Patient-reported outcomes in randomised controlled trials of gynaecological cancers: investigating...
17
Review Patient-reported outcomes in randomised controlled trials of gynaecological cancers: Investigating methodological quality and impact on clinical decision-making Fabio Efficace a,⇑ , Marc Jacobs b , Andrea Pusic c , Elfriede Greimel d , Alfonso Piciocchi a , Jacobien M. Kieffer e , Alexandra Gilbert f , Peter Fayers g , Jane Blazeby h , On behalf of EORTC Quality of Life Group (Patient Reported Outcome Measurements Over Time In ONcology-PROMOTION Registry) a Data Center and Health Outcomes Research Unit, Italian Group for Adult Hematologic Diseases (GIMEMA), Rome, Italy b Academic Medical Center, University of Amsterdam, Department of Medical Psychology, Amsterdam, The Netherlands c Department of Surgery, Memorial Sloan Kettering Cancer Center, New York, USA d Department of Obstetrics and Gynecology, Medical University of Graz, Graz, Austria e Division of Psychosocial Research & Epidemiology, The Netherlands Cancer Institute, Amsterdam, The Netherlands f Leeds Institute of Cancer Studies and Pathology, University of Leeds, Leeds, UK g Institute of Applied Health Sciences, University of Aberdeen, Aberdeen, UK h Centre for Surgical Research, University of Bristol and University Hospitals NHS Foundation Trust, Bristol, UK Received 5 February 2014; received in revised form 27 March 2014; accepted 4 April 2014 Available online 10 May 2014 KEYWORDS Gynaecologic cancer Patient-reported out- comes Clinical trials Quality of life Clinical decision-making Abstract Aim: The aim for this study is to investigate the methodological quality and potential impact on clinical decision making of patient reported outcome (PRO) assessment in randomised controlled trials (RCTs) in the gynaecological cancer sites. Methods: A systematic review identified RCTs published between January 2004 and June 2012. Relevant studies were evaluated using a pre-determined extraction form which included: (1) Trial demographics and clinical and PRO characteristics; (2) level of PRO reporting and (3) bias, assessed using the Cochrane Risk of Bias tool. All studies were additionally analysed in relation to their relevance in supporting clinical decision making. Results: Fifty RCTs enrolling 24,991 patients were identified. In eight RCTs (16%) a PRO was the primary end-point. Twenty-one studies (42%) were carried out in a multi-national context. Where statistically significant PRO differences between treatments were found, it related in http://dx.doi.org/10.1016/j.ejca.2014.04.005 0959-8049/Ó 2014 Elsevier Ltd. All rights reserved. ⇑ Corresponding author: Address: Head, Health Outcome Research Unit, Italian Group for Adult Hematologic Diseases (GIMEMA), GIMEMA Data Center, Via Benevento, 6, 00161 Rome, Italy. Tel.: +39 06 441 639831; fax: +39 06 4402516. E-mail address: f.effi[email protected] (F. Efficace). European Journal of Cancer (2014) 50, 1925– 1941 Available at www.sciencedirect.com ScienceDirect journal homepage: www.ejcancer.com
Transcript of Patient-reported outcomes in randomised controlled trials of gynaecological cancers: investigating...
European Journal of Cancer (2014) 50, 1925– 1941
A v a i l a b l e a t w w w . s c i e n c e d i r e c t . c o m
ScienceDirect
journa l homepag e : www.e j cancer . com
Review
Patient-reported outcomes in randomised controlledtrials of gynaecological cancers: Investigatingmethodological quality and impact on clinicaldecision-making
http://dx.doi.org/10.1016/j.ejca.2014.04.005
0959-8049/� 2014 Elsevier Ltd. All rights reserved.
⇑ Corresponding author: Address: Head, Health Outcome Research Unit, Italian Group for Adult Hematologic Diseases (GIMEMA), GIData Center, Via Benevento, 6, 00161 Rome, Italy. Tel.: +39 06 441 639831; fax: +39 06 4402516.
E-mail address: [email protected] (F. Efficace).
Fabio Efficace a,⇑, Marc Jacobs b, Andrea Pusic c, Elfriede Greimel d, Alfonso Piciocchi a,Jacobien M. Kieffer e, Alexandra Gilbert f, Peter Fayers g, Jane Blazeby h, On behalf ofEORTC Quality of Life Group (Patient Reported Outcome Measurements Over Time InONcology-PROMOTION Registry)
a Data Center and Health Outcomes Research Unit, Italian Group for Adult Hematologic Diseases (GIMEMA), Rome, Italyb Academic Medical Center, University of Amsterdam, Department of Medical Psychology, Amsterdam, The Netherlandsc Department of Surgery, Memorial Sloan Kettering Cancer Center, New York, USAd Department of Obstetrics and Gynecology, Medical University of Graz, Graz, Austriae Division of Psychosocial Research & Epidemiology, The Netherlands Cancer Institute, Amsterdam, The Netherlandsf Leeds Institute of Cancer Studies and Pathology, University of Leeds, Leeds, UKg Institute of Applied Health Sciences, University of Aberdeen, Aberdeen, UKh Centre for Surgical Research, University of Bristol and University Hospitals NHS Foundation Trust, Bristol, UK
Received 5 February 2014; received in revised form 27 March 2014; accepted 4 April 2014Available online 10 May 2014
KEYWORDS
Gynaecologic cancerPatient-reported out-comesClinical trialsQuality of lifeClinical decision-making
Abstract Aim: The aim for this study is to investigate the methodological quality andpotential impact on clinical decision making of patient reported outcome (PRO) assessmentin randomised controlled trials (RCTs) in the gynaecological cancer sites.Methods: A systematic review identified RCTs published between January 2004 and June2012. Relevant studies were evaluated using a pre-determined extraction form which included:(1) Trial demographics and clinical and PRO characteristics; (2) level of PRO reporting and(3) bias, assessed using the Cochrane Risk of Bias tool. All studies were additionally analysedin relation to their relevance in supporting clinical decision making.Results: Fifty RCTs enrolling 24,991 patients were identified. In eight RCTs (16%) a PRO wasthe primary end-point. Twenty-one studies (42%) were carried out in a multi-national context.Where statistically significant PRO differences between treatments were found, it related in
MEMA

1926 F. Efficace et al. / European Journal of Cancer 50 (2014) 1925–1941
most cases to both symptoms and domains other than symptoms (n = 17, 57%). The majorityof studies (n = 42, 84%) did not mention the mode of administration nor the methods of col-lecting PRO data. Statistical approaches for dealing with missing data were only explicitlymentioned in nine RCTs (18%). Sixteen RCTs (32%) were considered to be of high-qualityand thus able to inform clinical decision making. Higher-quality PRO studies were generallyassociated with RCTs that were at a low risk of bias.Conclusion: This study showed that RCTs with PROs were generally well designed and con-ducted. In a third the information was very informative to fully understand the pros and consof PROs treatment decision-making.
� 2014 Elsevier Ltd. All rights reserved.
1. Introduction
Gynaecological cancers arise from the cervix, ovary,endometrium, vulva or vagina and as well as affecting2.2% of the female population by the age of 65 theyare the second commonest cause of cancer death inwomen after breast cancer [1].
Gynaecological cancers are treated with differenttreatment modalities including surgery, radiotherapyand chemotherapy either alone or in combination.Whilst combinations of different treatments are knownto improve survival they also increase the risk of side-effects in both the short and long term with patientscontinuing to report more gastrointestinal and sexualdysfunction symptoms than women in the generalpopulation in the years following treatment [2]. Thesesymptoms are associated with considerable impairmentin health-related quality of life (HRQOL) [3–5] thatcan also persist over the long-term period [6].
It is increasingly recognised that a comprehensiveevaluation of treatment effectiveness should include apatient reported outcome (PRO) assessment to fullycapture patients’ perceptions of symptoms, functioningand general well-being [7]. Inclusion of PROs can beparticularly valuable in randomised controlled clinicaltrials (RCTs) as it can potentially generate unique datato help health physicians to make more informed treat-ment decisions. However, information derived fromPROs need to be based on well-planned RCTs to ensurethat results are solid enough to robustly inform clinicalpractice [8]. Several methodological aspects should befully considered when implementing PROs in a RCTsetting [9]. Some excellent examples of the importantinformation that can be drawn by including PROs ingynaecological RCTs are available. To illustrate, thePost Operative Radiation Therapy in Endometrial Car-cinoma (PORTEC) trial found a significant reduction inthe rate of local regional recurrence with the addition ofpost operative radiotherapy to standard surgical treat-ment of endometrial cancer. However, this reductiondid not translate into an overall survival advantageand patients treated with the additional radiotherapyreported higher rates of gastrointestinal toxicity [10].
The use of HRQOL in this RCT led to the decision torecommend postoperative radiotherapy only in high-risk patients where the risk of relapse is considered tooutweigh the potential treatment related toxicity [10].Although this represents a concrete example of PROimplementation in a RCT setting, previous data haveshown a number of methodological flaws, which havehampered drawing strong conclusions from many RCTsconducted in several cancer disease sites [11–13].
While previous work has investigated the methodo-logical quality of studies in cervical cancer survivors, itreported studies published up to 2005 and was notfocused on RCTs [6]. On this ground, the broad scopeof this systematic review was to provide evidence-baseddata to help health care policy makers and physiciansbetter appreciate the state-of-art of PRO research inmain gynaecological cancers. Specific objectives were:(1) assess the quality of PRO reporting and methodolog-ical quality of each RCT, (2) identify high-quality PROstudies most likely to inform clinical decision-making (3)synthesise main clinical and PRO findings from the highquality studies.
2. Materials and methods
2.1. Search strategy for identification of studies
A systematic literature search was conducted inMedline, the Cochrane Controlled Trials Register,PsycINFO, and PsycARTICLES to identify RCTspublished between January 2004 and June 2012. Thesearch strategy was restricted to RCTs. Only Englishlanguage articles were considered and no restrictionswere included in the search field description. Expertsin the field were contacted to identify potentiallyrelevant articles not retrieved in the electronic search.Key searching strategy is reported in the onlineAppendix A. Titles and abstracts of identified articleswere screened for inclusion. Additional publicationswere identified by scanning reference lists of relevantarticles. Details on searching strategy and selectionprocess were documented according to the PRISMAguidelines [14].

F. Efficace et al. / European Journal of Cancer 50 (2014) 1925–1941 1927
2.2. Selection criteria
2.2.1. Types of participants
Clinical trials in adult patients with a diagnosis ofcervical, ovarian, endometrial, vaginal or vulval cancerwere included regardless of disease stage. Studies ofpatients undergoing screening or with benign diseasewere excluded.
2.2.2. Types of intervention
All RCTs comparing conventional treatments wereincluded. Studies considering psychosocial interventionsor complementary therapies were not eligible.
2.2.3. Types of outcome measures examined
Studies including a PRO as a primary or secondaryoutcome were included. We included both RCTs thatevaluated either multi-dimensional patient-reportedHRQOL or other types of health outcomes as long asthey were reported by patients themselves. Studiesevaluating treatment satisfaction and adherence totherapy were not included.
2.2.4. Types of studies
We included all RCTs that (1) compared differentconventional treatment modalities and symptomsmanagement, and (2) had enrolled at least 50 patients.We restricted our review to RCTs because they arethe gold standard of research by which decisions aremade regarding the clinical effectiveness of treatments.Studies including a heterogeneous sample of cancersites were included if dealing with gynaecologicalcancers. Conference abstracts and case reports wereexcluded.
2.3. Data extraction and type of information extracted
Data extracted from the included RCTs were storedin predefined electronic data extraction forms (eDEFs)[15] and a web-based data collection system wasdeveloped for the purpose of this research (http://pro-motion.gimema.it/). Three reviewers (M.J., J.K. andA.P.) independently extracted data on: (1) basic trialdemographics (e.g. year, journal), (2) clinical and PROcharacteristics (e.g. number of patients enrolled, studylocation, treatments being compared, PRO instrumentused and clinical and PRO assessments). Summary offindings (i.e. PROs and clinical) was also extracted; (3)the quality of PRO reporting, based on the recently pub-lished guidelines by the International Society for Qualityof Life Research (ISOQOL) [16] and 4) risk of bias usingthe Cochrane Risk of Bias tool [17]. Results were cross-checked, and discrepancies were resolved by discussionwith the senior author (F.E.). In trials with multiplepublications, we obtained relevant data by combiningall trial publications.
2.4. Quality assessment and identification of high quality
studies
PRO quality assessment was based on the recentlydeveloped ISOQOL consensus-based recommendationsfor reporting of PROs in RCT publications [16]. Theseguidelines currently represent the highest quality criteriaavailable and they form the basis for the recentlypublished PRO extension of the CONSORT (CONsoli-dated Standards of Reporting Trials) guidelines [8]. TheISOQOL guidelines comprise up to 29 key criteria(depending on whether the PRO is a secondary orprimary end-point of the trial) that a study should doc-ument in order for the PRO data to be reliable. Each cri-terion was rated as either ‘yes’ (scored as 1) if the issuewas addressed or ‘no’ (scored as 0) if not. The higherthe score the higher the quality. In order to identifyhigh-quality studies that may have an impact on clinicaldecision-making, we a priori determined that at leasttwo thirds of the ISOQOL recommended criteria mustbe satisfied. Additional details on methodology usedhave been previously reported [15]. To assess internalvalidity (i.e. freedom from bias) of RCTs, we alsoapplied criteria from the Cochrane Risk of Bias tool.We thus evaluated each RCT for its adequacy ofsequence generation; allocation concealment; blindingof participants/personnel; completeness of outcomedata; blinding of outcome assessment; no selectivity ofoutcome reporting and other sources of bias [17].
3. Results
The systematic literature search yielded 2735 records(Fig. 1). Application of inclusion criteria identified 50RCTs enrolling overall 24,991 patients publishedbetween January 2004 and June 2012 (see Appendixfor the full list of papers retrieved). The majority ofthese (i.e. 32%) have been conducted on patients withovarian cancer.
3.1. Study demographics and PRO assessment
In eight RCTs (16%) a PRO was the primary end-point. Twenty-one studies (42%) were carried out in amulti-national context. Twenty-six studies (52%) wereat least partially supported by industry. Twenty-threestudies (46%) involved patients with mixed diseasestages, and 16 (32%) only recruited patients withadvanced/metastatic disease. Although 31 RCTs (62%)enrolled more than 200 patients, PROs were the primaryend-point in only two of these RCTs. The two most fre-quently used PRO instruments, used alone or in con-junction with other measures, were the EuropeanOrganization for Research and Treatment of Cancer(EORTC) QLQ-C30 in 24 RCTs (48%), and the

Fig. 1. Schematic breakdown of literature search results of Gynaecological Randomised Controlled Trials (preferred reporting items for systematicreviews and metaanalysis). PRO = patient-reported outcome.
1928 F. Efficace et al. / European Journal of Cancer 50 (2014) 1925–1941
Functional Assessment of Cancer Therapy (FACT)instruments in 16 (32%). Thirty studies (60%) found aPRO difference between treatment arms. When a PROdifference was found, this related to both symptomsand domains other than symptoms in 17 RCTs (57%).Further details are provided in Table 1.
3.2. Overview on PRO assessment methodology
The majority of publications (42 RCTs; 84%) did notreport the mode of administration of the PRO tool norwere the methods of collecting the data described. Inaddition, 43 RCTs (86%) did not state a PRO hypothesisnor did they specify to which PRO domain the hypoth-esis was relevant. Although the extent of missing datawas well documented in 30 RCTs (60%), only nineRCTs (18%) explicitly stated the statistical approachesapplied for dealing with missing data. In addition, 15RCTs (30%) explained the reasons for missing data. Six-teen RCTs (32%) provided a flow diagram that provideda description of the allocation of participants and thoselost to follow-up for PROs specifically. When discussingtheir findings, only 15 RCTs (30%) discussed the clinicalsignificance of their findings. Moreover, only 14 RCTs(28%) discussed the generalisability issues that wereuniquely related to the PRO results. The limitations ofthe PRO components of the trial were discussed in lessthan half of the RCTs included (46%). A complete over-view is provided in Table 2.
3.3. Overview on outcomes from higher-quality PRO
studies
Sixteen RCTs (32%) that were likely to providerobust PRO data to inform clinical decision-making(Table 3) were identified. Five RCTs (31%) focused onadvanced/metastatic disease, three (19%) reported onnon-metastatic disease stages and seven (44%) includedon mixed disease stages (both loco-regional and meta-static disease). One RCT did not explicitly state patients’disease stage. The majority of these studies were at a lowrisk of bias for sequence generation (n = 11, 69%), allo-cation concealment (n = 11, 69%), blinding of partici-pants/personnel (n = 3, 19%) and outcome (n = 11,69%), attrition (n = 10, 63%) and selective outcomereporting (n = 10, 62%). Conversely, the percentages oflow risk of bias RCTs were generally a bit lower in lowerquality PRO studies. Fig. 2 depicts risk of bias of allRCTs, classified by the PRO quality rating (high versuslow).
3.3.1. Summary outcomes from metastatic/advanced
disease
The largest RCT, with 976 patients [18–23], had pro-gression free survival as the primary end-point and usedthe EORTC QLQ-C30 and the ovarian specific module(OV-28) to assess HRQOL. This trial showed that theexperimental arm had significant improvements in pro-gression free survival and less peripheral neuropathy,

Table 1Randomised controlled trial (RCT) demographic characteristics.
Variable Patient-reportedoutcome (PRO)end-pointn (%)
Totaln (%)
Primary8 (16%)
Secondary42 (84%)
Basic RCT demographics
Anatomic site of cancer Cervical 2 (25) 7 (16.675) 9 (18)Endometrial 2 (25) 6 (14.29) 8 (16)Ovarian 1 (12.50) 15 (35.72) 16 (32)Multiple disease sites 3 (37.50) 14 (33.33) 17 (34)
International No 6 (75) 23 (54.76) 29 (58)Yes 2 (25) 19 (45.24) 21 (42)
Industry supported (fully or in part)* No 7 (87.5) 17 (40.48) 24 (48)Yes 1 (12.5) 25 (59.52) 26 (52)
Overall study sample size (regardless of patientsincluded in the PRO analysis)
6200 patients 6 (75) 13 (30.95) 19 (38)>200 patients 2 (25) 29 (69.05) 31 (62)
Disease stage Advanced/metastatic 2 (25) 14 (33.33) 16 (32)Locoregional/no distant metastasis 5 (62.5) 5 (11.9) 10 (20)Mixed disease stages 1 (12.5) 22 (52.38) 23 (46)Unclear 0 (0) 1 (2.38) 1 (2)
Broad treatment type Radiotherapy 2 (25) 7 (16.67) 9 (18)Surgery 4 (50) 6 (14.29) 10 (20)Chemotherapy 3 (37.50) 36 (85.71) 39 (78)Target therapy 2 (25) 1 (2.38) 3 (6)
Difference between treatment arms in the primaryend-point
No 0 (0) 20 (47.62) 20 (40)Yes 8 (100) 22 (52.38) 30 (60)
Overall survival (OS) difference favouringexperimental treatment
No 1 (12.5) 28 (66.67) 29 (58)Yes 0 (0) 7 (16.67) 7 (14)N/A (in case OS was not assessed) 7 (87.5) 7 (16.67) 14 (28)
PRO-related basic characteristics
PRO instrument used European Organization for Research andTreatment of Cancer (EORTC) instruments
3 (37.50) 21 (50) 24 (48)
Functional Assessment of Cancer Therapy(FACT) instruments
2 (25) 14 (33.33) 16 (32)
Visual analogue scale (VAS) 2 (25) 1 (2.38) 3 (6)Others 1 (12.5) 6 (14.29) 7 (14)
PRO difference between treatment arms No differences at all 1 (12.5) 18 (42.86) 19 (38)Yes broadly favouring experimental treatment� 7 (87.5) 12 (28.57) 19 (38)Yes broadly favouring standard treatment� 0 (0) 11 (26.19) 11 (22)N/A 0 (0) 1 (2.38) 1 (2)
If statistically significant PRO difference exists, inwhich domain?
Symptoms only 3 (42.86) 6 (26.09) 9 (30)PRO domains other than symptoms only (e.g.functional scales or global QoL)
0 (0) 4 (17.39) 4 (13.33)
Both domains (symptoms + domains other thansymptoms)
4 (57.14) 13 (56.52) 17(56.67)
Length of PRO assessment during RCT Up to 6 months 8 (100) 15 (35.71) 23 (46)Up to 1 year 0 (0) 13 (30.95) 13 (26)More than 1 year 0 (0) 14 (33.33) 14 (28)
Secondary paper on PRO� No 7 (87.5) 30 (71.43) 37 (74)Yes 1 (12.5) 12 (28.57) 13 (26)
* Assessed if explicitly stated or if one or more authors were affiliated to a pharmaceutical company. This evaluation is based solely on informationextracted from the paper.� Often, multiple PRO domains (e.g. from multidimensional HRQOL questionnaires) are analysed at the same time in longitudinal PRO–RCTs; toillustrate, difference in such domains might favour the experimental treatment arm at a given time-point and then favouring the control treatmentarm at a different time point over the course of the study. So, the term ‘broadly’ was inserted to account for this possible discrepancy.� Assessed as ‘yes’ if at least one paper was published in addition to the original RCT report.
F. Efficace et al. / European Journal of Cancer 50 (2014) 1925–1941 1929

Table 2Level of patient-reported outcomes (PROs) reporting by type of end-point (PRO primary versus secondary end-point of the trial).
PRO end-pointn (%)
Totaln (%)
Primary8 (16%)
Secondary42 (84%)
Title and abstractThe PRO should be identified as an outcome in the abstract No 2 (25) 10 (23.81) 12 (24)
Yes 6 (75) 32 (76.19) 38 (76)The title of the paper should be explicit as to the randomised controlled trial (RCT) including a PRO No 4 (50) – 4 (50)
Yes 4 (50) – 4 (50)
Introduction, background and objectivesThe PRO hypothesis should be stated and should specify the relevant PRO domain if applicable No 7 (87.5) 36 (85.71) 43 (86)
Yes 1 (12.5) 4 (9.52) 5 (10)N/A (if explorative) 0 (0) 2 (4.76) 2 (4)
The introduction should contain a summary of PRO research that is relevant to the RCT No 3 (37.5) – 3 (37.5)Yes 5 (62.5) – 5 (62.5)
Additional details regarding the hypothesis should be provided, including the rationale for the selected domain(s),the expected direction(s) of change and the time points for assessment
No 8 (100) – 8 (100)
MethodsOutcomes
The mode of administration of the PRO tool and the methods of collecting data should be described No 7 (87.5) 35 (83.33) 42 (84)Yes 1 (12.5) 7 (16.67) 8 (16)
Electronic mode of PRO administration* No 1 (12.5) 7 (16.67) 8 (16)N/A 7 (87.5) 35 (83.33) 42 (84)
The rationale for choice of the PRO instrument used should be provided No 8 (100) 34 (80.95) 42 (84)Yes 0 (0) 8 (19.05) 8 (16)
Evidence of PRO instrument validity and reliability should be provided or cited No� 4 (50) 8 (19.05) 12 (24)Yes 4 (50) 34 (80.95) 38 (76)
The intended PRO data collection schedule should be provided No 2 (25) 6 (14.29) 8 (16)Yes 6 (75) 36 (85.71) 42 (84)
PROs should be identified in the trial protocol post hoc analyses should be identified No 6 (75) 28 (66.67) 34 (68)Yes 2 (25) 14 (33.33) 16 (32)
The status of PRO as either a primary or secondary outcome should be stated No 1 (12.5) 0 (0) 1 (2)Yes 5 (62.5) 39 (92.86) 44 (88)Unclear 2 (25) 3 (7.14) 5 (10)
A citation for the original development of the PRO instrument should be provided No� 5 (62.5) – 5 (62.5)Yes 3 (37.5) – 3 (37.5)
Windows for valid PRO responses should be specified and justified as being appropriate for the clinical context No 7 (87.5) – 7 (87.5)Yes 1 (12.5) – 1 (12.5)
Sample size
There should be a power sample size calculation relevant to the PRO based on a clinical rationale No 5 (62.5) – 5 (62.5)Yes 3 (37.5) – 3 (37.5)
Statistical methods
1930F
.E
ffica
ceet
al./E
uro
pea
nJ
ou
rna
lo
fC
an
cer5
0(
20
14
)1
92
5–
19
41

There should be evidence of appropriate statistical analysis and tests of statistical significance for each PRO hypothesis tested Yes 1 (12.5) 4 (9.52) 5 (10)N/A (If PRO hypotheses werenot stated)
7 (87.5) 38 (90.48) 45 (90)
The extent of missing data should be stated� No 3 (37.5) 17 (40.48) 20 (40)Yes 5 (62.5) 25 (59.52) 30 (60)
Statistical approaches for dealing with missing data should be explicitly stated � No 7 (87.5) 34 (80.95) 41 (82)Yes 1 (12.5) 8 (19.05) 9 (18)
The manner in which multiple comparisons have been addressed should be provided No 5 (62.5) – 5 (62.5)Yes 3 (37.5) – 3 (37.5)
ResultsParticipant flow
A flow diagram or a description of the allocation of participants and those lost to follow-up should be provided for PROsspecifically
No 6 (75) 28 (66.67) 34 (68)Yes 2 (25) 14 (33.33) 16 (32)
The reasons for missing data should be explained No 3 (37.5) 32 (76.19) 35 (70)Yes 5 (62.5) 10 (23.81) 15 (30)
Baseline data
The study patients characteristics should be described including baseline PRO scores No 3 (37.5) 16 (38.1) 19 (38)Yes 5 (62.5) 26 (61.9) 31 (62)
Outcomes and estimation
Are PRO outcomes also reported in a graphical format?* No 4 (50) 22 (52.38) 26 (52)Yes 4 (50) 20 (47.62) 24 (48)
The analysis of PRO data should account for survival differences between treatment groups if relevant No 1 (12.5) – 1 (12.5)N/A (if not relevant) 7 (87.5) – 7 (87.5)
Results should be reported for all PRO domains(if multi-dimensional)and items identified by the reference instrument No 2 (25) – 2 (25)Yes 6 (75) – 6 (75)
The proportion of patients achieving pre-defined responder definitions should be provided where relevant No 4 (50) – 4 (50)Yes 1 (12.5) – 1 (12.5)N/A (if not relevant) 3 (37.5) – 3 (37.5)
DiscussionLimitations
The limitations of the PRO components of the trial should be explicitly discussed No 6 (75) 21 (50) 27 (54)Yes 2 (25) 21 (50) 23 (46)
Generalisability
Generalisability issues uniquely related to the PRO results should be discussed No 2 (25) 34 (80.95) 36 (72)Yes 6 (75) 8 (19.05) 14 (28)
Interpretation
Are PRO interpreted? (Not only re-stated)* No 3 (37.5) 19 (45.24) 22 (44)Yes 5 (62.5) 23 (54.76) 28 (56)
The clinical significance of the PRO findings should be discussed No 7 (87.5) 28 (66.67) 35 (70)Yes 1 (12.5) 14 (33.33) 15 (30)
Methodology used to assess clinical significance (in case this was addressed)* Anchor based 0 (0) 3 (21.43) 3 (20)Distribution based 1 (100) 9 (64.29) 10
(66.67)Other 0 (0) 2 (14.29) 2
(13.33)(continued on next page)
F.
Effi
cace
eta
l./Eu
rop
ean
Jo
urn
al
of
Ca
ncer
50
(2
01
4)
19
25
–1
94
11931

Tab
le3
(co
nti
nu
ed)
PR
Oen
d-p
oin
tn
(%)
To
tal
n(%
)
Pri
mar
y8
(16%
)S
eco
nd
ary
42(8
4%)
Th
eP
RO
resu
lts
sho
uld
be
dis
cuss
edin
the
con
text
of
the
oth
ercl
inic
altr
ial
ou
tco
mes
No
2(2
5)20
(47.
62)
22(4
4)Y
es6
(75)
22(5
2.38
)28
(56)
Oth
erin
form
atio
nP
roto
col
Aco
py
of
the
inst
rum
ent
sho
uld
be
incl
ud
edif
ith
asn
ot
bee
np
ub
lish
edp
revi
ou
sly
(It
cou
ldb
efo
un
din
the
arti
cle
Ap
pen
dix
or
inth
eo
nli
ne
vers
ion
)N
o8
(100
)–
8(1
00)
Fo
rd
escr
ipti
vep
urp
ose
s,su
bh
ead
ings
of
this
tab
lere
flec
tth
ato
fre
po
rted
inth
eIn
tern
atio
nal
So
ciet
yfo
rQ
ual
ity
of
Lif
eR
esea
rch
(IS
OQ
OL
)re
com
men
ded
stan
dar
ds,
ho
wev
er,
rati
ng
of
item
sw
asin
dep
end
ent
of
loca
tio
no
fth
ein
form
atio
nw
ith
inth
em
anu
scri
pt;
N/A
:n
ot
app
lica
ble
.–,
Ind
icat
esit
ems
that
are
no
tap
pli
cab
leas
thes
ear
ere
com
men
ded
tob
ere
po
rted
on
lyw
hen
PR
Ois
ap
rim
ary
end
-po
int.
*T
he
foll
ow
ing
item
sh
ave
no
tb
een
incl
ud
edin
the
ISO
QO
Lre
com
men
ded
stan
dar
ds
[16]
bu
th
ave
bee
nad
ded
inth
ista
ble
toh
ave
aw
ider
ou
tlo
ok
on
the
leve
lo
fre
po
rtin
g.�
We
eval
uat
edas
‘no
’if
all
PR
Om
easu
res
use
din
the
stu
dy
wer
en
ot
vali
dat
ed.
�T
hes
eit
ems
wer
eo
rigi
nal
lyco
mb
ined
inth
eIS
OQ
OL
reco
mm
end
edst
and
ard
s[1
6]b
ut
hav
eb
een
spli
tin
this
rep
ort
tob
ette
rin
vest
igat
ep
oss
ible
dis
crep
anci
esb
etw
een
do
cum
enta
tio
no
fP
RO
mis
sin
gd
ata
(i.e
.re
po
rtin
gh
ow
man
yp
atie
nts
did
no
tco
mp
lete
agi
ven
qu
esti
on
nai
reat
any
give
nti
me
po
int)
vers
us
actu
alre
po
rtin
go
fst
atis
tica
lm
eth
od
sto
add
ress
this
issu
e.A
lso
,w
ew
ante
dto
be
con
sist
ent
wit
hit
ems
rep
ort
edin
the
CO
Nso
lid
ated
Sta
nd
ard
so
fR
epo
rtin
gT
rial
s(C
ON
SO
RT
)P
RO
exte
nsi
on
(i.e
.st
ati
stic
al
ap
pro
ach
esfo
rd
eali
ng
wit
hm
issi
ng
da
taar
ere
po
rted
asa
stan
dal
on
eis
sue)
.
1932 F. Efficace et al. / European Journal of Cancer 50 (2014) 1925–1941
and other chemotherapy side-effects, and less impact onbody image than standard chemotherapy, althoughthese benefits were not translated into a difference inglobal quality of life scores. Other smaller RCTs thatused the FACT instruments did not show a cleardifference in HRQOL between chemotherapy-basedtreatment arms also.
3.3.2. Summary outcomes from non-metastatic disease
stageThe largest trial, with 429 patients, conducted by
Armstrong and colleagues [24–27] showed that intrave-nous therapy, when compared to intraperitonealtherapy, improved progression free survival. In addi-tion, after intravenous therapy, patients showed morephysical and functional well-being, less ovarian cancersymptoms and less abdominal discomfort using theFACT questionnaires.
3.3.3. Summary outcomes from mixed disease stage
The biggest study included in this systematic review,with 2616 patients overall, was conducted by Walkerand colleagues [28–30]. This trial randomised patientswith clinical stage I to stage IIA uterine cancer tolaparoscopy or open laparotomy with recurrence freesurvival as the primary outcome. This trial showed thatpatients treated by laparoscopy had fewer moderate tosevere post-operative adverse events, and a lower fre-quency of hospitalisation of more than 2 days. In addi-tion, results obtained mainly with the use of the FACTquestionnaires, showed that these patients had betterphysical functioning, body image, less pain and an ear-lier resumption of normal activities and return to workat 6 weeks after surgery. Further details and a summaryof key findings from other studies are reported inTable 3.
4. Discussion
In this systematic review, whose data has been gath-ered by the PROMOTION Registry, a large interna-tional initiative by the EORTC Quality of Life Group,all PRO-based RCTs conducted in gynaecological can-cers have been searched. The broad goal of our reviewwas to summarise the main findings stemming from thisstudy, to help health care policy makers and physiciansbetter appreciate the state-of-art in this field.
Some 25,000 patients with various gynaecologicalcancers have been enrolled in 50 RCTs over the lastfew years and, of these, at least one-third has providedreliable PRO data and has considered the informationalongside the clinical data to make treatment recom-mendations. We thus recommend that future trials con-tinue to do this and that PRO trial design and reportingis conducted in a robust manner so that patients can beinformed how treatments impact not only on survival

Table 3Randomised controlled trials with robust PRO design: basic study characteristics.
Study* International Age of patients (years)� Overall
study
sample
size
Baseline
PRO
sample
size
PRO instruments used Primary end-
point
Treatment outline Summary main clinical results Summary of PRO results/PRO
treatment recommendations
Anatomic
site of
cancer
Metastatic/advanced disease stage
Kurtz JE et al. Ann
Oncol
2011;22(11):2417–
23;
Alexandre J et al.
Br J Cancer
2012;106(4):633–7;
Brundage M et al.
Ann Oncol 2012;
23(8):2020–7;
Gladieff L et al.
Ann Oncol 2012;
23(5):1185–9;
Joly et al.; Gynecol
Oncol
2011;122(2):226–
32;
Pujade-Lauraine
et al. J Clin Oncol
2010; 28(20):3323–
9
Yes Median (range)
Carboplatin–pegylated
liposomal doxorubicin
(CD): 60.5 (24–82)
Carboplatin–paclitaxel
(CP): 61 (27–82)
976 879 EORTC QLQ-C30;
EORTC QLQ-OV28
Progression
free-survival
CD arm: combination of pegylated
liposomal doxorubicin (PLD) (30 mg/
m2 intravenously on day 1) and
carboplatin (AUC 5 based on the
Calvert formula using glomerular
filtration rate calculated from serum
creatinine values according to the
method of Cockroft and Gault,
administered intravenously on day 1 at
4-week intervals.
CP arm: combination of paclitaxel
(175 mg/m2 intravenously on day 1) and
carboplatin (AUC 5 intravenously on
day 1) at 3-week intervals. Random
assignment was performed in permuted
blocks of six cycles
With medi follow-up of 22 months,
Progressio ree-Survival for the
pegylated osomal doxorubicin with
carboplati rm was statistically
superior to he carboplatin and
paclitaxel (hazard ratio, 0.821; 95%
confidence terval (CI) = 0.72–0.94;
p = 0 .005 edian progression free
survival (P ) was 11.3 versus
9.4 months espectively. Overall severe
non-haema logic toxicity (36.8%
versus 28.4 ; p < 0.01) leading to early
discontinu on (15% versus 6%;
p < 0.001) curred more frequently in
the CP arm
Global quality of life (QoL) and
abdominal symptom scores
improved over time in both
arms; at 6 months, 36% of
patients met criteria for
improved symptoms. Treatment
with CD resulted in less
peripheral neuropathy (9.8
versus 24.2), fewer other
chemotherapy side-effects (9.5
versus 16.2) and less impact on
body image (3.8 versus 10.4)
versus CP (all p < 0.02) at
6 months
Multiple
disease sites
Cella D et al. Gynecol
Oncol
2010;119(3):531–7;
Monk BJ et al. J
Clin Oncol
2009;27(28): 4649–
55
No Median (range)
Vinorelbine (VC) = 49;
(24–76) gemcitabine
(GC) = 45; (20–89)
Topotecan (TC) = 48;
(25–75) paclitaxel
(PC) = 50; (29–81)
513 410 FACT-Cx TOI; FACT/
GOG-NTX; BPI
Overall
survival
Patients were randomly assigned to
paclitaxel 135 mg/m2 over 24 h plus Cis
50 mg/m2 day 2 every 3 weeks (PC,
reference arm); vinorelbine 30 mg/
m2 days 1 and 8 plus Cis 50 mg/m2 day
1 every 3 weeks (VC); gemcitabine
1000 mg/m2 day 1 and 8 plus Cis 50 mg/
m2 day 1 every 3 weeks (GC); or
topotecan 0.75 mg/m2 days 1, 2 and 3
plus Cis 50 mg/m2 day 1 every 3 weeks
(TC).
Duration: up to 6 months
No statisti lly significant difference No statistically significant
differences in health-related
quality of life (HRQOL),
neuropathy, or pain
Cervical
Long HJ et al. J Clin
Oncol 2005;23(21):
4626–33;
Monk BJ et al. J
Clin Oncol
2005;23(21): 4617–
25;
Long HJ et al.
Gynecol Oncol
2006;100(3): 537–
43
No Cisplatin–topotecan
(CT): 46(22–84)
Cisplatin (CPT): 48 (27–
76)
364 284 FACT-G, FACT-Cx,
FACT/GOG-NTX, BPI,
UNI
Overall
survival
Cisplatin 50 mg/m2 every 3 weeks
(CPT);
Cisplatin 50 mg/m2 IV day 1 plus
topotecan 0.75 mg/m2 days 1–3 every
21 days (CT) (methotrexate 30 mg/
m2 days 1, 15 and 22, vinblastine 3 mg/
m2 days 2, 15 and 22, doxorubicin
30 mg/m2 day 2, and cisplatin 70 mg/
m2 day 2 every 28 days.
Methotrexate, vinblastine, doxorubicin
and cisplatin (MVAC). Max six cycles
Patients re iving cisplatin and
topotecan had statistically superior
outcomes those receiving cisplatin
CPT, with edian overall survival of 9.4
and 6.5 mo ths (p = 0 .017), median
PFS of 4.6 nd 2.9 months (p = 0.014)
and respon rates of 27% and 13%,
respectivel
There was no statistical evidence
suggesting that reported QoL
and adverse effects scores
changed over time differently
across regimens.
Baseline FACT-G (p = 0.0016)
and BPI (p = 0.0001) scores were
significantly associated with
patient age; older patients had
better QOL and less pain.
Baseline UNI was positively
correlated with FACT-G
(r = 0.66; p < 0.001) and Cx
subscale (r = 0.29; p < 0.001),
and negatively related to BPI
(r = �0.41; p < 0.0001). Baseline
FACT-Cx (FACT-G + Cx
subscale) was associated with
survival
Cervical
(continued on next page)
F.
Effi
cace
eta
l./Eu
rop
ean
Jo
urn
al
of
Ca
ncer
50
(2
01
4)
19
25
–1
94
11933
of
an
n F
lip
n a
t
arm
in
); m
FS
, r
to
%
ati
oc
ca
ce
CT
to
m
n
a
se
y
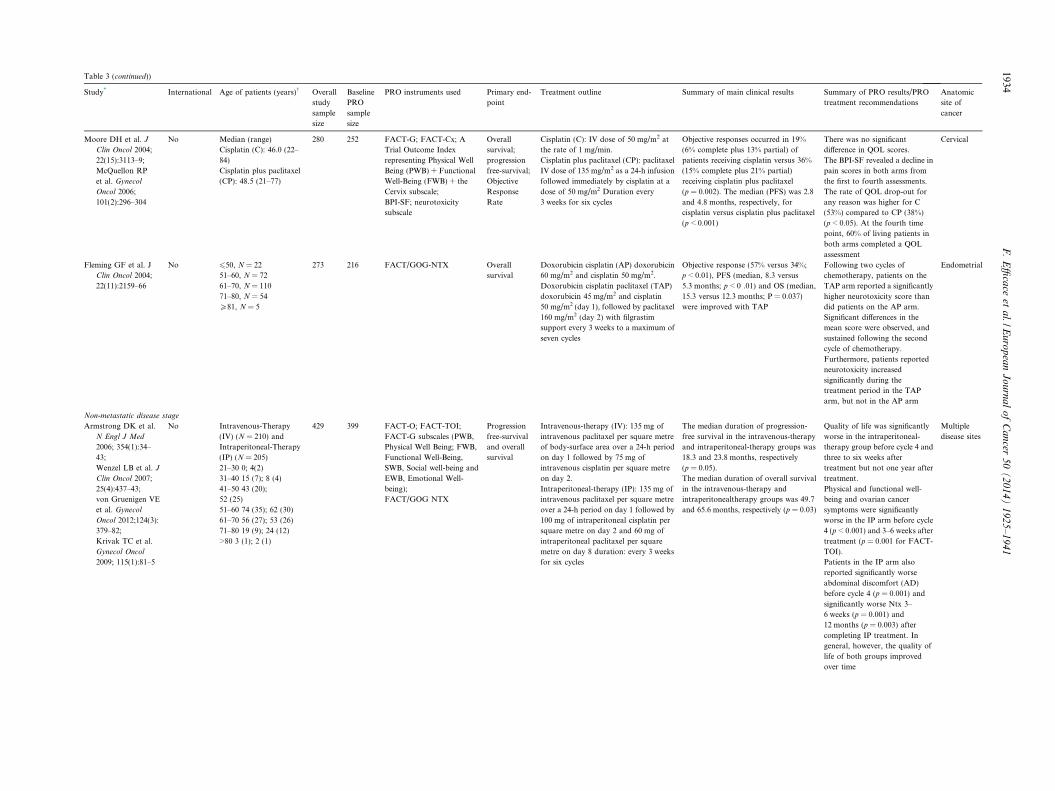
Table 3 (continued))
Study* International Age of patients (years)� Overall
study
sample
size
Baseline
PRO
sample
size
PRO instruments used Primary end-
point
Treatment outline Summary of m in clinical results Summary of PRO results/PRO
treatment recommendations
Anatomic
site of
cancer
Moore DH et al. J
Clin Oncol 2004;
22(15):3113–9;
McQuellon RP
et al. Gynecol
Oncol 2006;
101(2):296–304
No Median (range)
Cisplatin (C): 46.0 (22–
84)
Cisplatin plus paclitaxel
(CP): 48.5 (21–77)
280 252 FACT-G; FACT-Cx; A
Trial Outcome Index
representing Physical Well
Being (PWB) + Functional
Well-Being (FWB) + the
Cervix subscale;
BPI-SF; neurotoxicity
subscale
Overall
survival;
progression
free-survival;
Objective
Response
Rate
Cisplatin (C): IV dose of 50 mg/m2 at
the rate of 1 mg/min.
Cisplatin plus paclitaxel (CP): paclitaxel
IV dose of 135 mg/m2 as a 24-h infusion
followed immediately by cisplatin at a
dose of 50 mg/m2 Duration every
3 weeks for six cycles
Objective resp ses occurred in 19%
(6% complete us 13% partial) of
patients receiv g cisplatin versus 36%
(15% complet lus 21% partial)
receiving cispl in plus paclitaxel
(p = 0.002). T median (PFS) was 2.8
and 4.8 month respectively, for
cisplatin versu cisplatin plus paclitaxel
(p < 0.001)
There was no significant
difference in QOL scores.
The BPI-SF revealed a decline in
pain scores in both arms from
the first to fourth assessments.
The rate of QOL drop-out for
any reason was higher for C
(53%) compared to CP (38%)
(p < 0.05). At the fourth time
point, 60% of living patients in
both arms completed a QOL
assessment
Cervical
Fleming GF et al. J
Clin Oncol 2004;
22(11):2159–66
No 650, N = 22
51–60, N = 72
61–70, N = 110
71–80, N = 54
P81, N = 5
273 216 FACT/GOG-NTX Overall
survival
Doxorubicin cisplatin (AP) doxorubicin
60 mg/m2 and cisplatin 50 mg/m2.
Doxorubicin cisplatin paclitaxel (TAP)
doxorubicin 45 mg/m2 and cisplatin
50 mg/m2 (day 1), followed by paclitaxel
160 mg/m2 (day 2) with filgrastim
support every 3 weeks to a maximum of
seven cycles
Objective resp se (57% versus 34%;
p < 0.01), PFS median, 8.3 versus
5.3 months; p 0 .01) and OS (median,
15.3 versus 12 months; P = 0.037)
were improve ith TAP
Following two cycles of
chemotherapy, patients on the
TAP arm reported a significantly
higher neurotoxicity score than
did patients on the AP arm.
Significant differences in the
mean score were observed, and
sustained following the second
cycle of chemotherapy.
Furthermore, patients reported
neurotoxicity increased
significantly during the
treatment period in the TAP
arm, but not in the AP arm
Endometrial
Non-metastatic disease stage
Armstrong DK et al.
N Engl J Med
2006; 354(1):34–
43;
Wenzel LB et al. J
Clin Oncol 2007;
25(4):437–43;
von Gruenigen VE
et al. Gynecol
Oncol 2012;124(3):
379–82;
Krivak TC et al.
Gynecol Oncol
2009; 115(1):81–5
No Intravenous-Therapy
(IV) (N = 210) and
Intraperitoneal-Therapy
(IP) (N = 205)
21–30 0; 4(2)
31–40 15 (7); 8 (4)
41–50 43 (20);
52 (25)
51–60 74 (35); 62 (30)
61–70 56 (27); 53 (26)
71–80 19 (9); 24 (12)
>80 3 (1); 2 (1)
429 399 FACT-O; FACT-TOI;
FACT-G subscales (PWB,
Physical Well Being; FWB,
Functional Well-Being,
SWB, Social well-being and
EWB, Emotional Well-
being);
FACT/GOG NTX
Progression
free-survival
and overall
survival
Intravenous-therapy (IV): 135 mg of
intravenous paclitaxel per square metre
of body-surface area over a 24-h period
on day 1 followed by 75 mg of
intravenous cisplatin per square metre
on day 2.
Intraperitoneal-therapy (IP): 135 mg of
intravenous paclitaxel per square metre
over a 24-h period on day 1 followed by
100 mg of intraperitoneal cisplatin per
square metre on day 2 and 60 mg of
intraperitoneal paclitaxel per square
metre on day 8 duration: every 3 weeks
for six cycles
The median d ation of progression-
free survival i he intravenous-therapy
and intraperit eal-therapy groups was
18.3 and 23.8 onths, respectively
(p = 0.05).
The median d ation of overall survival
in the intraven us-therapy and
intraperitonea erapy groups was 49.7
and 65.6 mon , respectively (p = 0.03)
Quality of life was significantly
worse in the intraperitoneal-
therapy group before cycle 4 and
three to six weeks after
treatment but not one year after
treatment.
Physical and functional well-
being and ovarian cancer
symptoms were significantly
worse in the IP arm before cycle
4 (p < 0.001) and 3–6 weeks after
treatment (p = 0.001 for FACT-
TOI).
Patients in the IP arm also
reported significantly worse
abdominal discomfort (AD)
before cycle 4 (p = 0.001) and
significantly worse Ntx 3–
6 weeks (p = 0.001) and
12 months (p = 0.003) after
completing IP treatment. In
general, however, the quality of
life of both groups improved
over time
Multiple
disease sites
1934F
.E
ffica
ceet
al./E
uro
pea
nJ
ou
rna
lo
fC
an
cer5
0(
20
14
)1
92
5–
19
41
a
on
pl
in
e p
at
he
s,
s
on
(
<
.3
d w
ur
n t
on
m
ur
o
lth
ths

Janda M et al.
Contemp Clin
Trials
2006;27(4):353–63;
Janda M et al.
Lancet Oncol 2010;
11(8):772–80
Yes Total laparoscopic
hysterectomy (TLH):
mean (SD) 62.8 (10.0)
Total abdominal
hysterectomy (TAH):
Mean (SD) 62.7 (9.7)
361 332 FACT-G; EnWB (FACT
subscale Endometrial)
(FACT-
G + EnWB = FACT-
Endometrial) Body image
scale; EQ-5D (EuroQoL-
VAS)
Patient
Reported
Outcomes
(PRO)
(including
QOL or
symptoms
relief)
QoL at
6 months
Total laparoscopic hysterectomy
(TLH).
Total abdominal hysterectomy (TAH)
Operating me was significantly longer
in the TL group (138 min [SD 43])
than in th TAH group (109 min [SD
34]; p = 0 1).
Postopera ely, twice as many patients
in the TA group experienced adverse
events of ade 3 or higher (33 of 142
[23.2%] v us 22 of 190 [11.6%] in the
TLH gro p = 0.004).
Postopera e serious adverse events
occurred re in the TAH group (27 of
142 [19.0% than in the TLH group (16
of 190 [7. ]; p = 0.002)
Patients who had TLH reported
significantly greater
improvement in QoL from
baseline compared with those
that had TAH, in all subscales
apart from emotional and social
well-being. Improvements in
QoL up to 6 months after
surgery continued to favour
TLH, except in the emotional
and social well-being measures
of the FACT and the visual
analogue scaled of the EuroQol-
VAS.
The greatest differences were
noted in FWB (13% greater
improvement for patients with
TLH), PWB (11%), EnWB (6%),
and the overallFACT-G
summary score (7%; p = 0.001
for all comparisons).
Patients in the TLH group also
reported a 5% (p = 0.001)
greater improvement in body
image and 7.5% (p = 0.001)
greater improvement in overall
QoL (EuroQoL-VAS) than
patients in the TAH group.
During the late post-op recovery
phase (3–6 mths after surg),TLH
patients recovered significantly
more in their physical,
(p = 0.008), functional
(p = 0.009), endometrial cancer-
specific (p = 0.003) and overall
wellbeing (FACT-G; p = 0.03),
and also had better QoL
recovery with regard to body
image (p = 0.001)
Endometrial
Mourits MJ et al.
Lancet Oncol 2010;
11(8):763–71;
Bijen CB et al.
Gynecol Oncol
2011; 121(1):76–82
No Total abdominal
hysterectomy (TLH):
n = 185 median: 62 range
40–89;
Total abdominal
hysterectomy (TAH):
n = 94 median 63 range
39–86
283 Unclear SF-36, SAQ, BIS, VAS for
general health perception.
EQ-5D
Major
complication
rate
Total abdominal hysterectomy (TAH)
and bilateral salpingo-oophorectomy
versus Total laparoscopic hysterectomy
(TLH) and bilateral salpingo-
oophorectomy
The prop ion of major complications
was 14�6% 7 of 185) in the TLH group
versus 14 (14 of 94) in the TAH
group, wi a diff erence of –0.3% (95%
CI = �9. o 8.5; p = 0.95).TLH was
associated ith signifi cantly less blood
loss (p < 001), less use of pain
medicatio p < 0.0001), a shorter
hospital s (p < 0.0001), and a faster
recovery 0.002), but the procedure
took long than TAH (p < 0.0001)
A higher percentage of patients
in TLH group (76.3%) resumed
daily activities after 6 weeks
than in TAH group (62.2%).
Patients who had TLH scored
significantly higher on the
physical functioning subscale of
the SF-36 at 6 weeks, and on the
role-physical subscale at
3 months after the procedure.
Patients who had TAH scored
significantly higher on the
vitality subscale of the mental
dimension 3 months after
surgery
Endometrial
(continued on next page)
F.
Effi
cace
eta
l./Eu
rop
ean
Jo
urn
al
of
Ca
ncer
50
(2
01
4)
19
25
–1
94
11935
ti
H
e
.00
tiv
H
gr
ers
up;
tiv
mo
])
9%
ort
(2
�9%
th
1 t
w
0.0
n (
tay
(p =
er

Table 3 (continued))
Study* International Age of patients (years)� Overall
study
sample
size
Baseline
PRO
sample
size
PRO instruments used Primary end-
point
Treatment outline Summary of main clinical results Summary of PRO results/PRO
treatment recommendations
Anatomic
site of
cancer
Mixed disease stage (loco-regional disease and metastatic disease)
Walker JL et al. J Clin
Oncol 2009;
27(32):5331–6;
Kornblith AB
et al. J Clin Oncol
2009; 27(32):5337–
42;
Walker JL et al. J
Clin Oncol 2012;
30(7):695–700
Yes Median (Range)
Laparoscopy
62.8 (55.4–71.6)
Laparotomy
62.7 (54.9–70.6)
2616 727 FACT-G; AP
MOS-SF36; PF
BPI; BI
Recurrence
free survival
Patients with clinical stage I to IIA
uterine cancer were randomly assigned
to laparoscopy (n 1696) or open
laparotomy (n 920), including
hysterectomy, salpingo-oophorectomy,
pelvic cytology and pelvic and para-
aortic lymphadenectomy
Laparoscopy had fewer moderate to
severe postoperative adverse events than
laparotomy (14% versus 21%,
respectively; p < 0.0001); significantly
longer operative time (median, 204
versus 130 min, respectively; p < 0.001).
Hospitalisation of more than 2 days was
significantly lower in laparoscopy versus
laparotomy patients (52% versus 94%,
respectively; p < 0.0001).
Pelvic and para-aortic nodes were not
removed in 8% of laparoscopy patients
and 4% of laparotomy patients
(p < 0.0001)
In an intent-to-treat analysis,
laparoscopy patients reported
significantly higher Functional
Assessment of Cancer Therapy –
General (FACT-G) scores
(p = 0.001), better physical
functioning (p = 0.006), better
body image (BI; p < 0.001), less
pain (p < 0.001) and its
interference with QoL
(p < 0.001), and an earlier
resumption of normal activities
(p = 0.003) and return to work
(p = 0.04) over the 6-week
postsurgery period, as compared
with laparotomy patients.
By 6 months, the only difference
between arms was the better BI
in laparoscopy
Endometrial
Greimel ER et al. J
Clin Oncol 2006;
24(4):579–86;
du Bois AJ et al. J
Natl Cancer Inst.
2003;95(17):1320–
9.
Hilpert F et al. Ann
Oncol 2007;
18(2):282–7
Yes Mean 56.7, Standard
deviation (SD) 10.93;
range 20.8–77.4 and 57.7
SD 10.11; range 25.4–
83.6 in the paclitaxel plus
carboplatin (TC) and
paclitaxel plus cisplatin
(PT)
798 TC: 397
eligible,
366
forms
returned
PT: 386
eligible,
357
forms
returned
EORTC QLQ-C30 Progression
free-survival
Paclitaxel (185 mg/m2) + carboplatin
(AUC = 6) (TC arm) versus paclitaxel
(185 mg/m2) + cisplatin 75 mg/m2 (PT
arm) – all six courses per 3 weeks
The proportion of patients without
progression at 2 years was not
statistically significantly different
between the two treatment arms (40.0%
for PT versus 37.5% for TC,
difference = 2.5%, one-sided 95%
confidence interval [CI] = �1 to 8.2%).
Median progression-free survival time
in the TC arm (17.2 months, 95%
CI = 15.2–19.3 months) and the PT arm
(19.1 months, 95% CI = 16.7–
21.5 months) were also not statistically
significantly different; the same was true
of median overall survival time
(43.3 months, 95% CI = 37.2–
47.8 months versus 44.1 months, 95%
CI = 40.2–49.4 months, for the TC and
PT arms, respectively)
Patients in the TC arm showed
better means scores after
treatment on overall QoL
(p = 0.012), physical functioning
(p = 0.012), role functioning
(P = 0.005) and cognitive
functioning (p = 0.024),
compared with the PT arm.
Concerning symptom
experience, patients undergoing
TC showed less nausea and
vomiting (p < 0.001), less
appetite loss (p < 0.001) and less
fatigue (p = 0.033) after
completion of treatment
compared with patients
undergoing PT
Ovarian
Carey MS et al.
Gynecol Oncol
2008; 108(1):100–
5;
Butler L et al. J
Clin Oncol 2004;
22(12):2461–8;
Piccart MJ J Natl
Cancer Inst 2000;
92(9):699–708;
Bezjak A et al. J
Clin Oncol
2004;22(22):4595–
603
Yes Median (Range)
Cyclophosphamide (CP):
58 (22–85)
paclitaxel (TP): 58 (23–
79)
680 152 EORTC QLQ-C30 Progression
free-survival
TP arm = paclitaxel at a dose of
175 mg/m2 as a 3-h infusion followed by
cisplatin at a dose of 75 mg/m2
CP arm = cyclophosphamide at
750 mg/m2 followed by cisplatin at
75 mg/m2. Duration every 3 weeks
between 3 and 9 cycles
At a median follow-up of 38.5 months
and despite a high rate of crossover
(48%) from the cyclophosphamide arm
to the paclitaxel arm at first detection of
progression of disease, a longer
progression-free survival (log-rank
p = 0.0005; median of 15.5 months
versus 11.5 months) and a longer overall
survival (log-rank p = 0.0016; median of
35.6 months versus 25.8 months) were
seen in the paclitaxel regimen compared
with the cyclophosphamide regimen
Clinically meaningful
improvements compared with
baseline (change scores > 10)
were found in both arms during
the treatment period in a
number of domains and items,
including global QOL,
emotional function, social
function, fatigue, pain, sleep,
constipation, appetite,
abdominal swelling and
abdominal cramps.
Improvements in global QOL
persisted for the duration of
follow-up. More neurosensory
effects and myalgia were found
in the paclitaxel arm
Ovarian
1936F
.E
ffica
ceet
al./E
uro
pea
nJ
ou
rna
lo
fC
an
cer5
0(
20
14
)1
92
5–
19
41

Wenzel L et al. J Clin
Oncol 2005;
23(24):5605–12;
Rose PG et al. N
Engl J Med
2004;351(24):2489–
97.
No Median (range)
Secondary surgery plus
chemotherapy group:
58.1 (25.4–81.6)
Chemotherapy-alone
group: 57.0 (27.0–81.6)
550 376 FACT-G; FACT-O; GOG
(supplemental questions)
Overall
survival
Name drugs: paclitaxel + cisplatin
Doses: Chemo only: paclitaxel 135 mg/
m2 over 24 h followed by immediately
by cisplatin Cis 75 mg/m2;
Duration: maximum of six cycles of
3 weeks
Surgery + chemo: paclitaxel 135 mg/m2
over 24 h followed immediately by
cisplatin Cis 75 mg/m2 every 3 weeks for
max six cycles. Secondary cytoreduction
performed as soon as possible after
haematologic recovery of the 3rd cycle,
but within six weeks after the
completion of the third cycle
No statistically significant differences For all patients, QOL decreased
approximately 1 unit from the
first to second assessment.
Significant improvement
observed at 6 months (p < 0.001)
was sustained at 12 months, with
no appreciable between-group
difference (p = 0.048). The
baseline FACT-O score was
associated with overall survival
(p = 0.048) but not progression-
free survival. Less neurotoxicity
was reported among patients
who did (38.4%) versus did not
(54.0%) undergo interval
secondary cytoreduction at the
third assessment (p = 0.005) and
older patients experienced more
long-term effects
Ovarian
Nout RA et al. Lancet
2010;
375(9717):816–23;
Nout RA et al. Eur
J Cancer
2012;48(11):1638–
48;
Nout RA et al. J
Clin Oncol 2009;
27(21):3547–56
No Pelvic external beam
radiotherapy
(EBRT) = Median 69
(SD:7);
vaginal brachytherapy
(VBT) = Median:70
(SD:7)
427 Unclear EORTC QLQ-C30
Version 3.0; subscales for
bowel and bladder
symptoms from the prostate
cancer module (PR25) and
subscale for sexual
functioning and symptoms
from Ovarian Cancer
Module (OV28)
Vaginal
recurrence
Vaginal brachytherapy (VBT) = 1.
High–dose-rate (HDR). schedules
aimed at 45–50 Gy by schedules of
21 Gy in three fractions of 7 Gy, 1 week
apart for the high-dose rate;
2. Low-dose rate (LDR) schedules:
30 Gy at 50–70 cGy/h
3. Medium-dose-rate. (MDR)
schedules: 28 Gy at 100 cGy/h in one
session. pelvic external beam
radiotherapy (EBRT) = A dose of
46 Gy 2 Gy fractions, five times per
week, duration unclear
No significant differences between arms
regarding vaginal recurrence.
Rates of acute grade 1–2
gastrointestinal toxicity were signifi
cantly lower in the vaginal
brachytherapy VBT group than in the
pelvic external beam radiotherapy
EBRT group at completion of
radiotherapy (12.6% [27/215] versus
53.8% [112/208]
Patients in the VBT group
reported better social
functioning (p < 0.002) and
lower symptom scores for
diarrhoea, faecal leakage, the
need to stay close to the toilet
and limitation in daily activities
because of bowel symptoms
(p < 0.001). At baseline, 15% of
patients were sexually active;
this increased significantly to
39% during the first year
(p < 0.001). Sexual functioning
and symptoms did not differ
between the treatment groups
Endometrial
Randall ME et al. J
Clin Oncol 2006;
24(1):36–44;
Bruner DW et al.
Qual Life Res
2007;16(1):89–100
No Median = 63 422 317 FS; APN; FACE; FACT-G. Progression
free-survival
Whole-abdominal irradiation (WAI):
irradiation dose was 30Gyin 20 daily
fractions. After WAI, patients received
a boost to the true pelvis or to an
extended field encompassing pelvic
lymph nodes (PLNs) and positive para-
aortic lymph nodes (PALNs). The boost
dose was 15 Gy in eight fractions. All
fields were treated once daily, 5 days per
week.
AP: chemotherapy; doxorubicin 60 mg/
m2 plus cisplatin 50 mg/m2 every
3 weeks for seven cycles, followed by
one cycle of cisplatin.
The stage-adjusted hazard ratio for
progression was 0.71 favouring
doxorubicin-cisplatin AP (95%
CI = 0.55–0.91; p < 0.01). At
60 months, 50% of patients receiving AP
were predicted to be alive and disease
free adjusting for stage compared with
38% of patients receiving whole-
abdominal irradiation WAI. The stage-
adjusted death hazard ratio was 0.68
(95% CI = 0.52–0.89; p < 0.01)
favouring AP. At 60 months and
adjusting for stage, 55% of AP patients
were predicted to be alive compared
with 42% of WAI patients
WAI patients reported worse FS
(p < 0.001) and FACE
(p < 0.001) scores at end of
treatment and poorer FACE
scores 3 months post-treatment
(p = 0.004) compared to AP
patients. APN scores were
significantly worse among AP
patients at end of treatment, and
3 and 6 months post-treatment
(p < 0.001 for all). FACT-G
scores did not differ between the
two arms at any assessment
point.
Endometrial
(continued on next page)
F.
Effi
cace
eta
l./Eu
rop
ean
Jo
urn
al
of
Ca
ncer
50
(2
01
4)
19
25
–1
94
11937

Table 3 (continued))
Study* International Age of patients (years)� Overall
study
sample
size
Baseline
PRO
sample
size
PRO instruments used Primary end-
point
Treatment outline Summary of m in clinical results Summary of PRO results/PRO
treatment recommendations
Anatomic
site of
cancer
Wilkinson PM et al.
Br J Cancer 2006;
94(7):947–54
Yes Mean: Epoetin
alfa = 59.1 (±10.6)
(range 35–87)
Best standard
treatment = 60.3 (±11.2)
(range (30–79)
182 102 FACT-G, FACT-An,
CLAS; LASA
Changes in
haemoglobin
(Hb) level
from baseline
to study end
Epoetin alfa 10,000–20,000 IU three
times weekly plus best standard
treatment (BST = transfusion of red
blood cells, as needed)/BST only. The
planned duration of study treatment
was a maximum of 28 weeks, which
included 18– 24 weeks of chemotherapy
(maximum, six cycles) plus up to
4 weeks after the last chemotherapy
dose
For the epoet alfa group, mean Hb
increased by 1 g dl(raise to the -
1power) by w ks 4–6 and was
significantly in eased from baseline
through study nd (p < 0.001). The
mean change Hb from baseline was
significantly ( 0.001) greater for
epoetin alfa th n BST patients at all
postbaseline e luations. Significantly
fewer epoetin fa than BST patients
required trans sion(s) after the first
4 weeks of tre ment (7.9 versus 30.5%;
p < 0.001)
Significant differences from
baseline favouring epoetin alfa
over BST for all three CLAS
change scores (Energy Level,
Ability to Do Daily Activities,
Overall QOL) and the average
median CLAS change score
during chemotherapy
Ovarian
Unclear disease stage
Alvarez Secord A et al.
Cancer
2012;118(13):3283–
93;
Pokrzywinski R
et al. Gynecol
Oncol
2011;123(3):505–
10;
Havrilesky LJ
et al. Cancer 2012;
118(2):386–91
No Mean/median (SD)
(range)
Docetaxel and
Carboplatin (cDC): 63.8/
64 (10.2) (43–84)
Sequential
Docetaxel and
Carboplatin (sDC): 63.0/
64.5 (10.0) (39–82)
150 148 FACT-O Progression
free-survival
Name drugs: docetaxel and carboplatin
Doses: cDC: docetaxel (30 mg/m2 iv on
days 1 and 8) combined with
carboplatin (AUC = 6 mg/mL/minute
iv on day 1) every 3 weeks.
sDC: docetaxel (30 mg/m2 iv on days 1
and 8) every 3 weeks followed by
carboplatin at an AUC of six
intravenously every 3 weeks at first
progression or after six cycles of
docetaxel for stable disease or a partial
response.
Duration: six cycles of 3 weeks
The median p gression-free survival
(PFS) was 13. onths (95% confidence
interval [CI] = .9–16.8) for
combination d cetaxel and carboplatin
cDC and 8.4 nths (95% CI = 7.1–
11.0) for sequ tial docetaxel and
carboplatin sD
Sequential docetaxel followed by
carboplatin (sDC) was
associated with significant
improvements in the FACT-O
TOI (p = 0.013), FACT-O total
score (p = 0.033) and ovarian
cancer-specific (OCS) module
(p = 0.029) compared to the
combination docetaxel and
carboplatin group (cDC)
Multiple
disease sites
Abbreviations: EORTC QLQ-C30: European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core-30; EO TC QLQ-OV28: European Organization for Researchand Treatment of Cancer Quality of Life Questionnaire-Ovarian Module-28; AUC: area under the curve; FACT-G: Functional Assessmen of Cancer Therapy – General; FACT-Cx: FunctionalAssessment of Cancer Therapy – Cervix; TOI: Trial Outcome Index; FACT/GOG-NTX: Functional Assessment of Cancer Therapy/Gynaeco gic Oncology Group – Neurotoxicity four-item scale;UNI = UNISCALE; BPI-SF: Brief Pain Inventory – short form; FACT-O: Functional Assessment of Cancer Therapy – Ovarian; EQ-5D European Quality of Life-5 Dimensions; VAS: visualanalogue scale; SF-36: The Medical Outcomes Study Short Form 36-Item Health Survey; SAQ: the Sexual Activity Questionnaire; BIS: body image scale; MOS-SF36 PF: the Physical FunctioningSubscale of the Medical Outcome Study – short form; AP: additional treatment related symptoms; BI: body image; APN: assessment for eripheral neuropathy scale; FS: fatigue scale; FACE:functional alterations due to changes in elimination; FACT-An: the fact-anaemia; CLAS: cancer linear analogue scale; LASA: linear analogu scale assessment; PRO: patient-reported outcome.* No ranking was made based on level or reporting in this table. Studies are ordered by overall number of patients recruited in the study.� Reported data as available in the paper.
1938F
.E
ffica
ceet
al./E
uro
pea
nJ
ou
rna
lo
fC
an
cer5
0(
20
14
)1
92
5–
19
41
a
in
.8
ee
cr
e
in
p <
a
va
al
fu
at
ro
7 m
9
o
mo
en
C
Rtlo
:
pe

Fig. 2. Risk bar chart showing risk of bias across randomised controlled trials (RCTs) by quality of patient-reported outcome (PRO) studies.
F. Efficace et al. / European Journal of Cancer 50 (2014) 1925–1941 1939
and toxicity data but also on aspects that are essential totheir overall health and well being.
Including a PRO assessment in a RCT requires spe-cial consideration of a number of methodologicalaspects, and major efforts have been made to increasestandards of PRO reporting in RCT by internationalleading groups such as the CONSORT Group and theISOQOL [8,16]. With regard to the key items recentlysuggested by the CONSORT PRO extension [8], ourwork has highlighted specific areas most in need ofurgent improvement, such as the importance of docu-menting statistical methods used to handle missing data.While 60% of studies indeed documented the extent ofPRO missing data, only 18% further reported detailson how these were managed in the analysis. This is inline with what has been found in PRO-based RCTs inprostate cancer [15].
Another important result, previously identified insimilar analyses [15], is the association between higherquality PRO studies and lower risk of RCT bias(Fig. 2). This might support the concept that large andwell-designed trials, hence probably those that havebeen designed and led by expert methodological andclinical groups who have also received adequate finan-cial and practical support, are more likely to incorporatewell planned PRO assessment. However, this should beconfirmed in other cancer disease sites.
Another important issue that arose from this reviewis the importance of selecting an appropriate PRO mea-sure when designing an RCT. Several of the robustPRO-based RCTs used a site specific PRO instrumentalongside a generic one and nearly all used the EORTCand FACT instruments. Where cancer generic measuresmay not be sensitive enough, site-specific instruments
maybe better able to detect clinically meaningfulchanges in HRQOL, and allow for a better discrimina-tion between treatment arms. This is critical for treat-ment of a disease that has such an impact on personalaspects of health (e.g. sexual function and body image)as well as the traditional measures. It turns out to beespecially important with gynaecologic cancer therapiesbecoming increasingly tailored to individual risk factors,and with the evolution of new biological agents present-ing a prospect of maintenance therapy, possibly extend-ing treatment side-effects. These new therapeutic regimesmay have the risk of additional toxicities, and willhighlight the importance of selecting PRO instrumentstailored to the research questions. For gynaecologiconcology specific instruments have been developed forthe major cancer sites (ovarian, endometrial, cervical,vulva) that can be used in clinical trials. With the avail-ability of valid and sensitive site-specific measures,HRQOL measurement will continue to gain prominenceas a principal outcome measure in clinical trials.
The choice of PRO instruments is critical in RCTs asthis should be as sensitive as possible to detect changesin the specific research question being tested [31]. Thus,an important question that needs to be further investi-gated in future studies is the relationship betweenPRO results and questionnaires used. Whether PROresults are linked to the quality and suitability of theinstrument for the specific question or are more corre-lated to the quality of the trial in general, remains tobe clarified. We aim to further examine this issue withinour EORTC QLG PROMOTION Registry.
This review has limitations. Although we used a com-prehensive searching strategy, it is still possible thatsome RCTs with a PRO component might have been

1940 F. Efficace et al. / European Journal of Cancer 50 (2014) 1925–1941
missed. Also, as previously noted [15], our definition of‘high quality studies’ is somewhat arbitrary and does notconsider the relevance for PRO inclusion in the specificRCT context. Lastly, it should be noted that possiblehigh quality HRQOL reports published after the cut-off date of this systematic literature search, are notconsidered in current work. To illustrate, Greimel andcolleagues recently published a comprehensive HRQOLanalysis [32] of an RCT [33] that we reviewed. There-fore, the additional HRQOL information stemmingfrom this RCT could not be included. This is a moregeneral issue of RCTs with a HRQOL component,because, the large amount of data collected typicallyprevents the possibility of including all information intoa single paper. Hence, a separate publication onHRQOL analysis and outcomes is necessary to allowfor a critical appraisal of the robustness of HRQOLfindings in medical practice. Ideally, this additional pub-lication should be in the same journal to the one report-ing the main RCT findings in order to reach the samereaders and possibly have a major clinical impact.
This paper also has several notable strengths. PROmethodological evaluation was based on the most solidand up to date quality criteria [16]. Furthermore, everyRCT has been reviewed at least by two independentreviewers, permitting a calibrated assessment of allPRO-based RCTs in gynaecological cancer research.Also, this review not only provided data on methodo-logical aspects of PRO assessment but also synthesisedthe clinical and PRO outcomes stemming for higherquality studies in an attempt to provide medical commu-nity with concrete take home messages.
To conclude, quite a few RCTs have been conductedin patients with gynaecological cancers over the last fewyears and in at least some one-third of these, PRO out-comes have been very informative to fully understandpro and cons of the new treatment approaches beingtested. Investigators should pay particular attention tothe most frequently unmet methodological aspects iden-tified in this work to further improve the quality andtransparency of their PRO findings in future RCTpublications.
Conflict of interest statement
None declared.
Acknowledgements
This paper stems from a larger project (i.e. PatientReported Outcome Measurements Over Time InONcology-PROMOTION Project) funded by a researchgrant from the European Organisation for Research andTreatment of Cancer (EORTC) Quality of Life Group.Also, additional support for the conduct of the studywas provided by the Italian Group for Adult Hemato-
logic Diseases (GIMEMA). JMB is supported by theMRC ConDuCT Hub for Trials MethodologyResearch. We also acknowledge Alessandro Perrecaand Salvatore Soldati, from the GIMEMA, for theircontribution to data management.
Appendix A. Supplementary data
Supplementary data associated with this article canbe found, in the online version, at http://dx.doi.org/10.1016/j.ejca.2014.04.005.
References
[1] Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM.Estimates of worldwide burden of cancer in 2008: GLOBOCAN2008. Int J Cancer 2010;127(12):2893–917. http://dx.doi.org/10.1002/ijc.25516.
[2] Bergmark K, Avall-Lundqvist E, Dickman PW, Henningsohn L,Steineck G. Vaginal changes and sexuality in women with ahistory of cervical cancer. N Engl J Med 1999;340(18):1383–9.http://dx.doi.org/10.1056/NEJM199905063401802.
[3] Greimel ER, Winter R, Kapp KS, Haas J. Quality of life andsexual functioning after cervical cancer treatment: a long-termfollow-up study. Psychooncology 2009;18(5):476–82. http://dx.doi.org/10.1002/pon.1426.
[4] Janda M, Obermair A, Cella D, Crandon AJ, Trimmel M. Vulvarcancer patients’ quality of life: a qualitative assessment. Int JGynecol Cancer 2004;14(5):875–81. http://dx.doi.org/10.1111/j.1048-891X.2004.14524.x.
[5] Barker CL, Routledge JA, Farnell DJ, Swindell R, Davidson SE.The impact of radiotherapy late effects on quality of life ingynaecological cancer patients. Br J Cancer2009;100(10):1558–65. http://dx.doi.org/10.1038/sj.bjc.6605050.
[6] Vistad I, Fossa SD, Dahl AA. A critical review of patient-ratedquality of life studies of long-term survivors of cervical cancer.Gynecol Oncol 2006;102(3):563–72. http://dx.doi.org/10.1016/j.ygyno.2006.03.050, pii: S0090-8258(06)00316-7.
[7] Basch E, Abernethy AP, Mullins CD, et al. Recommendations forincorporating patient-reported outcomes into clinical compara-tive effectiveness research in adult oncology. J Clin Oncol2012;30(34):4249–55. http://dx.doi.org/10.1200/JCO.2012.42.5967.
[8] Calvert M, Blazeby J, Altman DG, Revicki DA, Moher D,Brundage MD. Reporting of patient-reported outcomes inrandomized trials: the CONSORT PRO extension. JAMA2013;309(8):814–22. http://dx.doi.org/10.1001/jama.2013.879.
[9] Chassany O, Sagnier P, Marquis P, et al. Patient-reportedoutcomes: the example of health related quality of life-a Europeanguidance document for the improved integration of health relatedquality of life assessment in the drug regulatory process. Drug InfJ 2002;36:209–38.
[10] Creutzberg CL, van Putten WL, Koper PC, et al. Surgery andpostoperative radiotherapy versus surgery alone for patients withstage-1 endometrial carcinoma: multicentre randomised trial.PORTEC Study Group. Post operative radiation therapy inendometrial carcinoma. Lancet 2000;355(9213):1404–11, pii:S0140673600021395.
[11] Efficace F, Bottomley A, van Andel G. Health related quality oflife in prostate carcinoma patients: a systematic review ofrandomized controlled trials. Cancer 2003;97(2):377–88. http://dx.doi.org/10.1002/cncr.11065.
[12] Claassens L, van Meerbeeck J, Coens C, et al. Health-relatedquality of life in non-small-cell lung cancer: an update of asystematic review on methodologic issues in randomized con-

F. Efficace et al. / European Journal of Cancer 50 (2014) 1925–1941 1941
trolled trials. J Clin Oncol 2011;29(15):2104–20. http://dx.doi.org/10.1200/JCO.2010.32.3683.
[13] Bottomley A, Therasse P. Quality of life in patients undergoingsystemic therapy for advanced breast cancer. Lancet Oncol2002;3(10):620–8, pii: S1470204502008768.
[14] Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reportingitems for systematic reviews and meta-analyses: the PRISMAstatement. PLoS Med 2009;6(7):e1000097. http://dx.doi.org/10.1371/journal.pmed.1000097.
[15] Efficace F, Feuerstein M, Fayers P, et al. Patient-reportedoutcomes in randomised controlled trials of prostate cancer:methodological quality and impact on clinical decision making.Eur Urol 2013. http://dx.doi.org/10.1016/j.eururo.2013.10.017,pii: S0302-2838(13)01090-7.
[16] Brundage M, Blazeby J, Revicki D, et al. Patient-reportedoutcomes in randomized clinical trials: development of ISOQOLreporting standards. Qual Life Res 2013;22(6):1161–75. http://dx.doi.org/10.1007/s11136-012-0252-1.
[17] Higgins JP, Altman DG, Gotzsche PC, et al. The CochraneCollaboration’s tool for assessing risk of bias in randomised trials.BMJ 2011;343:d5928. http://dx.doi.org/10.1136/bmj.d5928.
[18] Kurtz JE, Kaminsky MC, Floquet A, et al. Ovarian cancer inelderly patients: carboplatin and pegylated liposomal doxorubicinversus carboplatin and paclitaxel in late relapse: a GynecologicCancer Intergroup (GCIG) CALYPSO sub-study. Ann Oncol2011;22(11):2417–23. http://dx.doi.org/10.1093/annonc/mdr001.
[19] Alexandre J, Brown C, Coeffic D, et al. CA-125 can be part of thetumour evaluation criteria in ovarian cancer trials: experience ofthe GCIG CALYPSO trial. Br J Cancer 2012;106(4):633–7.http://dx.doi.org/10.1038/bjc.2011.593.
[20] Brundage M, Gropp M, Mefti F, et al. Health-related quality oflife in recurrent platinum-sensitive ovarian cancer – results fromthe CALYPSO trial. Ann Oncol 2012;23(8):2020–7. http://dx.doi.org/10.1093/annonc/mdr583.
[21] Gladieff L, Ferrero A, De Rauglaudre G, et al. Carboplatin andpegylated liposomal doxorubicin versus carboplatin and paclit-axel in partially platinum-sensitive ovarian cancer patients: resultsfrom a subset analysis of the CALYPSO phase III trial. AnnOncol 2012;23(5):1185–9. http://dx.doi.org/10.1093/annonc/mdr441.
[22] Joly F, Ray-Coquard I, Fabbro M, et al. Decreased hypersensi-tivity reactions with carboplatin–pegylated liposomal doxorubicincompared to carboplatin–paclitaxel combination: analysis fromthe GCIG CALYPSO relapsing ovarian cancer trial. GynecolOncol 2011;122(2):226–32. http://dx.doi.org/10.1016/j.ygyno.2011.04.019, pii: S0090-8258(11)00316-7.
[23] Pujade-Lauraine E, Wagner U, Aavall-Lundqvist E, et al. Pegy-lated liposomal Doxorubicin and Carboplatin compared withPaclitaxel and Carboplatin for patients with platinum-sensitiveovarian cancer in late relapse. J Clin Oncol 2010;28(20):3323–9.http://dx.doi.org/10.1200/JCO.2009.25.7519.
[24] Armstrong DK, Bundy B, Wenzel L, et al. Intraperitonealcisplatin and paclitaxel in ovarian cancer. N Engl J Med2006;354(1):34–43. http://dx.doi.org/10.1056/NEJMoa052985.
[25] Wenzel LB, Huang HQ, Armstrong DK, Walker JL, Cella D.Health-related quality of life during and after intraperitonealversus intravenous chemotherapy for optimally debulked ovariancancer: a Gynecologic Oncology Group Study. J Clin Oncol2007;25(4):437–43. http://dx.doi.org/10.1200/JCO.2006.07.3494.
[26] von Gruenigen VE, Huang HQ, Gil KM, Frasure HE, ArmstrongDK, Wenzel LB. The association between quality of life domainsand overall survival in ovarian cancer patients during adjuvantchemotherapy: a Gynecologic Oncology Group Study. GynecolOncol 2012;124(3):379–82. http://dx.doi.org/10.1016/j.ygyno.2011.11.032, pii: S0090-8258(11)00950-4.
[27] Krivak TC, Tian C, Rose GS, Armstrong DK, Maxwell GL. AGynecologic Oncology Group Study of serum CA-125 levels inpatients with stage III optimally debulked ovarian cancer treatedwith intraperitoneal compared to intravenous chemotherapy: ananalysis of patients enrolled in GOG 172. Gynecol Oncol2009;115(1):81–5. http://dx.doi.org/10.1016/j.ygyno.2009.06.021,pii: S0090-8258(09)00459-4.
[28] Walker JL, Piedmonte MR, Spirtos NM, et al. Laparoscopycompared with laparotomy for comprehensive surgical staging ofuterine cancer: Gynecologic Oncology Group Study LAP2. J ClinOncol 2009;27(32):5331–6. http://dx.doi.org/10.1200/JCO.2009.22.3248.
[29] Kornblith AB, Huang HQ, Walker JL, Spirtos NM, RotmenschJ, Cella D. Quality of life of patients with endometrial cancerundergoing laparoscopic international federation of gynecologyand obstetrics staging compared with laparotomy: a GynecologicOncology Group study. J Clin Oncol 2009;27(32):5337–42. http://dx.doi.org/10.1200/JCO.2009.22.3529.
[30] Walker JL, Piedmonte MR, Spirtos NM, et al. Recurrence andsurvival after random assignment to laparoscopy versus laparot-omy for comprehensive surgical staging of uterine cancer:Gynecologic Oncology Group LAP2 Study. J Clin Oncol2012;30(7):695–700. http://dx.doi.org/10.1200/JCO.2011.38.8645.
[31] Osoba D. Translating the science of patient-reported outcomesassessment into clinical practice. J Natl Cancer Inst Monogr2007;37:5–11. http://dx.doi.org/10.1093/jncimonographs/lgm002.
[32] Greimel E, Kristensen GB, van der Burg ME, et al. Quality of lifeof advanced ovarian cancer patients in the randomized phase IIIstudy comparing primary debulking surgery versus neo-adjuvantchemotherapy. Gynecol Oncol 2013;131(2):437–44. http://dx.doi.org/10.1016/j.ygyno.2013.08.014, pii: S0090-8258(13)01099-8.
[33] Vergote I, Trope CG, Amant F, et al. Neoadjuvant chemotherapyor primary surgery in stage IIIC or IV ovarian cancer. N Engl JMed 2010;363(10):943–53. http://dx.doi.org/10.1056/NEJMoa0908806.