Orthographically sensitive treatment for dysprosody in children with Childhood Apraxia of Speech...
14
2014 http://informahealthcare.com/pdr ISSN: 1751-8423 (print), 1751-8431 (electronic) Dev Neurorehabil, 2014; 17(2): 137–146 ! 2014 Informa UK Ltd. DOI: 10.3109/17518423.2014.906002 ORIGINAL ARTICLE Orthographically sensitive treatment for dysprosody in children with Childhood Apraxia of Speech using ReST intervention Patricia McCabe, Anita G. Macdonald-D’Silva, Lauren J. van Rees, Kirrie J. Ballard, & Joanne Arciuli Discipline of Speech Pathology, Faculty of Health Sciences, The University of Sydney, Sydney, NSW, Australia Abstract Objective: Impaired prosody is a core diagnostic feature of Childhood Apraxia of Speech (CAS) but there is limited evidence of effective prosodic intervention. This study reports the efficacy of the ReST intervention used in conjunction with bisyllabic pseudo word stimuli containing orthographic cues that are strongly associated with either strong-weak or weak-strong patterns of lexical stress. Methods: Using a single case AB design with one follow-up and replication, four children with CAS received treatment of four one-hour sessions per week for three weeks. Sessions contained 100 randomized trials of pseudo word treatment stimuli. Baseline measures were taken of treated and untreated behaviors; retention was measured at one day and four weeks post-treatment. Results: Children’s production of lexical stress improved from pre to post-treatment. Treatment effects and maintenance varied among participants. Conclusions: This study provides support for the treatment of prosodic deficits in CAS. Keywords Childhood apraxia of speech, lexical stress, orthography, prosody, dyspraxia, intervention History Received 5 January 2014 Revised 12 March 2014 Accepted 13 March 2014 Published online 2 April 2014 Introduction Dysprosody in Childhood Apraxia of Speech Atypical prosody is thought to be a key feature of Childhood Apraxia of Speech (CAS) [1, 2]. The production of lexical stress, in particular, is an area of weakness in CAS. While individuals with CAS have been shown to mark stress in similar ways to younger but typically developing children [3], they appear to use longer word and segment durations than their typically developing peers and tend not shorten duration of vowels in unstressed initial syllables [4]. This paper reports a study designed to examine use of Rapid Syllable Transition Training (ReST), in conjunction with orthographically biased stimuli, to treat disordered prosody in children with CAS. Prosody is realized acoustically through the manipulation of vowel duration (ms), vocal intensity (dB), and vocal pitch (i.e. fundamental frequency or F0 in Hz) [5]. In languages such as English, stressed syllables carry the longest vowel duration and higher peak F0 and intensity compared with other syllables within the word. The dominant lexical stress pattern for English nouns is strong-weak (SW) where stress is placed on the first syllable of words and subsequent syllables are shorter, softer or lower in pitch. English speaking children who are typically developing show a reliance on this pattern in their speech when learning other lexical contrasts such as weak-strong (WS) where the stress is placed on the second syllable of a word [6–8] and the preceding syllable carries weaker stress. Thus younger English speaking children having more success with SW words than WS ones [7, 9]. High levels of variability and inconsistency in the production of stress are noted in children with CAS when compared with other children or adults with speech impair- ments [9–11]. Atypical prosody has been said to differentiate children with CAS from other children with speech delay or phonological disorder and higher levels of dysprosody occur in younger children with CAS than children with other speech disorders [12]. In their repetition of both SW and WS nonwords, children with CAS are perceived to match lexical stress patterns less frequently than phonologically disordered children, even when no differences are detected on acoustic measures [13]. Munson and colleagues [14] also noted that children with CAS mark SW words with pitch and loudness contrasts and WS words with duration contrasts while other children do not make this distinction. Excessive, equal or misplaced stress has also been reported to occur more often in children with CAS when compared with other pediatric speech populations and adults with acquired Apraxia of Speech [13, 15]. These various stress differences between typically developing children and children with CAS may lead to the perceived significant difficulties in both understanding and treating the speech of these children [16]. Prosodic impairments impact significantly on overall speech intelligibility although relatively few studies consider prosody when discussing intelligibility. A review of the literature, looking at the interaction of prosody and speech intelligibility in disorders of speech such as dysarthria, emphasized the impact of prosody on overall speech intelli- gibility [16]. For example, in people with dysarthria, Correspondence: Dr. Patricia McCabe, Speech Pathology, Faculty of Health Sciences, University of Sydney, PO Box 170, Lidcombe, Sydney, NSW 1825, Australia. E-mail: [email protected] Dev Neurorehabil Downloaded from informahealthcare.com by University of Sydney on 04/03/14 For personal use only.
Transcript of Orthographically sensitive treatment for dysprosody in children with Childhood Apraxia of Speech...

2014
http://informahealthcare.com/pdrISSN: 1751-8423 (print), 1751-8431 (electronic)
Dev Neurorehabil, 2014; 17(2): 137–146! 2014 Informa UK Ltd. DOI: 10.3109/17518423.2014.906002
ORIGINAL ARTICLE
Orthographically sensitive treatment for dysprosody in children withChildhood Apraxia of Speech using ReST intervention
Patricia McCabe, Anita G. Macdonald-D’Silva, Lauren J. van Rees, Kirrie J. Ballard, & Joanne Arciuli
Discipline of Speech Pathology, Faculty of Health Sciences, The University of Sydney, Sydney, NSW, Australia
Abstract
Objective: Impaired prosody is a core diagnostic feature of Childhood Apraxia of Speech (CAS)but there is limited evidence of effective prosodic intervention. This study reports the efficacyof the ReST intervention used in conjunction with bisyllabic pseudo word stimuli containingorthographic cues that are strongly associated with either strong-weak or weak-strong patternsof lexical stress. Methods: Using a single case AB design with one follow-up and replication, fourchildren with CAS received treatment of four one-hour sessions per week for three weeks.Sessions contained 100 randomized trials of pseudo word treatment stimuli. Baseline measureswere taken of treated and untreated behaviors; retention was measured at one day and fourweeks post-treatment. Results: Children’s production of lexical stress improved from pre topost-treatment. Treatment effects and maintenance varied among participants. Conclusions:This study provides support for the treatment of prosodic deficits in CAS.
Keywords
Childhood apraxia of speech, lexical stress,orthography, prosody, dyspraxia,intervention
History
Received 5 January 2014Revised 12 March 2014Accepted 13 March 2014Published online 2 April 2014
Introduction
Dysprosody in Childhood Apraxia of Speech
Atypical prosody is thought to be a key feature of Childhood
Apraxia of Speech (CAS) [1, 2]. The production of lexical
stress, in particular, is an area of weakness in CAS. While
individuals with CAS have been shown to mark stress in
similar ways to younger but typically developing children [3],
they appear to use longer word and segment durations than
their typically developing peers and tend not shorten duration
of vowels in unstressed initial syllables [4]. This paper reports
a study designed to examine use of Rapid Syllable Transition
Training (ReST), in conjunction with orthographically biased
stimuli, to treat disordered prosody in children with CAS.
Prosody is realized acoustically through the manipulation
of vowel duration (ms), vocal intensity (dB), and vocal pitch
(i.e. fundamental frequency or F0 in Hz) [5]. In languages
such as English, stressed syllables carry the longest vowel
duration and higher peak F0 and intensity compared with
other syllables within the word. The dominant lexical stress
pattern for English nouns is strong-weak (SW) where stress is
placed on the first syllable of words and subsequent syllables
are shorter, softer or lower in pitch. English speaking children
who are typically developing show a reliance on this pattern
in their speech when learning other lexical contrasts such as
weak-strong (WS) where the stress is placed on the second
syllable of a word [6–8] and the preceding syllable carries
weaker stress. Thus younger English speaking children having
more success with SW words than WS ones [7, 9].
High levels of variability and inconsistency in the
production of stress are noted in children with CAS when
compared with other children or adults with speech impair-
ments [9–11]. Atypical prosody has been said to differentiate
children with CAS from other children with speech delay or
phonological disorder and higher levels of dysprosody occur
in younger children with CAS than children with other speech
disorders [12]. In their repetition of both SW and WS
nonwords, children with CAS are perceived to match lexical
stress patterns less frequently than phonologically disordered
children, even when no differences are detected on acoustic
measures [13]. Munson and colleagues [14] also noted that
children with CAS mark SW words with pitch and loudness
contrasts and WS words with duration contrasts while other
children do not make this distinction. Excessive, equal or
misplaced stress has also been reported to occur more often in
children with CAS when compared with other pediatric
speech populations and adults with acquired Apraxia of
Speech [13, 15]. These various stress differences between
typically developing children and children with CAS may lead
to the perceived significant difficulties in both understanding
and treating the speech of these children [16].
Prosodic impairments impact significantly on overall
speech intelligibility although relatively few studies consider
prosody when discussing intelligibility. A review of the
literature, looking at the interaction of prosody and speech
intelligibility in disorders of speech such as dysarthria,
emphasized the impact of prosody on overall speech intelli-
gibility [16]. For example, in people with dysarthria,
Correspondence: Dr. Patricia McCabe, Speech Pathology, Faculty ofHealth Sciences, University of Sydney, PO Box 170, Lidcombe, Sydney,NSW 1825, Australia. E-mail: [email protected]
Dev
Neu
rore
habi
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f Sy
dney
on
04/0
3/14
For
pers
onal
use
onl
y.

judgments of both impaired prosody and measures of
articulatory accuracy correlate highly with perceived speech
intelligibility [17]. Thus, prosodic impairment can affect
understanding of speech at similar levels to the loss of
intelligibility caused by the segmental speech impairment.
Additionally, we now know that, in English, both supraseg-
mental and segmental information assist lexical access during
the recognition of spoken words [18–20]. Incorrect placement
of stress has been shown to impede lexical access [21].
Treatment for CAS
Most existing interventions for CAS focus primarily on
articulatory parameters and little consideration has been given
to treatment of prosodic impairments and particularly to
measurement of resultant improved prosody in this disorder.
With the exception of the team led by Strand [22–24] who
described Dynamic Temporal and Tactile Cueing (DTTC)
intervention and the ReST intervention [25], no studies report
treatment for prosody specifically.
DTTC intervention includes instruction for varying pros-
ody within treatment trials while focusing on the articulatory
accuracy of target words. In DTTC, children imitate words or
phrases with varied intonation patterns following a model
provided by the clinician. This variation in prosody is not
variation in lexical stress but rather variation in sentence
stress. To date DTTC studies have not reported measurement
of prosody to document changes to prosodic accuracy as a
direct result of this approach.
By contrast, the ReST treatment specifically targets the
ability to control relative durations in the production of SW
and WS pseudo words while simultaneously producing
accurate speech segments at an age appropriate speech rate.
Thus, ReST involves targeting production of lexical stress.
Ballard and colleagues [25] reported that treatment stimuli
consisting of cloze sentences with target three syllable pseudo
words as the final word in the sentence were modeled by the
clinician in the pre-practice phase where the children imitated
the clinician. The stimuli were then read by the children
without a model in the practice phase [25]. All three
participants in that multiple baseline design study improved
prosodic control including duration, loudness, and/or pitch
contrasts for both SW and WS stress patterns and generaliza-
tion was noted to untreated but similar stimuli.
A separate body of work by Arciuli and colleagues has
demonstrated that there are orthographic markers for lexical
stress present in the spelling patterns of English words [8, 26–
28]. Analyses of both child and adult corpora have revealed
that the beginnings and endings of bisyllabic words are
indicators of stress position. Most recently, Arciuli et al. [8]
examined a database of almost 20 000 disyllabic words from
children’s reading materials in an effort to identify probabil-
istic orthographic cues to lexical stress. To illustrate the kinds
of findings they reported, the analyses revealed that most
bisyllabic words beginning with ‘‘be’’ and most bisyllabic
words ending with ‘‘oon’’ have WS stress. In behavioural
testing of 186 typically developing children aged 5–12 years
using carefully constructed pseudo words that contained these
probabilistic cues, Arciuli and colleagues demonstrated that
children are sensitive to these cues. That is, when presented
with an orthographically biased pseudo word such as
‘‘bedoon’’ the children tended to assign a WS pattern
during reading aloud. Older children were found to be more
sensitive to these cues than younger children and this
developmental trajectory was further explored using compu-
tational modeling. It was concluded that sensitivity to these
probabilistic orthographic cues is most likely the result of
implicit learning that grows over time with increasing
exposure to a broader range of written materials.
Van Rees and colleagues recently drew on Arciuli’s work
in their use of orthographic stimuli containing probabilistic
cues to lexical stress in a study examining explicit training of
stress assignment in typically developing children [29]. Using
the approach outlined by Ballard et al., Van Rees et al.
reported using explicit instruction to attend to the relative
length of each syllable as a part of the training and reported
perceptual judgment of stress production as the primary
outcome measure. Typically developing children were ran-
domly allocated to either learn the stimuli (the experimental
group) or be in a control group. Children in the experimental
group learnt to say the pseudo word stimuli in minimum time
while children in the control group did not. Van Rees et al.
concluded that this approach could be applied in future
studies, in an attempt to remediate dysprosody.
Indeed, no previous prosodic intervention for CAS has
been taken into account the biases toward different lexical
stress patterns that may arise with various orthographic
stimuli. It seems possible that the use of orthographic stimuli
may either enhance or hinder the treatment depending on
whether the stimuli contain spelling patterns that are in line
with the stress patterns that the child is being asked to
produce. This applies to studies using either real words or
pseudo words. However, pseudo words are especially
appropriate for use in treatment because they are not
influenced by previously learned motor plans, or differences
in frequency or familiarity across participants [30]. To
illustrate the role of orthographic bias, if a child was being
presented with a written pseudo word such as ‘‘bedoon’’ and
was being asked to produce SW stress, that child could,
potentially, struggle to overcome a preference for assigning
WS stress. Presentation of the written pseudo word
‘‘bedoon’’ in conjunction with instruction on the production
of a WS pattern might be likely to facilitate success in stress
production.
Here, we extend the ReST intervention for CAS [25] by
using Van Rees et al.’s [29] pseudo word stimuli. This is the
first prosody intervention study to use such treatment stimuli.
Hypotheses for this study were:
(1) Children with CAS will show significant improvement in
the ability to contrast SW and WS lexical stress patterns
in both treated and similar untreated exemplars of biased
two-syllable pseudo words.
(2) The effects of treatment will be retained up to four weeks
post-treatment and will generalize to similar untrained
stimuli.
(3) Treatment effects will generalise to connected speech as
a measure of ecological validity.
(4) Treatment effects will not generalize to improved recep-
tive vocabulary skills, demonstrating experimental
control.
138 P. McCabe et al. Dev Neurorehabil, 2014; 17(2): 137–146
Dev
Neu
rore
habi
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f Sy
dney
on
04/0
3/14
For
pers
onal
use
onl
y.

Method
Participants
This research was approved by The University of Sydney
Human Research Ethics Committee (number 11317).
Participants were recruited through electronic advertisements,
the university clinic and community speech language path-
ologists. Four children met the inclusion criteria: history and
current diagnosis of CAS; normal receptive language skills
(Clinical Evaluation of Language Fundamentals, 4th edition,
Australian Standardization CELF-4 [31]); Peabody Picture
Vocabulary Test, PPVT [32]; normal hearing acuity [33]; no
known other developmental or genetic diagnosis; and English
as their first language and at least one parent with English as
their first language. Oral motor examination [34] revealed no
abnormalities in orofacial structure, muscle strength, muscle
tone, or reflexes for any participant. Connected speech
samples were collected for each child, following McLeod’s
procedures [35], with at least 50 utterances collected for each
child, transcribed phonemically and entered into the
Computerized Profiling program to calculate speech accuracy
measures [36]. The ASHA core CAS features [37] were used
by two independent and experienced speech pathologists to
confirm CAS diagnosis from the single word, inconsistency
and connected speech samples reported in Table I. These
features included inconsistent sound errors on repetitions of
syllables or words (as scored on the DEAP inconsistency
subtest [38]); the presence of poor control of coarticulatory
transitions between sounds and syllables; and inappropriate
prosody, particularly of lexical or phrasal stress. Table I
contains a summary of test results for both eligibility and
description of participants.
Reading ability
As the treatment centered on visually presented stimuli,
reading ability was assessed using the Neale Analysis of
Reading Ability, 3rd edition (NARA-3) [39] and the Word
Table I. Pre-treatment assessment battery results for P1, P2, P3, and P4.
P1(male, 8 y; 6 m)
P2(male, 6 y; 7 m)
P3(male, 6 y;6 m)
P4(male, 5 y; 5 m)
Test (used for) Std CI Std CI Std CI Std CI
Peabody Picture Vocabulary Test – 4th edition Form A(receptive vocabulary)
90 83–97 90 83–97 91 84–98 117 109–124
Clinical Evaluation of Language Fundamentals – 4th edition (receptive & expressive language ability)Core Language Score 57* 49–55 81 74–88 76 69–83 89 84–94Receptive Language Index 103 93–113 96 87–105 103 94–112 105 97–103Expressive Language Index 53* 44–62 76* 68–84 74* 66–82 80* 74–86
Test of Auditory Processing – 3rd editionWord Discrimination(auditory discrimination of real words)
5* 3.7–6.3 8 6.4–9.6 8 6.4–9.6 9 7.3–11.6
Word Memory (verbal memory) 6* 4.6–7.4 10 8.6–11.4 6* 4.6–7.4 12 10.7–13.3
Woodcock Reading Mastery Test – RevisedBasic skills cluster 88 86–89 127 126–129 94 88–100 104 101–107
Word identification (reading level) 90 88–91 129 127–130 98 90–102 104 99–108Word attack (nonword reading) 89 87–91 121 119–122 81* 28–103 105 94–110
Lower Case Letters checklist percent(letter name knowledge)
89 – 94 – 48 – 59 –
Comprehensive Test of Phonological Processing Std ±SEM Std ±SEM Std ±SEM Std ±SEM
Phonological Awareness Composite score 64* 59–69 106 103–109 85 82–88 85 82–88Phonological Memory Composite score 70* 64–76 91 84–98 88 81–95 88 82–94
Memory For Digits (verbal memory) 6* 4–8 10 9–11 7 6–8 8 7–9Non-word Repetition (nonword repetition) 4* 3–5 7 6–8 9 8–10 8 7–9
Rapid Naming Composite score 91 86–96 94 89–99 118 113–123 136 131–141
Neale Analysis of Reading Ability – 3rd edition(reading level)
Readingage ±SEM
Readingage ±SEM
Accuracy 6.2 – 56.0–6.8 – 7.0 – 6.5–7.7 –Comprehension 6.11 – 6.3–7.3 – 6.9 – 6.3–7.5 –Rate 7.4 – 6.8–8.0 – 12.9 – 11.7–413 –
Connected speech % % % %
Percent Vowels Correct (PVC) 74 – 77 – 90 – 85 –Percent Consonants Correct (PCC) 81 – 95 – 70 – 60 –Stress pattern match percent (core CAS feature) 46 – 53 – 79 – 63 –Inconsistency percent (Dodd, 2002) (core CAS feature) 20 24 36 40
Standardized tests scores (Std) and 95% confidence intervals (CI) or Standard Errors of Measurement (SEM) are reported as appropriate forassessments.
– Refers to assessments and/or subtests not administered due to age/ability or where range scores not available.* Indicates a score 1 or more standard deviations below the mean.% indicates a percentage score.
DOI: 10.3109/17518423.2014.906002 Prosodic treatment of CAS 139
Dev
Neu
rore
habi
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f Sy
dney
on
04/0
3/14
For
pers
onal
use
onl
y.

Identification subtest of the Woodcock Reading Mastery Test-
Revised (WRMT-R) [40]. These were used to determine each
participant’s reading level. Nonword reading was assessed
using the WRMT-R Word Attack subtest. Nonword speech
repetition was assessed using the Comprehensive Test of
Phonological Processing (CTOPP) [41]. Participants P1 and
P2 were able to read passages from the NARA-3, identify
words in the Word Identification subtest, and decode
nonwords in the Word Attack subtest of the WRMT-R and
so judged capable of independently reading the stimuli
presented in treatment. Participants P3 and P4 were unable
to identify words or decode nonwords and so were not
administered the NARA-3 and were supported in treatment
with clinician spoken modeling of stimuli for direct imitation.
Experimental design
A single case AB design with one follow-up with replication
was employed to test treatment-related changes from pre- to
post-treatment in the four children. All participants completed
three baseline sessions, followed by 12 one-hour treatment
sessions over three weeks. Experimental probes were admin-
istered after every fourth session, on a separate day to
treatment, and a single probe was completed at four weeks
post-treatment. No feedback on production accuracy was
provided during these probes, which tested for acquisition and
retention of treated behaviors and generalization of treatment
effects to untrained stimuli. In addition, a connected speech
sample was collected at each testing point to evaluate
generalization of treatment effects in a more ecologically
valid context. Receptive vocabulary skills were tested pre-
and post-treatment as a measure of experimental control as
this treatment that uses pseudo words was not expected to
accelerate the development of receptive vocabulary.
Stimulus materials and equipment
Baseline/experimental probe and treatment stimuli consisted
of the same 30 bisyllabic pseudo words used in van Rees’ study
[29] which were orthographically biased to either a strong-
weak (SW; e.g., mandan) or a weak-strong (WS; e.g., bedoon)
stress pattern, based on the work of Arciuli and colleagues
[8,26] (Appendix). Pseudo words were used as these cannot be
influenced by learned motor or linguistic plans, which may be
related to frequency of use or familiarity, that are present when
using real words [25,30]. Speech interventions using pseudo
words have been shown to stimulate generalization of
treatment effects to real words [42].
Nineteen treatment pseudo words were selected randomly
from the list of 30 with the remaining 11 serving as probes to
assess acquisition of skills to untreated related stimuli. All
pseudo words were displayed orthographically on flash cards
in 72 point Times New Roman font on 13.2� 4.7 cm index
cards with a different picture of an alien accompanying each
word [43]. Pictures were provided for each pseudo word to
make them visually more interesting thereby enhancing the
distinctiveness of each of the pseudo words.
All baselines and experimental probes were digitally
recorded in a sound-treated booth using a Layla 24/96
Multitrack Recording System with C420III – PP Micro-Mic II
head-mounted microphone (AKG Acoustics) and Adobe
Audition 1.0 [44] with a sampling rate of 44 100 Hz [45].
A 5 cm microphone-to-mouth distance was used.
Treatment procedures
Following Ballard et al. [25] and van Rees et al. [29],
treatment sessions were of 60 min duration, four days per
week for three weeks (total 12 sessions per participant).
Participants and their parents were instructed to undertake no
additional practice of treatment targets outside of these
sessions. Neither children nor their parents were advised of
the hypotheses; however, it was not possible to blind
clinicians to the research hypotheses. Clinicians received a
treatment manual and explicit instruction, training, and
demonstration of treatment procedures prior to commencing
sessions [46]. All sessions were video-recorded for later
scoring of reliability on dependent measures. Consistent with
a PML approach [47], sessions consisted of a pre-practice
component (10–20 min) and a practice component (40–
50 min), as follows.
Pre-practice
During pre-practice, clinicians first presented a randomly
selected stimulus item and asked the child to identify whether
it had a SW (long-short) or a WS (short-long) pattern. If
necessary, the clinician corrected the response. Next, the
clinician modeled the pseudo word for imitation and provided
100% knowledge of performance (KP) feedback on stress
pattern (e.g., ‘‘Try to make the first part even shorter’’) to
shape further attempts. All models were presented with
sentence intonation pattern. Other cues were offered as
appropriate such as hand tapping to cue rhythm and target
length of syllables. This feedback and shaping cues allowed
participants to experience successful production. Although
knowledge of results (KR) feedback (i.e., indicating only the
correctness of a response) was given on segmental errors, no
specific articulatory or phonetic placement instructions were
provided. Participants were moved to the practice phase when
they had produced five consecutive correct trials, including
both SW and WS tokens.
Practice
The 19 orthographic treatment stimuli were presented in
random order with at least 100 trials per session, for a minimum
target of 1200 trials per child. Participants were instructed
either to read the word aloud or to repeat the word after the
clinician dependent on the presentation method assigned from
pretesting. KR feedback was given (i.e. ‘‘good’’/"not good’’)
for combined prosodic and segmental accuracy on 50% of all
trials, fading from high to low frequency across the session,
with a delay between response and provision of feedback of
3–5 s. No KP feedback was provided. Mastery was set at 80%
correct over three consecutive sessions. It should be noted that
typically developing children achieve this mastery on an
average within 3–4 sessions [29].
Variation to practice procedure
Across sessions one to five, it was noted that all participants
had consistent idiosyncratic, incorrect productions for some
140 P. McCabe et al. Dev Neurorehabil, 2014; 17(2): 137–146
Dev
Neu
rore
habi
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f Sy
dney
on
04/0
3/14
For
pers
onal
use
onl
y.

pseudo words. For example, P1 produced ‘‘mandan’’ as
/m"nd|d/ (a real word) instead of /mænd|n/ (a pseudo word).
Although the lexical stress pattern was correct, we decided to
eliminate these idiosyncratic productions with short blocks of
trials. This short-block procedure was triggered when the
error occurred on a trial that had, a priori, been randomly
selected to receive KR feedback. That is, a participant was
given KR feedback on prosodic and segmental accuracy on
the first attempt at the stimulus item; that is, if the production
was correct the child received KR feedback and was presented
with the next trial, but if the idiosyncratic production occurred
s/he received modified KR feedback (e.g. ‘‘good pattern,
wrong sounds’’) and was prompted to try again. Up to three
extra attempts were allowed with KR feedback on each
attempt. The block trials were interwoven with, but in
addition to, the 100 trials per session.
Dependent measures
Productions of pseudo word stimuli during baselines and
experimental probes and during treatment sessions were
judged perceptually as correct or incorrect based on the three
measures – (1) stress pattern correct; (2) all segments correct;
and (3) simultaneously correct stress and segments; the latter
having been shown in studies by Ballard et al. [25] and
McCabe et al. [48] to be harder than either separately. For
stress pattern, a response was judged as correct if the vowel in
the strong syllable was perceived as a full vowel (i.e. not
reduced) and the vowel in the weak syllable was perceived as
a schwa. For segmental accuracy, responses were further
subcategorized as percent vowels correct (PVC) and percent
consonants correct (PCC) as calculated in the PROPH module
of Computerized Profiling [36].
Connected speech samples were collected at each probe
session to examine for generalisation of treatment effects to a
functional speaking task. A minimum of 50 utterances were
phonemically transcribed and entered into Computerized
Profiling [36].
Data analysis
Perceptual treated and untreated probe item data were
graphed for visual analysis and treatment effects analyzed
using percent nonoverlapping data (PND). Scruggs and
Mastropieri [49] (p. 224) suggested that a value of over
70% datapoints nonoverlapping across baseline and treatment
phases of the study for treated or untreated stimuli suggests
a clear treatment or generalization effect, respectively, while
scores between 50 and 70 have questionable effect and scores
under 50 should be interpreted as no demonstration of treat-
ment effect. Sub-analysis of SW and WS accuracy is reported
as raw scores for each participant.
Reliability
Inter- and intra-rater reliability on dependent measures was
calculated for 20% of trials for each treatment session for all
participants; that is, inter-rater agreement on judgment of
response accuracy during treatment and intra- and inter- rater
agreement on phonemic transcription of responses. As per
Ballard et al. [25] and Van Rees et al. [29], to be recorded as
an accurate production, the pseudo word had to be correct for
both stress and segments. Intra-rater agreement on phonemic
transcription ranged from 95 to 97% across participants, and
inter-rater agreement from 83 to 90%.
Reliability of perceptual intra-rater and inter-rater agree-
ment was also calculated on a random 14% of baseline and
experimental probe data for each participant. The intra-rater
agreement was 93% and the inter-rater agreement was 88%.
Reliability of treatment provision (fidelity) was calculated
on compliance with the protocol during the practice phase.
A random block of 20 stimulus–response pairs was examined
for each session and scored for treatment fidelity. Trials were
considered to have fidelity if all components were correct
including: (1) correct presentation of stimulus, including
correct phonemic and prosodic spoken model for P3 and P4;
(2) provision of delayed feedback; (3) provision of KR
feedback only; and finally (4) provision of feedback only on
the pre-randomized items. Fidelity was as follows P1 mean
78% SD 13; P2 mean 76% SD 15, P3 mean 83% SD 16, and
p4 mean 70% SD 17. For the whole group, fidelity was
therefore mean 75% SD 16. Most lapses in fidelity were due
to errors in delaying feedback (both substantially shorter and
longer delays than the desired 3 s) and occurred more
frequently in earlier sessions than in later ones.
Results
Performance on treated pseudo words during practice
During treatment sessions, all participants demonstrated
improved prosodic and segmental accuracy of SW and WS
bisyllabic pseudo words, although none reached the mastery
criterion of 80% correct over three consecutive sessions
(Supplementary figures). P1 initially demonstrated both
prosodic and segmental accuracy below 10% correct and
steadily improved to 66% on both measures in the final
session. P2 initially had prosodic accuracy below 30% and
segmental accuracy below 10%; with prosodic accuracy
reaching 82% correct in the final session and segmental
accuracy fluctuating between 39 and 59% over the final three
sessions. Initially, the P3’s prosodic accuracy was 15% and
the segmental accuracy was about 50%. Both measures
improved over time, reaching a peak of 75% in the second last
session. P4 initially demonstrated prosodic accuracy around
30% and segmental accuracy around 50%. Prosodic accuracy
increased to an average of 58% in the final three sessions and
segmental accuracy increased to an average of 79%.
Treatment, retention, and generalization effects
As this was a within-subject experimental design study,
results are interpreted for each participant individually.
Figure 1 shows the perceptual measures of treated and
untreated probe items for each participant and Online
Supplementary Figures 2–5 show the analysis of SW and
WS items for each participant.
Participant 1
PND across three probes and retention on treated items was
75 and on untreated items was 25. With regard to SW and WS
stimuli, P1 improved from 0% accuracy to 50% correct for
DOI: 10.3109/17518423.2014.906002 Prosodic treatment of CAS 141
Dev
Neu
rore
habi
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f Sy
dney
on
04/0
3/14
For
pers
onal
use
onl
y.
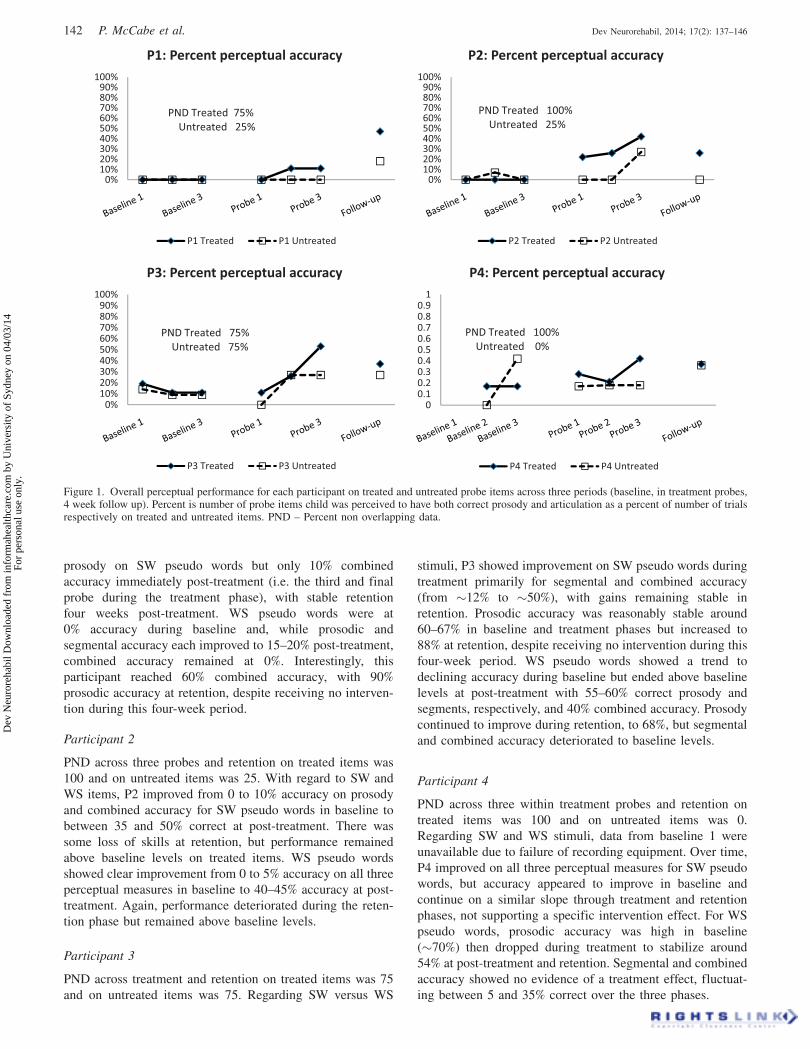
prosody on SW pseudo words but only 10% combined
accuracy immediately post-treatment (i.e. the third and final
probe during the treatment phase), with stable retention
four weeks post-treatment. WS pseudo words were at
0% accuracy during baseline and, while prosodic and
segmental accuracy each improved to 15–20% post-treatment,
combined accuracy remained at 0%. Interestingly, this
participant reached 60% combined accuracy, with 90%
prosodic accuracy at retention, despite receiving no interven-
tion during this four-week period.
Participant 2
PND across three probes and retention on treated items was
100 and on untreated items was 25. With regard to SW and
WS items, P2 improved from 0 to 10% accuracy on prosody
and combined accuracy for SW pseudo words in baseline to
between 35 and 50% correct at post-treatment. There was
some loss of skills at retention, but performance remained
above baseline levels on treated items. WS pseudo words
showed clear improvement from 0 to 5% accuracy on all three
perceptual measures in baseline to 40–45% accuracy at post-
treatment. Again, performance deteriorated during the reten-
tion phase but remained above baseline levels.
Participant 3
PND across treatment and retention on treated items was 75
and on untreated items was 75. Regarding SW versus WS
stimuli, P3 showed improvement on SW pseudo words during
treatment primarily for segmental and combined accuracy
(from �12% to �50%), with gains remaining stable in
retention. Prosodic accuracy was reasonably stable around
60–67% in baseline and treatment phases but increased to
88% at retention, despite receiving no intervention during this
four-week period. WS pseudo words showed a trend to
declining accuracy during baseline but ended above baseline
levels at post-treatment with 55–60% correct prosody and
segments, respectively, and 40% combined accuracy. Prosody
continued to improve during retention, to 68%, but segmental
and combined accuracy deteriorated to baseline levels.
Participant 4
PND across three within treatment probes and retention on
treated items was 100 and on untreated items was 0.
Regarding SW and WS stimuli, data from baseline 1 were
unavailable due to failure of recording equipment. Over time,
P4 improved on all three perceptual measures for SW pseudo
words, but accuracy appeared to improve in baseline and
continue on a similar slope through treatment and retention
phases, not supporting a specific intervention effect. For WS
pseudo words, prosodic accuracy was high in baseline
(�70%) then dropped during treatment to stabilize around
54% at post-treatment and retention. Segmental and combined
accuracy showed no evidence of a treatment effect, fluctuat-
ing between 5 and 35% correct over the three phases.
0%10%20%30%40%50%60%70%80%90%
100%
P1: Percent perceptual accuracy
P1 Treated P1 Untreated
PND Treated 75%Untreated 25%
0%10%20%30%40%50%60%70%80%90%
100%
P2: Percent perceptual accuracy
P2 Treated P2 Untreated
PND Treated 100%Untreated 25%
0%10%20%30%40%50%60%70%80%90%
100%
P3: Percent perceptual accuracy
P3 Treated P3 Untreated
PND Treated 75%Untreated 75%
00.10.20.30.40.50.60.70.80.9
1
P4: Percent perceptual accuracy
P4 Treated P4 Untreated
PND Treated 100%Untreated 0%
Figure 1. Overall perceptual performance for each participant on treated and untreated probe items across three periods (baseline, in treatment probes,4 week follow up). Percent is number of probe items child was perceived to have both correct prosody and articulation as a percent of number of trialsrespectively on treated and untreated items. PND – Percent non overlapping data.
142 P. McCabe et al. Dev Neurorehabil, 2014; 17(2): 137–146
Dev
Neu
rore
habi
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f Sy
dney
on
04/0
3/14
For
pers
onal
use
onl
y.

Generalization to connected speech
Changes in PVC, PCC and stress pattern matches obtained
from connected speech samples at pre-treatment (baseline 3),
post-treatment (1 day immediate post) and retention (4 weeks
post) probe time points are presented in Table II. All
participants increased in their ability to produce correct
stress patterns during connected speech from pre-treatment to
the retention probe. P1, P2, and P3 increased in stress matches
by 19–23 percentage points from pre-treatment to retention,
while P3 increased by 6 percentage points.
Segmental accuracy increased in connected speech for
some participants. Small positive changes in PVC over time
were noted for P1, P2, and P4, with these participants
showing increasing PVC values over time by 6–10 percentage
points. For PCC, P1 and P2 showed deterioration in accuracy
from pre-treatment to retention (27 and 7 points, respect-
ively). P3 and P4 showed small increases in PCC of 4 and 6
percentage points, respectively.
Experimental control
Results of post-treatment language assessment are reported in
Table III. While small improvements were noted for receptive
vocabulary scores on the PPVT [32], these were within the
95% confidence interval of the mean suggesting no systematic
change related to the treatment, as expected.
Discussion
This study evaluated a treatment protocol targeting improved
prosody and segmental accuracy in children with CAS.
Specifically, we examined the use of ReST intervention using
bisyllabic pseudo word stimuli orthographically biased for
particular lexical stress patterns. We hypothesized that (1)
children would improve in their ability to produce lexical
stress in novel two-syllable pseudo words; (2) treatment
effects would be retained up to four weeks post-treatment;
(3) treatment effects would generalise to connected speech;
and (4) experimental control would be demonstrated. The
hypotheses were supported, however, the magnitude of the
treatment effect, retention, and generalization varied across
participants. Based on perceptual judgments of prosodic,
segmental and combined accuracies (the ability to produce
both correct stress pattern and correct phonemes), all children
improved in their ability to produce both lexical stress
contrasts and segmental accuracy from the initial to final
treatment sessions in treated words, thus a treatment effect
occurred. Participants also produced noticeable differences
between SW and WS stimuli at more than one time point as
was expected with the focus of treatment being the vowel
length produced in the weak syllable with criterion set at
production of the schwa vowel.
Both children who read the stimuli (P1 and P2) improved
their production of treated words and the effects of treatment
generalized to untrained probe items and to connected speech.
Thus, reading orthographically biased stimuli may be a
functional approach to treatment of CAS and it may be that
imitation of a clinician model, which is common practice in
speech intervention, is not required by older children with
CAS. This finding may help ameliorate a number of the
problems reported by parents to be associated with regular
home practice including finding time for daily practice [50]
and knowing that they are providing an accurate model for their
child [51]. It should be noted, however, that reading ability and
difficulties decoding pseudo words may influence both stress
assignment and segmental accuracy of spoken stimuli. While it
is difficult to control for this effect during treatment (i.e.,
determining if errors are the result of misreading and/or
misarticulation), it needs to be considered when determining if
children are going to be asked directly to read treatment
stimuli. Gillon and colleagues have shown that children with
CAS may experience delays in reading ability [52,53] and,
therefore, clinicians should cautiously consider written-only
orthographically biased stimulus. This applies not only to
prosodic interventions but also to treatments targeting other
characteristics of CAS such as segmental errors.
Where written stimuli are used, particular attention should
be paid to the nature of these stimuli as it seems possible that
certain stimuli may enhance or hinder the treatment depend-
ing on whether the stimuli contain spelling patterns that are in
line with the stress patterns that the child is being asked to
produce. This applies to studies using either real words or
pseudo words. The combination of this study and that of Van
Rees et al. [29] suggests that the use of appropriately selected
written stimuli which are orthographically biased can enhance
production accuracy for children with CAS and those with
typical speech development.
Participants also made changes in segmental accuracy both
in therapy and in the generalization measure of connected
speech. This occurred even though only simple Knowledge
of Results [47] feedback on correct/incorrect production
was provided on segmental accuracy. That is, participants
were only told that sounds were correct or incorrect in the
pre-practice phase and not in the practice phase and no direct
teaching on sound accuracy was provided at any stage. This
finding echoes work with adults with acquired apraxia of
speech where both Mauszycki and Wambaugh [54] and
Table II. Percent vowels correct (PVC), percent consonants correct(PCC), and percent stress pattern matches (stress %) during connectedspeech at pre-treatment (Pre), post-treatment (Post) and retention (Ret)for each participant..
P1 P2 P3 P4
Pre Post Ret Pre Post Ret Pre Post Ret Pre Post Ret
PVC 74 81 80 78 87 87 90 88 92 85 84 91PCC 81 80 54 95 95 88 70 86 74 60 70 66Stress % 46 43 70 53 81 76 79 77 85 64 68 83
Table III. Post-treatment assessment results for P1, P2, P3, and P4.
P1 P2 P3 P4
Test Std CI Std CI Std CI Std CI
Peabody PictureVocabularyTest – 4th editionForm B
84 78–91 96 89–103 90 83–97 119 111–125
Standardized tests scores (Std) and 95% confidence intervals (CI) arereported, % indicates a percentage score.
DOI: 10.3109/17518423.2014.906002 Prosodic treatment of CAS 143
Dev
Neu
rore
habi
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f Sy
dney
on
04/0
3/14
For
pers
onal
use
onl
y.

Brendel and Zeigler [55] reported training rate or rhythm
alone also improved segmental accuracy.
All participants had difficulty synchronously producing
both correct stress patterns and correct segments. These
difficulties are reflected in the perceptual judgments of both
treatment and probe data where most participants had poor
performance on simultaneous production of the correct stress
pattern whilst maintaining segmental accuracy. This inability
to combine performance across speech elements may be
hypothesized as causally linked to an increased load on the
overall speech system. For example, P3 maintained only
prosodic accuracy after treatment and P4 was able to achieve
accurate prosody alone on most occasions with segmental
accuracy apparently sacrificed to achieve prosodic accuracy
[56]. Stress pattern matches during connected speech
increased while PCC values decreased for P1 and P2 also
suggesting a sacrifice of segmental accuracy to achieve
prosodic accuracy. Such a trade-off between development of
lexical stress and segmental accuracy is seen in the develop-
ment of polysyllabic words in typically developing children
with prosodic and/or segmental accuracy sacrificed at differ-
ent stages of development until an adult like production is
realized [57]. Therefore, participants in this study may be
following a normal developmental pattern in the development
of lexical stress with positive changes to stress production
triggered as a result of treatment [6].
Generalization
Generalization to non-treated pseudo word items mirrored the
results for treatment stimuli in all participants; however, the
changes were less pronounced. Generalization to connected
speech was also observed with change over time in measures
of stress pattern match and PVC. Prior to treatment all
children had prosodic impairments in connected speech in the
moderate to severe range. Although connected PCC measures
were mostly mild to moderate prior to treatment, in combin-
ation with poor prosody, this resulted in a high level of
perceived unintelligibility. The connected speech generaliza-
tion reported here is a highly desired outcome, as an increase
in matching prosodic patterns will lead to increased speech
intelligibility [58]. Additionally, generalization to connected
speech suggests that the use of orthographically biased pseudo
word stimuli may promote learning during treatment and
promote generalization to more complex untreated but
desirable behaviors. This suggestion requires further investi-
gation but such generalization from pseudo words has been
reported for other speech disorders in children [42].
Limitations
The design of the current study limits the generalization of
these results but provides preliminary evidence of treatment
efficacy. When combined with the extant Ballard et al. [26]
and Van Rees et al. [30] studies, the findings reported here
suggest that ReST intervention is a promising treatment
worthy of further investigation.
A number of additional constraints on the generalizability
of the research exist. Each child was treated by a different
clinician and so there may have been a confound of treating
clinician. However, participant–clinician pairs were randomly
assigned and all clinicians were required to demonstrate
treatment fidelity and so delivered the protocol as intended.
A ceiling effect was observed for P4 with the bisyllabic
stimuli in isolation being insufficiently challenging. Future
studies should manage this effect through the provision of
more complex orthographically biased stimuli and the use of
such stimuli in cloze sentences as per Ballard et al.’s
approach [25].
These four single cases provide evidence that a treatment
effect can be obtained using the current protocol. Additional
research is needed to further test this treatment approach in
a larger group of children with CAS using both imitation
and spontaneous reading of the stimuli and to assess the
effects of orthographically biased treatment stimuli in a range
of prosodic disorders. Further development of the protocol
and validation with a wider range of children with CAS is also
required before we can be assured of the efficacy of this
promising intervention.
Conclusions
Prosodic impairments can be treated in children with CAS
using ReST intervention in conjunction with orthographically
biased stimuli. The use of stimuli orthographically biased to
particular lexical stress patterns resulted in positive treatment
outcomes for all children with maintenance and generalization
of treatment skills.
Acknowledgements
Thanks to Tal Schwarzmann, Katrina Wu, Henna Chaudhry,
and Nicole Willcox for assistance with data collection and the
four children and their families.
Declaration of interest
The authors are not aware of any conflicts of interest
associated with this paper. The authors are solely responsible
for the content and writing of this paper. Parts of this study
were presented at the 2010 Conference on Motor Speech in
Savannah, GA, USA, and the 2010 Speech Pathology
Australia National Conference in Melbourne, VIC, Australia.
References
1. Shriberg LD, Green JR, Campbell TF, McSweeny JL, Scheer AR. Adiagnostic marker for childhood apraxia of speech: The coefficientof variation ratio. Clinical Linguistics & Phonetics 2003;17(7):575–595.
2. Sussman HM, Marquardt TP, Doyle J. An acoustic analysis ofphonemic integrity and contrastiveness in developmental apraxia ofspeech. Journal of Medical Speech Language Pathology 2000;8(4):301–313.
3. Maassen B. Issues contrasting adult acquired versus developmentalapraxia of speech. Seminars in Speech & Language 2002;23(4):257–266.
4. Stackhouse J. Developmental verbal dyspraxia I: A review andcritique. European Journal of Disorders of Communication 1992;27(1):19–34.
5. Thoonen G, Maassen B, Wit J, Gabreels F, Schreuder R. Theintegrated use of maximum performance tasks in differentialdiagnostic evaluations among children with motor speech disorders.Clinical Linguistics & Phonetics 1996;10(4):311–336.
6. Ballard KJ, Djaja D, Arciuli J, James DG, van Doorn JL.Developmental trajectory for production of prosody: Analysis oflexical stress contrastivity in children aged 3 to 7 years and adults.
144 P. McCabe et al. Dev Neurorehabil, 2014; 17(2): 137–146
Dev
Neu
rore
habi
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f Sy
dney
on
04/0
3/14
For
pers
onal
use
onl
y.

Journal of Speech Language and Hearing Research 2012;55(6):1822–1835.
7. James DGH. Hippopotamus is so hard to say: Children’s acquisitionof polysyllabic words. Sydney, Australia: The University of Sydney;2006.
8. Arciuli J, Monaghan P, Seva N. Learning to assign lexical stressduring reading aloud: Corpus, behavioral, and computationalinvestigations. Journal of Memory and Language 2010;63(2):180–196.
9. Hall PK, Jordan LS, Robin DA. Developmental apraxia of speech:Theory and clinical practice. Austin, TX: Pro-Ed; 1993.
10. Davis BL, Jakielski KJ, Marquardt TP. Developmental apraxia ofspeech: Determiners of differential diagnosis. Clinical Linguistics& Phonetics 1998;12(1):25–45.
11. Hickman LA. The apraxia profile. San Antonio, TX: ThePsychological Corporation; 1997.
12. Shriberg LD, Aram DM, Kwiatkowski J. Developmental apraxia ofspeech: II. Toward a diagnostic marker. Journal of Speech,Language, and Hearing Research 1997;40(2):286–312.
13. Odell KH, Shriberg LD. Prosody-voice characteristics of childrenand adults with apraxia of speech. Clinical Linguistics & Phonetics2001;15(4):275–307.
14. Munson B, Bjorum EM, Windsor J. Acoustic and perceptualcorrelates of stress in nonwords produced by children withsuspected developmental apraxia of speech and children withphonological disorder. Journal of Speech, Language, and HearingResearch 2003;46:189–202.
15. Guyette TW, Diedrich WM. A critical review of developmentalapraxia of speech. In: Lass N, editor. Speech and language:Advances in basic research and practice. Vol. 5. New York:Academic Press; 1981. pp 1–49.
16. Souza TN, Payao MC, Costa RC. Childhood speech apraxia infocus: Theoretical perspectives and present tendencies. Pro-fono:Revista de atualizacao cientıfica 2009;21(1):76–80.
17. Williams P, Stephens H. Nuffield Centre Dyspraxia Programme.Windsor, United Kingdom: The Miracle Factory; 2004.
18. Arciuli J, Slowiaczek LM. The where and when of linguistic word-level prosody. Neuropsychologia 2007;45(11):2638–2642.
19. Arciuli J, Cupples L. Effects of stress typicality during spoken wordrecognition by native and nonnative speakers of English: Evidencefrom onset gating. Memory and Cognition 2004;32(1):21–30.
20. Arciuli J, Cupples L. Effects of stress typicality during speededgrammatical classification. Language and Speech 2003;46(4):353–374.
21. Slowiaczek LM, Soltano EG, Bernstein HL. Lexical and metricalstress in word recognition: Lexical or pre-lexical influences?Journal of Psycholinguistic Research 2006;35(6):491–512.
22. Strand EA, Debertine P. The efficacy of integral stimulationintervention with developmental apraxia of speech. Journal ofMedical Speech Language Pathology 2000;8(4):295–300.
23. Strand EA, Skinder A. Treatment of developmental apraxia ofspeech: Integral stimulation methods. In: Caruso A, Strand E,editors. Clinical management of motor speech disorders in children.New York: Thieme Medical Publishers Inc.; 1999.
24. Strand EA, Stoeckel R, Baas BS. Treatment of severe childhoodapraxia of speech: A treatment efficacy study. Journal of MedicalSpeech-Language Pathology 2006;14(4):297–307.
25. Ballard KJ, Robin DA, McCabe P, McDonald J. A treatment fordysprosody in childhood apraxia of speech. Journal of Speech,Language, and Hearing Research 2010;53(5):1227–1245.
26. Arciuli J, Cupples L. The processing of lexical stress during visualword recognition: Typicality effects and orthographic correlates.Quarterly Journal of Experimental Psychology 2006;59(5):920–948.
27. Seva N, Monaghan P, Arciuli J. Stressing what is important:Orthographic cues and lexical stress assignment. Journal ofNeurolinguistics 2009;22(3):237–249.
28. Arciuli J, Cupples L. Would you rather ‘embert a cudsert’ or‘cudsert an embert’? How spelling patterns at the beginning ofEnglish disyllables can cue grammatical category. In: KhlentzosACSD, editor. Mental states, Vol. 2: Language and cognitivestructure, Studies in language companion series. Amsterdam,Netherlands: John Benjamins Publishing Company; 2007.pp 213–238.
29. van Rees LJ, Ballard KJ, McCabe P, Macdonald-D’Silva AG,Arciuli J. Training production of lexical stress in typicallydeveloping children with orthographically biased stimuli andprinciples of motor learning. American Journal of Speech-Language Pathology 2012;21(3):197–206.
30. Maas E, Barlow J, Robin D, Shapiro L. Treatment of sound errorsin aphasia and apraxia of speech: Effects of phonologicalcomplexity. Aphasiology 2002;16(4/5/6):609–622.
31. Semel E, Wiig E, Secord W. Clinical evaluation of languagefundamentals – 4th ed. Australian Standardised Edition (CELF-4Australian). Pearson Inc.; 2006.
32. Dunn LM, Dunn DM. Peabody picture vocabulary test.Minneapolis, MN: Pearson; 2007.
33. American Speech-Language-Hearing Association. Guidelines formanual pure tone threshold audiometry. ASHA 1978;20:297–301.
34. Robbins J, Klee T. Clinical assessment of oropharyngeal motordevelopment in young children. Journal of Speech and HearingDisorders 1987;52:217–277.
35. McLeod S. Sampling consonant clusters: Four procedures designedfor Australian children. Australian Communication Quarterly 1997;Autumn:9–12.
36. Long SH, Fey ME, Channell RW. Computerized profiling 9.7.0.Cleveland, OH: Case Western Reserve University; 2006.
37. American Speech-Language-Hearing Association. ChildhoodApraxia of Speech [Technical Report]. Available from: www.asha.org/policy. 2007.
38. Dodd B, Hua Z, Crosbie S, Holm A, Ozanne A. DiagnosticEvaluation of Articulation and Phonology (DEAP). London,England: The Psychological Corporation; 2002.
39. Neale MD. Neale analysis of reading ability. Melbourne, Australia:ACER Press; 1999.
40. Woodcock RW. Woodcock Reading Mastery Tests-Revised/Normative Update (WRMT-R/NU). Allen, TX: PearsonAssessments; 1998.
41. Wagner R, Torgesen JK, Rashotte CA. Comprehensive test ofphonological processing (CTOPP). Austin, TX: Pro-Ed; 1999.
42. Gierut JA, Morrisette ML, Ziemer SM. Nonwords and generaliza-tion in children with phonological disorders. American Journal ofSpeech-Language Pathology 2010;19(2):167–177.
43. Gupta P, Lipinski J, Abbs B, Lin P-H, Aktunc E, Ludden D, MartinN, Newman R. Space aliens and nonwords: Stimuli for investigatingthe learning of novel word-meaning pairs. Behavior ResearchMethods, Instruments, & Computers 2004;36(4):599–603.
44. Adobe Systems Incorporated. Adobe Audition 1.0 2003.45. Deliyski DD, Shaw HS, Evans MK. Influence of sampling rate on
accuracy and reliability of acoustic voice analysis. Logopedics,Phoniatrics, Vocology 2005;30:55–62.
46. Murray E, McCabe P, Ballard KJ. A comparison of two treatmentsfor childhood apraxia of speech: Methods and treatment protocolfor a parallel group randomised control trial. BMC Pediatrics 2012;12:112.
47. Maas E, Robin DA, Austermann Hula SN, Freedman SE, Wulf G,Ballard KJ, Schmidt RA. Principles of motor learning in treatmentof motor speech disorders. American Journal of Speech-LanguagePathology 2008;17(3):277–298.
48. McCabe P, Ballard KJ. An Innovative Syllable TransitionTreatment Trial for Childhood Apraxia of Speech. Motor SpeechConference. Monterey, CA, USA; 2008.
49. Scruggs TE, Mastropieri MA. Summarizing single-subjectresearch: Issues and applications. Behavior Modification 1998;22(3):221–242.
50. Ruggero L, McCabe P, Ballard KJ, Munro N. Paediatric speech-language pathology service delivery: An exploratory survey ofAustralian parents. International Journal of Speech-LanguagePathology 2012;14(4):338–350.
51. Thomas D, McCabe P, Ballard KJ. Parent training for rapid syllabletransitions treatment for childhood apraxia of speech: Fidelity ofparent conducted treatment. Motor Speech Symposium. Sarasota,FL, USA; 2014.
52. Gillon GT, Moriarty BC. Childhood apraxia of speech: Children atrisk for persistent reading and spelling disorder. Seminars in Speechand Language 2007;28(1):48–57.
53. McNeill BC, Gillon GT, Dodd B. Phonological awareness and earlyreading development in childhood apraxia of speech (CAS).
DOI: 10.3109/17518423.2014.906002 Prosodic treatment of CAS 145
Dev
Neu
rore
habi
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f Sy
dney
on
04/0
3/14
For
pers
onal
use
onl
y.

International Journal of Language & Communication Disorders2009;44(2):175–192.
54. Mauszycki SC, Wambaugh JL. The effects of rate control treatmenton consonant production accuracy in mild apraxia of speech.Aphasiology 2008;22(7-8):906–920.
55. Brendel B, Ziegler W. Effectiveness of metrical pacing in thetreatment of apraxia of speech. Aphasiology 2007;22(1):77–102.
56. Howard S. The interplay between articulation and prosody inchildren with impaired speech: Observations from electropalato-
graphic and perceptual analysis. International Journal of Speech-Language Pathology 2007;9(1):20–35.
57. James DGH, van Doorn J, McLeod S. The contribution ofpolysyllabic words in clinical decision making about children’sspeech. Clinical Linguistics & Phonetics 2008;22(4 and5):345–353.
58. Klopfenstein M. Interaction between prosody and intelligibility.International Journal of Speech-Language Pathology 2009;11(4):326–331.
Appendix
Table A1. Treatment and non-treatment stimuli set with treatment words in bold (based on Arciuli et al. [1] and used inVan Rees et al. [2]).
SW orthographyPhonemic transcription and
production used for imitation WSPhonemic transcription and
production used for imitation
coddol /kodFl/ adibe /Fdib/combol /kombFl/ adoon /Fdun/condan /kondFn/ amade /FmeId/condey /kondF/ apoon /Fpun/copet /kopFt/ bemade /bFmeId/covan /kovFn/ bemiss /bFmIs/mandan /mændFn/ bepade /bFpeId/mapet /mæpFt/ beribe /bFraIb/mappol /mæpFl/ bevade /bFveId/maran /mæ7Fn/ abade /FbeId/combet /kombFt/ amiss /FmIs/conol /konFl/ bedibe /bFdaIb/mambey /mæmbF/ bediss /bFdIs/mandol /mændFl bedoon /bFdun/manet /mænFt/ bemoon /bFmun/
References[1] Arciuli J, Monaghan P, Seva N. Learning to assign lexical stress during reading aloud: Corpus, behavioral, and
computational investigations. Journal of Memory and Language 2010;63(2):180-196.[2] van Rees LJ, Ballard KJ, McCabe P, Macdonald-D’Silva AG, Arciuli J. Training production of lexical stress in
typically developing children with orthographically biased stimuli and principles of motor learning. American Journalof Speech-Language Pathology 2012:1058-0360_2012_11-0008.
146 P. McCabe et al. Dev Neurorehabil, 2014; 17(2): 137–146
Dev
Neu
rore
habi
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f Sy
dney
on
04/0
3/14
For
pers
onal
use
onl
y.

Figure 2. P1s performance across the baseline and experimental probes. The panel shows percent correct for production of stress, segments, and
both combined, as perceptually judged, for treated strong-weak (SW) nonwords (A) and treated weak-strong (WS) nonwords (B).
A B

Figure 3. P2s performance across the baseline and experimental probes. The panel shows percent correct for production of stress, segments, and
both combined, as perceptually judged, for treated strong-weak (SW) nonwords (A) and treated weak-strong (WS) nonwords (B).

Figure 4. P3s performance across the baseline and experimental probes. The panel shows percent correct for production of stress, segments, and
both combined, as perceptually judged, for treated strong-weak (SW) nonwords (A) and treated weak-strong (WS) nonwords (B).
A B

Figure 5. P4s performance across the baseline and experimental probes. The top panel shows percent correct for production of stress, segments,
and both combined, as perceptually judged, for treated strong-weak (SW) nonwords (A) and treated weak-strong (WS) nonwords (B).
A B