
PATIENT NAME : MRS. KIRAN SHARMA - GiveIndia
24
Cert. No. MC-2461 PATIENT NAME : MRS. KIRAN SHARMA PATIENT ID : FH.10727635 ACCESSION NO : 0013UE004728 AGE : 60 Years SEX : Female DATE OF BIRTH : 01/01/1961 DRAWN : 21/05/2021 06:41 RECEIVED : 21/05/2021 07:15 REPORTED : 21/05/2021 08:58 REFERRING DOCTOR : DR. ER Doctor Charges CLIENT PATIENT ID : UID:10727635 CLIENT NAME : FLT LT RAJAN DHAL CHARITABLE TRUST IPD UID:10727635 REQNO-6397811 IPD-EMERGENCY IPID-63236/21/1301 CLINICAL INFORMATION : Final Results Biological Reference Interval Units Test Report Status HAEMATOLOGY COMPLETE BLOOD COUNT, EDTA WHOLE BLOOD/SMEAR BLOOD COUNTS HEMOGLOBIN 12.6 12.0 - 15.0 g/dL METHOD : PHOTOMETRIC RED BLOOD CELL COUNT 4.70 3.8 - 4.8 mil/µL METHOD : ELECTRICAL IMPEDANCE WHITE BLOOD CELL COUNT 23.26 4.0 - 10.0 thou/µL High METHOD : ELECTRICAL IMPEDANCE PLATELET COUNT 175 150 - 410 thou/µL METHOD : ELECTRICAL IMPEDANCE Comments GIANT PLATELET SEEN. RBC AND PLATELET INDICES HEMATOCRIT 37.47 36 - 46 % METHOD : MEASURED MEAN CORPUSCULAR VOL 79.7 83.0 - 101.0 fL Low METHOD : MEASURED MEAN CORPUSCULAR HGB. 26.7 27.0 - 32.0 pg Low METHOD : CALCULATED PARAMETER MEAN CORPUSCULAR HEMOGLOBIN CONCENTRATION 33.5 31.5 - 34.5 g/dL METHOD : CALCULATED PARAMETER RED CELL DISTRIBUTION WIDTH 17.5 11.6 - 14.0 % High METHOD : CALCULATED PARAMETER MEAN PLATELET VOLUME 12.5 6.8 - 10.9 fL High METHOD : CALCULATED PARAMETER WBC DIFFERENTIAL COUNT - NLR SEGMENTED NEUTROPHILS 89 40 - 80 % High METHOD : VCS TECHNOLOGY/ MICROSCOPY ABSOLUTE NEUTROPHIL COUNT 20.70 2.0 - 7.0 thou/µL High METHOD : CALCULATED PARAMETER LYMPHOCYTES 3 20 - 40 % Low METHOD : VCS TECHNOLOGY/ MICROSCOPY ABSOLUTE LYMPHOCYTE COUNT 0.70 1.0 - 3.0 thou/µL Low METHOD : CALCULATED PARAMETER NEUTROPHIL LYMPHOCYTE RATIO (NLR) 30.9 Page 1 Of 2 C/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ NEW DELHI, 110070 DELHI, INDIA Tel : 011-42776222, CIN - U74899PB1995PLC045956 SRL LIMITED C/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ NEW DELHI, 110070 DELHI, INDIA Tel : 011-42776222, CIN - U74899PB1995PLC045956 SRL LIMITED
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of PATIENT NAME : MRS. KIRAN SHARMA - GiveIndia
Cert. No. MC-2461
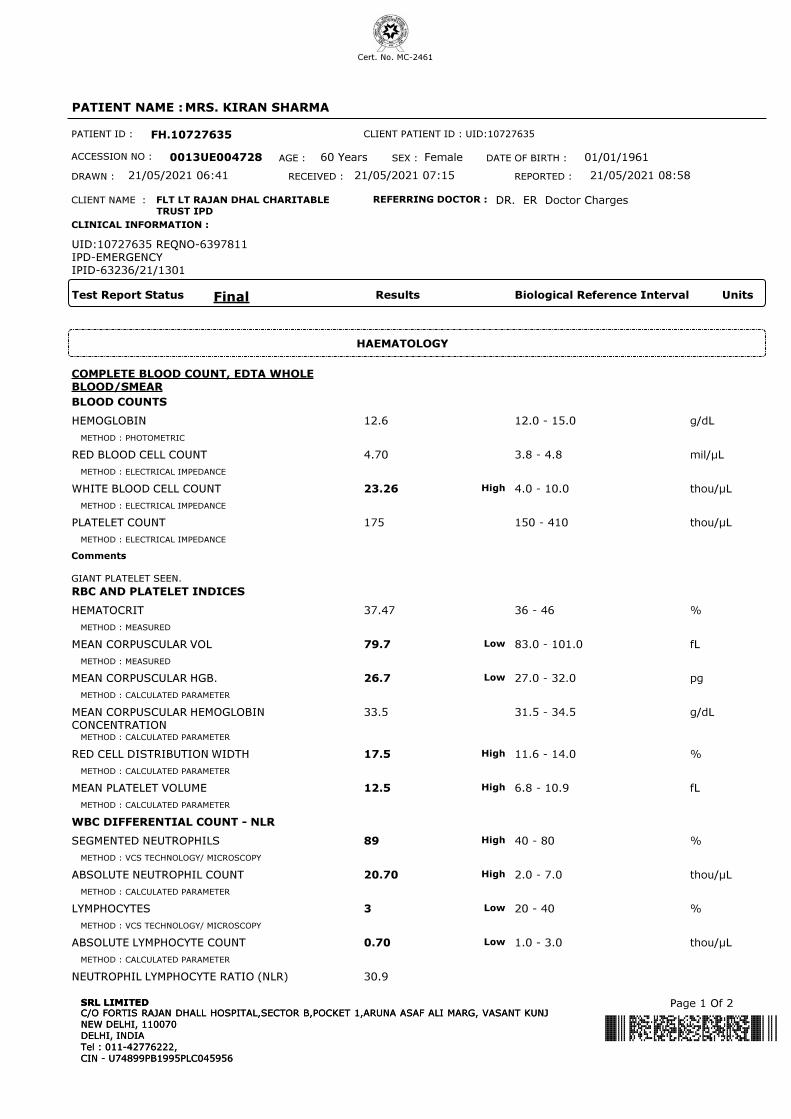
PATIENT NAME : MRS. KIRAN SHARMA
PATIENT ID : FH.10727635
ACCESSION NO : 0013UE004728 AGE : 60 Years SEX : Female DATE OF BIRTH : 01/01/1961
DRAWN : 21/05/2021 06:41 RECEIVED : 21/05/2021 07:15 REPORTED : 21/05/2021 08:58
REFERRING DOCTOR : DR. ER Doctor Charges
CLIENT PATIENT ID : UID:10727635
CLIENT NAME : FLT LT RAJAN DHAL CHARITABLE
TRUST IPD
UID:10727635 REQNO-6397811
IPD-EMERGENCY
IPID-63236/21/1301
CLINICAL INFORMATION :
Final Results Biological Reference Interval UnitsTest Report Status
HAEMATOLOGY
COMPLETE BLOOD COUNT, EDTA WHOLE
BLOOD/SMEAR
BLOOD COUNTS
HEMOGLOBIN 12.6 12.0 - 15.0 g/dL
METHOD : PHOTOMETRIC
RED BLOOD CELL COUNT 4.70 3.8 - 4.8 mil/µL
METHOD : ELECTRICAL IMPEDANCE
WHITE BLOOD CELL COUNT 23.26 4.0 - 10.0 thou/µLHigh
METHOD : ELECTRICAL IMPEDANCE
PLATELET COUNT 175 150 - 410 thou/µL
METHOD : ELECTRICAL IMPEDANCE
Comments
GIANT PLATELET SEEN.
RBC AND PLATELET INDICES
HEMATOCRIT 37.47 36 - 46 %
METHOD : MEASURED
MEAN CORPUSCULAR VOL 79.7 83.0 - 101.0 fLLow
METHOD : MEASURED
MEAN CORPUSCULAR HGB. 26.7 27.0 - 32.0 pgLow
METHOD : CALCULATED PARAMETER
MEAN CORPUSCULAR HEMOGLOBIN
CONCENTRATION
33.5 31.5 - 34.5 g/dL
METHOD : CALCULATED PARAMETER
RED CELL DISTRIBUTION WIDTH 17.5 11.6 - 14.0 %High
METHOD : CALCULATED PARAMETER
MEAN PLATELET VOLUME 12.5 6.8 - 10.9 fLHigh
METHOD : CALCULATED PARAMETER
WBC DIFFERENTIAL COUNT - NLR
SEGMENTED NEUTROPHILS 89 40 - 80 %High
METHOD : VCS TECHNOLOGY/ MICROSCOPY
ABSOLUTE NEUTROPHIL COUNT 20.70 2.0 - 7.0 thou/µLHigh
METHOD : CALCULATED PARAMETER
LYMPHOCYTES 3 20 - 40 %Low
METHOD : VCS TECHNOLOGY/ MICROSCOPY
ABSOLUTE LYMPHOCYTE COUNT 0.70 1.0 - 3.0 thou/µLLow
METHOD : CALCULATED PARAMETER
NEUTROPHIL LYMPHOCYTE RATIO (NLR) 30.9
Page 1 Of 2C/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITEDC/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITED

Cert. No. MC-2461
PATIENT NAME : MRS. KIRAN SHARMA
PATIENT ID : FH.10727635
ACCESSION NO : 0013UE004728 AGE : 60 Years SEX : Female DATE OF BIRTH : 01/01/1961
DRAWN : 21/05/2021 06:41 RECEIVED : 21/05/2021 07:15 REPORTED : 21/05/2021 08:58
REFERRING DOCTOR : DR. ER Doctor Charges
CLIENT PATIENT ID : UID:10727635
CLIENT NAME : FLT LT RAJAN DHAL CHARITABLE
TRUST IPD
UID:10727635 REQNO-6397811
IPD-EMERGENCY
IPID-63236/21/1301
CLINICAL INFORMATION :
Final Results Biological Reference Interval UnitsTest Report Status
EOSINOPHILS 1 1 - 6 %
METHOD : VCS TECHNOLOGY/ MICROSCOPY
ABSOLUTE EOSINOPHIL COUNT 0.23 0.02 - 0.50 thou/µL
METHOD : CALCULATED PARAMETER
MONOCYTES 3 2 - 10 %
METHOD : VCS TECHNOLOGY/ MICROSCOPY
ABSOLUTE MONOCYTE COUNT 0.70 0.2 - 1.0 thou/µL
METHOD : CALCULATED PARAMETER
BASOPHILS 0 < 1 - 2 %
ABSOLUTE BASOPHIL COUNT 0.00 0.02 - 0.10 thou/µLLow
METHOD : CALCULATED PARAMETER
BAND (STAB) CELLS 03 %
MYELOCYTES 01 %High
DIFFERENTIAL COUNT PERFORMED ON: EDTA SMEAR
METHOD : AUTOMATED ANALYZER / MICROSCOPY
DISCLAIMER: THE ABSOLUTE WHITE CELL COUNTS ARE OUTSIDE THE NABL ACCREDITED SCOPE OF THE LABORATORY.
Interpretation(s)
BLOOD COUNTS-
The cell morphology is well preserved for 24hrs. However after 24-48 hrs a progressive increase in MCV and HCT is observed leading to a decrease in MCHC. A direct smear is
recommended for an accurate differential count and for examination of RBC morphology.
RBC AND PLATELET INDICES-
The cell morphology is well preserved for 24hrs. However after 24-48 hrs a progressive increase in MCV and HCT is observed leading to a decrease in MCHC. A direct smear is
recommended for an accurate differential count and for examination of RBC morphology.
WBC DIFFERENTIAL COUNT - NLR-
The optimal threshold of 3.3 for NLR showed a prognostic possibility of clinical symptoms to change from mild to severe in COVID positive patients. When age = 49.5 years
old and NLR = 3.3, 46.1% COVID-19 patients with mild disease might become severe. By contrast, when age < 49.5 years old and NLR < 3.3, COVID-19 patients tend to
show mild disease.
(Reference to - The diagnostic and predictive role of NLR, d-NLR and PLR in COVID-19 patients ; A.-P. Yang, et al.; International Immunopharmacology 84 (2020) 106504
This ratio element is a calculated parameter and out of NABL scope.
**End Of Report**
Please visit www.srlworld.com for related Test Information for this accession
Dr Nitin Kumar Dumeer, M.D.
Senior pathologist,Lab head
Page 2 Of 2C/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITEDC/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITED

Cert. No. MC-2461
PATIENT NAME : MRS. KIRAN SHARMA
PATIENT ID : FH.10727635
ACCESSION NO : 0013UE004765 AGE : 59 Years SEX : Female DATE OF BIRTH : 23/06/1961
DRAWN : 21/05/2021 09:55 RECEIVED : 21/05/2021 10:14 REPORTED : 21/05/2021 10:44
REFERRING DOCTOR :
CLIENT PATIENT ID : UID:10727635
CLIENT NAME : FLT LT RAJAN DHAL CHARITABLE
TRUST IPD
UID:10727635 REQNO-6398686
IPD-ICU(4)
IPID-63236/21/1301
CLINICAL INFORMATION :
Final Results Biological Reference Interval UnitsTest Report Status
COAGULATION
ACT PARTIAL THROMBO PLASTIN TIME
(APTT), PLASMA
APTT 22.3 22.2 - 33.2 SECONDS
METHOD : CLOT DETECTION BY BALL OSCILATION
Comments
LOW OR HIGH HEMATOCRIT VALUES CAN ALTER PT & APTT VALUE.
KINDLY CORRELATE CLINICALLY.
PROTHROMBIN TIME, PLASMA
PROTHROMBIN TIME (PT) 15.0 11.6 - 14.6 SECONDSHigh
METHOD : CLOT DETECTION BY BALL OSCILATION
INTERNATIONAL NORMALIZED RATIO (INR) 1.18 < 1.4 RATIO
MEAN NORMAL PT 13.1 SECONDS
Interpretation(s)
ACT PARTIAL THROMBO PLASTIN TIME(APTT), PLASMA-
The activated partial thromboplastin time (APTT) reflects the activities of most of the coagulation factors, including factor XII and other ""contact factors"" (prekallikrein [PK]
and high molecular weight kininogen [HMWK]) and factors XI, IX, and VIII in the intrinsic coagulation pathway, as well as coagulation factors in the common coagulation
pathway that include factors X, V, II and fibrinogen (factor I). The APTT also depends on phospholipid (a partial thromboplastin) and ionic calcium, as well as the activator of
the contact factors (eg, silica) present in the reagent, but reflects neither the integrity of the extrinsic coagulantion pathway that includes factor VII and tissue factor, nor the
activity of factor XIII (fibrin stabilizing factor). The APTT is variably sensitive to the presence of specific and nonspecific inhibitors of the intrinsic and common coagulation
pathways, including lupus anticoagulants or antiphospholipid antibodies. It is useful for monitoring unfractionated heparin therapy, for screening for certain coagulation factor
deficiencies, detection of coagulation inhibitors such as lupus anticoagulant, specific factor inhibitors, and nonspecific inhibitors.
APTT “mixing” studies:
Poor or partial correction of the abnormal result by normal plasma may be observed in the presence of coagulation factor inhibitors, anticoagulant drugs such as heparin or
direct thrombin inhibitors. Total correction indicates coagulation factors deficiency.
PROTHROMBIN TIME, PLASMA-
Prothrombin Time measures the integrity of the extrinsic pathway and the adequacy of critical coagulation factors involved in it, namely, Factor VII. This test is therefore,
used for monitoring oral anticoagulation therapy which lowers the levels of multiple vitamin K dependent coagulation factors in blood (Factors II, VII, IX and X) including
Factor VII. The result of PT is expressed as International Normalized Ratio (INR) to neutralize the influence of variable sensitivity of the reagents (thromboplastin) used in the
assay by different laboratories.
Prolonged PT/INR is observed in hereditary or acquired deficiency of the relevant coagulation factors, vitamin K deficiency, liver disease, specific coagulation factor inhibitors
and nonspecific inhibitors of PT (eg, monoclonal immunoglobulins, elevated fibrin degradation products).
The following INR ranges are recommended for achieving optimal anticoagulation in different clinical conditions:
Diagnosis TargetINR
Treatment of venous thrombosis 2.0- 3.0
Treatment of pulmonary embolism 2.0- 3.0
Prevention of systemic embolism 2.0- 3.0
Tissue heart valves 2.0- 3.0
Hypercoagulable states 2.0- 3.0
Atrial fibrillation 2.0- 3.0
Mechanical prosthetic valves (high risk) 2.5- 3.5
Bileaflet mechanical valve in aortic position 2.0- 3.0
Page 1 Of 2C/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITEDC/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITED

Cert. No. MC-2461
PATIENT NAME : MRS. KIRAN SHARMA
PATIENT ID : FH.10727635
ACCESSION NO : 0013UE004765 AGE : 59 Years SEX : Female DATE OF BIRTH : 23/06/1961
DRAWN : 21/05/2021 09:55 RECEIVED : 21/05/2021 10:14 REPORTED : 21/05/2021 10:44
REFERRING DOCTOR :
CLIENT PATIENT ID : UID:10727635
CLIENT NAME : FLT LT RAJAN DHAL CHARITABLE
TRUST IPD
UID:10727635 REQNO-6398686
IPD-ICU(4)
IPID-63236/21/1301
CLINICAL INFORMATION :
Final Results Biological Reference Interval UnitsTest Report Status
**End Of Report**
Please visit www.srlworld.com for related Test Information for this accession
Dr Nitin Kumar Dumeer, M.D.
Senior pathologist,Lab head
Page 2 Of 2C/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITEDC/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITED

Cert. No. MC-2461
PATIENT NAME : MRS. KIRAN SHARMA
PATIENT ID : FH.10727635
ACCESSION NO : 0013UE004744 AGE : 60 Years SEX : Female DATE OF BIRTH : 01/01/1961
DRAWN : 21/05/2021 07:14 RECEIVED : 21/05/2021 07:32 REPORTED : 21/05/2021 10:48
REFERRING DOCTOR : DR. ER Doctor Charges
CLIENT PATIENT ID : UID:10727635
CLIENT NAME : FLT LT RAJAN DHAL CHARITABLE
TRUST IPD
UID:10727635 REQNO-6397939
IPD-EMERGENCY
IPID-63236/21/1301
CLINICAL INFORMATION :
Final Results Biological Reference Interval UnitsTest Report Status
KIDNEY PANEL - 1
SERUM BLOOD UREA NITROGEN
BLOOD UREA NITROGEN 15 8 - 23 mg/dL
METHOD : UREASE -GLDH
CREATININE EGFR- EPI
CREATININE 0.62 0.60 - 1.20 mg/dL
METHOD : MODIFIED JAFFE KINETIC
AGE 60 years
METHOD : MANUAL
GLOMERULAR FILTRATION RATE (FEMALE) 98.01 Refer Interpretation Below mL/min/1.73m2
METHOD : CALCULATED PARAMETER
BUN/CREAT RATIO
BUN/CREAT RATIO 24.19 5.00 - 15.00High
METHOD : CALCULATED PARAMETER
URIC ACID, SERUM
URIC ACID 4.6 2.6 - 6.0 mg/dL
METHOD : URICASE/ PAP
TOTAL PROTEIN, SERUM
TOTAL PROTEIN 5.8 6.4 - 8.2 g/dLLow
METHOD : BIURET
ALBUMIN, SERUM
ALBUMIN 2.2 3.4 - 5.0 g/dLLow
METHOD : BROMOCRESOL PURPLE
GLOBULIN
GLOBULIN 3.6 2.0 - 4.1 g/dL
METHOD : CALCULATED PARAMETER
ELECTROLYTES (NA/K/CL), SERUM
SODIUM 131 136 - 145 mmol/LLow
METHOD : ION SELECTIVE ELECTRODE TECHNOLOGY INDIRECT
POTASSIUM 3.40 3.50 - 5.10 mmol/LLow
METHOD : ION SELECTIVE ELECTRODE TECHNOLOGY INDIRECT
CHLORIDE 96 98 - 107 mmol/LLow
METHOD : ION SELECTIVE ELECTRODE TECHNOLOGY INDIRECT
URINALYSIS
COLOR PALE YELLOW
METHOD : MANUAL
APPEARANCE CLEAR
METHOD : MANUAL
Page 1 Of 4C/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITEDC/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITED

Cert. No. MC-2461
PATIENT NAME : MRS. KIRAN SHARMA
PATIENT ID : FH.10727635
ACCESSION NO : 0013UE004744 AGE : 60 Years SEX : Female DATE OF BIRTH : 01/01/1961
DRAWN : 21/05/2021 07:14 RECEIVED : 21/05/2021 07:32 REPORTED : 21/05/2021 10:48
REFERRING DOCTOR : DR. ER Doctor Charges
CLIENT PATIENT ID : UID:10727635
CLIENT NAME : FLT LT RAJAN DHAL CHARITABLE
TRUST IPD
UID:10727635 REQNO-6397939
IPD-EMERGENCY
IPID-63236/21/1301
CLINICAL INFORMATION :
Final Results Biological Reference Interval UnitsTest Report Status
PH 6.0 4.7 - 7.5
METHOD : DIPSTICK
SPECIFIC GRAVITY 1.015 1.003 - 1.035
METHOD : DIPSTICK
GLUCOSE NOT DETECTED NOT DETECTED
METHOD : DIPSTICK / MANUAL
PROTEIN NOT DETECTED NOT DETECTED
METHOD : DIPSTICK / MANUAL
KETONES NOT DETECTED NOT DETECTED
METHOD : DIPSTICK / MANUAL
BLOOD NOT DETECTED NOT DETECTED
METHOD : DIPSTICK
BILIRUBIN NOT DETECTED NOT DETECTED
METHOD : DIPSTICK / MANUAL
UROBILINOGEN NORMAL NORMAL
METHOD : DIPSTICK / MANUAL
NITRITE NOT DETECTED NOT DETECTED
METHOD : DIPSTICK
WBC 1-2 0-5 /HPF
METHOD : MICROSCOPIC EXAMINATION
EPITHELIAL CELLS 1-2 0-5 /HPF
METHOD : MICROSCOPIC EXAMINATION
RED BLOOD CELLS NOT DETECTED NOT DETECTED /HPF
METHOD : MICROSCOPIC EXAMINATION
CASTS NOT DETECTED
METHOD : MICROSCOPIC EXAMINATION
CRYSTALS NOT DETECTED
METHOD : MICROSCOPIC EXAMINATION
Comments
NOTE :- MICROSCOPIC EXAMINATION OF URINE IS PERFORMED BY CENTRIFUGED URINARY SEDIMENT.
Interpretation(s)
SERUM BLOOD UREA NITROGEN-
Causes of Increased levels
Pre renal
• High protein diet, Increased protein catabolism, GI haemorrhage, Cortisol, Dehydration, CHF Renal
• Renal Failure
Post Renal
• Malignancy, Nephrolithiasis, Prostatism
Causes of decreased levels
• Liver disease
• SIADH.
CREATININE EGFR- EPI-
GFR— Glomerular filtration rate (GFR) is a measure of the function of the kidneys. The GFR is a calculation based on a serum creatinine test. Creatinine is a muscle waste
Page 2 Of 4C/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITED
C/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITED

Cert. No. MC-2461
PATIENT NAME : MRS. KIRAN SHARMA
PATIENT ID : FH.10727635
ACCESSION NO : 0013UE004744 AGE : 60 Years SEX : Female DATE OF BIRTH : 01/01/1961
DRAWN : 21/05/2021 07:14 RECEIVED : 21/05/2021 07:32 REPORTED : 21/05/2021 10:48
REFERRING DOCTOR : DR. ER Doctor Charges
CLIENT PATIENT ID : UID:10727635
CLIENT NAME : FLT LT RAJAN DHAL CHARITABLE
TRUST IPD
UID:10727635 REQNO-6397939
IPD-EMERGENCY
IPID-63236/21/1301
CLINICAL INFORMATION :
Final Results Biological Reference IntervalTest Report Status
product that is filtered from the blood by the kidneys and excreted into urine at a relatively steady rate. When kidney function decreases, less creatinine is excreted and
concentrations increase in the blood. With the creatinine test, a reasonable estimate of the actual GFR can be determined.
A GFR of 60 or higher is in the normal range.
A GFR below 60 may mean kidney disease.
A GFR of 15 or lower may mean kidney failure.
Estimated GFR (eGFR) is the preferred method for identifying people with chronic kidney disease (CKD). In adults, eGFR calculated using the Modification of Diet in Renal
Disease (MDRD) Study equation provides a more clinically useful measure of kidney function than serum creatinine alone.
The CKD-EPI creatinine equation is based on the same four variables as the MDRD Study equation, but uses a 2-slope spline to model the relationship between estimated GFR
and serum creatinine, and a different relationship for age, sex and race. The equation was reported to perform better and with less bias than the MDRD Study equation,
especially in patients with higher GFR. This results in reduced misclassification of CKD.
The CKD-EPI creatinine equation has not been validated in children & will only be reported for patients = 18 years of age. For pediatric and childrens, Schwartz Pediatric
Bedside eGFR (2009) formulae is used. This revised "bedside" pediatric eGFR requires only serum creatinine and height.
URIC ACID, SERUM-
Causes of Increased levels
Dietary
• High Protein Intake.
• Prolonged Fasting,
• Rapid weight loss.
Gout
Lesch nyhan syndrome.
Type 2 DM.
Metabolic syndrome.
Causes of decreased levels
• Low Zinc Intake
• OCP’s
• Multiple Sclerosis
Nutritional tips to manage increased Uric acid levels
• Drink plenty of fluids
• Limit animal proteins
• High Fibre foods
• Vit C Intake
• Antioxidant rich foods
TOTAL PROTEIN, SERUM-
Serum total protein,also known as total protein, is a biochemical test for measuring the total amount of protein in serum..Protein in the plasma is made up of albumin and
globulin
Higher-than-normal levels may be due to: Chronic inflammation or infection, including HIV and hepatitis B or C, Multiple myeloma, Waldenstrom's disease
Lower-than-normal levels may be due to: Agammaglobulinemia, Bleeding (hemorrhage),Burns,Glomerulonephritis, Liver disease, Malabsorption, Malnutrition, Nephrotic
syndrome,Protein-losing enteropathy etc.
ALBUMIN, SERUM-
Human serum albumin is the most abundant protein in human blood plasma. It is produced in the liver. Albumin constitutes about half of the blood serum protein. Low blood
albumin levels (hypoalbuminemia) can be caused by: Liver disease like cirrhosis of the liver, nephrotic syndrome, protein-losing enteropathy, Burns, hemodilution, increased
vascular permeability or decreased lymphatic clearance,malnutrition and wasting etc.
ELECTROLYTES (NA/K/CL), SERUM-
Sodium levels are Increased in dehydration, cushing's syndrome, aldosteronism & decreased in Addison's disease, hypopituitarism,liver disease. Hypokalemia (low K) is
common in vomiting, diarrhea, alcoholism, folic acid deficiency and primary aldosteronism. Hyperkalemia may be seen in end-stage renal failure, hemolysis, trauma,
Addison's disease, metabolic acidosis, acute starvation, dehydration, and with rapid K infusion.Chloride is increased in dehydration, renal tubular acidosis (hyperchloremia
metabolic acidosis), acute renal failure, metabolic acidosis associated with prolonged diarrhea and loss of sodium bicarbonate, diabetes insipidus, adrenocortical hyperfuction,
salicylate intoxication and with excessive infusion of isotonic saline or extremely high dietary intake of salt.Chloride is decreased in overhydration, chronic respiratory acidosis,
salt-losing nephritis, metabolic alkalosis, congestive heart failure, Addisonian crisis, certain types of metabolic acidosis, persistent gastric secretion and prolonged vomiting,
URINALYSIS-Routine urine analysis assists in screening and diagnosis of various metabolic, urological, kidney and liver disorders
Protein: Elevated proteins can be an early sign of kidney disease. Urinary protein excretion can also be temporarily elevated by strenuous exercise, orthostatic proteinuria,
dehydration, urinary tract infections and acute illness with fever
Glucose: Uncontrolled diabetes mellitus can lead to presence of glucose in urine. Other causes include pregnancy, hormonal disturbances, liver disease and certain
medications.
Ketones: Uncontrolled diabetes mellitus can lead to presence of ketones in urine. Ketones can also be seen in starvation, frequent vomiting, pregnancy and strenuous
exercise.
Blood: Occult blood can occur in urine as intact erythrocytes or haemoglobin, which can occur in various urological, nephrological and bleeding disorders.
Leukocytes: An increase in leukocytes is an indication of inflammation in urinary tract or kidneys. Most common cause is bacterial urinary tract infection.
Nitrite: Many bacteria give positive results when their number is high. Nitrite concentration during infection increases with length of time the urine specimen is retained in
bladder prior to collection.
pH: The kidneys play an important role in maintaining acid base balance of the body. Conditions of the body producing acidosis/ alkalosis or ingestion of certain type of food
can affect the pH of urine.
Specific gravity: Specific gravity gives an indication of how concentrated the urine is. Increased specific gravity is seen in conditions like dehydration, glycosuria and
proteinuria while decreased specific gravity is seen in excessive fluid intake, renal failure and diabetes insipidus.
Bilirubin: In certain liver diseases such as biliary obstruction or hepatitis, bilirubin gets excreted in urine.
Page 3 Of 4C/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITED
C/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITED

Cert. No. MC-2461
PATIENT NAME : MRS. KIRAN SHARMA
PATIENT ID : FH.10727635
ACCESSION NO : 0013UE004744 AGE : 60 Years SEX : Female DATE OF BIRTH : 01/01/1961
DRAWN : 21/05/2021 07:14 RECEIVED : 21/05/2021 07:32 REPORTED : 21/05/2021 10:48
REFERRING DOCTOR : DR. ER Doctor Charges
CLIENT PATIENT ID : UID:10727635
CLIENT NAME : FLT LT RAJAN DHAL CHARITABLE
TRUST IPD
UID:10727635 REQNO-6397939
IPD-EMERGENCY
IPID-63236/21/1301
CLINICAL INFORMATION :
Final Results Biological Reference IntervalTest Report Status
Urobilinogen: Positive results are seen in liver diseases like hepatitis and cirrhosis and in cases of hemolytic anemia
**End Of Report**
Please visit www.srlworld.com for related Test Information for this accession
Dr. Rahul Bhardwaj,MD.
Pathologist
Dr Nitin Kumar Dumeer, M.D.
Senior pathologist,Lab head
Page 4 Of 4C/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITEDC/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITED

Cert. No. MC-2461
PATIENT NAME : MRS. KIRAN SHARMA
PATIENT ID : FH.10727635
ACCESSION NO : 0013UE004772 AGE : 59 Years SEX : Female DATE OF BIRTH : 23/06/1961
DRAWN : 21/05/2021 09:55 RECEIVED : 21/05/2021 10:38 REPORTED : 21/05/2021 11:53
REFERRING DOCTOR :
CLIENT PATIENT ID : UID:10727635
CLIENT NAME : FLT LT RAJAN DHAL CHARITABLE
TRUST IPD
UID:10727635 REQNO-6398686
IPD-ICU(4)
IPID-63236/21/1301
CLINICAL INFORMATION :
Final Results Biological Reference Interval UnitsTest Report Status
BIO CHEMISTRY
LIVER FUNCTION PROFILE, SERUM
BILIRUBIN, TOTAL 1.24 0.2 - 1.0 mg/dLHigh
METHOD : DIAZO METHOD
BILIRUBIN, DIRECT 0.42 0.0 - 0.2 mg/dLHigh
METHOD : DIAZO METHOD
BILIRUBIN, INDIRECT 0.47 0.1 - 1.0 mg/dL
METHOD : CALCULATED PARAMETER
TOTAL PROTEIN 5.9 6.4 - 8.2 g/dLLow
METHOD : BIURET
ALBUMIN 2.3 3.4 - 5.0 g/dLLow
METHOD : SPECTROPHOTOMETRY – BROMOCRESOL PURPLE
GLOBULIN 2.8 2.0 - 4.1 g/dL
METHOD : CALCULATED PARAMETER
ALBUMIN/GLOBULIN RATIO 0.3 1.0 - 2.1 RATIOLow
METHOD : CALCULATED PARAMETER
ASPARTATE AMINOTRANSFERASE (AST/SGOT) 23 15 - 37 U/L
METHOD : SPECTROPHOTOMETRIC-IFCC WITH UV WITH PYRIDOXAL-5-PHOSPHATE
ALANINE AMINOTRANSFERASE (ALT/SGPT) 21 < 34.0 U/L
METHOD : SPECTROPHOTOMETRIC-IFCC WITH UV WITH PYRIDOXAL-5-PHOSPHATE
ALKALINE PHOSPHATASE 124 30 - 120 U/LHigh
METHOD : SPECTROPHOTOMETRY, P-NPP (AMP BUFFER)
GAMMA GLUTAMYL TRANSFERASE (GGT) 28 5 - 55 U/L
METHOD : SPECTROPHOTOMETRIC-IFCC WITH UV WITH PYRIDOXAL-5-PHOSPHATE
LACTATE DEHYDROGENASE 342 100 - 190 U/LHigh
METHOD : LACTATE -PYRUVATE
CALCIUM, SERUM
CALCIUM 7.8 8.5 - 10.1 mg/dLLow
METHOD : O-CRESOLPHTHALEIN COMPLEXONE
MAGNESIUM, SERUM
MAGNESIUM 1.5 1.8 - 2.4 mg/dLLow
METHOD : METHYLTHYMOL BLUE
PHOSPHORUS, SERUM
PHOSPHORUS 3.9 2.5 - 4.9 mg/dL
METHOD : PHOSPHOMOLYBDATE UV FORMATION
Interpretation(s)
LIVER FUNCTION PROFILE, SERUM-
Page 1 Of 2C/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITEDC/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITED

Cert. No. MC-2461
PATIENT NAME : MRS. KIRAN SHARMA
PATIENT ID : FH.10727635
ACCESSION NO : 0013UE004772 AGE : 59 Years SEX : Female DATE OF BIRTH : 23/06/1961
DRAWN : 21/05/2021 09:55 RECEIVED : 21/05/2021 10:38 REPORTED : 21/05/2021 11:53
REFERRING DOCTOR :
CLIENT PATIENT ID : UID:10727635
CLIENT NAME : FLT LT RAJAN DHAL CHARITABLE
TRUST IPD
UID:10727635 REQNO-6398686
IPD-ICU(4)
IPID-63236/21/1301
CLINICAL INFORMATION :
Final Results Biological Reference Interval UnitsTest Report Status
LIVER FUNCTION PROFILE
Bilirubin is a yellowish pigment found in bile and is a breakdown product of normal heme catabolism. Bilirubin is excreted in bile and urine, and elevated levels may give
yellow discoloration in jaundice.Elevated levels results from increased bilirubin production (eg, hemolysis and ineffective erythropoiesis), decreased bilirubin excretion (eg,
obstruction and hepatitis), and abnormal bilirubinmetabolism (eg, hereditary and neonatal jaundice). Conjugated (direct) bilirubin is elevated more than unconjugated
(indirect) bilirubin in Viral hepatitis, Drug reactions, Alcoholic liver disease Conjugated (direct) bilirubin is also elevated more than unconjugated (indirect) bilirubin when
there is some kind of blockage of the bile ducts like in Gallstones getting into the bile ducts, tumors &Scarring of the bile ducts. Increased unconjugated (indirect) bilirubin
may be a result of Hemolytic or pernicious anemia, Transfusion reaction & a common metabolic condition termed Gilbert syndrome, due to low levels of the enzyme that
attaches sugar molecules to bilirubin.
AST is an enzyme found in various parts of the body. AST is found in the liver, heart, skeletal muscle, kidneys, brain, and red blood cells, and it is commonly measured
clinically as a marker for liver health. AST levels increase during chronic viral hepatitis, blockage of the bile duct, cirrhosis of the liver,liver cancer,kidney failure,hemolytic
anemia,pancreatitis,hemochromatosis. AST levels may also increase after a heart attack or strenuous activity.ALT test measures the amount of this enzyme in the blood.ALT
is found mainly in the liver, but also in smaller amounts in the kidneys,heart,muscles, and pancreas.It is commonly measured as a part of a diagnostic evaluation of
hepatocellular injury, to determine liver health.AST levels increase during acute hepatitis,sometimes due to a viral infection,ischemia to the liver,chronic hepatitis,obstruction
of bile ducts,cirrhosis.
ALP is a protein found in almost all body tissues.Tissues with higher amounts of ALP include the liver,bile ducts and bone.Elevated ALP levels are seen in Biliary obstruction,
Osteoblastic bone tumors, osteomalacia, hepatitis, Hyperparathyroidism, Leukemia, Lymphoma, Paget's disease,Rickets,Sarcoidosis etc. Lower-than-normal ALP levels seen
in Hypophosphatasia,Malnutrition,Protein deficiency,Wilson's disease.GGT is an enzyme found in cell membranes of many tissues mainly in the liver,kidney and pancreas.It is
also found in other tissues including intestine,spleen,heart, brain and seminal vesicles.The highest concentration is in the kidney,but the liver is considered the source of
normal enzyme activity.Serum GGT has been widely used as an index of liver dysfunction.Elevated serum GGT activity can be found in diseases of the liver,biliary system and
pancreas.Conditions that increase serum GGT are obstructive liver disease,high alcohol consumption and use of enzyme-inducing drugs etc.Serum total protein,also known as
total protein,is a biochemical test for measuring the total amount of protein in serum.Protein in the plasma is made up of albumin and globulin.Higher-than-normal levels may
be due to:Chronic inflammation or infection,includingHIV and hepatitis B or C,Multiple myeloma,Waldenstrom's disease.Lower-than-normal levels may be due to:
Agammaglobulinemia,Bleeding (hemorrhage),Burns,Glomerulonephritis,Liverdisease, Malabsorption,Malnutrition,Nephrotic syndrome,Protein-losing enteropathy etc.Human
serum albumin is the most abundant protein in human blood plasma.It is produced in the liver.Albumin constitutes about half of the blood serum protein.Low blood albumin
levels (hypoalbuminemia) can be caused by:Liver disease like cirrhosis of the liver, nephrotic syndrome,protein-losing enteropathy,Burns,hemodilution,increased vascular
permeability or decreased lymphatic clearance,malnutrition and wasting etc
CALCIUM, SERUM-
Commom causes of decreased value of calcium (hypocalcemia) are chronic renal failure, hypomagnesemia and hypoalbuminemia.
Hypercalcemia (increased value of calcium) can be caused by increased intestinal absorbtion (vitamin d intoxication), increased skeletal reasorption (immobilization),
or a combination of mechanisms (primary hyperparathyroidism). Primary hyperparathyroidism and malignancy accounts for 90-95% of all cases of hypercalcemia.
Values of total calcium is affected by serum proteins, particularly albumin thus, latter’s value should be taken into account when interpreting serum calcium
levels. The following regression equation may be helpful.
Corrected total calcium (mg/dl)= total calcium (mg/dl) + 0.8 (4- albumin [g/dl])*
because regression equations vary among group of patients in different physiological and pathological conditions, mathematical corrections are only
approximations. The possible mathematical corrections should be replaced by direct determination of free calcium by ISE (available with srl) a common and
important source of preanalytical error in the measurement of calcium is prolonged torniquet application during sampling. Thus, this along with fist clenching
should be avoided before phlebotomy.
MAGNESIUM, SERUM-
Moderate or severe magnesium deficiency is usually due to losses of magnesium from gastrointestinal tract or kidneys as in vomiting and diarrhoea in former
and alcohol, diabetes mellitus (osmotic diuresis), loop diuretics (furosemide) and aminoglycoside antibiotics in latter.
Symptomatic hypermagnesemia is almost always caused by excessive intake with concomitant renal failure, thereby decreasing the ability of the kidneys to
excrete excess magnesium.
Magnesium concentration in erythrocytes are approximately three times those of serum. Conversion factors for the units used to express magnesium
concentration are:
mg/dl= meq/l x 1.22 = mmol/l x 2.43
PHOSPHORUS, SERUM-
**End Of Report**
Please visit www.srlworld.com for related Test Information for this accession
Dr Nitin Kumar Dumeer, M.D.
Senior pathologist,Lab head
Page 2 Of 2C/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITEDC/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITED
Cert. No. MC-2461
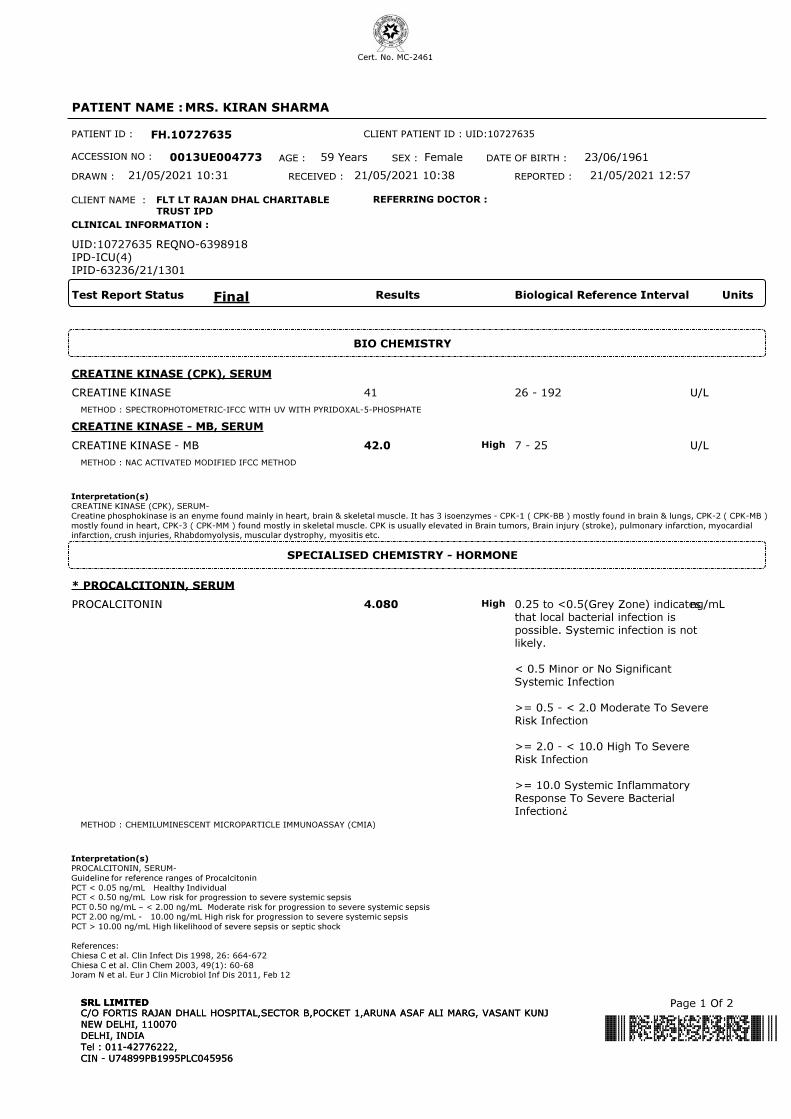
PATIENT NAME : MRS. KIRAN SHARMA
PATIENT ID : FH.10727635
ACCESSION NO : 0013UE004773 AGE : 59 Years SEX : Female DATE OF BIRTH : 23/06/1961
DRAWN : 21/05/2021 10:31 RECEIVED : 21/05/2021 10:38 REPORTED : 21/05/2021 12:57
REFERRING DOCTOR :
CLIENT PATIENT ID : UID:10727635
CLIENT NAME : FLT LT RAJAN DHAL CHARITABLE
TRUST IPD
UID:10727635 REQNO-6398918
IPD-ICU(4)
IPID-63236/21/1301
CLINICAL INFORMATION :
Final Results Biological Reference Interval UnitsTest Report Status
BIO CHEMISTRY
CREATINE KINASE (CPK), SERUM
CREATINE KINASE 41 26 - 192 U/L
METHOD : SPECTROPHOTOMETRIC-IFCC WITH UV WITH PYRIDOXAL-5-PHOSPHATE
CREATINE KINASE - MB, SERUM
CREATINE KINASE - MB 42.0 7 - 25 U/LHigh
METHOD : NAC ACTIVATED MODIFIED IFCC METHOD
Interpretation(s)
CREATINE KINASE (CPK), SERUM-
Creatine phosphokinase is an enyme found mainly in heart, brain & skeletal muscle. It has 3 isoenzymes - CPK-1 ( CPK-BB ) mostly found in brain & lungs, CPK-2 ( CPK-MB )
mostly found in heart, CPK-3 ( CPK-MM ) found mostly in skeletal muscle. CPK is usually elevated in Brain tumors, Brain injury (stroke), pulmonary infarction, myocardial
infarction, crush injuries, Rhabdomyolysis, muscular dystrophy, myositis etc.
SPECIALISED CHEMISTRY - HORMONE
* PROCALCITONIN, SERUM
PROCALCITONIN 4.080 0.25 to <0.5(Grey Zone) indicates
that local bacterial infection is
possible. Systemic infection is not
likely.
< 0.5 Minor or No Significant
Systemic Infection
>= 0.5 - < 2.0 Moderate To Severe
Risk Infection
>= 2.0 - < 10.0 High To Severe
Risk Infection
>= 10.0 Systemic Inflammatory
Response To Severe Bacterial
Infection¿
ng/mLHigh
METHOD : CHEMILUMINESCENT MICROPARTICLE IMMUNOASSAY (CMIA)
Interpretation(s)
PROCALCITONIN, SERUM-
Guideline for reference ranges of Procalcitonin
PCT < 0.05 ng/mL Healthy Individual
PCT < 0.50 ng/mL Low risk for progression to severe systemic sepsis
PCT 0.50 ng/mL – < 2.00 ng/mL Moderate risk for progression to severe systemic sepsis
PCT 2.00 ng/mL - 10.00 ng/mL High risk for progression to severe systemic sepsis
PCT > 10.00 ng/mL High likelihood of severe sepsis or septic shock
References:
Chiesa C et al. Clin Infect Dis 1998, 26: 664-672
Chiesa C et al. Clin Chem 2003, 49(1): 60-68
Joram N et al. Eur J Clin Microbiol Inf Dis 2011, Feb 12
Page 1 Of 2C/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITEDC/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITED

Cert. No. MC-2461
PATIENT NAME : MRS. KIRAN SHARMA
PATIENT ID : FH.10727635
ACCESSION NO : 0013UE004773 AGE : 59 Years SEX : Female DATE OF BIRTH : 23/06/1961
DRAWN : 21/05/2021 10:31 RECEIVED : 21/05/2021 10:38 REPORTED : 21/05/2021 12:57
REFERRING DOCTOR :
CLIENT PATIENT ID : UID:10727635
CLIENT NAME : FLT LT RAJAN DHAL CHARITABLE
TRUST IPD
UID:10727635 REQNO-6398918
IPD-ICU(4)
IPID-63236/21/1301
CLINICAL INFORMATION :
Final Results Biological Reference Interval UnitsTest Report Status
**End Of Report**
Please visit www.srlworld.com for related Test Information for this accession
TEST MARKED WITH '*' ARE OUTSIDE THE NABL ACCREDITED SCOPE OF THE LABORATORY.
Dr Nitin Kumar Dumeer, M.D.
Senior pathologist,Lab head
Page 2 Of 2C/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITEDC/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITED

Cert. No. MC-2461
PATIENT NAME : MRS. KIRAN SHARMA
PATIENT ID : FH.10727635
ACCESSION NO : 0013UE004794 AGE : 59 Years SEX : Female DATE OF BIRTH : 23/06/1961
DRAWN : 21/05/2021 10:35 RECEIVED : 21/05/2021 11:24 REPORTED : 21/05/2021 12:57
REFERRING DOCTOR : SELF
CLIENT PATIENT ID : UID:10727635
CLIENT NAME : FLT LT RAJAN DHAL CHARITABLE
TRUST IPD
UID:10727635 REQNO-6398952
IPD-ICU(4)
IPID-63236/21/1301
CLINICAL INFORMATION :
Final Results Biological Reference Interval UnitsTest Report Status
BIO CHEMISTRY
C-REACTIVE PROTEIN, SERUM
C-REACTIVE PROTEIN 191.2 < 10.0 mg/LHigh
SPECIALISED CHEMISTRY - ANEMIA
FERRITIN, SERUM
FERRITIN 215.2 4.63 - 204.00 ng/mLHigh
METHOD : CHEMILUMINESCENT MICROPARTICLE IMMUNOASSAY (CMIA)
Interpretation(s)
FERRITIN, SERUM-Ferritin is a high-molecular-weight protein that contains approximately 20% iron. It occurs normally in almost all tissues of the body but especially in
hepatocytes and reticuloendothelial cells, where it serves as an iron reserve. When needed, the iron molecules are released from the apoferritin shell and bind to transferrin,
the circulating plasma protein that transports iron to the erythropoietic cells.
A low serum ferritin value is thought to be the best laboratory indicator of iron depletion. Virtually all patients with low serum iron and low ferritin have iron deficiency. Serum
Ferritin concentration, when considered with other factors such as serum iron, iron-binding capacity and tissue iron stores is valuable in the diagnosis of iron deficiency
anemia, anemia of chronic infection and conditions such as thalassemia and hemochromatosis that are associated with iron overload. It is particularly useful in distinguishing
between iron-deficiency anemia (serum ferritin levels diminished) and "anemia of chronic disease" (serum ferritin levels usually normal or elevated).
Ferritin is an acute phase reactant. It can be found to be elevated in the following conditions and do not reflect actual body iron stores: 1.Inflammation 2.Significant tissue
destruction 3.Liver diseases 4.Malignancies such as acute leukemia and Hodgkin's disease 5.Therapy with iron supplements.
Interferences:
Heterophilic antibodies in human serum can react with reagent immunoglobulins, interfering with in vitro immunoassays. Patients routinely exposed to animals or to animal
serum products can be prone to this interference and anomalous values may be observed.
**End Of Report**
Please visit www.srlworld.com for related Test Information for this accession
Dr Nitin Kumar Dumeer, M.D.
Senior pathologist,Lab head
Page 1 Of 1C/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITEDC/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITED

PATIENT NAME : MRS. KIRAN SHARMA
PATIENT ID : FH.10727635
ACCESSION NO : 0013UE004794 AGE : 59 Years SEX : Female DATE OF BIRTH : 23/06/1961
DRAWN : 21/05/2021 10:35 RECEIVED : 21/05/2021 11:24 REPORTED : 21/05/2021 19:20
REFERRING DOCTOR : SELF
CLIENT PATIENT ID : UID:10727635
CLIENT NAME : FLT LT RAJAN DHAL CHARITABLE
TRUST IPD
UID:10727635 REQNO-6398952
IPD-ICU(4)
IPID-63236/21/1301
CLINICAL INFORMATION :
Final Results Biological Reference Interval UnitsTest Report Status
ENDOCRINOLOGY
INTERLEUKIN 6, SERUM
INTERLEUKIN 6 93.20 <3.4 pg/mLHigh
Interpretation(s)
INTERLEUKIN 6, SERUM-
Interleukin-6 (IL-6) is a pleiotropic cytokine with a wide range of functions, IL-6 is produced from a single gene encoding a product of 212 amino acids, which is cleaved at
the N-terminus to produce a 184 amino acid peptide with a molecular weight between 22-27 kDa.
IL-6 production is rapidly induced in the course of acute inflammatory reactions associated with injury, trauma, stress, infection, brain death, neoplasia and other situations.
IL-6 concentrations in trauma patients may predict later complications from additional surgical stress or indicate missed injuries or complications.
Sequential measurements of IL-6 in serum or plasma of patients admitted to the ICU (intensive care unit) showed to be useful in evaluating the severity of SIRS (systemic
inflammatory response syndrome), sepsis and septic shock and to predict the outcome of these patients. IL-6 is also useful as an early alarm marker for the detection of
neonatal sepsis.IL-6 also plays a role in chronic inflammation e.g. rheumatoid arthritis.
**End Of Report**
Please visit www.srlworld.com for related Test Information for this accession
Dr. Shakti Aggarwal
Senior Biochemist
Dr. Anurag Bansal
LAB DIRECTOR
Page 1 Of 1SRL,REFERENCE LAB, GP-26, MARUTI INDUSTRIAL ESTATE,UDYOG VIHAR,SECTOR-18,
GURGAON, 122015
HARYANA, INDIA
Tel : 9111591115, CIN - U74899PB1995PLC045956
Email : [email protected]
SRL LIMITEDSRL,REFERENCE LAB, GP-26, MARUTI INDUSTRIAL ESTATE,UDYOG VIHAR,SECTOR-18,
GURGAON, 122015
HARYANA, INDIA
Tel : 9111591115, CIN - U74899PB1995PLC045956
Email : [email protected]
SRL LIMITED

PATIENT NAME : MRS. KIRAN SHARMA
PATIENT ID : FH.10727635
ACCESSION NO : 0013UE004855 AGE : 59 Years SEX : Female DATE OF BIRTH : 23/06/1961
DRAWN : 21/05/2021 16:14 RECEIVED : 21/05/2021 16:29 REPORTED : 22/05/2021 06:01
REFERRING DOCTOR : SELF
CLIENT PATIENT ID : UID:10727635
CLIENT NAME : FLT LT RAJAN DHAL CHARITABLE
TRUST IPD
ICMR Registration No: SRLRL001
UID:10727635 REQNO-6401536
IPD-ICU(4)
IPID-63236/21/1301
CLINICAL INFORMATION :
Final Results Biological Reference Interval UnitsTest Report Status
MOLECULAR BIOLOGY
SARS COV -2 REAL TIME PCR
SARS-COV-2 RNA NEGATIVE
Interpretation(s)
SARS COV -2 REAL TIME PCR-
SARS-CoV-2, formerly known as 2019-nCoV, is the causative agent of the coronavirus disease 2019 (COVID-19). Main symptoms of the disease include fever, cough and
shortness of breath. The virus is spread via person-to-person contact through respiratory droplets produced when a person coughs or sneezes. The SARS-CoV-2 RNA is
generally detectable in nasopharyngeal/oropharyngeal swabs during the acute phase of infection. Positive results are indicative of active infection. Real Time PCR assay
targets specific genes and can be used for diagnosis of SARS-CoV-2 virus infection which contributes to severe upper respiratory distress and complications.
Positive result indicates that RNA from SARS-CoV-2 was detected in the specimen, and the patient is considered infected with the virus and presumed to be contagious.
Negative test result for this test means that SARS-CoV-2 RNA was not detected in the specimen above the limit of detection of the assay.
Limitations:
• Negative results do not preclude COVID-19 and should not be used as the sole basis for patient management decisions. Negative results must be combined with clinical
observations, patient history, and epidemiological information.
• Positive results do not rule out bacterial infection or co-infection with other viruses.
• Optimum specimen types and timing for peak viral levels during infections caused by 2019-nCoV have not been determined. Collection of multiple specimens (types and
time points) from the same patient may be necessary to detect the virus.
• Follow-up testing may particularly be important if patient has a clinical picture of viral pneumonia, a potential exposure history, and/or radiographic findings (chest CT or
MRI scan) consistent with COVID -19 pneumonia. However repeat testing in the near-term after clearance (within 90 days) should be avoided as prolonged shedding of
non-viable virus is not uncommon
• Ct values generated from different assay systems within the same laboratory, or from different laboratories, are not directly comparable and do not necessarily reflect the
same viral load due to inter-assay and inter-laboratory variability.
• Variation in timing of sample collection, fluctuations in virus shedding, and difference between detection limit of different testing methods within same or different labs could
lead to variation in results particularly during initial phase of infection.
• If the virus mutates in the rRT-PCR target region, 2019-nCoV may not be detected or may be detected less predictably. Inhibitors or other types of interference may
produce a false negative result.
• The performance of this test has not been established for monitoring treatment of 2019-nCoV infection.
Note: Test is performed using ICMR approved Kit.
References:
1. Laboratory testing for coronavirus disease 2019 (COVID-19) in suspected human cases. Interim guidance. World Health Organization.
2. Druce et al. JCM. 2011
3. N. Engl. J. Med. 2020, 382, 929–936
**End Of Report**
Please visit www.srlworld.com for related Test Information for this accession
Dr. Anurag Bansal
LAB DIRECTOR
Dr. Rashmi Talwar, PhD
Section Head- Genetics
Dr. Yoginder Pal Singh, Ph.D
Molecular Biologist
Page 1 Of 1SRL,REFERENCE LAB, GP-26, MARUTI INDUSTRIAL ESTATE,UDYOG VIHAR,SECTOR-18,
GURGAON, 122015
HARYANA, INDIA
Tel : 9111591115, CIN - U74899PB1995PLC045956
Email : [email protected]
SRL LIMITEDSRL,REFERENCE LAB, GP-26, MARUTI INDUSTRIAL ESTATE,UDYOG VIHAR,SECTOR-18,
GURGAON, 122015
HARYANA, INDIA
Tel : 9111591115, CIN - U74899PB1995PLC045956
Email : [email protected]
SRL LIMITED

Cert. No. MC-2461
PATIENT NAME : MRS. KIRAN SHARMA
PATIENT ID : FH.10727635
ACCESSION NO : 0013UE004941 AGE : 59 Years SEX : Female DATE OF BIRTH : 23/06/1961
DRAWN : 22/05/2021 05:12 RECEIVED : 22/05/2021 05:12 REPORTED : 22/05/2021 08:26
REFERRING DOCTOR :
CLIENT PATIENT ID : UID:10727635
CLIENT NAME : FLT LT RAJAN DHAL CHARITABLE
TRUST IPD
UID:10727635 REQNO-6406271
IPD-ICU(4)
IPID-63236/21/1301
CLINICAL INFORMATION :
Final Results Biological Reference Interval UnitsTest Report Status
KIDNEY PANEL - 1
SERUM BLOOD UREA NITROGEN
BLOOD UREA NITROGEN 17 6 - 20 mg/dL
METHOD : UREASE -GLDH
CREATININE EGFR- EPI
CREATININE 0.67 0.60 - 1.10 mg/dL
METHOD : MODIFIED JAFFE KINETIC
AGE 59 years
METHOD : MANUAL
GLOMERULAR FILTRATION RATE (FEMALE) 96.21 Refer Interpretation Below mL/min/1.73m2
METHOD : CALCULATED PARAMETER
BUN/CREAT RATIO
BUN/CREAT RATIO 25.37 5.00 - 15.00High
METHOD : CALCULATED PARAMETER
URIC ACID, SERUM
URIC ACID 3.6 2.6 - 6.0 mg/dL
METHOD : URICASE/ PAP
TOTAL PROTEIN, SERUM
TOTAL PROTEIN 5.1 6.4 - 8.2 g/dLLow
METHOD : BIURET
Comments
NOTE :- KINDLY CORRELATE CLINICALLY.
ALBUMIN, SERUM
ALBUMIN 1.9 3.4 - 5.0 g/dLLow
METHOD : BROMOCRESOL PURPLE
GLOBULIN
GLOBULIN 3.2 2.0 - 4.1 g/dL
METHOD : CALCULATED PARAMETER
ELECTROLYTES (NA/K/CL), SERUM
SODIUM 140 136 - 145 mmol/L
METHOD : ION SELECTIVE ELECTRODE TECHNOLOGY INDIRECT
POTASSIUM 4.20 3.50 - 5.10 mmol/L
METHOD : ION SELECTIVE ELECTRODE TECHNOLOGY INDIRECT
CHLORIDE 104 98 - 107 mmol/L
METHOD : ION SELECTIVE ELECTRODE TECHNOLOGY INDIRECT
URINALYSIS
COLOR PALE YELLOW
METHOD : MANUAL
Page 1 Of 5C/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITEDC/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITED

Cert. No. MC-2461
PATIENT NAME : MRS. KIRAN SHARMA
PATIENT ID : FH.10727635
ACCESSION NO : 0013UE004941 AGE : 59 Years SEX : Female DATE OF BIRTH : 23/06/1961
DRAWN : 22/05/2021 05:12 RECEIVED : 22/05/2021 05:12 REPORTED : 22/05/2021 08:26
REFERRING DOCTOR :
CLIENT PATIENT ID : UID:10727635
CLIENT NAME : FLT LT RAJAN DHAL CHARITABLE
TRUST IPD
UID:10727635 REQNO-6406271
IPD-ICU(4)
IPID-63236/21/1301
CLINICAL INFORMATION :
Final Results Biological Reference Interval UnitsTest Report Status
APPEARANCE HAZY
METHOD : MANUAL
PH 5.5 4.7 - 7.5
METHOD : DIPSTICK
SPECIFIC GRAVITY 1.030 1.003 - 1.035
METHOD : DIPSTICK
GLUCOSE DETECTED (+++) NOT DETECTED
METHOD : DIPSTICK / MANUAL
PROTEIN DETECTED (+) NOT DETECTED
METHOD : DIPSTICK / MANUAL
KETONES DETECTED (TRACE) NOT DETECTED
METHOD : DIPSTICK / MANUAL
BLOOD DETECTED (+) IN
URINE
NOT DETECTED
METHOD : DIPSTICK
BILIRUBIN NOT DETECTED NOT DETECTED
METHOD : DIPSTICK / MANUAL
UROBILINOGEN NORMAL NORMAL
METHOD : DIPSTICK / MANUAL
NITRITE NOT DETECTED NOT DETECTED
METHOD : DIPSTICK
WBC 8-10 0-5 /HPF
METHOD : MICROSCOPIC EXAMINATION
EPITHELIAL CELLS 2-3 0-5 /HPF
METHOD : MICROSCOPIC EXAMINATION
RED BLOOD CELLS 3 - 5 NOT DETECTED /HPF
METHOD : MICROSCOPIC EXAMINATION
CASTS GRANULAR CAST SEEN.
METHOD : MICROSCOPIC EXAMINATION
CRYSTALS NOT DETECTED
METHOD : MICROSCOPIC EXAMINATION
Comments
NOTE :- MICROSCOPIC EXAMINATION OF URINE IS PERFORMED BY CENTRIFUGED URINARY SEDIMENT.
NOTE :- KETONE IN URINE IN ABSENCE OF GLYCOSURIA MAY BE FOUND IN CASES OF
FEVER, VOMITING, DEHYDRATION ETC.
Interpretation(s)
SERUM BLOOD UREA NITROGEN-
Causes of Increased levels
Pre renal
• High protein diet, Increased protein catabolism, GI haemorrhage, Cortisol, Dehydration, CHF Renal
• Renal Failure
Page 2 Of 5C/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITED
C/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITED

Cert. No. MC-2461
PATIENT NAME : MRS. KIRAN SHARMA
PATIENT ID : FH.10727635
ACCESSION NO : 0013UE004941 AGE : 59 Years SEX : Female DATE OF BIRTH : 23/06/1961
DRAWN : 22/05/2021 05:12 RECEIVED : 22/05/2021 05:12 REPORTED : 22/05/2021 08:26
REFERRING DOCTOR :
CLIENT PATIENT ID : UID:10727635
CLIENT NAME : FLT LT RAJAN DHAL CHARITABLE
TRUST IPD
UID:10727635 REQNO-6406271
IPD-ICU(4)
IPID-63236/21/1301
CLINICAL INFORMATION :
Final Results Biological Reference IntervalTest Report Status
Post Renal
• Malignancy, Nephrolithiasis, Prostatism
Causes of decreased levels
• Liver disease
• SIADH.
CREATININE EGFR- EPI-
GFR— Glomerular filtration rate (GFR) is a measure of the function of the kidneys. The GFR is a calculation based on a serum creatinine test. Creatinine is a muscle waste
product that is filtered from the blood by the kidneys and excreted into urine at a relatively steady rate. When kidney function decreases, less creatinine is excreted and
concentrations increase in the blood. With the creatinine test, a reasonable estimate of the actual GFR can be determined.
A GFR of 60 or higher is in the normal range.
A GFR below 60 may mean kidney disease.
A GFR of 15 or lower may mean kidney failure.
Estimated GFR (eGFR) is the preferred method for identifying people with chronic kidney disease (CKD). In adults, eGFR calculated using the Modification of Diet in Renal
Disease (MDRD) Study equation provides a more clinically useful measure of kidney function than serum creatinine alone.
The CKD-EPI creatinine equation is based on the same four variables as the MDRD Study equation, but uses a 2-slope spline to model the relationship between estimated GFR
and serum creatinine, and a different relationship for age, sex and race. The equation was reported to perform better and with less bias than the MDRD Study equation,
especially in patients with higher GFR. This results in reduced misclassification of CKD.
The CKD-EPI creatinine equation has not been validated in children & will only be reported for patients = 18 years of age. For pediatric and childrens, Schwartz Pediatric
Bedside eGFR (2009) formulae is used. This revised "bedside" pediatric eGFR requires only serum creatinine and height.
URIC ACID, SERUM-
Causes of Increased levels
Dietary
• High Protein Intake.
• Prolonged Fasting,
• Rapid weight loss.
Gout
Lesch nyhan syndrome.
Type 2 DM.
Metabolic syndrome.
Causes of decreased levels
• Low Zinc Intake
• OCP’s
• Multiple Sclerosis
Nutritional tips to manage increased Uric acid levels
• Drink plenty of fluids
• Limit animal proteins
• High Fibre foods
• Vit C Intake
• Antioxidant rich foods
TOTAL PROTEIN, SERUM-
Serum total protein,also known as total protein, is a biochemical test for measuring the total amount of protein in serum..Protein in the plasma is made up of albumin and
globulin
Higher-than-normal levels may be due to: Chronic inflammation or infection, including HIV and hepatitis B or C, Multiple myeloma, Waldenstrom's disease
Lower-than-normal levels may be due to: Agammaglobulinemia, Bleeding (hemorrhage),Burns,Glomerulonephritis, Liver disease, Malabsorption, Malnutrition, Nephrotic
syndrome,Protein-losing enteropathy etc.
ALBUMIN, SERUM-
Human serum albumin is the most abundant protein in human blood plasma. It is produced in the liver. Albumin constitutes about half of the blood serum protein. Low blood
albumin levels (hypoalbuminemia) can be caused by: Liver disease like cirrhosis of the liver, nephrotic syndrome, protein-losing enteropathy, Burns, hemodilution, increased
vascular permeability or decreased lymphatic clearance,malnutrition and wasting etc.
ELECTROLYTES (NA/K/CL), SERUM-
Sodium levels are Increased in dehydration, cushing's syndrome, aldosteronism & decreased in Addison's disease, hypopituitarism,liver disease. Hypokalemia (low K) is
common in vomiting, diarrhea, alcoholism, folic acid deficiency and primary aldosteronism. Hyperkalemia may be seen in end-stage renal failure, hemolysis, trauma,
Addison's disease, metabolic acidosis, acute starvation, dehydration, and with rapid K infusion.Chloride is increased in dehydration, renal tubular acidosis (hyperchloremia
metabolic acidosis), acute renal failure, metabolic acidosis associated with prolonged diarrhea and loss of sodium bicarbonate, diabetes insipidus, adrenocortical hyperfuction,
salicylate intoxication and with excessive infusion of isotonic saline or extremely high dietary intake of salt.Chloride is decreased in overhydration, chronic respiratory acidosis,
salt-losing nephritis, metabolic alkalosis, congestive heart failure, Addisonian crisis, certain types of metabolic acidosis, persistent gastric secretion and prolonged vomiting,
URINALYSIS-Routine urine analysis assists in screening and diagnosis of various metabolic, urological, kidney and liver disorders
Protein: Elevated proteins can be an early sign of kidney disease. Urinary protein excretion can also be temporarily elevated by strenuous exercise, orthostatic proteinuria,
dehydration, urinary tract infections and acute illness with fever
Glucose: Uncontrolled diabetes mellitus can lead to presence of glucose in urine. Other causes include pregnancy, hormonal disturbances, liver disease and certain
medications.
Ketones: Uncontrolled diabetes mellitus can lead to presence of ketones in urine. Ketones can also be seen in starvation, frequent vomiting, pregnancy and strenuous
exercise.
Blood: Occult blood can occur in urine as intact erythrocytes or haemoglobin, which can occur in various urological, nephrological and bleeding disorders.
Page 3 Of 5C/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITED
C/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITED

Cert. No. MC-2461
PATIENT NAME : MRS. KIRAN SHARMA
PATIENT ID : FH.10727635
ACCESSION NO : 0013UE004941 AGE : 59 Years SEX : Female DATE OF BIRTH : 23/06/1961
DRAWN : 22/05/2021 05:12 RECEIVED : 22/05/2021 05:12 REPORTED : 22/05/2021 08:26
REFERRING DOCTOR :
CLIENT PATIENT ID : UID:10727635
CLIENT NAME : FLT LT RAJAN DHAL CHARITABLE
TRUST IPD
UID:10727635 REQNO-6406271
IPD-ICU(4)
IPID-63236/21/1301
CLINICAL INFORMATION :
Final Results Biological Reference IntervalTest Report Status
Leukocytes: An increase in leukocytes is an indication of inflammation in urinary tract or kidneys. Most common cause is bacterial urinary tract infection.
Nitrite: Many bacteria give positive results when their number is high. Nitrite concentration during infection increases with length of time the urine specimen is retained in
bladder prior to collection.
pH: The kidneys play an important role in maintaining acid base balance of the body. Conditions of the body producing acidosis/ alkalosis or ingestion of certain type of food
can affect the pH of urine.
Specific gravity: Specific gravity gives an indication of how concentrated the urine is. Increased specific gravity is seen in conditions like dehydration, glycosuria and
proteinuria while decreased specific gravity is seen in excessive fluid intake, renal failure and diabetes insipidus.
Bilirubin: In certain liver diseases such as biliary obstruction or hepatitis, bilirubin gets excreted in urine.
Urobilinogen: Positive results are seen in liver diseases like hepatitis and cirrhosis and in cases of hemolytic anemia
HAEMATOLOGY
COMPLETE BLOOD COUNT, EDTA WHOLE
BLOOD/SMEAR
BLOOD COUNTS
HEMOGLOBIN 10.5 12.0 - 15.0 g/dLLow
METHOD : PHOTOMETRIC
RED BLOOD CELL COUNT 4.05 3.8 - 4.8 mil/µL
METHOD : ELECTRICAL IMPEDANCE
WHITE BLOOD CELL COUNT 11.09 4.0 - 10.0 thou/µLHigh
METHOD : ELECTRICAL IMPEDANCE
PLATELET COUNT 155 150 - 410 thou/µL
METHOD : ELECTRICAL IMPEDANCE
RBC AND PLATELET INDICES
HEMATOCRIT 32.55 36 - 46 %Low
METHOD : MEASURED
MEAN CORPUSCULAR VOL 80.5 83.0 - 101.0 fLLow
METHOD : MEASURED
MEAN CORPUSCULAR HGB. 25.9 27.0 - 32.0 pgLow
METHOD : CALCULATED PARAMETER
MEAN CORPUSCULAR HEMOGLOBIN
CONCENTRATION
32.2 31.5 - 34.5 g/dL
METHOD : CALCULATED PARAMETER
RED CELL DISTRIBUTION WIDTH 17.7 11.6 - 14.0 %High
METHOD : CALCULATED PARAMETER
MEAN PLATELET VOLUME 11.2 6.8 - 10.9 fLHigh
METHOD : CALCULATED PARAMETER
WBC DIFFERENTIAL COUNT - NLR
SEGMENTED NEUTROPHILS 92 40 - 80 %High
METHOD : VCS TECHNOLOGY/ MICROSCOPY
ABSOLUTE NEUTROPHIL COUNT 10.20 2.0 - 7.0 thou/µLHigh
METHOD : CALCULATED PARAMETER
LYMPHOCYTES 4 20 - 40 %Low
METHOD : VCS TECHNOLOGY/ MICROSCOPY
Page 4 Of 5C/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITEDC/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITED

Cert. No. MC-2461
PATIENT NAME : MRS. KIRAN SHARMA
PATIENT ID : FH.10727635
ACCESSION NO : 0013UE004941 AGE : 59 Years SEX : Female DATE OF BIRTH : 23/06/1961
DRAWN : 22/05/2021 05:12 RECEIVED : 22/05/2021 05:12 REPORTED : 22/05/2021 08:26
REFERRING DOCTOR :
CLIENT PATIENT ID : UID:10727635
CLIENT NAME : FLT LT RAJAN DHAL CHARITABLE
TRUST IPD
UID:10727635 REQNO-6406271
IPD-ICU(4)
IPID-63236/21/1301
CLINICAL INFORMATION :
Final Results Biological Reference IntervalTest Report Status
ABSOLUTE LYMPHOCYTE COUNT 0.44 1.0 - 3.0 thou/µLLow
METHOD : CALCULATED PARAMETER
NEUTROPHIL LYMPHOCYTE RATIO (NLR) 23.2
EOSINOPHILS 1 1 - 6 %
METHOD : VCS TECHNOLOGY/ MICROSCOPY
ABSOLUTE EOSINOPHIL COUNT 0.11 0.02 - 0.50 thou/µL
METHOD : CALCULATED PARAMETER
MONOCYTES 3 2 - 10 %
METHOD : VCS TECHNOLOGY/ MICROSCOPY
ABSOLUTE MONOCYTE COUNT 0.33 0.2 - 1.0 thou/µL
METHOD : CALCULATED PARAMETER
BASOPHILS 0 < 1 - 2 %
ABSOLUTE BASOPHIL COUNT 0.00 0.02 - 0.10 thou/µLLow
METHOD : CALCULATED PARAMETER
DIFFERENTIAL COUNT PERFORMED ON: EDTA SMEAR
METHOD : AUTOMATED ANALYZER / MICROSCOPY
DISCLAIMER: THE ABSOLUTE WHITE CELL COUNTS ARE OUTSIDE THE NABL ACCREDITED SCOPE OF THE LABORATORY.
Interpretation(s)
BLOOD COUNTS-
The cell morphology is well preserved for 24hrs. However after 24-48 hrs a progressive increase in MCV and HCT is observed leading to a decrease in MCHC. A direct smear is
recommended for an accurate differential count and for examination of RBC morphology.
RBC AND PLATELET INDICES-
The cell morphology is well preserved for 24hrs. However after 24-48 hrs a progressive increase in MCV and HCT is observed leading to a decrease in MCHC. A direct smear is
recommended for an accurate differential count and for examination of RBC morphology.
WBC DIFFERENTIAL COUNT - NLR-
The optimal threshold of 3.3 for NLR showed a prognostic possibility of clinical symptoms to change from mild to severe in COVID positive patients. When age = 49.5 years
old and NLR = 3.3, 46.1% COVID-19 patients with mild disease might become severe. By contrast, when age < 49.5 years old and NLR < 3.3, COVID-19 patients tend to
show mild disease.
(Reference to - The diagnostic and predictive role of NLR, d-NLR and PLR in COVID-19 patients ; A.-P. Yang, et al.; International Immunopharmacology 84 (2020) 106504
This ratio element is a calculated parameter and out of NABL scope.
**End Of Report**
Please visit www.srlworld.com for related Test Information for this accession
Dr. Rahul Bhardwaj,MD.
Pathologist
Dr Nitin Kumar Dumeer, M.D.
Senior pathologist,Lab head
Page 5 Of 5C/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITEDC/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITED

Cert. No. MC-2461
PATIENT NAME : MRS. KIRAN SHARMA
PATIENT ID : FH.10727635
ACCESSION NO : 0013UE005176 AGE : 59 Years SEX : Female DATE OF BIRTH : 23/06/1961
DRAWN : 23/05/2021 02:34 RECEIVED : 23/05/2021 05:25 REPORTED : 23/05/2021 07:34
REFERRING DOCTOR :
CLIENT PATIENT ID : UID:10727635
CLIENT NAME : FLT LT RAJAN DHAL CHARITABLE
TRUST IPD
UID:10727635 REQNO-6414176
IPD-ICU(2)
IPID-63236/21/1301
CLINICAL INFORMATION :
Final Results Biological Reference Interval UnitsTest Report Status
HAEMATOLOGY
COMPLETE BLOOD COUNT, EDTA WHOLE
BLOOD/SMEAR
BLOOD COUNTS
HEMOGLOBIN 10.0 12.0 - 15.0 g/dLLow
METHOD : PHOTOMETRIC
RED BLOOD CELL COUNT 3.84 3.8 - 4.8 mil/µL
METHOD : ELECTRICAL IMPEDANCE
WHITE BLOOD CELL COUNT 6.47 4.0 - 10.0 thou/µL
METHOD : ELECTRICAL IMPEDANCE
PLATELET COUNT 150 150 - 410 thou/µL
METHOD : ELECTRICAL IMPEDANCE
Comments
GIANT PLATELETS SEEN.
RBC AND PLATELET INDICES
HEMATOCRIT 30.61 36 - 46 %Low
METHOD : MEASURED
MEAN CORPUSCULAR VOL 79.8 83.0 - 101.0 fLLow
METHOD : MEASURED
MEAN CORPUSCULAR HGB. 25.9 27.0 - 32.0 pgLow
METHOD : CALCULATED PARAMETER
MEAN CORPUSCULAR HEMOGLOBIN
CONCENTRATION
32.5 31.5 - 34.5 g/dL
METHOD : CALCULATED PARAMETER
RED CELL DISTRIBUTION WIDTH 17.1 11.6 - 14.0 %High
METHOD : CALCULATED PARAMETER
MEAN PLATELET VOLUME 11.4 6.8 - 10.9 fLHigh
METHOD : CALCULATED PARAMETER
WBC DIFFERENTIAL COUNT - NLR
SEGMENTED NEUTROPHILS 88 40 - 80 %High
METHOD : VCS TECHNOLOGY/ MICROSCOPY
ABSOLUTE NEUTROPHIL COUNT 5.69 2.0 - 7.0 thou/µL
METHOD : CALCULATED PARAMETER
LYMPHOCYTES 8 20 - 40 %Low
METHOD : VCS TECHNOLOGY/ MICROSCOPY
ABSOLUTE LYMPHOCYTE COUNT 0.52 1.0 - 3.0 thou/µLLow
METHOD : CALCULATED PARAMETER
NEUTROPHIL LYMPHOCYTE RATIO (NLR) 10.9
Page 1 Of 3C/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITEDC/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITED
Cert. No. MC-2461
PATIENT NAME : MRS. KIRAN SHARMA
PATIENT ID : FH.10727635
ACCESSION NO : 0013UE005176 AGE : 59 Years SEX : Female DATE OF BIRTH : 23/06/1961
DRAWN : 23/05/2021 02:34 RECEIVED : 23/05/2021 05:25 REPORTED : 23/05/2021 07:34
REFERRING DOCTOR :
CLIENT PATIENT ID : UID:10727635
CLIENT NAME : FLT LT RAJAN DHAL CHARITABLE
TRUST IPD
UID:10727635 REQNO-6414176
IPD-ICU(2)
IPID-63236/21/1301
CLINICAL INFORMATION :
Final Results Biological Reference Interval UnitsTest Report Status
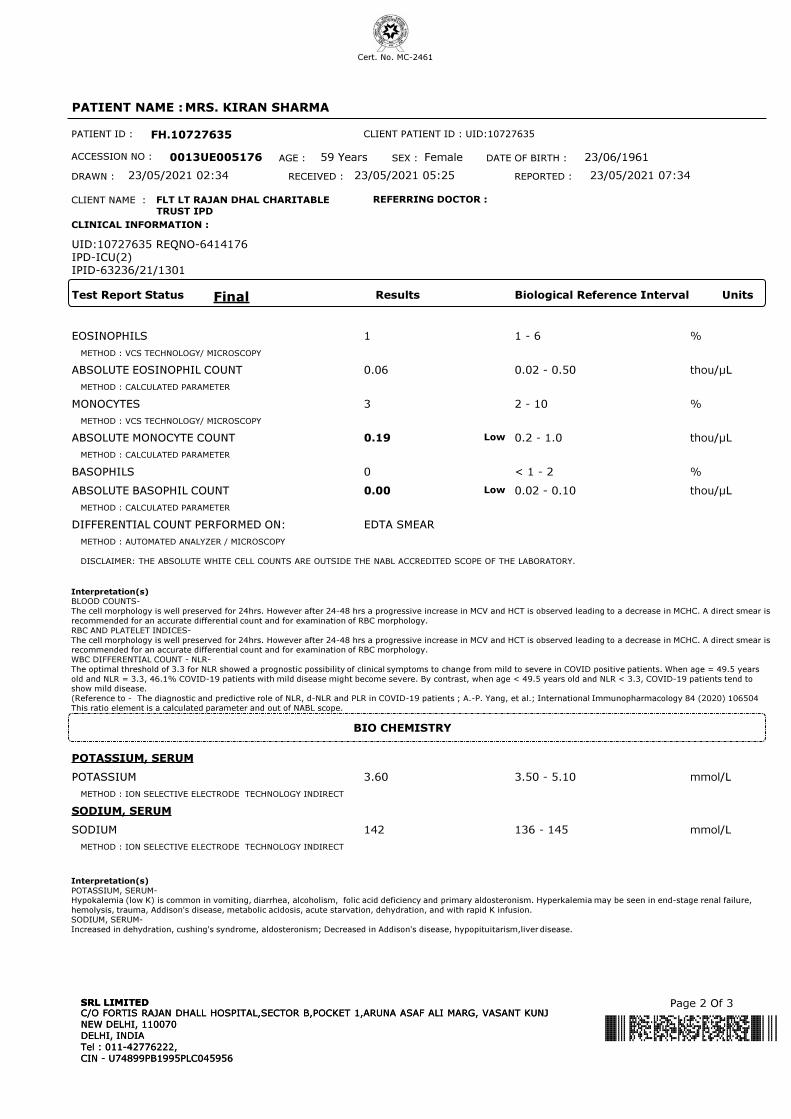
EOSINOPHILS 1 1 - 6 %
METHOD : VCS TECHNOLOGY/ MICROSCOPY
ABSOLUTE EOSINOPHIL COUNT 0.06 0.02 - 0.50 thou/µL
METHOD : CALCULATED PARAMETER
MONOCYTES 3 2 - 10 %
METHOD : VCS TECHNOLOGY/ MICROSCOPY
ABSOLUTE MONOCYTE COUNT 0.19 0.2 - 1.0 thou/µLLow
METHOD : CALCULATED PARAMETER
BASOPHILS 0 < 1 - 2 %
ABSOLUTE BASOPHIL COUNT 0.00 0.02 - 0.10 thou/µLLow
METHOD : CALCULATED PARAMETER
DIFFERENTIAL COUNT PERFORMED ON: EDTA SMEAR
METHOD : AUTOMATED ANALYZER / MICROSCOPY
DISCLAIMER: THE ABSOLUTE WHITE CELL COUNTS ARE OUTSIDE THE NABL ACCREDITED SCOPE OF THE LABORATORY.
Interpretation(s)
BLOOD COUNTS-
The cell morphology is well preserved for 24hrs. However after 24-48 hrs a progressive increase in MCV and HCT is observed leading to a decrease in MCHC. A direct smear is
recommended for an accurate differential count and for examination of RBC morphology.
RBC AND PLATELET INDICES-
The cell morphology is well preserved for 24hrs. However after 24-48 hrs a progressive increase in MCV and HCT is observed leading to a decrease in MCHC. A direct smear is
recommended for an accurate differential count and for examination of RBC morphology.
WBC DIFFERENTIAL COUNT - NLR-
The optimal threshold of 3.3 for NLR showed a prognostic possibility of clinical symptoms to change from mild to severe in COVID positive patients. When age = 49.5 years
old and NLR = 3.3, 46.1% COVID-19 patients with mild disease might become severe. By contrast, when age < 49.5 years old and NLR < 3.3, COVID-19 patients tend to
show mild disease.
(Reference to - The diagnostic and predictive role of NLR, d-NLR and PLR in COVID-19 patients ; A.-P. Yang, et al.; International Immunopharmacology 84 (2020) 106504
This ratio element is a calculated parameter and out of NABL scope.
BIO CHEMISTRY
POTASSIUM, SERUM
POTASSIUM 3.60 3.50 - 5.10 mmol/L
METHOD : ION SELECTIVE ELECTRODE TECHNOLOGY INDIRECT
SODIUM, SERUM
SODIUM 142 136 - 145 mmol/L
METHOD : ION SELECTIVE ELECTRODE TECHNOLOGY INDIRECT
Interpretation(s)
POTASSIUM, SERUM-
Hypokalemia (low K) is common in vomiting, diarrhea, alcoholism, folic acid deficiency and primary aldosteronism. Hyperkalemia may be seen in end-stage renal failure,
hemolysis, trauma, Addison's disease, metabolic acidosis, acute starvation, dehydration, and with rapid K infusion.
SODIUM, SERUM-
Increased in dehydration, cushing's syndrome, aldosteronism; Decreased in Addison's disease, hypopituitarism,liver disease.
Page 2 Of 3C/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITED
C/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITED

Cert. No. MC-2461
PATIENT NAME : MRS. KIRAN SHARMA
PATIENT ID : FH.10727635
ACCESSION NO : 0013UE005176 AGE : 59 Years SEX : Female DATE OF BIRTH : 23/06/1961
DRAWN : 23/05/2021 02:34 RECEIVED : 23/05/2021 05:25 REPORTED : 23/05/2021 07:34
REFERRING DOCTOR :
CLIENT PATIENT ID : UID:10727635
CLIENT NAME : FLT LT RAJAN DHAL CHARITABLE
TRUST IPD
UID:10727635 REQNO-6414176
IPD-ICU(2)
IPID-63236/21/1301
CLINICAL INFORMATION :
Final Results Biological Reference Interval UnitsTest Report Status
**End Of Report**
Please visit www.srlworld.com for related Test Information for this accession
Dr Nitin Kumar Dumeer, M.D.
Senior pathologist,Lab head
Page 3 Of 3C/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITEDC/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITED

Cert. No. MC-2461
PATIENT NAME : MRS. KIRAN SHARMA
PATIENT ID : FH.10727635
ACCESSION NO : 0013UE005268 AGE : 59 Years SEX : Female DATE OF BIRTH : 23/06/1961
DRAWN : 23/05/2021 14:45 RECEIVED : 23/05/2021 15:13 REPORTED : 23/05/2021 16:13
REFERRING DOCTOR :
CLIENT PATIENT ID : UID:10727635
CLIENT NAME : FLT LT RAJAN DHAL CHARITABLE
TRUST IPD
UID:10727635 REQNO-6417320
IPD-ICU(2)
IPID-63236/21/1301
CLINICAL INFORMATION :
Final Results Biological Reference Interval UnitsTest Report Status
MICRO BIOLOGY
GRAM STAIN
SPECIMEN SOURCE BRONCHOALVEOLAR LAVAGE (MINI)
METHOD : MICROSCOPIC EXAMINATION
GRAM STAIN SMEAR SHOWS FEW PUS CELLS, NO MICRO-ORGANISMS SEEN.
METHOD : MICROSCOPIC EXAMINATION
**End Of Report**
Please visit www.srlworld.com for related Test Information for this accession
Dr.Rahul Behl,M.D.
Microbiologist
Page 1 Of 1C/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITEDC/O FORTIS RAJAN DHALL HOSPITAL,SECTOR B,POCKET 1,ARUNA ASAF ALI MARG, VASANT KUNJ
NEW DELHI, 110070
DELHI, INDIA
Tel : 011-42776222,
CIN - U74899PB1995PLC045956
SRL LIMITED




















