Doctor Who Classics / Doctor Who 2005 - renouveau et continuité
Upload
khangminh22Category
view
5download
0
WHOChestRadiographyinEpidemiologicalStudies
PartB–StudyGuidelines
Contents
IntroductionObjectives1. Personnel2. Infrastructure
2.1 Climate2.2 DepartmentRooms2.3 ConsumableStorage2.4 PowerSupply
3. EquipmentSpecifications3.1 X-rayequipment3.2 Imageprocessors3.3 Equipmentprocurement,installationandservicing
4. Identification&imagelabeling4.1 Patientidentification4.2 Imageannotations
5. ChestX-rayimagingrecommendations5.1 Patientpositioning5.2 Technicalfactors5.3 Otherrequirements5.4 Thefinalimage
6. Imagearchivingandviewingrecommendations6.1 Imagestorage6.2 Digitizingimages6.3 Imagetransportationforstudypurposes6.4 Imageviewingforstudypurposes
AcknowledgementsGlossaryReferences

IntroductionInpediatricradiographicexaminations,radiationdoseisofparticularconcern.Pediatricpatientsarerelativelymoreradiosensitivethanadultpatients(1-4).Thisisduetothecombinationofthehigherradiationsensitivityofthedevelopingorgansandthelongerlifeexpectancy,givingalongertimeframeforanyradiation-inducedcancertobeexpressed(5-7).TheaverageeffectivedoseforachestX-rayona5-year-oldpatienthasbeenquotedas0.02milli-Sieverts(mSv),whichisequivalenttoapproximatelythreedaysofnaturalbackgroundradiation(8).Furthermore,aqualitativepresentationofcancerincidenceriskforachestX-rayforpatientsat1-yearand5-yearsofagedemonstratesthattheriskisnegligible(8).ThisdataisconsideredaworldwideaverageanddespitethislowradiationdoseproducedforpediatricchestX-rays,thewidespreaduseofmedicalradiationisincreasing,particularlyinchildren.Therefore,monitoringofradiationdosestopatientsisstillpertinenttoensurethatdosesaremaintainedatacceptablelevels.Thiscanbeachievedthroughthecomparisonoflocaldosestodosereferencelevels(DRL),whichwillbediscussedindetailinPartC–QualityControl.Diagnosticimagingchallengesarisefromtheneedforimagingtobeconductedbyqualifiedand/orexperiencedpersonnelinadditiontotheuseofequipmentthathasbeenproperlyinstalledandwellmaintained.Significantchallengesarepresentwhenprovidingdiagnosticimagingtochildren,particularlyindevelopingandremotecountrieswherethereisvariableaccesstodiagnosticimaging.Forexample,inmostSub-SaharanAfricancountries,accesstoimagingfacilitiesisseverelylimited,withaclearmajorityofimagingservicesbeingavailableinurbanareas.Additionally,radiationprotectionmeasuresarerarelyenforced,sparepartsforbreakdownsareoftenrareorunaffordable,electricitysupplycanbeerraticandimagequalitysubstandard(9).Intheacquisitionofradiographsofanybodypartofanypatient,theapplicationofradiationtothepatientmustbeoptimized.Optimizationofradiationinvolvesadjustingimagingequipmentparametersandimplementingprotectivemeasuresforpatients,staffandvisitorstoensurethatthelowestradiationdoseisutilizedtoachievethedesireddiagnosticoutcome(10).Therecommendationsincludedintheseguidelinesarecomponentsthataredeemedpertinenttoachievehighqualitypediatricchestradiographs.Additionally,acountry’sradiationprotectionandsafetyinfrastructurecouldbestrengthenedbyon-goingneedsassessment,practicestandarddevelopment,policyimplementation,trainingsupportandsystemevaluation(9).Whilsttheseguidelinesareintendedforuseacrossallhealthcarefacilities,regardlessoftheirresourcelimitations,therecommendationsaretheminimumrequiredtoensurethathighqualityimagescanbeachievedforthepurposesofepidemiologicalstudies.Theaspirationhereisforhighqualityimages,yetimagesthatareconsidered‘readable’canstillbeacceptableasthereadableimagecouldbecriticaltopatientcareandsurvivalinmanysettings.Itisexpectedthatsitesinvolvedinthesestudieswillmeettheminimumstandardswithrespecttothespecificationsoutlinedintheseguidelinestoensurethatthedesiredimagesareachievable.Allsiteswillneedtobeevaluatedtodeterminetheiradherencetothespecificationsandtheleveloftechnicalsupportrequiredtomeetthestandards.Examplesofsupportmayincludeon-siteassistanceofserviceengineersforequipmentmaintenanceor
upgradeandanelectricalevaluationofthesite,aswellastrainingofstaff,provisionofsoftwareanddevelopmentoflocalprotocolsforx-raytechniques.ObjectivesTheobjectiveoftheseguidelinesistoestablisharesourceforresearchers,studystaffandcollaboratingradiologydepartments,outliningmajorissuesfacedinobtaininghighqualitypediatricchestX-rayswithafocusonremoteandunder-resourcedregions.Experiencefrompreviousstudiessuggestthatearlycollaborationbetweenradiologydepartmentsandresearchstaffwillassistinmaximizingthequalityofchestradiographs.TheseguidelinesaimtoinformthedevelopmentofprotocolsforachievingqualitychestX-raysinstudiesinvolvingchildrenaged0-59months.Theclinicalsetting,projectgoalsandneedsoftheresearcherswillvarybetweenstudies,hencetheintentofthisdocumentistoproviderecommendationsflexibletoindividualcircumstances.Eachstudywillneedtotailorthenumberanddetailofprotocolsorstandardoperatingproceduresaccordingtothescopeandcomplexityoftheproject.TheseguidelinesreviewthemajorfactorscontributingtoaqualitypediatricchestX-raywithanemphasisonissuesthataremostimportantand/oreasilyadjustedbytheresearchteam.Therecommendationsareinkeepingwithacceptedradiologicalprinciplesofjustification,optimizationandlimitation(10).Theyhavebeendevelopedfrombestpracticetechniquesaccordingtocurrentliterature,inadditiontointernationalregulationsfromtheWorldHealthOrganization(WHO),theInternationalCommissionforRadiologicalProtection(ICRP),theInternationalAtomicEnergyAgency(IAEA)andtheEuropeanCommission.MinimumrequiredstandardsareidentifiedtoensureboththatfacilitieswithresourcelimitationscanprovidequalitychestX-raysforstudypurposes,andthatthereisconsistencybetweenfacilitiesinmulti-sitestudies.Theseguidelinesdonotnecessarilyaffectasite’sexistingstandardsandprotocols,noraretheyintendedforclinicaluse.However,theirusemaybebeneficialforwiderpatientcare.Theprimaryapplicationoftheseguidelinesistooptimizechestradiographsasadiagnostictoolinepidemiologicalstudies.Asummaryoftheguidelineswithrecommendedrequirements,measuresoftherequirementsandtherationalecanbefoundinappendix1.

1.Personnel“Adequatetraininginradiationsafetyisaprerequisiteforallstaffworkinginthemedicalimagingservice.Whererecognizednationalstandardsforradiationsafetytrainingexist,thesemustbeappliedbythemedicalimagingservice.”(11)Thesignificanceofadequatetraininginchestradiography,particularlyinchildren,isimportanttoensurethathighqualityimagesareacquiredunderthesafestconditions.Additionally,theseimagesshouldbeobtainedwithminimaldistresstothepatientandparentsorcarers.Thisismorelikelytobeachievedifthoseeitheracquiringtheimagesorsupervisingthoseacquiringtheimageshavesignificantexperience(forexample,aminimumof5-years)and/oraqualificationofatleasta6-monthcertificateinradiography.Whilstthisisrecommended,thesearenotalwaysfeasiblemandatoryoptionsanditisrecognizedthattherequiredqualificationsvarygreatlyfromcountrytocountry.Eachfacilitywillthereforeneedtoconsidertheirownconstraintswhenidentifyingappropriatestaff.Thecompetenciesoffacilitystaff,alongwithotherqualityissuescanbeevaluatedusingthesampleimagesthataresenttoexperiencedradiologistsandradiographersalongwiththeassessmentsurvey(PartA).Iffacilitystaffhaveverylittleexperienceorunderstandingoftechnicalinformation,researchersshouldconsiderbudgetingforexternaladviceandtechnicalassistance.Thoseacquiringtheimages,aswellasanyotherpersonnelworkingintheX-rayexaminationroomonadailybasisareencouragedtowearradiation-monitoringbadges,forexampleThermo-luminescentdosimeters(TLD)orBerylliumOxideOpticallyStimulatedLuminescence(OSL)meters.Themonitoringbadgesarerecommendedtobeissuedandassessedbyanapprovedregulatorybodyeverythreemonths,withassessmentdatafeedbackgiventothesite,aswellasanynecessaryactionresultingfromthedata.
2.InfrastructureItisdesirablethatthelayoutandspecificationsofthedepartmentconformtonationalorinternationalregulations,whilstmaintainingcomfortforthepatient.Thiswillensurethattheradiographicexaminationscanbeconductedinamannerthatissafeandefficient,aswellasallowforthefullcapabilitiesoftheequipment.ThefollowingdepartmentspecificationsaretheminimumrequiredforthepurposesoftheseguidelinesinkeepingwiththesafeconductofchestX-rayexaminationsonchildren.2.1ClimateIndoorclimatecontrolandgoodventilation,suchaswiththeuseofairconditioners,arerequiredifindoortemperaturesbelow15degrees,above28degreesand/orahumidityofgreaterthan80%isexpected.Thiswillalsoassistintheprotectionofthesolid-statecircuitsusedforX-rayproductionandwillensurethatreliableimagequalityismaintained(11).2.2DepartmentroomsItisexpectedthatadepartmentconsistofaminimumofthreerooms(12):
• X-rayexaminationroom• Darkroomforprocessing(ifX-rayfilmprocessingisrequired)• Viewingroom(orofficewhereviewingofimagescanoccur)
2.2.1X-rayexaminationroomTherequirementsofthesizeoftheX-rayexaminationroomneedtoallowappropriateaccessforallpatients,includingthosetravellingtothedepartmentonahospitalbed.Additionally,theroomsizemustallowfortherequiredfocal-filmdistance(seesection5.2technicalfactors).ItisrecognizedthatX-rayequipmentwillvarybetweenfacilitiesduetothenumberofmanufacturersonthemarket.Theminimumroomsizewillthereforebelargelydependentonthespecificationsoftheequipment.Itisrecommendedthatthefullcapabilitiesoftheequipmentareassessedpriortostudycommencementtoensuretherequiredimagescanbeacquired.ToallowforappropriatemovementofanX-rayunit,thefloorsshouldbecompletelylevel.Thebestmaterialtoachievethisisleveledconcrete,whichiscoveredbywoodorpolyvinylchloride(PVC).(12)Windowsintheexaminationroomareacceptable,butonlyiftheyarepositionedsothatnobodyoutsideoftheroomcanbeexposedtoradiationorlookintheroom.Toensureappropriateradiationprotectiontothoseoutsideoftheexaminationroom,theWorldHealthOrganizationgenerallyrecommendsthatthewallsneedtobeconstructedofconcreteorsolidbrick(12).However,roomdesignrequirementsaregenerallynotprescriptive,rathertherequirementtomeetdoselimitsforradiationworkersandfacilityvisitorsaretobekeptwithininternationallimits,suchasthoseoutlinedbytheInternationalCommissionforRadiologicalProtection(ICRP)(12).Themethodtoachievethisrequirementisatthediscretionofthefacilityandcanbeachievedinanumberofways,suchaswarninglights,leadshieldingorphysicalrestrictiontotheexaminationroom.Additionally,chestX-raysonchildrenisconsideredalowradiationworkload,therebyreducingtheneedforstringentrestrictionsonroomconstruction.Withintheexaminationroom,ifthereareanywallsandscreensseparatingtheoperatorfromtheX-raysourcetheyshouldallowforacontinual,unobstructedviewofthepatienttoensurethatthepatientisinthecorrectpositionatthepointofimageacquisition.(12)
Allexaminationroomsshouldhaveoxygensupply,aswellassuctionforusewithpatientswhererequired.Additionally,toreducetheriskofinfection,theseroomsshouldprovideappropriateprotectiveclothingforallstaffmembers,includingwhererelevant,masks,glovesandgowns(12).2.2.2DarkroomWhenusingfilm,inordertoachievehighqualityimagestheprocessingofthefilmsarejustasimportantastheimageacquisition.Itisthereforeimperativethatthesizeandconditionsofthedarkroomareappropriateforadequatefilmprocessing.ThefollowingdarkroomrecommendationsarebaseduponthosebytheWorldHealthOrganization’squalitysystemsformedicalimagingandtheconsumerguideforthepurchaseofX-rayequipment(11,12):
• Darkroomsshould:o Beentirelylightprooffromoutsidelight,includingtheentryareao Haveanavailable60Wincandescentwhitelight.Fluorescentlightwillhave
anafterglowandmayfogthefilmo Haveasafelightforfilmprocessingconditionswithamaximumof15Wand
colouredfilter,withthecolourdependingonthetypeoffilmused.Thisshouldalsobeatleast120cmabovethebench-top
o Beproperlyventilated,withatleast15air-changesperhourallowingairtobedrawninfromoutsideandhaveanadequateextractionfanthatfunctionswheneverthedarkroomisinuse
o Allowforadequatespacefortheprocessorandconsumables,aswellasforachievingtherequiredwork.Thisis6squaremetres,withaminimumdimensionof2metresifthedarkroomservesoneX-rayexaminationroom,but,8squaremetresifthedepartmentemploysadarkroomattendant.Theceilingheightshouldnotbelessthan3metres
o Haveaslopingfloortowardsadraininggutterincaseofachemicalspillo Haveanairexchangethatconformstolocalandnationalstandardsand
providingfreshairwherepossible.2.2.3Viewingroom/officeAdequateworkingspaceforadministrativeandimage-viewingdutieswithalightboxorcomputerisaminimumof10squaremetres.Thisspacewillneedtobemuchlargerifitisalsobeingusedforfilmstorage.TheentrancetotheofficeshouldneverbethroughtheX-rayexaminationroomasthisisnotsafepractice.(12)
2.3ConsumableStorageStorageofconsumableitems,suchasunexposedfilmorunusedchemicalsrequireasignificantamountofspace,aswellasappropriateclimatecontroltoavoiddamage(11).Thefollowingarerecommendationsonstorageofunexposedfilm,unusedchemicalsandimagingcassettes:
• StorageshouldneverbeintheX-rayexaminationroomastheyareeasilydamagedinthisenvironment.
• Areasofthedepartment,suchastheviewingroom,officeordarkroomaresuitableforstorage,providedthereisadequatespacethatwillnotposeanoccupationaltrippinghazard
• Filmboxesmustbestoredasperthemanufacturerinstructions,aswellasuprightandawayfromheat,humidityandradiation.
• Imagingcassettesshouldalwaysbestoreduprighttoavoiddustsettlingonthefilm.• Onceexposedtoair,chemicalsshouldbeplacedintheappropriatesectionofthe
filmprocessorimmediatelytoavoidoxidation.Chemicalhandlingshouldbeasperthemanufacturerguidelines,ensuringthattheydonotcomeintocontactwiththeskinoreyes,andarenotinhaledoringested.Inthecaseofaccidentalchemicalsplashintotheeyes,thereshouldbeemergencyeyewashkitsineachfacility.Storageofchemicalsshouldensurethattheyareinawell-ventilatedroom,awayfromanyfilmstorage.Thestorageshouldalsoincludearotationsystemtoensurethatchemicalsdonotreachtheirexpirydate.2.4PowersupplyTherequiredpowersupplytoanX-raydepartmentlargelydependsonboththetypeofequipmentandthenumberofitemsofelectricalequipmentusedtoefficientlyrunthedepartment.Asageneralrequirement,itisexpectedthatwherepossible,thepowersupplyisconstantandreliablefortheX-rayunitsthatitissupplyingandhaveasufficientback-upsupply(forexample,anACgenerator).AstandardX-raysystemneedsasymmetrical3-phasemainswithgroundingsupply.Amulti-peakgeneratorwithenergystorageinbatteriescanusea230V,10A‘household’walloutletandstilleasilyhandletherequired30kWforchestX-rays.Thisisalsonoproblemforageneratorwithenergystorageinacapacitor(see‘equipmentspecifications’below)(12).IfthelocalmainssupplysystemdiffersfromthepermittedmainssupplysystemsforaspecificX-raysystem,atransformerforconversionwillbeneeded.Itmustbenotedherethatthesevaluesareforadultchestradiographs.Thepowerrequirementsforchildrenarethatthegeneratorisatleast80kWtoallowforshorterexposuretimesaschildrenmaybeunabletokeepstillorholdtheirbreathfortheX-ray.Iftheelectricalmainssupplyissuspectedtobeunstableorofteninterrupted,itisrecommendedthatanUninterruptiblePowerSupply(UPS)beinstalled.TheUPSisonlyusedtopowertheX-raygeneratorandassociatedimageacquisitionequipmentandwillswitchovertotheback-upsupplyautomaticallyintheeventofapoweroutage.ThemainsimpedanceistheapparentelectricalresistanceofthepowerlineandmustbelessthanorequaltothespecificationoftheX-raygeneratormainsresistance.DespitewhichX-raygeneratorisused,theimpedanceofthesupplymainsshouldbenolargerthan3ohms(Ω).However,withenergystorageintheX-raygenerator,theimpedancevalueisnotcritical(12)Ordinarylighting,darkroomlight,lightboxesandfilmmarkingequipmentwillrequireanadditional2-3kWinpower.Furthermore,anautomaticprocessorneedsaseparate,verystablemainssupplyfor3-4kW.Therefore,forelectricalsafety,allstandardelectricalwalloutletsinthedepartmentsshouldfollowlocalregulationsandshallbefor230Vand10A,mustbedouble,groundedandsuitablyprotected(12).

3.EquipmentspecificationsTheequipmentusedintheacquisitionofchestradiographsonchildrenmustadheretoaminimumstandardandcomplywithanynationalregulationsofthecountryofpracticetoensureasafe,yethighqualityimageacquisitionprocess.Thefollowingspecificationsaretheminimumrequiredtobeabletoparticipatesafelyandefficientlyinanepidemiologicalstudy.Itisexpectedthatthepersonsoperatingeachofthesepiecesofequipmenthavebeentrainedintheirdailyuseandinbasicmaintenanceandthatthemainx-rayunitusedforacquiringimagesforthepurposesofastudyisastationaryunit(12).
3.1 X-rayEquipmentTheremaybeoccasionswheretheX-rayunitorimageprocessormalfunctionsandisunabletobeusedforaperiodoftime,whichmayaffectthecollectionofdataforthestudy.Inthesecircumstancesitisexpectedthatforasitetobeincludedinastudy,equipmentrepairmustbeabletobecarriedoutwithin24-hoursofthemalfunction.Ifthisisnotpossible,analternativesourcemustbeavailabletobeused.FortheX-rayunit,thisalternativemaybeamobileX-rayunitorback-upX-rayunit.
3.1.1 GeneratorMainrequirement:A12-pulseorhighfrequencymulti-phase(alsoknownasa‘converter’)generator.Modernsystemsrequirea3-phase80kWgeneratortoallowforthelowexposuretimesrequiredforpediatricchestX-rays.Rationale:
• Enablesshortexposuretimes,whicharerequiredinpediatricimagingtoallowforacquisitionduringnormalrespirationandavoidmotionartefact.
• Allowsforhighvoltages,whichreducespatientskinentrancedose.(13)Othergeneratorrequirements:
• Tubevoltagerangeof50-120kVwithavariationconsistencyoflessthan5%(13)
• AdjustablemAssettings,withaminimumpossiblevalueoflessthanorequalto0.5mAs(13)
• SeparatedisplayofmAandtime,withtheshortestexposuretimeat1ms.(13)
• Poweroutputofastationaryormobilegeneratorshouldbegreaterthanorequalto50kWforappropriateefficiency
• Stationarygenerator(12)o Integratedenergysourceo Multi-peakinvertertechnologyo Abilitytooperatefroma‘household’mainssupplyof230Vand
10A,orfromafuel-poweredACgenerator.• Mobilegenerator(12)
o Energystorage,forexamplealead/acidbattery(notNi-cad)orlargecapacitor
o Multi-peakinvertertechnology
NotethatthepowerrequirementsfortheX-raygeneratorislargelydependentonthetypeofgenerator.Differentgeneratorswillhavedifferentpowerrequirementsandtheabilitytomeettheserequirementsshouldbeconfirmedwiththemanufactureruponpurchaseofequipmentoracceptanceofdonatedequipment.
3.1.2 StationaryX-raysystem
ThestationaryX-raysystemisonethatisusedinafixedlocationwithinabuilding.ItisanX-rayfilmbasedsystemthatuseseitheranalogue,analogue-to-digitalordigitaltechniquesforimagecaptureanddisplay.Thesystemconsistsofmodularconfigurationsthatcanbeupgradedbytheadditionofhardwareorsoftwarecomponentsoraccessories.(14)Toensureeasyandsafeacquisitionofimages,theminimumrequirements,basedontheWHOEquipmentSpecifications(14)are:
• Useahorizontal,angulatedorverticalX-raybeamtoenableimagingofthepediatricchestinboththesupineanderectposition(12)
• Separatecontrolconsoleandgeneratorallowingforasafedistanceand/orshieldingfromtheoperatorandthepatient
• DigitaldisplayofmAs,kVandelectronictimerontheconsole• AkVrangeofatleast50kVto120kV,digitallydisplayed• AmArangeofatleast25mAto600mA,digitallydisplayed• Anexposuretimeofatleast1ms• X-raytubepowerratingofatleast50kW• X-raytubewitharotatinganodeandnominalfocalspotsizelessthan
1mm(mostmodernsystemscomewithfocalspotsizesof0.6mmand1.2mm)
• Anyanti-scattergridswithintheimagereceptorholdermustbeabletoberemovedortheunitsmusthaveimagereceptorholderstoenableimagereceptorstobeplacedinfrontofthegrids
• Heatstoragecapacityoftheanodeatleast300kilo-heatunits(kHU)• Visualandaudibleexposureindicatorsontheconsole• Emergencystopcontrolsintheeventofequipmentmalfunction• Adjustablemulti-leafcollimatorsforfieldsizealterationthatare
rotatable90-degreesinbothdirectionswithaworkingpatientcenteringlightorlightbeamdiaphragm(LBD)
• Concealedcablesonthepatienttable• Source-to-imagedistancerangeofatleast90cm-125cm• FullycounterbalancedX-raytubeheadforsafeandeasymovement• TheX-raytubemustbeabletorotatedindependentlyoftheimage
receptoranditsholders• Dose-area-product(DAP)meterinstalledwherepossibletomeasureand
displaytheDAPdoseandoptionally,theDAPrateanddoserateIftheX-raysystemisadigitalsystem,thefollowingspecificationsapply(14):
• MinimumJointPhotographicsExpertGroup(JPEG)compatibleimagestorageandtransfer
• Alphanumericannotationsofimages
• Imagedisplaytobecontrastandbrightnessadjustable,withadiagonalscreensizeofatleast18inches
• Theimagestobedisplayedimmediatelyafterexposure• Thesystemtobecapableofstoringatleast3000imageswithcapacityfor
removablestorage3.1.3 MobileX-raysystemThemobileX-raysystemisonethatisusedinavarietyoflocationswithinabuilding.Itisanassemblyofdevicesthatcompriseeitheranalogue,analogue-to-digitalordigitaltechniquesforimagecaptureanddisplay.Thesystemcanoperatebybatteryandbedrivenorpushedbyanoperatortovariouslocations.(14)IfamobileX-rayunitistobeusedasatemporaryreplacementintheeventofastationaryX-raysystemmalfunction,theminimumrequirements,basedontheWHOEquipmentSpecifications(14)are:
• Useahorizontal,angulatedorverticalX-raybeamtoenableimagingofthepediatricchestinboththesupineanderectposition(12)
• AkVrangeofatleast50kVto120kV,digitallydisplayed• AmArangeofatleast0.5mAsto200mAs,digitallydisplayed• Anexposuretimerangeofleast1msto5s• X-raytuberatingofatleast50kW• X-raytubewitharotatinganodeandnominalfocalspotsizelessthan1mm• Heatstoragecapacityoftheanodeofatleast300kHU• Adjustablemulti-leafcollimators,rotatable90-degreesinbothdirectionswitha
workingpatientcenteringlightorlightbeamdiaphragm(LBD)• Aworking‘low-battery’indicator• Exposuresmadebyremotecontrol,withtheswitchonacordatleast3metres
long• X-raytubestandfullycounterbalancedforrotationinalldirections• Anarticulatedarmforimagingpatientsinanyposition• Concealedcablesinthearmsystem• Animagereceptorstoragefacility• Motorbatteryofthesealedlead-acidtype,whichcanberechargedbythemain
unitpowerconnection• Afitted,resettableovercurrentbreakeronbothliveandneutralsupplylines• Avoltagecorrector/stabilizerallowingoperationat±30%ofthelocalrelated
voltage• Capabilityofbeingstoredcontinuouslyinanambienttemperatureof0-40
degreesandrelativehumidityof15-90%,andoperatingcontinuouslyinambienttemperatureof10-30degreesandrelativehumidityof15-90%
3.2 ImageProcessorsTheWHOManualofDiagnosticImagingstatesthatimageprocessingisasimportantasimageacquisitiontoobtainthebestimagequality(15).Intheprocessingofimages,thepreferenceisforsitestoemployacomputedradiography(CR)ordigitalradiography(DR)system,duetotheoverallcostsavings,archivingabilitiesandpostprocessingmanipulationofimages.However,theimplementationofthesesystemscanbedifficult,particularlyinremoteareaswithrespecttothehighinitialcostandongoingtechnicalsupport.Consequently,theminimumprocessingrequirementsoutlinedintheseguidelinesisfortheuseofautomaticfilm(i.e.analogue)processors,whethertheyaredarkroomprocessorsordaylightprocessors.Manualdarkroomprocessingisanoldtechniquethatrequiresmoreprecisionandattentionfromdarkroomtechnicians,particularlyinsuboptimalconditions,suchashighroomtemperatureandpoorventilation(15).Imagequalityisalsomuchmorevariableanditishighlyrecommendedthatstudiesdonotusethistechnique.Theminimumrequirementsintheseguidelinesthereforeareformanualdarkroomprocessingnottobeincluded.ThefollowingspecificationsaretakenfromtheWHOEquipmentSpecifications(14)toensurethattheprocessingofimagesismaintainedatoptimumlevels:3.2.1 DarkroomAutomaticProcessor
ThedarkroomautomaticprocessorisadeviceinwhichX-rayfilmmustbemanuallyremovedfromacassetteandloadedintotheprocessorinadarkroomsetting.Theprocessorthenautomaticallytransportsthefilmthroughthedeveloping,fixing,washinganddryingstagesalongaseriesofrollers.Italsoalertstheusertothecurrentprocessstage,timetocompletionandremainingamountofreagents(14).Theminimumspecificationsforthedarkroomautomaticprocessor,basedontheWHOEquipmentSpecifications(14)are:
• Allowingforatleast100filmsofmaximumsizetobeprocessedperhour• Automaticfilmtransferandcontrolprocesses• Volumeofthestoreddeveloper,fixerandwashertobeatleast4litres
each• Allowanceofsilverreclamationfromthechemicalsused• Displaysandalertsforchemicaltemperatureandamountsremaining• Sufficientdraincapacityforcontinuousoperationatmaximumload• Automaticfilmdetectiondevice• Standbymodewhennotinuse• Thetotalweightofprocessorwithchemicalsin-situshouldbenotgreater
than250kg• Regulateddriertemperature• Adjustablewaterconsumption• Capableofbeingstoredcontinuouslyinanambienttemperatureof0-40
degreesCelsiusandrelativehumidityof15-90%,andoperatingcontinuouslyinanambienttemperatureof10-40degreesCelsiusandrelativehumidityof15-90%
• Mountedeitheronatable-toporwithafloor-mountedstand

• Aconnectiontobothahotandcoldexternalrunningwatersupplywiththeprecisewaterrequirementsaspermanufacturerrecommendationsandwatershut-offvalvessupplied.Waterconsumptionnottobegreaterthan5litresperminuteandpassedthroughafiltertoeliminateanyimpurities
• Resettablecircuitbreakersinbothliveandneutralsupplylinesforelectricalprotection
• Powermainssupplyof3-4kW
3.2.2 DaylightAutomaticProcessor
Thedaylightautomaticprocessorworksjustasadarkroomautomaticprocessor,howeverwillautomaticallyunloadX-rayfilmfromcassettesdirectlyintotheautomaticfilmprocessorportionofthesystemandreloadfreshX-rayfilmbackintothecassette(14).Thisprocessorthereforehasthesamespecificationsasdescribedforthedarkroomautomaticprocessor,withtheexceptionofthecassetteloadingandunloadingrequirements.
3.2.3 ComputedRadiographyProcessor
Unlikemanyfilm-basedsystems,CRsystemsdonotrequiretheuseofadarkroom.CRimagingplatesareknownasphosphorplatescreateanimagebyexcitingtheelectronsintheplateintoahigherenergystatewhenexposedtoX-rays,formingalatentimage.ThisisthenreadintheCRreaderwithalaserspot,wheretheelectronsabsorbthelaserenergyandemitlightastheyreturntotheirgroundstate.Thislightiscollectedbyalightguideandsenttoaphotomultipliertube,whichproducesananaloguesignalthatisconvertedtoadigitalsignal.Theplateisthenexposedtoanerasinglight,removingtheresidualradiation.Insomecases,itispossibletousethestandardfilmcassetteswithCRphosphorplates.Therearevariationsinthemethodsdescribedabovedependingonthetypeofreaderandmanufacturer.However,thefollowingminimumspecificationsforaCRsystemisrequired:
• ApanelforindicatingonlinestatusoftheCRreaderincaseofmachinemalfunction
• Thespatialresolutionofthedigitalimageis6pixels/mmormore• Theimagesizeshouldbe12-bitsorhigher• Specificpediatricalgorithmsthatareweightdependentshouldbe
establishedandbeappliedtoallpediatricchestimages.• Theabilityforpost-processingofimages,suchasannotationsandgrey
scaleoptimizations,priortoimagesbeingsentforreading.• Theabilityforsingleexposurestohavemultiplepost-processingapplied
totherawdatacreatingmultipleimagesthatcanbearchivedorfilmed• Theabilitytore-processanarchivedimagewithanewalgorithmand
thenarchivethenewimage• Recordpatientidentificationdatadirectlyontotheimage• Retrieveandreproducehighqualityimagesfromstoreddatawithoutthe
lossofimagequality
• Harddiskcapacitylargeenoughtobeabletostoreimagescommensuratewiththeworkload
• Abilitytosendimagestoanexternalsource(e.g.PACS/USB)and/orprintontohardcopy
• Powerinputtobe220-240Vat50Hzandfittedwithaplugcommensuratewithfacility’selectricaloutlets.Thereisalsotobearesettableovercurrentbreakerfittedforprotection
• Theresolutionofthephosphorscreensshouldbeintheorderof1576x1976pixelsfora24x30cmcassetteor1770x2370pixelsfora18x24cmcassette
3.2.4 DigitalRadiographySystems
DRsystemsgenerallydonotuseaphysicalmediumforwhichanimageisstored,rathersendingtheimagetoacomputerscreendirectlyafterexposure.AnothersignificantadvantageofDRoverCRisthatsimilarimagequalitycharacteristicscanbeobtainedatupto60%lowerradiationdoses.Inadditiontotheexposuresettings,theappearanceofthefinalimagedisplayedonthescreenisdependentuponthealgorithmsthathavebeenestablishedandapplied.ThefollowingspecificationsaretheminimumrequiredforaDRsystem:
• Specificpediatricalgorithmsthatareweightdependentshouldbeestablishedandbeappliedtoallpediatricchestimages.
• Theabilityforpost-processingofimages,suchasannotationsandgreyscaleoptimizations,priortoimagesbeingsentforreading.
• Theabilityforsingleexposurestohavemultiplepost-processingappliedtotherawdatacreatingmultipleimagesthatcanbearchivedorfilmed
• Theabilitytore-processanarchivedimagewithanewalgorithmandthenarchivethenewimage
• Harddiskcapacitylargeenoughtobeabletostoreimagescommensuratewiththeworkload
• Abilitytosendimagestoanexternalsource(e.g.PACS/USB)
Theimagingspecificationsfordigitalradiographyvarywidelyacrossdifferentmanufacturers.ItisthereforedifficulttoproviderecommendationsontheminimumdetectorandX-rayrequirementswhenusingdigitalradiography.However,asanexample,inapaediatricsetting,thefollowingrelevantdigitaldetectorandX-rayrequirementswouldbesufficient:• HighDoseQuantumEfficiency(DQE)CesiumIodidedetectors.Thisenables
improvedimagequalitywithlowerdoses.• Paediatricimageoptimizationsoftware• DetectorMatrixminimum
o For35x43cmdetectors–2520x3032pixelmatrixo For25x30cmdetectors–1752x2130pixelmatrixo 14bitbit-depthforacquisition,12-bitforstorageo Pixelsizeof125micrometres
Forthedisplaymonitors,thefollowingspecificationsarerecommended:
• Resolutiono 1280x1024pixels
• Visualcontrast
o 1000:1• Brightness
o 220cd/m2Asaseparaterequirementforallportabledigitaldetectors,a“highshocktolerance”isrecommendedtoavoiddamageifthedetectorisaccidentallydropped.Foranyfixeddigitalimagereceptor,thefieldsizeshouldensurethattheentirechestcanbeimagedinoneradiograph.Additionally,calibrationofthedetectorsshouldbeperformedbytheserviceengineeratthetimeofthescheduledequipmentmaintenance.
3.3.Equipmentprocurement,installationandservicing
Regularmaintenanceofequipmentisessentialtoensureaconsistentqualityofimaging.EquipmentmaintenanceprocessesthatcanbecompletedbysitepersonnelwillbediscussedindetailinPartC-QualityControl.However,itisexpectedthatforasitetoparticipateinastudy,well-trainedandqualifiedpersonnelwillservicethefollowingequipmentatleastyearly:
• X-rayunitandgenerator• UninterruptedPowerSupply(ifapplicable)• Filmprocessor• CRreader• DRimagingreceptors
Itispreferablefortheservicingpersonneltobefromthesamemanufacturerasthespecificpieceofequipment.However,thisisnotalwayspossibleandanappropriateengineer(eitherfromthesite’scountryoforiginorinternational)deemedsuitablebytheresearcherscanbeaviablealternative.Maintenanceandrepairofequipmentisfurthercomplicatedwhereequipmentisdonated.Donatingequipmentmaynotnecessarilyhavethedesiredeffectofimprovingcare(16).Forexample,almost50%ofalldonatedx-rayequipmentinthedevelopingworldisoutofserviceduetopoorinfrastructureormissingequipment(17).Furthermore,fordigitalX-rayequipment,requiredinformationtechnologyinfrastructure,suchasinternetaccesscanoftenbeoverlooked.Donationofthisequipmentshouldonlybeconsideredwhenaservicecontractfromamanufacturer’srepresentativeispurchasedalongwiththedonation.However,thecontractcostsmayexceedthatofthepurchaseofusedequipment(16).Thefollowingpointsshouldbeconsideredinthedecisiontoacceptequipmentdonations(16);
• Itisrarefordonatedequipmenttoconformtothepowersupplyrequirementsofthetargetcountryandshouldthereforebeconsideredinthepreparationofequipment
• Theequipmentshouldconformwithgovernmentpoliciesandadministrativearrangementsofthetargetcountry
• Forthequalityoftheequipmenttobeacceptableinthetargetcountry,itshouldbeacceptableinthedonorcountry
• Thereshouldbeeffectivecommunicationbetweenthedonorandrecipient.Furthermore,alldonationsshouldbemadeaccordingtoaplanagreedtobyboththedonorandrecipient.
Inthecaseswherenewequipmentisrequiredtobepurchased,considerationshouldbegiventothefollowing(inadditiontothespecificationsoutlinedabove):
• Theimagingsystemmustbeeasytouseandmaintain.Filmbasedsystemsincurlargeongoingcostsduetoconsumablesandstorage.Adigitalsystemisthereforepreferable(18)
• Digitaldevicesthataredesignedtooptimizepediatricimaging,includingtheabilitytosegregatealgorithmsintospecificpatientsizesubgroups.Usingadultsettingsinapediatricenvironmentmayunnecessarilyresultinincreasedpatientradiationdoseorpoorimagequality.
• Imagingsystemsmustbeabletoelectronicallytransferimages.JPEGorAudioVideoInterleaved(AVI)canbeused,buttheimageidentificationwouldeitherhavetobetransferredasaseparatefileorbeimbeddedwithintheimage.Additionally,aphysicalmeansofimagetransport,suchasEthernet,aUSBorWi-fiisrequired(18).
• ImplementationoftheexposureindicatorstandardbytheInternationalElectrotechnicalCommission(IEC)62494-1(19)
Whetherequipmentispurchasedordonated,allequipmentistobeinstalledbythesupplier,whoshouldalsoperformsafetyandoperationchecksbeforehandingovertothedepartment(14).Afterinstallation,appropriateinspectionshouldoccurtoensuremechanicalandelectricalsafetyaswellasproperradiationlimits(14,20).Thesupplierisalsoresponsibleforprovidingtechnicaltrainingtousersintheoperationandbasicmaintenanceoftheequipment.Alistofequipmentandproceduresrequiredforlocalcalibrationandroutinemaintenanceoftheequipment,aswellasuserandtechnicalmaintenancemanualsshallbeprovided.Thesemanualsshouldalsobeprovidedinalanguageunderstoodbytheuser(14,16).Fullrecordsofallservicing,maintenanceandanyrepairsorreplacementpartsshouldbemaintainedforeachitemofequipment(10).Theperiodofmanufacturerwarranty,ifany,shouldalsobeevidentintheservicerecords.Contactdetailsofthemanufacturerandsupplier,aswellasanylocalserviceagentsaretobeprovidedtothedepartment(14).
Furthermore,tobeincludedinastudy,sitesshouldideallyhaveservicedtheirequipmentwithin12-monthsofthebeginningofaproject.
4.IdentificationandimagelabellingTherearespecificgeneralprinciplesthatareassociatedwithgoodimagingperformance.However,someoftheseprinciplesarerequiredtoensurethatimagesareappropriatelyidentified,arematchedtotherightpatientandthatimagescontaininformationabouthowtheywereacquiredforproperanalysisandreproducibility.
4.1 PatientIdentificationAllpatientsshouldbeproperlyidentifiedpriortoimagingtoensurethatthecorrectpatientandstudymatchtherequiredimaging.Theminimumrequirementisthatpatientsareidentifiedviathefacility’susualclinicalprocedure,whichmayincludethepatientnameanddateofbirthmatchingtherequestforimaging.Anyidentificationchecksshouldberecordedonboththeimagingrequestformandstudycasereportform.
4.2 ImageannotationAllimagesmusthavethefollowinginformationpresentandlegible.Theseannotationsmustnotobscureanyanatomyandshouldbeinthesamelocationontheimageeverytime.Theyshouldalsobeeitherincludedontheradiographordigitallyinscribedontheimage.Someoftheseannotationsmaybesubsequentlyobscuredorremovedtoensurethede-identificationofpatientdataintheinterpretationofchestX-rays:
• Nameanddateofbirthofthepatient• Dateofexamination• Anatomicalsidemarker(leftorright)• Whethertheimagewasacquiredinasupineorerectposition• Nameoffacility• Exposurefactorsusedtoacquiretheimage(preferredbutnotessential)
5.ChestX-rayImagingRecommendationsIntheacquisitionofchestX-rayimagesinpediatricpatients,thereisnotonlyaneedtostandardizethex-rayequipment,butalsotheradiologictechniquestoensureoptimizationofradiationdose(21).Forexample,somepartsofthedevelopingworldusefluoroscopyunitstoobtainreal-timeimagesofthechestasadiagnostictoolforpneumonia.Thisisahighlyunreliableexaminationthatinvolvesanincreasedradiationdose(11).ItisthereforerecommendedthatastandardX-raytechniquebeusedforepidemiologicalstudies.ManypathologicalprocessesrequiretheuseofboththeAPorPAandlateralchestX-raystoassistintheirdiagnosis.ItisalsounderstoodthatfacilityprotocolmayrequirebothoftheseprojectionsforallchestX-rays.However,forthepurposesoftheepidemiologicalstudiesthattheseguidelinesarewritten,anAPorPAchestalonewillsuffice.Formanyresearchquestions,thelateralchestX-rayisnotrequired,butmaystillbeusedifclinicallyindicatedoriftheresearchquestionspecificallyrequireslateralviews.Thepurposeoftheseguidelinesistotargetstudieswithacohortofpatientsbetween0and59months.Inthesecases,theAPchestispreferredoverthePAchest.ThepositioningmethodsofpatientsinthisagegrouparemuchsimplerfortheAPchestandarelikeliertoachievepatientco-operation.Furthermore,thedifferencesinmagnificationofinternalstructuresbetweentheAPandPAchestatthisagearenegligibleduetothecylindricalshapeofthepediatricchest.
5.1 PatientPositioning
PositioningchildrenforchestX-rayexaminationsisanimportanttaskthatcanbedifficultwherepatientsareuncooperative.However,itiscrucialthattheresultantimagebeofsufficientqualitythatitisdiagnostic.Itisthereforeimperativethatthemethodofpatientpositioningisexactandindependentofthelevelofcooperationofthepatient.FortheAPchestX-rayexamination,thetwomainmethodsofacquiringtheimagearewiththepatientinthesupineorerectposition.Theerectpositionofthepatientisthemoredifficulttobeachieved,particularlyifthepersonacquiringtheimageisnotwelltrainedinthisareaordoesnotregularlyacquireimagesonthesepatients.Consequently,itisexpectedthatifthefacilityconductserectchestX-raysonchildrendaily,anerectchestX-rayshouldbeperformed.Forallotherfacilities,orwherepositioningapatientforanerectchestX-rayisdifficult,asupinechestX-raywillsuffice.TheseguidelinesdescribethepositioningmethodsforboththeerectandsupinechestX-rays.InstructionalvideosofpositioningmethodsbyTheRoyalChildren’sHospitalinMelbourne,AustraliacanalsobefoundontheWHO-CRESwebsite.ThepatientistobepositionedinatrueAPposition,withtheirshouldersandanteriorsuperioriliacspines(ASIS)equidistantfromtheimagereceptor,ensuringthattheyarenotrotated.Themid-coronalplaneofthepatientshouldbepositionedsothatitisparalleltotheimagereceptor.Intheuncooperativepatient,thearmsaretobeimmobilizedabovethepatient’sheadtoensurethatthescapulaeareclearfromthelung-fields.Thiscanbealsoachievedinthecooperativepatientbyplacingthepatient’shandsontheirthighsandbringingtheelbowsanteriorly.Mostchildrenunder5-yearswillnotcooperatewhenbeingpositionedforchestX-rays,whichwillrequirethemtobeimmobilized.Intheimmobilizationofchildrenforchest
X-raysitneedstobearelativelyeasyprocessthatisnon-traumaticforthepatient.Furthermore,whilstitneedstobeensuredthatthepatientcannotmoveandthatthebeamcanbecentered,theusefulnessofanyimmobilizationneedstobeexplainedtotheparent,asthemethodsusedcanbedistressingtoaparent.Thereareanumberofspecificallydesignedimmobilizationdevicesavailabletobepurchasedonlineatareasonablecost.However,itmustbereiteratedherethatthesemustbenon-traumatictothechildandtheymustbequickandeasytouse.Forsitesthatdonotcurrentlyuseanimmobilizationdevice,patientscanbeimmobilizedthroughtheuseofassistants.Asdiscussedabove,thevideolinkoutlineshowassistantscanbeused.Thisisalsooutlinedinthefigure1,whichisaposterthatdescribestoassistantshowtoproperlyimmobilizethepatients.EachofthesemethodsuseaspecificchairwithaVelcrostrapthathasbeenconstructedforthespecificpurposeofimmobilizingchildrenforchestX-rays.However,themethodscanbeeasilyvariedifachairsuchasthisisunavailable.Forexample,anotherassistantmaybeusedtoholdthepatientatthelevelofthefemursorpelvistoensurenorotationofthelowerhalfofthebody(15).Intheuncooperativepatient,thepersonwhoisimmobilizingthepatientbythearmsshouldholdthepatient’sarmsattheleveloftheelbowstoavoidthepatientbeingabletomovetheirarms.Slightinwardpressuretowardsthepatient’sheadshouldalsobeappliedtoensurethattheheadisimmobilized,withthepatient’schinnotoverlyingtheupperchest.

Figure1AninstructionalposterforparentsandcaregiversondisplayatTheRoyalChildren’sHospital,MelbournethatdemonstrateshowtocorrectlypositionachildforachestX-ray(Source:CreativeStudio,TheRoyalChildren’sHospital,Melbourne)
Positioning children for chest X-rayYou are your child’s best support and comfort. Please help your child and assist in getting the clearest chest X-rays by following the instructions below. Before your baby/child has their X-ray: they need to be undressed from the waist up, they need to have their hair tied up on top of their head (if they have long hair) and the child’s helper (parent/guardian/friend) will be required to put on a lead apron.
1. Seat baby on the stool with their bottom right back against the screen.
2. Baby should be straight and facing forward.
3. With baby’s legs straight forward a waist strap is tightened around baby’s lap.
4. Helper stands to the side.
5. Helper lifts the baby’s arms up as straight as possible to either side of the baby’s face and supports the baby’s head upright between their arms.
6. Hold baby in this position until X-ray is complete.
Baby who is unable to support their head
1. Seat baby on the stool with their bottom right back against the screen.
2. Baby should be straight and facing forward.
3. Then a waist strap will be tightened around baby’s lap.
4. Helper stands to the side.
5. To help secure the stool the helper may place their foot on the stool’s base.
6. Helper holds both of baby’s arms at the elbow so that the arms are straight up, at either side of baby’s head at the level of their ears.
7. Hold baby in this position until X-ray is complete.
Baby who is able to sit
1. Seat toddler on the stool with their bottom right back against the screen.
2. Toddler should be straight and facing forward.
3. Then a waist strap will be tightened around toddler’s lap.
4. Helper stands to the side.
5. To help secure the stool the helper may place their foot on the stool’s base.
6. Then helper holds both of toddler’s arms at the elbow so that the arms are straight up and at either side of toddler’s head.
7. Hold baby in this position until X-ray is complete.
Toddler
ERC 121120
1. The child sits on the stool with their bottom right back against the screen.
2. The child needs to sit facing forward and straight.
3. A waist strap is placed around the child’s lap.
4. Helper stands close by for reassurance.
5. The child is asked to put their hands on their hips and lean their back against the screen.
6. The child needs to hold this position until the X-ray is complete.
Preschooler
ItisnotidealforthepersonacquiringtheimageorotherstaffmembersofthefacilitytoholdthepatientsforchestX-rays.Thisisduetothecumulativeeffectofscatteredradiationdosethattheywouldreceiveforholdingpatientsrepetitively.Therefore,theroleofholdingthepatientshouldbegiventotheparentorcaregiverofthepatient.Whenprovidedwithproperinstructions,parentsandcaregiverscanbeveryhelpful,althoughitisimportantthattheyknowexactlywhatisrequiredofthem(22).Incaseswheretheparentorcaregiverispregnant,orwheretheparentorcaregiverareincapableofholdingthepatientthisroleshouldthenbesharedamongstthefacilitystaff.Furthermore,tominimizethescatteredradiationdosetoothers,onlythosewhoarerequiredintheexaminationroomatthetimeofexposureshouldbeintheroom.Nomatterwhoisholdingthepatient,thescatteredradiationdosetoanypersonassistinginimmobilizingthepatientduringthechestX-rayexaminationmustbebelow1mSv(23).Consequently,thispersonistobeprotectedwithastandardleadapron(11).Thethicknessoftheleadapronisselectedbaseduponconsiderationofthetypeofexamination.Forgeneralradiography,includingpediatricchestX-ray,thisleadapronistobeofatleast0.25mmleadequivalence(24).
5.2 TechnicalFactors
Therearemanyfactorsinvolvedatatechnicallevelwhenacquiringtheimagethatcanaffectboththequalityoftheimageandtheradiationsafetyofthepatient.Patientradiationdosecanvarybetweensites,aswellaswithinasiteduetodifferentequipment,filtration,techniquesandpatientcharacteristics(22).Targetsinmeetingexposureindex,alongwithfactorsofshielding,griduseandincorrectpositioningalsohighlighttheregularchallengesfaced,particularlywhenimagingchildren(25).Whilstinclinicalpractice,severalvariationsexistbetweenthesetechnicalfactors,thefollowingaretherecommendedrequirementsforchestX-raysinchildren:5.2.1 Imagereceptorandprocessing
Theimagereceptortypeandimageprocessingrequirementsarelargelydependentonwhetherfilm,CRorDRisemployed.BothCRandDRhavesignificantbenefitswhencomparedwithconventionalfilm,particularlyintheirpostprocessingcapabilitiesandimprovedcontrastresolution.Ingeneral,CRandDRhavethepotentialfordosereductionwhileimprovingimagequalityanddiagnosticaccuracy.CRandDRcancompensateforunderoroverexposuresofthepatient,coveringarangeof300-400timesthatoffilm-screensystems.Thishasamajoradvantageofreducingrepeatimaging.However,unlessthesystemisfullyoptimised,dosereductionisnotachievedandoverexposureswillgoundetected.Thisisknownasthe“exposurecreep”phenomenon.Forexample,overexposuresof5-10timesanormalexposurewillhavetheappearanceofaproperlyexposedimageduetothecompensationbyadigitaldetector.Systemoptimizationcanbeachievedwithstafftrainingandcontinuousmonitoringofparametersandpractices.
ForCRandDR,intheprocessingofimagesthenomenclaturefordigitalimageprocessingalgorithmsandexposureindicesmustbestandardizedsothattheycanbeunderstoodbyallusers.Theseimageprocessingalgorithmsincludealteringbrightness,detail,contrastandlatitudetoimprovetheoverallqualityoftheimage.Additionally,anyexposureordoseinformation,aswellasthepatientrecordshouldbeabletobesenttoanyimagestoragemediuminaccessibleform.
5.2.1.1 FilmTheuseofX-rayfilmisverycomplexastherearemanyprocessingvariablesthatcanaffectthequalityoftheimage.Theseareoutlinedasfollows:
• Eachfilmcanbecoveredinoneortwoemulsionsofsilverhalidecrystalsofvaryingshapesanddistributions.Thesefactorsinfluencetheresolutionoftheimage,withasmallercrystalsizeincreasingtheresolution.However,asmallercrystalsizewillalsodecreasethespeedatwhichanimagecanbeacquired,whichisadisadvantageinpediatricchestimagingwhereshortexposuretimesarerequired.Filmwithemulsionsofacrystalsizeof3-5micro-meters(μm)issufficientforthedetailrequiredforpediatricchestX-raysandshouldthusbeused.Thesefilmsshouldalsohaveadoubleemulsion,whicheffectivelydoublestheamountofcrystalsandincreasesthespeedatwhichtheimagecanbeacquired.
• Insidethefilmcassettesareintensifyingscreens,whichareeither
blue-sensitive(e.g.calciumtungstate)orgreen-sensitive(e.g.rareearthor“Lanex”)dependingonthelightthattheyemit.Screensarecoatedwithafluorescentmaterialcalledphosphors,whichconvertX-rayphotonenergytolight.ThepurposeofthescreensistoassistintheexposureoffilmbyemittingsmallamountsoflightontothefilmemulsionswhenexposedtoX-rays,therebydramaticallyreducingtheamountofpatientexposure.Thescreenscanvaryintheirspeed,dependingonthethicknessofthephosphors(thickerphosphors=fasterscreen).Fasterscreensareidealastheyresultinbothshorterexposuretimes,whichisidealforpediatricchestimaging,andalowerradiationexposuretothepatient.However,thisalsoresultsinalowerimageresolution.Basedonthis,thefastestpossiblescreenspeedshouldbeused,providedthereissufficientsignal-to-noiseratioandnolossofdiagnosticinformation(11).Thenominalspeedclassisthereforeaminimumof200,withamaximumof400forpediatricchestX-rays(15).Blue-sensitivescreensaretypicallyslowerandmorereadilyavailableglobally,butareavailableintheserecommendedspeeds.
Theradiationexposurerequiredtoproduceadiagnosticimagewillvarydependingonthefilmsandscreenswhenusedinconjunctionwitheachother.Forexample,twofilmsfromdifferingmanufacturersusingthesamescreenfromonemanufacturermayrequiredifferentexposurestoproducetherequireddiagnosticimage.Consequently,itishighlyrecommendedthatthefilms,screensandcassettesusedataparticular
siteareallfromthesamemanufacturerandthatthecassettesarelabeledwiththescreenspeedandfilmtype.Inmostcases,thiswillhavetheaddedbenefitofquickreplacementofpartsifrequired.Furthermore,forefficientworkflowandcontingencyplanning,itisrecommendedthatthereareatleastthreecassettesofeachscreenspeedandfilmtypeavailable.
Theopticaldensityofthefilmisameasureofthefilmdarkening.ThiscanbemeasuredwithadensitometerandisoutlinedinPartC–QualityControl.Withoutphotonexposure,allfilmshaveanopticaldensitythatisknownasthebase-foglevel.Indiagnosticradiography,thebase-fogopticaldensityshouldnotexceed0.25(13).Afterexposure,therewillbearangeofopticaldensitiesonthefilmcorrespondingthebrightanddarkareasoftheimage.Forthediagnosticareasofimaging,theopticaldensitiesshouldbeintherangeof0.5to2.2(13).However,itmustbenotedthatthejudgmentofopticaldensitiesareusuallybasedonglobalimpressionsratherthanmeasurements.Theaestheticqualityoftheimageisdeterminedbythecassettesizeused.Forchildrenlessthan5-years,acassettesizeof24x30cmissufficienttoincludeallrelevantanatomy,whilstacassettesizeof18x24cmissufficientifthepatientislessthan10kg.
5.2.1.2 ComputedRadiography
Contrarytoscreen-filmradiography,CRsystemsdonotshowanyfixedrelationbetweentheimagereceptordoseandtheopticaldensityoftheresultingfilm.Moreover,theexposureordynamicrangeofimagingplatesusedinCRismuchwiderthanconventionalfilm.Therefore,itisnotpossibletogivespeednumbersforthiskindofimagereceptor.However,cassetteswithimagingplatesshouldnotbeexposedhigherthanscreen-filmcassettesforthesamemedicalapplication,providedtheconfigurationoftheX-raysystemisthesame.Thisisevenmoreevidentwhenfilm-screencassettesandimagingplatecassettesareusedinparallel,orwhenimagingplatecassettesdirectlyreplacescreen-filmcassettesinafacility.CassettesizesforCRimagingplatesaresimilartothoseofconventionalfilm.Forsomemanufacturers,thecassettesthatareusedforfilmareapplicabletoCR.TheaestheticprinciplesforCRarethereforealsoapplicableasforfilm.Finally,theimplementationanddisplayofanyexposureindicatorvaluesisrecommendedforsufficientmonitoringofpatientdoseincomparisonwithimagequality.
5.2.1.3 DigitalRadiographyEachoftherecommendedflatpaneldetectorandmonitorspecificationsforpediatricchestradiographyusingthedigitalsystemshavebeenoutlinedinsection3.2.4under“equipmentspecifications”.Toenableoptimalimageacquisitionanddisplay,itisrecommendedthatdigitalsystemsareconfiguredtoallowtheusertoselectabodysizeoragethatisappropriatetotheindividualpatient.Forexample,thefollowingwouldbeconsideredacceptedcategories:
• Lessthan1.5kg• 1.5kgto2.5kg• Birth(greaterthan2.5kg)to1-month• 1-monthto2-years• 2-yearsto5-years
Eachofthesecategorieswouldencompassthepediatricalgorithmsdiscussedin3.2.4.Additionally,whilstnotessential,arapiddisplayofapreviewimageisrecommendedforworkflowefficiency.Viewingmonitorsshouldallowforblacksurroundingsoftheimageforeaseofviewing.AsperCR,theimplementationanddisplayofanyexposureindicatorvaluesisrecommendedforsufficientmonitoringofpatientdoseincomparisonwithimagequality.
5.2.2 Filtration
“Thequalityofx-raybeamisimportantinthereductionofradiationexposureandisaffectedbyfiltration(inherentandadded)ontheX-raytube,bytheX-raygeneratorandbytheexposuretechniqueselected.”WorldHealthOrganisation(11).
Duringimageacquisition,thelowerenergyradiationontheradiationspectrumiscompletelyabsorbedbythepatientandthusaddstotheradiationdosetothepatientandisirrelevantintheproductionoftheimage(10).Avoidanceofthisisnecessarythroughfiltrationoftheradiationbeam.Theamountoffiltrationusedmustbeenoughtoavoidthelowerenergyradiationfromreachingthepatient,butnotbetoolargethatitabsorbssomeofthehigherenergyradiationthatwouldcontributetothequalityoftheimage.RecommendedinherentfiltrationrequirementsforallX-raytubesshouldbe2mmAlforuseofexposuresabove70kVp,withallowanceforaddedfiltration(20).TheaddedfiltrationallowsforanincreasedX-raybeamenergytobeusedwithshorteravailableexposuretimes,whichwillinherentlyresultinalowerpatientdose.
Inregardstoaddedfiltration,upto1mmAlplus0.1-0.2mmCuisappropriate(notethatevery0.1mmCuisequivalentto3mmAl),andcomplieswithInternationalstandards(10).
5.2.3 Anti-scattergrid
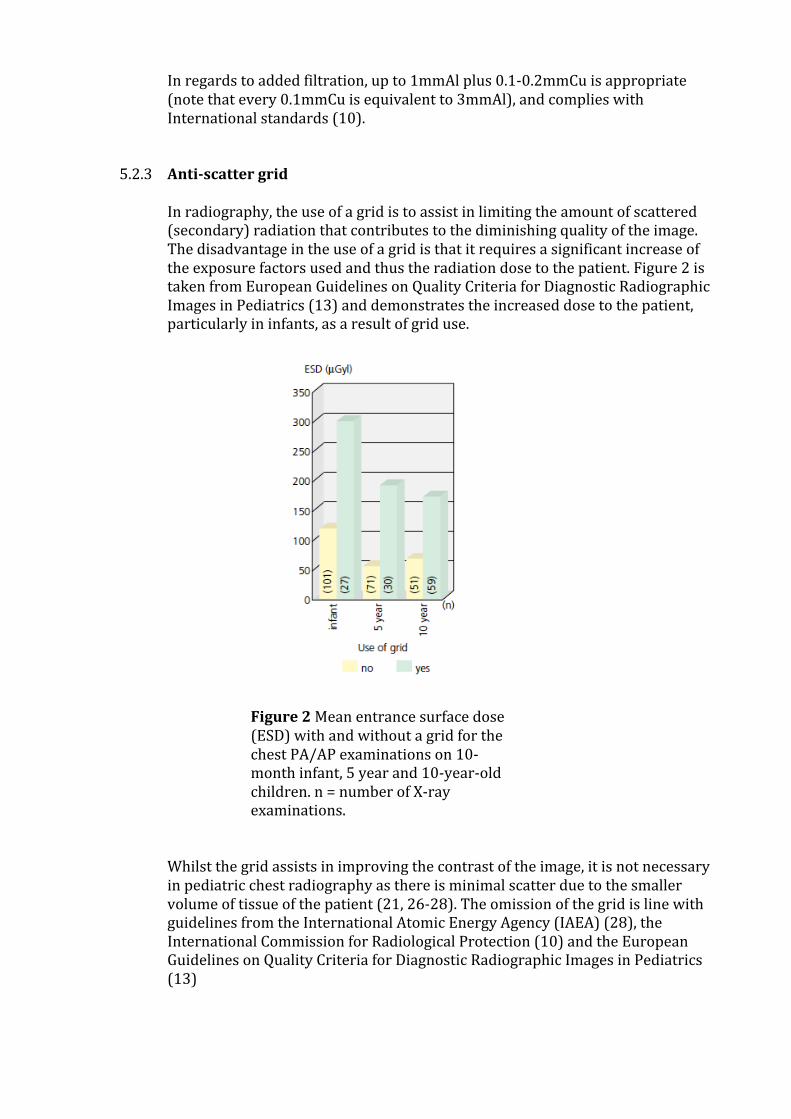
Inradiography,theuseofagridistoassistinlimitingtheamountofscattered(secondary)radiationthatcontributestothediminishingqualityoftheimage.Thedisadvantageintheuseofagridisthatitrequiresasignificantincreaseoftheexposurefactorsusedandthustheradiationdosetothepatient.Figure2istakenfromEuropeanGuidelinesonQualityCriteriaforDiagnosticRadiographicImagesinPediatrics(13)anddemonstratestheincreaseddosetothepatient,particularlyininfants,asaresultofgriduse.
Figure2Meanentrancesurfacedose(ESD)withandwithoutagridforthechestPA/APexaminationson10-monthinfant,5yearand10-year-oldchildren.n=numberofX-rayexaminations.
Whilstthegridassistsinimprovingthecontrastoftheimage,itisnotnecessaryinpediatricchestradiographyasthereisminimalscatterduetothesmallervolumeoftissueofthepatient(21,26-28).TheomissionofthegridislinewithguidelinesfromtheInternationalAtomicEnergyAgency(IAEA)(28),theInternationalCommissionforRadiologicalProtection(10)andtheEuropeanGuidelinesonQualityCriteriaforDiagnosticRadiographicImagesinPediatrics(13)
5.2.4 AutomaticExposureControl(AEC)
TheconceptoftheAECistoensuregoodimagequalitythroughtheuseofionizationchamberspositionedbehindtheimagereceptorthatallowanamountofradiationsufficienttoproduceapre-determinedhighqualityimage.However,inpediatricexaminations,theuseoftheAECislargelyimpracticalasitreliesheavilyoncooperationofthepatientforprecisepositioningandthechambers’large,fixedsizeandshapecannotcompensateforthevariationinthesizeofthepediatricpatient(13,26).Furthermore,theirusehasthepotentialtoincreasetheexposuretime,astheyareunreliableattherequiredlowexposuretimesusedforpediatricimaging,whichincreasestheriskofmovementartefactbeingpresentontheimage(13,25).InasurveyofcontributionstoradiationdoseforpediatricchestX-rayexaminations,itwasdiscoveredthatofthefoursitesthatusedtheAECforchestexaminations,threesiteshaddeliveredthelargesteffectivedosestopatientsintheentirecohort(27).Consequently,inlinewithbothEuropeanandIAEAGuidelines(13,29)andintheinterestofoptimizingtheradiationdosetothepatient,itisrecommendedthattheAECisnotusedforpediatricchestX-rayexaminations.
5.2.5 Exposurefactors
Theexposurefactorsthatcanbesetbytheoperatorallcontributetotheimagequality,whichcanbeachievedinasafemanner.The3exposurefactorsare:
o Kilo-voltage(kV),whichdeterminestheenergyandthereforepenetratingpoweroftheX-raybeamthroughthebody
o Milli-amperes(mA),whichdeterminesthenumberofX-rayphotonsthatareproduced,directlyaffectingthebrightnessoftheimage,and
o Time(s),whichdeterminestheamountoftimetheX-rayphotonsarebeingproduced.
ThemAandtimearedirectlyrelatedandarecommonlysetasonefactor(mAs),butcanoccasionallybesetseparately.Exposurefactorsettingsvarydependingonequipmentageandcharacteristics,aswellastheimage-processingmedium.Thus,itisnotpracticaltoproviderecommendedexposuresettings,asthiswouldnottranslatetoallsites.Asaguidingprinciple,itisrecommendedthat“Theradiationdosegiventopatientsshouldbeaslowasreasonablyachievable(ALARA),whilestillprovidinganimagequalitythatisadequatetoenableanaccuratediagnosis”(7,26,30,31).However,thefollowinginformationprovidesbestpracticerecommendationsforeachoftheexposurefactorsandhowtheycontributetoimagequalityanddosetothepatient.Itisexpectedfromthisinformationthataweight-dependentexposurechartforeachsiteisdevelopedforusebythesites’operators(11).ThekVdirectlyaffectstheimagecontrast,withahighcontrastatlowersettings,However,thiscomesattheexpenseofanincreasedpatientskinentrancedose.IncreasingthekVreducesthepatientskinentrancedose,butwillalsoreducetheimagecontrast(32).Furthermore,“asbeamenergyisincreased,X-raysbecomemorepenetrating,arelesslikelytobeattenuatedwithinthepatientandaremorelikelytoreachtheimagereceptorcomparedwithlowerbeamenergies.
Thisresultsinradiationdosereductionsover50%”(32,33).Thereisthereforeabalancethatmustbereachedtoensureanappropriateimagecontrastandpatientskinentrancedose.ThekVsettingmustbehighenoughthatthelungstructureandspinecanbediscerniblebehindtheheartandmediastinum.EuropeanguidelinessuggestthattheoptimalkVrangeforpediatricchestX-raysisbetween60kVand80kV(13)anditisrecommendedthatatleast70kVisusedatthenewbornlevelthatincreasestonomorethan80kVfor5-year-oldpatients.HigherkVsettingsalsoallowforlowermAssettings,inparticularexposuretimesettings,whichreducetheriskofmotionartefactinpediatricpatients.Dependingontheageandcharacteristicsoftheequipment,at70kVsettingsaslowas0.5mAscanbeusedfornewborns.WhenestablishingthecurrentandtimesettingsforpediatricchestX-raysthereneedstobetheabilitytoalterboththemAandtimeindependentofoneanother.Itisidealthattheexposuretimeisverylow,suchaslessthan10ms,orevenlessthan4msinthenewborn.Thistakesintoaccountthenon-cooperationofthepatientandwillminimizetheriskofmovementartefact.
5.2.6 Source-to-imagedistance(SID)
Alsoknownasthefocal-film-distance(FFD),theSIDisthedistancefromtheX-raytube’sfocalspottotheimagereceptor.ForchestX-raysthisistypicallyquitelargetominimizethemagnificationfactorofinternalcheststructures,suchastheheart.Inadults,thisvalueisanywherebetween150cmand200cm.ThelongSIDisalsosuggestedbytheIAEA(26)andisthoughttoassistincontrollingthepediatricpatientradiationdosebyusingairasanaturalfilter(27).Inchildren,thesmallerthicknessofthepatientmeansthatasmallerSIDisallowableinordertoachieveasimilarmagnificationfactor.TheEuropeanguidelinessuggestthattheSIDforchestX-raysinpediatricpatientsis150cmwhenthepatientispositionederectand100cmforsupine(13).However,tostandardizetherequirementsforsimplicity,itisrecommendedthattheSIDusedforpediatricchestx-raysis125cmregardlessofwhetherthepatientispositionederectorsupine.TheSIDalsodictatesthemAsthatisusedtoachieveanappropriateimagedensity.Theintensityofthesourceofradiationisinverselyproportionaltothesquareofthedistance.Thisisknownasthe“inversesquarelaw”.Forexample,if1mAswasusedat100cmSID,4mAswouldneedtobeusedat200cmSIDinordertoachievethesameopticaldensityontheimage.ItisunderstandablethatequipmentatsomesiteswilleitherhaveafixedSIDoronethatdoesnotallowforaSIDof125cm.Inthesecases,itisexpectedthatthemAswillbealteredinaccordancewiththeinversesquarelawinordertoachieveanimagewithoptimalopticaldensityandthatthereisconsistencyfromoneimagetothenext.
5.2.7 X-raybeamposition
Withthepatientinthecorrectpositionasdescribedpreviously,theX-raybeammustnowbepositionedcorrectlyinordertoachievethedesiredimage.AsthepatientstargetedintheseguidelinesareforanAPchestX-rayonly,usinganX-raybeamthatisnotangledwillprojectthemedialendsoftheclaviclestoosuperiorlyonthelung-fields,resultinginalordoticappearanceofthechest.ThereasonforthisisduetothelargedistancebetweenthemedialendsoftheclaviclesandtheimagereceptorinconjunctionwiththedivergentgeometryoftheX-raybeam.Consequently,theX-raytubeshouldbeangled10degreesinthecaudaldirection(towardsthepatient’sfeet)inordertobeperpendiculartothepatient’ssternum.Thecentreofthebeam(centralray)istobeinthemid-sagittalplaneofthepatientatthelevelofthepatient’snipples(15).WiththeX-raybeamcentredandangledcorrectly,thebeamcanbecollimated.
5.2.8 Beamcollimation
CollimationoftheX-raybeamallowstheoperatortolimitthefieldsizetotheareaofinterest.Asspecifiedintheequipmentspecifications,thefieldsizecanbeadjustedusingtheadjustablemulti-leafcollimators.Collimationisveryimportantasitreducestheirradiationofunnecessarystructuresandlimitstheamountofscatteredradiationthatalsocontributestothepatientdoseandpoorimagecontrastandresolution(10,22,26,34).Aninappropriatefieldsizeisoneofthemostimportantfaultsinpediatricradiationtechniques.Eventheinclusionofunnecessaryanatomywithintheradiationfielddoesnotsignificantlycontributetotheclinicalgainviaincidentalfindings(25).Itisthereforeimperativethatthefieldsizeisassmallaspossible,butmaintainsalltherequiredclinicalinformationandrelevantanatomy(11,20).Inpediatricpatients,tightcollimationcanbedifficultbecauseasubstantialproportionofthesepatientsareuncooperative(21,26).Recommendedtechniquesforadultsarenotapplicabletopediatricpatientsasitcanresultinunnecessaryradiationtonon-thoracicstructures(25,35).However,thisimagecriterionspecifiestheappropriatefieldsizelimitations.Whilstsomedegreeoflatitudeisnecessarytoensurethattheentirefieldofinterestisincluded,thiscannotbeacceptedasanexcuseforrepeatedlyusingtoolargeafieldsizeinpediatricpatients.AppropriatecollimationforpediatricchestX-rayscanbedescribedasfollows:
Withthearmselevated,thesuperiorborderofthepalpableacromio-clavicular(AC)jointgenerallyliesabovethelungapexandshouldbeusedasthesuperiorcollimationborder.Inferiorly,theribscanusuallybefelt,whichissufficientfortheinferiorcollimationborder(25).Laterally,thecollimationborderscanextendto1cmlateraloftheskinedgeinneonatesto2cmforallotherchildren.
Overall,thetopofthelungstothelowerpartsofthediaphragm,includingthecostophrenicanglesshouldbeincluded.Onthefinalimage,allfourbordersofcollimationshouldbepresent.WiththeuseofbothCRandDR,itispossiblefortheoperatortoaddartificialborderstotheimageduringthepost-processingphaseafteracquisition.Whilstthiscanimprovetheoverallappearanceoftheimage,itmisrepresentstheradiationfieldthatwasusedtoexposethepatient(8,10,26).Additionally,thehistogramanalysisalgorithmsoftheCRandDRsystemswillnothaveanticipatedanyunnecessaryanatomyincludedandcontrastwillbesacrificedtoappropriatelyrepresentthisanatomy(26).5.2.9OptimizingTechnicalFactors
Relevanttothetechnologicalinformationpresentedabove,Willis(26)outlinedfivecoursesofactionin2009thatcanresultindosereductionforaradiographicprojectionthatarerelevanthere:
1. Decreasedigitalreceptordose:
Whilstthisisonlyrelevantforthosesiteswithdigitalsystems,itallowsforlowerexposurefactorstobeused.Thelowerexposurefactorswillproducesmallerdetectorsignalsandthesecanbeamplifiedbythedigitalsystem.
2. Increasereceptorefficiency:ThismaybelimitedtotheavailablesoftwareofthesystembeingusedbutisrelevanttobothCRandDRsystems.
3. Increaseradiationpenetration:Thiscanbeachievedeitherbyincreasingthebeamenergy(kV)orusingaddedbeamfiltration.Asdiscussedabove,thiscausesadecreaseinsubjectcontrastandnoiseduetolessphotonsbeingrequiredtomaintaintheexposure.
4. Decreasescatteredradiation:Anexampleofhowtodecreasethescatteredradiationistouseadequatebeamcollimation.
5. Combinenoisyimages:Notcommonlyused,butavailableinsomeCRsystems,thisisaprocesswherebystimulatedluminescencefromboththefrontandbacksidesofacomputedradiographyimagingreceptorisacquired.
5.3 OtherRequirements
Onceacquired,theresultantimageshoulddemonstratetherelevantanatomyclearlyandwithnounnecessaryartefactsthatmayinterferewiththediagnosticvalueoftheimage.Manyobjectscanbeclassifiedasunnecessaryartefacts,forexamplejewelry,patientmonitoringleadsorevenbuttonsfromclothing.Artefactscanalsobecausedduringfilmhandlingorimageprocessing,soitisimperativethatfilmhandlingandimageprocessingisperformedcorrectly.Additionally,astechnologyimproves,sotoodoestheimagedetailandthisresultsinbasicchildren’sclothingbeingsometimesvisibleontheimages.Itisthereforerecommendedthatallclothingandotherremovableartefactsthatareanticipatedtobewithinthefieldofviewareremovedpriortopositioningthepatient.
Thefinalimageshouldalsodemonstratethechestintheinspiratoryphase(15).AchestX-rayacquiredwiththepatientintheinspiratoryphaseallowssufficientcontrasttovisualizeanyfluidorothermarkingswithinthelungsduetothelowdensityofthelungs.AchestX-rayacquiredintheexpiratoryphasealsoraisesthepositionofthediaphragms,leadingtoexaggerationoftheheartsize,aswellasobscuringthelungbases.ItnoteasytoachieveachestX-rayoninspirationintheuncooperativepediatricpatient,astheycannotsuspendrespirationintheinspiratoryphaseondemand.Consequently,itisuptotheoperatortohaveanuninterruptedviewofthepatientatthepointofexposuretoensurethattheexposureismadewhilstthepatientisattheinspiratorypointoftherespiratorycycle.Pediatricpatientstendtobreatheusingtheirabdominalmusclesandexposingatthepointofinspirationisgenerallyachievedthroughobservationoftheinwardandoutwardmotionofthepatient’sabdomen.Thisisalsomoreeasilyachievedifthepatient’supperhalfisnaked.
5.4 TheFinalImage
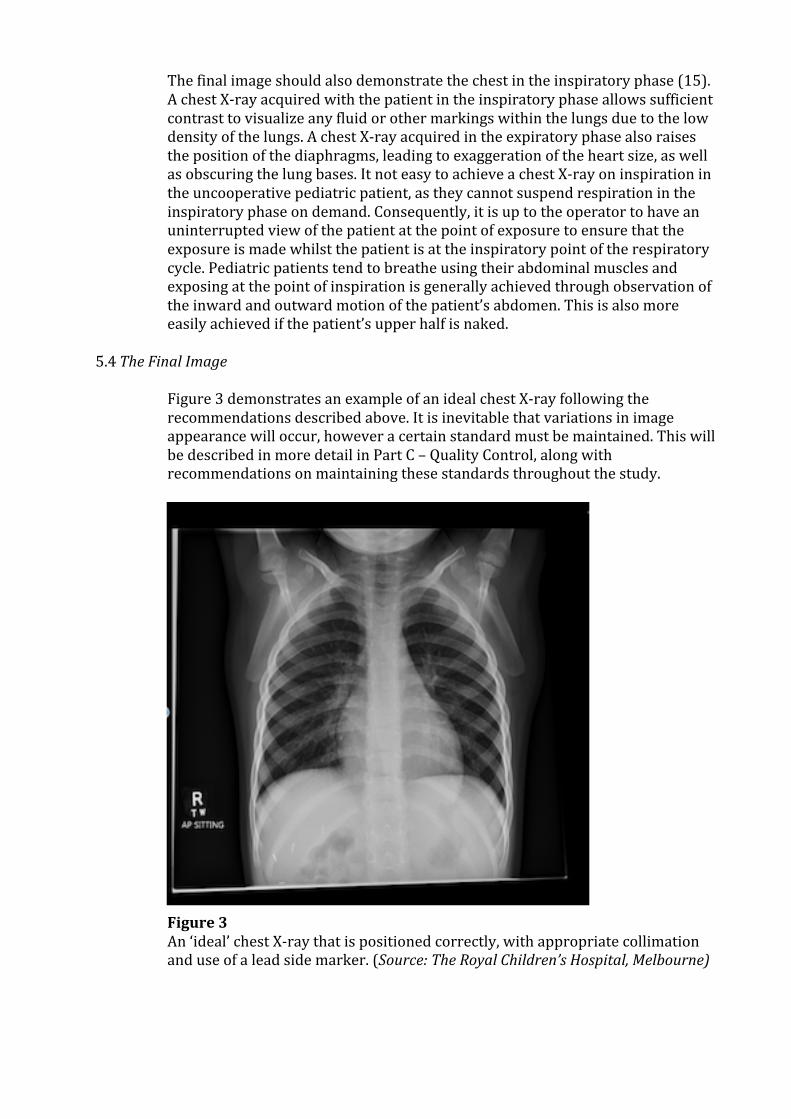
Figure3demonstratesanexampleofanidealchestX-rayfollowingtherecommendationsdescribedabove.Itisinevitablethatvariationsinimageappearancewilloccur,howeveracertainstandardmustbemaintained.ThiswillbedescribedinmoredetailinPartC–QualityControl,alongwithrecommendationsonmaintainingthesestandardsthroughoutthestudy.Figure3An‘ideal’chestX-raythatispositionedcorrectly,withappropriatecollimationanduseofaleadsidemarker.(Source:TheRoyalChildren’sHospital,Melbourne)

6.ImageArchivingandViewingRecommendations6.1ImagestorageArchivingofimagesisanimportantfactorintheongoingcareofpatients.Imagescontributetothepermanentrecordingofapatient’smedicalhistoryandinmanyinstances,patientsreturnforrepeatstudiesthatoftenrequireacomparisonwithpreviousstudies.Successfularchivingisalsoimportanttoensurethepermanenceoftheradiographforstudypurposes,allowingforre-examinationandcomparisonasresearchquestionsareinvestigated.Imagearchivingistheresponsibilityoftheimagingdepartmentatthefacilityandimagesshouldbearchivedinawaythattheycanbeeasilyretrieveddespitethetypeofimageprocessingused(film/CR/DR).Whilstimagesmaybestoredon-siteashard-copyfilmsorasdigitalimages,allimageswillneedtobeindigitalformatforthepurposesofepidemiologicalstudies(seebelowfordigitizingspecifications).Thiswillpreventproblemsassociatedwiththepotentiallossofhardcopyimagesandincreaseefficiencyinthephysicaltransportofimages.Evenininstanceswhereplainfilmsareconsideredthepropertyofthepatientandthusnotarchived,thesefilmsshouldbedigitizedbeforebeinggiventothepatient.Studyprotocolsshouldexplainaclearprocessforthenamingofdigitalfilesthathasasystematicandconsistentapproachtofilenamesandensurethecorrectradiographisassignedtoitsrelevantcase.APictureArchivingCommunicationSystem(PACS)networkisasystemfortheelectronicstorageofimagesandallowsthemtobeviewedonanyworkstationthatisconnectedtothesystem.PACSisidealforsitesthatcurrentlystoretheirimageselectronicallyasitallowsimagestobestoredinoneplacewithoutusingamplephysicalspace.Additionally,thereisanincreasingneedforfacilitatingthecommunicationbetweenradiologistsandreferringphysiciansandthisallowsreferringphysiciansinotherareasofafacilitytobeabletoviewimagesquickly(33).APACSnetworkshouldalsoconsistofaneffectivebackupprogram,therebypreventinglossofimages.SitesthatcurrentlyhaveorareabletoestablishaPACSnetworkwillrequireastorageareanetwork(SAN)capacitythatiscommensuratewithboththeworkloadandimagingmodalitiesthatareemployedbythesite.Theywillalsorequireaccesstoasufficientbroadbandnetwork,aswellasviewingstations.PACSisnotnecessarilyanoptionforallsitesduetothecostanddatastoragerestrictions.Intheseinstances,storingimagesoncompactdiscs(CDs)onlyarenotidealastheycanoftenbehardtoretrieveshouldapatientreturnforanewstudy(36).Themostpracticalmethodistosendthedatatoanetworkgateway,suchasaninexpensivelaptopcomputerthatisconnectedtothenetworkviaacellularmodem(18).Thishasthefollowingadvantages(18);
• Studiescanbebacked-uptoCDorUSB• Itcanconnecttoanexternalantennatoincreaseitssignalandthepower
consumptionisverylow• CommunicationbetweenthegatewayandtheX-raysystemcanbeeitherwired,
suchasanEthernetcable,orwireless• Inexpensivesmallcomputersystemsmakethereplacementofsystemsabetter
optionthanrepairofthesesystems• Supportforsoftwareisavailable,albeitinformalviatheinternet
Anothersimilarmethodistostoreimagesonacomputerhard-drive,withasufficientstoragecapacitythatdoesnotaffectthequalityoftheimages,aswellasaneffectivebackupsystem.Despitethemethod,adailysystemback-upisrecommendedwiththeback-upsystemappropriatelystored(18).Anyimagesstoredforstudypurposesshouldbecentralized,easilyretrievable,andhaveadequatebackupavailable.Inthedigitalstorageandtransferofimages,theamountofdataconstitutinganimageinfluencestheamountofdigitalstoragerequirements,particularlyinfacilitieswheremanyimagesareacquired.Thisnecessitatestheneedfordigitalcompressionwherethisamountofdatacanbereduced.Thishasanaddedadvantageinthetransferofimagesasthecompressionreducesthebandwidthrequirementsfortransfer(18).Thereare2maintypesofdigitalcompression,eachwiththeirownadvantagesanddisadvantages(37-41):
• Reversiblecompressionalgorithms(lossless)o Advantage:Informationinthedigitalimageisnotalteredo Disadvantage:Onlysmallcompressionratios(3:1)arepossible(38-40)
• Irreversiblecompressionalgorithms(lossy)o Advantage:Allowsforlargecompressionratiosandthusalowsizeo Disadvantage:Altersinformationinthedigitalimage(e.g.reducedimage
sharpness(42))
Inmostcases,wherethereisaneedforcompression,theuseofreversiblecompressionalgorithmsisinefficientduetothelimitedcompressionratios.Forstorageandtransmissioncoststobesignificantlyaffected,compressionratiosintheorderof20:1orhigherarerequired(43).Withtheincreasedexpectationforaccesstoimagingdataandthusincreasesinstorageandbandwidthrequirements,irreversiblecompressioncanbejustified(40).However,usingirreversiblecompressionalgorithmshasthepotentialtoomitvitalinformationwithintheimage,dependingonthecompressionratio.Thehighertheratio,themoreimagesthatcanbestoredinaspecificarea,butthehigherthelossofinformationwithintheimage(40).Whilstthelevelofacceptableimagedegradationisinmostcasessubjective,thefollowingisaguidetosomebestpracticelevelsofdigitalcompressionanditisrecommendedthattestingforindividualapplicationsofcompressioniscarriedouttodeterminethecompressionthresholdforeachstudy.Itisalsorecommendedthatwherepossible,thecompressionratioandtypeisdisplayedandthattheseimagescannotberecompressed(40).Ithasbeendemonstratedthatirreversibledigitalcompressionmethodscanbeappliedtohighresolutionskeletalimageswithoutsacrificingimagequality(42).Furthermore,differentlossycompressionalgorithmsareavailable,someofwhichcanminimizetheeffectonimagequalitybyreducingtheamountofnoiseandnon-criticalinformationintheimage(41,43,44).Forexample,JPEGtechniquesarethemostcommonlyusedstandard.However,theysufferfromblockingartefactsthatincreaseineffectwithincreasingcompressionratio(40,43,44).Alternatively,waveletcompressionalgorithmshavebeenshowntohavenoclinicallysignificantdegradationforcompressionratiosbelow30:1andhavebeensuggestedtobeasuitablealternativetoJPEGtechniques(40,43).JPEG2000isanothertypeofcompressionalgorithmthatcanprovidehighercompressionlevelsthanJPEGimagesatanequivalentorhigherimagequality(46,47).IncomparisontoJPEGimages,theJPEG2000algorithmismoreefficientwithasingleunifiedcodingframework,cansupportregionofinterest(ROI)codingandisrobusttobiterrorsinwirelesscommunicationapplications(40,44).Usingthisalgorithm,the
CanadianAssociationofRadiologists(CAR)Guidelinessuggestthatthereisscopeforirreversiblecompressioninpeediatricchestradiographsforbothcomputedanddigitalradiographytechniques,andthatthesuggestedcompressionratioisbetween20:1and30:1(40,46).
6.2DigitizingImagesForthepurposesofepidemiologicalstudies,allimageswillneedtobepresentedtoreadersindigitalformatforinterpretation.Thereareseveralmethodsbywhichradiographscanbedigitized,suchasscanningradiographsintoadigitizerortakingdigitalphotographsoftheimages.Eachmethodcomeswithawiderangeofrequiredexpenditureandquality.Regardlessofthemethodofdigitalacquisitionfromconventionalradiograph,itiswidelyrecognizedthatthedigitizedimagewillbeinferiorinquality.Takingdigitalphotographsofhardcopyimagesisamorecost-effectivemethodofdigitizingimageswhencomparedtoadigitalfilmscanner(48).Whilstdigitalphotographyhasbeendemonstratedtobeineffectiveduetothelimitationsofspatialresolution,decreasedlatitudeandincreasedimagenoise,morerecentstudiessuggestthatthedifferenceinqualitybetweenthetwomethodsisinsignificant(41,48-51).Inonestudy,digitalphotographsofimagesweretakenwithadigitalcamerausing3.3megapixelsand6xopticalzoom,withthephotographsacquiredofimagesthatwereplaced1metreawayonafilmlightbox.Imageswererecordedwitharesolutionof2048x1536pixels,withamanualfocusofthecamerasetto1metre,ISOtoauto,picturequalitytofineandsharpnessatzero(48).
Meanwhile,imagesvisualizedfromalow-cost,flatbedcommercialscannercanproducesimilarresultstoanoriginalimage,despiteasubjectivelowerimagequality(50).Nevertheless,themainobjectiveistoensurethatanylossofimagequalityiskepttoaminimum.Itisthereforerecommendedthatimagescapturedusingananaloguetechniqueandconvertedtodigitalmustnotbecompressed(40).Itisrecommendedthattheresponsibilityofscanningfalluponasfewpeoplepersiteaspossibletoensurethatappropriatetrainingondigitizingtechniquesiseffective.Thisstaffisalsoresponsibleforensuringthatthedigitizedimageisacorrectrepresentationoftheoriginalimage,forexamplecorrectorientationandnoobviousartefactsthathaveoccurredasaresultofthedigitizationprocess.6.3ImageTransportationforStudyPurposesImagetransfermethodologywillbelargelydirectedbyspecificstudyandethicsrequirements.Hencethereisnoparticularcorrectmethodofimagetransfermentionedintheseguidelines.Thespecificformatforwhichtheimagesaretobetransferredwillalsodependonthespecificstudy.Asaminimum,itisrecommendedthattheformatbeineitheraDICOMorJPEG/TIF/Bitmapformatasthesewillensureminimumlossofqualitycomparedtootherformats.However,onlyDICOMformatsallowforzooming,panningandwindowingofimageswithoutlossofdiagnosticinformation.Despitethetransfermethodologyused,thefollowingspecificationsarerequiredtomeettherequiredobjectivesandmaintainpatientprivacyandsafety:
• Allimagesaretobede-identifiedtoensurethataspecificpatientcannotbeidentified.Imagescanthenbenamedaccordingtothestudy’simageidentificationrequirements.Astudyprotocolforfilenamingisrecommendedtoensureaconsistentprocessisfollowedfortheidentificationofeachimagetothecorrectpatientidentifier,aswellasanyadditionalfactors,suchasthenumberoftheradiographinasequenceofimages(ifmorethanonearetaken)andtheprojectionoftheimage(suchassupineorerect).
• Allimagesbeingtransferredfromasinglesiteshouldbeofsimilarsize.Imagesbeingtransferredthathavealargevariationinfilesizesindicatesthataproblemexistsinthesavingortransferalprocess.
• Forallimages,includingthosethatareacquiredinadigitalformat,itisimportantthatthereisnotanylossofimagequalityinthetransportationprocessandthattheprocessiserrorfree.
Toensurethattheelectronictransmissionofimagesismosteffective,particularlyinlowresourcedregions,thefollowingrequirementsarerecommended(18):
• Compresstheimagestolimitthecommunicationbandwidthuse• Avoidanyconstantuseofanetworkconnection.Forexample,useofthe‘cloud’
willlimittheuseofanetworkconnection• Planforfrequentperiodsofnetworkunavailabilityinkeepingwithpower
limitations.Forexample,useasoftwarepackagethatadjuststhedatapacketsizesothatsmallerpacketsaresentduringtimesofnetworkinstability
• Weighthereliabilityofvarioustransfermethodswiththeirassociatedcost.
6.5 Imageviewingforstudypurposes
Theabilityofthereadertosufficientlyreportontheimagefindingscanbeaffectedbythreeissues:
• Theimageformat,suchasDICOMversusJPEG.Asdiscussedpreviously,theseformatsaresubjectedtodifferentcompressionandadjustmentcapabilities.
• Theviewingmonitor.Differingbrightnessandresolutionfromonemonitortoanothermayaffecttheabilitytodistinguishbetweensmallchangeswithintheimage.
• Thesurroundingenvironment,forexamplethebrightnessofbackgroundlight.Thesethreeissuesaremoreimportantinstudieswhereimagesarebeingviewedinmultiplelocations.Forexample,aprogramatonefacilitymayhavetheabilityforthereadertowindowimagestothedesiredquality,whilstadifferentfacilitycanonlyviewimageswithafixedquality.Hence,thereisaneedtostandardizetheviewingconditionsandworkstationcapabilitiestominimizethisvariation.Methodsforpediatricchestradiographinterpretationinepidemiologicalstudies,suchasthatdevelopedbytheWHO,areusuallyfocusedonhighspecificityandnotintendedtoprovideadetaileddiagnosisfortheindividualpatient.Assuch,studiesdonotgenerallyrequirehighqualitysoftwareandmonitorcapabilitiesthatmightbenecessarytoinformaccuratedecisionsregardingpatientcare.Withtherecommendationthatimagesaretransportedandthereforeviewedoncomputerworkstations,theconditionsbywhichthereaderinterpretstheimagesshouldberelativelyconsistentforallworkstationlocations.Incaseswhereimagesaretobeinterpretedbymultiplereaders,imagesthatarepresentedwithnocapabilitiesfor

adjustmentofbrightness,greylevelandzoomwillminimizevaryinginterpretations.Furthermore,itisessentialthatimagesareviewedinroomswithlowambientlight.(13)
AcknowledgementsJeffSolomano–RadiographicEngineer–PhilipsAustraliaStuartBaker–BusinessDevelopmentManager–AgfaHealthcareAustraliaMitaPedersen–ChiefRadiographer–TheRoyalChildren’sHospital,MelbourneAmandaPotter–GeneralX-raySupervisor-TheRoyalChildren’sHospital,MelbourneDrThomasCherian–Coordinator,Programme&ImpactMonitoringImmunization,Vaccines&Biologicals,WorldHealthOrganization–Geneva,SwitzerlandCynthiaCowling–SessionalLecturer,MedicalImaging–MonashUniversity,MelbourneBilalOmarjee–InformationandCommunicationTechnology–TheRoyalChildren’sHospital,MelbourneSimonPase-Director,CreativeStudio–TheRoyalChildren’sHospital,MelbourneRobGrant–SeniorVideoProducer,CreativeStudio–TheRoyalChildren’sHospital,MelbourneStephenJones–BusinessManager–CarestreamAustraliaDavidHalfpenny–BusinessDevelopmentExecutiveUK–TMCTelemedicineClinicGlossaryAEC AbbreviationforAutomaticExposureControl.Ionizationchambers
positionedbehindtheimagereceptorthatallowanamountofradiationsufficienttoproduceapre-determinedgoodqualityimage
Anti-scattergrid Adeviceconsistingofalternateradiopaqueandradiolucentstrips,designedtoallowtheprimaryX-raystopassthrough,butabsorbscatteredradiation
AP Abbreviationforantero-posterior,whichdescribestheprojectionwherebythex-raybeampathtravelsfromtheanteriortoposteriorpartsofthepatient
Artefact Anartificialappearanceonaradiographthatisnotnaturalandcanbecausedbyavarietyofmeans,includingstructuresormishandlingoffilm
Base-fog Densityofaprocessedfilmwithouttheeffectsoflightorradiation,causedbythemanufacturerandstorageofthefilm
Beam(X-ray) AspatialdistributionofX-raysemanatingfromtheX-raytubeBit(binarydigit) Smallestpieceofdigitalinformationthatacomputingdevicehandles.It
representsofforon(0or1).Alldataincomputingdevicesareprocessedasbitsorstringsofbits
Bucky AcommonlyusedabbreviationofthePotter-Buckymovinggridsystem,whichisdesignedtoreducetheamountofscatteredradiationreachingthefilm
Cassette Lighttightholderthatcontainsapairofintensifyingscreens(forfilm),betweenwhichisplacedthefilm
CentralRay ThecentreoftheX-raybeam,oftenusedtodefinethedirectionoftheX-raybeamrelativetoabodypartorimagereceptor
Collimator(s) Adeviceusedtocontrolthecoverageofthex-raybeamanddeterminethex-rayfieldsize.Alsoknownasthelightbeamdiaphragm(LBD)
Compressionratio Theaveragenumberofbitsperpixel(bpp)beforeimagecompressiondividedbythenumberofbppaftercompression
Contrast Differencebetween2ormoredensitiesonafilm.Highcontrastiswheretherearefewshadesofgreybetweenthelightestanddarkestareasoftheimage
CR Abbreviationforcomputedradiography,wheretransmittedX-raysareconvertedtolightviaasolid-stateimagingdevice,suchasa
photostimulablephosphorplate,andrecoveredandprocessedusingadigitalcomputer
Darkroom LighttightroominwhichtheprocessingofradiographsiscarriedoutDensitometer Adeviceusedtomeasuretheopticaldensityonofanyspotona
radiographbymeasuringthelightthatisallowedtopassthroughitDetail(image) Theamountandqualityofinformationcontainedinaradiographicimage,
whichisdeterminedbyimagesharpness,contrastanddensity Developer Thechemicaltreatmentthatconvertsthelatentfilmimageintoavisual
imageDistortion MisrepresentationofabodypartoutlineintheimageduetochangesinX-
raybeam/bodypartalignmentorunacceptableobject-imagedistanceDose Ageneraltermdenotingthequantityofradiationorenergyabsorbedina
targetDoseQuantum AmeasureoftheinformationtransferefficiencytoadigitaldetectorthatEfficiency(DQE) isdependentontheefficientabsorptionofX-raysaswellasthe
conversiontoausefulsignalwithminimumcorruptionbyotherdetectornoisesources
DR Abbreviationfordigitalradiography,wheretransmittedX-raysareconverteddirectlyintoadigitalimageusinganarrayofsolid-statedetectors
Effectivedose Thesumoftheproductsoftheabsorbedorgandoseandtherespectivetissue-weightingfactorforeachspecifiedorganasoutlinedbytheICRP.Thesumforallorgansinthebodyshouldbe1
Emulsion Theactivelayerofchemicalcrystalssuspendedinagelatinlayeroffilm,whichissensitivetolightandradiation.Itcanalsobeusedtodescribetheradiationsensitivelayerofintensifyingscreens.
Erect TermusedtodescribetheuprightpositionofthepatientExposure TheamountofradiationproducedfromtheX-raytubebyapre-
determinedsetofexposurefactors(voltage,current,time).Theterm‘exposure’isusuallyusedtomeanexposurefactors.
ExposureCreep AphenomenonwherebytheintroductionofimagemanipulationinCRandDRhasresultedinhigherpatientexposurestoavoidimageswithquantummottle
FFD Abbreviationforfocal-film-distance,thedistancefromthefocalpoint(origin)oftheX-raybeamtotheimagereceptor.Alsoknownasthesource-image-distance(SID)
Filmdensity Degreeofblackeningonafilm.Thisincreasesasexposuretothefilmincreases.Itcanberadiographic,wherethedegreeofblackeningiscausedbythedepositofmetallicsilver,ortissue,wherethegreaterdensityofthetissuecausesmoreattenuationofthex-raybeamandthusappearslighterontheradiograph
Filter(safelight) Aspecialized,colouredglasswindow,fittedtoasafelightinadarkroomthatenablesthesafehandlingofX-rayfilm
Filter(X-ray) Asheetofmetal(usuallyaluminium)fittedtotheportofanX-raytubetofilteroutthelowwavelengthX-rayphotons
Fixer DissolvesoffallunwantedfilmemulsionandmakestheimagepermanentFocalspot TheareaontheX-raytubeanodewheretheX-raysareproducedFog Unwantedblackeningofafilm,whichiscommonlycausedbyscattered
radiationreachingtheunprocessedfilmorlightfogcausedbyunwantedwhitelightreachingtheunprocessedfilm
Grayscale Thenumberofdifferentshadesorlevelsofgraythatcanbestoredanddisplayedbyacomputersystem.Thenumberofgraylevelsisdirectly
relatedtothenumberofbitsineachpixel:6bits=64graylevels,7bits=129graylevels,8bits=256graylevels,10bits=1024graylevelsand12bits=4096graylevels.
Grid See“Anti-scattergrid”Imagereceptor AdevicethatisusedtocapturethedifferenceinX-raybeamenergies
afterpassingthroughanobjectandthenconvertingittoanimage.Itmaybeafilmandcassette,phosphorescentscreen(forCR)oraflat-paneldetector(forDR)
Intensifyingscreen Radiationsensitivescreens,placedinsideacassetteoneithersideofthefilm,whichfluorescewhenstruckbyradiation,thelightemittedsignificantlycontributingtotheblackeningeffectonthefilm
kV Abbreviationforkilo-voltage,itisanX-rayexposurefactorthatcontrolsthepenetratingpowerandthusqualityoftheX-raybeam.Italsoaffectstheimagecontrast(higherkV=lowercontrast)
Lateral Adescriptionoftheprojectionwherebythex-raybeampathtravelseitherfromthelefttorightsideorrighttoleftsideofthepatient
LosslesscompressionAcompresseddigitalimagethatisperfectlyreconstructedandnumericallyidenticaltotheoriginal.
Lossycompression Acompressedimagewheresomedataarediscarded,nevertoberecovered.Thefrequencycontenttowhichthehumaneyeisinsensitiveisremoved.Theoriginalimageisnotidenticaltothedecompressedversion
mA Abbreviationformilli-amperes,itisanX-rayexposurefactorthatcontrolstheintensityofradiationandthereforefilmdensityandpatientdose(highermA=higherfilmdensity=higherpatientdose)
mAs Abbreviationformilli-ampereseconds,itisthemultipleofthemAandtheexposuretime(inseconds)andreferstothequantityordensityofradiationtowhichthepatientisexposed.ThedensitycanbecontrolledbysettingeitherthemAsasonefactororsettingthemAandtimeseparately
Naturalbackgroundradiation Theamountofradiationtowhichapopulationisexposedfromnaturalresources,suchasterrestrialradiationresultingfromnaturallyoccurringradionuclidesinthesoilandcosmicradiationoriginatinginouterspace
Oxidation Aweakeningofthedeveloperstrengthcausedbyprolongedexposuretoair
PA Abbreviationforpostero-anterior,whichdescribestheprojectionwherebythex-raybeampathtravelsfromtheposteriortoanteriorpartsofthepatient
Penetration TheabilityoftheX-raybeamtopenetratestructures,asdeterminedbytheenergyofthebeam(controlledbykV)
Primarybeam RadiationemittedfromtheX-raytubethathasnotreachedthepatientorobjectbeingimaged
Processing ThechemicaltreatmentofanexposedX-rayfilmthatresultsintheproductionofanX-rayimage
Quality(image) Theappropriatelevelofcontrast,definitionandpatientpositioninginthedemonstrationoftherequiredbodypartsofanimagetoallowtheimagetobeappropriatelyread
Radiolucent ThepropertyofastructuretowhollyorpartiallyallowthepassageofX-rays
Radiopaque ThepropertyofastructuretowhollyorpartiallystopthepassageofX-rays
Resolution Theabilityofanimagingsystemtodifferentiatebetweenobjects

Scatter(radiation) Secondaryradiationthathasbeenchangedindirectionfromtheprimarybeam
SID Abbreviationforsource-to-imagedistance,thedistancefromthefocalpoint(origin)oftheX-raybeamtotheimagereceptor.Alsoknownasthefocal-film-distance(FFD)
Sievert Theunitofequivalentdoseandeffectivedose,equalto1J/kgintheinternationalsystemofunits
Supine Atermusedtodescribeapatientlyinghorizontalontheirback
References:1. StevenD(2004)Radiosensitivityofchildren:potentialforoverexposureinCRandDR
andmagnitudeofdosesinordinaryradiographicexaminations.PeditrRadiol34:S167-S172
2. TomaP,RizzoF,StagnaroNetal(2001)MultisliceCTincongenitalbronchopulmonarymalformationsinchildren.RadiolMed116:133-151
3. KimBH,DoKH,GooHW,YangDH,OhSY,KimHJ,LeeKY,LeeJE,(2012)NationalsurveyofradiationdosesofpediatricchestradiographyinKorea:Analysisofthefactorsaffectingradiationdoses,KoreanJRadiol,13(5):610-617
4. GuoH,LiuWY,HeXY,ZhouXS,ZengQL,LiBY,(2013)Optimizingimagingqualityandradiationdosebytheage-dependentsettingoftubevoltageinpediatricchestdigitalradiography,KoreanJRadiol,14(1):126-131
5. NationalRadiologicalProtectionBoard(1993)Occupational,publicandmedicalexposure,Vol.4,No.2.NRPB
6. NationsScientificCommitteeontheEffectsofAtomicRadiation(2000)Sourceseffectsandrisksofionizingradiation.Vol.II:Effects.UNSCEAR2000Report.UnitedNations
7. Brenner,D.,Elliston,C.,Hall,E.andBordon,W.E.(2001)Estimatedrisksofradiation-inducedfatalcancerfrompediatricCT.Am.J.Roentgenol.176,289–296
8. WorldHealthOrganization(2016)Communicatingradiationrisksinpaediatricimaging,WHO,GenevaSwitzerland,ISBN9789241510349
9. KawooyaMG,HammouA,GharbiHA,LauL(2014)LeadershipandinnovationstoimprovequalityimagingandradiationsafetyinAfrica.InLauL,Kwan-HoongN(ed)RadiologicalSafetyandQuality:LeadershipandInnovation,Springer,p339-360
10. InternationalCommissiononRadiologicalProtection(2013)Radiologicalprotectioninpaediatricdiagnosticandinterventionalradiology.ICRPPublication121.Ann.ICRP42(2)
11. WorldHealthOrganization(1999)Qualitysystemsformedicalimaging:Guidelinesforimplementationandmonitoring.WHO,EasternMediterraneanRegionalOffice
12. WorldHealthOrganization(2000)Consumerguideforthepurchaseofx-rayequipment.WHOCollaboratingCentreforGeneralandContinuingRadiologicalEducation,UniversityofLund,Sweden,WHOreferencenumberWHO/DIL/00.1
13. EuropeanCommission(1996)Europeanguidelinesonqualitycriteriafordiagnosticradiographyimagesinpaediatrics.EUR16261EN,OfficeforOfficialPublicationsoftheEuropeanCommunities,Luxembourg
14. WorldHealthOrganization.Technicalspecificationsfor61medicaldevices.Availablefrom:http://www.who.int/medical_devices/management_use/mde_tech_spec/en/(accessed30thNovember2017)
15. SandstromS(2003)TheWHOmanualofdiagnosticimaging.WorldHealthOrganization.ISBN92-4-154608-5
16. MalkinR,TenintyB(2014)MedicalImagingintheglobalpublichealth:Donation,procurement,installationandmaintenance.InMolluraDJ,LungrenMP(ed)RadiologyinGlobalHealth:Strategies,ImplementationandApplications,Springer,p33-40
17. PerryL,MalkinR(2011)Effectivenessofmedicalequipmentdonationstoimprovehealthsystems:howmuchmedicalequipmentisbrokeninthedevelopingworld?MedBiolEngComput.49:719-22
18. GarraBS.(2014)Informationtechnologyinglobalhealthradiology.InMolluraDJ,LungrenMP(ed)RadiologyinGlobalHealth:Strategies,ImplementationandApplications,Springer,p61-74
19. InternationalStandardIEC62494-1(2008)Medicalelectricalequipment–exposureindexofdigitalX-rayimagingsystems–Part1:definitionsandrequirementsforgeneralradiography.InternationalElectrotechnicalCommission,ISBN2-8318-9944-3
20. DobbinsIIIJTD,FrushDP,KigongoCJN,MacfallJR,ReimanJrRE,TraheyGE.(2014)Medicalimagingsafetyinthedevelopingworld.InMolluraDJ,LungrenMP(ed)RadiologyininGlobalHealth:Strategies,ImplementationandApplications,Springer,p41-60
21. ParkHS,KimYS,ParkOS,KimST,JeonCW,KimHJ,(2014)EffectiveDQE(eDQE)anddosetooptimizeradiographictechnicalparameters:asurveyofpediatricchestX-rayexaminationsinKorea,Radiolmed,119:231-239
22. SuliemanA,VlychouM,TsougosI,TheodorouK,(2011)RadiationdosestopaediatricpatientsandcomfortersundergoingchestX-rays,RadiationProtectionDosimetry,147(1-2):171-175
23. ICRP(2007)The2007RecommendationsoftheInternationalCommissiononRadiologicalProtection.ICRPPublication103.Ann.ICRP37(2-4)
24. AustralianRadiationProtectionandNuclearSafetyAgency(ARPANSA).2008RadiationProtectioninDiagnosticandInterventionalRadiology.RadiationProtectionSeriesPublicationNo.14.1
25. SoboleskiD,TheriaultC,AckerA,DagnoneV,MansonD,(2006)Unnecessaryirradiationtonon-thoracicstructuresduringpediatricchestradiography,PediatrRadiol,36:22-25
26. MolluraDJ,LungrenMP.RadiologyinGlobalHealth:Strategies,ImplementationandApplications,Springer,2014p41-60Availableat:http://www.springer.com/gp/book/9781461406037(Accessed24thJune2017)
27. WillisCE,(2009)Optimizingdigitalradiographyofchildren,EuropeanJournalofRadiology,72:266-273
28. HintenlangKM,WilliamsJL,HintenlangDE,(2002)Asurveyofradiationdoseassociatedwithpediatricplain–filmchestX-rayexaminations,PediatrRadiol,32:771-777
29. Kostova-LefterovaD,TasevaD,IngilizovaK,Hristova-PopovaJ,VassilevaJ,(2011)PotentialforoptimizationofpaediatricchestX-rayexamination,RadiationProtectionDosimetry,147(1-2):168-170
30. InternationalAtomicEnergyAgency(2012)SafetyReportsSeriesNo.71:RadiationProtectioninPaediatricRadiology.IAEA1020-6450,Vienna.Availablefromhttp://www-pub.iaea.org/MTCD/Publications/PDF/Pub1543_web.pdf(Accessed24thFebruary2017)
31. VanoE.(2005)ICRPrecommendationson‘Managingpatientdoseindigitalradiology’.RadiatProtDosimetry114:126-130
32. BuschHP,PaulknerK.(2005)Imagequalityanddosemanagementindigitalradiography:anewparadigmforoptimization.RadiatProtDosimetry117:143-147
33. DohertyP,O’LearyD,BrennanPC.(2003)DoCECguidelinesunder-utilisethefullpotentialofincreasingkVpasadose-reducingtool?EurRadiol13:1992-1999
34. BrennanPC(1995)Adose-reducingexaminationofthefemalepelvis.RadiographyToday61:32-35
35. BrindhabanA,EzeCU(2006)EstimationofradiationdoseduringdiagnosticX-rayexaminationsofnewbornbabiesand1-year-oldinfants.Med.Princ.Pract.15(1),260–265
36. BallingerPW.Merrill’satlasofradiographicpositionsandradiologicprocedures,vol.3.Mosby-YearBook,St.Louis,2003,p190
37. RatibO,RoduitN,NidupD,DeGeerG,RossetA,GeisbuhlerA(2016)PACSforBhutan:acosteffectiveopensourcearchitectureforemergingcountries.InsightsImaging7:747-753
38. JainAK.(1981)Imagedatacompression:areview.ProcIEEE,69:349-38939. AberleDR,GleesonF,SayreJW,etal.(1993)Theeffectofirreversibleimage
compressionondiagnosticaccuracyinthoracicimaging.InvestRadiol,28:398-40340. ResnikoffHL.Waveletanalysisandapplications.NewYork:Springer-Verlag(inpress)
41. CanadianAssociationofRadiologists(2011)CARStandardsforIrreversibleCompressioninDigitalDiagnosticImagingwithRadiology.Availablefromhttps://car.ca/uploads/standards%20guidelines/Standard_Lossy_Compression_EN.pdf(Accessed14thJanuary2017)
42. KhodaieM,AskariA,BahaadingbeigyK.(2015)EvaluationofaVeryLow-CostandSimpleTeleradiologyTechnique.JDigitImaging,28:295-301
43. BrambleJM,CookLT,MurpheyMD,MartinNL,AndersonWH,HensleyKS.(1989)Imagedatacompressioninmagnificationhandradiographs,Radiology,170:133-136
44. GoldbergMA,PivovarovM,Mayo-SmithWW,BhallaMP,BlickmanJG,BramsonRT,BolandGWL,LlewellynHJ,HalpernE.(1994)Applicationofwaveletcompressiontodigitizedradiographs,AJR,163:463-468
45. KoffD,BakP,MatosA,NormalG.(2013)EvaluationsofIrreversibleCompressionRatiosforMedicalImagesThinSliceCTandUpdateofCanadianAssociationofRadiologists(CAR)Guidelines.JDigitImaging,26:440-446
46. HoBKT,TsengV,MaM,ChenD.(1993)AmathematicalmodeltoquantifyJPEGblockartifacvts.ProcSPIE,1987:269-274
47. DriggersRG.TheEncyclopediaofopticalengineering.Volume12,NewYork:Dekker,2003
48. IyribozTA,ZukoskiMJ,HopperKD,StaggPLA.(1999)AcomparisonofWaveletandJPEGlossycompressionmethodsappliedtomedicalimages.JDigitImaging,12(2)suppl1:14-17
49. JavadiM,SubhannachartP,LevineS,VijitsanguanC,TungsagunwattanaS,DowellSF,OlsenSJ.(2006)DiagnosingpneumoniainruralThailand:Digitalcamerasversusfilmdigitizersforchestradiographteleradiology.InternationalJournalofInfectiousDiseases10:129-135
50. SzotA,JacobsonFL,MunnS,JazayeriD,NardellE,HarrisonD.(2004)DiagnosticaccuracyofchestX-raysacquiredusingadigitalcameraforlow-costteleradiology.IntlJMedInform73:65-73
51. RuessL,UyeharaCFT,ShielsKC,ChoKH,O’ConnorSC,WhittonRK,PersonDA(2001)Digitizingpediatricchestradiographs:comparisonoflow-cost,commercialoff-the-shelftechnologies,PediatrRadiol,31:841-847
52. WhitehouseR,MouldingF(2000)Latitudeandnoisecomparisonsbetweendigitalcamerasandaradiographicfilmscanner.JTelemedTelecare6:S1:41-42
Appendix
1. Summaryofstudyrecommendations
Copyright © 2022 FDOKUMEN