
TIME REPRODUCTION DISTURBANCES IN ADHD CHILDREN: AN ERP STUDY

Attention deficit hyperactivity disorder (ADHD)and executive functioning in affected and unaffectedadolescents and their parents: challenging theendophenotype construct
A. J. A.M. Thissen1,2*, N. N. J. Rommelse1,2, P. J. Hoekstra3, C. Hartman3, D. Heslenfeld4, M. Luman4,M. van Lieshout4, B. Franke5, J. Oosterlaan4 and J. K. Buitelaar2,6
1Department of Psychiatry, Donders Institute for Brain, Cognition and Behaviour, Radboud University Medical Centre, Nijmegen, The Netherlands2Karakter Child and Adolescent Psychiatry University Centre, Nijmegen, The Netherlands3Department of Psychiatry, University Medical Centre Groningen, University of Groningen, The Netherlands4VU University, Amsterdam, The Netherlands5Departments of Human Genetics and Psychiatry, Radboud University Nijmegen Medical Centre, Nijmegen, The Netherlands6Department of Cognitive Neuroscience, Donders Institute for Brain, Cognition and Behaviour, Radboud University Medical Centre, Nijmegen,The Netherlands
Background. The results of twin and sibling studies suggest that executive functioning is a prime candidate endo-phenotype in attention deficit hyperactivity disorder (ADHD). However, studies have not assessed the co-segregationof executive function (EF) deficits from parents to offspring directly, and it is unclear whether executive functioningis an ADHD endophenotype in adolescents, given the substantial changes in prefrontal lobe functioning, EF andADHD symptoms during adolescence.
Method. We recruited 259 ADHD and 98 control families with an offspring average age of 17.3 years. All participantswere assessed for ADHD and EF [inhibition, verbal (VWM) and visuospatial working memory (VsWM)]. Data wereanalysed using generalized estimating equations (GEEs).
Results. Parental ADHD was associated with offspring ADHD and parental EF was associated with offspring EF butthere were no cross-associations (parental ADHD was not associated with offspring EF or vice versa). Similar resultswere found when siblings were compared. EF deficits were only found in affected adolescents and not in their unaffectedsiblings or (un)affected parents.
Conclusions. The core EFs proposed to be aetiologically related to ADHD, that is working memory and inhibition, seemto be aetiologically independent of ADHD in adolescence. EF deficits documented in childhood in unaffected siblingswere no longer present in adolescence, suggesting that children ‘grow out’ of early EF deficits. This is the first studyto document ADHD and EF in a large family sample with adolescent offspring. The results suggest that, after childhood,the majority of influences on ADHD are independent from those on EF. This has potential implications for currentaetiological models of causality in ADHD.
Received 2 November 2012; Revised 1 May 2013; Accepted 2 May 2013; First published online 31 May 2013
Key words: ADHD, adolescents, endophenotype, executive functioning.
Introduction
Attention deficit hyperactivity disorder (ADHD), ahighly prevalent (∼5%) and strongly heritable (70–75%)neurodevelopmental disorder, is often accompaniedby weaknesses in executive functions (EFs) (Willcuttet al. 2005). These functions are defined as neuro-cognitive processes that maintain an appropriate
problem-solving set to attain a future goal (Welsh &Pennington, 1988) and mainly encompass inhibitorycontrol, working memory, shifting and planning(Best et al. 2009). Meta-analyses indicate that work-ing memory (weighted effect sizes 0.47–0.85) andinhibition (weighted effect sizes 0.58–0.61) are stronglyassociated with ADHD (Lijffijt et al. 2005; Martinussenet al. 2005; Willcutt et al. 2005; Kasper et al. 2012).However, the causal role of EF deficits in ADHD isunclear, given that only about a third of patients sufferfrom such deficits (Nigg et al. 2005; Willcutt et al. 2005;Fair et al. 2012) and that about half of healthy control
* Address for correspondence: Ms. A. J. A. M. Thissen, ReinierPostlaan 12, 6525 GC Nijmegen, The Netherlands.
(Email: [email protected])
Psychological Medicine (2014), 44, 881–892. © Cambridge University Press 2013doi:10.1017/S0033291713001153
ORIGINAL ARTICLE

children have one or more EF impairments (Nigget al. 2005). This suggests that EF deficits are neithernecessary nor solely responsible for ADHD in allpatients (Willcutt et al. 2005), although they mayhave a causative role in a subset of patients.
Some key aspects in the relationship betweenADHD and EF are still underexplored, includingwhether EF deficits and ADHD co-segregate fromparent to offspring. To our knowledge, only onestudy addressed this question. In their study of pat-terns of inheritance of both ADHD and inhibitorycontrol, Goos et al. (2009) found that paternal inhibi-tory control was related to offspring inhibitory controlindependently of ADHD symptom severity. Similarly,we did not find EF in children to influence the associ-ation between parent and offspring ADHD symptoms(Thissen et al. 2012), which suggests that EF may notbe part of the causal pathway from genes to ADHDsymptoms. Other studies have reported EF to be mod-estly associated in parents and offspring (Nigg et al.2004; Jester et al. 2009) or ADHD (Nigg et al. 2004;Seidman et al. 2005; van Steijn et al. 2012) but thesestudies did not investigate whether ADHD and EFdeficits are transmitted together between generations,which would indicate an aetiological link betweenthe two. Despite familial associations being modest,the inclusion of EF endophenotypes can facilitate un-ravelling the aetiological nature of parent–offspringrelationships, which can lead to identification ofmore homogeneous aetiological subgroups in ADHDand/or parent-specific causal pathways underlyingcognitive deficits (Coghill et al. 2005; Thissen et al.2012).
Other study designs have found support for thehypothesis that ADHD and EF partly share aetio-logical factors. Twin modelling studies have shown amoderate/substantial overlap in genetic influences onADHD and EF measures of inhibition and work-ing memory (Kuntsi et al. 2006; Bidwell et al. 2007).Similarly, several family studies have providedevidence that ‘cool’ [inhibition, verbal (VWM) andvisuospatial working memory (VsWM)] and ‘hot’(delay aversion) EF impairments are also present inthe unaffected siblings of ADHD patients (Rommelse,2008; Bitsakou et al. 2009). Furthermore, reports onthe association between ADHD candidate genes andmeasures of EF suggest that some genes may indeedincrease the risk of both ADHD and EF deficits(Cummins et al. 2012; Gilsbach et al. 2012). However,on the basis of these studies it cannot be concludedthat EF deficits give rise to ADHD.
Another view on this issue is offered by studiesof patients with persisting or remitting ADHD. Coreneurocognitive deficits of ADHD are those deficitsthat are present in patients with remitting ADHD,
whereas deficits that are no longer present in thesepatients are seen as epiphenomena (Halperin &Schulz, 2006), that is, related to the same factors asADHD but not mediating between risk factors andADHD (Walters & Owen, 2007). However, it couldalso be argued that the deficits that disappear whensymptoms diminish are the ones that are aetiologicallyrelated to, or at least play an important role in main-taining, ADHD. One study found that patients withADHD in remission no longer had EF abnormalities(Halperin et al. 2008); however, in general, studieshave not reported inhibition or VWM to be associatedwith changes in symptoms (for an extensive review onthis topic, see van Lieshout et al. 2013). Given that theargument of EF being causal for ADHD cannot bebased solely on the concurrent improvement of EF per-formance and ADHD symptom decline throughoutdevelopment within an observational study design,more research is needed.
Because age clearly plays a significant role in bothADHD symptom decline and EF development, theinfluence of developmental factors needs to be takeninto account when studying both. In light of executivefunctioning relying significantly on frontal lobe func-tioning (Rubia et al. 2001, 2003), the relationshipbetween ADHD and EF in adolescence is of particularinterest because it is this area of the brain that showspronounced developmental changes during adoles-cence and young adulthood in healthy subjects(Blakemore & Choudhury, 2006) and also abnormalactivity in individuals with ADHD (Durston et al.2003). In healthy individuals, performance on EFtasks, such as inhibitory control and VWM, continuesto develop during adolescence (Leon-Carrion et al.2004; Luna et al. 2004; Luciana et al. 2005) and evenin young adulthood (De Luca et al. 2003). Never-theless, to what extent development may moderatethe relationship between ADHD and EF is still un-known.
The aim of the present study was to investigatethe association between ADHD and EF by determin-ing whether they have similar aetiological rootsduring adolescence. In this case it was expected that(a) ADHD and EF would co-segregate from parent tooffspring, (b) ADHD and EF would cross-correlatebetween siblings and (c) unaffected siblings wouldshow EF weaknesses comparable to those seen intheir affected siblings. This is the first study to investi-gate these issues in a large family sample of parentsand their adolescent offspring, using data obtainedwith robust EF tasks (a stop task, a verbal digit spantask and a visuospatial grid task) previously shownto be sensitive to EF impairments in children withADHD (Klingberg et al. 2002; Westerberg et al. 2004;Rommelse et al. 2008).
882 A. J. A.M. Thissen et al.

Method
Participants
Participants were selected from the Dutch follow-up(2009–2012) of the International Multicentre ADHDGenetics (IMAGE) study performed between 2003and 2006 (as described previously in Nijmeijer et al.2009). Inclusion criteria at enrolment for all parti-cipants were offspring age between 5 and 19 years,European Caucasian descent, IQ 570, and no dia-gnosis of autism, epilepsy, general learning difficulties,brain disorders or known genetic disorders (suchas Fragile X syndrome or Down syndrome). All familymembers were invited to a follow-up assessment, witha mean follow-up period of 5.9 (S.D.=0.72) years andno additional inclusion criteria, apart from a minimumage of 8 years for neuropsychological testing and im-aging. The current study involved 259 ADHD familiesand 98 control families with at least one family mem-ber with a complete neuropsychological assessment.The ADHD families consisted of 406 affected sib-lings (153 combined, 155 inattentive, 37 hyperactive-impulsive subtype and 61 subthreshold cases), 209unaffected siblings and 452 parents (174 affected, 278unaffected). The control families consisted of 193 chil-dren and 137 parents. The mean age of the offspringwas 17.3 (S.D.=3.7) years and that of the parents was48.6 (S.D.=5.0) years. Table 1 provides details of theparticipants’ characteristics.
ADHD diagnoses
All participants were reassessed using a semi-structured diagnostic interview [Dutch translation ofthe Schedule for Affective Disorders and Schizo-phrenia for School-Age Children – Present and Life-time Version (K-SADS-PL; Kaufman et al. 1997)] andConners’ ADHD questionnaires to determine currentADHD diagnoses. A diagnostic algorithm was appliedto combine symptom counts on the K-SADS-PL andConners’ questionnaire. A detailed description of thealgorithm is provided in Table 2.
Measures
Parent and offspring ADHD symptoms
Information concerning current ADHD symptoms wasobtained using the Dutch version of the Conners’Adult ADHD Rating Scale –Observer: Screen Ver-sion (CAARS-O:SV) for parents and the Conners’Parent Rating Scale –Revised: Long version (CPRS-R:L) for children (Conners et al. 1999). For each parent,the DSM Total Score was used as a measure of currentparental ADHD severity. Scores on the ADHD Inatten-tive and Hyperactive-Impulsive scales were used to
verify possible differential effects for inattention andhyperactivity-impulsivity. The same method was usedfor offspring, using the subscales DSM Total Score,ADHD Inattentive and ADHD Hyperactive-Impulsive.
Neuropsychological paradigms
Inhibition. A visual Stop task (Logan et al. 1984) wasused to measure inhibition of an ongoing response.Details of the task and its administration havebeen described elsewhere (Rommelse et al. 2008).Functional magnetic resonance imaging (fMRI) scanswere recorded while the children performed the task,which consisted of four experimental blocks of 48Go and 12 Stop trials. The delay between Go andStop signals was adapted online so as to lead tosuccessful inhibition in 50% of the trials. The out-come measure was the Stop Signal Reaction Time(SSRT), which reflects the latency of the inhibitoryprocess.
VsWM. VsWM grid tasks, including active rehearsaland dual-task requirements, were used to measureexecutive VsWM in parents (Westerberg et al. 2004)and children (Dumontheil & Klingberg, 2012).Parents had to reproduce sequences of circles appear-ing in a 4×4 grid by pointing to the corresponding pos-itions with an arrow driven by a computer mouse.Trials increased in sequence length from two to nine.At every level, the last two trials (sublevel B) containeda more complex spatial pattern than the first twotrials (sublevel A). The task was stopped whensubjects failed to complete both trials of a sublevel.The number of correct trials, taking into account bothlocation and order, was used as a measure of VsWMin parents.
Children performed a slightly different version ofthe task while fMRI scans were recorded. The task con-sisted of experimental and control trials, the latterbeing used to control for non-working-memory-relatedbrain activity in fMRI analyses (not part of this study).After each sequence, the children were presented witha number and a question mark in the grid, probingboth spatial and temporal positions in the sequence.With a yes/no response they had to indicate whetherthe probed location was indeed stimulated at that pos-ition in the sequence. The task consisted of four exper-imental blocks of 24 trials. In each block, two types oftask load (sequence length either three or six) were pre-sented, and within each task load 50% of the trialswere experimental or control. The number of correctexperimental trials, taking into account both locationand order, was used as a measure of VsWM in chil-dren, including both task loads because all groups
ADHD and EF in adolescents and their parents 883

differed equally on both low and high memory loads(van Ewijk et al. 2013).
VWM. The total number of correct trials (Total score)on the Digit Span Backwards of the Wechsler Intel-ligence Scale for Children (WISC; Wechsler, 2002) orthe Wechsler Adult Intelligence Scale – III (WAIS-III;Wechsler, 2000) was used as a measure of VWM inparents and children.
Intelligence. Full-scale IQ was estimated in parents andchildren by combining scores on the two subtests ofthe WISC/WAIS-III that show the highest correlationwith full-scale IQ score, namely Vocabulary andBlock Design (0.88 for WISC and 0.90 for WAIS)(Silverstein, 1975, 1982).
Procedure
This study was part of a comprehensive assessmentprotocol. Because of time constraints in recordingfMRI scans, the VsWM and Stop tasks were adminis-tered in a random 75% sample of all scans, with amaximum of two children per family. fMRI scanswere not recorded in parents. Participants were askednot to use psychostimulant drugs from 48 h beforethe assessment and not to use any other psychotropicmedication at least 3 days before the assessment.After the study procedures had been carefullyexplained, all participants gave their written informedconsent, with parents providing consent for childrenaged below 12 years. The study protocol was approvedby the local medical ethics committees of the Radboud
Table 1. Sample characteristics of parents and adolescents
ParentsAffected Unaffected Controls Group main
effectaPairwise groupcomparisons (p<0.05)bn=174 n=278 n=137
Age (years), mean (S.D.) 48.0 (5.2) 48.6 (5.2) 49.1 (4.2) N.S.% Male 54.0 41.0 43.1 7.8* 1>2=3Estimated IQ, mean (S.D.) 102.3 (17.2) 101.3 (16.5) 111.7 (16.0) 19.3** 1=2<3Conners’ Observer DSM-IVc
Inattention, mean (S.D.) 52.2 (10.7) 44.2 (7.5) 41.9 (4.4) 72.8** 1>2>3Hyperactive-Impulsive, mean (S.D.) 54.9 (11.1) 45.1 (7.1) 43.7 (5.1) 93.2** 1>2=3
ADHD diagnosisInattentive, n (%) 26 (15) – –Hyperactive-Impulsive, n (%) 15 (8) – –Combined, n (%) 65 (37) – –Subthreshold, n (%) 68 (39) – –
Adolescents n=406 n=209d n=193
Age (years), mean (S.D.) 17.4 (3.4) 17.4 (4.0) 16.8 (3.8) N.S.Age<12 years (%) 9.6 13.4 17.1 7.1* 1<3, 1=2/2=3% Male 70.9 39.7 39.9 80.2** 1>2=3Estimated IQ, mean (S.D.) 96.6 (16.3) 101.2 (15.4) 107.3 (14.5) 31.2** 1<2<3Conners’ Parent DSM-IVc
Inattention, mean (S.D.) 63.5 (11.8) 48.0 (6.6) 46.6 (5.9) 287.0** 1>2=3Hyperactive-Impulsive, mean (S.D.) 67.2 (48.8) 48.8 (7.9) 46.6 (5.0) 283.5** 1>2=3
ADHD diagnosis DSM-IVInattentive, n (%) 155 (37) – –Hyperactive-Impulsive, n (%) 37 (9) – –Combined, n (%) 153 (37) – –Subthreshold, n (%) 61 (17) – –
ADHD, Attention deficit hyperactivity disorder; S.D., standard deviation; N.S., not significant.a F statistic; group differences for % male were tested with χ2 tests.b 1=Affected, 2=Unaffected, 3=Control.c t scores based on American norm group; Dutch t scores are found to be lower [Dutch (Adult) Twin Register].d Twenty-three (11%) remitted cases, similar to the International Multicentre ADHD Genetics (IMAGE) approach; results
with and without remitted cases did not differ.* p<0.05, **p<0.001.
884 A. J. A.M. Thissen et al.

University Nijmegen Medical Centre and the VUMedical Centre Amsterdam.
Data analyses
MRI was contraindicated in about 25% of the children(for instance because of wearing braces), so that datawere available for the Stop task and the VsWM taskfor 460 (54%) and 475 (56%) children respectively(missing data not replaced). Children with andwithout data on the Stop task did not differ in age(mean=17.7 v. 17.2 years, p=0.053), sex (male 56%v. 55%, p=0.82), IQ (mean=101 v. 100, p=0.25) or pro-portion diagnosed with ADHD (50% v. 52%, p=0.36).This was also the case for children with and withoutVsWM task data (p’s between 0.14 and 0.95). Lessthan 6% of data for all other measures were missing
and seemed to be missing at random. The missingdata (i.e. <6%) were replaced by means of expectationmaximization. Cognitive and ADHD measures weresuccessfully normalized and standardized into z scores(van der Waerden transformation) for parents and off-spring separately. For SSRTs, z scores were mirrored,so that higher z scores for all measures would havethe same meaning: better EF performance or moresevere ADHD symptomatology. The results based onraw and standardized measures were similar.
To test whether parental ADHD and cognitive func-tions predicted offspring ADHD and cognitive func-tions, generalized estimating equations (GEEs) wereused with a linear regression model and robust esti-mators. To maximally correct for familial dependencewithin the data set (for example, two mother–childeffects were calculated in most families), family
Table 2. Diagnostic algorithm for attention deficit hyperactivity disorder (ADHD) in the International Multicentre ADHD Genetics(NeuroIMAGE) sample
To determine ADHD diagnoses, a combination of Conners’ ADHD questionnaires and a semi-structured diagnostic interviewwas used. Each participant was assessed with a parent-rated questionnaire [Conners’ Parent Rating Scale –Revised: Longversion (CPRS-R:L)] and either a teacher rating [Conners’ Teacher Rating Scale –Revised: Long version (CTRS-R:L) appliedfor children<18 years] or a self-report [Conners’ Adult ADHD Rating Scales – Self-Report: Long version (CAARS-S:L) appliedfor children 518 years]. Participants were administered the Dutch translation of the Schedule for Affective Disorders andSchizophrenia for School-Age Children – Present and Lifetime Version (K-SADS-PL: Kaufman et al. 1997) containingdevelopmentally appropriate questions to assess each of the 18 ADHD symptoms, compatible with DSM-IV-TR (APA, 2000).Parents, reporting on their children, and the children themselves, if 512 years old, were interviewed separately. Final scoreson each item of the K-SADS were determined by weighing all available information. Initially, all participants were administeredthe K-SADS ADHD screening interview. Participants with elevated scores on any of the screen items were administered the fullADHD supplement. For participants using medication, ratings were gathered of participants’ functioning off medication. Usinga diagnostic algorithm, a combined symptom count was calculated by adding symptom counts on the K-SADS and CTRS-R:L(for participants aged<18 years) or the CAARS-S:L (for participants aged 518 years), both providing operational definitionsof each of the 18 behavioural symptoms defined by DSM-IV. Symptoms of the CTRS-R:L or CAARS-S:L were only added tothe combined symptom count if at least two symptoms were reported to avoid the Conners’ score putting too much weighton the diagnosis.
From the Conners’ ADHD questionnaires the following scales were used: DSM Inattentive behaviour (scale L of the CTRS-R:L/CPRS-R:L; scale E of the CAARS-S:L), DSM Hyperactive/Impulsive behaviour (scale M of the CTRS-R:L/CPRS-R:L; scale F of theCAARS-S:L), and DSM Total (scale N of the CTRS-R:L/CPRS-R:L; scale G of the CAARS-S:L). Participants with a combinedsymptom count of at least six symptoms of hyperactive/impulsive behaviour and/or inattentive behaviour were diagnosed withADHD, provided they: (a) met the DSM-IV criteria for pervasiveness and impact of the disorder (measures derived from theK-SADS), (b) showed an age of onset before 12, and (c) received a t value 563 on at least one of three scales on at least oneof the Conners’ ADHD questionnaires (i.e. CPRS-R:L and/or CTRS-R:L for children<18 years and CPRS-R:L and/or CAARS-S:Lfor children 518 years), pertaining to a period without medication.
Participants with a combined symptom count of at least six symptoms who did not meet one or more of these criteria wereevaluated by a team of trained experts to derive a consensus decision on their diagnosis. Unaffected participants were requiredto receive a t <63 on each of the above-mentioned scales of each of the Conners’ ADHD questionnaires, and have a combinedsymptom count of up to three symptoms. For young adults (518 years), criteria were adapted slightly such that a combinedsymptom count of five instead of six symptoms was sufficient for a diagnosis (Kooij et al. 2005), and with up to two symptomson the combined symptom count they were labelled ‘unaffected’. Participants not meeting criteria for ADHD or unaffected statuswere labelled ‘subthreshold ADHD’. Diagnostic procedure for parents were similar to those applied for children 518 years.The ADHD questionnaire was completed by their partner [Conners’ Adult ADHD Questionnaire –Observer: Short version(CAARS-O:SV)]. A retrospective childhood diagnosis was established in addition to a current diagnosis, using the samediagnostic algorithm used for young adults. Parents with a current and/or childhood diagnosis were labelled as affected(n=7 having only a childhood diagnosis of ADHD).
ADHD and EF in adolescents and their parents 885

number was used as a repeated measure and thestructure for working correlation matrices was setat exchangeable. In all parent–offspring analyses (car-ried out separately for ADHD symptomatology, in-hibition, VWM, VsWM and IQ), age and sex ofthe child, parental age and their interactions withthe main predictor were implemented in the model.Maternal and paternal total ADHD symptomatology(which were not strongly correlated: r=0.19, p<0.001)were included simultaneously in the same models.The mediation effects of child EF on parent–offspringADHD relationships were computed using a multiplemediation bootstrap analysis (Preacher & Hayes,2004) and the moderation effects of parental EF wereinvestigated by examining the interaction between par-ental ADHD and EF in relation to offspring ADHD.Individual correlations between EF/IQ and ADHD,and sibling (first and second born) and spouse corre-lations for EF/IQ and ADHD were calculated withcorrection for age differences (spouse and sibling)and sex differences (siblings). Individual correlationswere calculated with GEEs to correct for familialdependence. Group differences [ADHD affected, un-affected (but related to affected sibling or child), control]were calculated for parents and offspring separately,using the aforementioned model with GEEs includinggroup and sex as factors and age as a covariate. ForEF measures, analyses were conducted with and with-out IQ as a covariate. Performance ceiling effects didnot occur on any of the tasks, as indicated by boxplotanalyses with raw data. Effect sizes in all modelswere defined in terms of standardized b (in parent–offspring analyses indicating the z score increase ofa dependent measure at the increase of one z scoreon an independent measure) or Cohen’s d (group com-parisons). A false discovery rate (FDR) correction wasused when there were multiple comparisons, using aq value setting of 0.05.
Results
Parental and adolescent EF and IQ group differences
The performance of the three parent groups is pre-sented in Fig. 1a. Group differences with medium tolarge effect sizes were found for VsWM, VWM andIQ. Affected and unaffected parents performed simi-larly on all EF measures. Control parents performedbetter than unaffected parents on VsWM and VWM(d=0.30, p=0.02 and d=0.27, p=0.01 respectively).After correction for IQ, group differences for VsWMand VWM were no longer significant. There were nointeractions between group and age or sex on any cog-nitive measure, except for VWM (group×age b=–0.04,p=0.03). Post-hoc tests revealed that age had only
a minor negative effect in the unaffected group(b=−0.02, p=0.01). Small negative main effectsfor age, but not sex, were found on VsWM (b=–0.04,p<0.001) and IQ (b=0.03, p=0.004).
The results for adolescent group comparisons arepresented in Fig. 1b. Medium to large group differ-ences were found for all EF measures and IQ.Unaffected siblings and controls performed similarlyon all EF measures (p’s between 0.60 and 0.87).Affected siblings performed worse than unaffectedsiblings on the inhibition task (d=0.24, p=0.02) andworse than unaffected siblings and controls on VsWM(d=0.23 and 0.24 respectively, p’s<0.03) and VWM(d=0.36 and 0.54 respectively, p’s<0.001) tasks. Aftercorrection for IQ, group differences for VsWM wereno longer significant. Small positive effects of age,but not sex, were found on all four measures(b’s between 0.02 and –0.09, p’s<0.03). There were nosignificant interaction effects with group, except for agroup×age effect on inhibition, with task performanceimproving significantly with age in the unaffectedadolescents only (b=0.06, p=0.004).
Similar results were obtained when patients withsubthreshold ADHD were excluded from the affectedgroup.
Parent–offspring relationships for ADHD and EF
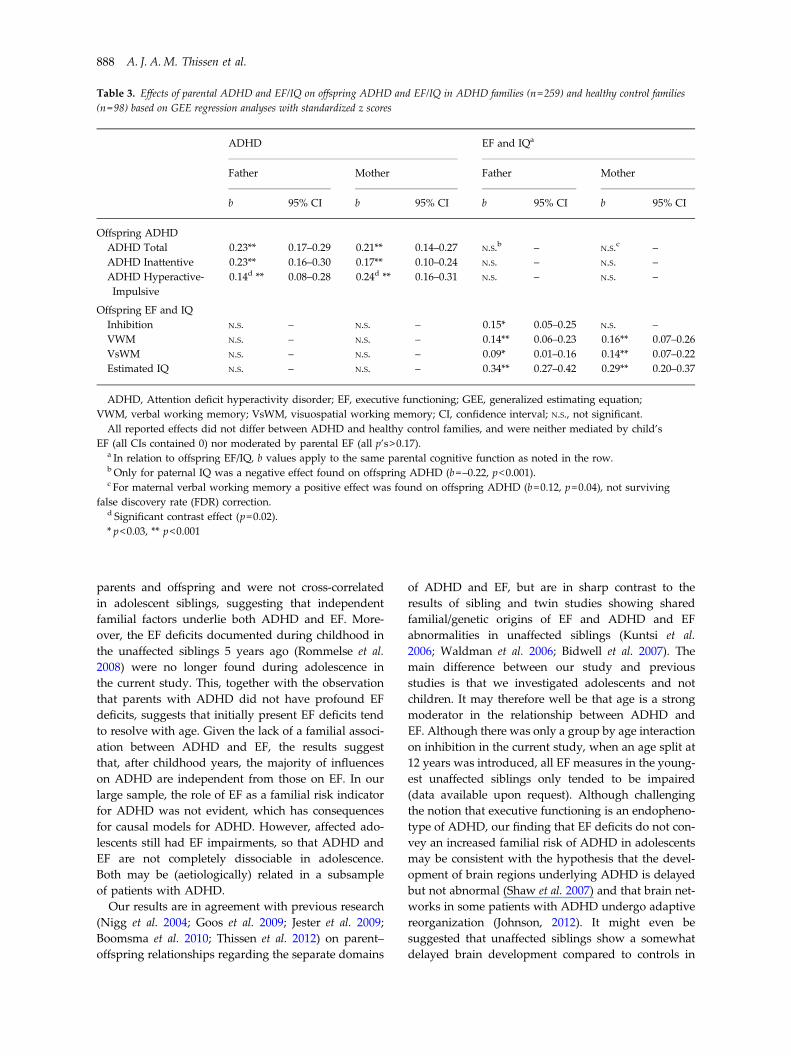
Table 3 shows the results for parent–offspring ana-lyses. The minor to moderately strong relationshipbetween parental and offspring ADHD (total and inat-tentive) was equally strong for fathers and mothers(p’s<0.001). The parent–offspring relationships forEF and IQ were positive for all measures and bothparents (father–offspring VsWM: p=0.026; all otherp’s<0.001) except for maternal inhibition (p=0.85).The largest effect size was found for IQ (b=0.34),followed by VWM, inhibition and VsWM (b=0.09).Testing for contrast effects revealed a strongermaternal than paternal parent–offspring relation-ship for hyperactive-impulsive symptoms, but therewere no other paternal and maternal differences inthe parent–offspring relationships for any of thecognitive measures (p’s between 0.15 and 0.75), illu-strating no effects of parental origin. None of theparent–offspring relationships interacted with child’sage, child’s sex or parental age (p’s between 0.06and 0.81).
To determine whether the aforementioned parent–offspring relationships for ADHD and EF/IQ differedbetween ADHD and control families, ‘family type’was included in the interaction with all independentparental measures. After FDR correction for multi-ple testing (14 interactions were tested), no significantresults remained (p’s between 0.03 and 0.97),
886 A. J. A.M. Thissen et al.

suggesting that parent–offspring effects were similar inADHD and healthy control families.
Co-segregation of EF and ADHD from parents tooffspring
Parental ADHD was not significantly associated withany offspring EF (p’s between 0.14 and 0.66) or IQ(p’s>0.30), nor was parental EF associated with off-spring ADHD (p’s between 0.17 and 0.93, and 0.04for maternal VWM, not surviving FDR correction),indicating that the transmission of ADHD and EFfrom parent to offspring was not associated in thissample. Multiple mediation bootstrapping revealednon-significant indirect effects of parental ADHD onoffspring ADHD through child EF and IQ (effectssizes between 0.005 and 0.01; all confidence intervalscontained 0). Including parental EF as a quantitativemeasure in the interaction with parental ADHDmeasures did not yield any significant results(p’s between 0.29 and 0.89). These findings suggestthat neither child EF nor parental EF influenced theparent–offspring ADHD relationship and that
therefore there was no co-segregation of ADHD andEF from parents to offspring.
Correlation analyses
Individual correlations between ADHD and EF/IQ arepresented in Table 4a. In offspring, EF/IQ was weaklyto moderately correlated with ADHD, whereas inparents almost none of the correlations were sig-nificant, except for a small effect for (inattentive)ADHD with inhibition. Table 4b shows correlationswithin families. Correlations between siblings wereminor for ADHD and around moderate for EF/IQ.Cross-correlations (ADHD sibling 1 – EF/IQ sibling 2and vice versa) were not significant (p’s between 0.17and 0.89), except for IQ (r=–0.13 p=0.02). Spouse cor-relations for ADHD and EF/IQ were overall small.
Discussion
In a large sample of ADHD affected and unaffectedadolescents and their parents, we observed thatADHD and EF were independently related between
(a) Inhibition Verbal working memory Visuospatial working memory Estimated IQ
Inhibition Verbal working memory Visuospatial working memory Estimated IQ(b)
0.40
Task
per
form
ance
(z s
core
s)Ta
sk p
erfo
rman
ce (z
sco
res)
–0.40
0.20
–0.20
0.00
0.40
–0.40
0.20
–0.20
0.00
ControlsUnaffected parents
Affectedparents
ControlsUnaffected parents
Affectedparents
ControlsUnaffected parents
Affectedparents
ControlsUnaffected siblings
Affectedsiblings
ControlsUnaffected siblings
Affectedsiblings
ControlsUnaffected siblings
Affectedsiblings
ControlsUnaffected siblings
Affectedsiblings
ControlsUnaffected parents
Affectedparents
p=0.004
p=0.02
p<0.0001
p<0.0001
p=0.02
p<0.001
p<0.001
p=0.005
p<0.0001
p<0.0001
p<0.0001
p=0.02
Fig. 1. Group differences on cognitive performance (a) between parents with attention deficit hyperactivity disorder (ADHD),unaffected parents of affected offspring and healthy control parents and (b) between adolescents with ADHD, their unaffectedsiblings and healthy controls. Higher z scores indicate better performance. Group differences indicated with dotted lines didnot reach significance after correction for IQ.
ADHD and EF in adolescents and their parents 887
parents and offspring and were not cross-correlatedin adolescent siblings, suggesting that independentfamilial factors underlie both ADHD and EF. More-over, the EF deficits documented during childhood inthe unaffected siblings 5 years ago (Rommelse et al.2008) were no longer found during adolescence inthe current study. This, together with the observationthat parents with ADHD did not have profound EFdeficits, suggests that initially present EF deficits tendto resolve with age. Given the lack of a familial associ-ation between ADHD and EF, the results suggestthat, after childhood years, the majority of influenceson ADHD are independent from those on EF. In ourlarge sample, the role of EF as a familial risk indicatorfor ADHD was not evident, which has consequencesfor causal models for ADHD. However, affected ado-lescents still had EF impairments, so that ADHD andEF are not completely dissociable in adolescence.Both may be (aetiologically) related in a subsampleof patients with ADHD.
Our results are in agreement with previous research(Nigg et al. 2004; Goos et al. 2009; Jester et al. 2009;Boomsma et al. 2010; Thissen et al. 2012) on parent–offspring relationships regarding the separate domains
of ADHD and EF, but are in sharp contrast to theresults of sibling and twin studies showing sharedfamilial/genetic origins of EF and ADHD and EFabnormalities in unaffected siblings (Kuntsi et al.2006; Waldman et al. 2006; Bidwell et al. 2007). Themain difference between our study and previousstudies is that we investigated adolescents and notchildren. It may therefore well be that age is a strongmoderator in the relationship between ADHD andEF. Although there was only a group by age interactionon inhibition in the current study, when an age split at12 years was introduced, all EF measures in the young-est unaffected siblings only tended to be impaired(data available upon request). Although challengingthe notion that executive functioning is an endopheno-type of ADHD, our finding that EF deficits do not con-vey an increased familial risk of ADHD in adolescentsmay be consistent with the hypothesis that the devel-opment of brain regions underlying ADHD is delayedbut not abnormal (Shaw et al. 2007) and that brain net-works in some patients with ADHD undergo adaptivereorganization (Johnson, 2012). It might even besuggested that unaffected siblings show a somewhatdelayed brain development compared to controls in
Table 3. Effects of parental ADHD and EF/IQ on offspring ADHD and EF/IQ in ADHD families (n=259) and healthy control families(n=98) based on GEE regression analyses with standardized z scores
ADHD EF and IQa
Father Mother Father Mother
b 95% CI b 95% CI b 95% CI b 95% CI
Offspring ADHDADHD Total 0.23** 0.17–0.29 0.21** 0.14–0.27 N.S.b – N.S.c –ADHD Inattentive 0.23** 0.16–0.30 0.17** 0.10–0.24 N.S. – N.S. –ADHD Hyperactive-Impulsive
0.14d ** 0.08–0.28 0.24d ** 0.16–0.31 N.S. – N.S. –
Offspring EF and IQInhibition N.S. – N.S. – 0.15* 0.05–0.25 N.S. –VWM N.S. – N.S. – 0.14** 0.06–0.23 0.16** 0.07–0.26VsWM N.S. – N.S. – 0.09* 0.01–0.16 0.14** 0.07–0.22Estimated IQ N.S. – N.S. – 0.34** 0.27–0.42 0.29** 0.20–0.37
ADHD, Attention deficit hyperactivity disorder; EF, executive functioning; GEE, generalized estimating equation;VWM, verbal working memory; VsWM, visuospatial working memory; CI, confidence interval; N.S., not significant.All reported effects did not differ between ADHD and healthy control families, and were neither mediated by child’s
EF (all CIs contained 0) nor moderated by parental EF (all p’s>0.17).a In relation to offspring EF/IQ, b values apply to the same parental cognitive function as noted in the row.b Only for paternal IQ was a negative effect found on offspring ADHD (b=–0.22, p<0.001).c For maternal verbal working memory a positive effect was found on offspring ADHD (b=0.12, p=0.04), not surviving
false discovery rate (FDR) correction.d Significant contrast effect (p=0.02).* p<0.03, ** p<0.001
888 A. J. A.M. Thissen et al.

childhood, yet accelerated compared to affectedsiblings in adolescence, with EF deficits during child-hood being markers of this delay. When compared totheir performance in childhood, we indeed foundsupport for an amelioration over time in unaffected,but not affected, adolescents’ performance, with un-affected siblings and controls not differing in ADHDsymptoms, comparable to the current findings(Rommelse et al. 2008), and with improved perform-ance in unaffected siblings on several EF domains(inhibition: d=0.19, p=0.048; VWM: d=0.20, p=0.02;VsWM: p=0.54), but not affected siblings (p’s between0.18 and 0.33) or controls (p’s between 0.06 and 0.35).
Alternatively or additionally, it may be that the samegenetic/familial mechanisms underlie EF deficits andADHD during childhood but not during adolescenceand possibly adulthood, which is in line with ourresults and many other studies showing no or onlysubtle impairments in adults with ADHD (Woodset al. 2002; Boonstra et al. 2005; but see Hervey et al.2004; Goos et al. 2009 for contrasting findings). How-ever, phenotypic correlations between ADHD symp-toms and EF task scores are typically found to be
small in childhood (population) samples as well(Willcutt et al. 2005; Crosbie et al. 2013), suggestingnon-EF factors play a role in the aetiology of ADHDthroughout the lifespan. Althoughwe cannot draw con-clusions about the role of genetics, the interpretation ofour results with regard to genetics is intriguing. It isknown that gene transcription is strongly influencedby developmental and the environment (Rutter et al.2006). Moreover, new, age-specific effects account formore than half of the familial (genetic and sharedenvironmental) influences on ADHD in early adoles-cence (Greven et al. 2011). Taken together, the resultsclearly indicate that the endophenotype construct ofexecutive functioning for ADHD is in any case depen-dent on developmental stage, a finding that shouldprompt reconsideration of our current understandingof the relationship between EF and ADHD.
Strengths and limitations
We improved upon previous studies by including alarge sample with cognitive data available for parentsand adolescent siblings and by performing careful
Table 4. (a) Individual correlations between ADHD symptomatology and cognitivefunctioning for parents and adolescents separately and (b) sibling and spouse correlations (r) forADHD symptomatology and cognitive functioning
(a) Inhibition VWM VsWM Estimated IQ
Parentsa
ADHD Inattentive −0.08** −0.02 −0.01 −0.02ADHD Hyperactive-Impulsive −0.03 −0.02 0.003 −0.01ADHD Total −0.07* −0.02 −0.004 −0.03
AdolescentsADHD Inattentive −0.13** −0.18** −0.15** −0.18**ADHD Hyperactive-Impulsive −0.11* −0.16** −0.15** −0.17**ADHD Total −0.13** −0.18** −0.15** −0.19**
(b) r
Sibling Spousea
ADHD Inattentive 0.16* 0.13*ADHD Hyperactive-Impulsive 0.05 0.12*ADHD Total 0.12* 0.19**Inhibition 0.13 0.08VWM 0.23** −0.04VsWM 0.28** −0.10*Estimated IQ 0.38** 0.22**
ADHD, Attention deficit hyperactivity disorder; VWM, verbal working memory;VsWM, visuospatial working memory.Significant correlations are indicated in bold.a ADHD scores obtained from observer reports.* p<0.05, **p<0.01.
ADHD and EF in adolescents and their parents 889

diagnostics. Furthermore, we investigated several EFparadigms and explicitly tested whether EF affectedthe relationship between parent–offspring ADHD.We also conducted all necessary analyses to investigatethe shared familiality of EF and ADHD and tooka thorough statistical approach by using GEEs foranalyses with correction for familial clustering. How-ever, some limitations should be acknowledged. Forexample, we included patients who were using medi-cation. Although participants were asked not to usetheir medication from 48 h prior to testing, there maystill have been confounding effects through medica-tion withdrawal and/or medication tolerance. Wealso used single measures of the EF constructs of inter-est. However, these measures were well validatedand have been shown to be robustly associated withADHD (Lijffijt et al. 2005; Martinussen et al. 2005; Will-cutt et al. 2005; Kasper et al. 2012). Another potentiallimitation is that inhibition and VsWM were measuredin offspring while they underwent fMRI, so that theyperformed tasks under different conditions fromthose of adults or from those when they were testedin childhood. This might have diminished thestrengths of the parent–offspring EF relationship andthe comparability of childhood and adolescent per-formance. However, with regard to parents and off-spring findings, if the different test environment isthe explanation for the absence of cross-relationshipsfor ADHD and EF, we would not expect to findparent–offspring relationships for the EF tasks either,which was clearly not the case. Concerning the differ-ential task conditions in childhood and adolescence,we consider that the different task conditions in child-hood and adolescence are unlikely to explain theobservation that EF deficits seemed to improve inunaffected offspring only (i.e. unaffected siblingswould then profit differentially from a test environ-ment normally experienced as more stressful). Thefinding that the youngest (below 12 years) unaffectedsiblings still showed EF deficits similar to those pre-viously reported in childhood supports the notionthat age, not task condition, is the most appropriateexplanation for the improved EF performance in theadolescent unaffected siblings. With regard to ourfindings in adults, it might be possible that no clearEF deficits were found in relation to ADHD becausereal-life EF difficulties cannot be detected with thestandard tasks (Torralva et al. 2013) used in our sampleof ADHD parents, who were recruited indirectlythrough their affected offspring. However, all taskscould detect EF deficits in affected adolescents,which suggests that the EF tasks used are sensitive toADHD pathology. Nevertheless, we recommend thatmore ecologically valid EF tasks be used in futurestudies as well.
Future directions
Our findings showing the importance of the effect ofage or developmental stage on the relationshipbetween executive functioning and ADHD have po-tential implications for current aetiological models ofcausality in ADHD. Therefore, a focus on age couldlead to greater insights concerning the relationshipbetween EF and ADHD. This paves the way for long-itudinal studies of developmental trajectories of,for example, EF in unaffected adult siblings and alsosibling (cross-)correlations in adult ADHD samples.We aim to follow up the current sample of adolescentsinto adulthood, to determine whether EF deficitswill eventually ameliorate in this sample of ADHDadolescents, and hence to establish a comprehensiveand sound model for EF and ADHD duringdevelopment.
Acknowledgements
We thank all the families and teachers who took part inthis study and all interns for their assistance in datacollection. We also thank R. Donders for his adviceon the statistical analyses.This work was supported by National Institutes ofHealth (NIH) Grant R01MH62873, The NetherlandsOrganization for Scientific Research (NOW) LargeInvestment Grant 1750102007010, and grants fromRadboud University Nijmegen Medical Centre, Uni-versity Medical Centre Groningen and Accare, andVU University Amsterdam.
Declaration of Interest
J. K. Buitelaar has been a consultant to/member ofadvisory board of/and/or speaker for Janssen CilagBV, Eli Lilly, Bristol–Myers Squibb, Organon/SheringPlough, UCB, Shire, Medice, Roche and Servier. P. J.Hoekstra has received advisory panel payments fromShire and Eli Lilly. All other authors have no conflictof interest to disclose.
References
APA (2000). Diagnostic and Statistical Manual of MentalDisorders, 4th edn, text revision (DSM-IV-TR). AmericanPsychiatric Association: Washington, DC.
Best JR, Miller PH, Jones LL (2009). Executive functionsafter age 5: changes and correlates. Developmental Review29, 180–200.
Bidwell LC, Willcutt EG, Defries JC, Pennington BF(2007). Testing for neuropsychological endophenotypesin siblings discordant for attention-deficit/hyperactivitydisorder. Biological Psychiatry 62, 991–998.
Bitsakou P, Psychogiou L, Thompson M, Sonuga-Barke EJ(2009). Delay aversion in attention deficit/hyperactivity
890 A. J. A.M. Thissen et al.

disorder: an empirical investigation of the broaderphenotype. Neuropsychologia 47, 446–456.
Blakemore SJ, Choudhury S (2006). Development of theadolescent brain: implications for executive function andsocial cognition. Journal of Child Psychology and Psychiatry47, 296–312.
Boomsma DI, Saviouk V, Hottenga JJ, Distel MA,de Moor MH, Vink JM, Geels LM, van Beek JH,Bartels M, de Geus EJ, Willemsen G (2010). Geneticepidemiology of attention deficit hyperactivity disorder(ADHD index) in adults. PLoS One 5, e10621.
Boonstra AM, Oosterlaan J, Sergeant JA, Buitelaar JK (2005).Executive functioning in adult ADHD: a meta-analyticreview. Psychological Medicine 35, 1097–1108.
Coghill D, Nigg J, Rothenberger A, Sonuga-Barke E,Tannock R (2005). Whither causal models in theneuroscience of ADHD? Developmental Science 8, 105–114.
Conners CK, Erhardt D, Sparrow EP (1999). Conners’ AdultADHD Rating Scales: CAARS. Multi-Health Systems: NorthTonawanda, NY.
Crosbie J, Arnold P, Paterson A, Swanson J, Dupuis A, Li X,Shan J, Goodale T, Tam C, Strug LJ, Schachar RJ (2013).Response inhibition and ADHD traits: correlates andheritability in a community sample. Journal of AbnormalChild Psychology 41, 497–507.
Cummins TD, Hawi Z, Hocking J, Strudwick M, Hester R,Garavan H, Wagner J, Chambers CD, Bellgrove MA(2012). Dopamine transporter genotype predictsbehavioural and neural measures of response inhibition.Molecular Psychiatry 17, 1086–1092.
De Luca CR, Wood SJ, Anderson V, Buchanan JA,Proffitt TM, Mahony K, Pantelis C (2003). Normative datafrom the CANTAB. I: Development of executive functionover the lifespan. Journal of Clinical and ExperimentalNeuropsychology 25, 242–254.
Dumontheil I, Klingberg T (2012). Brain activityduring a visuospatial working memory task predictsarithmetical performance 2 years later. Cerebral Cortex 22,1078–1085.
Durston S, Tottenham NT, Thomas KM, Davidson MC,Eigsti IM, Yang Y, Ulug AM, Casey BJ (2003). Differentialpatterns of striatal activation in young children with andwithout ADHD. Biological Psychiatry 53, 871–878.
Fair DA, Bathula D, Nikolas MA, Nigg JT (2012). Distinctneuropsychological subgroups in typically developingyouth inform heterogeneity in children with ADHD.Proceedings of the National Academy of Sciences USA 109,6769–6774.
Gilsbach S, Neufang S, Scherag S, Vloet TD, Fink GR,Herpertz-Dahlmann B, Konrad K (2012). Effects of theDRD4 genotype on neural networks associated withexecutive functions in children and adolescents.Developmental Cognitive Neuroscience 2, 417–427.
Goos LM, Crosbie J, Payne S, Schachar R (2009). Validationand extension of the endophenotype model in ADHDpatterns of inheritance in a family study of inhibitorycontrol. American Journal of Psychiatry 166, 711–717.
Greven CU, Asherson P, Rijsdijk FV, Plomin R (2011).A longitudinal twin study on the association between
inattentive and hyperactive-impulsive ADHD symptoms.Journal of Abnormal Child Psychology 39, 623–632.
Halperin JM, Schulz KP (2006). Revisiting the role ofthe prefrontal cortex in the pathophysiology ofattention-deficit/hyperactivity disorder. PsychologicalBulletin 132, 560–581.
Halperin JM, Trampush JW, Miller CJ, Marks DJ,Newcorn JH (2008). Neuropsychological outcome inadolescents/young adults with childhood ADHD: profilesof persisters, remitters and controls. Journal of ChildPsychology and Psychiatry 49, 958–966.
Hervey AS, Epstein JN, Curry JF (2004). Neuropsychologyof adults with attention-deficit/hyperactivity disorder: ameta-analytic review. Neuropsychology 18, 485–503.
Jester JM, Nigg JT, Puttler LI, Long JC, Fitzgerald HE,Zucker RA (2009). Intergenerational transmission ofneuropsychological executive functioning. Brain andCognition 70, 145–153.
Johnson MH (2012). Executive function and developmentaldisorders: the flip side of the coin. Trends in CognitiveSciences 16, 454–457.
Kasper LJ, Alderson RM, Hudec KL (2012). Moderators ofworking memory deficits in children with attention-deficit/hyperactivity disorder (ADHD): a meta-analytic review.Clinical Psychology Review 32, 605–617.
Kaufman J, Birmaher B, Brent D, Rao U, Flynn C, Moreci P,Williamson D, Ryan N (1997). Schedule for AffectiveDisorders and Schizophrenia for School-AgeChildren-Present and Lifetime Version (K-SADS-PL): initialreliability and validity data. Journal of the American Academyof Child and Adolescent Psychiatry 36, 980–988.
Klingberg T, Forssberg H, Westerberg H (2002). Training ofworking memory in children with ADHD. Journal of Clinicaland Experimental Neuropsychology 24, 781–791.
Kooij JJ, Buitelaar JK, van den Oord EJ, Furer JW, RijndersCA, Hodiamont PP (2005). Internal and external validity ofattention-deficit hyperactivity disorder in apopulation-based sample of adults. Psychological Medicine35, 817–827.
Kuntsi J, Rogers H, Swinard G, Borger N, van der Meere J,Rijsdijk F, Asherson P (2006). Reaction time, inhibition,working memory and ‘delay aversion’ performance: geneticinfluences and their interpretation. Psychological Medicine36, 1613–1624.
Leon-Carrion J, Garcia-Orza J, Perez-Santamaria FJ (2004).Development of the inhibitory component of the executivefunctions in children and adolescents. International Journal ofNeuroscience 114, 1291–1311.
Lijffijt M, Kenemans JL, Verbaten MN, van Engeland H(2005). A meta-analytic review of stopping performancein attention-deficit/hyperactivity disorder: deficientinhibitory motor control? Journal of Abnormal Psychology114, 216–222.
Logan GD, Cowan WB, Davis KA (1984). On the ability toinhibit simple and choice reaction time responses: a modeland a method. Journal of Experimental Psychology. HumanPerception and Performance 10, 276–291.
Luciana M, Conklin HM, Hooper CJ, Yarger RS (2005).The development of nonverbal working memory and
ADHD and EF in adolescents and their parents 891

executive control processes in adolescents. ChildDevelopment 76, 697–712.
Luna B, Garver KE, Urban TA, Lazar NA, Sweeney JA(2004). Maturation of cognitive processes from latechildhood to adulthood. Child Development 75, 1357–1372.
Martinussen R, Hayden J, Hogg-Johnson S, Tannock R(2005). A meta-analysis of working memory impairmentsin children with attention-deficit/hyperactivity disorder.Journal of the American Academy of Child and AdolescentPsychiatry 44, 377–384.
Nigg JT, Blaskey LG, Stawicki JA, Sachek J (2004).Evaluating the endophenotype model of ADHDneuropsychological deficit: results for parents and siblingsof children with ADHD combined and inattentive subtypes.Journal of Abnormal Psychology 113, 614–625.
Nigg JT, Willcutt EG, Doyle AE, Sonuga-Barke EJS (2005).Causal heterogeneity in attention-deficit/hyperactivitydisorder: do we need neuropsychologically impairedsubtypes? Biological Psychiatry 57, 1224–1230.
Nijmeijer JS, Hoekstra P, Minderaa R, Buitelaar J, Altink M,Buschgens CJM, Fliers E, Rommelse NNJ, Sergeant J,Hartman CA (2009). PDD symptoms in ADHD, anindependent familial trait? Journal of Abnormal ChildPsychology 37, 443–453.
Preacher KJ, Hayes AF (2004). SPSS and SAS proceduresfor estimating indirect effects in simple mediation models.Behaviour Research Methods, Instruments, and Computers 36,717–731.
Rommelse NN (2008). Endophenotypes in the geneticresearch of ADHD over the last decade: have they livedup to their expectations? Expert Review of Neurotherapeutics8, 1425–1429.
Rommelse NNJ, Altink ME, Oosterlaan J, Buschgens CJM,Buitelaar J, Sergeant JA (2008). Support for an independentfamilial segregation of executive and intelligenceendophenotypes in ADHD families. Psychological Medicine38, 1595–1606.
Rubia K, Russell T, Overmeyer S, Brammer MJ,Bullmore ET, Sharma T, Simmons A, Williams SCR,Giampietro V, Andrew CM, Taylor E (2001). Mappingmotor inhibition: conjunctive brain activations acrossdifferent versions of go/no-go and stop tasks. NeuroImage13, 250–261.
Rubia K, Smith AB, Brammer MJ, Taylor E (2003). Rightinferior prefrontal cortex mediates response inhibitionwhile mesial prefrontal cortex is responsible for errordetection. NeuroImage 20, 351–358.
Rutter M, Moffitt TE, Caspi A (2006). Gene-environmentinterplay and psychopathology: multiple varieties but realeffects. Journal of Child Psychology and Psychiatry 47, 226–261.
Seidman LJ, Biederman J, Monuteaux MC, Valera E,Doyle AE, Faraone SV (2005). Impact of gender and ageon executive functioning: do girls and boys with andwithout attention deficit hyperactivity disorder differneuropsychologically in preteen and teenage years?Developmental Neuropsychology 27, 79–105.
Shaw P, Eckstrand K, Sharp W, Blumenthal J, Lerch JP,Greenstein D, Clasen L, Evans A, Giedd J, Rapoport JL(2007). Attention-deficit/hyperactivity disorder is
characterized by a delay in cortical maturation. Proceedingsof the National Academy of Sciences USA 104, 19649–19654.
Silverstein AB (1975). Validity of WISC-R short forms. Journalof Clinical Psychology 31, 696–697.
Silverstein AB (1982). 2-Subtest and 4-subtest short formsof the Wechsler Adult Intelligence Scale-Revised. Journalof Consulting and Clinical Psychology 50, 415–418.
Thissen AJ, Rommelse NN, Altink ME, Oosterlaan J,Buitelaar JK (2012). Parent-of-origin effects in ADHD:distinct influences of paternal and maternal ADHD onneuropsychological functioning in offspring. Journal ofAttention Disorders. Published online: 24 May 2012. doi:10.1177/1087054712443159.
Torralva T, Gleichgerrcht E, Lischinsky A, Roca M, Manes F(2013). ‘Ecological’ and highly demanding executive tasksdetect real-life deficits in high-functioning adult ADHDpatients. Journal of Attention Disorders 17, 11–19.
van Ewijk H, Heslenfeld DJ, Luman M, Rommelse NN,Hartman CA, Hoekstra P, Franke B, Buitelaar JK,Oosterlaan J (2013). Visuospatial working memory inADHD patients, unaffected siblings, and healthy controls.Journal of Attention Disorders. Published online: 8 April 2013.doi: 10.1177/1087054713482582.
van Lieshout M, Luman M, Buitelaar J, Rommelse NN,Oosterlaan J (2013). Does neurocognitive functioningpredict future or persistence of ADHD? A systematicreview. Clinical Psychology Review 33, 539–560.
van Steijn DJ, Richards JS, Oerlemans AM, de Ruiter SW,van Aken MA, Franke B, Buitelaar JK, Rommelse NN(2012). The co-occurrence of autism spectrum disorderand attention-deficit/hyperactivity disorder symptoms inparents of children with ASD or ASD with ADHD.Journal of Child Psychology and Psychiatry 53, 954–963.
Waldman ID, Nigg JT, Gizer IR, Park L, Rappley MD,Friderici K (2006). The adrenergic receptor alpha-2A gene(ADRA2A) and neuropsychological executive functions asputative endophenotypes for childhood ADHD. Cognitive,Affective and Behavioral Neuroscience 6, 18–30.
Walters JT, Owen MJ (2007). Endophenotypes in psychiatricgenetics. Molecular Psychiatry 12, 886–890.
Wechsler D (2000). WAIS-III Nederlandstalige bewerking.Technische Handleiding. The Psychological Corporation:London.
Wechsler D (2002). WISC-III Handleiding. The PsychologicalCorporation: London.
Welsh MC, Pennington BF (1988). Assessing frontal-lobefunctioning in children: views from developmentalpsychology. Developmental Neuropsychology 4, 199–230.
Westerberg H, Hirvikoski T, Forssberg H, Klingberg T(2004). Visuo-spatial working memory span: a sensitivemeasure of cognitive deficits in children with ADHD.Child Neuropsychology 10, 155–161.
Willcutt EG, Doyle AE, Nigg JT, Faraone SV, Pennington BF(2005). Validity of the executive function theory ofattention-deficit/hyperactivity disorder: a meta-analyticreview. Biological Psychiatry 57, 1336–1346.
Woods SP, Lovejoy DW, Ball JD (2002). Neuropsychologicalcharacteristics of adults with ADHD: a comprehensivereview of initial studies. Clinical Neuropsychologist 16, 12–34.
892 A. J. A.M. Thissen et al.
Copyright © 2022 FDOKUMEN




















