Brain Abscesses in Children: Results of 24 Children From a Reference Center in Central Anatolia,...
11
http://jcn.sagepub.com/ Journal of Child Neurology http://jcn.sagepub.com/content/early/2014/09/12/0883073814549247 The online version of this article can be found at: DOI: 10.1177/0883073814549247 published online 15 September 2014 J Child Neurol Ozturk Selim Doganay, Hakan Gumus, Ekrem Unal, Mehmet Kose, Sureyya Burcu Gorkem, Ali Kurtsoy and Mustafa Kursat Mehmet Canpolat, Ozgur Ceylan, Huseyin Per, Gonca Koc, Abdulfettah Tumturk, Sefer Kumandas, Turkan Patiroglu, Turkey Brain Abscesses in Children: Results of 24 Children From a Reference Center in Central Anatolia, Published by: http://www.sagepublications.com can be found at: Journal of Child Neurology Additional services and information for http://jcn.sagepub.com/cgi/alerts Email Alerts: http://jcn.sagepub.com/subscriptions Subscriptions: http://www.sagepub.com/journalsReprints.nav Reprints: http://www.sagepub.com/journalsPermissions.nav Permissions: What is This? - Sep 15, 2014 OnlineFirst Version of Record >> at Erciyes Universitesi on September 15, 2014 jcn.sagepub.com Downloaded from at Erciyes Universitesi on September 15, 2014 jcn.sagepub.com Downloaded from
-
Upload
independent -
Category
Documents
-
view
6 -
download
0
Transcript of Brain Abscesses in Children: Results of 24 Children From a Reference Center in Central Anatolia,...

http://jcn.sagepub.com/Journal of Child Neurology
http://jcn.sagepub.com/content/early/2014/09/12/0883073814549247The online version of this article can be found at:
DOI: 10.1177/0883073814549247
published online 15 September 2014J Child NeurolOzturk
Selim Doganay, Hakan Gumus, Ekrem Unal, Mehmet Kose, Sureyya Burcu Gorkem, Ali Kurtsoy and Mustafa Kursat Mehmet Canpolat, Ozgur Ceylan, Huseyin Per, Gonca Koc, Abdulfettah Tumturk, Sefer Kumandas, Turkan Patiroglu,
TurkeyBrain Abscesses in Children: Results of 24 Children From a Reference Center in Central Anatolia,
Published by:
http://www.sagepublications.com
can be found at:Journal of Child NeurologyAdditional services and information for
http://jcn.sagepub.com/cgi/alertsEmail Alerts:
http://jcn.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- Sep 15, 2014OnlineFirst Version of Record >>
at Erciyes Universitesi on September 15, 2014jcn.sagepub.comDownloaded from at Erciyes Universitesi on September 15, 2014jcn.sagepub.comDownloaded from

Original Article
Brain Abscesses in Children: Results of24 Children From a Reference Centerin Central Anatolia, Turkey
Mehmet Canpolat, MD1, Ozgur Ceylan, MD2, Huseyin Per, MD1,Gonca Koc, MD3, Abdulfettah Tumturk, MD4, Sefer Kumandas, MD1,Turkan Patiroglu, MD5,6, Selim Doganay, MD3, Hakan Gumus, MD1,Ekrem Unal, MD5, Mehmet Kose, MD7, Sureyya Burcu Gorkem, MD3,Ali Kurtsoy, MD4, and Mustafa Kursat Ozturk, MD2
AbstractChildhood brain abscesses are a rare and potentially life-threatening condition requiring urgent diagnosis and treatment. This retro-spective study analyzed the clinical and radiologic findings of 24 (7 girl, 17 boys) cases with brain abscess. Mean age was 92.98+ 68.04months. The most common presenting symptoms were nausea-vomiting (45.8%) and headache (41.7%). Brain abscess was most com-monly located in the frontal region. Diffusion restriction was determined in 78.4% of lesions. The mean apparent diffusion coefficientvalue in these lesions was 0.511 + 0.23� 10–3 mm2/s. Cultures were sterile in 40% of cases. Antimicrobial therapy was given to only16.7% of cases. Predisposing factors were identified in 91.6% of cases (congenital heart disease in 20.8% and immunosuppression in20.8%). Mortality level was 12.5%. In conclusion, immunocompromised states, and congenital heart disease have become an importantpredisposing factor for brain abscesses. Effective and prompt management should ensure better outcome in childhood.
Keywordsbrain abscess, child, clinical and radiologic features
Received June 10, 2014. Received revised July 02, 2014. Accepted for publication August 02, 2014.
Brain abscesses in childhood are rare but serious infectious dis-
ease.1 It is difficult to assess the incidence of brain abscesses, but
it is probably 2 to 3 cases of every 10 000 hospital admissions.2
Approximately 25% of all brain abscesses are seen in childhood,
most commonly between the ages of 4 and 7.3-5 There is gener-
ally an underlying predisposing condition. The majority of brain
abscesses are associated with congenital heart defects and infec-
tions in the face, head, and brain. There is also a risk of brain
abscess in immunosuppressed children.3-7 Brain abscess may not
produce symptoms for weeks. Clinical findings may be mild and
may be affected by various factors such as age and location of
abscess. A classic triad characterized by headache, fever, and
focal neurologic deficit is seen in 9% to 28% of children.4,5 The
main micro-organisms responsible for brain abscess are
aerobic and anaerobic streptococci and staphylococci. The most
prevalent species in the viridans group are streptococci, espe-
cially Streptococcus milleri. Staphylococcus aureus generally
grows in cultures of abscesses developing after trauma. Other
microorganisms that cause brain abscesses are Bacteroides spe-
cies, Proteus species, Haemophilus influenzae, Escherichia coli,
Citrobacter group, Nocardia, Aspergillus, and Corynebacterium
species and Mycobacterium tuberculosis. No growth is
determined in more than 10% of cases, despite the latest culture
techniques.1-8
Management of brain abscesses is both medical and surgi-
cal, although medical treatment alone may be sufficient in
1 Division of Pediatric Neurology, Department of Pediatrics, Faculty of
Medicine, Erciyes University, Kayseri, Turkey2 Division of Pediatric Infectious diseases, Department of Pediatrics, Faculty of
Medicine, Erciyes University, Kayseri, Turkey3 Department of Pediatric Radiology, Faculty of Medicine, Erciyes University,
Kayseri, Turkey4 Department of Neurosurgery, Erciyes University, Faculty of Medicine,
Kayseri, Turkey5 Division of Hematology and Oncology, Department of Pediatrics, Faculty of
Medicine, Erciyes University, Kayseri, Turkey6 Division of Allergy and Immunology, Department of Pediatrics, Faculty of
Medicine, Erciyes University, Kayseri, Turkey7 Division of Pediatric Pulmonology, Department of Pediatrics, Faculty of
Medicine, Erciyes University, Kayseri, Turkey
Corresponding Author:
Huseyin Per, MD, Division of Pediatric Neurology, Department of Pediatrics,
Faculty of Medicine, Erciyes University, Talas, Kayseri 38039, Turkey.
Email: [email protected]
Journal of Child Neurology1-10ª The Author(s) 2014Reprints and permission:sagepub.com/journalsPermissions.navDOI: 10.1177/0883073814549247jcn.sagepub.com
at Erciyes Universitesi on September 15, 2014jcn.sagepub.comDownloaded from
some selected cases. Surgical drainage and antimicrobial ther-
apy are the preferred options in most cases of brain tumor. Sur-
gical drainage (aspiration) or excision is advised if the lesion
diameter is >2.5 cm or if it causes a mass effect.2-5,9-11
The death rate in brain abscesses used to be around 30% to
60%, although there has been a significant decrease in recent
years, to below 10%. Early diagnosis with neuroradiologic
imaging, rapid neurosurgical intervention, and broad spectrum
antimicrobial therapy including both aerobic and anaerobic
bacteria has led to positive outcomes.3-5
The purpose of this study was to analyze the clinical findings,
radiologic characteristics, risk factors, and prognoses of 24 cases
under observation in our clinic with a diagnosis of brain abscess.
Methods
Cases diagnosed with brain abscess between September 2003 and May
2014, and monitored by the Erciyes University Faculty of Medicine
Pediatric Neurology and Pediatric Infectious Diseases, Turkey, were
evaluated retrospectively. The demographic findings, presenting
symptoms, underlying medical conditions, predisposing risk factors,
abscess sites, radiologic findings, micro-organisms isolated, treatment
regimes, prognoses, and outcomes were recorded of 24 patients aged
between 1 month and 17 years diagnosed with brain abscess and for
which records were available.
Brain abscess cranial computed tomography (CT) or magnetic
resonance imaging (MRI) findings were assessed retrospectively.
These consisted of lesion number and site, perilesional edema, post-
contrast ring sign, shift, presence of hypointense rim on T2-
weighted MRI, and presence or not of diffusion restriction on
diffusion-weighted MRIs. Apparent diffusion coefficient (ADC) val-
ues from lesions were analyzed quantitatively.
Aspirate material collected during surgery was processed in the
microbiology laboratory for urgent aerobic and anaerobic culture. In
nonsurgical cases, diagnosis was confirmed with typical clinical
symptoms and response to treatment.
Results
Twenty-four cases, 7 (29.2%) female and 17 (71.8%) male,
were diagnosed with brain abscess in the 10-year study period.
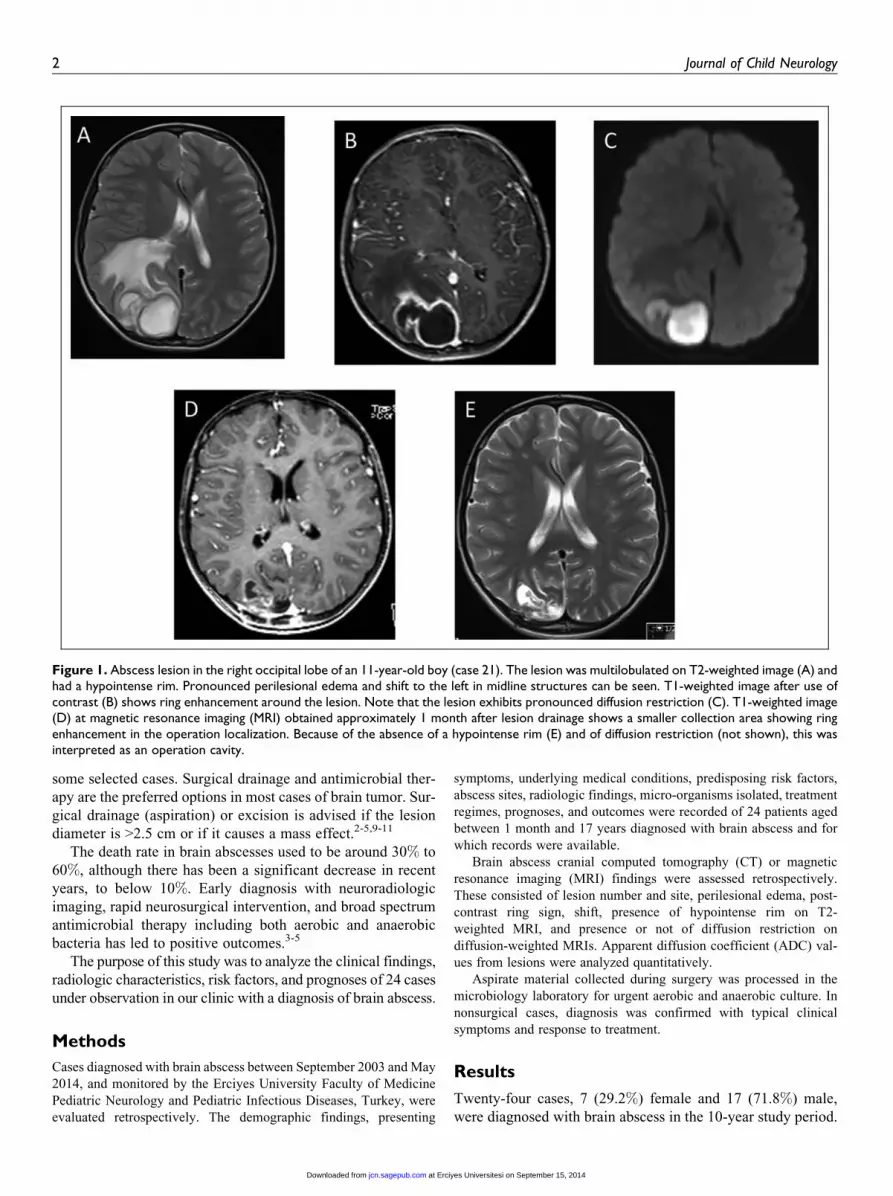
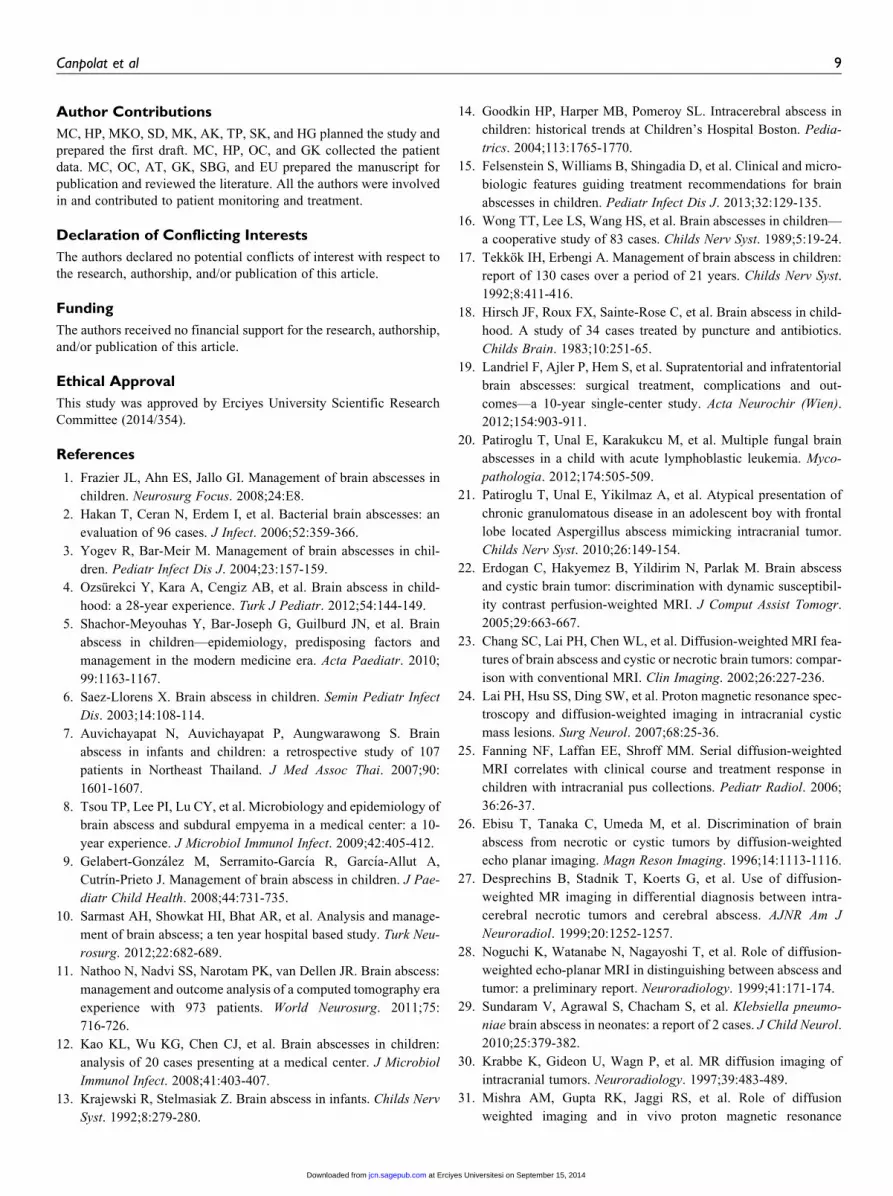
Figure 1. Abscess lesion in the right occipital lobe of an 11-year-old boy (case 21). The lesion was multilobulated on T2-weighted image (A) andhad a hypointense rim. Pronounced perilesional edema and shift to the left in midline structures can be seen. T1-weighted image after use ofcontrast (B) shows ring enhancement around the lesion. Note that the lesion exhibits pronounced diffusion restriction (C). T1-weighted image(D) at magnetic resonance imaging (MRI) obtained approximately 1 month after lesion drainage shows a smaller collection area showing ringenhancement in the operation localization. Because of the absence of a hypointense rim (E) and of diffusion restriction (not shown), this wasinterpreted as an operation cavity.
2 Journal of Child Neurology
at Erciyes Universitesi on September 15, 2014jcn.sagepub.comDownloaded from

Mean age of patients was 92.98 + 68.04 months (minimum 1
month to maximum 204 months). Four cases were referred to
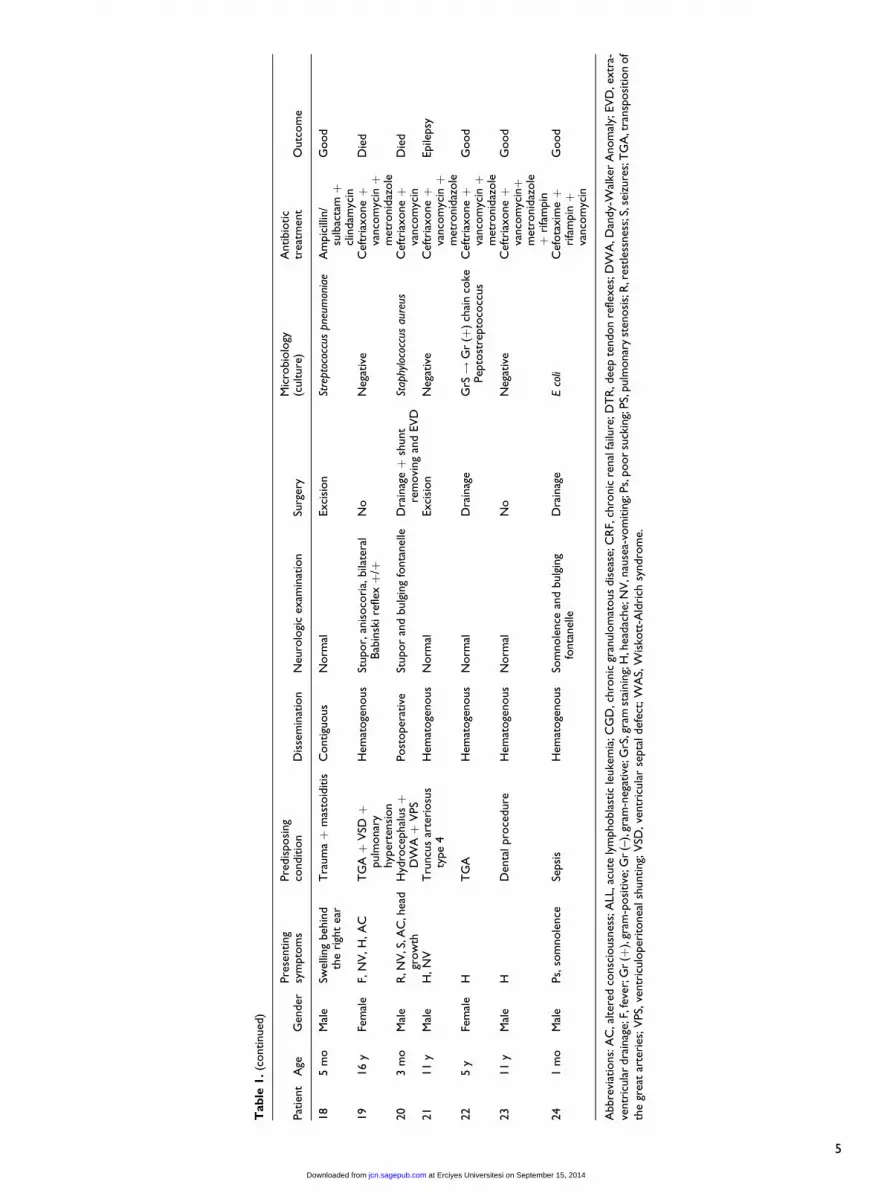
our clinic from other hospitals. General characteristics of cases
are shown in Table 1.
Clinical Features
The most common presenting symptoms were nausea-vomiting
in 11/24 (45.8%) cases, headache in 10/24 (41.7%), convulsion
in 9/24 (37.5%), fever in 7/24 (29.2%), and altered state of con-
sciousness in 7/24 (29.2%) (Table 1).
The most common findings at neurologic examination
were a normal neurologic appearance in 9/24 (37.5%) cases,
altered state of consciousness in 9/24 (37.5%) (stupor in 3 and
somnolence in 6), focal neurologic deficit in 6/24 (25.0%)
(aphasia in 1 case, facial paralysis in 1 case, hemiparesis in
2 cases, and anisocoria in 2 cases), bilateral positive Babinski
reflex in 3/24 (12.5%), papilledema in 1/24 (4.2%), and pos-
itive meningeal irritation findings in 1/24 (4.2%) (Table 1).
The classic triad of fever, headache, and focal neurologic
deficit was determined in 2/24 (8.4%) cases.
Predisposing Factors
Predisposing factors were identified in 22/24 (91.6%) cases.
The most common were congenital heart disease in 5/24
(20.8%) cases and immunosuppression in 5/24 (20.8%). Addi-
tionally, sinusitis was determined in 2/24 (8.3%) cases, dental
procedure in 2/24 (8.3%), autogenic factors in 2/24 (8.3%),
sepsis in 2/24 (8.3%), and trauma in 2/24 (8.3%), whereas the
condition developed postoperatively in 2/24 (8.3%). Pneumo-
nia was a predisposing factor in 1/24 (4.2%) cases and menin-
gitis in 1/24 (4.2%) cases. No predisposing factor was
determined in 2/24 (8.3%) cases (Table 1).
Dissemination
Postoperative spread was determined in 2/24 (8.3%) cases,
contiguous spread in 5/24 (20.8), and hematogenous spread
in 15/24 (62.5%). The 2 cases (8.3%) in which predisposing
factors were not identified were assessed as hematogenous
spread (Table 1).
Radiologic Findings
All cases underwent CT or MRI. Because preoperative images
for 4 cases referred to our clinic were not available from the
hospital records, these cases were evaluated from the records
in the files, and the other 20 cases were evaluated retrospec-
tively using the available images by 2 pediatric radiologists,
GK and SD. All cases were diagnosed radiologically with
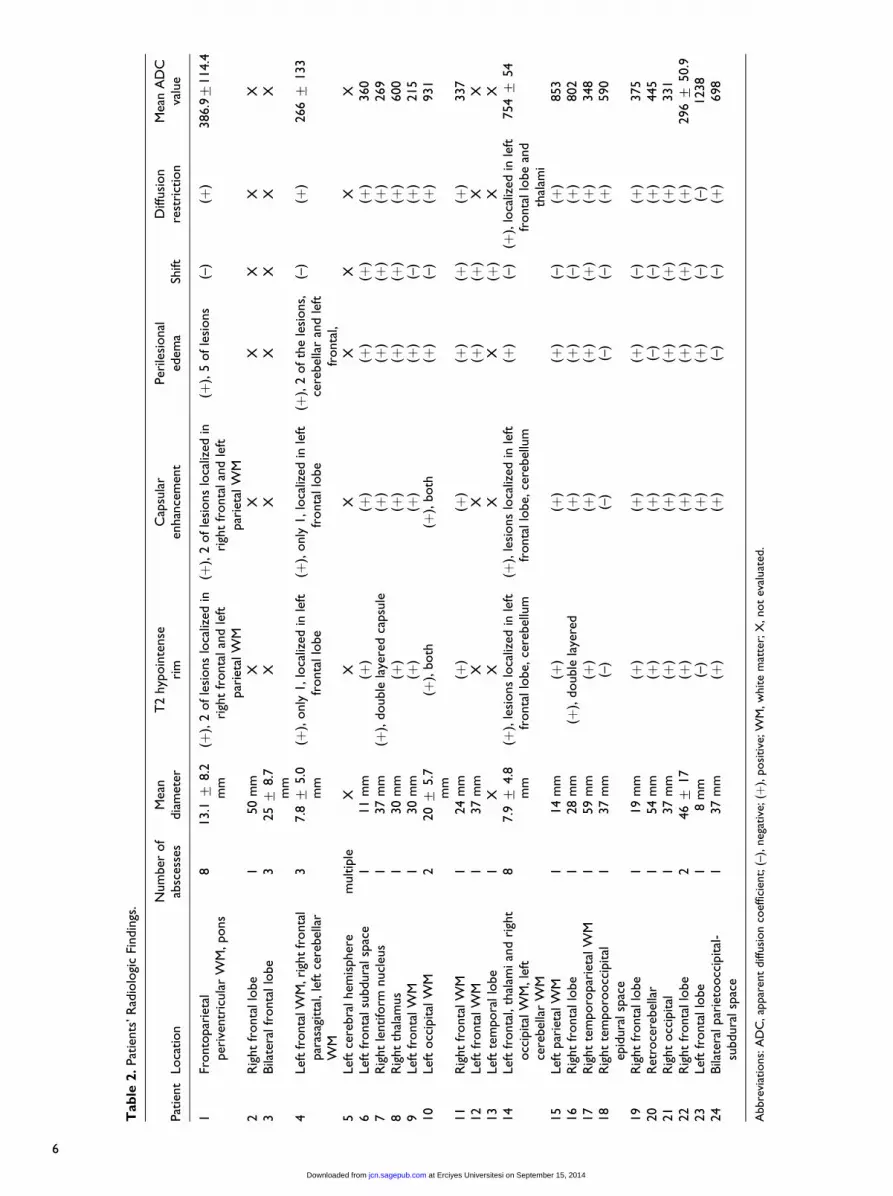
brain abscess before surgery. Radiologic findings are given
in Table 2, and sample case images are given in Figure 1.
Abscesses ranged between 3.4 and 54 mm in size (mean +standard deviation ¼ 32 + 14.7 mm). The most common
abscess locations were supratentorial, in 16/20 (80%) cases.
Abscesses were located infratentorially in 1/20 (5%) cases and
were located in both supra- and infratentorial regions in 3/20
(15%) cases. Abscesses were single in 15/20 (75%) cases and
multiple in 5/20 (25%). Abscesses were frontal in 8/20 (40%)
cases, parietal in 1/20 (5%), occipital in 2/20 (10%), fronto-
parietal in 1/20 (5%), parieto-occipital in 1/20 (5%), tempor-
oparietal in 1/20 (5%), temporooccipital in 1/20 (5%),
cerebellar in 2/20 (10%), in the brain stem in 1/20 (5%), and
in the basal ganglia in 3/20 (15%) cases. Lesions were intra-
parenchymal in 16/20 (80%) cases, subdural in 3/20 (15%), and
epidural in 1/20 (5%).
Total number of abscesses determined in the 20 cases was
38. Only CT images were available for 1 patient. T2 hypoin-
tense rim was determined in 21/37 (56.8%) lesions (2 lesions
had 2-layer hypointense rims), capsular enhancement in 22/
37 (59.5%) lesions, perilesional edema in 30/37 (81.1%)
lesions, and shift in 8/20 (40%) cases, and diffusion restriction
was determined qualitatively in 29/37 (78.4%). Mean apparent
diffusion coefficient value in these 29 abscesses was 0.511 +0.23 � 10–3 mm2/s. Mean apparent diffusion coefficient value
in the 8 lesions not exhibiting qualitative diffusion restriction
was 1.274 + 0.12 � 10–3 mm2/s.
Microbiology
No growth occurred in blood cultures of the 4/24 (16.7%)
nonsurgical cases. Bacteriological investigation was positive
in 13/20 (65.0%) of cases receiving surgery and from which
abscess specimens were taken.
Positive results were obtained in 3/20 (15.0%) cases at gram
staining. Gram-negative bacillus was observed in 1 case at
Gram staining, but culture was sterile. Gram-positive chain
coke was observed in 2 cases at Gram staining, and Peptostrep-
tococcus grew in culture.
Growth was determined in abscess culture in 12/20 (60.0%)
cases. Peptostreptococcus grew in abscess culture in 4 cases
and Aspergillus in 2 cases. Proteus, Pseudomonas, Bacter-
oides, Streptococcus pneumoniae, S aureus, and E coli grew
in abscess culture in 1 case each (Table 1).
Treatment
Antimicrobial therapy alone was administered in 4/24 (16.7%)
cases, and both surgical and antimicrobial therapy in 20/24
(83.3%). In surgical treatment, excision with craniotomy was
performed in 4/20 (20.0%) cases and drainage surgery with burr
hole in 16/20 (80.0%). Shunt removal surgery and extraventricu-
lar drainage surgery were performed in the same session in 1
case in which drainage was applied. Medical treatment was
administered as antibiotic therapy for 6 weeks. Empiric antimi-
crobial therapy was given in 4/24 (16.7%) cases in which sur-
gery could not be performed and abscess specimens could not
be obtained, on the basis of predisposing risk factor, assumed
origin of infection, or hospital- or community-acquired infection
status. Empiric antimicrobial therapy initiated in 20/24 (83.3%)
cases undergoing surgery was adjusted on the basis of microbio-
logical investigation (Table 1).
Canpolat et al 3
at Erciyes Universitesi on September 15, 2014jcn.sagepub.comDownloaded from

Tab
le1.
Pat
ients
’C
linic
alC
har
acte
rist
ics.
Pat
ient
Age
Gen
der
Pre
senting
sym
pto
ms
Pre
dis
posi
ng
conditio
nD
isse
min
atio
nN
euro
logi
cex
amin
atio
nSu
rger
yM
icro
bio
logy
(culture
)A
ntibio
tic
trea
tmen
tO
utc
om
e
117
yM
ale
F,N
V,A
CC
RF
(ren
altr
ansp
lant)
,se
condar
yim
munodef
icie
ncy
,pan
cyto
pen
ia,
hem
ophag
ocy
tosi
s
Hem
atoge
nous
Stupor,
Bab
insk
iþ
/þD
TR
hyp
erac
tive
No
Neg
ativ
eM
eropen
emþ
amik
acinþ
fluco
naz
oleþ
amphote
rici
nB
Die
d
213
yM
ale
H,N
VN
oH
emat
oge
nous
Pap
illed
ema
Dra
inag
eN
egat
ive
Cef
tria
xoneþ
met
ronid
azole
Good
31.5
yM
ale
F,N
V,S
Pneu
monia
Hem
atoge
nous
Som
nole
nce
Dra
inag
eN
egat
ive
Cef
tria
xoneþ
met
ronid
azole
þva
nco
myc
in
Good
44.5
yFe
mal
eF,
SA
LLH
emat
oge
nous
Norm
alD
rain
age
Asp
ergi
llus
nig
erA
mphote
rici
nBþ
vori
conaz
ole
Epile
psy
52.5
mo
Mal
eF,
Ps,
som
nole
nce
Uro
sepsi
sH
emat
oge
nous
Som
nole
nce
and
bulg
ing
fonta
nel
le,e
yes
dev
iate
dto
the
left
,ri
ght
hem
ipar
esis
Dra
inag
ePro
teus
Cef
ota
xim
eþ
amik
acinþ
mer
open
em
Epile
psy
,hem
ipar
esis
67.5
yM
ale
H,N
V,S
Max
illar
yan
dfr
onta
lsi
nusi
tis
Contigu
ous
Norm
alN
oN
egat
ive
Cef
tria
xoneþ
met
ronid
azole
þva
nco
myc
in
Epile
psy
714
yFe
mal
eF,
H,N
V,le
ftce
ntr
alfa
cial
par
alys
is
No
Hem
atoge
nous
Faci
alpar
alys
isD
rain
age
Neg
ativ
eM
eropen
emþ
met
ronid
azole
þri
fam
pin
Good
87
yM
ale
F,H
,so
mnole
nce
TG
Aþ
PS
Hem
atoge
nous
Som
nole
nce
Dra
inag
eG
rS!
Gr
(–)
bac
illus
Neg
ativ
eC
eftr
iaxoneþ
vanco
myc
inþ
met
ronid
azole
Epile
psy
99
yM
ale
HT
raum
a:fr
onta
lbone
frac
ture
Contigu
ous
Norm
alD
rain
age
Neg
ativ
eC
eftr
iaxoneþ
vanco
myc
inþ
met
ronid
azole
Good
10
4y
Mal
eS
Ara
chnoid
cyst
soper
ated
Post
oper
ativ
eN
orm
alExci
sion
Pse
udom
onas
Cef
tria
xoneþ
vanco
myc
inþ
met
ronid
azole
Epile
psy
11
16
yM
ale
S,par
esth
esia
inth
ele
ftle
gC
GD
Hem
atoge
nous
Unre
mar
kable
exce
pt
for
ora
lm
onili
asis
and
skin
scar
sat
axill
ary
and
per
ianal
regi
on
Dra
inag
eAsp
ergi
llus
fum
igat
usA
mphote
rici
nBþ
vori
conaz
ole
Good
12
14
yM
ale
Spee
chdis
ord
ers,
SSi
nusi
tis
Contigu
ous
Aphas
ia,so
mnole
nce
Dra
inag
eG
rS!
Gr
(þ)
chai
nco
kePep
tost
repto
cocc
us
Cef
tria
xoneþ
vanco
myc
inþ
met
ronid
azole
Epile
psy
13
12
yFe
mal
eH
,N
VO
titis
med
ia,
mas
toid
itis
,m
enin
gitis
Contigu
ous
Men
inge
alir
rita
tion
sign
sposi
tive
Dra
inag
eN
egat
ive
Cef
tria
xoneþ
mer
open
emþ
met
ronid
azole
Epile
psy
14
12
yM
ale
S,co
ugh
WA
S,m
uco
sitis,
lung
absc
ess
Hem
atoge
nous
Norm
alD
rain
age
Pep
tost
repto
cocc
us
Cef
tria
xoneþ
vanco
myc
inEpile
psy
15
3y
Fem
ale
S,so
mnole
nce
ALL
,fe
bri
leneu
tropen
iaH
emat
oge
nous
Som
nole
nce
anis
oco
ria,
Bab
insk
ire
flexþ
/þD
rain
age
Neg
ativ
eC
eftr
iaxoneþ
vanco
myc
inþ
met
ronid
azole
þam
phote
rici
nB
Good
16
3y
Fem
ale
NV
Fora
men
ova
leH
emat
oge
nous
Norm
alD
rain
age
Bac
tero
ides
Cef
tria
xoneþ
vanco
myc
inþ
met
ronid
azole
Good
17
4.5
yM
ale
R,N
VD
enta
lpro
cedure
Hem
atoge
nous
Left
hem
ipar
esis
Exci
sion
Pep
tost
repto
cocc
us
Am
pic
illin
/su
lbac
tamþ
amik
acinþ
met
ronid
azole
Epile
psy
,hem
ipar
esis
(con
tinue
d)
4
at Erciyes Universitesi on September 15, 2014jcn.sagepub.comDownloaded from
Tab
le1.
(continued
)
Pat
ient
Age
Gen
der
Pre
senting
sym
pto
ms
Pre
dis
posi
ng
conditio
nD
isse
min
atio
nN
euro
logi
cex
amin
atio
nSu
rger
yM
icro
bio
logy
(culture
)A
ntibio
tic
trea
tmen
tO
utc
om
e
18
5m
oM
ale
Swel
ling
beh
ind
the
righ
tea
rT
raum
aþ
mas
toid
itis
Contigu
ous
Norm
alExci
sion
Stre
ptoc
occu
spn
eum
onia
eA
mpic
illin
/su
lbac
tamþ
clin
dam
ycin
Good
19
16
yFe
mal
eF,
NV
,H
,A
CT
GAþ
VSDþ
pulm
onar
yhyp
erte
nsi
on
Hem
atoge
nous
Stupor,
anis
oco
ria,
bila
tera
lBab
insk
ire
flexþ
/þN
oN
egat
ive
Cef
tria
xoneþ
vanco
myc
inþ
met
ronid
azole
Die
d
20
3m
oM
ale
R,N
V,S
,AC
,hea
dgr
ow
thH
ydro
cephal
usþ
DW
Aþ
VPS
Post
oper
ativ
eSt
upor
and
bulg
ing
fonta
nel
leD
rain
ageþ
shunt
rem
ovi
ng
and
EV
DSt
aphy
loco
ccus
aure
usC
eftr
iaxoneþ
vanco
myc
inD
ied
21
11
yM
ale
H,N
VT
runcu
sar
teri
osu
sty
pe
4H
emat
oge
nous
Norm
alExci
sion
Neg
ativ
eC
eftr
iaxoneþ
vanco
myc
inþ
met
ronid
azole
Epile
psy
22
5y
Fem
ale
HT
GA
Hem
atoge
nous
Norm
alD
rain
age
GrS!
Gr
(þ)
chai
nco
kePep
tost
repto
cocc
us
Cef
tria
xoneþ
vanco
myc
inþ
met
ronid
azole
Good
23
11
yM
ale
HD
enta
lpro
cedure
Hem
atoge
nous
Norm
alN
oN
egat
ive
Cef
tria
xoneþ
vanco
myc
inþ
met
ronid
azole
þri
fam
pin
Good
24
1m
oM
ale
Ps,
som
nole
nce
Sepsi
sH
emat
oge
nous
Som
nole
nce
and
bulg
ing
fonta
nel
leD
rain
age
Eco
liC
efota
xim
eþ
rifa
mpinþ
vanco
myc
in
Good
Abbre
viat
ions:
AC
,alter
edco
nsc
iousn
ess;
ALL
,acu
tely
mphobla
stic
leuke
mia
;CG
D,c
hro
nic
gran
ulo
mat
ous
dis
ease
;CR
F,ch
ronic
renal
failu
re;D
TR
,dee
pte
ndon
refle
xes
;DW
A,D
andy-
Wal
ker
Anom
aly;
EV
D,e
xtr
a-ve
ntr
icula
rdra
inag
e;F,
feve
r;G
r(þ
),gr
am-p
osi
tive
;Gr
(–),
gram
-neg
ativ
e;G
rS,g
ram
stai
nin
g;H
,hea
dac
he;
NV
,nau
sea-
vom
itin
g;Ps,
poor
suck
ing;
PS,
pulm
onar
yst
enosi
s;R
,res
tles
snes
s;S,
seiz
ure
s;T
GA
,tra
nsp
osi
tion
of
the
grea
tar
teri
es;V
PS,
ventr
iculo
per
itonea
lsh
unting;
VSD
,ve
ntr
icula
rse
pta
ldef
ect;
WA
S,W
isko
tt-A
ldri
chsy
ndro
me.
5
at Erciyes Universitesi on September 15, 2014jcn.sagepub.comDownloaded from
Tab
le2.
Pat
ients
’R
adio
logi
cFi
ndin
gs.
Pat
ient
Loca
tion
Num
ber
of
absc
esse
sM
ean
dia
met
erT
2hyp
oin
tense
rim
Cap
sula
ren
han
cem
ent
Per
ilesi
onal
edem
aSh
iftD
iffusi
on
rest
rict
ion
Mea
nA
DC
valu
e
1Fr
onto
par
ieta
lper
iven
tric
ula
rW
M,pons
813.1
+8.2
mm
(þ),
2ofle
sions
loca
lized
inri
ght
fronta
lan
dle
ftpar
ieta
lW
M
(þ),
2ofle
sions
loca
lized
inri
ght
fronta
lan
dle
ftpar
ieta
lW
M
(þ),
5ofle
sions
(–)
(þ)
386.9+
114.4
2R
ight
fronta
llo
be
150
mm
XX
XX
XX
3Bila
tera
lfr
onta
llo
be
325+
8.7
mm
XX
XX
XX
4Le
ftfr
onta
lWM
,rig
ht
fronta
lpar
asag
itta
l,le
ftce
rebel
lar
WM
37.8
+5.0
mm
(þ),
only
1,lo
caliz
edin
left
fronta
llo
be
(þ),
only
1,lo
caliz
edin
left
fronta
llo
be
(þ),
2ofth
ele
sions,
cere
bel
lar
and
left
fronta
l,
(–)
(þ)
266+
133
5Le
ftce
rebra
lhem
ispher
em
ultip
leX
XX
XX
XX
6Le
ftfr
onta
lsu
bdura
lsp
ace
111
mm
(þ)
(þ)
(þ)
(þ)
(þ)
360
7R
ight
lentifo
rmnucl
eus
137
mm
(þ),
double
laye
red
capsu
le(þ
)(þ
)(þ
)(þ
)269
8R
ight
thal
amus
130
mm
(þ)
(þ)
(þ)
( þ)
(þ)
600
9Le
ftfr
onta
lW
M1
30
mm
(þ)
(þ)
(þ)
(–)
(þ)
215
10
Left
occ
ipital
WM
220+
5.7
mm
(þ),
both
(þ),
both
(þ)
(–)
(þ)
931
11
Rig
ht
fronta
lW
M1
24
mm
(þ)
(þ)
(þ)
(þ)
(þ)
337
12
Left
fronta
lW
M1
37
mm
XX
(þ)
(þ)
XX
13
Left
tem
pora
llo
be
1X
XX
X(þ
)X
X14
Left
fronta
l,th
alam
ian
dri
ght
occ
ipital
WM
,le
ftce
rebel
lar
WM
87.9
+4.8
mm
(þ),
lesi
ons
loca
lized
inle
ftfr
onta
llo
be,
cere
bel
lum
(þ),
lesi
ons
loca
lized
inle
ftfr
onta
llo
be,
cere
bel
lum
(þ)
(–)
(þ),
loca
lized
inle
ftfr
onta
llo
be
and
thal
ami
754+
54
15
Left
par
ieta
lW
M1
14
mm
(þ)
(þ)
(þ)
(–)
(þ)
853
16
Rig
ht
fronta
llo
be
128
mm
(þ),
double
laye
red
(þ)
(þ)
(–)
(þ)
802
17
Rig
ht
tem
poro
par
ieta
lW
M1
59
mm
(þ)
(þ)
(þ)
(þ)
(þ)
348
18
Rig
ht
tem
poro
occ
ipital
epid
ura
lsp
ace
137
mm
(–)
(–)
(–)
(–)
(þ)
590
19
Rig
ht
fronta
llo
be
119
mm
(þ)
(þ)
(þ)
(–)
(þ)
375
20
Ret
roce
rebel
lar
154
mm
(þ)
(þ)
(–)
(–)
(þ)
445
21
Rig
ht
occ
ipital
137
mm
(þ)
(þ)
(þ)
(þ)
(þ)
331
22
Rig
ht
fronta
llo
be
246+
17
(þ)
(þ)
(þ)
(þ)
(þ)
296+
50.9
23
Left
fronta
llo
be
18
mm
(–)
(þ)
(þ)
(–)
(–)
1238
24
Bila
tera
lpar
ieto
occ
ipital
-su
bdura
lsp
ace
137
mm
(þ)
(þ)
(–)
(–)
(þ)
698
Abbre
viat
ions:
AD
C,ap
par
ent
diff
usi
on
coef
ficie
nt;
(–),
neg
ativ
e;(þ
),posi
tive
;W
M,w
hite
mat
ter;
X,not
eval
uat
ed.
6
at Erciyes Universitesi on September 15, 2014jcn.sagepub.comDownloaded from

Outcomes
Three of the 24 patients (12.5%) died during treatment. No neu-
rologic sequelae were observed in 11/24 (45.8%) cases in the
first year of monitoring. Epilepsy was diagnosed in 8/24
(33.3%) cases and epilepsy and hemiparesis in 2/24 (8.3%) in
the first year of monitoring (Table 1).
Discussion
Brain abscess in children is rare. Clinical presentation is asso-
ciated with a large number of factors, including site of abscess,
number of abscesses, pathogen, presence or absence of accom-
panying meningitis or ventriculitis, the patient’s immune status
and stage of disease. Although fever, headache and vomiting
are seen in 60% to 70% of adults, clinical findings in children
may be nonspecific, especially as age decreases.2-5,9,12 Fever is
a nonspecific finding that may be generally seen at a level of
30% to 70% in various phases of the disease. Headache is seen
in 42% to 80% of adults, although this level may be lower in
children, at 30% to 50%. Nausea-vomiting is a finding of
increased intracranial pressure and is seen in approximately
25% to 50% of patients. Altered state of consciousness is seen
in approximately 2/3 of cases and may vary in degree from a
mild state of sleep to coma.1-7 Brain abscess in children may
lead to increased head circumference, bulging fontanel, and
separation of cranial sutures.1 Presenting symptoms in our
study were nausea-vomiting in 45.8% of cases, headache in
41.7%, convulsion in 37.5%, fever in 29.2%, and altered con-
sciousness in 29.2%. Our clinical findings were similar to those
of other studies involving the same age group.4,5,9,11-17
Focal neurologic deficit may be seen in 20% to 60% of
cases.4,5,9 Location of the abscess determined focal neurologic
deficits. If the abscess is in the parietal lobe, it leads to hemi-
paresis, to dysphagia if it is in the temporal lobe, and to vision
defects if it is in the occipital lobe.9 Cranial nerve paralysis,
nystagmus, and ataxia may also be seen, depending on the loca-
tion of the abscess.1 Papilledema is seen in 41% to 70% of
adults.9,16,18 However, that level decreases in childhood since
the fontanels are still open. In agreement with the literature,
in this study neurologic appearance was normal in 37.5% of
cases, altered consciousness was present in 37.5%, and focal
neurologic deficit in 25.0%, and bilateral Babinski reflex posi-
tivity was determined in 12.5%. The classic triad characterized
by headache, fever, and focal neurologic deficit was deter-
mined in 8.4% of children.4,5
No underlying predisposing factor is determined in 15% to
30% of brain abscesses.1 In this study, no predisposing factor
was identified in 8.4% of children. Predisposing factors in brain
abscesses are contiguous infections, hematogenous dissemina-
tion, and penetrating head injuries, including surgical interven-
tions.9 Neurosurgical procedures are responsible for some 8%to 10% of cases.16,18 In this study, postoperative spread was
present in 8.3% of cases, contiguous spread in 20.8%, and
hematogenous spread in 62.5%. Shachor-Meyouhas et al5
determined predisposing factors at a level of 81% in their
27-case series; sinusitis-mastoiditis-otitis at a level of 30%,
trauma at 15%, meningitis at 15%, anatomic brain cyst at
7%, pulmonary origin at 4%, congenital heart disease at 7%,
and other causes at 4%, whereas no predisposing factor was
identified in 18% of cases. Goodkin et al14 determined conge-
nital heart disease at a level of 51% and sinusitis-mastoiditis-
otitis at a level of 11% and identified no predisposing factor
in 7% of cases. Auvichayapat et al7 identified congenital heart
disease at a level of 35% and sinusitis-mastoiditis-otitis at a
level of 20%. In a 75-case series from Turkey, Ozsurekci
et al4 determined congenital heart disease at a level of
33.3%, sinusitis at 5.3%, mastoiditis-otitis at 16%, pulmonary
origin at 2.6%, trauma at 2.6%, and immunosuppression at
3.9%. Landriel et al19 determined an immunosuppression level
of 18% in their 59-case series. The most common predisposing
factors in this study were congenital heart disease in 20.8% of
cases, immunosuppression in 20.8%, sinusitis in 8.3%, dental
procedure in 8.3%, autogenic in 8.3%, sepsis in 8.3%, trauma
in 8.3%, neurosurgical procedures in 8.3%, pneumonia in
4.2%, and meningitis in 4.2%. Two cases identified as immu-
nosuppression were associated with acute lymphoblastic leuke-
mia and 1 with chronic renal failure and renal transplantation.
Wiskott-Aldrich syndrome was present in one case, and
chronic granulomatous disease–related immune deficiency in
the other. Brain abscess associated with immunosuppression/
immune deficiency has been increasingly frequently reported
in recent years.4,19-21 This may be related to the development
of diagnostic tests in rare immune deficiencies and the easy
availability of such tests.
Imaging techniques help determine abscess location, edema,
and mass effect.1 Cranial CT used to be widely employed in the
diagnosis of brain abscesses. Significant delays in diagnosis
occurred in the pre–CT scan era, leading to high morbidity and
mortality. Today, MRI may be regarded as the primary imaging
technique for intracranial lesions. Abscess lesions appear
hypointense on T1-weighted images and hyperintense on T2-
weighted images. Vasogenic edema is often determined around
the lesion and occupying a broader space than it. A hypointense
capsule may be observed around the abscess on T2-weighted
images, and an iso-hyperintense capsule on T1-weighted
images. Nathoo et al11 reported that 89.6% of abscesses were
supratentorial, 9.4% infratentorial, and 1% both supra- and
infratentorial. In a study of 75 cases, Ozsurekci et al4 deter-
mined single abscesses in 66.6% of cases and multiple
abscesses in 33.3%. The most frequent abscess locations were
25.3% frontal, 22.6% parietal, 14.6% temporal, 5.3% occipital,
14.6% frontoparietal, 6.6% parieto-occipital, 4% temporopar-
ietal, 4% temporoparieto-occipital, 13.3% cerebellum, and
8% brain stem. Other studies have reported that the most com-
mon abscess locations are parietal and/or frontal lobe.4,5,9 In
our study, and in agreement with the literature, 80% of
abscesses were supratentorial, 5% infratentorial, and 15% in
both supra- and infratentorial regions. Single abscess was pres-
ent in 75% of cases and multiple in 25%. The most common
location for abscesses was the frontal region. Underlying
immune deficiency, congenital heart diseases, sinusitis, and
Canpolat et al 7
at Erciyes Universitesi on September 15, 2014jcn.sagepub.comDownloaded from

facial infections such as dental infection in cases of frontally
located brain abscess (Tables 1 and 2) were noteworthy as
being compatible with the literature and the general study pop-
ulation as etiologic risk factors. Abscess usually appears in a
pronounced hyperintense form on diffusion-weighted images
and possesses low ADC values, indicating diffusion restriction.
Presence of diffusion restriction helps differentiate abscess
from other cystic lesions (e.g., cystic brain tumors).1,9,22-24
Fanning et al25 showed significantly low ADC signal values
in abscesses. Several studies have reported that diffusion-
weighted images are reliable in differentiating abscesses from
malign cystic tumors in particular. Generally, ADC values
decrease because of intense viscosity appearing because of
their high necrotic living cells, bacteria, and protein content,
whereas cystic-necrotic brain tumors have higher ADC values
because of their more serous structure than that of abscesses.
ADC values defined for abscesses in the literature range
between 0.28 and 0.7 (10–3 mm2/s).25-28 However, diffusion
restriction may not be determined in pyogenic abscess lesions
as presented in our study and relevant literature. There may
therefore be a need for advanced radiologic imaging tech-
niques in the differential diagnosis of cystic tumors.29,30 Dif-
fusion restriction may not appear in fungal abscesses and
abscess lesions containing sterile pus.
In agreement with the literature, T2 hypointense rim was
determined in 56.8% of lesions in this study, capsular enhance-
ment in 59.5%, perilesional edema in 81.1%, and shift in 40%.
Qualitative diffusion restriction was determined in 29 (78.4%)
lesions. Mean apparent diffusion coefficient value in these 29
abscesses was 0.511 + 0.23 � 10–3 mm2/s.
Sterile pus cultures were found in 40% of cases. The level of
sterile pus cultures in the literature ranges between 10% and
56%.3-9,12 Growth was determined in 60.0% of pus cultures
in this study. Peptostreptococcus grew in 4 abscess cultures
(20%) and Aspergillus in 2 (10%). Proteus, Pseudomonas, Bac-
teroides, S pneumoniae, S aureus, and E coli grew in 1 (5%)
abscess culture each. Aspergillus growth was present in 2 of our
immunosuppressed cases and Peptostreptococcus growth in 1.
This was compatible with the literature.1,14,20,21 Gram-negative
organisms such as Klebsiella, E coli, Proteus, and Citrobacter
have been reported to be capable of causing abscesses in new-
borns.1,14,31,32 E coli was determined in pus cultures as an agent
in a 1-month-old case in our study.
Although treatment of brain abscesses is still a subject of
debate in the literature, contemporary treatment is a combina-
tion of antimicrobial therapy and surgical intervention.9 Ther-
apeutic approach depends on several factors, such as stage of
the abscess, its location and origin, virulence of the pathogen
micro-organism, number of abscesses, patient response, and
degree of edema.9,12 Antimicrobial therapy alone is preferred
in abscesses <2 cm in size, in high-density lesions, in multiple
abscesses, in patients whose condition is too poor for surgery,
and if the abscess is located in a position inaccessible to sur-
gery.9 Auvichayapat et al7 used antimicrobial therapy alone in
14.7% of cases, Goodkin et al14 in 12.5%, and Ozsurekci et al4
in 24%. In our study, again in agreement with the literature,
16.7% of cases received antimicrobial therapy alone. There
are no randomized controlled trials about the effectiveness
of antibiotic regimens for treating children with brain
abscess.33 Empiric antimicrobial therapy is dictated by pre-
sumed source, but often includes nafcillin or vancomycin,
cefotaxime or ceftriaxone, and metronidazole. Therapy is
adjusted when the culture results are available. Patients usu-
ally receive a minimum 6- to 8-week course of intravenous
antibiotics, which may be prolonged depending on the clinical
context, such as in immunocompromised patients.1-3,15 In our
study, in agreement with the literature, the most preferred
drugs for combination treatment were vancomycin, third-
generation cephalosporin, and metronidazole (Table 1). There
is a need for a well-designed randomized controlled trial to
evaluate the effects of different antibiotic regimens on brain
abscess.
Generally, combination therapy is preferred. In this study,
83.3% of cases received both surgery and antimicrobial ther-
apy. The most common surgical approach is drainage.1,34 This
is particularly advised if the abscess is >2.5 cm in size.1 In
agreement with previous studies,4-12,14,15,19 craniotomy and
excision were performed in 20.0% of the cases in this study,
and drainage surgery in 80.0%.
Until the 1980s, brain abscess–related mortality rates in
children were 11% to 53%. Although some studies have
reported that mortality rates have decreased to 3.7% to 10%thanks to the use of CT and MRI, rapid advances in microbio-
logical tests, fast and effective antibiotherapy, and advances in
neurosurgery, the general mortality rate today is still approxi-
mately 15%.1-18 The mortality rate in our series was 12.5%.
Although our mortality rate was compatible with the literature,
it was higher than that in some recently published case
series.4,5,7,11,12 We attribute this to the predisposing factors in
fatal cases 1 and 19 and their general condition being too poor
for surgery.
The main limitation of this study is that preoperative radi-
ologic images for 4 cases were unavailable since the analysis
was retrospective.
In conclusion, despite advances in diagnosis and treatment,
brain abscesses in children are still associated with high
neurologic morbidity and mortality. Clinical findings may
sometimes be highly indistinct and diagnosis requires a high
index of suspicion. Diagnosis is made on the basis of a com-
bination of clinical and radiologic tests. In recent years,
immunocompromised states have become an important pre-
disposing factor for the development of brain abscesses.
Surgical drainage combined with specific antibiotic therapy
is recommended in these patients. Effective and prompt
management should ensure a much better outcome of brain
abscess in childhood.
Acknowledgments
We are most grateful to Prof Dr Ibrahim Suat Oktem, Prof Dr Abdul-
hakim Coskun, Dr Alper Ozcan, and Dr Huseyin Baz for their support
for this study. We also extend our grateful thanks to all the patients in
this study and their long-suffering families.
8 Journal of Child Neurology
at Erciyes Universitesi on September 15, 2014jcn.sagepub.comDownloaded from
Author Contributions
MC, HP, MKO, SD, MK, AK, TP, SK, and HG planned the study and
prepared the first draft. MC, HP, OC, and GK collected the patient
data. MC, OC, AT, GK, SBG, and EU prepared the manuscript for
publication and reviewed the literature. All the authors were involved
in and contributed to patient monitoring and treatment.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to
the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship,
and/or publication of this article.
Ethical Approval
This study was approved by Erciyes University Scientific Research
Committee (2014/354).
References
1. Frazier JL, Ahn ES, Jallo GI. Management of brain abscesses in
children. Neurosurg Focus. 2008;24:E8.
2. Hakan T, Ceran N, Erdem I, et al. Bacterial brain abscesses: an
evaluation of 96 cases. J Infect. 2006;52:359-366.
3. Yogev R, Bar-Meir M. Management of brain abscesses in chil-
dren. Pediatr Infect Dis J. 2004;23:157-159.
4. Ozsurekci Y, Kara A, Cengiz AB, et al. Brain abscess in child-
hood: a 28-year experience. Turk J Pediatr. 2012;54:144-149.
5. Shachor-Meyouhas Y, Bar-Joseph G, Guilburd JN, et al. Brain
abscess in children—epidemiology, predisposing factors and
management in the modern medicine era. Acta Paediatr. 2010;
99:1163-1167.
6. Saez-Llorens X. Brain abscess in children. Semin Pediatr Infect
Dis. 2003;14:108-114.
7. Auvichayapat N, Auvichayapat P, Aungwarawong S. Brain
abscess in infants and children: a retrospective study of 107
patients in Northeast Thailand. J Med Assoc Thai. 2007;90:
1601-1607.
8. Tsou TP, Lee PI, Lu CY, et al. Microbiology and epidemiology of
brain abscess and subdural empyema in a medical center: a 10-
year experience. J Microbiol Immunol Infect. 2009;42:405-412.
9. Gelabert-Gonzalez M, Serramito-Garcıa R, Garcıa-Allut A,
Cutrın-Prieto J. Management of brain abscess in children. J Pae-
diatr Child Health. 2008;44:731-735.
10. Sarmast AH, Showkat HI, Bhat AR, et al. Analysis and manage-
ment of brain abscess; a ten year hospital based study. Turk Neu-
rosurg. 2012;22:682-689.
11. Nathoo N, Nadvi SS, Narotam PK, van Dellen JR. Brain abscess:
management and outcome analysis of a computed tomography era
experience with 973 patients. World Neurosurg. 2011;75:
716-726.
12. Kao KL, Wu KG, Chen CJ, et al. Brain abscesses in children:
analysis of 20 cases presenting at a medical center. J Microbiol
Immunol Infect. 2008;41:403-407.
13. Krajewski R, Stelmasiak Z. Brain abscess in infants. Childs Nerv
Syst. 1992;8:279-280.
14. Goodkin HP, Harper MB, Pomeroy SL. Intracerebral abscess in
children: historical trends at Children’s Hospital Boston. Pedia-
trics. 2004;113:1765-1770.
15. Felsenstein S, Williams B, Shingadia D, et al. Clinical and micro-
biologic features guiding treatment recommendations for brain
abscesses in children. Pediatr Infect Dis J. 2013;32:129-135.
16. Wong TT, Lee LS, Wang HS, et al. Brain abscesses in children—
a cooperative study of 83 cases. Childs Nerv Syst. 1989;5:19-24.
17. Tekkok IH, Erbengi A. Management of brain abscess in children:
report of 130 cases over a period of 21 years. Childs Nerv Syst.
1992;8:411-416.
18. Hirsch JF, Roux FX, Sainte-Rose C, et al. Brain abscess in child-
hood. A study of 34 cases treated by puncture and antibiotics.
Childs Brain. 1983;10:251-65.
19. Landriel F, Ajler P, Hem S, et al. Supratentorial and infratentorial
brain abscesses: surgical treatment, complications and out-
comes—a 10-year single-center study. Acta Neurochir (Wien).
2012;154:903-911.
20. Patiroglu T, Unal E, Karakukcu M, et al. Multiple fungal brain
abscesses in a child with acute lymphoblastic leukemia. Myco-
pathologia. 2012;174:505-509.
21. Patiroglu T, Unal E, Yikilmaz A, et al. Atypical presentation of
chronic granulomatous disease in an adolescent boy with frontal
lobe located Aspergillus abscess mimicking intracranial tumor.
Childs Nerv Syst. 2010;26:149-154.
22. Erdogan C, Hakyemez B, Yildirim N, Parlak M. Brain abscess
and cystic brain tumor: discrimination with dynamic susceptibil-
ity contrast perfusion-weighted MRI. J Comput Assist Tomogr.
2005;29:663-667.
23. Chang SC, Lai PH, Chen WL, et al. Diffusion-weighted MRI fea-
tures of brain abscess and cystic or necrotic brain tumors: compar-
ison with conventional MRI. Clin Imaging. 2002;26:227-236.
24. Lai PH, Hsu SS, Ding SW, et al. Proton magnetic resonance spec-
troscopy and diffusion-weighted imaging in intracranial cystic
mass lesions. Surg Neurol. 2007;68:25-36.
25. Fanning NF, Laffan EE, Shroff MM. Serial diffusion-weighted
MRI correlates with clinical course and treatment response in
children with intracranial pus collections. Pediatr Radiol. 2006;
36:26-37.
26. Ebisu T, Tanaka C, Umeda M, et al. Discrimination of brain
abscess from necrotic or cystic tumors by diffusion-weighted
echo planar imaging. Magn Reson Imaging. 1996;14:1113-1116.
27. Desprechins B, Stadnik T, Koerts G, et al. Use of diffusion-
weighted MR imaging in differential diagnosis between intra-
cerebral necrotic tumors and cerebral abscess. AJNR Am J
Neuroradiol. 1999;20:1252-1257.
28. Noguchi K, Watanabe N, Nagayoshi T, et al. Role of diffusion-
weighted echo-planar MRI in distinguishing between abscess and
tumor: a preliminary report. Neuroradiology. 1999;41:171-174.
29. Sundaram V, Agrawal S, Chacham S, et al. Klebsiella pneumo-
niae brain abscess in neonates: a report of 2 cases. J Child Neurol.
2010;25:379-382.
30. Krabbe K, Gideon U, Wagn P, et al. MR diffusion imaging of
intracranial tumors. Neuroradiology. 1997;39:483-489.
31. Mishra AM, Gupta RK, Jaggi RS, et al. Role of diffusion
weighted imaging and in vivo proton magnetic resonance
Canpolat et al 9
at Erciyes Universitesi on September 15, 2014jcn.sagepub.comDownloaded from

spectroscopy in the differential diagnosis of ring enhancing intra-
cranial cystic mass lesions. J Comput Assit Tomogr. 2004;28:
540-547.
32. Phan H, Lehman D. Cerebral abscess complicating Proteus mir-
abilis meningitis in a newborn infant. J Child Neurol. 2012;27:
405-407.
33. Lumbiganon P, Chaikitpinyo A. Antibiotics for brain abscesses in
people with cyanotic congenital heart disease. Cochrane Data-
base Syst Rev. 2013;3:CD004469.
34. Ciurea AV, Stoica F, Vasilescu G, Nuteanu L. Neurosurgical
management of brain abscesses in children. Childs Nerv Syst.
1999;15:309-317.
10 Journal of Child Neurology
at Erciyes Universitesi on September 15, 2014jcn.sagepub.comDownloaded from