department often did, albeit ‘uninfluentially’, asChristopher Hamlin as shown, makes him emblematic of a practitioner who embodiedthe fullest expression of the scientific authority of epidemiology.18 Yet, the performancesof Victorian epidemiology were not static in this period. Insofar as its representativeness,Thorne’s 1879 studywas one investigation of a single—though critically important and ‘ex-emplary’—infectious disease by an epidemiologist at theMedical Department.19 It does notfully characterise, for example, all epidemiological research conducted by inspectors at the
13MichaelWorboys, ‘Practice and Science ofMedicine intheNineteenthCentury’, Isis, 2011,102,109–15,115.
14John Eyler, Sir Arthur Newsholme and StateMedicine,1885–1935 (Cambridge: Cambridge University Press,2002).
15Michael Brown’s recent use of performance as an ana-lytical category is a useful example, although in hisstudy, Brown conceives of performance as associationand knowledge. See, Michael Brown, PerformingMedicine: Medical Culture and Identity in ProvincialEngland, c.1760–1850 (Manchester:Manchester Uni-versity Press, 2011).
16Iwan Rhy Morus, ‘Placing Performance’, Isis, 2010,101, 775–8, 776.
17Vassiliki Betty Smocovitis, Unifying Biology: the Evolu-tionary Synthesis and Evolutionary Biology (Princeton:Princeton University Press, 1996), 86.
18ChristopherHamlin,AScienceof Impurity:WaterAna-lysis in Nineteenth Century Britain (Berkeley: Universityof California Press, 1990), 270.
19Lloyd G. Stevenson, ‘Exemplary Disease: The TyphoidPattern’, Journal of the History of Medicine andAllied Sciences, 1982, 37, 159–81.
Page 4 of 26 Jacob Steere-Williams
by guest on September 9, 2014
http://shm.oxfordjournals.org/
Dow
nloaded from

Medical Department, or epidemiological studies conducted by Medical Officers of Healthduring this period. Yet, in important ways, Thorne’s practices at Caterham, as well as theprocess bywhich his findingswere communicated, represent a visionof epidemiological au-thority that was widespread in the period. What makes this an especially interesting case,furthermore, is that it was conducted and communicated at a time before the widespreadacceptance of bacteriology. Carl Eberth only published his discovery of rodlike bacteriataken from typhoid patients in 1880, and Georg Gaffky isolated b.typhosus in 1884, itwill be recalled, a very short time after Thorne’s 1879 study. Even then, as James Starkhas reinforced in his recent study of anthrax in Britain, the Bacteriological Revolution didnot immediately constitute a major epistemic shift or reorganisation of medical practice.20
There has beenmuch historiographical debate in the past three decades about a waningepidemiology and a burgeoning bacteriology in the late nineteenth century. WilliamColeman in his classic account, Yellow Fever in the North, maintained that a ‘biomedicalorientation’ shaped epidemiological practice after 1880.21 Alfredo Morabia, who haswritten extensively on the subject, has posed the question rather succinctly, asking, ‘epi-demiology and bacteriology in 1900: who is the handmaid of whom?’22 Hardy andWorboys have pushed back on the claim that bacteriology overshadowed field-based bac-teriology, a position recently articulated in RosemaryWall’s Bacteria in Britain, 1880–1939,which suggests that ‘the dominance of epidemiology over bacteriology… appears to havecontinuedwell into the twentieth century’.23 Yet, crucial questions abound for the late Vic-torian period: under what circumstances did epidemiologists and bacteriologists cooperateon outbreak investigations? Where were disciplinary boundaries drawn between the twopublic health activities? Hardy, using the co-practices of epidemiology and bacteriology attheMedical Department for the period 1890–1905, has extrapolated that British epidemiol-ogists felt under threat from their bacteriological counterparts, even as competitionbetween the twopractices increasingly revealeda ‘close,butuneasy’ relationship inprevent-ivemedicine.24Thisarticle seeks tomovebeyondHardy’s characterisationofa trenchantanddichotomous relationship between epidemiology and bacteriology at the Medical Depart-ment in the last two decades of the nineteenth century. In this way this article contributesto Steve Sturdy’s critique that historians have tended to overstate the conflict between
20James F. Stark, The Making of Modern Anthrax,1875–1920: Uniting Local, National, and Global His-tories of Disease (London: Pickering & Chatto, 2013).Janet Greenless has recently added to the rich litera-ture on bacteriology and occupational health in thelate Victorian period. See, Janet Greenless, ‘“TheDangers Attending these Conditions are Evident”:Public Health and theWorking Environment of Lanca-shire Textile Communities, c.1870–1939’, SocialHistory of Medicine, 2013, 26, 672–94.
21David Lilienfeld, ‘The Greening of Epidemiology: Sani-tary Physicians and the London EpidemiologicalSociety (1830–1870)’, Bulletin of the History of Medi-cine, 1978, 52, 526; Mervyn Susser, ‘Does RiskFactor Epidemiology Put Epidemiology at Risk?Peering into the Future’, Journal of Epidemiology andCommunity Health, 1998, 52, 608–11; WilliamColeman, Yellow Fever in the North: the Methods of
Early Epidemiology (Madison: University of WisconsinPress, 1983), 173.
22A. Morabia, ‘Epidemiology and Bacteriology in 1900:Who is the Handmaid of Whom?’ Journal of Epidemi-ology and Community Health, 1998, 52, 617–8.
23Rosemary Wall, Bacteria in Britain: 1880–1939(London: Pickering & Chatto, 2013), 147; AnneHardy, ‘Methods of Outbreak Investigation in the“Era of Bacteriology”, 1820–1920’, in A. Morabia,ed.,AHistory of EpidemiologicMethods andConcepts(Berlin: Birkhauser Verlag, 2004), 199; MichaelWorboys, ‘Was There a Bacteriological Revolution inLate Nineteenth Century Medicine?’ Studies inHistory and Philosophy of Biological and BiomedicalScience, 2007, 38, 20–4; Anne Hardy, ‘On the Cusp’,328–46.
24Hardy, ‘On the Cusp’, 345.
The Local Government Board, 1870–1900 Page 5 of 26
by guest on September 9, 2014
http://shm.oxfordjournals.org/
Dow
nloaded from

science and medicine.25 The lens of performance nuances just why epidemiologists werewilling to incorporate—or eschew—bacteriological methods and practices, rather than itstheoretical underpinnings. In what follows I re-examine Thorne’s 1879 Caterham study inlight of what it reveals about the performance of science, paying particular attention tothe ways that Thorne defended epidemiological practices and presented epidemiologicalways of knowing to various audiences.26 In the second half of the article I turn towardsan investigation—also of an outbreak of typhoid fever—that occurred over fifteen yearslater, in 1896, by H. Timbrell Bulstrode, also of the Medical Department. Unlike Thorne’s1879 Caterham investigation, in addition to traditional field-based epidemiologicalmethods, Bulstrode relied extensively on bacteriology; he worked closely with EdwardKlein, who examined the bacteriological counts in the Chichester water supply, and SidneyMartin, who analysed the presence of typhoid bacteria in samples of Chichester soils. Bul-strode’s contemporaries praised the epidemiological investigation at Chichester, particularlyas a startling revelation of the continuing endemic threat of typhoid fever as the nineteenthcentury came to a close. Fully in themidst of the Bacteriological Revolution, Bulstrode’s epi-demiological practices were braced by bacteriological tests of soil and water. Examiningtheperformativeaspectsof Bulstrode’s epidemiology, as I dobelow, reveals two importantconclusions. The first is that the shoe-leather practices of epidemiology at theMedical De-partment emblematic in Throne’s 1879 study remained largely unchanged by the end ofthe century. The field-based, statistically-informed, andpopulation-centred epidemiologyof the 1870s was essentially that of the 1890s, suggesting a continuity of epidemiologicalpractice. The second is that despite a relative continuity of practice, the performance ofepidemiology was changing by the 1890s. Bulstrode sought to establish his credibilityand authority at the Medical Department, and by extension the credibility of epidemi-ology, in a disciplinarily and historically reflexive way, one that was especially politicised.Both Thorne and Bulstrode, practising essentially the same epidemiological methods insimilar institutional contexts, sought to confirm epidemiological ways of knowing andcajole audiences in different manners. This suggests, as I return to in the conclusion,both a reinterpretation of the relationship between epidemiology and bacteriology atthe Medical Department, as well as a novel approach to understanding the performanceof public health in this period.
‘via exclusionis’; RichardThorneThorne’s Performanceof Epidemiologyat Caterham in 1879
Addressing the Epidemiological Society of London in 1878, a year before his Caterham in-vestigation, Thorne admitted that he had ‘little acquaintance with the laboratory’, and thathe relied ‘for most of his data on experience gained in what I may perhaps term the field-work of epidemiology’.27 Such a programmatic dismissal of laboratory science bothreflected a shared disciplinary awareness amongst British epidemiologists and reified the
25Steve Sturdy, ‘Looking for Trouble: Medical Scienceand Clinical Practice in the Historiography of ModernMedicine’, Social History of Medicine, 2011, 24,734–57.
26My use of an epidemiological ‘way of knowing’ is anextension of John Pickstone, Ways of Knowing: A
New History of Science, Technology, and Medicine(Manchester: Manchester University Press, 2001).
27Richard Thorne Thorne, ‘Remarks on the Origin of In-fection’, Transactions of the Epidemiological Societyof London, Read 8 April 1878, vol. IV, (1875–1876 to1880–1881), 234–46.
Page 6 of 26 Jacob Steere-Williams
by guest on September 9, 2014
http://shm.oxfordjournals.org/
Dow
nloaded from
role of field-based knowledge-making over laboratory-based knowledge-making. In thiswaywe canmore fully understand the epidemiological practices Thorne employed atCater-ham in the course of his 1879 investigation.
That Thorne descended into theCaterhamwell and conducted an experimentwithwaterbuckets used for diarrhoeal dejections was tantamount to fulfilling the duties of whatThorne’s colleagueat theMedicalDepartment, JohnNettenRadcliffe, calleda ‘day labourer’or ‘journeymanworker’ in Victorian epidemiology.28 Althoughhehadnot previously servedas aMedical Officer of Health—his colleagues Edward Ballard, JohnBurdon Sanderson, andGeorge Buchanan, for example, had—Thornewas trained as amedical student on the con-tinent and at St Bartholomew’s Hospital. He qualified forMRCS in 1863 andMRCP in 1865.From themid 1860s, while working at the London Fever Hospital, he was called upon occa-sionally by John Simon to undertake investigations of local outbreaks of infectious diseases.He was hired by the department as a full-time inspector in 1871, until he was appointedChief Medical Officer in 1892 to replace George Buchanan.
Thorne’s 1879 practices of case-tracing to find and interview the index case, J.K., wereconstitutive performances of epidemiology that both guided practice, as well as provideda corporeal and gestural basis for how such practices were communicated to larger audi-ences.29 But how was Thorne’s study communicated, and how was the epistemic claimmade that Thorne ‘hasperfectly succeeded inprovinghis case’, as ErnestHart, the sagaciousmedical reformer and editor of the BritishMedical Journal, noted in 1879?30 In part, Thornehimself provided the agency for rationalising the epidemiological findings; his colleagues—at the Medical Department and in the wider community of epidemiologists and medicalwriters—also justified the conclusions and public health outcomes that followed the Cater-ham study.
Thorne’s report was published in theNinth Annual Report of Medical Officer of the LocalGovernment Board, and separately as a pamphlet. In his commentary,GeorgeBuchanan, asChiefMedicalOfficer, responsible for collatingandcommunicating inspector reports, notedthat Thorne’s investigation at Caterham had offered ‘conclusive proof of the manner of itsdistribution… from this one case [J.K.] the deep water was specifically contaminated, andfever was spread over a large district’.31 The legitimacy of Thorne’s study, judging from Bu-chanan, lay in Thorne’s ability to convince contemporaries that he had discovered the indexcase.Not onlywas such a finding integral to thebasis ofmakingepidemiological knowledgein thisperiod, itwasalso verymuchpredicatedon theperformative reality ofdescending intoawell, conducting experiments, and interviewing individuals. Such praisewas likewise seenin the contemporary medical press. The Medical Times and Gazette found it ‘difficult toescape from accepting the conclusion that the Caterham works were infected by thisworkman’.32 ‘The conditions of this huge and involuntary experiment’, the article noted,‘seem to have been as nearly perfect as may be, and the indictment against the implicated
28John Netten Radcliffe, ‘On the Recent Progress of Epi-demiology in England’, The Practitioner, 1875, 15,459–80, 459.
29Michael Wintroub, ‘Taking a Bow in the Theatre ofThings’, Isis, 2010, 101, 779–93, 779.
30Ernest Hart, ‘The Recent Epidemic of Enteric Fever inthe Caterham Valley’, BMJ, 1879, 1, 668–70.
31Ninth Annual Report of the Local Government Board,1879–80. Supplement Containing the Report of theMedical Officer for 1879, viii.
32Anon., ‘TheLateEpidemicof Enteric Fever atCaterhamand Redhill’,Medical Times and Gazette, Saturday 10May, 1879, 505–7, 507.
The Local Government Board, 1870–1900 Page 7 of 26
by guest on September 9, 2014
http://shm.oxfordjournals.org/
Dow
nloaded from

water-supply appears at least fair and justifiable’.33 This referred to thediscernable outcomeof Thorne’s Caterham investigation, namely public health action by the Caterham local au-thorities. Thorne was able—through persuasion that rested on the basis of his epidemio-logical methods—to convince the local Sanitary Authorities to issue public notices thatthe Caterham water had been ‘accidentally contaminated’.34 Residents were recom-mended not to use the company’s water until further notice, or, if necessary, to boilwater before use. Thorne also successfully prompted the Caterham WaterworksCompany to pump a large portion of their water to waste for three weeks, at an economicloss, and to thoroughly cleanse, scour, and disinfect the walls of the wells, adits, reservoirs,and surrounding soilwith chlorideof limeandpermanganateof potash. Thornenoted, innolittle triumphal tone, that ‘theCompany actedwith considerable energy andpromptitude inadopting allmeasureswhichwere foundpossible todoawaywith the results of theacciden-tal contamination to which their water had been subjected’.35 It is worth reflecting on thecomplex and delicate relationship between Thorne’s epidemiological field-practices, thecommunication of his methods and results, and the political outcome of his recommenda-tions. As an inspector for the Medical Department, Thorne could only make recommenda-tions to local authorities; that the Caterham authorities, as well as the local water company,fully compliedwithThornewas theproductof a sharedvaluationof Thorne’s epidemiologic-al methods, which rested on the performative nature of Thorne’s experiments, interviews,and statistical tabulations. The local authorities at Caterham and Redhill responded favour-ably toThorneeven though,orperhapsbecause,heonly reliedonanepidemiologicalwayofknowing to convince contemporaries of the necessary and sufficient cause of the local out-break.36 In this way, Thorne’s performances at Caterham, to further reflect, embody whatSteven Shapin has recently called the ‘practices of securing and maintaining credibility’.37
Much of the contemporary approbation of Thorne’s 1879 study focused on his method-ology, which, as we saw above, was dependent on routine epidemiological performance.The Practitionerwasdirect in praising Thorne’s epidemiologicalmethods, stating that his in-vestigationexhibited ‘inaperspicuousand intelligiblemanner themethodof inquirywhich isusually adopted by the Medical Inspectors of the Board, and which has hitherto beenattended with results which leave little to be desired’.38 Later that year Edward Ballard,Thorne’s colleague and close friend at the Medical Department, addressing the Section ofMedicine at the Annual Meeting of the British Medical Association held in Cork, echoedsuch remarks as were published in The Practitioner and Medical Times and Gazette.Ballard called Thorne’s epidemiological methodology at Caterham the ‘via exclusionis,the favouritemethod in thedepartment, and indeed theonly one applicable to suchdifficult
33Ibid., 507.34Thorne, ‘On an Extensive Epidemic of Enteric Fever atRed Hill”, 90.
35Ibid., 91.36Thorne’s1879 study in thisway fulfils RichardDoll’s cri-teria of an epidemiological study that provided, at leastaccording to Thorne’s 1879 contemporaries, proofbeyond reasonable doubt. See, Richard Doll, ‘Proofof Causality: Deduction from Epidemiological Obser-vation’, Perspectives in Biology and Medicine, 2002,45, 499–515.
37Steven Shapin, Never Pure: Historical Studies ofScience as if it was Produced by People with Bodies,Situated in Times, Space, Culture, and Society, andStruggling for Credibility and Authority (Baltimore:The Johns Hopkins University Press, 2010), 9.
38T. LauderBrunton., ‘Enteric Fever:ACrucial Instanceofits Spread Through the Medium of Drinking Water’,The Practitioner, January to June, 1879, xxii; 473–80,473.
Page 8 of 26 Jacob Steere-Williams
by guest on September 9, 2014
http://shm.oxfordjournals.org/
Dow
nloaded from

inquiries’.39 It was, put another way, quoting an early twentieth-century description, ‘theSherlockianmethod in epidemiology’, which typified the deductive basis of epidemiologicalpractice in the late Victorian period. To his contemporaries, Thorne’s success rested on asound methodology, one that in 1875 John Netten Radcliffe pronounced, signalled ‘thegold of scientific epidemiology’.40 Such professional back-patting of Thorne by his contem-poraries suggests important ways in which epidemiological methods were standardised inthis period. It is clear that the activities of infectious disease investigation conductedthrough the Medical Department were crucial to such standardisation of practice. So toowas the performativeways that local studiesweremade known towidermedical, scientific,and public audiences.
Evenoutsideofhis cadreof like-mindedpublichealthworkersat theMedicalDepartment,where we might expect praise, Thorne’s Caterham investigation garnered a great deal ofinterest and acclaim.41 This was due to the complex ways that Thorne projected epidemi-ology to larger audiences. In May of 1879, for example, he was requested to present apaper at the Annual Conference on National Water Supply, Sewage and Health, held inLondon by the Royal Society of Arts, a special conference at the request of the Prince ofWales.42 Thorne summarised his Caterham findings by noting that ‘in short there can benodoubt that thepollutionof thiswater, as the result of theman’s disease, and theepidemicin question, were related to each other as cause and effect; indeed the several essential inci-dents recorded are linked together in point of date, with a precision characteristic of theresultswhichmighthavebeenexpected tohave followedascientific inoculation’.43 Present-ing before a large and prestigious audience, Thornewas at pains to defend epidemiologicalways of knowing, particularly the authority of proving cause and effect. The eminent sani-tary engineer Baldwin Latham was supportive of Thorne’s claims, noting in the minutes ofthe meeting that Thorne’s was ‘a very valuable paper… the lessons to be drawn from itwould be of great use in the future’.44 Thus, Thorne’s 1879 Caterham study was both em-blematic of epidemiological practices, and one that many practitioners recognised as indi-cative of the power of epidemiological methodology.
In the lively discussion that followedhis presentationat theAnnualConferenceonNation-al Water Supply, Sewage and Health, Thorne was asked about the chemical state of theCaterham water. His response was that he had ‘specially avoided having the water ana-lysed’, as ‘you might have taken 100 samples and never found any evidence of specifically
39Ballard, ‘Observations on Some of the Ways in WhichDrinking-Water May Become Polluted’.
40Anon., ‘The Sherlockian Method in Epidemiology’,BMJ, 1936, 639; Radcliffe, ‘On the Recent Progressof Epidemiology in England’, 464.
41See, Anon., ‘Typhoid Fever Spread by Water’, TheBristol Mercury and Daily Post, 1897, 9669, 3. Seealso, John Tyndall, ‘Cholera and Disinfection’, DailyNews, 1883, 11641, 6. Edward Klein, presenting evi-dence before the Royal Commission to Inquire Intothe Water Supply of the Metropolis in 1893–94,argued that Thorne’s typhoid study at Caterham was‘perfectly sufficient to establish the proposition thatwater fouled with cholera dejecta or typhoid dejecta
may produce infection, the one with cholera, theother with typhoid fever’. Edward Klein, minutes ofevidence, Royal Commission to Inquire Into theWater Supply of the Metropolis, ParliamentaryPapers (London, 1894), 417.
42Anon., ‘Conference onNationalWater Supply, Sewer-age andHealth’, Journal of the Society of Arts, 20 June1879, 662.
43Richard Thorne Thorne, ‘The Recent Outbreak ofEnteric Fever atCaterhamandRedhill’,AnnualConfer-ence onNationalWater Supply, Sewerage andHealth,Royal Society of Arts, 1879, 117–19, 118.
44Ibid., Discussion of Minutes of Conference, 174.
The Local Government Board, 1870–1900 Page 9 of 26
by guest on September 9, 2014
http://shm.oxfordjournals.org/
Dow
nloaded from

diseasedmatter in it; but in the one hundred and first youmight have discovered it’.45 Suchapathy to the chemical analysis ofwaterwas common, asHamlin has shown.46W. F. Bynumhas claimed that ‘Britain remained a relative bacteriological backwater through the last thirdof the century, andclinical andepidemiological featuresofwhatwereoftencalled the ‘acutespecific fevers’ were just as important as the French, German and British laboratory evi-dence’.47 Assessing Bynum’s claim lies outside of the scope of this article, thoughThorne’s 1879 study—both his projection and self-fashioning of the investigation, as wellas its reception by contemporaries, including local political authorities and scientific collea-gues—is suggestive confirmatory evidence of such ‘bacteriological backwater’. By examin-ing the projection and reception of epidemiology, how Thorne and others defended,constructed, andmaintainedepidemiologicalwaysof knowing,wearebetter able tounder-stand the reasonswhy the Caterham local authorities placed trust and authority in Thorne’srecommendations, and to the larger significance of his study. Without the often-inconclu-sive practices of chemical or bacteriological analysis, Thorne could, through performance,command public health recommendations. To Thorne, a quintessential Victorian epidemi-ologist, ignoring bacteriology and chemistry was a deliberate strategy.
The public health lessons that contemporaries gleaned from Thorne’s Caterham studywere fourfold: (1) even aminute quantity of the germ, or poison of typhoid fever, under fa-vourable conditions when introduced into a water supply, could lead to an extensive out-break; (2) mild, or ‘perambulatory’ cases of typhoid fever represented a special publichealth danger, by reason of their intensely poisonous diarrhoea; (3) all sources of excremen-tal pollution near water sources should be extensively investigated, and; (4) no personssuffering from diarrhoeal complaints should work for the construction or storage ofwater.48 To contemporaries, Thorne’s 1879 investigation was one of a series of confirma-tions of the developing water-borne aetiological hypothesis; into the early twentiethcentury it remained a classic study in Victorian epidemiology.49 Late Victorian epidemio-logical investigations of typhoid fever reinforced the cultural assumptions that typhoidwas bred of filth, and, as Hamlin has argued, that the protection of water supplies andthe revamping of sewerage systems in rural and provincial areas was behind advancementsmade in numerous metropolitan ones.50 The image of Thorne, who only a few years laterbecame the administrative leader of British state medicine, climbing into a well in 1879forms more than just an interesting anecdote; it was a both routine epidemiological field-work, as well as a powerful performance that Thorne used to convince local authorities toact onhis powerless recommendations. SuchperformancesbyVictorian epidemiologists ac-companiedexperimentation, interviewing, case-tracing,map-makingand statistical tabula-tion, which we must also treat as performative. Field performances were accompaniedby rhetorical strategies of self-promotion by Victorian epidemiologists. Through his
45Ibid., 173.46ChristopherHamlin,AScienceof Impurity:WaterAna-lysis in Nineteenth Century Britain (Berkeley: Universityof California Press, 1990), esp. ch. 8.
47W. F. Bynum, ‘The Evolution of Germs and the Evolu-tion of Disease: Some British Debates, 1870–1900’,History and Philosophy of Science of the Life Sciences,2002, 24, 53–68, 54.
48Brunton., ‘Enteric Fever’, 480.49See, William Thompson Sedgwick’s 1922 study Princi-ples of Sanitary Science and Public Health (London:Macmillian, 1922), 191–200.
50ChristopherHamlin, ‘Muddling inBumbledom:On theEnormity of Large Sanitary Improvements in FourBritish Towns, 1855–1885’, Victorian Studies, 1988,32, 55–83.
Page 10 of 26 Jacob Steere-Williams
by guest on September 9, 2014
http://shm.oxfordjournals.org/
Dow
nloaded from

epidemiological methods, Thorne had also placed his finger on one of the more controver-sial aspects of statemedicine that continued into the twentieth century; the index case, J.K.,whose perambulatory case of typhoid fever enabled him to continue working in the Cater-ham well whilst being highly infectious, was the late Victorian precursor to the infamousTyphoid Mary, the latter being a healthy carrier.51 To Thorne and his contemporariesaround 1879 the perambulatory problem loomed larger than the identification of thetyphoid ‘germ’or ‘poison’. And,while thiswas a product of the belief in the epidemiologicalpractices employed by Thorne at Caterham, in the next two decades, American, French andGerman bacteriologists began to discover some of the specific microbes responsible formany major infectious diseases.
Endemic Typhoid Fever and the Emergence of Bacteriologyat the Medical Department
Hardy has argued that ‘reductionist bacteriological methods encountered criticism andresistance from an already well established [epidemiological] tradition’.52 My reading ofepidemiological investigations at the Medical Department in the last two decades of thenineteenth century, a period Hardy has concluded most historians still believe was ‘devoidof epidemiological enterprise’, confirms that while epidemiological practices remainedthe standard for outbreak investigation, there was significant room for cooperationbetween the two practices. As I articulate below, epidemiologists at the Medical Depart-ment began to seek bacteriological confirmation of their epidemiological studies only as astrategy of reaffirming the knowledge and authority of their emerging discipline.Thorne’s 1879 scoff at laboratory evidence is suggestive of the trend Hardy has articulated,though as I argued above, the reasons for resistance were part of a complex matrix of per-formative posturing, not necessarily a challenge to laboratory practices.While it is clear that‘the impact of bacteriology on the English epidemiological tradition was rather less impres-sive’ than on continental Europe or in North America, we still know very little about thecomplex ways British epidemiologists navigated the partial acceptance of bacteriologicalmethods and findings in the last two decades of the nineteenth century.53 Thorne’s pefor-mative act of having ‘little acquaintance with the laboratory’, and having ‘specially avoidedhaving the water analysed’ should not cloud the reality that auxiliary scientific, and particu-larly laboratory researchwas integral to the daily activities of medical science at theMedicalDepartment. Terrie Romano, for example, through an analysis of John Burdon Sanderson’sresearch activities, has detailed the Medical Department’s support of physiological andpathological research, particularly during the most intense period of debates overgerms.54 Even a cursory examination of Medical Department investigations from 1870 to1900 reveals that inspectors frequently sent water or milk to be analysed by the depart-ment’s scientific analysts, at times either BurdonSanderson, the chemist J. L.W.Thudichum,
51Judith Walzer Leavitt, Typhoid Mary: Captive to thePublic’s Health (Boston: Beacon Press, 1996). Seealso, Andrew Mendelsohn, ‘A Bacteriological Ap-proach to Controlling Typhoid’, in Deborah Brunton,ed., Health, Disease, and Society in Europe,1800–1930 (Manchester: Manchester UniversityPress, 2004), 185–8.
52Hardy, ‘Methods of Outbreak Investigation in the Eraof Bacteriology’, 206.
53Ibid.54Terrie Romano, Making Medicine Scientific: JohnBurdon Sanderson and the Culture of VictorianScience (Baltimore: The Johns Hopkins UniversityPress, 2002).
The Local Government Board, 1870–1900 Page 11 of 26
by guest on September 9, 2014
http://shm.oxfordjournals.org/
Dow
nloaded from

or later theproto-bacteriologist EdwardKlein.Hardy’s claim, in otherwords, that epidemiol-ogists were resistant to bacteriological approaches not only fails to address why, but moreimportantly, obscures the ways that the performative aspects of epidemiology often dic-tated whether a practitioner advocated for, or denounced laboratory evidence.
In the last twodecades of the century it became increasingly difficult for British epidemiol-ogists to simply ignorebacteriological practices theway Thornedid forwater analysis duringhis Caterham investigation. While epidemiologists at the Medical Department remainedcommitted to field-based, observational, and statistical practices, the investigation of epi-demic diseases became increasingly influenced by bacteriology. The second half of thisarticle explores theways inwhich British epidemiologists cautiously engagedwith bacterio-logical practices. Under focus in what follows is an investigation by H. Timbrell Bulstrode—who like Thornewas an inspector for theMedical Department—into anoutbreakof typhoidfever in Chichester in 1896. It is worth briefly exploring, however, why both investigationswere on typhoid fever.
After 1866, the final visitation of cholera in Britain, British epidemiologists believed thatinvestigations of typhoid fever held the key to answering unresolved debates over thenature of water-borne disease.55 Moreover, because of what John Simon called their‘close aetiological affinity’, protecting the country from typhoid, which continued inSimon’s mind to have a ‘deplorable and disgraceful power of spreading among our popu-lation’, would provide Britain with better security ‘against cholera than any imaginablesystem of quarantine’.56 Typhoid was an insidious endemic disease throughout the Victor-ian period; while outbreaks were often sporadic, at times they were highly virulent.57
William Stewart, Honorary Surgeon to the Beckett Hospital in Barnsley, put it best in1877, saying that typhoid was universally prevalent ‘in hot and cold climates, in town andcountry, in the houses of the rich and the hovels of the poor’.58 Typhoid was particularly re-markable to contemporaries because of its capacity to strike the rich and also the poor, theurban and the rural. It killed those who were atrociously dirty and those who were impec-cably clean. The disease was mapped onto the Victorian social body through the ubiquityof filth.59
55On cholera and quarantine, see, Krista Maglen, ‘“TheFirst Line of Defence” British Quarantine and the PortSanitary Authorities in the Nineteenth Century’,Social History of Medicine, 2002, 15, 413–28. On the1866 cholera outbreak, see, William Luckin, ‘TheFinal Catastrophe—Cholera in London, 1866’,Medical History, 1977, 21, 32–42. On the role oftyphoid, see Jacob Steere-Williams, ‘The Perfect Foodand the Filth Disease: Milk-borne Typhoid and Epi-demiological Practice in late Victorian Britain’,Journal of the History of Medicine and Allied Sciences,2010, 65, 514–45.
56Memo from John Simon to the Local GovernmentBoard, titled, re: Radcliffe’s ‘Diffusion of Cholera’,dated 30 June 1874. National Archives, Kew. MH113/12.
57Hardy and Luckin have shown that there was a slow,but unsteady post-1870 decline in the incidence of
the disease in Britain. By 1907, the Registrar-Generalclaimed that the mortality from typhoid fever fellfrom a rate of 384 per million in 1869 to 89 permillion in 1905. The use of such mortality statisticsshould be deployed with serious caution for most oftheVictorian period. Itwasnotuntil 1869 that theStat-istical Office of the Registrar-General officially distin-guished between typhoid, typhus, and simplecontinued fever. See, William Luckin, Pollution andControl: A Social History of the Thames in the Nine-teenth Century (Bristol: Adam Hilger Press, 1986), es-pecially ch. 6, and Hardy, Epidemic Streets, 152–4.
58W. Stewart, ‘A New Theory of the Origin of TyphoidFever’, BMJ, 1877, 1, 289–90, 289.
59Mary Poovey, Making A Social Body: British CulturalFormation, 1830–1864 (Chicago: Chicago UniversityPress, 1995).
Page 12 of 26 Jacob Steere-Williams
by guest on September 9, 2014
http://shm.oxfordjournals.org/
Dow
nloaded from

Tobe sure, linking typhoid fever to filthwasamoral gesture.GerryKearnsput it bestwhenhe noted, ‘the sewer and the slumwere part of a moral as well as a medical topography’.60
Alfred Haviland, Medical Officer of Health for Northamptonshire, famously quipped in theBritish Medical Journal that typhoid was ‘a national disgrace’, typifying the ways thattyphoid, as the preeminent filth disease, was connected to both material conditions suchas inadequate sewerage and water supply, and crucially, to behaviour and class.61 By the1880s though, the older Chadwickian notion of indiscriminate filth was gradually beingadapted to fit a multiplicity of germ theories. ‘Destroy the specific germs before they mixwith the filth’, Robert Hudson, Medical Officer of Health in Redruth noted, ‘look on filthas the agent for the dissemination of the poison, not the poison itself, and you are morelikely to be rewarded by success’.62 But whereas ‘it has long been an accepted doctrinethat filth was in some way related to the production of disease’, late Victorian epidemiolo-gists sought to show the specific ways that filth could cause disease.63
While typhoid fever became a model disease for epidemiological research in the secondhalf of the nineteenth century, British sanitarians remained puzzled by the nosological,pathological, and diagnostic aspects of the disease. As is well known in the history of medi-cine, pathological research dominated the study of fever in Britain in the middle decades ofthe nineteenth century. For many, Charles Murchison’s 1862 Treatise on the ContinuedFevers was the definitive work on sorting out the often-muddled nosological categoriesof fever.64 Murchison’s ‘pythogenic theory’ represented an aetiological compromise;typhoid feverwasadistinctdiseasecapableof transmission throughair,water,or foodstuffs,but only after it underwent a fermentation-like process in the soil. So contentious was thenosology and aetiology of typhoid—rural Britons were notoriously charged by their urbancounterparts in maintaining a belief in spontaneous generation— that many Britishmedical practitioners, particularly epidemiologists at the Medical Department, preferredto call the disease enteric fever, denoting the organs with which the lesions occurred.65
Here nomenclature mattered, as those physicians who preferred enteric fever allied them-selves with the French School of pathological specificity. Enteric remained the favouredname for many British public health officials throughout the second half of the nineteenthcentury, although by the 1880s most used typhoid and enteric interchangeably.
While the diagnosis of typhoid fever remained controversial throughout the second halfof thenineteenth century, anepidemiological—relating to theorigin and communicationofthe disease—approach dominated public health practice from the 1870s. Instead of avoid-ing the problematic diagnostic question regarding the fevers, this turn reinforced the need
60Gerry Kearns, ‘Biology, Class, and the Urban Penalty’,in Gerry Kearnes and CharlesW. J. Withers, eds,Urba-nising Britain: Essays on Class and the Community inthe Nineteenth century (Cambridge: Cambridge Uni-versity Press, 1991), 12.
61AlfredHaviland, ‘Abstract of Two Lectures on theGeo-graphical Distribution of Typhoid Fever in England andWales’, BMJ, 1872, 580, 148–9, 148.
62Robert H. Hudson, ‘TheGerm-Theory of Enteric Fever’,BMJ, 1877, 1, 740–1.
63Thorne, On the Progress of Preventive Medicine, 25.
64The definitive account remains Margaret Pelling,Cholera, Fever, and English Medicine, 1825–1865(Oxford: Oxford University Press, 1978).
65Benjamin Ward Richardson, ‘The Present Position andProspects of Epidemiological Science’, Transactions ofthe Epidemiological Society of London (London:Robert Hardwicke, 1867), 119. For a later account,see, William Corfield, The Etiology of Typhoid Feverand its Prevention (London: Gower Street, W.C.,1902), 2.
The Local Government Board, 1870–1900 Page 13 of 26
by guest on September 9, 2014
http://shm.oxfordjournals.org/
Dow
nloaded from

for proper diagnosis and death certification as paramount for making informed statisticalarguments and successful public health interventions.66
Interest in typhoid as a model disease was nowhere more apparent than at the MedicalDepartment. Nearly one-half of all department investigations from the 1870s to the1890s were local outbreaks of the disease.67 The Times, for example, noted in 1873 thatthese investigations ‘throw much light upon the particular conditions under which entericfever is developed and propagated both in towns and in rural districts’.68 The pressingpublic health question surrounding the disease in the last two decades of the nineteenthcentury was its persistent and endemic nature. This was framed as an epidemiologicalproblem; one of discovering the mediums with which typhoid fever spread, such aswater,milk, or, as itwas still oftenbelieved, sewergas.69 By the1890s, the threat of typhoid-charged soil was increasingly the focus of epidemiological and bacteriological inquiry at theMedical Department. As I demonstrate below, by examining an outbreakof typhoid fever atChichester in 1896, epidemiology and bacteriology could cooperate during outbreak inves-tigations at the Medical Department.
H. Timbrell Bulstrode and the Chichester Typhoid Study of 1896By the late1890sChichesterheldapoor sanitary reputationamongst the staff at theMedicalDepartment. The city possessed, asA.C.Houston later noted in 1904, ‘theunenviable repu-tation of being one of a number of places in England andWales in which enteric fever pre-vails in endemic and epidemic form to a notable extent’.70 Edward Seaton, one of thedepartment’s earliest inspectors hiredby JohnSimon,was the first to investigate the sanitarystate of Chichester, in 1865. Seaton, no doubt seeking to shock his readers, noted in hisreport that, the ‘death-rate which, for a small city well situated, not overcrowded, but com-prehendingwithin its bounds even fields andopen country, inwhich no largemanufacturesare carried on, gives strong evidence of something radically amiss in the sanitary conditionsof the place’.71 As of 1865 Chichester had no system of drainage and no extraneous watersupply; Seaton found nuisances of every sort, no little due to Chichester’s large cattlemarket, held every other Wednesday. Several years later, in 1879, when Seaton hadreplaced Simon as Chief Medical Officer, Hubert Airy visited Chichester to investigate anexplosive outbreak of typhoid fever. Airy’s investigation localised the 1879 outbreak to aninfected milk supply; he ended his report by noting that ‘there yet remain grave defects inthe sanitary condition of the city’.72
66JohnNetten Radcliffe, ‘The State of Epidemic, Epizoot-ic, and Epiphytic Disease in Great Britain, in 1861–62’,Transactions of the Epidemiological Society of London(London: Robert Hardwicke, 1863), 393.
67TheDepartment’s Annual Report for 1874 focused ex-clusively on Typhoid Fever, and included John Simon’sfamously reprinted, FilthDiseasesand their Prevention.
68Anon., ‘Enteric Fever’, The Times, Issue 27666, col. D(17 April 1873), 4.
69On sewer gas, see, H.Alfred Roechling, SewerGas andits Influence upon Health (London: Biggs and Co.,1898). For a more general discussion, particularly onthe American side, Tomes, The Gospel of Germs:Men, Women, and the Microbe in American Life
(Cambridge, Mass. Harvard University Press, 1998),24, 78–9.
70A. C. Houston, ‘Report on the Chemical and Bacterio-logical Examination of Tunbridge Wells Deep WellWater’, Thirty-SecondAnnual Report of the Local Gov-ernment Board, 1902–1903, Supplement Containingthe Report of the Medical Officer (London: Spotti-swoode, 1904), 581.
71Edward Seaton, ‘Report on Circumstances Endanger-ing the Public Health of Chichester’, in Eight Reportof the Medical Officer of the Privy Council (London:Spottiswoode, 1866), 220–6, 220.
72HubertAiry, ‘Report to theLocalGovernmentBoardonan Outbreak of Enteric Fever in Chichester’, 9.
Page 14 of 26 Jacob Steere-Williams
by guest on September 9, 2014
http://shm.oxfordjournals.org/
Dow
nloaded from

Between 1870 and 1890 vital statistics from the Registrar-General’s Office showed thatthe death-rate from typhoid fever in Chichester was one of the worst in England andWales. During both Decennial periods—1871–1880, and 1881–1890—Chichester hadthe highest death rate of all the Registration Districts in Sussex. Moreover, compared withall of England and Wales, only 31 of 630 Districts had a higher death rate from 1871 to1880. Chichester was worse-off in the decennial 1881–1890, whereby the city ranked inthe top twenty of districts with the highest incidence of typhoid fever. When therefore,Thorne, by then Chief Medical Officer, was informed by the Mayor of Chichester in July1896 that an explosive outbreak of typhoid fever was on the rise, he quickly respondedby sending a member of his epidemiological staff, H. Timbrell Bulstrode.
Herbert Timbrell Bulstrode served as an inspector at the Medical Department for nearlytwenty years, from 1892 and until his sudden death from heart failure in 1911. Thirtyyears old and fresh from a medical degree at Cambridge, Bulstrode was the first inspectorhired by Thorne, when the latter became Chief Medical Officer. ‘He had a notable charac-teristic of independently investigating’ his obituarist noted, and was part of a cadre of epi-demiologists who—following in the footsteps of Simon, Ballard, Netten-Radcliffe,Buchanan and Thorne—considered themselves professional epidemiologists. Althoughperhaps lesswell-known today,Bulstrode is best remembered forprovidingepidemiologicalconfirmationof the role of shellfish in transmitting typhoid fever, and, asMorabia andHardyhave shown, for using novel methods of epidemiological inquiry such as questionnaires.73
In 1896 the population of Chichester stood at just over 10,000. While typhoid was acommon occurrence, between July and August over 100 new cases of the disease werereported,most ofwhich occurred in ‘the same streets and areas inwhich hadbeen attackedwhen Seaton reported on the city 30 years ago’.74 Bulstrode’s Chichester investigationbegan much like the hundreds of others conducted by the inspectorate at the department.He convenedwithMr E. Prior, theMayor,Mr Davy, the Board’s General Inspector,membersof the local Sanitary Committee, andwith the Chairman of theWater Company, who com-bined to provide Bulstrode with an up-to-date list of fever cases, their addresses, and thesanitary condition and source ofwater supply of eachhouse. Such assistance from local offi-cials—although not always forthcoming—was a central feature of late nineteenth and es-pecially early twentieth century epidemiological investigations. Bulstrode visited andinterviewed individuals on the list, and also inspected the public waterworks.
Bulstrode’s initial focuswas on thewater supply and drainage of Chichester. The city wassupplied, he found, with water from both private shallow wells, and the Chichester Water-worksCompany. The shallowwells, ‘imperfectly protectedagainst filth soaking through thesoil’, were of particular concern, as many were located near privies or cesspools, and fittedwith loose, wooden lids.75 Chichester possessed a recently constructed sewer system, butprivies were still in wide use, Bulstrode found, and even in places where household privies
73AlfredoMorabia andAnneHardy, ‘The PioneeringUseof aQuestionnaire to Investigate a Food-BorneDiseaseOutbreak in Early 20th century Britain’, Journal ofEpdemiology andCommunity Health, 2005, 59, 94–9.
74Richard Thorne Thorne, ‘Enteric Fever at Chichester,’Twenty-Sixth Annual Report of the Local Government
Board, Supplement Containing the Report of theMedical Officer for 1896–97, xii.
75H. Timbrell Bulstrode, ‘Report Upon Prevalence ofEnteric Fever in the City of Chichester’, Twenty-SixthAnnual Report of the Local Government Board, Sup-plement Containing the Report of the MedicalOfficer for 1896–97, 93.
The Local Government Board, 1870–1900 Page 15 of 26
by guest on September 9, 2014
http://shm.oxfordjournals.org/
Dow
nloaded from

had been abandoned, ‘the privy vaults had, together with their contents, perhaps the accu-mulation of some years, been simply filled in, and not, as they should have been, carefullyemptied, their bricks removed, and their sites carefully cleansed’.76 ‘Chichester must, Ifear’, Bulstrode lamented in his report, ‘still be regarded as not differing substantiallyfrom an undrained city’.77
Bulstrode found nothing illuminating as to the distribution of the disease via sex, thoughhenoticed that63of the111attacksbelonged to thosebetween theagesof5and20.78 Thepublic water supply was largely free from suspicion, a conclusion Bulstrode reached usingepidemiological, chemical and bacteriological evidence. Of the 682 houses within thewalls of Chichester, 494 were supplied by the public water company. Of that number, Bul-strode found, only threewere invaded by typhoid. Altogether, of the 76 houses invaded, 39were supplied by private wells (2.9 per cent case incidence) and 37 (2.6 per cent case inci-dence) with water from the public company. Although the epidemiological evidence wasinconclusive to indict the public water supply, Bulstrode sent samples of Chichester waterto Edward Klein. On 29 July 1896, with the incidence of typhoid fever in Chichester onthe rise, Klein, at his laboratory at St Bartholomew’s Hospital, performed three routine bac-teriological tests on the Chichester water. He first made a gelatin plate with 1
4 c.c. water todetermine the number of aerobicmicrobes. After a 48 hour incubation period, Klein found,theplate yieldedonly 23 colonies, or 92aerobicmicrobesper 1 c.c., a small numberof harm-less bacteria.79 Klein then took 1,200 c.c. of Chichester water and forced it through a Ber-kefeld filter, using gelatin culture media—phenolated broth, phenolated gelatin, andiodised potato gelatin—to test for the typhoid bacillus. He found no typhoid microbes.Lastly, Klein took theparticulatematterof120c.c. and tested it for thepresenceofanaerobicmicrobes, noneofwhichwere found.Klein endedhis report,whichwas compiled at theendofBulstrode’s, by soundlydeclaring that ‘the sampleofwater deliveredherewasof excellentquality as far as bacteriological tests go’.80 Klein’s bacteriology, in other words, was suffi-cient in guiding epidemiological practice—it took Bulstrode’s attention away from thewaterworks company. But insofar as its applicability to epidemiology, bacteriology wasonly used here to confirm epidemiological methods.
Bulstrode’s rhetorical strategies at Chichester relied on a historical epidemiological claim,in which typhoid prevailed in 1896 in places where it had in former years. Neither the con-struction of a new sewerage system, or the public provision of water to parts of the city,affected the preventive change necessary to curb outbreaks of the disease. Seemingly pro-gressive sanitary improvement, Bulstrode suggested, had failed to prevent the disease.‘There would, indeed,’ Bulstrode concluded, ‘appear from consideration of the pasthistory of Chichester in respect to enteric fever, no need to seek out in explanation newagencies of dissemination, suchas, for instance, thepublicwater supply, or the recently con-structed sewerage’.81 It was clear that typhoid fever was endemic in Chichester, but that its
76Ibid.77Ibid, 92.78Although a higher incidence in children and youngadults suggested dissemination via milk, Bulstrodefound no evidence that milk played a role.
79EdwardKlein, ‘Report of BacteriologicalAnalysis of theChichester Public Water Supply’ Twenty Sixth Annual
Report of the Local Government Board, SupplementContaining the Report of the Medical Officer for1896–97, 105–6; Bulstrode, ‘Report Upon Prevalenceof Enteric Fever in the City of Chichester’, 105.
80Ibid.81Bulstrode, ‘Report Upon Prevalence of Enteric Fever inthe City of Chichester’, 104.
Page 16 of 26 Jacob Steere-Williams
by guest on September 9, 2014
http://shm.oxfordjournals.org/
Dow
nloaded from

cause, Bulstrode feared, ‘is not easy to determine’. With filthy cesspools and privies still inabundance, Bulstrode lamented that ‘not until the cesspits and cesspools of the placehave been abolished, and their sites and the soil in the neighbourhood thoroughly cleansed,can it be hoped that enteric fever will be banished from the city’.82
Compared to Thorne’s 1879 Caterham investigation, Bulstrode’s Chichester study failedto elicit a dramatic response from local authorities. This was partly, it seems, from the rhet-orical and performative strategies Bulstrode used to communicate his study. Like Thorne,Bulstrode provided a list of recommendations to the Chichester town council, issued 21July 1896. He included generic sanitary suggestions, such as the removal of all ‘accumula-tions of filth’, and specific remedial measures increasingly used to combat infectious dis-eases, such as the removal of early cases to the local isolation hospital. Bulstrode’s chiefconcern was the state and preponderance of privies in Chichester. He noted in his reportthat the Chichester Sanitary Committee adopted a formal resolution to ‘carry out theserecommendations in their entirety’, but further epidemiological study in 1900 by TheodoreThomson indicated that such measures largely went unfulfilled.83
In the course of Bulstrode’s investigation bacteriology was relied upon, but only in an an-cillary way. Klein’s analysis of the Chichester public water supply failed to detect the specificgermsof typhoid fever, andhenceall but rule out suspicionof the company. But, Bulstrode’sstatistical analysis satisfied him to the same conclusion. In thisway, the newmethods of bac-teriologydidnot serve topush theboundariesofdisease investigation. Itwas ratherquite theopposite; the defining feature of Bulstrode’s 1896Chichester investigationwas that it loca-lised theoutbreak to theendemicityofChichester soils. Thorne, for example, inhis summary,highlighted that Bulstrode’s study ‘goes to show that enteric fever, thoughmainly distribu-ted in epidemic form by means of water or of milk, is by no means always a ‘water-borne’disease; and it raises anew the question as to how far recurring prevalences of entericfever in one town or spot can be due to the persistence in more or less active form incertain soils of the organism of that disease’.84 Cotemporaries, such as William Henry Cor-field, saw Bulstrode’s 1896 study as a powerful example of the endemicity of typhoid fever,and one that provided aetiological clarity on the role of soil in transmitting the disease.85 Itwas epidemiological investigation—themethods and practices exhibited by both Thorne in1879andBulstrode in1896—thatpushedaetiological boundaries andpointed to the roleofsoil in maintaining outbreaks of typhoid fever. Yet, this was a matter left up to bacteriologyand microbiology to further investigate in the twentieth century.
It is worth reflecting on the performative aspects of Bulstrode’s 1896Chichester investiga-tion, especially as it compares to Thorne’s 1879Caterhamstudy. The shoe-leather practicesofVictorian epidemiology—what Ballard called the ‘via exclusionis’ method—was still at thecentre of disease investigation as the nineteenth century came to a close. And, while weusually claim that the ‘new’ public health of the early twentieth century was obsessed withindividuals—and the resultant public health practices of isolation and disinfection—Bul-strode’s epidemiology was firmly population-centred. But, unlike Thorne, Bulstrode was
82Ibid.83Theodore Thomson andCol. J. T.Marsh, ‘Enteric Feverin the city of Chichester,’ Twenty-Ninth Annual Reportof the Local Government Board, Supplement
Containing the Report of the Medical Officer for1899–1900, 52–88.
84Thorne, ‘Enteric Fever at Chichester’, xiii.85WilliamHenryCorfield, TheAetiology of Typhoid Feverand its Prevention (London: H.K. Lewis, 1902), 125.
The Local Government Board, 1870–1900 Page 17 of 26
by guest on September 9, 2014
http://shm.oxfordjournals.org/
Dow
nloaded from

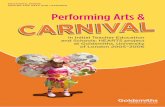
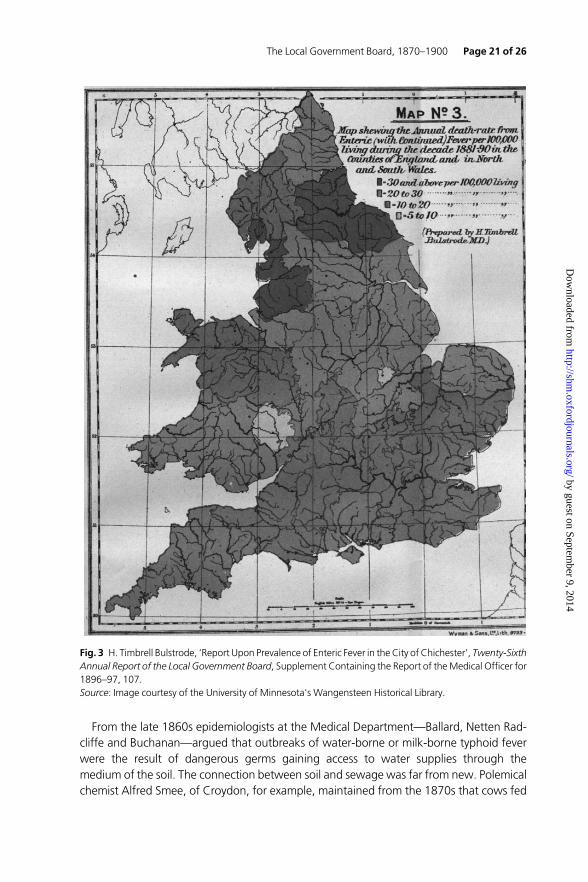
muchmore keen to use epidemiological findings to engage in politicised arguments. Perhapsbecause Thorne’s recommendations were actively pursued by the Caterham authorities,largely a result of his ability to provide causal proof using only epidemiological evidence, hefelt little need to engage in a larger debate over public health. Bulstrode, however, used therhetoric of historical epidemiology to substantiate the conclusions to be drawn from his1896 Chichester study. This positioning had important methodological and performativeramifications, and indicates that while the methods of epidemiological inquiry had not sub-stantially changed from the 1870s to the 1890s, the way in which epidemiologists at theMedical Department substantiated epidemiologicalways of knowingwere changing.Of par-ticular interest are three maps Bulstrode prepared for his 1896 report (Figures 1–3).86
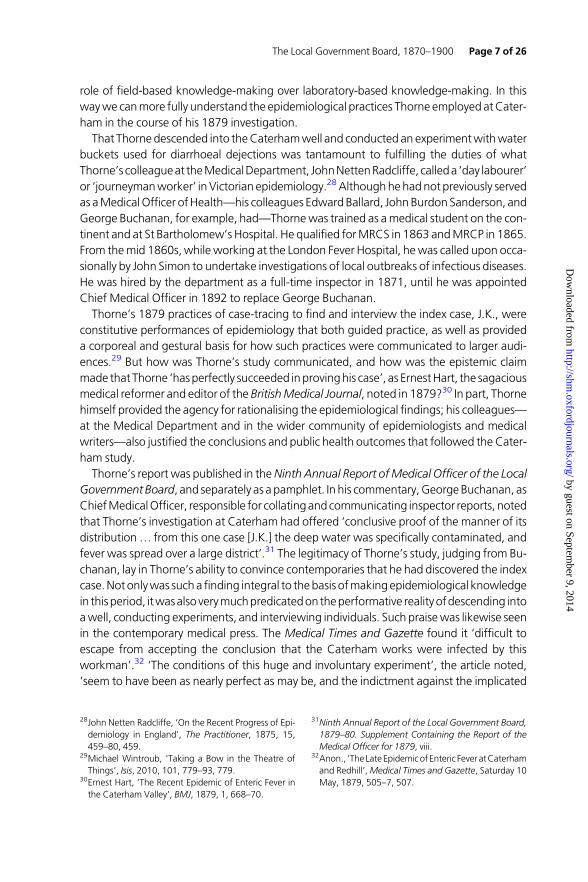
The maps depict the Registration Counties of England and Wales; Figure 1 shows theannual death-rate of typhoid fever per 100,000 persons during the decade 1871–1880,with the rates on different counties indicated by five sets of colours, and ranging from 70deaths ormore per 100,00 to under 30 deaths per 100,000. The secondmap (Figure 2) pro-vides the same data for the period 1881–1890; what is strikingwas that only two of the fivecolours in the firstmap remained, as three of the highest incidences of death had altogetherdisappeared. Bulstrode, and by extension Thorne, used the tools of epidemiology—including cartography—to depict what was seemingly a successful narrative of Victorianpublic health, namely, the dramatic decrease in the incidence of typhoid fever from 1860to1900. The rhetorical claimbehind the useof such representationswas that epidemiology,as the central science of state medicine, was in part responsible for the decrease in thedisease. Yet, Bulstrode used map three (Figure 3) to construct a rather different publichealth argument; it showed those Registration Districts in the period 1881–1890 whichhad the highest incidences of typhoid fever, and were thus lagging behind the generaltrend.87 This was no doubt also part of Bulstrode’s attempt to situate and self-present hisepidemiological practices at Caterham, and by extension, what he saw as the continualforging of the relationship between epidemiology and bacteriology. In his Annual Report,Thorne noticed that they served ‘to indicate that whilst enteric fever has been undergoingenormous diminution in this country, the areas of both its maximum and its minimum inci-dences have remained practically the same during the 20 years 1871–90’.88 The rhetoric ofcondemnation here is particularly interesting, especially in light of Keir Waddington’s ana-lysis of practices and conceptualisations of rural public health in late Victorian Wales.89
Thorne played a significant role in guiding the surge of soil-based studies of microorgan-isms in late nineteenth and early twentieth century Britain from his perch at theMedical De-partment. Although increasingly bacteriological, these studies remained committed to
86Medical geographers have recently made cogentclaims about the epistemic role of epidemiologicalmaps in making arguments about the causation andspread of disease. See, Tom Koch, Disease Maps: Epi-demics on theGround (Chicago: University of ChicagoPress, 2011).
87Graham Mooney has argued that ‘mortality compari-sonsbetweencountryside and townbecameaparticu-larly useful tool for demonstrating the shockingconditions of urban life’. See, Graham Mooney, ‘Pro-fessionalisation in Public Health and theMeasurement
of Sanitary Progress in Nineteenth Century Englandand Wales’, Social History of Medicine, 1997, 10,53–78, 53.
88Thorne, ‘Enteric Fever at Chichester’, Twenty-SixthAnnual Report of the Local Government Board, Sup-plement Containing the Report of the MedicalOfficer for 1896–97, xiii.
89Keir Waddington, ‘It Might Not be a Nuisance in aCountry Cottage: Sanitary Conditions and Images ofHealth in Victorian Rural Wales’, Rural History, 2012,23, 185–204.
Page 18 of 26 Jacob Steere-Williams
by guest on September 9, 2014
http://shm.oxfordjournals.org/
Dow
nloaded from

furthering epidemiological claims, although, as Thorne noted in his Twenty-Sixth AnnualReport in1897, ‘therehasbeen ratherdiscouragement’ofbacteriological evidence confirm-ing epidemiological suspicion.90 During the Chichester study, Bulstrode—instructed by
Fig. 1 H. Timbrell Bulstrode, ‘Report Upon Prevalence of Enteric Fever in the City of Chichester’, Twenty-SixthAnnual Report of the Local Government Board, Supplement Containing the Report of theMedical Officer for1896–97, 107.Source: Image courtesy of the University of Minnesota's Wangensteen Historical Library.
90Thorne, ‘Enteric Fever at Chichester’, xxi.
The Local Government Board, 1870–1900 Page 19 of 26
by guest on September 9, 2014
http://shm.oxfordjournals.org/
Dow
nloaded from

Thorne—sent samples of soils thought to be infected with typhoid microbes to SidneyMartin, the Jamaican-born, University College London and Viennese trained bacteriologistworking on a part-time basis for the department. The role of soil in spreading infectious dis-eases such as typhoid fever was not new to the 1890s, but resurged as a result of epidemio-logical studies such as Bulstrode’s.
Fig. 2 H. Timbrell Bulstrode, ‘Report Upon Prevalence of Enteric Fever in the City of Chichester’, Twenty-SixthAnnual Report of the Local Government Board, Supplement Containing the Report of theMedical Officer for1896–97, 108.Source: Image courtesy of the University of Minnesota's Wangensteen Historical Library.
Page 20 of 26 Jacob Steere-Williams
by guest on September 9, 2014
http://shm.oxfordjournals.org/
Dow
nloaded from
From the late 1860s epidemiologists at the Medical Department—Ballard, Netten Rad-cliffe and Buchanan—argued that outbreaks of water-borne or milk-borne typhoid feverwere the result of dangerous germs gaining access to water supplies through themedium of the soil. The connection between soil and sewage was far from new. Polemicalchemist Alfred Smee, of Croydon, for example, maintained from the 1870s that cows fed
Fig. 3 H. Timbrell Bulstrode, ‘Report Upon Prevalence of Enteric Fever in the City of Chichester’, Twenty-SixthAnnual Report of the Local Government Board, Supplement Containing the Report of theMedical Officer for1896–97, 107.Source: Image courtesy of the University of Minnesota's Wangensteen Historical Library.
The Local Government Board, 1870–1900 Page 21 of 26
by guest on September 9, 2014
http://shm.oxfordjournals.org/
Dow
nloaded from

with sewage-contaminated grasses could spread typhoid through their milk.91 Smee’saetiological theory combined Charles Murchison’s and Max von Pettenkofer’s belief thatdisease-causing germs had to undergo a period of fermentation, or incubation, in the soilto become infective.92 Early theories such as Murchison’s and Petterkofer’s, which wereenvironmentally-driven, have been chalked up to the lasting strength of localist doctrinein the late nineteenth century. AsWorboys has shown, there was amultiplicity of germ the-ories. Itwas still aetiologically viable, after all, to suggest that thegermsof typhoidandsimilardiseasesmultiplied in favourable soil conditions rather than in the bodies of patients, a viewwhich had crucial public health implications for stopping the spread of infectious diseasesthrough disinfection and isolation practices.93 Yet it would be misleading to think ofsoil-based aetiological theories that persisted into the 1890s as aligned with the Murchi-son/Pettenkofer camp, as aetiological hold-outs who maintained a belief in spontaneousgeneration long after it was scientifically fashionable. Instead, soil-based research wasundertaken by the vanguard of British bacteriologists—Sidney Martin, A. C. Houston andEdward Klein—often on a contractual basis with the Medical Department, who sought toprovemore exclusivist aetiological theories and to explore fundamental biological questionsabout the life cycle of germs.94 It was only in the 1890s that the role of soil was againconsidered, but it was in light of epidemiological specificity.
With the soil samples he received fromBulstrode atChichester,Martin began to testwhatsoil conditions—temperature, soil bacteria,water levels—were productive or inimical to thedevelopment of b. typhosus outside the human organism.95 Martin’s research demon-strates cooperation between epidemiologists and bacteriologists at the Medical Depart-ment. Martin received eight samples of soil; four from houses where typhoid had beenextensively present during the 1896 Chichester study and four from houses free of thedisease.
Martin found that the typhoid bacillus could remain alive and virulent for long periods oftime in sterilised cultivated soils (normal garden soil, for example that might be found nearhouseholds), but that ‘in virgin, uncultivated soil it rapidly dies’.96 Bacteriological testing of
91Alfred Smee, Milk, Typhoid Fever, and Sewage: ASeries of Letters (London: W.H. & L. Collingridge,1873), and Smee, Sewage, Sewage Produce, andDisease, (London: W.H. & L. Collingridge, 1873). Seealso, Alfred Carpenter, Some Points in the Physiologic-al and Medical Aspects of Sewage Irrigation (London:Hardwicke, 1870). Smee’s interest in the matter canbe dated to the late 1850s, when he sent a series ofletters to John Simon, then Medical Officer of Healthfor the City of London. See, Letters from Alfred Smeeto John Simon, dated 19 December 1859 and 20 De-cember 1859. Royal College of Surgeons of England,John Simon Collection, 67.h.5 Letters & Papers, re:College Affairs.
92Max von Pettenkofer, ‘Boden and Grundwasser inihren Beziehungen zuCholera und Typhus’, Zeitschriftfur Biologie, 1869, 2, 171–310. Bacteriological re-search in the 1880s and 1890s on the relationshipbetween soil and anthrax may have also contributedto Houston’s interest. On anthrax, see, James Stark,
The Making of Modern Anthrax, and Susan Jones,Death in a Small Package: A Short History of Anthrax(Baltimore: The Johns Hopkins University Press,2010), especially ch. 1.
93Aetiological debates on typhoid were at the centre ofthe Section of Medicine at the Annual Meeting ofthe British Medical Association in 1879 held in Cork.See, Alfred Carpenter, ‘A Consideration of Some ofthe Fallacies which are based upon a narrow view ofthe Germ-Theory’, BMJ, 1880, 994, 79–81.
94On Houston, see, A. C. Houston, ‘Enteric Fever in itsPublic Health Aspects’, The Lancet, 1901, 1, 468–9.
95Sidney Martin, ‘Preliminary Report on the Growth ofthe Typhoid Bacillus in Soil’, Twenty-Sixth AnnualReport of the Local Government Board, SupplementContaining the Report of the Medical Officer for1896–97, 231–42.
96Martin, ‘The Growth of the Typhoid Bacillus in Soil’,1278.
Page 22 of 26 Jacob Steere-Williams
by guest on September 9, 2014
http://shm.oxfordjournals.org/
Dow
nloaded from

b.typhosus in soils was a confirmation of the long-held doctrine by John Burdon Sandersonthat certain diseases ‘possess thewonderful property of passing into a state of persistent in-activity or latent vitality, in which they perform no function, but can at any moment bewakened up into active function, whenever they are brought under favourable circum-stances’.97 Reflecting on the importance of Martin’s soil-based studies of typhoid in hisAnnual Report for 1897, Thorne noted that, ‘whilst much of the diminution in entericfever has gone hand-in-hand with the abandonment of water services which, beingsubject to receive specific pollution, served for wide diffusions and sudden outbursts ofenter fever,-much of the persistent prevalence of that disease is associated with thosesystems for the disposal of excreta and refuse which still find favour in certain parts of thiscountry, and which inevitably involve organic pollution of the soil’.98
Soil-based research highlighted one of the most pressing public health problems thatoccurred in late nineteenth-century Britain, namely, sporadic but persistent outbreaks ofendemic diseases such as typhoid fever. This was, as Hardy has claimed, originally a ‘specificepidemiological problem’ and one to which ‘bacteriology had failed to provide theanswer’.99 Yet, in the last two decades of the nineteenth century bacteriological studiesat the Medical Department on disease-causing organisms in soil succeeded in elucidatingfurther aetiological clarity, and reinforcing remedialmeasures in publicworks. This confirmsWorboys’ claim that a ‘seed and soil’ botanical metaphor dominated the understanding ofgerms in the second half of the nineteenth century.100 Yet ‘seed and soil’ was more thansimply a metaphor; it guided epidemiological as well as bacteriological practice. WhereasHardy has seen the failure of bacteriology to confirm the aetiological role of soil in spreadingtyphoid as a plausible rationale for the growing ‘uneasiness’ between the two groups ofpractitioners, it is more likely that this episode confirms that epidemiological rather thanbacteriological practices dominated the scope of the Medical Department.
In his annual report for 1897, Thorne summarised Bulstrode’s epidemiological researchalongside Martin’s fledgling bacteriological research, noting,
these facts go to indicate the need for systematic study of a question which has grad-ually come toacquire considerable importance, andwhichmaybeput thus:—Whatarethe local conditions by reason of which certain areas, whether registration counties,town, or villages, have, for at least a generation, become identified with such persist-ence or periodic recrudescence of enteric fever, as has continued to secure for themdeath-rates from that disease in excess of other districts with some at least of whichthey may not unfairly be compared?101
Epidemiological practices played a key role in answering Thorne’s plea, but so too did thenew practices of bacteriology, particularly soil-related studies and those that sought tounderstand the survival of germs outside of the human body. That Bulstrode activelyyoked his epidemiological field-work to the practices of bacteriology signifies a shift in the
97John Burdon Sanderson, Lectures on the Occurrenceof Organic Forms in Connection with Contagious andInfective Diseases, quoted in Thorne, ‘Remarks onthe Origin of Infection’, 240.
98RichardThorneThorne, Twenty SixthAnnual Report ofthe LocalGovernmentBoard, 1896–1897Supplement
Containing the Report of the Medical Officer for1896–1897 (London: Eyre & Spottiswoode, 1897), xiv.
99Hardy, ‘On the Cusp’, 343.100Worboys, Spreading Germs, 6–7.101Thorne, Twenty SixthAnnual Report of the LocalGov-
ernment Board, 1896–1897, xiv.
The Local Government Board, 1870–1900 Page 23 of 26
by guest on September 9, 2014
http://shm.oxfordjournals.org/
Dow
nloaded from

performance of public health at theMedical Department. By the 1890s epidemiologists likeBulstrode could not claim, for example, that they had ‘little acquaintance’with the labora-tory. Increasingly, bacteriology and epidemiology sought to answer the tough questions inpublic health, such as the persistence of typhoid fever. Ultimately, however, from the per-spectiveof performance, Bulstrode’s inclusionof bacteriologyonlymuddied theaetiologicalwaters of his epistemological claims. Although he sought to ‘receive support at the hands ofthe bacteriologist’, he ultimately found little value in bacteriological justification.102 Epi-demiologyhadsuggested theendemicityof typhoid in theChichester soils, andbacteriologywas too premature to providemore than preliminary causal evidence. Unlike Hardy’s claim,this was not by itself reason for fissure between epidemiology and bacteriology. Hence Bul-strode’s appeal to historical epidemiology, and to the aesthetics ofmap-making. Relying onthe traditional posturing of epidemiologists, mutually intelligible to Thorne and Bulstrode,the Chichester study could be used to make a politicised argument that denouncedlaggard local authorities such as those in Chichester, and perhaps throughout Britain.
ConclusionHardy has called the last two decades of the nineteenth century a ‘neglected’ period in thehistory ofBritish epidemiology.WhereasGermanandAmericanpractitioners ofHighVictor-ian Epidemiology were more willing to incorporate the newmethods—and results—of theburgeoning field of bacteriology,Hardy has argued, English epidemiologists remained com-mitted to field-based, observational, and statistically-informed methods that focused onpopulations, as opposed to individuals.103 In the examples under scrutiny here, bothThorne in his 1879 Caterham investigation and Bulstrode in his 1896 Chichester investiga-tion relied on the widely practised traditions of field epidemiology. This suggests a confirm-ation of Hardy’s hypothesis. Yet, this article moves us beyond Hardy’s characterisation of aJanus-faced discipline. By focusing on the performative aspects of epidemiology at theMedical Department, a different picture emerges as to how,why andwhen epidemiologistschose to incorporate or eschew the claims, methods, and practices of laboratory science. Inthis light, Thorne appears less concerned that newbacteriological reductionismwouldover-take traditional, field-based methods of tracking disease.104 Where we have previouslyunderstood such statements as professional turf battles, perhaps they were instead partof a complex process of performing state medicine. Thorne’s official pronouncement thathe had ‘little acquaintance with the laboratory’ was thus part of a complex justification ofthe merits of epidemiological ways of knowing, not necessarily a growing rift betweenepidemiology and bacteriology, which appears less a late Victorian phenomenon than anEdwardian or even inter-war one. Thorne’s posturing reveals an epidemiology that wasself-reflexively confident in its ability to answer aetiological questions about public healthproblems. Thorne’s descending into the Caterham well to provide proof of the index casewas as much a part of that posturing as was his official testimony before scientific andpublic audiences. To the Medical Department of 1879, and to the epidemiological
102Bulstrode, ‘ReportUponPrevalenceof Enteric Fever inthe City of Chichester’, 101.
103Hardy, ‘Methods of Outbreak Investigation in the Eraof Bacteriology’, 200.
104Hardy, ‘On the Cusp’, 328–46.
Page 24 of 26 Jacob Steere-Williams
by guest on September 9, 2014
http://shm.oxfordjournals.org/
Dow
nloaded from

profession at large, Thorne’s Caterham study was a success, both methodologically andrhetorically.
By the 1890s, as the case of Bulstrode’s Chichester study demonstrates, epidemiologistsat theMedicalDepartmentwere re-fashioningepidemiologyalongsidebacteriology, not, asHardy suggests, against it. Therewas room, some thought, for bothways of knowing in thestate appropriation ofmedical science. As the case of soil-based bacteriological studies sug-gests, bacteriological approaches to understanding disease were rather unproblematicallyadopted to the problems traditionally handled by field epidemiology.105
The Medical Department is a useful site to begin a re-evaluation of the performances ofbroader trends in late Victorian public health. Although the department was one centralnode in the construction of epidemiological knowledge in Britain, we still need morestudies devoted to the ways in which Medical Officers of Health, particularly in ruralareas, practised and defended epidemiology. Not universally, but as the nineteenthcentury came to a close, the staff at the Medical Department was keen to deploy the newscience of bacteriology in answering still unresolved aetiological questions, although it isclear from this article that new approaches often followed epidemiological practice, notthe other way around. As I stated at the outset, the two narratives under examinationhere were part of a much larger set of epidemiological and bacteriological activities thatwere conducted through theMedical Department, and doubtless more studies of differentdisease practices are needed to draw definitive conclusions about the way that theMedicalDepartment represented epidemiology at large. Yet, these two studies nonetheless allowfor careful examination of the performative aspects of public health.
Examining the projection and reception of epidemiological ways of knowing in the periodwhenbacteriologywas ‘on the cusp’ suggests a reinterpretation of RoyMacLeod’s character-isation of theMedical Department.106 By following new tenets in the cultural history ofmedi-cine, such as the local production of scientific knowledge, and its performative posturing andappropriation, the epidemiologists at theMedical Department can beunderstood as having anew agency we have not afforded them in the past. Epidemiologists such as Thorne and Bul-strodewereat thecentreofepidemiologicalknowledge-makingandcirculation in the lateVic-torian period; although based out of the department’s Whitehall office, they travelledthroughoutBritain,and interactedwithawide rangeof localmedical practitioners, politicians,privatebusinessownersand,of course, everydayBritons.107Howthesepractitionersobtainedtheir authority, and how their knowledge was recognised by various local, regional, nationaland international groups are questions this article only begins to answer.Moreover, as I haveargued here, such practices—including the methods of epidemiology as well as how investi-gations were discussed, debated and disseminated—need to be understood as dynamic ac-tivities, and part of a widespread network of knowledge circulation in the Victorian period.By the early twentieth century Anglo-American epidemiology took a distinctly biostatisticalturn.108 As this article suggests, perhaps we ought to look more closely at the continuity of
105Ibid., 329. See also, Olga Amsterdamska, ‘Demarcat-ing Epidemiology’, Science, Technology, & HumanValues, 2005, 30, Special Issue: Demarcation Socia-lised: Constructing Boundaries and Recognising Dif-ference, 17–51.
106Roy MacLeod, ‘The Frustration of State Medicine,1880–1889’,Medical History, 1967, 1, 15–40.
107James Secord, ‘Knowledge in Transit’, Isis, 2004, 95,654–72.
108Anne Hardy and M. Elleen Magnello, ‘StatisticalMethods in Epidemiology: Karl Pearson, Ronald
The Local Government Board, 1870–1900 Page 25 of 26
by guest on September 9, 2014
http://shm.oxfordjournals.org/
Dow
nloaded from
lateVictorianepidemiological fieldpractice, asopposed toassuming—aswehave for the caseof bacteriology—that it too was overshadowed by the biostatistics ofMajor Greenwood andKarl Pearson.
AcknowledgementsMick Worboys, Chris Hamlin and Anne Hardy all provided generous support and poignantcommentary at various stages of this project. I would like to acknowledge especially thementorship that JohnEyler hasprovided formanyyears. Theeditors atSHMprovided incisiveguidance, and themanuscriptwasmade thebetter by the anonymous reviewers. Earlier ver-sionsof this articlewerepresentedat theAnnualMeetingof theAmericanAssociationof theHistory of Medicine in Baltimore.
Ross, Major Greenwood, and Austin Bradford Hill,1900–1945’, in Alfred Morabia, ed., A History of
Epidemiologic Methods and Concepts (Basel,Verlag, 2004), 80–9.
Page 26 of 26 Jacob Steere-Williams
by guest on September 9, 2014
http://shm.oxfordjournals.org/
Dow
nloaded from