
Peer-Reviewed, Evidence-Based Analysis of Vitamin D and Primary Hyperparathyroidism
11
Peer-Reviewed, Evidence-Based Analysis of Vitamin D and Primary Hyperparathyroidism Storm Weaver David B. Doherty Camilo Jimenez Nancy D. Perrier Published online: 24 March 2009 Ó Socie ´te ´ Internationale de Chirurgie 2009 Abstract Background Research into the actions of vitamin D on the human body has been increasing at an exponential rate, as has understanding of the impact of vitamin D on various aspects of the endocrine system. Primary hyperparathy- roidism (PHPT) is a disease of the endocrine system that can result in debility if not diagnosed. New understanding about the effect of vitamin D on parathyroid hormone regulation may provide an opportunity to better understand the coexistence of PHPT and vitamin D deficiency. Methods An evidence-based literature review was based on a PubMed search for research involving vitamin D and primary hyperparathyroidism, and evaluating existing research on vitamin D. The PubMed search included English-language articles published between 1977 and 2008, with a focus on research and analysis completed between 2005 and the present. This study examined recent developments in understanding the relationship between vitamin D and PHPT. This review of existing literature examined the impact of vitamin D insufficiency and defi- ciency, including the impact on diagnosis of vitamin D insufficiency/deficiency, diagnosis and management of PHPT, and the impact on overall health. The level of evi- dence was determined according to criteria proposed by Sackett et al. and the grade of recommendation according to the criteria proposed by Heinrich et al. Results Level III and level IV evidence predominates the vitamin D/PHPT based literature, with several notable Heinrich grade A, B, and C studies available. Additional evaluation of studies’ review is provided by reference and by section. Conclusions Vitamin D metabolism plays an important role in PHPT etiology, diagnosis, and management. Care of both conditions may have an important impact on overall health in humans. Introduction Vitamin D, once poorly understood has been shown to be highly involved in a number of human processes, from calcium regulation to blood lipid regulation [1 (V)] . A fat- soluble vitamin, vitamin D is present naturally in relatively few foods but is added to some foods as a supplement. In humans, vitamin D is produced through the conversion of cholesterol during exposure to ultraviolet (UV)B radiation on the skin. Vitamin D deficiency is a common condition in the United States and worldwide [2 (V), 3 (V), 4 (III)] likely caused by the combination of diets sparse in vitamin D, avoidance of ultraviolet B (UVB) sunlight, indoor con- finement, and an increasingly elderly population. Primary hyperparathyroidism (PHPT) is also common and largely affects the elderly. The low 25-hydroxyvitamin D level frequently seen in patients with PHPT is believed to be at least partly a result of the metabolic sequelae of inherent excess parathyroid hormone (PTH) converting 25-hydrox- yvitamin D to 1,25-dihydroxyvitamin D [5 (II), 6 (II)]. However, other factors seem to contribute to the coexis- tence of the two conditions [7 (III)]. S. Weaver Á D. B. Doherty Á N. D. Perrier (&) Department of Surgical Oncology, The University of Texas M. D. Anderson Cancer Center, PO Box 301402, Houston, TX 77230-1402, USA e-mail: [email protected] C. Jimenez Department of Endocrine Neoplasia, The University of Texas M. D. Anderson Cancer Center, Houston, TX, USA 123 World J Surg (2009) 33:2292–2302 DOI 10.1007/s00268-009-9966-9
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Peer-Reviewed, Evidence-Based Analysis of Vitamin D and Primary Hyperparathyroidism
Peer-Reviewed, Evidence-Based Analysis of Vitamin Dand Primary Hyperparathyroidism
Storm Weaver Æ David B. Doherty ÆCamilo Jimenez Æ Nancy D. Perrier
Published online: 24 March 2009
� Societe Internationale de Chirurgie 2009
Abstract
Background Research into the actions of vitamin D on
the human body has been increasing at an exponential rate,
as has understanding of the impact of vitamin D on various
aspects of the endocrine system. Primary hyperparathy-
roidism (PHPT) is a disease of the endocrine system that
can result in debility if not diagnosed. New understanding
about the effect of vitamin D on parathyroid hormone
regulation may provide an opportunity to better understand
the coexistence of PHPT and vitamin D deficiency.
Methods An evidence-based literature review was based
on a PubMed search for research involving vitamin D and
primary hyperparathyroidism, and evaluating existing
research on vitamin D. The PubMed search included
English-language articles published between 1977 and
2008, with a focus on research and analysis completed
between 2005 and the present. This study examined recent
developments in understanding the relationship between
vitamin D and PHPT. This review of existing literature
examined the impact of vitamin D insufficiency and defi-
ciency, including the impact on diagnosis of vitamin D
insufficiency/deficiency, diagnosis and management of
PHPT, and the impact on overall health. The level of evi-
dence was determined according to criteria proposed by
Sackett et al. and the grade of recommendation according
to the criteria proposed by Heinrich et al.
Results Level III and level IV evidence predominates the
vitamin D/PHPT based literature, with several notable
Heinrich grade A, B, and C studies available. Additional
evaluation of studies’ review is provided by reference and
by section.
Conclusions Vitamin D metabolism plays an important
role in PHPT etiology, diagnosis, and management. Care of
both conditions may have an important impact on overall
health in humans.
Introduction
Vitamin D, once poorly understood has been shown to be
highly involved in a number of human processes, from
calcium regulation to blood lipid regulation [1 (V)] . A fat-
soluble vitamin, vitamin D is present naturally in relatively
few foods but is added to some foods as a supplement. In
humans, vitamin D is produced through the conversion of
cholesterol during exposure to ultraviolet (UV)B radiation
on the skin.
Vitamin D deficiency is a common condition in the
United States and worldwide [2 (V), 3 (V), 4 (III)] likely
caused by the combination of diets sparse in vitamin D,
avoidance of ultraviolet B (UVB) sunlight, indoor con-
finement, and an increasingly elderly population. Primary
hyperparathyroidism (PHPT) is also common and largely
affects the elderly. The low 25-hydroxyvitamin D level
frequently seen in patients with PHPT is believed to be at
least partly a result of the metabolic sequelae of inherent
excess parathyroid hormone (PTH) converting 25-hydrox-
yvitamin D to 1,25-dihydroxyvitamin D [5 (II), 6 (II)].
However, other factors seem to contribute to the coexis-
tence of the two conditions [7 (III)].
S. Weaver � D. B. Doherty � N. D. Perrier (&)
Department of Surgical Oncology, The University of Texas
M. D. Anderson Cancer Center, PO Box 301402, Houston,
TX 77230-1402, USA
e-mail: [email protected]
C. Jimenez
Department of Endocrine Neoplasia, The University of Texas
M. D. Anderson Cancer Center, Houston, TX, USA
123
World J Surg (2009) 33:2292–2302
DOI 10.1007/s00268-009-9966-9

The effects of a low preoperative vitamin D level in the
setting of PHPT remain unclear, particularly in patients
with mild PHPT. Differentiating primary autonomous PTH
production in the setting of mild hypercalcemia from sec-
ondary PTH elevation due to vitamin D deficiency is not
always straightforward. Some studies suggest that vitamin
D deficiency may worsen the manifestations of PHPT by
promoting more pronounced parathyroid gland prolifera-
tion [8 (III)]. The result is higher PTH elevation, larger
adenomas, and more frequent fractures compared with
patients who have vitamin D sufficiency [9 (V), 10 (I), 11,
12 (V)].
Vitamin D
The generic appellation ‘‘vitamin D’’ comprises multiple
forms of the vitamin, metabolized in the body in the
intestines and liver. Although vitamin D is created through
conversion of cholesterol in the skin, during exposure to
UVB radiation on the skin, vitamin D also can be ingested,
most often in one of two major types (vitamin D2 and
vitamin D3). Research on the function and metabolism of
vitamin D comprises a number of studies, ranging from
Sackett Level II through Sackett Level V investigations,
including both human and animal studies. Sackett Level III
investigations predominate, with a number of Sackett Level
V reviews evaluating accumulated evidence present.
Ingested vitamin D is converted to useful forms through
synthesis in the liver and/or intestines, where D2 and
D3 are converted to calcifediol (25-hydroxycholecal-
ciferol, also called calcidiol) in the liver, and/or calcitriol
(1, 25-dihydrovitamin D) in the kidneys and intestines.
As previously noted, there are two major types of vita-
min D: vitamin D2 (ergocalciferol) and vitamin D3
(cholecalciferol), most often provided in supplementation,
including fortification of food and dairy products. Until
recently, the most commonly fortified food product was
milk, and milk was typically fortified with vitamin D2, also
known as ergocalciferol. Ergocalciferol is primarily a
plant-based version of vitamin D, with a slightly different
structure and less biological activity in the human body
than vitamin D3 (cholecalciferol), due to a more complex
molecular bonding system. Double bonds on two of the
carbon side chains (C23 and C24), as well as the addition
of a methyl group on C24 act as inhibitors and slow met-
abolic transformation of D2 in the body.
Despite its drawbacks, vitamin D2 is more commer-
cially accessible and less expensive to produce, making it
more suitable for large-scale fortification of foodstuffs.
Fortification of foodstuffs has increased over time, making
access and affordability of D2 a significant factor in
increasing availability of vitamin D in the food supply.
Whereas it was primarily milk that was fortified with
vitamin D, the increase in research concerning the impact
of vitamin D deficiency on populations over time has
resulted in an increase, in the western world, in fortification
of any number of food products, including dairy, fruit/
vegetable juices, and baked goods.
Vitamin D3, also known as cholecalciferol, is the type of
vitamin D synthesized in the human body during exposure
of the skin to UVB radiation. Cholecalciferol is also pro-
duced in other animals, and although more difficult to
obtain, is more easily converted to calcifediol—the active
form of vitamin D used within the human body.
The process of conversion of cholecalciferol in the skin
is a result of the interaction between 7-dehydrocholoesterol
and UVB light within certain wavelengths (typically 270
and 300 nm). Peak synthesis occurs in a much narrower
band between 295 and 297 nm [13 (V), 14 (II)]. The rel-
evance of the wavelengths is particularly important: these
wavelengths are only present in sunlight at sea level when
the sun is[45� above the horizon or when the UV index is
[3 [15 (III)].
Individuals with fair skin can synthesize sufficient
vitamin D through 10–15 min of exposure of the arms,
hands, face, and/or back without sunscreen each day, pro-
vided that the proper solar elevation and/or UV index is
met. This exposure enables the synthesis of sufficient
cholecalciferol to meet the daily requirement of 400–
1000 IU recommended by nutrition researchers [15 (III),
16 (V), 17 (I), 18 (V)]. People with darker skin require
longer UVB exposure to synthesize sufficient cholecalcif-
erol. Once the body has created sufficient cholecalciferol to
attain equilibrium, additional vitamin D is degraded or
converted to other photosynthesized products as quickly as
it is generated.
Interestingly, the human body is exceptionally efficient
at synthesizing vitamin D, yet individuals with extensive
exposure to sunlight do not suffer from vitamin D intoxi-
cation (which can occur in individuals obtaining excessive
vitamin D through supplementation). It has been noted that
once the human body has synthesized sufficient vitamin D,
the synthesizing products (previtamin D3 and vitamin D3)
respond to the presence of sunlight by synthesizing further
into other photoproducts [16 (V)].
Although we are still working to understand the body’s
need for vitamin D, and establish accurate reference values
for vitamin D levels at different ages and health statuses,
some guidelines have been set regarding what reference
ranges of vitamin D constitute ‘‘deficiency,’’ ‘‘insuffi-
ciency,’’ and ‘‘normal.’’ As we understand more about the
relationship between vitamin D and health, these reference
ranges are shifting, but current ranges for 25(OH)D are
typically considered optimal if, 32.0–100.0 ng/ml [19 (V),
20 (III)].
World J Surg (2009) 33:2292–2302 2293
123

Gross vitamin D deficiency, resulting in changes in the
body such as rickets, brought about the changes in the food
supply that encouraged supplementation. This was evident
especially in foods consumed by children.
As a fat-soluble vitamin, there has been concern among
medical practitioners over the level of vitamin D at which
vitamin D intoxication would occur. Side effects of vitamin
D intoxication, including hypercalcemia, can be serious,
and limited understanding of the metabolic cycle for vita-
min D possibly caused error on the side of caution where
fat-soluble vitamins were concerned. The current Recom-
mended Daily Allowance (RDA) of vitamin D, increased to
400 IU in 2007, but is still considered by some to be
insufficient for anything other than prevention of the most
visible side-effects of vitamin D deficiency. Holick and
others believe that the minimum requirements for vitamin
D are closer to 1000 IU per day [16 (V)]. In addition, with
the increased use of sunscreens and the reduced amount of
time spent outdoors for both children and adults, these
requirements must be met through supplementation, which
is a much less efficient method than the body’s own syn-
thetic process.
Due to supplementation at minimal values in the food
supply, which prevents the more visible symptoms of gross
vitamin D deficiency, vitamin D insufficiency, although
common, remains undetected in many patients. As we
understand more about the function of vitamin D in the
body, links are developing about the relevance of vitamin
D for immune function, maintenance of cognitive capacity
in elderly populations, cancer prevention and treatment,
and other vital matters of health. Despite the beneficial
aspects of campaigns to raise awareness about the dangers
of UV light, sun exposure, and the relationship to cancers,
such as melanoma, these campaigns, combined with
decreased exposure to natural sunlight, have contributed to
the prevalence of vitamin D insufficiency and chronic
marginal deficiency in western populations.
Vitamin D deficiency induces mild secondary hyper-
parathyroidism with a subsequent increase in bone
turnover, and, in elderly patients, an increased risk of
osteoporotic fracture, mainly at cortical sites [21 (IV)].
Typically, insufficiency is determined at that point at which
there is insufficient calcidiol present in the blood to allow
serum parathyroid hormone homeostasis, noted as the point
at which serum PTH levels start to increase. Currently,
serum calcidiol levels are usually considered normal
when C30 ng/ml, insufficient between 25–30 ng/ml, and
deficient when \25 ng/ml [13 (V), 22 (V)]. This reference
range is currently being analyzed and may change as fur-
ther developments in understanding the role of vitamin D
in multiple systems of the body takes shape. The estab-
lishment of new reference ranges will be discussed in
upcoming sections.
Even slight deficiencies in vitamin D can impact the
immune and musculoskeletal systems by affecting bone
density and muscle strength [23 (V), 24 (III)]. Vitamin D
deficiency also has been implicated in the development and
progression of some cancers and chronic disorders, including
melanoma and diabetes [25] (I), 26 (V), 27 (IV), 28 (IV)].
Primary hyperparathyroidism
PHPT is a metabolic disorder characterized by autonomous
overproduction of PTH [29 (I)]. A biochemical diagnosis is
made when a patient has an elevated or high-normal serum
calcium level and an inappropriately elevated intact PTH
level (serum Ca levels C 10.2 mg/dl, intact PTH level [80 pg/ml).
Approximately 100,000 patients in the United States are
diagnosed with PHPT each year [30] (IV)]. Increased
screening for abnormal serum calcium levels during rou-
tine medical examinations and the routine use of
multichannel autoanalyzers have resulted in earlier and
increased PHPT detection [31](V)]. Eighty percent of
patients with PHPT are now diagnosed biochemically
before they develop ‘‘classic’’ PHPT symptoms, such as
nephrolithiasis, pancreatitis, or osteitis fibrosis cystica.
Despite the greater tendency for testing that has provided
beneficial early diagnosis, nonclassic and early symptoms
of PHPT, including fatigue, bone/joint pain, cognitive
difficulty, and sleep disturbances, among others, may be
insufficiently problematic to elicit documentation. These
symptoms are commonly dismissed by the patient and not
mentioned. In addition, because the majority of these
symptoms are difficult to quantify and often are subjective,
patients with PHPT who exhibit these symptoms are
commonly referred to as ‘‘asymptomatic.’’
PHPT prevalence increases with age. Perimenopausal,
menopausal, and postmenopausal women are at the greatest
risk of developing PHPT [32] (IV), 33 (V), 34 (II), 35 (III),
36 (V)]. One screening study found that approximately
14% of women older than aged 65 years have PHPT [37
(I)]. Because the population of elderly patients continues to
increase, with 20% of the U.S. population predicted to
be older than aged 65 years by 2030, PHPT is becoming an
increasingly important health issue. Furthermore, because
elderly patients are more likely to be confined to their
homes or extended care facilities, to have restricted diets,
and to have little exposure to UV radiation, they also are
the population most likely to be deficient in vitamin D
[1 (V), 18 (V), 38 (II)]. Therefore, it is not surprising that
PHPT and vitamin D deficiency coexist in many elderly
patients. In fact, a recent study revealed that up to 75% of
elderly patients with PHPT also have vitamin D deficiency
[39 (V)].
2294 World J Surg (2009) 33:2292–2302
123

Mobility issues tend to increase as individuals age, and
loss of muscle strength and dexterity are more common in
elderly populations. Although inactivity and comorbidities
can contribute to loss of muscle strength in elderly patients,
some researchers have suggested that age-related changes
in hormonal status, specifically calcidiol and PTH, also
contribute to this loss. A substantial percentage of elderly
patients who experience loss of muscle strength, especially
those with weakness or fatigue and few additional symp-
toms, will have few overt symptoms of vitamin D
deficiency.
Untangling the connections between vitamin D
and PHPT
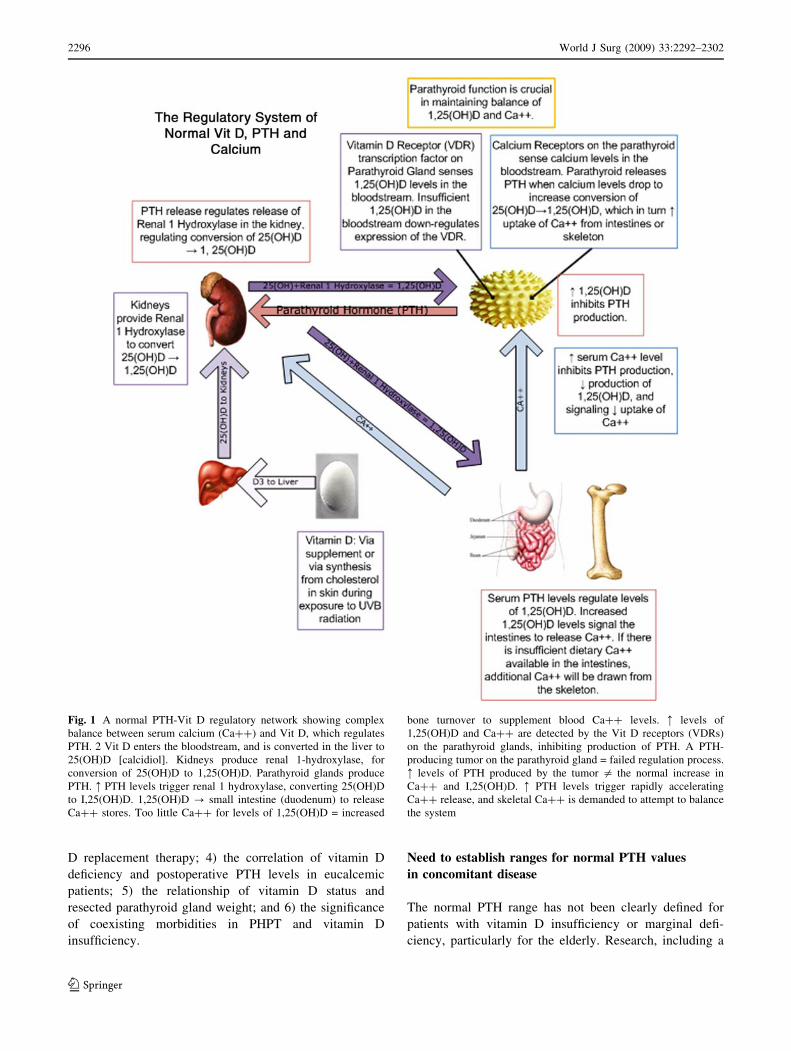
A complex regulatory network of vitamin D, calcium, and
PTH exists within the human endocrine system (Fig. 1) [2
(V)]. Vitamin D receptors on the parathyroid glands detect
levels of calcitriol, which inhibits the production of PTH,
the major regulator of renal 1-hydroxylase. In PHPT,
autonomous production of PTH, the result of tumor or
increased parathyroid glandular mass, supersedes the
normal feedback mechanism.
Current research by Sambrook et al., [40 (I)] among
others, recognizes the link between vitamin D insufficiency
and PHPT, and those individuals with undiagnosed vitamin
D insufficiency are being shown to have a more compli-
cated course in the resolution of PHPT.
This overview highlights a range of Sackett I-V evi-
dence in the examination of the connection between
vitamin D and PHPT. Some of the earliest studies of
vitamin D and PHPT investigated vitamin D metabolism
regulation by the parathyroid glands. In 1972, Garabedian
et al. found evidence that the removal of the parathyroid
glands significantly interfered with vitamin D metabolism
[41]. This group also found that replacing PTH with
parathyroid extract could nearly restore vitamin D metab-
olism. Furthermore, Garabedian et al. noted that vitamin D
levels controlled by release of PTH from the parathyroid
glands were independent of blood or intestinal calcium
levels, indicating that calcium homeostasis and the vitamin
D/PTH regulating mechanism are separate processes [41
(III)].
The search for novel ways to manage hypercalcemia—
the key symptom of PHPT—has led to further studies of
vitamin D and PHPT. In 1977, Kaplan et al. found that
increases in calcitriol levels were linked to increases in
fractional and urinary calcium levels, but that serum cal-
cium levels, serum phosphorus levels, and serum PTH
levels remained unaffected. The researchers also found that
abnormally high vitamin D levels are linked to increases in
intestinal calcium absorption, but they also noted that that
vitamin D metabolism related to parathyroid function may
have only a limited role in absorptive hypercalcemia.
Furthermore, Kaplan et al. [42 (II)] found that intestinal
calcium absorption exceeded the levels that would be
expected in the setting of increased serum calcitriol levels.
In 1991, Vieth et al. [30] found that serum calcitriol
levels are useful in the diagnosis of PHPT. Their study
revealed that vitamin D metabolites were not dependent on
PTH and were stable in patients diagnosed with PHPT as
well as in serum samples from patients without PHPT.
Metabolites of vitamin D did not fluctuate despite changes
in PTH. However, levels of 1,25(OH)2D were significantly
higher in patients with PHPT. Ninety-fifth percentile of
1,25(OH)2D levels were reached in 65% of patients with
PHPT. It was concluded that making the elevated levels of
1,25(OH)2D were a good tool for evaluating patients with
potential PHPT. Vieth et al. also found that the PTH-
dependent metabolite calcitriol increased 100-fold. The
group found a significant correlation between serum cal-
citriol levels and serum calcidiol levels in patients with
PHPT (r = 0.5; P \ 0.05) but not in patients who did not
have PHPT (r = 0.02), suggesting that high serum calci-
triol levels indicate the need for further testing for PHPT
[30 (IV)].
Several important questions about the complex rela-
tionship between vitamin D and PHPT have been
addressed, including questions about the role of vitamin D
in PHPT homeostasis and the impact of vitamin D on
serum calcium levels in patients with PHPT. It seems that
the severity of PHPT increases when the disease and
vitamin D insufficiency occur concurrently.
Among the questions being examined, there is the
question of whether PHPT may be a result of parathyroid
gland stimulation from vitamin D insufficiency. It is pos-
sible that vitamin D insufficiency could predispose patients
to PHPT, but not all patients with PHPT are vitamin D-
deficient. Decreased vitamin D levels can lead to fewer
vitamin D receptors (VDR), which are created in response
to active 1,25(OH)2D stimulating expression of the VDR
on the parathyroid glands. This impedes the feedback
inhibition by calcitriol on PTH [40 (I), 7 (III)].
To effectively manage concomitant PHPT with under-
lying vitamin D insufficiency or deficiency, there are
several other issues that need to be addressed, which are
being explored in current research or have yet to be
explored, including: 1) the definition of a ‘‘normal’’ PTH
value in patients with concomitant PHPT and vitamin D
insufficiency/deficiency, particularly elderly patients; 2)
the role and effect of preoperative vitamin D replacement
therapy in patients with concomitant PHPT and vitamin D
deficiency; 3) the role of post-parathyroidectomy vitamin
World J Surg (2009) 33:2292–2302 2295
123
D replacement therapy; 4) the correlation of vitamin D
deficiency and postoperative PTH levels in eucalcemic
patients; 5) the relationship of vitamin D status and
resected parathyroid gland weight; and 6) the significance
of coexisting morbidities in PHPT and vitamin D
insufficiency.
Need to establish ranges for normal PTH values
in concomitant disease
The normal PTH range has not been clearly defined for
patients with vitamin D insufficiency or marginal defi-
ciency, particularly for the elderly. Research, including a
Fig. 1 A normal PTH-Vit D regulatory network showing complex
balance between serum calcium (Ca??) and Vit D, which regulates
PTH. 2 Vit D enters the bloodstream, and is converted in the liver to
25(OH)D [calcidiol]. Kidneys produce renal 1-hydroxylase, for
conversion of 25(OH)D to 1,25(OH)D. Parathyroid glands produce
PTH. : PTH levels trigger renal 1 hydroxylase, converting 25(OH)D
to I,25(OH)D. 1,25(OH)D ? small intestine (duodenum) to release
Ca?? stores. Too little Ca?? for levels of 1,25(OH)D = increased
bone turnover to supplement blood Ca?? levels. : levels of
1,25(OH)D and Ca?? are detected by the Vit D receptors (VDRs)
on the parathyroid glands, inhibiting production of PTH. A PTH-
producing tumor on the parathyroid gland = failed regulation process.
: levels of PTH produced by the tumor = the normal increase in
Ca?? and I,25(OH)D. : PTH levels trigger rapidly accelerating
Ca?? release, and skeletal Ca?? is demanded to attempt to balance
the system
2296 World J Surg (2009) 33:2292–2302
123

full range of evidence in which Sackett III evidence pre-
dominates, marks a strong interest in this area.
Secondary hyperparathyroidism (SHPT), caused by low
serum calcidiol levels, may be misdiagnosed as eucalcemic
PHPT in patients who have a high normal serum calcium
level, an elevated intact PTH level, and concomitant vita-
min D insufficiency or deficiency. Several factors impact
proper diagnosis, and without thorough screening, can
result in borderline cases having improper management.
Established patient history of current or previous use of
agents known to affect bone and/or calcium metabolism,
such as glucocorticoids, anticonvulsants, thiazide diuretics,
furosemide, lithium, estrogen or estrogen/progesterone,
bisphosphonates, antiresorptive treatments, calcium sup-
plements, and/or vitamin D supplements, must be taken
into consideration, because these agents can impact serum
calcium levels and impede regulation of PTH. A thorough
medical history should be taken to elicit information about
fractures, nephrolithiasis, endocrinopathies, and any situa-
tion that induced a period of immobilization lasting more
than 2 months, particularly in elderly patients with poten-
tial diagnosis of SHPT or PHPT [43 (III)]. Laboratory
evaluation of vitamin D levels can assist in the process of
diagnosis, particularly for patients in whom significant
insufficiency or marginal deficiency may be impacting
symptomology, as demonstrated by Silverberg et al. in
1999 [7]. In this work, Silverberg et al. studied 124 patients
with mild hyperparathyroidism and found that patients in
the lowest vitamin D tertile had significantly higher PTH
levels than did patients in the other two tertiles. However,
there was no correlation between PTH and vitamin D levels
in patients with a vitamin D level [25 ng/ml, and no
correlations between PTH and calcidiol or calcitriol level
(III).
Souberbielle et al. [44 (II)] have performed considerable
research defining a normal reference range for PTH. His
group noted that there is a need to reevaluate current nor-
mative values, because developments in understanding the
association between vitamin D levels and PTH levels is
expanding. This sentiment was echoed by Bilezikian et al.,
who stated in a 2002 workshop on asymptomatic PHPT
that ‘‘better-defined normative values for age, gender,
menopausal status, and race for both PTH and calcium
would be helpful’’ [45 (V)].
Although serum PTH levels are typically higher in black
patients and elderly patients than in young and white
population, serum calcidiol levels are usually lower in
black and elderly patients [46] (II), 47 (III)]. This lower
vitamin D status may partly explain the higher PTH values
found in black patients and elderly patients [48 (III)].
Before 2004–2005, and recent reassessment of existing
PTH reference ranges based on developing information
about the relationship between PTH and vitamin D status,
the upper limit of the normative PTH range was set at
65 ng/ml. As information on the impact of vitamin D
insufficiency on PTH levels has become more apparent, it
has been realized that the reference ranges considered
‘‘normal’’ were based on insufficient information. On the
basis of a study of 708 consecutive, osteopenic, vitamin D-
sufficient patients, Souberbielle et al. proposed an upper
limit for the reference range for PTH of B46 ng/ml, by
Allegro assay. When 46 ng/ml was used as the cutoff for
‘‘normal’’ in patients the number of false negatives was
significantly reduced, compared with the number of false
negatives using the 65 ng/l upper limit. The number of
false positives did not increase in those patients. This
showed a net improvement in the percentage of patients
with surgically proven PHPT. Souberbielle et al. concluded
that this new range enabled diagnoses of normocalcemic
PHPT after all other possibilities, including malabsorptive
diseases, had been ruled out. The concept of the impact of
vitamin D on the previously accepted upper limit for nor-
mal serum PTH levels was further emphasized by Ozbey
et al., who also found that vitamin D may affect serum
calcium levels, leading to a normocalcemic presentation of
PHPT [49 (V)].
Souberbielle et al. [44] (II)] also sought to redefine
serum PTH reference ranges in elderly patients. Using two
different assays to measure PTH levels in 280 healthy 60-
to 79-year-old patients, Souberbielle et al. found that
vitamin D-deficient patients tended to be older and have
higher PTH levels and that patients with low vitamin D
levels had PTH levels above the 97th percentile. The
researchers concluded that the reference range for PTH
group may depend on vitamin D status.
Vitamin D deficiency and postoperative PTH levels
Untch et al. [50 (III)] evaluated the impact of calcidiol
deficiency (\25 ng/ml) on intraoperative and postoperative
PTH kinetics and outcomes after parathyroidectomy in 93
patients who underwent parathyroid adenoma resection for
PHPT. PTH and serum calcidiol levels were recorded at six
perioperative time points. Untch et al. found that calcidiol-
deficient patients had significantly higher preoperative
serum calcium, alkaline phosphatase, and PTH levels and
significantly higher PTH levels at incision and at 1 week
and 1–3 months after surgery. The mean decrease in
PTH ?tul?> level 5 minutes after resection was 79 ± 14% in
the calcidiol-deficient group and 72 ± 22% in the noncal-
cidiol-deficient group (P = 0.03). The researchers also
found that calcidiol levels were inversely correlated with
adenoma weight (P = 0.03) and postoperative PTH mea-
surements (P = 0.008). The authors concluded that
calcidiol-deficient patients have higher baseline and
World J Surg (2009) 33:2292–2302 2297
123

postoperative PTH levels but that calcidiol is not correlated
with alterations in intraoperative PTH kinetics. These find-
ings suggest that preoperative vitamin D deficiency is
associated with higher postoperative PTH levels, which can
indicate a higher risk for development of postoperative
hypocalcemia. Ozbey et al. also noted that postoperative
PTH levels were significantly higher in patients with low
preoperative vitamin D levels, suggesting a negative corre-
lation between serum PTH and serum calcidiol levels [49
(V)].
In a retrospective study, Wang et al. assessed persistently
elevated intraoperative and postoperative PTH levels in 816
patients who underwent parathyroidectomy [51 (IV)].
Patients’ preoperative vitamin D levels were unknown.
Wang concluded that patients with postoperative vitamin D
levels on the lower tertile of the reference range were likely
to have elevated postoperative PTH levels. Lower postop-
erative vitamin D levels also were correlated with smaller
percentage decreases in intraoperative PTH levels. The
authors suggested that a minimally invasive parathyroidecty
that depends on intraoperative PTH to determine extent of
surgery might not be as effective in patients with preexisting,
unresolved vitamin D insufficiency.
Beyer et al. [52 (II)] noted that after undergoing curative
parathyroidectomy for PHPT, as many as 43% of patients
have normocalcemia but elevated intact PTH levels that
could be due to an absolute or relative vitamin D defi-
ciency. In the study by Beyer et al., 86 patients who had
undergone parathyroidectomy for PHPT were divided into
two groups. Group 1 consisted of 26 patients who received
oral calcitriol and calcium carbonate postoperatively.
Group 2 consisted of 60 patients who did not receive cal-
citriol postoperatively (some received calcium carbonate at
the surgeon’s discretion). Eighty-five patients (99%)
achieved a postoperative cure with a sustained reduction in
serum calcium. At the 30-day postoperative evaluation,
serum PTH normalization was present in both group 1 and
group 2 (mean PTH, 41 ± 31 pg/ml and 39 ± 31 pg/ml,
respectively; P = 0.91). At 1–3 months postoperatively,
the mean serum calcium levels remained similar for group
1 and group 2 (9.5 ± 0.7 pg/ml and 9.3 ± 0.5 pg/ml,
respectively; P = 0.39), but the mean serum PTH level
was significantly higher in group 2 (67 ± 45 pg/ml, P =
0.02). At 4–6 months, the mean PTH remained higher in
group 2 (36 ± 22 pg/ml vs. 67 ± 35 pg/ml; P = 0.3),
even though the mean calcium levels remained normal in
both groups. The incidence of postoperative normocalce-
mic PTH elevation was therefore significantly higher in
group 2 at 1–3 months (39% vs. 14% in group 1; P = 0.04)
and at 7–12 months (83% vs. 22%; P = 0.04). Beyer et al.
concluded that vitamin D supplementation after parathy-
roidectomy for PHPT reduces the incidence of postoperative
eucalcemic PTH elevation.
Vitamin D deficiency also may be a risk factor for
postoperative hypocalcemia [53] (IV)]. In 2005, Stewart
et al. evaluated 190 patients with PHPT who had under-
gone minimally invasive parathyroidectomy for excision of
a single adenoma. Patients were divided into two groups:
those who were hypocalcemic after surgery (40% of
patients), and those who were not (60%). Stewart et al.
found that postoperative serum calcidiol levels were sig-
nificantly lower in patients who became hypocalcemic after
surgery. Sackett III, IV, and V level evidence are heavily
weighted in this area, and larger studies at the Sackett I and
II level are necessary to confirm existing evidence and
establish improved understanding of the involvement of
vitamin D in this area.
Vitamin D deficiency and increased gland weight
Some studies have examined the relationship between
vitamin D status and parathyroid gland weight in patients
with PHPT. Rao et al. [10] (I)] found a significant inverse
correlation between the mean serum calcidiol level and
mean parathyroid gland weight in 148 patients with PHPT.
The authors also noted a weak direct correlation between
parathyroid gland weight and calcitriol level and a weak
inverse correlation between gland weight and age. Serum
PTH levels and adjusted serum calcium levels were all
significantly higher in vitamin D-deficient patients. The
researchers concluded that parathyroid gland weight
depends on calcidiol levels in PHPT patients. Other studies
support this conclusion; for example, Beyer et al. found
that vitamin D-deficient patients had significantly larger
parathyroid glands (mean, 1757 g) than nonvitamin
D-deficient patients (mean, 524 g; P = 0.005) [52 (II)].
Moosgaard et al. [54] (II)] studied 170 patients with
surgically proven parathyroid adenomas and found that
parathyroid adenoma weight and calcidiol levels were
inversely correlated but that adenoma weight and calcitriol
levels were not related. Low calcidiol levels also were
related to higher PTH levels and higher PTH-to-adenoma
weight ratios. The group concluded that vitamin D defi-
ciency, particularly deficiency of circulating 25(OH)D,
calcidiol, potentially increases PTH secretion but that
neither PTH secretion nor adenoma weight is associated
with serum calcitriol levels. Similarly, Ozbey et al. found
an inverse relationship between parathyroid weight and
serum calcidiol levels [49 (V)]. In contrast, Silverberg et al.
found no correlation between vitamin D and gland weight
and noted that postoperative pathological examination of
parathyroid adenomas and glandular tissue did not show
any significant variation among patients with different
calcidiol levels [7 (III)]. Several strong (Sackett I or II)
studies confirm the strength of evidence in this area,
2298 World J Surg (2009) 33:2292–2302
123

backed by reviews that link evidence and present directions
for future research.
Vitamin D deficiency and PHPT severity
It is possible that vitamin D deficiency increases PHPT
severity, as postulated by Ozbey et al [49] (V)]. Silverberg
et al. [7 (III)] proposed that the PTH gene, which is abnor-
mally active in PHPT, is even less constrained in the setting
of vitamin D deficiency and that the lack of regulatory
feedback normally provided by vitamin D could account for
increased PHPT severity in vitamin D-deficient patients.
Raef et al. [55 (III)] studied the effect of vitamin D status
on the severity of bone disease and other PHPT features in
49 patients from a vitamin D-deficient region in Saudi
Arabia. Patients who had undergone bone mineral densi-
tometry were divided into two groups. Group A consisted of
19 patients who had severe bone changes indicating oste-
oporosis, and group B consisted of 23 patients with mild or
no bone changes. Ninety-four percent of the patients in
group A were in the bottom two vitamin D tertiles for the
general population. Patients in group A also were on aver-
age 14 years younger than patients in group B.
Furthermore, group A patients had higher PTH levels and
larger parathyroid tumors than group B patients and thus
required more medical treatment after parathyroidectomy.
Sambrook et al. [40 (I)] evaluated the effects of an
elevated PTH level and vitamin D deficiency in frail,
elderly PHPT patients. In this prospective study, 842
patients’ biochemical parameters, including serum
25(OH)D, serum calcium, serum PTH, and bone ultrasound
attenuation, were assessed in relation to 5-year mortality.
PTH was found to affect mortality independent of vitamin
D and kidney function. The authors concluded that aging is
associated with the decreased responsiveness of renal 1-
hydroxylase to PTH. The researchers also noted that
hypercalcemic patients, such as those with PHPT, feared
worsening their hypercalcemia with vitamin D and thus
avoided it.
Beyer et al. [52 (II)] also suggested that vitamin D
insufficiency in patients with PHPT may be associated
with greater disease severity, higher incidence of multi-
gland disease, and elevated postoperative serum PTH
levels. Patients with suboptimal serum vitamin D levels
(B20 ng/ml) had a significantly higher mean serum cal-
cium level (11.3 ± 1.2 mg/dl vs. 10.8 ± 0.9 mg/dl;
P = 0.012) and mean serum PTH level (204 ± 138 pg/ml
vs. 156 ± 179 pg/ml; P = 0.006) than patients with opti-
mal serum vitamin D levels ([ 20 ng/ml). Patients with
vitamin D insufficiency also had a significantly higher
mean bone-specific alkaline phosphatase level than patients
without vitamin D insufficiency (P = 0.006). However, the
two groups had similar postoperative serum calcium levels,
serum PTH levels, eucalcemia rates, and postoperative
eucalcemic PTH elevation rates. Beyer et al. concluded
that, based on preoperative serum calcium and PTH levels,
bone markers, and gland size, PHPT patients with vitamin
D insufficiency have significantly greater PHPT severity
than PHPT patients without vitamin D insufficiency. The
researchers also noted that postoperative achievement of
eucalcemia seems to be independent of vitamin D status.
Pradeep et al. [56 (V)] evaluated 82 Indian patients with
PHPT who underwent parathyroidectomy to ascertain the
impact of vitamin D on postoperative outcome. Preopera-
tive calcidiol levels were available for 70 patients; 59
(84%) of these patients were vitamin D-deficient. Of the 32
patients for whom postoperative calcidiol levels were
available, 24 (75%) were vitamin D-deficient. To assess
recovery patterns in target organs, patients underwent
biochemical (serum calcium, phosphorus, and alkaline
phosphatase measurements) and radiological (bone mineral
densitometry) investigations at 3 weeks, 3 months,
6 months, and annually thereafter. Ultrasonography was
used to assess renal and pancreatic changes at 6 months
and annually thereafter. Follow-up ranged from 2 to
13 (median, 3) years. After surgery, 24 (75%) of 32
patients had persistent vitamin D deficiency (mean,
12.15 ± 5.45 ng/ml). Radiologic evaluation of all patients
revealed vigorous but disorderly bone remineralization
during 3 months. Bone pain and weakness disappeared
quickly in all patients. Kidney disease was evaluated in 43
patients; of these, 31 (74%) became symptom-free during
follow-up, 9 (21%) had no change in renal symptoms, and
3 (7%) had progression to end-stage renal failure. Seven
patients developed pancreatitis postoperatively. Six
patients (94.6%) became symptom-free during follow-up.
Pradeep et al. concluded that, in India, PHPT presents as
advanced disease with concomitant vitamin D deficiency.
The authors also concluded that persistent vitamin D
deficiency delays bone recovery, and that supplementation
to maintain non-deficient vitamin D status is necessary on
an ongoing basis to improve chances of recovery from
advanced PHPT, including the attendant renal and pan-
creatic issues found in advanced cases. Although Sackett
III-V evidence predominates in this area, several Sackett I,
Grade A and Sackett II, Grade B studies show great
promise for understanding the role of vitamin D in PHPT
severity.
Vitamin D repletion in patients with PHPT undergoing
parathyroidectomy
The role of vitamin D replacement therapy before and/or
after parathyroidectomy in patients with biochemical
World J Surg (2009) 33:2292–2302 2299
123

evidence of PHPT and low serum calcidiol levels has been
debated.
In 1999, Silverberg et al. [7 (III)] recommended that
vitamin D repletion not be used in patients with concom-
itant PHPT and vitamin D deficiency, because severe
hypercalcemia could occur. In 2005, Grey et al. [8 (III)]
evaluated vitamin D repletion for 1 year in 21 vitamin D-
deficient patients with mild PHPT undergoing clinical,
nonoperative management. All patients had baseline serum
calcium levels \ 12 mg/dl. Patients’ serum vitamin D
levels were normal at 6 months and had not increased at
12 months, and their serum calcitriol levels and serum
calcium levels did not change significantly from baseline to
6 or 12 months. Although patients’ intact PTH levels
decreased 25% during vitamin D repletion, the levels
remained abnormally elevated.
Our group recently reported similar findings in a large
cohort of patients with PHPT. We queried a prospective
database of 301 patients with PHPT who were treated at
The University of Texas M. D. Anderson during a 3-year
period. Before parathyroidectomy, 118 patients (39%)
had a vitamin D level C30 ng/ml (sufficient), 71 (24%)
were vitamin D-deficient, and 112 (37%) were vitamin
D-deficient but underwent vitamin D replacement ther-
apy. The median duration of replacement was 28 days,
and the standard ergocalciferol dose given was 400,000
U. Of the 112 patients who underwent vitamin D
repletion, 91 (81%) had mean serum calcium levels that
decreased or remained relatively unchanged after reple-
tion. Parathyroid gland size was smallest in patients who
were vitamin D-sufficient before surgery and largest in
patients who were vitamin D-deficient and did not
undergo vitamin D replacement therapy. PTH levels
measured 1 and 6 months postoperatively were signifi-
cantly lower in the initially vitamin D-sufficient group
than in the other two groups (P = 0.05 and P = 0.009,
respectively). We did not observe any postoperative
differences in PTH levels between vitamin D-deficient
patients who did or did not undergo vitamin D repletion.
Only six patients developed worsened hypercalcemia, but
the highest increase in serum calcium was 0.6 mg/dl. We
concluded that preoperative vitamin D replacement
therapy is safe for patients with PHPT and does not
increase serum calcium levels. Although preoperative
vitamin D status affects gland size and postoperative
PTH level, vitamin D repletion in vitamin D-deficient
patients does not seem to have an effect that persists
postoperatively. Sackett III evidence predominates in this
area, and the relationship between vitamin D repletion,
when repletion may be effective, and the level of effect
it may have would benefit from extended high-Sackett-
level research.
Working toward the future
Efforts to understand the relationship of vitamin D and
various body systems are providing better understanding of
this once understudied vitamin. Even research that is not
directly related to PHPT is providing insights into symp-
tomology associated with vitamin D deficiency that can
coexist with, complicate, or confuse the diagnostic picture
for patients who are being examined for the possibility of
PHPT.
Dawson-Hughes has played a key role in researching the
impact of vitamin D levels on outcomes in patients, with
particularly interesting research on the issue of vitamin D
and elderly populations, which also is a key population
dealing with PHPT. She postulated that vitamin D has
measurable clinical benefits for elderly patients’ musculo-
skeletal systems and that bone mass, bone loss, muscle
performance, fall risk, and fracture incidence were associ-
ated with serum calcidiol levels [18 (V)]. She determined
that a mean serum vitamin D concentration C65 nmol/l
improves muscle performance and reduces the risk of falls
and that a serum vitamin D concentration of C75 nmol/l
reduces the risk of fractures. She proposed consistent ter-
minology to define vitamin D deficiency as serum calcidiol
concentrations \25 nmol/l, vitamin D insufficiency as
serum calcidiol concentrations of 25–74 nmol/l, and vitamin
D sufficiency as C75 nmol/l. Dawson-Hughes’ work cites
the National Health and Nutrition Examination Survey III,
which estimated that 30% of persons aged 60 years or older
who reside in lower latitudes (30� N and below) experience
vitamin D insufficiency during the winter months and that
26% of people aged 60 years or older who reside in higher
latitudes (45� N and above) experience vitamin D insuffi-
ciency, even during the summer months where sunlight
levels are highest. Dawson-Hughes and her colleagues
suggested that future research should more precisely define
how vitamin D affects muscles and identify the amount of
calcidiol needed to promote optimal muscle function and the
population of older patients who are most likely to respond
favorably to vitamin D supplementation.
Research impacting our understanding of the role of
vitamin D in endocrine function is developing, and our
understanding of this field is improving, in part through
ongoing research with potentially far-reaching impact on
our understanding of the links between nutrition and
endocrine function.
In one ongoing study, von Hurst et al. [57 (I)] have
determined that vitamin D receptors in the endocrine
pancreas may play a role in insulin secretion. The
researchers found limited evidence that vitamin D influ-
ences insulin resistance and early-stage type 2 diabetes.
Hannan et al. [17 (I)] examined the relationship between
2300 World J Surg (2009) 33:2292–2302
123

serum calcidiol levels and bone mineral density by eth-
nicity. In a population-based, observational study of 1,114
patients, the researchers found that compared with white
men, a higher percentage of black men (44%) and Hispanic
men (23%) had calcidiol levels in the lowest quartile
(P \ 0.001). The authors recommended further research
into biological mechanisms for the differences in serum
calcidiol levels between ethnic groups.
Conclusions
Although reduced vitamin D and calcium-sensing receptors
have been demonstrated in parathyroid adenomas, the ways
in which vitamin D depletion influences adenoma growth
in circumstances of suboptimal VDR development remains
unclear. Dietary restriction of calcium has a trivial effect
on serum calcium levels but is accompanied by increased
bone resorption. Much work remains to elucidate the
relationship between vitamin D, endocrine, and other dis-
eases of suboptimal nutrition, and diseases such as PHPT,
which appears to have a hitherto poorly explored nutri-
tional/environmental component in the impact of vitamin D
on the health of the parathyroid and the management of
PHPT.
Acknowledgments This work has been generously supported by
The American Geriatrics Society Jahnigen Scholars Program. The
authors thank Linda McGraw, Program Coordinator, Department of
Surgical Oncology, Section of Surgical Endocrinology for assistance
with manuscript preparation.
References
1. Bischoff-Ferrari HA (2008) Optimal serum 25-hydroxyvitamin D
levels for multiple health outcomes. Adv Exp Med Biol 624:55–71
2. Feldman D (1999) Vitamin D, parathyroid hormone, and calcium:
a complex regulatory network. Am J Med 107:637–639
3. Holick MF (2007) Vitamin D deficiency. N Engl J Med 357:266–
281
4. Chapuy MC, Preziosi P, Maamer M et al (1997) Prevalence of
vitamin D insufficiency in an adult normal population. Osteo-
poros Int 7:439–443
5. Davies M, Heys SE, Selby PL et al (1997) Increased catabolism
of 25-hydroxyvitamin D in patients with partial gastrectomy and
elevated 1,25-dihydroxyvitamin D levels. Implications for met-
abolic bone disease. J Clin Endocrinol Metab 82:209–212
6. Clements MR, Davies M, Hayes ME et al (1992) The role of
1,25-dihydroxyvitamin D in the mechanism of acquired vitamin
D deficiency. Clin Endocrinol (Oxf) 37:17–27
7. Silverberg SJ, Shane E, Dempster DW et al (1999) The effects of
vitamin D insufficiency in patients with primary hyperparathy-
roidism. Am J Med 107:561–567
8. Grey A, Lucas J, Horne A et al (2005) Vitamin D repletion in
patients with primary hyperparathyroidism and coexistent vita-
min D insufficiency. J Clin Endocrinol Metab 90:2122–2126
9. Rao DS, Agarwal G, Talpos GB et al (2002) Role of vitamin D
and calcium nutrition in disease expression and parathyroid tumor
growth in primary hyperparathyroidism: a global perspective.
J Bone Miner Res 17(Suppl 2):N75–80
10. Rao DS, Honasoge M, Divine GW et al (2000) Effect of vitamin
D nutrition on parathyroid adenoma weight: pathogenetic and
clinical implications. J Clin Endocrinol Metab 85:1054–1058
11. Nordenstrom E, Westerdahl J, Lindergard B et al (2002) Multifac-
torial risk profile for bone fractures in primary hyperparathyroidism.
World J Surg 26:1463–1467
12. Buchwald PC, Westin G, Akerstrom G (2005) Vitamin D in
normal and pathological parathyroid glands: new prospects for
treating hyperparathyroidism (review). Int J Mol Med 15:
701–706
13. Norman AW (1998) Sunlight, season, skin pigmentation, vitamin
D, and 25-hydroxyvitamin D: integral components of the vitamin
D endocrine system. Am J Clin Nutr 67:1108–1110
14. MacLaughlin JA, Anderson RR, Holick MF (1982) Spectral
character of sunlight modulates photosynthesis of previtamin D3
and its photoisomers in human skin. Science 216:1001–1003
15. Chen TC, Chimeh F, Lu Z et al (2007) Factors that influence the
cutaneous synthesis and dietary sources of vitamin D. Arch
Biochem Biophys 460:213–217
16. Holick MF (2004) Vitamin D: importance in the prevention of
cancers, type 1 diabetes, heart disease, and osteoporosis. Am J
Clin Nutr 79:362–371
17. Hannan MT, Litman HJ, Araujo AB et al (2008) Serum 25-hy-
droxyvitamin D and bone mineral density in a racially and
ethnically diverse group of men. J Clin Endocrinol Metab 93:40–46
18. Dawson-Hughes B (2008) Serum 25-hydroxyvitamin D and
functional outcomes in the elderly. Am J Clin Nutr 88:537S–
540S
19. Hollis BW (2005) Circulating 25-hydroxyvitamin D levels
indicative of vitamin D sufficiency: implications for establishing
a new effective dietary intake recommendation for vitamin D. J
Nutr 135:317–322
20. Hollis BW, Wagner CL (2005) Normal serum vitamin D levels. N
Engl J Med 352:515–516 (author reply 515–516)
21. Souberbielle JC, Lawson-Body E, Hammadi B et al (2003) The
use in clinical practice of parathyroid hormone normative values
established in vitamin D-sufficient subjects. J Clin Endocrinol
Metab 88:3501–3504
22. Vieth R (2006) What is the optimal vitamin D status for health?
Prog Biophys Mol Biol 92:26–32
23. Szodoray P, Nakken B, Gaal J et al (2008) The complex role of
vitamin D in autoimmune diseases. Scand J Immunol 68:261–269
24. Baeke F, Etten EV, Gysemans C et al (2008) Vitamin D signaling
in immune-mediated disorders: evolving insights and therapeutic
opportunities. Mol Aspects Med 29:376–387
25. Melamed ML, Michos ED, Post W et al (2008) 25-hydroxyvi-
tamin D levels and the risk of mortality in the general population.
Arch Intern Med 168:1629–1637
26. Mocellin S, Nitti D (2008) Vitamin D receptor polymorphisms
and the risk of cutaneous melanoma: a systematic review and
meta-analysis. Cancer 113:2398–2407
27. Lally RM (2008) Vitamin D and cancer: more questions than
answers remain. ONS Connect 23:23
28. Doro P, Grant WB, Benko R et al (2008) Vitamin D and the
seasonality of type 2 diabetes. Med Hypotheses 71:317–318
29. Sambrook PN, Chen JS, March LM et al (2004) Serum para-
thyroid hormone predicts time to fall independent of vitamin D
status in a frail elderly population. J Clin Endocrinol Metab 89:
1572–1576
30. Vieth R, Bayley TA, Walfish PG et al (1991) Relevance of
vitamin D metabolite concentrations in supporting the diagnosis
of primary hyperparathyroidism. Surgery 110:1043–1047
31. Younes NA, Shafagoj Y, Khatib F et al (2005) Laboratory
screening for hyperparathyroidism. Clin Chim Acta 353:1–12
World J Surg (2009) 33:2292–2302 2301
123

32. Doherty DA, Sanders KM, Kotowicz MA et al (2001) Lifetime and
five-year age-specific risks of first and subsequent osteoporotic
fractures in postmenopausal women. Osteoporos Int 12:16–23
33. Melton LJ III (2002) The epidemiology of primary hyperpara-
thyroidism in North America. J Bone Miner Res 17(Suppl
2):N12–N17
34. Lundgren E, Hagstrom EG, Lundin J et al (2002) Primary
hyperparathyroidism revisited in menopausal women with serum
calcium in the upper normal range at population-based screening
8 years ago. World J Surg 26:931–936
35. Lundgren E, Rastad J, Thurfjell E et al (1997) Population-based
screening for primary hyperparathyroidism with serum calcium
and parathyroid hormone values in menopausal women. Surgery
121:287–294
36. Bilezikian JP, Silverberg SJ (2000) Clinical spectrum of primary
hyperparathyroidism. Rev Endocr Metab Disord 1:237–245
37. Jorde R, Bonaa KH, Sundsfjord J (2000) Primary hyperparathy-
roidism detected in a health screening. The Tromso Study. J Clin
Epidemiol 53:1164–1169
38. Marcus R, Madvig P, Young G (1984) Age-related changes in
parathyroid hormone and parathyroid hormone action in normal
humans. J Clin Endocrinol Metab 58:223–230
39. Yetley EA (2008) Assessing the vitamin D status of the U.S.
population. Am J Clin Nutr 88:558S–564S
40. Sambrook PN, Chen JS, March LM et al (2004) Serum para-
thyroid hormone is associated with increased mortality
independent of 25-hydroxy vitamin d status, bone mass, and renal
function in the frail and very old: a cohort study. J Clin Endo-
crinol Metab 89:5477–5481
41. Garabedian M, Holick MF, Deluca HF et al (1972) Control of 25-
hydroxycholecalciferol metabolism by parathyroid glands. Proc
Natl Acad Sci U S A 69:1673–1676
42. Kaplan RA, Haussler MR, Deftos LJ et al (1977) The role of 1
alpha, 25-dihydroxyvitamin D in the mediation of intestinal hy-
perabsorption of calcium in primary hyperparathyroidism and
absorptive hypercalciuria. J Clin Invest 59:756–760
43. Pak CY, Oata M, Lawrence EC et al (1974) The hypercalciurias,
Causes, parathyroid functions, and diagnostic criteria. J Clin
Invest 54:387–400
44. Souberbielle JC, Cormier C, Kindermans C et al (2001) Vitamin
D status and redefining serum parathyroid hormone reference
range in the elderly. J Clin Endocrinol Metab 86:3086–3090
45. Bilezikian JP, Potts JT Jr, Fuleihan Gel H et al (2002) Summary
statement from a workshop on asymptomatic primary hyper-
parathyroidism: a perspective for the 21st century. J Clin
Endocrinol Metab 87:5353–5361
46. Bell NH, Greene A, Epstein S et al (1985) Evidence for alteration
of the vitamin D-endocrine system in blacks. J Clin Invest
76:470–473
47. Quesada JM, Coopmans W, Ruiz B et al (1992) Influence of
vitamin D on parathyroid function in the elderly. J Clin Endo-
crinol Metab 75:494–501
48. Souberbielle JC, Fayol V, Sault C et al (2005) Assay-specific
decision limits for two new automated parathyroid hormone and
25-hydroxyvitamin D assays. Clin Chem 51:395–400
49. Ozbey N, Erbil Y, Ademoglu E et al (2006) Correlations between
vitamin D status and biochemical/clinical and pathological
parameters in primary hyperparathyroidism. World J Surg 30:
321–326
50. Untch BR, Barfield ME, Dar M et al (2007) Impact of 25-hy-
droxyvitamin D deficiency on perioperative parathyroid hormone
kinetics and results in patients with primary hyperparathyroidism.
Surgery 142:1022–1026
51. Wang TS, Ostrower ST, Heller KS (2005) Persistently elevated
parathyroid hormone levels after parathyroid surgery. Surgery
138:1130–1136
52. Beyer TD, Solorzano CC, Prinz RA et al (2007) Oral vitamin D
supplementation reduces the incidence of eucalcemic PTH ele-
vation after surgery for primary hyperparathyroidism. Surgery
141:777–783
53. Stewart ZA, Blackford A, Somervell H et al (2005) 25-hydrox-
yvitamin D deficiency is a risk factor for symptoms of
postoperative hypocalcemia and secondary hyperparathyroidism
after minimally invasive parathyroidectomy. Surgery 138:1018–
1026
54. Moosgaard B, Vestergaard P, Heickendorff L et al (2006) Plasma
25-hydroxyvitamin D and not 1,25-dihydroxyvitamin D is associ-
ated with parathyroid adenoma secretion in primary hyperpara-
thyroidism: a cross-sectional study. Eur J Endocrinol 155:237–244
55. Raef H, Ingemansson S, Sobhi S et al (2004) The effect of
vitamin D status on the severity of bone disease and on the other
features of primary hyperparathyroidism (pHPT) in a vitamin D
deficient region. J Endocrinol Invest 27:807–812
56. Pradeep PV, Mishra A, Agarwal G et al (2008) Long-term out-
come after parathyroidectomy in patients with advanced primary
hyperparathyroidism and associated vitamin D deficiency. World
J Surg 32:829–835
57. von Hurst PR, Stonehouse W, Matthys C et al (2008) Study
protocol-metabolic syndrome, vitamin D and bone status in South
Asian women living in Auckland, New Zealand: a randomised,
placebo-controlled, double-blind vitamin D intervention. BMC
Public Health 8:267
2302 World J Surg (2009) 33:2292–2302
123




















