Central Nervous System Tuberculosis in Children - Pediatric ...
Upload
independentCategory
view
2download
0
Panniculitis in Children
AntonioTorrelo, MD*, Angela Hern�andez, MDKEYWORDS� Panniculitis � Children � Newborn � Fat necrosis � Nodules
The panniculitides are a group of heterogeneousinflammatory diseases that involve the subcutane-ous fat.1,2 Different pathomechanisms may resultin inflammation of the subcutaneous fatty tissue.Because most cases of panniculitis show thesame clinical appearance, a histopathologic studyis usually required for a correct diagnosis. The his-topathologic study of panniculitis is often difficult,however, because of a limited ability of the fattytissue to display multiple patterns of disease. Fur-thermore, the need for big size biopsy specimensand the nonspecific histopathologic findings usu-ally found in late-stage lesions of panniculitismake it even more difficult to reach a final diagno-sis. A good clinicopathologic correlation and a skil-ful dermatopathologist are very useful tools for theidentification of the causes of panniculitis.
The panniculitides in children are not a frequentconsultation. Indeed, besides erythema nodosum(EN), which is by far the most common form ofpanniculitis, there exist merely anecdotal reportsof most of the well-known panniculitides of adults.Some types of panniculitis, such as subcutaneousfat necrosis (SFN), appear only in children, buteven those disorders are rarely seen. Most typesof panniculitis have been reported to occur in chil-dren, however, and a diagnostic work-up must beperformed in every case to ascertain a definitecause, especially considering that some of themmay bear an uncertain prognosis or may even befatal if untreated. In the absence of specific diag-nostic algorithms for childhood panniculitis, clini-cians must rest on the diagnostic proceduresusually performed in adults. A skin biopsy is thebest tool for the diagnosis of panniculitis, and clini-cians must be wise in the election of the best timeand site to obtain a skin sample of enough size anddepth to permit an accurate diagnosis.
There are as many classifications of panniculitisas textbooks and articles. The most useful are
Department of Dermatology, Hospital del Nino Jesus, C/M* Corresponding author.E-mail address: [email protected] (A. Torrelo).
Dermatol Clin 26 (2008) 491–500doi:10.1016/j.det.2008.05.0100733-8635/08/$ – see front matter ª 2008 Elsevier Inc. All
those based on the classical histopathologic dis-tinction between lobular and septal panniculitis.An etiologic classification is more desirable, how-ever, from a clinical point of view (Box 1).
In this article the panniculitides are thoroughlyreviewed, and virtually all types of panniculitis aretreated elsewhere. The focus is on the specificpanniculitides of children. Discussed also are thepediatric aspects of the main types of panniculiti-des commonly seen in adults.
SPECIFIC PANNICULITIS OF CHILDRENFat Necrosis of the Newborn
SFN of the newborn is an uncommon, benign pan-niculitis usually found in full-term infants. The on-set of the disease may range throughout theneonatal period, and both early and late onsetcases have been reported.
Clinically, it is characterized by multiple indu-rate, nonpitting plaques or nodules with or withouterythema on the cheeks, buttocks, thighs, back,and extremities (Fig. 1).3–5 The lesions tend tospare the anterior trunk. The affected areas maybe mobile over the underlying tissues. The overly-ing skin may show some inflammation, leading toa red or brown hue, or a completely normalappearance (see Fig. 1). The lesions are betterdetected by palpation of the nodules; these maybe discrete or may be rather confluent, especiallyover the back. Many lesions may become fluctuantwith liquefied fat, which may eventually discharge.Mild atrophy or depression of the skin may be no-ticed after resolution of the inflammatory nodules.
The cause for this disorder is unknown. In manycases perinatal complications are recorded, suchas Rh factor incompatibility, meconium aspiration,umbilical cord prolapse, asphyxia, seizures, con-genital heart disease, intestinal perforation, hypo-thermia, sepsis, anemia, gestational diabetes,
enendez Pelayo 65, 28009 Madrid, Spain
rights reserved. derm
.thec
lini
cs.c
om

Fig.1. Subcutaneous fat necrosis of the newborn: ery-thematous indurate nodule on the external aspect ofthe left arm.
Box1Classification of the panniculitis of children
Specific panniculitis of children
Cold panniculitis
Subcutaneous fat necrosis of the newborn
Sclerema neonatorum
Poststeroid panniculitis
Adult-type panniculitis appearing in children
Erythema nodosum
Enzymatic panniculitis
a1-Antitrypsin panniculitis
Pancreatic disease
Infectious panniculitis
Bacterial
Mycobacterial
Fungal
Panniculitis in connective tissue disease
Lupus panniculitis
Deep morphea
Dermatomyositis
Polyarteritis nodosa
Granulomatous panniculitis
Subcutaneous granuloma annulare
Deep sarcoidosis
Physical panniculitis
Injections, iatrogenic, factitial
Extravasation
Blunt trauma
Malignant panniculitis
Histiocytic cytophagic panniculitis
Subcutaneous panniculitic T-cell lymphoma
Edematous, scarring vasculitic panniculitis(hydroa-like lymphoma)
Idiopathic panniculitides
Idiopathic lipoatrophic panniculitis (includ-ing connective tissue panniculitis, panniculitisassociated with autoimmune disorders, lipo-phagic panniculitis of childhood, atrophicconnective tissue panniculitis of the ankles,and recurrent lobular panniculitis)
Eosinophilic panniculitis (not a specific disease)
Torrelo & Hernandez492
preeclampsia, or maternal use or abuse ofdrugs.3,6 SFN has been reported independentlyof the modalities of delivery (vaginal versus cae-sarean section), and an obstetric trauma does
not seem to be a major cause of the disorder.6
Perinatal asphyxia and meconium aspirationseem to be the most crucial factors for the disor-der. In less than 5% of cases SFN appears in oth-erwise normal newborns. The pathogenesis ofSFN might be related to the subcutaneous fatcomposition in neonates, with a relatively highconcentration of saturated fatty acids in respectto adult fat, rich in unsaturated fatty acids. Satu-rated fatty acids have a higher melting point at64�C, which confers a greater propensity of neo-natal fat to undergo crystallization under coldstress, with consequent adipocyte necrosis.7
Other proposed mechanisms include immaturityof the enzymatic systems involved in fatty acidsmetabolism and hypoxic injury to subcutaneousfat.3
Histopathologically, SFN shows a mostly lobularpanniculitis, with a dense inflammatory infiltratecomposed of lymphocytes, histiocytes, lipoph-ages, multinucleated giant cells, and sometimeseosinophils interspersed among the adipocytesof the fat lobule.2 Many adipocytes are replacedby cells with finely eosinophilic granular cytoplasmthat contain narrow needle-shaped clefts radiallyarranged, which represent crystals of triglyceridesof the adipocytes (Fig. 2). Some of these cleftsmay also be seen within the cytoplasm of multinu-cleated giant cells. Although the needle-shapedcrystals within the cytoplasm of adipocytes andhistiocytes are quite characteristic of SFN, theymay not be seen, and similar crystals have beendescribed in cases of poststeroid panniculitisand sclerema neonatorum (SN) (see later). Inlate-stage lesions there is septal fibrosis and areasof calcification may appear within the fat lobule.
The course of SFN is usually uncomplicated andspontaneous resolution over several weeks is ex-pected. SFN may sometimes be complicated,however, with metabolic disbalances that may

Fig. 2. Histopathology of subcutaneous fatnecrosisof the newborn. (A) Scanningpower showing a mostly lobularpan-niculitis, with a dense inflammatory infiltrate Hematoxylin-eosin stain, original magnficiation �4. (B) The infiltrate iscomposed of lymphocytes, histiocytes, lipophages, and multinucleated giant cells. Many adipocytes are replaced bynarrow needle-shaped clefts radially arranged. Hematoxylin-eosin stain, original magnficiation �100. (C) Highermagnifications of the needle-shaped crystals. Hematoxylin-eosin stain, original magnficiation �400.
Panniculitis in Children 493
occur even several months after the resolution ofSFN. These metabolic complications includehypoglycemia, thrombocytopenia, hypertriglyceri-demia, anemia, and hypercalcemia.4,5,8 Hypogly-cemia and thrombocytopenia are the mostfrequent and their onset may precede in days orweeks the development of SFN. These complica-tions might be a consequence of perinatal distresscaused by the triggering factors usually associ-ated with SFN. They tend to resolve spontaneouslywithin a few weeks without complications. Hyper-trigliceridemia, which is a rare complication, usu-ally appears in concomitance with the skinlesions, and is supposed to be caused by mobili-zation of fatty acids from the necrotic adipocytes.The presence of anemia noted in one case of SFNmight have acted as a precipitating factor of SFNinstead of being as a consequence. Hypercalce-mia is the most consistent complication of SFN,which can even be lethal.5 Different hypothesesfor the development of hypercalcemia have beenproposed, including calcium release from theresolving necrotic subcutaneous lesions or boneresorption stimulation by elevated levels ofparathyroid hormone. An extrarenal production of1,25-dihydroxyvitamin D3 by macrophages in the
granuloma is the most plausible explanation.4,9 Insome cases of SFN and hypercalcemia, however,normal levels of 1,25-dihydroxyvitamin D3 havebeen detected.4 Because hypercalcemia mayhave a delayed onset, even up to 6 months afterthe development of the skin manifestations, a pro-longed follow-up with serial determination of se-rum calcium levels is mandatory. Symptoms ofhypercalcemia, such as lethargy, irritability, fever,vomiting, dehydration, failure to thrive, polyuria,and polydipsia, should be sought to avoid toxiceffects of calcium, both acute, such as cardiacarrest or renal failure, and chronic, such as calcifi-cations in the kidney, bone, falx cerebri, and car-diovascular system.5
The approach to the management of SFN itselfshould be conservative, mostly because of its ten-dency to spontaneous resolution. The main goalsare the prevention, early detection, and treatmentof metabolic complications of SFN, especially hy-percalcemia.4,5,8 Avoidance of calcium and vita-min D3 intake should be instituted as early aspossible, and maintenance of adequate hydrationwith intravenous normal saline. Loop diureticsare used to achieve increased calcium excretionby inhibiting calcium reabsorption, but a risk for
Torrelo & Hernandez494
dehydration and consequent worsening of hyper-calcemia exists. Glucocorticoids (prednisolone) in-terfere with the metabolism of vitamin D to itsactive form and also inhibit the production of 1,25-dihydroxyvitamin D3 by the macrophages involvedin the inflammatory process. Etidronate, a memberof the bisphosphonate group of drugs that de-crease bone resorption, has been reported to besuccessful in the management hypercalcemia as-sociated with SFN.8 It should be used as a sec-ond-line drug, because its effects on boneproduction, growth plates, and mineralization areyet unknown. Calcitonin and citrate may be usedas second-line therapy for resistant cases.
Sclerema Neonatorum
Under the term ‘‘sclerema neonatorum,’’ a subcuta-neous condition of the newborn is described in clas-sical textbooks. SN shares many clinical andpathologic similarities with SFN. Most cases of thisrare disorder have been described in very severelyill newborns with low weight or who are premature,in the setting of a wide variety of conditions, suchas infections, congenital heart disease, and othermajor developmental defects. SN was reported inthe past as a life-threatening complication and wasconsidered a sign of very poor prognosis; hence,its denomination as ‘‘preagonic induration.’’
The newborn affected with SN is severely ill atthe onset of the skin induration, and cutaneous le-sions appear during the first days of life.10,11 Theyusually begin on the buttocks and thighs, but rap-idly extend to involve large areas of the body, re-sulting in immobility of the extremities andextensive woody induration of the back. The prog-nosis is poor and most infants affected with SN diewithin a few days. The high ratio of saturated to un-saturated fatty acids in the adipose tissue of all ne-onates has been said to be even higher in infantswith SN, and this can be a predisposing factor.
From a histopathologic point of view, it is noto-rious that, despite striking clinical features, histo-pathology usually shows minimal changes.2,11 Inthe subcutaneous fat, the inflammatory infiltrateis sparse or even absent, and the process doesnot resemble a panniculitis. The poor immunologicresponse of the severely ill infant may be responsi-ble for this absence of striking histopathologic fea-tures. There is little evidence of fat necrosis, andthe most characteristic feature of SN is the pres-ence of radially arranged, needle-shaped clefts inadipocytes, and, occasionally, in some of the fewmultinucleated giant cells present in the sparseinflammatory infiltrate. Autopsy studies have iden-tified identical needle-shaped crystals in adipo-cytes of visceral fat in SN.
The prognosis of SN is poor. Infants who survivean episode of SN during the first week of life,however, have normal-appearing skin with no cal-cifications or other long-term complications.Treatment of SN is primarily directed to the under-lying disease. Systemic corticosteroids are inef-fective, but there is evidence that repeatedexchange transfusions may reduce mortality.
Surprisingly, no new cases of SN have been re-ported in the literature during the last years, evenfrom countries with poor health conditions andhigh neonatal mortality rates. Furthermore, theboundaries between SFN and NS are not veryclear; some cases in the literature are describedunder SN but show typical features of SFN, andthe co-occurrence of both disorders in the samepatient has been reported.12 Furthermore, theage of onset and the predisposing factors overlapin both disorders. Many of the differential criteriafor a diagnosis of SN and SFN are related to dis-ease severity, and both diseases share many his-topathologic features. Currently, as others do,the authors prefer to consider SN and SFN as var-iants of the same disease,6 with SN at the most se-vere pole and tending to appear in younger andpreterm newborns.
Poststeroid Panniculitis
Poststeroid panniculitis is a mostly lobular panni-culitis of children and infants on prolonged sys-temic corticosteroid treatment, and is related toa quick decrease or a sudden withdrawal of ste-roid therapy.
Poststeroid panniculitis only occurs in children.Although some cases have appeared in infants,older children have also been reported.13 It isa very rare disorder, with around 20 cases de-scribed in the literature. The lesions appear asasymptomatic, firm, subcutaneous nodules, oftenwith overlying erythema, measuring 0.5 to 4 cm,which appear on the cheeks, arms, or trunk.14
They usually appear 1 to 10 days after cessationof high doses of systemic corticosteroids.
The disorders for which a corticosteroid therapyis instituted are varied, and include rheumaticfever, leukemia, nephritic syndrome, and braintumors. Likewise, different oral or intravenous cor-ticosteroid agents, including prednisone, prednis-olone, and dexamethasone, have been associatedwith the disorder. A rapid reduction in the steroidadministration seems to predispose children topoststeroid panniculitis.14 Although sometimes re-institution of corticosteroids has induced improve-ment of panniculitis, other authors state that this isnot necessary for its resolution.14 It has been sug-gested that a sudden withdrawal of corticosteroids
Panniculitis in Children 495
may cause an increase in the ratio of saturated tounsaturated fatty acids, leading to crystal forma-tion.13 This mechanism is the same proposed forother panniculitis of the infant. The histopathologyof poststeroid panniculitis shows features similarto those of SFN of the newborn. They consist ofa mostly lobular panniculitis with an inflammatoryinfiltrate of foamy histiocytes and lymphocytes in-volving the fat lobules.2 Often, narrow strands ofneedle-shaped clefts are evident within the cyto-plasm of some histiocytes, although usually theyare not as numerous as in SFN of the newborn.
Lesions of poststeroid panniculitis usually dis-appear gradually without residual scarring duringsome weeks or months, even without resumingsteroid therapy. Complications are unusual; ulcer-ation seldom occurs, then leading to atrophicscars on the cheeks of the infant. No treatment isusually necessary, and it is doubtful if readminis-tration of high doses of systemic corticosteroidand a slower and gradual decrease of the doseis indicated.
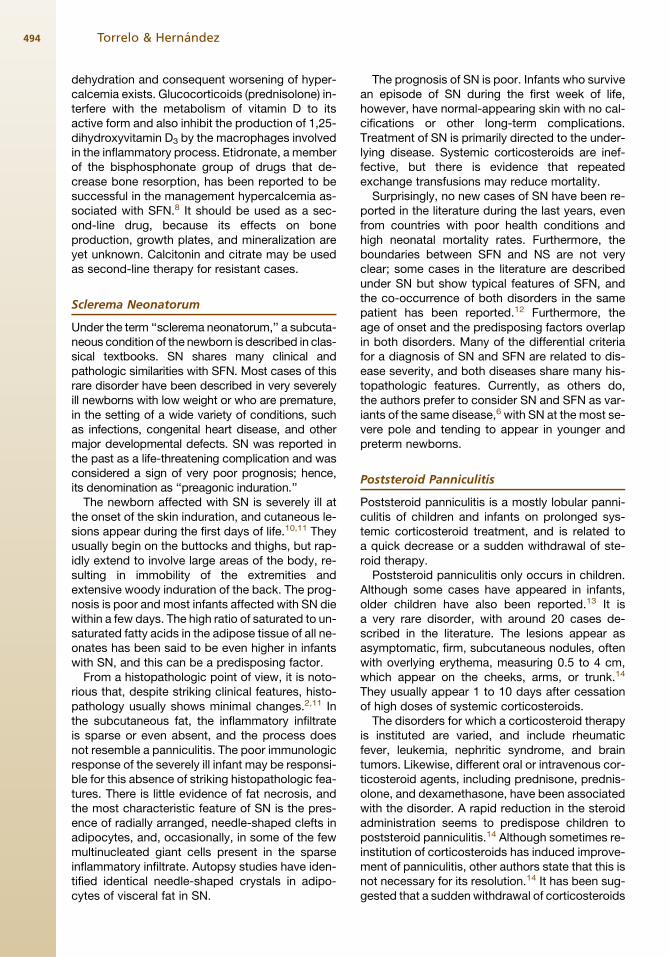
Fig. 3. Erythema nodosum on the anterior aspect ofthe legs of a 9-year-old girl.
Cold Panniculitis
Cold panniculitis (adiponecrosis a frigore) is a typeof panniculitis of newborns that appears 48 to 72hours after exposure to cold. Cold panniculitis isextensively reviewed in elsewhere in this issue.Briefly, cold panniculitis appears as indurate ery-thematous nodules with ill-defined margins. Theoverlying skin is usually intact, and the infant isusually in good general health. Exposure to freez-ing air and application of ice bags to the infant’scheeks for the treatment of supraventricular tachy-cardia are the most common causes in newborns.In older children, sucking ice cubes or ice lollies(popsicles) may induce cold panniculitis (popsiclepanniculitis). The prognosis is excellent and notreatment other than a warm temperature is re-quired for cold panniculitis.
Neonates have higher saturated fat content thanadults. More saturated fat has a higher meltingpoint, and temperature must be maintained abovethis point to preserve the normal composition ofthe fatty tissue. A small decrease in the infant’stemperature might result in crystallization of thefat, leading to cold panniculitis. Interestingly, hy-pothermia and cold exposure are also primary fac-tors in the pathophysiology of SFN and SN. Themore localized nature of cold panniculitis mightbe related to the local application or exposure tocold to a certain site of the infant’s skin insteadof to central or generalized hypothermia. In somecases, a clear distinction between cold panniculitisand SFN is difficult, and lesions that were initially
considered to be cold panniculitis have evolvedinto SFN.8
PEDIATRIC ASPECTS OF THE PANNICULITIDES
All the types of panniculitis that have been dis-cussed are extensively reviewed elsewhere inthis issue. For a more specific description of theirclinical and histopathologic features the reader isdirected to those articles. Next, the purely pediat-ric aspects and differential features of these disor-ders in children is discussed.
Erythema Nodosum
EN is the most common type of panniculitis in chil-dren. It is rare in children under 2 years, and peaksin adolescence both in boys and girls. Clinically,EN in children shows an identical appearance asin adults; however, a higher frequency of lesionson the anterior aspects of the thighs, upper limbs,trunk, and face has been reported (Fig. 3).15 Theassociated joint symptoms are rare in children.
Etiology of EN in children is essentially similar toadult EN. Overall, streptococcal and gastrointesti-nal infections are the main causes of EN in chil-dren, whereas tuberculosis is a rare cause of ENin children.16 Furthermore, sarcoidosis also isa rare cause of EN in children. Idiopathic casesrepresent as much as 40% of cases of EN in child-hood.15 A skin biopsy is not generally performed,but it should be taken in patients with an atypicalpresentation or a protracted course. For a correctidentification of the cause of EN, a work-up includ-ing complete blood cell count, liver function tests,throat swabs, stool culture, chest film, Mantoux
Torrelo & Hernandez496
test, ASO titer, and serologic tests for Yersinia in-fection is advisable.
Therapy of EN in children is essentially based onbed rest and nonsteroidal anti-inflammatorydrugs. In very painful cases, a short course oforal corticosteroids might be considered.
a1-Antitrypsin Deficiency
Panniculitis caused by a1-antitrypsin is a raredisorder, but it is even rarer in children. To the au-thors’ knowledge, only five cases of a1-antitrypsinin children have been reported.17–19 The age of on-set of the skin lesions ranges between 7 and 16years. In most pediatric cases, an antecedent oftrauma is clearly elicited from the history, and le-sions develop on the traumatized area. Areas oferythema and induration rapidly evolve into deep,painless, ulcers; these ulcers do not heal with an-tibiotics or corticosteroids, but respond well to oraldapsone (1–2 mg/kg/d), as in adults with a1-anti-trypsin deficiency. Oral doxycycline was of helpin a teenager.19 A pediatric onset of the diseasedoes not confer a better prognosis, because le-sions may continue to appear into adulthood.
Infectious Panniculitis
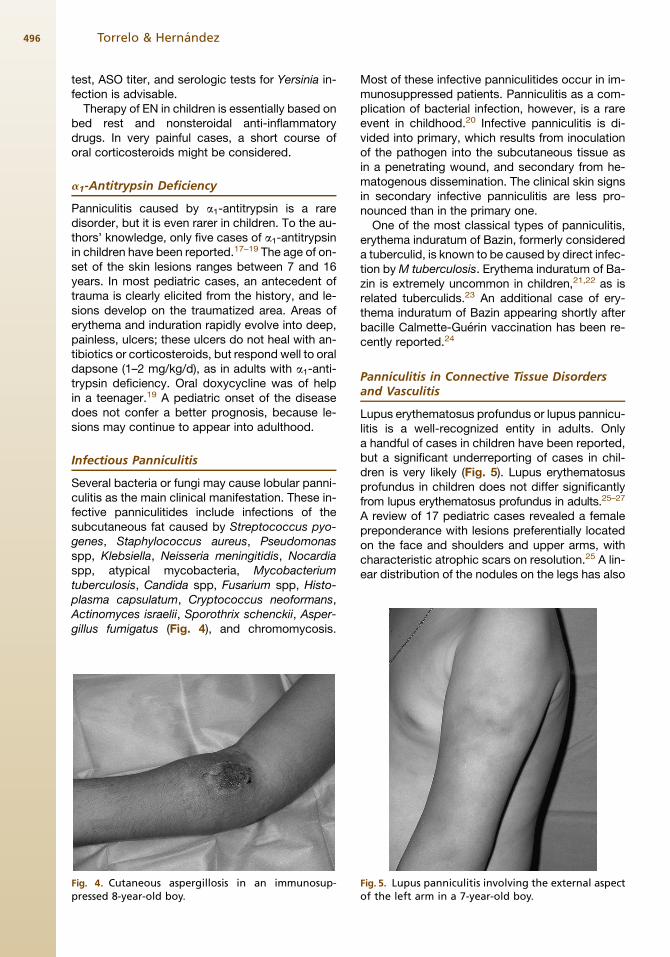
Several bacteria or fungi may cause lobular panni-culitis as the main clinical manifestation. These in-fective panniculitides include infections of thesubcutaneous fat caused by Streptococcus pyo-genes, Staphylococcus aureus, Pseudomonasspp, Klebsiella, Neisseria meningitidis, Nocardiaspp, atypical mycobacteria, Mycobacteriumtuberculosis, Candida spp, Fusarium spp, Histo-plasma capsulatum, Cryptococcus neoformans,Actinomyces israelii, Sporothrix schenckii, Asper-gillus fumigatus (Fig. 4), and chromomycosis.
Fig. 4. Cutaneous aspergillosis in an immunosup-pressed 8-year-old boy.
Most of these infective panniculitides occur in im-munosuppressed patients. Panniculitis as a com-plication of bacterial infection, however, is a rareevent in childhood.20 Infective panniculitis is di-vided into primary, which results from inoculationof the pathogen into the subcutaneous tissue asin a penetrating wound, and secondary from he-matogenous dissemination. The clinical skin signsin secondary infective panniculitis are less pro-nounced than in the primary one.
One of the most classical types of panniculitis,erythema induratum of Bazin, formerly considereda tuberculid, is known to be caused by direct infec-tion by M tuberculosis. Erythema induratum of Ba-zin is extremely uncommon in children,21,22 as isrelated tuberculids.23 An additional case of ery-thema induratum of Bazin appearing shortly afterbacille Calmette-Guerin vaccination has been re-cently reported.24
Panniculitis in Connective Tissue Disordersand Vasculitis
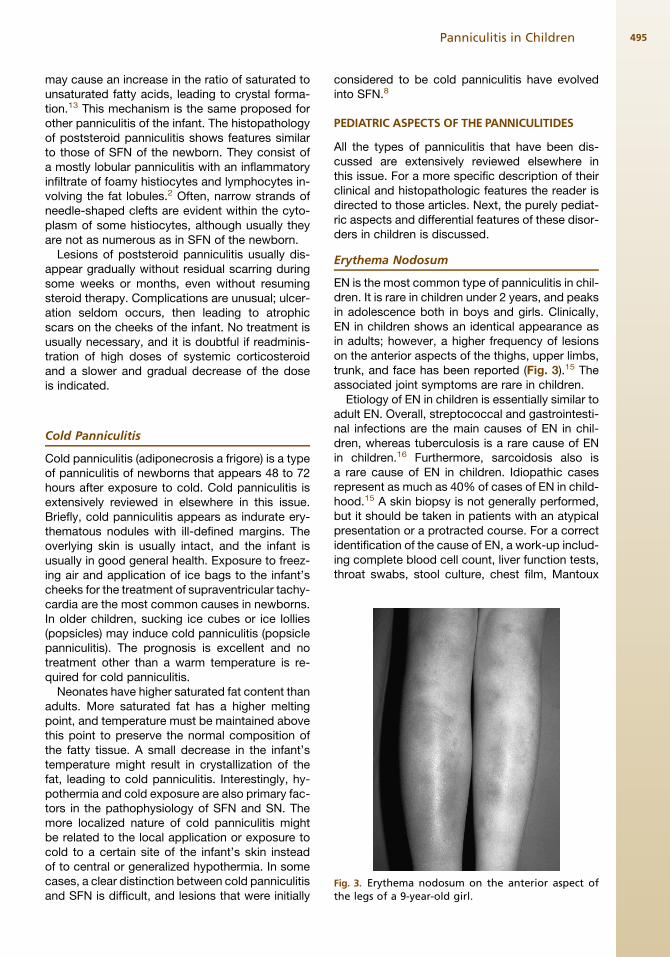
Lupus erythematosus profundus or lupus pannicu-litis is a well-recognized entity in adults. Onlya handful of cases in children have been reported,but a significant underreporting of cases in chil-dren is very likely (Fig. 5). Lupus erythematosusprofundus in children does not differ significantlyfrom lupus erythematosus profundus in adults.25–27
A review of 17 pediatric cases revealed a femalepreponderance with lesions preferentially locatedon the face and shoulders and upper arms, withcharacteristic atrophic scars on resolution.25 A lin-ear distribution of the nodules on the legs has also
Fig. 5. Lupus panniculitis involving the external aspectof the left arm in a 7-year-old boy.

Panniculitis in Children 497
been rarely reported. An association between lu-pus erythematosus profundus and complementfactors C2 and C4 deficiency has been observedin some children.25,27 A single report described lu-pus panniculitis in a patient with neonatal lupuserythematosus.28
Panniculitis is a rare clinical finding in juveniledermatomyositis (DM). Panniculitis may appearat the onset of the disease or the lesions may ap-pear months before DM is diagnosed, and can bedelayed even for 1 year or more after the diagnosisof DM. So far, panniculitis has been reported infour children with DM.29,30 It is also a very rare in-stance in adult DM. Focal subclinical panniculitishas been reported in 10% of patients with DM,however, which suggests the existence of a sub-clinical form of panniculitis.31 Interestingly, bothlocalized and partial lipodystrophy have been re-ported in a significant number of cases of juvenileDM, usually in the absence of clinical panniculitis.It is not known if lipoatrophy is an end stage ofsubclinical panniculitis.32 Calcification is a com-mon feature in many children with juvenile DM.A panniculitis associated with calcification of themuscle and deep tissue is much more commonthan pure panniculitis in DM.2
Panniculitis has also been described in otherautoimmune disorders, such as morphea (deepmorphea) and vasculitis (polyarteritis nodosa).The so-called ‘‘connective tissue panniculitis’’ isdiscussed later with the idiopathic lipoatrophicpanniculitides.
Malignant Panniculitis
Cytophagic histiocytic panniculitis and subcutane-ous panniculitis T-cell lymphoma are two clinicallyand histopathologically different disorders, poten-tially fatal, that usually appear in adults. Some au-thors consider that both disorders are part of thespectrum of T-cell lymphomas, however, becauseboth disorders may show the phenomenon of he-mophagocytosis both in the subcutaneous tissueand in the bone marrow. Cytophagic histiocyticpanniculitis is not a lymphoma itself, and subcuta-neous panniculitis T-cell lymphoma is not purelya panniculitis, but a malignant proliferation ofT cells involving the subcutaneous fat lobules.2
Patients with cytophagic histiocytic panniculitishave a prolonged clinical course of panniculitis,which usually ends in a terminal state character-ized by fever, hepatosplenomegaly, and pan-cytopenia secondary to hemocytophagocytosisinvolving the bone marrow. Some patients with cy-tophagic histiocytic panniculitis have a benign clin-ical behavior, even after many years of follow-up.Some anecdotal cases of cytophagic histiocytic
panniculitis have been reported in children olderthan 12 years.33,34
Subcutaneous panniculitis T-cell lymphomarepresents less than 1% of all the non-Hodgkinlymphomas. So far, only 12 cases of subcutane-ous panniculitis T-cell lymphoma have been re-ported in children from 3 to 17 years of age.35–38
The main features in these pediatric patients area slight female preponderance, a fatality rate of50%, and frequent systemic symptoms, particu-larly fever and malaise. Furthermore, bone marrowinvolvement with evidence of hemophagocytosisis found in 50% of the five children. The outcomeof the patients who had evidence of hemophago-cytic syndrome is poor (80% mortality rate). In chil-dren, as distinct from adults, the face is frequentlyinvolved and systemic symptoms are the more fre-quently presenting features. In contrast to adultswho were treated with chemotherapy, radiother-apy, or a combination of the two and experiencedremission in 41%, 83%, and 67%, respectively,with these treatments, all the children receivedchemotherapy and 50% of them experiencedremission.38 It has been proposed that early intro-duction of cyclosporine in combination withmultiagent chemotherapy may lead to a betterprognosis, even if the lymphoma is complicatedby hemophagocytic syndrome.37
The term ‘‘edematous, scarring vasculitic panni-culitis’’ was used to describe a striking condition ofMexican children, who showed clinical featuresreminiscent of a severe form of hydroa vaccinifor-mis along with malaise, fever, failure to thrive, andhepatosplenomegaly.39 On histopathology, the au-thors described a mostly septal panniculitis withvariable degrees of vasculitis. Unfortunately, no im-munophenotyping was performed. Even thoughthe authors considered this entity as an inflamma-tory process, three of their patients also carriedthe diagnosis of cutaneous lymphoma, and 2 ofthe 14 patients died of a non-Hodgkin’s lymphoma.Similar cases were later described from Japan andKorea, and from Mexico and Peru.40,41 All these pa-tients were considered to have a distinct type of cu-taneous lymphoma, called angiocentric cutaneousT-cell lymphoma of childhood or hydroa-like lym-phoma. It must be recognized, however, that al-though many of the patients have had a fatalcourse even after chemotherapy was instituted,some others have continued with a chronic coursefor many years and have not had a fatal outcome.Immunophenotyping of the lymphoid infiltrate ispredominantly CD3 and CD30 positive, and thereis a strong association of the disease withEpstein-Barr virus, which can be detected by insitu hybridization in the lesions of angiocentriccutaneous T-cell lymphoma of childhood.

Fig. 6. Idiopathic lipoatrophic panniculitis: subcutane-ous nodules on the legs. Lesions tend to regressionleaving areas of lipoatrophy.
Torrelo & Hernandez498
IDIOPATHIC LIPOATROPHIC PANNICULITISIN CHILDHOOD
This term encompasses a clinical presentation ofidiopathic lobar panniculitis usually beginning inchildhood associated with fever, systemic involve-ment from inflamed visceral fat, and lipoatrophy asan end stage of the inflammatory process. Ex-cluded from this group are patients with othertypes of panniculitis associated with fever and lip-oatrophy for which a diagnosis has been achieved.
Many of these cases were initially included un-der the eponym Weber-Christian disease; anothereponym was added, Rothmann-Makai syndrome,to describe patients with a similar condition butwith only cutaneous involvement. With time, how-ever, it became apparent that many of the cases ofWeber-Christian disease had another type of pan-niculitis that had not been correctly diagnosed,such as EN, superficial thromboflebitis, factitialpanniculitis, traumatic panniculitis, and cytopha-gic histiocytic panniculitis.42 It was proposed thatthe term ‘‘Weber-Christian disease’’ be jettisonedbecause it does not refer to a distinct entity, andthat such cases of idiopathic lobar panniculitisshould be reclassified to a more specific diagno-sis. Although the authors agree that the eponymis better abandoned, they have attended in theirclinics a number of patients with recurrent lobarpanniculitis with fever for whom a more specific di-agnosis cannot be attained, even after a thoroughlaboratory work-up. Peters and Winkelmann, andlater Winkelmann himself, proposed the terms‘‘connective tissue panniculitis’’43,44 and ‘‘lipopha-gic panniculitis of childhood’’45 for patients withrecurrent, progressive, lobular lymphocytic panni-culitis with intermittent fever because of the findingof occasional positive antinuclear antibody titers inthe serum. Billings and colleagues46 proposed thatlipoatrophic panniculitis is a form of autoimmunedisease of the fat, because of an association withinsulin-dependent diabetes mellitus, Hashimoto’sthyroiditis, and juvenile rheumatoid arthritis. Theterm ‘‘connective tissue panniculitis’’ is not veryfortunate, because it may lead to confusion withother typical forms of panniculitis that are associ-ated with connective tissue disorders (eg, lupuspanniculitis or panniculitis of dermatomyositis)and because many patients with identical clinicaland pathologic features do not have an associa-tion with antinuclear antibody titers or other auto-immune disorders. A further disorder, called‘‘annular lipoatrophy of the ankles,’’ was used todescribe a 6-year-old child with Graves’ disease,alopecia areata, and positive antinuclear antibodytiters who had circumferential bands of atrophy onthe ankles that had been preceded by a painless
violaceous plaque.47–49 The term ‘‘idiopathic lip-oatrophic panniculitis’’ better represents the dis-ease spectrum of these patients. It is possible,however, that at least some patients with idio-pathic lipoatrophic panniculitis may show withtime more specific forms of panniculitis.
Patients with idiopathic lipoatrophic panniculitisare usually children who show inflamed, tender,subcutaneous nodules that are mainly located onthe legs and arms.42–53 The overlying skin maylook normal or show a violaceous discoloration.The lesions appear in subsequent attacks of newlesions, whereas the older ones tend to subsideleaving a striking lipoatrophy (Fig. 6). The attacksare associated with fever and a slight degree ofmalaise. A visceral involvement has been reportedin some patients under the term ‘‘Weber-Christiandisease,’’ but it is not clear if those patients mighthave had another disorder, such as cytophagichistiocytic panniculitis, that could have accountedfor a fatal outcome or a protracted course. Histo-pathology in the cases described as connectivetissue panniculitis has shown a lobar panniculitiswith a mixed, predominantly lymphocytic infiltrate,which also contains histiocytes, eosinophils,plasma cells, and neutrophils, along with variabledegrees of lipoatrophy. Lipidized giant cells areusually seen in the so-called ‘‘lipophagic pannicu-litis of children’’ and in the ‘‘annular lipoatrophy ofthe ankles.’’ Laboratory investigations may showan elevated erythrocyte sedimentation rate, a slightanemia, leukocytosis and thrombocytosis, ele-vated AST or ALT levels, and sometimes positiveantinuclear antibody titers. An identical disorderas idiopathic lipoatrophic panniculitis has been re-ported to occur in a patient with Niemann-Pick dis-ease54 and in association with an abnormality in
Panniculitis in Children 499
chromosome 10q24-26, very close to the humanpancreatic lipase gene.55
The course of idiopathic lipoatrophic panniculi-tis is variable, and some patients show a verymild disease with a limited course, whereas othershave a severe febrile disease with continuous ac-tivity, leading to prostration and malaise. For mildcases, rest and nonsteroidal anti-inflammatorydrugs may suffice, but more aggressive casesmight need oral corticosteroids, which are usuallyeffective. Corticosteroid-sparing agents, such asmethotrexate and cyclosporine, are worth tryingin severe cases.
OTHER TYPES OF PANNICULITIS IN CHILDREN
There are anecdotal reports of children with painfulerythematous plantar nodules, which on histopa-thology show a septal and lobular panniculitiswith vasculitis. The course is acute, with spontane-ous resolution of the lesions within some weeks.This entity is differentiated from traumatic plantarurticaria and idiopathic plantar hydradenitis.56
A case report of neutrophilic panniculitis aftergranulocyte colony–stimulating factor has beenreported in a 13-year-old girl with chronic neutro-penia.57 She developed nodules on her legs,thighs, and buttocks, which on histopathologyshowed a mixed septal and lobar panniculitis. Asingle case of calcifying panniculitis has been re-ported in a 15-year-old boy after kidneytransplantation.58
REFERENCES
1. Requena L, Sanchez Yus E. Panniculitis. Part I.
Mostly septal panniculitis. J Am Acad Dermatol
2001;45:163–83.
2. Requena L, Sanchez Yus E. Panniculitis. Part II.
Mostly lobular panniculitis. J Am Acad Dermatol
2001;45:325–61.
3. Sharata H, Postellon DC, Hashimoto K. Subcutane-
ous fat necrosis, hypercalcemia, and prostaglandin
E. Pediatr Dermatol 1995;12:43–7.
4. Tran JT, Sheth AP. Complications of subcutaneous fat
necrosis of the newborn: a case report and review of
the literature. Pediatr Dermatol 2003;20:257–61.
5. Borgia F, De Pasquale L, Cacace C, et al. Subcuta-
neous fat necrosis of the newborn: be aware of
hypercalcaemia. J Paediatr Child Health 2006;42:
316–8.
6. Burden AD, Krafchik BR. Subcutaneous fat necrosis
of the newborn: a review of 11 cases. Pediatr
Dermatol 1999;16:384–7.
7. Katz DA, Huerter C, Bogard P, et al. Subcutaneous
fat necrosis of the newborn. Arch Dermatol 1984;
120:1517–8.
8. Wiadrowski TP, Marshman G. Subcutaneous fat ne-
crosis of the newborn following hypothermia and
complicated by pain and hypercalcaemia. Australas
J Dermatol 2001;42:207–10.
9. Norwood-Galloway A, Lebwohl M, Phelps RG, et al.
Subcutaneous fat necrosis of the newborn with hy-
percalcemia. J Am Acad Dermatol 1987;16:435–9.
10. Prendiville JS, Krol AL. Diseases of the dermis
and subcutaneous tissues. In: Schachner LA,
Hansen RC, editors. Pediatric dermatology. Phila-
delphia: Mosby; 2003. p. 713–67.
11. Fretzin DF, Arias AM. Sclerema neonatorum and
subcutaneous fat necrosis of the newborn. Pediatr
Dermatol 1987;4:112–22.
12. Jardine D, Atherton DJ, Trompeter RS. Sclerema neo-
natorum and subcutaneous fat necrosis of the new-
born in the same infant. Eur J Pediatr 1990;150:125–6.
13. Reichel M, Diaz Cascajo C. Bilateral jawline nodules
in a child with a brain-stem glioma: poststeroid panni-
culitis. Arch Dermatol 1995;131:1448–9, 1451–2.
14. Silverman RA, Newman AJ, LeVine MJ, et al. Post-
steroid panniculitis: a case report. Pediatr Dermatol
1988;5:92–3.
15. Labbe L, Perel Y, Maleville J, et al. Erythema nodo-
sum in children: a study of 27 patients. Pediatr Der-
matol 1996;13:447–50.
16. Laurance B, Stone GH, Philpott MG, et al. Aetiology
of erythema nodosum in children: a study by a group
of pediatricians. Lancet 1961;2:14–6.
17. Edmonds BK, Hodge JA, Rietschel RL. Alpha 1-anti-
trypsin deficiency-associated panniculitis: case re-
port and review of the literature. Pediatr Dermatol
1991;8:296–9.
18. Martinon Sanchez F, Fernandez Villar MC, Otero
Esteban JJ, et al. Paniculitis asociada a deficiencia
de alfa-1-antitripsina. An Esp Pediatr 1993;38:
269–70.
19. Chng WJ, Henderson CA. Suppurative panniculitis
associated with alpha 1-antitrypsin deficiency
(PiSZ phenotype) treated with doxycycline. Br J Der-
matol 2001;144:1282–3.
20. Kakourou T, Theodoridou M, Stefanaki K, et al. Two
cases of panniculitis complicating Neisseria menin-
gitidis serogroup A and Streptococcus pyogenes
bacteraemia, respectively. J Eur Acad Dermatol
Venereol 2006;20:1165–7.
21. Chang MW, Lawrence R, Orlow SJ. Erythema indu-
ratum of Bazin in an infant. Pediatrics 1999;103:498–9.
22. Leahy TR, Downey P, Ramsay B, et al. Erythema in-
duratum of Bazin and episcleritis in a 6 year old girl.
Arch Dis Child 2005;90:1132.
23. Jordaan HF, Schneider JW, Abdulla EA. Nodular tu-
berculid: a report of four patients. Pediatr Dermatol
2000;17:183–8.
24. Inoue T, Fukumoto T, Ansai S, et al. Erythema indu-
ratum of Bazin in an infant after bacille Calmette-
Guerin vaccination. J Dermatol 2006;33:268–72.
Torrelo & Hernandez500
25. Bachmeyer C, Aractingi S, Blanc F, et al. Lupus
erythemateux profound chez l’enfant. Ann Dermatol
Venereol 1992;119:535–41.
26. Muncaster A, Stewart G, Moss C, et al. Facial lupus
erythematosus profundus in a 9-year-old boy. J R
Soc Med 1998;91:207–8.
27. Nousari HC, Kimyai-Asadi A, Santana HM, et al.
Generalized lupus panniculitis and antiphospholipid
syndrome in a patient without complement defi-
ciency. Pediatr Dermatol 1999;16:273–6.
28. Nitta Y. Lupus erythematosus profundus associated
with neonatal lupus erythematosus. Br J Dermatol
1997;136:112–4.
29. Ghali FE, Reed AM, Groben PA, et al. Panniculitis in
juvenile dermatomyositis. Pediatr Dermatol 1999;16:
270–2.
30. Chao YY, Yang LJ. Dermatomyositis presenting as
panniculitis. Int J Dermatol 2000;39:141–4.
31. Janis JF, Winkelman RK. Histopathology of the skin
in dermatomyositis: a histopathologic study of 55
cases. Arch Dermatol 1968;97:640–50.
32. Pope E, Janson A, Khambalia A, et al. Childhood ac-
quired lipodystrophy: a retrospective study. J Am
Acad Dermatol 2006;55:947–50.
33. Garcia-Consuegra J, Barrio MI, Fonseca E, et al.
Histiocytic cytophagic panniculitis: report of a case
in a 12-year-old girl. Eur J Pediatr 1991;150:468–9.
34. Secmeer G, Sakalli H, Gok F, et al. Fatal cytophagic
histiocytic panniculitis. Pediatr Dermatol 2004;21:
246–9.
35. Thomson AB, McKenzie KJ, Jackson R, et al. Sub-
cutaneous panniculitic T-cell lymphoma in child-
hood: successful response to chemotherapy. Med
Pediatr Oncol 2001;37:549–52.
36. Chan YF, Lee KC, Llewellyn H. Subcutaneous T-cell
lymphoma presenting as panniculitis in children: re-
port of two cases. Pediatr Pathol 1994;14:595–608.
37. Shani-Adir A, Lucky AW, Prendiville J, et al. Subcu-
taneous panniculitic T-cell lymphoma in children: re-
sponse to combination therapy with cyclosporine
and chemotherapy. J Am Acad Dermatol 2004;
50(Suppl):S18–22.
38. Yim JH, Kim MY, Kim HO, et al. Subcutaneous pan-
niculitis-like T-cell lymphoma in a 26-month-old child
with a review of the literature. Pediatric Dermatol
2006;23:537–40.
39. Ruiz-Maldonado R, Parrilla FM, Orozco-
Covarrubias ML, et al. Edematous, scarring vasculitic
panniculitis: a new multisystemic disease with malig-
nant potential. J Am Acad Dermatol 1995;32:37–44.
40. Magana M, Sangueza P, Gil-Beristain J, et al. Angio-
centric cutaneous T-cell lymphoma of childhood (hy-
droa-like lymphoma): a distinctive type of cutaneous
T-cell lymphoma. J Am Acad Dermatol 1998;38:
574–9.
41. Barrionuevo C, Anderson VM, Zevallos-Giampietri E,
et al. Hydroa-like cutaneous T-cell lymphoma:
a clinicopathologic and molecular genetic study of
16 pediatric cases from Peru. Appl Immunohisto-
chem Mol Morphol 2002;10:7–14.
42. White JW, Winkelmann RK. Weber-Christian panni-
culitis: a review of 30 cases with this diagnosis.
J Am Acad Dermatol 1998;39:56–62.
43. Winkelmann RK. Panniculitis in connective tissue
disease. Arch Dermatol 1983;119:336–44.
44. Peters MS, Winkelmann RK. Localized lipoatrophy
(atrophic connective tissue disease panniculitis).
Arch Dermatol 1980;116:1363–8.
45. Winkelmann RK, McEvoy MT, Peters MS. Lipophagic
panniculitis in childhood. J Am Acad Dermatol 1989;
21:971–8.
46. Billings JK, Milgraum SS, Gupta AK, et al. Lipoatro-
phic panniculitis: a possible autoimmune inflamma-
tory disease of fat. Arch Dermatol 1987;123:1662–6.
47. Roth DE, Schikler KN, Callen JP. Annular atrophic
connective tissue panniculitis of the ankles. J Am
Acad Dermatol 1989;21:1152–6.
48. Dimson OG, Esterly NB. Annular lipoatrophy of the
ankles. J Am Acad Dermatol 2006;54(Suppl):S40–2.
49. Madasseri A, McDermott MB, Irvine AD. Lipoatro-
phic panniculitis of the ankles. Clin Exp Dermatol
2006;31:303–5.
50. Sorensen RU, Abramowsky CR, Stern RC. Ten-year
course of early-onset Weber-Christian syndrome
with recurrent pneumonia: a suggestion for patho-
genesis. Pediatrics 1986;78:115–20.
51. Falcini F, Simonini G, Battini ML, et al. Lipophagic
granulomatous panniculitis misdiagnosed as pur-
pura in an 8-year old girl. Clin Exp Rheumatol
2002;20:432.
52. Melchiorre LP Jr, Rose CD, Hyde PM, et al. Lipopha-
gic granulomatous panniculitis with lipoatrophy
mimicking arthritis with pitting edema. J Rheumatol
2000;27:504–6.
53. Mirza B, Muir J, Peake J, et al. Connective tissue
panniculitis in a child with vitiligo and Hashimoto’s
thyroiditis. Australas J Dermatol 2006;47:49–52.
54. Bukhari I. Idiopathic nodular panniculitis in Nie-
mann-Pick disease. J Eur Acad Dermatol Venereol
2005;19:600–2.
55. Martinez A, Malone M, Hoeger P, et al. Lipoatrophic
panniculitis and chromosome 10 abnormality. Br
J Dermatol 2000;142:1034–9.
56. Sandraps E, Blomme S, Demeester A, et al. Eryth-
eme nodulaire plantaire doloreux de l’enfant. Ann
Dermatol Venereol 1996;123:647–50.
57. Prendiville J, Thiessen P, Mallory SB. Neutrophilic
dermatoses in two children with idiopathic neutrope-
nia: association with granulocyte colony-stimulating
factor (G-CSF) therapy. Pediatr Dermatol 2001;18:
417–21.
58. Koch Nogueira PC, Giuliani C, Rey N, et al. Calcify-
ing panniculitis in a child after renal transplantation.
Nephrol Dial Transplant 1997;12:216–8.
Copyright © 2022 FDOKUMEN