On the Objectivity of the Scoring of Harvard Group Scale of Hypnotic Susceptibility
23
This article was downloaded by: [University of California, San Diego] On: 13 November 2012, At: 03:38 Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK International Journal of Clinical and Experimental Hypnosis Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/nhyp20 On the Objectivity of the Scoring of Harvard Group Scale of Hypnotic Susceptibility Katalin Varga a , Lajos Farkas a & László Mérő a a Eötvös Loránd University, Budapest, Hungary Version of record first published: 23 Aug 2012. To cite this article: Katalin Varga, Lajos Farkas & László Mérő (2012): On the Objectivity of the Scoring of Harvard Group Scale of Hypnotic Susceptibility, International Journal of Clinical and Experimental Hypnosis, 60:4, 458-479 To link to this article: http://dx.doi.org/10.1080/00207144.2012.675298 PLEASE SCROLL DOWN FOR ARTICLE Full terms and conditions of use: http://www.tandfonline.com/page/terms-and- conditions This article may be used for research, teaching, and private study purposes. Any substantial or systematic reproduction, redistribution, reselling, loan, sub- licensing, systematic supply, or distribution in any form to anyone is expressly forbidden. The publisher does not give any warranty express or implied or make any representation that the contents will be complete or accurate or up to date. The accuracy of any instructions, formulae, and drug doses should be independently verified with primary sources. The publisher shall not be liable for any loss, actions, claims, proceedings, demand, or costs or damages whatsoever or howsoever caused arising directly or indirectly in connection with or arising out of the use of this material.
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of On the Objectivity of the Scoring of Harvard Group Scale of Hypnotic Susceptibility

This article was downloaded by: [University of California, San Diego]On: 13 November 2012, At: 03:38Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
International Journal of Clinicaland Experimental HypnosisPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/nhyp20
On the Objectivity of the Scoringof Harvard Group Scale ofHypnotic SusceptibilityKatalin Varga a , Lajos Farkas a & László Mérő aa Eötvös Loránd University, Budapest, HungaryVersion of record first published: 23 Aug 2012.
To cite this article: Katalin Varga, Lajos Farkas & László Mérő (2012): On the Objectivityof the Scoring of Harvard Group Scale of Hypnotic Susceptibility, International Journal ofClinical and Experimental Hypnosis, 60:4, 458-479
To link to this article: http://dx.doi.org/10.1080/00207144.2012.675298
PLEASE SCROLL DOWN FOR ARTICLE
Full terms and conditions of use: http://www.tandfonline.com/page/terms-and-conditions
This article may be used for research, teaching, and private study purposes.Any substantial or systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyone is expresslyforbidden.
The publisher does not give any warranty express or implied or make anyrepresentation that the contents will be complete or accurate or up to date. Theaccuracy of any instructions, formulae, and drug doses should be independentlyverified with primary sources. The publisher shall not be liable for any loss,actions, claims, proceedings, demand, or costs or damages whatsoever orhowsoever caused arising directly or indirectly in connection with or arising outof the use of this material.

Intl. Journal of Clinical and Experimental Hypnosis, 60(4): 458–479, 2012Copyright © International Journal of Clinical and Experimental HypnosisISSN: 0020-7144 print / 1744-5183 onlineDOI: 10.1080/00207144.2012.675298
ON THE OBJECTIVITY OF THE SCORINGOF HARVARD GROUP SCALE OF
HYPNOTIC SUSCEPTIBILITY1
Katalin Varga, Lajos Farkas, and László Méro2
Eötvös Loránd University, Budapest, Hungary
Abstract: The authors analyzed the Harvard Group Scale of HypnoticSusceptibility, Form A, scores of 1,887 subjects. In addition to theusual self-scoring, trained observers also scored the behavioral man-ifestations of the subjects according to the same standardized criteriaduring the sessions. Self- and observer-scoring proved to be internallyconsistent and highly correlated (r = .832). Item-by-item analysis,however, yielded notable differences. Subjects and observers scoreditems differently in about 20% of the cases; only 3 items showed nosystematic bias toward pass or fail. Many subjects’ hypnotizabilitylevel would be classified differently according to observer cate-gorization (Cohen’s Kappa = .563). We suggest reconsidering the“objectivity” of self-scoring.
Hypnotizability and Its Measurement
Since it became obvious that people react differently to hypnosis, thenecessity to apply measures that reflect the level of hypnotic respon-siveness of individuals has been a central problem in modern hypnosisresearch and clinical practice (Hilgard, 1982). The general method ofmeasuring hypnotic responsiveness today is to apply a standardizedprotocol (induction and test suggestions) and to observe the reactionsof subjects along strict criteria. It is a common element of the standard-ized hypnotizability scales is that behavioral reactions of the personsare observed and scored. The scoring is based on the judgment whetheror not these overt responses reach certain criteria, for example, amountand direction of movement within a time limit.
Manuscript submitted September 26, 2011; final revision accepted September 29, 2011.1This work was supported by the Hungarian Scientific Research Fund (OTKA
T34454 to Éva I. Bányai). The authors are greatful to Anna C. Gosi-Greguss and ZackBoukydis for their valuable remarks on a previous version of the article.
2Address correspondence to Katalin Varga, Institute of Psychology, Eötvös LorándUniversity, Izabella utca 46. Pf. 755, Budapest, H-1384, Hungary. E-mail: [email protected]
458
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a, S
an D
iego
] at
03:
38 1
3 N
ovem
ber
2012

OBJECTIVITY OF SCORING THE HGSHS 459
Among the instruments of hypnotic responsiveness, the HarvardGroup Scale of Hypnotic Susceptibility, Form A (HGSHS:A), developedby Shor and Orne (1962, 1963), is a widely applied group methodfor a quick and comfortable way for selecting subjects for furtherexperiments.
The HGSHS:A was constructed on the basis of the Stanford scales(Weitzenhoffer & Hilgard, 1959). Some modifications were introduceddue to the group administration of the scale: Some items were changed(e.g., instead of “postural sway,” “head falling” was introduced), butthe basic logic of scoring remained the same. There is another modifi-cation compared to the individual scales that is more important fromthe viewpoint of the present analysis: Self-scoring became the standardway of scoring the responses. It is not the hypnotist (or an observer)who scores the reaction of the subjects, but rather, it is the subjectsthemselves who evaluate whether or not they met the given criteriaat each test-suggestion in a “Response booklet” immediately followingthe hypnosis session. For example, in the case of the “Right arm immo-bilization” suggestion, the booklet says: “You were next told how heavyyour right hand and arm felt and then told to try to lift your hand up.Would you estimate that an onlooker would have observed that youdid not lift your hand and arm up at least 1 inch (before you were toldto stop trying)? Circle one: A. I did not lift my hand and arm at least1 inch by then. B. I did lift my hand and arm 1 inch or more by then”(Shor & Orne, 1962, p. 5).
Bentler and Hilgard (1963) investigated, whether self-scoring yieldsa quantitative score of susceptibility similar to a score that could beobtained in an individual session scored by the hypnotist. In order tocheck the accuracy of self-scoring, HGSHS:A performance was scoredboth by the subjects and an observer (the hypnotist-observer or anassistant) in sessions of small groups of 4–6 subjects for a total sampleof 45 university students. A correlation of r = .83 showed that self-scores predicted the observers’ scores accurately. Bentler and Roberts(1963) replicated the same trend in larger groups (consisting of 52 and39 subjects).
Apparently, these studies are the only empirical bases of consider-ing self-scoring as a reliable and valid way of measuring the hypnoticresponsiveness of an individual; all later studies rely on the high pos-itive correlation between the self-score and observer-score reportedby Bentler and Hilgard (1963) and Bentler and Roberts (1963), andwhat the Hungarian version of the scale also showed (Greguss, Bányai,Mészáros, Csókay, & Gerber, 1975).
In spite of the fact that some later papers report lower correla-tions (r = .60 to .70) between self-scores and observer-scores (Hartman,1965; Levitt, Aronoff, & Morgan, 1974; O’Connell, 1964), the sci-entific community seems to accept that self-scoring is a valid ver-sion of observer-scoring. A recent comprehensive analysis of the
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a, S
an D
iego
] at
03:
38 1
3 N
ovem
ber
2012

460 KATALIN VARGA ET AL.
measurement of hypnotizability does not even mention how self-scoring of the HGSHS:A became the standard method (Laurence,Beaulieu-Prévost, & du Chéné, 2008), and many reports of nationalnorms of the HGSHS:A takes it as well-based evidence that self-scoringreflects overt-behavioral responding reliably (not even referring to the1963 study of Bentler and Hilgard; see, e.g., Bergman, Trenter, & Kallio,2003; Bongartz, 1985; Coe, 1964; David, Montgomery, & Holdevici,2003; De Pascalis, Russo, & Marucci, 2000; Kallio & Ihamuotila, 1999;Lichtemberg, 2008; Pyun & Kim, 2009; Siuta, 2010).
In the study of Younger, Kemmerer, Winkel, and Nash (2005), asopposed to the original situation—where the participants of the hyp-nosis session were aware of being observed and scored—confederatesmade surreptitious observations of subjects’ responding. In this“secret” scoring system, only moderate agreement was found betweenself-scoring and observer-scoring (see details later).
Based on the early studies, the standard (self) scoring of theHGSHS:A is called and considered to be an instrument that yields objec-tive data about the responsiveness of the individual, as opposed to thesubjective indices (e.g., hypnotic depth, involuntariness score, and so on,see, e.g., Bongartz, 1985; Gwynn, Spanos, Gabora, & Jarrett, 1988; Jupp,Collins, & McCabe, 1985; Kirsch, Council, & Wickless, 1990; Laurence &Perry, 1982, etc.).
It is surprising that even those who stress the importance of subjec-tive effects of hypnosis fail to recognize that self-score is not in fact anobjective measure. For example, Gwynn et al. (1988), as opposed to theconventional “objective” score on the HGSHS:A, introduce a subjectivedimension by asking the subjects to rate the experiences connected tothe test suggestions and calculate an involuntary and a compliance scoreas well. In their report, Gwynn et al. interpret the HGSHS:A self-score(referred to by them as an objective score) as a real objective index ofperformance, in contrast with the applied (really) subjective measures.Kirsch and his colleagues (1990) suggest to supplement the behavioralscoring on the HGSHS:A with subjective scoring: Where “behavioral”refers to the self-scoring of the subjects along with objective crite-ria, and subjective scoring is the based on new scale, developed bythese authors to measure the subjective experiences associated with thetest suggestions on the HGSHS:A (This new scale—called “SubjectiveExperience Scale for HGSHS:A”—words each item so as to capture theintended nature of the suggested effect, instead of facing the subjectswith the overt criteria, as is the case in the standard response booklet).
It is a general feature of hypnosis research—not a specific char-acteristic of the HGSHS:A—to consider the self-scoring of thesubjects using overt behavioral pass/fail criteria to be an objectivemeasure of hypnotizability. This is the case in the Carleton UniversityResponsiveness to Suggestion Scale (Spanos et al., 1983) where theso-called objective score is gathered in the same way as in the case of
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a, S
an D
iego
] at
03:
38 1
3 N
ovem
ber
2012

OBJECTIVITY OF SCORING THE HGSHS 461
the HGSHS:A, and to this “objective” score a (truly) subjective score isadded, leading to a combined objective-involuntary score, using con-junctive criterion (only when an enactment is reported as involuntaryis scored as a pass). In his theoretical paper on the hypnosis scales,Balthazard (1993) considers the combined scoring (behavioral scorecorrected by subjective report) one of the directions of future develop-ments of the hypnosis scales. In his arguments, the “behavioral” scoreis considered to be an objective measure of the effect of the suggestions,there is no word about the actual subjectivity of this index.
There were several critics regarding the standardized scales ofhypnotizability in the past decades, including the HGSHS:A (see, e.g.,lack of sensitivity for involuntariness, Farthing, Brown, & Venturino,1983; Bowers, Laurence, & Hart, 1988; for nonverbal communica-tion, Sacerdote, 1982; for fluctuating hypnotic depth, Tart, 1970,1978/1979; Perry & Laurence, 1980; for individual needs of subjects,Van Der Does, Van Dyck, Spinhoven, & Kloosman, 1989, and so on).Regarding scoring, mainly the scoring of the amnesia item is criticized(Kihlstrom & Register, 1984), or the differentiation between nonhyp-notic and hypnotic suggestibility (Kirsch, 1997; Kirsch & Braffman,2001; Weitzenhoffer, 1980). Regarding the HGSHS:A as a screeninginstrument, caution arose as it does not correlate well with the more dif-ficult scales (Barnes, Lynn, & Pekala, 2009; Laurence et al., 2008). Noneof the critics of the standardized scales address the issue of this false“supposed-objectivity” of the standardized group scales.
The analysis of the scoring procedure and some empirical resultsbring up the issue that the subjects in the standardized protocol of theHGSHS:A are forced to rate their own performance on a scale that isbased on externally observable, overt, behavioral criteria, which is thedimension that is not in the subjects’ immediate hypnotic experience.
The aim of the present article is to have a closer look on the relation-ship between observer-scoring and self-scoring of the HGSHS:A.
First of all, on the basis of the large (N = 1,887) sample of theHypnosis Research Laboratory at Eötvös Loránd University, whereboth the self-scores and observer-scores were available, we wanted toreplicate the early correlational study by Bentler and Hilgard (1963) andBentler and Roberts (1963).
Second, our database is appropriate to test the correspondence ofself-scoring and observer-scoring on an item-by-item basis and to runa statistical analysis on this correspondence.
Method
The documentation of the HGSHS:A sessions of 35 years (1975–2010)of the Hypnosis Research Laboratory at Eötvös Loránd Universityhas been analyzed. Volunteers were recruited at the Department of
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a, S
an D
iego
] at
03:
38 1
3 N
ovem
ber
2012

462 KATALIN VARGA ET AL.
Comparative Physiology (until 1986) and at the Institute of Psychology(from 1987) at Eötvös Loránd University. Subjects were screened by theHungarian version (Greguss et al., 1975) of the Harvard Group Scale ofHypnotic Susceptibility, Form A (Shor & Orne, 1962).
In addition to the usual self-scoring in the response booklets by thesubjects, trained observers also scored the behavioral manifestationsof the subjects according to the same standardized criteria during thesessions. These scores will be referred to as self-scores and observer-scores, respectively.
It must be remarked that the overall group of “trained observers”across the past more than three decades is rather heterogeneous. Whileevery observer—mostly upper class psychology majors, doing somehypnosis research themselves—was similarly trained for the crite-ria and possible response variations by the senior researchers of theHypnosis Research Laboratory either in small groups as an optionalpart of their studies or individually; some of them participated onlyin a few sessions while others gained great practice in many sessions.The number of subjects to be observed simultaneously also varied from1 to 10–12. Furthermore, in cases of uncertainty, the observers may haveintractably modified their evaluation in the direction of the self-score ofthe observed subjects.
Since the amnesia item of the HGSHS:A is scored on the basis ofa number of elements listed by the subjects in the response bookletbefore the lifting of the posthypnotic amnesia suggestion (accordingto the protocol described by Shor & Orne, 1962), self-scores and theobserver-scores were always the same in the case of this item.
ParticipantsOver 25 years, altogether 2,080 volunteer subjects participated in
hypnosis sessions in groups of 2 to 80 subjects. Out of the 2,080 sub-jects, 1,887 (793 males, 1,094 females, mean age: 24.5, SD = 6.58) hadboth observer-scores and self-scores. The data of these subjects formthe basis of this analysis.
Results
Due to the fact that the scoring of the Amnesia item (pass if subjectrecalls only 0 to 3 items from Suggestion Nos. 3 to 11) is always thesame in the case of subjects and observers, we calculated the resultsboth with and without this item. The scale with the Amnesia item willbe referred to as HGSHS:A-12, the one without this item will be calledHGSHS:A-11.
Both self-scoring and observer-scoring proved to be internally con-sistent: Cronbach’s Alphas for self-scoring were .671 (in the case of
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a, S
an D
iego
] at
03:
38 1
3 N
ovem
ber
2012

OBJECTIVITY OF SCORING THE HGSHS 463
HGSHS:A-12) and .674 (in the case of HGSHS:A-11), and those forobserver-scoring were .732 (in the case of HGSHS:A-12) and .734 (inthe case of HGSHS:A-11).
The comparison of the mean scores based on observer-scoring andself-scoring shows that due to the large sample size (N = 1,887),the difference between the means is statistically significant, both incases of the total scale (HGSHS:A-12: mean observer-score = 6.16,SD = 2.807, mean self-score = 5.92, SD = 2.687), t(1,886) = 6.705,p < .001, and the scale without the amnesia item (HGSHS:A-11: meanobserver-score = 5.73, SD = 2.659, mean self-score = 5.49, SD= 2.538),t(1,886) = 6.736, p < .001. The absolute difference between the means ofthe observer-scores and self-scores, however, is practically negligible asit is only 0.24.
The correlation between self-scores and observer-scores in the totalsample of 1,887 subjects is high and statistically significant (r = .832,p < .001, for the HGSHS:A-12, and r = .812, p < .001, for the HGSHS:A-11). These correlation values are very similar to those reported byBentler and Hilgard (1962) four decades ago.
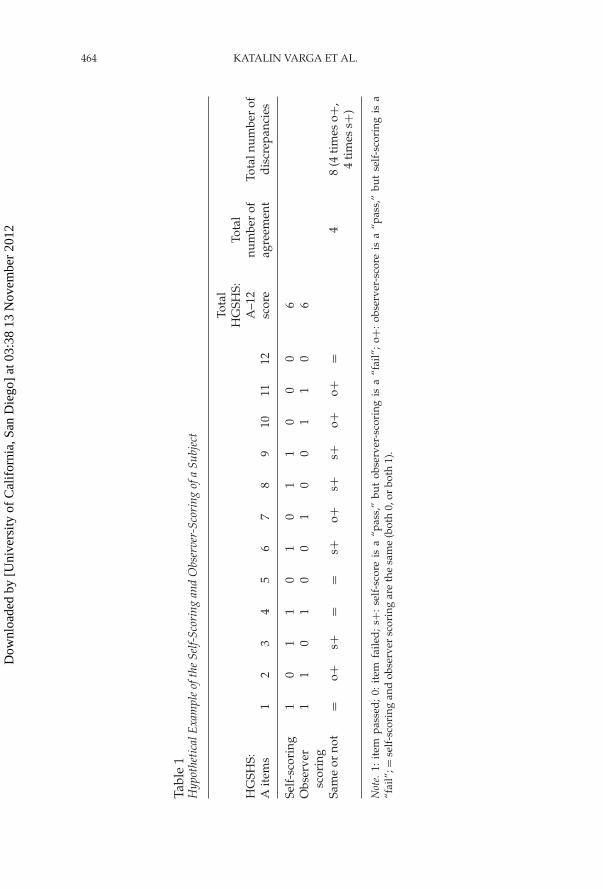
The correlations of the total scores, however, do not reflect if theindividual items were scored similarly or differently by the observerand the subject, although there can be notable differences between theirscoring. The observer and the subject can reach the same (or nearly thesame) total score (say: 6), but the actual items scored as pass can be dif-ferent in the two cases. A hypothetical example is presented in Table 1.In this case, the total HGSHS:A scores of self-scoring and observer-scoring are exactly the same (yielding a high correlation between thetotal scores), but the actual items are scored the same only in 6 of the12 items. In the remaining six items, either the self-score is a “pass” andthe observer-score is a “fail” (referred to as s+ from now on), or theother way around: self-score is a “fail,” and observer-score is a “pass”(referred to as o+ from now on).
The item-by-item analysis of our data revealed important discrepan-cies. Table 2 represents the percentage and total number of discrepantitems in our sample.
Table 3 shows the interrater-agreement measures (Cohen’s Kappavalues), the Corrected Item-Total Correlations, and Cronbach’s alphavalues for the self-scores and the observer-scores. It can be seen thatthe interrater agreement values are fluctuating, ranging from .333 upto .712. On the basis of the Corrected Item-Total Correlation we can seethat items Nos. 3 (Hand Lowering) and 11 (Posthypnotic Suggestion)are the weakest items of the test, their exclusion would dramaticallyimprove the internal consistency of the HGSHS:A.
Table 4 presents the scoring results of the HGSHS:A items. The num-ber of cases where self-scoring and observer-scoring were the same, justlike the frequency of the two types of discrepancies, is also presented.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a, S
an D
iego
] at
03:
38 1
3 N
ovem
ber
2012
464 KATALIN VARGA ET AL.
Tabl
e1
Hyp
othe
tica
lExa
mpl
eof
the
Self-
Scor
ing
and
Obs
erve
r-Sc
orin
gof
aSu
bjec
t
HG
SHS:
Ait
ems
12
34
56
78
910
1112
Tota
lH
GSH
S:A
–12
scor
e
Tota
lnu
mbe
rof
agre
emen
tTo
taln
umbe
rof
dis
crep
anci
es
Self
-sco
ring
10
11
01
01
10
00
6O
bser
ver
scor
ing
11
01
00
10
01
10
6
Sam
eor
not
=o+
s+=
=s+
o+s+
s+o+
o+=
48
(4ti
mes
o+,
4ti
mes
s+)
Not
e.1:
item
pass
ed;
0:it
emfa
iled
;s+
:se
lf-s
core
isa
“pas
s,”
but
obse
rver
-sco
ring
isa
“fai
l”;
o+:
obse
rver
-sco
reis
a“p
ass,
”bu
tse
lf-s
cori
ngis
a“f
ail”
;=se
lf-s
cori
ngan
dob
serv
ersc
orin
gar
eth
esa
me
(bot
h0,
orbo
th1)
.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a, S
an D
iego
] at
03:
38 1
3 N
ovem
ber
2012

OBJECTIVITY OF SCORING THE HGSHS 465
Table 2The Percentage and Total Number of Discrepant Items in Our Sample
Proportion ofdiscrepant items
Total number ofdiscrepancies
Total numberof items
Number ofSubjects
HGSHS:A–12 20.18% 4,569 22,644 N = 1,887HGSHS:A–11 22.01% 4,569 20,757 N = 1,887
It can be seen, that apart from the “by definition” same amnesia, onlyItem Numbers 4, 9, and 11 are the ones where there was no statisticallysignificant difference between self-and observer-scoring.
Items Numbers 1, 7, and 8 proved to be “s+”; that is, statisticallysignificant the way subjects tend to score this item as “pass,” whileobservers as “fail.” We have the other type: Item Numbers 2, 3, 5, 6, and10 where the observer-scores are statistically more frequently “pass,”while self-scoring more frequently “fail.” These items are called “o+”items.
The agreement in classification based on self-scores and observer-scores is presented in Table 5. It can be seen that many subjects wouldbelong to a different category, depending on the basis of categorization(self or observer). The agreement between the two categories is onlymoderate (Cohen’s Kappa = .563).
Discussion
The overall correlation between self-scoring and observer-scoring ofthe HGSHS:A in our study was practically the same as the result ofBentler and Hilgard (1963) and those of Bentler and Roberts (1963).There is a high (r = .83) correlation between self-scores and observer-scores for the total (12 items) HGSHS:A scores, which drops onlyslightly to r = .81 when the amnesia item (which is “by definition”scored the same in self-scoring and in observer-scoring) is excluded.Both self-scoring and observer-scoring proved to be internally consis-tent, showing acceptable Cronbach’s alphas. It is important, though,that the internal consistency of observer-scoring was higher than thatof self-scoring.
The means of the self-scores and the observer-scores were also prac-tically the same, showing only negligible differences (only 0.24 point),even if this difference was statistically significant.
We found, however, important discrepancies when performing item-by-item analysis. The items were scored differently by the subjects andthe observers in about 20% of the cases. This can well be in the range
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a, S
an D
iego
] at
03:
38 1
3 N
ovem
ber
2012

466 KATALIN VARGA ET AL.
Tabl
e3
Coh
en’s
Kap
pa,
Cor
rect
edIt
em-T
otal
Cor
rela
tion
s,an
dC
ronb
ach’
sA
lpha
ifIt
emD
elet
edV
alue
sfo
rth
eSe
lf-Sc
ores
and
the
Obs
erve
r-Sc
ores
(N=
1,88
7)
Self
-sco
reO
bser
ver-
scor
e
HG
SHS:
A–1
2H
GSH
S:A
–11
HG
SHS:
A–1
2H
GSH
S:A
–11
Item
Coh
en’s
Kap
pa
Cor
rect
edIt
em-T
otal
Cor
rela
tion
Cro
nbac
h’s
Alp
haif
Item
Del
eted
Cor
rect
edIt
em-T
otal
Cor
rela
tion
Cro
nbac
h’s
Alp
haif
Item
Del
eted
Cor
rect
edIt
em-T
otal
Cor
rela
tion
Cro
nbac
h’s
Alp
haif
Item
Del
eted
Cor
rect
edIt
em-T
otal
Cor
rela
tion
Cro
nbac
h’s
Alp
haif
Item
Del
eted
1.H
ead
falli
ng.4
85.2
84.6
59.2
86.6
55.3
72.7
13.3
75.7
162.
Eye
clos
ure
.430
.209
.671
.211
.669
.346
.716
.356
.718
3.H
and
low
erin
g.3
33.1
63.6
77.1
79.6
73.4
01.7
10.4
06.7
124.
Arm
imm
obili
zati
on.5
38.3
78.6
43.3
68.6
40.4
23.7
06.4
13.7
10
5.Fi
nger
lock
.633
.461
.630
.457
.624
.480
.699
.475
.702
6.A
rmri
gid
ity
.577
.502
.621
.502
.614
.532
.690
.532
.692
7.H
and
sm
ovin
g.5
10.2
48.6
64.2
58.6
60.3
88.7
11.4
02.7
128.
Com
mun
icat
ion
inhi
biti
on.4
08.4
45.6
32.4
37.6
27.3
40.7
17.3
39.7
20
9.H
allu
cina
tion
.481
.204
.669
.199
.667
.243
.728
.239
.732
10.E
yeca
tale
psy
.619
.509
.620
.504
.614
.519
.692
.525
.693
11.P
osth
ypno
tic
sugg
esti
on.7
12.1
21.6
84.1
13.6
84.1
31.7
44.1
25.7
50
12.A
mne
sia
n/a
.212
.671
––
.215
.734
––
Not
e.H
GSH
S:A
–12:
tota
lsca
le;H
GSH
S:A
–11:
scal
ew
itho
utth
eam
nesi
ait
em.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a, S
an D
iego
] at
03:
38 1
3 N
ovem
ber
2012

OBJECTIVITY OF SCORING THE HGSHS 467
Tabl
e4
The
Scor
ing
Res
ults
ofth
eH
GSH
S:A
Item
s
HG
SHS:
Ait
ems
1.H
ead
Falli
ng
2. Eye
Clo
sure
3.H
and
Low
erin
g
4.A
rmIm
mob
iliza
tion
5.Fi
nger
Loc
k
6.A
rmR
igid
ity
7.H
and
sM
ovin
g
8.C
omm
unic
atio
nIn
hibi
tion
9.H
allu
cina
tion
10.
Eye
Cat
alep
sy
11.
Post
hypn
otic
Sugg
esti
on
s=
o1,
402
(74.
3%)
1,38
6(7
3.4%
)1,
394
(73.
9%)
1,46
4(7
7.6%
)1,
585
(84.
0%)
1,48
8(7
8.9%
)1,
453
(77.
0%)
1,38
7(7
3.5%
)1,
572
(83.
3%)
1,52
5(8
0.8%
)1,
638
(86.
8%)
s+36
341
146
205
7016
727
737
514
796
111
o+12
246
034
721
823
223
215
712
516
826
613
8
X2
(bet
wee
ns+
and
o+)
119.
755
350.
421
81.9
490.
400
86.9
0110
.589
33.1
8012
5.0
1.40
079
.834
2.92
8
No.
ofd
iscr
epan
tsc
ores
485
501
493
423
302
399
434
500
315
362
249
Perc
ento
fd
iscr
epan
tsc
ores
25.7
%26
.6%
26.1
%22
.4%
16.0
%21
.1%
23.0
%26
.5%
16.7
%19
.2%
13.2
%
p<
.001
<.0
01<
.001
ns<
.001
<.0
1<
.001
<.0
01ns
<.0
01<
.1
Prev
alen
ceof
s+or
o+
s+o+
o+“n
opr
eva-
lenc
e”o+
o+s+
s+“n
opr
eva-
lenc
e”o+
“no
prev
a-le
nce”
Not
e.“N
opr
eval
ence
”:se
lf-s
cori
ngan
dob
serv
er-s
cori
ngar
eth
esa
me
(bot
h0,
orbo
th1)
;s+:
self
-sco
reis
a“p
ass,
”bu
tobs
erve
r-sc
orin
gis
a“f
ail”
;o+
:obs
erve
r-sc
ore
isa
“pas
s,”
buts
elf-
scor
ing
isa
“fai
l.T
heX
2va
lues
,alo
ngw
ith
the
leve
lofs
igni
fican
ce,a
real
sopr
esen
ted
.Ite
mN
o.12
(Am
nesi
a)is
notl
iste
d,a
sth
esc
orin
gof
this
item
isal
way
sth
esa
me.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a, S
an D
iego
] at
03:
38 1
3 N
ovem
ber
2012

468 KATALIN VARGA ET AL.
Table 5Classification of Low, Medium, and High Hypnotizable SubjectsBased on Self-Scores Versus Observer-Scores of HGSHS:A
HGSHS observer
0–4 5–7 8–12 Total
HGSHS self 0–4 438 140 15 5935–7 102 423 185 7108–12 2 105 477 584
Total 542 668 677 1,887
that is allowed by the overall correlation being “only” r = .83 (and notr = 1).
Having a closer look at the discrepancies, however, we foundthat three items (Head Falling, Hands Moving, CommunicationInhibition) were systematically (and statistically significantly) moreoften scored by the subjects’ self-scoring as pass (s+), while fiveothers (Eye Closure, Hand Lowering, Finger Lock, Arm Rigidity,And Eye Catalepsy) scored statistically significantly more often aspass by the observers (o+). In only three items of the HGSHS:A(Arm Immobilization, Hallucination and Posthypnotic Suggestion,not counting Amnesia) were there no systematic differences betweenobserver-scoring and self-scoring (neither prevailed over the other asstatistically significantly).
This implies that the HGSHS:A is a scale in which the o+ and s+items are almost balanced, so that an overall correspondence can bereached (there is a high positive correlation for the total score) in spiteof the fact that in only three items did we find no systematic bias towardpass/fail as compared to the other type of scoring when there was adiscrepancy between the two methods of scoring. This “construction”was probably involuntary, as the authors of the Stanford scale—andits derivates—report that the only basis of construction was the levelof difficulty (Hilgard, 1978/1979; Weitzenhoffer, 1980, 1997; Woody &Barnier, 2008).
What Is Common in the Three Types of Items (s+, o+, and “NoPrevalence”)?
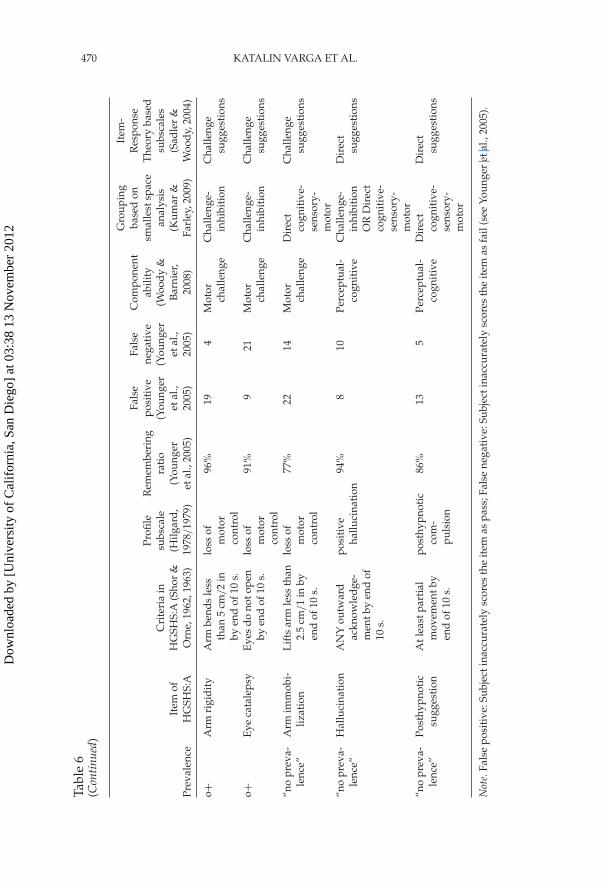
One may wonder what the common element can be in the itemsscored more often as pass by the subjects (s+), by the observers ( o+),and when neither prevailed over the other (“no prevalence”) whenthere was a discrepancy in scoring between subjects and observers?We can analyze our results from many viewpoints (see Table 6 fordetails).
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a, S
an D
iego
] at
03:
38 1
3 N
ovem
ber
2012

OBJECTIVITY OF SCORING THE HGSHS 469
Tabl
e6
The
s+,o
+,an
d“N
oP
reva
lenc
e”It
ems
and
Som
eR
elat
edE
arlie
rSt
udie
sor
Syst
ems
ofC
ateg
oriz
ing
the
Test
Sugg
esti
ons
Prev
alen
ceIt
emof
HG
SHS:
A
Cri
teri
ain
HG
SHS:
A(S
hor
&O
rne,
1962
,196
3)
Profi
lesu
bsca
le(H
ilgar
d,
1978
/19
79)
Rem
embe
ring
rati
o(Y
oung
eret
al.,
2005
)
Fals
epo
siti
ve(Y
oung
eret
al.,
2005
)
Fals
ene
gati
ve(Y
oung
eret
al.,
2005
)
Com
pone
ntab
ility
(Woo
dy
&B
arni
er,
2008
)
Gro
upin
gba
sed
onsm
alle
stsp
ace
anal
ysis
(Kum
ar&
Farl
ey,2
009)
Item
-R
espo
nse
The
ory
base
dsu
bsca
les
(Sad
ler
&W
ood
y,20
04)
s+H
ead
falli
ngA
tlea
st5
cm/2
info
rwar
dby
“Now
!”
loss
ofm
otor
cont
rol
98%
192
Dir
ectm
otor
Dir
ectm
otor
Dir
ect
sugg
esti
ons
s+H
and
sm
ovin
gH
and
sle
ssth
an15
cm/6
inap
artb
yen
dof
10s.
Los
sof
mot
orco
ntro
l
95%
137
Dir
ectm
otor
Dir
ectm
otor
Dir
ect
sugg
esti
ons
s+C
omm
unic
atio
nin
hibi
tion
No
reco
gniz
able
head
shak
eby
end
of10
s.
Los
sof
mot
orco
ntro
l
94%
218
Mot
orch
alle
nge
Cha
lleng
e-in
hibi
tion
Cha
lleng
esu
gges
tion
s
o+E
yecl
osur
eE
yes
clos
edby
“You
rey
esm
ayha
vecl
osed
byno
w.”
Los
sof
mot
orco
ntro
l
98%
319
Dir
ectm
otor
Dir
ectm
otor
Dir
ect
sugg
esti
ons
o+H
and
low
erin
gA
rmlo
wer
edat
leas
t15
cm/6
inby
end
of10
s.
loss
ofm
otor
cont
rol
98%
108
Dir
ectm
otor
Dir
ectm
otor
Dir
ect
sugg
esti
ons
o+Fi
nger
lock
Fing
ers
inco
mpl
etel
yse
para
ted
byen
dof
10s.
loss
ofm
otor
cont
rol
95%
915
Mot
orch
alle
nge
Cha
lleng
e-in
hibi
tion
Cha
lleng
esu
gges
tion
s
(Con
tinu
ed)
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a, S
an D
iego
] at
03:
38 1
3 N
ovem
ber
2012
470 KATALIN VARGA ET AL.
Tabl
e6
(Con
tinu
ed)
Prev
alen
ceIt
emof
HG
SHS:
A
Cri
teri
ain
HG
SHS:
A(S
hor
&O
rne,
1962
,196
3)
Profi
lesu
bsca
le(H
ilgar
d,
1978
/19
79)
Rem
embe
ring
rati
o(Y
oung
eret
al.,
2005
)
Fals
epo
siti
ve(Y
oung
eret
al.,
2005
)
Fals
ene
gati
ve(Y
oung
eret
al.,
2005
)
Com
pone
ntab
ility
(Woo
dy
&B
arni
er,
2008
)
Gro
upin
gba
sed
onsm
alle
stsp
ace
anal
ysis
(Kum
ar&
Farl
ey,2
009)
Item
-R
espo
nse
The
ory
base
dsu
bsca
les
(Sad
ler
&W
ood
y,20
04)
o+A
rmri
gid
ity
Arm
bend
sle
ssth
an5
cm/2
inby
end
of10
s.
loss
ofm
otor
cont
rol
96%
194
Mot
orch
alle
nge
Cha
lleng
e-in
hibi
tion
Cha
lleng
esu
gges
tion
s
o+E
yeca
tale
psy
Eye
sd
ono
tope
nby
end
of10
s.lo
ssof
mot
orco
ntro
l
91%
921
Mot
orch
alle
nge
Cha
lleng
e-in
hibi
tion
Cha
lleng
esu
gges
tion
s
“no
prev
a-le
nce”
Arm
imm
obi-
lizat
ion
Lif
tsar
mle
ssth
an2.
5cm
/1
inby
end
of10
s.
loss
ofm
otor
cont
rol
77%
2214
Mot
orch
alle
nge
Dir
ect
cogn
itiv
e-se
nsor
y-m
otor
Cha
lleng
esu
gges
tion
s
“no
prev
a-le
nce”
Hal
luci
nati
onA
NY
outw
ard
ackn
owle
dge
-m
entb
yen
dof
10s.
posi
tive
hallu
cina
tion
94%
810
Perc
eptu
al-
cogn
itiv
eC
halle
nge-
inhi
biti
onO
RD
irec
tco
gnit
ive-
sens
ory-
mot
or
Dir
ect
sugg
esti
ons
“no
prev
a-le
nce”
Post
hypn
otic
sugg
esti
onA
tlea
stpa
rtia
lm
ovem
entb
yen
dof
10s.
post
hypn
otic
com
-pu
lsio
n
86%
135
Perc
eptu
al-
cogn
itiv
eD
irec
tco
gnit
ive-
sens
ory-
mot
or
Dir
ect
sugg
esti
ons
Not
e.Fa
lse
posi
tive
:Sub
ject
inac
cura
tely
scor
esth
eit
emas
pass
;Fal
sene
gati
ve:S
ubje
ctin
accu
rate
lysc
ores
the
item
asfa
il(s
eeYo
unge
ret
al.,
2005
).
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a, S
an D
iego
] at
03:
38 1
3 N
ovem
ber
2012

OBJECTIVITY OF SCORING THE HGSHS 471
Almost all of the items of the HGSHS:A can be classified as “loss ofmotor control” (except for the Hallucination, Posthypnotic Suggestion)according to the Stanford Profile Scale of Hypnotic Susceptibility (SPS;Hilgard, 1978/1979). In this system, “loss of motor control” is defined as“Motor responses carried out automatically as a result of direct sugges-tion: loss of volitional control over movement as a result of suggestion”(Hilgard, 1978/1979, p. 74). None of the HGSHS:A items belong tothe further possible categories of the SPS (Agnosia and CognitiveDistortion, Negative Hallucination, or Dreams and Regression).
We assume that subjects cannot tell after the session if their move-ments were above or below the criteria that are provided in centimeters(both for the subjects, and the observers). All the three categories, how-ever, contain items with numeric criteria (15 cm/6 in. or 2.5 cm/1 in.).
The item groups in our study do not correspond with the factorsdescribed by Woody and Barnier (2008) either: Direct motor, motorchallenge, and perceptual-cognitive items are equally represented inthe s+, o+, and “no prevalence” groups. The same is true for the Item-Response Theory-based two subscales (direct and challenge sugges-tions, see Sadler & Woody, 2004). The smallest space analysis of Kumarand Farley (2009) finds a system very close to the factors described byWoody and Barnier (2008), neither showing correspondence with theitem groups of our study.
Younger et al. (2005) provide data on the frequency of false posi-tive scorings (the subject inaccurately scores the item as pass) and falsenegative ones (the subject inaccurately scores the item as fail) in theirsample of 79 university students. They do not analyze these discrepan-cies systematically; the categorization is based solely on the comparisonof the raw frequencies. As it can be seen in our cases, the s+ itemsare more often false positives than false negatives, but our o+ and ”noprevalence” items are mixed in this sense (see Table 6 for details).
Taken together, none of the systems or groupings of the HGSHS:Aare consistent with our item categories. The only correspondencebetween the earlier studies or systems and our results is that the sub-jects tend to score the items of Head Falling, Hands Moving, andCommunication Inhibition as positive more often than the observers(called “false positive” by Younger et al., 2005, and s+ by us). In theYounger et al. study, however, the majority of the test suggestions(seven items) were inaccurately scored as pass by the subjects, and onlyfour items were inaccurately reported as fail. In our study, the patternis the opposite: We have only three items as s+, and five as o+.
Why Self-Scoring Cannot Be Objective?If we agree that hypnosis is an altered state of consciousness (ASC),
many of the general characteristics of ASC lead to the theoretical
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a, S
an D
iego
] at
03:
38 1
3 N
ovem
ber
2012
472 KATALIN VARGA ET AL.
question if it is possible at all to get a behavioral self-score about thehypnotic performance.
As many theorists stress, the essence of the ASCs is the quali-tative shift in the subjective experience on the part of the individualbeing in the altered state (see Orne, 1959; Fromm, 1977; Ludwig, 1972;Tart, 1972). These experiences are unusual, unique, and many timesuncertain. During the altered state the subject temporarily relinquishesreality-control: he or she departs from the reality-testing objectivity; forexample, the perception of time and space may drastically change, notto mention the alterations in body image. In spite of this, the subjects areasked paradoxically, to judge “objectively” whether their overt move-ments reached a certain amount (e.g., 6 in./15 cm) or not, within a giventime limit (e.g., 10 s).
What makes the whole scoring even more questionable is the amnesiaitem (although amnesia can be spontaneous, it is a suggested item in theHGSHS:A): Just a few minutes after the amnesia suggestion is lifted,the subject is asked to retrospectively rate his or her own responsesconcerning a period about which they (at least some of them) had justbeen amnesic. Indeed, the study by Younger et al. (2005) showed that asurprisingly high number of subjects (32%) did not remember at leastone item of the HGSHS:A, and as much as six items were not remem-bered by 3% of their sample (see Table 6 for details). They concludedthat “accuracy of self-report is no better than chance when the individ-ual indicates that they do not remember the item” (Younger et al., 2005,p. 314). According to their analysis, not-remembering-items is not con-nected to the amnesia suggestion of the scale (there was no differencebetween those who passed and who failed the amnesia suggestion,either in their ratio of remembering, or in their level of accuracy).
It is worth mentioning the research of Bowers (Bowers et al., 1988),who described various mismatches between the behavioral and sub-jective measures of hypnosis: In some cases, for instance, the subjectscored his or her own response to be negative, but he or she reportedthat the same suggestion was performed and experienced involuntarily(see also Woody & Barnier, 2008). Sheehan and McConkey (1982) alsoreport that in some cases the objective feedback about the hypnosis ses-sion (the video-replay about the subject’s performance) is surprisingfor the subjects, as they do not remember their own behavioral mani-festations; nevertheless, they still have subjective feelings regarding thesame item. Younger et al. (2005) also conclude on the basis of their find-ings that “the internal experience of the hypnotized individual may bequite different from observable behaviors” (p. 316).
All these empirical observations imply that the behavioral and thesubjective level of hypnosis can be dissociated: The scoring asks to usethe former, while the dimension that is available for the subject is thelatter.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a, S
an D
iego
] at
03:
38 1
3 N
ovem
ber
2012

OBJECTIVITY OF SCORING THE HGSHS 473
To raise some practical questions as well. The scoring of the test sug-gestions is connected to a time limit: The continuous behavioral man-ifestation must be observed at a certain moment in time that is accu-rately specified by the standard protocol for the hypnotist/observer,but it is not known by the subjects. The same pass/fail criteria maybe a “pass” 3 seconds later (when, for instance, the lowering of the armreaches the extent/magnitude set by the criteria), but it must be scoredas “fail” at the moment of time limit. How does the subject know whatthe appropriate moment was, when he or she must judge the degree ofmovement to make retrospective scoring?
In 5 cases out of the 11 self-scored items, the criteria are specifiedby accuracy of length (2.5 cm / 1 in., 5 cm / 2 in., or 15 cm / 6 in.,depending on the suggestion). To test the ability of everyday peopleto accurately judge these distances, we asked 11 university studentsin their normal waking states (without any reference to hypnosis), toextend their dominant hand in front of them and to lower it by 15 cm(or to raise it from their laps by 2.5 cm) with their eyes closed. Inthe case of the expected 15 cm, the average actual performance was12.7 cm (SD = 5.3 cm), which is significantly different from the expectedvalue, t(10) = 1.414, p < .05. (The corresponding numbers in the case of2.5 cm were: x = 3.45 cm, SD = 1.94, t(10) = 1.631, p < .05, significantlydifferent from the expected 2.5 cm.)
All in all:, if we put together these considerations, it seems to bealmost impossible that a subject can retrospectively accurately judgehis or her behavioral performance on 11 hypnotic test suggestions. Buthe or she does, at least, on the whole scale! How?
What Can Be the Basis of the Subjects’ Self-Scoring?One obvious possibility is that both the self-scoring and the
observer-scoring are based on the same criteria. The scoring booklet (forself-scoring) provides the subject the description of the desired effect.Paraphrasing the analogy of Woody and Barnier (2008): This is as iftwo persons, whose mathematical ability should be measured wouldbe informed about the correct answer, their task would only be to indi-cate if they could solve it. In this system, a much higher correspondencecan be expected between the two judgments. The fact that the scor-ing of the HGSHS:A is dichotomous further raises the probability ofcorrespondence.
Shor, Pistole, Easton, and Kihlstrom’s (1984) study, however, showsthat it does not make any difference on the accuracy of predic-tion of their own hypnotic responsiveness whether the subjects areinformed or not about the behavioral scoring criteria that are appliedin the scoring of the HGSHS:A. Jupp et al. (1985) reported that the
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a, S
an D
iego
] at
03:
38 1
3 N
ovem
ber
2012

474 KATALIN VARGA ET AL.
correlation between hypnotic depth (as a general estimation of thesubject concerning their own hypnosis) and the standard score onthe HGSHS:A (self-scored by the same subject) is very high (aroundr = .71), whether or not the subjects are acquainted with the behavioralpass/fall criteria when they make the global depth estimates. Thesestudies suggest that the subjects’ experiences on the Harvard scale doesnot rely on the behavioral pass/fail criteria of their performance.
McConkey, Wende, and Barnier (1999) asked subjects of varioushypnotizability to indicate their subjective experiences on a dial (con-nected to a computer) during three test suggestions: an ideomotor (armlevitation), a challenge (arm rigidity), and a cognitive (anosmia) item.They found that “subjects who passed according to behavioral criteriaexperienced the suggested effect to a greater degree than those whofailed” (McConkey et al., 1999, p. 33). This could be the basis of self-scoring on the HGSHS:A too, supposing that the subject remembersthe nature and degree of the original experience retrospectively whilefilling out the response booklet. It is an important further problemthat the subjective experiences of high and medium hypnotizables inMcConkey et al.’s study did not differ from each other, only from thelows. Their conclusion that “in response to a given suggestion, mediumhypnotizable subjects are not necessarily less able than high hypnotiz-able subjects to have a successful and compelling hypnotic experience”(p. 34) makes it improbable that accurate self-scoring could solely bebased on this experiential aspect.
As Költo and his colleagues (in press) demonstrated (on the sameHungarian sample as our study), there is a slight but consistent risein the total HGSHS:A scores over time between 1973 and 2010. Thistrend appears both in self-scoring and in observer-scoring. Whateverlies behind the scoring accuracy of self-scoring and observer-scoring, itseems to influence both the subjects and the observers.
Conclusion
Scientific hypnosis research is based on the standardized measure-ment of individual differences in responding to hypnosis. Amongthe standardized scales, the HGSHS:A is used in nearly 70% of hyp-nosis research (Barnier & McConkey, 2004), as it is cost and timeeffectively applicable for screening subjects in group sessions. Theretrospective self-scoring of subjects became the standard scoring sys-tem of the HGSHS:A. This index is considered (and called) to be an“objective” index of the behavior of the subjects. But it is importantto realize that just because the Response Booklet of the HGSHS:A
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a, S
an D
iego
] at
03:
38 1
3 N
ovem
ber
2012

OBJECTIVITY OF SCORING THE HGSHS 475
acquaints the subjects with and requires them to use the same pass/failscoring criteria about responsiveness to suggestions as employed byexternal observers, the subjects’ judgments are nevertheless a subjectiveestimation, rather than an objective observation.
We probably need to face the fact that—even if the correla-tion between the total self-scores and observer-scores is as high asr = .83)—there might be notable discrepancies between self-scoringand observer-scoring. Even the classification of the subjects based onself-scoring and observer-scoring can be different, depending on thebasis of classification. Different subjects belong to the high, medium,and low categories depending on what scoring is used (see on thisalso Younger et al., 2005). The problem becomes even more complexif we consider the contradiction between behavioral responding andsubjective experience on the same scale. Pekala and Kumar (2007),for instance, described “pseudolows,” whose total score is low on theHGSHS:A, but whose reported phenomenological experiences wouldrank them as mediums.
The self-scoring of the HGSHS:A is not in fact an objective measureof hypnotic responsiveness (regardless of it being called so). Whateveris measured by this index, it seems to be independent of the effect ofhypnosis that is experienced subjectively by the hypnotized individual.Another possibility is that the self-score reflects a general estimation ofthe subject’s own hypnotic responding, “transformed” into the numericvalues that are asked for by the response booklet. In any case, it wouldbe more appropriate not to call the standard scoring of the HGSHS:A as“objective.” We recommend using the expression “self-scoring” insteadand consider it what it really is: a subjective, retrospective estimation.
Some further research is needed on large samples to test the actual(item-by-item) correspondence of objective observer-scoring and self-scoring of the HGSHS:A, even if it is used only for screening individ-uals of different hypnotizability to be confirmed later by individualmeasurement.
References
Balthazard, C. G. (1993). The hypnosis scales at their centenary: Some fundamental issuesstill unresolved. International Journal of Clinical and Experimental Hypnosis, 41, 47–73.
Barnier, A. M., McConkey, K. M. (2004). Defining and identifying the highly hypnoti-zable person. In M. Heap, R. J. Brown, & D. A. Oakley (Eds.), High Hypnotisability:Theoretical, Experimental and Clinical Issues (pp. 30–60). London, United Kingdom:Brunner-Routledge.
Barnes, S. M., Lynn, S. J., & Pekala, R. J. (2009). Not all group hypnotic suggestibilityscales are created equal: Individual differences in behavioral and subjective responses.Consciousness and Cognition, 18, 255–265.
Bentler, P. M., & Hilgard, E. R. (1963). A comparison of group and individual inductionof hypnosis with self-scoring and observer-scoring. International Journal of Clinical andExperimental Hypnosis, 11, 49–54.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a, S
an D
iego
] at
03:
38 1
3 N
ovem
ber
2012
476 KATALIN VARGA ET AL.
Bentler, P. M., & Roberts, M. R. (1963). Hypnotic susceptibility assessed in large groups.International Journal of Clinical and Experimental Hypnosis, 11, 93–97.
Bergman, M., Trenter, E., & Kallio, S. (2003). Swedish norms for the Harvard Group Scaleof Hypnotic Susceptibility, Form A. International Journal of Clinical and ExperimentalHypnosis, 51, 348–356.
Bongartz, W. (1985). German norms for the Harvard Group Scale of HypnoticSusceptibility, Form A. International Journal of Clinical and Experimental Hypnosis, 33,131–140.
Bowers, P. G., Laurence, J.-R., & Hart, D. (1988). The experience of hypnotic suggestions.International Journal of Clinical and Experimental Hypnosis, 36, 336–349.
Coe, W. C. (1964). Further norms on the Harvard Group Scale of Hypnotic Susceptibility,Form A. International Journal of Clinical and Experimental Hypnosis, 12, 184–190.
David, D., Montgomery, G., & Holdevici, I. (2003). Romanian norms for the HarvardGroup Scale of Hypnotic Susceptibility, Form A. International Journal of Clinical andExperimental Hypnosis, 51, 66–76.
De Pascalis, V., Russo, P., & Marucci, F. S. (2000). Italian norms for the HarvardGroup Scale of Hypnotic Susceptibility, Form A. International Journal of Clinical andExperimental Hypnosis, 48, 44–55.
Farthing, G. W., Brown, S. W., & Venturino, M. (1983). Involuntariness of response on theHarvard Group Scale of Hypnotic Susceptibility. International Journal of Clinical andExperimental Hypnosis, 31, 170–181.
Fromm, E. (1977). An ego-psychological theory of altered states of consciousness.International Journal of Clinical and Experimental Hypnosis, 25, 372–387.
Greguss, A. Cs., Bányai, É., Mészáros, I., Csókay, L., & Gerber A. (1975). A hipnózis irántiérzékenység standard vizsgálata magyar nyelven [The standardised investigation ofhypnotic susceptibility in Hungarian language]. In L. Benedek & T. Székely (Ed.),A Magyar Pszichológiai Társaság IV: Tudományos Jubileumi Nagygyulése [The ScientificMeeting of Hungarian Psychological Association] (pp. 61–62). Budapest, Hungary:Magyar Pszichológiai Társaság.
Gwynn, M. I., Spanos, N. P., Gabora, N. J., & Jarrett, L. E. (1988). Long-term and short-term follow-up on the Harvard Group Scale of Hypnotic Susceptibility: Form A.British Journal of Experimental and Clinical Hypnosis, 5, 117–124.
Hartman, B. J. (1965). Self-scoring and observer-scoring estimates of hypnotic suscepti-bility in a group situation. Perceptual and Motor Skills, 20, 452.
Hilgard, E. R. (1978/1979). The Stanford Hypnotic Susceptibility Scales as related toother measures of hypnotic responsiveness. American Journal of Clinical Hypnosis, 21,68–83.
Hilgard, E. R. (1982). Hypnotic susceptibility and implications for measurement.International Journal of Clinical and Experimental Hypnosis, 30, 394–403.
Jupp, J. J., Collins, J. K., & McCabe, M. P. (1985). Estimates of hypnotizability: Standardgroup scale versus subjective impression in clinical populations. International Journalof Clinical and Experimental Hypnosis, 33, 140–149.
Kallio, S., & Ihamuotila, M. J. (1999). Finnish norms for the Harvard Group Scale ofHypnotic Susceptibility, Form A. International Journal of Clinical and ExperimentalHypnosis, 47, 227–235.
Kihlstrom, J. F., & Register, P. A. (1984). Optimal scoring of amnesia on the HarvardGroup Scale of Hypnotic Susceptibility, Form A. International Journal of Clinical andExperimental Hypnosis, 32, 51–57.
Kirsch, I. (1997). Suggestibility or hypnosis: What do our scales really measure?International Journal of Clinical and Experimental Hypnosis, 45, 212–225.
Kirsch, I., & Braffman, W. (2001). Imaginative suggestibility and hypnotizability. CurrentDirections in Psychological Science, 10, 57–61.
Kirsch, I., Council, J. R., & Wickless, C. (1990). Subjective scoring for the HarvardGroup Scale of Hypnotic Susceptibility, Form A. International Journal of Clinical andExperimental Hypnosis, 38, 112–124.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a, S
an D
iego
] at
03:
38 1
3 N
ovem
ber
2012

OBJECTIVITY OF SCORING THE HGSHS 477
Kumar, V. K., & Farley, F. (2009). Structural aspects of three hypnotizability scales:Smallest space analysis. International Journal of Clinical and Experimental Hypnosis, 57,343–365.
Laurence, J.-R., Beaulieu-Prévost, D., & du Chéné, T. (2008). Measuring and understand-ing individual differences in hypnotizability. In M. R. Nash & A. J. Barnier (Eds.), TheOxford Handbook of Hypnosis: Theory, Research and Practice (pp. 225–253). New York,NY: Oxford University Press.
Laurence, J.-R., & Perry, C. (1982). Montreal norms for the Harvard Group Scale ofHypnotic Susceptibility, Form A. International Journal of Clinical and ExperimentalHypnosis, 30, 167–176.
Levitt, E. E., Aronoff, G., & Morgan, C. D. (1974). A note on possible limitations on the useof the Harvard Group Scale Of Hypnotic Suggestibility, Form A. International Journalof Clinical and Experimental Hypnosis, 22, 234–238.
Lichtenberg, P. (2008). Israeli norms for the Harvard Group Scale of HypnoticSusceptibility, Form A. International Journal of Clinical and Experimental Hypnosis, 56,384–393.
Ludwig, A. M. (1972). Altered states of consciousness. In C. T. Tart (Ed.), Altered states ofconsciousness (pp. 11–24). New York, NY: Anchor Book Doubleday.
McConkey, K. M., Wende, V., & Barnier, A. J. (1999). Measuring change in the subjectiveexperience of hypnosis. International Journal of Clinical and Experimental Hypnosis, 47,23–39.
O’Connell, D. N. (1964). An experimental comparison of hypnotic depth measured byself-ratings and by an objective scale. International Journal of Clinical and ExperimentalHypnosis, 12, 34–46.
Orne, M. T. (1959). The nature of hypnosis: Artifact and essence. Journal of Abnormal andSocial Psychology, 58, 277–299.
Pekala, R. J., & Kumar, V. K. (2007). An empirical-phenomenological approach to quan-tifying consciousness and states of consciousness: With particular reference to under-standing the nature of hypnosis. In G. Jamieson (Ed.), Towards a cognitive-neuroscienceof hypnosis and conscious states: A resource for researchers: Students and Clinicians (pp.167–194). London, United Kingdom: Oxford University Press.
Perry, C., & Laurence, J.-R. (1980). Hypnotic depth and hypnotic susceptibility: Areplicated finding. International Journal of Clinical and Experimental Hypnosis, 28,272–280.
Pyun, Y. D., & Kim, Y. J. (2009). Norms for the Korean version of the Harvard Group Scaleof Hypnotic Susceptibility, Form A. International Journal of Clinical and ExperimentalHypnosis, 57, 117–126.
Sacerdote, P. (1982). A non-statistical dissertation about hypnotizability scalesand clinical goals: Comparison with individualized induction and deepen-ing procedures. International Journal of Clinical and Experimental Hypnosis, 30,354–376.
Sadler, P., & Woody, E. (2004). Four decades of group hypnosis scales: What does itemresponse theory tell us about what we’ve been measuring? International Journal ofClinical and Experimental Hypnosis, 52, 132–158.
Sheehan, P. W., & McConkey, K. M. (1982). Hypnosis and experience: The exploration ofphenomena and process. Hillsdale, NJ: Lawrence Erlbaum.
Siuta, J. (2010). Polish norms for the Harvard Group Scale of Hypnotic Susceptibility,Form A. International Journal of Clinical and Experimental Hypnosis, 58,433–443.
Shor, R. E., & Orne, E. C. (1962). Harvard Group Scale of Hypnotic Susceptibility, Form A.Palo Alto, CA: Consulting Psychologists.
Shor, R. E., & Orne, E. C. (1963). Norms on the Harvard Group Scale of HypnoticSusceptibility, Form A. International Journal of Clinical and Experimental Hypnosis, 11,39–47.
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a, S
an D
iego
] at
03:
38 1
3 N
ovem
ber
2012

478 KATALIN VARGA ET AL.
Shor, R. E., Pistole, D. D., Easton, R. D., & Kihlstrom, J. F. (1984). Relation of predictedto actual hypnotic responsiveness, with special reference to posthypnotic amnesia.International Journal of Clinical and Experimental Hypnosis, 32, 376–387.
Spanos, N. P., Radtke, H. L., Hoodgins, D. C., Bertrand, L. D., Stam, H. J., & Dubreuil,D. L. (1983). The Carleton University Responsiveness to Suggestion Scale: Stability,reliability, and relationship with expectancy and “hypnotic experiences.” PsychologicalReports, 53, 555–563.
Tart, C. T. (1970). Self-report scales of hypnotic depth. International Journal of Clinical andExperimental Hypnosis, 18, 105–125.
Tart, C. T. (1972). Altered states of consciousness. New York, NY: Anchor Book Doubleday.Tart, C. T. (1978/1979). Quick and convenient assessment of hypnotic depth: Self-report
scales. American Journal of Clinical Hypnosis, 21, 186–207.Van Der Does, A. J. W., Van Dyck, R., Spinhoven, P., & Kloosman, A. (1989). The effective-
ness of standardized versus individualized hypnotic suggestions. International Journalof Clinical and Experimental Hypnosis, 37, 1–5.
Weitzenhoffer, A. M. (1980). Hypnotic susceptibility revisited. American Journal of ClinicalHypnosis, 22, 130–146.
Weitzenhoffer, A. M. (1997). Hypnotic susceptibility: A personal and historical noteregarding the development and naming of the Stanford scales. International Journalof Clinical and Experimental Hypnosis, 45, 126–143.
Weitzenhoffer, A. M., & Hilgard, L. R. (1959). Stanford Hypnotic Susceptibility Scale, FormsA and B. Palo Alto, CA: Consulting Psychologists Press.
Woody, E. Z., & Barnier, A. J. (2008). Hypnosis scales for the twenty-first century: Whatdo we need and how should we use them? In M. R. Nash & A. J. Barnier (Eds.), TheOxford handbook of hypnosis: Theory, research and practice (pp. 255–281). New York, NY:Oxford University Press.
Younger, J., Kemmerer, D. D., Winkel, J. D., & Nash, M. R. (2005). The Harvard GroupScale of Hypnotic Susceptibility: Accuracy of self-report and the memory for items.International Journal of Clinical and Experimental Hypnosis, 53, 306–320.
Über die Objektivität der Meßergebnisse der Harvard GruppenSkala zur Feststellung der Hypnotisierbarkeit
Katalin Varga, Lajos Farkas und László MéroAbstrakt: Die Autoren analysierten die Meßwerte von 1887 Probandenin der Harvard Gruppen Skala zur Feststellung der Hypnotisierbarkeit.Zusätzlich zu den gewohnten Selbsteinschätzungen bewerteten tranierteBeobachter ebenfalls die Verhaltensweisen der Probanden in bezug aufdieselben standardisierten Kriterien während der Sitzungen. Es zeigte sich,daß Selbsteinschätzung und Beobachterwerte intern konsistent waren undhoch korrelierten (r = 0,832). Die Merkmal für Merkmal-Analyse zeigtejedoch auffallende Unterschiede. Probanden und Beobachter bewerteteneinzelne Merkmale in 20% der Fälle unterschiedlich; nur drei Merkmalezeigten keinen systematischen Fehler bezüglich pass or fail. Oftmals würdeder Hypnotisierbarkeitslevel eines Probanden bezüglich der Einschätzungder Beobachter anders klassifiziert (Cohen´s Kappa = 0,563). Wir empfehlen,die “Objektivität” der Selbsteinschätzung noch einmal zu überdenken.
Stephanie Reigel, MD
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a, S
an D
iego
] at
03:
38 1
3 N
ovem
ber
2012

OBJECTIVITY OF SCORING THE HGSHS 479
Au sujet de l’objectivité de la notation de l’échelle desusceptibilité hypnotique du Groupe de Harvard
Katalin Varga, Lajos Farkas et László MéroRésumé: Les auteurs ont analysé les résultats obtenus par 1887 sujetsau questionnaire de l’échelle de susceptibilité hypnotique du Groupe deHarvard, formulaire A. En parallèle à l’auto-évaluation habituelle des sujets,des observateurs spécialement formés ont également coté les manifestationscomportementales de ces sujets en fonction des mêmes critères standardisés.Les résultats des sujets et ceux des observateurs se sont avérés intrinsèque-ment cohérents et présentaient une étroite corrélation (r = 0,832). Une analyseitem par item a toutefois donné des différences notables. Sujets et observa-teurs ont évalué les items différemment dans environ 20 % des cas; seuls3 items ne montraient aucun biais systématique en faveur d’un résultat posi-tif ou négatif. Le niveau d’hypnotisabilité de nombreux sujets serait classédifféremment selon la catégorisation des observateurs (coefficient Kappade Cohen = 0,563). Nous recommandons de reconsidérer «l’objectivité» del’autoévaluation.
Johanne ReynaultC. Tr. (STIBC)
Sobre la objetividad de la calificación de la Escala GrupalHarvard de Susceptibilidad Hipnótica
Katalin Varga, Lajos Farkas, y László MéroResumen: Los autores analizaron las calificaciones de 1887 sujetosen la Escala Grupal Harvard de Susceptibilidad Hipnótica, Forma A.Adicionalmente a la autocalificación usual, observadores entrenados tam-bién calificaron las manifestaciones conductuales de los sujetos siguiendolos mismos criterios estandarizados durante las sesiones. Las calificacionespropias y la de los observadores probaron ser internamente consistentesy estar altamente correlacionadas (r = .832). El análisis por reactivo,sin embargo, arrojó diferencias notables. Los sujetos y los observadoresdifirieron en las calificaciones de reactivos en el 20% de los casos; solo 3 reac-tivos no mostraron sesgo sistemático hacia la aprobación o reprobación. Elnivel de hipnotizabilidad de muchos sujetos se clasificaría distinto segúnla categorización de los observadores (Kappa de Cohen = .563). Sugerimosreconsiderar la “objetividad” de la autocalificación.
Omar Sánchez-Armáss Cappello, PhDAutonomous University of San Luis Potosi,Mexico
Dow
nloa
ded
by [
Uni
vers
ity o
f C
alif
orni
a, S
an D
iego
] at
03:
38 1
3 N
ovem
ber
2012