
Obesity and Psychiatric Disorder: Developmental Trajectories
11
DOI: 10.1542/peds.111.4.851 2003;111;851-859 Pediatrics and E. Jane Costello Sarah Mustillo, Carol Worthman, Alaattin Erkanli, Gordon Keeler, Adrian Angold Obesity and Psychiatric Disorder: Developmental Trajectories http://www.pediatrics.org/cgi/content/full/111/4/851 located on the World Wide Web at: The online version of this article, along with updated information and services, is rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275. Grove Village, Illinois, 60007. Copyright © 2003 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk publication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly at Duke University on September 25, 2007 www.pediatrics.org Downloaded from
Transcript of Obesity and Psychiatric Disorder: Developmental Trajectories
DOI: 10.1542/peds.111.4.851 2003;111;851-859 Pediatrics
and E. Jane Costello Sarah Mustillo, Carol Worthman, Alaattin Erkanli, Gordon Keeler, Adrian Angold
Obesity and Psychiatric Disorder: Developmental Trajectories
http://www.pediatrics.org/cgi/content/full/111/4/851located on the World Wide Web at:
The online version of this article, along with updated information and services, is
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275. Grove Village, Illinois, 60007. Copyright © 2003 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Duke University on September 25, 2007 www.pediatrics.orgDownloaded from

Obesity and Psychiatric Disorder: Developmental Trajectories
Sarah Mustillo, PhD*; Carol Worthman, PhD‡; Alaattin Erkanli, PhD*; Gordon Keeler, MS*;Adrian Angold, MRCPsych*; and E. Jane Costello, PhD*
ABSTRACT. Objectives. To identify age-related tra-jectories of obesity from childhood into adolescence, andto test the association of these trajectories with the de-velopment of psychiatric disorders (conduct disorder, op-positional defiant disorder, attention-deficit/hyperactiv-ity disorder, substance abuse, depression, and anxiety).
Methods. White children (N � 991) 9 to 16 years oldfrom the Great Smoky Mountains Study, a representativesample of rural youth, were evaluated annually over an8-year period for height, weight, psychiatric disorder,and vulnerabilities for psychiatric disorder. Longitudinalanalyses on the repeated measures data were conductedusing developmental trajectory models and generalizedestimating equation models.
Results. Obesity was 3 to 4 times more common thanexpected from national rates using Centers for DiseaseControl and Prevention 2000 criteria. Four developmentaltrajectories of obesity were found: no obesity (73%),chronic obesity (15%), childhood obesity (5%), and ado-lescent obesity (7%). Only chronic obesity was associatedwith psychiatric disorder: oppositional defiant disorderin boys and girls and depressive disorders in boys.
Conclusions. In a general population sample studiedlongitudinally, chronic obesity was associated withpsychopathology. Pediatrics 2003;111:851–859; obesity,psychopathology, developmental trajectories, depression,conduct disorder.
ABBREVIATIONS. GSMS, Great Smoky Mountains Study; BMI,body mass index; NHANES, National Health Interview Survey;CAPA, Child and Adolescent Psychiatric Assessment; ADHD,attention-deficit/hyperactivity disorder; SPMM, semiparametricmixture model; GEE, Generalized Estimation Equation; CDC,Centers for Disease Control and Prevention.
Obesity among children and adolescents is aserious public health issue in the UnitedStates. The percentage of children defined as
overweight has more than doubled since the 1970sand is still on the rise.1 Many studies have docu-mented a secular trend in childhood obesity that isassociated with increased health risks, both duringchildhood and later in adulthood.2–4 During child-hood, obesity is associated with neurologic, pulmo-nary, gastrointestinal, circulatory, and endocrine
conditions.5,6 In adulthood, a history of childhoodobesity is associated with an increased risk for car-diovascular disease, diabetes, colon cancer, and all-cause mortality.5,7
Overweight and obesity, or perceptions thereof,may also affect self-esteem, body image, and socialmobility,5,8 and it is well-known that adults who areoverweight or obese are at an increased risk forpsychological disorders.9,10 Less is known aboutwhether childhood obesity is associated with concur-rent psychopathology, or with specific types of psy-chiatric disorder. Most of the published research onobesity and psychopathology in children has usedclinical samples recruited because of obesity11–14 ordepression.15 The risk of psychiatric disorder inobese children in these referred samples may notreflect what is seen in the general population.
Among the structural, familial, and environmentalvulnerabilities associated with both obesity and psy-chopathology in childhood are being from a poor16,17
or single-parent household,17,18 having harsh or abu-sive parents,17,19,20 and, for some psychiatric disor-ders, being female.21 However, there is little researchthat establishes the direction of effect, or the role ofthese factors as mediators or moderators of the linkbetween obesity and psychopathology.
Weight fluctuations are common in childhood, andeven more so in adolescence.22 Because most studiesof childhood obesity and psychopathology are cross-sectional or retrospective, we do not know whetherthere are distinct patterns of obesity throughoutchildhood, nor do we know whether certain patternsare associated with particular outcomes. This studyprovides repeated measures of height and weighttaken annually over 8 years, together with annualinformation about family characteristics and mentalhealth. Longitudinal data permit identification ofdistinct developmental trajectories of obesity, sepa-rating the transiently obese from the chronicallyobese, and those whose obesity is confined to child-hood or adolescence.
The goals of this study are 1) to determine thenumber and type of distinct obesity trajectories in ageneral population sample of white children 9 to 16years old; 2) to examine whether trajectory member-ship is associated with family vulnerabilities such asgender, poverty, single-parent family, parentingstyle, parental history of mental illness or drugabuse, and life events; and 3) to test the relationshipbetween obesity trajectory membership and psycho-pathology, controlling for a range of potential medi-ators.
From the *Center for Developmental Epidemiology, Department of Psychi-atry and Behavioral Sciences, Duke University School of Medicine, Durham,North Carolina; and ‡Department of Anthropology, Emory University,Atlanta, Georgia.Received for publication May 22, 2002; accepted Oct 3, 2002.Address correspondence to Sarah Mustillo, PhD, Center for DevelopmentalEpidemiology, Duke University Medical Center, Box 3454, Durham, NC27710. E-mail: [email protected] (ISSN 0031 4005). Copyright © 2003 by the American Acad-emy of Pediatrics.
PEDIATRICS Vol. 111 No. 4 April 2003 851 at Duke University on September 25, 2007 www.pediatrics.orgDownloaded from

METHODS
Study Design and SampleA full description of the setting, sample, and data collection
methods can be found elsewhere.23 The Great Smoky MountainsStudy (GSMS) is a longitudinal study of the development ofpsychiatric disorder and need for mental health services in ruralyouth. A representative sample of 3 cohorts of children, 9, 11, and13 years old at intake was recruited from 11 counties in westernNorth Carolina. Potential participants were selected from the pop-ulation of some 20 000 children using a household equal proba-bility, accelerated cohort design.24 The accelerated cohort designmeans that over several years of data collection each cohortreaches a given age in a different year, which controls for cohorteffects.25
We used a 2-phase process to select the final sample for thelongitudinal study. A screening questionnaire was administeredto a parent (usually the mother) of the first stage random sample(N � 3896; 95% of those contacted). The questionnaire consistedmainly of the externalizing (behavioral) problems scale of theChild Behavior Checklist,26 and was administered by telephone orin person. All children scoring above a predetermined cut point(the top 25% of the total scores, in this case it was a score of 20)plus a 1-in-10 random sample of the remaining 75%, were re-cruited for detailed interviews. Eighty percent of those recruitedagreed to participate. The contribution of each participant wasweighted by the inverse of their selection probabilities, stratifiedby age and gender, to provide accurate prevalence estimates forthe population of the study area.27 Families were reinterviewedannually until the child was 16, and every 2 to 3 years thereafter.The data presented here, based on the first 8 annual waves of thestudy (1993–2000), consist of 4600 interviews with 991 non-His-panic white participants and their parents.
Fewer than 10% of the area residents and the sample wereAfrican American. Because racial/ethnic differences in adiposityand its correlates are well-documented,28,29 non-white childrenwere excluded from these analyses as power was not adequate forcomparisons.
The study protocol was approved by the Duke UniversitySchool of Medicine Institutional Review Board.
ProceduresTwo interviewers visited the family each year, either at home or
in a location convenient for them. Before the interviews began,parent and child signed informed consent forms. They were theninterviewed in separate rooms. Each parent and child was paid$10 after the interview.
Measures
ObesityHeight and weight were both assessed at 2 different points
during the interview, and the 2 averaged for these analyses. Par-ticipants wore normal clothing without shoes, socks, and belts.Height was measured to the nearest 0.1 cm using a stadiometer(CMS Weighing Equipment, London, United Kingdom) and stan-dard techniques.30 The measurement was repeated if the first 2measurements differed by �0.5 cm, and the nearest 2 of theresultant 3 were averaged. Participants were weighed twice to thenearest 0.1 kg on a portable digital scale (Soehnle, Murrhardt,Germany); a repeat measure was taken if the first 2 differed by�0.2 kg, and averaged as for height. Body mass index (BMI) wascalculated using the standard wt/ht2 formula.
For adults, obesity is generally defined as BMI �30 kg/m2; butno equivalent standard exists for children.30,31 In this study we useage- and sex-specific 95th percentiles from the revised (2000)growth charts of the Centers for Disease Control and Prevention(CDC), which are based on data from the National Health Inter-view Survey (NHANES).32 The reference values are based on USnational survey data and are intended for US children and ado-lescents.33 Because the GSMS children were weighed clothed, andthe NHANES children were weighed wearing only a gown, un-dergarments, and foam slippers, we subtracted 1 kg from weightbefore calculating the BMI.
PsychopathologyThe psychopathology outcomes were assessed using the Child
and Adolescent Psychiatric Assessment (CAPA), a psychiatric inter-
view for children 9 to 17 years old. The CAPA is an interviewer-based interview.34 The goal of interviews using this format is tocombine the advantages of clinical interviews with those of highlystructured epidemiologic interview methods.35 While using ahighly structured format of questions and probes, the interviewer-based approach trains the interviewer to ensure that the parent orchild being interviewed understands the construct under review,and provides enough detail and examples for a clear rating of theclinical severity of each symptom to be made. A detailed glossaryprovides the operational rules for identifying a clinically signifi-cant level of severity for each symptom.
The CAPA interviews parent and child separately, using dif-ferent interviewers. The presence of a symptom can be determinedon the basis of information from a single respondent, or using theeither/or rule common in clinical practice. For these analyses, wecounted a symptom as present if reported by either parent or childor both. The time frame of the CAPA for determining the presenceof most psychiatric symptoms is the past 3 months. Diagnoseswere based on Diagnostic and Statistical Manual of Mental Disorders,Fourth Edition criteria.36 For these analyses we combined psychi-atric diagnoses into 7 groups: conduct disorder, oppositional de-fiant disorder, depressive disorders (including major depression,dysthymia, and depression not otherwise specified), anxietydisorders (including separation anxiety, generalized anxiety dis-order, simple phobia, social phobia, agoraphobia, and panic),bulimia, substance abuse, and attention-deficit/hyperactivity dis-order (ADHD).
Background and Family VariablesPotential mediators and moderators of the relationship be-
tween obesity and psychopathology included in these analyseswere gender; family income (coded 0 � $0–$25 000, 1 � $25 001–$45 000, and 2 � 45 001�); 1 or both parents with less than an11th-grade education; single parent family; parental history oftreated mental illness, drug abuse, or criminal conviction; harsh oroverprotective parenting style; lax supervision; and traumatic lifeevents.
SeasonWe included in the trajectory models a variable to account for
the season when the child was weighed and measured. All par-ticipants were interviewed each year on a day as close as possibleto their birthday. Small seasonal variations in weight gain havebeen noted in 2 European samples,37,38 and studies relying onself-reports of weight have found that healthy adults believe theirweight increases by �5 pounds in the winter,39–41 although clin-ical research has failed to find support for seasonal weight gain.41
There is little literature on seasonal effects on children’s weight.Despite the lack of consensus on seasonal weight variation in
the literature, we noted a substantial seasonal weight variation inour sample. On average, 29% of children measured in the wintermonths (January, February, and March) were obese, comparedwith 20% during the remaining months, with a mean BMI differ-ence of 1. To correct for this, we included a 4-category variable forseason (January to March, April to June, July to September, andOctober to December) in the trajectory model as a time-dependentcovariate.
Interviewers and Interviewer TrainingInterviewers were residents of the area in which the study took
place. All had at least bachelor’s level degrees. They received 1month of training and constant quality control, maintained bypostinterview reviews of each schedule, notes, and tape record-ings by experienced interviewer supervisors and study faculty.Interviewers were trained by Department of Social Services staff inthe States requirements for reporting abuse or neglect.
Data Management and AnalysisScoring programs for the CAPA, written in SAS software (SAS
Institute, Inc, Cary, NC), combine information about the date ofonset, duration, and intensity of each event and symptom to createscale scores and diagnoses. Prevalence rates were calculated usingStata 7.0 (Stata Corporation, College Station, TX), taking the sur-vey design into account through weights and clustering. Signifi-cant differences were calculated using a design-based Pearson �2
with a second-order correction converted to an F statistic.
852 OBESITY AND PSYCHIATRIC DISORDER: DEVELOPMENTAL TRAJECTORIES at Duke University on September 25, 2007 www.pediatrics.orgDownloaded from
Obesity trajectories were determined by fitting a semiparamet-ric mixture model (SPMM) to the data, using PROC TRAJ inSAS.42 SPMMs identify distinct groups of individual trajectorieswithin the population. This approach to modeling growth curvesis different from traditional latent growth curve modeling in thatthe latter assumes the random parameters to be bivariate normaldistributed. In other words, all individuals belong to a single classof individuals who vary continuously on a latent trait. In contrast,the group-based method employed here assumes a number ofdiscrete classes, each having a specific intercept and age slope andan estimated population prevalence.42 Because we suspected thatindividuals do not vary continuously on obesity, but rather thatthere are a distinct number of obesity trajectories, the group-basedmethod was the most appropriate.
The logit model was used to model the presence or absence ofobesity predicted by age. By specifying the sampling weights, weinvoked the robust variance estimator (ie, sandwich type estima-tor) to adjust the standard errors of the parameter estimates toaccount for the 2-phase sampling design. Thus, the classes thatwere identified, and their estimated prevalences and correlates,relate to the entire population of white children in the 11-countyarea from which participants were sampled.
Children were classified into their most probable obesity tra-jectory class by the use of posterior probabilities. A posteriorprobability is the probability of each individual belonging to each
group.42 Thus, individuals are assigned to the group to which theyhave the highest probability of belonging. Once children wereassigned to a trajectory class, we conducted analyses in 3 stages.
First, we computed bivariate statistics to obtain prevalencerates of various background, familial, and psychopathologicalcharacteristics by obesity trajectory. An F test for each variabletested whether there was any difference among obesity groups.Second, we fit multinomial logit models to determine how thebackground and familial characteristics identified as significant inthe first stage distinguished children on the different obesity tra-jectories from the comparison group of never-obese children.Third, we fit Generalized Estimation Equation (GEE) models toestimate the relationship between the different obesity trajectoriesand psychiatric disorders, controlling for the background factorsidentified in the second stage. The GEE models were run usingbinary regression with logit link function for dichotomous out-comes, such as the presence or absence of a psychiatric diagnosis,using the Stata program xtgee. The use of multiwave data with theappropriate sample weights capitalized on the availability of mul-tiple observation points over time, while controlling for the effecton variance estimates of repeated measures on the same child, foroverlapping cohorts, and for design effects.
RESULTS
Obesity and AgeTable 1 shows the association between age and
mean BMI for boys and girls. Gender differences inmean BMI were small and insignificant. BMI rosesteadily through late childhood and adolescence, be-ginning at �18 for 9 year olds, and rising to �20 byage 12, 22 by age 14, and 24 by age 16.
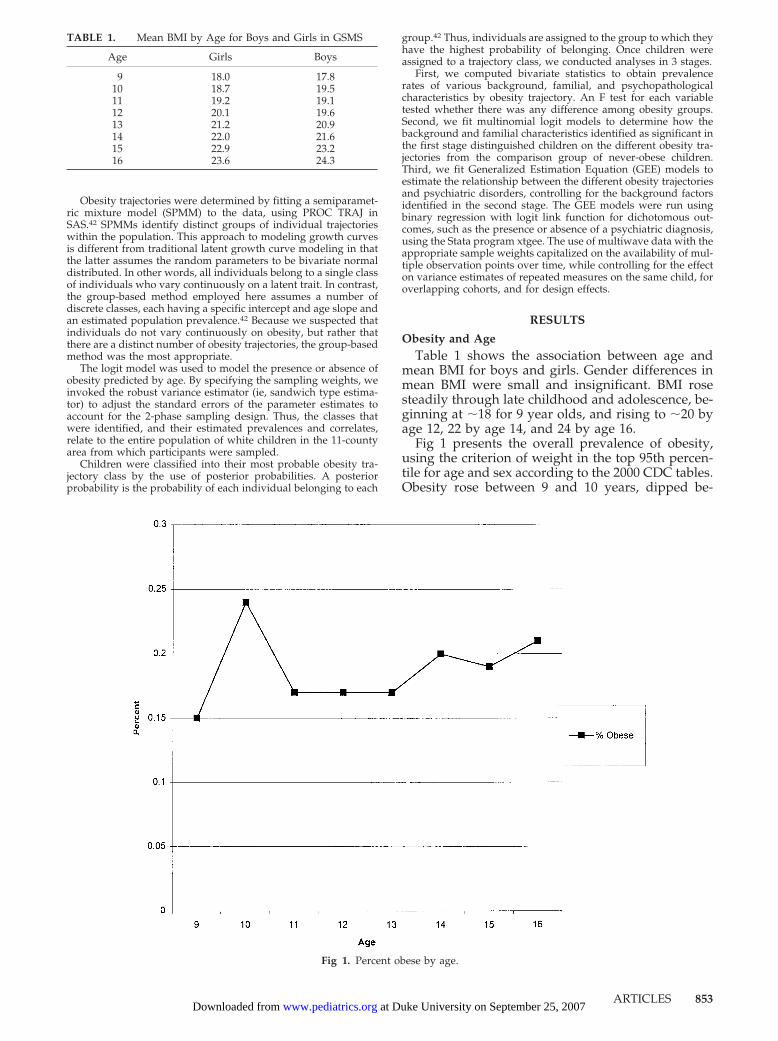
Fig 1 presents the overall prevalence of obesity,using the criterion of weight in the top 95th percen-tile for age and sex according to the 2000 CDC tables.Obesity rose between 9 and 10 years, dipped be-
Fig 1. Percent obese by age.
TABLE 1. Mean BMI by Age for Boys and Girls in GSMS
Age Girls Boys
9 18.0 17.810 18.7 19.511 19.2 19.112 20.1 19.613 21.2 20.914 22.0 21.615 22.9 23.216 23.6 24.3
ARTICLES 853 at Duke University on September 25, 2007 www.pediatrics.orgDownloaded from
tween 10 and 11 years, flattened out between 11 and13 years, then rose again steadily to 16 years, atwhich point �20% were obese. Generally, the prev-alence of obesity increased with age. These resultsshow that this rural, Southern sample was substan-tially heavier than the general population of childrenand adolescents in the United States, based on theCDC criteria, as 20% of the sample was above the95th percentile by 16 years.
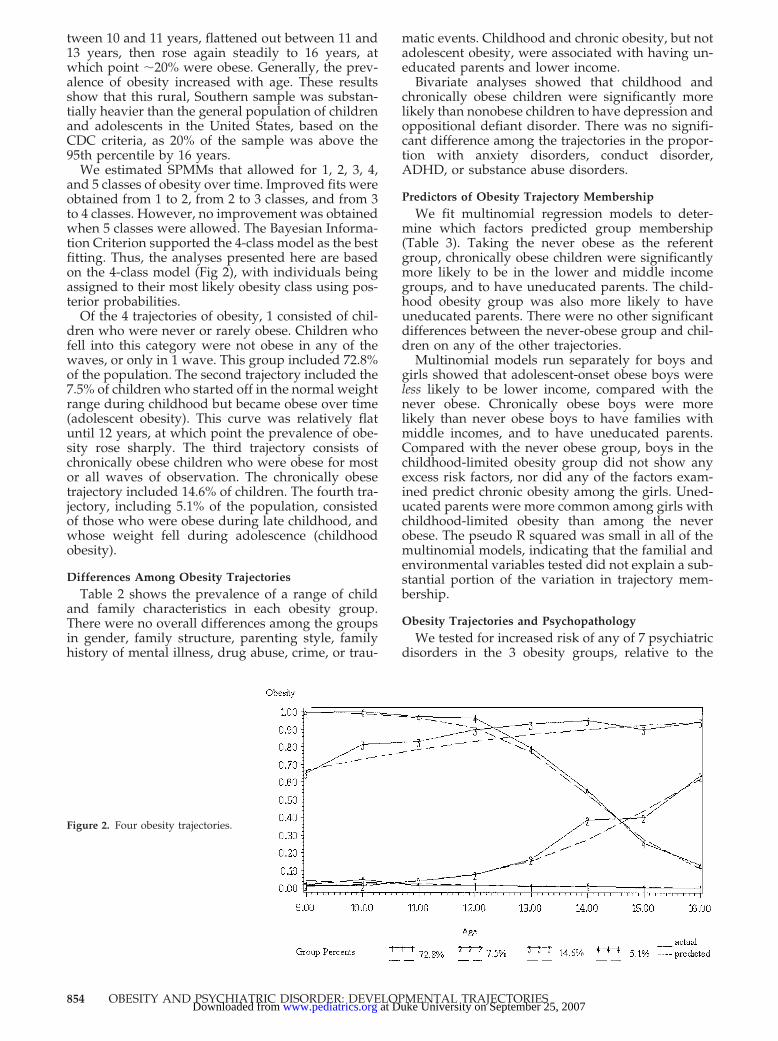
We estimated SPMMs that allowed for 1, 2, 3, 4,and 5 classes of obesity over time. Improved fits wereobtained from 1 to 2, from 2 to 3 classes, and from 3to 4 classes. However, no improvement was obtainedwhen 5 classes were allowed. The Bayesian Informa-tion Criterion supported the 4-class model as the bestfitting. Thus, the analyses presented here are basedon the 4-class model (Fig 2), with individuals beingassigned to their most likely obesity class using pos-terior probabilities.
Of the 4 trajectories of obesity, 1 consisted of chil-dren who were never or rarely obese. Children whofell into this category were not obese in any of thewaves, or only in 1 wave. This group included 72.8%of the population. The second trajectory included the7.5% of children who started off in the normal weightrange during childhood but became obese over time(adolescent obesity). This curve was relatively flatuntil 12 years, at which point the prevalence of obe-sity rose sharply. The third trajectory consists ofchronically obese children who were obese for mostor all waves of observation. The chronically obesetrajectory included 14.6% of children. The fourth tra-jectory, including 5.1% of the population, consistedof those who were obese during late childhood, andwhose weight fell during adolescence (childhoodobesity).
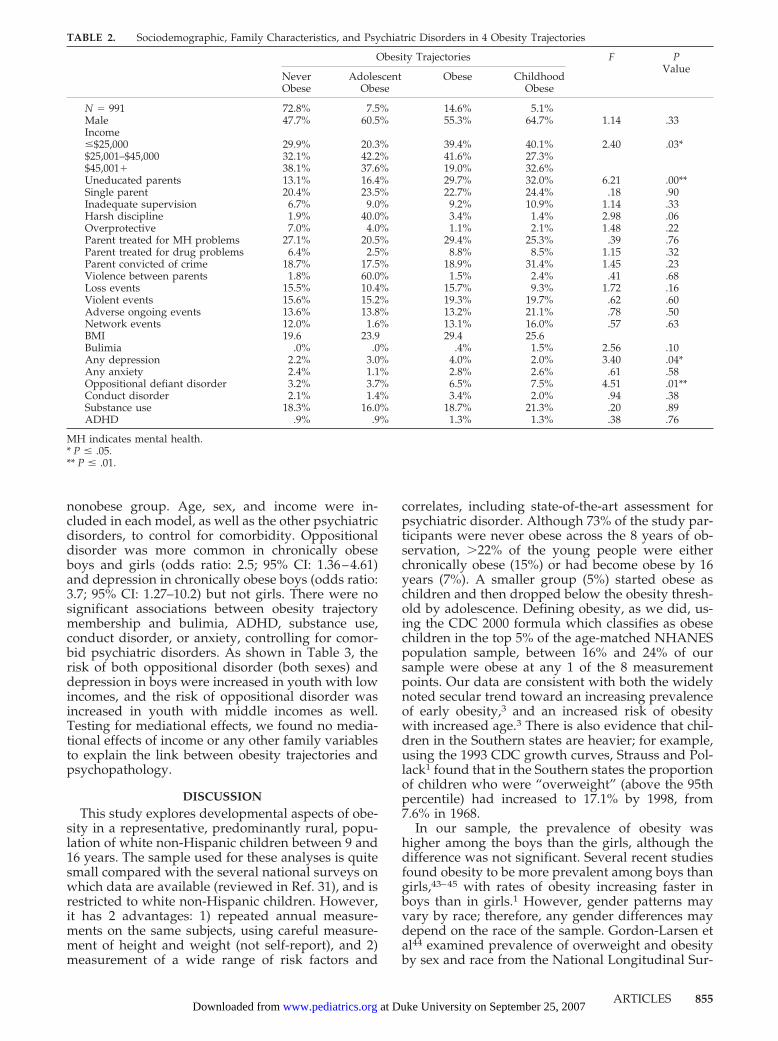
Differences Among Obesity TrajectoriesTable 2 shows the prevalence of a range of child
and family characteristics in each obesity group.There were no overall differences among the groupsin gender, family structure, parenting style, familyhistory of mental illness, drug abuse, crime, or trau-
matic events. Childhood and chronic obesity, but notadolescent obesity, were associated with having un-educated parents and lower income.
Bivariate analyses showed that childhood andchronically obese children were significantly morelikely than nonobese children to have depression andoppositional defiant disorder. There was no signifi-cant difference among the trajectories in the propor-tion with anxiety disorders, conduct disorder,ADHD, or substance abuse disorders.
Predictors of Obesity Trajectory MembershipWe fit multinomial regression models to deter-
mine which factors predicted group membership(Table 3). Taking the never obese as the referentgroup, chronically obese children were significantlymore likely to be in the lower and middle incomegroups, and to have uneducated parents. The child-hood obesity group was also more likely to haveuneducated parents. There were no other significantdifferences between the never-obese group and chil-dren on any of the other trajectories.
Multinomial models run separately for boys andgirls showed that adolescent-onset obese boys wereless likely to be lower income, compared with thenever obese. Chronically obese boys were morelikely than never obese boys to have families withmiddle incomes, and to have uneducated parents.Compared with the never obese group, boys in thechildhood-limited obesity group did not show anyexcess risk factors, nor did any of the factors exam-ined predict chronic obesity among the girls. Uned-ucated parents were more common among girls withchildhood-limited obesity than among the neverobese. The pseudo R squared was small in all of themultinomial models, indicating that the familial andenvironmental variables tested did not explain a sub-stantial portion of the variation in trajectory mem-bership.
Obesity Trajectories and PsychopathologyWe tested for increased risk of any of 7 psychiatric
disorders in the 3 obesity groups, relative to the
Figure 2. Four obesity trajectories.
854 OBESITY AND PSYCHIATRIC DISORDER: DEVELOPMENTAL TRAJECTORIES at Duke University on September 25, 2007 www.pediatrics.orgDownloaded from
nonobese group. Age, sex, and income were in-cluded in each model, as well as the other psychiatricdisorders, to control for comorbidity. Oppositionaldisorder was more common in chronically obeseboys and girls (odds ratio: 2.5; 95% CI: 1.36–4.61)and depression in chronically obese boys (odds ratio:3.7; 95% CI: 1.27–10.2) but not girls. There were nosignificant associations between obesity trajectorymembership and bulimia, ADHD, substance use,conduct disorder, or anxiety, controlling for comor-bid psychiatric disorders. As shown in Table 3, therisk of both oppositional disorder (both sexes) anddepression in boys were increased in youth with lowincomes, and the risk of oppositional disorder wasincreased in youth with middle incomes as well.Testing for mediational effects, we found no media-tional effects of income or any other family variablesto explain the link between obesity trajectories andpsychopathology.
DISCUSSIONThis study explores developmental aspects of obe-
sity in a representative, predominantly rural, popu-lation of white non-Hispanic children between 9 and16 years. The sample used for these analyses is quitesmall compared with the several national surveys onwhich data are available (reviewed in Ref. 31), and isrestricted to white non-Hispanic children. However,it has 2 advantages: 1) repeated annual measure-ments on the same subjects, using careful measure-ment of height and weight (not self-report), and 2)measurement of a wide range of risk factors and
correlates, including state-of-the-art assessment forpsychiatric disorder. Although 73% of the study par-ticipants were never obese across the 8 years of ob-servation, �22% of the young people were eitherchronically obese (15%) or had become obese by 16years (7%). A smaller group (5%) started obese aschildren and then dropped below the obesity thresh-old by adolescence. Defining obesity, as we did, us-ing the CDC 2000 formula which classifies as obesechildren in the top 5% of the age-matched NHANESpopulation sample, between 16% and 24% of oursample were obese at any 1 of the 8 measurementpoints. Our data are consistent with both the widelynoted secular trend toward an increasing prevalenceof early obesity,3 and an increased risk of obesitywith increased age.3 There is also evidence that chil-dren in the Southern states are heavier; for example,using the 1993 CDC growth curves, Strauss and Pol-lack1 found that in the Southern states the proportionof children who were “overweight” (above the 95thpercentile) had increased to 17.1% by 1998, from7.6% in 1968.
In our sample, the prevalence of obesity washigher among the boys than the girls, although thedifference was not significant. Several recent studiesfound obesity to be more prevalent among boys thangirls,43–45 with rates of obesity increasing faster inboys than in girls.1 However, gender patterns mayvary by race; therefore, any gender differences maydepend on the race of the sample. Gordon-Larsen etal44 examined prevalence of overweight and obesityby sex and race from the National Longitudinal Sur-
TABLE 2. Sociodemographic, Family Characteristics, and Psychiatric Disorders in 4 Obesity Trajectories
Obesity Trajectories F PValue
NeverObese
AdolescentObese
Obese ChildhoodObese
N � 991 72.8% 7.5% 14.6% 5.1%Male 47.7% 60.5% 55.3% 64.7% 1.14 .33Income�$25,000 29.9% 20.3% 39.4% 40.1% 2.40 .03*$25,001–$45,000 32.1% 42.2% 41.6% 27.3%$45,001� 38.1% 37.6% 19.0% 32.6%Uneducated parents 13.1% 16.4% 29.7% 32.0% 6.21 .00**Single parent 20.4% 23.5% 22.7% 24.4% .18 .90Inadequate supervision 6.7% 9.0% 9.2% 10.9% 1.14 .33Harsh discipline 1.9% 40.0% 3.4% 1.4% 2.98 .06Overprotective 7.0% 4.0% 1.1% 2.1% 1.48 .22Parent treated for MH problems 27.1% 20.5% 29.4% 25.3% .39 .76Parent treated for drug problems 6.4% 2.5% 8.8% 8.5% 1.15 .32Parent convicted of crime 18.7% 17.5% 18.9% 31.4% 1.45 .23Violence between parents 1.8% 60.0% 1.5% 2.4% .41 .68Loss events 15.5% 10.4% 15.7% 9.3% 1.72 .16Violent events 15.6% 15.2% 19.3% 19.7% .62 .60Adverse ongoing events 13.6% 13.8% 13.2% 21.1% .78 .50Network events 12.0% 1.6% 13.1% 16.0% .57 .63BMI 19.6 23.9 29.4 25.6Bulimia .0% .0% .4% 1.5% 2.56 .10Any depression 2.2% 3.0% 4.0% 2.0% 3.40 .04*Any anxiety 2.4% 1.1% 2.8% 2.6% .61 .58Oppositional defiant disorder 3.2% 3.7% 6.5% 7.5% 4.51 .01**Conduct disorder 2.1% 1.4% 3.4% 2.0% .94 .38Substance use 18.3% 16.0% 18.7% 21.3% .20 .89ADHD .9% .9% 1.3% 1.3% .38 .76
MH indicates mental health.* P � .05.** P � .01.
ARTICLES 855 at Duke University on September 25, 2007 www.pediatrics.orgDownloaded from

vey of Adolescent Health and found that boys had ahigher prevalence of overweight and obesity thangirls among whites and Asians, but girls had a higherprevalence among Hispanics and blacks.
Familial and environmental risk factors for chronicobesity were surprisingly few; of the �20 examined,only income and lack of parental education remainedsignificant in multivariable analyses. Children withchronic or childhood obesity were more than twiceas likely as other children to come from familieswhere 1 or both parents left school before the 11thgrade. Lack of parental education remained signifi-cant after controlling for having a single, unem-ployed, or teenage parent, and other correlated riskfactors (Table 3). An inverse relationship betweenincome and BMI has been observed in several stud-ies.46–48 The present study found a correlation be-tween BMI and income of between �.20 and �.25across each of the 8 annual assessments. However,this link between income and overweight may bespecific to white children in the United States,1 and isclearly a phenomenon of developed economies. Thisstudy found an inverse relationship between chronicobesity and socioeconomic status in the combinedsample, contrary to several previous studies, whichfind a stronger association among females thanmales.49 However, in our sample, different types ofobesity had different associations with income so theapparent inconsistencies may be attributed to thedifference between examining trajectories of obesityand obesity as a monolithic category.
Using developmental trajectory modeling, wewere able to show that chronic and childhood-onlyobesity were more common in the lowest incomegroup (annual family income below $25 000) than inthe middle or upper income groups. Chronic obesitywas also more common than expected in childrenfrom the middle income group ($25 000–$45 000).This inverse relationship between weight and pov-erty, beginning in childhood and, in the case of thepoorest children, persisting into adolescence, reflectsearlier studies.16,50 It is particularly troubling in thelight of evidence from the 1946 British birth cohort
TABLE 3. Comparison with Never Obese Trajectory: Multinomial Regression
Independent Variables Adolescent Obesity* Chronic Obesity* Childhood Obesity*
Relative Risk Ratios (Robust Standard Error)
Male 1.72 (.85) 1.28 (.37) 1.95 (1.13)Low income† .67 (.30) 2.16 (.74)‡ 1.05 (.73)Middle income† 1.27 (.49) 2.31 (.72)§ .80 (.50)Parental style 1.12 (.35) 1.24 (.23) 1.25 (.25)Parental history .74 (.13) .92 (.09) 1.09 (.15)Uneducated parents 1.61 (.78) 2.34 (.73)§ 3.20 (1.68)‡Life events 1.37 (.28) 1.01 (.15) .80 (.20)Wald �2 54.4§Pseudo R2 .04
Girls onlyLow income† 1.11 (.81) 2.25 (1.14) 1.39 (1.11)Middle income† .91 (.77) 1.79 (.86) 1.73 (1.02)Parental style 1.18 (.57) .80 (.23) 1.12 (.24)Parental history .89 (.18) .90 (.11) 1.16 (.24)Uneducated parents 2.37 (1.65) 2.08 (.97) 7.44 (4.39)§Life events 1.44 (.50) 1.29 (.30) 1.39 (.29)Wald �2 88.5§Pseudo R2 .05
Boys onlyLow income† .37 (.18)‡ 2.08 (.93) .93 (.83)Middle income† 1.53 (.60) 2.92 (1.10)§ .56 (.46)Parental style 1.08 (.44) 1.75 (.40) 1.27 (.41)Parental history .62 (.16) .95 (.16) 1.08 (.15)Uneducated parents 1.10 (.69) 2.51 (1.06)‡ 1.70 (1.32)Life events 1.25 (.33) .80 (.15) .50 (.16)‡Wald �2 47.5§Pseudo R2 .05
* Reference group is Group 1—Never/Rarely Obese.† Reference group is high income.‡ P � .05.§ P � .01.
TABLE 4. GEE Models of Association Between Obesity Tra-jectories and Oppositional Defiance Disorder (Both Sexes) andDepression (Boys) (Semirobust Standard Errors in Parentheses)
Independent Variables OppositionalDefiance Disorder
Total Sample
DepressionBoys Only
Sex 1.31 (.33)Low income† 2.85 (.85)§ 4.50 (2.23)§Middle income† 2.06 (.66)‡ 2.15 (1.08)Age 1.08 (.06) 1.17 (.11)Adolescent obese* .94 (.41) .24 (.26)Chronic obese* 2.57 (.79)§ 3.72 (1.94)§Childhood obese* 2.00 (.91) 1.68 (1.15)Wald �2 24.83§ 26.90§n (observations/subjects) 4288/983 2374/555
* Reference group is Group 1—Never/Rarely Obese.† Reference group is high income.‡ P � .05§ P � .01.
856 OBESITY AND PSYCHIATRIC DISORDER: DEVELOPMENTAL TRAJECTORIES at Duke University on September 25, 2007 www.pediatrics.orgDownloaded from

that the inverse association between socioeconomicstatus and BMI predicted higher BMI through tomiddle age48 and was impervious to the child’s lateracademic or economic achievements.
The present study shows first and foremost thatthere are different types of childhood obesity. Addi-tionally, this study shows that of the 4 basic weighttrajectories—never obese, chronically obese, increas-ing risk, and decreasing risk—only chronic obesitywas associated with a statistically significant increasein the risk of psychiatric disorder. The group withthe next-highest prevalence of psychiatric disorderwas in the small group who were obese in childhoodbut became less so as they moved through adoles-cence. Adolescent-onset obesity was not associatedwith increased risk of psychopathology.
Chronically obese children had significantlyhigher rates of oppositional defiant disorder, and (forboys) depression. This is, to our knowledge, the firststudy to show an association between chronic obe-sity and behavioral problems in children and adoles-cents. Several studies have linked child and adoles-cent obesity to depression, but the majority of theseare based on clinic samples, referred either becauseof obesity11–14 or depression.15 We cannot rule outthe possibility that the co-occurrence of the 2 condi-tions increased the likelihood of a clinical referral.51
Among epidemiologic studies, the evidence link-ing obesity and depression is much less clear. TheNew York longitudinal study52 found an inverse re-lationship between adolescent depression and youngadult obesity in males, and no relationship in fe-males. One study53 argued that the association be-tween overweight and depression may be caused bythe effects of dieting, or of poor health. Another54
demonstrated that any association between depres-sion and BMI in a sample of third graders was ex-plained by concern about being overweight. Ofcourse, this may be true across the whole populationbut not true for the smaller group of obese youth.
Some studies have found that obesity is associatedwith lower levels of psychopathology, as opposed tohigher levels.55 Friedman et al55 note that inconsis-tencies in prior studies of obesity and psychopathol-ogy may be attributed to methodological and sam-pling limitations. Additionally, we would add thatinconsistencies in prior findings may be caused, inpart, by the failure to consider developmental trajec-tories. In our sample, being obese at 1 point in timewas not associated with an increased risk in psycho-pathology, rather being in the chronically obese tra-jectory was.
One limitation of this study is that it does notaddress the issue of causality. Studies such as thisbeg the question, does obesity increase the risk ofpsychopathology or does psychopathology increasethe risk of obesity? DiPietro et al56 rely on epidemi-ologic data to examine changes in weight as a func-tion of changes in depressive symptoms and findthat depression plays a role in weight change.Younger men (�55 years old) who were depressed atbaseline gained more weight during the follow-upperiod than those not depressed, while youngwomen who were depressed at baseline gained less
weight than the nondepressed. In a small prospectivecase-control study, Pine et al15 found that depressionduring childhood was positively associated withBMI during adulthood. Conversely, Pine et al52
found an association with current but not prior de-pression in a large, population-based sample. Theseinconsistencies between prior depression and cur-rent BMI may be due to differences in type of sample,measurement of psychopathology, and the use ofself-report versus measured height and weight.
In this study, we examine the association betweenobesity and psychopathology; however, we draw noconclusions about causal ordering. If psychopathol-ogy increases the risk of obesity, we would expect anassociation in the chronic and adolescent-onsetgroups. If obesity increases the risk of psychopathol-ogy, we would expect an association in the chronicand childhood-limited groups. Our findings showthat psychopathology is most common in the chron-ically obese group first, and the childhood-limitedgroup second. Therefore, these results could be sug-gestive of obesity increasing the risk of psychopa-thology; however, that conclusion is purely specula-tive. Future research investigating the sequence ofevents is necessary to draw any conclusions aboutcausation. It is also possible that rather than 1 in-creasing the risk of the other, they are both associ-ated with the same physiologic mechanisms.
Evidence, largely from adults, links obesity anddepression through underlying neuro-endocrinesubstrates. Specifically, activity of the hypothalamo-pituitary adrenal axis appears to be altered in bothdepressed57–59 and obese60,61 adults, although evi-dence from depressed obese adults is contradicto-ry,62 and little is known about children. The trajecto-ries of obesity identified here may manifest in partsequelae of suboptimal conditions for early develop-ment. For example, a growing body of research doc-uments the role of maternofetal stress in later mentaland physical health risk. Prenatal stress followed bypostnatal overnutrition leads to childhood over-weight63 and adult obesity64 as well as adult depres-sion65 and increased hypothalamo-pituitary adrenalactivity.66,67 Overall, relevant findings are more sug-gestive than definitive, leaving etiologic interrela-tionships between obesity and mood or behaviordisorders and their possible common neuroendo-crine mediators a subject for further investigation.
Although chronic obesity and bulimia were linkedin bivariate analyses, there were very few cases ofbulimia in this sample, and all but 2 were comorbidfor oppositional disorder and/or depression. Inter-estingly, bulimia was only associated with obesitywhen it was comorbid with a psychiatric disorder.Bulimia is clearly an important clinical problem, andthe fact that in this population of 9 to 16 year olds itwas seen almost exclusively in children with otherpsychiatric disorders argues for vigilance on the partof clinicians to identify these comorbid childrenearly.
There is debate about the accuracy of BMI as ameasure of the prevalence of obesity.68,69 For exam-ple, Frankenfield et al69 compared BMI to percentbody fat as measures of obesity, and found that BMI
ARTICLES 857 at Duke University on September 25, 2007 www.pediatrics.orgDownloaded from
underidentified obesity. Defining obesity as a BMI�30 or at least 25% body fat for men and 30% forwomen, 30% of men and 40% of women who hadBMI �30 had obesity-level body fat. In adolescents,however, Malina68 found BMI to be a highly sensi-tive and specific marker of obesity, if not of over-weight.
A technical limitation of this study is that thechildren were weighed and measured clothed exceptfor their shoes, socks, and belts. A constant 1 kg wassubtracted from their weight before BMIs were cal-culated. The seasonal difference in weight observedin this study may have been caused in part by extraclothing worn in the winter, although Americanhomes tend to be kept to a fairly even temperaturethroughout the year. Another limitation is that al-though the GEE models used repeated measures,they did not deal with the relative timing of obesityand psychiatric disorder. Thus, we could determineif an association existed between the obesity trajec-tories and Diagnostic and Statistical Manual of MentalDisorders, Fourth Edition diagnoses, but not whetheran association was more likely to occur at a particu-lar age or if the association existed over time.
CONCLUSIONSChronic obesity across 8 years from 9 to 16 years of
age was observed in almost 15% of a general popu-lation sample of rural white youth, 3 times the ratepredicted using the most recent CDC criteria. A fur-ther 7% became obese in adolescence, while 5% whohad been obese in childhood moved out of obesity byadolescence. Chronic obesity was more common inchildren from poor and less-educated families, and ithad implications for mental health. New methods ofdata analysis that permit the modeling of develop-mental trajectories offer the opportunity to deepenour understanding of pathways to health and illnessacross childhood and adolescence.
ACKNOWLEDGMENTSWork contributing to these analyses was supported by
MH01167, MH57731, and MH48085 from the National Institute ofMental Health, and DA11301 from the National Institute on DrugAbuse.
We are most grateful to the people of western North Carolinafor their collaboration in the GSMS, to Dan Nagin and Mike Ezellfor their methodological assistance, and to the reviewers for theirhelpful comments.
REFERENCES1. Strauss RS, Pollack HA. Epidemic increase in childhood overweight,
1986–1998. JAMA. 2001;286:2845–28482. Gidding SS, Bao W, Srinivasan SR, Berenson GS. Effects of secular
trends in obesity on coronary risk factors in children: the BogalusaHeart Study. J Pediatr. 1995;127:868–874
3. Tremblay MS, Willms JD. Secular trends in the body mass index ofCanadian children. Can Med Assoc J. 2000;163:1429–1433
4. Eisenmann JC, Katzmarzyk PT, Arnall DA, Kanuha V, Interpreter C,Malina RM. Growth and overweight of Navajo youth: secular changesfrom 1955 to 1997. Int J Obes Relat Metab Disord. 2000;24:211–218
5. Must S, Strauss RS. Risks and consequences of childhood and adoles-cent obesity. Int J Obes Relat Metab Disord. 1999;23:S2–11
6. Deckelbaum RJ, Williams CL. Childhood obesity: the health issue. ObesJ. 2001;9:239S–243S
7. Dietz WH. Childhood weight affects adult mortality. J Nutr. 1998;128:411S–414S
8. Ge X, Elder GH, Regnerus M, Cox C. Pubertal transitions, perceptions
of being overweight, and adolescents’ psychological maladjustment:gender and ethnic differences. Soc Psychol Q. 2001;64:363–375
9. National Institutes of Health National Heart, Lung, and Blood Institute.Clinical guidelines on the identification, evaluation, and treatment ofoverweight and obesity in adults. 1998
10. Stunkard AJ, Wadden TA. Obesity: Theory and Therapy, 2nd ed. NewYork, NY: Raven Press; 1993
11. Britz B, Siegfried W, Ziegler A, et al. Rates of psychiatric disorders in aclinical study group of adolescents with extreme obesity and in obeseadolescents ascertained via a population based study. Int J Obes. 2000;24:1707–1714
12. Zipper E, Vila G, Dabbas M, et al. Obesity in children and adolescents,mental disorders and familial psychopathology. Presse Med. 2001;30:1489–1495
13. Sheslow D, Hassink S, Wallace W, DeLancey E. The relationship be-tween self-esteem and depression in obese children. Ann N Y Acad Sci.1993;699:289–291
14. Csabi G, Tenyi T, Molnar D. Depressive symptoms among obese chil-dren. Eat Weight Disord. 2000;5:43–45
15. Pine DS, Goldstein RB, Wolk S, Weissman MM. The association be-tween childhood depression and adulthood body mass index. Pediatrics.2001;107:1049–1056
16. Stunkard AJ, Sorensen TIA. Obesity and socioeconomic status—a com-plex relation. N Engl J Med. 1993;329:1036–1037
17. Costello EJ, Keeler GP, Angold A. Poverty, race/ethnicity and psychi-atric disorder: a study of rural children. Am J Public Health. 2001;91:1494–1498
18. Racelli GP, Belmont L. Obesity in nineteen year old men: family sizeand birth order associations. Am J Epidemiol. 1975;109:66–77
19. Felitti VJ, Anda RF, Nordenberg D, et al. Relationship of childhoodabuse and household dysfunction to many of the leading causes ofdeath in adults. Am J Prev Med. 1998;14:245–258
20. Jacoby A, Altman DG, Cook J, Holland WW, Elliot A. Influence of somesocial and environmental factors of the nutrient intake and nutritionalstatus of school children. Am J Public Health. 1975;29:1494–1498
21. Ambrosius WT, Newman SA, Pratt JH. Rates of change in measures ofbody size vary by ethnicity and gender. Ethn Dis. 2001;11:303–310
22. Guo S, Huang C, Maynard L, et al. Body mass index during childhood,adolescence, and young adulthood in relation to adult overweight andadiposity: the Fels Longitudinal Study. Int J Obes Relat Metab Disord.2000;24:1628–1635
23. Costello EJ, Angold A, Burns BJ, et al. The Great Smoky MountainsStudy of Youth: goals, designs, methods, and the prevalence of DSM-III-R disorders. Arch Gen Psychiatry. 1996;53:1129–1136
24. Schaie KW. A general model for the study of developmental problems.Psychol Bull. 1965;64:92–107
25. Willett JB, Singer JD, Martin NC. The design and analysis of longitudi-nal studies of development and psychopathology in context: statisticalmodels and methodological recommendations. Dev Psychopathol. 1998;10:395–426
26. Achenbach TM, Edelbrock CS. Behavorial problems and competenciesreported by parents of normal and disturbed children aged fourthrough sixteen. Monogr Soc Res Child Dev. 1981;46:1–82
27. Cochran WG. Sampling Techniques. New York, NY: Wiley; 199528. Kimm SY, Barton BA, Obarzanek E, et al. Racial divergence in adiposity
during adolscence: the NHLBI growth and health study. Pediatrics.2001;107(3). Available at: www.pediatrics.org/cgi/content/full/107/3/e34
29. Must A, Gortmaker SL, Dietz WH. Risk factors for obesity in youngadults: Hispanics, African Americans and whites in the transition years,age 16–28 years. Biomed Pharmacother. 1994;48(3–4):143–56
30. Frisancho R. Anthropometric Standards for the Assessment of Growth andNutritional Status. Ann Arbor, MI: University of Michigan Press; 1990
31. Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standarddefinition for child overweight and obesity worldwide internationalsurvey. BMJ. 2000;320:1–6
32. Kuczmarski RJ, Ogden CL, Grummer-Strawn LM, et al. CDC GrowthCharts: United States advance data from vital and health statistics, no314. National Center for Health Statistics. 2000
33. Flegal KM, Ogden CL, Wei R, Kuczmarski RL, Johnson CL. Prevalenceof overweight in US children: comparison of US growth charts from theCenters of Disease Control and Prevention with other reference valuesfor body mass index. Am J Clin Nutr. 2001;73:1086–1093
34. Angold A, Fisher PW. Interviewer-based interviews. In: Shaffer D,Lucas C, Richters J, eds. Diagnostic Assessment in Child and AdolescentPsychopathology. New York, NY: Guilford Press; 1999:34–64
35. Wing JK, Cooper JE, Sartorius N. Present State Examination (PSE). In:Wing JK, Cooper JE, Sartorius N, eds. The Measurement and Classification
858 OBESITY AND PSYCHIATRIC DISORDER: DEVELOPMENTAL TRAJECTORIES at Duke University on September 25, 2007 www.pediatrics.orgDownloaded from

of Psychiatric Symptoms. Cambridge, England: Cambridge UniversityPress; 1974
36. American Psychiatric Association. Diagnostic and Statistical Manual ofMental Disorders, Fourth Edition. Washington, DC: American PsychiatricPress, Inc; 1994
37. Andersson I, Rossner S. The Christmas factor in obesity therapy. Int JObes Relat Metab Disord. 1992;16:1013–1015
38. Van Staveren WA, Seurenberg P, Burema J, DeGroot LC, Hautvast JG.Seasonal variation in food intake, pattern of physical activity andchange in body weight in a group of young adult Dutch womenconsuming self-selected diets. Int J Obes. 1986;10:133–145
39. Rosenthal N, Genhart M, Jacobsen F, Skwerer R, Wehr T. Disturbancesof appetite and weight regulation in seasonal affective disorder. AnnN Y Acad Sci. 1987;499:216–230
40. Thompson C, Stinson D, Fernandez M, Fine J, Isaacs G. A comparisonof normal, bipolar, and seasonal affective disorder subjects using theSeasonal Pattern Assessment Questionnaire. J Affect Disord. 1988;14:257–264
41. Yanovski J, Yanovski S, Sovik K, Nguyen T, O’Neil P, Sebring N. Aprospective study of holiday weight gain. N Engl J Med. 2000;342:861–867
42. Nagin DS. Analyzing developmental trajectories: a semiparametric,group-based approach. Psychol Methods. 1999;4:139–157
43. Crespo CJ, Smit E, Troiano RP, Bartlett SJ, Macera CA, Andersen RE.Television watching, energy intake, and obesity in US children. ArchPediatr Adolesc Med. 2001;155:360–365
44. Gordon-Larsen P, McMurray RG, Popkin B. Adolescent physical activ-ity and inactivity vary by ethnicity: The National Longitudinal Study ofAdolescent Health. J Pediatr. 1999;135:301–306
45. Gauthier BM, Hickner JM, Ornstein S. High prevalence of overweightchildren and adolescents in the Practice Partner Research Network. ArchPediatr Adolesc Med. 2000;154:625–628
46. Seidell JC, Flegal KM. Assessing obesity: classification and epidemiol-ogy. Br Med Bull. 1997;53:238–252
47. Goodman E. The role of socioeconomic status gradients in explainingdifferences in US adolescents’ health. Am J Public Health. 1999;89:1522–1528
48. Hardy R, Wadworth M, Kuh D. The influence of childhood weight andsocioeconomic status on change in adult body mass index in a Britishnational birth cohort. Int J Obes. 2000;24:725–734
49. Sobal J, Stunkard AJ. Socioeconomic status and obesity: a review of theliterature. Psychol Bull. 1989;105:260–275
50. Braddon FE, Rodgers B, Wadsworth ME, Davies JM. Onset of obesity ina 36 year birth cohort study. Br Med J Clin Res Ed. 1986;293:299–303
51. Berkson J. Limitations of the application of fourfold table analysis tohospital data. Biometrics Bull. 1946;2:47–52
52. Pine DS, Cohen P, Brook J, Coplan JD. Psychiatric symptoms in ado-lescence as predictors of obesity in early adulthood: a longitudinalstudy. Am J Public Health. 1997;87:1303–1310
53. Ross CE. Overweight and depression. J Health Soc Behav. 1994;35:63–7954. Erickson SJ, Robinson TN, Haydel KF, Killen JD. Are overweight chil-
dren unhappy? Body mass index, depressive symptoms, and over-weight concerns in elementary school children. Arch Pediatr AdolescMed. 2000;154:931–935
55. Friedman MA, Brownell KD. Psychological correlates of obesity: mov-ing to the next research generation. Psychol Bull. 1995;117:3–20
56. Di Pietro L, Anda RF, Williamson DF, Stunkard AJ. Depressive symp-toms and weight change in a national cohort of adults. Int J Obes.1992;16:745–753
57. Rubin RT, Phillips JJ, McCracken JT, Sadow TF. Adrenal gland volumein major depression: relationship to basal and stimulated pituitary-adrenal cortical axis function. Biol Psychiatry. 1996;40:89–97
58. Yehuda R, Teicher MH, Trestman RL, Levengood RA, Siever LJ. Corti-sol regulation in posttraumatic stress disorder and major depression: achronological analysis. Biol Psychiatry. 1996;40:79–88
59. Young EA, Lopez JF, Murphy-Weinberg V, Watson SJ, Akil H. Hor-monal evidence for altered responsiveness to social stress in majordepression. Neuropsychopharmacology. 2000;23:411–418
60. Rosmond R, Bouchard C, Bjorntorp P. Tsp509I polymorphism in exon 2of the glucocorticoid receptor gene in relation to obesity and cortisolsecretion: a cohort study. Br Med J. 2001;322:652–653
61. Bjorntorp R, Rosmond R. Obesity and cortisol. Nutrition. 2000;16:924–936
62. Katz JR, Taylor NF, Goodrick S, Perry L, Yudkin JS, Coppack SW.Central obesity, depression and hypothalamo-pituitary-adrenal axis inmen and postmenopausal women. Int J Obes. 2000;24:246–251
63. Okosum IS, Liao Y, Rotimi CNM, Dever GE, Cooper RS. Impact of birthweight on ethnic variations in subcutaneous and central adiposity inAmerican children aged 5–11 years: a study from the Third NationalHealth and Nutrition Examination Survey. Int J Obes. 2000;24:479–484
64. Eriksson J, Forsen T, Tuomilehto J, Osmond C, Barker D. Size at birth,childhood growth and obesity in adult life. Int J Obes. 2001;25:735–740
65. Thompson C, Syddall H, Rodin I, Osmond C, Barker DJ. Birth weightand the risk of depressive disorder in late life. Br J Psychiatry. 2001;179:450–455
66. Phillips DI, Walker BR, Reynolds RM, et al. Low birth weight predictselevated plasma cortisol concentrations in adults from 3 populations.Hypertension. 2000;35:1301–1306
67. Welberg LA, Seckl JR, Holmes MC. Inhibition of 11 �-hydroxysteroiddehydrogenase, the foeto-placental barrier to maternal glucocorticoids,permanently programs amygdala GR mRNA expression and anxiety-like behavior in the offspring. Eur J Neurosci. 2000;12:1047–1054
68. Malina RM, Katzmarzyk PT. Validity of the body mass index as anindicator of the risk and presence of overweight adolescents. Am J ClinNutr. 1999;70:131S–136S
69. Frankenfield DC, Rowe WA, Cooney RN, Smith JS, Becker D. Limits ofbody mass index to detect obesity and predict body composition. Nu-trition. 2000;17:26–30
NEONATOLOGY: PLEASE COPY
“People will keep claiming to have created cloned babies and eventually some-one will succeed, but at what cost? A lot of damaged children and disappointedparents.”
The New York Times, January 19, 2003
—Thomas Murray, Bioethicist
ARTICLES 859 at Duke University on September 25, 2007 www.pediatrics.orgDownloaded from

DOI: 10.1542/peds.111.4.851 2003;111;851-859 Pediatrics
and E. Jane Costello Sarah Mustillo, Carol Worthman, Alaattin Erkanli, Gordon Keeler, Adrian Angold
Obesity and Psychiatric Disorder: Developmental Trajectories
& ServicesUpdated Information
http://www.pediatrics.org/cgi/content/full/111/4/851including high-resolution figures, can be found at:
References
http://www.pediatrics.org/cgi/content/full/111/4/851#BIBLat: This article cites 49 articles, 20 of which you can access for free
Citations
shttp://www.pediatrics.org/cgi/content/full/111/4/851#otherarticleThis article has been cited by 8 HighWire-hosted articles:
Rs)3Peer Reviews (PPost-Publication
http://www.pediatrics.org/cgi/eletters/111/4/851R has been posted to this article: 3One P
Subspecialty Collections
mhttp://www.pediatrics.org/cgi/collection/nutrition_and_metabolis
Nutrition & Metabolismfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.pediatrics.org/misc/Permissions.shtmltables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://www.pediatrics.org/misc/reprints.shtml
Information about ordering reprints can be found online:
at Duke University on September 25, 2007 www.pediatrics.orgDownloaded from




















