
On the nature of nighttime ionisation enhancements observed ...
Upload
independentCategory
view
2download
0
Journal of Adolescence 32 (2009) 1059e1074
www.elsevier.com/locate/jado
Nighttime sleep and daytime functioning correlates of theinsomnia complaint in young adults
Julio Fernandez-Mendoza a,b, Antonio Vela-Bueno a,*, Alexandros N. Vgontzas c,Sara Olavarrieta-Bernardino a, Marıa Jose Ramos-Platon b, Edward O. Bixler c,
Juan Jose De la Cruz-Troca d
a Department of Psychiatry, School of Medicine, Universidad Autonoma de Madrid, c/ Arzobispo Morcillo s/n, 28029Madrid, Spain
b Department of Psychobiology, School of Psychology, Universidad Complutense de Madrid, Campus de Somosaguas s/n,28223 Madrid, Spain
c Sleep Research & Treatment Center, Department of Psychiatry, College of Medicine, Penn State University, Hershey,PA 17033, United States
d Department of Preventive Medicine, School of Medicine, Universidad Autonoma de Madrid, c/ Arzobispo Morcillo s/n,28029 Madrid, Spain
Abstract
The nighttime and daytime correlates of the insomnia complaint (IC) were assessed in an in-classsurvey on a sample of 1238 first year university students (18.85� 1.45 years) at the UniversidadAutonoma of Madrid, Spain. Evidence was found that the likelihood of complaining of insomnia wasincreased by perceiving difficulties with initiating and maintaining sleep, reporting low quality ofnocturnal sleep, having a long sleep onset latency and having an evening circadian preference. The moststrongly related daytime variables to IC being perceived difficulties in concentrating, feelings of irrita-bility and fatigue, and symptoms of anxiety and depression. The data, in addition to confirm those of
* Corresponding author at: Laboratory of Human Sleep and Applied Chronobiology, Department of Psychiatry, Schoolof Medicine, Universidad Autonoma de Madrid, c/ Arzobispo Morcillo s/n, 28029 Madrid, Spain. Tel.: þ34 914975492;
fax: þ34 914975353.E-mail address: [email protected] (A. Vela-Bueno).
0140-1971/$36.00� 2009TheAssociation for Professionals in Services forAdolescents. Published byElsevier Ltd.All rights reserved.doi:10.1016/j.adolescence.2009.03.005

1060 J. Fernandez-Mendoza et al. / Journal of Adolescence 32 (2009) 1059e1074
clinical studies on subjects complaining of insomnia, suggest that having an evening chronotypeincreases the vulnerability of adolescents and young adults to complain of insomnia.� 2009 The Association for Professionals in Services for Adolescents. Published by Elsevier Ltd. Allrights reserved.
Keywords: Insomnia complaint; Nighttime sleep; Sleepiness and fatigue; Mood and cognition; Young adults
Introduction
There is a growing interest about inadequate sleep in subjects who are in the first decades of thelife cycle, with the main focus of sleep research being mainly on the problems associated withinsufficient sleep and the ensuing excessive daytime sleepiness (EDS) in both adolescents andyoung adults (Millman, 2005). There are some surveys on chronic insomnia and poor sleep inadolescents (Roberts, Roberts, & Chan, 2008; Roberts, Roberts, & Duong, 2008) and youngadults (Chang, Ford, Mead, Cooper-Patrick, & Klag, 1997; Yang, Wu, Hsieh, Liu, & Lu, 2003)that have examined some of the correlates of such conditions.
Both clinical and pathophysiological evidence have contributed to characterize insomnia asa 24-hour disorder. Clinically, insomniac patients present with both nighttime and daytimemanifestations (Kales et al., 1984; Kloss, 2003; Moul, Nofzinger, Pilkonis, Houck, Mielwald, &Buysse, 2002). Current criteria in the two main sleep disorders classifications in use (AmericanPsychiatric Association, 2000; American Academy of Sleep Medicine, 2005) include both night-time and daytime manifestations. The first group is made of difficulty initiating and/or main-taining sleep, as well as waking up too early and non-restorative sleep. The daytime impairmentsinvolve: cognitive functions (attention, concentration, and memory), mood (mainly dysphoria andirritability); EDS and fatigue; motivation, energy and/or initiative reduction; proneness for errorsor accidents; various somatic complaints; sequelae in the social relations; vocational dysfunctionsor poor school performance (American Psychiatric Association, 2000; American Academy ofSleep Medicine, 2005).
From the pathophysiological standpoint, a variety of studies have shown that subjects withinsomnia have a higher activity of different physiological and cognitive-emotional systems (Basta,Chrousos, Vela-Bueno, & Vgontzas, 2007). These findings have given support to the notion ofinsomnia as a disorder of hyperarousal extending to the 24 h. The daytime correlates of insomniahave been considered as direct sequelae of the nighttime sleep difficulties (Kloss, 2003) or asmanifestations of the same pathophysiological mechanism (i.e. hyperarousal; Bonnet & Arand,1997; Basta et al., 2007). Both views have created a growing awareness that the daytime correlatesshould be addressed and studied in insomnia among all age groups (Basta et al., 2007; Kloss,2003). Older and more recent studies give support to the need of integrating both nighttime anddaytime correlates of insomnia for epidemiological, evaluation and therapeutic purposes (Kaleset al., 1984; Moul et al., 2002; Moul, Hall, Pilkonis, & Buysse, 2004).
We were interested in confirming in a non-clinical sample of young adults the findings ofclinical studies (American Psychiatric Association, 2000; American Academy of Sleep Medicine,2005; Kales et al., 1984; Kloss, 2003; Moul et al., 2002) and those of epidemiological surveys

1061J. Fernandez-Mendoza et al. / Journal of Adolescence 32 (2009) 1059e1074
among general population (LeBlanc, Beaulieu-Bonneau, Merette, Savard, Ivers, & Morin, 2007;Ohayon, 2002; Ohayon & Paiva, 2005; Roth & Ancoli-Israel, 1999; Stewart et al., 2006; Zammit,Weiner, Damato, Sillup, & McMillan, 1999). The main purpose of this study was to assess thevarious self-reported nighttime and daytime correlates of the insomnia complaint in youngadulthood, a period of life in which insomnia often begins (American Psychiatric Association,2000). Thus, we hypothesized that the complaint of insomnia is characterized by specific nighttimeand daytime manifestations among non-clinical young adult individuals from the community.Our data were obtained from a survey conducted on a sample of first year university students.
Methods
Participants and procedure
The current study is a part of a project assessing the sleep habits and disorders, as well as theirhealth and life style correlates among a sample of young adults of Madrid (Spain). Self-reportedinformation was obtained from an anonymous self-developed questionnaire (Vela-Bueno et al.,2008) administered to first year students of the Universidad Autonoma de Madrid (UAM), Spainbetween November 2002 and March 2003. The ethical committee of the UAM granted thefulfillment of international ethical standards. Informed consent was obtained from participantsafter the nature of the procedures was explained. A total of 1714 questionnaires were given in anin-class survey in a total of 29 classes; at the end 1271 were collected, giving a response rate of74.5%. The final sample comprised a 26% of males and a 74% of females; given the lowerproportion of males in the sample as compared to that of the target population (35.45%),the sample was weighted for gender as to be representative of the first-year UAM students’population. The mean age was 18.85 (�1.45) years with a range of 16e25.
Measures
The survey package distributed consisted of three parts: (1) a self-developed questionnaire(Vela-Bueno et al., 2008); (2) the Spanish version of the MorningnesseEveningness Questionnaire(MEQ) (Adan & Almirall, 1990); and (3) the Spanish version of the Epworth Sleepiness Scale(ESS) (Izquierdo-Vicario, Ramos-Platon, Conesa-Peraleja, Lozano-Parra, & Espinar-Sierra,1997). All information was referred to the last twelve months, except as otherwise stated. Thesections of the self-developed questionnaire used in this study were as follows.
Socio-demographic informationEight open questions were used to record information on sex, age, weight, height, parent’s
marital status and their academic background, and number of brothers and sisters. In the presentstudy sex, age, and body mass index [BMI; weight (kg)/height (m2)] were submitted to analyses.
Sleep habits and sleep durationRecording of estimated bedtime and rising time (during weekdays and weekends) was made by
using 4 open ended questions recorded in an ‘‘hour:minutes’’ format: ‘‘At what time do you usually
1062 J. Fernandez-Mendoza et al. / Journal of Adolescence 32 (2009) 1059e1074
go to bed during the week?’’, ‘‘At what time do you usually go to bed during the weekend?’’, ‘‘At whattime do you usually wake up during the week?’’, and ‘‘At what time do you usually wake up duringthe weekend?’’. In order to assess napping behavior participants were asked ‘‘Do you take naps atanytime during the day?’’ in a dichotomized way (yes, no). Weekday’s and weekend’s actual sleepand desired sleep length were reported by 4 open ended questions recorded in minutes: ‘‘Howmany hours of sleep do you usually get during the week?’’, ‘‘How many hours of sleep do you usuallyget during the weekend?’’, ‘‘How many hours of sleep would you desire to get during the week?’’, and‘‘How many hours of sleep would you desire to get during the weekend?’’.
Sleep difficulties and sleep disordersBy using definitions regarding 22 sleep disorders from the International Classification of Sleep
Disorders (ICSD) (American Sleep Disorders Association, 1997), self-reported presence of sleepdisorders was assessed and all of them were answered in a dichotomized way (yes, no). In order toassess sleep difficulties experienced during the previous 12 months participants were asked: ‘‘Doyou have difficulty initiating sleep?’’, ‘‘Do you have difficulty maintaining sleep?’’, and ‘‘Do you wakeup too early in the morning before desired?’’. Another question assessed the subjective insomniacomplaint (IC): ‘‘Do you have insomnia?’’. Irregular SleepeWake Pattern was assessed by usingthe ICSD definition (American Sleep Disorders Association, 1997): ‘‘Irregular sleepewake pattern(ISWP) consists of temporally disorganized and variable episodes of sleeping and waking behavior,being unpredictable the time of sleep onset even at any particular time of the day. ¿Do you haveISWP?’’.
Quality of nighttime sleepThis section included 3 questions regarding perceived quality of nighttime sleep: ‘‘How is the
quality of your current sleep?’’, ‘‘How deep is your current sleep?’’, ‘‘How restorative is your currentsleep?’’. The latter was used to estimate non-restorative sleep (NRS) as responses were scored ina 7-point Likert scale (from extremely restorative to extremely non-restorative). In this finalquestion, if a subject gave an answer from ‘‘little restorative’’ to ‘‘extremely non-restorative’’, heor she was defined as a subject with NRS.
Mixed anxious and depressive symptoms checklistThe presence of anxiety, depressive, and somatic symptoms associated with both anxiety and
depression was assessed with a dichotomic option response (yes, no). These symptoms were drawnfrom the ones included in the DSM-IV-TR (American Psychiatric Association, 2000) for majordepression, generalized anxiety, and panic disorder. A quantitative index (MADS) of the presenceof mixed anxious, depressive, and somatic-associated symptoms was obtained by assigning 0 (no)and 1 (yes) values to each symptom and adding them in a total score, where higher score meanthigher number of symptoms (range 0e24).
Academic and cognitive performanceSubjective perception of impact of poor sleep on academic performance was assessed in each
individual by a question asking ‘‘Do you think that your academic performance would improve ifgetting better sleep?’’ this question was answered in a dichotomized way (yes, no). Also conse-quences of sleep on academic performance and daytime functioning were assessed by 5 groups of

1063J. Fernandez-Mendoza et al. / Journal of Adolescence 32 (2009) 1059e1074
questions regarding the perceived grade of dysfunction in class (mood, alertness, memory, classattendance, and sleepiness). These questions were: ‘‘Do you feel (restless, irritable, bad-tempered,angry, aggressive, violent, and less sociable) in class?’’ answered in a dichotomized way (yes/no);‘‘Do you have poorer memory (i.e. problems remembering events or tasks)?’’, and ‘‘Do you havea decreased ability to concentrate’’ both answered in a dichotomized way (yes/no); ‘‘Do you missclasses due to oversleeping?’’, and ‘‘Do you miss classes due to excessive tiredness’’ also answered ina dichotomized way (yes/no); ‘‘Do you fall asleep in class?’’, ‘‘Do you have the need for sleep inclass?’’, and ‘‘Do you need to do something to avoid falling asleep in class?’’ all answered ina dichotomized way (yes/no). In addition, 10 items regarding the perceived ability to concentrate(‘‘Do you have less ability to concentrate.?’’) at certain daytime periods (1st and 2nd hour of themorning and of the afternoon) were also included in the assessment of perceived cognitiveperformance.
The MEQ (Horne & Ostberg, 1976) consists of 19 separate questions to determine the circadianpreference of individuals. The three major chronotypes in which participants can be classified intoare: morning, neither and evening. The Spanish version of the MEQ was used in this study, whichhas shown high internal consistency and reliability (r¼ .733, p¼ .00001) (Adan & Almirall, 1990).
The ESS (Johns, 1992) requires participants to rate the likelihood that they would fall asleep inany of 8 different situations (e.g. ‘‘sitting and reading,’’ ‘‘watching television’’) on a 4-point ratingscale. The level of sleepiness was obtained by adding the scores pertaining to each question, thefinal result was categorized into two groups of low and high level of sleepiness (scores of �10 or>10). The Spanish version of the ESS was used in this study, which has demonstrated highinternal consistency and reliability (a¼ .88) and good testeretest consistency (r¼ .82 with a 5-month interval) (Izquierdo-Vicario et al., 1997).
Statistical analyses
The relationship between qualitative variables and the insomnia complaint (IC) was analyzedwith Pearson chi-square test and Yates’ correction or Fisher exact probability test if necessary.Effect sizes for chi-square tests were measured by Cohen’s 4 (phi) statistic; by convention, valuesof .10, .30, and .50 are defined as small, medium, and large effects, respectively (Cohen, 1988). Tostudy mean differences in quantitative variables between the IC group and the non-IC group, thet-Student test was used; p values uncorrected for multiple comparisons are reported. Effect sizesfor t-Student tests were measured by Cohen’s d statistic; by convention, values of .20, .50, and .80are defined as small, medium, and large effects, respectively (Cohen, 1988). Multivariate logisticregression models were applied to explore the association between the IC and all other variables ofthe study as covariates. Results were presented as mutually adjusted odds ratios (OR) and 95%confidence intervals (CI). The final multivariate logistic regression models, using the forwardstepwise method (‘‘p’’ of entry <.05 and ‘‘p’’ of removing <.1) included all variables that retainedstatistical significance, after controlling for the confounding effects of other variables. In order toeliminate possible confounding effects between nighttime and daytime variables when exploringtheir independent association with the IC, two-fold regression models were run out: one fornighttime sleep correlates and one for daytime functioning correlates. The significance level wasestablished at p< .05. All the analyses were performed by using SPSS 14.0 for Windows (SPSS,Inc., Chicago, IL).
1064 J. Fernandez-Mendoza et al. / Journal of Adolescence 32 (2009) 1059e1074
Results
Characteristics of participants complaining of insomnia
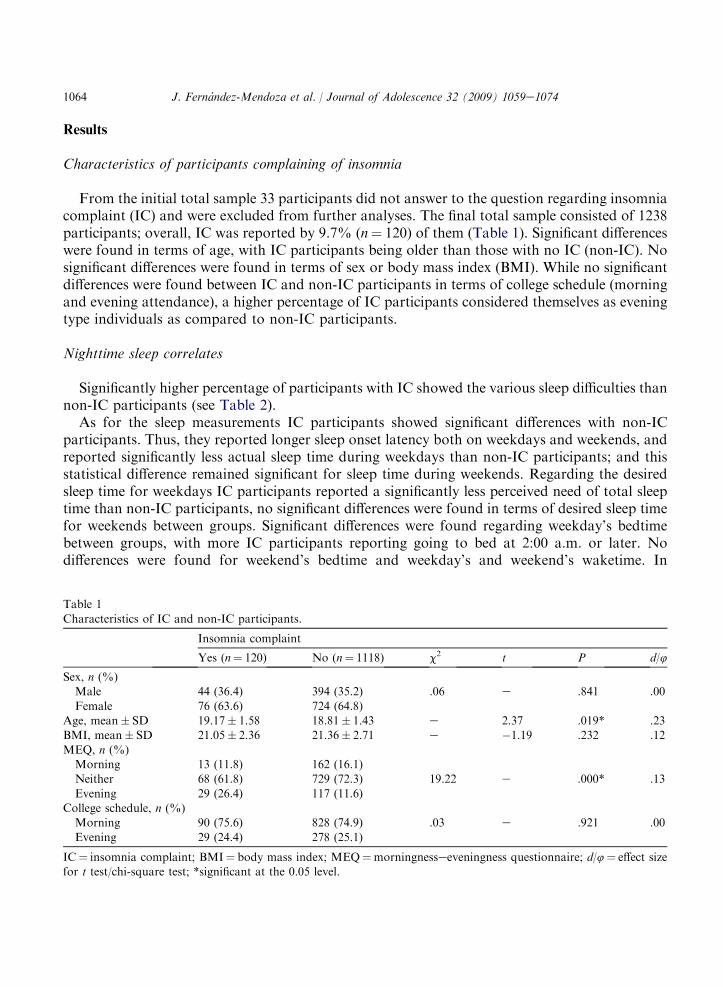
From the initial total sample 33 participants did not answer to the question regarding insomniacomplaint (IC) and were excluded from further analyses. The final total sample consisted of 1238participants; overall, IC was reported by 9.7% (n¼ 120) of them (Table 1). Significant differenceswere found in terms of age, with IC participants being older than those with no IC (non-IC). Nosignificant differences were found in terms of sex or body mass index (BMI). While no significantdifferences were found between IC and non-IC participants in terms of college schedule (morningand evening attendance), a higher percentage of IC participants considered themselves as eveningtype individuals as compared to non-IC participants.
Nighttime sleep correlates
Significantly higher percentage of participants with IC showed the various sleep difficulties thannon-IC participants (see Table 2).
As for the sleep measurements IC participants showed significant differences with non-ICparticipants. Thus, they reported longer sleep onset latency both on weekdays and weekends, andreported significantly less actual sleep time during weekdays than non-IC participants; and thisstatistical difference remained significant for sleep time during weekends. Regarding the desiredsleep time for weekdays IC participants reported a significantly less perceived need of total sleeptime than non-IC participants, no significant differences were found in terms of desired sleep timefor weekends between groups. Significant differences were found regarding weekday’s bedtimebetween groups, with more IC participants reporting going to bed at 2:00 a.m. or later. Nodifferences were found for weekend’s bedtime and weekday’s and weekend’s waketime. In
Table 1
Characteristics of IC and non-IC participants.
Insomnia complaint
Yes (n¼ 120) No (n¼ 1118) c2 t P d/4
Sex, n (%)Male 44 (36.4) 394 (35.2) .06 e .841 .00
Female 76 (63.6) 724 (64.8)Age, mean� SD 19.17� 1.58 18.81� 1.43 e 2.37 .019* .23BMI, mean� SD 21.05� 2.36 21.36� 2.71 e �1.19 .232 .12
MEQ, n (%)Morning 13 (11.8) 162 (16.1)Neither 68 (61.8) 729 (72.3) 19.22 e .000* .13
Evening 29 (26.4) 117 (11.6)College schedule, n (%)
Morning 90 (75.6) 828 (74.9) .03 e .921 .00
Evening 29 (24.4) 278 (25.1)
IC¼ insomnia complaint; BMI¼ body mass index; MEQ¼morningnesseeveningness questionnaire; d/4¼ effect sizefor t test/chi-square test; *significant at the 0.05 level.

Table 2Mean scores of IC and non-IC participants on self-reported nighttime sleep variables.
Insomnia complaint
Yes (n¼ 120) No (n¼ 1118) c2 t P d/4
Sleep DifficultiesDifficulty initiating sleep, n (%) 102 (85.7) 244 (21.9) 216.86 e .000* .42
Difficulty maintaining sleep, n (%) 45 (38.5) 75 (6.7) 121.44 e .000* .31Early morning awakening, n (%) 51 (42.9) 295 (26.4) 14.43 e .000* .11Non-restorative sleep, n (%) 58 (50.9) 228 (21.2) 49.76 e .000* .20
Sleep DurationSleep onset latency (weekdays), mean� SDa 0:49� 0:27 0:25� 0:23 e 9.31 .000* .95Sleep onset latency (weekends), mean� SDa 0:20� 0:20 0:14� 0:16 e 3.16 .002* .33
Actual sleep time (weekdays), mean� SDb 6:54� 1:08 7:31� 1:00 e �6.28 .000* .74Actual sleep time (weekends), mean� SDb 8:02� 1:22 8:22� 1:32 e �2.18 .031* .16Desired sleep time (weekdays), mean� SDb 8:47� 1:13 9:05� 1:26 e �2.21 .027* .48
Desired sleep time (weekends), mean� SDb 9:45� 1:14 9:47� 1:32 e �.23 .819 .00
Sleep Habits and Pattern
Bedtime on weekdays, n (%)21:00e23:59 36 (30.3) 378 (33.9)24:00e24:59 51 (42.9) 550 (49.4) 8.90 e .031* .0501:00e01:59 22 (18.5) 142 (12.7)
�02:00 10 (8.4) 44 (3.9)
Bedtime on weekends, n (%)23:00e01:59 20 (17.4) 217 (19.8)02:00e02:59 23 (20) 247 (22.5) 5.62 e .229 .03
03:00e03:59 29 (25.2) 247 (22.5)04:00e04:59 13 (11.3) 181 (16.5)�05:00 30 (26.1) 205 (18.7)
Waketime on weekdays, n (%)
05:15e06:59 10(8.4) 101 (9.1)07:00e07:59 60 (50.4) 525 (47.3) 2.19 e .700 .0208:00e08:59 26 (21.8) 256 (23)09:00e09:59 12 (10.1) 152 (13.7)
10:00e13:30 11 (9.2) 77 (6.9)
Waketime on weekends, n (%)06:00e09:59 16 (13.6) 193 (17.5)10:00e11:59 60 (50.8) 548 (49.8) 4.38 e .223 .03
12:00e13:59 28 (23.7) 282 (25.6)14:00e18:00 14 (11.9) 78 (7.1)
Irregular sleepewake pattern, n (%) 20 (16.8) 84 (7.6) 11.87 e .002* .10
Sleep Quality and Depth
Quality of nighttime sleep, n (%)Low 50 (42.4) 68 (6.1) 178.70 e .30Average 42 (35.6) 327 (29.5) .000*
(continued on next page)
1065J. Fernandez-Mendoza et al. / Journal of Adolescence 32 (2009) 1059e1074

Table 2 (continued )
Insomnia complaint
Yes (n¼ 120) No (n¼ 1118) c2 t P d/4
High 26 (22) 714 (64.4)
Depth of nighttime sleep, n (%)
Low 39 (33.6) 115 (10.4) 56.07 eAverage 33 (28.4) 298 (26.8) .000* .15High 44 (37.9) 697 (62.8)
IC¼ insomnia complaint; SD¼ standard deviation.a Mean and SD values in hours:minutes.b Mean and SD values in hours:minutes; d/4¼ effect size for t test/chi-square test; *significant at the 0.05 level.
1066 J. Fernandez-Mendoza et al. / Journal of Adolescence 32 (2009) 1059e1074
addition, a higher percentage of IC participants reported having an irregular sleepewake pattern.A greater proportion of IC participants reported a low quality and a low depth of nighttime sleepthan non-IC participants.
Daytime functioning correlates
A higher percentage of IC participants than non-IC participants reported feelings of fatigue,missing classes due to tiredness and due to oversleeping (see Table 3).
In contrast, no significant differences between IC and non-IC participants were found in eitherthe total score of the ESS or when the score was split into two groups, with a total score higherthan 10 in the ESS meaning EDS. Moreover, when the participants were asked about theirnapping behavior non-significant differences were found between IC and non-IC participants.Furthermore, several other questions regarding indirect manifestations of EDS did not showsignificant differences between groups (see Table 3).
IC participants reported significantly more symptoms of anxiety and depression than non-ICparticipants, and they also reported more often feeling irritable in class and feeling angry in class.On the other hand, no significant differences between groups were found for several questionsregarding perceived mood and behavior in class (see Table 3).
A significantly greater proportion of ICparticipants as compared to non-ICparticipants reportedadecreased ability to concentrate andpoorermemory. In addition, ICparticipantswere significantlymore likely to report less ability to concentrate during the first hour in the morning than non-ICparticipants. In contrast, a significant relationship was found in terms of less ability to concentrateduring the secondhour in the afternoon,where non-ICparticipants reported it in ahigher percentagethan IC participants. When other daytime periods were taken into account (i.e. second hour in themorning, and first hour in the afternoon) no significant differences were found between both groups(see Table 3). Finally, more IC participants than non-IC participants reported that they consideredgetting better sleep as necessary to improve their academic performance.
Logistic regression analyses
In order to assess the independent contribution of all significant self-reported nighttime sleepand daytime functioning variables for the IC, two logistic regression analyses were carried out.
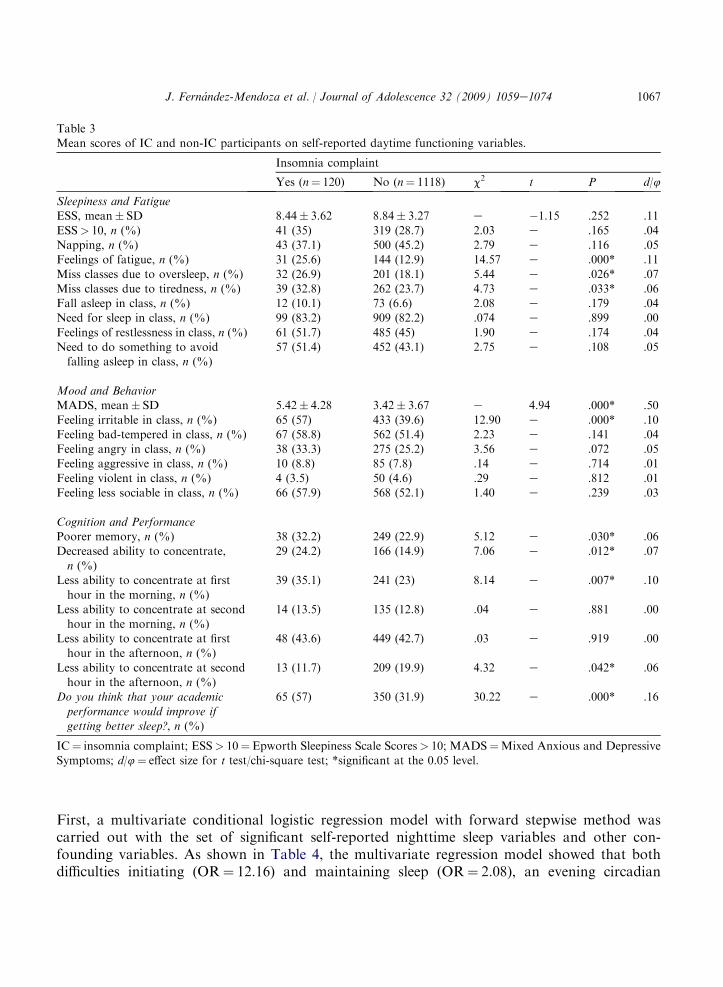
Table 3Mean scores of IC and non-IC participants on self-reported daytime functioning variables.
Insomnia complaint
Yes (n¼ 120) No (n¼ 1118) c2 t P d/4
Sleepiness and FatigueESS, mean� SD 8.44� 3.62 8.84� 3.27 e �1.15 .252 .11
ESS> 10, n (%) 41 (35) 319 (28.7) 2.03 e .165 .04Napping, n (%) 43 (37.1) 500 (45.2) 2.79 e .116 .05Feelings of fatigue, n (%) 31 (25.6) 144 (12.9) 14.57 e .000* .11
Miss classes due to oversleep, n (%) 32 (26.9) 201 (18.1) 5.44 e .026* .07Miss classes due to tiredness, n (%) 39 (32.8) 262 (23.7) 4.73 e .033* .06Fall asleep in class, n (%) 12 (10.1) 73 (6.6) 2.08 e .179 .04Need for sleep in class, n (%) 99 (83.2) 909 (82.2) .074 e .899 .00
Feelings of restlessness in class, n (%) 61 (51.7) 485 (45) 1.90 e .174 .04Need to do something to avoidfalling asleep in class, n (%)
57 (51.4) 452 (43.1) 2.75 e .108 .05
Mood and BehaviorMADS, mean� SD 5.42� 4.28 3.42� 3.67 e 4.94 .000* .50
Feeling irritable in class, n (%) 65 (57) 433 (39.6) 12.90 e .000* .10Feeling bad-tempered in class, n (%) 67 (58.8) 562 (51.4) 2.23 e .141 .04Feeling angry in class, n (%) 38 (33.3) 275 (25.2) 3.56 e .072 .05Feeling aggressive in class, n (%) 10 (8.8) 85 (7.8) .14 e .714 .01
Feeling violent in class, n (%) 4 (3.5) 50 (4.6) .29 e .812 .01Feeling less sociable in class, n (%) 66 (57.9) 568 (52.1) 1.40 e .239 .03
Cognition and PerformancePoorer memory, n (%) 38 (32.2) 249 (22.9) 5.12 e .030* .06Decreased ability to concentrate,
n (%)
29 (24.2) 166 (14.9) 7.06 e .012* .07
Less ability to concentrate at firsthour in the morning, n (%)
39 (35.1) 241 (23) 8.14 e .007* .10
Less ability to concentrate at secondhour in the morning, n (%)
14 (13.5) 135 (12.8) .04 e .881 .00
Less ability to concentrate at firsthour in the afternoon, n (%)
48 (43.6) 449 (42.7) .03 e .919 .00
Less ability to concentrate at secondhour in the afternoon, n (%)
13 (11.7) 209 (19.9) 4.32 e .042* .06
Do you think that your academic
performance would improve ifgetting better sleep?, n (%)
65 (57) 350 (31.9) 30.22 e .000* .16
IC¼ insomnia complaint; ESS> 10¼Epworth Sleepiness Scale Scores> 10; MADS¼Mixed Anxious and DepressiveSymptoms; d/4¼ effect size for t test/chi-square test; *significant at the 0.05 level.
1067J. Fernandez-Mendoza et al. / Journal of Adolescence 32 (2009) 1059e1074
First, a multivariate conditional logistic regression model with forward stepwise method wascarried out with the set of significant self-reported nighttime sleep variables and other con-founding variables. As shown in Table 4, the multivariate regression model showed that bothdifficulties initiating (OR¼ 12.16) and maintaining sleep (OR¼ 2.08), an evening circadian

Table 4Summary of multiple stepwise logistic regression analysesa for participants complaining of insomnia (IC): nighttime
sleep variables.
b Sig. OR CI (95.0%)
Lower Upper
Age e 0.064 e e eSex e 0.440 e e eDifficulty initiating sleep 2.498 0.000 12.16 5.931 24.937Difficulty maintaining sleep 0.735 0.019 2.086 1.126 3.863
Evening chronotype 0.676 0.005 1.966 1.233 3.134Low qualityof nighttime sleep
0.476 0.015 1.610 1.099 2.359
Sleep onset
latency: weekdays
0.012 0.010 1.012 1.003 1.021
Actual sleeptime: weekdays
e 0.099 e e e
Actual sleeptime: weekends
e 0.965 e e e
Desired sleep
time: weekdays
e 0.880 e e e
Early morning awakening e 0.790 e e eNon-restorative sleep e 0.910 e e eLow depth
of nighttime sleep
e 0.089 e e e
Irregular sleep pattern e 0.391 e e e
OR¼ odd ratio; CI¼ confidence interval; IC¼ insomnia complaint.a HosmereLemeshow Goodness-of-Fit test> 0.05. The model provides a good fit for the data.
1068 J. Fernandez-Mendoza et al. / Journal of Adolescence 32 (2009) 1059e1074
preference (OR¼ 1.96), a low quality of nighttime sleep (OR¼ 1.61) and a long sleep onsetlatency (OR¼ 1.01) increased the likelihood of complaining of insomnia, adjusted by sex and age.
Furthermore, another multivariate conditional logistic stepwise forward regression analysiswas performed with significant daytime functioning variables in chi-square analyses to adjust forthe confounding effects of other variables (see Table 5). Results of this analysis showed thathaving less ability to concentrate at first hour in the morning remained as the most importantvariable related to the IC (OR¼ 1.69), followed by feeling irritable in class (OR¼ 1.64), havingfeelings of fatigue (OR¼ 1.40), and the presence of mixed anxious and depressive symptoms(OR¼ 1.09).
To examine the possible confounding effect of delayed sleep phase patterns, these multivariateregression models were re-run including this variable taken from the sleep disorders section of thequestionnaire [assessed by the item: ‘‘Delayed Sleep Phase Syndrome (DSPS) is a disorder inwhich the nighttime sleep episode is delayed in relation to the desired clock time, resulting in sleep-onset difficulty or difficulty in awakening at the desired time, but little difficulty in maintaining sleeponce sleep has begun ¿Do you have DSPS?’’ answered in a dichotomized way (yes, no)]. Thisvariable resulted to be a non-significant predictor of the IC early in the first step of the forwardconditional regression method (b¼ .20; OR¼ 1.22; CI95%¼ .68e2.19; p¼ .498). Thus, themodels remained with the same significant predictors while controlling for this variable.

Table 5Summary of multiple stepwise logistic regression analysesa for participants complaining of insomnia (IC): daytime
functioning variables.
b Sig. OR CI (95.0%)
Lower Upper
Age e 0.110 e e eSex e 0.312 e e eLess abilityto concentrate at first
hour in the morning
0.528 0.017 1.695 1.099 2.614
Feel irritablein class
0.497 0.018 1.644 1.087 2.486
Feelings of fatigue 0.692 0.005 1.405 1.102 2.388
MADS 0.098 0.007 1.087 1.022 1.156Decreased abilityto concentrate
e 0.741 e e e
Miss classesdue to sleep
e 0.349 e e e
Miss classes
due to tiredness
e 0.495 e e e
Less abilityto concentrate at secondhour in the afternoon
e 0.134 e e e
Poorer memory e 0.334 e e e
OR¼ odd ratio; CI¼ confidence interval; MADS¼Mixed Anxious and Depressive Symptoms.a HosmereLemeshow Goodness-of-Fit test> 0.05. The model provides a good fit for the data.
1069J. Fernandez-Mendoza et al. / Journal of Adolescence 32 (2009) 1059e1074
Discussion
This study aimed at defining the nighttime and daytime correlates of the IC in a sample of firstyear university students aged 18.85 (�1.45) years. Regarding the prevalence of the IC in our data(9.7%) were similar to those reported for the same age group in surveys of the general populationof different countries (Ancoli-Israel & Roth, 1999; Ohayon, 2002; Ohayon & Paiva, 2005; Stewartet al., 2006). A large body of evidence has suggested that women of all ages complain morefrequently of insomnia than do men, with a recent meta-analysis showing also sex differences inyoung adults (15e30 years) (Zhang & Wing, 2006). The absence of sex differences in our studycould probably be due to the narrower age range (16e25), which agrees with the results ofa previous study (Ohayon & Paiva, 2005). Although the age difference was statistically significant,it was small in terms of their absolute values and statistical effect size (d¼ .23). There were notinter-group differences in terms of BMI, which rules out the possible confounding effect of thisvariable.
No differences were found in terms of college schedule. It should be taken into account that theschedules in Spanish university students are randomly assigned. Significantly more IC participantsin our sample reported an evening circadian preference, which is in agreement with reportingmore often going to bed later than 2:00 a.m. during weekdays. Studies on adolescents have shown

1070 J. Fernandez-Mendoza et al. / Journal of Adolescence 32 (2009) 1059e1074
that those subjects with an evening preference are more likely to have a poorer quality and lesssleep than morning individuals (Giannotti, Cortesi, Sebastiani, & Ottaviano, 2002; Warner,Murray, & Meyer, 2008). Moreover, two recent studies have concluded that certain factors, suchas the sleepewake irregularity, associated with an evening circadian preference may contribute tothe perpetuation of insomnia (Adan, Fabbri, Natale, & Prat, 2006; Ong, Huang, Kuo, & Manber,2007). Actually, in our sample a higher proportion of IC participants reported having an irregularsleepewake pattern.
The participants complaining of insomnia reported a poorer sleep both in terms of quantity andquality. The prevalence of all sleep difficulties was much higher in IC participants, although theprevalence of sleep difficulties was still relatively important in the non-IC group. It is well knownthat many individuals with sleep difficulties do not complain of insomnia. Difficulty initiatingsleep was by far (almost 86%) the one most frequently reported by IC participants, with figuressimilar to those of clinical studies with a larger range of age (Kales et al., 1984; Roth, Kramer, &Lutz, 1976). It also agrees with the fact that younger adults tend to experience greater difficulty ininitiating sleep, whereas, older adults tend to have difficulty in maintaining sleep (Alapin, Fichten,Libman, Creti, Bailes, & Wright, 2000). Consistent with the report of more difficulty initiatingsleep, the IC participants also reported a sleep onset latency that was twice of that of non-ICparticipants, also showing a large effect size (d¼ .95). Whereas sleep onset latency showed in bothgroups a shortening over the weekend, IC participants still reported a longer latency than that ofnon-complaining participants, although small in terms of effect size (d¼ .33). Also, actual sleeptime was significantly shorter both on weekdays (d¼ .74) and on weekend days (d¼ .16) in ICparticipants. That is, IC participants although demonstrating recovery over the weekend still havea shorter actual sleep time and a longer sleep onset latency. IC participants showed not only worsenighttime sleep from a quantitative standpoint but, they reported significantly worse quality ofsleep as well as less depth of sleep.
Our data on EDS and fatigue are in agreement with those of the literature (Riedel & Lichstein,2000). Thus, no differences between groups were found in terms of EDS, when this symptom wasassessed with the ESS or through direct or indirect manifestations. These general findings aresimilar to those from clinical samples (Buysse et al., 2007; Chambers & Keller, 1993; Moul et al.,2002; Riedel & Lichstein, 2000). Furthermore, significant differences were found between groupsin several items indicating fatigue (having feelings of fatigue and missing classes due to tiredness).This fact is in agreement with previous literature reporting that the complaint of fatigue iscommon among insomniacs (Buysse et al., 2007; Moul et al., 2002; Riedel & Lichstein, 2000).These findings are consistent with the model proposed by Vgontzas et al. (2002) that insomnia isassociated with fatigue and not with EDS.
The prevalence of anxious and depressive symptoms was higher and showed a medium effectsize for IC participants (d¼ .50). Multiple studies have extensively documented a relationshipbetween insomnia and depression and anxiety (Bixler, Vgontzas, Lin, Vela-Bueno, & Kales, 2002;Chang et al., 1997; Eller, Aluoja, Vasar, & Veldi, 2006; Ford & Kamerow, 1989; Kloss, 2003;Riedel & Lichstein, 2000; Taylor, Lichstein, Durrence, Reidel, & Bush, 2005; Vollrath, Wicki, &Angst, 1989). The IC participants of the present study reported feeling irritable more often thannon-IC participants; however those feelings related to aggression and negative social interactions(feeling angry, aggressive, violent or less sociable in class) did not show significant differencesbetween groups, which suggest internalization of negative feelings. It has been demonstrated that

1071J. Fernandez-Mendoza et al. / Journal of Adolescence 32 (2009) 1059e1074
insomniacs handle stress through internalization of emotions, which leads to emotional arousal,and, in turn, to physiologic hyperarousal before and during sleep (Basta et al., 2007). Furtherstudies should examine the relationship between such internalization of emotions and physio-logical indices of hyperarousal in subjects complaining of insomnia.
In a different realm, insomnia patients often perceive their daytime performance as impairedand they report decrements in their cognitive performance (e.g. memory, attention, concentration)(Kloss, 2003). However, these subjective complaints are almost never corroborated by objectivefindings (Riedel & Lichstein, 2000). The lack of objective findings in daytime performance ininsomnia is at variance with the objective findings of impaired performance after sleep restriction(Vgontzas et al., 2004), which further suggests that insomnia is not a result of sleep loss (Bastaet al., 2007). In our sample, clear-cut differences were observed in terms of perceived cognitiveperformance, with poorer memory and decreased concentration being more often reported in ICparticipants, less ability to concentrate at first hour in the morning being the most frequentlyreported. In agreement with the fact that IC participants reported more often an evening circadianpreference, is the finding that non-IC participants reported less ability to concentrate at secondhour of the afternoon than IC participants. Higher college absenteeism (missing classes due tooversleeping and due to tiredness) was reported by IC participants; although these variables didnot entered into the final daytime multivariate model, it did the item on a more general decreasedability to concentrate at first hour in the morning, confirming the impact of insomnia in perceivedcognitive performance and academic functioning (Millman, 2005; Roth & Ancoli-Israel, 1999).Furthermore, it is difficult to ascertain if this perceived oversleeping is ‘‘actual oversleeping’’ orjust ‘‘staying in bed without getting up’’. Nevertheless, our data on waketimes showed nosignificant differences between the IC group and the participants not complaining of insomnia.Thus, we can argue that this absenteeism due to oversleeping might be caused by disturbed sleep(difficulties initiating and maintaining it). Moreover, a higher proportion of IC participantsthought that their school performance would improve with a better sleep.
The overall results of this study show that young adults complaining of insomnia reportsignificantly worse nighttime sleep and perceive more impairments in functioning during the daythan those individuals non-complaining of insomnia. Multivariate regression analyses showedthat difficulties initiating and maintaining sleep, low quality of nighttime sleep, long sleep onsetlatency and having an evening circadian preference were the most significant nighttime correlatesof the IC. Highly significant daytime correlates of the IC were fatigue, irritability, difficulty inconcentrating during the day, and symptoms of anxiety and depression. Thus, it appears that thecomplaint of insomnia is a good indicator of current insomnia e considered as a whole picture ofnighttime and daytime manifestations e and not merely a global dissatisfaction with nighttimesleep (Ohayon & Paiva, 2005). For example, in a very well conducted study by Ohayon and Zulley(2001), correlates of ‘‘global sleep dissatisfaction’’ were: short sleep duration (<6 h), long sleeplatency (>30 min), older age (65e74 years), upper airway disease, anxiety symptoms, too hotbedroom, the need of a particular object in order to fall asleep, and excessive daytime sleepiness;a set of correlates that are very different to those found in the present non-clinical study and inprevious clinical studies of individuals complaining of insomnia.
The data presented here suggest the need of integrating both nighttime and daytime manifes-tations when assessing insomnia among clinical and non-clinical young adult populations as earlydetection and prevention of further chronic insomnia is an important matter with a negative

1072 J. Fernandez-Mendoza et al. / Journal of Adolescence 32 (2009) 1059e1074
impact on both health and academic performance. However, some limitations of the present studymust be pointed out. First, the participants of the study belong to a special population group,thus, further research is required to establish whether or not these findings can be generalized toother samples; second, the measurements in the current study were based solely on self-reports,which increase the possibility that the relationships between nighttime and daytime variables withthe IC might be due to common method variance; third, the results of the present study are basedon cross-sectional data, therefore no conclusions can be drawn about causality or directions ofinfluence; fourth, our study did not include recordings of grade point averages (GPAs) whichwould help better understand the impact of the insomnia complaint among this population; fifth,although the way we asked about insomnia has been used in widely quoted papers on the subject(Chang et al., 1997), some authors consider it inadequate or useless (Moul et al., 2004), because itdoes not specify about the severity, duration and frequency of insomnia. However, our data onnighttime and daytime correlates of the self-reported insomnia complaint resemble those obtainedfrom clinical (Buysse et al., 2007; Moul et al., 2004) and epidemiological (LeBlanc et al., 2007;Roberts et al., 2008) samples of chronic insomniacs using structured instruments based onstandardized diagnostic criteria.
References
Adan, A., & Almirall, H. (1990). Adaptation and standardization of a Spanish version of the morningnesseeveningnessquestionnaire: individual differences. Personality and Individual Differences, 11, 1123e1130.
Adan, A., Fabbri, M., Natale, V., & Prat, G. (2006). Sleep Beliefs Scale (SBS) and circadian typology. Journal of Sleep
Research, 15, 125e132.Alapin, I., Fichten, C. S., Libman, E., Creti, L., Bailes, S., & Wright, J. (2000). How is good and poor sleep in older
adults and college students related to daytime sleepiness, fatigue, and ability to concentrate? Journal of Psychoso-matic Research, 49, 381e390.
American Sleep Disorders Association. (1997). International classification of sleep disorders. Revised Edition: Diag-nostic and Coding Manual. Rochester, Minnesota: American Sleep Disorders Association.
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (4th ed.). Washington,
DC: American Psychiatric Association. text revision (DSM-IV-TR).American Academy of Sleep Medicine. (2005). International classification of sleep disorders. Diagnostic and Coding
Manual (2nd ed.). Westchester, Illinois: American Academy of Sleep Medicine.
Ancoli-Israel, S., & Roth, T. (1999). Characteristics of insomnia in the United States: results of the 1991 National SleepFoundation Survey I. Sleep, 22, S347eS353.
Basta, M., Chrousos, G. P., Vela-Bueno, A., & Vgontzas, A. N. (2007). Chronic insomnia and the stress system. SleepMedicine Clinics, 2, 279e291.
Bixler, E. O., Vgontzas, A. N., Lin, H. M., Vela-Bueno, A., & Kales, A. (2002). Insomnia in central Pennsylvania.Journal of Psychosomatic Research, 53, 589e592.
Bonnet, M. H., & Arand, D. L. (1997). Hyperarousal and insomnia. Sleep Medicine Reviews, 1, 97e108.
Buysse, D. J., Thompson, W., Scott, J., Franzen, P. L., Germain, A., Hall, M., et al. (2007). Daytime symptoms inprimary insomnia: a prospective analysis using ecological momentary assessment. Sleep Medicine, 8, 198e208.
Chambers, M. J., & Keller, B. (1993). Alert insomniacs: are they really sleep deprived? Clinical Psychology Reviews, 13,
649e666.Chang, P. P., Ford, D. E., Mead, L. A., Cooper-Patrick, L., & Klag, M. J. (1997). Insomnia in young men and
subsequent depression. The Johns Hopkins Precursors Study. American Journal of Epidemiology, 146, 105e114.
Cohen, J. (1988). Statistical power analysis (2nd ed.). Hillsdale, NJ: Lawrence Erlbaum.Eller, T., Aluoja, A., Vasar, V., & Veldi, M. (2006). Symptoms of anxiety and depression in Estonian medical students
with sleep problems. Depression and Anxiety, 23, 250e256.

1073J. Fernandez-Mendoza et al. / Journal of Adolescence 32 (2009) 1059e1074
Ford, D. E., & Kamerow, D. B. (1989). Epidemiologic study of sleep disturbances and psychiatric disorders. An
opportunity for prevention? Journal of the American Medical Association, 262, 1479e1484.Giannotti, F., Cortesi, F., Sebastiani, T., & Ottaviano, S. (2002). Circadian preference, sleep and daytime behaviour in
adolescence. Journal of Sleep Research, 11, 191e199.
Horne, J. A., & Ostberg, O. (1976). A self-assessment questionnaire to determine morningnesseeveningness in humancircadian rhythms. International Journal of Chronobiology, 4, 97e110.
Izquierdo-Vicario, Y., Ramos-Platon, M. J., Conesa-Peraleja, D., Lozano-Parra, A. B., & Espinar-Sierra, J. (1997).Epworth Sleepiness Scale in a sample of the Spanish population. Sleep, 20, 676e677.
Johns, M. W. (1992). Reliability and factor analysis of the Epworth Sleepiness Scale. Sleep, 15, 376e381.Kales, J. D., Kales, A., Bixler, E. O., Soldatos, C. R., Cadieux, R. J., Kashurba, G. J., et al. (1984). Biopsy-
chobehavioral correlates of insomnia, V: clinical characteristics and behavioral correlates. American Journal of
Psychiatry, 141, 1371e1376.Kloss, J. D. (2003). Daytime sequelae of insomnia. In M. P. Szuba, J. D. Kloss, & D. F. Dinges (Eds.), Insomnia:
Principles and management (pp. 23e42). Cambridge: Cambridge University Press.
LeBlanc, M., Beaulieu-Bonneau, S., Merette, C., Savard, J., Ivers, H., & Morin, C. M. (2007). Psychological andhealth-related quality of life factors associated with insomnia in a population-based sample. Journal of Psychoso-matic Research, 63, 157e166.
Millman, R. P.Working Group on Sleepiness in Adolescents/Young AdultsAAP Committee on Adolescence (2005).
Excessive sleepiness in adolescents and young adults: causes, consequences, and treatment strategies. Pediatrics, 115,1774e1786.
Moul, D. E., Hall, M., Pilkonis, P. A., & Buysse, D. J. (2004). Self-report measures of insomnia in adults: rationales,
choices, and needs. Sleep Medicine Reviews, 8, 177e198.Moul, D. E., Nofzinger, E. A., Pilkonis, P. A., Houck, P. R., Miewald, J. M., & Buysse, D. J. (2002). Symptom reports
in severe chronic insomnia. Sleep, 25, 553e563.
Ohayon, M. M. (2002). Epidemiology of insomnia: what we know and what we still need to learn. Sleep MedicineReviews, 6, 97e111.
Ohayon, M. M., & Paiva, T. (2005). Global sleep dissatisfaction for the assessment of insomnia severity in the general
population of Portugal. Sleep Medicine, 6, 435e441.Ohayon, M. M., & Zulley, J. (2001). Correlates of global sleep dissatisfaction in the German population. Sleep, 24,
780e787.Ong, J. C., Huang, J. S., Kuo, T. F., & Manber, R. (2007). Characteristics of insomniacs with self-reported morning
and evening chronotypes. Journal of Clinical Sleep Medicine, 3, 289e294.Riedel, B. W., & Lichstein, K. L. (2000). Insomnia and daytime functioning. Sleep Medicine Reviews, 4, 277e298.Roberts, R. E., Roberts, C. R., & Chan, W. (2008). Persistence and change in symptoms of insomnia among adoles-
cents. Sleep, 31, 177e184.Roberts, R. E., Roberts, C. R., & Duong, H. T. (2008). H.T. Chronic insomnia and its negative consequences for health
and functioning of adolescents: a 12-month prospective study. Journal of Adolescent Health, 42, 294e302.
Roth, T., & Ancoli-Israel, S. (1999). Daytime consequences and correlates of insomnia in the United States: results ofthe 1991 National Sleep Foundation Survey II. Sleep, 22, S354eS358.
Roth, T., Kramer, M., & Lutz, T. (1976). The nature of insomnia: a descriptive summary of a sleep clinic population.Comprehensive Psychiatry, 17, 217e220.
Stewart, R., Besset, A., Bebbington, P., Brugha, T., Lindesay, J., Jenkins, R., et al. (2006). Insomnia comorbidityand impact and hypnotic use by age group in a national survey population aged 16 to 74 years. Sleep, 29,1391e1397.
Taylor, D. J., Lichstein, K. L., Durrence, H. H., Reidel, B. W., & Bush, A. J. (2005). Epidemiology of insomnia,depression, and anxiety. Sleep, 28, 1457e1464.
Vela-Bueno, A., Fernandez-Mendoza, J., Olavarrieta-Bernardino, S., Vgontzas, A. N., Bixler, E. O., de la Cruz-
Troca, J. J., et al. (2008). Sleep and behavioral correlates of napping among young adults: a survey of first-yearuniversity students in Madrid, Spain. Journal of American College Health, 57, 150e158.
Vgontzas, A. N., Zoumakis, E., Bixler, E. O., Lin, H. M., Follett, H., Kales, A., et al. (2004). Adverse effects of modest
sleep restriction on sleepiness, performance, and inflammatory cytokines. Journal of Clinical Endocrinology andMetabolism, 89, 2119e2126.

1074 J. Fernandez-Mendoza et al. / Journal of Adolescence 32 (2009) 1059e1074
Vgontzas, A. N., Zoumakis, M., Papanicolaou, D. A., Bixler, E. O., Prolo, P., Lin, H. M., et al. (2002). Chronic
insomnia is associated with a shift of interleukin-6 and tumor necrosis factor secretion from nighttime to daytime.Metabolism, 51, 887e892.
Vollrath, M., Wicki, W., & Angst, J. (1989). The Zurich study. VIII. Insomnia: association with depression,
anxiety, somatic syndromes, and course of insomnia. European Archives of Psychiatry and Neurological Sciences,239, 113e124.
Warner, S., Murray, G., & Meyer, D. (2008). Holiday and school-term sleep patterns of Australian adolescents. Journalof Adolescence, 31, 595e608.
Yang, C. M., Wu, C. H., Hsieh, M. H., Liu, M. H., & Lu, F. H. (2003). Coping with sleep disturbances among youngadults: a survey of first-year college students in Taiwan. Behavioral Medicine, 29, 133e138.
Zammit, G. K., Weiner, J., Damato, N., Sillup, G. P., & McMillan, C. A. (1999). Quality of life in people with
insomnia. Sleep, 22, S379eS385.Zhang, B., & Wing, Y. K. (2006). Sex differences in insomnia: a meta-analysis. Sleep, 29, 85e93.
Copyright © 2022 FDOKUMEN




















