
Nonablative Fractional Laser Resurfacing of Nonfacial Photodamage: Clinical and Histochemical...
10
56 Original Article Nonablative Fractional Laser Resurfacing of Nonfacial Photodamage: Clinical and Histochemical Evaluation. Neveen Fouad M. Hassan, M.D.* and Hamada Mohamed El-tabak, M.D.† *Department of Dermatology and Venereology, Faculty of Medicine, Ain-Shams university, Egypt and † Department of Pathology, Riyad Care Hospital, KSA Background. Ultraviolet irradiation from the sun has deleterious effects on human skin. Photoaging results from accumulated damage caused by repeated exposures. Rejuvenation treatment options include topical preparations, chemical peels, dermabrasion and microdermabrasion. Ablative laser resurfacing although highly effective had several disadvantages. To overcome these disadvantages, a variety of non-ablative techniques have been developed. Although non-ablative techniques are associated with less downtime, efficacy is often limited. Fractional photothermolysis is a new concept in laser treatment that results in the placement of numerous microscopic zones of thermal damage, microscopic thermal zones (MTZs), leaving the majority of the skin tissue intact. Objective. To clinically evaluate the effect of 1440-nm, non-ablative, fractional photothermolysis on non-facial rhytides induced by photodamage. Furthermore, it entails immunochemical and immunohistochemical assessment of procollagen I production before and following laser treatment sessions, to determine whether the reduction in collagen I in photodamaged human skin is restored by 1440 nm fractional photothermolysis therapy. Patients and methods. The study included twenty female participants. Subjects received six treatments at two-week intervals using the Combined Apex Pulse (CAP) enabled, 1440-nm, Nd:YAG, Laser System. Participants were evaluated clinically, punch biopsies were obtained from photodamaged skin, as well as from a sun-protected area (negative control). The punches were used for immunohistochemical and quantitative assessment of type I procollagen levels. Results. Significant clinical improvement in wrinkling by comparing pre- treatment and post-treatment photographs. Type I procollagen production increased significantly in photodamaged skin post treatment in comparison to pretreatment levels. Conclusion. 1440-nm fractional resurfacing treatment is safe and is associated with positive clinical, chemical and histochemical changes in the photodamaged skin. (J Egypt Women Dermatol Soc 2009; 6: 56-65) Keywords. Photodamage, fractional photothermolysis, type I procollagen. Corresponding Author. Neveen Fouad M. Hassan, M.D., Assistant Professor of Dermatology and Venereology, Faculty of Medicine, Ain- Shams university, Egypt. E-mail. [email protected] Conflict of interest. None declared. Copyright © 2009 Egyptian Women Dermatologic Society. All rights reserved. U and premature aging (photoaging). Sunburn and immune suppression occur acutely in response to excessive exposure to the sun, whereas skin cancer and photoaging result from accumulated damage caused by repeated exposures 1,2 . Photoaged skin is characterized by wrinkles, laxity, uneven pigmentation, brown spots and a leathery appearance. In contrast, chronologically aged skin that has been protected from the sun is thin and has reduced elasticity but is otherwise smooth and unblemished 3 . Rejuvenation treatment options include the topical application of various natural and synthetic preparations to the skin 4-6 , chemical peels 7,8 and dermabrasion 9 . Later, microdermabrasion 10 became widely accepted. Peeling methods and microdermabrasion techniques were refined and standardized as much as possible and in some cases combined in an attempt to limit morbidity and obtain safety and consistency 11 . The development of the pulsed CO 2 laser/ computerized pattern generator and the flash scanner in the early 1990’s, and the erbium (Er:YAG) laser made it possible to obtain more consistent and predictable results than with the peels and dermabrasion and led to the widespread acceptance of ablative laser resurfacing by dermatologists, cosmetic surgeons, and patients alike 12-15 . Although highly effective for wrinkles, brown spots and even sagging skin, the disadvantages of the ablative laser resurfacing include discomfort, a large, oozing wound needing meticulous postoperative care for a week or more, as well as the long-term risk of scarring and changes in skin color 16 . To overcome these disadvantages, a variety of non- ablative techniques have been developed. During the late 1990’s, non-ablative laser resurfacing became ltraviolet irradiation from the sun has deleterious effects on human skin, including sunburn, immune suppression, cancer
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Nonablative Fractional Laser Resurfacing of Nonfacial Photodamage: Clinical and Histochemical...

56
Original Article
Nonablative Fractional Laser Resurfacing of Nonfacial Photodamage: Clinical and Histochemical Evaluation.
Neveen Fouad M. Hassan, M.D.* and Hamada Mohamed El-tabak, M.D.†*department of dermatology and Venereology, Faculty of medicine,
Ain-Shams university, Egypt and † department of Pathology, Riyad care Hospital, KSA
Background. Ultraviolet irradiation from the sun has deleterious effects on human skin. Photoaging results from accumulated damage caused by repeated exposures. Rejuvenation treatment options include topical preparations, chemical peels, dermabrasion and microdermabrasion. Ablative laser resurfacing although highly effective had several disadvantages. To overcome these disadvantages, a variety of non-ablative techniques have been developed. Although non-ablative techniques are associated with less downtime, efficacy is often limited. Fractional photothermolysis is a new concept in laser treatment that results in the placement of numerous microscopic zones of thermal damage, microscopic thermal zones (mTZs), leaving the majority of the skin tissue intact. Objective. To clinically evaluate the effect of 1440-nm, non-ablative, fractional photothermolysis on non-facial rhytides induced by photodamage. Furthermore, it entails immunochemical and immunohistochemical assessment of procollagen I production before and following laser treatment sessions, to determine whether the reduction in collagen I in photodamaged human skin is restored by 1440 nm fractional photothermolysis therapy. Patients and methods. The study included twenty female participants. Subjects received six treatments at two-week intervals using the combined Apex Pulse (cAP) enabled, 1440-nm, Nd:YAG, Laser System. Participants were evaluated clinically, punch biopsies were obtained from photodamaged skin, as well as from a sun-protected area (negative control). The punches were used for immunohistochemical and quantitative assessment of type I procollagen levels. Results. Significant clinical improvement in wrinkling by comparing pre-treatment and post-treatment photographs. Type I procollagen production increased significantly in photodamaged skin post treatment in comparison to pretreatment levels. Conclusion. 1440-nm fractional resurfacing treatment is safe and is associated with positive clinical, chemical and histochemical changes in the photodamaged skin. (J Egypt Women Dermatol Soc 2009; 6: 56-65)
Keywords. Photodamage, fractional photothermolysis, type I procollagen.
Corresponding Author. Neveen Fouad m. Hassan, m.d., Assistant Professor of dermatology and Venereology, Faculty of medicine, Ain-Shams university, Egypt. E-mail. [email protected]
Conflict of interest. None declared.Copyright © 2009 Egyptian Women dermatologic Society. All rights reserved.
Uand premature aging (photoaging). Sunburn and immune suppression occur acutely in response to excessive exposure to the sun, whereas skin cancer and photoaging result from accumulated damage caused by repeated exposures1,2. Photoaged skin is characterized by wrinkles, laxity, uneven pigmentation, brown spots and a leathery appearance. In contrast, chronologically aged skin that has been protected from the sun is thin and has reduced elasticity but is otherwise smooth and unblemished3.
Rejuvenation treatment options include the topical application of various natural and synthetic preparations to the skin4-6, chemical peels7,8
and dermabrasion9. Later, microdermabrasion10 became widely accepted. Peeling methods and microdermabrasion techniques were refined and
standardized as much as possible and in some cases combined in an attempt to limit morbidity and obtain safety and consistency11.
The development of the pulsed cO2 laser/computerized pattern generator and the flash scanner in the early 1990’s, and the erbium (Er:YAG) laser made it possible to obtain more consistent and predictable results than with the peels and dermabrasion and led to the widespread acceptance of ablative laser resurfacing by dermatologists, cosmetic surgeons, and patients alike12-15. Although highly effective for wrinkles, brown spots and even sagging skin, the disadvantages of the ablative laser resurfacing include discomfort, a large, oozing wound needing meticulous postoperative care for a week or more, as well as the long-term risk of scarring and changes in skin color16.
To overcome these disadvantages, a variety of non-ablative techniques have been developed. during the late 1990’s, non-ablative laser resurfacing became
ltraviolet irradiation from the sun has deleterious effects on human skin, including sunburn, immune suppression, cancer

Neveen Fouad M. Hassan and Hamada Mohamed El-tabak
J Egypt Women Dermatol Soc. vol. 6, No. 2, 2009
57
popular. Using a variety of laser wavelengths, as well as intense pulsed light; some acting more towards the skin surface, some deeper in the collagen layers, non-Ablative techniques are capable of improving skin texture, pigment abnormalities and even some tightening occasionally, with no or minimal risk and without any downtime17-19. One example is the 1064 Nd:YAG laser which produces gradual and subtle improvement in skin tone and texture by a thermally mediated mechanism. However, multiple treatments are needed and with a few, unpredictable exceptions, the results are limited20. In all resurfacing techniques, chemical, mechanical, or light-based, the potential for improvement is related to the depth and degree of the injury, regardless of the method used. Although non-ablative techniques are associated with less downtime, efficacy is often limited21,22.
Fractional photothermolysis is a new concept in laser applications in which infrared laser treatment results in the placement of numerous microscopic zones of thermal damage, microscopic thermal zones (mTZs), leaving the majority of the skin tissue intact. The remaining untreated skin serves as a reservoir for healing. The depth and the diameter of each microthermal zone are determined by the energy setting. The proportion of the surface area treated depends on the densities and the number of passes. Fraxel SR laser was among the first used machines in the technology of fractional photothermolysis, it utilizes a 1550-nm diode pumped erbium fiber laser to produce arrays of microscopic, thermal epidermal necrosis and dermal collagen denaturation. The stratum corneum is mostly spared, by its low water content. Tissues surrounding the mTZs are not heated or damaged, and the epidermal tiny wounds form microepidermal necrotic debris (mENds), which give the treated area a “bronzed” appearance until they shed and heal within a few days to a week later. This approach has also been called “microrejuvenation” and has been used to treat superficial photoaging. Drawbacks are time consuming pre-and post-treatment procedures, multiple passes, tracking topical blue dye application and the need for anaesthesia to relieve patient discomfort during treatment23. Recently, the advent of second generation “micro-rejuvenation” approaches, 1440-nm Nd:YAG fractional lasers have shown that outcomes for superficial photoaging and like conditions can be improved by creating small, localized zones of significant thermal injury, apexes of high-fluence, surrounded by untreated skin zones, bases of low-fluence. This approach minimizes much of the inflammatory wound healing response and associated side-effects of the first generation fractional rejuvenation methods24.
Histologic and ultrastructural studies have proved that alterations in photoaged skin are found in dermal connective tissue. The extracellular
matrix in the dermis is composed primarily of type I collagen, with lesser amounts of type III collagen, elastin, proteoglycans, and fibronectin. Thus, studies of collagen are more easily accomplished if directed at collagen I. Collagen fibrils are responsible for the strength and resiliency of skin25. The biosynthesis of collagen I in the dermis begins with the formation of procollagen I within dermal fibroblasts. After its secretion from fibroblasts, procollagen I is enzymatically cleaved of its aminopropeptide and carboxypropeptide; the presence of propeptide provides an index of collagen I synthesis26. Therefore, an antibody that can recognize the carboxypropeptide
portion of procollagen I or its distal derivatives will both identify precursors of collagen I and provide an indirect measure of collagen I formation27.
dermal damage induced by ultraviolet irradiation is principally manifested histologically as the disorganization of collagen fibrils and the accumulation of abnormal elastin-containing
material28. Photoaged skin includes reduced levels of types I and III collagen precursors and cross-links, an increased ratio of type III to type I collagen and an increased level of elastin29. Improvement in the appearance of photoaged skin after treatment is associated with the restoration of type I procollagen to levels approaching those in skin that has not been exposed to sun3. These observations have led to the belief that the aged appearance of sun-exposed
skin results from alterations in the structure and composition of collagen and elastin in the dermal extracellular matrix30, 31.
The clinically observed ability of fractional photothermolysis to improve fine wrinkles associated with damage caused by exposure to sunlight
(photodamage)23,24, has ignited considerable interest in the mechanisms of this process. Although there is no established histologic correlate of a wrinkle, a reduction in collagen levels in areas of skin exposed to the sun is believed to be an etiologic component. This belief is based on the known property of collagen to provide strength and resiliency to skin25,28.
Aim of workThis study aimed at clinically evaluating
the effect of 1440-nm, non-ablative, fractional photothermolysis on non-facial rhytides induced by photodamage. Furthermore, it entails immunochemical and immunohistochemical assessment of procollagen I production before and following laser treatment sessions, to determine whether the reduction in collagen I in
photodamaged human skin is restored by 1440 nm fractional photothermolysis therapy. The effect of treatment on collagen I levels in treated
photodamaged skin might point out one of the mechanisms that underlie clinical improvement reported by this novel non-ablative treatment tool.
Nonablative Fractional Laser Resurfacing of Nonfacial Photodamage: Clinical and Histochemical Evaluation.
J Egypt Women Dermatol Soc. vol. 6, No. 2, 2009
58
PAtiENts ANd MEtHOds
Participants and fractional laser treatment protocol
This study was conducted between January and July 2008, in Riyad care Hospital, KSA. Twenty female participants (n=20), aging between 42-60 years, with Fitzpatrick skin types II, III, IV; with the clinical diagnosis of moderate to severe, non-facial photoaging (but otherwise healthy) involving the hands, forearms, neck and/or the V-area of the chest were enrolled in this study (Table1). An explanation including the risks, benefits, and potential complications was given to the participants and written informed consents were obtained. All participants had been previously treated with topical agents (tretinoin, glycolic acid, α-hydroxy acids, salicylic acid), chemical peels, microdermabrasion, intense pulsed light (IPL) and/or laser resurfacing without appreciable patient satisfaction (Table1). All participants did not receive any treatment for their photoaging for at least two years before contributing to this study.
table 1: demographic criteria of the participants.
demographic Criteria No. of
participants(n = 20)
Treatment Areas
Neck 2
Hands 5
Hands & Forearms 10
V-area of chest 3
Skin Types
II 5
III 13
IV 2
Previous TreatmentTopical preparations (T.p) only 8
T.p & Peels 6
T.p & microdermabrasion 2
T.p & IPL 3
T.p & Nd:YAG (1064 nm) 1
Participants had to have a baseline, treatment-area, overall integrated assessment (OIA) of photodamage; to select subjects with at least moderate photodamage. Evaluated elements included the following: fine wrinkling, mottled hyperpigmentation, lentigines, tactile roughness, coarse wrinkling, telangiectasia, pore size, elastoses and actinic keratoses. OIA scoring was derived according to a photonumeric guideline illustrating the OIA grades of minimal, mild, moderate, severe
and very severe. A score of at least 4, on a 9-point scale, (0: indicates no photodamage and 9: very severe photodamage), was a prerequisite for participation32.
Subjects were evaluated and photographed prior initiation of treatment, and three months after the final treatment. Subjects received six treatments at two-week intervals. No preoperative preparation was required. Prior to treatment the skin was cleaned and any makeup was removed. Subjects were treated using the combined Apex Pulse (cAP) enabled AFFIRm, Nd:YAG, Laser System (cynosure Inc., Westford, mA) at 1440-nm wavelength, 3 msec pulse duration and 10-mm diameter cAP array. The initial treatment fluence was 4 J /cm² and fluences were increased 0.5 to 1 J/cm² at subsequent sessions to a maximum of 7 J/cm² and 1 Hz pulse repetition rate. Treatment areas received two passes. All treatments were delivered in conjunction with only Smart cool (cynosure, Inc., Westford, mA) cold-air cooling, with fan speed between 3-5. The cAP array was always kept in full contact with the skin throughout the procedure for optimal efficacy. Neither local anaesthesia, nor tracking blue dye was applied to the areas of laser treatment. Participants were instructed to exercise effective sun protection during the whole period of the study. Sun protection guidelines were thoroughly explained to all of them. Physical sun protection was recommended whether by avoidance of exposure to sun and/or by protective clothing. chemical sun protection was obligatory and broad-spectrum sun screens were granted to all participants.
Participants were evaluated clinically for their wrinkles by comparing before and three-months after the last treatment photographs. The wrinkles´ improvement was rated according to four categories: 0%, 1-25%, 26-50%, 51-75%, and more than 75%. Three months after the last treatment session, patients were asked to report on their level of satisfaction with non-ablative, fractional laser treatment according to the following scale: very satisfied, satisfied, slightly satisfied, and unsatisfied. They also reported on average pain scores according to a scale of 1-10, with 1 describing mild pain and 10 describing severest pain.
skin Biopsies 3 mm punch biopsies were obtained from each
individual, from photodamaged skin at baseline (week 0) and three months after the end of treatment (week 24) as well as from a sun-protected area (the buttock) (negative control). The punches were placed in isotonic saline and transported immediately to the laboratory in an ice box, to be used for immunohistochemical and quantitative assessment of type I procollagen levels. On arrival
in the laboratory, biopsies were immediately frozen in optimal cutting temperature embedding (OcT)

Neveen Fouad M. Hassan and Hamada Mohamed El-tabak
J Egypt Women Dermatol Soc. vol. 6, No. 2, 2009
59
medium (miles Laboratories, Naperville, Ill.), frozen in liquid nitrogen and stored at -70 °c until use. All biopsies were obtained after receiving informed consent.
immunochemical assessment of type i procollagen production
Serial frozen sections were prepared from OcT-embedded skin biopsies. Samples of 200, and 7 µm thickness were obtained. Areas of the sections from the 200-µm samples were measured using Image ProPlus software to calculate the volume of the 200-µm sample. Soluble protein extracts were prepared from the 200-µm samples, which were homogenized in ice-cold extraction buffer (50 mmol/L Tris-Hcl, pH 7.4, 0.15 mol/L Nacl, 1% Triton X-100, and protease inhibitors [complete mini, Hoffmann-LaRoche, Nutley, NJ]), and vortexed in the presence of glass beads (Biospec, Bartlesville, OK). After centrifugation for 10 minutes at 10,000 x g and 4°c, supernatants were assayed for procollagen I using a commercial enzyme-linked immunosorbent assay kit (Panvera, madison, WI)27 . The procollagen assay uses an antibody to the c-terminal propeptide region that is part of the collagen molecule as it is synthesized and secreted
(before being proteolytically cleaved). As such, this assay is a measure of newly synthesized collagen. Type I procollagen concentrations were normalized to the volume of tissue used for the preparation of each sample.
immunohistochemical analysis of type i procollagen
For the immunohistochemical analysis, 7 µm cryostat sections were placed on triple-welled microslides (Carlson Scientific, Peotone, Ill.) coated with poly-l-lysine transparent microslide adhesive (Sigma Chemical, St. Louis). The sections were fixed
in chilled acetone and then incubated with a well-characterized mouse monoclonal IgG1 antibody (SP1.d8) that recognizes a 19-amino-acid portion of the aminopropeptide-cleavage site of human procollagen
I33. This antibody recognizes the aminopropeptide whether it is cleaved from or still a part of procollagen I molecules “i.e., collagen I precursors” but does not recognize the triple helix of collagen I or the carboxypropeptide fragment. Appropriately diluted mouse IgG1 was used as a control. The samples were processed for staining with an immunoperoxidase
technique (Vectastain ABc Kit, Vector Laboratories, Burlingame, calif.), with 3-amino-9-ethyl carbazole (Sigma) as the chromogen, counterstained with hematoxylin (Lerner Laboratories, Pittsburgh) and wet-mounted with Aquamount (Lerner Laboratories).
Quantification of immunohistochemical staningThe intensity and extent of staining were assessed
with a six-point scale in which a score of 0 indicated no staining, a score of 1 minimal staining, a score of 2 low-
to-moderate levels of staining, a score of 3 moderate staining, a score of 4 high levels of staining and a score of 5 maximal staining. The pattern of collagen I immunohisto-chemical staining was extracellular, in a papillary dermal band (a narrow zone immediately beneath the epidermis). Four high-power fields from each section were graded under light microscopy.
statistical analysis The data obtained were analyzed using microsoft
Excel and SAS analytic software. The paired t-test was used to compare staining patterns in skin protected from the sun (buttocks) and photodamaged skin. The differences in the collagen I immuno-histochemical staining between pre- and post-treatment photodamaged skin were assessed with the two-tailed t-test. All p values are two-sided. Percentages were determined before rounding of the means. Summary data are expressed as means ±Sd. The correlation between the clinical severity of photodamage, degree of post-treatment clinical improvement and the intensity of collagen I immunostaining was assessed with the Pearson correlation analysis.
REsULts
All twenty participants completed the study. They were all females with mean age ± Sd of 47.4 ± 3 years. Twenty-five percent of the study group was Fitzpatrick skin type II, whereas 65% were skin type III, and 10% were skin type IV. The cAP technology provided a dense pattern of energy distribution, creating a more uniform treatment. This allowed treatment with fewer passes and shortened the treatment time. Typical initial response to treatment was limited to a sunburn-like erythema and oedema, which resolved within few hours to three days. Participants reported an average pain score of 4.6 on a scale of 1 to 10, with 10 signifying pain similar to a bee sting. Participants, in addition, reported on their level of satisfaction regarding treatment outcome; 55% were very satisfied, 25% were satisfied, 15% reported as slightly satisfied, and 5% as unsatisfied. The whole study group could resume normal activities immediately after treatment, none of them required time-off their work. None of the study group developed post-treatment abrasions, hyperpigmentation, hypopigmentation, and/or scarring.
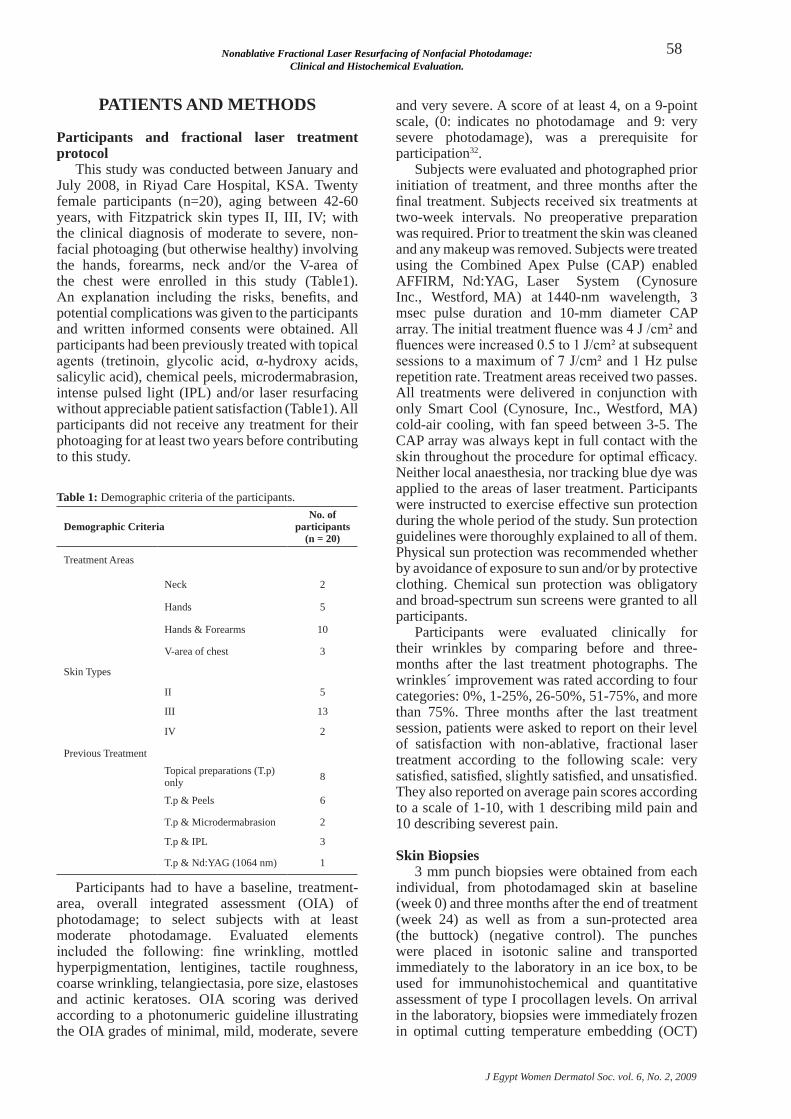
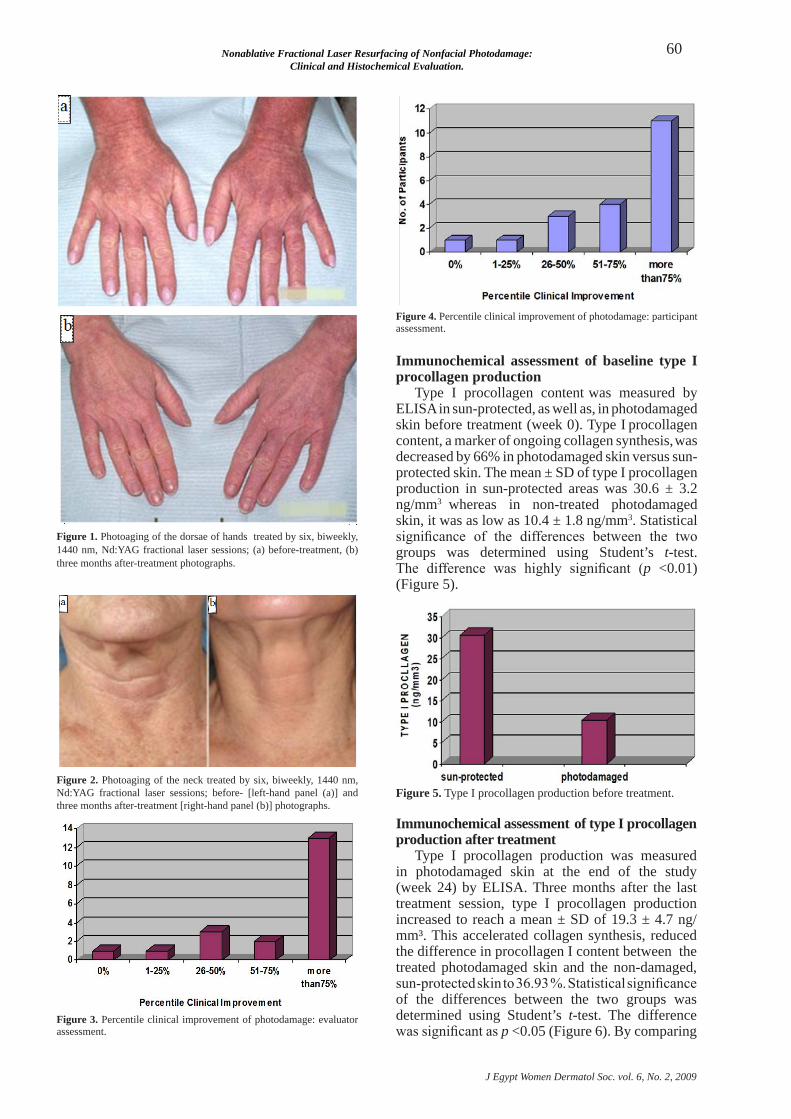
clinical improvement in photodamage was evaluated by comparing pre-treatment (baseline, week 0) and post-treatment (12-weeks after the sixth treatment session, week 24) photographs (Figure 1, 2). Sixty-five percent of the study group was assessed to achieve more than 75% improvement of their photoaging according to the evaluator assessment of pre- and post-treatment photographs (Figure 3). Fifty-five percent of the participants rated themselves as having more than 75% wrinkle improvement (Figure 4).
Nonablative Fractional Laser Resurfacing of Nonfacial Photodamage: Clinical and Histochemical Evaluation.
J Egypt Women Dermatol Soc. vol. 6, No. 2, 2009
60
Figure 1. Photoaging of the dorsae of hands treated by six, biweekly, 1440 nm, Nd:YAG fractional laser sessions; (a) before-treatment, (b) three months after-treatment photographs.
Figure 2. Photoaging of the neck treated by six, biweekly, 1440 nm, Nd:YAG fractional laser sessions; before- [left-hand panel (a)] and three months after-treatment [right-hand panel (b)] photographs.
Figure 3. Percentile clinical improvement of photodamage: evaluator assessment.
Figure 4. Percentile clinical improvement of photodamage: participant assessment.
immunochemical assessment of baseline type i procollagen production
Type I procollagen content was measured by ELISA in sun-protected, as well as, in photodamaged skin before treatment (week 0). Type I procollagen content, a marker of ongoing collagen synthesis, was decreased by 66% in photodamaged skin versus sun-protected skin. The mean ± Sd of type I procollagen production in sun-protected areas was 30.6 ± 3.2 ng/mm3 whereas in non-treated photodamaged skin, it was as low as 10.4 ± 1.8 ng/mm3. Statistical significance of the differences between the two groups was determined using Student’s t-test. The difference was highly significant (p <0.01) (Figure 5).
Figure 5. Type I procollagen production before treatment.
immunochemical assessment of type i procollagen production after treatment
Type I procollagen production was measured in photodamaged skin at the end of the study (week 24) by ELISA. Three months after the last treatment session, type I procollagen production increased to reach a mean ± Sd of 19.3 ± 4.7 ng/mm³. This accelerated collagen synthesis, reduced the difference in procollagen I content between the treated photodamaged skin and the non-damaged, sun-protected skin to 36.93 %. Statistical significance of the differences between the two groups was determined using Student’s t-test. The difference was significant as p <0.05 (Figure 6). By comparing

Neveen Fouad M. Hassan and Hamada Mohamed El-tabak
J Egypt Women Dermatol Soc. vol. 6, No. 2, 2009
61
type I procollagen production in photodamaged skin before treatment (week 0), and at the end of the study (week 24); post-treatment synthesis increased by 85.55 %. The statistical significance of the differences between the two groups was determined using Student’s t-test. The difference was highly significant as p <0.01 (Figure 7).
Figure 6. Type I procollagen production after treatment.
Figure 7. Type I procollagen production in photodamaged skin before and after treatment.
Comparison between procollagen i immunostaining in photodamaged and sun-protected skin at baseline
The average clinical severity of photodamage in treatment areas was 5.4 ± 0.3 (on the scale used, a grade of 9 indicated the most severe photodamage).
comparison of the intensity of procollagen I immunostaining in photodamaged skin from the treatment areas at baseline with the skin from the buttocks, which represents a sun-protected area, demonstrated a 56% less staining in the former. Pro
collagen I immunostaining within photodamaged papillary dermis, showed minimal staining (1.2 ± 0.2) and moderate staining was observed (2.7 ± 0.3) in protected skin (p <0.001) (Figure 8). There was a significant correlation between the clinical severity
of photodamage and the intensity of procollagen I immunostaining in the papillary dermis (r = -0.58, p = 0.002), implying that the more severe the photodamage the greater the reduction in procollagen I formation (Figure 9). multiple linear regression
modeling showed that the partial correlation
between the clinical severity of photodamage and procollagen I immunohistochemical staining, after adjustment for patient age, was significant (partial r = -0.55, p = 0.005). conversely, however, the partial correlation of age was not significant after adjustment for the clinical severity of photodamage (partial r = 0.22, p = 0.3) suggesting that the degree of photodamage is a better predictor of collagen I formation than chronologic age.
Figure 8. Procollagen I immunohistochemical staining in sun- protected skin and photodamaged skin from a single patient (x60). Skin from the buttocks, which had been protected from the sun, shows grade 3 staining within the papillary dermis [left-hand panel (a)]. In photodamaged skin from the extensor aspect of the forearm, staining is markedly reduced to grade 1, representing decreased formation of collagen I [right-hand panel (b)].
Figure 9. Relation between the clinical severity of photodamage and the extent of procollagen I immunohistochemical staining in the papillary dermis. As the clinical severity of photodamage increased, the extent of procollagen I formation in the papillary dermis decreased (the best linear fit is shown by the line).(r = -0.58, p = 0.002).
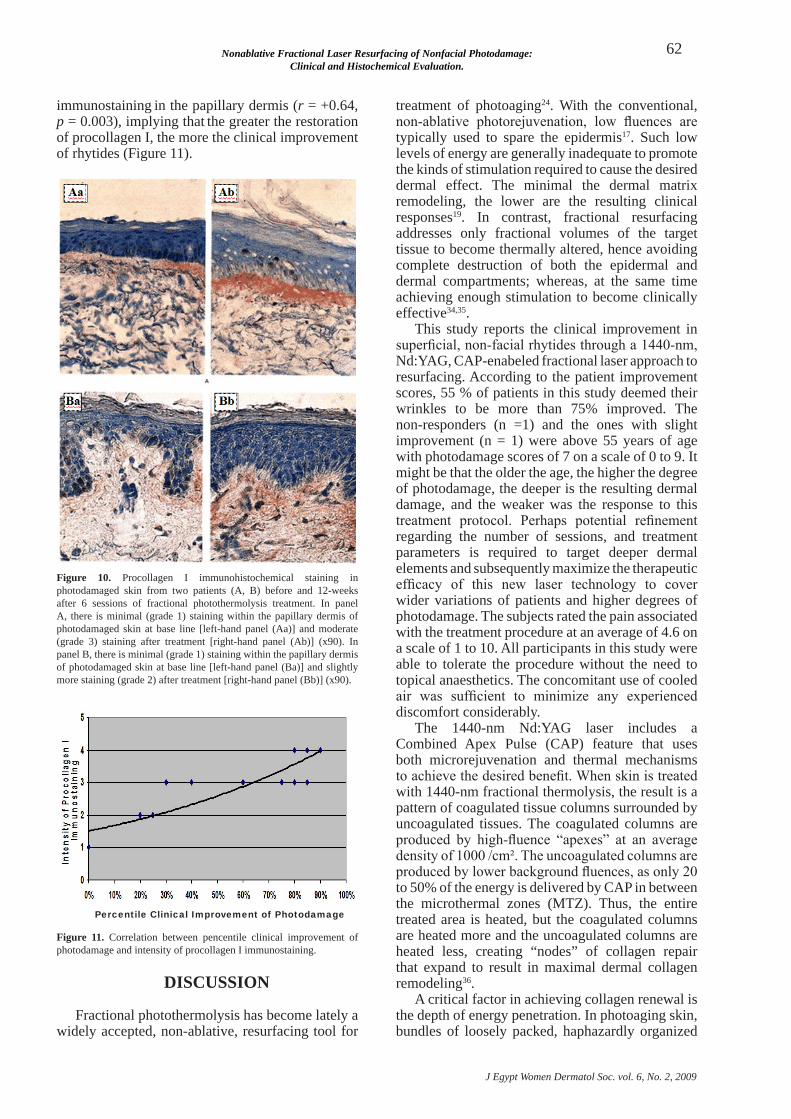
Comparison of procollagen i immunostaining pre- and post-treatment in photodamaged skin
Treatment of photodamaged skin with fractional photothermolysis produced increased procollagen I immunostaining within the papillary dermis by 80
percent (from 1.1 ± 0.2 at base line to 2.0 ± 0.3 after treatment), (p = 0.006) (Figure 10). There was a significant positive correlation between the evaluator assessment of the percentile clinical improvement of wrinkles and the intensity of procollagen I
Nonablative Fractional Laser Resurfacing of Nonfacial Photodamage: Clinical and Histochemical Evaluation.
J Egypt Women Dermatol Soc. vol. 6, No. 2, 2009
62
immunostaining in the papillary dermis (r = +0.64, p = 0.003), implying that the greater the restoration of procollagen I, the more the clinical improvement of rhytides (Figure 11).
Figure 10. Procollagen I immunohistochemical staining in photodamaged skin from two patients (A, B) before and 12-weeks after 6 sessions of fractional photothermolysis treatment. In panel A, there is minimal (grade 1) staining within the papillary dermis of photodamaged skin at base line [left-hand panel (Aa)] and moderate (grade 3) staining after treatment [right-hand panel (Ab)] (x90). In panel B, there is minimal (grade 1) staining within the papillary dermis of photodamaged skin at base line [left-hand panel (Ba)] and slightly more staining (grade 2) after treatment [right-hand panel (Bb)] (x90).
Figure 11. correlation between pencentile clinical improvement of photodamage and intensity of procollagen I immunostaining.
treatment of photoaging24. With the conventional, non-ablative photorejuvenation, low fluences are typically used to spare the epidermis17. Such low levels of energy are generally inadequate to promote the kinds of stimulation required to cause the desired dermal effect. The minimal the dermal matrix remodeling, the lower are the resulting clinical responses19. In contrast, fractional resurfacing addresses only fractional volumes of the target tissue to become thermally altered, hence avoiding complete destruction of both the epidermal and dermal compartments; whereas, at the same time achieving enough stimulation to become clinically effective34,35.
This study reports the clinical improvement in superficial, non-facial rhytides through a 1440-nm, Nd:YAG, cAP-enabeled fractional laser approach to resurfacing. According to the patient improvement scores, 55 % of patients in this study deemed their wrinkles to be more than 75% improved. The non-responders (n =1) and the ones with slight improvement (n = 1) were above 55 years of age with photodamage scores of 7 on a scale of 0 to 9. It might be that the older the age, the higher the degree of photodamage, the deeper is the resulting dermal damage, and the weaker was the response to this treatment protocol. Perhaps potential refinement regarding the number of sessions, and treatment parameters is required to target deeper dermal elements and subsequently maximize the therapeutic efficacy of this new laser technology to cover wider variations of patients and higher degrees of photodamage. The subjects rated the pain associated with the treatment procedure at an average of 4.6 on a scale of 1 to 10. All participants in this study were able to tolerate the procedure without the need to topical anaesthetics. The concomitant use of cooled air was sufficient to minimize any experienced discomfort considerably.
The 1440-nm Nd:YAG laser includes a combined Apex Pulse (cAP) feature that uses both microrejuvenation and thermal mechanisms to achieve the desired benefit. When skin is treated with 1440-nm fractional thermolysis, the result is a pattern of coagulated tissue columns surrounded by uncoagulated tissues. The coagulated columns are produced by high-fluence “apexes” at an average density of 1000 /cm². The uncoagulated columns are produced by lower background fluences, as only 20 to 50% of the energy is delivered by cAP in between the microthermal zones (mTZ). Thus, the entire treated area is heated, but the coagulated columns are heated more and the uncoagulated columns are heated less, creating “nodes” of collagen repair that expand to result in maximal dermal collagen remodeling36.
A critical factor in achieving collagen renewal is the depth of energy penetration. In photoaging skin, bundles of loosely packed, haphazardly organized
disCUssiON
Fractional photothermolysis has become lately a widely accepted, non-ablative, resurfacing tool for
Percentile Clinical Improvement of Photodamage

Neveen Fouad M. Hassan and Hamada Mohamed El-tabak
J Egypt Women Dermatol Soc. vol. 6, No. 2, 2009
63
collagen3 are present in the dermis at depths ranging from 100 to 400 microns37. The cO2 laser induces thermal changes in collagen at 100 to nearly 300 microns38. This indicates that a laser whose energy penetrates up to 300 microns would effectively induce restoration of photodamaged collagen and consequently result in clinical improvement of wrinkles, and that deeper penetration would be unnecessary since cO2 laser energy typically does not penetrate deeper than 300 microns. 1440-nm cAP energy was reported to penetrate up to 300 microns into the papillary dermis, where most sun damage occurs39. This depth of penetration is comparable to cO2 laser, the gold standard modality for effective ablative resurfacing12.
Fractional microrejuvenation lasers with longer wavelengths had proved effective in the treatment of acne scars40,41, surgical, atrophic and hypopigmented scars34,42,43, melasma44, lentigines, poikiloderma of civatte45 and dyspigmentation46. Ablative photothermolysis, in addition, improved the signs of photodamage and was accepted as a resurfacing tool for rejuvenation therapy47. manstein and colleagues reported improvement in periorbital rhytides in 96% of patients, with improvement in wrinkle scores in thirty subjects treated with Fraxel SR laser23. This laser penetrates as deep as 350 to 750 microns48. This depth of penetration might appear higher than required to achieve clinical benefit, when compared to the depth of penetration of cO2 laser energy49. Furthermore, the deeper the penetration the higher will be the incidence of untoward side-effects, including the severity of pain experienced during the procedure, the necessity to use local anaesthetics, post-treatment abrasions, prolonged erythma and oedema, as well as longer down-time periods. moreover, the session set-up, and post-treatment procedures are time consuming and sometimes messy35. However, and by observing the results of the current work, one can assume that fractional lasers with deeper penetration might be of more benefit in subjects with higher degrees of photodamage affecting the deepest dermal compartment, as represented by the non-responder and the slightly responding group of this study.
Reduction of type I collagen is a characteristic
feature of chronologically aged skin and is enhanced in photodamage. This has been well described using histological and ultrastructural approaches in the past3. mechanisms underlying the loss of collagen synthesis in photodamaged skin have not been fully delineated. Although destruction of existing collagen is, undoubtedly, central to the deleterious changes observed in aged/photoaged skin, failure to replace damaged collagen with newly synthesized material is also critical to the overall pathophysiology. There is a sustained down-regulation in collagen synthesis in photodamaged skin relative to what occurs in healthy sun-protected skin25,26. The significant correlation
of reduced levels of collagen I immunostaining with the severity of photodamage and the known property of collagen to provide cutaneous tensile strength and resiliency raise the possibility that the reduction in collagen I restoration may contribute to
the production of wrinkles27,28.
This study detected increased collagen I immunostaining three months after six, biweekly treatments with 1440-nm fractional laser. This observation points to a laser-induced increase in collagen I formation in photodamaged human dermis and suggest that the clinical improvement reported in this study may result from this increase. By correlating the degree of clinical improvement, as assessed by the evaluator, directly with the formation of collagen I, a significant positive correlation pointed-out that the higher the degree of clinical improvement of wrinkles, the more collagen I is restored. Interestingly, it was noted during histopathological examination of all biopsies included in this study that healing of the dermal layers after fractional photothermolysis seems to lack an “inflammatory” phase; although there were clear evidence of collagen remodeling. more interestingly, although near and mid-infrared laser wavelengths are poorly absorbed by melanin, post-treatment clinical improvement of pigmentation was observed by the evaluator and appreciated by the participants. These observations were not targeted as end points in the current study design, yet they were worth mentioning as they might deserve further assessment in future researches.
Finally, the results of the current study are an indication that reduced dermal collagen formation in photodamaged skin is partly restored by treatment with fractional photothermolysis. 1440-nm fractional laser was shown to be effective in the amelioration of the signs of photodamage. Significant improvement was seen for superficial rhytides three months after six, biweekly treatment sessions in most of the subjects. There were significantly higher rates of clinical improvement in the OIA of photodamage, as assessed by the evaluator of pre- and post-treatment photographs, as well as by the participants themselves. The fractional treatment induced favorable immunochemical (ELISA), and immunohistochemical (type I procollagen) changes in the production of type I collagen in photodamaged skin. These changes were significant when compared with baseline and non-photoaged, sun-protected skin of the same patient. Therefore, the ability of this novel laser to reduce the effects of photodamage clinically is
not simply cosmetic but rather is probably based on the active repair of dermal collagen. However, the small number of participants enrolled in this study invites larger-scale studies for further evaluation of this novel, non-ablative, resurfacing tool.

Nonablative Fractional Laser Resurfacing of Nonfacial Photodamage: Clinical and Histochemical Evaluation.
J Egypt Women Dermatol Soc. vol. 6, No. 2, 2009
64
Conclusion.The new cAP enabled 1440-nm Nd:YAG laser
represents a new development in non-ablative treatment of wrinkles.1440-nm fractional resurfacing treatment is safe and is associated with positive clinical, chemical, and histochemical changes in the photodamaged skin. It reduced the severity of fine wrinkles, and ameliorated the overall condition of photoaged skin when compared to baseline and sun-protected skin. For pain sensation, 1440-nm laser rejuvenating treatment was well tolerated, although a concomitant air-cooling hand-piece was used for more convenience of the participants.
REFERENCEs
cooper Kd, Oberhelman L, Hamilton TA, 1. Baadsgaard O, Terhune m, LeVee G, et al. UV exposure reduces immunization rates and promotes tolerance to epicutaneous antigens in humans: Relationship to dose, cd1a-dR+ epidermal macrophage induction and Langerhans cell depletion. Proc Natl Acad Sci U S A 1992; 89: 8497-1501.Weinstock mA. Epidemiology of nonmelanoma skin 2. cancer: Clinical issues, definitions and classification. J Invest Dermatol 1994; 102 (suppl): 4-5.Gilchrest BA, Yaar m. Ageing and photoageing of 3. the skin: Observations at the cellular and molecular level. Br J Dermatol 1992; 127 (suppl 41): 25-30.Stiller mJ, Bartolone J, Stern R, Smith S, Kollias 4. N, Gillies R, et al. Topical 8% glycolic acid and 8% L-lactic acid creams for the treatment of photodamaged skin. A double-blind vehicle-controlled clinical trial. Arch Dermatol 1996; 132: 631-6.Thibault PK, Wlodarczyk J, Wenck A. A double-blind 5. randomized clinical trial on the effectiveness of a daily glycolic acid 5% formulation in the treatment of photoaging. Dermatol Surg 1998; 24: 573-8.Weiss JS, Ellis cN, Headington JT, Tincoff T, 6. Hamilton TA, Voorhees JJ. Topical tretinoin improves photoaged skin. A double-blind vehicle-controlled study. JAMA 1988; 259: 527-32. [Erratum JAmA 1988; 260: 926].Witheiler dd, Lawrence N, cox SE, cruz c, cockerell 7. CJ, Freemen RG. Long-term efficacy and safety of Jessner’s solution and 35% trichloroacetic acid vs 5% fluorouracil in the treatment of widespread facial actinic keratoses. Dermatol Surg 1997; 23: 191-6.drake LA, dinehart Sm, Goltz RW, Graham GF, 8. Hordinsky mK, Lewis cW, et al. Guidelines of care for chemical peeling. J Am Acad Dermatol 1995; 33: 497-503.Roenigk HH. dermabrasion: State of the art. 9. J Cosmet Dermatol 2002; 1: 72-87.Hernandez-Perez E, Ibiett EV. Gross and microscopic 10. findings in patients undergoing microdermabrasion for facial rejuvenation. Dermatol Surg 2001; 27: 637-40.
Spencer Jm, Kurtz ES. Approaches to document the 11. efficacy and safety of microdermabrasion procedure. Dermatol Surg 2006; 32: 1353-7.Raulin c, Grema H. Single-pass carbon dioxide laser 12. skin resurfacing combined with cold-air cooling: Efficacy and patient satisfaction of a prospective side-by-side study. Arch Dermatol 2004; 140: 1333-6.Roy d. Ablative facial resurfacing. 13. Dermatol Clin 2005; 23: 549-59.Railan d, Kilmer S. Ablative treatment of photoaging. 14. Dermatol Ther 2005; 18: 227-41.Trelles mA. Laser ablative resurfacing for 15. photorejuvenation based on more than a decade’s experience and 1200 patients: Personal observations. J Cosmet Dermatol 2003; 2: 2-13.Batra RS. Ablative laser resurfacing - postoperative 16. care. Skin Therapy Lett 2004; 9: 6-9.Nikolaou VA, Stratigos AJ, dover JS. Nonablative 17. skin rejuvenation. J Cosmet Dermatol 2005; 4: 301-7.Trelles mA. Phototherapy in anti-aging and its 18. photobiologic basics: A new approach to skin rejuvenation. J Cosmet Dermatol 2006; 5: 87-91.Trelles mA, mordon S, calderhead RG. Facial 19. rejuvenation and light: our personal experience. Lasers Med Sci 2007; 22: 93-9.Bhatia Ac, dover JS, Arndt KA, Stewart B, Alam m. 20. Patient satisfaction and reported long-term therapeutic efficacy associated with 1064 nm Nd:YAG laser treatment of acne scarring and photoaging. Dermatol Surg 2006; 32: 346-52.Shook BA, Hruza GJ. Periorbital ablative and 21. nonablative resurfacing. Facial Plast Surg Clin North Am 2005; 13: 571-82.Hedelund L, Bjerring P, Egekvist H, Haedersdal m. 22. Ablative versus non-ablative treatment of perioral rhytides. A randomized controlled trial with long-term blinded clinical evaluations and non-invasive measurements. Lasers Surg Med 2006; 38: 129-36.manstein d, Herron GS, Sink RK, Tanner H, Anderson 23. RR. Fractional photothermolysis: a new concept for cutaneous remodeling using microscopic patterns of thermal injury. Lasers Surg Med 2004; 34: 426-38.Geronemus RG. Fractional photothermolysis: current 24. and future applications. Lasers Surg Med 2006; 38: 169-76.Schwartz E, cruickshank FA, christensen cc, Perlish 25. JS, Lebwohl m. collagen alterations in chronically sun-damaged human skin. Photochem Photobiol 1993; 58: 841-4.Birkedal Hansen H. catabolism and turnover of 26. collagens: collagenases. Methods Enzymol 1987; 144: 140-71.Risteli J, Elomaa I, Niemi S, Novamo A, Risteli L. 27. Radioimmunoassay for the pyridinoline cross-linked carboxy-terminal telopeptide of type I collagen: A new serum marker of bone collagen degradation. Clin Chem 1993; 39: 635-40.

Neveen Fouad M. Hassan and Hamada Mohamed El-tabak
J Egypt Women Dermatol Soc. vol. 6, No. 2, 2009
65
Warren R, Gartstein V, Kligman Am, montagna W, 28. Allendorf RA, Ridder Gm. Age, sunlight and facial skin: a histologic and quantitative study. J Am Acad Dermatol 1991; 25: 751-60. [Erratunm: J Am Acad Dermatol 1992; 26: 558-65].Yamauchi m, Prisayanh P, Haque Z, Woodley dT. 29. collagen cross-linking in sun-exposed and unexposed sites of aged human skin. J Invest Dermatol 1991; 97: 938-41.Uitto J. Understanding premature skin aging. 30. N Engl J Med 1997; 337: 1463-5.Ellis cN, Weiss JS, Hamilton TA, Headington JT, 31. Zelickson AS, Voorhees JJ. Sustained improvement with prolonged topical tretinoin (retinoic acid) for photoaged skin. J Am Acad Dermatol 1990; 23: 629-37.Kappes UP. Skin ageing and wrinkles: clinical and 32. photographic scoring. J Cosmet Dermatol 2004; 3: 23-5.Foellmer HG, Kawahara K, madri JA, Furthmayr 33. H, Timpl R, Tuderman L. A monoclonal antibody specific for the amino terminal cleavage site of procollagen type I. Eur J Biochem 1983; 134: 183-9.Alster TS, Tanzi EL, Lazarus m. The use of fractional 34. laser photothermolysis for the treatment of atrophic scars. Dermatol Surg 2007; 33: 295-9.Jih mH, Kimyai-Asadi A. Fractional 35. photothermolysis: A review and update. Semin Cutan Med Surg 2008; 27: 63-71.Weiss RA. comparison of histological features of 36. 1550 nm fractional resurfacing and microlens array scattering of 1440 nm. Lasers Surg Med 2006; 38 (suppl 18).Hardaway cA, Ross EV, Barnette dJ, Paithankar 37. dY. Non-ablative cutaneous remodeling with a 1.45 microm mid-infrared diode laser: Phase I. J Cosmet Laser Ther 2002; 4: 3-8.Nanni cA, Alster TS. complications of carbon 38. dioxide laser resurfacing. An evaluation of 500 patients. Dermatol Surg 1998; 24: 315-20.Bedi VP, chan KF, Sink RK, Hantash Bm, Herron 39.
GS, Rahman Z, et al. The effects of pulse energy variations on the dimensions of microscopic thermal treatment zones in nonablative fractional resurfacing. Lasers Surg Med 2007; 39: 145-55.Hasegawa T, matsukura T, mizuno Y, Suga Y, 40. Ogawa H, Ikeda S. clinical trial of a laser device called fractional photothermolysis system for acne scars. J Dermatol 2006; 33: 623-7.Walgrave SE, Ortiz AE, macFalls HT, Elkeeb L, 41. Truitt AK, Tournas JA, et al. Evaluation of a novel fractional resurfacing device for treatment of acne scarring. Lasers Surg Med 2009; 41: 122-7.Behroozan dS, Goldberg LH, dai T, Geronemus 42. RG, Friedman Pm. Fractional photothermolysis for the treatment of surgical scars: a case report. J Cosmet Laser Ther 2006; 8: 35-8.Glaich AS, Rahman Z, Goldberg LH, Friedman 43. Pm. Fractional resurfacing for the treatment of hypopigmented scars: a pilot study. Dermatol Surg 2007; 33: 289-94.Rokhsar cK, Fitzpatrick RE. The treatment of 44. melasma with fractional photothermolysis: a pilot study. Dermatol Surg 2005; 31: 1645-50.Behroozan dS, Goldberg LH, Glaich AS, dai T, 45. Friedman Pm. Fractional photothermolysis for treatment of poikiloderma of civatte. Dermatol Surg 2006; 32: 298-301.Rahman Z, Alam m, dover JS. Fractional 46. Laser treatment for pigmentation and texture improvement. Skin Therapy Lett 2006; 11: 7-11.Wanner m, Tanzi EL, Alster TS. Fractional 47. photothermolysis: treatment of facial and nonfacial cutaneous photodamage with a 1550-nm erbium-doped fiber laser. Dermatol Surg 2007; 33: 23-8.Bass LS. Rejuvenation of the aging face using 48. Fraxel laser treatment. Aesthet Surg J 2005; 25: 307-9.Rokhsar cK, ciocon dH. Fractional 49. photothermolysis for the treatment of postinflammatory hyperpigmentation after carbon dioxide laser resurfacing. Dermatol Surg 2009; 35: 535-7.










![The Resurfacing of Arabic Qaf [q] in the Speech of Young ...](https://static.fdokumen.com/doc/165x107/6327fe736d480576770d8d74/the-resurfacing-of-arabic-qaf-q-in-the-speech-of-young-.jpg)









