Paed Mag Jan to March 2014.p65 - CiteSeerX
38
Karnataka Paediatric Journal Vol. 29, No. 1 Jan - March 2014 1 Karnataka Paediatric Journal Vol. 29, No. 4 Jan - March 2014 Journal of the IAP Karnataka State Branch CONTENTS 1. Presidents Message 3 2. Oral Care Practices In Intensive Care Units - Dr.Aswathy Rajan 4 Dr.Ashivj Shriyan 3. Ellis Van Creveld Syndrome With Hydrocephalus- A Rare Association 8 Dr. Palled V Dr. Pujar M S 4. Infective Tropical Acute Kidney Injury In An Adolescent From 11 Rural Coastal Karnataka - A Case Report. Dr Sandeep Kumar Dr Shrikiran Aroor, Dr Suneel Mundkur, R. Dr Maneesh Kumar 5. Vaccine Preventable Disease Death: Tip Of The Iceberg. 14 Dr.Ramya Bandi Dr. Ramesh H 6. Study Of Correlation Of Low Birth Weight With Selected 17 Anthropometric Variables Dr Anil Narayanan, Dr Prakash Saldanha, Dr Mithun 7. Neumanns Tumor - A Rare Dental Tumor In Newborn 23 Dr.Venkatesh. H.A 8. Correlation Of Clinical And Radiological Findings In The Children With 25 Lower Respiratory Tract Infections. Dr.Ansar Murtuza Hussain, Dr.Prakash Saldanha, Dr.Shamshad Khan 9. Serum Creatinine Monitoring In Birth Asphyxiated Newborns 31 Dr. Shamim Amanulla Khan, Dr. Shyam Sudhir, Dr. Faheem 10. Rickettsial Fever- An Incidence Study In A Tertiary Care Centre In South India 36 Dr.Nirmalavineethapinto Dr.Sudharudrappa Dr.Suresh R. . EDITORIAL BOARD Editor in Chief : Editor Dr. B. Sanjeev Rai Dr. Sudharshan S E-mail : [email protected] E mail: [email protected] Mob. : 94481-33494 Mob: 9880008471 EDITORIAL OFFICE Medicare Centre, Karangalpady, Mangalore - 575 003 MEMBERS : Dr. Santhosh Soans Dr. Sridhar Avabratha Dr. Kamalakshi Bhat Dr. Vijay Kulkarnia Dr. Basavaraj Dr.Mahendrappa Dr. G K Gupta Dr.A N Tobbi Dr. Veerashanker Dr. Amarnath K Dr. Srinivasa S PAGE No.
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Paed Mag Jan to March 2014.p65 - CiteSeerX

Karnataka Paediatric Journal Vol. 29, No. 1 Jan - March 2014
1
Karnataka Paediatric Journal Vol. 29, No. 4 Jan - March 2014
Journal of the IAP Karnataka State BranchCONTENTS
1. Presidents Message 3
2. Oral Care Practices In Intensive Care Units - Dr.Aswathy Rajan 4
Dr.Ashivj Shriyan
3. Ellis Van Creveld Syndrome With Hydrocephalus- A Rare Association 8
Dr. Palled V Dr. Pujar M S
4. Infective Tropical Acute Kidney Injury In An Adolescent From 11
Rural Coastal Karnataka - A Case Report.
Dr Sandeep Kumar Dr Shrikiran Aroor, Dr Suneel Mundkur, R. Dr Maneesh Kumar
5. Vaccine Preventable Disease Death: Tip Of The Iceberg. 14
Dr.Ramya Bandi Dr. Ramesh H
6. Study Of Correlation Of Low Birth Weight With Selected 17
Anthropometric Variables
Dr Anil Narayanan, Dr Prakash Saldanha, Dr Mithun
7. Neumann�s Tumor - A Rare Dental Tumor In Newborn 23
Dr.Venkatesh. H.A
8. Correlation Of Clinical And Radiological Findings In The Children With 25
Lower Respiratory Tract Infections.
Dr.Ansar Murtuza Hussain, Dr.Prakash Saldanha, Dr.Shamshad Khan
9. Serum Creatinine Monitoring In Birth Asphyxiated Newborns 31
Dr. Shamim Amanulla Khan, Dr. Shyam Sudhir, Dr. Faheem
10. Rickettsial Fever- An Incidence Study In A Tertiary Care Centre In South India 36
Dr.Nirmalavineethapinto Dr.Sudharudrappa Dr.Suresh R.
.EDITORIAL BOARD
Editor in Chief : Editor
Dr. B. Sanjeev Rai Dr. Sudharshan SE-mail : [email protected] E mail: [email protected]. : 94481-33494 Mob: 9880008471
EDITORIAL OFFICEMedicare Centre, Karangalpady, Mangalore - 575 003
MEMBERS : Dr. Santhosh Soans Dr. Sridhar Avabratha Dr. Kamalakshi Bhat
Dr. Vijay Kulkarnia Dr. Basavaraj Dr.Mahendrappa Dr. G K Gupta Dr.A N Tobbi
Dr. Veerashanker Dr. Amarnath K Dr. Srinivasa S
PAGE No.

Karnataka Paediatric Journal Vol. 29, No. 1 Jan - March 2014
2
INDAN ACADEMY OF PAEDIATRCSKarnataka State BranchSociety Reg No: EKM � S460-2006-2007
Dr. NARAYANAPPA D. Dr. GHFTAK K.B. Dr. P. SUBBARAO
President Secretary Treasurer
M:9845112560 M : 9844778712 M :9845872653
Dr. SANTOSH SOANS Dr. KIRAN BALIGA Dr. B. SANJEEV RAI
President Elect-2015 & Historian Joint Secretary Editor in Chief K.P.J.
M:9886332179 M:9886198991 M:9448133494
Executive Board Members
Bagalkot Dr. Ramesh Pattar
Bangalore Urban Dr. Ravishanker M
Belgaum Dr. Tanmaya Metgud
Bellary Dr. B K Srikanth
Bidar Dr.Sanjeev Biradar
Bijapur Dr Sadashiv Ukkali
Chikkamagalur Dr.Ramesh.M.B.
Chitradurga Dr. Basanth P
Dakshina Kannada Dr. Ashv�rl Shriyan
Davangere Dr. Madhu Pujar
Dharwad Dr. Fateppur
Gadag Dr.Shivkumar I Manvi
Gulburga Dr. Rohit Bandari
Hassan Dr. Prasanna Kumar
Haveri Dr.Anand Ingalgavi
Kodagu Dr. Krishnananda
Kolar Dr.Arun
Kollegal Dr.Sridhar M
Koppal Dr. Anand Kumar.
Mandya Dr.G K Gupta
Mysore Dr. Cherak K.B.
Raichur Dr. Vijay Sukhani
Address for Correspondence:
Dr. CHETAK. K.B.# 1409, Navagraha Temple Road, K.R. Mohalla, Mysore
Mob. : 9844778712, Email : [email protected]
Shimoga Dr. Yateesh
Tumkur Dr. Kumar
Udupi Dr. Leslie Lewis
Uttar Kannada Dr Anrita D'Souza.
Yadir
Ex . Officio�s
Dr. Mrs. N.S. MahantashettiDr. Babanna K. Hukkeri
Central IAP Executive Board Members
Dr. Srinivasa S. Mob:9341 288129
Dr. Basavaraja. G.V. Mob:9448 1 53754
Dr. Deepak Chiradoni Mob:9880629906
Zonal Co-ordinators
Bangalore Dr. Venkatachalapathy
Dharwad Dr. Vijay Kulkarni
Gulbarga Dr. M.M. Patil
Davanagere Dr. Madhu Pujar
Mysore Dr. Prashanth S.N.

Karnataka Paediatric Journal Vol. 29, No. 1 Jan - March 2014
3
DR.D.NARAYANAPPA, MBBS, MD, FIAP
Dear Fellow Pediatricians of Karnataka state,
Greetings from the IAP Karnataka State Branch. I Sincerely thank all our fellowpediatricians for having faith in me and electing me for this prestigious post. We as a team are readyto shoulder the responsibility bestowed on us and would like to keep up the standards setby our peers. Hope the co-operation, advice and suggestion continues in the future.
Inspite of being advanced in technology and one of the largest countries for humanresources, India contributes to nearly one fifth of the child mortality in the world. As a driveto reduce the Infant mortality rate and Under 5 mortality rate, IAP in collaboration withGovernment of Karnataka has implemented several programs like IYCF, public privatepartnerships and has been conducting regular workshops, CMEs.
As the antibiotic resistance is on the rise in our country, there is an urgent need tospread awareness regarding the rational antibiotic policy and rational investigation practices.This is also one of the action plans of central IAP and we plan to implement it effectively inour state.
To reduce the Neonatal mortality Rate, Central IAP has adopted a perfect publicprivate partnership - NSSK and NRPFGM. We need to strengthen these programs by regulartraining at all district places. Our team plans to work towards the same with active supportof state NNF members. Central IAP has very high regards about our state branch for itsexcellent academic activities. I extend full co-operation from our team to all the presidentsand secretaries of the district branches to continue to hold regular academic activities andupdate the knowledge. I also request to enroll maximum members from your districts so thatthe number of our state pediatricians in Central IAP increases and remains a great asset.
With the continued support and co-operation from Central IAP, fellow pediatriciansand our enthusiastic team members, I plan to achieve all our goals for this year. We believein unity is the strength and wish to take the standards of our state to the highest level withthe aim of� Moving towards ���..comprehensive care preventive, promotive, curative�To conclude.......Team work - a fuel that allows common man to achieve uncommon results
JAI IAPJAI KARNATAKA
DR. NARAYANAPPA. D,PRESIDENT, IAPKSB,PROF & HOD OF PAEDIATRICSJ.S.S. MEDICAL COLLEGE,J.S.S. UNIVERSITY,MYSORE.
Presidents Message

Karnataka Paediatric Journal Vol. 29, No. 1 Jan - March 2014
4
*Dept of Pediatrics ,AJ Institute of Medical Scinences, Kuntikana Mangalore
ORAL CARE PRACTICES IN INTENSIVE CARE UNITSDr.Aswathy Rajan, Dr.Ashivj Shriyan*
ABSTRACT
Background � Oral hygiene is essential
to minimize the risk of infection and
significantly affects the child�s well-being.
Although nurses recognize the oral hygiene
as an integral part of the care in the ICU,
the relationship between oral hygiene and
reduction of VAP is less recognized.
Aim of the study � The study has
aimed to evaluate nurse�s opinions on oral
hygiene in mechanically ventilated ICU
patients.
Methods � A prospective, cross sectional
study was conducted on 50 ICU nursing
staff in A. J. Institute of Medical Sciences,
Mangalore. A five-part questionnaire filled in by
the same was assessed.
Results � Methods of providing oral
care and frequency varied in the same unit.
Nurses did not hold oral care as a priority
amongst their nursing interventions. Only
32% (n=16) of the nurses are aware that the
goal of providing oral care is to prevent
ventilator associated pneumonia. A total of
18% (n=9) of the participants have identified
oral care as the first priority in comparison
with other nursing care provided to ICU
patients, third to tracheal suctioning opined
by 46% (n=23) of them.
Conclusions � This survey helps to
bring to light the current oral care practices
in our institution and should be a step
towards improving the practices in ICU.
Keywords � Oral care, nursing
opinions, ventilator associated pneumonia
INTRODUCTION
Oral hygiene is essential to minimize
the risk of infection and significantly affects
the child�s well-being.1 Oral care has been a
low priority intervention in the intensive
care unit (ICU).2 In the critical care setting,
poor oral hygiene is associated with higher
nosocomial infection rates.2 The oro-
pharyngeal colonization with pathogenic
organism contributes to development of
ventilator associated pneumonia (VAP)3
which delays recovery and increases
patient�s mortality rates.4
Although nurses recognize the oral
hygiene as an integral part of the care in the
ICU, the relationship between oral hygiene
and reduction of VAP is less recognized.
Blamoun et al4 have shown that the
application of ventilator care bundle, oral
care protocol and subglottic suctioning
together significantly reduce the rate of VAP.
MATERIALS AND METHODS
The study has aimed to evaluate
nurse�s opinions on oral hygiene in
mechanically ventilated ICU patients. A
prospective, cross sectional study was
conducted on 50 ICU nursing staff in A. J.
Institute of Medical Sciences, Mangalore. All
nursing staff working in neonatal and
pediatric ICU, medical ICU and cardiac ICU
of the institute were included. A two part
questionnaire was prepared after appropriate
approval from the institution, which was
reviewed by one anesthesiologist, two pediatric/
neonatal intensivists and two nurses with
post basic critical care qualification.

Karnataka Paediatric Journal Vol. 29, No. 1 Jan - March 2014
5
The questionnaire (Annexure 1)
consisted of five parts. The first part had
questions regarding the qualification of the
participants and their training in oral care.
Second part consists of questions on oral
care protocol in the institution and the
frequency and goal of providing oral care to
mechanically ventilated patients. Third part
asked the participants to grade from 1 to 4,
a list of 4 essential nursing care parameters
(tracheal suctioning, eye care, oral care and
writing reports), where 1 was given to the
one with most importance. Fourth part
assesses the nurse�s attitudes toward oral
care in mechanically ventilated patients.
They were asked to score from 1 to 4,
keeping 1 as the most likely cause for
ineffective oral care being provided to
patients. The questions assessed the basic
barriers nurses come across in the ICU
including documentation work, lack of time,
presence of the endotracheal tube and
difficulty to clean. The last part asks them to
score the most commonly used material for
providing oral care in the ICU (plain cotton
swab/gauze, chlorhexidine, physiological
salt solution, toothbrush/paste, betadine).
RESULTS
Among a total of 50 nurses, 84%
(n=42) have a bachelor degree, while 10%
(n=3) have a diploma in nursing and only
6% (n=5) have a master�s degree in nursing.
38% (n=19) of the nurses responded they
have had specialized training other than
their basic nursing training in oral care/
hygiene. 92% (n=46) of them understood
the importance and requirement of an oral
care protocol in the institution. A study
found that without a protocol for oral
hygiene, oral care was performed infrequently.
Here, majority of the nurses support the
provision of oral hygiene in ICU twice a
day, which accounts for 66% (n=14) of the
total participants. 28% (n=14) provide oral
care only once a day while 4% (n=2)
provide care thrice a day and 2% (n=1)
more than 3 times a day (Graph 1).
Graph 1. Frequency of oral care
Only 32% (n=16) of the nurses are
aware that the goal of providing oral care is
to prevent ventilator associated pneumonia
while 68% (n=34) assume that it is done to
provide comfort to the mechanically
ventilated patient. A total of 18% (n=9) of
the participants have identified oral care as
the first priority in comparison with other
nursing care provided to ICU patients, third
to tracheal suctioning opined by 46%
(n=23) of them. A high percentage of nurses
voted writing reports (32%) as their first
priority while eye care again was a priority
only for 4% (n=2). Oral care was second
priority again only to 12% (n=6) as writing
reports was a high second priority for them
(56%). Majority of nurses voted oral care as
only a third priority with 58% of them
voting for the same. Eye care remained a 4th
priority for 72% of the nurses (Graph 2).
Graph 2. Knowledge of goal of oral care

Karnataka Paediatric Journal Vol. 29, No. 1 Jan - March 2014
6
80% (n=40) of the nurses reported
spending time in documentation was the
main barrier to providing oral care. 8%
(n=4) of them claimed lack of time as a
hindrance to oral care only second to
documentation, while 6% (n=3) of them
voted the simultaneous presence of an
endotracheal tube as a major factor to not
provide oral to the children and another 6%
(n=3) claimed they find provision of oral
care a difficult task (Graph 3).
Graph 3. Nursing attitudes
None of the participants opine that
cotton swabs and gauze are materials for
providing oral care. Unfortunately, only 42%
(n=21) use chlorhexidine for the same.
Physiological salt solution (normal saline)
was voted for by 46% (n=23) of them, while
8% (n=4) use betadine. Toothbrush and
toothpaste are used by only 4% (n=2) of
them (Graph 4).
Graph 4. Use of equipment by the nurses
DISCUSSION
This survey aimed to assess the
quality, knowledge and practices of oral care
in mechanically ventilated patients in the
ICU. The results revealed that the frequency,
method and attitude toward oral care
differed widely among nurses. Thereby,
successfully analyzing and identifying areas
for improvement.
Many nurses showed that the only
training that they had received in oral care
had been their basic training. Oral care for
mechanically ventilated patients requires
specialized skills and knowledge. Many of
the nurses in this study believed that oral
care was provided to promote patient�s
comfort rather than to prevent VAP. This is
consistent with previous studies, that
suggests that nurses do not have up-to-date
knowledge of oral care for ICU patients and
the educational course has not prepared
them for providing quality oral care.4
A study found that approximately
93% of nurses practice oral care more than
four times per shift after the implementation
of a new oral care protocol showing the
importance of the presence of a standard
protocol which can be established by the
institution to guide the nurses and provide
better oral care.4
Tracheal suctioning was given the
most importance amongst nursing
interventions in this study. Provision of oral
care was given only a third priority
probably due to the false perception that
oral care is less contributory to the patient�s
health than other nursing care activities for
the mechanically ventilated patients.5
ICU nurses were found to have too
much of documentation work and lack of
time assumed due to staff shortage as the
main obstacles for oral care. In a study

Karnataka Paediatric Journal Vol. 29, No. 1 Jan - March 2014
7
done by Schwartz and Powell6, nurses also
fear dislodgement of endotracheal tube and
are therefore hesitant to provide a variety of
oral interventions.
Foam and cotton swabs generally are
not effective for removing debris and
plaque.3 Physiological salt solution (normal
saline), because of its tendency to cause
drying, has limited use as a mouth rinse in
critical care settings.3 Toothbrush was used
only in 4% of the cases despite the
recommendation that it is the best method
for removing plaques in the ICU patients. A
reason for not using toothbrushes could be
the nurses� lack of knowledge of up-to-date
research findings. Chlorhexidine gluconate
is a commonly used broad-spectrum anti-
bacterial mouth rinse that decontaminated
the oropharynx and reduces dental plaque.
The anti-plaque activity of chlorhexidine is
superior to that of other antiseptic
mouthwashes. It has better antibacterial
properties as once it fixes to the oral
surfaces, chlorhexidine gluconate is released
between 8 to 24 hours. Therefore, a twelfth
hourly chlorhexidine gluconate use is
recommended.1
CONCLUSION
Oral care is an essential nursing
intervention in the ICU. The existence of
various oral care practices indicates that
there is a need of a standardized oral care
protocol. Providing protocol based oral care
may decrease the incidence of VAP in
mechanically ventilated patients in the ICU.
Nurses seem to lack evidence based
knowledge of the importance and correct
manner of oral care. This survey helps to
bring to light the current oral care practices
in our institution and should be a step
towards improving the practices in ICU.
REFERENCES
1. Johnstone L, Spence D, Koziol-McLain
J. Oral Hygiene Care in the Pediatric
Intensive Care Uint: Practice
Recommendations. Pediatric Nursing
2010; 36(2):85-96
2. Perrie H, Windsor S. A survey of oral
care practices in South African
Intensive care units. South Asian J Crit
Care 2011; 27 (2): 42-6.
3. Berry AM, Davidson PM, Masters J,
Rolls K. Systematic Literature Review of
Oral Hygeine Practices for Intensice
Care Patients Receiving Mechanical
Ventilation. Am J Crit Care 2007;
16:552-562.
4. Soh KL, Ghazail SS, Soh KG, Raman
RA, Abdullah SSS, Ong SL. Oral care
practice for the ventilated patients in
intensive care units: a pilot survey. J
Infect Crit Ctries 2012; 6(4):333-339.
5. Munro CL, Grap MJ. Oral Health and
Care in the Intensive Care Unit: State of
the Science. Am J Crit Care 2004; 13:25-
34.
6. Adib-Hajbaghery M, Ansari A, Azizi-
Fini I. Intensive care nurses� opinions
and practice for oral care of
mechanically ventilated patients.
Indian J Crit Care Med 2013; 17:23-7

Karnataka Paediatric Journal Vol. 29, No. 1 Jan - March 2014
8
ABSTRACT
Ellis van Creveld syndrome is a
chondroectodermal dysplasia with autosomal
recessive inheritance characterized by short
ribs, polydactyly, growth retardation,
ectodermal and heart defects. We report
a stillborn baby with Ellis van Creveld
Syndrome with hydrocephalus which is an
unusual feature and briefly review the
literature.
KEY WORDS: Ellis van Creveld
Syndrome, Hydrocephalus
INTRODUCTION
Ellis van Creveld syndrome is a
chondroectodermal dysplasia with autosomal
recessive inheritance characterized by short
ribs, polydactyly, growth retardation, ectodermal
and heart defects[1]. It is a rare disease
first described in 1940 by Richard W.B.
Ellis and Simon van Creveld [2], with more than
200 cases reported worldwide till now [3]. We
present a stillborn baby with features
suggestive of Ellis van Creveld Syndrome
with hydrocephalus which is an unusual
feature.
CASE REPORT
A single stillborn term female
baby was delivered via naturalis at CG
Hospital, Davangere, Karnataka with
birth weight 2.5kgs and length 45cms.
Head circumference could not be
measured at birth as craniocentesis was
done during labour to facilitate vaginal
delivery due to which skull bones had
collapsed. But antenatally measured
Ellis Van Creveld Syndrome With Hydrocephalus-
A Rare Association
Dr. Palled V Dr. Pujar MS*
JJM Medical College, Davangere. *1955, �Madhumann�, MCC �A� Block, Davangere.
Email- [email protected]
head circumference at 39wks through
ultrasonography was 42.7cms. Placental
calcification was seen.
Clinically, baby had collapsedskull bones, large clover shaped head,hypertelorism, wide nasal bridge, cleftlip and cleft palate, neonatal tooth,short bilateral upper and lower limbs,polysyndactyly in all 4 limbs,hypoplastic nails, saddle gap in rightlower limb and bilateral great toe stood
out[Fig1, 2].
Fig1- Large head, hypetelorism, short
broad nose, cleft lip, short limbs
Fig2- Nail hypoplasia, Polysyndactyly,
Standing out of great toe.
Infantogram revealed two neonatal
teeth, narrow thorax, shortened long
bones, bowing of bilateral radii and left
ulna, polydactyly, shortening of middle

Karnataka Paediatric Journal Vol. 29, No. 1 Jan - March 2014
9
and distal phalanges of hand, pubic
diastasis, short and squared iliac wings,
horizontal acetabulum[Fig3].
Fig3- Short humeri and femurs, Short
ribs and Narrow thorax
Autopsy findings were as follows- heart
showed atrial septal defect 0.6 x 0.6cm,
small intestine showed 2.5cm constriction
at 5cm distance from ileoceacal junction,
Microscopy of laryngeal and thyroid cartilage
showed >3 cells in single lacuna, vesicular
nuclei, large chondrocytes and irregularly
spaced lacunae[Fig4] suggestive of
chondrodysplasia.
Fig4- Abnormally large chondrocytes, large
lacunae with 2-3 chondrocytes in single
lacuna
DISCUSSION
Ellis van Creveld syndrome is a
rare autosomal recessive disorder which
affects the ectodermal, mesodermal and
endodermal derivatives [4], characterized
by short ribs, short limbs, postaxial
polydactyly, and dysplastic teeth and
nails [1]. In Amish population its prevalence
is 1 in 5000 live births whereas in
non-Amish population it occurs in 1 in
1,000,000 live births [5]. It occurs in
two thirds [6] of the patients due to
mutations in the EVC1 and EVC2
genes located on chromosome 4p16 [1, 3]
lying in a head to head configuration[7].
In the first trimester scan, at 13th
week of gestation, there is increased
thickness of fetal nuchal translucency[1,8]. After 18th week, narrow thorax,
marked shortening of the long bones,
hexadactyly of hands and feet and
cardiac defect can be identified.
Clinical features include small
stature, neonatal teeth, small teeth,
delayed eruption, short upper lip bound
by frenula to alveolar ridge, irregularly
short extremities, polysyndactyly in all 4
limbs, hypoplastic nails, cardiac defects
(approx. 60%) most commonly atrial
septal defect, often with single atrium
(40%) [1, 2]. Cardiac defect is the main
determinant of longevity. Although most
patients have normal intelligence and
normal head circumference, occasional
CNS anomalies and hydrocephaly have
been noted with Dandy-Walker malformation
in some rare cases [2].
Histologically cartilaginous changes
include irregularly spaced lacunae,
abnormal chondrocyte nuclei, islands of
cartilage in metaphyseal bone, protrusion
of bone into the epiphyseal cartilage.
Chondro-osseous tissue from supernumery
digits show irregular column formation
and vascular invasion, concavity of the
epiphyseal line protruding into the
cartilage, and islands of cartilage along
the periosteum and within the metaphyseal
bone. In rib and iliac crest, the resting
cartilage contains abnormally large
chondrocytes, often with several cells
per lacuna (normally 1-2), increased

Karnataka Paediatric Journal Vol. 29, No. 1 Jan - March 2014
10
vascularity of the cartilage, and a
particularly fibrous-appearing matrix with
areas of degeneration [9].
Radiological features include
postaxial polysyndactyly, short ribs,
short iliac wings, horizontal acetabulum
with medial and lateral spurs (trident
pelvis), premature ossification of femoral
capital epiphyses, proximal tibial
epiphysis is hypoplastic laterally with
dome shaped metaphysis, medial tibial
diaphyseal exostosis, genu valgum and
fibular shortening may be seen at knee.
Carpal development is delayed and
carpal fusions are seen especially
between capitate and hamate. In
addition, polycarpyly with ninth carpal
bone may appear in distal row in
some [10].
Prognosis: Approximately 50%
babies die in early infancy due to
cardiorespiratory problems [3].
fWHAT IS THE SIGNIFICANCE OF
THIS REPORT?
Hydrocephalus in Ellis van Creveld
syndrome is a rare entity. This report adds to
the list of such cases.
REFERENCES
1. Baujat G and Merrer ML- Ellis van
Creveld syndrome, Orphanet Journal
of Rare Diseases 2007, 2:27.
2. A. Amin, T. Ahmed, M. Ashraf, Z.
Lone, I. Wani: Chondroectodermal
Dysplasia (Ellis-van Creveld Syndrome):
A case report. The Internet Journal
of Pediatrics and Neonatology. 2009
Volume 10 Number 1.3.
Jones KL.
Smith�s recognizable patterns of
human malformation. 6th ed. Elsevier
Saunders ; chapter J p422.
4. Hegde K, Puthran RN, Nair G,
Nair PP. Ellis van Creveld syndrome�
a report of two siblings; BMJ Case
Reports 2011.
5. KM Veena, H Jagadishchandra, Rao
PK, Chatra L. Ellis van Creveld
syndrome in an Indian child: a case
report. Imaging Sci Dent. 2011
December; 41(4): 167�170.
6. Tompson SW, Ruiz-Perez VL, Blair HJ,
Barton S, Navarro V, Robson JL,
Wright MJ, Goodship JA: Sequencing
EVC1 and EVC2 identifies mutations
in two-thirds of Ellis van Creveld
syndrome patients. Hum Genet 2007,
120:663-670.
7. Ruiz-Perez V, Tompson S, Blair H,
Espinoza-Valdez C, Lapunzina P, Silva
E, Hamel B, Gibbs J, Young I,
Wright M, Goodship J: Mutations in
two nonhomologous genes in a
head-to-head configuration cause Ellis
van Creveld syndrome. Am J Hum
Genet 2003, 72:728-732.
8. Venkat-Raman N, Sebire N, Murphy
K: Increased first-trimester fetal nuchal
translucenty thickness in association
with chondroectodermal dysplasia (Ellis
van Creveld). Ultrasound Obstet
Gynecol 2005,25:412-414.
9. Sillence DO, Horton WA and Rimoin
DL. Morphologic Studies in the
Skeletal Dysplasias: A Review, Am J
Pathol 96:811-870, 1979.
10. Haque F, Ahmed SA: Ellis van
Creveld Syndrome- Letter to the
editor, Indian Pediatrics, Vol41, 867-
868.
AKNOWLEDGEMENTS
We thank the baby�s family for
handing over the baby to the
Department of Pediatrics, JJM Medical
College, Davangere for academic study.
We also thank the Department of
Pathology, JJM Medical College,
Davangere for actively participating in
establishing the diagnosis by autopsy
and histopathologic study.

Karnataka Paediatric Journal Vol. 29, No. 1 Jan - March 2014
11
Abstract:Tropical acute kidney injury
refers to acute kidney injury secondary to
diseases prevalent in the tropical region.
Factorsthat contribute to poor outcome of
tropical AKI include low socioeconomic
status, poor access to treatment, and delay
in seeking medical attention. Early clinical
diagnosis and appropriate treatment can
minimize fatal outcome. We report an
adolescent with leptospirosis who presented
with non-oliguricrenal failure requiring
hemodialysis and he recovered.
Key words:Tropical infection, acute
kidney injury, Leptospirosis, Adolescent
Introduction:
Tropical infectious diseases in
association with acute kidney injury (AKI)
are given importance during recent years in
the era of enormous expansion of travel and
immigration [1]. The epidemiology of
community-acquired AKI in developing
tropical countries is markedly different from
AKI in developed countries with a temperate
climate. Leptospirosis is a common etiology
of tropical AKI in Indian subcontinent. We
report an adolescent with leptospiral
nephropathy with class 3 AKI and
recovered completely.
Case report:
A 14-year-old boy hailing from rural
village of coastal Karnataka presented with
fever for 10 days, vomiting for 4 days and
gum bleedingalong with altered sensorium
noticed since 2 days. There was no oliguria
or hematuria. His father was an
agriculturist. His past history was not
significant.
His height was 163cm, weight was
40kg. He had a pulse rate of 110 beats /
min, respiratory rate 20 cycles/min and a
blood pressure of 122/70 mmHg. Examination
revealed moderate pallor, icterus and diffuse
conjunctival suffusion with evidence of
glossitis and oral mucosal bleed.Abdominal
examination revealed tender hepatomegaly.
Examination of other systems was unremarkable.
Investigations showed anemia and
thrombocytopenia with hemoglobin of 9.7
gm/dl and platelet count of 70,000/cmm
respectively. He had leukocytosis with
raised ESR and CRP.There was no evidence
of hemolysis in peripheral smear. He had
grossly elevated renal function tests
(creatinine � 14 mg/dL; urea 810mg/dl)
with hyperkalemia.He was categorized to
class 3 AKI (failure) as per modified
pediatric RIFLE (risk,injury,failure,loss, end
stage) criteriabut without oliguria.Urine
analysis revealed microscopic hematuria
and proteinuria (1+) with granular casts.
His serum LDH and complement level was
normal. Liver function tests were deranged
withhyperbilirubinemia(Total bilirubin: 31.7
mg/dL, Direct: 23.5 mg/dL), marginally
INFECTIVE TROPICAL ACUTE KIDNEY INJURY IN ANADOLESCENT FROM RURAL COASTAL KARNATAKA -A CASE REPORT.Dr SANDEEP KUMAR *Dr SHRIKIRAN AROOR, Dr SUNEEL MUNDKUR, r.
Dr MANEESH KUMAR
Department of pediatrics, Kasturba Medical College, Manipal University, Manipal.
Email: [email protected].

Karnataka Paediatric Journal Vol. 29, No. 1 Jan - March 2014
12
elevated liver enzymes,hypoalbuminemia,
and coagulopathy (INR-1.9).Urine dark
ground microscopy for leptospira was
negative. IgM Leptospira test by enzyme
immune assay (EIA) was positive. Abdominal
ultrasonography showed hepatomegaly with
bilateral grade I renal parenchymal changes.
Workup for malaria, dengue and rickettsial
infections were negative. Blood and urine
cultures were sterile. Serological markers of
hepatotrophic viruses were negative.
He was treated with IV crystalline
penicillin for 10 days, along with anti-hyperkalemic
measures and fluid management as per AKI
protocol. He required 4 cycles of hemodialysis.
He responded clinically and renal
parameters were normalized over next
9days as depicted in line diagram (fig 1 and
2). He was followedup for next 3 months
and he remained asymptomatic with normal
blood count, renal and liver function tests.
Discussion:
Tropical nephropathies causing AKI
are broadly classified as infective or
toxic.The infective nephropathies that are
commonly prevalent in Indian subcontinent
include diarrheal diseases, bacterial sepsis,
malaria, leptospirosis, dengue fever, enteric
fever, kalaazar and rickettsial fever [2].
Factors that contribute to poor outcome
include to low levels of income, poor access
to health care, and social or cultural
practices leading to delay in seeking
medical intervention.The incidence of
tropical glomerulonephritis is found to be
up to 4% of pediatric hospitaladmissions [3].
Leptospirosis is a zooanthroponosis
caused by a spirochete of genus Leptospira,
the species being L. interrogans and
L.biflexa. Leptospira infect many species of
domestic animals including pets, livestock,
birds and fish. Rat is the principal source
of human infection. Occupational groups
with a high incidence of leptospirosis
include agriculturists and others that require
contact with animals. Leptospira enter
humans through abrasions and cuts in the
skin or through mucous membranes.The
incidence of AKI in adults with severe
leptospirosis as per literature varies from
40% to 60% [4].Renal involvement is
predominantly a result of tubular damage
and interstitial nephritis is the basic lesion
reported in leptospirosis.However rarely
renal involvement may be attributable to
widespread vasculitis and hypovolemia
secondary to myocarditis[5].
Clinical manifestations are classically
biphasic, with an initial septicemic phase
lasting for 3 to 7 days followed by an
immune phase, during which nephropathy
occurs. In its mild formoften referred to as
anicteric leptospirosis seen in majority of
cases, presents as any acute febrile illness
with headache and myalgia.Severe form as
in our case is characterized by jaundice,
renal dysfunction and hemorrhagic diathesis
referred to as hepatorenal syndrome or
Weil�s syndrome that accounts for only 5-10
% [6].The diagnosis of leptospirosis should
be considered in febrile patients with evidence

Karnataka Paediatric Journal Vol. 29, No. 1 Jan - March 2014
13
ofrenal, hepatic and mucous membrane
changes. AKI in leptospirosis is primarily
non-oliguric, as in the present case.
Clinical features compatible with
Leptospira along with positive serological
test usually establish the diagnosis [6]. It
was the typical ocular manifestation of
icterus along with conjunctival suffusion
which gave us a clue to suspect leptospirosis.
AKI in Leptospirosis usually leads to rapid
elevation of renal parameters often to high
levels. Conjugated hyperbilirubinemia in the
present case is explained by the frequent
association of intrahepatic cholestasis in
leptospirosis. Less frequently diagnosis is
done by demonstration of organism in urine
by phase contract or dark field microscopy,
but is less sensitive [6]. Serologic tests like
microscopic slide-agglutination test (MAT),
dipstick ELISA and dot ELISA for IgM
antibodies are available. Antibody titers
usually appear by the 12th day of illness
and reach a maximum by the 3rd week.
General management principles of
AKI with careful fluid and electrolyte
balance along with specific antimicrobial
therapy is the cornerstone of management
[7]. Intravenous penicillin Gin the dose of 6-
8 millionU/m2/day every 4-6 hours for
duration of 7-10 days remains the drug of
choice [8]. Treatment initiated before the 7th
day of illness is shown to shorten the
clinical course and complications. Other
antimicrobials include 3rd generation
cephalosporins, amoxycillin, doxycycline
and erythromycin [8]. Poor prognostic
factors include oliguric renal failure,
pulmonary complications, hypotension and
serum creatinine more than 3 mg/dL,
requiring dialysis [9, 10]. Complete recovery
from renal failure is typical among
survivors.
This case has been reported to
highlight the importance of tropical AKI
where early intervention often prevents the
progression of AKI and long term renal
damage.Most causes of tropical AKI are
preventable and strategies to reduce the
burden of tropical AKI require both
improvements in basic public health,
achieved through effective interventions, and
increased access to effective medical care.
REFERENCES:
1. Barsoum R, Sitprija V. Tropical Nephrology.
In: Diseases of the Kidney, Schrier
RW,Gottaschalk CW, Eds, 6th Edn, Boston,
Little,Brown & Co. 1997; 2221-2268.
2. Banerjee S. Tropical acute kidney injury -
Recognition and management. Indian J
PractPediatr 2012; 14:133-142.
3. Herberg J, Pahari A, Walters S, Levin
M.Infectious Diseases and the Kidney. In:
Pediatric Nephrology, Avner ED, et al.
Eds, 6th Edn,Berlin: Springer Verlag 2009;
1235-1274.
4. Andrade L, Daher EF, Seguro AC.
Leptospiral nephropathy. Semin Nephrol.
2008; 28:383�94.
5. Lai KN, Aarnos I, Woodroffe AJ, Clarkson
AR.Renal lesions in Leptospirosis. Aust N
Z M Med1982; 12:276.
6. Sunil Karande, Hemantkulkarni, Madhuri
Kulkarni, Anuradha De, Ami Varaiya.
Leptospirosis in children in Mumbai slums.
Indian J Pediatr 2002; 69 (10): 855-858.
7. Abboud O. Tropical renal failure. J
TroNephro-Urol 2007; 5:11 -13.
8. H. Dele Davies and Melissa Beth
Rosenberg.Leptospira.In Behrman RE,
Kliegman RM et al. Nelson Textbook of
Pediatrics, 19thedn. Philadelphia: W.B.
Saunders Company; 2011; p 1023-1026.
9. Ricaldi JN, Vinetz JM. Leptospirosis in the
tropics and in travellers.Curr Infect Dis
Rep.2006; 8:51�8.
10. Covic A, Goldsmith DJ, Gusbeth-Tatomir P,
Seica A, Covic M. A retrospective 5 year
study in Moldova of acute renal failure
due to leptospirosis: 58 cases and a review
of the literature.Nephrol Dial Transplant.2003;
18:112

Karnataka Paediatric Journal Vol. 29, No. 1 Jan - March 2014
14
Abstract
Diphtheria is one of the vaccine
preventable disease for which effectiveness
of vaccine exceeds 95% after three doses.We
report an unimmunized case who died
due to complications of diphtheria. There is
a huge disparity between the reported
figures and WHO estimated figures of DPT3
coverage in India and reflects the poor
immunization coverage status in our
country responsible for such deaths.
Introduction
Diphtheria is one of the vaccine
preventable disease for which effectiveness
of vaccine exceeds 95% after three doses[1].
We report an unimmunized case who died
due to complications of diphtheria and the
current state of immunization coverage in
our country.
Case Report
A 4 year old boy was referred to our
hospital with fever since 8 days and pain
and swelling of neck since 4days.He was
the third child of non consanguineousparents.
Mother had no antenatal checkups done. He
was delivered normally at home by an
untrained dhai. He had normal developmental
milestones. He was never immunized since
birth. His elder sibling, 6year old female
child also had similar complaints of fever
and pain in the throat. On examination
there was bull neck and dirty white
membrane over the tonsils extending into
soft palate and posterior pharyngeal wall.
Child was suspected to havetonsillar and
pharyngeal diphtheria was investigated
VACCINE PREVENTABLE DISEASE DEATH: TIP OF THE ICEBERGDr.RAMYA BANDI* Dr. RAMESH H
Department of Pediatrics,JJM medical college,Bapuji Child Health Institute and Research Centre,Davangere, Karnataka-577004. Email:[email protected].
accordingly. A throat swab was taken which
was positive for albert�s stain and bacilli
with metachromatic granules were seen. He
was treated with crystalline penicillin and
antidiphtheric antitoxin. His blood counts
revealed leukocytosis. On second day of
admission diagnosis was confirmed as the
culture grew corynebacterium diphtheria
bacillus(sub species: intermedia).Child also
had stridor and arrhythmias with heart
blocks and t wave abnormalities after 48
hours of admission. Later for the worsening
respiratory distress he was ventilated with
endotracheal tube. There was no evidence of
laryngeal membrane as observed during
intubation. Child developed congestive heart
failure, pulmonary odema and despite of
supportive care succumbed to death after six
hours of ventilation.His final diagnosis was
Pharyngeal and Tonsillar diphtheria with
myocarditis and congestive cardiac failure.
Fig 1: Bull neck appearance
Fig 2 : Heart block recording due to myocarditis

Karnataka Paediatric Journal Vol. 29, No. 1 Jan - March 2014
15
DISCUSSION
Diphtheria is an acute toxic infection
caused by Corynebacteriumdiphtheriae, an
aerobic, non-encapsulated, gram positive
bacillus. It is an endemic disease in India[2].
Diphtheria occurs by entry of C. diphtheriae
into the nose or mouth and after a 2-4 day
incubation period, toxins are secreted which
leads to toxin-mediated tissue necrosis. This
coupled with local inflammatory response
produces patchy exudates which later forms
fibrinous exudates and a tough adherent
membrane. In tonsillar and pharyngeal
diphtheria, sore throat is a universal early
symptom. Underlying soft tissue edema and
enlarged lymphnodescan cause a bull-neck
appearance. Respiratory embarrassment may
follow extension of disease into larynx or
tracheobronchial tree. The main complications
of the disease are toxin mediated.Toxin is
distributed via blood stream &lymphatics
throughout the body. Major respiratory
complications like airway obstruction,
stridor are due to pseudomembrane
formation while the toxin mediated effects
are seen mainly on the heart and nervous
system[3]. Toxic cardiomayopathy occurs in
10-25% of cases with respiratory diphtheria.
Myocarditis is a poor prognosticating sign
as about 60% of death in diphtheria are due
to it. Myocarditis most commonly occurs in
the second week of the disease but can
appear as early as the first or as late as the
sixth week of illness. In our case myocarditis
presented in second week of illness. . A
prolonged PR interval and changes in the
ST-T wave on an electrocardiographic
tracing are relatively frequent findings.
Single or progressive cardiac dysrhythmias
can occur, including 1st-, 2nd-, and 3rd-
degree heart block. This child also had
progressive cardiac arrhythmias in the form
of varying heart blocks. Specific antitoxin is
the mainstay of therapy and should be
administered on the basis of clinical
diagnosis and dosage depends on the
extent of the membrane. Because it
neutralizes only free toxin, antitoxin efficacy
diminishes with elapsed time after the onset of
mucocutaneoussymptoms. The role of
antimicrobial therapy is to halt toxin
production, treat localized infection, and
prevent transmission of the organism to
contacts. Only erythromycin or penicillin is
recommended; erythromycin is marginally
superior to penicillin for eradication of
nasopharyngeal carriage. Appropriate
therapy is erythromycin (40-50 mg/kg/day
divided every 6 hr by mouth [PO] or
intravenously [IV]; maximum 2 g/day),
aqueous crystalline penicillin G (100,000-
150,000 U/kg/day divided every 6 hr IV or
intramuscularly [IM]), or procaine penicillin
(25,000-50,000 U/kg/day divided every 12
hr IM) for 14 days[3].This child received
crystalline penicillin as antibiotic. Antibiotic
therapy is not a substitute for antitoxin
therapy. The prognosis for patients with
diphtheria depends on the virulence of the
organism, patient age, immunization status,
site of infection, and speed of administration
of the antitoxin. The poor prognosis factors
in this child include age < 5years, unimmunized
status,delay in antitoxin administration. At
recovery, administration of diphtheria toxoid
is indicated to complete the primary series

Karnataka Paediatric Journal Vol. 29, No. 1 Jan - March 2014
16
or booster doses of immunization, because
not all patients develop antibodies to
diphtheritic toxin after infection[3].
This case is reported to highlight the
prevailing health system scenario in
India.This child was delivered at home.
Parents were unaware of the immunization
programme and other siblings were also
unimmunized. They were also not registered
in any anganawadicentre. Other siblings
were vaccinated appropriately at our health
service and sent.According to WHO/
UNICEF [4]estimates the national
immunization coverage rate for the year
2011for India was 72% for DPT3. This
coverage rate is a good indicator of the
health system prevailing in a country. It is
expected to be atleast at and above 80%
according to WHO/UNICEF.Our neighbouring
country SriLanka has a coverage of more
than 80%. According to the figures reported
by our country 87% of districts had DPT3
coverage at or greater than 80%. This huge
disparitywould reflect the poor reporting
system in our country which is far from
reality.
According to reported statistics from
all countries WHO[5] has published
incidence time series for all vaccine
preventable diseases. According to that
2,525 cases of diphtheria were reported from
India for the year 2012 ,wherein majority of
the countries have not even reported in
hundreds. According to WHO reported
values are usually underestimates of actual
cases. So the burden of these vaccine
preventable diseases in our country is large
and masked. The health system and the
immunization coverage is not �good
enough� at the grass root level for which
may lives are lost, otherwise could have
been saved.This case truly represents the tip
of iceberg because innumerable such
incidents do occur and are undereported.
Strengthening of the health system is the
only solution for such deaths and everyone
should contribute to it with in their scope of
reach.
REFERENCES
1. Vijay Y, Choudhary P, Thacker N. IAP
guide book on Immunization. Indian
Academy of Pediatrics; 2011.p61.
2. Patil Y Diphtheria. In :Parthasarthy A,
Kundu R, Agarwal R. Textbook of
Pediatric Infectious Diseases. Jaypee;
2013.p.225.
3. Buescher ES Diphtheria(corynebacterium
diphtheria). In :Kleigman RM, Behrman
RE, SchorNF,Geme JW, Stanton BF,
editors. Nelson Textbook of Pediatrics.
Philadelphia:Saunders Elsevier; 2011.
p.928.
4. Immunization summary 2013 edition.
Available at http://www.who.int/
entity/immunization_ monitoring/en/
5. Vaccine preventable diseases. Available
at http://www.who.int/immunization
_monitoring/burden/estimates_burden/
en/index.html

Karnataka Paediatric Journal Vol. 29, No. 1 Jan - March 2014
17
Abstract
Objective: To study correlation of low
birth-weight with selected anthropometric
measures of newborns, such as mid-upper
arm circumference (MUAC), chest circumference,
head circumference, and crown-heel length
to identify the best predictor among them
and also with its cut off value .
Studydesign: Case control study of
100 in each group of newborn babies were
done in a tertiary referral centre, in Mangalore
city to examine the correlation between
birth-weight and selected anthropometric
parameters of newborns.
Results & Conclusion: The mean
birth-weight of low-birth-weight (<2,500 g)
babies were 2084 ± 265 gms and that of
babies taken as control were 2782 ± 185
gms. All key anthropometric parameters of
low-birth-weight (<2,500 g) babies were
significantly different from those of the
controls (2700g)(p<0.001). Chest circumference
was the best detector of birth-weight with
area under the graph in ROC curve was
0.848, followed by head circumference 0.824
and MUAC 0.823. We found that these
anthropometric variables can easily be used
to identify the low birth babies at the time of
birth.
Key words: Low birth-weight;
Anthropometry
INTRODUCTION
Birth weight is regarded as one of the
most sensitive and reliable predictors of
health of any community. India, a large
number of deliveries take place outside
health facilities. In the absence of adequate
resources and trained man power for timely
diagnosis and management of low birth
babies, there has been a requirement of
simpler method for identification of low
birth-weight babies even by untrained health
personals. Low birth weight has been
defined by the World Health Organization
(WHO) as weight at birth of less than 2,500
grams (5.5 pounds)1 irrespective of
gestational age. It is an important public
health problem because of its association
with poorer outcomes when compared
normal birth weight babies. The national
neonatal perinatal database reported that
nearly about one third of all neonates born
in major hospitals of India every year are
LBW. Of all neonatal death, nearly 82%
occur among LBW, which is highest in the
world. An early identification and
immediate direct interventions, such as
extra nutrition, can result in low-birth-
weight infants catching up with their
heavier contemporaries1. Screening for low-
birth-weight babies warrants proxy
indicators which can be used for low birth-
weight and for preventing infant mortality.
These include the circumferences of the
newborn�s head, chest, and mid-arm, and
crown-heel length. Different studies from
developing countries have suggested
different anthropometric surrogates to
identify LBW babies and recommended
various cut off values19,20. This study was
conducted to indentify appropriate alternate
indices for low birth-weight which can be
used in situations where accurate weight
measurement at birth is not feasible. Aims
Yenepoya Medical College, Yenepoya University, Mangalore
STUDY OF CORRELATION OF LOW BIRTH WEIGHTWITH SELECTED ANTHROPOMETRIC VARIABLESDr Anil Narayanan, Dr Prakash Saldanha, Dr Mithun

Karnataka Paediatric Journal Vol. 29, No. 1 Jan - March 2014
18
and objectives of the study was 1) corelating
low birth-weight with selected anthropometric
measures of newborns, such as mid-upper
arm circumference (MUAC), chest circumference,
head circumference, and crown-heel length
and identify the best predictor among them
2)to determine its cut off value to identify
LBW babies.
Materials and Methods: This was a
hospital based prospective, Case Control
Study done in Department of Pediatrics in
the Labour room, Yenepoya Medical College,
Mangalore, India between January 2012 To
December 2012. A simple random-sampling
technique was adopted to recruit the study
subjects. All cases are managed as per the
protocol for treatment of low birth weight
babies. There was no follow-up of patients
for study purpose. A total of 100
consecutive low birth babies(<2500g), were
selected as cases for enrollment in the study.
Still births, patients born elsewhere and
referred to Yenepoya Medical College,
Mangalore, were excluded from the study.
An equal number of normal birth weight
babies (>2700gms) irrespective of gestational
age selected as controls during the period of
study. Accurate weighing of the baby was
done on a regularly calibrated electronic
weighing machine with a sensitivity <5 gm.
The birth weight was recorded up to the
first digit after the decimal. The babies
having their birth weight recorded with
rounding up and down,which produces an
inaccurate birth weight recording were
excluded from the study. The study included
both term and pre-term babies. Gestational
age was calculated as total duration of
pregnancy in weeks from the first date of
the last menstrual period (LMP) to birth of
the baby. Gestational ages of these infants
ranged from 31 to 44 weeks. The
anthropometric parameters of the newborns
recorded were using standard techniques as
described by DB Jelliffe 7. MUAC was
measured at the midpoint between the tip of
acromion process and olecranon process in
the left upper arm with a fibre-glass
measuring tape to the nearest of 0.1 cm.
Head circumference was also measured
with the help of a fibre-glass measuring tape
21 to the nearest of 0.1 cm. Maximum
occipito-frontal circumference of head was
recorded. Crown-heel length was recorded
to the nearest of 0.1 cm on an infantometer
with the baby supine, knees fully extended,
and soles of feet held firmly against the foot
board and head touching the fixed board.
Chest circumference was measured at the
level of nipple by a fibre-glass measuring
tape to the nearest of 0.1 cm at the end
phase of expiration.
Datas were analyzed using standard
statistical methods, which included paired t
test to compare the data among two groups.
Receiver operating characteristic curve
(ROC) was prepared to analyze the validity
of using the anthropometric parameters of
the newborns for diagnosing low birth
weight). Specificity and sentivity of
individual anthropometric parameters of the
newborns for diagnosing low birth weight
was calculated using confidence interval of
10% and confidence limit of 95%. All the
data was analyzed with SPSS 17 software8,9,10 .
Results:
A total of 200 cases inclusive of cases
and controls(49%males and 51% females)
studied of which , the mean birth-weight of
low birth weight babies was 2,084 ± 265 g
and that of controls were 2,782 ± 185 g. All
the mean anthropometric values (Table 1)
were found to be significant differences than
those for the control babies. The mean
MUAC, chest circumference, crown to heel
length and head circumference of the cases
were found to be lower than the mean

Karnataka Paediatric Journal Vol. 29, No. 1 Jan - March 2014
19
MUAC, chest circumference, crown to heel
length and head circumference of the
controls. ROC graph (Table 2 and Graph 1)
of the mean MUAC, chest circumference,
crown to heel length and head circumference
of the cases and control showed graphs
skewed to the top left corner.. The area
under the graph for MUAC, chest
circumference, crown to heel length and
head circumference of the cases and control
were 0.848, 0.823, 0.750 and 0.824, which
established validity of anthropometric
values for diagnosis of low birth weight.
Sensitivity and specificity analyses were
carried out with different cut-off points for
MUAC, chest circumference, and head
circumference of the cases to identify low
birth-weight babies (Table 3). The aim of
selecting cut off points was to identify
correctly all the low-birth weight babies
with a least number of false-positive case.
Table 1 the mean anthropometric values of
the newborns.
Table 2 : ROC curve characteristics and
correlation coefficient value for various
variables.
1-chest circumference 2-head circumference
3-mid arm circumference 4-crown heel
length 5-birth weight
ROC Curve for various anthropometric
parameters of low birth weight babies
Table 3: Sensitivity and specificity with
different cut-off points for MUAC, chest
circumference, and head circumference of
the cases to identify low birth weight babies
1-chest circumference 2-head circumference
3-mid arm circumference 4-crown heel
length
Anthropometric variables
Case/ Control Number Mean
Std. Deviation t value
P value
case 100 27.98. 2.78 -9.603 0.00 CC1(mm)
control 100 32.63 3.96
case 100 28.65 2.83 -9.414 0.00 HC2(mm)
control 100 32.91 3.52
case 100 8.65 1.09 -10.641 0.00 MAC3(mm)
control 100 10.51 1.36
case 100 44.37 3.00 -6.902 0.00 CHL4(mm)
control 100 47.45 3.30
case 100 2084 265 -21.559 0.00 BWT5(gms)
control 100 2782 185
Test Result Variables Area
Std. Error
Asymptotic Sig.
Correlation coefficient
CC1 0.848 0.031 0.000 0.837
HC2 0.824 0.029 0.000 0.802
MAC3 0.823 0.029 0.000 0.650
CHL4 0.750 0.035 0.000 0.403
Test Result Variable(s)
Positive if Greater Than or Equal To Sensitivity Specificity
Positive likelihood ratio of the
cut off value
27.95 0.820 0.610 2.10
29.35* 0.820 0.873 6.43
29.95 0.780 0.800 3.90
CC1
30.50 0.740 0.840 4.6
29.90 0.800 0.701 2.67
30.15 0.760 0.706 2.58
30.95 0.760 0.820 4.22
HC2
31.60* 0.700 0.870 5.38
9.20 0.800 0.780 6.15
9.55 0.800 0.820 4.44
MAC3
9.85* 0.800 0.880 6.66
40.80 0.970 0.890 8.88
41.25 0.970 0.820 5.38
41.75 0.940 0.800 4.50
CHL4
42.50 0.830 0.690 2.76

Karnataka Paediatric Journal Vol. 29, No. 1 Jan - March 2014
20
* cut off values of anthrometric variables for
LBW babies in order of significance
Discussion
Present study is first of its type in
Daksin Kannada with respect to correlation
of low birth eight with anthropometric
variables and predicting the cut off value
for the identification of the same. The
findings of this study are comparable with
the findings of these South Asian countries.
The mean birth-weight of new born normal
birth weight babies was 2,782 ± 185 g
which is comparable to the mean birth-
weight in the multi-centre study was 2,630
g, 2,780 g, and 2,840 g, respectively, for
India, Nepal, and Sri Lanka 11, 12. The present
study revealed that all anthropometric
parameters of the new-borns significantly
correlated with one another. For an early
identification of low-birth-weight babies, we
considered arm, chest and head circumferences
as surrogates and found that all were
significantly linked to birth-weight. Most
studies used cut-off points of 28, 29, and 30
cm for chest circumference for a proxy
indicator for birth-weights 2. A comparative
analysis using these and cut-off values of
27.95, 29.35 and 30.5 cm for this study is
shown in Table 3. The cut off value of 29.35
cm, can identify 87 % low birth babies with
sensitivity of 83% with high accuracy as
shown by positive likelihood ratio of test at
6.43. Results of similar studies in India
also showed a chest circumference of <30
cm, and MUAC of <8.7 cm to have the best
sensitivity and specificity for identifying
low-birth-weight infants 3, 13, 14. In a Brazilian
study, head circumference of 33 cm and
chest circumference of 31 cm had been
identified as cut-off points for identifying
low-birth-weight pre-term babies 15. In Egypt,
two cut-off points of 29 to <30 and <29 cm
were selected for chest circumference to
identify �at-risk� and �high-risk� infants
respectively1. As with other parameters
concerned, high sensitivity, specificity and
high positive likelihood ratio was shown by
MUAC and crown to heel length values
9.85comes and 40.80 cm respectively
Linear Regression analysis found the entire
four variables to independently predict the
occurrence of low birth weight in the babies.
The findings of the present study revealed
that, of four parameters 16, 17, 18, chest
circumference and head circumference have
high correlation coefficient (0.837 and 0.802),
are the best one to identify low-birth-weight
infants. Highest correlation (0.837) was
between chest circumference and birth-
weight. So the chest circumference should be
preferred in most cases; as measurement of
head circumference at birth would not be
accurate due to moulding of head, particularly
in cases of prolonged and obstructed
labour19, 20.
Trained birth attendants and health
and family-planning workers working in
rural areas can easily be provided with a
measuring tape, it would be logical to
assume that these substitute measurements
would be useful in predicting neonatal
outcome. Since it is a simple tool to measure
babies and also to detect low-birth-weight
babies, grassroots-level health and family-
planning workers and trained birth
attendants, can identify infants with low
birth-weight with a fair degree of accuracy
and can play a significant role in
identifying low-birth-weight babies and in
giving proper advice to mothers and other
caretakers21-24. Furthermore, in the certain
religious community, where taboos exist
regarding weighing of newborns, these
measurements can be used without any

Karnataka Paediatric Journal Vol. 29, No. 1 Jan - March 2014
21
obstruction from the community to identify
low ¬birth-weight babies. In conclusion, we
recommend the use of chest circumference
rather than mid arm or head circumferences
as a surrogate for birth-weight.25
References
1. Diamond ID, Abd EL-Aleem AM, Ali
MY, Mostafa SAM, El-Nashar SMA,
Guidotti RJ. The relationship between
birth weight, and arm and chest
circumference in Egypt (brief report). J
Trop Paediatr 1991;37:323-6.
2. Use of a simple anthropometric
measurement to predict birth weight.
WHO collaborative study of birth
weight surrogates. Bull World Health
Organ 1993;71:157-63.
3. Bhargava SK, Ramji S, Kumar A,
Mohan M, Marwah J, Sachdev HP. Mid-
upper arm and chest circumferences at
birth as predictors of low birth weight
and neonatal mortality in the
community. Br Med J 1985;291:1617-9.
4. Sharma JN, Saxena S, Sharma U.
Relationship between birth weight and
other neonatal anthropometric
parameters, v Joypur: Department of
Paediatric Medicine, Sir Pandmpat
Mother and Child Health Institute,
SMS Medical College, 1988:244-8.
5. Khanam ST, Shahidullah M. A study of
correlation of thigh and mid-arm
circumference of newborns and birth-
weight. Bangladesh Med J 1990;19: 45-
50.
6. Alves JG, Lima GM, Azevedo GN,
Cabral VB, Moggi RS, Nunes R.
Evaluation of newborn arm circumference
as an indicator of low birth weight.
Bull Pan Am Health Organ
1991;25:207-9.
7. Jelliffe DB. The assessment of the
nutritional status of the community
(with special reference to field surveys
in developing regions of the world).
Geneva: World Health Organization,
1966:64-76. (WHO monograph series
no. 53).
8. Reitsma JB, Glas AS, Rutjes AW,
Scholten RJ, Bossuyt PM, Zwinderman
AH. Bivariate analysis of sensitivity
and specificity produces informative
summary measures in diagnostic
reviews. J ClinEpidemiol. 2005;58:982�
90.
9. Akobeng AK. Understanding diagnostic
test 3: Receiver operating characteristic
curves. ActaPaediatr. 2007;96:644�7.
10. Deeks JJ, Macaskill P, Irwig L. The
performance of tests of publication bias
and other sample size effects in
systematic reviews of diagnostic
accuracy was assessed. J ClinEpidemiol.
2005;58:882�93.
11. Karim E, Mascie-Taylor CG. The
association between birthweight,
sociodemographic variables and
maternal anthropometry in an urban
sample from Dhaka, Bangladesh. Ann
Hum Biol 1997; 24:387-401.
12. World Health Organization. Multicentre
study on low birth weight and infant
mortality in India, Nepal and Sri
Lanka. New Delhi: Southeast Asia

Karnataka Paediatric Journal Vol. 29, No. 1 Jan - March 2014
22
Regional Office, World Health
Organization, 1994. 78 p. (SEARO
regional health paper no. 25).
13. Raymond EG, Tafari N, Troendle JF,
Clemens J. Development of a practical
screening tool to identify preterm, low-
birthweight neonates in Ethiopia.
Lancet 1994;344:524-7.
14. Bhargava SK, Sachdev HP, Iyer PU,
Ramji S. Current status of infant
growth measurements in the perinatal
period in India. ActaPaediatrScand
1985;319(Suppl):103-10.
15. Pjoda J, Kelley L. Low birthweight; a
report based on the International Low
Birthweight Symposium and Workshop,
Dhaka, 14-17 June 1999. Geneva:
United Nations Administrative Committee
on Coordination/Sub-Committee on
Nutrition, World Health Organization,
2000:30. (ACC/SCN nutritionpolicy
paper no. 18).
16. Ahmed FU, Karim E, Bhuiyan SN.
Mid-arm circumference at birth as
predictor of low birth weight and
neonatal mortality. J Biosoc Sci.
2000;32:487�93.
17. Ezeaka VC, Egri-Okwaji MT, Renner JK,
Grange AO. Anthropometric measurements
in detection of low birth weight infants
in Lagos. Niger Postgrad Med J.
2003;10:168�72.
18. Fok TF, Hon KL, Wong E, Ng PC, So
HK, Lau J, et al. Trunk anthropometry
of Hong Kong Chinese infants. Early
Hum Dev. 2005;81:781�90.
19. Kulkarni AP, Sathe PV. Relationship
between birthweight and anthropometric
measurement of newborn. Indian J
Community Med. 1993;18:141�8.
20. Mullany LC, Darmstadt GL, Khatry SK,
Leclerq SC, Tielsch JM. Relationship
between the surrogate anthropometric
measurements, foot length and chest
circumference and birth weight among
newborns of Sarlahi Nepal. Eur J
ClinNutr. 2007;61:40�6.
21. Singh M, Paul VK, Deorari AD,
Anandalakshmi PN, Sundaram KR.
Simple tricoloured measuring tapes for
identification of low birthweight babies
by community health workers. Ann
Trop Paediatr. 1988;8:87�91.
22. Arisoy AE, Sarman G. Chest and mid-
arm circumferences: identification of
low birth weight newborns in Turkey.
J Trop Pediatr. 1995;41:34�7.
23. Ngowi JA, Redding-Lallinger R, Hirji
KF. An assessment of the use of
anthropometric measures for predicting
low birth weight. J Trop Pediatr.
1993;39:356�60.
24. Das JC, Afroze A, Khanam ST, Paul N.
Mid-arm circumference: an alternative
measure for screening low birth weight
babies. Bangladesh Med Res Counc
Bull. 2005;31:1�6.
25. Goto E. Meta-analysis to estimate the
correlation coefficients between
birthweight and other anthropometric
measurements at birth. Indian J Pediatr.
2011;78:311�8.

Karnataka Paediatric Journal Vol. 29, No. 1 Jan - March 2014
23
Abstract
Neumann�s tumor also called as
Epulis tumor is a rare and benign dental
lesion seen exclusively in newborn. This
tumor arises from mucosa of the maxillary
alveolar ridge and characterized by smooth
surfaced sessile or pedunculated mass with
normal to reddish color. We report a case of
a new born presenting with pedunculated
reddish mass arising from maxillary
alveolar ridge.
Key words: Neumann�s tumor:
congenital Epulis: benign : neonate
Neumann�s tumor, a rare benign
tumor of dental interest is exclusively seen
in new born with preponderance to
females(10:1)1-3 arises from right maxillary
anterior alveolar ridge and rarely from
mandibular area. Its size varies from several
centimeters to few millimeters. Aetiology of
this tumor is unknown but certain theories
like myogenic, neurogenic,odontogenic,
fibroblastic are suggested . This tumor is
usually not associated with any other
congenital malformations4 except mild mid
facial hypoplasia. Bigger masses produce
feeding and breathing difficulties needing
emergency intervention. The diagnosis is
mainly clinical. Histologically it is similar to
granulosa cell tumor. This benign tumor
needs surgical excision as spontaneous
regression is rare
Consultant neonatologist, Manipal hospital, Bangalore
Case report
A term 4 days female neonate
appropriate for gestational age was
presented to out patient department with
complaints of a swelling in the oral cavity.
she was born vaginally to nonconsanguinous
union and hemodynamically stable. Parents
were surprised to look at the mass and they
were very anxious. Weight ,length and
head circumference were at 50th percentile.
Clinical diagnosis of Neumann�s tumor
also called as congenital epulis was made
.The mass was measuring 2.5 cm in length
,reddish and pedunculated (as shown in
picture 1) . This mass was not causing
feeding and breathing difficulties. There
were no other congenital malformations
noted. Dental opinion was sought and
parents were reassured .
Neumann�s tumor in new born
Discussion
Neumann�s tumor also called as
granulosa tumor was first published in
the year 18715 by Neumann. the usual site
of tumor is future maxillary canine area.
The clinical presentation consists of lobular
, sessile or pedunculated mass. some times
presents with multiple tumors covered by a
smooth mucosal surface. when lesion is
NEUMANN�S TUMOR - A RARE DENTAL TUMOR
IN NEWBORNDr. Venkatesh. H.A

Karnataka Paediatric Journal Vol. 29, No. 1 Jan - March 2014
24
large unlike in our case as depicted in the
picture 1, it causes feeding and breathing
difficulty warranting immediate surgical
excision. Recurrence following incomplete
excision is not published. some small
lesions will undergo spontaneous
regression6-7 as it has happened in our case
. The mass disappeared slowly with in a
year. The lesion probably develops late in
utero hence not usually picked up by
antenatal ultrasound.The differential
diagnosis of a mass in oral cavity includes
dermoid cysts, haemangioma, lymphatic
malformations.
References
1. Chami RG, Wang HS. Large congenital
Epulis of new born. J pediatr Surg
1986: 21(11):929-30
2. Inan M.Yalcin O.Pul M.Congenital
fibrous epulis in the infant.Yonsei Med
J 2002:43(5):675-7
3. Bernhoft CH,Gihuus-Moe O,Bang
G.Congenital epulis in the new born.Int
J Pediatr otorhinolaryngol 1987;
13(1):25-9
4. Koch BL ,Myer C 3rd,Egelhoff JC.
Congenital epulis. AJNR Am J
Neuroradiol 1997;18(4):739-41
5. Neumann E. Elin fall von congaliter
epulis. Arch Helik 1871;12:189
6. Kusuwaka J, Kuhara S. Koga C, Inoue
T, Congenital granular cell tumor
(congenital epulis) in the fetus : a case
report. J Oral Maxillofacial Surg
1997,55(11):1356-9
7. Bork M, Hoede N, Korting GW,
Burgdorf WH, Young SK. Disease of
the oral mucosa and the lips.
Philadephia, PA: WB Saunders;
1996.p.293
Lakeside Education Trust
and
Rajiv Gandhi Institute of Public health and
Center for Diseases Control
Jointly Organises32nd Annual CME Programme
Sunday 27th July 2014
at
Hotel Atria, Bangalore
Vector Borne Diseases and Food Borne Syndromes
C o - S p o n s o r sIAP Karnataka State Branch IAP Bangalore Branch (BPS)
IMA Bangalore � East Branch Pediatric Association of India (PAI)
Lakeside Medical Center & Hospital Pediatric Allergy Association of India (PAAI)
For further details contact
Dr. H Paramesh
#33/4, Meanee Avenue Road ,Near Ulsoor Lake, Bangalore � 560 042
Phones: Mobile: 098450 22689, Office 080 � 25360823, 25303677, Fax: 080 �25512934

Karnataka Paediatric Journal Vol. 29, No. 1 Jan - March 2014
25
ABSTRACT
Objective: To identify differences in
clinical features of children with acute lower
respiratory tract infection between those with
and without radio graphically abnormalities.
Material and methods: It was a
prospective case series conducted on 50
consecutive children aged between 2 and 60
months admitted as cases of acute LRTI who
underwent CXR for diagnosis.
Results: Among the clinical findings,
we observed that there was a statistical
difference in the chest x-ray finding of the
patients with symptoms of wheezing and
refusal to feed, and signs of fever,
tachypnoea, wheezing, crackles and chest in
drawing (Pearson chi square 0.001- 0.01).
Among the clinical signs and symptoms at
the time of admission, we observed that
symptoms of wheezing and refusal to feed
and signs of crackles and chest in drawing
were found to be independently affecting the
presence in the chest x-ray finding of the
patients (Multinomial logistic regression
analysis (0.001- 0.016).
Conclusion: Radiological findings
more accurately correlates with clinical
symptoms like wheezing, refusal to feed,
signs of crackles and chest in drawing,
reflecting a more severe inflammatory
process. Patients in the early stages of acute
lower respiratory tract infections with
clinical finding primarily as cough and
fever may not have specific chest x-ray
findings.
Key Words � LRTI, chest X rays, chest in
drawing
INTRODUCTION
Lower respiratory tract infections
have been identified as a leading cause of
mortality in children in developing countries
and a cause of significant morbidity
worldwide1. The World Health Organization
(WHO) proposed the use of a standardized
management based on the detection of
simple signs2, in clinical and chest X-ray
(CXR) findings on admission.3Particularly in
primary health centres and rural settings,
major difficulty in diagnosing lower
respiratory tract infections promptly, is the
absence of an easily identifiable and gold-
standard diagnostic criterion4. Better
understanding of correlation between
clinical finding and radiological finding of a
case of lower respiratory tract infections, is
extremely helpful in paediatric emergency
set-up5.In this study, we aimed to identify
differences in clinical features of children
with acute lower respiratory tract infection
between those with and without radio
graphical abnormalities.
METHODS: This was a prospective
case series studied on 50 consecutive
Children aged between 2 and 60 months
admitted from January 2013 to June2013, as
cases of acute LRTI who underwent CXR
for diagnosis. The study protocol was
approved by the Ethics Committee of
Yenepoya Medical College. Acute LRTI was
defined as child presenting with symptoms
Yenepoya Medical College, Yenepoya University, Mangalore
CORRELATION OF CLINICAL AND RADIOLOGICAL FINDINGS IN
THE CHILDREN WITH LOWER RESPIRATORY TRACT INFECTIONSDr.Ansar Murtuza Hussain, Dr.Prakash Saldanha, Dr.Shamshad Khan
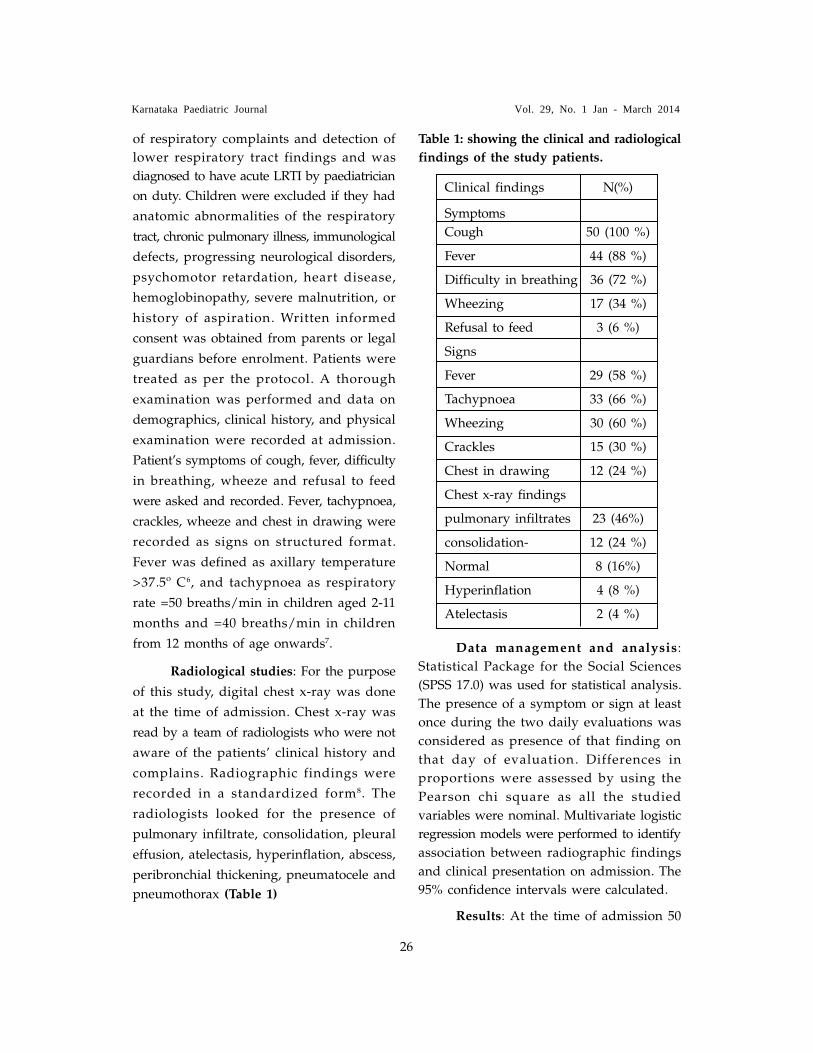
Karnataka Paediatric Journal Vol. 29, No. 1 Jan - March 2014
26
of respiratory complaints and detection of
lower respiratory tract findings and was
diagnosed to have acute LRTI by paediatrician
on duty. Children were excluded if they had
anatomic abnormalities of the respiratory
tract, chronic pulmonary illness, immunological
defects, progressing neurological disorders,
psychomotor retardation, heart disease,
hemoglobinopathy, severe malnutrition, or
history of aspiration. Written informed
consent was obtained from parents or legal
guardians before enrolment. Patients were
treated as per the protocol. A thorough
examination was performed and data on
demographics, clinical history, and physical
examination were recorded at admission.
Patient�s symptoms of cough, fever, difficulty
in breathing, wheeze and refusal to feed
were asked and recorded. Fever, tachypnoea,
crackles, wheeze and chest in drawing were
recorded as signs on structured format.
Fever was defined as axillary temperature
>37.5º C6, and tachypnoea as respiratory
rate =50 breaths/min in children aged 2-11
months and =40 breaths/min in children
from 12 months of age onwards7.
Radiological studies: For the purpose
of this study, digital chest x-ray was done
at the time of admission. Chest x-ray was
read by a team of radiologists who were not
aware of the patients� clinical history and
complains. Radiographic findings were
recorded in a standardized form8. The
radiologists looked for the presence of
pulmonary infiltrate, consolidation, pleural
effusion, atelectasis, hyperinflation, abscess,
peribronchial thickening, pneumatocele and
pneumothorax (Table 1)
Table 1: showing the clinical and radiological
findings of the study patients.
Clinical findings N(%)
Symptoms
Cough 50 (100 %)
Fever 44 (88 %)
Difficulty in breathing 36 (72 %)
Wheezing 17 (34 %)
Refusal to feed 3 (6 %)
Signs
Fever 29 (58 %)
Tachypnoea 33 (66 %)
Wheezing 30 (60 %)
Crackles 15 (30 %)
Chest in drawing 12 (24 %)
Chest x-ray findings
pulmonary infiltrates 23 (46%)
consolidation- 12 (24 %)
Normal 8 (16%)
Hyperinflation 4 (8 %)
Atelectasis 2 (4 %)
Data management and analysis:
Statistical Package for the Social Sciences
(SPSS 17.0) was used for statistical analysis.
The presence of a symptom or sign at least
once during the two daily evaluations was
considered as presence of that finding on
that day of evaluation. Differences in
proportions were assessed by using the
Pearson chi square as all the studied
variables were nominal. Multivariate logistic
regression models were performed to identify
association between radiographic findings
and clinical presentation on admission. The
95% confidence intervals were calculated.
Results: At the time of admission 50

Karnataka Paediatric Journal Vol. 29, No. 1 Jan - March 2014
27
(100 %) children had cough and 44 (88 %)
had fever. Difficulty in breathing, wheezing
and refusal to feed was present in 36 (72
%), 17 (34 %) and 3 (6 %) cases. Signs of
fever, tachypnoea, wheezing, crackles, chest
in drawing was present in 29 (58 %), 33 (66
%), 30 (60 %), 15 (30 %) and 12 (24 %) cases
respectively. Chest x-ray findings included
pulmonary infiltrates, consolidation,
hyperinflation, atelectasis, pleural effusion
in 23 (46%), 12 (24 %), 8 (100%), 2 (4 %)
and 1 (2 %) respectively. 4 (8 %) of the
patients had no abnormalities in chest x-
ray.(Table 1)
Among the clinical symptoms at the
time of admission, we observed that there
was a statistical difference in the chest x-ray
finding of the patients with symptoms of
wheezing and refusal to feed (Pearson chi
square 0.001- 0.01). Among the clinical signs
at the time of admission, we observed that
there was a statistical difference in the chest
x-ray finding of the patients with signs of
fever, tachypnoea, wheezing, crackles and
chest in drawing (Pearson chi square 0.000-
0.001). Among the clinical signs and
symptoms at the time of admission, we
observed that symptoms of wheezing and
refusal to feed and signs of crackles and
chest in drawing were found to be
independently affecting the presence in the
chest x-ray finding of the patients
(Multinomial logistic regression analysis
(sig) 0.001- 0.016).(Table 2 and 3)
Table 2: Showing Cross tabulation of the Chest x-ray findings of the patients with the
clinical presentations at the time of admission.
Chest x-ray
findings
Fever (sympto
m)
Cough (symptom) Difficult
y in breathin
g
(symptom)
Wheezing
(symptom)
Refusal to feed
(symptom)
Fever
(sign)
Tachypnoea
(sign)
Wheezing
(sign)
Crackles
(sign)
Chest in drawing
(sign)
pulmonary
infiltrates
23(46%) 20 (45.4 %) 14(38.8
%) 2 (11.7
%) 0 (0.0 %) 8(16 %) 12(36.4
%) 8(26.7
%) 2(13.3
%) 2(16.6
%)
consolidation
13 (26%) 13 (29.5 %) 13 (36.1
%) 8 (47.1
%) 0 (0.0 %) 13(26 %) 13(39.4
%) 13(43.3
%) 6(40.0
%) 3(25 %)
no abnormali
ty detected
7 (14%) 4 (9.1 %) 3 (8.3 %) 0(0.0 %) 0 (0.0 %) 1(2 %) 1(3.03
%) 2(6.7 %) 0(0.0 %) 0(0.0 %)
hyperinflation
4 (8 %) 4 (9.1 %) 3 (8.3 %) 4 (23.5
%) 0 (0.0 %) 4(8 %) 4(12.1
%) 4(13.4
%) 4(26.6
%) 4(33.3
%)
atelectasis 2 (4 %) 2 (4.5 %) 2 (5.5 %) 2 (11.7
%) 2
(66.6%) 2(4 %) 2(6.05
%) 2(6.7 %) 2(13.3
%) 2(16,6
%)
pleural effusion
1 (2 %) 1 (2.3 %) 1 (2.7 %) 1(5.8 %) 1 (33.3
%) 1(2 %) 1(3.03
%) 1(3.3 %) 1(6.7
%)
1(8.3 %)
total 50 44 36 17 3 29 33 30 15 12

Karnataka Paediatric Journal Vol. 29, No. 1 Jan - March 2014
28
confirmed that tachypnea and lower chest
in drawing when applied by health workers
and paediatricians as a diagnostic tool had
the sensitivity of 70% and 81% respectively9.
In the Vellore study10 lower chest wall in
drawing correctly predicts 79 percent of
children with LRI who were hospitalized by
a paediatrician. These criteria have proved
effective in reducing ARI mortality in
children below 5 years in community by
56% in Abbottabad, Pakistan11.
We observed that the patients of
acute lower respiratory tract infections the
x-ray finding of the cases with sign and
symptoms like fever cough and difficulty in
breathing were not very different from those
without these signs. This is similar to the
observation in earlier reports that cough or
difficulty breathing plus tachypnea12, are not
always sensitive indicator of pneumonia
has been published13. In a clinical trial of
treatment of non-severe pneumonia
conducted by Hazir T et al14, author
reported that out of 891 cases only 6.8% had
radiographic feature of pneumonia. Similar
finding were reported by Shann Fet al15 use
of radiographs does not have that level of
sensitivity signs like respiratory rate and
Chest x-ray findings
Fever (symptom)
Cough (symptom)
Difficulty in breathing
(symptom)
Wheezing
(symptom)
Refusal to feed
(symptom)
Fever
(signs)
Tachypnoea
(signs)
Wheezing
(signs)
Crackles
(signs)
Chest in drawing
(signs)
Pearson chi square
1.00 0.107 0.060 0.000 0.000 1.00 0.001 0.000 0.000 0.000
Multinomial logistic regression analysis (sig)
0.931 0.845 0.300 0.001 0.010 0.752 0.845 0.821 0.016 0.012
Table 3: Pearson chi square and multinomial logistic regression analysis of study variable.
Discussion:
The clinical presentation of pneumonia
varies with the age of the patient, the extent
of the disease, and the etiologic agent. Non�
specific signs and symptoms include fever,
chills, headache, malaise, restlessness and
irritability. General signs of lower respiratory
tract disease include cough, fever,
tachypnea, refusal to feed and retractions of
the accessory intercostal and abdominal
muscles. Chest in drawing is a particularly
useful sign as it appears early and yet has
a high specificity and a reasonable
sensitivity. Respiratory rates to be measured
in all infants thought to be ill or to have
acute feeding problems. Cough with
expectoration of sputum is more common in
older children. Decreased breath sounds
may be present but the presence of crackles,
characteristic of pneumonia in older
children. Rapid breathing as defined by
WHO, detects about 85 percent of children
with pneumonia, and more than 80 percent
of children with potentially fatal pneumonia
are probably successfully identified and
treated using the WHO diagnostic criteria.
Mulholland et al in Philippines have

Karnataka Paediatric Journal Vol. 29, No. 1 Jan - March 2014
29
chest in drawing. Finally, there is a
considerable overlap in the clinical and
radiological features of bacterial and viral
pneumonias15, 16.
We observed that children with a
clinical diagnosis of lower respiratory tract
infection and having wheezing, refusal to
feed and chest in drawing, crackles were
found to have different radiological finding
as compared to those which lack them.
More over the presence of wheezing, refusal
to feed, signs of crackles and chest in
drawing were found to be independently
affecting the chest x-ray finding of the
patients. The accuracy of the chest
radiograph in predicting the etiologic agent
causing pneumonia has been disputed. The
radiologic pattern has a relation with the
clinical condition and a routine chest x-ray
is necessary at the initiation treatment.
Staphylococcal pneumonia is frequently
associated with pneumatoceles and pleural
effusion that subsequently evolve to
empyema17 these findings might be
explained by the overlap on clinical
presentation of children with bronchiolitis
and pneumonia. Chest radiographs remain
the diagnostic mainstay in childhood
pneumonia providing support to the clinical
impression and defining the extent of the
inflammatory process. Although it is not
possible to decide from a radiograph
whether a child is suffering from a bacterial
or viral infection and intraobserver and
interobserver variation among radiologists is
common, a high quality chest film can be
useful in the differential diagnosis between
these entities.
Conclusion: we concluded that
radiological findings more accurately
correlates with clinical findings like
wheezing, refusal to feed, signs of crackles
and chest in drawing , reflecting a more
severe inflammatory process. Moreover,
patients in the early stages of acute lower
respiratory tract infections with clinical
finding primarily as cough and fever may
not have specific chest x-ray findings.
REFERENCES:
1. Ranganathan SC, Sonnappa S.
Pneumonia and other respiratory
infections. PediatrClin North Am.
2009;56:135-56.
2. World Health Organization. Acute
Respiratory Infections in Children:
Case Management in Small Hospitals
in Developing Countries. A Manual for
Doctors and Other Senior Health
Workers. World Health Organization:
Programme for the Control of Acute
Respiratory Infections. Geneva,
Switzerland: 1990.
3. Puumalainen T, Quiambao B, Abucejo-
Ladesma E, et al. Clinical case review:
a method to improve identification of
true clinical and radiographic
pneumonia in children meeting the
World Health Organization definition
for pneumonia. BMC Infect Dis.
2008;8:95.
4. Wilkins TR, Wilkins RL. Clinical and
radiographic evidence of pneumonia.
Radiol Technol. 2005;77:106-10.
5. Mahabee-Gittens EM, Grupp-Phelan J,
Brody AS, et al. Identifying children
with pneumonia in the emergency
department. ClinPediatr. 2005;44:427-35.

Karnataka Paediatric Journal Vol. 29, No. 1 Jan - March 2014
30
6. El-Radhi AS, Barry W. Thermometry in
paediatric practice. Arch Dis Child.
2006;91:351-6.
7. World Health Organization. Integrated
management of childhood illness chart
booklet. (WC 503.2). Geneva: WHO,
2008. Available at: http:// whqlibdoc.
who.int/ publications/2008/9789241
597289_eng.pdf. Accessed on January
15; 2009.
8. Cherian T, Mulholland EK, Carlin JB, et
al. Standardized interpretation of
paediatric chest radiographs for the
diagnosis of pneumonia in epidemiological
studies. Bull World Health Organ.
2005;83(5):353-9.
9. Mulholland EK, Simoes EAF, Costales
MO, McGrath EJ, Manalac EM, Gove
S.Standardized diagnosis of pneumonia
in developing countries.Pediatric Infect
Dis J1992;11(2):77-81.
10. Shan F. Etiology of Severe Pneumonia
in Children in Developing Countries.
Pediatr Infect Dis. 1986;5(2):247-52.
11. Shaikh QamaruddinNizami, Zulfiqar
Ahmed Bhutta, Rumina Hasan, Yousuf
A Husen.Role of Chest X-ray in
diagnosis of lower respiratory tract
infections in children less than five
years of age in Community. Pak J Med
Sci 2005 Vol. 21 No. 4 417-421.
12. World Health Organization. Integrated
management of childhood illness chart
booklet. (WC 503.2). Geneva: WHO,
2008. Available at: http://
whqlibdoc.who.int/ publications/
2 0 0 8 / 9 7 8 9 2 4 1 5 9 7 2 8 9 _ e n g . p d f .
Accessed on January 15; 2009.
13. Shah S, Bachur R, Kim D, Neuman MI.
Lack of predictive value of tachypnea
in the diagnosis of pneumonia in
children. Pediatr Infect Dis J.
2010;29:406-9.
14. Hazir T, Qazi SA, Bin Nisar Y, et al.
Comparison of standard versus double
dose of amoxicillin in the treatment of
non-severe pneumonia in children aged
2-59 months: a multi-centre, double
blind, randomised controlled trial in
Pakistan. Arch Dis Child. 2007;92(4):
291-7.
15. Shann F, Hart K, Thomas D. Acute
lower respiratory tract infections in
children: possible criteria for selection
of patients for antibiotic therapy and
hospital admission. Bull World Health
Org1984;62(5):749-53.
16. Wall RA, Corrah PT, Mabey DC,
Greenwood BM.Theetiology of lobar
pneumonia in the Gambia. Bull World
Health Org1986;64(4):553-8.
17. Caffey�sPediatric Diagnostic Imaging
10th Edition Vol.I, 994-1006.

Karnataka Paediatric Journal Vol. 29, No. 1 Jan - March 2014
31
ABSTRACT
Objective: To understand the need for
monitoring creatinine levels in Birth
asphyxiated neonates to evaluate the
possibility of Acute Kidney Injury in them.
Study Design: prospective hospital
based observational study done in
Department of Pediatrics, Yenepoya Medical
College, and Mangalore, India between Jan
2013 � June 2013.
Patients: 25 newborns born with an
Apgar score (A/S) of =5 at 5 min and
admitted in the NICU were studied, renal
function parameters�blood urea, serum
creatinine, serum electrolytes were monitored
initially within 24 hours of birth and then
serially everyday up to day 5 of life.
Results: The newborns were divided
in two groups. Asphyxiated babies with
normal renal functions were selected as
group A and with impaired renal functions,
as Group B. The renal function parameters
of group A did not show any significant
variation in the serial estimation, which
though was elevated on Day 1 of life
became normalised by Day 3, whereas in
group B, renal function parameters exhibited
progressively higher levels in the serial
estimation of the values from day 1 to day 5.
Conclusion: Monitoring of serum
creatinine is recommended in asphyxiated
neonates with altered renal parameters on
day 1 of life to evaluate the possibility of
acute kidney injury in them.
Key Words: Birth Aphyxia, Creatinine,
monitoring
INTRODUCTION:
Asphyxia remains a common problem
in paediatric intensive care. The incidence
of asphyxia is estimated to be between 1
and 10 per 1000 live births and is a
significant cause of morbidity and death in
the term and preterm neonate1. Asphyxia is
known to lead to multi-organ dysfunction
and a redistribution of cardiac output
which compromises renal perfusion 2, 3, 4, 5.
Renal system is involved in about 50% of
the cases of perinatal asphyxia. Perinatal
asphyxia results in fetal hypoxemia and
hypercarbia1 which further contributes to
renal insult. Moreover perinatal asphyxia
producing ischemia is the commonest cause
of neonatal renal failure5, 6. A high incidence
of altered renal function has been reported
in many studies7, 8, 9.There are not many
reports which elaborates on the pattern of
change in routinely measured renal function
in the cases of birth asphyxia. An accurate
estimate of the pattern of variation in
routinely measured renal function
parameters will help us in early diagnosis
and management renal abnormalities in the
cases of birth asphyxia.
METHODS
This was a hospital based prospective,
observational study done in Department of
Pediatrics, Yenepoya Medical College
Mangalore, and India between January 2013
SERUM CREATININE MONITORING IN BIRTH
ASPHYXIATED NEWBORNSDr. Shamim Amanulla Khan, Dr. Shyam Sudhir, Dr. Faheem
Yenepoya Medical College,Yenepoya University, Mangalore

Karnataka Paediatric Journal Vol. 29, No. 1 Jan - March 2014
32
� June 2013. Neonates with an Apgar score
(A/S) of =5 at 5 min of life were included
in the study. Neonates diagnosed with
heart disease, congenital abnormality of
kidneys and urinary tract, perinatal
exposure to medicine that might change
renal hemodynamic, polycythemia, and
twins were excluded from the study10. All
cases were managed as per the clinical
condition, and data was recorded by
treating pediatrician blinded for study
outcome. Gestational age, birth weight,
relevant perinatal history, findings on
physical examination and systemic
examination were recorded on a
predesigned proforma. Daily weight
recordings were taken on an electronic scale,
24 hours urine output measurement done by
applying plastic collection bags and urine
examination performed daily. Renal function
parameters�blood urea, serum creatinine,
serum electrolytes were monitored initially
within 24 hours of birth and then serially
everyday up to day 5 of life by drawing 1
mL of blood with aseptic precautions and a
disposable syringe from any large peripheral
vein, for various tests. After 5 days, babies
having abnormal renal functions had their
laboratory parameters monitored and were
managed accordingly till recovery. Twenty
four hour urine output was measured using
self-adhesive plastic urine collecting bags
and sent for routine examination. Neonates
who developed renal failure were managed
conservatively as per the clinical decision of
the paediatrician incharge. Arterial blood
gas analysis was done as and when
required for the management of the
particular case. Criteria adopted for labelling
an asphyxiated neonate as having renal
failure were , serum creatinine >1mg/dL
plus two of the following three (1) urine
output <0.5 mL/kg/hour,(2) blood urea
>40mg/dL,(3) presence of significant
hematuria or proteinuria. These criteria
were, applied on day 3 of life and the
criteria when fulfilled were considered as
indication of renal failure 12. For blood
urea- diacetyl monoxime13 (DAM) Method;
serum creatinine-Jaff�s reaction 13 (picric acid
reaction); and Serum electrolytes (S·Na +
S·K +)-electronic analyzer, were used. Renal
USG was advised if clinically required.
Asphyxiated babies with normal renal
functions were grouped as group A and
babies with birth asphyxia with impaired
renal functions were grouped as Group B.
Stastical analysis
Data was analyzed using SPSS 17
software. The statistical difference in the
mean value of basic demographic factors
was assessed using unpaired t test of chi
square test as per variable. The statistical
difference in the serial values of the serum
parameters were analyzed using one way
ANOVA for confidence level of 95%, p <
0.05 were considered significant.
RESULTS
25 birth asphyxiated newborns were
studied out of which 14(56%) were girls
with a mean birth weight of 2.63 ± 0.43 kg
and mean gestational age of 39.15 ±3.7
weeks. The patients were divided into two
groups: Group A with normal renal function
(n-14) (M/F 8:6) and Group B renal failure
(n-11) (M/F 6:5)(table 1). No statistical
difference in the mean age (p=0.564) and
gestational age (p=0.433) were noted among
the two group of patients.

Karnataka Paediatric Journal Vol. 29, No. 1 Jan - March 2014
33
Table 1: showing the basic demographic
parameters of the two groups of study
patients.
Group A
Group B
Statistical method
Significance
N 14 11
Male/female 8/6 6/5 chi-square with one degree of freedom
p = 0.828
Birth weight (Kg) 2.67 ±0.32
2.59 ±0.73
unpaired t test
0.564
Gestational age( weeks)
39.43 ± 3.4
38.79 ± 3.7
Paired t test 0.433
The renal function parameters of
group A with normal renal function were
statistically different from the corresponding
values for group B (p=0.000-0.012). The
renal function parameters of group A with
normal renal function did not show any
variation in the serial estimation of the
values from day 1 to day 5(p=0.32-0.48). In
Group B neonates, renal function
parameters exhibited progressively higher
levels in the serial estimation of the values
from day 1 to day 5, which was statistically
significant (p=0.000-0.0043) (Table 2).
Table 2: showing the serial renal function parameters of the two groups of patients
DAY 1 DAY 2
DAY 3 DAY 4
DAY 5 p DAY 1 DAY 2 DAY 3 DAY 4 DAY 5
P value
Serum urea
23.4±3.8
24.7±2.7
26.5±6.2
24.4±5.
25.3±5.1
0.482
42.4±3.9
44.8±3.6
49.5±4.3
51.1±15.
55.02±5
0.0043
Serum creatinine
0.9±0.64
1.1±0.45
1.2±0.27
1.1±0.7
1.3±0.24
0.728
1.69±1.25
1.93±2.12
2.32±1.4
2.43±2.1
3.11±1.4
0.0023
Urine output(ml/kg/hr)
0.49±0.16
0.45±0.12
0.51±0.06
0.49±01
0.48±0.12
0.793
0.45±0.24
0.39±0.16
0.36±0.3
0.33±0.1
0.37±0.2
0.0012
Urine routine
P �
H -
P �
H -
P �
H -
P-
H-
P-
H-
P +
H -
P +
H -
P �
H-
P �
H -
P �
H -
0.000
Fig 1.Chart showing the variation in the serial serum creatinine levels in the two groups of
patients.

Karnataka Paediatric Journal Vol. 29, No. 1 Jan - March 2014
34
DISCUSSION
11 (44%) of the studied newborn with
birth asphyxia had renal failure. Even those
babies who did not qualify the diagnostic
criteria of birth asphyxia had renal function
parameters higher than those for healthy
newborn 8.This reflects a mild injury to the
kidneys in the majority of them14. However,
kidneys are very sensitive to oxygen
deprivation and injury may result in
permanent renal impairment in up to 40%
of survivors7. Hence, renal function should
be closely monitored in all asphyxiated
neonates, as renal dysfunction is the most
common involvement during perinatal
asphyxia15.
Incidence of renal failure was
seen in 44% of the asphyxiated neonates
which is quite comparable to the incidence
of renal failure reported in earlier studies7, 8,
9. However, Dauber et al 16 studied seven
infants born with A/S of =5 at 1 min, for
renal parameters and observed that 57%
developed ARF. Furthermore, Mohan et al 17
reported an incidence of 72% in asphyxiated
neonates with an overall mortality of 36%,
which could be because of employing
highly sensitive tests, such as measurements
of â2 M, fractional excretion of sodium, and
renal failure index along with urine/plasma
ratio of creatinine.
Out of 25 asphyxiated neonates 11
(44%) developed ARF, which showed the
worsening of the renal parameters on serial
estimation. The fact that levels of the renal
function parameters were similar to study
done by Gupta et al 7 , Saili et al 8 and
Dauber et al 16 the latter studies do not
provide the serial profile of five days values
so exact comparison is not possible.
In conclusion, renal function abnormalities
represent a significant problem among
asphyxiated neonates, and these neonates
have a higher risk to develop renal failure.
We recommend kidney functions to be done
routinely in asphyxiated neonates to
evaluate the possibility of acute kidney
injury in them.
REFERENCES
1. Lisa MA, Papile LA., Cloherty JP,
Eichenwald EC, Stark AR (Eds):
Manual of neonatal care, 6 th Ed. New
Delhi, Wolters Kluwer India Pvt Ltd
2008; 518-35.
2. Bhargava M, Bhargava SK. Impairment
of platelet functions in birth anoxia.
Indian J Med Res 1978; 68:976-9.
3. Costello AM, Mananethar DS. Perinatal
asphyxia in less developed countries.
Arch Dis Child 1994; 71:F1-3. Volpe
JJ. Hypoxia ischemic encephalopathy.
In Volpe JJ (Eds): Neurology of
newborn, 3rd Ed. Philadelphia:
Saunders 2000, 217,277,296,331
4. Volpe JJ. Hypoxia ischemic encephalopathy.
In Volpe JJ (Eds): Neurology of
newborn, 3rd Ed. Philadelphia:
Saunders 2000, 217,277,296,331.
5. Chevalier RL, Campbell F, Noorman A.
Prognostic factors in neonatal acute
renal failure. Pediatrics 1984; 74:265-72.
6. Guinard JP. Renal functions in new
born infant. Pediatr Clin Am 1982;
29:777-89.
7. Gupta BD, Sharma P, Bagla J, Parakh
M, Soni J P. Renal failure in
asphyxiated neonates: Indian Pediatr
2005;42:928-34
8. Saili A, Sarna MS, Dutta AK. Acute

Karnataka Paediatric Journal Vol. 29, No. 1 Jan - March 2014
35
renal failure in asphyxiated newborns.
Indian Pediatr 1990; 28:19-23.
9. Kojima T, Kobayashi T, Matsuzaki S,
Iwase I, Kobayashi Y. Effects of
perinatal asphyxia and myoglobinuria
on development of acute neonatal renal
failure. Arch Dis Child 1985; 60:908-12.
10. Jenic AG, Cernadas JM, Gorenstein A,
et al. A randomized, double-blind,
placebo-controlled trial of effects of
prophylactic theophylline on renal
functions in term-neonates with
perinatal asphyxia. Pediatrics
2000;105(4): e45-54
11. Costello A, Ellis M. Birth asphyxia.
Apgar score and neonatal
encephalopathy: Editorial. Indian
Pediatr 1997; 34:975-7.
12. Misra PK, Kumar A, Natu SM, Kapoor
RK, Srivastava KL, Das K. Renal
failure in symptomatic perinatal
asphyxia. Indian Pediatr 1991; 28:
1147-1151.
13. Varely H, Gowenlock AH, McMurray
JC. Creatinine, Urate and Urea. In
Practical Clin Biochem, William
Heinemann Med Books 1988:350-67.
14. Martin-Ancel A, Garcia-Alix A, Goya F,
Cabanas F, Buergueros M, Guero J.
Multiple organ involvement in
perinatal asphyxia. J Pediatr 1995;
127:786-93.
15. Sabrine N, Singh J, Sinha SK. Medical
management of birth asphyxia. Indian
Pediatr 1999;36:
16. Dauber IM, Krauss AN, Synchych PS.
Renal failure following perinatal
anoxia. J Pediatr 1976;88:851-5
17. Mohan PV, Pai PM. Renal insult in
asphyxia neonatorum. Indian Pediatr
2000; 37:1102-6.

Karnataka Paediatric Journal Vol. 29, No. 1 Jan - March 2014
36
Abstract:
Aim: This study was done to measure
the incidence of rickettsial fever in a tertiary
care hospital in Mysore Karnataka.Settings:
Pediatric ward of Cheluvamba Hospital
Mysore Methods: This study included all
children between the age group 1year to 14
years who were admitted in Cheluvamba
Hospital Mysore from 1st July 2012 to 31st
June 2013 .The Case records of all children
with a clinical diagnosis of rickettsial fever
and who tested positive for Weil Felix
reaction were reviewed. Weil Felix test was
done by the tube agglutination method .A
titre of 1/160 and above was considered
significant. RGA Scoring system for spotted
fever group of Rickettsial fever was used
(Score above 9 was taken as positive).
Statistical Analysis used was SPSS version
17 for windows and data analysis was by
descriptive analysis and chi square
test.Results:In our study a total of 13
children (4.56% of viral exanthematous
fever) were found to have rickettsial fever.
Age ranged from 1 y to 14 years with
maximum incidence below 5 years (46.2%)
and male predominance (M:F = 1.6:1).
Major presenting symptoms were fever (100
% with mean of 8.76 days) and rash (100%),
followed by oedema (38.5%), hepatosplenomegaly
(21%). Conclusions: Rickettsial fever should
to be considered in children with presenting
complaints of fever with rash. A positive
Weil Felix reaction in the presence of clinical
suspicion and the RGA scoring above 9 can
be regarded as diagnostic for rickettsial
fever where facilities for confirmatory tests
are not available. Early diagnosis and
treatment is associated with reduced
morbidity and mortality.Key words:
Rickettsial Fever, RGA scoring system, Weil
Felix reaction.
Introduction:
Rickettsial Fever is an acute febrile
zoonotic illness transmitted by bite of mites
and ticks with varied clinical manifestations
presenting as fever with rash or
accompanied with gastrointestinal
,respiratory orcentral nervous system
involvement.The main agent causing
rickettsial infection in our country is
Orientiatsutsugamushi,which is the
etiological agent for scrub typhus1.Often
labeled as viral �Exanthematous fever��2.
Rickettsial infection can lead onto serious
end organ damage which includes
pneumonitis, ARDS, acute renal failure,
myocarditis, disseminated intravascular
coagulation (DIC)3 and septic shock.4 The
presence of Rickettsial fever and its re-
emergence have been established in various
parts of India- Jammu and Kashmir,
Himachal Pradesh, Uttaranchal, Rajasthan,
Assam, West Bengal, Maharashtra, Kerala,
Tamil Nadu and Karnataka.
Diagnosis of the disease is often
challenging due to non-availability of
confirmatory laboratory tests and cost factor.
Diagnosis and confirmation of this
disease is based on Serological tests like
Micro Immunofluorescence,Latex agglutination,
RICKETTSIAL FEVER- AN INCIDENCE STUDY IN A
TERTIARY CARE CENTRE IN SOUTH INDIADr. NirmalaVineethaPinto, Dr. SudhaRudrappa, Dr. Suresh R.
Department of Pediatrics, Mysore Medical College and Research Institute,Mysore.

Karnataka Paediatric Journal Vol. 29, No. 1 Jan - March 2014
37
Indirecthemagglutination, ELISA and
Immunoperoxidase3 .Gold standard test for
diagnosis isimmunofluorescence assay.
The Weil-Felix (WF) test is based on
the detection of antibodies to various
Proteus species which contain antigens
with cross-reacting epitopes to antigens from
members of the genus Rickettsia. Whole cells
of Proteus vulgaris OX-2 react strongly with
sera from persons infected with SFG
rickettsiae,and whole cells of P. vulgaris
OX-19 reacts with sera from persons
infected with typhus group rickettsiae.
The OX-K strain of Proteus mirabilis
was demonstrated to agglutinate with sera
from scrub typhus patients5. By the WF test,
agglutinating antibodies are detectable after
5 to 10 days following the onset of
symptoms, with the antibodies being mainly
of the immunoglobulin M (IgM) type. The
poor sensitivity of the WF test is now well
demonstrated but a good correlation
between the results of the WF test and detection
of IgM antibodies by an immunofluorescence
assay (IFA) is often observed.
The RGA scale was devised by Rathi
GoodmanAghai et al. includes clinical and
laboratory findings in scrub typus6.Total
score is 35 (25 clinical and 10 laboratory).
TABLE 1 shows the RGA scoring system for
spotted fever
Highest accuracy was found at a
score of 14 with a sensitivity and specificity
at 96.15 % and 98.84%. A score of 17 had
100% specificity and score of 9 had 100%
sensitivity
Observations:
In our study from July 2012 to June 2013,
13 children (4.56% of viral exanthematous
fever) satisfied our inclusion criteria. Age
ranged from 1 year to 14 years with
maximum incidence below 5 years age
group (46.2%) and male predominance (M:F=1.6:1).
Major presenting symptoms were fever (100
% with mean of 8.76 days) and rash
(100%), followed by oedema (38.5%),
hepatosplenomegaly (21%).
TABLE- 2 Observations of the study
On Weil Felix test, 8 children showed
titres = 1:160 for OX2 antigen and 8children
for OX-19 antigen = 1:160, while 4children
showed titre =1:320 for both the antigens at
presentation 1child showed a titre of 1:640.
RGA scores had a median of 14.
Discussion:
This study documents that rickettsial
fever is prevalent in Karnataka and needs to
be considered as an essential differential
diagnosis in children presenting with

Karnataka Paediatric Journal Vol. 29, No. 1 Jan - March 2014
38
exanthematous fever. In our study 13
children met our inclusion criteria and had
a positive Weil Felix test and RGA scores
were above 9.Incidence being 4.29 % with a
male preponderance and maximum in age
group less than five years. Weil Felix test
even with low sensitivity can be used in a
set up where confirmatory tests are not
available,however it should be correlated
with clinical features and the RGA scoring
system can be applied.
The clinical features indicating strong
suspicion for diagnosis includes rashes
involving palm and soles, edema of hands
and soles, hepatosplenomegaly and
arthralgia.
The importance of rapid diagnosis is
the prompt response to antimicrobial
therapy and reduced mortality in children
with early treatment. The treatment given in
our set up was oral doxycycline 4 mg/kg/
day7till 3 days after being afebrile, to which
all the children responded and there was
no morbidity.
Delay in diagnosis and treatment has
been associated with death and grave
neurological sequelae.
References
1 Isaac R, Verghese GM, Mathai E et al,
Scrub typhus : prevalence and
diagnostic issues in rural southern
India, Clinical Infectious diseases, 2004
Nov, vol 39, pp. 1395 � 1396
2 N.Murali , Swathi Pillai, Thomas
Cherian et al ,Rickettsial infections in
South India- How to spot the Spotted
fever, IndianPediatrics, 2001 ,vol
38:1393-1396
3 Tsay RW, Chang F Y, Serious
complications in scrub typhus, Journal
of Microbiology, Immunology and
Infection, 1998, vol 31(4), pp. 240 - 244
4 Mohd Ashraf, Arshad Farooq,
SaikaBashiaet al, Renal failure
association with scrub typhus, JK
Science, 2010 april-june, vol 12 (2).
5 SK Mahajan*, R Kashyap*, A Kanga**,
V Sharma**, BS Prasher*, LS
Pal;Relevance of Weil-Felix Test in
Diagnosis of Scrub Typhus in India
JAPI � vol. 54 � august 2006
6 Narendra b rathi, *akanksha n rathi,
#michael h goodman, and #zubair h
aghaiRickettsial Diseases in Central
India: Proposed Clinical Scoring System
for Early Detection of Spotted Fever
indianpediatricsvolume 48; November
17, 2011
7 David H. Walker, J. Stephen Dumler,
Thomas Marrie. Harrison�s Principles
of InternalMedicine 18th edition.
McGraw-Hill Companies Inc.; 2012.
Chapter 174 The Rickettsial Diseases.
pp.1407 � 1417