Prognostic Factors After Repeat Hepatectomy for Recurrent Hepatocellular Carcinoma
Upload
independentCategory
view
0download
0
60
One-stage ultrasonographically guidedhepatectomy for multiple bilobarcolorectal metastases: A feasible andeffective alternative to the 2-stageapproachGuido Torzilli, MD, PhD, Fabio Procopio, MD, Florin Botea, MD, Matteo Marconi, MD,Daniele Del Fabbro, Matteo Donadon, MD, Angela Palmisano, MD, Antonino Spinelli, MD,and Marco Montorsi, MD, Milan, Italy
Background. Two-stage hepatectomy with or without portal vein embolization allows treatment ofmultiple bilobar metastases, thereby expanding operative indications for these patients. Two operationsare needed, however, and some patients are not able to complete the treatment strategy because of diseaseprogression. Using experience gained from our policy of ultrasonographically guided resection, weexplored the safety and effectiveness of 1-stage operative procedures in patients otherwise recommended forthe 2-stage approach.Methods. A total of 29 patients with multiple ($4) bilobar colorectal liver metastases (CLM) were se-lected from 100 consecutive patients submitted to surgical resection. The total number of preoperativeCLM was 163 (median, 5; range, 2--20). The operative strategy was based on tumor-vessel relationshipsat intraoperative ultrasonography (IOUS) and on findings at color Doppler IOUS.Results. There was no in-hospital mortality. Tumor removal was feasible with 1-stage operativeprocedures in all but 3 patients who underwent laparotomy. The overall morbidity rate was 23%(6/26); none of the patients required reoperation. Major morbidity occurred in 1 patient (4%). Bloodtransfusions were administered in 4 patients (15%). After a mean follow-up of 17 months (median, 14;range, 6--54), 3 patients had died from systemic recurrence, 12 patients were alive without disease, and11 were alive with disease. No local recurrences were observed at the resection margin.Conclusion. IOUS-guided resection based on strict criteria allows a 1-stage operative treatment in selectedpatients with multiple bilobar CLM. This strategy decreases the need for a two-stage hepatectomy, therebyavoiding the disadvantages of a 2-stage approach. (Surgery 2009;146:60-71.)
From the Third Department of General Surgery, University of Milan, IRCCS Istituto Clinico Humanitas,Rozzano, Milan, Italy
OPERATIVE TREATMENT OF COLORECTAL LIVER METASTASES
(CLM) remains the gold standard therapy, limitedonly by its technical feasibility.1 The key to the proce-dure’s success is leaving enough remnant liver to en-sure patient survival. In cases of multiple and bilobar
Supported in part by a research grant from the Cesare BannoFoundation for Cancer Research.
Accepted for publication February 13, 2009.
Reprint requests: Guido Torzilli, MD, PhD, Associate Professorof Surgery, Chief, Liver Surgery Unit, Third Department of Sur-gery, University of Milan, IRCCS Istituto Clinico Humanitas, ViaManzoni 56, 20089 Rozzano, Milan, Italy. E-mail: [email protected].
0039-6060/$ - see front matter
� 2009 Mosby, Inc. All rights reserved.
doi:10.1016/j.surg.2009.02.017
SURGERY
CLM, the most commonly used operative approachis a 2-stage hepatectomy.2 This multistep strategyuses limited resections and major hepatectomieswith or without preresection portal vein emboliza-tion (PVE).2,3 This method also allows extendingoperative indications to those patients previouslyjudged to be unresectable, because the metastaticdisease would demand the removal of too muchliver parenchyma for the resection to be curative.This approach, however, has some drawbacks. Twooperations are needed, each of which is associatedwith mortality and morbidity. In addition, somepatients do not complete this treatment approachbecause of tumor progression during the intervalbetween the 2 surgical procedures or after PVE.
A possible alternative, however, does exist. Wehave shown, both for primary and metastatic liver

SurgeryVolume 146, Number 1
Torzilli et al 61
CLM
HV
DL
CLM
PB
AG
DL
CLM
PB
AG
DL
A B C
CLM
HV
DLCLM
PB
AG
DL
D E
Fig 1. Operative strategy based on intra-operative ultrasonography tumor type, appearance, and relation betweencolorectal liver metastases (CLM) and major hepatic vessels: (A) <0.5 cm distance between the CLM and the Glissonianpedicle (G); (B) <0.5 cm distance between the CLM and the hepatic vein (HV); (C) contact <1/3 circumferencebetween the CLM and G; (D) contact >1/3 circumference between the CLM and G; (E) contact between the CLMand HV. The dotted line shows the dissection line (DL). A, Artery; B, bile duct; P, portal branch.
neoplasms, that a well-defined policy of ultrason-ically guided hepatectomy allows us to carry outradical operations safely and without major re-moval of liver parenchyma in the vast majority ofpatients, even when the tumors have complexpresentations such as multiplicity and vascularinvasion.4-7 Using information gleaned from thisexperience, we explored the feasibility, safety,and effectiveness of a 1-stage operative procedurein a prospective cohort of patients who otherwisewould have undergone the 2-stage approach.
METHODS
Terminology. The terminology for liver anatomyand resections used in this study is based on theBrisbane classification.8 Hepatic resections areconsidered major when at least 3 adjacent segmentsare removed. The hepatic vein (HV) at the cavalconfluence, the so-called hepatocaval confluence,was defined as the last 4 cm of the HV before itsconfluence into the inferior vena cava (IVC). Post-operative death was analyzed at 30 days and 90 daysafter operation. Any adverse event that requiredadditional operative treatment or any invasivecorrective procedure was considered a majorpostoperative morbidity. Liver failure was consid-ered mild when the total serum bilirubin concen-tration ranged from 2 to 5 mg/dL for >3 dayspostoperatively, medium when it ranged from 5 to
10 mg/dL for >3 days postoperatively, and severewhen it exceeded 10 mg/dL for >3 days postoper-atively.9 Local tumor recurrence was defined asrecurrence at the cut-edge (true local recurrence),and was analyzed after a minimum follow-up of6 months.
Eligibility criteria. Inclusion criteria for thecurrent study were as follows: (1) patients present-ing with resectable CLM; (2) 4 or more lesions;(3) bilobar involvement of the liver; (4) contact orclose adjacency (<0.5 cm) of at least 1 CLM with amajor intrahepatic vascular structures (first- orsecond-order portal branches and/or HV at cavalconfluence). A criterion for nonresectability wasthe presence of bilateral tumor involvement of thefirst-order portal branches for $1/3 vessel circum-ference, even with minimal bile duct dilation atany imaging modality.
Pre-operative work-up. Preoperative imagingwork-up consisted of abdominal transcutaneousultrasonography (US), computed tomography(CT), or magnetic resonance imaging (MRI), andchest spiral CT for every patient. From 2004,18-fluoro-2-deoxy-glucose positron emission tomog-raphy (18F FDG-PET) imaging was also included.Patients were selected for 1-stage resection basedon technical feasibility, regardless of size or numberof metastases, after a multidisciplinary meetingwith our medical oncologists. Technical feasibility
SurgeryJuly 2009
62 Torzilli et al
was established if residual liver volume (RLV) withoptimal blood inflow and outflow and biliarydrainage was expected to be sufficient. RLV wasconsidered sufficient if it represented 40% of thewhole liver volume in the case of normal (oreven steatotic) liver, if it represented $50% ofthe whole liver volume in the presence of cirrhoticliver, or if the total serum bilirubin level rangedbetween 1 and 1.5 mg/dL. In the event of diseasedliver parenchyma and a total serum bilirubinlevel ranging between 1.5 and 2 mg/dL, tumorec-tomy alone was considered acceptable. In addi-tion, hepatic resection was contraindicated ifserum bilirubin level was $2 mg/dL. Using CTor MRI, surgeons calculated the liver volume byadding together the liver areas determined foreach slice.
Operative technique. A J-shaped laparotomy wasusually performed. For those patients with tu-mor(s) close to the hepatocaval confluence or inthe paracaval portion of segment 1, a J-shapedthoracoabdominal incision was carried out. Intra-operative ultrasonography (IOUS) was performedusing an Aloka SDD 5500 and, more recently, anAloka Alpha 10 (Aloka, Tokyo, Japan), bothequipped with the standard 2--6 MHz convexprobe, 5--10 MHz T-shaped, and the 5--10 MHzmicroconvex probe. The staging was completed
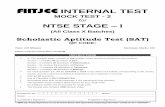
Fig 2. The inferior right hepatic vein (IRHV) as it ap-pears at intraoperative ultrasonography. The main fea-ture is that it runs behind the main right (RPV) andright sectional (P5-8 and P6-7) portal branches. IVC, In-ferior vena cava.
with contrast-enhanced intraoperative ultrasonog-raphy (CEIOUS); the contrast agent consisted of4.8 mL of microbubbles filled with sulfur hexa-fluoride (SonoVue; Bracco Imaging, Italy), whichwas injected intravenously.10,11
At this point, based on the IOUS criteria fortumor--vessel relations reported previously,4,5 theoperative strategy was defined. In particular, ves-sels were spared if IOUS showed the following:(1) the portal branch or HV was separated by athin layer of liver parenchyma (detectable byIOUS even if < 5 mm) from a CLM (Fig 1, Aand B); or (2) the portal branch was in contactwith a CLM without vessel wall discontinuation,with contact < 1/3 of the vessel diameter, andwithout proximal bile duct dilation (Fig 1, C). Inall the other conditions (Type C), Vessel resectionwas carried out (Fig 1, D and E), In particular, in acondition similar to type B (Fig 1, C), but betweena CLM and an HV, the vessel was considered in-vaded and therefore resected (Type Cb) (Fig 1, E).
To determine the extent of resection, paren-chyma fed by the portal branch that is to beresected must be considered.4 In the case of resect-ing an HV, the extension of the resection to thewhole liver parenchyma drained theoretically bythat vein was considered only in the absence ofat least one of these conditions:
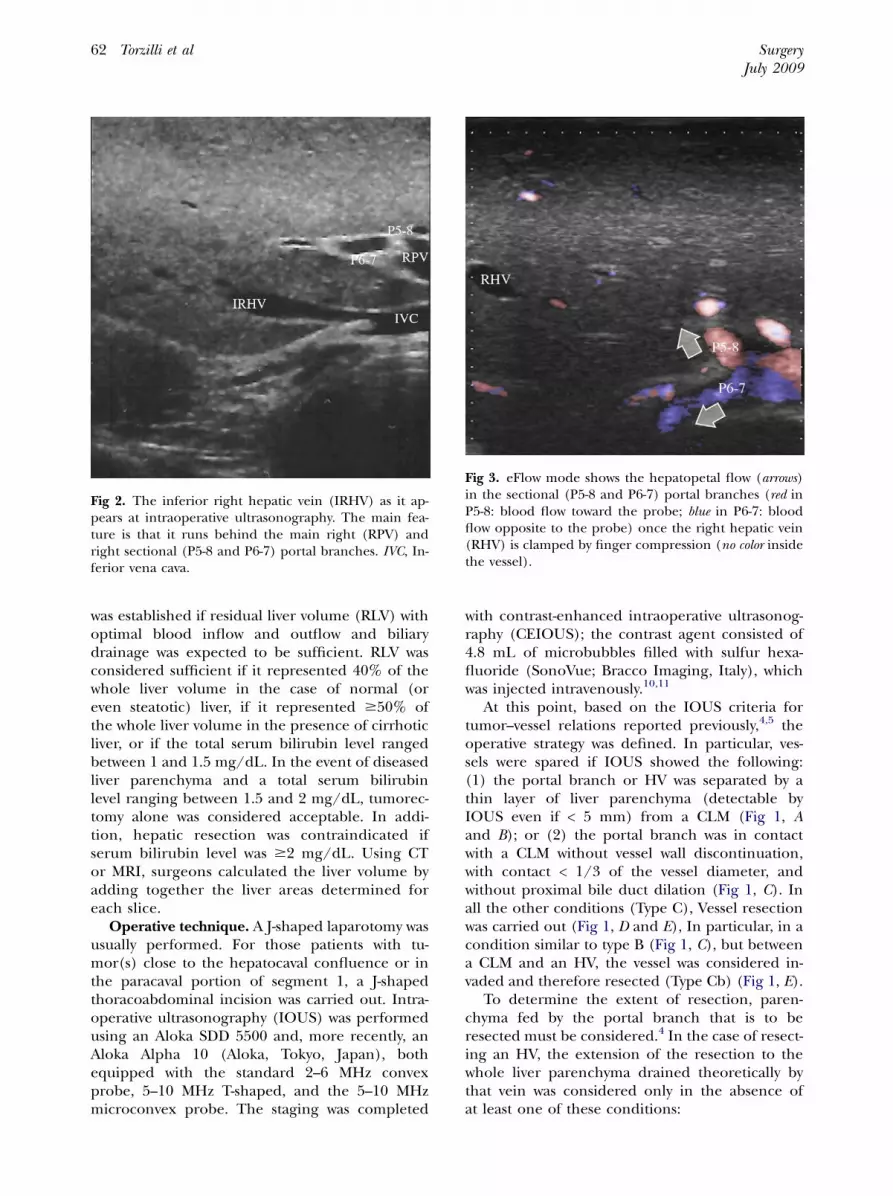
Fig 3. eFlow mode shows the hepatopetal flow (arrows)in the sectional (P5-8 and P6-7) portal branches (red inP5-8: blood flow toward the probe; blue in P6-7: bloodflow opposite to the probe) once the right hepatic vein(RHV) is clamped by finger compression (no color insidethe vessel).
SurgeryVolume 146, Number 1
Torzilli et al 63
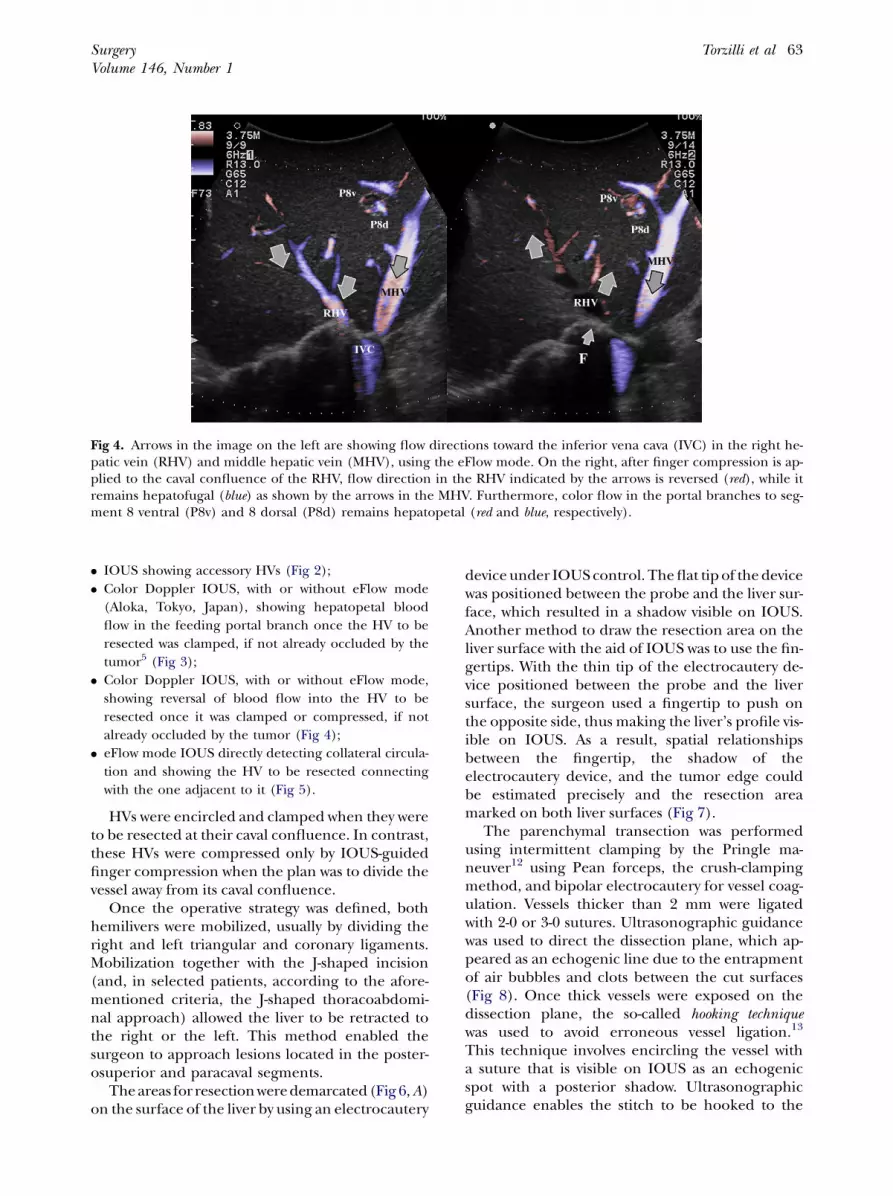
Fig 4. Arrows in the image on the left are showing flow directions toward the inferior vena cava (IVC) in the right he-patic vein (RHV) and middle hepatic vein (MHV), using the eFlow mode. On the right, after finger compression is ap-plied to the caval confluence of the RHV, flow direction in the RHV indicated by the arrows is reversed (red), while itremains hepatofugal (blue) as shown by the arrows in the MHV. Furthermore, color flow in the portal branches to seg-ment 8 ventral (P8v) and 8 dorsal (P8d) remains hepatopetal (red and blue, respectively).
d IOUS showing accessory HVs (Fig 2);d Color Doppler IOUS, with or without eFlow mode
(Aloka, Tokyo, Japan), showing hepatopetal blood
flow in the feeding portal branch once the HV to be
resected was clamped, if not already occluded by the
tumor5 (Fig 3);d Color Doppler IOUS, with or without eFlow mode,
showing reversal of blood flow into the HV to be
resected once it was clamped or compressed, if not
already occluded by the tumor (Fig 4);d eFlow mode IOUS directly detecting collateral circula-
tion and showing the HV to be resected connecting
with the one adjacent to it (Fig 5).
HVs were encircled and clamped when they wereto be resected at their caval confluence. In contrast,these HVs were compressed only by IOUS-guidedfinger compression when the plan was to divide thevessel away from its caval confluence.
Once the operative strategy was defined, bothhemilivers were mobilized, usually by dividing theright and left triangular and coronary ligaments.Mobilization together with the J-shaped incision(and, in selected patients, according to the afore-mentioned criteria, the J-shaped thoracoabdomi-nal approach) allowed the liver to be retracted tothe right or the left. This method enabled thesurgeon to approach lesions located in the poster-osuperior and paracaval segments.
The areas for resection were demarcated (Fig 6, A)on the surface of the liver by using an electrocautery
device under IOUS control. The flat tip of the devicewas positioned between the probe and the liver sur-face, which resulted in a shadow visible on IOUS.Another method to draw the resection area on theliver surface with the aid of IOUS was to use the fin-gertips. With the thin tip of the electrocautery de-vice positioned between the probe and the liversurface, the surgeon used a fingertip to push onthe opposite side, thus making the liver’s profile vis-ible on IOUS. As a result, spatial relationshipsbetween the fingertip, the shadow of theelectrocautery device, and the tumor edge couldbe estimated precisely and the resection areamarked on both liver surfaces (Fig 7).
The parenchymal transection was performedusing intermittent clamping by the Pringle ma-neuver12 using Pean forceps, the crush-clampingmethod, and bipolar electrocautery for vessel coag-ulation. Vessels thicker than 2 mm were ligatedwith 2-0 or 3-0 sutures. Ultrasonographic guidancewas used to direct the dissection plane, which ap-peared as an echogenic line due to the entrapmentof air bubbles and clots between the cut surfaces(Fig 8). Once thick vessels were exposed on thedissection plane, the so-called hooking techniquewas used to avoid erroneous vessel ligation.13
This technique involves encircling the vessel witha suture that is visible on IOUS as an echogenicspot with a posterior shadow. Ultrasonographicguidance enables the stitch to be hooked to the
SurgeryJuly 2009
64 Torzilli et al
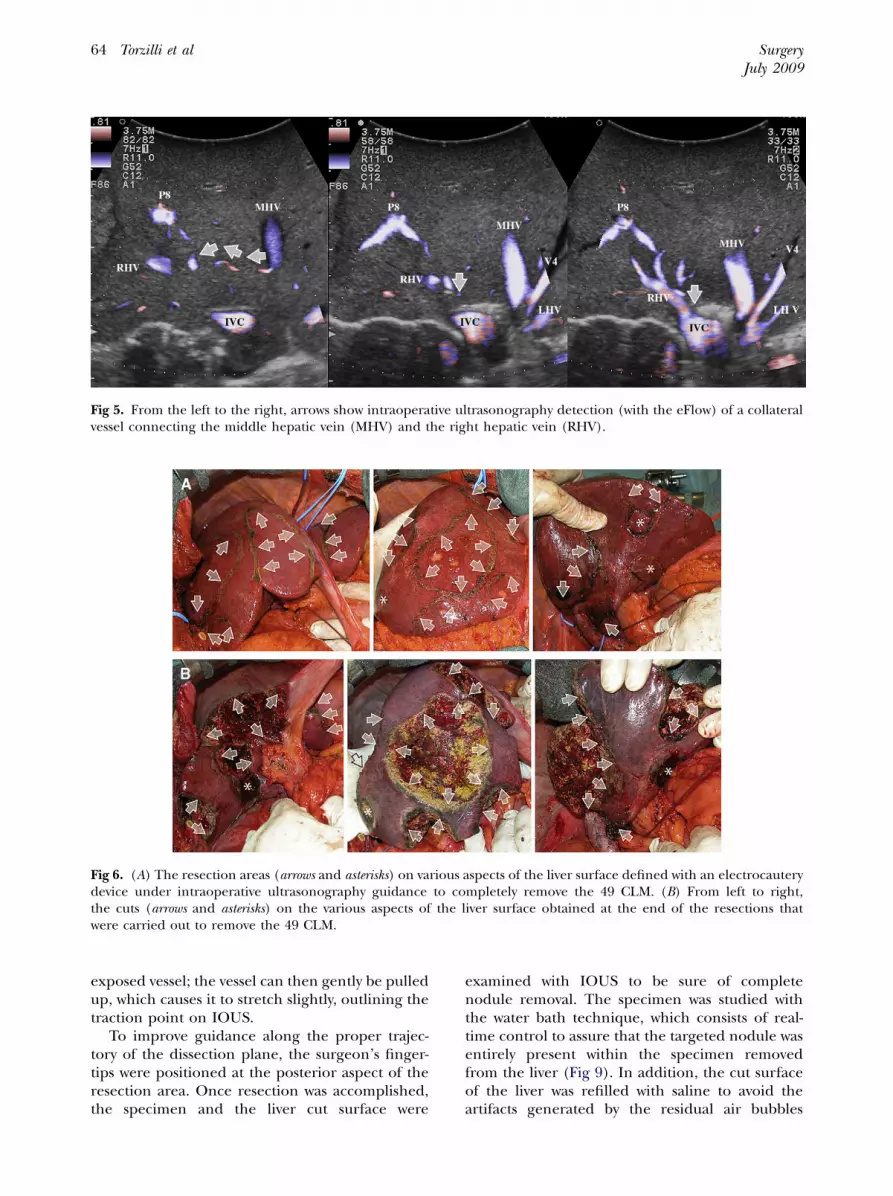
Fig 5. From the left to the right, arrows show intraoperative ultrasonography detection (with the eFlow) of a collateralvessel connecting the middle hepatic vein (MHV) and the right hepatic vein (RHV).
Fig 6. (A) The resection areas (arrows and asterisks) on various aspects of the liver surface defined with an electrocauterydevice under intraoperative ultrasonography guidance to completely remove the 49 CLM. (B) From left to right,the cuts (arrows and asterisks) on the various aspects of the liver surface obtained at the end of the resections thatwere carried out to remove the 49 CLM.
exposed vessel; the vessel can then gently be pulledup, which causes it to stretch slightly, outlining thetraction point on IOUS.
To improve guidance along the proper trajec-tory of the dissection plane, the surgeon’s finger-tips were positioned at the posterior aspect of theresection area. Once resection was accomplished,the specimen and the liver cut surface were
examined with IOUS to be sure of completenodule removal. The specimen was studied withthe water bath technique, which consists of real-time control to assure that the targeted nodule wasentirely present within the specimen removedfrom the liver (Fig 9). In addition, the cut surfaceof the liver was refilled with saline to avoid theartifacts generated by the residual air bubbles

SurgeryVolume 146, Number 1
Torzilli et al 65
and clots, and then re-imaged with IOUS. If resid-ual lesions were observed, the same procedure ofdemarcation was repeated on the cut surface,and resection was accomplished (Fig 10).
Finally, the cut surfaces of the liver (Fig 6, B)were secured by suture control of vessels and, ifnecessary, by electrocautery, fibrillar-oxidated re-generated cellulose (Fibrillar Tabotamp; Ethicon,Somerville, NJ) and/or fibrin glue (either Tissucolpurchased from Baxter [Deerfield, IL] or Quixilobtained from Ethicon). To rule out bile leakage,we performed a careful examination of the resec-tion area, but did not routinely perform intraoper-ative cholangiography.14 Multihole, 19-French,closed-suction drains were always left near the re-section area. Drains were removed on the 7th post-operative day (POD) or when the bilirubin level inthe drain discharge (sampled routinely on the 3rd,5th, and 7th POD) showed a decrement, asdescribed previously.15 A chest tube was left inpatients undergoing thoracoabdominal incision.
Outcome measures. We studied the morbidity,mortality, amount of blood loss, and rate of bloodtransfusions, as well as the serum levels of totalbilirubin, aspartate aminotransferase (AST), andalanine aminotransferase (ALT) on the 1st, 3rd,5th, and 7th POD. Because the secondary outcomefor this study was the reliability of the procedure
Fig 7. At intraoperative ultrasonography, the electrocau-tery device positioned between the liver surface (arrows)and the surgeon’s fingertip positioned on the oppositeside of the liver (F) allow the surgeon to draw an idealplane for dissection (white arrows).
from an oncologic standpoint, we studied therate of true local recurrence (at the resection mar-gin) after a minimum follow-up of 6 months. Thepatients were followed in our institution by an ex-pert hepatobiliary team every 3 months with aphysical examination, liver function tests, serumcarcinoembryonic antigen levels, US (twice ayear), and CT or MRI (twice a year). Re-resectionof recurrences was always considered without orwith resectable extrahepatic disease. Percutaneousablation therapy was proposed when hepatic recur-rence was visible at US, < 2 cm, and not close to anyvisceral cavities such as the stomach or colon.
Patients. Among 144 consecutive patients re-ferred to our unit between September 2001 andDecember 2007, 100 (69%) underwent liver resec-tion. A total of 44 patients were excluded becauseof massive liver involvement in 13, multiple distantmetastases in 23, or lymph node metastases in 8.Based on the above criteria, we selected 29 patients(29%) including 16 males and 13 females with amean age of 63 years (range, 36--82). The totalnumber of preoperative metastatic lesions was163, with a median of 5 lesions per patient (range,2--20). The median size of the largest CLM was4 cm (range, 2--13).
Of the 29 patients, 19 (66%) received chemo-therapy before resection; 2 patients underwent1 limited resection at the same time as the colonresection, and 2 underwent intraoperative ablationtherapy at the time of the colon resection. Che-motherapy was associated with disease progressionin 10 patients, stable disease in 7, and tumor
Fig 8. The dissection plane (arrows) is visible at intrao-perative ultrasonography and is passing just adjacent tothe portal branch to segment 5 and 8 (P5-8) along a sys-tematic extended right posterior sectionectomy (SERPS)procedure.

Surgery66 Torzilli et al
Fig 9. Once the specimen is removed, the presence of the tiny CLM (arrows) is confirmed with intraoperative ultraso-nography (A) and with the water bath technique (B). G, Gauze.
July 2009
reduction in 2. At follow-up, 1 patient underwentpercutaneous ablation for 2 CLM with incompletetumor necrosis, and 2 patients were referred to ourUnit without any previous treatment. All the pre-operative treatments were carried out in othercenters before referral.
Statistical analysis. Continuous variables arepresented as medians and ranges, whereas propor-tions are presented as numbers and percentages.
RESULTS
Feasibility and intraoperative findings. One-stage, complete resection of CLM was feasible in
Fig 10. A tiny residual CLM (asterisk) is visualized with in-traoperative ultrasonography (IOUS) exploring the cutsurface (arrows) after tissue removal was accomplished;transparent arrows indicate the resection margin that isdefined on the cut surface with the electrocautery deviceunder IOUS guidance.
26 of 29 patients. At exploratory laparotomy, 3patients had diffuse peritoneal carcinomatosis.After IOUS, 103 new lesions were detected in 18patients. In 14 of the 21 patients studied withCEIOUS, 9 additional lesions were found, all ofwhich were confirmed at pathology together withthe 157 lesions detected preoperatively. Therefore,the total number of resected lesions was 269, corre-sponding to a median of 6 lesions per patient(range, 4--49).
Of the 26 patients, 16 (61%) had tumors at thehepatocaval confluence. In 20 patients (77%),IOUS confirmed 29 CLM with macrovascular inva-sion (28 type C and 1 Cb subtype, according to theIOUS criteria for tumor--vessel relations4,5). IOUSdisclosed a type A relation for 27 CLM in 17 pa-tients, a type B relation for 5 CLM in 4 patients,and type A + C combined relations for 6 CLM in6 patients. There were 67 tumor--vessel relationsclassified at IOUS (Table).
Operative procedures. All procedures, includ-ing operations, IOUS, and CEIOUS, were performedby the same surgeon (G.T.). A thoracoabdominalincision was carried out in 7 patients (27%). Themedian operation time was 555 minutes (range, 299--958). Median clamping time was 116 minutes (range,65--348). In 1 patient, an overall clamping time of 348minutes was required to resect 49 lesions (Fig 6, Aand B). Preconditioning was never used. Theoverall median blood loss was 500 mL (range, 50--1,000 mL). Only 4 patients (15%) received bloodtransfusions.
Each type of operative resection is outlined inthe Table. Only 1 of 26 patients (4%) underwent aright hepatectomy associated with 2 limited left-sided resections, which represents the only majorhepatectomy. An extended right posterior sectio-nectomy (a so-called systematic extended right posteriorsectionectomy [SERPS procedure]),7 was performed in
SurgeryVolume 146, Number 1
Torzilli et al 67
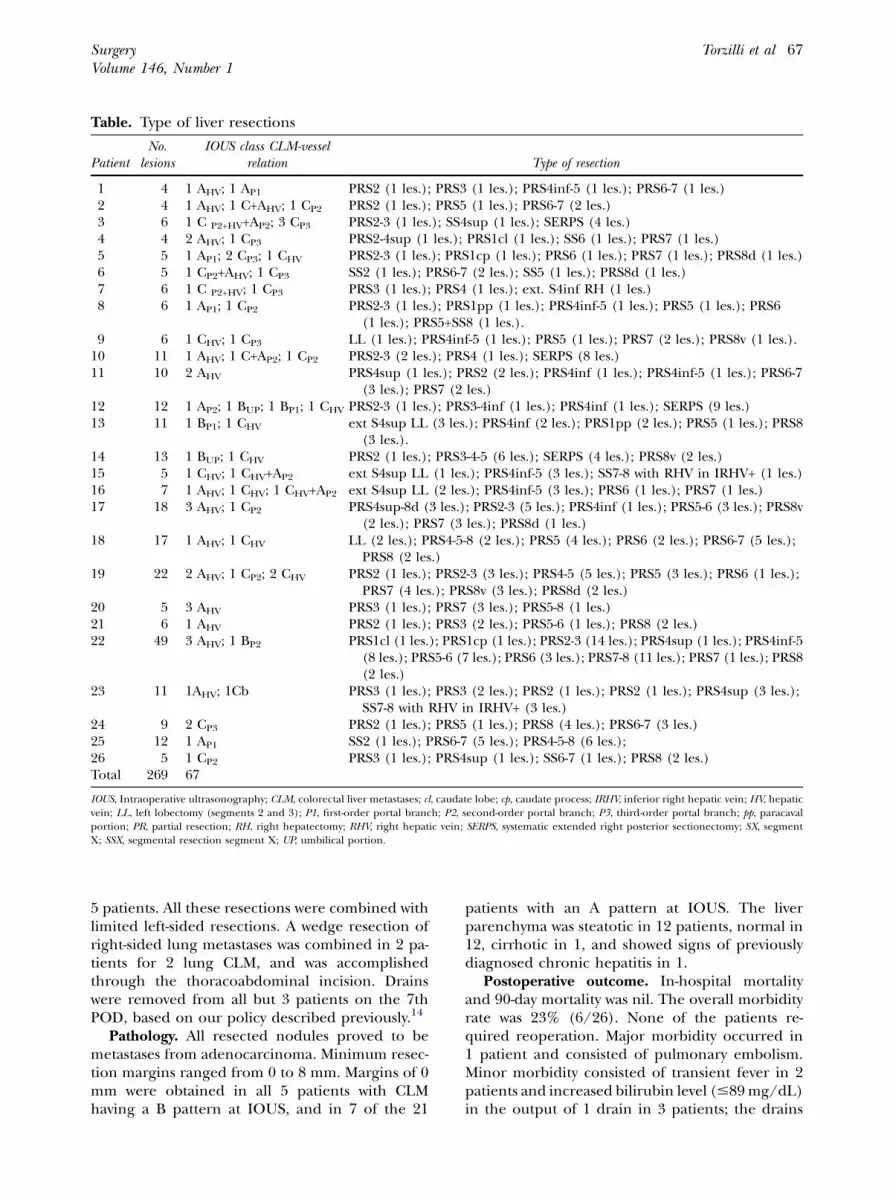
Table. Type of liver resections
PatientNo.
lesionsIOUS class CLM-vessel
relation Type of resection
1 4 1 AHV; 1 AP1 PRS2 (1 les.); PRS3 (1 les.); PRS4inf-5 (1 les.); PRS6-7 (1 les.)2 4 1 AHV; 1 C+AHV; 1 CP2 PRS2 (1 les.); PRS5 (1 les.); PRS6-7 (2 les.)3 6 1 C P2+HV+AP2; 3 CP3 PRS2-3 (1 les.); SS4sup (1 les.); SERPS (4 les.)4 4 2 AHV; 1 CP3 PRS2-4sup (1 les.); PRS1cl (1 les.); SS6 (1 les.); PRS7 (1 les.)5 5 1 AP1; 2 CP3; 1 CHV PRS2-3 (1 les.); PRS1cp (1 les.); PRS6 (1 les.); PRS7 (1 les.); PRS8d (1 les.)6 5 1 CP2+AHV; 1 CP3 SS2 (1 les.); PRS6-7 (2 les.); SS5 (1 les.); PRS8d (1 les.)7 6 1 C P2+HV; 1 CP3 PRS3 (1 les.); PRS4 (1 les.); ext. S4inf RH (1 les.)8 6 1 AP1; 1 CP2 PRS2-3 (1 les.); PRS1pp (1 les.); PRS4inf-5 (1 les.); PRS5 (1 les.); PRS6
(1 les.); PRS5+SS8 (1 les.).9 6 1 CHV; 1 CP3 LL (1 les.); PRS4inf-5 (1 les.); PRS5 (1 les.); PRS7 (2 les.); PRS8v (1 les.).
10 11 1 AHV; 1 C+AP2; 1 CP2 PRS2-3 (2 les.); PRS4 (1 les.); SERPS (8 les.)11 10 2 AHV PRS4sup (1 les.); PRS2 (2 les.); PRS4inf (1 les.); PRS4inf-5 (1 les.); PRS6-7
(3 les.); PRS7 (2 les.)12 12 1 AP2; 1 BUP; 1 BP1; 1 CHV PRS2-3 (1 les.); PRS3-4inf (1 les.); PRS4inf (1 les.); SERPS (9 les.)13 11 1 BP1; 1 CHV ext S4sup LL (3 les.); PRS4inf (2 les.); PRS1pp (2 les.); PRS5 (1 les.); PRS8
(3 les.).14 13 1 BUP; 1 CHV PRS2 (1 les.); PRS3-4-5 (6 les.); SERPS (4 les.); PRS8v (2 les.)15 5 1 CHV; 1 CHV+AP2 ext S4sup LL (1 les.); PRS4inf-5 (3 les.); SS7-8 with RHV in IRHV+ (1 les.)16 7 1 AHV; 1 CHV; 1 CHV+AP2 ext S4sup LL (2 les.); PRS4inf-5 (3 les.); PRS6 (1 les.); PRS7 (1 les.)17 18 3 AHV; 1 CP2 PRS4sup-8d (3 les.); PRS2-3 (5 les.); PRS4inf (1 les.); PRS5-6 (3 les.); PRS8v
(2 les.); PRS7 (3 les.); PRS8d (1 les.)18 17 1 AHV; 1 CHV LL (2 les.); PRS4-5-8 (2 les.); PRS5 (4 les.); PRS6 (2 les.); PRS6-7 (5 les.);
PRS8 (2 les.)19 22 2 AHV; 1 CP2; 2 CHV PRS2 (1 les.); PRS2-3 (3 les.); PRS4-5 (5 les.); PRS5 (3 les.); PRS6 (1 les.);
PRS7 (4 les.); PRS8v (3 les.); PRS8d (2 les.)20 5 3 AHV PRS3 (1 les.); PRS7 (3 les.); PRS5-8 (1 les.)21 6 1 AHV PRS2 (1 les.); PRS3 (2 les.); PRS5-6 (1 les.); PRS8 (2 les.)22 49 3 AHV; 1 BP2 PRS1cl (1 les.); PRS1cp (1 les.); PRS2-3 (14 les.); PRS4sup (1 les.); PRS4inf-5
(8 les.); PRS5-6 (7 les.); PRS6 (3 les.); PRS7-8 (11 les.); PRS7 (1 les.); PRS8(2 les.)
23 11 1AHV; 1Cb PRS3 (1 les.); PRS3 (2 les.); PRS2 (1 les.); PRS2 (1 les.); PRS4sup (3 les.);SS7-8 with RHV in IRHV+ (3 les.)
24 9 2 CP3 PRS2 (1 les.); PRS5 (1 les.); PRS8 (4 les.); PRS6-7 (3 les.)25 12 1 AP1 SS2 (1 les.); PRS6-7 (5 les.); PRS4-5-8 (6 les.);26 5 1 CP2 PRS3 (1 les.); PRS4sup (1 les.); SS6-7 (1 les.); PRS8 (2 les.)Total 269 67
IOUS, Intraoperative ultrasonography; CLM, colorectal liver metastases; cl, caudate lobe; cp, caudate process; IRHV, inferior right hepatic vein; HV, hepaticvein; LL, left lobectomy (segments 2 and 3); P1, first-order portal branch; P2, second-order portal branch; P3, third-order portal branch; pp, paracavalportion; PR, partial resection; RH, right hepatectomy; RHV, right hepatic vein; SERPS, systematic extended right posterior sectionectomy; SX, segmentX; SSX, segmental resection segment X; UP, umbilical portion.
5 patients. All these resections were combined withlimited left-sided resections. A wedge resection ofright-sided lung metastases was combined in 2 pa-tients for 2 lung CLM, and was accomplishedthrough the thoracoabdominal incision. Drainswere removed from all but 3 patients on the 7thPOD, based on our policy described previously.14
Pathology. All resected nodules proved to bemetastases from adenocarcinoma. Minimum resec-tion margins ranged from 0 to 8 mm. Margins of 0mm were obtained in all 5 patients with CLMhaving a B pattern at IOUS, and in 7 of the 21
patients with an A pattern at IOUS. The liverparenchyma was steatotic in 12 patients, normal in12, cirrhotic in 1, and showed signs of previouslydiagnosed chronic hepatitis in 1.
Postoperative outcome. In-hospital mortalityand 90-day mortality was nil. The overall morbidityrate was 23% (6/26). None of the patients re-quired reoperation. Major morbidity occurred in1 patient and consisted of pulmonary embolism.Minor morbidity consisted of transient fever in 2patients and increased bilirubin level (#89 mg/dL)in the output of 1 drain in 3 patients; the drains

SurgeryJuly 2009
68 Torzilli et al
were left in place until the bilirubin level in thedrain output decreased to <10 mg/dL. The drainwas then removed, and the patients were dischargedon the 13th, 16th, and 23rd POD, respectively.Serum levels of bilirubin, AST, and ALT returnedto normal usually by POD 5. The median hospitalstay was 9 days (range, 8--33).
Long-term outcome. After a median follow-upof 14 months (mean, 17; range, 6--54), 3 patientsdied from both liver and extrahepatic recurrence(12%), but we did not observe any local recurrenceat the resection margin. Of the 26 patients, 12(46%) are alive without disease, and 11 (42%) arealive with disease. Among the latter, 5 patients havehad both liver and extrahepatic recurrences: 5hepatic recurrences only and 1 extrahepatic recur-rence only. Liver recurrences occurred bilaterallyin 7 patients, in the side where more CLM wereremoved in 3, and in the opposite side in theremaining 3 patients.
Of those 10 patients operated for CLM who hadprogression during chemotherapy, 1 patient(10%) died; 5 (50%) are alive with disease; and 4(40%) are alive disease-free. The median follow-upfor this subgroup was 8 months. Re-resection wascarried out in 2 of the 5 patients who had only liverrecurrences; for the other 3 patients, percutaneousablation was carried out in 2, and the third patientrefused any other treatment. Of the 8 patients whohad hepatic relapses combined with extrahepaticdisease, liver resection was combined with totalabdominal hysterectomy and salpingo-oophorec-tomy in 1; percutaneous ablation was carried out in3; and systemic chemotherapy was administered inthe remaining 4. Systemic chemotherapy was alsogiven to the patient with extrahepatic relapsesonly.
DISCUSSION
Two-stage hepatectomy combining limited re-section and major hepatectomies with or withoutPVE is a multistep strategy for the treatment ofotherwise unresectable multiple bilobar CLM.However, 19--24% of patients do not completethe treatment strategy.2,3 Furthermore, major hep-atectomies are still associated with appreciablerates of mortality and major morbidity includingliver failure,2,8,16 although more recent series de-scribe greater levels of safety.17 PVE itself is associ-ated with morbidity; although reported at only2%,18 it still results in additional morbidity forthe treatment strategy as a whole. In addition,15% of patients do not benefit from PVE, mainlybecause of disease progression or insufficient
remnant liver hypertrophy,18 whereas others havea worse outcome because of a greater rate of newlesions in the remnant liver compared withpatients who did not undergo PVE.3,19-23
Using the experience gained from our estab-lished policy,4-6 we herein explored the possibilityof providing at least the same therapeutic resultsof the 2-stage approach with a 1-stage approach.Rather than making major resections safer, ouraim was to establish a surgical procedure thatmaximizes parenchymal-sparing and allows cura-tive resection in 1 stage. Indeed, following andexpanding on previous experiences,24 we haveshown how, with the aid of IOUS, it is possible tospare liver parenchyma in most circumstances, de-spite complex presentations.4-7 For this reason, itwas feasible to limit the use of a formal right hep-atectomy to just 1 of the 26 patients (4%) in ourseries, with no need for a two-stage approach.This policy, however, often resulted in resectionmargins of 0 mm.
It is noteworthy that, although we never achieveda minimal resection margin of 1 cm, there was norecurrence at the resection margin during a meanfollow-up similar to that of the 2 major reports on2-stage hepatectomies: 17 (median, 14) of our seriesversus 22 (median, not reported),2 and 19 (median,12),3 respectively. Moreover, contrary to the 2 majorreports on 2-stage hepatectomies,2,3 we never adop-ted intraoperative ablation therapies, which webelieve are suboptimal even when compared with0-mm margin resection.25
In contrast, several studies have demonstratedthat a limited tumor-free margin is not a contra-indication for resection by showing that the risk ofrecurrence at the resection margin does not ap-pear to be greater.26,27 Based on precise crite-ria,4,5,7 IOUS guidance helps maximize thepossibility of getting closer to the tumor. Indeed,other authors in the 1990s showed that 16% to18% of patients with hepatocellular carcinomawho underwent liver resection without IOUSguidance had positive margins, whereas none ofthe patients who underwent liver resectionunder the guidance of IOUS had residualtumor.28,29
Performing more conservative hepatic resec-tions allows for repeat hepatectomies should anew CLM be detected.1 Indeed, in cases of recur-rence, procedures that preserve major vascularstructures allow more surgical options than a ma-jor hepatectomy. As a consequence, re-resectionwas possible in 2 of the 5 patients with hepaticrelapses only in our series, and in 1 patient withhepatic recurrences and resectable extrahepatic

SurgeryVolume 146, Number 1
Torzilli et al 69
disease. Furthermore, all 5 patients with hepaticrelapses only, except the 1 patient who refusedboth reoperation and percutaneous ablation ther-apy, were able to receive local treatment withradical intent. In this sense, the multimodalapproach has a fundamental role that should bediscussed with every patient with multiple CLMwhen obtaining informed consent for the firstoperative treatment. Patients should agree to theirwillingness for re-treatment to not invalidate thisapproach.
Sparing a substantial amount of the liver pa-renchyma by our aggressive parenchymal-sparingtechnique does not seem to expose patients to agreater risk of recurrence. We noted that 54% ofpatients developed disease during the follow-up(50% involving the liver) in our study comparedto 64% (48% involving the liver) reported byJaeck et al3 and 69% (61% involving the liver)reported by Adam et al.2 Furthermore, in thespared hemiliver with the greatest number ofCLM to be removed, there did not appear to bea greater rate of liver recurrence, and recurrenceswere bilateral.
The 1-stage procedure may also be safer thanthe 2-stage approach with or without PVE; therewas no mortality or increased incidence of majormorbidity.2,3,19-23 The operative technique we pro-posed herein is not simple because it involves mul-tiple combined procedures that account for thelong durations of the operative procedure andthe long clamping times. Such long operationshave often been associated with those series featur-ing the best results in terms of safety,1,30 even incirrhotic patients.6,31 A long and careful proceduremay be required to achieve optimal hemostasis andthe prevention of biliary leak.4,5,7 Intermittent he-patic inflow clamping has been shown in several se-ries to be safe and effective compared to noclamping and to continuous clamping with orwithout preconditioning.32-34 We were able to ob-tain good results with up to 348 minutes of clamp-ing time similar to that of 322 minutes reported bySakamoto et al.35 Although these intermittentclamping times are quite long, serum levels of bil-irubin, AST, and ALT returned to normal usuallyby POD 5. Furthermore, the inflow occlusion,which minimized blood transfusion rates (15% inthis series), has beneficial effects on both short-and long-term outcomes.36,37
This prospective cohort of patients was com-pared with historic data reported by other centers.The resectability rate of our series from outpatientclinic to exploration is rather high (>60%). Ourseries includes those patients with unfavorable
conditions compared with those considered forthe 2-stage procedure.2,3 We included patients witha minimum of 4 bilobar CLM, patients with CLMhaving relations with major intrahepatic vascularstructures, and patients with disease progressionafter chemotherapy. Furthermore, the 3 patientssubmitted to exploratory laparotomy for diffusecarcinomatosis also would not have been consid-ered suitable for the 2-stage operation. All theseconsiderations should help in the concerns aboutmajor selection bias and, furthermore, show thatthis approach is not just an alternative to the2-stage policy, but may allow the opportunity to oper-ate on patients otherwise considered unresectableby the conventional approaches.
A possible criticism of our approach is thatthe procedure is based on intraoperative findingsand, for this reason, cannot be applied systemati-cally. Our approach, however, does not ignore thepreoperative findings. In fact, the preoperativeworkup was crucial in allowing us to expect thefeasibility of a 1-stage approach by means ofaggressive parenchymal sparing.4-7 By using the cri-teria we have outlined, many lesions that wouldappear to require a major hepatic resection byconventional criteria can actually be resected with-out a major hepatic resection as shown in the hereinpresented series. With our approach, a completeresection using a 1-stage, parenchymal-sparing ap-proach may even lead to a greater overall resectionrate than a 2-stage approach, although we acknowl-edge that we have not included a comparable con-trol group undergoing a 2-stage approach.
The intraoperative detection of 112 new lesionsby IOUS and CEIOUS, representing 42% of all thelesions removed, is worthy of discussion. MultipleCLM lesions are associated generally with a greaterrate of missed lesions at preoperative imaging.38,39
PET, however, seems inadequate for accurate intra-hepatic staging,39 especially for those patients un-dergoing operation after chemotherapy,40 whorepresented 66% of our series. These consider-ations highlight the central and crucial role playedby IOUS and CEIOUS in treating these patients.
There are limitations of IOUS and CEIOUS,including the cost of state-of-the-art ultrasoundmachines and the need for hepatic surgeons to bewell trained in their use. However, a wide range ofprices for suitable ultrasound machine exists, andcourses are available to train surgeons in the use ofultrasound in surgical practice. The American Col-lege of Surgeons has recognized recently the needfor specifically trained surgeons in the United Statesand, similarly, we have started a School for SurgicalUltrasonography in Europe.

SurgeryJuly 2009
70 Torzilli et al
In conclusion, we have shown that IOUS-guidedresection based on strict criteria allows a radicalbut parenchymal-sparing, 1-stage hepatectomy/metastasectomy in patients with multiple bilobarCLM. This strategy limits the need for 2-stagehepatectomy and, in so doing, may rise abovemany of the limitations and consequences of a2-stage approach.
The authors thank Ms Rosalind Roberts for hereditorial assistance during manuscript preparation.
REFERENCES
1. Minagawa M, Makuuchi M, Torzilli G, Takayama T, KawasakiS, Kosuge T, et al. Extension of the frontiers of surgical in-dications in the treatment of liver metastases from colorec-tal cancer: long-term results of our experience. Ann Surg2000;231:487-99.
2. Adam R, Laurent A, Azoulay D, Castaing D, Bismuth H.Two-stage hepatectomy: a planned strategy to treat irresect-able liver tumors. Ann Surg 2000;232:777-85.
3. Jaeck D, Oussoultzoglou E, Rosso E, Greget M, Weber JC,Bachellier P. A two-stage hepatectomy procedure combinedwith portal vein embolization to achieve curative resectionfor initially unresectable multiple and bilobar colorectalliver metastases. Ann Surg 2004;240:1037-49.
4. Torzilli G, Montorsi M, Donadon M, Palmisano A, Del Fab-bro D, Gambetti A, et al. ‘‘Radical but conservative’’ is themain goal for ultrasonography-guided liver resection: pro-spective validation of this approach. J Am Coll Surg 2005;201:517-28.
5. Torzilli G, Montorsi M, Del Fabbro D, Palmisano A, Dona-don M, Makuuchi M. Ultrasonographically-guided surgicalapproach to liver tumours involving the hepatic veins closeto the caval confluence. Br J Surg 2006;93:1238-46.
6. Torzilli G, Donadon N, Marconi M, Palmisano A, Del Fab-bro D, Spinelli A, et al. Hepatectomy for stage B and stageC hepatocellular carcinoma in the Barcelona Clinic LiverCancer classification: results of a prospective analysis.Arch Surg 2008;143:1082-90.
7. Torzilli G, Donadon M, Marconi M, Botea F, Palmisano A,Del Fabbro D, et al. Systematic extended right posterior sec-tionectomy: a safe and effective alternative to right hepatec-tomy. Ann Surg 2008;247:603-11.
8. The terminology committee of the IHPBA. The Brisbane2000 terminology of hepatic anatomy and resections. HPB2002;2:333-9.
9. Vauthey JN, Pawlik TM, Abdalla EK, Arens JF, Nemr RA, Wei SH,et al. Is extended hepatectomy for hepatobiliary malignancyjustified? Ann Surg 2004;239:722-39.
10. Torzilli G, Palmisano A, Del Fabbro D, Marconi M, Dona-don M, Spinelli A, et al. Contrast-enhanced intraoperativeultrasonography during surgery for hepatocellular carci-noma in liver cirrhosis: is it useful or useless? A prospectivecohort study of our experience. Ann Surg Oncol 2007;14:1347-55.
11. Torzilli G, Del Fabbro D, Palmisano A, Donadon M, Bianchi P,Roncalli M, et al. Contrast-enhanced intraoperative ultra-sonography during hepatectomies for colorectal cancerliver metastases. J Gastrointest Surg 2005;9:1148-53.
12. Pringle JH. Notes on the arrest of hepatic hemorrhage dueto trauma. Ann Surg 1908;48:541-9.
13. Torzilli G, Takayama T, Hui AM, Kubota K, Harihara Y, Ma-kuuchi M. A new technical aspect of ultrasound-guided liversurgery. Am J Surg 1999;178:341-3.
14. Ijichi M, Takayama T, Toyoda H, Sano K, Kubota KMakuuchi M. Randomized trial of the usefulness of a bileleakage test during hepatic resection. Arch Surg 2000;135:1395-400.
15. Torzilli G, Olivari N, Del Fabbro D, Gambetti A, Leoni P,Gendarini A, Makuuchi M. Bilirubin level fluctuation indrain discharge after hepatectomies justifies long-termdrain maintenance. Hepatogastroenterology 2005;52:1206-10.
16. Hemming AW, Reed AI, Howard RJ, Fujita S, Hochwald SN,Caridi JG, et al. Preoperative portal vein embolization forextended hepatectomy. Ann Surg 2003;237:686-93.
17. Kianmanesh R, Farges O, Abdalla EK, Sauvanet A, Rusz-niewski P, Belghiti J. Right portal vein ligation: a newplanned two step all-surgical approach for complete resec-tion of primary gastrointestinal tumors with multiple bilat-eral metastases. J Am Coll Surg 2003;197:164-70.
18. Abulkhir A, Limongelli P, Healey AJ, et al. Preoperative por-tal vein embolization for major liver resection: a meta-analysis. Ann Surg 2008;247:49-57.
19. Aoki T, Imamura H, Hasegawa K, Matsukura A, Sano K, Su-gawara Y, et al. Sequential preoperative arterial and portalvenous embolizations in patients with hepatocellular carci-noma. Arch Surg 2004;139:766-74.
20. Jaeck D, Oussoultzoglou E, Rosso E, Greget M, Weber JC,Bachellier P. A two-stage hepatectomy procedure combinedwith portal vein embolization to achieve curative resectionfor initially unresectable multiple and bilobar colorectalliver metastases. Ann Surg 2004;240:1037-49.
21. Di Stefano DR, de Baere T, Denys A, et al. Preoperative per-cutaneous portal vein embolization: evaluation of adverseevents in 188 patients. Radiology 2005;234:625-30.
22. Azoulay D, Castaing D, Smail A, Adam R, Cailliez V, LaurentA, et al. Resection of nonresectable liver metastases from co-lorectal cancer after percutaneous portal vein embolization.Ann Surg 2000;231:480-6.
23. Elias D, Ouellet JF, De Baere T, Lasser P, Roche A. Preoper-ative selective portal vein embolization before hepatectomyfor liver metastases: long-term results and impact on sur-vival. Surgery 2002;131:294-9.
24. Makuuchi M, Hasegawa H, Yamazaki S, Takayasu K. Fournew hepatectomy procedures for resection of the right he-patic vein and preservation of the inferior right hepaticvein. Surg Gynecol Obstet 1987;164:68-72.
25. Abdalla EK, Vauthey JN, Ellis LM, Ellis V, Pollock R, BroglioKR, et al. Recurrence and outcomes following hepatic resec-tion, radiofrequency ablation, and combined resection/ab-lation for colorectal liver metastases. Ann Surg 2004;239:818-25.
26. Pawlik TM, Scoggins CR, Zorzi D, Abdalla EK, Andres A,Eng C, et al. Effect of surgical margin status on survivaland site of recurrence after hepatic resection for colorectalmetastases. Ann Surg 2005;241:715-22.
27. Kokudo N, Miki Y, Sugai S, Yanagisawa A, Kato Y, SakamotoY, et al. Genetic and histological assessment of surgical mar-gins in resected liver metastases from colorectal carcinoma:minimum surgical margins for successful resection. ArchSurg 2002;137:833-40.
28. Lai EC, Ng IO, Ng MM, Lok AS, Tam PC, Fan ST, et al.Long-term results of resection for large hepatocellular car-cinoma: a multivariate analysis of clinicopathological fea-tures. Hepatology 1990;11:815-8.
SurgeryVolume 146, Number 1
Torzilli et al 71
29. Lau WY, Leung KL, Lee TW, et al. Ultrasonography during liverresection for hepatocellular carcinoma. Br J Surg 1993;80:493-4.
30. Imamura H, Seyama Y, Kokudo N, Maema A, Sugawara Y,Sano K, et al. One thousand fifty-six hepatectomies withoutmortality in 8 years. Arch Surg 2003;138:1198-206.
31. Torzilli G, Makuuchi M, Inoue K, et al. No-mortality liver re-section for hepatocellular carcinoma in cirrhotic and non-cirrhotic patients: is there a way? A prospective analysis ofour approach. Arch Surg 1999;134:984-92.
32. Man K, Fan ST, Ng IO, Lo CM, Liu CL, Wong J. Prospectiveevaluation of Pringle maneuver in hepatectomy for liver tu-mors by a randomized study. Ann Surg 1997;226:704-13.
33. Belghiti J, Noun R, Malafosse R, Jagot P, et al. Continuousversus intermittent portal triad clamping for liver resection:a controlled study. Ann Surg 1999;229:369-75.
34. Petrowsky H, McCormack L, Trujillo M, et al. A prospective,randomized, controlled trial comparing intermittent portaltriad clamping versus ischemic preconditioning with con-tinuous clamping for major liver resection. Ann Surg2006;244:921-30.
35. Sakamoto Y, Makuuchi M, Takayama T, Minagawa M, Kita Y.Pringle’s maneuver lasting 322 min. Hepatogastroenterol-ogy 1999;46:457-8.
36. Torzilli G, Gambetti A, Del Fabbro D, Leoni P, Donadon M,Montorsi M, et al. Techniques for hepatectomies withoutblood transfusion focusing on interpretation of postopera-tive anemia. Arch Surg 2004;139:1061-5.
37. Yamamoto J, Kosuge T, Takayama T, et al. Perioperativeblood transfusion promotes recurrence of hepatocellularcarcinoma after hepatectomy. Surgery 1994;115:303-9.
38. Wang X, Hershman DL, Abrams JA, Feingold D, Grann VR,Jacobson JS, et al. Predictors of survival after hepatic resec-tion among patients with colorectal liver metastasis. Br JCancer 2007;97:1606-12.
39. Torzilli G, Botea F, Procopio F, et al. Use of contrast-en-hanced intraoperative ultrasonography during liver surgeryfor colorectal cancer liver metastases -- its impact on opera-tive outcome. Analysis of a prospective cohort study. Eur JCancer 2008;6:16-23.
40. Lubezky N, Metser U, Geva R, et al. The role and limitationsof 18-fluoro-2-deoxy-D-glucose positron emission tomogra-phy (FDG-PET) scan and computerized tomography (CT)in restaging patients with hepatic colorectal metastases fol-lowing neoadjuvant chemotherapy: comparison with opera-tive and pathological findings. J Gastrointest Surg 2007;11:472-8.
Copyright © 2022 FDOKUMEN