Polymorphic microsatellite loci for primitively eusocial Stenogastrine wasps

ORIGINAL ARTICLE 543J o u r n a l o fJ o u r n a l o f
CellularPhysiologyCellularPhysiology
P53 Mutations in ColorectalCancer From Northern Iran:Relationships With Site of TumorOrigin, Microsatellite Instabilityand K-ras Mutations
MAHBOOBEH MAHDAVINIA,1,2 FARAZ BISHEHSARI,1,2 FABIO VERGINELLI,1ALBANA CUMASHI,1 ROSSANO LATTANZIO,1 MASOUD SOTOUDEH,2,3 REZA ANSARI,2
DANIELA SEMERARO,4 MAHSHID HORMAZDI,4 HAFEZ FAKHERI,5 NASER RAKHSHANI,2
LAURA DE LELLIS,1 MARIA CRISTINA CURIA,1 ALESSANDRO CAMA,1 MAURO PIANTELLI,1
REZA MALEKZADEH,2 STEFANO IACOBELLI,1 AND RENATO MARIANI-COSTANTINI1*1Department of Oncology and Neurosciences, University G. d’Annunzio, and Center of Excellence on Aging (CeSI),
G. d’Annunzio University Foundation, Chieti, Italy2Digestive Disease Research Center (DDRC), Shariati Hospital, Medical Sciences/University of Tehran, Tehran, Iran3Department of Pathology, Shariati Hospital, Medical Sciences/University of Tehran, Tehran, Iran4Department of Pathology, Mehr Hospital, Tehran, Iran5Department of Medicine, Mazandran University of Medical Sciences, Sari, Iran
CRC-associated P53 mutations have not been studied extensively in non-Western countries at relatively low CRC risk. We examined, forthe first time, 196 paraffin-embedded CRC cases from Northern Iran for mutations in P53 exons 5–8 using PCR-direct sequencing. P53status and mutation site/type were correlated with nuclear protein accumulation, clinicopathologic variables and data on K-ras mutationsand high-level microsatellite instability (MSI-H). We detected 96 P53 mutations in 87 (44.4%) cases and protein accumulation in 84 cases(42.8%). P53 mutations correlated directly with stage and inversely with MSI-H. Distal CRCs were more frequently mutated at major CpGhotspot codons [248 (8/66, 12.1%), 175 (7/66, 10.6%), and 245 (7/66, 10.6%)], while in proximal tumors codon 213, emerged as mostfrequently mutated (5/28, 17.9% vs. 3/66, 4.5%, P¼ 0.048). Transitions at CpGs, the most common mutation type, were more frequent innon-mucinous (25% vs. 10.4% in mucinous, P¼ 0.032), and distal CRC (27% vs. 12.5% in proximal, P¼ 0.02), and correlated with K-rastransversions. Transitions at non-CpGs, second most common P53 mutation, were more frequent in proximal tumors (15.6% vs. 4.7% indistal, P¼ 0.01), and correlated with K-ras transitions and MSI-H. Overall frequency and types of mutations and correlations with P53accumulation, stage and MSI-H were as reported for non-Iranian patients. However P53 mutation site/type and correlations between P53and K-ras mutation types differed between proximal and distal CRC. The codon 213 P53 mutation that recurred in proximal CRC waspreviously reported as frequent in esophageal cancer from Northern Iran.
J. Cell. Physiol. 216: 543–550, 2008. � 2008 Wiley-Liss, Inc.
M. Mahdavinia and F. Bishehsari contributed equally to this work.
Contract grant sponsor: Faculty of Medicine, G. d’AnnunzioUniversity, Chieti.Contract grant sponsor: Digestive Disease Research Center(DDRC)—Tehran University of Medical Sciences, Tehran, Iran.
*Correspondence to: Renato Mariani-Costantini, Unit of MolecularPathology, Center of Excellence on Ageing (CeSI), G. d’AnnunzioUniversity Foundation, 66100 Chieti, Italy. E-mail: [email protected]
Received 4 November 2007; Accepted 30 January 2008
DOI: 10.1002/jcp.21428
Colorectal cancer (CRC) is the third most common cancerworldwide, but age-standardized incidence rates (ASRs) varywidely between different geographical regions, a phenomenonwhich may reflect variation in exposure to environmentalcarcinogens (Potter, 1999; Kamangar et al., 2006). In particular,CRC ASRs are low (3–7/100,000) in countries of Central-WestAsia, the Middle East and Africa when compared to high-riskareas such as North America, Australia, North-WesternEurope, and Japan (30–50/100,000) (Ferlay et al., 2004). Thelimited data available for CRC in countries at lower risk suggestthat differences in the frequencies of pathologic and molecularCRC phenotypes of clinical relevance could occur compared tohigh risk countries (Hayashi et al., 1996; Qing et al., 2003; Chanet al., 2005).
Mutations in the P53 gene are major genetic alterationsinvolved in CRC progression (Arnold et al., 2005). Suchmutations play specific biological roles (Samowitz et al., 2002;Russo et al., 2005), provide clues about mechanisms of geneticdamage (Greenblatt et al., 1994; Hussain and Harris, 2000), tendto be differentially associated with other cancer-related geneticalterations and have prognostic and clinical relevance (Soong
� 2 0 0 8 W I L E Y - L I S S , I N C .
et al., 1997; Kim et al., 2007). P53 mutations have not beenstudied extensively in non-Western countries at lower CRCrisk.
In Iran CRC incidence is relatively low (6–8/100,000) (Sadjadiet al., 2003; Ansari et al., 2006), although it may be rapidly

544 M A H D A V I N I A E T A L .
increasing (Hosseini et al., 2004; Semnani et al., 2006). Theyoung age structure of the population and the low CRC rates inolder age groups may account for the high proportions of youngcases and of familial and right-sided tumors in Iranian CRCseries (Hosseini et al., 2004; Mahdavinia et al., 2005; Ansari et al.,2006).
In an earlier study, we characterized a retrospective paraffin-embedded series of 182 CRC cases from the capital city,Tehran, Northern Iran, for mutations in the K-ras gene andhigh-level microsatellite instability (MSI-H) status. This revealedMSI-H and K-ras mutation frequencies in the range of thosefound in non-Iranian CRC series, but highlighted differences intype and codon distribution of K-ras mutations (Bishehsari et al.,2006).
In the present study, the same CRC series (Bishehsari et al.,2006), upgraded to 196 cases, was analyzed for mutations in themost frequently mutated region of the P53 gene, that is, exons5–8, which encode the DNA binding domain. P53 mutationswere correlated with P53 protein accumulation, as revealed byimmunohistochemistry (IHC), with clinicopathologic variablesand with previously described data on K-ras mutations and MSI-H (Bishehsari et al., 2006).
Obtained results agree with those reported for non-IranianCRC with regard to overall frequency and types of P53mutations and to correlations between P53 mutations, proteinaccumulation, tumor stage, and MSI-H (McDermott et al., 2002;Diep et al., 2003; Iacopetta, 2003; Klump et al., 2004; Russoet al., 2005; Soreide et al., 2006). However P53 mutation siteand type significantly differed between proximal and distal CRC,and codon 213, a mutation hotspot previously reported inNorthern Iran for esophageal squamous cell carcinoma (ESCC)(Biramijamal et al., 2001), was by far the commonest mutationsite in proximal tumors. Correlations between P53 and K-rasmutation types also emerged. These results suggest that inNorthern Iran different mutational mechanisms couldcontribute to P53 mutation load in proximal versus distalcolorectal carcinogenesis.
Patients and MethodsCRC cases and DNA preparation
The study was reviewed and approved by the Ethics Committeeof the Digestive Disease Research Center (DDRC) of TehranUniversity of Medical Sciences. As previously described(Bishehsari et al., 2006) a series of 211 formalin-fixed, paraffin-embedded CRC cases accessioned from February 1998 throughSeptember 2003 was retrieved from the pathology archives ofMehr and Atieh Hospitals, two major CRC referral centers inTehran. Patients with CRC associated to inflammatory boweldisease or familial adenomatous polyposis and those whounderwent preoperative chemo- and/or radio-therapy wereexcluded, while patients who fulfilled the Amsterdam II criteriafor hereditary non-polyposis colorectal cancer (HNPCC) wereincluded (13 cases). Data collected for each case included age atCRC diagnosis, site of the primary tumor in the colorectum[proximal or distal to the splenic flexure (Iacopetta, 2002)],disease stage, mucin production, and histological grade.
The demographic and pathological characteristics of thestudy series were consistent with those previously reported inrecent epidemiologic studies conducted in Iran (Sadjadi et al.,2003; Hosseini et al., 2004; Ansari et al., 2006). Samples from196 out of 211 CRC patients were successfully scanned formutations in exons 5–8 of P53, including 85 women and 111men, with male to female ratio of 1.3, and mean age of 53.4 years(�15.5). Sixty-four tumors (32.7%) were proximal to thesplenic flexure, 67 (34.2%) were in the left colon and 59 (30.1%)in the rectum, location of 6 tumors (3%) was unspecified. Thedistribution of the cases according to the modified Dukes’classification was as follows: Duke A, 5; Duke B, 94; Duke C, 64;
JOURNAL OF CELLULAR PHYSIOLOGY
and Duke D, 23 cases. Tumors were graded according to theWHO histological classification (Hamilton and Aaltonen,2000). Archival slides were reviewed by a pathologist at DDRC(M.S.). CRC diagnosis was independently confirmed on newly-cut slides by a pathologist at CeSI (M.P.). For each case an areawith at least 50% cancer cells was defined on standard sectionsstained with hematoxylin and eosin (H&E) and used to guidemanual microdissection for DNA extraction. Areas exclusivelycomprising normal colorectal muscular wall were similarlyidentified for normal DNA extraction. Serial 15-mm-thicksections were prepared for DNA extraction. For each casematched normal and tumor areas were dissected from de-waxed slides and digested for 1–2 days at 568C in 100 mlof buffer (50 mM TRIS pH 8.5, 1 mM EDTA, 0.5% TWEEN 20)containing proteinase K (20 mg/ml). DNA was purified using theQIAamp DNA minikit (Qiagen, Hilden, Germany).
Mutational analyses
De-waxing, microdissection, DNA extraction, and PCR set-upwere all performed in a dedicated laboratory, free ofcontamination from PCR products. Exons 5–8 of P53 wereamplified by GenAmp PCR System 9700 (Applied Biosystems,Foster City, CA). PCR conditions were: 10 min at 958Cfollowed by 35–40 cycles of 1500 at annealing temperature, 3000
at 728C (extension), and 1500 at 958C (denaturation). Thereaction was ended by a 10 min extension at 728C. Annealingtemperatures varied between 578C and 608C according toprimer set. Primers’ sequences and PCR annealingtemperatures (8C) are detailed as follows;
Exon5: Forward 50-CCCTGAAAGTTGAGACAGAGGAA-30 and reverse 50-CCAGCCCTGTCGTCTCTCCAG-30
(608C),Exon6: Forward 50-CCGGAGACTAAGGAGTGACT-30
and reverse 50-CTTAACCCCTCCTCCCAGAGA-30
(578C),Exon 7: Forward 50-CGGAGTAGAACCCGGACACA-30
and reverse 50-GGGGCACAGCAGGCCAGTG-30 (608C),Exon 8: Forward 50-CGGAATGACGGAGAACGAAG-30
and reverse 50-CCAGGCATAACTGCACCCTTG-30
(608C).
The reaction mixture (30 ml) contained 1.5 U of AmpliTaqGoldTM (Perkin-Elmer Corp., Foster City, CA), theaccompanying PCR buffer, 1.5 mM MgCl2, 200 mM of eachdeoxynucleoside triphosphate and 0.5mM of each primer. Afterelectrophoresis on ethidium bromide-stained 2% agarose gelPCR products were purified with Montage PCR microfilters(Millipore Corporation, Bedford, MA), sequenced directly usingthe ABI PRISM Big Dye_Terminator v3.1 Cycle SequencingReady Reaction Kit (Applied Biosystems) and visualized bycapillary electrophoresis with an ABI 310 Genetic Analyzer.Samples with mutations were verified by at least twoindependent PCR reactions and sequence analysis of both DNAstrands. Parallel analysis of matched DNAs from CRC andnormal colorectal muscular wall excluded germlinepolymorphisms.
Data on mutations at codons 12, 13, and 61 of K-ras and onMSI-H status were from our previous study, to which we referfor methodology (Bishehsari et al., 2006). Here we extendedMSI analyses from 182 originally tested cases to all the 196 casesanalyzed for P53 mutations. MSI analysis was based on twomononucleotide repeats, BAT25 and BAT26, considered themost sensitive markers of MSI-H (Hatch et al., 2005).
Immunohistochemistry
Formalin fixed, paraffin embedded, 5-mm-thick sections weredewaxed, rehydrated in graded alcohols, and processed using

P 5 3 A N D C O L O R E C T A L C A N C E R I N I R A N 545
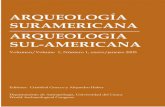
the streptavidin–biotin–immunoperoxidase method. Briefly,antigen retrieval was performed by 10 min microwave heattreatment in 10 mM sodium citrate buffer pH 6.0. Sections werethen incubated with 1% hydrogen peroxide for 15 min, to blockendogenous peroxidase activity, and subsequently with 1%bovine serum albumin diluted in Tris buffered saline (TBS) at pH7.6 for 20 min, to block non-specific binding. Sections wereincubated with primary mouse anti-P53 antibody (NCL-p53-DO7; Novocastra Laboratories Ltd, Newcastle Upon Tyne,UK; 1/50 dilution) for 30 min, then with the Vectastain ABCperoxidase kit (Vector Laboratories, Burlingame, CA)according to the manufacturer’s instructions and using 3,30-diaminobenzidine as chromogen. All slides werecounterstained with Mayer hematoxylin, dehydrated, cleared,and mounted. Tumor sections previously known to be positivefor P53 nuclear accumulation served as positive control.Omission of the primary antibody was included as a negativecontrol. Five hundred cells were randomly selected andcounted from five representative fields of each section by twoindependent observers who had no prior knowledge of theclinicopathologic variables. P53 expression was consideredpositive if seen in >10% of tumor cell nuclei (Fig. 1). Cases withevaluation scores differing by >10% between the twoobservers were re-evaluated until consensus was achieved.IHC analyses were blinded to mutational data.
Statistical analyses
Statistical comparisons were performed by Student’s t-test forcontinuous and Chi-square for categorical variables. When theexpected value was<5, two-tailed Fisher’s exact test was used.SPSS for IBM PC (Chicago, IL) was adopted for all analyses. Allcited P values are two-sided; P< 0.05 was considered asstatistically significant.
ResultsP53 mutations and protein accumulation
Of 211 CRCs for which paraffin-embedded blocks wereretrieved, 196 yielded DNA qualitatively and quantitativelyadequate for the analysis of mutations in exons 5–8 of the P53gene. Mutations were detected in 87/196 cases (44.4%), whichincluded 9 cases with 2 mutations each, for a total of 96 tumor-associated P53 mutations. Table 1 details mutations for eachmutation-positive case in proximal and distal tumors,respectively.
As predicted based on literature (Soussi and Beroud, 2003;Olivier et al., 2004; Russo et al., 2005) most mutations were base
Fig. 1. Nuclear P53 protein accumulation in a colorectal cancer case carmucosa (b). Bar U 50 mm.
JOURNAL OF CELLULAR PHYSIOLOGY
substitutions (84/96, 87.5%), among which G:A transitions atCpG dinucleotides were the commonest type (42/96, 43.7%),followed by G:A transitions at non-CpGs (16/96, 16.6%).Deletions/insertions comprised 12.5% (12/96) of the mutations.The codons with the highest mutation rates were 248 (9, 9.4%),213 (8, 8.3%), 245 (8, 8.3%), 175 (7, 7.2%), and273 (5, 5.2%). Fourof these, that is, codons 248, 175, 273, and 245, are majormutation hotspots in primary CRC, with frequencies of 11%,10.9%, 8.9%, and 5.6%, respectively, as determined among exons5–8 mutations associated with primary CRC in the IARC TP53mutation database (R12 update, November 2007, http://www.iarc.fr/ p53), while codon 213 is less frequently mutated(1.9%) in that database (Petitjean et al., 2007).
P53 mutations may increase protein half-life and are oftenassociated with protein accumulation in the nucleus(McDermott et al., 2002). All the 196 cases analyzed for P53mutations were immunostained for P53. Overall 84 cases(42.8%) scored positive for p53 nuclear accumulation. Therewas a general concordance between protein accumulation andmutation status (77%, Spearman test; P< 0.0001, Table 2), with80.7% specificity (88 negative by IHC of 109 cases with noevidence of P53 mutation) and 72.4% sensitivity (63 positive byIHC of 87 mutated cases). These results are in the range ofthose reported in the literature (Soong et al., 1996; McDermottet al., 2002; Curtin et al., 2004; Klump et al., 2004). Eighteen ofthe 24 cases with detected P53 mutations that did not show P53accumulation carried mutations predicted to result in theexpression of a truncated protein (including 10 nonsense, 6frame-shift, and 2 splice-site mutations). Only six tumors withan identified P53 missense mutation scored negative for P53accumulation. On the other hand, no P53 mutations weredetected in 21/84 cases positive for P53 accumulation (25%), afrequently reported discrepancy which could be explained byseveral factors, including mutations outside screened exons,formation of complexes between P53 and other cellularproteins and alterations in processes that control P53stabilization (Kaserer et al., 2000; Bazan et al., 2002; Munroet al., 2005). Table 2 correlates P53 immunostaining with genemutation.
P53 status and clinicopathologic variables
The frequency and spectrum of P53 mutations and the presenceof P53 nuclear accumulation were correlated with individual andclinicopathologic variables, including age, gender, tumorlocation, grade, stage, and mucin production. Consistent withsome previous reports (Samowitz et al., 2002; Russo et al., 2005)
rying a deleterious P53 mutation (a), compared to matched normal

TABLE 1. P53 gene mutations (n U 96) in proximal (n U 26), distal (n U 59) and location-unspecified (n U 2) colorectal carcinomas from Northern Iran,
sorted by exon, codon, and number of mutations per tumor
Case number Age/sex Exon Codon Genetic alteration Aminoacid alteration P53 nuclear accumulation
ProximalCases with one mutation
73 65/male 5 127 TCC!TTC Ser! Phe Positive2 36/male 5 135 TGC!TTC Cys! Phe Positive63 75/female 5 135 TGC!TAC Cys!Tyr Negative7 43/female 5 163 TAC!TGC Tyr!Cys Positive26 41/male 5 168 CAC!TAC His!Tyr Positive27 23/female 5 173 GTG!TTG Val! Leu Negative37 56/female 6 195 ATC!ACC Ile!Thr Positive13 33/male 6 213 CGA!TGA Arg! STOP Positive61 64/female 6 213 CGA!CTA Arg! Leu Positive71 73/male 6 213 CGA!TGA Arg! STOP Negative16 27/male 6 220 5 bp del TATGAG!/�/G Frameshift Negative25 37/female 7 225 GTT!GCT Val!Ala Negative42 50/male 7 245 GGC!GAC Gly!Asp Positive18 46/female 7 248 CGG!CTG Arg! Leu Positive31 65/female 8 271 GAG!AAG Glu! Lys Positive6 43/male 8 272 GTG!ATG Val!Met Positive68 75/male 8 278 CCT!ACT Pro!Thr Negative15 47/male 8 282 CGG!TGG Arg!Trp Positive28 38/male 8 282 CGG!TGG Arg!Trp Positive11 44/male 8 283 CGC!TGC Arg!Cys Positive1 40/male 8 297 1 bp del CAC!/AC Frameshift Negative67 76/male i6-intron 0 Non-coding Splice Negative75 82/male i6-intron 0 Non-coding Splice Negative
Cases with two mutations80 35/male 7 250 CCC!CTC Pro! Leu Positive
6 213 CGA!TGA Arg! STOP83 39/female 8 302 GGG!AGG Gly!Arg Positive
8 273 CGT!CAT Arg!His84 59/female 8 293 GGG!GGA Gly!Gly Positive
6 213 CGA!TGA Arg! STOPDistal
32 61/female 5 126 9 bp del TACTCCCCTGCC!/�/GCC In frame Positive69 69/female 5 133 ATG!AAG Met! Lys Positive59 74/male 5 135 TGC!TAC Cys!Tyr Positive46 50/female 5 143 GTG!ATG Val!Met Positive57 55/male 5 152 CCG!CTG Pro! Leu Positive51 73/female 5 159 1 bp ins GCC!GC(A)C Frameshift Positive54 61/male 5 173 GTG!TTG Val! Leu Positive3 38/female 5 175 CGC!CAC Arg!His Positive17 40/male 5 175 CGC!CAC Arg!His Positive20 43/male 5 175 CGC!CAC Arg!His Positive52 68/male 5 175 CGC!CAC Arg!His Positive65 68/male 5 175 CGC!CAC Arg!His Positive29 36/male 5 179 CAT!CGT His!Arg Positive58 63/male 6 195 ATC!ACC Ile!Thr Positive22 37/female 6 196 CGA!TGA Arg! STOP Negative23 36/female 6 196 CGA!TGA Arg! STOP Negative66 70/male 6 196 CGA!TGA Arg! STOP Negative77 88/male 6 196 CGA!TGA Arg! STOP Negative10 41/male 6 209 2bp de AGA!A// Frameshift Negative35 58/female 6 213 CGA!TGA Arg! STOP Positive50 65/male 6 213 CGA!TGA Arg! STOP Negative60 65/female 6 213 CGA!TGA Arg! STOP Negative56 78/male 6 216 GTG!TTG Val! Leu Positive76 55/male 6 220 TAT!TGT Tyr!Cys Positive12 42/male 7 236 TAC!TGC Tyr!Cys Positive41 47/male 7 236 TAC!TGC Tyr!Cys Positive4 32/male 7 242 6 bp ins TCCTGC!TCC(AGTTCC)TGC In frame Positive78 78/male 7 242 TGC!TCC Cys! Ser Positive19 43/female 7 244 GGC!AGC Gly! Ser Positive5 42/male 7 245 GGC!AGC Gly! Ser Positive30 42/male 7 245 GGC!AGC Gly! Ser Positive44 55/female 7 245 GGC!AGC Gly! Ser Positive45 57/male 7 245 GGC!AGC Gly! Ser Positive53 83/female 7 245 GGC!AGC Gly! Ser Positive72 73/male 7 245 GGC!GAC Gly!Asp Positive34 62/male 7 248 CGG!CTG Arg! Leu Negative47 59/female 7 248 CGG!CAG Arg!Gln Positive55 73/male 7 248 CGG!TGG Arg!Trp Positive70 75/male 7 248 CGG!TGG Arg!Trp Positive74 71/male 7 248 CGG!CAG Arg!Gln Positive21 33/female 7 253 ACC!CCC Thr! Pro Negative39 50/female 7 253 3 bp del ACCATC!A///TC In frame Positive43 61/male 7 253 6 bp ins ACC!A(TCCTCA)CC In frame Positive24 42/male 8 266 1 bp ins GGA!G(A)GA Frameshift Negative
(Continued)
JOURNAL OF CELLULAR PHYSIOLOGY
546 M A H D A V I N I A E T A L .

TABLE 1. (Continued )
Case number Age/sex Exon Codon Genetic alteration Aminoacid alteration P53 nuclear accumulation
33 61/female 8 266 GGA!GG(TACTCTATGCT)A Frameshift Negative14 42/male 8 273 CGT!TGT Arg!Cys Positive36 58/male 8 273 CGT!TGT Arg!Cys Positive62 68/male 8 273 CGT!TGT Arg!Cys Positive64 53/female 8 273 CGT!CAT Arg!His Positive48 54/female 8 277 TGT!TGA Cys! STOP Negative38 56/male 8 282 CGG!TGG Arg!Trp Positive8 27/female 8 286 GAA!GTA Glu!Val Positive49 61/male 8 294 GAG!TAG Glu! STOP Negative9 43/female 8 306 CGA!TGA Arg! STOP NegativeCases with two mutations
79 37/male 5 173 GTG!TTG Val! Leu Positive7 248 CGG!TGG Arg!Trp
85 56/female 5 175 CGC!CAC Arg!His Positive7 235 3 bp del AACTAC!///TAC In frame
87 75/male 5 175 CGC!CAC Arg!His Positive7 248 CGG!CAG Arg!Gln
81 30/female 7 236 TAC!TAT Tyr!Tyr Positive7 245 GGC!AGC Gly! Ser
86 68/male 7 260 TCC!TCT Ser! Ser Positive7 248 CGG!CAG Arg!Gln
Unspecified location82 43/female 7 258 GAA!GGA Glu!Gly Positive82 8 301 CCA!CCG Pro! Pro40 59/male 8 269 20 bp ins AGC!AG(CACAAACACGCACCTCAAGC)C Frameshift Negative
TABLE 3. Frequency of P53 alterations (mutation and nuclear
accumulation) in relation to clinicopathologic and molecular characteristics
in 196 colorectal cancer cases from Northern Iran
No. ofpatients
P53 genemutation, n (%)
P53 nuclearaccumulation,
n (%)
Overall series 196 87 (44.38%) 84 (42.86%)Age
Age mean W (SD) 53.4 W (15.5) Present:54.1 W 15.4
Positive:53.6 W 14.1
GenderFemale 85 35 (42.00%) 34 (40.00%)Male 111 52 (46.8%) 50 (45.04%)
Locationa,b P < 0.01Proximal 64 25 (39.06%) 17 (26.56%)Distal 126 60 (47.62%) 65 (51.58%)
Grade P < 0.001Well 39 18 (46.15%) 10 (25.64%)Moderate 128 61 (47.65%) 68 (53.12%)Poor 29 8 (27.58%) 6 (20.68%)
Stagec
A 5 P U 0.04B 94 36 (38.29%) 38 (40.42%)C 64 33 (51.56%) 31 (48.43%)D 23 15 (65.22%) 12 (52.17%)
P 5 3 A N D C O L O R E C T A L C A N C E R I N I R A N 547
the frequency of P53 mutations increased significantly withtumor stage (36/94, 38.3%; 33/64, 51.5%, and 15/23, 65.2% instages B, C, and D respectively, P for trend <0.05). We did notfind significant relationships between presence/absence of P53mutations and other variables (Table 3). Also, no significantcorrelations between P53 nuclear accumulation andclinicopathologic and individual variables emerged, except thatdistal CRCs were more frequently positive than proximaltumors (51.6% vs. 26.6%). The frequency of P53 mutations wasalsohigher indistal relative toproximal tumorsbut thedifferencedid not reach statistical significance (47.6% vs. 39%) (Table 3).
The analysis of P53 mutation type in relation toclinicopathologic variables revealed that G to A transitions atCpG sites were more frequent in non-mucinous versusmucinous CRCs [37/148 (25%) vs. 5/48 (10.4%), P¼ 0.032].With regard to tumor location there was a higher frequency ofG to A transitions at CpGs in distal CRCs [34/126 (27%) vs. 8/64(12.5%) in proximal, P¼ 0.023] whereas G to A transitions atnon-CpGs were more frequent in proximal tumors [10/64(15.6%) vs. 6/126 (4.7%) in distal, P¼ 0.011].
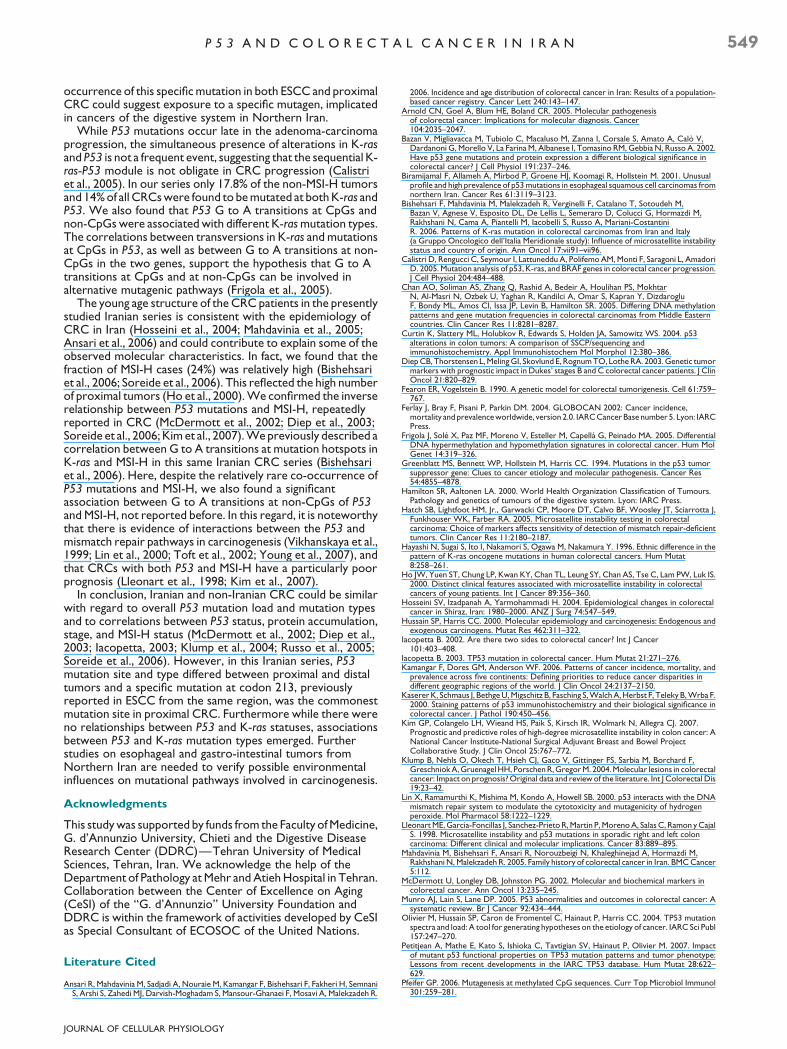
We next compared the distribution of mutated codonsbetween proximal and distal tumors (Fig. 2). In distal CRCs thethree most frequently mutated codons, all major P53 hotspots(Soussi and Beroud, 2003; Olivier et al., 2004), were 248 (8/66,12.1%), 175 (7/66, 10.6%), and 245 (7/66, 10.6%).
By contrast codon 213 clearly emerged as the mostfrequently mutated site in proximal tumors (5/28, 17.9% vs. 3/66, 4.5% in distal, Fisher’s exact test P¼ 0.048). Notably, inseven out of eight cases, mutations at codon 213 were G to Atransitions at the first nucleotide (Table 1).
TABLE 2. Nuclear P53 protein accumulation and P53 mutation status in
196 colorectal cancer cases from Northern Iran
P53 mutation
Detected Not detected
p53 accumulation (%)Positive 63 (72.4%) 21 (19.3%)Negative 24 (27.5%) 88 (80.7%)
JOURNAL OF CELLULAR PHYSIOLOGY
Relationships between P53, MSI-H, and K-ras statuses
Forty-seven of the 196 CRCs (24%) showed MSI-H. Asexpected MSI-H cases included most of the cases that fulfilledthe Amsterdam II criteria for HNPCC (i.e., 12/13, 92%).
HistotypeMucinous 48 17 (35.41%) 18 (37.50%)Non-mucinous 148 70 (47.30%) 66 (44.59%)
Microsatellite instability P < 0.001MSI-H 47 8 (17.02%) 5 (10.64%)Non-MSI-H 149 79 (53.02%) 79 (53.02%)
K-rasd
Mutated 68 26 (38.23%) 28 (41.17%)Non-mutated 114 57 (50.00%) 50 (43.86%)
aProximal or distal to the splenic flexure (Iacopetta, 2002).bIn six samples the location was not specified.cIn 10 cases the stage was not specified.dThe analyses on K-ras are in 182 of samples.

Fig. 2. Mutation frequencies in exons 5–8 of P53 in proximal (&) (27mutations) and distal (&) (64 mutations) colorectal cancer cases fromNorthern Iran, plotted by codon. Mutations at splice sites (n U 2) havenot been considered for this plot.
548 M A H D A V I N I A E T A L .
P53 was mutated in 53% (79/149) of the non-MSI-H casesversus 17.2% (8/47) of the MSI-H cases (P< 0.001) (Table 3).Consistently, P53 nuclear accumulation was more oftenassociated with non-MSI-H tumors (53% vs. 10.6%, P< 0.001).Eight of the nine P53 mutations detected in MSI-H tumors wereG to A transitions (four at CpGs and four at non-CpGs). Theanalysis of P53 mutation type revealed an association betweenG to A transitions at non-CpGs and MSI-H [4/9 (44.4%) in MSI-H vs. 12/87 (13.8%) in non-MSI-H, Fisher’s exact test P¼ 0.04].
Of the 13 cases meeting Amsterdam II criteria, only 2 (15.4%)revealed a deleterious P53 mutation (frame-shift and missense,respectively). P53 nuclear accumulation was detected in onlyone of these putative HNPCC cases (7.7%), that is, the case withan identified missense P53 mutation.
Of the 196 CRCs analyzed for P53 mutations, 182 had beenpreviously characterized for mutations in exons 1–2 of K-ras,which include the hotspot codons 12, 13, and 61 (Bishehsariet al., 2006). Figure 3 shows the proportions of cases with
Fig. 3. Percentages of P53 and K-ras mutations and MSI-H statusdetermined in 182 CRC cases from Northern Iran.
JOURNAL OF CELLULAR PHYSIOLOGY
different combinations of P53, K-ras and MSI-H statuses. Therewas no significant difference in the frequency of P53 mutationsbetween tumors with and without K-ras mutation (38.2% vs.50%, respectively, P¼ 0.12). Mutations at P53 and K-ras co-occurred in 26 tumors (14% of total and 17.8% of non-MSI-Htumors).
Analysis of mutation types in tumors mutated in both K-rasand P53 showed that G to A transitions at CpGs and non-CpGsof P53 were associated with different K-ras mutation types.While transversions in K-ras prevailed in the CRCs with P53mutations at CpGs (9/12 cases), G to A transitions in K-raswere observed in the three cases with a P53 transition at non-CpGs (Fisher’s exact test, P¼ 0.04). Other associations couldnot be tested due to low number of cases.
Discussion
We describe here for the first time the P53 mutational profile ofa CRC series from Iran, a country with relatively low CRCincidence (Ansari et al., 2006). We found that 87 out of 196cases (44.4%) carried a pathogenic P53 mutation, a frequencysimilar to those reported for non-Iranian CRC (McDermottet al., 2002; Iacopetta, 2003; Klump et al., 2004; Russo et al.,2005). Correlations between P53 mutations and tumor stagewere in agreement with the notion that P53 mutationsaccumulate during CRC progression (Fearon and Vogelstein,1990). Consistently with the literature and with databasecompilations (Soussi and Beroud, 2003; Olivier et al., 2004;Russo et al., 2005), the majority of the detected mutations(43.7%) were G to A transitions at CpGs, a type of mutationthat could reflect spontaneous deamination or preferentialadduct formation at methylated CpGs (Greenblatt et al., 1994;Soussi and Beroud, 2003; Pfeifer, 2006), followed by G to Atransitions at non-CpGs (16.6%).
Several studies reported that P53 alterations (either genemutations or nuclear accumulation) are more frequent in distalthan in proximal CRC (Iacopetta, 2003; Russo et al., 2005). Inthe current study, distal CRC showed a significantly higherfrequency of P53 nuclear protein accumulation. We alsoobserved a higher percentage of P53 mutations in distal relativeto proximal tumors but the difference did not reach statisticalsignificance. Data about the influence of tumor location on P53mutation site/type are limited, but a recent meta-analysis of caseseries from 17 different countries found that P53 mutationsites/types were comparable in proximal and distal CRC (Russoet al., 2005), which suggests similar mutagenic factorsthroughout the large intestine. Interestingly, in our Iranianseries proximal CRCs showed a significantly higher frequencyof mutations at codon 213, a CpG site not comprised among thefive most prevalent P53 mutation hotspots (Soussi and Beroud,2003; Olivier et al., 2004; Petitjean et al., 2007), while othermutations were quite dispersed. Furthermore transitions atnon-CpGs were more frequent in proximal tumors. DistalCRCs were more frequently mutated at four of the five classicalCpG hotspots, that is, codons 175, 245, 248, and 273, and,consistently, transitions at CpGs were more frequent in distaltumors.
Information on cancer-associated P53 mutations availablefor Iran is limited to ESCC, which has one of the highest worldprevalences in the northern part of the country (Biramijamalet al., 2001; Sepehr et al., 2001). Two studies conducted onESCC series sampled in Tehran and on the Caspian littoralrevealed a high frequency of P53 mutations and an unusualmutational profile, with an excess of transition mutations,including mutations at CpG hotspots (Biramijamal et al., 2001;Sepehr et al., 2001). Intriguingly in one of these two studies theC to T transition at codon 213 that we found at high frequencyin proximal CRC recurred in 5/48 (10.4%) ESCC cases thatresulted mutated in P53 (Biramijamal et al., 2001). A frequent
P 5 3 A N D C O L O R E C T A L C A N C E R I N I R A N 549
occurrence of this specific mutation in both ESCC and proximalCRC could suggest exposure to a specific mutagen, implicatedin cancers of the digestive system in Northern Iran.
While P53 mutations occur late in the adenoma-carcinomaprogression, the simultaneous presence of alterations in K-rasand P53 is not a frequent event, suggesting that the sequential K-ras-P53 module is not obligate in CRC progression (Calistriet al., 2005). In our series only 17.8% of the non-MSI-H tumorsand 14% of all CRCs were found to be mutated at both K-ras andP53. We also found that P53 G to A transitions at CpGs andnon-CpGs were associated with different K-ras mutation types.The correlations between transversions in K-ras and mutationsat CpGs in P53, as well as between G to A transitions at non-CpGs in the two genes, support the hypothesis that G to Atransitions at CpGs and at non-CpGs can be involved inalternative mutagenic pathways (Frigola et al., 2005).
The young age structure of the CRC patients in the presentlystudied Iranian series is consistent with the epidemiology ofCRC in Iran (Hosseini et al., 2004; Mahdavinia et al., 2005;Ansari et al., 2006) and could contribute to explain some of theobserved molecular characteristics. In fact, we found that thefraction of MSI-H cases (24%) was relatively high (Bishehsariet al., 2006; Soreide et al., 2006). This reflected the high numberof proximal tumors (Ho et al., 2000). We confirmed the inverserelationship between P53 mutations and MSI-H, repeatedlyreported in CRC (McDermott et al., 2002; Diep et al., 2003;Soreide et al., 2006; Kim et al., 2007). We previously described acorrelation between G to A transitions at mutation hotspots inK-ras and MSI-H in this same Iranian CRC series (Bishehsariet al., 2006). Here, despite the relatively rare co-occurrence ofP53 mutations and MSI-H, we also found a significantassociation between G to A transitions at non-CpGs of P53and MSI-H, not reported before. In this regard, it is noteworthythat there is evidence of interactions between the P53 andmismatch repair pathways in carcinogenesis (Vikhanskaya et al.,1999; Lin et al., 2000; Toft et al., 2002; Young et al., 2007), andthat CRCs with both P53 and MSI-H have a particularly poorprognosis (Lleonart et al., 1998; Kim et al., 2007).
In conclusion, Iranian and non-Iranian CRC could be similarwith regard to overall P53 mutation load and mutation typesand to correlations between P53 status, protein accumulation,stage, and MSI-H status (McDermott et al., 2002; Diep et al.,2003; Iacopetta, 2003; Klump et al., 2004; Russo et al., 2005;Soreide et al., 2006). However, in this Iranian series, P53mutation site and type differed between proximal and distaltumors and a specific mutation at codon 213, previouslyreported in ESCC from the same region, was the commonestmutation site in proximal CRC. Furthermore while there wereno relationships between P53 and K-ras statuses, associationsbetween P53 and K-ras mutation types emerged. Furtherstudies on esophageal and gastro-intestinal tumors fromNorthern Iran are needed to verify possible environmentalinfluences on mutational pathways involved in carcinogenesis.
Acknowledgments
This study was supported by funds from the Faculty of Medicine,G. d’Annunzio University, Chieti and the Digestive DiseaseResearch Center (DDRC)—Tehran University of MedicalSciences, Tehran, Iran. We acknowledge the help of theDepartment of Pathology at Mehr and Atieh Hospital in Tehran.Collaboration between the Center of Excellence on Aging(CeSI) of the ‘‘G. d’Annunzio’’ University Foundation andDDRC is within the framework of activities developed by CeSIas Special Consultant of ECOSOC of the United Nations.
Literature Cited
Ansari R, Mahdavinia M, Sadjadi A, Nouraie M, Kamangar F, Bishehsari F, Fakheri H, SemnaniS, Arshi S, Zahedi MJ, Darvish-Moghadam S, Mansour-Ghanaei F, Mosavi A, Malekzadeh R.
JOURNAL OF CELLULAR PHYSIOLOGY
2006. Incidence and age distribution of colorectal cancer in Iran: Results of a population-based cancer registry. Cancer Lett 240:143–147.
Arnold CN, Goel A, Blum HE, Boland CR. 2005. Molecular pathogenesisof colorectal cancer: Implications for molecular diagnosis. Cancer104:2035–2047.
Bazan V, Migliavacca M, Tubiolo C, Macaluso M, Zanna I, Corsale S, Amato A, Calo V,Dardanoni G, Morello V, La Farina M, Albanese I, Tomasino RM, Gebbia N, Russo A. 2002.Have p53 gene mutations and protein expression a different biological significance incolorectal cancer? J Cell Physiol 191:237–246.
Biramijamal F, Allameh A, Mirbod P, Groene HJ, Koomagi R, Hollstein M. 2001. Unusualprofile and high prevalence of p53 mutations in esophageal squamous cell carcinomas fromnorthern Iran. Cancer Res 61:3119–3123.
Bishehsari F, Mahdavinia M, Malekzadeh R, Verginelli F, Catalano T, Sotoudeh M,Bazan V, Agnese V, Esposito DL, De Lellis L, Semeraro D, Colucci G, Hormazdi M,Rakhshani N, Cama A, Piantelli M, Iacobelli S, Russo A, Mariani-CostantiniR. 2006. Patterns of K-ras mutation in colorectal carcinomas from Iran and Italy(a Gruppo Oncologico dell’Italia Meridionale study): Influence of microsatellite instabilitystatus and country of origin. Ann Oncol 17:vii91–vii96.
Calistri D, Rengucci C, Seymour I, Lattuneddu A, Polifemo AM, Monti F, Saragoni L, AmadoriD. 2005. Mutation analysis of p53, K-ras, and BRAF genes in colorectal cancer progression.J Cell Physiol 204:484–488.
Chan AO, Soliman AS, Zhang Q, Rashid A, Bedeir A, Houlihan PS, MokhtarN, Al-Masri N, Ozbek U, Yaghan R, Kandilci A, Omar S, Kapran Y, DizdarogluF, Bondy ML, Amos CI, Issa JP, Levin B, Hamilton SR. 2005. Differing DNA methylationpatterns and gene mutation frequencies in colorectal carcinomas from Middle Easterncountries. Clin Cancer Res 11:8281–8287.
Curtin K, Slattery ML, Holubkov R, Edwards S, Holden JA, Samowitz WS. 2004. p53alterations in colon tumors: A comparison of SSCP/sequencing andimmunohistochemistry. Appl Immunohistochem Mol Morphol 12:380–386.
Diep CB, Thorstensen L, Meling GI, Skovlund E, Rognum TO, Lothe RA. 2003. Genetic tumormarkers with prognostic impact in Dukes’ stages B and C colorectal cancer patients. J ClinOncol 21:820–829.
Fearon ER, Vogelstein B. 1990. A genetic model for colorectal tumorigenesis. Cell 61:759–767.
Ferlay J, Bray F, Pisani P, Parkin DM. 2004. GLOBOCAN 2002: Cancer incidence,mortality and prevalenceworldwide, version 2.0. IARC Cancer Base number 5. Lyon: IARCPress.
Frigola J, Sole X, Paz MF, Moreno V, Esteller M, Capella G, Peinado MA. 2005. DifferentialDNA hypermethylation and hypomethylation signatures in colorectal cancer. Hum MolGenet 14:319–326.
Greenblatt MS, Bennett WP, Hollstein M, Harris CC. 1994. Mutations in the p53 tumorsuppressor gene: Clues to cancer etiology and molecular pathogenesis. Cancer Res54:4855–4878.
Hamilton SR, Aaltonen LA. 2000. World Health Organization Classification of Tumours.Pathology and genetics of tumours of the digestive system. Lyon: IARC Press.
Hatch SB, Lightfoot HM, Jr., Garwacki CP, Moore DT, Calvo BF, Woosley JT, Sciarrotta J,Funkhouser WK, Farber RA. 2005. Microsatellite instability testing in colorectalcarcinoma: Choice of markers affects sensitivity of detection of mismatch repair-deficienttumors. Clin Cancer Res 11:2180–2187.
Hayashi N, Sugai S, Ito I, Nakamori S, Ogawa M, Nakamura Y. 1996. Ethnic difference in thepattern of K-ras oncogene mutations in human colorectal cancers. Hum Mutat8:258–261.
Ho JW, Yuen ST, Chung LP, Kwan KY, Chan TL, Leung SY, Chan AS, Tse C, Lam PW, Luk IS.2000. Distinct clinical features associated with microsatellite instability in colorectalcancers of young patients. Int J Cancer 89:356–360.
Hosseini SV, Izadpanah A, Yarmohammadi H. 2004. Epidemiological changes in colorectalcancer in Shiraz, Iran: 1980–2000. ANZ J Surg 74:547–549.
Hussain SP, Harris CC. 2000. Molecular epidemiology and carcinogenesis: Endogenous andexogenous carcinogens. Mutat Res 462:311–322.
Iacopetta B. 2002. Are there two sides to colorectal cancer? Int J Cancer101:403–408.
Iacopetta B. 2003. TP53 mutation in colorectal cancer. Hum Mutat 21:271–276.Kamangar F, Dores GM, Anderson WF. 2006. Patterns of cancer incidence, mortality, and
prevalence across five continents: Defining priorities to reduce cancer disparities indifferent geographic regions of the world. J Clin Oncol 24:2137–2150.
Kaserer K, Schmaus J, Bethge U, Migschitz B, Fasching S, Walch A, Herbst F, Teleky B, Wrba F.2000. Staining patterns of p53 immunohistochemistry and their biological significance incolorectal cancer. J Pathol 190:450–456.
Kim GP, Colangelo LH, Wieand HS, Paik S, Kirsch IR, Wolmark N, Allegra CJ. 2007.Prognostic and predictive roles of high-degree microsatellite instability in colon cancer: ANational Cancer Institute-National Surgical Adjuvant Breast and Bowel ProjectCollaborative Study. J Clin Oncol 25:767–772.
Klump B, Nehls O, Okech T, Hsieh CJ, Gaco V, Gittinger FS, Sarbia M, Borchard F,Greschniok A, Gruenagel HH, Porschen R, Gregor M. 2004. Molecular lesions in colorectalcancer: Impact on prognosis? Original data and review of the literature. Int J Colorectal Dis19:23–42.
Lin X, Ramamurthi K, Mishima M, Kondo A, Howell SB. 2000. p53 interacts with the DNAmismatch repair system to modulate the cytotoxicity and mutagenicity of hydrogenperoxide. Mol Pharmacol 58:1222–1229.
Lleonart ME, Garcia-Foncillas J, Sanchez-Prieto R, Martin P, Moreno A, Salas C, Ramon y CajalS. 1998. Microsatellite instability and p53 mutations in sporadic right and left coloncarcinoma: Different clinical and molecular implications. Cancer 83:889–895.
Mahdavinia M, Bishehsari F, Ansari R, Norouzbeigi N, Khaleghinejad A, Hormazdi M,Rakhshani N, Malekzadeh R. 2005. Family history of colorectal cancer in Iran. BMC Cancer5:112.
McDermott U, Longley DB, Johnston PG. 2002. Molecular and biochemical markers incolorectal cancer. Ann Oncol 13:235–245.
Munro AJ, Lain S, Lane DP. 2005. P53 abnormalities and outcomes in colorectal cancer: Asystematic review. Br J Cancer 92:434–444.
Olivier M, Hussain SP, Caron de Fromentel C, Hainaut P, Harris CC. 2004. TP53 mutationspectra and load: A tool for generating hypotheses on the etiology of cancer. IARC Sci Publ157:247–270.
Petitjean A, Mathe E, Kato S, Ishioka C, Tavtigian SV, Hainaut P, Olivier M. 2007. Impactof mutant p53 functional properties on TP53 mutation patterns and tumor phenotype:Lessons from recent developments in the IARC TP53 database. Hum Mutat 28:622–629.
Pfeifer GP. 2006. Mutagenesis at methylated CpG sequences. Curr Top Microbiol Immunol301:259–281.

550 M A H D A V I N I A E T A L .
Potter JD. 1999. Colorectal cancer: Molecules and populations. J Natl Cancer Inst91:916–932.
Qing SH, Rao KY, Jiang HY, Wexner SD. 2003. Racial differences in the anatomicaldistribution of colorectal cancer: A study of differences between American and Chinesepatients. World J Gastroenterol 9:721–725.
Russo A, Bazan V, Iacopetta B, Kerr D, Soussi T, Gebbia N. 2005. The TP53 colorectal cancerinternational collaborative study on the prognostic and predictive significance of p53mutation: Influence of tumor site, type of mutation, and adjuvant treatment. J Clin Oncol23:7518–7528.
Sadjadi A, Malekzadeh R, Derakhshan MH, Sepehr A, Nouraie M, Sotoudeh M, Yazdanbod A,Shokoohi B, Mashayekhi A, Arshi S, Majidpour A, Babaei M, Mosavi A, Mohagheghi MA,Alimohammadian M. 2003. Cancer occurrence in Ardabil: Results of a population-basedcancer registry from Iran. Int J Cancer 107:113–118.
Samowitz WS, Curtin K, Ma KN, Edwards S, Schaffer D, Leppert MF, Slattery ML. 2002.Prognostic significance of p53 mutations in colon cancer at the population level. Int JCancer 99:597–602.
Semnani S, Sadjadi A, Fahimi S, Nouraie M, Naeimi M, Kabir J, Fakheri H, Saadatnia H,Ghavamnasiri MR, Malekzadeh R. 2006. Declining incidence of esophageal cancer in theTurkmen Plain, eastern part of the Caspian Littoral of Iran: A retrospective cancersurveillance. Cancer Detect Prev 30:14–19.
Sepehr A, Taniere P, Martel-Planche G, Zia’ee AA, Rastgar-Jazii F, Yazdanbod M, Etemad-Moghadam G, Kamangar F, Saidi F, Hainaut P. 2001. Distinct pattern of TP53
JOURNAL OF CELLULAR PHYSIOLOGY
mutations in squamous cell carcinoma of the esophagus in Iran. Oncogene 20:7368–7374.
Soong R, Robbins PD, Dix BR, Grieu F, Lim B, Knowles S, Williams KE, Turbett GR,House AK, Iacopetta BJ. 1996. Concordance between p53 protein overexpression andgene mutation in a large series of common human carcinomas. Hum Pathol 27:1050–1055.
Soong R, Grieu F, Robbins P, Dix B, Chen D, Parsons R, House A, Iacopetta B. 1997. p53alterations are associated with improved prognosis in distal colonic carcinomas. ClinCancer Res 3:1405–1411.
Soreide K, Janssen EA, Soiland H, Korner H, Baak JP. 2006. Microsatellite instability incolorectal cancer. Br J Surg 93:395–406.
Soussi T, Beroud C. 2003. Significance of TP53 mutations in human cancer: A critical analysisof mutations at CpG dinucleotides. Hum Mutat 21:192–200.
Toft NJ, Curtis LJ, Sansom OJ, Leitch AL, Wyllie AH, te Riele H, Arends MJ, Clarke AR. 2002.Heterozygosity for p53 promotes microsatellite instability and tumourigenesis on a Msh2deficient background. Oncogene 21:6299–6306.
Vikhanskaya F, Colella G, Valenti M, Parodi S, D’Incalci M, Broggini M. 1999. Cooperationbetween p53 and hMLH1 in a human colocarcinoma cell line in response to DNA damage.Clin Cancer Res 5:937–941.
Young LC, Keuling AM, Lai R, Nation PN, Tron VA, Andrew SE. 2007. The associatedcontributions of p53 and the DNA mismatch repair protein Msh6 to spontaneoustumorigenesis. Carcinogenesis 28:2131–2138.
Copyright © 2022 FDOKUMEN