
Interruption and patient satisfaction in resident-patient consultations
Upload
khangminh22Category
view
0download
0
San Antonio Breast Cancer Symposium®, December 8-11, 2020
This presentation is the intellectual property of the author/presenter. Contact [email protected] for permission to reprint and/or distribute. Mittendorf et al, IMpassion031 PRO analys
Patient-Reported Outcomes From the Phase 3 IMpassion031 Trial of Neoadjuvant Atezolizumab Plus Chemotherapy in Early Triple-Negative Breast CancerElizabeth A. Mittendorf, MD, PhD
Elizabeth A. Mittendorf,1 Nadia Harbeck,2 Hong (Amy) Zhang,3 Shigehira Saji,4 Kyung Hae Jung,5 Sheetal Patel,6 Shilpen Patel,6 Anh Nguyen Duc,7Mario Liste-Hermoso,7 Stephen Y. Chui,6 Carlos H. Barrios8
1Dana-Farber/Brigham and Women’s Cancer Center, Boston, MA; 2Breast Center, Ludwig-Maximilians-University, Munich, Germany; 3Memorial Sloan Kettering Cancer Center, New York, NY; 4Fukushima Medical University, Fukushima, Japan; 5Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea; 6Genentech Inc, South San Francisco, CA; 7F. Hoffmann-La Roche Ltd, Basel, Switzerland; 8Oncology Research Center, Hospital São Lucas, Pontifical Catholic University of Rio Grande do Sul, Porto Alegre, RS, Brazil
San Antonio Breast Cancer Symposium®, December 8-11, 2020
This presentation is the intellectual property of the author/presenter. Contact [email protected] for permission to reprint and/or distribute. Mittendorf et al, IMpassion031 PRO analys
Disclosures
Dr Mittendorf has the following to disclose:• Research support from GlaxoSmithKline• Honoraria from Physicians’ Education Resource• Compensation for serving on advisory boards for AstraZeneca, Exact Sciences, Merck,
Peregrine Pharmaceuticals, Roche/Genentech, SELLAS Life Sciences and TapImmune• Institutional support from AstraZeneca, EMD Serono, Galena Biopharma and
Roche/Genentech• Uncompensated steering committee member for Bristol Myers Squibb, Lilly and
Roche/Genentech
San Antonio Breast Cancer Symposium®, December 8-11, 2020
This presentation is the intellectual property of the author/presenter. Contact [email protected] for permission to reprint and/or distribute. Mittendorf et al, IMpassion031 PRO analys
Background
• The IMpassion031 study (NCT03197935), combining atezolizumab with nab-paclitaxel, followed by doxorubicin plus cyclophosphamide for the neoadjuvant treatment of early-stage TNBC, showed improved pCR with a safety profile that was similar between arms1
– Atezolizumab-chemotherapy resulted in a +16.5% increase in pCR rate vs placebo-chemotherapy (57.6% vs 41.1%) in the ITT population (P=0.0044) and pCR benefit was seen regardless of PD-L1 status
• Since early breast cancer is largely asymptomatic, treatment-related symptoms and their impact define the patient experience
• Toxicities of neoadjuvant chemotherapy considered clinically manageable by physicians may significantly increase patients’ distress and interfere with daily life, leading to reduced adherence or early discontinuation2
• This is the first analysis measuring the treatment burden of checkpoint inhibitor therapy for early-stage breast cancer using patient-reported outcomes (PROs)
pCR, pathologic complete response.1. Mittendorf EA, et al. Lancet 2020;396:1090-100; 2. Hall E, et al. Eur J Cancer 2014;50:2375-89.
San Antonio Breast Cancer Symposium®, December 8-11, 2020
This presentation is the intellectual property of the author/presenter. Contact [email protected] for permission to reprint and/or distribute. Mittendorf et al, IMpassion031 PRO analys
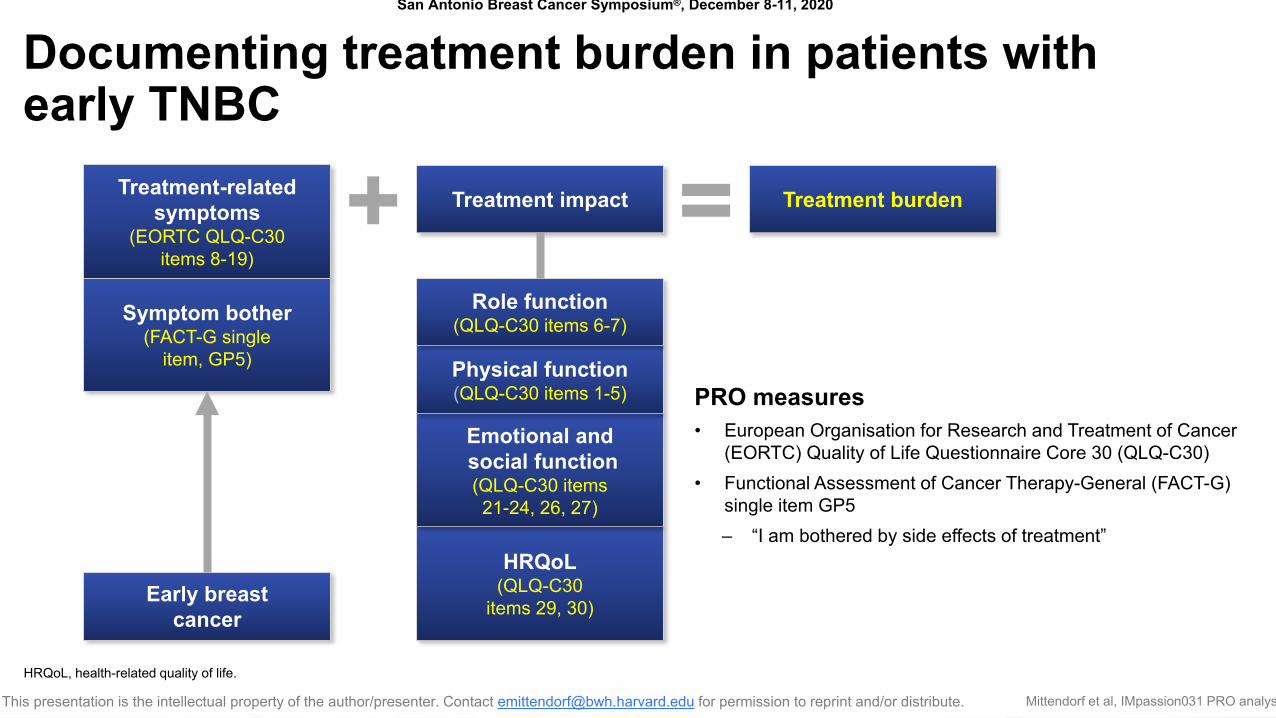
Documenting treatment burden in patients with early TNBC
PRO measures• European Organisation for Research and Treatment of Cancer
(EORTC) Quality of Life Questionnaire Core 30 (QLQ-C30)• Functional Assessment of Cancer Therapy-General (FACT-G)
single item GP5 – “I am bothered by side effects of treatment”
Treatment-related symptoms
(EORTC QLQ-C30items 8-19)
Symptom bother(FACT-G single
item, GP5)
Early breast cancer
HRQoL(QLQ-C30
items 29, 30)
Emotional andsocial function(QLQ-C30 items 21-24, 26, 27)
Physical function(QLQ-C30 items 1-5)
Role function(QLQ-C30 items 6-7)
Treatment impact Treatment burden+ =
HRQoL, health-related quality of life.
San Antonio Breast Cancer Symposium®, December 8-11, 2020
This presentation is the intellectual property of the author/presenter. Contact [email protected] for permission to reprint and/or distribute. Mittendorf et al, IMpassion031 PRO analys
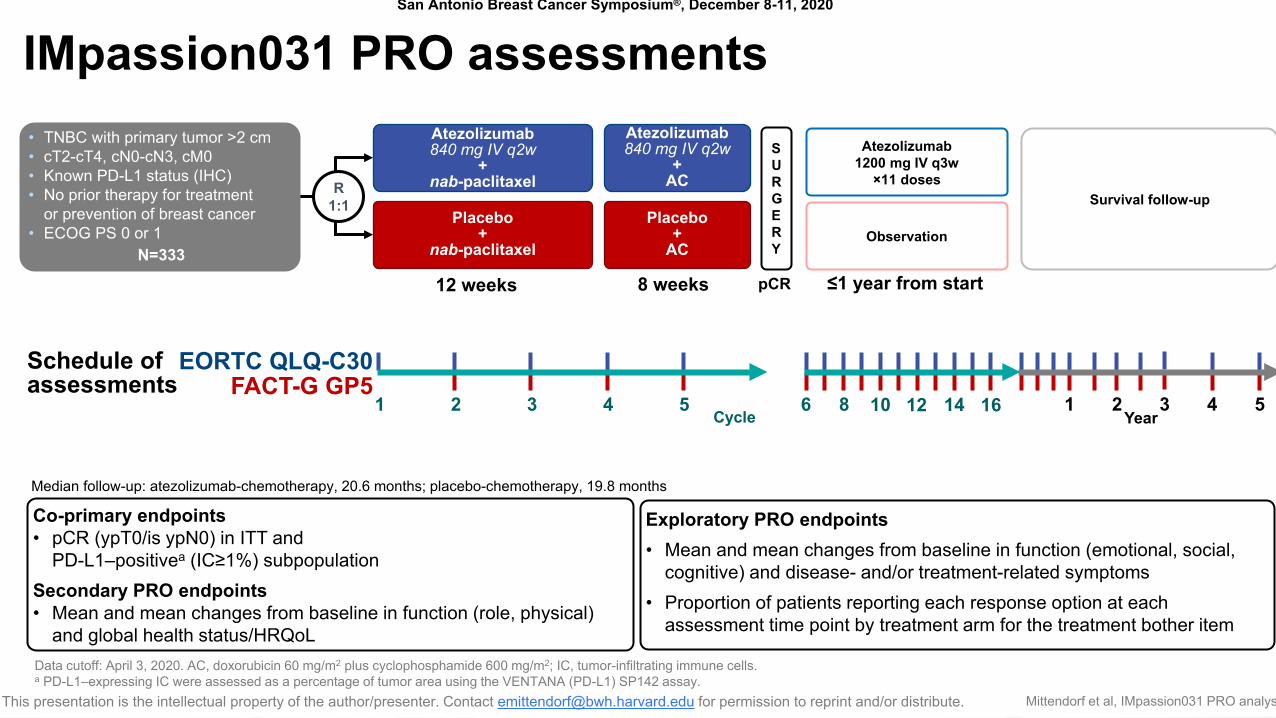
IMpassion031 PRO assessments
Placebo +
nab-paclitaxel
Atezolizumab840 mg IV q2w
+ nab-paclitaxelR
1:1
12 weeks
SURGERY
Atezolizumab1200 mg IV q3w
×11 doses
• TNBC with primary tumor >2 cm• cT2-cT4, cN0-cN3, cM0• Known PD-L1 status (IHC)• No prior therapy for treatment
or prevention of breast cancer• ECOG PS 0 or 1
N=333
Placebo +
AC
Atezolizumab 840 mg IV q2w
+AC
8 weeks pCR
Observation
Survival follow-up
≤1 year from start
Cycle1 2 3 4 5 6 8 12 1610 14
Year1 2 3 4 5
EORTC QLQ-C30Schedule of assessments FACT-G GP5
Data cutoff: April 3, 2020. AC, doxorubicin 60 mg/m2 plus cyclophosphamide 600 mg/m2; IC, tumor-infiltrating immune cells.a PD-L1–expressing IC were assessed as a percentage of tumor area using the VENTANA (PD-L1) SP142 assay.
Co-primary endpoints• pCR (ypT0/is ypN0) in ITT and
PD-L1–positivea (IC≥1%) subpopulationSecondary PRO endpoints• Mean and mean changes from baseline in function (role, physical)
and global health status/HRQoL
Exploratory PRO endpoints• Mean and mean changes from baseline in function (emotional, social,
cognitive) and disease- and/or treatment-related symptoms• Proportion of patients reporting each response option at each
assessment time point by treatment arm for the treatment bother item
Median follow-up: atezolizumab-chemotherapy, 20.6 months; placebo-chemotherapy, 19.8 months
San Antonio Breast Cancer Symposium®, December 8-11, 2020
This presentation is the intellectual property of the author/presenter. Contact [email protected] for permission to reprint and/or distribute. Mittendorf et al, IMpassion031 PRO analys
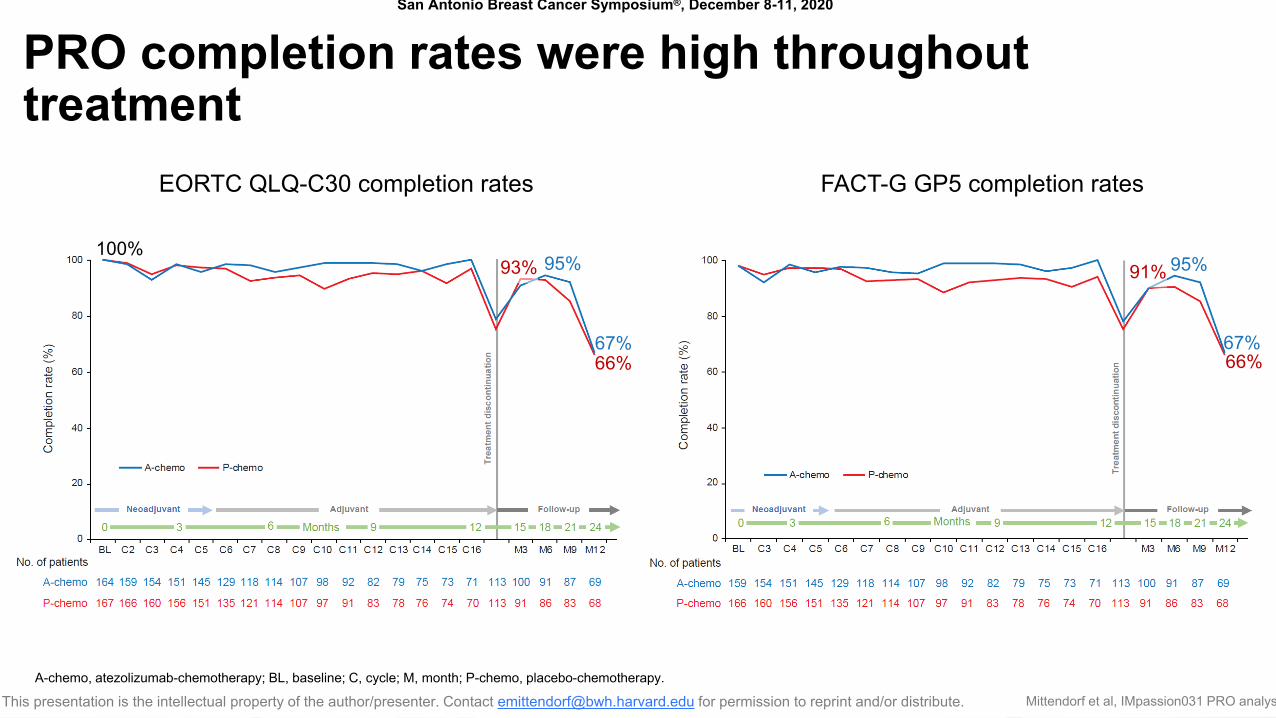
PRO completion rates were high throughout treatment
EORTC QLQ-C30 completion rates FACT-G GP5 completion rates
67%66%
95%93%100%
67%66%
95%91%
A-chemo, atezolizumab-chemotherapy; BL, baseline; C, cycle; M, month; P-chemo, placebo-chemotherapy.
San Antonio Breast Cancer Symposium®, December 8-11, 2020
This presentation is the intellectual property of the author/presenter. Contact [email protected] for permission to reprint and/or distribute. Mittendorf et al, IMpassion031 PRO analys
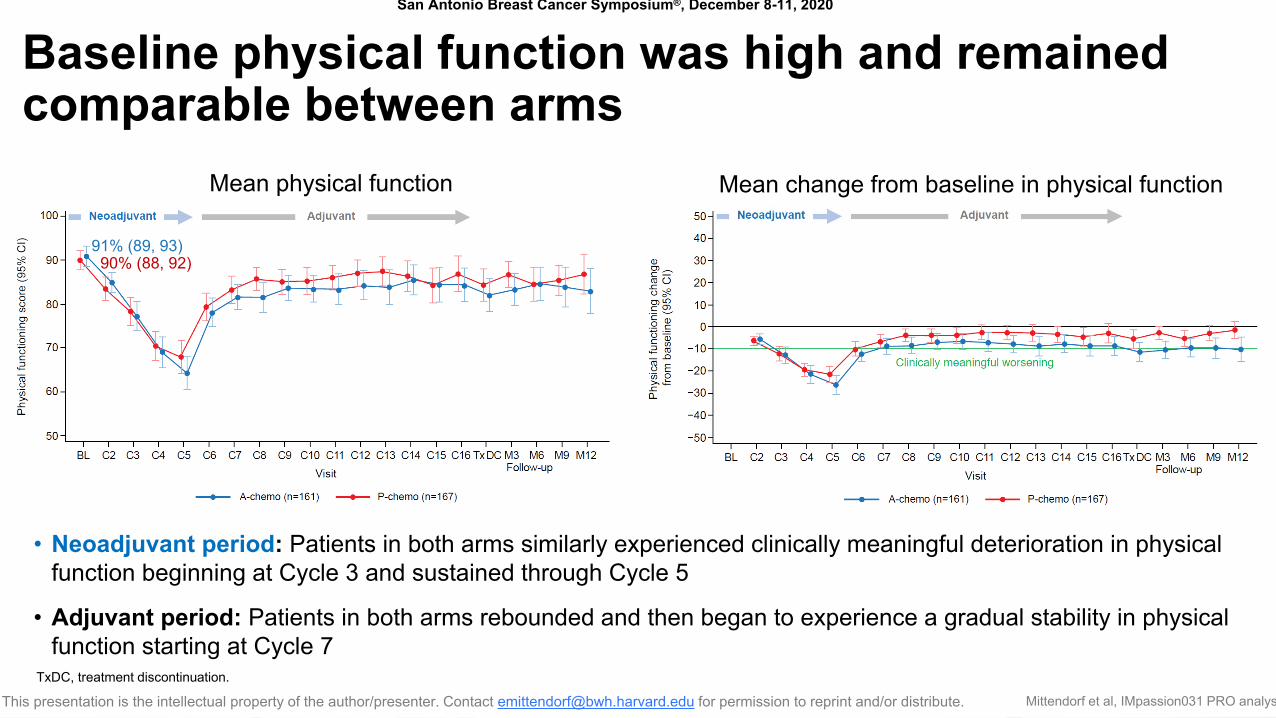
Baseline physical function was high and remained comparable between arms
• Neoadjuvant period: Patients in both arms similarly experienced clinically meaningful deterioration in physical function beginning at Cycle 3 and sustained through Cycle 5
• Adjuvant period: Patients in both arms rebounded and then began to experience a gradual stability in physical function starting at Cycle 7
Mean physical function
90% (88, 92)91% (89, 93)
TxDC, treatment discontinuation.
Mean change from baseline in physical function
San Antonio Breast Cancer Symposium®, December 8-11, 2020
This presentation is the intellectual property of the author/presenter. Contact [email protected] for permission to reprint and/or distribute. Mittendorf et al, IMpassion031 PRO analys
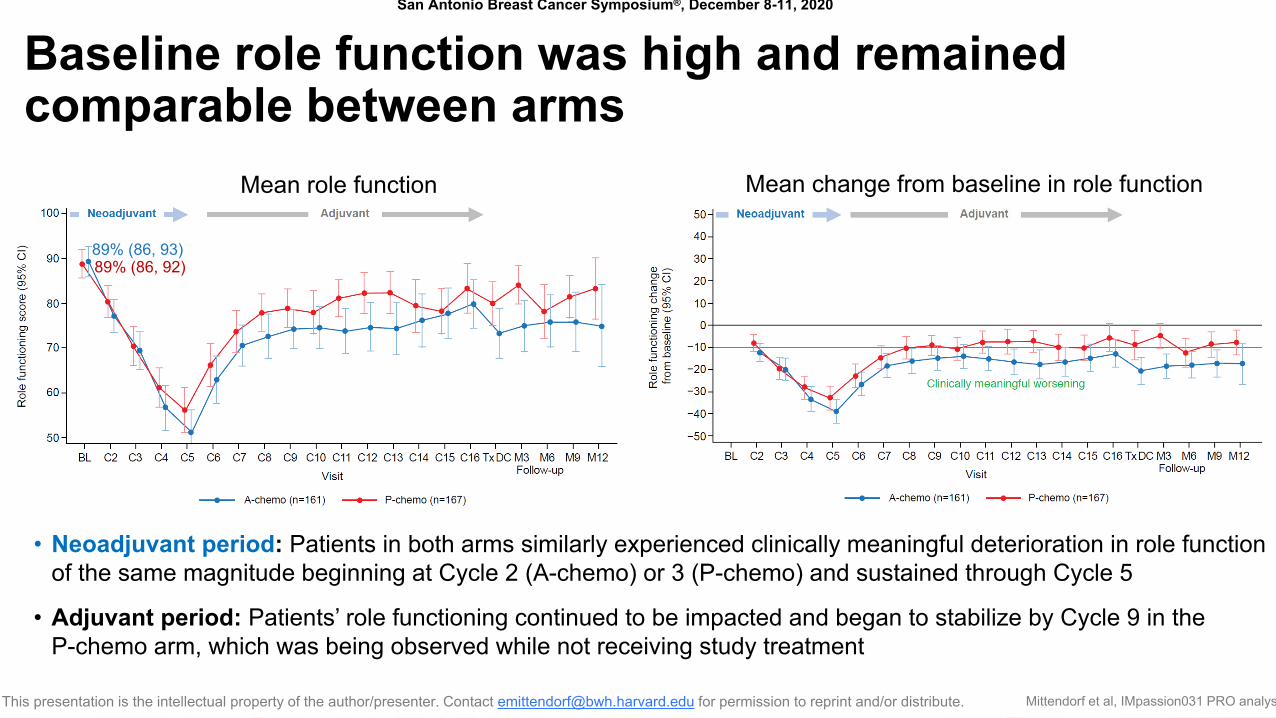
Baseline role function was high and remained comparable between arms
• Neoadjuvant period: Patients in both arms similarly experienced clinically meaningful deterioration in role function of the same magnitude beginning at Cycle 2 (A-chemo) or 3 (P-chemo) and sustained through Cycle 5
• Adjuvant period: Patients’ role functioning continued to be impacted and began to stabilize by Cycle 9 in the P-chemo arm, which was being observed while not receiving study treatment
Mean change from baseline in role functionMean role function
89% (86, 92)89% (86, 93)
San Antonio Breast Cancer Symposium®, December 8-11, 2020
This presentation is the intellectual property of the author/presenter. Contact [email protected] for permission to reprint and/or distribute. Mittendorf et al, IMpassion031 PRO analys
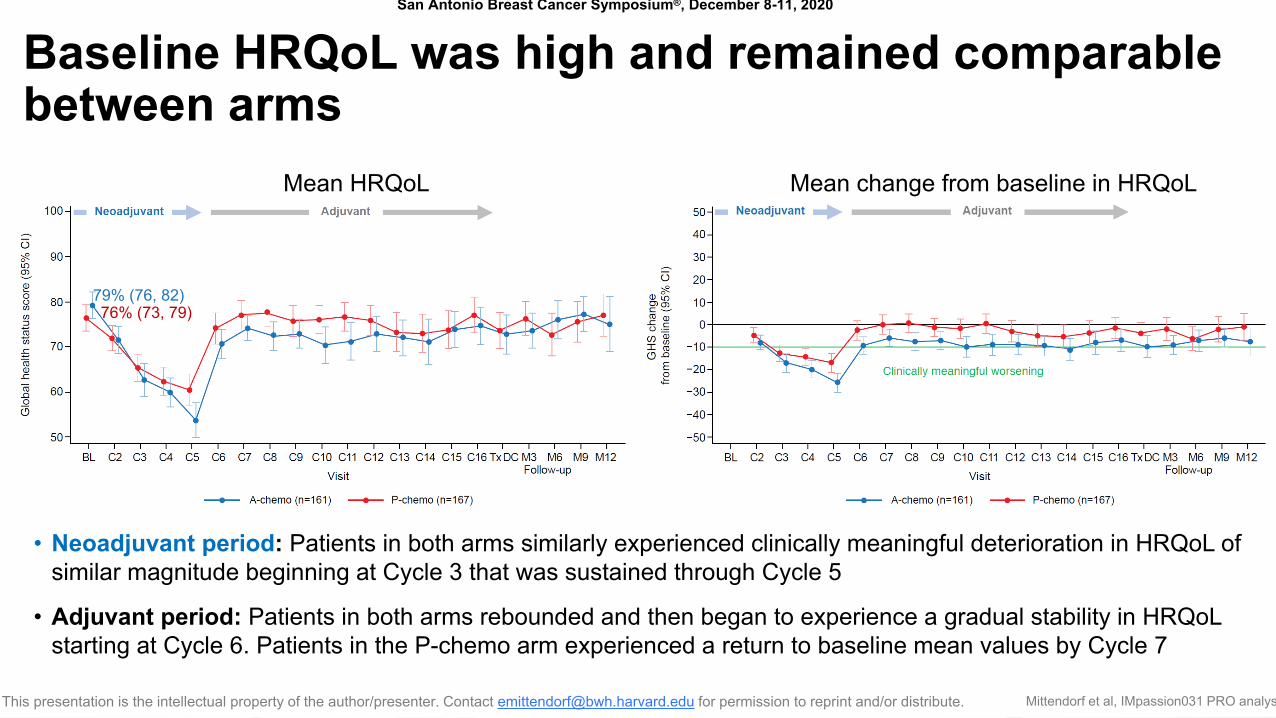
Baseline HRQoL was high and remained comparable between arms
• Neoadjuvant period: Patients in both arms similarly experienced clinically meaningful deterioration in HRQoL of similar magnitude beginning at Cycle 3 that was sustained through Cycle 5
• Adjuvant period: Patients in both arms rebounded and then began to experience a gradual stability in HRQoLstarting at Cycle 6. Patients in the P-chemo arm experienced a return to baseline mean values by Cycle 7
Mean change from baseline in HRQoLMean HRQoL
76% (73, 79)79% (76, 82)
San Antonio Breast Cancer Symposium®, December 8-11, 2020
This presentation is the intellectual property of the author/presenter. Contact [email protected] for permission to reprint and/or distribute. Mittendorf et al, IMpassion031 PRO analys
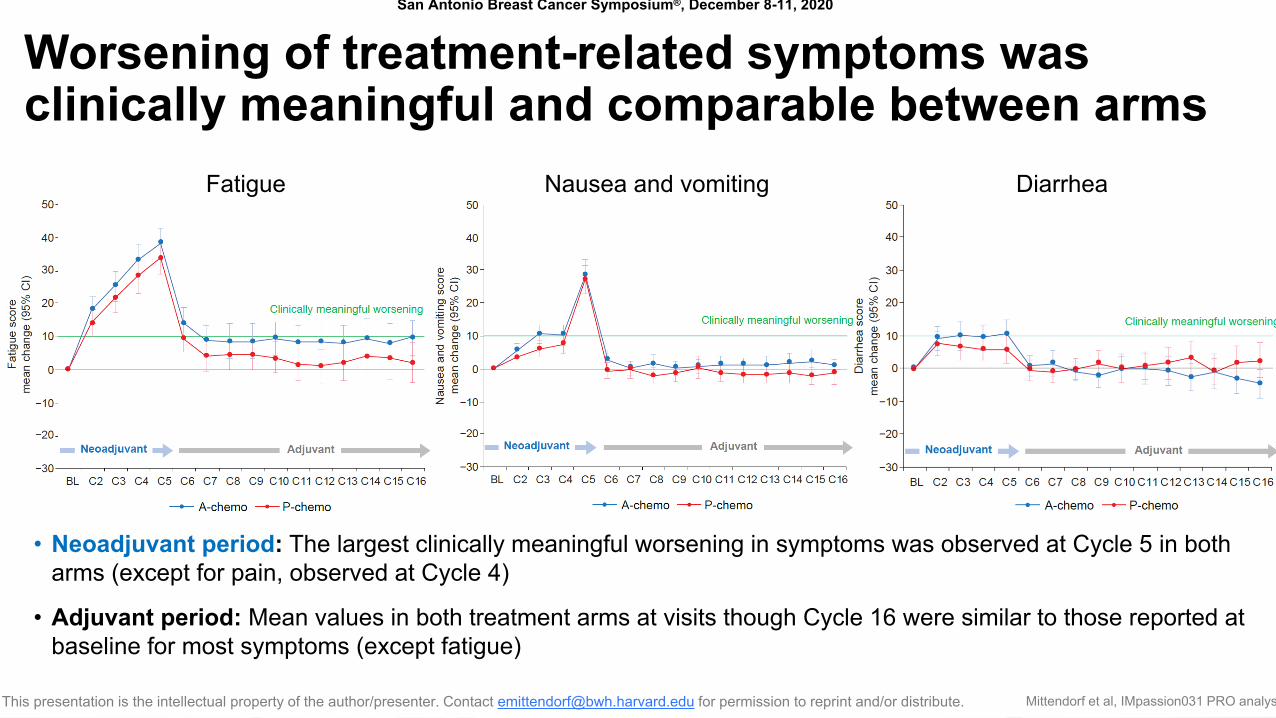
Worsening of treatment-related symptoms was clinically meaningful and comparable between arms
• Neoadjuvant period: The largest clinically meaningful worsening in symptoms was observed at Cycle 5 in both arms (except for pain, observed at Cycle 4)
• Adjuvant period: Mean values in both treatment arms at visits though Cycle 16 were similar to those reported at baseline for most symptoms (except fatigue)
Fatigue Nausea and vomiting Diarrhea
San Antonio Breast Cancer Symposium®, December 8-11, 2020
This presentation is the intellectual property of the author/presenter. Contact [email protected] for permission to reprint and/or distribute. Mittendorf et al, IMpassion031 PRO analys
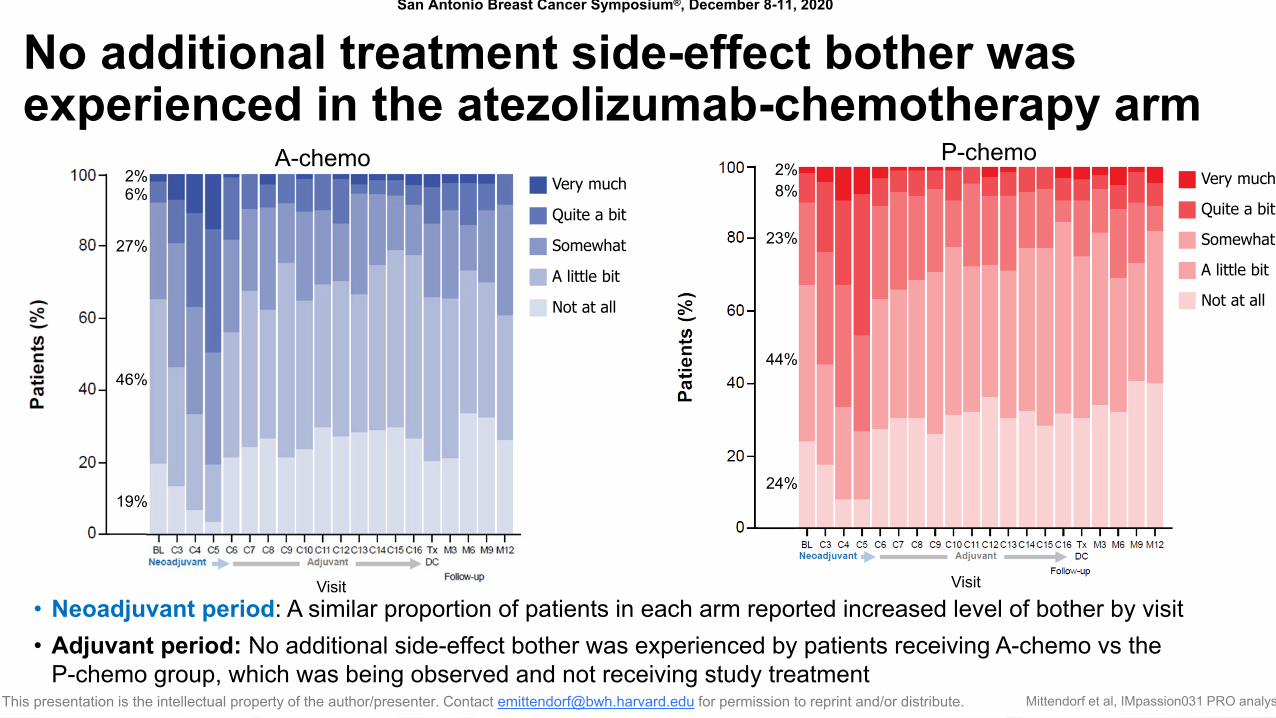
No additional treatment side-effect bother was experienced in the atezolizumab-chemotherapy arm
• Neoadjuvant period: A similar proportion of patients in each arm reported increased level of bother by visit• Adjuvant period: No additional side-effect bother was experienced by patients receiving A-chemo vs the
P-chemo group, which was being observed and not receiving study treatment
A-chemo
Not at all
A little bit
Somewhat
Quite a bit
Very much2%6%
27%
46%
19%
Visit
P-chemo
Not at all
A little bit
Somewhat
Quite a bit
Very much2%8%
23%
44%
24%
Visit
San Antonio Breast Cancer Symposium®, December 8-11, 2020
This presentation is the intellectual property of the author/presenter. Contact [email protected] for permission to reprint and/or distribute. Mittendorf et al, IMpassion031 PRO analys
Summary
• In this first analysis of PROs for checkpoint inhibitor therapy for patients with treatment-naive early-stage TNBC being treated with curative intent:– Patients who received atezolizumab plus chemotherapy during the neoadjuvant treatment period in IMpassion031 did not
experience additional detrimental impact on their day-to-day functioning or HRQoL compared with patients in the placebo plus chemotherapy arm
– Patients’ physical and role functioning and HRQoL began to stabilize and return to baseline levels in both arms during the adjuvant treatment period, although role function continued to be impacted for patients in the atezolizumab plus chemotherapy arm who resumed study treatment after surgery
• Treatment-related symptoms experienced by patients in both arms were similar, and the addition of atezolizumab to chemotherapy was tolerable with no additional treatment side-effect bother reported
• The analysis of PROs from IMpassion031 demonstrated that adding atezolizumab to neoadjuvant chemotherapy with nab-paclitaxel followed by AC improved pCR rate1 without imposing additional treatment burden on patients
1. Mittendorf EA, et al. Lancet 2020;396:1090-100.
San Antonio Breast Cancer Symposium®, December 8-11, 2020
This presentation is the intellectual property of the author/presenter. Contact [email protected] for permission to reprint and/or distribute. Mittendorf et al, IMpassion031 PRO analys
Acknowledgments
• The patients and their families
• The investigators and clinical study sites
• This study is sponsored by F. Hoffmann-La Roche Ltd
• Medical writing assistance for this presentation was provided by Chris Lum, PhD, of Health Interactions and funded by F. Hoffmann-La Roche Ltd
Copyright © 2022 FDOKUMEN




















