Cognitive performance and sleep quality in the elderly suffering from chronic insomnia
11
Cognitive performance and sleep quality in the elderly suffering from chronic insomnia Relationship between objective and subjective measures Ce ´lyne H. Bastien*, E ´ milie Fortier-Brochu, Isabelle Rioux, Me ´lanie LeBlanc, Meagan Daley, Charles M. Morin E ´ cole de Psychologie and Centre d’E ´ tude des Troubles du Sommeil, Universite ´ Laval, Ste-Foy, Que ´bec, Canada G1K 7P4 Abstract Objective: The objective of the present study was to evaluate the relationship between objective and subjective sleep quality and objective and subjective evaluation of cognitive performance in older adults suffering of chronic insomnia (using or not benzodiazepines, BZs) or self-reported good sleepers. Methods: Three groups of participants 55 years and older were evaluated: 20 insomnia sufferers using BZs chronically, 20 drug-free insomnia sufferers and 20 good sleepers. Objective sleep (PSG) and subjective sleep (sleep diaries, SD) were measured. Objective measures of cognitive performance (attention/concen- tration, verbal/visual memory, executive function and psycho- motor speed) and subjective perception of daily performance were evaluated. Results: Correlational analysis revealed that objective and subjective measures of daytime performance are differentially related to sleep quality for the three groups. An objective good night of sleep is associated with better cognitive performance in good sleepers and drug-free individuals. On the other hand, the impression of having slept well is related to better cognitive performance in good sleepers and chronic insomnia sufferers using BZs. Conclusion: Daytime perform- ance and sleep quality are related, but differently so for a good sleeper, an insomnia sufferer without treatment, or one using BZs to alleviate sleep difficulties. D 2003 Elsevier Science Inc. All rights reserved. Keywords: Insomnia; Performance; Sleep quality; Hypnotics; Benzodiazepines Introduction According to available epidemiological data, 12 – 25% of people 65 years of age and older complain of insomnia on a regular basis [1,2]. The elderly report greater difficulty maintaining sleep whereas younger adults complain more frequently of difficulties initiating sleep [3]. Pharmacother- apy remains the most frequently used treatment for elderly insomnia sufferers [4]. According to Mellinger et al. [2], 14% of the elderly consume hypnotics, compared to 7.4% of adults under 65. Elsewhere, 11% of people over the age of 65 were found to have been using hypnotic medication regularly during the previous year and 4% had been con- suming hypnotics for more than 10 years [5]. The sedative medications most frequently prescribed to facilitate sleep are GABAergic substances like benzodiaze- pines (BZs). In the short-term, BZs have the effect of reducing sleep latency and the length and frequency of nocturnal awakenings, and of increasing the total duration of sleep and its quality [3]. Furthermore, the occurrence of the EEG ‘‘speeding’’ in association with BZs use is gen- erally thought to represent the intensification of processes associated with sensory inhibition (i.e., increase in sleep spindle activity) [6,7]. However, these improvements in sleep continuity are paralleled by an increase in the amount of time spent in light sleep (Stage 2), by a moderate reduction in the time spent in REM sleep and by substantial reduction in the time spent in deep sleep (Stages 3 and 4). Recently, Vignola et al. [8] found that the sleep patterns of elderly insomnia sufferers using BZs on a chronic basis (1– 34 years of use) was as disturbed as those of elderly suffering of chronic insomnia who had not received treat- ment for their sleep difficulties [8]. 0022-3999/03/$ – see front matter D 2003 Elsevier Science Inc. All rights reserved. PII:S0022-3999(02)00544-5 * Corresponding author. E ´ cole de Psychologie, Universite ´ Laval, Ste- Foy, Que ´bec, Canada G1K 7P4. Tel.: +1-418-656-2131x8344; fax: +1-418- 656-5152. E-mail address: [email protected] (C.H. Bastien). Journal of Psychosomatic Research 54 (2003) 39 – 49
Transcript of Cognitive performance and sleep quality in the elderly suffering from chronic insomnia

Cognitive performance and sleep quality in the elderly suffering
from chronic insomnia
Relationship between objective and subjective measures
Celyne H. Bastien*, Emilie Fortier-Brochu, Isabelle Rioux,Melanie LeBlanc, Meagan Daley, Charles M. Morin
Ecole de Psychologie and Centre d’Etude des Troubles du Sommeil, Universite Laval, Ste-Foy, Quebec, Canada G1K 7P4
Abstract
Objective: The objective of the present study was to evaluate
the relationship between objective and subjective sleep quality
and objective and subjective evaluation of cognitive performance
in older adults suffering of chronic insomnia (using or not
benzodiazepines, BZs) or self-reported good sleepers. Methods:
Three groups of participants 55 years and older were evaluated:
20 insomnia sufferers using BZs chronically, 20 drug-free
insomnia sufferers and 20 good sleepers. Objective sleep
(PSG) and subjective sleep (sleep diaries, SD) were measured.
Objective measures of cognitive performance (attention/concen-
tration, verbal/visual memory, executive function and psycho-
motor speed) and subjective perception of daily performance
were evaluated. Results: Correlational analysis revealed that
objective and subjective measures of daytime performance are
differentially related to sleep quality for the three groups. An
objective good night of sleep is associated with better cognitive
performance in good sleepers and drug-free individuals. On the
other hand, the impression of having slept well is related to
better cognitive performance in good sleepers and chronic
insomnia sufferers using BZs. Conclusion: Daytime perform-
ance and sleep quality are related, but differently so for a good
sleeper, an insomnia sufferer without treatment, or one using
BZs to alleviate sleep difficulties. D 2003 Elsevier Science Inc.
All rights reserved.
Keywords: Insomnia; Performance; Sleep quality; Hypnotics; Benzodiazepines
Introduction
According to available epidemiological data, 12–25% of
people 65 years of age and older complain of insomnia on a
regular basis [1,2]. The elderly report greater difficulty
maintaining sleep whereas younger adults complain more
frequently of difficulties initiating sleep [3]. Pharmacother-
apy remains the most frequently used treatment for elderly
insomnia sufferers [4]. According to Mellinger et al. [2],
14% of the elderly consume hypnotics, compared to 7.4% of
adults under 65. Elsewhere, 11% of people over the age of
65 were found to have been using hypnotic medication
regularly during the previous year and 4% had been con-
suming hypnotics for more than 10 years [5].
The sedative medications most frequently prescribed to
facilitate sleep are GABAergic substances like benzodiaze-
pines (BZs). In the short-term, BZs have the effect of
reducing sleep latency and the length and frequency of
nocturnal awakenings, and of increasing the total duration
of sleep and its quality [3]. Furthermore, the occurrence of
the EEG ‘‘speeding’’ in association with BZs use is gen-
erally thought to represent the intensification of processes
associated with sensory inhibition (i.e., increase in sleep
spindle activity) [6,7]. However, these improvements in
sleep continuity are paralleled by an increase in the amount
of time spent in light sleep (Stage 2), by a moderate
reduction in the time spent in REM sleep and by substantial
reduction in the time spent in deep sleep (Stages 3 and 4).
Recently, Vignola et al. [8] found that the sleep patterns of
elderly insomnia sufferers using BZs on a chronic basis (1–
34 years of use) was as disturbed as those of elderly
suffering of chronic insomnia who had not received treat-
ment for their sleep difficulties [8].
0022-3999/03/$ – see front matter D 2003 Elsevier Science Inc. All rights reserved.
PII: S0022 -3999 (02 )00544 -5
* Corresponding author. Ecole de Psychologie, Universite Laval, Ste-
Foy, Quebec, Canada G1K 7P4. Tel.: +1-418-656-2131x8344; fax: +1-418-
656-5152.
E-mail address: [email protected] (C.H. Bastien).
Journal of Psychosomatic Research 54 (2003) 39–49

Besides their effects on sleep, BZs are associated with
certain undesirable secondary effects, most notably depend-
ence, daytime sleepiness, sedation and anterograde amnesia
[9–12]. A number of studies investigating the cognitive
effects of chronic BZs use in adults with anxiety strongly
suggest an alteration in verbal learning, memory, visuo-
spatial ability and psychomotor capacity [13,14]. On the
other hand, research looking at the effects of BZs on
cognitive function in patients with insomnia has produced
different results. As such, no performance deficit was
detected in elderly insomnia sufferers using BZs chronically
relative to a sample of good sleepers [8].
After a poor night of sleep, individuals suffering of
insomnia usually report disruption of mood, alteration of
motor abilities, social discomfort and a certain cognitive
inefficiency that is accompanied by sleepiness [15]. These
daytime consequences represent an important concern for
individuals with insomnia [16]. Objectively, an alteration of
neuropsychological function has been found in adult insom-
nia sufferers relative to good sleepers. More specifically,
people with insomnia exhibit alterations in tasks measuring
balance, attention and reaction time [16], and access to
information stored in semantic memory [17]. However, no
difference has been detected for psychomotor function
[17,18], episodic memory [16] divided attention [16], verbal
learning and recognition of figures and words [18]. Contrary
to Hauri [16], Broman et al. [18] found no alteration in
reaction time in insomnia sufferers. In elderly with insom-
nia, some studies suggest a deterioration in attention and
concentration [8].
Investigation into other characteristics of insomnia points
to a more negative subjective evaluation of performance by
individuals with insomnia than by good sleepers. As such,
adults with insomnia have weaker expectations of their
performance, evaluate their performance more negatively
and report having performed less well than individuals of
similar age and actual capability level [18]. Available data
suggest that, even in the absence of objective deficits, such a
negative evaluation of performance also exists in drug-free
elderly suffering of insomnia as compared to good sleepers
and elderly insomnia sufferers using BZs [8].
A relationship also appears between objective sleep
quality and performance in insomnia sufferers. As such,
longer nocturnal awakening periods are associated with
reduced objective performance at tasks measuring psycho-
motor ability [17,18]. Furthermore, the duration of sleep is
positively correlated with the subjective evaluation of per-
formance [18]. However, these results were obtained using
small samples (e.g., 10 per group) [17] in which a large
proportion of individuals were experiencing psychological
distress (e.g., 16/26 participants).
In insomnia sufferers 55 years and older, subjectively
evaluated poor sleep quality is associated with reduced
performance in tasks measuring vigilance, psychomotor
speed, recall, problem resolution and speed and accuracy
in complex decision-making [19]. On the other hand,
objectively evaluated poor sleep quality appears to be
more closely linked short-term memory functions. A
formal comparison between the performance observed in
elderly with insomnia and that of elderly good sleepers
was not undertaken.
Considering the widespread use of BZs in the elderly
population suffering of insomnia, it is important to deepen
our understanding of the impact of chronic use of BZs on
cognitive function. Furthermore, understanding the relation-
ship between sleep quality and cognitive performance has
important clinical implications both in terms of better
understanding insomnia sufferers’ complaints of daytime
consequences, as well as in terms of treatment planning and
implementation. In regards to the cognitive performance,
analysis will be based on the same sample data obtained by
Vignola et al. [8]. Their results did not investigate any
relationships between the subjective and objective perform-
ance of sleep and cognitive functions. In the Vignola et al.’s
[8] study, objective sleep was measured with two nights
following the neuropsychological testing and subjective
sleep was measured from the completion of 2 weeks of
sleep diary (SD). As such, the purpose of the present study
is to expend previous findings and, with the use of a
correlational approach, to examine the relationship between
the objective and subjective evaluation of sleep and cog-
nitive performance in elderly insomnia sufferers who do or
not use BZs on a chronic basis, as well as in good sleepers.
By targeting the night just before the evaluation of cognit-
ive performance, one should better understand the relation-
ship between cognitive functioning and the preceding night
of sleep.
Methods
Participants
The 60 participants in this study were divided into
three groups of 20, including a group of 20 insomnia
sufferers utilizing BZs chronically as sleep aids (INSBZ;
10 males and 10 females), 20 insomnia sufferers not
taking medication (INS; 9 males and 11 females) and
20 good sleepers (GS; 11 males and 9 females). All
participants were 55 years of age or older, with a mean
age of 62.5 years (S.D. = 5.8). Inclusion criteria for both
groups of insomnia sufferers were: (a) presence of a
subjective complaint of insomnia defined by difficulty
initiating sleep (sleep latency > 30 min) and/or maintain-
ing sleep (nocturnal awakenings >30 min), (b) presence of
insomnia at least three nights per week, (c) problems
present for a minimum of 6 months, (d) presence of at
least one complaint of a negative consequence associated
with daytime functioning due to insomnia and (e) pres-
ence of marked psychological distress and/or disruption of
occupational and social functioning due to insomnia. The
participants in the INSBZ group had been using BZs to
C.H. Bastien et al. / Journal of Psychosomatic Research 54 (2003) 39–4940
facilitate sleep at least four nights per week for more than
3 months, while the INS group had to be drug-free for at
least 1 month before entering the study. Finally, partic-
ipants in the GS group did not meet any criteria for
insomnia and were not using any medication to aid sleep.
For each group, the presence or absence of insomnia
complaints was confirmed by information obtained from
SD [20] over a period of 2 weeks. The exclusion criteria for
all participants were: (a) presence of a major medical
condition (e.g., cancer) or of a degenerative neurological
condition (e.g., dementia), (b) presence of major psycho-
pathology (e.g., depression), (c) presence of another sleep
disorder (e.g., sleep apnea), (d) a score of 23 or higher on
the Beck Depression Inventory (BDI) [21], (e) a score
lower than 27 on the Folstein Mini-Mental State Exam
(FMMSE) [22] or (f) use of psychotropic medication or any
other medication that alters sleep. For the two insomnia
groups, inclusion and exclusion criteria were taken from the
International Classification of Sleep Disorders (ICSD-10)
[23] and the Diagnostic and Statistical Manual of Mental
Disorders (DSM-IV) [24].
Participants had a mean education level of 12.9 years
(S.D. = 4.0). In addition, the majority were married (76.7%)
and retired (70.0%). The mean duration of insomnia was
25.8 years (S.D. = 15.7). On average, participants in the
INSBZ condition had been using BZs as sleep aid for
13.5 years (S.D. = 10.0, range 1–34). The mean frequency
of BZs use was 6.6 nights per week (S.D. = 1.1).
Sleep measures
Data for objective sleep were obtained using polysom-
nographic recording (PSG). This included data obtained
from electroencephalogram (EEG), electrooculogram
(EOG) and electromyogram (EMG). Sleep latency, fre-
quency of nocturnal awakenings, sleep efficiency, total
sleep time, total wake time and the proportion of time
spent in each sleep stage were used as clinical sleep
variables. Data collected on the first night of sleep in the
laboratory, prior to neuropsychological analysis, were used
in the present analysis.
The SD [20] measures the subjective quality of sleep. It
is completed in the morning, upon wakening, and permits
collection of diverse information concerning the perception
of sleep, such as sleep latency, the frequency of nocturnal
awakenings, total wake time, total sleep time, sleep quality,
subjective sleep depth and feeling of being well-rested. The
SD obtained following the first night of sleep in the
laboratory was used in this analysis.
The Insomnia Severity Index (ISI) [20] is composed of
seven items that evaluate: (a) the severity of sleep-onset
(initial), (b) sleep maintenance (middle), (c) early morning
awakening (terminal) problems, (d) satisfaction with current
sleep pattern, (e) interference with daily functioning, (f)
noticeability of impairment attributed to the sleep problem
and (g) level of distress caused by the sleep problem. Each
of these items is rated on a five-point Likert scale (‘‘0’’= not
at all, ‘‘4’’= extremely) and the time interval is ‘‘in the last
2 weeks.’’ Total scores range from 0 to 28, with high scores
indicating greater insomnia severity. The ISI is available in
three different versions: patient (self-administered), signific-
ant other (usually a spouse) and clinician. The ISI has
adequate internal consistency and correlates adequately with
subjective and objective sleep measures [25]. In the present
study, only the patient version of the ISI was computed.
Table 1
Neuropsychological instruments used to measure each factor
Factor Neuropsychological instruments
Verbal and visual
memory (VVM)
Verbal Paired Associates I
(immediate recall)
Verbal Paired Associates II
(delayed recall)
Visual Reproduction I
(immediate recall)
Visual Reproduction II
(delayed recall)
Psychomotor speed (PS) Digit Symbol Substitution Test
Purdue Pegboard
Trail Making Tests A and B
Wilkinson’s Four-Choice
Reaction Time
Attention and concentration (AC) Digit Span Forward
Digit Span Backward
Executive functions (EF) Wisconsin Card Sorting Test
Table 2
Means and standard deviations of descriptive variables
INS, n= 20 INSBZ, n= 20 GS n= 20F ratio
Variable M (S.D.) M (S.D.) M (S.D.) (2,57)
Sociodemographic
Age (years) 61.70 (6.43) 62.30 (5.89) 63.35 (5.15) 0.41
Education (years) 13.60 (5.15) 11.65 (2.76) 13.35 (3.67) 1.42
Mental abilities
Mini-Mental
State (MMS)
29.10 (1.12) 28.75 (1.25) 28.85 (1.04) 0.50
Vocabulary
(standard score)
12.65 (3.84) 12.00 (3.09) 13.30 (2.36) 0.85
Information
(standard score)
10.15 (3.51) 10.00 (3.01) 11.50 (3.40) 1.24
Sleep
Sleep Impairment
Index (SII)
17.90 (4.85)a 16.85 (4.55)b 1.60 (1.88) 104.59*
Psychological
BDI 9.00 (4.48)a 9.40 (7.16)b 1.75 (1.68) 15.01*
BAI 9.10 (8.38)a 8.60 (5.44)b 1.20 (1.47) 11.51*
INS = Insomniacs without benzodiazepine, INSBZ = insomniacs with
benzodiazepine, GS = good sleepers.
Adapted from Vignola et al. [8].a Significant difference between INS and GS ( P < .01).b Significant difference between INSBZ and GS ( P < .01).
* P< .01.
C.H. Bastien et al. / Journal of Psychosomatic Research 54 (2003) 39–49 41
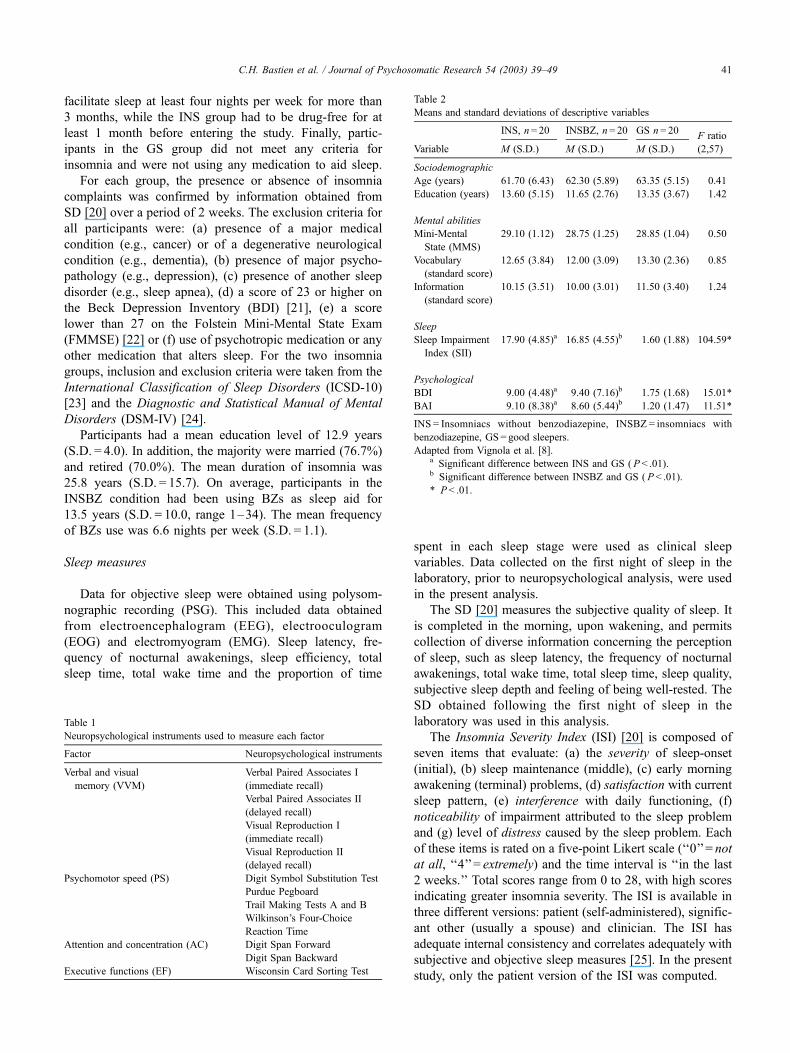
Neuropsychological measures
Factorial analysis described by Vignola et al. permits the
grouping of cognitive function measures used in the battery
of tests into four factors. A comprehensive list of the
neuropsychological instruments used in the present study
are noted in Table 1.
Memory was evaluated using the Verbal Paired Asso-
ciates Tests I and II [26] and Visual Reproduction Tests I
and II [26], which measure, respectively, verbal and visual
memory. The first administration of these two tests requires
immediate recall of the items presented, whereas the second
tests delayed recall. Attention and concentration were eval-
uated through the aid of Digit Span tests [26] in which
repetition of numbers in order (Digit Span Forward) and in
inverse order (Digit Span Backward) was required. Inverse
order recall is also a measure of the ability to perform an
operation in working memory. Psychomotor speed was
measured using four different tests. The Digit Symbol
Substitution Test [27] measures visuo-motor speed and
coordination. The Purdue Pegboard [28] was used to meas-
ure manual dexterity. The Trail Making Tests A and B [29]
require complex visual surveying and measure psychomotor
speed, agility, alternating visual attention and mental flex-
Table 4
Means and standard deviations of subjective sleep variables
INS INSBZ GS
Variable M S.D. n M S.D. n M S.D. n df F
SOL 78.00 78.19 20 66.55 59.11 20 39.00 37.19 20 2, 57 2.19
WASO 54.44 45.67 18 70.79 83.72 19 33.8 39.50 20 2, 54 1.89
TWT 172.00 126.93 20 185.89 109.31 19 97.75 102.73 20 2, 56 3.44*
TST 286.40 115.63 20 264.21a 113.84 19 372.35 107.12 20 2, 56 5.10**
Freshness upon awakening 2.58b 0.79 12 3.00a 1.13 12 3.18 1.25 11 2, 32 9.41**
Soundness 2.08 0.79 12 3.08 1.32 13 3.18 1.25 11 2, 33 3.32*
SE 63.32 25.48 20 58.60a 24.15 19 80.96 21.38 20 2, 33 4.86*
FNA 2.78 1.35 18 2.12 1.90 17 3.37 2.93 19 2, 56 1.47
INS= Insomniacs without benzodiazepine, INSBZ= insomniacs with benzodiazepine, GS = good sleepers.a Difference between INSBZ and GS.b Difference between INS and GS.
* P < .05.
** P < .01.
Table 5
Correlations between objective and subjective measures of sleep
SubjectiveObjective measures
measures SL TWT TST FEN SE % S 1 % S 2
Good sleepers (GS)
SL
WASO
TWT
TST
Fre
Sou
SQ
SE
FNA
Drug-free insomniacs (INS)
SL .66** .45*
WASO .47*
TWT .57**
TST � .61**
Fre
Sou
SQ
SE � .57**
FNA
SOL TWT TST FEN SE % S 1 % S 2
Benzodiazepine users (INSBZ)
SOL
WASO
TWT .52* � .48*
TST .46*
Fre
Sou
SQ
SE � .48* .46*
FNA
SOL=Sleep-onset latency, WASO=wake after sleep-onset, TWT= total
wake time, TST= total sleep time, FNA= frequency of night awakening,
SE = sleep efficiency, % S 1 = time spent in Stage 1, % S 2 = time spent in
Stage 2, Fre = freshness upon awakening, Sou = soundness of sleep,
SQ= sleep quality.
* P< .05.
** P< .01.
Table 3
Means and standard deviations of objective sleep variables
INS, n= 20 INSBZ, n= 20 GS, n= 20F ratio
Variable M (S.D.) M (S.D.) M (S.D.) (2,57)
SOL 29.07 (23.61) 27.06 (15.50) 27.54 (19.91) 0.06
TWT 127.91 (58.59) 126.06 (58.59) 100.79 (47.01) 1.62
FNA 3.90 (3.24) 3.25 (2.20) 2.75 (2.15) 0.99
SE 91.78 (88.26) 72.61 (11.96) 80.60 (8.55) 0.69
TST 319.66 (81.29) 329.33 (60.51) 372.52 (38.12) 4.05
% Stage 1 11.85 (5.90) 10.56 (4.91) 10.61 (6.32) 0.32
% Stage 2 62.79 (10.08) 60.98 (9.07) 66.35 (9.86) 1.57
INS = Insomniacs without benzodiazepine, INSBZ = insomniacs with
benzodiazepine, GS =Good sleepers.
C.H. Bastien et al. / Journal of Psychosomatic Research 54 (2003) 39–4942
ibility. Wilkinson’s Four-Choice Reaction Time Test [30]
was used to evaluate reaction time and vigilance. Finally,
executive function was measured with the Wisconsin Card
Sorting Test [31] that measures abstraction skills, mental
flexibility and the ability to maintain a pattern of responses.
Several instruments permitted the measurement of sub-
jective perception of daytime functioning. Participants used
a visual analogue scale (VAS) of 100 mm to indicate their
level of wakefulness, energy and mood. While the actual
state scale (ASS) permitted participants to evaluate their
level of fatigue, anxiety, motivation, concentration as well
as their performance expectations, the evaluation of per-
formance scale (EPS) asked participants to indicate the
quality of their performance and their satisfaction with their
performance, and to compare their performance with that of
other individuals of the same age who possess the same
actual capacities.
Procedures
Recruitment, informed consent and remuneration
Participants were recruited by placing advertisements in
local newspapers. After completing a telephone interview,
interested individuals were scheduled for a in-house inter-
view during which they were asked to sign a consent form
and to then complete several questionnaires and assess-
ment procedures aimed at screening them for their eligib-
ility. The in-house screening included a psychological
evaluation in order to determine the presence of psycho-
pathology, a clinical sleep evaluation and a medical exam.
Evaluations were performed by a variety of examiners,
including graduate students in psychology and a physician.
Eligible participants were enrolled into the study and were
compensated for their participation. A sum of CAN$150
was offered to GS to compensate them for their participa-
tion in the study, while a nonpharmacological treatment
for insomnia was offered to members of the other groups
at no cost.
In lab study procedures
Participants retained for the study then spent three
consecutive nights in the sleep laboratory. Subjects arrived
at the lab at 8:00 p.m. and slept according to their normal
schedule (i.e., they selected their bedtime and rise time).
Upon awakening, participants completed a SD. The battery
of neuropsychological tests was administered after the first
of the three nights in the laboratory, approximately 1 h after
Table 6
Correlations between objective measures of performance and objective sleep quality
Objective measures
Functions SOL TWT TST FNA SE % S 1 % S 2 % S 4
Good sleepers (GS)
VVM � .48a,* � .45a,* .51b,*
� .53b,* � .45b,*
PS � .48c,*
AC
EF � .79d,**
Drug-free insomniacs (INS)
VVM � .53b,* .52a,* � .59a,**
PS .69e,** � .46c,* .61d,**
.56c,*
AC � .58f,**
EF
Benzodiazepine users (INSBZ)
VVM .49b,* .60a,**
PS .48c,*
AC
EF
SL=Sleep-onset latency, TWT= total wake time (SOL+TWT1), TST= total sleep time, FNA= frequency of night awakening, SE = sleep efficiency,
% S 1 = time spent in Stage 1, % S 2 = time spent in Stage 2, % S 4 = time spent in Stage 4, VVM=visual and verbal memory, PS = psychomotor speed,
AC= attention and concentration, EF = executive functions.a Delayed recall.b Immediate recall.c Purdue Board.d Wisconsin Card Sorting Test.e Wilkinson reaction time.f Digit Span (Backward).
* P < .05.
** P < .01.
C.H. Bastien et al. / Journal of Psychosomatic Research 54 (2003) 39–49 43
rising (between 7:30 and 9:00). The EASS and the VAS
were administered prior to neuropsychological evaluation.
The EPS was administered after each test as well as at the
end of the neuropsychological evaluation. This evaluation
lasted between 1.5 and 2 h.
Results
Descriptive analysis
Demographic and clinical profile data
Descriptive statistics for each of the sociodemographic,
psychological, general ability and sleep variables for the
three groups of participants are presented in Vignola et al.
[8] and are adapted in Table 2. Univariate analysis of
variance performed for each of these variables demonstrates
equivalence of age, occupation, education and general
mental abilities. Differences between groups were identified
for measures of insomnia severity, anxiety and depression.
Tukey multiple comparison tests revealed that the two
insomnia groups, as compared to good sleepers, exhibited
greater symptom severity on the ISI (P < .01), Beck Anxiety
Inventory (BAI; P < .01) and the BDI (P < .01). The two
insomnia groups did not differ in terms of scores obtained
on the ISI, BAI or BDI.
A MANOVA was computed on the objective sleep
measures to determine whether the three groups differed
for those variables. Means and standard deviations for those
variables are presented in Table 3. There was no significant
difference among the three groups on PSG measures,
including sleep onset latency, total wake time, total sleep
time, frequency of night awakening, sleep efficiency and the
percentages of time spent in Stages 1 and 2.
One-way ANOVAs computed on the subjective sleep
measures revealed significant differences between group.
Means and standard deviations for those variables are
presented in Table 4. Post-hoc comparisons revealed that
INSBZ had a longer total wake time, a shorter total sleep
time, a lower score for freshness upon awakening and
soundness of sleep than GS. INS had a lower score than
GS for freshness upon awakening.
Group differences on the subjective and objective meas-
ures of cognitive performance have been reported in Vignola
et al. [8]. In general, their results showed that individuals
with insomnia, both medicated and unmedicated, performed
Table 7
Correlations between objective measures of performance and subjective sleep quality
Subjective sleep measures
Functions SOL TWT TST Fre Sou SQ SE FNA
Good sleepers (GS)
VVM � .52a,* � .61b,* .51a,*
.52c,*
PS � .49d,* � .58d,* .57d,** .63d,*
AC � .53e,* .76e,** .66f,* .56e,*
.67f,* .69e,*
EF
Drug-free insomniacs (INS)
VVM .45c,* � .52c,* � .60c,* � .48c,*
PS
AC
EF
Benzodiazepine users (INSBZ)
VVM � .49c,* � .57c,* .46c,*
� .55a,**
PS
AC
EF
SOL= sleep-onset latency, TWT= total wake time, TST= total sleep time, Fre = freshness upon awakening, Sou = soundness of sleep, SQ= sleep quality,
SE = sleep efficiency, FNA= frequency of night awakening, VVM=visual and verbal memory, PS = psychomotor speed, AC= attention and concentration,
EF = executive functions.a Delayed visual reproduction.b Delayed verbal memory.c Immediate visual reproduction.d Trail Making Test.e Digit Span (Backward).f Digit Span (Forward).
* P < .05.
** P < .01.
C.H. Bastien et al. / Journal of Psychosomatic Research 54 (2003) 39–4944
worse than good sleepers on the attention/concentration
factor. There were no other objective evidence of perform-
ance impairments. Subjectively, unmedicated insomniacs
had lower performance expectancies and rated their perform-
ance more negatively relative to medicated insomniacs and
good sleepers. Again, although interesting, these results did
not investigate any interrelationships between the subjective
and objective performance of sleep and cognitive functions
among the three groups.
Correlational analyses: the associations between sleep and
neuropsychological measures
These data were analyzed using a correlational approach.
The significance level used was .05 (a= .05). The Spearman
coefficient was utilized for the four nonparametric variables
(Visual Reproduction I and II, Forward Digit Span and
Backward Digit Span), while the Pearson coefficient was
used for the remaining parametric measures.
Objective and subjective quality of sleep
Significant correlation coefficients between objective and
subjective measures of sleep are presented for each group
separately in Table 5. Absolute values of significant cor-
relation coefficients vary between .45 and .66. In INSBZ,
subjective evaluation of sleep parameters is not associated
with objective measures of these same parameters. In INS,
objective difficulties in maintaining sleep are associated
with subjective difficulties initiating and maintaining sleep.
Also, objective difficulties initiating sleep are associated
with subjective difficulties initiating sleep. In INSBZ,
objective difficulties maintaining sleep are associated with
subjective difficulties maintaining sleep.
Table 8
Correlations between subjective performance and subjective quality of sleep
Daytime functioning Cognitive performance
VAS EASS EPS
Sleep Ev En Hu Fa An Mo Co AP Qu Sa Au Re
Good sleepers (GS)
SOL
TWT
TST
Fre � .61* � .78**
Sou � .64* � .66 * .61*
SQ � .65*
FNA
SE
Drug-free insomniacs (INS)
SOL
TWT .50* .46*
TST � .59** .48*
Fre .71** � .85**
Sou
SQ � .63* � .45*
FNA
SE � .50*
Al En Mo Ti An Mo Co Pe Qu Sa Ot Re
Benzodiazepine users (INSBZ)
SOL � .46* � .56*
TWT � .60*
TST
Fre
Sou
SQ
FNA � .59** � .50* � .52* .52* � .50*
SE .49* .57*
VAS= visual analogue scale, EASS= evaluation of actual state mood, EPS = evaluation of performance scale, Al = alertness, En = energy, Mo=mood,
Ti = tiredness, An = anxiety, Mo =motivation, Co = concentration, Pe = performance expectancy, Qu = quality of performance, Sa = satisfaction with
performance, Ot = compared with others, Re = compared to real capacities, SOL= sleep-onset latency, TWT= total wake time, TST= total sleep time,
Fre = freshness upon awakening, Sou = soundness of sleep, SQ= sleep quality, FNA= frequency of night awakening, SE = sleep efficiency.
* P < .05.
** P < .01.
C.H. Bastien et al. / Journal of Psychosomatic Research 54 (2003) 39–49 45
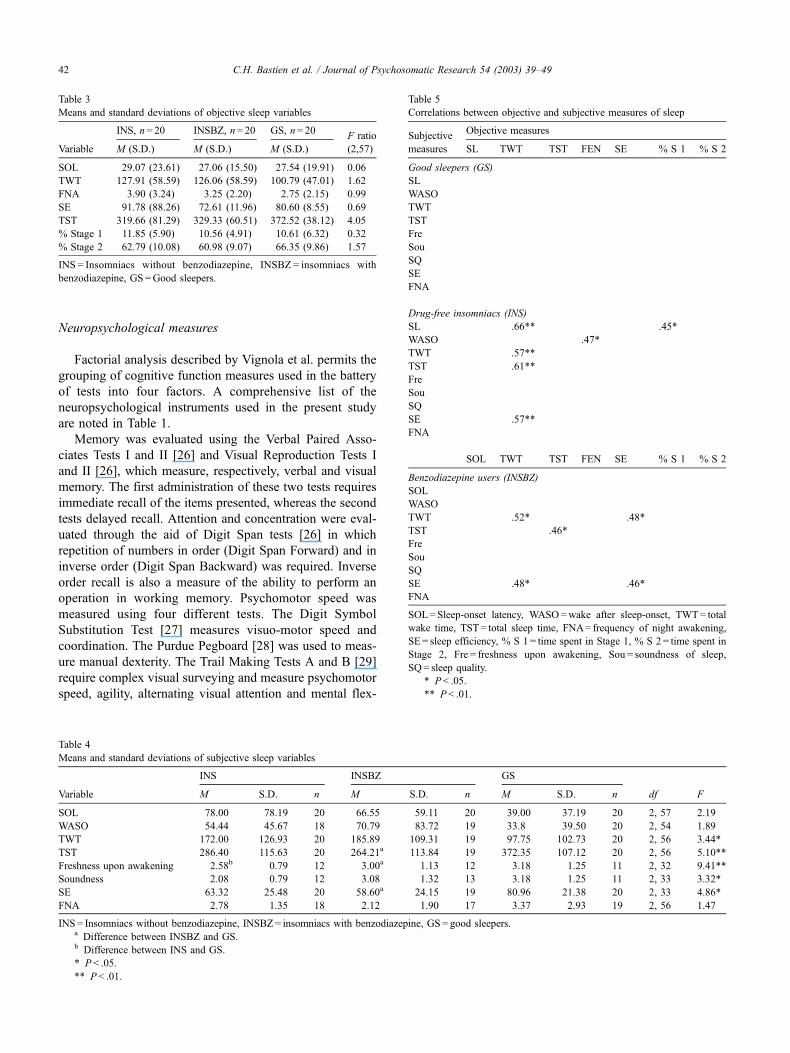
Objective performance and objective sleep quality
Significant correlation coefficients identified between
objective performance measures and quality of sleep
measures are depicted in Table 6. The correlations
observed between objective performance measures and
the percentage of time spent in Stages 3–4 sleep are
not presented due to the low proportion of time spent in
these stages in participants. Absolute values for the
significant correlation coefficients vary between .45 and
.79. For GS and INS, difficulties in initiating sleep are
associated with an alteration of verbal memory. This
difficulty is also associated with poorer performance on
executive function tests in GS and a change in psycho-
motor speed, attention and concentration in INS. Difficult-
ies maintaining sleep are associated with alterations in
psychomotor speed in GS and INS, and deterioration of
verbal memory in GS. In INSBZ, difficulties initiating
sleep appear to be associated with better performance in
verbal memory tasks.
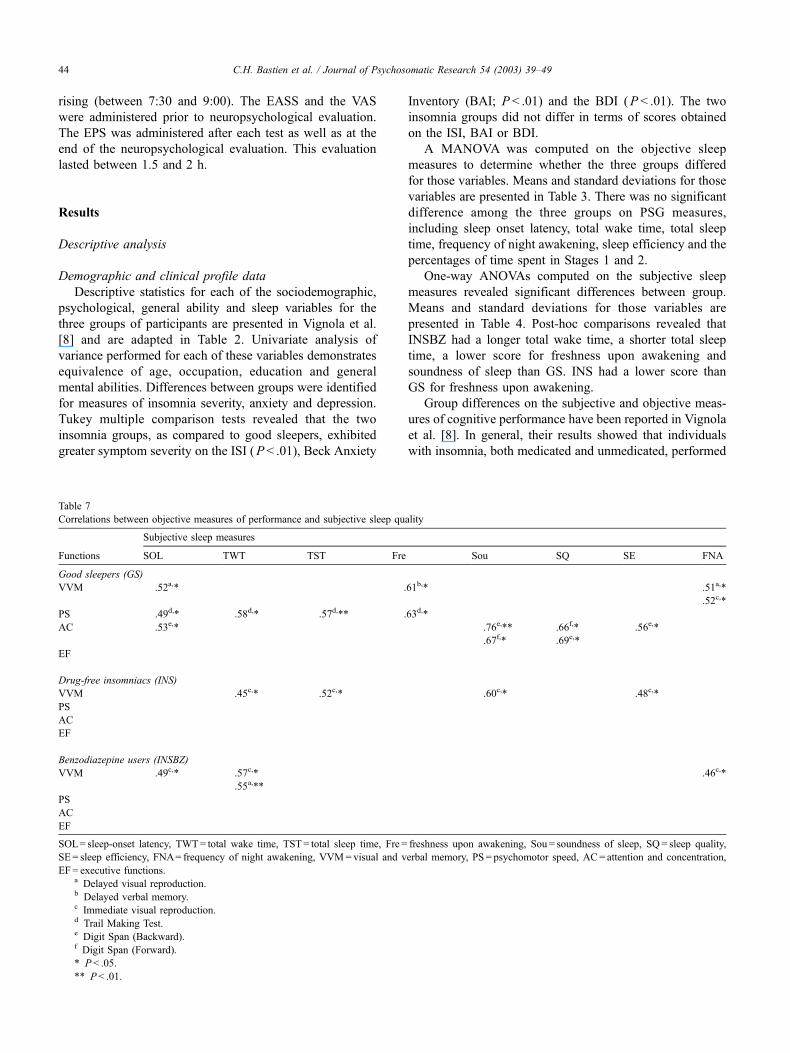
Objective performance and subjective sleep quality
Significant correlation coefficients between subjective
sleep parameters and objective measures of cognitive per-
formance and significant relationships are illustrated in
Table 9
Correlations between objective and subjective measures of performance
Daytime functioning Cognitive performance
VAS EASS EPS
Functions Al En Mo Ti An Mo Co Pe Qu Sa Ot Re
Good sleepers (GS)
VVM .54a,* .63b,** .49b,* .45c,* .46c,*
.46c,*
PS � .54d,* � .52e,* .45f,* .48f,* .52f,* � .47d,*
� .48e,* � .60d,**
.44d,*
AC � .48g,* .46h,*
� .47h,*
EF .67i,** � .60j,** � .52j,* � .70j,** � .48j,*
� .54j,*
Drug-free inomniacs (INS)
VVM .70c,** .59c,** .52c,*
PS
AC .52j, *
EF
Benzodiazepine users (INSBZ)
VVM � .62c,** .48b,* .50k,* .46b,*
.56b,*
PS � .46l, * � .60l,**
AC .45h,*
EF
VAS= visual analogue scale, EASS= evaluation of actual state mood, EPS = evaluation of performance scale, Al = alertness, En = energy, Mo=mood,
Ti = tiredness, An = anxiety, Mo =motivation, Co = concentration, Pe = performance expectancy, Qu = quality of performance, Sa = satisfaction with
performance, Ot = compared with others, Re = compared to real capacities, VVM=visual and verbal memory, PS = psychomotor speed, AC= attention and
concentration, EF = executive functions.a Immediate visual recall.b Delayed verbal recall.c Delayed visual reproduction.d Trail Making Test B.e Trail Making Test A.f Purdue Board.g Digit Span (Forward).h Digit Span (Backward).i Wisconsin (number of categories).j Wisconsin (perseveration).k Immediate verbal recall.l Wilkinson Reaction Time Test.
* P < .05.
** P < .01.
C.H. Bastien et al. / Journal of Psychosomatic Research 54 (2003) 39–4946

Table 7. Absolute values of significant correlation coef-
ficients vary between .45 and .76. In GS, the subjective
depth, quality and efficiency of sleep are associated with
better performance on attention and concentration tests,
but poorer memory performance. Subjective difficulties
in initiating sleep are associated with alterations in
memory, attention and concentration. In GS, subjective
difficulties in initiating and maintaining sleep appear to
be associated with better psychomotor speed. Finally,
subjective difficulties maintaining sleep are associated
with memory alterations. In INS, visual memory
improves when subjective sleep depth increases, but
diminishes when subjective difficulties in maintaining
sleep increase. In INSBZ, subjective difficulties initiating
and maintaining sleep are associated with an alteration in
visual memory.
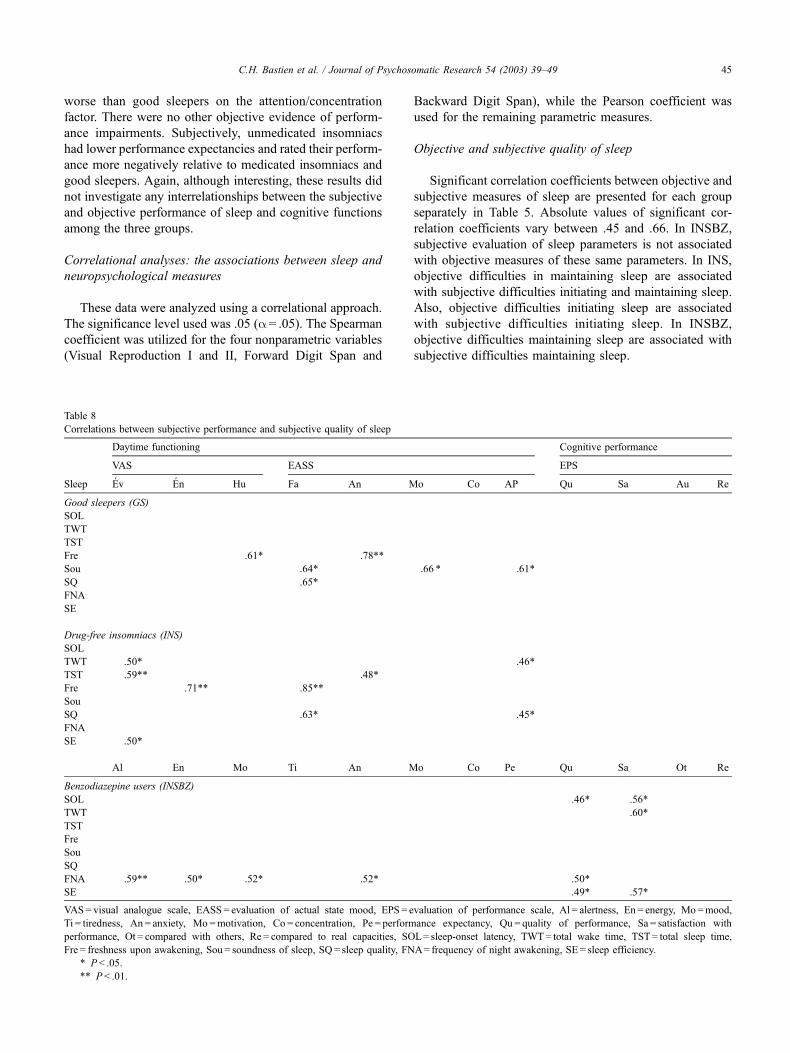
Subjective performance and subjective quality of sleep
Table 8 illustrates the significant relationships between
subjective measures of sleep quality and subjective meas-
ures of daytime function. Absolute values of significant
correlation coefficients vary between .45 and .85. In INSBZ
and INS, the impression of having experienced deep restor-
ative sleep is associated with a better evaluation of daytime
functioning. For INS, temporal indicators of sleep quality
are associated with a more negative evaluation of daytime
functioning. As well, expectations of INS towards their
performance increase when they have the impression of
having slept poorly. For INSBZ, only the number of
nocturnal awakenings is associated with a more negative
evaluation of daytime functioning. On the other hand,
subjective difficulties initiating and maintaining sleep are
associated with a more negative subjective evaluation of
performance on neuropsychological tests.
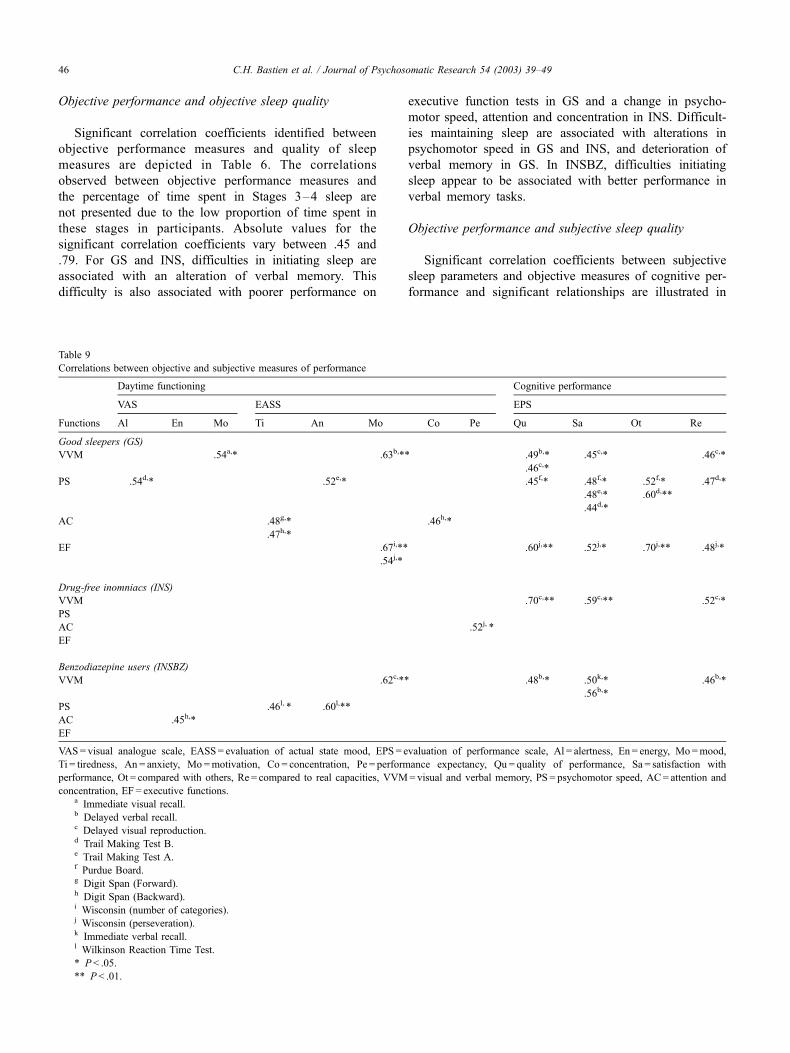
Objective performance and subjective performance
Significant relationships and correlation coefficients
between subjective measures of daytime functioning and
performance on tests, and objective measures of perform-
ance on tests are presented in Table 9. Absolute values of
significant correlation coefficients vary between .44 and .70.
In INSBZ, good performance on tests of memory, attention,
concentration and executive function is associated with a
higher subjective evaluation of daytime functioning. Per-
formance on memory, psychomotor speed and executive
function tasks was also related to a higher subjective
evaluation of performance on neuropsychological tests.
For the two insomnia groups (INS and INSBZ), however,
better subjective evaluation of daytime functioning was not
associated with better cognitive performance, and only
performance on memory tasks was associated with subject-
ive evaluation of performance on tests. In addition, for
INSBZ, a subjective negative evaluation of daytime func-
tioning was associated with better objective performance.
Discussion
The goal of the present study was to examine the
relationship between objective and subjective sleep quality
and daytime performance in elderly good sleepers, or suffer-
ing from chronic insomnia and who were either using or not
BZs as a sleep aid. The first goal was to verify the presence
of a positive relationship between cognitive performance and
objective sleep quality. It would appear that certain objective
sleep parameters are associated with different aspects of
cognitive performance. In good sleepers and drug-free
insomniacs, a good night’s sleep is associated with better
cognitive performance. These results correspond with earlier
studies that have shown an association between the quality of
sleep and performance on certain tasks [16–18]. The obser-
vation that a shorter sleep latency is associated with poorer
performance on verbal memory tasks in BZ users could be
attributable to the persistence of the drugs’ sedative effect at
the moment of test completion. However, Vignola et al. [8]
found that BZs did not affect sleep after prolonged use,
suggesting the development of a tolerance to the drugs. Other
authors, on the other hand, have suggested continued effec-
tiveness of BZs even after long-term use [9]. In addition, it
seems that only partial tolerance to some effects of BZs on
memory occurs [32].
The hypothesis that subjective sleep quality is associated
with better cognitive performance is also supported by the
results of the present study. In fact, it appears that good
sleepers and chronic insomnia sufferers using BZs perform
better on certain tasks when they have the impression of
having slept well. The relationship between performance on
attention tasks and subjective sleep quality in good sleepers
supports results obtained by Vignola et al. [8]. However, in
insomnia sufferers, better performance on visual memory
tasks following a subjective bad night could be due to the
fact that these individuals invest more effort in maintaining
good performance when they think they have slept poorly.
These results corroborate those obtained by Broman et al.
[18] and Schneider-Helmert [34], according to whom,
people suffering of insomnia have a tendency to compensate
for their cognitive deficits by increasing their efforts, par-
ticularly where visual tasks are concerned. In fact, the
results indicate that untreated insomnia sufferers base their
evaluation of their overall cognitive performance on their
judgment of performance on a single visual memory task.
The third objective of this study was to test for a
relationship between cognitive performance and subjective
evaluation of daytime performance. It seems that the three
groups of participants subjectively evaluate their daytime
functioning in a way that corresponds with certain aspects of
their actual performance, but the nature of this relationship
varies as a function of group. In good sleepers, a stronger
correspondence between their evaluation of daytime per-
formance and actual performance appears. In the two groups
of insomnia sufferers, the absence of a relationship between
daytime functioning and performance on tests indicates that,
C.H. Bastien et al. / Journal of Psychosomatic Research 54 (2003) 39–49 47

even though there is an objective alteration of performance
that appears to be related to a poorer objective sleep quality
in these individuals, subjective complaints of daytime func-
tioning, regardless of medication use, do not appear to be
associated with an objective cognitive alteration. This phe-
nomenon of discrepant subjective and objective evaluations
could be related to false beliefs concerning daytime con-
sequences of insomnia [8,20].
Finally, the hypothesis that subjective sleep quality is
associated with subjective evaluation of daytime perform-
ance was also supported by the observed correlations. Once
again, this relationship varies as a function of group
observed. In good sleepers and unmedicated insomnia
sufferers, the impression of having slept well appears more
important than subjective sleep duration in terms of its
influence on functioning upon awakening. However, the
fact that the level of alertness is associated with a shorter
sleep duration in people with insomnia could reflect the
phenomenon of cortical activation described by Bonnet and
Arand [33]. Some researchers propose that this activation
could further interfere with certain aspects of cognitive
performance as well as the ability to channel energy [8]. It
appears, in fact, that insomnia sufferers expend more energy
than good sleepers to overcome their fatigue [18]. As such,
they report investing greater effort than do good sleepers to
maintain performance levels rather than succumb to fatigue
after a poor night of sleep [18]. The phenomenon of
compensation could explain the fact that the expectations
insomnia sufferers have regarding their performance
increase when the feel they have slept poorly [18,34].
Furthermore, BZ users evaluate their performance on neuro-
psychological tests more favourably when they have the
impression of having slept well. Some authors have in fact
suggested that prolonged use of BZs leads to overestimation
of sleep time and mental capabilities [11]. This effect on the
perception of sleep and performance could be attributable to
anterograde amnesia associated with BZ use.
Results of the present study also indicate that the rela-
tionship between objective and subjective measures of sleep
quality differ from one group to another. While untreated
insomnia sufferers correctly subjectively identify their
objective difficulties initiating and maintaining sleep,
chronic BZs users only subjectively recognize their dif-
ficulties maintaining sleep. In good sleepers, no relationship
appears to exist between subjective and objective sleep
difficulties. It is thus possible that people with insomnia
perceive variations in their sleep better than good sleepers.
This could be the result of elevated cortical activity observed
in insomnia sufferers. Similarly, BZs used in the treatment of
insomnia could diminish cortical activation levels and, con-
sequently, alter the perception of sleep [33].
The generalizability of the present results may be limited
owing to several factors. First, the moderately small sample
size per group limits the power of the statistical analyses
used to detect significant relationships between the varia-
bles. In addition, the participants consisted of elderly
persons in excellent physical and psychological health
who are not likely representative of the general population
of elderly individuals. Furthermore, several authors have
demonstrated that the sleep of individuals evaluated in a
laboratory setting is different than that observed in their
home [35]. More specifically, the first night spent in the
laboratory is usually considered a period of adaptation.
Consequently, the sleep measures obtained at this time are
probably not representative of the typical sleep quality of
participants. This procedure increases reactivity to the
experimental context and could be responsible for factors
such as the increase in psychomotor speed witnessed in
good sleepers after a bad night’s sleep. The desire to
perform well on tests, despite the impression of not having
slept well, may have contributed to increased efforts put
forth by the participants on the tasks in question.
Despite these limitations, it is still possible to conclude
that daytime performance and sleep quality are related, but
in a manner that differs depending upon whether individuals
are good sleepers, insomnia sufferers without treatment, or
those using BZs to treat their insomnia. Some of the
observed relationships support the hypothesis of a height-
ened activation level in both groups of insomnia sufferers.
Furthermore, support was found for the hypothesis that
people with insomnia compensate for their daytime dif-
ficulties by investing greater effort. It is thus important to
consider the phenomena of cortical activation and com-
pensation when considering treatment. Given the secondary
effects associated with long-term utilization of BZs, it is
particularly pertinent to question their actual efficacy in
improving sleep and daytime performance. Results obtained
in this study highlight the importance of examining non-
pharmacologic alternatives to treatment. For example, beha-
vioural-cognitive treatment represents a viable alternative in
so far as it addresses the modification of sleep habits and
false beliefs surrounding sleep.
Acknowledgments
Preparation of this article was supported in part by the
National Institute of Mental Health Grant #MH55469 and
Fonds de la recherche en sante du Quebec (FRSQ).
References
[1] Ford DE, Kamerow DB. Epidemiologic study of sleep disturbances
and psychiatric disorders. JAMA 1989;262:1479–84.
[2] Mellinger GD, Balter MB, Uhlenhuth EH. Insomnia and its treatment.
Prevalence and correlates. Arch Gen Psychiatry 1995;42(3):225–32.
[3] Morin CM, Blais FC, Mimeault V. Sleep disturbances in late life. In:
Hersen M, Van Hasselt VB, editors. Handbook of clinical geropsy-
chology. New York: Plenum, 1998. pp. 273–99.
[4] Morin CM, Baillargeon L, Bastien CH. Treatment of hypnotic-
dependent insomnia. In: Lichstein KL, Morin CM, editors. Treatment
of late-life insomnia. Oakland: Sage Publications, 2000. pp. 271–96.
C.H. Bastien et al. / Journal of Psychosomatic Research 54 (2003) 39–4948
[5] Morgan K, Dallosso H, Ebrahim S, Arie T, Fentem PH. Prevalence,
frequency, and duration of hypnotic drug use among elderly living at
home. Br Med J (Clin Res Ed) 1988;296(6622):601–2 (Feb. 27).
[6] Aeschbach D, Dijk D-J, Trachsel L, Brunner DP, Borbely AA. Dy-
namics of slow-wave activity and spindle frequency activity in the
human sleep EEG: effect of midazolam and zopiclone. Neuropsycho-
pharmacology 1994;11:237–44.
[7] Borbely A, Mattmann P, Loepfe M, Strauch I, Lehmann D. Effect of
benzodiazepine hypnotics on all-night sleep EEG spectra. Hum Neu-
robiol 1985;4:189–94.
[8] Vignola A, Lamoureux C, Bastien CH, Morin CM. Effects of chronic
insomnia and use of benzodiazepines on daytime performance in older
adults. J Gerontol 2000;55B(1):P54–62.
[9] Buysse DJ, Reynolds CF. Pharmacologic treatment. In: Lichstein KL,
Morin CM, editors. Treatment of late-life insomnia. Thousand Oaks:
Sage Publications, 2000. pp. 231–67.
[10] Roth T, Hartse KM, Saab PG, Piccione PM, Kramer M. The effects of
flurazepam, lorazepam, and triazolam on sleep and memory. Psycho-
pharmacology 1980;70:231–7.
[11] Schneider-Helmert D. Why low-dose benzodiazepine-dependent in-
somniacs can’t escape their sleeping pills. Acta Psychiatr Scand
1988;78:706–11.
[12] Spinweber CL, Johnson LC. Effects of triazolam (0.5 mg) on sleep,
performance, memory, and arousal threshold. Psychopharmacology
1982;76:5–12.
[13] Golombok S, Moodley P, Lader M. Cognitive impairment in long-term
benzodiazepine users. Psychol Med 1988;18:365–74.
[14] Tata PR, Rollings J, Collins M, Pickering A, Jacobson RR. Lack of
cognitive recovery following withdrawal from long-term benzodiaze-
pine use. Psychol Med 1994;14:203–13.
[15] Zammit GK. Subjective ratings of the characteristics and sequelae of
good and poor sleep in normals. J Clin Psychol 1988;44:123–30.
[16] Hauri P. Cognitive deficits in insomnia patients. Acta Neurol Belg
1997;97(2):113–7.
[17] Mendelson WB, Garnett D, Gillin JC, Weingartner H. The experience
of insomnia and daytime and nighttime functioning. Psychiatr Res
1984;12:235–50.
[18] Broman JE, Lundh LG, Aleman K, Hetta J. Subjective and objective
performance in patients with persistent insomnia. Scand J Behav Ther
1992;21:115–26.
[19] Hart RP, Morin CM, Best AM. Neuropsychological performance in
elderly insomnia patients. Aging Cognit 1995;2:268–78.
[20] Morin CM. Insomnia: psychological assessment and management.
New York: Guilford Press, 1993.
[21] Beck AT, Steer RA, Garbin MG. Psychometric properties of the Beck
Depression Inventory: twenty-five years of evaluation. Clin Psychol
Rev 1988;8:77–100.
[22] Folstein MF, Folstein SE, McHugh PR. ‘‘Mini-mental state.’’ A prac-
tical method for grading the cognitive state of patients for the clini-
cian. J Psychiatr Res 1975;12:189–98.
[23] American Sleep Disorders Association. International classification of
sleep disorders: diagnostic and coding manual. Rochester, MN: Amer-
ican Sleep Disorders Association, 1990.
[24] American Psychiatric Association. Diagnostic and statistical manual
of mental disorders. 4th ed. Washington, DC: American Psychiatric
Association, 1994.
[25] Bastien CH, Vallieres A, Morin CM. Validation of the insomnia se-
verity index as a clinical outcome measure for insomnia research.
Sleep Med 2001;2:297–307.
[26] Wechsler D. Wechsler Memory Scale-Revised manual. San Antonio:
Psychological, 1987.
[27] Wechsler D. Wechsler Adult Intelligence Scale-Revised manual. New
York: Psychological, 1981.
[28] Tiffin J. Purdue Pegboard examiner’s manual. Rosemont: London
House, 1968.
[29] Reitan RM. Validity of the trail making test as an indicator of organic
brain damage. Percept Mot Skills 1958;8:271–6.
[30] Wilkinson RT, Houghton D. Portable Four-Choice Reaction Time
Test with magnetic tape memory. Behav Res Meth Instrum 1975;7:
441–6.
[31] Grant DA, Berg EA. The Wisconsin Card Sorting Test: systemic lay-
out. Madison, WI: University of Wisconsin, 1948.
[32] Gorenstein C, Bernik MA, Pompeia S. Differential acute psychomotor
and cognitive effects of diazepam on long-term benzodiazepine users.
Int Clin Psychopharmacol 1994;9(3):145–53.
[33] Bonnet MH, Arand DL. Hyperarousal and insomnia. Sleep Med Rev
1997;1(2):97–108.
[34] Schneider-Helmert D. Twenty-four-hour sleep–wake function and
personality patterns in chronic insomniacs and healthy controls. Sleep
1987;10(5):452–62.
[35] Edinger JD, Fins AI, Sullivan RJ, Marsh GR, Dailey DS, Hope TV,
Young M, Shaw E, Carlson D, Vasilas D. Sleep in the laboratory and
sleep at home: comparisons of older insomniacs and normal sleepers.
Sleep 1997;20(12):1119–26.
C.H. Bastien et al. / Journal of Psychosomatic Research 54 (2003) 39–49 49