p065 Artifacts, Anatomical and Physiological Variants, and Unrelated Diseases That Might Cause...
18
Artifacts, Anatomical and Physiological Variants, and Unrelated Diseases That Might Cause False-Positive Whole-Body 131-I Scans in Patients With Thyroid Cancer Brahm Shapiro, Vittoria Rufini, Ayman Jarwan, Onelio Geatti, Kimberlee J. Kearfott, Lorraine M. Fig, lan D. Kirkwood, and Milton D. Gross The whole body 131-1 scan remains an important component in the postoperative treatment of patients with well-differentiated thyroid cancer, Because nor- mal thyroid tissue remnants and residual or meta- static loci of well-differentiated thyroid cancer have the unique ability to concentrate, orgsnify, and store 131-1, the whole body scan provides a depiction of those tissues that can be ablated with therapeutic doses of 131-1. Over time, it has become obvious that the whole body scan may also reveal foci of 131-1 uptake owing to a wide variety of other causes. We provide a detailed pathophysiological classification of the artifacts, anatomic and physiological variants, and nonthyroidal diseases that may give rise to false- positive whole body scans in postoperative patients with thyroid cancer. These include ectopic foci of normal thyroid tissue; nonthyroidal physiological sites (eg, choroid plexus, salivary glands, gastric mucosa, urinary tract); contamination by physiological sec- tions; ectopic gastric mucosa; other gastrointestinal abnormalities; urinary tract abnormalities; mammary abnormalities; serous cavities and cysts; inflammation and infection; nonthyroidal neoplasms; and currently unexplained causes. This article also provides a de- tailed review of the widely scattered English language literature in which these phenomena were originally described. Copyright 2000 by W.B. Saunders Company W rHOLE BODY 131-1 scanning of patients with thyroid cancer after a thyroidectomy has been widely accepted as a central component of the treatment of this disease for over 4 decades. 1-12 The value of the technique lies in its ability to detect loci of residual normal thyroid tissue and tumor and metastatic spread to remote sites. The modality may depict disease that is otherwise undetectable by any other modality. 6,8-1~ Further- more, uptake of 13 I-I on diagnostic studies permits the selection of patients for whom 131-I therapy is appropriate. 6,8,9,13 All of this rests on the unique property of thy- roid tissue to concentrate, organify, and retain 131-I. 2,7-9,11-17 Many thyroid cancers retain this characteristic property and, thus, foci of uptake on postthyroidectomy scans are considered highly specific for thyroid tissue, be it residual remnant, normal, or cancerous tissue in the neck or else- where in metastatic f o c i . 2'7"9'11"17 This specificity is unfortunately degraded by uptake in other tissues that can concentrate 131-I but do not retain it in or- ganic form (Fig 1). These include the choroid plexus, salivary glands, nasopharynx, and stomach; furthermore, excretion via the kidney, liver, and gut may depict these organs and the bladder, z,6-9,II,14,I5,17 The literature is replete with an ever-growing collection of reports of uptake in these organs and tissues and their associated diseases, as well as other pathological processes. 1,4,6,8,12-14,18-21 The accurate interpretation of postthyroidec- tomy whole body 131-I images requires a thorough knowledge and understanding of all these potential confounding phenomena. 1,2,4,6-9,13,18,19,21 Imaging af- ter the therapeutic administration of large activities of 131-I permits verification of the biodistribution of the therapeutic dose and may depict an otherwise greater extent of disease. 6-9 The same problem of interpretation applies in this posttherapeutic situa- tion as in the diagnostic images. Unfortunately the literature is widely scattered and consists primarily of isolated case reports, very small series, or it is hidden within larger works as anecdotal descrip- tions. 1'3,4'6'8'12,14J8-21 We have sought to approach this daunting problem by means of a detailed review with the available data organized according to first principles based on the underlying physi- ological principles governing the biodistribution of radioactive iodine. This permits a logical classi- fication and pathophysiological interpretation of From the University of Michigan, Department of Veterans' Affairs Health Systems, Department of Internal Medicine, Division of Nuclear Medicine, Ann Arbor, MI; Instituto di Medicina Nucleate, Universita Cattolica del Sacro Cuote, Rome, Italy; Department of Nuclear Engineering and Radiological Sciences, University of Michigan, Ann Arbor, MI; and Servizio di Medicina Nucleate, Ospedale Maggiore, Trieste, Italy. Address reprint requests to Brahm Shapiro, MB, ChB, PhD, Division of Nuclear Medicine, University of Michigan Medical Center, 1500 East Medical Center Drive, Ann Arbor, M148109-0028. Copyright 2000 by W.B. Saunders Company 0001-2998/00/3002-00065 l 0.00/0 doi: 10.1053/nm. 2000.5414 Seminars in Nuclear Medicine, Vol XXX, No 2 (April), 2000: pp 115-132 115
Transcript of p065 Artifacts, Anatomical and Physiological Variants, and Unrelated Diseases That Might Cause...

Artifacts, Anatomical and Physiological Variants, and Unrelated Diseases That Might Cause False-Positive
Whole-Body 131-I Scans in Patients With Thyroid Cancer
Brahm Shapiro, Vittoria Rufini, Ayman Jarwan, Onelio Geatti, Kimberlee J. Kearfott, Lorraine M. Fig, lan D. Kirkwood, and Milton D. Gross
The whole body 131-1 scan remains an important component in the postoperative t reatment of patients with well-differentiated thyroid cancer, Because nor- mal thyroid tissue remnants and residual or meta- static loci of well-differentiated thyroid cancer have the unique abil i ty to concentrate, orgsnify, and store 131-1, the whole body scan provides a depiction of those tissues that can be ablated w i th therapeutic doses of 131-1. Over t ime, it has become obvious that the whole body scan may also reveal foci of 131-1 uptake owing to a wide variety of other causes. We provide a detailed pathophysiological classification of the artifacts, anatomic and physiological variants, and nonthyroidal diseases that may give rise to false-
positive whole body scans in postoperative patients w i th thyroid cancer. These include ectopic foci of normal thyroid tissue; nonthyroidal physiological sites (eg, choroid plexus, salivary glands, gastric mucosa, urinary tract); contamination by physiological sec- tions; ectopic gastric mucosa; other gastrointestinal abnormalit ies; urinary tract abnormalit ies; mammary abnormalit ies; serous cavities and cysts; inf lammation and infection; nonthyroidal neoplasms; and currently unexplained causes. This article also provides a de- tailed review of the widely scattered English language literature in which these phenomena were originally described. Copyright �9 2000 by W.B. Saunders Company
W rHOLE BODY 131-1 scanning of patients with thyroid cancer after a thyroidectomy
has been widely accepted as a central component of the treatment of this disease for over 4 decades. 1-12 The value of the technique lies in its ability to detect loci of residual normal thyroid tissue and tumor and metastatic spread to remote sites. The modality may depict disease that is otherwise undetectable by any other modality. 6,8-1~ Further- more, uptake of 13 I-I on diagnostic studies permits the selection of patients for whom 131-I therapy is appropriate. 6,8,9,13
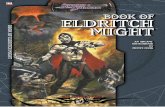
All of this rests on the unique property of thy- roid tissue to concentrate, organify, and retain 131-I. 2,7-9,11-17 Many thyroid cancers retain this characteristic property and, thus, foci of uptake on postthyroidectomy scans are considered highly specific for thyroid tissue, be it residual remnant, normal, or cancerous tissue in the neck or else- where in metastatic foc i . 2'7"9'11"17 This specificity is unfortunately degraded by uptake in other tissues that can concentrate 131-I but do not retain it in or- ganic form (Fig 1). These include the choroid plexus, salivary glands, nasopharynx, and stomach; furthermore, excretion via the kidney, liver, and gut may depict these organs and the bladder, z,6-9,II,14,I5,17 The literature is replete with an ever-growing collection of reports of uptake in these organs and tissues and their associated diseases, as well as other pathological processes. 1,4,6,8,12-14,18-21
The accurate interpretation of postthyroidec-
tomy whole body 131-I images requires a thorough knowledge and understanding of all these potential confounding phenomena. 1,2,4,6-9,13,18,19,21 Imaging af- ter the therapeutic administration of large activities of 131-I permits verification of the biodistribution of the therapeutic dose and may depict an otherwise greater extent of disease. 6-9 The same problem of interpretation applies in this posttherapeutic situa- tion as in the diagnostic images. Unfortunately the literature is widely scattered and consists primarily of isolated case reports, very small series, or it is hidden within larger works as anecdotal descrip- tions. 1'3,4'6'8'12,14J8-21 We have sought to approach this daunting problem by means of a detailed review with the available data organized according to first principles based on the underlying physi- ological principles governing the biodistribution of radioactive iodine. This permits a logical classi- fication and pathophysiological interpretation of
From the University of Michigan, Department of Veterans' Affairs Health Systems, Department of Internal Medicine, Division of Nuclear Medicine, Ann Arbor, MI; Instituto di Medicina Nucleate, Universita Cattolica del Sacro Cuote, Rome, Italy; Department of Nuclear Engineering and Radiological Sciences, University of Michigan, Ann Arbor, MI; and Servizio di Medicina Nucleate, Ospedale Maggiore, Trieste, Italy.
Address reprint requests to Brahm Shapiro, MB, ChB, PhD, Division of Nuclear Medicine, University of Michigan Medical Center, 1500 East Medical Center Drive, Ann Arbor, M148109-0028.
Copyright �9 2000 by W.B. Saunders Company 0001-2998/00/3002-00065 l 0.00/0 doi: 10.1053/nm. 2000.5414
Seminars in Nuclear Medicine, Vol XXX, No 2 (April), 2000: pp 115-132 115

116 SHAPIRO ET AL
Feces I Sweat I" Expired breath I"
> Inorganic iodine pathways
D O ~ c iodine pathways
the disparate literature of the host of artifacts, anatomical and physiological variants, and nonthy- roidal diseases that are responsible for false- positive whole body 131-1 scans in thyroid cancer. In the references, we provide a comprehensive compilation of the primary sources of the literature on this subject.
The administration of large activities of 131-I for the treatment of residual or metastatic well-differenti- ated thyroid cancer is a uniquely effective systemic therapy when applied to appropriate patients. 3,5-9,11 Recognition of the multiple causes of false-positive diagnostic studies will prevent the inappropriate delivery of this therapy. Similarly the correct interpretation of posttherapy images will prevent incorrect prognostic inferences from being drawn.
ARTIFACTS RELATED TO ECTOPIC NORMAL THYROID TISSUE
The embryological origin of the thyroid gland from the foramen cecum at the junction between the anterior two thirds and the posterior one third of
Milk I" Uri .e I"
Fig 1. A schematic represen- tation of iodine metabolism.
the tongue, with its subsequent descent and bifurca- tion in the neck, gives rise to a wide variety of abnormalities owing to embryological maldevelop- ment (Table 1). 4,22-56 Thus, complete failure to migrate leads to a lingual thyroid (Fig 2) and incomplete migration leads to a high cervical thyroid, whereas excessive migration causes a superior mediastinal thyroid or even a paracardiac gland. 4,22-4~ Foci of functioning tissue may remain anywhere along the embryological thyroglossal d u c t tract. 4,22-24,29,39-41 Abnormal migration results in widely divergent ectopic foci (eg, esophageal, intratracheal, and intrahepatic). 4,22-24,31,32,42,43,57-59 The so-called lateral aberrant thyroid tissue is highly controversial and many believe that it is, in fact, well-differentiated thyroid cancer metastatic to and completely replacing cervical lymph nodes, with the thyroidal primary being completely oc- cult. 4'23,24,52,5456 Finally, normally differentiated thy- roid tissue may occur in the ovary (struma ovari i) . 4,23,24,44"53 This may represent the thyroidal

131-1 SCAN ARTIFACTS 117
Table 1. Ectopic Normal Thyroid Tissue
Comments Regarding Abnormal Embryonic Ectopic Normal Thyroid 13ssue Sites Mechanism for 131-1 Uptake Thyroid Migration/Development
Lingual thyroid 4,23-2s,4~ Owing to normal processes Failure to migrate (descend) of thyroidal 131-1 uptake and organificetion
" Incomplete migration Excessive migration Excessive migration
High cervical thyroid ~,~3,=3,~4,~7,2a,30,3~.4~
Thoracic superior mediastinal thyroid ".zz,z4,~-z> Paracardiac thyroid ~,2~,33,3",37,3s
Intracardiac ( S t ruma cordis) Pericardial
Functioning thyroid tissue in the thyroglossal tract 4̀~3'z~,2~,39,40's9
Esophageal thyroid 4,23,24,32,4~ Intratracheal thyroid 4.23,32,42
Ovarian thyroid ( St ruma ovarit~ ~,~3,2~,~
Lateral aberrant thyroid tissue rests 4.14,z3,24,54-56
lntrahepatic thyroid tissue 4.~3.~4̀31's'/'ss
Small foci of functioning thyroid tissue along route of migration may be stimulated by high TSH levels after thyroidectomy
Abnormal migration Abnormal migration Differentiation of thyroid tissue in a benign ovarian
teratoma Current knowledge suggests many or all are owing to
metastases to cervical lymph nodes Need to be distinguished from biliary tract
component of a teratoma or it may exist in isola- tion.
ARTIFACTS RELATED TO PHYSIOLOGICAL SITES OF NONTHYROIDAL UPTAKE OR
BIODISTRIBUTION
Although thyroid tissue is unique in its ability to organify iodide and synthesize thyroid hormones, a variety of glandular tissues share with the thyroid gland the ability to actively transport 131-I against a chemical gradient from the plasma into their
secretory lumen (Table 2). 2'16'60 Concentration gra- dients of up to 20:1 can be achieved. Tissues that share this property include gastric mucosa, nasal mucosa, salivary glands, lachrymal gland, and the lactating or nonlactating breast (Fig 3). 2'4"~3"16'60"90
The choroid plexus, although not a glandular epithelium, is nevertheless a site of secretory function for the formation of cerebrospinal fluid (CSF) and also shows 13 I-I uptake. 4
Iodide, being a small ion, is readily cleared by glomerular filtration and subsequently subject to a
< =
, , ~',, ~., .~, ~ ,. �9 ~ '., , .,.~.,, .., ' ~ - , ,
Fig 2. (A) Anterior and (B) lateral views of the head, neck, and upper chest, 24 hours after 2 mCi of 131-1 after a total thyroidectomy for papillary thyroid cancer. There w a s a small thyroid bed remnant (arrowhead) and normal uptake of 131-1 in the N, nose; M, mouth; and P, parotid glands. The intense midline focus of uptake below the floor of the mouth was owing to s lingual thyroid remnant in the base of the tongue (arrow).

118 SHAPIRO ET AL
Table 2. Physiological Sites of Nonthyroidal Uptake or Biodistribution
Physiological Sites of Nonthyroidal Mechanism for 131-1 Uptake (owing to Uptake/Distribution Normal Processes of 131-1Biodistribution) Comments Regarding Normal Biodistdbutien
Normal cardiac blood pool displaced by pectus excavatum 4,1~
Carotid ectasia 4Js,7~176
Salivary gland uptake 4.6,16.26,6~
Gastric mucosal uptake 4A6,69 Nasal mucosal uptake 4,63,69,70,73,74,82
Gut activity 4,69
Urinary tract excret ion 4,21,91,92
Choroid plexus uptake 4
Cardiac and great vessel blood pool may persist 2,4,7~
Nonlactating breast uptake 4,16,sT,el,83,84
Lactating breast uptake (see Figure 3) 4'13'16'61'64-66'68'69'72'77-79'82'84'90
Liver uptake 4,73,98,99,1~
Gallbladder uptake 4,73,91,1~
Swallowed saliva in pharynx and esophagus 4,62,8~
Lacrimal gland 4,s8
131-1 transported from site of absorption Activity fades as blood pool clears with via circulation time (not to be confused with lung
lesions) 131-1 transported from site of absorption Activity fades as blood pool clears with
via circulation time (not to be confused with tumor
Site of active 131-1 transport
Site of active 131-1 tra nsport Site of active 131-1 transport Translocation of activity secreted by
gastric mucosa Major route of clearance Site of active 131-1 transport
Slow renal clearance in renal disease or absent renal clearance in renal failure and on dialysis
Site of active 131-1 transport
Site of active 131-1 transport
Hepatic u pta ke of 131-1-1a beled thyroid hormones synthesized by functioning normal or neoplastic thyroid tissue
Enterohepatic excretion of 131-1 thyroid hormone and metabolites
Activity translated from site of secretion in salivary glands
Site of active 131-1 transport
spread to cervical lymph nodes) Knowledge of normal biodistribution
required for image interpretation n
Notto be confused with brain or skull metastases
Slow or absent renal clearance from blood pool owing to kidney disease
Usually faint but intensity may be quite variable (not to be confused with lung metastases)
Uptake may be intense, breast feeding must cease before scintigraphy as signifi- cant 131-1 may be transferred to the infant
The uptake by normal residual thyroid tissue or functioning thyroid cancer deposits is usually very obvious
Unusual cause for focal uptake in right upper quadrant may be discharged into gut by gallbladder contraction
Knowledge of normal biodiatribution required for image interpretation, restudy after swallow of water
Secretion in tears
balance between tubular secretion and reabsorption such that the urine is the principal route of 131-1 excretion. 2,4,2],91-93 Clearance of 131-I is delayed in patients on dialysis. 93-97 Urinary iodide concentra- tion or excretion rates are a good index of the state of iodine nutrition.
Thyroid hormones undergo metabolic degrada- tion and excretion in conjugated form into the gut. 4,69 Hence, 131-1 uptake by the liver several days after 131-1 administration is an index of the amount of functioning (hormone synthesizing) tis- sue present. 4,69,73,91,98-101 The gallbladder may occa- sionally be depicted when biliary excretion is extensive. 4,73,91,1~ The majority of the various io- dine-containing compounds excreted via the liver undergo further metabolism and reabsorption with reutilization in an enterohepatic circulation. 4,73,91,98-1~
After the prompt and efficient absorption of 131-I in the upper gastrointestinal tract, the anion is carried to all tissues of the body via the circulation and, particularly at earlier imaging time points, 131-I within the vascular compartment may be visualized. ~,a~ Examples of artifactual cardiovascu- lar depictions include the heart and great vessels, particularly in the presence of pectus excavatum and carotid ectasia. 2,4,18,7~176 In the face of renal insufficiency, clearance from the vascular compart- ment will be delayed.
ARTIFACTS RELATED TO CONTAMINATION BY PHYSIOLOGICAL SECRETIONS
A wide variety of potentially misleading artifacts can arise from contamination by physiological or pathological secretions derived from those organs that

131-1 SCAN ARTIFACTS 119
A �9 -.c ~
C , . , . . : .
Fig 3. Diagnostic scan of 2 mCi of 131-1 in a patient 1 week after weaning after 18 months of lactation. Some milk could sti l l be expressed from the breasts. (A) Anterior, (B) lef t lateral, and (C) right lateral images of the neck and chest, showing {B) intense bilateral breast uptake, and ST, normal gastric uptake. This clearly showed that a delay of much longer than 1 week after weaning is required for resolution of breast uptake of 131-1.
are capable of uptake and excretion of 131-1 (Table 3). These include urine, saliva (Fig 4), nasal secretions, other respiratory tract secretions, sweat, vomit, and breast milk. 1,10,19,61,63-65,68-70,72-75,77,79,82,87,88,90,92,105-123 Any
focus of 131-I uptake for which there is not an obvious physiological or pathological causation must be sus- pected as arising from contamination by secretions. The patient should always be imaged in a clean gown and, if necessary, this should be replaced after an attempt is made to wash away any unex- plained 131-I foci. 92'106'113'124"126
Irritants or foreign bodies may exaggerate this phenomenon such as tracheostomy tubes, bronchitis, nose rings, ocular prosthesis, chewing gum, or chewing tobacco, tt,88,112,t13:t8,119 Unless sweating is excessive and owing to fever or high environmental temperature, this route of excretion is seldom prominent but may be increased in cystic fibrosis. 1~176176176
ARTIFACTS RELATED TO ECTOPIC GASTRIC MUCOSA
The ability of gastric mucosa to concentrate 131-1 is a prominent feature on whole body 131-1 scintigraphy and this property is retained by ectopic gastric mucosa (Table 4). 4'16'18'69'86'127"138 Ectopic
gastric mucosa may arise de novo as an abnormal- ity of embryological development in diverticuli (eg, Meckel's), or in duplication cysts almost anywhere along the foregut and midgut, or as a component of ovarian or other teratomas.41.86,127,129 Chronic inflammatory changes may cause meta- plastic transformation of gastrointestinal epithe- lium of various types to gastric mucosa (eg, squamous to gastric mucosa in Barrett's esophagus and gastric metaplasia in chronic colitis). 138 Finally, normal gastric mucosa may be anatomically dis- placed to abnormal anatomic sites. Mechanisms for this phenomenon include a hiatus hernia (Fig 5A and B) and surgeries such as a gastric pull- through.4,16,18,86A29-133,135-137
ARTIFACTS RELATED TO ABNORMALITIES OF GASTROINTESTINAL UPTAKE OTHER THAN
ECTOPIC GASTRIC MUCOSA
A variety of pathophysiological processes other than active gastric transport of 131-1 may result in altered 131-I biodistribution (Table 5). These in- clude active concentration by salivary glands with secretion into saliva with subsequent abnormal transfer of the radioactivity into upper gastrointesti- nal diverticuli, delay by mechanical esophageal stric- ture, or dysmotility. 4,14,16,28,62,69,80,86,113,119,126,139-142 When
131-I is used in capsule form rather than in solu- tion, poorly dissolved capsules may be retained

120 SHAPIRO ET AL
Table 3. Contamination by Physiological Secretions
Mechanism for 131-1 Uptake (Consequence Sources of Contamination by of Normal Physiological Concentration Comments Regarding
Physiological Secretions or Route of Excretion) Normal 131-1 Biodistribution
Urine (see Figure 1 )19,92,105-115 Major route of 131-1 excretion Clothing must be changed just before scanning, attempts to wash away unex- plained foci should always be made if there is any suspicion of contamination (not to be confused with pathological uptake)
Typically onto hair, skin, clothing; may be seen on neurosurgical immobilization frame
Saliva (see Figure 1 )60,75,90,112,113,115-117
Nasal secretions 63,70,73,74,82,90,110,111,113"115
Nasal secretions on nose ring TM
Respiratory secretions (especially if there is a tracheostomy) (see Figure 9)113.~1s.119
Sweat 105,108.109,113,120
Vomit89.113
Breast mi l k 1,61,64,65,68,69,72,77,87,88,121"123
Lacrimal, on artificial eye ss.9~ Chewing gum and chewing tobacco 1~2
External contamination (source unknown) 92,1~
Active 131-1 transport into saliva
Active 131-1 transport by mucus glands Active 131-1 transport by mucus glands
and drying on ring Active 131-1 transport by mucus glands
Active 131-1 transport into sweat
Active 131-1 transport into gastric secre- tions
Active 131-1 transport into milk (iodine is an essential micronutrient for the infant)
Active 131-1 transport into tears Stimulate salivation with transport of 131-1
saliva Origin of skin or clothing contamination not
always obvious
Sweat iodide excretion may be greater in cystic fibrosis
Vomiting may occur as a side effect of 131-1 therapy
Activity may be transmitted to infant
Could be washed off prosthesis Gum, tobacco quid, and expectorated saliva
may cause extensive contamination Contamination above the waist usually
saliva or nasal secretion, below waist often urine
in the esophagus under these circumstances. 143 Asymmetrical depiction of the salivary glands them- selves may follow ductal obstruction owing to stone (Fig 6), stricture, or tUlTIOr. 4'6'8'14'16'28'60'69,71,143-148 Prior
surgery or radiotherapy may reduce salivary gland 13 1-I uptake and this may be asymmetrical, lntralumi-
nal 13 1-I within the upper gastrointestinal tract is derived from swallowed saliva or active gastric secretion and can be refluxed into the esopha- gus. 4'16'62'69'80'86'127'142'144'145 This phenomenon is ex-
tremely common and to distinguish esophageal reflux activity from mediastinal nodal metastases,
Fig 4. (A) Anterior and (B) posterior views of the neck and chest in a patient 6 weeks after a near-total thyroidectomy for papillary thyroid cancer obtained 24 hours after 2 mCi 131-1 tracer dose shows (s) normal salivary gland uptake and (M) mouth activity. There was extensive salivary contamination of the shirt over the patient's shoulder (arrowhead) and a prominent halo around the heart owing to a pericardial effusion caused by hypothyroidism (small arrows).

131-1 SCAN ARTIFACTS 121
Table 4. Uptake by Ectopic Gastric Mucosa
Comments Regarding Normal Function of Gastric Sites of Uptake by Mucosal (Normal Gastric Mucosal Uptake Is One of the
Ectopic Gastric Mucosa Mechanism for 131-1 Uptake Most Prominent Features on the Postthyroidectomy 131-1 Scan)
Meckel's diverticulum 4,1z7 Owing to normal active 131-I Gastric mucosa at abnormal site
transport into gastric
secretions n Gastric duplication cysts (may occur in
esophagus, duodenum, small bowel)4,86,129
Normal stomach in abnormal locations (hiatus hernia, gastric pull through) (see Figure 5A and [3) 4"1e.18,e6A2~'137
Ba rrett's esophagus 13s
Gastric mucosa at abnormal site
Displacement of stomach from normal site
Gastric mucosa present at abnormal site in esophagus
studies must be performed after a drink of wa- ter. 3'4'6'8'14'86'138 In resistant cases, the patient may have to be studied while sitting upright.
Radioiodine secreted by the stomach, 131-I- labeled metabolites of thyroxine metabolism ex- creted into the bile, and possible direct secretion by colonic mucosa together will often result in promi- nent depicti on of the col on. 1,3,4,7,8,14,91,98,99, i 01,102,149.150
When extensive, this degrades the quality of im- ages owing to possible masking of metastatic sites and decreasing information density elsewhere in
the scan, as well as increasing colonic radiation exposure. 150 The decreased colonic motility, which almost always accompanies the hypothyroidism required for whole body 131-I studies is a major contributing factor. 15o The appropriate use of laxa- tives will remedy this phenomenon. Is~
ARTIFACTS RELATED TO URINARY TRACT ABNORMALITIES
The urinary tract is the principal route of iodide excretion after glomerular filtration of the small
Fig 5. (A) Whole body anterior image obtained 24 hours after a dose of 2 mCi of 131-1 in a patient wi th papillary thyroid carcinoma after a total thyro idectomy and radioiodine abla- tion of thyroid remnants. There is normal uptake of 131-1 in the nasopharynx and salivary glands, stomach (s), and gut (G), and excretion via the bladder (B) as well as a focus above the stomach (arrow) owing to a hiatus hernia_ (This was con- f irmed by a barium study, see Figure 5B.) (B) Barium study showing the presence of a small hiatus hernia.

122 SHAPIRO ET AL
Table 5. Abnormalities of Gastrointestinal Uptake Other Than Ectopic Gastric Mucosa
Mechanism for 131-1 Uptake Sites of Other Abnormalities (Owing to Normal Active 131-1 Comments Regarding Abnormal of Gastrointestinal Uptake Transport Into Secretions) Motility or Structure
Zenker's diverticulum ~39,~4~ Active 131-1 transport into saliva Owing to retention of activity in swal- lowed saliva in diverticulum
Retention of saliva above stricture Delayed clearance from esophagus
Stricture of esophagus 8~176 Achalasia and other causes of esopha-
geal dysmotil ity zs,s2,~ 2s,~4~,~ 4s,147
Poorly dissolved 131-] capsule ~43
Colonic bypass graft of the esopha- gus131,13 7
Gastroesophageal reflux 14,sg,ss,13s
Abnormal location of bowel with normal 131-1 content (eg, diaphrag- matic or other hernias) 69,128,133
Constipation 150
Parotid gland uptake 148
Asymmetrical retention of saliva in sali- vary glands 1'~
Active 131-1 transport into saliva Active 131-1 transport into saliva
Lack of absorption and retention in the esophagus
Active 131-1 transport into saliva and gastric secretions
Active 131-1 transport into gastric secre- tions
Active 13%1 transport into gastric secre- tions and translocation by luminal transport
Active 131-1 transport into gastric secre- tions and translocation by luminal transport to small bowel and colon
Active 131-1 secreted into the lumen in patients with ectasia
Active 131-1 transport into saliva
Often combined with retention of saliva above stricture and delayed clearance from esophagus
Delayed clearance and reflux from stomach
Reflux of gastric activity into esophagus is very common, always rescan after drink of water if mediastinal activity is present
Luminal 131-1 activity observed at abnormal location
Delayed transport of luminal 131-1 activity owing to abnormal colonic motility (may be a result of hypothy- roidism)
Pooling of activity in dilated duct as dis- tinct from diffuse uptake in gland
Owing to obstruction of salivary duct by stone, stricture, or tumor (or absence of normal gland owing to prior sur- gical removal or injury by radiation therapy)
Fig 6. Anterior view of head, neck, and chest 24 hours after a dose of 2 mCi of 131-I after a near-total thyroidectomy for pap- illary thyroid cancer. There was a large thyroid remnant (large ar- row), normal 131-I uptake in the nose (N), mouth (M), parotid glands (P), and right submendibu- lar gland (s). There was increased 131-1 uptake in the left suhman- dibular gland owing to an ob- structing stone (small arrow).

131-1 SCAN ARTIFACTS 123
Table 6. Urinary Tract Abnormalities
Comments Regarding Slow Clearance From Urinary Tract Sites of Urinary Tract Abnormalities Mechanism for 131-1 Uptake or Abnormal Structures in Communication With Urinary Tract*
Hydronephrosis, extrarenal pelvis, and calyectasis 3̀4,6,e,~s,2L24
Renal cysts 2Llsl
Urinary tract diverticuli (eg, affecting renal pelvis, ureter, and bladder) 4,s,s.ls,2~,z4
Urinary tract f istulae ",s,s.ls.2~,9~
Atonic or dilated bladder 4,6's,~s,21,24
Ectopic kidney or transplanted kidney ~.4,s,z~,z4,s~
Renal clearance of 131-1
into the urine as the
major route of
excretion e
Slow clearance from dilated and/or obstructed renal col- lecting system
Cyst communicates with urinary tract or nephrons
Delayed clearance from diverticuli
131-1 in urine transferred to abnormal locations by fistu-
lous communications
Delayed clearance from bladder owing to obstruction or abnormal moti l i ty
Normal renal handling of 131-1 at abnormal location
*Simultaneous imaging of urinary tract with suitable radiopharmaceutical (eg, Tc-99m-DTPA or Tc-99m MAG3) may be helpful.
anion and a balance between tubular secretion and reabsorpfion (Table 6). 2-4J5'~7"21"86 Thus, the urine within the bladder is often the most radioactive site on the whole body 131-I scan, particularly at 24 and 48 hours postadministration. 2,3,~-8,14,18,2L86J16 As a consequence of this, all dilations, diverticuli, and fistulae of the kidney, ureter, and bladder may show focal 131-I retention.3,4,6-8,14.21:24,86,116 The same is true of ectopic, horseshoe and transplanted kidneys. 21 Renal cysts may show 131-I uptake if they communicate with the urinary tract or if the epithelium, which lines them, has the capacity to concentrate and secrete iodide. 21,151 The simulta- neous depiction of the urinary tract with a suitable renal tract-imaging agent such as 99mTc-DTPA or 99mTc-MAG3 may be useful in characterizing the nature of these urinary tract abnormalities.
ARTIFACTS RELATED TO MAMMARY VARIATIONS AND ABNORMALITIES
The glandular epithelium of the breast during lactation is capable of actively transporting the
essential micronutrient iodide from plasma into milk with an efficiency of 20 to 1 (Table 7) . 15,16,61,64.65,68,69,72,77,79,87,88,12 I- 123,156-158 The lactat-
ing breast shows intense 131-I uptake. 4,13, i 6,61,64- 66,68,69,72,77-79,82,84,90 This is under systemic hormonal
influence including priming by estrogens, secretory stimulation by prolactin, and milk ejection by oxytocin, which acts on both breasts. In addition, local reflex secretory stimulation occurs in that 131-I uptake is greater in the breast which is stimulated in asymmetrical or unilateral suckling. The phenomenon of breast uptake persists for weeks or even months after lactation ceases, Faint to moderate 13 I-I uptake is also seen in nonlactat- ing breast tissue presumably owing to the same epithelial mechanism that operates in lacta- tion.4,]6.67.st,83,84 This phenomenon may be symmetri-
cal or asymmetrical and may also be seen in unilateral mammary hypertrophy, supernumery breasts, and lactational duct cysts (Figs 7 and 8).81,83.89.152-155
Table 7. Mammary Abnormalities
Mechanism for 131-1 Uptake Sites of (Breast Duct Epithelium Actively Comments Regarding Related
Mammary Abnormalities Transports 131-1 Into the Lumen) Abnormalities of Location or Structure
Unilateral mammary hyper- Site of active 131-1 transport Asymmetrical exaggeration of normal breast uptake t rophySLSS.ls2.1ss
Supernumerary breast s9 Site of active 131-1 transport
Site of active 131-1 transport
Site of active 131-1 transport
Asymmetrical lactation sS,ls2.1~
Lactational duct cyst ls5
Additional foci of breast tissue may be found from axilla
to groin
Asymmetrical suckling may stimulate 131-1 uptake into
breast with greatest milk secretion Cyst may be lined with epithelium able to transport 131-1
into cyst lumen

124 SHAPIRO ET AL
B
Fig 7, Diagnostic 131-1 scans. of the chest performed 24 hours after a 2 mCi tracer dose in a pat ient w i th a previously re- sected papil lary thyroid carci- noma (A, anterior, B, left lateral). There is a small intense focus of activity that corresponded to a palpable breast cyst. After aspira- t ion of the cyst f luid contents the uptake disappeared as shown in C (anterior) and D (left lateral}, which are images obtained for lesser total counts. This indi- cates that the vast majori ty of the 131-1 activity was in the cyst fluid. Normal gastric uptake (s).
ARTIFACTS RELATED TO UPTAKE IN SEROUS CAVITIES AND CYSTS
The epithelia lining pleura, peritoneum, and pericar- dium are not able to actively transport 131-I but may be permeable to passive diffusion even in the absence of
inflammation (Table 8). This leads to the accumulation of 131-I in pleural, peritoneal and pericardial effusions, scrotal hydroceles, and pleuropericardial cystS. 19'159-163
Similar processes appear to operate in ovarian cysts and lymphoepithelial cysts. 161'162
Fig 8. (A) Anter ior and (B) poster ior head, neck, and chest views 24 hours after administrat ion of a dose of 2 mCi of 131-1 in a patient wi th papil lary thyroid cancer after a prior thyroidectomy. Note thyroidal bed 131-1 uptake (arrow) and normal stomach (ST), salivary gland (s), and mouth (M) uptake. There is intense 131-1 uptake in the right breast (B) (note clear visualization anteriorly and not posteriorly). The patient had ceased breast feeding just before tracer administrat ion but for months had only been feeding her infant on the r ight breast, Thus, al though the hormonal miiMu of both breasts was the same (eg, prolactin levels) the local effect of suckling was important in 131-1 uptake by the lactating breast.

131-1 SCAN ARTIFACTS 125
Table 8. Uptake in Serous Cavities and Cysts
Sites of Uptake in Comments Regarding Diverse Locations and Serous Cavities or Cysts Mechanism for 131-1 Uptake Factors That May Be Involved
Pericardial effusion (not associated with Cysts are lined by epithelia not able to May be associated with hypothyroidism inflammation; also see Table 9) ~6,~69,~6~ actively transport 131-1; passive diffu-
sion into cyst fluid with subsequent slow c l e a r a n c e
Scrotal hydrocele ls~
Lymphoepithelial cysts 161 Ovarian cysts ~62
Pleuropericardial cysts ~63
Must be distinguished from urinary contamination
This does not include lesions (terato- mas) with ectopic gastric, salivary gland, or thyroid epithelium
ARTIFACTS RELATED TO UPTAKE IN SITES OF INFLAMMATION OR INFECTION
Inflammation, whether it be sterile (autoimmune, traumatic, or ischemic) or owing to infection, results in increased blood flow caused by vasodila- tion, increased capillary permeability owing to the complex interplay of various inflammatory cells, immune mediators, lymphokines, and other sys- temic and paracrine mediatory factors (Table 9).
This results in the accumulation of 131-1 at the sites of a wide variety of inflammatory and infectious processes in which increased blood flow delivers increased levels of 131-1 to the site, which then diffuses through the capillaries that are rendered highly permeable and then accumulates in the increased extracellular water space (edema fluid) (Fig 9). 1.6,12,19,20,90,117,145,160,161,164"175 These pro-
cesses seem to be independent of the active iodide
Table 9. Uptake in Sites of Inflammation or Infection
Comments Regarding Diverse Uptake in Sites of Locations Possible (Inflammatory
Inflammation/Infection Mechanism for 131-1 Uptake Process Need Not Be Infectious in Cause)
Pulmonary (eg, rheumatoid lung, Inflammation results in increased perfu- Increased production of mucus may be an bronchiectasis, fungal infection, sion, vasodilation, end capillary perme- additional factor or acute respiratory tract infec- ability tion)2O,9O,164-1s6
Perica rditislg, llT,lSo,~s~ Skin burns ~61 "
Dental disease/peridontal surgery ~z.167"169 ArthrRis (eg, rheumatoid) ~ss Chronic sinusitis 1,9~176
Dacryocystitis ~,90
Psoriatic plaques s Acute or chronic cholecystitis ~7~ Scalp folliculitis ~72 Sialoadenitis 14s Recent myocardial infarct ~v3
Infected sebaceous cyst 171,174
Frontal sinus mucocele 17~
Site of needle biopsy 175
r
Increased capillary permeability and inflammation in region of infarcted myo- cardium implies coronary redistribution
Inflammation results in increased perfu- sion, vasodilation, and capillary perme- ability
Frequently autoimmune in cause Need not be infected to show 131-1 uptake May not be clinically evident Usually noninfected inflammatory lesion Increased production of mucus may be an
additional factor Increased uptake in gland beyond that
owing to concentration in tears Noninfected inflammatory lesion Biliary excretion may also occur
Should not be confused with normal gastric uptake of 131-1 or activity in a hiatus hernia
Sebaceous glands may also concentrate 131-1
Sinus mucosa capable of iodide transport To be distinguished from acute or chronic sinusitis
Inflammation at site of trauma Uninfected inflammation

126 SHAPIRO ET AL
Fig 9. (A) Anterior and (B) posterior head, neck, and chest views obtained 3 days after a 175-mCi therapy dose of 131-1 6 weeks after a total thyroidectomy and tracheostomy for an invasive papillary carcinoma that had infiltrated the larynx. There was normal uptake of 131-1 in the salivary glands (s) and nasopharynx (N). There was intense uptake of 131-1 in the region of the thyroid bed and tracheostomy (large arrowheads) and faint abnormal uptake of 131-1 throughout the tracheobronchial tree, which had the appearance of an inverted Y (small arrows). This was caused by tracheobronchitis associated with the tracheostomy.
transport seen in thyroid, gastric, salivary, and other �9 " 16 specialized epltheha.
ARTIFACTS RELATED TO UPTAKE BY NONTHYROIDAL NEOPLASMS
A wide variety of nonthyroidal neoplasms have been shown to have 131-1 uptake, albeit per-
haps only in a minority of such lesions (Table 1 0 ) . 44-51'53'64'67'161"162"t76-19! The mechanisms for this
uptake are probably diverse and include (1) the increased vascularity and capillary permeability similar to that seen in inflammation and infection (these include meningiomas, ovarian adenocarci- noma and cystadenoma, uterine fibroma [Fig 10],
Table 10. Uptake by Nonthyroidal Neoplasms
Comments Regarding Both Primary and Sites of Nonthyroidal Neoplasms Mechanism for 131-1 Uptake* Metastatic Tumors
Gastric adenocarcinoma 67,~76,177 Gastric mucosa actively transports 131-1 Probably owing to preservation of
Meningioma17S, 17~ Lung cancer (adenocarcinoma, oat cell
carcinoma, and squamous cell carci- noma)iS1.176,180-183
Salivary adenocarcinoma (Warthin's tumor} 184
Ovarian adenocarcinoma and ovarian cystadenoma 162
Ovarian teratoma (benign or malig- nant)44-s1.53.185-188
normal gastric mucosal active iodide uptake mechanisms
This would explain uptake in adenocar- cinoma but not squamous or oat cell cancers
Other salivary tumors are less likely to show 131-1 uptake; must be distin- guished from uptake owing to ductal obstruction
Mechanism differs from that in ovarian teratomas
"nssues that normally take up 131-1 may differentiate in such tumors
Teratomas at other sites (benign or malignant) 189
Uterine f ibromyoma (see Figure 10)
Abdominal neurilemoma 67,19~
Mechanism unclear (highly vascular) Bronchial mucus glands actively trans-
port 131-1
Salivary glands actively transport 131-1
Mechanism unclear
Owing to uptake of 131-1 into salivary gland, gastric mucosa, or thyroid gland tissue present in tumor
Owing to uptake of 131-1 into salivary gland, gastric mucosa, or thyroid gland tissue present
Mechanism unclear
Mechanism unclear
33ssues that normally take up 131-1 may differentiate in such tumors
May be difficult to separate from bladder and bowel activity
May be difficult to separate from bladder and bowel activity
*Some, by no means all, of these tumors are derived from tissues that can normally concentrate 131-1,

131-1 SCAN ARTIFACTS 127
B C
Fig 10. Diagnostic studies performed 24 hours after a dose of 2 mCi of 131-1 as part of a metastatic survey in a patient after a total thyroidectomy for papillary thyroid cancer. There was intense and extensive gut radioactivity (G) owing to the constipation caused by the hypothyroidism required in preparation for the scan. There was normal urinary excretion of 131-1 through the bladder (B) and urinary contamination of the vulva. There was also a large abnormal focus of 131-1 uptake in the anterior pelvis (T), which was quite separate from the gut and bladder and best seen on the (A) anterior and (C) right anterior oblique projections. On the (B) posterior projection the focus was much fainter, indicating a relatively anterior location. The abnormal 131-1 uptake was in a large fibroid uterus, which rose out of the pelvis.
neurilemoma)67,162,179,187,19~ and (2) many of the
tumors are derived from epithelia that show normal physiological iodide transportJ 6 These include gastric adenocarcinoma, bronchial adenocarcinoma, salivary adenocarcinoma, ovarian and other teratomas con- taining gastric, salivary, thyroid, and similar tis- sues.44-51,53,65,161,176,177,180-184,186-189
CURRENTLY UNEXPLAINED SITES OF ARTIFACTUAL UPTAKE
There remain a few reports of focal 131-I uptake in postthyroidectomy patients for which there re- mains no obvious physiological or pathophysiologi- cal explanation (Table 11). The uptake of 131-I in normal or hyperplastic thymic tissue remains unex- plained because there does not seem to be a well-defined iodine uptake mechanism in the thy- mus. 192-2~176 Focal uptake of 131-I at sites of poren- cephaly and cerebral malacia occurring up to 25 years after the original cerebral injury remain
unexplained but may relate to ongoing chronic inflammation.2~176176
CONCLUSIONS
This classification and organization of artifacts, anatomic and physiological variants, and non- thyroidal d i seases caus ing f a l s e - p o s i t i v e whole body 131-I scans in thyroid cancer patients and in the correct interpretation of both diagnostic and posttherapeutic 131-I studies gives access to an extensive and scattered literature. This pro- vides a single compendium of the available English language literature on the subject at the millenium. This organizational schema is offered as a means to interpret and clarify additional future observations in this area, which will undoubtedly continue to accrue.
Acknowledgement: The authors wish to thank Judith A. Csoka for assistance in the preparation of the text.
Table 11, Currently Unexplained Sites of Uptake
Factors to Be Considered in Other Sites and Causes Mechanisms for 131-1 Uptake Otherwise Unexplained Thoracic 131-1
Unexplained thymic uptake 192-2~176 Currently unexplained May be associated with a mediastinal mass at CT scan owing to thymic hyperplasia
" To be considered in otherwise unexplained thoracic 131-1
Trauma occurred 25 years earlier
Unexplained mediastinal uptake (? normal variant) 19s,197
Unexplained uptake at site of porencephaly TM
Posttraumatic cerebral malacia 2~176 Possible chronic inflammation of cerebral or overlying tissues
Prior surgery for cerebral abscess 25 years earlier

128 SHAPIRO ET AL
REFERENCES 1. Bakheet SM, Hammami MM: False positive radioiodine
whole-body scan in thyroid cancer patients due to unrelated pathology. C/in Nucl Med 19:325-329, 1994
2. Berson SA, Yallow RS: Quantitative aspects of iodine metabolism: The exchangeable organic iodine pool and the rates of thyroid secretion, peripheral degradation and fecal excretion of endogenously synthesized organically bound iodine. J Clin Invest 33:1533-1552, 1954
3. Cavalieri RR: Nuclear imaging in the management of thyroid carcinoma. Thyroid 6:485-492, 1996
4. Datz FL: Gamuts in Nuclear Medicine (ed 3). St. Louis, MO, Mosby-Yearbook, 1995, pp 14-15, 27-34
5. Echenique R, Kasi L, Haynie TP, et al: Critical evaluation of serum thyroglobulin levels and 1-131 scans in post-therapy patients with differentiated thyroid carcinoma: Concise commu- nication. J Nucl Meal 23:235-240, 1982
6. Fogelman I, Maisey MN: The thyroid scan in the manage- ment of thyroid disease, in Freeman LM, Weissmann HS (eds): Nuclear Medicine Annual, New York, Raven Press, 1989, pp 1
7. Freitas JE, Gross MD, Ripley S, et al: Radionuclide diagnosis and therapy of thyroid cancer: Current status report. Semin Nucl Med 15:106-131, 1985
8. Johnson PM: Thyroid and whole-body scanning, in Werner SC, Ingbar SH (eds): The Thyroid, A Fundamental and Clinical Text, ed 4, Harper & Row, Hagerston, PA, 1978, pp 247-297
9. Maxon RH; Smith HS: Radioiodine-131 in the diagnosis and treatment of metastatic well differentiated thyroid cancer. Endocrinol Metab Clin North Am 19:685-718, 1990
10. Ramanna L, Waxman AD, Brachman MB, et al: Correla- tion of thyroglobulin measurements and radioiodine scans in the follow-up of patients with differentiated thyroid cancer. Cancer 55:1525-1529, 1985
11. Riggs DS: Quantitative aspects of iodine metabolism in man. Pharmacol Rev 4:283-293, 1952
12. Sutter CW, Masilungan BG, Stadalnik RC: False-positive results of 1-131 whole-body scans in patients with thyroid cancer. Semin Nucl Med 25:279-282, 1995
13. Zalis ED, Ellison RB, Captain MC, et al: A diagnostic pitfall with radioiodine scanning. Am J Roentgeno194:837-838, 1965
14. Wu S, Brown T, Milne N, et al: Iodine-131 total body scan: Extrathyroidal uptake of radioiodine. Semin Nncl Med 16:82-84, 1986
15. Wolff J: Iodide Concentrating Mechanisms, in Roll JE, Kopin IJ, Berson SA (eds): The Thyroid and Biogenic Amines: Methods in Investigative and Diagnostic Endocrinology, vol 1, Amsterdam, North-Holland Publishing Co, 1972, pp 115-203
16. Spitzweg C, Joba W, Eisenmenger W, et al: Analysis of human sodium iodide symporter gene expression in extrathyroi- dal tissues and cloning of its complementary deoxyribonucleic acids from salivary gland, mammary gland, and gastric mucosa. J Clin Endocrinol Metab 83:1746-1751, 1998
17. Wayne EJ, Koutras DA, Alexander WD (eds): Clinical Aspects of Iodine Metabolism. Philadelphia, FA Davis Com- pany, 1964, pp 1-303
18. Greenler DR Klein HA: The scope of false-positive iodine-131 images for thyroid carcinoma. Clin Nucl Med 14:111-117, 1989
19. Geatti O, Shapiro B, Orsolon PG, et al: An unusual false
positive scan in a patient with pericardial effusion. Clin Nucl Med 19:678-682, 1994
20. Bakheet S, Powe J, Hammami M: Radioiodine uptake in the chest. J Nucl Med 38:984-986, 1997
21. Bakheet S, Harnmami M, Powe J: False-positive radioio- dine uptake in the abdomen and the pelvis: Radioiodine retention in the kidneys and review of the literature. Clin Nucl Med 21:932-937, 1996
22. Turlington B: Embryology and anatomy of the thyroid and parathyroid glands, in Eisenberg B (ed): Imaging of the Thyroid and Parathyroid Glands, Churchill Livingstone Inc, New York, 1991, pp 1-8
23. Larochelle D, Arcand P, Belzile M, et al: Ectopic thyroid tissue: A review of the literature. J Otolaryngol 8:523-530, 1979
24. Sloan LW, Feind CR: Clinical aspects of anomalous development, in Weruer SC, Ingbar SH (eds): The Thyroid, Harper & Row, New York, 1971, pp 317-333
25. Weider D J, Parker W: Lingual thyroid. Ann Otol Rhinol Laryngol 86:841-848, 1977
26. Strain J, Oates E, Nejad A: Unusual appearance of lingual thyroid in congenital hypothyroidism. Clin Nucl Med 23:460, 1998
27. Coover L: False-positive result of a total-body scan caused by benign thyroidal tissue after I-131 ablation. Clin Nucl Med 24:182-183, 1999
28. Lin DS: Thyroid imaging--mediastinal uptake in thyroid imaging. Semin Nucl IVied 13:395-396, 1983
29. Leung AKC, Wong AL, Robson WLM: Ectopic thyroid gland simulating a thyroglossal duct cyst: A case report. Can J Surg 38:87-89, 1995
30. Sironi M, Assi A, Andruccioli M, et al: Submandibular ectopic thyroid gland. Clin Nucl Med 21:585, 1996
31. Touliopoulos P, to tes E: Autonomously functioning thyroid rests following total thyroidectomy for Graves' disease. Clin Nucl Med 18:914, 1993
32. Dowling EA, Johnson IM, Collier FCD: Intratracheal goiter: A clinico-pathologic review. Ann Surg 156:258-267, 1962
33. Dundas P: Intrathoracic aberrant goiter. Acta Chir Scand 128:729-736, 1964
34. Fogelfeld L, Rubinstein U, Bar-On J, et al: Severe thyrotoxicosis caused by an ectopic intrathoracic goiter. Clin Nucl Med 11:20-22, 1986
35. Salvatore M, Gallo A: Accessory thyroid in the anterior mediastinum: Case report. J Nucl Med 16:1135-1136, 1975
36. Salvatore M, Rufini V, Corsello SM, et al: Thyrotoxicosis due to ectopic retrotracheal adenoma treated with radioiodine. J Nucl Biol Med 37:69-72, 1993
37. Thakore K, Vansant J: Hyperthyroidism due to toxic, intrathoracic thyroid tissue with absent cervical thyroid gland. Clin Nucl Med 18:535-536, 1993
38. Rieser GD, Ober KP, Cowan R J, et al: Radioiodine imaging of struma cordis. Clin Nucl Med 13:421-422, 1988
39. Aldasouqi S, Edmondson J, Prince M, et al: Carcinoma of thyro-glossal duct remnants: Report of three cases and a review of the literature. The Endocrinologist 6:238-244, 1996
40. Gaby M: The rote of thyroid dysgenesis and maldescent in the etiology of sporadic cretinism. J Pediatr 60:830-835, 1962
41. Gorbman A, Dickhoff WW, Vigna SR, et al: The thyroid

131-1 SCAN ARTIFACTS 129
gland, in Gorbman A (ed): Comparative Endocrinology, John Wiley and Sons, New York, 1983, pp 185-202
42. Myers EN, Pantangco IP: Intratracheal thyroid. Laryngo- scope 85:1833-1840, 1975
43. Postlethwait RN, Detmer DE: Ectopic thyroid nodule in the esophagus. Ann Thorac Surg 19:98-100, 1975
44. Braun WW, Shetty KR, Rosenfeld PS: Hyperthyroidism due to struma ovarii: Demonstration by radioiodine scan. Acta Endocrinol 73:266-272, 1973
45. Falsetti L, Schivardi MR, Maira G, et al: Riscontro di struma ovarii in una paziente in trattamento per carcinoma tiroideo. Ann Ost Gin Med Perin 106:290-293, 1985
46. March DE, Desai AG, Park CH, et al: Struma ovarii:
Hyperthyroidism in a postmenopausal woman. J Nucl Med 29:263-265, 1988
47. Salvatore M, Rufini V, Daudone MS, et ah Occasional detection of "struma ovarii" in a patient with thyroid cancer. Radiol Med (Torino) 81:744-767, 1991
48. Thomas RD, Batty VB: Metastatic malignant struma
ovarii: Two case reports. Clin Nucl Med 17:577-578, 1992 49. Yeh E-L, Meade RC, Reutz PP: Radionuclide study of
struma ovarii. J Nucl Med 14:118-121, 1973 50. Yeh E-L, Meade RC, Ruetz PP: Radionuclide study of
struma ovarii. J Nucl Med 14:118-121, 1973 51. Zwas ST, Heyman Z, Lieberman LM: 1311 ovarian uptake
in a whole-body scan for thyroid carcinoma. Semin Nucl Med 19:340-342, 1989
52. Ziessman HA, Bahar H, Fahey FH, et al: Hepatic visualization on iodine-131 whole-body thyroid cancer scans. J Nucl Med 28:1408-1411, 1987
53. Joja I, Asakawa T, Mitsumori A, et al: 1-123 uptake in non-functional struma ovarii. Clin Nucl Med 23:10-12, 1998
54. Moses DC, Thompson NW, Nishiyama RH, et ah Ectopic thyroid tissue in the neck, benign or malignant? Cancer 38:361- 365, 1976
55. Ryo UY, Stachura ME, Schneider AB, et al: Significance of extrathyroidal uptake of Tc-99m and 1-123 in the thyroid scan: Concise communication. J Nucl Med 22:1039-1042, 1981
56. Sud AM, Gross MD: Radioiodine uptake following thyroidectomy for thyroid cancer: Recurrence or ectopic tissue? Clin Nucl Med 16:894-897, 1991
57. Todino V, Pacella CM, Crescenzi A, et al: Ectopic thyroid tissue in the liver: Case report. Eur J Nucl Med 23:1055, 1996 (abstract)
58. Bakheet S, Powe J, Hammami MM, et al: Isolated porta hepatis metastasis of papillary thyroid cancer. J Nucl Med 37:993-994, 1996
59. Feuerstein IM, Harbert JC: Hypertrophied thyroid tissue in a thyroglossal duct remnant. Clin Nucl Med 11:135, 1986
60. Freinkel KA, Ingbar SH: Concentration gradients for inorganic iodide 1-131 and chloride in mixed human saliva. J Clin Invest 32:1077-1084, 1953
61. Ahlgren L, Ivarsson S, Johansson L, et al: Excretion of radionuclides in human breast milk after the administration of radiopharmaceuticals. J Nucl Med 26:1085-1090, 1985
62. Bakheet S, Hammami MM: False positive thyroid cancer metastasis on whole body radioiodine scanning due to retained radioactivity in the oesophagus. Eur J Nucl Med 20:415-419, 1993
63. Boxen I, Zhang M: Nasal secretion of iodine-131. Clin Nucl Med 15:610-611, 1990
64. Coakley A J, Mountford PJ: Nuclear medicine and the nursing mother. Br Med J 291:159-160, 1985
65. Clode WH, Sobral JMV, Lima-Basto E, et al: Elective uptake of radioiodine by cancer of the stomach. Surgery 50:725-727, 1961
66. Duong RB, Fernandez-Ulloa M, Planitz MK, et ah J231 breast uptake in a young primipara with postpartum transient thyrotoxicosis. Clin Nucl Med 8:35, 1983
67. Ganatra RD, Atmaram SH, Sharma SM: An unusual site of radioiodine concentration in a patient with thyroid cancer (letter). J Nucl Med 13:777, 1972
68. Hedrick WR, DiSimone RN, Keen RL: Radiation dosim- etry from breast milk excretion of radioiodine and pertechnetate. J Nucl Med 27:1569-1571, 1986
69. Honour AJ, Myant NB, Rowlands EN: Secretion of radioiodine in digestive juices and milk in man. Clin Sci (Colch) 11:447-462, 1952
70. Lopez OL, Maisano ER: Vascular retention of Tc-99m pertechnetate simulating ectopic or metastatic thyroid tissue. Clin Nucl Med 8:503-504, 1983
71. Malpani BL, Samuel AM, Ray S: Differential kinetics of parotid and submandibular gland function as demonstrated by scintigraphic means and its possible implications. Nucl Med Commun 16:706-709, 1995
72. Mountford PJ, Coakley AJ: A review of the secretion of radioactivity in human breast milk: Data, quantitative analysis and recommendations. Nucl Med Commun 10:15-27, 1989
73. Neutze JA, Norby EH, VanNostrand D, et al: Nasal radioiodine uptake: A prospective study of frequency, degree, and pattern. Presented at the 34th Annual Meeting. J Nucl Med 28:686, 1987 (Abstract 542)
74. Norby EH, Neutze J, van Nostrand D, et ah Nasal radioiodine activity: A prospective study of frequency, intensity and pattern. J Nucl Med 31:52-54, 1990
75. Park HM, Tarver RD, Schauwecker DS, et al: Spurious thyroid cancer metastasis: Saliva contamination artifact in high dose lodine-131 metastases survey. J Nucl Med 27:634-636, 1986
76. Riccabona G: Differentiated thyroid carcinoma, in Mur- ray IPC, Ell PJ (eds): Nuclear Medicine in Clinical Diagnosis and Treatment. Churchill Livingstone, 1998, pp 941-957
77. Romney B, NicholoffEF, Esser PD: Excretion of radioio- dine in breast milk. J Nucl Med 30:124-126, 1989
78. Romney BM, NicholoffEF: Diagnostic nuclear medicine and the nursing mother. App Radiology 16:51-56, 1987
79. Romney BM, Nickoloff EL, Esser PD, et ah Radionu- clide administration to nursing mothers: Mathematically derived guidelines. Radiology 160:549-554, 1986
80. Schuster DM, Alazraki N: Esophageal scarfing causing false-positive uptake on 1-131 whole-body imaging. Clin Nucl Med 23:334, 1998
81. Hammami MM, Bakheet S: Radioiodine breast uptake in non-breast feeding women. Clinical and scintigraphic character- istics. J Nucl Med 37:26-31, 1996
82. Park HM, Wellman H: Hot nose after 1-131 sodium iodide thyroablation therapy. Clin Nucl Med 17:130-131, 1992
83. Allen T, Wiest P, Vela S, et ah 1-131 uptake in the breast for thyroid cancer surveillance with biopsy-proven benign tissue. Clin Nucl Med 23:585-587, 1998
84. Baemler GR, Joo KG: Radioactive iodine uptake by breasts (letter). J Nucl Med 27:149-151, 1986

130 SHAPIRO ET AL
85. Watanabe N, Matsumoto M, Ohtake H, et al: Bilateral breast uptake of T 1-201 chloride in a nursing woman. Clin Nucl Med 21:818-819, 1996
86. McDougaU IR: Whole body scintigraphy with radioiodine- 131: A comprehensive list of false-positives with some ex- amples. Clin Nucl Med 20:869-875, 1995
87. Robinson PS, Barker P, Campbell A, et al: Iodine-131 in breast milk following therapy for thyroid carcinoma. J Nucl Med 35:1797-1801, 1994
88. Bakheet S, Hammami M, Hemidan A, et al: Radioiodine secretion in tears. J Nucl Med 39:1452-1454, 1998
89. Bakheet SM, Hammami MM: Patterns of radioiodine uptake by the lactating breast. Eur J Nucl Med 21:604-608, 1994
90. Howarth DV, Forstrom LA, O'Connor MK, et al: Patient- related and pitfalls artifacts in nuclear medicine imaging. Semin Nucl Med 26:295-307, 1996
91. Achong DM, Oates E, Lee SL, et al: Gallbladder visualization during post-therapy iodine- 131 imaging of thyroid carcinoma. J Nucl Med 32:2275-2277, 1991
92. Nishizawa K, Ohara K, Ohshima M, et al: Monitoring of iodine excretions and used materials of patients treated with 13 li. Health Phy 38:467-481, 1980
93. Daumerie C, Vynckier S, Caussin J, et al: Radioiodine treatment of thyroid carcinoma in patients on maintenance hemodialysis. Thyroid 6:301-304, 1996
94. Howard N, Glasser M: Iodine-131 ablation therapy for a patient on maintenance haemodialysis. Br J Radio154:259-261, 1981
95. Mello AM, Isaacs R, Petersen J, et al: Management of thyroid papillary carcinoma with radioiodine in a patient with end-stage renal disease on hemodialysis. Clin Nucl Med 19:776- 781, 1994
96. Morrish DW, Filipow JL, McEwan AJ, et al: 131I treat- ment of thyroid papillary carcinoma in a patient with renal failure. Cancer 66:2509-2513, 1990
97. Nibhanupudy JR, Hamilton W, Sridhar R, et al: Iodine- 131 treatment of hyperthyroidism in a patient on dialysis for chronic renal failure. Am J Nephrol 13:214-217, 1993
98. Rosenbaum RC, Johnston GS, Valente WA: Frequency of hepatic visualization during 13!I imaging for metastatic thyroid carcinoma. Clin Nucl Med 13:657-660, 1988
99. Schober B, Cohen P, Lyster D, et al: Diffuse liver uptake of 13/I (letter). J Nucl Med 31:1575-1576, 1990
100. Nodine JH, Maldia G: Pseudostruma ovarii. Obstet Gynecol 17:460-463, 1961
101. You DL, Tzen KY, Chert JF, et al: False-positive whole-body iodine-131 scan due to intrahepatic duct dilatation. J Nucl Med 38:1977-1979, 1997
102. Chung JK, Lee YJ, Jeong JM, et al: Clinical significance of hepatic visualization on 1-131 whole-body scan in patients with thyroid carcinoma. J Nucl Med 38:1191-1195, 1997
103. Muherji S, Ziessman HA, Earll JM, et al: False-positive iodine-131 whole-body scan due to pectus excavatum. Clin Nucl Med 13:207-208, 1988
104. Giuffrida D, Garofalo MR, Cacciaguerra G, et al: False positive 1-131 total body scan due to an ectasia of the common carotids. J Endocrinol Invest 16:207-211, 1993
105. Abdel-Dayem HM, Halker K, E1 Sayed M: The radioac- tive wig in iodine-131 whole-body imaging. Clin Nucl Med 9:454-455, 1984
106. Bakheet SM, Hammami MM: Spurious thyroid cancer
bone metastases on radioiodine scan due to external contamina- tion. Eur J Radiol 16:239-242, 1993
107. Bakheet S, Hammami MM: Spurious lung metastases on radioiodine thyroid and whole body imaging. Clin Nucl Med 18:307-312, 1993
108. Brodkey JS, Gibbs GE: Sweat iodide excretion in patients with cystic fibrosis of the pancreas. J Appl Physiol 15:501-502, 1960
109. Camponovo EJ, Goyer PF, Silverman ED, et al: Axillary iodine-131 accumulation due to perspiration. C/in Nucl Med 14:762-763, 1989
110. Chandramouly BS, Scagnelli T, Burgess CK: Artifact on iodine-131 whole body scan due to contaminated handkerchief. Clin Nucl Med 14:301-302, 1989
111. Dick C, Mudun A, Alazraki NP: False-positive 1-131 images mimicking thyroid cancer metastasis: The nose ring sign. Clin Nucl Med 20:876-877, 1995
112. Gritters LS, Wissing J, Gross MD, et al: Extensive salivary contamination due to concurrent use of chewing tobacco during 1-131 radioablative therapy. Clin Nucl Med 18:115-117, 1993
113. Ibis E, Wilson CR, Collier BD, et al: Iodine-131 contamination from thyroid cancer patients. J Nucl Med 33:2110- 2115, 1992
114. Pochis WT, Krasnow AZ, Isitman AT, et al: The radioactive handkerchief sign: A contamination artifact in I-131 imaging for metastatic thyroid carcinoma. Clin Nucl Med t5:491-494, 1990
115. Carey JE, Kumpuris TM, Wrobel MC: Release of patients containing therapeutic dosages of iodine-131 from hospitals. J Nucl Med Techno123:144-149, 1995
116. Ryo UY, Alavi A, Collier BD, et al: (editors). The thyroid, in Atlas of Nuclear Medicine Artifacts and Variants, Yearbook Medical Publishers, Chicago, 1995, pp 23-33
117. Silva F, Negron JA: Unusual contamination after a therapeutic dose of iodine-131. J Nucl Med 37:70, 75, 1996
118. Ain KB, Shih WJ: False-positive 1-131 uptake at a tracheostomy site: discernment with TI-201 imaging. Clin Nucl Med 19:619-621, 1994
119. Kirk GA, Schulz EE: Post-laryngectomy localization of 1-131 at tracheostomy site on a total body scan. Clin Nucl Med 9:409-411, 1984
120. Joyce WT, Cowan R J: A potential false-positive post- therapy radioiodine scan secondary to I-131 excretion in perspi- ration. Clin Nucl Med 20:368-369, 1995
121. Lawes SC. 123I excertion in breast milk-additional data. Nucl Med Commun 13:570-572, 1992
122. Weaver JC, Kamm ML, Dobson RL: Excretion of radioiodine in human milk. JAMA 173:872-875, 1960
123. Spencer RP, Spitznagle LA, Karimeddini MK, et al: Breast milk content of 131I in a hypothyroid patient. Nucl Med Biol 13:585, 1986
124. Wiseman J: Bony metastasis from thyroid carcinoma or contamination? Clin Nucl Med 9:363, 1984
125. Schechter D, Krausz Y, Moshe S, et al: Radioiodine hot hand sign. Clin Nucl Med 23:378-379, 1998
126. Barzel US, Chun KJ: Artifact of 1-131 whole-body scan with thoracic vertebral uptake in a patient with papillary thyroid carcinoma. Clin Nucl Med 22:855, 1997
127. Caplan RH, Gundersen GA, Abellera M, et al: Uptake

131-1 SCAN ARTIFACTS 131
of iodine- 131 by a Meckel's diverticulum mimicking metastatic thyroid cancer. Clin Nucl Med 12:760-762, 1987
128. Ho Y, Hicks R: Hiatus hernia: A potential cause of false-positive iodine-131 scan in thyroid carcinoma. Clin Nucl Med 23:621-622, 1998
129. Kamoi I, Nishitani H, Oshiumi Y, et al: Intrathoracic gastric cyst demonstrated by Tc-99m pertechnetate scintigraphy. AJR Am J Roentgenol 134:1080-1081, 1980
130. McNamara M, Tsang H: Hiatal hernia with reflux resulting in false positive 1-131 scan. Clin Nucl Med 23:178- 179, 1998
131. Misaki T, Iida Y, Kasayi K, et al: First impressions: Unusual extrathyroidal uptake. J Nucl Med 39:1650, 1998
132. Schneider JA, Divgi CR, Scott AM, et al: Hiatal hernia on whole-body radioiodine survey mimicking metastic thyroid cancer. Clin Nucl Med 18:751-753, 1993
133. Unal S, Oguz H, Alagol F, et al: Misinterpretation of I- 131 scintigraphy because of diaphragmatic hernia. Clin Nucl Med 21:151-152, 1996
134. White JE, Flickinger FW, Morgan ME: 1311 accumula- tion in gastric pull-up simulating pulmonary metastases on total-body scan for thyroid cancer. Clin Nuc Med 15:809-810, 1990
135. Willis LL, Cowan RJ: Mediastinal uptake of 1-131 in a hiatal hernia mimicking recurrence of papillary thyroid carci- noma. Clin Nucl Med 18:961-963, 1993
136. Bekis R, Durak H: Intrathoracic stomach causing a pitfall on thyroid imaging. Clin Nucl Med 23:848-849, 1998
137. Ceccarelli C, Pancini F, Lippi E et al: An unusual case of a false-positive iodine- 131 whole-body scan in a patient with papillary thyroid cancer. Clin Nucl Med 3:192-193, 1987
138. Berquist TH, Nolan NG, Stephens DM, et ah Radioiso- tope scintigraphy in diagnosis of Barrett's esophagus. A JR Am J Roentgenol 123:401-411, 1971
139. Boulahdour H, Meignan M, Melliere D, et al: False- positive 1-131 scan induced by Zenker's diverticulum. Clin Nucl Med 17:243-244, 1992
140. Dhawan VM, Kaess KR, Spencer RP: False positive thyroid scan due to Zenker's diverticulum. J Nucl Med 19:1231- 1232, 1978
140a. Kistler AM, Yudt WM, Bakalar RS, et al: Retained esophageal activity on iodine- 131 survey in patient with benign esophageal stricture. Clin Nucl Med 18:908-909, 1993
141. Ozdemir A, Gungor F, Ozugur S, et al: Abnormal iodine-131 uptake in the mediastinum caused by achalasia. Clin Nucl Med 23:706-707, 1998
142. Grossman M: Gastroesophageal reflux: A potential source of confusion in technetium thyroid scanning: Case report. J Nucl Med 18:548-549, 1977
143. Robertson JS, Verhasseet M, Wahnet HW: Use of 1231 for thyroid uptake measurements and depression of 131I thyroid uptake by incomplete dissolution of capsule filler. J Nucl Med 15:770-774, 1974
144. Kipper MS, Krohn LD: Increased submandibular gland uptake on thyroid scintigraphy due to Wharton's duct stone. Clin Nucl Med 21:881-882, 1996
145. Kolla IS, Alazraki NP, Watts NB: Sialoadenitis mimick- ing metastatic thyroid carcinoma. Clin Nucl Med 14:564-566, 1989
146. Tyson JW, Wilkinson RH, Witherspoon LR, et al:
False-positive 1-131 total body scans. J Nucl Med 15:1052- 1053, 1974
147. Wendell TJ, Wilkinson RH, Witherspoon LR, et al: False positive 1311 total-body scans. J Nucl Med 15:1052-1053, 1974
148. Wolff H, Breda DJ, DaSilva N, et ah False-positive I-131 deposition in a parotid gland duct ectasia. Clin Nucl Med 23:257-259, 1998
149. CarlisleM, CortesA, McDougalllR: Uptake ofl-131 in the biliary tract: A potential cause of a false-positive result of scintiscan. Clin Nucl Med 23:524-527, 1998
150. Schall GL, Temple R: Importance of proper bowel cleansing before 1-131 whole body scan or retention study. J Nucl Med 13:181-182, 1972
151. Brachman MB, Rothman BJ, Ramanna L, et al: False- positive iodine-131 body scan caused by a large renal cyst. Clin Nucl Med 13:416-418, 1988
152. Bakheet MS, Powe J, Hammami MM: Unilateral radio- iodine breast uptake. Clin Nucl Med 23:170-171, 1998
153. Robinson PS, Surveyor I: Response to letter: Unilateral iodine-131 uptake in the lactating breast. J Nucl Med 36:1725, 1995
154. Griinwald F, Palmedo H, Biersack HJ: Unilateral iodine- 131 uptake in the lactating breast. J Nucl Med 36:1724-1725, 1995
155. Serafini A, Sfakianakis G, Georgiou M, et al: Breast cyst simulating metastases of iodine-131 imaging in thyroid carci- noma. J Nucl Med 39:1910-1912, 1998
156. Blue PW, Dydek GJ, Ghaed N, et al: Radiation dosim- etry from breast milk excretion of iodine-123. J Nucl Med 28:544-545, 1987
157. Numberger CE, Lipscomb A: Transmission of radioio- dine (I-131) to infants through human maternal milk. JAMA 150:1398-1400, 1952
158. Rubow S, Klopper J: Excretion of radioiodine in human milk following a therapeutic dose of 13tl. Eur J Nucl Med 14:632-633, 1988
159. Maslack MM, Wilson CA: Iodine-131 accumulation in a pericardial effusion (letter). J Nucl Med 28:133, 1987
160. Silva F, Garcia L, Flores C, et al: Pericardial effusion: Unusual complication in thyroid cancer. Clin Nucl Med 21:218- 220, 1996
161. Haubold-Reuter BG, Landolt U, Schulthess GKV: Bron- chogenic carcinoma mimicking metastatic thyroid carcinoma. J Nucl Med 34:809-811, 1993
162. Kim EE, Pjura G, Gobuty A, et al: 131-I uptake in a benign serous cystadenoma of the ovary. Eur J Nucl Med 9:433-435, 1984
163. Francese C, Schlumberger M, Travagli JP, et al: Iodine- 131 uptake in a pleuropericardial cyst: Case report of a false-positive radioiodine total body scan result in a patient with a thyroid cancer. Eur J Nucl Med 18:779-780, 1991
164. Bakheet SM, Hammami MM, Powe J: Radioiodine bronchogram in acute respiratory tract infection. Clin Nucl Med 22:308-309, 1997
165. Bakheet SM, Hammami MM, Powe J: Radioiodine uptake in rheumatoid arthritis-associated lung disease mimick- ing thyroid cancer metastases. Clin Nucl Med 23:319-320, 1998
166. Hrschl R, Choy DHL, Grandevia B: Iodine-131 uptake in inflammatory lung disease: A potential pitfall in treatment of thyroid carcinoma. J Nucl Med 29:701-706, 1988

132 SHAPIRO ET AL
167. Herzog G, Kisling G, Bekerman C: Diagnostic signifi- cance of dental history in the clinical evaluation of patients with thyroid carcinoma: Periodontal surgery mimicking a metastasis on 1-131 whole-body survey. Clin Nucl Med 17:589-590, 1992
168. Wadhwa SS, Mansberg R: Benign oral disease as a cause of false-positive iodine- 131 scans. Clin Nucl Med 23:747- 749, 1998
169. Otsuka N, Fukunaga M, Morita K, et al: 131I uptake in patient with thyroid cancer and rheumatoid arthritis during acupuncture treatment. Clin Nucl Med 15:29-31, 1990
170. Matheja R Lerch H, Schmid K, et al: Frontal sinus mucocele mimicking a metastasis of papillary thyroid carci- noma. J Nucl Med 38:1022-1024, 1997
171. Brucker-Davis F, Reynolds JC, Skarulis MC, et al: False-positive iodine-131 whole-body scans due to cholecystitis and sebaceous cyst. J Nucl Med 37:1690-1693, 1996
172. Kinuya S, Yokoyama K, Michigishi T, et al: 1-131 accumulation in folliculitis of the scalp. Clin Nncl Med 21:807- 808, 1996
173. Froncova K, et al: Uptake of radioiodine by myocar- dium following infarction. Cas Lek Cesk 103:64, 1964, quoted by Bmcer M, in: Nuclear Cardiology-coronary and myocardial phase. Vignettes in Nuclear Medicine No. 89, Mallinkrodt Inc, St. Louis, MO, 1978, p 9
174. Turoglu HT, Naddaf S, Young I, et al: Infected seba- ceous cyst: A cause for false-positive total-body I- 123 metastatic survey for thyroid cancer. Clin Nucl Med 23:887, 1996
175. Naddaf S, Akisik MF, Omar WS, et al: 1-123 uptake in the chest wall after needle biopsy of a pulmonary nodule. Clin Nucl Med 22:572-573, 1997
176. Langsteger W, Ktiltringer E Meister E, et al: False- positive scans in papillary thyroid carcinoma (letter). J Nucl Med 34:2280, 1993
177. Wu S, Kollin J, Coodley E, et al: 1-131 total body scan: Localization of disseminated gastric adenocarcinoma. Case report and survey of the literature. J Nucl Med 25:1204-1209, 1984
178. Berding G, Forsting M, Georgi P: Unspezifische spei- chergung in J-131-Ganzk6rperszintigramm bei de Nachsorge eines metasterierienden papill~en SchilddriJsencarcinoms bed- ingt durch ein meningeom. Nuc Compact 21:163-164, 1990
179. Preisman RA, Halpern SE, Shishido R, et al: Uptake of 131-1 by a papillary meningioma. AJR Am J Roentgenol 128:349-350, 1977
180. Acosta J, Chitkara R, Kahn F, et al: Radioactive iodine uptake by a large ceil undifferentiated bronchogenic carcinoma. Clin Nucl Med 7:368-369, 1982
181. Femandez-Ulloa M, Maxon HR, Mehta S, et al: Iodine- 131 uptake by primary lung adenocarcinoma, misinterpretation of 13lI scan. JAMA 236:857-858, 1976
182. Langsteger W, Lind R K61tringer R et al: Misinterpreta- tion of iodine uptake in papillary thyroid carcinoma and primary lung adenocarcinmna. J Cancer Res Clin Oncol 116:8-12, 1990
183. Misaki T, Takeuchi R, Miyamoto S, et al: Radioiodine uptake by squamous-cell carcinoma of the lung. J Nncl Med 35:474-475, 1994
184. Burt RW: Accumulation of 123-1 in a Warthin's tumor. Clin Nucl Med 3:155-156, 1978
185. Harbert JC: Radio iodine therapy of differentiated thyroid carcinoma, in Harbert JC, Robertson JS, Held KID (eds): Nuclear Medicine Therapy, Thieme Medical Publishers Inc, New York, 1987, pp 37-89
186. Wynne HMN, McCartney JC, McClendon JF: Struma ovarii. Am J Obstet Gyneco139:263-275, 1940
187. Willemse PHB, Oosterhuis JW, Aalders JG, et al: Malignant struma ovarii treated by ovariectomy, thyroidectomy and 1-131 administration. Cancer 60:178- t 82, 1987
188. Brenner W, Bohuslavizki KH, Wolf H, et al: Radio- therapy with iodine-131 in recurrent malignant stmma ovarii. Eur J Nucl Med 23:91-94, 1996
189. Lakshmanan M, Reynolds JC, DelVecchio S, et al: Pelvic radioiodine uptake in a rectal wall teratoma after thyroidectomy for papillary carcinoma. J Nucl Med 33:1848- 1850, 1992
190. Wang PW, Chen HY, Li CH, et al: Uptake of 1-131 by an abdominal neurilemoma mimicking metastatic thyroid carci- noma. Clin Nucl Med 18:964-966, 1993
191. Wilson RL, Cowan R J: Tc-99m pertechnetate uptake in a thymoma: Case report. Clin Nucl Med 7:149-150, 1982
192. Bestagno M, Pagliavni R, Maira G, et al: Mediastinal uptake of 131I in patients with thyroid cancer: may it be referred to normal thymus? Eur J Nucl Med 20:648, 1993 (ahstr)
193. Goldman M, Bauer SR: A comparative study of iodine uptake by thyroid and thymus glands of male and female Sprague-Dawley rats of different ages. Acta Endocrinol 85:64- 70, 1977
194. Jackson GL, Graham WR Flickinger FW, et al: Thymus accumulation of radioactive iodine. Pennsylvania Medicine 82:37-38, 1979
195. Michigishi T, Mizukami Y, Shuke N, et al: Visualization Of the thymus with therapeutic doses of radioiodine in patients with thyroid cancer. Ear J Nucl Med 20:75-79, 1993
196. Veronikis IE, Simkin R Braverman LE: Thymic uptake of iodine-131 in the anterior mediastinum. J Nucl Med 37:991- 992, 1996
197. Vermiglio F, Baudin E, Travagli JR et al: Iodine concentration by the thymus in thyroid carcinoma. J Nucl Med 37:1830-1831, 1996
198. Wilson L, Barrington SF, Kettle AG, et al: Physiological uptake occurs in the thymus of young patients treated with radioiodine for thyroid carcinoma. J Nucl Med 38:152R 1997 (abstr)
199. Wilson LM, Barrington SE Morrison ID, et al: Therapeu- tic implications of thymic uptake of radioiodine in thyroid carcinoma. Enr J Nucl Med 25:622-628, 1998
200. Salvatore M, Saletmich I, Rufini V, et al: Unusual false-positive radioiodine whole-body scans in patients with differentiated thyroid carcinoma. Clin Nucl Med 22:380-384, 1997
201. Andreas J, Brtihl K, Eissmer D: False-positive 1-131 whole body imaging after 1-131 therapy for a follicular carci- noma. Clin Nucl Med 22:123-124, 1997