
Prefrontal hyperactivity in older people during motor planning
Upload
independentCategory
view
0download
0
Child Neuropsychology, 13: 276–304, 2007http://www.psypress.com/childneuropsychISSN: 0929-7049 print / 1744-4136 onlineDOI: 10.1080/09297040600770761
© 2007 Taylor & Francis Group, LLC, an Informa business
PERFORMANCE OF CHILDREN WITH ATTENTION DEFICIT HYPERACTIVITY DISORDER (ADHD) ON A TEST BATTERY OF IMPULSIVENESS
Katya Rubia, Anna Smith, and Eric TaylorDepartment of Child and Adolescent Psychiatry, Institute of Psychiatry, KingsCollege, London, UK
Children with ADHD were compared to healthy controls on a task battery of cognitivecontrol, measuring motor inhibition (Go/No-Go and Stop tasks), cognitive inhibition(motor Stroop and Switch tasks), sustained attention and time discrimination. Childrenwith ADHD showed an inconsistent and premature response style across all 6 tasks. Inaddition they showed task-specific impairments in measures of sustained attention, timediscrimination, and motor inhibition, but spared cognitive inhibition. Measures of impair-ment correlated with behavioral hyperactivity and with each other, suggesting that theymeasure interrelated aspects of a multifaceted construct of cognitive impulsiveness. Thetask battery as a whole showed 76% correct discrimination of cases and controls.
Keywords: attention deficit/hyperactivity disorder (ADHD), impulsiveness, motorinhibition, continuous performance task (CPT), attention, time estimation
INTRODUCTION
Impulsiveness is being considered to be a core symptom of attention deficit/hyperactivity disorder (ADHD) by the DSM-IV (American Psychiatric Association,1994). Impulsivity is characterized by an inappropriately speedy, premature, highlychangeable, and nonpersistent, poorly controlled, unreflective, and immediacy-boundresponse style that affects predominantly the output level of behavior (Rubia, 2002).
We have previously hypothesized that the characteristic symptoms of ADHD fit thecriteria of a generalized impulsivity disorder that expresses itself at the motor level (over-activity), cognitive level (i.e., an impulsive cognitive and attentional style that results inpoor performance on tasks of cognitive control), emotional level (uncontrolled irritabletemperament), and social level (social disinhibition) (Rubia, 2002). Behavioral impair-ments that have been observed in children with ADHD include a speed-accuracy trade-offfavoring speed (Dykman, Ackerman, & Oglesby, 1979), an inconsistent response style(Leth-Steenson, Elbaz, & Douglas, 2000; Rubia, Taylor, Smith, Oksannen, & Newman,2001a), problems with inhibiting a motor response in Go/No-Go and Stop tasks (for overview
We thank Raoul Horbe-Forbes, Dr. John Wang and Maxine Sinclair for their help with the data collectionand Serena Maja for programming the task battery.
Address correspondence to Dr. Katya Rubia, Dept of Child and Adolescent Psychiatry, Institute ofPsychiatry, 16 De Crespigny Park, London, SE5 8AJ. E-mail: [email protected]

ADHD AND A TEST BATTERY OF IMPULSIVENESS 277
see Sergeant, Geurts, & Oosterlaan, 2002; Willcutt, Doyle, Nigg, Faraone, & Pennington,2005), deficits in sustaining attention as measured on the continuous performance task (foroverview see Losier, McGrath, & Klein, 1996; Willcutt et al., 2005), problems withmotivational control and reward related behaviors (Luman, Oosterlaan, & Sergeant, 2005),and abnormal timing behavior including delay aversion (Sonuga-Barke & Taylor, 1992),clumsy motor timing (Rubia, Sergeant, Taylor, & Taylor, 1999; Rubia, Smith, Noorlos,Gunning, & Sergeant, 2003), and time estimation deficits (Mullins, Bellgrove, Gill, &Robertson, 2005; Rubia, Smith, Noorlos et al., 2003; Smith, Taylor, Warner-Rogers, &Rubia, 2002).
In short, several functions of cognitive, attentional, and motivational control andtiming abnormalities have thus been related to ADHD pathology; and each one of themhas been suggested to be the underlying primary cause for the other deficits. In this way,impulsiveness in patients with ADHD has thus been suggested by some authorities in thefield to be the result of an inability to inhibit responses (Barkley, 1997), or motivationalproblems with delaying reward-related responses (Sonuga-Barke & Taylor, 1992), or def-icits in timing functions (Rubia et al., 1999; Rubia & Smith, 2001), or attention deficits(Banaschewski et al., 2004; Brandeis et al., 2002). Recently, dual (Sonuga-Barke, 2005)and multiple pathway models (Nigg, Willcutt, Alysa, Doyle, & Sonuga-Barke 2005) havebeen proposed, suggesting different neurobiological and neuropsychological pathways toADHD aetio-pathophysiology. We have previously argued that impulsiveness is essen-tially characterized by two main problem domains: problems with self-control functions,leading to poor inhibitory and attentional functions, and problems with timing behavior,leading to temporal myopia, present-boundedness, and aversion to delay of rewards(Rubia, 2002).
In this study we wanted to test the hypothesis that the cognitive style of ADHD ischaracterized by deficits in several specific cognitive functions, including inhibitory,attentional, and motivational control and perceptual temporal processes, and by task-unspecific deficits such as a general premature and inconsistent response style.
In most studies the above mentioned cognitive function domains thought to underlieADHD aetiology such as timing, reward, and inhibitory and attentional control functionshave been measured in isolation. It is crucial, however, to understand whether and howthese different domains of hypothesized impairment relate to each other within the samesample. In this study we combine tests of these different cognitive domains in one singletask battery and within one subject population in order to test whether the same ADHDpopulation would show deficits in all hypothesized “deficit domains” or only specificones, to explore their relative sensitivity and specificity, and to explore the relationshipbetween deficits in these different cognitive domains. We have chosen the umbrella termof “cognitive control functions” for the different cognitive domains we aimed to test inchildren with ADHD, which involve functions of attentional, inhibitory and motivationcontrol, and time management. “Cognitive control functions” measure a subset of execu-tive functions, which usually include more general tests of output control such asplanning, goal-directed behavior, verbal fluency, working memory, and selective atten-tion. In order to measure these different impulsiveness-related cognitive control functionsin one single battery of homogenously designed visual tests, we designed a task battery,the Maudsley Attention and Response Suppression Task battery (MARS). The MARStask battery consists of 6 tasks measuring key functions that have been shown to beimpaired in children with ADHD and have been related to impulsiveness: (1) selectivemotor response inhibition, requiring the inhibition of a motor response in 30% of trials

278 K. RUBIA ET AL.
(Go/No-Go task; Rubia, Taylor et al., 2001), (2) the ability to unexpectedly withhold amotor response that is already being triggered by a go-stimulus (Stop task; Rubia, Smith,Brammer, & Taylor, 2003), (3) a motor version of a Stroop-like interference inhibitiontask, requiring the participant to override a prepotent response tendency towards spatiallycompatible cues for action that interfere with the primary intended action (motor Strooptask; Rubia, Smith et al., in press), (4) the ability to switch between stimulus-responseassociations of two alternating spatial dimensions, requiring the inhibition of previouslyvalid visual-spatial stimulus-response associations in order to switch to a new one (Switchtask; Smith, Taylor, Brammer, & Rubia, 2004), (5) sustained attention and the effect ofmotivation on this function (rewarded continuous performance task), and (6) a task of timediscrimination, requiring the discrimination between time intervals of about a secondduration that differ by several hundreds of milliseconds (Temporal Discrimination task;Smith et al., 2002; Smith, Lidzba, Taylor, & Rubia, 2003).
Some of the tasks designed for this study were faster, simpler, and purely visualmodifications of previously used task versions; others, such as the spatial switch task andthe rewarded CPT, have never previously been applied to children with ADHD. All taskshave been made as homogenous as possible in their motor requirements (all tasks requires aspeeded two-choice motor response), inter-trial-intervals (ITI), and total task durations inorder to compare between variables and provide some common measures (such as meanreaction time, intrasubject variability, and premature responding) across tasks. Further-more, all tasks were about half the typical duration for tests of this type, of cognitive controltasks with the shortest task being the CPT with an ITI of 1s. The fast speed was aimed toadapt the tasks to this particularly delay-averse patient group in order to avoid task-unrelated performance decline caused by problems with sustaining attention, delayaversion, or boredom. We have previously shown that faster versions of Go/No-Go andStop tasks elicit the same inhibitory deficits as slower versions (Rubia, Taylor et al., 2001).
We used a visual stop signal for the Stop task (Rubia, Oosterlaan, Sergeant,Brandeis, & van Leeuwen, 1998; Rubia, Taylor et al., 2001), as opposed to the auditorystop signal that has been used in most previous studies, in order to eliminate the confoundof two different modalities for executive and inhibitory processes (Nigg, 2000) and toprovide the same (visual) modality for all tasks. Furthermore, we designed a motor Stroopversion to measure interference inhibition as opposed to the Color-Word Stroop task thathas been measured previously in children with ADHD (Sergeant et al., 2002), in order toavoid confounds with reading problems and make the task comparable to the motor inhibi-tion tasks. A novel Switch task requiring switching between two spatial dimensions wasdesigned to keep other confounding cognitive functions such as working memory andrule-learning requirements to a minimum (Smith et al., 2004). The effect of reward wasmeasured in a CPT task by rewarding half of the target trials. Finally, the key perceptualtask was a Temporal Discrimination task to replicate our own previous findings of timediscrimination deficits in children with ADHD (Smith et al., 2002) and to explore for thefirst time the relationship between perceptual time estimation deficits and deficits in theother, more predominantly, executive tasks.
We hypothesized that children with ADHD would be impaired on the task-specificmeasures of these 6 different tasks and would also show deficits in measures that arecommon across all tasks such as intrasubject variability and premature responding.Increased intrasubject variability of response has been one of the most consistent findingsin patients with ADHD (Leth-Steenson et al., 2000; Castellanos et al., 2005) and has beenobserved during a wide range of tasks including motor response inhibition (Rubia et al.,

ADHD AND A TEST BATTERY OF IMPULSIVENESS 279
1998; Rubia, Taylor et al., 2001; Schachar, Tannock, Marriot, & Logan, 1995), sustainedattention (Leth-Steenson et al., 2000), motor timing (Rubia, Sergeant et al., 1999a; Rubia,Smith et al., 2003), and time estimation (Mullins et al., 2005; Rubia Sergeant et al., 1999;Rubia, Smith et al., 2003; Toplak, Rucklidge, Hetherington, John, & Tannock, 2003).Premature responding has rarely been measured in cognitive tasks, but the few studies thathave measured it have observed a higher rate of premature responses in patients withADHD compared to healthy controls during time estimation (Sonuga-Barke, Saxton, &Hall, 1998; Smith et al., 2002), the Matching Familiar Figures Task (Cambell, Endmann, &Bernfield, 1977; Rosenbaum & Baker, 1984), and the Stop task (Bedard et al., 2003;Rubia, Smith et al., 2001). The relatively speedy and premature response style of ADHDis, however, not to be confounded with an absolute speed superiority. Hyperactive chil-dren tend to show slower reaction times in cognitive tasks (Pennington & Ozonoff, 1996;Sergeant, Geurts, Huijbregts, Scheres, & Oosterlaan, 2003) and in tasks where speed isrequested, such as reaction time tasks (Carte, Nigg, & Hinshaw, 1996; Rhodes, Coghill, &Matthews, 2005), as they seem to be less able to adjust their own motor response to therequested speed level (Rubia, Sergeant et al., 1999; Rubia, Smith, Noorlos et al., 2003).However, in task situations where they can self-pace their own speed of performance, theywill typically trade speed for accuracy (Dykman et al., 1979) and it is this particularspeed-accuracy trade-off that causes the relatively “fast” and premature response style,rather than a speed-superiority in absolute terms.
One of the main hypotheses of this study was therefore that children with ADHDwould show a task-unspecific premature and inconsistent response style across all 6 cog-nitive tasks, in line with our hypothesis that a task-independent and generic premature andinconsistent response style is a main feature of impulsiveness (Rubia, 2002). We further-more hypothesized task-specific deficits in children with ADHD within each of theselected tasks: we expected an increased number of commission errors in the Go/No-Gotask, a slower speed of the inhibitory process in the Stop task, a larger switch effect (asmeasured by a larger difference between switch and repeat reaction times), a largerinterference effect in the motor Stroop task (as measured by a larger difference betweenincongruent and congruent reaction times), higher rates of omission and commissionerrors in the rewarded CPT task, and higher error rates in the Time Estimation task. Wehypothesized that the effect of reward in the CPT task would be more pronounced in chil-dren with ADHD than in controls, normalizing impaired task performance.We alsohypothesized that the dependent measures of these 6 tasks and the inconsistent and prema-ture response style across all 6 tasks would correlate with the behavioral hyperactivityscores. Finally, we hypothesized that the different measures on the selected tasks wouldcorrelate with each other, because we consider them to be interrelated functions some ofwhich overlap and share underlying basic functions. In particular, we expected that motorand cognitive inhibition measures, commission errors on the CPT, and prematureresponses would correlate with each other, reflecting functions of inhibitory control. Fortime estimation errors, we hypothesized that they would be a more isolated perceptual def-icit and would correlate only with premature responding (because we consider prematureerrors a reflection of problems with both temporal and inhibitory processes). Discriminantanalysis should explore which of the dependent variables would be the most sensitive todistinguish between the groups.
An additional advantage of the MARS task battery is that we have established thebiological substrates of task performance on these tests in healthy adults and adolescentsfrom an adaptation of the MARS task battery for functional magnetic resonance imaging

280 K. RUBIA ET AL.
(fMRI) (Rubia, Overmeyer et al., 2001; Rubia, Smith, Brammer, & Taylor, 2003; Rubiaet al., in press; Rubia, Smith, Brammer, Toone, & Taylor, 2005; Smith, Lidzba, Taylor, &Rubia, 2003; Smith et al., 2004). All tasks have shown to elicit activation in prefrontalcortical areas, with some overlap, but also distinct and task-specific fronto-striatal andfronto-parieto-temporal brain activation patterns. Deficits in performance on these tasks inchildren with ADHD would, therefore, also be informative with respect to potentiallycompromised function of mediating underlying neural brain substrates.
METHOD
Participants
Sixty-six boys and girls participated in the study. Patients were 32 children andadolescents in the age range from 7 to 15 years (M = 11.1, SD = 2.6), two of themfemales, with the diagnosis made by an experienced psychiatrist of hyperkinetic disorder(using the ICD-10) and of ADHD-combined type (using the DSM-IV criteria of theAmerican Psychiatric Association (APA, 1994). Exclusion criteria were the presence ofspecific learning or reading disabilities, or another psychiatric disorder, neurologicalabnormalities, epilepsy, drug or substance abuse. The only exception was conduct disor-der, which can be seen as a complication of the disorder (Taylor, Chadwick, Heptinstall, &Danckaerts, 1996) and was present in 7 children with ADHD. None of the patients metcriteria for Oppositional Defiant Disorder. Patients scored above threshold on the parentratings of the hyperactivity scale of the Strengths and Difficulties Questionnaire (SDQ;Goodman, 1997). The Strengths and Difficulties Questionnaire is a brief validated behav-ioral screening questionnaire that can be completed by the parents or teachers of childrenaged 4 to 16 (Goodman 1997; Goodman, Ford, Simmons, Gatward, & Meltzer, 2000b;Goodman, Renfrew, & Mullik, 2000a). The SDQ consists of 25 items, either positive ornegative, divided into 5 scales of emotional symptoms, conduct problems, hyperactivity-inattention problems, peer-relationship problems, and prosocial behavior. For each of the5 scales the scores can range from 0 to 10, with 10 being the most impaired score. Scoresfrom the SDQ have been shown to be highly correlated with scores from the ChildBehavior Checklist (CBCL) and are equally able to discriminate clinical cases fromhealthy controls. As judged against a semistructured interview, the SDQ has been shownto be significantly better than the CBCL at detecting inattention and hyperactivity, and atleast as good at detecting internalizing and externalizing problems (Goodman & Scott,1999). The SDQ identifies 81–91% of the children with a clinical diagnosis and is partic-ularly sensitive with respect to conduct and hyperactivity symptoms (Goodman, Fordet al., 2000; Goodman, Renfrew, et al., 2000a).
Patients also scored above the 5th percentile rank (equivalent to IQ of 75) on theRaven’s Standard Progressive Matrices Intelligence Questionnaire (IQ) (Raven, 1960).Patients had no history of neurotropic medication except stimulant medication of half life< 12 hours, no drug or substance abuse and were medication free for 24 hours prior to testing.
Control participants were 34 healthy children and adolescents in the same age rangeand age-matched (M = 11, SD = 2.5), four of them girls, with no history of prior diagnosisof ADHD or any other mental or neurological disorder. They scored below threshold onthe SDQ in total score and component scales in hyperactivity, conduct problems, andemotional problems. They scored above the 5th percentile rank on the Raven’s IQ and hadno history of neurotropic medication or drug and substance abuse.

ADHD AND A TEST BATTERY OF IMPULSIVENESS 281
The children received a reward of £5.- for their performance on the reward task atthe end of testing. All children received the same reward of £5.-, although they were toldthat the full amount was only to be obtained for a 100% success rates on the reward task.
The study was approved by the Ethical Committee of the Institute of Psychiatry.
Mars Task Battery
Go/no-go task. The Go/No-Go task is a selective motor response inhibition taskwhere a motor response has to be either executed or not. In order to make the task more chal-lenging, we divided the test in two subtests of 2 min and 32 s each, blocked for a right- and aleft-handed response, respectively, that would increase the prepotent response tendency.
(a) Left-handed response: Green space ships of 300ms duration each pointing left appearin the middle of the screen and participants have to make a left-handed buttonresponse. After the display of the airplane, there is a 1.3s blank screen. In 26.3% of tri-als, green enemy planets (of 300ms duration each) appear in the middle of the screeninstead of the space ships and participants have to inhibit their motor response. 95 tri-als in total, 70 Go trials and 25 No-Go trials.
(b) Right-handed response: The task is identical in number of trials, except that all greenspace ships point to the right side and a right-handed response is required. In 26.3% oftrials, green enemy planets appear on the screen and participants have to inhibit theirmotor response.
The dependent variable of the task is the number of commission errors to the No-Gostimuli. Total task duration was 5 minutes and 4 seconds.
Stop task. The more challenging Stop task requires the withholding of an alreadytriggered go response by a stop signal that appears unexpectedly and shortly after the go sig-nal, converting the go signal after its presentation into a stop signal. This task version is avisual and faster modification (Rubia, Smith, Brammer et al., 2003) of the tracking stop signaltask (Logan, Schachar, & Tannock, 1997), which by comparison to the version of Logan et al.(1997) contains an algorithm that makes sure that every participant at every moment of thetask has 50% of successful and failed inhibition trials (Rubia, Smith, Brammer et al., 2003).
Green airplanes (go signals) of 1s duration each, pointing left or right, appear in themiddle of the screen, and participants have to make congruent button responses on agamepad, i.e., press the left or right button. After the airplane there is a blank screen of700ms, resulting in a total trial time of 1.7s. On 27% of trials, the duration of the airplanesis interrupted by a red explosion (stop signal) about 250ms later (of 300ms duration), andparticipants have to inhibit the motor response that was triggered by the airplane. Thedelay between go signal and stop signal changes according to the participant’s perfor-mance in steps of 50ms. If the participant’s success rate is 50%, the stop signal delayremains 250ms. If the participant is successful in the previous trials, the success rate willgo higher than 50% and the delay between airplane and explosion becomes longer in stepsof 50ms, making it harder for the participant to inhibit. If the participant then fails toinhibit for several trials, the success rate will fall below 50% and the delay will becomeshorter in steps of 50ms, making it easier for the participant to inhibit. This algorithmtherefore makes sure that by changing the stop signal delay, every participant will haveexactly 50% of successful and 50% of unsuccessful stop trials at the end of the task, with a

282 K. RUBIA ET AL.
mean probability of inhibition of 50%. There were 178 trials in total, with 48 stop trials,24 after a left-handed go response and 24 after a right-handed go response. Task durationis 5 minutes. Forty-eight stop trials exceed the suggested number of 40 stop trials toestimate SSRT reliably (Band, van der Molen, & Logan, 2003).
The main dependent variable in this task is the stop signal reaction time, calculatedby subtracting the mean stop signal delay (i.e. the average time between airplane andexplosion, at which the participant managed to inhibit to 50% of trials) from the meanreaction time to go trials (Logan et al., 1997).
Motor Stroop task. The motor version of the Stroop task, also called the direc-tional Stroop task, investigates the ability to inhibit interfering information in a simplestimulus response incompatibility setting. Participants have to respond to the iconic infor-mation provided by the stimulus (i.e. to execute a left hand response if the stimulus pointsto the left side). Incompatible stimuli provide spatial information that is incompatible withtheir iconic information (i.e. they appear on the screen side that is opposite to the directionin which they point). The tendency to respond to the same side as the stimulus appearancehas been documented as “spatial incompatibility” or the “Simon effect” (Simon andBerbaum, 1988, 1990). Yellow airplanes pointing left or right appear on the left or right sideof the screen with a duration of 300ms, followed by a blank screen of 1700ms, resulting inan ITI of 2s. On 72.7% of trials the airplanes are congruent, i.e. the direction of where theypoint and the side of the screen is congruent. Participants are instructed to make a left orright button response on the gamepad, according to where the airplanes are pointing. In27.3% of trials the airplanes pointing right appear on the left side of the screen or the air-planes pointing left appear on the right side of the screen, presenting the difficult incon-gruent “Stroop” conditions. There are 154 trials in total, 112 congruent trials to either sideand 42 incongruent trials to either side. Task duration was 5 minutes and 8 seconds.
The dependent variable of this task is the Stroop effect (mean reaction time tocongruent trials subtracted from mean reaction time to incongruent trials) and the numberof errors to Stroop and non-Stroop trials.
Switch task. We designed a modified version of a visual-spatial Switch task(Meiran, 1996) to investigate attention shifting between two different spatial dimensions(Smith et al., 2004). Previously valid visual-spatial stimulus-response associations need tobe inhibited in order to shift attention to currently valid stimulus-response associationsand to change between both sets. This task thus requires pure attentional switchingbetween two spatial dimensions and avoids the working memory confounds of otherSwitch tasks such as the Wisconsin Card Sorting Task (Smith et al., 2004). Participantswere presented with a grid divided into four squares in the center of which was a double-headed arrow positioned either horizontally or vertically. The grid with the double-headedarrow was presented for 1600ms. Then, 200ms after presentation of the grid and arrows, ared dot appeared on the screen for 1400ms in any one of the four squares of the grid. Ahorizontally pointing double-headed arrow indicated that the participant had to indicatewhether the circle was in either of the two left or the two right squares of the grid, bypressing the left or right button. After the 1600ms of presentation time, there was a blankscreen for 800ms, in which participants made their button response. This presentation wasrepeated for several repeat trials with a total trial time of 2.4s. These repeat trials werefollowed by a switch trial, in which the arrow changed to a vertical position, and theparticipant had to indicate whether the circle was in either of the two upper or two lower

ADHD AND A TEST BATTERY OF IMPULSIVENESS 283
squares of the grid by pressing the top or bottom button. This instruction was maintainedfor several repeat trials, followed by another switch trial in which the arrow changed backto a horizontal position, and so on. For their button responses, participants used a 4-buttongamepad. This pattern continued for 128 trials with high frequency repeat trials (91 trials:72.1%) interspersed with low frequency switch trials (37 trials: 27.9%). There were aminimum number of 2 repeat trials before every switch trial. Task duration was 5 minutesand 7.2 seconds.
The dependent variable of this task is the Switch effect (mean reaction time to repeattrials subtracted from mean reaction time to switch trials).
Rewarded-CPT task. A rewarded CPT-AX task was used to measure the effectof reward on sustained attention. A string of letters was presented to the participants fromthe alphabet from A to L with a trial time of 1s. The duration of the letters was 300ms, fol-lowed by a blank screen. Participants had to ignore all letters except for the target letters.Target letters were either an “A” followed by an “X” or an “A” followed by an “O”. Halfof the targets among a string of letters (i.e. “A-X”) were rewarded and half were notrewarded (“A-O”) to investigate the effect of reward on reaction times. The reward wascounterbalanced across participants, so that half of the participants were rewarded for “A-X”and the other half for “A-O.” There were 480 trials in total, with 30 rewarded and 30nonrewarded targets, i.e. 12% of response trials, 6% of them rewarded and 6% of themunrewarded. Total task duration was 8 min. Participants were told they would win 50pence for every three rewarded trials, which would amount to £5.- if they had a 100%success rate. To reinforce the effect of reward the amount that was won during the taskwas displayed visually throughout the task by a reward bar (and a nonreward bar) on theright hand side of the screen. For every three successful hits, a reward bar with 10 unitswas being filled, every unit representing the 50 pence won in the task. There was also abar for the nonrewarded hits. The rewarded bar was red for those children rewarded forA-X and blue for those rewarded for A-O, and the opposite was the case for the othergroup of children (i.e. reward bar blue (A-O), nonreward bar red (A-X).
The dependent variables of this task are the number of omission errors to targettrials and the number of commission errors, i.e. false hits, to nontarget items.
Time discrimination task. This task is a modification of the Time Discrimi-nation Task used by Smith et al. (2002, 2003). Time intervals differing by several hun-dreds of milliseconds need to be discriminated. Participants were presented with a red andgreen circle, 5 cm in diameter, appearing consecutively with no interspersed pause and inrandom order. The red circle was consistently presented on the left side and the greencircle consistently on the right side of the center of the computer screen, with a gap of 1cm separating their positions. One of these circles was randomly presented for a standardduration of 1000 milliseconds, and the comparison circle for either 1300, 1400, or 1500milliseconds. After presentation of a standard interval and a comparison interval, therewas a blank screen for 2.1s in which participants made their response. The participantshad to decide which of the two circles stayed on the screen for the longest time. They weretold to respond using a left-sided button if they thought the red circle, displayed on the leftside of the screen, lasted longest, or a right-sided button if they believed the green circle,displayed to the right side, lasted the longest. Children were instructed to decide whichcircle lasted longer by counting, in order to provide a consistent and homogenous strategy.The standard interval was 1s; the comparison intervals were either 1.3, 1.4, or 1.5 s long

284 K. RUBIA ET AL.
and the response time 2.1s; So, the total trial times were either 4.4, 4.5, or 4.6s. Sixty pairsof stimuli were presented for a total task duration of 4.5min.
The dependent variable for this task is the number of time discrimination (TD) errors.In all tasks we also analyzed mean reaction times, intrasubject standard deviations
of mean reaction times, and premature responses. Premature responses were defined asresponses made 200ms before and 100ms after stimulus onset. Responses that fall into thistime window have been made before the type of stimulus that appeared on the screencould be seen (200ms before stimulus appearance) or registered (100ms after stimulusonset is too short to be considered an average normal reaction time). It is important toanalyze premature responses separately, as they could confound inhibitory and executivemeasures. In inhibition tasks, for example, a premature response before the stimulusappears on the screen would prevent the participant from either successfully executing aresponse to a go signal or inhibiting to a no-go signal.
Testing Procedure
For all tasks, participants used a 4-button gamepad. The whole testing procedurelasted about 1 hour. The task order was fixed in the following order: Go/No-Go, Stop,Stroop, Switch, Rewarded CPT, and Time Discrimination tasks. All task variables werescored in a positive direction, so that a greater impairment on the task is shown in greatervalues on the different dependent task variables.
Sample Size Estimation & Calculation of Statistical Power
The effect size estimate (Cohen’s d; Cohen, 1988) was based on previous studiesthat have used similar tasks, i.e. the Gonogo and Stop tasks (Rubia, Taylor et al., 2001;Cohen’s d = 1) and the Time Discrimination task (Smith et al., 2002; Cohen’s d = .82) andon average effect sizes from a meta-analysis of executive function in children with ADHD(Pennington & Ozonoff, 1996; Cohen’s d = .7). An effect size of .8 and p value of < .05was selected for the power analysis to identify the number of participants necessary to findsignificant differences in key outcome variables of the neuropsychological MARS tasks.The minimum aggregate sample size estimated was 25 for the ADHD group and 23 for theControl group.
Data Analysis
Two outliers showing extreme scores (deviating more than 3 times the standarddeviation of the group mean) on one or more of the task variables were excluded from theanalysis (the data of one female control child were excluded from the Time Discrimina-tion task and the data of one male child with ADHD were excluded from the Reward andStroop tasks). Some of the children did not complete all tasks due to time constraints withan average of 3 missing values per task (5%), which was not significantly related to age,IQ, or group status. The missing data were missing completely at random (MCAR) andthe analysis was therefore conducted on the available data only. Wherever the data did notfulfill the assumptions necessary for analyses using parametric statistics, appropriatetransformations were applied. Several of the variables were thus transformed in order tonormalize their distribution: composite premature responses were normalized by transforming

ADHD AND A TEST BATTERY OF IMPULSIVENESS 285
to the power of .601 as suggested using a spread by level plot. Coefficients of variancewere transformed by reciprocal transformation. Go/No-Go commission errors, Stop signalreaction times, Stroop effect, and Stroop errors were subject to square root transformation.CPT commission and omission errors were transformed by ranking. Independent t-testswere used to measure for group differences in age, handedness, IQ, and SDQ hyperactiv-ity scores. To test for between-group differences in performance on the task battery, inde-pendent t-tests were conducted on the following dependent variables: mean reaction times,variability of mean reaction times and premature responding combined across all 6 tasks,SSRT for the Stop task, Commission errors in the GNG task, Stroop effect and Strooperrors, Switch cost, omission and commission errors on the CPT task, and Time discrimi-nation errors. To test for an effect of reward on the CPT task performance, repeated mea-sures ANOVA was used with group as the between-subject factor and reward as thewithin subject factor.
Pearson correlation analyses were used to investigate the correlations between thecognitive dependent variables and the scores on the hyperactivity scale of the SDQ and ageand to investigate correlations between different task variables. Effect sizes were calculated
for all dependent measure comparisons using
(Cohen, 1988). Discriminant analysis was used to explore sensitivity and specificity of themain task variables. Positive and negative predictive values were calculated based on theprevalence rate of .04 of children with ADHD in the United Kingdom (Taylor, Sandberg,Thorley, & Giles, 1991). For correlation analysis between tasks variables and discriminantanalysis, only the main variables that were specific for each task were used (i.e. overallerror rates on the Stroop task were not included in the analysis as they were not specificto the Stroop trials). In order to control for multiple testing, the p-value was adjustedaccording to the False Discovery Rates, which has been shown to be a more powerfuladjustment for multiple testing than the Bonferroni correction when more than 4 pairwisecomparisons are being conducted (Benjamini & Hochberg, 1995; Nakagawa, 2004; Millis,2003; Keselman, Cribbie, & Hollan, 2002; Perneger, 1998).
RESULTS
IQ and Behavioral Ratings
Independent t-tests showed no significant group differences in gender, handedness,IQ, or age. Mean IQ scores on Raven’s SPM (SD) were: Controls: 39(7) (equivalent tononverbal IQ of 103 (13)); Patients with ADHD 35(11) (equivalent to nonverbal IQ of 99(16)); df = 64, t = 1.6; p = ns. Mean age of Controls (SD): 11(2); Mean age of patientswith ADHD (SD): 11 (2); df = 64, t = .98, p = ns. As expected, patients and controlsdiffered significantly on the SDQ hyperactivity ratings: Mean SDQ rating (SD) Controls:2.31(1.6); Patients with ADHD: 8.1(2); df = 64, t = −13, p < .00.
Performance on MARS Task Battery
Premature responding and intra-subject variability across all tasks.
We had hypothesized that intrasubject variability and premature responding were task-unspecific characteristics of an impulsive response style during tests of cognitive control,so these variables were combined for all 6 tasks. To make the data comparable across
Cohen s d M M’ / / = ⎡⎣
⎤⎦1 2 1
22
2 2− +√ ( )s s

286 K. RUBIA ET AL.
tasks, premature responding was expressed as a percentage of the correct responses foreach task, and variability of response was expressed as coefficient of variation (a measureof relative variability, equal to the ratio of standard deviation to mean, expressed as thepercentage: CV = (SD/mean reaction time)*100. A composite score across all 6 tasks wasalso used for MRT. The group measures of MRT, intrasubject variability of response andpremature responses for each of the tasks are shown in the Appendix Table. In the individ-ual tasks, the effects sizes for differences in MRT were small, while the effect sizes fordifferences in premature responses reached from d = .4 to d = .8 and those for differencesin variable responses ranged between d = .3 to d = .8.
Independent t-tests for the combined measures across all tasks showed no group dif-ferences in MRT, but increased intrasubject variability of response and increased prema-ture responses for the ADHD compared to the control group (Table 1). The effect sizeswere large for intrasubject response variability and medium for premature responses. Bothvariables correlated significantly with the hyperactivity scores of the SDQ (Table 1).
Go/No-Go Task (GNG)
Children with ADHD made significantly more commission errors to no-go signalswith a large effect size (Table 1).
Stop Task
Hyperactive children showed significant impairments in the speed of the inhibitoryprocess, reflected in SSRT (MRT-SSD). The effect size for the SSRT differences waslarge (Table 1).
As expected, no group differences were observed in the probability of inhibition,suggesting that the tracking algorithm was successful (Probability of inhibition (SD):Controls = 50(3)%; ADHD: 49(4)%; df = 60, t = 1.3, p < ns).
Motor Stroop Task
Children with ADHD made more errors to both congruent and noncongruent trialswith a medium effect size. There was, however, no significant group difference for theStroop effect (Table 1).
Switch Task
Children with ADHD showed a trend for a larger Switch cost than controls with asmall effect size (Table 1).
Rewarded CPT
Repeated measures analysis of variance showed that there was no group by rewardinteraction on any of the dependent measures, suggesting that reward had no differentialeffect on the performance of the two groups on the CPT task. There was, however, a sig-nificant effect of reward alone on MRT (F = 11, df = 1, p < .00) and SD of MRT (F = 7,df = 1, p < .01). Thus, over all participants, reward reduced both MRT (MRT reward (SD):379(69), MRT nonreward: 413(97)) and intrasubject variability of response (intrasubject

287
Tab
le 1
MA
NO
VA
s fo
r th
e M
ain
Tas
k va
riab
les
of th
e Si
x T
asks
of
the
MA
RS
Tas
k B
atte
ry b
y G
roup
.
TA
SK
ME
AS
UR
EC
ontr
ols
Mea
n (S
D)
AD
HD
Mea
n (S
D)
dft
Cor
rect
ed p
-val
ueE
ffec
t siz
e d
Cor
rela
tions
with
SD
Q h
yper
activ
ity r
; p c
orre
cted
Cor
rela
tions
wit
h ag
e r;
p c
orre
cted
All
task
sM
RT
(m
s)53
9(79
)54
6(69
)64
−.4
ns.0
9ns
−.5;
.00
All
task
sC
V30
(8)
38(9
)64
4.0
0.9
4.5
; .00
−.3;
ns
All
task
sPR
EM
(%
)1(
2)3(
3)64
−4.0
0.7
8.4
; .00
−.4;
.02
Go/
no-g
oC
OM
(%
)19
(15)
28(1
4)61
−3.0
2.6
2.3
; .02
−.4;
.00
Sto
pS
SR
T (
ms)
214(
75)
279(
105)
60−3
.02
.71
.3; .
06ns
Mot
or S
troo
pS
troo
p ef
fect
(m
s)75
(29)
77(5
6)60
.5ns
.09
nsns
Str
oop
erro
rs (
%)
14(1
0)20
(11)
60−2
.03
.56
.3; .
03−.
6; .0
0S
wit
chSw
itch
cos
t (m
s)34
(47)
61(6
8)60
−2.0
8.4
6ns
nsC
PT
OM
(%
)7(
8)13
(11)
60−3
.02
.62
.4; .
00−.
3; .0
9C
OM
(%
)3(
6)7(
10)
60−3
.01
.48
.3; .
01ns
TD
Err
ors
26(1
4)40
(18)
51−3
.01
.87
.4; .
01ns
Not
e. M
RT
= c
ompo
site
mea
n re
actio
n tim
e (m
s) a
vera
ged
acro
ss t
asks
; C
V =
com
posi
te m
ean
coef
fici
elnt
of
vari
ance
ave
rage
d ac
ross
tas
ks.
PRE
M =
pre
mat
ure
resp
onse
sac
ross
all
task
s in
per
cent
age.
GN
G C
OM
= c
omis
sion
err
ors
in p
erce
ntag
e; S
SRT
= s
top
sign
al r
eact
ion
time
(ms)
, cal
cula
ted
as M
RT
to g
o tr
ials
-sto
p si
gnal
del
ay;
CPT
(C
)OM
= (
c)om
issi
on e
rror
s. C
orre
latio
ns r
efer
to P
ears
on c
orre
latio
ns r
; SD
Q h
yper
acti
vity
: sco
res
for
atte
ntio
n de
fici
t/hy
pera
ctiv
ity
on th
e S
tren
gth
and
Dif
ficu
lty
Que
stio
nnai
re. A
ll s
tati
stic
san
d p
valu
es s
how
n he
re a
re b
ased
on
tran
sfor
med
dat
a w
here
app
licab
le. p
cor
rect
ed =
p-v
alue
cor
rect
ed f
or m
ulti
ple
test
ing
acco
rdin
g to
the
met
hod
of F
alse
Dis
cove
ry R
ate
ofB
enja
min
i & H
ochb
erg
(199
5).

288 K. RUBIA ET AL.
SD of MRT reward (SD): 95(30), intrasubject SD of MRT to nonreward: 106(32)) but hadno effect on the number of omission errors.
Considering that the ITI for this task was relatively short, we investigated the possi-bility that long reaction times (RT) to target stimuli could have been confounded withpremature responses to the next trial. The inspection of the reaction time distribution,however, makes this possibility unlikely, as the mean reaction time for the CPT was400ms, and the most extreme value (i.e. the slowest RT) was 620ms. If longer RTmeasures had been observed up to the upper limit of measurement of 800ms, there couldindeed have been a confound between late reaction times and premature responses. Theunlikelihood of this confound was further confirmed by an extremely weak correlationbetween MRT and premature responses (r = .09, N = 62, p < .5).
For the between-group comparisons, the measures were collapsed for the rewardedand nonrewarded conditions. Children with ADHD showed significantly more omissionerrors to targets with a medium effect size and more commission errors to nontargets witha small effect size (Table 1).
Time Discrimination Task
Hyperactive children made more errors in the time discrimination task with a largeeffect size (Table 1).
Clinical Correlations
There were significant positive Pearson correlations between all those dependentvariables that differed between the groups and the SDQ hyperactivity scores (r > .3). Thecorrelation between SSRT and SDQ was, however, only significant at a trend level aftercorrecting for multiple testing (Table 1).
Correlations Between Tasks
Table 2 shows the Pearson correlations between all task variables. Intrasubject vari-ability of response correlated with premature responding, commission errors on the GNGtask, ommission errors on the CPT and TD errors, and at an uncorrected p value withSSRT. Premature responding was correlated with the inhibitory measures of SSRT andGNG commission errors, but also with Time Discrimination errors. SSRT correlated withMRT, with commission errors on the GNG task, and with premature responding. At anuncorrected p value, the inhibitory measures of SSRT and GNG commission errors corre-lated with time discrimination errors. Omission and commission errors on the CPT task andcommission errors on the GNG task correlated with each other. At an uncorrected p value,CPT omission errors also correlated with time discrimination errors. The Switch effect didnot correlate with any other measure and the Stroop effect only correlated with MRT.
Correlations With Age
There was a significant correlation between age and some of the performancemeasures, including mean reaction times, premature responding, Go/No-Go commissionerrors and Stroop errors. There was a trend for a correlation between age and omissionerrors on the CPT (see Table 2).

ADHD AND A TEST BATTERY OF IMPULSIVENESS 289
Group differences in the correlations between age and performance, suggestive of amaturational delay, were observed only at an uncorrected p value for the time discriminationerrors (r Controls = −.6, r ADHD = −.07, p = .02), variability of response (r Controls = −.5,r ADHD = .01, p < .02), and MRT (r Controls = −.7, rADHD = −.3, p = .04).
Discriminant Validity
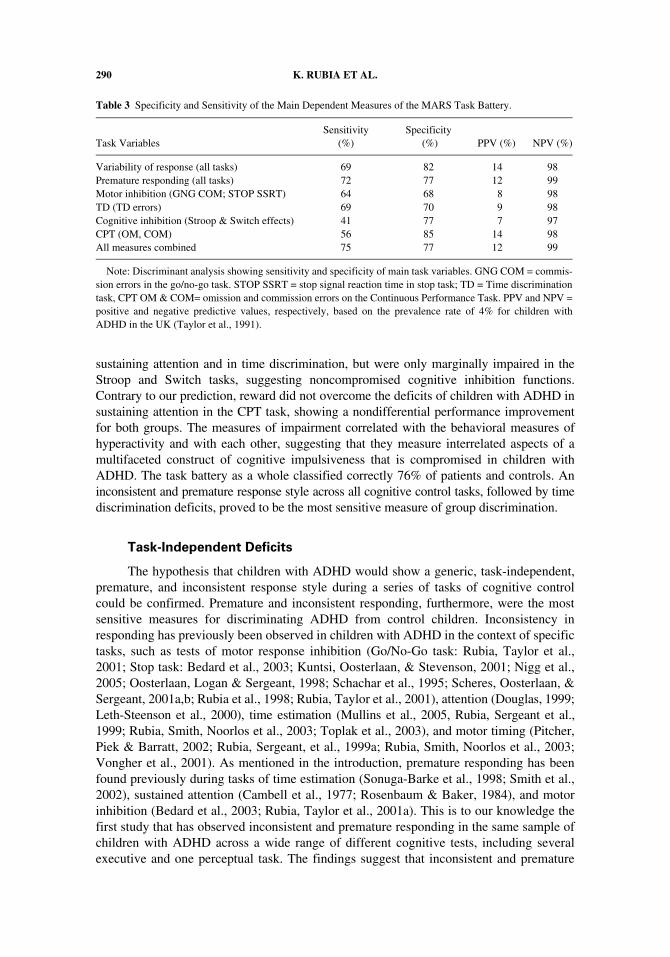
Discriminant analysis on the combination of all task measures showed a relativelygood sensitivity for the whole task battery of 75% for correct classification of patients andof 77% for correct classification of controls (Table 3). From the task-specific measures,premature responding showed the highest sensitivity of 72% and specificity of 77%, fol-lowed by response variability and time discrimination errors both with 69% sensitivity(82% and 70% specificity, respectively). Motor response inhibition (measured as commis-sion errors on the GNG task and SSRT on the Stop task) showed only moderate sensitivityof 64% and specificity of 68% (see Table 3).
DISCUSSION
Children with ADHD showed some context-independent deficits—increased intra-subject variability and premature responding—across all tasks of the MARS task battery.They also showed task-specific impairments in the two motor response inhibition tasks, in
Table 2 Correlations Between the Main Variables of the Six Tasks of the MARS Task Battery.
Correlation r/p-value CV PREM
GNG COM SSRT
Stroop effect Switch cost CPT OM CPT COM TD Errors
MRT −.2 .4** .3 .3* .3* .1 .1 .1 .2ns .00 .02 .01 .01 ns ns ns ns
CV .7** .5** .3 −.2 .1 .3* .1 .6**.00 .00 .04 ns ns .01 ns .00
PREM .5** .5** −.1 .1 .3 .2 .4**.00 .00 ns ns .03 ns .00
GNG COM .4* .0 .1 .4* .3* .3.00 ns ns .00 .02 .03
SSRT .1 .3 .2 .2 .3ns .04 ns ns .03
Stroop effect −.1 −.1 .0 −.0ns ns ns ns
Switch cost .1 .2 .2ns ns ns
CPT OM .2 .3.05 .03
CPT COM .1ns
Note. Pearson correlation coefficients (r) across the six tasks of the MARS task battery and corresponding(uncorrected) p-values. MRT = MRT across all six tasks. CV = Coefficient of variance across all six tasks.PREM = Premature responses across all six tasks. GNG COM = Commission errors to no-go signals. STOPSSRT = stop signal reaction time (ms); STR effect = Stroop effect: (MRT to stroop trials – MRT congruenttrials). Switch effect: (MRT to switch trials - MRT to repeat trials). CPT OM: Number of omissions of targettrials. CPT COM: Number of commission errors. TD Errors: Number of incorrect time discriminations. Nranged from 50 to 66. *Correlation is significant after correction for multiple testing using FDR (*p corrected <.05; **p corrected < .01).
290 K. RUBIA ET AL.
sustaining attention and in time discrimination, but were only marginally impaired in theStroop and Switch tasks, suggesting noncompromised cognitive inhibition functions.Contrary to our prediction, reward did not overcome the deficits of children with ADHD insustaining attention in the CPT task, showing a nondifferential performance improvementfor both groups. The measures of impairment correlated with the behavioral measures ofhyperactivity and with each other, suggesting that they measure interrelated aspects of amultifaceted construct of cognitive impulsiveness that is compromised in children withADHD. The task battery as a whole classified correctly 76% of patients and controls. Aninconsistent and premature response style across all cognitive control tasks, followed by timediscrimination deficits, proved to be the most sensitive measure of group discrimination.
Task-Independent Deficits
The hypothesis that children with ADHD would show a generic, task-independent,premature, and inconsistent response style during a series of tasks of cognitive controlcould be confirmed. Premature and inconsistent responding, furthermore, were the mostsensitive measures for discriminating ADHD from control children. Inconsistency inresponding has previously been observed in children with ADHD in the context of specifictasks, such as tests of motor response inhibition (Go/No-Go task: Rubia, Taylor et al.,2001; Stop task: Bedard et al., 2003; Kuntsi, Oosterlaan, & Stevenson, 2001; Nigg et al.,2005; Oosterlaan, Logan & Sergeant, 1998; Schachar et al., 1995; Scheres, Oosterlaan, &Sergeant, 2001a,b; Rubia et al., 1998; Rubia, Taylor et al., 2001), attention (Douglas, 1999;Leth-Steenson et al., 2000), time estimation (Mullins et al., 2005, Rubia, Sergeant et al.,1999; Rubia, Smith, Noorlos et al., 2003; Toplak et al., 2003), and motor timing (Pitcher,Piek & Barratt, 2002; Rubia, Sergeant, et al., 1999a; Rubia, Smith, Noorlos et al., 2003;Vongher et al., 2001). As mentioned in the introduction, premature responding has beenfound previously during tasks of time estimation (Sonuga-Barke et al., 1998; Smith et al.,2002), sustained attention (Cambell et al., 1977; Rosenbaum & Baker, 1984), and motorinhibition (Bedard et al., 2003; Rubia, Taylor et al., 2001a). This is to our knowledge thefirst study that has observed inconsistent and premature responding in the same sample ofchildren with ADHD across a wide range of different cognitive tests, including severalexecutive and one perceptual task. The findings suggest that inconsistent and premature
Table 3 Specificity and Sensitivity of the Main Dependent Measures of the MARS Task Battery.
Task VariablesSensitivity
(%)Specificity
(%) PPV (%) NPV (%)
Variability of response (all tasks) 69 82 14 98Premature responding (all tasks) 72 77 12 99Motor inhibition (GNG COM; STOP SSRT) 64 68 8 98TD (TD errors) 69 70 9 98Cognitive inhibition (Stroop & Switch effects) 41 77 7 97CPT (OM, COM) 56 85 14 98All measures combined 75 77 12 99
Note: Discriminant analysis showing sensitivity and specificity of main task variables. GNG COM = commis-sion errors in the go/no-go task. STOP SSRT = stop signal reaction time in stop task; TD = Time discriminationtask, CPT OM & COM= omission and commission errors on the Continuous Performance Task. PPV and NPV =positive and negative predictive values, respectively, based on the prevalence rate of 4% for children withADHD in the UK (Taylor et al., 1991).

ADHD AND A TEST BATTERY OF IMPULSIVENESS 291
responding is typical of patients with ADHD beyond specific task-settings and should beseen as context-independent. This confirms our hypothesis that impulsiveness is character-ized by a task-independent, premature, and inconsistent response style (Rubia, 2002).
Variability of responding discriminated children with ADHD from controls betterthan other, more typical measures of impairment such as inhibitory control. This supportsrecent suggestions that response variability might represent an ubiquitous and etiologicallyimportant characteristic of ADHD (Castellanos & Tannock, 2002; Castellanos et al., 2005).An inconsistent response style has been suggested to reflect problems with sustainingattention and concentration (Leth-Steenson et al., 2000), with motor timing (Rubia,Sergeant et al., 1999; Rubia, Taylor et al., 2001; Rubia, Smith, Noorlos et al., 2003) andwith response regulation (Sergeant, Oosterlaan & van der Meere, 1999). Motor responsevariability has been found to correlate with the accuracy of perceptual timing (Keele,Polorny, Corcos, & Ivry, 1985; Pastor, Artieda, Jahanshahi, & Obeso, 1992; Smith, 1957)and has been shown to be strongly elicited in children with ADHD during motor timingtasks (Rubia, Sergeant, et al., 1999; Rubia, Smith, Noorlos et al., 2003). An associationwith sustained attention, however, has also been suggested both in a meta-analysis of CPTstudies in children with ADHD (Leth-Steenson et al., 2000) and on the basis of evokedpotential studies (Segalowitz, Dywan, & Unsal, 1997); the hypothesis of a link betweenvariability of response and sustained attention could be confirmed by recent findings of acorrelation between variability of time reproduction of longer seconds intervals and mea-sures of sustained attention in children with ADHD (Mullins et al., 2005); other theorieshave suggested that problems with effort and response regulation are the underlying causefor increased response variability (Sergeant et al., 1999, 2003). In this study, response vari-ability appeared to be related to all three: timing, response regulation, and sustained attentionfunctions. It correlated with time estimation errors and premature responding (suggestive ofa relationship with poor perceptive and motor timing functions), with commission errors inthe GNG task (suggestive of an association with poor response control), and with omissionerrors in the CPT (suggestive of a relationship with suboptimal attention functions).
Premature responding gave the most sensitive discrimination between children withADHD and controls. A premature response style has more typically been related to thetiming aspects of impulsiveness such as a relatively fast cognitive tempo and a speed-accu-racy trade-off, favoring speed (Dykman et al., 1979; Rubia, Smith, Noorlos et al., 2001). Acontext-independent, pervasive premature response style is consistent with the behavioraldefinition of impulsiveness as a premature, rapid, and unplanned response style, in whichacts are executed before all consequences have been fully considered (Moeller, Barratt,Dougherty, Schmitz, & Swann, 2001; Rubia, 2002). Premature responding was in facthighly correlated with time estimation errors, supporting the view that it reflects deficitswith timing processes. Interestingly, premature responding also correlated strongly withthe two motor inhibitory measures of the Stop and the GNG tasks, suggesting that it mightbe related to both an abnormal timing process and poor inhibitory response regulation.Prepotent responses could thus be due to an interaction between poor inhibitory controland abnormal timing functions. This would be in line with a definition of impulsiveness asa poorly timed and poorly controlled response style (Rubia, 2002; White et al., 1994).
Task-Specific Deficits
Our study confirms deficits in motor response inhibition, which is one of the mostconsistent findings in the neuropsychology of children with ADHD (Banaschewski et al.,

292 K. RUBIA ET AL.
2005; Nigg, 2001; Willcutt et al., 2005). The finding of poor inhibitory performance in theGo/No-Go task replicates previous studies (Ge et al., 2000; Hartung, Milich, Lynam, &Martin, 2002; Iaboni, Douglas, & Baker, 1995; Rubia, Taylor, Smith et al., 2001) as doesthe finding of slower SSRT (Chhabildas, Pennington, & Willcutt, 2001; Nigg, 1999;Oosterlaan et al., 1998; Pliszka, Borcherding, Spratley, Leon, & Irick, 1997; Rubia et al.,1998; Schachar et al., 1995; Schachar, Mota, Logan, Tannock, & Klim, 2000; Sergeantet al., 2002). There have, however, also been negative findings (Kuntsi et al., 2001;Manassis, Tannock, & Barbosa, 2000; Pliszka, Liotti, & Woldorff, 2000; Scheres et al.,2001a,b). A recent meta-analysis showed that 82% of 27 studies using the stop signal taskfound impairment in SSRT in children with ADHD with a mean effect size of .62, whichis slightly lower than that observed in this study (Willcutt et al., 2005). As expected, thetwo inhibitory measures were strongly correlated with each other, suggesting that they tapinto similar motor inhibitory processes. GNG commission errors also correlated with com-mission errors on the CPT, confirming the commonly held view that commission errors onthe CPT reflect disinhibitory impulsiveness (Halperin, 1991). Interestingly, however,GNG commission errors also correlated with omission errors on the CPT, thought toreflect inattentiveness (Leth-Steenson et al., 2000; Halperin, 1991). This is in line with thesuggestion that the ability to sustain attention may be an important underlying basic func-tion for the performance of inhibition tasks (Aron & Poldrack, 2005; Nigg, 2001). It ispossible that the higher rate of premature responding in children with ADHD might haveinfluenced the calculation of the SSRT, as a premature response during a stop signal trialwould lead to a longer SSD. However, there was only a trend for a correlation betweenpremature responses during stop trials and SSD (r = .3, p < .07). Furthermore, it is verylikely that response prematurity and poor inhibitory control are closely interconnecteddeficits, possibly caused by a common underlying cognitive deficit, since overall responseprematurity across all tasks correlated with both the likelihood to inhibit in the GNG taskand with SSRT.
As opposed to the motor inhibitory functions, cognitive inhibitory control was onlymarginally impaired in children with ADHD. The motor Stroop task as a whole appearedto be difficult for the children with ADHD, as shown in increased error rates to bothcongruent and noncongruent trials, which makes the negative finding on group differ-ences in the Stroop effect not very reliable. However, there was no differential erroreffect for incongruent as opposed to congruent trials and the deficits in this task cantherefore not be considered specific to the interference effect. Findings on the Color-Word Stroop interference effect in children with ADHD have been controversial sincemost of the earlier studies did not control for reading and naming speed and those that didfound no deficits (Gaultney, Kipp, Weistein, & Neill, 1999; Milich, Balentine, & Lynam,2001; Nigg, Blaskey, Huang-Pollock, & Rappley, 2002; Schmitz et al., 2002; for a meta-analysis see van Mourik, Oosterlaan, & Sergeant, 2005). Impairments in the interferenceeffect in the Eriksen Flanker task (which is similar to the interference effect measured inour motor Stroop task) have also been controversial, with some studies finding animpairment (Crone, Jennings, & van der Molen, 2003), but others not (Jonkman et al.,1999; Scheres et al., 2004).
The impairment in children with ADHD in the Switch cost was only significant at atrend level. It is possible that this may reflect a lack of statistical power. Alternatively, it isalso possible that our simplified Switch task version, which was purposely designed toisolate “pure” switching and reduce confounding functions such as working memory andrule learning to a minimum (Smith et al., 2004), elicits only marginal impairments,

ADHD AND A TEST BATTERY OF IMPULSIVENESS 293
suggesting that “pure” switching is not a typical deficit of children with ADHD. Theliterature on switching deficits in children with ADHD in more difficult task versions,however, has been rather inconsistent, with both positive and negative findings on theWisconsin Card Sorting Test (WCST) (for overview, see Sergeant et al., 2002 andWillcutt et al., 2005). The meta-analysis of Willcutt et al. (2005) found that only 46% of24 studies found children with ADHD to make perseverative errors in this task with aneffect size of .46, which is identical to the effect size observed in this study for the Switchcost. Other studies, however, using easier visual-spatial set shifting tasks that wererelatively unconfounded by additional cognitive functions, have shown impairments inchildren with ADHD (Cepeda, Cepeda, & Kramer, 2000; Itami & Uno, 2002; Kempton et al.,1999; Koschak, Kunert, Derichs, Weniger, & Irle, 2003; Rubia, Tayor, Smith et al., 2001).
It is interesting that the two cognitive inhibition measures did not correlate with anyof the other task-specific measures of impairment, suggesting that they may be measuringdifferent underlying cognitive processes that may have only a minor, if any, effect on thecognitive impulsiveness of children with ADHD. The negative finding of no correlationbetween motor and interference inhibition is in line with previous findings of no correla-tion between the SSRT and the interference effects of both the Color-Word Stroop(Pennington, 1997; Scheres et al., 2004) and the Eriksen Flanker test (Scheres et al., 2004).A deficit in children with ADHD in motor, but not interference inhibition, and the lack ofan intercorrelation between tasks are in line with the taxonomy of inhibition functions ofNigg (2000, 2001) who advocates a clear distinction between motor response inhibition assuppression of a primary response and attentional interference control as suppression of asecondary, competing response. It thus appears from our own findings and the evidencefrom the literature that cognitive inhibitory functions such as interference inhibition andcognitive flexibility may be only marginally impaired in children with ADHD and areprobably not part of the core underlying cognitive deficits (Barkley, 1997; Nigg, 2001).
The increased levels of omission and commission errors during the CPT in childrenwith ADHD compared to controls confirm consistent findings in the literature of deficitswith sustained attention in children with ADHD (for overview see Losier et al., 1996;Willcutt et al., 2005). The meta-analysis of Willcutt et al. (2005) on 83 studies of execu-tive functions in children with ADHD found that increased omission errors on the CPT,together with increased SSRT, were the most consistent findings in the literature. Themean effect sizes for omission (d = .64) and commission errors (d = .51) of about 30studies were strikingly similar to those of this study (Willcutt et al., 2005).
Contrary to our prediction, however, the presence of reward did not improve the defi-cits, which does not support the view that ADHD is a motivational problem (Sonuga-Barke& Taylor, 1992) or is characterized by a hypersensitivity to reward (Douglas & Parry, 1994).Our negative findings are in line with two previous studies that also did not find an effect ofreward on sustaining attention in children with ADHD (Solanto, Wender, & Bartell, 1997;van der Meere, Shalev, Borger, & Grosstsur, 1995). Out of nine previous studies that haveused reward conditions with cognitive tests, only three have found a differential effect ofreward on the performance of children with ADHD, using tasks of temporal reproduction(McInerney, & Kerns, 2003), arithmetics (Carlson, Mann & Alexander, 2000) or a FigureMatching Task (Carlson & Tamm, 2000; for overview see Luman et al., 2005). Hypersensi-tivity to reward in children with ADHD is not confirmed by this study and may depend onthe amount of reward, specific task requirements, and initial level of impairment.
Of all task-specific measures, time perception deficits were the second mostsensitive group discriminator, correctly classifying up to 70% of cases and controls. The

294 K. RUBIA ET AL.
findings of time discrimination deficits replicate our own and other researcher’s recentfindings of temporal discrimination deficits in children with ADHD in the range of milli-seconds (Smith et al., 2002; Toplak et al., 2003) and seconds (Rubia, Smith, Noorlos et al.,2003). Other related timing deficits that have been observed in children with ADHDinclude time estimation deficits in the range of seconds (Barkley et al., 2001; Kerns,McInerney & Wilde, 2001; Mullins et al., 2005; Smith et al., 2002; Sonuga-Barke et al.,1998; West et al., 2000) and problems with motor timing (Rubia, Sergeant, Taylor et al.,1999; Rubia, Smith, Noorlos et al., 2003). Deficits in fine temporal perception have beenrelated to deficits in motor timing (Ivry, 1996; Keele et al., 1985; Rubia & Smith, 2004)and to behavioral impulsiveness (Rubia, Schuri, von Cramon, & Poeppel, 1997; Rubia,Sergeant, Taylor et al., 1999; Smith et al., 2002). Both associations are supported in thisstudy by the findings of an intercorrelation between time discrimination errors and prema-ture responding (which has been conceptualized as an abnormal timing process by Rubia,Taylor, Smith et al., 2001), and between temporal discrimination problems and behavioralimpulsiveness as measured on the SDQ. The positive intercorrelation between time dis-crimination deficits and typical and ubiquitous problems such as a premature and incon-sistent response style suggests that perceptual timing is not an isolated deficit in childrenwith ADHD, but is related to at least some of the other, pervasive executive dysfunctionsof response prematurity and variability. The association between time perception andmeasures of motor inhibition and sustained attention needs to be further explored in futurestudies, given that it only reached significance in this study at an uncorrected p value andwas not hypothesized. Problems with temporal processes, including perceptual timedeficits and a premature response style, therefore, appear to be a crucial branch of a multi-faceted complex of impairments forming the typical cognitive style of children withADHD.
All measures of impairment correlated significantly with the SDQ, confirming arelationship between specific cognitive deficits on the MARS task battery and behavioralimpulsiveness. From all measures of impairment, SSRT correlated with SDQ only at atrend level after correction for multiple testing. The correlation was, however, predictedand is unlikely to be a chance finding.
In conclusion, we found that children with ADHD show a generic, task-indepen-dent, premature, and inconsistent response style, and problems with motor inhibitorycontrol, time estimation, and sustained attention. These different cognitive functions ofimpairment appeared to be interrelated with each other and with behavioral measures ofimpulsiveness, suggesting they form a cognitive construct of impulsiveness underlyingADHD symptomatology. We could not confirm the hypothesis that cognitive inhibitionfunctions, in the form of interference inhibition and cognitive flexibility, form part of thisconstruct of impulsiveness. We also could not confirm the hypothesis that potential moti-vational causes of attention deficits could be ameliorated with incentives nor that therewas hypersensitivity to reward in ADHD compared to control children. In light of thefindings of an intercorrelation between impaired functions, although some of them wererelatively weak, we hypothesize that timing, motor inhibition, and sustained, but notselective, attention are interconnected cognitive functions underlying the impulsive cogni-tive style of children with ADHD, and that they may possibly be responsible for the perva-sive premature, and variable response style. The findings support the notion that thecognitive style of children with ADHD is characterized more by deficits in motor than incognitive inhibition functions and in executive inhibitory rather than motivational regula-tory functions (Nigg, 2001).

ADHD AND A TEST BATTERY OF IMPULSIVENESS 295
Support for the hypothesis of an interrelatedness of these different cognitive func-tions is provided by functional neuroimaging studies. Right inferior prefrontal cortex hasbeen found to be a crucial brain region for inhibitory motor control in Go/No-Go and Stoptasks (Rubia, Lee et al., 2005; Rubia, Overmeyer et al., 2001; Rubia, Smith, Brammer, &Taylor, 2003; Rubia et al., in press; Aron & Poldrack, 2005), but it is also a key area forsustained attention (Lawrence, Ross, Hoffmann, Garavan, & Stein 2003; Voisin, Bidet-Caulet, Bertrand, & Fonlupt, 2006) and for time discrimination of milliseconds (Maquetet al., 1996; Ortuno et al., 2002; Rubia & Smith, 2004; Smith et al., 2003). The most parsi-monious explanation for a common neural substrate for these different cognitive functionsmay be that sustaining attention or even more basic attention functions (Brandeis et al.,1998; Banaschewski et al., 2004) are necessary for the performance of higher order inhibi-tion tasks (Aron & Poldrack, 2005; Nigg, 2001) and for the ability to discriminate tempo-ral intervals that requires sustained attention to time (Pardo, Fox, & Raichle, 1991; Coull,2004, Coull, Frackowiak & Frith, 1998; Coull, Vidal, Nazarian, & Macar, 2004; Smithet al., 2002, 2003; Rubia & Smith, 2005). On the other hand, inhibitory mechanisms havealso been suggested to be important for higher order attention and executive functions(Barkley, 1997; Nigg, 2000). Evidence exists for a common neural substrate in right infe-rior prefrontal cortex for the inhibitory processes involved during motor response inhibitionand cognitive flexibility (Konishi et al., 1999; Rubia et al., in press; Smith et al., 2004).
Unfortunately we do not have functional imaging data on this particular patientgroup. However, abnormalities in these right prefrontal lobe mediated cognitive functionsof motor inhibition, attention, and time estimation in children with ADHD are in line withevidence for structural (Sowell et al., 2003; Bush, Valera, & Seidman, 2005; Swansonet al., 2004) and functional abnormalities in other groups of children and adolescents withADHD in right inferior prefrontal cortex during motor response inhibition (Rubia, Overmeyer,Taylor, Brammer et al., 1999; Rubia, Overmeyer, Taylor et al., 2000; Rubia, Taylor et al.,2001; Rubia, Smith, Brammer et al., 2005; Booth et al., 2005), attentional flexibility(Smith, Taylor, Brammer, & Rubia, 2006; Silk et al., 2005), and time estimation (Smithet al., 2006).
There is also evidence for different neural substrates for motor and interferenceinhibition functions, supporting the behavioral distinction between these two functions(Nigg, 2000) and the findings of a differential impairment in children with ADHD. Perfor-mance on the motor Stroop task has been shown to be mediated by a predominantly lefthemispheric network of prefrontal, parietal, and temporal cortices (Liu, Banich, Jacobson& Tanabe, 2004; Rubia et al., in press), in striking similarity to the left hemispheric net-work mediating Color-Word Stroop task performance (Banich et al., 2000; Fan, Flombaum,McCandliss, Thomas, & Posner, 2003), and in contrast to the predominantly right prefron-tal lobe mediated functions of motor response inhibition, timing, and sustained attention(see references above). The absence of abnormalities in the Stroop effect in children withADHD in this and other studies (Sergeant et al., 2003; van Mourik et al., 2005) may beexplained by the left hemispheric laterality effect of interference inhibition, becauseADHD has been associated more predominantly with right prefrontal structural and func-tional deficits (Aron & Poldrack, 2005; Bush, Valera, & Seidman, 2005; Swanson et al.,2004). The negative behavioral findings are also in line with our fMRI findings of normalbrain activation in adolescents with ADHD during unimpaired motor Stroop task performance(Smith et al., 2006).
Unfortunately not much is known about the neural substrates of variability ofresponse and premature responding. Some evidence has suggested a key role of prefrontal

296 K. RUBIA ET AL.
cortex in response variability, which would be in line with the evidence for functional andstructural frontal lobe deficits in children with ADHD. Lesion studies have suggested a roleof lateral prefrontal cortex in response consistency (Stuss, Murphy, Binns, & Alexander,2003); and a study using fMRI found a correlation between response variability in a stoptask and prefrontal and parietal brain regions mediating inhibitory control (Bellgrove et al.,2004).
Our findings of an interrelationship of the cognitive functions that are impaired inchildren with ADHD are consistent with a multifactorial cognitive aetiology model ofADHD, in which an impulsive cognitive style is attributable to an additive or interactivedysfunction in multiple, but probably related, cognitive systems and their closely relatedmediating neural networks (Sergeant et al., 2003; Willcutt et al., 2005). Our data,however, do not exclude the possibility that subtypes of children with ADHD may bequantitatively or qualitatively more impaired in one or the other functions, or be moremotivationally than cognitively impaired, as has been suggested by theories of dual ormultiple separate aetiological pathways to ADHD (Nigg, Blaskey, Stawicki, & Sachek2004; Nigg, Goldsmith, & Sachek 2004; Nigg 2005; Solanto et al., 2001; Sonuga-Barke,2005). Studies using larger sample sizes and different subtypes of children with ADHD,including patients with pure attention deficits, will be needed to clarify this issue.
Age Effects
Several of the variables that were impaired in children with ADHD correlatednegatively with age, suggesting that ADHD children may show developmental differ-ences. This is in line with our neurofunctional studies showing reduced activation inADHD adolescents in the same frontal brain region that show a linear correlation with agein the transition from childhood to adulthood (Rubia et al., 2000; Rubia, Smith, Brammeret al., 2005b; Rubia et al., in press; Smith et al., 2006). It is possible that insufficient powermay have accounted for the negative finding of no age effect on the SSRT that has beenshown in other studies to develop progressively with age (Williams, Ponesse, Schachar,Logan, & Tannock, 1999; Bedard et al., 2003).
Limitations
We are aware that the sample size of this study was relatively small, which in particularlimits the statistical power of the discriminant analysis that needs to be considered prelim-inary. Nevertheless, the positive findings were in the expected direction and in line withthe apriori hypotheses. A replication in a larger sample will be needed to corroborate thenegative findings.
The discriminant power of the MARS task battery as a whole showed 76% correctclassification of cases and controls, which compares favorably to standard neuropsycho-logical test measures of executive functions (Grodzinsky & Barkley, 1999) and test batteriesused as diagnostic aides (Rielly, Cunningham, Richards, Elbard, & Mahoney, 1999).Although the sensitivity and specificity of the task battery was considerably high, thepositive predictive value (PPV) was rather poor. This is related to the low prevalence ofADHD in the general population. A widely recognized limitation of the PPV is its strongdependence on the prevalence of the disorder; a low disease prevalence leads to a lowPPV, even in the presence of high diagnostic test sensitivity (Brenner & Gefeller, 1997). Ifthe findings can be replicated in a larger sample, the MARS task battery might potentially

ADHD AND A TEST BATTERY OF IMPULSIVENESS 297
be useful as a differentiated and biologically informed measurement tool of a cognitiveconstruct of impulsiveness.
In summary, performance of children with ADHD on a task battery of several testsof prefrontal lobe-mediated functions of cognitive control showed that behavioral impul-siveness in children with ADHD appears to be related to a generic, task-independentinconsistent, and premature response style and to task-specific deficits in motor inhibi-tion, sustaining attention, and time perception. These coexisting cognitive deficits in tim-ing, attentional, and inhibitory domains appear to be interrelated aspects of amultifaceted construct of cognitive impulsiveness that together show a group discrimi-nant power of 76%.
Original manuscript received October 11, 2005Revised manuscript accepted April 21, 2006
First published online October 20, 2006
REFERENCES
American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders,4th ed. Washington DC: American Psychiatric Association.
Aron, A. R., & Poldrack, R. A. (2005). The cognitive neuroscience of response inhibition:Relevance for genetic research in attention-deficit/hyperactivity disorder. Biological Psychiatry,57, 1285–1292.
Banaschewski, T., Brandeis, D., Heinrich, H., Albrecht, B., Brunner, E., & Rothenberger, A. (2004).Questioning inhibitory control as the specific deficit of ADHD: Evidence from brain electricalactivity. Journal of Neural Transmission, 111, 841–864.
Banaschewski, T., Hollis C., Oosterlaan J., Royers H., Rubia K., Willcutt E., & Taylor E. (2005).Towards an understanding of unique and shared pathways in the psychopathophysiology ofADHD. Developmental Science, 8, 132–140.
Band, G. P. H., van der Molen, M. W., & Logan, G. D. (2003). Horse-race model simulations of thestop signal procedure. Acta Psychologica, 112, 105–142.
Banich, M. T., Milham, M. P., Atchley, R., Cohen, N. J., Webb, A., Wszalek, T., Kramer, A. F.,Liang, Z-P., Wright, A., Shenker, J., & Margin, A. (2000). fMRI studies of Stroop tasks revealunique roles of anterior and posterior brain systems in attentional selection. Journal ofCognitive Neuroscience, 12, 988–1000.
Barkley, R. A. (1997). Behavioral inhibition, sustained attention, and executive functions:Constructing a unifying theory of ADHD. Psychological Bulletin, 121, 65–94.
Barkley, R. A., Edwards, G., Laneri, M., Fletcher, K., & Metevia, L. (2001). Executive functioning,temporal discounting, and sense of time in adolescents with Attention Deficit HyperactivityDisorder (ADHD) and Oppositional Defiant Disorder (ODD). Journal of Abnormal ChildPsychology, 29, 541–556.
Bedard, A. C., Ickowicz, A., Logan, G. D., Hogg-Johnson, S., Schachar, R., & Tannock, R. (2003).Selective inhibition in children with attention-deficit hyperactivity disorder off and on stimu-lant medication. Journal of Abnormal Child Psychology, 31, 315–327.
Bellgrove M. A., Hester R., & Garavan, H. (2004). The functional neuroanatomical correlates ofresponse variability: Evidence from a response inhibition task. Neuropsychologia, 42,1910–1916.
Benjamini, Y., & Hochberg, Y. (1995). Controlling the false discovery rate: A practical andpowerful approach to multiple testing. Journal of the Royal Statistical Society B Met, 57,289–300.
Booth, J. R., Burman, D. D., Meyer, J. R., Lei, Z., Trommer, B. L., Davenport, N. D., Li, W.,Parrish, T. B., Gitelman, D. R., & Mesulam, M. M. (2005). Larger deficits in brain networks for

298 K. RUBIA ET AL.
response inhibition than for visual selective attention in attention deficit hyperactivity disorder(ADHD). Journal of Child Psychology and Psychiatry, 46, 94–111.
Brandeis, D., Banaschewski, T., Baving, L., Georgiewa, P., Blanz, B., Warnke, A., Steinhausen, H. C.,Rothenberger A., & Scheuerflug, P. (2002). Multicenter P300 brain mapping of impaired atten-tion to cues in hyperkinetic children. J Am Acad Child Adolesc Psychiatry, 41, 990–998.
Brandeis, D., v. Leeuwen, T. H., Rubia, K., Vitacco, D., Steger, J., Borntraeger, E., & Steinhausen,H. C. (1998). Neuroelectric precursors of stop failures in children with attention problems.Behavioural Brain Research, 94, 111–125.
Brenner, H., & Gefeller, O. (1997). Variation of sensitivity, specificity, likelihood ratios andpredictive values with disease prevalence. Statistics in Medicine, 16, 981–991.
Bush, G., Valera, E., & Seidman, L. J. (2005). Functional neuroimaging of attention-deficit/hyperac-tivity disorder: A review and suggested future directions. Biological Psychiatry, 57, 1273–1284.
Cambell, S. B., Endmann, M. W., & Bernfield, G. (1977). A three year follow-up of hyperactivepreschoolers into elementary school. Journal of Child Psychology and Psychiatry, 18, 239–243.
Carlson, C. L., Mann, M., & Alexander, D. K. (2000). Effects of reward and response cost on the per-formance and motivation of children with ADHD. Cognitive Therapy and Research, 24, 87–98.
Carlson, C. L., & Tamm, L. (2000). Responsiveness of children with attention deficit-hyperactivitydisorder to reward and response cost: Differential impact on performance and motivation. Journalof Consulting and Clinical Psychology, 68, 73–83.
Carte, E. T., Nigg, J. T., & Hinshaw, S. P. (1996). Neuropsychological functioning, motor speed,and language processing in boys with and without ADHD. Journal of Abnormal Child Psychol-ogy, 24, 481–498.
Castellanos, F. X., Sonuga-Barke, E. J. S., Scheres, A., Di Martino, A., Hyde, C., & Walters, J. R.(2005). Varieties of attention-deficit/hyperactivity disorder-related intra-individual variability.Biological Psychiatry, 57, 1416–1423.
Castellanos, F. X., & Tannock, R. (2002). Neuroscience of attention-deficit/hyperactivity disorder:The search for endophenotypes. Nature Reviews Neuroscience 3, 617–628.
Cepeda, N. J., Cepeda, M. L., & Kramer, A. F. (2000). Task switching and Attention Deficit Hyper-activity Disorder. Journal of Abnormal Child Psychology, 28, 213–226.
Chhabildas, N., Pennington, B. F., & Willcutt, E. G. (2001). A comparison of the neuropsy-chological profiles of the DSM-IV subtypes of ADHD Journal of Abnormal Child Psychology,29, 529–540.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.). Hillsdale, NJ:Lawrence Erlbaum Associates.
Coull, J. T. (2004). fMRI studies of temporal attention: Allocating attention within, or towards, time.Cognitive Brain Research, 21, 216–226.
Coull, J. T., Frackowiak, R. S. J., & Frith, C. D. (1998). Monitoring for target objects: Activationof right frontal and parietal cortices with increasing time on task. Neuropsychologia, 36,1325–1334.
Coull, J. T., Vidal, F., Nazarian, B., & Macar, F. (2004). Functional anatomy of the attentionalmodulation of time estimation. Science, 303, 1506–1508.
Crone, E. A., Jennings, J. R., & van der Molen, M. W. (2003). Sensitivity to interference andresponse contingencies in attention-deficit/hyperactivity disorder. Journal of Child Psychologyand Psychiatry and Allied Disciplines, 44, 214–226.
Douglas, V. I. (1999). Cognitive control processes in attention deficit hyperactivity disorder. In H.C. Quay, & A. E. Hogan (Eds.), Handbook of disruptive behaviour disorders (pp. 105–138).New York: Plenum Press.
Douglas, V. I., & Parry, P. A. (1994). Effects of reward and nonreward on frustration and attentionin attention deficit disorder. Journal of Abnormal Child Psychology, 22, 313–326.
Dykman, R. A., Ackerman, P. T., & Oglesby, D. M. (1979). Selective and sustained attention inhyperactive, learning-disabled and normal boys. Journal of Nervous and Mental Disease, 167,288–297.

ADHD AND A TEST BATTERY OF IMPULSIVENESS 299
Fan, J., Flombaum, J. I., McCandliss, B. D., Thomas, K. M., & Posner, M. I. (2003). Cognitive andbrain consequences of conflict. Neuroimage, 18, 42–57.
Gaultney, J. F., Kipp, K., Weinstein J. A., & McNeill, J. (1999). Inhibition and mental effort in attentiondeficit hyperactivity disorder. Journal of Developmental Physical Disabilities, 11, 105–114.
Ge, Y. L., Robaey, P., Karayanidis, F., Bourassa, M., Pelletier, G., & Geoffrey, G. (2000). ERPs andbehavioural inhibition in a Go/No-go task in children with attention-deficit hyperactivity disorder.Brain and Cognition, 43, 215–220.
Goodman, R. (1997) The Strengths and Difficulties Questionnaire: A research note. Journal ofChild Psychology & Psychiatry, 38, 581–586.
Goodman, R., Ford, T., Simmons, H., Gatward, R., & Meltzer, H. (2000b). Using the Strengths andDifficulties Questionnaire (SDQ) to screen for child psychiatric disorders in a communitysample. British Journal of Psychiatry, 177, 534–539.
Goodman, R., Renfrew, D., & Mullick, M. (2000a). Predicting type of psychiatric disorder fromStrengths and Difficulties Questionnaire (SDQ) scores in child mental health clinics in Londonand Dhaka. European Child and Adolescent Psychiatry, 9, 129–134.
Goodman, R., & Scott, S. (1999). Comparing the Strengths and Difficulties Questionnaire and the ChildBehaviour Checklist: Is small beautiful? Journal of Abnormal Child Psychology, 27, 17–24.
Grodzinsky, G. M., & Barkley, R. A. (1999). Predictive power of frontal lobe tests in the diagnosisof attention deficit hyperactivity disorder. Clinical Neuropsychologist, 13, 12–21.
Halperin, J. M. (1991). The clinical-assessment of attention. International Journal of Neuroscience,58, 171–182.
Hartung, C. M., Milich, G., Lynam, D. R., & Martin, C. A. (2002). Understanding the relationsamong gender, disinhibition, and disruptive behavior in adolescents. Journal of AbnormalPsychology, 111, 659–664.
Iaboni, F., Douglas, V. I., & Baker, A. G. (1995). Effects of reward and response costs on inhibitionin ADHD children. Journal of Abnormal Psychology 104, 232–240.
Itami, S., & Uno, H. (2002). Orbitofrontal cortex dysfunction in attention-deficit hyperactivitydisorder revealed by reversal and extinction tasks. NeuroReport, 13, 2453–2457.
Ivry, R. B. (1996). The representation of temporal information in perception and motor control.Current Opinion in Neurobiology, 6, 851–857.
Jonkman, L. M., Kemner, C., Verbaten, M. N., Van Engeland, H., Kenemans, J. L., Camfferman,G., Buitelaar, J.K., & Koelega, H.S. (1999). Perceptual and response interference in childrenwith attention-deficit hyperactivity disorder, and the effects of methylphenidate. Psychophysiol-ogy, 36, 419–429.
Keele, S., Polorny, R., Corcos, D., & Ivry, R. (1985). Do perception and motor production sharecommon timing mechanisms: A correlational analysis. Acta Psychologia, 60, 173–191.
Kempton, S., Vance, A., Maruff, P., Luk, E., Costin, J., & Pantelis C. (1999). Executive functionand attention deficit hyperactivity disorder: Stimulant medication and better executive functionperformance in children. Psychological Medicine, 29, 527–538.
Kerns, K. A., McInerney, R. J., & Wilde, N. J. (2001). Time reproduction, working memory, andbehavioral inhibition in children with ADHD. Child Neuropsychology, 7, 21–31.
Keselman, H. J., Cribbie, R., & Holland, B. (2002). Controlling the rate of Type I error over a largeset of statistical tests. British Journal of Mathematical Statistics and Psychology, 55, 27–39.
Konishi, S., Nakajima, K., Uchida, I., Kikyo, H., Kameyama, M., & Miyashita, Y. (1999). Commoninhibitory mechanism in human inferior prefrontal cortex revealed by event-related functionalMRI. Brain, 122, 981–991.
Koschack, J., Kunert, H. J., Derichs, G., Weniger, G., & Irle, E. (2003) Impaired and enhancedattentional function in children with attention deficit/hyperactivity disorder. PsychologicalMedicine, 33, 481–489.
Kuntsi, J., Oosterlaan, J., & Stevenson, J. (2001). Psychological mechanisms in hyperactivity: Iresponse inhibition deficit, working memory impairment, delay aversion, or something else?Journal of Child Psychology and Psychiatry, 42, 199–210.

300 K. RUBIA ET AL.
Lawrence, N. S., Ross, T. J., Hoffmann, R., Garavan, H., & Stein, E. A. (2003). Multiple neuronalnetworks mediate sustained attention. Journal of Cognitive Neuroscience, 15, 1028–1038.
Leth-Steenson, C., Elbaz, Z. K., & Douglas, V. I. (2000). Mean response times, variability and skewin the responding of ADHD children: A response time distributional approach. Acta Psychologica,104, 167–190.
Liu, X., Banich, M. T., Jacobson, B. L., & Tanabe, J. L. (2004). Common and distinct neuralsubstrates of attentional control in an integrated Simon and spatial Stroop task as assessed byevent-related fMRI. Neuroimage, 22, 1097–1106.
Logan, G. D., Schachar, R., & Tannock, R. T. (1997). Impulsivity and inhibitory control. Psycholog-ical Science, 8, 60–64.
Losier, B. J., McGrath, P. J., & Klein, R. M. (1996). Error patterns of the Continuous PerformanceTest in non-medicated and medicated samples of children with and without ADHD: A meta-analytic review. Journal of Child Psychology & Psychiatry, 37, 971–987.
Luman, M., Oosterlaan, J., & Sergeant, J. A. (2005). The impact of reinforcement contin-gencies on AD/HD: A review and theoretical appraisal. Clinical Psychology Review, 25,183–213.
Manassis, K., Tannock, R., & Barbosa, J. (2000). Dichotic listening and response inhibition inchildren with comorbid anxiety disorders and ADHD. Journal of the American Academy ofChild Psychiatry 39, 1152–1159.
Maquet, P., Lejeune, H., Pouthas, V., Bonnet, M., Casini, L., Macar, F., Timsit-Berthier, M., Vidal,F., Ferrara, A., Degueldre, C., Quaglia, L., Delfiore, G., Luxen, A., Woods, R., Mazziotta, J. C.,& Comar, D. (1996). Brain activation induced by estimation of duration: A PET study.Neuroimage, 3, 119–126.
McInerney, R. J., & Kerns, K. A. (2003). Time reproduction in children with ADHD: Motivationmatters. Child Neuropsychology, 9, 91–108.
Meiran, N. (1996). Reconfiguration of processing mode prior to task performance. Journal of Exper-imental Psychology: Learning, Memory and Cognition, 22, 1423–1442.
Milich, R., Balentine, A. C., & Lynam, D. R. (2001). ADHD combined type and ADHD predomi-nantly inattentive type are distinct and unrelated disorder. Clinical Psychology: Science andPractice, 8, 463–488.
Millis, S. R. (2003). Statistical practices: The seven deadly sins. Child Neuropsychology, 9,221–223.
Moeller, F. G., Barratt, E. S., Dougherty, D. M., Schmitz, J. M., & Swann, A. C. (2001). Psychiatricaspects of impulsivity. American Journal of Psychiatry, 158, 1783–1793.
Mullins, C., Bellgrove, M. A., Gill, M., Robertson, I. H. (2005). Variability in time reproduction:Difference in ADHD combined and inattentive subtypes. Journal of the American Academy ofChild & Adolescent Psychiatry, 44, 169–176.
Nakagawa, S. (2004). A farewell to Bonferroni: The problems of low statistical power and publica-tion bias. Behavioral Ecology, 15, 1044–1045.
Nigg, J. T. (1999). The ADHD response-inhibition deficit as measured by the stop task: Replicationwith DSM-IV combined type, extension, and qualification Journal of Abnormal Child Psychol-ogy, 27, 393–402.
Nigg, J. T. (2000). On inhibition/disinhibition in developmental psychopathology: Views fromcognitive and personality psychology and a working inhibition taxonomy. Psychological Bulle-tin, 126(2), 220–246.
Nigg, J. T. (2001). Is ADHD a disinhibitory disorder? Psychological Bulletin, 127(5), 571–598.Nigg, J. T. (2005). Neuropsychologic theory and findings in attention-deficit/hyperactivity disorder:
The state of the field and salient challenges for the coming decade. Biological Psychiatry, 57,1424–1435.
Nigg, J. T., Blaskey, L. G., Huang-Pollock, C. L., & Rappley, M. D. (2002). Neuropsychologicalexecutive functions and DSM-IV ADHD subtypes. JAMA-Journal of the American MedicalAssociation, 41, 59–66.

ADHD AND A TEST BATTERY OF IMPULSIVENESS 301
Nigg, J. T., Blaskey, L. G., Stawicki, J. A., & Sachek, J. (2004). Evaluating the endophenotypemodel of ADHD neuropsychological deficit: Results for parents and siblings of childrenwith ADHD combined and inattentive subtypes. Journal of Abnormal Psychology, 113,614–625.
Nigg, J. T., Goldsmith, H. H., & Sachek, J. (2004). Temperament and attention deficit hyperactivitydisorder: The development of a multiple pathway model. Journal of Clinical Child and Adoles-cent Psychology, 33, 42–53.
Nigg, J. T., Willcutt, E. G., Alysa, E., Doyle, A. E., & Sonuga-Barke, E. J. S. (2005). Causal hetero-geneity in attention-deficit/hyperactivity disorder: Do we need neuropsychologically impairedsubtypes? Biological Psychiatry, 57, 1224–1230.
Oosterlaan, J., Logan, G. D., & Sergeant, J. A. (1998). Response inhibition in AD/HD, CD, comor-bid AD/HD + CD, anxious, and control children: A meta-analysis of studies with the stop task.Journal of Child Psychology & Psychiatry, 39, 411–425.
Ortuno, F., Ojeda, N., Arbizu, J., Lopez, P., Marti-Climent, J. M., Penuelas, I., & Cervera, S. (2002).Sustained attention in a counting task: Normal performance and functional neuroanatomy.Neuroimage, 17, 411–420.
Pardo, J. V., Fox, P. T., & Raichle, M. E. (1991). Localization of a human system for sustainedattention by positron emission tomography. Nature, 349, 61–64.
Pastor, M. A., Artieda, J., Jahanshahi, M., & Obeso, J. A. (1992). Time estimation and reproductionis abnormal in Parkinson’s disease. Brain, 115, 211–225.
Pennington, P. F. (1997). Dimensions of executive functions in normal and abnormal development.In N. A. Krasnegor, G. R. Lyon, & P. S. Goldman-Rakic (Eds.), Development of the prefrontalcortex: Evolution, neurobiology and behaviour (pp. 265–281). Baltimore: P.H. Brookes.
Pennington, P. F., & Ozonoff, S. (1996). Executive functions and developmental psychopathology.Journal of Child Psychology & Psychiatry, 37, 51–87.
Perneger, T. V. (1998). What’s wrong with Bonferroni adjustments. British Medical Journal, 316,1236–1238.
Pitcher, T. M., Piek, J. P., & Barratt, N. C. (2002). Timing and force control in boys with attentiondeficit hyperactivity disorder: Subtype differences and the effect of comorbid developmentalcoordination disorder. Human Movement Science, 21, 919–945.
Pliszka, S. R., Borcherding, S. H., Spratley, K., Leon, S., & Irick, S. (1997). Measuring inhibitorycontrol in children. Journal of Developmental and Behavioural Pediatrics, 18, 254–259.
Pliszka, S. R., Liotti, M., & Woldorff, M. G. (2000). Inhibitory control in children with attention-deficit/hyperactivity disorder: Event-related potentials identify the processing component andtiming of an impaired right-frontal response-inhibition mechanism. Biological Psychiatry, 48,238–246.
Raven, J. C. (1960). Guide to the standard progressive matrices. London: HK Lewis.Rhodes, S. M., Coghill, D. R., & Matthews, K. (2005). A neuropsychological investigation of psy-
chostimulant drug treatment-naive boys with hyperkinetic disorder (ADHD). PsychologicalMedicine, 35, 1–12.
Rielly, N. E., Cunningham, C. E., Richards, J. E., Elbard, H., & Mahoney, W. J. (1999). Detectingattention deficit hyperactivity disorder in a communications clinic: Diagnostic utility of theGordon diagnostic system. Journal of Clinical and Experimental Neuropsychology, 21,685–700.
Rosenbaum, M., & Baker, E. (1984). Self-control behavior in hyperactive and nonhyperactivechildren. Journal of Abnormal Child Psychology, 12, 303–317.
Rubia, K. (2002). The dynamic approach to neurodevelopmental psychiatric disorders: Use of fMRIcombined with neuropsychology to elucidate the dynamics of psychiatric disorders, exemplifiedin ADHD and schizophrenia. Behavioural Brain Research, 130, 47–56.
Rubia, K., Lee F., Cleare, A., Tunstall, N., Fu, C., & McGuire, P. (2005). Acute TryptophanDepletion reduces right inferior prefrontal activation during response inhibition in fast, eventrelated fMRI. Psychopharmacology, 179, 791–803.

302 K. RUBIA ET AL.
Rubia, K., Oosterlaan, J., Sergeant, J., Brandeis, D., & v. Leeuwen T. H. (1998). Inhibitorydysfunction in hyperactive boys. Behavioural Brain Research, 94, 25–32.
Rubia, K., Overmeyer, S., Taylor, E., Brammer, M., Williams, S. C. R., Simmons, A., Andrew, C.,& Bullmore, E. T. (1999). Hypofrontality in Attention Deficit Hyperactivity Disorder duringhigher order motor control: A study with fMRI. American Journal of Psychiatry, 156, 891–896.
Rubia, K., Overmeyer, S., Taylor, E., Brammer, M., Williams, S. C. R., Simmons, A., Andrew, C., &Bullmore, E. T. (2000). Frontalisation with age: Mapping neurodevelopmental trajectories withfMRI. Neuroscience Biobehavioural Review, 24, 13–21.
Rubia, K., Overmeyer, S., Taylor, E., Brammer, M., Williams, S. C. R., Simmons, A., Andrew, C.,Giampietro, V., & Bullmore, E. T. (2001). Mapping motor inhibition: Conjunctive brainactivations across different versions of go/no-go and stop tasks. NeuroImage, 13, 250–261.
Rubia, K., Schuri, U., v. Cramon, I., & Poeppel, E. (1997). Time estimation as a neuronal networkproperty: A lesion study. NeuroReport, 8, 1273–1276.
Rubia, K., Sergeant, J., Taylor, A., & Taylor, E. (1999). Synchronization, anticipation and consis-tency of motor timing in dimensionally defined children with Attention Deficit HyperactivityDisorder. Perceptual and Motor Skills, 89, 1237–1258.
Rubia, K., & Smith, A. (2001). Attention deficit-hyperactivity disorder: Current findings andtreatment. Current Opinion in Psychiatry, 14, 309–316.
Rubia, K., & Smith, A. (2004). The neural correlates of cognitive time management: A review. ActaNeurobiologiae, 64, 329–340.
Rubia, K., Smith, A., Brammer, M., & Taylor, E. (2003). Right inferior prefrontal cortex mediatesresponse inhibition while mesial prefrontal cortex is responsible for error detection. NeuroImage,20, 351–358.
Rubia, K., Smith, A. B., Brammer, M. J., Toone, B., & Taylor, E. (2005). Medication-naïveadolescents with Attention-Deficit Hyperactivity Disorder show abnormal brain activationduring inhibition and error detection. Am J Psych, 162, 1067–1075.
Rubia, K., Smith, A., Noorlos, J., Gunning, W., & Sergeant, J. A. (2003). Motor timing deficits incommunity and clinical boys with hyperactive behaviour: The effect of Methylphenidate onmotor timing. Journal of Abnormal Psychology and Psychiatry, 31, 301–131.
Rubia, K., Smith, A. B., Woolley J., Nosarti, C., Heyman I., Brammer M., & Taylor E. (in press).Progressive increase of fronto-striatal brain activation from childhood to adulthood duringevent related tasks of cognitive control. Human Brain Mapping.
Rubia, K., Taylor, E., Smith, A. B, Oksannen, H., & Newman, S. (2001). Neuropsychologicalanalyses of impulsiveness in childhood hyperactivity. British Journal of Psychiatry, 179,138–143.
Schachar, R., Mota, V. L., Logan, G. D., Tannock, R., & Klim, P. (2000). Confirmation of an inhib-itory control deficit in attention-deficit/hyperactivity disorder. Journal of Abnormal ChildPsychology, 28, 227–235.
Schachar, R., Tannock, R., Marriot, M., & Logan, G. (1995). Deficient inhibitory control in atten-tion deficit hyperactivity disorder. Journal of Abnormal Child Psychology, 23, 411–437.
Scheres, A., Oosterlaan, J., Geurts, H., Morein-Zamir, S., Meiran, N., Schut, H., Vlasveld, L.,Sergeant (2004). Executive functioning in boys with ADHD: Primarily an inhibition deficit?Archives of Clinical Neuropsychology, 19, 569–594.
Scheres, A., Oosterlaan, J., & Sergeant, J. A. (2001a). Response execution and inhibition in childrenwith AD/HD and other disruptive disorders: The role of behavioural activation. J Child PsycholPsyc 42, 347–357.
Scheres, A., Oosterlaan, J., & Sergeant, J. A. (2001b). Response inhibition in children with DSM-IVsubtypes of AD/HD and related disruptive disorders: The role of reward. Child Neuropsychology7, 172–189.
Segalowitz, S. J., Dywan, J., & Unsal, A. (1997). Attentional factors in response time variabilityafter traumatic brain injury: An ERP study. Journal of the International NeuropsychologicalSociety, 3, 95–107.

ADHD AND A TEST BATTERY OF IMPULSIVENESS 303
Sergeant, J. A., Geurts, H., Huijbregts, S., Scheres, A., & Oosterlaan, J. (2003). The top and the bot-tom of ADHD: A neuropsychological perspective. Neuroscience and Biobehavioral Reviews,27, 583–592.
Sergeant, J. A., Geurts, H., & Oosterlaan, J. (2002). How specific is a deficit of executivefunctioning for Attention-Deficit/Hyperactivity Disorder? Behavioural Brain Research,130, 3–28.
Sergeant, J. A., Oosterlaan, J., & van der Meere, J. (1999). Information processing and energeticfactors in attention deficits/hyperactivity disorder. In H. C. Quay & A. E. Hogan (Eds.), Hand-book of disruptive behaviour disorder (pp. 75–104). New York: Kluwer/Plenum.
Schmitz, M., Cadore, L., Paczko, M., Kipper, L., Chaves, M., Rohde, L. A., Moura, C., & Knijnik,M. (2002). Neuropsychological performance in DSM-IV ADHD subtypes: An exploratorystudy with untreated adolescents. Canadian Journal of Psychiatry, 47, 863–869.
Silk, T., Vance, A., Rinehart, N., Egan, G., O’Boyle, M., Bradshaw, J. L., & Cunnington, R. (2005).Fronto-parietal activation in attention-deficit hyperactivity disorder, combined type: Functionalmagnetic resonance imaging study. British Journal of Psychiatry, 187, 282–283.
Simon, J. R., & Berbaum, K. (1988). Effect of irrelevant information on retrieval time for relevantinformation. Acta Psychologica, 61, 33–57.
Simon, J. R., & Berbaum, K. (1990). Effect of conflicting cues on information-processing: TheStroop Effect vs the Simon Effect. Acta Psychologica 73(2), 159–170.
Smith A., Lidzba K., Taylor, E., & Rubia, K. (2003). A right hemispheric fronto-striatal network fortemporal discrimination. NeuroImage, 20, 344–350.
Smith, A., Taylor, E., Brammer, M., & Rubia, K. (2004). The neural correlates associated withswitching set as measured using fast, event-related functional magnetic resonance imaging.Human Brain Mapping, 21, 247–256.
Smith, A., Taylor, E., Brammer M., & Rubia, K. (2006). Task specific hypoactivation in prefrontaland temporo-parietal brain regions in medication-naïve children and adolescents with AttentionDeficit/Hyperactivity Disorder during motor inhibition and task switching. American Journalof Psychiatry, 163, 957–960.
Smith, A., Taylor, E., Warner-Rogers, J., & Rubia, K. (2002). Temporal processing in children withADHD: Evidence for a pure time perception deficit in ADHD. Journal of Child Psychologyand Psychiatry 43, 529–542.
Smith, O. W. (1957). Relationship between rhythm discrimination to motor rhythm performance.Journal of Applied Psychology, 41, 365–369.
Solanto, M. V., Abikoff, H., Sonuga-Barke, E., Schachar, R., Logan, G. D., Wigal, T., Hechtman,L., Hinshaw, S., & Turkel, E. (2001). The ecological validity of delay aversion and responseinhibition as measures of impulsivity in AD/HD: A supplement to the NIMH multimodaltreatment study of AD/HD. Journal of Abnormal Child Psychology, 29, 215–228.
Solanto, M. V., Wender, E. H., & Bartell, S. S. (1997). Effects of Methylphenidate and behav-ioural contingencies on sustained attention in attention-deficit hyperactivity disorder: A testof the reward dysfunction hypothesis. Journal of Child and Adolescent Psychopathology, 7,123–136.
Sonuga-Barke, E. J. S. (2005). Causal models of Attention-Deficit/Hyperactivity Disorder: fromsimple deficits to multiple developmental pathways. Biological Psychiatry, 57, 1231–1238.
Sonuga-Barke, E. J., & Taylor, E. (1992). The effect of delay on hyperactive and non-hyperactivechildren’s response times: A research note. Journal of Child Psychology and Psychiatry, 33,1091–1096.
Sonuga-Barke, E. J., Saxton, T., & Hall, M. (1998). The role of interval underestimation in hyper-active children’s failure to suppress responses over time. Behavioural Brain Research, 94,45–50.
Sowell, E. R., Thompson, P. M., Welcome, S. E., Henkenius, A. L., Toga, A. W., & Peterson, B. S.(2003). Cortical abnormalities in children and adolescents with attention-deficit hyperactivitydisorder. Lancet, 362, 1699–1707.

304 K. RUBIA ET AL.
Stuss, D. T., Murphy, K. J., Binns, M. A., & Alexander, M. P. (2003). Staying on the job: The fron-tal lobes control individual performance variability. Brain, 126, 2363–2380.
Swanson, J. M., Casey, B. J., Nigg, J., Castellanos, E. X., Volkow, N. D., & Taylor, E. (2004).Clinical and cognitive definitions of attention deficits in children with attention-deficit/hyper-activity disorder. In M. I. Posner (Ed.) Cognitive neuroscience of attention (pp. 430–445).New York: Guilford Press.
Taylor, E., Chadwick, O., Heptinstall, E., & Danckaerts, M. (1996). Hyperactivity and conductproblems as risk factors for adolescent development. Journal of the American Academy ofChild Psychiatry, 35, 1213–1226.
Taylor, E., Sandberg, E., Thorley, G. & Giles, S. (1991). The epidemiology of childhoodhyperactivity. Maudsley Monograph No. 33. Oxford: Oxford University Press.
Toplak, M. E., Rucklidge, J. J., Hetherington, R., John, S. C. F., & Tannock, R. (2003). Timeperception deficits in attention-deficit/hyperactivity disorder and comorbid reading difficultiesin child and adolescent samples. J Child Psychology and Psychiatry, 44, 888–903.
Van der Meere, J., Shalev, R., Borger, N., & Grosstsur, V. (1995). Sustained attention, activationand MPH in ADHD: A research note. Journal of Child Psychology and Psychiatry and AlliedDisciplines, 36, 697–703.
van Mourik, R., Oosterlaan, J., & Sergeant, J. A. (2005). The Stroop revisited: A meta-analysis ofinterference control in AD/HD. Journal of Child Psychology and Psychiatry, 46, 150–165.
Voisin, J., Bidet-Caulet, A., Bertrand, O., & Fonlupt, P. (2006). Listening in silence activates auditoryareas: A functional magnetic resonance imaging study. Journal of Neuroscience, 26, 273–278.
Vongher, J. M., Vassileva, J. L., Fischer, M., Conant, L., Risinger, R. C., Salmeron, B. J., Stein, E.A., Barkley, R. A., & Rao, S. M. (2001). Behavioral inhibition and motor timing in ADHDadults. Brain and Cognition, 47, 219–222.
West, J., Douglas, G., Houghton, S., Lawrence, V., Whiting, K., & Glasgow, K. (2000). Timeperception in boys with attention-deficit/hyperactivity disorder according to time duration,distraction and mode of presentation. Child Neuropsychology 6, 241–250.
White, J. L., Moffitt, T. E., Caspi, A., Bartusch, D. J., Needles, D. J., & Stouthamerloeber, M.(1994). Measuring impulsivity and examining its relationship to delinquency. Journal ofAbnormal Psychology, 103, 192–205.
Willcutt, E. G., Doyle, A. E., Nigg, J. T., Faraone, S. V., & Pennington, B. F. (2005). Validity of theexecutive function theory of Attention Deficit/Hyperactivity Disorder: A meta-analytic review.Biological Psychiatry, 57, 1336–1346.
Williams, B. R., Ponesse, J. S., Schachar, R. J., Logan, G. D., & Tannock, R. (1999). Developmentof inhibitory control across the life span. Developmental Psychology, 35, 205–213.
Copyright © 2022 FDOKUMEN




















