Patterns of senescence in human cardiovascular fitness: VO 2 max in subsistence and industrialized...
14
Original Research Article Patterns of Senescence in Human Cardiovascular Fitness: VO 2 max in Subsistence and Industrialized Populations ANNE C. PISOR, 1 * MICHAEL GURVEN, 1 AARON D. BLACKWELL, 1 HILLARD KAPLAN, 2 AND GANDHI YETISH 2 1 Department of Anthropology, University of California, Santa Barbara, California 2 Department of Anthropology, University of New Mexico, Albuquerque, New Mexico ABSTRACT: Objectives: This study explores whether cardiovascular fitness levels and senescent decline are simi- lar in the Tsimane of Bolivia and Canadians, as well as other subsistence and industrialized populations. Among Tsi- mane, we examine whether morbidity predicts lower levels and faster decline of cardiovascular fitness, or whether their lifestyle (e.g., high physical activity) promotes high levels and slow decline. Alternatively, high activity levels and morbidity might counterbalance such that Tsimane fitness levels and decline are similar to those in industrialized populations. Methods: Maximal oxygen uptake (VO 2 max) was estimated using a step test heart rate method for 701 participants. We compared these estimates to the Canadian Health Measures Survey and previous studies in industrialized and sub- sistence populations. We evaluated whether health indicators and proxies for market integration were associated with VO 2 max levels and rate of decline for the Tsimane. Results: The Tsimane have significantly higher levels of VO 2 max and slower rates of decline than Canadians; initial evidence suggests differences in VO 2 max levels between other subsistence and industrialized populations. Low hemo- globin predicts low VO 2 max for Tsimane women while helminth infection predicts high VO 2 max for Tsimane men, though results might be specific to the VO 2 max scaling parameter used. No variables tested interact with age to moder- ate decline. Conclusions: The Tsimane demonstrate higher levels of cardiovascular fitness than industrialized populations, but levels similar to other subsistence populations. The high VO 2 max of Tsimane is consistent with their high physical activity and few indicators of cardiovascular disease, measured in previous studies. Am. J. Hum. Biol. 00:000–000, 2013. V C 2013 Wiley Periodicals, Inc. Physical fitness, or the ability to perform “daily tasks [...] without undue fatigue” (Centers for Disease Control and Prevention, 2011), declines with age in both humans and nonhuman animals [e.g., dogs, (Haidet, 1989); horses (Walker et al., 2010)]. In humans, even elite athletes exhibit physical fitness declines (Sagiv et al., 2007) and these declines from higher peak fitness may be steeper than the decline of their more sedentary counterparts (Fitzgerald et al., 1997). Although the decline in physical fitness appears universal in industrialized nations (Fitz- gerald et al., 1997; Hawkins and Wiswell, 2003), an out- standing question is whether similar declines are observed in subsistence level populations. Individuals in subsistence populations often engage in physically demanding work well into old-age, yet these populations also often carry high burdens of pathogens and parasites, which may result in conditions that limit physical capacity, such as anemia (B en efice and Ndiaye, 2005; Panter-Brick et al., 1992). As a consequence, age related decline in physical fitness may be accelerated in subsist- ence populations due to systemic stress and disease or decelerated due to high demand for physical capacity. Alternatively, decline may be similar to those observed in industrialized populations if senescence in physical fit- ness follows a species-typical pattern. This article: (1) investigates age-related decline in cardiovascular fit- ness—a component of physical fitness determined by oxy- gen transport and use—in a subsistence population, the Tsimane of Bolivia; (2) examines factors mediating cardio- vascular fitness, including anemia, physical condition, and market integration; and (3) compares the rates of decline in the Tsimane with those of an industrialized nation to explore whether both exhibit similar patterns of decline. Although other factors contribute to physical fitness, individual fitness is determined primarily by the cardio- vascular system, and in particular cardiac output (Ameri- can College of Sports Medicine, 2006; Sagiv et al., 2007). The key molecule in this larger system is oxygen, which allows the conversion of adenosine triphosphate to avail- able energy in muscle cells (Wagner, 1996). Thus, we quantify cardiovascular fitness by estimating the maxi- mum volume of oxygen an individual is able to use per minute, often called aerobic capacity (VO 2 max; Howley et al., 1995; Wagner, 1996). The cardiovascular system is flexible in its development, responding to features of an individual’s early environment (Rowland and Boyajian, 1995) such as fetal testosterone exposure (Manning et al., 2007) and the elevation above sea level experienced dur- ing childhood (Frisancho et al., 1995). In populations where food production, processing, childcare, and other Contract grant sponsor: National Science Foundation (NSF); Contract grant number: BCS-0422690; Contract grant sponsor: National Institutes of Health/National Institute on Aging (NIH/NIA); Contract grant num- bers: R01AG024119-01; R01AG024119-04; R01AG024119-07. *Correspondence to: Anne C. Pisor, Department of Anthropology, Uni- versity of California, Santa Barbara, CA 93106-3210, USA. E-mail: [email protected] Additional Supporting Information may be found in the online version of this article. Received 10 April 2013; Revision received 17 July 2013; Accepted 2 August 2013 DOI: 10.1002/ajhb.22445 Published online 00 Month 2013 in Wiley Online Library (wileyonlinelibrary.com). V C 2013 Wiley Periodicals, Inc. AMERICAN JOURNAL OF HUMAN BIOLOGY 00:00–00 (2013)
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of Patterns of senescence in human cardiovascular fitness: VO 2 max in subsistence and industrialized...
Original Research Article
Patterns of Senescence in Human Cardiovascular Fitness VO2max inSubsistence and Industrialized Populations
ANNE C PISOR1 MICHAEL GURVEN1 AARON D BLACKWELL1 HILLARD KAPLAN2 AND GANDHI YETISH2
1Department of Anthropology University of California Santa Barbara California2Department of Anthropology University of New Mexico Albuquerque New Mexico
ABSTRACT Objectives This study explores whether cardiovascular fitness levels and senescent decline are simi-lar in the Tsimane of Bolivia and Canadians as well as other subsistence and industrialized populations Among Tsi-mane we examine whether morbidity predicts lower levels and faster decline of cardiovascular fitness or whethertheir lifestyle (eg high physical activity) promotes high levels and slow decline Alternatively high activity levels andmorbidity might counterbalance such that Tsimane fitness levels and decline are similar to those in industrializedpopulations
Methods Maximal oxygen uptake (VO2max) was estimated using a step test heart rate method for 701 participantsWe compared these estimates to the Canadian Health Measures Survey and previous studies in industrialized and sub-sistence populations We evaluated whether health indicators and proxies for market integration were associated withVO2max levels and rate of decline for the Tsimane
Results The Tsimane have significantly higher levels of VO2max and slower rates of decline than Canadians initialevidence suggests differences in VO2max levels between other subsistence and industrialized populations Low hemo-globin predicts low VO2max for Tsimane women while helminth infection predicts high VO2max for Tsimane menthough results might be specific to the VO2max scaling parameter used No variables tested interact with age to moder-ate decline
Conclusions The Tsimane demonstrate higher levels of cardiovascular fitness than industrialized populations butlevels similar to other subsistence populations The high VO2max of Tsimane is consistent with their high physicalactivity and few indicators of cardiovascular disease measured in previous studies Am J Hum Biol 00000ndash0002013 VC 2013 Wiley Periodicals Inc
Physical fitness or the ability to perform ldquodaily tasks[ ] without undue fatiguerdquo (Centers for Disease Controland Prevention 2011) declines with age in both humansand nonhuman animals [eg dogs (Haidet 1989) horses(Walker et al 2010)] In humans even elite athletesexhibit physical fitness declines (Sagiv et al 2007) andthese declines from higher peak fitness may be steeperthan the decline of their more sedentary counterparts(Fitzgerald et al 1997) Although the decline in physicalfitness appears universal in industrialized nations (Fitz-gerald et al 1997 Hawkins and Wiswell 2003) an out-standing question is whether similar declines areobserved in subsistence level populations Individuals insubsistence populations often engage in physicallydemanding work well into old-age yet these populationsalso often carry high burdens of pathogens and parasiteswhich may result in conditions that limit physicalcapacity such as anemia (Benefice and Ndiaye 2005Panter-Brick et al 1992) As a consequence age relateddecline in physical fitness may be accelerated in subsist-ence populations due to systemic stress and disease ordecelerated due to high demand for physical capacityAlternatively decline may be similar to those observed inindustrialized populations if senescence in physical fit-ness follows a species-typical pattern This article (1)investigates age-related decline in cardiovascular fit-nessmdasha component of physical fitness determined by oxy-gen transport and usemdashin a subsistence population theTsimane of Bolivia (2) examines factors mediating cardio-vascular fitness including anemia physical conditionand market integration and (3) compares the rates ofdecline in the Tsimane with those of an industrialized
nation to explore whether both exhibit similar patterns ofdecline
Although other factors contribute to physical fitnessindividual fitness is determined primarily by the cardio-vascular system and in particular cardiac output (Ameri-can College of Sports Medicine 2006 Sagiv et al 2007)The key molecule in this larger system is oxygen whichallows the conversion of adenosine triphosphate to avail-able energy in muscle cells (Wagner 1996) Thus wequantify cardiovascular fitness by estimating the maxi-mum volume of oxygen an individual is able to use perminute often called aerobic capacity (VO2max Howleyet al 1995 Wagner 1996) The cardiovascular system isflexible in its development responding to features of anindividualrsquos early environment (Rowland and Boyajian1995) such as fetal testosterone exposure (Manning et al2007) and the elevation above sea level experienced dur-ing childhood (Frisancho et al 1995) In populationswhere food production processing childcare and other
Contract grant sponsor National Science Foundation (NSF) Contractgrant number BCS-0422690 Contract grant sponsor National Institutesof HealthNational Institute on Aging (NIHNIA) Contract grant num-bers R01AG024119-01 R01AG024119-04 R01AG024119-07
Correspondence to Anne C Pisor Department of Anthropology Uni-versity of California Santa Barbara CA 93106-3210 USA E-mailpisorumailucsbeduAdditional Supporting Information may be found in the online version ofthis article
Received 10 April 2013 Revision received 17 July 2013 Accepted 2August 2013
DOI 101002ajhb22445Published online 00 Month 2013 in Wiley Online Library
(wileyonlinelibrarycom)
VC 2013 Wiley Periodicals Inc
AMERICAN JOURNAL OF HUMAN BIOLOGY 0000ndash00 (2013)
daily tasks require high levels of physical activity earlydemand may favor early investment in oxygen transportfunction leading to greater peak cardiovascular fitness(eg Frisancho et al 1995 Malina 2001) Additionallycardiovascular fitness may remain high if high levels ofactivity are sustained throughout adulthood or may beup-regulated by training (Finch and Lenfant 1972 Hoff-man 2002 Sagiv et al 2007 Wagner 1996) leading toslower decline with age
In subsistence populations individuals experience highenergy demand in conjunction with both work and leisureactivities (eg Malina and Little 2008 Panter-Brick et al1992 Walker and Hill 2003) It appears that any differen-ces in physical fitness performance may arise from differ-ences in levels of sedentary activity between subsistenceand industrialized populations as subsistence groups inte-grate to national markets sedentism may increase leadingto reductions in cardiovascular fitness (Katzmarzyk et al1994 Rode and Shephard 1994) However studies employ-ing factorial methods accelerometry and doubly labeledwater suggest considerable overlap in measured activitylevels and energy expenditure among members of subsist-ence and industrialized populations (Gurven et al 2013Madimenos et al 2011 Pontzer et al 2012) Among theTsimane our focal group women age 20ndash70 have averagephysical activity levels (PALs defined as total daily ener-getic expenditure divided by basal metabolic rate) of 173ndash185 over a 24 h period (Gurven et al 2013) while a sameage nonoverweight American sample has a similar aver-age of 178 (Blair et al 2004) Tsimane men are morephysically active than their American counterparts (Tsi-mane males 202-215 American males 173) though bothAmerican and Tsimane males fall within the range ofcross-population PALs reported by Gurven et al (2013)
The few studies that have examined cardiovascular fit-ness in subsistence populations show mixed evidence for adecline in fitness with age Turkana men engaging in pas-toralism do not exhibit a consistent decline in VO2max byage 45 (Curran-Everett 1994) Ache women living on a res-ervation and practicing a combination of gathering andhorticulture do not exhibit a decline in cardiovascular fit-ness by age 60 (Walker and Hill 2003) However thesefindings are based on relatively small samples and may beunduly influenced by outliers In contrast Inuit still livinga traditional lifestyle do show significant declines with age(Shepard 1978) as do small-scale farmers in Kenya(Christensen et al 2012) Given these mixed resultsshould we expect a cardiovascular fitness decline in all sub-sistence level societies and if so of the same steepness asthe decline among industrialized nations
Although sustained subsistence activity muscularityand leanness should help promote cardiorespiratory fit-ness throughout life other features of subsistence soci-eties may instead hinder performance especially at laterages Cardiovascular fitness level may be curbed by lim-ited energy reserves and food shortages The benefits of alarge capacity for physical activity may be age specificinvestments in cardiovascular fitness may be high earlyin the lifespan however higher adult mortality in subsist-ence societies may discount investments that maintainfunctionality in old age Limited energy budgets in sub-sistence societies might make such tradeoffs betweenadult functionality and late age maintenance more severeEven in industrialized societies the diminished ability tomaintain muscle with age results in lower muscle mass
or sarcopenia Although central limiting factors such ascardiac output are primarily responsible for age-relateddecline (Carrick-Ranson et al 2013 Ogawa et al 1992)muscle mass is also a predictor of slowed decline (Carrick-Ranson et al 2013 Sanada et al 2007 Stones andKozma 1985) as muscles consume 95 of oxygen used bythe body during exercise (Fleg and Lakatta 1988)
Another physical limit on the transport system is imposedby hemoglobin-bearing red blood cells which carry oxygenfrom lungs to muscles Individuals with anemia (low hemo-globin) do worse than nonanemic individuals on cardiovas-cular fitness tests (Buzina et al 1989 Panter-Brick et al1992 Wagner 1996) as do individuals who experience bloodloss from chronic helminth infections (King et al 2005Panter-Brick et al 1992) Anemia and helminth infectionsare more common in subsistence populations than industri-alized populations (Hotez et al 2008) The Tsimane have amuch higher prevalence of both helminths (Blackwell et al2011) and anemia than North Americans do Giardia andother protozoal bacterial and viral infections are also prev-alent (Blackwell et al 2013) Likewise respiratory ailmentscurb oxygen uptake (Collins 1999 Wagner 1996) and areoften common in subsistence groups While asthma andallergies are prevalent in the United States (Sondik et al2012) tuberculosis pneumonias and upper respiratoryinfections are not uncommon among the Tsimane (Eid et al2007) Together these factors might place an upper limit oncardiovascular fitness even for individuals engaged in fre-quent and intensive activity
This study investigates senescent changes in cardiovas-cular fitness among a large sample of Tsimane adults andtests whether predicted factors described above mediatethese changes To explore differences between subsistencegroups and industrialized nations Tsimane values arecompared with data from the Canadian Health MeasuresSurvey which employed a similar method for measuringcardiovascular fitness We first test whether Tsimanehave higher peak VO2max than Canadians Second weexamine whether Tsimane show similar senescentdeclines as Canadians given demands on Tsimane forphysical activity into older adulthood and increased stresson the cardiovascular system which are expected to haveopposing effects on fitness Tsimane and Canadian per-formance is compared with previous work in industrial-ized and subsistence groups to provide additional contextThird we examine the impact of mediating health andanthropometric factors on cardiovascular fitness includ-ing anemia respiratory illness helminth infections andproxy measures of market integration (distance to thelocal town Spanish-speaking ability) Due to competingdemands for somatic resources we predict that indicatorsof poor health will predict lower physical fitness levelsand faster age-related decline Though other populationsevidence lower levels of physical activity with increasingmarket integration Tsimane living closer to town andthose fluent in Spanish do not appear to become more sed-entary (Gurven et al 2013) we therefore expect that car-diovascular fitness will not differ between more and lessmarket integrated individuals
METHODS
Measuring cardiovascular fitness maximal oxygen uptake
Performance of the oxygen transport system can bemeasured by maximal oxygen uptake Oxygen uptake
2 AC PISOR ET AL
American Journal of Human Biology
(volume O2 or VO2) is calculated as the differencebetween the percentages of oxygen in inhaled (about 21)and exhaled gases multiplied by the volume of gasexhaled (Howley et al 1995) Maximal oxygen uptake(VO2max) refers to the peak oxygen uptake possible for agiven individual achieved during exercise to exhaustionBecause exercise to exhaustion can be potentially danger-ous in individuals with significant underlying cardiovas-cular disease VO2max is often estimated at asubmaximal level of exercise (eg 85 of age-specificmaximal heart rate HR) Additionally the use of a gascollection bag can be inconvenient or expensive for fieldand large scale projects (eg Shephard 1970) For thesereasons estimation of VO2max from a participantrsquos sub-maximal heart rate is often employed (eg Astrand andRyhming 1954) HR estimation methods were used forthe Canadian and Tsimane samples although only in thecase of the Canadians was the routine for calculatingVO2max derived from laboratory studies with the samepopulation
Study populations
Tsimane The Tsimane are a forager-horticulturalistgroup living in the Bolivian Amazon The Tsimane have apopulation of 11000 spanning 901 villages ranging insize from 40 to 550 individuals Villages near the localtown (San Borja population 24000) or near roads havemore extensive market access and greater participation inwage labor Although PALs are often predicted to declinewith market integration Tsimane women and men livingnear the local town are not less active than Tsimane fromother regions perhaps because of the physical activityrequired in wage labor (eg logging and cash croppingGurven et al 2013) Men in all regions have higher PALsthan women although menrsquos activity exhibits more sea-sonal variation Aging Tsimane remain active (Gurvenet al 2013) although these individuals may engage inless physically demanding subsistence activities becauseof increases in infirmity with age (Schniter 2009)
Tsimane data were collected as part of the TsimaneHealth and Life History Project (THLHP httpwwwun-medutsimane) from 2002ndash2010 Patients were seen byTHLHP physicians either during annual visits to villagesor at the THLHP medical office in San Borja Self-reported ailments were considered together with physicalexamination fecal and blood test results to assist in diag-nosis and treatment Sampling procedures for the exercisetest were designed to ensure a sample representative ofthe Tsimane population Participantsrsquo ages range from 10to 88 years old (n 5 766 55 female)
Pretest exclusion Tsimane Tsimane participants werenot automatically excluded from the study for having aparticular condition but any complaints or conditionswere recorded Our study protocol did not exclude partici-pants for any reason However some individuals whojudged themselves unable to participate or who experi-enced discomfort during exercise opted out The mostcommon reason given by participants for opting out waspain although this was rare (65 total excluded remainingn 5 701) Nonparticipation rates in this population werebelow 10 until after age 70 (Supporting Information FigS1) Although frailty may have constrained participation
at late ages the final sample below age 70 includes Tsi-mane at various levels of health and ability allowing us tobetter explore the correlates of fitness decline (eg paininfection) in this population Pregnant and lactatingwomen were included in the Tsimane sample as womenare pregnant or lactating for much of their adult lives
Experimental protocol Tsimane Participants were askedto complete a modified submaximal Harvard step test(Astrand and Ryhming 1954) at a bench height of 20 cmfor 5 min at 30 ascents per minute (Walker and Hill2003) The pace of stepping was recorded for each partici-pant regardless of whether the participant attained 30steps per minute VO2max was estimated using Shep-hardrsquos (1970) HR-based calculation routine for step testsWe first estimated VO2 with the following equation
E 979 3 W 3 H 3 Neth THORNL
1 kcal
4184 Joules 1 ml O2
200 kcal(1)
where W is weight in kilograms H is the step height inmeters N is number of ascents during the exercise testand L is the length of the test in minutes The conversionfactor adjusts for the efficiency of stepping Stepping isabout 16 efficientmdashonly 16 of the work done duringstepping contributes to vertical displacement (Shephardet al 1976)mdashand thus work done must be multiplied by669 (Shephard 1970) to account for the amount of effortrequired by participants The work (in Joules) required tocomplete the exercise test was calculated as 979 ms2 W xH x N where 979 ms2 is the acceleration due to gravity(Powers and Howley 2009) Kilocalories per minute weredivided by 200 to convert kilocalories to mlmin of O2
(ACSM 2006)Equations for estimating VO2max from submaximal
VO2 at peak HR during the test (P taken to be the lastminute of exercise) were drawn from Shephard (1970)These are based on age and sex specific regressions thatrely on assumptions about maximal HR by age
Females EethVO 2maxTHORN5 VO 2 198272eth THORNP272
1 VO 2max
00114age 1077 1
kg
(2a)
Males EethVO 2maxTHORN5 VO 2 198261eth THORNP261
1 VO 2max
00137age 10668 1
kg
(2b)
The estimates of VO2max produced by Eqs 2ab are inunits of ml of oxygen per minute per kilogram (ml min21
kg21) also called relative VO2max Another common mea-sure of VO2max absolute VO2max (l min21) was calcu-lated by multiplying VO2max in l min21 kg21 byparticipant body weight
Post-test exclusion Tsimane The Shepard equations forestimating VO2max depend on individuals achieving aheart rate within a certain range 120ndash172 for femalesand 122ndash170 for males Typical protocols call for excluding
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 3
American Journal of Human Biology
individuals who do not meet this level However manyTsimane (55 of females 81 of males) did not achievethis criterion either because the age-specific maximalHRs derived from industrialized populations are inaccu-rate for the Tsimane or because higher fitness allowedthese Tsimane to perform the step test with less effort Wetherefore evaluated several exclusion criteria for the Tsi-mane sample including the HR range specified by Shep-hard (1970) for the calculation routine a HR increase oflt5 beats per minute during exercise (National Healthand Nutrition Examination Survey 2004) different per-centages [65 (Siconolfi et al 1985) 70 (American Collegeof Sports Medicine 2006 Canadian Society for ExercisePhysiology 2003) 75 (NHANES 2004)] of age-specificmaximal HR (Tanaka et al 2001) achieved the 95th cen-tile obtained from a Generalized Additive Model for Loca-tion Scale and Shape (Rigby and Stasinopoulos 2005)and a rate of HR increase from the beginning to the end ofexercise that is beyond the 95 confidence interval (CI)from the 20 year age- and sex-specific mean The samplesize remaining after these exclusions varies from 4(75 of age-specific maximal HR) to 79 (increase lt5beats per minute during exercise) of our original sample(for sample sizes under each criterion considered see Sup-porting Information Table S1) We interpreted exclusioncriteria that excluded the vast majority of participants asnot giving a representative sample of the Tsimane Theuse of centiles or CIs enables us to compare each partici-pant against a metric from the same population Becausethe centile and CI approaches led to about the same rela-tively small number of participants excluded we adoptedthe CI exclusion for ease of interpretation
To evaluate the accuracy of HR estimation for the Tsi-mane population we compare VO2max estimated fromHR with VO2max estimated from the ratio of inhaled toexhaled O2 collected in a smaller subset of Tsimane Anadditional strength of the O2 method is that the VO2 andHR measured for a given individual is extrapolated to pre-dict their VO2max at their predicted age-specific maximalHR without reliance on additional assumptions beyondthat of an age-specific maximal HR Methods used in O2
measurement are described in the Supporting Informa-tion (Appendix A)
Tsimane model covariates Fat-free mass (FFM) was esti-mated by subtracting body fat mass from total mass Bodyfat percentage was estimated with bioimpedance using aportable Tanita scale and with skinfold measurementtaken at four sites (bicep tricep subscapular suprailiac)body fat percentage was estimated from skinfold measure-ment with equations from Durnin and Womersley (1974)Arthritis and respiratory ailments were diagnosed byTHLHP physicians during routine medical exams Hemo-globin levels in g dl21 were attained using the QBC Auto-read Plus Dry Hematology System (QBC DiagnosticsPort Matilda PA) anemia was defined using Centers forDisease Control (CDC) criteria (CDC 1998) and for agesfor which CDC criteria were not available World HealthOrganization (2001) criteria Helminth and giardia infec-tions were diagnosed in wet slide mounts and using amodified Percoll technique as has been previouslydescribed (Blackwell et al 2011 Eberl et al 2002) Wecoded helminth infection as bivariate (presence or absenceof helminths) combining diagnoses with hookworm
roundworm (Ascaris lumbricoides and Strongyloides ster-coralis) and whipworm (Trichuris trichiura) Because ofan established relationship between helminth infectionand anemia helminths and giardia are considered sepa-rately in this analyses Self-reported pain was included asa binary measure indexing the presence of back kneebone or connective tissue pain Spanish-speaking abilitywas treated as dichotomous where individuals rated asspeaking more than ldquosomerdquo Spanish by THLHP projectstaff were considered Spanish speakers Additional cova-riates include pregnancy status and as-the-crow-flies dis-tance of home village to the market town of San Borja
Because of a concern that leg length relative to benchheight may affect performance during step tests (Shahna-waz 1978) we considered including leg length in allwithin-population regressions Leg length was calculatedby subtracting participant seated height (minus chairheight) from standing height Including leg length wors-ened model fits perhaps because mass and leg length aremoderately correlated (for females Pearsonrsquos r 5 042 formales r 5 041) and mass is already controlled for by ouruse of relative (rather than absolute) VO2max addition-ally use of the leg length variable eliminated participantsfor whom seated height data were unavailable As suchwe decided to not control for leg length in the analysesbelow
Canadian health measures survey Canadian fitness datawere collected during the first wave of the CanadianHealth Measures Survey (CHMS wwwstatcangccaimdb-bmdi5071-enghtm) from 2007 to 2009 Canadianswere selected as a comparison group since VO2max in theCHMS was assessed using a step test procedure withVO2max estimated based on HR Individuals weresampled with the goal of representing 97 of the Cana-dian population from all provinces (Giroux 2007) Asmeasured with tri-axial accelerometers Canadian chil-dren in this sample are sedentary for 64 of their wakinghours (Colley et al 2011a) adult (ages 20ndash79) females aresedentary for 69 of the day and adult males are seden-tary for 68 (Colley et al 2011b)
Pretest exclusion CHMS CHMS participants wereexcluded from fitness testing if they had a heart conditionchest pain high blood pressure (systolic blood pressurehigher than 144) or heart rate (higher than 100) or weretaking medication for any of these conditions (Bryan et al2007) across all ages a total of 267 of potential partici-pants were excluded including 56 of 60ndash69 year olds(Shields et al 2010) Participants who experienced discom-fort during testing could stop at any time Women morethan 12 weeks pregnant were not allowed to participate
Experimental protocol CHMS Participants completed astep test developed by Bailey et al (1976 modified byWeller et al 1993) on a bench with two steps each 203cm tall Individuals began stepping at a rate expected torequire 65ndash70 of VO2max for a same-sex individual 10years their senior (Canadian Society for Exercise Physiol-ogy 2003) After a 3 min exercise interval researchersmeasured HR to ascertain whether the participant hadachieved 85 of his or her age-specific maximal HR If
4 AC PISOR ET AL
American Journal of Human Biology
85 of maximal HR was reached exercise testing wasstopped if 85 of maximal HR was not reached partici-pants proceeded to the next stage of exercise stepping ata faster cadence
VO2max was estimated using a regression equationdeveloped by Weller et al (1993)
E VO2maxeth THORN532116a2024b2017c (3)
where a is the estimated VO2 at the end of the finalstage of exercise (Weller et al 1993) b is age in yearsand c is body weight in kg If a participant could not stepat the prescribed cadence during a given stage of exerciseVO2max was estimated based on the last completed exer-cise stage (Shields et al 2010) About 1 of participantseligible for the test did not complete it Participants didnot proceed beyond the eighth level of exercise regardlessof whether they had attained 85 of their age-specificmaximal HR The result is estimated relative VO2max (mlmin21 kg21)
Skinfold measurements used to calculate absoluteFFM in this article were taken before the cardiovascularfitness test at four sites (bicep tricep subscapular andsuprailiac) using Harpenden calipers (Baty InternationalUK Shields et al 2010) but only for individuals with abody mass index under 30 kg m22
Statistical analyses
All statistical analyses were performed with the R soft-ware package version 2153 (R Development Core Team2011) Smooth fits used generalized additive models(GAM) which regress a predictor on the response andsmooth the residuals (Venables and Ripley 2002) in thepackage used for the present analyses (mgcv Wood2006) the degree of smoothness was determined by apenalized likelihood technique The result is a model thathas both linear and non-linear elements allowing a closefit to the data while also providing interpretable parame-ter estimates Where appropriate model fits were eval-uated using the Akaike Information Criterion (AIC) amaximum likelihood measure of goodness-of-fit
Exploratory models indicate sex differences in VO2maxin the Tsimane population and so each sex is modeledseparately in all analyses Because data for both popula-tions only exist for ages 11ndash69 all cross-population com-parative analyses (linear models t-tests) are limited tothis age group Age in years is included in all analysesWithin-population comparisons (linear models) use theTsimane subsample age 20 and older an age group inwhich both males and females are close to their peakVO2max and include individuals up to age 70 compara-ble to the Canadians and before the age at which optingout removed large portions of the sample For the subsam-ple between 20 and 69 females and males evidence a lin-ear decline although female VO2max is curvilinear whenall ages are considered because all within-populationcomparisons (linear models) are performed on this sub-sample age2 terms were not included Publically availableCHMS data are limited to VO2max mean and standarddeviation for age categories of variable size (for categoriessee Table 3) Cross-population comparisons use the sameage categories to explore differences between Canadiansand Tsimane
Covariates could not be included in between-populationcomparisons as the latter are based on binned data how-ever extensive individual-level Tsimane data allow fordetailed examination of factors that may mediate physicalfitness decline For these within-population linear modelswe only included participants aged 20ndash69 for whom medi-cal and anthropometric data were available during thesame medical round (about a calendar year in lengthTable 1)
To explore the possibility of a non-linear relationshipbetween mass and VO2max and how this might affectany differences between the Tsimane and Canadians we1) allometrically scaled Tsimane VO2max and 2) projectedrelative VO2max for the Tsimane using Canadian fatmass and FFM from same-sex same-age categories Toallometrically scale VO2max we calculated a the scalingparameter in allometric equations for the Tsimane(Calder 1987) To project VO2max for the Tsimaneassuming the same body composition as the Canadianswe regressed absolute VO2max on absolute fat mass abso-lute FFM and age (and age2 for the Tsimane females) inthe Tsimane female and male subsamples With theresulting parameter estimates we predicted whether Tsi-mane would perform at rates similar to those observed inour study if the Tsimane had the average fat mass andFFM exhibited in each of the four Canadian cohorts (ages12ndash19 20ndash39 40ndash59 and 60ndash79) The results of these cal-culations are discussed below Hereafter VO2max willrefer to relative VO2max unless otherwise stated
RESULTS
Age at peak VO2max and levels across the lifespan
Tsimane Predicted values of absolute (l min21) and rela-tive VO2max (ml min21 kg21) for the Tsimane appear inFigure 1 Both Tsimane females and males exhibit a peakin absolute VO2max A peak in absolute VO2max is char-acteristic across populations but appears in late adoles-cence in industrialized nations concurrent with peakabsolute FFM (Armstrong 2001) In the Tsimane as wellpeak absolute VO2max and peak absolute FFM areroughly concurrent using smoothed fits of predicted val-ues female VO2max peaks at age 31 at 295 l min21 and
TABLE 1 Descriptive statistics for the Tsimane after exclusion (ages20ndash69)
Variables
Tsimane Females Tsimane Males
Mean(and SD)or Percent n
Mean(and SD)or Percent n
Age 413 (143) 203 436 (152) 280Body weight (kg) 534 (93) 203 624 (74) 280FFM (kg) 397 (43) 203 520 (58) 280Perc FFM 075 (008) 203 084 (005) 280Distance to town in 10 km 44 (24) 196 42 (24) 273Hemoglobin 129 (14) 117 143 (12) 157Arthritis 11 133 4 185Helminths 51 92 58 128Giardia 38 92 40 128Nonarthritic Pain 54 133 75 138Respiratory Ailments 27 133 15 185Spanish-speaking Ability 17 271 42 271Pregnant 3 203 ndash ndash
Two-level factors are reported as percentage of the subsample with a givenailment
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 5
American Journal of Human Biology
absolute FFM at age 34 at 405 kg for males VO2maxpeaks at age 24 at 344 l min21 and FFM at age 29 at 544kg Estimated peak VO2max is relatively robust to thesmoothing parameter selected with the peak shifting nomore than 1 year for females and two years for malesunder different methods of smoothing Average level ofVO2max may appear higher in females but a median fitreveals that Tsimane females and males have roughlysimilar VO2max (see Supporting Information Fig S2)
Relative (ml min21 kg21) VO2max estimation controlsfor the effect of body mass (and by extension partiallycontrols for percent FFM correlation between the two forfemales r 5 2075 for males r 5 2043) Removing theeffects of body mass by using a relative measure does notremove the peaks exhibited by females or males in earlyadulthood (Fig 1) Tsimane females peak at age 28 (5379ml min21 kg21) and Tsimane males peak at age 22 (at5489 ml min21 kg21) Indeed this peak also remainswhen we scale by absolute FFM (ml min21 fat-free kg21see Supporting Information Table S2)
To evaluate whether Tsimane participants performedsimilarly under the O2 method we compared age-matched subsamples to O2 method participants Tsimanemales performed significantly worse under the HRmethod relative to the O2 method (O2 mean 5 695 mlmin21 kg21 HR mean 5 590 ml min21 kg21 t 5 629Plt 0001) There is no significant difference between Tsi-mane females tested under the HR and O2 methods (O2
mean 5 529 HR mean 5 543 t 5 2077 P 5 044) For acomparison of smooths from the two samples see Sup-porting Information Figure S3Mediators of Levels Across the Tsimane Lifespan Weidentified and investigated several health-related factorsthat might affect level of VO2max achieved by eitherdiminishing resources available to the body or hamperingthe cardiovascular system directly We posit that thesevariables may mediate the effect of age on VO2max Can-didate mediators include the presence of anemia infectionwith helminths or giardia arthritis or nonarthritic painrespiratory ailments distance from the local market
Fig 1 Predicted Tsimane VO2max by age Predicted values are drawn from GAM models regressing smooths of log age on VO2max Inter-vals are 95 prediction intervals Age was smoothed using restricted maximum likelihood Other smoothing parameters (such as Mallowrsquos Cpand maximum likelihood) varied the age at peak absolute VO2max by up to 1 year for females and up to 2 years for males Points represent theraw data for Tsimane A Absolute VO2max by age for females B Absolute VO2max by age for males C Relative VO2max by age for femalesD Relative VO2max by age for males [Color figure can be viewed in the online issue which is available at wileyonlinelibrarycom]
6 AC PISOR ET AL
American Journal of Human Biology
town and Spanish speaking ability Although percentFFM generally predicts absolute rather than relativeVO2max we test it as a potential mediator Pregnancywas included as a control in female models While a highmacroparasite load may increase the likelihood of havinglow hemoglobin (and thus anemia) an interaction termbetween presence of helminths and presence of anemiawas not included because they are not significantlyrelated in this sample only 26 participants of the 92 withhelminths have anemia while 14 of the 86 without hel-minths have anemia (for females v2 5 052 P 5 047 formales v2 5 200 P 5 016)
To evaluate whether these candidate mediators affectedVO2max levels we conducted linear regressions on rela-tive VO2max (see Table 2) We first examined each predic-tor independently Females with higher hemoglobin levelshad significantly higher cardiovascular fitness perform-ance for an increase in 1 g dl21 concentration of hemoglo-bin a Tsimane woman is predicted to have 293 ml min21
kg21 higher VO2max (t 5 268 Plt 001) Helminth infec-tion mediated the relationship between age and VO2maxfor males such that men with a helminth infection arepredicted to have 616 ml min21 kg21 higher VO2max(t 5 231 Plt 005) A best fit model approach (fit on thesubset of females for whom all measures are available)provides similar results to fitting a separate model for
each potential mediating variable When a stepwise AICprocedure was used with data on all health and marketintegration measures hemoglobin level was the only sig-nificant predictor that remained in the female model(n 5 82 standardized b 5 022 Plt 005) For males hel-minth infection remained in the model as well (n 5 116standardized b 5 023 Plt 005)
Scaling VO2max by FFM (ml min21 fat-free kg21)rather than body mass produced similar results hemoglo-bin levels remained a significant positive predictor ofVO2max for females (standardized b 5 030 Plt 001) andhelminth infection a positive predictor for males (standar-dized b 5 020 Plt005) See Supporting InformationTable S3 for all regression results with ml min21 fat-freekg21 as the outcome
Anemia was initially included in model fits howevertreating hemoglobin level as a covariate in place of pres-ence of anemia improved model fit for Tsimane females(anemia AIC 5 10027 hemoglobin AIC 5 98963)Although no association was found between presence ofanemia and helminth infection there is a significant asso-ciation between hemoglobin levels and helminth infectionControlling for age a helminth diagnosis is a significantnegative predictor of hemoglobin levels for females (stand-ardized b 5 2031 Plt 001) Replacing presence of ane-mia with hemoglobin level for males did not improve or
TABLE 3 Comparison of Tsimane and Canadian relative VO2max by age category and sex
Sex Age group
Tsimane Canadians
t-Statistic P-valueMean (ml min21 kg21) n Mean (ml min21 kg21) n
Females 11ndash14 435 7 487 534 2118 02815ndash19 476 33 423 500 310 00020ndash39 510 72 383 662 908 00040ndash59 431 69 314 655 1005 00060ndash69 412 5 242 554 340 003
Males 11ndash14 415 4 548 542 2300 00615ndash19 516 31 508 514 046 06520ndash39 511 96 442 526 527 00040ndash59 432 68 362 584 380 00060ndash69 381 26 275 546 509 000
TABLE 2 Linear models exploring whether mediators affect the level (main effects models) of relative VO2max for Tsimane females and males
Sex Candidate mediatorAge effect est
(P-value)
Main effect models
Sample sizeMediator main effect
est (P-value) Age main effect est (P-value)
Females Perc FFM 2023 (000) 000 (097) 2023 (000) 203Hemoglobin 2013 (028) 024 (001) 2011 (022) 117Helminths 2019 (007) 003 (077) 2020 (006) 92Giardia 2019 (007) 011 (028) 2019 (007) 92Lung ailment 2017 (006) 2005 (060) 2018 (005) 133Reported pain 2017 (006) 2001 (094) 2017 (006) 133Arthritis 2017 (006) 2002 (083) 2016 (007) 133Distance to town 2023 (000) 002 (081) 2023 (000) 196Spanish speaking 2023 (000) 2008 (056) 2024 (000) 197
Males Perc FFM 2037 (000) 009 (012) 2034 (000) 280Hemoglobin 2029 (000) 2002 (076) 2029 (000) 157Helminths 2030 (000) 019 (002) 2027 (000) 128Giardia 2030 (000) 006 (049) 2030 (000) 128Lung ailment 2030 (000) 2007 (033) 2031 (000) 185Reported pain 2030 (000) 011 (013) 2031 (000) 185Arthritis 2030 (000) 2006 (044) 2028 (000) 185Distance to town 2037 (000) 2003 (059) 2037 (000) 273Spanish speaking 2038 (000) 008 (050) 2037 (000) 271
All parameter estimates are standardized
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 7
American Journal of Human Biology
worsen model fit and there is no significant relationshipbetween hemoglobin levels and helminth infection formales (standardized b 5 2010 P 5 028) Parameter esti-mates for anemia were not significant in models for eitherfemales or males
Between-group Table 3 presents Tsimane and Canadianestimated VO2max binned into age categories used byCHMS These data suggest that Canadian females andmales achieve peak VO2max between the ages of 11 and14 while Tsimane males peak between ages 15 and 19Tsimane females peak later between age 20 and 39Across comparable age categories Tsimane have signifi-cantly higher VO2max than Canadians at all ages exceptbetween 11 and 15 for females and 11 and 19 for males(Table 3) However the sample size of Tsimane teenagersunder age 15 is quite small As aforementioned to controlfor the influence of a small number of data points for theyoungest and oldest Tsimane individuals we used GAMto predict VO2max across logged age Predicted valuessuggest that Tsimane females peak at age 28 and Tsimanemales peak at age 22 (see Fig 1c d) These estimates areconsistent with scatterplots of the raw data (plotted onFig 1) and mask fewer fine-grained effects of age thanTable 3 as each CHMS adult age category spans twodecades
It is possible the difference between the Tsimane andCanadians reflects a greater increase in body mass acrossages in the Canadian population or different trajectoriesof change in body composition The former could occurbecause body mass appears in the denominator and cantherefore scale down VO2max while the latter implies dif-ferential changes in FFM when FFM is a predictor ofVO2max in many studies To explore these possibilitieswe performed two calculations we allometrically scaledTsimane VO2max and we projected Tsimane VO2maxassuming the Tsimane had equivalent fat mass and FFMas Canadians from same-sex same-age categories Con-trolling for age the allometric scaling coefficient a wasslightly greater than 1 for both sexes (females a 5 111males a 5 118) This suggests that any disparity inVO2max between Canadians and the Tsimane cannot beexplained solely by mass differences Indeed assumingthe Tsimane have the same body composition as Cana-dians projected VO2max differs little from observedVO2max The Tsimane outperform the Canadians in everycohort by at least 35 ml min21 kg21 except among theyoungest males who perform similarly (see SupportingInformation Fig S4)
To control for possible disparities in changes in bodycomposition by age within each population as these mightalso influence differences between the Tsimane and Cana-dians we scaled VO2max by absolute FFM from the samepopulation to obtain ml min21 fat-free kg21 BecauseCanadian body composition data were only available viaskinfolds (bicep tricep subscapular and suprailiac) weused the subset of Tsimane (n 5 246) for which the samefour skinfolds measurements were available We calcu-lated average absolute FFM for each cohort using averageweight and average summed skinfolds (Durnin andWomersley 1974) and scaled average VO2max in mlmin21 by this number to obtain ml min21 fat-free kg21Under this method of scaling the Tsimane outperformCanadians in every cohort over age 20 by at least 165 ml
min21 fat-free kg21 (see Supporting Information TableS2) Canadian females and males in the 12ndash19 cohortsoutperform Tsimane of the same age
We next compared Tsimane to other subsistence popula-tions reported in the literature (Table 4) Consistent withcommon practice in the literature we report means foreach group but when possible we also predicted VO2maxat age 25 to provide age-corrected comparisons Weselected age 25 as it is the age of peak relative VO2max inthis study and for female Kamba and Maasai in Christen-sen et als (2012) recent study To predict VO2max at age25 we regressed the median ages on mean VO2max acrossthe available age categories Tsimane females and maleshave roughly the same predicted VO2max at age 25 asseveral other subsistence populations but higher VO2maxthan industrialized populations To test for differencesbetween industrialized and subsistence populations weconducted a linear regression on predicted VO2max at age25 this is not a meta-analysis and results should beinterpreted with caution Overall subsistence populationsdisplay higher peak VO2max than in industrialized popu-lations controlling for sex (440 vs 367 ml min21 kg21
[Plt 001]) The Tsimane O2 and indigenous Siberian sam-ples were excluded Tsimane O2 to avoid the problem ofnon-independence with Tsimane HR data and Siberiansbecause the sample has a limited age range comparedwith the other studies
Pace of decline slope of VO2max decline across thelifespan
Tsimane To evaluate whether Tsimane participants per-formed similarly under different methods we comparedage-matched subsamples of participants from the presentstudy with O2 method participants Despite a higher level(intercept) of VO2max in the O2 sample Tsimane malesdeclined marginally significantly faster under the O2
method relative to the HR method (O2 5 68 per decadeHR 5 47 decline per decade t 5 2195 P 5 005) Thereis no significant difference between Tsimane femalestested under the O2 and HR methods (O2 5 60 per dec-ade HR 5 48 decline per decade t 5 2055 P 5 058)Mediators of Slope Across the Lifespan We fit a series oflinear models to test for interactions between the candi-date mediators and age-related decline in TsimaneVO2max There are no variables that significantly inter-act with age to predict VO2max (see Supporting Informa-tion Table S4) An AIC selection approach and scaling byabsolute FFM (see Supporting Information Table S3) pro-vides the same results no variables significantly interactwith age to predict VO2max
Between-group VO2max is most often reported as a lin-ear decline across the adult lifespan though Hawkins andWiswell (2003) dispute whether the decline is actually lin-ear For example a linear approximation is not appropri-ate for Tsimane females if ages 11ndash80 are consideredFigure 2 contrasts linear declines in VO2max for Cana-dians and Tsimane males as well as a curvilinear fit forTsimane females with declines in industrialized nationsderived from meta-analyses (Fitzgerald et al 1997 Wil-son and Tanaka 2000) To explore whether rates ofdecline in VO2max among Tsimane and Canadians weredifferent we regressed average VO2max by age category
8 AC PISOR ET AL
American Journal of Human Biology
TA
BL
E4
Mea
nV
O2m
ax
esti
ma
ted
VO
2m
ax
at
age
25a
nd
dec
lin
ein
VO
2m
ax
per
dec
ad
efr
omth
isst
ud
ya
nd
pre
vio
us
rese
arc
ha
Pop
ula
tion
Fem
ale
Male
Pu
bli
cati
onM
ean
VO
2m
ax
VO
2m
ax
Age
25
bP
erce
nt
Dec
lin
eA
ge
Ran
ge
(n)
Mea
nV
O2m
ax
VO
2m
ax
Age
25
bP
erce
nt
Dec
lin
eA
ge
Ran
ge
(n)
Ind
ust
riali
zed
Can
ad
ac
312
400
73
20ndash69
(2905)
361
458
68
20ndash69
(2712)
Jap
an
d357
414
39
20ndash69
(656)
417
473
38
20ndash69
(807)
San
ad
aet
al
2007
Sw
eden
e330
g409
80
20ndash65
324
g388
75
20ndash65
Ek
blo
met
al
2007
Th
ail
an
d(i
nd
ust
ry)e
275
293
54
16ndash55
(56)
389
415
57
16ndash53
(70)
Yoo
pat
etal
2002
US
(H
erit
age)
f273
17ndash65
(360)
359
17ndash65
(293)
Sk
inn
eret
al
2003
US
(N
HA
NE
S)d
356
363
24
20ndash49
(1312)
444
438
39
20ndash49
(1481)
Su
bsi
sten
ceT
sim
an
e(H
R)c
498
521
h16
h20ndash69
471
538
h61
h20ndash69
Tsi
man
e(O
2)c
436
74
h36ndash69
540
25
h36ndash69
Ifalu
k(1
969ndash70)c
429
488
69
20ndash59
(43)
49
597
75
20ndash69
(75)
Rod
ean
dS
hep
hard
1994
Ach
ec465
434
257
20ndash59
(62)
519
614
84
20ndash59
(65)
Walk
eran
dH
ill
2003
Lu
oc378
372
39
17ndash68
(209)
429
48
54
17ndash68
(172)
Ch
rist
ense
net
al
2012
b
Kam
ba
c377
371
45
17ndash68
(283)
431
516
34
17ndash68
(94)
Ch
rist
ense
net
al
2012
Maasa
ic389
410
45
17ndash68
(178)
431
528
69
17ndash68
(163)
Ch
rist
ense
net
al
2012
Ind
igen
ous
Sib
eria
nsc
338
341
22
220ndash39
(14)
462
471
66
20ndash39
(30)
Katz
marz
yk
etal
1994
Ru
ral
Nep
alc
187
15ndash60
(39)
221
15ndash60
(35)
Pan
ter-
Bri
cket
al
1992
Ngis
onyok
aT
urk
an
af
38
387
18
20ndash44
(19)
Cu
rran
-Ever
ett
1994
aV
alu
esm
issi
ng
wh
enn
otavail
able
from
ap
art
icu
lar
stu
dy
Per
cen
td
ecli
ne
(per
cen
tof
pea
kvalu
elo
st)
per
dec
ad
ew
as
calc
ula
ted
as
by
regre
ssin
gre
lati
ve
VO
2m
ax
by
age
mu
ltip
lyin
gth
ep
ara
met
eres
tim
ate
for
age
by
10
an
dd
ivid
ing
this
nu
mber
by
the
inte
rcep
t(p
resu
med
pea
k
ass
um
ing
ali
nea
rd
ecli
ne
inV
O2m
ax
acr
oss
age)
B
ecau
seof
lack
ofacc
ess
tora
wd
ata
re
gre
ssio
ns
wer
efi
tw
ith
mea
nV
O2m
ax
an
dm
edia
nage
by
coh
ort
bA
ge
25
valu
esw
ere
esti
mate
dby
regre
ssin
gre
lati
ve
VO
2m
ax
by
age
then
usi
ng
the
resu
ltin
gp
ara
met
eres
tim
ate
sto
pre
dic
tV
O2m
ax
at
age
25
the
pea
kin
rece
ntl
yst
ud
ied
pop
ula
tion
s(e
g
Kam
ba
an
dM
aasa
ife
male
sC
hri
sten
sen
etal
2012fe
male
san
dm
ale
sin
this
art
icle
)B
ecau
seof
lack
ofacc
ess
tora
wd
ata
re
gre
ssio
ns
wer
efi
tw
ith
mea
nV
O2m
ax
an
dm
edia
nage
by
coh
ort
cS
ubm
axim
alst
epte
st
dS
ubm
axim
altr
ead
mil
lte
st
eS
ubm
axim
aler
gom
eter
test
f M
axim
al
ergom
eter
test
gS
wed
ish
data
wer
ere
por
ted
as
med
ian
sfo
rea
chage
cate
gor
yth
evalu
esre
por
ted
her
eare
mea
ns
ofth
ese
med
ian
s2006
ind
ivid
uals
part
icip
ate
dbu
tn
um
ber
by
sex
was
not
rep
orte
d
hF
orco
mp
ara
bil
ity
we
bin
ned
the
Tsi
man
eH
Ran
dO
2d
ata
into
10
yea
rage
cate
gor
ies
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 9
American Journal of Human Biology
on median age (for a given age category) population andtheir interaction term For comparability Tsimane werebinned into the Canadian age categories and averageswere computed for these categories leading to estimateddeclines slightly different from those in Table 4 for thepurposes of this test we treat the Tsimane female declineas linear Because within-population variance in declineis not available these regressions should be treated asdescriptive comparisons rather than statistical tests ofdifferences between the two groups The rate of decline inVO2max is steeper for Canadian females (69 per decadefaster decline per decade) and males (42 faster declineper decade) compared with Tsimane females and males
The rate of cardiovascular fitness decline between theTsimane and Canadians is different but this differencedoes not extend to industrialized and subsistence popula-tions (see Table 4) Controlling for sex subsistence groupshave about one quarter of a percent lower declines perdecade Again because the variance in decline is not rep-resented in this regression results should be interpretedas comparative rather than as a statistical test As beforeTsimane O2 results were not included in the analysis toavoid nonindependence and the indigenous Siberianswere excluded because of discrepancy in ages sampled
DISCUSSION
Our comparisons demonstrate that across a wide varietyof societies cardiovascular fitness senesces with age Car-diovascular fitness is higher on average among members ofsubsistence societies than among industrialized societiesbut rates of fitness decline from peak are not slower Ourmore detailed comparison between the Tsimane a subsist-ence population and Canadians an industrialized popula-tion reveals differences in cardiovascular fitness levelsand rate of fitness decline Cardiovascular fitness levelswere higher among the Tsimane than among Canadiansand the rate of decline across the lifespan was significantlyslower among Tsimane women and men Potential Cana-
dian participants were excluded due to many health con-cerns including pregnancy and history of high bloodpressure whereas Tsimane were only excluded if they self-identified as unable to participate This suggests the Cana-dian sample is a relatively healthy subsample of Canadayet the Tsimane still outperform them in cardiovascular fit-ness It may be that the higher demand for cardiovascularfitness in late ages among the Tsimane outweighs anyeffects of poor health Another possibility is that greaterself-selection among Tsimane due to higher adult mortalityleaves more robust older adult survivors thereby reducingthe observed slope of fitness decline at the population level(Vaupel et al 1979) perhaps this is partially why fewerTsimane older adults opted out of the exercise test thanCanadian older adults were screened out (ages 60ndash69Canadian females 5 56 Tsimane females 5 15 Cana-dian males 5 57 Tsimane males 5 5)
Consistent with prior research on age-related changesin cardiovascular fitness the Tsimane do evidence a lin-ear decline in VO2max with age but not as steep a declineas typically seen in industrialized populations Based oncomparisons with the Canadians and with other industri-alized populations we believe the Tsimane data from thepresent study and the pilot O2 data combined indicatethat the Tsimane perform better on tests of cardiovascularfitness than the average individual from an industrializednation
To further explore the potential effects of health factorson cardiovascular fitness level and rate of decline weinvestigated predictors of individual differences in fitnesswithin the Tsimane population Overall we found thatmost health indicators among the Tsimane did not hinderVO2max levels or rates of decline Lower hemoglobin lev-els were associated with lower VO2max levels in womenbut not men consistent with the notion that compromisedblood oxygen transport curbs cardiovascular fitness(Buzina et al 1989 Panter-Brick et al 1992) In the USlow hemoglobin is more common in active women thanactive men (Sinclair and Hinton 2005) hemoglobin is
Fig 2 Linear changes in VO2max with age for Canadians and the Tsimane Intercepts and slopes for Canadians and Tsimane can be foundin Table 4 Because age2 is significant for the full sample of Tsimane females their change in VO2max across age is curvilinear Slopes forendurance trained active and sedentary individuals from industrialized nations are drawn from a meta-analysis performed by Fitzgeraldet al (1997) for females and Wilson and Tanaka (2000) for males Endurance trained individuals are represented by the top dotted line abovefollowed by active individuals below and sedentary on the bottom Trained individuals engage in 31 sessions of endurance exercise per weekfor at least a year while active individuals engage in 2 or fewer sessions per week of cardiovascular exercise [Color figure can be viewed in theonline issue which is available at wileyonlinelibrarycom]
10 AC PISOR ET AL
American Journal of Human Biology
also lower in Tsimane women than Tsimane men(female 5 129 [sd 13] g ml21 males 5 142 [13] g ml21)Even mild (non-anemic) iron deficiencies impacts womenrsquosexercise performance (Zhu and Haas 1997) Inconsistentwith findings from Panter-Brick et al (1992) among ruralNepalese helminth infection did not diminish levels ofVO2max for Tsimane men helminth infection wasactually a predictor of higher VO2max There are severalreasons why this might be the case First we only testedwhether presence or absence of helminths mediated theeffect of age on VO2max rather than parasite load (egnumber of worms egg counts) it is possible that helminthinfection only affects VO2max at high parasite loads Sec-ond blood loss (and thus low hemoglobin levels) resultingfrom helminth infection may be partially offset by theamount of iron in the Tsimane adult diet Tsimane ironintake is an estimated 166 of the US Dietary ReferenceIntake (Martin et al 2012) and Tsimane hemoglobin lev-els are higher than in the Nepalese (females 129 vs 109males 1424 vs 120 Panter-Brick et al 1992) Thirdthese analyses consider helminth infection at the time ofexercise test rather than past infections It may be thatthe cumulative burden of past infection has a larger effecton cardiovascular fitness if so this would suggest thatthe surprising positive effect of helminth infection onVO2max levels in men is either spurious or capturing athird variable
Secular declines in VO2max are expected with increasingmarket integration and lifestyle change because ofincreased sedentism (Katzmarzyk et al 1994 Rode andShephard 1994) Two proxies for market integration in thispopulationmdashdistance to San Borja and the ability to speakSpanishmdashwere not significant predictors of VO2max levelsor decline This is consistent with our predictions as Tsi-mane females and males that live near town do not appearto have lower activity levels (Gurven et al 2013) Wageopportunities near town primarily include working asranch hands collecting and weaving palm thatch panelscash cropping and working for logging companies Each ofthese involves extensive activity furthermore transporta-tion to town often involves bicycling walking and polingdugout canoes Cash cropping of rice and corn also involvesthe clearing and weeding of larger fields Except for cashcropping and palm thatch manufacture most wage laboropportunities are currently restricted to men
This study makes several unique contributions to theexisting literature It offers the first systematic compari-son of cardiovascular fitness level and rate of declinebetween subsistence and industrialized societies Resultscompiled from previous studies support the general claimthat despite greater pathogen stress the greater activityregime of subsistence societies helps support higher peakVO2max Additionally this is one of the first studies toexplore senescent changes in cardiovascular fitnesswithin a large sample from a subsistence population Thelarge number of health measures and proxies of marketintegration available permitted testing whether these fac-tors mediated age-related variation and whether theymodulated the rate of decline Despite reports that healthstatus and market integration have been important inother studies (eg Buzina et al 1989 Katzmarzyk et al1994 Panter-Brick et al 1992 Rode and Shephard1994) their overall net effect was small among the Tsi-mane most apparent in measures of hemoglobin levelsamong women and helminth infection among men
The results of these analyses may also shed light onindividual and population level differences in chronic dis-ease In industrialized populations meta-analyses demon-strate that cardiovascular fitness is protective againstcardiovascular disease (Jette et al 1992 Hawkins andWiswell 2003) Prior studies among Tsimane suggest rel-atively few deaths from heart attacks or strokes (Gurvenet al 2007) a low prevalence of common cardiovasculardisease risk factors like obesity high blood low-densitylipoprotein levels hypertension and peripheral arterialdisease and the existence of additional protective factorslike lean diet and physical activity (Gurven et al 20092013 Vasunilashorn et al 2010) Market foods such ascooking oil sugar and pasta represent only 6 of theaverage Tsimane diet and Tsimane also consume a greatdeal of lean meat and omega-3 fatty acids (Martin et al2012) This study complements these findings by demon-strating that Tsimane show relatively high VO2max anindicator of strong cardiorespiratory health TsimaneVO2max declines with age as it does everywhere whichsuggests declining muscle mass with age (Fleg andLakatta 1988) and lowered cardiac output (American Col-lege of Sports Medicine 2006 Sagiv et al 2007) ratherthan increased cardiovascular disease risk
Limitations
The Canadians were selected as a comparison industri-alized population because of the similarity of the CHMSand Tsimane protocols very few studies of industrializedpopulations have large sample sizes sample across thelife course and use a step test Several aspects of theCHMS and Tsimane protocols remain potentially incom-parable The Canadians experienced more stringentexclusion criteria than the Tsimane meaning that the Tsi-mane sample may be more representative of cardiovascu-lar condition in the Tsimane population than theCanadian sample of the Canadian population Again ifthe Tsimane sample was subjected to these criteria wemight expect the differences in VO2max between popula-tions to only increase On the other hand Canadian par-ticipants were assigned stepping cadences based on theirage and sex and cadence was increased across the exer-cise test if a participant did not reach 85 of his or herage-specific maximal HR all Tsimane were asked to com-plete 30 ascents per minute with no increase based ontheir achieved HRs Few Tsimane reached 75 of theirage-specific maximal HR (see Supporting InformationTable S1) perhaps because the age-specific maximal HRsderived from industrialized populations are inaccurate forthe Tsimane or because higher fitness allowed these Tsi-mane to perform the step test of 30 ascents per minutewith less effort Due to these discrepancies in protocolwhich may lead to errors in estimating VO2max we alsoincorporated Tsimane data collected using the O2 methodas a check because the O2 method estimates VO2max onthe relationship between HR and VO2 in a givenparticipant
Indeed it is an open question as to whether typicalmethods for indirectly estimating cardiovascular fitnessfrom HR are appropriate for subsistence level popula-tions Common routines for VO2max estimation assumeage-specific declines in cardiovascular fitness (eg Shep-hard 1970) but these methods have only been validatedwith samples from industrialized populations which are
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 11
American Journal of Human Biology
often self-selected (Beall et al 1985) Additionally regres-sions drawn from laboratory studies require participantsachieve a HR within a certain range for accurate VO2maxestimation however the appropriateness of these rangesgiven slight modifications to protocol and inclusion of par-ticipants of different ages different populations and bothsexes is questionable For example the maximal HRexhibited by young men varies across subsistence popula-tions (Shephard 1978) Use of these criteria is compli-cated by the fact that the most commonly used equationfor estimating maximal possible HR by age 220-age maybe inaccurate (Robergs and Landwehr 2002) and particu-larly inappropriate for older adults (see Tanaka et al2001) For these reasons we chose to use an exclusion cri-terion for the Tsimane that evaluates individual increasein HR across exercise relative to the mean increase in HRfor Tsimane of the same sex and age
The pattern of Tsimane fitness decline differs moder-ately by the choice of exclusion criterion for participants(see Supporting Information Table S1) and by method oftesting However this is a common finding Lee et al(2011) predicted VO2max from submaximal exercise usingthe O2 method and the HR-based American College ofSports Medicine calculation routine in a US sample Theyfound that (1) the HR-based routine predicts higherVO2max across the sexes than does the O2 routine and(2) the two methods have a correlation of only 077 Whenevaluating different testing procedures Shephard et al(1968) found differences in VO2max estimation by type oftest used (eg bicycle ergometer versus step test) and cal-culation routine Exercise tests exclusion criteria andcalculation routines combine to provide an estimate ofactual VO2max for a given individual and as such varia-tion in estimation is to be expected However such varia-tion may affect cross-population comparisons inunforeseen ways thus the comparisons presented hereshould be interpreted with caution
While population-level variation in cardiovascular fit-ness decline may reflect the differences in the demands ofendurance-based physical activity muscularity and com-promised oxygen transport it is possible that genetic fac-tors may also play a potential role (Collins 1999) In oneindustrialized sample maternal cardiovascular fitnessexhibited a heritability of 30 which is attributed toinheritance of the maternal mitochondrial genome (Bou-chard et al 2000) We do not have the relevant geneticdata for the populations considered here however andthus operate under the simplifying assumption thatinheritance should not affect population-level patternsand will not consistently bias individual-level compari-sons in any particular direction
This study is further limited by its cross-sectionaldesign Cross-sectional data present well-known problemsfor the measurement of individual aging (Crimmins andSeeman 2001) Mortality selection in which individualsin poorer condition are likely to die at younger ages pro-duces a downward bias in the estimation of aging rates atthe individual level (Vaupel and Yashin 1985 Vaupelet al 1979) Cohort effects if present also produce com-plicated and non-monotonic biases in estimation (Carnesand Olshansky 2001) Due to the problem of between-individual heterogeneity and the within-individual pro-cess of senescence a recent overview of aging studies con-cludes that ldquoonly longitudinal studies [ ] provide reliablesources of information in the study of senescencerdquo (Nussey
et al 2008) To date there are no longitudinal studies ofcardiovascular fitness in subsistence populations We arecurrently re-testing participants under the O2 methodallowing a better grasp of the within-individual variationthat shapes patterns of senescent decline
ACKNOWLEDGMENTS
The authors thank Paul Hooper Steven Gaulin JohnTooby Patricia Kramer the Human Evolution and Biode-mography laboratory and the Center for EvolutionaryPsychology at UCSB for helpful advice and feedback thestaff at the Tsimane Health and Life History Project andthe Tsimane for their participation and patience
LITERATURE CITED
American College of Sports Medicine 2006 ACSMrsquos Guidelines for Exer-cise Testing and Prescription 7th ed Philadelphia Lippincott Williamsamp Wilkins
Armstrong N 2001 Peak oxygen uptake in relation to growth and matura-tion in 11- to 17-year-old humans Eur J Appl Physiol 85546ndash551
Astrand PO Ryhming I 1954 A nomogram for calculation of aerobiccapacity (physical fitness) from pulse rate during submaximal work JAppl Physiol 7218ndash221
Bailey DA Shephard RJ Mirwald RL 1976 Validation of a self-administered home test of cardio-respiratory fitness Can J Appl SportSci 167ndash78
Beall CM Goldstein MC and Feldman ES 1985 The physical fitness ofelderly Nepalese farmers residing in rugged mountain and flat terrainJ Gerontol 40529ndash535
Benefice E Ndiaye G 2005 Relationships between anthropometry cardi-orespiratory fitness indices and physical activity levels in different ageand sex groups in rural Senegal (West Africa) Ann Hum Biol 32366ndash382 Available from httpwwwncbinlmnihgovpubmed16099780
Blackwell AD Gurven MD Sugiyama LS Madimenos FC Liebert MAMartin MA Kaplan HS Snodgrass JJ 2011 Evidence for a peak shift in ahumoral response to helminths age profiles of IgE in the Shuar of Ecuadorthe Tsimane of Bolivia and the US NHANES PLoS Negl Trop Dis 5e1218 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid53125146amptool5pmcentrezamprendertype5abstract
Blackwell AD Martin M Kaplan H Gurven M Evidence for an antagonis-tic relationship between Giardia lamblia and helminth infections impli-cations for treatment of helminth infections in developing populations
Blair SN LaMonte MJ Nichaman MZ 2004 The evolution of physicalactivity recommendations how much is enough Am J Clin Nutr 79913Sndash920S Available at httpwwwncbinlmnihgovpubmed15113739
Bouchard C Rankinen T Chagnon YC Rice T Perusse L Gagnon JBorecki I An P Leon a S et al 2000 Genomic scan for maximal oxygenuptake and its response to training in the HERITAGE Family Study JAppl Physiol 88551ndash559 Available at httpwwwncbinlmnihgovpubmed10658022
Bryan S St-Denis M Wojtas D 2007 Canadian Health Measures Surveyclinic operations and logistics Health Rep 1853ndash69
Buzina R Bates CJ van der Beek J Brubacher G Chandra RK HallbergL Heseker J Mertz W Pietrzik K et al 1989 Workshop on FunctionalSignificance of Mild-to-Moderate Malnutrition Am J Clin Nutrition 50172ndash176
Calder WA 1987 Scaling energetics of homeothermic vertebrates anoperational allometry Annu Rev Physiol 49107ndash120
Canadian Society for Exercise Physiology 2003 The Canadian PhysicalActivity Fitness amp Lifestyle Approach (CPAFLA) CSEP-Health amp Fit-ness Programrsquos Health-Related Appraisal and Counselling Strategy 3rded
Carnes BA Olshansky SJ 2001 Heterogeneity and its biodemographicimplications for longevity and mortality Exp Gerontol 36419ndash430Available at httpwwwncbinlmnihgovpubmed11250115
Carrick-Ranson G Hastings JL Bhella PS Shibata S Fujimoto N PalmerD Boyd K Levine BD 2013 The effect of age-related differences inbody size and composition on cardiovascular determinants of VO2max JGerontol A Biol Sci Med Sci 68608ndash616 Available at httpwwwncbinlmnihgovpubmed23160363
Centers for Disease Control and Prevention 1998 Recommendations toPrevent and Control Iron Deficiency in the United States MMWRRecomm Rep 471ndash36 Available at httpwwwcdcgovmmwrpreviewmmwrhtml00051880htm
12 AC PISOR ET AL
American Journal of Human Biology
Centers for Disease Control and Prevention 2011 Glossary of TermsPhysical Activity for Everyone [Internet] Available from httpwwwcdcgovphysicalactivityeveryoneglossary
Christensen DL Faurholt-Jepsen D Boit MK Mwaniki DL Kilonzo BTetens I Kiplamai FK Cheruiyot SC Friis H et al 2012 Cardiorespira-tory fitness and physical activity in Luo Kamba and Maasai of ruralKenya Am J Hum Biol 24723ndash729 Available at httpwwwncbinlm-nihgovpubmed22836508
Colley RC Garriguet D Janssen I Craig CL Clarke J Tremblay MS2011a Physical activity of Canadian children and youth accelerometerresults from the 2007 to 2009 Canadian Health Measures SurveyHealth Rep 2215ndash23
Colley RC Garriguet D Janssen I Craig CL Clarke J Tremblay MS2011b Physical activity of Canadian adults accelerometer results fromthe 2007 to 2009 Canadian Health Measures Survey Health Rep 227ndash14 Available at httpwwwncbinlmnihgovpubmed21510585
Collins KJ 1999 Physiological variation and adaptability in human popu-lations Ann Hum Biol 2619ndash38
Crimmins E Seeman T 2001 Integrating Biology into DemographicResearch on Health and Aging (With a Focus on the MacArthur Study ofSuccessful Aging) Cells and Surveys Should Biological Measures beIncluded in Social Science Research Washington DC National Acad-emy Press p 9ndash41
Curran-Everett LS 1994 Accordance Between VO2max and Behavior inNgisonyoka Turkana Am J Hum Biol 6761ndash771
Durnin JVGA Womersley J 1974 Body fat assessed from total body den-sity and its estimation from skinfold thickness measurements on 481men and women aged from 16 to 72 years Br J Nutr 3277ndash97
Eberl M Al-Sherbiny M Hagan P Ljubojevic S Thomas AW Wilson RA2002 A novel and sensitive method to monitor helminth infections byfaecal sampling Acta Trop 83183ndash187
Eid D Gurven M Kaplan H Winking J 2007 Enfermedades infecciosas alo largo de la vida y en el envejecimiento en indıgenas sudamericanos dela etnia Tsimane Aging in Developing Countries Building Bridges forIntegrated Research Agendas Santiago Chile
Ekblom B Engstreuroom L-M Ekblom O 2007 Secular trends of physical fit-ness in Swedish adults Scand J Med Sci Sports 17267ndash273 Availableat httpwwwncbinlmnihgovpubmed17501867
Finch CA Lenfant C 1972 Oxygen Transport in Man N Engl J Med 286407ndash415
Fitzgerald MD Tanaka H Tran ZV Seals DR 1997 Age-related declinesin maximal aerobic capacity in regularly exercising vs sedentarywomen a meta-analysis J Appl Physiol (Bethesda Md 1985) 83160ndash165 Available at httpwwwncbinlmnihgovpubmed9216959
Fleg JL Lakatta EG 1988 Role of muscle loss in the age-associated reduc-tion in VO2max J Appl Physiol 651147ndash1151
Frisancho AR Frisancho HG Milotich M Brutsaert T Albalak RSpielvogel H Villena M Vargas E Soria R 1995 Developmentalgenetic and environmental components of aerobic capacity at high alti-tude Am J Phys Anthropol 96431ndash442 Available at httpwwwncbinlmnihgovpubmed7604895
Giroux S 2007 Canadian health measures survey sampling strategyoverview Health Rep 1831ndash36
Gurven M Jaeggi A V Kaplan H Cummings D 2013 Physical activityand modernization among Bolivian Amerindians PLoS ONE 81ndash13
Gurven M Kaplan H Winking J Rodriguez DE Vasunilashorn S KimJK Finch C Crimmins E 2009 Inflammation and infection do not pro-mote arterial aging and cardiovascular disease risk factors among leanhorticulturalists PLoS ONE 41ndash12
Haidet GC 1989 Dynamic exercise in senescent beagles oxygen consump-tion and hemodynamic responses The Am J Physiol 257H1428ndash1437Available at httpwwwncbinlmnihgovpubmed2589499
Hawkins S Wiswell R 2003 Rate and mechanism of maximal oxygen con-sumption decline with aging implications for exercise training SportsMed 33877ndash888 Available at httpwwwncbinlmnihgovpubmed12974656
Hoffman J 2002 Physiological aspects of sport training and performance1st ed Champaign IL Human Kinetics Publishers
Hotez PJ Bottazzi ME Franco-Paredes C Ault SK Periago MR 2008 Theneglected tropical diseases of Latin America and the Caribbean a review ofdisease burden and distribution and a roadmap for control and eliminationPLoS Negl Trop Dis 2e300 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid52553488amptool5pmcentrezamprendertype5abstract
Howley ET Bassett DR Welch HG 1995 Criteria for maximal oxygenuptake review and commentary Med Sci Sports Exerc 271292ndash1301Available at httpwwwncbinlmnihgovpubmed8531628
Jette M Sidney K Quenneville J Landry F 1992 Relation between cardi-orespiratory fitness and selected risk factors for coronary heart diseasein a population of Canadian men and women CMAJ 1461353ndash1360Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid51488567amptool5pmcentrezamprendertype5abstract
Katzmarzyk PT Leonard WR Crawford MH 1994 Predicted maximaloxygen consumption of Indigenous Siberians Am J Hum Biol 6783ndash790
King CH Dickman K Tisch DJ 2005 Reassessment of the cost of chronichelmintic infection a meta-analysis of disability-related outcomes inendemic schistosomiasis Lancet 3651561ndash1569 Available at httpwwwncbinlmnihgovpubmed15866310
Lee J-M Bassett D Jr Thompson D Fitzhugh E 2011 Validation of thecosmed fitmate for predicting maximal oxygen consumption J StrengthCond Res 252573ndash2579
Madimenos FC Snodgrass JJ Blackwell AD Liebert MA Sugiyama LS2011 Physical activity in an indigenous Ecuadorian forager-horticulturalist population as measured using accelerometry Am J HumBiol 23488ndash497 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid53110644amptool5pmcentrezamprendertype5abstract
Malina RM 2001 Physical activity and fitness pathways from childhoodto adulthood Am J Hum Biol 13162ndash172 Available at httpwwwncbinlmnihgovpubmed11460860
Malina RM Little BB 2008 Physical activity the present in the contextof the past Am J Hum Biol 20373ndash391 Available at httpwwwncbinlmnihgovpubmed18433002
Manning JT Morris L Caswell N 2007 Endurance running and digitratio (2D 4D) implications for fetal testosterone effects on runningspeed and vascular health Am J Hum Biol 19416ndash421
Martin Ma Lassek WD Gaulin SJC Evans RW Woo JG Geraghty SRDavidson BS Morrow AL Kaplan HS et al 2012 Fatty acid composi-tion in the mature milk of Bolivian forager-horticulturalists controlledcomparisons with a US sample Matern Child Nutr 8404ndash418 Availableat httpwwwncbinlmnihgovpubmed22624983
National Health and Nutrition Examination Survey 2004 CardiovascularFitness Procedures Manual
Nussey D Coulson T Festa-Bianchet M Gaillard J-M 2008 Measuringsenescence in wild animal populations towards a longitudinal approachFunction Ecol 22393ndash406
Ogawa T Spina RJ Martin WHI Kohrt WM Schechtman KB HolloszyJO Ehsani AA 1992 Effects of aging sex and physical training cardio-vascular responses to exercise Circulation 86494ndash503
Panter-Brick C Miller UG Eggerman M 1992 Hemoglobin levels andstep test performance of men and women in Nepal Am J Hum Biol 4481ndash491
Pontzer H Raichlen Da Wood BM Mabulla AZP Racette SB MarloweFW 2012 Hunter-gatherer energetics and human obesity PLoS ONE 7e40503 Available at httpcdxplosorg101371journalpone0040503
R Development Core Team 2011 R A language and environment for sta-tistical computing R Development Core Team
Rigby R Stasinopoulos D 2005 Generalize additive models for locationscale and shape (with discussion) Appl Stat 54507ndash554
Robergs RA Landwehr R 2002 The surprising history of theldquoHRmax5220-agerdquo equation J Exerc Physiol 51ndash10
Rode A Shephard RJ 1994 Physiological consequences of acculturation a20-year study of fitness in an Inuit community Eur J Appl Physiol 69516ndash524
Rowland TW Boyajian A 1995 Aerobic response to endurance training inchildren Pediatrics 96654ndash658
Sagiv M Ben-sira D Amir R 2007 What maintains energy supply atpeak aerobic exercise in trained and untrained older men Gerontology53357ndash361
Sanada K Kuchiki T Miyachi M Mcgrath K Higuchi M Ebashi H 2007Effects of age on ventilatory threshold and peak oxygen uptake normal-ised for regional skeletal muscle mass in Japanese men and womenaged 20 ndash 80 years Eur J Appl Physiol 99475ndash483
Schniter E 2009 Why Old Age Non-Material Contributions and Patternsof Aging Among Older Adult Tsimanersquo 607
Shahnawaz H 1978 Influence of limb length on a stepping exercise JAppl Physiol 44346ndash349
Shephard RJ 1970 Computer programs for solution of the Astrand nomo-gram and the calculation of body surface area J Sports Med 10206ndash210
Shephard RJ Allen C Benade AJS Davies CT Di Prampero PE HedmanR Merriman JE Myhre K Simmons R 1968 Standardization of sub-maximal exercise tests Bull World Health Organ 38765ndash775 Availableat httpwwwpubmedcentralnihgovarticlerenderfcgiartid52554690amptool5pmcentrezamprendertype5abstract
Shephard RJ Bailey Da Mirwald RL 1976 Development of the CanadianHome Fitness Test Can Med Assoc J 114675ndash679 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid51956906amptool5pmcentrezamprendertype5abstract
Shields M Tremblay MS Laviolette M Craig CL Janssen I Gorber SC2010 Fitness of Canadian adults results from the 2007ndash2009 canadianhealth measures survey Health Rep 2121ndash35 Available at httpwwwncbinlmnihgovpubmed20426224
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 13
American Journal of Human Biology
Siconolfi SF Garber CE Lasater TM Carleton RA 1985 A simple validstep test for estimating maximal oxygen uptake in epidemiologic stud-ies Am J Epidemiol 121382ndash390 Available at httpwwwncbinlm-nihgovpubmed4014128
Sinclair LM Hinton PS 2005 Prevalence of iron deficiency with and with-out anemia in recreationally active men and women J Am Diet Assoc105975ndash978 Available from httpwwwncbinlmnihgovpubmed15942552
Skinner JS Gaskill SE Rankinen T Leon AS Rao DC Wilmore JHBouchard C 2003 Heart rate versus VO2max age sex race initial fit-ness and training response-HERITAGE Med Sci Sports Exerc 351908ndash1913 Available at httpwwwncbinlmnihgovpubmed14600558
Sondik EJ Madans JH Gentlemand JF 2012 Summary health statisticsfor US adults National Health Interview Survey 2010 Vital Health Stat101ndash80 Available at httpwwwncbinlmnihgovpubmed20687424
Stones MJ Kozma A 1985 Physical performance Aging and Human Per-formance New York Wiley p 261ndash292
Tanaka H Monahan KD Seals DR 2001 Age-predicted maximal heartrate revisited J Am Coll Cardiol] 37153ndash156 Available at httpwwwncbinlmnihgovpubmed11153730
Vasunilashorn S Crimmins EM Kim JK Winking J Gurven M KaplanH Finch CE 2010 Blood lipids infection and inflammatory markers inthe Tsimane of Bolivia Am J Hum Biol 22731ndash740 Available at httpwwwncbinlmnihgovpubmed20721985
Vaupel JV Manton KG Stallard E 1979 The impact of heterogeneity inindividual frailty on the dynamics of mortality Demography 16439ndash454
Vaupel JW Yashin AI 1985 Heterogeneityrsquos ruses some surprising effectsof selection on population dynamics Am Stat 39176ndash185
Venables WN Ripley BD 2002 Modern Applied Statistics with S FourthNew York Springer
Wagner PD 1996 Determinants of maximal oxygen transport and utiliza-tion Annu Rev Physiol 5821ndash50 Available at httpwwwncbinlmnih-govpubmed8815793
Walker A Arent SM McKeever KH 2010 Maximal aerobic capacity(VO2max) in horses a retrospective study to identify the age-relateddecline Comparative Exerc Physiol 6177ndash181 Available at httpwwwjournalscambridgeorgabstract_S1755254010000073
Walker R Hill K 2003 Modeling growth and senescence in physical per-formance among the Ache of Eastern Paraguay Am J Hum Biol 208196ndash208
Weller IM Thomas SG Corey PN Cox MH 1993 Prediction of maximaloxygen uptake from a modified Canadian aerobic fitness test Can JAppl Physiol 18175ndash188 Available at httpwwwncbinlmnihgovpubmed8513290
Wilson TM Tanaka H 2000 Meta-analysis of the age-associated declinein maximal aerobic capacity in men relation to training status Am JPhysiol Heart Circ Physiol 278H829ndash834 Available at httpwwwncbinlmnihgovpubmed10710351
Wood SN 2006 Generalized Additive Models An Introduction with RBoca Raton Florida Chapman and HallCRC Press
World Health Organization 2001 Iron deficiency anaemia assessmentprevention and control a guide for programme managers Available athttpwhqlibdocwhointhq2001WHO_NHD_013pdf
Yoopat P Toicharoen P Boontong S Glinsukon T Vanwonterghem KLouhevaara V 2002 Cardiorespiratory capacity of Thai workers in dif-ferent age and job categories J Physiol Anthropol Appl Hum Sci 21121ndash128 Available at httpwwwncbinlmnihgovpubmed12056179
Zhu YI Haas JD 1997 Iron depletion without anemia and physical per-formance in young women Am J Clin Nutr 66334ndash341 Available athttpwwwncbinlmnihgovpubmed9250112
14 AC PISOR ET AL
American Journal of Human Biology

daily tasks require high levels of physical activity earlydemand may favor early investment in oxygen transportfunction leading to greater peak cardiovascular fitness(eg Frisancho et al 1995 Malina 2001) Additionallycardiovascular fitness may remain high if high levels ofactivity are sustained throughout adulthood or may beup-regulated by training (Finch and Lenfant 1972 Hoff-man 2002 Sagiv et al 2007 Wagner 1996) leading toslower decline with age
In subsistence populations individuals experience highenergy demand in conjunction with both work and leisureactivities (eg Malina and Little 2008 Panter-Brick et al1992 Walker and Hill 2003) It appears that any differen-ces in physical fitness performance may arise from differ-ences in levels of sedentary activity between subsistenceand industrialized populations as subsistence groups inte-grate to national markets sedentism may increase leadingto reductions in cardiovascular fitness (Katzmarzyk et al1994 Rode and Shephard 1994) However studies employ-ing factorial methods accelerometry and doubly labeledwater suggest considerable overlap in measured activitylevels and energy expenditure among members of subsist-ence and industrialized populations (Gurven et al 2013Madimenos et al 2011 Pontzer et al 2012) Among theTsimane our focal group women age 20ndash70 have averagephysical activity levels (PALs defined as total daily ener-getic expenditure divided by basal metabolic rate) of 173ndash185 over a 24 h period (Gurven et al 2013) while a sameage nonoverweight American sample has a similar aver-age of 178 (Blair et al 2004) Tsimane men are morephysically active than their American counterparts (Tsi-mane males 202-215 American males 173) though bothAmerican and Tsimane males fall within the range ofcross-population PALs reported by Gurven et al (2013)
The few studies that have examined cardiovascular fit-ness in subsistence populations show mixed evidence for adecline in fitness with age Turkana men engaging in pas-toralism do not exhibit a consistent decline in VO2max byage 45 (Curran-Everett 1994) Ache women living on a res-ervation and practicing a combination of gathering andhorticulture do not exhibit a decline in cardiovascular fit-ness by age 60 (Walker and Hill 2003) However thesefindings are based on relatively small samples and may beunduly influenced by outliers In contrast Inuit still livinga traditional lifestyle do show significant declines with age(Shepard 1978) as do small-scale farmers in Kenya(Christensen et al 2012) Given these mixed resultsshould we expect a cardiovascular fitness decline in all sub-sistence level societies and if so of the same steepness asthe decline among industrialized nations
Although sustained subsistence activity muscularityand leanness should help promote cardiorespiratory fit-ness throughout life other features of subsistence soci-eties may instead hinder performance especially at laterages Cardiovascular fitness level may be curbed by lim-ited energy reserves and food shortages The benefits of alarge capacity for physical activity may be age specificinvestments in cardiovascular fitness may be high earlyin the lifespan however higher adult mortality in subsist-ence societies may discount investments that maintainfunctionality in old age Limited energy budgets in sub-sistence societies might make such tradeoffs betweenadult functionality and late age maintenance more severeEven in industrialized societies the diminished ability tomaintain muscle with age results in lower muscle mass
or sarcopenia Although central limiting factors such ascardiac output are primarily responsible for age-relateddecline (Carrick-Ranson et al 2013 Ogawa et al 1992)muscle mass is also a predictor of slowed decline (Carrick-Ranson et al 2013 Sanada et al 2007 Stones andKozma 1985) as muscles consume 95 of oxygen used bythe body during exercise (Fleg and Lakatta 1988)
Another physical limit on the transport system is imposedby hemoglobin-bearing red blood cells which carry oxygenfrom lungs to muscles Individuals with anemia (low hemo-globin) do worse than nonanemic individuals on cardiovas-cular fitness tests (Buzina et al 1989 Panter-Brick et al1992 Wagner 1996) as do individuals who experience bloodloss from chronic helminth infections (King et al 2005Panter-Brick et al 1992) Anemia and helminth infectionsare more common in subsistence populations than industri-alized populations (Hotez et al 2008) The Tsimane have amuch higher prevalence of both helminths (Blackwell et al2011) and anemia than North Americans do Giardia andother protozoal bacterial and viral infections are also prev-alent (Blackwell et al 2013) Likewise respiratory ailmentscurb oxygen uptake (Collins 1999 Wagner 1996) and areoften common in subsistence groups While asthma andallergies are prevalent in the United States (Sondik et al2012) tuberculosis pneumonias and upper respiratoryinfections are not uncommon among the Tsimane (Eid et al2007) Together these factors might place an upper limit oncardiovascular fitness even for individuals engaged in fre-quent and intensive activity
This study investigates senescent changes in cardiovas-cular fitness among a large sample of Tsimane adults andtests whether predicted factors described above mediatethese changes To explore differences between subsistencegroups and industrialized nations Tsimane values arecompared with data from the Canadian Health MeasuresSurvey which employed a similar method for measuringcardiovascular fitness We first test whether Tsimanehave higher peak VO2max than Canadians Second weexamine whether Tsimane show similar senescentdeclines as Canadians given demands on Tsimane forphysical activity into older adulthood and increased stresson the cardiovascular system which are expected to haveopposing effects on fitness Tsimane and Canadian per-formance is compared with previous work in industrial-ized and subsistence groups to provide additional contextThird we examine the impact of mediating health andanthropometric factors on cardiovascular fitness includ-ing anemia respiratory illness helminth infections andproxy measures of market integration (distance to thelocal town Spanish-speaking ability) Due to competingdemands for somatic resources we predict that indicatorsof poor health will predict lower physical fitness levelsand faster age-related decline Though other populationsevidence lower levels of physical activity with increasingmarket integration Tsimane living closer to town andthose fluent in Spanish do not appear to become more sed-entary (Gurven et al 2013) we therefore expect that car-diovascular fitness will not differ between more and lessmarket integrated individuals
METHODS
Measuring cardiovascular fitness maximal oxygen uptake
Performance of the oxygen transport system can bemeasured by maximal oxygen uptake Oxygen uptake
2 AC PISOR ET AL
American Journal of Human Biology
(volume O2 or VO2) is calculated as the differencebetween the percentages of oxygen in inhaled (about 21)and exhaled gases multiplied by the volume of gasexhaled (Howley et al 1995) Maximal oxygen uptake(VO2max) refers to the peak oxygen uptake possible for agiven individual achieved during exercise to exhaustionBecause exercise to exhaustion can be potentially danger-ous in individuals with significant underlying cardiovas-cular disease VO2max is often estimated at asubmaximal level of exercise (eg 85 of age-specificmaximal heart rate HR) Additionally the use of a gascollection bag can be inconvenient or expensive for fieldand large scale projects (eg Shephard 1970) For thesereasons estimation of VO2max from a participantrsquos sub-maximal heart rate is often employed (eg Astrand andRyhming 1954) HR estimation methods were used forthe Canadian and Tsimane samples although only in thecase of the Canadians was the routine for calculatingVO2max derived from laboratory studies with the samepopulation
Study populations
Tsimane The Tsimane are a forager-horticulturalistgroup living in the Bolivian Amazon The Tsimane have apopulation of 11000 spanning 901 villages ranging insize from 40 to 550 individuals Villages near the localtown (San Borja population 24000) or near roads havemore extensive market access and greater participation inwage labor Although PALs are often predicted to declinewith market integration Tsimane women and men livingnear the local town are not less active than Tsimane fromother regions perhaps because of the physical activityrequired in wage labor (eg logging and cash croppingGurven et al 2013) Men in all regions have higher PALsthan women although menrsquos activity exhibits more sea-sonal variation Aging Tsimane remain active (Gurvenet al 2013) although these individuals may engage inless physically demanding subsistence activities becauseof increases in infirmity with age (Schniter 2009)
Tsimane data were collected as part of the TsimaneHealth and Life History Project (THLHP httpwwwun-medutsimane) from 2002ndash2010 Patients were seen byTHLHP physicians either during annual visits to villagesor at the THLHP medical office in San Borja Self-reported ailments were considered together with physicalexamination fecal and blood test results to assist in diag-nosis and treatment Sampling procedures for the exercisetest were designed to ensure a sample representative ofthe Tsimane population Participantsrsquo ages range from 10to 88 years old (n 5 766 55 female)
Pretest exclusion Tsimane Tsimane participants werenot automatically excluded from the study for having aparticular condition but any complaints or conditionswere recorded Our study protocol did not exclude partici-pants for any reason However some individuals whojudged themselves unable to participate or who experi-enced discomfort during exercise opted out The mostcommon reason given by participants for opting out waspain although this was rare (65 total excluded remainingn 5 701) Nonparticipation rates in this population werebelow 10 until after age 70 (Supporting Information FigS1) Although frailty may have constrained participation
at late ages the final sample below age 70 includes Tsi-mane at various levels of health and ability allowing us tobetter explore the correlates of fitness decline (eg paininfection) in this population Pregnant and lactatingwomen were included in the Tsimane sample as womenare pregnant or lactating for much of their adult lives
Experimental protocol Tsimane Participants were askedto complete a modified submaximal Harvard step test(Astrand and Ryhming 1954) at a bench height of 20 cmfor 5 min at 30 ascents per minute (Walker and Hill2003) The pace of stepping was recorded for each partici-pant regardless of whether the participant attained 30steps per minute VO2max was estimated using Shep-hardrsquos (1970) HR-based calculation routine for step testsWe first estimated VO2 with the following equation
E 979 3 W 3 H 3 Neth THORNL
1 kcal
4184 Joules 1 ml O2
200 kcal(1)
where W is weight in kilograms H is the step height inmeters N is number of ascents during the exercise testand L is the length of the test in minutes The conversionfactor adjusts for the efficiency of stepping Stepping isabout 16 efficientmdashonly 16 of the work done duringstepping contributes to vertical displacement (Shephardet al 1976)mdashand thus work done must be multiplied by669 (Shephard 1970) to account for the amount of effortrequired by participants The work (in Joules) required tocomplete the exercise test was calculated as 979 ms2 W xH x N where 979 ms2 is the acceleration due to gravity(Powers and Howley 2009) Kilocalories per minute weredivided by 200 to convert kilocalories to mlmin of O2
(ACSM 2006)Equations for estimating VO2max from submaximal
VO2 at peak HR during the test (P taken to be the lastminute of exercise) were drawn from Shephard (1970)These are based on age and sex specific regressions thatrely on assumptions about maximal HR by age
Females EethVO 2maxTHORN5 VO 2 198272eth THORNP272
1 VO 2max
00114age 1077 1
kg
(2a)
Males EethVO 2maxTHORN5 VO 2 198261eth THORNP261
1 VO 2max
00137age 10668 1
kg
(2b)
The estimates of VO2max produced by Eqs 2ab are inunits of ml of oxygen per minute per kilogram (ml min21
kg21) also called relative VO2max Another common mea-sure of VO2max absolute VO2max (l min21) was calcu-lated by multiplying VO2max in l min21 kg21 byparticipant body weight
Post-test exclusion Tsimane The Shepard equations forestimating VO2max depend on individuals achieving aheart rate within a certain range 120ndash172 for femalesand 122ndash170 for males Typical protocols call for excluding
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 3
American Journal of Human Biology
individuals who do not meet this level However manyTsimane (55 of females 81 of males) did not achievethis criterion either because the age-specific maximalHRs derived from industrialized populations are inaccu-rate for the Tsimane or because higher fitness allowedthese Tsimane to perform the step test with less effort Wetherefore evaluated several exclusion criteria for the Tsi-mane sample including the HR range specified by Shep-hard (1970) for the calculation routine a HR increase oflt5 beats per minute during exercise (National Healthand Nutrition Examination Survey 2004) different per-centages [65 (Siconolfi et al 1985) 70 (American Collegeof Sports Medicine 2006 Canadian Society for ExercisePhysiology 2003) 75 (NHANES 2004)] of age-specificmaximal HR (Tanaka et al 2001) achieved the 95th cen-tile obtained from a Generalized Additive Model for Loca-tion Scale and Shape (Rigby and Stasinopoulos 2005)and a rate of HR increase from the beginning to the end ofexercise that is beyond the 95 confidence interval (CI)from the 20 year age- and sex-specific mean The samplesize remaining after these exclusions varies from 4(75 of age-specific maximal HR) to 79 (increase lt5beats per minute during exercise) of our original sample(for sample sizes under each criterion considered see Sup-porting Information Table S1) We interpreted exclusioncriteria that excluded the vast majority of participants asnot giving a representative sample of the Tsimane Theuse of centiles or CIs enables us to compare each partici-pant against a metric from the same population Becausethe centile and CI approaches led to about the same rela-tively small number of participants excluded we adoptedthe CI exclusion for ease of interpretation
To evaluate the accuracy of HR estimation for the Tsi-mane population we compare VO2max estimated fromHR with VO2max estimated from the ratio of inhaled toexhaled O2 collected in a smaller subset of Tsimane Anadditional strength of the O2 method is that the VO2 andHR measured for a given individual is extrapolated to pre-dict their VO2max at their predicted age-specific maximalHR without reliance on additional assumptions beyondthat of an age-specific maximal HR Methods used in O2
measurement are described in the Supporting Informa-tion (Appendix A)
Tsimane model covariates Fat-free mass (FFM) was esti-mated by subtracting body fat mass from total mass Bodyfat percentage was estimated with bioimpedance using aportable Tanita scale and with skinfold measurementtaken at four sites (bicep tricep subscapular suprailiac)body fat percentage was estimated from skinfold measure-ment with equations from Durnin and Womersley (1974)Arthritis and respiratory ailments were diagnosed byTHLHP physicians during routine medical exams Hemo-globin levels in g dl21 were attained using the QBC Auto-read Plus Dry Hematology System (QBC DiagnosticsPort Matilda PA) anemia was defined using Centers forDisease Control (CDC) criteria (CDC 1998) and for agesfor which CDC criteria were not available World HealthOrganization (2001) criteria Helminth and giardia infec-tions were diagnosed in wet slide mounts and using amodified Percoll technique as has been previouslydescribed (Blackwell et al 2011 Eberl et al 2002) Wecoded helminth infection as bivariate (presence or absenceof helminths) combining diagnoses with hookworm
roundworm (Ascaris lumbricoides and Strongyloides ster-coralis) and whipworm (Trichuris trichiura) Because ofan established relationship between helminth infectionand anemia helminths and giardia are considered sepa-rately in this analyses Self-reported pain was included asa binary measure indexing the presence of back kneebone or connective tissue pain Spanish-speaking abilitywas treated as dichotomous where individuals rated asspeaking more than ldquosomerdquo Spanish by THLHP projectstaff were considered Spanish speakers Additional cova-riates include pregnancy status and as-the-crow-flies dis-tance of home village to the market town of San Borja
Because of a concern that leg length relative to benchheight may affect performance during step tests (Shahna-waz 1978) we considered including leg length in allwithin-population regressions Leg length was calculatedby subtracting participant seated height (minus chairheight) from standing height Including leg length wors-ened model fits perhaps because mass and leg length aremoderately correlated (for females Pearsonrsquos r 5 042 formales r 5 041) and mass is already controlled for by ouruse of relative (rather than absolute) VO2max addition-ally use of the leg length variable eliminated participantsfor whom seated height data were unavailable As suchwe decided to not control for leg length in the analysesbelow
Canadian health measures survey Canadian fitness datawere collected during the first wave of the CanadianHealth Measures Survey (CHMS wwwstatcangccaimdb-bmdi5071-enghtm) from 2007 to 2009 Canadianswere selected as a comparison group since VO2max in theCHMS was assessed using a step test procedure withVO2max estimated based on HR Individuals weresampled with the goal of representing 97 of the Cana-dian population from all provinces (Giroux 2007) Asmeasured with tri-axial accelerometers Canadian chil-dren in this sample are sedentary for 64 of their wakinghours (Colley et al 2011a) adult (ages 20ndash79) females aresedentary for 69 of the day and adult males are seden-tary for 68 (Colley et al 2011b)
Pretest exclusion CHMS CHMS participants wereexcluded from fitness testing if they had a heart conditionchest pain high blood pressure (systolic blood pressurehigher than 144) or heart rate (higher than 100) or weretaking medication for any of these conditions (Bryan et al2007) across all ages a total of 267 of potential partici-pants were excluded including 56 of 60ndash69 year olds(Shields et al 2010) Participants who experienced discom-fort during testing could stop at any time Women morethan 12 weeks pregnant were not allowed to participate
Experimental protocol CHMS Participants completed astep test developed by Bailey et al (1976 modified byWeller et al 1993) on a bench with two steps each 203cm tall Individuals began stepping at a rate expected torequire 65ndash70 of VO2max for a same-sex individual 10years their senior (Canadian Society for Exercise Physiol-ogy 2003) After a 3 min exercise interval researchersmeasured HR to ascertain whether the participant hadachieved 85 of his or her age-specific maximal HR If
4 AC PISOR ET AL
American Journal of Human Biology
85 of maximal HR was reached exercise testing wasstopped if 85 of maximal HR was not reached partici-pants proceeded to the next stage of exercise stepping ata faster cadence
VO2max was estimated using a regression equationdeveloped by Weller et al (1993)
E VO2maxeth THORN532116a2024b2017c (3)
where a is the estimated VO2 at the end of the finalstage of exercise (Weller et al 1993) b is age in yearsand c is body weight in kg If a participant could not stepat the prescribed cadence during a given stage of exerciseVO2max was estimated based on the last completed exer-cise stage (Shields et al 2010) About 1 of participantseligible for the test did not complete it Participants didnot proceed beyond the eighth level of exercise regardlessof whether they had attained 85 of their age-specificmaximal HR The result is estimated relative VO2max (mlmin21 kg21)
Skinfold measurements used to calculate absoluteFFM in this article were taken before the cardiovascularfitness test at four sites (bicep tricep subscapular andsuprailiac) using Harpenden calipers (Baty InternationalUK Shields et al 2010) but only for individuals with abody mass index under 30 kg m22
Statistical analyses
All statistical analyses were performed with the R soft-ware package version 2153 (R Development Core Team2011) Smooth fits used generalized additive models(GAM) which regress a predictor on the response andsmooth the residuals (Venables and Ripley 2002) in thepackage used for the present analyses (mgcv Wood2006) the degree of smoothness was determined by apenalized likelihood technique The result is a model thathas both linear and non-linear elements allowing a closefit to the data while also providing interpretable parame-ter estimates Where appropriate model fits were eval-uated using the Akaike Information Criterion (AIC) amaximum likelihood measure of goodness-of-fit
Exploratory models indicate sex differences in VO2maxin the Tsimane population and so each sex is modeledseparately in all analyses Because data for both popula-tions only exist for ages 11ndash69 all cross-population com-parative analyses (linear models t-tests) are limited tothis age group Age in years is included in all analysesWithin-population comparisons (linear models) use theTsimane subsample age 20 and older an age group inwhich both males and females are close to their peakVO2max and include individuals up to age 70 compara-ble to the Canadians and before the age at which optingout removed large portions of the sample For the subsam-ple between 20 and 69 females and males evidence a lin-ear decline although female VO2max is curvilinear whenall ages are considered because all within-populationcomparisons (linear models) are performed on this sub-sample age2 terms were not included Publically availableCHMS data are limited to VO2max mean and standarddeviation for age categories of variable size (for categoriessee Table 3) Cross-population comparisons use the sameage categories to explore differences between Canadiansand Tsimane
Covariates could not be included in between-populationcomparisons as the latter are based on binned data how-ever extensive individual-level Tsimane data allow fordetailed examination of factors that may mediate physicalfitness decline For these within-population linear modelswe only included participants aged 20ndash69 for whom medi-cal and anthropometric data were available during thesame medical round (about a calendar year in lengthTable 1)
To explore the possibility of a non-linear relationshipbetween mass and VO2max and how this might affectany differences between the Tsimane and Canadians we1) allometrically scaled Tsimane VO2max and 2) projectedrelative VO2max for the Tsimane using Canadian fatmass and FFM from same-sex same-age categories Toallometrically scale VO2max we calculated a the scalingparameter in allometric equations for the Tsimane(Calder 1987) To project VO2max for the Tsimaneassuming the same body composition as the Canadianswe regressed absolute VO2max on absolute fat mass abso-lute FFM and age (and age2 for the Tsimane females) inthe Tsimane female and male subsamples With theresulting parameter estimates we predicted whether Tsi-mane would perform at rates similar to those observed inour study if the Tsimane had the average fat mass andFFM exhibited in each of the four Canadian cohorts (ages12ndash19 20ndash39 40ndash59 and 60ndash79) The results of these cal-culations are discussed below Hereafter VO2max willrefer to relative VO2max unless otherwise stated
RESULTS
Age at peak VO2max and levels across the lifespan
Tsimane Predicted values of absolute (l min21) and rela-tive VO2max (ml min21 kg21) for the Tsimane appear inFigure 1 Both Tsimane females and males exhibit a peakin absolute VO2max A peak in absolute VO2max is char-acteristic across populations but appears in late adoles-cence in industrialized nations concurrent with peakabsolute FFM (Armstrong 2001) In the Tsimane as wellpeak absolute VO2max and peak absolute FFM areroughly concurrent using smoothed fits of predicted val-ues female VO2max peaks at age 31 at 295 l min21 and
TABLE 1 Descriptive statistics for the Tsimane after exclusion (ages20ndash69)
Variables
Tsimane Females Tsimane Males
Mean(and SD)or Percent n
Mean(and SD)or Percent n
Age 413 (143) 203 436 (152) 280Body weight (kg) 534 (93) 203 624 (74) 280FFM (kg) 397 (43) 203 520 (58) 280Perc FFM 075 (008) 203 084 (005) 280Distance to town in 10 km 44 (24) 196 42 (24) 273Hemoglobin 129 (14) 117 143 (12) 157Arthritis 11 133 4 185Helminths 51 92 58 128Giardia 38 92 40 128Nonarthritic Pain 54 133 75 138Respiratory Ailments 27 133 15 185Spanish-speaking Ability 17 271 42 271Pregnant 3 203 ndash ndash
Two-level factors are reported as percentage of the subsample with a givenailment
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 5
American Journal of Human Biology
absolute FFM at age 34 at 405 kg for males VO2maxpeaks at age 24 at 344 l min21 and FFM at age 29 at 544kg Estimated peak VO2max is relatively robust to thesmoothing parameter selected with the peak shifting nomore than 1 year for females and two years for malesunder different methods of smoothing Average level ofVO2max may appear higher in females but a median fitreveals that Tsimane females and males have roughlysimilar VO2max (see Supporting Information Fig S2)
Relative (ml min21 kg21) VO2max estimation controlsfor the effect of body mass (and by extension partiallycontrols for percent FFM correlation between the two forfemales r 5 2075 for males r 5 2043) Removing theeffects of body mass by using a relative measure does notremove the peaks exhibited by females or males in earlyadulthood (Fig 1) Tsimane females peak at age 28 (5379ml min21 kg21) and Tsimane males peak at age 22 (at5489 ml min21 kg21) Indeed this peak also remainswhen we scale by absolute FFM (ml min21 fat-free kg21see Supporting Information Table S2)
To evaluate whether Tsimane participants performedsimilarly under the O2 method we compared age-matched subsamples to O2 method participants Tsimanemales performed significantly worse under the HRmethod relative to the O2 method (O2 mean 5 695 mlmin21 kg21 HR mean 5 590 ml min21 kg21 t 5 629Plt 0001) There is no significant difference between Tsi-mane females tested under the HR and O2 methods (O2
mean 5 529 HR mean 5 543 t 5 2077 P 5 044) For acomparison of smooths from the two samples see Sup-porting Information Figure S3Mediators of Levels Across the Tsimane Lifespan Weidentified and investigated several health-related factorsthat might affect level of VO2max achieved by eitherdiminishing resources available to the body or hamperingthe cardiovascular system directly We posit that thesevariables may mediate the effect of age on VO2max Can-didate mediators include the presence of anemia infectionwith helminths or giardia arthritis or nonarthritic painrespiratory ailments distance from the local market
Fig 1 Predicted Tsimane VO2max by age Predicted values are drawn from GAM models regressing smooths of log age on VO2max Inter-vals are 95 prediction intervals Age was smoothed using restricted maximum likelihood Other smoothing parameters (such as Mallowrsquos Cpand maximum likelihood) varied the age at peak absolute VO2max by up to 1 year for females and up to 2 years for males Points represent theraw data for Tsimane A Absolute VO2max by age for females B Absolute VO2max by age for males C Relative VO2max by age for femalesD Relative VO2max by age for males [Color figure can be viewed in the online issue which is available at wileyonlinelibrarycom]
6 AC PISOR ET AL
American Journal of Human Biology
town and Spanish speaking ability Although percentFFM generally predicts absolute rather than relativeVO2max we test it as a potential mediator Pregnancywas included as a control in female models While a highmacroparasite load may increase the likelihood of havinglow hemoglobin (and thus anemia) an interaction termbetween presence of helminths and presence of anemiawas not included because they are not significantlyrelated in this sample only 26 participants of the 92 withhelminths have anemia while 14 of the 86 without hel-minths have anemia (for females v2 5 052 P 5 047 formales v2 5 200 P 5 016)
To evaluate whether these candidate mediators affectedVO2max levels we conducted linear regressions on rela-tive VO2max (see Table 2) We first examined each predic-tor independently Females with higher hemoglobin levelshad significantly higher cardiovascular fitness perform-ance for an increase in 1 g dl21 concentration of hemoglo-bin a Tsimane woman is predicted to have 293 ml min21
kg21 higher VO2max (t 5 268 Plt 001) Helminth infec-tion mediated the relationship between age and VO2maxfor males such that men with a helminth infection arepredicted to have 616 ml min21 kg21 higher VO2max(t 5 231 Plt 005) A best fit model approach (fit on thesubset of females for whom all measures are available)provides similar results to fitting a separate model for
each potential mediating variable When a stepwise AICprocedure was used with data on all health and marketintegration measures hemoglobin level was the only sig-nificant predictor that remained in the female model(n 5 82 standardized b 5 022 Plt 005) For males hel-minth infection remained in the model as well (n 5 116standardized b 5 023 Plt 005)
Scaling VO2max by FFM (ml min21 fat-free kg21)rather than body mass produced similar results hemoglo-bin levels remained a significant positive predictor ofVO2max for females (standardized b 5 030 Plt 001) andhelminth infection a positive predictor for males (standar-dized b 5 020 Plt005) See Supporting InformationTable S3 for all regression results with ml min21 fat-freekg21 as the outcome
Anemia was initially included in model fits howevertreating hemoglobin level as a covariate in place of pres-ence of anemia improved model fit for Tsimane females(anemia AIC 5 10027 hemoglobin AIC 5 98963)Although no association was found between presence ofanemia and helminth infection there is a significant asso-ciation between hemoglobin levels and helminth infectionControlling for age a helminth diagnosis is a significantnegative predictor of hemoglobin levels for females (stand-ardized b 5 2031 Plt 001) Replacing presence of ane-mia with hemoglobin level for males did not improve or
TABLE 3 Comparison of Tsimane and Canadian relative VO2max by age category and sex
Sex Age group
Tsimane Canadians
t-Statistic P-valueMean (ml min21 kg21) n Mean (ml min21 kg21) n
Females 11ndash14 435 7 487 534 2118 02815ndash19 476 33 423 500 310 00020ndash39 510 72 383 662 908 00040ndash59 431 69 314 655 1005 00060ndash69 412 5 242 554 340 003
Males 11ndash14 415 4 548 542 2300 00615ndash19 516 31 508 514 046 06520ndash39 511 96 442 526 527 00040ndash59 432 68 362 584 380 00060ndash69 381 26 275 546 509 000
TABLE 2 Linear models exploring whether mediators affect the level (main effects models) of relative VO2max for Tsimane females and males
Sex Candidate mediatorAge effect est
(P-value)
Main effect models
Sample sizeMediator main effect
est (P-value) Age main effect est (P-value)
Females Perc FFM 2023 (000) 000 (097) 2023 (000) 203Hemoglobin 2013 (028) 024 (001) 2011 (022) 117Helminths 2019 (007) 003 (077) 2020 (006) 92Giardia 2019 (007) 011 (028) 2019 (007) 92Lung ailment 2017 (006) 2005 (060) 2018 (005) 133Reported pain 2017 (006) 2001 (094) 2017 (006) 133Arthritis 2017 (006) 2002 (083) 2016 (007) 133Distance to town 2023 (000) 002 (081) 2023 (000) 196Spanish speaking 2023 (000) 2008 (056) 2024 (000) 197
Males Perc FFM 2037 (000) 009 (012) 2034 (000) 280Hemoglobin 2029 (000) 2002 (076) 2029 (000) 157Helminths 2030 (000) 019 (002) 2027 (000) 128Giardia 2030 (000) 006 (049) 2030 (000) 128Lung ailment 2030 (000) 2007 (033) 2031 (000) 185Reported pain 2030 (000) 011 (013) 2031 (000) 185Arthritis 2030 (000) 2006 (044) 2028 (000) 185Distance to town 2037 (000) 2003 (059) 2037 (000) 273Spanish speaking 2038 (000) 008 (050) 2037 (000) 271
All parameter estimates are standardized
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 7
American Journal of Human Biology
worsen model fit and there is no significant relationshipbetween hemoglobin levels and helminth infection formales (standardized b 5 2010 P 5 028) Parameter esti-mates for anemia were not significant in models for eitherfemales or males
Between-group Table 3 presents Tsimane and Canadianestimated VO2max binned into age categories used byCHMS These data suggest that Canadian females andmales achieve peak VO2max between the ages of 11 and14 while Tsimane males peak between ages 15 and 19Tsimane females peak later between age 20 and 39Across comparable age categories Tsimane have signifi-cantly higher VO2max than Canadians at all ages exceptbetween 11 and 15 for females and 11 and 19 for males(Table 3) However the sample size of Tsimane teenagersunder age 15 is quite small As aforementioned to controlfor the influence of a small number of data points for theyoungest and oldest Tsimane individuals we used GAMto predict VO2max across logged age Predicted valuessuggest that Tsimane females peak at age 28 and Tsimanemales peak at age 22 (see Fig 1c d) These estimates areconsistent with scatterplots of the raw data (plotted onFig 1) and mask fewer fine-grained effects of age thanTable 3 as each CHMS adult age category spans twodecades
It is possible the difference between the Tsimane andCanadians reflects a greater increase in body mass acrossages in the Canadian population or different trajectoriesof change in body composition The former could occurbecause body mass appears in the denominator and cantherefore scale down VO2max while the latter implies dif-ferential changes in FFM when FFM is a predictor ofVO2max in many studies To explore these possibilitieswe performed two calculations we allometrically scaledTsimane VO2max and we projected Tsimane VO2maxassuming the Tsimane had equivalent fat mass and FFMas Canadians from same-sex same-age categories Con-trolling for age the allometric scaling coefficient a wasslightly greater than 1 for both sexes (females a 5 111males a 5 118) This suggests that any disparity inVO2max between Canadians and the Tsimane cannot beexplained solely by mass differences Indeed assumingthe Tsimane have the same body composition as Cana-dians projected VO2max differs little from observedVO2max The Tsimane outperform the Canadians in everycohort by at least 35 ml min21 kg21 except among theyoungest males who perform similarly (see SupportingInformation Fig S4)
To control for possible disparities in changes in bodycomposition by age within each population as these mightalso influence differences between the Tsimane and Cana-dians we scaled VO2max by absolute FFM from the samepopulation to obtain ml min21 fat-free kg21 BecauseCanadian body composition data were only available viaskinfolds (bicep tricep subscapular and suprailiac) weused the subset of Tsimane (n 5 246) for which the samefour skinfolds measurements were available We calcu-lated average absolute FFM for each cohort using averageweight and average summed skinfolds (Durnin andWomersley 1974) and scaled average VO2max in mlmin21 by this number to obtain ml min21 fat-free kg21Under this method of scaling the Tsimane outperformCanadians in every cohort over age 20 by at least 165 ml
min21 fat-free kg21 (see Supporting Information TableS2) Canadian females and males in the 12ndash19 cohortsoutperform Tsimane of the same age
We next compared Tsimane to other subsistence popula-tions reported in the literature (Table 4) Consistent withcommon practice in the literature we report means foreach group but when possible we also predicted VO2maxat age 25 to provide age-corrected comparisons Weselected age 25 as it is the age of peak relative VO2max inthis study and for female Kamba and Maasai in Christen-sen et als (2012) recent study To predict VO2max at age25 we regressed the median ages on mean VO2max acrossthe available age categories Tsimane females and maleshave roughly the same predicted VO2max at age 25 asseveral other subsistence populations but higher VO2maxthan industrialized populations To test for differencesbetween industrialized and subsistence populations weconducted a linear regression on predicted VO2max at age25 this is not a meta-analysis and results should beinterpreted with caution Overall subsistence populationsdisplay higher peak VO2max than in industrialized popu-lations controlling for sex (440 vs 367 ml min21 kg21
[Plt 001]) The Tsimane O2 and indigenous Siberian sam-ples were excluded Tsimane O2 to avoid the problem ofnon-independence with Tsimane HR data and Siberiansbecause the sample has a limited age range comparedwith the other studies
Pace of decline slope of VO2max decline across thelifespan
Tsimane To evaluate whether Tsimane participants per-formed similarly under different methods we comparedage-matched subsamples of participants from the presentstudy with O2 method participants Despite a higher level(intercept) of VO2max in the O2 sample Tsimane malesdeclined marginally significantly faster under the O2
method relative to the HR method (O2 5 68 per decadeHR 5 47 decline per decade t 5 2195 P 5 005) Thereis no significant difference between Tsimane femalestested under the O2 and HR methods (O2 5 60 per dec-ade HR 5 48 decline per decade t 5 2055 P 5 058)Mediators of Slope Across the Lifespan We fit a series oflinear models to test for interactions between the candi-date mediators and age-related decline in TsimaneVO2max There are no variables that significantly inter-act with age to predict VO2max (see Supporting Informa-tion Table S4) An AIC selection approach and scaling byabsolute FFM (see Supporting Information Table S3) pro-vides the same results no variables significantly interactwith age to predict VO2max
Between-group VO2max is most often reported as a lin-ear decline across the adult lifespan though Hawkins andWiswell (2003) dispute whether the decline is actually lin-ear For example a linear approximation is not appropri-ate for Tsimane females if ages 11ndash80 are consideredFigure 2 contrasts linear declines in VO2max for Cana-dians and Tsimane males as well as a curvilinear fit forTsimane females with declines in industrialized nationsderived from meta-analyses (Fitzgerald et al 1997 Wil-son and Tanaka 2000) To explore whether rates ofdecline in VO2max among Tsimane and Canadians weredifferent we regressed average VO2max by age category
8 AC PISOR ET AL
American Journal of Human Biology
TA
BL
E4
Mea
nV
O2m
ax
esti
ma
ted
VO
2m
ax
at
age
25a
nd
dec
lin
ein
VO
2m
ax
per
dec
ad
efr
omth
isst
ud
ya
nd
pre
vio
us
rese
arc
ha
Pop
ula
tion
Fem
ale
Male
Pu
bli
cati
onM
ean
VO
2m
ax
VO
2m
ax
Age
25
bP
erce
nt
Dec
lin
eA
ge
Ran
ge
(n)
Mea
nV
O2m
ax
VO
2m
ax
Age
25
bP
erce
nt
Dec
lin
eA
ge
Ran
ge
(n)
Ind
ust
riali
zed
Can
ad
ac
312
400
73
20ndash69
(2905)
361
458
68
20ndash69
(2712)
Jap
an
d357
414
39
20ndash69
(656)
417
473
38
20ndash69
(807)
San
ad
aet
al
2007
Sw
eden
e330
g409
80
20ndash65
324
g388
75
20ndash65
Ek
blo
met
al
2007
Th
ail
an
d(i
nd
ust
ry)e
275
293
54
16ndash55
(56)
389
415
57
16ndash53
(70)
Yoo
pat
etal
2002
US
(H
erit
age)
f273
17ndash65
(360)
359
17ndash65
(293)
Sk
inn
eret
al
2003
US
(N
HA
NE
S)d
356
363
24
20ndash49
(1312)
444
438
39
20ndash49
(1481)
Su
bsi
sten
ceT
sim
an
e(H
R)c
498
521
h16
h20ndash69
471
538
h61
h20ndash69
Tsi
man
e(O
2)c
436
74
h36ndash69
540
25
h36ndash69
Ifalu
k(1
969ndash70)c
429
488
69
20ndash59
(43)
49
597
75
20ndash69
(75)
Rod
ean
dS
hep
hard
1994
Ach
ec465
434
257
20ndash59
(62)
519
614
84
20ndash59
(65)
Walk
eran
dH
ill
2003
Lu
oc378
372
39
17ndash68
(209)
429
48
54
17ndash68
(172)
Ch
rist
ense
net
al
2012
b
Kam
ba
c377
371
45
17ndash68
(283)
431
516
34
17ndash68
(94)
Ch
rist
ense
net
al
2012
Maasa
ic389
410
45
17ndash68
(178)
431
528
69
17ndash68
(163)
Ch
rist
ense
net
al
2012
Ind
igen
ous
Sib
eria
nsc
338
341
22
220ndash39
(14)
462
471
66
20ndash39
(30)
Katz
marz
yk
etal
1994
Ru
ral
Nep
alc
187
15ndash60
(39)
221
15ndash60
(35)
Pan
ter-
Bri
cket
al
1992
Ngis
onyok
aT
urk
an
af
38
387
18
20ndash44
(19)
Cu
rran
-Ever
ett
1994
aV
alu
esm
issi
ng
wh
enn
otavail
able
from
ap
art
icu
lar
stu
dy
Per
cen
td
ecli
ne
(per
cen
tof
pea
kvalu
elo
st)
per
dec
ad
ew
as
calc
ula
ted
as
by
regre
ssin
gre
lati
ve
VO
2m
ax
by
age
mu
ltip
lyin
gth
ep
ara
met
eres
tim
ate
for
age
by
10
an
dd
ivid
ing
this
nu
mber
by
the
inte
rcep
t(p
resu
med
pea
k
ass
um
ing
ali
nea
rd
ecli
ne
inV
O2m
ax
acr
oss
age)
B
ecau
seof
lack
ofacc
ess
tora
wd
ata
re
gre
ssio
ns
wer
efi
tw
ith
mea
nV
O2m
ax
an
dm
edia
nage
by
coh
ort
bA
ge
25
valu
esw
ere
esti
mate
dby
regre
ssin
gre
lati
ve
VO
2m
ax
by
age
then
usi
ng
the
resu
ltin
gp
ara
met
eres
tim
ate
sto
pre
dic
tV
O2m
ax
at
age
25
the
pea
kin
rece
ntl
yst
ud
ied
pop
ula
tion
s(e
g
Kam
ba
an
dM
aasa
ife
male
sC
hri
sten
sen
etal
2012fe
male
san
dm
ale
sin
this
art
icle
)B
ecau
seof
lack
ofacc
ess
tora
wd
ata
re
gre
ssio
ns
wer
efi
tw
ith
mea
nV
O2m
ax
an
dm
edia
nage
by
coh
ort
cS
ubm
axim
alst
epte
st
dS
ubm
axim
altr
ead
mil
lte
st
eS
ubm
axim
aler
gom
eter
test
f M
axim
al
ergom
eter
test
gS
wed
ish
data
wer
ere
por
ted
as
med
ian
sfo
rea
chage
cate
gor
yth
evalu
esre
por
ted
her
eare
mea
ns
ofth
ese
med
ian
s2006
ind
ivid
uals
part
icip
ate
dbu
tn
um
ber
by
sex
was
not
rep
orte
d
hF
orco
mp
ara
bil
ity
we
bin
ned
the
Tsi
man
eH
Ran
dO
2d
ata
into
10
yea
rage
cate
gor
ies
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 9
American Journal of Human Biology
on median age (for a given age category) population andtheir interaction term For comparability Tsimane werebinned into the Canadian age categories and averageswere computed for these categories leading to estimateddeclines slightly different from those in Table 4 for thepurposes of this test we treat the Tsimane female declineas linear Because within-population variance in declineis not available these regressions should be treated asdescriptive comparisons rather than statistical tests ofdifferences between the two groups The rate of decline inVO2max is steeper for Canadian females (69 per decadefaster decline per decade) and males (42 faster declineper decade) compared with Tsimane females and males
The rate of cardiovascular fitness decline between theTsimane and Canadians is different but this differencedoes not extend to industrialized and subsistence popula-tions (see Table 4) Controlling for sex subsistence groupshave about one quarter of a percent lower declines perdecade Again because the variance in decline is not rep-resented in this regression results should be interpretedas comparative rather than as a statistical test As beforeTsimane O2 results were not included in the analysis toavoid nonindependence and the indigenous Siberianswere excluded because of discrepancy in ages sampled
DISCUSSION
Our comparisons demonstrate that across a wide varietyof societies cardiovascular fitness senesces with age Car-diovascular fitness is higher on average among members ofsubsistence societies than among industrialized societiesbut rates of fitness decline from peak are not slower Ourmore detailed comparison between the Tsimane a subsist-ence population and Canadians an industrialized popula-tion reveals differences in cardiovascular fitness levelsand rate of fitness decline Cardiovascular fitness levelswere higher among the Tsimane than among Canadiansand the rate of decline across the lifespan was significantlyslower among Tsimane women and men Potential Cana-
dian participants were excluded due to many health con-cerns including pregnancy and history of high bloodpressure whereas Tsimane were only excluded if they self-identified as unable to participate This suggests the Cana-dian sample is a relatively healthy subsample of Canadayet the Tsimane still outperform them in cardiovascular fit-ness It may be that the higher demand for cardiovascularfitness in late ages among the Tsimane outweighs anyeffects of poor health Another possibility is that greaterself-selection among Tsimane due to higher adult mortalityleaves more robust older adult survivors thereby reducingthe observed slope of fitness decline at the population level(Vaupel et al 1979) perhaps this is partially why fewerTsimane older adults opted out of the exercise test thanCanadian older adults were screened out (ages 60ndash69Canadian females 5 56 Tsimane females 5 15 Cana-dian males 5 57 Tsimane males 5 5)
Consistent with prior research on age-related changesin cardiovascular fitness the Tsimane do evidence a lin-ear decline in VO2max with age but not as steep a declineas typically seen in industrialized populations Based oncomparisons with the Canadians and with other industri-alized populations we believe the Tsimane data from thepresent study and the pilot O2 data combined indicatethat the Tsimane perform better on tests of cardiovascularfitness than the average individual from an industrializednation
To further explore the potential effects of health factorson cardiovascular fitness level and rate of decline weinvestigated predictors of individual differences in fitnesswithin the Tsimane population Overall we found thatmost health indicators among the Tsimane did not hinderVO2max levels or rates of decline Lower hemoglobin lev-els were associated with lower VO2max levels in womenbut not men consistent with the notion that compromisedblood oxygen transport curbs cardiovascular fitness(Buzina et al 1989 Panter-Brick et al 1992) In the USlow hemoglobin is more common in active women thanactive men (Sinclair and Hinton 2005) hemoglobin is
Fig 2 Linear changes in VO2max with age for Canadians and the Tsimane Intercepts and slopes for Canadians and Tsimane can be foundin Table 4 Because age2 is significant for the full sample of Tsimane females their change in VO2max across age is curvilinear Slopes forendurance trained active and sedentary individuals from industrialized nations are drawn from a meta-analysis performed by Fitzgeraldet al (1997) for females and Wilson and Tanaka (2000) for males Endurance trained individuals are represented by the top dotted line abovefollowed by active individuals below and sedentary on the bottom Trained individuals engage in 31 sessions of endurance exercise per weekfor at least a year while active individuals engage in 2 or fewer sessions per week of cardiovascular exercise [Color figure can be viewed in theonline issue which is available at wileyonlinelibrarycom]
10 AC PISOR ET AL
American Journal of Human Biology
also lower in Tsimane women than Tsimane men(female 5 129 [sd 13] g ml21 males 5 142 [13] g ml21)Even mild (non-anemic) iron deficiencies impacts womenrsquosexercise performance (Zhu and Haas 1997) Inconsistentwith findings from Panter-Brick et al (1992) among ruralNepalese helminth infection did not diminish levels ofVO2max for Tsimane men helminth infection wasactually a predictor of higher VO2max There are severalreasons why this might be the case First we only testedwhether presence or absence of helminths mediated theeffect of age on VO2max rather than parasite load (egnumber of worms egg counts) it is possible that helminthinfection only affects VO2max at high parasite loads Sec-ond blood loss (and thus low hemoglobin levels) resultingfrom helminth infection may be partially offset by theamount of iron in the Tsimane adult diet Tsimane ironintake is an estimated 166 of the US Dietary ReferenceIntake (Martin et al 2012) and Tsimane hemoglobin lev-els are higher than in the Nepalese (females 129 vs 109males 1424 vs 120 Panter-Brick et al 1992) Thirdthese analyses consider helminth infection at the time ofexercise test rather than past infections It may be thatthe cumulative burden of past infection has a larger effecton cardiovascular fitness if so this would suggest thatthe surprising positive effect of helminth infection onVO2max levels in men is either spurious or capturing athird variable
Secular declines in VO2max are expected with increasingmarket integration and lifestyle change because ofincreased sedentism (Katzmarzyk et al 1994 Rode andShephard 1994) Two proxies for market integration in thispopulationmdashdistance to San Borja and the ability to speakSpanishmdashwere not significant predictors of VO2max levelsor decline This is consistent with our predictions as Tsi-mane females and males that live near town do not appearto have lower activity levels (Gurven et al 2013) Wageopportunities near town primarily include working asranch hands collecting and weaving palm thatch panelscash cropping and working for logging companies Each ofthese involves extensive activity furthermore transporta-tion to town often involves bicycling walking and polingdugout canoes Cash cropping of rice and corn also involvesthe clearing and weeding of larger fields Except for cashcropping and palm thatch manufacture most wage laboropportunities are currently restricted to men
This study makes several unique contributions to theexisting literature It offers the first systematic compari-son of cardiovascular fitness level and rate of declinebetween subsistence and industrialized societies Resultscompiled from previous studies support the general claimthat despite greater pathogen stress the greater activityregime of subsistence societies helps support higher peakVO2max Additionally this is one of the first studies toexplore senescent changes in cardiovascular fitnesswithin a large sample from a subsistence population Thelarge number of health measures and proxies of marketintegration available permitted testing whether these fac-tors mediated age-related variation and whether theymodulated the rate of decline Despite reports that healthstatus and market integration have been important inother studies (eg Buzina et al 1989 Katzmarzyk et al1994 Panter-Brick et al 1992 Rode and Shephard1994) their overall net effect was small among the Tsi-mane most apparent in measures of hemoglobin levelsamong women and helminth infection among men
The results of these analyses may also shed light onindividual and population level differences in chronic dis-ease In industrialized populations meta-analyses demon-strate that cardiovascular fitness is protective againstcardiovascular disease (Jette et al 1992 Hawkins andWiswell 2003) Prior studies among Tsimane suggest rel-atively few deaths from heart attacks or strokes (Gurvenet al 2007) a low prevalence of common cardiovasculardisease risk factors like obesity high blood low-densitylipoprotein levels hypertension and peripheral arterialdisease and the existence of additional protective factorslike lean diet and physical activity (Gurven et al 20092013 Vasunilashorn et al 2010) Market foods such ascooking oil sugar and pasta represent only 6 of theaverage Tsimane diet and Tsimane also consume a greatdeal of lean meat and omega-3 fatty acids (Martin et al2012) This study complements these findings by demon-strating that Tsimane show relatively high VO2max anindicator of strong cardiorespiratory health TsimaneVO2max declines with age as it does everywhere whichsuggests declining muscle mass with age (Fleg andLakatta 1988) and lowered cardiac output (American Col-lege of Sports Medicine 2006 Sagiv et al 2007) ratherthan increased cardiovascular disease risk
Limitations
The Canadians were selected as a comparison industri-alized population because of the similarity of the CHMSand Tsimane protocols very few studies of industrializedpopulations have large sample sizes sample across thelife course and use a step test Several aspects of theCHMS and Tsimane protocols remain potentially incom-parable The Canadians experienced more stringentexclusion criteria than the Tsimane meaning that the Tsi-mane sample may be more representative of cardiovascu-lar condition in the Tsimane population than theCanadian sample of the Canadian population Again ifthe Tsimane sample was subjected to these criteria wemight expect the differences in VO2max between popula-tions to only increase On the other hand Canadian par-ticipants were assigned stepping cadences based on theirage and sex and cadence was increased across the exer-cise test if a participant did not reach 85 of his or herage-specific maximal HR all Tsimane were asked to com-plete 30 ascents per minute with no increase based ontheir achieved HRs Few Tsimane reached 75 of theirage-specific maximal HR (see Supporting InformationTable S1) perhaps because the age-specific maximal HRsderived from industrialized populations are inaccurate forthe Tsimane or because higher fitness allowed these Tsi-mane to perform the step test of 30 ascents per minutewith less effort Due to these discrepancies in protocolwhich may lead to errors in estimating VO2max we alsoincorporated Tsimane data collected using the O2 methodas a check because the O2 method estimates VO2max onthe relationship between HR and VO2 in a givenparticipant
Indeed it is an open question as to whether typicalmethods for indirectly estimating cardiovascular fitnessfrom HR are appropriate for subsistence level popula-tions Common routines for VO2max estimation assumeage-specific declines in cardiovascular fitness (eg Shep-hard 1970) but these methods have only been validatedwith samples from industrialized populations which are
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 11
American Journal of Human Biology
often self-selected (Beall et al 1985) Additionally regres-sions drawn from laboratory studies require participantsachieve a HR within a certain range for accurate VO2maxestimation however the appropriateness of these rangesgiven slight modifications to protocol and inclusion of par-ticipants of different ages different populations and bothsexes is questionable For example the maximal HRexhibited by young men varies across subsistence popula-tions (Shephard 1978) Use of these criteria is compli-cated by the fact that the most commonly used equationfor estimating maximal possible HR by age 220-age maybe inaccurate (Robergs and Landwehr 2002) and particu-larly inappropriate for older adults (see Tanaka et al2001) For these reasons we chose to use an exclusion cri-terion for the Tsimane that evaluates individual increasein HR across exercise relative to the mean increase in HRfor Tsimane of the same sex and age
The pattern of Tsimane fitness decline differs moder-ately by the choice of exclusion criterion for participants(see Supporting Information Table S1) and by method oftesting However this is a common finding Lee et al(2011) predicted VO2max from submaximal exercise usingthe O2 method and the HR-based American College ofSports Medicine calculation routine in a US sample Theyfound that (1) the HR-based routine predicts higherVO2max across the sexes than does the O2 routine and(2) the two methods have a correlation of only 077 Whenevaluating different testing procedures Shephard et al(1968) found differences in VO2max estimation by type oftest used (eg bicycle ergometer versus step test) and cal-culation routine Exercise tests exclusion criteria andcalculation routines combine to provide an estimate ofactual VO2max for a given individual and as such varia-tion in estimation is to be expected However such varia-tion may affect cross-population comparisons inunforeseen ways thus the comparisons presented hereshould be interpreted with caution
While population-level variation in cardiovascular fit-ness decline may reflect the differences in the demands ofendurance-based physical activity muscularity and com-promised oxygen transport it is possible that genetic fac-tors may also play a potential role (Collins 1999) In oneindustrialized sample maternal cardiovascular fitnessexhibited a heritability of 30 which is attributed toinheritance of the maternal mitochondrial genome (Bou-chard et al 2000) We do not have the relevant geneticdata for the populations considered here however andthus operate under the simplifying assumption thatinheritance should not affect population-level patternsand will not consistently bias individual-level compari-sons in any particular direction
This study is further limited by its cross-sectionaldesign Cross-sectional data present well-known problemsfor the measurement of individual aging (Crimmins andSeeman 2001) Mortality selection in which individualsin poorer condition are likely to die at younger ages pro-duces a downward bias in the estimation of aging rates atthe individual level (Vaupel and Yashin 1985 Vaupelet al 1979) Cohort effects if present also produce com-plicated and non-monotonic biases in estimation (Carnesand Olshansky 2001) Due to the problem of between-individual heterogeneity and the within-individual pro-cess of senescence a recent overview of aging studies con-cludes that ldquoonly longitudinal studies [ ] provide reliablesources of information in the study of senescencerdquo (Nussey
et al 2008) To date there are no longitudinal studies ofcardiovascular fitness in subsistence populations We arecurrently re-testing participants under the O2 methodallowing a better grasp of the within-individual variationthat shapes patterns of senescent decline
ACKNOWLEDGMENTS
The authors thank Paul Hooper Steven Gaulin JohnTooby Patricia Kramer the Human Evolution and Biode-mography laboratory and the Center for EvolutionaryPsychology at UCSB for helpful advice and feedback thestaff at the Tsimane Health and Life History Project andthe Tsimane for their participation and patience
LITERATURE CITED
American College of Sports Medicine 2006 ACSMrsquos Guidelines for Exer-cise Testing and Prescription 7th ed Philadelphia Lippincott Williamsamp Wilkins
Armstrong N 2001 Peak oxygen uptake in relation to growth and matura-tion in 11- to 17-year-old humans Eur J Appl Physiol 85546ndash551
Astrand PO Ryhming I 1954 A nomogram for calculation of aerobiccapacity (physical fitness) from pulse rate during submaximal work JAppl Physiol 7218ndash221
Bailey DA Shephard RJ Mirwald RL 1976 Validation of a self-administered home test of cardio-respiratory fitness Can J Appl SportSci 167ndash78
Beall CM Goldstein MC and Feldman ES 1985 The physical fitness ofelderly Nepalese farmers residing in rugged mountain and flat terrainJ Gerontol 40529ndash535
Benefice E Ndiaye G 2005 Relationships between anthropometry cardi-orespiratory fitness indices and physical activity levels in different ageand sex groups in rural Senegal (West Africa) Ann Hum Biol 32366ndash382 Available from httpwwwncbinlmnihgovpubmed16099780
Blackwell AD Gurven MD Sugiyama LS Madimenos FC Liebert MAMartin MA Kaplan HS Snodgrass JJ 2011 Evidence for a peak shift in ahumoral response to helminths age profiles of IgE in the Shuar of Ecuadorthe Tsimane of Bolivia and the US NHANES PLoS Negl Trop Dis 5e1218 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid53125146amptool5pmcentrezamprendertype5abstract
Blackwell AD Martin M Kaplan H Gurven M Evidence for an antagonis-tic relationship between Giardia lamblia and helminth infections impli-cations for treatment of helminth infections in developing populations
Blair SN LaMonte MJ Nichaman MZ 2004 The evolution of physicalactivity recommendations how much is enough Am J Clin Nutr 79913Sndash920S Available at httpwwwncbinlmnihgovpubmed15113739
Bouchard C Rankinen T Chagnon YC Rice T Perusse L Gagnon JBorecki I An P Leon a S et al 2000 Genomic scan for maximal oxygenuptake and its response to training in the HERITAGE Family Study JAppl Physiol 88551ndash559 Available at httpwwwncbinlmnihgovpubmed10658022
Bryan S St-Denis M Wojtas D 2007 Canadian Health Measures Surveyclinic operations and logistics Health Rep 1853ndash69
Buzina R Bates CJ van der Beek J Brubacher G Chandra RK HallbergL Heseker J Mertz W Pietrzik K et al 1989 Workshop on FunctionalSignificance of Mild-to-Moderate Malnutrition Am J Clin Nutrition 50172ndash176
Calder WA 1987 Scaling energetics of homeothermic vertebrates anoperational allometry Annu Rev Physiol 49107ndash120
Canadian Society for Exercise Physiology 2003 The Canadian PhysicalActivity Fitness amp Lifestyle Approach (CPAFLA) CSEP-Health amp Fit-ness Programrsquos Health-Related Appraisal and Counselling Strategy 3rded
Carnes BA Olshansky SJ 2001 Heterogeneity and its biodemographicimplications for longevity and mortality Exp Gerontol 36419ndash430Available at httpwwwncbinlmnihgovpubmed11250115
Carrick-Ranson G Hastings JL Bhella PS Shibata S Fujimoto N PalmerD Boyd K Levine BD 2013 The effect of age-related differences inbody size and composition on cardiovascular determinants of VO2max JGerontol A Biol Sci Med Sci 68608ndash616 Available at httpwwwncbinlmnihgovpubmed23160363
Centers for Disease Control and Prevention 1998 Recommendations toPrevent and Control Iron Deficiency in the United States MMWRRecomm Rep 471ndash36 Available at httpwwwcdcgovmmwrpreviewmmwrhtml00051880htm
12 AC PISOR ET AL
American Journal of Human Biology
Centers for Disease Control and Prevention 2011 Glossary of TermsPhysical Activity for Everyone [Internet] Available from httpwwwcdcgovphysicalactivityeveryoneglossary
Christensen DL Faurholt-Jepsen D Boit MK Mwaniki DL Kilonzo BTetens I Kiplamai FK Cheruiyot SC Friis H et al 2012 Cardiorespira-tory fitness and physical activity in Luo Kamba and Maasai of ruralKenya Am J Hum Biol 24723ndash729 Available at httpwwwncbinlm-nihgovpubmed22836508
Colley RC Garriguet D Janssen I Craig CL Clarke J Tremblay MS2011a Physical activity of Canadian children and youth accelerometerresults from the 2007 to 2009 Canadian Health Measures SurveyHealth Rep 2215ndash23
Colley RC Garriguet D Janssen I Craig CL Clarke J Tremblay MS2011b Physical activity of Canadian adults accelerometer results fromthe 2007 to 2009 Canadian Health Measures Survey Health Rep 227ndash14 Available at httpwwwncbinlmnihgovpubmed21510585
Collins KJ 1999 Physiological variation and adaptability in human popu-lations Ann Hum Biol 2619ndash38
Crimmins E Seeman T 2001 Integrating Biology into DemographicResearch on Health and Aging (With a Focus on the MacArthur Study ofSuccessful Aging) Cells and Surveys Should Biological Measures beIncluded in Social Science Research Washington DC National Acad-emy Press p 9ndash41
Curran-Everett LS 1994 Accordance Between VO2max and Behavior inNgisonyoka Turkana Am J Hum Biol 6761ndash771
Durnin JVGA Womersley J 1974 Body fat assessed from total body den-sity and its estimation from skinfold thickness measurements on 481men and women aged from 16 to 72 years Br J Nutr 3277ndash97
Eberl M Al-Sherbiny M Hagan P Ljubojevic S Thomas AW Wilson RA2002 A novel and sensitive method to monitor helminth infections byfaecal sampling Acta Trop 83183ndash187
Eid D Gurven M Kaplan H Winking J 2007 Enfermedades infecciosas alo largo de la vida y en el envejecimiento en indıgenas sudamericanos dela etnia Tsimane Aging in Developing Countries Building Bridges forIntegrated Research Agendas Santiago Chile
Ekblom B Engstreuroom L-M Ekblom O 2007 Secular trends of physical fit-ness in Swedish adults Scand J Med Sci Sports 17267ndash273 Availableat httpwwwncbinlmnihgovpubmed17501867
Finch CA Lenfant C 1972 Oxygen Transport in Man N Engl J Med 286407ndash415
Fitzgerald MD Tanaka H Tran ZV Seals DR 1997 Age-related declinesin maximal aerobic capacity in regularly exercising vs sedentarywomen a meta-analysis J Appl Physiol (Bethesda Md 1985) 83160ndash165 Available at httpwwwncbinlmnihgovpubmed9216959
Fleg JL Lakatta EG 1988 Role of muscle loss in the age-associated reduc-tion in VO2max J Appl Physiol 651147ndash1151
Frisancho AR Frisancho HG Milotich M Brutsaert T Albalak RSpielvogel H Villena M Vargas E Soria R 1995 Developmentalgenetic and environmental components of aerobic capacity at high alti-tude Am J Phys Anthropol 96431ndash442 Available at httpwwwncbinlmnihgovpubmed7604895
Giroux S 2007 Canadian health measures survey sampling strategyoverview Health Rep 1831ndash36
Gurven M Jaeggi A V Kaplan H Cummings D 2013 Physical activityand modernization among Bolivian Amerindians PLoS ONE 81ndash13
Gurven M Kaplan H Winking J Rodriguez DE Vasunilashorn S KimJK Finch C Crimmins E 2009 Inflammation and infection do not pro-mote arterial aging and cardiovascular disease risk factors among leanhorticulturalists PLoS ONE 41ndash12
Haidet GC 1989 Dynamic exercise in senescent beagles oxygen consump-tion and hemodynamic responses The Am J Physiol 257H1428ndash1437Available at httpwwwncbinlmnihgovpubmed2589499
Hawkins S Wiswell R 2003 Rate and mechanism of maximal oxygen con-sumption decline with aging implications for exercise training SportsMed 33877ndash888 Available at httpwwwncbinlmnihgovpubmed12974656
Hoffman J 2002 Physiological aspects of sport training and performance1st ed Champaign IL Human Kinetics Publishers
Hotez PJ Bottazzi ME Franco-Paredes C Ault SK Periago MR 2008 Theneglected tropical diseases of Latin America and the Caribbean a review ofdisease burden and distribution and a roadmap for control and eliminationPLoS Negl Trop Dis 2e300 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid52553488amptool5pmcentrezamprendertype5abstract
Howley ET Bassett DR Welch HG 1995 Criteria for maximal oxygenuptake review and commentary Med Sci Sports Exerc 271292ndash1301Available at httpwwwncbinlmnihgovpubmed8531628
Jette M Sidney K Quenneville J Landry F 1992 Relation between cardi-orespiratory fitness and selected risk factors for coronary heart diseasein a population of Canadian men and women CMAJ 1461353ndash1360Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid51488567amptool5pmcentrezamprendertype5abstract
Katzmarzyk PT Leonard WR Crawford MH 1994 Predicted maximaloxygen consumption of Indigenous Siberians Am J Hum Biol 6783ndash790
King CH Dickman K Tisch DJ 2005 Reassessment of the cost of chronichelmintic infection a meta-analysis of disability-related outcomes inendemic schistosomiasis Lancet 3651561ndash1569 Available at httpwwwncbinlmnihgovpubmed15866310
Lee J-M Bassett D Jr Thompson D Fitzhugh E 2011 Validation of thecosmed fitmate for predicting maximal oxygen consumption J StrengthCond Res 252573ndash2579
Madimenos FC Snodgrass JJ Blackwell AD Liebert MA Sugiyama LS2011 Physical activity in an indigenous Ecuadorian forager-horticulturalist population as measured using accelerometry Am J HumBiol 23488ndash497 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid53110644amptool5pmcentrezamprendertype5abstract
Malina RM 2001 Physical activity and fitness pathways from childhoodto adulthood Am J Hum Biol 13162ndash172 Available at httpwwwncbinlmnihgovpubmed11460860
Malina RM Little BB 2008 Physical activity the present in the contextof the past Am J Hum Biol 20373ndash391 Available at httpwwwncbinlmnihgovpubmed18433002
Manning JT Morris L Caswell N 2007 Endurance running and digitratio (2D 4D) implications for fetal testosterone effects on runningspeed and vascular health Am J Hum Biol 19416ndash421
Martin Ma Lassek WD Gaulin SJC Evans RW Woo JG Geraghty SRDavidson BS Morrow AL Kaplan HS et al 2012 Fatty acid composi-tion in the mature milk of Bolivian forager-horticulturalists controlledcomparisons with a US sample Matern Child Nutr 8404ndash418 Availableat httpwwwncbinlmnihgovpubmed22624983
National Health and Nutrition Examination Survey 2004 CardiovascularFitness Procedures Manual
Nussey D Coulson T Festa-Bianchet M Gaillard J-M 2008 Measuringsenescence in wild animal populations towards a longitudinal approachFunction Ecol 22393ndash406
Ogawa T Spina RJ Martin WHI Kohrt WM Schechtman KB HolloszyJO Ehsani AA 1992 Effects of aging sex and physical training cardio-vascular responses to exercise Circulation 86494ndash503
Panter-Brick C Miller UG Eggerman M 1992 Hemoglobin levels andstep test performance of men and women in Nepal Am J Hum Biol 4481ndash491
Pontzer H Raichlen Da Wood BM Mabulla AZP Racette SB MarloweFW 2012 Hunter-gatherer energetics and human obesity PLoS ONE 7e40503 Available at httpcdxplosorg101371journalpone0040503
R Development Core Team 2011 R A language and environment for sta-tistical computing R Development Core Team
Rigby R Stasinopoulos D 2005 Generalize additive models for locationscale and shape (with discussion) Appl Stat 54507ndash554
Robergs RA Landwehr R 2002 The surprising history of theldquoHRmax5220-agerdquo equation J Exerc Physiol 51ndash10
Rode A Shephard RJ 1994 Physiological consequences of acculturation a20-year study of fitness in an Inuit community Eur J Appl Physiol 69516ndash524
Rowland TW Boyajian A 1995 Aerobic response to endurance training inchildren Pediatrics 96654ndash658
Sagiv M Ben-sira D Amir R 2007 What maintains energy supply atpeak aerobic exercise in trained and untrained older men Gerontology53357ndash361
Sanada K Kuchiki T Miyachi M Mcgrath K Higuchi M Ebashi H 2007Effects of age on ventilatory threshold and peak oxygen uptake normal-ised for regional skeletal muscle mass in Japanese men and womenaged 20 ndash 80 years Eur J Appl Physiol 99475ndash483
Schniter E 2009 Why Old Age Non-Material Contributions and Patternsof Aging Among Older Adult Tsimanersquo 607
Shahnawaz H 1978 Influence of limb length on a stepping exercise JAppl Physiol 44346ndash349
Shephard RJ 1970 Computer programs for solution of the Astrand nomo-gram and the calculation of body surface area J Sports Med 10206ndash210
Shephard RJ Allen C Benade AJS Davies CT Di Prampero PE HedmanR Merriman JE Myhre K Simmons R 1968 Standardization of sub-maximal exercise tests Bull World Health Organ 38765ndash775 Availableat httpwwwpubmedcentralnihgovarticlerenderfcgiartid52554690amptool5pmcentrezamprendertype5abstract
Shephard RJ Bailey Da Mirwald RL 1976 Development of the CanadianHome Fitness Test Can Med Assoc J 114675ndash679 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid51956906amptool5pmcentrezamprendertype5abstract
Shields M Tremblay MS Laviolette M Craig CL Janssen I Gorber SC2010 Fitness of Canadian adults results from the 2007ndash2009 canadianhealth measures survey Health Rep 2121ndash35 Available at httpwwwncbinlmnihgovpubmed20426224
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 13
American Journal of Human Biology
Siconolfi SF Garber CE Lasater TM Carleton RA 1985 A simple validstep test for estimating maximal oxygen uptake in epidemiologic stud-ies Am J Epidemiol 121382ndash390 Available at httpwwwncbinlm-nihgovpubmed4014128
Sinclair LM Hinton PS 2005 Prevalence of iron deficiency with and with-out anemia in recreationally active men and women J Am Diet Assoc105975ndash978 Available from httpwwwncbinlmnihgovpubmed15942552
Skinner JS Gaskill SE Rankinen T Leon AS Rao DC Wilmore JHBouchard C 2003 Heart rate versus VO2max age sex race initial fit-ness and training response-HERITAGE Med Sci Sports Exerc 351908ndash1913 Available at httpwwwncbinlmnihgovpubmed14600558
Sondik EJ Madans JH Gentlemand JF 2012 Summary health statisticsfor US adults National Health Interview Survey 2010 Vital Health Stat101ndash80 Available at httpwwwncbinlmnihgovpubmed20687424
Stones MJ Kozma A 1985 Physical performance Aging and Human Per-formance New York Wiley p 261ndash292
Tanaka H Monahan KD Seals DR 2001 Age-predicted maximal heartrate revisited J Am Coll Cardiol] 37153ndash156 Available at httpwwwncbinlmnihgovpubmed11153730
Vasunilashorn S Crimmins EM Kim JK Winking J Gurven M KaplanH Finch CE 2010 Blood lipids infection and inflammatory markers inthe Tsimane of Bolivia Am J Hum Biol 22731ndash740 Available at httpwwwncbinlmnihgovpubmed20721985
Vaupel JV Manton KG Stallard E 1979 The impact of heterogeneity inindividual frailty on the dynamics of mortality Demography 16439ndash454
Vaupel JW Yashin AI 1985 Heterogeneityrsquos ruses some surprising effectsof selection on population dynamics Am Stat 39176ndash185
Venables WN Ripley BD 2002 Modern Applied Statistics with S FourthNew York Springer
Wagner PD 1996 Determinants of maximal oxygen transport and utiliza-tion Annu Rev Physiol 5821ndash50 Available at httpwwwncbinlmnih-govpubmed8815793
Walker A Arent SM McKeever KH 2010 Maximal aerobic capacity(VO2max) in horses a retrospective study to identify the age-relateddecline Comparative Exerc Physiol 6177ndash181 Available at httpwwwjournalscambridgeorgabstract_S1755254010000073
Walker R Hill K 2003 Modeling growth and senescence in physical per-formance among the Ache of Eastern Paraguay Am J Hum Biol 208196ndash208
Weller IM Thomas SG Corey PN Cox MH 1993 Prediction of maximaloxygen uptake from a modified Canadian aerobic fitness test Can JAppl Physiol 18175ndash188 Available at httpwwwncbinlmnihgovpubmed8513290
Wilson TM Tanaka H 2000 Meta-analysis of the age-associated declinein maximal aerobic capacity in men relation to training status Am JPhysiol Heart Circ Physiol 278H829ndash834 Available at httpwwwncbinlmnihgovpubmed10710351
Wood SN 2006 Generalized Additive Models An Introduction with RBoca Raton Florida Chapman and HallCRC Press
World Health Organization 2001 Iron deficiency anaemia assessmentprevention and control a guide for programme managers Available athttpwhqlibdocwhointhq2001WHO_NHD_013pdf
Yoopat P Toicharoen P Boontong S Glinsukon T Vanwonterghem KLouhevaara V 2002 Cardiorespiratory capacity of Thai workers in dif-ferent age and job categories J Physiol Anthropol Appl Hum Sci 21121ndash128 Available at httpwwwncbinlmnihgovpubmed12056179
Zhu YI Haas JD 1997 Iron depletion without anemia and physical per-formance in young women Am J Clin Nutr 66334ndash341 Available athttpwwwncbinlmnihgovpubmed9250112
14 AC PISOR ET AL
American Journal of Human Biology

(volume O2 or VO2) is calculated as the differencebetween the percentages of oxygen in inhaled (about 21)and exhaled gases multiplied by the volume of gasexhaled (Howley et al 1995) Maximal oxygen uptake(VO2max) refers to the peak oxygen uptake possible for agiven individual achieved during exercise to exhaustionBecause exercise to exhaustion can be potentially danger-ous in individuals with significant underlying cardiovas-cular disease VO2max is often estimated at asubmaximal level of exercise (eg 85 of age-specificmaximal heart rate HR) Additionally the use of a gascollection bag can be inconvenient or expensive for fieldand large scale projects (eg Shephard 1970) For thesereasons estimation of VO2max from a participantrsquos sub-maximal heart rate is often employed (eg Astrand andRyhming 1954) HR estimation methods were used forthe Canadian and Tsimane samples although only in thecase of the Canadians was the routine for calculatingVO2max derived from laboratory studies with the samepopulation
Study populations
Tsimane The Tsimane are a forager-horticulturalistgroup living in the Bolivian Amazon The Tsimane have apopulation of 11000 spanning 901 villages ranging insize from 40 to 550 individuals Villages near the localtown (San Borja population 24000) or near roads havemore extensive market access and greater participation inwage labor Although PALs are often predicted to declinewith market integration Tsimane women and men livingnear the local town are not less active than Tsimane fromother regions perhaps because of the physical activityrequired in wage labor (eg logging and cash croppingGurven et al 2013) Men in all regions have higher PALsthan women although menrsquos activity exhibits more sea-sonal variation Aging Tsimane remain active (Gurvenet al 2013) although these individuals may engage inless physically demanding subsistence activities becauseof increases in infirmity with age (Schniter 2009)
Tsimane data were collected as part of the TsimaneHealth and Life History Project (THLHP httpwwwun-medutsimane) from 2002ndash2010 Patients were seen byTHLHP physicians either during annual visits to villagesor at the THLHP medical office in San Borja Self-reported ailments were considered together with physicalexamination fecal and blood test results to assist in diag-nosis and treatment Sampling procedures for the exercisetest were designed to ensure a sample representative ofthe Tsimane population Participantsrsquo ages range from 10to 88 years old (n 5 766 55 female)
Pretest exclusion Tsimane Tsimane participants werenot automatically excluded from the study for having aparticular condition but any complaints or conditionswere recorded Our study protocol did not exclude partici-pants for any reason However some individuals whojudged themselves unable to participate or who experi-enced discomfort during exercise opted out The mostcommon reason given by participants for opting out waspain although this was rare (65 total excluded remainingn 5 701) Nonparticipation rates in this population werebelow 10 until after age 70 (Supporting Information FigS1) Although frailty may have constrained participation
at late ages the final sample below age 70 includes Tsi-mane at various levels of health and ability allowing us tobetter explore the correlates of fitness decline (eg paininfection) in this population Pregnant and lactatingwomen were included in the Tsimane sample as womenare pregnant or lactating for much of their adult lives
Experimental protocol Tsimane Participants were askedto complete a modified submaximal Harvard step test(Astrand and Ryhming 1954) at a bench height of 20 cmfor 5 min at 30 ascents per minute (Walker and Hill2003) The pace of stepping was recorded for each partici-pant regardless of whether the participant attained 30steps per minute VO2max was estimated using Shep-hardrsquos (1970) HR-based calculation routine for step testsWe first estimated VO2 with the following equation
E 979 3 W 3 H 3 Neth THORNL
1 kcal
4184 Joules 1 ml O2
200 kcal(1)
where W is weight in kilograms H is the step height inmeters N is number of ascents during the exercise testand L is the length of the test in minutes The conversionfactor adjusts for the efficiency of stepping Stepping isabout 16 efficientmdashonly 16 of the work done duringstepping contributes to vertical displacement (Shephardet al 1976)mdashand thus work done must be multiplied by669 (Shephard 1970) to account for the amount of effortrequired by participants The work (in Joules) required tocomplete the exercise test was calculated as 979 ms2 W xH x N where 979 ms2 is the acceleration due to gravity(Powers and Howley 2009) Kilocalories per minute weredivided by 200 to convert kilocalories to mlmin of O2
(ACSM 2006)Equations for estimating VO2max from submaximal
VO2 at peak HR during the test (P taken to be the lastminute of exercise) were drawn from Shephard (1970)These are based on age and sex specific regressions thatrely on assumptions about maximal HR by age
Females EethVO 2maxTHORN5 VO 2 198272eth THORNP272
1 VO 2max
00114age 1077 1
kg
(2a)
Males EethVO 2maxTHORN5 VO 2 198261eth THORNP261
1 VO 2max
00137age 10668 1
kg
(2b)
The estimates of VO2max produced by Eqs 2ab are inunits of ml of oxygen per minute per kilogram (ml min21
kg21) also called relative VO2max Another common mea-sure of VO2max absolute VO2max (l min21) was calcu-lated by multiplying VO2max in l min21 kg21 byparticipant body weight
Post-test exclusion Tsimane The Shepard equations forestimating VO2max depend on individuals achieving aheart rate within a certain range 120ndash172 for femalesand 122ndash170 for males Typical protocols call for excluding
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 3
American Journal of Human Biology
individuals who do not meet this level However manyTsimane (55 of females 81 of males) did not achievethis criterion either because the age-specific maximalHRs derived from industrialized populations are inaccu-rate for the Tsimane or because higher fitness allowedthese Tsimane to perform the step test with less effort Wetherefore evaluated several exclusion criteria for the Tsi-mane sample including the HR range specified by Shep-hard (1970) for the calculation routine a HR increase oflt5 beats per minute during exercise (National Healthand Nutrition Examination Survey 2004) different per-centages [65 (Siconolfi et al 1985) 70 (American Collegeof Sports Medicine 2006 Canadian Society for ExercisePhysiology 2003) 75 (NHANES 2004)] of age-specificmaximal HR (Tanaka et al 2001) achieved the 95th cen-tile obtained from a Generalized Additive Model for Loca-tion Scale and Shape (Rigby and Stasinopoulos 2005)and a rate of HR increase from the beginning to the end ofexercise that is beyond the 95 confidence interval (CI)from the 20 year age- and sex-specific mean The samplesize remaining after these exclusions varies from 4(75 of age-specific maximal HR) to 79 (increase lt5beats per minute during exercise) of our original sample(for sample sizes under each criterion considered see Sup-porting Information Table S1) We interpreted exclusioncriteria that excluded the vast majority of participants asnot giving a representative sample of the Tsimane Theuse of centiles or CIs enables us to compare each partici-pant against a metric from the same population Becausethe centile and CI approaches led to about the same rela-tively small number of participants excluded we adoptedthe CI exclusion for ease of interpretation
To evaluate the accuracy of HR estimation for the Tsi-mane population we compare VO2max estimated fromHR with VO2max estimated from the ratio of inhaled toexhaled O2 collected in a smaller subset of Tsimane Anadditional strength of the O2 method is that the VO2 andHR measured for a given individual is extrapolated to pre-dict their VO2max at their predicted age-specific maximalHR without reliance on additional assumptions beyondthat of an age-specific maximal HR Methods used in O2
measurement are described in the Supporting Informa-tion (Appendix A)
Tsimane model covariates Fat-free mass (FFM) was esti-mated by subtracting body fat mass from total mass Bodyfat percentage was estimated with bioimpedance using aportable Tanita scale and with skinfold measurementtaken at four sites (bicep tricep subscapular suprailiac)body fat percentage was estimated from skinfold measure-ment with equations from Durnin and Womersley (1974)Arthritis and respiratory ailments were diagnosed byTHLHP physicians during routine medical exams Hemo-globin levels in g dl21 were attained using the QBC Auto-read Plus Dry Hematology System (QBC DiagnosticsPort Matilda PA) anemia was defined using Centers forDisease Control (CDC) criteria (CDC 1998) and for agesfor which CDC criteria were not available World HealthOrganization (2001) criteria Helminth and giardia infec-tions were diagnosed in wet slide mounts and using amodified Percoll technique as has been previouslydescribed (Blackwell et al 2011 Eberl et al 2002) Wecoded helminth infection as bivariate (presence or absenceof helminths) combining diagnoses with hookworm
roundworm (Ascaris lumbricoides and Strongyloides ster-coralis) and whipworm (Trichuris trichiura) Because ofan established relationship between helminth infectionand anemia helminths and giardia are considered sepa-rately in this analyses Self-reported pain was included asa binary measure indexing the presence of back kneebone or connective tissue pain Spanish-speaking abilitywas treated as dichotomous where individuals rated asspeaking more than ldquosomerdquo Spanish by THLHP projectstaff were considered Spanish speakers Additional cova-riates include pregnancy status and as-the-crow-flies dis-tance of home village to the market town of San Borja
Because of a concern that leg length relative to benchheight may affect performance during step tests (Shahna-waz 1978) we considered including leg length in allwithin-population regressions Leg length was calculatedby subtracting participant seated height (minus chairheight) from standing height Including leg length wors-ened model fits perhaps because mass and leg length aremoderately correlated (for females Pearsonrsquos r 5 042 formales r 5 041) and mass is already controlled for by ouruse of relative (rather than absolute) VO2max addition-ally use of the leg length variable eliminated participantsfor whom seated height data were unavailable As suchwe decided to not control for leg length in the analysesbelow
Canadian health measures survey Canadian fitness datawere collected during the first wave of the CanadianHealth Measures Survey (CHMS wwwstatcangccaimdb-bmdi5071-enghtm) from 2007 to 2009 Canadianswere selected as a comparison group since VO2max in theCHMS was assessed using a step test procedure withVO2max estimated based on HR Individuals weresampled with the goal of representing 97 of the Cana-dian population from all provinces (Giroux 2007) Asmeasured with tri-axial accelerometers Canadian chil-dren in this sample are sedentary for 64 of their wakinghours (Colley et al 2011a) adult (ages 20ndash79) females aresedentary for 69 of the day and adult males are seden-tary for 68 (Colley et al 2011b)
Pretest exclusion CHMS CHMS participants wereexcluded from fitness testing if they had a heart conditionchest pain high blood pressure (systolic blood pressurehigher than 144) or heart rate (higher than 100) or weretaking medication for any of these conditions (Bryan et al2007) across all ages a total of 267 of potential partici-pants were excluded including 56 of 60ndash69 year olds(Shields et al 2010) Participants who experienced discom-fort during testing could stop at any time Women morethan 12 weeks pregnant were not allowed to participate
Experimental protocol CHMS Participants completed astep test developed by Bailey et al (1976 modified byWeller et al 1993) on a bench with two steps each 203cm tall Individuals began stepping at a rate expected torequire 65ndash70 of VO2max for a same-sex individual 10years their senior (Canadian Society for Exercise Physiol-ogy 2003) After a 3 min exercise interval researchersmeasured HR to ascertain whether the participant hadachieved 85 of his or her age-specific maximal HR If
4 AC PISOR ET AL
American Journal of Human Biology
85 of maximal HR was reached exercise testing wasstopped if 85 of maximal HR was not reached partici-pants proceeded to the next stage of exercise stepping ata faster cadence
VO2max was estimated using a regression equationdeveloped by Weller et al (1993)
E VO2maxeth THORN532116a2024b2017c (3)
where a is the estimated VO2 at the end of the finalstage of exercise (Weller et al 1993) b is age in yearsand c is body weight in kg If a participant could not stepat the prescribed cadence during a given stage of exerciseVO2max was estimated based on the last completed exer-cise stage (Shields et al 2010) About 1 of participantseligible for the test did not complete it Participants didnot proceed beyond the eighth level of exercise regardlessof whether they had attained 85 of their age-specificmaximal HR The result is estimated relative VO2max (mlmin21 kg21)
Skinfold measurements used to calculate absoluteFFM in this article were taken before the cardiovascularfitness test at four sites (bicep tricep subscapular andsuprailiac) using Harpenden calipers (Baty InternationalUK Shields et al 2010) but only for individuals with abody mass index under 30 kg m22
Statistical analyses
All statistical analyses were performed with the R soft-ware package version 2153 (R Development Core Team2011) Smooth fits used generalized additive models(GAM) which regress a predictor on the response andsmooth the residuals (Venables and Ripley 2002) in thepackage used for the present analyses (mgcv Wood2006) the degree of smoothness was determined by apenalized likelihood technique The result is a model thathas both linear and non-linear elements allowing a closefit to the data while also providing interpretable parame-ter estimates Where appropriate model fits were eval-uated using the Akaike Information Criterion (AIC) amaximum likelihood measure of goodness-of-fit
Exploratory models indicate sex differences in VO2maxin the Tsimane population and so each sex is modeledseparately in all analyses Because data for both popula-tions only exist for ages 11ndash69 all cross-population com-parative analyses (linear models t-tests) are limited tothis age group Age in years is included in all analysesWithin-population comparisons (linear models) use theTsimane subsample age 20 and older an age group inwhich both males and females are close to their peakVO2max and include individuals up to age 70 compara-ble to the Canadians and before the age at which optingout removed large portions of the sample For the subsam-ple between 20 and 69 females and males evidence a lin-ear decline although female VO2max is curvilinear whenall ages are considered because all within-populationcomparisons (linear models) are performed on this sub-sample age2 terms were not included Publically availableCHMS data are limited to VO2max mean and standarddeviation for age categories of variable size (for categoriessee Table 3) Cross-population comparisons use the sameage categories to explore differences between Canadiansand Tsimane
Covariates could not be included in between-populationcomparisons as the latter are based on binned data how-ever extensive individual-level Tsimane data allow fordetailed examination of factors that may mediate physicalfitness decline For these within-population linear modelswe only included participants aged 20ndash69 for whom medi-cal and anthropometric data were available during thesame medical round (about a calendar year in lengthTable 1)
To explore the possibility of a non-linear relationshipbetween mass and VO2max and how this might affectany differences between the Tsimane and Canadians we1) allometrically scaled Tsimane VO2max and 2) projectedrelative VO2max for the Tsimane using Canadian fatmass and FFM from same-sex same-age categories Toallometrically scale VO2max we calculated a the scalingparameter in allometric equations for the Tsimane(Calder 1987) To project VO2max for the Tsimaneassuming the same body composition as the Canadianswe regressed absolute VO2max on absolute fat mass abso-lute FFM and age (and age2 for the Tsimane females) inthe Tsimane female and male subsamples With theresulting parameter estimates we predicted whether Tsi-mane would perform at rates similar to those observed inour study if the Tsimane had the average fat mass andFFM exhibited in each of the four Canadian cohorts (ages12ndash19 20ndash39 40ndash59 and 60ndash79) The results of these cal-culations are discussed below Hereafter VO2max willrefer to relative VO2max unless otherwise stated
RESULTS
Age at peak VO2max and levels across the lifespan
Tsimane Predicted values of absolute (l min21) and rela-tive VO2max (ml min21 kg21) for the Tsimane appear inFigure 1 Both Tsimane females and males exhibit a peakin absolute VO2max A peak in absolute VO2max is char-acteristic across populations but appears in late adoles-cence in industrialized nations concurrent with peakabsolute FFM (Armstrong 2001) In the Tsimane as wellpeak absolute VO2max and peak absolute FFM areroughly concurrent using smoothed fits of predicted val-ues female VO2max peaks at age 31 at 295 l min21 and
TABLE 1 Descriptive statistics for the Tsimane after exclusion (ages20ndash69)
Variables
Tsimane Females Tsimane Males
Mean(and SD)or Percent n
Mean(and SD)or Percent n
Age 413 (143) 203 436 (152) 280Body weight (kg) 534 (93) 203 624 (74) 280FFM (kg) 397 (43) 203 520 (58) 280Perc FFM 075 (008) 203 084 (005) 280Distance to town in 10 km 44 (24) 196 42 (24) 273Hemoglobin 129 (14) 117 143 (12) 157Arthritis 11 133 4 185Helminths 51 92 58 128Giardia 38 92 40 128Nonarthritic Pain 54 133 75 138Respiratory Ailments 27 133 15 185Spanish-speaking Ability 17 271 42 271Pregnant 3 203 ndash ndash
Two-level factors are reported as percentage of the subsample with a givenailment
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 5
American Journal of Human Biology
absolute FFM at age 34 at 405 kg for males VO2maxpeaks at age 24 at 344 l min21 and FFM at age 29 at 544kg Estimated peak VO2max is relatively robust to thesmoothing parameter selected with the peak shifting nomore than 1 year for females and two years for malesunder different methods of smoothing Average level ofVO2max may appear higher in females but a median fitreveals that Tsimane females and males have roughlysimilar VO2max (see Supporting Information Fig S2)
Relative (ml min21 kg21) VO2max estimation controlsfor the effect of body mass (and by extension partiallycontrols for percent FFM correlation between the two forfemales r 5 2075 for males r 5 2043) Removing theeffects of body mass by using a relative measure does notremove the peaks exhibited by females or males in earlyadulthood (Fig 1) Tsimane females peak at age 28 (5379ml min21 kg21) and Tsimane males peak at age 22 (at5489 ml min21 kg21) Indeed this peak also remainswhen we scale by absolute FFM (ml min21 fat-free kg21see Supporting Information Table S2)
To evaluate whether Tsimane participants performedsimilarly under the O2 method we compared age-matched subsamples to O2 method participants Tsimanemales performed significantly worse under the HRmethod relative to the O2 method (O2 mean 5 695 mlmin21 kg21 HR mean 5 590 ml min21 kg21 t 5 629Plt 0001) There is no significant difference between Tsi-mane females tested under the HR and O2 methods (O2
mean 5 529 HR mean 5 543 t 5 2077 P 5 044) For acomparison of smooths from the two samples see Sup-porting Information Figure S3Mediators of Levels Across the Tsimane Lifespan Weidentified and investigated several health-related factorsthat might affect level of VO2max achieved by eitherdiminishing resources available to the body or hamperingthe cardiovascular system directly We posit that thesevariables may mediate the effect of age on VO2max Can-didate mediators include the presence of anemia infectionwith helminths or giardia arthritis or nonarthritic painrespiratory ailments distance from the local market
Fig 1 Predicted Tsimane VO2max by age Predicted values are drawn from GAM models regressing smooths of log age on VO2max Inter-vals are 95 prediction intervals Age was smoothed using restricted maximum likelihood Other smoothing parameters (such as Mallowrsquos Cpand maximum likelihood) varied the age at peak absolute VO2max by up to 1 year for females and up to 2 years for males Points represent theraw data for Tsimane A Absolute VO2max by age for females B Absolute VO2max by age for males C Relative VO2max by age for femalesD Relative VO2max by age for males [Color figure can be viewed in the online issue which is available at wileyonlinelibrarycom]
6 AC PISOR ET AL
American Journal of Human Biology
town and Spanish speaking ability Although percentFFM generally predicts absolute rather than relativeVO2max we test it as a potential mediator Pregnancywas included as a control in female models While a highmacroparasite load may increase the likelihood of havinglow hemoglobin (and thus anemia) an interaction termbetween presence of helminths and presence of anemiawas not included because they are not significantlyrelated in this sample only 26 participants of the 92 withhelminths have anemia while 14 of the 86 without hel-minths have anemia (for females v2 5 052 P 5 047 formales v2 5 200 P 5 016)
To evaluate whether these candidate mediators affectedVO2max levels we conducted linear regressions on rela-tive VO2max (see Table 2) We first examined each predic-tor independently Females with higher hemoglobin levelshad significantly higher cardiovascular fitness perform-ance for an increase in 1 g dl21 concentration of hemoglo-bin a Tsimane woman is predicted to have 293 ml min21
kg21 higher VO2max (t 5 268 Plt 001) Helminth infec-tion mediated the relationship between age and VO2maxfor males such that men with a helminth infection arepredicted to have 616 ml min21 kg21 higher VO2max(t 5 231 Plt 005) A best fit model approach (fit on thesubset of females for whom all measures are available)provides similar results to fitting a separate model for
each potential mediating variable When a stepwise AICprocedure was used with data on all health and marketintegration measures hemoglobin level was the only sig-nificant predictor that remained in the female model(n 5 82 standardized b 5 022 Plt 005) For males hel-minth infection remained in the model as well (n 5 116standardized b 5 023 Plt 005)
Scaling VO2max by FFM (ml min21 fat-free kg21)rather than body mass produced similar results hemoglo-bin levels remained a significant positive predictor ofVO2max for females (standardized b 5 030 Plt 001) andhelminth infection a positive predictor for males (standar-dized b 5 020 Plt005) See Supporting InformationTable S3 for all regression results with ml min21 fat-freekg21 as the outcome
Anemia was initially included in model fits howevertreating hemoglobin level as a covariate in place of pres-ence of anemia improved model fit for Tsimane females(anemia AIC 5 10027 hemoglobin AIC 5 98963)Although no association was found between presence ofanemia and helminth infection there is a significant asso-ciation between hemoglobin levels and helminth infectionControlling for age a helminth diagnosis is a significantnegative predictor of hemoglobin levels for females (stand-ardized b 5 2031 Plt 001) Replacing presence of ane-mia with hemoglobin level for males did not improve or
TABLE 3 Comparison of Tsimane and Canadian relative VO2max by age category and sex
Sex Age group
Tsimane Canadians
t-Statistic P-valueMean (ml min21 kg21) n Mean (ml min21 kg21) n
Females 11ndash14 435 7 487 534 2118 02815ndash19 476 33 423 500 310 00020ndash39 510 72 383 662 908 00040ndash59 431 69 314 655 1005 00060ndash69 412 5 242 554 340 003
Males 11ndash14 415 4 548 542 2300 00615ndash19 516 31 508 514 046 06520ndash39 511 96 442 526 527 00040ndash59 432 68 362 584 380 00060ndash69 381 26 275 546 509 000
TABLE 2 Linear models exploring whether mediators affect the level (main effects models) of relative VO2max for Tsimane females and males
Sex Candidate mediatorAge effect est
(P-value)
Main effect models
Sample sizeMediator main effect
est (P-value) Age main effect est (P-value)
Females Perc FFM 2023 (000) 000 (097) 2023 (000) 203Hemoglobin 2013 (028) 024 (001) 2011 (022) 117Helminths 2019 (007) 003 (077) 2020 (006) 92Giardia 2019 (007) 011 (028) 2019 (007) 92Lung ailment 2017 (006) 2005 (060) 2018 (005) 133Reported pain 2017 (006) 2001 (094) 2017 (006) 133Arthritis 2017 (006) 2002 (083) 2016 (007) 133Distance to town 2023 (000) 002 (081) 2023 (000) 196Spanish speaking 2023 (000) 2008 (056) 2024 (000) 197
Males Perc FFM 2037 (000) 009 (012) 2034 (000) 280Hemoglobin 2029 (000) 2002 (076) 2029 (000) 157Helminths 2030 (000) 019 (002) 2027 (000) 128Giardia 2030 (000) 006 (049) 2030 (000) 128Lung ailment 2030 (000) 2007 (033) 2031 (000) 185Reported pain 2030 (000) 011 (013) 2031 (000) 185Arthritis 2030 (000) 2006 (044) 2028 (000) 185Distance to town 2037 (000) 2003 (059) 2037 (000) 273Spanish speaking 2038 (000) 008 (050) 2037 (000) 271
All parameter estimates are standardized
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 7
American Journal of Human Biology
worsen model fit and there is no significant relationshipbetween hemoglobin levels and helminth infection formales (standardized b 5 2010 P 5 028) Parameter esti-mates for anemia were not significant in models for eitherfemales or males
Between-group Table 3 presents Tsimane and Canadianestimated VO2max binned into age categories used byCHMS These data suggest that Canadian females andmales achieve peak VO2max between the ages of 11 and14 while Tsimane males peak between ages 15 and 19Tsimane females peak later between age 20 and 39Across comparable age categories Tsimane have signifi-cantly higher VO2max than Canadians at all ages exceptbetween 11 and 15 for females and 11 and 19 for males(Table 3) However the sample size of Tsimane teenagersunder age 15 is quite small As aforementioned to controlfor the influence of a small number of data points for theyoungest and oldest Tsimane individuals we used GAMto predict VO2max across logged age Predicted valuessuggest that Tsimane females peak at age 28 and Tsimanemales peak at age 22 (see Fig 1c d) These estimates areconsistent with scatterplots of the raw data (plotted onFig 1) and mask fewer fine-grained effects of age thanTable 3 as each CHMS adult age category spans twodecades
It is possible the difference between the Tsimane andCanadians reflects a greater increase in body mass acrossages in the Canadian population or different trajectoriesof change in body composition The former could occurbecause body mass appears in the denominator and cantherefore scale down VO2max while the latter implies dif-ferential changes in FFM when FFM is a predictor ofVO2max in many studies To explore these possibilitieswe performed two calculations we allometrically scaledTsimane VO2max and we projected Tsimane VO2maxassuming the Tsimane had equivalent fat mass and FFMas Canadians from same-sex same-age categories Con-trolling for age the allometric scaling coefficient a wasslightly greater than 1 for both sexes (females a 5 111males a 5 118) This suggests that any disparity inVO2max between Canadians and the Tsimane cannot beexplained solely by mass differences Indeed assumingthe Tsimane have the same body composition as Cana-dians projected VO2max differs little from observedVO2max The Tsimane outperform the Canadians in everycohort by at least 35 ml min21 kg21 except among theyoungest males who perform similarly (see SupportingInformation Fig S4)
To control for possible disparities in changes in bodycomposition by age within each population as these mightalso influence differences between the Tsimane and Cana-dians we scaled VO2max by absolute FFM from the samepopulation to obtain ml min21 fat-free kg21 BecauseCanadian body composition data were only available viaskinfolds (bicep tricep subscapular and suprailiac) weused the subset of Tsimane (n 5 246) for which the samefour skinfolds measurements were available We calcu-lated average absolute FFM for each cohort using averageweight and average summed skinfolds (Durnin andWomersley 1974) and scaled average VO2max in mlmin21 by this number to obtain ml min21 fat-free kg21Under this method of scaling the Tsimane outperformCanadians in every cohort over age 20 by at least 165 ml
min21 fat-free kg21 (see Supporting Information TableS2) Canadian females and males in the 12ndash19 cohortsoutperform Tsimane of the same age
We next compared Tsimane to other subsistence popula-tions reported in the literature (Table 4) Consistent withcommon practice in the literature we report means foreach group but when possible we also predicted VO2maxat age 25 to provide age-corrected comparisons Weselected age 25 as it is the age of peak relative VO2max inthis study and for female Kamba and Maasai in Christen-sen et als (2012) recent study To predict VO2max at age25 we regressed the median ages on mean VO2max acrossthe available age categories Tsimane females and maleshave roughly the same predicted VO2max at age 25 asseveral other subsistence populations but higher VO2maxthan industrialized populations To test for differencesbetween industrialized and subsistence populations weconducted a linear regression on predicted VO2max at age25 this is not a meta-analysis and results should beinterpreted with caution Overall subsistence populationsdisplay higher peak VO2max than in industrialized popu-lations controlling for sex (440 vs 367 ml min21 kg21
[Plt 001]) The Tsimane O2 and indigenous Siberian sam-ples were excluded Tsimane O2 to avoid the problem ofnon-independence with Tsimane HR data and Siberiansbecause the sample has a limited age range comparedwith the other studies
Pace of decline slope of VO2max decline across thelifespan
Tsimane To evaluate whether Tsimane participants per-formed similarly under different methods we comparedage-matched subsamples of participants from the presentstudy with O2 method participants Despite a higher level(intercept) of VO2max in the O2 sample Tsimane malesdeclined marginally significantly faster under the O2
method relative to the HR method (O2 5 68 per decadeHR 5 47 decline per decade t 5 2195 P 5 005) Thereis no significant difference between Tsimane femalestested under the O2 and HR methods (O2 5 60 per dec-ade HR 5 48 decline per decade t 5 2055 P 5 058)Mediators of Slope Across the Lifespan We fit a series oflinear models to test for interactions between the candi-date mediators and age-related decline in TsimaneVO2max There are no variables that significantly inter-act with age to predict VO2max (see Supporting Informa-tion Table S4) An AIC selection approach and scaling byabsolute FFM (see Supporting Information Table S3) pro-vides the same results no variables significantly interactwith age to predict VO2max
Between-group VO2max is most often reported as a lin-ear decline across the adult lifespan though Hawkins andWiswell (2003) dispute whether the decline is actually lin-ear For example a linear approximation is not appropri-ate for Tsimane females if ages 11ndash80 are consideredFigure 2 contrasts linear declines in VO2max for Cana-dians and Tsimane males as well as a curvilinear fit forTsimane females with declines in industrialized nationsderived from meta-analyses (Fitzgerald et al 1997 Wil-son and Tanaka 2000) To explore whether rates ofdecline in VO2max among Tsimane and Canadians weredifferent we regressed average VO2max by age category
8 AC PISOR ET AL
American Journal of Human Biology
TA
BL
E4
Mea
nV
O2m
ax
esti
ma
ted
VO
2m
ax
at
age
25a
nd
dec
lin
ein
VO
2m
ax
per
dec
ad
efr
omth
isst
ud
ya
nd
pre
vio
us
rese
arc
ha
Pop
ula
tion
Fem
ale
Male
Pu
bli
cati
onM
ean
VO
2m
ax
VO
2m
ax
Age
25
bP
erce
nt
Dec
lin
eA
ge
Ran
ge
(n)
Mea
nV
O2m
ax
VO
2m
ax
Age
25
bP
erce
nt
Dec
lin
eA
ge
Ran
ge
(n)
Ind
ust
riali
zed
Can
ad
ac
312
400
73
20ndash69
(2905)
361
458
68
20ndash69
(2712)
Jap
an
d357
414
39
20ndash69
(656)
417
473
38
20ndash69
(807)
San
ad
aet
al
2007
Sw
eden
e330
g409
80
20ndash65
324
g388
75
20ndash65
Ek
blo
met
al
2007
Th
ail
an
d(i
nd
ust
ry)e
275
293
54
16ndash55
(56)
389
415
57
16ndash53
(70)
Yoo
pat
etal
2002
US
(H
erit
age)
f273
17ndash65
(360)
359
17ndash65
(293)
Sk
inn
eret
al
2003
US
(N
HA
NE
S)d
356
363
24
20ndash49
(1312)
444
438
39
20ndash49
(1481)
Su
bsi
sten
ceT
sim
an
e(H
R)c
498
521
h16
h20ndash69
471
538
h61
h20ndash69
Tsi
man
e(O
2)c
436
74
h36ndash69
540
25
h36ndash69
Ifalu
k(1
969ndash70)c
429
488
69
20ndash59
(43)
49
597
75
20ndash69
(75)
Rod
ean
dS
hep
hard
1994
Ach
ec465
434
257
20ndash59
(62)
519
614
84
20ndash59
(65)
Walk
eran
dH
ill
2003
Lu
oc378
372
39
17ndash68
(209)
429
48
54
17ndash68
(172)
Ch
rist
ense
net
al
2012
b
Kam
ba
c377
371
45
17ndash68
(283)
431
516
34
17ndash68
(94)
Ch
rist
ense
net
al
2012
Maasa
ic389
410
45
17ndash68
(178)
431
528
69
17ndash68
(163)
Ch
rist
ense
net
al
2012
Ind
igen
ous
Sib
eria
nsc
338
341
22
220ndash39
(14)
462
471
66
20ndash39
(30)
Katz
marz
yk
etal
1994
Ru
ral
Nep
alc
187
15ndash60
(39)
221
15ndash60
(35)
Pan
ter-
Bri
cket
al
1992
Ngis
onyok
aT
urk
an
af
38
387
18
20ndash44
(19)
Cu
rran
-Ever
ett
1994
aV
alu
esm
issi
ng
wh
enn
otavail
able
from
ap
art
icu
lar
stu
dy
Per
cen
td
ecli
ne
(per
cen
tof
pea
kvalu
elo
st)
per
dec
ad
ew
as
calc
ula
ted
as
by
regre
ssin
gre
lati
ve
VO
2m
ax
by
age
mu
ltip
lyin
gth
ep
ara
met
eres
tim
ate
for
age
by
10
an
dd
ivid
ing
this
nu
mber
by
the
inte
rcep
t(p
resu
med
pea
k
ass
um
ing
ali
nea
rd
ecli
ne
inV
O2m
ax
acr
oss
age)
B
ecau
seof
lack
ofacc
ess
tora
wd
ata
re
gre
ssio
ns
wer
efi
tw
ith
mea
nV
O2m
ax
an
dm
edia
nage
by
coh
ort
bA
ge
25
valu
esw
ere
esti
mate
dby
regre
ssin
gre
lati
ve
VO
2m
ax
by
age
then
usi
ng
the
resu
ltin
gp
ara
met
eres
tim
ate
sto
pre
dic
tV
O2m
ax
at
age
25
the
pea
kin
rece
ntl
yst
ud
ied
pop
ula
tion
s(e
g
Kam
ba
an
dM
aasa
ife
male
sC
hri
sten
sen
etal
2012fe
male
san
dm
ale
sin
this
art
icle
)B
ecau
seof
lack
ofacc
ess
tora
wd
ata
re
gre
ssio
ns
wer
efi
tw
ith
mea
nV
O2m
ax
an
dm
edia
nage
by
coh
ort
cS
ubm
axim
alst
epte
st
dS
ubm
axim
altr
ead
mil
lte
st
eS
ubm
axim
aler
gom
eter
test
f M
axim
al
ergom
eter
test
gS
wed
ish
data
wer
ere
por
ted
as
med
ian
sfo
rea
chage
cate
gor
yth
evalu
esre
por
ted
her
eare
mea
ns
ofth
ese
med
ian
s2006
ind
ivid
uals
part
icip
ate
dbu
tn
um
ber
by
sex
was
not
rep
orte
d
hF
orco
mp
ara
bil
ity
we
bin
ned
the
Tsi
man
eH
Ran
dO
2d
ata
into
10
yea
rage
cate
gor
ies
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 9
American Journal of Human Biology
on median age (for a given age category) population andtheir interaction term For comparability Tsimane werebinned into the Canadian age categories and averageswere computed for these categories leading to estimateddeclines slightly different from those in Table 4 for thepurposes of this test we treat the Tsimane female declineas linear Because within-population variance in declineis not available these regressions should be treated asdescriptive comparisons rather than statistical tests ofdifferences between the two groups The rate of decline inVO2max is steeper for Canadian females (69 per decadefaster decline per decade) and males (42 faster declineper decade) compared with Tsimane females and males
The rate of cardiovascular fitness decline between theTsimane and Canadians is different but this differencedoes not extend to industrialized and subsistence popula-tions (see Table 4) Controlling for sex subsistence groupshave about one quarter of a percent lower declines perdecade Again because the variance in decline is not rep-resented in this regression results should be interpretedas comparative rather than as a statistical test As beforeTsimane O2 results were not included in the analysis toavoid nonindependence and the indigenous Siberianswere excluded because of discrepancy in ages sampled
DISCUSSION
Our comparisons demonstrate that across a wide varietyof societies cardiovascular fitness senesces with age Car-diovascular fitness is higher on average among members ofsubsistence societies than among industrialized societiesbut rates of fitness decline from peak are not slower Ourmore detailed comparison between the Tsimane a subsist-ence population and Canadians an industrialized popula-tion reveals differences in cardiovascular fitness levelsand rate of fitness decline Cardiovascular fitness levelswere higher among the Tsimane than among Canadiansand the rate of decline across the lifespan was significantlyslower among Tsimane women and men Potential Cana-
dian participants were excluded due to many health con-cerns including pregnancy and history of high bloodpressure whereas Tsimane were only excluded if they self-identified as unable to participate This suggests the Cana-dian sample is a relatively healthy subsample of Canadayet the Tsimane still outperform them in cardiovascular fit-ness It may be that the higher demand for cardiovascularfitness in late ages among the Tsimane outweighs anyeffects of poor health Another possibility is that greaterself-selection among Tsimane due to higher adult mortalityleaves more robust older adult survivors thereby reducingthe observed slope of fitness decline at the population level(Vaupel et al 1979) perhaps this is partially why fewerTsimane older adults opted out of the exercise test thanCanadian older adults were screened out (ages 60ndash69Canadian females 5 56 Tsimane females 5 15 Cana-dian males 5 57 Tsimane males 5 5)
Consistent with prior research on age-related changesin cardiovascular fitness the Tsimane do evidence a lin-ear decline in VO2max with age but not as steep a declineas typically seen in industrialized populations Based oncomparisons with the Canadians and with other industri-alized populations we believe the Tsimane data from thepresent study and the pilot O2 data combined indicatethat the Tsimane perform better on tests of cardiovascularfitness than the average individual from an industrializednation
To further explore the potential effects of health factorson cardiovascular fitness level and rate of decline weinvestigated predictors of individual differences in fitnesswithin the Tsimane population Overall we found thatmost health indicators among the Tsimane did not hinderVO2max levels or rates of decline Lower hemoglobin lev-els were associated with lower VO2max levels in womenbut not men consistent with the notion that compromisedblood oxygen transport curbs cardiovascular fitness(Buzina et al 1989 Panter-Brick et al 1992) In the USlow hemoglobin is more common in active women thanactive men (Sinclair and Hinton 2005) hemoglobin is
Fig 2 Linear changes in VO2max with age for Canadians and the Tsimane Intercepts and slopes for Canadians and Tsimane can be foundin Table 4 Because age2 is significant for the full sample of Tsimane females their change in VO2max across age is curvilinear Slopes forendurance trained active and sedentary individuals from industrialized nations are drawn from a meta-analysis performed by Fitzgeraldet al (1997) for females and Wilson and Tanaka (2000) for males Endurance trained individuals are represented by the top dotted line abovefollowed by active individuals below and sedentary on the bottom Trained individuals engage in 31 sessions of endurance exercise per weekfor at least a year while active individuals engage in 2 or fewer sessions per week of cardiovascular exercise [Color figure can be viewed in theonline issue which is available at wileyonlinelibrarycom]
10 AC PISOR ET AL
American Journal of Human Biology
also lower in Tsimane women than Tsimane men(female 5 129 [sd 13] g ml21 males 5 142 [13] g ml21)Even mild (non-anemic) iron deficiencies impacts womenrsquosexercise performance (Zhu and Haas 1997) Inconsistentwith findings from Panter-Brick et al (1992) among ruralNepalese helminth infection did not diminish levels ofVO2max for Tsimane men helminth infection wasactually a predictor of higher VO2max There are severalreasons why this might be the case First we only testedwhether presence or absence of helminths mediated theeffect of age on VO2max rather than parasite load (egnumber of worms egg counts) it is possible that helminthinfection only affects VO2max at high parasite loads Sec-ond blood loss (and thus low hemoglobin levels) resultingfrom helminth infection may be partially offset by theamount of iron in the Tsimane adult diet Tsimane ironintake is an estimated 166 of the US Dietary ReferenceIntake (Martin et al 2012) and Tsimane hemoglobin lev-els are higher than in the Nepalese (females 129 vs 109males 1424 vs 120 Panter-Brick et al 1992) Thirdthese analyses consider helminth infection at the time ofexercise test rather than past infections It may be thatthe cumulative burden of past infection has a larger effecton cardiovascular fitness if so this would suggest thatthe surprising positive effect of helminth infection onVO2max levels in men is either spurious or capturing athird variable
Secular declines in VO2max are expected with increasingmarket integration and lifestyle change because ofincreased sedentism (Katzmarzyk et al 1994 Rode andShephard 1994) Two proxies for market integration in thispopulationmdashdistance to San Borja and the ability to speakSpanishmdashwere not significant predictors of VO2max levelsor decline This is consistent with our predictions as Tsi-mane females and males that live near town do not appearto have lower activity levels (Gurven et al 2013) Wageopportunities near town primarily include working asranch hands collecting and weaving palm thatch panelscash cropping and working for logging companies Each ofthese involves extensive activity furthermore transporta-tion to town often involves bicycling walking and polingdugout canoes Cash cropping of rice and corn also involvesthe clearing and weeding of larger fields Except for cashcropping and palm thatch manufacture most wage laboropportunities are currently restricted to men
This study makes several unique contributions to theexisting literature It offers the first systematic compari-son of cardiovascular fitness level and rate of declinebetween subsistence and industrialized societies Resultscompiled from previous studies support the general claimthat despite greater pathogen stress the greater activityregime of subsistence societies helps support higher peakVO2max Additionally this is one of the first studies toexplore senescent changes in cardiovascular fitnesswithin a large sample from a subsistence population Thelarge number of health measures and proxies of marketintegration available permitted testing whether these fac-tors mediated age-related variation and whether theymodulated the rate of decline Despite reports that healthstatus and market integration have been important inother studies (eg Buzina et al 1989 Katzmarzyk et al1994 Panter-Brick et al 1992 Rode and Shephard1994) their overall net effect was small among the Tsi-mane most apparent in measures of hemoglobin levelsamong women and helminth infection among men
The results of these analyses may also shed light onindividual and population level differences in chronic dis-ease In industrialized populations meta-analyses demon-strate that cardiovascular fitness is protective againstcardiovascular disease (Jette et al 1992 Hawkins andWiswell 2003) Prior studies among Tsimane suggest rel-atively few deaths from heart attacks or strokes (Gurvenet al 2007) a low prevalence of common cardiovasculardisease risk factors like obesity high blood low-densitylipoprotein levels hypertension and peripheral arterialdisease and the existence of additional protective factorslike lean diet and physical activity (Gurven et al 20092013 Vasunilashorn et al 2010) Market foods such ascooking oil sugar and pasta represent only 6 of theaverage Tsimane diet and Tsimane also consume a greatdeal of lean meat and omega-3 fatty acids (Martin et al2012) This study complements these findings by demon-strating that Tsimane show relatively high VO2max anindicator of strong cardiorespiratory health TsimaneVO2max declines with age as it does everywhere whichsuggests declining muscle mass with age (Fleg andLakatta 1988) and lowered cardiac output (American Col-lege of Sports Medicine 2006 Sagiv et al 2007) ratherthan increased cardiovascular disease risk
Limitations
The Canadians were selected as a comparison industri-alized population because of the similarity of the CHMSand Tsimane protocols very few studies of industrializedpopulations have large sample sizes sample across thelife course and use a step test Several aspects of theCHMS and Tsimane protocols remain potentially incom-parable The Canadians experienced more stringentexclusion criteria than the Tsimane meaning that the Tsi-mane sample may be more representative of cardiovascu-lar condition in the Tsimane population than theCanadian sample of the Canadian population Again ifthe Tsimane sample was subjected to these criteria wemight expect the differences in VO2max between popula-tions to only increase On the other hand Canadian par-ticipants were assigned stepping cadences based on theirage and sex and cadence was increased across the exer-cise test if a participant did not reach 85 of his or herage-specific maximal HR all Tsimane were asked to com-plete 30 ascents per minute with no increase based ontheir achieved HRs Few Tsimane reached 75 of theirage-specific maximal HR (see Supporting InformationTable S1) perhaps because the age-specific maximal HRsderived from industrialized populations are inaccurate forthe Tsimane or because higher fitness allowed these Tsi-mane to perform the step test of 30 ascents per minutewith less effort Due to these discrepancies in protocolwhich may lead to errors in estimating VO2max we alsoincorporated Tsimane data collected using the O2 methodas a check because the O2 method estimates VO2max onthe relationship between HR and VO2 in a givenparticipant
Indeed it is an open question as to whether typicalmethods for indirectly estimating cardiovascular fitnessfrom HR are appropriate for subsistence level popula-tions Common routines for VO2max estimation assumeage-specific declines in cardiovascular fitness (eg Shep-hard 1970) but these methods have only been validatedwith samples from industrialized populations which are
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 11
American Journal of Human Biology
often self-selected (Beall et al 1985) Additionally regres-sions drawn from laboratory studies require participantsachieve a HR within a certain range for accurate VO2maxestimation however the appropriateness of these rangesgiven slight modifications to protocol and inclusion of par-ticipants of different ages different populations and bothsexes is questionable For example the maximal HRexhibited by young men varies across subsistence popula-tions (Shephard 1978) Use of these criteria is compli-cated by the fact that the most commonly used equationfor estimating maximal possible HR by age 220-age maybe inaccurate (Robergs and Landwehr 2002) and particu-larly inappropriate for older adults (see Tanaka et al2001) For these reasons we chose to use an exclusion cri-terion for the Tsimane that evaluates individual increasein HR across exercise relative to the mean increase in HRfor Tsimane of the same sex and age
The pattern of Tsimane fitness decline differs moder-ately by the choice of exclusion criterion for participants(see Supporting Information Table S1) and by method oftesting However this is a common finding Lee et al(2011) predicted VO2max from submaximal exercise usingthe O2 method and the HR-based American College ofSports Medicine calculation routine in a US sample Theyfound that (1) the HR-based routine predicts higherVO2max across the sexes than does the O2 routine and(2) the two methods have a correlation of only 077 Whenevaluating different testing procedures Shephard et al(1968) found differences in VO2max estimation by type oftest used (eg bicycle ergometer versus step test) and cal-culation routine Exercise tests exclusion criteria andcalculation routines combine to provide an estimate ofactual VO2max for a given individual and as such varia-tion in estimation is to be expected However such varia-tion may affect cross-population comparisons inunforeseen ways thus the comparisons presented hereshould be interpreted with caution
While population-level variation in cardiovascular fit-ness decline may reflect the differences in the demands ofendurance-based physical activity muscularity and com-promised oxygen transport it is possible that genetic fac-tors may also play a potential role (Collins 1999) In oneindustrialized sample maternal cardiovascular fitnessexhibited a heritability of 30 which is attributed toinheritance of the maternal mitochondrial genome (Bou-chard et al 2000) We do not have the relevant geneticdata for the populations considered here however andthus operate under the simplifying assumption thatinheritance should not affect population-level patternsand will not consistently bias individual-level compari-sons in any particular direction
This study is further limited by its cross-sectionaldesign Cross-sectional data present well-known problemsfor the measurement of individual aging (Crimmins andSeeman 2001) Mortality selection in which individualsin poorer condition are likely to die at younger ages pro-duces a downward bias in the estimation of aging rates atthe individual level (Vaupel and Yashin 1985 Vaupelet al 1979) Cohort effects if present also produce com-plicated and non-monotonic biases in estimation (Carnesand Olshansky 2001) Due to the problem of between-individual heterogeneity and the within-individual pro-cess of senescence a recent overview of aging studies con-cludes that ldquoonly longitudinal studies [ ] provide reliablesources of information in the study of senescencerdquo (Nussey
et al 2008) To date there are no longitudinal studies ofcardiovascular fitness in subsistence populations We arecurrently re-testing participants under the O2 methodallowing a better grasp of the within-individual variationthat shapes patterns of senescent decline
ACKNOWLEDGMENTS
The authors thank Paul Hooper Steven Gaulin JohnTooby Patricia Kramer the Human Evolution and Biode-mography laboratory and the Center for EvolutionaryPsychology at UCSB for helpful advice and feedback thestaff at the Tsimane Health and Life History Project andthe Tsimane for their participation and patience
LITERATURE CITED
American College of Sports Medicine 2006 ACSMrsquos Guidelines for Exer-cise Testing and Prescription 7th ed Philadelphia Lippincott Williamsamp Wilkins
Armstrong N 2001 Peak oxygen uptake in relation to growth and matura-tion in 11- to 17-year-old humans Eur J Appl Physiol 85546ndash551
Astrand PO Ryhming I 1954 A nomogram for calculation of aerobiccapacity (physical fitness) from pulse rate during submaximal work JAppl Physiol 7218ndash221
Bailey DA Shephard RJ Mirwald RL 1976 Validation of a self-administered home test of cardio-respiratory fitness Can J Appl SportSci 167ndash78
Beall CM Goldstein MC and Feldman ES 1985 The physical fitness ofelderly Nepalese farmers residing in rugged mountain and flat terrainJ Gerontol 40529ndash535
Benefice E Ndiaye G 2005 Relationships between anthropometry cardi-orespiratory fitness indices and physical activity levels in different ageand sex groups in rural Senegal (West Africa) Ann Hum Biol 32366ndash382 Available from httpwwwncbinlmnihgovpubmed16099780
Blackwell AD Gurven MD Sugiyama LS Madimenos FC Liebert MAMartin MA Kaplan HS Snodgrass JJ 2011 Evidence for a peak shift in ahumoral response to helminths age profiles of IgE in the Shuar of Ecuadorthe Tsimane of Bolivia and the US NHANES PLoS Negl Trop Dis 5e1218 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid53125146amptool5pmcentrezamprendertype5abstract
Blackwell AD Martin M Kaplan H Gurven M Evidence for an antagonis-tic relationship between Giardia lamblia and helminth infections impli-cations for treatment of helminth infections in developing populations
Blair SN LaMonte MJ Nichaman MZ 2004 The evolution of physicalactivity recommendations how much is enough Am J Clin Nutr 79913Sndash920S Available at httpwwwncbinlmnihgovpubmed15113739
Bouchard C Rankinen T Chagnon YC Rice T Perusse L Gagnon JBorecki I An P Leon a S et al 2000 Genomic scan for maximal oxygenuptake and its response to training in the HERITAGE Family Study JAppl Physiol 88551ndash559 Available at httpwwwncbinlmnihgovpubmed10658022
Bryan S St-Denis M Wojtas D 2007 Canadian Health Measures Surveyclinic operations and logistics Health Rep 1853ndash69
Buzina R Bates CJ van der Beek J Brubacher G Chandra RK HallbergL Heseker J Mertz W Pietrzik K et al 1989 Workshop on FunctionalSignificance of Mild-to-Moderate Malnutrition Am J Clin Nutrition 50172ndash176
Calder WA 1987 Scaling energetics of homeothermic vertebrates anoperational allometry Annu Rev Physiol 49107ndash120
Canadian Society for Exercise Physiology 2003 The Canadian PhysicalActivity Fitness amp Lifestyle Approach (CPAFLA) CSEP-Health amp Fit-ness Programrsquos Health-Related Appraisal and Counselling Strategy 3rded
Carnes BA Olshansky SJ 2001 Heterogeneity and its biodemographicimplications for longevity and mortality Exp Gerontol 36419ndash430Available at httpwwwncbinlmnihgovpubmed11250115
Carrick-Ranson G Hastings JL Bhella PS Shibata S Fujimoto N PalmerD Boyd K Levine BD 2013 The effect of age-related differences inbody size and composition on cardiovascular determinants of VO2max JGerontol A Biol Sci Med Sci 68608ndash616 Available at httpwwwncbinlmnihgovpubmed23160363
Centers for Disease Control and Prevention 1998 Recommendations toPrevent and Control Iron Deficiency in the United States MMWRRecomm Rep 471ndash36 Available at httpwwwcdcgovmmwrpreviewmmwrhtml00051880htm
12 AC PISOR ET AL
American Journal of Human Biology
Centers for Disease Control and Prevention 2011 Glossary of TermsPhysical Activity for Everyone [Internet] Available from httpwwwcdcgovphysicalactivityeveryoneglossary
Christensen DL Faurholt-Jepsen D Boit MK Mwaniki DL Kilonzo BTetens I Kiplamai FK Cheruiyot SC Friis H et al 2012 Cardiorespira-tory fitness and physical activity in Luo Kamba and Maasai of ruralKenya Am J Hum Biol 24723ndash729 Available at httpwwwncbinlm-nihgovpubmed22836508
Colley RC Garriguet D Janssen I Craig CL Clarke J Tremblay MS2011a Physical activity of Canadian children and youth accelerometerresults from the 2007 to 2009 Canadian Health Measures SurveyHealth Rep 2215ndash23
Colley RC Garriguet D Janssen I Craig CL Clarke J Tremblay MS2011b Physical activity of Canadian adults accelerometer results fromthe 2007 to 2009 Canadian Health Measures Survey Health Rep 227ndash14 Available at httpwwwncbinlmnihgovpubmed21510585
Collins KJ 1999 Physiological variation and adaptability in human popu-lations Ann Hum Biol 2619ndash38
Crimmins E Seeman T 2001 Integrating Biology into DemographicResearch on Health and Aging (With a Focus on the MacArthur Study ofSuccessful Aging) Cells and Surveys Should Biological Measures beIncluded in Social Science Research Washington DC National Acad-emy Press p 9ndash41
Curran-Everett LS 1994 Accordance Between VO2max and Behavior inNgisonyoka Turkana Am J Hum Biol 6761ndash771
Durnin JVGA Womersley J 1974 Body fat assessed from total body den-sity and its estimation from skinfold thickness measurements on 481men and women aged from 16 to 72 years Br J Nutr 3277ndash97
Eberl M Al-Sherbiny M Hagan P Ljubojevic S Thomas AW Wilson RA2002 A novel and sensitive method to monitor helminth infections byfaecal sampling Acta Trop 83183ndash187
Eid D Gurven M Kaplan H Winking J 2007 Enfermedades infecciosas alo largo de la vida y en el envejecimiento en indıgenas sudamericanos dela etnia Tsimane Aging in Developing Countries Building Bridges forIntegrated Research Agendas Santiago Chile
Ekblom B Engstreuroom L-M Ekblom O 2007 Secular trends of physical fit-ness in Swedish adults Scand J Med Sci Sports 17267ndash273 Availableat httpwwwncbinlmnihgovpubmed17501867
Finch CA Lenfant C 1972 Oxygen Transport in Man N Engl J Med 286407ndash415
Fitzgerald MD Tanaka H Tran ZV Seals DR 1997 Age-related declinesin maximal aerobic capacity in regularly exercising vs sedentarywomen a meta-analysis J Appl Physiol (Bethesda Md 1985) 83160ndash165 Available at httpwwwncbinlmnihgovpubmed9216959
Fleg JL Lakatta EG 1988 Role of muscle loss in the age-associated reduc-tion in VO2max J Appl Physiol 651147ndash1151
Frisancho AR Frisancho HG Milotich M Brutsaert T Albalak RSpielvogel H Villena M Vargas E Soria R 1995 Developmentalgenetic and environmental components of aerobic capacity at high alti-tude Am J Phys Anthropol 96431ndash442 Available at httpwwwncbinlmnihgovpubmed7604895
Giroux S 2007 Canadian health measures survey sampling strategyoverview Health Rep 1831ndash36
Gurven M Jaeggi A V Kaplan H Cummings D 2013 Physical activityand modernization among Bolivian Amerindians PLoS ONE 81ndash13
Gurven M Kaplan H Winking J Rodriguez DE Vasunilashorn S KimJK Finch C Crimmins E 2009 Inflammation and infection do not pro-mote arterial aging and cardiovascular disease risk factors among leanhorticulturalists PLoS ONE 41ndash12
Haidet GC 1989 Dynamic exercise in senescent beagles oxygen consump-tion and hemodynamic responses The Am J Physiol 257H1428ndash1437Available at httpwwwncbinlmnihgovpubmed2589499
Hawkins S Wiswell R 2003 Rate and mechanism of maximal oxygen con-sumption decline with aging implications for exercise training SportsMed 33877ndash888 Available at httpwwwncbinlmnihgovpubmed12974656
Hoffman J 2002 Physiological aspects of sport training and performance1st ed Champaign IL Human Kinetics Publishers
Hotez PJ Bottazzi ME Franco-Paredes C Ault SK Periago MR 2008 Theneglected tropical diseases of Latin America and the Caribbean a review ofdisease burden and distribution and a roadmap for control and eliminationPLoS Negl Trop Dis 2e300 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid52553488amptool5pmcentrezamprendertype5abstract
Howley ET Bassett DR Welch HG 1995 Criteria for maximal oxygenuptake review and commentary Med Sci Sports Exerc 271292ndash1301Available at httpwwwncbinlmnihgovpubmed8531628
Jette M Sidney K Quenneville J Landry F 1992 Relation between cardi-orespiratory fitness and selected risk factors for coronary heart diseasein a population of Canadian men and women CMAJ 1461353ndash1360Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid51488567amptool5pmcentrezamprendertype5abstract
Katzmarzyk PT Leonard WR Crawford MH 1994 Predicted maximaloxygen consumption of Indigenous Siberians Am J Hum Biol 6783ndash790
King CH Dickman K Tisch DJ 2005 Reassessment of the cost of chronichelmintic infection a meta-analysis of disability-related outcomes inendemic schistosomiasis Lancet 3651561ndash1569 Available at httpwwwncbinlmnihgovpubmed15866310
Lee J-M Bassett D Jr Thompson D Fitzhugh E 2011 Validation of thecosmed fitmate for predicting maximal oxygen consumption J StrengthCond Res 252573ndash2579
Madimenos FC Snodgrass JJ Blackwell AD Liebert MA Sugiyama LS2011 Physical activity in an indigenous Ecuadorian forager-horticulturalist population as measured using accelerometry Am J HumBiol 23488ndash497 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid53110644amptool5pmcentrezamprendertype5abstract
Malina RM 2001 Physical activity and fitness pathways from childhoodto adulthood Am J Hum Biol 13162ndash172 Available at httpwwwncbinlmnihgovpubmed11460860
Malina RM Little BB 2008 Physical activity the present in the contextof the past Am J Hum Biol 20373ndash391 Available at httpwwwncbinlmnihgovpubmed18433002
Manning JT Morris L Caswell N 2007 Endurance running and digitratio (2D 4D) implications for fetal testosterone effects on runningspeed and vascular health Am J Hum Biol 19416ndash421
Martin Ma Lassek WD Gaulin SJC Evans RW Woo JG Geraghty SRDavidson BS Morrow AL Kaplan HS et al 2012 Fatty acid composi-tion in the mature milk of Bolivian forager-horticulturalists controlledcomparisons with a US sample Matern Child Nutr 8404ndash418 Availableat httpwwwncbinlmnihgovpubmed22624983
National Health and Nutrition Examination Survey 2004 CardiovascularFitness Procedures Manual
Nussey D Coulson T Festa-Bianchet M Gaillard J-M 2008 Measuringsenescence in wild animal populations towards a longitudinal approachFunction Ecol 22393ndash406
Ogawa T Spina RJ Martin WHI Kohrt WM Schechtman KB HolloszyJO Ehsani AA 1992 Effects of aging sex and physical training cardio-vascular responses to exercise Circulation 86494ndash503
Panter-Brick C Miller UG Eggerman M 1992 Hemoglobin levels andstep test performance of men and women in Nepal Am J Hum Biol 4481ndash491
Pontzer H Raichlen Da Wood BM Mabulla AZP Racette SB MarloweFW 2012 Hunter-gatherer energetics and human obesity PLoS ONE 7e40503 Available at httpcdxplosorg101371journalpone0040503
R Development Core Team 2011 R A language and environment for sta-tistical computing R Development Core Team
Rigby R Stasinopoulos D 2005 Generalize additive models for locationscale and shape (with discussion) Appl Stat 54507ndash554
Robergs RA Landwehr R 2002 The surprising history of theldquoHRmax5220-agerdquo equation J Exerc Physiol 51ndash10
Rode A Shephard RJ 1994 Physiological consequences of acculturation a20-year study of fitness in an Inuit community Eur J Appl Physiol 69516ndash524
Rowland TW Boyajian A 1995 Aerobic response to endurance training inchildren Pediatrics 96654ndash658
Sagiv M Ben-sira D Amir R 2007 What maintains energy supply atpeak aerobic exercise in trained and untrained older men Gerontology53357ndash361
Sanada K Kuchiki T Miyachi M Mcgrath K Higuchi M Ebashi H 2007Effects of age on ventilatory threshold and peak oxygen uptake normal-ised for regional skeletal muscle mass in Japanese men and womenaged 20 ndash 80 years Eur J Appl Physiol 99475ndash483
Schniter E 2009 Why Old Age Non-Material Contributions and Patternsof Aging Among Older Adult Tsimanersquo 607
Shahnawaz H 1978 Influence of limb length on a stepping exercise JAppl Physiol 44346ndash349
Shephard RJ 1970 Computer programs for solution of the Astrand nomo-gram and the calculation of body surface area J Sports Med 10206ndash210
Shephard RJ Allen C Benade AJS Davies CT Di Prampero PE HedmanR Merriman JE Myhre K Simmons R 1968 Standardization of sub-maximal exercise tests Bull World Health Organ 38765ndash775 Availableat httpwwwpubmedcentralnihgovarticlerenderfcgiartid52554690amptool5pmcentrezamprendertype5abstract
Shephard RJ Bailey Da Mirwald RL 1976 Development of the CanadianHome Fitness Test Can Med Assoc J 114675ndash679 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid51956906amptool5pmcentrezamprendertype5abstract
Shields M Tremblay MS Laviolette M Craig CL Janssen I Gorber SC2010 Fitness of Canadian adults results from the 2007ndash2009 canadianhealth measures survey Health Rep 2121ndash35 Available at httpwwwncbinlmnihgovpubmed20426224
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 13
American Journal of Human Biology
Siconolfi SF Garber CE Lasater TM Carleton RA 1985 A simple validstep test for estimating maximal oxygen uptake in epidemiologic stud-ies Am J Epidemiol 121382ndash390 Available at httpwwwncbinlm-nihgovpubmed4014128
Sinclair LM Hinton PS 2005 Prevalence of iron deficiency with and with-out anemia in recreationally active men and women J Am Diet Assoc105975ndash978 Available from httpwwwncbinlmnihgovpubmed15942552
Skinner JS Gaskill SE Rankinen T Leon AS Rao DC Wilmore JHBouchard C 2003 Heart rate versus VO2max age sex race initial fit-ness and training response-HERITAGE Med Sci Sports Exerc 351908ndash1913 Available at httpwwwncbinlmnihgovpubmed14600558
Sondik EJ Madans JH Gentlemand JF 2012 Summary health statisticsfor US adults National Health Interview Survey 2010 Vital Health Stat101ndash80 Available at httpwwwncbinlmnihgovpubmed20687424
Stones MJ Kozma A 1985 Physical performance Aging and Human Per-formance New York Wiley p 261ndash292
Tanaka H Monahan KD Seals DR 2001 Age-predicted maximal heartrate revisited J Am Coll Cardiol] 37153ndash156 Available at httpwwwncbinlmnihgovpubmed11153730
Vasunilashorn S Crimmins EM Kim JK Winking J Gurven M KaplanH Finch CE 2010 Blood lipids infection and inflammatory markers inthe Tsimane of Bolivia Am J Hum Biol 22731ndash740 Available at httpwwwncbinlmnihgovpubmed20721985
Vaupel JV Manton KG Stallard E 1979 The impact of heterogeneity inindividual frailty on the dynamics of mortality Demography 16439ndash454
Vaupel JW Yashin AI 1985 Heterogeneityrsquos ruses some surprising effectsof selection on population dynamics Am Stat 39176ndash185
Venables WN Ripley BD 2002 Modern Applied Statistics with S FourthNew York Springer
Wagner PD 1996 Determinants of maximal oxygen transport and utiliza-tion Annu Rev Physiol 5821ndash50 Available at httpwwwncbinlmnih-govpubmed8815793
Walker A Arent SM McKeever KH 2010 Maximal aerobic capacity(VO2max) in horses a retrospective study to identify the age-relateddecline Comparative Exerc Physiol 6177ndash181 Available at httpwwwjournalscambridgeorgabstract_S1755254010000073
Walker R Hill K 2003 Modeling growth and senescence in physical per-formance among the Ache of Eastern Paraguay Am J Hum Biol 208196ndash208
Weller IM Thomas SG Corey PN Cox MH 1993 Prediction of maximaloxygen uptake from a modified Canadian aerobic fitness test Can JAppl Physiol 18175ndash188 Available at httpwwwncbinlmnihgovpubmed8513290
Wilson TM Tanaka H 2000 Meta-analysis of the age-associated declinein maximal aerobic capacity in men relation to training status Am JPhysiol Heart Circ Physiol 278H829ndash834 Available at httpwwwncbinlmnihgovpubmed10710351
Wood SN 2006 Generalized Additive Models An Introduction with RBoca Raton Florida Chapman and HallCRC Press
World Health Organization 2001 Iron deficiency anaemia assessmentprevention and control a guide for programme managers Available athttpwhqlibdocwhointhq2001WHO_NHD_013pdf
Yoopat P Toicharoen P Boontong S Glinsukon T Vanwonterghem KLouhevaara V 2002 Cardiorespiratory capacity of Thai workers in dif-ferent age and job categories J Physiol Anthropol Appl Hum Sci 21121ndash128 Available at httpwwwncbinlmnihgovpubmed12056179
Zhu YI Haas JD 1997 Iron depletion without anemia and physical per-formance in young women Am J Clin Nutr 66334ndash341 Available athttpwwwncbinlmnihgovpubmed9250112
14 AC PISOR ET AL
American Journal of Human Biology

individuals who do not meet this level However manyTsimane (55 of females 81 of males) did not achievethis criterion either because the age-specific maximalHRs derived from industrialized populations are inaccu-rate for the Tsimane or because higher fitness allowedthese Tsimane to perform the step test with less effort Wetherefore evaluated several exclusion criteria for the Tsi-mane sample including the HR range specified by Shep-hard (1970) for the calculation routine a HR increase oflt5 beats per minute during exercise (National Healthand Nutrition Examination Survey 2004) different per-centages [65 (Siconolfi et al 1985) 70 (American Collegeof Sports Medicine 2006 Canadian Society for ExercisePhysiology 2003) 75 (NHANES 2004)] of age-specificmaximal HR (Tanaka et al 2001) achieved the 95th cen-tile obtained from a Generalized Additive Model for Loca-tion Scale and Shape (Rigby and Stasinopoulos 2005)and a rate of HR increase from the beginning to the end ofexercise that is beyond the 95 confidence interval (CI)from the 20 year age- and sex-specific mean The samplesize remaining after these exclusions varies from 4(75 of age-specific maximal HR) to 79 (increase lt5beats per minute during exercise) of our original sample(for sample sizes under each criterion considered see Sup-porting Information Table S1) We interpreted exclusioncriteria that excluded the vast majority of participants asnot giving a representative sample of the Tsimane Theuse of centiles or CIs enables us to compare each partici-pant against a metric from the same population Becausethe centile and CI approaches led to about the same rela-tively small number of participants excluded we adoptedthe CI exclusion for ease of interpretation
To evaluate the accuracy of HR estimation for the Tsi-mane population we compare VO2max estimated fromHR with VO2max estimated from the ratio of inhaled toexhaled O2 collected in a smaller subset of Tsimane Anadditional strength of the O2 method is that the VO2 andHR measured for a given individual is extrapolated to pre-dict their VO2max at their predicted age-specific maximalHR without reliance on additional assumptions beyondthat of an age-specific maximal HR Methods used in O2
measurement are described in the Supporting Informa-tion (Appendix A)
Tsimane model covariates Fat-free mass (FFM) was esti-mated by subtracting body fat mass from total mass Bodyfat percentage was estimated with bioimpedance using aportable Tanita scale and with skinfold measurementtaken at four sites (bicep tricep subscapular suprailiac)body fat percentage was estimated from skinfold measure-ment with equations from Durnin and Womersley (1974)Arthritis and respiratory ailments were diagnosed byTHLHP physicians during routine medical exams Hemo-globin levels in g dl21 were attained using the QBC Auto-read Plus Dry Hematology System (QBC DiagnosticsPort Matilda PA) anemia was defined using Centers forDisease Control (CDC) criteria (CDC 1998) and for agesfor which CDC criteria were not available World HealthOrganization (2001) criteria Helminth and giardia infec-tions were diagnosed in wet slide mounts and using amodified Percoll technique as has been previouslydescribed (Blackwell et al 2011 Eberl et al 2002) Wecoded helminth infection as bivariate (presence or absenceof helminths) combining diagnoses with hookworm
roundworm (Ascaris lumbricoides and Strongyloides ster-coralis) and whipworm (Trichuris trichiura) Because ofan established relationship between helminth infectionand anemia helminths and giardia are considered sepa-rately in this analyses Self-reported pain was included asa binary measure indexing the presence of back kneebone or connective tissue pain Spanish-speaking abilitywas treated as dichotomous where individuals rated asspeaking more than ldquosomerdquo Spanish by THLHP projectstaff were considered Spanish speakers Additional cova-riates include pregnancy status and as-the-crow-flies dis-tance of home village to the market town of San Borja
Because of a concern that leg length relative to benchheight may affect performance during step tests (Shahna-waz 1978) we considered including leg length in allwithin-population regressions Leg length was calculatedby subtracting participant seated height (minus chairheight) from standing height Including leg length wors-ened model fits perhaps because mass and leg length aremoderately correlated (for females Pearsonrsquos r 5 042 formales r 5 041) and mass is already controlled for by ouruse of relative (rather than absolute) VO2max addition-ally use of the leg length variable eliminated participantsfor whom seated height data were unavailable As suchwe decided to not control for leg length in the analysesbelow
Canadian health measures survey Canadian fitness datawere collected during the first wave of the CanadianHealth Measures Survey (CHMS wwwstatcangccaimdb-bmdi5071-enghtm) from 2007 to 2009 Canadianswere selected as a comparison group since VO2max in theCHMS was assessed using a step test procedure withVO2max estimated based on HR Individuals weresampled with the goal of representing 97 of the Cana-dian population from all provinces (Giroux 2007) Asmeasured with tri-axial accelerometers Canadian chil-dren in this sample are sedentary for 64 of their wakinghours (Colley et al 2011a) adult (ages 20ndash79) females aresedentary for 69 of the day and adult males are seden-tary for 68 (Colley et al 2011b)
Pretest exclusion CHMS CHMS participants wereexcluded from fitness testing if they had a heart conditionchest pain high blood pressure (systolic blood pressurehigher than 144) or heart rate (higher than 100) or weretaking medication for any of these conditions (Bryan et al2007) across all ages a total of 267 of potential partici-pants were excluded including 56 of 60ndash69 year olds(Shields et al 2010) Participants who experienced discom-fort during testing could stop at any time Women morethan 12 weeks pregnant were not allowed to participate
Experimental protocol CHMS Participants completed astep test developed by Bailey et al (1976 modified byWeller et al 1993) on a bench with two steps each 203cm tall Individuals began stepping at a rate expected torequire 65ndash70 of VO2max for a same-sex individual 10years their senior (Canadian Society for Exercise Physiol-ogy 2003) After a 3 min exercise interval researchersmeasured HR to ascertain whether the participant hadachieved 85 of his or her age-specific maximal HR If
4 AC PISOR ET AL
American Journal of Human Biology
85 of maximal HR was reached exercise testing wasstopped if 85 of maximal HR was not reached partici-pants proceeded to the next stage of exercise stepping ata faster cadence
VO2max was estimated using a regression equationdeveloped by Weller et al (1993)
E VO2maxeth THORN532116a2024b2017c (3)
where a is the estimated VO2 at the end of the finalstage of exercise (Weller et al 1993) b is age in yearsand c is body weight in kg If a participant could not stepat the prescribed cadence during a given stage of exerciseVO2max was estimated based on the last completed exer-cise stage (Shields et al 2010) About 1 of participantseligible for the test did not complete it Participants didnot proceed beyond the eighth level of exercise regardlessof whether they had attained 85 of their age-specificmaximal HR The result is estimated relative VO2max (mlmin21 kg21)
Skinfold measurements used to calculate absoluteFFM in this article were taken before the cardiovascularfitness test at four sites (bicep tricep subscapular andsuprailiac) using Harpenden calipers (Baty InternationalUK Shields et al 2010) but only for individuals with abody mass index under 30 kg m22
Statistical analyses
All statistical analyses were performed with the R soft-ware package version 2153 (R Development Core Team2011) Smooth fits used generalized additive models(GAM) which regress a predictor on the response andsmooth the residuals (Venables and Ripley 2002) in thepackage used for the present analyses (mgcv Wood2006) the degree of smoothness was determined by apenalized likelihood technique The result is a model thathas both linear and non-linear elements allowing a closefit to the data while also providing interpretable parame-ter estimates Where appropriate model fits were eval-uated using the Akaike Information Criterion (AIC) amaximum likelihood measure of goodness-of-fit
Exploratory models indicate sex differences in VO2maxin the Tsimane population and so each sex is modeledseparately in all analyses Because data for both popula-tions only exist for ages 11ndash69 all cross-population com-parative analyses (linear models t-tests) are limited tothis age group Age in years is included in all analysesWithin-population comparisons (linear models) use theTsimane subsample age 20 and older an age group inwhich both males and females are close to their peakVO2max and include individuals up to age 70 compara-ble to the Canadians and before the age at which optingout removed large portions of the sample For the subsam-ple between 20 and 69 females and males evidence a lin-ear decline although female VO2max is curvilinear whenall ages are considered because all within-populationcomparisons (linear models) are performed on this sub-sample age2 terms were not included Publically availableCHMS data are limited to VO2max mean and standarddeviation for age categories of variable size (for categoriessee Table 3) Cross-population comparisons use the sameage categories to explore differences between Canadiansand Tsimane
Covariates could not be included in between-populationcomparisons as the latter are based on binned data how-ever extensive individual-level Tsimane data allow fordetailed examination of factors that may mediate physicalfitness decline For these within-population linear modelswe only included participants aged 20ndash69 for whom medi-cal and anthropometric data were available during thesame medical round (about a calendar year in lengthTable 1)
To explore the possibility of a non-linear relationshipbetween mass and VO2max and how this might affectany differences between the Tsimane and Canadians we1) allometrically scaled Tsimane VO2max and 2) projectedrelative VO2max for the Tsimane using Canadian fatmass and FFM from same-sex same-age categories Toallometrically scale VO2max we calculated a the scalingparameter in allometric equations for the Tsimane(Calder 1987) To project VO2max for the Tsimaneassuming the same body composition as the Canadianswe regressed absolute VO2max on absolute fat mass abso-lute FFM and age (and age2 for the Tsimane females) inthe Tsimane female and male subsamples With theresulting parameter estimates we predicted whether Tsi-mane would perform at rates similar to those observed inour study if the Tsimane had the average fat mass andFFM exhibited in each of the four Canadian cohorts (ages12ndash19 20ndash39 40ndash59 and 60ndash79) The results of these cal-culations are discussed below Hereafter VO2max willrefer to relative VO2max unless otherwise stated
RESULTS
Age at peak VO2max and levels across the lifespan
Tsimane Predicted values of absolute (l min21) and rela-tive VO2max (ml min21 kg21) for the Tsimane appear inFigure 1 Both Tsimane females and males exhibit a peakin absolute VO2max A peak in absolute VO2max is char-acteristic across populations but appears in late adoles-cence in industrialized nations concurrent with peakabsolute FFM (Armstrong 2001) In the Tsimane as wellpeak absolute VO2max and peak absolute FFM areroughly concurrent using smoothed fits of predicted val-ues female VO2max peaks at age 31 at 295 l min21 and
TABLE 1 Descriptive statistics for the Tsimane after exclusion (ages20ndash69)
Variables
Tsimane Females Tsimane Males
Mean(and SD)or Percent n
Mean(and SD)or Percent n
Age 413 (143) 203 436 (152) 280Body weight (kg) 534 (93) 203 624 (74) 280FFM (kg) 397 (43) 203 520 (58) 280Perc FFM 075 (008) 203 084 (005) 280Distance to town in 10 km 44 (24) 196 42 (24) 273Hemoglobin 129 (14) 117 143 (12) 157Arthritis 11 133 4 185Helminths 51 92 58 128Giardia 38 92 40 128Nonarthritic Pain 54 133 75 138Respiratory Ailments 27 133 15 185Spanish-speaking Ability 17 271 42 271Pregnant 3 203 ndash ndash
Two-level factors are reported as percentage of the subsample with a givenailment
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 5
American Journal of Human Biology
absolute FFM at age 34 at 405 kg for males VO2maxpeaks at age 24 at 344 l min21 and FFM at age 29 at 544kg Estimated peak VO2max is relatively robust to thesmoothing parameter selected with the peak shifting nomore than 1 year for females and two years for malesunder different methods of smoothing Average level ofVO2max may appear higher in females but a median fitreveals that Tsimane females and males have roughlysimilar VO2max (see Supporting Information Fig S2)
Relative (ml min21 kg21) VO2max estimation controlsfor the effect of body mass (and by extension partiallycontrols for percent FFM correlation between the two forfemales r 5 2075 for males r 5 2043) Removing theeffects of body mass by using a relative measure does notremove the peaks exhibited by females or males in earlyadulthood (Fig 1) Tsimane females peak at age 28 (5379ml min21 kg21) and Tsimane males peak at age 22 (at5489 ml min21 kg21) Indeed this peak also remainswhen we scale by absolute FFM (ml min21 fat-free kg21see Supporting Information Table S2)
To evaluate whether Tsimane participants performedsimilarly under the O2 method we compared age-matched subsamples to O2 method participants Tsimanemales performed significantly worse under the HRmethod relative to the O2 method (O2 mean 5 695 mlmin21 kg21 HR mean 5 590 ml min21 kg21 t 5 629Plt 0001) There is no significant difference between Tsi-mane females tested under the HR and O2 methods (O2
mean 5 529 HR mean 5 543 t 5 2077 P 5 044) For acomparison of smooths from the two samples see Sup-porting Information Figure S3Mediators of Levels Across the Tsimane Lifespan Weidentified and investigated several health-related factorsthat might affect level of VO2max achieved by eitherdiminishing resources available to the body or hamperingthe cardiovascular system directly We posit that thesevariables may mediate the effect of age on VO2max Can-didate mediators include the presence of anemia infectionwith helminths or giardia arthritis or nonarthritic painrespiratory ailments distance from the local market
Fig 1 Predicted Tsimane VO2max by age Predicted values are drawn from GAM models regressing smooths of log age on VO2max Inter-vals are 95 prediction intervals Age was smoothed using restricted maximum likelihood Other smoothing parameters (such as Mallowrsquos Cpand maximum likelihood) varied the age at peak absolute VO2max by up to 1 year for females and up to 2 years for males Points represent theraw data for Tsimane A Absolute VO2max by age for females B Absolute VO2max by age for males C Relative VO2max by age for femalesD Relative VO2max by age for males [Color figure can be viewed in the online issue which is available at wileyonlinelibrarycom]
6 AC PISOR ET AL
American Journal of Human Biology
town and Spanish speaking ability Although percentFFM generally predicts absolute rather than relativeVO2max we test it as a potential mediator Pregnancywas included as a control in female models While a highmacroparasite load may increase the likelihood of havinglow hemoglobin (and thus anemia) an interaction termbetween presence of helminths and presence of anemiawas not included because they are not significantlyrelated in this sample only 26 participants of the 92 withhelminths have anemia while 14 of the 86 without hel-minths have anemia (for females v2 5 052 P 5 047 formales v2 5 200 P 5 016)
To evaluate whether these candidate mediators affectedVO2max levels we conducted linear regressions on rela-tive VO2max (see Table 2) We first examined each predic-tor independently Females with higher hemoglobin levelshad significantly higher cardiovascular fitness perform-ance for an increase in 1 g dl21 concentration of hemoglo-bin a Tsimane woman is predicted to have 293 ml min21
kg21 higher VO2max (t 5 268 Plt 001) Helminth infec-tion mediated the relationship between age and VO2maxfor males such that men with a helminth infection arepredicted to have 616 ml min21 kg21 higher VO2max(t 5 231 Plt 005) A best fit model approach (fit on thesubset of females for whom all measures are available)provides similar results to fitting a separate model for
each potential mediating variable When a stepwise AICprocedure was used with data on all health and marketintegration measures hemoglobin level was the only sig-nificant predictor that remained in the female model(n 5 82 standardized b 5 022 Plt 005) For males hel-minth infection remained in the model as well (n 5 116standardized b 5 023 Plt 005)
Scaling VO2max by FFM (ml min21 fat-free kg21)rather than body mass produced similar results hemoglo-bin levels remained a significant positive predictor ofVO2max for females (standardized b 5 030 Plt 001) andhelminth infection a positive predictor for males (standar-dized b 5 020 Plt005) See Supporting InformationTable S3 for all regression results with ml min21 fat-freekg21 as the outcome
Anemia was initially included in model fits howevertreating hemoglobin level as a covariate in place of pres-ence of anemia improved model fit for Tsimane females(anemia AIC 5 10027 hemoglobin AIC 5 98963)Although no association was found between presence ofanemia and helminth infection there is a significant asso-ciation between hemoglobin levels and helminth infectionControlling for age a helminth diagnosis is a significantnegative predictor of hemoglobin levels for females (stand-ardized b 5 2031 Plt 001) Replacing presence of ane-mia with hemoglobin level for males did not improve or
TABLE 3 Comparison of Tsimane and Canadian relative VO2max by age category and sex
Sex Age group
Tsimane Canadians
t-Statistic P-valueMean (ml min21 kg21) n Mean (ml min21 kg21) n
Females 11ndash14 435 7 487 534 2118 02815ndash19 476 33 423 500 310 00020ndash39 510 72 383 662 908 00040ndash59 431 69 314 655 1005 00060ndash69 412 5 242 554 340 003
Males 11ndash14 415 4 548 542 2300 00615ndash19 516 31 508 514 046 06520ndash39 511 96 442 526 527 00040ndash59 432 68 362 584 380 00060ndash69 381 26 275 546 509 000
TABLE 2 Linear models exploring whether mediators affect the level (main effects models) of relative VO2max for Tsimane females and males
Sex Candidate mediatorAge effect est
(P-value)
Main effect models
Sample sizeMediator main effect
est (P-value) Age main effect est (P-value)
Females Perc FFM 2023 (000) 000 (097) 2023 (000) 203Hemoglobin 2013 (028) 024 (001) 2011 (022) 117Helminths 2019 (007) 003 (077) 2020 (006) 92Giardia 2019 (007) 011 (028) 2019 (007) 92Lung ailment 2017 (006) 2005 (060) 2018 (005) 133Reported pain 2017 (006) 2001 (094) 2017 (006) 133Arthritis 2017 (006) 2002 (083) 2016 (007) 133Distance to town 2023 (000) 002 (081) 2023 (000) 196Spanish speaking 2023 (000) 2008 (056) 2024 (000) 197
Males Perc FFM 2037 (000) 009 (012) 2034 (000) 280Hemoglobin 2029 (000) 2002 (076) 2029 (000) 157Helminths 2030 (000) 019 (002) 2027 (000) 128Giardia 2030 (000) 006 (049) 2030 (000) 128Lung ailment 2030 (000) 2007 (033) 2031 (000) 185Reported pain 2030 (000) 011 (013) 2031 (000) 185Arthritis 2030 (000) 2006 (044) 2028 (000) 185Distance to town 2037 (000) 2003 (059) 2037 (000) 273Spanish speaking 2038 (000) 008 (050) 2037 (000) 271
All parameter estimates are standardized
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 7
American Journal of Human Biology
worsen model fit and there is no significant relationshipbetween hemoglobin levels and helminth infection formales (standardized b 5 2010 P 5 028) Parameter esti-mates for anemia were not significant in models for eitherfemales or males
Between-group Table 3 presents Tsimane and Canadianestimated VO2max binned into age categories used byCHMS These data suggest that Canadian females andmales achieve peak VO2max between the ages of 11 and14 while Tsimane males peak between ages 15 and 19Tsimane females peak later between age 20 and 39Across comparable age categories Tsimane have signifi-cantly higher VO2max than Canadians at all ages exceptbetween 11 and 15 for females and 11 and 19 for males(Table 3) However the sample size of Tsimane teenagersunder age 15 is quite small As aforementioned to controlfor the influence of a small number of data points for theyoungest and oldest Tsimane individuals we used GAMto predict VO2max across logged age Predicted valuessuggest that Tsimane females peak at age 28 and Tsimanemales peak at age 22 (see Fig 1c d) These estimates areconsistent with scatterplots of the raw data (plotted onFig 1) and mask fewer fine-grained effects of age thanTable 3 as each CHMS adult age category spans twodecades
It is possible the difference between the Tsimane andCanadians reflects a greater increase in body mass acrossages in the Canadian population or different trajectoriesof change in body composition The former could occurbecause body mass appears in the denominator and cantherefore scale down VO2max while the latter implies dif-ferential changes in FFM when FFM is a predictor ofVO2max in many studies To explore these possibilitieswe performed two calculations we allometrically scaledTsimane VO2max and we projected Tsimane VO2maxassuming the Tsimane had equivalent fat mass and FFMas Canadians from same-sex same-age categories Con-trolling for age the allometric scaling coefficient a wasslightly greater than 1 for both sexes (females a 5 111males a 5 118) This suggests that any disparity inVO2max between Canadians and the Tsimane cannot beexplained solely by mass differences Indeed assumingthe Tsimane have the same body composition as Cana-dians projected VO2max differs little from observedVO2max The Tsimane outperform the Canadians in everycohort by at least 35 ml min21 kg21 except among theyoungest males who perform similarly (see SupportingInformation Fig S4)
To control for possible disparities in changes in bodycomposition by age within each population as these mightalso influence differences between the Tsimane and Cana-dians we scaled VO2max by absolute FFM from the samepopulation to obtain ml min21 fat-free kg21 BecauseCanadian body composition data were only available viaskinfolds (bicep tricep subscapular and suprailiac) weused the subset of Tsimane (n 5 246) for which the samefour skinfolds measurements were available We calcu-lated average absolute FFM for each cohort using averageweight and average summed skinfolds (Durnin andWomersley 1974) and scaled average VO2max in mlmin21 by this number to obtain ml min21 fat-free kg21Under this method of scaling the Tsimane outperformCanadians in every cohort over age 20 by at least 165 ml
min21 fat-free kg21 (see Supporting Information TableS2) Canadian females and males in the 12ndash19 cohortsoutperform Tsimane of the same age
We next compared Tsimane to other subsistence popula-tions reported in the literature (Table 4) Consistent withcommon practice in the literature we report means foreach group but when possible we also predicted VO2maxat age 25 to provide age-corrected comparisons Weselected age 25 as it is the age of peak relative VO2max inthis study and for female Kamba and Maasai in Christen-sen et als (2012) recent study To predict VO2max at age25 we regressed the median ages on mean VO2max acrossthe available age categories Tsimane females and maleshave roughly the same predicted VO2max at age 25 asseveral other subsistence populations but higher VO2maxthan industrialized populations To test for differencesbetween industrialized and subsistence populations weconducted a linear regression on predicted VO2max at age25 this is not a meta-analysis and results should beinterpreted with caution Overall subsistence populationsdisplay higher peak VO2max than in industrialized popu-lations controlling for sex (440 vs 367 ml min21 kg21
[Plt 001]) The Tsimane O2 and indigenous Siberian sam-ples were excluded Tsimane O2 to avoid the problem ofnon-independence with Tsimane HR data and Siberiansbecause the sample has a limited age range comparedwith the other studies
Pace of decline slope of VO2max decline across thelifespan
Tsimane To evaluate whether Tsimane participants per-formed similarly under different methods we comparedage-matched subsamples of participants from the presentstudy with O2 method participants Despite a higher level(intercept) of VO2max in the O2 sample Tsimane malesdeclined marginally significantly faster under the O2
method relative to the HR method (O2 5 68 per decadeHR 5 47 decline per decade t 5 2195 P 5 005) Thereis no significant difference between Tsimane femalestested under the O2 and HR methods (O2 5 60 per dec-ade HR 5 48 decline per decade t 5 2055 P 5 058)Mediators of Slope Across the Lifespan We fit a series oflinear models to test for interactions between the candi-date mediators and age-related decline in TsimaneVO2max There are no variables that significantly inter-act with age to predict VO2max (see Supporting Informa-tion Table S4) An AIC selection approach and scaling byabsolute FFM (see Supporting Information Table S3) pro-vides the same results no variables significantly interactwith age to predict VO2max
Between-group VO2max is most often reported as a lin-ear decline across the adult lifespan though Hawkins andWiswell (2003) dispute whether the decline is actually lin-ear For example a linear approximation is not appropri-ate for Tsimane females if ages 11ndash80 are consideredFigure 2 contrasts linear declines in VO2max for Cana-dians and Tsimane males as well as a curvilinear fit forTsimane females with declines in industrialized nationsderived from meta-analyses (Fitzgerald et al 1997 Wil-son and Tanaka 2000) To explore whether rates ofdecline in VO2max among Tsimane and Canadians weredifferent we regressed average VO2max by age category
8 AC PISOR ET AL
American Journal of Human Biology
TA
BL
E4
Mea
nV
O2m
ax
esti
ma
ted
VO
2m
ax
at
age
25a
nd
dec
lin
ein
VO
2m
ax
per
dec
ad
efr
omth
isst
ud
ya
nd
pre
vio
us
rese
arc
ha
Pop
ula
tion
Fem
ale
Male
Pu
bli
cati
onM
ean
VO
2m
ax
VO
2m
ax
Age
25
bP
erce
nt
Dec
lin
eA
ge
Ran
ge
(n)
Mea
nV
O2m
ax
VO
2m
ax
Age
25
bP
erce
nt
Dec
lin
eA
ge
Ran
ge
(n)
Ind
ust
riali
zed
Can
ad
ac
312
400
73
20ndash69
(2905)
361
458
68
20ndash69
(2712)
Jap
an
d357
414
39
20ndash69
(656)
417
473
38
20ndash69
(807)
San
ad
aet
al
2007
Sw
eden
e330
g409
80
20ndash65
324
g388
75
20ndash65
Ek
blo
met
al
2007
Th
ail
an
d(i
nd
ust
ry)e
275
293
54
16ndash55
(56)
389
415
57
16ndash53
(70)
Yoo
pat
etal
2002
US
(H
erit
age)
f273
17ndash65
(360)
359
17ndash65
(293)
Sk
inn
eret
al
2003
US
(N
HA
NE
S)d
356
363
24
20ndash49
(1312)
444
438
39
20ndash49
(1481)
Su
bsi
sten
ceT
sim
an
e(H
R)c
498
521
h16
h20ndash69
471
538
h61
h20ndash69
Tsi
man
e(O
2)c
436
74
h36ndash69
540
25
h36ndash69
Ifalu
k(1
969ndash70)c
429
488
69
20ndash59
(43)
49
597
75
20ndash69
(75)
Rod
ean
dS
hep
hard
1994
Ach
ec465
434
257
20ndash59
(62)
519
614
84
20ndash59
(65)
Walk
eran
dH
ill
2003
Lu
oc378
372
39
17ndash68
(209)
429
48
54
17ndash68
(172)
Ch
rist
ense
net
al
2012
b
Kam
ba
c377
371
45
17ndash68
(283)
431
516
34
17ndash68
(94)
Ch
rist
ense
net
al
2012
Maasa
ic389
410
45
17ndash68
(178)
431
528
69
17ndash68
(163)
Ch
rist
ense
net
al
2012
Ind
igen
ous
Sib
eria
nsc
338
341
22
220ndash39
(14)
462
471
66
20ndash39
(30)
Katz
marz
yk
etal
1994
Ru
ral
Nep
alc
187
15ndash60
(39)
221
15ndash60
(35)
Pan
ter-
Bri
cket
al
1992
Ngis
onyok
aT
urk
an
af
38
387
18
20ndash44
(19)
Cu
rran
-Ever
ett
1994
aV
alu
esm
issi
ng
wh
enn
otavail
able
from
ap
art
icu
lar
stu
dy
Per
cen
td
ecli
ne
(per
cen
tof
pea
kvalu
elo
st)
per
dec
ad
ew
as
calc
ula
ted
as
by
regre
ssin
gre
lati
ve
VO
2m
ax
by
age
mu
ltip
lyin
gth
ep
ara
met
eres
tim
ate
for
age
by
10
an
dd
ivid
ing
this
nu
mber
by
the
inte
rcep
t(p
resu
med
pea
k
ass
um
ing
ali
nea
rd
ecli
ne
inV
O2m
ax
acr
oss
age)
B
ecau
seof
lack
ofacc
ess
tora
wd
ata
re
gre
ssio
ns
wer
efi
tw
ith
mea
nV
O2m
ax
an
dm
edia
nage
by
coh
ort
bA
ge
25
valu
esw
ere
esti
mate
dby
regre
ssin
gre
lati
ve
VO
2m
ax
by
age
then
usi
ng
the
resu
ltin
gp
ara
met
eres
tim
ate
sto
pre
dic
tV
O2m
ax
at
age
25
the
pea
kin
rece
ntl
yst
ud
ied
pop
ula
tion
s(e
g
Kam
ba
an
dM
aasa
ife
male
sC
hri
sten
sen
etal
2012fe
male
san
dm
ale
sin
this
art
icle
)B
ecau
seof
lack
ofacc
ess
tora
wd
ata
re
gre
ssio
ns
wer
efi
tw
ith
mea
nV
O2m
ax
an
dm
edia
nage
by
coh
ort
cS
ubm
axim
alst
epte
st
dS
ubm
axim
altr
ead
mil
lte
st
eS
ubm
axim
aler
gom
eter
test
f M
axim
al
ergom
eter
test
gS
wed
ish
data
wer
ere
por
ted
as
med
ian
sfo
rea
chage
cate
gor
yth
evalu
esre
por
ted
her
eare
mea
ns
ofth
ese
med
ian
s2006
ind
ivid
uals
part
icip
ate
dbu
tn
um
ber
by
sex
was
not
rep
orte
d
hF
orco
mp
ara
bil
ity
we
bin
ned
the
Tsi
man
eH
Ran
dO
2d
ata
into
10
yea
rage
cate
gor
ies
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 9
American Journal of Human Biology
on median age (for a given age category) population andtheir interaction term For comparability Tsimane werebinned into the Canadian age categories and averageswere computed for these categories leading to estimateddeclines slightly different from those in Table 4 for thepurposes of this test we treat the Tsimane female declineas linear Because within-population variance in declineis not available these regressions should be treated asdescriptive comparisons rather than statistical tests ofdifferences between the two groups The rate of decline inVO2max is steeper for Canadian females (69 per decadefaster decline per decade) and males (42 faster declineper decade) compared with Tsimane females and males
The rate of cardiovascular fitness decline between theTsimane and Canadians is different but this differencedoes not extend to industrialized and subsistence popula-tions (see Table 4) Controlling for sex subsistence groupshave about one quarter of a percent lower declines perdecade Again because the variance in decline is not rep-resented in this regression results should be interpretedas comparative rather than as a statistical test As beforeTsimane O2 results were not included in the analysis toavoid nonindependence and the indigenous Siberianswere excluded because of discrepancy in ages sampled
DISCUSSION
Our comparisons demonstrate that across a wide varietyof societies cardiovascular fitness senesces with age Car-diovascular fitness is higher on average among members ofsubsistence societies than among industrialized societiesbut rates of fitness decline from peak are not slower Ourmore detailed comparison between the Tsimane a subsist-ence population and Canadians an industrialized popula-tion reveals differences in cardiovascular fitness levelsand rate of fitness decline Cardiovascular fitness levelswere higher among the Tsimane than among Canadiansand the rate of decline across the lifespan was significantlyslower among Tsimane women and men Potential Cana-
dian participants were excluded due to many health con-cerns including pregnancy and history of high bloodpressure whereas Tsimane were only excluded if they self-identified as unable to participate This suggests the Cana-dian sample is a relatively healthy subsample of Canadayet the Tsimane still outperform them in cardiovascular fit-ness It may be that the higher demand for cardiovascularfitness in late ages among the Tsimane outweighs anyeffects of poor health Another possibility is that greaterself-selection among Tsimane due to higher adult mortalityleaves more robust older adult survivors thereby reducingthe observed slope of fitness decline at the population level(Vaupel et al 1979) perhaps this is partially why fewerTsimane older adults opted out of the exercise test thanCanadian older adults were screened out (ages 60ndash69Canadian females 5 56 Tsimane females 5 15 Cana-dian males 5 57 Tsimane males 5 5)
Consistent with prior research on age-related changesin cardiovascular fitness the Tsimane do evidence a lin-ear decline in VO2max with age but not as steep a declineas typically seen in industrialized populations Based oncomparisons with the Canadians and with other industri-alized populations we believe the Tsimane data from thepresent study and the pilot O2 data combined indicatethat the Tsimane perform better on tests of cardiovascularfitness than the average individual from an industrializednation
To further explore the potential effects of health factorson cardiovascular fitness level and rate of decline weinvestigated predictors of individual differences in fitnesswithin the Tsimane population Overall we found thatmost health indicators among the Tsimane did not hinderVO2max levels or rates of decline Lower hemoglobin lev-els were associated with lower VO2max levels in womenbut not men consistent with the notion that compromisedblood oxygen transport curbs cardiovascular fitness(Buzina et al 1989 Panter-Brick et al 1992) In the USlow hemoglobin is more common in active women thanactive men (Sinclair and Hinton 2005) hemoglobin is
Fig 2 Linear changes in VO2max with age for Canadians and the Tsimane Intercepts and slopes for Canadians and Tsimane can be foundin Table 4 Because age2 is significant for the full sample of Tsimane females their change in VO2max across age is curvilinear Slopes forendurance trained active and sedentary individuals from industrialized nations are drawn from a meta-analysis performed by Fitzgeraldet al (1997) for females and Wilson and Tanaka (2000) for males Endurance trained individuals are represented by the top dotted line abovefollowed by active individuals below and sedentary on the bottom Trained individuals engage in 31 sessions of endurance exercise per weekfor at least a year while active individuals engage in 2 or fewer sessions per week of cardiovascular exercise [Color figure can be viewed in theonline issue which is available at wileyonlinelibrarycom]
10 AC PISOR ET AL
American Journal of Human Biology
also lower in Tsimane women than Tsimane men(female 5 129 [sd 13] g ml21 males 5 142 [13] g ml21)Even mild (non-anemic) iron deficiencies impacts womenrsquosexercise performance (Zhu and Haas 1997) Inconsistentwith findings from Panter-Brick et al (1992) among ruralNepalese helminth infection did not diminish levels ofVO2max for Tsimane men helminth infection wasactually a predictor of higher VO2max There are severalreasons why this might be the case First we only testedwhether presence or absence of helminths mediated theeffect of age on VO2max rather than parasite load (egnumber of worms egg counts) it is possible that helminthinfection only affects VO2max at high parasite loads Sec-ond blood loss (and thus low hemoglobin levels) resultingfrom helminth infection may be partially offset by theamount of iron in the Tsimane adult diet Tsimane ironintake is an estimated 166 of the US Dietary ReferenceIntake (Martin et al 2012) and Tsimane hemoglobin lev-els are higher than in the Nepalese (females 129 vs 109males 1424 vs 120 Panter-Brick et al 1992) Thirdthese analyses consider helminth infection at the time ofexercise test rather than past infections It may be thatthe cumulative burden of past infection has a larger effecton cardiovascular fitness if so this would suggest thatthe surprising positive effect of helminth infection onVO2max levels in men is either spurious or capturing athird variable
Secular declines in VO2max are expected with increasingmarket integration and lifestyle change because ofincreased sedentism (Katzmarzyk et al 1994 Rode andShephard 1994) Two proxies for market integration in thispopulationmdashdistance to San Borja and the ability to speakSpanishmdashwere not significant predictors of VO2max levelsor decline This is consistent with our predictions as Tsi-mane females and males that live near town do not appearto have lower activity levels (Gurven et al 2013) Wageopportunities near town primarily include working asranch hands collecting and weaving palm thatch panelscash cropping and working for logging companies Each ofthese involves extensive activity furthermore transporta-tion to town often involves bicycling walking and polingdugout canoes Cash cropping of rice and corn also involvesthe clearing and weeding of larger fields Except for cashcropping and palm thatch manufacture most wage laboropportunities are currently restricted to men
This study makes several unique contributions to theexisting literature It offers the first systematic compari-son of cardiovascular fitness level and rate of declinebetween subsistence and industrialized societies Resultscompiled from previous studies support the general claimthat despite greater pathogen stress the greater activityregime of subsistence societies helps support higher peakVO2max Additionally this is one of the first studies toexplore senescent changes in cardiovascular fitnesswithin a large sample from a subsistence population Thelarge number of health measures and proxies of marketintegration available permitted testing whether these fac-tors mediated age-related variation and whether theymodulated the rate of decline Despite reports that healthstatus and market integration have been important inother studies (eg Buzina et al 1989 Katzmarzyk et al1994 Panter-Brick et al 1992 Rode and Shephard1994) their overall net effect was small among the Tsi-mane most apparent in measures of hemoglobin levelsamong women and helminth infection among men
The results of these analyses may also shed light onindividual and population level differences in chronic dis-ease In industrialized populations meta-analyses demon-strate that cardiovascular fitness is protective againstcardiovascular disease (Jette et al 1992 Hawkins andWiswell 2003) Prior studies among Tsimane suggest rel-atively few deaths from heart attacks or strokes (Gurvenet al 2007) a low prevalence of common cardiovasculardisease risk factors like obesity high blood low-densitylipoprotein levels hypertension and peripheral arterialdisease and the existence of additional protective factorslike lean diet and physical activity (Gurven et al 20092013 Vasunilashorn et al 2010) Market foods such ascooking oil sugar and pasta represent only 6 of theaverage Tsimane diet and Tsimane also consume a greatdeal of lean meat and omega-3 fatty acids (Martin et al2012) This study complements these findings by demon-strating that Tsimane show relatively high VO2max anindicator of strong cardiorespiratory health TsimaneVO2max declines with age as it does everywhere whichsuggests declining muscle mass with age (Fleg andLakatta 1988) and lowered cardiac output (American Col-lege of Sports Medicine 2006 Sagiv et al 2007) ratherthan increased cardiovascular disease risk
Limitations
The Canadians were selected as a comparison industri-alized population because of the similarity of the CHMSand Tsimane protocols very few studies of industrializedpopulations have large sample sizes sample across thelife course and use a step test Several aspects of theCHMS and Tsimane protocols remain potentially incom-parable The Canadians experienced more stringentexclusion criteria than the Tsimane meaning that the Tsi-mane sample may be more representative of cardiovascu-lar condition in the Tsimane population than theCanadian sample of the Canadian population Again ifthe Tsimane sample was subjected to these criteria wemight expect the differences in VO2max between popula-tions to only increase On the other hand Canadian par-ticipants were assigned stepping cadences based on theirage and sex and cadence was increased across the exer-cise test if a participant did not reach 85 of his or herage-specific maximal HR all Tsimane were asked to com-plete 30 ascents per minute with no increase based ontheir achieved HRs Few Tsimane reached 75 of theirage-specific maximal HR (see Supporting InformationTable S1) perhaps because the age-specific maximal HRsderived from industrialized populations are inaccurate forthe Tsimane or because higher fitness allowed these Tsi-mane to perform the step test of 30 ascents per minutewith less effort Due to these discrepancies in protocolwhich may lead to errors in estimating VO2max we alsoincorporated Tsimane data collected using the O2 methodas a check because the O2 method estimates VO2max onthe relationship between HR and VO2 in a givenparticipant
Indeed it is an open question as to whether typicalmethods for indirectly estimating cardiovascular fitnessfrom HR are appropriate for subsistence level popula-tions Common routines for VO2max estimation assumeage-specific declines in cardiovascular fitness (eg Shep-hard 1970) but these methods have only been validatedwith samples from industrialized populations which are
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 11
American Journal of Human Biology
often self-selected (Beall et al 1985) Additionally regres-sions drawn from laboratory studies require participantsachieve a HR within a certain range for accurate VO2maxestimation however the appropriateness of these rangesgiven slight modifications to protocol and inclusion of par-ticipants of different ages different populations and bothsexes is questionable For example the maximal HRexhibited by young men varies across subsistence popula-tions (Shephard 1978) Use of these criteria is compli-cated by the fact that the most commonly used equationfor estimating maximal possible HR by age 220-age maybe inaccurate (Robergs and Landwehr 2002) and particu-larly inappropriate for older adults (see Tanaka et al2001) For these reasons we chose to use an exclusion cri-terion for the Tsimane that evaluates individual increasein HR across exercise relative to the mean increase in HRfor Tsimane of the same sex and age
The pattern of Tsimane fitness decline differs moder-ately by the choice of exclusion criterion for participants(see Supporting Information Table S1) and by method oftesting However this is a common finding Lee et al(2011) predicted VO2max from submaximal exercise usingthe O2 method and the HR-based American College ofSports Medicine calculation routine in a US sample Theyfound that (1) the HR-based routine predicts higherVO2max across the sexes than does the O2 routine and(2) the two methods have a correlation of only 077 Whenevaluating different testing procedures Shephard et al(1968) found differences in VO2max estimation by type oftest used (eg bicycle ergometer versus step test) and cal-culation routine Exercise tests exclusion criteria andcalculation routines combine to provide an estimate ofactual VO2max for a given individual and as such varia-tion in estimation is to be expected However such varia-tion may affect cross-population comparisons inunforeseen ways thus the comparisons presented hereshould be interpreted with caution
While population-level variation in cardiovascular fit-ness decline may reflect the differences in the demands ofendurance-based physical activity muscularity and com-promised oxygen transport it is possible that genetic fac-tors may also play a potential role (Collins 1999) In oneindustrialized sample maternal cardiovascular fitnessexhibited a heritability of 30 which is attributed toinheritance of the maternal mitochondrial genome (Bou-chard et al 2000) We do not have the relevant geneticdata for the populations considered here however andthus operate under the simplifying assumption thatinheritance should not affect population-level patternsand will not consistently bias individual-level compari-sons in any particular direction
This study is further limited by its cross-sectionaldesign Cross-sectional data present well-known problemsfor the measurement of individual aging (Crimmins andSeeman 2001) Mortality selection in which individualsin poorer condition are likely to die at younger ages pro-duces a downward bias in the estimation of aging rates atthe individual level (Vaupel and Yashin 1985 Vaupelet al 1979) Cohort effects if present also produce com-plicated and non-monotonic biases in estimation (Carnesand Olshansky 2001) Due to the problem of between-individual heterogeneity and the within-individual pro-cess of senescence a recent overview of aging studies con-cludes that ldquoonly longitudinal studies [ ] provide reliablesources of information in the study of senescencerdquo (Nussey
et al 2008) To date there are no longitudinal studies ofcardiovascular fitness in subsistence populations We arecurrently re-testing participants under the O2 methodallowing a better grasp of the within-individual variationthat shapes patterns of senescent decline
ACKNOWLEDGMENTS
The authors thank Paul Hooper Steven Gaulin JohnTooby Patricia Kramer the Human Evolution and Biode-mography laboratory and the Center for EvolutionaryPsychology at UCSB for helpful advice and feedback thestaff at the Tsimane Health and Life History Project andthe Tsimane for their participation and patience
LITERATURE CITED
American College of Sports Medicine 2006 ACSMrsquos Guidelines for Exer-cise Testing and Prescription 7th ed Philadelphia Lippincott Williamsamp Wilkins
Armstrong N 2001 Peak oxygen uptake in relation to growth and matura-tion in 11- to 17-year-old humans Eur J Appl Physiol 85546ndash551
Astrand PO Ryhming I 1954 A nomogram for calculation of aerobiccapacity (physical fitness) from pulse rate during submaximal work JAppl Physiol 7218ndash221
Bailey DA Shephard RJ Mirwald RL 1976 Validation of a self-administered home test of cardio-respiratory fitness Can J Appl SportSci 167ndash78
Beall CM Goldstein MC and Feldman ES 1985 The physical fitness ofelderly Nepalese farmers residing in rugged mountain and flat terrainJ Gerontol 40529ndash535
Benefice E Ndiaye G 2005 Relationships between anthropometry cardi-orespiratory fitness indices and physical activity levels in different ageand sex groups in rural Senegal (West Africa) Ann Hum Biol 32366ndash382 Available from httpwwwncbinlmnihgovpubmed16099780
Blackwell AD Gurven MD Sugiyama LS Madimenos FC Liebert MAMartin MA Kaplan HS Snodgrass JJ 2011 Evidence for a peak shift in ahumoral response to helminths age profiles of IgE in the Shuar of Ecuadorthe Tsimane of Bolivia and the US NHANES PLoS Negl Trop Dis 5e1218 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid53125146amptool5pmcentrezamprendertype5abstract
Blackwell AD Martin M Kaplan H Gurven M Evidence for an antagonis-tic relationship between Giardia lamblia and helminth infections impli-cations for treatment of helminth infections in developing populations
Blair SN LaMonte MJ Nichaman MZ 2004 The evolution of physicalactivity recommendations how much is enough Am J Clin Nutr 79913Sndash920S Available at httpwwwncbinlmnihgovpubmed15113739
Bouchard C Rankinen T Chagnon YC Rice T Perusse L Gagnon JBorecki I An P Leon a S et al 2000 Genomic scan for maximal oxygenuptake and its response to training in the HERITAGE Family Study JAppl Physiol 88551ndash559 Available at httpwwwncbinlmnihgovpubmed10658022
Bryan S St-Denis M Wojtas D 2007 Canadian Health Measures Surveyclinic operations and logistics Health Rep 1853ndash69
Buzina R Bates CJ van der Beek J Brubacher G Chandra RK HallbergL Heseker J Mertz W Pietrzik K et al 1989 Workshop on FunctionalSignificance of Mild-to-Moderate Malnutrition Am J Clin Nutrition 50172ndash176
Calder WA 1987 Scaling energetics of homeothermic vertebrates anoperational allometry Annu Rev Physiol 49107ndash120
Canadian Society for Exercise Physiology 2003 The Canadian PhysicalActivity Fitness amp Lifestyle Approach (CPAFLA) CSEP-Health amp Fit-ness Programrsquos Health-Related Appraisal and Counselling Strategy 3rded
Carnes BA Olshansky SJ 2001 Heterogeneity and its biodemographicimplications for longevity and mortality Exp Gerontol 36419ndash430Available at httpwwwncbinlmnihgovpubmed11250115
Carrick-Ranson G Hastings JL Bhella PS Shibata S Fujimoto N PalmerD Boyd K Levine BD 2013 The effect of age-related differences inbody size and composition on cardiovascular determinants of VO2max JGerontol A Biol Sci Med Sci 68608ndash616 Available at httpwwwncbinlmnihgovpubmed23160363
Centers for Disease Control and Prevention 1998 Recommendations toPrevent and Control Iron Deficiency in the United States MMWRRecomm Rep 471ndash36 Available at httpwwwcdcgovmmwrpreviewmmwrhtml00051880htm
12 AC PISOR ET AL
American Journal of Human Biology
Centers for Disease Control and Prevention 2011 Glossary of TermsPhysical Activity for Everyone [Internet] Available from httpwwwcdcgovphysicalactivityeveryoneglossary
Christensen DL Faurholt-Jepsen D Boit MK Mwaniki DL Kilonzo BTetens I Kiplamai FK Cheruiyot SC Friis H et al 2012 Cardiorespira-tory fitness and physical activity in Luo Kamba and Maasai of ruralKenya Am J Hum Biol 24723ndash729 Available at httpwwwncbinlm-nihgovpubmed22836508
Colley RC Garriguet D Janssen I Craig CL Clarke J Tremblay MS2011a Physical activity of Canadian children and youth accelerometerresults from the 2007 to 2009 Canadian Health Measures SurveyHealth Rep 2215ndash23
Colley RC Garriguet D Janssen I Craig CL Clarke J Tremblay MS2011b Physical activity of Canadian adults accelerometer results fromthe 2007 to 2009 Canadian Health Measures Survey Health Rep 227ndash14 Available at httpwwwncbinlmnihgovpubmed21510585
Collins KJ 1999 Physiological variation and adaptability in human popu-lations Ann Hum Biol 2619ndash38
Crimmins E Seeman T 2001 Integrating Biology into DemographicResearch on Health and Aging (With a Focus on the MacArthur Study ofSuccessful Aging) Cells and Surveys Should Biological Measures beIncluded in Social Science Research Washington DC National Acad-emy Press p 9ndash41
Curran-Everett LS 1994 Accordance Between VO2max and Behavior inNgisonyoka Turkana Am J Hum Biol 6761ndash771
Durnin JVGA Womersley J 1974 Body fat assessed from total body den-sity and its estimation from skinfold thickness measurements on 481men and women aged from 16 to 72 years Br J Nutr 3277ndash97
Eberl M Al-Sherbiny M Hagan P Ljubojevic S Thomas AW Wilson RA2002 A novel and sensitive method to monitor helminth infections byfaecal sampling Acta Trop 83183ndash187
Eid D Gurven M Kaplan H Winking J 2007 Enfermedades infecciosas alo largo de la vida y en el envejecimiento en indıgenas sudamericanos dela etnia Tsimane Aging in Developing Countries Building Bridges forIntegrated Research Agendas Santiago Chile
Ekblom B Engstreuroom L-M Ekblom O 2007 Secular trends of physical fit-ness in Swedish adults Scand J Med Sci Sports 17267ndash273 Availableat httpwwwncbinlmnihgovpubmed17501867
Finch CA Lenfant C 1972 Oxygen Transport in Man N Engl J Med 286407ndash415
Fitzgerald MD Tanaka H Tran ZV Seals DR 1997 Age-related declinesin maximal aerobic capacity in regularly exercising vs sedentarywomen a meta-analysis J Appl Physiol (Bethesda Md 1985) 83160ndash165 Available at httpwwwncbinlmnihgovpubmed9216959
Fleg JL Lakatta EG 1988 Role of muscle loss in the age-associated reduc-tion in VO2max J Appl Physiol 651147ndash1151
Frisancho AR Frisancho HG Milotich M Brutsaert T Albalak RSpielvogel H Villena M Vargas E Soria R 1995 Developmentalgenetic and environmental components of aerobic capacity at high alti-tude Am J Phys Anthropol 96431ndash442 Available at httpwwwncbinlmnihgovpubmed7604895
Giroux S 2007 Canadian health measures survey sampling strategyoverview Health Rep 1831ndash36
Gurven M Jaeggi A V Kaplan H Cummings D 2013 Physical activityand modernization among Bolivian Amerindians PLoS ONE 81ndash13
Gurven M Kaplan H Winking J Rodriguez DE Vasunilashorn S KimJK Finch C Crimmins E 2009 Inflammation and infection do not pro-mote arterial aging and cardiovascular disease risk factors among leanhorticulturalists PLoS ONE 41ndash12
Haidet GC 1989 Dynamic exercise in senescent beagles oxygen consump-tion and hemodynamic responses The Am J Physiol 257H1428ndash1437Available at httpwwwncbinlmnihgovpubmed2589499
Hawkins S Wiswell R 2003 Rate and mechanism of maximal oxygen con-sumption decline with aging implications for exercise training SportsMed 33877ndash888 Available at httpwwwncbinlmnihgovpubmed12974656
Hoffman J 2002 Physiological aspects of sport training and performance1st ed Champaign IL Human Kinetics Publishers
Hotez PJ Bottazzi ME Franco-Paredes C Ault SK Periago MR 2008 Theneglected tropical diseases of Latin America and the Caribbean a review ofdisease burden and distribution and a roadmap for control and eliminationPLoS Negl Trop Dis 2e300 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid52553488amptool5pmcentrezamprendertype5abstract
Howley ET Bassett DR Welch HG 1995 Criteria for maximal oxygenuptake review and commentary Med Sci Sports Exerc 271292ndash1301Available at httpwwwncbinlmnihgovpubmed8531628
Jette M Sidney K Quenneville J Landry F 1992 Relation between cardi-orespiratory fitness and selected risk factors for coronary heart diseasein a population of Canadian men and women CMAJ 1461353ndash1360Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid51488567amptool5pmcentrezamprendertype5abstract
Katzmarzyk PT Leonard WR Crawford MH 1994 Predicted maximaloxygen consumption of Indigenous Siberians Am J Hum Biol 6783ndash790
King CH Dickman K Tisch DJ 2005 Reassessment of the cost of chronichelmintic infection a meta-analysis of disability-related outcomes inendemic schistosomiasis Lancet 3651561ndash1569 Available at httpwwwncbinlmnihgovpubmed15866310
Lee J-M Bassett D Jr Thompson D Fitzhugh E 2011 Validation of thecosmed fitmate for predicting maximal oxygen consumption J StrengthCond Res 252573ndash2579
Madimenos FC Snodgrass JJ Blackwell AD Liebert MA Sugiyama LS2011 Physical activity in an indigenous Ecuadorian forager-horticulturalist population as measured using accelerometry Am J HumBiol 23488ndash497 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid53110644amptool5pmcentrezamprendertype5abstract
Malina RM 2001 Physical activity and fitness pathways from childhoodto adulthood Am J Hum Biol 13162ndash172 Available at httpwwwncbinlmnihgovpubmed11460860
Malina RM Little BB 2008 Physical activity the present in the contextof the past Am J Hum Biol 20373ndash391 Available at httpwwwncbinlmnihgovpubmed18433002
Manning JT Morris L Caswell N 2007 Endurance running and digitratio (2D 4D) implications for fetal testosterone effects on runningspeed and vascular health Am J Hum Biol 19416ndash421
Martin Ma Lassek WD Gaulin SJC Evans RW Woo JG Geraghty SRDavidson BS Morrow AL Kaplan HS et al 2012 Fatty acid composi-tion in the mature milk of Bolivian forager-horticulturalists controlledcomparisons with a US sample Matern Child Nutr 8404ndash418 Availableat httpwwwncbinlmnihgovpubmed22624983
National Health and Nutrition Examination Survey 2004 CardiovascularFitness Procedures Manual
Nussey D Coulson T Festa-Bianchet M Gaillard J-M 2008 Measuringsenescence in wild animal populations towards a longitudinal approachFunction Ecol 22393ndash406
Ogawa T Spina RJ Martin WHI Kohrt WM Schechtman KB HolloszyJO Ehsani AA 1992 Effects of aging sex and physical training cardio-vascular responses to exercise Circulation 86494ndash503
Panter-Brick C Miller UG Eggerman M 1992 Hemoglobin levels andstep test performance of men and women in Nepal Am J Hum Biol 4481ndash491
Pontzer H Raichlen Da Wood BM Mabulla AZP Racette SB MarloweFW 2012 Hunter-gatherer energetics and human obesity PLoS ONE 7e40503 Available at httpcdxplosorg101371journalpone0040503
R Development Core Team 2011 R A language and environment for sta-tistical computing R Development Core Team
Rigby R Stasinopoulos D 2005 Generalize additive models for locationscale and shape (with discussion) Appl Stat 54507ndash554
Robergs RA Landwehr R 2002 The surprising history of theldquoHRmax5220-agerdquo equation J Exerc Physiol 51ndash10
Rode A Shephard RJ 1994 Physiological consequences of acculturation a20-year study of fitness in an Inuit community Eur J Appl Physiol 69516ndash524
Rowland TW Boyajian A 1995 Aerobic response to endurance training inchildren Pediatrics 96654ndash658
Sagiv M Ben-sira D Amir R 2007 What maintains energy supply atpeak aerobic exercise in trained and untrained older men Gerontology53357ndash361
Sanada K Kuchiki T Miyachi M Mcgrath K Higuchi M Ebashi H 2007Effects of age on ventilatory threshold and peak oxygen uptake normal-ised for regional skeletal muscle mass in Japanese men and womenaged 20 ndash 80 years Eur J Appl Physiol 99475ndash483
Schniter E 2009 Why Old Age Non-Material Contributions and Patternsof Aging Among Older Adult Tsimanersquo 607
Shahnawaz H 1978 Influence of limb length on a stepping exercise JAppl Physiol 44346ndash349
Shephard RJ 1970 Computer programs for solution of the Astrand nomo-gram and the calculation of body surface area J Sports Med 10206ndash210
Shephard RJ Allen C Benade AJS Davies CT Di Prampero PE HedmanR Merriman JE Myhre K Simmons R 1968 Standardization of sub-maximal exercise tests Bull World Health Organ 38765ndash775 Availableat httpwwwpubmedcentralnihgovarticlerenderfcgiartid52554690amptool5pmcentrezamprendertype5abstract
Shephard RJ Bailey Da Mirwald RL 1976 Development of the CanadianHome Fitness Test Can Med Assoc J 114675ndash679 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid51956906amptool5pmcentrezamprendertype5abstract
Shields M Tremblay MS Laviolette M Craig CL Janssen I Gorber SC2010 Fitness of Canadian adults results from the 2007ndash2009 canadianhealth measures survey Health Rep 2121ndash35 Available at httpwwwncbinlmnihgovpubmed20426224
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 13
American Journal of Human Biology
Siconolfi SF Garber CE Lasater TM Carleton RA 1985 A simple validstep test for estimating maximal oxygen uptake in epidemiologic stud-ies Am J Epidemiol 121382ndash390 Available at httpwwwncbinlm-nihgovpubmed4014128
Sinclair LM Hinton PS 2005 Prevalence of iron deficiency with and with-out anemia in recreationally active men and women J Am Diet Assoc105975ndash978 Available from httpwwwncbinlmnihgovpubmed15942552
Skinner JS Gaskill SE Rankinen T Leon AS Rao DC Wilmore JHBouchard C 2003 Heart rate versus VO2max age sex race initial fit-ness and training response-HERITAGE Med Sci Sports Exerc 351908ndash1913 Available at httpwwwncbinlmnihgovpubmed14600558
Sondik EJ Madans JH Gentlemand JF 2012 Summary health statisticsfor US adults National Health Interview Survey 2010 Vital Health Stat101ndash80 Available at httpwwwncbinlmnihgovpubmed20687424
Stones MJ Kozma A 1985 Physical performance Aging and Human Per-formance New York Wiley p 261ndash292
Tanaka H Monahan KD Seals DR 2001 Age-predicted maximal heartrate revisited J Am Coll Cardiol] 37153ndash156 Available at httpwwwncbinlmnihgovpubmed11153730
Vasunilashorn S Crimmins EM Kim JK Winking J Gurven M KaplanH Finch CE 2010 Blood lipids infection and inflammatory markers inthe Tsimane of Bolivia Am J Hum Biol 22731ndash740 Available at httpwwwncbinlmnihgovpubmed20721985
Vaupel JV Manton KG Stallard E 1979 The impact of heterogeneity inindividual frailty on the dynamics of mortality Demography 16439ndash454
Vaupel JW Yashin AI 1985 Heterogeneityrsquos ruses some surprising effectsof selection on population dynamics Am Stat 39176ndash185
Venables WN Ripley BD 2002 Modern Applied Statistics with S FourthNew York Springer
Wagner PD 1996 Determinants of maximal oxygen transport and utiliza-tion Annu Rev Physiol 5821ndash50 Available at httpwwwncbinlmnih-govpubmed8815793
Walker A Arent SM McKeever KH 2010 Maximal aerobic capacity(VO2max) in horses a retrospective study to identify the age-relateddecline Comparative Exerc Physiol 6177ndash181 Available at httpwwwjournalscambridgeorgabstract_S1755254010000073
Walker R Hill K 2003 Modeling growth and senescence in physical per-formance among the Ache of Eastern Paraguay Am J Hum Biol 208196ndash208
Weller IM Thomas SG Corey PN Cox MH 1993 Prediction of maximaloxygen uptake from a modified Canadian aerobic fitness test Can JAppl Physiol 18175ndash188 Available at httpwwwncbinlmnihgovpubmed8513290
Wilson TM Tanaka H 2000 Meta-analysis of the age-associated declinein maximal aerobic capacity in men relation to training status Am JPhysiol Heart Circ Physiol 278H829ndash834 Available at httpwwwncbinlmnihgovpubmed10710351
Wood SN 2006 Generalized Additive Models An Introduction with RBoca Raton Florida Chapman and HallCRC Press
World Health Organization 2001 Iron deficiency anaemia assessmentprevention and control a guide for programme managers Available athttpwhqlibdocwhointhq2001WHO_NHD_013pdf
Yoopat P Toicharoen P Boontong S Glinsukon T Vanwonterghem KLouhevaara V 2002 Cardiorespiratory capacity of Thai workers in dif-ferent age and job categories J Physiol Anthropol Appl Hum Sci 21121ndash128 Available at httpwwwncbinlmnihgovpubmed12056179
Zhu YI Haas JD 1997 Iron depletion without anemia and physical per-formance in young women Am J Clin Nutr 66334ndash341 Available athttpwwwncbinlmnihgovpubmed9250112
14 AC PISOR ET AL
American Journal of Human Biology

85 of maximal HR was reached exercise testing wasstopped if 85 of maximal HR was not reached partici-pants proceeded to the next stage of exercise stepping ata faster cadence
VO2max was estimated using a regression equationdeveloped by Weller et al (1993)
E VO2maxeth THORN532116a2024b2017c (3)
where a is the estimated VO2 at the end of the finalstage of exercise (Weller et al 1993) b is age in yearsand c is body weight in kg If a participant could not stepat the prescribed cadence during a given stage of exerciseVO2max was estimated based on the last completed exer-cise stage (Shields et al 2010) About 1 of participantseligible for the test did not complete it Participants didnot proceed beyond the eighth level of exercise regardlessof whether they had attained 85 of their age-specificmaximal HR The result is estimated relative VO2max (mlmin21 kg21)
Skinfold measurements used to calculate absoluteFFM in this article were taken before the cardiovascularfitness test at four sites (bicep tricep subscapular andsuprailiac) using Harpenden calipers (Baty InternationalUK Shields et al 2010) but only for individuals with abody mass index under 30 kg m22
Statistical analyses
All statistical analyses were performed with the R soft-ware package version 2153 (R Development Core Team2011) Smooth fits used generalized additive models(GAM) which regress a predictor on the response andsmooth the residuals (Venables and Ripley 2002) in thepackage used for the present analyses (mgcv Wood2006) the degree of smoothness was determined by apenalized likelihood technique The result is a model thathas both linear and non-linear elements allowing a closefit to the data while also providing interpretable parame-ter estimates Where appropriate model fits were eval-uated using the Akaike Information Criterion (AIC) amaximum likelihood measure of goodness-of-fit
Exploratory models indicate sex differences in VO2maxin the Tsimane population and so each sex is modeledseparately in all analyses Because data for both popula-tions only exist for ages 11ndash69 all cross-population com-parative analyses (linear models t-tests) are limited tothis age group Age in years is included in all analysesWithin-population comparisons (linear models) use theTsimane subsample age 20 and older an age group inwhich both males and females are close to their peakVO2max and include individuals up to age 70 compara-ble to the Canadians and before the age at which optingout removed large portions of the sample For the subsam-ple between 20 and 69 females and males evidence a lin-ear decline although female VO2max is curvilinear whenall ages are considered because all within-populationcomparisons (linear models) are performed on this sub-sample age2 terms were not included Publically availableCHMS data are limited to VO2max mean and standarddeviation for age categories of variable size (for categoriessee Table 3) Cross-population comparisons use the sameage categories to explore differences between Canadiansand Tsimane
Covariates could not be included in between-populationcomparisons as the latter are based on binned data how-ever extensive individual-level Tsimane data allow fordetailed examination of factors that may mediate physicalfitness decline For these within-population linear modelswe only included participants aged 20ndash69 for whom medi-cal and anthropometric data were available during thesame medical round (about a calendar year in lengthTable 1)
To explore the possibility of a non-linear relationshipbetween mass and VO2max and how this might affectany differences between the Tsimane and Canadians we1) allometrically scaled Tsimane VO2max and 2) projectedrelative VO2max for the Tsimane using Canadian fatmass and FFM from same-sex same-age categories Toallometrically scale VO2max we calculated a the scalingparameter in allometric equations for the Tsimane(Calder 1987) To project VO2max for the Tsimaneassuming the same body composition as the Canadianswe regressed absolute VO2max on absolute fat mass abso-lute FFM and age (and age2 for the Tsimane females) inthe Tsimane female and male subsamples With theresulting parameter estimates we predicted whether Tsi-mane would perform at rates similar to those observed inour study if the Tsimane had the average fat mass andFFM exhibited in each of the four Canadian cohorts (ages12ndash19 20ndash39 40ndash59 and 60ndash79) The results of these cal-culations are discussed below Hereafter VO2max willrefer to relative VO2max unless otherwise stated
RESULTS
Age at peak VO2max and levels across the lifespan
Tsimane Predicted values of absolute (l min21) and rela-tive VO2max (ml min21 kg21) for the Tsimane appear inFigure 1 Both Tsimane females and males exhibit a peakin absolute VO2max A peak in absolute VO2max is char-acteristic across populations but appears in late adoles-cence in industrialized nations concurrent with peakabsolute FFM (Armstrong 2001) In the Tsimane as wellpeak absolute VO2max and peak absolute FFM areroughly concurrent using smoothed fits of predicted val-ues female VO2max peaks at age 31 at 295 l min21 and
TABLE 1 Descriptive statistics for the Tsimane after exclusion (ages20ndash69)
Variables
Tsimane Females Tsimane Males
Mean(and SD)or Percent n
Mean(and SD)or Percent n
Age 413 (143) 203 436 (152) 280Body weight (kg) 534 (93) 203 624 (74) 280FFM (kg) 397 (43) 203 520 (58) 280Perc FFM 075 (008) 203 084 (005) 280Distance to town in 10 km 44 (24) 196 42 (24) 273Hemoglobin 129 (14) 117 143 (12) 157Arthritis 11 133 4 185Helminths 51 92 58 128Giardia 38 92 40 128Nonarthritic Pain 54 133 75 138Respiratory Ailments 27 133 15 185Spanish-speaking Ability 17 271 42 271Pregnant 3 203 ndash ndash
Two-level factors are reported as percentage of the subsample with a givenailment
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 5
American Journal of Human Biology
absolute FFM at age 34 at 405 kg for males VO2maxpeaks at age 24 at 344 l min21 and FFM at age 29 at 544kg Estimated peak VO2max is relatively robust to thesmoothing parameter selected with the peak shifting nomore than 1 year for females and two years for malesunder different methods of smoothing Average level ofVO2max may appear higher in females but a median fitreveals that Tsimane females and males have roughlysimilar VO2max (see Supporting Information Fig S2)
Relative (ml min21 kg21) VO2max estimation controlsfor the effect of body mass (and by extension partiallycontrols for percent FFM correlation between the two forfemales r 5 2075 for males r 5 2043) Removing theeffects of body mass by using a relative measure does notremove the peaks exhibited by females or males in earlyadulthood (Fig 1) Tsimane females peak at age 28 (5379ml min21 kg21) and Tsimane males peak at age 22 (at5489 ml min21 kg21) Indeed this peak also remainswhen we scale by absolute FFM (ml min21 fat-free kg21see Supporting Information Table S2)
To evaluate whether Tsimane participants performedsimilarly under the O2 method we compared age-matched subsamples to O2 method participants Tsimanemales performed significantly worse under the HRmethod relative to the O2 method (O2 mean 5 695 mlmin21 kg21 HR mean 5 590 ml min21 kg21 t 5 629Plt 0001) There is no significant difference between Tsi-mane females tested under the HR and O2 methods (O2
mean 5 529 HR mean 5 543 t 5 2077 P 5 044) For acomparison of smooths from the two samples see Sup-porting Information Figure S3Mediators of Levels Across the Tsimane Lifespan Weidentified and investigated several health-related factorsthat might affect level of VO2max achieved by eitherdiminishing resources available to the body or hamperingthe cardiovascular system directly We posit that thesevariables may mediate the effect of age on VO2max Can-didate mediators include the presence of anemia infectionwith helminths or giardia arthritis or nonarthritic painrespiratory ailments distance from the local market
Fig 1 Predicted Tsimane VO2max by age Predicted values are drawn from GAM models regressing smooths of log age on VO2max Inter-vals are 95 prediction intervals Age was smoothed using restricted maximum likelihood Other smoothing parameters (such as Mallowrsquos Cpand maximum likelihood) varied the age at peak absolute VO2max by up to 1 year for females and up to 2 years for males Points represent theraw data for Tsimane A Absolute VO2max by age for females B Absolute VO2max by age for males C Relative VO2max by age for femalesD Relative VO2max by age for males [Color figure can be viewed in the online issue which is available at wileyonlinelibrarycom]
6 AC PISOR ET AL
American Journal of Human Biology
town and Spanish speaking ability Although percentFFM generally predicts absolute rather than relativeVO2max we test it as a potential mediator Pregnancywas included as a control in female models While a highmacroparasite load may increase the likelihood of havinglow hemoglobin (and thus anemia) an interaction termbetween presence of helminths and presence of anemiawas not included because they are not significantlyrelated in this sample only 26 participants of the 92 withhelminths have anemia while 14 of the 86 without hel-minths have anemia (for females v2 5 052 P 5 047 formales v2 5 200 P 5 016)
To evaluate whether these candidate mediators affectedVO2max levels we conducted linear regressions on rela-tive VO2max (see Table 2) We first examined each predic-tor independently Females with higher hemoglobin levelshad significantly higher cardiovascular fitness perform-ance for an increase in 1 g dl21 concentration of hemoglo-bin a Tsimane woman is predicted to have 293 ml min21
kg21 higher VO2max (t 5 268 Plt 001) Helminth infec-tion mediated the relationship between age and VO2maxfor males such that men with a helminth infection arepredicted to have 616 ml min21 kg21 higher VO2max(t 5 231 Plt 005) A best fit model approach (fit on thesubset of females for whom all measures are available)provides similar results to fitting a separate model for
each potential mediating variable When a stepwise AICprocedure was used with data on all health and marketintegration measures hemoglobin level was the only sig-nificant predictor that remained in the female model(n 5 82 standardized b 5 022 Plt 005) For males hel-minth infection remained in the model as well (n 5 116standardized b 5 023 Plt 005)
Scaling VO2max by FFM (ml min21 fat-free kg21)rather than body mass produced similar results hemoglo-bin levels remained a significant positive predictor ofVO2max for females (standardized b 5 030 Plt 001) andhelminth infection a positive predictor for males (standar-dized b 5 020 Plt005) See Supporting InformationTable S3 for all regression results with ml min21 fat-freekg21 as the outcome
Anemia was initially included in model fits howevertreating hemoglobin level as a covariate in place of pres-ence of anemia improved model fit for Tsimane females(anemia AIC 5 10027 hemoglobin AIC 5 98963)Although no association was found between presence ofanemia and helminth infection there is a significant asso-ciation between hemoglobin levels and helminth infectionControlling for age a helminth diagnosis is a significantnegative predictor of hemoglobin levels for females (stand-ardized b 5 2031 Plt 001) Replacing presence of ane-mia with hemoglobin level for males did not improve or
TABLE 3 Comparison of Tsimane and Canadian relative VO2max by age category and sex
Sex Age group
Tsimane Canadians
t-Statistic P-valueMean (ml min21 kg21) n Mean (ml min21 kg21) n
Females 11ndash14 435 7 487 534 2118 02815ndash19 476 33 423 500 310 00020ndash39 510 72 383 662 908 00040ndash59 431 69 314 655 1005 00060ndash69 412 5 242 554 340 003
Males 11ndash14 415 4 548 542 2300 00615ndash19 516 31 508 514 046 06520ndash39 511 96 442 526 527 00040ndash59 432 68 362 584 380 00060ndash69 381 26 275 546 509 000
TABLE 2 Linear models exploring whether mediators affect the level (main effects models) of relative VO2max for Tsimane females and males
Sex Candidate mediatorAge effect est
(P-value)
Main effect models
Sample sizeMediator main effect
est (P-value) Age main effect est (P-value)
Females Perc FFM 2023 (000) 000 (097) 2023 (000) 203Hemoglobin 2013 (028) 024 (001) 2011 (022) 117Helminths 2019 (007) 003 (077) 2020 (006) 92Giardia 2019 (007) 011 (028) 2019 (007) 92Lung ailment 2017 (006) 2005 (060) 2018 (005) 133Reported pain 2017 (006) 2001 (094) 2017 (006) 133Arthritis 2017 (006) 2002 (083) 2016 (007) 133Distance to town 2023 (000) 002 (081) 2023 (000) 196Spanish speaking 2023 (000) 2008 (056) 2024 (000) 197
Males Perc FFM 2037 (000) 009 (012) 2034 (000) 280Hemoglobin 2029 (000) 2002 (076) 2029 (000) 157Helminths 2030 (000) 019 (002) 2027 (000) 128Giardia 2030 (000) 006 (049) 2030 (000) 128Lung ailment 2030 (000) 2007 (033) 2031 (000) 185Reported pain 2030 (000) 011 (013) 2031 (000) 185Arthritis 2030 (000) 2006 (044) 2028 (000) 185Distance to town 2037 (000) 2003 (059) 2037 (000) 273Spanish speaking 2038 (000) 008 (050) 2037 (000) 271
All parameter estimates are standardized
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 7
American Journal of Human Biology
worsen model fit and there is no significant relationshipbetween hemoglobin levels and helminth infection formales (standardized b 5 2010 P 5 028) Parameter esti-mates for anemia were not significant in models for eitherfemales or males
Between-group Table 3 presents Tsimane and Canadianestimated VO2max binned into age categories used byCHMS These data suggest that Canadian females andmales achieve peak VO2max between the ages of 11 and14 while Tsimane males peak between ages 15 and 19Tsimane females peak later between age 20 and 39Across comparable age categories Tsimane have signifi-cantly higher VO2max than Canadians at all ages exceptbetween 11 and 15 for females and 11 and 19 for males(Table 3) However the sample size of Tsimane teenagersunder age 15 is quite small As aforementioned to controlfor the influence of a small number of data points for theyoungest and oldest Tsimane individuals we used GAMto predict VO2max across logged age Predicted valuessuggest that Tsimane females peak at age 28 and Tsimanemales peak at age 22 (see Fig 1c d) These estimates areconsistent with scatterplots of the raw data (plotted onFig 1) and mask fewer fine-grained effects of age thanTable 3 as each CHMS adult age category spans twodecades
It is possible the difference between the Tsimane andCanadians reflects a greater increase in body mass acrossages in the Canadian population or different trajectoriesof change in body composition The former could occurbecause body mass appears in the denominator and cantherefore scale down VO2max while the latter implies dif-ferential changes in FFM when FFM is a predictor ofVO2max in many studies To explore these possibilitieswe performed two calculations we allometrically scaledTsimane VO2max and we projected Tsimane VO2maxassuming the Tsimane had equivalent fat mass and FFMas Canadians from same-sex same-age categories Con-trolling for age the allometric scaling coefficient a wasslightly greater than 1 for both sexes (females a 5 111males a 5 118) This suggests that any disparity inVO2max between Canadians and the Tsimane cannot beexplained solely by mass differences Indeed assumingthe Tsimane have the same body composition as Cana-dians projected VO2max differs little from observedVO2max The Tsimane outperform the Canadians in everycohort by at least 35 ml min21 kg21 except among theyoungest males who perform similarly (see SupportingInformation Fig S4)
To control for possible disparities in changes in bodycomposition by age within each population as these mightalso influence differences between the Tsimane and Cana-dians we scaled VO2max by absolute FFM from the samepopulation to obtain ml min21 fat-free kg21 BecauseCanadian body composition data were only available viaskinfolds (bicep tricep subscapular and suprailiac) weused the subset of Tsimane (n 5 246) for which the samefour skinfolds measurements were available We calcu-lated average absolute FFM for each cohort using averageweight and average summed skinfolds (Durnin andWomersley 1974) and scaled average VO2max in mlmin21 by this number to obtain ml min21 fat-free kg21Under this method of scaling the Tsimane outperformCanadians in every cohort over age 20 by at least 165 ml
min21 fat-free kg21 (see Supporting Information TableS2) Canadian females and males in the 12ndash19 cohortsoutperform Tsimane of the same age
We next compared Tsimane to other subsistence popula-tions reported in the literature (Table 4) Consistent withcommon practice in the literature we report means foreach group but when possible we also predicted VO2maxat age 25 to provide age-corrected comparisons Weselected age 25 as it is the age of peak relative VO2max inthis study and for female Kamba and Maasai in Christen-sen et als (2012) recent study To predict VO2max at age25 we regressed the median ages on mean VO2max acrossthe available age categories Tsimane females and maleshave roughly the same predicted VO2max at age 25 asseveral other subsistence populations but higher VO2maxthan industrialized populations To test for differencesbetween industrialized and subsistence populations weconducted a linear regression on predicted VO2max at age25 this is not a meta-analysis and results should beinterpreted with caution Overall subsistence populationsdisplay higher peak VO2max than in industrialized popu-lations controlling for sex (440 vs 367 ml min21 kg21
[Plt 001]) The Tsimane O2 and indigenous Siberian sam-ples were excluded Tsimane O2 to avoid the problem ofnon-independence with Tsimane HR data and Siberiansbecause the sample has a limited age range comparedwith the other studies
Pace of decline slope of VO2max decline across thelifespan
Tsimane To evaluate whether Tsimane participants per-formed similarly under different methods we comparedage-matched subsamples of participants from the presentstudy with O2 method participants Despite a higher level(intercept) of VO2max in the O2 sample Tsimane malesdeclined marginally significantly faster under the O2
method relative to the HR method (O2 5 68 per decadeHR 5 47 decline per decade t 5 2195 P 5 005) Thereis no significant difference between Tsimane femalestested under the O2 and HR methods (O2 5 60 per dec-ade HR 5 48 decline per decade t 5 2055 P 5 058)Mediators of Slope Across the Lifespan We fit a series oflinear models to test for interactions between the candi-date mediators and age-related decline in TsimaneVO2max There are no variables that significantly inter-act with age to predict VO2max (see Supporting Informa-tion Table S4) An AIC selection approach and scaling byabsolute FFM (see Supporting Information Table S3) pro-vides the same results no variables significantly interactwith age to predict VO2max
Between-group VO2max is most often reported as a lin-ear decline across the adult lifespan though Hawkins andWiswell (2003) dispute whether the decline is actually lin-ear For example a linear approximation is not appropri-ate for Tsimane females if ages 11ndash80 are consideredFigure 2 contrasts linear declines in VO2max for Cana-dians and Tsimane males as well as a curvilinear fit forTsimane females with declines in industrialized nationsderived from meta-analyses (Fitzgerald et al 1997 Wil-son and Tanaka 2000) To explore whether rates ofdecline in VO2max among Tsimane and Canadians weredifferent we regressed average VO2max by age category
8 AC PISOR ET AL
American Journal of Human Biology
TA
BL
E4
Mea
nV
O2m
ax
esti
ma
ted
VO
2m
ax
at
age
25a
nd
dec
lin
ein
VO
2m
ax
per
dec
ad
efr
omth
isst
ud
ya
nd
pre
vio
us
rese
arc
ha
Pop
ula
tion
Fem
ale
Male
Pu
bli
cati
onM
ean
VO
2m
ax
VO
2m
ax
Age
25
bP
erce
nt
Dec
lin
eA
ge
Ran
ge
(n)
Mea
nV
O2m
ax
VO
2m
ax
Age
25
bP
erce
nt
Dec
lin
eA
ge
Ran
ge
(n)
Ind
ust
riali
zed
Can
ad
ac
312
400
73
20ndash69
(2905)
361
458
68
20ndash69
(2712)
Jap
an
d357
414
39
20ndash69
(656)
417
473
38
20ndash69
(807)
San
ad
aet
al
2007
Sw
eden
e330
g409
80
20ndash65
324
g388
75
20ndash65
Ek
blo
met
al
2007
Th
ail
an
d(i
nd
ust
ry)e
275
293
54
16ndash55
(56)
389
415
57
16ndash53
(70)
Yoo
pat
etal
2002
US
(H
erit
age)
f273
17ndash65
(360)
359
17ndash65
(293)
Sk
inn
eret
al
2003
US
(N
HA
NE
S)d
356
363
24
20ndash49
(1312)
444
438
39
20ndash49
(1481)
Su
bsi
sten
ceT
sim
an
e(H
R)c
498
521
h16
h20ndash69
471
538
h61
h20ndash69
Tsi
man
e(O
2)c
436
74
h36ndash69
540
25
h36ndash69
Ifalu
k(1
969ndash70)c
429
488
69
20ndash59
(43)
49
597
75
20ndash69
(75)
Rod
ean
dS
hep
hard
1994
Ach
ec465
434
257
20ndash59
(62)
519
614
84
20ndash59
(65)
Walk
eran
dH
ill
2003
Lu
oc378
372
39
17ndash68
(209)
429
48
54
17ndash68
(172)
Ch
rist
ense
net
al
2012
b
Kam
ba
c377
371
45
17ndash68
(283)
431
516
34
17ndash68
(94)
Ch
rist
ense
net
al
2012
Maasa
ic389
410
45
17ndash68
(178)
431
528
69
17ndash68
(163)
Ch
rist
ense
net
al
2012
Ind
igen
ous
Sib
eria
nsc
338
341
22
220ndash39
(14)
462
471
66
20ndash39
(30)
Katz
marz
yk
etal
1994
Ru
ral
Nep
alc
187
15ndash60
(39)
221
15ndash60
(35)
Pan
ter-
Bri
cket
al
1992
Ngis
onyok
aT
urk
an
af
38
387
18
20ndash44
(19)
Cu
rran
-Ever
ett
1994
aV
alu
esm
issi
ng
wh
enn
otavail
able
from
ap
art
icu
lar
stu
dy
Per
cen
td
ecli
ne
(per
cen
tof
pea
kvalu
elo
st)
per
dec
ad
ew
as
calc
ula
ted
as
by
regre
ssin
gre
lati
ve
VO
2m
ax
by
age
mu
ltip
lyin
gth
ep
ara
met
eres
tim
ate
for
age
by
10
an
dd
ivid
ing
this
nu
mber
by
the
inte
rcep
t(p
resu
med
pea
k
ass
um
ing
ali
nea
rd
ecli
ne
inV
O2m
ax
acr
oss
age)
B
ecau
seof
lack
ofacc
ess
tora
wd
ata
re
gre
ssio
ns
wer
efi
tw
ith
mea
nV
O2m
ax
an
dm
edia
nage
by
coh
ort
bA
ge
25
valu
esw
ere
esti
mate
dby
regre
ssin
gre
lati
ve
VO
2m
ax
by
age
then
usi
ng
the
resu
ltin
gp
ara
met
eres
tim
ate
sto
pre
dic
tV
O2m
ax
at
age
25
the
pea
kin
rece
ntl
yst
ud
ied
pop
ula
tion
s(e
g
Kam
ba
an
dM
aasa
ife
male
sC
hri
sten
sen
etal
2012fe
male
san
dm
ale
sin
this
art
icle
)B
ecau
seof
lack
ofacc
ess
tora
wd
ata
re
gre
ssio
ns
wer
efi
tw
ith
mea
nV
O2m
ax
an
dm
edia
nage
by
coh
ort
cS
ubm
axim
alst
epte
st
dS
ubm
axim
altr
ead
mil
lte
st
eS
ubm
axim
aler
gom
eter
test
f M
axim
al
ergom
eter
test
gS
wed
ish
data
wer
ere
por
ted
as
med
ian
sfo
rea
chage
cate
gor
yth
evalu
esre
por
ted
her
eare
mea
ns
ofth
ese
med
ian
s2006
ind
ivid
uals
part
icip
ate
dbu
tn
um
ber
by
sex
was
not
rep
orte
d
hF
orco
mp
ara
bil
ity
we
bin
ned
the
Tsi
man
eH
Ran
dO
2d
ata
into
10
yea
rage
cate
gor
ies
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 9
American Journal of Human Biology
on median age (for a given age category) population andtheir interaction term For comparability Tsimane werebinned into the Canadian age categories and averageswere computed for these categories leading to estimateddeclines slightly different from those in Table 4 for thepurposes of this test we treat the Tsimane female declineas linear Because within-population variance in declineis not available these regressions should be treated asdescriptive comparisons rather than statistical tests ofdifferences between the two groups The rate of decline inVO2max is steeper for Canadian females (69 per decadefaster decline per decade) and males (42 faster declineper decade) compared with Tsimane females and males
The rate of cardiovascular fitness decline between theTsimane and Canadians is different but this differencedoes not extend to industrialized and subsistence popula-tions (see Table 4) Controlling for sex subsistence groupshave about one quarter of a percent lower declines perdecade Again because the variance in decline is not rep-resented in this regression results should be interpretedas comparative rather than as a statistical test As beforeTsimane O2 results were not included in the analysis toavoid nonindependence and the indigenous Siberianswere excluded because of discrepancy in ages sampled
DISCUSSION
Our comparisons demonstrate that across a wide varietyof societies cardiovascular fitness senesces with age Car-diovascular fitness is higher on average among members ofsubsistence societies than among industrialized societiesbut rates of fitness decline from peak are not slower Ourmore detailed comparison between the Tsimane a subsist-ence population and Canadians an industrialized popula-tion reveals differences in cardiovascular fitness levelsand rate of fitness decline Cardiovascular fitness levelswere higher among the Tsimane than among Canadiansand the rate of decline across the lifespan was significantlyslower among Tsimane women and men Potential Cana-
dian participants were excluded due to many health con-cerns including pregnancy and history of high bloodpressure whereas Tsimane were only excluded if they self-identified as unable to participate This suggests the Cana-dian sample is a relatively healthy subsample of Canadayet the Tsimane still outperform them in cardiovascular fit-ness It may be that the higher demand for cardiovascularfitness in late ages among the Tsimane outweighs anyeffects of poor health Another possibility is that greaterself-selection among Tsimane due to higher adult mortalityleaves more robust older adult survivors thereby reducingthe observed slope of fitness decline at the population level(Vaupel et al 1979) perhaps this is partially why fewerTsimane older adults opted out of the exercise test thanCanadian older adults were screened out (ages 60ndash69Canadian females 5 56 Tsimane females 5 15 Cana-dian males 5 57 Tsimane males 5 5)
Consistent with prior research on age-related changesin cardiovascular fitness the Tsimane do evidence a lin-ear decline in VO2max with age but not as steep a declineas typically seen in industrialized populations Based oncomparisons with the Canadians and with other industri-alized populations we believe the Tsimane data from thepresent study and the pilot O2 data combined indicatethat the Tsimane perform better on tests of cardiovascularfitness than the average individual from an industrializednation
To further explore the potential effects of health factorson cardiovascular fitness level and rate of decline weinvestigated predictors of individual differences in fitnesswithin the Tsimane population Overall we found thatmost health indicators among the Tsimane did not hinderVO2max levels or rates of decline Lower hemoglobin lev-els were associated with lower VO2max levels in womenbut not men consistent with the notion that compromisedblood oxygen transport curbs cardiovascular fitness(Buzina et al 1989 Panter-Brick et al 1992) In the USlow hemoglobin is more common in active women thanactive men (Sinclair and Hinton 2005) hemoglobin is
Fig 2 Linear changes in VO2max with age for Canadians and the Tsimane Intercepts and slopes for Canadians and Tsimane can be foundin Table 4 Because age2 is significant for the full sample of Tsimane females their change in VO2max across age is curvilinear Slopes forendurance trained active and sedentary individuals from industrialized nations are drawn from a meta-analysis performed by Fitzgeraldet al (1997) for females and Wilson and Tanaka (2000) for males Endurance trained individuals are represented by the top dotted line abovefollowed by active individuals below and sedentary on the bottom Trained individuals engage in 31 sessions of endurance exercise per weekfor at least a year while active individuals engage in 2 or fewer sessions per week of cardiovascular exercise [Color figure can be viewed in theonline issue which is available at wileyonlinelibrarycom]
10 AC PISOR ET AL
American Journal of Human Biology
also lower in Tsimane women than Tsimane men(female 5 129 [sd 13] g ml21 males 5 142 [13] g ml21)Even mild (non-anemic) iron deficiencies impacts womenrsquosexercise performance (Zhu and Haas 1997) Inconsistentwith findings from Panter-Brick et al (1992) among ruralNepalese helminth infection did not diminish levels ofVO2max for Tsimane men helminth infection wasactually a predictor of higher VO2max There are severalreasons why this might be the case First we only testedwhether presence or absence of helminths mediated theeffect of age on VO2max rather than parasite load (egnumber of worms egg counts) it is possible that helminthinfection only affects VO2max at high parasite loads Sec-ond blood loss (and thus low hemoglobin levels) resultingfrom helminth infection may be partially offset by theamount of iron in the Tsimane adult diet Tsimane ironintake is an estimated 166 of the US Dietary ReferenceIntake (Martin et al 2012) and Tsimane hemoglobin lev-els are higher than in the Nepalese (females 129 vs 109males 1424 vs 120 Panter-Brick et al 1992) Thirdthese analyses consider helminth infection at the time ofexercise test rather than past infections It may be thatthe cumulative burden of past infection has a larger effecton cardiovascular fitness if so this would suggest thatthe surprising positive effect of helminth infection onVO2max levels in men is either spurious or capturing athird variable
Secular declines in VO2max are expected with increasingmarket integration and lifestyle change because ofincreased sedentism (Katzmarzyk et al 1994 Rode andShephard 1994) Two proxies for market integration in thispopulationmdashdistance to San Borja and the ability to speakSpanishmdashwere not significant predictors of VO2max levelsor decline This is consistent with our predictions as Tsi-mane females and males that live near town do not appearto have lower activity levels (Gurven et al 2013) Wageopportunities near town primarily include working asranch hands collecting and weaving palm thatch panelscash cropping and working for logging companies Each ofthese involves extensive activity furthermore transporta-tion to town often involves bicycling walking and polingdugout canoes Cash cropping of rice and corn also involvesthe clearing and weeding of larger fields Except for cashcropping and palm thatch manufacture most wage laboropportunities are currently restricted to men
This study makes several unique contributions to theexisting literature It offers the first systematic compari-son of cardiovascular fitness level and rate of declinebetween subsistence and industrialized societies Resultscompiled from previous studies support the general claimthat despite greater pathogen stress the greater activityregime of subsistence societies helps support higher peakVO2max Additionally this is one of the first studies toexplore senescent changes in cardiovascular fitnesswithin a large sample from a subsistence population Thelarge number of health measures and proxies of marketintegration available permitted testing whether these fac-tors mediated age-related variation and whether theymodulated the rate of decline Despite reports that healthstatus and market integration have been important inother studies (eg Buzina et al 1989 Katzmarzyk et al1994 Panter-Brick et al 1992 Rode and Shephard1994) their overall net effect was small among the Tsi-mane most apparent in measures of hemoglobin levelsamong women and helminth infection among men
The results of these analyses may also shed light onindividual and population level differences in chronic dis-ease In industrialized populations meta-analyses demon-strate that cardiovascular fitness is protective againstcardiovascular disease (Jette et al 1992 Hawkins andWiswell 2003) Prior studies among Tsimane suggest rel-atively few deaths from heart attacks or strokes (Gurvenet al 2007) a low prevalence of common cardiovasculardisease risk factors like obesity high blood low-densitylipoprotein levels hypertension and peripheral arterialdisease and the existence of additional protective factorslike lean diet and physical activity (Gurven et al 20092013 Vasunilashorn et al 2010) Market foods such ascooking oil sugar and pasta represent only 6 of theaverage Tsimane diet and Tsimane also consume a greatdeal of lean meat and omega-3 fatty acids (Martin et al2012) This study complements these findings by demon-strating that Tsimane show relatively high VO2max anindicator of strong cardiorespiratory health TsimaneVO2max declines with age as it does everywhere whichsuggests declining muscle mass with age (Fleg andLakatta 1988) and lowered cardiac output (American Col-lege of Sports Medicine 2006 Sagiv et al 2007) ratherthan increased cardiovascular disease risk
Limitations
The Canadians were selected as a comparison industri-alized population because of the similarity of the CHMSand Tsimane protocols very few studies of industrializedpopulations have large sample sizes sample across thelife course and use a step test Several aspects of theCHMS and Tsimane protocols remain potentially incom-parable The Canadians experienced more stringentexclusion criteria than the Tsimane meaning that the Tsi-mane sample may be more representative of cardiovascu-lar condition in the Tsimane population than theCanadian sample of the Canadian population Again ifthe Tsimane sample was subjected to these criteria wemight expect the differences in VO2max between popula-tions to only increase On the other hand Canadian par-ticipants were assigned stepping cadences based on theirage and sex and cadence was increased across the exer-cise test if a participant did not reach 85 of his or herage-specific maximal HR all Tsimane were asked to com-plete 30 ascents per minute with no increase based ontheir achieved HRs Few Tsimane reached 75 of theirage-specific maximal HR (see Supporting InformationTable S1) perhaps because the age-specific maximal HRsderived from industrialized populations are inaccurate forthe Tsimane or because higher fitness allowed these Tsi-mane to perform the step test of 30 ascents per minutewith less effort Due to these discrepancies in protocolwhich may lead to errors in estimating VO2max we alsoincorporated Tsimane data collected using the O2 methodas a check because the O2 method estimates VO2max onthe relationship between HR and VO2 in a givenparticipant
Indeed it is an open question as to whether typicalmethods for indirectly estimating cardiovascular fitnessfrom HR are appropriate for subsistence level popula-tions Common routines for VO2max estimation assumeage-specific declines in cardiovascular fitness (eg Shep-hard 1970) but these methods have only been validatedwith samples from industrialized populations which are
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 11
American Journal of Human Biology
often self-selected (Beall et al 1985) Additionally regres-sions drawn from laboratory studies require participantsachieve a HR within a certain range for accurate VO2maxestimation however the appropriateness of these rangesgiven slight modifications to protocol and inclusion of par-ticipants of different ages different populations and bothsexes is questionable For example the maximal HRexhibited by young men varies across subsistence popula-tions (Shephard 1978) Use of these criteria is compli-cated by the fact that the most commonly used equationfor estimating maximal possible HR by age 220-age maybe inaccurate (Robergs and Landwehr 2002) and particu-larly inappropriate for older adults (see Tanaka et al2001) For these reasons we chose to use an exclusion cri-terion for the Tsimane that evaluates individual increasein HR across exercise relative to the mean increase in HRfor Tsimane of the same sex and age
The pattern of Tsimane fitness decline differs moder-ately by the choice of exclusion criterion for participants(see Supporting Information Table S1) and by method oftesting However this is a common finding Lee et al(2011) predicted VO2max from submaximal exercise usingthe O2 method and the HR-based American College ofSports Medicine calculation routine in a US sample Theyfound that (1) the HR-based routine predicts higherVO2max across the sexes than does the O2 routine and(2) the two methods have a correlation of only 077 Whenevaluating different testing procedures Shephard et al(1968) found differences in VO2max estimation by type oftest used (eg bicycle ergometer versus step test) and cal-culation routine Exercise tests exclusion criteria andcalculation routines combine to provide an estimate ofactual VO2max for a given individual and as such varia-tion in estimation is to be expected However such varia-tion may affect cross-population comparisons inunforeseen ways thus the comparisons presented hereshould be interpreted with caution
While population-level variation in cardiovascular fit-ness decline may reflect the differences in the demands ofendurance-based physical activity muscularity and com-promised oxygen transport it is possible that genetic fac-tors may also play a potential role (Collins 1999) In oneindustrialized sample maternal cardiovascular fitnessexhibited a heritability of 30 which is attributed toinheritance of the maternal mitochondrial genome (Bou-chard et al 2000) We do not have the relevant geneticdata for the populations considered here however andthus operate under the simplifying assumption thatinheritance should not affect population-level patternsand will not consistently bias individual-level compari-sons in any particular direction
This study is further limited by its cross-sectionaldesign Cross-sectional data present well-known problemsfor the measurement of individual aging (Crimmins andSeeman 2001) Mortality selection in which individualsin poorer condition are likely to die at younger ages pro-duces a downward bias in the estimation of aging rates atthe individual level (Vaupel and Yashin 1985 Vaupelet al 1979) Cohort effects if present also produce com-plicated and non-monotonic biases in estimation (Carnesand Olshansky 2001) Due to the problem of between-individual heterogeneity and the within-individual pro-cess of senescence a recent overview of aging studies con-cludes that ldquoonly longitudinal studies [ ] provide reliablesources of information in the study of senescencerdquo (Nussey
et al 2008) To date there are no longitudinal studies ofcardiovascular fitness in subsistence populations We arecurrently re-testing participants under the O2 methodallowing a better grasp of the within-individual variationthat shapes patterns of senescent decline
ACKNOWLEDGMENTS
The authors thank Paul Hooper Steven Gaulin JohnTooby Patricia Kramer the Human Evolution and Biode-mography laboratory and the Center for EvolutionaryPsychology at UCSB for helpful advice and feedback thestaff at the Tsimane Health and Life History Project andthe Tsimane for their participation and patience
LITERATURE CITED
American College of Sports Medicine 2006 ACSMrsquos Guidelines for Exer-cise Testing and Prescription 7th ed Philadelphia Lippincott Williamsamp Wilkins
Armstrong N 2001 Peak oxygen uptake in relation to growth and matura-tion in 11- to 17-year-old humans Eur J Appl Physiol 85546ndash551
Astrand PO Ryhming I 1954 A nomogram for calculation of aerobiccapacity (physical fitness) from pulse rate during submaximal work JAppl Physiol 7218ndash221
Bailey DA Shephard RJ Mirwald RL 1976 Validation of a self-administered home test of cardio-respiratory fitness Can J Appl SportSci 167ndash78
Beall CM Goldstein MC and Feldman ES 1985 The physical fitness ofelderly Nepalese farmers residing in rugged mountain and flat terrainJ Gerontol 40529ndash535
Benefice E Ndiaye G 2005 Relationships between anthropometry cardi-orespiratory fitness indices and physical activity levels in different ageand sex groups in rural Senegal (West Africa) Ann Hum Biol 32366ndash382 Available from httpwwwncbinlmnihgovpubmed16099780
Blackwell AD Gurven MD Sugiyama LS Madimenos FC Liebert MAMartin MA Kaplan HS Snodgrass JJ 2011 Evidence for a peak shift in ahumoral response to helminths age profiles of IgE in the Shuar of Ecuadorthe Tsimane of Bolivia and the US NHANES PLoS Negl Trop Dis 5e1218 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid53125146amptool5pmcentrezamprendertype5abstract
Blackwell AD Martin M Kaplan H Gurven M Evidence for an antagonis-tic relationship between Giardia lamblia and helminth infections impli-cations for treatment of helminth infections in developing populations
Blair SN LaMonte MJ Nichaman MZ 2004 The evolution of physicalactivity recommendations how much is enough Am J Clin Nutr 79913Sndash920S Available at httpwwwncbinlmnihgovpubmed15113739
Bouchard C Rankinen T Chagnon YC Rice T Perusse L Gagnon JBorecki I An P Leon a S et al 2000 Genomic scan for maximal oxygenuptake and its response to training in the HERITAGE Family Study JAppl Physiol 88551ndash559 Available at httpwwwncbinlmnihgovpubmed10658022
Bryan S St-Denis M Wojtas D 2007 Canadian Health Measures Surveyclinic operations and logistics Health Rep 1853ndash69
Buzina R Bates CJ van der Beek J Brubacher G Chandra RK HallbergL Heseker J Mertz W Pietrzik K et al 1989 Workshop on FunctionalSignificance of Mild-to-Moderate Malnutrition Am J Clin Nutrition 50172ndash176
Calder WA 1987 Scaling energetics of homeothermic vertebrates anoperational allometry Annu Rev Physiol 49107ndash120
Canadian Society for Exercise Physiology 2003 The Canadian PhysicalActivity Fitness amp Lifestyle Approach (CPAFLA) CSEP-Health amp Fit-ness Programrsquos Health-Related Appraisal and Counselling Strategy 3rded
Carnes BA Olshansky SJ 2001 Heterogeneity and its biodemographicimplications for longevity and mortality Exp Gerontol 36419ndash430Available at httpwwwncbinlmnihgovpubmed11250115
Carrick-Ranson G Hastings JL Bhella PS Shibata S Fujimoto N PalmerD Boyd K Levine BD 2013 The effect of age-related differences inbody size and composition on cardiovascular determinants of VO2max JGerontol A Biol Sci Med Sci 68608ndash616 Available at httpwwwncbinlmnihgovpubmed23160363
Centers for Disease Control and Prevention 1998 Recommendations toPrevent and Control Iron Deficiency in the United States MMWRRecomm Rep 471ndash36 Available at httpwwwcdcgovmmwrpreviewmmwrhtml00051880htm
12 AC PISOR ET AL
American Journal of Human Biology
Centers for Disease Control and Prevention 2011 Glossary of TermsPhysical Activity for Everyone [Internet] Available from httpwwwcdcgovphysicalactivityeveryoneglossary
Christensen DL Faurholt-Jepsen D Boit MK Mwaniki DL Kilonzo BTetens I Kiplamai FK Cheruiyot SC Friis H et al 2012 Cardiorespira-tory fitness and physical activity in Luo Kamba and Maasai of ruralKenya Am J Hum Biol 24723ndash729 Available at httpwwwncbinlm-nihgovpubmed22836508
Colley RC Garriguet D Janssen I Craig CL Clarke J Tremblay MS2011a Physical activity of Canadian children and youth accelerometerresults from the 2007 to 2009 Canadian Health Measures SurveyHealth Rep 2215ndash23
Colley RC Garriguet D Janssen I Craig CL Clarke J Tremblay MS2011b Physical activity of Canadian adults accelerometer results fromthe 2007 to 2009 Canadian Health Measures Survey Health Rep 227ndash14 Available at httpwwwncbinlmnihgovpubmed21510585
Collins KJ 1999 Physiological variation and adaptability in human popu-lations Ann Hum Biol 2619ndash38
Crimmins E Seeman T 2001 Integrating Biology into DemographicResearch on Health and Aging (With a Focus on the MacArthur Study ofSuccessful Aging) Cells and Surveys Should Biological Measures beIncluded in Social Science Research Washington DC National Acad-emy Press p 9ndash41
Curran-Everett LS 1994 Accordance Between VO2max and Behavior inNgisonyoka Turkana Am J Hum Biol 6761ndash771
Durnin JVGA Womersley J 1974 Body fat assessed from total body den-sity and its estimation from skinfold thickness measurements on 481men and women aged from 16 to 72 years Br J Nutr 3277ndash97
Eberl M Al-Sherbiny M Hagan P Ljubojevic S Thomas AW Wilson RA2002 A novel and sensitive method to monitor helminth infections byfaecal sampling Acta Trop 83183ndash187
Eid D Gurven M Kaplan H Winking J 2007 Enfermedades infecciosas alo largo de la vida y en el envejecimiento en indıgenas sudamericanos dela etnia Tsimane Aging in Developing Countries Building Bridges forIntegrated Research Agendas Santiago Chile
Ekblom B Engstreuroom L-M Ekblom O 2007 Secular trends of physical fit-ness in Swedish adults Scand J Med Sci Sports 17267ndash273 Availableat httpwwwncbinlmnihgovpubmed17501867
Finch CA Lenfant C 1972 Oxygen Transport in Man N Engl J Med 286407ndash415
Fitzgerald MD Tanaka H Tran ZV Seals DR 1997 Age-related declinesin maximal aerobic capacity in regularly exercising vs sedentarywomen a meta-analysis J Appl Physiol (Bethesda Md 1985) 83160ndash165 Available at httpwwwncbinlmnihgovpubmed9216959
Fleg JL Lakatta EG 1988 Role of muscle loss in the age-associated reduc-tion in VO2max J Appl Physiol 651147ndash1151
Frisancho AR Frisancho HG Milotich M Brutsaert T Albalak RSpielvogel H Villena M Vargas E Soria R 1995 Developmentalgenetic and environmental components of aerobic capacity at high alti-tude Am J Phys Anthropol 96431ndash442 Available at httpwwwncbinlmnihgovpubmed7604895
Giroux S 2007 Canadian health measures survey sampling strategyoverview Health Rep 1831ndash36
Gurven M Jaeggi A V Kaplan H Cummings D 2013 Physical activityand modernization among Bolivian Amerindians PLoS ONE 81ndash13
Gurven M Kaplan H Winking J Rodriguez DE Vasunilashorn S KimJK Finch C Crimmins E 2009 Inflammation and infection do not pro-mote arterial aging and cardiovascular disease risk factors among leanhorticulturalists PLoS ONE 41ndash12
Haidet GC 1989 Dynamic exercise in senescent beagles oxygen consump-tion and hemodynamic responses The Am J Physiol 257H1428ndash1437Available at httpwwwncbinlmnihgovpubmed2589499
Hawkins S Wiswell R 2003 Rate and mechanism of maximal oxygen con-sumption decline with aging implications for exercise training SportsMed 33877ndash888 Available at httpwwwncbinlmnihgovpubmed12974656
Hoffman J 2002 Physiological aspects of sport training and performance1st ed Champaign IL Human Kinetics Publishers
Hotez PJ Bottazzi ME Franco-Paredes C Ault SK Periago MR 2008 Theneglected tropical diseases of Latin America and the Caribbean a review ofdisease burden and distribution and a roadmap for control and eliminationPLoS Negl Trop Dis 2e300 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid52553488amptool5pmcentrezamprendertype5abstract
Howley ET Bassett DR Welch HG 1995 Criteria for maximal oxygenuptake review and commentary Med Sci Sports Exerc 271292ndash1301Available at httpwwwncbinlmnihgovpubmed8531628
Jette M Sidney K Quenneville J Landry F 1992 Relation between cardi-orespiratory fitness and selected risk factors for coronary heart diseasein a population of Canadian men and women CMAJ 1461353ndash1360Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid51488567amptool5pmcentrezamprendertype5abstract
Katzmarzyk PT Leonard WR Crawford MH 1994 Predicted maximaloxygen consumption of Indigenous Siberians Am J Hum Biol 6783ndash790
King CH Dickman K Tisch DJ 2005 Reassessment of the cost of chronichelmintic infection a meta-analysis of disability-related outcomes inendemic schistosomiasis Lancet 3651561ndash1569 Available at httpwwwncbinlmnihgovpubmed15866310
Lee J-M Bassett D Jr Thompson D Fitzhugh E 2011 Validation of thecosmed fitmate for predicting maximal oxygen consumption J StrengthCond Res 252573ndash2579
Madimenos FC Snodgrass JJ Blackwell AD Liebert MA Sugiyama LS2011 Physical activity in an indigenous Ecuadorian forager-horticulturalist population as measured using accelerometry Am J HumBiol 23488ndash497 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid53110644amptool5pmcentrezamprendertype5abstract
Malina RM 2001 Physical activity and fitness pathways from childhoodto adulthood Am J Hum Biol 13162ndash172 Available at httpwwwncbinlmnihgovpubmed11460860
Malina RM Little BB 2008 Physical activity the present in the contextof the past Am J Hum Biol 20373ndash391 Available at httpwwwncbinlmnihgovpubmed18433002
Manning JT Morris L Caswell N 2007 Endurance running and digitratio (2D 4D) implications for fetal testosterone effects on runningspeed and vascular health Am J Hum Biol 19416ndash421
Martin Ma Lassek WD Gaulin SJC Evans RW Woo JG Geraghty SRDavidson BS Morrow AL Kaplan HS et al 2012 Fatty acid composi-tion in the mature milk of Bolivian forager-horticulturalists controlledcomparisons with a US sample Matern Child Nutr 8404ndash418 Availableat httpwwwncbinlmnihgovpubmed22624983
National Health and Nutrition Examination Survey 2004 CardiovascularFitness Procedures Manual
Nussey D Coulson T Festa-Bianchet M Gaillard J-M 2008 Measuringsenescence in wild animal populations towards a longitudinal approachFunction Ecol 22393ndash406
Ogawa T Spina RJ Martin WHI Kohrt WM Schechtman KB HolloszyJO Ehsani AA 1992 Effects of aging sex and physical training cardio-vascular responses to exercise Circulation 86494ndash503
Panter-Brick C Miller UG Eggerman M 1992 Hemoglobin levels andstep test performance of men and women in Nepal Am J Hum Biol 4481ndash491
Pontzer H Raichlen Da Wood BM Mabulla AZP Racette SB MarloweFW 2012 Hunter-gatherer energetics and human obesity PLoS ONE 7e40503 Available at httpcdxplosorg101371journalpone0040503
R Development Core Team 2011 R A language and environment for sta-tistical computing R Development Core Team
Rigby R Stasinopoulos D 2005 Generalize additive models for locationscale and shape (with discussion) Appl Stat 54507ndash554
Robergs RA Landwehr R 2002 The surprising history of theldquoHRmax5220-agerdquo equation J Exerc Physiol 51ndash10
Rode A Shephard RJ 1994 Physiological consequences of acculturation a20-year study of fitness in an Inuit community Eur J Appl Physiol 69516ndash524
Rowland TW Boyajian A 1995 Aerobic response to endurance training inchildren Pediatrics 96654ndash658
Sagiv M Ben-sira D Amir R 2007 What maintains energy supply atpeak aerobic exercise in trained and untrained older men Gerontology53357ndash361
Sanada K Kuchiki T Miyachi M Mcgrath K Higuchi M Ebashi H 2007Effects of age on ventilatory threshold and peak oxygen uptake normal-ised for regional skeletal muscle mass in Japanese men and womenaged 20 ndash 80 years Eur J Appl Physiol 99475ndash483
Schniter E 2009 Why Old Age Non-Material Contributions and Patternsof Aging Among Older Adult Tsimanersquo 607
Shahnawaz H 1978 Influence of limb length on a stepping exercise JAppl Physiol 44346ndash349
Shephard RJ 1970 Computer programs for solution of the Astrand nomo-gram and the calculation of body surface area J Sports Med 10206ndash210
Shephard RJ Allen C Benade AJS Davies CT Di Prampero PE HedmanR Merriman JE Myhre K Simmons R 1968 Standardization of sub-maximal exercise tests Bull World Health Organ 38765ndash775 Availableat httpwwwpubmedcentralnihgovarticlerenderfcgiartid52554690amptool5pmcentrezamprendertype5abstract
Shephard RJ Bailey Da Mirwald RL 1976 Development of the CanadianHome Fitness Test Can Med Assoc J 114675ndash679 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid51956906amptool5pmcentrezamprendertype5abstract
Shields M Tremblay MS Laviolette M Craig CL Janssen I Gorber SC2010 Fitness of Canadian adults results from the 2007ndash2009 canadianhealth measures survey Health Rep 2121ndash35 Available at httpwwwncbinlmnihgovpubmed20426224
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 13
American Journal of Human Biology
Siconolfi SF Garber CE Lasater TM Carleton RA 1985 A simple validstep test for estimating maximal oxygen uptake in epidemiologic stud-ies Am J Epidemiol 121382ndash390 Available at httpwwwncbinlm-nihgovpubmed4014128
Sinclair LM Hinton PS 2005 Prevalence of iron deficiency with and with-out anemia in recreationally active men and women J Am Diet Assoc105975ndash978 Available from httpwwwncbinlmnihgovpubmed15942552
Skinner JS Gaskill SE Rankinen T Leon AS Rao DC Wilmore JHBouchard C 2003 Heart rate versus VO2max age sex race initial fit-ness and training response-HERITAGE Med Sci Sports Exerc 351908ndash1913 Available at httpwwwncbinlmnihgovpubmed14600558
Sondik EJ Madans JH Gentlemand JF 2012 Summary health statisticsfor US adults National Health Interview Survey 2010 Vital Health Stat101ndash80 Available at httpwwwncbinlmnihgovpubmed20687424
Stones MJ Kozma A 1985 Physical performance Aging and Human Per-formance New York Wiley p 261ndash292
Tanaka H Monahan KD Seals DR 2001 Age-predicted maximal heartrate revisited J Am Coll Cardiol] 37153ndash156 Available at httpwwwncbinlmnihgovpubmed11153730
Vasunilashorn S Crimmins EM Kim JK Winking J Gurven M KaplanH Finch CE 2010 Blood lipids infection and inflammatory markers inthe Tsimane of Bolivia Am J Hum Biol 22731ndash740 Available at httpwwwncbinlmnihgovpubmed20721985
Vaupel JV Manton KG Stallard E 1979 The impact of heterogeneity inindividual frailty on the dynamics of mortality Demography 16439ndash454
Vaupel JW Yashin AI 1985 Heterogeneityrsquos ruses some surprising effectsof selection on population dynamics Am Stat 39176ndash185
Venables WN Ripley BD 2002 Modern Applied Statistics with S FourthNew York Springer
Wagner PD 1996 Determinants of maximal oxygen transport and utiliza-tion Annu Rev Physiol 5821ndash50 Available at httpwwwncbinlmnih-govpubmed8815793
Walker A Arent SM McKeever KH 2010 Maximal aerobic capacity(VO2max) in horses a retrospective study to identify the age-relateddecline Comparative Exerc Physiol 6177ndash181 Available at httpwwwjournalscambridgeorgabstract_S1755254010000073
Walker R Hill K 2003 Modeling growth and senescence in physical per-formance among the Ache of Eastern Paraguay Am J Hum Biol 208196ndash208
Weller IM Thomas SG Corey PN Cox MH 1993 Prediction of maximaloxygen uptake from a modified Canadian aerobic fitness test Can JAppl Physiol 18175ndash188 Available at httpwwwncbinlmnihgovpubmed8513290
Wilson TM Tanaka H 2000 Meta-analysis of the age-associated declinein maximal aerobic capacity in men relation to training status Am JPhysiol Heart Circ Physiol 278H829ndash834 Available at httpwwwncbinlmnihgovpubmed10710351
Wood SN 2006 Generalized Additive Models An Introduction with RBoca Raton Florida Chapman and HallCRC Press
World Health Organization 2001 Iron deficiency anaemia assessmentprevention and control a guide for programme managers Available athttpwhqlibdocwhointhq2001WHO_NHD_013pdf
Yoopat P Toicharoen P Boontong S Glinsukon T Vanwonterghem KLouhevaara V 2002 Cardiorespiratory capacity of Thai workers in dif-ferent age and job categories J Physiol Anthropol Appl Hum Sci 21121ndash128 Available at httpwwwncbinlmnihgovpubmed12056179
Zhu YI Haas JD 1997 Iron depletion without anemia and physical per-formance in young women Am J Clin Nutr 66334ndash341 Available athttpwwwncbinlmnihgovpubmed9250112
14 AC PISOR ET AL
American Journal of Human Biology
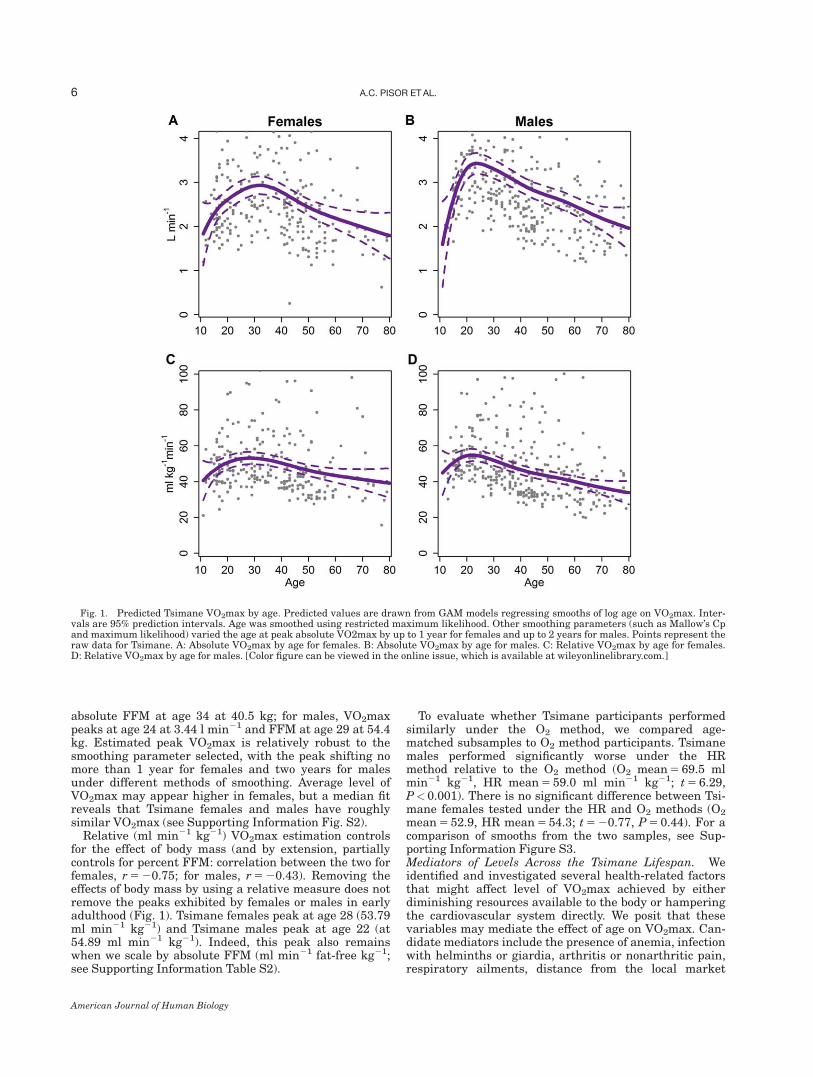
absolute FFM at age 34 at 405 kg for males VO2maxpeaks at age 24 at 344 l min21 and FFM at age 29 at 544kg Estimated peak VO2max is relatively robust to thesmoothing parameter selected with the peak shifting nomore than 1 year for females and two years for malesunder different methods of smoothing Average level ofVO2max may appear higher in females but a median fitreveals that Tsimane females and males have roughlysimilar VO2max (see Supporting Information Fig S2)
Relative (ml min21 kg21) VO2max estimation controlsfor the effect of body mass (and by extension partiallycontrols for percent FFM correlation between the two forfemales r 5 2075 for males r 5 2043) Removing theeffects of body mass by using a relative measure does notremove the peaks exhibited by females or males in earlyadulthood (Fig 1) Tsimane females peak at age 28 (5379ml min21 kg21) and Tsimane males peak at age 22 (at5489 ml min21 kg21) Indeed this peak also remainswhen we scale by absolute FFM (ml min21 fat-free kg21see Supporting Information Table S2)
To evaluate whether Tsimane participants performedsimilarly under the O2 method we compared age-matched subsamples to O2 method participants Tsimanemales performed significantly worse under the HRmethod relative to the O2 method (O2 mean 5 695 mlmin21 kg21 HR mean 5 590 ml min21 kg21 t 5 629Plt 0001) There is no significant difference between Tsi-mane females tested under the HR and O2 methods (O2
mean 5 529 HR mean 5 543 t 5 2077 P 5 044) For acomparison of smooths from the two samples see Sup-porting Information Figure S3Mediators of Levels Across the Tsimane Lifespan Weidentified and investigated several health-related factorsthat might affect level of VO2max achieved by eitherdiminishing resources available to the body or hamperingthe cardiovascular system directly We posit that thesevariables may mediate the effect of age on VO2max Can-didate mediators include the presence of anemia infectionwith helminths or giardia arthritis or nonarthritic painrespiratory ailments distance from the local market
Fig 1 Predicted Tsimane VO2max by age Predicted values are drawn from GAM models regressing smooths of log age on VO2max Inter-vals are 95 prediction intervals Age was smoothed using restricted maximum likelihood Other smoothing parameters (such as Mallowrsquos Cpand maximum likelihood) varied the age at peak absolute VO2max by up to 1 year for females and up to 2 years for males Points represent theraw data for Tsimane A Absolute VO2max by age for females B Absolute VO2max by age for males C Relative VO2max by age for femalesD Relative VO2max by age for males [Color figure can be viewed in the online issue which is available at wileyonlinelibrarycom]
6 AC PISOR ET AL
American Journal of Human Biology
town and Spanish speaking ability Although percentFFM generally predicts absolute rather than relativeVO2max we test it as a potential mediator Pregnancywas included as a control in female models While a highmacroparasite load may increase the likelihood of havinglow hemoglobin (and thus anemia) an interaction termbetween presence of helminths and presence of anemiawas not included because they are not significantlyrelated in this sample only 26 participants of the 92 withhelminths have anemia while 14 of the 86 without hel-minths have anemia (for females v2 5 052 P 5 047 formales v2 5 200 P 5 016)
To evaluate whether these candidate mediators affectedVO2max levels we conducted linear regressions on rela-tive VO2max (see Table 2) We first examined each predic-tor independently Females with higher hemoglobin levelshad significantly higher cardiovascular fitness perform-ance for an increase in 1 g dl21 concentration of hemoglo-bin a Tsimane woman is predicted to have 293 ml min21
kg21 higher VO2max (t 5 268 Plt 001) Helminth infec-tion mediated the relationship between age and VO2maxfor males such that men with a helminth infection arepredicted to have 616 ml min21 kg21 higher VO2max(t 5 231 Plt 005) A best fit model approach (fit on thesubset of females for whom all measures are available)provides similar results to fitting a separate model for
each potential mediating variable When a stepwise AICprocedure was used with data on all health and marketintegration measures hemoglobin level was the only sig-nificant predictor that remained in the female model(n 5 82 standardized b 5 022 Plt 005) For males hel-minth infection remained in the model as well (n 5 116standardized b 5 023 Plt 005)
Scaling VO2max by FFM (ml min21 fat-free kg21)rather than body mass produced similar results hemoglo-bin levels remained a significant positive predictor ofVO2max for females (standardized b 5 030 Plt 001) andhelminth infection a positive predictor for males (standar-dized b 5 020 Plt005) See Supporting InformationTable S3 for all regression results with ml min21 fat-freekg21 as the outcome
Anemia was initially included in model fits howevertreating hemoglobin level as a covariate in place of pres-ence of anemia improved model fit for Tsimane females(anemia AIC 5 10027 hemoglobin AIC 5 98963)Although no association was found between presence ofanemia and helminth infection there is a significant asso-ciation between hemoglobin levels and helminth infectionControlling for age a helminth diagnosis is a significantnegative predictor of hemoglobin levels for females (stand-ardized b 5 2031 Plt 001) Replacing presence of ane-mia with hemoglobin level for males did not improve or
TABLE 3 Comparison of Tsimane and Canadian relative VO2max by age category and sex
Sex Age group
Tsimane Canadians
t-Statistic P-valueMean (ml min21 kg21) n Mean (ml min21 kg21) n
Females 11ndash14 435 7 487 534 2118 02815ndash19 476 33 423 500 310 00020ndash39 510 72 383 662 908 00040ndash59 431 69 314 655 1005 00060ndash69 412 5 242 554 340 003
Males 11ndash14 415 4 548 542 2300 00615ndash19 516 31 508 514 046 06520ndash39 511 96 442 526 527 00040ndash59 432 68 362 584 380 00060ndash69 381 26 275 546 509 000
TABLE 2 Linear models exploring whether mediators affect the level (main effects models) of relative VO2max for Tsimane females and males
Sex Candidate mediatorAge effect est
(P-value)
Main effect models
Sample sizeMediator main effect
est (P-value) Age main effect est (P-value)
Females Perc FFM 2023 (000) 000 (097) 2023 (000) 203Hemoglobin 2013 (028) 024 (001) 2011 (022) 117Helminths 2019 (007) 003 (077) 2020 (006) 92Giardia 2019 (007) 011 (028) 2019 (007) 92Lung ailment 2017 (006) 2005 (060) 2018 (005) 133Reported pain 2017 (006) 2001 (094) 2017 (006) 133Arthritis 2017 (006) 2002 (083) 2016 (007) 133Distance to town 2023 (000) 002 (081) 2023 (000) 196Spanish speaking 2023 (000) 2008 (056) 2024 (000) 197
Males Perc FFM 2037 (000) 009 (012) 2034 (000) 280Hemoglobin 2029 (000) 2002 (076) 2029 (000) 157Helminths 2030 (000) 019 (002) 2027 (000) 128Giardia 2030 (000) 006 (049) 2030 (000) 128Lung ailment 2030 (000) 2007 (033) 2031 (000) 185Reported pain 2030 (000) 011 (013) 2031 (000) 185Arthritis 2030 (000) 2006 (044) 2028 (000) 185Distance to town 2037 (000) 2003 (059) 2037 (000) 273Spanish speaking 2038 (000) 008 (050) 2037 (000) 271
All parameter estimates are standardized
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 7
American Journal of Human Biology
worsen model fit and there is no significant relationshipbetween hemoglobin levels and helminth infection formales (standardized b 5 2010 P 5 028) Parameter esti-mates for anemia were not significant in models for eitherfemales or males
Between-group Table 3 presents Tsimane and Canadianestimated VO2max binned into age categories used byCHMS These data suggest that Canadian females andmales achieve peak VO2max between the ages of 11 and14 while Tsimane males peak between ages 15 and 19Tsimane females peak later between age 20 and 39Across comparable age categories Tsimane have signifi-cantly higher VO2max than Canadians at all ages exceptbetween 11 and 15 for females and 11 and 19 for males(Table 3) However the sample size of Tsimane teenagersunder age 15 is quite small As aforementioned to controlfor the influence of a small number of data points for theyoungest and oldest Tsimane individuals we used GAMto predict VO2max across logged age Predicted valuessuggest that Tsimane females peak at age 28 and Tsimanemales peak at age 22 (see Fig 1c d) These estimates areconsistent with scatterplots of the raw data (plotted onFig 1) and mask fewer fine-grained effects of age thanTable 3 as each CHMS adult age category spans twodecades
It is possible the difference between the Tsimane andCanadians reflects a greater increase in body mass acrossages in the Canadian population or different trajectoriesof change in body composition The former could occurbecause body mass appears in the denominator and cantherefore scale down VO2max while the latter implies dif-ferential changes in FFM when FFM is a predictor ofVO2max in many studies To explore these possibilitieswe performed two calculations we allometrically scaledTsimane VO2max and we projected Tsimane VO2maxassuming the Tsimane had equivalent fat mass and FFMas Canadians from same-sex same-age categories Con-trolling for age the allometric scaling coefficient a wasslightly greater than 1 for both sexes (females a 5 111males a 5 118) This suggests that any disparity inVO2max between Canadians and the Tsimane cannot beexplained solely by mass differences Indeed assumingthe Tsimane have the same body composition as Cana-dians projected VO2max differs little from observedVO2max The Tsimane outperform the Canadians in everycohort by at least 35 ml min21 kg21 except among theyoungest males who perform similarly (see SupportingInformation Fig S4)
To control for possible disparities in changes in bodycomposition by age within each population as these mightalso influence differences between the Tsimane and Cana-dians we scaled VO2max by absolute FFM from the samepopulation to obtain ml min21 fat-free kg21 BecauseCanadian body composition data were only available viaskinfolds (bicep tricep subscapular and suprailiac) weused the subset of Tsimane (n 5 246) for which the samefour skinfolds measurements were available We calcu-lated average absolute FFM for each cohort using averageweight and average summed skinfolds (Durnin andWomersley 1974) and scaled average VO2max in mlmin21 by this number to obtain ml min21 fat-free kg21Under this method of scaling the Tsimane outperformCanadians in every cohort over age 20 by at least 165 ml
min21 fat-free kg21 (see Supporting Information TableS2) Canadian females and males in the 12ndash19 cohortsoutperform Tsimane of the same age
We next compared Tsimane to other subsistence popula-tions reported in the literature (Table 4) Consistent withcommon practice in the literature we report means foreach group but when possible we also predicted VO2maxat age 25 to provide age-corrected comparisons Weselected age 25 as it is the age of peak relative VO2max inthis study and for female Kamba and Maasai in Christen-sen et als (2012) recent study To predict VO2max at age25 we regressed the median ages on mean VO2max acrossthe available age categories Tsimane females and maleshave roughly the same predicted VO2max at age 25 asseveral other subsistence populations but higher VO2maxthan industrialized populations To test for differencesbetween industrialized and subsistence populations weconducted a linear regression on predicted VO2max at age25 this is not a meta-analysis and results should beinterpreted with caution Overall subsistence populationsdisplay higher peak VO2max than in industrialized popu-lations controlling for sex (440 vs 367 ml min21 kg21
[Plt 001]) The Tsimane O2 and indigenous Siberian sam-ples were excluded Tsimane O2 to avoid the problem ofnon-independence with Tsimane HR data and Siberiansbecause the sample has a limited age range comparedwith the other studies
Pace of decline slope of VO2max decline across thelifespan
Tsimane To evaluate whether Tsimane participants per-formed similarly under different methods we comparedage-matched subsamples of participants from the presentstudy with O2 method participants Despite a higher level(intercept) of VO2max in the O2 sample Tsimane malesdeclined marginally significantly faster under the O2
method relative to the HR method (O2 5 68 per decadeHR 5 47 decline per decade t 5 2195 P 5 005) Thereis no significant difference between Tsimane femalestested under the O2 and HR methods (O2 5 60 per dec-ade HR 5 48 decline per decade t 5 2055 P 5 058)Mediators of Slope Across the Lifespan We fit a series oflinear models to test for interactions between the candi-date mediators and age-related decline in TsimaneVO2max There are no variables that significantly inter-act with age to predict VO2max (see Supporting Informa-tion Table S4) An AIC selection approach and scaling byabsolute FFM (see Supporting Information Table S3) pro-vides the same results no variables significantly interactwith age to predict VO2max
Between-group VO2max is most often reported as a lin-ear decline across the adult lifespan though Hawkins andWiswell (2003) dispute whether the decline is actually lin-ear For example a linear approximation is not appropri-ate for Tsimane females if ages 11ndash80 are consideredFigure 2 contrasts linear declines in VO2max for Cana-dians and Tsimane males as well as a curvilinear fit forTsimane females with declines in industrialized nationsderived from meta-analyses (Fitzgerald et al 1997 Wil-son and Tanaka 2000) To explore whether rates ofdecline in VO2max among Tsimane and Canadians weredifferent we regressed average VO2max by age category
8 AC PISOR ET AL
American Journal of Human Biology
TA
BL
E4
Mea
nV
O2m
ax
esti
ma
ted
VO
2m
ax
at
age
25a
nd
dec
lin
ein
VO
2m
ax
per
dec
ad
efr
omth
isst
ud
ya
nd
pre
vio
us
rese
arc
ha
Pop
ula
tion
Fem
ale
Male
Pu
bli
cati
onM
ean
VO
2m
ax
VO
2m
ax
Age
25
bP
erce
nt
Dec
lin
eA
ge
Ran
ge
(n)
Mea
nV
O2m
ax
VO
2m
ax
Age
25
bP
erce
nt
Dec
lin
eA
ge
Ran
ge
(n)
Ind
ust
riali
zed
Can
ad
ac
312
400
73
20ndash69
(2905)
361
458
68
20ndash69
(2712)
Jap
an
d357
414
39
20ndash69
(656)
417
473
38
20ndash69
(807)
San
ad
aet
al
2007
Sw
eden
e330
g409
80
20ndash65
324
g388
75
20ndash65
Ek
blo
met
al
2007
Th
ail
an
d(i
nd
ust
ry)e
275
293
54
16ndash55
(56)
389
415
57
16ndash53
(70)
Yoo
pat
etal
2002
US
(H
erit
age)
f273
17ndash65
(360)
359
17ndash65
(293)
Sk
inn
eret
al
2003
US
(N
HA
NE
S)d
356
363
24
20ndash49
(1312)
444
438
39
20ndash49
(1481)
Su
bsi
sten
ceT
sim
an
e(H
R)c
498
521
h16
h20ndash69
471
538
h61
h20ndash69
Tsi
man
e(O
2)c
436
74
h36ndash69
540
25
h36ndash69
Ifalu
k(1
969ndash70)c
429
488
69
20ndash59
(43)
49
597
75
20ndash69
(75)
Rod
ean
dS
hep
hard
1994
Ach
ec465
434
257
20ndash59
(62)
519
614
84
20ndash59
(65)
Walk
eran
dH
ill
2003
Lu
oc378
372
39
17ndash68
(209)
429
48
54
17ndash68
(172)
Ch
rist
ense
net
al
2012
b
Kam
ba
c377
371
45
17ndash68
(283)
431
516
34
17ndash68
(94)
Ch
rist
ense
net
al
2012
Maasa
ic389
410
45
17ndash68
(178)
431
528
69
17ndash68
(163)
Ch
rist
ense
net
al
2012
Ind
igen
ous
Sib
eria
nsc
338
341
22
220ndash39
(14)
462
471
66
20ndash39
(30)
Katz
marz
yk
etal
1994
Ru
ral
Nep
alc
187
15ndash60
(39)
221
15ndash60
(35)
Pan
ter-
Bri
cket
al
1992
Ngis
onyok
aT
urk
an
af
38
387
18
20ndash44
(19)
Cu
rran
-Ever
ett
1994
aV
alu
esm
issi
ng
wh
enn
otavail
able
from
ap
art
icu
lar
stu
dy
Per
cen
td
ecli
ne
(per
cen
tof
pea
kvalu
elo
st)
per
dec
ad
ew
as
calc
ula
ted
as
by
regre
ssin
gre
lati
ve
VO
2m
ax
by
age
mu
ltip
lyin
gth
ep
ara
met
eres
tim
ate
for
age
by
10
an
dd
ivid
ing
this
nu
mber
by
the
inte
rcep
t(p
resu
med
pea
k
ass
um
ing
ali
nea
rd
ecli
ne
inV
O2m
ax
acr
oss
age)
B
ecau
seof
lack
ofacc
ess
tora
wd
ata
re
gre
ssio
ns
wer
efi
tw
ith
mea
nV
O2m
ax
an
dm
edia
nage
by
coh
ort
bA
ge
25
valu
esw
ere
esti
mate
dby
regre
ssin
gre
lati
ve
VO
2m
ax
by
age
then
usi
ng
the
resu
ltin
gp
ara
met
eres
tim
ate
sto
pre
dic
tV
O2m
ax
at
age
25
the
pea
kin
rece
ntl
yst
ud
ied
pop
ula
tion
s(e
g
Kam
ba
an
dM
aasa
ife
male
sC
hri
sten
sen
etal
2012fe
male
san
dm
ale
sin
this
art
icle
)B
ecau
seof
lack
ofacc
ess
tora
wd
ata
re
gre
ssio
ns
wer
efi
tw
ith
mea
nV
O2m
ax
an
dm
edia
nage
by
coh
ort
cS
ubm
axim
alst
epte
st
dS
ubm
axim
altr
ead
mil
lte
st
eS
ubm
axim
aler
gom
eter
test
f M
axim
al
ergom
eter
test
gS
wed
ish
data
wer
ere
por
ted
as
med
ian
sfo
rea
chage
cate
gor
yth
evalu
esre
por
ted
her
eare
mea
ns
ofth
ese
med
ian
s2006
ind
ivid
uals
part
icip
ate
dbu
tn
um
ber
by
sex
was
not
rep
orte
d
hF
orco
mp
ara
bil
ity
we
bin
ned
the
Tsi
man
eH
Ran
dO
2d
ata
into
10
yea
rage
cate
gor
ies
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 9
American Journal of Human Biology
on median age (for a given age category) population andtheir interaction term For comparability Tsimane werebinned into the Canadian age categories and averageswere computed for these categories leading to estimateddeclines slightly different from those in Table 4 for thepurposes of this test we treat the Tsimane female declineas linear Because within-population variance in declineis not available these regressions should be treated asdescriptive comparisons rather than statistical tests ofdifferences between the two groups The rate of decline inVO2max is steeper for Canadian females (69 per decadefaster decline per decade) and males (42 faster declineper decade) compared with Tsimane females and males
The rate of cardiovascular fitness decline between theTsimane and Canadians is different but this differencedoes not extend to industrialized and subsistence popula-tions (see Table 4) Controlling for sex subsistence groupshave about one quarter of a percent lower declines perdecade Again because the variance in decline is not rep-resented in this regression results should be interpretedas comparative rather than as a statistical test As beforeTsimane O2 results were not included in the analysis toavoid nonindependence and the indigenous Siberianswere excluded because of discrepancy in ages sampled
DISCUSSION
Our comparisons demonstrate that across a wide varietyof societies cardiovascular fitness senesces with age Car-diovascular fitness is higher on average among members ofsubsistence societies than among industrialized societiesbut rates of fitness decline from peak are not slower Ourmore detailed comparison between the Tsimane a subsist-ence population and Canadians an industrialized popula-tion reveals differences in cardiovascular fitness levelsand rate of fitness decline Cardiovascular fitness levelswere higher among the Tsimane than among Canadiansand the rate of decline across the lifespan was significantlyslower among Tsimane women and men Potential Cana-
dian participants were excluded due to many health con-cerns including pregnancy and history of high bloodpressure whereas Tsimane were only excluded if they self-identified as unable to participate This suggests the Cana-dian sample is a relatively healthy subsample of Canadayet the Tsimane still outperform them in cardiovascular fit-ness It may be that the higher demand for cardiovascularfitness in late ages among the Tsimane outweighs anyeffects of poor health Another possibility is that greaterself-selection among Tsimane due to higher adult mortalityleaves more robust older adult survivors thereby reducingthe observed slope of fitness decline at the population level(Vaupel et al 1979) perhaps this is partially why fewerTsimane older adults opted out of the exercise test thanCanadian older adults were screened out (ages 60ndash69Canadian females 5 56 Tsimane females 5 15 Cana-dian males 5 57 Tsimane males 5 5)
Consistent with prior research on age-related changesin cardiovascular fitness the Tsimane do evidence a lin-ear decline in VO2max with age but not as steep a declineas typically seen in industrialized populations Based oncomparisons with the Canadians and with other industri-alized populations we believe the Tsimane data from thepresent study and the pilot O2 data combined indicatethat the Tsimane perform better on tests of cardiovascularfitness than the average individual from an industrializednation
To further explore the potential effects of health factorson cardiovascular fitness level and rate of decline weinvestigated predictors of individual differences in fitnesswithin the Tsimane population Overall we found thatmost health indicators among the Tsimane did not hinderVO2max levels or rates of decline Lower hemoglobin lev-els were associated with lower VO2max levels in womenbut not men consistent with the notion that compromisedblood oxygen transport curbs cardiovascular fitness(Buzina et al 1989 Panter-Brick et al 1992) In the USlow hemoglobin is more common in active women thanactive men (Sinclair and Hinton 2005) hemoglobin is
Fig 2 Linear changes in VO2max with age for Canadians and the Tsimane Intercepts and slopes for Canadians and Tsimane can be foundin Table 4 Because age2 is significant for the full sample of Tsimane females their change in VO2max across age is curvilinear Slopes forendurance trained active and sedentary individuals from industrialized nations are drawn from a meta-analysis performed by Fitzgeraldet al (1997) for females and Wilson and Tanaka (2000) for males Endurance trained individuals are represented by the top dotted line abovefollowed by active individuals below and sedentary on the bottom Trained individuals engage in 31 sessions of endurance exercise per weekfor at least a year while active individuals engage in 2 or fewer sessions per week of cardiovascular exercise [Color figure can be viewed in theonline issue which is available at wileyonlinelibrarycom]
10 AC PISOR ET AL
American Journal of Human Biology
also lower in Tsimane women than Tsimane men(female 5 129 [sd 13] g ml21 males 5 142 [13] g ml21)Even mild (non-anemic) iron deficiencies impacts womenrsquosexercise performance (Zhu and Haas 1997) Inconsistentwith findings from Panter-Brick et al (1992) among ruralNepalese helminth infection did not diminish levels ofVO2max for Tsimane men helminth infection wasactually a predictor of higher VO2max There are severalreasons why this might be the case First we only testedwhether presence or absence of helminths mediated theeffect of age on VO2max rather than parasite load (egnumber of worms egg counts) it is possible that helminthinfection only affects VO2max at high parasite loads Sec-ond blood loss (and thus low hemoglobin levels) resultingfrom helminth infection may be partially offset by theamount of iron in the Tsimane adult diet Tsimane ironintake is an estimated 166 of the US Dietary ReferenceIntake (Martin et al 2012) and Tsimane hemoglobin lev-els are higher than in the Nepalese (females 129 vs 109males 1424 vs 120 Panter-Brick et al 1992) Thirdthese analyses consider helminth infection at the time ofexercise test rather than past infections It may be thatthe cumulative burden of past infection has a larger effecton cardiovascular fitness if so this would suggest thatthe surprising positive effect of helminth infection onVO2max levels in men is either spurious or capturing athird variable
Secular declines in VO2max are expected with increasingmarket integration and lifestyle change because ofincreased sedentism (Katzmarzyk et al 1994 Rode andShephard 1994) Two proxies for market integration in thispopulationmdashdistance to San Borja and the ability to speakSpanishmdashwere not significant predictors of VO2max levelsor decline This is consistent with our predictions as Tsi-mane females and males that live near town do not appearto have lower activity levels (Gurven et al 2013) Wageopportunities near town primarily include working asranch hands collecting and weaving palm thatch panelscash cropping and working for logging companies Each ofthese involves extensive activity furthermore transporta-tion to town often involves bicycling walking and polingdugout canoes Cash cropping of rice and corn also involvesthe clearing and weeding of larger fields Except for cashcropping and palm thatch manufacture most wage laboropportunities are currently restricted to men
This study makes several unique contributions to theexisting literature It offers the first systematic compari-son of cardiovascular fitness level and rate of declinebetween subsistence and industrialized societies Resultscompiled from previous studies support the general claimthat despite greater pathogen stress the greater activityregime of subsistence societies helps support higher peakVO2max Additionally this is one of the first studies toexplore senescent changes in cardiovascular fitnesswithin a large sample from a subsistence population Thelarge number of health measures and proxies of marketintegration available permitted testing whether these fac-tors mediated age-related variation and whether theymodulated the rate of decline Despite reports that healthstatus and market integration have been important inother studies (eg Buzina et al 1989 Katzmarzyk et al1994 Panter-Brick et al 1992 Rode and Shephard1994) their overall net effect was small among the Tsi-mane most apparent in measures of hemoglobin levelsamong women and helminth infection among men
The results of these analyses may also shed light onindividual and population level differences in chronic dis-ease In industrialized populations meta-analyses demon-strate that cardiovascular fitness is protective againstcardiovascular disease (Jette et al 1992 Hawkins andWiswell 2003) Prior studies among Tsimane suggest rel-atively few deaths from heart attacks or strokes (Gurvenet al 2007) a low prevalence of common cardiovasculardisease risk factors like obesity high blood low-densitylipoprotein levels hypertension and peripheral arterialdisease and the existence of additional protective factorslike lean diet and physical activity (Gurven et al 20092013 Vasunilashorn et al 2010) Market foods such ascooking oil sugar and pasta represent only 6 of theaverage Tsimane diet and Tsimane also consume a greatdeal of lean meat and omega-3 fatty acids (Martin et al2012) This study complements these findings by demon-strating that Tsimane show relatively high VO2max anindicator of strong cardiorespiratory health TsimaneVO2max declines with age as it does everywhere whichsuggests declining muscle mass with age (Fleg andLakatta 1988) and lowered cardiac output (American Col-lege of Sports Medicine 2006 Sagiv et al 2007) ratherthan increased cardiovascular disease risk
Limitations
The Canadians were selected as a comparison industri-alized population because of the similarity of the CHMSand Tsimane protocols very few studies of industrializedpopulations have large sample sizes sample across thelife course and use a step test Several aspects of theCHMS and Tsimane protocols remain potentially incom-parable The Canadians experienced more stringentexclusion criteria than the Tsimane meaning that the Tsi-mane sample may be more representative of cardiovascu-lar condition in the Tsimane population than theCanadian sample of the Canadian population Again ifthe Tsimane sample was subjected to these criteria wemight expect the differences in VO2max between popula-tions to only increase On the other hand Canadian par-ticipants were assigned stepping cadences based on theirage and sex and cadence was increased across the exer-cise test if a participant did not reach 85 of his or herage-specific maximal HR all Tsimane were asked to com-plete 30 ascents per minute with no increase based ontheir achieved HRs Few Tsimane reached 75 of theirage-specific maximal HR (see Supporting InformationTable S1) perhaps because the age-specific maximal HRsderived from industrialized populations are inaccurate forthe Tsimane or because higher fitness allowed these Tsi-mane to perform the step test of 30 ascents per minutewith less effort Due to these discrepancies in protocolwhich may lead to errors in estimating VO2max we alsoincorporated Tsimane data collected using the O2 methodas a check because the O2 method estimates VO2max onthe relationship between HR and VO2 in a givenparticipant
Indeed it is an open question as to whether typicalmethods for indirectly estimating cardiovascular fitnessfrom HR are appropriate for subsistence level popula-tions Common routines for VO2max estimation assumeage-specific declines in cardiovascular fitness (eg Shep-hard 1970) but these methods have only been validatedwith samples from industrialized populations which are
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 11
American Journal of Human Biology
often self-selected (Beall et al 1985) Additionally regres-sions drawn from laboratory studies require participantsachieve a HR within a certain range for accurate VO2maxestimation however the appropriateness of these rangesgiven slight modifications to protocol and inclusion of par-ticipants of different ages different populations and bothsexes is questionable For example the maximal HRexhibited by young men varies across subsistence popula-tions (Shephard 1978) Use of these criteria is compli-cated by the fact that the most commonly used equationfor estimating maximal possible HR by age 220-age maybe inaccurate (Robergs and Landwehr 2002) and particu-larly inappropriate for older adults (see Tanaka et al2001) For these reasons we chose to use an exclusion cri-terion for the Tsimane that evaluates individual increasein HR across exercise relative to the mean increase in HRfor Tsimane of the same sex and age
The pattern of Tsimane fitness decline differs moder-ately by the choice of exclusion criterion for participants(see Supporting Information Table S1) and by method oftesting However this is a common finding Lee et al(2011) predicted VO2max from submaximal exercise usingthe O2 method and the HR-based American College ofSports Medicine calculation routine in a US sample Theyfound that (1) the HR-based routine predicts higherVO2max across the sexes than does the O2 routine and(2) the two methods have a correlation of only 077 Whenevaluating different testing procedures Shephard et al(1968) found differences in VO2max estimation by type oftest used (eg bicycle ergometer versus step test) and cal-culation routine Exercise tests exclusion criteria andcalculation routines combine to provide an estimate ofactual VO2max for a given individual and as such varia-tion in estimation is to be expected However such varia-tion may affect cross-population comparisons inunforeseen ways thus the comparisons presented hereshould be interpreted with caution
While population-level variation in cardiovascular fit-ness decline may reflect the differences in the demands ofendurance-based physical activity muscularity and com-promised oxygen transport it is possible that genetic fac-tors may also play a potential role (Collins 1999) In oneindustrialized sample maternal cardiovascular fitnessexhibited a heritability of 30 which is attributed toinheritance of the maternal mitochondrial genome (Bou-chard et al 2000) We do not have the relevant geneticdata for the populations considered here however andthus operate under the simplifying assumption thatinheritance should not affect population-level patternsand will not consistently bias individual-level compari-sons in any particular direction
This study is further limited by its cross-sectionaldesign Cross-sectional data present well-known problemsfor the measurement of individual aging (Crimmins andSeeman 2001) Mortality selection in which individualsin poorer condition are likely to die at younger ages pro-duces a downward bias in the estimation of aging rates atthe individual level (Vaupel and Yashin 1985 Vaupelet al 1979) Cohort effects if present also produce com-plicated and non-monotonic biases in estimation (Carnesand Olshansky 2001) Due to the problem of between-individual heterogeneity and the within-individual pro-cess of senescence a recent overview of aging studies con-cludes that ldquoonly longitudinal studies [ ] provide reliablesources of information in the study of senescencerdquo (Nussey
et al 2008) To date there are no longitudinal studies ofcardiovascular fitness in subsistence populations We arecurrently re-testing participants under the O2 methodallowing a better grasp of the within-individual variationthat shapes patterns of senescent decline
ACKNOWLEDGMENTS
The authors thank Paul Hooper Steven Gaulin JohnTooby Patricia Kramer the Human Evolution and Biode-mography laboratory and the Center for EvolutionaryPsychology at UCSB for helpful advice and feedback thestaff at the Tsimane Health and Life History Project andthe Tsimane for their participation and patience
LITERATURE CITED
American College of Sports Medicine 2006 ACSMrsquos Guidelines for Exer-cise Testing and Prescription 7th ed Philadelphia Lippincott Williamsamp Wilkins
Armstrong N 2001 Peak oxygen uptake in relation to growth and matura-tion in 11- to 17-year-old humans Eur J Appl Physiol 85546ndash551
Astrand PO Ryhming I 1954 A nomogram for calculation of aerobiccapacity (physical fitness) from pulse rate during submaximal work JAppl Physiol 7218ndash221
Bailey DA Shephard RJ Mirwald RL 1976 Validation of a self-administered home test of cardio-respiratory fitness Can J Appl SportSci 167ndash78
Beall CM Goldstein MC and Feldman ES 1985 The physical fitness ofelderly Nepalese farmers residing in rugged mountain and flat terrainJ Gerontol 40529ndash535
Benefice E Ndiaye G 2005 Relationships between anthropometry cardi-orespiratory fitness indices and physical activity levels in different ageand sex groups in rural Senegal (West Africa) Ann Hum Biol 32366ndash382 Available from httpwwwncbinlmnihgovpubmed16099780
Blackwell AD Gurven MD Sugiyama LS Madimenos FC Liebert MAMartin MA Kaplan HS Snodgrass JJ 2011 Evidence for a peak shift in ahumoral response to helminths age profiles of IgE in the Shuar of Ecuadorthe Tsimane of Bolivia and the US NHANES PLoS Negl Trop Dis 5e1218 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid53125146amptool5pmcentrezamprendertype5abstract
Blackwell AD Martin M Kaplan H Gurven M Evidence for an antagonis-tic relationship between Giardia lamblia and helminth infections impli-cations for treatment of helminth infections in developing populations
Blair SN LaMonte MJ Nichaman MZ 2004 The evolution of physicalactivity recommendations how much is enough Am J Clin Nutr 79913Sndash920S Available at httpwwwncbinlmnihgovpubmed15113739
Bouchard C Rankinen T Chagnon YC Rice T Perusse L Gagnon JBorecki I An P Leon a S et al 2000 Genomic scan for maximal oxygenuptake and its response to training in the HERITAGE Family Study JAppl Physiol 88551ndash559 Available at httpwwwncbinlmnihgovpubmed10658022
Bryan S St-Denis M Wojtas D 2007 Canadian Health Measures Surveyclinic operations and logistics Health Rep 1853ndash69
Buzina R Bates CJ van der Beek J Brubacher G Chandra RK HallbergL Heseker J Mertz W Pietrzik K et al 1989 Workshop on FunctionalSignificance of Mild-to-Moderate Malnutrition Am J Clin Nutrition 50172ndash176
Calder WA 1987 Scaling energetics of homeothermic vertebrates anoperational allometry Annu Rev Physiol 49107ndash120
Canadian Society for Exercise Physiology 2003 The Canadian PhysicalActivity Fitness amp Lifestyle Approach (CPAFLA) CSEP-Health amp Fit-ness Programrsquos Health-Related Appraisal and Counselling Strategy 3rded
Carnes BA Olshansky SJ 2001 Heterogeneity and its biodemographicimplications for longevity and mortality Exp Gerontol 36419ndash430Available at httpwwwncbinlmnihgovpubmed11250115
Carrick-Ranson G Hastings JL Bhella PS Shibata S Fujimoto N PalmerD Boyd K Levine BD 2013 The effect of age-related differences inbody size and composition on cardiovascular determinants of VO2max JGerontol A Biol Sci Med Sci 68608ndash616 Available at httpwwwncbinlmnihgovpubmed23160363
Centers for Disease Control and Prevention 1998 Recommendations toPrevent and Control Iron Deficiency in the United States MMWRRecomm Rep 471ndash36 Available at httpwwwcdcgovmmwrpreviewmmwrhtml00051880htm
12 AC PISOR ET AL
American Journal of Human Biology
Centers for Disease Control and Prevention 2011 Glossary of TermsPhysical Activity for Everyone [Internet] Available from httpwwwcdcgovphysicalactivityeveryoneglossary
Christensen DL Faurholt-Jepsen D Boit MK Mwaniki DL Kilonzo BTetens I Kiplamai FK Cheruiyot SC Friis H et al 2012 Cardiorespira-tory fitness and physical activity in Luo Kamba and Maasai of ruralKenya Am J Hum Biol 24723ndash729 Available at httpwwwncbinlm-nihgovpubmed22836508
Colley RC Garriguet D Janssen I Craig CL Clarke J Tremblay MS2011a Physical activity of Canadian children and youth accelerometerresults from the 2007 to 2009 Canadian Health Measures SurveyHealth Rep 2215ndash23
Colley RC Garriguet D Janssen I Craig CL Clarke J Tremblay MS2011b Physical activity of Canadian adults accelerometer results fromthe 2007 to 2009 Canadian Health Measures Survey Health Rep 227ndash14 Available at httpwwwncbinlmnihgovpubmed21510585
Collins KJ 1999 Physiological variation and adaptability in human popu-lations Ann Hum Biol 2619ndash38
Crimmins E Seeman T 2001 Integrating Biology into DemographicResearch on Health and Aging (With a Focus on the MacArthur Study ofSuccessful Aging) Cells and Surveys Should Biological Measures beIncluded in Social Science Research Washington DC National Acad-emy Press p 9ndash41
Curran-Everett LS 1994 Accordance Between VO2max and Behavior inNgisonyoka Turkana Am J Hum Biol 6761ndash771
Durnin JVGA Womersley J 1974 Body fat assessed from total body den-sity and its estimation from skinfold thickness measurements on 481men and women aged from 16 to 72 years Br J Nutr 3277ndash97
Eberl M Al-Sherbiny M Hagan P Ljubojevic S Thomas AW Wilson RA2002 A novel and sensitive method to monitor helminth infections byfaecal sampling Acta Trop 83183ndash187
Eid D Gurven M Kaplan H Winking J 2007 Enfermedades infecciosas alo largo de la vida y en el envejecimiento en indıgenas sudamericanos dela etnia Tsimane Aging in Developing Countries Building Bridges forIntegrated Research Agendas Santiago Chile
Ekblom B Engstreuroom L-M Ekblom O 2007 Secular trends of physical fit-ness in Swedish adults Scand J Med Sci Sports 17267ndash273 Availableat httpwwwncbinlmnihgovpubmed17501867
Finch CA Lenfant C 1972 Oxygen Transport in Man N Engl J Med 286407ndash415
Fitzgerald MD Tanaka H Tran ZV Seals DR 1997 Age-related declinesin maximal aerobic capacity in regularly exercising vs sedentarywomen a meta-analysis J Appl Physiol (Bethesda Md 1985) 83160ndash165 Available at httpwwwncbinlmnihgovpubmed9216959
Fleg JL Lakatta EG 1988 Role of muscle loss in the age-associated reduc-tion in VO2max J Appl Physiol 651147ndash1151
Frisancho AR Frisancho HG Milotich M Brutsaert T Albalak RSpielvogel H Villena M Vargas E Soria R 1995 Developmentalgenetic and environmental components of aerobic capacity at high alti-tude Am J Phys Anthropol 96431ndash442 Available at httpwwwncbinlmnihgovpubmed7604895
Giroux S 2007 Canadian health measures survey sampling strategyoverview Health Rep 1831ndash36
Gurven M Jaeggi A V Kaplan H Cummings D 2013 Physical activityand modernization among Bolivian Amerindians PLoS ONE 81ndash13
Gurven M Kaplan H Winking J Rodriguez DE Vasunilashorn S KimJK Finch C Crimmins E 2009 Inflammation and infection do not pro-mote arterial aging and cardiovascular disease risk factors among leanhorticulturalists PLoS ONE 41ndash12
Haidet GC 1989 Dynamic exercise in senescent beagles oxygen consump-tion and hemodynamic responses The Am J Physiol 257H1428ndash1437Available at httpwwwncbinlmnihgovpubmed2589499
Hawkins S Wiswell R 2003 Rate and mechanism of maximal oxygen con-sumption decline with aging implications for exercise training SportsMed 33877ndash888 Available at httpwwwncbinlmnihgovpubmed12974656
Hoffman J 2002 Physiological aspects of sport training and performance1st ed Champaign IL Human Kinetics Publishers
Hotez PJ Bottazzi ME Franco-Paredes C Ault SK Periago MR 2008 Theneglected tropical diseases of Latin America and the Caribbean a review ofdisease burden and distribution and a roadmap for control and eliminationPLoS Negl Trop Dis 2e300 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid52553488amptool5pmcentrezamprendertype5abstract
Howley ET Bassett DR Welch HG 1995 Criteria for maximal oxygenuptake review and commentary Med Sci Sports Exerc 271292ndash1301Available at httpwwwncbinlmnihgovpubmed8531628
Jette M Sidney K Quenneville J Landry F 1992 Relation between cardi-orespiratory fitness and selected risk factors for coronary heart diseasein a population of Canadian men and women CMAJ 1461353ndash1360Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid51488567amptool5pmcentrezamprendertype5abstract
Katzmarzyk PT Leonard WR Crawford MH 1994 Predicted maximaloxygen consumption of Indigenous Siberians Am J Hum Biol 6783ndash790
King CH Dickman K Tisch DJ 2005 Reassessment of the cost of chronichelmintic infection a meta-analysis of disability-related outcomes inendemic schistosomiasis Lancet 3651561ndash1569 Available at httpwwwncbinlmnihgovpubmed15866310
Lee J-M Bassett D Jr Thompson D Fitzhugh E 2011 Validation of thecosmed fitmate for predicting maximal oxygen consumption J StrengthCond Res 252573ndash2579
Madimenos FC Snodgrass JJ Blackwell AD Liebert MA Sugiyama LS2011 Physical activity in an indigenous Ecuadorian forager-horticulturalist population as measured using accelerometry Am J HumBiol 23488ndash497 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid53110644amptool5pmcentrezamprendertype5abstract
Malina RM 2001 Physical activity and fitness pathways from childhoodto adulthood Am J Hum Biol 13162ndash172 Available at httpwwwncbinlmnihgovpubmed11460860
Malina RM Little BB 2008 Physical activity the present in the contextof the past Am J Hum Biol 20373ndash391 Available at httpwwwncbinlmnihgovpubmed18433002
Manning JT Morris L Caswell N 2007 Endurance running and digitratio (2D 4D) implications for fetal testosterone effects on runningspeed and vascular health Am J Hum Biol 19416ndash421
Martin Ma Lassek WD Gaulin SJC Evans RW Woo JG Geraghty SRDavidson BS Morrow AL Kaplan HS et al 2012 Fatty acid composi-tion in the mature milk of Bolivian forager-horticulturalists controlledcomparisons with a US sample Matern Child Nutr 8404ndash418 Availableat httpwwwncbinlmnihgovpubmed22624983
National Health and Nutrition Examination Survey 2004 CardiovascularFitness Procedures Manual
Nussey D Coulson T Festa-Bianchet M Gaillard J-M 2008 Measuringsenescence in wild animal populations towards a longitudinal approachFunction Ecol 22393ndash406
Ogawa T Spina RJ Martin WHI Kohrt WM Schechtman KB HolloszyJO Ehsani AA 1992 Effects of aging sex and physical training cardio-vascular responses to exercise Circulation 86494ndash503
Panter-Brick C Miller UG Eggerman M 1992 Hemoglobin levels andstep test performance of men and women in Nepal Am J Hum Biol 4481ndash491
Pontzer H Raichlen Da Wood BM Mabulla AZP Racette SB MarloweFW 2012 Hunter-gatherer energetics and human obesity PLoS ONE 7e40503 Available at httpcdxplosorg101371journalpone0040503
R Development Core Team 2011 R A language and environment for sta-tistical computing R Development Core Team
Rigby R Stasinopoulos D 2005 Generalize additive models for locationscale and shape (with discussion) Appl Stat 54507ndash554
Robergs RA Landwehr R 2002 The surprising history of theldquoHRmax5220-agerdquo equation J Exerc Physiol 51ndash10
Rode A Shephard RJ 1994 Physiological consequences of acculturation a20-year study of fitness in an Inuit community Eur J Appl Physiol 69516ndash524
Rowland TW Boyajian A 1995 Aerobic response to endurance training inchildren Pediatrics 96654ndash658
Sagiv M Ben-sira D Amir R 2007 What maintains energy supply atpeak aerobic exercise in trained and untrained older men Gerontology53357ndash361
Sanada K Kuchiki T Miyachi M Mcgrath K Higuchi M Ebashi H 2007Effects of age on ventilatory threshold and peak oxygen uptake normal-ised for regional skeletal muscle mass in Japanese men and womenaged 20 ndash 80 years Eur J Appl Physiol 99475ndash483
Schniter E 2009 Why Old Age Non-Material Contributions and Patternsof Aging Among Older Adult Tsimanersquo 607
Shahnawaz H 1978 Influence of limb length on a stepping exercise JAppl Physiol 44346ndash349
Shephard RJ 1970 Computer programs for solution of the Astrand nomo-gram and the calculation of body surface area J Sports Med 10206ndash210
Shephard RJ Allen C Benade AJS Davies CT Di Prampero PE HedmanR Merriman JE Myhre K Simmons R 1968 Standardization of sub-maximal exercise tests Bull World Health Organ 38765ndash775 Availableat httpwwwpubmedcentralnihgovarticlerenderfcgiartid52554690amptool5pmcentrezamprendertype5abstract
Shephard RJ Bailey Da Mirwald RL 1976 Development of the CanadianHome Fitness Test Can Med Assoc J 114675ndash679 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid51956906amptool5pmcentrezamprendertype5abstract
Shields M Tremblay MS Laviolette M Craig CL Janssen I Gorber SC2010 Fitness of Canadian adults results from the 2007ndash2009 canadianhealth measures survey Health Rep 2121ndash35 Available at httpwwwncbinlmnihgovpubmed20426224
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 13
American Journal of Human Biology
Siconolfi SF Garber CE Lasater TM Carleton RA 1985 A simple validstep test for estimating maximal oxygen uptake in epidemiologic stud-ies Am J Epidemiol 121382ndash390 Available at httpwwwncbinlm-nihgovpubmed4014128
Sinclair LM Hinton PS 2005 Prevalence of iron deficiency with and with-out anemia in recreationally active men and women J Am Diet Assoc105975ndash978 Available from httpwwwncbinlmnihgovpubmed15942552
Skinner JS Gaskill SE Rankinen T Leon AS Rao DC Wilmore JHBouchard C 2003 Heart rate versus VO2max age sex race initial fit-ness and training response-HERITAGE Med Sci Sports Exerc 351908ndash1913 Available at httpwwwncbinlmnihgovpubmed14600558
Sondik EJ Madans JH Gentlemand JF 2012 Summary health statisticsfor US adults National Health Interview Survey 2010 Vital Health Stat101ndash80 Available at httpwwwncbinlmnihgovpubmed20687424
Stones MJ Kozma A 1985 Physical performance Aging and Human Per-formance New York Wiley p 261ndash292
Tanaka H Monahan KD Seals DR 2001 Age-predicted maximal heartrate revisited J Am Coll Cardiol] 37153ndash156 Available at httpwwwncbinlmnihgovpubmed11153730
Vasunilashorn S Crimmins EM Kim JK Winking J Gurven M KaplanH Finch CE 2010 Blood lipids infection and inflammatory markers inthe Tsimane of Bolivia Am J Hum Biol 22731ndash740 Available at httpwwwncbinlmnihgovpubmed20721985
Vaupel JV Manton KG Stallard E 1979 The impact of heterogeneity inindividual frailty on the dynamics of mortality Demography 16439ndash454
Vaupel JW Yashin AI 1985 Heterogeneityrsquos ruses some surprising effectsof selection on population dynamics Am Stat 39176ndash185
Venables WN Ripley BD 2002 Modern Applied Statistics with S FourthNew York Springer
Wagner PD 1996 Determinants of maximal oxygen transport and utiliza-tion Annu Rev Physiol 5821ndash50 Available at httpwwwncbinlmnih-govpubmed8815793
Walker A Arent SM McKeever KH 2010 Maximal aerobic capacity(VO2max) in horses a retrospective study to identify the age-relateddecline Comparative Exerc Physiol 6177ndash181 Available at httpwwwjournalscambridgeorgabstract_S1755254010000073
Walker R Hill K 2003 Modeling growth and senescence in physical per-formance among the Ache of Eastern Paraguay Am J Hum Biol 208196ndash208
Weller IM Thomas SG Corey PN Cox MH 1993 Prediction of maximaloxygen uptake from a modified Canadian aerobic fitness test Can JAppl Physiol 18175ndash188 Available at httpwwwncbinlmnihgovpubmed8513290
Wilson TM Tanaka H 2000 Meta-analysis of the age-associated declinein maximal aerobic capacity in men relation to training status Am JPhysiol Heart Circ Physiol 278H829ndash834 Available at httpwwwncbinlmnihgovpubmed10710351
Wood SN 2006 Generalized Additive Models An Introduction with RBoca Raton Florida Chapman and HallCRC Press
World Health Organization 2001 Iron deficiency anaemia assessmentprevention and control a guide for programme managers Available athttpwhqlibdocwhointhq2001WHO_NHD_013pdf
Yoopat P Toicharoen P Boontong S Glinsukon T Vanwonterghem KLouhevaara V 2002 Cardiorespiratory capacity of Thai workers in dif-ferent age and job categories J Physiol Anthropol Appl Hum Sci 21121ndash128 Available at httpwwwncbinlmnihgovpubmed12056179
Zhu YI Haas JD 1997 Iron depletion without anemia and physical per-formance in young women Am J Clin Nutr 66334ndash341 Available athttpwwwncbinlmnihgovpubmed9250112
14 AC PISOR ET AL
American Journal of Human Biology
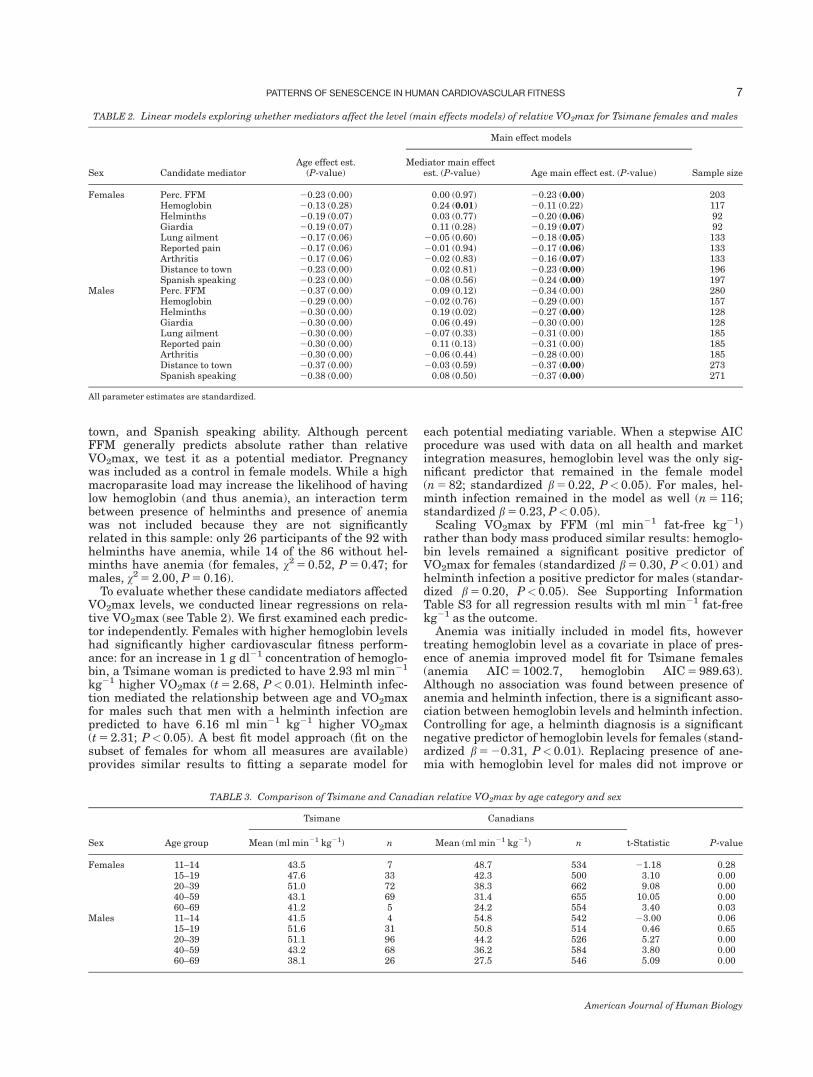
town and Spanish speaking ability Although percentFFM generally predicts absolute rather than relativeVO2max we test it as a potential mediator Pregnancywas included as a control in female models While a highmacroparasite load may increase the likelihood of havinglow hemoglobin (and thus anemia) an interaction termbetween presence of helminths and presence of anemiawas not included because they are not significantlyrelated in this sample only 26 participants of the 92 withhelminths have anemia while 14 of the 86 without hel-minths have anemia (for females v2 5 052 P 5 047 formales v2 5 200 P 5 016)
To evaluate whether these candidate mediators affectedVO2max levels we conducted linear regressions on rela-tive VO2max (see Table 2) We first examined each predic-tor independently Females with higher hemoglobin levelshad significantly higher cardiovascular fitness perform-ance for an increase in 1 g dl21 concentration of hemoglo-bin a Tsimane woman is predicted to have 293 ml min21
kg21 higher VO2max (t 5 268 Plt 001) Helminth infec-tion mediated the relationship between age and VO2maxfor males such that men with a helminth infection arepredicted to have 616 ml min21 kg21 higher VO2max(t 5 231 Plt 005) A best fit model approach (fit on thesubset of females for whom all measures are available)provides similar results to fitting a separate model for
each potential mediating variable When a stepwise AICprocedure was used with data on all health and marketintegration measures hemoglobin level was the only sig-nificant predictor that remained in the female model(n 5 82 standardized b 5 022 Plt 005) For males hel-minth infection remained in the model as well (n 5 116standardized b 5 023 Plt 005)
Scaling VO2max by FFM (ml min21 fat-free kg21)rather than body mass produced similar results hemoglo-bin levels remained a significant positive predictor ofVO2max for females (standardized b 5 030 Plt 001) andhelminth infection a positive predictor for males (standar-dized b 5 020 Plt005) See Supporting InformationTable S3 for all regression results with ml min21 fat-freekg21 as the outcome
Anemia was initially included in model fits howevertreating hemoglobin level as a covariate in place of pres-ence of anemia improved model fit for Tsimane females(anemia AIC 5 10027 hemoglobin AIC 5 98963)Although no association was found between presence ofanemia and helminth infection there is a significant asso-ciation between hemoglobin levels and helminth infectionControlling for age a helminth diagnosis is a significantnegative predictor of hemoglobin levels for females (stand-ardized b 5 2031 Plt 001) Replacing presence of ane-mia with hemoglobin level for males did not improve or
TABLE 3 Comparison of Tsimane and Canadian relative VO2max by age category and sex
Sex Age group
Tsimane Canadians
t-Statistic P-valueMean (ml min21 kg21) n Mean (ml min21 kg21) n
Females 11ndash14 435 7 487 534 2118 02815ndash19 476 33 423 500 310 00020ndash39 510 72 383 662 908 00040ndash59 431 69 314 655 1005 00060ndash69 412 5 242 554 340 003
Males 11ndash14 415 4 548 542 2300 00615ndash19 516 31 508 514 046 06520ndash39 511 96 442 526 527 00040ndash59 432 68 362 584 380 00060ndash69 381 26 275 546 509 000
TABLE 2 Linear models exploring whether mediators affect the level (main effects models) of relative VO2max for Tsimane females and males
Sex Candidate mediatorAge effect est
(P-value)
Main effect models
Sample sizeMediator main effect
est (P-value) Age main effect est (P-value)
Females Perc FFM 2023 (000) 000 (097) 2023 (000) 203Hemoglobin 2013 (028) 024 (001) 2011 (022) 117Helminths 2019 (007) 003 (077) 2020 (006) 92Giardia 2019 (007) 011 (028) 2019 (007) 92Lung ailment 2017 (006) 2005 (060) 2018 (005) 133Reported pain 2017 (006) 2001 (094) 2017 (006) 133Arthritis 2017 (006) 2002 (083) 2016 (007) 133Distance to town 2023 (000) 002 (081) 2023 (000) 196Spanish speaking 2023 (000) 2008 (056) 2024 (000) 197
Males Perc FFM 2037 (000) 009 (012) 2034 (000) 280Hemoglobin 2029 (000) 2002 (076) 2029 (000) 157Helminths 2030 (000) 019 (002) 2027 (000) 128Giardia 2030 (000) 006 (049) 2030 (000) 128Lung ailment 2030 (000) 2007 (033) 2031 (000) 185Reported pain 2030 (000) 011 (013) 2031 (000) 185Arthritis 2030 (000) 2006 (044) 2028 (000) 185Distance to town 2037 (000) 2003 (059) 2037 (000) 273Spanish speaking 2038 (000) 008 (050) 2037 (000) 271
All parameter estimates are standardized
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 7
American Journal of Human Biology
worsen model fit and there is no significant relationshipbetween hemoglobin levels and helminth infection formales (standardized b 5 2010 P 5 028) Parameter esti-mates for anemia were not significant in models for eitherfemales or males
Between-group Table 3 presents Tsimane and Canadianestimated VO2max binned into age categories used byCHMS These data suggest that Canadian females andmales achieve peak VO2max between the ages of 11 and14 while Tsimane males peak between ages 15 and 19Tsimane females peak later between age 20 and 39Across comparable age categories Tsimane have signifi-cantly higher VO2max than Canadians at all ages exceptbetween 11 and 15 for females and 11 and 19 for males(Table 3) However the sample size of Tsimane teenagersunder age 15 is quite small As aforementioned to controlfor the influence of a small number of data points for theyoungest and oldest Tsimane individuals we used GAMto predict VO2max across logged age Predicted valuessuggest that Tsimane females peak at age 28 and Tsimanemales peak at age 22 (see Fig 1c d) These estimates areconsistent with scatterplots of the raw data (plotted onFig 1) and mask fewer fine-grained effects of age thanTable 3 as each CHMS adult age category spans twodecades
It is possible the difference between the Tsimane andCanadians reflects a greater increase in body mass acrossages in the Canadian population or different trajectoriesof change in body composition The former could occurbecause body mass appears in the denominator and cantherefore scale down VO2max while the latter implies dif-ferential changes in FFM when FFM is a predictor ofVO2max in many studies To explore these possibilitieswe performed two calculations we allometrically scaledTsimane VO2max and we projected Tsimane VO2maxassuming the Tsimane had equivalent fat mass and FFMas Canadians from same-sex same-age categories Con-trolling for age the allometric scaling coefficient a wasslightly greater than 1 for both sexes (females a 5 111males a 5 118) This suggests that any disparity inVO2max between Canadians and the Tsimane cannot beexplained solely by mass differences Indeed assumingthe Tsimane have the same body composition as Cana-dians projected VO2max differs little from observedVO2max The Tsimane outperform the Canadians in everycohort by at least 35 ml min21 kg21 except among theyoungest males who perform similarly (see SupportingInformation Fig S4)
To control for possible disparities in changes in bodycomposition by age within each population as these mightalso influence differences between the Tsimane and Cana-dians we scaled VO2max by absolute FFM from the samepopulation to obtain ml min21 fat-free kg21 BecauseCanadian body composition data were only available viaskinfolds (bicep tricep subscapular and suprailiac) weused the subset of Tsimane (n 5 246) for which the samefour skinfolds measurements were available We calcu-lated average absolute FFM for each cohort using averageweight and average summed skinfolds (Durnin andWomersley 1974) and scaled average VO2max in mlmin21 by this number to obtain ml min21 fat-free kg21Under this method of scaling the Tsimane outperformCanadians in every cohort over age 20 by at least 165 ml
min21 fat-free kg21 (see Supporting Information TableS2) Canadian females and males in the 12ndash19 cohortsoutperform Tsimane of the same age
We next compared Tsimane to other subsistence popula-tions reported in the literature (Table 4) Consistent withcommon practice in the literature we report means foreach group but when possible we also predicted VO2maxat age 25 to provide age-corrected comparisons Weselected age 25 as it is the age of peak relative VO2max inthis study and for female Kamba and Maasai in Christen-sen et als (2012) recent study To predict VO2max at age25 we regressed the median ages on mean VO2max acrossthe available age categories Tsimane females and maleshave roughly the same predicted VO2max at age 25 asseveral other subsistence populations but higher VO2maxthan industrialized populations To test for differencesbetween industrialized and subsistence populations weconducted a linear regression on predicted VO2max at age25 this is not a meta-analysis and results should beinterpreted with caution Overall subsistence populationsdisplay higher peak VO2max than in industrialized popu-lations controlling for sex (440 vs 367 ml min21 kg21
[Plt 001]) The Tsimane O2 and indigenous Siberian sam-ples were excluded Tsimane O2 to avoid the problem ofnon-independence with Tsimane HR data and Siberiansbecause the sample has a limited age range comparedwith the other studies
Pace of decline slope of VO2max decline across thelifespan
Tsimane To evaluate whether Tsimane participants per-formed similarly under different methods we comparedage-matched subsamples of participants from the presentstudy with O2 method participants Despite a higher level(intercept) of VO2max in the O2 sample Tsimane malesdeclined marginally significantly faster under the O2
method relative to the HR method (O2 5 68 per decadeHR 5 47 decline per decade t 5 2195 P 5 005) Thereis no significant difference between Tsimane femalestested under the O2 and HR methods (O2 5 60 per dec-ade HR 5 48 decline per decade t 5 2055 P 5 058)Mediators of Slope Across the Lifespan We fit a series oflinear models to test for interactions between the candi-date mediators and age-related decline in TsimaneVO2max There are no variables that significantly inter-act with age to predict VO2max (see Supporting Informa-tion Table S4) An AIC selection approach and scaling byabsolute FFM (see Supporting Information Table S3) pro-vides the same results no variables significantly interactwith age to predict VO2max
Between-group VO2max is most often reported as a lin-ear decline across the adult lifespan though Hawkins andWiswell (2003) dispute whether the decline is actually lin-ear For example a linear approximation is not appropri-ate for Tsimane females if ages 11ndash80 are consideredFigure 2 contrasts linear declines in VO2max for Cana-dians and Tsimane males as well as a curvilinear fit forTsimane females with declines in industrialized nationsderived from meta-analyses (Fitzgerald et al 1997 Wil-son and Tanaka 2000) To explore whether rates ofdecline in VO2max among Tsimane and Canadians weredifferent we regressed average VO2max by age category
8 AC PISOR ET AL
American Journal of Human Biology
TA
BL
E4
Mea
nV
O2m
ax
esti
ma
ted
VO
2m
ax
at
age
25a
nd
dec
lin
ein
VO
2m
ax
per
dec
ad
efr
omth
isst
ud
ya
nd
pre
vio
us
rese
arc
ha
Pop
ula
tion
Fem
ale
Male
Pu
bli
cati
onM
ean
VO
2m
ax
VO
2m
ax
Age
25
bP
erce
nt
Dec
lin
eA
ge
Ran
ge
(n)
Mea
nV
O2m
ax
VO
2m
ax
Age
25
bP
erce
nt
Dec
lin
eA
ge
Ran
ge
(n)
Ind
ust
riali
zed
Can
ad
ac
312
400
73
20ndash69
(2905)
361
458
68
20ndash69
(2712)
Jap
an
d357
414
39
20ndash69
(656)
417
473
38
20ndash69
(807)
San
ad
aet
al
2007
Sw
eden
e330
g409
80
20ndash65
324
g388
75
20ndash65
Ek
blo
met
al
2007
Th
ail
an
d(i
nd
ust
ry)e
275
293
54
16ndash55
(56)
389
415
57
16ndash53
(70)
Yoo
pat
etal
2002
US
(H
erit
age)
f273
17ndash65
(360)
359
17ndash65
(293)
Sk
inn
eret
al
2003
US
(N
HA
NE
S)d
356
363
24
20ndash49
(1312)
444
438
39
20ndash49
(1481)
Su
bsi
sten
ceT
sim
an
e(H
R)c
498
521
h16
h20ndash69
471
538
h61
h20ndash69
Tsi
man
e(O
2)c
436
74
h36ndash69
540
25
h36ndash69
Ifalu
k(1
969ndash70)c
429
488
69
20ndash59
(43)
49
597
75
20ndash69
(75)
Rod
ean
dS
hep
hard
1994
Ach
ec465
434
257
20ndash59
(62)
519
614
84
20ndash59
(65)
Walk
eran
dH
ill
2003
Lu
oc378
372
39
17ndash68
(209)
429
48
54
17ndash68
(172)
Ch
rist
ense
net
al
2012
b
Kam
ba
c377
371
45
17ndash68
(283)
431
516
34
17ndash68
(94)
Ch
rist
ense
net
al
2012
Maasa
ic389
410
45
17ndash68
(178)
431
528
69
17ndash68
(163)
Ch
rist
ense
net
al
2012
Ind
igen
ous
Sib
eria
nsc
338
341
22
220ndash39
(14)
462
471
66
20ndash39
(30)
Katz
marz
yk
etal
1994
Ru
ral
Nep
alc
187
15ndash60
(39)
221
15ndash60
(35)
Pan
ter-
Bri
cket
al
1992
Ngis
onyok
aT
urk
an
af
38
387
18
20ndash44
(19)
Cu
rran
-Ever
ett
1994
aV
alu
esm
issi
ng
wh
enn
otavail
able
from
ap
art
icu
lar
stu
dy
Per
cen
td
ecli
ne
(per
cen
tof
pea
kvalu
elo
st)
per
dec
ad
ew
as
calc
ula
ted
as
by
regre
ssin
gre
lati
ve
VO
2m
ax
by
age
mu
ltip
lyin
gth
ep
ara
met
eres
tim
ate
for
age
by
10
an
dd
ivid
ing
this
nu
mber
by
the
inte
rcep
t(p
resu
med
pea
k
ass
um
ing
ali
nea
rd
ecli
ne
inV
O2m
ax
acr
oss
age)
B
ecau
seof
lack
ofacc
ess
tora
wd
ata
re
gre
ssio
ns
wer
efi
tw
ith
mea
nV
O2m
ax
an
dm
edia
nage
by
coh
ort
bA
ge
25
valu
esw
ere
esti
mate
dby
regre
ssin
gre
lati
ve
VO
2m
ax
by
age
then
usi
ng
the
resu
ltin
gp
ara
met
eres
tim
ate
sto
pre
dic
tV
O2m
ax
at
age
25
the
pea
kin
rece
ntl
yst
ud
ied
pop
ula
tion
s(e
g
Kam
ba
an
dM
aasa
ife
male
sC
hri
sten
sen
etal
2012fe
male
san
dm
ale
sin
this
art
icle
)B
ecau
seof
lack
ofacc
ess
tora
wd
ata
re
gre
ssio
ns
wer
efi
tw
ith
mea
nV
O2m
ax
an
dm
edia
nage
by
coh
ort
cS
ubm
axim
alst
epte
st
dS
ubm
axim
altr
ead
mil
lte
st
eS
ubm
axim
aler
gom
eter
test
f M
axim
al
ergom
eter
test
gS
wed
ish
data
wer
ere
por
ted
as
med
ian
sfo
rea
chage
cate
gor
yth
evalu
esre
por
ted
her
eare
mea
ns
ofth
ese
med
ian
s2006
ind
ivid
uals
part
icip
ate
dbu
tn
um
ber
by
sex
was
not
rep
orte
d
hF
orco
mp
ara
bil
ity
we
bin
ned
the
Tsi
man
eH
Ran
dO
2d
ata
into
10
yea
rage
cate
gor
ies
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 9
American Journal of Human Biology
on median age (for a given age category) population andtheir interaction term For comparability Tsimane werebinned into the Canadian age categories and averageswere computed for these categories leading to estimateddeclines slightly different from those in Table 4 for thepurposes of this test we treat the Tsimane female declineas linear Because within-population variance in declineis not available these regressions should be treated asdescriptive comparisons rather than statistical tests ofdifferences between the two groups The rate of decline inVO2max is steeper for Canadian females (69 per decadefaster decline per decade) and males (42 faster declineper decade) compared with Tsimane females and males
The rate of cardiovascular fitness decline between theTsimane and Canadians is different but this differencedoes not extend to industrialized and subsistence popula-tions (see Table 4) Controlling for sex subsistence groupshave about one quarter of a percent lower declines perdecade Again because the variance in decline is not rep-resented in this regression results should be interpretedas comparative rather than as a statistical test As beforeTsimane O2 results were not included in the analysis toavoid nonindependence and the indigenous Siberianswere excluded because of discrepancy in ages sampled
DISCUSSION
Our comparisons demonstrate that across a wide varietyof societies cardiovascular fitness senesces with age Car-diovascular fitness is higher on average among members ofsubsistence societies than among industrialized societiesbut rates of fitness decline from peak are not slower Ourmore detailed comparison between the Tsimane a subsist-ence population and Canadians an industrialized popula-tion reveals differences in cardiovascular fitness levelsand rate of fitness decline Cardiovascular fitness levelswere higher among the Tsimane than among Canadiansand the rate of decline across the lifespan was significantlyslower among Tsimane women and men Potential Cana-
dian participants were excluded due to many health con-cerns including pregnancy and history of high bloodpressure whereas Tsimane were only excluded if they self-identified as unable to participate This suggests the Cana-dian sample is a relatively healthy subsample of Canadayet the Tsimane still outperform them in cardiovascular fit-ness It may be that the higher demand for cardiovascularfitness in late ages among the Tsimane outweighs anyeffects of poor health Another possibility is that greaterself-selection among Tsimane due to higher adult mortalityleaves more robust older adult survivors thereby reducingthe observed slope of fitness decline at the population level(Vaupel et al 1979) perhaps this is partially why fewerTsimane older adults opted out of the exercise test thanCanadian older adults were screened out (ages 60ndash69Canadian females 5 56 Tsimane females 5 15 Cana-dian males 5 57 Tsimane males 5 5)
Consistent with prior research on age-related changesin cardiovascular fitness the Tsimane do evidence a lin-ear decline in VO2max with age but not as steep a declineas typically seen in industrialized populations Based oncomparisons with the Canadians and with other industri-alized populations we believe the Tsimane data from thepresent study and the pilot O2 data combined indicatethat the Tsimane perform better on tests of cardiovascularfitness than the average individual from an industrializednation
To further explore the potential effects of health factorson cardiovascular fitness level and rate of decline weinvestigated predictors of individual differences in fitnesswithin the Tsimane population Overall we found thatmost health indicators among the Tsimane did not hinderVO2max levels or rates of decline Lower hemoglobin lev-els were associated with lower VO2max levels in womenbut not men consistent with the notion that compromisedblood oxygen transport curbs cardiovascular fitness(Buzina et al 1989 Panter-Brick et al 1992) In the USlow hemoglobin is more common in active women thanactive men (Sinclair and Hinton 2005) hemoglobin is
Fig 2 Linear changes in VO2max with age for Canadians and the Tsimane Intercepts and slopes for Canadians and Tsimane can be foundin Table 4 Because age2 is significant for the full sample of Tsimane females their change in VO2max across age is curvilinear Slopes forendurance trained active and sedentary individuals from industrialized nations are drawn from a meta-analysis performed by Fitzgeraldet al (1997) for females and Wilson and Tanaka (2000) for males Endurance trained individuals are represented by the top dotted line abovefollowed by active individuals below and sedentary on the bottom Trained individuals engage in 31 sessions of endurance exercise per weekfor at least a year while active individuals engage in 2 or fewer sessions per week of cardiovascular exercise [Color figure can be viewed in theonline issue which is available at wileyonlinelibrarycom]
10 AC PISOR ET AL
American Journal of Human Biology
also lower in Tsimane women than Tsimane men(female 5 129 [sd 13] g ml21 males 5 142 [13] g ml21)Even mild (non-anemic) iron deficiencies impacts womenrsquosexercise performance (Zhu and Haas 1997) Inconsistentwith findings from Panter-Brick et al (1992) among ruralNepalese helminth infection did not diminish levels ofVO2max for Tsimane men helminth infection wasactually a predictor of higher VO2max There are severalreasons why this might be the case First we only testedwhether presence or absence of helminths mediated theeffect of age on VO2max rather than parasite load (egnumber of worms egg counts) it is possible that helminthinfection only affects VO2max at high parasite loads Sec-ond blood loss (and thus low hemoglobin levels) resultingfrom helminth infection may be partially offset by theamount of iron in the Tsimane adult diet Tsimane ironintake is an estimated 166 of the US Dietary ReferenceIntake (Martin et al 2012) and Tsimane hemoglobin lev-els are higher than in the Nepalese (females 129 vs 109males 1424 vs 120 Panter-Brick et al 1992) Thirdthese analyses consider helminth infection at the time ofexercise test rather than past infections It may be thatthe cumulative burden of past infection has a larger effecton cardiovascular fitness if so this would suggest thatthe surprising positive effect of helminth infection onVO2max levels in men is either spurious or capturing athird variable
Secular declines in VO2max are expected with increasingmarket integration and lifestyle change because ofincreased sedentism (Katzmarzyk et al 1994 Rode andShephard 1994) Two proxies for market integration in thispopulationmdashdistance to San Borja and the ability to speakSpanishmdashwere not significant predictors of VO2max levelsor decline This is consistent with our predictions as Tsi-mane females and males that live near town do not appearto have lower activity levels (Gurven et al 2013) Wageopportunities near town primarily include working asranch hands collecting and weaving palm thatch panelscash cropping and working for logging companies Each ofthese involves extensive activity furthermore transporta-tion to town often involves bicycling walking and polingdugout canoes Cash cropping of rice and corn also involvesthe clearing and weeding of larger fields Except for cashcropping and palm thatch manufacture most wage laboropportunities are currently restricted to men
This study makes several unique contributions to theexisting literature It offers the first systematic compari-son of cardiovascular fitness level and rate of declinebetween subsistence and industrialized societies Resultscompiled from previous studies support the general claimthat despite greater pathogen stress the greater activityregime of subsistence societies helps support higher peakVO2max Additionally this is one of the first studies toexplore senescent changes in cardiovascular fitnesswithin a large sample from a subsistence population Thelarge number of health measures and proxies of marketintegration available permitted testing whether these fac-tors mediated age-related variation and whether theymodulated the rate of decline Despite reports that healthstatus and market integration have been important inother studies (eg Buzina et al 1989 Katzmarzyk et al1994 Panter-Brick et al 1992 Rode and Shephard1994) their overall net effect was small among the Tsi-mane most apparent in measures of hemoglobin levelsamong women and helminth infection among men
The results of these analyses may also shed light onindividual and population level differences in chronic dis-ease In industrialized populations meta-analyses demon-strate that cardiovascular fitness is protective againstcardiovascular disease (Jette et al 1992 Hawkins andWiswell 2003) Prior studies among Tsimane suggest rel-atively few deaths from heart attacks or strokes (Gurvenet al 2007) a low prevalence of common cardiovasculardisease risk factors like obesity high blood low-densitylipoprotein levels hypertension and peripheral arterialdisease and the existence of additional protective factorslike lean diet and physical activity (Gurven et al 20092013 Vasunilashorn et al 2010) Market foods such ascooking oil sugar and pasta represent only 6 of theaverage Tsimane diet and Tsimane also consume a greatdeal of lean meat and omega-3 fatty acids (Martin et al2012) This study complements these findings by demon-strating that Tsimane show relatively high VO2max anindicator of strong cardiorespiratory health TsimaneVO2max declines with age as it does everywhere whichsuggests declining muscle mass with age (Fleg andLakatta 1988) and lowered cardiac output (American Col-lege of Sports Medicine 2006 Sagiv et al 2007) ratherthan increased cardiovascular disease risk
Limitations
The Canadians were selected as a comparison industri-alized population because of the similarity of the CHMSand Tsimane protocols very few studies of industrializedpopulations have large sample sizes sample across thelife course and use a step test Several aspects of theCHMS and Tsimane protocols remain potentially incom-parable The Canadians experienced more stringentexclusion criteria than the Tsimane meaning that the Tsi-mane sample may be more representative of cardiovascu-lar condition in the Tsimane population than theCanadian sample of the Canadian population Again ifthe Tsimane sample was subjected to these criteria wemight expect the differences in VO2max between popula-tions to only increase On the other hand Canadian par-ticipants were assigned stepping cadences based on theirage and sex and cadence was increased across the exer-cise test if a participant did not reach 85 of his or herage-specific maximal HR all Tsimane were asked to com-plete 30 ascents per minute with no increase based ontheir achieved HRs Few Tsimane reached 75 of theirage-specific maximal HR (see Supporting InformationTable S1) perhaps because the age-specific maximal HRsderived from industrialized populations are inaccurate forthe Tsimane or because higher fitness allowed these Tsi-mane to perform the step test of 30 ascents per minutewith less effort Due to these discrepancies in protocolwhich may lead to errors in estimating VO2max we alsoincorporated Tsimane data collected using the O2 methodas a check because the O2 method estimates VO2max onthe relationship between HR and VO2 in a givenparticipant
Indeed it is an open question as to whether typicalmethods for indirectly estimating cardiovascular fitnessfrom HR are appropriate for subsistence level popula-tions Common routines for VO2max estimation assumeage-specific declines in cardiovascular fitness (eg Shep-hard 1970) but these methods have only been validatedwith samples from industrialized populations which are
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 11
American Journal of Human Biology
often self-selected (Beall et al 1985) Additionally regres-sions drawn from laboratory studies require participantsachieve a HR within a certain range for accurate VO2maxestimation however the appropriateness of these rangesgiven slight modifications to protocol and inclusion of par-ticipants of different ages different populations and bothsexes is questionable For example the maximal HRexhibited by young men varies across subsistence popula-tions (Shephard 1978) Use of these criteria is compli-cated by the fact that the most commonly used equationfor estimating maximal possible HR by age 220-age maybe inaccurate (Robergs and Landwehr 2002) and particu-larly inappropriate for older adults (see Tanaka et al2001) For these reasons we chose to use an exclusion cri-terion for the Tsimane that evaluates individual increasein HR across exercise relative to the mean increase in HRfor Tsimane of the same sex and age
The pattern of Tsimane fitness decline differs moder-ately by the choice of exclusion criterion for participants(see Supporting Information Table S1) and by method oftesting However this is a common finding Lee et al(2011) predicted VO2max from submaximal exercise usingthe O2 method and the HR-based American College ofSports Medicine calculation routine in a US sample Theyfound that (1) the HR-based routine predicts higherVO2max across the sexes than does the O2 routine and(2) the two methods have a correlation of only 077 Whenevaluating different testing procedures Shephard et al(1968) found differences in VO2max estimation by type oftest used (eg bicycle ergometer versus step test) and cal-culation routine Exercise tests exclusion criteria andcalculation routines combine to provide an estimate ofactual VO2max for a given individual and as such varia-tion in estimation is to be expected However such varia-tion may affect cross-population comparisons inunforeseen ways thus the comparisons presented hereshould be interpreted with caution
While population-level variation in cardiovascular fit-ness decline may reflect the differences in the demands ofendurance-based physical activity muscularity and com-promised oxygen transport it is possible that genetic fac-tors may also play a potential role (Collins 1999) In oneindustrialized sample maternal cardiovascular fitnessexhibited a heritability of 30 which is attributed toinheritance of the maternal mitochondrial genome (Bou-chard et al 2000) We do not have the relevant geneticdata for the populations considered here however andthus operate under the simplifying assumption thatinheritance should not affect population-level patternsand will not consistently bias individual-level compari-sons in any particular direction
This study is further limited by its cross-sectionaldesign Cross-sectional data present well-known problemsfor the measurement of individual aging (Crimmins andSeeman 2001) Mortality selection in which individualsin poorer condition are likely to die at younger ages pro-duces a downward bias in the estimation of aging rates atthe individual level (Vaupel and Yashin 1985 Vaupelet al 1979) Cohort effects if present also produce com-plicated and non-monotonic biases in estimation (Carnesand Olshansky 2001) Due to the problem of between-individual heterogeneity and the within-individual pro-cess of senescence a recent overview of aging studies con-cludes that ldquoonly longitudinal studies [ ] provide reliablesources of information in the study of senescencerdquo (Nussey
et al 2008) To date there are no longitudinal studies ofcardiovascular fitness in subsistence populations We arecurrently re-testing participants under the O2 methodallowing a better grasp of the within-individual variationthat shapes patterns of senescent decline
ACKNOWLEDGMENTS
The authors thank Paul Hooper Steven Gaulin JohnTooby Patricia Kramer the Human Evolution and Biode-mography laboratory and the Center for EvolutionaryPsychology at UCSB for helpful advice and feedback thestaff at the Tsimane Health and Life History Project andthe Tsimane for their participation and patience
LITERATURE CITED
American College of Sports Medicine 2006 ACSMrsquos Guidelines for Exer-cise Testing and Prescription 7th ed Philadelphia Lippincott Williamsamp Wilkins
Armstrong N 2001 Peak oxygen uptake in relation to growth and matura-tion in 11- to 17-year-old humans Eur J Appl Physiol 85546ndash551
Astrand PO Ryhming I 1954 A nomogram for calculation of aerobiccapacity (physical fitness) from pulse rate during submaximal work JAppl Physiol 7218ndash221
Bailey DA Shephard RJ Mirwald RL 1976 Validation of a self-administered home test of cardio-respiratory fitness Can J Appl SportSci 167ndash78
Beall CM Goldstein MC and Feldman ES 1985 The physical fitness ofelderly Nepalese farmers residing in rugged mountain and flat terrainJ Gerontol 40529ndash535
Benefice E Ndiaye G 2005 Relationships between anthropometry cardi-orespiratory fitness indices and physical activity levels in different ageand sex groups in rural Senegal (West Africa) Ann Hum Biol 32366ndash382 Available from httpwwwncbinlmnihgovpubmed16099780
Blackwell AD Gurven MD Sugiyama LS Madimenos FC Liebert MAMartin MA Kaplan HS Snodgrass JJ 2011 Evidence for a peak shift in ahumoral response to helminths age profiles of IgE in the Shuar of Ecuadorthe Tsimane of Bolivia and the US NHANES PLoS Negl Trop Dis 5e1218 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid53125146amptool5pmcentrezamprendertype5abstract
Blackwell AD Martin M Kaplan H Gurven M Evidence for an antagonis-tic relationship between Giardia lamblia and helminth infections impli-cations for treatment of helminth infections in developing populations
Blair SN LaMonte MJ Nichaman MZ 2004 The evolution of physicalactivity recommendations how much is enough Am J Clin Nutr 79913Sndash920S Available at httpwwwncbinlmnihgovpubmed15113739
Bouchard C Rankinen T Chagnon YC Rice T Perusse L Gagnon JBorecki I An P Leon a S et al 2000 Genomic scan for maximal oxygenuptake and its response to training in the HERITAGE Family Study JAppl Physiol 88551ndash559 Available at httpwwwncbinlmnihgovpubmed10658022
Bryan S St-Denis M Wojtas D 2007 Canadian Health Measures Surveyclinic operations and logistics Health Rep 1853ndash69
Buzina R Bates CJ van der Beek J Brubacher G Chandra RK HallbergL Heseker J Mertz W Pietrzik K et al 1989 Workshop on FunctionalSignificance of Mild-to-Moderate Malnutrition Am J Clin Nutrition 50172ndash176
Calder WA 1987 Scaling energetics of homeothermic vertebrates anoperational allometry Annu Rev Physiol 49107ndash120
Canadian Society for Exercise Physiology 2003 The Canadian PhysicalActivity Fitness amp Lifestyle Approach (CPAFLA) CSEP-Health amp Fit-ness Programrsquos Health-Related Appraisal and Counselling Strategy 3rded
Carnes BA Olshansky SJ 2001 Heterogeneity and its biodemographicimplications for longevity and mortality Exp Gerontol 36419ndash430Available at httpwwwncbinlmnihgovpubmed11250115
Carrick-Ranson G Hastings JL Bhella PS Shibata S Fujimoto N PalmerD Boyd K Levine BD 2013 The effect of age-related differences inbody size and composition on cardiovascular determinants of VO2max JGerontol A Biol Sci Med Sci 68608ndash616 Available at httpwwwncbinlmnihgovpubmed23160363
Centers for Disease Control and Prevention 1998 Recommendations toPrevent and Control Iron Deficiency in the United States MMWRRecomm Rep 471ndash36 Available at httpwwwcdcgovmmwrpreviewmmwrhtml00051880htm
12 AC PISOR ET AL
American Journal of Human Biology
Centers for Disease Control and Prevention 2011 Glossary of TermsPhysical Activity for Everyone [Internet] Available from httpwwwcdcgovphysicalactivityeveryoneglossary
Christensen DL Faurholt-Jepsen D Boit MK Mwaniki DL Kilonzo BTetens I Kiplamai FK Cheruiyot SC Friis H et al 2012 Cardiorespira-tory fitness and physical activity in Luo Kamba and Maasai of ruralKenya Am J Hum Biol 24723ndash729 Available at httpwwwncbinlm-nihgovpubmed22836508
Colley RC Garriguet D Janssen I Craig CL Clarke J Tremblay MS2011a Physical activity of Canadian children and youth accelerometerresults from the 2007 to 2009 Canadian Health Measures SurveyHealth Rep 2215ndash23
Colley RC Garriguet D Janssen I Craig CL Clarke J Tremblay MS2011b Physical activity of Canadian adults accelerometer results fromthe 2007 to 2009 Canadian Health Measures Survey Health Rep 227ndash14 Available at httpwwwncbinlmnihgovpubmed21510585
Collins KJ 1999 Physiological variation and adaptability in human popu-lations Ann Hum Biol 2619ndash38
Crimmins E Seeman T 2001 Integrating Biology into DemographicResearch on Health and Aging (With a Focus on the MacArthur Study ofSuccessful Aging) Cells and Surveys Should Biological Measures beIncluded in Social Science Research Washington DC National Acad-emy Press p 9ndash41
Curran-Everett LS 1994 Accordance Between VO2max and Behavior inNgisonyoka Turkana Am J Hum Biol 6761ndash771
Durnin JVGA Womersley J 1974 Body fat assessed from total body den-sity and its estimation from skinfold thickness measurements on 481men and women aged from 16 to 72 years Br J Nutr 3277ndash97
Eberl M Al-Sherbiny M Hagan P Ljubojevic S Thomas AW Wilson RA2002 A novel and sensitive method to monitor helminth infections byfaecal sampling Acta Trop 83183ndash187
Eid D Gurven M Kaplan H Winking J 2007 Enfermedades infecciosas alo largo de la vida y en el envejecimiento en indıgenas sudamericanos dela etnia Tsimane Aging in Developing Countries Building Bridges forIntegrated Research Agendas Santiago Chile
Ekblom B Engstreuroom L-M Ekblom O 2007 Secular trends of physical fit-ness in Swedish adults Scand J Med Sci Sports 17267ndash273 Availableat httpwwwncbinlmnihgovpubmed17501867
Finch CA Lenfant C 1972 Oxygen Transport in Man N Engl J Med 286407ndash415
Fitzgerald MD Tanaka H Tran ZV Seals DR 1997 Age-related declinesin maximal aerobic capacity in regularly exercising vs sedentarywomen a meta-analysis J Appl Physiol (Bethesda Md 1985) 83160ndash165 Available at httpwwwncbinlmnihgovpubmed9216959
Fleg JL Lakatta EG 1988 Role of muscle loss in the age-associated reduc-tion in VO2max J Appl Physiol 651147ndash1151
Frisancho AR Frisancho HG Milotich M Brutsaert T Albalak RSpielvogel H Villena M Vargas E Soria R 1995 Developmentalgenetic and environmental components of aerobic capacity at high alti-tude Am J Phys Anthropol 96431ndash442 Available at httpwwwncbinlmnihgovpubmed7604895
Giroux S 2007 Canadian health measures survey sampling strategyoverview Health Rep 1831ndash36
Gurven M Jaeggi A V Kaplan H Cummings D 2013 Physical activityand modernization among Bolivian Amerindians PLoS ONE 81ndash13
Gurven M Kaplan H Winking J Rodriguez DE Vasunilashorn S KimJK Finch C Crimmins E 2009 Inflammation and infection do not pro-mote arterial aging and cardiovascular disease risk factors among leanhorticulturalists PLoS ONE 41ndash12
Haidet GC 1989 Dynamic exercise in senescent beagles oxygen consump-tion and hemodynamic responses The Am J Physiol 257H1428ndash1437Available at httpwwwncbinlmnihgovpubmed2589499
Hawkins S Wiswell R 2003 Rate and mechanism of maximal oxygen con-sumption decline with aging implications for exercise training SportsMed 33877ndash888 Available at httpwwwncbinlmnihgovpubmed12974656
Hoffman J 2002 Physiological aspects of sport training and performance1st ed Champaign IL Human Kinetics Publishers
Hotez PJ Bottazzi ME Franco-Paredes C Ault SK Periago MR 2008 Theneglected tropical diseases of Latin America and the Caribbean a review ofdisease burden and distribution and a roadmap for control and eliminationPLoS Negl Trop Dis 2e300 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid52553488amptool5pmcentrezamprendertype5abstract
Howley ET Bassett DR Welch HG 1995 Criteria for maximal oxygenuptake review and commentary Med Sci Sports Exerc 271292ndash1301Available at httpwwwncbinlmnihgovpubmed8531628
Jette M Sidney K Quenneville J Landry F 1992 Relation between cardi-orespiratory fitness and selected risk factors for coronary heart diseasein a population of Canadian men and women CMAJ 1461353ndash1360Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid51488567amptool5pmcentrezamprendertype5abstract
Katzmarzyk PT Leonard WR Crawford MH 1994 Predicted maximaloxygen consumption of Indigenous Siberians Am J Hum Biol 6783ndash790
King CH Dickman K Tisch DJ 2005 Reassessment of the cost of chronichelmintic infection a meta-analysis of disability-related outcomes inendemic schistosomiasis Lancet 3651561ndash1569 Available at httpwwwncbinlmnihgovpubmed15866310
Lee J-M Bassett D Jr Thompson D Fitzhugh E 2011 Validation of thecosmed fitmate for predicting maximal oxygen consumption J StrengthCond Res 252573ndash2579
Madimenos FC Snodgrass JJ Blackwell AD Liebert MA Sugiyama LS2011 Physical activity in an indigenous Ecuadorian forager-horticulturalist population as measured using accelerometry Am J HumBiol 23488ndash497 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid53110644amptool5pmcentrezamprendertype5abstract
Malina RM 2001 Physical activity and fitness pathways from childhoodto adulthood Am J Hum Biol 13162ndash172 Available at httpwwwncbinlmnihgovpubmed11460860
Malina RM Little BB 2008 Physical activity the present in the contextof the past Am J Hum Biol 20373ndash391 Available at httpwwwncbinlmnihgovpubmed18433002
Manning JT Morris L Caswell N 2007 Endurance running and digitratio (2D 4D) implications for fetal testosterone effects on runningspeed and vascular health Am J Hum Biol 19416ndash421
Martin Ma Lassek WD Gaulin SJC Evans RW Woo JG Geraghty SRDavidson BS Morrow AL Kaplan HS et al 2012 Fatty acid composi-tion in the mature milk of Bolivian forager-horticulturalists controlledcomparisons with a US sample Matern Child Nutr 8404ndash418 Availableat httpwwwncbinlmnihgovpubmed22624983
National Health and Nutrition Examination Survey 2004 CardiovascularFitness Procedures Manual
Nussey D Coulson T Festa-Bianchet M Gaillard J-M 2008 Measuringsenescence in wild animal populations towards a longitudinal approachFunction Ecol 22393ndash406
Ogawa T Spina RJ Martin WHI Kohrt WM Schechtman KB HolloszyJO Ehsani AA 1992 Effects of aging sex and physical training cardio-vascular responses to exercise Circulation 86494ndash503
Panter-Brick C Miller UG Eggerman M 1992 Hemoglobin levels andstep test performance of men and women in Nepal Am J Hum Biol 4481ndash491
Pontzer H Raichlen Da Wood BM Mabulla AZP Racette SB MarloweFW 2012 Hunter-gatherer energetics and human obesity PLoS ONE 7e40503 Available at httpcdxplosorg101371journalpone0040503
R Development Core Team 2011 R A language and environment for sta-tistical computing R Development Core Team
Rigby R Stasinopoulos D 2005 Generalize additive models for locationscale and shape (with discussion) Appl Stat 54507ndash554
Robergs RA Landwehr R 2002 The surprising history of theldquoHRmax5220-agerdquo equation J Exerc Physiol 51ndash10
Rode A Shephard RJ 1994 Physiological consequences of acculturation a20-year study of fitness in an Inuit community Eur J Appl Physiol 69516ndash524
Rowland TW Boyajian A 1995 Aerobic response to endurance training inchildren Pediatrics 96654ndash658
Sagiv M Ben-sira D Amir R 2007 What maintains energy supply atpeak aerobic exercise in trained and untrained older men Gerontology53357ndash361
Sanada K Kuchiki T Miyachi M Mcgrath K Higuchi M Ebashi H 2007Effects of age on ventilatory threshold and peak oxygen uptake normal-ised for regional skeletal muscle mass in Japanese men and womenaged 20 ndash 80 years Eur J Appl Physiol 99475ndash483
Schniter E 2009 Why Old Age Non-Material Contributions and Patternsof Aging Among Older Adult Tsimanersquo 607
Shahnawaz H 1978 Influence of limb length on a stepping exercise JAppl Physiol 44346ndash349
Shephard RJ 1970 Computer programs for solution of the Astrand nomo-gram and the calculation of body surface area J Sports Med 10206ndash210
Shephard RJ Allen C Benade AJS Davies CT Di Prampero PE HedmanR Merriman JE Myhre K Simmons R 1968 Standardization of sub-maximal exercise tests Bull World Health Organ 38765ndash775 Availableat httpwwwpubmedcentralnihgovarticlerenderfcgiartid52554690amptool5pmcentrezamprendertype5abstract
Shephard RJ Bailey Da Mirwald RL 1976 Development of the CanadianHome Fitness Test Can Med Assoc J 114675ndash679 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid51956906amptool5pmcentrezamprendertype5abstract
Shields M Tremblay MS Laviolette M Craig CL Janssen I Gorber SC2010 Fitness of Canadian adults results from the 2007ndash2009 canadianhealth measures survey Health Rep 2121ndash35 Available at httpwwwncbinlmnihgovpubmed20426224
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 13
American Journal of Human Biology
Siconolfi SF Garber CE Lasater TM Carleton RA 1985 A simple validstep test for estimating maximal oxygen uptake in epidemiologic stud-ies Am J Epidemiol 121382ndash390 Available at httpwwwncbinlm-nihgovpubmed4014128
Sinclair LM Hinton PS 2005 Prevalence of iron deficiency with and with-out anemia in recreationally active men and women J Am Diet Assoc105975ndash978 Available from httpwwwncbinlmnihgovpubmed15942552
Skinner JS Gaskill SE Rankinen T Leon AS Rao DC Wilmore JHBouchard C 2003 Heart rate versus VO2max age sex race initial fit-ness and training response-HERITAGE Med Sci Sports Exerc 351908ndash1913 Available at httpwwwncbinlmnihgovpubmed14600558
Sondik EJ Madans JH Gentlemand JF 2012 Summary health statisticsfor US adults National Health Interview Survey 2010 Vital Health Stat101ndash80 Available at httpwwwncbinlmnihgovpubmed20687424
Stones MJ Kozma A 1985 Physical performance Aging and Human Per-formance New York Wiley p 261ndash292
Tanaka H Monahan KD Seals DR 2001 Age-predicted maximal heartrate revisited J Am Coll Cardiol] 37153ndash156 Available at httpwwwncbinlmnihgovpubmed11153730
Vasunilashorn S Crimmins EM Kim JK Winking J Gurven M KaplanH Finch CE 2010 Blood lipids infection and inflammatory markers inthe Tsimane of Bolivia Am J Hum Biol 22731ndash740 Available at httpwwwncbinlmnihgovpubmed20721985
Vaupel JV Manton KG Stallard E 1979 The impact of heterogeneity inindividual frailty on the dynamics of mortality Demography 16439ndash454
Vaupel JW Yashin AI 1985 Heterogeneityrsquos ruses some surprising effectsof selection on population dynamics Am Stat 39176ndash185
Venables WN Ripley BD 2002 Modern Applied Statistics with S FourthNew York Springer
Wagner PD 1996 Determinants of maximal oxygen transport and utiliza-tion Annu Rev Physiol 5821ndash50 Available at httpwwwncbinlmnih-govpubmed8815793
Walker A Arent SM McKeever KH 2010 Maximal aerobic capacity(VO2max) in horses a retrospective study to identify the age-relateddecline Comparative Exerc Physiol 6177ndash181 Available at httpwwwjournalscambridgeorgabstract_S1755254010000073
Walker R Hill K 2003 Modeling growth and senescence in physical per-formance among the Ache of Eastern Paraguay Am J Hum Biol 208196ndash208
Weller IM Thomas SG Corey PN Cox MH 1993 Prediction of maximaloxygen uptake from a modified Canadian aerobic fitness test Can JAppl Physiol 18175ndash188 Available at httpwwwncbinlmnihgovpubmed8513290
Wilson TM Tanaka H 2000 Meta-analysis of the age-associated declinein maximal aerobic capacity in men relation to training status Am JPhysiol Heart Circ Physiol 278H829ndash834 Available at httpwwwncbinlmnihgovpubmed10710351
Wood SN 2006 Generalized Additive Models An Introduction with RBoca Raton Florida Chapman and HallCRC Press
World Health Organization 2001 Iron deficiency anaemia assessmentprevention and control a guide for programme managers Available athttpwhqlibdocwhointhq2001WHO_NHD_013pdf
Yoopat P Toicharoen P Boontong S Glinsukon T Vanwonterghem KLouhevaara V 2002 Cardiorespiratory capacity of Thai workers in dif-ferent age and job categories J Physiol Anthropol Appl Hum Sci 21121ndash128 Available at httpwwwncbinlmnihgovpubmed12056179
Zhu YI Haas JD 1997 Iron depletion without anemia and physical per-formance in young women Am J Clin Nutr 66334ndash341 Available athttpwwwncbinlmnihgovpubmed9250112
14 AC PISOR ET AL
American Journal of Human Biology

worsen model fit and there is no significant relationshipbetween hemoglobin levels and helminth infection formales (standardized b 5 2010 P 5 028) Parameter esti-mates for anemia were not significant in models for eitherfemales or males
Between-group Table 3 presents Tsimane and Canadianestimated VO2max binned into age categories used byCHMS These data suggest that Canadian females andmales achieve peak VO2max between the ages of 11 and14 while Tsimane males peak between ages 15 and 19Tsimane females peak later between age 20 and 39Across comparable age categories Tsimane have signifi-cantly higher VO2max than Canadians at all ages exceptbetween 11 and 15 for females and 11 and 19 for males(Table 3) However the sample size of Tsimane teenagersunder age 15 is quite small As aforementioned to controlfor the influence of a small number of data points for theyoungest and oldest Tsimane individuals we used GAMto predict VO2max across logged age Predicted valuessuggest that Tsimane females peak at age 28 and Tsimanemales peak at age 22 (see Fig 1c d) These estimates areconsistent with scatterplots of the raw data (plotted onFig 1) and mask fewer fine-grained effects of age thanTable 3 as each CHMS adult age category spans twodecades
It is possible the difference between the Tsimane andCanadians reflects a greater increase in body mass acrossages in the Canadian population or different trajectoriesof change in body composition The former could occurbecause body mass appears in the denominator and cantherefore scale down VO2max while the latter implies dif-ferential changes in FFM when FFM is a predictor ofVO2max in many studies To explore these possibilitieswe performed two calculations we allometrically scaledTsimane VO2max and we projected Tsimane VO2maxassuming the Tsimane had equivalent fat mass and FFMas Canadians from same-sex same-age categories Con-trolling for age the allometric scaling coefficient a wasslightly greater than 1 for both sexes (females a 5 111males a 5 118) This suggests that any disparity inVO2max between Canadians and the Tsimane cannot beexplained solely by mass differences Indeed assumingthe Tsimane have the same body composition as Cana-dians projected VO2max differs little from observedVO2max The Tsimane outperform the Canadians in everycohort by at least 35 ml min21 kg21 except among theyoungest males who perform similarly (see SupportingInformation Fig S4)
To control for possible disparities in changes in bodycomposition by age within each population as these mightalso influence differences between the Tsimane and Cana-dians we scaled VO2max by absolute FFM from the samepopulation to obtain ml min21 fat-free kg21 BecauseCanadian body composition data were only available viaskinfolds (bicep tricep subscapular and suprailiac) weused the subset of Tsimane (n 5 246) for which the samefour skinfolds measurements were available We calcu-lated average absolute FFM for each cohort using averageweight and average summed skinfolds (Durnin andWomersley 1974) and scaled average VO2max in mlmin21 by this number to obtain ml min21 fat-free kg21Under this method of scaling the Tsimane outperformCanadians in every cohort over age 20 by at least 165 ml
min21 fat-free kg21 (see Supporting Information TableS2) Canadian females and males in the 12ndash19 cohortsoutperform Tsimane of the same age
We next compared Tsimane to other subsistence popula-tions reported in the literature (Table 4) Consistent withcommon practice in the literature we report means foreach group but when possible we also predicted VO2maxat age 25 to provide age-corrected comparisons Weselected age 25 as it is the age of peak relative VO2max inthis study and for female Kamba and Maasai in Christen-sen et als (2012) recent study To predict VO2max at age25 we regressed the median ages on mean VO2max acrossthe available age categories Tsimane females and maleshave roughly the same predicted VO2max at age 25 asseveral other subsistence populations but higher VO2maxthan industrialized populations To test for differencesbetween industrialized and subsistence populations weconducted a linear regression on predicted VO2max at age25 this is not a meta-analysis and results should beinterpreted with caution Overall subsistence populationsdisplay higher peak VO2max than in industrialized popu-lations controlling for sex (440 vs 367 ml min21 kg21
[Plt 001]) The Tsimane O2 and indigenous Siberian sam-ples were excluded Tsimane O2 to avoid the problem ofnon-independence with Tsimane HR data and Siberiansbecause the sample has a limited age range comparedwith the other studies
Pace of decline slope of VO2max decline across thelifespan
Tsimane To evaluate whether Tsimane participants per-formed similarly under different methods we comparedage-matched subsamples of participants from the presentstudy with O2 method participants Despite a higher level(intercept) of VO2max in the O2 sample Tsimane malesdeclined marginally significantly faster under the O2
method relative to the HR method (O2 5 68 per decadeHR 5 47 decline per decade t 5 2195 P 5 005) Thereis no significant difference between Tsimane femalestested under the O2 and HR methods (O2 5 60 per dec-ade HR 5 48 decline per decade t 5 2055 P 5 058)Mediators of Slope Across the Lifespan We fit a series oflinear models to test for interactions between the candi-date mediators and age-related decline in TsimaneVO2max There are no variables that significantly inter-act with age to predict VO2max (see Supporting Informa-tion Table S4) An AIC selection approach and scaling byabsolute FFM (see Supporting Information Table S3) pro-vides the same results no variables significantly interactwith age to predict VO2max
Between-group VO2max is most often reported as a lin-ear decline across the adult lifespan though Hawkins andWiswell (2003) dispute whether the decline is actually lin-ear For example a linear approximation is not appropri-ate for Tsimane females if ages 11ndash80 are consideredFigure 2 contrasts linear declines in VO2max for Cana-dians and Tsimane males as well as a curvilinear fit forTsimane females with declines in industrialized nationsderived from meta-analyses (Fitzgerald et al 1997 Wil-son and Tanaka 2000) To explore whether rates ofdecline in VO2max among Tsimane and Canadians weredifferent we regressed average VO2max by age category
8 AC PISOR ET AL
American Journal of Human Biology
TA
BL
E4
Mea
nV
O2m
ax
esti
ma
ted
VO
2m
ax
at
age
25a
nd
dec
lin
ein
VO
2m
ax
per
dec
ad
efr
omth
isst
ud
ya
nd
pre
vio
us
rese
arc
ha
Pop
ula
tion
Fem
ale
Male
Pu
bli
cati
onM
ean
VO
2m
ax
VO
2m
ax
Age
25
bP
erce
nt
Dec
lin
eA
ge
Ran
ge
(n)
Mea
nV
O2m
ax
VO
2m
ax
Age
25
bP
erce
nt
Dec
lin
eA
ge
Ran
ge
(n)
Ind
ust
riali
zed
Can
ad
ac
312
400
73
20ndash69
(2905)
361
458
68
20ndash69
(2712)
Jap
an
d357
414
39
20ndash69
(656)
417
473
38
20ndash69
(807)
San
ad
aet
al
2007
Sw
eden
e330
g409
80
20ndash65
324
g388
75
20ndash65
Ek
blo
met
al
2007
Th
ail
an
d(i
nd
ust
ry)e
275
293
54
16ndash55
(56)
389
415
57
16ndash53
(70)
Yoo
pat
etal
2002
US
(H
erit
age)
f273
17ndash65
(360)
359
17ndash65
(293)
Sk
inn
eret
al
2003
US
(N
HA
NE
S)d
356
363
24
20ndash49
(1312)
444
438
39
20ndash49
(1481)
Su
bsi
sten
ceT
sim
an
e(H
R)c
498
521
h16
h20ndash69
471
538
h61
h20ndash69
Tsi
man
e(O
2)c
436
74
h36ndash69
540
25
h36ndash69
Ifalu
k(1
969ndash70)c
429
488
69
20ndash59
(43)
49
597
75
20ndash69
(75)
Rod
ean
dS
hep
hard
1994
Ach
ec465
434
257
20ndash59
(62)
519
614
84
20ndash59
(65)
Walk
eran
dH
ill
2003
Lu
oc378
372
39
17ndash68
(209)
429
48
54
17ndash68
(172)
Ch
rist
ense
net
al
2012
b
Kam
ba
c377
371
45
17ndash68
(283)
431
516
34
17ndash68
(94)
Ch
rist
ense
net
al
2012
Maasa
ic389
410
45
17ndash68
(178)
431
528
69
17ndash68
(163)
Ch
rist
ense
net
al
2012
Ind
igen
ous
Sib
eria
nsc
338
341
22
220ndash39
(14)
462
471
66
20ndash39
(30)
Katz
marz
yk
etal
1994
Ru
ral
Nep
alc
187
15ndash60
(39)
221
15ndash60
(35)
Pan
ter-
Bri
cket
al
1992
Ngis
onyok
aT
urk
an
af
38
387
18
20ndash44
(19)
Cu
rran
-Ever
ett
1994
aV
alu
esm
issi
ng
wh
enn
otavail
able
from
ap
art
icu
lar
stu
dy
Per
cen
td
ecli
ne
(per
cen
tof
pea
kvalu
elo
st)
per
dec
ad
ew
as
calc
ula
ted
as
by
regre
ssin
gre
lati
ve
VO
2m
ax
by
age
mu
ltip
lyin
gth
ep
ara
met
eres
tim
ate
for
age
by
10
an
dd
ivid
ing
this
nu
mber
by
the
inte
rcep
t(p
resu
med
pea
k
ass
um
ing
ali
nea
rd
ecli
ne
inV
O2m
ax
acr
oss
age)
B
ecau
seof
lack
ofacc
ess
tora
wd
ata
re
gre
ssio
ns
wer
efi
tw
ith
mea
nV
O2m
ax
an
dm
edia
nage
by
coh
ort
bA
ge
25
valu
esw
ere
esti
mate
dby
regre
ssin
gre
lati
ve
VO
2m
ax
by
age
then
usi
ng
the
resu
ltin
gp
ara
met
eres
tim
ate
sto
pre
dic
tV
O2m
ax
at
age
25
the
pea
kin
rece
ntl
yst
ud
ied
pop
ula
tion
s(e
g
Kam
ba
an
dM
aasa
ife
male
sC
hri
sten
sen
etal
2012fe
male
san
dm
ale
sin
this
art
icle
)B
ecau
seof
lack
ofacc
ess
tora
wd
ata
re
gre
ssio
ns
wer
efi
tw
ith
mea
nV
O2m
ax
an
dm
edia
nage
by
coh
ort
cS
ubm
axim
alst
epte
st
dS
ubm
axim
altr
ead
mil
lte
st
eS
ubm
axim
aler
gom
eter
test
f M
axim
al
ergom
eter
test
gS
wed
ish
data
wer
ere
por
ted
as
med
ian
sfo
rea
chage
cate
gor
yth
evalu
esre
por
ted
her
eare
mea
ns
ofth
ese
med
ian
s2006
ind
ivid
uals
part
icip
ate
dbu
tn
um
ber
by
sex
was
not
rep
orte
d
hF
orco
mp
ara
bil
ity
we
bin
ned
the
Tsi
man
eH
Ran
dO
2d
ata
into
10
yea
rage
cate
gor
ies
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 9
American Journal of Human Biology
on median age (for a given age category) population andtheir interaction term For comparability Tsimane werebinned into the Canadian age categories and averageswere computed for these categories leading to estimateddeclines slightly different from those in Table 4 for thepurposes of this test we treat the Tsimane female declineas linear Because within-population variance in declineis not available these regressions should be treated asdescriptive comparisons rather than statistical tests ofdifferences between the two groups The rate of decline inVO2max is steeper for Canadian females (69 per decadefaster decline per decade) and males (42 faster declineper decade) compared with Tsimane females and males
The rate of cardiovascular fitness decline between theTsimane and Canadians is different but this differencedoes not extend to industrialized and subsistence popula-tions (see Table 4) Controlling for sex subsistence groupshave about one quarter of a percent lower declines perdecade Again because the variance in decline is not rep-resented in this regression results should be interpretedas comparative rather than as a statistical test As beforeTsimane O2 results were not included in the analysis toavoid nonindependence and the indigenous Siberianswere excluded because of discrepancy in ages sampled
DISCUSSION
Our comparisons demonstrate that across a wide varietyof societies cardiovascular fitness senesces with age Car-diovascular fitness is higher on average among members ofsubsistence societies than among industrialized societiesbut rates of fitness decline from peak are not slower Ourmore detailed comparison between the Tsimane a subsist-ence population and Canadians an industrialized popula-tion reveals differences in cardiovascular fitness levelsand rate of fitness decline Cardiovascular fitness levelswere higher among the Tsimane than among Canadiansand the rate of decline across the lifespan was significantlyslower among Tsimane women and men Potential Cana-
dian participants were excluded due to many health con-cerns including pregnancy and history of high bloodpressure whereas Tsimane were only excluded if they self-identified as unable to participate This suggests the Cana-dian sample is a relatively healthy subsample of Canadayet the Tsimane still outperform them in cardiovascular fit-ness It may be that the higher demand for cardiovascularfitness in late ages among the Tsimane outweighs anyeffects of poor health Another possibility is that greaterself-selection among Tsimane due to higher adult mortalityleaves more robust older adult survivors thereby reducingthe observed slope of fitness decline at the population level(Vaupel et al 1979) perhaps this is partially why fewerTsimane older adults opted out of the exercise test thanCanadian older adults were screened out (ages 60ndash69Canadian females 5 56 Tsimane females 5 15 Cana-dian males 5 57 Tsimane males 5 5)
Consistent with prior research on age-related changesin cardiovascular fitness the Tsimane do evidence a lin-ear decline in VO2max with age but not as steep a declineas typically seen in industrialized populations Based oncomparisons with the Canadians and with other industri-alized populations we believe the Tsimane data from thepresent study and the pilot O2 data combined indicatethat the Tsimane perform better on tests of cardiovascularfitness than the average individual from an industrializednation
To further explore the potential effects of health factorson cardiovascular fitness level and rate of decline weinvestigated predictors of individual differences in fitnesswithin the Tsimane population Overall we found thatmost health indicators among the Tsimane did not hinderVO2max levels or rates of decline Lower hemoglobin lev-els were associated with lower VO2max levels in womenbut not men consistent with the notion that compromisedblood oxygen transport curbs cardiovascular fitness(Buzina et al 1989 Panter-Brick et al 1992) In the USlow hemoglobin is more common in active women thanactive men (Sinclair and Hinton 2005) hemoglobin is
Fig 2 Linear changes in VO2max with age for Canadians and the Tsimane Intercepts and slopes for Canadians and Tsimane can be foundin Table 4 Because age2 is significant for the full sample of Tsimane females their change in VO2max across age is curvilinear Slopes forendurance trained active and sedentary individuals from industrialized nations are drawn from a meta-analysis performed by Fitzgeraldet al (1997) for females and Wilson and Tanaka (2000) for males Endurance trained individuals are represented by the top dotted line abovefollowed by active individuals below and sedentary on the bottom Trained individuals engage in 31 sessions of endurance exercise per weekfor at least a year while active individuals engage in 2 or fewer sessions per week of cardiovascular exercise [Color figure can be viewed in theonline issue which is available at wileyonlinelibrarycom]
10 AC PISOR ET AL
American Journal of Human Biology
also lower in Tsimane women than Tsimane men(female 5 129 [sd 13] g ml21 males 5 142 [13] g ml21)Even mild (non-anemic) iron deficiencies impacts womenrsquosexercise performance (Zhu and Haas 1997) Inconsistentwith findings from Panter-Brick et al (1992) among ruralNepalese helminth infection did not diminish levels ofVO2max for Tsimane men helminth infection wasactually a predictor of higher VO2max There are severalreasons why this might be the case First we only testedwhether presence or absence of helminths mediated theeffect of age on VO2max rather than parasite load (egnumber of worms egg counts) it is possible that helminthinfection only affects VO2max at high parasite loads Sec-ond blood loss (and thus low hemoglobin levels) resultingfrom helminth infection may be partially offset by theamount of iron in the Tsimane adult diet Tsimane ironintake is an estimated 166 of the US Dietary ReferenceIntake (Martin et al 2012) and Tsimane hemoglobin lev-els are higher than in the Nepalese (females 129 vs 109males 1424 vs 120 Panter-Brick et al 1992) Thirdthese analyses consider helminth infection at the time ofexercise test rather than past infections It may be thatthe cumulative burden of past infection has a larger effecton cardiovascular fitness if so this would suggest thatthe surprising positive effect of helminth infection onVO2max levels in men is either spurious or capturing athird variable
Secular declines in VO2max are expected with increasingmarket integration and lifestyle change because ofincreased sedentism (Katzmarzyk et al 1994 Rode andShephard 1994) Two proxies for market integration in thispopulationmdashdistance to San Borja and the ability to speakSpanishmdashwere not significant predictors of VO2max levelsor decline This is consistent with our predictions as Tsi-mane females and males that live near town do not appearto have lower activity levels (Gurven et al 2013) Wageopportunities near town primarily include working asranch hands collecting and weaving palm thatch panelscash cropping and working for logging companies Each ofthese involves extensive activity furthermore transporta-tion to town often involves bicycling walking and polingdugout canoes Cash cropping of rice and corn also involvesthe clearing and weeding of larger fields Except for cashcropping and palm thatch manufacture most wage laboropportunities are currently restricted to men
This study makes several unique contributions to theexisting literature It offers the first systematic compari-son of cardiovascular fitness level and rate of declinebetween subsistence and industrialized societies Resultscompiled from previous studies support the general claimthat despite greater pathogen stress the greater activityregime of subsistence societies helps support higher peakVO2max Additionally this is one of the first studies toexplore senescent changes in cardiovascular fitnesswithin a large sample from a subsistence population Thelarge number of health measures and proxies of marketintegration available permitted testing whether these fac-tors mediated age-related variation and whether theymodulated the rate of decline Despite reports that healthstatus and market integration have been important inother studies (eg Buzina et al 1989 Katzmarzyk et al1994 Panter-Brick et al 1992 Rode and Shephard1994) their overall net effect was small among the Tsi-mane most apparent in measures of hemoglobin levelsamong women and helminth infection among men
The results of these analyses may also shed light onindividual and population level differences in chronic dis-ease In industrialized populations meta-analyses demon-strate that cardiovascular fitness is protective againstcardiovascular disease (Jette et al 1992 Hawkins andWiswell 2003) Prior studies among Tsimane suggest rel-atively few deaths from heart attacks or strokes (Gurvenet al 2007) a low prevalence of common cardiovasculardisease risk factors like obesity high blood low-densitylipoprotein levels hypertension and peripheral arterialdisease and the existence of additional protective factorslike lean diet and physical activity (Gurven et al 20092013 Vasunilashorn et al 2010) Market foods such ascooking oil sugar and pasta represent only 6 of theaverage Tsimane diet and Tsimane also consume a greatdeal of lean meat and omega-3 fatty acids (Martin et al2012) This study complements these findings by demon-strating that Tsimane show relatively high VO2max anindicator of strong cardiorespiratory health TsimaneVO2max declines with age as it does everywhere whichsuggests declining muscle mass with age (Fleg andLakatta 1988) and lowered cardiac output (American Col-lege of Sports Medicine 2006 Sagiv et al 2007) ratherthan increased cardiovascular disease risk
Limitations
The Canadians were selected as a comparison industri-alized population because of the similarity of the CHMSand Tsimane protocols very few studies of industrializedpopulations have large sample sizes sample across thelife course and use a step test Several aspects of theCHMS and Tsimane protocols remain potentially incom-parable The Canadians experienced more stringentexclusion criteria than the Tsimane meaning that the Tsi-mane sample may be more representative of cardiovascu-lar condition in the Tsimane population than theCanadian sample of the Canadian population Again ifthe Tsimane sample was subjected to these criteria wemight expect the differences in VO2max between popula-tions to only increase On the other hand Canadian par-ticipants were assigned stepping cadences based on theirage and sex and cadence was increased across the exer-cise test if a participant did not reach 85 of his or herage-specific maximal HR all Tsimane were asked to com-plete 30 ascents per minute with no increase based ontheir achieved HRs Few Tsimane reached 75 of theirage-specific maximal HR (see Supporting InformationTable S1) perhaps because the age-specific maximal HRsderived from industrialized populations are inaccurate forthe Tsimane or because higher fitness allowed these Tsi-mane to perform the step test of 30 ascents per minutewith less effort Due to these discrepancies in protocolwhich may lead to errors in estimating VO2max we alsoincorporated Tsimane data collected using the O2 methodas a check because the O2 method estimates VO2max onthe relationship between HR and VO2 in a givenparticipant
Indeed it is an open question as to whether typicalmethods for indirectly estimating cardiovascular fitnessfrom HR are appropriate for subsistence level popula-tions Common routines for VO2max estimation assumeage-specific declines in cardiovascular fitness (eg Shep-hard 1970) but these methods have only been validatedwith samples from industrialized populations which are
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 11
American Journal of Human Biology
often self-selected (Beall et al 1985) Additionally regres-sions drawn from laboratory studies require participantsachieve a HR within a certain range for accurate VO2maxestimation however the appropriateness of these rangesgiven slight modifications to protocol and inclusion of par-ticipants of different ages different populations and bothsexes is questionable For example the maximal HRexhibited by young men varies across subsistence popula-tions (Shephard 1978) Use of these criteria is compli-cated by the fact that the most commonly used equationfor estimating maximal possible HR by age 220-age maybe inaccurate (Robergs and Landwehr 2002) and particu-larly inappropriate for older adults (see Tanaka et al2001) For these reasons we chose to use an exclusion cri-terion for the Tsimane that evaluates individual increasein HR across exercise relative to the mean increase in HRfor Tsimane of the same sex and age
The pattern of Tsimane fitness decline differs moder-ately by the choice of exclusion criterion for participants(see Supporting Information Table S1) and by method oftesting However this is a common finding Lee et al(2011) predicted VO2max from submaximal exercise usingthe O2 method and the HR-based American College ofSports Medicine calculation routine in a US sample Theyfound that (1) the HR-based routine predicts higherVO2max across the sexes than does the O2 routine and(2) the two methods have a correlation of only 077 Whenevaluating different testing procedures Shephard et al(1968) found differences in VO2max estimation by type oftest used (eg bicycle ergometer versus step test) and cal-culation routine Exercise tests exclusion criteria andcalculation routines combine to provide an estimate ofactual VO2max for a given individual and as such varia-tion in estimation is to be expected However such varia-tion may affect cross-population comparisons inunforeseen ways thus the comparisons presented hereshould be interpreted with caution
While population-level variation in cardiovascular fit-ness decline may reflect the differences in the demands ofendurance-based physical activity muscularity and com-promised oxygen transport it is possible that genetic fac-tors may also play a potential role (Collins 1999) In oneindustrialized sample maternal cardiovascular fitnessexhibited a heritability of 30 which is attributed toinheritance of the maternal mitochondrial genome (Bou-chard et al 2000) We do not have the relevant geneticdata for the populations considered here however andthus operate under the simplifying assumption thatinheritance should not affect population-level patternsand will not consistently bias individual-level compari-sons in any particular direction
This study is further limited by its cross-sectionaldesign Cross-sectional data present well-known problemsfor the measurement of individual aging (Crimmins andSeeman 2001) Mortality selection in which individualsin poorer condition are likely to die at younger ages pro-duces a downward bias in the estimation of aging rates atthe individual level (Vaupel and Yashin 1985 Vaupelet al 1979) Cohort effects if present also produce com-plicated and non-monotonic biases in estimation (Carnesand Olshansky 2001) Due to the problem of between-individual heterogeneity and the within-individual pro-cess of senescence a recent overview of aging studies con-cludes that ldquoonly longitudinal studies [ ] provide reliablesources of information in the study of senescencerdquo (Nussey
et al 2008) To date there are no longitudinal studies ofcardiovascular fitness in subsistence populations We arecurrently re-testing participants under the O2 methodallowing a better grasp of the within-individual variationthat shapes patterns of senescent decline
ACKNOWLEDGMENTS
The authors thank Paul Hooper Steven Gaulin JohnTooby Patricia Kramer the Human Evolution and Biode-mography laboratory and the Center for EvolutionaryPsychology at UCSB for helpful advice and feedback thestaff at the Tsimane Health and Life History Project andthe Tsimane for their participation and patience
LITERATURE CITED
American College of Sports Medicine 2006 ACSMrsquos Guidelines for Exer-cise Testing and Prescription 7th ed Philadelphia Lippincott Williamsamp Wilkins
Armstrong N 2001 Peak oxygen uptake in relation to growth and matura-tion in 11- to 17-year-old humans Eur J Appl Physiol 85546ndash551
Astrand PO Ryhming I 1954 A nomogram for calculation of aerobiccapacity (physical fitness) from pulse rate during submaximal work JAppl Physiol 7218ndash221
Bailey DA Shephard RJ Mirwald RL 1976 Validation of a self-administered home test of cardio-respiratory fitness Can J Appl SportSci 167ndash78
Beall CM Goldstein MC and Feldman ES 1985 The physical fitness ofelderly Nepalese farmers residing in rugged mountain and flat terrainJ Gerontol 40529ndash535
Benefice E Ndiaye G 2005 Relationships between anthropometry cardi-orespiratory fitness indices and physical activity levels in different ageand sex groups in rural Senegal (West Africa) Ann Hum Biol 32366ndash382 Available from httpwwwncbinlmnihgovpubmed16099780
Blackwell AD Gurven MD Sugiyama LS Madimenos FC Liebert MAMartin MA Kaplan HS Snodgrass JJ 2011 Evidence for a peak shift in ahumoral response to helminths age profiles of IgE in the Shuar of Ecuadorthe Tsimane of Bolivia and the US NHANES PLoS Negl Trop Dis 5e1218 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid53125146amptool5pmcentrezamprendertype5abstract
Blackwell AD Martin M Kaplan H Gurven M Evidence for an antagonis-tic relationship between Giardia lamblia and helminth infections impli-cations for treatment of helminth infections in developing populations
Blair SN LaMonte MJ Nichaman MZ 2004 The evolution of physicalactivity recommendations how much is enough Am J Clin Nutr 79913Sndash920S Available at httpwwwncbinlmnihgovpubmed15113739
Bouchard C Rankinen T Chagnon YC Rice T Perusse L Gagnon JBorecki I An P Leon a S et al 2000 Genomic scan for maximal oxygenuptake and its response to training in the HERITAGE Family Study JAppl Physiol 88551ndash559 Available at httpwwwncbinlmnihgovpubmed10658022
Bryan S St-Denis M Wojtas D 2007 Canadian Health Measures Surveyclinic operations and logistics Health Rep 1853ndash69
Buzina R Bates CJ van der Beek J Brubacher G Chandra RK HallbergL Heseker J Mertz W Pietrzik K et al 1989 Workshop on FunctionalSignificance of Mild-to-Moderate Malnutrition Am J Clin Nutrition 50172ndash176
Calder WA 1987 Scaling energetics of homeothermic vertebrates anoperational allometry Annu Rev Physiol 49107ndash120
Canadian Society for Exercise Physiology 2003 The Canadian PhysicalActivity Fitness amp Lifestyle Approach (CPAFLA) CSEP-Health amp Fit-ness Programrsquos Health-Related Appraisal and Counselling Strategy 3rded
Carnes BA Olshansky SJ 2001 Heterogeneity and its biodemographicimplications for longevity and mortality Exp Gerontol 36419ndash430Available at httpwwwncbinlmnihgovpubmed11250115
Carrick-Ranson G Hastings JL Bhella PS Shibata S Fujimoto N PalmerD Boyd K Levine BD 2013 The effect of age-related differences inbody size and composition on cardiovascular determinants of VO2max JGerontol A Biol Sci Med Sci 68608ndash616 Available at httpwwwncbinlmnihgovpubmed23160363
Centers for Disease Control and Prevention 1998 Recommendations toPrevent and Control Iron Deficiency in the United States MMWRRecomm Rep 471ndash36 Available at httpwwwcdcgovmmwrpreviewmmwrhtml00051880htm
12 AC PISOR ET AL
American Journal of Human Biology
Centers for Disease Control and Prevention 2011 Glossary of TermsPhysical Activity for Everyone [Internet] Available from httpwwwcdcgovphysicalactivityeveryoneglossary
Christensen DL Faurholt-Jepsen D Boit MK Mwaniki DL Kilonzo BTetens I Kiplamai FK Cheruiyot SC Friis H et al 2012 Cardiorespira-tory fitness and physical activity in Luo Kamba and Maasai of ruralKenya Am J Hum Biol 24723ndash729 Available at httpwwwncbinlm-nihgovpubmed22836508
Colley RC Garriguet D Janssen I Craig CL Clarke J Tremblay MS2011a Physical activity of Canadian children and youth accelerometerresults from the 2007 to 2009 Canadian Health Measures SurveyHealth Rep 2215ndash23
Colley RC Garriguet D Janssen I Craig CL Clarke J Tremblay MS2011b Physical activity of Canadian adults accelerometer results fromthe 2007 to 2009 Canadian Health Measures Survey Health Rep 227ndash14 Available at httpwwwncbinlmnihgovpubmed21510585
Collins KJ 1999 Physiological variation and adaptability in human popu-lations Ann Hum Biol 2619ndash38
Crimmins E Seeman T 2001 Integrating Biology into DemographicResearch on Health and Aging (With a Focus on the MacArthur Study ofSuccessful Aging) Cells and Surveys Should Biological Measures beIncluded in Social Science Research Washington DC National Acad-emy Press p 9ndash41
Curran-Everett LS 1994 Accordance Between VO2max and Behavior inNgisonyoka Turkana Am J Hum Biol 6761ndash771
Durnin JVGA Womersley J 1974 Body fat assessed from total body den-sity and its estimation from skinfold thickness measurements on 481men and women aged from 16 to 72 years Br J Nutr 3277ndash97
Eberl M Al-Sherbiny M Hagan P Ljubojevic S Thomas AW Wilson RA2002 A novel and sensitive method to monitor helminth infections byfaecal sampling Acta Trop 83183ndash187
Eid D Gurven M Kaplan H Winking J 2007 Enfermedades infecciosas alo largo de la vida y en el envejecimiento en indıgenas sudamericanos dela etnia Tsimane Aging in Developing Countries Building Bridges forIntegrated Research Agendas Santiago Chile
Ekblom B Engstreuroom L-M Ekblom O 2007 Secular trends of physical fit-ness in Swedish adults Scand J Med Sci Sports 17267ndash273 Availableat httpwwwncbinlmnihgovpubmed17501867
Finch CA Lenfant C 1972 Oxygen Transport in Man N Engl J Med 286407ndash415
Fitzgerald MD Tanaka H Tran ZV Seals DR 1997 Age-related declinesin maximal aerobic capacity in regularly exercising vs sedentarywomen a meta-analysis J Appl Physiol (Bethesda Md 1985) 83160ndash165 Available at httpwwwncbinlmnihgovpubmed9216959
Fleg JL Lakatta EG 1988 Role of muscle loss in the age-associated reduc-tion in VO2max J Appl Physiol 651147ndash1151
Frisancho AR Frisancho HG Milotich M Brutsaert T Albalak RSpielvogel H Villena M Vargas E Soria R 1995 Developmentalgenetic and environmental components of aerobic capacity at high alti-tude Am J Phys Anthropol 96431ndash442 Available at httpwwwncbinlmnihgovpubmed7604895
Giroux S 2007 Canadian health measures survey sampling strategyoverview Health Rep 1831ndash36
Gurven M Jaeggi A V Kaplan H Cummings D 2013 Physical activityand modernization among Bolivian Amerindians PLoS ONE 81ndash13
Gurven M Kaplan H Winking J Rodriguez DE Vasunilashorn S KimJK Finch C Crimmins E 2009 Inflammation and infection do not pro-mote arterial aging and cardiovascular disease risk factors among leanhorticulturalists PLoS ONE 41ndash12
Haidet GC 1989 Dynamic exercise in senescent beagles oxygen consump-tion and hemodynamic responses The Am J Physiol 257H1428ndash1437Available at httpwwwncbinlmnihgovpubmed2589499
Hawkins S Wiswell R 2003 Rate and mechanism of maximal oxygen con-sumption decline with aging implications for exercise training SportsMed 33877ndash888 Available at httpwwwncbinlmnihgovpubmed12974656
Hoffman J 2002 Physiological aspects of sport training and performance1st ed Champaign IL Human Kinetics Publishers
Hotez PJ Bottazzi ME Franco-Paredes C Ault SK Periago MR 2008 Theneglected tropical diseases of Latin America and the Caribbean a review ofdisease burden and distribution and a roadmap for control and eliminationPLoS Negl Trop Dis 2e300 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid52553488amptool5pmcentrezamprendertype5abstract
Howley ET Bassett DR Welch HG 1995 Criteria for maximal oxygenuptake review and commentary Med Sci Sports Exerc 271292ndash1301Available at httpwwwncbinlmnihgovpubmed8531628
Jette M Sidney K Quenneville J Landry F 1992 Relation between cardi-orespiratory fitness and selected risk factors for coronary heart diseasein a population of Canadian men and women CMAJ 1461353ndash1360Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid51488567amptool5pmcentrezamprendertype5abstract
Katzmarzyk PT Leonard WR Crawford MH 1994 Predicted maximaloxygen consumption of Indigenous Siberians Am J Hum Biol 6783ndash790
King CH Dickman K Tisch DJ 2005 Reassessment of the cost of chronichelmintic infection a meta-analysis of disability-related outcomes inendemic schistosomiasis Lancet 3651561ndash1569 Available at httpwwwncbinlmnihgovpubmed15866310
Lee J-M Bassett D Jr Thompson D Fitzhugh E 2011 Validation of thecosmed fitmate for predicting maximal oxygen consumption J StrengthCond Res 252573ndash2579
Madimenos FC Snodgrass JJ Blackwell AD Liebert MA Sugiyama LS2011 Physical activity in an indigenous Ecuadorian forager-horticulturalist population as measured using accelerometry Am J HumBiol 23488ndash497 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid53110644amptool5pmcentrezamprendertype5abstract
Malina RM 2001 Physical activity and fitness pathways from childhoodto adulthood Am J Hum Biol 13162ndash172 Available at httpwwwncbinlmnihgovpubmed11460860
Malina RM Little BB 2008 Physical activity the present in the contextof the past Am J Hum Biol 20373ndash391 Available at httpwwwncbinlmnihgovpubmed18433002
Manning JT Morris L Caswell N 2007 Endurance running and digitratio (2D 4D) implications for fetal testosterone effects on runningspeed and vascular health Am J Hum Biol 19416ndash421
Martin Ma Lassek WD Gaulin SJC Evans RW Woo JG Geraghty SRDavidson BS Morrow AL Kaplan HS et al 2012 Fatty acid composi-tion in the mature milk of Bolivian forager-horticulturalists controlledcomparisons with a US sample Matern Child Nutr 8404ndash418 Availableat httpwwwncbinlmnihgovpubmed22624983
National Health and Nutrition Examination Survey 2004 CardiovascularFitness Procedures Manual
Nussey D Coulson T Festa-Bianchet M Gaillard J-M 2008 Measuringsenescence in wild animal populations towards a longitudinal approachFunction Ecol 22393ndash406
Ogawa T Spina RJ Martin WHI Kohrt WM Schechtman KB HolloszyJO Ehsani AA 1992 Effects of aging sex and physical training cardio-vascular responses to exercise Circulation 86494ndash503
Panter-Brick C Miller UG Eggerman M 1992 Hemoglobin levels andstep test performance of men and women in Nepal Am J Hum Biol 4481ndash491
Pontzer H Raichlen Da Wood BM Mabulla AZP Racette SB MarloweFW 2012 Hunter-gatherer energetics and human obesity PLoS ONE 7e40503 Available at httpcdxplosorg101371journalpone0040503
R Development Core Team 2011 R A language and environment for sta-tistical computing R Development Core Team
Rigby R Stasinopoulos D 2005 Generalize additive models for locationscale and shape (with discussion) Appl Stat 54507ndash554
Robergs RA Landwehr R 2002 The surprising history of theldquoHRmax5220-agerdquo equation J Exerc Physiol 51ndash10
Rode A Shephard RJ 1994 Physiological consequences of acculturation a20-year study of fitness in an Inuit community Eur J Appl Physiol 69516ndash524
Rowland TW Boyajian A 1995 Aerobic response to endurance training inchildren Pediatrics 96654ndash658
Sagiv M Ben-sira D Amir R 2007 What maintains energy supply atpeak aerobic exercise in trained and untrained older men Gerontology53357ndash361
Sanada K Kuchiki T Miyachi M Mcgrath K Higuchi M Ebashi H 2007Effects of age on ventilatory threshold and peak oxygen uptake normal-ised for regional skeletal muscle mass in Japanese men and womenaged 20 ndash 80 years Eur J Appl Physiol 99475ndash483
Schniter E 2009 Why Old Age Non-Material Contributions and Patternsof Aging Among Older Adult Tsimanersquo 607
Shahnawaz H 1978 Influence of limb length on a stepping exercise JAppl Physiol 44346ndash349
Shephard RJ 1970 Computer programs for solution of the Astrand nomo-gram and the calculation of body surface area J Sports Med 10206ndash210
Shephard RJ Allen C Benade AJS Davies CT Di Prampero PE HedmanR Merriman JE Myhre K Simmons R 1968 Standardization of sub-maximal exercise tests Bull World Health Organ 38765ndash775 Availableat httpwwwpubmedcentralnihgovarticlerenderfcgiartid52554690amptool5pmcentrezamprendertype5abstract
Shephard RJ Bailey Da Mirwald RL 1976 Development of the CanadianHome Fitness Test Can Med Assoc J 114675ndash679 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid51956906amptool5pmcentrezamprendertype5abstract
Shields M Tremblay MS Laviolette M Craig CL Janssen I Gorber SC2010 Fitness of Canadian adults results from the 2007ndash2009 canadianhealth measures survey Health Rep 2121ndash35 Available at httpwwwncbinlmnihgovpubmed20426224
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 13
American Journal of Human Biology
Siconolfi SF Garber CE Lasater TM Carleton RA 1985 A simple validstep test for estimating maximal oxygen uptake in epidemiologic stud-ies Am J Epidemiol 121382ndash390 Available at httpwwwncbinlm-nihgovpubmed4014128
Sinclair LM Hinton PS 2005 Prevalence of iron deficiency with and with-out anemia in recreationally active men and women J Am Diet Assoc105975ndash978 Available from httpwwwncbinlmnihgovpubmed15942552
Skinner JS Gaskill SE Rankinen T Leon AS Rao DC Wilmore JHBouchard C 2003 Heart rate versus VO2max age sex race initial fit-ness and training response-HERITAGE Med Sci Sports Exerc 351908ndash1913 Available at httpwwwncbinlmnihgovpubmed14600558
Sondik EJ Madans JH Gentlemand JF 2012 Summary health statisticsfor US adults National Health Interview Survey 2010 Vital Health Stat101ndash80 Available at httpwwwncbinlmnihgovpubmed20687424
Stones MJ Kozma A 1985 Physical performance Aging and Human Per-formance New York Wiley p 261ndash292
Tanaka H Monahan KD Seals DR 2001 Age-predicted maximal heartrate revisited J Am Coll Cardiol] 37153ndash156 Available at httpwwwncbinlmnihgovpubmed11153730
Vasunilashorn S Crimmins EM Kim JK Winking J Gurven M KaplanH Finch CE 2010 Blood lipids infection and inflammatory markers inthe Tsimane of Bolivia Am J Hum Biol 22731ndash740 Available at httpwwwncbinlmnihgovpubmed20721985
Vaupel JV Manton KG Stallard E 1979 The impact of heterogeneity inindividual frailty on the dynamics of mortality Demography 16439ndash454
Vaupel JW Yashin AI 1985 Heterogeneityrsquos ruses some surprising effectsof selection on population dynamics Am Stat 39176ndash185
Venables WN Ripley BD 2002 Modern Applied Statistics with S FourthNew York Springer
Wagner PD 1996 Determinants of maximal oxygen transport and utiliza-tion Annu Rev Physiol 5821ndash50 Available at httpwwwncbinlmnih-govpubmed8815793
Walker A Arent SM McKeever KH 2010 Maximal aerobic capacity(VO2max) in horses a retrospective study to identify the age-relateddecline Comparative Exerc Physiol 6177ndash181 Available at httpwwwjournalscambridgeorgabstract_S1755254010000073
Walker R Hill K 2003 Modeling growth and senescence in physical per-formance among the Ache of Eastern Paraguay Am J Hum Biol 208196ndash208
Weller IM Thomas SG Corey PN Cox MH 1993 Prediction of maximaloxygen uptake from a modified Canadian aerobic fitness test Can JAppl Physiol 18175ndash188 Available at httpwwwncbinlmnihgovpubmed8513290
Wilson TM Tanaka H 2000 Meta-analysis of the age-associated declinein maximal aerobic capacity in men relation to training status Am JPhysiol Heart Circ Physiol 278H829ndash834 Available at httpwwwncbinlmnihgovpubmed10710351
Wood SN 2006 Generalized Additive Models An Introduction with RBoca Raton Florida Chapman and HallCRC Press
World Health Organization 2001 Iron deficiency anaemia assessmentprevention and control a guide for programme managers Available athttpwhqlibdocwhointhq2001WHO_NHD_013pdf
Yoopat P Toicharoen P Boontong S Glinsukon T Vanwonterghem KLouhevaara V 2002 Cardiorespiratory capacity of Thai workers in dif-ferent age and job categories J Physiol Anthropol Appl Hum Sci 21121ndash128 Available at httpwwwncbinlmnihgovpubmed12056179
Zhu YI Haas JD 1997 Iron depletion without anemia and physical per-formance in young women Am J Clin Nutr 66334ndash341 Available athttpwwwncbinlmnihgovpubmed9250112
14 AC PISOR ET AL
American Journal of Human Biology
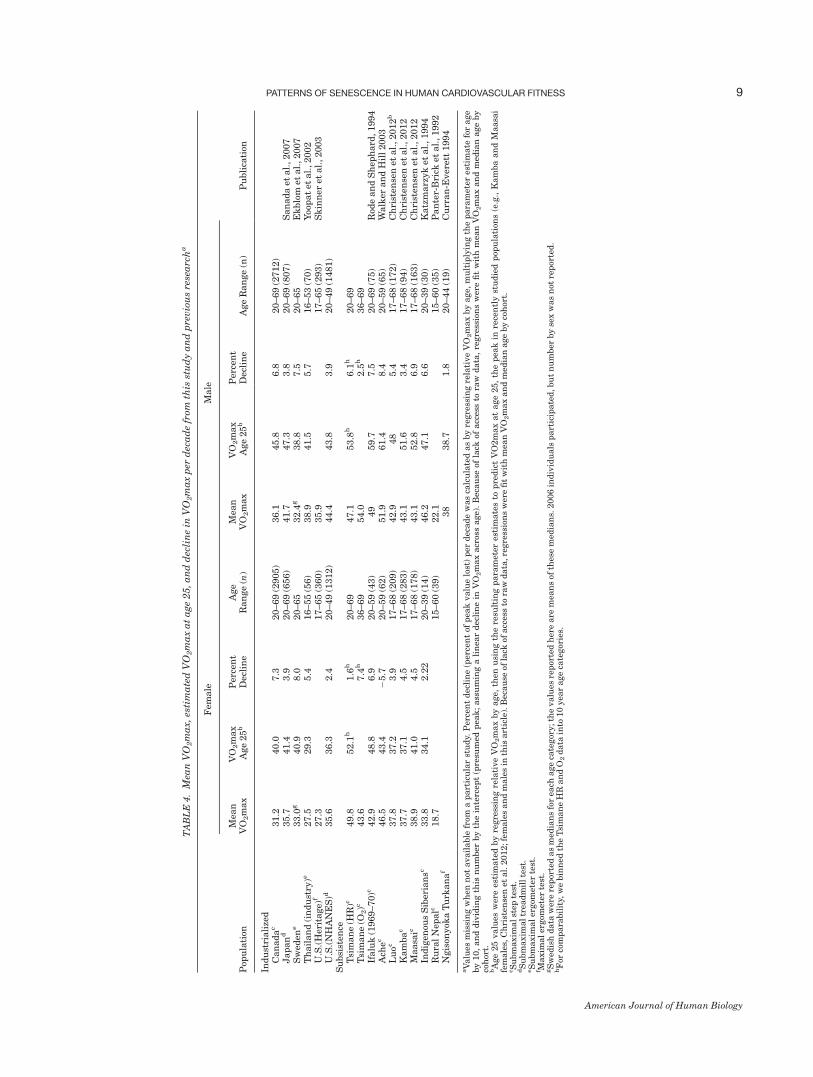
TA
BL
E4
Mea
nV
O2m
ax
esti
ma
ted
VO
2m
ax
at
age
25a
nd
dec
lin
ein
VO
2m
ax
per
dec
ad
efr
omth
isst
ud
ya
nd
pre
vio
us
rese
arc
ha
Pop
ula
tion
Fem
ale
Male
Pu
bli
cati
onM
ean
VO
2m
ax
VO
2m
ax
Age
25
bP
erce
nt
Dec
lin
eA
ge
Ran
ge
(n)
Mea
nV
O2m
ax
VO
2m
ax
Age
25
bP
erce
nt
Dec
lin
eA
ge
Ran
ge
(n)
Ind
ust
riali
zed
Can
ad
ac
312
400
73
20ndash69
(2905)
361
458
68
20ndash69
(2712)
Jap
an
d357
414
39
20ndash69
(656)
417
473
38
20ndash69
(807)
San
ad
aet
al
2007
Sw
eden
e330
g409
80
20ndash65
324
g388
75
20ndash65
Ek
blo
met
al
2007
Th
ail
an
d(i
nd
ust
ry)e
275
293
54
16ndash55
(56)
389
415
57
16ndash53
(70)
Yoo
pat
etal
2002
US
(H
erit
age)
f273
17ndash65
(360)
359
17ndash65
(293)
Sk
inn
eret
al
2003
US
(N
HA
NE
S)d
356
363
24
20ndash49
(1312)
444
438
39
20ndash49
(1481)
Su
bsi
sten
ceT
sim
an
e(H
R)c
498
521
h16
h20ndash69
471
538
h61
h20ndash69
Tsi
man
e(O
2)c
436
74
h36ndash69
540
25
h36ndash69
Ifalu
k(1
969ndash70)c
429
488
69
20ndash59
(43)
49
597
75
20ndash69
(75)
Rod
ean
dS
hep
hard
1994
Ach
ec465
434
257
20ndash59
(62)
519
614
84
20ndash59
(65)
Walk
eran
dH
ill
2003
Lu
oc378
372
39
17ndash68
(209)
429
48
54
17ndash68
(172)
Ch
rist
ense
net
al
2012
b
Kam
ba
c377
371
45
17ndash68
(283)
431
516
34
17ndash68
(94)
Ch
rist
ense
net
al
2012
Maasa
ic389
410
45
17ndash68
(178)
431
528
69
17ndash68
(163)
Ch
rist
ense
net
al
2012
Ind
igen
ous
Sib
eria
nsc
338
341
22
220ndash39
(14)
462
471
66
20ndash39
(30)
Katz
marz
yk
etal
1994
Ru
ral
Nep
alc
187
15ndash60
(39)
221
15ndash60
(35)
Pan
ter-
Bri
cket
al
1992
Ngis
onyok
aT
urk
an
af
38
387
18
20ndash44
(19)
Cu
rran
-Ever
ett
1994
aV
alu
esm
issi
ng
wh
enn
otavail
able
from
ap
art
icu
lar
stu
dy
Per
cen
td
ecli
ne
(per
cen
tof
pea
kvalu
elo
st)
per
dec
ad
ew
as
calc
ula
ted
as
by
regre
ssin
gre
lati
ve
VO
2m
ax
by
age
mu
ltip
lyin
gth
ep
ara
met
eres
tim
ate
for
age
by
10
an
dd
ivid
ing
this
nu
mber
by
the
inte
rcep
t(p
resu
med
pea
k
ass
um
ing
ali
nea
rd
ecli
ne
inV
O2m
ax
acr
oss
age)
B
ecau
seof
lack
ofacc
ess
tora
wd
ata
re
gre
ssio
ns
wer
efi
tw
ith
mea
nV
O2m
ax
an
dm
edia
nage
by
coh
ort
bA
ge
25
valu
esw
ere
esti
mate
dby
regre
ssin
gre
lati
ve
VO
2m
ax
by
age
then
usi
ng
the
resu
ltin
gp
ara
met
eres
tim
ate
sto
pre
dic
tV
O2m
ax
at
age
25
the
pea
kin
rece
ntl
yst
ud
ied
pop
ula
tion
s(e
g
Kam
ba
an
dM
aasa
ife
male
sC
hri
sten
sen
etal
2012fe
male
san
dm
ale
sin
this
art
icle
)B
ecau
seof
lack
ofacc
ess
tora
wd
ata
re
gre
ssio
ns
wer
efi
tw
ith
mea
nV
O2m
ax
an
dm
edia
nage
by
coh
ort
cS
ubm
axim
alst
epte
st
dS
ubm
axim
altr
ead
mil
lte
st
eS
ubm
axim
aler
gom
eter
test
f M
axim
al
ergom
eter
test
gS
wed
ish
data
wer
ere
por
ted
as
med
ian
sfo
rea
chage
cate
gor
yth
evalu
esre
por
ted
her
eare
mea
ns
ofth
ese
med
ian
s2006
ind
ivid
uals
part
icip
ate
dbu
tn
um
ber
by
sex
was
not
rep
orte
d
hF
orco
mp
ara
bil
ity
we
bin
ned
the
Tsi
man
eH
Ran
dO
2d
ata
into
10
yea
rage
cate
gor
ies
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 9
American Journal of Human Biology
on median age (for a given age category) population andtheir interaction term For comparability Tsimane werebinned into the Canadian age categories and averageswere computed for these categories leading to estimateddeclines slightly different from those in Table 4 for thepurposes of this test we treat the Tsimane female declineas linear Because within-population variance in declineis not available these regressions should be treated asdescriptive comparisons rather than statistical tests ofdifferences between the two groups The rate of decline inVO2max is steeper for Canadian females (69 per decadefaster decline per decade) and males (42 faster declineper decade) compared with Tsimane females and males
The rate of cardiovascular fitness decline between theTsimane and Canadians is different but this differencedoes not extend to industrialized and subsistence popula-tions (see Table 4) Controlling for sex subsistence groupshave about one quarter of a percent lower declines perdecade Again because the variance in decline is not rep-resented in this regression results should be interpretedas comparative rather than as a statistical test As beforeTsimane O2 results were not included in the analysis toavoid nonindependence and the indigenous Siberianswere excluded because of discrepancy in ages sampled
DISCUSSION
Our comparisons demonstrate that across a wide varietyof societies cardiovascular fitness senesces with age Car-diovascular fitness is higher on average among members ofsubsistence societies than among industrialized societiesbut rates of fitness decline from peak are not slower Ourmore detailed comparison between the Tsimane a subsist-ence population and Canadians an industrialized popula-tion reveals differences in cardiovascular fitness levelsand rate of fitness decline Cardiovascular fitness levelswere higher among the Tsimane than among Canadiansand the rate of decline across the lifespan was significantlyslower among Tsimane women and men Potential Cana-
dian participants were excluded due to many health con-cerns including pregnancy and history of high bloodpressure whereas Tsimane were only excluded if they self-identified as unable to participate This suggests the Cana-dian sample is a relatively healthy subsample of Canadayet the Tsimane still outperform them in cardiovascular fit-ness It may be that the higher demand for cardiovascularfitness in late ages among the Tsimane outweighs anyeffects of poor health Another possibility is that greaterself-selection among Tsimane due to higher adult mortalityleaves more robust older adult survivors thereby reducingthe observed slope of fitness decline at the population level(Vaupel et al 1979) perhaps this is partially why fewerTsimane older adults opted out of the exercise test thanCanadian older adults were screened out (ages 60ndash69Canadian females 5 56 Tsimane females 5 15 Cana-dian males 5 57 Tsimane males 5 5)
Consistent with prior research on age-related changesin cardiovascular fitness the Tsimane do evidence a lin-ear decline in VO2max with age but not as steep a declineas typically seen in industrialized populations Based oncomparisons with the Canadians and with other industri-alized populations we believe the Tsimane data from thepresent study and the pilot O2 data combined indicatethat the Tsimane perform better on tests of cardiovascularfitness than the average individual from an industrializednation
To further explore the potential effects of health factorson cardiovascular fitness level and rate of decline weinvestigated predictors of individual differences in fitnesswithin the Tsimane population Overall we found thatmost health indicators among the Tsimane did not hinderVO2max levels or rates of decline Lower hemoglobin lev-els were associated with lower VO2max levels in womenbut not men consistent with the notion that compromisedblood oxygen transport curbs cardiovascular fitness(Buzina et al 1989 Panter-Brick et al 1992) In the USlow hemoglobin is more common in active women thanactive men (Sinclair and Hinton 2005) hemoglobin is
Fig 2 Linear changes in VO2max with age for Canadians and the Tsimane Intercepts and slopes for Canadians and Tsimane can be foundin Table 4 Because age2 is significant for the full sample of Tsimane females their change in VO2max across age is curvilinear Slopes forendurance trained active and sedentary individuals from industrialized nations are drawn from a meta-analysis performed by Fitzgeraldet al (1997) for females and Wilson and Tanaka (2000) for males Endurance trained individuals are represented by the top dotted line abovefollowed by active individuals below and sedentary on the bottom Trained individuals engage in 31 sessions of endurance exercise per weekfor at least a year while active individuals engage in 2 or fewer sessions per week of cardiovascular exercise [Color figure can be viewed in theonline issue which is available at wileyonlinelibrarycom]
10 AC PISOR ET AL
American Journal of Human Biology
also lower in Tsimane women than Tsimane men(female 5 129 [sd 13] g ml21 males 5 142 [13] g ml21)Even mild (non-anemic) iron deficiencies impacts womenrsquosexercise performance (Zhu and Haas 1997) Inconsistentwith findings from Panter-Brick et al (1992) among ruralNepalese helminth infection did not diminish levels ofVO2max for Tsimane men helminth infection wasactually a predictor of higher VO2max There are severalreasons why this might be the case First we only testedwhether presence or absence of helminths mediated theeffect of age on VO2max rather than parasite load (egnumber of worms egg counts) it is possible that helminthinfection only affects VO2max at high parasite loads Sec-ond blood loss (and thus low hemoglobin levels) resultingfrom helminth infection may be partially offset by theamount of iron in the Tsimane adult diet Tsimane ironintake is an estimated 166 of the US Dietary ReferenceIntake (Martin et al 2012) and Tsimane hemoglobin lev-els are higher than in the Nepalese (females 129 vs 109males 1424 vs 120 Panter-Brick et al 1992) Thirdthese analyses consider helminth infection at the time ofexercise test rather than past infections It may be thatthe cumulative burden of past infection has a larger effecton cardiovascular fitness if so this would suggest thatthe surprising positive effect of helminth infection onVO2max levels in men is either spurious or capturing athird variable
Secular declines in VO2max are expected with increasingmarket integration and lifestyle change because ofincreased sedentism (Katzmarzyk et al 1994 Rode andShephard 1994) Two proxies for market integration in thispopulationmdashdistance to San Borja and the ability to speakSpanishmdashwere not significant predictors of VO2max levelsor decline This is consistent with our predictions as Tsi-mane females and males that live near town do not appearto have lower activity levels (Gurven et al 2013) Wageopportunities near town primarily include working asranch hands collecting and weaving palm thatch panelscash cropping and working for logging companies Each ofthese involves extensive activity furthermore transporta-tion to town often involves bicycling walking and polingdugout canoes Cash cropping of rice and corn also involvesthe clearing and weeding of larger fields Except for cashcropping and palm thatch manufacture most wage laboropportunities are currently restricted to men
This study makes several unique contributions to theexisting literature It offers the first systematic compari-son of cardiovascular fitness level and rate of declinebetween subsistence and industrialized societies Resultscompiled from previous studies support the general claimthat despite greater pathogen stress the greater activityregime of subsistence societies helps support higher peakVO2max Additionally this is one of the first studies toexplore senescent changes in cardiovascular fitnesswithin a large sample from a subsistence population Thelarge number of health measures and proxies of marketintegration available permitted testing whether these fac-tors mediated age-related variation and whether theymodulated the rate of decline Despite reports that healthstatus and market integration have been important inother studies (eg Buzina et al 1989 Katzmarzyk et al1994 Panter-Brick et al 1992 Rode and Shephard1994) their overall net effect was small among the Tsi-mane most apparent in measures of hemoglobin levelsamong women and helminth infection among men
The results of these analyses may also shed light onindividual and population level differences in chronic dis-ease In industrialized populations meta-analyses demon-strate that cardiovascular fitness is protective againstcardiovascular disease (Jette et al 1992 Hawkins andWiswell 2003) Prior studies among Tsimane suggest rel-atively few deaths from heart attacks or strokes (Gurvenet al 2007) a low prevalence of common cardiovasculardisease risk factors like obesity high blood low-densitylipoprotein levels hypertension and peripheral arterialdisease and the existence of additional protective factorslike lean diet and physical activity (Gurven et al 20092013 Vasunilashorn et al 2010) Market foods such ascooking oil sugar and pasta represent only 6 of theaverage Tsimane diet and Tsimane also consume a greatdeal of lean meat and omega-3 fatty acids (Martin et al2012) This study complements these findings by demon-strating that Tsimane show relatively high VO2max anindicator of strong cardiorespiratory health TsimaneVO2max declines with age as it does everywhere whichsuggests declining muscle mass with age (Fleg andLakatta 1988) and lowered cardiac output (American Col-lege of Sports Medicine 2006 Sagiv et al 2007) ratherthan increased cardiovascular disease risk
Limitations
The Canadians were selected as a comparison industri-alized population because of the similarity of the CHMSand Tsimane protocols very few studies of industrializedpopulations have large sample sizes sample across thelife course and use a step test Several aspects of theCHMS and Tsimane protocols remain potentially incom-parable The Canadians experienced more stringentexclusion criteria than the Tsimane meaning that the Tsi-mane sample may be more representative of cardiovascu-lar condition in the Tsimane population than theCanadian sample of the Canadian population Again ifthe Tsimane sample was subjected to these criteria wemight expect the differences in VO2max between popula-tions to only increase On the other hand Canadian par-ticipants were assigned stepping cadences based on theirage and sex and cadence was increased across the exer-cise test if a participant did not reach 85 of his or herage-specific maximal HR all Tsimane were asked to com-plete 30 ascents per minute with no increase based ontheir achieved HRs Few Tsimane reached 75 of theirage-specific maximal HR (see Supporting InformationTable S1) perhaps because the age-specific maximal HRsderived from industrialized populations are inaccurate forthe Tsimane or because higher fitness allowed these Tsi-mane to perform the step test of 30 ascents per minutewith less effort Due to these discrepancies in protocolwhich may lead to errors in estimating VO2max we alsoincorporated Tsimane data collected using the O2 methodas a check because the O2 method estimates VO2max onthe relationship between HR and VO2 in a givenparticipant
Indeed it is an open question as to whether typicalmethods for indirectly estimating cardiovascular fitnessfrom HR are appropriate for subsistence level popula-tions Common routines for VO2max estimation assumeage-specific declines in cardiovascular fitness (eg Shep-hard 1970) but these methods have only been validatedwith samples from industrialized populations which are
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 11
American Journal of Human Biology
often self-selected (Beall et al 1985) Additionally regres-sions drawn from laboratory studies require participantsachieve a HR within a certain range for accurate VO2maxestimation however the appropriateness of these rangesgiven slight modifications to protocol and inclusion of par-ticipants of different ages different populations and bothsexes is questionable For example the maximal HRexhibited by young men varies across subsistence popula-tions (Shephard 1978) Use of these criteria is compli-cated by the fact that the most commonly used equationfor estimating maximal possible HR by age 220-age maybe inaccurate (Robergs and Landwehr 2002) and particu-larly inappropriate for older adults (see Tanaka et al2001) For these reasons we chose to use an exclusion cri-terion for the Tsimane that evaluates individual increasein HR across exercise relative to the mean increase in HRfor Tsimane of the same sex and age
The pattern of Tsimane fitness decline differs moder-ately by the choice of exclusion criterion for participants(see Supporting Information Table S1) and by method oftesting However this is a common finding Lee et al(2011) predicted VO2max from submaximal exercise usingthe O2 method and the HR-based American College ofSports Medicine calculation routine in a US sample Theyfound that (1) the HR-based routine predicts higherVO2max across the sexes than does the O2 routine and(2) the two methods have a correlation of only 077 Whenevaluating different testing procedures Shephard et al(1968) found differences in VO2max estimation by type oftest used (eg bicycle ergometer versus step test) and cal-culation routine Exercise tests exclusion criteria andcalculation routines combine to provide an estimate ofactual VO2max for a given individual and as such varia-tion in estimation is to be expected However such varia-tion may affect cross-population comparisons inunforeseen ways thus the comparisons presented hereshould be interpreted with caution
While population-level variation in cardiovascular fit-ness decline may reflect the differences in the demands ofendurance-based physical activity muscularity and com-promised oxygen transport it is possible that genetic fac-tors may also play a potential role (Collins 1999) In oneindustrialized sample maternal cardiovascular fitnessexhibited a heritability of 30 which is attributed toinheritance of the maternal mitochondrial genome (Bou-chard et al 2000) We do not have the relevant geneticdata for the populations considered here however andthus operate under the simplifying assumption thatinheritance should not affect population-level patternsand will not consistently bias individual-level compari-sons in any particular direction
This study is further limited by its cross-sectionaldesign Cross-sectional data present well-known problemsfor the measurement of individual aging (Crimmins andSeeman 2001) Mortality selection in which individualsin poorer condition are likely to die at younger ages pro-duces a downward bias in the estimation of aging rates atthe individual level (Vaupel and Yashin 1985 Vaupelet al 1979) Cohort effects if present also produce com-plicated and non-monotonic biases in estimation (Carnesand Olshansky 2001) Due to the problem of between-individual heterogeneity and the within-individual pro-cess of senescence a recent overview of aging studies con-cludes that ldquoonly longitudinal studies [ ] provide reliablesources of information in the study of senescencerdquo (Nussey
et al 2008) To date there are no longitudinal studies ofcardiovascular fitness in subsistence populations We arecurrently re-testing participants under the O2 methodallowing a better grasp of the within-individual variationthat shapes patterns of senescent decline
ACKNOWLEDGMENTS
The authors thank Paul Hooper Steven Gaulin JohnTooby Patricia Kramer the Human Evolution and Biode-mography laboratory and the Center for EvolutionaryPsychology at UCSB for helpful advice and feedback thestaff at the Tsimane Health and Life History Project andthe Tsimane for their participation and patience
LITERATURE CITED
American College of Sports Medicine 2006 ACSMrsquos Guidelines for Exer-cise Testing and Prescription 7th ed Philadelphia Lippincott Williamsamp Wilkins
Armstrong N 2001 Peak oxygen uptake in relation to growth and matura-tion in 11- to 17-year-old humans Eur J Appl Physiol 85546ndash551
Astrand PO Ryhming I 1954 A nomogram for calculation of aerobiccapacity (physical fitness) from pulse rate during submaximal work JAppl Physiol 7218ndash221
Bailey DA Shephard RJ Mirwald RL 1976 Validation of a self-administered home test of cardio-respiratory fitness Can J Appl SportSci 167ndash78
Beall CM Goldstein MC and Feldman ES 1985 The physical fitness ofelderly Nepalese farmers residing in rugged mountain and flat terrainJ Gerontol 40529ndash535
Benefice E Ndiaye G 2005 Relationships between anthropometry cardi-orespiratory fitness indices and physical activity levels in different ageand sex groups in rural Senegal (West Africa) Ann Hum Biol 32366ndash382 Available from httpwwwncbinlmnihgovpubmed16099780
Blackwell AD Gurven MD Sugiyama LS Madimenos FC Liebert MAMartin MA Kaplan HS Snodgrass JJ 2011 Evidence for a peak shift in ahumoral response to helminths age profiles of IgE in the Shuar of Ecuadorthe Tsimane of Bolivia and the US NHANES PLoS Negl Trop Dis 5e1218 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid53125146amptool5pmcentrezamprendertype5abstract
Blackwell AD Martin M Kaplan H Gurven M Evidence for an antagonis-tic relationship between Giardia lamblia and helminth infections impli-cations for treatment of helminth infections in developing populations
Blair SN LaMonte MJ Nichaman MZ 2004 The evolution of physicalactivity recommendations how much is enough Am J Clin Nutr 79913Sndash920S Available at httpwwwncbinlmnihgovpubmed15113739
Bouchard C Rankinen T Chagnon YC Rice T Perusse L Gagnon JBorecki I An P Leon a S et al 2000 Genomic scan for maximal oxygenuptake and its response to training in the HERITAGE Family Study JAppl Physiol 88551ndash559 Available at httpwwwncbinlmnihgovpubmed10658022
Bryan S St-Denis M Wojtas D 2007 Canadian Health Measures Surveyclinic operations and logistics Health Rep 1853ndash69
Buzina R Bates CJ van der Beek J Brubacher G Chandra RK HallbergL Heseker J Mertz W Pietrzik K et al 1989 Workshop on FunctionalSignificance of Mild-to-Moderate Malnutrition Am J Clin Nutrition 50172ndash176
Calder WA 1987 Scaling energetics of homeothermic vertebrates anoperational allometry Annu Rev Physiol 49107ndash120
Canadian Society for Exercise Physiology 2003 The Canadian PhysicalActivity Fitness amp Lifestyle Approach (CPAFLA) CSEP-Health amp Fit-ness Programrsquos Health-Related Appraisal and Counselling Strategy 3rded
Carnes BA Olshansky SJ 2001 Heterogeneity and its biodemographicimplications for longevity and mortality Exp Gerontol 36419ndash430Available at httpwwwncbinlmnihgovpubmed11250115
Carrick-Ranson G Hastings JL Bhella PS Shibata S Fujimoto N PalmerD Boyd K Levine BD 2013 The effect of age-related differences inbody size and composition on cardiovascular determinants of VO2max JGerontol A Biol Sci Med Sci 68608ndash616 Available at httpwwwncbinlmnihgovpubmed23160363
Centers for Disease Control and Prevention 1998 Recommendations toPrevent and Control Iron Deficiency in the United States MMWRRecomm Rep 471ndash36 Available at httpwwwcdcgovmmwrpreviewmmwrhtml00051880htm
12 AC PISOR ET AL
American Journal of Human Biology
Centers for Disease Control and Prevention 2011 Glossary of TermsPhysical Activity for Everyone [Internet] Available from httpwwwcdcgovphysicalactivityeveryoneglossary
Christensen DL Faurholt-Jepsen D Boit MK Mwaniki DL Kilonzo BTetens I Kiplamai FK Cheruiyot SC Friis H et al 2012 Cardiorespira-tory fitness and physical activity in Luo Kamba and Maasai of ruralKenya Am J Hum Biol 24723ndash729 Available at httpwwwncbinlm-nihgovpubmed22836508
Colley RC Garriguet D Janssen I Craig CL Clarke J Tremblay MS2011a Physical activity of Canadian children and youth accelerometerresults from the 2007 to 2009 Canadian Health Measures SurveyHealth Rep 2215ndash23
Colley RC Garriguet D Janssen I Craig CL Clarke J Tremblay MS2011b Physical activity of Canadian adults accelerometer results fromthe 2007 to 2009 Canadian Health Measures Survey Health Rep 227ndash14 Available at httpwwwncbinlmnihgovpubmed21510585
Collins KJ 1999 Physiological variation and adaptability in human popu-lations Ann Hum Biol 2619ndash38
Crimmins E Seeman T 2001 Integrating Biology into DemographicResearch on Health and Aging (With a Focus on the MacArthur Study ofSuccessful Aging) Cells and Surveys Should Biological Measures beIncluded in Social Science Research Washington DC National Acad-emy Press p 9ndash41
Curran-Everett LS 1994 Accordance Between VO2max and Behavior inNgisonyoka Turkana Am J Hum Biol 6761ndash771
Durnin JVGA Womersley J 1974 Body fat assessed from total body den-sity and its estimation from skinfold thickness measurements on 481men and women aged from 16 to 72 years Br J Nutr 3277ndash97
Eberl M Al-Sherbiny M Hagan P Ljubojevic S Thomas AW Wilson RA2002 A novel and sensitive method to monitor helminth infections byfaecal sampling Acta Trop 83183ndash187
Eid D Gurven M Kaplan H Winking J 2007 Enfermedades infecciosas alo largo de la vida y en el envejecimiento en indıgenas sudamericanos dela etnia Tsimane Aging in Developing Countries Building Bridges forIntegrated Research Agendas Santiago Chile
Ekblom B Engstreuroom L-M Ekblom O 2007 Secular trends of physical fit-ness in Swedish adults Scand J Med Sci Sports 17267ndash273 Availableat httpwwwncbinlmnihgovpubmed17501867
Finch CA Lenfant C 1972 Oxygen Transport in Man N Engl J Med 286407ndash415
Fitzgerald MD Tanaka H Tran ZV Seals DR 1997 Age-related declinesin maximal aerobic capacity in regularly exercising vs sedentarywomen a meta-analysis J Appl Physiol (Bethesda Md 1985) 83160ndash165 Available at httpwwwncbinlmnihgovpubmed9216959
Fleg JL Lakatta EG 1988 Role of muscle loss in the age-associated reduc-tion in VO2max J Appl Physiol 651147ndash1151
Frisancho AR Frisancho HG Milotich M Brutsaert T Albalak RSpielvogel H Villena M Vargas E Soria R 1995 Developmentalgenetic and environmental components of aerobic capacity at high alti-tude Am J Phys Anthropol 96431ndash442 Available at httpwwwncbinlmnihgovpubmed7604895
Giroux S 2007 Canadian health measures survey sampling strategyoverview Health Rep 1831ndash36
Gurven M Jaeggi A V Kaplan H Cummings D 2013 Physical activityand modernization among Bolivian Amerindians PLoS ONE 81ndash13
Gurven M Kaplan H Winking J Rodriguez DE Vasunilashorn S KimJK Finch C Crimmins E 2009 Inflammation and infection do not pro-mote arterial aging and cardiovascular disease risk factors among leanhorticulturalists PLoS ONE 41ndash12
Haidet GC 1989 Dynamic exercise in senescent beagles oxygen consump-tion and hemodynamic responses The Am J Physiol 257H1428ndash1437Available at httpwwwncbinlmnihgovpubmed2589499
Hawkins S Wiswell R 2003 Rate and mechanism of maximal oxygen con-sumption decline with aging implications for exercise training SportsMed 33877ndash888 Available at httpwwwncbinlmnihgovpubmed12974656
Hoffman J 2002 Physiological aspects of sport training and performance1st ed Champaign IL Human Kinetics Publishers
Hotez PJ Bottazzi ME Franco-Paredes C Ault SK Periago MR 2008 Theneglected tropical diseases of Latin America and the Caribbean a review ofdisease burden and distribution and a roadmap for control and eliminationPLoS Negl Trop Dis 2e300 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid52553488amptool5pmcentrezamprendertype5abstract
Howley ET Bassett DR Welch HG 1995 Criteria for maximal oxygenuptake review and commentary Med Sci Sports Exerc 271292ndash1301Available at httpwwwncbinlmnihgovpubmed8531628
Jette M Sidney K Quenneville J Landry F 1992 Relation between cardi-orespiratory fitness and selected risk factors for coronary heart diseasein a population of Canadian men and women CMAJ 1461353ndash1360Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid51488567amptool5pmcentrezamprendertype5abstract
Katzmarzyk PT Leonard WR Crawford MH 1994 Predicted maximaloxygen consumption of Indigenous Siberians Am J Hum Biol 6783ndash790
King CH Dickman K Tisch DJ 2005 Reassessment of the cost of chronichelmintic infection a meta-analysis of disability-related outcomes inendemic schistosomiasis Lancet 3651561ndash1569 Available at httpwwwncbinlmnihgovpubmed15866310
Lee J-M Bassett D Jr Thompson D Fitzhugh E 2011 Validation of thecosmed fitmate for predicting maximal oxygen consumption J StrengthCond Res 252573ndash2579
Madimenos FC Snodgrass JJ Blackwell AD Liebert MA Sugiyama LS2011 Physical activity in an indigenous Ecuadorian forager-horticulturalist population as measured using accelerometry Am J HumBiol 23488ndash497 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid53110644amptool5pmcentrezamprendertype5abstract
Malina RM 2001 Physical activity and fitness pathways from childhoodto adulthood Am J Hum Biol 13162ndash172 Available at httpwwwncbinlmnihgovpubmed11460860
Malina RM Little BB 2008 Physical activity the present in the contextof the past Am J Hum Biol 20373ndash391 Available at httpwwwncbinlmnihgovpubmed18433002
Manning JT Morris L Caswell N 2007 Endurance running and digitratio (2D 4D) implications for fetal testosterone effects on runningspeed and vascular health Am J Hum Biol 19416ndash421
Martin Ma Lassek WD Gaulin SJC Evans RW Woo JG Geraghty SRDavidson BS Morrow AL Kaplan HS et al 2012 Fatty acid composi-tion in the mature milk of Bolivian forager-horticulturalists controlledcomparisons with a US sample Matern Child Nutr 8404ndash418 Availableat httpwwwncbinlmnihgovpubmed22624983
National Health and Nutrition Examination Survey 2004 CardiovascularFitness Procedures Manual
Nussey D Coulson T Festa-Bianchet M Gaillard J-M 2008 Measuringsenescence in wild animal populations towards a longitudinal approachFunction Ecol 22393ndash406
Ogawa T Spina RJ Martin WHI Kohrt WM Schechtman KB HolloszyJO Ehsani AA 1992 Effects of aging sex and physical training cardio-vascular responses to exercise Circulation 86494ndash503
Panter-Brick C Miller UG Eggerman M 1992 Hemoglobin levels andstep test performance of men and women in Nepal Am J Hum Biol 4481ndash491
Pontzer H Raichlen Da Wood BM Mabulla AZP Racette SB MarloweFW 2012 Hunter-gatherer energetics and human obesity PLoS ONE 7e40503 Available at httpcdxplosorg101371journalpone0040503
R Development Core Team 2011 R A language and environment for sta-tistical computing R Development Core Team
Rigby R Stasinopoulos D 2005 Generalize additive models for locationscale and shape (with discussion) Appl Stat 54507ndash554
Robergs RA Landwehr R 2002 The surprising history of theldquoHRmax5220-agerdquo equation J Exerc Physiol 51ndash10
Rode A Shephard RJ 1994 Physiological consequences of acculturation a20-year study of fitness in an Inuit community Eur J Appl Physiol 69516ndash524
Rowland TW Boyajian A 1995 Aerobic response to endurance training inchildren Pediatrics 96654ndash658
Sagiv M Ben-sira D Amir R 2007 What maintains energy supply atpeak aerobic exercise in trained and untrained older men Gerontology53357ndash361
Sanada K Kuchiki T Miyachi M Mcgrath K Higuchi M Ebashi H 2007Effects of age on ventilatory threshold and peak oxygen uptake normal-ised for regional skeletal muscle mass in Japanese men and womenaged 20 ndash 80 years Eur J Appl Physiol 99475ndash483
Schniter E 2009 Why Old Age Non-Material Contributions and Patternsof Aging Among Older Adult Tsimanersquo 607
Shahnawaz H 1978 Influence of limb length on a stepping exercise JAppl Physiol 44346ndash349
Shephard RJ 1970 Computer programs for solution of the Astrand nomo-gram and the calculation of body surface area J Sports Med 10206ndash210
Shephard RJ Allen C Benade AJS Davies CT Di Prampero PE HedmanR Merriman JE Myhre K Simmons R 1968 Standardization of sub-maximal exercise tests Bull World Health Organ 38765ndash775 Availableat httpwwwpubmedcentralnihgovarticlerenderfcgiartid52554690amptool5pmcentrezamprendertype5abstract
Shephard RJ Bailey Da Mirwald RL 1976 Development of the CanadianHome Fitness Test Can Med Assoc J 114675ndash679 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid51956906amptool5pmcentrezamprendertype5abstract
Shields M Tremblay MS Laviolette M Craig CL Janssen I Gorber SC2010 Fitness of Canadian adults results from the 2007ndash2009 canadianhealth measures survey Health Rep 2121ndash35 Available at httpwwwncbinlmnihgovpubmed20426224
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 13
American Journal of Human Biology
Siconolfi SF Garber CE Lasater TM Carleton RA 1985 A simple validstep test for estimating maximal oxygen uptake in epidemiologic stud-ies Am J Epidemiol 121382ndash390 Available at httpwwwncbinlm-nihgovpubmed4014128
Sinclair LM Hinton PS 2005 Prevalence of iron deficiency with and with-out anemia in recreationally active men and women J Am Diet Assoc105975ndash978 Available from httpwwwncbinlmnihgovpubmed15942552
Skinner JS Gaskill SE Rankinen T Leon AS Rao DC Wilmore JHBouchard C 2003 Heart rate versus VO2max age sex race initial fit-ness and training response-HERITAGE Med Sci Sports Exerc 351908ndash1913 Available at httpwwwncbinlmnihgovpubmed14600558
Sondik EJ Madans JH Gentlemand JF 2012 Summary health statisticsfor US adults National Health Interview Survey 2010 Vital Health Stat101ndash80 Available at httpwwwncbinlmnihgovpubmed20687424
Stones MJ Kozma A 1985 Physical performance Aging and Human Per-formance New York Wiley p 261ndash292
Tanaka H Monahan KD Seals DR 2001 Age-predicted maximal heartrate revisited J Am Coll Cardiol] 37153ndash156 Available at httpwwwncbinlmnihgovpubmed11153730
Vasunilashorn S Crimmins EM Kim JK Winking J Gurven M KaplanH Finch CE 2010 Blood lipids infection and inflammatory markers inthe Tsimane of Bolivia Am J Hum Biol 22731ndash740 Available at httpwwwncbinlmnihgovpubmed20721985
Vaupel JV Manton KG Stallard E 1979 The impact of heterogeneity inindividual frailty on the dynamics of mortality Demography 16439ndash454
Vaupel JW Yashin AI 1985 Heterogeneityrsquos ruses some surprising effectsof selection on population dynamics Am Stat 39176ndash185
Venables WN Ripley BD 2002 Modern Applied Statistics with S FourthNew York Springer
Wagner PD 1996 Determinants of maximal oxygen transport and utiliza-tion Annu Rev Physiol 5821ndash50 Available at httpwwwncbinlmnih-govpubmed8815793
Walker A Arent SM McKeever KH 2010 Maximal aerobic capacity(VO2max) in horses a retrospective study to identify the age-relateddecline Comparative Exerc Physiol 6177ndash181 Available at httpwwwjournalscambridgeorgabstract_S1755254010000073
Walker R Hill K 2003 Modeling growth and senescence in physical per-formance among the Ache of Eastern Paraguay Am J Hum Biol 208196ndash208
Weller IM Thomas SG Corey PN Cox MH 1993 Prediction of maximaloxygen uptake from a modified Canadian aerobic fitness test Can JAppl Physiol 18175ndash188 Available at httpwwwncbinlmnihgovpubmed8513290
Wilson TM Tanaka H 2000 Meta-analysis of the age-associated declinein maximal aerobic capacity in men relation to training status Am JPhysiol Heart Circ Physiol 278H829ndash834 Available at httpwwwncbinlmnihgovpubmed10710351
Wood SN 2006 Generalized Additive Models An Introduction with RBoca Raton Florida Chapman and HallCRC Press
World Health Organization 2001 Iron deficiency anaemia assessmentprevention and control a guide for programme managers Available athttpwhqlibdocwhointhq2001WHO_NHD_013pdf
Yoopat P Toicharoen P Boontong S Glinsukon T Vanwonterghem KLouhevaara V 2002 Cardiorespiratory capacity of Thai workers in dif-ferent age and job categories J Physiol Anthropol Appl Hum Sci 21121ndash128 Available at httpwwwncbinlmnihgovpubmed12056179
Zhu YI Haas JD 1997 Iron depletion without anemia and physical per-formance in young women Am J Clin Nutr 66334ndash341 Available athttpwwwncbinlmnihgovpubmed9250112
14 AC PISOR ET AL
American Journal of Human Biology

on median age (for a given age category) population andtheir interaction term For comparability Tsimane werebinned into the Canadian age categories and averageswere computed for these categories leading to estimateddeclines slightly different from those in Table 4 for thepurposes of this test we treat the Tsimane female declineas linear Because within-population variance in declineis not available these regressions should be treated asdescriptive comparisons rather than statistical tests ofdifferences between the two groups The rate of decline inVO2max is steeper for Canadian females (69 per decadefaster decline per decade) and males (42 faster declineper decade) compared with Tsimane females and males
The rate of cardiovascular fitness decline between theTsimane and Canadians is different but this differencedoes not extend to industrialized and subsistence popula-tions (see Table 4) Controlling for sex subsistence groupshave about one quarter of a percent lower declines perdecade Again because the variance in decline is not rep-resented in this regression results should be interpretedas comparative rather than as a statistical test As beforeTsimane O2 results were not included in the analysis toavoid nonindependence and the indigenous Siberianswere excluded because of discrepancy in ages sampled
DISCUSSION
Our comparisons demonstrate that across a wide varietyof societies cardiovascular fitness senesces with age Car-diovascular fitness is higher on average among members ofsubsistence societies than among industrialized societiesbut rates of fitness decline from peak are not slower Ourmore detailed comparison between the Tsimane a subsist-ence population and Canadians an industrialized popula-tion reveals differences in cardiovascular fitness levelsand rate of fitness decline Cardiovascular fitness levelswere higher among the Tsimane than among Canadiansand the rate of decline across the lifespan was significantlyslower among Tsimane women and men Potential Cana-
dian participants were excluded due to many health con-cerns including pregnancy and history of high bloodpressure whereas Tsimane were only excluded if they self-identified as unable to participate This suggests the Cana-dian sample is a relatively healthy subsample of Canadayet the Tsimane still outperform them in cardiovascular fit-ness It may be that the higher demand for cardiovascularfitness in late ages among the Tsimane outweighs anyeffects of poor health Another possibility is that greaterself-selection among Tsimane due to higher adult mortalityleaves more robust older adult survivors thereby reducingthe observed slope of fitness decline at the population level(Vaupel et al 1979) perhaps this is partially why fewerTsimane older adults opted out of the exercise test thanCanadian older adults were screened out (ages 60ndash69Canadian females 5 56 Tsimane females 5 15 Cana-dian males 5 57 Tsimane males 5 5)
Consistent with prior research on age-related changesin cardiovascular fitness the Tsimane do evidence a lin-ear decline in VO2max with age but not as steep a declineas typically seen in industrialized populations Based oncomparisons with the Canadians and with other industri-alized populations we believe the Tsimane data from thepresent study and the pilot O2 data combined indicatethat the Tsimane perform better on tests of cardiovascularfitness than the average individual from an industrializednation
To further explore the potential effects of health factorson cardiovascular fitness level and rate of decline weinvestigated predictors of individual differences in fitnesswithin the Tsimane population Overall we found thatmost health indicators among the Tsimane did not hinderVO2max levels or rates of decline Lower hemoglobin lev-els were associated with lower VO2max levels in womenbut not men consistent with the notion that compromisedblood oxygen transport curbs cardiovascular fitness(Buzina et al 1989 Panter-Brick et al 1992) In the USlow hemoglobin is more common in active women thanactive men (Sinclair and Hinton 2005) hemoglobin is
Fig 2 Linear changes in VO2max with age for Canadians and the Tsimane Intercepts and slopes for Canadians and Tsimane can be foundin Table 4 Because age2 is significant for the full sample of Tsimane females their change in VO2max across age is curvilinear Slopes forendurance trained active and sedentary individuals from industrialized nations are drawn from a meta-analysis performed by Fitzgeraldet al (1997) for females and Wilson and Tanaka (2000) for males Endurance trained individuals are represented by the top dotted line abovefollowed by active individuals below and sedentary on the bottom Trained individuals engage in 31 sessions of endurance exercise per weekfor at least a year while active individuals engage in 2 or fewer sessions per week of cardiovascular exercise [Color figure can be viewed in theonline issue which is available at wileyonlinelibrarycom]
10 AC PISOR ET AL
American Journal of Human Biology
also lower in Tsimane women than Tsimane men(female 5 129 [sd 13] g ml21 males 5 142 [13] g ml21)Even mild (non-anemic) iron deficiencies impacts womenrsquosexercise performance (Zhu and Haas 1997) Inconsistentwith findings from Panter-Brick et al (1992) among ruralNepalese helminth infection did not diminish levels ofVO2max for Tsimane men helminth infection wasactually a predictor of higher VO2max There are severalreasons why this might be the case First we only testedwhether presence or absence of helminths mediated theeffect of age on VO2max rather than parasite load (egnumber of worms egg counts) it is possible that helminthinfection only affects VO2max at high parasite loads Sec-ond blood loss (and thus low hemoglobin levels) resultingfrom helminth infection may be partially offset by theamount of iron in the Tsimane adult diet Tsimane ironintake is an estimated 166 of the US Dietary ReferenceIntake (Martin et al 2012) and Tsimane hemoglobin lev-els are higher than in the Nepalese (females 129 vs 109males 1424 vs 120 Panter-Brick et al 1992) Thirdthese analyses consider helminth infection at the time ofexercise test rather than past infections It may be thatthe cumulative burden of past infection has a larger effecton cardiovascular fitness if so this would suggest thatthe surprising positive effect of helminth infection onVO2max levels in men is either spurious or capturing athird variable
Secular declines in VO2max are expected with increasingmarket integration and lifestyle change because ofincreased sedentism (Katzmarzyk et al 1994 Rode andShephard 1994) Two proxies for market integration in thispopulationmdashdistance to San Borja and the ability to speakSpanishmdashwere not significant predictors of VO2max levelsor decline This is consistent with our predictions as Tsi-mane females and males that live near town do not appearto have lower activity levels (Gurven et al 2013) Wageopportunities near town primarily include working asranch hands collecting and weaving palm thatch panelscash cropping and working for logging companies Each ofthese involves extensive activity furthermore transporta-tion to town often involves bicycling walking and polingdugout canoes Cash cropping of rice and corn also involvesthe clearing and weeding of larger fields Except for cashcropping and palm thatch manufacture most wage laboropportunities are currently restricted to men
This study makes several unique contributions to theexisting literature It offers the first systematic compari-son of cardiovascular fitness level and rate of declinebetween subsistence and industrialized societies Resultscompiled from previous studies support the general claimthat despite greater pathogen stress the greater activityregime of subsistence societies helps support higher peakVO2max Additionally this is one of the first studies toexplore senescent changes in cardiovascular fitnesswithin a large sample from a subsistence population Thelarge number of health measures and proxies of marketintegration available permitted testing whether these fac-tors mediated age-related variation and whether theymodulated the rate of decline Despite reports that healthstatus and market integration have been important inother studies (eg Buzina et al 1989 Katzmarzyk et al1994 Panter-Brick et al 1992 Rode and Shephard1994) their overall net effect was small among the Tsi-mane most apparent in measures of hemoglobin levelsamong women and helminth infection among men
The results of these analyses may also shed light onindividual and population level differences in chronic dis-ease In industrialized populations meta-analyses demon-strate that cardiovascular fitness is protective againstcardiovascular disease (Jette et al 1992 Hawkins andWiswell 2003) Prior studies among Tsimane suggest rel-atively few deaths from heart attacks or strokes (Gurvenet al 2007) a low prevalence of common cardiovasculardisease risk factors like obesity high blood low-densitylipoprotein levels hypertension and peripheral arterialdisease and the existence of additional protective factorslike lean diet and physical activity (Gurven et al 20092013 Vasunilashorn et al 2010) Market foods such ascooking oil sugar and pasta represent only 6 of theaverage Tsimane diet and Tsimane also consume a greatdeal of lean meat and omega-3 fatty acids (Martin et al2012) This study complements these findings by demon-strating that Tsimane show relatively high VO2max anindicator of strong cardiorespiratory health TsimaneVO2max declines with age as it does everywhere whichsuggests declining muscle mass with age (Fleg andLakatta 1988) and lowered cardiac output (American Col-lege of Sports Medicine 2006 Sagiv et al 2007) ratherthan increased cardiovascular disease risk
Limitations
The Canadians were selected as a comparison industri-alized population because of the similarity of the CHMSand Tsimane protocols very few studies of industrializedpopulations have large sample sizes sample across thelife course and use a step test Several aspects of theCHMS and Tsimane protocols remain potentially incom-parable The Canadians experienced more stringentexclusion criteria than the Tsimane meaning that the Tsi-mane sample may be more representative of cardiovascu-lar condition in the Tsimane population than theCanadian sample of the Canadian population Again ifthe Tsimane sample was subjected to these criteria wemight expect the differences in VO2max between popula-tions to only increase On the other hand Canadian par-ticipants were assigned stepping cadences based on theirage and sex and cadence was increased across the exer-cise test if a participant did not reach 85 of his or herage-specific maximal HR all Tsimane were asked to com-plete 30 ascents per minute with no increase based ontheir achieved HRs Few Tsimane reached 75 of theirage-specific maximal HR (see Supporting InformationTable S1) perhaps because the age-specific maximal HRsderived from industrialized populations are inaccurate forthe Tsimane or because higher fitness allowed these Tsi-mane to perform the step test of 30 ascents per minutewith less effort Due to these discrepancies in protocolwhich may lead to errors in estimating VO2max we alsoincorporated Tsimane data collected using the O2 methodas a check because the O2 method estimates VO2max onthe relationship between HR and VO2 in a givenparticipant
Indeed it is an open question as to whether typicalmethods for indirectly estimating cardiovascular fitnessfrom HR are appropriate for subsistence level popula-tions Common routines for VO2max estimation assumeage-specific declines in cardiovascular fitness (eg Shep-hard 1970) but these methods have only been validatedwith samples from industrialized populations which are
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 11
American Journal of Human Biology
often self-selected (Beall et al 1985) Additionally regres-sions drawn from laboratory studies require participantsachieve a HR within a certain range for accurate VO2maxestimation however the appropriateness of these rangesgiven slight modifications to protocol and inclusion of par-ticipants of different ages different populations and bothsexes is questionable For example the maximal HRexhibited by young men varies across subsistence popula-tions (Shephard 1978) Use of these criteria is compli-cated by the fact that the most commonly used equationfor estimating maximal possible HR by age 220-age maybe inaccurate (Robergs and Landwehr 2002) and particu-larly inappropriate for older adults (see Tanaka et al2001) For these reasons we chose to use an exclusion cri-terion for the Tsimane that evaluates individual increasein HR across exercise relative to the mean increase in HRfor Tsimane of the same sex and age
The pattern of Tsimane fitness decline differs moder-ately by the choice of exclusion criterion for participants(see Supporting Information Table S1) and by method oftesting However this is a common finding Lee et al(2011) predicted VO2max from submaximal exercise usingthe O2 method and the HR-based American College ofSports Medicine calculation routine in a US sample Theyfound that (1) the HR-based routine predicts higherVO2max across the sexes than does the O2 routine and(2) the two methods have a correlation of only 077 Whenevaluating different testing procedures Shephard et al(1968) found differences in VO2max estimation by type oftest used (eg bicycle ergometer versus step test) and cal-culation routine Exercise tests exclusion criteria andcalculation routines combine to provide an estimate ofactual VO2max for a given individual and as such varia-tion in estimation is to be expected However such varia-tion may affect cross-population comparisons inunforeseen ways thus the comparisons presented hereshould be interpreted with caution
While population-level variation in cardiovascular fit-ness decline may reflect the differences in the demands ofendurance-based physical activity muscularity and com-promised oxygen transport it is possible that genetic fac-tors may also play a potential role (Collins 1999) In oneindustrialized sample maternal cardiovascular fitnessexhibited a heritability of 30 which is attributed toinheritance of the maternal mitochondrial genome (Bou-chard et al 2000) We do not have the relevant geneticdata for the populations considered here however andthus operate under the simplifying assumption thatinheritance should not affect population-level patternsand will not consistently bias individual-level compari-sons in any particular direction
This study is further limited by its cross-sectionaldesign Cross-sectional data present well-known problemsfor the measurement of individual aging (Crimmins andSeeman 2001) Mortality selection in which individualsin poorer condition are likely to die at younger ages pro-duces a downward bias in the estimation of aging rates atthe individual level (Vaupel and Yashin 1985 Vaupelet al 1979) Cohort effects if present also produce com-plicated and non-monotonic biases in estimation (Carnesand Olshansky 2001) Due to the problem of between-individual heterogeneity and the within-individual pro-cess of senescence a recent overview of aging studies con-cludes that ldquoonly longitudinal studies [ ] provide reliablesources of information in the study of senescencerdquo (Nussey
et al 2008) To date there are no longitudinal studies ofcardiovascular fitness in subsistence populations We arecurrently re-testing participants under the O2 methodallowing a better grasp of the within-individual variationthat shapes patterns of senescent decline
ACKNOWLEDGMENTS
The authors thank Paul Hooper Steven Gaulin JohnTooby Patricia Kramer the Human Evolution and Biode-mography laboratory and the Center for EvolutionaryPsychology at UCSB for helpful advice and feedback thestaff at the Tsimane Health and Life History Project andthe Tsimane for their participation and patience
LITERATURE CITED
American College of Sports Medicine 2006 ACSMrsquos Guidelines for Exer-cise Testing and Prescription 7th ed Philadelphia Lippincott Williamsamp Wilkins
Armstrong N 2001 Peak oxygen uptake in relation to growth and matura-tion in 11- to 17-year-old humans Eur J Appl Physiol 85546ndash551
Astrand PO Ryhming I 1954 A nomogram for calculation of aerobiccapacity (physical fitness) from pulse rate during submaximal work JAppl Physiol 7218ndash221
Bailey DA Shephard RJ Mirwald RL 1976 Validation of a self-administered home test of cardio-respiratory fitness Can J Appl SportSci 167ndash78
Beall CM Goldstein MC and Feldman ES 1985 The physical fitness ofelderly Nepalese farmers residing in rugged mountain and flat terrainJ Gerontol 40529ndash535
Benefice E Ndiaye G 2005 Relationships between anthropometry cardi-orespiratory fitness indices and physical activity levels in different ageand sex groups in rural Senegal (West Africa) Ann Hum Biol 32366ndash382 Available from httpwwwncbinlmnihgovpubmed16099780
Blackwell AD Gurven MD Sugiyama LS Madimenos FC Liebert MAMartin MA Kaplan HS Snodgrass JJ 2011 Evidence for a peak shift in ahumoral response to helminths age profiles of IgE in the Shuar of Ecuadorthe Tsimane of Bolivia and the US NHANES PLoS Negl Trop Dis 5e1218 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid53125146amptool5pmcentrezamprendertype5abstract
Blackwell AD Martin M Kaplan H Gurven M Evidence for an antagonis-tic relationship between Giardia lamblia and helminth infections impli-cations for treatment of helminth infections in developing populations
Blair SN LaMonte MJ Nichaman MZ 2004 The evolution of physicalactivity recommendations how much is enough Am J Clin Nutr 79913Sndash920S Available at httpwwwncbinlmnihgovpubmed15113739
Bouchard C Rankinen T Chagnon YC Rice T Perusse L Gagnon JBorecki I An P Leon a S et al 2000 Genomic scan for maximal oxygenuptake and its response to training in the HERITAGE Family Study JAppl Physiol 88551ndash559 Available at httpwwwncbinlmnihgovpubmed10658022
Bryan S St-Denis M Wojtas D 2007 Canadian Health Measures Surveyclinic operations and logistics Health Rep 1853ndash69
Buzina R Bates CJ van der Beek J Brubacher G Chandra RK HallbergL Heseker J Mertz W Pietrzik K et al 1989 Workshop on FunctionalSignificance of Mild-to-Moderate Malnutrition Am J Clin Nutrition 50172ndash176
Calder WA 1987 Scaling energetics of homeothermic vertebrates anoperational allometry Annu Rev Physiol 49107ndash120
Canadian Society for Exercise Physiology 2003 The Canadian PhysicalActivity Fitness amp Lifestyle Approach (CPAFLA) CSEP-Health amp Fit-ness Programrsquos Health-Related Appraisal and Counselling Strategy 3rded
Carnes BA Olshansky SJ 2001 Heterogeneity and its biodemographicimplications for longevity and mortality Exp Gerontol 36419ndash430Available at httpwwwncbinlmnihgovpubmed11250115
Carrick-Ranson G Hastings JL Bhella PS Shibata S Fujimoto N PalmerD Boyd K Levine BD 2013 The effect of age-related differences inbody size and composition on cardiovascular determinants of VO2max JGerontol A Biol Sci Med Sci 68608ndash616 Available at httpwwwncbinlmnihgovpubmed23160363
Centers for Disease Control and Prevention 1998 Recommendations toPrevent and Control Iron Deficiency in the United States MMWRRecomm Rep 471ndash36 Available at httpwwwcdcgovmmwrpreviewmmwrhtml00051880htm
12 AC PISOR ET AL
American Journal of Human Biology
Centers for Disease Control and Prevention 2011 Glossary of TermsPhysical Activity for Everyone [Internet] Available from httpwwwcdcgovphysicalactivityeveryoneglossary
Christensen DL Faurholt-Jepsen D Boit MK Mwaniki DL Kilonzo BTetens I Kiplamai FK Cheruiyot SC Friis H et al 2012 Cardiorespira-tory fitness and physical activity in Luo Kamba and Maasai of ruralKenya Am J Hum Biol 24723ndash729 Available at httpwwwncbinlm-nihgovpubmed22836508
Colley RC Garriguet D Janssen I Craig CL Clarke J Tremblay MS2011a Physical activity of Canadian children and youth accelerometerresults from the 2007 to 2009 Canadian Health Measures SurveyHealth Rep 2215ndash23
Colley RC Garriguet D Janssen I Craig CL Clarke J Tremblay MS2011b Physical activity of Canadian adults accelerometer results fromthe 2007 to 2009 Canadian Health Measures Survey Health Rep 227ndash14 Available at httpwwwncbinlmnihgovpubmed21510585
Collins KJ 1999 Physiological variation and adaptability in human popu-lations Ann Hum Biol 2619ndash38
Crimmins E Seeman T 2001 Integrating Biology into DemographicResearch on Health and Aging (With a Focus on the MacArthur Study ofSuccessful Aging) Cells and Surveys Should Biological Measures beIncluded in Social Science Research Washington DC National Acad-emy Press p 9ndash41
Curran-Everett LS 1994 Accordance Between VO2max and Behavior inNgisonyoka Turkana Am J Hum Biol 6761ndash771
Durnin JVGA Womersley J 1974 Body fat assessed from total body den-sity and its estimation from skinfold thickness measurements on 481men and women aged from 16 to 72 years Br J Nutr 3277ndash97
Eberl M Al-Sherbiny M Hagan P Ljubojevic S Thomas AW Wilson RA2002 A novel and sensitive method to monitor helminth infections byfaecal sampling Acta Trop 83183ndash187
Eid D Gurven M Kaplan H Winking J 2007 Enfermedades infecciosas alo largo de la vida y en el envejecimiento en indıgenas sudamericanos dela etnia Tsimane Aging in Developing Countries Building Bridges forIntegrated Research Agendas Santiago Chile
Ekblom B Engstreuroom L-M Ekblom O 2007 Secular trends of physical fit-ness in Swedish adults Scand J Med Sci Sports 17267ndash273 Availableat httpwwwncbinlmnihgovpubmed17501867
Finch CA Lenfant C 1972 Oxygen Transport in Man N Engl J Med 286407ndash415
Fitzgerald MD Tanaka H Tran ZV Seals DR 1997 Age-related declinesin maximal aerobic capacity in regularly exercising vs sedentarywomen a meta-analysis J Appl Physiol (Bethesda Md 1985) 83160ndash165 Available at httpwwwncbinlmnihgovpubmed9216959
Fleg JL Lakatta EG 1988 Role of muscle loss in the age-associated reduc-tion in VO2max J Appl Physiol 651147ndash1151
Frisancho AR Frisancho HG Milotich M Brutsaert T Albalak RSpielvogel H Villena M Vargas E Soria R 1995 Developmentalgenetic and environmental components of aerobic capacity at high alti-tude Am J Phys Anthropol 96431ndash442 Available at httpwwwncbinlmnihgovpubmed7604895
Giroux S 2007 Canadian health measures survey sampling strategyoverview Health Rep 1831ndash36
Gurven M Jaeggi A V Kaplan H Cummings D 2013 Physical activityand modernization among Bolivian Amerindians PLoS ONE 81ndash13
Gurven M Kaplan H Winking J Rodriguez DE Vasunilashorn S KimJK Finch C Crimmins E 2009 Inflammation and infection do not pro-mote arterial aging and cardiovascular disease risk factors among leanhorticulturalists PLoS ONE 41ndash12
Haidet GC 1989 Dynamic exercise in senescent beagles oxygen consump-tion and hemodynamic responses The Am J Physiol 257H1428ndash1437Available at httpwwwncbinlmnihgovpubmed2589499
Hawkins S Wiswell R 2003 Rate and mechanism of maximal oxygen con-sumption decline with aging implications for exercise training SportsMed 33877ndash888 Available at httpwwwncbinlmnihgovpubmed12974656
Hoffman J 2002 Physiological aspects of sport training and performance1st ed Champaign IL Human Kinetics Publishers
Hotez PJ Bottazzi ME Franco-Paredes C Ault SK Periago MR 2008 Theneglected tropical diseases of Latin America and the Caribbean a review ofdisease burden and distribution and a roadmap for control and eliminationPLoS Negl Trop Dis 2e300 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid52553488amptool5pmcentrezamprendertype5abstract
Howley ET Bassett DR Welch HG 1995 Criteria for maximal oxygenuptake review and commentary Med Sci Sports Exerc 271292ndash1301Available at httpwwwncbinlmnihgovpubmed8531628
Jette M Sidney K Quenneville J Landry F 1992 Relation between cardi-orespiratory fitness and selected risk factors for coronary heart diseasein a population of Canadian men and women CMAJ 1461353ndash1360Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid51488567amptool5pmcentrezamprendertype5abstract
Katzmarzyk PT Leonard WR Crawford MH 1994 Predicted maximaloxygen consumption of Indigenous Siberians Am J Hum Biol 6783ndash790
King CH Dickman K Tisch DJ 2005 Reassessment of the cost of chronichelmintic infection a meta-analysis of disability-related outcomes inendemic schistosomiasis Lancet 3651561ndash1569 Available at httpwwwncbinlmnihgovpubmed15866310
Lee J-M Bassett D Jr Thompson D Fitzhugh E 2011 Validation of thecosmed fitmate for predicting maximal oxygen consumption J StrengthCond Res 252573ndash2579
Madimenos FC Snodgrass JJ Blackwell AD Liebert MA Sugiyama LS2011 Physical activity in an indigenous Ecuadorian forager-horticulturalist population as measured using accelerometry Am J HumBiol 23488ndash497 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid53110644amptool5pmcentrezamprendertype5abstract
Malina RM 2001 Physical activity and fitness pathways from childhoodto adulthood Am J Hum Biol 13162ndash172 Available at httpwwwncbinlmnihgovpubmed11460860
Malina RM Little BB 2008 Physical activity the present in the contextof the past Am J Hum Biol 20373ndash391 Available at httpwwwncbinlmnihgovpubmed18433002
Manning JT Morris L Caswell N 2007 Endurance running and digitratio (2D 4D) implications for fetal testosterone effects on runningspeed and vascular health Am J Hum Biol 19416ndash421
Martin Ma Lassek WD Gaulin SJC Evans RW Woo JG Geraghty SRDavidson BS Morrow AL Kaplan HS et al 2012 Fatty acid composi-tion in the mature milk of Bolivian forager-horticulturalists controlledcomparisons with a US sample Matern Child Nutr 8404ndash418 Availableat httpwwwncbinlmnihgovpubmed22624983
National Health and Nutrition Examination Survey 2004 CardiovascularFitness Procedures Manual
Nussey D Coulson T Festa-Bianchet M Gaillard J-M 2008 Measuringsenescence in wild animal populations towards a longitudinal approachFunction Ecol 22393ndash406
Ogawa T Spina RJ Martin WHI Kohrt WM Schechtman KB HolloszyJO Ehsani AA 1992 Effects of aging sex and physical training cardio-vascular responses to exercise Circulation 86494ndash503
Panter-Brick C Miller UG Eggerman M 1992 Hemoglobin levels andstep test performance of men and women in Nepal Am J Hum Biol 4481ndash491
Pontzer H Raichlen Da Wood BM Mabulla AZP Racette SB MarloweFW 2012 Hunter-gatherer energetics and human obesity PLoS ONE 7e40503 Available at httpcdxplosorg101371journalpone0040503
R Development Core Team 2011 R A language and environment for sta-tistical computing R Development Core Team
Rigby R Stasinopoulos D 2005 Generalize additive models for locationscale and shape (with discussion) Appl Stat 54507ndash554
Robergs RA Landwehr R 2002 The surprising history of theldquoHRmax5220-agerdquo equation J Exerc Physiol 51ndash10
Rode A Shephard RJ 1994 Physiological consequences of acculturation a20-year study of fitness in an Inuit community Eur J Appl Physiol 69516ndash524
Rowland TW Boyajian A 1995 Aerobic response to endurance training inchildren Pediatrics 96654ndash658
Sagiv M Ben-sira D Amir R 2007 What maintains energy supply atpeak aerobic exercise in trained and untrained older men Gerontology53357ndash361
Sanada K Kuchiki T Miyachi M Mcgrath K Higuchi M Ebashi H 2007Effects of age on ventilatory threshold and peak oxygen uptake normal-ised for regional skeletal muscle mass in Japanese men and womenaged 20 ndash 80 years Eur J Appl Physiol 99475ndash483
Schniter E 2009 Why Old Age Non-Material Contributions and Patternsof Aging Among Older Adult Tsimanersquo 607
Shahnawaz H 1978 Influence of limb length on a stepping exercise JAppl Physiol 44346ndash349
Shephard RJ 1970 Computer programs for solution of the Astrand nomo-gram and the calculation of body surface area J Sports Med 10206ndash210
Shephard RJ Allen C Benade AJS Davies CT Di Prampero PE HedmanR Merriman JE Myhre K Simmons R 1968 Standardization of sub-maximal exercise tests Bull World Health Organ 38765ndash775 Availableat httpwwwpubmedcentralnihgovarticlerenderfcgiartid52554690amptool5pmcentrezamprendertype5abstract
Shephard RJ Bailey Da Mirwald RL 1976 Development of the CanadianHome Fitness Test Can Med Assoc J 114675ndash679 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid51956906amptool5pmcentrezamprendertype5abstract
Shields M Tremblay MS Laviolette M Craig CL Janssen I Gorber SC2010 Fitness of Canadian adults results from the 2007ndash2009 canadianhealth measures survey Health Rep 2121ndash35 Available at httpwwwncbinlmnihgovpubmed20426224
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 13
American Journal of Human Biology
Siconolfi SF Garber CE Lasater TM Carleton RA 1985 A simple validstep test for estimating maximal oxygen uptake in epidemiologic stud-ies Am J Epidemiol 121382ndash390 Available at httpwwwncbinlm-nihgovpubmed4014128
Sinclair LM Hinton PS 2005 Prevalence of iron deficiency with and with-out anemia in recreationally active men and women J Am Diet Assoc105975ndash978 Available from httpwwwncbinlmnihgovpubmed15942552
Skinner JS Gaskill SE Rankinen T Leon AS Rao DC Wilmore JHBouchard C 2003 Heart rate versus VO2max age sex race initial fit-ness and training response-HERITAGE Med Sci Sports Exerc 351908ndash1913 Available at httpwwwncbinlmnihgovpubmed14600558
Sondik EJ Madans JH Gentlemand JF 2012 Summary health statisticsfor US adults National Health Interview Survey 2010 Vital Health Stat101ndash80 Available at httpwwwncbinlmnihgovpubmed20687424
Stones MJ Kozma A 1985 Physical performance Aging and Human Per-formance New York Wiley p 261ndash292
Tanaka H Monahan KD Seals DR 2001 Age-predicted maximal heartrate revisited J Am Coll Cardiol] 37153ndash156 Available at httpwwwncbinlmnihgovpubmed11153730
Vasunilashorn S Crimmins EM Kim JK Winking J Gurven M KaplanH Finch CE 2010 Blood lipids infection and inflammatory markers inthe Tsimane of Bolivia Am J Hum Biol 22731ndash740 Available at httpwwwncbinlmnihgovpubmed20721985
Vaupel JV Manton KG Stallard E 1979 The impact of heterogeneity inindividual frailty on the dynamics of mortality Demography 16439ndash454
Vaupel JW Yashin AI 1985 Heterogeneityrsquos ruses some surprising effectsof selection on population dynamics Am Stat 39176ndash185
Venables WN Ripley BD 2002 Modern Applied Statistics with S FourthNew York Springer
Wagner PD 1996 Determinants of maximal oxygen transport and utiliza-tion Annu Rev Physiol 5821ndash50 Available at httpwwwncbinlmnih-govpubmed8815793
Walker A Arent SM McKeever KH 2010 Maximal aerobic capacity(VO2max) in horses a retrospective study to identify the age-relateddecline Comparative Exerc Physiol 6177ndash181 Available at httpwwwjournalscambridgeorgabstract_S1755254010000073
Walker R Hill K 2003 Modeling growth and senescence in physical per-formance among the Ache of Eastern Paraguay Am J Hum Biol 208196ndash208
Weller IM Thomas SG Corey PN Cox MH 1993 Prediction of maximaloxygen uptake from a modified Canadian aerobic fitness test Can JAppl Physiol 18175ndash188 Available at httpwwwncbinlmnihgovpubmed8513290
Wilson TM Tanaka H 2000 Meta-analysis of the age-associated declinein maximal aerobic capacity in men relation to training status Am JPhysiol Heart Circ Physiol 278H829ndash834 Available at httpwwwncbinlmnihgovpubmed10710351
Wood SN 2006 Generalized Additive Models An Introduction with RBoca Raton Florida Chapman and HallCRC Press
World Health Organization 2001 Iron deficiency anaemia assessmentprevention and control a guide for programme managers Available athttpwhqlibdocwhointhq2001WHO_NHD_013pdf
Yoopat P Toicharoen P Boontong S Glinsukon T Vanwonterghem KLouhevaara V 2002 Cardiorespiratory capacity of Thai workers in dif-ferent age and job categories J Physiol Anthropol Appl Hum Sci 21121ndash128 Available at httpwwwncbinlmnihgovpubmed12056179
Zhu YI Haas JD 1997 Iron depletion without anemia and physical per-formance in young women Am J Clin Nutr 66334ndash341 Available athttpwwwncbinlmnihgovpubmed9250112
14 AC PISOR ET AL
American Journal of Human Biology

also lower in Tsimane women than Tsimane men(female 5 129 [sd 13] g ml21 males 5 142 [13] g ml21)Even mild (non-anemic) iron deficiencies impacts womenrsquosexercise performance (Zhu and Haas 1997) Inconsistentwith findings from Panter-Brick et al (1992) among ruralNepalese helminth infection did not diminish levels ofVO2max for Tsimane men helminth infection wasactually a predictor of higher VO2max There are severalreasons why this might be the case First we only testedwhether presence or absence of helminths mediated theeffect of age on VO2max rather than parasite load (egnumber of worms egg counts) it is possible that helminthinfection only affects VO2max at high parasite loads Sec-ond blood loss (and thus low hemoglobin levels) resultingfrom helminth infection may be partially offset by theamount of iron in the Tsimane adult diet Tsimane ironintake is an estimated 166 of the US Dietary ReferenceIntake (Martin et al 2012) and Tsimane hemoglobin lev-els are higher than in the Nepalese (females 129 vs 109males 1424 vs 120 Panter-Brick et al 1992) Thirdthese analyses consider helminth infection at the time ofexercise test rather than past infections It may be thatthe cumulative burden of past infection has a larger effecton cardiovascular fitness if so this would suggest thatthe surprising positive effect of helminth infection onVO2max levels in men is either spurious or capturing athird variable
Secular declines in VO2max are expected with increasingmarket integration and lifestyle change because ofincreased sedentism (Katzmarzyk et al 1994 Rode andShephard 1994) Two proxies for market integration in thispopulationmdashdistance to San Borja and the ability to speakSpanishmdashwere not significant predictors of VO2max levelsor decline This is consistent with our predictions as Tsi-mane females and males that live near town do not appearto have lower activity levels (Gurven et al 2013) Wageopportunities near town primarily include working asranch hands collecting and weaving palm thatch panelscash cropping and working for logging companies Each ofthese involves extensive activity furthermore transporta-tion to town often involves bicycling walking and polingdugout canoes Cash cropping of rice and corn also involvesthe clearing and weeding of larger fields Except for cashcropping and palm thatch manufacture most wage laboropportunities are currently restricted to men
This study makes several unique contributions to theexisting literature It offers the first systematic compari-son of cardiovascular fitness level and rate of declinebetween subsistence and industrialized societies Resultscompiled from previous studies support the general claimthat despite greater pathogen stress the greater activityregime of subsistence societies helps support higher peakVO2max Additionally this is one of the first studies toexplore senescent changes in cardiovascular fitnesswithin a large sample from a subsistence population Thelarge number of health measures and proxies of marketintegration available permitted testing whether these fac-tors mediated age-related variation and whether theymodulated the rate of decline Despite reports that healthstatus and market integration have been important inother studies (eg Buzina et al 1989 Katzmarzyk et al1994 Panter-Brick et al 1992 Rode and Shephard1994) their overall net effect was small among the Tsi-mane most apparent in measures of hemoglobin levelsamong women and helminth infection among men
The results of these analyses may also shed light onindividual and population level differences in chronic dis-ease In industrialized populations meta-analyses demon-strate that cardiovascular fitness is protective againstcardiovascular disease (Jette et al 1992 Hawkins andWiswell 2003) Prior studies among Tsimane suggest rel-atively few deaths from heart attacks or strokes (Gurvenet al 2007) a low prevalence of common cardiovasculardisease risk factors like obesity high blood low-densitylipoprotein levels hypertension and peripheral arterialdisease and the existence of additional protective factorslike lean diet and physical activity (Gurven et al 20092013 Vasunilashorn et al 2010) Market foods such ascooking oil sugar and pasta represent only 6 of theaverage Tsimane diet and Tsimane also consume a greatdeal of lean meat and omega-3 fatty acids (Martin et al2012) This study complements these findings by demon-strating that Tsimane show relatively high VO2max anindicator of strong cardiorespiratory health TsimaneVO2max declines with age as it does everywhere whichsuggests declining muscle mass with age (Fleg andLakatta 1988) and lowered cardiac output (American Col-lege of Sports Medicine 2006 Sagiv et al 2007) ratherthan increased cardiovascular disease risk
Limitations
The Canadians were selected as a comparison industri-alized population because of the similarity of the CHMSand Tsimane protocols very few studies of industrializedpopulations have large sample sizes sample across thelife course and use a step test Several aspects of theCHMS and Tsimane protocols remain potentially incom-parable The Canadians experienced more stringentexclusion criteria than the Tsimane meaning that the Tsi-mane sample may be more representative of cardiovascu-lar condition in the Tsimane population than theCanadian sample of the Canadian population Again ifthe Tsimane sample was subjected to these criteria wemight expect the differences in VO2max between popula-tions to only increase On the other hand Canadian par-ticipants were assigned stepping cadences based on theirage and sex and cadence was increased across the exer-cise test if a participant did not reach 85 of his or herage-specific maximal HR all Tsimane were asked to com-plete 30 ascents per minute with no increase based ontheir achieved HRs Few Tsimane reached 75 of theirage-specific maximal HR (see Supporting InformationTable S1) perhaps because the age-specific maximal HRsderived from industrialized populations are inaccurate forthe Tsimane or because higher fitness allowed these Tsi-mane to perform the step test of 30 ascents per minutewith less effort Due to these discrepancies in protocolwhich may lead to errors in estimating VO2max we alsoincorporated Tsimane data collected using the O2 methodas a check because the O2 method estimates VO2max onthe relationship between HR and VO2 in a givenparticipant
Indeed it is an open question as to whether typicalmethods for indirectly estimating cardiovascular fitnessfrom HR are appropriate for subsistence level popula-tions Common routines for VO2max estimation assumeage-specific declines in cardiovascular fitness (eg Shep-hard 1970) but these methods have only been validatedwith samples from industrialized populations which are
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 11
American Journal of Human Biology
often self-selected (Beall et al 1985) Additionally regres-sions drawn from laboratory studies require participantsachieve a HR within a certain range for accurate VO2maxestimation however the appropriateness of these rangesgiven slight modifications to protocol and inclusion of par-ticipants of different ages different populations and bothsexes is questionable For example the maximal HRexhibited by young men varies across subsistence popula-tions (Shephard 1978) Use of these criteria is compli-cated by the fact that the most commonly used equationfor estimating maximal possible HR by age 220-age maybe inaccurate (Robergs and Landwehr 2002) and particu-larly inappropriate for older adults (see Tanaka et al2001) For these reasons we chose to use an exclusion cri-terion for the Tsimane that evaluates individual increasein HR across exercise relative to the mean increase in HRfor Tsimane of the same sex and age
The pattern of Tsimane fitness decline differs moder-ately by the choice of exclusion criterion for participants(see Supporting Information Table S1) and by method oftesting However this is a common finding Lee et al(2011) predicted VO2max from submaximal exercise usingthe O2 method and the HR-based American College ofSports Medicine calculation routine in a US sample Theyfound that (1) the HR-based routine predicts higherVO2max across the sexes than does the O2 routine and(2) the two methods have a correlation of only 077 Whenevaluating different testing procedures Shephard et al(1968) found differences in VO2max estimation by type oftest used (eg bicycle ergometer versus step test) and cal-culation routine Exercise tests exclusion criteria andcalculation routines combine to provide an estimate ofactual VO2max for a given individual and as such varia-tion in estimation is to be expected However such varia-tion may affect cross-population comparisons inunforeseen ways thus the comparisons presented hereshould be interpreted with caution
While population-level variation in cardiovascular fit-ness decline may reflect the differences in the demands ofendurance-based physical activity muscularity and com-promised oxygen transport it is possible that genetic fac-tors may also play a potential role (Collins 1999) In oneindustrialized sample maternal cardiovascular fitnessexhibited a heritability of 30 which is attributed toinheritance of the maternal mitochondrial genome (Bou-chard et al 2000) We do not have the relevant geneticdata for the populations considered here however andthus operate under the simplifying assumption thatinheritance should not affect population-level patternsand will not consistently bias individual-level compari-sons in any particular direction
This study is further limited by its cross-sectionaldesign Cross-sectional data present well-known problemsfor the measurement of individual aging (Crimmins andSeeman 2001) Mortality selection in which individualsin poorer condition are likely to die at younger ages pro-duces a downward bias in the estimation of aging rates atthe individual level (Vaupel and Yashin 1985 Vaupelet al 1979) Cohort effects if present also produce com-plicated and non-monotonic biases in estimation (Carnesand Olshansky 2001) Due to the problem of between-individual heterogeneity and the within-individual pro-cess of senescence a recent overview of aging studies con-cludes that ldquoonly longitudinal studies [ ] provide reliablesources of information in the study of senescencerdquo (Nussey
et al 2008) To date there are no longitudinal studies ofcardiovascular fitness in subsistence populations We arecurrently re-testing participants under the O2 methodallowing a better grasp of the within-individual variationthat shapes patterns of senescent decline
ACKNOWLEDGMENTS
The authors thank Paul Hooper Steven Gaulin JohnTooby Patricia Kramer the Human Evolution and Biode-mography laboratory and the Center for EvolutionaryPsychology at UCSB for helpful advice and feedback thestaff at the Tsimane Health and Life History Project andthe Tsimane for their participation and patience
LITERATURE CITED
American College of Sports Medicine 2006 ACSMrsquos Guidelines for Exer-cise Testing and Prescription 7th ed Philadelphia Lippincott Williamsamp Wilkins
Armstrong N 2001 Peak oxygen uptake in relation to growth and matura-tion in 11- to 17-year-old humans Eur J Appl Physiol 85546ndash551
Astrand PO Ryhming I 1954 A nomogram for calculation of aerobiccapacity (physical fitness) from pulse rate during submaximal work JAppl Physiol 7218ndash221
Bailey DA Shephard RJ Mirwald RL 1976 Validation of a self-administered home test of cardio-respiratory fitness Can J Appl SportSci 167ndash78
Beall CM Goldstein MC and Feldman ES 1985 The physical fitness ofelderly Nepalese farmers residing in rugged mountain and flat terrainJ Gerontol 40529ndash535
Benefice E Ndiaye G 2005 Relationships between anthropometry cardi-orespiratory fitness indices and physical activity levels in different ageand sex groups in rural Senegal (West Africa) Ann Hum Biol 32366ndash382 Available from httpwwwncbinlmnihgovpubmed16099780
Blackwell AD Gurven MD Sugiyama LS Madimenos FC Liebert MAMartin MA Kaplan HS Snodgrass JJ 2011 Evidence for a peak shift in ahumoral response to helminths age profiles of IgE in the Shuar of Ecuadorthe Tsimane of Bolivia and the US NHANES PLoS Negl Trop Dis 5e1218 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid53125146amptool5pmcentrezamprendertype5abstract
Blackwell AD Martin M Kaplan H Gurven M Evidence for an antagonis-tic relationship between Giardia lamblia and helminth infections impli-cations for treatment of helminth infections in developing populations
Blair SN LaMonte MJ Nichaman MZ 2004 The evolution of physicalactivity recommendations how much is enough Am J Clin Nutr 79913Sndash920S Available at httpwwwncbinlmnihgovpubmed15113739
Bouchard C Rankinen T Chagnon YC Rice T Perusse L Gagnon JBorecki I An P Leon a S et al 2000 Genomic scan for maximal oxygenuptake and its response to training in the HERITAGE Family Study JAppl Physiol 88551ndash559 Available at httpwwwncbinlmnihgovpubmed10658022
Bryan S St-Denis M Wojtas D 2007 Canadian Health Measures Surveyclinic operations and logistics Health Rep 1853ndash69
Buzina R Bates CJ van der Beek J Brubacher G Chandra RK HallbergL Heseker J Mertz W Pietrzik K et al 1989 Workshop on FunctionalSignificance of Mild-to-Moderate Malnutrition Am J Clin Nutrition 50172ndash176
Calder WA 1987 Scaling energetics of homeothermic vertebrates anoperational allometry Annu Rev Physiol 49107ndash120
Canadian Society for Exercise Physiology 2003 The Canadian PhysicalActivity Fitness amp Lifestyle Approach (CPAFLA) CSEP-Health amp Fit-ness Programrsquos Health-Related Appraisal and Counselling Strategy 3rded
Carnes BA Olshansky SJ 2001 Heterogeneity and its biodemographicimplications for longevity and mortality Exp Gerontol 36419ndash430Available at httpwwwncbinlmnihgovpubmed11250115
Carrick-Ranson G Hastings JL Bhella PS Shibata S Fujimoto N PalmerD Boyd K Levine BD 2013 The effect of age-related differences inbody size and composition on cardiovascular determinants of VO2max JGerontol A Biol Sci Med Sci 68608ndash616 Available at httpwwwncbinlmnihgovpubmed23160363
Centers for Disease Control and Prevention 1998 Recommendations toPrevent and Control Iron Deficiency in the United States MMWRRecomm Rep 471ndash36 Available at httpwwwcdcgovmmwrpreviewmmwrhtml00051880htm
12 AC PISOR ET AL
American Journal of Human Biology
Centers for Disease Control and Prevention 2011 Glossary of TermsPhysical Activity for Everyone [Internet] Available from httpwwwcdcgovphysicalactivityeveryoneglossary
Christensen DL Faurholt-Jepsen D Boit MK Mwaniki DL Kilonzo BTetens I Kiplamai FK Cheruiyot SC Friis H et al 2012 Cardiorespira-tory fitness and physical activity in Luo Kamba and Maasai of ruralKenya Am J Hum Biol 24723ndash729 Available at httpwwwncbinlm-nihgovpubmed22836508
Colley RC Garriguet D Janssen I Craig CL Clarke J Tremblay MS2011a Physical activity of Canadian children and youth accelerometerresults from the 2007 to 2009 Canadian Health Measures SurveyHealth Rep 2215ndash23
Colley RC Garriguet D Janssen I Craig CL Clarke J Tremblay MS2011b Physical activity of Canadian adults accelerometer results fromthe 2007 to 2009 Canadian Health Measures Survey Health Rep 227ndash14 Available at httpwwwncbinlmnihgovpubmed21510585
Collins KJ 1999 Physiological variation and adaptability in human popu-lations Ann Hum Biol 2619ndash38
Crimmins E Seeman T 2001 Integrating Biology into DemographicResearch on Health and Aging (With a Focus on the MacArthur Study ofSuccessful Aging) Cells and Surveys Should Biological Measures beIncluded in Social Science Research Washington DC National Acad-emy Press p 9ndash41
Curran-Everett LS 1994 Accordance Between VO2max and Behavior inNgisonyoka Turkana Am J Hum Biol 6761ndash771
Durnin JVGA Womersley J 1974 Body fat assessed from total body den-sity and its estimation from skinfold thickness measurements on 481men and women aged from 16 to 72 years Br J Nutr 3277ndash97
Eberl M Al-Sherbiny M Hagan P Ljubojevic S Thomas AW Wilson RA2002 A novel and sensitive method to monitor helminth infections byfaecal sampling Acta Trop 83183ndash187
Eid D Gurven M Kaplan H Winking J 2007 Enfermedades infecciosas alo largo de la vida y en el envejecimiento en indıgenas sudamericanos dela etnia Tsimane Aging in Developing Countries Building Bridges forIntegrated Research Agendas Santiago Chile
Ekblom B Engstreuroom L-M Ekblom O 2007 Secular trends of physical fit-ness in Swedish adults Scand J Med Sci Sports 17267ndash273 Availableat httpwwwncbinlmnihgovpubmed17501867
Finch CA Lenfant C 1972 Oxygen Transport in Man N Engl J Med 286407ndash415
Fitzgerald MD Tanaka H Tran ZV Seals DR 1997 Age-related declinesin maximal aerobic capacity in regularly exercising vs sedentarywomen a meta-analysis J Appl Physiol (Bethesda Md 1985) 83160ndash165 Available at httpwwwncbinlmnihgovpubmed9216959
Fleg JL Lakatta EG 1988 Role of muscle loss in the age-associated reduc-tion in VO2max J Appl Physiol 651147ndash1151
Frisancho AR Frisancho HG Milotich M Brutsaert T Albalak RSpielvogel H Villena M Vargas E Soria R 1995 Developmentalgenetic and environmental components of aerobic capacity at high alti-tude Am J Phys Anthropol 96431ndash442 Available at httpwwwncbinlmnihgovpubmed7604895
Giroux S 2007 Canadian health measures survey sampling strategyoverview Health Rep 1831ndash36
Gurven M Jaeggi A V Kaplan H Cummings D 2013 Physical activityand modernization among Bolivian Amerindians PLoS ONE 81ndash13
Gurven M Kaplan H Winking J Rodriguez DE Vasunilashorn S KimJK Finch C Crimmins E 2009 Inflammation and infection do not pro-mote arterial aging and cardiovascular disease risk factors among leanhorticulturalists PLoS ONE 41ndash12
Haidet GC 1989 Dynamic exercise in senescent beagles oxygen consump-tion and hemodynamic responses The Am J Physiol 257H1428ndash1437Available at httpwwwncbinlmnihgovpubmed2589499
Hawkins S Wiswell R 2003 Rate and mechanism of maximal oxygen con-sumption decline with aging implications for exercise training SportsMed 33877ndash888 Available at httpwwwncbinlmnihgovpubmed12974656
Hoffman J 2002 Physiological aspects of sport training and performance1st ed Champaign IL Human Kinetics Publishers
Hotez PJ Bottazzi ME Franco-Paredes C Ault SK Periago MR 2008 Theneglected tropical diseases of Latin America and the Caribbean a review ofdisease burden and distribution and a roadmap for control and eliminationPLoS Negl Trop Dis 2e300 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid52553488amptool5pmcentrezamprendertype5abstract
Howley ET Bassett DR Welch HG 1995 Criteria for maximal oxygenuptake review and commentary Med Sci Sports Exerc 271292ndash1301Available at httpwwwncbinlmnihgovpubmed8531628
Jette M Sidney K Quenneville J Landry F 1992 Relation between cardi-orespiratory fitness and selected risk factors for coronary heart diseasein a population of Canadian men and women CMAJ 1461353ndash1360Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid51488567amptool5pmcentrezamprendertype5abstract
Katzmarzyk PT Leonard WR Crawford MH 1994 Predicted maximaloxygen consumption of Indigenous Siberians Am J Hum Biol 6783ndash790
King CH Dickman K Tisch DJ 2005 Reassessment of the cost of chronichelmintic infection a meta-analysis of disability-related outcomes inendemic schistosomiasis Lancet 3651561ndash1569 Available at httpwwwncbinlmnihgovpubmed15866310
Lee J-M Bassett D Jr Thompson D Fitzhugh E 2011 Validation of thecosmed fitmate for predicting maximal oxygen consumption J StrengthCond Res 252573ndash2579
Madimenos FC Snodgrass JJ Blackwell AD Liebert MA Sugiyama LS2011 Physical activity in an indigenous Ecuadorian forager-horticulturalist population as measured using accelerometry Am J HumBiol 23488ndash497 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid53110644amptool5pmcentrezamprendertype5abstract
Malina RM 2001 Physical activity and fitness pathways from childhoodto adulthood Am J Hum Biol 13162ndash172 Available at httpwwwncbinlmnihgovpubmed11460860
Malina RM Little BB 2008 Physical activity the present in the contextof the past Am J Hum Biol 20373ndash391 Available at httpwwwncbinlmnihgovpubmed18433002
Manning JT Morris L Caswell N 2007 Endurance running and digitratio (2D 4D) implications for fetal testosterone effects on runningspeed and vascular health Am J Hum Biol 19416ndash421
Martin Ma Lassek WD Gaulin SJC Evans RW Woo JG Geraghty SRDavidson BS Morrow AL Kaplan HS et al 2012 Fatty acid composi-tion in the mature milk of Bolivian forager-horticulturalists controlledcomparisons with a US sample Matern Child Nutr 8404ndash418 Availableat httpwwwncbinlmnihgovpubmed22624983
National Health and Nutrition Examination Survey 2004 CardiovascularFitness Procedures Manual
Nussey D Coulson T Festa-Bianchet M Gaillard J-M 2008 Measuringsenescence in wild animal populations towards a longitudinal approachFunction Ecol 22393ndash406
Ogawa T Spina RJ Martin WHI Kohrt WM Schechtman KB HolloszyJO Ehsani AA 1992 Effects of aging sex and physical training cardio-vascular responses to exercise Circulation 86494ndash503
Panter-Brick C Miller UG Eggerman M 1992 Hemoglobin levels andstep test performance of men and women in Nepal Am J Hum Biol 4481ndash491
Pontzer H Raichlen Da Wood BM Mabulla AZP Racette SB MarloweFW 2012 Hunter-gatherer energetics and human obesity PLoS ONE 7e40503 Available at httpcdxplosorg101371journalpone0040503
R Development Core Team 2011 R A language and environment for sta-tistical computing R Development Core Team
Rigby R Stasinopoulos D 2005 Generalize additive models for locationscale and shape (with discussion) Appl Stat 54507ndash554
Robergs RA Landwehr R 2002 The surprising history of theldquoHRmax5220-agerdquo equation J Exerc Physiol 51ndash10
Rode A Shephard RJ 1994 Physiological consequences of acculturation a20-year study of fitness in an Inuit community Eur J Appl Physiol 69516ndash524
Rowland TW Boyajian A 1995 Aerobic response to endurance training inchildren Pediatrics 96654ndash658
Sagiv M Ben-sira D Amir R 2007 What maintains energy supply atpeak aerobic exercise in trained and untrained older men Gerontology53357ndash361
Sanada K Kuchiki T Miyachi M Mcgrath K Higuchi M Ebashi H 2007Effects of age on ventilatory threshold and peak oxygen uptake normal-ised for regional skeletal muscle mass in Japanese men and womenaged 20 ndash 80 years Eur J Appl Physiol 99475ndash483
Schniter E 2009 Why Old Age Non-Material Contributions and Patternsof Aging Among Older Adult Tsimanersquo 607
Shahnawaz H 1978 Influence of limb length on a stepping exercise JAppl Physiol 44346ndash349
Shephard RJ 1970 Computer programs for solution of the Astrand nomo-gram and the calculation of body surface area J Sports Med 10206ndash210
Shephard RJ Allen C Benade AJS Davies CT Di Prampero PE HedmanR Merriman JE Myhre K Simmons R 1968 Standardization of sub-maximal exercise tests Bull World Health Organ 38765ndash775 Availableat httpwwwpubmedcentralnihgovarticlerenderfcgiartid52554690amptool5pmcentrezamprendertype5abstract
Shephard RJ Bailey Da Mirwald RL 1976 Development of the CanadianHome Fitness Test Can Med Assoc J 114675ndash679 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid51956906amptool5pmcentrezamprendertype5abstract
Shields M Tremblay MS Laviolette M Craig CL Janssen I Gorber SC2010 Fitness of Canadian adults results from the 2007ndash2009 canadianhealth measures survey Health Rep 2121ndash35 Available at httpwwwncbinlmnihgovpubmed20426224
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 13
American Journal of Human Biology
Siconolfi SF Garber CE Lasater TM Carleton RA 1985 A simple validstep test for estimating maximal oxygen uptake in epidemiologic stud-ies Am J Epidemiol 121382ndash390 Available at httpwwwncbinlm-nihgovpubmed4014128
Sinclair LM Hinton PS 2005 Prevalence of iron deficiency with and with-out anemia in recreationally active men and women J Am Diet Assoc105975ndash978 Available from httpwwwncbinlmnihgovpubmed15942552
Skinner JS Gaskill SE Rankinen T Leon AS Rao DC Wilmore JHBouchard C 2003 Heart rate versus VO2max age sex race initial fit-ness and training response-HERITAGE Med Sci Sports Exerc 351908ndash1913 Available at httpwwwncbinlmnihgovpubmed14600558
Sondik EJ Madans JH Gentlemand JF 2012 Summary health statisticsfor US adults National Health Interview Survey 2010 Vital Health Stat101ndash80 Available at httpwwwncbinlmnihgovpubmed20687424
Stones MJ Kozma A 1985 Physical performance Aging and Human Per-formance New York Wiley p 261ndash292
Tanaka H Monahan KD Seals DR 2001 Age-predicted maximal heartrate revisited J Am Coll Cardiol] 37153ndash156 Available at httpwwwncbinlmnihgovpubmed11153730
Vasunilashorn S Crimmins EM Kim JK Winking J Gurven M KaplanH Finch CE 2010 Blood lipids infection and inflammatory markers inthe Tsimane of Bolivia Am J Hum Biol 22731ndash740 Available at httpwwwncbinlmnihgovpubmed20721985
Vaupel JV Manton KG Stallard E 1979 The impact of heterogeneity inindividual frailty on the dynamics of mortality Demography 16439ndash454
Vaupel JW Yashin AI 1985 Heterogeneityrsquos ruses some surprising effectsof selection on population dynamics Am Stat 39176ndash185
Venables WN Ripley BD 2002 Modern Applied Statistics with S FourthNew York Springer
Wagner PD 1996 Determinants of maximal oxygen transport and utiliza-tion Annu Rev Physiol 5821ndash50 Available at httpwwwncbinlmnih-govpubmed8815793
Walker A Arent SM McKeever KH 2010 Maximal aerobic capacity(VO2max) in horses a retrospective study to identify the age-relateddecline Comparative Exerc Physiol 6177ndash181 Available at httpwwwjournalscambridgeorgabstract_S1755254010000073
Walker R Hill K 2003 Modeling growth and senescence in physical per-formance among the Ache of Eastern Paraguay Am J Hum Biol 208196ndash208
Weller IM Thomas SG Corey PN Cox MH 1993 Prediction of maximaloxygen uptake from a modified Canadian aerobic fitness test Can JAppl Physiol 18175ndash188 Available at httpwwwncbinlmnihgovpubmed8513290
Wilson TM Tanaka H 2000 Meta-analysis of the age-associated declinein maximal aerobic capacity in men relation to training status Am JPhysiol Heart Circ Physiol 278H829ndash834 Available at httpwwwncbinlmnihgovpubmed10710351
Wood SN 2006 Generalized Additive Models An Introduction with RBoca Raton Florida Chapman and HallCRC Press
World Health Organization 2001 Iron deficiency anaemia assessmentprevention and control a guide for programme managers Available athttpwhqlibdocwhointhq2001WHO_NHD_013pdf
Yoopat P Toicharoen P Boontong S Glinsukon T Vanwonterghem KLouhevaara V 2002 Cardiorespiratory capacity of Thai workers in dif-ferent age and job categories J Physiol Anthropol Appl Hum Sci 21121ndash128 Available at httpwwwncbinlmnihgovpubmed12056179
Zhu YI Haas JD 1997 Iron depletion without anemia and physical per-formance in young women Am J Clin Nutr 66334ndash341 Available athttpwwwncbinlmnihgovpubmed9250112
14 AC PISOR ET AL
American Journal of Human Biology
often self-selected (Beall et al 1985) Additionally regres-sions drawn from laboratory studies require participantsachieve a HR within a certain range for accurate VO2maxestimation however the appropriateness of these rangesgiven slight modifications to protocol and inclusion of par-ticipants of different ages different populations and bothsexes is questionable For example the maximal HRexhibited by young men varies across subsistence popula-tions (Shephard 1978) Use of these criteria is compli-cated by the fact that the most commonly used equationfor estimating maximal possible HR by age 220-age maybe inaccurate (Robergs and Landwehr 2002) and particu-larly inappropriate for older adults (see Tanaka et al2001) For these reasons we chose to use an exclusion cri-terion for the Tsimane that evaluates individual increasein HR across exercise relative to the mean increase in HRfor Tsimane of the same sex and age
The pattern of Tsimane fitness decline differs moder-ately by the choice of exclusion criterion for participants(see Supporting Information Table S1) and by method oftesting However this is a common finding Lee et al(2011) predicted VO2max from submaximal exercise usingthe O2 method and the HR-based American College ofSports Medicine calculation routine in a US sample Theyfound that (1) the HR-based routine predicts higherVO2max across the sexes than does the O2 routine and(2) the two methods have a correlation of only 077 Whenevaluating different testing procedures Shephard et al(1968) found differences in VO2max estimation by type oftest used (eg bicycle ergometer versus step test) and cal-culation routine Exercise tests exclusion criteria andcalculation routines combine to provide an estimate ofactual VO2max for a given individual and as such varia-tion in estimation is to be expected However such varia-tion may affect cross-population comparisons inunforeseen ways thus the comparisons presented hereshould be interpreted with caution
While population-level variation in cardiovascular fit-ness decline may reflect the differences in the demands ofendurance-based physical activity muscularity and com-promised oxygen transport it is possible that genetic fac-tors may also play a potential role (Collins 1999) In oneindustrialized sample maternal cardiovascular fitnessexhibited a heritability of 30 which is attributed toinheritance of the maternal mitochondrial genome (Bou-chard et al 2000) We do not have the relevant geneticdata for the populations considered here however andthus operate under the simplifying assumption thatinheritance should not affect population-level patternsand will not consistently bias individual-level compari-sons in any particular direction
This study is further limited by its cross-sectionaldesign Cross-sectional data present well-known problemsfor the measurement of individual aging (Crimmins andSeeman 2001) Mortality selection in which individualsin poorer condition are likely to die at younger ages pro-duces a downward bias in the estimation of aging rates atthe individual level (Vaupel and Yashin 1985 Vaupelet al 1979) Cohort effects if present also produce com-plicated and non-monotonic biases in estimation (Carnesand Olshansky 2001) Due to the problem of between-individual heterogeneity and the within-individual pro-cess of senescence a recent overview of aging studies con-cludes that ldquoonly longitudinal studies [ ] provide reliablesources of information in the study of senescencerdquo (Nussey
et al 2008) To date there are no longitudinal studies ofcardiovascular fitness in subsistence populations We arecurrently re-testing participants under the O2 methodallowing a better grasp of the within-individual variationthat shapes patterns of senescent decline
ACKNOWLEDGMENTS
The authors thank Paul Hooper Steven Gaulin JohnTooby Patricia Kramer the Human Evolution and Biode-mography laboratory and the Center for EvolutionaryPsychology at UCSB for helpful advice and feedback thestaff at the Tsimane Health and Life History Project andthe Tsimane for their participation and patience
LITERATURE CITED
American College of Sports Medicine 2006 ACSMrsquos Guidelines for Exer-cise Testing and Prescription 7th ed Philadelphia Lippincott Williamsamp Wilkins
Armstrong N 2001 Peak oxygen uptake in relation to growth and matura-tion in 11- to 17-year-old humans Eur J Appl Physiol 85546ndash551
Astrand PO Ryhming I 1954 A nomogram for calculation of aerobiccapacity (physical fitness) from pulse rate during submaximal work JAppl Physiol 7218ndash221
Bailey DA Shephard RJ Mirwald RL 1976 Validation of a self-administered home test of cardio-respiratory fitness Can J Appl SportSci 167ndash78
Beall CM Goldstein MC and Feldman ES 1985 The physical fitness ofelderly Nepalese farmers residing in rugged mountain and flat terrainJ Gerontol 40529ndash535
Benefice E Ndiaye G 2005 Relationships between anthropometry cardi-orespiratory fitness indices and physical activity levels in different ageand sex groups in rural Senegal (West Africa) Ann Hum Biol 32366ndash382 Available from httpwwwncbinlmnihgovpubmed16099780
Blackwell AD Gurven MD Sugiyama LS Madimenos FC Liebert MAMartin MA Kaplan HS Snodgrass JJ 2011 Evidence for a peak shift in ahumoral response to helminths age profiles of IgE in the Shuar of Ecuadorthe Tsimane of Bolivia and the US NHANES PLoS Negl Trop Dis 5e1218 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid53125146amptool5pmcentrezamprendertype5abstract
Blackwell AD Martin M Kaplan H Gurven M Evidence for an antagonis-tic relationship between Giardia lamblia and helminth infections impli-cations for treatment of helminth infections in developing populations
Blair SN LaMonte MJ Nichaman MZ 2004 The evolution of physicalactivity recommendations how much is enough Am J Clin Nutr 79913Sndash920S Available at httpwwwncbinlmnihgovpubmed15113739
Bouchard C Rankinen T Chagnon YC Rice T Perusse L Gagnon JBorecki I An P Leon a S et al 2000 Genomic scan for maximal oxygenuptake and its response to training in the HERITAGE Family Study JAppl Physiol 88551ndash559 Available at httpwwwncbinlmnihgovpubmed10658022
Bryan S St-Denis M Wojtas D 2007 Canadian Health Measures Surveyclinic operations and logistics Health Rep 1853ndash69
Buzina R Bates CJ van der Beek J Brubacher G Chandra RK HallbergL Heseker J Mertz W Pietrzik K et al 1989 Workshop on FunctionalSignificance of Mild-to-Moderate Malnutrition Am J Clin Nutrition 50172ndash176
Calder WA 1987 Scaling energetics of homeothermic vertebrates anoperational allometry Annu Rev Physiol 49107ndash120
Canadian Society for Exercise Physiology 2003 The Canadian PhysicalActivity Fitness amp Lifestyle Approach (CPAFLA) CSEP-Health amp Fit-ness Programrsquos Health-Related Appraisal and Counselling Strategy 3rded
Carnes BA Olshansky SJ 2001 Heterogeneity and its biodemographicimplications for longevity and mortality Exp Gerontol 36419ndash430Available at httpwwwncbinlmnihgovpubmed11250115
Carrick-Ranson G Hastings JL Bhella PS Shibata S Fujimoto N PalmerD Boyd K Levine BD 2013 The effect of age-related differences inbody size and composition on cardiovascular determinants of VO2max JGerontol A Biol Sci Med Sci 68608ndash616 Available at httpwwwncbinlmnihgovpubmed23160363
Centers for Disease Control and Prevention 1998 Recommendations toPrevent and Control Iron Deficiency in the United States MMWRRecomm Rep 471ndash36 Available at httpwwwcdcgovmmwrpreviewmmwrhtml00051880htm
12 AC PISOR ET AL
American Journal of Human Biology
Centers for Disease Control and Prevention 2011 Glossary of TermsPhysical Activity for Everyone [Internet] Available from httpwwwcdcgovphysicalactivityeveryoneglossary
Christensen DL Faurholt-Jepsen D Boit MK Mwaniki DL Kilonzo BTetens I Kiplamai FK Cheruiyot SC Friis H et al 2012 Cardiorespira-tory fitness and physical activity in Luo Kamba and Maasai of ruralKenya Am J Hum Biol 24723ndash729 Available at httpwwwncbinlm-nihgovpubmed22836508
Colley RC Garriguet D Janssen I Craig CL Clarke J Tremblay MS2011a Physical activity of Canadian children and youth accelerometerresults from the 2007 to 2009 Canadian Health Measures SurveyHealth Rep 2215ndash23
Colley RC Garriguet D Janssen I Craig CL Clarke J Tremblay MS2011b Physical activity of Canadian adults accelerometer results fromthe 2007 to 2009 Canadian Health Measures Survey Health Rep 227ndash14 Available at httpwwwncbinlmnihgovpubmed21510585
Collins KJ 1999 Physiological variation and adaptability in human popu-lations Ann Hum Biol 2619ndash38
Crimmins E Seeman T 2001 Integrating Biology into DemographicResearch on Health and Aging (With a Focus on the MacArthur Study ofSuccessful Aging) Cells and Surveys Should Biological Measures beIncluded in Social Science Research Washington DC National Acad-emy Press p 9ndash41
Curran-Everett LS 1994 Accordance Between VO2max and Behavior inNgisonyoka Turkana Am J Hum Biol 6761ndash771
Durnin JVGA Womersley J 1974 Body fat assessed from total body den-sity and its estimation from skinfold thickness measurements on 481men and women aged from 16 to 72 years Br J Nutr 3277ndash97
Eberl M Al-Sherbiny M Hagan P Ljubojevic S Thomas AW Wilson RA2002 A novel and sensitive method to monitor helminth infections byfaecal sampling Acta Trop 83183ndash187
Eid D Gurven M Kaplan H Winking J 2007 Enfermedades infecciosas alo largo de la vida y en el envejecimiento en indıgenas sudamericanos dela etnia Tsimane Aging in Developing Countries Building Bridges forIntegrated Research Agendas Santiago Chile
Ekblom B Engstreuroom L-M Ekblom O 2007 Secular trends of physical fit-ness in Swedish adults Scand J Med Sci Sports 17267ndash273 Availableat httpwwwncbinlmnihgovpubmed17501867
Finch CA Lenfant C 1972 Oxygen Transport in Man N Engl J Med 286407ndash415
Fitzgerald MD Tanaka H Tran ZV Seals DR 1997 Age-related declinesin maximal aerobic capacity in regularly exercising vs sedentarywomen a meta-analysis J Appl Physiol (Bethesda Md 1985) 83160ndash165 Available at httpwwwncbinlmnihgovpubmed9216959
Fleg JL Lakatta EG 1988 Role of muscle loss in the age-associated reduc-tion in VO2max J Appl Physiol 651147ndash1151
Frisancho AR Frisancho HG Milotich M Brutsaert T Albalak RSpielvogel H Villena M Vargas E Soria R 1995 Developmentalgenetic and environmental components of aerobic capacity at high alti-tude Am J Phys Anthropol 96431ndash442 Available at httpwwwncbinlmnihgovpubmed7604895
Giroux S 2007 Canadian health measures survey sampling strategyoverview Health Rep 1831ndash36
Gurven M Jaeggi A V Kaplan H Cummings D 2013 Physical activityand modernization among Bolivian Amerindians PLoS ONE 81ndash13
Gurven M Kaplan H Winking J Rodriguez DE Vasunilashorn S KimJK Finch C Crimmins E 2009 Inflammation and infection do not pro-mote arterial aging and cardiovascular disease risk factors among leanhorticulturalists PLoS ONE 41ndash12
Haidet GC 1989 Dynamic exercise in senescent beagles oxygen consump-tion and hemodynamic responses The Am J Physiol 257H1428ndash1437Available at httpwwwncbinlmnihgovpubmed2589499
Hawkins S Wiswell R 2003 Rate and mechanism of maximal oxygen con-sumption decline with aging implications for exercise training SportsMed 33877ndash888 Available at httpwwwncbinlmnihgovpubmed12974656
Hoffman J 2002 Physiological aspects of sport training and performance1st ed Champaign IL Human Kinetics Publishers
Hotez PJ Bottazzi ME Franco-Paredes C Ault SK Periago MR 2008 Theneglected tropical diseases of Latin America and the Caribbean a review ofdisease burden and distribution and a roadmap for control and eliminationPLoS Negl Trop Dis 2e300 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid52553488amptool5pmcentrezamprendertype5abstract
Howley ET Bassett DR Welch HG 1995 Criteria for maximal oxygenuptake review and commentary Med Sci Sports Exerc 271292ndash1301Available at httpwwwncbinlmnihgovpubmed8531628
Jette M Sidney K Quenneville J Landry F 1992 Relation between cardi-orespiratory fitness and selected risk factors for coronary heart diseasein a population of Canadian men and women CMAJ 1461353ndash1360Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid51488567amptool5pmcentrezamprendertype5abstract
Katzmarzyk PT Leonard WR Crawford MH 1994 Predicted maximaloxygen consumption of Indigenous Siberians Am J Hum Biol 6783ndash790
King CH Dickman K Tisch DJ 2005 Reassessment of the cost of chronichelmintic infection a meta-analysis of disability-related outcomes inendemic schistosomiasis Lancet 3651561ndash1569 Available at httpwwwncbinlmnihgovpubmed15866310
Lee J-M Bassett D Jr Thompson D Fitzhugh E 2011 Validation of thecosmed fitmate for predicting maximal oxygen consumption J StrengthCond Res 252573ndash2579
Madimenos FC Snodgrass JJ Blackwell AD Liebert MA Sugiyama LS2011 Physical activity in an indigenous Ecuadorian forager-horticulturalist population as measured using accelerometry Am J HumBiol 23488ndash497 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid53110644amptool5pmcentrezamprendertype5abstract
Malina RM 2001 Physical activity and fitness pathways from childhoodto adulthood Am J Hum Biol 13162ndash172 Available at httpwwwncbinlmnihgovpubmed11460860
Malina RM Little BB 2008 Physical activity the present in the contextof the past Am J Hum Biol 20373ndash391 Available at httpwwwncbinlmnihgovpubmed18433002
Manning JT Morris L Caswell N 2007 Endurance running and digitratio (2D 4D) implications for fetal testosterone effects on runningspeed and vascular health Am J Hum Biol 19416ndash421
Martin Ma Lassek WD Gaulin SJC Evans RW Woo JG Geraghty SRDavidson BS Morrow AL Kaplan HS et al 2012 Fatty acid composi-tion in the mature milk of Bolivian forager-horticulturalists controlledcomparisons with a US sample Matern Child Nutr 8404ndash418 Availableat httpwwwncbinlmnihgovpubmed22624983
National Health and Nutrition Examination Survey 2004 CardiovascularFitness Procedures Manual
Nussey D Coulson T Festa-Bianchet M Gaillard J-M 2008 Measuringsenescence in wild animal populations towards a longitudinal approachFunction Ecol 22393ndash406
Ogawa T Spina RJ Martin WHI Kohrt WM Schechtman KB HolloszyJO Ehsani AA 1992 Effects of aging sex and physical training cardio-vascular responses to exercise Circulation 86494ndash503
Panter-Brick C Miller UG Eggerman M 1992 Hemoglobin levels andstep test performance of men and women in Nepal Am J Hum Biol 4481ndash491
Pontzer H Raichlen Da Wood BM Mabulla AZP Racette SB MarloweFW 2012 Hunter-gatherer energetics and human obesity PLoS ONE 7e40503 Available at httpcdxplosorg101371journalpone0040503
R Development Core Team 2011 R A language and environment for sta-tistical computing R Development Core Team
Rigby R Stasinopoulos D 2005 Generalize additive models for locationscale and shape (with discussion) Appl Stat 54507ndash554
Robergs RA Landwehr R 2002 The surprising history of theldquoHRmax5220-agerdquo equation J Exerc Physiol 51ndash10
Rode A Shephard RJ 1994 Physiological consequences of acculturation a20-year study of fitness in an Inuit community Eur J Appl Physiol 69516ndash524
Rowland TW Boyajian A 1995 Aerobic response to endurance training inchildren Pediatrics 96654ndash658
Sagiv M Ben-sira D Amir R 2007 What maintains energy supply atpeak aerobic exercise in trained and untrained older men Gerontology53357ndash361
Sanada K Kuchiki T Miyachi M Mcgrath K Higuchi M Ebashi H 2007Effects of age on ventilatory threshold and peak oxygen uptake normal-ised for regional skeletal muscle mass in Japanese men and womenaged 20 ndash 80 years Eur J Appl Physiol 99475ndash483
Schniter E 2009 Why Old Age Non-Material Contributions and Patternsof Aging Among Older Adult Tsimanersquo 607
Shahnawaz H 1978 Influence of limb length on a stepping exercise JAppl Physiol 44346ndash349
Shephard RJ 1970 Computer programs for solution of the Astrand nomo-gram and the calculation of body surface area J Sports Med 10206ndash210
Shephard RJ Allen C Benade AJS Davies CT Di Prampero PE HedmanR Merriman JE Myhre K Simmons R 1968 Standardization of sub-maximal exercise tests Bull World Health Organ 38765ndash775 Availableat httpwwwpubmedcentralnihgovarticlerenderfcgiartid52554690amptool5pmcentrezamprendertype5abstract
Shephard RJ Bailey Da Mirwald RL 1976 Development of the CanadianHome Fitness Test Can Med Assoc J 114675ndash679 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid51956906amptool5pmcentrezamprendertype5abstract
Shields M Tremblay MS Laviolette M Craig CL Janssen I Gorber SC2010 Fitness of Canadian adults results from the 2007ndash2009 canadianhealth measures survey Health Rep 2121ndash35 Available at httpwwwncbinlmnihgovpubmed20426224
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 13
American Journal of Human Biology
Siconolfi SF Garber CE Lasater TM Carleton RA 1985 A simple validstep test for estimating maximal oxygen uptake in epidemiologic stud-ies Am J Epidemiol 121382ndash390 Available at httpwwwncbinlm-nihgovpubmed4014128
Sinclair LM Hinton PS 2005 Prevalence of iron deficiency with and with-out anemia in recreationally active men and women J Am Diet Assoc105975ndash978 Available from httpwwwncbinlmnihgovpubmed15942552
Skinner JS Gaskill SE Rankinen T Leon AS Rao DC Wilmore JHBouchard C 2003 Heart rate versus VO2max age sex race initial fit-ness and training response-HERITAGE Med Sci Sports Exerc 351908ndash1913 Available at httpwwwncbinlmnihgovpubmed14600558
Sondik EJ Madans JH Gentlemand JF 2012 Summary health statisticsfor US adults National Health Interview Survey 2010 Vital Health Stat101ndash80 Available at httpwwwncbinlmnihgovpubmed20687424
Stones MJ Kozma A 1985 Physical performance Aging and Human Per-formance New York Wiley p 261ndash292
Tanaka H Monahan KD Seals DR 2001 Age-predicted maximal heartrate revisited J Am Coll Cardiol] 37153ndash156 Available at httpwwwncbinlmnihgovpubmed11153730
Vasunilashorn S Crimmins EM Kim JK Winking J Gurven M KaplanH Finch CE 2010 Blood lipids infection and inflammatory markers inthe Tsimane of Bolivia Am J Hum Biol 22731ndash740 Available at httpwwwncbinlmnihgovpubmed20721985
Vaupel JV Manton KG Stallard E 1979 The impact of heterogeneity inindividual frailty on the dynamics of mortality Demography 16439ndash454
Vaupel JW Yashin AI 1985 Heterogeneityrsquos ruses some surprising effectsof selection on population dynamics Am Stat 39176ndash185
Venables WN Ripley BD 2002 Modern Applied Statistics with S FourthNew York Springer
Wagner PD 1996 Determinants of maximal oxygen transport and utiliza-tion Annu Rev Physiol 5821ndash50 Available at httpwwwncbinlmnih-govpubmed8815793
Walker A Arent SM McKeever KH 2010 Maximal aerobic capacity(VO2max) in horses a retrospective study to identify the age-relateddecline Comparative Exerc Physiol 6177ndash181 Available at httpwwwjournalscambridgeorgabstract_S1755254010000073
Walker R Hill K 2003 Modeling growth and senescence in physical per-formance among the Ache of Eastern Paraguay Am J Hum Biol 208196ndash208
Weller IM Thomas SG Corey PN Cox MH 1993 Prediction of maximaloxygen uptake from a modified Canadian aerobic fitness test Can JAppl Physiol 18175ndash188 Available at httpwwwncbinlmnihgovpubmed8513290
Wilson TM Tanaka H 2000 Meta-analysis of the age-associated declinein maximal aerobic capacity in men relation to training status Am JPhysiol Heart Circ Physiol 278H829ndash834 Available at httpwwwncbinlmnihgovpubmed10710351
Wood SN 2006 Generalized Additive Models An Introduction with RBoca Raton Florida Chapman and HallCRC Press
World Health Organization 2001 Iron deficiency anaemia assessmentprevention and control a guide for programme managers Available athttpwhqlibdocwhointhq2001WHO_NHD_013pdf
Yoopat P Toicharoen P Boontong S Glinsukon T Vanwonterghem KLouhevaara V 2002 Cardiorespiratory capacity of Thai workers in dif-ferent age and job categories J Physiol Anthropol Appl Hum Sci 21121ndash128 Available at httpwwwncbinlmnihgovpubmed12056179
Zhu YI Haas JD 1997 Iron depletion without anemia and physical per-formance in young women Am J Clin Nutr 66334ndash341 Available athttpwwwncbinlmnihgovpubmed9250112
14 AC PISOR ET AL
American Journal of Human Biology
Centers for Disease Control and Prevention 2011 Glossary of TermsPhysical Activity for Everyone [Internet] Available from httpwwwcdcgovphysicalactivityeveryoneglossary
Christensen DL Faurholt-Jepsen D Boit MK Mwaniki DL Kilonzo BTetens I Kiplamai FK Cheruiyot SC Friis H et al 2012 Cardiorespira-tory fitness and physical activity in Luo Kamba and Maasai of ruralKenya Am J Hum Biol 24723ndash729 Available at httpwwwncbinlm-nihgovpubmed22836508
Colley RC Garriguet D Janssen I Craig CL Clarke J Tremblay MS2011a Physical activity of Canadian children and youth accelerometerresults from the 2007 to 2009 Canadian Health Measures SurveyHealth Rep 2215ndash23
Colley RC Garriguet D Janssen I Craig CL Clarke J Tremblay MS2011b Physical activity of Canadian adults accelerometer results fromthe 2007 to 2009 Canadian Health Measures Survey Health Rep 227ndash14 Available at httpwwwncbinlmnihgovpubmed21510585
Collins KJ 1999 Physiological variation and adaptability in human popu-lations Ann Hum Biol 2619ndash38
Crimmins E Seeman T 2001 Integrating Biology into DemographicResearch on Health and Aging (With a Focus on the MacArthur Study ofSuccessful Aging) Cells and Surveys Should Biological Measures beIncluded in Social Science Research Washington DC National Acad-emy Press p 9ndash41
Curran-Everett LS 1994 Accordance Between VO2max and Behavior inNgisonyoka Turkana Am J Hum Biol 6761ndash771
Durnin JVGA Womersley J 1974 Body fat assessed from total body den-sity and its estimation from skinfold thickness measurements on 481men and women aged from 16 to 72 years Br J Nutr 3277ndash97
Eberl M Al-Sherbiny M Hagan P Ljubojevic S Thomas AW Wilson RA2002 A novel and sensitive method to monitor helminth infections byfaecal sampling Acta Trop 83183ndash187
Eid D Gurven M Kaplan H Winking J 2007 Enfermedades infecciosas alo largo de la vida y en el envejecimiento en indıgenas sudamericanos dela etnia Tsimane Aging in Developing Countries Building Bridges forIntegrated Research Agendas Santiago Chile
Ekblom B Engstreuroom L-M Ekblom O 2007 Secular trends of physical fit-ness in Swedish adults Scand J Med Sci Sports 17267ndash273 Availableat httpwwwncbinlmnihgovpubmed17501867
Finch CA Lenfant C 1972 Oxygen Transport in Man N Engl J Med 286407ndash415
Fitzgerald MD Tanaka H Tran ZV Seals DR 1997 Age-related declinesin maximal aerobic capacity in regularly exercising vs sedentarywomen a meta-analysis J Appl Physiol (Bethesda Md 1985) 83160ndash165 Available at httpwwwncbinlmnihgovpubmed9216959
Fleg JL Lakatta EG 1988 Role of muscle loss in the age-associated reduc-tion in VO2max J Appl Physiol 651147ndash1151
Frisancho AR Frisancho HG Milotich M Brutsaert T Albalak RSpielvogel H Villena M Vargas E Soria R 1995 Developmentalgenetic and environmental components of aerobic capacity at high alti-tude Am J Phys Anthropol 96431ndash442 Available at httpwwwncbinlmnihgovpubmed7604895
Giroux S 2007 Canadian health measures survey sampling strategyoverview Health Rep 1831ndash36
Gurven M Jaeggi A V Kaplan H Cummings D 2013 Physical activityand modernization among Bolivian Amerindians PLoS ONE 81ndash13
Gurven M Kaplan H Winking J Rodriguez DE Vasunilashorn S KimJK Finch C Crimmins E 2009 Inflammation and infection do not pro-mote arterial aging and cardiovascular disease risk factors among leanhorticulturalists PLoS ONE 41ndash12
Haidet GC 1989 Dynamic exercise in senescent beagles oxygen consump-tion and hemodynamic responses The Am J Physiol 257H1428ndash1437Available at httpwwwncbinlmnihgovpubmed2589499
Hawkins S Wiswell R 2003 Rate and mechanism of maximal oxygen con-sumption decline with aging implications for exercise training SportsMed 33877ndash888 Available at httpwwwncbinlmnihgovpubmed12974656
Hoffman J 2002 Physiological aspects of sport training and performance1st ed Champaign IL Human Kinetics Publishers
Hotez PJ Bottazzi ME Franco-Paredes C Ault SK Periago MR 2008 Theneglected tropical diseases of Latin America and the Caribbean a review ofdisease burden and distribution and a roadmap for control and eliminationPLoS Negl Trop Dis 2e300 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid52553488amptool5pmcentrezamprendertype5abstract
Howley ET Bassett DR Welch HG 1995 Criteria for maximal oxygenuptake review and commentary Med Sci Sports Exerc 271292ndash1301Available at httpwwwncbinlmnihgovpubmed8531628
Jette M Sidney K Quenneville J Landry F 1992 Relation between cardi-orespiratory fitness and selected risk factors for coronary heart diseasein a population of Canadian men and women CMAJ 1461353ndash1360Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid51488567amptool5pmcentrezamprendertype5abstract
Katzmarzyk PT Leonard WR Crawford MH 1994 Predicted maximaloxygen consumption of Indigenous Siberians Am J Hum Biol 6783ndash790
King CH Dickman K Tisch DJ 2005 Reassessment of the cost of chronichelmintic infection a meta-analysis of disability-related outcomes inendemic schistosomiasis Lancet 3651561ndash1569 Available at httpwwwncbinlmnihgovpubmed15866310
Lee J-M Bassett D Jr Thompson D Fitzhugh E 2011 Validation of thecosmed fitmate for predicting maximal oxygen consumption J StrengthCond Res 252573ndash2579
Madimenos FC Snodgrass JJ Blackwell AD Liebert MA Sugiyama LS2011 Physical activity in an indigenous Ecuadorian forager-horticulturalist population as measured using accelerometry Am J HumBiol 23488ndash497 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid53110644amptool5pmcentrezamprendertype5abstract
Malina RM 2001 Physical activity and fitness pathways from childhoodto adulthood Am J Hum Biol 13162ndash172 Available at httpwwwncbinlmnihgovpubmed11460860
Malina RM Little BB 2008 Physical activity the present in the contextof the past Am J Hum Biol 20373ndash391 Available at httpwwwncbinlmnihgovpubmed18433002
Manning JT Morris L Caswell N 2007 Endurance running and digitratio (2D 4D) implications for fetal testosterone effects on runningspeed and vascular health Am J Hum Biol 19416ndash421
Martin Ma Lassek WD Gaulin SJC Evans RW Woo JG Geraghty SRDavidson BS Morrow AL Kaplan HS et al 2012 Fatty acid composi-tion in the mature milk of Bolivian forager-horticulturalists controlledcomparisons with a US sample Matern Child Nutr 8404ndash418 Availableat httpwwwncbinlmnihgovpubmed22624983
National Health and Nutrition Examination Survey 2004 CardiovascularFitness Procedures Manual
Nussey D Coulson T Festa-Bianchet M Gaillard J-M 2008 Measuringsenescence in wild animal populations towards a longitudinal approachFunction Ecol 22393ndash406
Ogawa T Spina RJ Martin WHI Kohrt WM Schechtman KB HolloszyJO Ehsani AA 1992 Effects of aging sex and physical training cardio-vascular responses to exercise Circulation 86494ndash503
Panter-Brick C Miller UG Eggerman M 1992 Hemoglobin levels andstep test performance of men and women in Nepal Am J Hum Biol 4481ndash491
Pontzer H Raichlen Da Wood BM Mabulla AZP Racette SB MarloweFW 2012 Hunter-gatherer energetics and human obesity PLoS ONE 7e40503 Available at httpcdxplosorg101371journalpone0040503
R Development Core Team 2011 R A language and environment for sta-tistical computing R Development Core Team
Rigby R Stasinopoulos D 2005 Generalize additive models for locationscale and shape (with discussion) Appl Stat 54507ndash554
Robergs RA Landwehr R 2002 The surprising history of theldquoHRmax5220-agerdquo equation J Exerc Physiol 51ndash10
Rode A Shephard RJ 1994 Physiological consequences of acculturation a20-year study of fitness in an Inuit community Eur J Appl Physiol 69516ndash524
Rowland TW Boyajian A 1995 Aerobic response to endurance training inchildren Pediatrics 96654ndash658
Sagiv M Ben-sira D Amir R 2007 What maintains energy supply atpeak aerobic exercise in trained and untrained older men Gerontology53357ndash361
Sanada K Kuchiki T Miyachi M Mcgrath K Higuchi M Ebashi H 2007Effects of age on ventilatory threshold and peak oxygen uptake normal-ised for regional skeletal muscle mass in Japanese men and womenaged 20 ndash 80 years Eur J Appl Physiol 99475ndash483
Schniter E 2009 Why Old Age Non-Material Contributions and Patternsof Aging Among Older Adult Tsimanersquo 607
Shahnawaz H 1978 Influence of limb length on a stepping exercise JAppl Physiol 44346ndash349
Shephard RJ 1970 Computer programs for solution of the Astrand nomo-gram and the calculation of body surface area J Sports Med 10206ndash210
Shephard RJ Allen C Benade AJS Davies CT Di Prampero PE HedmanR Merriman JE Myhre K Simmons R 1968 Standardization of sub-maximal exercise tests Bull World Health Organ 38765ndash775 Availableat httpwwwpubmedcentralnihgovarticlerenderfcgiartid52554690amptool5pmcentrezamprendertype5abstract
Shephard RJ Bailey Da Mirwald RL 1976 Development of the CanadianHome Fitness Test Can Med Assoc J 114675ndash679 Available at httpwwwpubmedcentralnihgovarticlerenderfcgiartid51956906amptool5pmcentrezamprendertype5abstract
Shields M Tremblay MS Laviolette M Craig CL Janssen I Gorber SC2010 Fitness of Canadian adults results from the 2007ndash2009 canadianhealth measures survey Health Rep 2121ndash35 Available at httpwwwncbinlmnihgovpubmed20426224
PATTERNS OF SENESCENCE IN HUMAN CARDIOVASCULAR FITNESS 13
American Journal of Human Biology
Siconolfi SF Garber CE Lasater TM Carleton RA 1985 A simple validstep test for estimating maximal oxygen uptake in epidemiologic stud-ies Am J Epidemiol 121382ndash390 Available at httpwwwncbinlm-nihgovpubmed4014128
Sinclair LM Hinton PS 2005 Prevalence of iron deficiency with and with-out anemia in recreationally active men and women J Am Diet Assoc105975ndash978 Available from httpwwwncbinlmnihgovpubmed15942552
Skinner JS Gaskill SE Rankinen T Leon AS Rao DC Wilmore JHBouchard C 2003 Heart rate versus VO2max age sex race initial fit-ness and training response-HERITAGE Med Sci Sports Exerc 351908ndash1913 Available at httpwwwncbinlmnihgovpubmed14600558
Sondik EJ Madans JH Gentlemand JF 2012 Summary health statisticsfor US adults National Health Interview Survey 2010 Vital Health Stat101ndash80 Available at httpwwwncbinlmnihgovpubmed20687424
Stones MJ Kozma A 1985 Physical performance Aging and Human Per-formance New York Wiley p 261ndash292
Tanaka H Monahan KD Seals DR 2001 Age-predicted maximal heartrate revisited J Am Coll Cardiol] 37153ndash156 Available at httpwwwncbinlmnihgovpubmed11153730
Vasunilashorn S Crimmins EM Kim JK Winking J Gurven M KaplanH Finch CE 2010 Blood lipids infection and inflammatory markers inthe Tsimane of Bolivia Am J Hum Biol 22731ndash740 Available at httpwwwncbinlmnihgovpubmed20721985
Vaupel JV Manton KG Stallard E 1979 The impact of heterogeneity inindividual frailty on the dynamics of mortality Demography 16439ndash454
Vaupel JW Yashin AI 1985 Heterogeneityrsquos ruses some surprising effectsof selection on population dynamics Am Stat 39176ndash185
Venables WN Ripley BD 2002 Modern Applied Statistics with S FourthNew York Springer
Wagner PD 1996 Determinants of maximal oxygen transport and utiliza-tion Annu Rev Physiol 5821ndash50 Available at httpwwwncbinlmnih-govpubmed8815793
Walker A Arent SM McKeever KH 2010 Maximal aerobic capacity(VO2max) in horses a retrospective study to identify the age-relateddecline Comparative Exerc Physiol 6177ndash181 Available at httpwwwjournalscambridgeorgabstract_S1755254010000073
Walker R Hill K 2003 Modeling growth and senescence in physical per-formance among the Ache of Eastern Paraguay Am J Hum Biol 208196ndash208
Weller IM Thomas SG Corey PN Cox MH 1993 Prediction of maximaloxygen uptake from a modified Canadian aerobic fitness test Can JAppl Physiol 18175ndash188 Available at httpwwwncbinlmnihgovpubmed8513290
Wilson TM Tanaka H 2000 Meta-analysis of the age-associated declinein maximal aerobic capacity in men relation to training status Am JPhysiol Heart Circ Physiol 278H829ndash834 Available at httpwwwncbinlmnihgovpubmed10710351
Wood SN 2006 Generalized Additive Models An Introduction with RBoca Raton Florida Chapman and HallCRC Press
World Health Organization 2001 Iron deficiency anaemia assessmentprevention and control a guide for programme managers Available athttpwhqlibdocwhointhq2001WHO_NHD_013pdf
Yoopat P Toicharoen P Boontong S Glinsukon T Vanwonterghem KLouhevaara V 2002 Cardiorespiratory capacity of Thai workers in dif-ferent age and job categories J Physiol Anthropol Appl Hum Sci 21121ndash128 Available at httpwwwncbinlmnihgovpubmed12056179
Zhu YI Haas JD 1997 Iron depletion without anemia and physical per-formance in young women Am J Clin Nutr 66334ndash341 Available athttpwwwncbinlmnihgovpubmed9250112
14 AC PISOR ET AL
American Journal of Human Biology
Siconolfi SF Garber CE Lasater TM Carleton RA 1985 A simple validstep test for estimating maximal oxygen uptake in epidemiologic stud-ies Am J Epidemiol 121382ndash390 Available at httpwwwncbinlm-nihgovpubmed4014128
Sinclair LM Hinton PS 2005 Prevalence of iron deficiency with and with-out anemia in recreationally active men and women J Am Diet Assoc105975ndash978 Available from httpwwwncbinlmnihgovpubmed15942552
Skinner JS Gaskill SE Rankinen T Leon AS Rao DC Wilmore JHBouchard C 2003 Heart rate versus VO2max age sex race initial fit-ness and training response-HERITAGE Med Sci Sports Exerc 351908ndash1913 Available at httpwwwncbinlmnihgovpubmed14600558
Sondik EJ Madans JH Gentlemand JF 2012 Summary health statisticsfor US adults National Health Interview Survey 2010 Vital Health Stat101ndash80 Available at httpwwwncbinlmnihgovpubmed20687424
Stones MJ Kozma A 1985 Physical performance Aging and Human Per-formance New York Wiley p 261ndash292
Tanaka H Monahan KD Seals DR 2001 Age-predicted maximal heartrate revisited J Am Coll Cardiol] 37153ndash156 Available at httpwwwncbinlmnihgovpubmed11153730
Vasunilashorn S Crimmins EM Kim JK Winking J Gurven M KaplanH Finch CE 2010 Blood lipids infection and inflammatory markers inthe Tsimane of Bolivia Am J Hum Biol 22731ndash740 Available at httpwwwncbinlmnihgovpubmed20721985
Vaupel JV Manton KG Stallard E 1979 The impact of heterogeneity inindividual frailty on the dynamics of mortality Demography 16439ndash454
Vaupel JW Yashin AI 1985 Heterogeneityrsquos ruses some surprising effectsof selection on population dynamics Am Stat 39176ndash185
Venables WN Ripley BD 2002 Modern Applied Statistics with S FourthNew York Springer
Wagner PD 1996 Determinants of maximal oxygen transport and utiliza-tion Annu Rev Physiol 5821ndash50 Available at httpwwwncbinlmnih-govpubmed8815793
Walker A Arent SM McKeever KH 2010 Maximal aerobic capacity(VO2max) in horses a retrospective study to identify the age-relateddecline Comparative Exerc Physiol 6177ndash181 Available at httpwwwjournalscambridgeorgabstract_S1755254010000073
Walker R Hill K 2003 Modeling growth and senescence in physical per-formance among the Ache of Eastern Paraguay Am J Hum Biol 208196ndash208
Weller IM Thomas SG Corey PN Cox MH 1993 Prediction of maximaloxygen uptake from a modified Canadian aerobic fitness test Can JAppl Physiol 18175ndash188 Available at httpwwwncbinlmnihgovpubmed8513290
Wilson TM Tanaka H 2000 Meta-analysis of the age-associated declinein maximal aerobic capacity in men relation to training status Am JPhysiol Heart Circ Physiol 278H829ndash834 Available at httpwwwncbinlmnihgovpubmed10710351
Wood SN 2006 Generalized Additive Models An Introduction with RBoca Raton Florida Chapman and HallCRC Press
World Health Organization 2001 Iron deficiency anaemia assessmentprevention and control a guide for programme managers Available athttpwhqlibdocwhointhq2001WHO_NHD_013pdf
Yoopat P Toicharoen P Boontong S Glinsukon T Vanwonterghem KLouhevaara V 2002 Cardiorespiratory capacity of Thai workers in dif-ferent age and job categories J Physiol Anthropol Appl Hum Sci 21121ndash128 Available at httpwwwncbinlmnihgovpubmed12056179
Zhu YI Haas JD 1997 Iron depletion without anemia and physical per-formance in young women Am J Clin Nutr 66334ndash341 Available athttpwwwncbinlmnihgovpubmed9250112
14 AC PISOR ET AL
American Journal of Human Biology