ISRAEL, JORDAN, MOROCCO, OMAN, U.A.E - African Wildlife Safaris
Upload
khangminh22Category
view
6download
0
i
Patient Safety Culture in Primary Health Care
Muscat, Oman
Muna Habib Al Lawati
MBBS (Krishna Institute of Medical Sciences, India)
Master of Quality Improvement in Health Care (University of Newcastle, Australia)
This thesis is submitted in fulfilment of the requirements
for the degree of Doctor of Philosophy
Discipline of Behavioral and Social Sciences in Health,
Faculty of Health Sciences
2019
ii
CANDIDATE’S CERTIFICATE
I, Muna Habib AL Lawati, hereby state that the work presented in my thesis is my own and
has not been submitted to any other Universities or higher degree institutions and the content
of my thesis is the result of the work I have carried out since the commence of my degree
candidature.
I, Muna Habib AL Lawati, hereby affirm that I was the key researcher of the work contained
in this thesis, including work published with several authors.
I, Muna Habib AL Lawati, acknowledge that an electronic copy of my thesis Patient Safety
Culture in Primary Health Care Muscat, Oman will be lodged in the University library.
Muna Habib AL Lawati
15th June 2019
iii
SUPERVISOR’S CERTIFICATE This is to certify that the thesis Patient Safety Culture in Primary Health Care Muscat, Oman
by Muna Habib AL Lawati in completion of the requirements for the degree of Doctor of
Philosophy is in a form ready for examination.
Professor Stephanie Short
Discipline of Behavioural & Social Sciences in Health
University of Sydney
15th June 2019
iv
ACKNOWLEDGEMENTS
First and foremost, I would like to acknowledge my limitless thanks to Allah, the Ever-
Magnificent and the Ever-Thankful for all the help and blessings.
I am grateful to my principal supervisor, Professor Stephanie Short, who has provided me
with all the support and guidance throughout my candidacy journey. I am very thankful to her
inspiration, encouragement and motivation to my work for such an important topic for my
beloved country Oman.
I would like to extend my thanks to my associate Supervisor, Sarah Dennis for her support
and guidance for the direction of my thesis and her valuable and precious comments. I also
wish to thank my local supervisor Dr Nadia Noor, for her advice and comments and for her
genuine and fruitful support. All my supervisors have made my PhD journey a delightful and
enjoyable experience.
I would like to thank Mr Sathiya Murthi Panchatcharam who participated in statistical
analysis for phase 2 of my research.
A very special thanks to Dr Cherry Russell, social researcher, provided expert proofreading
and editing of this thesis with publication.
This research work would have not been possible without the contribution of the field work
research teams in the data collection phase, my gratitude goes to all the health care
professionals who participated in this study.
My sincere thanks to the Ministry of Higher Education for providing me a scholarship to
accomplish my research and Ministry of Health for supporting me in that regard.
v
I would like to express my greatest gratitude to my friends and colleagues at the Directorate
General of Health Services, Muscat Region, for their support and encouragement for the
competition of my PhD.
My wholehearted sincere thanks to my family for their generous support that they provided
me thought my PhD journey because of their unconditional love and support I have the
chance to complete my thesis. I owe profound gratitude to my Husband, Ali whose constant
and limitless encouragement and great sacrifice helped me to accomplish this degree. I thank
my three adorable children Hussain, Heba and Hassan for their kindness, understanding and
patience for their support.
Last but not the least, sincere thanks to all the people who took park in making this thesis
from vison to reality.
vi
TABLE OF CONTENTS CANDIDATE’S CERTIFICATE ........................................................................................................ ii
SUPERVISOR’S CERTIFICATE...................................................................................................... iii
ACKNOWLEDGEMENTS ................................................................................................................ iv
TABLE OF CONTENTS .................................................................................................................... vi
ABSTRACT .......................................................................................................................................... ix
OVERVIEW OF THE THESIS.......................................................................................................... xi
DISSEMINATION OF THE RESEARCH ...................................................................................... xiii
PEER REVIEWED PAPRERS ........................................................................................................ xiii
PRESENTATION ARISING FROM THE THESIS ...................................................................... xiv
ABBREVIATION ............................................................................................................................... xv
Chapter 1 Preface ................................................................................................................................. 1
1.1 Structure of the Thesis ............................................................................................................ 1
1.2 Rationale for the thesis ............................................................................................................ 2
1.3 References ............................................................................................................................... 6
Chapter 2 Patient Safety in Health Care ................................................................................................. 7
2 Patient Safety ...................................................................................................................................... 8
2.1 What is safety culture in health care? ................................................................................... 13
2.2 What is safety climate in health care? ................................................................................... 18
2.3 Tools to assess safety culture in primary healthcare ............................................................. 18
2.4 Patient Safety culture in the Eastern Mediterranean Region................................................. 23
2.5 The Omani Context ............................................................................................................... 25
2.5.1 Country profile .............................................................................................................. 25
2.5.2 Demographic indicators ................................................................................................ 26
2.6 Healthcare system in Oman .................................................................................................. 27
2.6.1 Primary health care in Oman ........................................................................................ 32
2.6.2 Characteristics of primary health care........................................................................... 32
2.7 Establishing patient safety in Oman ...................................................................................... 34
2.8 Research on patient safety in Oman ...................................................................................... 35
2.9 Patient safety gap in primary health care in Oman ............................................................... 36
2.10 References ............................................................................................................................. 38
Chapter 3 A mixed methods research design ................................................................................... 42
3.1 Background ........................................................................................................................... 42
3.2 Phase 1: Systematic review ................................................................................................... 44
3.3 Phase Two: Questionnaire-based survey .............................................................................. 45
The study participants in phase two: ................................................................................................. 46
vii
3.4 Phase three: Qualitative focus group discussions ................................................................. 47
3.5 Summary ............................................................................................................................... 49
3.6 References ............................................................................................................................. 50
Chapter 4 Patient safety and safety culture in primary health care: a systematic review ........... 51
4 Authorship statement ......................................................................................................................... 52
4.1 Abstract ................................................................................................................................. 53
4.2 Background ........................................................................................................................... 53
4.3 Methods................................................................................................................................. 54
4.4 Results ................................................................................................................................... 54
4.5 Discussion ............................................................................................................................. 61
4.6 Conclusion ............................................................................................................................ 62
4.7 References ............................................................................................................................. 63
Chapter 5 Assessment of patient safety culture in primary health care in Muscat, Oman: a questionnaire -based survey ............................................................................................................... 64
5 Authorship statement ......................................................................................................................... 65
5.1 Abstract ................................................................................................................................. 66
5.2 Background ........................................................................................................................... 66
5.3 Methods................................................................................................................................. 66
5.4 Results ................................................................................................................................... 67
5.5 Discussion ............................................................................................................................. 70
5.6 Conclusion ............................................................................................................................ 71
5.7 References ............................................................................................................................. 72
Chapter 6 Health professionals’ perceptions of patient safety culture in primary care in Oman: A qualitative study ................................................................................................................. 73
6 Authorship statement ......................................................................................................................... 74
6.1 Abstract ................................................................................................................................. 77
6.2 Introduction ........................................................................................................................... 79
6.3 Methods................................................................................................................................. 79
6.4 Results ................................................................................................................................... 81
6.5 Discussion ............................................................................................................................. 86
6.6 Conclusion ............................................................................................................................ 88
6.7 References ............................................................................................................................. 89
Chapter 7 Consolidation and Conclusion ..................................................................................... 90
7 Purpose of the thesis .......................................................................................................................... 91
7.1 Overview of the key findings ................................................................................................ 91
7.2 Limitations of the thesis ........................................................................................................ 96
viii
7.3 Originality and significance of the study .............................................................................. 96
7.4 Policy Recommendations ...................................................................................................... 97
7.4.1 Policy makers ................................................................................................................ 97
7.4.2 At the level of the health center the main implications are as follows:......................... 98
7.5 Research .............................................................................................................................. 100
7.6 Final conclusions ................................................................................................................ 100
7.7 References ........................................................................................................................... 101
APPENDICES .................................................................................................................................... 102
APPENDIX A Institutional ethics approval letter .............................................................................. 103
Ethical approval .................................................................................................................................. 104
APPENDIX B Information sheet for participants in phase 2, the questionnaire-based survey .......... 105
APPENDIX C Questionnaire used in phase 2, the questionnaire-based survey ................................. 106
APPENDIX D Study participant information and consent form used in Phase 3, the focus group discussions .......................................................................................................................................... 114
APPENDIX E Interview schedule used in the focus group discussions ............................................. 115
APPENDIX F The “Health Vision 2050” ........................................................................................... 116
ix
ABSTRACT
Patient safety is a foremost concern worldwide and is a developing field of research with a
growing evidence base in western countries, but little has been explored in the Middle East.
The aim of this thesis was to conduct the first study to explore patient safety in primary health
care in Muscat Oman. The results will inform and fill an evidence gap and contribute to
implementation of the Sultanate of Oman Ministry of Health Vision 2050. This study uses
mixed method design in three phases, with each phase building on the previous phase to
develop a deeper understanding of the phenomenon under study.
The phase 1 systematic review of the published literature identified that the most important
first step is the assessment of safety culture in an organization. The most commonly used tool
was the Hospital Survey on Patient Safety Culture survey (HSOPSC) which had also been used
in Kuwait, Turkey, and Iran.
In the second phase the HSOPC tool was used to provide a basic understanding of the safety-
related perceptions of health care professionals. The number of respondents was 186 out of 198
in the questionnaire-based survey (response rate: 94%). Overall, the survey revealed a strong
sense of teamwork, organization learning for continuous improvement, and teamwork across
the units. The four dimensions which received the lowest scores were communication
problems, non-punitive response to errors, frequency of event reporting and errors occurring
when transferring patients to higher levels of health care during handoffs and transitions.
Two focus group discussions with health care professionals were conducted to explore the root
cause of poor scores achieved in phase 2. The results highlighted that error reporting in primary
care needs to encourage an atmosphere where a non-punitive response to error reporting is
promoted without the fear of blame.
x
The conceptualisation, mixed method design and findings that emerged from this first study of
patient safety culture in primary health care in Muscat Oman will provide a base for a national
study, and will be used by the Ministry of Health in Oman to inform policies, guidelines and
training to strengthen patient safety in primary health care in line with Health Vision 2050.
xi
OVERVIEW OF THE THESIS
The broad aim of this thesis was to understand the patient safety culture in Muscat, Oman. To
accomplish this aim, this thesis presents several studies which employed a variety of research
designs and is composed into seven chapters, each one of them dealing with different aspect of
the thesis. Chapter One, is an introduction to the thesis and provides the background to the
development of the research questions. Chapter two is the literature review which provides
the milestones of development of patient safety system by the World Health Organization, I
discuss the difference between safety culture and safety climate, illustrate various tools that
have been used to assess patient safety and common tools used in primary health care.
Chapter three examines the varies methodologies used during my PhD candidature, it draws
on mixed methods design and is divided into three phases, with each phase building on the
previous phase to develop a deeper understanding of patient safety culture in primary health
care in Muscat, Oman.
Chapter four is a systematic review of the literature were searches were commenced using
Medline, EMBASE, CINAHL and Scopus from the year 2000 to 2014. The themes identified
safety culture in primary care, incident reporting, safety climate and adverse events and the
most common theme from 2011 onwards was the assessment of safety culture in primary care.
The most commonly used safety culture assessment tool is the Hospital survey on patient safety
culture (HSOPSC) which has been used in developing countries in the Middle East.
This systematic review identified that the most significant first step is the assessment of safety
culture in primary care that will provide a basic understanding to safety-related perceptions of
health care providers and the HSOPSC has been commonly used in Kuwait, Turkey, and Iran.
xii
The outcome of this formed the basis of chapter 5 which used the Hospital survey on patient
safety culture (HSOPSC). The response rate was high, and the ultimate areas of strength were
teamwork within the units with positivity and organization learning and continuous
improvement. The weaknesses were nonpunitive response to errors, inadequate staffing and
hand offs and transition.
In order to understand the perception of patient safety among the health care professionals’
chapter six illustrates the focus group discussions to understand the culture of blame and
identify the training needs and recommendations to establish patient safety in Muscat. Oman.
Conclusions and consolidation are drawn in chapter seven which provides an overview of the
thesis with limitations and recommendations.
xiii
DISSEMINATION OF THE RESEARCH
I would like to sincerely acknowledge the feedback I received from the journal reviewers,
editors and feedback from conference presentations. Portions of the work presented in this
thesis have been published and/or presented in the following journals and conferences,
PEER REVIEWED PAPRERS Chapter 4:
Scholarly Publication 1
• Patient safety and safety culture in primary health care: a systematic review
Lawati, M., Dennis, S., Short, S. D., & Abdulhadi, N. N. (2018). Patient safety and safety culture in primary health care: a systematic review. BMC family practice, 19(1), 104. doi:10.1186/s12875-018-0793-7
Chapter 5:
Scholarly Publication 2
• Assessment of patient safety culture in primary health care in Muscat, Oman: a questionnaire -based survey
Al Lawati, M. H., Short, S. D., Abdulhadi, N. N., Panchatcharam, S. M., & Dennis, S. (2019). Assessment of patient safety culture in primary health care in Muscat, Oman: a questionnaire -based survey. BMC family practice, 20(1), 50. doi:10.1186/s12875-019-0937-4
Chapter 6:
(Manuscript submitted and under peer review)
Primary health care professional’s perception of patient safety and safety culture in Muscat, Oman: a qualitative study
xiv
PRESENTATION ARISING FROM THE THESIS
• Patient safety in primary health care setting: A systematic review Muna Habib AL
Lawati, Dr Sarah Dennis, Professor Stephanie D. Short, Dr Nadia Noor ,Primary
Health Care Research Conference, PHC Research Matters, Adelaide 29 to 31 July
2015, Adelaide Convention Center, Australia.
• Patient safety in primary health care setting: A systematic review Muna Habib AL
Lawati, Dr Sarah Dennis, Professor Stephanie D. Short, Dr Nadia Noor, Isqua 32rd
International Conference, building quality and safety in the health care system, Doha,
from 4th to 7th October, 2015, National Convention Center, Qatar.
• Patient Safety culture in primary care in Muscat, Oman Muna Habib AL Lawati, Dr
Muna AL Lawati, D r Sarah Dennis , Professor Stephanie D. Short, Dr Nadia Noor,
Sathiya Murthi P, Patient Safety Congress, 5-6th July 2016, Manchester Convention
Center, United Kingdom.
• Patient Safety culture in primary care in Muscat, Oman Muna Habib AL Lawati, Dr
Muna AL Lawati, D r Sarah Dennis , Professor Stephanie D. Short, Dr Nadia Noor,
Sathiya Murthi P, 3rd Annual Congress & Medicare Expo on Primary Healthcare,
Clinical & Medical Case Reports, Primary Healthcare Conference, 17-19th April
2017 Dubai, United Arab Emirates.
• PhD thesis presentation , Patient Safety Culture in Primary Health Care in
Muscat, Oman, 18th April 2019, Directorate General of Health Services of Muscat
Region. Stephanie Short and Sarah Denis attended on ZOOM, Oman.
xv
ABBREVIATION
Abbreviation Meaning AHRC Agency for Healthcare Research and Quality CAGR Compounded annual growth rate DGQAC Directorate General of Quality Assurance Centre EMRO Eastern Mediterranean Region FraTix Frankfurt Patient Safety Matrix GCC Gulf Cooperation Council HSOPSC Hospital Survey on Patient Safety Culture IOM Institute of Medicine MaPSaF Manchester Patient Safety Framework MoH Ministry of Health PSFHI Patient Safety Friendly Hospital Initiative’ PHC Primary health care SAQ Safety Attitudes Questionnaire

1
Chapter 1 Preface
1
This chapter provides the structure and the study rationale of this thesis on patient safety in
primary health care in Oman.
This thesis is organized into seven chapters. The University of Sydney allows published
manuscripts that arise from the candidature to be included in the thesis. The first chapter is
the preface and rationale and the second chapter are the literature review, the third chapter is
the mixed methods design and the last chapter is the consolidation and conclusion.
The other chapters which are chapter four, five and six are published papers and a manuscript
submitted for publication. Ethics approval was obtained before the start of the studies. Each
chapter contains its own reference list and can be read independently yet contributing to the
whole thesis.
1.1 Structure of the Thesis
In Chapter 1, I have broadly outlined the background to the study and focused on challenges
faced in Oman regarding patient safety.
In Chapter 2, I have emphasized issues related to patient safety, what is the culture of health
care, described the differences between safety culture and safety climate, different models of
safety culture, and various tools used to assess safety culture in primary care. Then I have
discussed patient safety in the Middle East, followed by background on Oman, research on
patient safety and establishment of patient safety in Oman including in hospitals, and then in
primary health care.
In Chapter 3, I have described the social scientific mixed methods design in three phases.
2
In Chapter 4, my first scholarly publication was a systematic review which aimed to
evaluate the literature on the safety culture and patient safety measures used globally to
enlighten the development of safety culture among health care workers in primary care with a
focus on the Middle East. This was published in BMC Family Practice.
Chapter 5 is based on the results of the second scholarly publication which assessed the
understanding of frontline primary health care professionals regarding patient safety culture
in primary health care in Oman. A validated Hospital Survey of Patient Safety Culture tool
was used since it was the most commonly used tool in primary health care in the Gulf
Cooperation Council (GCC) Countries. This paper was published in BMC Family Practice.
In Chapter 6, (a manuscript submitted for publication) I explored the understanding of
patient safety among primary health care professionals working in Muscat, Oman. In this
qualitative study, in addition, I identified areas for improvement in order to inform a
framework to guide patient safety policy in primary health care in Oman into the future.
Chapter 7, the consolidation and conclusion, provides a summary of the whole study and
includes a discussion of its limitations. It reviews the contribution of each of the scholarly
publications to the study overall and explains the originality and significance of those
contributions.
1.2 Rationale for the thesis
Quality and patient safety are an essential goal for health care organizations and safety is
dependent on the safety culture. Quality begins with safety, let us not forget the Hippocratic
principle: “First, do no harm”. While efforts to improve patient safety and quality of care are
a global concern, many efforts have been unsuccessful due to the lack of implementation of
health plans and policies (1). Most of the research is based in hospitals, although primary
3
health care is the first line of contact with the patients. In Oman, furthermore, it has been
identified that a significant proportion of errors that occur in hospitals actually originate from
earlier levels of care (2).
In this thesis I examine the perception of the primary health care professionals to safety
culture because assessment of patient safety culture is the most essential first step in
achieving high quality health care organizations.
The current thinking on patient safety recognizes the growing need for developing a patient
safety culture to improve patient safety and quality of care (3). Establishing an environment
for patient safety may be challenging because it is associated with a change of behavior. The
perception one may draw from the literature is that, once a health care organization succeeds
in changing the perception of the frontline health care professionals towards patient safety, it
can be assured of having the most reliable and effective strategy for improving the quality of
care. Therefore a positive patient safety culture should reduce adverse events (4). Similarly,
safety culture assessment helps in auditing the integrity of the health care system and for
provision of health care improvement and benchmarking furthermore, safety culture
assessment allows health care organizations to identify the strengths and weakness of their
safety culture. Safety culture of an organization is defined as the product of individual and
group values, attitudes, perceptions, competencies and patterns of behaviors that determine the
commitment of the organizations health and safety management (5).
As health care organizations continually strive to improve, there is a growing recognition of
the importance of establishing a culture of safety. Achieving a culture of safety requires an
understanding of the values, beliefs, and norms about what is important in an organization and
what attitudes and behaviors related to patient safety are expected and appropriate.
Organizations with a positive safety culture are characterized by communications founded on
mutual trust, by shared perceptions of the importance of safety, and by confidence in the
4
efficacy of preventive measures. As primary care centers continually strive to improve, there
is a growing recognition of the importance of establishing a culture of safety. Achieving a
culture of safety requires an understanding of the values, beliefs, and norms about what is
important in an organization (6). Furthermore, patient safety in primary care is an emerging
field with a growing evidence base in the western countries, but as Chapter 4 shows, little has
been published from Oman and other Gulf Cooperation Countries (GCC).
The Ministry of Health in Oman has been working since 2002 at different levels to improve
the quality of health care services and its safety. A national working team was established to
develop a national action plan, guidelines, and mechanisms for monitoring and follow-up of
different patient safety aspects in Oman (7). A situational analysis of patient safety systems in
the Ministry of Health institutions was conducted from February to May 2009. An assessment
using patient safety indicators was carried out at different levels of the health care system
namely primary, secondary and tertiary levels (8). The key findings of this situational analysis
were that there were no vision and mission statements either at national, regional or institutional
levels. In addition, in those institutions which did have vision and mission statements, safety
was not mentioned as an essential dimension of quality. Those institutions which developed
these values did not communicate them to staff or the community adequately. The primary
health care have yearly objectives to improve the care provided, there were in general and not
related to patient safety (8).
Primary health care had scattered and poorly coordinated systems to monitor quality of care
for example, surveys on staff and patient satisfaction were conducted alternatively every two
years. They had an on-going system for auditing primary health care programs by using a
manual checklist developed by the Ministry of Health by an intensive comprehensive audit
used to be carried out yearly and the health centres prepare a corrective action plan with time
frame for the non-conformity detected by the auditors during these audits. The auditors were
5
primary health care professionals who were locally trained by the Quality Management
Department in the Ministry of Health. A recheck audit is carried out by the nursing in charge
in the health centre to make sure that action plan was implemented, and non-conformity are
corrected. Another form of monitoring was the Top Management Reviews. This is a form of
a meeting conducted yearly at the level of different regions in Oman where top officials from
the Ministry of Health attend and discuss the audit reports from each primary health care centre
and the incident reports concerning the health centre. It is basically a platform to discuss
achievements, and unresolved administrative issues concerning primary health care in the
region and the reports.
Three C Card reports are reports conducted in primary health care centres quarterly. This is
where the patient fills out a form which includes Comments, Compliments and Complaints,
these are then submitted and analysed by the Quality Management section in the region and
presented in the Top Management Review meeting. To date there is no specify system to
monitor patient safety in primary care.
In line with this scattered and fragmented system the aims of this thesis are:
1- Discover the processes or systems which facilitate a safety culture in primary care
2- Explore the measures used globally to assess the effectiveness of safety culture in
primary care and its impact on safety culture in primary care.
3- Explore the understanding of primary health care professionals regarding patient
safety culture in primary health care facilities in Oman, in order to establish a baseline
for the strengthening of patient safety in primary health care in Oman.
4- Outline areas for improvement in order to develop a framework for patient safety in
primary health care in Oman.
6
1.3 References
1. Shannon D. Special report: quality of care survey. Challenges in patient safety and quality: replacing discouragement with hope. Physician executive. 2007;33(3):16-7. 2. Medical Protection Society. How to create a patient safety culture. 2012;4(2):12-3. 3. Muna Habib AL Lawati, Sarah Dennis, Stephanie D Short, Nadia Noor Abdulhadi. Patient safety and safety culture in primary health care: a systematic review. BMC Family Practice. 2018;19:104. 4. Joann Sorra P, Kabir Khanna, MA, Naomi Dyer, PhD, Russ Mardon, PhD, and Theresa Famolaro, MPS. Exploring relationships between patient safety culture and patients' assessments of hospital care. Patient safety journal Volume 8(Number 3 ). 5. Maha Mohamed Ghobashi, Hanan Abdel Ghani El-Ragehy, Fatma Abdullah Al-Doseri , Hanan Mosleh. Assessment of patient safety culture in primary health care settings in Kuwait. Epidemiol Biostat Public Health. 2014;11(3):e9101-1-e-9. 6. World Health Organization. Conceptual Framework for the International Classification for Patient Safety. Geneva; 2009. 7. World Health Organization. Regional Launch of the WHO Multi-Professional Patient Safety Curriculum Guide in the Eastern Mediterranean Region Geneva; 2012. 8. Al-Mandhari DA. Situational Analysis of Patient Safety System in Ministry of Health Institutions, Muscat, Oman. Ministry of Health Oman, World Health Organization; 2009.
7
Chapter 2 Patient Safety in Health Care
8
2 Patient Safety
This critical analysis of the grey and academic literature presented in this thesis takes us on a
chronological journey thorough the relevant developments in patient safety internationally and
within the Eastern Mediterranean Region of the World Health Organization, of which Oman is
a member state, until 2014 when this doctoral study commenced.
This story starts with the landmark report published in 1999, by the Institute of Medicine (IOM)
in the United States “To Err is Human: Building a Safer Health System”, emphasized that patient
safety should be a key fundamental concern on the agenda of all nations (1). The publication
was a revolutionary document for patient safety and was an alarm against errors in health care
and patient harm. In the intervening two decades much has been published on patient safety in
the hospital setting, although more recently research has been emerging in other settings such as
primary care.
Patient safety is a universal issue which can affect countries at each stage of development. It is
expected that millions of patients globally suffer disabilities, injuries or death annually due to
unsafe medical practices.
In 2002, the World Health Organization, through a World Health Assembly Resolution, urged
member states to focus on importance of patient safety as a universal health care issue, this was
the first global approach to patient safety. Then, two years later, in 2004, the World Health
Organization launched a patient safety program, and established the World Alliance for Patient
Safety (2). This program emphasized the importance of patient safety as a worldwide health
care concern. In 2005-2006, the World Health Organization formulated the First Global Patient
Safety Challenge under the heading “Clean Care Safer Care” its main objection was to reinforce
the member state’s commitments in order to reduce health care-related infections. The key
elements were to increase awareness of the impact of adverse events on patient safety and to
9
develop improvement strategies. Member states committed formally to address infections
related to health care in their countries and implement the World Health Organization’s
guidelines (3). The Joint Commission on Accreditation of Healthcare Organizations and the
Joint Commission International were officially chosen as a World Health Organization team to
focus on patient safety solutions in 2005 (4).
In 2007, nine patient safety solutions were introduced to be used in health care, these solutions
were: look-alike, sound-alike medication names; patient identification; communication during
patient hand-overs; performance of correct procedure at correct body site; control of
concentrated electrolyte solutions; assuring medication accuracy at transitions in care; avoiding
catheter and tubing misconnections; single use of injection devices; and improved hand hygiene
to prevent health care-associated infection (4). During the same year, the first reginal meeting
on patient safety in the Eastern Mediterranean Region was conducted in Cairo (5). This meeting
stressed the importance of patient safety in developing countries since unavoidable patient harm
was more likely in developing countries compared to developed countries. This is due
inadequacy of resources, poor information system, lack of transparency from the health care
providers and insufficient trust from the patients themselves. All these factors added to the
magnitude and the importance of patient safety in the Eastern Mediterranean Region (5).
The Second Global Patient Safety Challenge launched in 2008 by the World Health Organization
under the heading “Safe Surgery Saves Lives” was introduced and aimed at reducing health care
infections and surgical risks in hospitals (6). It also identified core competencies required for
undertaking patient safety research and improving patient safety in an organized way (7).
In 2008, the World Health Organization identified a set of core competencies needed for
conducting patient safety research as a basis for improvement. These core competencies would
strengthen the health professionals needs to facilitate improvement in patient safety
10
internationally. Following on, in 2009, the international classification for patient safety was
developed as a conceptual framework (8) which outlined internationally agreed classifications
of patient safety and described various patient safety incidents. Alongside this the WHO
published Human Factors in Patient Safety Review of Topics and Tools (9) in order to improve
the understanding of the human factors related to patient safety. Human factors were defined
as “environmental, organizational and job factors, and human and individual characteristics
which influence behavior at work in a way which can affect health and safety. A simple way to
view human factors is to think about three aspects: the job, the individual and the organization
and how they impact on people’s health and safety-related behavior” (9). These factors are
divided into four categories: organization, team, individual and work-related environment. The
main aim of the framework is to describe how these categories influence patient safety.
Another important milestone in the history of patient safety was introduction of the Multi-
Professional Patient Safety Curriculum Guide by the Wold Health Organization in 2011 (10)
This is a guide to support the teaching of patient safety in universities and in areas such as
pharmacy, nursing, midwifery, medicine and dentistry. . Subsequently, the First Patient Safety
Assessment Manual was published which includes a set of standards for various patient safety
domains in hospitals (11). They provide a framework for patient care under the umbrella of
patient safety. This benchmarking tool enables hospitals to identify areas for improvement.
These standards were pilot tested in seven countries within the WHO Eastern Mediterranean
Region (Egypt, Jordan, Morocco, Pakistan, Sudan, Tunisia and Yemen) (11).
Following this, in 2012, the World Health Organization developed Patient Safety Research: A
guide for developing training programs This valuable document emphasizes the importance of
evidence in understanding existing problems, so that improvement strategies can be
11
implemented. It further highlighted the need for research on patient safety, and how the needs
differ across different countries (7).
Hospitals have received more attention on patient safety compared to primary care (12)
however more recently there has been more research developing in primary care (13-16).
Attaining a culture of safety requires an understanding of the values, attitudes, beliefs and
norms that are significant to health care organization and what attitudes and behaviors are
suitable and projected for patient safety (16) that is to understand to understand the safety
culture of an organization (15) . Likewise assessment of safety culture benefits health care
organizations to evaluate areas for improvement and evaluate these changes over time
which is the first most important strategy to improve quality of health care (17).
The most common theme evolving from 2011 onwards was the assessment of safety culture
in primary care, followed by incident reporting, safety climate and adverse event. The most
commonly used tool used in primary care to measure safety culture are the Manchester
Patient Safety Framework (MaPSaF) (18), the Hospital Survey on Patient Safety Culture
(HSOPSC) (19) and the Safety Attitudes Questionnaire (SAQ) (20). These tools are further
discussed in depth below.
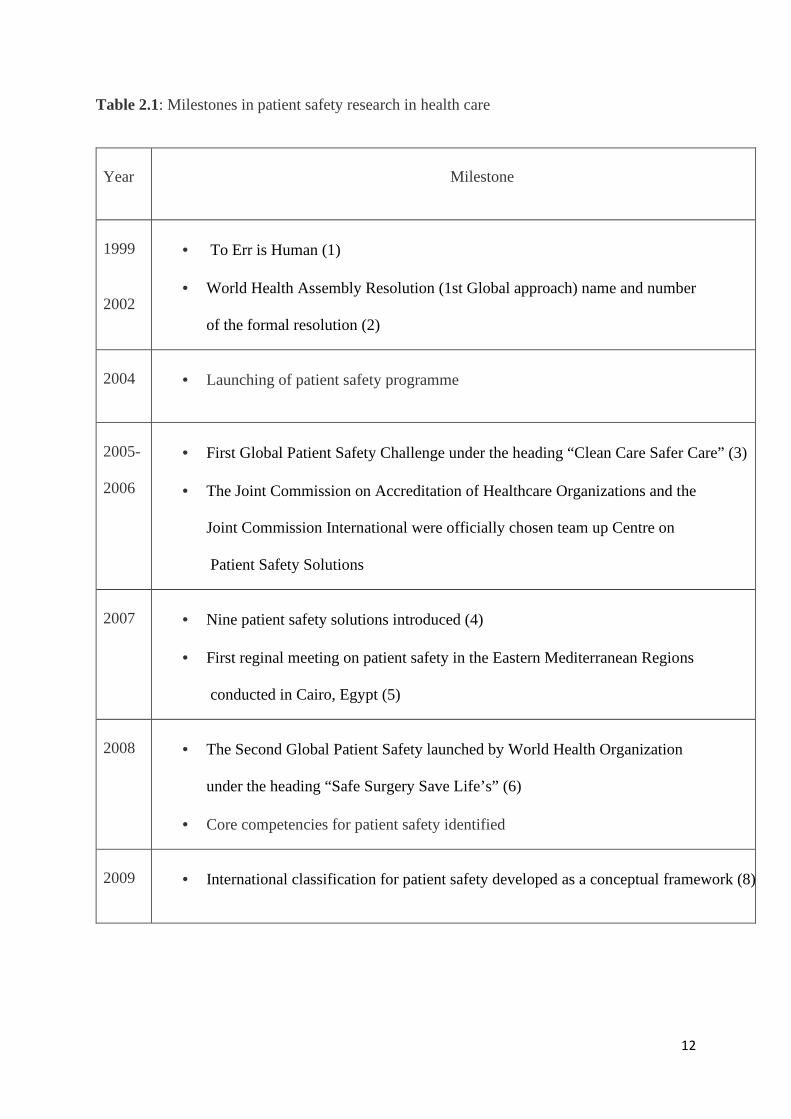
We summarise the development of expertise and action in relation to patient safety in health care
in Table 2.1 below.
12
Table 2.1: Milestones in patient safety research in health care
Year Milestone
1999
2002
• To Err is Human (1)
• World Health Assembly Resolution (1st Global approach) name and number
of the formal resolution (2)
2004 • Launching of patient safety programme
2005-
2006
• First Global Patient Safety Challenge under the heading “Clean Care Safer Care” (3)
• The Joint Commission on Accreditation of Healthcare Organizations and the
Joint Commission International were officially chosen team up Centre on
Patient Safety Solutions
2007 • Nine patient safety solutions introduced (4)
• First reginal meeting on patient safety in the Eastern Mediterranean Regions
conducted in Cairo, Egypt (5)
2008 • The Second Global Patient Safety launched by World Health Organization
under the heading “Safe Surgery Save Life’s” (6)
• Core competencies for patient safety identified
2009 • International classification for patient safety developed as a conceptual framework (8)
13
2011 • Multi-Professional Patient Safety Curriculum Guide developed (10)
• First Patient Safety Assessment Manual published, which includes set of
standards for patient safety domains in hospitals (11)
2012 • Patient Safety Research: A guide for developing training programs published (7)
We will now examine more closely the concepts most relevant to this study: safety culture,
characteristic of the safety culture model and ‘the Swiss cheese model of accident causation’
that has been used to assess patient safety culture in health care.
2.1 What is safety culture in health care?
The concept of ‘safety culture’ was first proposed after the Chernobyl nuclear power disaster
in 1986 and adapted by different other organizations such as aviation industry, a highly
reliable industry. While the concept was introduced over three decades ago, Dominic Cooper
a British psychologist and behavioral researcher, defined culture as the “product of multiple
goal oriented interactions between people (psychological), jobs (behavioral), and the
organizational (situational), whereas safety culture is the combination of the dynamic inter-
relationships between individuals 'attitudes, their safety behavior organization’s safety
systems support to improve safety on daily basis” (21).
In the intervening years there have been varying definitions in the literature concerning safety
culture, however the most widely cited definition in the context of health care is that used by
Agency for Healthcare Research and Quality (AHRC), an agency within the United States
Department of Health and Human Services.
14
“The safety culture of an organization is the product of individual and group values, attitudes,
perceptions, competencies, and patterns of behavior that determine the commitment to, and the
style and proficiency of, an organization’s health and safety management. Organizations with
a positive safety culture are characterized by communications founded on mutual trust, by
shared perceptions of the importance of safety, and by confidence in the efficacy of preventive
measures” (22) (23).
This has clearly influenced the definition of safety culture used by the World Health
Organization which is:
“… a culture that exhibits the following five high-level attributes that health-care
professionals strive to operationalize through the implementation of strong safety management
systems; a culture where all health-care workers (including front-line staff, physicians, and
administrators) accept responsibility for the safety of themselves, their co-workers, patients,
and visitors; a culture that prioritizes safety above financial and operational goals; a culture
that encourages and rewards the identification, communication, and resolution of safety
issues; a culture that provides for organizational learning from accidents; a culture that
provides appropriate resources, structure, and accountability to maintain effective safety
systems” (24).
Thus, within the context of health care, safety culture reflects the attitudes and values of people
working in an environment, including management’s obligation to safety, work practices
related to safety, adherence to safety rules and adverse events. Safety culture affects the
behavior of a person in relation to patient safety.
James Reason, another British psychologist (25) described five essential characteristics which
are required to develop a culture of safety. This is outlined in Figure 2.2 an organisation can
accomplish a strong, positive safety culture if these elements are embedded in the
organization.
15
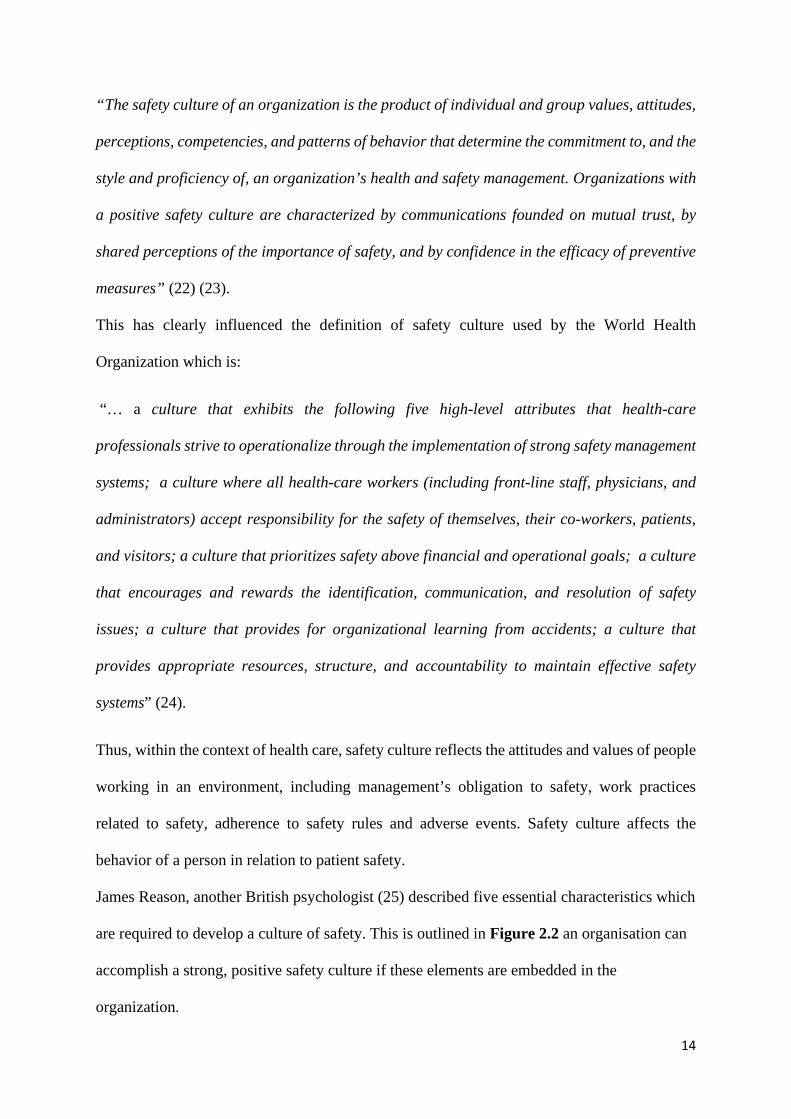
Figure 2.2: Characteristics of a safety culture model, as developed by James Reason
Source: Jilcha, Kassu & Kitaw, Daniel. (2016). A literature review on global occupational
safety and health practice & accidents severity. International Journal for Quality Research.
In order to achieve and accomplish a strong positive safety culture organization must
consider these five elements. Informed culture , where health care professions in an
organization have the knowledge that determines the safety of an organization as a whole
with an effective information system that can analyze , collect data on adverse events, and
report adverse events freely without being blamed as in reporting culture and they are
encouraged to do so in just culture. A learning culture were staff take adverse events as
areas for improvements and a flexible culture were staff can report correctly in a speedy
environment.
There is an interrelationship among these, an informed culture must count on a good
reporting culture, which it turns rely upon a just culture. role of management in establishing
the policies, procedures and tools to establish those are essential for its success. These
Safety culture characteristics
Informed culture
Reporting culture
Just culture
Learning culture
Flexible culture
16
characteristics, if united together, can lead to a strong , positive culture with trust that
support organizations to achieve incident reporting, failure to do so, can demotivate
employees to report errors, adverse events or incidents (26).
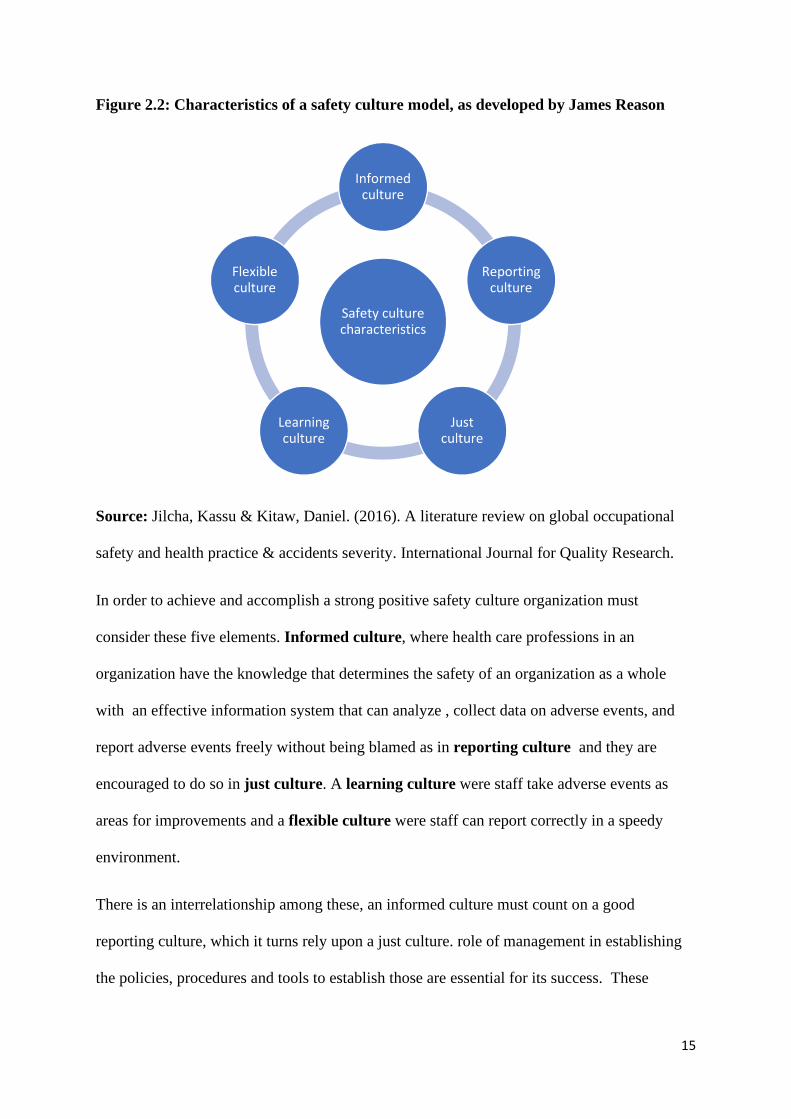
A common model that helps to understand system failure, the incidence of adverse events and
incidents is the ‘Swiss cheese model of safety incidents’, developed by James Reason (27).
This graphic model has been widely adopted by patient safety professionals and the World
Health Organization (27), and is illustrated in Figure 2.3. This model proposes that adverse
events can be prevented by defensive barriers with holes which are inconsistent and can open
and close randomly representing the swiss cheese. If all the holes are aligned by any chance, a
risk will reach to a patient which can cause adverse event (27).
Figure 2.3: The Swiss cheese model of safety incidents developed by James Reason
Source ( https://psnet.ahrq.gov/primers/primer/21 accessed on 22nd May 2019)
As the model indicates, health care is a very complex environment and expecting errors from
humans is likely, as their work is a stressful and dynamic environment. This approach helps in
identifying errors before they occur that can lead to patient harm. There were two terms used
by Reason ‘active term’ and ‘latent term’ to differentiate between human errors and system
17
errors (27). Reason defines error "as a general term covering all those occasions in which a
traced sequence of mental or physical activities fails to achieve the expected result, and when
these failures cannot be attributed to the intervention of chance" (28).
Active errors occur when a human encounter a larger system and usually involves the frontline
personnel. They are unsafe acts that represent the sharp end for example failure to identify the
patient before blood investigation. On the other hand, latent errors, represented by the blunt
end, occur because of organization failures. This blunt end represents the systems in the health
care that are not in-patient contacts but can impact the personnel, for example policies. The
sharp end is further divided into slips and mistakes, which draws on cognitive psychology.
Slips occur when a set of a plan is carried out incorrectly for example the pharmacist dispensed
flucloxacillin instead of amoxicillin occur due to stress, emotional disruption and fatigue.
Mistakes occur due to a lack experience, inadequate training, or negligence and can be reduced
by enhancing competences, career pathways and training.
Latent errors involve a more intensive approach that assesses how policies and protocols are
designed, how individuals relate in a system and depends on the availability of resources
(personal, finance and time) and severity of an error. Therefore, in order to improve a system,
we need to pay attention to the human factors which includes design of protocols, policies and
guidelines. Furthermore, reporting of active errors need to be encouraged since it helps to
identify flaws in the system.
We turn now in the next section to discuss safety climate, the term that denotes a snap shot of
safety culture.
18
2.2 What is safety climate in health care?
Safety climate is defined as “a summary of perceptions that employees share about their work
environment” (29), it is a reflection of safety culture in an organization (26).
The terms safety culture and safety climate have been used frequently in healthcare
organizations. These twin terms derive from an iceberg metaphor, safety climate is the
perception across the workforce at a given time and place and refers to what is happening in an
organization. It is the way things are done which can be seen. Whereas the safety culture is the
underlying values, ideas, behaviours and working practices that influence the health and safety
performance of an organization (30).It explains the reason behind why it is happening and
represents long term attitudes and beliefs.
In short, safety climate describes what is happening in an organization which is more
superficial whereas safety culture explains why it is happening which is more in dept (31).
I will now address, in the following section, various tools which have been used in assessing
safety culture and safety climate in health care, and primary health care.
2.3 Tools to assess safety culture in primary healthcare
Around the globe there are many tools which have been used to assess safety culture and safety
climate, these tools are mainly for hospital use but some have been used in other settings such
as primary health care, nursing homes, surgical wards and emergency units (32).
Based on the systematic review (33), that was conducted for this study, which is discussed in
depth in Chapter 4, the three most commonly used tools used to assess patient safety in primary
health care research are as follows:
1. Hospital Survey on Patient Safety (19, 22)
19
2. Safety Attribute Questionnaire (20)
3. Manchester Patient Safety Assessment framework (18)
We now examine the relative relevance and usefulness of these three tools for the purposes of
this study.
First, the Hospital Survey on Patient Safety Culture (HSOPSC) was developed by the
Agency of Health Care and Research for Hospitals in 2004 in the USA (22). It has since been
adapted and modified for use other health care settings (22). It measures healthcare
professionals’ perspectives of safety culture. The tool was developed after an extensive
literature review on safety, accidents, medical errors, safety climate and culture and
organizational climate and culture. There were also interviews with hospital staff and surveys.
The instrument includes fourteen dimensions, twelve are multiple item dimensions (two safety
culture dimensions and two outcome dimensions) and the last two are single item dimensions
used to check the validity. The dimensions are: manager’s expectations and actions promoting
safety, organizational learning, and teamwork within units, communication openness, feedback
and communication about errors, non-punitive response to errors, staffing, and management
support for patient safety, teamwork across units and handoffs and transitions. The scale used
is a five-point Likert scale which ranges from ‘Strongly disagree’ to ‘Strongly agree’, or from
‘Never’ to ‘Always’ when relevant. A global safety grade between ‘poor’ and ‘excellent’ and
the numbers of reported incidents in the past 12 months were also assessed. The dimensions
of the tool are communication openness, feedback and communication about errors, frequency
of events, handoff and transitions, management support, non-punitive response to errors,
organizational learning, overall perception of patient safety, staffing, supervisor expectations
and teamwork within and across the units.
In terms of reliability and validity the Hospital Survey on Patient Safety Culture tool was found
20
to be “psychometrically sound at the individual, unit and hospital level analysis” (34) in
primary health care settings, it has been used in studies from the USA, UK and Europe in the
hospital setting (33, 35). It has been adapted and validated for primary care use in Portugal (36)
and Switzerland (37). It is a valid and a reliable tool developed based on previous literature,
cognitive tests and factor analysis. Safety culture variations have been reported across
healthcare facilities, departments and occupational categories of healthcare workers in North
America, Europe, Asia, and the Middle East (38).
This tool has been used in the primary health care settings in the Middle East including Kuwait
(16), Turkey (14), Iran (13) and Yemen (15) . Furthermore, the tool has been used in Saudi
Arabia ( 6 studies), Egypt ( 4 Studies), Oman ( 2 studies), Kuwait ( 1 study), Lebanon (1 study)
and Palestine (1 study) and out of these sixteen were in hospital settings and only two in
primary care setting (39).
We turn now to consider the second tool, the Safety Attitudes Questionnaire (SAQ) (20),
which is a modification of the Intensive Care Unit Management Attitudes Questionnaire (20) .
This questionnaire derives from the Flight Management Attitudes Questionnaire commonly
used in aviation. It was developed based on that fact that aviation accidents occur due to a break
down in teamwork, leadership, communication issues and combined decision machining.
Therefore, it measures the attitudes of staff based on these domains (20). The tool was
developed by a team from the University of Texas in 2000 (40).
The Safety Attitudes Questionnaire is based upon two conceptual models, the Vincent's (41)
framework for analyzing risk and safety and Donabedian's (42) conceptual model for assessing
quality. This creates four themes: safety climate, teamwork climate, stress recognition, and
organizational climate, it’s a user-friendly questionnaire and can be used to monitor changes
over a period.
The tool can measure six patient safety-related domains which are teamwork climate, safety
21
climate, perceptions of management, job satisfaction, working conditions, and stress
recognition (20).
In terms of primary health care, it has been used in Brazil (43) the study assesses attitudes to
safety culture in Brazilian primary care and used in Germany general practice where it was
modified to a German version called as the Frankfurt Patient Safety Climate Questionnaire
(44). The theoretical framework behind this questionnaire focuses on human factors which
makes the tool flexible to adapt the context of the country where its used in. The main weakness
of the tool is that it cannot explore differences in attitudes it can only pin point differences in
attitudes (20) and some respondents found the questionnaire quite long (32).
We now move to the third most commonly used tool used in primary health care safety
research, The Manchester Patient Safety Assessment framework (MaPSaF). The
Manchester Patient Safety assessment Framework was developed by researchers at the
University of Manchester to assist National Health Service organizations to monitor their
processes in safety culture. This tool was promoted by the National Patient Safety Agency
(NPSA) in the National Health Service in the UK. The typology of organizational culture used
in the development of Manchester Patient Safety Culture Assessment Tool (MaPSCAT) (45)
assesses organizations as either pathological, bureaucratic or generative (46). However, this
was again further modified to five-levels of organizational culture (18) which are: (1)
pathological organizational culture where this form of organizational culture they are certain
that there is no need to waste time on risk management and safety issues. (2) Reactive
organization culture is confidence that risk should be taken seriously, and something needs to
be done if an incident occurred. (3) The calculative organization culture has systems in place
to manage all possible risks. (4) The proactive organizational culture is always on the alert,
thinking of risks that might emerge and take actions before the risk occur. (5) The fifth and last
type of organizational culture is a generative organizational culture, which believes that risk
22
management is an integral part of everything in an organization.
the Manchester Patient Safety assessment Framework has ten domain (18) which are as:
continues improvement; priority given to safety, system errors and individual responsibility,
recording incidents, evaluation incidents, learning and effective change, communications with
in the organization, personal development and management, staff education, training and team
work.
The Manchester Patient Safety Assessment Framework is a validated tool (47), that can be used
to assist organizations to reflect on safety culture. It can be used to assess an organization’s
culture maturity as a site for improvement. The MaPSaF was also modified for use in the
German health system and was renamed the Frankfurt Patient Safety Matrix (FraTix) (48) .
FraTix appeared to be a good tool for self-assessments aimed at improving safety culture but
did not lead to measurable improvements in error management. The tool was altered and tested
in the New Zealand (49) context to facilitate learning about safety culture and facilitate team
communication.
The tool can be easily adapted to the context as seen in German and New Zealand primary care
but to accurately learn about strengths and weakness of safety culture validated quantitative
and qualitative methods to be used together to assess safety culture in primary care (48).
As the above discussion suggests, there is no single tool used for assessing patient safety
climate or culture within health care organizations. Each tool has its strengths and
weaknesses. Most of the tools have been developed for usage in the hospital setting but can
be adapted to primary health care. All the three tools can be used in primary care in order to
improve patient safety culture. There is no tool that offers a quick fix to patient safety culture.
Each tool requires time and commitment so that the health care organization can benefit.
We now turn to examine patient safety in the Middle East.

23
2.4 Patient Safety culture in the Eastern Mediterranean Region
There are 22 countries in the Eastern Mediterranean Region of WHO: these are Afghanistan,
Bahrain, Djibouti, Egypt, Iran, Iraq, Jordan, Kuwait, Lebanon, Libya, Morocco, Oman,
Pakistan, Palestine, Qatar, Saudi Arabia, Somalia, Sudan, Syria, Tunisia, United Arabs
Emirates and Yemen. In 2007 these member states were encouraged by the World Health
Organization Eastern Mediterranean Region to improve patient safety through the introduction
of the ‘Patient Safety Friendly Hospital Initiative’ (PSFHI) (11) (5). The Eastern
Mediterranean Region of the World Health Organization is illustrated in Figure 2.4.
Figure 2.4: Map of the Eastern Mediterranean Region of the World Health Organization.
(Source: https://www.iapb.org/iapb-regions/eastern-mediterranean/ accessed on 15th May
2019)
The following s suggest that patient safety is a major concern for the health policy agenda in
Arab countries (EMRO) and it is vital that the causes of harm to patients are identified and
understood to develop strategies for improvement.
24
The Patient Safety Friendly Hospital Initiative involved one hospital each from seven
developing countries (Egypt, Jordan, Morocco, Pakistan, Sudan, Tunisia and Yemen) being
assessed using the Patient Safety Friendly Hospital Initiative (39).
The initiative found that none of the hospitals selected achieved a baseline score due to a lack
of leadership and management commitment. In addition, it was also found that patients were
not involved nor did they have any involvement in the management of their own treatment
plans which is a part of the standard (39).
The Patient Safety Friendly Hospital Initiative provide a framework that allows hospitals to
evaluate patient care from a patient safety perception, capacity building in patient safety and
involve patients to improve the care provided. the standards are divided under five domains
which are: 1) Leadership and management; 2) Patient and public involvement; 3) Safe
evidence-based clinical practice; 4) Safe environment; and 5) Lifelong learning (11). There are
140 patient safety standards under the domains, and these were developed based on the World
Health Organizations clinical guidelines, systematic reviews on patient safety, varies countries
accreditation standards (Arab League for Quality in Health care) and published papers on
patient safety.
Accreditation of an organization suggests that the organization is complying with the
international or national standards to provide a quality health care. There are various
accreditation body using different standards are available globally. The World Health
Organization carried out another study in the Eastern Mediterranean Region on the
accreditation programs and found that there were no accreditation system, this encouraged the
health care institutions to start introducing accreditation in the health care system in 2000 (50).
25
A further study was performed in hospitals in Egypt, Jordan, Kenya, Morocco, South Africa,
Sudan, Tunisia and Yemen to evaluate the frequency and nature of adverse events to patients
of these countries, 83% of adverse events reported in these countries were avoidable (39).
One of the greatest challenges for patient safety in the Arab word especially the Gulf
Cooperation Council (GCC) comprises of six countries, Bahrain, Kuwait, Oman, Qatar, Saudi
Arabia, and United Arab Emirates is the diverse health care workforce. The majority of the
health care professionals working in the GCC are graduates from many different countries with
varied cultures and training backgrounds (51). For example, in Ras Al Khaimah in the United
Arab Emirates over 90 per cent of nurses and doctors are internationally qualified despite the
policy of ‘Emiratization’(52). Emiratization is the term used as an initiative by the government
of the United Arab Emirates to hire its citizens in the public and private sectors. In Oman we
use the term Omanization which means the same.
We now focus on the context within which this mixed methods design was conducted: Oman.
We examine its geography and history briefly, and its demographic profile.
2.5 The Omani Context
2.5.1 Country profile
The Sultanate of Oman is in the south-eastern corner of the Arabian Peninsula, bordering the
Arabian Sea, Gulf of Oman, and Persian Gulf, between Yemen and the United Arab
Emirates, Muscat is the capital of Oman. The Sultanate of Oman is a high-income oil-
producing country in the Arabian Gulf. It follows the Al Busaidi ruling dynasty, all Omani
are Muslims and follow the culture of Islam. Its renaissance, that is its social and economic
transformation, began in 1970 with the ascent of His Majesty Sultan Qaboos Bin Said to
power. Oil was discovered in Oman in mid 1960s. The population is concentrated in major
26
urban centers, with few people dispersed in isolated small areas. The economy is dependent
currently on oil, agriculture, fishing and tourism.
2.5.2 Demographic indicators
Oman has a young population with median age of 19 years and age-dependency ratio of 0.7,
It has been placed by the World Bank as a high income country (53), this classification is
based on the fact that Oman has a gross national income per capita of more than US$12,056.
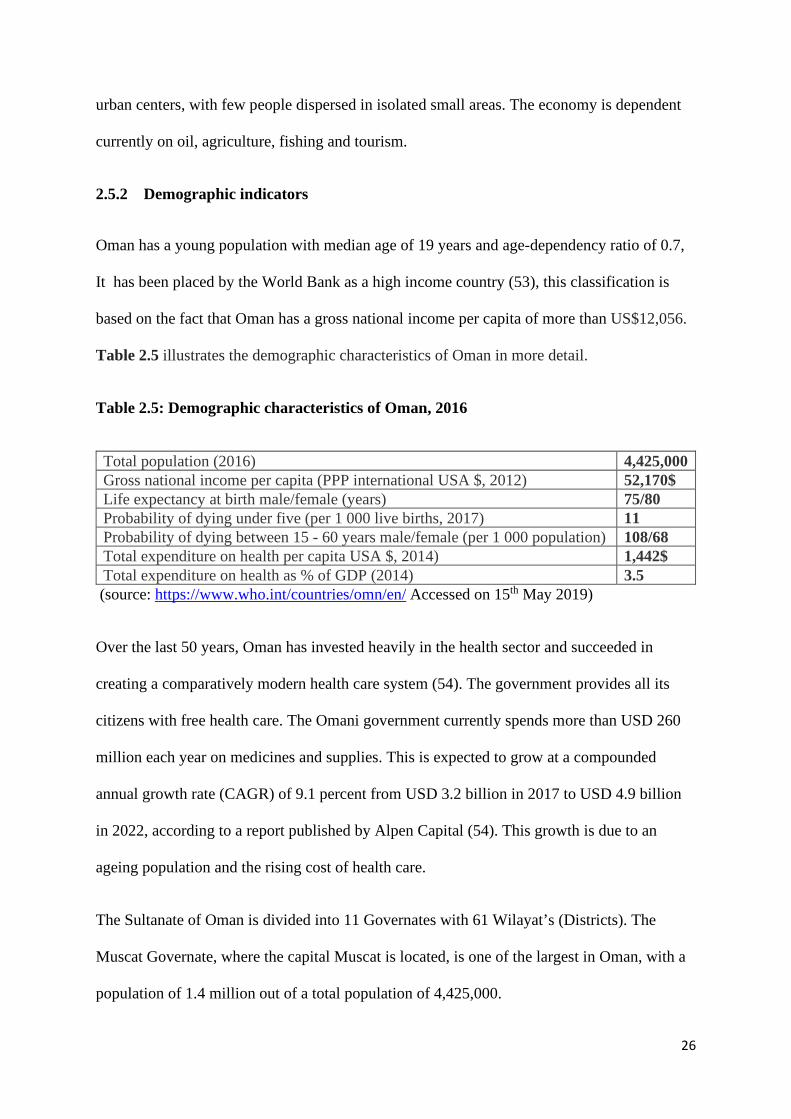
Table 2.5 illustrates the demographic characteristics of Oman in more detail.
Table 2.5: Demographic characteristics of Oman, 2016
Total population (2016) 4,425,000 Gross national income per capita (PPP international USA $, 2012) 52,170$ Life expectancy at birth male/female (years) 75/80 Probability of dying under five (per 1 000 live births, 2017) 11 Probability of dying between 15 - 60 years male/female (per 1 000 population) 108/68 Total expenditure on health per capita USA $, 2014) 1,442$ Total expenditure on health as % of GDP (2014) 3.5
(source: https://www.who.int/countries/omn/en/ Accessed on 15th May 2019)
Over the last 50 years, Oman has invested heavily in the health sector and succeeded in
creating a comparatively modern health care system (54). The government provides all its
citizens with free health care. The Omani government currently spends more than USD 260
million each year on medicines and supplies. This is expected to grow at a compounded
annual growth rate (CAGR) of 9.1 percent from USD 3.2 billion in 2017 to USD 4.9 billion
in 2022, according to a report published by Alpen Capital (54). This growth is due to an
ageing population and the rising cost of health care.
The Sultanate of Oman is divided into 11 Governates with 61 Wilayat’s (Districts). The
Muscat Governate, where the capital Muscat is located, is one of the largest in Oman, with a
population of 1.4 million out of a total population of 4,425,000.
27
2.6 Healthcare system in Oman
The healthcare system in Oman has developed rapidly in the last 50 years. Before the 1970s,
there were only two hospitals in Muscat with a total of 12 beds, owned and administered by
the American Mission (Provided by American health care professionals). The health service
was very limited with few physicians and nurses. The Omani population mainly used
traditional methods for treatment.
There are four distinct phases in the development of the Omani health system:
First phase 1971-80: There were significant advances in the health care system. This decade
heralded the beginning of Oman’s phase one of the Health System Infrastructure
Development. In 1975, His Majesty the Sultan Qaboos established the Ministry of Health by
a Royal Decree (No. 26/75). The Ministry took over two hospitals: 1) Al Koula Hospital
which was run by the Petroleum Development Oman since it was close to the Petroleum port
and 2) AL Rahma Hospital was run by the American Mission ( hospital run by a American
health care professionals) (55). It mainly treated the locals and expatriates during that time.
Second phase, 1981-1990: In phase 2 of the Health System Infrastructure Development,
there was continued expansion of the health care system. New hospitals were built with
modern tertiary medical care facilities, and the College of Medicine and Hospital of the
Sultan Qaboos University was established, Oman’s first medical school, in 1986 with
guidance and support of the Royal court (55).
Third phase, 1991-2000: Oman’s Health Infrastructure Development Phase 3 was
characterized by the replacement of old hospitals by new modern hospitals and well-designed
health centers. The Wilayat’s (districts) approach was introduced, which aids in the
formulation, monitoring and implementation of the health development plans. Furthermore,
28
the Wilayat health supervisors’ offices where set up for leading the Wilayat Health System
and to serve as a link between the Ministry of Health and the community. In addition, there
was considerable strengthening of the health system organization and management. Human
resources production within Oman’s health care system entered the consolidation phase with
the advent of the 21st century.
Fourth phase post-2000: This phase has been characterized by the consolidation in which
primary care was reinforced through the expansion of primary care centers to provide
primary health care to all Omani population .This has been further strengthened by the
expansion of the primary health care network of health centers and extended health centers
such as hospitals and nursing homes, further development of super specialty health care, for
example the National Oncology Center, and the proposed National and Regional Cardiac
Centers, as well as a series of organizational and managerial reforms and refinements.
In 2002, the Omani quality management system was piloted in one of the primary health
centers. By 2005 all the primary health care centers in Muscat Oman had established the
Omani quality management system.
The implementation of the quality management system was carried out in four stages:
1- Introduction and preparatory stage:
The purpose of the introductory phase was to ensure that the key ministry of Health officials
was acquainted with and approved the Quality Assurance/Improvement systems vision, goals
strategies and approaches. During this phase, a comprehensive assessment of the situation of
the health care system was done.
29
2- Early Implementation Stage:
In this phase the Quality Assurance/Improvement was implemented in 2002 in selected
regions and Muscat was one of them. The regional Quality Committee developed; a lot of
training activities conducted to all the level of the health care workers to ensure that all the
elements were understood in order to carry out the quality system. This phase provided the
basis for future planning and implementation of the expansion phase.
3- Expansion stage:
Quality Assurance/Improvement system was expanded to other primary health care centers in
Muscat region. Areas for improvement were recognized during the early implementation
phase were addressed, priorities agreed, and policies for expansion were developed.
4- Consolidation stage:
Here was institutionalization of the quality management system to the Muscat health
Governate which was under the umbrella of the Ministry of Health. This was attained by
continuously monitoring and evaluating processes in health care institutes.
In order to continue the achievements made in health care status in Oman over the last fifty
years the Ministry of Health (MoH) developed a long-term vision for the development and
enhancement of the health care system in Oman. In 2012, a long-term vision was named as
“Health Vision 2050” (56) which was developed through a number of well-thought-out
scientific activities which comprehensively examined all the factors that affect the health
system: political, economic, social, technological, environmental and legal factors. It is based
on the six building blocks of the health system: leadership or governance, financing, human
resources for health, service delivery, information, and medical products, vaccines and
30
technology that used the “World Health Organizations Framework for Action on Health
System (56).
The Ministry of Health established a Directorate General of Quality Assurance Centre
(DGQAC) in 2014 to meet the need of the striving 2050 plan. The mission of the department
is “to raise the level of quality of healthcare services and patient safety in all Ministry of
Health institutions in collaboration with these institutions through the application of
international standards appropriate to the local realities”. (57)
The objectives for the Quality Assurance and Patient Safety Department under the umbrella
of the Directorate General of Quality Assurance Centre at the Ministry of Health that is based
on the “Health Vision 2050” are:
• To establish a centralized documentation system in accordance with international
standards.
• To establish a national accreditation system will be in collaboration with international
accreditation institutions.
• To establish an integrated risk management system based on international standards.
• To establish an integrated system to ensure patient safety based on international
standards.
• To establish a system to motivate health workers and empower patients in health
institutions under the Ministry of Health.
Prior to the development of the “Health Vision 2050”, there were strategic health development
plans for each five-year health development in Oman from the year of 1976, these plans had
substantial impact on health services and health status and it reflects the commitment of the
government towards health care and health services since renaissance.
31
Since then, nine five year plans have been implemented , The first segment of the health
planning in Oman was from 1976 to 1990, wherein three five-year plans were implemented
(1976-1980), (1981-1985), (1986- 1990), these plans were based on infrastructure building of
health services since during that time there were limited health institutions.
The second segment of health planning began in 1991 this encompassed three five-year health
plans: (1991-1995), (1996-2000), (2001-2005), this phase was characterised by
“Decentralization of health services” through the formation of directorates general of health
services for each region in Oman. The decentralization policy in health services smoothed in
promoting the health services at the reginal level and resulted in rise in health services all over
Oman.
The third segment of health plans includes the seventh and eight five-year health plans (2006-
2010), (2011-2015). These plans were based on health visions, goals, objectives and strategies
were developed at the national level. these health plans projected expected results using
evidence-based-management philosophy and included the targets, the operational activities, the
resources needed and indicators for monitoring and evaluation.
A Fourth segment of health plans started in 2011 at the time of development of "Health Vision
2050". This stage projected vision of health services in the coming forty years. These strategic
health plans in the "Health Vision 2050" were interpreted in the development of the ninth five
years health plan that started in 2015. The current updated plan (2016-2020) is based on the
“World Health Organizations Framework for Action on Health System” which is the main
framework for the “Health Vision 2050”.
The quality management system was introduced in the seventh five-year plan (2006-2010) and
patient safety was introduced in this domain in the eighth five-year plan (2011-2015). The main
32
aim of the quality and patient safety plan is to improve the quality of services provided at all
the levels of care that is primary, secondary and tertiary.
As of 2019, the Quality Assurance/Improvement activities and programs were concurrently
reinforced and included standard organizational operations. This study commenced in 2014
with the aim of contributing to fulfilment of the “Health Vision 2050” with ideas and
evidence to inform the strengthening of patient safety policies, guidelines and training in
primary health care in Oman.
This brings us to the primary health care system in Oman.
2.6.1 Primary health care in Oman
Primary health care (PHC) is the is the first line of care provided to the community. It is a
whole-of-society approach to health and well-being focused on the requirements of
individuals, families and communities (58). The World Health Organization described
Primary Health Care as meeting the people’s health needs, by promoting preventive,
protective, curative, rehabilitative and palliative care for all the individuals in the community
(59). It further address the social, economic, environmental policies of the community in
addition to empowering communities, families, individuals to help and protect health and
social services for all (59). Most of the research on patient safety in recent years has been on
hospitals however, since 2018, the research has been extended to primary healthcare as well,
highlighting the importance of patient safety in primary care (33).
2.6.2 Characteristics of primary health care
Primary health care (PHC) are considered as the essential entry point for treatment for other
levels of care for a patient to be transferred secondary and tertiary care the patient must go
through primary health care. It acts as a connection between the public and service provider
33
and reflects the expansion of the health system. It is known that the optimal use of primary
health care centres will reduce the workload of other higher level of care in Oman (60).
In Oman a range of services are provided in the primary health care centers, general
outpatient departments, mother and child care, school health, immunization, elderly care,
health education, communicable and non-communicable disease, dentistry, X-ray services,
laboratory services and pharmacy. Each primary health care centers services a population of
around 10-15 thousand, and as at 2019 there were 38 primary health care centers across
Muscat.
The services are provided by general medical practitioners from different nationalities,
dentists, nurses health educators, X-ray technicians, pharmacists and dietitians. In the remote
areas in Muscat facilities like X-ray and dental clinics are generally not available. The staff
work in two shifts in the morning and in the afternoons including certain hours during the
weekends (60).
There are some unique characteristics to primary health care that make of patient safety
initiatives quite challenging. In hospitals for instance, the care is provided within one system,
unlike primary health care where the patient is referred to other specialties secondary or
tertiary care for further treatment and management. In addition, primary health care offers
treatment which is less invasive compared to hospitals. Adverse events reporting in hospital
is more advanced and complex where as in primary healthcare the reporting system is manual
and not automated (61).
34
2.7 Establishing patient safety in Oman
Patient safety is the absence of avoidable harm to a patient and reduction of unnecessary risk
which are associated to the health of the patients. The Ministry of Health of Oman considers
that patient safety is an essential factor in delivery of high-quality health services to the
community. In order to improve the patient safety programs in Oman, the regional office
developed and adopted a strategic plan to improve the overall performance of safety issue in
patients. In 2007, a team was established for improving patient safety by conducting a patient
safety training program for all health care organization, this was organized by the department
of Quality Assurance and Improvement at the Ministry of Health. Patient safety has been
implemented in health care institutions in the following phases as proposed by the strategic
health plans (62):
Developmental stage 1 (2009-2010)
• Health care systems to be assessed for safe health care in primary, secondary and
tertiary care. Corrective action plans were implemented.
• Patient safety culture and awareness to be assessed among health care professional
Developmental stage 2 (2010-2011)
● Develop a safety training schedule for key members as well as selected staffs at
institutional levels.
● Training of the national key figures on patient’s safety.
● Raise awareness among to service providers and general public for improving
patient’s safety.
● Conduct risk management and assessment.
35
Developmental stage 3 (2012-2013)
● Develop and launch national safety indicators
● Implement national patient’s safety solution (3-4 solutions)
● Develop national safety standards
There are a set of indicators developed by the Ministry of Health for assessment of Quality
Assurance and Improvement system in Oman for all health institutions, and the indicators
related to Patient Safety as per the plan (2016-2020) are (63): (1) By the end of 2020, an
integrated system will be established to ensure patient safety based on international standards,
(2) an integrated system established to motivate health workers and empower patients and (3)
establish an integrated risk management system based on international standards. Until 2019,
none of these indicators have been established in primary care.
I will now further discuss research on patient safety in Oman till date
2.8 Research on patient safety in Oman
Oman aims to expand the health and wellbeing of its people by adapting the best available and
evidence based health practices and system and it attempts to be the research centre and the
research leader that addresses health priorities in order to enhance and improve the health care
system in Oman to fulfil the “Health Vision 2050” .Oman ranks ninth among the fifteen
countries in the middle east region in terms of research (64).
There are four papers on patient safety in Oman till date published in various nation and
international journals. The first study published in 2014 on patient safety culture assessments
in hospitals in Oman and the study explored patient safety culture among nurses (61) identified
that communication about errors, teamwork and management support are major patient safety
culture predictors and investing in improving these aspects will no doubt enrich patient safety
36
culture in Omani health care system (65). The second one, in 2016 was shown to compare self-
estimated awareness and practice of the World Health Organization’s nine “Life-saving Patient
Safety Solutions” in Oman including hospital and primary health care (67).
The third paper (33) and the fourth paper (68) are scholarly publication and are part of this
thesis that are discussed in depth in chapter four and five. The next paragraph will discuss
about patient safety gap in primary health care.
2.9 Patient safety gap in primary health care in Oman
The Ministry of Health is very keen to see Oman as an example for other countries in practicing
patient safety. It implemented the Patient Safety Friendly Hospital Initiative by the WHO in
the Government and the private hospital across Oman in 2011and aimed at enhancing the
prominence and application of patient safety practices in health care facilities. It delivers an
outstanding framework to guide hospitals in establishing a patient safety improvement process.
these standards included, leadership/management, patient and public involvement, safe
evidence-based clinical practices, safe environment and life learning measure (69).
There is a limited understanding to patient safety culture in primary health care and the
perception of primary health care professionals in Oman has not be studied before the
commencement of this thesis hence it will help to understand their attitudes and behaviours
towards patient safety thus providing an opportunity to enhance patient safety in Oman since
there is a lack of knowledge about patient safety culture and no previous studies have examined
this aspect in the Omani primary health care.
As at the time of writing, in 2019, the primary health care system in Oman does not have an
established system of patient safety even though the Ministry of Health initiated development
37
of patient safety which was mainly seen in hospitals. The main aim of this thesis is to
establish a baseline for the development of patient safety in primary care.
In progressing this the next Chapter will discuss the 1st Phase which will help us to develop
the patient safety policy for primary care. The next chapter describes different methodologies
used in this study that addresses the research questions developed in my thesis.
38
2.10 References
1. Linda TK, Corrigan JM, Donaldson MS. To err is human: building a safer health system. Washington DC: National Academy Press; 1999 1999//. 2. World Health Organization. World Alliance for Patient Safety. Geneva: WHO; 2004 October 2004. 3. WORLD HEALTH ORGANIZATION G. GLOBAL PATIENT SAFETY CHALLENGE. 2006. 4. Organization WH. WHO launches 'Nine patient safety solutions' 2007 [Available from: https://www.who.int/mediacentre/news/releases/2007/pr22/en/. 5. World Health Organization. Report on the first regional workshop on patients for patient safety in the Eastern Mediterranean Region. Cairo, Egypt,: Regional Office for the Eastern Mediterranean; 2007. 6. Organization WH. The Second Global Patient Safety Challenge, Safe Surgery Save Lives Geneva 2008.
7. Organization WH. Patient Safety Research, A guide for developing training programmes. Genva 2012. 8. World Health Organization. Conceptual Framework for the International Classification for Patient Safety. Geneva; 2009. 9. WORLD HEALTH ORGANIZATION G. Human Factors in Patient safety Review of Topics and Tools 2009. 10. Organization WH. WHO Multi-professional Patient Safety Curriculum Guide Geneva 2011 [Available from: https://www.who.int/patientsafety/education/mp_curriculum_guide/en/. 11. Organization WH. Patient safety assessment manual first edition Geneva; 2011. 12. Dorien LM Zwart, Elizabeth LJ Van Rensen, Cor J Kalkman, Theo JM Verhei. Central or local incident reporting? A comparative study in Dutch GP out-of-hours services. Pubmed. 2011(Br J Gen Pract. 2011 Mar;61(584):183-7. doi: 10.3399/bjgp11X561168). 13. Tabrizchi N, Sedaghat M. The first study of patient safety culture in Iranian primary health centers. Acta Med Iran. 2012;50(7):505-10. 14. Bodur S, Filiz E. A survey on patient safety culture in primary healthcare services in Turkey. Int J Qual Health Care. 2009;21(5):348-55. 15. Hana H Webair, Salwa S Al Assani, Reema H Al Haddad, Wafa H Al Shaeeb, Manal A Bin Selm, Abdulla S Alyamani. Assessment of patient safety culture in primary care setting, Al-Mukala, Yemen. BMC Fam Pract. 2015;16:136. 16. Maha Mohamed Ghobashi, Hanan Abdel Ghani El-Ragehy, Fatma Abdullah Al-Doseri , Hanan Mosleh. Assessment of patient safety culture in primary health care settings in Kuwait. Epidemiol Biostat Public Health. 2014;11(3):e9101-1-e-9.
17. Joann Sorra P, Kabir Khanna, MA, Naomi Dyer, PhD, Russ Mardon, PhD, and Theresa Famolaro, MPS. Exploring relationships between patient safety culture and patients' assessments of hospital care. Patient safety journal Volume 8(Number 3 ). 18. Kirk S, Parker D, Claridge T, Esmail A, Marshall M. Patient safety culture in primary care: developing a theoretical framework for practical use. Quality & Safety in Health Care. 2007;16(4):313-20. 19. Westat R, Sorra J, Nieva V. Hospital Survey on Patient Safety Culture2004 2004//. 20. Sexton JB, Helmreich RL, Neilands TB, Rowan K, Vella K, Boyden J, et al. The Safety Attitudes Questionnaire: psychometric properties, benchmarking data, and emerging research. BMC health services research. 2006;6:44-.
39
21. Cooper Dominic. Towards a Model of Safety Culture2000. 111-36 p. 22. Agency for Healthcare Research and Quality. Hospital Survey on Patient Safety Culture 2016 [Available from: https://www.ahrq.gov/sites/default/files/wysiwyg/professionals/quality-patient-safety/patientsafetyculture/hospital/resources/hospscanform.pdf. 23. Christine E. Sammer R, Phd, Kristine Lykens, Phd, Karan P. Singh, Phd, Douglas A.Mains. What is patient safety culture? A review of literature. Journal of Nursing Scholarship. 2010(42:2):156-65. 24. World Health Organization. Definitions of Key Concepts from the WHO Patient Safety Curriculum Guide Geneva; 2011. 25. Reason J, Clarke D. Managing the risks of organizational accidents. In: Reason J, Clarke D, editors. 2003. p. 285-8. 26. Jilcha K, Kitaw D. A literature review on global occupational safety and health practice & accidents severity2016. 279-310 p. 27. Perneger TV. The Swiss cheese model of safety incidents: are there holes in the metaphor? BMC health services research. 2005;5:71-. 28. Ribeiro GdSR, Silva RCd, Ferreira MdA, Silva GRd. Slips, lapses and mistakes inthe use of equipment by nurses in an intensive care unit. Revista da Escola de Enfermagem da USP. 2016;50:419-26. 29. Guldenmund FW. The nature of safety culture: a review of theory and research 2000. 215-57 p.30. Accreditation A. Safety climate 2012 [Available from: https://acclaimaccreditation.co.uk/safety-climate-tool/safety-culture. 31. Hadyn Ellis , Neil Macrae. Validation in Psychology: Research Perspectives2001. 32. Foundation TH. Measuring safety culture London Evidence scan 2011. 33. Muna Habib AL Lawati, Sarah Dennis, Stephanie D Short, Nadia Noor Abdulhadi. Patient safety and safety culture in primary health care: a systematic review. BMC Family Practice. 2018;19:104. 34. Westat R, MD, Joann Sorra, Ph.D, Laura Gray, M.P.H, Suzanne Streagle, M.A, Theresa Famolaro, M.P.S. Naomi Yount, Ph.D,Jessica Behm, M.A. AHRQ Hospital Survey on Patient Safety Culture: User’s Guide AHRQ Publication No. 15(16)-0049-EF; 2004.
35. Marleen Smits, Ingrid Christiaans Dingelhoff, Cordula Wagner, Gerrit van der Wal , Peter P Groenewegen. The psychometric properties of the 'Hospital Survey on Patient Safety Culture' in Dutch hospitals. BMC health services research. 2008;8(230). 36. Ornelas M D, Pais D, Sousa P. Patient Safety Culture in Portuguese Primary Healthcare. Quality in Primary Care 2016;24(5):214-5. 37. Mats Hedsköld, Karin Pukk-Härenstam, Elisabeth Berg, Marion Lindh, Michael Soop, John Øvretveit, et al. Psychometric properties of the hospital survey on patient safety culture, HSOPSC,applied on a large Swedish health care sample. BMC health services research. 2013;13(332). 38. Joris Giai, Basten Boussat, Pauline Occelli, Garald Gandon, Arnaud Seigneurin, Philippe Michel, et al. Hospital survey on patient safety culture (HSOPS): variability of scoring strategies. Int J Qual Health Care. 2017;29(5):685-92. 39. Mustafa Elmontsri AA, Ricky Banarsee, Azeem Majeed. Status of patient safety culture in Arab countries: a systematic review. BMJ open. 2017;7(e013487). 40. Sexton JB, Thomas EJ, Helmreich RL. Error, stress, and teamwork in medicine and aviation: cross sectional surveys. BMJ. 2000;320(7237):745-9. 41. Vincent C, Taylor-Adams S, Stanhope N. Framework for analysing risk and safety in clinical medicine. BMJ (Clinical research ed). 1998;316(7138):1154-7.
40
42. Donabedian A. The Quality of Care: How Can It Be Assessed? JAMA. 1988;260(12):1743-8. 43. Paese F, Sasso GTMDS. Patient safety culture in primary health care [Portuguese]. Texto & Contexto Enfermagem. 2013;22(2):302-10. 44. Hoffmann B. The Frankfurt patient safety climate questionnaire for general practices (FraSiK): analysis of psychometric properties. BMJ Qual Saf. 2011;20. 45. Parker D. Managing risk in healthcare: understanding your safety culture using the Manchester Patient Safety Framework (MaPSaF. Journal of Nursing Management. 2009;17(2):218-22. 46. Westrum R. A typology of organisational cultures. Qual Saf Health Care. 2004(13(Suppl II):ii22–7). 47. Susan Kirk DP, Tanya Claridge, Aneez Esmail, Martin Marshall. Patient safety culture in primary care: developing a theoretical framework for practical use. Qual Saf Health Care 2007;16(313):320. 48. Hoffmann B, Müller V, Rochon J, Gondan M, Müller B, Albay Z, et al. Effects of a team-based assessment and intervention on patient safety culture in general practice: An open randomised controlled trial. BMJ Quality and Safety. 2014;23(1):35-46. 49. Wallis K, Dovey S. Assessing patient safety culture in New Zealand primary care: a pilot study using a modified Manchester Patient Safety Framework in Dunedin general practices. Journal of Primary Health Care. 2011;3(1):35-40. 50. Organization WH. World Health Organization, Quality and Accreditation in Health Care Services: A Global Review Geneve World Health Organization 2003 [Available from: https://www.who.int/hrh/documents/en/quality_accreditation.pdf. 51. Khoja T, Rawaf S, Qidwai W, Rawaf D, Nanji K, Hamad A. Health Care in Gulf Cooperation Council Countries: A Review of Challenges and Opportunities. Cureus. 2017;9(8):e1586-e. 52. Stephanie Short, Nikhil Hawal, Albusaidi NS. Streamlining and Modernizing Medical Workforce Governance: A Case Study of Ras Al Khaimah, United Arab Emirates The Sheikh Saud bin Saqr Al Qasimi Foundation for Policy Research 2018;Policy Paper No. 27 53. Bank W. Oman: The World Bank 2019 [Available from: https://data.worldbank.org/country/oman. 54. Commerce USDo. Oman - Healthcare: United States Department of Commerce 2018 [Available from: https://www.export.gov/article?id=Oman-Healthcare. 55. Organization WH. Health Systems Profile- Oman Geneve Regional Health Systems Observatory- EMRO 56. Dr Ali Taleb Al Hinai, Dr Ahmed Mohamed Al Qasmi, Dr Medhat K El Sayed, Mr Mohamed Hussein Fahmy Bayoumi, Dr Adhra Hilal Al Mawali, Dr Halima Qalm Al Hinai, et al. Health Vision 2050. Sultanate of Oman: Ministry of Health 2014. Contract No.: 1. 57. Health Mo. Directorate General of Quality Assurance Center Oman 2019 [Available from: https://www.moh.gov.om/en/web/directorate-quality-assurance-center/about-us. 58. WORLD HEALTH ORGANIZATION G. Oman Primary Health Care in Action. 2008. 59. World Health Organization G. Primary health care: 30 years since Alma-Ata. World health organization 2008. 60. Oman MoH. Primary health care 2019 [Available from: https://www.moh.gov.om/en/web/general-directorate-of-primary-health-care/introduction. 61. Ahmed Al-Mandhari, Ibrahim Al-Zakwani, Moosa Al-Kindi, Jihane Tawilah, Atsu S S Dorvlo, Samir Al-Adawi. Patient Safety Culture Assessment in Oman. Oman medical journal. 22 May 2014.
41
62. Organization WH. Patient Safety Oman Geneve The World Health Organization 2019 [Available from: http://www.emro.who.int/patient-safety/countries/country-activities-oman.html. 63. studies Dopa. Operational Plan for the Ninth Five Year Plan for Health Development. In: studies Dopa, editor. Oman Ministry of Health Oman 2017. 64. SCImago. SCImago Journal & Country Rank [Portal] 2019 [Available from: https://www.scimagojr.com/countryrank.php. 65. Ammouri AA, Tailakh AK, Muliira JK, Geethakrishnan R, Al Kindi SN. Patient safety culture among nurses. International Nursing Review 2015;62 102–10. 66. Muna Habib A. L. Lawati, Stephanie D. Short, Nadia Noor Abdulhadi, Sathiya Murthi Panchatcharam, Sarah Dennis. Assessment of patient safety culture in primary health care in Muscat, Oman: a questionnaire -based survey. BMC Family Practice. 2019. 67. Ahmed Al-Mandhari, Ibrahim Al-Zakwani, Samir Al-Adawi , Samra Al-Barwani, Lakshmanan Jeyaseelan. Awareness and implementation of nine World Health Organization’s patient safety solutions among three groups of healthcare workers in Oman. BMC Health Services Research (2016) 16:533. 2016. 68. AL Lawati MH, Short SD, Abdulhadi NN, Panchatcharam SM, Dennis S. Assessment of patient safety culture in primary health care in Muscat, Oman: a questionnaire -based survey. BMC Family Practice. 2019;20(1):50. 69. Organization WH. Patient Safety Friendly Hospital Initiative in Oman 2019 [Available from: http://www.emro.who.int/omn/oman-news/patient-safety-friendly-hospital-initiative-in-oman.html.
42
Chapter 3 A mixed methods research design
3.1 Background
In late 2014, I started my PhD candidature. I had been discussing and exploring the idea of
patient safety culture in primary health care in Oman with my supervisor and with relevant
experts at the Ministry of Health in Muscat, Oman. This thesis represents work commenced
during my candidature as a doctoral student in the Faculty of Health Sciences at the
University of Sydney. It also aims to inform and fill a policy gap that exists in Oman; patient
safety in primary care as outlined in Vision 2050 for Oman. This study draws on a mixed
methods research design. The study is divided into three phases, with each phase building on
the previous phase to develop a deeper understanding of patient safety culture in primary
health care in Muscat, Oman. The analytical activity associated with the results of these
studies is reflected in the scholarly publications which are included in the thesis, as
highlighted in Figure 4.
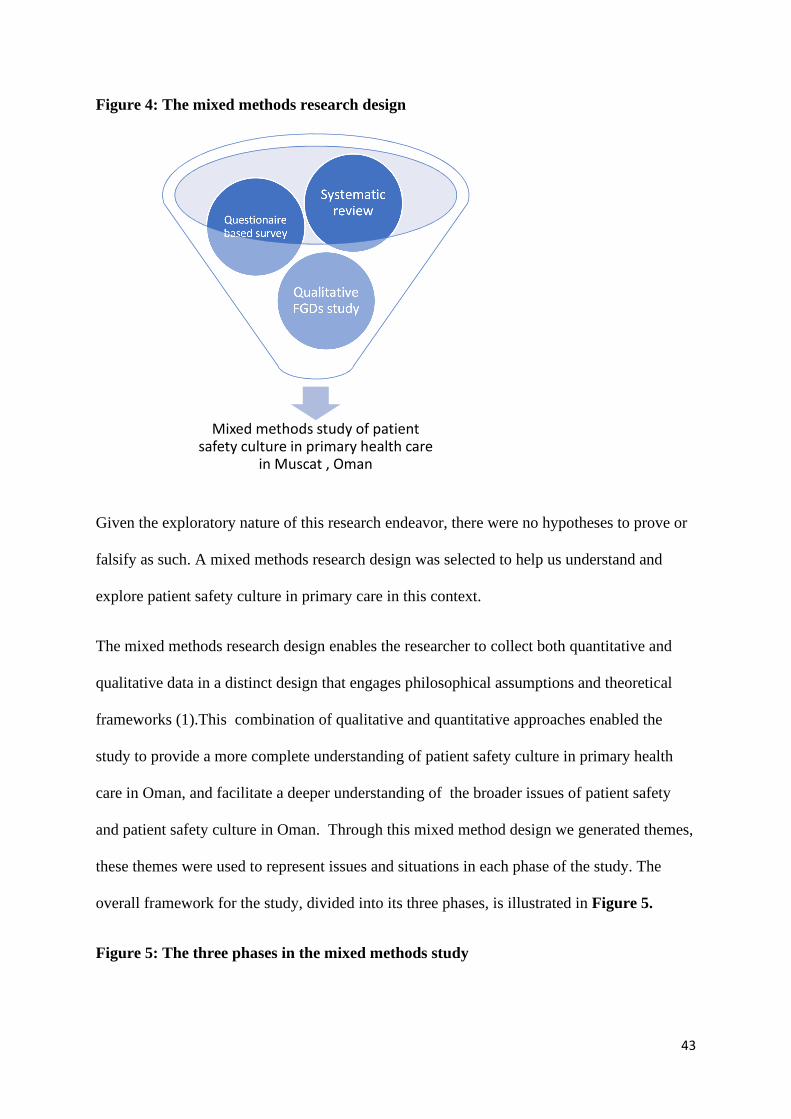
43
Figure 4: The mixed methods research design
Given the exploratory nature of this research endeavor, there were no hypotheses to prove or
falsify as such. A mixed methods research design was selected to help us understand and
explore patient safety culture in primary care in this context.
The mixed methods research design enables the researcher to collect both quantitative and
qualitative data in a distinct design that engages philosophical assumptions and theoretical
frameworks (1).This combination of qualitative and quantitative approaches enabled the
study to provide a more complete understanding of patient safety culture in primary health
care in Oman, and facilitate a deeper understanding of the broader issues of patient safety
and patient safety culture in Oman. Through this mixed method design we generated themes,
these themes were used to represent issues and situations in each phase of the study. The
overall framework for the study, divided into its three phases, is illustrated in Figure 5.
Figure 5: The three phases in the mixed methods study
Mixed methods study of patient safety culture in primary health care
in Muscat , Oman
Qualitative FGDs study
Questionaire based survey
Systematic review
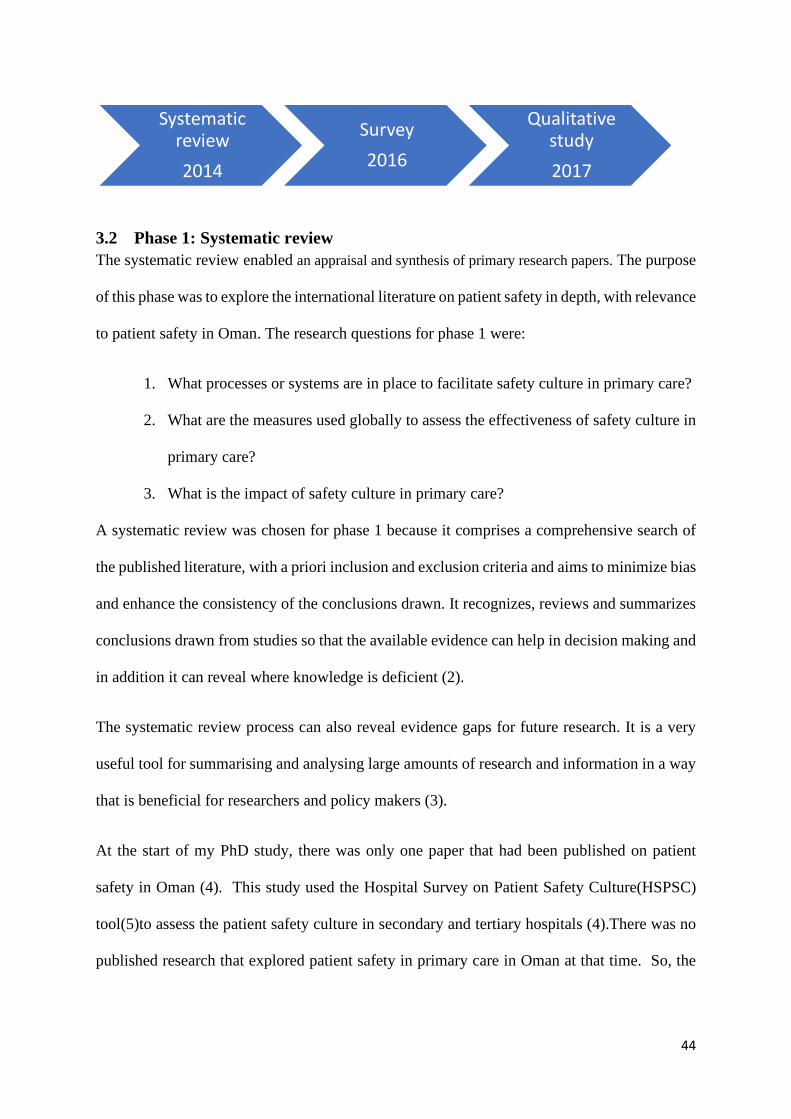
44
3.2 Phase 1: Systematic review The systematic review enabled an appraisal and synthesis of primary research papers. The purpose
of this phase was to explore the international literature on patient safety in depth, with relevance
to patient safety in Oman. The research questions for phase 1 were:
1. What processes or systems are in place to facilitate safety culture in primary care?
2. What are the measures used globally to assess the effectiveness of safety culture in
primary care?
3. What is the impact of safety culture in primary care?
A systematic review was chosen for phase 1 because it comprises a comprehensive search of
the published literature, with a priori inclusion and exclusion criteria and aims to minimize bias
and enhance the consistency of the conclusions drawn. It recognizes, reviews and summarizes
conclusions drawn from studies so that the available evidence can help in decision making and
in addition it can reveal where knowledge is deficient (2).
The systematic review process can also reveal evidence gaps for future research. It is a very
useful tool for summarising and analysing large amounts of research and information in a way
that is beneficial for researchers and policy makers (3).
At the start of my PhD study, there was only one paper that had been published on patient
safety in Oman (4). This study used the Hospital Survey on Patient Safety Culture(HSPSC)
tool(5)to assess the patient safety culture in secondary and tertiary hospitals (4).There was no
published research that explored patient safety in primary care in Oman at that time. So, the
Systematic review
2014
Survey
2016
Qualitative study
2017
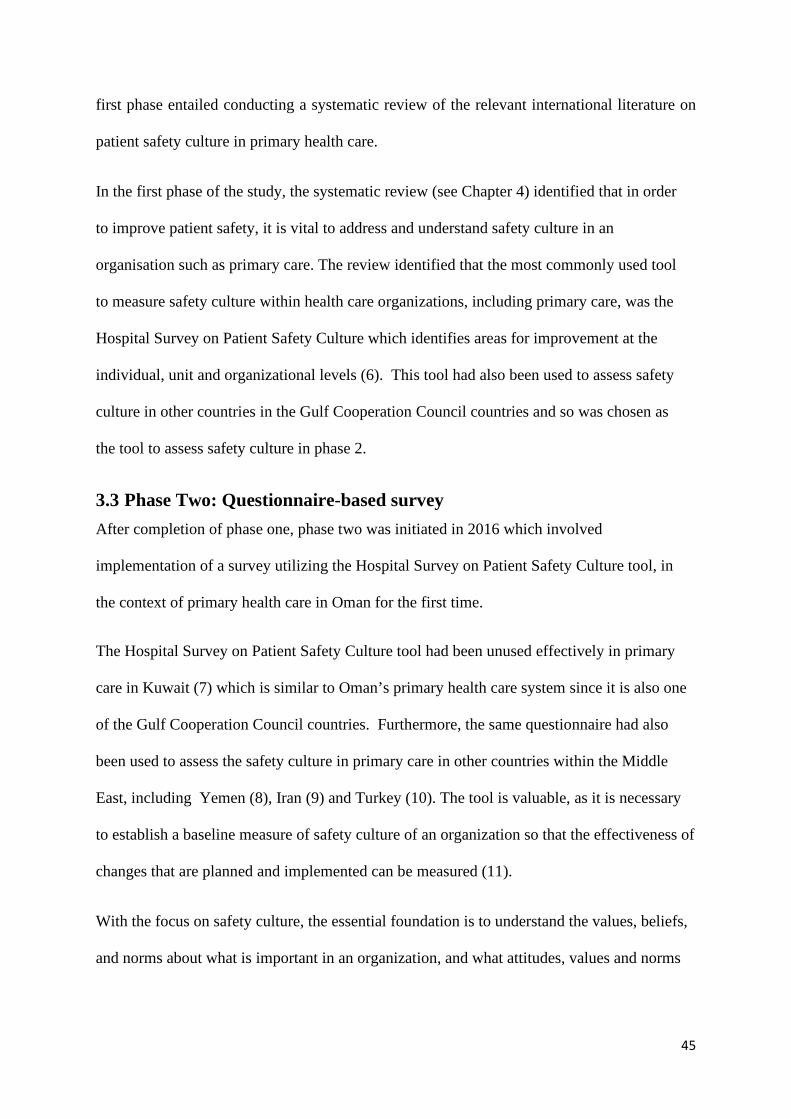
45
first phase entailed conducting a systematic review of the relevant international literature on
patient safety culture in primary health care.
In the first phase of the study, the systematic review (see Chapter 4) identified that in order
to improve patient safety, it is vital to address and understand safety culture in an
organisation such as primary care. The review identified that the most commonly used tool
to measure safety culture within health care organizations, including primary care, was the
Hospital Survey on Patient Safety Culture which identifies areas for improvement at the
individual, unit and organizational levels (6). This tool had also been used to assess safety
culture in other countries in the Gulf Cooperation Council countries and so was chosen as
the tool to assess safety culture in phase 2.
3.3 Phase Two: Questionnaire-based survey
After completion of phase one, phase two was initiated in 2016 which involved
implementation of a survey utilizing the Hospital Survey on Patient Safety Culture tool, in
the context of primary health care in Oman for the first time.
The Hospital Survey on Patient Safety Culture tool had been unused effectively in primary
care in Kuwait (7) which is similar to Oman’s primary health care system since it is also one
of the Gulf Cooperation Council countries. Furthermore, the same questionnaire had also
been used to assess the safety culture in primary care in other countries within the Middle
East, including Yemen (8), Iran (9) and Turkey (10). The tool is valuable, as it is necessary
to establish a baseline measure of safety culture of an organization so that the effectiveness of
changes that are planned and implemented can be measured (11).
With the focus on safety culture, the essential foundation is to understand the values, beliefs,
and norms about what is important in an organization, and what attitudes, values and norms
46
relevant to patient safety are evident in primary health care in Oman. The research questions
in this second phase aimed to:
1. Understand the attitudes, beliefs, perceptions and values that employees share in
relation to safety culture in the Omani health care settings.
2. Does the safety culture in Omani primary health care setting help in the reduction of
medical errors?
3. What are the appropriate indicators for assessing safety culture in primary health
care?
4. Does the safety culture focus on the health care professionals, patients and/or
managers?
Using the mixed method research design enabled a comprehensive exploration of patient
safety in primary care within a real life context (12). This approach provides powerful
understandings about many significant aspects of health and healthcare delivery systems (13).
Furthermore, the outcomes of the study can act as a reference for organizations or individuals
who face a similar issue or problem. The main limitation was that conclusions regarding the
cause of an issue or problem cannot be generalised beyond the specific study. The detailed
methodology is provided in Chapter five.
The study participants in phase two:
The population for the survey were health care professionals in primary health care in the
Muscat governorate (N =1984), and total number of health care professionals working in
primary health care in Muscat included in the study (N =1164). This population reflects the
22 out of 28 health centers which were included in the study. The 22 out of 28 healthcare
centers were selected on the basis of services which includes general practice, nursing care
and pharmacy these services are functional 7 times a week in addition to services such as
47
laboratory, X ray services and dentistry care provided 5days a week excluding weekends. We
aimed to survey a representative sample of 10% of the total from each occupational category.
From each center we sampled the following: Nurses (n =3), Physicians (n =2), Radiographers
(n =1), Laboratory technicians (n=1), Dentists (n=1) and Pharmacists (n=1) (9 in total from
each center). Thus, the sample size for this study was (9×22=198) health professionals from
the selected primary care centers
3.4 Phase three: Qualitative focus group discussions
Phase two of the study revealed four dimensions which scored the lowest scores. These were
associated with communication problems between the staff (23%), non-punitive response to
errors (27%), frequency of event reporting (40%), and errors occurring when transferring
patients to higher levels of health care during handoffs and transitions (46%) (14). As the
reasons behind these low scores cannot be identified using survey methodology, qualitative
focus group discussions were planned and executed. Two focus group discussions were
conducted with a purposive sample of Ministry of Health professionals and officials in
Muscat in 2017, in order to explore the following research questions:
1. What is the understanding of patient safety among the primary health care staff?
2. How confident are the staff to report the error and what is the process to report errors
in primary health care?
3. Is there any training in patient safety in primary health care?
4. Are there any policies or guidelines for patient safety in primary care?
5. What are the recommendations to improve patient safety in primary care?
This focus group discussion method was considered as appropriate for this phase since it can
simplify the organisation of interviews with participants and obtain maximum information
from participants in the limited time available (15). Furthermore, open ended questions
allowed issues to emerge rather than assume what that issues are in closed ended questions.
48
The participants selected as they acted as focal points in the quality system in primary care
in Muscat, and they shared similar interests and were concerned about patient safety even
though they had different opinions on the topics discussed. The foremost limitation of this
methodology is that participants can be influenced by the presence of other people which
can lead them to formulate answers which are more desirable and socially accepted (15).
Further details regarding this method of social scientific research are provided in Chapter
six.
Overall, phases two and three helped to recognize the blunt and the sharp ends in the swiss
cheese model of accident causation (16) as outlined in the previous Chapter. The blunt end in
accident causation that was investigated in the survey, identified the latent errors which are
factors in the organization which impact the causes of errors such as availability of policies,
guidelines and procedures in primary health care. In addition, it also brings to light the
environmental factors for example staffing issues and team factors that affect safety culture.
The sharp end in the swiss cheese model of accident causation are the active errors where there
is a contact between individuals and organization which are identified as training needs,
capacity building and implications for future recommendations, as identified in the focus group
discussions.
The study participants in phase 3
A total of 27 primary health care professionals were approached, from the 22 eligible primary
health care centers, and invited to participate. Of these, 20 health care professionals agreed to
participate while six were unable to participate on the days of focus group discussion because
of work commitments and/or time constrains. However, those who declined had broadly
similar characteristics to those who attended in terms of work experience in primary health care
and quality management activities in the health centers.
49
3.5 Summary
The methodological pluralism adopted for this study aimed to enhance our overall
understanding of patient safety culture in primary health care in Muscat, Oman. The systematic
review enabled the definition of the core concept in this study ‘patient safety culture.’It
identified the most commonly tool used to assess patient safety culture, namely the Hospital
Survey on Patient Safety Culture tool (5). This tool was used in phase two as a basis for the
survey that was implemented in 22 primary health centers in Muscat in 2016 in order to
comprehend the values, beliefs, and norms within the organization relevant to patient safety.
Phase three, the focus group discussion held with with health care professionals in Muscat in
2017, then facilitated identification of the root causes of the poor scores achieved in phase two.
This final phase of the study also enabled identification of the training needs of health
professionals within the Ministry of Health in Oman, and the recommendations for
strengthening patient safety in primary health care in line with fulfilling the “Vision 2050” aim
for Oman.
50
3.6 References
1. John W. Creswell, Vicki L. Plano Clark. Research design: qualitative, quantitative, and mixed
methods approaches. 4th edition ed. California: SAGE Publications: Thousand Oaks; 2014.
2. University of York Centre for Reviews Dissemination. Systematic reviews : CRD's guidance for
undertaking reviews in health care. York: CRD, University of York; 2009.
3. Gopala krishnan S, Ganesh kumar P. Systematic Reviews and Meta-analysis: Understanding
the Best Evidence in Primary Healthcare. J Family Med Prim Care. 2013;2(1):9-14.
4. Al-Mandhari A, Al-Zakwani I, Al-Kindi M, Tawilah J, Dorvlo ASS, Al-Adawi S. Patient Safety
Culture Assessment in Oman. Oman medical journal. 2014;29.
5. Westat R, MD, Joann Sorra, Ph.D, Laura Gray, M.P.H, Suzanne Streagle, M.A, Theresa
Famolaro, M.P.S. Naomi Yount, Ph.D,Jessica Behm, M.A. AHRQ Hospital Survey on Patient Safety
Culture: User’s Guide AHRQ Publication No. 15(16)-0049-EF; 2004.
6. Muna Habib AL Lawati, Sarah Dennis, Stephanie D Short, Nadia Noor Abdulhadi. Patient
safety and safety culture in primary health care: a systematic review. BMC Family Practice.
2018;19:104.
7. Ghobashi MM, El-Ragehy HAG, Al-Doseri FA, Mosleh H. Assessment of patient safety culture
in primary health care settings in Kuwait. Epidemiol Biostat Public Health. 2014;11(3):e9101-1-e-9.
8. Hana H Webair, Salwa S Al Assani, Reema H Al Haddad, Wafa H Al Shaeeb, Manal A Bin Selm,
Abdulla S Alyamani. Assessment of patient safety culture in primary care setting, Al-Mukala, Yemen.
BMC Fam Pract. 2015;16:136.
9. Tabrizchi N, Sedaghat M. The first study of patient safety culture in Iranian primary health
centers. Acta Med Iran. 2012;50.
10. Bodur S, Filiz E. A survey on patient safety culture in primary healthcare services in Turkey.
Int J Qual Health Care. 2009;21.
11. Agency for Healthcare Research and Quality. Hospital survey on patient safety culture 2016
[Available from: https://www.ahrq.gov/sites/default/files/wysiwyg/professionals/quality-patient-
safety/patientsafetyculture/hospital/userguide/hospcult.pdf.
12. Robert K Yin. Case study research; design and methods, 4th ed.(Brief article)(Book
review)2009; 24(1).
13. Crowe S, Cresswell K, Robertson A, Huby G, Avery A, Sheikh A. The case study approach.
BMC Medical Research Methodology. 2011;11(1):100.
14. Muna Habib A. L. Lawati, Stephanie D. Short, Nadia Noor Abdulhadi, Sathiya Murthi
Panchatcharam, Sarah Dennis. Assessment of patient safety culture in primary health care in
Muscat, Oman: a questionnaire -based survey. BMC Family Practice. 2019.
15. Acocella I. The focus groups in social research: advantages and disadvantages. Quality &
Quantity. 2012;46(4):1125-36.
16. Perneger TV. The Swiss cheese model of safety incidents: are there holes in the metaphor?
BMC health services research. 2005;5:71-.
51
Chapter 4 Patient safety and safety culture in primary health care: a systematic review

RESEARCH ARTICLE Open Access
Patient safety and safety culture in primaryhealth care: a systematic reviewMuna Habib AL. Lawati1,2* , Sarah Dennis3,4, Stephanie D. Short1 and Nadia Noor Abdulhadi5
Abstract
Background: Patient safety in primary care is an emerging field of research with a growing evidence base inwestern countries but little has been explored in the Gulf Cooperation Council Countries (GCC) including theSultanate of Oman. This study aimed to review the literature on the safety culture and patient safety measures usedglobally to inform the development of safety culture among health care workers in primary care with a particularfocus on the Middle East.
Methods: A systematic review of the literature. Searches were undertaken using Medline, EMBASE, CINAHL andScopus from the year 2000 to 2014. Terms defining safety culture were combined with terms identifying patientsafety and primary care.
Results: The database searches identified 3072 papers that were screened for inclusion in the review. After the screeningand verification, data were extracted from 28 papers that described safety culture in primary care. The global distributionof the articles is as follows: the Netherlands (7), the United States (5), Germany (4), the United Kingdom (1), Australia,Canada and Brazil (two for each country), and with one each from Turkey, Iran, Saudi Arabia and Kuwait. Thecharacteristics of the included studies were grouped under the following themes: safety culture in primary care, incidentreporting, safety climate and adverse events. The most common theme from 2011 onwards was the assessment of safetyculture in primary care (13 studies, 46%). The most commonly used safety culture assessment tool is the Hospital surveyon patient safety culture (HSOPSC) which has been used in developing countries in the Middle East.
Conclusions: This systematic review reveals that the most important first step is the assessment of safety culture inprimary care which will provide a basic understanding to safety-related perceptions of health care providers. The HSOPSChas been commonly used in Kuwait, Turkey, and Iran.
Keywords: Patent safety, Safety culture, Primary care, Gulf countries, Oman
BackgroundThe World Health Organization (WHO) defines patientsafety as “the prevention of errors and adverse effects topatients associated with health care” and “to do no harmto patients” [1, 2]. There are millions of patients globallywho suffer disabilities, injuries or death each year due tounsafe medical practices [3]. This has led to the widerrecognition of the importance of patient safety, the in-corporation of patient safety approaches into the stra-tegic plans of health care organizations and a growing
body of research in this field [4]. “To Err is Human:Building a Safer Health System” was published in 1999by the Institute of Medicine (IOM), it emphasized thatsafety was the key fundamental concern. This was alandmark publication for patient safety and warned oferrors in health care and the potential for patient harm[5]. Patient safety in primary care has not been exploredto the same extent as in the hospital settings [6] howevermore recently there has been more research emerging inprimary care [7–10]. Achieving a culture of safety re-quires an understanding of the values, attitudes, beliefsand norms that are important to health care organizationand what attitudes and behaviors are appropriate and ex-pected for patient safety [10].
* Correspondence: [email protected] of Health Sciences, Discipline of Behavioral and Social Sciences inHealth, The University of Sydney, Science Road, Sydney, NSW 2006, Australia2Department of Quality Assurance and Patient Safety, Ministry of Health,P.O.Box, 626, Wadi Al Kabir, 117 Muscat, PC, OmanFull list of author information is available at the end of the article
© The Author(s). 2018 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, andreproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link tothe Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver(http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
Lawati et al. BMC Family Practice (2018) 19:104 https://doi.org/10.1186/s12875-018-0793-7

This systematic review aimed to identify the patientsafety measures used globally to assess the effectivenessof safety culture in primary care. The outcome of thisstudy will help to inform strategies for patient safety forprimary care in Oman in order to accomplish the 2050 vi-sion. The specific research questions for this review were:
1. What processes or systems are in place to facilitatea safety culture in in primary care?
2. What are the measures used globally to assess theeffectiveness of safety culture in primary care?
3. What is the impact of safety culture in primary care?
MethodsA systematic review of the published literature from2000 to 2014 was conducted. This date range was chosenbecause it followed the publication of “To Err is Human”in 1999 [5]. The databases used to identify the articles wereMedline, Embase, CINAHL and Scopus. The terms used inMedline search were Health System, Safety Culture, PatientSafety, Primary Health care, Adverse Event, Health CareProfessionals and Health Care Managers.There were several key definitions used to scope the
review and inform the inclusion and exclusion criteria:
1. Patient Safety: WHO defines patient safety “as theabsence of preventable harm to a patient during theprocess of health care” [1].
2. Safety Culture: Defined “as shared values, attitudes,perceptions, competencies and patterns of behaviors”.
3. Primary Care: WHO defined primary care “associally appropriate, universally accessible,scientifically sound first level care provided by asuitably trained workforce supported by integratedreferral systems (to secondary care or tertiary care)and in a way that gives priority to those most needed,maximizes community and individual self-relianceand participation and involves collaboration withother sectors. It includes the following: healthpromotion, illness prevention, care of the sick,advocacy and community development” [11].
Articles were included in the review if they were pub-lished in the year 2000 or later and met the followingfour inclusion criteria:
1. They reported on the use of patient safety tools orapproaches or mechanisms or procedures used inprimary health care with an impact on patient care(outcome) measured.
2. If they were contained any of the followingmethodologies; systematic review, interventionstudy (randomized controlled trials), descriptivestudy or qualitative design.
3. They discussed patient safety in primary care, orsafety culture in primary care.
4. Published in English.
Articles were excluded if they were opinion papers/es-says, editorial reviews, interviews, comments or narrativereviews.After removal of the duplicates and papers with no ab-
stracts, the titles and abstracts of 61 papers werescreened by two researchers (MA and NN). The full textof all articles remaining were obtained and reviewed by tworesearchers (MA and NN). The full text articles were readand those that met the inclusion criteria were included inthe review. The flow chart in Additional file 1 illustrates theselection process by using Preferred Reporting Itemsfor Systematic Reviews and Meta-Analyses (PRISMA)flowchart [12].The following information was extracted from the in-
cluded articles: authors, year of publication, title andaims, objectives, methods, country and key findings. Toassess the quality three different tools were used accordingto study design. Systematic reviews were evaluated byAssessing Methodological Quality of Systematic Review(AMSTAR), quantitative studies were assessed by EffectivePublic Health Practice Project (EPHPP) and cross sec-tional studies were evaluated by using Strengthening theReporting of Observational studies in Epidemiology(STROBE) [13].
ResultsThe database searches identified 3072 papers that werescreened for inclusion in the review. After title and abstractscreening there were 61 remaining papers that described in-terventions in safety culture in primary care. Following veri-fication and data extraction there were a total number of 28articles included in the systematic review (Additional file 1).The global distribution of the articles are as follows: theNetherlands (7), the United States (5), Germany (4),Australia, Canada and Brazil (two for each country), theUnited Kingdom (1), and with one each from Turkey, Iran,Saudi Arabia and Kuwait. The characteristics of the in-cluded studies grouped under the following themes: safetyculture in primary care, incident reporting, safety climateand adverse events are specified in Table 1.
Safety culture in primary careThirteen studies addressed safety culture and tools to as-sess safety culture in general practice and most (9/13)were cross sectional studies [7, 8, 10, 14–19], the otherstudies were qualitative interviews [20], a systematic re-view [21], a retrospective audit [22], randomized controltrial [22], mixed methods [23] and a case study [24].The definition of patient safety culture varied among
the articles. A common definition of safety culture was
Lawati et al. BMC Family Practice (2018) 19:104 Page 2 of 12
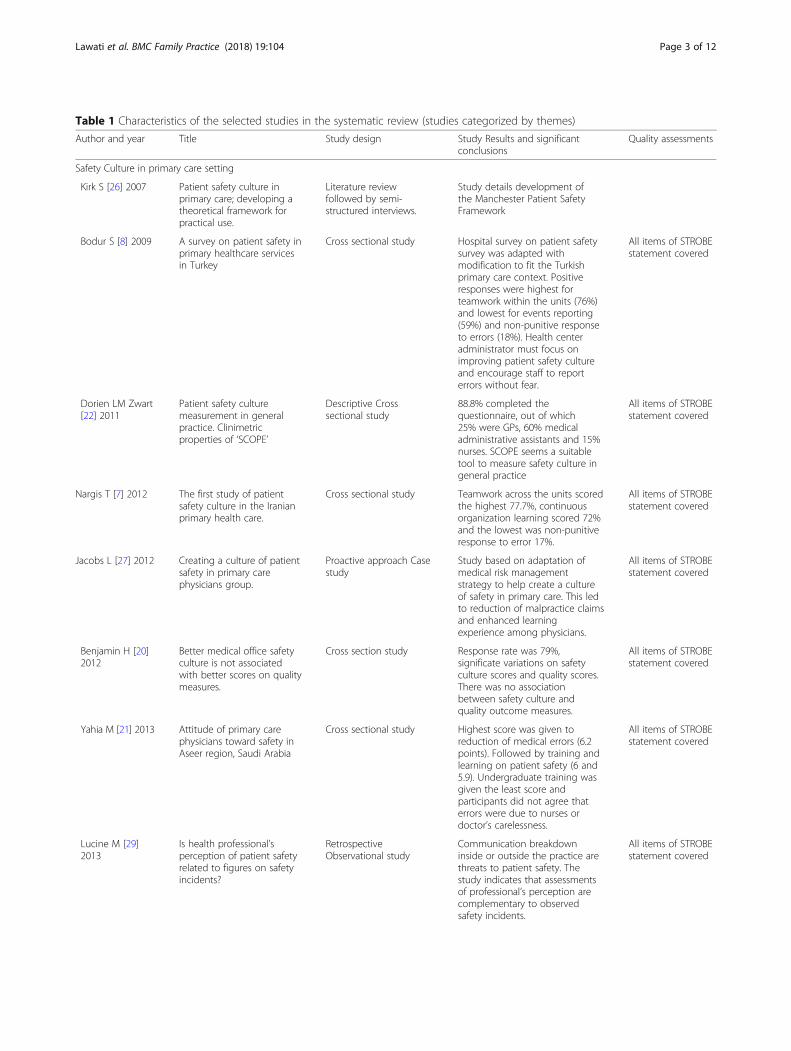
Table 1 Characteristics of the selected studies in the systematic review (studies categorized by themes)
Author and year Title Study design Study Results and significantconclusions
Quality assessments
Safety Culture in primary care setting
Kirk S [26] 2007 Patient safety culture inprimary care; developing atheoretical framework forpractical use.
Literature reviewfollowed by semi-structured interviews.
Study details development ofthe Manchester Patient SafetyFramework
Bodur S [8] 2009 A survey on patient safety inprimary healthcare servicesin Turkey
Cross sectional study Hospital survey on patient safetysurvey was adapted withmodification to fit the Turkishprimary care context. Positiveresponses were highest forteamwork within the units (76%)and lowest for events reporting(59%) and non-punitive responseto errors (18%). Health centeradministrator must focus onimproving patient safety cultureand encourage staff to reporterrors without fear.
All items of STROBEstatement covered
Dorien LM Zwart[22] 2011
Patient safety culturemeasurement in generalpractice. Clinimetricproperties of ‘SCOPE’
Descriptive Crosssectional study
88.8% completed thequestionnaire, out of which25% were GPs, 60% medicaladministrative assistants and 15%nurses. SCOPE seems a suitabletool to measure safety culture ingeneral practice
All items of STROBEstatement covered
Nargis T [7] 2012 The first study of patientsafety culture in the Iranianprimary health care.
Cross sectional study Teamwork across the units scoredthe highest 77.7%, continuousorganization learning scored 72%and the lowest was non-punitiveresponse to error 17%.
All items of STROBEstatement covered
Jacobs L [27] 2012 Creating a culture of patientsafety in primary carephysicians group.
Proactive approach Casestudy
Study based on adaptation ofmedical risk managementstrategy to help create a cultureof safety in primary care. This ledto reduction of malpractice claimsand enhanced learningexperience among physicians.
All items of STROBEstatement covered
Benjamin H [20]2012
Better medical office safetyculture is not associatedwith better scores on qualitymeasures.
Cross section study Response rate was 79%,significate variations on safetyculture scores and quality scores.There was no associationbetween safety culture andquality outcome measures.
All items of STROBEstatement covered
Yahia M [21] 2013 Attitude of primary carephysicians toward safety inAseer region, Saudi Arabia
Cross sectional study Highest score was given toreduction of medical errors (6.2points). Followed by training andlearning on patient safety (6 and5.9). Undergraduate training wasgiven the least score andparticipants did not agree thaterrors were due to nurses ordoctor’s carelessness.
All items of STROBEstatement covered
Lucine M [29]2013
Is health professional’sperception of patient safetyrelated to figures on safetyincidents?
RetrospectiveObservational study
Communication breakdowninside or outside the practice arethreats to patient safety. Thestudy indicates that assessmentsof professional’s perception arecomplementary to observedsafety incidents.
All items of STROBEstatement covered
Lawati et al. BMC Family Practice (2018) 19:104 Page 3 of 12
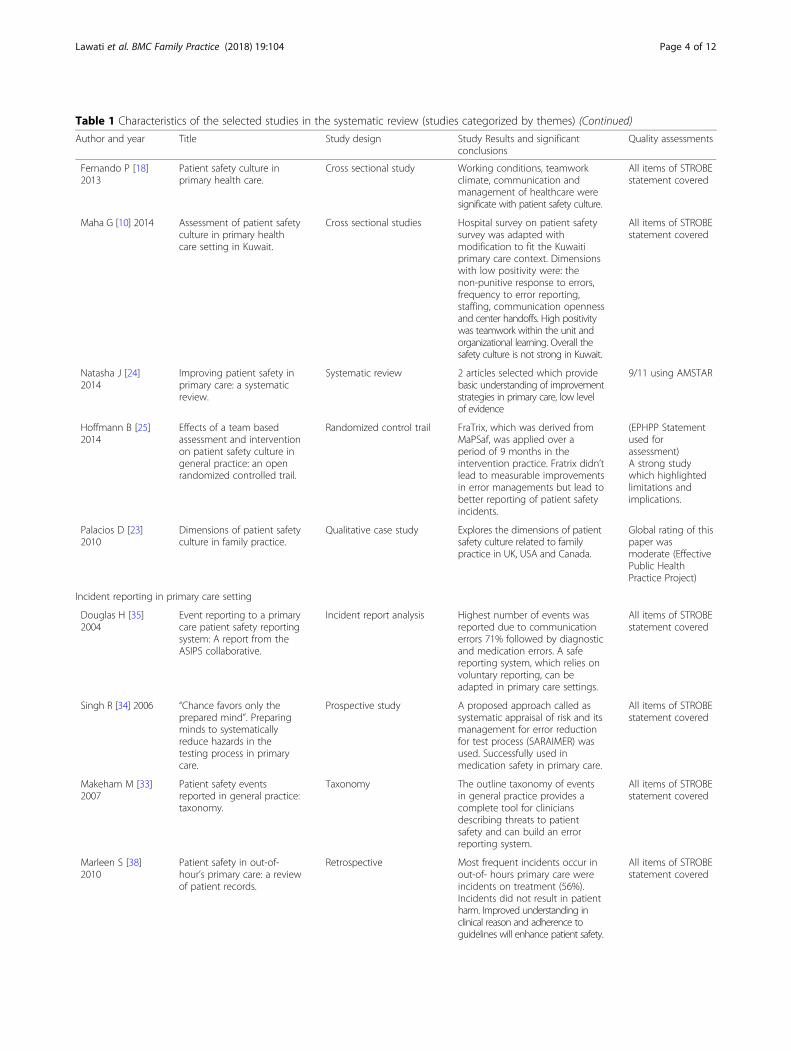
Table 1 Characteristics of the selected studies in the systematic review (studies categorized by themes) (Continued)
Author and year Title Study design Study Results and significantconclusions
Quality assessments
Fernando P [18]2013
Patient safety culture inprimary health care.
Cross sectional study Working conditions, teamworkclimate, communication andmanagement of healthcare weresignificate with patient safety culture.
All items of STROBEstatement covered
Maha G [10] 2014 Assessment of patient safetyculture in primary healthcare setting in Kuwait.
Cross sectional studies Hospital survey on patient safetysurvey was adapted withmodification to fit the Kuwaitiprimary care context. Dimensionswith low positivity were: thenon-punitive response to errors,frequency to error reporting,staffing, communication opennessand center handoffs. High positivitywas teamwork within the unit andorganizational learning. Overall thesafety culture is not strong in Kuwait.
All items of STROBEstatement covered
Natasha J [24]2014
Improving patient safety inprimary care: a systematicreview.
Systematic review 2 articles selected which providebasic understanding of improvementstrategies in primary care, low levelof evidence
9/11 using AMSTAR
Hoffmann B [25]2014
Effects of a team basedassessment and interventionon patient safety culture ingeneral practice: an openrandomized controlled trail.
Randomized control trail FraTrix, which was derived fromMaPSaf, was applied over aperiod of 9 months in theintervention practice. Fratrix didn’tlead to measurable improvementsin error managements but lead tobetter reporting of patient safetyincidents.
(EPHPP Statementused forassessment)A strong studywhich highlightedlimitations andimplications.
Palacios D [23]2010
Dimensions of patient safetyculture in family practice.
Qualitative case study Explores the dimensions of patientsafety culture related to familypractice in UK, USA and Canada.
Global rating of thispaper wasmoderate (EffectivePublic HealthPractice Project)
Incident reporting in primary care setting
Douglas H [35]2004
Event reporting to a primarycare patient safety reportingsystem: A report from theASIPS collaborative.
Incident report analysis Highest number of events wasreported due to communicationerrors 71% followed by diagnosticand medication errors. A safereporting system, which relies onvoluntary reporting, can beadapted in primary care settings.
All items of STROBEstatement covered
Singh R [34] 2006 “Chance favors only theprepared mind”. Preparingminds to systematicallyreduce hazards in thetesting process in primarycare.
Prospective study A proposed approach called assystematic appraisal of risk and itsmanagement for error reductionfor test process (SARAIMER) wasused. Successfully used inmedication safety in primary care.
All items of STROBEstatement covered
Makeham M [33]2007
Patient safety eventsreported in general practice:taxonomy.
Taxonomy The outline taxonomy of eventsin general practice provides acomplete tool for cliniciansdescribing threats to patientsafety and can build an errorreporting system.
All items of STROBEstatement covered
Marleen S [38]2010
Patient safety in out-of-hour’s primary care: a reviewof patient records.
Retrospective Most frequent incidents occur inout-of- hours primary care wereincidents on treatment (56%).Incidents did not result in patientharm. Improved understanding inclinical reason and adherence toguidelines will enhance patient safety.
All items of STROBEstatement covered
Lawati et al. BMC Family Practice (2018) 19:104 Page 4 of 12
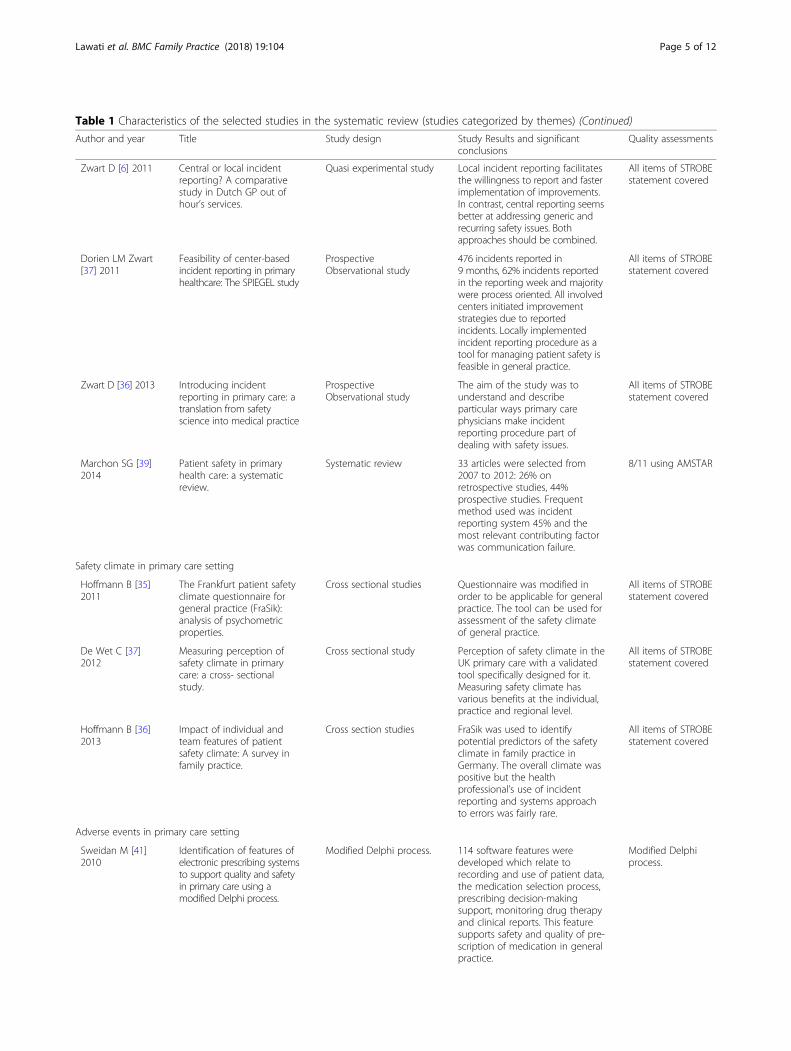
Table 1 Characteristics of the selected studies in the systematic review (studies categorized by themes) (Continued)
Author and year Title Study design Study Results and significantconclusions
Quality assessments
Zwart D [6] 2011 Central or local incidentreporting? A comparativestudy in Dutch GP out ofhour’s services.
Quasi experimental study Local incident reporting facilitatesthe willingness to report and fasterimplementation of improvements.In contrast, central reporting seemsbetter at addressing generic andrecurring safety issues. Bothapproaches should be combined.
All items of STROBEstatement covered
Dorien LM Zwart[37] 2011
Feasibility of center-basedincident reporting in primaryhealthcare: The SPIEGEL study
ProspectiveObservational study
476 incidents reported in9 months, 62% incidents reportedin the reporting week and majoritywere process oriented. All involvedcenters initiated improvementstrategies due to reportedincidents. Locally implementedincident reporting procedure as atool for managing patient safety isfeasible in general practice.
All items of STROBEstatement covered
Zwart D [36] 2013 Introducing incidentreporting in primary care: atranslation from safetyscience into medical practice
ProspectiveObservational study
The aim of the study was tounderstand and describeparticular ways primary carephysicians make incidentreporting procedure part ofdealing with safety issues.
All items of STROBEstatement covered
Marchon SG [39]2014
Patient safety in primaryhealth care: a systematicreview.
Systematic review 33 articles were selected from2007 to 2012: 26% onretrospective studies, 44%prospective studies. Frequentmethod used was incidentreporting system 45% and themost relevant contributing factorwas communication failure.
8/11 using AMSTAR
Safety climate in primary care setting
Hoffmann B [35]2011
The Frankfurt patient safetyclimate questionnaire forgeneral practice (FraSik):analysis of psychometricproperties.
Cross sectional studies Questionnaire was modified inorder to be applicable for generalpractice. The tool can be used forassessment of the safety climateof general practice.
All items of STROBEstatement covered
De Wet C [37]2012
Measuring perception ofsafety climate in primarycare: a cross- sectionalstudy.
Cross sectional study Perception of safety climate in theUK primary care with a validatedtool specifically designed for it.Measuring safety climate hasvarious benefits at the individual,practice and regional level.
All items of STROBEstatement covered
Hoffmann B [36]2013
Impact of individual andteam features of patientsafety climate: A survey infamily practice.
Cross section studies FraSik was used to identifypotential predictors of the safetyclimate in family practice inGermany. The overall climate waspositive but the healthprofessional’s use of incidentreporting and systems approachto errors was fairly rare.
All items of STROBEstatement covered
Adverse events in primary care setting
Sweidan M [41]2010
Identification of features ofelectronic prescribing systemsto support quality and safetyin primary care using amodified Delphi process.
Modified Delphi process. 114 software features weredeveloped which relate torecording and use of patient data,the medication selection process,prescribing decision-makingsupport, monitoring drug therapyand clinical reports. This featuresupports safety and quality of pre-scription of medication in generalpractice.
Modified Delphiprocess.
Lawati et al. BMC Family Practice (2018) 19:104 Page 5 of 12

utilized in eight studies, which referred to shared values,perceptions, attitudes, competencies and behaviorswithin an organization [8, 10, 14, 15, 19–23]. The defin-ition of safety culture was lacking in two articles butthey defined patient safety and patient safety incidentsrespectively [18]. There was one study where patientsafety culture was defined as acceptance and actions of pa-tient safety as the first priority in the organization [7] andfour articles did not define safety culture [17, 24–26].Two studies of safety culture utilized a qualitative ap-
proach, followed by a survey or an audit. The othereleven studies utililized quantitative tools to assess safetyculture. The systematic review included a study by Gaalet al. in the Netherlands that explored the views of pri-mary care doctors and nurses to identify aspects of carelinked to patient safety in a qualitative study [16]. Medi-cation safety was most frequently mentioned with inci-dents occurring in diagnosis and treatment, errors incommunication and poor patient doctor relationshipwere the most common errors in primary care [25]. Theaspects that were considered essential for patient safetywere; the availability of medical instruments, telephoneaccessibility and safe electric sockets. General practi-tioners relied on the skills and knowledge of the practicenurses since most of the patients were seen by them.The GPs did not supervise the practice nurses whenproviding advice to patients over the phone which theyfelt was a threat to patient safety. The results of thisqualitative study were used to develop a web-based sur-vey, which was one of the first to assess the views ofgeneral practitioners (GPs) on patient safety [16] in theNetherlands. They found that GPs were concerned about
the maintenance of medical records, prescription andmonitoring of medication.Another Dutch study identified that health care pro-
fessionals who had a perception and understanding of pa-tient safety had more incidents recorded [26]. All thehealth professionals surveyed felt that communicationbreakdown inside and outside the practice was a threat topatient safety and was associated with more incidents [26].A systematic review on the use of interventions of pa-
tient safety that affect safety culture in primary care onlyincluded two studies [21]. One of the included studiesdescribed the implementation of an electronic medicalrecords system in general practice using the safety attri-bute questionnaire as a part of patient safety improve-ments [21]. The authors facilitated two workshops forgeneral practice on risk management and significantaudit analysis. The authors concluded that further re-search was required to assess the effect of interventionson safety culture in primary care [21].Two main tools were used to measure safety culture;
the Manchester Patient Safety Framework (MaPSaF) andthe Hospital Survey on Patient Safety Culture (HSOPSC).The Manchester Patient Safety Framework (MaPSaF) [23]was developed to measure the multidimensional and dy-namic nature of safety culture and enabled recognition ofsubcultures within a single organization because subcul-tures act as a powerful influence on error detection andlearning. In addition, the tool provided insights into pa-tient safety culture, facilitated interactive self-reflectionabout safety culture of an organization, explored differ-ences in perception among different staff categories,helped understand how mature an organization was in
Table 1 Characteristics of the selected studies in the systematic review (studies categorized by themes) (Continued)
Author and year Title Study design Study Results and significantconclusions
Quality assessments
Wong K [40] 2010 A systematic review ofmedication safety outcomesrelated to drug interactionsoftware.
Systematic review No study addressed the benefitsand harms or cost effectiveness ofdrug interactions. The evidencedoes not support a benefit ofsoftware on medication safety orsupport any practice in this policy.
7/11 using AMSTAR
Singh R [42] 2004 Estimation impacts on safetycaused by the introductionof the electronic medicalrecords in primary care.
FMEA Hazard score was calculated foreach error before and 1 year afterimplementation of electronicmedical records. Hazardsperceived by staffs decreased indomains of physician –nurses andphysicians –chart. But increase inphysician- patient and nurse-chart domain.
All items of STROBEstatement covered
Joachim S [43]2011
Effectiveness of a qualityimprovement program inimproving management ofprimary care practices
Cross sectional study Primary care practices thatcompleted the European Practiceassessments twice over a period of3 yrs showed overall improvementsin practice management, qualityand safety and complaintmanagement.
All items of STROBEstatement covered
Lawati et al. BMC Family Practice (2018) 19:104 Page 6 of 12

terms of safety culture and evaluated interventions whichwere aimed at improving safety culture. The MaPSaF isfounded on Westrum’s typology of organizational com-munication from 1992, which defined how different typesof organizations process information. This typology wasexpanded upon by Parker and Hudson to describe fivelevels of progressively maturing organizational safety cul-ture. The MaPSaF measures ten dimensions of safety cul-ture, derived from a literature review on patient safety inprimary care and in-depth interviews and focus group dis-cussions with health care professionals and managers. Thedimensions are commitment to overall safety, prioritygiven to safety; system errors and individual responsibility;recording incidents and best practice; evaluation incidentsand best practice; learning and effecting change; commu-nication about safety issues; staff education and trainingand team work approach. The tool helped to acknowledgethat patient safety was multidimensional and complex, of-fered insights and demonstrated strengths and weaknessesof a patient safety culture, provided differences in percep-tion among and helped the organization to understandwhat a mature safety culture in health care might looklike. It should not be used to conduct performance man-agement nor to divide or attribute blame when the organi-zation’s safety culture is not sufficiently mature [27]. Thistool is best used as a facilitative educational tool for healthcare providers and managers.The Manchester Patient Safety Framework (MaPSaF)
[14, 22] has been adapted for use in different health sys-tems. The MaPSaF was modified and tested in the NewZealand context to facilitate learning about safety cultureand facilitate team communication mentioned in thesystematic review [15]. The MaPSaF has been modifiedfor use in the German health system and was renamedthe Frankfurt Patient Safety Matrix (FraTix) [22]. Thistool was validated and used in a randomized control trialof 60 general practices to determine safety culture at dif-ferent levels. There were no differences between thegeneral practice physicians’ groups but the interventiongroup showed improved reporting and management ofpatient safety incidents than the control group. FraTixappeared to be a good tool for self-assessments aimed atimproving safety culture but did not lead to measurableimprovements in error management.The Hospital Survey on Patient Safety Culture
(HSOPSC) was developed by the Agency of Health Careand Research for Hospitals in 2004, and has beenadapted and modified for other health care settings. Itmeasures healthcare professional’s perspectives towardssafety culture at the individual, unit and organizationallevel. It was pilot tested with more than 1400 hospitalemployees from 21 hospitals across the USA [28]. Thetool was developed after an extensive literature reviewon safety, accidents, medical errors, safety climate and
culture and organizational climate and culture. Therewere also interviews with hospital staff and surveys. Theinstrument includes fourteen dimensions, twelve aremultiple item dimensions (two safety culture dimensionsand two outcome dimensions) and the last two are sin-gle item dimensions used to check the validity. This toolhas a broad spectrum of applicability has been com-pleted by all types of hospital staff from security guardsto nurses, paramedical staff and physicians employed bythe organization. In terms of reliability and validity theHSOPSC was found to be “psychometrically sound atthe individual, unit and hospital level analysis” [29] inprimary care settings. It has since been used in Kuwait,Turkey, the Netherlands and Iran [7, 8, 10, 19]. The di-mension most commonly scored among Kuwait, Turkeyand Iran was teamwork within the units and the leastwas non-punitive response to errors. Similarly, theHSOPSC has since been adapted and validated for usein Dutch general practice, and was renamed SCOPE[19], a Dutch abbreviation for systematic culture on pa-tient safety in primary care. Table 2 compares the char-acteristics of the MaPSaF and HSOPSC.Paese [15] used the Safety Attitudes Questionnaire
(SAQ) to assess attitudes to safety culture in Brazilianprimary care. The survey was conducted among com-munity health agents, nursing technicians and nurses.The SAQ assesses the quality of safety and teamworkstandards in a given time in a health care organization.Nine attributes are assessed which are: job satisfaction,teamwork climate, perception of work environment,communication, patient safety, ongoing education, man-agement of the healthcare center, recognition of stress,error prevention by using preventive measures. Patientsafety attribute was considered to be an important attri-bute among the respondents whereas prevention mea-sures to avoid errors were viewed as being a lessimportant attribute.A case study in a primary care physician practice in
the USA explored the impact of a comprehensive riskmanagement program from 2003 to 2009. The programresulted in fewer insurance claims and considerable costsavings thereby enhancing patient safety culture inprimary care by implementing risk management pro-gram, the program further provided the physicians’ asense of control over the treatment of malpractice andencouraged them to provide the best care for theirpatients [24].
Incident reporting in primary careIncident reporting to assess patient safety in primarycare has grown in importance. There were two types ofstudy under this theme; 1) studies that explored differentapproaches to incident reporting [6, 30–34] and 2) dif-ferent mechanism to report incidents [35, 36].
Lawati et al. BMC Family Practice (2018) 19:104 Page 7 of 12

A number of studies have looked at incident reportingmechanisms and no one method was found to be super-ior. A mixture of methods was required to identify ad-verse events in primary care. The feasibility of a locallyimplemented incident reporting procedure (IRP) in pri-mary health centers was evaluated [33]. Introducing IRPin primary care to manage patient safety seemed to beless suitable for dealing with serious adverse events sinceit neglected the emotional needs of the healthcareworkers involved in the medical error [33]. This studyfurther compared the number and the nature of incidentreports collected locally (IRP) and from the existing cen-tralized incident reporting procedure. They found thatthe local incident reporting procedure enabled the healthcare professionals to control the assessments of their in-cident reports since the reports remained within thehealth center. This facilitated organizational learningand in turn increased the willingness to report and facili-tated quicker implementation of improvement. The cen-tral procedure that collected reports from many settings,appeared to address common and recurrent safety issuesmore effectively. Therefore, they concluded that both ap-proaches were necessary and should be combined [37].A systematic review reported on the methodologies to
evaluate incidents in primary care, types of incidents,contributing factors and solutions to make a safer pri-mary care. There were 33 included articles and the mostuniversally used method was incident analysis from inci-dent reports (45%). The review did not report on the ef-fectiveness of any specific method for incident reportingnor were specific tools mentioned. The most frequenttypes of incident were associated with medication anddiagnosis errors and the most relevant contributing fac-tor was communication failure among healthcare team[15]. Reviewing medical reports as an approach to
incident reporting in primary healthcare was examinedin a Dutch study mentioned in the systematic review.This retrospective review identified records with evidenceof a potential patient safety incident in out-of-hours pri-mary care and reviewed the type, causes and conse-quences of the incident. They found that incidents didoccur in out-of-hours primary care but that most (70%)did not result in patient harm. The most frequent incidentwas treatment errors (56%). All incidents were attributedto failures in clinical reasoning because of lack of access tothe patient’s medical history, insufficient medical know-ledge, high workload, age and being high risk (patientswith one or more conditions such as cardiac and vasculardisease, asthma/COPD, diabetes, pregnancy, malignancyand immune disease). The mean age for patients withincidents was 52 years compared to 36 years for pa-tients without incidents. Logistic regression analysisidentified that the likelihood of an incident increasedby 1.03 (95% confidence interval: 1.01 to 1.04) for eachyear increase in patient age the baseline age used wasless or more then 50 [15].
Safety climate in primary careSafety climate was assessed in three cross sectional studiesusing similar definitions of safety climate and safety culture[38–40]. Safety climate was defined as “shared employeeperceptions of the priority of safety at their unit andorganization at large” [38]. The safety climate was referredto as what was happening in an organization whereas;safety culture explained why it was happening [41].There was no tool to assess safety climate so Hoffman
et al. evaluated the use of the existing Safety AttributeQuestionnaire, Ambulatory version which was piloted andmodified to be used in general practice. It was renamedthe Frankfurt patient safety climate questionnaire for
Table 2 Comparision of Manchester Patient Safety Framework (MaPSaF) and Hospital Survey on Patient Safety Culture (HSOPSC)
The Manchester Patient Safety Framework (MaPSaF) The Hospital Survey on Patient Safety Culture (HSOPSC)
Developed by University of Manchester Developed by the US agency for Healthcare and Research
Defined patient safety culture according to 10 dimensions:• Continuous improvement• Priority given to staff• System errors and individual responsibility• Recording incidents• Evaluation incidents• Learning and effecting change• Communication personnel management• Staff education• teamwork
Defined patient safety culture according to 12 dimensions:• Frequency of error reporting• Number or error reporting• Supervisors expectations and actions• Organizational learning• Teamwork within units• Communication openness• Feedback and communication about errors\• Non-punitive response to errors• Staffing• Management support• Teamwork across units• Handoffs and transitions
Reflects on safety culture, highlights differences in perceptionbetween staff groups help understand what a mature safetyculture might look like and monitor changes over time
The tool can assess safety culture at individual, unit andorganizational level.
Deigned to be used in the UK context Designed to be used globally
Lawati et al. BMC Family Practice (2018) 19:104 Page 8 of 12

general practice (FraSik) and was used to assess the safetyclimate in German general practice [38]. FraSik was furtherassessed in a survey which recongnises strengths and weak-nesses of the safety climate of general practice and inaddition too, individual and practical features that affect thesafety climate perception of health care professionals in pri-mary care [39]. Doctors and health care assistants perceivedthat safety climate in German general practice was positiveand highlighted areas for improvement in patient safety,reporting incidents and cause of errors. A limitation of thestudy was a low response rate because those that respondedto the survey might have an interest in patient safety andtherefore more positive response and may not reflect theviews other health professionals working in the system [39].Interestingly, the terms safety climate and safety cul-
ture in the studies mentioned above have been usedinterchangeably although they mean different things.Safety climate is defined as “surface features of the safetyculture from attitudes and perceptions of individuals at agiven point in time” and “the measurable components ofsafety culture” [42]. Whereas, a safety culture is the“product of individual and group values, attitudes, com-petencies and patterns of behavior that determine thecommitment to, and the style and proficiency of an or-ganization’s health and safety programs” [14].
Adverse events in primary careTwo papers reported on adverse events with a focus onmedication error [43, 44]. Both the papers related to infor-mation technology to improve patient safety and qualityof care. A systematic review, which reviewed literature onthe use of drug interaction detection software (DIS) [43].Only four studies met the inclusion criteria and they werenot able to address the benefits and harms of drug inter-action software for medication safety. There was no pub-lished evidence to supports these systems or policies.An Australian study aimed to identify the features of
e-prescribing software that best supported patient safetyand quality of care in primary care. A list of 114 featureswas identified by literature review, key informant andexpert groups (Delphi Process). These features could beused to develop software standards by policy makers andcould be adapted in other settings and countries, butwere not evaluated [44]. Another paper discussed theintroduction of an electronic medical record system intoprimary care because of its impact to improve healthcare quality. The electronic medical system further in-cludes current practice knowledge, which can supportdecision making, eventually leading to reduction to prac-tice expenses and further increasing revenues by accur-ate billing and customer satisfaction [45].The European Practice Assessment tool was used in a
German study to assess the primary care practice focusingon the five domains in primary care practice (infrastructure,
people, finance, quality and safety). Two groups where se-lected, the intervention group is the one which had a previ-ous training in the tool and showed improvement in all thefive domains compared to the comparative group whichgroup which didn’t have any previous trainings. Thishighlighted that there is a benefit to quality improvementwhen accreditation tools are introduced as a bench-mark assessment to improve the health care profes-sional’s performance [46].
DiscussionPatient safety is critical to health care quality and re-mains a developmental challenge in primary care inmany countries. In addition interventions addressing pa-tient safety culture in primary care are limited comparedto secondary care [21].To improve patient safety, an important first step is to
address and understand the safety culture of anorganization. Similarly assessment of safety culture helpshealth care organizations to assess areas for improvementand analyze changes over time [9]. This systematic reviewhas recognized that the most common theme emergingfrom 2011 onwards was the assessment of safety culturein primary care. An important first strategy to improve allaspects of health care quality is creating a culture of safetywithin health care organizations [47].An understanding of the safety culture is vital to im-
prove the problematic practices or attitudes such as mis-communication, adverse events and a non-punitiveresponse to errors, which can lead to an improvement inthe safety culture of primary care. Likewise, the measure-ment of safety culture in primary care can help in theidentification of areas for improvement which might causeadverse events and errors. Patient care follow-up, commu-nication openness and work pressure were essential to im-prove patient safety in primary care [2]. Secondly, anotherkey area for improvement seen in the systematic reviewwas the issue of inadequate numbers of staff and providersto handle patients in primary care, highlighting this as anarea that requires attention [7, 8, 10].Communication breakdown, which affects both safety
culture and acts as a contributing factor for incidents,needs to be emphasized and addressed to help strengthenpatient safety culture in primary care [19]. Communica-tion openness was seen in the Kuwaiti and Turkey studiesas an area of concern [8, 10] unlike in the Iranian and theDutch studies [7, 19]. The inconsistency between out-comes regarding communication openness might be asso-ciated with differences in cultural background wheredisparagement and disagreement is regarded as blame andthus can lead to loss of occupation or personal relation-ships among staff and therefore staff tend to avoid it. Ingeneral communication openness was found to be a prob-lem in developing and Middle Eastern countries due to
Lawati et al. BMC Family Practice (2018) 19:104 Page 9 of 12

the blame culture [9]. Organizations with a positive safetyculture constituted a communication policy, establishedthe importance of safety in health care and developed pre-ventive measures.This systematic review brings to light an emerging lit-
erature on patient safety culture in primary care frommiddle to low income countries. As health care organi-zations attempt to improve, there is a need to establish aculture of safety an example seen in primary care inOman.To to achive that, its essential to understand theculture of safety which requires an understanding of thevalues, beliefs, and norms about what is significant in anorganization and what attitudes and behaviors related topatient safety are importand and suitable. Establishingan environment for patient safety may be challenging inOman because no studies on patient safety have beenundertaken in primary care, only hospital care. A furthercomplication is that the health centers are scattered un-like hospitals which is a single unit and in addition thehealth care workforce includes many nationalities andbackgrounds with varying understandings of patientsafety from different health care systems.The insight one may draw from the literature is that,
the most reliable and effective strategy for improving thequality of care is in changing the perception of the front-line health care professionals towards patient safetywhich in-turn will result in reduced adverse events andcommunication breakdown [47].The safety of the staff and patients in a health care
organization was affected by the extent of safety per-ceived across the organization. This concept wasassessed by two frequently used tools in the systematicreview which assessed safety culture in primary care: theManchester Patient Safety Framework (MaPSAF) andHospital Survey on Patient Safety Culture (HSOPSC).The HSOPSC tool emerged as the most likely tool to beused in the GCC to assess the safety culture in primarycare for the following reasons; firstly, it was used success-fully in Kuwait and more recently in Yemen and bothcountries have a similar GCC primary health systems. Sec-ondly, the same questionnaire has been used to assess thehospital safety culture in other countries in the GCC [48].Incident reporting is an important aspect for achieving
patient safety [6]. There is a need to develop an incidentreporting system in primary care in the Middle Eastwithin the health centers, similar to hospitals, which iscomputerized and helps in tracking and following up theincidents. The findings from this systematic review sug-gest that the system developed should include a local in-cident reporting system which will record and monitorincidents within the health center along with a central-ized reporting system at the ministry of health whichcan address and monitor incidents which are recurrentand common in primary care [49]. A local approach aids
in willingness to report and facilitate quicker implemen-tation whereas a central approach addresses the com-mon and recurrent safety issues [49].Patient safety in primary care is an emerging field of re-
search in western countries but little has been publishedfrom Oman and the other Gulf Cooperation Council Coun-tries (GCC). The Ministry of Health (MOH) in Oman hasbeen working for many years at different levels to improvethe quality of health care services and its safety.Patient safety in primary care can be enhanced in the
GCC by introducing 5 yrs plans across primary care.This such example was seen in Oman where they devel-oped a “Vision 2050” which is updated every 5 yrs. Poten-tial areas for improvement are introduced for the next2020–2025 five-year plan for patient safety in primary careacross all the regions of Oman. With the aid of these plansthe Ministry of Health, in partnership with the Ministry ofInformation Technology, are working together to achieveinformation transfer, linkage of patient information be-tween health centers, secondary care and hospitals so thatthe civil identification number can be used as a singleidentification number to access all patient health informa-tion across the health institutions.
ConclusionThis systematic review reveals that the most importantfirst step is the assessment of safety culture in primarycare which will provide basic understanding to safetyre-lated perceptions of the health care providers. The mostcommonly used safety culture assessment tool is theHSOPSC which aids in identifying areas for improve-ment at the individual, unit and organizational level.This review recognized that safety culture in primarycare should be assessed on a regular basis to evaluatethe effectiveness of safety in health institutions.Furthermore, results from this review will be used to
inform an empirical study of safety culture in primarycare in Oman using the Hospital Survey on PatientSafety Culture (HSOPSC) tool, with a view to developinga template for the development of safety culture in pri-mary care in the context of rapid economic growth.
Additional file
Additional file 1: PRISMA flowchart. The completed PRISMA flowchartfor the systematic review. (DOC 57 kb)
AbbreviationsAMSTAR: Assessing Methodological Quality of Systematic Review;EPHPP: Quantitative studies were assessed by Effective Public Health PracticeProject; GCC: Gulf Cooperation Council; HSOPSC: Hospital survey on patientsafety culture; IOM: International Institute of Medicine; MOH: Ministry ofHealth; PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses; SAQ: Safety attribute questionnaire; STROBE: Cross sectional studieswere evaluated by using Strengthening the Reporting of Observationalstudies in Epidemiology; WHO: World Health Organization
Lawati et al. BMC Family Practice (2018) 19:104 Page 10 of 12
Availability of data and materialsThe databases used to identify the articles were Medline, Embase, CINAHLand Scopus. Published literature were selected from 200o to 1014. The termsused in Medline search were Health System, Safety Culture, Patient Safety, PrimaryHealth care, Adverse Event, Health Care Professionals and Health Care Managers.
Authors’ contributionsMA and NN screened the titles and abstracts of all remaining papers and thefull text of all articles remaining were obtained and reviewed by two researchersMA and NN. All Authors participated in developing study method, definitionsand criteria. All authors participated in the sequence in drafting the manuscript.All authors read and approved the final manuscript.
Authors informationPhD Student at the University of Sydney, Head of Quality and Patient Safety atthe Directorate General of Health Services, Ministry of Health, Muscat, Oman.
Ethics approval and consent to participateEthical approval was obtained from Research and Ethical Review andApproval Committee in Oman.
Consent for publicationNot applicable.
Competing interestsThe authors declare that they have no competing interests.
Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims inpublished maps and institutional affiliations.
Author details1Faculty of Health Sciences, Discipline of Behavioral and Social Sciences inHealth, The University of Sydney, Science Road, Sydney, NSW 2006, Australia.2Department of Quality Assurance and Patient Safety, Ministry of Health,P.O.Box, 626, Wadi Al Kabir, 117 Muscat, PC, Oman. 3Ingham Institute forApplied Medical Research, Campbell Street, Liverpool, NSW 2170, Australia.4Faculty of Health Sciences, Discipline of Physiotherapy, The University ofSydney, 71 East Street, Lidcombe, NSW 2141, Australia. 5Directorate Generalof Planning and Studies, Ministry of Health, Muscat, Oman.
Received: 26 February 2018 Accepted: 8 June 2018
References1. World Health Organization, G. Conceptual framework for the international
classification for patient safety. In: Version 1.1 final technical report January2009; 2009.
2. Gaal S, Verstappen W, Wensing M. What do primary care physicians andresearchers consider the most important patient safety improvementstrategies? BMC Health Serv Res. 2011;11:102.
3. Sorra J, Nieva VF. Safety culture assessment. A tool for improving patient safetyin healthcare organizations. Qual Saf Health Care. 2003;12(Suppl II):ii17–23.
4. Gonzalez-Formoso C, et al. Adverse events analysis as an educational tool toimprove patient safety culture in primary care: a randomized trial. BMC FamPract. 2011;12:50.
5. Linda TK, Corrigan JM, Donaldson MS. To err is human: building a saferhealth system. Washington DC: National Academy Press; 1999.
6. Zwart DL, Van Rensel EL, Kalkman CJ, Verheij TJ. Central or local incidentreporting? A comparative study in Dutch GP out-of-hours services. Br J GenPract. 2011;61(584):183–7. https://doi.org/10.3399/bjgp11X561168.
7. Tabrizchi N, Sedaghat M. The first study of patient safety culture in Iranianprimary health centers. Acta Med Iran. 2012;50(7):505–10.
8. Bodur S, Filiz E. A survey on patient safety culture in primary healthcareservices in Turkey. Int J Qual Health Care. 2009;21(5):348–55.
9. Webair HH, Al-Assani SS. Reema H. Al-Haddad, Wafa H. Al-Shaeeb, Manal A.Selm, and A.S. Alyamani. Assessment of patient safety culture in primarycare setting, Al-Mukala, Yemen. BMC Fam Pract. 2015;16:136.
10. Ghobashi MM, et al. Assessment of patient safety culture in primary healthcare settings in Kuwait. Epidemiol Biostat Public Health. 2014;11(3):e9101–9.
11. World Health Organization. Conceptual Framework for the InternationalClassification for Patient Safety. GENEVA: WHO; 2009. Contract No.: WHO/IER/PSP/2010.2.
12. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC, JPA I, et al. ThePRISMA statement for reporting systematic reviews and meta-analyses ofstudies that evaluate healthcare interventions: explanation and elaboration.BMJ. 2009;339(1):b2700.
13. STROBE. Strengthening the Reporting of OBservational studies in Epidemiology( STROBE). 2009; Available from: http://www.strobe-statement.org/.
14. Wallis K, Dovey S. Assessing patient safety culture in New Zealand primarycare: a pilot study using a modified Manchester patient safety framework inDunedin general practices. J Prim Health Care. 2011;3(1):35–40.
15. Paese F, Sasso GT. Patient safety culture in primary health care [Portuguese].Texto & Contexto Enfermagem. 2013;22(2):302–10.
16. Gaal S, Verstappen W, Wensing M. Patient safety in primary care: a survey ofgeneral practitioners in the Netherlands. BMC Health Serv Res. 2010;10:21.
17. Hagopian B, et al. Better medical office safety culture is not associated withbetter scores on quality measures. J Patient Saf. 2012;8(1):15–21.
18. Al-Khaldi YM. Attitude of primary care physicians toward patient safety in Aseerregion, Saudi Arabia. Journal of Family & Community Medicine. 2013;20(3):153–8.
19. Zwart DLM, et al. Patient safety culture measurement in general practice.Clinimetric properties of ‘SCOPE’. BMC Fam Pract. 2011;12(1):117.
20. Palacios-Derflingher L, et al. Dimensions of patient safety culture in familypractice. Healthc Q. 2010;13:121–7.
21. Verbakel NJ LM, Verheij TJ, Wagner C, Zwart DL. Improving Patient SafetyCulture in Primary Care: A Systematic Review. PubMed. 2014;00(00).
22. Hoffmann B, et al. Effects of a team-based assessment and intervention onpatient safety culture in general practice: an open randomised controlledtrial. BMJ Qual Saf. 2014;23(1):35–46.
23. Kirk S, et al. Patient safety culture in primary care: developing a theoreticalframework for practical use. Qual Saf Health Care. 2007;16(4):313–20.
24. Jacobs L, et al. Creating a culture of patient safety in a primary-carephysician group. Conn Med. 2012;76(5):291–7.
25. Gaal S, et al. Patient safety in primary care has many aspects: an interviewstudy in primary care doctors and nurses. J Eval Clin Pract. 2010;16(3):639–43.
26. Martijn L, et al. Are health professionals’ perceptions of patient safetyrelated to figures on safety incidents? J Eval Clin Pract. 2013;19(5):944–7.
27. Parker D, Kirk S, Claridge T, Lawrie M, Ashcroft DM. The Manchester PatientSafety Framework (MaPSaF). In Patient Safety Research: shaping theEuropean agenda - International Conference Porto, Portugal. 2007.
28. Westat R, Joann Sorra, and Veronica Nieva, Hospital Survey on Patient SafetyCulture. 2004.
29. Sorra JS, Dyer N, Multilevel psychometric properties of the AHRQ hospitalsurvey on patient safety culture. BMC Health Serv Res. 2011;10(199).
30. Makeham MA, et al. Patient safety events reported in general practice: ataxonomy. Qual Saf Health Care. 2008;17(1):53–7.
31. Singh R, et al. “Chance favors only the prepared mind”: preparing minds tosystematically reduce hazards in the testing process in primary care. JPatient Saf. 2014;10(1):20–8.
32. Fernald DH, et al. Event reporting to a primary care patient safety reportingsystem: a report from the ASIPS collaborative. Ann Fam Med. 2004;2(4):327–32.
33. Zwart DLM, de Bont AA. Introducing incident reporting in primary care: atranslation from safety science into medical practice. Health. Risk andSociety. 2013;15(3):265–78.
34. Zwart DLM, et al. Feasibility of Centre-based incident reporting in primaryhealthcare: the SPIEGEL study. BMJ Qual Saf. 2011;20(2):121–7.
35. Smits M, et al. Patient safety in out-of-hours primary care: a review ofpatient records. BMC Health Serv Res. 2010;10:335.
36. Marchon SG, Mendes Junior WV. Patient safety in primary health care: asystematic review. Cadernos de Saúde Pública. 2014;30:1815–35.
37. De Wet C, Johnson P, Mash R, McConnachie A, Bowie P. Measuringperceptions of safety climate in primary care: A cross-sectional study. J EvalClin Pract. 2012;18(1):135–42.
38. Hoffmann B, et al. The Frankfurt patient safety climate questionnaire forgeneral practices (FraSiK): analysis of psychometric properties. BMJ Qual Saf.2011;20(9):797–805.
39. Hoffmann B, et al. Impact of individual and team features of patient safetyclimate: a survey in family practices. Ann Fam Med. 2013;11(4):355–62.
40. De Wet C, et al. Measuring perceptions of safety climate in primary care: across-sectional study. J Eval Clin Pract. 2012;18(1):135–42.
41. Ellis Hadyn, N Macrae., Validation in psychology: research Perspectives 2001.
Lawati et al. BMC Family Practice (2018) 19:104 Page 11 of 12

42. Gaba David M, Singer SJ, Sinaiko Anna D, Bowen Jennie D, CiavarelliAnthony P. Differences in safety climate between hospital personnel andnaval aviators. Hum factors. 2003;45(2):173–85.
43. Wong K, Yu SKH, Holbrook A. A systematic review of medication safetyoutcomes related to drug interaction software. Canadian Journal of ClinicalPharmacology. 2010;17(2):e243–55.
44. Sweidan M, et al. Identification of features of electronic prescribing systemsto support quality and safety in primary care using a modified Delphiprocess. BMC Med Inform Decis Mak. 2010;10:21.
45. Singh R, et al. Estimating impacts on safety caused by the introduction ofelectronic medical records in primary care. Inform Prim Care. 2004;12(4):235–42.
46. Szecsenyi J, et al. Effectiveness of a quality-improvement program inimproving management of primary care practices. CMAJ. 2011;183(18):E1326–33.
47. Joann Sorra P, Kabir Khanna MA, Dyer N, Mardon R, Famolaro T. Exploringrelationships between patient safety culture and patients’ assessments ofhospital care. J Patient Saf. 2012;8(3):131–9.
48. Al-Mandhari A, Al-Zakwani I, Al-Kindi M, Tawilah J, Dorvlo ASS, Al-Adawi S.Patient Safety Culture Assessment in Oman. Oman Med J. 2014;29(4):264.
49. Wetzels R, et al. Mix of methods is needed to identify adverse events ingeneral practice: a prospective observational study. BMC Fam Pract. 2008;9(1):35.
Lawati et al. BMC Family Practice (2018) 19:104 Page 12 of 12
64
Chapter 5 Assessment of patient safety culture in primary health care in Muscat, Oman: a questionnaire -based survey
RESEARCH ARTICLE Open Access
Assessment of patient safety culture inprimary health care in Muscat, Oman: aquestionnaire -based surveyMuna Habib AL Lawati1,2* , Stephanie D. Short1, Nadia Noor Abdulhadi2, Sathiya Murthi Panchatcharam3 andSarah Dennis1,4,5
Abstract
Background: Patient safety is a universal issue which affects countries at all stages of health system development.Patient safety research in primary care reveals that globally millions of people suffer disabilities, injuries, or deathdue to unsafe medical practices. This study aims to explore the understanding of frontline primary health careprofessionals regarding patient safety culture in health care facilities in Oman.
Methods: A questionnaire–based survey was conducted using a validated Hospital Survey of Patient Safety Culturetool. Invitations were sent to all 198 health professionals from each occupational category from each primary carecenter in Muscat, Oman.
Results: The total number of respondents was 186 participants out of 198 (response rate: 94%). Overall, the staffhad a strong sense of teamwork within the units (85%), they reported organization learning for continuousimprovement (84%) and teamwork across the units (82%). However, the four dimensions which received the lowestscores were related to communication problems between the staff (23%), non-punitive response to errors (27%),frequency of event reporting (40%), and errors occurring when transferring patients to higher levels of health careduring handoffs and transitions (46%).
Conclusions: Overall, the participants rated patient safety in the primary health care setting as excellent or verygood and the perception of patient safety was moderately positive. The core areas of strength were teamworkwithin the units with positivity and organization learning and continuous improvement. The weaknesses were non-punitive response to errors, inadequate staffing and hand offs and transition. The results of this study will providepolicy makers and health care professionals with a detailed understanding of the current patient safety culture inprimary care in Muscat, Oman. The results will be used by the Ministry of Health to inform policy and strategies tostrengthen patient safety within primary health care in Oman.
Keywords: Patient safety, Safety culture, Primary health care, medical errors, Oman
BackgroundUnsafe medical practices lead to disabilities, injuries anddeath each year to millions of patients worldwide [1] . TheWorld Health Organization (WHO) defines patient safetyas “the prevention of errors and adverse effects to patientsassociated with health care” and “to do no harm to
patients” [2]. The aim is to reduce the risk of unnecessaryharm associated with health care to an acceptable mini-mum. The acceptable minimum is context specific, basedon current knowledge, resources available and balancedagainst the risk of alternative treatment options [3].“To Err is Human: Building a Safer Health System”
was published in 1999 by the Institute of Medicine(IOM), it highlighted that safety was an important con-cern. Patient safety in hospitals has received more atten-tion as compared to primary care [4]. However, in mosthealthcare systems the majority of patient consultations
© The Author(s). 2019 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, andreproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link tothe Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver(http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
* Correspondence: [email protected] of Physiotherapy, Faculty of Health Sciences, The University ofSydney, Sydney, Australia2Ministry of Health, P.O.Box, 626, PC 117 Wadi Al Kabir, Muscat, OmanFull list of author information is available at the end of the article
AL Lawati et al. BMC Family Practice (2019) 20:50 https://doi.org/10.1186/s12875-019-0937-4

take place in primary care and many of the incidentsidentified in hospitals may have originated in primarycare, making the need for primary care patient safety re-search even more important.There is no single standard to identify patient safety
incidents in primary care [5]. The literature suggests that24 - 85% of all harmful events occurring in primary arepreventable [6]. This varies with research suggesting thatin high income countries 50% of harm in primary care ispreventable increasing to 60% in low income countries[7]. Attaining a culture of safety is a vital first step andrequires an understanding of the values, beliefs, andnorms about what is significant in an organizations, andwhat attitudes and behaviors applicable to patient safetyare anticipated [8]. Organizations with a positive safetyculture are characterized by communications foundedon mutual trust, shared perceptions of the importanceof safety, and by confidence in the efficacy of preventivemeasures [8].There has been little research on patient safety
published from Oman and other Gulf CooperationCouncil (GCC) countries. There has been one pub-lished study in patient safety culture in primaryhealthcare in Kuwait [9] and three studies in theEastern Mediterranean Region (EMRO) [9–11]. TheMinistry of Health (MOH) in Oman has been work-ing for many years at different levels to improve thequality and safety of health care services. A nationalworking team was established in 2012 to develop anational action plan, guidelines, and mechanisms formonitoring and follow-up of aspects of patient safetyin Oman [12]. Research into patient safety was identi-fied as an important priority by the MOH, Oman, inits 2050 vision [13]. This study was conducted in thisfertile context for research. Muscat is the capital ofOman, and the pilot region for new proposals andinitiatives from the MOH since it covers a wide arearanging from a modern cosmopolitan population toremote areas where access to health care is limited[14]. The Sultanate of Oman is a high-income Arabcountry. It has experienced a rapid economic and so-cial transformation since the 1970s which has re-sulted in better quality living standards [15]. Thetotal population of Oman is 4.4 million and a thirdof the total population of Oman live in the capitalcity Muscat [16]. Primary health care centers(PHCCs) are the entry point for most patients withdifferent health conditions in the publicly-fundedOmani healthcare system.The aim of this study was to explore the understand-
ing of primary health care professionals regarding pa-tient safety culture in primary health care facilities inOman, in order to establish a baseline for the strength-ening of patient safety in primary health care in Oman.
MethodsA cross-sectional survey was undertaken to assess thepatient safety culture in primary health care in Muscat,the capital of Oman between January and June 2016. Avalidated self-administered questionnaire, the HospitalSurvey on Patient Safety Culture (HSOPSC) developedby the Agency of healthcare Research (AHRQ) [17] wasused to assess the current patient safety culture amonghealthcare professionals in primary care [18].The HSOPSC has been used in studies from the USA,
UK and Europe in the hospital setting [19, 20]. It hasalso been used in the hospital setting in in the MiddleEast including Kuwait [9], Turkey [21], Iran [10] andYemen [11]. It has been adapted and validated for pri-mary care use in Portugal [22] and Switzerland [23]. It isa valid and a reliable tool developed on the basis of pre-vious literature, cognitive tests and factor analysis. Safetyculture variations have been reported across healthcarefacilities, departments and occupational categories ofhealthcare workers in North America, Europe, Asia, andthe Middle East [24]. The instrument includes 42 itemsgrouped into 12 composite measures. It includes alsotwo questions that ask respondents to provide an over-all grade on patient safety for their work and to indicatethe number of events they reported over the past 12months. The scale used is a five-point Likert scalewhich ranges from ‘Strongly disagree’ to ‘Stronglyagree’, or from ‘Never’ to ‘Always’ when relevant. A glo-bal safety grade between ‘poor’ and ‘excellent’ and thenumbers of reported incidents in the past 12 monthswere also assessed.
Pre-test/pilot studyPretesting of the questionnaire was conducted with sixfrontline health care professionals who were family phy-sicians, nurses and policy makers working in the MOH,Oman. The questionnaire was not translated into Arabicbecause all health professionals in Oman speak English.This was followed by modifications of the questionnairefor the primary health care setting in Oman. The termhospital was replaced by primary health care centers andthe name of the districts, locally known as (wilayats)were included following their feedback from the primaryhealth care professionals and the policy makers (Add-itional file 1).Primary health care centers in Muscat, the capital of
Oman, were included if they had the following services:general practice, nursing care and pharmacy and theseservices were functional seven days a week in additionto services of laboratory, radiology and dentistry careprovided five days a week, excluding weekends. A sys-tematic random sampling scheme was used in each primary health center, with assistance from an administra-tor, to select a sample of 10% condition sampling from
AL Lawati et al. BMC Family Practice (2019) 20:50 Page 2 of 8

each health professional category which represented theprimary health care workforce. Health professionals wereeligible for inclusion if they were full-time frontlinehealth care professionals working in primary health carecenters in the Muscat region (There are no part-timehealth care professionals working in the Ministry ofHealth in Oman). The health professions included doc-tors, nurses, dentists, pharmacists, radiographers, and la-boratory technicians.The selected health professionals were invited by an
intermediary, a head nurse, and the principal investiga-tor (MAL) explained the importance of the survey andits potential impact on safety in primary health care inaddition to importance of their participation. The surveywas given to the selected participants in a sealed enve-lope during working hours. Surveys were collected in asealed envelope two to three days after distribution. Atotal of 198 health professionals from primary healthcare centers in the Muscat region were invited to takepart in the survey and verbal consent was taken fromthe participant. All the sealed envelopes were collectedfrom each health center by the intermediary. The partic-ipants were advised not to discuss the questionnaire witheach other to avoid peer influence. The intermediarywas not included as a participant.
Sample sizeThe population of the survey was health care profes-sionals in primary health care in the Muscat governor-ate (N = 1984). The total number of health careprofessionals working in primary health care inMuscat included in the study (N = 1164) this popula-tion reflects the 22 out of 28 health centers whichwere included in the study. The 22 out of 28 health-care centers were selected on the basis of serviceswhich includes general practice, nursing care andpharmacy these services are functional 7 times a weekin addition to services such as laboratory, X ray ser-vices and dentistry care provided 5 days a week ex-cluding weekends. We aimed to survey arepresentative sample of 10% of the total from eachoccupational category. From each center we sampledthe following: Nurses (n = 3), Physicians (n = 2),Radiographers (n = 1), Laboratory technicians (n = 1),Dentists (n = 1) and Pharmacists (n = 1) (9 in totalfrom each center). Thus, the sample size for this studywas (9 × 22 = 198) health professionals from the se-lected primary care centers.
Data managementThe principal investigator (MAL) entered the datainto the University of Sydney’s REDCAP database[25]. No identifying information was obtained from
the participants, confidentially and anonymity wereassured and maintained.
Statistical analysisData were analyzed using SPSS 22 statistical software(IBM Corp. Released 2013. IBM SPSS Statistics forWindows, Version 22.0. Armonk, NY: IBM Corp). De-scriptive statistics were used to explore the characteris-tics of the respondents. Calculation of the compositefrequency for the twelve patient safety dimensions mea-sured by the HSOPSC data collection tool was con-ducted as per the user guidelines published by AHRQ[26]. Items were worded in negative and positive direc-tions. The composite frequency was calculated by divid-ing the total number of positive responses of all theitems constituting a dimension (numerator) by the totalnumber of the responses to all the items of that dimen-sion excluding missing responses (denominator) times100. The resulting number represents a positive re-sponse on that specific dimension [26]. The responsesfor each item in the dimensions were strongly disagree,disagree, neither, agree and strongly agree, and from‘never’ to ‘always’ when relevant. Positive responseswere considered whenever strongly agree and agreewhere chosen. Composite frequencies of the total per-centage of the positive responses of each dimensionwere calculated in addition to each item and primaryhealth care center.
Ethical considerationThe study protocol was approved by the Research andEthical Review and Approval Committee at the Centreof Research and Studies in the Ministry of Health on2nd February 2016, Muscat, Oman. A permission letterwas further sent to all the health centers and verbal in-formed consent was obtained from each participant. SeeAdditional file 2 for the research ethics approval letter.
ResultsDemographic dataOut of the 28 operating primary health care centers inthe Muscat area, 22 met the inclusion criteria. Therewere 186 completed questionnaires from the 198 healthprofessionals invited to participate (response rate of94%). The demographic characteristics of the participat-ing health professionals are detailed in Table 1.Overall, 74% (139/186) of the staff who participated
in the survey graded patient safety as excellent or verygood, and 63% (116/186) of staff in the health centershad not reported any events in the past 12 months andonly a third (60/186) had reported one to five events,see Table 2.
a. Unit level (Department level)
AL Lawati et al. BMC Family Practice (2019) 20:50 Page 3 of 8
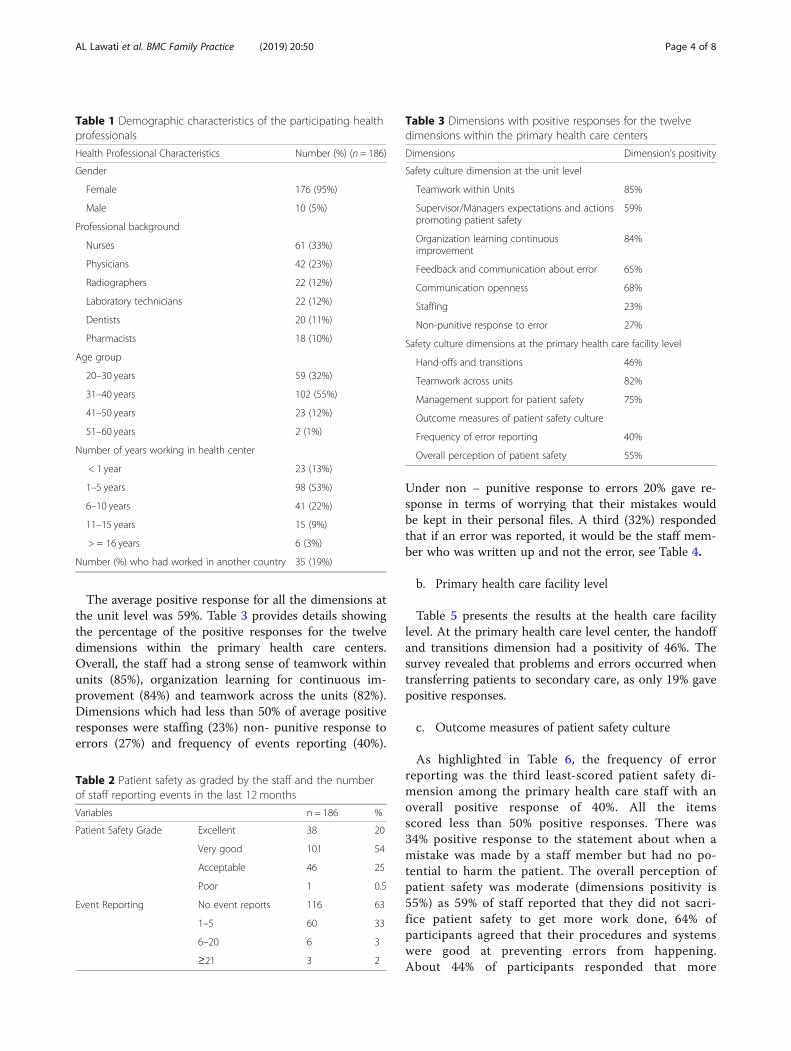
The average positive response for all the dimensions atthe unit level was 59%. Table 3 provides details showingthe percentage of the positive responses for the twelvedimensions within the primary health care centers.Overall, the staff had a strong sense of teamwork withinunits (85%), organization learning for continuous im-provement (84%) and teamwork across the units (82%).Dimensions which had less than 50% of average positiveresponses were staffing (23%) non- punitive response toerrors (27%) and frequency of events reporting (40%).
Under non – punitive response to errors 20% gave re-sponse in terms of worrying that their mistakes wouldbe kept in their personal files. A third (32%) respondedthat if an error was reported, it would be the staff mem-ber who was written up and not the error, see Table 4.
b. Primary health care facility level
Table 5 presents the results at the health care facilitylevel. At the primary health care level center, the handoffand transitions dimension had a positivity of 46%. Thesurvey revealed that problems and errors occurred whentransferring patients to secondary care, as only 19% gavepositive responses.
c. Outcome measures of patient safety culture
As highlighted in Table 6, the frequency of errorreporting was the third least-scored patient safety di-mension among the primary health care staff with anoverall positive response of 40%. All the itemsscored less than 50% positive responses. There was34% positive response to the statement about when amistake was made by a staff member but had no po-tential to harm the patient. The overall perception ofpatient safety was moderate (dimensions positivity is55%) as 59% of staff reported that they did not sacri-fice patient safety to get more work done, 64% ofparticipants agreed that their procedures and systemswere good at preventing errors from happening.About 44% of participants responded that more
Table 1 Demographic characteristics of the participating healthprofessionals
Health Professional Characteristics Number (%) (n = 186)
Gender
Female 176 (95%)
Male 10 (5%)
Professional background
Nurses 61 (33%)
Physicians 42 (23%)
Radiographers 22 (12%)
Laboratory technicians 22 (12%)
Dentists 20 (11%)
Pharmacists 18 (10%)
Age group
20–30 years 59 (32%)
31–40 years 102 (55%)
41–50 years 23 (12%)
51–60 years 2 (1%)
Number of years working in health center
< 1 year 23 (13%)
1–5 years 98 (53%)
6–10 years 41 (22%)
11–15 years 15 (9%)
> = 16 years 6 (3%)
Number (%) who had worked in another country 35 (19%)
Table 2 Patient safety as graded by the staff and the numberof staff reporting events in the last 12 months
Variables n = 186 %
Patient Safety Grade Excellent 38 20
Very good 101 54
Acceptable 46 25
Poor 1 0.5
Event Reporting No event reports 116 63
1–5 60 33
6–20 6 3
≥21 3 2
Table 3 Dimensions with positive responses for the twelvedimensions within the primary health care centers
Dimensions Dimension’s positivity
Safety culture dimension at the unit level
Teamwork within Units 85%
Supervisor/Managers expectations and actionspromoting patient safety
59%
Organization learning continuousimprovement
84%
Feedback and communication about error 65%
Communication openness 68%
Staffing 23%
Non-punitive response to error 27%
Safety culture dimensions at the primary health care facility level
Hand-offs and transitions 46%
Teamwork across units 82%
Management support for patient safety 75%
Outcome measures of patient safety culture
Frequency of error reporting 40%
Overall perception of patient safety 55%
AL Lawati et al. BMC Family Practice (2019) 20:50 Page 4 of 8
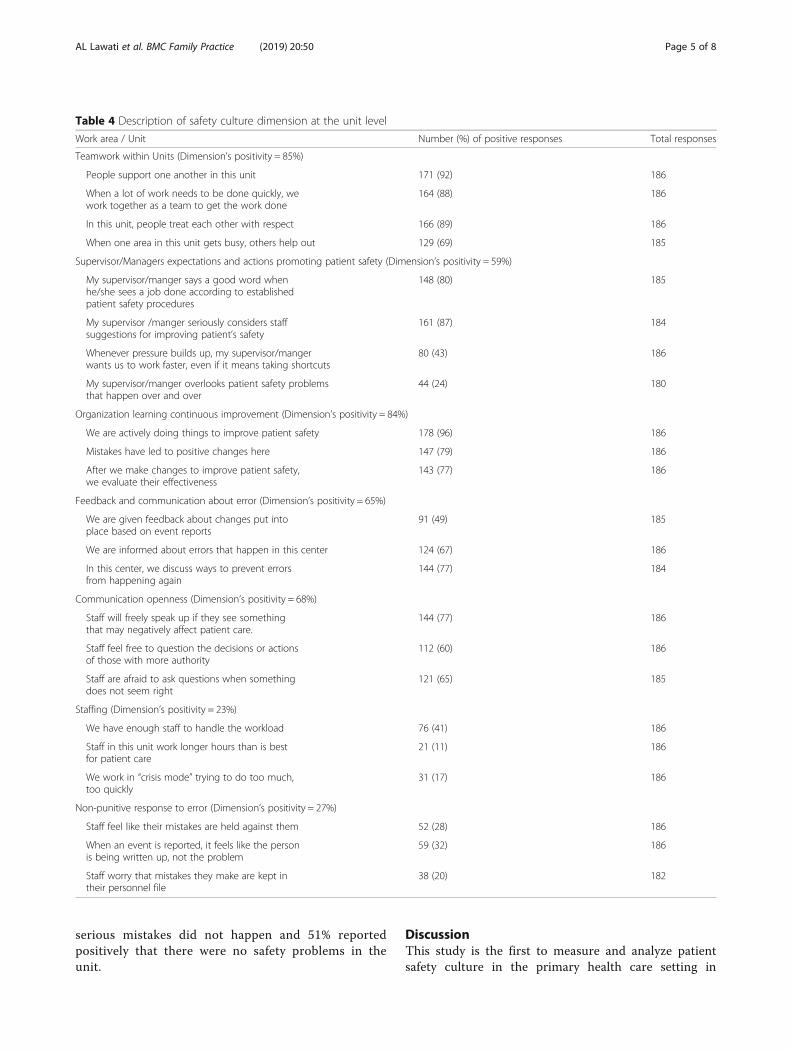
serious mistakes did not happen and 51% reportedpositively that there were no safety problems in theunit.
DiscussionThis study is the first to measure and analyze patientsafety culture in the primary health care setting in
Table 4 Description of safety culture dimension at the unit level
Work area / Unit Number (%) of positive responses Total responses
Teamwork within Units (Dimension’s positivity = 85%)
People support one another in this unit 171 (92) 186
When a lot of work needs to be done quickly, wework together as a team to get the work done
164 (88) 186
In this unit, people treat each other with respect 166 (89) 186
When one area in this unit gets busy, others help out 129 (69) 185
Supervisor/Managers expectations and actions promoting patient safety (Dimension’s positivity = 59%)
My supervisor/manger says a good word whenhe/she sees a job done according to establishedpatient safety procedures
148 (80) 185
My supervisor /manger seriously considers staffsuggestions for improving patient’s safety
161 (87) 184
Whenever pressure builds up, my supervisor/mangerwants us to work faster, even if it means taking shortcuts
80 (43) 186
My supervisor/manger overlooks patient safety problemsthat happen over and over
44 (24) 180
Organization learning continuous improvement (Dimension’s positivity = 84%)
We are actively doing things to improve patient safety 178 (96) 186
Mistakes have led to positive changes here 147 (79) 186
After we make changes to improve patient safety,we evaluate their effectiveness
143 (77) 186
Feedback and communication about error (Dimension’s positivity = 65%)
We are given feedback about changes put intoplace based on event reports
91 (49) 185
We are informed about errors that happen in this center 124 (67) 186
In this center, we discuss ways to prevent errorsfrom happening again
144 (77) 184
Communication openness (Dimension’s positivity = 68%)
Staff will freely speak up if they see somethingthat may negatively affect patient care.
144 (77) 186
Staff feel free to question the decisions or actionsof those with more authority
112 (60) 186
Staff are afraid to ask questions when somethingdoes not seem right
121 (65) 185
Staffing (Dimension’s positivity = 23%)
We have enough staff to handle the workload 76 (41) 186
Staff in this unit work longer hours than is bestfor patient care
21 (11) 186
We work in “crisis mode” trying to do too much,too quickly
31 (17) 186
Non-punitive response to error (Dimension’s positivity = 27%)
Staff feel like their mistakes are held against them 52 (28) 186
When an event is reported, it feels like the personis being written up, not the problem
59 (32) 186
Staff worry that mistakes they make are kept intheir personnel file
38 (20) 182
AL Lawati et al. BMC Family Practice (2019) 20:50 Page 5 of 8
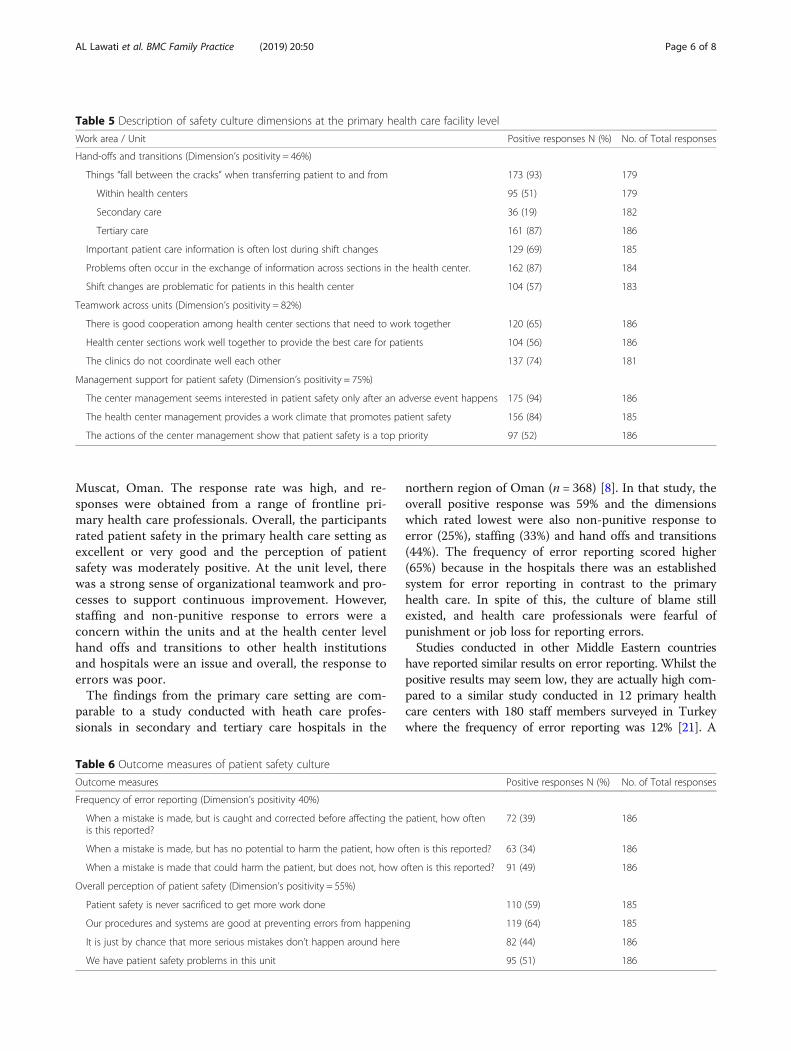
Muscat, Oman. The response rate was high, and re-sponses were obtained from a range of frontline pri-mary health care professionals. Overall, the participantsrated patient safety in the primary health care setting asexcellent or very good and the perception of patientsafety was moderately positive. At the unit level, therewas a strong sense of organizational teamwork and pro-cesses to support continuous improvement. However,staffing and non-punitive response to errors were aconcern within the units and at the health center levelhand offs and transitions to other health institutionsand hospitals were an issue and overall, the response toerrors was poor.The findings from the primary care setting are com-
parable to a study conducted with heath care profes-sionals in secondary and tertiary care hospitals in the
northern region of Oman (n = 368) [8]. In that study, theoverall positive response was 59% and the dimensionswhich rated lowest were also non-punitive response toerror (25%), staffing (33%) and hand offs and transitions(44%). The frequency of error reporting scored higher(65%) because in the hospitals there was an establishedsystem for error reporting in contrast to the primaryhealth care. In spite of this, the culture of blame stillexisted, and health care professionals were fearful ofpunishment or job loss for reporting errors.Studies conducted in other Middle Eastern countries
have reported similar results on error reporting. Whilst thepositive results may seem low, they are actually high com-pared to a similar study conducted in 12 primary healthcare centers with 180 staff members surveyed in Turkeywhere the frequency of error reporting was 12% [21]. A
Table 5 Description of safety culture dimensions at the primary health care facility level
Work area / Unit Positive responses N (%) No. of Total responses
Hand-offs and transitions (Dimension’s positivity = 46%)
Things “fall between the cracks” when transferring patient to and from 173 (93) 179
Within health centers 95 (51) 179
Secondary care 36 (19) 182
Tertiary care 161 (87) 186
Important patient care information is often lost during shift changes 129 (69) 185
Problems often occur in the exchange of information across sections in the health center. 162 (87) 184
Shift changes are problematic for patients in this health center 104 (57) 183
Teamwork across units (Dimension’s positivity = 82%)
There is good cooperation among health center sections that need to work together 120 (65) 186
Health center sections work well together to provide the best care for patients 104 (56) 186
The clinics do not coordinate well each other 137 (74) 181
Management support for patient safety (Dimension’s positivity = 75%)
The center management seems interested in patient safety only after an adverse event happens 175 (94) 186
The health center management provides a work climate that promotes patient safety 156 (84) 185
The actions of the center management show that patient safety is a top priority 97 (52) 186
Table 6 Outcome measures of patient safety culture
Outcome measures Positive responses N (%) No. of Total responses
Frequency of error reporting (Dimension’s positivity 40%)
When a mistake is made, but is caught and corrected before affecting the patient, how oftenis this reported?
72 (39) 186
When a mistake is made, but has no potential to harm the patient, how often is this reported? 63 (34) 186
When a mistake is made that could harm the patient, but does not, how often is this reported? 91 (49) 186
Overall perception of patient safety (Dimension’s positivity = 55%)
Patient safety is never sacrificed to get more work done 110 (59) 185
Our procedures and systems are good at preventing errors from happening 119 (64) 185
It is just by chance that more serious mistakes don’t happen around here 82 (44) 186
We have patient safety problems in this unit 95 (51) 186
AL Lawati et al. BMC Family Practice (2019) 20:50 Page 6 of 8

similar study in Kuwait [9] surveyed 223 health profes-sionals in 22 centers, they reported 24% non-punitive re-sponse to errors compared to 27% in the current Omanistudy, which is quite similar possibly due to relatively highpositivity of the organizational learning 74% in Kuwait and79% in current Omani study. Health center hand offs andtransitions showed similar results to Kuwait, indicatingthere were issues with safe continuity of care when pa-tients were transferred to secondary and tertiary care.Additionally, teamwork across the units was scoredequally between the Omani and the Kuwaiti primaryhealth care. The area with the lowest positive score in thisstudy was inadequate staffing (23%). This was low com-pared to results from Iran (38%), Kuwait (41%), Turkey(49%) and Yemen (50%). A possible reason for this is thatthe number of staffs in each health center in Muscat isstandardized. However, due to population movements tothe suburbs there have been increases in the population ofthe catchment area corresponding to the health centersplacing more demands on the available staff. Furthermore,in the last three years no new health centers have beenbuilt by the MOH in Muscat.The MOH has developed a long-term vision for the de-
velopment and strengthening of the health care system inOman. In 2012, “Vision 2050” was issued and distributed.Vision 2050 comprehensively examined the health systemfunctions, namely the political; economic; social; techno-logical; environmental; and legal environments (PESTELanalysis) [13]. Furthermore, Oman’s Quality Assuranceand Patient Safety vision for 2050 specified that “the qual-ity and patient safety health care in Oman will be recog-nized internationally as a top healthcare system thatresponds to community needs through communityempowerment and partnership and provides quality, sus-tainable and innovative health care services through com-mitted competent and efficient staff” [13]. The results ofthis survey will be used to inform progress towardsrealization of these objectives in patient safety in primaryhealth care in Oman.The culture of an organization needs to be assessed first,
before effective change in an organization can occur [13].Falling under the umbrella of “vision 2050” are thenational five years’ health development plans. Outcome ofthis study is expected to be taken into consideration forthe next five years (2020–2025), develop plan for estab-lishing of a national survey to assess the perception of pa-tient safety in primary care across all the regions of Oman.The results of this study will assist the Ministry of Healthto implement key strategies for improvement. Further-more, the Ministry of Health will further take necessarysteps for partnership with other Ministries if required.This survey had a few limitations that need to be con-
sidered. The language of the survey was English, eventhough English was not the native language of all
participants, but is the language used among health careprofessionals and most of the medical college and tech-nical schools teach in English.The data were analyzed by calculating the percentage
of positive responses but averaging individual means hasbeen found to give a better precision [24]. Some criticsmight recommend using the Safety Attitudes Question-naire to assess patient safety culture but it has beennoted that the HSPSC has similar psychometric proper-ties [27]. The HSPSC has in addition similar psychomet-ric properties in various population settings, includingthe Arabic speaking one [28] however, they were nottested in this study. Another possible limitation is thatthe Medical Office Survey on Patient Safety Culture(MOSOPSC) tool which was designed for use in primarycare and used in the Portuguese Primary Healthcare [22]could have been used however the aim was to use a toolwhich had previously been used in the Gulf region.
ConclusionsThis survey of patient safety culture in primary health carein Muscat, Oman, has identified that the core areas ofstrength are teamwork within the units and organizationlearning and continuous improvement. Areas which re-quire improvement are non-punitive response to errors,inadequate staffing and hand offs and transition. The find-ings from this study will provide policy makers and healthcare professionals with a detailed understanding of thecurrent patient safety culture in Muscat, Oman as a foun-dation for improvements in patient safety, led by the Min-istry of Health in Oman. A well-designed national patientsafety initiative is required which should be integrated intoprimary health care center policies and in the upcomingfive-year organizational plan which aims to improvecommunication openness and to establish an automatedincidence reporting system. Staffing levels and handoffsand transitions also demand closer attention.
Additional files
Additional file 1: The questionnaire. (PDF 872 kb)
Additional file 2: Approval letter. (PDF 32 kb)
AbbreviationsAHRQ: Agency of healthcare Research and Quality; EMRO: Eastern MediterraneanRegion; GCC: Gulf Cooperation Council Countries; HSOPSC: Hospital Survey ofPatient Safety Culture tool; MOH: Ministry of Health; WHO: World HealthOrganization
AcknowledgementsThe Authors are grateful to the managers and the primary health care professionalswho participated in the survey.
FundingScholarship for the research was provided from the Ministry of Higher Educationin Oman. They further funded my PhD education and provide me with anallowance for my research.
AL Lawati et al. BMC Family Practice (2019) 20:50 Page 7 of 8
Availability of data and materialsThe data are stored in a personal hard drive. They are available from thecorresponding author on request.
Authors’ contributionsMA and NN undertook the pilot study and data collection. SS and SD oversawthe methodology and analysis of the results and made significant contributionsto the manuscript SP participated in statistical analysis. All authors participatedin developing the study hypothesis, objectives and study design. All authorsparticipated in drafting the manuscript. All authors read and approved the finalmanuscript.
Authors’ informationPhD Student at the University of Sydney, Head of Quality and Patient Safetyat the Directorate General of Health Services, Muscat Oman, Ministry ofHealth.
Ethics approval and consent to participateThe study protocol was approved by the “Research and Ethical Review andApproval Committee” at the Centre of Research and Studies in the Ministryof Health, Muscat, Oman on 2nd February 2016. Informed verbal consentwas obtained by all the participants and approved by the committee sincethe participants are heath care professionals who are aware of the scientificresearch and its implication for improvement, no personal informationwould be identified in any publication arising from the study. Theparticipants were allowed to call the principal researcher if they had anyquestions or information. The participation was voluntary and anonymous.This was approved by the “Research and Ethical Review and ApprovalCommittee” at the Centre of Research and Studies in the Ministry of Health,Muscat, Oman.
Consent for publicationNot applicable.
Competing interestsThe authors declare that they have no competing interests.
Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims in publishedmaps and institutional affiliations.
Author details1Discipline of Physiotherapy, Faculty of Health Sciences, The University ofSydney, Sydney, Australia. 2Ministry of Health, P.O.Box, 626, PC 117 Wadi AlKabir, Muscat, Oman. 3Statistical Department, Oman Medical Specialty Board,Way # 4443, Bld. 18, Block 244, Plot 404, North Azaiba, Muscat, Oman. 4SouthWestern Sydney Local Health District, Liverpool, NSW 2171, Australia.5Ingham Institute of Applied Medical Research, 1 Campbell Street, Liverpool,NSW 2171, Australia.
Received: 16 December 2018 Accepted: 25 March 2019
References1. Nieva VF, Sorra J. Safety culture assessment. A tool for improving patient safety
in healthcare organizations. Qual Saf Health Care. 2003;12(Suppl II):ii17–23.2. World Health Organization. Conceptual framework for the international
classification for patient safety. Geneva; 2009.3. World Health Organization. World Alliance for patient safety. Geneva: WHO;
2004. p. 2004.4. Dorien LM Zwart, Elizabeth LJ Van Rensen, Cor J Kalkman, Theo JM Verhei.
Central or local incident reporting? A comparative study in Dutch GP out-of-hours services. Pubmed. 2011(Br J Gen Pract 2011;61(584):183–187. doi:https://doi.org/10.3399/bjgp11X561168).
5. Gaal S, Verstappen W, Wolters R, Lankveld H, van Weel C, Wensing M.Prevalence and consequences of patient safety incidents in general practicein the Netherlands: a retrospective medical record review study. ImplementSci. 2011;6:37.
6. O’Beirne M, Sterling PD, Zwicker K, Hebert P, Norton PG. Safety incidents infamily medicine. BMJ Qual Safety. 2011;20(12):1005–10.
7. Luke Slawomirski, Ane Auraaen, Niek Klazinga. The economics of-patientsafety in primary and ambulatory care April 2018. 3rd Global MinisterialSummit on Patient Safety 2018 April 2018.
8. Ahmed Al-Mandhari, Ibrahim Al-Zakwani, Moosa Al-Kindi, Jihane Tawilah,Atsu S S Dorvlo, Samir Al-Adawi. Patient safety culture assessment in Oman.Oman Med J 22 May 2014.
9. Ghobashi MM, El-Ragehy HAG, Al-Doseri FA, Mosleh H. Assessment ofpatient safety culture in primary health care settings in Kuwait. EpidemiolBiostat Public Health. 2014;11(3):e9101–1-e-9.
10. Tabrizchi N, Sedaghat M. The first study of patient safety culture in Iranianprimary health centers. Acta Med Iran. 2012;50(7):505–10.
11. Webair HH, Al Assani SS, Al Haddad RH, Al Shaeeb WH, Selm MAB, AlyamaniAS. Assessment of patient safety culture in primary care setting, Al-Mukala,Yemen. BMC Fam Pract. 2015;16:136.
12. World Health Organization. Regional launch of the WHO multi-professionalpatient safety curriculum guide in the eastern Mediterranean region.Geneva; 2012.
13. Dr Ali Taleb Al Hinai, Dr Ahmed Mohamed Al Qasmi, Dr Medhat K El Sayed,Mr Mohamed Hussein Fahmy Bayoumi, Dr Adhra Hilal Al Mawali, Dr HalimaQalm Al Hinai, et al. Health Vision 2050. Ministry of Health , Sultanate ofOman; 2014. Contract No.: 1.
14. Ministry of Health. Annual health report Muscat, Oman 2014.15. Ganguly SS, Al-Lawati A, Al-Shafaee MA, Duttagupta KK. Epidemiological
transition of some diseases in Oman: a situational analysis. East MederrHealth J. 2009;45(1):26–31.
16. Department of Information and Statistics Annual Health Report. Oman:Ministry of Health; 2016.
17. Agency for Healthcare Research and Quality. Hospital survey on patientsafety culture 2016 [Available from: https://www.ahrq.gov/sites/default/files/wysiwyg/professionals/quality-patient-safety/patientsafetyculture/hospital/userguide/hospcult.pdf.
18. Sorra J S, Nieva V F. Measuring Patient Safety Culture Manual, Part I: GettingStarted & Planning Your Survey Process Hospital Survey on Patient SafetyCulture AHRQ Publication 2004 [.
19. Marleen Smits, Ingrid Christiaans Dingelhoff, Cordula Wagner, Gerrit van derWal, Peter P Groenewegen. The psychometric properties of the 'Hospitalsurvey on patient safety Culture' in Dutch hospitals. BMC Health Serv Res2008;8(230).
20. Muna Habib AL Lawati, Sarah Dennis, Stephanie D Short, Nadia NoorAbdulhadi. Patient safety and safety culture in primary health care: asystematic review. BMC Family Practice. 2018;19:104.
21. Bodur S, Filiz E. A survey on patient safety culture in primary healthcareservices in Turkey. Int J Qual Health Care. 2009;21(5):348–55.
22. Ornelas MD, Pais D, Sousa P. Patient safety culture in Portuguese primaryhealthcare. Qual Prim Care. 2016;24(5):214–5.
23. Hedsköld M, Pukk-Härenstam K, Berg E, Lindh M, Soop M, Øvretveit J, et al.Psychometric properties of the hospital survey on patient safety culture,HSOPSC,applied on a large Swedish health care sample. BMC Health ServRes. 2013;13(332).
24. Giai J, Boussat B, Occelli P, Gandon G, Seigneurin A, Michel P, et al. Hospitalsurvey on patient safety culture (HSOPS): variability of scoring strategies. IntJ Qual Health Care. 2017;29(5):685–92.
25. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Conde,research electronic data capture (REDCap) – a metadata-drivenmethodology and workflow process for providing translational researchinformatics support. J Biomed Inform. 2009;42(2):377–81.
26. AHRQ. ISNA Bulletin 2008;34(2):11–12.27. Etchegaray JM, Thomas EJ. Comparing two safety culture surveys: safety
attitudes questionnaire and hospital survey on patient safety. BMJ Qual Saf.2012;21(6):490–8.
28. El-Jardali F, Jaafar M, Dimassi H, Jamal D, Hamdan R. The current state ofpatient safety culture in Lebanese hospitals: a study at baseline. Int J QualHealth Care. 2010;22(5):386–95.
AL Lawati et al. BMC Family Practice (2019) 20:50 Page 8 of 8
73
Chapter 6 Health professionals’ perceptions of patient safety culture in primary care in Oman: A qualitative study
Oman Medical Journal
Health professionals’ perceptions of patient safety culture in primary care in Oman: Aqualitative study--Manuscript Draft--
Manuscript Number:
Full Title: Health professionals’ perceptions of patient safety culture in primary care in Oman: Aqualitative study
Article Type: Original Article
Keywords: patient safety; safety culture; primary health care; teamwork; communication errors;guidelines; Oman
Corresponding Author: Muna Al LawatiDirectorate General of Health Services , Muscat RegionOMAN
Corresponding Author SecondaryInformation:
Corresponding Author's Institution: Directorate General of Health Services , Muscat Region
Corresponding Author's SecondaryInstitution:
First Author: Muna Al Lawati
First Author Secondary Information:
Order of Authors: Muna Al Lawati
Dr Nadia Noor Abdulhadi
Professor Stephanie D. Short
Associate Professor Sarah Dennis
Order of Authors Secondary Information:
Manuscript Region of Origin: OMAN
Abstract: Objective
Patient safety culture is a vital component of quality health care and is a fundamentalconcern for healthcare organizations around the world. Little has been published onpatient safety in primary health care (PHC) in Oman. Hence, the aim of this study wasto explore the understanding of patient safety by primary health care professionalsworking in Muscat, Oman. A specific objective was to identify areas for improvement inorder to inform the development of a framework for patient safety policy in primaryhealth care in Oman.Methods
Two focus group discussions were conducted among 14 participants from 22 primaryhealth care centers in Muscat, Oman. Qualitative content analysis wasemployed.Findings
Healthcare professionals reported that improvements were needed in current patientsafety practice in the PHC, particularly in relation to collaboration among staff. Theparticipants expressed a range of understandings of safety culture. Four main themeswere identified. These were: safety culture in primary health care; safety climate;adverse events; and training to improve the safety of patients and staff working inPHCs.Conclusions
Initiatives need to be implemented to improve teamwork, error reporting and thesystem response to errors, development and monitoring of polices and communicationamong staff. The outcomes of this study will be used by the Ministry of Health in Omanto develop policies and guidelines for patient safety in primary health care.
Powered by Editorial Manager® and ProduXion Manager® from Aries Systems Corporation
Suggested Reviewers: Dr. Thamra Al [email protected] reseach background
Dr Qamra AL [email protected] General of Quality and Patient Safety ,she has extensive background onpatient safety.
Powered by Editorial Manager® and ProduXion Manager® from Aries Systems Corporation
Health professionals’ perceptions of patient safety culture in primary care
in Oman: A qualitative study
Dr Muna Habib AL Lawati
1. The University of Sydney
Discipline of Behavioral and Social Sciences in Health, Faculty of Health Sciences
New South Wales 2006, Australia
2. Ministry of Health, Oman
P.O.Box 626, PC 117 Wadi Al Kabir, Muscat, Oman
Email: [email protected]
Dr Nadia Noor Abdulhadi
Directorate General of Planning and Studies, Ministry of Health, Oman
P.O.Box 358 PC 116, Mina Al Fahal , Oman
Email: [email protected], [email protected]
Professor Stephanie D. Short
The University of Sydney
Discipline of Behavioral and Social Sciences in Health, Faculty of Health Sciences
New South Wales 2006, Australia
Email: [email protected]
Associate Professor Sarah Dennis
1. The University of Sydney,
Discipline of Physiotherapy, Faculty of Health Sciences
New South Wales 2006, Australia
Cover Page Only
1. South Western Sydney Local Health District,
Liverpool NSW 2171, Australia
2. Ingham Institute of Applied Medical Research
1 Campbell Street
Liverpool NSW 2171, Australia
Email: [email protected]
Corresponding author
Dr Muna Habib AL Lawati
1. The University of Sydney
Discipline of Behavioral and Social Sciences in Health, Faculty of Health Sciences
New South Wales 2006, Australia
2. Ministry of Health, Oman
P.O.Box, 626, PC 117 Wadi Al Kabir ,Muscat, Oman
Email: [email protected]

Abstract
Objective: Patient safety culture is a vital component of quality health care and is a
fundamental concern for healthcare organizations around the world. Little has been published
on patient safety in primary health care (PHC) in Oman. Hence, the aim of this study was to
explore the understanding of patient safety by primary health care professionals working in
Muscat, Oman. A specific objective was to identify areas for improvement in order to inform
the development of a framework for patient safety policy in primary health care in Oman.
Methods: Two focus group discussions were conducted among 14 participants from 22
primary health care centers in Muscat, Oman. Qualitative content analysis was employed.
Findings: Healthcare professionals reported that improvements were needed in current
patient safety practice in the PHC, particularly in relation to collaboration among staff. The
participants expressed a range of understandings of safety culture. Four main themes were
identified. These were: safety culture in primary health care; safety climate; adverse events;
and training to improve the safety of patients and staff working in PHCs.
Conclusions: Initiatives need to be implemented to improve teamwork, error reporting and
the system response to errors, development and monitoring of polices and communication
among staff. The outcomes of this study will be used by the Ministry of Health in Oman to
develop policies and guidelines for patient safety in primary health care.
Words: 238
Key words: patient safety; safety culture; primary health care; teamwork; communication
errors; guidelines; Oman
Manuscript (Without cover page) Click here to access/download;Manuscript (Without coverpage);OMJ Manuscript .doc
Introduction
Patient safety is an important concern in the health systems of countries at all stages of
development. Worldwide, millions of people suffer disabilities, injuries or death annually due
to unsafe medical practices (1). To date, most of the patient safety research has been
conducted in hospitals rather than primary health care (2). Yet many incidents related to
patient safety in hospitals have their origins in primary care (3).
A recent systematic review of the literature on safety culture in Arab countries identified only
18 studies. A key finding was that health professionals in a number of countries were
concerned about punitive responses to error reporting (4). A recent study in primary care in
Muscat, Oman used the Hospital Survey on Patient Safety Culture (HSPSC) which was
adapted for use in primary care (2). Respondents rated the dimension of teamwork highly and
strongly supported the need for non-punitive responses to errors, as was found in the
systematic review (4). The use of qualitative research methods may help to provide deeper
understanding of the issues and identify potential solutions to progress patient safety culture
in Arab countries (4).
The Ministry of Health (MoH) in Oman has recognized the importance of delivering quality
health care to the community. In response to an initiative from the World Health Organization
(WHO) in 2007, a national patient safety team was established in Oman and workshops on
patient safety were conducted in many health care institutions (5). The resulting patient safety
initiatives focused on hospital autonomy and infection control programs. More recently, a
focus on primary health care has emerged (5).
Given the paucity of research on patient safety culture in primary health care in Oman, the
main aim of this study was to explore the understanding of patient safety among health care
professionals working in primary health care in Muscat, Oman. A secondary aim was to
identify areas for training and improvement in order to develop a framework for patient safety
in primary health care in Oman.
Methods
Given the exploratory nature of this study, a qualitative, phenomenological approach was
chosen (6, 7). Focus group discussions (FGDs) were conducted with primary health care
professionals in Muscat (6). The topic guide for the FGDs was informed by the research
team’s earlier systematic review (8) and survey conducted in 22 primary health care centers
in Muscat, Oman (9).
A purposive sampling strategy was used to select participants from 22 of the 28 primary
health care centers (PHCCs) within the Muscat region. These centers were selected they
provided a full range of primary health care services, including laboratory; dental, pharmacy
and radiographic facilities. The inclusion criteria for staff were: five years or more work
experience in primary health care and involvement as a quality focal point in the health center
(Table 1). The participants were invited personally by telephone.
The two focus group discussions were conducted in September 2017 by two researchers
(MAL, NN) in a meeting room in the Directorate General of Health Services in Muscat. This
was a central location and a convenient venue for all participants. The FGDs were conducted
in English as all the participants, Omani and non-Omani, were fluent English speakers. The
FGDs were digitally recorded on an iPad and transcribed verbatim. All health care
professionals gave their written informed consent to participate and for the discussion to be
recorded.
As previously noted, the topic guide was developed based on available literature and previous
studies conducted by the research team (8-10). It was piloted with six health professionals.
Six key issues were explored: 1) understanding of patient safety; 2) awareness of patient
safety procedures in PHCCs; 3) reporting errors in PHCCs; 4) communication between
medical and paramedical staff; 5) training in patient safety; and 6) suggestions for future
improvements in patient safety (Appendix A). Each FGD lasted about two hours, including
20 minutes for greetings and introductory remarks, and was followed by a debriefing between
the researchers. Similarities and differences were noted and, despite the small sample size,
the two FGDs provided rich information and data saturation was achieved.
Inductive qualitative content analysis was employed (11). The transcripts were read several
times to obtain a sense of the whole content. The text was divided into meaningful units,
which were labeled with codes. The second stage of analysis was conducted using the codes
to identify similar opinions and perceptions. The codes were sorted into categories, which
were examined for differences and similarities and finally condensed into four broad themes:
safety culture; safety climate, adverse events, and recommendations for training to improve
the safety of patients and staff working in primary health care centers. The content of the
themes was discussed and verified by all the authors. Disagreements were resolved through
discussion among the authors until consensus was reached.
Results
A total of 27 primary health care professionals from the 22 eligible PHCCs were invited to
participate. Of these, 20 agreed to participate, of whom 6 were unable to participate because
of work commitments and/or time constraints on the days scheduled for the FGD. However,
those who declined had broadly similar characteristics to those who attended in terms of work
experience in primary health care and quality management activities in the health centers.
The demographic characteristics of the participating health care professionals are detailed in
Table 1. Nurses were oversampled because they constitute the largest segment of the
primary health care workforce in Muscat, Oman
Each of the four main themes that were considered important for patient safety and for safety
culture among the staff at the PHCCs is elaborated below.
1. Safety culture
Shared responsibility and teamwork approach
The participants understood the importance of patient safety culture and recognized that
patient safety also included the safety of health care professionals.
In my point of view patient safety starts from staff safety.
We as an institution we are responsible for the patient's safety.
There were a range of views about the role of different health care professionals and their
responsibilities for patient safety in primary health care centres. Doctors and nurses
emphasized teamwork and shared responsibility. This responsibility started from the time the
patient entered the health centre, even before they saw a health care professional.
Yes, we definitely agree, patient safety is a shared responsibility, patient safety starts
from the time the patient enters the main gate of the health centre.
Despite this agreement about the importance of teamwork to ensuring patient safety, this was
not always the case in practice. Doctors expressed the view that employees the medical
records department and the medical orderlies did not perceive themselves as part of the team
with regard to safety issues and did not always follow safety procedures.
The medical record staff and the medical orderly usually deal with documentation of the
patient’s visits and they think they are not part of patient safety.
The participants reported that patient safety was not on the agenda at center meetings, which
only discussed administrative issues.
The patient safety issues never come up in these meetings. It is mostly administration
issues.
Clean work environment and hazard control
The importance of cleanliness in relation to patient safety was emphasized. Health
professionals were critical of the standard of cleaning in the centers and the poor behaviour of
some of the cleaners. They reported that the cleaning companies were selected and contracted
by the Ministry of Health and were not operating at the high standards required for infection
control. This was putting health care professionals, cleaning staff and patients at risk.
In my health center, I never touch a door with bare hands, I am using tissue papers.
Yeah, because myself I saw the cleaners. They use the same gloves and the same tools
from the laboratory and clean all health centers with the same tools.
They are using the same mop for different contaminated areas and non-contaminated
areas.
Another example was unsafe handling by cleaners of the sharps’ containers:
The cleaner took a sharp container which was not tightly closed. Everything in
that, inside the sharp container fell. What he did, by his hand, no gloves he
took all the needles from the floor back to the container.
All participants agreed that hazard control is an important safety practice and essential for a
clean and healthy environment. In this context, they noted that blood containers and other
biological samples were frequently taken to the laboratory by the patients themselves. Often
the containers leaked blood or urine into the plastic bags, putting patients and staff at risk.
The radiographers highlighted the need for safety procedures such as checking the radiation
detection badge.
The doctors should train the patients about proper way for handling of blood
samples; the doctor should put it in a clear plastic bag not just give it in the
patients hands.
Patient confidentiality
The laboratory technicians emphasized the importance of confidentiality and informed consent
as an essential component of safety when performing blood tests to confirm conditions such as
hepatitis or HIV (AIDS). They felt that these safety measures were compromised when the
health center was crowded and the clinics were busy.
We should keep confidentiality of all data. Also, be sure that the results are released
to this specific patient in the right way, in the right time, to be delivered in the right
time and to be sure that quality control result is acceptable. Also, to keep
confidentiality of all information, whatever the result.
I feel these things are missed when there are too many patients and its very crowded.
It is not intentionally missed, the doctor is busy, the nurse is busy, and they are just
missed.
2. Safety climate
Communication
Appropriate and effective communication between health care professionals, with patients
and with administration staff is essential to ensure patient safety in a safety culture. The
participants identified areas of weakness in communication, such as poor documentation of
patient data and mistakes with information transfer between health care professionals and
patients.
We, in our laboratory, were having one sample for testing HIV, in September
2015. We sent the first sample and we got a request for another sample. Our
role is to inform the treating doctor and he will inform the patient and collect
another sample. So, we informed the doctor. Then in July 2017 we received
results confirming the retest, and the first sample was also positive.
I don't know what the situation for the patient is, so I tried to call the patient
again. I asked my staff to call the patient but no reply until now. So, we
documented this incident. I also informed the doctor. She told me we called
no reply, so I requested to have guidance how to manage and who is
responsibility is that and whom we should call.
Yes, there is a communication problem with the central laboratory.
Communication among health services, administrative staff and health care providers
The participants reported communication problems or misunderstandings regarding the
availability of policies and guidelines for patients and health care professionals. While
doctors were aware of safety guidelines for patients and staff, other health care providers
were not
I think there is a communication problem. I think yes, we do have a form. But no
incident policy.
Some health professionals, particularly dentists and pharmacists, reported feeling
marginalised:
‘We as dentists are isolated in the health centres. We feel we are left alone. They have not
included us in the meetings in the health center. I have rotated in so many health centers,
and it is the same issue.
3. Adverse events
Non-punitive responses to errors and error reporting
Non-medical staff participants said they were afraid to report errors out of concern that they
would be held seen responsible and mistakes would be recorded in their personal files.
Some staff feel blamed when reporting yeah, what we are giving our nurses
awareness to report and not to feel bad but when the problem is with the staff that the
staff definitely feel blamed. Even though we counsel them.
Doctors, however, said they had no concerns about reporting incidents.
Of course, we are confident, and we are competent, we can report errors, this is easy.
Most of the error reporting in primary health care centers took place verbally unless the error
was serious enough to cause patient harm.
Mostly verbally but if it continues or reported repeated many times then the staff is asked to
write a report.
There was no formal system, such as those used in hospitals, to report incidents in primary
health care.
We also need a computerized system to report errors like hospitals.
The participants described incident reporting and documentation as ad hoc and dependent on
those in charge.
I think it’s personal, if the head of the health center feels she wants to
do it than it will happen, it is a personal choice. There is no system or
protocol to form a committee and discuss problems or errors.
Despite this, there were some examples of this haphazard system working well.
Big things like for example we don’t have side rails for patients to climb when
they entered the health centers. One patient fell, and it was a big thing, so we
documented, and the side rails were put. This is a big thing. Now in summer
when the weather is 50 degrees the patients can’t hold the metal rail, so we
again documented, and it was covered by a cloth.
Errors during patient transitions
Shift transition was identified as a time when errors were commonly made, contributing to
poor patient safety. There was a lack of feedback from management in response to an error so
that systems could be improved to prevent it happening again.
One day the working staff left one patient inside the health center with an
intravenous fluid inside the treatment room and left the health center by the
end of the evening shift. That patient was left alone and when the cleaner went
to close the rooms he found the patient and her husband inside the room.
What they did the husband called the police and then they came. The police
came and took the patient. Then when that cleaner saw the police, he was
surprised. They called the health center in charge. Then she came. Nobody
from the health centre informed us, not even the nurse, and the issue passed as
if nothing had happened’
4. Recommendations for training to improve safety practice
Training on patient safety issues
Interviewees agreed that there was a lack of training in patient safety and no safety-related
programs were conducted in primary health care.
Increase professional and patient involvement in safety-related issues
They emphasized the need to raise awareness of safety issues among both staff and patients
and to have a system in place to disseminate relevant information to all staff.
We need to increase awareness of patient safety for patients and for staff also
and increase awareness of staff to write the incident reports.
Having teams with responsibility for patient safety and the promotion of safety culture among
primary health care providers was also suggested.
There has to be a proper system for patient safety in the health centers
with a team for patient safety who can follow up on patient safety
issues.
A further recommendation was to involve patients in discussions about safety, including the
safe use of medicines and reporting adverse events:
So, we should involve patients in the patient safety issues even for use of
medicines and to inform them about expected adverse events.
Discussion
The findings show that primary health care professionals believe patient safety to be
important but that it is inadequate in the current system. There were varied and
multidimensional understandings of safety culture among health professionals.
Only doctors were aware of the existence of guidelines and policies for patient safety in
primary health care. These had been developed by the Ministry of Health in Oman for use in
primary health care centers in 2011 (12) and were disseminated to doctors but not to other
staff. These guidelines include Standard Operation Procedures (SOP) for commonly
performed procedures in primary health care but do not explicitly discuss patient safety..
Guidelines and policies for patient safety are important to facilitate a sense of accountability
and responsibility. Ensuring their availability to all staff would be a simple strategy to
increase awareness of patient safety and inform practice.
All healthcare professionals in this study recognized the importance of teamwork in primary
health care and the impact this has on patient safety. However, some participants felt that
they were not part of the health care team. Teamwork will ensure better health care, minimise
errors, a encourage better health care outcomes and provide ideas to enhance patient safety
(13, 14).
Good communication among staff in important for effective teamwork. It fosters the
development of networks among different health care providers, helps to prevent errors,
improves patient care and increases organizational trust (15). Communication among the
team is important to eliminate threats to the safety of patients (16). A systematic approach to
patient safety education and training is essential in order to develop a culture of open
communication rather than the existing culture of blame (17). When communication between
the different departments in the health center is suboptimal, this can affect continuity of care
(18) and patient safety (15). This needs to be supported by a blame-free system for reporting
and addressing errors if patient safety is to be guaranteed.
Patient handover is known to be a high risk period for errors due to ineffective
communication (19), a fact highlighted by the WHO (20). Organizational trust is also
essential, not only trust physicians and patients but also between health professionals and
management (21). Research shows that organizational trust leads to better organizational
effectiveness and that an environment that focuses on learning from errors will lead to better
patient care (21). Health care professionals need to learn from errors and take appropriate
action without assigning blame (22), as a perceived culture of blame adversely affects the
health care environment and patient safety (23).
Better understanding the safety culture and safety climate in health care will enable us to
build on strengths and focus on areas for improvement. This will in turn lead to a more
competent workforce that is motivated and engaged in patient safety and eventually reduce
the number of errors in the organization. This study has highlighted the need for a clear focus
on patient safety in primary care that includes: (1) comprehensive operationalization of core
concepts relating to safety in primary care; (2) clear guidelines for monitoring, detection and
reporting of errors; (3) effective dissemination of this information to all primary care staff,
along with an action plan; (4) adoption of a non- punitive response to errors based on the
development of an electronic event system for primary care.
Strengths and limitations of the study
The dependability (truth value in relation to data) of our results is high because the entire
team contributed to the analysis and interpretation of data. The usefulness or transferability of
our results depends on how well we have been able to capture the perceptions of participants.

One possible limitation is that the participants’ responses might have been influenced by fear
of disclosure since the principal investigator once worked among the team in one of the
primary health care centers.
Conclusions
A patient safety culture is not yet fully established in primary health care. Initiatives are
required to improve teamwork and communication among staff, develop a system for
reporting and responding to errors, and develop and implement appropriate policies. The
results of this study will be used by the Ministry of Health in Oman to develop policies and
systems to improve patient safety in primary health care.
Declarations
Ethical approval
The study was approved by the Research and Ethical Review and Approval Committee at the
Centre of Research and Studies in the Ministry of Health on 2nd February 2016, Muscat,
Oman. All participants provided their written informed consent to participate after clarifying
the aims and conduct of the study, and their anonymity was guaranteed.
Consent to participate
Consent was given by each participant
Consent to publish
Not applicable
Availability of data
The datasets used and/or analyzed during the current study are available from the
corresponding author on reasonable request.
Competing Interests
The author(s) declare that they have no competing interest.
Funding
The Omani PhD scholarship Fund
Author’s contributions
The authors jointly designed the study, analyzed the data and prepared the manuscript. MA
and NN conducted the interviews. MA and NN coded the data independently. All authors
read and contributed to and approved the final manuscript.
Author details
PhD Student at the University of Sydney,
Head of the Department of Quality and Patient Safety at the Directorate General of Health
Services, Ministry of Health, Muscat, Oman.
Abbreviations
World Health Organization (WHO)
The Ministry of Health (MoH)
Hospital Survey on Patient Safety Culture (HSPSC)
Focus group discussions (FGDs)
Primary Health Care Centers (PHCCs)
References
1. V F Nieva, J Sorra. Safety culture assessment. A tool for improving patient safety in healthcare organizations. Qual Saf Health Care. 2003;12(Suppl II):ii17–ii23. 2. AL Lawati MH, Short SD, Abdulhadi NN, Panchatcharam SM, Dennis S. Assessment of patient safety culture in primary health care in Muscat, Oman: a questionnaire -based survey. BMC Family Practice. 2019;20(1):50. 3. Ignacio Ricci-Cabelloa, Enriqueta Pujol-Riberab, Mariona Pons-Viguésb, Sarah Patricia Slightd, Anna Berenguerab. Patients’ perceptions and experiences of patient safety in primary care in England. Qxford Family Practice Journal. 2016;Vol. 33, (No. 5):535–42. 4. Mustafa Elmontsri AA, Ricky Banarsee, Azeem Majeed. Status of patient safety culture in Arab countries: a systematic review. BMJ open. 2017;7(e013487). 5. World Health Organization. Patient Safety 2018 [Available from: http://www.who.int/patientsafety/en/. 6. Marcus K, Quimson G, Short SD. Source country perceptions, experiences, and recommendations regarding health workforce migration: a case study from the Philippines. Hum Resour Health. 2014;12(1):62. 7. Matua GA, Seshan V, Savithri R, Fronda DC. Challenges and Strategies for Building and Maintaining Effective Preceptor-Preceptee Relationships among Nurses. Sultan Qaboos University medical journal. 2014;14(4):e530-e6. 8. Muna Habib AL Lawati, Sarah Dennis, Stephanie D Short, Nadia Noor Abdulhadi. Patient safety and safety culture in primary health care: a systematic review. BMC Family Practice. 2018;19:104. 9. Muna Habib A. L. Lawati, Stephanie D. Short, Nadia Noor Abdulhadi, Sathiya Murthi Panchatcharam, Sarah Dennis. Assessment of patient safety culture in primary health care in Muscat, Oman: a questionnaire -based survey. BMC Family Practice. 2019. 10. Marzieh Pazokian, Borhani F. Nurses’ Perspectives on Factors Affecting Patient Safety: A Qualitative Study. Evidence Based Care Journal 2017;7(3): 76-81. 11. Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Education Today
February 2004;Volume 24(Issue 2):Pages 105-12. 12. Ministry of Health. Policies for Primary Health Care. In: Care DoPH, editor. Muscat,Oman: Ministry of Health 2011. 13. Noronha JA, Seshan V, Raman S, Ramasubramaniam S, Madavan G, Muliira RS, et al. Patient Safety - A shared responsibility for ensuring quality care
SQU Med J. 2011;11(3):428-35. 14. Jones A, Jones D. Improving teamwork, trust and safety: An ethnographic study of an interprofessional initiative. Journal of Interprofessional Care. 2011;25(3):175-81. 15. Burgener AM. Enhancing Communication to Improve Patient Safety and to Increase Patient Satisfaction. The Health Care Manager. 2017;36(3):238-43. 16. Fadi El-Jardali, Hani Dimassi, Diana Jamal, Maha Jaafar, Nour Hemadeh. Predictors and outcomes of patient safety culture in hospitals BMC Health Services Research 2011. 2011;11:45. 17. Leotsakos A, Ardolino A, Cheung R, Zheng H, Barraclough B, Walton M. Educating future leaders in patient safety. Journal of multidisciplinary healthcare. 2014;7:381-8. 18. Alazri M, Heywood P, Neal RD, Leese B. Continuity of Care: Literature review and implications. Sultan Qaboos University medical journal. 2007;7(3):197-206. 19. Patterson ES, Roth EM, Woods DD, Chow R, Gomes JO. Handoff strategies in settings with high consequences for failure: lessons for health care operations. Int J Qual Health Care 2004;4(2):125-32.
20. Organization WH. Call for more research on patient safety Geneve World Health Organization 2007 [Available from: https://www.who.int/mediacentre/news/releases/2007/pr52/en/. 21. J Firth Cozens. Organisational trust: the keystone to patient safety. Qual Saf Health Care 2004;13:56–61. doi: 10.1136/qshc.2003.007971. 22. Mrayyan M, Shishani K, Al-Faouri I, Ammouri A. Nurses' perceptions of medication errors in Jordan2008. 94-105 p. 23. Ashish Jha. Summary of the evidence on patinet safety: implications for research
In: Organization WH, editor. Geneve 2008.
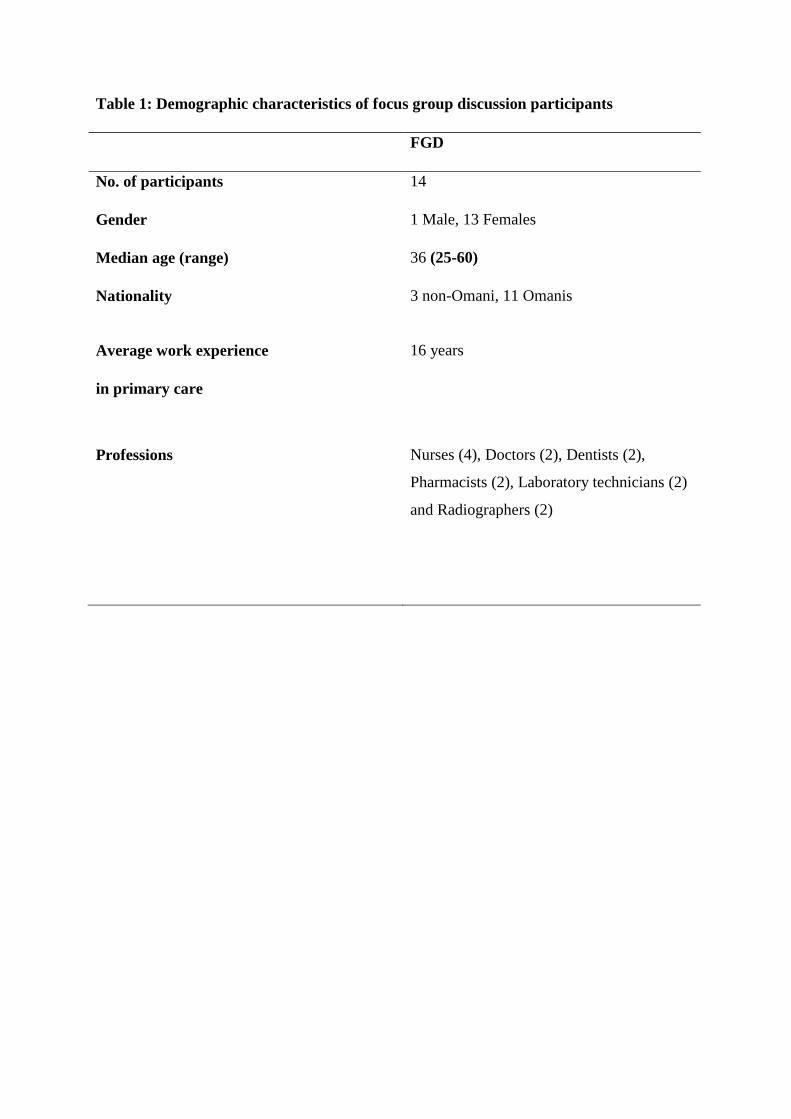
Table 1: Demographic characteristics of focus group discussion participants
FGD
No. of participants 14
Gender 1 Male, 13 Females
Median age (range) 36 (25-60)
Nationality 3 non-Omani, 11 Omanis
Average work experience
in primary care
16 years
Professions Nurses (4), Doctors (2), Dentists (2),
Pharmacists (2), Laboratory technicians (2)
and Radiographers (2)
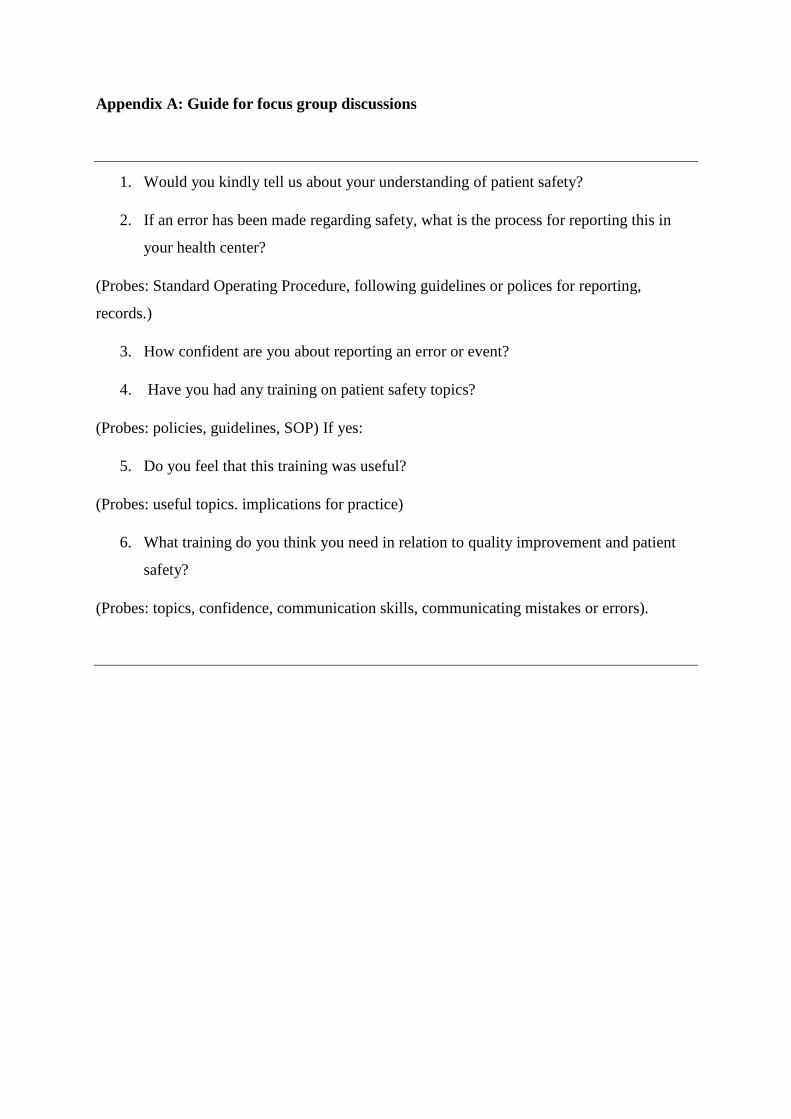
Appendix A: Guide for focus group discussions
1. Would you kindly tell us about your understanding of patient safety?
2. If an error has been made regarding safety, what is the process for reporting this in
your health center?
(Probes: Standard Operating Procedure, following guidelines or polices for reporting,
records.)
3. How confident are you about reporting an error or event?
4. Have you had any training on patient safety topics?
(Probes: policies, guidelines, SOP) If yes:
5. Do you feel that this training was useful?
(Probes: useful topics. implications for practice)
6. What training do you think you need in relation to quality improvement and patient
safety?
(Probes: topics, confidence, communication skills, communicating mistakes or errors).
90
Chapter 7 Consolidation and Conclusion
91
7 Purpose of the thesis
The current thinking on patient safety identifies the growing need for developing a patient
safety culture to improve patient safety and quality of care. Establishing an environment for
patient safety may be challenging because it is associated with a change of behavior. The
perception one may draw from the literature is that, once a health care organization succeeds
in changing the perception of the frontline health care professionals towards patient safety, it
can be assured of having the most reliable and effective strategy for improving the quality of
care. Similarly, culture assessment helps in auditing the integrity of the health care system and
for provision of health care improvement and benchmarking furthermore, safety culture
assessment allows health care organizations to identify the strengths and weakness of their
safety culture and further recognize the understanding of the values, beliefs, and norms about
what is important in an organization and what attitudes and behaviors related to patient safety
are expected and appropriate.
The broad aim of this thesis was to assess the understanding of primary health care staff
regarding safety culture and their awareness of safety measures that should be followed during
encounters with patients in Muscat, Oman. In order to fulfil the “Health Vision 2050” strategy,
the Ministry of Health aims to use the current evidence in patient safety around the world to
develop a national patient safety template for the Omani primary health care system.
7.1 Overview of the key findings
The thesis highlighted that assessment of patient safety culture is the foremost essential theme
to assess the quality of the health care organization by using the Hospital Survey On Patient
92
Safety Culture (HSOPSC) tool which is a questionnaire bases survey that was commonly used
in primary health care. The use of focus group discussion with health care professionals in
primary health care further enhanced identification of root causes for communication problems
between the staff, non-punitive response to errors and frequency of event reporting. It further
added insights on recommendations in order to establish patient safety system in primary health
care in Oman.
This thesis has examined patient safety culture in primary health care in Muscat Oman, by
using the commonly used safety culture assessment tool which is the Hospital survey on
patient safety culture (HSOPSC) which has been used in developing countries in the Middle
East and it was evident in the systematic review which is discussed in Chapter 4. The key
finding from the systematic review are that the study results were grouped under the
following themes: safety culture in primary care, incident reporting, safety climate and
adverse events. The most common theme from 2011 onwards was the assessment of safety
culture in primary care and the most commonly used assessment tool used was the Hospital
Survey on Patient Safety Culture (HSOPSC) which has been used previously in developing
countries in the Middle East. With the questionnaire-based survey using the Hospital Survey
on Patient Safety Culture (HSOPSC) the response rate was 94%. Respondents generally
regarded patient safety as excellent or very good in the primary health care setting and the
perception of patient safety was moderately positive. The key areas of strength were
teamwork within the units with positivity and organization learning and continuous
improvement. The weaknesses were non-punitive response to errors, inadequate staffing and
hand offs and transition, as discussed in depth is Chapter 5. the survey highlighted some
important findings, and these were explored further in the qualitative project. The focus
group discussions helped in identifying the root cause of the poor scores which highlighted in
the survey. The qualitative study identified four main themes that were considered important
93
for patient safety and safety culture. These were: safety culture in primary health care, safety
climate, adverse events and recommendations to improve the safety of patients and staff
working in primary health care centers (PHCCs) which is highlighted in Chapter 6.
With the help of multiple methods of data collection used to collect evidence to discover the
phenomenon from a number of different perspectives, such as systematic reviews, surveys,
individual interviews and focus group discussions (1). This mixed methods design was
chosen to facilitate a deeper understanding of the broader issue of patient safety and patient
safety culture in Oman.
Since the publication of our systematic review in 2018 there has been a further systematic
review published which has focused on patient safety in Arab countries (2) .The review
included studies from several Arab countries including Saudi Arabia, Egypt, Jordan, Oman,
Lebanon, Kuwait and Palestine and included both primary and secondary care although most
(16/18) were from secondary care. The review concluded that patient safety culture needs to
be encouraged in order to improve patient safety in the Arab world (2). The results of this
review were broadly consistent with the findings from our survey study (3). For example,
concerns about non-punitive response to errors was identified as an issue in all the countries
ranging from lowest 16% in Saudi Arabia and the highest 66.7% in Egypt. This highlights that
across the Arab world there is a need to address the culture of blame to create an environment
where clinicians can confidently and safely report errors. The study from Kuwait (4) reported
24% non-punitive response to errors related to 27% in the current Omani study, which is quite
comparable perhaps due to relatively high positivity of the organizational learning 74% in
Kuwait and 79% in current Omani study. There were quite marked differences in the responses
to inadequate staffing ranging from 23% in the Kuwaiti to 49% in Turkey (5) and 50% in
Yemen (6). These levels were higher than 33% reported in our study and this may reflect
94
policy in Oman which standardizes the number of staffs in each health center. However, due
to population movements to the suburbs there have been increases in the population of the
catchment area to the health centers which leads to more demand on the health center staff.
The review emphasized that to further identify root causes in relation to poor safety culture,
the use of qualitative research would provide more insights to safety culture in the Arab world.
Another paper was followed on developing a patient safety system using the WHO tool in
Hospitals in 2018 in Oman (34) which describes implementation of the Patient Safety
Friendly Hospital Initiative (PSFHI) in 11 Omani hospitals. The results are based on a the
World Health Organizations initiative that assigned teams from different hospitals to
implement the Patient Safety Friendly Hospital Standards. Since then almost 90% of the main
hospitals in Oman have been enrolled in this initiative, a total of 26 hospitals (16 out of 18
public and 10 private hospitals). The hospitals enrolled had regular assessment from the
internal teams from the Ministry of Health and external teams from the World Health
Organization. The last assessment by the World Health Organization was from 5 to 26 April
2018, in 3 public (Khoula hospital, Ibra and Sohar hospitals) and one private hospital (Badr
Al Salamaa hospital). Each was assessed and successfully accredited (7).
By the year 2020, Oman aims to have 90% of its main hospitals evaluated and accredited by
the World Health Organization for patient safety (8)
The Patient Safety Friendly Hospital Initiative which is implement in hospital has shown that
Oman strives for and regards patient safety an important element in providing quality health care
and with the outcome of this thesis a template for patient safety in primary health care will be
established. The World Health Organization addressed ten facts which are relevant to this study
(9) in order to ensure a safer health care environment by incorporating patient safety , these 10
facts are:
95
Fact 1: Patient safety harm in the 14th most leading cause of morbidity and mortality compared
to tuberculosis and malaria, 42.7 million adverse events occur during hospitalization around the
world.
Fact 2: 1 in 10 patients is harmed in high income countries when hospitalized and 50% of them
is preventable. In low- and middle-income countries, the rate of adverse event is 8 % of which
83% in preventable.
Fact 3: Unsafe usage of medication leads to patient harm, which is preventable and costs millions
of dollars, it is estimated that $42 million dollars is associated with medication error.
Fact 4: Adverse vents leads to 15 % increase in health care expenditure.
Fact 5: Financial savings can be achieved if patient safety in implement in health care in addition
better patient outcome.
Fact 6: Out of 100 Patients admitted, 14 out of them acquire hospital infections.
Fact 7: Surgical complication leads to more than 1 million death annually.
Fact 8: Diagnostic errors account for 6-17% of adverse events annually.
Fact 9: In appropriate use of radiation can lead to harm not only to patients but to health care
professionals.
Fact 10: Administrative errors, due to system is the most frequently reported error in primary
health care, it is estimated that 5-50 per 100000 consultations.
The relevance of these ten facts for the future of patient safety in primary health care in Oman
is establishing patient safety system in all primary health care centres. The very common saying
96
"a process that is not measured cannot be managed" emphasized that monitoring patient safety
is an integral part of any quality health care system.
7.2 Limitations of the thesis
The thesis used varies types of methods to enhance the reliability and validity of the study but
nevertheless several limitations were encountered in the research process which are essential
to be acknowledged as follows:
• One of the main limitations was that the researcher was once a part of the primary
health care center and one of the department leaders in Muscat region. Providing the
significance and the nature of the study to the health care professional was importance
to conduct the research. Confidentiality was highly protected and maintained
throughout the research.
• Another possible limitation is that the Medical Office Survey on Patient Safety Culture
(MOSOPSC) tool which was designed for use in primary care and used in the
Portuguese Primary Healthcare (10) could have been used however the aim was to use
a tool which had previously been used in the Gulf region within the Middle East.
7.3 Originality and significance of the study
This is the first in-depth study to explore patient safety and safety culture in primary health
care in Muscat, Oman. Using mixed methods design we have aimed to understand the
perception of the primary health care professions to patient safetyy quantitatively and
qualitatively to understand the root cause of poor scores highlighted in the survey. Though
the scholarly papers presented in the thesis, the literature on the safety culture and patient
safety measures used globally was evaluated to enlighten the development of safety culture
97
among health care workers in primary care. Founded on the results of the systematic review
the second scholarly publication assessed the understanding of frontline primary health care
professionals regarding patient safety culture in primary health care in Oman.
A validated Hospital Survey of Patient Safety Culture tool was used since it was the most
commonly used tool in primary health care in the Gulf Cooperation Council (GCC)
Countries, by using this tool we have been able to benchmark against other countries.
Following this, in the third paper I explored the understanding of patient safety by primary
health care professionals working in Muscat, Oman and explored the areas in the survey to
find the root cause of the dimensions which were graded low. In addition, this study enabled
me to identify areas for improvement and recommendations in order to form a framework to
guide patient safety policy in primary health care in Oman. This contribution has significant
implications in the area of safety culture in Oman, the Gulf Co-operation Council countries
and the Middle East countries to help formulate research, policies and guidelines for patient
safety into the future.
7.4 Policy Recommendations
The results from this work will be used to strengthen patient safety in primary health care in
Oman. This requires an integrated approach at different levels, at the level of the health
center, with policy makers, researchers and clinicians.
7.4.1 Policy makers
• The Ministry of Health should establish a communication system with health center
staff and provide feedback through evidence-based practices so that safety culture in
enhanced in primary health care as the core principle for patient safety is leadership,
98
through their commitment, top management will create an enviorment were the health
care professionals are fully involved in patient safety system.
• Establishing a culture of openness, teamwork, communication and strong leadership
that supports patient safety at all the levels of the health care system since work in
organizations is accomplished through systems and processes.
• Administrators need to enhance a culture of blame free so that staff can report
incidents and that they can learn from each other’s experiences as a learing process.
• That educators incorporate patient safety into health professional curricula for all
health care professionals, including utilizing the World Health Organization Patient
Safety Curriculum Guide.
• Establishing patient safety representatives at the reginal level to ensure that patient
safety in integrated in all the levels of the health care system.
• Establishing an accreditation system because accreditation of an health care
organization implies the organization to comply with present standards. A local
Omani national accreditation system should be established that meets the requirement
of primary health care which incorporates patient safety as an essential element. The
accreditation center should be responsible for approving the standards, policies and
guidelines and taking into account that these standards are communicated to all the
health care professionals by licensing and accrediting the primary health care.
7.4.2 At the level of the health center the main implications are as follows:
• The need to establish a system to learn from errors, analyze the errors, establish
feedback and evaluate these errors, and discuss them with staff as a learning process
99
so that everyone in the health center can learn in order to eliminate the culture of
blame.
• Establishment of a system to educate staff regarding available policies so that
everyone in the health center is aware of the policies and guidelines since we have
found that only the doctors were awere of the policies available.
• The need to strengthen team work across the units, with other departments in the
health center, to enhance communication and promote patient safety because the
dentist and the pharmacists felt left out in the primary health care centers.
• Continuous monitoring of the safety culture in primary health care by establishing a
patient safety team or focal point and reassessment of patient safety culture every two
or three years across Oman.
• Establishing patient safety training for primary health care professionals on a regular
basis to so that primary health care professionals are up to date to the latest trends in
patient safety.
• Establishment of an automated incident reporting system like the one in hospitals for
primary health care because the incident reporting is manual and subjective.
• Finally, patients to be placed at the center of the health care process since they can
provide valuable information to help improve health care practices, services and the
process of decision making reflecting their experiences and perceptions. They can act
as a source of information to provide insights on policies and approaches of care.
100
7.5 Research
That a follow-up study be conducted in two years’ time with the same tool, the Hospital
Survey on Patient Safety Culture tool so that the primary health care can benchmark the
health care centers, nationally, among the Gulf Cooperation Council countries and then
compare themselves among the EMRO region. Furthermore, by maintaining a systematic
method of follow up represents a challenge then just completion of a single survey. This
Hospital Survey on Patient Safety Culture tool to be part of the five-year plan and conducted
all over Oman as a basis for benchmarking the culture of patient safety in primary health care
in Oman.
7.6 Final conclusions
The findings of this thesis have enhanced our scholarly understanding of patient safety
culture in primary health care in Muscat, Oman, in terms of how best to measure patient
safety culture by using a quantitative approach supported by qualitative focus group
discussions at the health centre level to understand the concept of patient safety culture
among healthcare providers. This mixed methods design has implications for primary health
centres, policy makers and research in Oman into the future within the context of the “Health
Vision 2050”. The Omani Ministry of Health would benefit from creating an integrated
approach towards patient safety that creates an environment for continuous monitoring, open
communication and an environment free from the culture of blame. Strong leadership and
commitment towards achieving improved patient safety is required at all levels of the
organization, including the level of primary health care into the future. It is anticipated that
the findings from this innovative social scientific mixed methods design will contribute to
achievement of this goal.
101
7.7 References
1. Robert K Yin. Case study research; design and methods, 4th ed.(Brief article)(Book review)2009; 24(1). 2. Mustafa Elmontsri AA, Ricky Banarsee, Azeem Majeed. Status of patient safety culture in Arab countries: a systematic review. BMJ open. 2017;7(e013487). 3. Muna Habib A. L. Lawati, Stephanie D. Short, Nadia Noor Abdulhadi, Sathiya Murthi Panchatcharam, Sarah Dennis. Assessment of patient safety culture in primary health care in Muscat, Oman: a questionnaire -based survey. BMC Family Practice. 2019. 4. Maha Mohamed Ghobashi, Hanan Abdel Ghani El-Ragehy, Fatma Abdullah Al-Doseri , Hanan Mosleh. Assessment of patient safety culture in primary health care settings in Kuwait. Epidemiol Biostat Public Health. 2014;11(3):e9101-1-e-9.
5. Bodur S, Filiz E. A survey on patient safety culture in primary healthcare services in Turkey. Int J Qual Health Care. 2009;21. 6. Hana H Webair, Salwa S Al Assani, Reema H Al Haddad, Wafa H Al Shaeeb, Manal A Bin Selm, Abdulla S Alyamani. Assessment of patient safety culture in primary care setting, Al-Mukala, Yemen. BMC Fam Pract. 2015;16:136. 7. Organization WH. Patient Safety Friendly Hospital Initiative in Oman 2019 [Available from: http://www.emro.who.int/omn/oman-news/patient-safety-friendly-hospital-initiative-in-oman.html. 8. Al-Mandhar A. Oman leads the way in patient safety: improving service delivery for UHC. Geneve World Health Organization 2019. 9. Organization WH. 10 facts about patinet safety Geneva2019 [Available from: https://www.who.int/features/factfiles/patient_safety/en/. 10. Ornelas Marta Dora P, Sousa. Patient Safety Culture in Portuguese Primary Healthcare. Quality in Primary Care 2016;24(5):214-8.
102
APPENDICES
103
APPENDIX A Institutional ethics approval letter
104
Ethical approval
The study protocol was approved by the “Research and Ethical Review and Approval
Committee” at the Centre of Research and Studies in the Ministry of Health, Muscat, Oman
on 2nd February 2016 for all the phases of the research. Informed verbal consent was
obtained by all the participants and approved by the Committee as the participants are heath
care professionals who are aware of scientific research and its implications for improvement.
No personal information was identified in any publication arising from the study. The
participants could call the principal researcher if they had any questions or sought further
information. The participation was voluntary and anonymous.

105
APPENDIX B Information sheet for participants in phase 2, the questionnaire-based survey
Information sheet for safety culture in primary health care centres in Muscat region.
Title of Research Study:
“Patient Safety culture Survey”
INFORMATION SHEET FOR PARTICIPANTS
Dear Client You are invited to take part in a research study to examine the safety culture of primary care in the Muscat Region. You will be requested to fill out a questionnaire which is self-administered. Before you decide whether to take part in the study it is important that you understand what the research is for and what you will be asked to do. Please take time to read the following information and discuss it with others if you wish. It is up to you to decide whether to take part or not. If you decide to take part, you will be given this information sheet to keep. The purpose of the research study is to explore patient safety culture in primary care centres in Muscat. The information gained from this research will be used to make recommendations for best practice and will offer insights to plan policies and guidelines for best practices in primary care in Oman. The questionnaire is confidential, and no identity will be revealed. This research is part of a PhD thesis at University of Sydney, Australia. Please do not hesitate to contact me if you need further information Thanking you in anticipation, Yours sincerely, Dr Muna Habib AL Lawati 99467686
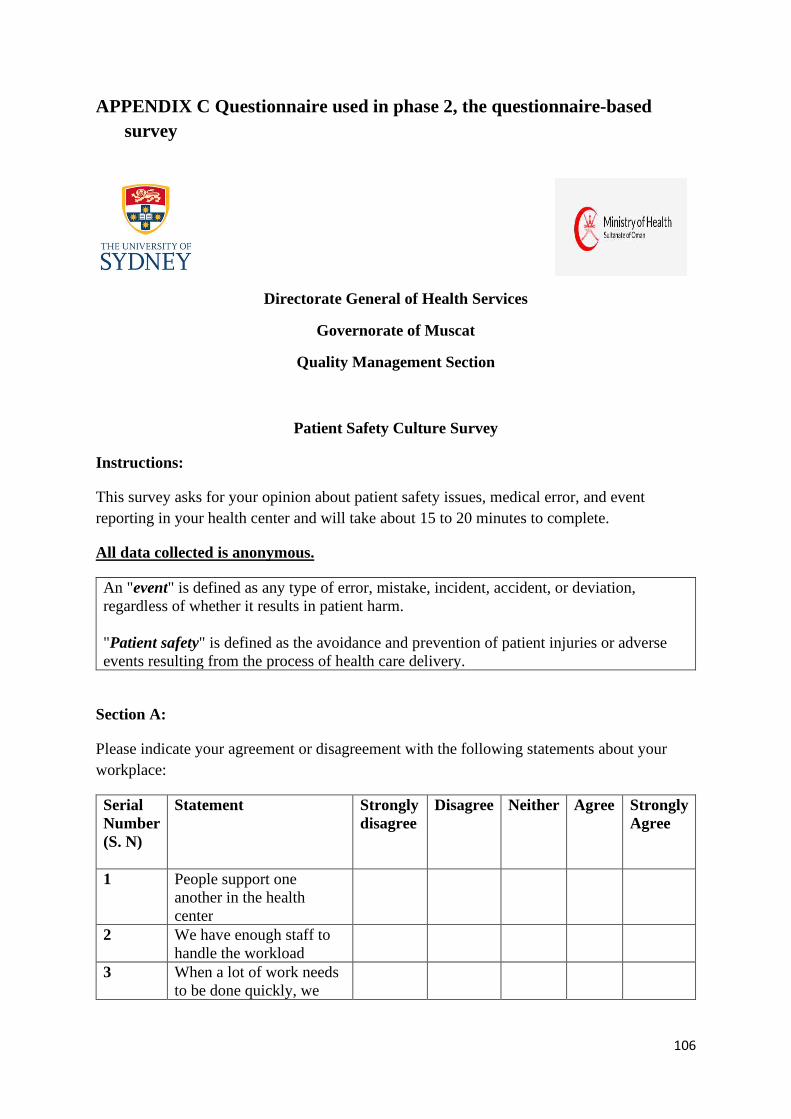
106
APPENDIX C Questionnaire used in phase 2, the questionnaire-based survey
Directorate General of Health Services
Governorate of Muscat
Quality Management Section
Patient Safety Culture Survey
Instructions:
This survey asks for your opinion about patient safety issues, medical error, and event reporting in your health center and will take about 15 to 20 minutes to complete.
All data collected is anonymous.
An "event" is defined as any type of error, mistake, incident, accident, or deviation, regardless of whether it results in patient harm. "Patient safety" is defined as the avoidance and prevention of patient injuries or adverse events resulting from the process of health care delivery.
Section A:
Please indicate your agreement or disagreement with the following statements about your workplace:
Serial Number (S. N)
Statement Strongly disagree
Disagree Neither Agree Strongly Agree
1 People support one another in the health center
2 We have enough staff to handle the workload
3 When a lot of work needs to be done quickly, we
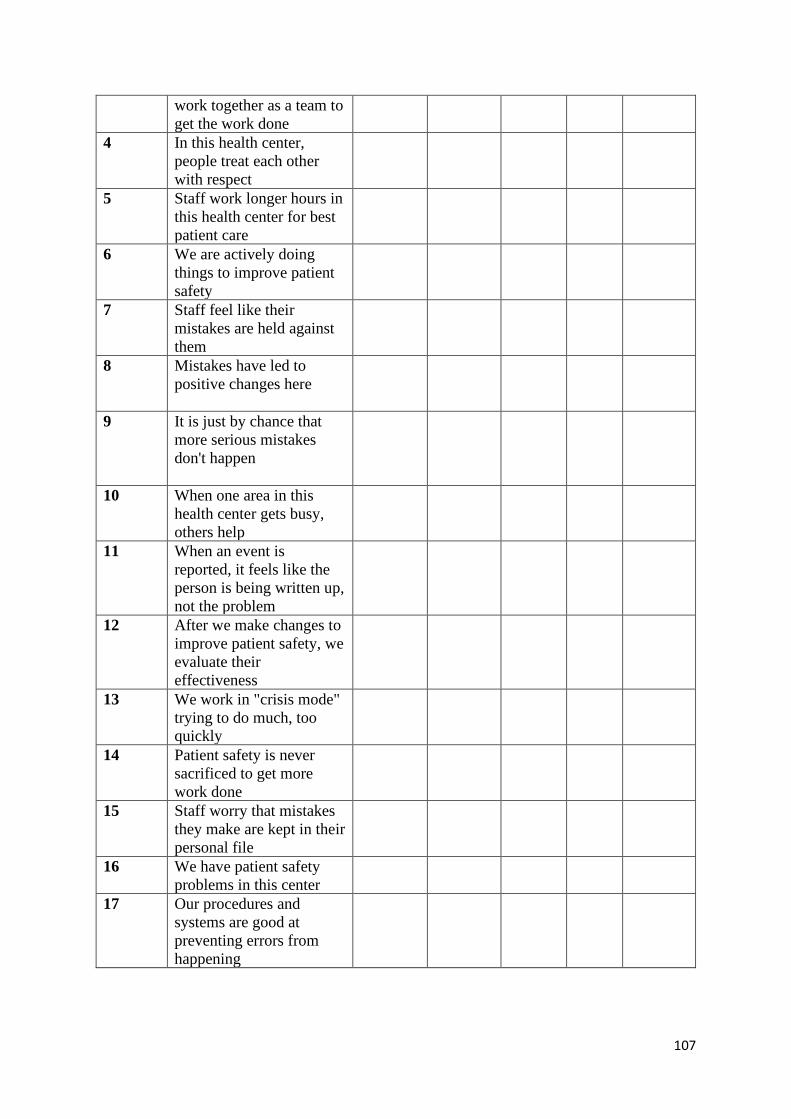
107
work together as a team to get the work done
4 In this health center, people treat each other with respect
5 Staff work longer hours in this health center for best patient care
6 We are actively doing things to improve patient safety
7 Staff feel like their mistakes are held against them
8 Mistakes have led to positive changes here
9 It is just by chance that more serious mistakes don't happen
10 When one area in this health center gets busy, others help
11 When an event is reported, it feels like the person is being written up, not the problem
12 After we make changes to improve patient safety, we evaluate their effectiveness
13 We work in "crisis mode" trying to do much, too quickly
14 Patient safety is never sacrificed to get more work done
15 Staff worry that mistakes they make are kept in their personal file
16 We have patient safety problems in this center
17 Our procedures and systems are good at preventing errors from happening
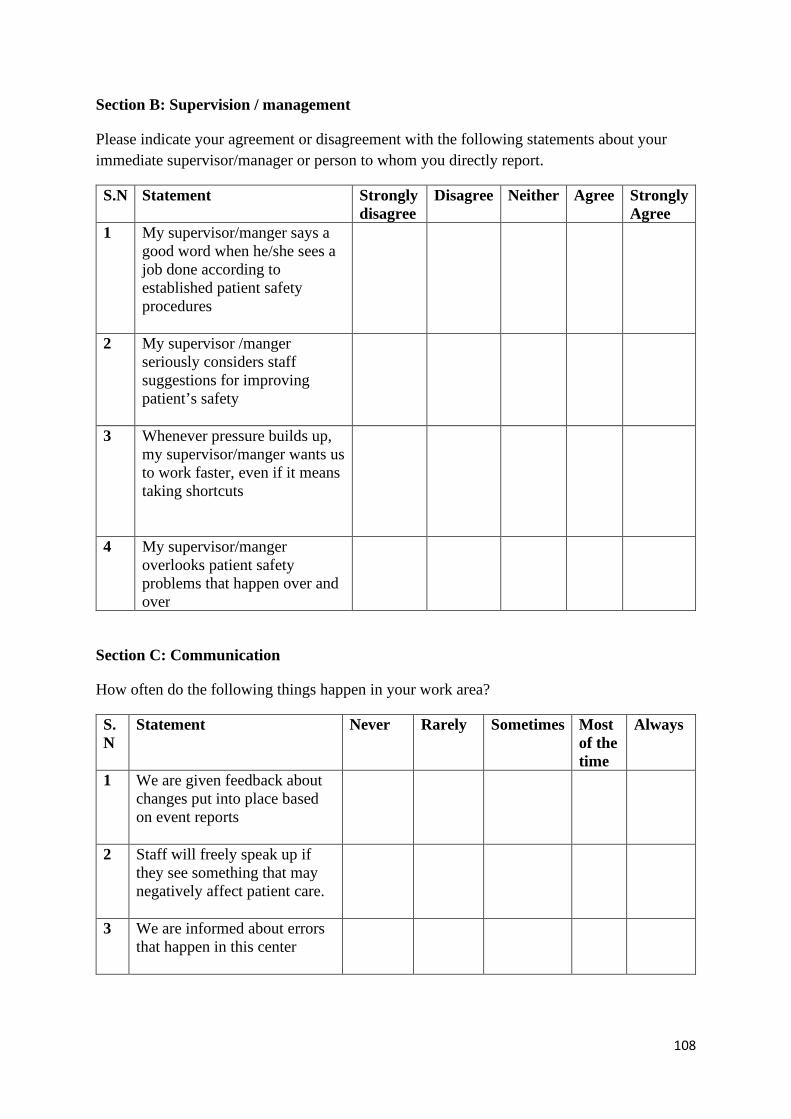
108
Section B: Supervision / management
Please indicate your agreement or disagreement with the following statements about your immediate supervisor/manager or person to whom you directly report.
S.N Statement Strongly disagree
Disagree Neither Agree Strongly Agree
1 My supervisor/manger says a good word when he/she sees a job done according to established patient safety procedures
2 My supervisor /manger seriously considers staff suggestions for improving patient’s safety
3 Whenever pressure builds up, my supervisor/manger wants us to work faster, even if it means taking shortcuts
4 My supervisor/manger overlooks patient safety problems that happen over and over
Section C: Communication
How often do the following things happen in your work area?
S. N
Statement Never Rarely Sometimes Most of the time
Always
1 We are given feedback about changes put into place based on event reports
2 Staff will freely speak up if they see something that may negatively affect patient care.
3 We are informed about errors that happen in this center
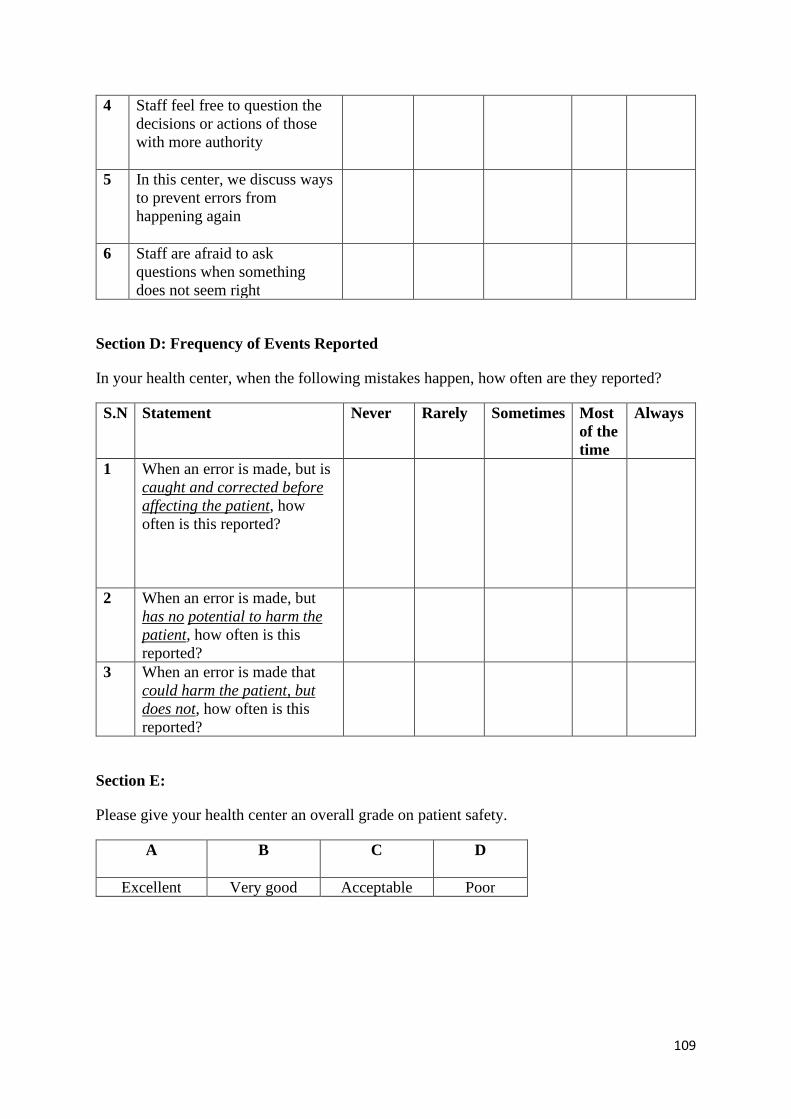
109
4 Staff feel free to question the decisions or actions of those with more authority
5 In this center, we discuss ways to prevent errors from happening again
6 Staff are afraid to ask questions when something does not seem right
Section D: Frequency of Events Reported
In your health center, when the following mistakes happen, how often are they reported?
S.N Statement Never Rarely Sometimes Most of the time
Always
1 When an error is made, but is caught and corrected before affecting the patient, how often is this reported?
2 When an error is made, but has no potential to harm the patient, how often is this reported?
3 When an error is made that could harm the patient, but does not, how often is this reported?
Section E:
Please give your health center an overall grade on patient safety.
A
B
C
D
Excellent Very good Acceptable Poor
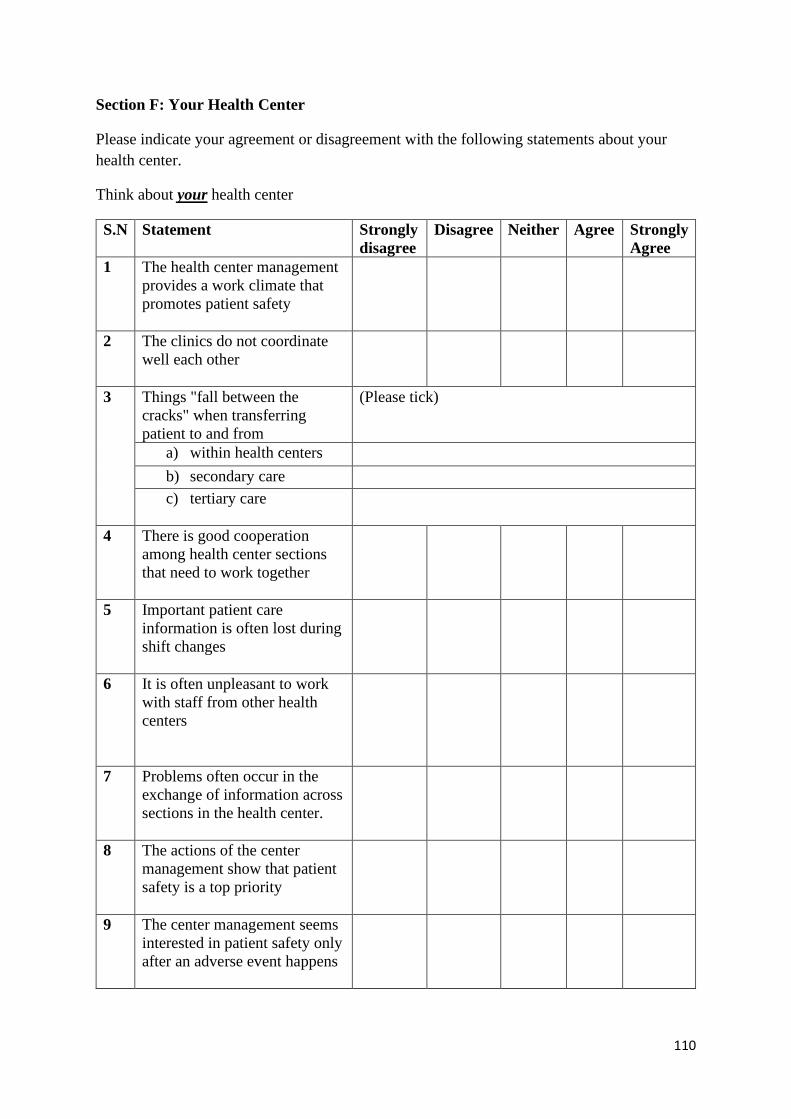
110
Section F: Your Health Center
Please indicate your agreement or disagreement with the following statements about your health center.
Think about your health center
S.N Statement Strongly disagree
Disagree Neither Agree Strongly Agree
1 The health center management provides a work climate that promotes patient safety
2 The clinics do not coordinate well each other
3 Things "fall between the cracks" when transferring patient to and from
(Please tick)
a) within health centers
b) secondary care c) tertiary care
4 There is good cooperation among health center sections that need to work together
5 Important patient care information is often lost during shift changes
6 It is often unpleasant to work with staff from other health centers
7 Problems often occur in the exchange of information across sections in the health center.
8 The actions of the center management show that patient safety is a top priority
9 The center management seems interested in patient safety only after an adverse event happens
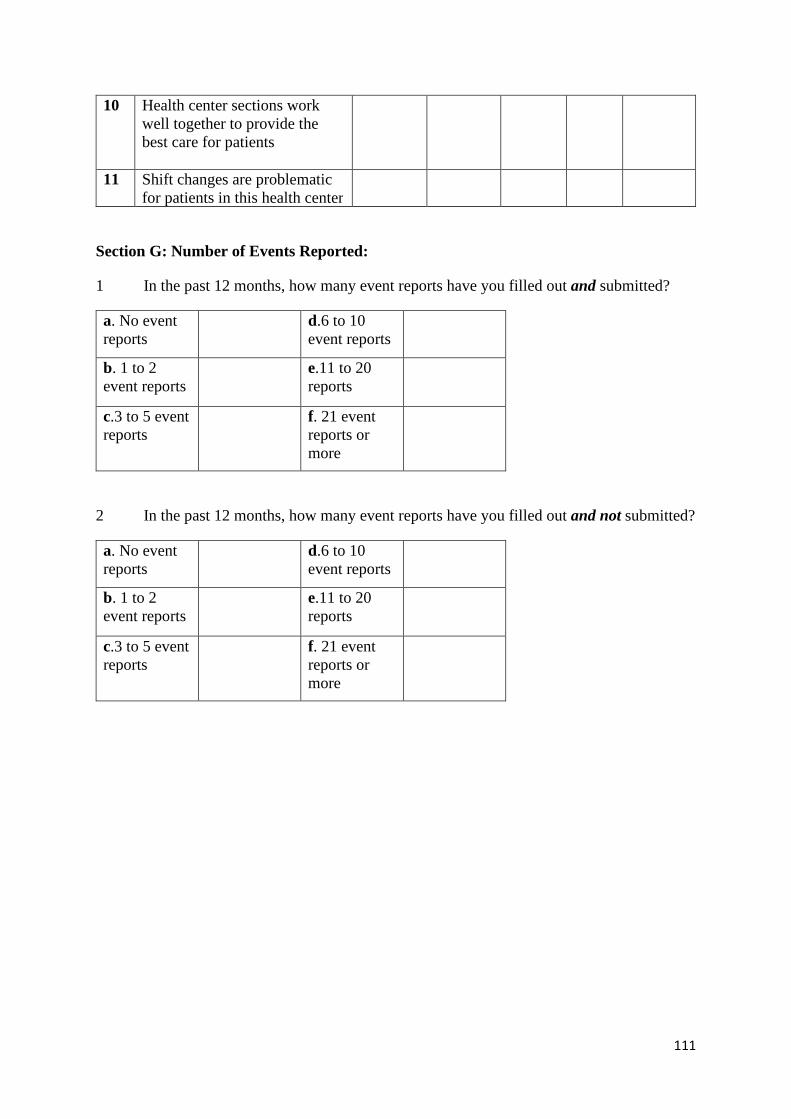
111
10 Health center sections work well together to provide the best care for patients
11 Shift changes are problematic for patients in this health center
Section G: Number of Events Reported:
1 In the past 12 months, how many event reports have you filled out and submitted?
a. No event reports
d.6 to 10 event reports
b. 1 to 2 event reports
e.11 to 20 reports
c.3 to 5 event reports
f. 21 event reports or more
2 In the past 12 months, how many event reports have you filled out and not submitted?
a. No event reports
d.6 to 10 event reports
b. 1 to 2 event reports
e.11 to 20 reports
c.3 to 5 event reports
f. 21 event reports or more
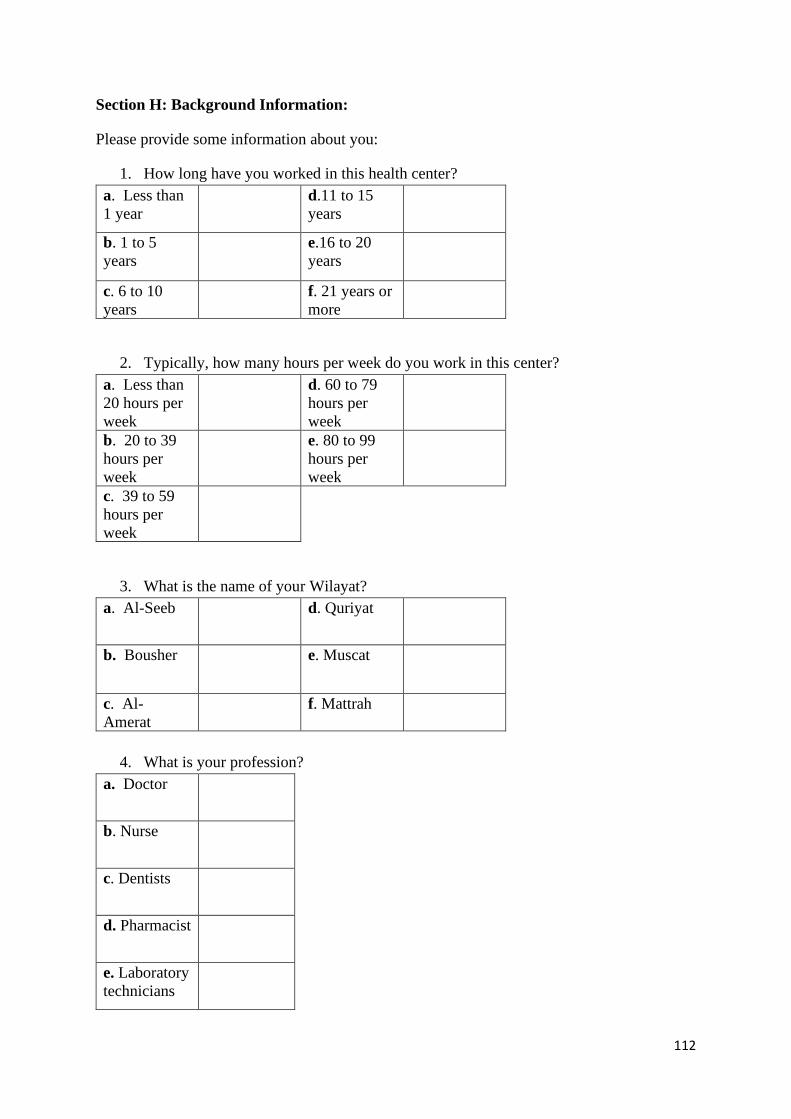
112
Section H: Background Information:
Please provide some information about you:
1. How long have you worked in this health center? a. Less than 1 year
d.11 to 15 years
b. 1 to 5 years
e.16 to 20 years
c. 6 to 10 years
f. 21 years or more
2. Typically, how many hours per week do you work in this center? a. Less than 20 hours per week
d. 60 to 79 hours per week
b. 20 to 39 hours per week
e. 80 to 99 hours per week
c. 39 to 59 hours per week
3. What is the name of your Wilayat? a. Al-Seeb d. Quriyat
b. Bousher e. Muscat
c. Al-Amerat
f. Mattrah
4. What is your profession?
a. Doctor
b. Nurse
c. Dentists
d. Pharmacist
e. Laboratory technicians

113
f. Radiographer
5 Please specify your age group
a. 20-30
b. 31-40
c. 41-50
d. 51-60
e. 61+
6 Please specify your gender
a. Male
b. Female
Thank you for taking the time to complete this survey
114
APPENDIX D Study participant information and consent form used in Phase 3, the focus group discussions
Guide topics for FGDs
Foreword/preface: Dear colleagues
Thank you for your agreement to participate in these discussions. It is a great pleasure to have
you all here for the discussions regarding safety culture and patient safety at the primary health
care in Muscat, as explained to you before. Your participation is highly important and will be
useful for further improvement of health care for the benefit of the patients and community. I
would like to assure you that your participation is highly confidential, and no names will be
shown at all and no harm will affect you at your work place or job. Your participation is
voluntary, and you have the right to refrain at any stage of the study if you felt you want to do
so. It is a free discussion, please feel comfortable.
This project is aiming at:
1- Determining the learning needs of primary healthcare staff in relation to quality
improvement and patient safety.
2- Determining what health system level changes are required so that PHC staff feel
confident / safe to report events.
3- Understanding the concept of patient safety in primary care
115
APPENDIX E Interview schedule used in the focus group discussions The questions and props:
1. Would you kindly tell us about your understanding to patient safety?
2. If an error has been made regarding safety, what is the process for reporting this in
your health centre?
(Probes: SOP, guidelines, policy, record)
3. How confident are you about reporting an error or event?
4. Did you take any training on patient safety topics?
(Probes: policies, guidelines, SOP)
5. Do you feel/think that this training was useful?
(Probes: useful topics)
6. What training do you think you need in relation to quality improvement and patient
safety?
(Probes: topics, confidence, communication skills, communicating mistakes or
errors).
How do u consider the culture of error reporting in your practice?
(Probe: Blame culture, open communication)
7. What needs to change so that primary healthcare staffs feel confident to report a
mistake?
(Probes: staffing levels, or administrating level)
8. Is there any sort of patient safety projects are underway in the health centre?
(Probes; centre level, regional etc, and who are involved?)
116
APPENDIX F The “Health Vision 2050”
Source: Sultanate of Oman, Ministry of Health (2014), Health Vison 2050, retrieved 1st June 1019, http://www.nationalplanningcycles.org/sites/default/files/planning_cycle_repository/oman/health_vision_2050_oman.pdf
Copyright © 2022 FDOKUMEN