Orthodontic diagnosis of long face syndrome - Renstrom ...
6
Orthodontic diagnosis of long face syndrome An important aspect of comprehensive orthodontic therapy is managing the vertical dimension of the patient's face. Many of the most difficult orthodontic cases involve long face syndrome. Characteristics include excessive eruption of posterior teeth, normal or excessive eruption of anterior teeth, short posterior facial height, and a steep mandibular plane angle.' Common diagnostic criteria for long face syndrome include a gonion (Go) to gnathion (Gn) to sella-nasion (SN) line angle (mandibular plane angle) of 37 or greater, and a posterior (S to Go) to anterior facial height (N to menton [Me]) ratio of 0.65 or less.' In Figure 1, the skeletal differences between normal and long-faced patients are illustrated. Causes and management The primary cause of long face syndrome is an unfavorable growth pattern? However, extrinsic factors such as large adenoids, finger habits, or improperly applied orthodontic mechanics can cause characteristics of long face syndrome. Limiting the extrusion of the posterior teeth is critical in orthodontic management of long face syndrome.' If the posterior teeth extrude more than normal, the bite opens. This increases the mandibular plane angle and reduces the ratio of posterior to anterior facial height. These changes cause characteristics of long face syndrome. Because the mandible opens along an arc, excessive bite opening results in a retruded mandibular position (Fig. 2). Sassouni' and Prahl-Anderson et al. showed that a retruded mandible combined with characteristics of long face syndrome result in poor facial esthetics.' McNamara showed that more than 60 percent of patients with Class II malocclusions exhibit 1 or more symptoms of long face syndrome.,
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Orthodontic diagnosis of long face syndrome - Renstrom ...

Orthodontic diagnosis of long face syndrome An important aspect of comprehensive orthodontic therapy is managing the vertical dimension of the patient's face. Many of the most difficult orthodontic cases involve long face syndrome. Characteristics include excessive eruption of posterior teeth, normal or excessive eruption of anterior teeth, short posterior facial height, and a steep mandibular plane angle.' Common diagnostic criteria for long face syndrome include a gonion (Go) to gnathion (Gn) to sella-nasion (SN) line angle (mandibular plane angle) of 37 or greater, and a posterior (S to Go) to anterior facial height (N to menton [Me]) ratio of 0.65 or less.' In Figure 1, the skeletal differences between normal and long-faced patients are illustrated. Causes and management The primary cause of long face syndrome is an unfavorable growth pattern? However, extrinsic factors such as large adenoids, finger habits, or improperly applied orthodontic mechanics can cause characteristics of long face syndrome. Limiting the extrusion of the posterior teeth is critical in orthodontic management of long face syndrome.' If the posterior teeth extrude more than normal, the bite opens. This increases the mandibular plane angle and reduces the ratio of posterior to anterior facial height. These changes cause characteristics of long face syndrome. Because the mandible opens along an arc, excessive bite opening results in a retruded mandibular position (Fig. 2). Sassouni' and Prahl-Anderson et al. showed that a retruded mandible combined with characteristics of long face syndrome result in poor facial esthetics.' McNamara showed that more than 60 percent of patients with Class II malocclusions exhibit 1 or more symptoms of long face syndrome.,

Fig. 1. Cephalometric illustrations of differences between a normal and long- faced patient. The patient with long face syndrome (A) has a Go-Gn to SN angle of 41 and a S-Go to N-Me ratio of .58. These measurements are diagnostic criteria for long face syndrome. The patient shown in (13) has more normal cephalometric measurements a Go-Gn to SN measurement of 26 and a S-Go to N-Me ratio of .71.
Fig. 2. The relationship between lower anterior facial height and effective mandibular length: an excessive vertical dimension of 15 mm produces an effective mandibular retrusion of 13 mm.
Fig. 3. The variability in growth at the mandibular condyle in relation to the posterior border of the ramus (R1).
Long face syndrome patients with malocclusions are the most difficult cases to treat. General practitioners who perform orthodontics must recognize patients with long face syndrome, and patients with the potential to develop characteristics of long face syndrome due to improper or inappropriately applied orthodontic mechanics. These cases should be referred to an orthodontist. Most orthodontic systems primarily affect the teeth and alveolar processes. Bands, brackets, and wires cause extrusion of teeth.' However, this bite-opening tendency is expressed differently among patients. Some patients' stomatognathic systems resist vertical dimension changes, and many months often are required to erupt teeth. Tooth eruption in other patients proceeds dramatically with only a month or two of leveling and aligning mechanics. A major challenge in performing orthodontic procedures is predicting a patient's response to extrusive forces. Bjork provided a reliable, convenient method of determining a patient's response to orthodontic appliances in terms of vertical dimension.' Patients who may have excessive posterior eruption and develop characteristics of long face syndrome can be recognized before treatment. Bjork, former chairman of the orthodontic department of the Royal College of Dentistry in Copenhagen, did his research in the 1950s and 60s. He placed metallic implants in the maxillas and mandibles of 240 growing patients and observed their growth for 10 to 15 years.' He performed no treatment but kept annual diagnostic records. His study cannot be duplicated because supervised neglect (not treating malocclusions) and placement of metallic implants for observation violate today's medical ethics. Superimposing a patient's lateral cephalometric x-rays on the stable metallic implants permits study of growth mechanics and direction. Most mandibular growth occurs at the condylar head.' Any change in mandibular shape results from apposition and resorption of surface bone. Bjork discovered that surface remodeling disguises about 50 percent of the growth rotation of the lower jaw.' Untreated patients have a wide range of condylar-growth direction." In Figure 3, condylar-growth direction is shown in some patients in Bjork's study. The majority of patients show slight anterior condylar growth. Many patients deviate from this pattern. Some patients have more anterior condylar growth, which results in more

horizontal mandibular growth. Some patients show more posterior condylar growth, which results in more vertical direction of mandibular growth (Fig. 4). No one knows why these differences occur. According to a widely accepted theory, different locations of growth cells on the condylar head produce different growth rotations, and location of growth cells-an inherited trait-determines mandibular-growth direction." Although the reasons for growth differences are not well understood, these differences affect the entire craniofacial complex. The muscles of mastication act in different directions in horizontal and vertical growers, and produce different muscular pressures and tensions in the two types of growth. This results in different apposition and resorption of surface bone and, therefore, different mandibular morphology in horizontal and vertical growers.
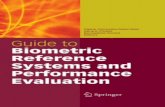
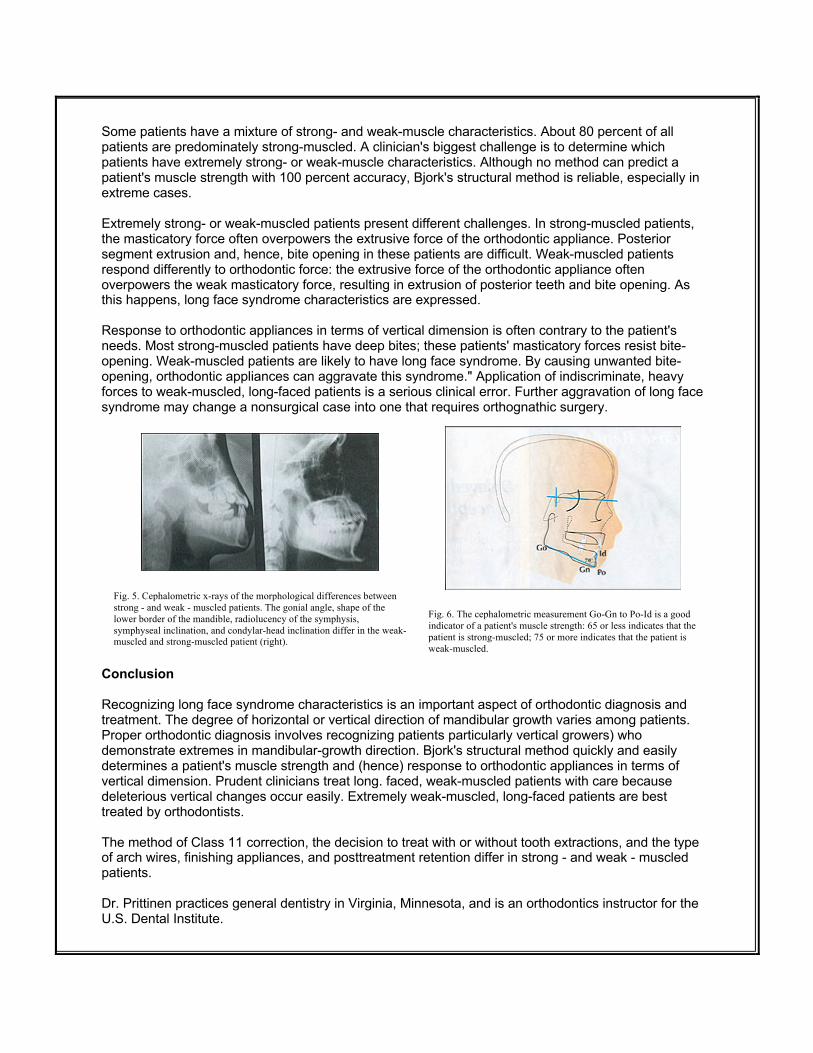
Fig. 4. (A): mandibular growth rotation produced by posterior cellular apposition on the condyle. (B): mandibular growth rotation produced by anterior cellular apposition on the condyle. Strong - and weak - muscle factors Why are these differences in mandibular morphology important? In horizontal growers, the angles at which the muscles work produce much masticatory force. In vertical growers, the angles at which the muscles work produce much less force.,' Therefore, horizontal growers can be referred to as strong-muscled patients, and vertical growers can be referred to as weak-muscled patients. Long face syndrome patients are usually weak-muscled, vertical growers. In Figure 5, the morphological differences are highlighted between the two growth patterns as viewed on lateral cephalometric x-rays. The morphological differences are numerous, but five are especially diagnostic. First, strong-muscled patients have relatively acute gonial angles; in weak-muscled patients, the gonial angle tends to be obtuse."," Second, the shape of the lower border of the mandible differs in the two types of patients. In strong-muscled patients, a double curvature on the lower border consists of a concavity near the gonial angle and a convexity near the anterior portion of the lower border. Weak-muscled patients lack this double curvature and instead exhibit a concave lower border. Third, strong-muscled patients have a radiopaque symphysis; in weak-muscled patients, this area is more radiolucent.2 Fourth, the more acute the symphyseal inclination, the more the patient tends to be strong-muscled. This can be quantified by a simple cephalometric measurement of the angle between Go-Gn and the chin line (the line from pogonion [P01 to infradentale [1d]-the most anterosuperior point on the mandibular alveolar ridge) (Fig. 6)." A range of 70 ± 4 is normal: 65 or less indicates that the patient is strong-muscled; 75 or more indicates that the patient is weak-muscled. Finally, condylar-head inclination indicates muscle strength. Strong-muscled patients have an anterior condylar-head inclination; weak-muscled patients have a posterior condylar-head inclination. Due to superimposition of the zygomatic process over the condylar area, condylar inclination sometimes is not visible on a cephalometric radiograph.
Some patients have a mixture of strong- and weak-muscle characteristics. About 80 percent of all patients are predominately strong-muscled. A clinician's biggest challenge is to determine which patients have extremely strong- or weak-muscle characteristics. Although no method can predict a patient's muscle strength with 100 percent accuracy, Bjork's structural method is reliable, especially in extreme cases. Extremely strong- or weak-muscled patients present different challenges. In strong-muscled patients, the masticatory force often overpowers the extrusive force of the orthodontic appliance. Posterior segment extrusion and, hence, bite opening in these patients are difficult. Weak-muscled patients respond differently to orthodontic force: the extrusive force of the orthodontic appliance often overpowers the weak masticatory force, resulting in extrusion of posterior teeth and bite opening. As this happens, long face syndrome characteristics are expressed. Response to orthodontic appliances in terms of vertical dimension is often contrary to the patient's needs. Most strong-muscled patients have deep bites; these patients' masticatory forces resist bite-opening. Weak-muscled patients are likely to have long face syndrome. By causing unwanted bite-opening, orthodontic appliances can aggravate this syndrome." Application of indiscriminate, heavy forces to weak-muscled, long-faced patients is a serious clinical error. Further aggravation of long face syndrome may change a nonsurgical case into one that requires orthognathic surgery.
Fig. 5. Cephalometric x-rays of the morphological differences between strong - and weak - muscled patients. The gonial angle, shape of the lower border of the mandible, radiolucency of the symphysis, symphyseal inclination, and condylar-head inclination differ in the weak-muscled and strong-muscled patient (right).
Fig. 6. The cephalometric measurement Go-Gn to Po-Id is a good indicator of a patient's muscle strength: 65 or less indicates that the patient is strong-muscled; 75 or more indicates that the patient is weak-muscled.
Conclusion Recognizing long face syndrome characteristics is an important aspect of orthodontic diagnosis and treatment. The degree of horizontal or vertical direction of mandibular growth varies among patients. Proper orthodontic diagnosis involves recognizing patients particularly vertical growers) who demonstrate extremes in mandibular-growth direction. Bjork's structural method quickly and easily determines a patient's muscle strength and (hence) response to orthodontic appliances in terms of vertical dimension. Prudent clinicians treat long. faced, weak-muscled patients with care because deleterious vertical changes occur easily. Extremely weak-muscled, long-faced patients are best treated by orthodontists. The method of Class 11 correction, the decision to treat with or without tooth extractions, and the type of arch wires, finishing appliances, and posttreatment retention differ in strong - and weak - muscled patients. Dr. Prittinen practices general dentistry in Virginia, Minnesota, and is an orthodontics instructor for the U.S. Dental Institute.

Address correspondence to: James R. Prittinen, DDS, 216 North Fifth Avenue, Virginia, MN 55792. Acknowledgement The author thanks Ann Marie Larson for helping prepare this manuscript References 1. Graber I, Swain B. Orthodontics: current principles and techniques. St. Louis: C.V. Mdshy Co.;1985:81:408. 2. Viazis A. Atlas of orthodontics, principles and clinical applications. Philadelphia: W.B. Saunders;1993:66. 3. Sassouni V. A radiographic cephalometric analysis of cephalofacial dental relationships. Am J Orthod 1965;41:735-764. 4. Prahl-Anderson B, Boersma H, Vander Linden F, Moore AW. Perceptions of dentofacial morphology by laypersons, general dentists, and orthodontists. JADA 1979; 98:209-212. 5. McNamara I. Integrated treatment of the orthodontic patient. Ann Arbor: University of Michigan Press;1 986:410-411. 6. Bennet JC, McLaughlin RP. Orthodontic treatment mechanics and the preadjusted appliance. Aylesbury, England: Wolfe Publishing;1 993:1 23. 7. Bjork A. Prediction of mandibular growth rotation. Am J Orthod 1969; 55:283-299. 8. Proffit W. Contemporary orthodontics. St. Louis: C.V. Mosby Co.; 1986:32, 88. 9. Bjork A, Skeiller V. Facial development and tooth eruption. Am J Orthod 1972; 62:339-383. 10. Bjork A. Sutural growth of the upper face studied by the implant method. Acta Odontol Scand 1966;24: 109-127. 11. [itt R. Comprehensive orthodontics. Presented at the Faculty for Orthodontic Research and Continuing Education (FORCE) Session 4; January 18, 1991; Winnipeg, Manitoba, Canada. 12. Litt R. Comprehensive orthodontics. Presented at FORCE Session 1; July 20, 1990; Montreal. 13. Viazis A. Atlas of orthodontics, principles and clinical applications, pp. 66, 70. 14. Bjork A. The face in profile: an anthropological x-ray investigation on Swedish children and conscripts. Svensk Tandlakare-Tidskrift 1947;40 (suppl) :27. 15. Burstone C, Nanda R. Retention and stability in orthodontics. Philadelphia: W.B. Saunders;1993:13,14. General Dentistry, 1996 vol. 44, no. 4, pp. 348-351. Dr. Jim Prittinen, DDS