
Adherence to maintenance medication in asthma in patients admitted with acute asthma

Overall asthma control: The relationship between currentcontrol and future risk
Eric D. Bateman, MD,a Helen K. Reddel, MBBS, PhD, FRACP,b G€oran Eriksson, MB, PhD,c,d Stefan Peterson, PhD,c
Ollie Ostlund, PhD,c Malcolm R. Sears, MB, FRACP, FRCPC,e Christine Jenkins, MD, FRACP,b Marc Humbert, MD,g
Roland Buhl, MD,h Tim W. Harrison, MD,i Santiago Quirce, MD, PhD,j and Paul M. O’Byrne, MB, FRCP(C)f Cape Town,
South Africa, Sydney, Australia, Lund, Sweden, Hamilton, Ontario, Canada, Clamart, France, Mainz, Germany, Nottingham, United Kingdom,
and Madrid, Spain
Background: Asthma guidelines emphasize both maintainingcurrent control and reducing future risk, but the relationshipbetween these 2 targets is not well understood.Objective: This retrospective analysis of 5 budesonide/formoterol maintenance and reliever therapy (Symbicort
From athe Division of Pulmonology, Department of Medicine, University of Cape Town;bthe Clinical Management Group, Woolcock Institute of Medical Research, Sydney;cAstraZeneca Research and Development, Lund; dthe Department of Respiratory
Medicine and Allergology, University Hospital, Lund; ethe Department of Medicine
and fthe Michael G. DeGroote School of Medicine, Faculty of Health Sciences,
McMaster University, Hamilton; gUniversite Paris-Sud 11, Service de Pneumologie
et Reanimation Respiratoire, Hopital Antoine Beclere, APHP, Clamart; hthe Pulmo-
nary Department, Mainz University Hospital, Mainz; ithe Respiratory Biomedical Re-
search Unit, City Hospital Campus, Nottingham University, Nottingham; and jthe
Department of Allergy, Hospital La Paz, Comunidad Autonoma de Madrid, Madrid.
Supported by AstraZeneca AB, Lund, Sweden.
Disclosure of potential conflict of interest: E. D. Bateman is on advisory boards for and
has received speakers’ honoraria from AstraZeneca, GlaxoSmithKline, and Boeh-
ringer Ingelheim; is on advisory boards for Nycomed, Merck, ALK-Abello, Hoffmann
la Roche (Data Safety Board), and Almirall/Forest Pharmaceuticals; and has received
research support from AstraZeneca, GlaxoSmithKline, Merck, Morris Pharmaceuti-
cals, Pfizer, Replidyne Inc, Almirall, Aeras, and Eumedic Inc. P. M. O’Byrne is on
advisory boards for and has received speakers’ honoraria from AstraZeneca and
GlaxoSmithKline; is on advisory boards for Topigen, Wyeth, and Schering; and has
received research support from AstraZeneca, GlaxoSmithKline, Merck, Wyeth,
Schering, and Alexion. M. R. Sears holds a chair endowed by AstraZeneca; has
received consultation fees from AstraZeneca, Merck Frosst, and Schering-Plough; and
has received research support from GlaxoSmithKline. T. W. Harrison has received
honoraria from AstraZeneca and has received research support from GlaxoSmithKline
and Boehringer Ingelheim. R. Buhl has received speakers’ fees and consultants’ fees,
as well as reimbursement for attending scientific conferences from AstraZeneca, and
his department has received research support from the Deutsche Forschungsgemein-
schaft, Almirall, AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, and
Novartis. S. Quirce is on advisory boards for and has received speakers’ honoraria from
AstraZeneca and has received research support from Ciber de Enfermedades
Respiratorias (CIBERES), Madrid. G. Eriksson, S. Peterson, and O. Ostlund are
employed by AstraZeneca. M. Humbert has consulted for Actelion, AstraZeneca,
Amgen, Chiesi, GlaxoSmithKline, MSD, Novartis, and Pfizer. C. Jenkins has received
speakers’ honoraria from GlaxoSmithKline, Novartis, and AstraZeneca and has
received research support from GlaxoSmithKline and AstraZeneca. H. K. Reddel is on
advisory boards for and has received research support from AstraZeneca and
GlaxoSmithKline and has received speakers’ honoraria from AstraZeneca, Getz
Pharma, and MerckSharp & Dohme.
Received for publication May 6, 2009; revised November 2, 2009; accepted for publica-
tion November 5, 2009.
Available online February 12, 2010.
Reprint requests: Eric D. Bateman, MD, Division of Pulmonology, Department of Med-
icine, University of Cape Town, George Street, Mowbray 7700, Cape Town, South
Africa. E-mail: [email protected].
0091-6749/$36.00
� 2010 American Academy of Allergy, Asthma & Immunology
doi:10.1016/j.jaci.2009.11.033
600
SMART Turbuhaler*) studies assessed the relationship betweenasthma control questionnaire (ACQ-5) and Global Initiative forAsthma-defined clinical asthma control and future risk ofinstability and exacerbations.Methods: The percentage of patients with Global Initiative forAsthma–defined controlled asthma over time was assessed forbudesonide/formoterol maintenance and reliever therapy versusthe 3 maintenance therapies; higher dose inhaled corticosteroid(ICS), same dose ICS/long-acting b2-agonist (LABA), andhigher dose ICS/LABA plus short-acting b2-agonist. Therelationship between baseline ACQ-5 and exacerbations wasinvestigated. A Markov analysis examined the transitionalprobability of change in control status throughout the studies.Results: The percentage of patients achieving asthma controlincreased with time, irrespective of treatment; the percentageControlled/Partly Controlled at study end was at least similar tobudesonide/formoterol maintenance and reliever therapy versusthe 3 maintenance therapies: higher dose ICS (56% vs 45%),same dose ICS/LABA (56% vs 53%), and higher dose ICS/LABA (54% vs 54%). Baseline ACQ-5 score correlatedpositively with exacerbation rates. A Controlled or PartlyControlled week predicted at least Partly Controlled asthma thefollowing week ($80% probability). The better the control, thelower the risk of an Uncontrolled week. The probability of anexacerbation was related to current state and was lower withbudesonide/formoterol maintenance and reliever therapy.Conclusions: Current control predicts future risk of instabilityand exacerbations. Budesonide/formoterol maintenance andreliever therapy reduces exacerbations versus comparators andachieves at least similar control. (J Allergy Clin Immunol2010;125:600-8.)
Key words: Asthma control, ACQ, exacerbations, GINA
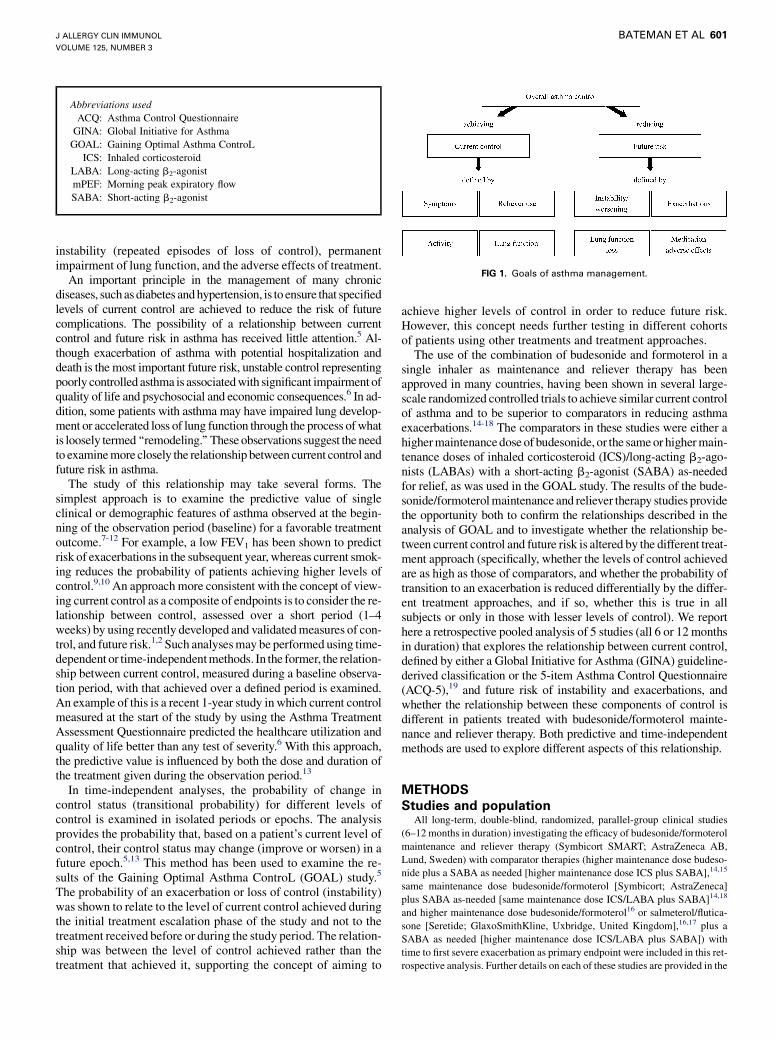
Recently published asthma guidelines1,2 and a recent Task Forcereport by the American Thoracic Society/European RespiratorySociety3,4 recommend changes in the definition of and methodsfor measuring asthma control. As in other chronic diseases, it is rec-ognized that control of asthma involves current control and long-term components referred to as ‘‘risk’’1 or ‘‘future risk’’3 (Fig 1).Current control (termed ‘‘impairment’’ in the National Asthma Ed-ucation and Prevention Program guidelines [page 36]1) is the pa-tient’s current and recent level of symptoms and functionalstatus. Longer-term components are the risk of exacerbations,
*Symbicort SMART and Turbuhaler are trademarks owned by AstraZeneca. Neither the
Symbicort SMART posology nor the dry powder formulation Turbuhaler are currently
approved in the United States.
J ALLERGY CLIN IMMUNOL
VOLUME 125, NUMBER 3
BATEMAN ET AL 601
Abbreviations used
ACQ: A
sthma Control QuestionnaireGINA: G
lobal Initiative for AsthmaGOAL: G
aining Optimal Asthma ControLICS: In
haled corticosteroidLABA: L
ong-acting b2-agonistmPEF: M
orning peak expiratory flowSABA: S
hort-acting b2-agonistFIG 1. Goals of asthma management.
instability (repeated episodes of loss of control), permanentimpairment of lung function, and the adverse effects of treatment.
An important principle in the management of many chronicdiseases, such as diabetes and hypertension, is to ensure that specifiedlevels of current control are achieved to reduce the risk of futurecomplications. The possibility of a relationship between currentcontrol and future risk in asthma has received little attention.5 Al-though exacerbation of asthma with potential hospitalization anddeath is the most important future risk, unstable control representingpoorly controlled asthma is associated with significant impairment ofquality of life and psychosocial and economic consequences.6 In ad-dition, some patients with asthma may have impaired lung develop-ment or accelerated loss of lung function through the process of whatis loosely termed ‘‘remodeling.’’ These observations suggest the needto examine more closely the relationship between current control andfuture risk in asthma.
The study of this relationship may take several forms. Thesimplest approach is to examine the predictive value of singleclinical or demographic features of asthma observed at the begin-ning of the observation period (baseline) for a favorable treatmentoutcome.7-12 For example, a low FEV1 has been shown to predictrisk of exacerbations in the subsequent year, whereas current smok-ing reduces the probability of patients achieving higher levels ofcontrol.9,10 An approach more consistent with the concept of view-ing current control as a composite of endpoints is to consider the re-lationship between control, assessed over a short period (1–4weeks) by using recently developed and validated measures of con-trol, and future risk.1,2 Such analyses may be performed using time-dependent or time-independent methods. In the former, the relation-ship between current control, measured during a baseline observa-tion period, with that achieved over a defined period is examined.An example of this is a recent 1-year study in which current controlmeasured at the start of the study by using the Asthma TreatmentAssessment Questionnaire predicted the healthcare utilization andquality of life better than any test of severity.6 With this approach,the predictive value is influenced by both the dose and duration ofthe treatment given during the observation period.13
In time-independent analyses, the probability of change incontrol status (transitional probability) for different levels ofcontrol is examined in isolated periods or epochs. The analysisprovides the probability that, based on a patient’s current level ofcontrol, their control status may change (improve or worsen) in afuture epoch.5,13 This method has been used to examine the re-sults of the Gaining Optimal Asthma ControL (GOAL) study.5
The probability of an exacerbation or loss of control (instability)was shown to relate to the level of current control achieved duringthe initial treatment escalation phase of the study and not to thetreatment received before or during the study period. The relation-ship was between the level of control achieved rather than thetreatment that achieved it, supporting the concept of aiming to
achieve higher levels of control in order to reduce future risk.However, this concept needs further testing in different cohortsof patients using other treatments and treatment approaches.
The use of the combination of budesonide and formoterol in asingle inhaler as maintenance and reliever therapy has beenapproved in many countries, having been shown in several large-scale randomized controlled trials to achieve similar current controlof asthma and to be superior to comparators in reducing asthmaexacerbations.14-18 The comparators in these studies were either ahigher maintenance dose of budesonide, or the same or higher main-tenance doses of inhaled corticosteroid (ICS)/long-acting b2-ago-nists (LABAs) with a short-acting b2-agonist (SABA) as-neededfor relief, as was used in the GOAL study. The results of the bude-sonide/formoterol maintenance and reliever therapy studies providethe opportunity both to confirm the relationships described in theanalysis of GOAL and to investigate whether the relationship be-tween current control and future risk is altered by the different treat-ment approach (specifically, whether the levels of control achievedare as high as those of comparators, and whether the probability oftransition to an exacerbation is reduced differentially by the differ-ent treatment approaches, and if so, whether this is true in allsubjects or only in those with lesser levels of control). We reporthere a retrospective pooled analysis of 5 studies (all 6 or 12 monthsin duration) that explores the relationship between current control,defined by either a Global Initiative for Asthma (GINA) guideline-derived classification or the 5-item Asthma Control Questionnaire(ACQ-5),19 and future risk of instability and exacerbations, andwhether the relationship between these components of control isdifferent in patients treated with budesonide/formoterol mainte-nance and reliever therapy. Both predictive and time-independentmethods are used to explore different aspects of this relationship.
METHODS
Studies and populationAll long-term, double-blind, randomized, parallel-group clinical studies
(6–12 months in duration) investigating the efficacy of budesonide/formoterol
maintenance and reliever therapy (Symbicort SMART; AstraZeneca AB,
Lund, Sweden) with comparator therapies (higher maintenance dose budeso-
nide plus a SABA as needed [higher maintenance dose ICS plus SABA],14,15
same maintenance dose budesonide/formoterol [Symbicort; AstraZeneca]
plus SABA as-needed [same maintenance dose ICS/LABA plus SABA]14,18
and higher maintenance dose budesonide/formoterol16 or salmeterol/flutica-
sone [Seretide; GlaxoSmithKline, Uxbridge, United Kingdom],16,17 plus a
SABA as needed [higher maintenance dose ICS/LABA plus SABA]) with
time to first severe exacerbation as primary endpoint were included in this ret-
rospective analysis. Further details on each of these studies are provided in the

TABLE I. Baseline demographics
Higher maintenance
dose ICS 1 SABA
Same maintenance
dose ICS/LABA 1 SABA
Higher maintenance
dose ICS/LABA 1 SABA
BUD/FORM maintenance
1 reliever therapy
N 1869 2050 3383 5246
Male, n (%) 821 (44) 844 (41) 1376 (41) 2173 (41)
Age, y 40 (4-80) 40 (4-83) 38 (12-83) 39 (4-89)
ICS dose at entry, mg/d 685 (100-2000) 683 (200-1600) 738 (100-3200) 715 (160-2000)
LABA use at entry, % 35 45 49 47
Median asthma duration, y 11 (0-71) 10 (0-69) 11 (0-77) 11 (0-70)
FEV1, % predicted normal 71.6 (37-100) 72.3 (39-108) 72.1 (30-222) 71.7 (29-131)
As-needed inh/d 2.2 (0-9.2) 2.1 (0-13.5) 2.3 (0-10.8) 2.1 (0-15.6)
Symptom-free days, % 16.7 (0-100) 17.1 (0-100) 9.5 (0-100) 12.8 (0-100)
Night-time awakenings, % 22.1 (0-100) 25.9 (0-100) 32.2 (0-100) 28.8 (0-100)
BUD/FORM, Budesonide/formoterol; inh, inhalations.
Data are means (ranges) unless otherwise indicated. For the purpose of baseline demographics, all available data for each treatment group are pooled. For individual demographic
data, please see the following references: higher maintenance dose ICS plus SABA,14,15 same maintenance dose ICS/LABA plus SABA,14,18 higher maintenance dose ICS/LABA
plus SABA,16,17 and BUD/FORM maintenance and reliever therapy.14-18 For night-time awakenings, % is percentage of nights with awakenings.
J ALLERGY CLIN IMMUNOL
MARCH 2010
602 BATEMAN ET AL
Studies and Population section and Table E1 in this article’s Online Repository
at www.jacionline.org.
All studies were performed in accordance with the Declaration of Helsinki
and Good Clinical Practice guidelines and were approved by independent
ethics committees. Written informed consent was obtained from each adult
patient; for underage patients, informed consent from both the patient and the
patient’s legal guardian was obtained.
AssessmentsSevere asthma exacerbations. A severe exacerbation was
defined as deterioration in asthma resulting in hospitalization/emergency
room treatment and/or oral steroid use. Two of the studies originally included a
fall in morning peak expiratory flow (mPEF) to �70% baseline on 2
consecutive days in the definition,14,15 but to harmonize, exacerbations based
only on a fall in mPEF were excluded when pooling the data.
Overall asthma control as defined by GINA criteria.For each of the 5 studies, GINA-defined asthma control was determined for
each week of the study by evaluation of the exacerbation data and patient diary
card data: (1) night-time symptoms or awakenings/week (none allowed); (2)
daytime symptoms (�2 d/wk); (3) reliever use (�2 d/wk with up to 2
inhalations each day, or alternatively, up to 4 inhalations on�1 day during the
week); (4) mPEF (�80% predicted normal before medication on every
morning of the week) and (5) freedom from activity limitation as determined
from daytime symptoms (daytime symptom score <2 on every day of the
week; see the Assessments section of the Online Repository at www.jacionline.
org for definition of scores). A week for any patient was considered Controlled
if, during that week, all 5 diary card subcriteria were controlled and no severe
exacerbation was recorded. The week was defined as Partly Controlled if any
1 or 2 of the subcriteria were uncontrolled and no exacerbation was recorded. If
the week had �3 uncontrolled subcriteria or an exacerbation, the week was
termed Uncontrolled. Control of subcriteria had to be positively demonstrated
by diary data; if not, subcriteria were considered Uncontrolled.
Asthma control as assessed by ACQ-5. In 3 studies
(budesonide/formoterol maintenance and reliever therapy vs same maintenance
dose ICS/LABA plus SABA18 and vs higher maintenance dose ICS/LABA plus
SABA16,17), the ACQ-5,19-21 a shortened version of 7-item Asthma Control
Questionnaire (ACQ-7),21,22 was self-assessed at clinic visits. The ACQ is a val-
idated method for distinguishing different levels of asthma control19,20 recom-
mended in asthma management guidelines.1,2 Each of the 5 questions on
symptom control were scored on a scale of 0 to 6, where 0 represents good con-
trol and 6, poor control. The overall score from the ACQ-5 was the mean of the 5
responses. For further details on the methodologies, please see the Methods sec-
tion in this article’s Online Repository at www.jacionline.org.
Statistical analysisChanges in asthma control over time. The proportion of
patients achieving Controlled or Partly Controlled asthma by GINA criteria
each week in the studies was plotted for budesonide/formoterol maintenance
and reliever therapy and the 3 comparators. Time courses for exacerbations
each week were also plotted.
The proportion of patients achieving asthma control over time based on
ACQ-5 cut-points, defined by the limits 0.50, 0.75, 1.00, 1.25, and 1.50, was
plotted for budesonide/formoterol maintenance and reliever therapy and the
comparators same maintenance dose ICS/LABA plus SABA and higher
maintenance dose ICS/LABA plus SABA. All plots were drawn using the Last
Value Extended principle to obtain the same number of patients each week, for
GINA control, or each visit, for ACQ cut-points.
Stability of asthma control: probability of changing
level of GINA-defined weekly control. Stability of asthma
control was assessed in a Markov analysis investigating transitional proba-
bility of change in control status (excluding exacerbations), as defined by
GINA. Results from all 5 studies were included in the Markov model5,13 to cal-
culate the weekly transition probability between control states defined as the
probability of a patient, during the next week, moving from one level of con-
trol (Controlled, Partly Controlled, or Uncontrolled) to another or remaining at
the same level of control or experiencing an exacerbation. Transition probabil-
ities, estimated by the observed transition frequencies, were tabulated and the
probabilities achieved with budesonide/formoterol maintenance and reliever
therapy compared with comparators. The odds of having an exacerbation
the week following a Controlled, Partly Controlled, or Uncontrolled week
were analyzed in a logistic regression model by using a generalized estimating
equation approach.
ACQ-5 at randomization as a predictor of exacerba-
tions. Exacerbation data from all patients in the two 6-month studies
comparing budesonide/formoterol maintenance and reliever therapy versus
higher maintenance dose ICS/LABA plus SABA16,17 were pooled and the
mean number of exacerbations stratified according to ACQ-5 cut-points at ran-
domization (before first dose of study medication). For a patient to be included
in these calculations, both an assessment of ACQ-5 at randomization and an
assessment of exacerbation status had to be available. The mean number of se-
vere exacerbations over time, stratified by ACQ-5 cut-point at randomization,
was described by using Kaplan–Meier plots and a Poisson regression model.
For further details on the statistical analyses, see the Statistical Analysis
section of this article’s Online Repository at www.jacionline.org.
RESULTS
Studies and populationBaseline characteristics were comparable between the 4 treat-
ment groups within this pooled analysis (Table I). At baseline, pa-tients had a mean FEV1, percentage predicted normal of 71.6% to72.3%; 35% to 49% of patients were using a LABA at entry.

FIG 2. Proportion of patients with Controlled and Controlled/Partly Controlled asthma by week according to
GINA criteria (A) and exacerbations (B), by week. Percentage of patients achieving Controlled (week with all
5 diary card subcriteria controlled and no severe exacerbations) and Controlled/Partly Controlled asthma
(week with no exacerbation and �2 subcriteria uncontrolled) by week (A); with �1 exacerbation requiring
medical intervention during the week (excluding peak expiratory flow) (B). Pooled data from higher main-
tenance dose ICS plus SABA,14,15 same maintenance dose ICS/LABA plus SABA,14,18 and higher mainte-
nance dose ICS/LABA plus SABA.16,17 *P values refer to analyses at last week of treatment (end of
treatment). BUD/FORM, budesonide/formoterol.
J ALLERGY CLIN IMMUNOL
VOLUME 125, NUMBER 3
BATEMAN ET AL 603
Time course to achieve GINA control targetsThe percentage of patients achieving a week of Controlled or
Controlled/Partly Controlled asthma, as defined by GINA criteria,increased throughout the study periods, irrespective of treatmentused, although most of the increase occurred during the first 3 to 6months (Fig 2, A). At the last week of study, 17.1% and 55.8% ofpatients randomized to budesonide/formoterol maintenance andreliever therapy achieved Controlled asthma and Controlled/Partly Controlled asthma versus 12.2% and 45.0% of patients ran-domized to higher maintenance dose ICS plus SABA, respec-tively (P < .001; see this article’s Table E2 in the OnlineRepository at www.jacionline.org). The percentage of patientsachieving Controlled or Controlled/Partly Controlled asthmawith budesonide/formoterol maintenance and reliever therapy atstudy end was at least comparable to same maintenance doseICS/LABA plus SABA (Controlled, 17.4% vs 16.8%, P 5 .73;Controlled/Partly Controlled, 55.7% vs 52.9%, P 5 .076) andhigher maintenance dose ICS/LABA plus SABA (Controlled,17.8% vs 18.8%, P 5 .56; Controlled/Partly Controlled, 54.3%vs 54.5%, P 5 .86). Similar trends were seen for the individualdiary card assessments (data not shown).
Exacerbation incidence remained similar over time during thestudy for all treatments (Fig 2, B). Consistently for all weeks instudy, fewer patients in the budesonide/formoterol maintenanceand reliever therapy group tended to experience exacerbations re-quiring medical intervention versus all 3 comparator groups.
Time course of ACQ-5 improvementIn the one 12-month study, analysis of the proportion of
patients at each ACQ-5 cut-point over time indicated that morepatients reached better control over 12 months with no obviousdifferences in the proportions of patients achieving variousACQ-5 cut-points for higher levels of control on budesonide/formoterol maintenance and reliever therapy versus same main-tenance dose ICS/LABA plus SABA (Fig 3). For the two6-month studies, similar numbers of patients showed improve-ment over time for budesonide/formoterol maintenance andreliever therapy versus higher maintenance dose ICS/LABAplus SABA (see Fig E1 in this article’s Online Repository atwww.jacionline.org). Overall, the data indicated that controlcontinued to improve over time, irrespective of treatments,with increasing percentages of patients achieving higher levelsof control.
Probability of moving to or remaining at a given
level of GINA-defined weekly control statusRegardless of treatment group, patients with Controlled or
Partly Controlled asthma in any given week had a similar(approximately 75%) estimated probability of remaining Con-trolled or Partly Controlled, respectively, the following week(Table II). The probability of deteriorating to a lesser level of con-trol (Partly Controlled or Uncontrolled, respectively) was

FIG 3. Proportion of patients below each ACQ-5 cut-point level over time, randomized to budesonide/
formoterol maintenance and reliever therapy (n 5 963 patients with a baseline ACQ-5 value and at least
1 value on treatment) versus same maintenance dose ICS/LABA plus SABA (n 5 984). Data from Rabe et al.18
BUD/FORM, budesonide/formoterol.
TABLE II. Transitional probability (%) of control status with pairwise comparison of treatments in any week according to GINA-defined
control status in the previous week
Control status in index week
C P U C P U
Control status in
following week Higher maintenance dose ICS 1 SABA BUD/FORM maintenance and reliever therapy
C 75 6.4 1.2 74 8.6 2.0
P 19 74 13 20 73 16
U 6.0 19 85 6.1 18 81
Ex 0.18 0.33 0.92 0.14 0.20 0.59
Same maintenance dose ICS/LABA 1 SABA BUD/FORM maintenance and reliever therapy
C 75 8.1 1.8 74 8.9 1.9
P 19 73 13 20 73 15
U 5.8 18 84 5.9 18 83
Ex 0.09 0.35 1.1 0.16 0.20 0.49
Higher maintenance dose ICS/LABA 1 SABA BUD/FORM maintenance and reliever therapy
C 74 10 2.3 73 10 2.1
P 20 71 15 21 72 15
U 5.7 18 82 5.7 18 83
Ex 0.18 0.31 0.98 0.08 0.21 0.66
BUD/FORM, Budesonide/formoterol; C, Controlled; Ex, exacerbation; P, Partly Controlled; U, Uncontrolled.
Transitional probability of control status in any week (state in the left column) according to control status in the previous week (state in the top row) in patients randomized to higher
maintenance dose ICS plus SABA and BUD/FORM maintenance and reliever therapy,14,15 same maintenance dose ICS/LABA plus SABA and BUD/FORM maintenance and
reliever therapy,14,18 and higher maintenance dose ICS/LABA plus SABA and BUD/FORM maintenance and reliever therapy.16,17 Underlined data indicate the probability of
remaining in the current state in subsequent weeks.
J ALLERGY CLIN IMMUNOL
MARCH 2010
604 BATEMAN ET AL
approximately 20%. For Controlled asthma, the probability of be-ing Uncontrolled the next week was approximately 6% for alltreatments. On the other hand, patients who were Partly Con-trolled or Uncontrolled in any week had a 6% to 16% chance of
improving (13% to 16% for Uncontrolled to Partly Controlledand 6.4% to 10% from Partly Controlled to Controlled).
The estimated probability of having an exacerbation in anyweek was higher the more uncontrolled the asthma was the

TABLE III. Treatment comparison of probability of exacerbation for each of 3 treatments, in any week according to GINA-defined
control status in the previous week
BUD/FORM maintenance and reliever therapy versus
Higher maintenance dose
ICS 1 SABA*
Same maintenance dose
ICS/LABA 1 SABAy
Higher maintenance dose
ICS/LABA 1 SABAzOR (95% CI) P value OR (95% CI) P value OR (95% CI) P value
C 0.77 (0.37-1.59) .473 1.8 (0.82-3.95) .146 0.48 (0.19-1.22) .124
P 0.61 (0.44-0.86) .004 0.57 (0.40-0.81) .002 0.69 (0.45-1.04) .074
U 0.64 (0.53-0.78) <.001 0.46 (0.38-0.56) <.001 0.69 (0.56-0.85) <.001
The OR is the ratio of the probability of an exacerbation the following week in the budesonide/formoterol maintenance and reliever therapy arm and the probability of an exacerbation
the following week in the comparator arm.
Treatment comparison of exacerbation risk by control status in the previous week.
BUD/FORM, Budesonide/formoterol; C, Controlled; OR, odds ratio; P, Partly Controlled; U, Uncontrolled.
*O’Byrne et al,14 Scicchitano et al15: 168,586 weeks, 861 with exacerbation.
�O’Byrne et al,14 Rabe et al18: 189,170 weeks, 964 with exacerbation.
�Kuna et al,16 Bousquet et al17: 129,123 weeks, 713 with exacerbation.
J ALLERGY CLIN IMMUNOL
VOLUME 125, NUMBER 3
BATEMAN ET AL 605
previous week (Table II). Improved control gave similar risk re-ductions for all treatments, although the absolute risks differedbetween treatments. The odds ratio for experiencing an exacerba-tion in subsequent weeks, for all treatments pooled, was 1.97(95% CI, 1.53–2.54) for a Partly Controlled versus Controlledweek (P < .001) and 2.91 (95% CI, 2.59–3.28) for an Uncon-trolled versus Partly Controlled week (P < .001), yielding anodds ratio of 5.74 (95% CI, 4.52–7.29) for an Uncontrolled versusControlled week (P < .001).
While the probability of remaining Controlled or Partly Con-trolled was similar between treatments, the probability of experi-encing an exacerbation differed (Table III). In theweek following anUncontrolled week, the probability of an exacerbation was signifi-cantly lower in patients treated with budesonide/formoterol mainte-nance and reliever therapy versus all 3 comparator groups. Asignificant risk reduction was also seen for budesonide/formoterolmaintenance and reliever therapy in patients who had in the previ-ous week experienced a Partly Controlled week, except for the com-parison with higher maintenance dose ICS/LABA plus SABA. Thenumber of exacerbations in the week following a Controlled weekwas small (83 in total) and showed no clear treatment pattern.
ACQ-5 at randomization as a predictor of
exacerbation riskThe risk of exacerbations during treatment increased with
increasing ACQ-5 cut-point at randomization (see Fig E2 in thisarticle’s Online Repository at www.jacionline.org). The exacerba-tion rate was higher in patients with ACQ-5� 0.75 versus patientswith an ACQ-5 <0.50 at randomization (P < .05). A marked in-crease in future risk of exacerbations was also observed forACQ-5 �1.50 versus ACQ-5 <0.50 (0.36 events/patient/12 mo[95% CI, 0.34–0.39] vs 0.13 events/patient/12 mo [95% CI,0.09–0.20]; P < .001). Analysis of exacerbation rates by treatmentgroup and ACQ-5 stratum showed that the exacerbation ratereduction for budesonide/formoterol maintenance and relievertherapy versus higher maintenance dose ICS/LABA was 12%for ACQ-5 <1.50 (P 5 .4) and 33% for ACQ-5�1.50 (P < .001).
DISCUSSIONThe management of chronic diseases requires an approach to
both the current manifestations and the long-term effects ofdisease. The focus of asthma management has shifted from
treatment of an acute disease to that of long-term control andprevention of future risks. With improvements in controllertherapy, it is now recognized that highly satisfactory levels ofcurrent control can be achieved and maintained for long pe-riods.23 It is thus relevant to consider different strategies for main-taining control and to identify those that are most effective inreducing future risk. The current study provides several usefulinsights on both current control and future risk.
First, in the pooled analysis of 5 studies,14-18 the proportion ofpatients achieving GINA-defined levels of Controlled/Partly Con-trolled asthma each week was approximately 10% higher with allICS/LABA combination regimens than with an ICS maintenancedose alone. These findings are consistent with the results of theGOAL study.23 However, the current study permitted a compari-son of the proportion of patients achieving control with theLABA-containing regimens involving regular maintenance dos-ing with ICS and LABA plus SABA for rescue as studied inGOAL and budesonide/formoterol as both maintenance and re-liever therapy. At equivalent maintenance doses of fixed-doseICS/LABA, the results were similar. Even doubling the mainte-nance dose did not improve control further; up to 60% achievedat least Partly Controlled asthma and fewer than 20% achievedControlled asthma at study end. These results are similar in mag-nitude to those patients in Stratum 3 in the GOAL study who, atstudy entry, were Uncontrolled on moderate doses of ICS.23
The analysis also confirms the value of sustained treatment inthe study cohorts, because the proportion of patients achievinghigher levels of both ACQ-5-defined and GINA-defined controlincreased over time. Most improvement occurred within the first 3months, but a further percentage of patients achieved higher levelsof control during sustained treatment.24,25 This benefit of sustainedtreatment was reported in the GOAL study,23 but unlike that study,in which treatment was increased at 3-monthly intervals, the cur-rent analysis demonstrated further improvement related to dura-tion of treatment alone. This conclusion is supported by theobservation that patients who received a higher maintenancedose of ICS/LABA plus SABA did not achieve better results.
Third, our analysis provides insights into the relationshipbetween current control and future risk. Current control atrandomization (ACQ-5 score) predicted risk of exacerbationduring the study. This finding is consistent with recent reports thatcomposite measures such as the Asthma Treatment AssessmentQuestionnaire predict healthcare use and exacerbations.12,26
However, in our analysis, this relationship differed in patients

J ALLERGY CLIN IMMUNOL
MARCH 2010
606 BATEMAN ET AL
receiving budesonide/formoterol maintenance and reliever ther-apy; in patients with an ACQ-5 score >1.50 at randomization,this treatment resulted in a 33% lower exacerbation risk comparedwith even those receiving higher maintenance dose ICS/LABAplus SABA as needed (P < .001).
The analysis of week-by-week exacerbation rates also con-firmed differences by treatment and treatment strategy. Althoughfewer patients treated with the higher maintenance dose of ICSalone (plus SABA) achieved control each week, the exacerbationrate was similar to that in patients receiving the lower mainte-nance doses of fixed-dose ICS/LABA, confirming the efficacy ofhigh maintenance doses of ICS in lowering the risk of exacerba-tions. Increasing the fixed maintenance dose of ICS/LABAreduced the rate of exacerbations further, but in all comparisons,the greatest reduction was observed with budesonide/formoterolmaintenance and reliever therapy (a 54% reduction in exacerba-tions versus same maintenance dose ICS/LABA plus SABA;P < .001; Table III).
These results, which suggest differences in the relationshipbetween current control and risk of exacerbations in differenttreatment groups, are better understood by considering the resultsof the Markov analysis, which provides the time-independentprobability of a patient’s status, or level of control, changing fromone week to another. Although the predictions apply to the weekthat follows, the predictions are made on the basis of a very largedatabase (composed of more than 129,000 weeks of follow-up)and may be used to estimate the probabilities for any week in thefuture, although with increasing uncertainty. This method haspreviously been used in a post hoc analysis of the results of theGOAL study, in which the authors confirmed a negative relation-ship between the level of asthma control achieved and future riskof instability, and demonstrated that the probability of becomingUncontrolled was inversely related to the level of controlachieved.5 Better stability was associated with reduced probabil-ity of unscheduled healthcare resource use and improved patientquality of life. The authors concluded that these data supportedthe guideline recommendation to aim for the highest level ofasthma control achievable as a strategy to reduce future risk of ex-acerbations. A limitation of their analysis, however, was a smallersample size and a relatively small number of exacerbations onwhich these conclusions were made.5
The current analysis supports these general conclusions butprovides additional information. First, for all 4 treatment ap-proaches, a high level of asthma control was associated with ahigh probability of maintaining this level of control in futureweeks—that is, clinical stability—and the probability of controlstatus changing was similar between the treatments. Patients with aControlled week had a 94% probability of remaining Controlled orPartly Controlled inother weeks of the study (Table II), regardless oftreatment category. Thus, stability is a feature of the level of controlachieved, regardless of the treatment that achieved it.5 Partly Con-trolled weeks were associated with a >80% probability of at leastPartly Controlled weeks in the future (Partly Controlled or Con-trolled) and a smaller probability of an Uncontrolled week—alsoa highly satisfactory outcome of treatment. Again, in those achiev-ing this, the probability did not differ with different treatments.
Furthermore, the Markov analysis confirmed that the better thelevel of control, the lower the risk of having an exacerbation.However, although the transitional probability of an exacerbationwas similarly low after a Controlled week, regardless of treat-ment, the probability differed between treatments in those who
were only Partly Controlled or Uncontrolled. Compared with the3 other treatment groups, budesonide/formoterol maintenanceand reliever therapy was associated with a reduced probability ofan exacerbation, confirming a selective benefit of the approach ofthis component on future risk.
Although it demonstrates a strong relationship between currentcontrol and exacerbation risk, the current analysis does notprovide an estimate of the amount of treatment-related improve-ment in current control that reduces the risk of an exacerbation inindividual patients. Use of a control measure such as the ACQ-5,which expresses control as a continuous variable, would be moreresponsive and suitable for an assessment of this than the GINAclassification, which is limited to 3 categories of control. In thestudies included in our analysis, the ACQ-5 was recorded on onlya few visits and in only some of the studies (3), whereas the GINAlevels of control were derived from daily diary card data for eachweek in every study.
The fact that steady improvements in levels of asthma controlobserved throughout the studies in all the treatment arms were notassociated with a further improvement in exacerbation riskappears to be contradictory to the hypothesis that improvedcurrent control is associated with reduced future risk. This may bebecause the increase in control was gradual and slow, and thereduction in exacerbations that followed might have been toosmall for the trend to become apparent during the 6 to 12 months’duration of the studies. Survival curves for time to first exacer-bation in the individual studies indicate a clear trend for adecreased risk over time. Most likely, patients with repeatedexacerbations (about a third of the exacerbating patients) dimin-ish this signal, and studies of 2 to 3 years’ duration would beneeded to assess such an effect.
The apparent limit or ceiling effect of the treatments used onthe achievement of current control in around 40% of the patientsincluded in these studies reflects the relatively refractory nature oftheir asthma and the limitations of the treatments used. Theinclusion criteria selected patients with Uncontrolled asthma inspite of regular treatment with ICS 6 LABA. It was thus notsurprising that many would fail to achieve guideline-based goalsof treatment. It was, however, surprising that 40% to 50% wereUncontrolled at the end of the study. Their refractoriness is furtherillustrated in the Markov analysis, which revealed that anUncontrolled week is highly likely to be followed by furtherUncontrolled weeks (>80% probability; see Table II), regardlessof treatment. Clearly, such patients represent a cohort of severeasthma with a high risk of exacerbations and require additionaltreatments. However, it is gratifying to note that, even in these pa-tients, the risk of exacerbations was significantly reduced by theuse of budesonide/formoterol maintenance and reliever therapy;in fact, the largest benefit of this approach was seen in this group.
In this analysis, we have followed the approach recommendedin recent guidelines of defining current asthma control from aclinical symptom-based perspective supplemented by measuresof lung function and expressed this as a composite.6,12,26,27 Stud-ies evaluating the relative predictive roles of these measures arelimited but agree that although a symptom-based measure ofcontrol may be adequate for the majority of patients, discordancebetween current control and future risk is evident in manypatients and may vary according to the treatment given.28-31 Inthese circumstances, and particularly in relatively treatment-refractory patients, measures that reflect other elements of thecondition—bronchial hyperresponsiveness and markers of

J ALLERGY CLIN IMMUNOL
VOLUME 125, NUMBER 3
BATEMAN ET AL 607
airway inflammation (eg, levels of exhaled nitric oxide32 andeosinophils in induced sputum33,34)—may be instructive.
These findings have several practical implications. The datasupport the recommendation that having a high level of currentcontrol improves stability and reduces the risk of exacerbationswhile on a regimen that includes an ICS. In some treatments, forexample, use of regular maintenance doses of LABA or SABAtherapy alone might promote a ‘‘high level of current control’’without also improving stability and the risk of exacerbations.29,30
Thus, although variability is a hallmark of Uncontrolled asthma,Controlled asthma may be stable for long periods—an importantmessage for patients and physicians. The results also confirm thehigher proportion of patients that achieve Controlled asthma withICS/LABA maintenance treatment compared with a higher main-tenance dose of ICS. Furthermore, the results support the impor-tance of sustained treatment, because additional patients,particularly those who entered these studies with a poor level ofcontrol and regardless of treatment regimen, continued to im-prove beyond 6 months. Finally, the data support the additionalbenefit of budesonide/formoterol maintenance and reliever ther-apy on exacerbations. Although exacerbation frequency con-tinues to relate to level of control, a further reduction isachieved, presumably because of the timely administration of bu-desonide/formoterol when used for relief. The data also suggestthat increasing the dose of maintenance ICS/LABA therapy toproduce maximal levels of control is not sufficient to provideoptimal outcomes for exacerbations.
This analysis has several limitations. It is a post hoc analysis inwhich the GINA control classification variables obtained from di-ary cards were analyzed retrospectively. In addition, the activitylimitation question was based on a general symptom questionrather than specific enquiry. A further limitation is that the pa-tients recruited in these studies represent the more severe end ofthe asthma spectrum. This might explain the relatively large pro-portion of patients that remained Uncontrolled during the studies.Prospective studies that also include steroid-naive patients andcontrolled patients on lower doses of ICS are required to test theserelationships between current control achieved and future risk.
In the current analysis, we have not attempted to study otheraspects of future risk such as lung function decline (for which thedata are not adequate) or the adverse effects of treatment. Ingeneral, the latter were mild, but a consistent favorable featurewas the significantly lower exposure to systemic corticosteroids,and in some studies, ICS in the budesonide/formoterol mainte-nance and reliever therapy group. This, over time, may result in adiminished risk of adverse outcomes.
In conclusion, this analysis provides new insights on therelationship between current control and future risk, whichtogether represent overall asthma control. Treatment with bude-sonide/formoterol maintenance and reliever therapy further re-duces exacerbations and achieves at least similar current controlcompared with comparator therapies.
Editorial assistance was provided by Dr Jessica Sample from MediTech
Media Ltd, who provided medical writing assistance on behalf of AstraZeneca.
Clinical implications: The use of budesonide/formoterol asmaintenance and reliever therapy achieves at least similar cur-rent control and greater reductions in exacerbations, reflectingbetter overall asthma control.
REFERENCES
1. NAEPP (National Asthma Education and Prevention Program). Expert Panel report
3: guidelines for the diagnosis and management of asthma. 2007. Available at:
http://www.nhlbi.nih.gov/guidelines/asthma/asthgdln.pdf. Accessed January 11,
2010.
2. Global Initiative for Asthma (GINA). Global strategy for asthma management and
prevention: NHLBI/WHO workshop report. Bethesda: National Institutes of
Health, National Heart, Lung and Blood Institute. Updated 2008. Available at:
http://www.ginasthma.com. Accessed January 11, 2010.
3. Taylor DR, Bateman ED, Boulet LP, Boushey HA, Busse WW, Casale TB, et al. A
new perspective on concepts of asthma severity and control. Eur Respir J 2008;32:
545-54.
4. Reddel HK, Taylor DR, Bateman ED, Boulet LP, Boushey HA, Busse WW, et al.
An official American Thoracic Society/European Respiratory Society statement:
asthma control and exacerbations: standardizing endpoints for clinical asthma
trials and clinical practice. Am J Respir Crit Care Med 2009;180:59-99.
5. Bateman ED, Bousquet J, Busse WW, Clark TJ, Gul N, Gibbs M, et al. Stability of
asthma control with regular treatment: an analysis of the Gaining Optimal Asthma
controL (GOAL) study. Allergy 2008;63:932-8.
6. Peters D, Chen C, Markson LE, Allen-Ramey FC, Vollmer WM. Using an asthma
control questionnaire and administrative data to predict health-care utilization.
Chest 2006;129:918-24.
7. Wakefield M, Ruffin R, Campbell D, Staugas R, Beilby J, McCaul K. A risk
screening questionnaire for adult asthmatics to predict attendance at hospital emer-
gency departments. South Australian Asthma Reference Panel. Chest 1997;112:
1527-33.
8. Li D, German D, Lulla S, Thomas RG, Wilson SR. Prospective study of hospital-
ization for asthma: a preliminary risk factor model. Am J Respir Crit Care Med
1995;151:647-55.
9. Fuhlbrigge AL, Kitch BT, Paltiel AD, Kuntz KM, Neumann PJ, Dockery DW, et al.
FEV(1) is associated with risk of asthma attacks in a pediatric population. J Allergy
Clin Immunol 2001;107:61-7.
10. Kitch BT, Paltiel AD, Kuntz KM, Dockery DW, Schouten JP, Weiss ST, et al. A
single measure of FEV1 is associated with risk of asthma attacks in long-term fol-
low-up. Chest 2004;126:1875-82.
11. Dorinsky PM, Edwards LD, Yancey SW, Rickard KA. Use of changes in symptoms
to predict changes in lung function in assessing the response to asthma therapy.
Clin Ther 2001;23:701-14.
12. Osborne ML, Pedula KL, O’Hollaren M, Ettinger KM, Stibolt T, Buist AS, et al.
Assessing future need for acute care in adult asthmatics: the Profile of Asthma
Risk Study: a prospective health maintenance organization-based study. Chest
2007;132:1151-61.
13. Combescure C, Chanez P, Saint-Pierre P, Daures JP, Proudhon H, Godard P.
Assessment of variations in control of asthma over time. Eur Respir J 2003;22:
298-304.
14. O’Byrne PM, Bisgaard H, Godard PP, Pistolesi M, Palmqvist M, Zhu Y, et al.
Budesonide/formoterol combination therapy as both maintenance and reliever
medication in asthma. Am J Respir Crit Care Med 2005;171:129-36.
15. Scicchitano R, Aalbers R, Ukena D, Manjra A, Fouquert L, Centanni S, et al. Ef-
ficacy and safety of budesonide/formoterol single inhaler therapy versus a higher
dose of budesonide in moderate to severe asthma. Curr Med Res Opin 2004;20:
1403-18.
16. Kuna P, Peters MJ, Manjra AI, Jorup C, Naya IP, Martinez-Jimenez NE, et al. Ef-
fect of budesonide/formoterol maintenance and reliever therapy on asthma exacer-
bations. Int J Clin Pract 2007;61:725-36.
17. Bousquet J, Boulet LP, Peters MJ, Magnussen H, Quiralte J, Martinez-Aguilar NE,
et al. Budesonide/formoterol for maintenance and relief in uncontrolled asthma vs.
high-dose salmeterol/fluticasone. Respir Med 2007;101:2437-46.
18. Rabe KF, Atienza T, Magyar P, Larsson P, Jorup C, Lalloo UG. Effect of budeso-
nide in combination with formoterol for reliever therapy in asthma exacerbations: a
randomised controlled, double-blind study. Lancet 2006;368:744-53.
19. Juniper EF, Bousquet J, Abetz L, Bateman ED. Identifying ‘‘well-controlled’’ and
‘‘not well-controlled’’ asthma using the Asthma Control Questionnaire. Respir Med
2006;100:616-21.
20. Juniper EF, O’Byrne PM, Guyatt GH, Ferrie PJ, King DR. Development and val-
idation of a questionnaire to measure asthma control. Eur Respir J 1999;14:902-7.
21. Juniper EF, Svensson K, M€ork AC, Stahl E. Measurement properties and interpre-
tation of three shortened versions of the asthma control questionnaire. Respir Med
2005;99:553-8.
22. Svensson K, Mork AC, Juniper EF. ACQ—is five out of seven items acceptable in
large clinical studies? Qual Life Res 2003;12:771. Abstract 1276.
23. Bateman ED, Boushey HA, Bousquet J, Busse WW, Clark TJ, Pauwels RA, et al.
Can guideline-defined asthma control be achieved? The Gaining Optimal Asthma
ControL study. Am J Respir Crit Care Med 2004;170:836-44.

J ALLERGY CLIN IMMUNOL
MARCH 2010
608 BATEMAN ET AL
24. Bateman ED, Clark TJ, Frith L, Bousquet J, Busse WW, Pedersen SE. Rate of re-
sponse of individual asthma control measures varies and may overestimate asthma
control: an analysis of the goal study. J Asthma 2007;44:667-73.
25. Reddel HK, Jenkins CR, Marks GB, Ware SI, Xuan W,Salome CM, et al. Optimal asthma
control, starting with high doses of inhaled budesonide. Eur Respir J 2000;16:226-35.
26. Vollmer WM, Markson LE, O’Connor E, Sanocki LL, Fitterman L, Berger M, et al.
Association of asthma control with health care utilization and quality of life. Am
J Respir Crit Care Med 1999;160:1647-52.
27. Vollmer WM, Markson LE, O’Connor E, Frazier EA, Berger M, Buist AS. Asso-
ciation of asthma control with health care utilization: a prospective evaluation. Am
J Respir Crit Care Med 2002;165:195-9.
28. Rosi E, Ronchi MC, Grazzini M, Duranti R, Scano G. Sputum analysis, bronchial
hyperresponsiveness, and airway function in asthma: results of a factor analysis.
J Allergy Clin Immunol 1999;103:232-7.
29. Lazarus SC, Boushey HA, Fahy JV, Chinchilli VM, Lemanske RF Jr, Sorkness CA,
et al. Long-acting beta2-agonist monotherapy vs continued therapy with inhaled
Harry Bernton (1885-1979Provident and Freedman’s Hoin populations within the lowhis consideration that inhalafly, mushroom fly) might hawith Halla Brown (1911-1993took a controlled study of hoand contamination of inadeqvomitus were demonstrated study, seven and five-tenths tests with extracts of cockrogroup of 114 allergic patientssera of skin test positive reprovoke constitutional reactifood substances, they conclinhalant, should be given crthe advisability of adding coas indicated.
Bernton HS, Brown H. InsecJ Allergy 1964;35:506-13.
AL
INNER CITY AS
corticosteroids in patients with persistent asthma: a randomized controlled trial.
JAMA 2001;285:2583-93.
30. Jenkins CR, Thien FC, Wheatley JR, Reddel HK. Traditional and patient-
centred outcomes with three classes of asthma medication. Eur Respir J
2005;26:36-44.
31. Gibson PG, Powell H, Ducharme FM. Differential effects of maintenance long-act-
ing beta-agonist and inhaled corticosteroid on asthma control and asthma exacer-
bations. J Allergy Clin Immunol 2007;119:344-50.
32. Harkins MS, Fiato KL, Iwamoto GK. Exhaled nitric oxide predicts asthma exacer-
bation. J Asthma 2004;41:471-6.
33. Green RH, Brightling CE, McKenna S, Hargadon B, Parker D, Bradding P, et al.
Asthma exacerbations and sputum eosinophil counts: a randomised controlled trial.
Lancet 2002;360:1715-21.
34. Jayaram L, Pizzichini MM, Cook RJ, Boulet LP, Lemiere C, Pizzichini E, et al.
Determining asthma treatment by monitoring sputum cell counts: effect on exacer-
bations. Eur Respir J 2006;27:483-94.
), MD, of Howard University and Washington’s spitals allergy clinics, noted the prevalence of asthma est social and economic strata. His observation led to
nt route allergenicity of flying insects (May fly, sand ve an indigenous indoor insect counterpart. In 1964, ), MD, of George Washington University, they under-
useholds that revealed endemic cockroach infestation uately protected food. Dead insects, their feces, and to be sources of allergens. In Bernton and Brown’s percent of 253 normal persons showed positive skin aches, compared with 28 percent of an unselected
. Skin-sensitizing antibodies were present in the blood actors and cockroach allergen had the capacity to
ons in these reactors. Since cockroaches contaminate uded that derivative allergens, whether ingestant or itical consideration. Accordingly, they recommended ckroach extract to the routine tests of allergic patients
t allergy—Preliminary studies of the cockroach.
LERGY ARCHIVES
THMA, ENDEMIC COCKROACH INFESTATION

J ALLERGY CLIN IMMUNOL
VOLUME 125, NUMBER 3
BATEMAN ET AL 608.e1
METHODS
Studies and populationAll long-term, double-blind, randomized, parallel-group clinical studies
(6–12 months in duration) investigating the efficacy of budesonide/formoterol
maintenance and reliever therapy (Symbicort SMART; AstraZeneca AB, Lund,
Sweden) with comparator therapies (higher maintenance dose budesonide plus
a SABA as needed [higher maintenance dose ICS plus SABA],E1,E2 same
maintenance dose budesonide/formoterol [Symbicort; AstraZeneca] plus
SABA as-needed [same maintenance dose ICS/LABA plus SABA]E1,E3 and
higher maintenance dose budesonide/formoterolE4 or salmeterol/fluticasone
[Seretide; GlaxoSmithKline, Uxbridge, United Kingdom] plus SABA as-
needed [higher maintenance dose ICS/LABA plus SABA]E4,E5 were included
in this retrospective analysis. The 1 exception was the study by Rabe et alE6 (bu-
desonide/formoterol maintenance and reliever therapy vs higher maintenance
dose budesonide plus SABA as needed), which had mPEF as the primary vari-
able. Further detail on each of these studies is summarized in Table E1. The
methodologies of the 5 studies have been published in detail previously.E1-E5
Two 12-month studies by O’Byrne et alE1 and Scicchitano et alE2 compared
budesonide/formoterol maintenance and reliever therapy (80/4.5 mg twice
daily [BID]E1 and 160/4.5 mg 2 inhalations once dailyE2) with higher mainte-
nance dose budesonide (Pulmicort; AstraZeneca; 320 mg BID,E1 160 mg 2 in-
halations BIDE2) plus terbutaline as needed (Bricanyl; AstraZeneca; 0.4 mg/
inhalation). In a third 12-month study by Rabe et al,E3 and in a further treat-
ment arm in the study by O’Byrne et al,E1 the comparator arm was the same
maintenance dose of ICS/LABA as used in the budesonide/formoterol main-
tenance and reliever therapy arm (budesonide/formoterol: 160/4.5 mg BIDE3
and 80/4.5 mg BID,E1 respectively) plus formoterol 4.5 mg (Oxis; Astra-
Zeneca)E3 or terbutaline (0.4 mg)E1,3 as needed. Only data from the terbutaline
as-needed arm were included in the current analysis; data from the formoterol
as-needed arm were excluded. Data from two 6-month studies that compared
budesonide/formoterol maintenance and reliever therapy (160/4.5 mg BIDE4
and 160/4.5 mg 2 inhalations BIDE5) with a higher maintenance dose ICS in
combination with LABA (Kuna et alE4: budesonide/formoterol 320/9 mg
BID or salmeterol/fluticasone 25/125 mg 2 inhalations BID; Bousquet et
alE5: salmeterol/fluticasone 50/500 mg BID) plus terbutaline (0.4 mg/inhala-
tion) were also pooled. All aforementioned drugs were administered via Tur-
buhaler (AstraZeneca) except for salmeterol/fluticasone, which was delivered
via either DiskusE5 or EvohalerE4 (GlaxoSmithKline).
The inclusion and exclusion criteria in each of these studies were similar. In
general, male and female patients aged �12 years with a diagnosis of asthma
were eligible for inclusion if they had a history of�1 asthma exacerbation in 12
months before study entry, use of ICS �3 months before study entry, FEV1
�50% of predicted normal (prebronchodilator), and�12% reversibility in in-
crease from baseline FEV1 15 minutes after inhalation of terbutaline 1 mg (Bri-
canyl Turbuhaler; AstraZeneca). For patients age �18 years, an increase in
basal FEV1�200 mL after inhalation of terbutaline 1 mg was required at study
entry.E2,3 Exclusion criteria included any respiratory infection affecting the
patient’s asthma or use of oral corticosteroids within 1 month of study entry.
The primary endpoint of all 5 studies was time to first severe exacerbation,
defined as deterioration in asthma resulting in hospitalization/emergency room
treatment and/or oral steroid use. In addition, 2 of the studies originally included
a fall in mPEF to�70% baseline on 2 consecutive days in the definition.E1,2 To
harmonize, exacerbations based only on a fall in mPEF were excluded when
pooling the data. Secondary measures included the rate of severe exacerbations
and measures of daily asthma control from daily diaries, which included home-
monitored PEF, reliever use, asthma symptoms, and nights with awakenings
caused by asthma symptoms. Daytime and night-time asthma symptom scores,
graded on a scale of 0 to 3 (where 0 5 no symptoms; 1 5 aware of symptoms but
can easily tolerate them; 2 5 asthma causing enough discomfort to cause prob-
lems with normal activities/sleep; 3 5 unable to do normal activities/sleep be-
cause of asthma), were also recorded in the daily diaries.
All studies were performed in accordance with the Declaration of Helsinki
and Good Clinical Practice guidelines and were approved by independent
ethics committees. Written informed consent was obtained from each adult
patient; for underage patients, informed consent from both the patient and the
patient’s legal guardian was obtained.
AssessmentsOverall asthma control as defined by GINA criteria.
For each of the 5 studies, GINA-defined asthma control was determined for
each week of the study by evaluation of the exacerbation data and patient diary
card data: (1) night-time symptoms or awakenings/week (none allowed); (2)
daytime symptoms (� 2 d/wk); (3) reliever use (�2 d/wk with up to 2
inhalations each day, or alternatively, up to 4 inhalations on�1 day during the
week); (4) mPEF (�80% predicted normal before medication on every
morning of the week); and (5) freedom from activity limitation as determined
from daytime symptoms (daytime symptom score <2 on every day of the week
where 0 5 no asthma symptoms; 1 5 aware of asthma symptoms but can
easily tolerate them; 2 5 asthma causes enough discomfort to cause problems
with normal activities; 3 5 unable to do normal activities because of
symptoms).
Aweek for any patient was considered Controlled if, during that week, all 5
of the diary card subcriteria were controlled and no severe exacerbation was
recorded. The week was defined as Partly Controlled if any 1 or 2 of the
subcriteria were uncontrolled and no exacerbation was recorded. If the week
had�3 Uncontrolled subcriteria and/or an exacerbation, the week was termed
Uncontrolled. Control of subcriteria had to be positively demonstrated by
diary data; if not, subcriteria were considered Uncontrolled.
Asthma control as assessed by ACQ-5. In 3 studies
(budesonide/formoterol maintenance and reliever therapy vs same mainte-
nance dose ICS/LABA plus SABAE3 and vs higher maintenance dose ICS/
LABA plus SABAE4,E5), the ACQ-5,E7-E9 a shortened version of the
ACQ-7,E8,E10 was self-assessed at clinic visits. The ACQ is a validated method
for distinguishing different levels of asthma controlE7,E9 recommended in
asthma management guidelines.E11,E12 Because ACQ-5 data were collected
in these studies, these data were used in this retrospective pooled analysis
and analyzed for their value in predicting achievement of control and asthma
exacerbations. It is important to note that the ACQ-5 is a widely used clinical
measure of asthma control and provides very similar outcomes to the ACQ-7,
which includes 2 additional questions concerning reliever use and lung
function.E8,E10
Each of the 5 questions on symptom control were scored on a scale of 0 to 6,
where 0 represents good control and 6, poor control. The overall score from the
ACQ-5 was the mean of the 5 responses.
Statistical analysisChanges in asthma control over time. The proportion of
patients achieving Controlled or Partly Controlled asthma by GINA criteria
each week in the studies was plotted for the budesonide/formoterol mainte-
nance and reliever therapy arm and the 3 comparators. Time courses for
exacerbations each week were also plotted. The proportion of patients
achieving asthma control over time on the basis of ACQ-5 cut-points, defined
by the limits 0.50, 0.75, 1.00, 1.25, and 1.50, was plotted for budesonide/
formoterol maintenance and reliever therapy and the comparators same
maintenance dose ICS/LABA plus SABA and higher maintenance dose ICS/
LABA plus SABA. All plots were drawn by using the Last Value Extended
principle to obtain the same number of patients each week for GINA control,
or each week for ACQ-5 cut-points, thus allowing for withdrawals and missing
data. Incomplete last weeks were removed together with weeks ending with
the last recorded day, because that day generally did not contain evening data.
The baseline week (week 0) was taken to be the 7 days up to the day before
randomization, whereas week 1 started with the day after randomization. Last
Value Extended was also used when assessing the percentage of patients with
ACQ-5 below different cut-points at different visits.
For each of the outcomes, the number of patients who were Controlled, and
the number of patients who were at least Partly Controlled in their last week in
study, was analyzed by using logistic regression with treatment and study as
factors.
Stability of asthma control: probability of changing
level of GINA-defined weekly control. Stability of asthma
control was assessed in a Markov analysis investigating transitional proba-
bility of change in control status (excluding exacerbations) as defined by

REFERENCES
E1. O’Byrne PM, Bisgaard H, Godard PP, Pistolesi M, Palmqvist M, Zhu Y, et al. Bu-
desonide/formoterol combination therapy as both maintenance and reliever med-
ication in asthma. Am J Respir Crit Care Med 2005;171:129-36.
E2. Scicchitano R, Aalbers R, Ukena D, Manjra A, Fouquert L, Centanni S, et al. Ef-
ficacy and safety of budesonide/formoterol single inhaler therapy versus a higher
dose of budesonide in moderate to severe asthma. Curr Med Res Opin 2004;20:
1403-18.
E3. Rabe KF, Atienza T, Magyar P, Larsson P, Jorup C, Lalloo UG. Effect of bude-
sonide in combination with formoterol for reliever therapy in asthma exacerba-
tions: a randomised controlled, double-blind study. Lancet 2006;368:744-53.
E4. Kuna P, Peters MJ, Manjra AI, Jorup C, Naya IP, Martinez-Jimenez NE, et al.
Effect of budesonide/formoterol maintenance and reliever therapy on asthma
exacerbations. Int J Clin Pract 2007;61:725-36.
E5. Bousquet J, Boulet LP, Peters MJ, Magnussen H, Quiralte J, Martinez-Aguilar
NE, et al. Budesonide/formoterol for maintenance and relief in uncontrolled
asthma vs. high-dose salmeterol/fluticasone. Respir Med 2007;101:2437-46.
E6. Rabe KF, Pizzichini E, Stallberg B, Romero S, Balanzat AM, Atienza T, et al.
Budesonide/formoterol in a single inhaler for maintenance and relief in mild-
to-moderate asthma: a randomized, double-blind trial. Chest 2006;129:246-56.
E7. Juniper EF, O’Byrne PM, Guyatt GH, Ferrie PJ, King DR. Development and vali-
dation of a questionnaire to measure asthma control. Eur Respir J 1999;14:902-7.
E8. Juniper EF, Svensson K, M€ork AC, Stahl E. Measurement properties and inter-
pretation of three shortened versions of the asthma control questionnaire. Respir
Med 2005;99:553-8.
E9. Juniper EF, Bousquet J, Abetz L, Bateman ED. Identifying ‘‘well-controlled’’ and
‘‘not well-controlled’’asthma using the Asthma Control Questionnaire. Respir
Med 2006;100:616-21.
E10. Svensson K, Mork AC, Juniper EF. ACQ—is five out of seven items acceptable in
large clinical studies? Qual Life Res 2003;12:771. Abstract 1276.
E11. NAEPP (National Asthma Education and Prevention Program). Expert Panel re-
port 3: guidelines for the diagnosis and management of asthma. 2007. Available
at: http://www.nhlbi.nih.gov/guidelines/asthma/asthgdln.pdf. Accessed January
11, 2010.
E12. Global Initiative for Asthma (GINA). Global strategy for asthma management
and prevention: NHLBI/WHO Workshop Report. Bethesda: National Institutes
of Health, National Heart, Lung and Blood Institute. Updated 2008. Available
at: http://www.ginasthma.com. Accessed January 11, 2010.
E13. Bateman ED, Bousquet J, Busse WW, Clark TJ, Gul N, Gibbs M, et al. Stability
of asthma control with regular treatment: an analysis of the Gaining Optimal
Asthma controL (GOAL) study. Allergy 2008;63:932-8.
E14. Combescure C, Chanez P, Saint-Pierre P, Daures JP, Proudhon H, Godard P. Assess-
ment of variations in control of asthma over time. Eur Respir J 2003;22:298-304.
J ALLERGY CLIN IMMUNOL
MARCH 2010
608.e2 BATEMAN ET AL
GINA. ACQ data that were not measured every week were not included in the
Markov analysis. Results from all 5 studies were included in the Markov
modelE13,E14 to calculate the weekly transition probability between control
states defined as the probability of a patient, during the next week, moving
from one level of control (Controlled, Partly Controlled, or Uncontrolled) to
another or remaining at the same level of control or experiencing an exacerba-
tion. Transition probabilities, estimated by the observed transition frequen-
cies, were tabulated and the probabilities achieved with budesonide/
formoterol maintenance and reliever therapy compared with comparators.
The Markov model is a form of time series model in which the response is dis-
crete and independent of time. The predictions provided relate to the week that
follows. However, the calculations are based on data collected from all weeks
in these 6-month or 12-month studies, and although more complex patterns
may apply, the Markov model may be used to estimate the probability of con-
trol for any pattern and for any week in the future.
To assess the impact of control state, treatment, and interaction on the risk of
exacerbation the following week, the outcome ‘‘exacerbation in week/no
exacerbation in week’’ was modeled with a logistic regression model with
factors treatment, previous control state (Controlled, Partly Controlled, or
Uncontrolled), treatment–control interaction, and study. Weeks with ongoing
exacerbation were removed from the analysis, and the model was fitted by using
a generalized estimating equation approach under a working independence
assumption. The results were stable under other choices of working covariance
structures. To obtain treatment comparisons between budesonide/formoterol
maintenance and reliever therapy and comparators, based on concurrent data
while avoiding an excessive number of model parameters, a separate analysis
was performed for each of the 3 comparators on a subset of the data.
To obtain a pooled estimate over all studies and treatments of the impact of
control state on exacerbation risk, the same data (all arms in all studies) were
analyzed by using a similar model with factors previous control state,
treatment, and study.
As an estimate of the transition probability from one weekly control state to
another, the fraction of classified weeks with each previous state that
transitioned to each following state was calculated for each comparator and
each set of concurrent budesonide/formoterol maintenance and reliever
therapy data. Weeks were classified as GINA Controlled, Partly Controlled,
or Uncontrolled, or a week with an exacerbation.
ACQ-5 at randomization as a predictor of
exacerbations. Exacerbation data from all patients in the two 6-month
studies comparing budesonide/formoterol maintenance and reliever therapy
versus higher maintenance dose ICS/LABA plus SABAE4,E5 were pooled and
the mean number of exacerbations stratified according to ACQ-5 cut-points at
randomization (before the first dose of study medication). For a patient to be
included in these calculations, both an assessment of ACQ-5 at randomization
and an assessment of exacerbation status had to be available.
The mean number of severe exacerbations over time, stratified by ACQ-5
cut-point at randomization, was described by using Kaplan–Meier plots and a
Poisson regression model, with adjustments performed for the study factor and
overdispersion.
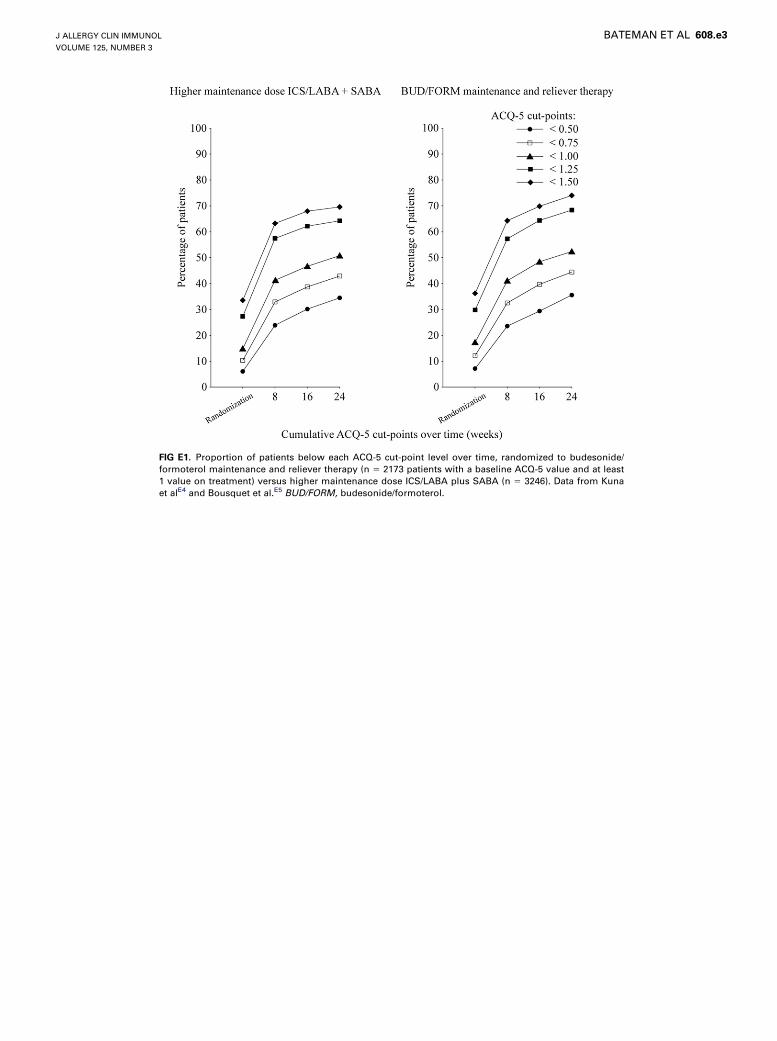
FIG E1. Proportion of patients below each ACQ-5 cut-point level over time, randomized to budesonide/
formoterol maintenance and reliever therapy (n 5 2173 patients with a baseline ACQ-5 value and at least
1 value on treatment) versus higher maintenance dose ICS/LABA plus SABA (n 5 3246). Data from Kuna
et alE4 and Bousquet et al.E5 BUD/FORM, budesonide/formoterol.
J ALLERGY CLIN IMMUNOL
VOLUME 125, NUMBER 3
BATEMAN ET AL 608.e3
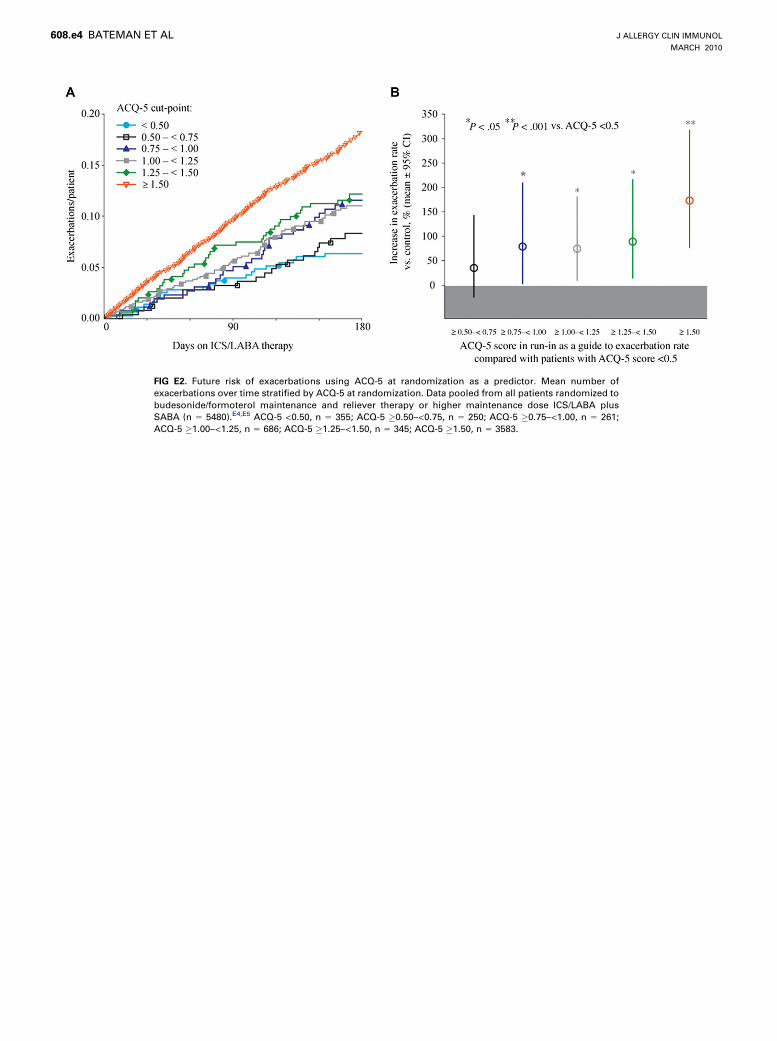
FIG E2. Future risk of exacerbations using ACQ-5 at randomization as a predictor. Mean number of
exacerbations over time stratified by ACQ-5 at randomization. Data pooled from all patients randomized to
budesonide/formoterol maintenance and reliever therapy or higher maintenance dose ICS/LABA plus
SABA (n 5 5480).E4,E5 ACQ-5 <0.50, n 5 355; ACQ-5 �0.50–<0.75, n 5 250; ACQ-5 �0.75–<1.00, n 5 261;
ACQ-5 �1.00–<1.25, n 5 686; ACQ-5 �1.25–<1.50, n 5 345; ACQ-5 �1.50, n 5 3583.
J ALLERGY CLIN IMMUNOL
MARCH 2010
608.e4 BATEMAN ET AL

TABLE E1. Summary of the budesonide/formoterol maintenance and reliever therapy clinical trials used in this retrospective analyses
Study duration Study intervention No. of patients Mean ICS mg/d (BDP equivalent)*y
Comparison with higher maintenance dose ICS therapy plus SABA
O’Byrne et alE1 12 mo BUD/FORM maintenance 1 reliever
(80/4.5 mg BID 1 as needed)
925 240 (375)
BUD (320 mg BID) plus SABA 926 640 (1000)
Scicchitano et alE2 12 mo BUD/FORM maintenance 1 reliever
(2 3 160/4.5 mg QD 1 as needed)
947 466 (728)
BUD (2 3 160 mg BID) plus SABA 943 640 (1000)
Comparison with same maintenance dose ICS/LABA therapy plus SABA
O’Byrne et alE1 12 mo BUD/FORM maintenance 1 reliever
(80/4.5 mg BID 1 as needed)
925 240 (375)
BUD/FORM (80/4.5 mg BID) plus SABA 909 160 (250)
Rabe et alE3 12 mo BUD/FORM maintenance 1 reliever
(160/4.5 mg BID 1 as needed)
1113 483 (755)
BUD/FORM (160/4.5 mg BID) plus
reliever�2281 320 (500)
Comparison with higher maintenance dose ICS/LABA therapy plus SABA
Kuna et alE4 6 mo BUD/FORM maintenance 1 reliever
(160/4.5 mg BID 1 as needed)
1107 483 (755)
BUD/FORM (320/9 mg BID) plus SABA 1105 640 (1000)
SAL/FLU (2 3 25/125 mg BID) plus SABA 1123 500 (1000)
Bousquet et alE5 6 mo BUD/FORM maintenance 1 reliever
(2 3 160/4.5 mg BID 1 as needed)
1154 792 (1238)
SAL/FLU (50/500 mg BID) plus SABA 1155 1000 (2000)
BDP, Beclomethasone dipropionate; BID, twice daily; BUD, budesonide; FLU, fluticasone; FORM, formoterol; QD, once daily; SAL, salmeterol.
In patients on BUD/FORM maintenance and reliever therapy, the additional mean dose of ICS taken as needed as recorded in the patient diary has been added to the regular daily
dose.
*Microgram dose of ICS is stated as prescribed regular daily dose.
�Mean ICS doses converted to BDP equivalents based on GINA guidelines.E12
�Only data from the terbutaline as-needed arm were included in the present analysis (n 5 1141); data from the formoterol as-needed arm (n 5 1140) were excluded.
J ALLERGY CLIN IMMUNOL
VOLUME 125, NUMBER 3
BATEMAN ET AL 608.e5

TABLE E2. Treatment odds ratios for being Controlled and at least Partly Controlled, according to GINA criteria, last week in study
Control status
BUD/FORM maintenance and reliever therapy versus
Higher maintenance dose
ICS 1 SABA*
Same maintenance dose
ICS/LABA 1 SABAy
Higher maintenance dose
ICS/LABA 1 SABAzOR (95% CI) P value OR (95% CI) P value OR (95% CI) P value
C 1.44 (1.20-1.74) <.001 1.03 (0.87-1.21) .73 0.96 (0.83-1.10) .56
C/P 1.56 (1.37-1.78) <.001 1.12 (0.99-1.27) .076 0.99 (0.89-1.10) .86
BUD/FORM, Budesonide/formoterol; C, Controlled; C/P, Partly Controlled; OR, odds ratio.
The OR is the ratio of the probability of being C or at least C/P in the BUD/FORM maintenance and reliever therapy arm and the probability of being C or least C/P in the
comparator arm.
*O’Byrne et al,E1 Scicchitano et alE2: N 5 3681.
�O’Byrne et al,E1 Rabe et alE3: N 5 4054.
�Kuna et al,E4 Bousquet et alE5: N 5 5586.
J ALLERGY CLIN IMMUNOL
MARCH 2010
608.e6 BATEMAN ET AL
Copyright © 2022 FDOKUMEN




















