ohpd_2009_02_s0107.pdf - Quintessence Publishing!
21
C o p y r i g h t b y N o t f o r Q u i n t e s s e n c e Not for Publication The Relationship Between Diabetes Mellitus and Destructive Periodontal Disease: A Meta-Analysis Nilo Guliberto Martins Chávarry a,b /Mario Vianna Vettore c / Carmelo Sansone a /Aubrey Sheiham d Purpose: The aim of this study was to systematically review the studies on the association between diabetes mellitus (DM) and destructive periodontal disease. Methods: The methods applied include a literature search strategy, inclusion and exclusion criteria for selecting the studies, characteristics of the studies, quality assessment and meta-analysis. Data sources included PubMed, EMBASE, SciELO and LILACS. Selected papers were articles relating to human studies investigating whether or not diabetes is a risk factor for periodontitis and if it influences the response to periodontal therapy. Those papers that were published between January 1980 and June 2007 were retrieved. Results: Of the 2440 identified studies, 49 cross-sectional and eight longitudinal studies met the inclusion criteria. Twenty-seven of the 49 cross-sectional studies that are included in this review detected more periodontal disease in diabetic subjects compared with non-diabetic subjects. The greater risk of periodontal disease progression was associated with type 2 DM, and one study associated DM with response to periodontal therapy. Methodological flaws of most of the studies included inadequate control for confounders, insufficient statistical analysis and lack of information about sampling design. Random effect model showed a significant association with clinical attachment level (mean difference = 1.00 [CI 95% = 0.15 to 1.84]) and periodontal pocket depth (mean difference = 0.46 [CI 95% = 0.01 to 0.91]) between type 2 diabetics and non-diabetics. Conclusions: Type 2 DM can be considered a risk factor for periodontitis. More studies are needed to confirm the harmful effects of type 1 DM on periodontal disease. Key words: diabetes mellitus, meta-analysis, periodontal disease, periodontitis, systematic review Oral Health Prev Dent 2009; 7: 107–127. Submitted for publication: 24.12.07; accepted for publication: 03.03.08. M oderate chronic periodontal disease is common in most countries (Albandar, 2002a, b; Sheiham and Netuveli, 2002). Poor oral hygiene and bacterial biofilms composed of anaerobic Gram negative microorganisms are the main causative factors for periodontal breakdown (Christersson, 1993). In addi- tion, the habit of smoking and diabetes mellitus (DM) have been described as the risk factors for periodon- tal disease initiation and progression (Obeid and Bercy, 2000; Albandar, 2002a, b). Other putative risk factors for periodontal disease include psychosocial factors, socioeconomic conditions and age (Albandar, 2002a, b; Vettore et al, 2003). Most narrative review papers claim an association between DM and periodontal disease (Belting et al, 1964; Campbell, 1967; Hugoson and Jordan, 1982; Mealey and Oates, 2006). However, these review papers did not follow adequate protocols that are applied in systematic reviews (Alderson et al, a Division of Graduate Periodontics, Federal University of Rio de Janeiro, Rio de Janeiro, Brazil. b Department of Prosthodontics Dentistry, UNIGRANRIO, Duque de Caxias, Brazil. c Department of Epidemiology and Quantitative Methods in Health, National School of Public Health, Oswaldo Cruz Foundation, Rio de Janeiro, Brazil. d Department of Epidemiology and Public Health, University College London, London, England. Correspondence: Mario Vianna Vettore, Department of Epidemiology and Quantitative Methods in Health, National School of Public Health, Oswaldo Cruz Foundation, Rio de Janeiro, Brazil. Tel: +55 21 25982620. Fax: +55 21 22706772. Email: mario@ensp.fiocruz.br ORIGINAL ARTICLE Vol 7, No 2, 2009 107
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of ohpd_2009_02_s0107.pdf - Quintessence Publishing!

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
The Relationship Between Diabetes Mellitusand Destructive Periodontal Disease: A Meta-Analysis
Nilo Guliberto Martins Chávarrya,b/Mario Vianna Vettorec/Carmelo Sansonea/Aubrey Sheihamd
Purpose: The aim of this study was to systematically review the studies on the association between diabetes mellitus(DM) and destructive periodontal disease.
Methods: The methods applied include a literature search strategy, inclusion and exclusion criteria for selecting thestudies, characteristics of the studies, quality assessment and meta-analysis. Data sources included PubMed, EMBASE,SciELO and LILACS. Selected papers were articles relating to human studies investigating whether or not diabetes is arisk factor for periodontitis and if it influences the response to periodontal therapy. Those papers that were publishedbetween January 1980 and June 2007 were retrieved.
Results: Of the 2440 identified studies, 49 cross-sectional and eight longitudinal studies met the inclusion criteria.Twenty-seven of the 49 cross-sectional studies that are included in this review detected more periodontal disease indiabetic subjects compared with non-diabetic subjects. The greater risk of periodontal disease progression wasassociated with type 2 DM, and one study associated DM with response to periodontal therapy. Methodological flaws ofmost of the studies included inadequate control for confounders, insufficient statistical analysis and lack of informationabout sampling design. Random effect model showed a significant association with clinical attachment level (meandifference = 1.00 [CI 95% = 0.15 to 1.84]) and periodontal pocket depth (mean difference = 0.46 [CI 95% = 0.01 to0.91]) between type 2 diabetics and non-diabetics.
Conclusions: Type 2 DM can be considered a risk factor for periodontitis. More studies are needed to confirm theharmful effects of type 1 DM on periodontal disease.
Key words: diabetes mellitus, meta-analysis, periodontal disease, periodontitis, systematic review
Oral Health Prev Dent 2009; 7: 107–127. Submitted for publication: 24.12.07; accepted for publication: 03.03.08.
MModerate chronic periodontal disease is commoninmost countries (Albandar, 2002a, b; Sheiham
and Netuveli, 2002). Poor oral hygiene and bacterial
biofilms composed of anaerobic Gram negativemicroorganisms are the main causative factors forperiodontal breakdown (Christersson, 1993). In addi-tion, the habit of smoking and diabetes mellitus (DM)have been described as the risk factors for periodon-tal disease initiation and progression (Obeid andBercy, 2000; Albandar, 2002a, b). Other putative riskfactors for periodontal disease include psychosocialfactors, socioeconomic conditionsandage (Albandar,2002a, b; Vettore et al, 2003).Most narrative review papers claim an association
between DM and periodontal disease (Belting et al,1964; Campbell, 1967; Hugoson and Jordan,1982; Mealey and Oates, 2006). However, thesereview papers did not follow adequate protocols thatare applied in systematic reviews (Alderson et al,
a Division of Graduate Periodontics, Federal University of Rio deJaneiro, Rio de Janeiro, Brazil.
b Department of Prosthodontics Dentistry, UNIGRANRIO, Duque deCaxias, Brazil.
c Department of Epidemiology and Quantitative Methods in Health,National School of Public Health, Oswaldo Cruz Foundation, Rio deJaneiro, Brazil.
d Department of Epidemiology and Public Health, University CollegeLondon, London, England.
Correspondence: Mario Vianna Vettore, Department of Epidemiologyand Quantitative Methods in Health, National School of Public Health,Oswaldo Cruz Foundation, Rio de Janeiro, Brazil. Tel: +55 2125982620. Fax: +55 21 22706772. Email: [email protected]
ORIGINAL ARTICLE
Vol 7, No 2, 2009 107

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
2004). The need for an adequate methodology forconducting systematic reviews is essential to avoidbias in selecting studies and to appraise the scien-tific literature critically. To overcome the possibleshortcomings of the previous reviews, a systematicreview was performed to assess if DM is a possiblerisk factor for destructive periodontal disease. Thefocused questions are: (i) do type 1 and 2 DMincrease the risk for periodontitis? (ii) do type 1and 2 DM influence the response to periodontaltherapy?
RESEARCH DESIGN AND METHODS
Development of a protocol
A protocol was developed to answer the selected andfocused questions, which included all aspects of thereviewmethodology (Alderson et al, 2004). Themeth-ods applied in this review included a literature searchstrategy, inclusion and exclusion criteria for selectingthe studies, selection process and data extraction,quality assessment and quantitative data synthesis.
Literature search strategy
The data sources included PubMed, EMBASE, SciELOandLILACS. Standardisedmethodological filterswereused to identify analytical studies. First, two themeswere derived that were then combined using the Bool-ean operator ‘AND’. Each theme was created usingthe operator ‘OR’, to search for terms appearing asboth exploded medical subject headings (MeSH)and text words. The first themewas created for ‘diabe-tes mellitus’, or ‘diabetes’, or ‘insulin resistance’, or‘glucose intolerance’, or ‘metabolic control’, or‘impaired glycaemia’ and the second for ‘periodontaldisease’, or ‘periodontitis’, or ‘periodontal’.Manual searching of the identified articles was
also conducted. The search was limited to humanstudies written in English.
Inclusion and exclusion criteria for selectingstudies
Studies were considered for inclusion if they ad-dressed clinical measures of destructive periodontaldisease and/or radiography of periodontal tissues.The analytical studies had to include an estimateof the effect of diabetes on periodontal diseaseand/or the statistical tests for comparison of
groups. The selected studies were published bet-ween January 1980 and June 2007.Case reports describing periodontal conditions in
diabetic subjects, ecological studies, experimentalanimal studies and previous reviews were excluded.In addition, published studies showing repeatedresults from the same original study were excluded.Studies that had inadequate or unclear scoring
systems for the measurement of destructive peri-odontal disease and those in which the type of dia-betes was not reported were excluded. Measuresof destructive periodontal disease were classifiedas adequate when clinical measures were basedon periodontal pocket depths and/or clinical at-tachment loss measures, or alveolar bone lossassessed using radiographs. Scoring measures ofdestructive periodontal disease were consideredinadequate if indices with unsatisfactory reliabilitywere used to assess periodontal status. The indicesincluded community periodontal index of treatmentneeds (CPITN), Ramfjord index and periodontal dis-ease index. Studies that did not report the methodof periodontal assessment and those that did notpresent the results of periodontal measures werescored as unclear.
Selection process and data extraction
Two reviewers (NGMCandCS) independently retrievedand evaluated the articles for eligibility. The extractionof information from studies was conducted by thesame reviewers, and the information included therange of duration of diabetes, type of periodontal dis-ease, definition of periodontitis, type of periodontalprobe used, number of patients, patient characteristicdata, confounders taken into account and the mainresults. Any discrepancies between reviewers werediscussed with a third reviewer (MVV) and resolvedby consensus.
Quality assessment
It was decided a priori that methodological quality forthe studies that were included would be assessedwith a predetermined appraisal form, focusing onthe following issues: sampling calculation, adjust-ment for potential confounders, statistical analysis,sampling design/selection of control group, res-ponse rate and blindness of outcome assessment.Longitudinal studies were also assessed for com-pleteness of follow-up. For quality assessment of clin-ical trials, the Revised CONSORT Statement for
Chávarry et al
108 Oral Health & Preventive Dentistry

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
Reporting Randomized Trials (Moher et al, 2001)was used, which included allocation concealment,method of randomisation, blindness of patients, clini-cian and examiners and completeness of follow-up.The following factors were assessed and the crite-
ria below were used.
Sampling calculationIt was noted if the sample size had been previouslydetermined.
Measures of diabetes
Diabetes was classified as adequate when it wasassessed through glycosylated haemoglobin, fast-ing blood glucose level or oral glucose tolerancetest and as inadequate when it was self-reported.
Were the examiners calibrated for periodontalassessment?• Adequate-level 1: when results on clinical cali-bration were presented.
• Adequate-level 2: when clinical calibration wasperformed, but the results were not reported.
• Inadequate: when clinical calibration was notperformed.
Adjustment for potential confounders• Adequate: when all the following variables weretaken into account: age, smoking, ethnicity,socioeconomic status, previous periodontal ther-apy, number of teeth, immunological and neuro-logical diseases.
• Inadequate: when any of the above variableswere not considered.
• Unclear: when control for confounders was notadequately explained.
Statistical analysis• Adequate: when estimates of association (oddsratio or relative risk) were provided or could becalculated and when multivariate analysis wasconducted.
• Inadequate: when only bivariate analysis wasperformed.
Sampling design/selection of the control group• Was the sample drawn randomly so that it is rep-resentative of the population it reports torepresent?
• Was the control/unexposed group selected fromthe same population that produced the cases/exposed group?
• Was the definition of case/exposed group expli-cit?
• Was the exposure assessed in the same mannerbetween groups?
• Was the outcome assessed in the same mannerbetween groups?
• Was the objective outcome criteria applied tocontrols to exclude cases in the control group?
• Was the objective exposure criteria applied to theunexposed group to exclude exposed persons inthe unexposed group?
Response rate• Was the non-response rate reported?• Were the non-response rates and reasons fornon-response similar in both groups?
Blindness of outcome assessment• Was the outcome assessment blind to exposurestatus?
• Was the level of exposure blind to outcomestatus?
Completeness of follow-up (longitudinal studiesonly)The following criteria were assessed.• Was the number of patients at baseline and atcompletion of the follow-up interval reported forboth groups?
• Were drop-out rates and reasons for drop-outsimilar between groups?
• Was exposure updated in studies with long-termfollow up?
• Was the dose–effect relationship between peri-odontitis and outcome noted?
Quantitative data synthesis and statisticalmethodsFor quantitative data synthesis, studies that pro-vided information on mean differences of periodontalpocket depth (PPD) and/or clinical attachment level(CAL) between diabetics and non-diabetics wereincluded. The data should be presented by the typeof diabetes and periodontal clinical measure. The
Chávarry et al
Vol 7, No 2, 2009 109

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
data were combined to estimate the pooled differ-ence of mean values with confidence interval at95% (CI 95%) using the inverse variance method.Homogeneity among studies was tested by Coch-ran’s Q test. Potential publication bias was testedfor using the rank correlation of Begg’s test (Beggand Berlin, 1994) and Egger’s test (Egger et al,1997). All statistical analyses were performed usingcommercial statistical software, version STATA6(Strata Corp, TX, USA). The significance level thatwas established for analyses was 5% (P � 0.05).
RESULTS
Search results
Of the 2440 identified studies, 57 met the inclusioncriteria. Selected papers included 49 cross-sectional
studies; 17 papers on type 1 DM, 26 on type 2 DMand 6 on type 1 and 2 DM. In addition, eight longitudi-nal studies were included; 3 papers on type 1 DM, 3on type 2 DM and 2 on type 1 and 2 DM (Fig 1).Epidemiological characteristicsandquality assess-
ment results of the analytical studies that wereincluded are presented according to the studydesign: cross-sectional and longitudinal studies, andtype of diabetes: type 1 DM, type 2 DM and type 1and 2 DM.
Cross-sectional studies
The epidemiological characteristics of the cross-sectional studies on the relationship betweendiabetes and periodontal disease are presented inTable 1 (type 1 DM), Table 2 (type 2 DM) and Table 3(type 1 and 2 DM). Of the 49 studies that compared
Potentially relevant publications identified and screened for retrieval: n = 2440
Full text retrieved for more detailed evaluation: n = 129
Studies included in systematic review: n = 57
Selected studies: n = 364
Papers excluded for not addressing different aspects and measures of destructive periodontal disease: n = 2076
Exclusion for other reasons: • No controls (non-diabetics): n = 21 • Periodontal disease considered as a risk factor
for diabetes: n = 18 • Measures of periodontal disease were classified
as inadequate and/or type of diabetes were unclear: n = 72
Papers identified through manual searching: n = 12
Papers excluded based on the exclusion criteria: • Case reports: n = 25 • Comments: n = 4 • Animal studies: n = 9 • Review articles: n = 121 • Duplicated study: n = 23 • Not in English language: n = 63 • Acute necrotising ulcerative gingivitus,
acute necrotising ulcerative periodontitis and endodontic–periodontal lesions: n = 2
Fig 1 Flow chart of stud-ies through the review.
Chávarry et al
110 Oral Health & Preventive Dentistry

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
the parameters of periodontal disease between dia-betic and non-diabetic patients, 27 found significantdifferences between groups in at least one periodon-tal parameter.The range of duration of diabetes was between 1
and 29 years for type 1 DM (seven studies), 1 to17 years for type 2 DM (17 studies) and 4 to17 years for type 1 and 2 DM (three studies). Moststudies considered periodontitis as the periodontaldisease under study. However, the definition of peri-odontitis varied considerably among studies, and ineight studies the criteria used to define periodontitiswere unclear.Six different types of periodontal probeswere used
in studies on type 1 DM. In six studies on type 1 DMand in 12 studies on type 2 DM, there was no infor-mation about the type of periodontal probe used. Ofthe seven studies on type 1 and 2 DM, only onereported on the type of periodontal probe.The sample size of the selected studies varied
from 16 to 15,246. The number of confounders
taken into account varied from 0 to 9, but most stud-ies considered only a few confounders.
Type 1 DMType 1DMwas considered in 17 cross-sectional stud-ies (Table 1). Eight of the 17 studies found an associ-ation between type 1 DM and periodontal disease.Seven studies showed differences in periodontalprobing depth (PPD) measures between groups, andfour studies found significantly more clinical attach-ment loss (CAL) in diabetics compared with non-diabetics. Five studies investigated the relationshipbetween type 1 DM and periodontal disease usingalveolar bone loss. One study detected differencesbetween diabetic and non-diabetic groups using alve-olar bone loss.
Type 2 DMThere were 26 studies on the relationship betweentype 2 DM and periodontal disease (Table 2). Of the
1 CAL
2 PPD
Morton 1995
Alpagot 2001
Yuan 2001
Alley 1993 Firatli 1994 Pinson 1995 Firatli 1996 Firatli 1997 Salvi 1997b
Alpagot 2001 Guthmiller 2001
Yucekal-Tuncer 2003 Aren 2003
Morton 1995
Alpagot 2001
Yuan 2001
Bulut 2001
Orbak 2002
mean difference-1 0 1
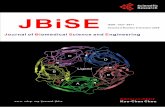
Combined0.26 (-0.004–0.533) p = 0.054
Manouchehr-Pour 1981
Alley 1993
Firatli 1994
Pinson 1995
Firatli 1996
Firatli 1997
Alpagot 2001
Guthmiller 2001
Yucekal-Tuncer 2003
-1 0 1
Combined0.11 (-0.03–0.245) p = 0.137
-1 0 1
Combined
1.00 (0.15–1.84) p = 0.021
-1 0 1
Combined
0.46 (0.01–0.91) p = 0.046
1a Type 1 DM 1b Type 2 DM
2a Type 1 DM 2b Type 2 DM
mean difference
mean difference mean difference
Fig 2 Mean differences in CAL and PPD between diabetics and non-diabetics according to the type of diabetes.CAL, clinical attachment loss; DM, diabetes mellitus; PPD, periodontal probing depth.
Chávarry et al
Vol 7, No 2, 2009 111

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
Table1
Cha
racteristics
ofcros
s-se
ctiona
lstud
ieson
type
1DM
andpe
riod
ontaldise
ase
Referen
ces
Ran
geof
duration
ofdiab
etes
Type
sof
period
ontal
dise
ase
Defi
nition
ofpe
riod
ontitis
Type
ofpe
riod
ontal
prob
e
Num
ber
ofpa
tien
tsAge
(yea
rs)
Variables
controlle
dRes
ults
Manouchehr-Pour
etal(1981)
�5.0
years
Adult
periodontitis
Severe
periodontitis:
meanvalueof
CAL
�4mm
and�6teeth
with
>50%ABL
Unclear
TotalN=32,
DsP
n=8,
DmPn=6,
nDsP
n=7,
nDmPn=11
DsP
=49,
DmP=51,
nDsP
=48,
nDmP=31
None
NSDforCAL
Nocorrelation
amongCAL,
FBGL,DOSorDUR
Rylander
etal(1986)*
�10.0
years
Periodontitis
Unclear
Unclear
TotalN=87,
Dn=46,
nDn=41
D=22.1
(19–25),
nD=22.3
(18–26)
Age
SDforCAL
�2mm
NSDforPPD4–5
mm,
PPD>5mmandABL
NocorrelationofDUR,
DOSandHbA
1c
with
periodontal
parameters
Sandholm
etal(1989)
5.2
±3.5
years
Periodontitis
Unclear
Standard
probe
(Hilm
ing,
0.6
mm)
TotalN=170,
Dn=85,
nDn=85
15.1
Ageandgender
NSDforPPD�4mm
Nosubjectswith
PPD�6mmand
ABL�1mm
Hugoson
etal(1989)*
Long
duration
28.9
±10.2;
shortduration
5.2
±1.9
Periodontitis
Based
onclinicaland
radiographical
criteria
modified
from
Hugoson
and
Jordan
(1982)
Unclear
TotalN=231,
Dlong
durationn=82,
Dshort
durationn=72,
nDn=77
20–70
Ageandgender
NSDforPPD�4mm,
PPD4–5
mmandABL
SDforPPD�4mm
insubjects
aged
<45years
SDforPPD�6mm
insubjectswith
long
durationof
diabetes
DePommereau
etal(1992)
1–14years
Unclear
Periodontitis:
loss
ofperiodontal
attachment�1
siteadjacentto2
ormoreteeth
WHO
periodontal
probe
TotalN=123,
Dn=85,
nDn=38
D=15.1,
nD:unclear
Age,durationof
diabetes
anddegree
ofmetaboliccontrol
ofdiabetes
NSDforperiodontitis
prevalence
andABL
Harber
etal(1993)*
Unclear
Periodontitis
Periodontitis:
�1
site,
PPD�5mm,
CAL
�2mm
Michigan
type
‘0’probe
with
Williams
TotalN=227,
Dn=132,
nDn=95
19–40
Pregnancy,
HIV,age,gender
andsm
oking
OR1.8
forformer
smokers,
OR6.9
current
smokers
NSDfornon-sm
okers
Thorstensson
and
Hugoson
(1993)*
>7.0
years
Unclear
Based
onclinicaland
radiographical
criteria
modified
from
Hugoson
and
Jordan
(1982)
Hilm
ingprobe
TotalN=182,
Dn=83,
nDn=99
40–69
Age,gender,duration
ofdiabetes,
numberofteeth
SDforABL
SDforPPD�4mm
and4–5
mm
SDfornumberofsites
PPD�6mmand
ABLin40–49
agegroup
Chávarry et al
112 Oral Health & Preventive Dentistry

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
Table1Cha
racteristics
ofcros
s-se
ctiona
lstud
ieson
type
1DM
andpe
riod
ontaldise
ase(C
ontinu
ed)
Referen
ces
Ran
geof
duration
ofdiab
etes
Type
sof
period
ontal
dise
ase
Defi
nition
ofpe
riod
ontitis
Type
ofpe
riod
ontal
prob
e
Num
ber
ofpa
tien
tsAge
(yea
rs)
Variables
controlle
dRes
ults
Alleyetal
(1993)
Unclear
Moderateto
severe
periodontitis
�4sitesinmultiple
quadrantswith
PPD
andCAL
�5mm,
BOPandABL
Unclear
TotalN=60,
DPn=15,
DnP
n=15,
nDPn=15,
nDnP
n=15
D=35.5,
nD=36.4
Ageandgender,previous
antibiotic
therapy,
previous
periodontal
therapyandrace
NSDforPPDandCAL
Firatlietal
(1994)
Unclear
Periodontitis
andgingivitis
Unclear
Williamsprobe
TotalN=68,
Dn=48,
nDn=20
D=11.6,
nD=12.5
Age
NSDCAL
andPPD
Thereareno
subjects
with
periodontitis
Pinson
etal
(1995)
Mean
6.6
years
Unclear
Unclear
Vine
valleyprobe
TotalN=50,
Dn=26,
nDn=24
D=13.5
±3.4,
nD=13.5
±3.1
Race,age,gender,previous
antibioticstherapy,any
severesystem
icillness,
numberofteethand
previous
ketosis
NSDformeanPPD
andmeanCAL
Nocorrelationof
clinicalvariables
andGHb
Sbordone
etal(1995)
Unclear
Unclear
Unclear
Michiganprobe
TotalN=32,
Dn=16,
nDn=16
D=11.3,
nD=13.2
Age,genderandnumber
ofperiodontalsites
NSDfor
PPDandCAL
Thorstensson
etal(1995)*
>7year/
mean
24.6
years
Periodontitis
ABL�1/3
ofnormal
bone
height
Unclear
TotalN=62,
Dn=28,
nDn=34
Unclear
Ageandgender
SDforPPD
of4and5mm
andPPD�4mm
Firatlietal
(1996)*
48.3
±23.7
months
Periodontitis
and
gingivitis
Unclear
Williamsprobe
TotalN=154,
Dn=77,
nDn=77
D=12.5,
nD=12.6
Age,gender,sm
oking,
ethnicity
andSES
SDforPPDandCAL
Salvietal
(1997)
Unclear
Adult
periodontitis
AAP
Unclear
TotalN=103,
Dn=39,
nDPn=43,
nDn=21
D=48.8,
nD=34.9
Pregnancy,Crohn’sdisease,
previous
antibiotic
therapy,
non-steroidalanti-inflammatory
drug
andsystem
icdisease
NSDforPPD
Guthm
iller
etal(2001)*
Unclear
Unclear
Unclear
Vine
valleyprobe
TotalN=33,
Dn=13,
nDn=20
D=27.0
±7.3,
nD=28.5
±7.1
Gender,ageandgestational
period
SDformeanPPD
andmeanCAL
Yucekal-Tuncer
etal(2003)*
Unclear
Chronic
periodontitis
CAL
�2mm
Borodontic
periodontal
probe
TotalN=16,
Dn=8,
nDn=8
Unclear
Smoking,previous
periodontal
treatmentandantibiotic
therapy
SDforPPD(patient
and
site-based
analysis)
SDforCAL
(site-based
analysis)
Aren
etal(2003)*
4.0
years
Periodontitis
Unclear
Williamsprobe
TotalN=48,
sDn=16,
lDn=16,
nDn=16
sDn=12.8
±5.8,
lDn=12.7
±3.8,
nDn=12.4
±1.9
Age,
gender
andSES
SDforPPD:lD
versus
sDandlD
versus
nD,
NSDforPPD:sD
versus
nD
ABL,alveolar
bone
loss;CEJ,cementoenam
eljunction;
AAP,
American
Academ
yofPeriodontology;D,diabetics;nD,non-diabetics;DsP,diabeticswith
severe
periodontitis;DmP,
diabeticswith
mild
periodontitis;nDsP,non-diabeticswith
severeperiodontitis;nDmP,non-diabeticswith
mild
periodontitis;DP,diabeticswith
periodontitis;sD,shortdurationofdiabetes;lD,long
durationofdiabetes;
nDP,
non-diabetes
with
periodontitis;
nDnP,non-diabetes
withoutperiodontitis;
DnP,diabeticswithoutperiodontitis;
FBGL,fastingbloodglucoselevel;DOS,insulin
dosage;DUR,diabeticduration;
SD,significantdifferencesbetweendiabeticsandnon-diabeticsgroups;NSD,non-significantdifferencesbetweendiabeticsandnon-diabeticsgroups;OR,odds
ratio;WHO,WorldHealth
Organization.
*Studies
with
atleastoneclinicalparameterthatisstatisticallydifferentbetweendiabeticsandnon-diabetics.
Chávarry et al
Vol 7, No 2, 2009 113

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
Table2
Epidem
iologica
lch
arac
teristicsof
cros
s-se
ctiona
lstud
ieson
type
2DM
andpe
riod
ontaldise
ase
Referen
ceRan
geof
diab
etes
duration
Type
ofpe
riod
ontal
dise
ase
Defi
nition
ofpe
riod
ontitis
Type
ofpe
riod
ontal
prob
e
Num
ber
ofpa
tien
tsAge
(yea
rs)
Variables
controlle
dRes
ults
Nelson
etal(1990)
Unclear
CP
<24teethor
�6
teethwith
�25%of
ABLor
�1tooth
with
�50%ABL
Unclear
701
�15
Ageandgender
NSDfor
Periodontal
disease,OR:
2.6
(1.0–6.6)
Emrich
etal(1991)*
Unclear
Periodontitis
CAL
�5mm,
ABL,Score2
(25–49%)Score3
(50–74%)Score
4(�
75%)
Unclear
Total
N=1342,
Dn=254,
Igtn=158,
nDn=930
�15
Ageandgender
SDforCAL
�5mm
OR:2.81SD
forABL�Score
2OR:3.43
Cherry-Peppers
andShip
(1993)
7.7
years
Periodontitis
Unclear
Unclear
TotalN=86,
Dn=11,
IGTn=32,
nDn=43
D=67.9
±11.1,
IGT=60.7
±19.1,
nD=60.2
±18.8
Age,gender,SES,
medicines
andsystem
icdiseases
NSDforPPD
andCAL
Morton
etal(1995)*
>2years/
mean7.9
years
Unclear
Unclear
Williamsprobe
Total
N=48,
Dn=24,
nDn=24
nD45.8
±10.7,
D46.8
±11.9
Ageandany
medicalproblems
SDforCAL
andPPD
Collin
etal(1998)
Unclear
Moderate-to-
advanced
periodontitis
Advanced:
meanABL>50%,
or�2teeth
PPD�6mm
Moderate:mean
ABL25–50%,or
�1
PPD�6mmor
�1
PPD3–6
mm
WHO
periodontal
probe
Total
N=65,
Dn=25,
nDn=40
D=58–76,
nD=59–77
Ageandsm
oking
NSDforABL
andCAL,
%ofsiteswith
PPD3mm
to<6mm
or�6mm
Pwas
seen
in40%Dand13%nD
Kawam
ura
etal(1998)
�1year
Unclear
Unclear
TG-SP5
Total
N=200,
Dn=102,
nDN=98
nD=52±7.9,
D=53±9.3
Cerebrovascular
disease,system
icdisease,taking
medications
which
mightaltercognitive
function,age,gender
andoccupation
NSDforPPD
Cutler
etal(1999)
Unclear
Adult
periodontitis
�4periodontal
pockets�6mm
with
BOPand
radiographical
evidence
of>50%
bone
loss
atthesameteeth
Floridaprobe,
constant
force,
automated
electronic
probe,20g
TotalN=35,
nDUnclear
n=6,
nDPn=7,wDUnclear
n=6,wDPn=5,
poorDUnclear
n=5,
poorDP:
n=6
nDUnclear=28.2
nDP=42.9
wDUnclear=52
wDP=65.8
poorDUnclear
=45,
poorDP=42.5
Tobaccoproducts,
antibiotic
and
system
icdisease
NSDfor
PPDandCAL
Fontana
etal(1999)*
17±4years
Periodontitis
Unclear
WHOperiodontal
probewith
standardised
pressure
of20–25g
TotalN=80,
Dn=40,
nDn=40
D=56±8,
nD=56±6
Age,gender,system
icillness,infections,
inflammation,sm
oking
andcurrentuseofdrugs
SDforABLand
CAL
Parameters
andbone
loss
Chávarry et al
114 Oral Health & Preventive Dentistry

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
Table2Ep
idem
iologica
lch
arac
teristicsof
cros
s-se
ctiona
lstud
ieson
type
2DM
andpe
riod
ontaldise
ase(C
ontinu
ed)
Referen
ceRan
geof
diab
etes
duration
Type
ofpe
riod
ontal
dise
ase
Defi
nition
ofpe
riod
ontitis
Type
ofpe
riod
ontal
prob
e
Num
ber
ofpa
tien
tsAge
(yea
rs)
Variables
controlle
dRes
ults
Kurtis
etal(1999)
Unclear
Adult
periodontitis
CAL
and
PPD>3mm
Williamsprobe
TotalN=72,
DPn=24,
nDPn=24,
nDUnclear
n=24
DP=37–65,
nDP=35–60,
nDUnclear
=17–22
Antim
icrobialagents
andperiodontal
treatmentinthe
previous
6months
NSDfor
PPDandCAL
Collin
etal(2000)
Unclear
Periodontitis
�1sitewith
PPD>4mm
WHO
periodontal
probe
Total
N=122,
Dn=45,
nDn=77
D=67±5.2,
nD=68±5.9
Age
NSDforPPD
Sandberg
etal(2000)*
9.9
years
SD(6.1)
Periodontitis
Advanced:
ABL:3(�
1/3)or
4(angulardefects
andfurcation
involvem
ent)
andPPD>4mm
Unclear
Total
N=204,
Dn=102,
nDn=102
D=64.8,
nD=64.9
Ageandgender
SDfornumberof
PPDof4–5
mm,
NSDforPPD�6mm
SDfornumberof
subjectswith
sites
with
advanced
periodontitis
Bulut
etal(2001)
Unclear
APAP,accordingto
Page
and
Shroeder(1976)
Unclear
TotalN=51,
Dn=17,
nDn=17,
nDUnclear
n=17
nDUnclear
=45.3,
D=52.5,
nDP=42.5
None
NSDformeanPPD
Yuan
etal(2001)
Unclear
Periodontitis
Site
with
PPD>3mm
Williams
Total
N=246,
D=105,
nD=141
D=57.1
±12.0
nD=57.1
±11.7
Ageandgender
NSDforPPD
andCAL
Orbak
etal(2002)*
Unclear
Unclear
Unclear
Unclear
Total
N=60sm
okers
Dn=21,
non-sm
okers
Dn=19,
non-sm
okers
nDn=20
Smokers
D=46±1.4
non-sm
okers
D=43±4.6
non-sm
okers
nD=41±3.9
Age,gender,drugs
thataffectthe
mouthflora,
immunesystem
orinflammatory
response,previous
periodontal
treatmentand
apicalpathology
oftheteeth
SDformean
CAL
NSDfor
meanPPD
Tsai
etal(2002)*
Unclear
Severe
periodontitis
�2siteswith
CAL
�6mm
and�1site
with
PPD�5mm
inoneofthese
sites
Unclear
TotalN=4343
45–90
Age,gender,
education,
race,income,
smokingstatus,
andextent
ofsubgingival
calculus
PoorD
·nD:
OR=2.90
(1.40–6.03)
andbetter
D·nD:
OR=1.56
(0.90–2.28)
Chávarry et al
Vol 7, No 2, 2009 115

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
Table2Ep
idem
iologica
lch
arac
teristicsof
cros
s-se
ctiona
lstud
ieson
type
2DM
andpe
riod
ontaldise
ase(C
ontinu
ed)
Referen
ceRan
geof
diab
etes
duration
Type
ofpe
riod
ontal
dise
ase
Defi
nition
ofpe
riod
ontitis
Type
ofpe
riod
ontal
prob
e
Num
ber
ofpa
tien
tsAge
(yea
rs)
Variables
controlle
dRes
ults
Zielinski
etal(2002)
5–15years
Periodontitis
BOPand
PD>3mm
Severe:
�2
teethwith
PPD�6mm
Moderate:1
site
with
PPD�6mm
or�1site
with
PPD3–6
mm
Michigan
type
‘0’
probe
TotalN=72,
Dn=32,
nDn=40
D=71±7,
nD=74±8
Age,numberofteeth,
severedementia,
anticoagulants,
antibiotic
prophylaxisor
taking
antibiotics
onthedayof
exam
ination,sm
oking,
regularcheckups
anddrymouth
NSDforprevalence
ofsevereand
moderateperiodontitis
Marugam
eetal(2003)
Unclear
Periodontitis
Moderate
ABL:
�1
toothwith
ABS<50%
andno
sites<25%
SevereABL:
�1
site
with
ABS<25%
Notused
Total
N=664
46–57
Unclear
NSDforABL
adjusted
OR=2.55
(0.86–7.54)
Saito
etal(2003)*
Unclear
Periodontitis
Tertilesofmean
ABL(the
ratio
ofthe
distance
ofCEJ
toalveolar
crestby
CEJ
torootapex)
low:10–20.7%,
medium:20.8–28.6%,
high:28.7–55.9%
Notused
Total
N=179
50–54
Gastritis,parotitis,
anti-inflammatory
drugs,
age,sm
oking
history,
systolicblood
pressure,BMI,
triglyceride
andHDL
cholesterol
Correlation:
ABL·CRP
Thehighesttertile
ofABLhada
significant
risk
ofCRPelevation
(�1.3
mg/L)
OR:8.2
(1.6–40.7)P=0.01
Ünlü
etal(2003)*
�5years
Periodontitis
PPD>3mm
Unclear
TotalN=30,
DPn=10,
nDPn=10,
nDUnclear
n=10
D=56,
nDP=49.3,
nDUnclear:
unclear
Systemicdisease,
smoking,nottaking
anymedication,
ageandgender
NSDforPPD
SDforCAL
Güneri
etal(2004)
�5years
Periodontitis
Sites>3mm
Unclear
TotalN=30,
DPn=10,
nDPn=10,
nDUnclear
n=10
DP=56,
nDP=49.3,
nDUnclear=50.3
Smoking,
system
icdiseases
andmedications
NSDforPPD
andCAL
Luand
Yang
(2004)*
Unclear
Periodontitis
Unclear
Unclear
Total
N=164
Dn=72,
nDn=92
D=54.3,
nD=54.9
Ageand
numberof
teeth
SDforCAL
Chávarry et al
116 Oral Health & Preventive Dentistry

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
Table2Ep
idem
iologica
lch
arac
teristicsof
cros
s-se
ctiona
lstud
ieson
type
2DM
andpe
riod
ontaldise
ase(C
ontinu
ed)
Referen
ceRan
geof
diab
etes
duration
Type
ofpe
riod
ontal
dise
ase
Defi
nition
ofpe
riod
ontitis
Type
ofpe
riod
ontal
prob
e
Num
ber
ofpa
tien
tsAge
(yea
rs)
Variables
controlle
dRes
ults
Saito
etal(2004)*
Unclear
Moderate-to-
advanced
periodontitis
MeanPPD
persubjects>2mm:
high
category;
1.3–2.0
mm:
intermediate
category:Mean
CAL
per
subjects>2.5
mm:
high
category;
1.5–2.5
mm:
intermediate
category
Unclear
Total
N=860,
nDn=679,
Dn=181
40–79
Age,gender,BMI,
exercise
frequency,
alcoholconsum
ption,
andsm
okinghabits
MeanPPD
intermediate/
high
OR:1.9
(1.0–3.4)/
OR:2.6
(1.3–5.0),
respectively
MeanCAL
intermediate/
high
OR:1.1
(0.6–2.0)/OR:2.0
(1.0–3.9),
respectively
Cam
pus
etal(2005)
18.2
±5years
Periodontitis
ADAcriteria
(24),
Moderate:PPD4–6
mm,
Advanced:PPD>6mm
Unclear
Total
N=212,
Dn=71,
nDn=141
35–75,
D=61,
nD=59.1
Num
ber
ofteethand
smoking
D·nD
and
gmc·bm
candbm
c·nD
SDfornumber
andpercent
ofPPD>4mm
Mansourand
Abd-Al-Sada
(2005)*
Unclear
Periodontitis
Advanced:�2teeth
with
PPD�5mm
(or30%ofteeth)
or�4teethwith
PPD�4mm
(or60%ofteeth)
Moderate:
�1
teethwith
PPD�5mm
or�2teeth
with
PPD�4mm
(or�30%ofteeth)
PCP-11
Total
N=1593,
Dn=633,
nDn=960
�40,
D=56.7,
nD=56.9
Num
berofteeth,
ageandsm
oking
SDformoderate
periodontitis
(PPD
)
Mattout
etal(2006)*
Unclear
CP
Unclear
Williams
periodontal
probePD
T20gpressure
Total
N=2144,
Dn=71
35–65
Age,sm
oking,
SES
andgender
SDforCAL
NSDforPPD
Borges-Yáñez
etal(2006)
Unclear
Periodontitis
Moderate:at
least2sites
with
CAL
�4mm
Severe:atleast
onesitewith
CAL
�6mm
Michigan
periodontal
probe
TotalN=170
>60
Age,gender,
edentulousness,
smokingand
calculus
NSDforCAL
ABL,alveolarbone
loss;CEJ,cem
entumenam
eljunction;WHO,W
orldHealth
Organisation;DsP,diabeticswith
severeperiodontitis;DmP,diabeticswith
mild
periodontitis;nDsP,non-diabeticswith
severeperiodontitis;
nDmP,non-diabeticswith
mild
periodontitis;D,diabetics;nD,non-diabetics;DP,diabeticswith
periodontitis;sD,shortdurationofdiabetes;lD,longdurationofdiabetes;IGT,impairedglucosetolerance;wDUnclear,well-
controlleddiabetes
withoutperiodontitis;wDP,well-controlleddiabetes
with
periodontitis;poorDUnclear,poorlycontrolleddiabetes
with
periodontitis;PoorDP,poorlycontrolleddiabetes
with
periodontits;nDP,non-diabetes
with
periodontitis;nDUnclear,non-diabeteswithoutperiodontitis;SES,socioeconom
icstatus;FBGL,fastingbloodglucoselevel;DOS,insulindosage;DUR,diabeticduration;SD,significantdifferencesbetweendiabeticand
non-diabeticgroups;N
SD,non-significantdifferencesbetweendiabeticsandnon-diabetics.
*Studies
with
atleastoneclinicalparameterthatisstatisticallydifferentbetweendiabeticsandnon-diabetics.
Chávarry et al
Vol 7, No 2, 2009 117

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
Table3
Epidem
iologica
lch
arac
teristicsof
cros
s-se
ctiona
lstud
ieson
type
1an
d2DM
andpe
riod
ontaldise
ase
Referen
ceRan
geof
diab
etes
duration
Type
ofpe
riod
ontal
dise
ase
Defi
nition
ofpe
riod
ontitis
Type
ofprob
eNum
ber
ofpa
tien
tsAge
(yea
rs)
Variables
controlle
dRes
ults
Oliverand
Tervonen
(1993)*
Mean13.8
years
Periodontitis
Unclear
Unclear
GP=15,132,
D=114
20–64,
D=40.6,
GP=40
Age,gender,
rheumatoid
arthritis,AIDS,
malignant
blooddisorders
andlong-term
medications
such
ascortisone,
phenytoin,
non-steroidal
anti-inflammatory
drugsandprevious
immunosuppressives
orantim
icrobialtherapy
SDforprevalence
andextentof
PPD�4mmNSD
forprevalence
and
extentofCAL
�3mm
and�5mmNSDof
PPDbetween1and2
Yavuzyilm
azetal(1996)*
Unclear
Unclear
Unclear
Unclear
TotalN=34,
Dtype
2n=10,
Dtype
2n=7,
nDn=17
nD=23.2
±3.3,
D=54.2
±15.8
Antibiotics,no
periodontaltreatment
withinthepast6months
SDformean
PPDandNSD
forPPD
between1and2
Alpagot
etal(2001)*
Type
110.03±5.73,
type
28.28±3.75
Unclear
Unclear
Unclear
TotalN=177
Dtype
2n=30
Dtype
1n=30
nDn=117
nD=36.0
±11.0,
Dtype
1=39.1
±12.7,
Dtype
2=45.2
±12.1
Unclear
SDformean
PPDandCAL
Persson
etal(2003)*
Unclear
Periodontitis
Siteswith
CAL
�4mm
andPPD�5mm
in>5%of
totalsites
UNCprobe
TotalN=1084,
Dtype
2n=100,
Dtype
1n=31,
nDn=953
60–75
Age,numberof
teeth(�
4),
smokingand
gender
SDfornumber
andproportion
ofsitesof
PPD�5mm
NSDfor
CAL
�4mm
andABL
OR:1.8
(1.1–3.1)
ofperiodontitis
Lalla
etal(2004)*
Unclear
Unclear
Notdefined
Notused
TotalN=300
Dtype
1n=23
Dtype
2n=103,
Unclear=24,
nD=150
nD=55±14.2,
D=56±13.1
Genderandage
SDforABL
Lalla
etal(2007)*
3.96±3.39
Periodontitis
�2teeth
with
�1site
with
CAL
>2mm
and/orbleeding
Unclear
TotalN=700
Dtype
1n=325
Dtype
2n=25
nDn=350
6–18
Age,gender,
ethnicity
andSES
SDformean
and%of
sites>2mm
ofCAL
Unclear,notpresented;GP,generalpopulationofem
ployed
American
adults;SD,significantdifferencesbetweendiabeticandnon-diabeticgroups;N
SD,non-significantdifferencesbetweendiabeticand
non-diabeticgroups;CAL,clinicalattachmentloss;D,diabetics;Ig,immunoglobulin;nD,non-diabetics;ELISA,
enzyme-linkedimmunosorbent
assay;CPITN,community
periodontalindexoftreatment
needs;GCF,gingivalcrevicularfluid;PMN,polym
orphonuclearperipheralblood;ABL,alveolarbone
loss;ABS,alveolarbone
support;WHO,W
orldHealth
Organization;OR,oddsratio;PKC,proteinkinase
C;CRP,C-reactiveprotein.
*Studies
with
atleastoneclinicalparameter
thatisstatisticallydifferentbetweendiabeticsandnon-diabetics.
Chávarry et al
118 Oral Health & Preventive Dentistry

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
16studies that comparedCALmeasuresbetweendia-betics and non-diabetics, seven detected a positiveassociation between DM and periodontal disease.Of the 19 studies that assessed PPD measures, 6on type 2 DM found significant differences of PPDmeasures between diabetics and non-diabetics.Periodontal disease was assessed radiographi-
cally in seven studies that tested the hypothesis thattype 2 DM increased the risk for periodontitis. Threestudies reported more alveolar bone loss in diabet-ics compared with non-diabetics.
Type 1 and 2 DMThere were six studies on the relationship betweentype 1 and 2 DM and periodontal disease (Table 3).Of the four studies that compared PPD measuresbetween diabetics and non-diabetics, all found asso-ciationswith PPD. In four studies, CALmeasureswereused; in two studies significant differences werereported. Alveolar bone loss was compared between
diabetics and non-diabetics in two studies. One studydetected more alveolar bone loss in diabetics.
Quality assessment: results of 49 cross-sectional studies
Sampling calculationOne study on type 2 DM determined the sample size(Lu and Yang, 2004).
Were the examiners trained and calibrated for
periodontal assessment?Thirteen studies were considered adequate for clini-cal calibration of periodontal disease; four type 1DM (Hugoson et al, 1989; Harber et al, 1993; Pinsonet al, 1995; Guthmiller et al, 2001), six type 2 DM(Marugame et al, 2003; Lu and Yang, 2004; Campuset al, 2005;Mansour and Abd-Al-Sada, 2005; Borges-Yáñez et al, 2006;Mattout et al, 2006) and three type
CAL
PPD
Type 1 DM Type 2 DM
stan
dard
ised
eff
ect
precision0 20 40 60
0
2
4
6
Type 1 DM Type 2 DM
stan
dard
ised
eff
ect
precision0 20 40 60 80
-10
0
10
stan
dard
ised
eff
ect
precision0 1 2 3 4
-40
-20
0
20
40
stan
dard
ised
eff
ect
precision0 5 10
-5
0
5
10
Fig 3 Egger’s Publication Bias Plots: mean differences in CALs and PPD in diabetics and non-diabetics, according to the type ofdiabetes. CAL, clinical attachment level; DM, diabetes mellitus; PPD, periodontal probing depth.
Chávarry et al
Vol 7, No 2, 2009 119

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
Table4
Epidem
iologica
lch
arac
teristicsof
long
itud
inal
stud
iesbe
twee
ndiab
etes
andpe
riod
ontaldise
ase
Referen
cePeriodo
ntal
therap
yDefi
nition
ofpe
riod
ontitis
Type
ofpe
riod
ontal
prob
e
Sam
plesize
Age
Variables
controlle
dNum
berof
patien
tsDuration
(mon
ths)
Res
ults
Diabe
tics
Non
-diabe
tics
Ran
geBas
eline
Fina
l
Firatli(1997)§*
No
Unclear
Williams
probe
TotalN=64,
Dn=44,
nDn=20
12.2
±3.9
12.3
±4.3
Unclear
Age,
smoking,
system
icdiseases,
race
and
SES
64
64
60
SDformean
CAL,Significant
correlation:
DURversus
CAL,NSD
formeanPPD
Tervonen
and
Karjalainen
(1997)§
Yes
Unclear
Unclear
Total
N=46,
Dn=36,
nDn=10
29.4
±3.7
30.1
±3.8
24–36
Ageand
number
ofteeth
46
43
36
NSDfor%PPD
and%CAL
Sbodorne
etal(1998)§
No
Unclear
Michigan
type
‘0’probe
Total
N=32,
Dn=16,
nDn=16
9–17
9–17
9–17
RaceandSES
16
16
36
NSDfor
meanCAL
andmeanPPD
Novaes
etal(1996,1997)�*
No
Adult
periodontitis
Michigan
type
‘0’probe
Total
N=60,
Dn=30,
nDn=30
52.3
44.6
30–77
Previous
periodontaltherapy,
antibioticsuse
60
60
12
SDformean
CAL,NSDfor
meanPPD
PoorD
versus
nD:
SDforCAL
andPPD
Taylor
etal(1998)�*
No
Unclear
Unclear
Total
N=362,
Dn=24,
nDn=338
Median=21.2
Median=25.7
15–57
Age,gender,
number
ofteeth
362
362
24
OR=4.2
(1.8–9.9)
Faria-Almeida
etal(2006)�*
Yes
Moderate
chronic
periodontitis:
4–6
mmof
CAL
inall
quadrants
NorthCarolina
periodontal
probe
Total
N=20,
type
2D
n=10,
nDn=10
Unclear
Unclear
35–70
Ageandgender
20
20
6SDforPPD
NSDforCAL
Westfelt
etal(1996)�
Yes
Unclear
Unclear
Total
N=40
type
1D
n=14,
type
2D
n=6,
nDn=20
Unclear
Unclear
46–65
Age,
gender,severity
ofperiodontal
disease,number
ofteeth,DURand
dentalplaque
40
38
60
NSDfor%
PPD�4mm
and�7mm
Chávarry et al
120 Oral Health & Preventive Dentistry

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
1 and 2 DM (Oliver and Tervonen, 1993; Perssonet al, 2003; Lalla et al, 2004).
Adjustment for potential confoundersAll the citations had an inadequate score for theadjustment of potential confounders.
Statistical analysisIn 14 studies, the statistical analysis was consid-ered adequate; 3 type 1 DM (Hugoson et al, 1989,Thorstensson and Hugoson, 1993; Yucekal-Tunceret al, 2003), 10 type 2 DM (Nelson et al, 1990; Em-rich et al, 1991; Cutler et al, 1999; Tsai et al, 2002;Marugame et al, 2003; Saito et al, 2003; Lu andYang, 2004; Saito et al, 2004; Campus et al,2005; Mattout et al, 2006) and 1 type 1 and 2DM (Persson et al, 2003).
Sampling design/selection of control groupThe sample was drawn randomly in five studies ontype 1 DM (Rylander et al, 1986; Hugoson et al,1989; Harber et al, 1993; Pinson et al, 1995; Firatliet al, 1996), in 16 studies on type 2 DM (Nelsonet al, 1990; Morton et al, 1995; Kawamura et al,1998; Kurtis et al, 1999; Sandberg et al, 2000; Bu-lut et al, 2001; Yuan et al, 2001; Tsai et al, 2002;Zielinski et al, 2002; Marugame et al, 2003; Saitoet al, 2003; Güneri et al, 2004; Saito et al, 2004;Mansour and Abd-Al-Sada, 2005; Borges-Yáñezet al, 2006; Mattout et al, 2006) and in three stud-ies on type 1 and 2 DM (Oliver and Tervonen, 1993;Persson et al, 2003; Lalla et al, 2004).The exposed and unexposed groups were from
the same population in seven studies on type 1DM (Rylander et al, 1986; Hugoson et al, 1989; Pin-son et al, 1995; Sbordone et al, 1995; Thorstens-son et al, 1995; Guthmiller et al, 2001; Aren et al,2003), in 19 studies on type 2 DM (Nelson et al,1990; Emrich et al, 1991; Cherry-Peppers and Ship,1993; Kawamura et al, 1998, Cutler et al, 1999;Kurtis et al, 1999; Sandberg et al, 2000; Yuanet al, 2001; Tsai et al, 2002; Zielinski et al, 2002;Marugame et al, 2003; Saito et al, 2003; Ünlüet al, 2003; Güneri et al, 2004; Saito et al, 2004;Campus et al, 2005; Mansour and Abd-Al-Sada,2005; Borges-Yáñez et al, 2006; Mattout et al,2006) and in one study on type 1 and 2 DM (Perssonet al, 2003)The definition of exposed and unexposed groups
was not clearly explained in one study on type 1DM (Harber et al, 1993), in three studies on type2 DM (Morton et al, 1995; Saito et al, 2003; Mat-tout et al, 2006) and in four studies on type 1 andC
hristgau
etal(1998)�
Yes
Moderate-
to-advanced
periodontitis:
�6
teethwith
PPD�4mm
NorthCarolina
periodontalprobe
Total
N=40,
type
1D
n=7,
type
2D
n=13,
nDn=20
Median=
54.5
(30–67)
Median=
50.5
(30–66)
Unclear
Age,gender,
antibioticsuse,
numberofteeth,
smokingand
system
icdiseases
40
40
4NSDfor
median%
PPDandCAL
Unclear,notpresented;
D,diabetics;
nD,non-diabetics;
SES,socioeconomicstatus;DUR,diabeticduration;
SD,significant
differencesbetweendiabeticsandnon-diabetics;
NSD,non-significant
differencesbetweendiabeticsandnon-diabetics;Dtype
1,diabetes
type
1;Dtype
2,diabetes
type
2;PoorD,poorlycontrolleddiabetes.Studies
accordingtotype
ofDM:§type
1;�type
2;�type
1and2.
*Studies
with
atleastoneclinicalparameterthatisstatisticallydifferentbetweendiabeticsandnon-diabetics.
Table4Ep
idem
iologica
lch
arac
teristicsof
long
itud
inal
stud
iesbe
twee
ndiab
etes
andpe
riod
ontaldise
ase(C
ontinu
ed)
Chávarry et al
Vol 7, No 2, 2009 121

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
2 DM (Oliver and Tervonen, 1993; Yavuzyilmaz et al,1996; Alpagot et al, 2001; Lalla et al, 2004).In three studies on type 1 DM (Firatli et al, 1994;
Firatli et al, 1996; Aren et al, 2003) and in two stud-ies on type 1 and 2 DM (Persson et al, 2003; Lallaet al, 2004), the exposure was assessed in thesame manner between the groups. Of the 23 studieson type 2 DM, only six assessed the exposure in thesame manner between the groups (Morton et al,1995; Sandberg et al, 2000; Ünlü et al, 2003;Güneri et al, 2004; Borges-Yáñez et al, 2006; Mat-tout et al, 2006).In all studies on type 1 and 2 DM, the outcome
was assessed similarly between the groups, andthe objective outcome criteria that were establishedfor periodontal disease assessment to excludecases in the controls were similar for both thegroups. In two of the five studies on type 1 and 2DM, these criteria were considered unclear (Oliverand Tervonen, 1993; Alpagot et al, 2001).The objective exposure criteria that were applied
to the unexposed group to exclude the exposed inthe unexposed groups was used in five studies ontype 1 DM (Thorstensson and Hugoson, 1993; Firatliet al, 1996; Guthmiller et al, 2001; Aren et al, 2003;Ünlü et al, 2003), in 16 studies on type 2 DM (Nel-son et al, 1990; Emrich et al, 1991; Cherry-Peppersand Ship, 1993; Collin et al, 1998; Kawamura et al,1998; Cutler et al, 1999; Fontana et al, 1999; Kurtiset al, 1999; Yuan et al, 2001; Orbak et al, 2002;Tsai et al, 2002; Marugame et al, 2003; Saitoet al, 2004; Borges-Yáñez et al, 2006; Mattoutet al, 2006) and in one study on type 1 and 2 DM(Alpagot et al, 2001).
Response ratesThe response rates were reported in three studieson type 1 DM (Hugoson et al, 1989; Harber et al,1993; Thorstensson and Hugoson, 1993), in threestudies on type 2 DM (Sandberg et al, 2000; Yuanet al, 2001; Tsai et al, 2002) and in one study ontype 1 and 2 DM (Persson et al, 2003).
Response rates and reasons for non-responsesimilar between groupsOnly one study on type 1 DM reported similarresponse rates and reasons for non-responsebetween groups (Thorstensson and Hugoson,1993).
Blindness of outcome assessmentSix studies on type 1 DM (Thorstensson and Hugo-son, 1993; Pinson et al, 1995; Firatli et al, 1996;
Guthmiller et al, 2001; Aren et al, 2003; Yucekal-Tuncer et al, 2003), seven studies on type 2 DM(Nelson et al, 1990; Emrich et al, 1991; Mortonet al, 1995; Kawamura et al, 1998; Yuan et al,2001; Zielinski et al, 2002; Marugame et al,2003) and no studies on type 1 and 2 DM had theoutcome assessment blinded to the exposurestatus.
Blindness of exposure assessmentFour studies on type 1 DM (Pinson et al, 1995; Firatliet al, 1996; Guthmiller et al, 2001; Aren et al,2003), seven studies on type 2 DM (Nelson et al,1990; Emrich et al, 1991; Morton et al, 1995; Ka-wamura et al, 1998; Yuan et al, 2001; Zielinskiet al, 2002; Marugame et al, 2003) and one studyon type 1 and 2 DM (Oliver and Tervonen, 1993)had the exposure assessment blinded to outcomestatus.
Meta-analysis of cross-sectional studies
Meta-analyses were conducted involving studies inwhich the mean differences of PPD and CAL werereported or could be extracted. The mean differ-ences for PPD and CAL measures between groupswere calculated as the mean value in diabetic groupminus the mean value in non-diabetic group. Positivedifferences between diabetics and non-diabetics forPPD and CAL measures revealed more periodontaldisease in the diabetic groups.The meta-analysis was performed according to the
type of diabetes (Fig 2). For the calculation of thepooled mean difference, each study was assigneda weight consisting of the reciprocal of variance ofdifference between two mean values. Estimates ofthe overall difference in each of the periodontalparameters and their corresponding CI 95% were cal-culated using the random-effect model.Type 1 diabetics were compared with non-diabet-
ics with respect to CAL measures in eight studies(Manouchehr-Pour et al, 1981; Alley et al, 1993; Pin-son et al, 1995; Firatli et al, 1996; Alpagot et al,2001; Guthmiller et al, 2001; Ünlü et al, 2003;Yucekal-Tuncer et al, 2003). The overall differenceof CAL between type 1 diabetics and non-diabeticswas not statistically significant (CAL mean differ-ence = 0.26 (�0.004 to 0.533), P = 0.054) (Fig2.1a). Type 2 diabetics were compared with non-diabetics with respect to CAL measures in threestudies (Morton et al, 1995; Alpagot et al, 2001;Yuan et al, 2001). There were statistically significant
Chávarry et al
122 Oral Health & Preventive Dentistry

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
differences for CAL measures between type 2 diabet-ics and non-diabetics (mean difference = 1.00 (0.15to 1.84), P = 0.021) (Fig 2.1b).The average differences in PPD were compared
between type 1 diabetics and non-diabetics in tenstudies (Alley et al, 1993; Pinson et al, 1995; Firatliet al, 1996; Firatli, 1997; Salvi et al, 1997; Alpagotet al, 2001; Guthmiller et al, 2001; Aren et al, 2003;Ünlü et al, 2003; Yucekal-Tuncer et al, 2003), andtype 2 diabetics and non-diabetics in five studies(Morton et al, 1995; Alpagot et al, 2001; Bulutet al, 2001; Yuan et al, 2001; Orbak et al, 2002).The overall difference in the average of PPDbetween type 1 diabetics and non-diabetics wasnot statistically different (mean difference = 0.11(�0.03 to 0.245), P = 0.137) (Fig 2.2a). The aver-age difference of PPD between type 2 diabeticsand non-diabetics was statistically different (meandifference = 0.46 (0.01 to 0.91, P = 0.046)(Fig 2.2b).Significant statistical heterogeneity was not found
across studies in all analyses: type 1 DM for meanof CAL: Q = 11.526, P = 0.17; type 2 DM for meanof CAL: Q = 2.416, P = 0.2990; type 1 DM for meanof PPD: Q = 7.220, P = 0.614 and type 2 DM formean of PPD: Q = 5.147, P = 0.273.
Publication bias
The results of Begg’s test with continuity correctionand Egger’s test confirmed that there was no evi-dence of publication bias. The results of the Begg’stest for type 1 DM for mean CAL: P = 0.754 and type2 DM for mean CAL: P = 1.000; type 1 DM for meanof PPD: P = 0.371 and type 2 DM for mean of PPD:P = 0.806. The results of Egger’s test for type 1DM for mean CAL: coefficient = 2.52, P = 0.015;type 2 DM for mean CAL: coefficient = �1.30,P = 0.719; type 1 DM for mean of PPD: coeffi-cient = 2.85, P = 0.220 and type 2 DM for meanof PPD: coefficient = 0.99, P = 0.640. Egger’s publi-cation bias plots were used to graphically show noevidence of publication bias (Fig 3). The values ofmean differences were plotted versus variancedifferences.
Longitudinal studies
The epidemiological characteristics of the eight longi-tudinal studies included in this review are describedin Table 4. Two papers were considered to be one
study, as they reported clinical and microbiologicalfindings of the same sample in separate papers(Novaes et al, 1996, 1997). No clinical trial wasidentified in the literature search, as no study ana-lysed the effect of glycaemic control on periodontalstatus. Of the eight selected longitudinal studies,four compared the progression of periodontal dis-ease between diabetics and non-diabetics and fourstudies investigated the effect of diabetes on theresponse to periodontal treatment (Table 4).The duration of diabetes was reported in two stud-
ies on type 1 and 2 DM (Westfelt et al, 1996; Christ-gau et al, 1998) and in one study on type 1 DM(Tervonen and Karjalainen, 1997). The duration ofdiabetes varied from 11 to 16.9 years. Three differ-ent types of periodontal probes were used. In gen-eral, few confounders were considered. Thenumbers ranged from 2 to 6 and the length of thestudies varied from 4 to 60 months.
Type 1 DMOf the three longitudinal studies on type 1 DM, twostudies compared periodontal disease progression(Firatli, 1997; Sbordone et al, 1998), and in onestudy the progression of periodontal disease wasmore pronounced in diabetics (Firatli, 1997). Inone study that investigated the relationship betweentype 1 DM and the response to periodontal therapy,no significant difference in the reduction of periodon-tal measures was observed between diabetics andnon-diabetics (Tervonen and Karjalainen, 1997).
Type 2 DMThree studies were conducted on type 2 DM and onthe progression of periodontal disease (Novaeset al, 1996, 1997; Taylor et al, 1998; Faria-Almeidaet al, 2006). One study found a significant increaseof CAL in diabetics compared with non-diabetics(Novaes et al, 1996). The other study showed thatthe progression of alveolar bone loss over timewas higher in diabetics compared with non-diabetics.The odds ratio was 4.2 (1.8 to 9.9) (Taylor et al,1998). The study that analysed the effect of diabe-tes on periodontal treatment showed a significantincrease of PPD in diabetics compared with non-dia-betics after 6 months of follow up (Faria-Almeidaet al, 2006).
Type 1 and 2 DMTwo studies included subjects with type 1 and 2 DMand analysed the effect of DM on the response toperiodontal therapy (Westfelt et al, 1996; Christgau
Chávarry et al
Vol 7, No 2, 2009 123

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
et al, 1998). No differences were reported in clinicalperiodontal measures between diabetics and non-diabetics after 4 months (Christgau et al, 1998)and after 5 years (Westfelt et al, 1996).
Quality assessment: results of eightlongitudinal studies
Sampling calculationNone of the eight studies determined the samplesize before the study.
Were the examiners trained and calibrated for
periodontal assessment?Of the eight studies, three had examiners who weretrained and calibrated for periodontal assessment(Firatli, 1997; Tervonen and Karjalainen, 1997; Tay-lor et al, 1998).
Adjustment for potential confoundersAll the citations received an inadequate score foradjustment of potential confounders.
Statistical analysisStatistical analysis was scored adequate in onestudy (Taylor et al, 1998).
Sampling design/selection of control groupIn one study, the sample was drawn randomly (Tayloret al, 1998). In five studies, the exposed and unex-posed groups came from the same population (Nov-aes et al, 1996, 1997; Tervonen and Karjalainen,1997; Christgau et al, 1998; Sbordone et al,1998; Taylor et al, 1998). The definition of exposedand unexposed groups was explicit in four citations(Westfelt et al, 1996; Christgau et al, 1998; Sbor-done et al, 1998; Taylor et al, 1998). The assess-ment of exposure was similar between the groupsin one study (Novaes et al, 1996, 1997). The expo-sure was assessed in the same manner in the samegroups in another study (Novaes et al, 1996, 1997).In all longitudinal studies, the outcome wasassessed in the same manner between the groups.The objective outcome criteria that were establishedfor assessed periodontitis for excluded cases in thecontrols were similar for both groups in all citations.Two studies (Novaes et al, 1996, 1997; Taylor et al,1998) had the objective exposure criteria applied tothe unexposed group to exclude exposed in the unex-posed groups.
Response rateFour studies reported the response rate (Firatli,1997; Tervonen and Karjalainen, 1997; Christgauet al, 1998; Taylor et al, 1998).
Blindness of outcome assessmentIn two studies, the examiners who conducted theperiodontal assessment were blinded to the diabeticstatus of the subjects (Tervonen and Karjalainen,1997; Taylor et al, 1998).
Blindness of exposure assessmentIn four studies, the examiners who tested the levelof glycaemic control were blinded for the periodontalstatus of the subjects (Firatli, 1997; Tervonen andKarjalainen, 1997; Sbordone et al, 1998; Tayloret al, 1998).
Updated exposureThe exposure was updated in seven studies (Novaeset al, 1996, 1997; Westfelt et al, 1996; Firatli,1997; Tervonen and Karjalainen, 1997; Sbordoneet al, 1998, Taylor et al, 1998, Faria-Almeida et al,2006).
Dropout ratesTwo studies reported dropouts (Westfelt et al, 1996;Tervonen and Karjalainen, 1997).
Dose–effect relationshipOne study reported dose–effect findings (Taylor et al,1998).
DISCUSSION
This meta-analysis of 57 peer-reviewed studiesleads to the conclusion that type 2 DM is a risk fac-tor for periodontitis. The overall difference for CAL of1.0 mm (CI 95%: 0.15 to 1.84, P < 0.021) was sig-nificant. In addition, longitudinal studies revealedsignificantly more progression of periodontal diseaseamong type 2 diabetics compared with non-diabet-ics. However, the evidence for an associationbetween type 1 DM and periodontitis is insufficient.Pooled differences of clinical measures of periodon-tal disease did not differ significantly between type 1diabetics and non-diabetics, and longitudinal studiesshowed conflicting findings.The lack of association between type 1 DM and
periodontal disease can be explained by the lowmean age of the subjects, namely, between 11
Chávarry et al
124 Oral Health & Preventive Dentistry

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
and 15 years. Even diabetic subjects in this agerange do not frequently develop destructive periodon-tal disease. As the prevalence of destructive peri-odontal disease would be apparent after the age of25 to 30 years (Albandar, 2002a, b), future studieson the relationship between type 1 DM and periodon-tal disease should select adult subjects.Most of the previous review papers on the associ-
ation between DM and periodontal disease did notuse an appropriate protocol for conducting system-atic reviews (Belting et al, 1964; Campbell, 1967;Hugoson and Jordan, 1982; Petersen and Ogawa,2005; Mealey and Oates, 2006; Tan et al, 2006).The limitations in such reviews include the lack ofinformation about the strategies used for searchingthe papers, the criteria used to select the papersand how the selection process and data extractionwere performed. Furthermore, the methodologicalquality of epidemiological studies was not taken intoaccount; for example, in this review, studies in whichthe type of diabetes were not reported and studieswith inadequate measures of periodontal diseasewere excluded. Applying those criteria resulted inthe exclusion of 72 papers and decreased the num-ber of studies considerably. However, the studieswith potential bias of exposure and outcome assess-ment might have been included in other reviews.Only one systematic review on the relationship
between diabetes and periodontal disease has beenconducted using quantitative data analysis (Khaderet al, 2006). Several features distinguish theauthors’ study from the previous meta-analysis byKhader et al (2006). First, the authors’ included farmore studies (57 versus 18). This occurred becausethe meta-analysis was conducted 4 years later andthe search strategy was not restricted to one data-base (MEDLINE). Second, the studies were com-bined according to the type of DM. In Khader et al(2006), the estimates of differences in meta-analy-sis were summarised for type 1 and 2 DM together.As type 1 and 2 DM are heterogeneous conditions,the conflation of the results generates unjustifiedassociations. Third, in this study clear criteria wereused to select studies with adequate assessmentof diabetes and periodontal disease, avoiding theinclusion of poor quality studies. Fourth, potentialpublication bias was assessed through Egger’s testand Begg’s test. There was no evidence of publica-tion bias. Finally, the quality assessment that wasconducted provided an adequate evaluation of themethodology of the selected studies.One limitation of this study is the use of observa-
tional studies in the meta-analysis as randomisedcontrolled trials (RCTs) were not identified. Although
RCTs provide the highest level of evidence, dueto ethical and logistical limitations, they cannotalways be performed. As no RCT was identified inthe authors’ search, observational studies wereincluded in this meta-analysis.The use of pooled estimates from observational
studies is controversial because they do not reachthe level of confidence of meta-analyses of random-ised controlled trials. The result of the meta-analysisin the present review can be considered appropriatebecause some precautions were used to reduce themethodological variability among studies that is fre-quently present in observational studies. Another lim-itation in this review is the inclusionof studieswith fewconfounders taken into account and the variability inthe sampling design and selection of control group.Although thedurationofdiabeteshasbeen reported
in some studies, relevant characteristics of DM suchas medical treatment, body mass index and systemiccomplications were not reported. Future studiesshould collect these data using accurate methods.Most of the reviews on diabetes and periodontal
disease supported the conclusions based on thePima Indian population study, an indigenous commu-nity with a high propensity to diabetes (Nelson et al,1990; Emrich et al, 1991). The conclusions basedon the Pima Indian population are relevant becausethe model minimised the potential confounders. Inaddition, the criteria used for periodontal diseaseassessment was based on alveolar bone loss thatwasassessed radiographically,which isa very reason-able method to detect periodontal disease. However,studies conducted on general populations are alsoimportant because of the differences in their genetic,environmental and behavioural characteristics.In conclusion, there is enough evidence to con-
sider type 2 DM as a risk factor for destructiveperiodontal disease. More studies are needed toassess if type 1 DM is a true risk factor for periodon-tal disease. In future studies on type 1 DM the inclu-sion of population aged 25 years and above isrecommended.
REFERENCES
1. Albandar JM. Periodontal diseases in North America.Periodontol 2000 2002a;29:31–69.
2. Albandar JM. Global risk factors and risk indicators forperiodontal diseases. Periodontol 2000 2002b;29:77–206.
3. Alderson P, Green S, Higgins JPT (eds). Cochrane review-ers’ handbook 4.2.2 (updated March 2004). In: TheCochrane Library, Issue 1. Chichester, UK: John Wiley &Sons, Ltd, 2004.
Chávarry et al
Vol 7, No 2, 2009 125

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
4. Alley CS, Reinhardt RA, Maze CA, DuBois LM, Wahl TO,Duckworth WC et al. HLA-D and T lymphocyte reactivity tospecific periodontal pathogens in type 1 diabetic periodon-titis. J Periodontol 1993;64:974–979.
5. Alpagot T, Silverman S, Lundergan W, Bell C, ChambersDW. Crevicular fluid elastase levels in relation to periodon-titis and metabolic control of diabetes. J Periodontal Res2001;36:169–174.
6. Aren G, Sepet E, Özdemir D, Dinççag N, Güvener B, Firatli E.Periodontal health, salivary status and metabolic control inchildren with type 1 diabetes mellitus. J Periodontol2003;74:1789–1795.
7. Begg CB, Berlin JA. Operating characteristics of a rankcorrelation test for publication bias. Biometrics1994;50:1088–1101.
8. Belting CM, Hiniker JJ, Dummett CO. Influence of diabetesmellitus on the severity of periodontal disease. J Period-ontol 1964;35:476–480.
9. Borges-Yáñez SA, Irigoyen-Camacho ME, Maupome G. Riskfactors and prevalence of periodontitis in community-dwelling elders in Mexico. J Clin Periodontol 2006;33:184–194.
10. Bulut S, Develioglu H, Taner IL, Berker E. Interleukin-1 betalevels in gingival crevicular fluid in type 2 diabetes mellitusand adult periodontitis. J Oral Sci 2001;43:161–177.
11. Campbell MJ. Periodontal disease in the diabetic patientand its treatment. Aust Dent J 1967;12:117–122.
12. Campus G, Salem A, Uzzau S, Baldoni E, Tonolo G.Diabetes and periodontal disease: a case-control study.J Periodontol 2005;76:418–425.
13. Cherry-Peppers G, Ship JA. Oral health in patients with typeII diabetes and impaired glucose tolerance. Diabetes Care1993;16:638–641.
14. Christersson LA. Actinobacillus actinomycetemcomitansand localized juvenile periodontitis, clinical, microbio-logic and histologic studies. Swed Dent J Suppl 1993;90:6–46.
15. Christgau M, Palitzsch K-D, Schmalz G, Kreiner U, Frenzel S.Healing response to non-surgical periodontal therapyin patients with diabetes mellitus: clinical, microbiological,and immunologic results. J Clin Periodontol 1998;25:112–124.
16. Collin HL, Sorsa T, Meurman JH, Niskanen L, Salo T, RonkaH et al. Salivary matrix metalloproteinase (MMP-8)levels and gelatinase (MMP-9) activities in patients withtype 2 diabetes mellitus. J Periodontal Res 2000;35:259–265.
17. Collin H-L, Uusitupa M, Niskanen L, Kontturi Närhi V,Markkanen H, Koivisto A-M et al. Periodontal findings inelderly patients with non-insulin dependent diabetes mel-litus. J Periodontol 1998;69:962–966.
18. Cutler CW, Machen RL, Jotwani R, Iacopino AM. Heightenedgingival inflammation and attachment loss in type 2diabetics with hyperlipidemia. J Periodontol 1999;70:1313–1321.
19. De Pommereau V, Dargent-Paré C, Robert JJ, Brion M.Periodontal status in insulin-dependent diabetic adoles-cents. J Clin Periodontol 1992;19:628–632.
20. Egger M, Smith GD, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997;315:629–634.
21. Emrich LJ, Shlossman M, Genco RJ. Periodontal disease innon-insulin-dependent diabetes mellitus. J Periodontol1991;62:123–130.
22. Faria-Almeida R, Navarro A, Bascones A. Clinical andmetabolic changes after conventional treatment of type 2diabetic patient with chronic periodontitis. J Periodontol2006;77:591–598.
23. Firatli E. The relationship between clinical periodontalstatus and insulin-dependent diabetes mellitus. Resultsafter 5 years. J Periodontol 1997;68:136–140.
24. Firatli E, Ünal T, Saka N, Onan U, Sivas A, Öz H. Serumfructosamine correlates with gingival index in children withinsulin-dependent diabetes mellitus (IDDM). J Clin Period-ontol 1994;21:565–568.
25. Firatli E, Yilmaz O, Onan U. The relationship betweenclinical attachment loss and the duration of insulin-depen-dent diabetes mellitus (IDDM) in children and adolescents.J Clin Periodontol 1996;23:362–366.
26. Fontana G, Lapolla A, Sanzari M, Piva E, Mussap M, DeToni S et al. An immunological evaluation of type II diabeticpatients with periodontal disease. J Diabetes Complica-tions 1999;13:23–30.
27. Güneri P, Unlu F, Yesilbek B, Bayraktar F, Kokuludag A,Hekimgil M et al. Vascular endothelial growth factor ingingival tissues and crevicular fluids of diabetic and healthyperiodontal patients. J Periodontol 2004;75:91–97.
28. Guthmiller JM, Hassebroek-Johnson JR, Weenig DR, John-son GK, Kirchner HL, Kohout FJ et al. Periodontal diseasein pregnancy complicated by type 1 diabetes mellitus. JPeriodontol 2001;72:1485–1490.
29. Harber J, Wattles J, Crowley M, Mandell R, Joshipura K,Kent RL. Evidence for cigarette smoking as a major riskfactor for periodontitis. J Periodontol 1993;64:16–23.
30. Hugoson A, Jordan T. Frequency distribution of individualsaged 20–70 years according to severity of periodontaldisease. Community Dent Oral Epidemiol 1982;10:187–192.
31. Hugoson A, Thorstensson H, Falk H, Kuylenstierna J.Periodontal conditions in insulin-dependent diabetics.J Clin Periodontol 1989;16:215–223.
32. Kawamura M, Fukuda S, Kawabata K, Iwamoto Y. Compar-ison of health behaviour and oral/medical conditions innon-insulin-dependent (type II) diabetics and non-diabetics.Aust Dent J 1998;43:315–320.
33. Khader YS, Kauod AS, El-Qaderi SS, Alkafajei A, BatayhaWQ. Periodontal status of diabetics compared with non-diabetics: a meta-analysis. J Diabetes Complications2006;20:59–68.
34. Kurtis B, Develioglu H, Taner IL, Balos K, Tekin IO. IL-6 levelsin gingival crevicular fluid (GCF) from patients with non-insulin dependent diabetes mellitus (NIDDM), adult peri-odontitis and healthy subjects. J Oral Sci 1999;41:63–67.
35. Lalla E, Cheng B, Lal S, Kaplan S, Softness B, Greenberg Eet al. Diabetes mellitus promotes periodontal destructionin children. J Clin Periodontol 2007;34:294–298.
36. Lalla E, Park DB, Papapanou PN, Lamster IB. Oral diseaseburden in Northern Manhattan patients with diabetesmellitus. Am J Public Health 2004;94:755–758.
37. Lu HK, Yang PC. Cross-sectional analysis of differentvariables of patients with non-insulin dependent diabetesand their periodontal status. Int J Periodontics RestorativeDent 2004;24:71–79.
38. Manouchehr-Pour M, Spagnuolo PJ, Rodman HM, BissadaNF. Comparison of neutrophil chemotactic response indiabetic patients with mild and severe periodontal disease.J Periodontol 1981;52:410–415.
Chávarry et al
126 Oral Health & Preventive Dentistry

Copyrig
ht
by
N
otfor
Qu
in
tessence
Not
forPublication
39. Mansour AA, Abd-Al-Sada N. Periodontal disease amongdiabetics in Iraq. Med Gen Med 2005;7:2.
40. Marugame T, Hayasaki H, Lee K, Eguchi H, Matsumoto S.Alveolar bone loss associated with glucose tolerance inJapanese men. Diabet Med 2003;20:746–751.
41. Mattout C, Bourgeois D, Bouchard P. Type 2 diabetes andperiodontal indicators: epidemiology in France 2002–2003. J Periodontal Res 2006;41:253–258.
42. Mealey BL, Oates TW. Diabetes mellitus and periodontaldisease. J Periodontol 2006;77:1289–1303.
43. Moher D, Schulz KF, Altman D. CONSORT group (Consol-idated Standards of Reporting Trials). The CONSORTstatement: revised recommendations for improving thequality of reports of parallel-group randomized trials. JAMA2001;285:1987–1991.
44. Morton AA, Williams RW, Watts LP. Initial study ofperiodontal status in non-insulin-dependent diabetics inMauritius. J Dent 1995;23:343–345.
45. Nelson RG, Shlossman M, Budding LM, Pettitt DJ, SaadMF, Genco RJ et al. Periodontal disease and NIDDM inPima Indians. Diabetes Care 1990;13:836–840.
46. Novaes AB Jr, Gutierrez FG, de Moraes Grisi MF, NovaesAB. Periodontal disease progression in type II non-insulin-dependent diabetes mellitus patients (NIDDM). Part II –Microbiological analysis using the bana test. Braz Dent J1997;8:27–33.
47. Novaes AB Jr, Gutierrez FG, Novaes AB. Periodontaldisease progression in type II non-insulin-dependent dia-betes mellitus patients (NIDDM). Part I – Probing pocketdepth and clinical attachment. Braz Dent J 1996;7:65–73.
48. Obeid P, Bercy P. Effects of smoking on periodontal healtha review. Adv Ther 2000;17:230–237.
49. Oliver RC, Tervonen T. Periodontitis and tooth loss. J AmDent Assoc 1993;124:71–75.
50. Orbak R, Tezel A, Çanakçi V, Demir T. The influence ofsmoking and non-insulin-dependent diabetes mellitus onperiodontal disease. J Int Med Res 2002;30:116–125.
51. Persson RE, Hollender LF, MacEntee MI, Wyatt CCL, KiyakGA, Persson GR. Assessment of periodontal conditions andsystemic disease in older subjects. J Clin Periodontol2003;30:207–213.
52. Petersen PE, Ogawa H. Strengthening the prevention ofperiodontal disease: the WHO approach. J Periodontol2005;76:2187–2193.
53. Pinson M, Hoffman WH, Garnick JJ, Litaker MS. Periodontaldisease and type I diabetes mellitus in children andadolescents. J Clin Periodontol 1995;22:118–123.
54. Rylander H, Ramberg P, Blohmé G, Lindhe J. Prevalence ofperiodontal disease in young diabetics. J Clin Periodontol1986;14:38–43.
55. Saito T, Murakami M, Shimazaki Y, Oobayashi K, Matsum-oto S, Koga T. Association between alveolar bone loss andelevated serum C-reactive protein in Japanese men. JPeriodontol 2003;74:1741–1746.
56. Saito T, Shimazaki Y, Kiyohara Y, Kato I, Kubo M, Lida Met al. The severity of periodontal disease is associated withthe development of glucose intolerance in non-diabetics:the Hisayama study. J Dent Res 2004;83:485–490.
57. Salvi GE, Yalda B, Collins JG, Jones BH, Smith FW, Arnold RRet al. Inflammatory mediator response as a potential riskmarker for periodontal diseases in insulin-dependent diabe-tes mellitus patients. J Periodontol 1997;68:127–135.
58. Sandberg GE, Sundberg HE, Fjellstrom CA, Wilkblad KF.Type 2 diabetes and oral health. A comparison betweendiabetic and non-diabetic subjects. Diabetes Res Clin Pract2000;50:27–34.
59. Sandholm L, Swanljung O, Rytömaa I, Kaprio EA, MäenpääJ. Periodontal status of Finnish adolescents with insulin-dependent diabetes mellitus. J Clin Periodontol 1989;16:617–620.
60. Sbordone L, Ramaglia L, Barone A, Ciaglia RN, Iacono VJ.Periodontal status and subgingival microbiota of insulin-dependent juvenile diabetics: a 3-year longitudinal study. JPeriodontol 1995;69:120–128.
61. Sbordone L, Ramaglia L, Barone A, Ciaglia RN, Tenore A,Iacono VJ. Periodontal status and selected cultivableanaerobic microflora of insulin-dependent juvenile diabet-ics. J Periodontol 1998;66:452–461.
62. Sheiham A, Netuveli GS. Periodontal diseases in Europe.Periodontol 2000 2002;29:104–121.
63. Tan WC, Tay FB, Lim LP. Diabetes as a risk factor forperiodontal disease: current status and future consider-ations. Ann Acad Med Singapore 2006;35:571–581.
64. Taylor GW, Burt BA, Becker MP, Genco RJ, Sholssman M,Knowler WC et al. Non-insulin dependent diabetes mellitusand alveolar bone loss progression over 2 years. J Period-ontol 1998;69:76–83.
65. Tervonen T, Karjalainen K. Periodotal disease related todiabetic status a pilot study of the response to periodontaltherapy in type 1 diabetes. J Clin Periodontol1997;24:505–510.
66. Thorstensson H, Dahlén G, Hugoson A. Some suspectedperiodontopathogens and serum antibody response inadult long-duration insulin-dependent diabetics. J ClinPeriodontol 1995;22:449–458.
67. Thorstensson H, Hugoson A. Periodontal disease experi-ence in adult long-duration insulin-dependent diabetics. JClin Periodontol 1993;20:352–358.
68. Tsai C, Hayes C, Taylor GW. Glycemic control of type 2diabetes and severe periodontal disease in the US adultpopulation. Community Dent Oral Epidemiol 2002;30:182–192.
69. Ünlü F, Güneri PG, Hekimgil M, Yesilbek B, Boyacioglu H.Expression of vascular endothelial growth factor in humanperiodontal tissues: comparison of healthy and diabeticpatients. J Periodontol 2003;74:181–187.
70. Vettore MV, Leao AT, Monteiro da Silva AM, Quintanilha RS,Lamarca GA. The relationship of stress and anxiety withchronic periodontitis. J Clin Periodontol 2003;30:394–402.
71. Westfelt E, Rylander G, Blohmé, Jonasson P, Lindhe J. Theeffect of periodontal therapy in diabetics results after5 years. J Clin Periodontol 1996;23:92–100.
72. Yavuzyilmaz E, Yumak Ö, Akdoganli T, Yamalik N, Özer N,Ersoy F et al. The alterations of whole saliva constituents inpatients with diabetes mellitus. Aust Dent J 1996;41:193–197.
73. Yucekal-Tuncer B, Uygur C, Firatli E. Gingival crevicular fluidlevels of aspartate amino transferase, sulfide ions and N-benzoyl-DL-arginine-2-naphthylamide in diabetic patientswith chronic periodontitis. J Clin Periodontol 2003;30:1053–1060.
74. Yuan K, Chang CJ, Hsu PC, Sun HS, Tseng CC, Wang JR.Detection of putative periodontal pathogens in non-insulin-dependent diabetes mellitus and non-diabetes mellitus bypolymerase chain reaction. J Periodontal Res 2001;36:18–24.
75. Zielinski MB, Fedele D, Forman LJ, Pomerantz SC. Oralhealth in the elderly with non-insulin-dependent diabetesmellitus. Spec Care Dentist 2002;22:94–98.
Chávarry et al
Vol 7, No 2, 2009 127