
Pediatric D ysphagia Treatm ent: The How & W hy - The ...
77
Pediatric Dysphagia Treatment: The How & Why Presented to The 20 th Annual Loretta G. Brown Symposium at the Memorie M. Gosa, PhD, CCC-SLP, BCS-S Pediatric Speech-Language Pathologist, Assistant Professor [email protected]
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Pediatric D ysphagia Treatm ent: The How & W hy - The ...

Pediatric Dysphagia Treatment:
The How &
Why
Presented to The 20thAnnual Loretta G.
Brown Sym
posium at the
Mem
orieM
. Gosa, PhD, CCC-SLP, BCS-SPediatric Speech-Language Pathologist, Assistant Professor
mem

Review of Feeding and sw
allowing problem
s in pediatric populations8:15 -9:45
09/21/182
Image from
: https://nouvelles.umontreal.ca/en/article/2017/12/14/eating-together-as-a-fam
ily-helps-children-feel-better/

9/17/18
1
http://www.craftsy.com/blog/2013/08/childs-face-mastering-proportions/ http://www.new-vis.com/fym/papers/p-feed10.htm
Developmental vs Acquired Dysphagia
• Relearning vs. basic acquisition of skills• Critical/Sensitive periods for learning• Cognitive skills for applying strategies
Early Nutrition for Growth & Long-Term Development
http://secondinnocence.blogspot.com/2008_10_01_archive.html

9/17/18
2
Children vs Adults: Feeding Skills• Early suckling– Oral phase is reflexive– Intake is single consistency (fluid)– Plane of movement in uni-directional– Brainstem mediated – Central pattern generator
• Later transition to solids– Oral phase is volitional– Intake is of variable consistency– Plane of movement in multi-directional– Greater cortical input is required
Sensory Integration
• Hyposensitive• Hypersensitive
• Stimulation– Tactile– Thermal– Chemo
Sensory Integration
• Hyposensitive– High threshold for
registering sensory input
– Reduced response to stimuli
– Actively seeks extra stimulation
http://noahsdad.com/first-tim-tam-balance-parenting/

9/17/18
3
Sensory Integration
• Hypersensitive– Low threshold for registering sensory input– Increased response to stimulus–May actively avoid stimulation
http://www.dailymail.co.uk/news/article-2085776/Moment-baby-tries-lemon-time--love-hate-time.html
Food Aversion
– Behavioral response to stimulus–May persist beyond initial sensory integration
problem
http://thetherapeuticresourcesblog.blogspot.com/2011/08/picky-eater-or-sensory-food-aversion.html
Learning to EatSynchrony of systems
Gut maturation
Oral anatomy
Neurology
Posture
Behaviour
Milk> solid foods
Small oral cavity> large
Reflexes> voluntary skills
Requiring support> independent
Passive> independent
• “Dysphagia is a swallowing disorder characterized by difficulty in oral preparation for the swallow or in moving material from the mouth to the stomach. Subsumed in this definition are problems in positioning food in the mouth and in the oral manipulation preceding the swallow including suckling, sucking, and mastication.”
ASHA, 1987, p. 57

9/17/18
4
Dysphagia
• Dysphagia exists if:– Feeding problems interfere with airway protection– Compromise adequate nutrition/hydration– (Peds) Compromise enjoyment for either parent
or child
Variable Incidence & Prevalence
• 25% - 45% of typically developing children (Arvedson, 2008;
Bernard-Bonnin, 2006; Brackett, Arvedson, & Manno, 2006; Burklow, Phelps, Schultz, McConnell, & Rudolph, 1998; Lefton-Greif, 2008; Linscheid, 2006; Manikam & Perman, 2000; Rudolph & Link, 2002)
• 30%-80% for children with developmental disorders (Arvedson, 2008; Brackett, Arvedson, & Manno, 2006; Lefton-Greif, 2008; Manikam & Perman, 2000)
• 3%-10% of children have severe consequences-Higher prevalence (10%-49%) in children with history of prematurity, medical illness and (26%-90%) physical disabilities (Manikam & Perman, 2000)
Consequences of Pediatric Dysphagia
1) Malnutrition-Managed successfully with supplemental nutrition
2) Aspiration with resulting respiratory compromise-Management is more complex-Airway problems may result from dysphagia but airway problems might also create dysphagia
Consequences of Pediatric Dysphagia
• Texture of food/fluid aspirated linked to respiratory outcomes
• Taniguchi and Moyer, 1994: – Pureed consistencies 9x increase in risk of
developing pneumonia– Thickened liquids, second greatest risk of
developing pneumonia– Thin liquids, not statistically significant increase in
risk for developing pneumonia

9/17/18
5
Causes of Pediatric Feeding Problems Disorders
of Appetite
Metabolic Diseases
Sensory Defects
Conditioned
Dysphagia
Anatomic Abnormalities of the Orophary
nx, Larynx,
Trachea, &
Esophagus
Disorders affecting Sucking-
Swallowing-
Breathing
Disorders affecting
Neuromuscular
Coordination of
Swallowing
Mucosal Infections
& Inflamma
tory Disorders
Rudolph CD & Link DT (2002) Feeding Disorders in Infants and Children. Pediatric Gastroenterology & Nutrition, 49(1), 97-112.
Clinical Signs
• Arvedson et al., 1994– Poor predictive values for aspiration: choke,
respiratory problems, concern for aspiration, and dependence on others for feeding
– 94% are silent aspirators• Perlman (1990)– Not having one or all clinical signs does not
suggest that patient is a safe feeder
09/21/18 20
Clinical Signs• Vary from child to child• Dependent upon age and type of underlying
disorder• Response to aspiration is age dependent• Coordination of swallowing mechanism improves
with age, protective reflexes– Cough in older children– Apnea in neonates– Desensitization from frequent aspiration/neurologic
impairment
09/21/18 21
Clinical Signs
• Knowledge of underlying diagnosis is important but vigilance is key!
• BPD, asthma, and cystic fibrosis often have GER and are at higher risk for respiratory complications of dysphagia
• Differences between infants and children:– Apnea and bradycardia more common than
cough, congestion, wheezing, bronchitis, atelectasis, & pneumonia
09/21/18 22

9/17/18
6
Oral Impairment• Lack of energy/endurance• Significant amount of oral residue• Excessive drooling• Prolonged mealtimes• Excessive gagging on secretions• Lip retraction/limited upper lip movement• Poor labial seal/anterior spillage• Jaw thrust/clench/retraction/instability/tonic or phasic bite
reflex• Reduced buccal tone/sensory awareness• Poor bolus formation/transport• Difficult initiation of swallow• Multiple swallows to clear oral cavity
09/21/18 23
Pharyngeal Impairment• Nasopharyngeal backflow• Slowed initiation of swallow• Multiple swallows to clear single bolus• Piecemeal deglutition• Hyper/Hypo active gag• Aspiration before/during/after swallow• Most commonly aspirate on liquids• Absent or reduced cough reflex• Cricopharyngeal dysmotility
09/21/18 24
Red Flags: Adult vs Pediatric Red Flags
• Adults• Recurrent Pneumonia• Head and Neck Cancer• Anoxia• Progressive Neurologic Disease• Anterior Cervical Spinal Fusion• Weight Loss• Diet Modifications• Brainstem Stroke• Guillain Barre• Laryngeal Trauma• Intubation• Ongoing respiratory problems
• Pediatrics• Issues affecting appetite• Metabolic Disease• Sensory defects• Craniofacial anomalies• Congenital conditions of
trachea/larynx• Abnormalities of esophagus
or lower GI tract• S:S:B Coordination Difficulty• Neuromuscular Disorders• Mucosal
infections/Inflammatory Disorders
• History of prematurity
09/21/18 25
Prematurity

9/17/18
7
Prematurity
1. Difficult S:S:B coordination2. Poor endurance due to respiratory problems3. Reduced strength/control of oral structures4. Poor state modulation/alertness5. Reduced control of oral-motor activities6. Oral hypersensitivity
Wolf & Glass, 1992
Intraventricular Hemorrhage– 40% in infants born prior
to 32 weeks (Volpe, 1997)– May lead to long-term
neurological impairment & decreased survival rate
– May impact on oral & pharyngeal functioning dependent on site of bleed and resulting neuropathology (hydrocephalus, etc…). (Ward & Beechy, 2003)
Necrotizing Enterocolitis (NEC)– GI disease, pathology unknown– Bowel injury in the neonate due
to pathogenic organism, enteral feedings and bowel compromise
– Symptoms range from mild feeding intolerance and abdominal distention to bowel perforation & additional system involvement
– Complicates nutritional support, creates LONG TERM feeding problems(Ward & Beechy, 2003)
09/21/18 29
Bronchopulmonary Dysplasia– Chronic lung disease– Secondary to infant respiratory
distress syndrome, barotrauma from positive pressure ventilation, oxygen toxicity, & respiratory infection
– 23-31 weeks gestation at greatest risk– Lung function improves during
childhood– Significant impact on growth, 30-67%
have growth failure in months following discharge
(Ward & Beechy, 2003; Vohr et al,. 1982; Kurzner et al., 1988)
09/21/18 30

9/17/18
8
Bronchopulmonary Dysplasia• Physiologically based feeding
problems & problems of mother-infant interaction– Poor sucking patterns, aspiration
during feeding (Pridham et al., 1989)
– Failure to develop anticipated suck/swallow rhythms at 32-40 weeks (Gewolb et al., 2001)
– Feeding interactions may be compromised
– Mothers report more depression & anxiety (Singer et al., 1996)
09/21/18 31
Congenital Heart Disease• Congenital Heart Disease– Higher risk for FTT/growth failure (Hofner et al., 2000)– 3 main categories
1. Acyanotic2. Cyanotic3. Obstructive heart defects
– Presence of hypoxia & pulmonary hypertension are predicting factors for feeding problems in this population
– Physiological problems & infant-mother feeding problems (Varan et al., 1999)
09/21/18 32
Congenital Neurologic Disorders
• Dysphagia common among children with CND and DD
• Both groups have predisposition to oral-motor dysfunction and GERD (Gisel et al., 2003)
• DD characteristically show food refusal, food selectivity by type or texture, oral-motor delay and dysphagia (any problem with swallowing) (Field et al., 1993)
09/21/18 33
Cerebral Palsy (CP) and Feeding/Swallowing
• 75% of patients with CP have some sign/symptom of dysphagia
• Malnutrition, dehydration, and respiratory complications can result from dysphagia
• Assessment of their feeding/swallowing abilities is an important part of their overall care

9/17/18
9
CP and Feeding/Swallowing• 45-50% of patients with CP are undernourished• Respiratory complications and pneumonia-- 90%
of deaths in patients with severe CP are caused by pneumonia
• Feeding/Swallowing difficulties due to:– Poor oral motor control– Poor pharyngeal movements– Persistence of primitive reflexes– Delayed gastric emptying– Abnormal posturing– Poor head control– Poor trunk stability
CP and Feeding/Swallowing• Poor growth seen in CP is frequently due to malnutrition• Pharyngeal dysphagia puts children with CP at risk for
multiple episodes of aspiration/pneumonia• GERD may also be associated with aspiration and
esophagitis• This combined with delayed gastric emptying may all
contribute to reduced oral intake
CP and Feeding/Swallowing• Chronic constipation present in 74% of patients– Secondary to prolonged transit at level of proximal
segments of the colon
• GERD present in more than 90% of children with CP– Also had prolonged gastric emptying
– Abnormal esophageal motility
• Oral motor dysfunction in children with CP is more than 90%-- with 1/3 of those presenting with severe OMD
• Results in:– Abnormal formation of bolus
– Defects in propulsion of bolus
CP and Feeding/Swallowing
• Feeding/Swallowing Functional Influences– Oral Issues– Pharyngeal Issues– Gastrointestinal Issues– Respiratory/Airway Issues

9/17/18
10
Aerodigestive Tract Anomalies
09/21/18 39
Nasopharynx Oropharynx Larynx Pharynx Trachea/Esophagus
Micellaneous
Choanal atresia
Nasal cysts
Tumors
Deviated
septum
Midface
hypoplasia
Cleft lip
Mandibular
hypoplasia
Adenotonsillar
hyperplasia
Epiglottitis
Penetrating
trauma
Tumor
Cyst
Laryngeal
Subglottic
stenosis
Laryngom
alacia
Vfpara.
Laryngeal
cleft
Laryngeal
web
Pharyng.
Paralysis
Pharyngit.
Peritonsill
ar absces
Retrophar
yngeal
abcess
TEF/Eso Atre
Esophageal
Mass
Mechanical
obstruction
LES/UES dysf.
Esophagitis
Esophageal
compression
NMJun
Disease
Muscular
disorders
Neoplastic
causes
Traumatic
Injury
Foreign body
ingestion
Nasopharynx
• Obstruct the nasal cavity- most impact on infants
• Bilateral/partial obstruction & stenosis• Stridor, labored breathing• Strained breathing increases during oral
feeding- disrupting coordination of breathing and swallowing
(Arvedson & Lefton-Greif, 1998) (Brodsky, 1997)
09/21/18 40
Oropharynx
• Cleft lip & palate–Most commonly occurring craniofacial anomalies– Palate=inability to generate adequate intraoral
pressure for sucking– Lip=may effect ability to produce intraoral
pressure due to lip seal inadequacy– Pierre Robin sequence most commonly presents
with a U-shaped cleft palate(Kosko et al., 1998)
09/21/18 41
Larynx
• Laryngomalacia–Most common cause of stridor, respiratory
distress, and airway obstruction in infants– High pitched inspiratory stridor during feeding
and/or crying– Commonly occurs with GERD– Typically resolves within first year of life
(Brodsky, 1997)
09/21/18 42

9/17/18
11
Larynx
• Vocal fold paralysis– Frequently leads to aspiration– Second most common congenital anomaly – Unilateral, bilateral, congenital, or acquired– Functional voicing but inspiratory stridor– Unilateral paralysis: aspiration & hoarseness– Bilateral paralysis: inspiratory or biphasic stridor;
worsens with feeding– Spontaneous recovery or tracheostomy
(Kosko et al., 1998) & (Friedman et al., 2001)
09/21/18 43
Larynx• Posterior laryngeal cleft– Rare congenital anomalies– Failure of posterior cricoid lamina to fuse– Association between laryngeal cleft and TEF
09/21/18 44
Trachea and Esophagus• Tracheosophageal fistula/Esophageal atresia
– Most common congenital aerodigestive tract anomalies– Surgical repair– May exist separately, frequently seen togetherTEF:– Communication between trachea and esophagus allow
food/fluid to pass directly to lungs– Congenital or acquired– Coughing, choking, cyanosis, and hyperreactive airway-
recurrent aspiration pneumonia(Brodsky and Volk, 1993)
09/21/18 45
Trachea and Esophagus• Tracheostomy– Surgical opening running from neck through to
trachea– Typically placed between 2-3 cervical vertebrae– May inhibit laryngeal excursion– Granulation tissue accumulation is common– Chronic bronchitis, wheezing, congestion, and
recurrent bacterial tracheitis should raise concern about chronic recurrent aspiration
– Aspiration is common complication(Loughlin and Lefton-Greif, 1994) & (Brodsky, 1997)
09/21/18 46

9/17/18
12
GERD• 2 main causes:
1. Failure of normal means of preventing reflux2. Failure of means to clear occurring refluxo Infants: LES, esophageal peristalsis, and anatomy of esophagus
matures with ageo Infants with normal development of LES can maintain
pressure, preventing reflux between swallowso Infants with GERD, transient relaxation of LES between
swallows (seconds-minutes), most significant etiology of GERD in children
(Kawahara el al., 1997) (Putnam, 1997)
GERD• Two hallmark clinical symptoms
(Carr et al., 2000) (Carr and Brodsky, 1999)Respiratory Feeding
Stridor *Frequent vomiting during & after feeding
Wheeze *Growth Faltering
Cough *Choking/gagging
Nasal Congestion Drooling
Hoarseness Irritability with feeding
Aspiration Wet burps
Reflux central apnea Back arching
Reflux-induced laryngospasm
Reflux bronchospasm
GERD
• Treatment– Pharmacological: medicines either neutralize acid or
prevent acid production– Nonpharmacological: Upright positioning, thickened
feeds– Surgical: Nissen fundoplication
(Sullivan, 1997) (Putnam, 1997) (Orenstein, 1983)
GERD• Feeding Problems
– Prolonged presence of refluxed material in esophagus leads to inflammation of mucosa & bleeding
– Pain associated with esophagus leads to food refusal (Pain association with Feeding)
– Reduced oral intake Failure to thrive– Irritability, arching, grimacing, head turning, physical refusal,
and gagging/wretching– Reports of globus/food stuck in throat- result of non-specific
disruptions in esophageal peristalsis– Chronic inflammation may lead to thickening & development
of a fibrous stricture: food impaction &/or vomiting (Putnam, 1997) (Cucchiara et al., 1990) (Hyman 1994)

9/17/18
13
GERD• Oral Phase
– Food refusal– Reduced self-feeding and readiness behaviors for solids– Oral hypersensitivity– Immature lip, tongue and jaw control– Food loss, poor lip closure/bolus containment– Difficulty with puree/semisolid foods– Delayed oral transit
• Pharyngeal Phase– Silent aspiration– Delayed pharyngeal transit times
(Mathisen et al., 1999)
Behavioral Feeding Problems
• Can arise as part of a number of other
comorbidities
• High prevalence (up to 85%)
• Reduced oral intake, poor/reduced weight
gain, malnutrition, FTT Effecting
neurological and physical development
• Disruptions in feeding routine impacts
intellectual, social and emotional growth of
the child AND overall family functioning
(Chatoor et al., 1988) (Palmer et al., 1975)
Behavioral Feeding ProblemsCommon clinical signs of behavioral feeding problems:
– Frowning/falling asleep, expressions of resistance/fear of accepting foods or liquids
– Panic in response to feeding utensil approaching
– Head turning– Hiding face– Struggling to avoid being fed– Gradual/sudden onset of
“difficult” mealtime behaviors
– Selective food refusal/food resistance
– Reduced appetite/lack of oral intake
– Failure to accept age-appropriate foods
– Excessive adaptations– Sudden refusal to
eat/drink– Sudden loss of appetite– Gradual change in eating
habits/patterns
Behavioral Feeding Problems• Causes
– Complex, multifactorial– Organic: physiological abnormalities, neuromuscular conditions,
allergies and acute infections, & various syndromes– Defining feature: medical/organic causes ruled out as being
significant enough to explain problems persistence– Non-organic environmental factors
• Two main etiologies1) Delayed development, lack of oral experience,failure to move into transitional period of feeding atnormal, developmentally appropriate time2) Psychological issues: negative patterns of mother-child
interaction and/or behavioral mismanagement

9/17/18
14
Behavioral Feeding Problems• Lack of oral experience/developmental delay– Critical period for taste: 4-6 m– Critical period for texture advancement: 6-7 m– Late development results in inadequate mastication for
chewing = aversive gagging or choking, further refusal– Populations at risk: prolonged NG feedings, children with
severe medical illness/prolonged hospitalization– Combination of oral restrictions and aversive oral
stimulation during developmentally critical periods promotes dysfunctional feeding abilities
(Skuse, 1993) (Morris, 1989) (Willging 2000)
Behavioral Feeding Problems• Psychosocial Factors– Successful feeding relies heavily on both child’s
OM skills and parent’s skill in interpreting child’s needs
– Failure of caregiver to understand child’s needs and their own role during feeding process often leads to AVERSIVE FEEDING PRACTICES & subsequent behavioral feeding problems
– Reaches beyond physical growth and into child’s cognitive and linguistic competence & attachment to major caregivers
(Arvedson, 1997)

9:45 –10:00
09/21/1869

Motor, Sensory, &
Behavioral Approaches to Feeding10:00 –
11:30
09/21/181

9/17/18
1
Multidisciplinary Management
Speech Language
Pathologist
Dietician
PCP
OTPT
Teacher
GIPulmonology
Social Worker
PedsDysphagia
Dysphagia TreatmentWhy treat Dysphagia?
• To facilitate safe oral feeding needed to sustain appropriate health and nutrition
Or• To transition patients to oral feedings as
appropriate
Successful Feeding
Medical Management
Nutrition
Skill
Environment
Behavior

9/17/18
2
Oral Sensory Motor Therapy
ORAL SENSORIMOTOR THERAPY• Oral sensorimotor therapy is a broad term,
encompassing many different therapy techniques aimed at improving the function of the structures involved in the skills of eating (and speaking)
• SLPs are taught the basic principles of OSM therapy as part of their training
• However, a range of new OSM therapy texts, equipment resources, and therapy programs become available each year
ORAL SENSORIMOTOR THERAPY
o Acquired knowledge and judgement are required to: o Set therapy goals
o Determine which specific OSM techniques to use to achieve goals
o Implement the OSM techniques
o Measure relevant outcomes
o Modify therapy techniques, as necessary, in order to achieve goals
ORAL SENSORIMOTOR THERAPY
• Aims of OSM therapy
– Main aim • To achieve an individual’s maximal functional
capacity for feeding and speech
– Target areas • Oral structures (lips, tongue, cheeks, jaw,
palate)
• Neck, chest, posture, respiration

9/17/18
3
ORAL SENSORIMOTOR THERAPY
• Goals of OSM therapy– Depending on the individual, goal may be to
achieve:• Skills appropriate to age • Skills appropriate to level of development / physical
capacity
– At different times during therapy specific goals may be to:• Acquire new skills• Develop existing skills• ‘Normalize’ skills the individual already
demonstrates
ORAL SENSORIMOTOR THERAPY
• Individual goals for OSM therapy
• Increased/decreased oral sensitivity to touch/ taste/ temperature
• Increased awareness of oral structures and movements
• Appropriate levels of arousal/ preparation for oral-motor tasks
• Co-ordinated oral movement sequences
ORAL SENSORIMOTOR THERAPY
• Individual goals for OSM therapy• Increased/ decreased oral muscle tone
• Increased/ decreased range of movement of oral structures
• Increased oral muscle strength
• Increased rate of movement of oral structures
• Increased precision of oral movements
• Facilitating appropriate oral reflexes, integrating/ inhibiting any abnormal oral reflexes
• Establishing functional oral movement patterns by guiding/ facilitating oral movements
ORAL SENSORIMOTOR THERAPY
• Specific goals for OSM therapy - Feeding– Decreased oral hypersensitivity/ increased oral
awareness– Increased oral self-exploration – Improved oral skills for feeding
(sucking/ chewing/ biting) – Safe swallowing – Improved saliva control – Assist in the transition from non-oral to oral feeding– Improve mealtime participation

9/17/18
4
ORAL SENSORIMOTOR THERAPY
• Specific OSM therapy techniques often involve:
– Utilizing equipment (purpose-specific or adapting non-specific equipment)
– Using taught strategies
– Cueing (tactile/ visual/ auditory)
– Games to make the task more appealing to children
ORAL SENSORIMOTOR THERAPY• Features essential to the success of OSM
therapy include:
– Individualized program– Graded tasks– Direct/ hands on– Involve repetitive practice– Often intensive/ short-term– Only forms part of an overall therapy plan– Skills worked on during OSM therapy must be
necessary /relevant to functional activities important to the individual’s life
Thickened Liquids
Image from: https://cdn-sg.theasianparent.com/wp-content/uploads/2013/08/shutterstock_116855842.jpg
THICKENED FLUIDSThe use of thickened fluids is routinely recommended for two main pediatric populations:
� (a) children with oral-pharyngeal dysphagia
� (b) children who display regurgitation
It is important that thickened fluids are prepared correctly.
� If thickened fluids are too thin, they may not assist in managing the underlying problem (i.e. aspiration during swallowing and/or reflux)
� If thickened fluids are too thick, they may cause additional problems (e.g. increased work of breathing, reduced intake due to fatigue)

9/17/18
5
THICKENED FLUIDSBottle feed provides infants with both nutrition and hydrationBottle-fed infants should be able to suck the feed through a nipple on a bottle in 20-30 minutes, in order to meet their nutritional and fluid requirements without expending excess energy
� If a bottle-fed infant requires thickened fluids, they may need to be switched to a faster flowing nipple to accommodate the thicker fluid.
THICKENED FLUIDSThickened bottle feeds are generally served heated, but will cool over the duration of a feed, and will likely get thicker. If the feed is re-heated, it may get thinner
Be aware that an infant with dysphagia who shows no clinical signs of aspiration with one type of thickened fluid may not manage another thickened fluid in the same way.
� Clinicians recommending thickened fluids need to be aware of potential variation in the viscosity or thickness of thickened fluids, as infants may be consuming liquids more or less viscous than assumed. Check that the recipe being used makes the correct thickness.
� Caregivers should be alert to clinical signs of fatigue and/or aspiration demonstrated during feeding (e.g. coughing, wet vocalizations, increased work of breathing), as this may indicate the thickness of the feed needs to be adjusted.
THICKENED FLUIDS
Expected measurements for thickened fluids
of different degrees of thickness are listed
below.
Thickened fluids Radius (mean) Radius (range) Reference
Pudding thick 2.2 cm 1.50- 2.89 cm QHealth (2006)
Honey thick 3.2 cm 2.90- 3.89 cm QHealth (2006)
Nectar thick 4.2 cm 3.90- 5.00 cm QHealth (2006)
Infant formula 9.7 cm Dodrill et al (2007, 2008)
THICKENING AGENTSThickening agents used for children with dysphagia should be labelled as suitable for use with patients with dysphagia. In addition, the packaging should contain clear instructions on how much thickening agent is required to prepare fluids that are consistent with the levels set out in the National Standards and/or to thicken bottle feeds.
In addition to speech pathology staff, dietetic, pharmacy, and medical staff should be involved in deciding which types of thickening agents are suitable for use with children.
Be aware that some thickening agents may contain allergens. Take particular care if a child has an allergy/ intolerance to corn, wheat, or gluten, or if they have eosinophilic esophagitis.

9/17/18
6
THICKENING AGENTSBe aware that most suppliers of thickening agents do not recommend the use of their products with infants prior to term age (i.e. premature babies), or if the child has certain types of gut pathology, as some kinds of thickening agent may not be digested by the premature/ pathological gut, and may possibly cause gut complications.
Many suppliers of xanthan gum do not recommend the use of their product with children under 1-2 years of age (Simply Thick & Thicken Up Clear)
THICKENING AGENTSSimply Thick Xanthan gum, citric acid and potassium sorbateThick & Easy (Hormel) Modified maize starch, maltodextrinResource ThickenUp (Nestle) Modified maize starchResource ThickenUp Clear (Nestle)
Maltodextrin, xanthan gum, potassium chloride (may contain traces of milk)
GelMix Maltodextrin, Organic Carob Bean Gum, Calcium Lactate
Rice Cereal (Gerber) Rice flour, tri- and di-calcium phosphate, soybean oil, soy lecithin, mixed tocopherols, electrolytic iron sulphate, alpha tocopherylacetate (vitamin A), pyridoxine hydrochloride (vitamin B6), thiamin mononitrate (vitamin B1), folic acid (vitamin B9), cyanocobalamin(vitamin B12)
Enfamil AR Rice starch, maltodextrinSimilac Sensitive for Spit Up Rice starch
RICE CEREAL
Can separate to thin fluid and solid mass
Can block teat
Increases energy content of feed
Contains potential allergens

9/17/18
7
Behavioral Feeding Management
09/21/18 28
Medical Skill Behavioral
Rommel, N., De Meyer, A. M., Feenstra, L., & Veereman-Wauters, G. (2003). The complexity of feeding problems in 700 infants and young children presenting to a tertiary care institution. Journal of pediatric gastroenterology and nutrition, 37(1), 75-84.

9/17/18
8
Classification System
700 children age 10 and under seen by a multi-disciplinary feeding clinic
• Medical: 86% • Oropharyngeal dysfunction: 61% • Behavioral: 18%
Rommel, N., De Meyer, A. M., Feenstra, L., & Veereman-Wauters, G. (2003). The complexity of feeding problems in 700 infants and young children presenting to a tertiary care institution. Journal of pediatric gastroenterology and nutrition, 37(1), 75-84.
Romm
el, N., De Meyer, A. M
., Feenstra, L., & Veerem
an-Wauters, G. (2003). The com
plexity of feeding problem
s in 700 infants and young children presenting to a tertiary care institution. Journal of pediatric gastroenterology and nutrition, 37(1), 75-84.
Feeding problems that can result from GI Issues
• Inappropriate mealtime behaviors• Refusal to self feed• Food selectivity • Inability to advance texture• Food refusal• Oral motor dysfunction/immaturity• Dysphagia/Aspiration• Frequent vomitingKerwin, M. E. (1999). Empirically supported treatments in pediatric psychology: severe feeding problems. Journal of Pediatric Psychology, 24(3), 193-214.
Food Neophobia
• Reluctance to eat and/or avoidance of new foods
• Peaks between 2-6 years of age
Dovey, Staples, Gibson, & Halford (2008). Food neophobia and picky/fussy eating in children: A review. Appetite, 50: 181-193.

9/17/18
9
KEY INDICATORS OF FEEDING DIFFICULTIES• Limited range of textures – Often reliance on ‘easy to eat foods’– Puree, dissolvable vs. lumpy, mechanical
• Limited range of foods– < 30 foods– <10 proteins, <10 fruit/ veg, <10 starches
• Prolonged mealtime duration– >30 mins at mealtimes, >2hrs a day spent trying to feed
child• Battles/ problematic behavior at mealtimes• Family stress related to the child’s eating patterns
BEHAVIORAL FEEDING• Promote a positive feeding relationship
between caregiver and child
– Where possible, step back from causes of any
unpleasant interactions
– Create opportunities for pleasant interactions
– Establish familiarity and comfort around food
and feeding environment
– Provide pleasurable oral stimulation
• Determine feeding readiness
– Gut
– Swallowing
– Breathing
BEHAVIORAL FEEDING• Normalize feeding
– Graded oral sensory tasks during feeding
– Graded oral motor tasks during feeding
• Initiate a behavioral feeding plan
– Set goals
– Follow routine
– Provide clear instructions
– Reward desirable feeding behaviors
– Do not reward undesirable feeding behaviors
– Be consistent
BEHAVIORAL FEEDING• ‘ABC’
• Antecedent
– Prompt: Verbal, visual, tactile, modelling
• Behavior
– Desirable vs undesirable
• Consequence
– Reinforcement – done to increase the likelihood of a
behaviour occurring again
– Punishment – done to decrease the likelihood of a
behaviour occurring again

9/17/18
10
Behavioral Approaches• Operant conditioning therapy
– Focus on changing behaviors related to eating– May also incorporate information on general parenting skills– Generally aimed at clinical populations
• Generally run in hospital-based feeding clinics• Usually run by therapists• E.g. Kennedy Kreiger, Medical College Wisconsin
Behavioral Approaches
• Differential Attention (with or without shaping)
– Positive attention for appropriate feeding behavior
and ignoring inappropriate behavior
• Contingent reinforcement
– Praise for the target response & ignoring all other
responses
• Punishment
– Attempting to reduce or eliminate unwanted
behaviors Kerwin, M. E. (1999). Empirically supported treatments in pediatric psychology: severe feeding problems. Journal of Pediatric Psychology, 24(3), 193-214.
Behavioral Approaches
• Positive reinforcement– Praise after an appropriate feeding response regardless of
whether it occurred independently, after a verbal prompt, or after a modeled response
• Manual guidance of the appropriate feeding response(s)– Physically, verbally, or manually directing
• 3-step guided compliance– Hierarchy of instruction and prompting: 1) Providing
verbal instruction; 2) if no response after a specific amount of time, modeling w/ the verbal instruction, & 3) if still no response, manual guidance
Kerwin, M. E. (1999). Empirically supported treatments in pediatric psychology: severe feeding problems. Journal of Pediatric Psychology, 24(3), 193-214.
Behavioral Approaches• Extinction
– Removing the reinforcer of a response
• Food refusal can be negatively reinforced by removing the spoon after refusal, thereby increasing the probability of food refusal
• Extinction procedure would require that the spoon remain at the child’s lips until it is accepted in to the mouth
• Increased acceptance and volume consumed in 10 – 130 sessions
• Behavior likely to worsen before it improves• Can be combined with positive reinforcement
Kerwin, M. E. (1999). Empirically supported treatments in pediatric psychology: severe feeding problems. Journal of Pediatric Psychology, 24(3), 193-214.

9/17/18
11
Behavioral Approaches
• Systematic desensitization therapy– Focus on improving willingness to interact with food– May also incorporate information on general
parenting skills– Generally aimed at clinical populations
• Generally run in hospital-based feeding clinics• Usually run by therapists• E.g. SOS Approach to Feeding
https://theoriesinpsychologyf10.wikispaces.com/file/view/Desensitization.gif/177474605/Desensitization.gif
Operant conditioning– Feeder determines
how much is eaten
Goals:– Improved volumes
taken– Reduced number of
refusal behaviors
Systematic desensitization
– Child determines how much is eaten
Goals:– Increased willingness
to try foods – Increased range of
foods tolerated
Comparing Programs
SOS APPROACH TO FEEDING
– Dr Kay Toomey and colleagues– Formal training is required to use this
approach
– Multi-disciplinary– Systematic desensitization – graded
hierarchies and games for learning and to minimise anxiety
– Social modelling – family, other children– Family focused – parent education– Family meals vs. therapy meals
FACTORS TO CONSIDER•Child’s health•Family issues•Service delivery issues

9/17/18
12
BEHAVIORAL FEEDING• Set realistic, step-wise goals
• Provide positive reinforcement
– Reward desirable behaviour
– Provide reinforcement immediately
– Provide specific feedback with reinforcement
– Be consistent in rewarding
¨ Ignore undesired behaviour (when safe to do so)
BEHAVIORAL FEEDING• Gradually fade the prompt
• Gradually thin the reinforcement
– Increase the number of times the desired task
has to be performed before a reward is given
– e.g. once then reward, then 2x, 3x etc,
before the reward
BEHAVIORAL FEEDING• Shaping/ chaining– Gradually increase the demands of the
task:• Smell a new food, then lick a new food, then taste
a new food• Hold a piece of new food in the mouth, then spit it
out• Bite a piece of new food, then spit it out• Bite a piece of new food, hold it in the mouth,
then spit it out• Bite a piece of new food, move it to the side of the
mouth, then spit it out• Chew a piece of new food, then spit it out• Chew and swallow a piece of new food• Increase the amount of time that the food has to
stay in the mouth (Count out loud to encourage the task to seem like a competition)

Lunch on your own
11:30 –12:45
09/21/1850

Practice scenarios for Motor, Sensory, and Behavioral
Approaches to Feeding & Sw
allowing Problem
s12:45 –
2:15
09/21/181

9/17/18
1
Four Case Scenarios• Please divide into groups of 5-6• Review and then select a case scenario from the
following 4 options• For Cases 1-3, considering the treatment options
reviewed this morning, document how you would address the feeding/swallowing issues for each individual case
• For Case 4- please use the provided thickeners and tools to determine the appropriate ratio of thickener to formula for this family
• We will review each case and have input from each group after ~30 minutes of discussion
09/21/18 2
Case 1: 2 y.o., 17p-syndrome with hypotonia, developmental delay, visual
impairment, and dysphagia• G-tube @ 1 month
secondary to difficulty eating
• H/o vocal stridor, severe GERD with copious vomiting and coughing during G-tube feedings until 1 year of age
• Viral pneumonia 3 months before evaluation- otherwise good respiratory health
09/21/18 3
• Satisfactory growth• MBS @ 5m revealed
laryngeal penetration with thin liquids but no aspiration. Subsequent initiation of transition to oral feedings began using pureed foods
• At this eval: Student taking pureed, baby foods (fruits & veggies)– two times daily in 1-2 oz portionsSheppard, J.J. (1997).Pediatric Dysphagia and Related Medical, Behavioral, and
Developmental Issues. In B.C. Sonies (Ed), Dysphagia: A Continuum of Care (p. 67). Gaithersburg, Maryland: Aspen Publishers, Inc.

9/17/18
2
Case 1- 2 y.o., 17p-syndrome with hypotonia, developmental delay, visual
impairment, and dysphagia• Smith-Magenis syndrome is a developmental disorder that affects many parts of the body. The
major features of this condition include mild to moderate intellectual disability, delayed speech and language skills, distinctive facial features, sleep disturbances, and behavioral problems.Most people with Smith-Magenis syndrome have a broad, square-shaped face with deep-set eyes, full cheeks, and a prominent lower jaw. The middle of the face and the bridge of the nose often appear flattened. The mouth tends to turn downward with a full, outward-curving upper lip. These facial differences can be subtle in early childhood, but they usually become more distinctive in later childhood and adulthood. Dental abnormalities are also common in affected individuals.Disruptedsleep patterns are characteristic of Smith-Magenis syndrome, typically beginning early in life. Affected people may be very sleepy during the day, but have trouble falling asleep and awaken several times each night.People with Smith-Magenis syndrome have affectionate, engaging personalities, but most also have behavioral problems. These include frequent temper tantrums and outbursts, aggression, anxiety, impulsiveness, and difficulty paying attention. Self-injury, including biting, hitting, head banging, and skin picking, is very common. Repetitive self-hugging is a behavioral trait that may be unique to Smith-Magenis syndrome. People with this condition also compulsively lick their fingers and flip pages of books and magazines (a behavior known as "lick and flip").Other signs and symptoms of Smith-Magenis syndrome include short stature, abnormal curvature of the spine (scoliosis), reduced sensitivity to pain and temperature, and a hoarse voice. Some people with this disorder have ear abnormalities that lead to hearing loss. Affected individuals may have eye abnormalities that cause nearsightedness (myopia) and other vision problems. Although less common, heart and kidney defects also have been reported in people with Smith-Magenis syndrome.
09/21/18 4
Case 1- 2 y.o., 17p-syndrome with hypotonia, developmental delay, visual impairment, and dysphagia• Clinical findings:
– Piecemeal swallowing of spooned boluses
– Poorly coordinated breathing & swallowing while eating pureed foods
– Increased respiratory rate after a few tastes, then refusal to continue accepting boluses
– Slightly wet breath sounds after bolus swallows
– Apparent anxiety during bolus swallowing and during NN mouthing tasks
Modified Barium Swallow:– Safe bolus swallows on puree
and thin liquid– No evidence of laryngeal
penetration or tracheal aspiration
– Bolus size was restricted by piecemeal delivery of the bolus into the pharynx
– Swallows became less organized as feeding progressed
Nutritional Evaluation:– Heavier than desired weight
for height
Sheppard, J.J. (1997).Pediatric Dysphagia and Related Medical, Behavioral, and Developmental Issues. In B.C. Sonies (Ed), Dysphagia: A Continuum of Care (p. 67). Gaithersburg, Maryland: Aspen Publishers, Inc.

9/17/18
3
Case 1- 2 y.o., 17p-syndrome with hypotonia, developmental delay, visual impairment, and dysphagia
• Clinical impression is dysphagia with impairment of oral preparation, oral initiation, and pharyngeal phases of swallowing. Contributing causes are:1) Traumatically conditioned effects of GERD2) Inadequate amount of practice for acquisition of the skills
needed for oral feeding
Sheppard, J.J. (1997).Pediatric Dysphagia and Related Medical, Behavioral, and Developmental Issues. In B.C. Sonies (Ed), Dysphagia: A Continuum of Care (p. 67). Gaithersburg, Maryland: Aspen Publishers, Inc.
http://graceriddell.com/

9/17/18
4
Case 2
• 4y, 3m with diagnoses of – Static encephalopathy with microcephaly– Cerebral palsy spastic quadriplegia– Profound cognitive impairment– Alternating exotropia– Scoliosis– Seizure disorder– Dysphagia
Sheppard, J.J. (1997).Pediatric Dysphagia and Related Medical, Behavioral, and Developmental Issues. In B.C. Sonies (Ed), Dysphagia: A Continuum of Care (p. 67). Gaithersburg, Maryland: Aspen Publishers, Inc.
Case 2: 4y, 3m: Microcephaly, CP spastic quadriplegia
• Hip adductor release surgery
• Selective posterior rhizotomy
• Tegretol and Depakote for seizure management, continues to have modified
complex partial seizures many times each day
• Asthma triggered by URI and takes Ventolin orally PRN for wheezing
• Multiple episodes of pneumonia- most recent episode 1 year ago
• Senokot and glycerine suppositories for constipation
• Reglan on a trial basis- family found it to be helpful. Discontinued b/c of concern
about side effects
• Weight for height is below 5th percentile
• Current diet is pureed table foods by spoon and liquids by cup– fed in another
person’s lap or in feeder seat
• Meal times are prolonged at 30-60 minutes
• Sounds congested during feedings
• Limited oral intake and crying after eating
• Referred for assessment secondary to coughing and gagging associated with eating
• Mother requests that recommendations focus on improving oral feeding
• Patient has G-tube, family attempting to wean from G-tube. Patient hasn’t used G-
tube in ~6 months
Sh
ep
pa
rd,
J.J.
(1
99
7).
Pe
dia
tric
Dysp
ha
gia
an
d R
ela
ted
Me
dic
al,
Be
ha
vio
ral,
an
d
De
ve
lop
me
nta
l Is
su
es.
In B
.C.
So
nie
s(E
d),
Dys
phag
ia: A
Con
tinuu
m o
f Car
e(p
.
67
). G
ait
he
rsb
urg
, M
ary
lan
d:
Asp
en
Pu
blish
ers
, In
c.

9/17/18
5
Case 2: 4y, 3m: Microcephaly, CP spastic quadriplegia• Clinical findings:
– Special chair and assistance needed to stabilize head-neck and thorax in sitting position during feeding– Small mandible and marked distoclusion (Malocclusion of the teeth in which those of the lower jaw
are in distal relation to the upper teeth– Pooled oral secretions in mouth and oropharynx– Reduced mouth opening and tongue blocking– Slow oral transit – Multiple swallows to clear each bolus– Congested breath sounds during and after each feedingDietician:– 861 calories/day– 50% of daily needsMBS:– Poor posterior containment of the bolus before swallow initiation– Spillover to pyriform sinuses before the swallow and residue in the valleculae and pyriform
sinuses after the swallow– Multiple swallows used to clear each bolus from the phayrnx– With pureed bolus, large laryngeal penetration & tracheal aspiration after the swallow– With liquid, laryngeal penetration with trace tracheal aspiration after the swallow
• Diminished pharyngeal contraction and ineffectual on all swallows• No coughing or gagging• Chest X-ray revealed barium in the left lower lobe bronchi
Sheppard, J.J. (1997).Pediatric Dysphagia and Related Medical, Behavioral, and Developmental Issues. In B.C. Sonies (Ed), Dysphagia: A Continuum of Care (p. 67). Gaithersburg, Maryland: Aspen Publishers, Inc.
Case 2: 4y, 3m: Microcephaly, CP spastic quadriplegia
Clinical Impressions• Severe dysphagia with involvement in oral
preparatory, oral initiation, and pharyngeal phases of swallow
• Severe malnutrition• Reactive Airway Disease• Contributing causes include
– Static encephalopathy– CP– Break through seizures– Oral and thoracic skeletal deformations
Sheppard, J.J. (1997).Pediatric Dysphagia and Related Medical, Behavioral, and Developmental Issues. In B.C. Sonies (Ed), Dysphagia: A Continuum of Care (p. 67). Gaithersburg, Maryland: Aspen Publishers, Inc.

9/17/18
6
Case 2: 4y, 3m: Microcephaly, CP spastic quadriplegia
Case 3- 11 month old infant with reflux and dysphagia
• 11 month old infant, born at term following uncomplicated delivery
• Significant reflux and ongoing unresolved respiratory issues
• Upper GI documented reflux • Modified barium swallow shows aspiration
with thin liquids, improved with slightly thick consistency
09/21/18 13

9/17/18
7
Case 3- 11 month old infant with reflux and dysphagia
• Referred to your clinic to determine appropriate thickening recommendations
• Determine if any of the provided formulas are the Slightly Thick consistency at rest with IDDSI Flow Test
• Use the provided thickening agents to determine the appropriate recipe for each formula provided- confirm with the IDDSI Flow Test
09/21/18 14
Case 3- IDDSI Flow Test
Copyright 2017 - Used with permission from IDDSI

9/17/18
8
Case Study #4: Cory• 2-year old boy with a normal birth• 6 weeks: began projectile vomiting during breast
feeding, was given medication, and the problem was resolved
• 6 months: refused introduction of baby foods, but still breastfeeding well
• 9 months: growth was slowing down and vomiting increased again
• 11 months: hospitalized for growth faltering and diagnosed with �behavioral feeding aversion�, placed on a gastronomy tube
• Now, parents want him enrolled in intensive behavioral feeding program to wean off the tube feeding
JusticeC
omm
unication Sciences and Disorders: An Introduction
Copyright ©
2006 by Pearson Education, Inc.U
pper Saddle River, N
ew Jersey 07458
All rights reserved.
Case Study 4- Cory
• What type of behavioral approach will you take?
• What will your goals be?• What else do you need to know? Whom else
might need to be involved?• What specific strategies might work well for
Cory?
09/21/18 17

Review of Case Scenarios
1:15 –2:15
09/21/1818

Break 2:15 –
2:30
09/21/1819
Review of the Evidence
2:30 –4:00
09/21/181

9/17/18
1
• Oral motor interventions include exercises and activities designed to influence the actions of the tongue, lips, soft palate, jaws, larynx, and/or respiratory muscles for improved strength, tone, range of motion, or coordination during feeding/swallowing and include traditional muscle exercises (active or passive), stretching, and/or sensory stimulation to the articulators and related structures
Treatment: Motor/Skill
Treatment: Motor/Skill

9/17/18
2
• Oral- Phase interventions impact on functional feeding ability, drooling, swallowing physiology, and pulmonary health in populations other than preterm infants.
• 16 studies included– none reported on pulmonary health outcomes
• Studies published before 2008
Treatment: Motor/Skill for Pediatric Populations
Arvedson, J., Clark, H., Lazarus, C., Schooling, T., & Frymark, T. (2010a). The effects of oral-motor exerciseson swallowing in children: an evidence-based systematic review. Developmental Medicine & Child Neurology,52(11), 1000–1013. doi:10.1111/j.1469-8749.2010.03707.x

9/17/18
3
• Clinical question 1: what is the effect of OME on swallowing physiology outcomes in children?– 8 studies addressed this question
– 3- effects of an intra-oral stimulating plate
– 3- impact of a tongue thrust treatment or lip & tongue exercises
– 2- use of oral, perioral, and facial stimulation
Treatment: Motor/Skill for Pediatric Populations
Arvedson, J., Clark, H., Lazarus, C., Schooling, T., & Frymark, T. (2010a). The effects of oral-motor exerciseson swallowing in children: an evidence-based systematic review. Developmental Medicine & Child Neurology,52(11), 1000–1013. doi:10.1111/j.1469-8749.2010.03707.x
• Clinical question 1: what is the effect of OME on swallowing physiology outcomes in children?– 3- effects of an intra-oral stimulating plate on
swallowing physiology outcomes in children with CP• Large positive impact on chewing, smaller impact on
swallowing and mouth clearing• 1 year follow-up no changes noted by the group that
continued to wear the device• Conclusions- during 1 year follow-up previous treatment
gains were maintained & maturation alone was equally as effective as the treatment
Treatment: Motor/Skill for Pediatric Populations
Arvedson, J., Clark, H., Lazarus, C., Schooling, T., & Frymark, T. (2010a). The effects of oral-motor exerciseson swallowing in children: an evidence-based systematic review. Developmental Medicine & Child Neurology,52(11), 1000–1013. doi:10.1111/j.1469-8749.2010.03707.x

9/17/18
4
• Clinical question 1: what is the effect of OME on swallowing physiology outcomes in children?– 3- impact of a tongue thrust treatment or lip & tongue exercises– None of the studies provide effect sizes– OME+ artic tx made greater gains than those receiving artic tx alone
on a 3 point tongue-thrust severity scale– Tongue thrust tx group performed significantly better than a no-tx
group on a 3 point tongue thrust severity scale 5 years after tx– Children completing the Face Former tx program had significantly
greater improvement in swallowing patterns than those receiving traditional myofunctional tx
Treatment: Motor/Skill for Pediatric Populations
Arvedson, J., Clark, H., Lazarus, C., Schooling, T., & Frymark, T. (2010a). The effects of oral-motor exerciseson swallowing in children: an evidence-based systematic review. Developmental Medicine & Child Neurology,52(11), 1000–1013. doi:10.1111/j.1469-8749.2010.03707.x
• Clinical question 1: what is the effect of OME on swallowing physiology outcomes in children?– 2- use of oral, perioral, and facial stimulation – Both used single subject designs, and only one provided
statistical analysis– Subjects for each study were classified as having multiple
disabilities– Significant reduction in tongue thrusting with solid foods
and semi-solid foods during treatment– 2-week return to baseline treatment, significant increase
in tongue thrusting with solid foods but not with semi-solid foods
Treatment: Motor/Skill for Pediatric Populations
Arvedson, J., Clark, H., Lazarus, C., Schooling, T., & Frymark, T. (2010a). The effects of oral-motor exerciseson swallowing in children: an evidence-based systematic review. Developmental Medicine & Child Neurology,52(11), 1000–1013. doi:10.1111/j.1469-8749.2010.03707.x

9/17/18
5
• Clinical question 3: what is the effect of OME on functional swallowing outcomes in children?
• 6 studies– 4- effects of an intra-oral stimulating plate in 58
participants with spastic CP ranging in age from 4y 5m – 15y 5m
– 2- effects of oral stimulation & neuromuscular facilitation procedures on weight gain in young people with severe to profound mental disability and neuromotor disability
Treatment: Motor/Skill for Pediatric Populations
Arvedson, J., Clark, H., Lazarus, C., Schooling, T., & Frymark, T. (2010a). The effects of oral-motor exerciseson swallowing in children: an evidence-based systematic review. Developmental Medicine & Child Neurology,52(11), 1000–1013. doi:10.1111/j.1469-8749.2010.03707.x
• Clinical question 3: what is the effect of OME on
functional swallowing outcomes in children?
– 4- effects of an intra-oral stimulating plate in 58
participants with spastic CP ranging in age from 4y
5m – 15y 5m
• 3 studies used single subject design with treatment for 12
months and found no difference in weight gain
• 1 study looked at long term impact of OME with the device
over an additional 1 year period compared with those who
did not wear the device for an additional year and found
no significant effect on weight or growth
Treatment: Motor/Skill for Pediatric
Populations
Arvedson, J., Clark, H., Lazarus, C., Schooling, T., & Frymark, T. (2010a). The effects of oral-motor exercises
on swallowing in children: an evidence-based systematic review. Developmental Medicine & Child Neurology,
52(11), 1000–1013. doi:10.1111/j.1469-8749.2010.03707.x

9/17/18
6
• Clinical question 4: what is the effect of OME on drooling management in children?– 5 total studies addressed this question
• 3- use of oral stim and facilitation in children and young adults with CP (one with statistical analysis)
• 1- use of chin cup intervention and OME classes in children and adolescents with CP (no statistical analysis)
• 1- use of oral stimulating plates in children with Down syndrome
Treatment: Motor/Skill for Pediatric Populations
Arvedson, J., Clark, H., Lazarus, C., Schooling, T., & Frymark, T. (2010a). The effects of oral-motor exerciseson swallowing in children: an evidence-based systematic review. Developmental Medicine & Child Neurology,52(11), 1000–1013. doi:10.1111/j.1469-8749.2010.03707.x
• Clinical question 4: what is the effect of OME on drooling management in children?– 1- use of oral stimulating plates in children
with Down syndrome– Negligible effect compared with OME alone
on parental perception of daytime drooling– Small effect on night time drooling
Treatment: Motor/Skill for Pediatric Populations
Arvedson, J., Clark, H., Lazarus, C., Schooling, T., & Frymark, T. (2010a). The effects of oral-motor exerciseson swallowing in children: an evidence-based systematic review. Developmental Medicine & Child Neurology,52(11), 1000–1013. doi:10.1111/j.1469-8749.2010.03707.x

9/17/18
7
• Clinical question 4: what is the effect of OME on drooling management in children?– 3- use of oral stim and facilitation in children
and young adults with CP• Only one provided statistical analysis- but did not
report effect sizes• OME had significant effect on pre/post saliva bib
weight for one participant but not the other
Treatment: Motor/Skill for Pediatric Populations
Arvedson, J., Clark, H., Lazarus, C., Schooling, T., & Frymark, T. (2010a). The effects of oral-motor exerciseson swallowing in children: an evidence-based systematic review. Developmental Medicine & Child Neurology,52(11), 1000–1013. doi:10.1111/j.1469-8749.2010.03707.x
• Conclusions• Insufficient evidence to determine the
effects of OME on children with oral sensorimotor deficits and swallowing problems
• Well designed studies are needed to provide evidence that can be incorporated into the treatment paradigm
Treatment: Motor/Skill for Pediatric Populations
Arvedson, J., Clark, H., Lazarus, C., Schooling, T., & Frymark, T. (2010a). The effects of oral-motor exerciseson swallowing in children: an evidence-based systematic review. Developmental Medicine & Child Neurology,52(11), 1000–1013. doi:10.1111/j.1469-8749.2010.03707.x
9/17/18
8
But surely in the last 10 years better research has been published on this
topic…

9/17/18
9
• This evidence based systematic review (EBSR) examined the published evidence for the use of common strategies used by clinicians across disciplines to treat pediatric swallowing and feeding problems.
1. What is the effect of oral motor interventions on functional oral feeding outcomes in children?
*Functional feeding outcomes = feeding behaviors, volume of oral intake, variety of oral intake, days to wean tube feeding, weight gain, and/or growth
Treatment: Motor/Skill for Pediatric Populations
Gosa, M. M., Carden, H. T., Jacks, C. C., Threadgill, A. Y., & Sidlovsky, T. C. (2017). Evidence to support treatment options for children with swallowing and feeding disorders: A systematic review. Journal of pediatric rehabilitation medicine, 10(2), 107-136.
1. What is the effect of oral motor interventions on functional oral feeding outcomes in children?
• 1 of the 61 studies • 20 participants in this experimental, randomized control trial
study had profound intellectual disability or neuromuscular disorders, lived in a residential care facility
• Oral motor program that included manual intervention, direct guidance, stretches, pressure, and oral desensitization administered 30–40 minutes daily, five times a week for nine weeks for the experimental group (n=10)
Treatment: Motor/Skill for Pediatric Populations
Gosa, M. M., Carden, H. T., Jacks, C. C., Threadgill, A. Y., & Sidlovsky, T. C. (2017). Evidence to support treatment options for children with swallowing and feeding disorders: A systematic review. Journal of pediatric rehabilitation medicine, 10(2), 107-136.

9/17/18
10
1. What is the effect of oral motor interventions on functional oral feeding outcomes in children?
• Analysis of the nine experimental subjects that had pre and post treatment oral motor function testing revealed no significant change following treatment.
• Statistical analysis of the full sample (n =20) revealed no significant difference in body weight gains between the experimental and the control group at discharge
Treatment: Motor/Skill for Pediatric Populations
Gosa, M. M., Carden, H. T., Jacks, C. C., Threadgill, A. Y., & Sidlovsky, T. C. (2017). Evidence to support treatment options for children with swallowing and feeding disorders: A systematic review. Journal of pediatric rehabilitation medicine, 10(2), 107-136.
Thickened FluidsPediatrics Literature
Gosa, Schooling, & Coleman, (2011). Thickened liquids as a treatment for children with dysphagia and associated adverse effects: A systematic review. ICAN: Infant, Child, & Adolescent Nutrition. Published online 5 May 2011.
• Clinical Question 1: For children with a diagnosis of dysphagia, what is the effect of thickened liquids on swallowing physiology (eg, aspiration, feeding efficiency), oral feeding development, weight gain and growth, hydration, or pulmonary health (eg, aspiration pneumonia, wheezing)?
• Clinical Question 2: Is there an increased occurrence of adverse effects (ie, NEC, gut adhesion, bowel obstruction, diarrhea, constipation, weight loss, failure to thrive, dehydration, aspiration, & cough) associated with the use of thickened liquids or certain thickening agents in children with or without dysphagia?

9/17/18
11
Thickened FluidsPediatrics LiteratureClinical Question 1: Summary
• 6 of the 22 identified studies• The 6 studies investigated swallowing physiology or oral
feeding outcomes & 1 study also examined pulmonary health
• Elimination of laryngeal or tracheal penetration (n=5)• Elimination of laryngeal penetration in 71% (22/31) • Half of the participants (60/121) from 5 studies
reported elimination of aspiration w/ the use of thickened liquids
• Elimination of nasopharyngeal reflux (n=2)• Improved initiation or resolution of delayed swallow in
20% (2/10)
Thickened FluidsPediatrics LiteratureClinical Question 2: Summary
• 16 of the identified 22 studies• 757 participants total in the 16 studies (ss ranged 18-104)• Adverse effects examined in these studies included weight loss,
cough, aspiration, constipation, & diarrhea
• 8 studies examined weight status; overall thickened formula had no effect or positive effect on weight gain
• 8 studies examined cough; mixed results with some reporting resolution of cough & some reporting no change in coughing
• 1 study examined aspiration; no instances of aspiration under either thickened or non-thickened feeding condition

9/17/18
12
Thickened FluidsPediatrics LiteratureClinical Question 2: Summary
• 3 studies examined constipation; no significant differences in constipation rate were reported
• 2 studies examined diarrhea; compared to standard formula, rice starch-thickened formula had no effect on the incidence of diarrhea among study participants
• Complication rate: overall rate of adverse events or unspecified complications were examined & all of the 16 investigations indicated that no infant experienced any complication during the study period
Thickened Fluids
Pediatrics Literature
• A systematic review by Steele and colleagues
(2015) investigating the influence of liquid
consistency modification on swallowing
physiology and function found that thicker
liquids reduce the risk of laryngeal penetration
and aspiration, but also increase the risk of
post-swallow residue in the pharynx. Steele, C. M., Alsanei, W. A., Ayanikalath, S., Barbon, C. E., Chen, J., Cichero, J. A., ... & Wang, H. (2014). The influence of food
texture and liquid consistency modification on swallowing physiology and function: A systematic review. Dysphagia, 30(1), 2-26.

9/17/18
13
Treatment :Sensory
2. What is the effect of sensory-based interventions (exercises and activities that are designed to promote sensory integration such as using a brushing or vibration protocol, a weighted vest, or deep pressure in the joints) on functional oral feeding outcomes in children
• None of the 61 articles included examined only sensory-based interventions.
Treatment: Sensory
Gosa, M. M., Carden, H. T., Jacks, C. C., Threadgill, A. Y., & Sidlovsky, T. C. (2017). Evidence to support treatment options for children with swallowing and feeding disorders: A systematic review. Journal of pediatric rehabilitation medicine, 10(2), 107-136.

9/17/18
14
• 3. What is the effect of behavioral-based interventions (including approaches that incorporate techniques with elements from operant conditioning, systematic desensitization, etc.. . . ) on functional oral feeding outcomes in children?
• 37 studies• 919 pooled participants, 86% were between 2
and 7 years old• 70% were small sample size (N of 1-13), 30% had
sample sizes from 24 – 490
Treatment: Behavioral
Gosa, M. M., Carden, H. T., Jacks, C. C., Threadgill, A. Y., & Sidlovsky, T. C. (2017). Evidence to support treatment options for children with swallowing and feeding disorders: A systematic review. Journal of pediatric rehabilitation medicine, 10(2), 107-136.
• 11/37 studies• Escape extinction (behavioral technique used to
treat behaviors that are maintained by escaping or avoiding; removing the possibility of escaping from the challenging stimulus)
• Reinforcement (the use of any stimulus which should increase the probability of a desired response, can be positive or negative)
• Single subject & small cohort designs• Impact on acceptance, intake, and presence of
undesirable behaviors at mealtimes
Treatment: Behavioral Positive Reinforcement & Extinction
Gosa, M. M., Carden, H. T., Jacks, C. C., Threadgill, A. Y., & Sidlovsky, T. C. (2017). Evidence to support treatment options for children with swallowing and feeding disorders: A systematic review. Journal of pediatric rehabilitation medicine, 10(2), 107-136.

9/17/18
15
• Escape extinction with – differential reinforcement increased oral intake & mouth clean
(n=3)– or without reinforcement increased mouth clean and decreased
undesirable mealtime behaviors (n=5)– representation of expelled bites increased acceptance of non-
preferred foods (n=3)– attention extinction combination decreased inappropriate
mealtime behaviors and increased food acceptance (n=4)– Chin prompt & representation of expulsion per bite decreased
rates of expulsion and increased volume of intake (n=4)– meal & taste probing resulted in increase in the volume and
variety of foods and decrease in undesirable mealtime behaviors maintained for up to 1 month post treatment (n=3)
Treatment: Behavioral Positive Reinforcement & Extinction
Gosa, M. M., Carden, H. T., Jacks, C. C., Threadgill, A. Y., & Sidlovsky, T. C. (2017). Evidence to support treatment options for children with swallowing and feeding disorders: A systematic review. Journal of pediatric rehabilitation medicine, 10(2), 107-136.
• Positive reinforcement with– non-contingent reinforcement and extinction of disruptive behavior decreased
undesirable feeding behavior and increased volume of food eaten (n=3)– negative reinforcement, self-feeding, parent education, structured mealtimes
and repeated presentation of novel foods resulted in improvements in variety and volume of oral intake, reduction of undesirable behaviors, improved parent-child interactions during mealtimes, & increases in both height and weight (n=1)
– escape extinction, & caregiver training for increased mastication, mouth clean, and acceptance
– escape extinction, & caregiver training with mixed results– 2 had increased self-feeding behavior and 1 had no improvement
– peer modeling for increased volume and variety of accepted foods, significant weight gain with 1 participant weaning tube feeding by two months’ post treatment
Treatment: Behavioral Positive Reinforcement & Extinction
Gosa, M. M., Carden, H. T., Jacks, C. C., Threadgill, A. Y., & Sidlovsky, T. C. (2017). Evidence to support treatment options for children with swallowing and feeding disorders: A systematic review. Journal of pediatric rehabilitation medicine, 10(2), 107-136.

9/17/18
16
• 11/37 studies• Shaping- behavior training that uses differential
reinforcement of successive approximations of the desired behavior
• Fading- initial prompting to perform behavior is gradually withdrawn, ensuring the child does not become dependent on the stimulus
• Impact on food refusal & discontinuation of tube feeding
Treatment: Behavioral Stimulus Shaping & Fading
Gosa, M. M., Carden, H. T., Jacks, C. C., Threadgill, A. Y., & Sidlovsky, T. C. (2017). Evidence to support treatment options for children with swallowing and feeding disorders: A systematic review. Journal of pediatric rehabilitation medicine, 10(2), 107-136.
• Shaping & fading – Generalization of oral acceptance in a case series with
discontinuation of tube feeding– Increases in oral intake with the reduction of G-tube
feedings and addition of oral feeding meals – Increases in acceptance of bites and decreased number
of disruptive responses– With visual cueing & positive reinforcement resulted in
tube weaning and full oral feeding with 2 pound weight gain
– With positive reinforcement, escape extinction, and flooding resulted in majority increase in some aspect of oral intake (n=86 ex-preterm)
Treatment: Behavioral Stimulus Shaping & Fading
Gosa, M. M., Carden, H. T., Jacks, C. C., Threadgill, A. Y., & Sidlovsky, T. C. (2017). Evidence to support treatment options for children with swallowing and feeding disorders: A systematic review. Journal of pediatric rehabilitation medicine, 10(2), 107-136.

9/17/18
17
• Shaping & fading – With escape extinction resulted in improving acceptance,
mouth clean, and decreasing inappropriate behaviors during mealtime
– With escape extinction and bite representation and Nukbrush resulted in increased mouth clean and acceptance and decreased packing & expulsions per bite
– With non-contingent access resulted in significant improvements in food variety, consumption, and appropriate mealtime behaviors
– With behavioral principles in teaching, parent education, & concurrent presentations of preferred foods with target foods resulted in increased height, weight, & BMI
Treatment: Behavioral Stimulus Shaping & Fading
Gosa, M. M., Carden, H. T., Jacks, C. C., Threadgill, A. Y., & Sidlovsky, T. C. (2017). Evidence to support treatment options for children with swallowing and feeding disorders: A systematic review. Journal of pediatric rehabilitation medicine, 10(2), 107-136.
• 13/37 studies• Focused on parent education & involvement
in combination with behavioral strategies (primarily: reinforcement, escape extinction, & fading)
• Approximately ½ reported on case studies• Positive reported impact on all functional
oral feeding outcomes
Treatment: Behavioral Caregiver Involvement & Education
Gosa, M. M., Carden, H. T., Jacks, C. C., Threadgill, A. Y., & Sidlovsky, T. C. (2017). Evidence to support treatment options for children with swallowing and feeding disorders: A systematic review. Journal of pediatric rehabilitation medicine, 10(2), 107-136.

9/17/18
18
* Determine whether OC or SysD intervention results in greater improvements in dietary variety/intake and greater reductions in difficult mealtime behaviors* Children, 2-6 years w/ ASD or NMC à randomized to receive 10 OC or SysD sessions at 1x/week or for 1 week
Treatment: Behavioral Comparison of Operant Conditioning
& Systematic Desensitization Gosa, M. M., Carden, H. T., Jacks, C. C., Threadgill, A. Y., & Sidlovsky, T. C. (2017). Evidence to support treatment options for children with swallowing and feeding disorders: A systematic review. Journal of pediatric rehabilitation medicine, 10(2), 107-136.Marshall, J., Path, B. S., & Hill, R. J. JPGN Journal of Pediatric Gastroenterology and Nutrition Publish Ahead of Print.
• Differences between OC & SysD• In OC group:• Trend towards greater increase in total number of
foods consumed & total number of unprocessed fruits and vegetables
• In SysD Group• Trend towards greater reduction of difficult mealtime
behaviors
Treatment: Behavioral Comparison of Operant Conditioning
& Systematic Desensitization Gosa, M. M., Carden, H. T., Jacks, C. C., Threadgill, A. Y., & Sidlovsky, T. C. (2017). Evidence to support treatment options for children with swallowing and feeding disorders: A systematic review. Journal of pediatric rehabilitation medicine, 10(2), 107-136.Marshall, J., Path, B. S., & Hill, R. J. JPGN Journal of Pediatric Gastroenterology and Nutrition Publish Ahead of Print.

9/17/18
19
• Differences between ASD & NMC• In ASD group:• Greater improvement in overall dietary quality
• In NMC group:• Slightly better improvement to dietary variety
(total proteins)
Treatment: Behavioral Comparison of Operant Conditioning
& Systematic Desensitization Gosa, M. M., Carden, H. T., Jacks, C. C., Threadgill, A. Y., & Sidlovsky, T. C. (2017). Evidence to support treatment options for children with swallowing and feeding disorders: A systematic review. Journal of pediatric rehabilitation medicine, 10(2), 107-136.Marshall, J., Path, B. S., & Hill, R. J. JPGN Journal of Pediatric Gastroenterology and Nutrition Publish Ahead of Print.
Differences between Intensive & Weekly • In weekly arm:• Greater reductions in difficult mealtime
behaviors• Greater reductions in number of problem
behaviors outside of mealtime
Treatment: Behavioral Comparison of Operant Conditioning
& Systematic Desensitization Gosa, M. M., Carden, H. T., Jacks, C. C., Threadgill, A. Y., & Sidlovsky, T. C. (2017). Evidence to support treatment options for children with swallowing and feeding disorders: A systematic review. Journal of pediatric rehabilitation medicine, 10(2), 107-136.Marshall, J., Path, B. S., & Hill, R. J. JPGN Journal of Pediatric Gastroenterology and Nutrition Publish Ahead of Print.

9/17/18
20
Treatment :Mixed Modality
• 5. What is the effect of applying mixed modality
interventions on functional oral feeding outcomes in
children?
• 23 of the 61 studies
• 395 pooled participants; majority of studies featured small
sample sizes (less than 10 participants)
• 95% of participants were between 2-10 years of age
• Mixed diagnostic population that included Down syndrome,
ASD, Goldenhar syndrome, Rett syndrome, CP, rubella
syndrome, & feeding complications due to major organ
system impairments
Treatment: Mixed Modality
Gosa, M. M., Carden, H. T., Jacks, C. C., Threadgill, A. Y., & Sidlovsky, T. C. (2017). Evidence to support treatment
options for children with swallowing and feeding disorders: A systematic review. Journal of pediatric rehabilitation medicine, 10(2), 107-136.

9/17/18
21
• Behavioral & OMI• 12/23, with pooled participants = 30• All studies utilized case study or single subject designs• Resulted in:
– G-tube feedings were significantly reduced or eliminated with significant reduction or elimination of undesirable mealtime behaviors and an overall increase in desirable parent behavior
– Reduced rates of expulsions and increased mouth cleans– Improved variety, texture, and volume of food eaten – Decreased packing, increased oral coordination &
participation in mealtimes
Treatment: Mixed Modality
Gosa, M. M., Carden, H. T., Jacks, C. C., Threadgill, A. Y., & Sidlovsky, T. C. (2017). Evidence to support treatment options for children with swallowing and feeding disorders: A systematic review. Journal of pediatric rehabilitation medicine, 10(2), 107-136.
• Behavioral & Sensory Intervention• 4/23• Sensory techniques included: light, rocking motion,
sensory play, and individualized sensory diets• Resulted in:
– Increased acceptance of solid foods– Increased acceptance of non-preferred foods & calories
consumed, decrease in undesirable behaviors– Caregiver satisfaction
Treatment: Mixed Modality
Gosa, M. M., Carden, H. T., Jacks, C. C., Threadgill, A. Y., & Sidlovsky, T. C. (2017). Evidence to support treatment options for children with swallowing and feeding disorders: A systematic review. Journal of pediatric rehabilitation medicine, 10(2), 107-136.

9/17/18
22
• Behavioral & OMI & Sensory Interventions• 5/23, Multidisciplinary approach• Resulted in:
– Increased acceptance of non-preferred foods & calories consumed, decrease in undesirable behaviors
– Weaning from tube feedings– Increase in lingual range of motion and duration of meal
times– Weaning of high calorie supplement use and weight gain– Caregiver satisfaction
Treatment: Mixed Modality
Gosa, M. M., Carden, H. T., Jacks, C. C., Threadgill, A. Y., & Sidlovsky, T. C. (2017). Evidence to support treatment options for children with swallowing and feeding disorders: A systematic review. Journal of pediatric rehabilitation medicine, 10(2), 107-136.
• Results demonstrated positive outcomes across all primary outcomes measured, regardless of randomization, intensity or group
• This suggests that, overall, intervention delivered by experienced therapists to a standardized protocol is effective in increasing dietary quality and variety, and decreasing difficult behaviors at mealtimes.
• Further research is required in examining other cohorts of children with feeding difficulties, and exploring outcomes after longer periods post intervention
Treatment: Behavioral Comparison of Operant Conditioning
& Systematic Desensitization Gosa, M. M., Carden, H. T., Jacks, C. C., Threadgill, A. Y., & Sidlovsky, T. C. (2017). Evidence to support treatment options for children with swallowing and feeding disorders: A systematic review. Journal of pediatric rehabilitation medicine, 10(2), 107-136.Marshall, J., Path, B. S., & Hill, R. J. JPGN Journal of Pediatric Gastroenterology and Nutrition Publish Ahead of Print.

9/17/18
23
• Lack of evidence to support the singular use of OMI or Sensory Based Interventions
• Moderate amounts of published evidence to support the use of behavioral interventions (37/61 articles) and the use of mixed method interventions (23/61 articles)
• Various levels of evidence available to support the use of behavioral (32/27, 86% were found to be phase one research) and combined treatment options (all phase one research)
Conclusions
Gosa, M. M., Carden, H. T., Jacks, C. C., Threadgill, A. Y., & Sidlovsky, T. C. (2017). Evidence to support treatment options for children with swallowing and feeding disorders: A systematic review. Journal of pediatric rehabilitation medicine, 10(2), 107-136.
• Clinical utility of findings about OMI and Mixed
Modality limited due to the primarily descriptive
nature of the evidence
• Moderate amount of published, phase one
evidence on mixed method interventions does
call for further investigation of these strategies
with greater scientific rigor to establish the full
dimensions of the therapeutic effect and
ultimately determine the internal and external
validity of these treatment options as an initial
therapeutic effect has been established
Conclusions
Gosa, M. M., Carden, H. T., Jacks, C. C., Threadgill, A. Y., & Sidlovsky, T. C. (2017). Evidence to support treatment
options for children with swallowing and feeding disorders: A systematic review. Journal of pediatric rehabilitation medicine, 10(2), 107-136.

9/17/18
24
• From this EBSR, clinicians recognize the importance of behavioral therapy techniques for remediating feeding disorders (60/61 articles)
• Clinicians must be trained in the appropriate application of the various behavioral therapy techniques
• 5/60 articles were RCT and met criteria of phase IV evidence
Conclusions
Gosa, M. M., Carden, H. T., Jacks, C. C., Threadgill, A. Y., & Sidlovsky, T. C. (2017). Evidence to support treatment options for children with swallowing and feeding disorders: A systematic review. Journal of pediatric rehabilitation medicine, 10(2), 107-136.
http://www.asha.org/members/ebp/EBSRs/
49

9/17/18
25
http://www.asha.org/members/ebp/EBSRs/
50
51

9/17/18
26
52
Framing the Question: PICOPopulation Intervention Comparison Outcome
Pediatric Patients
(0-18 yoa)
Thickened Fluids Regular (Thin)
Fluids
Swallowing
Function/Develop
ment, Nutrition, &
Pulmonary Health
Pediatric Patients
(0-18 yoa)
Thickened Fluids Regular (Thin)
Fluids
Constipation,
Diarrhea, NEC,
etc…
53
Clinical Question 1: For children with a diagnosis of dysphagia, what is the
effect of thickened liquids on swallowing physiology (eg, aspiration, feeding
efficiency), oral feeding development, weight gain and growth, hydration, or
pulmonary health (eg, aspiration pneumonia, wheezing)?
Clinical Question 2: Is there an increased occurrence of adverse effects (ie, NEC,
gut adhesion, bowel obstruction, diarrhea, constipation, weight loss, failure to
thrive, dehydration, aspiration, & cough) associated with the use of thickened
liquids or certain thickening agents in children with or without dysphagia?

9/17/18
27
Finding the Evidence: ASHA’s Evidence Maps (www.ncepmaps.org)
54
55
Finding the Evidence: ASHA’s Evidence Maps (www.ncepmaps.org)
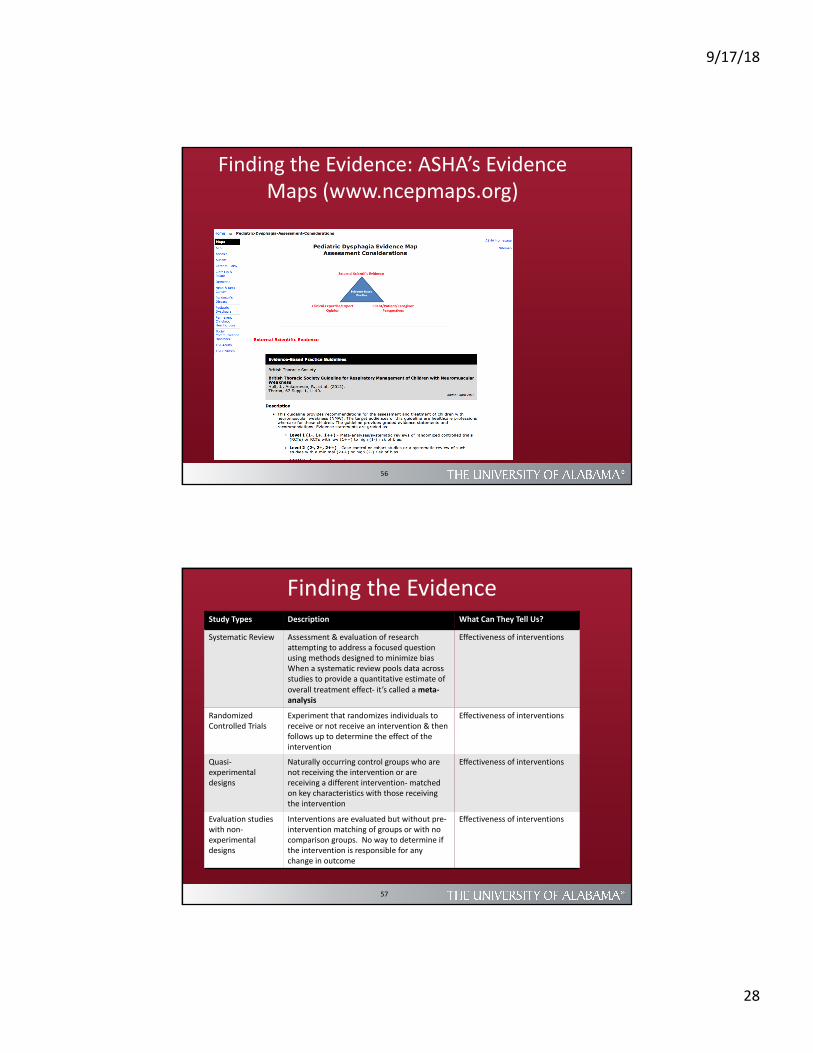
9/17/18
28
56
Finding the Evidence: ASHA’s Evidence Maps (www.ncepmaps.org)
Finding the EvidenceStudy Types Description What Can They Tell Us?
Systematic Review Assessment & evaluation of research attempting to address a focused question using methods designed to minimize biasWhen a systematic review pools data across studies to provide a quantitative estimate of overall treatment effect- it’s called a meta-analysis
Effectiveness of interventions
RandomizedControlled Trials
Experiment that randomizes individuals to receive or not receive an intervention & then follows up to determine the effect of the intervention
Effectiveness of interventions
Quasi-experimental designs
Naturally occurring control groups who are not receiving the intervention or are receiving a different intervention- matched on key characteristics with those receiving the intervention
Effectiveness of interventions
Evaluation studies with non-experimental designs
Interventions are evaluated but without pre-intervention matching of groups or with no comparison groups. No way to determine if the intervention is responsible for any change in outcome
Effectiveness of interventions
57

9/17/18
29
Finding the Evidence
Study Types Description What Can They Tell Us?
Case-controlstudies
Subjects with problem are matched with controls w/o the problem. Exposure of two groups to possible causes is compared
Risk Factors
Cohort studies Collect information longitudinally at intervals; often from birth into adulthood
Associations btwn early development & experiences, and later outcomes
Population Surveys Sample of the population asked to provide responses to questions on subject of interest
Prevalence of problems
QualitativeResearch
Concerned with the meanings people give to their experiences and how they make sense of the world
About social processes and what matters to people, how these vary in different circumstances, and why
Practice Guidelines Consist of systematically developed statements to assist practitioners and service users in making decisions about services. Should be based on high quality research.
58
Finding the Evidence:Hierarchy of Levels of Evidence
Level DescriptionIa Well designed meta-analysis of >1 RCTIb Well designed RCTIIa Well designed controlled study without randomizationIIb Well-designed quasi-experimental studyIII Well-designed non-experimental studies (case studies)IV Expert committee report, consensus conference, clinical
experience of respected authorities
59

9/17/18
30
Finding the Evidence
• Medline: Best place to start for health care studies
• Largest online bibliographic database of health care studies
• Cites over 12 million articles • Articles from 4,000 peer reviewed journals
60
Finding the Evidence
Cumulative Index to Nursing and Allied Health (CINAHL)
• More likely to contain studies with negative findings
• European database; studies in all languages
“Grey” Literature
• Not published in peer-reviewed literature
• Technical reports, conference proceedings, testimony
and other unpublished evidence
• Typically requires conversation with content experts,
relevant professional groups/organizations, and
internet search engines
61

9/17/18
31
Finding the Evidence: Key Words & Controlled Vocabulary
• Key words: describe the characteristics of a subject you are reviewing – Looking for the word(s) in the title and/or abstract of the article – Key word searching helpful when looking for a new drug or a
new procedure that has not been introduced into the controlled vocabulary of the database
• Controlled vocabulary: organized list of approved terms or key words that indexers of the journal or set of journals used to describe the same journal articles– Controlled vocabulary using the terms that indexers used when
they indexed the articles– MEDLINE/PubMed MESH- medical subject headings– MESH heading for cancer is controlled vocabulary term
neoplasms
62
Finding the Evidence:Controlled Vocabulary in Abstracts
63

9/17/18
32
Finding the Evidence:Snowballing Technique
64
Goal: use references in the appears or books you have read to gather more references
Build a list of references until you begin to see the same references over and over again
You own the literature when you read a few sentences about a study cited by an author and you know the article before you see the reference
Assessing the Evidence• Relevance of the article/review to your specific clinical question
• Who wrote & published the article/review– Some are produced by advocacy groups or payors– To what extent would they be affected by positive or negative
findings?
• Level of evidence and study quality– Establishment of a hierarchy of study designs based on the ability of
the design to protect against bias (no one universally accepted hierarchy)
– Assessment of the extent to which a study was designed and implemented appropriately (no universally accepted set of criteria) http://www.sign.ac.uk/guidelines/fulltext/50/annexc.html
65

9/17/18
33
Making Decisions• Synthesize clinical expertise/experience, patient’s
perspective, and available scientific evidence• EB clinical guidelines may have already been developed on
topics related to your question; do you follow them?1) How relevant are the guidelines to your specific clinical
question(s)?2) To what extent are the clinical practice guidelines truly
evidence-based?a) The methodology by which evidence was identified and evaluated should be
transparentb) Appraisal of Guidelines Research and Evaluation II (AGREE II)- evaluates the
process of practice guideline development and the quality of reporting
3) Who wrote and published the guideline?
66
Making Decisions
• When guidelines do not meet expectations or do not exist, clinicians must rely on the evidence they identified and assessed to make clinical decisions
• Other factors will come into play- patient preference, cost effectiveness, potential harm, availability
67




















