
p100 Comparison of Methods of Estimation of Lifetime Cancer Risk due to Chronic Environmental...
10
Paper COMPARISON OF METHODS OF ESTIMATION OF LIFETIME CANCER RISK DUE TO CHRONIC EXPOSURE TO TRANSURANICS Kyle L. McMillan, William R. Kaye, and Kimberlee J. Kearfott* Abstract—The cancer risk due to chronic transuranic intakes is properly calculated using an integration over multiple years of intake of the annual effective dose rates arising each year following an intake multiplied by age-dependent risk functions for the year during which the dose is actually received. Approximate computations of risk involving sums of the products of committed effective dose and the age-dependent risk functions for each year of intake indicate the appropri- ateness of the committed effective dose as a surrogate quantity for risk when applied to different circumstances. The assump- tions that all dose is received at the time of intake with committed effective dose and that risk is uniform over a range of ages both lead to a misuse of the available age-dependent risk functions and thus contribute to a divergence from the true risk associated with an intake over multiple years. Com- parison of the correctly integrated risk functions with the approximations gives insights into how the current committed effective dose models used for regulatory purposes are not necessarily indicative of the risk for chronic intakes of radio- nuclides with long biological and radiological half-lives. A summary and comparison of such computations for tran- suranic intakes was prepared for the ingestion of water and the inhalation of different particle sizes by both males and females. Risk results for committed effective dose consistently overes- timated risks by approximately 100% for all transuranics for ingestion models and approximately 75% for all transuranics for Type M inhalation models considering age-dependent risk models. For constant risk as a function of age, the committed effective dose integration underestimated the actual risk situ- ation by nearly 60% for ingestion and 50% for Type M inhalation during the first 20 y. Health Phys. 101(6):693–702; 2011 Key words: 241 Am; children; dose, internal; radiation risk INTRODUCTION QUANTIFYING THE risks of radionuclide intakes is essential for many aspects of public and occupational radiation exposure. These include nuclear industrial impacts eval- uations, regulatory compliance schemes, risk minimiza- tion for exposed populations, and the evaluation of radiation health risks. Biokinetic and internal dose mod- els for anatomically and physiologically stylized phan- toms provide reproducible and standardized estimates of the radiation absorbed dose associated with an intake. These dose estimates may be weighted for the relative risks of radiation type and summed across various tissues and organs using standardized radiation health-risk re- lated factors. A time integral of such assessments for the dose yields the committed effective dose (CED), a useful regulatory quantity when applied to radionuclide intakes (ICRP 2007). The CED is not only typically based upon averaged anatomy and physiology and stylized radiation absorp- tion models, but assigns, in a philosophical sense, the total integrated effective dose over the individual’s life, presumed proportional to the risk to the individual in the year the intake occurred. This is an appropriate simpli- fication justifiable for regulatory purposes. Such an assumption is also accurate for radionuclides whose effective half-lives are short relative to 1 y and thus deliver their dose during that timeframe. However, not all radionuclides fall into that category. It should also be noted that radiation risk per unit effective dose may vary significantly as a function of age. Based on atomic bomb survivor data, the solid cancer risk is nearly three times greater for a 10-y-old than a 50-y-old adult (UNSCEAR 2006). While it was never the intent of the CED to represent actual risks, the quantity is not only potentially misleading to the public concerning risks, but it may also misinform policy decisions for prolonged public intakes of radionuclides whose effective half-lives are long. Such cases occur for radionuclide spills, naturally occurring environmental radionuclides, and nuclear facilities that * University of Michigan, Department of Nuclear Engineering and Radiological Sciences, 2355 Bonisteel Boulevard, Ann Arbor, MI 48109-2104. The authors declare no conflicts of interest. For correspondence contact: Kimberlee J. Kearfott, University of Michigan, Department of Nuclear Engineering and Radiological Sci- ences, 2355 Bonisteel Blvd, Ann Arbor, MI 48109-2104, or email at [email protected]. (Manuscript accepted 29 April 2011) 0017-9078/11/0 Copyright © 2011 Health Physics Society DOI: 10.1097/HP.0b013e318222249f www.health-physics.com 693
Transcript of p100 Comparison of Methods of Estimation of Lifetime Cancer Risk due to Chronic Environmental...

Paper
COMPARISON OF METHODS OF ESTIMATION OFLIFETIME CANCER RISK DUE TO CHRONIC EXPOSURE
TO TRANSURANICS
Kyle L. McMillan, William R. Kaye, and Kimberlee J. Kearfott*
Abstract—The cancer risk due to chronic transuranic intakesis properly calculated using an integration over multiple yearsof intake of the annual effective dose rates arising each yearfollowing an intake multiplied by age-dependent risk functionsfor the year during which the dose is actually received.Approximate computations of risk involving sums of theproducts of committed effective dose and the age-dependentrisk functions for each year of intake indicate the appropri-ateness of the committed effective dose as a surrogate quantityfor risk when applied to different circumstances. The assump-tions that all dose is received at the time of intake withcommitted effective dose and that risk is uniform over a rangeof ages both lead to a misuse of the available age-dependentrisk functions and thus contribute to a divergence from thetrue risk associated with an intake over multiple years. Com-parison of the correctly integrated risk functions with theapproximations gives insights into how the current committedeffective dose models used for regulatory purposes are notnecessarily indicative of the risk for chronic intakes of radio-nuclides with long biological and radiological half-lives. Asummary and comparison of such computations for tran-suranic intakes was prepared for the ingestion of water and theinhalation of different particle sizes by both males and females.Risk results for committed effective dose consistently overes-timated risks by approximately 100% for all transuranics foringestion models and approximately 75% for all transuranicsfor Type M inhalation models considering age-dependent riskmodels. For constant risk as a function of age, the committedeffective dose integration underestimated the actual risk situ-ation by nearly 60% for ingestion and 50% for Type Minhalation during the first 20 y.Health Phys. 101(6):693–702; 2011
Key words: 241Am; children; dose, internal; radiation risk
INTRODUCTION
QUANTIFYING THE risks of radionuclide intakes is essentialfor many aspects of public and occupational radiationexposure. These include nuclear industrial impacts eval-uations, regulatory compliance schemes, risk minimiza-tion for exposed populations, and the evaluation ofradiation health risks. Biokinetic and internal dose mod-els for anatomically and physiologically stylized phan-toms provide reproducible and standardized estimates ofthe radiation absorbed dose associated with an intake.These dose estimates may be weighted for the relativerisks of radiation type and summed across various tissuesand organs using standardized radiation health-risk re-lated factors. A time integral of such assessments for thedose yields the committed effective dose (CED), a usefulregulatory quantity when applied to radionuclide intakes(ICRP 2007).
The CED is not only typically based upon averagedanatomy and physiology and stylized radiation absorp-tion models, but assigns, in a philosophical sense, thetotal integrated effective dose over the individual’s life,presumed proportional to the risk to the individual in theyear the intake occurred. This is an appropriate simpli-fication justifiable for regulatory purposes. Such anassumption is also accurate for radionuclides whoseeffective half-lives are short relative to 1 y and thusdeliver their dose during that timeframe. However, notall radionuclides fall into that category. It should also benoted that radiation risk per unit effective dose may varysignificantly as a function of age. Based on atomic bombsurvivor data, the solid cancer risk is nearly three timesgreater for a 10-y-old than a 50-y-old adult (UNSCEAR2006). While it was never the intent of the CED torepresent actual risks, the quantity is not only potentiallymisleading to the public concerning risks, but it may alsomisinform policy decisions for prolonged public intakesof radionuclides whose effective half-lives are long. Suchcases occur for radionuclide spills, naturally occurringenvironmental radionuclides, and nuclear facilities that
* University of Michigan, Department of Nuclear Engineeringand Radiological Sciences, 2355 Bonisteel Boulevard, Ann Arbor, MI48109-2104.
The authors declare no conflicts of interest.For correspondence contact: Kimberlee J. Kearfott, University of
Michigan, Department of Nuclear Engineering and Radiological Sci-ences, 2355 Bonisteel Blvd, Ann Arbor, MI 48109-2104, or email [email protected].
(Manuscript accepted 29 April 2011)0017-9078/11/0Copyright © 2011 Health Physics Society
DOI: 10.1097/HP.0b013e318222249f
www.health-physics.com 693

might release radionuclides over extended time periods,such as nuclear power plants or waste storage facilities.
Recent work highlighted the chronic intake of nat-urally occurring radioactive materials (NORM) (namelyradionuclides of uranium, thorium, and actinium) usingsimplified dose calculations not accounting for riskvarying as a function of age (Beauvais et al. 2009). Forthe chronic intake of radionuclides having non-trivialradiological and biological half-lives, the proper analyticapproach is to compute the dose delivered to an individ-ual each year following an intake due to that intake andweight that with an age-dependent risk factor corre-sponding to the age of the individual during the year thatthe dose is delivered. Integration is then performedacross all years of intake (Kaye et al. 2011). A simplified,approximate method of estimating the risk from chronicintake situations would consist of summing, over allyears of intake, the products of the CED for each year ofintake with the age-dependent risk factors for the year ofthe intake. If the integrated doses are performed over thenext 50 y for adults and 70 y for children (ICRP 1990,2007), then the results would represent the risk “impres-sion” caused by use of the CED quantity. The approxi-mation corresponding to the CED risk representation wasfound to overestimate the appropriate risk integration byup to 80% for the dose due to 137Cs in milk in a nuclearincident scenario and overestimate by up to 50% the riskfor a chronic natural uranium ingestion.
Transuranics are long-lived radionuclides havinglong biological half-lives that are produced as a result ofneutron capture reactions. This paper limits itself toradionuclides classifiable as transuranic waste, namelyalpha emitters having half-lives exceeding 20 y (U.S.NRC 2004). Concern about these would likely includechronic intakes from long-term waste repositories, weap-ons production facilities, and nuclear reactors.
Seventeen radionuclides of americium, californium,curium, neptunium, plutonium, and berkelium are con-sidered. Significant dose per unit activity from tran-suranic intakes is not only restricted to organs involvedin uptake (lungs for inhalation and the gastrointestinaltrack for ingestion) but also occurs for the liver and theskeleton (ICRP 1988). Each of these transuranics has abiological half-life on the order of 20 and 50 y, respec-tively (ICRP 1990, 2007). An analysis of 238Pu incadavers concluded that the inhalation of 238Pu in theform of a highly insoluble ceramic resulted in theaccumulation of activity an order of magnitude greater inthe liver and skeleton than in the lungs (James et al.2003). Additionally, it had been well established throughinvestigations of human and animal subjects that most ofthe systematic burden of a plutonium intake is in the liver
and skeleton at all times after exposure (Eckerman et al.2007).
The work presented in this paper focuses on bothdoses and risks due to chronic intakes of transuranicradionuclides for different particle sizes, inhalationtypes, and ages of individuals. Within each scenario, therisks for both males and females are presented. Foringestion, an age-dependent water consumption rate isused. For inhalation, an age-dependent breathing rate isused. The consumption and breathing rates are takenfrom Environmental Protection Agency Federal Guid-ance Report 13 (Eckerman et al. 1999). Type F, Type M,and Type S absorptions for different particle sizedaerosols are all investigated as the chemical and physicalnature of transuranics results in a variety of possibleinhalation intakes (U.S. DOE 2008).
It is important to note that the risk estimates are onlyas good as the risk function data used. This paper is notintended to be a definitive, or even contributing, paper onthe actual magnitude of the radiation risks associatedwith transuranics and the details of exposure scenarios.Instead, this paper aims to draw attention to the relativeerrors introduced into the perceived risk representationspromoted by the use of the CED quantity; i.e., by notproperly considering the age-dependency of risks due tochronic transuranic intakes. Differences would roughlyrepresent the misimpression caused by usage of theregulatory quantity CED.
THEORY
When the risk is independent of age, the total risk ofcancer death in a lifetime, Rtotal, is modeled as:
Rtotal � R �ainitial
afinal
I�t� �t
tlifetime
F�a�, t�da�dt, (1)
where R is the age-independent risk, ainitial and afinal
represent the age of the individual at the beginning andend of the exposure period, tlifetime is the average lifetimeof an individual, I(t) is the intake rate at any given timet, and F(a, t) is the dose quantity received at age a perunit intake that occurred at time t.
The correct approach to the computation of the risksdue to exposure to radiation uses the effective dose rate(EDR). With this approach the total risk is given by:
Rtotal � �ainitial
afinal
I�t� �t
tlifetime
R�a�� F�a�, t�da�dt, (2)
694 Health Physics December 2011, Volume 101, Number 6
www.health-physics.com

where R(a) is the risk per unit dose quantity received atage a. This rigorous approach applies age-dependent riskfunctions to all ages that for each year that the dose isactually received post intake.
An approximate way of estimating the total riskinvolves assigning the dose to the year of the intake,similar to the way the CED is treated, and weighting withthe risk factor corresponding to the age of the individualat the year of the intake. With this approach, the total riskis given by:
Rtotal � �ainitial
afinal
R�a�I�t� �t
treg
F�a�, t�da�dt, (3)
where age-dependent risk functions are applied only tothe ages at which intakes are received. The upper limit ofthe dose integral has been changed to treg, which repre-sents the integration period specified by the appropriateregulation for a scenario of interest. Furthermore, itshould be noted that the age of the individual appears inthe risk term outside the dose integral. While this is notmathematically correct, the equation must be written inthis way to communicate the fundamental problem withusing the CED to evaluate risk. This less rigorousapproach is an approximation of regulatory data (Kaye etal. 2011).
The foundation of the proposed technique lieswithin eqns (1), (2), and (3). In the case of no age-dependence of risk, eqn (1) will yield accurate results,and the CED will track actual risk very well. For anage-dependent risk, but for radionuclides having shorteffective half-lives, eqn (3) will represent an accurateapproximation, and the CED will similarly represent thesituation adequately. Because transuranics exhibit longeffective half-lives and there are likely to be age-dependent risk coefficients, eqn (2) is the most appropri-ate representation of risk. This work will investigate eqns(1), (2), and (3) as applied to transuranics.
Within this paper, risk will be reported in terms ofexcess relative risk, ERR, of death from all solid cancers.For a given dose quantity, Q, the ERR is expressed as:
ERR�Q� �h�Q� � h�O�
h�O�, (4)
where h(Q) is the probability of death or disease for anindividual who receives the dose quantity Q, and h(0) isthe probability of death or disease for an individualwho receives no additional dose (UNSCEAR 2006).An ERR value of 1 would indicate that an exposedindividual of a particular age is twice as likely to die
of solid cancer as a person of the same age who hasreceived no dose.
METHODS
First, the F(a, t) term in eqns (1), (2), and (3) isdetermined by calculating dose as a function of time foran acute intake. Dose coefficients for the public fordifferent ages of intake are derived in InternationalCommission of Radiation Protection and Measurements(ICRP) Reports 69 and 71 (ICRP 1995a and b). Asoftware tool published by the ICRP (Eckerman et al.2001) is used to calculate the effective dose as a functionof time after intake for various intake types, radionu-clides, chemical forms, and particulate size. This soft-ware tool applies the proper ICRP transport models andthus correctly incorporates the translocation of a radio-nuclide intake from organ to organ to give an accurateportrayal of the continuously changing organ burdensthroughout the chronic situations under consideration.Once the effective dose is compiled, an intake function isapplied. The intake function gives intake rates for bothwater and air for specified age divisions. Rather thanusing continuous functions, the problem is discretized asa series of acute intakes corresponding to age ranges forwhich dose coefficients are available. Intake rates arespecified for both males and females. Water intake ratesfor both males and females are modeled as steadilyincreasing over an individual’s lifetime. Air intake ratesfollow a similar trend for both males and females, but theintake rates are modeled as steady state following theteenage years of an individual’s life (Eckerman et al.1999).
To best quantify cancer risks due to chronic tran-suranic intakes, the study used to generate risk datashould be based upon similar conditions of total dose,dose rate, radiation type, age, and gender. By far the mostcomprehensively studied radiation-exposed populationsare the atomic bomb survivors. A relationship betweenERR and the dose received for atomic bomb survivors ofa variety of ages (UNSCEAR 2006) has been developed(Preston et al. 2004). Notably, the atomic bomb survivorsreceived acute external photon exposures and notlower dose-rate chronic internal exposure from alphaemitters. The data are admittedly thus not ideal in thetransuranic case.
Other studies of interest are those of the exposure ofminers to radon progeny and the exposure of radium dialworkers to 226Ra and 228Ra. Epidemiologic studies ofunderground miners are the principal basis for estimatingthe quantitative risk of lung-cancer associated with ex-posure to radon progeny (National Research Council1999), a scenario much closer to that associated with
695Estimation of lifetime cancer risk ● K. L. MCMILLAN ET AL.
www.health-physics.com

chronic inhalation of alpha-emitting transuranics. Al-though the study of the miners exposed to radon progenyis well suited for dealing with chronic exposure scenariosassociated with alpha particles, the majority of subjectsare adult males. Using these data to determine risk to agegroups other than adult males, such as children, isproblematic since they contain no substantive informa-tion about age-dependency of risk. Like the study ofunderground workers, the investigation of the exposureof radium dial workers to alpha-emitting 226Ra and 228Raoffers a scenario very closely matched to that of thechronic inhalation of transuranics (Carnes et al. 1997).This investigation, though, like the underground workerstudy, contained far less information about age-dependency of risk than the atomic bomb survivor data.Because the women within the study entered the radiumindustry during their late teens, risk for young children isnot represented. With the high variation in risk betweenchildren and adults, it is imperative that the study ofradiation-exposed populations chosen to for this investi-gation contain distinct risk data for such ages.
In the same sense that the studies of the exposure ofminers to radon progeny and the exposure of radium dialworkers to 226Ra and 228Ra offer scenarios more closelymatched to the chronic inhalation of transuranics, it isalso possible to offer more specific organ cancer risks asopposed to all solid cancer risk as quoted in the atomicbomb survivor data. However, if a more specific scenariois chosen, there will be less information available todescribe the age-dependency of the cancer risk. The cruxof this investigation is the age-dependency of cancer risk;thus the authors have selected the data set that providesthe most substantial set of data for a wide variety of ages.
The data from the atomic bomb survivors incorpo-rate a variety of ages of exposure. Those models werethus chosen for application to this study as models ofage-dependency of risk, bearing in mind that this work’sgoal is not to present absolute risk but to approximateproblems introduced through improper temporal integra-tions of risk functions. ERR is calculated for the atomicbomb survivor data as:
ERR�e� � � � exp�k1 � k2 � log�e��, (5)
where � � 2.30272 [1/Sv], �1 � 0.7335, �2 � �0.6195,and e is the age of intake (UNSCEAR 2006).
Eqn (5) is used to calculate the risk per unit dose asa function of age at which the dose is received, desig-nated R in eqn (1). An adjustment could be made for theage at which cancer is attained, but in this paper, theoverall probability of death from cancer is considered.For the age-dependent methods, eqn (5) represents theF(a) term. For the CED method, the risk is calculated for
the total dose received using the initial age of intake forthe e term in the equation. For the EDR method, risk iscalculated for each dose received using the age that thedose is received. Additionally, uniform risk is calculatedby using the adult age of 30 y for each intake. Bysumming the risk due to the dose at each time interval,the total risk associated with the intake of a transuranicradionuclide is then calculated as illustrated in eqns (1),(2), and (3). The resultant risk is quoted as ERR.
This treatment of the effective dose computed in theICRP software is done computationally using a programpreviously implemented for risk calculations associatedwith dietary contamination (Kaye et al. 2011). Quantify-ing errors introduced by using age-independent riskfunctions instead of age-dependent risk functions is doneby comparing total risk calculated using eqns (1) and (2).Quantifying errors introduced by using the CED approx-imation method instead of the more rigorous EDRmethod is done by comparing total risk calculated usingeqns (2) and (3).
The computational procedure for calculating thechronic intake of a transuranic radionuclide will beapplied to all 17 transuranics of interest. For both malesand females, ingestion and inhalation calculations areperformed. Inhalation AMAD (activity median aerody-namic diameter) sizes are varied from 0.01–10 �m.Additionally, for inhalation intakes, Type F, Type M, andType S aerosols are investigated.
RESULTS
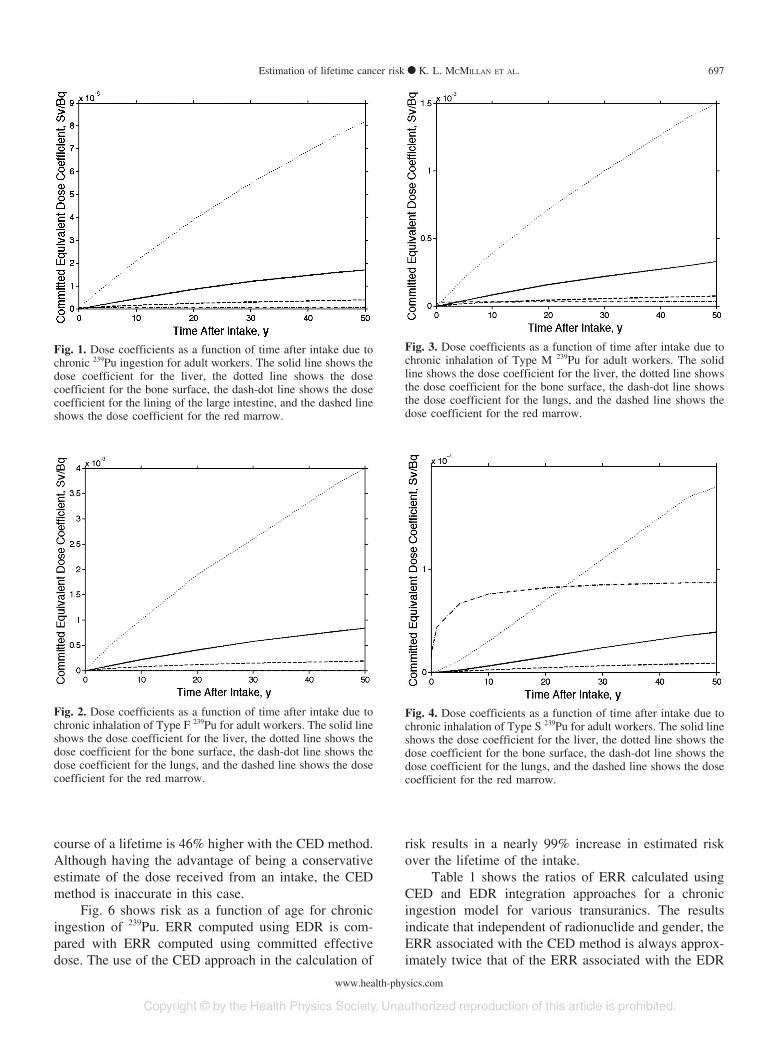
Fig. 1 shows the dose coefficient as a function oftime post intake for a chronic ingestion of 239Pu. It isnoted that the bone surface and the liver both have dosecoefficients greater than the lining of the large intestine,selected for comparison because it was the component ofthe gastrointestinal system with highest dose coefficient.
Figs. 2–4 show the dose coefficient as a function oftime post intake for chronic inhalations of Type F, TypeM, and Type S 239Pu, respectively. Once again, the bonesurface and the liver both have dose coefficients greaterthan the lungs (the component of the respiratory systemwith the highest dose coefficient) for Type F and Type Mchemical forms. For Type S, the bone surface continuesto have a dose coefficient greater than that of the lungs,but the dose coefficient of the lungs is slightly greaterthan that of the liver.
Fig. 5 shows the dose rate as a function of age forchronic 239Pu ingestion. When using the CED method,the dose is overestimated by 72% during the first 63 y oflife. Additionally, because CED is calculated to 50 or70 y beyond the current age, the total dose over the
696 Health Physics December 2011, Volume 101, Number 6
www.health-physics.com
course of a lifetime is 46% higher with the CED method.Although having the advantage of being a conservativeestimate of the dose received from an intake, the CEDmethod is inaccurate in this case.
Fig. 6 shows risk as a function of age for chronicingestion of 239Pu. ERR computed using EDR is com-pared with ERR computed using committed effectivedose. The use of the CED approach in the calculation of
risk results in a nearly 99% increase in estimated riskover the lifetime of the intake.
Table 1 shows the ratios of ERR calculated usingCED and EDR integration approaches for a chronicingestion model for various transuranics. The resultsindicate that independent of radionuclide and gender, theERR associated with the CED method is always approx-imately twice that of the ERR associated with the EDR
Fig. 1. Dose coefficients as a function of time after intake due tochronic 239Pu ingestion for adult workers. The solid line shows thedose coefficient for the liver, the dotted line shows the dosecoefficient for the bone surface, the dash-dot line shows the dosecoefficient for the lining of the large intestine, and the dashed lineshows the dose coefficient for the red marrow.
Fig. 2. Dose coefficients as a function of time after intake due tochronic inhalation of Type F 239Pu for adult workers. The solid lineshows the dose coefficient for the liver, the dotted line shows thedose coefficient for the bone surface, the dash-dot line shows thedose coefficient for the lungs, and the dashed line shows the dosecoefficient for the red marrow.
Fig. 3. Dose coefficients as a function of time after intake due tochronic inhalation of Type M 239Pu for adult workers. The solidline shows the dose coefficient for the liver, the dotted line showsthe dose coefficient for the bone surface, the dash-dot line showsthe dose coefficient for the lungs, and the dashed line shows thedose coefficient for the red marrow.
Fig. 4. Dose coefficients as a function of time after intake due tochronic inhalation of Type S 239Pu for adult workers. The solid lineshows the dose coefficient for the liver, the dotted line shows thedose coefficient for the bone surface, the dash-dot line shows thedose coefficient for the lungs, and the dashed line shows the dosecoefficient for the red marrow.
697Estimation of lifetime cancer risk ● K. L. MCMILLAN ET AL.
www.health-physics.com
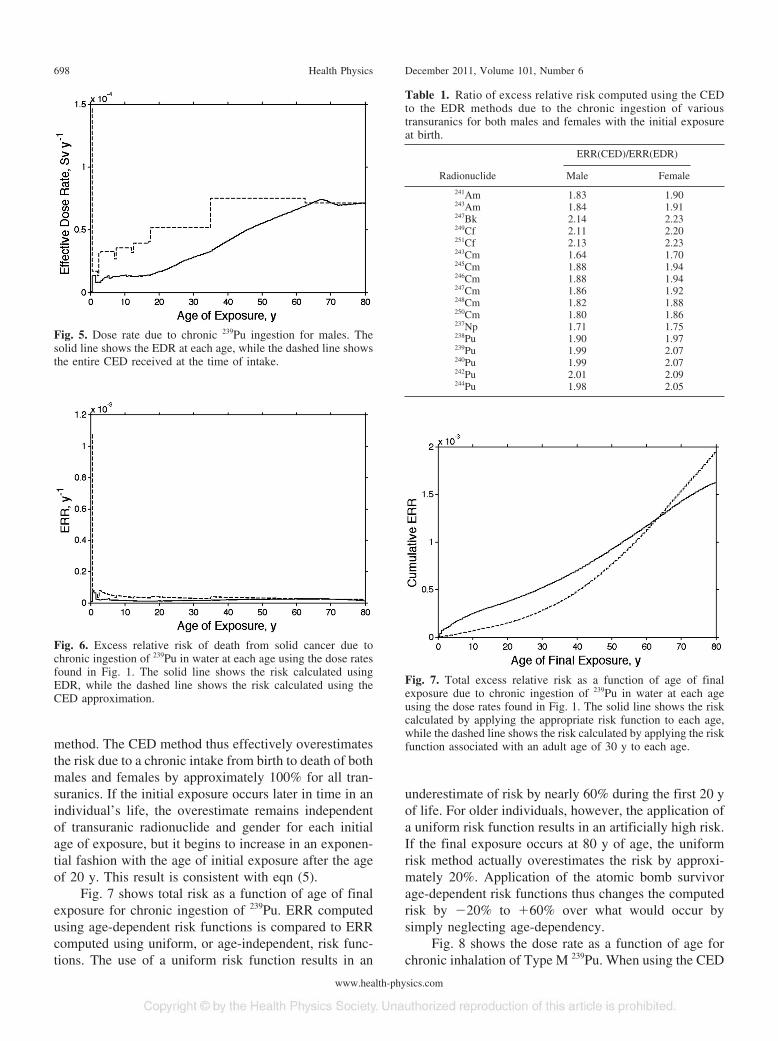
method. The CED method thus effectively overestimatesthe risk due to a chronic intake from birth to death of bothmales and females by approximately 100% for all tran-suranics. If the initial exposure occurs later in time in anindividual’s life, the overestimate remains independentof transuranic radionuclide and gender for each initialage of exposure, but it begins to increase in an exponen-tial fashion with the age of initial exposure after the ageof 20 y. This result is consistent with eqn (5).
Fig. 7 shows total risk as a function of age of finalexposure for chronic ingestion of 239Pu. ERR computedusing age-dependent risk functions is compared to ERRcomputed using uniform, or age-independent, risk func-tions. The use of a uniform risk function results in an
underestimate of risk by nearly 60% during the first 20 yof life. For older individuals, however, the application ofa uniform risk function results in an artificially high risk.If the final exposure occurs at 80 y of age, the uniformrisk method actually overestimates the risk by approxi-mately 20%. Application of the atomic bomb survivorage-dependent risk functions thus changes the computedrisk by �20% to �60% over what would occur bysimply neglecting age-dependency.
Fig. 8 shows the dose rate as a function of age forchronic inhalation of Type M 239Pu. When using the CED
Fig. 5. Dose rate due to chronic 239Pu ingestion for males. Thesolid line shows the EDR at each age, while the dashed line showsthe entire CED received at the time of intake.
Fig. 6. Excess relative risk of death from solid cancer due tochronic ingestion of 239Pu in water at each age using the dose ratesfound in Fig. 1. The solid line shows the risk calculated usingEDR, while the dashed line shows the risk calculated using theCED approximation.
Table 1. Ratio of excess relative risk computed using the CEDto the EDR methods due to the chronic ingestion of varioustransuranics for both males and females with the initial exposureat birth.
ERR(CED)/ERR(EDR)
Radionuclide Male Female
241Am 1.83 1.90243Am 1.84 1.91247Bk 2.14 2.23249Cf 2.11 2.20251Cf 2.13 2.23243Cm 1.64 1.70245Cm 1.88 1.94246Cm 1.88 1.94247Cm 1.86 1.92248Cm 1.82 1.88250Cm 1.80 1.86237Np 1.71 1.75238Pu 1.90 1.97239Pu 1.99 2.07240Pu 1.99 2.07242Pu 2.01 2.09244Pu 1.98 2.05
Fig. 7. Total excess relative risk as a function of age of finalexposure due to chronic ingestion of 239Pu in water at each ageusing the dose rates found in Fig. 1. The solid line shows the riskcalculated by applying the appropriate risk function to each age,while the dashed line shows the risk calculated by applying the riskfunction associated with an adult age of 30 y to each age.
698 Health Physics December 2011, Volume 101, Number 6
www.health-physics.com
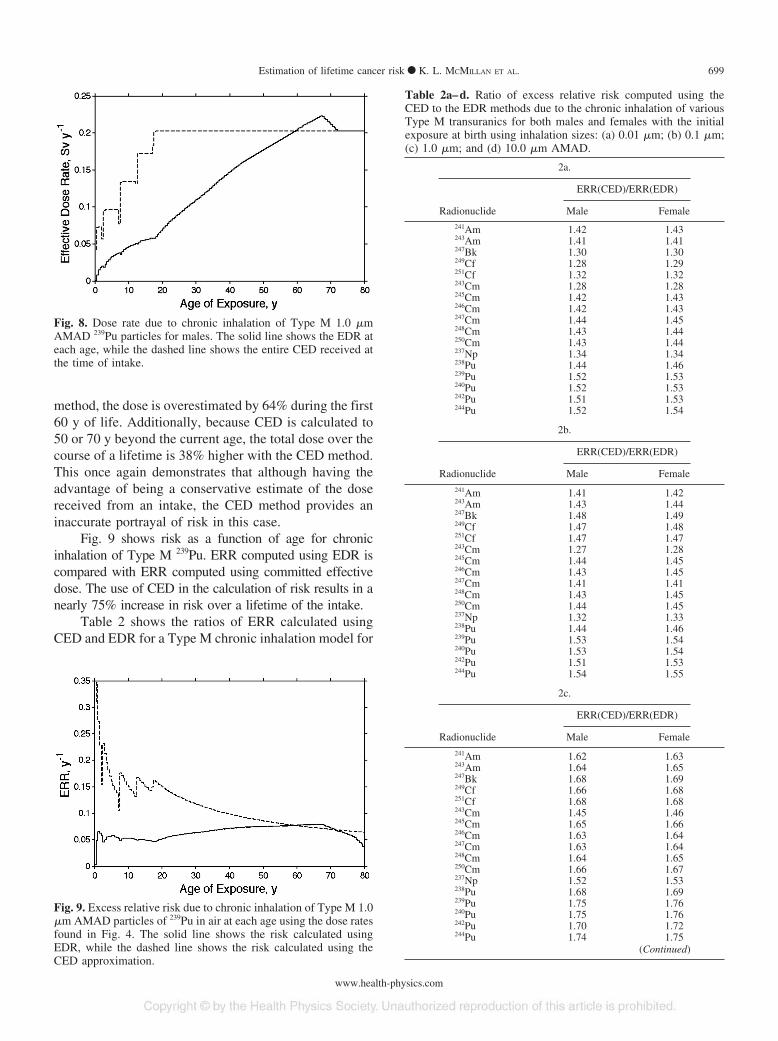
method, the dose is overestimated by 64% during the first60 y of life. Additionally, because CED is calculated to50 or 70 y beyond the current age, the total dose over thecourse of a lifetime is 38% higher with the CED method.This once again demonstrates that although having theadvantage of being a conservative estimate of the dosereceived from an intake, the CED method provides aninaccurate portrayal of risk in this case.
Fig. 9 shows risk as a function of age for chronicinhalation of Type M 239Pu. ERR computed using EDR iscompared with ERR computed using committed effectivedose. The use of CED in the calculation of risk results in anearly 75% increase in risk over a lifetime of the intake.
Table 2 shows the ratios of ERR calculated usingCED and EDR for a Type M chronic inhalation model for
Fig. 8. Dose rate due to chronic inhalation of Type M 1.0 �mAMAD 239Pu particles for males. The solid line shows the EDR ateach age, while the dashed line shows the entire CED received atthe time of intake.
Fig. 9. Excess relative risk due to chronic inhalation of Type M 1.0�m AMAD particles of 239Pu in air at each age using the dose ratesfound in Fig. 4. The solid line shows the risk calculated usingEDR, while the dashed line shows the risk calculated using theCED approximation.
Table 2a–d. Ratio of excess relative risk computed using theCED to the EDR methods due to the chronic inhalation of variousType M transuranics for both males and females with the initialexposure at birth using inhalation sizes: (a) 0.01 �m; (b) 0.1 �m;(c) 1.0 �m; and (d) 10.0 �m AMAD.
2a.
ERR(CED)/ERR(EDR)
Radionuclide Male Female241Am 1.42 1.43243Am 1.41 1.41247Bk 1.30 1.30249Cf 1.28 1.29251Cf 1.32 1.32243Cm 1.28 1.28245Cm 1.42 1.43246Cm 1.42 1.43247Cm 1.44 1.45248Cm 1.43 1.44250Cm 1.43 1.44237Np 1.34 1.34238Pu 1.44 1.46239Pu 1.52 1.53240Pu 1.52 1.53242Pu 1.51 1.53244Pu 1.52 1.54
2b.
ERR(CED)/ERR(EDR)
Radionuclide Male Female
241Am 1.41 1.42243Am 1.43 1.44247Bk 1.48 1.49249Cf 1.47 1.48251Cf 1.47 1.47243Cm 1.27 1.28245Cm 1.44 1.45246Cm 1.43 1.45247Cm 1.41 1.41248Cm 1.43 1.45250Cm 1.44 1.45237Np 1.32 1.33238Pu 1.44 1.46239Pu 1.53 1.54240Pu 1.53 1.54242Pu 1.51 1.53244Pu 1.54 1.55
2c.
ERR(CED)/ERR(EDR)
Radionuclide Male Female
241Am 1.62 1.63243Am 1.64 1.65247Bk 1.68 1.69249Cf 1.66 1.68251Cf 1.68 1.68243Cm 1.45 1.46245Cm 1.65 1.66246Cm 1.63 1.64247Cm 1.63 1.64248Cm 1.64 1.65250Cm 1.66 1.67237Np 1.52 1.53238Pu 1.68 1.69239Pu 1.75 1.76240Pu 1.75 1.76242Pu 1.70 1.72244Pu 1.74 1.75
(Continued)
699Estimation of lifetime cancer risk ● K. L. MCMILLAN ET AL.
www.health-physics.com
various transuranics. The results indicate that regardlessof transuranic type, individual’s gender, and aerosolparticle size, the ERR associated with the CED method isalways approximately 1.75 times that of the ERR asso-ciated with the EDR method. In other words, the CEDmethod overestimates that risk by approximately 75% forall cases. Again, this overestimate was calculated forchronic intake over the lifetime of an individual with theinitial exposure occurring at birth. As in the case ofchronic ingestion, for chronic inhalation the overestimatebegins to increase in an exponential fashion for an initialexposure after the age of 20 y.
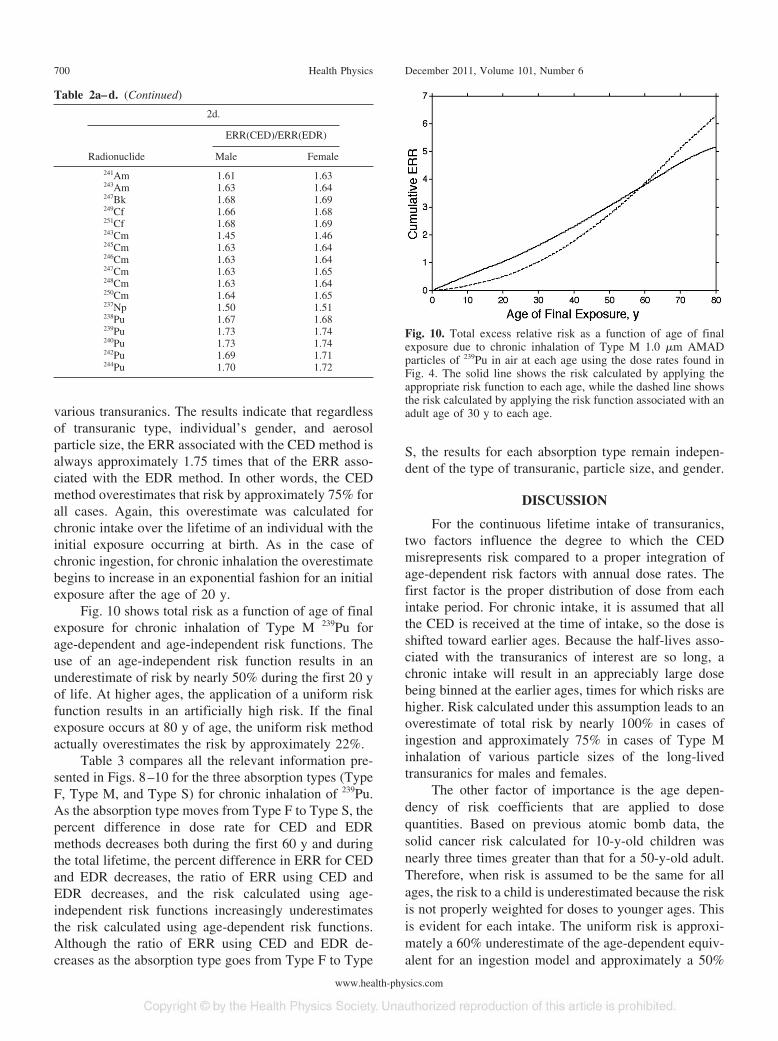
Fig. 10 shows total risk as a function of age of finalexposure for chronic inhalation of Type M 239Pu forage-dependent and age-independent risk functions. Theuse of an age-independent risk function results in anunderestimate of risk by nearly 50% during the first 20 yof life. At higher ages, the application of a uniform riskfunction results in an artificially high risk. If the finalexposure occurs at 80 y of age, the uniform risk methodactually overestimates the risk by approximately 22%.
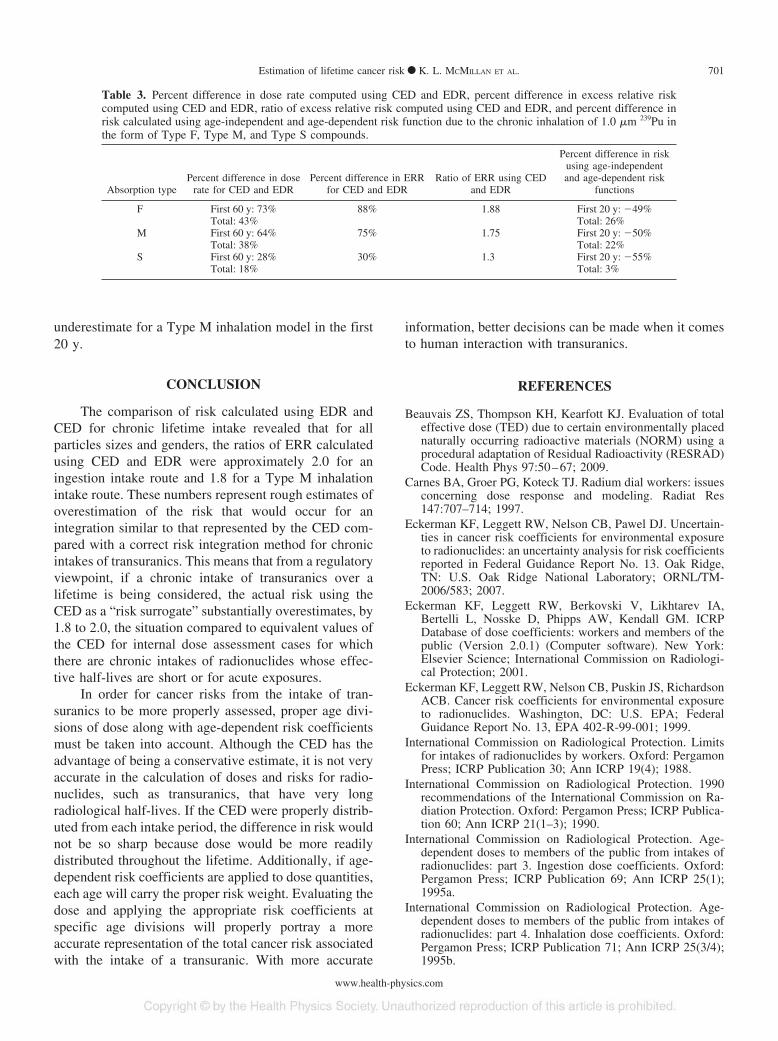
Table 3 compares all the relevant information pre-sented in Figs. 8–10 for the three absorption types (TypeF, Type M, and Type S) for chronic inhalation of 239Pu.As the absorption type moves from Type F to Type S, thepercent difference in dose rate for CED and EDRmethods decreases both during the first 60 y and duringthe total lifetime, the percent difference in ERR for CEDand EDR decreases, the ratio of ERR using CED andEDR decreases, and the risk calculated using age-independent risk functions increasingly underestimatesthe risk calculated using age-dependent risk functions.Although the ratio of ERR using CED and EDR de-creases as the absorption type goes from Type F to Type
S, the results for each absorption type remain indepen-dent of the type of transuranic, particle size, and gender.
DISCUSSION
For the continuous lifetime intake of transuranics,two factors influence the degree to which the CEDmisrepresents risk compared to a proper integration ofage-dependent risk factors with annual dose rates. Thefirst factor is the proper distribution of dose from eachintake period. For chronic intake, it is assumed that allthe CED is received at the time of intake, so the dose isshifted toward earlier ages. Because the half-lives asso-ciated with the transuranics of interest are so long, achronic intake will result in an appreciably large dosebeing binned at the earlier ages, times for which risks arehigher. Risk calculated under this assumption leads to anoverestimate of total risk by nearly 100% in cases ofingestion and approximately 75% in cases of Type Minhalation of various particle sizes of the long-livedtransuranics for males and females.
The other factor of importance is the age depen-dency of risk coefficients that are applied to dosequantities. Based on previous atomic bomb data, thesolid cancer risk calculated for 10-y-old children wasnearly three times greater than that for a 50-y-old adult.Therefore, when risk is assumed to be the same for allages, the risk to a child is underestimated because the riskis not properly weighted for doses to younger ages. Thisis evident for each intake. The uniform risk is approxi-mately a 60% underestimate of the age-dependent equiv-alent for an ingestion model and approximately a 50%
Table 2a–d. (Continued)
2d.
ERR(CED)/ERR(EDR)
Radionuclide Male Female
241Am 1.61 1.63243Am 1.63 1.64247Bk 1.68 1.69249Cf 1.66 1.68251Cf 1.68 1.69243Cm 1.45 1.46245Cm 1.63 1.64246Cm 1.63 1.64247Cm 1.63 1.65248Cm 1.63 1.64250Cm 1.64 1.65237Np 1.50 1.51238Pu 1.67 1.68239Pu 1.73 1.74240Pu 1.73 1.74242Pu 1.69 1.71244Pu 1.70 1.72
Fig. 10. Total excess relative risk as a function of age of finalexposure due to chronic inhalation of Type M 1.0 �m AMADparticles of 239Pu in air at each age using the dose rates found inFig. 4. The solid line shows the risk calculated by applying theappropriate risk function to each age, while the dashed line showsthe risk calculated by applying the risk function associated with anadult age of 30 y to each age.
700 Health Physics December 2011, Volume 101, Number 6
www.health-physics.com
underestimate for a Type M inhalation model in the first20 y.
CONCLUSION
The comparison of risk calculated using EDR andCED for chronic lifetime intake revealed that for allparticles sizes and genders, the ratios of ERR calculatedusing CED and EDR were approximately 2.0 for aningestion intake route and 1.8 for a Type M inhalationintake route. These numbers represent rough estimates ofoverestimation of the risk that would occur for anintegration similar to that represented by the CED com-pared with a correct risk integration method for chronicintakes of transuranics. This means that from a regulatoryviewpoint, if a chronic intake of transuranics over alifetime is being considered, the actual risk using theCED as a “risk surrogate” substantially overestimates, by1.8 to 2.0, the situation compared to equivalent values ofthe CED for internal dose assessment cases for whichthere are chronic intakes of radionuclides whose effec-tive half-lives are short or for acute exposures.
In order for cancer risks from the intake of tran-suranics to be more properly assessed, proper age divi-sions of dose along with age-dependent risk coefficientsmust be taken into account. Although the CED has theadvantage of being a conservative estimate, it is not veryaccurate in the calculation of doses and risks for radio-nuclides, such as transuranics, that have very longradiological half-lives. If the CED were properly distrib-uted from each intake period, the difference in risk wouldnot be so sharp because dose would be more readilydistributed throughout the lifetime. Additionally, if age-dependent risk coefficients are applied to dose quantities,each age will carry the proper risk weight. Evaluating thedose and applying the appropriate risk coefficients atspecific age divisions will properly portray a moreaccurate representation of the total cancer risk associatedwith the intake of a transuranic. With more accurate
information, better decisions can be made when it comesto human interaction with transuranics.
REFERENCES
Beauvais ZS, Thompson KH, Kearfott KJ. Evaluation of totaleffective dose (TED) due to certain environmentally placednaturally occurring radioactive materials (NORM) using aprocedural adaptation of Residual Radioactivity (RESRAD)Code. Health Phys 97:50–67; 2009.
Carnes BA, Groer PG, Koteck TJ. Radium dial workers: issuesconcerning dose response and modeling. Radiat Res147:707–714; 1997.
Eckerman KF, Leggett RW, Nelson CB, Pawel DJ. Uncertain-ties in cancer risk coefficients for environmental exposureto radionuclides: an uncertainty analysis for risk coefficientsreported in Federal Guidance Report No. 13. Oak Ridge,TN: U.S. Oak Ridge National Laboratory; ORNL/TM-2006/583; 2007.
Eckerman KF, Leggett RW, Berkovski V, Likhtarev IA,Bertelli L, Nosske D, Phipps AW, Kendall GM. ICRPDatabase of dose coefficients: workers and members of thepublic (Version 2.0.1) (Computer software). New York:Elsevier Science; International Commission on Radiologi-cal Protection; 2001.
Eckerman KF, Leggett RW, Nelson CB, Puskin JS, RichardsonACB. Cancer risk coefficients for environmental exposureto radionuclides. Washington, DC: U.S. EPA; FederalGuidance Report No. 13, EPA 402-R-99-001; 1999.
International Commission on Radiological Protection. Limitsfor intakes of radionuclides by workers. Oxford: PergamonPress; ICRP Publication 30; Ann ICRP 19(4); 1988.
International Commission on Radiological Protection. 1990recommendations of the International Commission on Ra-diation Protection. Oxford: Pergamon Press; ICRP Publica-tion 60; Ann ICRP 21(1–3); 1990.
International Commission on Radiological Protection. Age-dependent doses to members of the public from intakes ofradionuclides: part 3. Ingestion dose coefficients. Oxford:Pergamon Press; ICRP Publication 69; Ann ICRP 25(1);1995a.
International Commission on Radiological Protection. Age-dependent doses to members of the public from intakes ofradionuclides: part 4. Inhalation dose coefficients. Oxford:Pergamon Press; ICRP Publication 71; Ann ICRP 25(3/4);1995b.
Table 3. Percent difference in dose rate computed using CED and EDR, percent difference in excess relative riskcomputed using CED and EDR, ratio of excess relative risk computed using CED and EDR, and percent difference inrisk calculated using age-independent and age-dependent risk function due to the chronic inhalation of 1.0 �m 239Pu inthe form of Type F, Type M, and Type S compounds.
Absorption typePercent difference in dose
rate for CED and EDRPercent difference in ERR
for CED and EDRRatio of ERR using CED
and EDR
Percent difference in riskusing age-independentand age-dependent risk
functions
F First 60 y: 73% 88% 1.88 First 20 y: �49%Total: 43% Total: 26%
M First 60 y: 64% 75% 1.75 First 20 y: �50%Total: 38% Total: 22%
S First 60 y: 28% 30% 1.3 First 20 y: �55%Total: 18% Total: 3%
701Estimation of lifetime cancer risk ● K. L. MCMILLAN ET AL.
www.health-physics.com

International Commission on Radiological Protection. The2007 recommendations of the International Commission onRadiation Protection. Oxford: Pergamon Press; ICRP Pub-lication 103; Ann ICRP 37(2–4); 2007.
James AC, Filipy RE, Russell JJ, McInroy JF. USTUR case0259 whole body donation: a comprehensive test of thecurrent ICRP models for the behavior of inhaled 238PuO2ceramic particles. Health Phys 84:2–33; 2003.
Kaye WR, Beauvais ZS, Kearfott KJ. Method of estimatinglifetime cancer risk due to chronic radionuclide intake.Health Phys 100:165–175; 2011.
National Research Council. Biological Effects of IonizingRadiation (BEIR) Report VI: the health effects of expo-sure to indoor radon. Washington, DC: National Academy Press;1999.
Preston DL, Pierce DA, Shimizu Y, Cullings HM, Fujita S,Funamotoa S, Kodamab K. Effect of recent changes in
atomic bomb survivor dosimetry on cancer mortality riskestimates. Radiat Res 162:377–389; 2004.
U.S. Department of Energy. Guide of good practices foroccupational radiological protection in plutonium facili-ties. Washington, DC: U.S. Department of Energy Officeof Health, Safety and Security; DOE-STD-1128-2008;2008.
United Nations Scientific Committee on the Effects of AtomicRadiation. United Nations Scientific Committee on theEffects of Atomic Radiation: sources and effects of ionizingradiation. Vienna: United Nations; 2006.
U.S. Nuclear Regulatory Commission. Environmental radia-tion protection standards for management and disposal ofspent nuclear fuel, high-level and transuranic radioactivewastes. Washington, DC: U.S. NRC; 40 Code of FederalRegulations, part 191; 2004.
f f
702 Health Physics December 2011, Volume 101, Number 6
www.health-physics.com



















