OPSPO ORING VAN BORSTKANKER TUSSEN 70 EN 74 J AAR
84
2012 KCE REPORT 1 OPSPO 76A ORING VAN BO ORSTK KANKER R TUSS EN 70 E EN 74 J www.kce.fgo AAR ov.be
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of OPSPO ORING VAN BORSTKANKER TUSSEN 70 EN 74 J AAR

2012
KCE REPORT 1
OPSPO
76A
ORING VAN BOORSTKKANKERR TUSSEN 70 EEN 74 J
www.kce.fgo
AAR
ov.be

Het Federa
Raad van B
aal Kennisce
Bestuur
entrum vooHet progrMinisbeleid
VoorzLeideVoorzVoorz(vice-AdminVerteg Verteg Verteg Interm Beroe Beroe Zieke Socia Kame
r de GezondFederaal Kennrammawet (1) vaster van Volksgdsondersteunen
zitter nd ambtenaar RIZ
zitter FOD Volksgezitter FOD Socialevoorzitter) nistrateur-generaagenwoordigers M
genwoordigers M
genwoordigers M
mutualistisch Agen
epsverenigingen v
epsverenigingen v
nhuisfederaties
ale partners
er van Volksverteg
dheidszorg iscentrum vooran 24 december gezondheid en de studies binne
ZIV (vice-voorzitteezondheid (vice-v
e Zekerheid
al FAGG inister van Volksg
inister van Sociale
inisterraad
ntschap
van de artsen
van de verpleegku
genwoordigers
r de Gezondher 2002 (artikelen
Sociale Zaken.en de sector van
Eff
Pieer) Jo voorzitter) Dir
Fra
Xagezondheid Be
Mae Zaken Oli
Ri JeaDaMicPaXaMaJea
undigen MicMyJohJeaRitPaLie
eidszorg is ee259 tot 281) die
. Het Centrum de gezondheids
fectieve Leden
erre Gillet De Cock
rk Cuypers ank Van Massenh
avier De Cuyper ernard Lange arco Schetgen ver de Stexhe De Ridder an-Noël Godin
aniel Devos chiel Callens
atrick Verertbruggeavier Brenez arc Moens an-Pierre Baeyenchel Foulon yriam Hubinon han Pauwels an-Claude Praetta Thys
aul Palsterman eve Wierinck
n parastatale, e onder de bevo
is belast metszorg en de ziekt
Plaats
Benoît Chris D
hove Jan Be
Greet M Franço Annick Karel V Lambe Frédér Bart Oo Frank D
en Yoland Geert M Roland
s Rita Cu Ludo M Olivier Katrien Pierre Leo Ne Celien
opgericht doooegdheid valt va
het realiseren teverzekering.
vervangende Le
Collin Decoster ertels
Musch ois Perl k Poncé Vermeyen ert Stamatakis ric Lernoux oghe De Smet de Husden Messiaen d Lemye uypers Meyers
Thonon n Kesteloot Smiets
eels Van Moerkerke
r de an de
van
den

Controle
Directie
Contact
Rege
AlgemAdjunProgr
FedeDoorbKruidB-100BelgiT +32F +32info@http://
ringscommissaris
meen Directeur nct Algemeen Direrammadirectie
raal Kenniscentrubuilding (10e verd
dtuinlaan 55 00 Brussel um 2 [0]2 287 33 88 2 [0]2 287 33 85
@kce.fgov.be /www.kce.fgov.be
s
ecteur
um voor de Gezonieping)
e
Yv
RaJea
ChKri
ndheidszorg (KCE
es Roger
af Mertens an-Pierre Closon
hristian Léonardstel De Gauquier
E)


2012
KCE REPORT 1GOOD CLINICA
OPSPO FRANÇOISE M
76A AL PRACTICE
ORING
MAMBOURG, JO R
VAN BO
ROBAYS, SOPHI
ORSTK
IE GERKENS
KANKERR TUSSEN 70 EEN 74 J
www.kce.fgo
AAR
ov.be

COLOFONTitel:
Auteurs:
Reviewers:
Externe experte
Externe Validat
Belangenconflic
Layout:
Disclaimer:
Publicatiedatum
Domein:
MeSH:
NLM classificat
Taal:
N
en:
toren:
ct:
m:
tie:
Opsp
Fran
Fran
Marc(ASBNeveVand
Philip
Geen
Ine V
• Draw
• Vuw
• To• A
al
26 ap
Good
Brea
WP 8
Nede
poring van borstka
çoise Mambourg
k Hulstaert (KCE)
c Arbijn (WIV - ISBL Brummammo)en (UZ Leuven), Mdenbroucke (UCL
ppe Autier (IPRI-L
n gemeld
Verhulst
De externe expertapport. Hun opm
wetenschappelijkervolgens werd it een consensu
wetenschappelijkot slot werd dit r
Alleen het KCE islsook voor de aa
pril 2012
d Clinical Practice
st Neoplasms ; M
870 - Breast - Neo
erlands, Engels
anker tussen 70 e
(KCE), Jo Robays
), Pascale Jonckh
SP), Martine Berli, Joëlle Desreux
Myriam Provost (SSaint-Luc), Geert
Lyon), Geert Page
rten werden geramerkingen werdee rapport en gingeen (finale) vers
us of een meerde rapport en ging
rapport unaniems verantwoordel
anbevelingen aan
e (GCP)
Mammography ; M
oplasms
en 74 jaar
s (KCE), Sophie G
heer (KCE), Nancy
ière (UCL Saint-Lx (CHU Liège), ASSMG), Hubert Tht Villeirs (UZ Gent
e (Jan Yperman Z
aadpleegd over een tijdens vergadgen niet noodza
sie aan de validaderheidsstem tusgen niet noodza goedgekeurd dolijk voor de even de overheid.
ass Screening
Gerkens (KCE)
y Thiry (KCE)
Luc), Hilde BosmAndré-Robert Grivhierens (UGent), Rt).
Ziekenhuis), Chant
een (preliminairederingen besprokelijk akkoord m
atoren voorgelegssen de validatokelijk alle drie akoor de Raad van ntuele resterend
ans (UZ Leuven)vegnée (Institut JReinhilde Van Ee
tal Van Ongeval (
e) versie van heoken. Zij zijn gee
met de inhoud ervd. De validatie v
oren. Zij zijn geekkoord met de inBestuur.
de vergissingen
), Jean-Benoit BuJules Bordet), Paeckhoudt (WVG), A
(KU Leuven)
t wetenschappeen coauteur vanvan. van het rapport ven coauteur vannhoud ervan.
of onvolledighe
urrion atrick Anne
lijke n het
volgt het
eden
Formaat:
Wettelijk depot:
Copyright:
Hoe refereren n
:
naar dit document
Adob
D/20
De Khttp:/
t? MamPractRepo
Dit Gezo
be® PDF™ (A4)
12/10.273/18
KCE-rapporten w//kce.fgov.be/nl/co
mbourg F, Robays
tice (GCP). Brusort 176A. D/2012/
document is beondheidszorg.
worden gepubliceontent/de-copyrigh
J, Gerkens S. Ossel: Federaal Ke10.273/18.
eschikbaar op
eerd onder de Lhts-van-de-kce-ra
psporing van borsenniscentrum voo
de website van
Licentie Creativeapporten
stkanker tussen 7or de Gezondhei
n het Federaal
e Commons « b
70 en 74 jaar. Goidszorg (KCE). 2
Kenniscentrum
by/nc/nd »
od Clinical 2012. KCE
voor de


KCE Report 176
VOOR
6A
RWOORD KeuzHoe hartingoedgevoMet tussehier egezoprimuOok immemet dwordmissondeen heOok fundemet dverw
JeanAdjun
zes maken in de zkan men bijvoo
ngreep te ontzegde algemene toesoed vanuit soms ddeze studie overen de 70 en 74 jaextra waakzaam
ondheidsklachten um non nocere is op het vlak van
ers doorgaans vedeze van screenin
dt duidelijk ook aen van een diag
erschat. Bovendieet ligt (dus) ook poal mobiliseert meeren, toch kan medit rapport beantw
wachten.
n-Pierre CLOSONnct Algemeen Dir
Opsporing borstk
zorg – het lijkt sneorbeeld verantwogen, louter omwi
stand? Dergelijke iametraal tegenov
r het al dan niet aaar begeven we ozijn. Zoals bij elkhebben en dus ohier dus des te bhet te gebruiken
eel vertrouwder mng. In het eerste gls minder belanggnose. Dit verklan laat het onderwolitiek gevoelig.
en alle op dit momen niet hopen datwoorden aan wat
ecteur
kanker
el op discriminatieoorden om aan lle van een leeftijdenkpistes roepever mekaar staanaanbieden van e
ons dus andermaae georganiseerdeook niet noodzakeelangrijker. argumentarium s
met de logica van geval is het risico grijk gezien dan haart mede waaro
werp de publieke o
ment voorhanden zt hiermee de contmen in een derge
e, zeker wanneer deen oudere patijdscriterium, ook
en steevast een vde waardensysteen georganiseerdal op glad ijs. Maae opsporing richt elijk om dit onder
staan we voor eede diagnosestellop vals positieve het risico op eenom de nadelen
opinie zeker niet o
zijnde wetenschatroverse zal ophoelijk debat van ee
de keuze gebeurtënt de terugbetaal is hij of zij voo
verhitte maatschamen. de borstkankerscrar ook om anderemen zich tot menrzoek gevraagd h
en bijzondere uitdling bij een persoresultaten niet all
n vals negatief revan screening s
onberoerd, er word
ppelijke bevindingouden. Alleen durven wetenschappel
t op basis van leealing voor een dor het overige noppelijke discussie
reening aan vroue redenen moetennsen die a priori ghebben. Het adag
daging. De clinicuoon met klachten leen kleiner, maaesultaat, namelijksystematisch wodt druk rond gelob
gen om een advieven we hopen daijk adviesorgaan
Raf MERTENS Algemeen Directe
i
eftijd. dure
og in e op,
uwen n we geen gium
us is dan
r het k het rden bbyd
es te at we mag
eur

ii
KORTTE SAMEENVATTTING
Opsporing borstk
IDvraggnBnedkmDle(odVcdOkegoegDdhin
kanker
NLEIDINGDit werk maakt devan het rapport:apport nr. 11). H
georganiseerde scgeen enkel sympnoch enige specifiBorstkankerscreennadelen inhoudt. Deen daling van ddaling van de morkan worden gegevminder vaak het gDe voornaamste evenskwaliteit. Eoverdiagnose) ge
diagnose kunnen dVals-positieve rescircuit van angdiagnostische ondOverdiagnose kakankergevallen dieen de frequentiegescreende popuoverdiagnose. Omeen kanker verdgediagnosticeerdeDoor screening kodoor klinische diahaar leven geconfnvasieve behande
G eel uit van een g
"BorstkankerscreHet gaat hier mecreening naar vrotoom vertonen deke risicofactor hning is een comDe voornaamste vde mortaliteit en rbiditeit houdt ofwven, ofwel dat er emetastaseerde snadelen van de
Een vals-positief evolgd door een bde levenskwaliteitsultaten doen gegstwekkende, enderzoeken. an worden gee zonder screenine neemt toe nalatie lager wordt
mdat het op dit moer zal evolueren
e kankers behandomen kankers tweagnose. Hierdoor fronteerd met hetelingen ertegen.
groter project meteening", gepubliceer bepaald om uwen van 70 tot 7at op borstkankeebben.
mplex proces dat voordelen van bor
de morbiditeit dwel in dat een mind
minder recidievenstadium bereikt.
screening hebbresultaat, een
behandeling en ht inderdaad negatezonde vrouwen n soms zelfs
edefinieerd als ng nooit klinisch zaarmate de levet. Overbehandelinoment onmogelijkn, wordt het oveld. ee tot drie jaar eewordt de vrouw
t feit dat zij aan
KCE Report 1
t als doel het updceerd in 2005 (de uitbreiding va74 jaar die voor deer zou kunnen w
t zowel voordelerstkankerscreenindoor borstkanker.der zware behandn optreden of de z
ben te maken meonterechte diag
het vervroegen vatief beïnvloeden. terechtkomen ininvasieve (biop
de opsporing zouden zijn opgemensverwachting ing is een gevolgk is te voorspellenvergrote deel va
erder aan het lichdus reeds vroeg
kanker lijdt en m
176A
daten (KCE-an de e rest
wijzen,
n als ng zijn Een
deling ziekte
et de gnose an de
n een psies)
van merkt, n de
g van n hoe
an de
ht dan ger in
met de

KCE Report 176
ONDERZDit rapport onborstkankerscreAls het antwoovraag: welk aleeftijdscategor
METHODHet onderzoek een literatuurovDARE. In dit ovNederlands en2011. De evaluatie vgebaseerd op Embase, NHS die werden gepjanuari 2000 totOm de risico’s/werd een specwerd in Medlinenaar onderzoebehandeling vabeschikbare BeTenslotte werdpraktijkaanbevewerd geen enke
6A
ZOEKSVRAderzoekt volgendeening uitbreiden rd op deze vraag antwoord moet rie die om een scr
DOLOGIE van de klinische
verzicht uitgevoerverzicht werden ar Frans werden g
van de risico’s/been overzicht vaEED en Econlit. Ipubliceerd in het t september 2011/baten-verhoudingcifiek model uitgee, Embase, HTA
eken rond de levan borstkanker. Helgische gegevensen op basis van elingen uitgewerkel belangenconflic
AGEN de vraag: moet tot de groep vrou negatief is, stelt men geven aa
reening vraagt?
voordelen van scrd in OVID Medlrtikels opgenomengepubliceerd van
baten-verhouding an modelleringson dit overzicht weEngels, Duits, Ne.
g in de Belgischeewerkt. Voor het o
EED en Psycinfovenskwaliteit tijde
Het model maakt ms. het verkregen be
kt en aan externe ct gemeld.
men de georganuwen van 70 tot 74zich nog een bijkan een vrouw
creening is gebasine, EMBASE, Cn die in het Engel
naf januari 2004
van deze screeonderzoeken uit Merden artikels opgederlands en Fran
context te kwantopbouwen van d
o (1950-10/2011) ens en na screemaximaal gebruik
ewijsmateriaal eeexperten voorge
Opsporing borstk
niseerde 4 jaar?
komende uit die
seerd op DSR en s, Duits, tot april
ening is Medline,
genomen ns vanaf
tificeren, it model gezocht
ening en k van de
n aantal elegd. Er
ROMDv•
•
Brevm
MNmbtuBo1mvraeAume
kanker
RESULTATONDERZOMortaliteit De beschikbare volgende feiten aa Screening gaa
een follow-up-de twee jaar e
De daling vantot uiting. Dezgemiddelde leop 70 jaar en
Bij de interpretatekening mee hou
vrouwen dat aan mortaliteit kon voo
Morbiditeit Naast het aantal gmen van screenibehandelingen te umoren aan hetBelgische gegevenom deze bewering
50) maken gewamastectomieën in van de vrouwen dadiotherapie, 38%
een hormonale beAnderzijds gaven uitsluitsel over hemetastatische stadeen daling van d
TEN VAN HEK
gerandomiseerdean het licht: at gepaard met ee-periode van 13 jaeen screening ondn de sterfte komt ze gegevens zijnevensverwachting13 jaar op 74 jaa
tie van deze buuden dat in de leede studies deelne
or hen niet statistis
gewonnen levensing verwacht dekunnen instellen,t licht te brengens waarover wij mg te valideren. Deag van 58% borsde minder gevor
die een borstspar% van hen kregenehandeling.
de gerandomiseeet percentage redia van de ziektede morbiditeit no
HET LITER
e en gecontrolee
en daling van de aar bij vrouwen bodergingen. tussen de 4 en 7
n te bekijken in hg in deze leeftijdr (Belgische gege
uitenlandse studieeftijdsgroep van 70eemt niet erg hoosch worden aange
sjaren is het voore mogelijkheid o aangezien screeen wanneer ze
momenteel beschie meest recente gstsparende chirurgrderde stadia (Starende ingreep ondn neo-adjuvante c
erde gecontroleerecidieven, noch o. Op deze basis ch worden ontkr
RATUUR-
erde studies bra
mortaliteit van 23oven de 50 jaar d
7 jaar na de screhet perspectief vascategorie, nl. 16
evens voor 2009). es moet men e0 tot 74 jaar het aog is; het effect oetoond.
rnaamste voordeem minder agres
ening tot doel heenog kleiner zijnkken laten ons nieegevens (KCE-ragie versus 38%
adia I en II). Bijnadergingen, kregenchemotherapie en
rde onderzoeken over de evolutie kan de hypothese
racht, noch beve
iii
chten
3% op ie om
ening an de 6 jaar
r wel aantal op de
el dat ssieve eft om n. De et toe
apport totale
a 90% n ook
n 41%
geen naar
e van stigd.
iv
Daarentegen wkanker wel in he
MODELLDe voornaamsCISNET-projecHet doel van dvan screening daling van de Staten van 197van het Breast De resultaten vlevensjaren perapport wordenvan de CISNETDeze modellen aangezien het werd een nieuw
EEN COHMethodologieHet model dat evolueert via javrouwen ouder uitnodiging vooworden vrouweVoor het deelnopgespoorde kals in de leeftijdDe bedoeling vhet licht te bren(metastatisch sbij de opgespootegelijkertijd het
werd het verlies vaet model opgenom
ERING ste modelleringsot (Cancer Interveeze modellen wadoor mammografmortaliteit door
74 tot 2000. Ze mCancer Screening
van deze modellener 1000 gescree ook andere mod
T-methodologie. zijn niet zonder minvoegen van Be
w, specifiek model
HORTMODe voor dit rapport
aarcycli. In dit moddan 70 jaar met
or een screeningen verder uitgenoemingspercentag
kankers versus ddsgroep van 50-69van screening is tngen teneinde ee
stadium) dat ongeorde kankers het t aantal gevorderd
an levenskwaliteit men (zie hieronde
onderzoeken weention and Surveias het evalueren vfie resp. van adjuborstkanker vastmaakten gebruik g Consortium. n wijzen op een wende vrouwen. dellen beschreven
meer aanpasbaar elgische gegevenl ontwikkeld.
DEL VOOR
werd ontworpendel worden twee t
elkaar vergelekeg (huidige situatiodigd om deel te
ge en de verdeline intervalkankers9 jaar genomen. umoren in een vren evolutie te vooeneeslijk is. Dezeaantal vroege stade stadia (II en IV
bij een gemetaster).
erden uitgevoerd llane Modeling Nvan het relatieve uvante behandelintgesteld in de Vevan gegevens af
winst gaande van In het wetensch
n die geen gebruik
aan de Belgischens onmogelijk is.
BELGIE
, is een cohortmotheoretische cohoen. Eén cohort krie), in de anderee nemen aan scg van de door sc
s worden dezelfd
roeg stadium (I enorkomen naar sta ‘stage shift’ houd
adia (I, II) toeneemV) vermindert.
Opsporing borstk
taseerde
in het Network).
aandeel ng in de erenigde fkomstig
9 tot 22 happelijk k maken
e situatie Daarom
odel dat orten van jgt geen
e cohort creening. creening e cijfers
n II) aan adium IV dt in dat mt terwijl
Vletupvo
PDg(2GppfuGorepli
MDagDgkbDd•
kanker
Verder hebben wevenskwaliteit afumorstadium. Deprognose van de van klinisch opgoptreden bij vrouw
Parameters Dit model maaktgemiddelde leven2009), de geg
Gemeenschap), dprogramma (50-69positief resultaat (unctie van het stGemeenschap wopportunistische sest van het land
percentage oveteratuuranalyse.
Meting van de lDe gegevens overafkomstig uit gezondheidstoestaDimensions) insgevaloriseerd dookonden niet over bevolking. De veranderingende modellen werde Het verlies aa
wordt geraam
we de hypotheshangen van de
eze hypothese hodoor screening
gespoorde kankewen die niet aan sc
t maximaal gebrnsverwachting vaevens van hetde gegevens af9 jaar), de tijd no(IMA/AIM) en de gtadium (kankerre
werden gebruiktscreening na 70 jd. Hoeveel vroegrdiagnose werd
levenskwaliteitr de levenskwalitede literatuur.
and werd hetstrument gebruor de algemene gegevens besch
in levenskwaliteien gebruikt, zijn d
an levenskwaliteit md op 16%, gedure
se vooropgesteldleeftijd van de
oudt geen rekeninopgespoorde kaners (intervalkankcreening deelnem
ruik van Belgiscan de vrouwen t kankerregisterkomstig van het
odig voor het ontkgegevens over ovgister). De gegevomdat ze vollejaar er minder va
ger de diagnose den bepaald o
t eit tijdens screenin
Voor het bEQ-5D (Europea
uikt; deze beengelse bevolki
hikken met betrek
it van vrouwen oude volgende: na een vals-positende 45 dagen.
KCE Report 1
d dat overlevingpatiënte en van
ng met het feit dnkers beter is dakers en kankersmen).
che gegevens, nvolgens hun le(voor de Vla
t huidige screenkrachten van een verleving na vijf javens van de Vladiger zijn en oaak gebeurt dan wordt gesteld e
op basis van
ng en behandelineschrijven van an Quality of schrijvingen weing ("UK tariffs")kking tot de Belg
uder dan 70 jaar
tief screeningsres
176A
g en n het at de
an die s die
nl. de eeftijd amse nings-
vals-aar in amse
omdat in de n het
de
g zijn de
Life-5 erden ). We gische
die in
ultaat

KCE Report 176
• Voor de kdiagnose levenskwade stadia levenskwastationair (
Omdat aan demoeten deze ci
Resultaten Het basisscenazou kunnen vodaling van de gewonnen leve3,9. Omdat er veeldetails, zie desensitiviteitsanapessimistisch sHet pessimistioverdiagnoselevenskwaliteit tijd nodig om dwerd de verdemomenteel woscreening (50-6winst van 8,7 vrouwen die aaomstandighedeleiden tot een d
6A
kankerpatiënten e(ongeacht het tyliteit geraamd op
IV. Tijdens de liteit geraamd op 18%) voor de stad
eze benadering vjfers met de nodig
ario toont dat screoorkomen per 10
sterfte met 21%nsjaren wordt ger
l onzekerheid is bespreking in halyse op het modcenario en een opsch scenario gen 10% vals-poptreedt van 0,1
de resultaten te ling van de opgeordt vastgesteld 69 jaar) in Vlaandlevensjaren, maaan de screening en - en we blijven daling van de leve
en tijdens het eeype behandeling16% voor de stadvolgende jaren
6% voor de staddia IV.
verschillende bepege omzichtigheid
eening tussen 70 000 deelnemende% vertegenwoordraamd op 13,1 en
met betrekking thet wetenschappdel uitgevoerd. Dptimistisch scenaraat uit van eepositieven, waar9 dat gedurendeontkrachten). Voespoorde kankers
in het kader eren. Dit pessimis
ar een verlies vadeelnamen. Dit bhierbij zeker realinskwaliteit.
erste jaar volgend) wordt het verldia I,II,III en op 1 wordt het verldia I,II,III. Dit ver
erkingen verbondworden geïnterpr
en 74 jaar 1,3 ove vrouwen, hetgedigt. Het globaan de winst aan QA
tot deze ramingepelijk rapport), wDeze analyse omrio. n hypothese mrdoor een verlie 54 dagen aanhoor de gescreends per stadia gebvan de georganstisch scenario raan 3,1 QALY’s pbetekent dat in bistisch - de screen
Opsporing borstk
d op de lies aan 8% voor ies aan
rlies blijft
den zijn, eteerd.
verlijden een een
al aantal ALY’s op
en (voor erd een
mvat een
et 20% es van oudt (de
de groep ruikt die niseerde
aamt een per 1000 bepaalde ning kan
Holeov(les6
CHwUhlelebrelebdEu
kanker
Het optimistisch overdiagnose enevenskwaliteit opop de gescreendevastgesteld in het70-74 jaar). Ditevensjaren en eescreening deelnam67 vrouwen voor e
CONCLUSHet doel van het welzijn van de Uiteraard zou het het mogelijk maevensjaren te winevenskwaliteit isbewijskracht, waealistische hypoevenskwaliteit kubalans tussen de doorslaan naar deEr wordt dus niet auit te breiden tot d
scenario gaatn 2% vals-posirtreedt van 0,13 g
e groep de verdelt kader van de int optimistisch s
en winst van 16,3men. Dit betekenteen screening uit t
IE organiseren van
bevolking door uitbreiden van de
aken om voor ennen. De invloeds echter veel nt gebaseerd othesen zou dez
unnen veroorzakevoor- en nadelen
e kant van een veraanbevolen om de groep vrouwen
uit van een itieven, waardoogedurende 36 daing per stadia toen Nederland geocenario raamt e
3 QALY’s per 100t dat het nodig is te nodigen om éé
n screenings is hvoortijdige overlie screening naar een bepaald aad van georganise
onzekerder (ergop een model)ze interventie zeen. In deze omn van screening grlies van welzijn ve georganiseerdevan 70 tot 74 jaar
hypothese metor een verlies agen. Dit scenarioe die momenteel wrganiseerde screeen winst van
00 vrouwen die aaom gedurende vij
én QALY te winne
et verbeteren vaijdens te voorkode leeftijd van 74
antal vrouwen eeerde screening og laag niveau ). Volgens bepelfs een verliesstandigheden zoglobaal eerder kuan de bevolking.
e borstkankerscrer.
v
t 3% van
o past wordt ening 17,0
an de jf jaar n.
n het omen. 4 jaar
enkele op de
van aalde van
ou de unnen
ening

vi
AANB
a Het KCE b
BEVELIN
blijft als enige veran
NGENa
ntwoordelijk voor de
• Het sygeorg
• Als eescreenvoord
• Elke svan kwregistom ekwalit
• Om heminimverder
e aanbevelingen die
Opsporing borstk
ystematisch uitnaniseerde borstk
en vrouw bovenning zal de arts eelen en mogelijk
screeningsmammwaliteit, met namratie en de optimeen screening eitsvereisten bea
et risico op een maliseren is het
r onderzoek zo la
e aan de overheid w
kanker
nodigen van vrokankerscreening
n de 70 jaar vrerover waken dake nadelen die de
mografie moet bme: de controle emalisering van he
vraagt, doorantwoordt.
verlies aan levebelangrijk dat daag mogelijk is e
worden geformuleerd
ouwen tussen 70g wordt niet aanb
raagt om een mat de vrouw goedeze screening me
eantwoorden aaen kwaliteit van et recall-percentarverwijzen naar
enskwaliteit te wde proportie vroen onder de Euro
d.
0 en 74 jaar ombevolen.
mammografie ind op de hoogte wet zich mee kan
an de Europese vde installaties, dage. Daarom zalr een structu
wijten aan vals pouwen die teruggopese vereisten
KCE Report 1
m deel te nemen
n het kader vanwordt gebracht va
brengen.
vereisten op hetde dubbele lezin de arts de vrouw
uur die aan
ositieve resultatgeroepen wordt blijft (<5%).
176A
n aan
n een an de
t vlak g, de w die deze
ten te voor

KCE Report 176
TABL
6
LE OF COONTENTLILILI
1.2.3.3.3.
4.4.
4.
4.
5.6.
S
TS ST OF FIGURESST OF TABLES .ST OF ABBREVI
SYNTHESCONTEXTONDERZOBESCHRI
1. INTUÏTIEV2. EPIDEMIO
3.2.1. D3.2.2. U3.2.3. VMETHODO
1. RAMING V4.1.1. D4.1.2. V
2. RAMING V4.2.1. V
3. BENADER4.3.1. M4.3.2. B4.3.3. B4.3.4. G4.3.5. SRESULTABESPREK
Screening Breast C
S .......................................................IATIONS .............
SE ........................T ...........................OEKSVRAGEN ...JVING VAN DE P
VE BENADERINGOLOGISCHE BENDoel op korte termUiteindelijk doel ....Vals-positieven enOLOGIE ..............VAN DE VOORDE
Daling van de morVerbetering van deVAN DE NADELE
Vermindering van RING DOOR MODMeting van de leveBeschrijving van hBasishypothesen ..Gegevensinvoer voSensitiviteitsanalysATEN ....................KING ....................
Cancer
............................
............................
............................
............................
............................
............................PROBLEMATIEKG ..........................NADERING..........
mijn ................................................... overtollige diagn............................ELEN VAN SCRErtaliteit ..................e levenskwaliteit vEN VAN SCREENde levenskwaliteit
DELLISERING ....enskwaliteit .........et product .......................................oor het model .....se ................................................................................
............................
............................
............................
............................
............................
............................K ...........................
............................
............................
............................
............................osen ................................................
EENING ...........................................
van patiënten .......ING .....................t van patiënten ....................................................................................................................................................................................................................................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
1
...... 4
...... 4
...... 5
...... 7
...... 7
...... 7
...... 8
...... 8
...... 8
...... 9
...... 9
...... 9
.... 11
.... 11
.... 11
.... 11
.... 12
.... 12
.... 12
.... 12
.... 13
.... 15
.... 15
.... 15
.... 16
.... 16

2
6.6.
7.7.7.7.8.
1.1.1.1.1.1.2.2.
2.
S
1. LEVENSJA2. TOEVOEG
6.2.1. M6.2.2. V6.2.3. OCONCLUS
1. MOET ME2. WAT MOE3. KERNBOO
REFEREN
SCIENTIFINTRODU
1. CONTEXT2. SCOPE O3. BREAST C4. CLINICAL5. SCIENTIF
LITERATU1. REVIEW O
2.1.1. M2.1.2. D2.1.3. D2.1.4. S2.1.5. K2.1.6. C
2. REVIEW O2.2.1. L2.2.2. S
Screening Breast C
AREN TOEVOEGGEN VAN LEVENMinder agressieveVals-positieven .....Overtollige diagnosSIES ....................
EN DE SCREENINET MEN ZEGGENODSCHAPPEN ...NTIES ...................
FIC REPORT ........CTION ................
T OF THIS REPOOF THIS REPORTCANCER SCREE QUESTIONS .....
FIC APPROACH ..URE REVIEWS ...OF CLINICAL STUMethodology .........Description of screDescription of screScreening conditioKey data ...............Conclusion ............OF MODELING SLiterature search sSelection criteria ...
Cancer
GEN? ...................NSKWALITEIT AAe behandelingen?............................ses en behandelin............................NG UITBREIDEN N TEGEN EEN PE........................................................
............................
............................RT ......................
T ...........................ENING IN BELGIU....................................................................................UDIES .............................................
eening benefit ......eening harms .......ons ...............................................................................
STUDIES ..............strategy ...........................................
............................AN LEVENSJARE
............................
............................ngen ................................................TOT DE LEEFTIJ
ERSOON DIE OM........................................................
............................
............................
............................
............................UM ....................................................................................................................................................................................................................................................................................................................................................................................................
............................N? ......................................................................................................................................JD VAN 74 JAAR
M SCREENING VR........................................................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
KCE Report
............................
............................
............................
............................
............................
............................R? .........................RAAGT? ......................................................................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
t 176
.... 16
.... 17
.... 17
.... 17
.... 17
.... 17
.... 17
.... 18
.... 18
.... 19
.... 20
.... 20
.... 20
.... 20
.... 20
.... 21
.... 21
.... 22
.... 22
.... 22
.... 23
.... 26
.... 28
.... 29
.... 30
.... 30
.... 30
.... 30
KCE Report 176
6
2.
3.3.3.3.
3.3.4.4.4.4.4.4.4.4.
S
2.2.3. Q2.2.4. S2.2.5. C
3. REVIEW O2.3.1. M2.3.2. R2.3.3. DDECISION
1. DATA SOU2. MODEL D3. DESCRIPT
3.3.1. A3.3.2. B3.3.3. P3.3.4. P3.3.5. R3.3.6. S3.3.7. S3.3.8. Q
4. RESULTS5. DISCUSS
ANSWER 1. BREAST C2. DELAY BE3. OVERALL4. MORBIDIT5. FALSE PO6. ADDITION7. OVER-DIA
Screening Breast C
Quantity of researcSelected studies ...Conclusion ............OF QUALITY OFMethods ................Results .................Discussion ............N ANALYSIS .......URCES ...............
DESCRIPTION .....TION OF THE PA
Age specific overaBreast cancer incidParticipation rate ..Proportion of screeRecall rate ............Stage distribution aStage specific relaQALY ....................S ...........................ION .....................TO CLINICAL Q
CANCER RELATEETWEEN THE SCL MORTALITY .....TY ........................OSITIVE OR FALSNAL DIAGNOSTICAGNOSIS AND O
Cancer
ch available .................................................................LIFE STUDIES ...........................................................................................................................................................................ARAMETERS ......all survival ............dence ..............................................en detected breas............................and stage shift ....
ative survival ............................................................................................
QUESTIONS .........ED MORTALITY .
CREENING AND T........................................................SE NEGATIVE RC TESTS .............
OVER-TREATMEN
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................st cancers ............................................................................................................................................................................................................................................THE MORTALITY........................................................ESULTS ..........................................
NT ........................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................Y REDUCTION ...............................................................................................................................................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
............................
3
.... 31
.... 31
.... 34
.... 34
.... 35
.... 36
.... 44
.... 44
.... 45
.... 45
.... 49
.... 49
.... 49
.... 49
.... 49
.... 49
.... 50
.... 51
.... 52
.... 55
.... 59
.... 61
.... 61
.... 61
.... 61
.... 61
.... 61
.... 61
.... 61

4
LIST OF F
LIST OF T
FIGURES
TABLES
4.5.
FiFiFiFi
TaTaTaTawoTaTaTaTaTapaTaTaTa
S
8. WHAT ATREFEREN
gure 2.1: Health sgure 2.2: Percentgure 3.1: Compargure 3.2: Compar
able 2.1: Data issuable 2.2: Selectionable 2.3: Modelingable 2.4: results omen screened foable 2.5: Article seable 2.6: Health stable 2.7: Descriptable 2.8: Descriptable 3.1: Stage diarticipants, age 50able 3.2: Parametable 3.3 Modelingable 3.4 Modeling
Screening Breast C
TTITUDE SHOULDNCES ...................
states for which uttage change in utirison of the two cortments in the two
ued from clinical ln criteria ..............g studies excludedof the different m
or the different moelection criteria ....tates descriptionsion of a “false posion of the selectedistribution among 0-69, Flemish screters used in the m results: baseline results: sensitivit
Cancer
D BE RECOMME............................
tilities are neededlities ....................
ohorts with and wo cohorts and the t
iterature review ..............................d after full-text assmodels in terms oodels ................................................s for the study of Lsitive” state (Gerad utilities .............screen detected
eening program 2model ....................
, worst and best cty analysis. ..........
NDED FOR WOM............................
d (reflection proce............................ithout a screeningtransitions betwee
............................
............................sessment ............of mortality reduc........................................................
Lidgren et al. ........rd et al)83 .........................................breast cancers, i001-2006. .......................................
case scenario. .................................
MEN IN CASE OF............................
ss) ..................................................g program ............en them ..............
............................
............................
............................ction and years o............................................................................................................................................nterval cancers a................................................................................................................
KCE Report
F SELF REFERRA............................
............................
............................
............................
............................
............................
............................
............................of life gained per............................................................................................................................................
and cancers amon................................................................................................................
t 176
AL?62 .... 63
.... 37
.... 43
.... 47
.... 48
.... 29
.... 31
.... 31 r 1000 .... 33 .... 35 .... 39 .... 40 .... 41 ng non .... 50 .... 53 .... 56 .... 57
KCE Report 176
LIST OF A
6
ABBREVIAATIONS AB
CPCCCIDCDEBCAHBCDNCIIMINICKCMMNINBNBNHNHNCQAQoRCRR
S
BBREVIATION
PG CRT I CIS ET CSC HRQ CR NETB ISNET
MA/AIM NAMI/RIZIV CER CE ST -A IS BSS BCSP HS HS EED CI ALY oL CT R
Screening Breast C
DEFINITION
Clinical PracticCochrane CenConfidence IntDuctal CarcinoData ExtractioBreast CancerAgency for HeBelgian CanceDutch NationaCancer InterveIntermutualistiNational InstituIncremental coBelgian HealthMean Sojourn Meta-analysisNational InstituCanadian NatiNorwegian BreNational HealtNHS EconomiNational CancQuality AdjusteQuality of LifeRandomized CRelative Risk
Cancer
ce Guideline ntral Register of Cterval oma in situ on Table r Surveillance Con
ealth Care Researer Registry al Evaluation Teamention and Surveic Agency ute for Health andost-effectiveness rhcare Knowledge
Time
ute for Statistics ional Breast Canceast Cancer Screeth Service (UK) c Evaluation Data
cer Institute (USA)ed Life Year
Controlled Trial
Controlled Trials
nsortium (USA) rch and Quality
m for Breast cancellance Modelling N
d Disability Insuranratio Centre
cer Screening Stuening Programme
abase )
er screening Network
nce
dy es
5

6
SESRSTTTUKUSUS
S
EER R T TO K SA SPSTF
Screening Breast C
Surveillance, ESystematic ReSojourn TimeTime-trade-offUnited KingdoUnites States US Preventive
Cancer
Epidemiology andeview
f om of America
e Services Task F
d End Results (US
orce
SA)
KCE Reportt 176

KCE Report 176
SYNT
6
THESE
SScreening Breast C
1Hbbr4ggdpbg7DlegoENnh
2MlemDe
Cancer
1. CONTEXHet KCE publicebasisrapport, geborstkankerscreenisicofactoren. Bor
40-49 jaar was gepubliceerd in 20geen systematiscderde rapport (KCprobleem van deborstkanker hebbgeorganiseerde b70 tot 74 jaar. Deze vraag wordtevensverwachtinggroepen die actieopenbare instantieEuropese Unie ricNederland, Spanjenoodzakelijk is omhen te nemen.
2. ONDERZMoet de georganeeftijd van 74 jaamen dan zeggen tDe eerste vraag hen de tweede op d
XT erde al drie rappubliceerd in
ning in het arstkankerscreenin
het onderwerp010. In dit rapporhe screening aanCE-rapport nr. 1
e opsporing van ben. In dit raporstkankerscreen
t vaak gesteld aang van de vrouwef zijn bij screenes hierover mindechten zich op de e en Zweden)1. D
m de vrouwen te i
ZOEKSVRiseerde borstkanr? Als het antwootegen een persooneeft meer specifie
de zorgverleners.
porten over bors2005 (KCE-rapplgemeen, in d
ng bij vrouwen in p van een gert (KCE-rapport nn bij vrouwen jon72), gepubliceerdvrouwen die ee
pport wordt onding moet uitbreid
n politici omwille welijke bevolking.ning deze uitbre
er unaniem. Slechleeftijdsgroep van
De andere landennformeren en de
RAGEN kerscreening wor
ord op deze vraagn die om deze screk betrekking op d
skankerscreeningport nr. 11) be bevolking zode leeftijdsklasse
edeeltelijke bijwer. 129) beval het nger dan 50 jaard in 2012, stelde
en verhoogd risicderzocht of menden naar vrouwen
van de stijging va. Hoewel de m
eiding vragen, zijts vier lidstaten va
n 70-74 jaar (Frann benadrukken da
beslissing samen
rden uitgebreid tg negatief is, wat reening vraagt? de openbare insta
7
. Het betrof onder e van erking
KCE r. Het e het co op n de n van
an de eeste jn de an de nkrijk, at het n met
ot de moet
anties

8
3. BESCHPROB
3.1. IntuïtievOp intuïtief vlameestal erg endoor Schwartz Staten toonde screening een verklaarde dat hgevallen levensdat voor de memaar een moreDeze algemen"vroegtijdige opverwachtingen interviews om tscreening via mborstkanker alskankers beginnvrouwen warendoor een mamvermeerdert enuit dat gevordekankers) samenSchwartz beklekankers kan opvan de responvoor een persooHet medisch komanier. Daardpercentage geuiteindelijke doAnderzijds lijke
HRIJVING LEMATIEKve benadering ak heeft borstkanthousiast over scbegin 21ste eeuw2
aan dat 87% vagoed idee is. Dr
het opsporen vans redt. Het enthoueesten van hen s
ele verplichting3. ne houding die
psporing van kankwekken bij vrou
te evalueren hoe mammografie ziens een uniform prnen met een genen van oordeel dat
mmografie en vroen doodt. Omwille verde kankers (en nhangen met het
emtoonde dat 94%psporen die zich nndenten ervan ovon die geen borstorps zelf begrijpt door blijven talrediagnosticeerde oel van de opspen clinici gevoelig
VAN DE K nkerscreening zecreening. Deze h2. Een enquête uian de volwassenrie vierde van de kanker in een vrosiasme van de rescreening geen t
e we als volgkers kan levens reuwen. Silverman vrouwen borstka
n. De meeste resrogressieve ziekt
eesbare en stille vindien borstkank
egtijdig behandeldvan deze opvattin
zonder enige twfalen van vroegtij
% van de vrouwennooit zullen ontwikvertuigd dat mamtkanker heeft5. de screening nie
rijke clinici zichkankers (tusse
oring het verlageer voor het risico
S
eker zin. De meouding werd aantgevoerd in de Veen van oordeel
e ondervraagde poeg stadium in de
espondenten was te nemen besliss
t kunnen sameedden", kan onrea
realiseerde telefnker en het voord
spondenten beschte en geloofden vorm4. Samengevker niet wordt opgd, de kanker grogen, gaan vrouwe
wijfel de meeste ddige opsporing.
n niet weten dat sckkelen. Bovendien
mmografie ongeva
et altijd op een ah concentreren ntijds doel), teren van de mortao van het misken
Screening Breast C
edia zijn ngetoond erenigde was dat
personen e meeste zo groot
sen was,
envatten alistische fonische deel van houwden
dat alle vat, deze gespoord oeit, zich en ervan dodelijke
creening n is 92% aarlijk is
adequate op het
rwijl het aliteit is. nen van
ep
3BwdvintoNb1vgp6v
E
1
2
3
4
Wtu
Cancer
een kanker (vals-npositieve resultate
3.2. EpidemiolBorstkanker is dewerden 10.849 gedan drie vierde vavan 50 jaar. Het ncidentie van borot 75 jaar6. Nochtans verschilborstkanker in het
999 was borstkavrouwen van 50 togroep van 70 topercentage 14% v60 tot 64 jaar, 7%van 75 tot 79 jaar6
Essentiële kenmer
. Screening istegenstellingeen klacht opersoon die die wordt op
2. Screening heziekte te beve
3. Screening hesamenhangt m
4. Het principe “vooral van toe
Wij wensen eraaussen 70 en 74 ja
negatief) dan vooren.
logische benade meest voorkomevallen van borstkan de borstkanker
gemiddelde ogerstkanker is 370,7
t het relatieve aat totale percentaganker verantwoorot 54 jaar, 13% in ot 74 jaar (KCEvoor vrouwen van
% voor de groep v6.
rken van screenin
s bedoeld voor g tot een patiëntof een symptoodeelneemt aan e
pgespoord. eeft als doel om oestigen.
eeft als uiteindemet de ziekte te v
“primum non noceepassing op scree
n te herinneren aar, meer dan 990
r de risico's die sa
dering mende kanker bijkanker gediagnosrs wordt gediagno
enblik van de dia7/100.000 in de g
andeel van mortae mortaliteit in fun
rdelijk voor 18% de groep van 60
E-rapport nr.11). n 50 tot 54 jaar, 1van 70 tot 74 jaar
ng:
personen in gt die zijn arts raaom, wordt ervaneen screening n
op korte termijn d
elijk doel de moverminderen.
ere” (in ieder gevaening.
dat op duizend 0 geen borstkanke
KCE Report
amenhangen met
j de vrouw. In Bsticeerd in 2008. osticeerd na de leagnose is 62 jaagroep vrouwen va
aliteit veroorzaakt nctie van de leeftvan de overlijdentot 64 jaar en 6% In 2006 bedroe2% voor de groep
r en 5% voor de g
goede gezondheadpleegt omwillen uitgegaan dat
niet lijdt aan de z
de afwezigheid va
ortaliteit/morbiditei
al geen kwaad do
gescreende vroer hebben.
t 176
t vals-
België Meer
eeftijd r. De an 70
door ijd. In ns bij in de
eg dit p van groep
id In e van t een ziekte
an de
it die
en) is
ouwen

KCE Report 176
3.2.1. Doel oScreening heefDe persoon dieonschuld" wat arts raadpleegt opgemerkt, "vehiertoe worden elkaar. In het gde plicht om allklacht of het syarts de plicht obedoeling hiervvrouwen die geOmdat de oplezieken gaat dezvan een clinicus3.2.2. UiteindDiagnosticeren kan ontwikkeleborstkankerscredie specifiek gede totale mortagevorderde, envormt een tussevoorwaarde dieMen kan ook dgepaard gaat mminder invasievin plaats van progressie naar
6
op korte termijn ft als doel om dee aan screening dbetreft borstkankomdat hij een klardacht" van ziektegebruikt, staan in
geval van het schle middelen in te
ymptoom. In het gom alleen de onovan is om de risicoeen borstkanker heeiding van artseze verandering vas. delijk doel
van kanker in eeen en uitzaaien eening. Daarom vekoppeld is aan dliteit. Het feit dat d
n dus mogelijk noenstap in dit proc
e echter onvoldoende hypothese voomet de ziekte veve behandelingentotale mastectom
r metastatische fa
afwezigheid vandeelneemt, geniet ker. Daarentegen acht heeft of omdae. Het doel van den deze twee situaerpstellen van eezetten om een et
geval van screeniontbeerlijke onderzo's en ongemakkeebben zo gering mn voornamelijk g
an gezichtspunt vo
en vroeg stadium(metastasen) is
verwacht men dae ziekte zal vermde gebruikte techog geneesbare laces. Het betreft hinde is7. ropstellen dat scr
ermindert, doordan te gebruiken (gmie) en doordat asen kan voorkom
S
n de ziekte te bevvan "het vermoewordt de patiënt
at hij iets ongewoe arts en de middties diametraal te
en diagnose heefttiologie te vinden ng daarentegen, zoeken uit te voeen van screening mogelijk te houdegebeurt in hospitolledig in tegen de
m vooraleer de zies het basisprincat screening de m
minderen, en bijgevnologie toelaat omaesies te diagnoser dus een noodz
reening de morbidat het mogelijk wgedeeltelijke mast
men een deel men.
Screening Breast C
vestigen. eden van t die zijn oon heeft delen die egenover t de arts voor de heeft de
eren. De voor de
n. talen bij e intuïtie
ekte zich ipe van
mortaliteit volg ook m weinig sticeren, zakelijke
diteit die wordt om tectomie van de
3VvndvDzgpbMotodkptrrinwgDvzv
Cancer
3.2.3. Vals-posiVooraleer een geovan te zijn dat denaar de kant van daling van de mveroorzaakt door oDe zogenaamd "vzonder de aanwgevolgen van borspositieve resultatebijkomende onderzMeer nog dan dovertollige diagnosot 74 jaar. Ovediagnosticeren vanklinisch zou manplaatsgevonden8. raag evolueert enisico is weinig bnderdaad dat soworden ze niet gezondheid9. Dit rapport heeft tvan deze screeninzorgen dat de voovan levenskwalitei
itieven en overtoorganiseerde scree verhouding voo
de voordelen. Omortaliteit het verongemakken en rivals-positieve" resezigheid van kastkankerscreeningen zorgen voor zoeken. de vals-positievese het grootste riertollige diagnosn kanker waarvannifesteren wanneDit risico is des
n de levensverwacbekend bij de beommige kankers behandeld, ze g
tot doel om de vong om ze in perspordelen grotendeeit.
ollige diagnoseneening in te voerenordelen/nadelen vOm dit te doen mrlies aan levenskisico's van de scresultaten (vermoedanker) zijn de og die het vaakst vheel veel angst
e resultaten is visico van screenin
se kan worden n de evolutie zodaeer er geen scte groter naarm
chting van de persevolking. Zeer wzo langzaam ev
geen invloed zo
oor- en nadelen tpectief te kunnenels opwegen tege
n n, is het nodig er van screening oveoet de grootte vakwaliteit compenseening. den van kankerlaongewenste negavoorkomen. Deze en het uitvoeren
vooral het risicong bij vrouwen vagedefinieerd als
anig is dat ze zich creening zou heate de kanker slsoon laag is. Voo
weinig vrouwen wvolueren dat, zeouden hebben o
te bepalen (zie F plaatsen en ervon het risico van v
9
zeker erhelt an de seren
aesies atieve
vals-n van
o van an 70 s het nooit
ebben echts ral dit weten lfs al
op de
Fig. 1) oor te verlies

10
Figuur 1 - mog
Opsporimamm
gelijke voor- en d
ing door mografie
de nadelen van s
Normaal
Abnormaal
S
screening.
Vals negatie
Resultaat +
Vals positie
Resultaat -
Screening Breast C
ef
ef
-
Ongeru
Geru
Bijko
Invasiecarcin
In s
carci
Cancer
nterecht stgesteld
ustgesteld
omende onderzoe
ef noma
Vb
situ
noma Vrbe
Diagnose laatti
eken
Vroegtijdige behandeling
roegtijdige ehandeling
jdiger
Verminderdemortaliteit
Overbehand
KCE Report
e
eling
t 176

KCE Report 176
4. METHWe hebben egezocht in de kinternationale gbij het KCE gelhoofdstuk 2 van
4.1. Raming4.1.1. Daling De meest borstkankerscrestudies. Op basworden gedaan1. Screening
opvolgingselke twee j
2. Deze dalinuiting. Dit levensverwlevensverw13 jaar op
De bewijskrachstudies kunnenenkele gerandoook vrouwen izeventigjarigentwee groepen) kunnen aantomethodologisch
6
ODOLOGIlementen voor e
klinische literatuurgegevens. Dit opzldende proceduren het wetenschap
g van de voordg van de mortalite
bewijskrachtigeeening komen usis van deze studn: zorgt voor een d
speriode van 13 jaar een screening
ng van de mortalimoet in perspect
wachting van wachting in deze 74 jaar (Belgische
htige gegevens van geen antwoord omiseerde studie, n de leeftijdscate dat aan deze stuom een statistis
onen. Bovendienhe bias.
E een antwoord opr, in modelleringsszoekingswerk wees. Ze worden gepelijk rapport.
elen van screeeit
e gegevens uit acht gerandomies kunnen twee
aling van de morjaar voor vrouweg ondergingen. iteit komt 4 tot 7 tief geplaatst wor
de doelpopulaleeftijdscategorie
e gegevens voor 2an deze gerandogeven op onze de Zweedse "Tw
egorie van 70 toudie deelnam wassch significant efn werd deze
S
p voorgenoemde studies en in natiord uitgevoerd voldetailleerd besch
ening
met betrekkinmiseerde gecontbelangrijke vastst
rtaliteit met 23% oen ouder dan 50
jaar na de screerden ten opzichteatie. De gem
e is 16 jaar op 702009).
omiseerde gecontbasisvraag. Slec
wo County"-studie,ot 74 jaar en hes te laag (10.000 ffect op de mortstudie gehinder
Screening Breast C
vragen onale en gens de reven in
ng tot troleerde tellingen
over een jaar die
ening tot e van de middelde 0 jaar en
troleerde chts één , bevatte et aantal
voor de aliteit te rd door
4HdbgvGpzvDhDtorato9okh
Cancer
4.1.2. VerbeteriHoewel screeningde verwachte vobehandelingen tgerandomiseerde verzameld in BelgGerandomiseerdepercentage recidieziekte gekwantificvan de morbiditDaarentegen werdhet hieronder bescDe Belgische gegeoe om deze bewapport 150) makeotale mastectomie90% van de vrondergingen, kregkregen een neo-ahormonale behand
ing van de leveng als doel heeft kloordelen dat hette gebruiken.
gecontroleerde ië laten toe om de gecontroleerdeeven, noch de evoeerd. Op deze bteit dus noch d een verlies van chreven model opevens waarover w
wering te validereen gewag van 58eën in de minder rouwen die eengen ook een behaadjuvante behanddeling.
nskwaliteit van pleine tumoren aat zal toelaten omNoch de gege
studies, noch eze verwachtingene onderzoeken olutie naar metasasis kan de hypoworden ontkraclevenskwaliteit d
pgenomen. wij momenteel besen. De meest rec8% conservatievegevorderde stadi
n conservatieve ndeling met radio
deling met chemo
patiënten n te tonen, is eenm minder agresevens afkomstig feitelijke gegen te bevestigen.
hebben noch statische stadia vaothese van een dcht, noch bevedoor metastasen w
schikken laten oncente gegevens (e chirurgie versusa (Stadia I en II). chirurgische ing
therapie, 38% vanotherapie en 41%
11
n van ssieve g uit evens
het an de daling stigd. wel in
s niet (KCE-s 38%
Bijna greep n hen
% een

12
4.2. Raming4.2.1. VerminScreening verodeel van de greeks factoren:1. De vals-po
ervaren alsonderzoekeongerustheprocedures
2. De overtoldiagnose wetenschabehandelinop de over
3. Een voortilevensjarenvroeger opwordt hierdpatiënte ovkanker, duenkele jarvoortijdige haar levens
g van de nadelendering van de loorzaakt een vermescreende perso
ositieve resultatens terecht-positieveen ze niet hebbeid met betrekks zoals puncties. llige diagnoses e
en overbehanappelijk rapport), lngen waaronder brleving van de perijdige diagnose kn in goede gezonp te sporen dan door vroeger in hverlijdt aan een ous voordat die kaen te vroeg "aadiagnose en be
sverwachting10.
en van screenilevenskwaliteit vmindering van de
onen. Dit kan wo
n van screening we resultaten gezie
ben kunnen ontkrking tot borstka
en behandelingendeling (voor mleiden tot ernstigeborstamputaties drsoon. kan leiden tot hedheid. Screening met een klinischaar leven ziek va
oorzaak die nietsnker de kans kre
an kanker geledehandeling geensz
S
ing van patiënten e levenskwaliteit vrden verklaard d
worden door de pen zolang de bijkrachten. Ze veroanker en de in
n die erop volgemeer details ze ongerustheid edie geen invloed
et verlies van mheeft als doel om
he diagnose. De an kanker. Wannete maken heeft m
eeg te evolueren,en hebben" terwzins een invloed
Screening Breast C
van een oor een
patiënten komende oorzaken nvasieve
n (over-zie het n zware hebben
meerdere m kanker
patiënte eer deze met haar , zou ze
wijl deze had op
4Mvsnti4ElezleOhhnreg(leDdvlemampppbbosg
Cancer
4.3. BenaderinMet voornoemde voor- en nadelenspecifiek model unodig studies te zoijdens de screenin4.3.1. Meting vaEr zijn verschillenevenskwaliteit. Beziekte zoals bijevenskwaliteit vanOrganization for hulpmiddelen evalhaar pyschologiscniet mogelijk omekening te houde
globale index voQALY). De QAevenskwaliteit. De farmaco-econode vragenlijst EQ-voor het evaluerevenskwaliteit gemet vijf elementeactiviteiten, pijn/himeerdere antwooprobleem (geen pproblemen). Dezpopulatie, dus vooborstkanker lijdenborstkanker. Via opgespoord die astudies worden degeraamd:
ng door modellliteratuuronderzoe
n niet afwegen uitgewerkt. Voor oeken met betrekng en de levenskwan de levenskwande instrumentenepaalde instrumejvoorbeeld de n patiënten die aResearch and Tlueren het beeld dch functioneren, dm met deze muen in een mode
oor levenskwaliteALY's zijn het
omische aanbeve-5D een van de bren van de QAkoppeld aan de gen: mobiliteit, aunder, angst/depre
orden mogelijk. Drobleem, enkele
ze vragenlijst wor screening aan e, en voor de ziekt
het literatuurovaan onze inclusiee variaties in leve
isering eken konden we en daarom hebbhet uitwerken va
kking tot de levenswaliteit van patiënaliteit n beschikbaar voenten zijn specifie
vragenlijst met an borstkanker lij
Treatment of Cadat de patiënte hde angst voor heultidimensionele l. Ze moeten wo
eit, nl. de Qualaantal levensjar
elingen van het Keste hulpmiddele
ALY's. Met dit gezondheidstoestautonomie van deessie. Voor elk vaDie verwijzen naproblemen, matig
wordt voorgelegdeen populatie vante zelf aan een p
verzicht konden ecriteria voldedenenskwaliteit bij ze
KCE Report
de verhouding tuben we hiervooran dit model waskwaliteit van vro
nten tijdens hun zi
oor het meten vaek aangepast aa
betrekking totjden van de Euro
ancer (EORTC). eeft van haar lichrvallen... Het is egezondheidsgege
orden omgezet inity-Adjusted Liferen met een g
CE gaan ervan un is die beschikbahulpmiddel wordand rekening houe persoon, dagean deze elementeaar de ernst vange problemen, ernd aan de betron vrouwen die nie
populatie patiëntendrie studies wo
n. Op basis van eventigjarigen als
t 176
ussen r een s het
ouwen ekte.
an de an de t de
opean Deze
haam, echter evens n een -Year
goede
uit dat aar is dt de udend elijkse n zijn n het nstige okken et aan n met orden deze volgt

KCE Report 176
1. Het verlie
screeningrnodig is omdie periodegegevens
2. Voor de kdiagnose (levenskwade stadiumlevenskwastationair (
Omdat aan demoeten deze cHet betreft hivragenlijst, nl. Ede dimensies betrekking tot dde impact op vragenlijst werdervan weerspipatiënten die zvan de gebruiktverklaren die walgemene popumetastasen ont4.3.2. BeschrHet model bevsamengesteld uaan hun overlweergeeft.
6
s aan levenskwresultaat wordt gm dit vals-positieve gemiddeld 45 dvan het Intermutu
kankerpatiënten, e(bij om het even wliteit geraamd op m IV. Tijdens deliteit geraamd op 18%) voor de stad
eze benadering vijfers met de noder resultaten uitEQS-5D, meet dedie specifiek zijnde patiënten houd
korte termijn vad gebruikt tijdensegelen dus nie
zich niet meer kunte studie zou de gwerd vastgesteld ulatie of tussen ptwikkelden. rijving van het pvat twee theoretiuit 100.000 vrouwijden. Hieronder
waliteit voortvloeiegeraamd op 16%ve resultaat te onagen (min. 36, m
ualistisch Agenschen tijdens het eewelke behandelin16% voor de stad
e volgende jaren 6% voor de staddium IV.
verschillende bepeige omzichtigheidt Angelsaksische
e algemene gezonn voor borstkankden slechts in gean de diagnose
s ambulante const de levenskwannen verplaatsengeringe wijziging tussen patiënten
patiënten met me
product sche cohorten. D
wen waarvan de evindt u het sch
S
end uit een vals% tijdens de peri
tkrachten. In Belgax. 54 dagen) volhap (IMA). erste jaar volgendng), wordt het verdia I,II,III en op 1n wordt het verldia I,II,III. Dit ver
erkingen verbondd worden geïnterpe landen. De gndheidsdimensieser. De maatrege
eringe mate rekenen de chirurgie
sultaties en de realiteit van ernsti. Het bijzondere in levenskwaliteit
n met borstkankeetastasen en zij d
Deze twee cohorevolutie wordt gevhema dat deze
Screening Breast C
s-positief iode die gië duurt lgens de
d op de rlies aan 8% voor lies aan rlies blijft
den zijn, preteerd. gebruikte s en niet elen met ning met e. Deze esultaten g zieke karakter
t kunnen er en de die geen
rten zijn volgd tot evolutie
Cancer 13

14
Coh
Co
Uitgenodigde Vr
Niet uitgenodigvrouwen
hort A
ohort B
rouwen
gde
S
(1) )Invasieve kagevonden door screening
(4) Ductal Carciin Situ
(2) Interval kankniet gescreendevrouwen
(3) Invasieve kbij niet gescreevrouwen
(6) Invasieve kbij niet gescreevrouwen
(7) Ductal Carcin Situ
Screening Breast C
IIIIIIIV
IIIIIIIV
IIIIIIIV
IIIIIIIV
anker
noma
ker bij e
anker ende
anker ende
cinoma
Cancer
(5) Overlijden (aloorzaken)
(8) Overlijden (aoorzaken)
lle
alle
KCE Reportt 176

KCE Report 176
Cohort A illugeorganiseerdevrouwen die uSommigen van(uitgenodigd/niewerden geïnvgediagnosticeegediagnosticeegediagnosticeedeelnemers (3voorkomen in dvan de uitgenode vrouwen daandoening danCohort B (contrvan dit cohortvrouwen werdeductaal carcinodie dit cohort borstkanker (8)Borstkanker evgevorderde stabehandeling is in een meer gev4.3.3. BasishDe basishypothdoor screeningII) groter dan bivan screening stadia (stage-shDe andere wlevenskwaliteit van de tumor eof dit nu al dan
6
ustreert de hype screening tot 7uitgenodigd werd hen namen deeet-deelnemer). Deventariseerd. Herd tijdens de srd in het interval trd werden in 3). De ductale de groep uitgenodigden/niet-deelndie dit cohort un borstkanker (5).role-cohort) komt t werden niet uien getroffen door eoom in situ (7). D
uitmaakten over.
volueert in vier stadium. Overlevindes te zwaarder vorderd stadium b
hypothesen hese is de volgen, is het percentagij kanker die kliniskomen voort uit dhift) volgend op deweerhouden hypvan de vrouwen n de leeftijd van dniet volgt op een
pothese van ee74 jaar. Het cohden om deel te l (uitgenodigd/deee kankers die zichet betreft hier screening (1), otussen twee screede groep van carcinomen in
digden/deelnemenemers (4). De ovuitmaakten overl. overeen met de htgenodigd voor een invasieve kane overgrote meerleden aan een
tadia (I, II, III, IVng is per definit
en meer invasiefbevindt op het mo
de: bij de kankersge weinig gevordesch gediagnosticede verschillen tuse screening.
pothese is dat uitsluitend afhan
de vrouw op het oscreening.
S
en uitbreiding vhort is samenges
nemen aan scelnemer) en andeh voordeden in he
kankers die of kankers die enings (2), of kan
de uitgenodigdsitu tenslotte
rs net zoals bij dvergrote meerderhleden aan een
huidige situatie. Dde screening. Snker (6), andere drderheid van de vandere aandoen
). Stadium I is htie minder goedf wanneer de kanoment van de diag
s die worden opgerde kankers (sta
eerd wordt. Alle vossen de verdeling
de overleving nkelijk is van het ogenblik van de di
Screening Breast C
van de steld uit
creening. eren niet et cohort
werden werden
nkers die den/niet-
kunnen de groep heid van
andere
De leden Sommige door een vrouwen
ning dan
et minst en de
nker zich gnose.
gespoord adia I en oordelen g van de
en de stadium
iagnose,
Do(4OBgDoles(VzWVHm“4Inhnkhinkuvh
a
Cancer
De cohorten weovergangsparameincidentie) en het
4.3.4. GegevenOm deze oefeninBelgische gegevegedetailleerd bescDe levensverwachoverlevingstabelleeeftijdsgroep. Destadia van de zVlaamse Gemee
zijn afkomstig uit Wallonië, Brussel Voor elk compartHet model bevat emeest aannemelijk“In wezen zijn alle 4.3.5. Sensitivitn ons model zijnhypothesen omwinoodzaak om te keuze veroorzaakhet model, met denformatie. Om aakunnen bieden, uitgevoerd waarbijverschillende scenhet wetenschappe
citaat toegesc
erden jaar na eters zoals het aan
overlevingspercensinvoer voor heng te kunnen doens in ons modechreven in hoofdsthting van de onden van de v incidentie van k
ziekte is afkomsnschap). De geg
de huidige progen de Vlaamse Giment van het meen basisscenarioke situatie. modellen vals, m
teitsanalyse n we uitgegaan ille van de gegevermijden een t
kt onzekerheid diee goede keuze vanan deze verschille
hebben we ej we gebruik maanario's worden geelijk rapport.
chreven aan de sta
jaar opgevolgd ntal vrouwen dat eentage in functie vt model
oen, hebben we l ingevoerd. Deztuk 3.3 van het raerzochte populatirouwelijke popu
kanker in functie stig van het Beevens met betrekgramma's (vrouw
Gemeenschap). odel werd de levo (base case) dat
maar sommige zijn
van een zeker evens waarover wte complex modee verband houdt n de parameters ende soorten onzeeen diepgaandekten van verschill
edetailleerd besch
tisticus George Box
in functie vanelk jaar getroffen wvan het kankerstad
zo goed mogelijze parameters woapport. ie is afkomstig vaulatie van dezvan de leeftijd e
elgisch Kankerrekking tot de scre
wen van 50-69 ja
venskwaliteit gemt overeenstemt m
n nuttig”a
aantal simplificerwe beschikten, eel te gebruiken.
met de structuuen met de bron va
ekerheden het hooe sensitiviteitsanlende scenario's. hreven in tabel 3.2
x.
15
n de wordt dium.
jk de orden
an de zelfde en de gister ening
aar in
meten. met de
rende en de Deze r van an de ofd te
nalyse Deze 2 van

16
5. RESUHet basisscenaoverlijdens zouhetgeen een dagewonnen leve3,9. Deze sensitivitoptimistisch sceHet pessimistisdiagnose van 2verlies van lev54 dagen aanhgescreende grostadia die momgeorganiseerdescenario raamtQALY per 100dat in bepaaldede screening kaHet optimistischdiagnose van 3verlies van levedagen aanhoudper stadia toe Nederland geoscenario raamtQALY per 1000dat het nodig iste nodigen om e
LTATEN ario toont dat uitbu kunnen voorkoaling van de sterfensjaren wordt ge
teitsanalyse omvenario. sch scenario gaat 20%, een percentavenskwaliteit woroudt (de tijd nodioep werd de ver
menteel wordt vaste screening (50t een winst van 80 vrouwen die aae omstandighedenan leiden tot een dh scenario gaat u3%, een percentaenskwaliteit worddt. Dit scenario pdie momenteel worganiseerde sct een winst van 0 vrouwen die aas om gedurende veen QALY te winn
breiding van de somen per 1000fte met 21% verteraamd op 13,1
vat een pessimi
uit van een hypoage vals-positieverdt veroorzaakt vg om de resultaterdeling van de otgesteld in het ka
0-69 jaar), toege8,7 levensjaren, man de screening n - en we blijven daling van de leveuit van een hypotage vals-positievet veroorzaakt van
past op de gescrewordt vastgesteldcreening (70-74 17,0 levensjarenan de screening vijf jaar 62 vrouwenen.
S
screening tot 74 deelnemende v
egenwoordigt. Heen de winst in Q
stisch scenario
these met een oven van 10% waardvan 0,19 dat geen te ontkrachtenopgespoorde kankder van de in Vlaepast. Dit pessimaar een verlies
deelnamen. Dit bhierbij zeker rea
enskwaliteit. these met een oven van 2% waardn 0,13 dat gedureeende groep de vd in het kader va
jaar). Dit optin en een winst v
deelnamen. Dit ben voor een scree
Screening Breast C
jaar 1,3 vrouwen, et aantal
QALY op
en een
vertollige door een durende ). Op de kers per anderen imistisch van 3,1
betekent listisch -
vertollige door een ende 36
verdeling an de in imistisch van 16,2 betekent ening uit
6Dbgsvvle
6DatovkhHtwBja2Dpnmehle
Cancer
6. BESPREDe resultaten van basissituatie betregescreende vrouwsensitiviteitsanalysvan de gekozen hvolgens sommigevenskwaliteit.
6.1. LevensjarDe verhoging vanargumenten die wot vrouwen die overonderstelling kenmerken heeft ahet geval voor het Het aantal overlijdweeënhalf keer zBelgische populataar, 8% tussen 602009). De oorzaken van percentage overlijnaar 6% van alle mortaliteit door kaen elk verantwoorhet overlijdenspereeftijd (KCE-rappo
EKING het hierboven be
eft, de winst in lewen. Dit resultaase. De QALY daahypothesen, gaan
ge geloofwaardi
ren toevoegen?n de levensverw
worden gebruikt oouder zijn dan 6dat de populatals de populatie vaantal vrouwen d
dens vastgesteld zo hoog als die itie verliest 4% va0 à 69 jaar en 20%
het overlijden verjdens door borstkoverlijdens tusse
anker, en de cardrdelijk voor meer rcentage daalt heort nr. 11).
schreven model wevensjaren 13 jat blijft betrouwba
arentegen variërende van een relage hypothesen,
? wachting van de om borstkankersc69 jaar. Dit argumie van de zev
van de zestigjarigedat overlijdt en hu
in de leeftijdsgron de leeftijdsgroen haar effectieve % tussen 70 à 79
rschillen eveneenkanker van 13% en 70 en 75 jaar. diovasculaire mordan een derde v
et aandeel van bo
KCE Report
wijzen erop dat, waar bedraagt per aar doorheen gann aanzienlijk in fuatief geringe wins, een verlies
vrouw is één vacreening uit te brment gaat uit vaventigjarigen dezen. Dit is helemaan doodsoorzaak. oep van 70-79 jaep van 60-69 jaa
leden tussen 509 jaar (Belgian life
ns. In België wijzigtussen 60 en 64Op die leeftijd z
rtaliteit praktisch van alle overlijdenorstkanker dus m
t 176
wat de 1000
ns de unctie st tot,
aan
an de eiden
an de zelfde al niet
aar is ar. De à 59 table
gt het 4 jaar ijn de gelijk
ns. In met de

KCE Report 176
6.2. Toevoe6.2.1. MinderNaast de winsverwacht van behandelingen gerandomiseerdwerden verzam6.2.2. Vals-pIn ons model belangrijke brovals-positieve reen relatief lanonderzoeken ktermen van QAEuropese normhet land (in Vlaa6.2.3. OvertoHet risico van voor zeventigjatoepassen, kanvrouwen, 108 ben waarschijnpercentage oveAnderzijds worgesteld door migeval van een kwaliteit van de
6
egen van levenr agressieve behst in levensjaren
screening de toe te passen. E
de gecontroleerdmeld in België, kon
ositieven vertegenwoordig
on van verlies aaresultaten (dat tonge wachtperiodekan leiden tot eALY. Als men e
men te houden (3,anderen), is de w
ollige diagnoses overtollige diagn
arigen. Wanneer wn men zich eraan bijkomende vrouwlijk een behand
er-diagnose van 1rden alle vrouweiddel van screeninklinische diagnos
e levensjaren die z
skwaliteit aan handelingen?
is het voornaammogelijkheid o
Echter, noch de e studies, noch d
nden deze verwac
gden de "vals-poan levenskwaliteiot 10% kan bedrae (gemiddeld 45 een totaal negaterin slaagt om d5%) zoals dit het
winst aan QALY 3 en behandelingoses is het groowe een percentagverwachten dat i
wen een diagnose deling zullen on0% toepassen, stn bij wie de diagng, twee tot drie jase. Dit heeft een zij nog hebben.
S
levensjaren?
mste voordeel daom minder aggegevens afkom
de feitelijke gegevchting bevestigen.
ositieve" diagnost. Een hoog peragen) gecombinedagen) voor bijkief screeningresuit percentage bingeval is in één re
op 1 000 vrouwengen
tste risico van scge over-diagnosen elk cohort van van kanker zullen
ndergaan. Als wtijgt dit aantal tot 3gnose van kankeaar eerder ziek danegatieve invloe
Screening Breast C
at wordt ressieve stig van vens die
sen een rcentage eerd met komende ultaat in nnen de egio van n.
creening van 3% 100.000 n krijgen we een 367. er wordt an in het
ed op de
77
DDamveezgdsnzgbHgdwpcmaHwreteoob
Cancer
7. CONCLU7.1. Moet men
jaar? De conclusie van Deze uitspraak is anderzijds op de smodel tonen eenvrouwen. Sommiger echter op dat heen algemeen verzijn dus als zodangeorganiseerde sdefinitie op een inspecificiteit houdt nemen op het vlazijn met name op geen schade toebillijkheid en het pHet principe van gedefinieerd: "Tendoen (primum noweldoen die samprincipe van rechtcollectieve dimensmet van een achtergestelden12”Het doel van hetwelzijn van de beesultaten die via e sluiten dat in sonderzochte leeftomstandigheden basisprincipe: “prim
USIES n de screening
deze studie is daenerzijds gebase
specifieke context winst van 13 lee hypothesen, die
het netto-resultaarlies in levenskwa
nig niet doorslaggescreening. Georgndividu die geen
in dat men des ak van ethische p
screening van toebrengen, het principe van respeweldoen of gee
n eerste geen kwon nocere) Dit mmengaat met eentvaardigheid of bsie van gezondhe
voorkeur voor ”. t organiseren vanevolking door vohet model werdensommige gevalletijdsgroep negatiezou dit kunnen
mum non nocere”
uitbreiden tot d
at het antwoord oeerd op de resultat van deze vraag.evensjaren aan e helemaal niet on
at van een uitbreidaliteit kan veroorzevend in de bijzoganiseerde screeenkele klacht, no te meer waakza
principes11. Drie eoepassing: het prprincipe van recct voor autonomie
en schade toebrewaad doen, in iedmoet gepaard gaan houding van illijkhkeid is: "dezeidsproblemen laa
de meest z
n screening is heortijdige overlijden verkregen lietenn screening de lef zou kunnen leiden tot een
” (in ieder geval ge
de leeftijd van
op deze vraag neeaten van het mod De resultaten vaper 1000 gescrenrealistisch zijn, wding van de screzaken. Deze resundere context vanening richt zichoch vraag heeft. aamheid moet inethische basisprinrincipe van weldochtvaardigheid ofe12. engen wordt als der geval geen kan met een plichwelwillendheid"12
ze bezorgdheid dat tussenbeide ko
zwakken, de m
et verbeteren vaens te voorkomenn echter niet toe olevenskwaliteit vabeïnvloeden. In
n schending vaneen kwaad doen)
17
74
en is. del en an het eende wijzen ening ltaten n een
h per Deze acht
ncipes oen of f van
volgt kwaad ht tot . Het
die de omen meest
n het n. De om uit an de deze
n het .

18
Anderzijds is seen lagere levzeker ook bij drespecteren vaeen bijkomendevraag.
7.2. Wat moscreeni
De context vanpunten: het indindividueel vlakde autonomie wordt als volgbasisprincipe, hhieruit voort; hindividuele persvrije keuze) en persoon een vduidelijk en coscreening in zijhet recht op gewet betreffendevan de patiëninformatieblad. uitwisseling vanTevens is het neen strategie ueen houding in • Specifieke • Het neme
beoordeling• Oriëntatie
waarvan de
screening duidelijvensverwachting. de andere leeftijdsan het principe vae reden te zijn o
oet men zeggeng vraagt?
n deze vraag onddividu zelf is hier k worden geëvalueis zeer goed vant gedefinieerd: "het respecteren vhet gaat om hesoon om keuzes tom zijn handelwij
vrije keuze zou orrect geïnformeen persoonlijke situ
eïnformeerde toese de rechten van dnte kan slechts
Het gaat om n ideeën met de znuttig dat de arts uitwerkt die de nadrie stappen wordinformatie voor d
en van een besg van de patiëntevan de persoon e modaliteiten de
jk minder doeltreDit verschil in
sgroepen, maar man rechtvaardighem negatief te ant
n tegen een pe
derscheidt zich vvragende partij e
eerd. Het principen toepassing in d"het respecteren van de autonomi
et erkennen vante maken voor zicjze te beheersen kunnen maken,
erd wordt over duatie. Het recht ostemming zijn besde patiënt. De geï
worden verkregeen proces wa
zorgverlener moetvoor zijn patiënte
adelen tot een miden aanbevolen: e leeftijdsgroep slissing in funct14. die screening wenadelen tot een m
S
effend voor vrouwdoeltreffendheid
minder uitgesprokeid of billijkheid btwoorden op de g
ersoon die om
an vorige vraag en het probleem e van het respectedeze situatie. Dit
van de persoonie van de persoo
het vermogen chzelf (zelfbeschik(zelfbestuur)12”. Ois het belangrijke voor- en nade
op informatie (artikschreven in de Bïnformeerde toestgen na lezing vaarbij idealiter ot plaatsvinden e die om screeninnimum beperkt13.
tie van de pers
enst, naar een scminimum beperke
Screening Breast C
wen met bestaat
ken. Het blijkt dus gestelde
op twee moet op eren van principe
n is het on vloeit van de
kking en Opdat de k dat hij elen van kel 7) en elgische temming van een ook een
g vraagt . Zo kan
soonlijke
creening en.
Dpdemcvo
7HwUhvVlebdb
Cancer
De criteria die wprogramma voorzide gebruikte appaeen optimalisatie vmammografische criteria in het kadvrouwen die uitdroriënteren.
7.3. KernboodHet doel van hetwelzijn van de Uiteraard zou het het mogelijk makevan deze maatreVolgens billijke hevenskwaliteit kubalans tussen ddoorslaan naar dbevolking.
werden gedefinieien met name hetaratuur, een dubbvan het trefpercen
afdelingen moeder van het Eurrukkelijk om scre
dschappen t organiseren vanbevolking door uitbreiden van de
en om enkele levegel op de leveypothesen zou d
unnen veroorzakee voor- en nade kant van een
eerd in het kadet toezicht op de tebele lezing van dntage1. Aangezieneten beantwoordropese programmeening vragen na
n screening is hevoortijdige overlie screening naar vensjaren te winnnskwaliteit is dudeze interventie en. In deze omdelen van screealgemeen verlie
KCE Report
er van het Euroechnische kwalitede mammografieën in België de erken aan welbep
ma, is het logischaar deze structur
et verbeteren vaijdens te voorkode leeftijd van 74en. Echter, de in
uidelijk meer onzzelfs een verliesstandigheden zoening eerder kus van welzijn va
t 176
opese it van ën en kende aalde h om en te
n het omen. 4 jaar vloed
zeker. s van ou de unnen an de

KCE Report 176
8. REFER1. Perry N
L. EuroscreeniOncol.
2. Schwarmammoprevent
3. Schwarfor can8.
4. SilvermFischhomammo2001;2
5. Schwarwomendetectio2000;32
6. Belgian2004-2
7. Paulus Good KnowleAvailabhttp://kc
6
RENTIES N, Broeders M, deopean guidelinesing and diagnosis2008;19(4):614-2rtz LM, Woloshinography for womtion of breast canrtz LM, Woloshin cer screening in
man E, Woloshin off B. Women's vography: a qualit1(3):231-40. rtz LM, Woloshin
n's attitudes to faon of ductal carci20(7250):1635-40n Cancer Registr005. Brussels; 20D, Mambourg F
Clinical Practice edge Centre (KCble ce.fgov.be/index_
e Wolf C, Tornbergs for quality assus. Fourth edition--22. n S. News mediaen in their 40s acer. JAMA. 2002;S, Fowler FJ, Jr.the United States
S, Schwartz LMviews on breast ctative interview st
S, Sox HC, Fiscalse positive manoma in situ: cros0. ry, editor. Cance
008. F, Bonneux L. [B
(GCP). BrusselCE); 2005 02/05/
_en.aspx?SGREF
S
g S, Holland R, vourance in breast-summary docume
a coverage of scand tamoxifen for 287(23):3136-42.., Welch HG. Ents. JAMA. 2004;29
M, Byram SJ, Wecancer risk and sctudy. Med Decis
chhoff B, Welch ammography resuss sectional surve
er incidence in B
Breast cancer scrls: Belgian Heal/2005. KCE Rep
=5221&CREF=93
Screening Breast C
on Karsa t cancer ent. Ann
creening primary
. husiasm
91(1):71-
elch HG, creening Making.
HG. US ults and ey. BMJ.
Belgium,
reening]. th Care
ports 11 from:
348
8
9
1
1
1
1
1
Cancer
8. MandelblaDraisma different benefits a19;152(2):
9. Woloshin HG. Womdebate. Ar
0. Mandelbladecisions among theClin Onco
1. Doumont organisé.
2. Gallois. DUNAFORM
3. USPSTF. Task ForMedicine 2
4. Woloshin mammogr2010;303(
att JS, Cronin KAG, et al. Effectscreening schednd harms.[Erratum:136]. Ann Intern S, Schwartz LM,
men's understandrch Intern Med. 20att JS, Silliman about the benefitse oldest old withol. 2009;27(4):487-D, Verstraeten
Santé en CommuDépister les caMEC, editor. MédScreening for Br
rce Recommend2011(151):716-26
S, Schwartz raphy screening: (2):164-5.
A, Bailey S, Berrs of mammogradules: model esm appears in AnnMed. 2009;151(10Byram SJ, Sox H
ding of the mam000;160(10):1434R. Hanging in s and harms of br
out a safety net o-90. K. Enjeux éth
unauté Française.ancers, mais à ecine. Paris; 2005reast Cancer: U.Sdation Statement6.
LM. The beneunderstanding t
ry DA, de Koningaphy screening ustimates of pot
n Intern Med. 20100):738-47.
HC, Fischhoff B, Wmmography scre4-40.
the balance: mreast cancer scre
of scientific eviden
hiques du dépi 2012(7):3-7. quelle condition
5. p. 72-7. S. Preventive Sert Annals of Int
efits and harmthe trade-offs. JA
19
g HJ, under tential 0 Jan
Welch ening
aking ening
nce. J
stage
n In:
rvices ternal
ms of AMA.

20
SCIENTIFIC RREPORT
S
T
Screening Breast C
11TbmRthreqoboos
1Tww
1Taaa2ecreinoddbth
Cancer
1. INTROD1.1. Context oThis report is a pbreast cancer scrmade a list of cRepresentatives ohe choice and theelated to each
questions(see KCover three KCE rebreast cancer screof 40-49 years (KCof women at risk foscreening (KCE re
1.2. Scope of This report focusewith mammograpwomen between 7
1.3. Breast caThe Belgian fedagreement in 200aged 50-69 yearsappropriate financ2001, Flanders, theach introduced acontext of alreademains quite freqn the age-group 5older women (>7dominant in the agdrops, mainly becaby means of diagnhat substitution o
DUCTION of this report artial update of teening publishedclinical questionsof stakeholders’ ore wording of the q
question and CE report 172)2. eports. A first KCEeening with mamCE report 129)3. or breast cancer aeport 172)2.
this report es on the extensiohy to older wom
70-74 years of age
ancer screeningderal and regio01 for an organis, to be organiz
cial resources suphe Walloon regionan organized scredy existing practquent in the Wallo50-69, but also a
70 years). In Flage-group 50-69. Iause organized scnostic mammograf screening mamm
he clinical practicd in 20051. Theres related to brearganizations wereuestions, to highlito score the
Selected questioE report published
mmography for woThe second is foand technical met
on of organized brmen. Eligible pope with average ris
g in Belgium nal governmentszed screening p
zed by the regiopplied by the feden and the Brusseeening programmtices. Indeed, opoon and Brussels among younger (4nders, screeningn the age-group 7creening stops at
aphy decreases amography by opp
KCE Report
ce guideline (CPGfore, the KCE exast cancer screee then invited to reight the main probrelevance of cl
ons were then did in 2010 is focuseomen in the age gcused on identificthods for breast ca
reast cancer screpulation is definek of breast cance
s signed a prorogramme for wonal governments
eral government. Sels capital region me within their sppportunistic screregion among wo
40-49 years of ag mammographies70-79 overall coveage 69. The covelso with 3%, indic
portunistic screeni
t 176
G) on xperts ening. eview blems linical vided ed on group cation ancer
ening ed as r.
otocol omen
s with Since have
pecific ening omen ge) or s are erage erage cating ing at

KCE Report 176
the age of 70 (including both screening) remWalloon region
1.4. ClinicaThis specific re1. What are c
screening i1.1. What
organi1.2. How lo
breast1.3. What
organi1.4. What
organi2. What are
organized sterms
2.2. Harms2.3. Harms2.4. Harms
3. What attitureferral?
6
is not frequent diagnostic or foll
mains at 18% in F(KCE report 172)
l questions port addresses thclinical benefits ofin women betweeis the effect of anzed screening onong is the delay bt cancer related mis the effect of anzed screening onis the effect of anzed screening onthe specific ha
screening in womof false positive o
s in terms of addits in terms of over-s in terms of overtude should be re
in Flanders. At low up mammogr
Flanders, 33% in )2.
he following questif an extension of
en 70 and 74 yearsn extension (70-74 the breast cancebetween the scree
mortality reduction?n extension (70-74 the overal mortal
n extension (70-74 morbidity? rms of an exte
men between 70 or false negative reional diagnostic te-diagnosis? treatment? ecommended for
S
this age, total craphies and oppoBrussels and 30%
ions: f breast cancer ors? 4 years) of breas
er related mortalityening and the as? 4 years) of breaslity? 4 years) of breas
ension of breast and 74 years?H
esults? ests?
women in case
Screening Breast C
coverage ortunistic % in the
rganized
st cancer y? sociated
st cancer
st cancer
cancer Harms in
e of self
1FpthemB(tacT
Cancer
1.5. Scientific For each clinical performed and disheir scientific coepidemiology, or models. To quanBelgian situation IMA/AIM), cancerables and construcycles. The methodology
approach question, a sys
scussed with the ompetency in se
health economicntify what the im
we applied dar registry and datucted a simple tim
used and the resu
stematic search support of extern
everal fields: gycs. For question
mplications of ourata from the Inta from the literat
me dependent Ma
ults are described
of the literaturenal experts choseynaecology, radion 3, we searcher findings are ontermutualistic Agure on the Belgiarkov chain with a
d in each chapter.
21
was en for ology, ed for n the gency an life nnual

22
2. LITER2.1. Review2.1.1. Metho2.1.1.1. SouA broad searcCDSR and DARfor systematic r2.1.1.2. SeaFor searching oin combination screening (or eEMBASE, the 'breast cancer'combined with (SR) or meta-an2.1.1.3. In- Databases werGerman. This r2004), thus wrestriction (Engselection basedwithout breastintervention (mdiagnosis testsanalysis or RC<75 years), anindependently b
RATURE REw of clinical studodology urces ch of the electroRE was conductedreviews (SR) and arch terms on Medline databwith usual langua
early detection) (following Emtre
and 'mammograpa standard searc
nalysis (M-A). and exclusion crre searched for Sreport is a update
we used a date lish, Dutch, Frencd on title, abstrat cancer and w
mammography), o, over diagnosis
CT), key questiond original publicaby 2 reviewers (FM
EVIEWS dies
nic databases Od in April 2011. Semeta-analysis (M
ase, the followingage: Breast neop(MESH) and mame terms were u
phy'. These MESHch strategy to ide
riteria SR and M-A in Ee of previous KCE
restriction (2004ch and German).act or full text wwithout particulaoutcome (mortaland over treatme (screening), age
ation. Relevant puM, JR).
S
OVID Medline, EMearch was conduc
M-A).
g MeSH terms welasms (MESH) an
mmography (MESused: 'cancer scrH and Emtree termentify systematic
English, French, DE report1 (search 4-2011) and a laInclusion criteria
were: population ar breast canceity, morbidity, a
ent), design (SR oe of population (>ublications were
Screening Breast C
MBASE, cted first
ere used nd mass SH). For reening', ms were reviews
Dutch or made in anguage used for (women
er risk), dditional or meta->70 and selected
2WquR2eresTeaTs2Tb(wwTu(wT2InwefuwTmd
Cancer
2.1.1.4. AdditioWe identified twoquestion 2. Therupdated by searchReviews from the2008). Additional hensure that no poeference lists of
screening3. The identified stueligible studies, available, the studThe description asearch are in Appe2.1.1.5. QualityThe methodologicbias were rated www.cochrane.nl
was conducted byThe methodologicusing the adeqwww.cochrane.nl
The results of the 2.1.1.6. Identifn the systematic were identified inexcluded on the bull and reviewed were included4-8. The reviews writtemortality as outcodiagnosis and the
onal evidence SR4, 5 as the mrefore the evidehing Medline and search date of thand searching otentially relevant f SR and of ou
dies were selectethe full-text was
dy was not taken innd results of the endix 1.1. ty appraisal cal quality of syst
using the check). The assessmen
y a team of two revcal quality of selecquate checklists ). quality appraisal afied systematic r
search for literan database searbasis of title and in more detail. O
en by Götzsche ome, those from review of Virnig8
more extensive soence-identified th the Cochrane Dthe two SR’s on
of reference lists wstudies were misur previous repo
ed based on titles retrieved. In cnto account. literature searche
tematic reviews aklists of the Dunt of the risk of bviewers (FM, JR).cted additional ev
of the Dutc
are in Appendix 1reviews ture reviews, 53
rches. The majoabstract; 10 citat
On the basis of t
and Nelson4, 5 aBiesheuvel and Jon ductal carcino
KCE Report
ource for the reserough those SRatabase of Syste(search date Nov
was also undertaksed. We also scaort on breast ca
e and abstract. Fcase no full-text
es and flow of st
and associated ritch Cochrane C
bias in the include. vidence was also h Cochrane C
.5.
citations on the ority of citations tions were retrievthe full text, 5 rev
are mainly focuseJorgensen6, 7 on ma in situ (DCIS)
t 176
earch R-was matic v-Dec ken to anned ancer
For all was
tudies
isk of Centre ed SR
rated Centre
topic were
ved in views
ed on over-.

KCE Report 176
As a first step,determine theirjudged to be ofupdate of onePreventive Tasquality and useThe review writappraisal of seJorgensen7 waswas also judged2.1.1.7. IdenThe evidence wsearching Medfrom the searchsearch for relevApril 2011) idenon the basis offull and reviewstudies were exthe flow of randBy hand searcSwedish RCT’sonly RCT tharandomization. their suitability fquality by Nelsanalysis10. 2.1.1.8. IdenFor diagnostic July 2011 identon the basis oretrieved in fullthose two stucomments on th
6
, a quality apprar suitability for incf high quality withe other review sk Force9. Humphd here as completten by Biesheuvelected trials not ss judged to be ofd to be of high quntified RCT
was updated usingdline and the Coch date of this SR vant RCTs carrientified 432 citationf title and abstract
wed in more detaxcluded because
domized controlledching of referencs were identified. at includes wom
Quality appraisalfor inclusion. Theon and of low qu
ntified additionaerrors and over-tifying 10 citationof title and abstr and reviewed indies were excluhe two main SR4,
isal of all the revclusion. Götzsche a low risk of biasperformed by H
hrey review was aementary informatel6 was judged to bsufficiently describf high quality. Theality.
g the key words rchrane Databaseon (search date d out in Medline,ns. The majority ot; the other paper
ail. On the basis of the study desd trials from selecce lists of GötzsAmong those, the
men aged 70-74l of this RCT was Two County trial
uality by Götzsche
l evidence -diagnosis, this us. The majority oract; 2 papers on more detail. On ded. Most pape5.
S
views was carriee and Nelson SR4
s. Nelson review5
Humphrey for thalso judged to beion source. be of good qualitybed) and those we review written b
eported in Nelsone of Systematic RNov 2008). The l EMBASE and C
of citations were ers (n=8) were retrof the full text,
sign (not an RCTction to in-or exclusche and Nelsone Two County tria
years at the s carried out to des was judged to be and included fo
pdate was carrieof citations were en diagnostic errothe basis of the
ers are discussio
Screening Breast C
d out to 4, 5 were 5 was an he U.S. e of high
y (quality written by by Virnig
n SR5 by Reviews iterature
CCRT (in excluded rieved in all eight
T) shows sion. 4, 5, the
als is the time of
etermine be of fair or further
ed out in excluded ors were full text,
ons and
FAFcoobsSin2Ins‘smrecp2Ded22Incth((trIn8in
Cancer
For DCIS, this updAll citations were eFor overtreatmentcitations on Medlinof citations were eovertreatment werbasis of the full teselected one pubScreening Programn Appendix 1.4. 2.1.1.9. Ongoin addition to the searched for clinicscreening’ and ‘mmajority of searchelevant trials (NC
considered as ouprotocol. 2.1.1.10. Data eData from systemextraction table (Ddata extraction tab2.1.2. Descript2.1.2.1. Sourcn the years 196conducted randomhe HIP trial (N =phase I and II, N Kopparberg and rial (N= 60 117) inn Canada, the Na835) were initiatedn 1979 in 1980 (N
date was carried excluded on the bt, this update wasne and 7 citationsexcluded on the bre retrieved in fu
ext, we retrieved ablication presentimme11. The desc
ing clinical trials database search
cal trials. The seamammography’ wh results (n=135CT00963911, NCt of scope after
extraction matic reviews andDET) summarizinble are in Appendition of screeningces 60-1980, USA, Smized controlled tr= 60 995) started= 60 076) startedOstergötland, N=
n 1980 and finallyational Breast Scd in 1980. In UniteN=44 268) and th
out in July 2011 basis of title and as carried out in Jus on the Cochranebasis of title and ll and reviewed iagain the SR writing data issued ription and results
hes, the ClinicalTarch terms ‘breastwere used to se5) were ongoing CT00247442) wer
receiving more i
from trials wereng key design feaix 1.6.
g benefit
Sweden, Canada rials of mammograd in 1963. In Sw in 1976 and 1978= 133 065) in 19y the Göteborg triacreening Trials (Ned Kingdom, the Ehe UK Age Trial i
identifying 7 citabstract. uly 2011 identifyine Library. The maabstract; 2 papen more detail. Otten by Götzschefrom the UK B
s of those update
Trials.gov websitet neoplasm’ as warch for studies.trials. Two potenre identified but information on th
e extracted into aatures and result
and United Kingaphy screening. In
weden, the Malmö8, the Two county977-78, the Stockal (N= 51 611) in NBSS-1 and 2, N Edinburgh, trial stin 1991 (trial limit
23
tions.
ng 19 ajority ers on n the 4 and
Breast es are
e was well as
. The ntially were
he full
data ts. All
gdom n US, ö trial y Trial kholm 1981. = 89
tarted ted to

24
women aged summarizing thThis part is baPreventive Servon the CochranSwedish Two-CSR10,13,14. Both reviews inMalmö I and Stockholm trialstudy was ratedNelson updatedabout youngerHumphrey pubfrom 50 to 74 women 39 to 74younger than 50Two-County trWe analysedinformation on County trial is therefore threepublication of thby Nelson and Two-County triHealth and WKopparberg andyears were clstratified by socluster. Finallythose, they werand 7 462 in tscreening rounclosed in 1984
40-49 years)12. eirs results are noased on the SRvices Task Forcene SR 4. We anaCounty trial (Ost
ncluded the sameII, the Two coun, the Göteborg trd as poor quality bd the meta-analys
women (40-49 yblication for morta
years. Götzsche4 years of age. T0 years and for w
rial the Swedish Tour specific popthe largest of th
e publications thahe initiator10, the pthe last publicatial was commiss
Welfare and includ Östergötland. Inuster-randomized
ocioeconomic stat, 78 085 womenre 10 568 womenthe control groupnds with a screenafter approximate
Numerous publow available.
R (2002) commisse (USPTSF) and alysed more in detergötland) which
e trials in their menty trial, the NBSrial and the UK Aby both authors ansis from Humphreyyears of age). Thality analysis pere4 performed firstThen he did a sepwomen older than 5
Two-County trial ulation (70-74 ye
he first eight randat describe this spublication of Nyson of Tabar publioned by the Swuded women in n 1977-78, 134 8d by geographictus, urban or ruran were invited ton aged 70-74 yea. At this age, woning interval of 3ely 7 years of scre
S
lications and so
sioned to assist its update of 200
etail one RCT nah was included
eta-analysis: the HSS trials (1 and Age Trial. The Ednd excluded therey9 to include new herefore, we referformed on womet a meta-analysisparate analysis for50 years.
in order to finears). The Swedisdomized trials. Wstudy. We used ström13 who was sished in July 201
wedish National Btwo Swedish c
67 women aged 4 area. They weal residency, ando the screening. rs in the screenin
omen were invited33 months. The teening10.
Screening Breast C
ome SR
the US 095,9 and med the by both
HIP trial, 2), the
dinburgh efore4, 9.
findings er to the en aged s among r women
nd more sh Two-
We used the first selected 114. The
Board of counties: 40 to 74 ere also d size of
Among ng group d to two trial was
InthKthmfrUoeFoTAadaNloSnseaOwavCtoca
Cancer
n 2002, Nyström he Malmö, OsteKopparberg trial whe age-dependenmortality relative rrom the OstergötUnfortunately, withof women 70 to 74each group)13. Finally, we found on mammographicTrials quality andAll studies includeas fair5, 9. Götzsdivided his resultsand results based Nevertheless, the ow risk of bias (seSome publicationsnumbers of womesome studies anaexact age at randas suboptimally raOstergötland, a puwitnesses were pralmost twice as hversus 0.0012, p County trial and cao that the validitycommittee (nameda doubtful cause o
performed one rergötland, Stockhwere not availablency of the effectrisks for consecuttland trial. The mhout the Kopparbe4 years of aged e
one publication sc screening effectd bias ed by Humphrey ische assessed ths on results based
on suboptimally rthird meta-analy
ee Appendix 1.5.1s based on The n enrolled. To exalysed results bydomization13. Nevandomized and lublic notary allocaresent. Breast cahigh in Kopparbe
= 0.02). The auause-of-death ass
y of local end poind consensus comof death14.
review of the Swholm, Göteborg e at this time. Thist of screening. Tive 5-years age g
median follow-up erg part of the Swenrolled was low (
summarizing longt on mortality14.
in 2002 and later he randomizationd on adequately rarandomized controyses were judged
). Swedish Two-Coplain this variation
y year-of-birth whvertheless, Götzscikely to be biase
ated the clusters bancer mortality in erg compared to utopsy rate was sessments were nnt committee datamittee) reviewed
KCE Report
wedish RCT’s incltrials. Results os publication asseThe author calcugroup based on retime was 17.9 y
wedish trial, the nu(approximately 50
g term data (29 y
by Nelson were n quality. This aandomized controol trial4. of high quality w
ounty reported van, Nyström replied
hile some others che assessed thised. He argued thby tossing a coin the control groupOstergötland (036% for all the
not blinded4. Accoa was criticized, athe records conta
t 176
uding of the essed ulated esults years. umber 000 in
years)
rated author ol trial
with a
arying d that used
s trial at for while
p was .0021 Two-
ording a third aining

KCE Report 176
2.1.2.2. BreFor women ageup, the Humphra significant re(RR) 0.84, 95%Risk (RR) 0.81,For women agcontrol trial sho15.8 years (me0.70 to 0.89). Tin terms of brrange13. For women agerandomization mortality at 13 ytrials with subbreast cancer mseven trials comThe review oconservative deat randomizatiomortality at 17.this age group group) and thistogether with N2.1.2.3. DelTabar publisheSwedish Two-Cmortality reductissued from locpresented. Thepresent here cpublication sho(CI) 0.62 to 1.0respectively 10
6
east cancer related 39 to 74 yearsrey meta-analysiseduction in breas% confidence inte, 95% (CI) (0.74, 0ged 39 to 74 yeowed a significan
edian follow up) oThis study showedreast cancer mor
ed at least 50 y adid not show a
years (Relative Roptimal randomizmortality (RR of 0mbined was 0.77 (of Swedish randetermination of caon, did not show4 years ((RR) 1.1was relatively sm
study is underpoelson that data arlay between screed in July 2011 County Trial14. Ttion in function of cal end point com validity of local econsensus data.
owed specific mor05), 27% ((RR) 00, 15 and 20 to 2
ted mortality reds and at approxims (M-A)9 and the Cst cancer mortaliterval (CI) 0.77 to0.87) respectivelyars, the Review nt reduction in b
of 21% (Relative Rd that the effect ofrtality reduction
at randomization, ta significant redisk (RR) 0.94, 95%zation showed a
0.77 (95% CI 0.67(95% CI 0.69 to 0
domized control ause of death for ww a significant re12, 95% (CI) 0.73mall (approximate
owered13. Conseqre insufficient for teening and specthe last follow-up
This publication mlength of follow u
mmittees and conend point committe
For women agertality reductions 0.73, 95% (CI) 0.29 years of follow
S
duction mately 13 years oCochrane review4
ty of 16% (Relat0.91) and 19% (
y. of Swedish rand
reast cancer moRisk (RR) 0.79, 9f breast cancer scvaries according
three trials with auction in breast % (CI) 0.77 to 1.1
a significant redu7 to 0.83)). The R0.86)4.
trial, applying women aged at leduction in breast3 to 1.72)). Unfortely 5000 womenuently, we must cthis age group5. cific mortality redp result (29-yearmodulated breastup. In this report bnsensus-based daee data was criticed 39 to 74 yeaof 20% ((RR) 0.8.59 to 0.92), and w up. In the sam
Screening Breast C
of follow-showed
ive Risk (Relative
domized rtality at
95% (CI) creening to age
adequate cancer
5). Four uction in RR for all
a more east 70 y t cancer tunately, in each
conclude
duction r) of the t cancer
both data ata were ized, we ars, this 80, 95% 27% at
me time,
dledinpfuaAs(wthsfrAinw2Ta(ysre1Umfrre2Wss
Cancer
deaths from breasength of follow-udeaths prevented ncluded in this sprevents deaths muture. So most oabsence of screenAuthors did not separately. Result77 080 in the scre
were 10 568 womehe control groupscreening rounds rom these cases wAs cited on previon the Swedish Twwomen in each gro2.1.2.4. All-cauThe Cochrane SRaged at least 50 y n=73654) did not
years (Relative Risuboptimal randoeduction in all-ca.02))4.
Unfortunately studmortality reductionraction of all-causeduction would re
2.1.2.5. MorbidWe found no datasources. In other screening reduces
st cancer preventup. They were reat 10, 15, 20, 25
study. Author empmore in the mediuf the breast canc
ning) more than 10calculate mortalits presented are eening group anden aged 70-74 yep. In Kopparberin women aged
were still includedous point, the grouwo-County Trial woup) and this studuse mortality R has reported d
at randomizationt show a significask (RR) 1.00, 95%
omization (n=982use breast cance
dies did not haven. According to thse mortality in caequire inclusion ofdity reduction a related to the cwords, we do no
s the morbidity of t
ted in the study gespectively 50, 9and 29 years of fphasized that breum to long term cer deaths would 0 years after randity relative risks based on 133 06 55 985 in the con
ears in the screenrg, cancers diag70-74 years and
d in the results14.up of women agedwas relatively smady is underpowere
ata on all-cause, two trials with adnt reduction in al% (CI) 0.95 to 1.0
261) also did noer mortality (RR of
statistical power hat disease specincer screening trf millions of subjec
cancer related moot accept or rejethe breast cancer
group increased 99, 114, 122 andfollow-up for all woeast cancer screthan in the immehave occurred (i
domization. for each age g
65 women aged 4ntrol group), whileing group and 7 4
gnosed after the breast cancer d
d 70-74 years incall (approximately ed13.
mortality. For wodequate randomizl-cause mortality 04). The two trialsot show a signif 0.99 (95% CI 0.
to detect an all-cific mortality is a rials, detect a moct.
orbidity in our select the hypothesisr disease.
25
along d 126 omen ening
ediate in the
group 40-74 e they 462 in e two eaths
luded 5000
omen zation at 13
s with ficant .97 to
cause small
ortality
ected s that

26
2.1.3. Descr2.1.3.1. SouThis part is basin part 2.3.5, wesearch date. Se2.1.3.2. StuSR written by reviews writtendiagnosis and different methoissued from thpublicly organizwas focused on2.1.3.3. PerThe sensitivity 81% in the Twdifficult to intebecause they replacement th(quality of mamfactors (the exresults of an esensibility mayspecificity of a aged 40-74 yecancer underwvalue of one-timfurther evaluatibiopsy. Positiveto 20% among Nelson reporte(USA) BCSC foa single screencommon amon
ription of screenurces sed on the 5 SR see updated those iee more details in
udy description Götzsche and N
n by Biesheuvel asubsequently on
ods to address e first RCTs whized screening prn ductal carcinomarformance of maof first mammog
wo County trial. Trpret. This data are not adjuste
herapy, mammogmmography, numxperience of radioexamination abnoy vary between
single mammogrears. This indicatewent further diagnme mammographion and from 50e predictive valuewomen 70 years
ed data from theor regularly screenning round. False
ng women aged
ing harms
elected in our main July 2011 starti appendix 1.4.
Nelson are descrand Jorgensen6,
n overtreatment. this issue. Biesile Jorgensen anrogrammes. The a in situ (DCIS)8.
ammography graphy for womenThis includes ovecannot be appli
ed for patient fagraphic breast deber of mammogrologists and thei
ormal)9. Provider countries4. In thraphic examinatioes that 4% of wnostic evaluationhy was 12% for a% to 75% for ab increases with aof age or older9. Breast Cancer ned women that ae-positive mamm70-79 years (68
S
in search4-8. As exing from the last l
ribed in point 3.17 were focused oEach author us
heuvel analysed nalysed data issu
review written b
n aged 70-74 yeer-diagnosis and ed to individual actors (use of hensity), technicalraphic views) or r propensity to lafactors may expe Two County t
on was 95.6% forwomen who did n
. The positive pabnormal results rbnormal results r
age and ranged fro
Surveillance Conare based on resuography results .8 per 1000 wom
Screening Breast C
xplained iterature
1.1. The on over-sed very
reports ued from by Virnig
ears was may be patients
hormone factors provider abel the lain that trial, the r women not have redictive requiring requiring om 18%
nsortium ults from are less men per
sliw2Ryhsoswoao2OddaNwebsGRsthbUBYENo
Cancer
screening round). ttle more commo
women per screen2.1.3.4. AdditioRates of additionayears (64.03 per higher among woscreening round) of screen detectedscreen-detected inwomen per screenof invasive breast aged 70 to 79 yeaother imaging test2.1.3.5. Over-dOver-diagnosis ofdetection with screduring the womanabsence of screenNelson reported rawith most from 1exclusion of DCISby age. She conclstatistically5. Götzsche reportedRCT’s that did nosomewhat larger ihe control group.breast cancer in oUSA after beginninBiesheuvel analyYork/HIP, Malm IIEdinburgh) and froNetherlands and over-detection of
Conversely, falseon among womening round)5. onal diagnostic t
al imaging are rela1000 women pe
omen aged 70 tothan among youn
d cancer is highesnvasive cancer aning round. The B
cancer detected ars, 154 women h, and 2 have biopdiagnosis f breast cancer eening of cancer n’s lifetime (and thning)6. ates of over-diagn1% to 10%. She
S cases, by whethluded that the stu
d that the level oot introduce earln the sub optimal He found also a
observational studng of the screeninysed publicationsI, Two County, Com four populatioItaly). He selectinvasive breast
e-negative mammn aged 70 to 79
tests atively low amonger screening rou
o 79 years (12.2nger women. As st in this age ground 1.4 screen-de
BCSC results indicby mammograph
have additional msies5.
at screening mathat would not haherefore would no
nosis varying frome explained variaher cases are inciudies are too hete
f over-diagnosis wy screening in thly randomized tria
a 40% to 60% incdies performed in ng4. s issued from tCanada a and b, on-based programed papers that acancer by mam
KCE Report
mography results 9 years (1.5 per
women aged 70 nd). Biopsy ratesper 1000 womeexpected, the nu
up. Results indicatetected DCIS per cate that for everyhy screening in woammography, 10
ay be defined asave presented clinot be diagnosed i
m less than 1% toations by inclusioident or prevalent
erogeneous to com
was about 30% ihe control groupals before screencrease in incidenAustralia, Europe
the first RCTs Stockholm, Göte
mme (Sweden, Noattempted to est
mmography scree
t 176
are a 1000
to 79 s are n per
umber te 6.5 1000
y case omen have
s the nically in the
o 30% on or t, and mbine
in the , and ing of
nce of e and
(New eborg, orway, imate
ening.

KCE Report 176
Note that he publications. Bscreened and uand high particcontrol group btime. After excseveral (some being based (definitions of tdescribed befoExcluding DCISaged 60–69 yeaJorgensen anaprogrammes. Hbreast cancer screening. Notehe estimated tscreened popuscreening, he screening withscreened and nmammography for women agebreast cancer Surprisingly, litincidence of bcalculated thatover-diagnosis CI 46% to 58%Discrepancies have led to a loThe approach BZahl, Jorgensewere substantiahypothetical inc
6
did not include Bias were descriunscreened popucipation in non-scbefore or during foclusion, he selec
overlapping) soon cumulative
terms are in appere, he selected t
S cases, over-detars6. alysed data issHe selected pape
before and afe that when data that they would clation. After exclucompared data
data covering non screened age
screening prograd 70 to 79 years
was closely rettle of this increareast cancer in over-diagnosis foincluding DCIS c)7. between results
ot of controversial Biesheuvel et al. ten and Götzche ally downwardly crease in incidenc
DCIS. He excibed as: differenlation, low participcreening group, oollow up, inappropcted 22 estimatesurces. Publicatio
e-incidence or endix 1.4.3). Excthe least biased otection ranged fro
ued from publicers that publishefter the introduwere present, DC
contribute to 10%usion of the impl
covering at leaat least seven y
e groups. The moammes was 50-6are available. The
elated to the intase was compenwomen older th
for invasive cancecases was 52% in
reported by Biesdiscussions. to adjusting for lea(2008), who statbiased, due to oce based on theo
S
luded potentiallynt breast cancer pation in screeninoffering screeningpriate adjustment s of over-detecti
ons were categorincidence-rate m
cluding biased stuover-detection es
om 7% to 21% for
cly organized scd trends in incidction of mammCIS were included% of the diagnoslementation phasast seven yearsyears after screest common age-r9 years. No data e increase in incidtroduction of scnsated for by a an 70 years. Joer was 35%. Then this meta-analys
sheuvel or by Jo
ad time was conteed that their est
over-adjustment, uretical models an
Screening Breast C
y biased r risk in ng group g to the for lead
on from rized as methods udies as stimates. r women
creening dence of
mography d. If not, ses in a e of the
s before ening in ange for specific
dence of creening.
drop in orgensen e rate of sis (95%
orgensen
ested by imations use of a d use of
locJinstrtoninw2HsinodUsswRTDSccro2uin
Cancer
ong term followconsidered estimaJorgensen & Göncidence with a screening. They arends, following too young to be scnot, the graphs ncidences beforewhom no explanat2.1.3.6. DCIS Historically, DCISsuspicious breasncreasing numbeof the disease is database (SurveilUnited States Nasurvival rate of 9screening was pewhen screening wRecent changes iThis author perfoDCIS in name of She included 63 compared data ocentury data colleose there from 1
2004. Incidence inuse of mammogrncidence8.
w up data that ation unhelpfully wötzsche used line
in an (hypothetassume a linear inhe same pattern creened. It is diffi
the authors pre screening was tion was given.
S was rare and t mass. Since rs of patients werexcellent. Maasslance, Epidemiolotional Cancer Ins96.6% for cases
erformed. The ratewas performed3, 15.
in DCIS incidencormed a SR on
Agency for Heapublications ad
btained before thcted in US where.87 per 100 000
ncreased most in raphy may expla
are considerablywide. ear regression ttical) population ncrease extrapolaas the linear trencult to judge if thiresent show nointroduced in the
diagnosed by sthe wide use
re diagnosed withs reported data isogy and End Restitute). Those das between 1978 e was 98.1% bet
ce in USA were eincidence, treatmlthcare Research
ddressing incidenhe screening (19e screening is com in 1973–1975 towomen older thain some but not
y diluted. They
to compare obsethat did not und
ated from prescrend observed in wois assumption hol
on-linear increasee UK and Norwa
surgical removal of mammograph
h DCIS. The progssued from the S
esults database oata showed a 10
and 1983, whetween 1984 and
emphasized by Vment and outcomh and Quality (AHnce for analysis. 973-1975) with cummon. DCIS incido 32.5 per 100 0an 50 years. Incret all of this incre
27
also
erved dergo ening omen lds or es in ay for
of a hy, a gnosis SEER of the 0-year en no 1989,
Virnig. es of
HRQ). She
urrent dence 000 in eased eased

28
2.1.3.7. OveGötzsche repowas significantlrandomization lumpectomies (with suboptima(RR of 1.42 (951.35 (95% CI 1Based on receemphasized ththere were app3500 cases. Aconserving surmethod has remincreasing incidhaving mastect900 in 2007/081
2.1.4. ScreeThe sojourn timdetectable phasimple mathem(mainly Markovthe lead time attainable lead in higher numbgained and high2.1.4.1. LiteIn a first stagMedline was csearch terms Mammography/limited to paperlists of the seleSee more detai
ertreatment rted that the numly larger in the sc
showed a sign(Relative Risk (RRl randomization s
5% CI 1.26 to 1.61.26 to 1.44)4. nt data from the e increasing num
proximately 1500 Although, most rgery, the percenmained constant dence of DCIS tretomies has increa11.
ening conditions me (ST) is the avse. Estimation ofmatical estimatev Models)12. Sojou
obtainable. If ttime is correspon
ber of additional her number of yeaerature search e, studies asses
consulted from 19(MESH) were: /. Sojourn time wrs written in Engli
ected studies werels in appendix 1.4
mber of mastectocreened groups. Tnificant increaseR) 1.31, 95% (CI)showed the same1)). The RR for al
UK Breast Screembers of patientscases, but in 200DCIS cases ma
ntage of patientsat 30% during th
eatments, the abssed from just und
verage duration of sojourn time cas or using mic
urn time provides he sojourn time nding long16. A lo
breast cancer dars with cancer du
ssing sojourn tim948 to October WBreast Neoplasm
was included in frish, Dutch, Frence checked for add4.4.
S
omies and lumpeThree trials with ae in mastectomi) 1.22 to 1.42). Tw increase in intervll five trials combi
ening Programmes with DCIS. In 07/08 there were ay be treat by
s being treated wis period. Becaus
solute numbers ofder 500 in 1998/99
of the preclinical an be performed crosimulation tecan absolute uppe
is long, the monger sojourn timedetected, more liue to lead-time17.
me were searcheWeek 1 2011. Thms/ Mass Screeree text. The seach, or German. Reditional relevant c
Screening Breast C
ectomies adequate ies and wo trials ventions ned was
e, Dixon 1998/99 close to breast-
with this se of the f women 9 to over
screen-by from
chniques er limit to maximum e results ife-years
ed. Ovid he main ning/ or
arch was eference citations.
SAc1kEedcreareOscddtwae2SWTeaminsdtoey
Cancer
Selection criteriaAll retrieved refecriteria (in terms o
) in a two-step keywords; followeEstimation of sojexcluding of 3 dudatabases. Of thiscriteria based on etained for full-tex
and 1 did not fetained16, 17, 25-32
Our search was bseveral publicationcited as referencedata published bydata29. Therefore,wo or more artiaccurate for our sextraction table (se2.1.4.2. ResultSojourn times caWe found 4 studiTwo- County Triaestimates of sojouapproximately themodel, but resultsn estimates publisstatistical methodsdeveloped statistico data from the Tearly detection myears (SD, 0.76)27
a erences were asof population, inteprocedure: initial
ed by full-text asjourn time not buplicates, 40 unis total of 40 refetitle and abstra
xt assessment, 6ulfill the outcom
based on ST durans were ST estims by the author. F
y Tabar in 199529
we used originacles based on t
study30, 31. Finally,ee appendix 1.6.7ts
alculated on RCTes based on the
al is described inurn time publishe same data. Both
s were not the samshed by the two as or by discrepanccal methods baseTwo County Trial
modalities as 0.92.
ssessed against ervention, outcom
assessment of ssessment of thebased on data que citations we
erences, 23 did nct evaluation. Am
6 did not fulfill theme criteria24. Fina
ation estimations mations were issueFor example, Zap. Duffy in 200526
al publications. Ifthe same data, 7 publications ar
7).
T’s data results of the Twn chapter 2 (poied by Tabar and h authors used thme. Shen underlinauthors25, 29 may cy in the data. Shed on the maximul. Authors estima
2 (SD, 0.09) and
KCE Report
pre-defined inclmes, and design-Tthe title, abstract
e selected referewere excluded.
ere identified fromnot meet the inclmong the 17 cita population criterally, 10 studies
as search. We fed from others stpa in 200332referrreferred also to one author publwe choose the re summarized in
wo- County Trialint 2.2.1.1.)10, 13. Duffy were base
he same Markov ned that the differbe caused by diffen applied his rec
um likelihood estimated the sensitiviti
the mean ST a
t 176
usion Table t and
ences. After
m the usion ations ia18-23 were
found tudies red to those ished most
n data
. The First
ed on chain rence ferent cently mates ies of
as 4.4
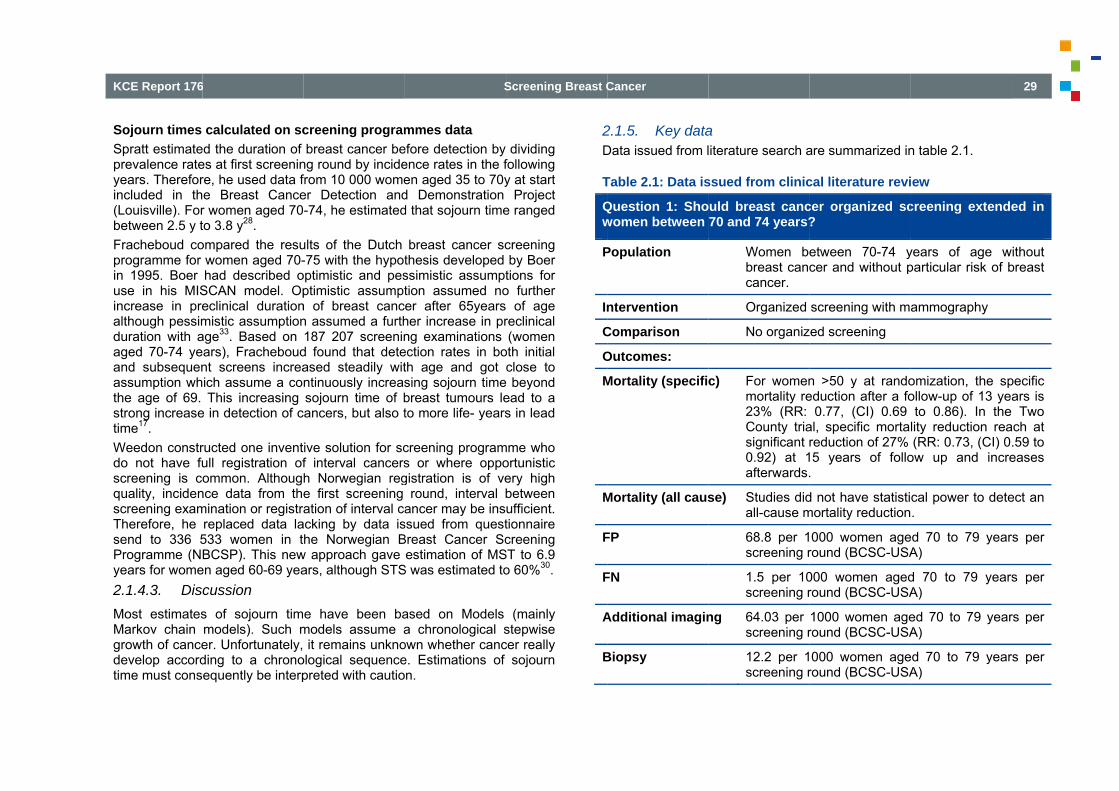
KCE Report 176
Sojourn times Spratt estimateprevalence rateyears. Thereforincluded in th(Louisville). Forbetween 2.5 y tFracheboud coprogramme for in 1995. Boer use in his MISincrease in prealthough pessimduration with aaged 70-74 yeand subsequenassumption whthe age of 69. strong increasetime17. Weedon constrdo not have fuscreening is cquality, incidenscreening examTherefore, he send to 336 5Programme (Nyears for wome2.1.4.3. DisMost estimatesMarkov chain growth of cancedevelop accordtime must cons
6
calculated on sced the duration of es at first screeninre, he used data fe Breast Cancer women aged 70to 3.8 y28. ompared the resu
women aged 70-had described o
SCAN model. Opeclinical durationmistic assumptionage33. Based on ars), Fracheboudnt screens increaich assume a coThis increasing
e in detection of c
ructed one inventull registration ofommon. Although
nce data from themination or registrareplaced data la533 women in tBCSP). This new
en aged 60-69 yeacussion s of sojourn timmodels). Such mer. Unfortunately, ding to a chronoequently be interp
creening programbreast cancer be
ng round by incidefrom 10 000 womeer Detection and-74, he estimated
ults of the Dutch -75 with the hypot
optimistic and pesptimistic assumpt
n of breast cancn assumed a furth187 207 screenin
d found that deteased steadily witntinuously increassojourn time of bancers, but also t
ive solution for scf interval cancersh Norwegian rege first screening ation of interval ca
acking by data ishe Norwegian B
w approach gave ars, although STS
e have been bamodels assume a
it remains unknoological sequencepreted with cautio
S
mmes data efore detection by ence rates in the fen aged 35 to 70yd Demonstration d that sojourn time
breast cancer scthesis developed ssimistic assumpttion assumed noer after 65yearsher increase in prng examinationsection rates in both age and got sing sojourn timebreast tumours leto more life- years
creening programs or where oppogistration is of ve
round, interval bancer may be ins
ssued from questBreast Cancer Sc
estimation of MSS was estimated to
ased on Models a chronological s
own whether cance. Estimations of n.
Screening Breast C
dividing following y at start
Project e ranged
creening by Boer tions for o further of age reclinical (women
oth initial close to
e beyond ead to a s in lead
mme who ortunistic ery high between ufficient. tionnaire creening
ST to 6.9 o 60%30.
(mainly stepwise cer really
sojourn
2D
T
Qw
P
In
C
O
M
M
F
F
A
B
Cancer
2.1.5. Key dataData issued from l
Table 2.1: Data is
Question 1: Showomen between
Population
ntervention
Comparison
Outcomes:
Mortality (specifi
Mortality (all caus
FP
FN
Additional imagin
Biopsy
a literature search a
ssued from clinic
ould breast canc70 and 74 years?
Women bebreast canccancer.
Organized
No organiz
c) For womenmortality re23% (RR: County triasignificant r0.92) at 1afterwards.
se) Studies didall-cause m
68.8 per 1screening r
1.5 per 10screening r
ng 64.03 per screening r
12.2 per 1screening r
are summarized in
cal literature revi
cer organized sc?
etween 70-74 ycer and without p
screening with m
ed screening
n >50 y at randoeduction after a fo
0.77, (CI) 0.69 al, specific mortareduction of 27%
15 years of follo.
d not have statistimortality reduction
000 women ageround (BCSC-USA
000 women agedround (BCSC-USA
1000 women ageround (BCSC-USA
000 women ageround (BCSC-USA
n table 2.1.
iew
creening extende
years of age wparticular risk of b
ammography
omization, the spollow-up of 13 yeato 0.86). In the
lity reduction rea(RR: 0.73, (CI) 0
ow up and incre
cal power to dete.
ed 70 to 79 yearA)
d 70 to 79 yearsA)
ed 70 to 79 yearA)
ed 70 to 79 yearA)
29
ed in
ithout breast
pecific ars is
Two ach at .59 to eases
ect an
rs per
s per
rs per
rs per

30
DCIS
Over-diagnosi
Over-treatmen
2.1.6. ConclAt this age groadditional imagspecific mortalmortality reducspecific mortaliafter screeningreduction must in our country.On the other pertinent to discin this age-groucancer screenitime bias althoScreening diagthe end of “the diagnosed brea
1.4 scre70 to 79
s Over-defrom (7%women a
nt The numwas sig(RR:1.35
lusion oup, performance
ging are relativelyity reduction of tion did not appeity reduction is ng ((RR) 0.80, (Cbe put in perspec
hand, aspects recussion of the benup. First, over-diagng, the risk of o
ough difficult to esnosed breast canlife in good health
ast cancer34.
een-detected DCIS9 years per screen
etection (excludin% to 21%) to 35aged 70 to 79 yea
mber of mastectognificantly larger 5 (95% CI 1.26 to
e of mammograpy low. Breast canc23% to 27% acear in the first yeot statistically sigI) 0.62 to 1.05). ctive with life-expe
elated to quality nefit and harms ognosis being an invertreatment persstimate, may be
ncer and consecuh condition” some
S
S per 1000 womening round (BCSC
g DCIS cases),5% (no data spears are available).
omies and lumpein the screened
o 1.44).
phy is high and cer screening achcording to autho
ears after screenignificant before 1
Breast cancer mectancy for this ag
of life raises qf breast cancer scnevitable consequsists. Secondly, tcrucial for older
utive treatment ma years earlier than
Screening Breast C
en aged C-USA)
ranged ecific for .
ectomies groups
rates of hieves a ors. This ing. The 10 years mortality ge-group
uestions creening uence of the lead women.
ay mean n clinical
22InoessMJliRcTs•••
2Ac2ksdin
Cancer
2.2. Review o2.2.1. Literaturn a first stage, ranon morbidity and meffectiveness of scsources to corresearched35. Medline, Embase,January 2000 up tmited to papers
Reference lists of citations. The keywords usesearch terms (MES Breast Neopla Mass Screeni Mammograph
2.2.2. SelectionAll retrieved refecriteria (in terms o2.2.) in a two-stepkeywords; followeshould be noted digital mammogran KCE report 1722
of modeling studre search strategndomized clinical mortality were seacreening require a
ectly inform deci
, NHS EED and to September 20written in Englishthe selected stud
ed and the resultsSH) were: asms; and ng or Early Detec
hy; and n criteria
erences were asof population, intep procedure: initiaed by full-text ass
that studies assphy) were exclude2.
dies gy trials analysing th
arched (see abova lot of informationsion makers, m
Econlit databases11 (see appendixh, Dutch, French,ies were checked
s are detailed in a
ction of Cancer ; a
ssessed against ervention, outcomeal assessment of sessment of the sessing screeninged because such
KCE Report
he impact of screve). Then, becausn from a wide ranodeling studies
s were consultedx 2.1). The search, Spanish, or Gerd for additional rel
ppendix 2.1. The
and
pre-defined selees, and design - Tf the title, abstracselected referenc
g techniques (suctopic was investig
t 176
ening se the nge of
were
from h was rman. evant
main
ection Table
ct and ces. It ch as gated

KCE Report 176
Table 2.2: Sele
Population
Intervention
Outcomes
Design
LYG: life-year ga
2.2.3. QuanAfter excluding the databases.citations. Of thicriteria based retained for full15 did not fulfilretained, conceCISNET, 2 appdeveloped by publications17, 3
appendix 2.2.
6
ection criteria
Inclusion crite
caucasian wombreast cancer particular risk
Screening mam
Morbidity and(e.g. LYG and Q
Modeling studie
ained; QALY: Quality
tity of research a195 duplicates,
. Hand searchings total of 1058 reon title and abs-text assessmentl the design criter
erning 6 models dplications of theseother groups or 36-59. The flow ch
eria Ex
men without and without
OtAs
mmography Otma(e
d Mortality QALYs)
Otdia
es Ot
y-adjusted life-year
available 1058 unique citatg did not allow eferences, 1016 dstract evaluation. t, 2 did not fulfill thria. Finally, 25 modeveloped by mo models on differeauthors, as som
hart of this selec
S
xclusion criteria
ther (e.g. womansian women, etc.)
ther, iammography tec.g. digital mammo
ther outcomes (eagnosis)
ther designs
gained
tions were identifus to identify ad
did not meet the iAmong the 42
he population critodeling publicatiodeling groups invent context and 7
me models have ction is presented
Screening Breast C
n at risk,
ncluding chniques ography)
e.g. over
fied from dditional nclusion citations teria and ons were volved in 7 models
several d in the
T
E
P
In
O
D
22T((cfotodmC(aTcre2eu
Cancer
Table 2.3: Modeli
Exclusion criteria
Population
ntervention
Outcome
Design
2.2.4. Selected2.2.4.1. The CThe Cancer Interhttp://cisnet.canceNCI)-sponsored
cancer control inteor breast cancer. o help determindeveloped their omodeling philosopCenter model37, UMISCAN) model5
and Stanford modThe seven modecontributions of seduction in brea
200077. Mandelblaestimates of poteunder different scr
ing studies exclu
a Studies
Messecar 2
Advisory CAnonymouBonneux 2Koning 20Habbema Rautenstra
d studies CISNET Projectrvention and Surer.gov) is a coninvestigators who
erventions on popThese models are optimal cance
own breast cancphies: The UniverUniversity of Wisc57, Dana-Farber mel51). ls were first usecreening mammost-cancer mortaliatt et all48 used 6ential benefits anreening schedules
uded after full-tex
2000; Wen 20056
Committee on Bus 2000; Barratt 22009; Caplan 20000; Feuer 2002006; Mandelblat
auch 2000, Xu 200
rveillance Modelinnsortium of Natiose focus is moulation trends in i
re also used to prer control strateger models spannrsity of Texas M.consin model, Ge
model44 University
d to assess the ography and adjuity in the United 6 of those CISN
nd harms of mams. One of the 7 mo
xt assessment
0, 61.
Breast Cancer 22002a; Barratt 2001; Carney 2007
04; Grivegnee 2tt 2003; Prevost 20062-76.
ng Network (CISonal Cancer Insodeling the impancidence and mo
roject future trendsgies40. Seven grning a wide rang. D. Anderson Caeorgetown47, Era
y of Rochester mo
relative and absuvant treatment t
States from 197ET models to prmmography screodels, the Univers
31
2006; 002b; 7; De 2001; 2000;
SNET) stitute act of ortality s and roups ge of ancer smus odel43
solute o the 75 to rovide ening sity of
32
Texas M. D. Apurely descriptiThe models wethey were comprocess, they aUS datasets B(Surveillance, eand the BerkeleA detailed dispublications anddetail, but sumdiscuss the maThe models espresent the recomparison of policy screeningFeuer et al.40
surveillance mosimulation modthrough the mnumber is gemechanistic orequations desctumor growth aCancer Centermodels could Farber model cmodels (Univehaving some characterizationobservable quaprogression of disease procesThe models statrends without screening use a
Anderson Cancer ve. ere developed by
mpared, discussealso used a commBCSC (Breast Caepidemiology andey mortality Databscussion of eachd on the CISNET
mmarize the pooleain limitations anstimated a large
esults of the parta screening pol
g age 50-74. identifies two d
odels used heredels at one end oodel one at a tinerated and indr analytic modelcribe the relationand metastasis. Tr, University of be characterizedcould be charactersity of Rochesteaspects of ea
n runs from bioantities to model t
disease, to epids is modeled (usuart with estimatesscreening and t
and improvements
Center model37
y different grouped and adapted mon set of variabancer Surveillancd end results), Cobase. h of this modelswebsite, we will n
ed comparison ofnd implications foe number of scet relevant to ourlicy screening ag
dimensions to ch. The first dimen
of the spectrum, wime, where at edividual life histols, where a set
nships between kThe University ofWisconsin, Geo
as micro simulaerized as analyticer and Stanford)ch. The secondologic, where ththe underlying disdemiologic, wherually the observabs of breast cancetreatment and ths in survival assoc
S
was not used as
s but not indepeduring the deve
bles and inputs, bce Consortium), Sonnecticut Tumor
s can be foundnot discuss each mf Mandelblatt et aor our research qenarios, but we wr research questge 50-69 to a sc
haracterize the tnsion incorporatewhere individuals ach transition a ories are generat of analytically key health statesf Texas M. D. Aorgetown, and Eation models; thec; and the remain) could be descrd dimension ofhe model goes sease onset, growre only a portionble portion). er incidence and mhen look at the eciated with treatm
Screening Breast C
s it was
endently, elopment ased on SEER 9 r registry
d in the model in al.48 and question. will only tion, the creening
types of es micro
are run random
ated, to derived
s and/or Anderson Erasmus e Dana-ning two ribed as f model
beyond wth, and n of the
mortality effect of
ment.
BpmdidceinoaccasthgTmmmwbotedredpTreligdTmIn
Cancer
Breast cancer is period (sojourn tmammography sedisease in the prdentification of eaclinical detection, estrogen receptor ndependent effecother causes. as age-specific variacharacteristics, trecompeting causesas preclinical detestages of diseasehat followed fromgrowth. The stage distribumodels were alsomodels that use thmodel reductions were used. The habiopsies and overobserved input waerms of QALYs. Mdisease or decreesults living with
diagnosis was notpurposes. Table 2.4 gives teduction and yeamited and there
gained per 1000 deaths averted ranThis class of modemodels are indivndependent valid
assumed to haime) and a clin
ensitivity (or thresreclinical screeninarlier-stage or sm
resulting in redustatus, and tumo
cts on mortality. Wmentioned before
ables for breast eatment algorithms of death. On theectable times (soje, were in these the model struct
utions in unscreeo intermediate ouhis observable vain mortality, life yearmful effects falsr diagnosis followas used, no attemMorbidity associa
ements in qualityh earlier knowlet considered, whic
he results of thears of life gained f
is some variabilitwomen screenednging from 4 to 6.els relies heavily ovidual bases theation was made
ave a preclinical,ical detection poholds of detectionng-detection perioaller tumors than uction in breast cr size– or stage–sWomen can die oe, the 6 models cancer incidence
ms and effects, a other hand, unobourn time), lead models estimatedture and assumpt
ened versus screetcomes, this in c
ariable as input. Aears gained werese positive mamm
wed from the modpt was made to q
ated with surgery y of life associatedge of a cancech makes the mod
e different modelsfor the different mty between moded ranging from 9
on unobservable vey are not alwadifficult because
KCE Report
, screening-detecoint. On the basn), screening idenod and results i might be identifiecancer mortality. specific treatment of breast cancer use a common s
e, mammographyand non-breast cabserved variablestime, dwell time wd intermediate outions concerning t
ened women in tcontrast to some As end output frome calculated, no Qmograms, unneceel, also here no
quantify those harfor screening-detted with false-poer diagnosis or dels less useful fo
s in terms of momodels. Gains are els, with number
to 17 and numb
variables, and as ays very transparesults from trials
t 176
ctable sis of ntifies n the ed by Age, have or of
set of y test ancer such within utputs tumor
these other
m the QALYs essary direct
rms in ected
ositive over
or our
ortality fairly
years ber of
most arent. s and
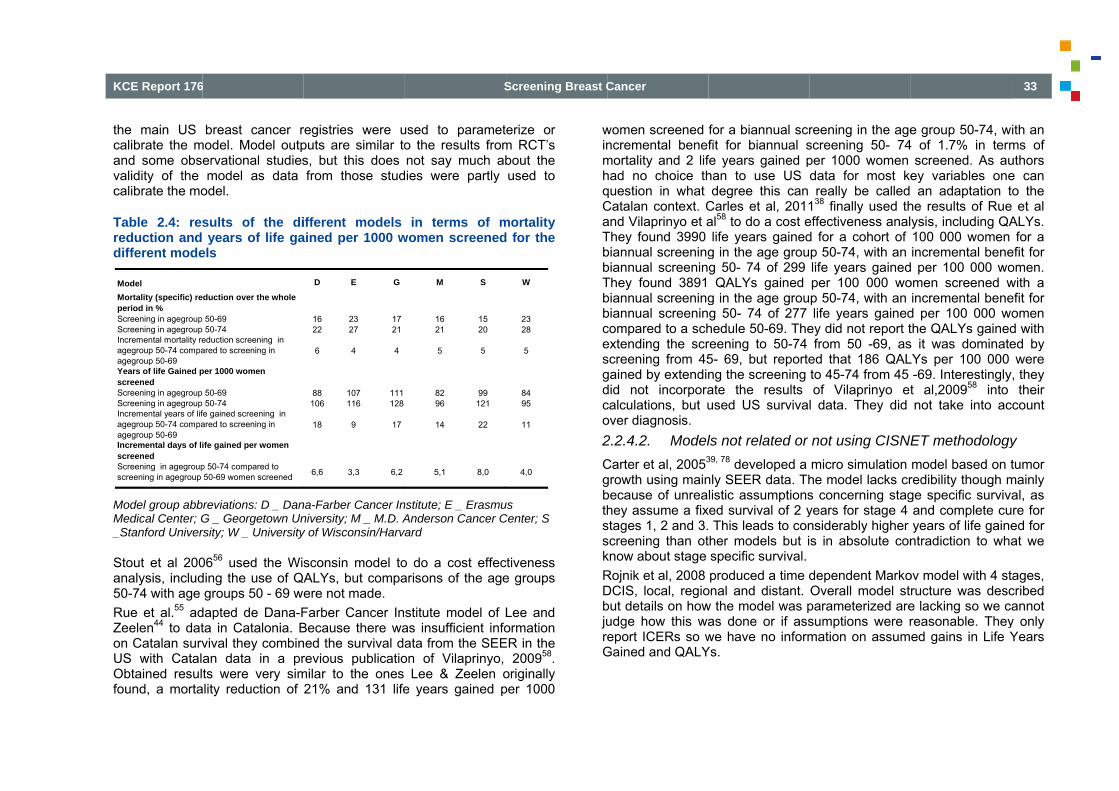
KCE Report 176
the main US calibrate the mand some obsvalidity of the calibrate the mo
Table 2.4: resreduction and different mode
Model group abbMedical Center; G_Stanford Univer
Stout et al 200analysis, includ50-74 with age Rue et al.55 adZeelen44 to daton Catalan survUS with CatalObtained resulfound, a morta
ModelMortality (specific) reperiod in %Screening in agegroup Screening in agegroup Incremental mortality reagegroup 50-74 compaagegroup 50-69Years of life Gained pscreenedScreening in agegroup Screening in agegroup Incremental years of lifagegroup 50-74 compaagegroup 50-69 Incremental days of liscreenedScreening in agegroupscreening in agegroup
6
breast cancer rmodel. Model outp
ervational studiesmodel as data
odel.
sults of the di years of life ga
els
breviations: D _ DanG _ Georgetown Unrsity; W _ University
0656 used the Wisding the use of QAgroups 50 - 69 w
dapted de Dana-Fta in Catalonia. Bvival they combinan data in a prts were very sim
ality reduction of
eduction over the whole
50-69 50-74eduction screening in ared to screening in
per 1000 women
50-69 50-74fe gained screening in ared to screening in
ife gained per women
p 50-74 compared to 50-69 women screened
registries were uputs are similar tos, but this does from those stud
ifferent models ained per 1000 w
na-Farber Cancer Inniversity; M _ M.D. Ay of Wisconsin/Harv
sconsin model toALYs, but compaere not made. Farber Cancer InBecause there waned the survival darevious publicatio
milar to the ones 21% and 131 life
D E G
16 23 1722 27 21
6 4 4
88 107 111106 116 128
18 9 17
6,6 3,3 6,2
S
used to parameto the results fromnot say much ab
dies were partly
in terms of mwomen screened
nstitute; E _ ErasmuAnderson Cancer C
vard
o do a cost effecarisons of the age
stitute model of Las insufficient infoata from the SEE
on of Vilaprinyo, Lee & Zeelen o
e years gained p
M S
16 1521 20
5 5
82 9996 121
14 22
5,1 8,0
Screening Breast C
erize or m RCT’s bout the used to
mortality d for the
us Center; S
ctiveness e groups
Lee and ormation
ER in the 200958.
originally per 1000
winmhqCaTbbTbbcesgdco2CgbthsskRDbjureG
W
2328
5
8495
11
4,0
Cancer
women screened ncremental benefmortality and 2 lifhad no choice thquestion in what Catalan context. Cand Vilaprinyo et aThey found 3990 biannual screeningbiannual screeninThey found 3891 biannual screeningbiannual screenincompared to a schextending the scrscreening from 45gained by extendindid not incorporacalculations, but uover diagnosis. 2.2.4.2. ModelCarter et al, 20053
growth using mainbecause of unreahey assume a fixstages 1, 2 and 3.screening than otknow about stage Rojnik et al, 2008 DCIS, local, regiobut details on howudge how this waeport ICERs so w
Gained and QALY
for a biannual scrfit for biannual sfe years gained phan to use US degree this can
Carles et al, 2011al58 to do a cost elife years gained
g in the age groug 50- 74 of 299 QALYs gained g in the age groug 50- 74 of 277 hedule 50-69. Thereening to 50-74 5- 69, but reporteng the screening ate the results used US survival
ls not related or 39, 78 developed a nly SEER data. Thlistic assumptions
xed survival of 2 y This leads to con
ther models but ispecific survival.produced a time d
onal and distant.w the model was pas done or if asswe have no informYs.
reening in the agescreening 50- 74per 1000 women data for most kereally be called
138 finally used theffectiveness anald for a cohort of p 50-74, with an life years gainedper 100 000 wop 50-74, with an life years gained
ey did not report tfrom 50 -69, as
ed that 186 QALto 45-74 from 45 of Vilaprinyo et
l data. They did
not using CISNEmicro simulation he model lacks crs concerning stagyears for stage 4 nsiderably higher s in absolute con
dependent MarkoOverall model stparameterized aresumptions were rmation on assum
e group 50-74, w4 of 1.7% in term
screened. As auey variables one
an adaptation the results of Rueysis, including QA100 000 women incremental bene
d per 100 000 woomen screened wincremental bene
d per 100 000 wothe QALYs gaineds it was dominateLYs per 100 000
-69. Interestinglyt al,200958 into not take into ac
ET methodologymodel based on tredibility though mge specific survivaand complete cuyears of life gainentradiction to wha
ov model with 4 structure was desce lacking so we careasonable. Theyed gains in Life Y
33
ith an ms of uthors e can o the et al ALYs. for a
efit for omen. with a efit for omen d with ed by were
, they their
count
y tumor
mainly al, as re for ed for at we
ages, cribed annot
y only Years

34
Neeser et al dscreening with coverage of 20breast cancer munclear how thranging from 5 years screeninrelevant for ouscreening wouldays) per womsimplistic by nreductions immwas not taken iRauner et al, 2only evaluated rather experimehow they actuaMahnken et al,length bias andonly adjusted HRijnsburger et developed by tCanadian CNB50–59, so their Barratt et al 2cohorts, with oother not, assuthe outcomes oscreening. Thereduction fromlinearly to maxthat benefit descreening. For of 70s, two fewwomen who stonumber of diag
developed a sima coverage of
0%. They assummortality with 15%hey come to this
to 20%. They cang beginning at ur research quesd save 41 lives p
men screened for not taking into amediately. No QAnto account.
2010 developed athe effect of scr
ental model is notlly modeled stage, 200846 develope
d over-detection aHazard ratio’s.
al, 200453 usethe Rotterdam57 SS-2 trial on breafindings are not r
200536 constructeone cohort womeming 100% partic
of women over 70ey assume a 37% for non compli
ximal level over fieclines linearly towomen who cont
wer women per op screening (sixnoses of breast c
mple Markov mod70% with opported that the orga% based on the s figure as IARCalculated the yea70 (they evaluat
stion as well. Thper 100 000 and 10 years. The mccount lead time
ALYs were used
an ant colonizatioreening amongst t useful for our pue specific survival.ed a method to and applied this to
ed the MISCAN (see above) to rast cancer screenreally useful for oued a Markov moen undergoing biecipation. Within th
0 years old underg% mortality reducance, and assumrst five years afteo nothing over ftinue screening fothousand die fro
x v eight deaths fcancer in screene
S
del comparing ortunistic screening
anized screening IARC handbook,
C postulates a rears of life gained ted other scheduey found that oradd 0.008 life ye
model is somewhae but applying aand effects on m
on optimization mwomen 50-70 a
urposes. It is also. adjust for lead timSEER data, but p
micro-simulationreplicate the dataning among womur purposes. odel for two hypennial screening his model, they evgoing 10 years of ction, adjusting tme that benefiter starting screenfive years after sor 10 years after m breast cancerfrom breast cancd women is abou
Screening Breast C
rganizes g with a reduces but it is
eduction for a 10 ules not rganized ears (2.9 at overly assumed morbidity
odel but and their o unclear
me bias, provided
n model a of the en aged
othetical and the valuated biennial
the 25% accrues
ning and stopping the age than in
cer). The t 41 and
th5Tin2Matoli
2BimdinhTaeafoDre1
Cancer
he number in uns50% brings the nuThis simple modento account the ef2.2.5. ConclusiModels described adapt them to the o parameterize thfe between 9 an 2
2.3. Review oBecause breast cmpact on the qudimensional healthnformative. It is health outcomes iTo value these madjusted life-year expected length adjustments are mor different healthDetermination of equires two steps. The health s
guidelines of health statessystem. Idealusing a genestates descrdescriptions fr
screened women umber of deaths el has the advantaffects of lead timeion are give useful inBelgian situation
hem. The CISNET22 years per 1000
of quality of life cancer screening
uality of life (QoLh-outcome measuimportant to taken the assessmenultidimensional ou
(QALY) must bof life by the
made using utilitieh states.
utility values, ns: tate description.
f the Belgian Hes should be deslly, the descriptioeric descriptive sriptions from Brom similar patien
about 26. assumin the screened gage of transparen
e and stage-shifts
nsights and elemen as we do not haT models give a m0 women screene
studies g programs are L) of the patientsure in terms of sue into account alnt of breast canceutcomes into a sibe used. QALYs
health-related qes derived from i
eeded for the c
According to theealth Care Knowscribed on a staon should be donsystem, such as Belgian patients nts in other countr
KCE Report
ming a risk reductigroup down 6.2 toncy, but does noton morbidity.
ents but it is difficave the necessarymodest gain in ye
ed.
expected to havs, models with a urvival are not enl the multidimens
er screening progrngle measure, qupermit to adjus
quality of life. Tindividuals’ prefer
calculation of QA
e pharmaco-econwledge Centre (Kandardized descrne by Belgian pa
the EQ-5D. If hare not avai
ries may be used7
t 176
ion of o 5.1. t take
cult to y data ear of
ve an one-
nough sional rams. uality-st the These rence
ALYs,
nomic KCE), riptive atients health lable,
79.

KCE Report 176
2. The valuat
economic gon a 0 (=vrepresentavalued by collected, discussed7
In this section,describing the treatment) is as2.3.1. Metho2.3.1.1. LiteElectronic dataestimates for screening and end of OctobeEmbase (via E(via OVID). Searches usingheading or texstrategies and t2.3.1.2. SelIdentified refere(in terms of poptwo-step procedfollowed by fuabstract was acitation was asthe selected stu
6
tion of these heguidelines of the Kvalue for death) toative sample of th
the Belgian popuvaluations from
79. the availability aburden of disea
ssessed. ods erature search stabases were con
different health treatment. System
er 2011 in the fombase.com), HTA
g various qualifierxt word. See appterms used. lection criteria ences were assespulation, intervendure: initial assesll-text assessmen
available and thesessed based on
udies were scrutin
ealth states. AccoKCE, health stateo 1 (=value for phe general publiculation but if no
m other countrie
and the quality oase due to breas
trategy nsulted for origin
states associatmatic searches wollowing databasA and EED (via
rs for “quality of lipendix 3.1 for an
ssed against pre-tion, outcome andssment of the titlent of the selecte
e citation was unn keywords and funized for additiona
S
ording to the phe values should beperfect health) scac. Ideally, they shoriginal Belgian des can be use
of published utilityst cancer (screen
nal publications oted with breast
were carried out uses: Medline (viaCRD NHS) and P
fe” were used asn overview of the
-defined selectiond design –Table 2e, abstract and keed references. Wnclear or ambiguoull-text. Referenceal relevant citation
Screening Breast C
armaco-e valued ale by a hould be data are ed and
y values ning and
on utility cancer
up to the a OVID), Psycinfo
Subject e search
n criteria 2.5) in a eywords;
When no ous, the e lists of
ns.
T
P
In
O
D
QQeHa
Cancer
Table 2.5: Article
I
Population Spcor
ntervention At
Outcome Ua(
Design Do6ms
QoL: Quality of Life. Quality of Life. DALYequivalent; TTO: TimHUI: Health Utility Inanalysis. VAS: visua
selection criteri
Inclusion criteria
Screened or treatpatients for breascancer, with a Caorigin and withoutrisk factors
Any intervention rto the Belgian set
Unique QoL weigallowing to derive(=utilities)
Direct (TTO, PTOor indirect (EQ-5D6D, HUI, QWB) vamethods in primastudies
QALY: Quality adjuY: Disability-Adjusteme-Trade-Off. PTO:ndex. QWB: Quality al analogue scale
ia
a Exclus
ted t ucasian t high
Other dCauca
relevant ttings
InterveBelgium
hts QALYs
Multi-dscores
O, SG) D, SF-aluation ry
LettersCUA wfrom thDirect (not reKCE pguideli
usted life year. HRQed Life-Years. HYE: : Person Trade-Off. of Well Being scale
sion criteria
diseases, non sian, high risk wo
entions not used inm
dimension HRQoLs, DALYs, HYEs, …
s, secondary studiwith QALYs derivehe literature, … valuations using Vcommended in thharmaco-economnes)79.
QoL: Health-Related healthy-years- SG: Standard-Gam
e. CUA: cost-utility
35
omen
n
L …
ies, ed
VAS e
mic
d
mble.

36
2.3.1.3. SelThe flowchart osearches on thduplicates, 352searching allowninety (290) ref65 references fat this stage, mOverall, we sele2.3.2. ResulA summary of tbe noted that values and theireported in the The selection o• Determinat• Selection o
Selection oSelection o
• Pooling of 2.3.2.1. DetHealth states foIt should be noreflection proce
lection process of the selection p
he databases retu2 unique citationswed us to identifyferences were disfor full-text evaluamostly because ofected 16 primary slts the selected studithis summary onr results. If other summary.
of utilities was dontion of health stateof utilities of a basecase studof other studies selected utilities atermination of heor which utility valuoted that this figess but not the
process is presenurned 524 citations were left (see ay 3 additional citacarded based on tion. Another 49 rf the unmet desigstudies (see appe
ies can be found nly report methoparameters were
ne according to thees for which utilitie
dy
and calculation of ealth states ues are needed a
gure is a schemamodel itself (de
S
nted in appendix 3ns. After exclusionalso appendix 3.2ations. Two-hundtitle and abstract
references were egn and populationendix 3.2).
in appendix 3.3. Iods used to deriv
measured, they w
e following stageses were needed
percentage chan
are listed in Figureatic representationescribed in secti
Screening Breast C
3.2. The n of 172 2). Hand dred and , leaving excluded criteria.
It should ve utility were not
s:
ges
e 2.1. n of the on 3.2).
Cancer KCE Reportt 176
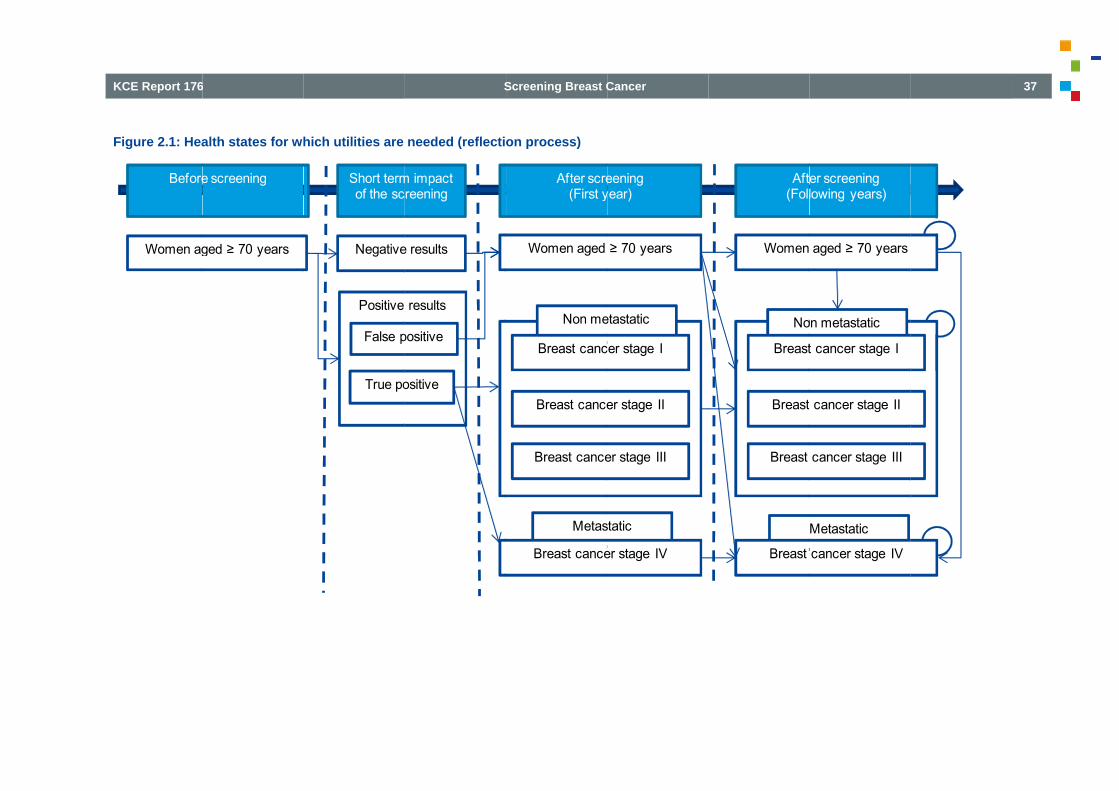
KCE Report 176
Figure 2.1: Hea
Women ag
Before
6
alth states for wh
ged ≥ 70 years
e screening
hich utilities are
Positive
Negative
False p
True po
Short termof the sc
S
needed (reflecti
results
e results
positive
ositive
m impact reening
Screening Breast C
on process)
Metas
Women aged
Breast cance
Breast cance
Breast cance
After scre(First y
Non me
Breast canc
Cancer
static
≥ 70 years
er stage II
er stage III
er stage IV
eeningyear)
etastatic
cer stage I
Women
Breast
Breast
Breast
Aft(Foll
No
Breast
Metastatic
aged ≥ 70 years
cancer stage II
cancer stage III
cancer stage IV
er screeninglowing years)
on metastatic
t cancer stage I
37

38
2.3.2.2. SelTo select utility by the pharmacdata could be foThen, we triedmodel. The aiminstruments andthe pharmaco-eto use the samquality of life weHowever, no st2.3.2.1 with thestudy with the gand to use it at Selection of th
We found onlymetastatic and the chance thaccording to th5D79. This studyUtility values imethods, i.e. technique) by Sgeneric instrumeconomic guidethese valuationTTO). In this stvalued using UKavailable). Heavalues for nontreatment) and patients are desThis study had
lection of utilities values, we first tco-economic guidound. to find the mos
m was to avoid d multiple populaeconomic guidelinme descriptive inseights coming fromtudy assessing ae same design wgreatest number othe starting point
he base case stu
y one study havimetastatic patienat this study als
he pharmaco-econy was therefore thin the study of a direct valuatioSwedish patients ment (i.e. the Eelines of the KCEs were retained (tudy, health statesK tariffs (because
alth states descri-metastatic patiethe following yea
scribed in Table 2the following limit
s tried to find Belgiadelines of the KCE
st complete studyas much as pos
ations to derive thnes of the KCE, it strument and them different studiesll of the heath sta
was found. We thof health states coof the selection pdy
ing assessed utints, i.e. the study oso used the betnomic guidelines he starting point oLidgren et al.80
on method (i.e. and an indirect v
EQ-5D instrumenE recommend thei.e. utility values fs were described
e no tariffs from thptions can be fonts in the first yars as well as ut2.8. tations:
S
an data as recomE79. However, no
y which best fit wsible the use of em. Indeed, accois strongly recom
e same set of vas79. ates described inherefore tried to orresponding to ouprocess.
lity values for boof Lidgren et al80.tter available insof the KCE, i.e. f our selection prowere derived fr
the time-trade-ofvaluation method nt). Because phe use of the EQ-5from EQ-5D and by Swedish patiee Swedish popula
ound in Table 2.6year (i.e. the yeaility values for m
Screening Breast C
mmended Belgian
with our multiple
ording to mmended alues for
n section find the
ur model
oth non-We had
strument the EQ-
ocess. rom two ff (TTO) using a
armaco-5D, only not from ents and ation are 6. Utility
ar of the etastatic
•
•
•
Cancer
Utility values cancer outpatfollowing limitaUtility values f
the shortthis shorttime and
Utility values palliative only reflefirst year
The short term(not measthis studythe valua
Non-metastatyear of diagnthat after the assumption idifference in uyear 5, 10 and
It should also (primary breapatients werinconstistencyMetastatic p
consultatGeneric instru
relevant specific ionly be uthese ins
were measuringtient clinic (Karolations: for non-metastatict term impact of st term impact wawas therefore notfor metastatic p
care. It was therected the quality of diagnosis.
m impact of diagnsured at the momy reported that thisation (measured thtic patients were dosis and the folloyear of treatmenis supported by utility values (fromd 1581. This US stbe noted that util
ast cancer in the re similar (0.6y may be due to thpatients only incions (best cases)uments such as tchanges in healtinstruments. How
used if validated mtruments are avai
g during out-patieinska University
c patients did not surgery. Howevers expected to cot included in the mpatients did not refore assumed thof life of metasta
nosis is also not fment of the diagnos impact was exphe year of diagnosdivided in only twowing years. It wt, utility values re
an US study m EQ-5D using Utudy is described ity estimates for nfirst year of diag96 and 0.685 he following reasoclude patients . he EQ-5D are lesth in a specific d
wever, diease-spemapping functionsilable, which was
KCE Report
ent visits at a bhospital), implyin
fully take into acr, on an annual b
over a limited lengmodel.
represent patienhat these utility v
atic patients durin
fully taken into acosis), even if authoected to be includsis). wo groups, i.e. thewas therefore assuemained constant
where no signiUS tariffs) was fou
in the appendix 3non metastatic pagnosis) and meta
respectivelly). ons: going in out-p
ss sensitive to cadisease than diseecific instrumentss to derive utilitiesnot the case79.
t 176
breast g the
count basis, gth of
nts in values ng the
count ors of ded in
e first umed . This ficant
und at .3.
atients astatic
This
atient
apture ease-s can s from

KCE Report 176
Table 2.6: Hea
Primary bcancer (year 0
Recurrence (y1)
Primary bcancer recurrence following year
Metastatic patSelection of otFor other heainstruments for us to identify apopulation stratwith UK tariffs),therefore used For the short tusing the EQ-5assessed utilitytrue negative. Hthe Swedish postates (as in positive” state is
6
lth states descri
breast -1)
Patients cancer wquestiondisease
year 0- Patients regional prior to metastat
breast and
rs
Patients breast cayear priometastat
ients Patients ther studies lth states, we trthe same popula
a study assessintified by age and , i.e. the study of for women aged 7term impact of p5D instrument way values for false Health states wereopulation) but UKthe other selects given in Table 2
ptions for the st
who had primawithin 1 year or lennaire, no recurre
who had at leaand/or contra-lateanswering the
tic disease.
who had been dancer or their lasor to answering thtic disease.
who had metasta
ried to find studation. The study ong utility values gender using the Burström et al.82
70 and over (see positive results afas identified (Gepositive, true po
e described by thK tariffs were usedted studies). A d2.7.
S
udy of Lidgren e
ary diagnosis bress prior to answeence and no m
st one recurrenceral) within 1 yea
questionnaire,
diagnosed with a t recurrence morehe questionnaire,
atic disease
dies having usedof Lidgren et al.80
for the general Ssame instrument These utility valuTable 2.8).
fter screening, onrard et al.)83. Thsitive, false negae UK population d to valuate thesdescription of th
Screening Breast C
et al.
reast of ering the etastatic
ce (loco-r or less and no
primary e than 1 , and no
d similar allowed
Swedish (EQ-5D
ues were
ne study his study ative and (and not e health e “false
Ainreoaareufawthd•
•
•
UIt3cpDCc•
Cancer
As showed in thisnvited for screenecalled for furth
obtention of a dassessment, only activity; pain/discoemaining two di
unaffected. The qalse positives laswere measured fherefore not be udecided to make th True negativ
population. The short term
the percentag This impact is
screening accet al.82 (generet al.80 (non mwere used.
Utility values for fat should be noted3.3 assessed the complexity and bepositive” in the stuDomeyer et al.84 inConcerning the evcancer in the long
s table, the descrining, having a brher examinationiagnosis, i.e. nothree of the five E
omfort; and anxietmensions (i.e. m
quality of life effecsted 12 months for the remainin
used to measure the following assu
ve patients have
m impact of positge change betwees present until the cording to IMA daral population for metastatic or met
alse positive and t that the study of short term impa
ecause the biopsyudy of Gerard et anto account. volution of utility vterm, no study wa
ption include the reast screen, wais, having furthe
o evidence of brEQ-5D dimensionty/distress and it
mobility and abilcts associated wwhile true positivg life expectancthe short term immptions:
e utility values e
ive results at screen true negative a
diagnosis, i.e. onata. After, either v
false positive) ortastatic disease y
true negative can Domeyer et al.84
ct of biopsy. Howy is included in theal.83, we decided t
alues for patientsas found.
following stage: iting for results, er examinations reast cancer. Fos were used, i.e. was assumed thaity of self-care) ith true negativesve and false neg
cy. These valuesmpact of screening
equal to the ge
eening is measurend false positive.
n average 45 daysvaluations of Bursr valuations of Lid
year 1 for true po
be found in Tabledescribed in app
wever, to avoid me description of a to not take the stu
s with metastatic b
39
being being
and or the usual at the were
s and gative s can g. We
eneral
ed by
s after ström dgren
ostive)
e 2.8. pendix model “false
udy of
breast
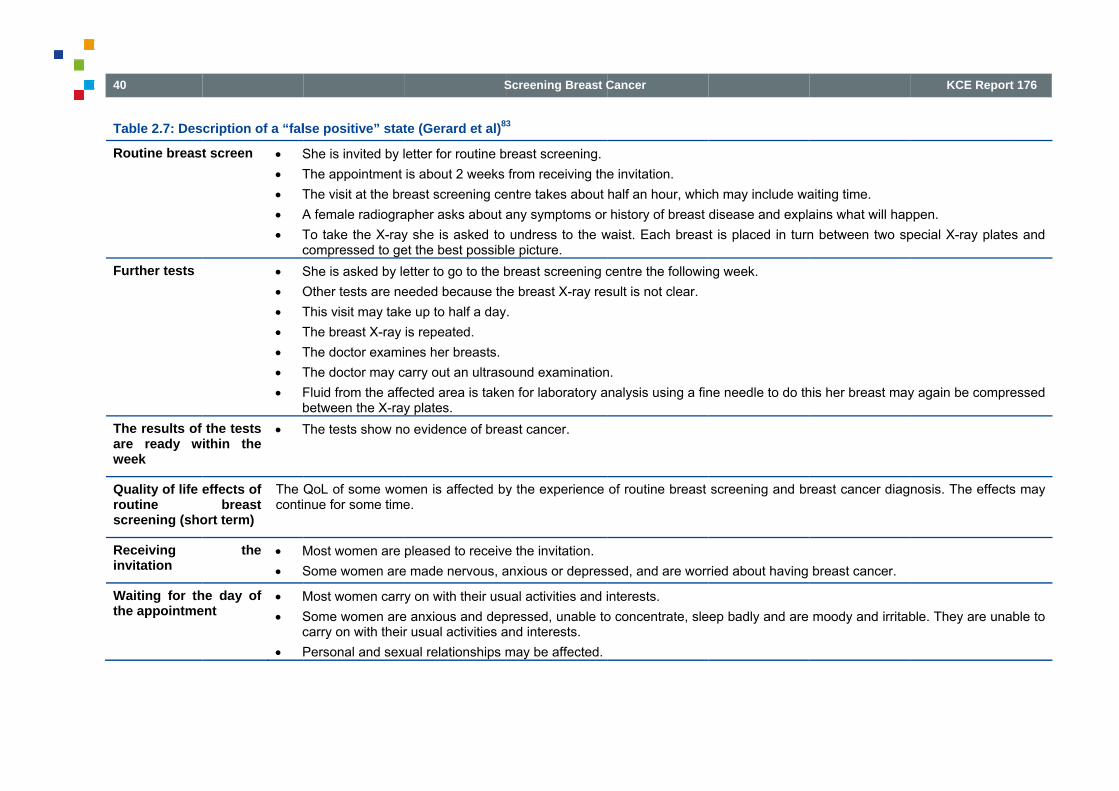
40
Table 2.7: Des
Routine breast
Further tests
The results of are ready wweek
Quality of life eroutine screening (sho
Receiving invitation
Waiting for ththe appointme
cription of a “fal
t screen • S• T• T• A• T
c• S• O• T• T• T• T• F
bthe tests
ithin the • T
effects of breast
ort term)
The Qconti
the • M• S
he day of ent
• M• S
c• P
lse positive” stat
She is invited by lThe appointment The visit at the breA female radiograTo take the X-raycompressed to geShe is asked by leOther tests are neThis visit may takeThe breast X-ray The doctor examiThe doctor may cFluid from the affebetween the X-rayThe tests show no
QoL of some womnue for some time
Most women are Some women are
Most women carrySome women arecarry on with theirPersonal and sex
S
te (Gerard et al)8
etter for routine bis about 2 weeks east screening ce
apher asks about ay she is asked to et the best possibletter to go to the beeded because the up to half a dayis repeated. nes her breasts.arry out an ultrasoected area is takey plates. o evidence of brea
men is affected bye.
pleased to receivee made nervous, a
y on with their usue anxious and depr usual activities aual relationships m
Screening Breast C
3
breast screening.from receiving the
entre takes about any symptoms or undress to the w
le picture. breast screening ce breast X-ray res.
ound examinationen for laboratory a
ast cancer.
y the experience
e the invitation. anxious or depres
ual activities and ipressed, unable toand interests. may be affected.
Cancer
e invitation. half an hour, whichistory of breast
waist. Each breas
centre the followinsult is not clear.
n. analysis using a fin
of routine breast
sed, and are worr
interests. o concentrate, sle
ch may include wadisease and explat is placed in turn
ng week.
ne needle to do th
screening and br
ried about having
ep badly and are
aiting time. ains what will hapn between two sp
his her breast may
reast cancer diag
breast cancer.
moody and irritab
KCE Report
ppen. pecial X-ray plates
y again be compre
nosis. The effects
ble. They are una
t 176
s and
essed
s may
ble to

KCE Report 176
At the breast sclinic
Waiting for the
Clear results test
Table 2.8: Des
Author (year)
Lidgren et al. (2007)80
Burström et al. (2001)82
Gerard et al. (1999)83
6
screening • M• M• M• M• S
e results • M• S
t• PIf rec
• M• O
after the • M• S
cription of the se
Instrument Pd
EQ-5D
S(
EQ-5D S(
EQ-5D Wy
Most women are Most women are Most women are Most women find Some women findMost women carrySome women areto carry on with thPersonal and sexcalled for further te
Most women are vOne of the tests, wMost women are Some women rem
elected utilitiesPopulation for hedescription
Sweden patients(Mean age: see h
Sweden patients(Mean age: see h
Women from UK ayears (eligible for
S
nervous, but are nnot embarrassed not unduly worriedthe breast X-ray i
d the breast X-rayy on with their usue anxious and depheir usual activitiesual relationships oests:
very anxious at bewhere the doctor reassured by the
main anxious for u
ealth state Po
ealth states) UK
UK
UK
ealth states) UK
aged 40-64 screening) UK
Screening Breast C
not anxious or depby the screening d about breast cais uncomfortable a
y very uncomfortabual activities and ipressed, un-able s and interests. of some women m
eing recalled for fremoves fluid fromclear results.
up to a year before
opulation for valu
K tariffs (general p
K tariffs (general p
K tariffs (general p
K tariffs (general p
K tariffs (general p
Cancer
pressed. procedure.
ancer developing.and slightly painfuble and painful. interests. to concentrate, s
may be affected.
urther tests. m the affected are
e they are back to
uation Hea
population) Prim
population) Brea
population) Meta
population) WomWomWom
population) True
ul, but this is short
leep badly and ar
ea, is painful.
o their usual self.
alth state
mary breast cance
ast cancer (follow
astatic patients; M
men aged 50-59men aged 70-79men aged 80-88
e negative
t lived.
re moody and irrit
er (Year 0-1); Mea
wing years); Mean
Mean age 56
table. They are u
Meavalu
an age: 56 0.69
age: 58 0.77
0.68
0.830.790.74
0.94
41
nable
n ue
6
9
5
3 2 0
0

42
2.3.2.3. Poo
chaA summary of can be found inal.82 were chos(A)). These valchange relativepercentage chaThe next stageassumed that uvalues in the gutilities betweecalculated, i.e.negative womeafter screening utilities will be m
oling of selectedanges selected utilities n Figure 2.2. Theen as the initial vues varied accord
e to these valuesanges did not varye concerns the shutility values for tgeneral populatioen true negative -16% (B). Initia
en and decreased(false or true pos
maintained for 45
d studies and cal
and of calculatioe utility values of alues of the modeding to women ag
s was applied. It y according to the hort term impact true negative wom
on (A). Then, the women and fal
al values were td by 16% for womsitive). As mentiondays.
S
lculation of perc
n of percentage cthe study of Burs
el (first state of thge. Then, the perwas assumed thwomen age (no dof the screening
men were equal percentage decr
se positive womthus maintained men with a positivned in the section
Screening Breast C
entage
changes ström et
he model rcentage at these data). g. It was to utility rease in
men was for true
ve result 0, these
Fvoscwb(Fn1pcth(
Cancer
For the first year values equal to thof the study of Lidstudy of Lidgren changes between women aged 50-5by 16% ((0.696-0.(0.685-0.833)/0.8
For the next yearnon-metastatic or
6% (C) and 18%patients who staycompared to the ghe years after (DG).
of screening, wohe general populadgren et al. wereet al.80 and the values for the sa
59 (and UK tariffs.833)/0.833) for n33) for metastaticrs, people from tmetastatic breas
% (E) respectivelyyed in this staggeneral populatio
D). Metastatic pat
omen without breation (A). For true used.80 To makestudy of Burström
ame population ws). Utility values wnon metastatic pac patients (E). the general popust cancer had utiy (as calculated age had their utilin ((0.779-0.833)/0ients maintained
KCE Report
east cancer had e positive, utility ve the link betweem et al.82, perce
were used, i.e. Swwere therefore redatients (C) and by
ulation who develity values reduce
above). Non-metaity decreased by0.833) and mainttheir utility until d
t 176
utility values en the ntage
wedish duced y 18%
loped ed by
astatic y 6% ained death

KCE Report 176
Figure 2.2: Per
Women age
Before
6
rcentage change
ed = 70 years
e screening
A
e in utilities
P
Short termscreeni
S
Positive results
True negative
False positive
True positive
m impact of theing (45 days)
B
A
Screening Breast C
Wome
Brea
Brea
A
N
Brea
Brea
Cancer
en aged = 70 yea
ast cancer stage II
ast cancer stage II
After screening(First year)
C
A
Non metastatic
ast cancer stage I
Metastatic
ast cancer stage IV
F
rs
I
I
VMetastatic
Women aged = 7
Breast cancer st
Breast cancer st
Breast cancer st
After screeni(Following yea
F G
C D
A
Non metasta
Breast cancer s
c
70 years
tage II
tage III
tage IV
ingars)
E
atic
stage I
43
44
2.3.3. DiscuTo include thevalues for eachthis chapter waon the KCE phamultiple instrumderived from the• The analys• No Belgian
possible (nUK tariffs results, Be
• The short taccount be
• Even if thethese utilitithis instrumConsequensuch as aimportant instrument low percenwomen in metastatic specific insbecause th
• Finally, thebetween reappendix 3parametersthese para
ussion quality of life im
h health state of tas therefore to searmaco-economic
ments and multiple EQ-5D instrume
sis had the followin data were availano access to priminstead of Belgialgian data would bterm impact of su
ecause no valid dae EQ-5D is one oies (according to ment is less senntly, it can be expa mastectomy (pif a disease sphad been used.
ntage change bethe general pop
patients. The assstruments was nehese instruments de review of the eported utility esti3.3), revealing as. Because of thmeters should be
mpact of screeninthe model had to lect these valuesc guidelines79. Wee valuations and ent. ng limitations: able and a transf
mary data). Even ian valuations wobe interesting for urgery and of diagata were availableof the best availathe KCE pharma
nsitive than diseapected that the impartial or total) pecific instrumen This lack of senetween patients pulation or betwsessment of the qevertheless not indo not permit to dliterature showedmates for breast
a high level of uhis uncertainty, a
e done in the chap
S
ng in the analysibe identified. The. The method wae tried to avoid th
focused on utility
ferability analysis if we expected th
ould not greatly infuture models. gnosis was not tae. able instrument toaco-economic guidase specific instrmpact of some cowould have bee
nt instead of a nsitivity could expwith breast caneen metastatic a
quality of life from vestigated in this erive QALYs.
d an important vcancer health sta
uncertainty arouna sensitivity ana
pter on model resu
Screening Breast C
is, utility e aim of
as based e use of y values
was not hat using nfluence
aken into
o assess delines), ruments. onditions en more
generic plain the cer and and non disease chapter
variability ates (see nd these lysis on
ults.
3TsacbwWthsnfiUWththbuh••
•
Cancer
3. DECISIOTo quantify whatsituation we consapproaches. For cancer registry anbelow). For the sewith annual cyclesWe consider perfohan trying to adasituation. Indeed, not available andindings of these mUS) data. We look at the effehe currently existhe current level. Tbaseline without huse of an additionhere: Available data Additional lite
screening and The model us
ON ANALYt the implicationsstructed a decisiothe first simple
nd data from the lecond, we constr
s. orming one Belgiaapt the models dBelgian data nee
d we would memodels, as we wo
ect of introducing ing situation with This has the advahaving to modify nal number of no
a used in this decierature review focd to the breast cansed for this decisio
YSIS s of our findingson analysis modapproach, we apliterature on the Bructed a simple t
an decision analydiscussed in chaeded to parameterely reproduce t
ould be obliged to
mammography sthe opportunistic
antage that we cathen, as this can
on verifiable assu
ision analysis; cused on qualityncer as such; on analysis.
KCE Report
s are on the Beel using two diff
pplied data from Belgian life tablestime dependent c
ysis a better apprapter 2 to the Beerize these modelthe already publo use the same (m
screening in additscreening going
an use Belgian da only be done m
umptions. We des
y of life related t
t 176
elgian ferent IMA,
s (see cohort
roach elgian ls are ished
mainly
ion to on at
ata as aking scribe
o the

KCE Report 176
3.1. Data soBelgian life tabOverall survivabe.STAT (http:/Belgian CanceThe Belgian Ccollects data cstatistics from tBelgian organAs recommendorganized screeprogram are woprograms ahttp://www.brumdépistage desFrançaise) andhttp://www.zorgIntermutualistiThe Intermutuasickness fundsnational screendefined by theinformation on focus on the tconfirmation anDutch Nation(DNETB)85. The Dutch Npublished a recontaining inforpopulation.
6
ources ble (2009) al was taken fro//statbel.fgov.be) er Registry (BCRCancer Registry Fconcerning new chese data (http://wized screening
ded by Europeanening programmeomen aged 50 to are organizedmammo.be/), Cens cancers (CCRd BorstKankerOpg-en-gezondheid.bic Agency (IMA)
alistic Agency (IMAs. IMA compiledning program cone program (50-6
persons outsidetests used, delaynd treatments follonal Evaluation
ational Evaluatioeport with their rmation on age s
om the Belgian
R) Foundation is ancancer cases in www.kankerregist
Commission, Bee. The target age 69 years. Belgiand by: Br
ntre CommunautaRef: http://www.cpsporing (BKO) (be/).
A) centralises dat and published
ntaining data on t69 years). IMA e the target ageys between screeowing testing (http
Team for Bre
on Team for Bfindings covering
specific stage dist
S
life table of 200
n public institutioBelgium and ma
ter.org/).
elgium started a groups as define
n breast cancer scrumammo (Baire de Référenceccref.org/) (Comm(Vlaamse Gemee
a coming from allseveral reports
the target age grcomplemented t-group, with a pening tests and p://www.nic-ima.beeast cancer sc
Breast cancer scg the period 19tributions in the s
Screening Breast C
09 from
n which akes up
national d by the creening ruxelles,
e pour le munauté enschap:
Belgian on the
roups as his with
particular possible e/).
creening
creening 90-2007
screened
STNin(lointh
3InmfrB7folelisaaacTdtiT•
Cancer
SEER database The Surveillance, National Cancer Inn an effort to redhttp://seer.cancerocations and sourn 1973. As they hese in the mode
3.2. Model den a first simple amortality caused brom the results oBelgian life table.74 is similar to tollowing Barratt eevel over first fivenearly to nothing
saved can then band effects on quaand stage-shift is approach was onlcomplex approachThe second apprdata on incidenceime dependent stThe model compa A cohort of w
the populationparticipates inby screening,screening. Thcases (intervaThe screen dthan the canc
Epidemiology, annstitute works to duce the burden r.gov/). SEER collrces throughout thused an outdatel.
escription approach we appby screening comof the meta-analWe assume herethe reduction in et al 200536 that e years after startg over five yearse derived from thality of life resultinmore difficult to a
ly used for cross h that makes use oroach makes usee of invasive cancate transition cohres 2 cohorts:
women starting at n in the age gron the screening an, depending on p
here is a mix of scal cancers and cdetected cancers ers not detected b
nd End Results (Sprovide informatioof cancer amon
lects data on canche United States.d distribution we
plied the 22% reduming from RCT alysis of Gøtzschee that the reductio
other age groupbenefit accrues
ting screening ans after stopping he life table. Howng from earlier diaassess in this apvalidation by com
of the stage-shift e of the Belgian Ccer and DCIS forort model with an
age 70 where scup 70-74, where nd where a part oparticipation rate creen detected ancancers amongstwill have a diffe
by screening.
SEER) Program oon on cancer statg the U.S. Popucer cases from va Data collection bcould not incorp
uction in breast cand its range, rese et al, 20084 oon in women ageps. We also asslinearly to a mad that benefit decscreening. Life
wever, effects of hagnosis, over-diagpproach. Thereforemparing it with a caused by screen
Cancer Registry (r the constructionnual cycles.
reening is extenda part of the wo
of the cancers is fand sensitivity o
nd not screen dett unscreend womerent stage distrib
45
of the tistics lation
arious began porate
ancer sulting n the
ed 70-sume, aximal clines years
harms gnosis e this more
ning. BCR)
n of a
ded to omen found of the ected
mens). bution

46
• A cohort o
extended bthe stage d
All women are number of QAcompared. OveWe assume tha• Survival an
the tumor women, an
• All benefit in stage-dis
Harm caused accounted for sinterval in theproportion womthe screening roFigure 3.1 showtransitions betwIn the unscreenyear are determ• Incidence o• Stage distr• Stage spec• Age specifOn top of that, fdetermined by s• Lead time a• The propo
found by sc
of women startinbeyond the age ofdistribution of the followed to deathLYs and deaths
erall mortality is noat: nd quality of life oat the moment t
nd not on the presof the screening rstribution caused by false positiv
separately, by asse participation wmen that are alive ound actually takews the different c
ween them. ned cohort, transi
mined by: of breast cancer; ribution of unscreecific survival; and ic overall mortalityfor the cohort whesome aspects of tas part of the can
ortion of cancers creening and thei
g at age 70 whef 69 years. For thnon screened.
h. The cumulativeto breast cance
ot compared as in
f the women depethe tumor is detesence or absence results from the sby the screening.
ves at the momesuming 3 screeniomen and applyand without brea
es place. compartments in
itions between co
ened cancers;
y due to other cauere screening takethe screening: cers will be foundfound by scree
r respective stage
S
ere the screeninhis cohort all wom
number of life yer of the two coh
n the end everybod
ends only on the ected and the agof screening; tage-shift, the diff. ent of the screeng rounds with a ying recall ratesast cancer at the
the two cohorts
ompartments from
uses. es place, transitio
d earlier; ening and propore distributions.
Screening Breast C
g is not men have
ears, the horts are dy dies.
stage of e of the
ferences
ening is 2 years
s at the moment
and the
m year to
n is also
rtion not
AddsymTmea
Cancer
As survival and diagnosis in the mdiagnosis and stscreening is applieyears (or 3 in senmanageable. Transitions betweemoment the diagnevolves after treaanymore.
quality of life dmodel, a separateage, and stage ed during 5 years nsitivity analysis)
en stages are notnosis is made follatment it does no
epends on both e compartment is
specific survivaland there is an athe number of co
t included as stagelowed by treatme
ot necessarily go
KCE Report
age and time made for each a
l is than appliedassumed lead timeompartments rem
es are assessed aent. Even if the ca
through the 4 s
t 176
since age of d. As e of 2 ained
at the ancer tages

KCE Report 176
Figure 3.1: Co
Cohorscree
Cow
scre
6
mparison of the
Healthy women
Healthy women
rt with ening
ohortwithout eening
two cohorts with
Id
is
S
h and without a s
Invasive cancer detected by screeni
DCIS
interval cancer in screened women
Invasive cancer in unscreened wome
Invasive cancer in unscreened wome
DCIS
Screening Breast C
screening progra
IIIIIIIV
IIIIIIIV
IIIIIIIV
IIIIIIIV
ing
en
en
Cancer
am
All c
All c
cause deaths
cause deaths
47

48
Figure 3.2: Co
mpartments in th
Healthy women
he two cohorts a
d
S
and the transition
Breastcancer stage I
Breastcancer stage IV
Breastcancer stage II
Breastcancer stage III
DCIS &over‐
diagnosed
Screening Breast C
ns between them
Death
Cancer
m
KCE Reportt 176

KCE Report 176
3.3. Descrip3.3.1. Age sOverall survivabe.STAT (http:/mortality based3.3.2. BreasFor the baselinethe 4 stages fowere used. Thethe IMA data wmammography 172 on breastassume that anpurposes, so ware less contamFor the situatiogroup will increa• Lead time
because onumber of this shift dused 2 yeaanalysis.
• Over diagbased on review abodiagnosis e
• Over diagdifferent wDCIS per 1place comlimited amcontrast widrop in DC
6
ption of the parspecific overall sal was taken fro//statbel.fgov.be) on data from thest cancer incidene without screeninr invasive for the
ere is some opporwe infer that in in the past 2 yea
t cancer screenin important part owe choose to useminated by opportuon where screenase with a numbe, cancers that wo
of lead time. This cases in the foll
depends on the aars lead time in t
gnosis invasive the findings in th
ove under 2.1.3.5.excluding DCIS.
gnosis DCIS, weway: we use the o100 000 is twice
mpared to the agemount of opportu
th the Brussels caCIS is much less p
rameters urvival
om the Belgian after adjusting fo Belgian Cancer rnce ng the BCR data oage group 70-74
rtunistic screeningFlanders the covars is 18% (for deng in risk group
of this is also for de data issued fromunistic screening.ning takes place,er of cancers comuld have appearewill lead to a co
lowing years. Theassumed lead timthe baseline and
cancer, we modhe literature as d. We assume a ra
e model the overobservation that iin the group 60-6e-groups 70-74 anistic screening apital region and Wronounced. So we
S
life table of 200or breast cancer register.
on incidence of D4 of the period 20g in that age grouverage with at leetails see the KCps)2. Given that diagnostic and fom Flanders becau , incidence in thing from two sour
ed later but are fouompensatory dece moment and deme (see point 3.2
3 years in the se
deled the over ddescribed in the lange of 2 to 30%
r diagnosis of DCn Flanders the in
69 where screeninand 75-79 wheretakes place. Th
Walloon region we take as an estim
Screening Breast C
09 from specific
DCIS and 04-2008
up. From east one
CE report we can llows up use they
e 70-74 rces: und now rease in egree of 2.2). We ensitivity
iagnosis iterature for over
CIS in a ncidence ng takes e only a his is in
where the mation of
3W3T6c7Ws3WsbsthmApaTthp
Cancer
over diagnosithe age-groupfact that screeDCIS. This brwomen per ye
3.3.3. ParticipaWe used a 70% pa3.3.4. ProportioThe data of the Be69, 49% of the cascancer or not part75% of the found We used a proporscreening of 70%3.3.5. Recall raWe assume a recscreening programbe an extension sensitivity analysishe more pessimmoment in certain As a baseline we plausible range foand adding 20%). The short term imhe percentage chpositive results.
s the difference ips 60-69 and 70-ening coverage isrings us to an oveear. ation rate articipation (plauson of screen detelgian screening pses are found by ticipating in the sccancers are screertion of cancers fo(plausible range 6ate call rate of 3.5%m concerning folloof the screening
s we used 2% in aistic scenario (1regions). assume a delay
or the sensitivity a
mpact of positive rhange in utility va
in DCIS incidence-74, augmented b only 60% as a prer diagnosis of DC
sible range 60% totected breast caprogram show thascreening, and thcreening. Among en-detected and 2ound among the w60% to 80%).
% based on the dow up rounds (as
g among women an optimistic scen0% recall rates
of 45 days, baseanalysis of 36 and
results at screenialues between tr
e in Flanders betby 1.5 to adjust foroxy for overdiagnCIS of 40 per 100
o 80%) as baselinancers at in the age grouhe rest is either in
the screened wo25% is interval cawomen participat
data from the Fles the screening waged 50-69. Fo
nario and 5 and 10are observed fo
ed on IMA data, wd 45 days (subtra
ing were measurerue negative and
49
tween or the nosed 0 000
ne.
up 50-terval
omen, ancer. ing in
emish would or the 0% in
or the
with a acting
ed by false

50
3.3.6. StageWe take estimascreened and uprovided by theFor the stage dstage distributioyears 2004 - underestimatedgoing on, see aFor stage distriis based on thecancer screeninfor the age gdistributions frostage shift we tnot have date stage distributiobe the same, baThe Flemish sscreen detecteparticipants, coperiod 2001-20non participants
e distribution andations of the stagunscreened from
e Flemish screenindistribution in the on amongst wom2008 a good es
d as there is somabove. bution in the scree data from the Dng report of 2009group 70-74 froom different sourthink this approximon screen detecton of cases amonased on the data screening prograed cancers, interollected amongst06. Stage distribus is very similar.
d stage shift ge distribution fothe BCR data o
ng program. unscreened wom
men in the group 7stimation. The stme opportunistic
eened population, Dutch National Ev9 (DNETB)85 whom 1998-2007. Arces is a suboptmates best the Beted cancer in thisng the non screenfrom the Flemish m provided datarval cancers andt women who gaution of interval ca
S
r breast cancer aon the Flanders a
men, we can cons70-74 in Flandersage shift will bescreening in tha
the base case esvaluation Team foo provide data speAlthough using 2timal way of modelgian situation, as age group. We ned and interval cscreening progra
a on the stagesd cancers amonave their consenancers and cance
Screening Breast C
amongst and data
sider the s for the
e slightly at group
stimation or Breast ecifically 2 stage deling a
as we do assume
cancer to m. among gst non
nt in the r among
TinF
S
I
II
II
IV
T
T
ScsBp2S
Cancer
Table 3.1: Stage nterval cancers Flemish screenin
Screencancer
Stage n
2586
I 1306
II 232
V 15
TOTAL 4139
This baseline stag
Stage distributioncancers not founscreening BCR data (Flemispopulation,70-74y2008) Stage %
I 31.6II 42.3III 16.6IV 9.5
distribution amoand cancers a
ng program 2001
n detected rs
In
% n
62.5% 62
31.6% 65
5.6% 20
0.4% 24
100% 15
ge shift we call Sce
n of nd by
sh y, 2004-
%
6%
3% 6% 5%
ong screen deteamong non part-2006.
nterval cancers
%
24 41.5%
56 43.6%
00 13.3%
4 1.6%
504 100%
enario 1:
StacanscrDascrSt
KCE Report
ected breast canticipants, age 5
Cancers amonon participan
n %
1454 41.8%
1460 42.0%
493 14.2%
71 2.0%
3478 100%
age distribution oncers found by reening
ata of the DNETBreening report 20tage %
I 80%II 18.7III 0.8%IV 0.5%
t 176
ncers, 50-69,
ngst nts
%
%
%
%
%
of
B 009
% % % %

KCE Report 176
Important remscreen detectecancers and nfound by screeother parameteFor the sensitivAs the stage dBreast cancer scan be achievethe stage-distribfrom the FlemisThis we call Sce
Stage distributcancers not foscreening BCR data (Flempopulation,70-2004-2008) Stage
I 3II 4III 1IV
In a third scenaInstead of usinwomen, we assthe stage distribthe stage distrifor Flanders fro
6
mark: It is imported cancers and
nonparticipants kening. In most cas
er values of the scvity analysis we usdistribution from screening report od in the Belgian cbution for screen sh cancer screeninenario 2:
tion of ound by
mish -74 years,
%
31.6%
42.3% 16.6% 9.5%
ario we use a slighng stage distributsume that introdubution amongst albution of the wom
om the Belgian bre
tant to note that that in the coho
eep the stage dses this is around creening and variese 2 supplementathe Dutch Natioof 2009 may be mcontext, we used a
detected patientsng program.
htly different modetions amongst sccing screening in ll breast cancer cmen 60-69 in the east cancer regist
S
this shift concerrt with screeningistribution of can50% but depend
es in time. ry scenario’s: nal Evaluation Tmore favorable thas an alternative ss of the age grou
Stage distribucancers foundscreening (Flescreening pro(50-69 years)Stage
I 62II 31III 5IV 0
eling approach. creened and unsthe group 69-74
cases in the popusame period, us
try.
Screening Breast C
rns only interval ncer not s on the
Team for han what scenario up 50-69
ution of d by emish ogramme
%
2.5% 1.6% 5.6% 0.4%
screened will shift
ulation to ing data
T
ScsBp2S
3Ssywasw•
•
Cancer
This we call scena
Stage distributioncancers not founscreening BCR data (Flemispopulation,70-742004-2008) Stage %
I 31.6II 42.3III 16.6IV 9.5%
3.3.7. Stage spStage specific susurvival data (takeyears. We used website (http://wwappendix 4.1). Wescreened and unswe used also: Entirely the
stagegroup. Tfor women areflect the facwell but it is aMoreover, theyears ago, thi
British surviv(http://info.canbut survival isof the problemsurvival of pevolution in br
ario 3
n of nd by
sh years,
6%
3% 6% %
pecific relative survival was takenen from KCE repodata from the D
ww.cijfersoverkanke assumed that sscreened breast c
Dutch survival dThe relative survivbove 70 compar
ct that older womealso possible thate data include pas may also explaival data comingncerresearchuk.ors considerably lowms with 10 year ersons treated areast cancer treat
StaamcanlevlevFlaSta
IIIIIV
urvival n from Belgian ort 150A)86. We oDutch cancer regker.nl) to supplemurvival conditiona
cancer patients. A
data for women val curve shows aed with the overen support the invt there is undertreatients that were in the lower relativg from breast rg/) They provide
wer than the Dutchsurvival data is t
at least 11 yearstment this is a lon
age distribution mongst all breast
ncers if screeninvels are similar tovels among 60-69anders age %
I 45.7% I 35.9% II 12.5% V 5.9%
stage specific aonly have data upgister taken from
ment until 7 yearsal on stage is simAs a sensitivity ana
above 70 yearsa lower relative surall survival. Thisvasive treatmentseatment of the eltreated more tha
ve survival. cancer research10 years surviva
h or Belgian datathe fact that it res ago, given theg time.
51
ng o 9 in
nnual p to 5 m the s (see ilar in alysis
s per urvival s may s less derly. an 20
h UK l data . One
eflects e fast

52
• Belgian su
coming frotreatment a
We did not useso that survivaland difficult to iThe survival cu3.3.8. QALYNumber of life was adjusted fo(see point 2.3).We made some• Utility value
age but penot vary acthis). For increase.
• Patients wpopulation.
• In the asseresults, moby screenin
urvival data supplom87. The problapply here as for te US SEER data l curves per stagencorporate in the rves can be found
Y years was calculor the quality of l
e assumptions: es at start of the mrcentage changesccording to the agthe sensitivity a
with negative resu. essment of utility obility and ability ong.
emented by Frenlem of the evothe British data. as they use an o
e are not comparmodel.
d in the annex.
lated for each stalife (QALYs), bas
model (before scrs relative to thesege of the women analysis, we app
lts had utility val
values for true neof self-care were a
S
nch 10 year surviolution in breast
outdated staging rable to the other
age and a stage sed on a literature
reening) were strae values were ass(we did not have
ply a 20% redu
ues equal to the
egative and false assumed to be un
Screening Breast C
val data cancer
method, sources
and this e search
atified by sumed to
data on ction or
general
positive naffected
•
•
•
P
Cancer
In the study oonly two grouTherefore papatients) weresupported by same for patquality indicatchange this ptreated by coassumption aimpact of pcorresponding
Utility values fmetastatic paFor non-metastudy showinNevertheless,QALYs for tak
At baseline, wdiscount rates
Parameters used i
of Lidgren et al.80, ps, i.e. the first ye
atients in stage e assumed to hathe fact that for yients in stage I, tors in breast canicture because monservative surge
are not available partial versus tog to our inclusion for non-metastatic
atients were assuastatic patients, thng no significant , as a sensitivity king into account awe did not discous of 1.5%, 3% andin the model are s
non-metastatic pear of diagnosis aI, II, III (groupeve the same utili
years 2001-2006, II, III according
ncer86. Note that any cancer foundery. Neverthelessand we found nootal mastectomycriteria. c patients (after thumed to remain chis assumption isdifferences at y
analysis we applya variation of utilitunt QALYs. For thd 5% were appliedshown in table 3.2
KCE Report
patients were dividand the following yed as non metaty. This assumptthe treatment wato the KCE repomore recent data
d by screening ares, data to proveo study compariny on quality of
he year of surgeryconstant across ys supported by ayear 5, 10, and y a 20% decremety values across yhe sensitivity anad. 2.
t 176
ded in years. astatic ion is
as the ort on a may e now e this g the f life
y) and years. n US 1581.
ent in years. alysis,

KCE Report 176
Table 3.2: Para
Parame
3.3.1 Age spe
3.3.2 Breast c
Lead tim Over-dia
cancer Over-dia
3.3.3 Participa3.3.4 Proporti
detected3.3.5 Recall r
Durationpositive
QALYs
3.3.6 Stage d
Stage I Stage II
6
ameters used in
eters
ecific overall surviv
cancer incidence
me agnosis invasive
agnosis DCIS
ation rate ion of screened d cancers ate
n of period after result lost in this period
istribution
the model
No screenin
val Belgian life-
BCR data (Flanders population, 2008)
BCR data (Fpopulation, 74years, 202008)
31.6% 42.3%
S
ng Base c
table Belgian
2004-
BCR dpopulaincreasover-diinvasivDCIS 2 years10.0%
40/100year 70.0%70.0%
3.5% (screen45 day
16.0%
Flemish 70-04-
Data oscreen
80.0%18.7%
Screening Breast C
case
n life-table
ata (Flemish ation, 2004-2008) sed by lead time.iagnosis ve cancer of
s
0 000 women per
Flemish ning program) ys
f the DNETB ning report 2009
Cancer
Sensitivity ana
Belgian life-tabl
BCR data (Flemincreased by leacancer of DCIS
3 years range from 3 to
40/100 000 wom
range from 60%range from 60%
range from 2%
range from 36 t
estimated betw
Scenario 2 Stage distributioFlemish screenprogramme (50
62.5% 31.6%
alysis
le
mish population, 2ad time. over-diag
30%
men per year
% to 80% % to 80%
to 10%
to 54 days
een 13% to 19%
Sceon of ing
0-69)
StagBCR60-6not
45.735.9
2004-2008) gnosis invasive
nario 3 ge distribution of R (Flemish women69 (screened and screened)
7% 9%
n
53

54
Stage I Stage IV
3.3.7 Stage s
survival
3.3.8 QALY Stage II
Stage II
Stage IV
Age rela
Discoun
II V
pecific relative
III IV
I IV
V
ated QALY
nted QALY
16.6% 9.5%
Belgian stagspecific annsurvival datasupplement7 years by Ddata -constant
-constant
-constant
-constant
S
0.8% 0.5%
ge nual a ed until Dutch
Belgianannualsuppleyears b
- const
-consta
-consta
-consta
Screening Breast C
n stage specific l survival data mented until 7 by Dutch data
tant
ant
ant
ant
Cancer
5.6% 0.4%
Dutch survival osurvival
-20.0% -20.0% -20.0% range from + 20 discounting rate
12.55.9%
or British survival
0% to -20%
e + 1.5%. 3% and
5% %
or Belgian/French
5%
KCE Report
h
t 176

KCE Report 176
3.4. ResultsIn the baseline of life saved pe395 per 100 00deaths would bbeing a reductioBecause of themodel structureis not due to rasource of inforsensitivity anaprobability-distrTable 3.4 showused for this anand justificationThe number of assumptions. Tdifferent assumuncertain or vagained rather thapart from the vAssumed degreand under the QALY would bslightly, this duenew case in thebut the effect isRecall rates of Ten per cent reAssumptions onimpact on yeaBritish survival loss of QALYs French 10 year
6
s scenario the mod
er 100 000 (13,1 p00 (3.9 per 1000) be averted per 1on of 21% (numbee considerable une we did an extenandom error but drmation on the palysis, as it waributions in a mea
ws the results of thnalysis was discun of chosen valuesf years of life gainThe number of QAmptions. This is ariable parametehan on mortality, values accorded tee of over-diagno
higher assumedbe lost instead oe to the fact that e model, one couls very small.
10% also can shecall rates are actun the choice of thrs of life gained data increase thein certain scenari
r survival is somew
del predicts that thper 1000) women QALYs. The mod00 000 women ser needed to be oncertainty surrounnsive sensitivity adue to issues relaparameter. We das not possible ningful way.
he sensitivity analussed in 3.3, descs. ned remains fairlyALY gained or lost
partly due to thrs have an impasuch as high rec
to the QALYs. osis has a strong d values of 20%of gained. Years an over diagnosed argue that this i
hift the balance toually found in somhe appropriate sur
and QALYs gaie number of life yos. Belgian survivwhere in between
S
here would be 130invited for screen
del also predicts screened (1.3 pe
offered screening:nding the parametanalysis. Most uncating to the right cid not do a probto choose app
ysis, the plausiblecription of the par
y constant under t varies much mohe fact the a lotact on the qualitcall rates, over dia
impact on QALYsor 30% even imof life gained in
ed case cannot beis somewhat of an
owards a loss of me parts of Belgiumrvival curve have ned. The Dutch
years gained but lval data suppleme.
Screening Breast C
07 years ning and that 128
er 1000), 782). ters and certainty
choice of babilistic propriate
e ranges rameters
different re under t of the y of life agnosis,
s gained mply that ncreases ecome a n artifact
QALYs. m. both an and the ead to a ented by
InoTththQTndsIIegainAQAredp3Aredp1AGsy
Cancer
ncreasing the assof life gained and QThe model’s estimhe valuation of thhe decrease in qQALYs gained, asThe estimations conot vary much in decrement in quascenarios: (i) decrII and IV with 20effect of increasingains in QALYs duas persons in stagn contrast to the LAs could be expecQALYs gained. As a worst case secall rate at 10%
days and using thprogram (scenario307 QALYs per 10As a best case scecall rate at 2%,
days and using thprogram (scenario
626 QALYs per 1Applying the 22%Götzsche et al. tosimilar result, 139 years of life saved
sumed lead time tQALYs.
mation of the numbhese QALYs. Dimquality of life dues could be expecteoming from the Lfunction of the d
ality of life due toreasing stage II II0% or (iii) decreag the number of ue to the stage shge I have in this sLidgren data. cted, introducing d
scenario, we set th%, loss of QALYs he stage distributio 2). This gives a00 000. cenario, we set tloss of QALYs p
he stage distribuo 1). This gives a 100 000. % reduction in mo the Belgian life t
cancers deaths dd.
to 3 years has an
ber of QALYs gainminishing the age e to old age, deced. idgren’s paper areifferent stages. W
o increasing stageI and IV with 20%
asing stage IV wQALYs gained, bhift alone outside cenario a better a
discount rates de
he estimation of oper recall at 0.19ion coming from gain of 872 Yea
he estimation of per recall at 0.13 tion coming fromgain of 1704 Yea
mortality from thtable, as describedue to breast can
n impact on both
ned or lost depenrelated QALYs, t
creases the numb
e fairly uniform anWe introduced a le at diagnosis, w
%, (ii) decreasing ith 20%. This ha
because there arethe effect on mor
assumed quality o
creases the numb
over diagnosis at 9 during a period the Flemish scrers of Life but a lo
over-diagnosis aduring a period
m the Dutch scrers of Life and a g
e meta-analysis ed above, gives ancer avoided and
55
years
ds on this is ber of
nd do larger with 3 stage
as the e also rtality, of life,
ber of
20%, of 54 ening
oss of
t 3%, of 36 ening ain of
from a very
1145

56
Table 3.3 Mode
Scenario
Baseline
Worst case
Best case
eling results: bas
Assump
Over recall loss of Qduring astage Dutch (scenarioOver recall loss of Qduring astage Flemish (scenarioOver recall loss of Qduring astage Dutch (scenario
seline, worst and
ptions
diagnosis: rate at 3
QALYs per recall a period of 45 distribution comscreening prog
o 1) diagnosis: rate at
QALYs per recall a period of 54 distribution comscreening prog
o 2) diagnosis: rate at
QALYs per recall a period of 36 distribution comscreening prog
o 1)
S
d best case scen
Years of lPer 100 00women
10%3.5%0.16days ming gram
1307 gaine
20%10%0.19 days ming gram
872 gained
3%2%
0.13 days ming gram
1704 gaine
Screening Breast C
nario.
ife 00
Quality adPer 100 00women
ed 395 gained
d 307 lost
ed 1626 gaine
Cancer
djusted years of l00
d
ed
life
KCE Reportt 176

KCE Report 176
Table 3.4 Mode
Baseline Assumed over0.03 0.05 0.1 0.2 0.3 Recall rate 0.02 0.035 0.05 0.1 Period betweeduration 36 days 45 days 54 days Period betweeQALYs lost QALYs loss peQALYs loss peQALYs loss peParticipation r0.6
6
eling results: sen
rdiagnosis
en false positive
en false positive
eriod 13% eriod 16% er period 19% rate
nsitivity analysis
e and confirmat
and confirmatio
S
s.
Stagescena
Years1307 13041305130713101314 1307130713071307
ion test:
130713071307
on test:%
130713071307 1120
Screening Breast C
eshift ario 1
s of life QALYs395 526 489 395 208 22 442 395 348 190
417 395 373
416 395 374 281
Cancer
Stageshift scenario 2
Years of life1014 1011 1012 1014 1018 1022 1014 1014 1014 1014
1014 1014 1014
1014 1014 1014 869
Stsc
QALYs Ye186 12 317 12280 12186 120 12-187 12 234 12186 12139 12-19 12
208 12186 12164 12
207 12186 12166 12 102 na
tageshift cenario 3
ears of life QA246 420
245 551245 514246 420249 232251 45
246 459246 420246 380246 249
246 438246 420246 401
246 449246 434246 420
a na
ALYs 0
1 4 0 2
9 0 0 9
8 0 1
9 4 0
57

58
0.7 0.8 Effectiveness 0.6 0.7 0.8 Survival curveDutch survivalBritisch survivBelgian survivAssumed leadAll QALYs minAll QALYs plusStage II III IV -2Stage III IV -20Stage IV -20 Discounted QADiscount rate Discount rate 3Discount rate 5
screening amon
e by stage from ol val val supplementedd time 3 years nus 20% s 20% 20 0
ALYs 1.5% for QALYs 3% for QALYs 5% for QALYs
ngst participants
other sources
d by French data
S
13071493 112013071493 16071714
a 1460109813071307130713071307 130713071307
Screening Breast C
395 509 281 395 509 710 399 473 118 -948 1587 903 648 450 297 215 138
Cancer
1014 1159 869 1014 1159 1181 1148 1045 875 1014 1014 1014 1014 1014 1014 1014 1014
186 na270 na 102 na186 na270 na 310 14-3 1596 1377 11-1089 121310 12465 12370 12241 12 121 1267 1215 12
a naa na
a naa naa na
481 505585 374365 477169 187246 -78246 153246 na246 na246 na
246 274246 193246 114
KCE Report
5 4 7 7 7
34
4 3 4
t 176

KCE Report 176
3.5. DiscusUnder baselinelimited impact osaved, amountiin that period andays of life gainThis results fallfound as reportranged from 9 tthat completelyYears of life gachoose a worstfrom 872 to 170on the meta-anthat this estimaestimation methgained are fairlyThe gain in quonly 3.9 QALYwomen) offereddata in anothescreening for 5shows that undin this age groimportant of thcertain parts of addressed befoThe worst casescreened, we mare still reasonelements wereeffect is sometquality of life pQALYs gained This is due to false positives a
6
sion e assumptions, son breast cancer ding to 1.4 death and 13 years of lifened per women ofl within the rangeted by Mandelblatto 22 per thousan
y different data andained remained fat and best case s04. It correspondsalysis of Götzsch
ation comes from hod. This indicatey robust and consality adjusted life
Ys per 1000 womd screening and uer way by statin5 years to gain
der certain assumoup would actualese is an assum
f Belgium, so thesore proceeding. e scenario would made sure that thnable assumption not considered imes mixed. Brin
per age-group incdepending on ththe fact that intr
and over diagnosi
screening in the deaths avoided a
avoided per 1000 e saved per 1000 ffered screening. e that the modelett et al in 200948, wnd women screend model structureirly constant in thscenario, with yeas also with the sime et al.4 and the Ba completely diff
es that the estimasistent with other s years (QALYs) i
men (1.4 quality ncertainty is large
ng that 250 womone year of life.ptions introducinglly generate a lo
med recall rate ofse high recall rate
imply a loss of 3 e assumptions of
ns and not undulin the worst casging down the bacreases or decreae chosen values
roducing screeninis but gains due to
S
age group 70-74nd number of yeawomen offered scwomen, amountin
ers of the CISNETwhere years of lifened. This, despites were used. e sensitivity analyars of life gained mplified estimatioBelgian life tables,ferent source of dations of the yeastudies. is considerably leadjusted day of
er. One can presemen need to be The sensitivity
g breast cancer scoss of QALYs. Thf 10%, as is the
es should certainly
QALYs per 1000f this worst case sy extreme. A nuse scenario becaaseline estimationases the final nuof the other para
ng induces losseso the stage shift.
Screening Breast C
4 has a ars of life creening ng to 4.7
T project e gained the fact
ysis. We ranging
on based , despite data and rs of life
ess, with life per
ent these offered
analysis creening he most case in
y first be
0 women scenario
umber of ause the n for the umber of ameters. s due to
UsTyupocuuccatooisCZlin51freTitcbandoTsina
Cancer
Under the best cascreened. The higher variabyears of life losuncertainty arounparticular concernother hand rather countries and in uncertainty arounduncertainty concecancer states but cost-effectivenessaddressed if we wo stage IV has onor lost as survival s low. Carles et al. 201Zeelen, found an fe years gained p
not report the QA50-69, as it was
.86 QALYs per 1rom 45-69. Intereet al, 201158 into thThe model takes it does not take cancers would habecause screeninare not life threatenon screen detectdetected cases is of stage, and thatThis indicates thaselection of less anterval cancers hattending screenin
ase scenario one w
bility seen in the t has a numbed key parameter
ning over-diagnosreflects real undBelgium betwee
d the valuation oferning the qualitalso age specific analyses are
want to have meanly a limited impain this stage is s
138, in an adaptincremental bene
per 1000 women cALYs gained with
dominated by sc1 000 were gaineestingly, they did nheir calculations, nto account over-into account leng
ave a slower cling tends to pick-uening. Follow up sted cancer in thebetter than case
t survival of intervat there may indaggressive cancehave a better sung indicates that
would gain 16 QA
estimation of theer of reasons. Trs that determineis. Variability due
derlying differencen regions. Theref the quality of lify of life surrounquality of life in Bconsidered, this
aningful results. Qct on overall numhort and proportio
ation of the CISefit for biannual sccompared to a schextending the screening from 45-
ed by extending tnot incorporate thbut used US surv-diagnosis and leagth bias, the factical course and
up slow growing tstudies of screen
e literature show tes among non parval cases is somdeed be a lengtrs by screening.
urvival than canceother factors also
ALYs per 1000 wo
e QALYs comparThere is considee a loss of QALYe to recall rates oes in practice bete is also considefe, and this is notnding different bBelgium. If in the fs problem shoulQuality of life attribmbers of QALYs g
on of stage IV pa
NET model of Lcreening 50-74 ofhedule 50-69. Thecreening to 50-74- 69, but reportedthe screening to 4he results of Vilapvival data. ad time bias. Howt that screen-dethave a better sutumors some of wdetected cancers
that survival of scrticipants, indepenewhat in betweenth time bias, thrHowever, the facer among womeo play a role, suc
59
omen
red to erable Ys, in on the tween erable t only breast future d be buted ained
atients
Lee & f 2.78 ey did from
d that 45-74 prinyo
wever, ected
urvival which s and creen ndent n88-91. rough ct that n not ch as

60
selection bias amongst womeadjustment for sand on effectinecessarily negthreatening canimpact on efficand greater cosWe unfortunateunscreened woMoreover, therecurves that will survival may beAnother majordistributions of on stage distrcancers and thscreening are vWe choose a mshift and its coessentially tumoto stay closer incorporating pathat the model overall effect odetected basedcan only evaluaBelgium, we cahowever needeto use the samewe would just mIn conclusion, tchoice of the pthe results. ThYears of Life gthere is eviden
(such as the soen non attending stage. However leveness, as detegatively correlatencers at an earlierciency, as detectist for no benefit toely did not have domen, tumors foe is in general coapply in the futur
e outdated. r source of uncthe diagnosed c
ibution show thae cancer amongs
very similar. modeling approac
onsequences, in cor growth modelsto the data and arameters based is less flexible an
of screening on td on Belgian dataate the effect of thannot vary the sced to parameterizee parameters that
merely replicate ththere is considera
parameters, so a is uncertainty is
gained and QALYce that continuing
ocial class or othscreening) and reength time has no
ection of slow gre with the ability r stage. Length timon of indolent tu
o women. ata on stage spec
ound by screeninonsiderable uncerte, as treatment ev
certainty is the cancers and stageat the stage distst the people who
ch that is essentcontrast to most s. This has the adv
make less use on Belgian data, nd has more simpthe proportion of a in the group 50he screening schereening interval. We the CISNET mot are already usedhem. able structural unlot of caution is nreflected in the
Ys gained in the eg screening until
S
er health relatedesidual confoundo direct impact onrowing tumors dto detect potenti
me has indeed a numors means mo
cific survival for tung and interval ctainty around thevolves and actual
right choice oe-shift. The Flemtributions of the o do not participat
tially based on thCISNET models vantage that it alloof unobserved vabut has the disadplifications. We mcancers that are-69. This implies
edules actually in We do not have
odels and would bd in the published
certainty around needed when intewide range of esend result. Neverthe age of 74 ye
Screening Breast C
d factors ing after efficacy oes not ially life-negative
ore harm
umors in cancers. survival data on
of stage ish data interval
te in the
he stage that are owed us ariables,
dvantage model an e screen
that we place in the data
be forced models,
the right erpreting stimated rtheless, ears has
muthloa
Cancer
modest effect on tuncertainty on thehat under reasonoss of quality adjuacceptable level b
the number of Lifee effect on qualitynable assumptionusted life years. Itefore extending s
e Years Saved buy adjusted life yeas the interventiont is important to b
screening.
KCE Report
ut there is considears, and the data n may even leadbring the recall rat
t 176
erable show
d to a tes to

KCE Report 176
4. ANSWWhat are clinbreast canceryears?
4.1. Breast What is the effescreening on thfor breast cancobtain an extra predicts that 12(1.3 per 1000),
4.2. Delay bHow long is thcancer relatedbetween 4 and
4.3. OveralWhat is the effescreening on tyears) of breasunclear. Studiemortality reduct
4.4. MorbidWhat is the effescreening on min randomized cor reject the hycancer diseasemorbidity may bcurrently at ourthe most recentconservative sadvanced stage
6
WER TO CLnical benefits anr organized scre
cancer relatedect of an extensiohe breast cancer rcer between the 13 years of life fo
28 deaths would being a reduction
between the sce delay between
d mortality reduc7 years after scre
l mortality ect of an extensiothe overall mortast cancer organizes did not have tion.
ity ect of an extensio
morbidity? We foucontrol trials. In o
ypothesis that scre. Aim of screeninbe diminish by lesr disposal do not t data (KCE repor
surgery versus 3es (C Stage I an
LINICAL QUnd specific harmeening in wome
d mortality n (70-74 years) orelated mortality?ages of 70 and
or 1,000 women sbe averted per 1
n of 21%.
creening and th the screening action? The morteening
n (70-74 years) oality? The effect zed screening onstatistical power
n (70-74 years) ond no data relatether words, on theening reduces thg is to detect minss aggressive treenable us to ratifrt 150)86 show 58%38% of total mand II). Nearly 90%
S
UESTIONSms of an extenen between 70
f breast cancer orThe continued sc74 makes it pos
screened. The mo00 000 women s
he mortality rednd the associatedtality reduction
f breast cancer orof an extension
n the overall mor to detect an a
f breast cancer ored to the cancer mis basis we do nohe morbidity of thor tumors. Conseatment. The Belgfy this assertion. A% of the interventastectomies in th% of patients und
Screening Breast C
S nsion of
and 74
rganized creening ssible to odel also screened
duction d breast appears
rganized n (70-74 ortality is all-cause
rganized morbidity ot accept e breast
equently, gian data Actually, tions are he least dergoing
ctrtr
4Wre3sans
4Wtoo
4Wtrc7mgTmtoinfi
Cancer
conservative surgereatment of neoreatment.
4.5. False posWhat are the speesults? The Belg
3,5% in Flandersscreening round. Aand rates of false negative results screening round (B
4.6. AdditionaWhat are the speco forty additional offered screening
4.7. Over-diagWhat are the spreatment? Basedcases), ranged fro70 to 79 years amastectomies andgroups (no data sThree trials with amastectomies ando 1.42). Two trincrease in interveive trials combine
ery also receive ro-adjuvant chemo
sitive or false necific harms in tegian data currentlys and of 10% At this age groupnegative results aare 1.5 per 100BCSC-USA).
al diagnostic tescific harms in termpunctures or biop(three rounds).
gnosis and ovepecific harms ind on selected stom (7% to 21%) toare available). Gd lumpectomies wspecific for womeadequate randomid lumpectomies (Rals with subopti
entions (RR of 1.4d was 1.35 (95%
adiotherapy treatmotherapy, and 4
negative resultserms of false posy at our disposalin Walloon and , performance ofare relatively low.00 women aged
sts ms of additional diapsies may be expe
er-treatment n terms of overudies, over-deteco 35% (no data spGötzsche reportedwas significantly len aged 70 to 79ization showed a Relative Risk (RRmal randomizatio
42 (95% CI 1.26 toCI 1.26 to 1.44).
ment, 38% are giv1% receive hor
s sitive or false negl show a recall ra
Brussels regionmammography is For USA, rate of
70 to 79 years
agnostic tests? Twected per 1000 wo
r-diagnosis and ction (excluding pecific for women d that the numblarger in the scre9 years are availa
significant increaR) 1.31, 95% (CI)on showed the o 1.61)). The RR f
61
ven a mone
gative ate of n per s high f false s per
wenty omen
over-DCIS aged
ber of eened able). ase in ) 1.22 same for all
62
4.8. What acase of
It is advisable doctor should dIn this way, recommended:• Information• Decision m• Steering of
methods thThe criteria defmake provisionused, the doubthe recall rate95
criteria laid dowtherefore logicatowards these s
attitude should f self referral? that when a pat
develop a strategyan attitude stru
n specific to the agmaking according t
f the person whohat minimize the dfined in the frame for the monitorin
ble reading of the5. In Belgium, thewn in the contexal to steer those wstructures.
be recommend tient asks her doy minimizing the ductured around
ge bracket93 to the patient pers
o so wishes towardrawbacks. ework of the Eurong of the technicae mammographiese approved mammxt of the Europeawomen who expl
S
ded for women
ctor for a screendrawbacks of scre
three phases
sonal assessmentrds a screening i
pean Programmel quality of the eqs, and an optimizmography units man Programme, aicitly request a sc
Screening Breast C
n in
ning, the eening92. can be
t94 nvolving
e notably quipment zation of meet the and it is creening
Cancer
KCE Reportt 176

KCE Report 176
5. REFER1. Paulus
Good KnowleAvailabhttp://kc
2. Verleyerisk foscreenid'experAvailabhttp://wrisk-for-
3. Mambocancer of 40-4Health reports http://kc
4. Gotzscmammo2011(1
5. Nelson ScreenServiceW237-4
6. Bieshestudy moverdetLancet
7. Jorgensmammoinciden
6
RENCES D, Mambourg F
Clinical Practice edge Centre (KCble ce.fgov.be/index_e L, Desomer A, or breast canceing]. Good clinicartise des soins dble www.kce.fgov.be/p
-breast-cancertecourg F, Robays j,
screening with m49 years ]. Good Care Knowledge
129ce.fgov.be/index_he PC, Nielsenography. Cochra). HD, Tyne K, Naiing for breast ca
es Task Force. 42. uvel C, Barratt A,
methods and biastection with mamOncol. 2007;8(12sen KJ, Götzscheography screenice trends. Bmj. 20
F, Bonneux L. [B(GCP). Brussel
CE); 2005 02/05
_en.aspx?SGREFGailly J, Robays
er/technical methl Practice (GCP).
de santé (KCE);
publication/report/chnical-methods-fo, Camberlin C, V
mammography forClinical Practice e Centre (KCE);9 Av_en.aspx?SGREF M. Screening ane Database o
k A, Bougatsos Cancer: an update
Ann Intern Me
Howard K, Houssses on estimates mography screen
2):1129-38. e PC. Overdiagnong programmes009;339.
S
Breast cancer scrls: Belgian Heal
5/2005. KCE rep
=5221&CREF=93s j. [Identifying wohods for breast
Bruxelles: Centre2012. KCE Repo
identifying-womenor-breast-cancer-slayen J, Gailly J.r women in the a(GCP). Brussels:2010 07/07/201
ailable =14851&CREF=1for breast canc
of Systematic R
C, Chan BK, Hume for the U.S. Preed. 2009;151(10)
sami N, Irwig L. Eof invasive breas
ning: a systematic
osis in publicly or: systematic re
Screening Breast C
reening]. th Care
ports 11 from:
348 omen at
cancer e fédéral orts 172
from: n-at-sc . [Breast gegroup Belgian
10. KCE from:
16581 cer with Reviews.
phrey L. eventive :727-37,
Effects of st cancer c review.
rganised view of
8
9
1
1
1
1
1
1
1
1
Cancer
8. Virnig BA,situ of theoutcomes
9. HumphreyscreeningServices T
0. Tabar L, Grontoft Omass screBreast CaBoard of H
1. Dixon JMmastectom
2. Smith RArandomizelearned? R
3. Nystrom LRutqvist updated 2002;359(
4. Tabar L, Swedish Ton Breast
5. Maass N,Heerlein Ibreast. Arc
6. Duffy SW,time in brboth entryMed. 1995
7. FrachebouVerbeek Alimit for po2006;118(
, Tuttle TM, Sham breast: a system. J Natl Cancer Iny LL, Helfand M: a summary of Task Force. Ann I
Fagerberg CJ, O, et al. Reductioeening with mamancer Screening WHealth and WelfarM. Breast screemies. Breast Canc, Duffy SW, Gabed trials of breaRadiol Clin North L, Andersson I, LE. Long-term overview of the(9310):909-19. Vitak B, Chen T
Two-County TrialCancer Mortality Alkasi O, Baue. Actual managemch Gynecol Obste, Chen HH, Tabarreast cancer screy to and exit from5;14(14):1531-43.ud J, GroenewoudAL, et al. Seventyopulation-based m(8):2020-5.
mliyan T, Kane RLmatic review of incnst. 2010;102(3):1, Chan BK, Woothe evidence fo
ntern Med. 2002;Gad A, Baldeto
on in mortality frommography. RandWorking Group ofre. Lancet. 1985;1ning has increa
cer Res. 2009;11 e R, Tabar L, Ye
ast cancer screeAm. 2004;42(5):7Bjurstam N, Friseeffects of mam Swedish rando
TH, Yen AM, Col: Impact of Mamduring 3 Decades
er M, Jonat W, Sment of ductal caet. 2009;280(5):69r L, Day NE. Estimeening using a Mm the preclinical d. d JH, Boer R, Dra
y-five years is an mammography sc
L. Ductal carcinomcidence, treatment70-8. olf SH. Breast car the U.S. Preve137(5 Part 1):347orp L, Holmbergom breast cancerdomised trial fromf the Swedish Na1(8433):829-32. ased the numbeSuppl 3:S19.
en AM, Chen THening: what have793-806, v. ell J, Nordenskjo
mmography screeomised trials. La
ohen A, Tot T, mmographic Scres. Radiology. 201Souchon R, Meinarcinoma in situ o99-705. mation of mean soMarkov chain moddetectable phase
aisma G, de Bruijappropriate uppe
creening. Int J Ca
63
ma in t, and
ancer entive 7-60. g LH, r after m the tional
er of
. The e we
old B, ening: ancet.
et al. ening 1.
nhold-of the
ojourn del of . Stat
n AE, er age ancer.

64
18. Fett MJ
mammoscreeni
19. Shen estimatBiostat
20. Wu JCEstimatnon-raneffects on redTreatm
21. Olsen Overdiamammo2006;12
22. Frisell breast Breast
23. Paci Escreeniin the Journa
24. Boer RcarcinoCancer
25. Duffy Sof breathe Nat
26. Duffy Sin brea2005;92
27. Shen Ybreast
J. Computer modographic screenining interval. JournY, Zelen M. Rtion of sensitivity istics. 2005;6(4):6, Hakama M, Antttion of natural hisndomized organizof inter-screeninguction of advancent. 2010;122(2):AH, Agbaje O
agnosis, sojourn ography scree2(4):338-42. J, Eklund G, Hecarcinomas in a Cancer Research
E, Duffy SW. Ming programmes: Florence Distric
l of EpidemiologyR, de Koning Homa screening intr. 1999;86(8):1506SW, Day NE, Tabast tumor progresstional Cancer Inst
SW, Gabe R. Whaast screening p2(3):597-600. Y, Zelen M. Screcancer early de
delling of the Swng and trade offs bnal of Medical ScreRobust modelingy and preclinical 604-14. tila A, Yen AM, Mtory parameters o
zed screening dag interval, sensiticed cancer. Bre553-66.
OF, Myles JP, time, and sensit
ening program
ellstrom L, Somerandomized scre
h & Treatment. 19Modelling the an
sensitivity, lead tct Programme (1. 1991;20(4):852-
HJ, van der Maaerval for women 6-10. ar L, Chen HH, Ssion: some age-stitute. Monographsat should the deterogrammes? Brit
eening sensitivityetection clinical tr
S
wedish two countybetween participaeening. 2001;8(1)
g in screening sojourn time dist
Malila N, Sarkeala of breast cancer bta: subsidiary anavity, and attendaast Cancer Rese
Lynge E, Duftivity in the Copem. Breast
ll A. Analysis of eening trial in Sto987;9(3):219-25. alysis of breast time and predictiv1975-1986). Inter8. as PJ. A longerage older than 65
Smith TC. Markovspecific results. Jos. 1997;22:93-7.ection rates of cantish Journal of
y and sojourn timrials: mammogra
Screening Breast C
y trial of ation and ):39-45. studies:
tribution.
T, et al. based on alysis of nce rate earch &
ffy SW. enhagen Journal.
interval ockholm.
cancer ve value rnational
r breast 5 years?
v models ournal of
ncers be Cancer.
me from ams and
2
2
3
3
3
3
3
3
3
3
Cancer
physical 2001;19(1
28. Spratt JS,duration odetection
29. Tabar L, Fal. Efficacthe Swedi
30. Weedon-FEstimatingquestionnaMedical S
31. Weedon-FEstimatingbreast caMedical S
32. Zappa M, women: eReviews in
33. Boer R, dsearch of J Cancer.
34. Mandelbladecisions among theClin Onco
35. Karnon J, et al. A designing 2007;11(5
36. Barratt A,outcomes informed c
37. Berry DA,Modeling
examinations. 5):3490-9. Greenberg RA, Hof cancer and caby screening. CanFagerberg G, Checy of breast cancesh Two-County T
Fekjaer H, Lindqvg mean sojourn aire data on timecreening. 2008;15
Fekjaer H, Vatteng mean sojourn ncer mammograpcreening. 2005;12Visioli CB, Ciatto
efficacy and cost-n Oncology Hemae Koning HJ, vanthe best upper ag1995;31A(12):20
att JS, Silliman about the benefitse oldest old withol. 2009;27(4):487-Goyder E, Tappereview and crit
screening pro52):iii-iv, ix-xi, 1-14 Howard K, Irwig
of screening mchoices. BMJ. 200, Inoue L, Shen Ythe impact of tre
Journal of
Heuser LS. Geomarcinoma in situ ncer Research. 19en HH, Duffy SWer screening by arial. Cancer. 1995
vist BH, Vatten Ltime and scree
e since previous 5(2):83-90. n LJ, Aalen OO, time and screen
phy screening: n2(4):172-8. o S. Mammograph-effectiveness. Reatology. 2003;46(3n Oortmarssen GJge limit for breast 40-3. R. Hanging in s and harms of br
out a safety net o-90. enden P, McPhie tique of modellinogrammes. Heal45. g L, Salkeld G, Hmammography: in05;330(7497):936Y, Venier J, Coheatment and scre
KCE Report
Clinical Onco
metry, growth ratesof the breast b
986;46(2):970-4. , Smart CR, Gad age. New results5;75(10):2507-17.J, Aalen OO, Tre
ening sensitivity screening. Journ
Lindqvist B, Trening test sensitivew results. Journ
hy screening in eeview 16 refs. C3):235-9. J, van der Maas Pcancer screening
the balance: mreast cancer scre
of scientific eviden
S, Towers I, Brazng in prioritisinglth Technol As
Houssami N. Modnformation to su6. en D, Bondy M, eening on U.S. b
t 176
ology.
s, and before
A, et from . etli S. using nal of
etli S. vity in nal of
elderly Critical
PJ. In g. Eur
aking ening
nce. J
zier J, and
ssess.
del of upport
et al. breast

KCE Report 176
cancer 2006;M
38. Carles Cost-ef(Spain)
39. Carter and en2005;27
40. Feuer Emammo2000: 2006;M
41. FrybacKuruchEpidem2006;M
42. Gyrd-Hin DenmHealth
43. Hanin RochesCancer
44. Lee S, breast 2006;M
45. Lee SJAnn On
46. Mahnkethe effeevaluatapproa
47. MandeSPECTtreatme
6
mortality: a BayeMonographs.(36):3
M, Vilaprinyo E, ffectiveness of ea). BMC Cancer. 20KJ, Castro F, Kend ages for ma7(1):40-7. EJ. Modeling the ography on U.S. introduction to th
Monographs.(36):2k DG, Stout Nittham V, Remin
miology SimulatioMonographs.(36):3Hansen D. Cost-bemark based on diCare. 2000;16(3)LG, Miller A, Zo
ster model of brer Inst Monogr. 200Zelen M. A stoch
cancer. JMonographs.(36):7J, Zelen M. Modencol. 2003;14(8):1en JD, Chan W, ects of lead-timeting screening mch. Stat Methods lblatt J, Schechte
TRUM populationent on U.S. bre
esian approach. J 30-6. Cots F, Gregori A
arly detection of b011;11.
essler E, Ericksonmmography scre
impact of adjuvabreast cancer mohe problem. J N2-6. NK, Rosenberg ngton PL. The Won Model. J Na37-47. enefit analysis of iscrete ranking da:811-21.
orin AV, Yakovleeast cancer detec06;Monographs.(3hastic model for pJ Natl Can79-86. elling the early de
199-202. Freeman DH, Jr
e bias, length biamammography: a
Med Res. 2008;1er CB, Lawrencen model of the ieast cancer trend
S
Natl Cancer Inst
A, Pla R, Roman breast cancer in C
n BA. Simulation eening. J Health
ant therapy and scortality between 1atl Cancer Inst
MA, Trentham-DWisconsin Breast atl Cancer Inst
mammography scata. Int J Technol
v AY. The Univection and surviva36):66-78. predicting the moncer Inst
etection of breast
., Freeman JL. Ras and over-detecensored bivaria7(6):643-63. W, Yi B, Cullenmpact of screends from 1975 to
Screening Breast C
Monogr.
R, et al. Catalonia
of begin hc Qual.
creening 975 and Monogr.
Dietz A, Cancer
Monogr.
creening l Assess
ersity of l. J Natl
ortality of Monogr.
cancer.
Reducing ection in ate data
n J. The ning and o 2000:
4
4
5
5
5
5
5
5
Cancer
principles Monogr. 2
48. MandelblaDraisma different benefits a19;152(2):
49. MandelblaJ, Extermolder womscreening 2005;20(6
50. Neeser K,effectivenescreening perspectiv(Structure
51. Plevritis Sstochasticfrom 192006;Mon
52. Rauner MDynamic Based IdOperation
53. RijnsburgeMiller AB,Breast Sc2004;110(
54. Rojnik KProbabilisscreening
55. Rue M, VMarcos-G
and practice of t2006;Monographsatt JS, Cronin KAG, et al. Effectscreening schednd harms.[Erratum:136]. Ann Intern att JS, Schechter
mann M, et al. Tomen: Costs, beby age, biology,
6):487-96. , Szucs T, Bulliardess analysis of
program fromve: quantitative asd abstract). 2007;
SK, Sigal BM, Sc simulation mode975 to 2000. ographs.(36):86-9
MS, Gutjahr WJ, Policy Modeling
dentification of Ps Research. 2010er AJ, van Oortm et al. Mammogrcreening Study-2(5):756-62. , Naversnik K, tic cost-effectivenpolicies in Sloven
Vilaprinyo E, Leeragera R, et al. Ef
the model method.(36):47-55.
A, Bailey S, Berrs of mammogradules: model esm appears in AnnMed. 2009;151(10CB, Yabroff KR,
oward optimal scnefits, and harmand health status
d JL, Bachmann f a quality-cont
m the Swiss ssessment of the ;10(1):42-53.
Salzman P, Roseel of U.S. breast c
J Natl Ca95. Heidenberger Kfor Chronic Dis
Pareto-Optimal S0;58(5):1269-86.
marssen GJ, Boerraphy benefit in t2: a model eval
Mateovic-Rojnikness modeling of nia. Value Health.e S, Martinez-Alffectiveness of ea
ds. J Natl Cance
ry DA, de Koningaphy screening ustimates of pot
n Intern Med. 20100):738-47. Lawrence W, Dig
creening strategiems of breast cas. J. Gen. Intern.
G, Schramm W. trolled mammogrstatutory healthmost influential fa
enberg J, Glynn cancer mortality trncer Inst Mo
, Wagner J, Passeases: MetaheuScreening Strate
r R, Draisma G, Tthe Canadian Nauation. Int J Ca
k T, Primiczakedifferent breast ca 2008;11(2):139-4lonso M, Carles
arly detection on b
65
er Inst
g HJ, under tential 0 Jan
gnam es for ancer Med.
Cost-raphy
h-care actors
P. A rends
onogr.
sia J. ristic-egies.
To T, tional
ancer.
lj M. ancer 48.
MD, breast

66
cancer 2009;9
56. Stout NSM, Frscreeni
57. Tan SYJD. Thecancer.
58. VilaprinEstimatsurvivaCancer
59. Wang screenicountiescreeni
60. Messecwithoutquiz 52
61. Wen YPcase o2005;24
62. Advisorcancer 61.
63. Anonymvolledig1997. LBorstka
64. Barratt K, et alBased
65. Barratt Benefit
mortality reduct(326).
NK, Rosenberg MAryback DG. Retring mammographY, van Oortmarsse MISCAN-Fadia . J Natl Cancer Innyo E, Rue M, tion of age- an
al functions usingr. 2009;9(98). H, Karesen R, ing in Norway: Re
es and cost-effing. Cancer Causcar DC. Mammogt cognitive impair2-3. P, Sheu ML. A coof breast cance4(6):519-28. ry Committee onin England: past
mous. Landelijk g ingevoerd; resLandelijk Evaluatanker. Ned TijdschA, Irwig L, Glaszi. Relative benefit Healthc. 2002;6(4AL, Les Irwig M
s, harms and cos
tion in Catalonia
A, Trentham-Dietrospective cost-ey. J Natl Cancer I
sen GJ, de Konincontinuous tumost Monogr. 2006;MMarcos-Gragera
nd stage-specific g US and Cata
Hervik A, Thoreesults from the firsfectiveness of es Control. 2001;
graphy screening frment. J Gerontol
ost-benefit analysr screening. Ta
n Breast Cancer and future. J Me
bevolkingsonderultaten van de tie Team voor behr Geneeskd. 200iou P, Salkeld G, of mammography
4):156-7. M, Glasziou PP, S
sts of screening m
S
a (Spain). BMC
tz A, Smith MA, Reffectiveness anaInst. 2006;98(11):ng HJ, Boer R, Hr growth model foMonographs.(36)
R, Martinez-AloCatalan breast
alan survival data
esen SA. Mammst screening rouna modeled na12(1):39-45. for older women wl Nurs. 2000;26(4
is of preventive caiwain J. Public
S. Screening foed Screen. 2006;1
rzoek naar borsimplementatiefaseevolkingsonderzo00;144(23):1124-9Houssami N, Kerly reduces with ag
Salkeld GP, Housmammography in
Screening Breast C
Cancer.
Robinson alysis of 774-82.
Habbema or breast :56-65. onso M.
cancer a. BMC
mography d in four tionwide
with and 4):14-24;
are: The Health.
or breast 13(2):59-
stkanker e 1990-
oek naar 9. likowske e. Evid.-
ssami N. n women
6
6
6
6
7
7
7
7
7
7
Cancer
70 years2002;176(
66. Bonneux voor evidGeneesku
67. Caplan LSscreening 40.
68. Carney PABuist DSMevents umammogr
69. De KoningEur J Rad
70. Feuer EJ, understanfrom mam2004;13(6
71. Grivegneecancer du
72. Habbema U.S. breasmeasures2006;Mon
73. Mandelblaal. The co65 years: Task Forc
74. Prevost Tgeneralizeof breast c
75. Rautenstrawaste of m
s and over: a(6):266-71. L. De voor- en n
dence-based infounde. 2009;153. S. To screen or n
in older women.
A, Abraham LA, M, et al. Factors aused to detecraphy. Am. J. Roeg HJ. Breast canciol. 2000;33(1):32Etzioni R, Cronind the impact of
mmography and 6):421-42. e AR, Autier P. A sein en BelgiqueJD, Tan SY, Cr
st cancer mortality informative? ographs.(36):105
att J, Saha S, Teuost-effectiveness o
a systematic rece. Ann Intern MedTC, Abrams KRed synthesis of evcancer screening.auch J. Is mam
money? MMW-Fo
systematic re
nadelen van borsormatie. Nederla
ot to screen: the . Public Health R
Miglioretti DL, Yaassociated with imct breast cancentgenol. 2007;18cer screening; cos2-7. n KA, Mariotto A. Tscreening on U.SPSA testing. Sta
Approche econome. Rev Med Brux. 2ronin KA. Impact y, 1975-2000: are
J Natl Can5-11. utsch S, Hoerger of screening mameview for the U.Sd. 2003;139(10):8
R, Jones DR. Hvidence: an exam Stat Med. 2000;1
mmography screertschr. Med. 2000
KCE Report
view. Med J
stkankerscreeningands Tijdschrift
issue of breast caRev. 2001;29(2-4)
abroff KR, Sicklesmaging and procecer after scre8(2):385-92.
st-effective in prac
The use of modelS. mortality: examat Methods Med
mique du depistag2001;22(4):A277-
of mammographe intermediate outncer Inst Mo
T, Siu AL, Atkins mography beyond
S. Preventive Ser835-42. ierarchical mode
mple based on st19(24):3359-76. ning only a poin
0;142(12):4-10.
t 176
Aust.
g: tijd voor
ancer ):231-
s EA, edural ening
ctice?
ing to mples
Res.
ge du -81. hy on come
onogr.
D, et d age rvices
els in tudies
ntless

KCE Report 176
76. Xu W,
women77. Berry D
et al. Ebreast c
78. Carter the stud
79. CleempRecomBelgiqufédéral 78B (D/
80. Lidgrenquality 2007;16
81. Freedmstates ocancer.
82. Burstroof life populat
83. Gerard attributespecific
84. Domeyrelated effects,Outcom
85. Borstkabevolki2010.
86. StordeuEyckenClinicalCentre
6
Vnenchak P, Sn aged 70 to 79 yeDA, Cronin KA, PleEffect of screenincancer. N Engl J KJ, Castro F, Kesdy of breast canceput I, Van Wilder mandations pour
ue. Health technod'expertise des s
/2008/10.273/24) n M, Wilking N, of life in differen6(6):1073-81.
man GM, Li T, Anof women after co. Breast Cancer R
om K, Johannessoby disease and
tion in Sweden. H K, Johnston K, e health classific health state descyer PJ, Sergentan
quality of life in v, long-term effect
mes. 2010;8(11):2anker LETvbngsonderzoek na
ur S, Vrijens F, n E. Quality indicl Practice (GCP).
(KCE); 2010.
Smucny J. Screears. J. 2000;49(3evritis SK, Frybac
ng and adjuvant tMed. 2005;353(17ssler E, Erickson er. Comput Biol MP, Vrijens F, Huybles évaluations plogy Assessment soins de santé (K Jonsson B, Reh
nt states of breas
nderson PR, Nicoonservative surgerRes Treat. 2010;12on M, Diderichsend socio-economic
Health Policy. 2001Brown J. The roication measure criptions. Health Enis TN, Zagouri vacuum-assisted ts and predictors.2010. bn. Landelijkeaar borstkanker i
Beirens K, Vlaycators in oncologBrussels: BelgianKCE reports 15
S
eening mammogr3):266-7. ck DG, Clarke L, Ztherapy on morta7):1784-92. B. A computer m
Med. 2003;33(4):3brechts M, Ramae
pharmacoéconomi(HTA). Bruxelles
KCE); 2008. KCE
hnberg C. Healthst cancer. Qual L
laou N, Konski Ary and radiation fo21(2):519-26. n F. Health-relatedc group in the 1;55(1):51-69.
ole of a pre-scorein validating co
Econ. 1999;8(8):6F, Zografos GC. breast biopsy: sh Health & Quality
e evaluatie n Nederland 199
yen J, Devriese gy: breast bancen Health Care Kn50C (D/2010/10.2
Screening Breast C
raphy in
Zelen M, lity from
model for 45-60. ekers D. iques en
s: Centre Reports
h related Life Res.
A. Health or breast
d quality general
ed multi-ondition-
685-99. Health-
hort-term y of Life
van 90-2007.
S, Van er. Good owledge 273/101)
8
8
8
9
9
9
9
9
9
Cancer
Available http://kce.f
87. INC. Survétat des lie
88. Mook S, Vvan Leeuwdetection 2011;103(
89. Cortesi L, Prognosispopulation
90. Joensuu HT, Kataja detected 2004;292(
91. Olsson A,J. Tumourby screen
92. PhysiciansPreventive
93. Woloshin mammogr2010;303(
94. Jorgensenfunded sc
95. Perry N, BL. Europescreening Oncol. 200
fgov.be/index_envie attendue des peux. 2010.
Van 't Veer LJ, Ruwen FE, et al. In
in invasive br(7):585-97. Chiuri VE, Rusce
s of screen-deten based study. BMH, Lehtimaki T, Ho
V, et al. Risk foby mammograph(9):1064-73. Borgquist S, Butr-related factors aing. Br J Surg. 20s AAoF. Summae Services. In: AA
S, Schwartz raphy screening: (2):164-5. n KJ, Gotzsche reening mammog
Broeders M, de Wean guidelines fo
and diagnosis. F08;19(4):614-22.
.aspx?SGREF=52patients atteints d
utgers EJ, Ravdin ndependent prognreast cancer. J
elli S, Bellelli V, Nected breast ca
MC Cancer. 2006;olli K, Elomaa L, Tor distant recurre
hy screening or o
tt S, Zackrisson Sand prognosis in b012;99(1):78-87. ary of Recomme
AFP Policy Action LM. The beneunderstanding t
PC. Content of graphy. BMJ. 2006
Wolf C, Tornberg Sor quality assuraFourth edition--sum
211&CREF=1884de cancers en Fra
PM, van de Veldenostic value of scJ Natl Cancer
Negri R, Rashid I, ancers: results 6:17. Turpeenniemi-Hujence of breast caother methods. J
S, Landberg G, Mbreast cancer det
endations for ClAAFP; 2010. efits and harmthe trade-offs. JA
invitations for pu6;332(7540):538-4, Holland R, von K
ance in breast cammary document
67
from: 47 ance :
e AO, creen
Inst.
et al. of a
janen ancer Jama.
Manjer ected
linical
ms of AMA.
ublicly 41. Karsa ancer t. Ann

68
cancer 2009;9
56. Stout NSM, Frscreeni
57. Tan SYJD. Thecancer.
58. VilaprinEstimatsurvivaCancer
59. Wang screenicountiescreeni
60. Messecwithoutquiz 52
61. Wen YPcase o2005;24
62. Advisorcancer 61.
63. Anonymvolledig1997. LBorstka
64. Barratt K, et alBased
65. Barratt Benefit
mortality reduct(326).
NK, Rosenberg MAryback DG. Retring mammographY, van Oortmarsse MISCAN-Fadia . J Natl Cancer Innyo E, Rue M, tion of age- an
al functions usingr. 2009;9(98). H, Karesen R, ing in Norway: Re
es and cost-effing. Cancer Causcar DC. Mammogt cognitive impair2-3. P, Sheu ML. A coof breast cance4(6):519-28. ry Committee onin England: past
mous. Landelijk g ingevoerd; resLandelijk Evaluatanker. Ned TijdschA, Irwig L, Glaszi. Relative benefit Healthc. 2002;6(4AL, Les Irwig M
s, harms and cos
tion in Catalonia
A, Trentham-Dietrospective cost-ey. J Natl Cancer I
sen GJ, de Konincontinuous tumost Monogr. 2006;MMarcos-Gragera
nd stage-specific g US and Cata
Hervik A, Thoreesults from the firsfectiveness of es Control. 2001;
graphy screening frment. J Gerontol
ost-benefit analysr screening. Ta
n Breast Cancer and future. J Me
bevolkingsonderultaten van de tie Team voor behr Geneeskd. 200iou P, Salkeld G, of mammography
4):156-7. M, Glasziou PP, S
sts of screening m
S
a (Spain). BMC
tz A, Smith MA, Reffectiveness anaInst. 2006;98(11):ng HJ, Boer R, Hr growth model foMonographs.(36)
R, Martinez-AloCatalan breast
alan survival data
esen SA. Mammst screening rouna modeled na12(1):39-45. for older women wl Nurs. 2000;26(4
is of preventive caiwain J. Public
S. Screening foed Screen. 2006;1
rzoek naar borsimplementatiefaseevolkingsonderzo00;144(23):1124-9Houssami N, Kerly reduces with ag
Salkeld GP, Housmammography in
Screening Breast C
Cancer.
Robinson alysis of 774-82.
Habbema or breast :56-65. onso M.
cancer a. BMC
mography d in four tionwide
with and 4):14-24;
are: The Health.
or breast 13(2):59-
stkanker e 1990-
oek naar 9. likowske e. Evid.-
ssami N. n women
6
6
6
6
7
7
7
7
7
7
Cancer
70 years2002;176(
66. Bonneux voor evidGeneesku
67. Caplan LSscreening 40.
68. Carney PABuist DSMevents umammogr
69. De KoningEur J Rad
70. Feuer EJ, understanfrom mam2004;13(6
71. Grivegneecancer du
72. Habbema U.S. breasmeasures2006;Mon
73. Mandelblaal. The co65 years: Task Forc
74. Prevost Tgeneralizeof breast c
75. Rautenstrawaste of m
s and over: a(6):266-71. L. De voor- en n
dence-based infounde. 2009;153. S. To screen or n
in older women.
A, Abraham LA, M, et al. Factors aused to detecraphy. Am. J. Roeg HJ. Breast canciol. 2000;33(1):32Etzioni R, Cronind the impact of
mmography and 6):421-42. e AR, Autier P. A sein en BelgiqueJD, Tan SY, Cr
st cancer mortality informative? ographs.(36):105
att J, Saha S, Teuost-effectiveness o
a systematic rece. Ann Intern MedTC, Abrams KRed synthesis of evcancer screening.auch J. Is mam
money? MMW-Fo
systematic re
nadelen van borsormatie. Nederla
ot to screen: the . Public Health R
Miglioretti DL, Yaassociated with imct breast cancentgenol. 2007;18cer screening; cos2-7. n KA, Mariotto A. Tscreening on U.SPSA testing. Sta
Approche econome. Rev Med Brux. 2ronin KA. Impact y, 1975-2000: are
J Natl Can5-11. utsch S, Hoerger of screening mameview for the U.Sd. 2003;139(10):8
R, Jones DR. Hvidence: an exam Stat Med. 2000;1
mmography screertschr. Med. 2000
KCE Report
view. Med J
stkankerscreeningands Tijdschrift
issue of breast caRev. 2001;29(2-4)
abroff KR, Sicklesmaging and procecer after scre8(2):385-92.
st-effective in prac
The use of modelS. mortality: examat Methods Med
mique du depistag2001;22(4):A277-
of mammographe intermediate outncer Inst Mo
T, Siu AL, Atkins mography beyond
S. Preventive Ser835-42. ierarchical mode
mple based on st19(24):3359-76. ning only a poin
0;142(12):4-10.
t 176
Aust.
g: tijd voor
ancer ):231-
s EA, edural ening
ctice?
ing to mples
Res.
ge du -81. hy on come
onogr.
D, et d age rvices
els in tudies
ntless

KCE Report 176
76. Xu W,
women77. Berry D
et al. Ebreast c
78. Carter the stud
79. CleempRecomBelgiqufédéral 78B (D/
80. Lidgrenquality 2007;16
81. Freedmstates ocancer.
82. Burstroof life populat
83. Gerard attributespecific
84. Domeyrelated effects,Outcom
85. Borstkabevolki2010.
86. StordeuEyckenClinicalCentre
6
Vnenchak P, Sn aged 70 to 79 yeDA, Cronin KA, PleEffect of screenincancer. N Engl J KJ, Castro F, Kesdy of breast canceput I, Van Wilder mandations pour
ue. Health technod'expertise des s
/2008/10.273/24) n M, Wilking N, of life in differen6(6):1073-81.
man GM, Li T, Anof women after co. Breast Cancer R
om K, Johannessoby disease and
tion in Sweden. H K, Johnston K, e health classific health state descyer PJ, Sergentan
quality of life in v, long-term effect
mes. 2010;8(11):2anker LETvbngsonderzoek na
ur S, Vrijens F, n E. Quality indicl Practice (GCP).
(KCE); 2010.
Smucny J. Screears. J. 2000;49(3evritis SK, Frybac
ng and adjuvant tMed. 2005;353(17ssler E, Erickson er. Comput Biol MP, Vrijens F, Huybles évaluations plogy Assessment soins de santé (K Jonsson B, Reh
nt states of breas
nderson PR, Nicoonservative surgerRes Treat. 2010;12on M, Diderichsend socio-economic
Health Policy. 2001Brown J. The roication measure criptions. Health Enis TN, Zagouri vacuum-assisted ts and predictors.2010. bn. Landelijkeaar borstkanker i
Beirens K, Vlaycators in oncologBrussels: BelgianKCE reports 15
S
eening mammogr3):266-7. ck DG, Clarke L, Ztherapy on morta7):1784-92. B. A computer m
Med. 2003;33(4):3brechts M, Ramae
pharmacoéconomi(HTA). Bruxelles
KCE); 2008. KCE
hnberg C. Healthst cancer. Qual L
laou N, Konski Ary and radiation fo21(2):519-26. n F. Health-relatedc group in the 1;55(1):51-69.
ole of a pre-scorein validating co
Econ. 1999;8(8):6F, Zografos GC. breast biopsy: sh Health & Quality
e evaluatie n Nederland 199
yen J, Devriese gy: breast bancen Health Care Kn50C (D/2010/10.2
Screening Breast C
raphy in
Zelen M, lity from
model for 45-60. ekers D. iques en
s: Centre Reports
h related Life Res.
A. Health or breast
d quality general
ed multi-ondition-
685-99. Health-
hort-term y of Life
van 90-2007.
S, Van er. Good owledge 273/101)
8
8
8
9
9
9
9
9
9
Cancer
Available http://kce.f
87. INC. Survétat des lie
88. Mook S, Vvan Leeuwdetection 2011;103(
89. Cortesi L, Prognosispopulation
90. Joensuu HT, Kataja detected 2004;292(
91. Olsson A,J. Tumourby screen
92. PhysiciansPreventive
93. Woloshinmammogr2010;303(
94. Jorgensenfunded sc
95. Perry N, BL. Europescreening Oncol. 200
fgov.be/index_envie attendue des peux. 2010.
Van 't Veer LJ, Ruwen FE, et al. In
in invasive br(7):585-97. Chiuri VE, Rusce
s of screen-deten based study. BMH, Lehtimaki T, Ho
V, et al. Risk foby mammograph(9):1064-73. Borgquist S, Butr-related factors aing. Br J Surg. 20s AAoF. Summae Services. In: AA
S, Schwartz raphy screening: (2):164-5. n KJ, Gotzsche reening mammog
Broeders M, de Wean guidelines fo
and diagnosis. F08;19(4):614-22.
.aspx?SGREF=52patients atteints d
utgers EJ, Ravdin ndependent prognreast cancer. J
elli S, Bellelli V, Nected breast ca
MC Cancer. 2006;olli K, Elomaa L, Tor distant recurre
hy screening or o
tt S, Zackrisson Sand prognosis in b012;99(1):78-87. ary of Recomme
AFP Policy Action LM. The beneunderstanding t
PC. Content of graphy. BMJ. 2006
Wolf C, Tornberg Sor quality assuraFourth edition--sum
211&CREF=1884de cancers en Fra
PM, van de Veldenostic value of scJ Natl Cancer
Negri R, Rashid I, ancers: results 6:17. Turpeenniemi-Hujence of breast caother methods. J
S, Landberg G, Mbreast cancer det
endations for ClAAFP; 2010. efits and harmthe trade-offs. JA
invitations for pu6;332(7540):538-4, Holland R, von K
ance in breast cammary document
69
from: 47 ance :
e AO, creen
Inst.
et al. of a
janen ancer Jama.
Manjer ected
linical
ms of AMA.
ublicly 41. Karsa ancer t. Ann