NEWCASTLE-UNDER-LYME PRIMARY CARE TRUST
212
NSCCG GOVERNING BOARD – PUBLIC SESSION Meeting to be held on the 6 th January 2016 from 2.00pm until 5.00pm Council Chambers, Merrial Street, Newcastle, Staffordshire AGENDA NO AGENDA ITEM PURPOSE LEAD/S ENC TIME PROCEDURAL ITEMS 1 Chairs welcome and to receive apologies Dr M Shapley Verbal 2.00pm 2 New Conflicts of interest (available on website) If any member of the Governing Board has any pecuniary interest, in any contract, proposed contract or other matter under consideration at this meeting he/she shall disclose the fact to the Chairman and shall not take part in the consideration or discussion of the matter or vote on any question with respect to it Additions/ Amendments Dr M Shapley Verbal 3 Minutes of the meeting held on Wednesday 4 th November Approve Dr M Shapley Enclosed 4 Matters arising Update Dr M Shapley Enclosed 5 Matters discussed within the Closed session Information Dr M Shapley Verbal 6 Accountable Officers Report Information Mr M Warnes Enclosed 2.10pm 7 EPRR Assurance Mr M Warnes Verbal 2.20pm 8 Equality and Inclusion Progress Report Assurance Mr M Warnes Enclosed 2.30pm 9 Annual Equality and Inclusion Report Approve Mr M Warnes Enclosed 2.40pm QUALITY AND SAFETY 10 Quality Report Assurance Mrs J Downey Enclosed 2.50pm 11 Patient Congress / Second Citizens Jury Decision Prof N Chambers Enclosed 3.10pm COMFORT BREAK STRATEGIC 12 PAN Staffordshire Transformation Programme “together we are better” Decision Mrs R Symons/ Mr M Warnes Enclosed 3.30pm PERFORMANCE/FINANCE 13 Integrated Performance Report Information Mr I Stoddart To be tabled 4.00pm 14 Finance Report Information Mr I Stoddart Enclosed 4.10pm 15 Allocations Information Mr I Stoddart Enclosed 4.20pm PARTNER ISSUES 16 Staffordshire County Council (Care) Update Information Ms N Glover-Edge To be tabled 4.30pm
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of NEWCASTLE-UNDER-LYME PRIMARY CARE TRUST

NSCCG GOVERNING BOARD – PUBLIC SESSION
Meeting to be held on the 6th January 2016 from 2.00pm until 5.00pm Council Chambers, Merrial Street, Newcastle, Staffordshire
AGENDA
NO AGENDA ITEM PURPOSE LEAD/S ENC
TIME
PROCEDURAL ITEMS
1 Chairs welcome and to receive apologies Dr M Shapley
Verbal 2.00pm
2 New Conflicts of interest (available on website)
If any member of the Governing Board has any pecuniary interest, in any contract, proposed contract or other matter under consideration at this meeting he/she shall disclose the fact to the Chairman and shall not take part in the consideration or discussion of the matter or vote on any question with respect to it
Additions/ Amendments
Dr M Shapley Verbal
3 Minutes of the meeting held on Wednesday 4th November
Approve Dr M Shapley Enclosed
4 Matters arising Update Dr M Shapley
Enclosed
5 Matters discussed within the Closed session
Information Dr M Shapley
Verbal
6 Accountable Officers Report Information Mr M Warnes
Enclosed 2.10pm
7 EPRR Assurance Mr M Warnes
Verbal 2.20pm
8 Equality and Inclusion Progress Report Assurance Mr M Warnes Enclosed
2.30pm
9 Annual Equality and Inclusion Report Approve
Mr M Warnes Enclosed 2.40pm
QUALITY AND SAFETY
10 Quality Report Assurance Mrs J Downey
Enclosed 2.50pm
11 Patient Congress / Second Citizens Jury Decision Prof N Chambers
Enclosed 3.10pm
COMFORT BREAK
STRATEGIC
12 PAN Staffordshire Transformation Programme “together we are better”
Decision Mrs R Symons/ Mr M Warnes
Enclosed 3.30pm
PERFORMANCE/FINANCE
13 Integrated Performance Report Information Mr I Stoddart
To be tabled 4.00pm
14 Finance Report
Information Mr I Stoddart Enclosed 4.10pm
15 Allocations Information Mr I Stoddart Enclosed
4.20pm
PARTNER ISSUES
16 Staffordshire County Council (Care) Update
Information Ms N Glover-Edge
To be tabled 4.30pm

GOVERNANCE
17 Audit Committee Report
Information/ Assurance
Mr N McFadden Enclosed 4.40pm
18 Governance update includes Constitution and Terms of reference updates (Planning Committee, Finance & Performance committee & Joint Commissioning Arrangements)
Approve Mrs A Palethorpe Enclosed 4.45pm
QUESTIONS FROM THE PUBLIC
19 Questions from the public
--- Dr M Shapley --- 4.50pm
DATE AND TIME OF NEXT MEETING
20 Wednesday 2nd March, Churnet Room, Moorlands House, Stockwell Street, Leek, Staffordshire
Note
The Clinical Chair and Members of the Governing Board will be glad to meet with members of the public and representatives of the press following the meeting to discuss and comment on any agenda items, or other issues which may be of current interest.
Members of the press/media are asked to contact the Communications and Marketing Department, tel: 01782 401048, with any requests for further
information and comment

NSCCG - Board - PUBLIC 4
th November 2015 Page 1 of 12
Approval of minutes - Initital of Chair - …………….
NORTH STAFFORDSHIRE CLINICAL COMMISSIONING GROUP
GOVERNING BOARD - PUBLIC SECTION
Minutes of the meeting held on Wednesday 4th November 2015
Seminar Rooms 2 – 5, Medical Institute, Hartshill, Newcastle, Staffordshire Commencing at 2.00pm
Present: Dr M Shapley Clinical Chair (CHAIR) (MSh) Prof N Chambers Lay Member, Patient Experience (NC) Mrs N Dowd Interim Director of Strategy, Planning &
Performance (co-opted) (ND) Mrs J Downey Director of Nursing and Quality (JD)
Dr L Hussain Non Executive GP Board Member (LH) Mr N McFadden Lay Member, Governance (NMcF) Dr R Page Non Executive GP Board Member (RP) Mrs S Parkin Clinical Director - Quality Partnerships & Engagement (SP) Mr I Stoddart Chief Finance Officer (Joint) (IS) Dr E Sutton Clinical Director - Primary Care (ES)
Dr P Unyolo Clinical Director – Commissioning (PU) Mr M Warnes Interim Accountable Officer (MW) In Attendance: Mrs L Ellis Board and Committee Manager (LE) Mrs A Palethorpe Head of Governance (AP) Ms F St Aubin d'Ancey Communications Team (FS) Observers Mr D Hardy Patient Representative (DH) 8 members of the public present (signed in)
2015.099
Chairs welcome and apologies for absence MSh welcomed members of the Governing Board and members of the public to the CCG Governing Board meeting, held in public. On behalf of the Governing Board, MSh formally welcomed JD to her first meeting of the Governing Board in her capacity as Director of Nursing and Quality. Apologies for absence were received from: Dr A Bradley Non Executive GP Board Member Mrs T Cork Local Pharmaceutical Representative Dr D Robertson Secondary Care Doctor Dr P Scott LMC representative Members of the Governing Board expressed concern regarding the lack of Local Authority representation and MSh agreed to write to Local Authority colleagues expressing the concerns.
ACTION MSh

NSCCG - Board - PUBLIC 4
th November 2015 Page 2 of 12
Approval of minutes - Initital of Chair - …………….
2015.100
A quorum of the Board was present and members had been given formal written notice of this meeting in accordance with the CCG’s constitution. Declarations of Interest No additional declaration or conflicts of interest were received.
ACTION
2015.101
Minutes of the last meeting held on the 1st July 2015 The minutes from the meeting held on the 2nd September, were approved as an accurate record of the meeting, with the following exception agenda item 2015.093, in which member of the public Bas Pickering referred to Kniveden Hall. LE agreed to obtain a progress update on the current status.
LE
2015.102
Matters Arising In addition to the items noted on the action tracker, the following reports were noted: Clinical Accountable Officers Report NMcF referred to the assurance meetings with NHS England and requested that formal feedback is shared with colleagues. MSh confirmed that he has shared the report with all Non-Executive Director colleagues. MW agreed to make reference to the assurance meetings in his Accountable officers report, when required. Strategic Planning At the last meeting it was requested that the draft strategy was presented to the Patient Congress. ND confirmed that this took place on the 21st October and members of the Patient Congress have requested that a progress update is provided at the meeting in December. Integrated Performance/Finance Report At the last meeting PU referred to the backlog position and asked if services commissioned by other providers can be included in the report. ND stated that provider organisations are not required to report on follow up data, however referral to treatment (RTT) can be included and agreed to work with colleagues. At the last meeting concern was expressed re performance information and it was noted that the CSU Business Intelligence Team are reviewing performance information to highlight a variety of performance information for the Governing Board. NC referred to the outpatient backlog position and noted that funding will be not released until the action plan is received and requested an update. ND stated that the current backlog stands at 33,069, of which 22,406 patients have been waiting for over five weeks, 5,049 patients have scheduled appointments, which equates to 12% of patients waiting for over 26 weeks. She advised that there is a joint action plan, but overall 4% under plan. It was noted that a working group has been established who are looking at other initiatives, for example none face to face appointments. LH asked if the CCG are paying twice for appointments. ND confirmed that the CCG will not pay over the contracted level.
MW ND

NSCCG - Board - PUBLIC 4
th November 2015 Page 3 of 12
Approval of minutes - Initital of Chair - …………….
2015.103 2015.104
Matters Discussed within the Closed Session MSh advised that the Governing Board in closed session discussed the financial position, quality, cancer and end of life. Accountable Officers Report MW advised that the CCG continues to face close scrutiny from NHS England due to its financial position and performance against its Financial Recovery Plan, performance against NHS Constitution standards, its leadership capacity and capability, following which the CCG has been given a ‘not assured’ status. He added that the CCG has agreed a plan with NHS England. MW advised that the urgent care system continues to attract national attention due to the continued failure to achieve the A&E 4 hour target. He added that the CCG is one of 26 organisations that have an emergency care improvement plan. MW referred to the referral to treatment (RTT) which continues to be below target and as a result a new remedial action plan has been requested. MW advised that the CCG continues to make good progress in the delivery of its financial plan and at month 6 is on track to deliver its £2 million deficit control total. MW advised that the Staffordshire CCGs’ application for Level 2 co-commissioning has been accepted by NHS England and there is a view nationally that it is the intention of NHS England that all CCGs have achieved level 3 by April 2016. MW referred to “my care, my way, home first” and advised that the formal public consultation exercise commenced in September and will end in mid-January, following which findings will be presented to the Overview and Scrutiny Committee. MW stated work continues to strengthen the collaborative working between the CCG and NHS Stoke-on-Trent CCG and progress is being made. MW advised that Governing Board members are kept updated regarding the Pan Staffordshire Transformation Programme and advised that a case for change is being prepared and led by Rita Symons, Programme Director, which will be submitted to NHS England late December and subject to its approval, a period of consultation will follow prior to the implementation of the programme later in the year.
MW advised that the CCG hosts the Primary Care Research Consortium, based at
Keele University and is an active member of the Staffordshire and Shropshire
Research, Development, Innovation and Evaluation (ReDIE) Group. He added that this partnership delivers an extensive research programme and continues to
support the further development of clinical academic research locally; ensuring the
commissioning and provision of evidence based clinical care to local residents. It was noted that work has been recognised by the Health Service Journal (HSJ),
which has shortlisted the ReDIE Group’s, and winners will be announced at the HSJ Awards evening on 18 November 2015.
MW provided an update regarding executive staffing and advised that initially ND’s appointment was for 6 months, however this has been extended to ensure that the CCG has the required senior leadership through the forthcoming annual planning round. He added that the CCG will be appointing their Accountable Officer early December.
ACTION
NSCCG - Board - PUBLIC 4
th November 2015 Page 4 of 12
Approval of minutes - Initital of Chair - …………….
On behalf of the Governing Board, MW thanked Rosie Trainor, Interim Director of Nursing for her hard work and support, who left the CCG at the end of October, following the permanent recruitment to the post. MSh referred to the Research Consortium and thanked MW and SP for their hard work and commitment. NMcF referred to “my care, my way, home first” and noted that a formal public consultation has commenced and requested details of dates and venues. FS stated that all details are available on the CCGs website. It was noted that findings will be presented to members of the Governing Board at an informal seminar. MSh referred to the quarterly assurance meetings and asked if a formal report will be shared. MW agreed to make the request. NC referred to the Pan Staffordshire Transformation Programme and noted that the programme is led by the Staffordshire Commissioning Congress and asked to what extent is there clinical leadership. MW stated that the Programme is led by the Staffordshire Commissioning Congress and includes a clinical leaders’ forum and a provider forum, in which there is representation, which also include public health representation. Member of the public Mr Syme referred to the 4 hour A&E target and stated that UHNM have indicated that they expect to achieve the 95% trajectory, as noted in their Board papers. He also referred to the wider plans and asked if the CCGs are factoring in the beds at Longton Cottage. MW stated that the beds at Longton Cottage will not be factored into the winter plans. Member of the public, Mr Williams referred to the collaborative working and if this would lead to a postcode lottery. MW stated that the CCGs commission the vast majority of services, however, there are differences, which are reflected in the difference of population and the needs of the population. He advised that the CCG has a robust prioritisation programme and noted that there are areas of difference. He advised that there are no national commissioning specifications for services and CCGs are best placed to make the decisions for the population they serve. Member of the public, Mr Pickering asked if there is public involvement with the Pan Staffordshire work. MW confirmed that there is significant patient and public involvement. He added that the CCG has a strong public and patient engagement mechanism in place. Members of the Governing Board noted the update.
ACTION MW
2015.105
Emergency, Preparedness, Resilience and Response (EPRR) MW advised that the CCG has completed the 2015/16 EPRR Self-Assessment and have been appraised as ‘Substantially Compliant (green)’ by NHS England. He added that the CCG has an EPPR work plan in place which will attain full compliance of the EPRR Core Standards by the 1st December 2015. He added that the CCG has also completed the EPRR Assurance Process for UHNM (Fully Compliant), NSCHT (Substantially Compliant) and SSOTP (Fully Compliant). Members of the Governing Board noted the update.

NSCCG - Board - PUBLIC 4
th November 2015 Page 5 of 12
Approval of minutes - Initital of Chair - …………….
2015.106 2015.107
Equality and Inclusion (E&I) MW presented the report and advised that the CCG had its first joint EDS annual public grading event in October and advised that much work has been carried out by the CCG in gathering largely retrospective evidence for EDS Goals 1 and 4 and work is continuing to gather evidence for EDS Goal 2 for 2016 grading i.e. engagement goal. SP advised that she attended the grading event, which was a joint event with Stoke CCG and advised that a summary was presented on the day, however detailed evidence is available on the CCGs website. She added that the CCGs were challenged and is content with the ratings. Members of the Governing Board received and noted the report. Quality Report SP presented the report and advised that constitutional/contractual breaches impact on patient experience and potentially on the effectiveness of care and advised that the Quality Committee has asked that an information request is issued to University Hospital of North Midlands NHS Trust for each area where the NHS Constitution is being breached or where the Trust is a significant outlier for performance breaches to confirm what systems and processes are in place to ensure that no patients are coming to harm whilst waiting, and what mitigating actions the Trust are taking to minimise poorer outcomes. She stated that the CCG will continue to undertake announced and unannounced quality visits to ascertain if patients have had a poor experience or sustained harm. North Staffordshire Combined Healthcare NHS Trust (NSCHT) SP advised that the Safety Thermometer ‘harm free care’ rate for July 2015 is 95.31% and no new harms were recorded. She also added that latest Friends and Family Test (FFT) results highlight that 87% of patients would recommend NSCHT, 74% of staff would recommend NSCHT as a place to receive care and 44% of staff would recommend NSCHT as a place to work. SP stated that the CCG undertook an unannounced quality visit to the Access Service on 25th August and advised that the visiting team recognised the improvements that the service have made and there were no immediate concerns raised with the Trust. She also added that the Care Quality Commission carried out a comprehensive inspection which included an announced inspection visit week commencing the 7th September and representatives from North Staffordshire CCG and Stoke-on-Trent CCG met with the CQC inspectors to share soft intelligence, areas of good practice and areas for development ahead of the announced inspection. Staffordshire and Stoke on Trent Partnership NHS Trust (SSOTP) SP advised that the Safety Thermometer ‘harm free care’ rate for July 2015 is 91.56% and 96.58% and no new harms recorded. She added that the highest rate of harm over the twelve months is pressure ulcers and the majority of these are existing Grade 2 pressure ulcers. It was noted that the number of new harm pressure ulcers remains constant between a high of 2.03% in July 2015 and a low of 1.2% in May 2015.
ACTION

NSCCG - Board - PUBLIC 4
th November 2015 Page 6 of 12
Approval of minutes - Initital of Chair - …………….
SP stated that the Trust continue to work towards the elimination of avoidable pressure ulcers and initiatives undertaken and include a training programme for pressure ulcer prevention, draft pressure ulcer guidelines, introduction of a visual and narrative grading scale and a DVD for equipment advice and guidance has also available. SP referred to the District Nursing service and advised that the Trust has appointed 29 band 5 district nurses in September & October within the North Division. There are 8.4 remaining vacancies for district nurses in the North Division and further interviews are scheduled. She advised that the Trust acknowledge that the retention of staff is key to continued progress and have assured the CCG that a strong induction has been put in place for all new recruits including welcome pack, IT in place, training, buddying, mentorship & preceptorship and peer support networks. Further, a Recruitment & Retention Strategy has been introduced and an implementation plan is in development. SP advised that the Care Quality Commission commenced their comprehensive inspection visits week commencing the 2nd November and representatives from North Staffordshire CCG and Stoke-on-Trent CCG met with the CQC inspectors to share soft intelligence, areas of good practice and areas for development ahead of the announced inspection. University Hospital of North Midlands NHS Trust (UHNM) SP referred to the discharge processes and timeliness, which have been highlighted as an area of development from patient feedback and within the CQC comprehensive inspection report. She added that the Trust have identified discharge as one of their quality priorities for 2015/16: Infection Prevention and Control (IPC) It was noted that North Staffordshire CCG is over trajectory at Month 5 with 60 clostridium difficile infections (CDI) cases reported against a cumulative tolerance of 25. Of the 60 CDI cases, 16 occurred within an acute setting and 44 in a non-acute setting (e.g. sample sent from a Nursing Home, General Practice or within 48 hours of admission to an acute or bedded community facility other than a Care Home). SP advised that a working group has been established, which includes representatives from all stakeholders. She added that discussions have taken place with Medicines Optimisations colleagues with regard to antibiotic prescribing to ensure effective prescribing. It was noted that prescribing guidelines have been issued and a significant amount of work is taking place. Safeguarding Adults, Children and Young People As noted in the report, SP advised that there is no further update. MSh referred to infection prevention and control and the high number of CDI cases and asked how we compare with other Trusts. JD stated that there are very robust action plans in place, however highlighted issues outside the control of the CCG, which include care homes and in the community setting. LH stated that there have recently been two antibiotic master classes and advised that his clinical experience has given rise to concerns regarding appropriate prescribing in the community and at the hospital interface. JD stated that there is a pharmacist based within A&E ensuring appropriate prescribing. SP advised that work is ongoing and is focusing on high prescribers and suggested that LH advises colleagues within the Medicines Optimisation Team.
ACTION

NSCCG - Board - PUBLIC 4
th November 2015 Page 7 of 12
Approval of minutes - Initital of Chair - …………….
2015.108
MW referred to the recent district nursing recruitment campaign and the training programme and stated that there is a need to ensure that the training includes management of complex needs of the community, including mental health needs. NC stated that there are workforce challenges within primary care and stated that there is a staff recruitment campaign in the future and suggested that this could be an early task for the federation to provide support and assistance. ES agreed and stated that there are recruitment issues, which not only refer to GPs, but nursing staff and added that the Joint Commissioning Committee has established a recruitment sub-group, which will link into the Pan Staffordshire work and the North Staffordshire delivery to ensure that all parties work more effectively together ensuring the best outcome for the patient. NC asked how the CCG will ensure that general practices who are struggling receive support are not left behind. ES stated that there is an element of practice awareness and support is also available from NHS England NC thanked SP for preparing the report and advised colleagues that there is a significant amount of background work behind the production of the report. NMcF echoed NC comments. Members of the Governing Board received and noted the report. Patient Congress NC provided a verbal update and advised that following each meeting of the Patient Congress, members receive a one page summary, which is also displayed on the CCG website. She advised that members of the Patient Congress received an update on the Keele University GP Access Audit, which overall showed access to be good, with the average wait times to see a doctor being 0- 3 days in most cases. She added that the findings will be shared with the CCG’s primary care team. NC advised that members received the Citizen Jury Final Report and Recommendations. It was noted that all recommendations have been taken on board by the CCG and a task and finish group has been established to monitor work taking place and the action plan to monitor this work was shared with Patient Congress. NC advised that PU was in attendance at the last meeting of the Patient Congress and provided an update to members regarding dementia and members were informed that as a result of the ongoing dementia awareness work and it was noted that dementia diagnosis rates within North Staffordshire are now at 70%, above the national average of 67%. NC were advised that the members were asked to consider the following questions regarding the developing joint CCG strategy:
Who should we be listening to?
What should we bear in mind?
What would you like to see included within the strategy?
Members provided feedback, which included; the strategy should be clear and evidence based with alignment to localities within North Staffordshire and Stoke-on-Trent, the CCG should consider listening to the voluntary sector as well as professional bodies who might specialise in specific conditions / services, e.g. Age
ACTION

NSCCG - Board - PUBLIC 4
th November 2015 Page 8 of 12
Approval of minutes - Initital of Chair - …………….
UK, Healthwatch, faith groups and listen to ethnic minorities, those from the 9 protected groups and members from more rural based communities. NC advised that members received an update regarding an extension to the out of hours GP contract and the proposals to review how the out of hours contract might be integrated with the Front of House service provided at the hospital Accident and Emergency department. Members of the Governing Board noted the update.
ACTION
2015.109
Prioritisation Programme MSh advised that the CCG has recently received a letter from Staffordshire County Council, which acknowledged the public concerns and those of our Partners and advised that a response will be provided to Staffordshire County Council. MW advised that eligibility criteria was introduced as from the 1st October this year and was communicated to all providers. He added that the CCG is fully aware of the views of the public. He advised that CCGs within the Staffordshire area are looking at adopting a similar policy. He assured the board that commissioning decisions are reviewed and where appropriate any additional evidence if taken into account and stated that the CCG is working closely with the Local Authority regarding prioritising services. NC referred to the clinical evidence which was considered by the Clinical Priority Advisory Group. IS stated that there is an issue with sustainability and not only the needs of the public, but also the wants of the public. MW stated that the CCG needs to ensure that it has a robust and clear communication process in relation to any commissioning decisions and stated that the CCG will have to make difficult decisions. RP raised concern regarding the lack of information available on the CCG website, as it has been agreed to have a dedicated page and stated that as of yesterday CSU colleagues still have not completed this task and asked if there is anything the Governing Board can do, as this information is necessary for public engagement. SP stated that the delay is disappointing and stated colleagues are close to completing and the information will be on the website imminently. FS stated that colleagues are working on the information and it is expected to be completed by early next week. Member of the public, Mr Pickering stated that guidance is not clear as to who is eligible under the new criteria and the CCG has not stipulated decibel range and asked how patients can measure if they meet the criteria as there is no comparison. SP stated that we are able to measure the degree of hearing loss and it is very clear in the new contract what is the cut-off point and advised that it is about the functional impact on the individual, not just about the hearing loss and advised that all information will be available on the website. Member of the media, Mr Blackhurst asked if it is possible to establish how many patients have failed the criteria in the first month and asked if any patients have requested this via the individual funding request route. MW stated that monthly monitoring has not taken place and stated that he is not aware of any patients requesting this via the individual funding route, however the new criteria was only implemented on the 1st October, so it is early days.
MW

NSCCG - Board - PUBLIC 4
th November 2015 Page 9 of 12
Approval of minutes - Initital of Chair - …………….
2015.110 2015.111
Members of the Governing Board received and noted the update and supported a response being provided to Staffordshire County Council. Research Consortium SP provided a verbal update and advised that various meetings have taken place between the CCG and Keele University and advised that work continues in relation to the governance of the Consortium, which included a revision of our service level agreement, which will clarify responsibilities and accountabilities and ensures a robust governance process is in place, together with adequate reporting arrangements. Colleagues continue to work together to strengthen the relationship between Keele University and the CCG. In addition colleagues are exploring better ways of communicating and publicising the outputs and outcomes from our research partnership and the recent HSJ Innovation award is an example of the work being undertaken. MSh asked if regular meetings will take place between CCG and Keele University colleagues. SP confirmed that regular meetings have been scheduled. IS advised that the CCG host the service level agreement and all information and updates are provided at the Audit Committee, in which all the information is provided in detail. He added that delegated responsibility has been given to the Director of Finance at Keele University. Members of the Governing Board received and update the update. Integrated Performance/Finance Report ND presented the performance element of the report and advised that colleagues are working on a new report format, which will be more comprehensive and will include a whole range of elements, one of which will focus on provider organisation performance and colleagues are in the process of liaising with Business Intelligence colleagues. She referred to the referral to treatment and advised that the target has been consistently failed and contract notices have been issued, in which the Trust has 10 days to respond and a remedial action plan has been requested. She added that the CCG continue to withhold 2% of the contract value. ND referred to the four hour A&E wait target and advised that the target fails to be achieved and stated that performance notices have been raised, following which a RAP (remedial action plan) was agreed. ND referred to the cancer waits and advised that the two week waits target is being met, with the exception of breast and advised that a recovery action plan has been compiled. She advised that the 31 day wait is not being achieved, however it is anticipated that trajectory will be achieved in January. It was noted that the 62 day wait is also not being achieved, however, it is anticipated that trajectory will be achieved by the end of the financial year. She advised that patients have been offered alternative appointments, however, patient choice is difficult to manage. It was noted that a remedial action plan is in place. She stated that UHNM are one of 19 providers nationally, who have been requested to submit an improvement plan to deliver the 62 day standard. She added that the plan has been agreed at the System Resilience Group (SRG), following which it was submitted to NHS England at the end of August.
ACTION MW
NSCCG - Board - PUBLIC 4
th November 2015 Page 10 of 12
Approval of minutes - Initital of Chair - …………….
NMcF referred to the A&E four hour wait and acknowledged the deterioration in the target. ND stated that this is of significant concern and stated that colleagues are working to set a local target of 90%. She added that domiciliary care is of concern and advised that additional resources have been received. MW advised that the SRG meet every two weeks and provided assurance that additional focus is provided to ensure progress is being made. MSh stated that there is an issue with patient flow throughout the healthcare system and asked if provider organisations are receiving support. MW stated that the Trust Development Agency (TDA) are working with all three local providers. IS confirmed that additional funding has been received to assist the domiciliary care service and advised that a remedial action plan is in place, which is reviewed at SRG. NC referred to the possibility of 7 day working and asked to what extend is the CCG in dialogue with voluntary sector organisations, specifically to make full use of the social capital to support patients as part of their discharge process. MW stated that this is an underutilised resource in the third sector and stated that there are 200 high intensive users, for example alcohol mis-use, mental health, loneliness and frequent flyers and stated that it is essential to look at the underlying cause, not the symptoms and working with the third sector is a vital part. SP stated that there is a pilot voluntary sector hub which accepts referrals from clinicians, one of which is a befriending service and stated that it is essential to have a systematic way of working with the voluntary sector. She advised that the Patient Congress will be devoting time to discuss how the CCG can work with the third sector. IS presented the finance element of the report and advised that the CCG continues to work to deliver the forecasted £2 million deficit plan. He added that activity and costs are below where expected IS advised that the CCG’s cumulative financial position as of the end of September (month 6) is reported at £1.558 million deficit, which is an improvement of £234,000 on the planned position which was expected at £1.792 million deficit. He added that the CCG’s forecast outturn position is still expected to be in line with forecasted £2 million deficit plan. IS stated for the CCG to deliver against the plan in full and achieve the year end position it is essential to deliver the QIPP programme of £7.66 million in full (the vast majority of which is scheduled to be achieved in the latter part of the year) and to maintain current expenditures to planned levels. He added that the CCG set a QIPP programme for 2015/16 of £7.66 million (net) with the majority of the savings profiled to be achieved in the latter part of the year and advised that performance to month 6 is behind trajectory but monitoring information suggests this slippage will be recovered in year. The QIPP programme continues to be monitored bi-weekly through the Finance Recovery Group. Work is now in place to identify Plan B schemes to deliver additional savings in year It was noted that the CCG have now received reporting information up to month 4 for Prescribing, which indicates spend to be above plan, forecast reporting is that spend will continue to be a levels above plan however delivery result of the QIPP programme savings in full would reduce this forecast overspend to £1.1 million.
ACTION

NSCCG - Board - PUBLIC 4
th November 2015 Page 11 of 12
Approval of minutes - Initital of Chair - …………….
NC stated that the biggest risk for the CCG is the delivery of the QIPP programme and requested more detail for the next meeting, to ensure assurance and ensure that the CCG is clear that we pay for services we receive from provider organisations. IS stated that further information is highlighted on page 12 of the report and stated that further information will be contained in the next report. He added that colleagues will go back to provider organisations to make sure that what the CCG invest is being delivered and also to ensure that all the contracts are robust. ND stated that work is progressing to align provider cost improvement plans with the QIPP and advised that this will be undertaken during the contract negotiation period. Member of the public, Mr Pickering referred to the recent report which has given to his Patient Participation Group regarding a patient who was discharged too early and was re-admitted and asked if the CCG will have to pay twice for this. ND stated that this is unfortunate, especially for the patient experience and confirmed that it would be two payments, as they would be classed as two separate admissions. However, she advised if a patient is re-admitted within 30 days there is a 30% reduction in cost. IS stated that the quality of discharge needs to be understood and stated concerns can be feedback via the contract route. Members of the Governing Board received and noted the report.
ACTION
2015.112 2015.113
Staffordshire County Council (Care) update In the absence of no representative from the Local Authority, members of the Governing Board received the report. Members of the Governing Board expressed concern regarding the lack of Local Authority representation and MSh agreed to write to Local Authority colleagues expressing the concerns. Risk Register/Assurance Framework AP presented that Risk Register/Assurance Framework and advised that the CCG has been working with Stoke on Trent CCG to align those risks that are applicable to both CCG’s to enable one risk register to be maintained and to avoid duplication. AP advised that it has been agreed at a previous Govenrning Board that risk scoring 15 or over would be presented, however, due to the new format of the report all risks are included in today’s report. JD asked why the CCG is not using the DATIX system. AP stated that the CCG does not pay for this element of the model. NC welcomed the format and asked if colleagues have considered the risks in relation to secondary care capacity and social care and the impact on the NHS, for example reduction in funding. Member of the public, Mr Syme referred to the national spending review and stated that this should be taken into account on the risk register. IS stated that the CCG has to consider the National economic climate and the potential impact on the NHS. He added that the CCG is in dialogue with the Local Authority and stated that this is not currently highglighted as a risk, however the CCG are fully aware and assured that is will be reflected as a risk if required.

NSCCG - Board - PUBLIC 4
th November 2015 Page 12 of 12
Approval of minutes - Initital of Chair - …………….
2015.114
Members of the Governing Board received and noted the report and recognised the work being undertaken with Stoke CCG to align the assurance framework and risk register. Chairs and Accountable Officers Urgent Action Request AP requested that the Governing Board formally ratify decisions made outside of the Governing Board forum. LH referred to the inclusion of the Termination of Pregnancy services (TOPS) in the integrated sexual health tender led by Stoke public Health and requested additional information. AP stated that work is being undertaken with Stoke on Trent CCG to establish a more integrated service and advised that notice has been provided to the current provider. ND stated that details have yet to be determined and confirmed that it is part of the integrated services initiative. MW stated that historically the service was commissioned by Stoke on Trent Primary Care Trust for both Stoke on Trent and North Staffordshire, following which it was transferred to Public Health and advised that work is progressing to establish a North Staffordshire and Stoke approach as part of the integrated service for North Staffordshire. Members of the Governing Board formally ratified the decisions made by the Clinical Chair, (Vice chair were applicable) and the Accountable Officer, in line with the Constitution.
ACTION
2015.115 2015.116
Any Other Business No issues raised. To receive additional questions from the members of the public Mr Syme referred to frequent flyers, specifically the five year forward view and pump prime investment for 24/7 mental health liaison, minimum standards of care, which refers to a specific amount of whole time equivalent staff being employed at all levels (nursing, psychiatrists) and referred to the difference in employed staff and that numbers stated in the standards. PU stated that colleagues are aware and stated that the CCG is in dialogue with the provider organisations and stated that no formal specification has been received. ND stated that the CCG have been requested to submit a plan of action by the 9th November and assured that the CCG is aware and discussions are taking place with the acute trust.
2015.117 Date and time of next meeting The next meeting will take place on Wednesday 6th January 2016 in the Council Chambers, Merrial Street, Newcastle, Staffordshire.
All parties should note that the minutes of the meeting are for record purposes only. Any action required should be noted by the parties concerned during the course of the meeting and action carried
out promptly without waiting for the issue of the minutes
These minutes are signed as being a true record of the meeting Signed:……………………………………………………………… Position:……………………………… Date:……………………

Meeting Action Tracker - CCG Board – HELD IN PUBLIC
Actions from the meeting held on the 4th November, update to be provided at the meeting scheduled on the 6th January
Item Action Lead
Progress
Minutes of the last meeting
The minutes from the meeting held on the 2nd September, were approved as an accurate record of the meeting, with the following exception agenda item 2015.093, in which member of the public Bas Pickering referred to Kniveden Hall. LE agreed to obtain a progress update on the current status.
LE E-mailed on the 5th November, chased 12th November,
response received stating “please be informed that we are we are currently looking at a number of options for Knivedon and will continue to update when we have further information”.
Matters Arising Integrated Performance/Finance Report At the last meeting PU referred to the backlog position and asked if services commissioned by other providers can be included in the report. ND stated that provider organisations are not required to report on follow up data, however referral to treatment (RTT) can be included and agreed to work with colleagues.
ND
Accountable Officers Report
MSh referred to the quarterly assurance meetings and asked if a formal report will be shared. MW agreed to make the request.
MW
Prioritisation Programme – hearing aids
MSh advised that the CCG has recently received a letter from Staffordshire County Council and advised that a response will be provided to Staffordshire County Council.
MSh/MW

Local Authority Members of the Governing Board expressed concern regarding the lack of Local Authority representation and MSh agreed to write to Local Authority colleagues expressing the concerns.
MSh Communication sent on the 10th November, response received stating that Staffordshire County Council are very committed to attending the Governing Board and provided assured that representation will be constant.

1
ENCLOSURE: 6
AUTHOR
REPORTING OFFICER /DIRECTOR
Name Marcus Warnes Name Marcus Warnes
Title Accountable Officer Title Accountable Officer
REPORT TO North Staffordshire CCG Governing Board
TITLE OF REPORT Accountable Officer’s Report
DATE OF THE MEETING Wednesday 6 January 2016
WHAT OTHER CCG COMMITTEE/GROUP/INDIVIDUALHASCONSIDERED THIS REPORT? None.
COMMITTEE/GROUP
INDIVIDUAL
ACTION REQUIRED FROM COMMITTEE/GROUP/ GOVERNING BOARD (please identify all applicable and provide details below)
Approve
Assurance
Discussion
For noting
X
RECOMMENDATION The Board is requested to note the contents of the report.
STRATEGIC GOALS SUPPORTED BY THIS PAPER (identify appropriate goals)
YES NO
1. Increase life expectancy and reduce inequality
X
2. Improve prevention, early detection and effective management of those at increased risk
X
3. Enhance quality of life and improve health outcomes for people with LTCs
X
4. Ensure people receive the right care in the right place
X
PURPOSE OF THE REPORT, KEY POINTS, OUTCOMES, EXECUTIVE SUMMARY (supporting information to be included, if applicable)

2
In this report I provide some context about the environment we have been operating in over the last month as well as describe progress with regard to A&E performance, financial recovery and Primary Care. I provide an update about the new model of care as well as matters of local and national interest. In addition I describe how we are progressing with collaborative working and strengthening our executive structure.
SUMMARY OF RISKS RELATING TO THE PROPOSAL
None.
ANY STATUTORY / REGULATORY / LEGAL / NHS CONSTITUTION/ASSURANCE / GOVERNANCE / PRESCRIBING IMPLICATIONS
None.
QUALITY IMPACT ASSESSMENT AND/OR EQUALITY IMPACT ASSESSMENT
N/a.
ANY RELATED WORK WITH STAKEHOLDERS/PRACTICES/PUBLIC AND PATIENT ENGAGEMENT
None.
ACRONYMS
Explained in the report.
3
1.0 Introduction
1.1 I am delighted to report that following a final interview on 9 December 2015, my application for the post of Accountable Officer for the CCG was successful and I commenced in post on 10 December. My appointment was subject to confirmation by NHS England, which has now been received. I would like to thank my colleagues on the Board and across the CCG and its membership for the support I received in my term as Interim Accountable Officer from 3 July 2015.
1.2 I welcome the confidence shown in me to carry out such a critical and challenging role. North
Staffordshire is a great place to work and I have enjoyed the support and friendship of CCG colleagues in my previous roles in the organisation. My immediate priorities are to continue working with our partners to improve performance against NHS Constitution Standards, particularly in A&E and hospital referral to treatment times; to secure the CCG’s finances this year so we go into next year in a strong position; and to ensure that the CCG has the necessary capacity and capability to operate effectively.
1.3 I look forward to working with the clinical leadership of the CCG to ensure that our member
practices are fully engaged in our commissioning activities and with our patients and wider population to secure the best possible health outcomes with the resources available to us.
1.4 In what has been a very difficult year for the CCG, wider health and social care economy and
nationally for the NHS, I would again like to acknowledge the outstanding efforts across the CCG and our partners. We continue collectively to respond to the pressures on urgent care, NHS constitutional targets, our financial position, delivery of our financial recovery plan, and the Pan Staffordshire Transformation Programme. These continue to be our key priorities, with reports for information and discussion within this Board meeting.
1.5 Further progress has been made since the last Board meeting on collaborative working with
our neighbouring CCGs, notably NHS Stoke-on-Trent CCG regarding integrating our workforce, and our providers in a collaborative and supportive way to respond to the challenges that we collectively have been experiencing. The CCGs’ Management of Change process concluded at the end of October and staff will transition into the structure and organisational arrangements from 1 January 2016.
1.6 As ever, I am grateful to the hard work and dedication of our staff and those in the front line in
primary, community and hospital settings. I would like to thank everyone for their professionalism and for the support that is being offered to colleagues and myself; it makes me really proud to be a member of this CCG and makes my job as Accountable Officer whilst challenging, an enjoyable one.
1.7 As I have reported previously, we continue to face close scrutiny from NHS England due to
our financial position and performance against our Financial Recovery Plan, performance against NHS Constitution standards and our leadership capacity and capability. These remain the reasons for our ‘not assured’ status and must remain the focus of our collective attention. We have a plan in place with NHS England to address this. Given our good performance towards financial recovery and implementation of proposals to strengthen our senior leadership, we continue to receive positive feedback and support from NHS England through the assurance process, and will be aiming to move on from our ‘not assured’ status this Quarter.
2.0 NHS Constitution Standards 2.1 A&E Performance 2.1.1 The urgent care system continues to attract national attention due to the continued failure to
achieve the A&E 4 hour target. Contractual processes are being followed with performance

4
notices issued and remedial action plans requested and through the System Resilience Group (SRG), recovery plans submitted.
2.1.2 You will note from the Integrated Performance Report that performance has not improved significantly and whilst fluctuating week to week, performance against the target of 95% remains around the high 80s% mark. The Recovery Plan requires a performance of at least 90% so we are behind trajectory. Significant measures have been taken by system partners during the year to address the challenges in the urgent care system, but the sustained improvements expected have not happened as we planned. The urgent care system remains under sustained pressure and now that winter is upon us we cannot afford to relax our focus on the continued improvements necessary to bring the system back into balance.
2.1.3 Winter plans have been implemented to provide the required resilience over the coming months. Particular attention is being given to out of hospital health and social care services, to ensure that discharge from the Royal Stoke University Hospital and flow through the system is maintained.
2.1.4 In the weeks leading up to Christmas, provider Chief Executives, CCG Accountable Officers
and system leaders from the local authorities and our regulators have participated in daily conference calls to ensure that everything possible is done to ensure patient care over the holiday period and to provide the resilience required to match capacity to predicted demand, facilitate timely discharge and maintain flow. An update on the success of these measures will be given at the Board meeting.
2.1.5 As stated previously, everyone needs to play their part in using our acute services
appropriately. A clear system wide communication strategy has been implemented to enable those in need of services to access the most appropriate care. Many problems can be managed effectively through self-care or a visit to the pharmacy or the GP. If in doubt, patients should ring the 111 service.
2.2 Referral to Treatment (RTT) 2.2.1 Both 18 Weeks and Cancer RTT performance remain areas of concern. The focus for 18
Weeks RTT is on the incomplete pathways, which is that 92% of patients on all waiting lists must have waited less than 18 weeks.
2.2.2 You will note from the Integrated Performance Report that performance falls short of the
required standard, which was not achieved in November. A verbal update on December’s position will be given at the Board meeting. Trusts were required to complete an Improvement Plan by 10 December 2015 for sign off by CCGs and submission to NHS England. The CCGs will continue to work with UHNM and our other providers to ensure this is successfully implemented and delivers the required improvements.
2.2.3 UHNM breached the agreed Remedial Action Plan (RAP), which has resulted in further
contractual sanctions. A further RAP has been submitted by the Trust, which at the time of writing this report has not yet been agreed by the CCGs. An update will be provided at the meeting.
2.2.4 The Cancer 62 Day RTT standard also remains a continued cause for concern as is
performance against some other cancer standards. Relatively small numbers of breaches have a significant impact on performance and we do recognise that due to the short waiting times involved some patients do choose to wait longer or in some cases do not attend appointments. This makes rebooking appointments difficult to achieve waiting time standards, but we must continue to work with our providers to ensure that all cancer patients receive timely treatment to ensure their care and longer term outcomes are not compromised due to waiting list pressures and management. Again, more detail can be found in the Integrated Performance Report.

5
2.2.5 A cancer RAP is in place with clear actions, trajectories and targets for improvement detailed. This is being monitored through the contract management arrangements with UHNM. An update on performance will be given at the Board meeting.
3.0 Financial Recovery
3.1 The CCG continues to make good progress on the delivery of its financial plan and at month 8 is on track to deliver its £2m deficit control total. Whilst we are performing better than planned for the year to date, due to the fact that many of our QIPP/financial recovery schemes impact in the second half of the year, we will remain focussed on the delivery of our planned deficit total.
3.2 We need to ensure key initiatives such as step up and step down services deliver the
required savings and we do have the requirement from NHS England to strive to improve our predicted end of year position from a £2m deficit to break even. Iain Stoddart, Chief Financial Officer provides more detail in his finance report later in the agenda.
3.3 The CCG continues to maintain a tight grip on its financial position through a fortnightly Financial Recovery Group, which is run jointly with Stoke CCG and chaired by myself. This enables close scrutiny of performance against the Financial Recovery Plan (FRP) and provides the opportunity for deep dives into areas of concern. In addition, we have voluntarily brought in an internal Turnaround Director, Alistair Mulvey, until the end of March 2016 to provide increased focus both on the achievement of this year’s FRP and the development of robust plans for 2016/17 and 2017/18. Alistair chairs the Performance and Delivery Steering Group, which meets weekly to both support and hold to account the leads for the schemes that constitute the FRP.
3.4 It is important to note that because we have a deficit plan, we are subject to much more
scrutiny by NHS England. Senior executives of Stoke and North Staffs CCGs attend monthly financial risk meeting with the North Midlands Area Team where progress against our plans is assessed. As such, we can make the Area Team aware of progress and provide early warning regarding areas that are not delivering as planned. This will ensure that we do not repeat the situation we faced last year, where our financial plans and position changed without NHS England being fully sighted.
4.0 Primary Care
4.1 Primary care remains a priority area for the CCG, given its critical importance to the delivery of new, community focussed models of care across the system. We continue to support the North Staffordshire GP Federation, which was established on 1 August 2015, whilst it develops its vision and plans. The Federation covers both Stoke and North Staffordshire and our 85 practices. The Federation is one of three in Staffordshire, with GP First and Alexin operating in the south of the County.
4.2 The Federation will play a key role in the northern Staffordshire provider landscape. The Federation is working with other providers, the CCGs and NHS England to develop and implement new models of care as set out in the Five Year Forward View. For example, the Federation is working with SSOTP to implement place based approaches to primary and community care provision in localities in Leek and Stoke, in line with the multi-specialty community provider model. The CCG will be working closely with the Federation and our providers to make this happen over the coming year.
4.3 The Staffordshire CCGs’ will be working towards Level 3 delegated commissioning across Staffordshire by April 2017 at the latest. The Staffordshire CCGs will work ever more closely through co-commissioning with the NHS England North Midlands Area Team to enable primary care to play an even more pivotal and effective role in shaping and providing healthcare services, recognising that it is critical given the increasing pressure on primary care that practices are adequately resourced to do so.

6
4.4 North Staffordshire and Stoke CCGs are making good progress on developing a primary care strategy that will sit within a broader pan Staffordshire primary care strategy. The strategy will provide a clear vision for primary care and co-commissioning and the role that the Federation and the primary care professions will play in the development and delivery of new models of care across Staffordshire.
5.0 My Care, My Way – Home First 5.1 I have regularly updated the Board at previous meetings on progress in developing and
implementing the new model of care for step up and step down services across the system, ‘My Care, My Way – Home First’, as well as the importance of securing agreements from our providers for its effective implementation. Furthermore, the importance we place on effectively engaging with stakeholders on the new model of care and the potential impact on the future configuration of community services.
5.2 The formal consultation exercise on My Care, My Way – Home First commenced in
September and will end in mid-January. Six public consultation meetings were held during October and November. I attended all six events, presenting our proposals and fielding questions. The events were independently chaired by Stoke and Staffordshire Healthwatch representatives, supported by commissioning managers and our comms team and generally went well.
5.3 The consultation concerns the new model of care and the shift of community services and in
particular intermediate care, into the community and people’s homes. Whilst this will impact on the use of community beds for intermediate care, any consultation on community beds and hospitals will now be part of the consultation on the Staffordshire transformation programme, ‘We’re Better Together’, which will be the vehicle to drive provider transformation and configuration across Staffordshire and Stoke on Trent. The first draft ‘We’re Better Together’ Case for Change was submitted to NHS England at the end of December 2015 and the Board will be updated at the meeting.
5.4 The step down contract has been signed by UHNM and commissioners and was
implemented from 1 December 2015. A further verbal update on progress will be provided at the Board meeting.
6.0 Collaborative Working 6.1 The strengthening of collaborative working between the CCG and NHS Stoke-on-Trent CCG
continues and the proposals for closer working and shared structures and workforce between the CCGs are being implemented.
6.2 The formal Management of Change process concluded at the end of October, all CCG
employees having been consulted on the proposed shared structure and any changes to roles and responsibilities. Following the staff consultation, feedback has been considered, proposals finalised and implementation of the shared structures will commence from 1 January 2016.
6.3 The revised structure includes an expanded executive management function shared with
Stoke whilst ensuring there is no dilution of clinical leadership at executive level. The revised senior leadership structure has been shared with NHS England to satisfy their concerns regarding the leadership capacity and capability in the CCG and to provide the required assurance that the CCG is able to meet the current demands it is facing.
6.4 Whilst the executive, clinical and managerial workforce and committee structures will be
shared by both CCGs, this is not a merger and both CCGs will remain sovereign bodies with their own governing bodies and accountable officers.

7
7.0 Pan Staffordshire Transformation Programme – ‘We’re Better Together’ 7.1 The high level, draft Case for Change was shared with NHS England on 23 December 2015.
This is a key document that will set out the challenging transformation programme that will be delivered across Staffordshire and Stoke on Trent over the coming years. Rita Symons, Programme Director will present an update report to the Board at its January meeting.
8.0 Update on Executive Staffing 8.1 Now that the Accountable Officer appointment has been made, the CCGs will commence the
recruitment of the Director of Commissioning and Director of Strategy, Planning and Performance posts in January.
8.2 Noreen Dowd will continue as Interim Director of Strategy, Planning and Performance until at
least the end of March 2015 or until a substantive appointment has been made. This will ensure that we have the required senior leadership through the forthcoming annual planning round.
8.3 We have advertised the Director of Commissioning post internally to senior staff on an interim
basis until a substantive appointment is made. We have some very capable senior managers for whom this will provide a valuable development opportunity. Interviews for the interim post will be in early January. This will provide further backfill development opportunities for other CCG managers.
9.0 Recommendation 9.1 The Board is requested to: 9.2 Note the contents of the report.

ENCLOSURE: 8
AUTHOR
REPORTING OFFICER /DIRECTOR
Name Julia Allen Name Alex Palethorpe Title Equality & Inclusion Business Partner Title Head of Governance
REPORT TO Governing Board
TITLE OF REPORT Equality & Inclusion (standing agenda) updates for (1) EDS and (2) WRES DATE OF THE MEETING 6 January 2016
WHAT OTHER CCG COMMITTEE/GROUP/INDIVIDUALHASCONSIDERED THIS REPORT?
COMMITTEE/GROUP Record which committee/group have already seen this report, note date and comments (if applicable)
INDIVIDUALPlease indicate name of individual and date agreed/approved (as necessary), for example HR, Finance, Quality, Medicines Optimisation or other
Joint ODC 17/11/15
ACTION REQUIRED FROM COMMITTEE/GROUP/ GOVERNING BOARD (please identify all applicable and provide details below)
Approve Assurance
xDiscussion
For noting
x
RECOMMENDATIONS The Governing Board is asked to:
Note the outcome of the joint EDS annual Public Grading, and in particular the: EDS Grading Report (Appendix 1); EDS CCGs mini Dashboard (Appendix 2); and EDS Summary Dashboard annual submission to NHS England (Appendix 3).
Note the progress in relation to WRES in particular the approval of the WRES action Plan by Joint ODC and by Marcus Warnes (Appendix 4)
EDS: Equality Delivery System v2
Note website display of all NSCCG EDS evidence for Goals 1: Better health outcomes; and Goal 4: Inclusive leadership (7 days in advance of public grading event i.e. by 20 October 2015)
Note that EDS evidence of CCG’s equality performance was presented by senior staff and clinical leads for Goal 1 (Better health outcomes): This year evidence focused mainly on joint commissioning work between both CCGs i.e. specific priority care pathways for: Long term conditions; Frail complex care; Neuro-community services; Hearing Aid service review (NSCCG); Dementia Strategy (SOTCCG); Transforming Cancer / End of life care; Datix – GP concerns reporting re providers / Complaints and PALs monitoring.
For information Goal 4 (Inclusive leadership at all levels). This year evidence focused on senior level planning and
decision making processes including support to Governing Board / Body re recognising and managing equality related business risk to support assurances for risk and inclusive ways of working.
9 EDS informal volunteer stakeholders attended. 12 CCG staff also attended to present summary evidence and to answer Q&A sessions at 27 October 2015 (1 day) annual public grading event.
A joint EDS Grading Report has been produced from this event and includes: recommendations from stakeholders on how CCGs can improve their grading to the next level, over the coming 12 months; as well as ‘lessons learnt’.
An annual EDS Action Plan (joint CCG) has been developed from recommendations made. This will be presented for consideration and approval at 19 January 2016 Joint ODC meeting.

WRES: For information
A WRES Action Plan has been approved by Marcus Warnes at 17 September 2015 meeting, from findings using ethnicity data gathered across all pay bands
NHS England has introduced a requirement as part of its Workforce Race Equality Standard which applies to NHS organisations or NHS funded organisations (excluding primary care and those with contract values of less than £200k) to record non-mandatory learning to ensure opportunities for development and progression are being applied fairly and consistently. The requirement to report on ‘Relative likelihood of BME staff accessing non mandatory training and CPD compared to White staff’ was not calculable in April 2015. HR and OD have now drafted a short guide for all staff members and sets out how to input a form to enable the CSU to log and record staff’s professional development and learning on ESR. This data should therefore be available for reporting in April 2016.
Nothing further to report on data until CCG workforce data is scrutinised annually at 1 April 2016.
STRATEGIC GOALS SUPPORTED BY THIS PAPER (identify appropriate goals) YES NO1. Increase life expectancy and reduce inequality
Yes
2. Improve prevention, early detection and effective management of those at increased risk
Yes
3. Enhance quality of life and improve health outcomes for people with LTCs
Yes
4. Ensure people receive the right care in the right place
PURPOSE OF THE REPORT, KEY POINTS, EXECUTIVE SUMMARY(supporting information to be included, if applicable) Key Headlines EDS Equality Delivery System v2 North Staffs CCG held its first EDS annual grading event jointly with Stoke CCG on the 27th October
2015.
Senior clinicians and staff presented summarised evidence to a group of 12 volunteer EDS informal stakeholders – from both localities of North Staffs and Stoke on Trent. For EDS Goals 1- Better Health outcomes and Goal 4- inclusive leadership at all levels. This year evidence focused on senior level planning and decision making processes including support to Governing Board / Body re recognising and managing equality related business risk to support assurances for risk and inclusive ways of working
Joint evidence of CCGs equality performance has for the first time been transparently displayed on EDS webpages to provide advance access to EDS evidence being presented on 27 October.
An EDS planning meeting on 22 December 2015 will consider next steps including continuing to gather evidence in ‘real time’ for EDS Goal 2 for 2016 grading on Tuesday 17 May 2016 i.e. to evidence the patient engagement goal. Goal 2 only will be addressed during 2016 and Goal 3 (workforce issues) in 2017.
CCGs worked hard to gather together volunteer stakeholders across each of the 9 protected groups and
evidence of working closely in partnership with: Healthwatch Stoke; Healthwatch Staffordshire; VAST; Support Staffordshire to provide opportunity for patient representatives to take part in the public grading and to achieve a representative spread of attendees at the annual event.
It is noted that representatives from Black Minority Ethnic groups did not attend on the day. Further work
is required with Engagement colleagues to go out to include local group reps in this process and to gain their feedback. BME representation in Stoke on Trent is 13.6% (2011 Census) mainly from the Pakistani community.
A joint EDS Grading Report has been produced from this event and includes: recommendations from stakeholders on how CCGs can improve their grading to the next level, over the coming 12 months; as well as ‘lessons learnt’.
An annual EDS Action Plan (joint CCG) has been developed from recommendations made. This will be presented for consideration and approval at 19 January 2016 Joint ODC meeting.
WRES: A WRES Action Plan has been approved by the CCG, from findings using ethnicity data gathered across
all pay bands
NHS England has introduced a requirement as part of its Workforce Race Equality Standard which applies to NHS organisations or NHS funded organisations (excluding primary care and those with contract values of less than £200k) to record non-mandatory learning to ensure opportunities for development and progression are being applied fairly and consistently. The requirement to report on ‘Relative likelihood of BME staff accessing non mandatory training and CPD compared to White staff’ was not calculable in April 2015. HR and OD have now drafted a short guide for all staff members and sets out how to complete a form to enable the CSU to log and record staff’s professional development and learning on ESR. This data should therefore be available for reporting in April 2016.
Nothing further to report on data until CCG workforce data is scrutinised annually at 1 April 2016.
SUMMARY OF RISKS RELATING TO THE PROPOSALHighlight any implications, including finance, quality, reputation, governance, strategic workforce, clinical, medicines optimisation, equality related or other CCGs are continuing to develop different ways of trying to involve protected group reps to provide regular feedback re any adverse impacts arising from healthcare changes being considered by CCG. Our larger provider partners are also required to submit their evidence of compliance for EDS annual public grading of equality evidence by local communities of interest representatives (not an internal grading of evidence) by 31 March 2016, as well as their WRES reporting and findings from workforce data for ethnicity by 1 July 2015. An annual website display of compliance information has been carried out in September and November with our larger (public sector) providers now displaying as a result, improved PSED compliance information on their websites. Cheryl Hardisty is looking at contract managers pursuing via cyclical contract meetings any significant gaps in timely data display for compliance which supports the wider requirements of the Public Sector Equality Duty. If any of our larger providers (including private sector) are not seen to be compliant, then the lead CCG is also not compliant in this area of meeting the PSED. EDS and WRES were mandated by NHS England from April 2015 as one means of evidencing how a commissioner and provider organisation is meeting the PSED. ANY STATUTORY / REGULATORY / LEGAL / NHS CONSTITUTION/ASSURANCE / GOVERNANCE / PRESCRIBING IMPLICATIONS Public Sector Equality Duty Equality Act Human Rights Act QUALITY IMPACT ASSESSMENT AND/OR EQUALITY IMPACT ASSESSMENT Date completed, please highlight any direct or indirect implications N/A ANY RELATED WORK WITH STAKEHOLDERS/PRACTICES/PUBLIC AND PATIENT ENGAGEMENTProvide further information, including dates if applicable N/A
ACRONYMS If not listed in the report, please list EDS Equality Delivery System WRES Workplace Race Equality Standard

EDS grading report for North Staffs CCG and Stoke on Trent CCG 27 October 2015 first joint annual public grading event 1
Appendix 2
EDS Joint Annual Public Grading Attendance Record 27 October 2015 (North Staffs CCG & Stoke on Trent CCG)
Executive Summary
Contents
1. EDS Executive Summary Report including ‘lessons learnt’ and ‘EDS Action Planning’
2. EDS detailed report 27 October 2015 public grading event
3. List of EDS Stakeholders and CCG staff / clinicians attending public grading event
4. Summary overview of commissioning evidence focus for Goal 1 & Goal 4
5. Reminder that all 2015 equality performance evidence is displayed on both CCG EDS webpages
6. Grading awarded / Detailed comments and feedback from EDS stakeholders by Goals 1 & 4 and for each required Outcome
7. Any additional comments / feedback received
Appendix 1: Evaluation Summary of EDS grading event
Evaluation comments received
Appendix 2: Embedded documents
What is commissioning in a CCG? (presentation)
EDS stakeholder training in how to carry out an EDS public grading of CCG evidence (presentation)
EDS grader notes template
EDS evaluation form template
EDS equality monitoring form template

EDS grading report for North Staffs CCG and Stoke on Trent CCG 27 October 2015 first joint annual public grading event 2
PSED requirement – giving ‘due regard’ to protected groups according to the Brown Principles (EHRC 2012).
EDS Executive Summary Report 27 October 2015 annual grading event North Staffs and Stoke on Trent CCGs
Nine EDS stakeholders and thirteen staff from both CCGs attended the first joint EDS annual public grading event. Stakeholders were invited to
attend as volunteer trained critical friends to support CCGs in identifying improvements and good outcomes specifically for people from
protected characteristic groups. Stakeholders received a capacity building session with ‘questions and answers’ (‘What is commissioning in a
CCG?’) and training re (‘How to carry out an EDS public grading of evidence’) on the day. This was to evaluate evidence presented by CCG
staff on their equality performance and learning journey during 2014, and 2015 to date, with next steps included. Senior staff presented
summary evidence for each required Outcome. Senior Clinicians attended to provide answers at each Q&A session with stakeholders.
Summary evidence and key documents were displayed publicly on both CCG EDS webpages 7 days before the grading. Stakeholders were
provided with this information and were encouraged to view available evidence in advance of the grading event.
EDS (Equality Delivery System v2) equality performance framework has been mandated by NHS England for all CCGs and their larger provider
partners from April 2015. Evidence is required to be transparently presented to a representative spread of local protected group volunteer
stakeholders on ‘how do local people from protected groups fare compared to people overall [in healthcare]?’ This means CCG gathering
specific evidence on the healthcare experience of local people from groups protected by the Equality Act 2010. For CCGs this information is
accessed through patient experience feedback at engagement opportunities with local communities of interest. Evidence can also be provided
through discussions around evidencing taking ‘due regard’ at Board meetings; which protected groups were targeted for their feedback on key
healthcare changes under consideration; patient experience stories; good outcomes for protected groups e.g. where CCG mitigate following
feedback to make services more inclusive and with fair access to local people from protected groups (fair access to information, services,
premises, and any employment / training opportunities).
Goal 1 (Better health outcomes): This year evidence focused mainly on joint commissioning work between both CCGs i.e. specific priority care
pathways i.e. Long term conditions; Frail complex care; Neuro-community services; Hearing Aid service review (NSCCG); Dementia Strategy
(SOTCCG); Transforming Cancer / End of life care; Datix – GP concerns reporting re providers / Complaints and PALs monitoring.
Goal 4 (Inclusive leadership at all levels). This year evidence focused on senior level planning and decision making processes including
support to Governing Board / Body re recognising and managing equality related business risk to support assurances for risk and inclusive
ways of working.

EDS grading report for North Staffs CCG and Stoke on Trent CCG 27 October 2015 first joint annual public grading event 3
The grading of evidence was as follows:
EDS Goal Required Outcome
Grading % Numbers Underdeveloped Developing Achieving Excelling
1 1.1 75% 6/8 √
1 1.2 75% 6/8+ √
1 1.3 50%+ 4/8+ √
1 1.4 63%+ 5/8+ √
4 4.1 63%+ 5/8+ √
4 4.2 88%+ 7/8+ √
4 4.3 75%+ 6/8+ √
Note: 1 EDS stakeholder was not present throughout the entire grading event.
Key recommendations to CCG:
CCGs will develop an EDS action plan from recommendations and lessons learnt to bring in improvements over the next 12 months.
1. Transgender care and health inequalities – GPs are still not treating Gender Reassignment patients fairly / correctly re healthcare /
support needs and accessing services. There are too many GPs who do not know enough about gender reassignment. Therefore
maybe have some specialised GPs who have that expertise.
2. Spread the EDS based learning in terms of all 9 protected groups.
Really good work and maybe doing a disservice in not measuring all the groups, would like to know who we are getting feedback
from at engagement events.
Fail to see how all the protected groups are being included and how do we demonstrate we are reaching those groups? Need to
monitor who is feedback back / attending engagement events and by other means. Also which protected groups and how are CCG
targeting for their feedback?
Neuro community services feedback 3. Ensuring this model (Outcome 1.2) is translated further across all commissioned services. Evidence from Neurological Alliance deserves a green / purple grading for showing inclusion, BUT …. Does this apply to all other areas
of clinical service commissioning? Re-assured by Dave Sanzeri’s assurance re all other LTCs and patient involvement from protected
groups.

EDS grading report for North Staffs CCG and Stoke on Trent CCG 27 October 2015 first joint annual public grading event 4
Outcome 1.2: For commissioners to persist in ensuring patient led specification development is transacted and that work with providers
is on-going to make this happen.
1.2: Again some really good engagement happening – but little mention again of any other than the ‘obvious’ protected groups – need
to measure the other protected groups i.e. what extent they were represented in the engagement?
1.2: You do all the engagement and come up with a solution but it comes across as though nothing has changed – this needs to be
addressed.
1.2: Really good work and maybe doing a disservice in not measuring all the groups, would like to know who we are getting feedback
from at engagement events.
1.2: Fail to see how all the protected groups are being included and how do we demonstrate we are reaching those groups? Also
ensuring this engagement model with protected groups is translated across all commissioned services.
1.2: Bridges between health and social care and housing – this is crucial to people’s health and wellbeing such as accommodation with
the right kind of support attached to it.
4. Build more sustainable bridges between health and social care and housing – think broadly around things that are crucial to people’s
health such as accommodation with the right kind of support attached to it (integration of health, social care and housing / support).
Hearing Aid service review & Dementia Strategy (1.3 Outcome) 5. Hearing Aids service: Ensure evidence presented reflects the required Outcome. (That in future evidence of one service to another
rather than as evolving or engagement service is considered. Also, that this particular required Outcome and what it is asking to measure, is clarified.) Clarify what the EDS required Outcome is asking us to measure, some good examples but needs translating into what we need to
do or a set of ‘inclusive ways of working’ principles
Relook at the evidence that has been presented, examples weren’t particularly clear re linking to required Outcome.
Definitions of transitions needs to be explained a bit better in particular hearing aids, and dementia strategy.
6. Look at the media and the public will claim to be unaware of the changes, we need to carry on informing the public of what we are
doing.
Generic recommendations continued
7. Need appropriate audit trail: Equality monitoring and patient satisfaction option to declare by protected groups is required to be
provided routinely - as an ‘option to declare’, when seeking feedback at engagement events or on line.
Ensure protected characteristics of engaged individual are recorded, so that this can inform engagement activity and consideration
going forward.
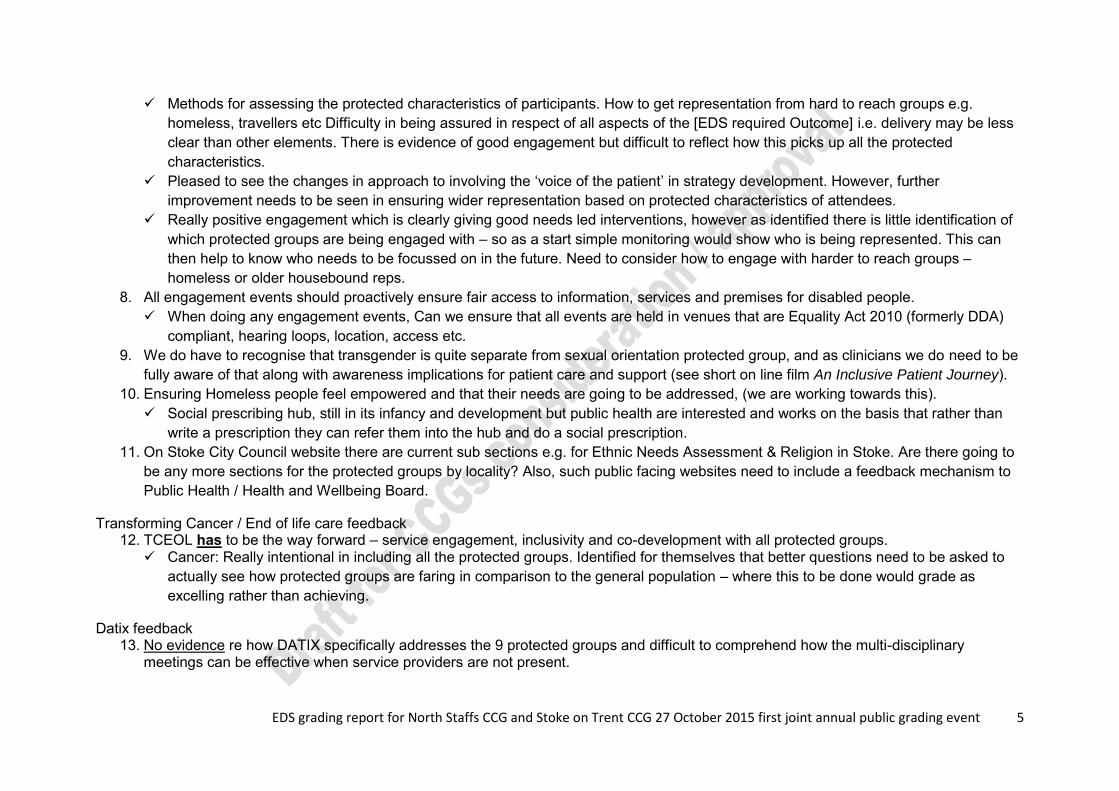
EDS grading report for North Staffs CCG and Stoke on Trent CCG 27 October 2015 first joint annual public grading event 5
Methods for assessing the protected characteristics of participants. How to get representation from hard to reach groups e.g.
homeless, travellers etc Difficulty in being assured in respect of all aspects of the [EDS required Outcome] i.e. delivery may be less
clear than other elements. There is evidence of good engagement but difficult to reflect how this picks up all the protected
characteristics.
Pleased to see the changes in approach to involving the ‘voice of the patient’ in strategy development. However, further
improvement needs to be seen in ensuring wider representation based on protected characteristics of attendees.
Really positive engagement which is clearly giving good needs led interventions, however as identified there is little identification of
which protected groups are being engaged with – so as a start simple monitoring would show who is being represented. This can
then help to know who needs to be focussed on in the future. Need to consider how to engage with harder to reach groups –
homeless or older housebound reps.
8. All engagement events should proactively ensure fair access to information, services and premises for disabled people.
When doing any engagement events, Can we ensure that all events are held in venues that are Equality Act 2010 (formerly DDA)
compliant, hearing loops, location, access etc.
9. We do have to recognise that transgender is quite separate from sexual orientation protected group, and as clinicians we do need to be
fully aware of that along with awareness implications for patient care and support (see short on line film An Inclusive Patient Journey).
10. Ensuring Homeless people feel empowered and that their needs are going to be addressed, (we are working towards this).
Social prescribing hub, still in its infancy and development but public health are interested and works on the basis that rather than
write a prescription they can refer them into the hub and do a social prescription.
11. On Stoke City Council website there are current sub sections e.g. for Ethnic Needs Assessment & Religion in Stoke. Are there going to
be any more sections for the protected groups by locality? Also, such public facing websites need to include a feedback mechanism to
Public Health / Health and Wellbeing Board.
Transforming Cancer / End of life care feedback 12. TCEOL has to be the way forward – service engagement, inclusivity and co-development with all protected groups.
Cancer: Really intentional in including all the protected groups. Identified for themselves that better questions need to be asked to
actually see how protected groups are faring in comparison to the general population – where this to be done would grade as
excelling rather than achieving.
Datix feedback 13. No evidence re how DATIX specifically addresses the 9 protected groups and difficult to comprehend how the multi-disciplinary
meetings can be effective when service providers are not present.

EDS grading report for North Staffs CCG and Stoke on Trent CCG 27 October 2015 first joint annual public grading event 6
Datix Complaints & PALS: opportunity lost within review process to consider against the protected groups not just the individual
complainant.
Datix: How joined up are the systems? If it is identified through these systems that one of the protected groups is particularly
suffering would that feed into more engagement with that group within whichever area it is?
Goal 4 feedback 14. 4.1: Seems that much is being done to ensure compliance with EDS v2, but it is difficult to ascertain just how far it is really embedded,
and not just through a 4 Goal requirement. Need to have tangible evidence. Sounds good. Too many anachronisms. 15. 4.2: Evidencing good outcomes for protected groups: You said. We listened. We did. – need to know more on how do senior decision
makers show this?
16. 4.2: Recognise CCGs are on a learning journey and the need for more work to ensure needs of protected groups represented clearly
within all Board / Senior Committee Papers.
Recognise more needs to be done. Good example of how CCG are obtaining information e.g. Equality Impact scrutiny and patient
story with You said. We listened. We did. - all discussed within Board Papers. Papers to get pushed back if more evidence [of CCG
taking due regard] needed.
4.2: Important to use voluntary sector / community groups to engage those who would not come to formal engagement meetings.
However, there is no substitute for feedback from local protected group reps themselves. Build frequent communication bridges to
gain more feedback. Show local communities how they can do this / a number of different ways. Keep it simple.
17. 4.3: Good examples of targeted training and Briefings for staff awareness raising. Proactive response to training needs of all staff is
evident. Recommendation: It would be good to include specific examples of where managers have translated training e.g. on
reasonable adjustments or the new Accessible Information Standard, into practice.
18. How do we approach recruitment around protected groups? This links with EDS Goal 3 in 2016 CCG evidence and evidence of fair
recruitment training for all recruiting managers / senior staff.

EDS grading report for North Staffs CCG and Stoke on Trent CCG 27 October 2015 first joint annual public grading event 7
Grading Underdeveloped Developing Achieving Excelling
People from all protected groups fare poorly compared with people overall OR evidence is not available
People from only some (2 or less) protected groups fare as well as people overall
People from most (3 to 5) protected groups fare as well as people overall
People from all (9) protected groups fare as well as people overall
2 2 2
3
1
2
3
4
Outcome 1.1 Outcome 1.2 Outcome 1.3 Outcome 1.4
EDS Goal 1 Grading 2015: Developing / Achieving
EDS Goal 1 Grading 2015:Developing / Achieving
3 3 3
0
1
2
3
4
Outcome 4.1 Outcome 4.2 Outcome 4.3
EDS Goal 4 Grading 2015: Achieving
EDS Goal 4 Grading 2015:Achieving
EDS grading report for North Staffs CCG and Stoke on Trent CCG 27 October 2015 first joint annual public grading event 8
Lessons learnt:
1. Engagement with protected group representatives by locality, and gathering differential satisfaction levels of patient experience at
engagement events and by other means, are key areas of focus for the CCGs
2. Further development of the EDS stakeholder group and how this group could be encouraged to provide regular feedback to CCG
commissioners to be explored further
3. Contact BME group representatives in 2015, to provide opportunity for feedback to CCG on current EDS evidence
4. This was the 2 CCG’s first joint annual public grading event. It is important to ensure any evidence / improvements are evidenced as
equally embedded and led at a senior level, by each CCG
5. CCGs should consider what is becoming more frequent wider commissioning across Staffordshire and how assurances can be
achieved in terms of managing equality related business risk by all participating CCGs
6. Greater focus on JSNA and protected group sub groups.
7. Ensure CCG branding is displayed at engagement events where practical
8. EDS evidence to be gathered by end April 2016 and suggest next EDS annual public grading takes place end May 2016. Room
booking to be made as early as practical i.e. in 2015.
9. Consider which priority areas should be focused on to lead evidence collection by key staff
10. Senior staff presenting evidence to have an opportunity for a practice run before grading event takes place. 11. Add watermark to all pdf evidence documents on website – both CCG names – show who owns the documents. 12. EDS should be led by senior clinicians and other senior CCG lead staff. 13. Suggest monthly review and quality check of evidence gathered for next public grading event. 14. CCGs should continue to annually track the EDS performance of our larger provider partners, as a means of continuing to give
assurances of their own contract monitoring performance. This includes annual public grading event, as well as the quality / robustness of their EDS evidence provided for public scrutiny
15. Less abbreviations / Plain English / early proof read of all documents used.

Appendix 1
EDS Annual Public Grading Dashboard Oct 2015 North Staffs CCG and Stoke on Trent CCG (first joint grading of equality performance evidence)
‘How do patients from protected groups fare compared to people overall [in healthcare]?’
Grading level key: Underdeveloped Developing Achieving Excelling
Goal 1: Better health outcomes (2015-16) Grading Goal 2: Improved patient access and experience (2016-17) Grading
1.1 Services are commissioned, procured, designed and delivered to meet the health needs of local communities
2.1 People, carers and communities can readily access hospital, community health or primary care services and should not be denied access on unreasonable grounds
1.2 Individual people’s health needs are assessed and met in appropriate and effective ways
2.2 People are informed and supported to be as involved as they wish to be in decisions about their care
1.3 Transitions from one service to another, for people on care pathways, are made smoothly with everyone well-informed
2.3 People report positive experiences of the NHS
1.4 When people use NHS services their safety is prioritised and they are free from mistakes, mistreatment and abuse
2.4 People’s complaints about services are handled respectfully and efficiently
Goal 3: A representative and supported workforce (2017-18) Grading Goal 4: Inclusive leadership at all levels (2015-16) Grading
3.1 Fair NHS recruitment and selection processes lead to a more representative workforce at all levels
4.1 Boards and senior leaders routinely demonstrate their commitment to promoting equality within and beyond their organisations
3.2 The NHS is committed to equal pay for work of equal value and expects employers to use equal pay audits to help fulfil their legal obligations
4.2 Papers that come before the Board and other major Committees identify equality-related impacts including risks, and say how these risks are managed
3.3 Training and development opportunities are taken up and positively evaluated by all staff
4.3 Middle managers and other line managers support their staff to work in culturally competent ways within a work environment free from discrimination
3.4 When at work, staff are free from abuse, harassment, bullying and violence from any source
3.5 Flexible working options are available to all staff consistent with the needs of the service and the way people lead their lives

Grading Underdeveloped Developing Achieving Excelling
People from all protected groups fare poorly compared with people overall OR evidence is not available
People from only some (2 or less) protected groups fare as well as people overall
People from most (3 to 5) protected groups fare as well as people overall
People from all (9) protected groups fare as well as people overall
Who are groups protected under the Equality Act 2010?
3.6 Staff report positive experiences of their membership of the workforce

Equality Delivery System for the NHS EDS2 Summary ReportImplementation of the Equality Delivery System – EDS2 is a requirement on both NHS commissioners and NHS providers. Organisations are encouraged to follow the implementation of EDS2 in accordance with the ‘9 Steps for EDS2 Implementation’ as outlined in the 2013 EDS2 guidance document. The document can be found at: http://www.england.nhs.uk/wp-content/uploads/2013/11/eds-nov131.pdf
This EDS2 Summary Report is designed to give an overview of the organisation’s most recent EDS2 implementation. It is recommended that once completed, this Summary Report is published on the organisation’s website.
Headline good practice examples of EDS2 outcomes (for patients/community/workforce):
Level of stakeholder involvement in EDS2 grading and subsequent actions:
Organisation’s EDS2 lead (name/email):
Organisation’s Board lead for EDS2:
NHS organisation name: Organisation’s Equality Objectives (including duration period):
Publication Gateway Reference Number: 03247
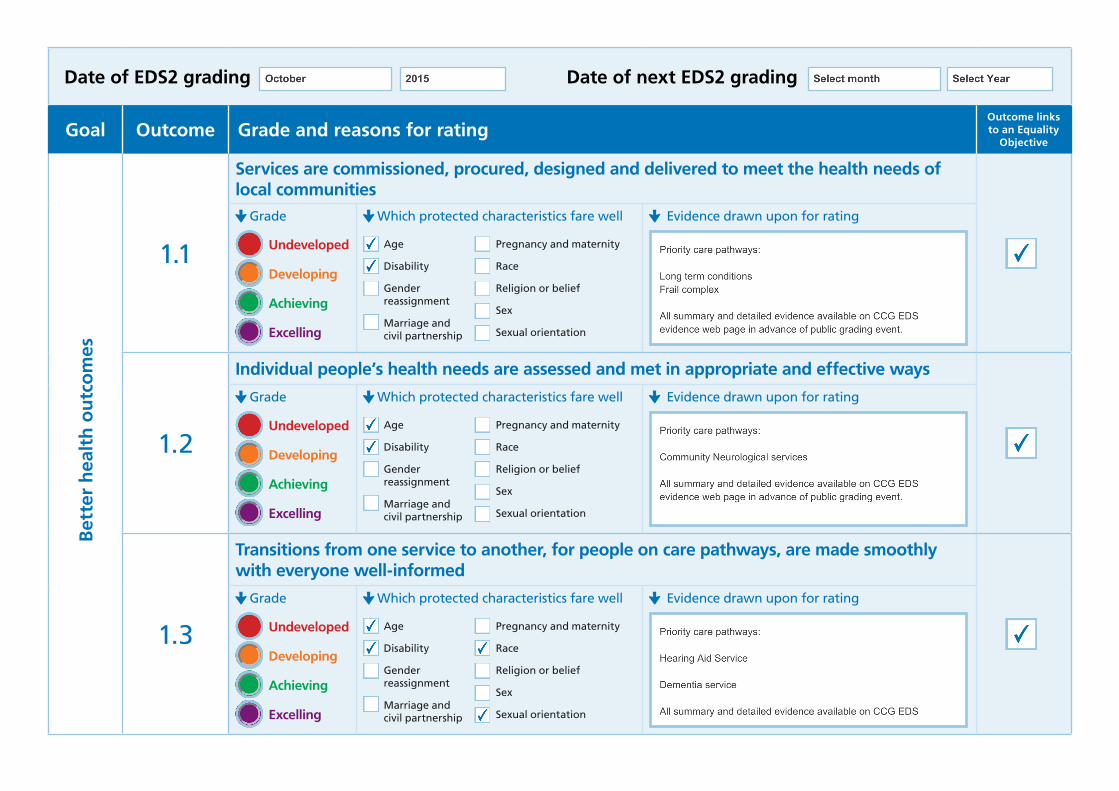
Date of EDS2 grading Date of next EDS2 grading
Goal Outcome Grade and reasons for ratingOutcome links to an Equality
Objective
Bet
ter
hea
lth
ou
tco
mes
1.1
Services are commissioned, procured, designed and delivered to meet the health needs of local communities
Grade
Undeveloped
Developing
Achieving
Excelling
Which protected characteristics fare well
Age
Disability
Gender reassignment
Marriage and civil partnership
Pregnancy and maternity
Race
Religion or belief
Sex
Sexual orientation
Evidence drawn upon for rating
1.2
Individual people’s health needs are assessed and met in appropriate and effective ways Grade
Undeveloped
Developing
Achieving
Excelling
Which protected characteristics fare well
Age
Disability
Gender reassignment
Marriage and civil partnership
Pregnancy and maternity
Race
Religion or belief
Sex
Sexual orientation
Evidence drawn upon for rating
1.3
Transitions from one service to another, for people on care pathways, are made smoothly with everyone well-informed
Grade
Undeveloped
Developing
Achieving
Excelling
Which protected characteristics fare well
Age
Disability
Gender reassignment
Marriage and civil partnership
Pregnancy and maternity
Race
Religion or belief
Sex
Sexual orientation
Evidence drawn upon for rating

Goal Outcome Grade and reasons for ratingOutcome links to an Equality
ObjectiveB
ette
r h
ealt
h o
utc
om
es, c
on
tin
ued
1.4
When people use NHS services their safety is prioritised and they are free from mistakes, mistreatment and abuse
Grade
Undeveloped
Developing
Achieving
Excelling
Which protected characteristics fare well
Age
Disability
Gender reassignment
Marriage and civil partnership
Pregnancy and maternity
Race
Religion or belief
Sex
Sexual orientation
Evidence drawn upon for rating
1.5
Screening, vaccination and other health promotion services reach and benefit all local communities
Grade
Undeveloped
Developing
Achieving
Excelling
Which protected characteristics fare well
Age
Disability
Gender reassignment
Marriage and civil partnership
Pregnancy and maternity
Race
Religion or belief
Sex
Sexual orientation
Evidence drawn upon for rating
Imp
rove
d
pat
ien
t ac
cess
an
d e
xper
ien
ce
2.1
People, carers and communities can readily access hospital, community health or primary care services and should not be denied access on unreasonable grounds
Grade
Undeveloped
Developing
Achieving
Excelling
Which protected characteristics fare well
Age
Disability
Gender reassignment
Marriage and civil partnership
Pregnancy and maternity
Race
Religion or belief
Sex
Sexual orientation
Evidence drawn upon for rating

Goal Outcome Grade and reasons for ratingOutcome links to an Equality
ObjectiveIm
pro
ved
pat
ien
t ac
cess
an
d e
xper
ien
ce 2.2
People are informed and supported to be as involved as they wish to be in decisions about their care
Grade
Undeveloped
Developing
Achieving
Excelling
Which protected characteristics fare well
Age
Disability
Gender reassignment
Marriage and civil partnership
Pregnancy and maternity
Race
Religion or belief
Sex
Sexual orientation
Evidence drawn upon for rating
2.3
People report positive experiences of the NHS Grade
Undeveloped
Developing
Achieving
Excelling
Which protected characteristics fare well
Age
Disability
Gender reassignment
Marriage and civil partnership
Pregnancy and maternity
Race
Religion or belief
Sex
Sexual orientation
Evidence drawn upon for rating
2.4
People’s complaints about services are handled respectfully and efficiently Grade
Undeveloped
Developing
Achieving
Excelling
Which protected characteristics fare well
Age
Disability
Gender reassignment
Marriage and civil partnership
Pregnancy and maternity
Race
Religion or belief
Sex
Sexual orientation
Evidence drawn upon for rating

Goal Outcome Grade and reasons for ratingOutcome links to an Equality
ObjectiveA
rep
rese
nta
tive
an
d s
up
po
rted
wo
rkfo
rce 3.1
Fair NHS recruitment and selection processes lead to a more representative workforce at all levels
Grade
Undeveloped
Developing
Achieving
Excelling
Which protected characteristics fare well
Age
Disability
Gender reassignment
Marriage and civil partnership
Pregnancy and maternity
Race
Religion or belief
Sex
Sexual orientation
Evidence drawn upon for rating
3.2
The NHS is committed to equal pay for work of equal value and expects employers to use equal pay audits to help fulfil their legal obligations
Grade
Undeveloped
Developing
Achieving
Excelling
Which protected characteristics fare well
Age
Disability
Gender reassignment
Marriage and civil partnership
Pregnancy and maternity
Race
Religion or belief
Sex
Sexual orientation
Evidence drawn upon for rating
3.3
Training and development opportunities are taken up and positively evaluated by all staff Grade
Undeveloped
Developing
Achieving
Excelling
Which protected characteristics fare well
Age
Disability
Gender reassignment
Marriage and civil partnership
Pregnancy and maternity
Race
Religion or belief
Sex
Sexual orientation
Evidence drawn upon for rating

Goal Outcome Grade and reasons for ratingOutcome links to an Equality
ObjectiveA
rep
rese
nta
tive
an
d s
up
po
rted
wo
rkfo
rce 3.4
When at work, staff are free from abuse, harassment, bullying and violence from any source Grade
Undeveloped
Developing
Achieving
Excelling
Which protected characteristics fare well
Age
Disability
Gender reassignment
Marriage and civil partnership
Pregnancy and maternity
Race
Religion or belief
Sex
Sexual orientation
Evidence drawn upon for rating
3.5
Flexible working options are available to all staff consistent with the needs of the service and the way people lead their lives
Grade
Undeveloped
Developing
Achieving
Excelling
Which protected characteristics fare well
Age
Disability
Gender reassignment
Marriage and civil partnership
Pregnancy and maternity
Race
Religion or belief
Sex
Sexual orientation
Evidence drawn upon for rating
3.6
Staff report positive experiences of their membership of the workforce Grade
Undeveloped
Developing
Achieving
Excelling
Which protected characteristics fare well
Age
Disability
Gender reassignment
Marriage and civil partnership
Pregnancy and maternity
Race
Religion or belief
Sex
Sexual orientation
Evidence drawn upon for rating
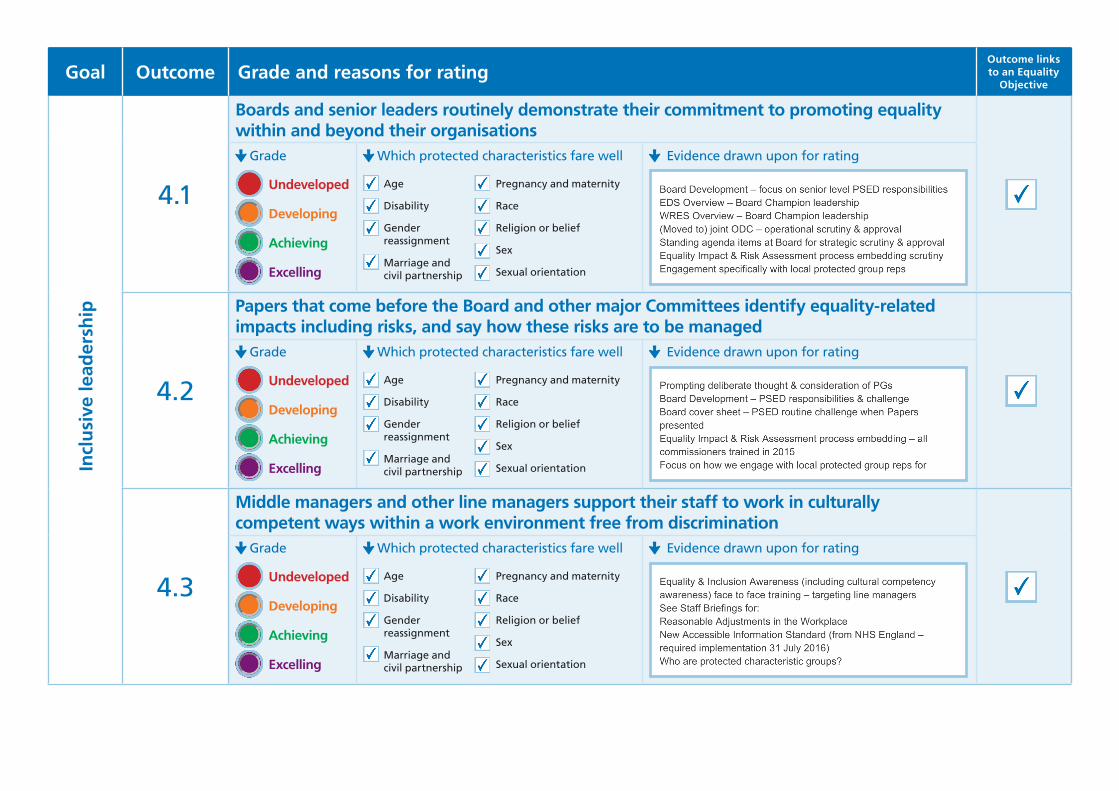
Goal Outcome Grade and reasons for ratingOutcome links to an Equality
ObjectiveIn
clu
sive
lead
ersh
ip
4.1
Boards and senior leaders routinely demonstrate their commitment to promoting equality within and beyond their organisations
Grade
Undeveloped
Developing
Achieving
Excelling
Which protected characteristics fare well
Age
Disability
Gender reassignment
Marriage and civil partnership
Pregnancy and maternity
Race
Religion or belief
Sex
Sexual orientation
Evidence drawn upon for rating
4.2
Papers that come before the Board and other major Committees identify equality-related impacts including risks, and say how these risks are to be managed
Grade
Undeveloped
Developing
Achieving
Excelling
Which protected characteristics fare well
Age
Disability
Gender reassignment
Marriage and civil partnership
Pregnancy and maternity
Race
Religion or belief
Sex
Sexual orientation
Evidence drawn upon for rating
4.3
Middle managers and other line managers support their staff to work in culturally competent ways within a work environment free from discrimination
Grade
Undeveloped
Developing
Achieving
Excelling
Which protected characteristics fare well
Age
Disability
Gender reassignment
Marriage and civil partnership
Pregnancy and maternity
Race
Religion or belief
Sex
Sexual orientation
Evidence drawn upon for rating

Date of report: month/year
Template for completion
Name of provider organisation
Name and title of Board lead for the Workforce Race Equality Standard
Name and contact details of lead manager compiling this report
Names of commissioners this report has been sent to
Name and contact details of co-ordinating commissioner this report has been sent to
Unique URL link on which this report will be found (to be added after submission)
This report has been signed off by on behalf of the Board on (insert name and date)
Publications Gateway Reference Number: 03496
Workforce Race Equality StandardREPORTING TEMPLATE

Report on the WRES indicators
1. Background narrative
2. Total numbers of staff
a. Any issues of completeness of data
a. Employed within this organisation at the date of the report
b. Any matters relating to reliability of comparisons with previous years
b. Proportion of BME staff employed within this organisation at the date of the report

Report on the WRES indicators, continued
4. Workforce dataa. What period does the organisation’s workforce data refer to?
3. Self reportinga. The proportion of total staff who have self–reported their ethnicity
b. Have any steps been taken in the last reporting period to improve the level of self-reporting by ethnicity
c. Are any steps planned during the current reporting period to improve the level of self reporting by ethnicity

Report on the WRES indicators, continued
5. Workforce Race Equality IndicatorsFor ease of analysis, as a guide we suggest a maximum of 150 words per indicator.
Indicator Data for reporting year
Data for previous year
Narrative – the implications of the data and any additional background explanatory narrative
Action taken and planned including e.g. does the indicator link to EDS2 evidence and/or a corporate Equality Objective
For each of these four workforce indicators, the Standard compares the metrics for White and BME staff.
1 Percentage of BME staff in Bands 8-9, VSM (including executive Board members and senior medical staff) compared with the percentage of BME staff in the overall workforce
2 Relative likelihood of BME staff being appointed from shortlisting compared to that of White staff being appointed from shortlisting across all posts.
3 Relative likelihood of BME staff entering the formal disciplinary process, compared to that of White staff entering the formal disciplinary process, as measured by entry into a formal disciplinary investigation* *Note: this indicator will be based on data from a two year rolling average of the current year and the previous year.
4 Relative likelihood of BME staff accessing non-mandatory training and CPD as compared to White staff

Report on the WRES indicators, continued
Indicator Data for reporting year
Data for previous year
Narrative – the implications of the data and any additional background explanatory narrative
Action taken and planned including e.g. does the indicator link to EDS2 evidence and/or a corporate Equality Objective
For each of these four staff survey indicators, the Standard compares the metrics for each survey question response for White and BME staff.
5 KF 18. Percentage of staff experiencing harassment, bullying or abuse from patients, relatives or the public in last 12 months
White
BME
White
BME
6 KF 19. Percentage of staff experiencing harassment, bullying or abuse from staff in last 12 months
White
BME
White
BME
7 KF 27. Percentage believing that trust provides equal opportunities for career progression or promotion
White
BME
White
BME
8 Q23. In the last 12 months have you personally experienced discrimination at work from any of the following? b) Manager/team leader or other colleagues
White
BME
White
BME
Does the Board meet the requirement on Board membership in 9?
9 Boards are expected to be broadly representative of the population they serve
Note 1. All provider organisations to whom the NHS Standard Contract applies are required to conduct staff surveys though those surveys for organisations that are not NHS Trusts may not follow the format of the NHS Staff Survey
Note 2. Please refer to the Technical Guidance for clarification on the precise means of each indicator.

Report on the WRES indicators, continued
7. If the organisation has a more detailed Plan agreed by its Board for addressing these and related issues you are asked to attach it or provide a link to it. Such a plan would normally elaborate on the steps summarised in section 5 above setting out the next steps with milestones for expected progress against the metrics. It may also identify the links with other work streams agreed at Board level such as EDS2.
6. Are there any other factors or data which should be taken into consideration in assessing progress? Please bear in mind any such information, action taken and planned may be subject to scrutiny by the Co-ordinating Commissioner or by regulators when inspecting against the “well led domain.”
Produced by NHS England, May 2015

ENCLOSURE: 9
AUTHOR
REPORTING OFFICER /DIRECTOR
Name Julia Allen Name Marcus Warnes Title Equality & Inclusion Business Partner Title Accountable Officer
REPORT TO Governing Board
TITLE OF REPORT Equality & Inclusion: Annual E&I Publication (Jan 2016) DATE OF THE MEETING 6 January 2016
WHAT OTHER CCG COMMITTEE/GROUP/INDIVIDUALHASCONSIDERED THIS REPORT?
COMMITTEE/GROUP Record which committee/group have already seen this report, note date and comments (if applicable) Joint ODC 17/11/15
INDIVIDUALPlease indicate name of individual and date agreed/approved (as necessary), for example HR, Finance, Quality, Medicines Optimisation or other
ACTION REQUIRED FROM COMMITTEE/GROUP/ GOVERNING BOARD (please identify all applicable and provide details below)
Approve Y Assurance Y Discussion
For noting Y
RECOMMENDATIONS The Governing Board is asked to:
Ratify the Annual Equality and Inclusion Publication following review by the Joint ODC and note this will be made publicly available on the CCG website by 31 January 2016. Appendix 1.
Note that Equality and Inclusion is delegated to the Joint ODC who review and monitor progress on a regular basis and report to Governing Board as appropriate.
Note that Equality Impact & Risks Assessments (EI&RA) are a primary source for demonstrating how CCG have considered legal duties under the Human Rights Act 1998, The Equality Act 2010 and the Public Sector Equality Duty 2011 – for employment and service delivery issues.
STRATEGIC GOALS SUPPORTED BY THIS PAPER (identify appropriate goals) YES NO1. Increase life expectancy and reduce inequality
Yes
2. Improve prevention, early detection and effective management of those at increased risk
Yes
3. Enhance quality of life and improve health outcomes for people with LTCs
Yes
4. Ensure people receive the right care in the right place
PURPOSE OF THE REPORT, KEY POINTS, EXECUTIVE SUMMARY(supporting information to be included, if applicable)

Attached is the CCG’s Annual Equality and Inclusion Publication which was reviewed by the Joint Organisational Development Committee at its meeting in November 2015. The Committee approved the report and agreed to recommend that the Governing Board ratify the document for publication. The report will be made publicly available on the CCG website by 31 January 2016. (Appendix 1) In summary:- The specific equality duties require CCGs to:
Publish information to show their compliance with the Equality Duty at least annually; and Set and publish Equality Objectives at least once every 4 years.
All information must be published in a way that makes it easy for people to access it. The Annual Equality and Inclusion Publication (January 2016) sets out North Staffordshire CCG’s evidence of how we are meeting these legal compliance requirements. Information we publish must show that CCG had ‘due regard’ to the 3 aims of the public sector Equality Duty (PSED):
1. Eliminate unlawful discrimination, harassment and victimisation 2. Advance equality of opportunity between different groups 3. Foster good relations between different groups.
Additionally, through the adoption of the NHS Equality Delivery System equality performance framework and Equality Impact and Risk Assessment process the CCG aims to demonstrate to the people we serve how we are meeting the three aims of the Equality Duty. CCG have drafted 3 new Equality Objectives (as part of a draft new Equality and Inclusion Strategy 2015 to 2017) and these will be issued in early 2016 (electronic engagement) for feedback from representatives of local communities of interest / protected characteristic groups. The general equality duty covers the following characteristics protected by the Equality Act 2010: age (including children and young people), disability, gender reassignment, pregnancy and maternity, race, religion or belief, gender, and sexual orientation. Gender reassignment includes people who are considering, undergoing or have undergone gender reassignment. Public bodies like CCGs also need to have due regard to the need to eliminate unlawful discrimination against someone because of their marriage or civil partnership status. This means that the first aim of the general equality duty applies to this characteristic but the other two aims do not. This applies only in relation to work, not to any other part of the Equality Act 2010. Equality Impact & Risk Assessments (EI&RA) Equality Impact & Risks Assessments (EI&RA) are a primary source for demonstrating how the CCG have considered legal duties under the Human Rights Act 1998, The Equality Act 2010 and the Public Sector Equality Duty 2011 – for employment and service delivery issues.
They evaluate the likely impact in a given scenario on people with a protected characteristic to ensure that employment practices and service provision do not discriminate and promote equality of opportunity. They provide an evidence trail from inception to decision making should an organisation be legally challenged or for Freedom of Information requests
Whilst they are not a means for ensuring or delivering legal compliance they are a receptacle for capturing all the considerations made and evidence during key activities such as;
Policy Development and Review Budget planning and allocation Service planning, review and re design Projects and work programmes Commissioning and procurement.
EI&RA process should capture evidence of CCG meeting the requirements of both the Brown Principles (‘due regard’ - deliberate consideration of protected groups in all we do), and the Gunning Principles (for engagement) – see Appendix 2 for details of the 4 Gunning Principles.
SUMMARY OF RISKS RELATING TO THE PROPOSALHighlight any implications, including finance, quality, reputation, governance, strategic workforce, clinical, medicines optimisation, equality related or other CCGs are continuing to develop different ways of trying to specifically involve protected group reps to provide regular early stage feedback re any adverse impacts arising from healthcare changes being considered by CCG.

The Gunning Principles (for engagement) are shown in Appendix 2. ANY STATUTORY / REGULATORY / LEGAL / NHS CONSTITUTION/ASSURANCE / GOVERNANCE / PRESCRIBING IMPLICATIONS The public sector Equality Duty (section 149 of the Act) came into force on 5 April 2011. The Equality Duty applies to public bodies (CCGs) and others carrying out public functions on their behalf. It supports good decision making by ensuring public bodies consider how different people will be affected by their activities, helping them to deliver policies and services which are efficient and effective; accessible to all; and which meet people’s needs. The Equality Duty is supported by specific duties, set out in regulations which came into force on 10 September 2011. The specific duties require public bodies to publish relevant, proportionate information demonstrating their compliance with the Equality Duty; and to set themselves specific, measurable equality objectives. Publishing relevant information will make public bodies transparent about their decision making processes, and accountable to their patients / service users. It will give the public the information they need to hold public bodies accountable for their performance on equality. The Equality Delivery System (EDS v2) is the NHS wide equality performance framework. NHS England mandated the framework from April 2015. It provides a means of CCG (and their larger combined annual contract value provider public and private sector partners) evidencing how they are meeting the public sector equality duty – through their annual equality performance re how do local people from protected groups fare compared to people overall [in healthcare]? CCG annually agree priority care pathways as the focus of EDS evidence, which is then publicly evaluated by the EDS stakeholder group over a 4 year delivery cycle set by NHS England. QUALITY IMPACT ASSESSMENT AND/OR EQUALITY IMPACT ASSESSMENT Date completed, please highlight any direct or indirect implications N/A ANY RELATED WORK WITH STAKEHOLDERS/PRACTICES/PUBLIC AND PATIENT ENGAGEMENTProvide further information, including dates if applicable N/A
ACRONYMS If not listed in the report, please list None


EDS grading report for North Staffs CCG and Stoke on Trent CCG 27 October 2015 first joint annual public grading event 1
EDS Joint Annual Public Grading Attendance Record 27 October 2015 (North Staffs CCG & Stoke on Trent CCG)
Executive Summary
Contents
1. EDS Executive Summary Report including ‘lessons learnt’ and ‘EDS Action Planning’
2. EDS detailed report 27 October 2015 public grading event 3. List of EDS Stakeholders and CCG staff / clinicians attending public grading
event 4. Summary overview of commissioning evidence focus for Goal 1 & Goal 4 5. Reminder that all 2015 equality performance evidence is displayed on both
CCG EDS webpages 6. Grading awarded / Detailed comments and feedback from EDS stakeholders
by Goals 1 & 4 and for each required Outcome 7. Any additional comments / feedback received
Appendix 1: Evaluation Summary of EDS grading event
Evaluation comments received
Appendix 2: Embedded documents
What is commissioning in a CCG? (presentation) EDS stakeholder training in how to carry out an EDS public grading of CCG
evidence (presentation) EDS grader notes template EDS evaluation form template EDS equality monitoring form template PSED requirement – giving ‘due regard’ to protected groups according to the
Brown Principles (EHRC 2012).
EDS Executive Summary Report 27 October 2015 annual grading event North Staffs and Stoke on Trent CCGs
Nine EDS stakeholders and thirteen staff from both CCGs attended the first joint EDS annual public grading event. Stakeholders were invited to attend as volunteer trained critical friends to support CCGs in identifying improvements and good outcomes specifically for people from protected characteristic groups. Stakeholders received a capacity building session with ‘questions and answers’ (‘What is commissioning in a CCG?’) and training re (‘How to carry out an EDS public grading of evidence’) on the day. This was to evaluate evidence

EDS grading report for North Staffs CCG and Stoke on Trent CCG 27 October 2015 first joint annual public grading event 2
presented by CCG staff on their equality performance and learning journey during 2014, and 2015 to date, with next steps included. Senior staff presented summary evidence for each required Outcome. Senior Clinicians attended to provide answers at each Q&A session with stakeholders. Summary evidence and key documents were displayed publicly on both CCG EDS webpages 7 days before the grading. Stakeholders were provided with this information and were encouraged to view available evidence in advance of the grading event.
EDS (Equality Delivery System v2) equality performance framework has been mandated by NHS England for all CCGs and their larger provider partners from April 2015. Evidence is required to be transparently presented to a representative spread of local protected group volunteer stakeholders on ‘how do local people from protected groups fare compared to people overall [in healthcare]?’ This means CCG gathering specific evidence on the healthcare experience of local people from groups protected by the Equality Act 2010. For CCGs this information is accessed through patient experience feedback at engagement opportunities with local communities of interest. Evidence can also be provided through discussions around evidencing taking ‘due regard’ at Board meetings; which protected groups were targeted for their feedback on key healthcare changes under consideration; patient experience stories; good outcomes for protected groups e.g. where CCG mitigate following feedback to make services more inclusive and with fair access to local people from protected groups (fair access to information, services, premises, and any employment / training opportunities).
Goal 1 (Better health outcomes): This year evidence focused mainly on joint commissioning work between both CCGs i.e. specific priority care pathways i.e. Long term conditions; Frail complex care; Neuro-community services; Hearing Aid service review (NSCCG); Dementia Strategy (SOTCCG); Transforming Cancer / End of life care; Datix – GP concerns reporting re providers / Complaints and PALs monitoring.
Goal 4 (Inclusive leadership at all levels). This year evidence focused on senior level planning and decision making processes including support to Governing Board / Body re recognising and managing equality related business risk to support assurances for risk and inclusive ways of working.
The grading of evidence was as follows:
EDS Goal
Required Outcome
Grading %
Numbers
Underdeveloped
Developing
Achieving
Excelling
1 1.1 75% 6/8 √ 1 1.2 75% 6/8+ √ 1 1.3 50%+ 4/8+ √ 1 1.4 63%+ 5/8+ √
4 4.1 63%+ 5/8+ √ 4 4.2 88%+ 7/8+ √ 4 4.3 75%+ 6/8+ √
Note: 1 EDS stakeholder was not present throughout the entire grading event.
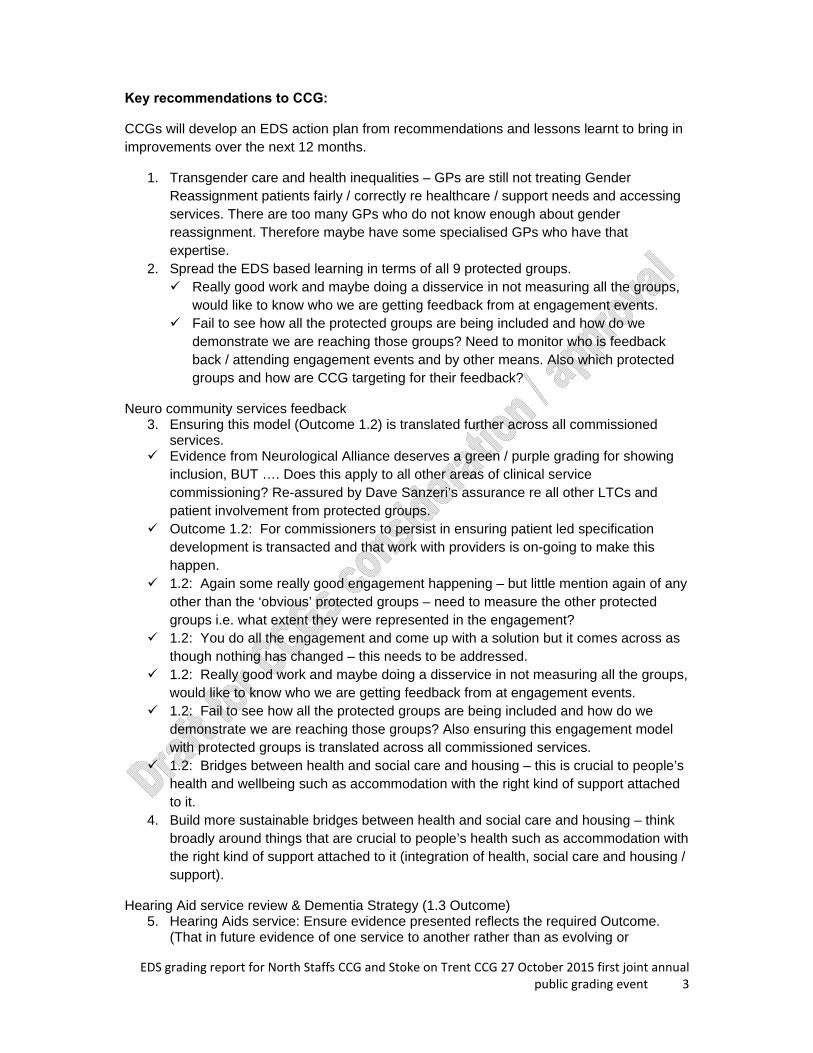
EDS grading report for North Staffs CCG and Stoke on Trent CCG 27 October 2015 first joint annual public grading event 3
Key recommendations to CCG:
CCGs will develop an EDS action plan from recommendations and lessons learnt to bring in improvements over the next 12 months.
1. Transgender care and health inequalities – GPs are still not treating Gender Reassignment patients fairly / correctly re healthcare / support needs and accessing services. There are too many GPs who do not know enough about gender reassignment. Therefore maybe have some specialised GPs who have that expertise.
2. Spread the EDS based learning in terms of all 9 protected groups. Really good work and maybe doing a disservice in not measuring all the groups,
would like to know who we are getting feedback from at engagement events. Fail to see how all the protected groups are being included and how do we
demonstrate we are reaching those groups? Need to monitor who is feedback back / attending engagement events and by other means. Also which protected groups and how are CCG targeting for their feedback?
Neuro community services feedback 3. Ensuring this model (Outcome 1.2) is translated further across all commissioned
services. Evidence from Neurological Alliance deserves a green / purple grading for showing
inclusion, BUT …. Does this apply to all other areas of clinical service commissioning? Re-assured by Dave Sanzeri’s assurance re all other LTCs and patient involvement from protected groups.
Outcome 1.2: For commissioners to persist in ensuring patient led specification development is transacted and that work with providers is on-going to make this happen.
1.2: Again some really good engagement happening – but little mention again of any other than the ‘obvious’ protected groups – need to measure the other protected groups i.e. what extent they were represented in the engagement?
1.2: You do all the engagement and come up with a solution but it comes across as though nothing has changed – this needs to be addressed.
1.2: Really good work and maybe doing a disservice in not measuring all the groups, would like to know who we are getting feedback from at engagement events.
1.2: Fail to see how all the protected groups are being included and how do we demonstrate we are reaching those groups? Also ensuring this engagement model with protected groups is translated across all commissioned services.
1.2: Bridges between health and social care and housing – this is crucial to people’s health and wellbeing such as accommodation with the right kind of support attached to it.
4. Build more sustainable bridges between health and social care and housing – think broadly around things that are crucial to people’s health such as accommodation with the right kind of support attached to it (integration of health, social care and housing / support).
Hearing Aid service review & Dementia Strategy (1.3 Outcome) 5. Hearing Aids service: Ensure evidence presented reflects the required Outcome.
(That in future evidence of one service to another rather than as evolving or

EDS grading report for North Staffs CCG and Stoke on Trent CCG 27 October 2015 first joint annual public grading event 4
engagement service is considered. Also, that this particular required Outcome and what it is asking to measure, is clarified.) Clarify what the EDS required Outcome is asking us to measure, some good
examples but needs translating into what we need to do or a set of ‘inclusive ways of working’ principles
Relook at the evidence that has been presented, examples weren’t particularly clear re linking to required Outcome.
Definitions of transitions needs to be explained a bit better in particular hearing aids, and dementia strategy.
6. Look at the media and the public will claim to be unaware of the changes, we need to carry on informing the public of what we are doing.
Generic recommendations continued
7. Need appropriate audit trail: Equality monitoring and patient satisfaction option to declare by protected groups is required to be provided routinely - as an ‘option to declare’, when seeking feedback at engagement events or on line. Ensure protected characteristics of engaged individual are recorded, so that this
can inform engagement activity and consideration going forward. Methods for assessing the protected characteristics of participants. How to get
representation from hard to reach groups e.g. homeless, travellers etc Difficulty in being assured in respect of all aspects of the [EDS required Outcome] i.e. delivery may be less clear than other elements. There is evidence of good engagement but difficult to reflect how this picks up all the protected characteristics.
Pleased to see the changes in approach to involving the ‘voice of the patient’ in strategy development. However, further improvement needs to be seen in ensuring wider representation based on protected characteristics of attendees.
Really positive engagement which is clearly giving good needs led interventions, however as identified there is little identification of which protected groups are being engaged with – so as a start simple monitoring would show who is being represented. This can then help to know who needs to be focussed on in the future. Need to consider how to engage with harder to reach groups – homeless or older housebound reps.
8. All engagement events should proactively ensure fair access to information, services and premises for disabled people. When doing any engagement events, Can we ensure that all events are held in
venues that are Equality Act 2010 (formerly DDA) compliant, hearing loops, location, access etc.
9. We do have to recognise that transgender is quite separate from sexual orientation protected group, and as clinicians we do need to be fully aware of that along with awareness implications for patient care and support (see short on line film An Inclusive Patient Journey).
10. Ensuring Homeless people feel empowered and that their needs are going to be addressed, (we are working towards this). Social prescribing hub, still in its infancy and development but public health are
interested and works on the basis that rather than write a prescription they can refer them into the hub and do a social prescription.
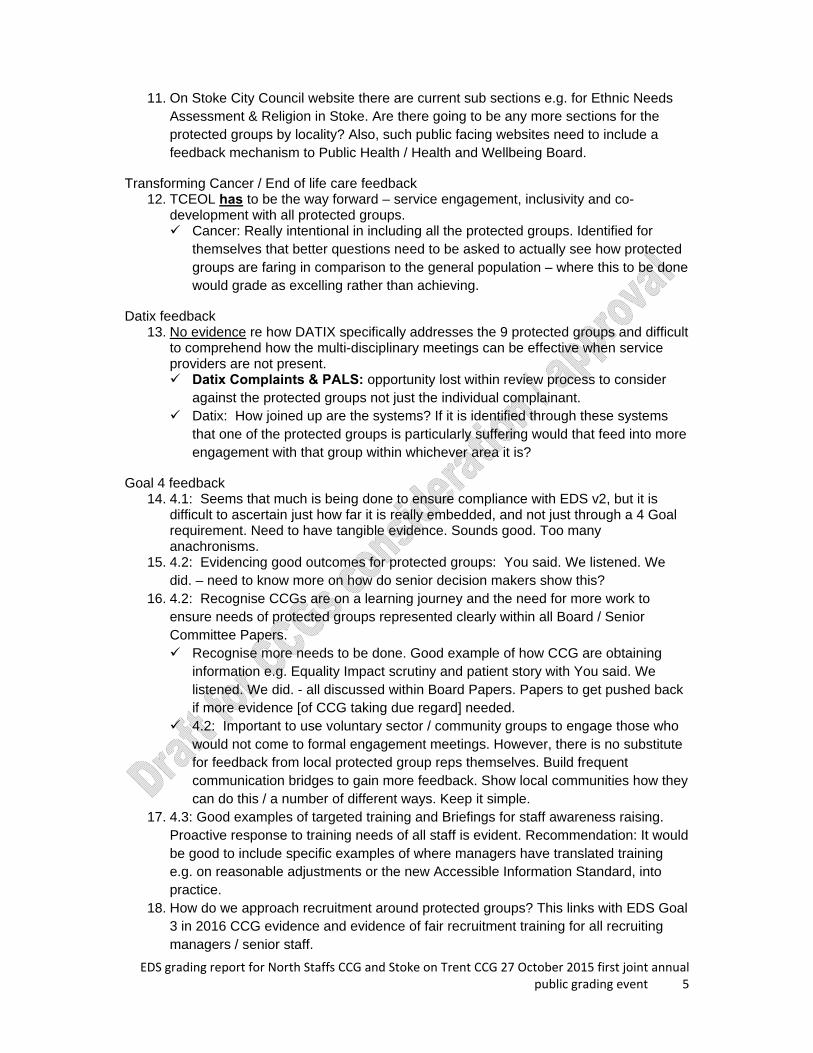
EDS grading report for North Staffs CCG and Stoke on Trent CCG 27 October 2015 first joint annual public grading event 5
11. On Stoke City Council website there are current sub sections e.g. for Ethnic Needs Assessment & Religion in Stoke. Are there going to be any more sections for the protected groups by locality? Also, such public facing websites need to include a feedback mechanism to Public Health / Health and Wellbeing Board.
Transforming Cancer / End of life care feedback 12. TCEOL has to be the way forward – service engagement, inclusivity and co-
development with all protected groups. Cancer: Really intentional in including all the protected groups. Identified for
themselves that better questions need to be asked to actually see how protected groups are faring in comparison to the general population – where this to be done would grade as excelling rather than achieving.
Datix feedback 13. No evidence re how DATIX specifically addresses the 9 protected groups and difficult
to comprehend how the multi-disciplinary meetings can be effective when service providers are not present. Datix Complaints & PALS: opportunity lost within review process to consider
against the protected groups not just the individual complainant. Datix: How joined up are the systems? If it is identified through these systems
that one of the protected groups is particularly suffering would that feed into more engagement with that group within whichever area it is?
Goal 4 feedback 14. 4.1: Seems that much is being done to ensure compliance with EDS v2, but it is
difficult to ascertain just how far it is really embedded, and not just through a 4 Goal requirement. Need to have tangible evidence. Sounds good. Too many anachronisms.
15. 4.2: Evidencing good outcomes for protected groups: You said. We listened. We did. – need to know more on how do senior decision makers show this?
16. 4.2: Recognise CCGs are on a learning journey and the need for more work to ensure needs of protected groups represented clearly within all Board / Senior Committee Papers. Recognise more needs to be done. Good example of how CCG are obtaining
information e.g. Equality Impact scrutiny and patient story with You said. We listened. We did. - all discussed within Board Papers. Papers to get pushed back if more evidence [of CCG taking due regard] needed.
4.2: Important to use voluntary sector / community groups to engage those who would not come to formal engagement meetings. However, there is no substitute for feedback from local protected group reps themselves. Build frequent communication bridges to gain more feedback. Show local communities how they can do this / a number of different ways. Keep it simple.
17. 4.3: Good examples of targeted training and Briefings for staff awareness raising. Proactive response to training needs of all staff is evident. Recommendation: It would be good to include specific examples of where managers have translated training e.g. on reasonable adjustments or the new Accessible Information Standard, into practice.
18. How do we approach recruitment around protected groups? This links with EDS Goal 3 in 2016 CCG evidence and evidence of fair recruitment training for all recruiting managers / senior staff.

EDS grading report for North Staffs CCG and Stoke on Trent CCG 27 October 2015 first joint annual public grading event 6
Grading Underdeveloped Developing Achieving Excelling People from all protected groups fare poorly compared with people overall OR evidence is not available
People from only some (2 or less) protected groups fare as well as people overall
People from most (3 to 5) protected groups fare as well as people overall
People from all (9) protected groups fare as well as people overall
Lessons learnt:
1. Engagement with protected group representatives by locality, and gathering differential satisfaction levels of patient experience at engagement events and by other means, are key areas of focus for the CCGs
2. Further development of the EDS stakeholder group and how this group could be
encouraged to provide regular feedback to CCG commissioners to be explored further
3. Contact BME group representatives in 2015, to provide opportunity for feedback
to CCG on current EDS evidence
2 2 2
3
1
2
3
4
Outcome 1.1 Outcome 1.2 Outcome 1.3 Outcome 1.4
EDS Goal 1 Grading 2015: Developing / Achieving
EDS Goal 1 Grading 2015:Developing / Achieving
3 3 3
0
1
2
3
4
Outcome 4.1 Outcome 4.2 Outcome 4.3
EDS Goal 4 Grading 2015: Achieving
EDS Goal 4 Grading 2015:Achieving

EDS grading report for North Staffs CCG and Stoke on Trent CCG 27 October 2015 first joint annual public grading event 7
4. This was the 2 CCG’s first joint annual public grading event. It is important to ensure any evidence / improvements are evidenced as equally embedded and led at a senior level, by each CCG
5. CCGs should consider what is becoming more frequent wider commissioning
across Staffordshire and how assurances can be achieved in terms of managing equality related business risk by all participating CCGs
6. Greater focus on JSNA and protected group sub groups. 7. Ensure CCG branding is displayed at engagement events where practical 8. EDS evidence to be gathered by end April 2016 and suggest next EDS annual
public grading takes place end May 2016. Room booking to be made as early as practical i.e. in 2015.
9. Consider which priority areas should be focused on to lead evidence collection by
key staff 10. Senior staff presenting evidence to have an opportunity for a practice run before
grading event takes place. 11. Add watermark to all pdf evidence documents on website – both CCG names –
show who owns the documents. 12. EDS should be led by senior clinicians and other senior CCG lead staff. 13. Suggest monthly review and quality check of evidence gathered for next public
grading event. 14. CCGs should continue to annually track the EDS performance of our larger
provider partners, as a means of continuing to give assurances of their own contract monitoring performance. This includes annual public grading event, as well as the quality / robustness of their EDS evidence provided for public scrutiny
15. Less abbreviations / Plain English / early proof read of all documents used.

EquAnn2015 –�
North E&I AnnuNSCCG GoEquality & I
ualitnual– 2016 (
Staffoal Report_overning BoInclusion: A
ty &l Pu(Janua
ordshir_v0.3_231oard meetinAnnual E&I
��
& Incublic
ry 2016
re Clin1214_jw g 6 JanuaryPublication
clusicatio6)�
nical Co
y 2016 n (Jan 2016
ion on�
ommis
) – Append
ssionin
ix 1
ng Gro
1
up
1
�

P a g e | 2
fairness
respect
equality
dignity
autonomy
Goal 1
Better Health Outcomes for ALL
Goal 2
Improved Patient & Carer Access and Experience
Goal 3
Empowered, Engaged and included staff
Goal 4
Inclusive Leadership at ALL
Levels

P a g e | 3
Contents Page
Foreword
4
1.0 Introduction and Aims of the Report 8 1.1 What is ‘Due Regard’? 8 1.2 The local context 8 1.3 Workforce Profile
Staff training
9
2.0 Compliance with the Public Sector Equality Duty 11 2.1 Protected Characteristics 11 2.2 Involving local people in decision making
Patient Participation Groups Patient Congress Membership Patient & Public Engagement
11
2.3 Equality Impact and Risk Assessment (EI&RA)
13
3.0 Outcomes of our Equality Objectives 14 3.1 Progress made on our Equality Objectives
15
4.0 Equality Delivery System Grading 2015 Public Grading 2015
18
5.0 Performance Monitoring our providers
20
6.0 Meeting statutory Human Rights requirements
21
7.0 Findings
21
8.0 Conclusions
22
9.0 Actions going forward
24
Appendix 1 CCG Workforce Profile
27
Appendix 2 The Outcomes of EDS v2 Grading 2015
34
Appendix 3 EDS Grading Dashboard 2015
36
P a g e | 4
Foreword
Meeting and exceeding our legal obligations to local protected groups:
NHS North Staffordshire Clinical Commissioning Group (CCG) are pleased to present our
third Annual Equality Publication which reflects CCG’s equality data performance in meeting
its legal duties set out in the Equality Act 2010 and the Human Rights Act 1998. This
January 2016 Publication follows on from last
year’s Annual Equality Data Publication
(31 January 2015), and will be displayed on our
website by 31 January and renewed annually.
We know that different patients, carers and staff
take up healthcare services, information and
employment opportunities differently. Health
inequalities exist within the vulnerable local
communities we serve. This publication sets out
what equality data we are aware of in 2015-16 for local protected groups and highlights any
significant gaps or trends with links to our agreed Equality Objectives (October 2012 -17
overall delivery cycle as set for CCGs by NHS England). CCG buys healthcare services for
our local community through contracts with approved provider partner organisations. Our
main provider partners hold and are required to similarly publish their (1) workforce and (2)
service delivery equality data of who is taking up services from protected groups, and
differential satisfaction levels in patient experience of healthcare services. All data held is
subject to the Data Protection Act 1998. This developing data is scrutinised for information
and service improvement purposes by both CCG and their provider partner organisations,
with assurance of recognising and managing equality business risk, given to CCG.
Through embedding of the NHS Equality Delivery System (NHS equality performance
framework) the CCG aims to demonstrate to the people we serve how we are meeting the
three aims of the Equality Duty (as required in the Equality Act 2010), and Public Sector
Equality Duty (PSED) 2011. North Staffs CCG and our larger provider partner organisations
publicly monitor their equality performance annually using the NHS wide Equality Delivery
System (EDS v2). This involves a transparent annual public grading of our equality
performance evidence across 4 Goals and 18 required Outcomes - over a 4 year delivery
cycle (2013 –17). The external grading is carried out by trained local communities of
We will work with our patients and provider partners to listen to the local vulnerable patient voice to help the CCG to shape services to be more inclusive of people from protected groups. We are a membership organisation of 33 GP Practices and 136 GPs.

P a g e | 5
interest, including volunteer patient and carer representatives from protected groups and
other interested stakeholders from local communities of interest. A grading dashboard is
displayed publicly on our CCG website and an action plan is developed to show
improvements at our next annual public grading.
The CCG is also required to monitor the EDS (Equality Delivery System) and WRES
(Workforce Race Equality Standard) performance of their larger provider partners. Both
EDS and WRES have become mandated by NHS England from April 2015, for all NHS
commissioning organisations and their larger provider partners. In addition, the CCG
displays our own WRES annual report on the WRES CCG webpage (showing data at
1 April 2015).
As a CCG, we take our responsibilities in this area of workforce and service delivery
information very seriously. Using processes including the EDS framework; robust provider
contract management; a developing Equality and Inclusion Strategy in 2015-16; Equality
Impact and Risk Assessment scrutiny of key healthcare changes; cyclical governance
arrangements; and our Annual Equality and Inclusion Publication, the CCG aims to
evidence the requirement to show ‘due regard’ or deliberate consideration and thought
about local protected groups in our planning and decision making. This includes the EDS
evidence requirement of ‘how do people from local protected groups fare compared to
people in general, [in healthcare services]?’
As a relatively new CCG (formed in shadow form April 2012), we are therefore at the early
stages of responding to the need to provide transparent reporting on what equality data is
held about local protected characteristic groups. This includes monitoring by provider
partners on: who is taking up services from protected groups? (with the option in place for
patients to declare their protected group profiles across different healthcare settings);
differential satisfaction levels with healthcare services, by protected group patients. The
equality monitoring of patients and staff is through the option to declare their demographic
profiles.
As a CCG we are keen to understand which protected groups (protected by the Equality Act
2010) we are reaching out to for feedback, at engagement / consultation and EDS public

P a g e | 6
grading events. We routinely provide the option at engagement and EDS grading events,
for those attending to anonymously declare their profiles.
We use various processes to help us to achieve and evidence good outcomes for those
groups protected under the Act. How we show ‘due regard’ in our planning and decision
making processes i.e. consistently provide fair access to information, healthcare services,
premises, and any employment opportunities for all vulnerable people under the Equality
Act 2010 and the Health and Social Care Act 2012, is our key concern within this publicly
available publication.
The CCG wants to work closely with local communities of interest to gather feedback on
any adverse impacts or unintended consequences from the changes CCG are considering.
There is much work for us to do to continue to develop our approach as a CCG to
successfully engaging specifically with protected group representatives across North
Staffordshire.
We recognise that this presents CCG with some challenges as we continue to develop our
ways of working locally with these sometimes ‘seldom heard’, more marginalised protected
groups. A range of engagement approaches is required, including: face to face engagement
seeking feedback from the earliest stages of consideration by CCG, on any barriers to
inclusion from key healthcare changes; providing the option to anonymously declare
demographic profiles by people attending engagement meetings or feeding back by other
means; working with Healthwatch Staffordshire to reach out across representatives of the 9
protected groups seeking feedback for the CCG.
In this publication it is important for us to acknowledge that in relation to equality and
diversity, the CCG this year has continued to focus on getting systems and processes in
place. We are not however complacent and realise there is much work to be done in the
coming year for us to continue to make fair progress. North Staffordshire CCG knows that a
robust equality and inclusion approach makes sound ethical and business sense. Our
Publication is a transparent report of some of the key outcomes achieved for people from
local protected groups.

P a g e | 7
Dr Mark Shapley Marcus Warnes Clinical Chair Interim Accountable Officer

P a g e | 8
1.0 Introduction This is the Clinical Commissioning Group’s (CCG) annual Equality & Inclusion Publication
which sets out how the CCG has been demonstrating ‘due regard’ to the public sector
equality duty’s three aims and will provide evidence for
meeting the specific equality duty, which requires all public
sector organisations to publish their equality information
annually.
1.1 What is ‘due regard’?
Due regard means that the Clinical Commissioning Group has
given advanced deliberate consideration to issues of equality and discrimination before
making any key healthcare decision that may be affected by them. That is a valuable
requirement that is seen as an integral and important part of the mechanisms for ensuring
the fulfilment of the aims of anti-discrimination legislation set out in the Equality Act 2010
and the Public Sector Equality Duty or PSED (2011).
1.2 A Local Context
North Staffordshire CCG serves a population of 213,000 across the main districts of
Newcastle-under-Lyme and the Staffordshire Moorlands.
Mixture of sparsely populated rural areas (Staffordshire Moorlands) and more
densely populated urban areas (Newcastle-under-Lyme, Leek and Biddulph).
Gap in life expectancy of nearly 10 years between those people living in the most
affluent and the most disadvantaged localities
Women in the Moorlands Rural and Werrington locality live 15 months longer and
women in Newcastle-under-Lyme South live 26 months longer than the England
average
Men in Newcastle-under-Lyme South live 13 months longer than national average
Men in Newcastle-under-Lyme Central live 14 months less than average
Women in Newcastle-under-Lyme Central live 32 months less than average
Ageing population, with the number of people aged over 75 years expected to
increase significantly over the next eight years
There will be more people living with long term conditions
A higher than average number of people die prematurely from largely preventable
illness and disease
“We will make equality core
to our business planning”

P a g e | 9
Circulatory diseases, cancer and respiratory disease account for three quarters of all
deaths
10,660 people from a minority ethnic group in North Staffordshire (5% of the
population, up from 3% in 2001 Census but lower than the England average of 20%)
15 out of 134 local authority wards ranked amongst most deprived nationally (11% of
the population)
Newcastle-under-Lyme North (20%) and Newcastle-under-Lyme Central (17%) have
the highest proportions of people living in the most deprived areas.
1.3 Workforce Profile
The CCG is supported by Midlands and Lancashire Commissioning Support Unit’s (CSU)
Human Resources and Equality and Inclusion Team in ensuring that it has in place fair and
equitable employment and recruitment practices. The CCG and CSU are committed to
holding up to date information about the CCG workforce, in line with Data Protection
legislation, and to ensure strategic decisions affecting the workforce are based on accurate
reporting and data.
The CCG aims to fully understand the diversity of the workforce so that the CCG can
ensure non-discriminatory practice, working with staff and staff representatives to identify
and eliminate barriers and discrimination in line with the Public Sector Equality Duty and the
Equality Act 2010 Employment Statutory Code of Practice. CCG also scrutinise workforce
data to monitor how we are representing the local communities we serve as required in
EDS Outcome 3.1: Fair NHS recruitment and selection processes lead to a more
representative workforce at all levels. See Appendix 1 for Workforce Profile.
We monitor our workforce and where employees identify as having a disability or long term
condition, as set out in the Equality Act 2010, access audits and reasonable adjustments
are put in place to support the employees. The CCG also carries out fair and equitable
access to recruitment. This means that where an applicant indicates they have a disability
or long term condition as set out in the Equality Act 2010 reasonable adjustments are put in
place to support the applicant, where required.

P a g e | 10
Staff Training
During 2015 all CCG employees have undertaken the mandatory training in Equality and
Diversity Awareness and this will also be a feature in our induction and development of
staff, including board members as they are appointed.
38.1% of CCG staff have completed the on-line e learning for Equality in 2015. This module
is required to be completed once every 3 years and within year 1 for new starters.
The CCG’s Governing Body received Equality and Inclusion development as part of their
overall development programme and this session was tailored to their needs and meets the
mandatory training requirement for 2015/16 financial year, in October 2015.
Commissioning Managers also received additional training in undertaking Equality Impact
and Risk Assessment (EI&RA) scrutiny and considering the Public Sector Equality Duty in
the form of EI&RA Workshop training in 2015. The targeted training aims to support the
CCG in its statutory duties for Equality and Inclusion, Information Governance, and
supports CCG Staff in undertaking Privacy Impact Assessments, Equality Impact scrutiny,
Human Rights screening for commissioning and decommissioning services, redesigning
services, strategy and policy development, and project planning.
The EI&RA training learning outcomes are to enable CCG staff to:
• develop an understanding of the EI&RA scrutiny process and evidencing how CCG
meet their PSED responsibilities
• identify the business, ethical and legal cases for undertaking equality impact and risk
assessment of key healthcare changes under early consideration by CCG
• understand and apply evidence of taking ‘due regard’ according to the Brown Principles
and to follow the Gunning Principles for engagement
• recognise and manage equality related business risk.

P a g e | 11
2.0 Compliance with the Public Sector Equality Duty
The CCG has worked to show due regard to the aims of the Public Sector General Equality
duty as set out in the Equality Act as set out below:
Aim 1 Eliminate unlawful discrimination, harassment and victimisation
Aim 2 Advance equality of opportunity between different groups
Aim 3 Foster good relations between different groups
Through the adoption of the NHS Equality Delivery System equality performance framework
and Equality Impact and Risk Assessment process the CCG aims to demonstrate to the
people we serve how we are meeting the three aims of the Equality Duty.
2.1 Protected characteristics The general equality duty covers the following
protected characteristics: age (including children and
young people), disability, gender reassignment,
pregnancy and maternity, race, religion or belief,
gender and sexual orientation. Gender reassignment
includes people who are considering, undergoing or
have undergone gender reassignment. Public
bodies like CCGs also need to have due regard to
the need to eliminate unlawful discrimination against someone because of their marriage or
civil partnership status. This means that the first aim of the general equality duty applies to
this characteristic but the other two aims do not. This applies only in relation to work, not to
any other part of the Equality Act 2010.
2.2 Involving local people in decision making
Patient Participation Groups
GP Practices have established patient participation groups (PPGs) in 31 out of our 33 GP
practices. CCG have supported where needed. We now have locality groups in all 5 areas:
Newcastle South, Newcastle Central and North, Leek and Biddulph, Moorlands rural and
Werrington.
“Our Vision is to ensure that local people from protected groups
have fair access to information, services,
premises and employment
opportunities”

P a g e | 12
Anyone registered with that practice is entitled to become a member of the PPG. In two of
the CCG’s five localities, the PPGs have worked collaboratively to establish locality groups
and these are currently under development in the other three localities.
Members of the PPGs have the opportunity to work with doctors and practice managers to:
Influence decisions about services and facilities
Help practices make the best use of resources
Improve communications between staff and patients
Make sure patient views are properly represented.
Members also have an opportunity to take part in practical tasks such as carrying out
surveys or giving advice at flu clinics.
Patient Congress
North Staffordshire CCG has established a vibrant and effective Patient Congress to involve
patients in commissioning decisions at a strategic level. Its 18 members represent PPGs
from all five localities in North Staffordshire, as well as a number of voluntary and
community sector groups. Members are able to provide a voice for those patients who are
seldom heard, including people with mental health problems such as misuse and dementia.
It is made up of people who have a real desire to see health services improve in the
communities where they live and is chaired by the Board’s Lay Member for Patient and
Public Involvement (PPI).
Members commit to spending about 50 hours per year, including attendance at bi-monthly
meetings. Patient Congress members provide a respected and credible voice at a wide
variety of internal and external events and groups, such as Clinical Directors and Senior
CCG Managers attend Congress meetings regularly to ensure members are well informed
and to gain insight to inform the work of the CCG.
In November 2015 Patient Congress members are being given the option to anonymously
declare their demographic profiles. The CCG are keen to understand who they are reaching
out to in terms representation of the nine characteristics protected by the Equality Act 2010,
for feedback from engagement and consultation to CCG on the impacts of healthcare
changes under consideration.

P a g e | 13
Membership
Anyone registered with a doctor within North Staffordshire is entitled to join the Patient
Membership Scheme. By March 2015 there were around 1,439 members and as a CCG
we are keen to continue to expand this membership group. We communicate with our
patient membership via a monthly newsletter, which has been developed to be North
Staffordshire focused with features on priority areas for the CCG and articles written by
CCG Board members. We use the newsletter to advertise opportunities for patients to get
involved and to disseminate information about local support groups.
Patient and Public Engagement
The North Staffordshire CCG Governing Board receives an annual Patient and Public
Engagement Report from the CSU which provides a “You Said, We Listened, We Did”
account of how services are being transformed through listening to what patients and the
public tell us are their health priorities.
We have a strong and effective relationship with Healthwatch Staffordshire, which builds
upon the positive co-working with the CCG previously established with LINK. Healthwatch
provides expertise and public representation at five strategic CCG groups including the
Quality Committee.
Our commissioning team has a track record of engaging with patients and clinicians. The
Clinical Director for Partnerships and Patient Engagement surveys commissioning
managers on a twice yearly basis regarding the engagement opportunities that they have
organised relating to specific commissioning tasks and this, combined with the report from
the CSU, provides an overview of patient and clinical engagement which is discussed at the
PPI steering group.
The CCG’s website provides an easily accessible wide range of information about the CCG
and ‘contact us’ feature, as well as providing links to local health services and community
groups. We also have a Facebook page and a Twitter account as part of our commitment
to widen our communications and involvement.
2.3 Equality Impact and Risk Assessment (EI&RA)
The Clinical Commissioning Group has adopted the EI&RA scrutiny process which provides
a framework for undertaking equality impact, privacy impact assessments and human rights

P a g e | 14
screening. Equality Impact & Risks Assessments (EI&RA) are a primary source for
demonstrating how CCG have considered legal duties under the Human Rights Act 1998,
The Equality Act 2010 and the Public Sector Equality Duty 2011.
They evaluate the likely impact in a given scenario on people with a protected characteristic
to ensure that employment practices and service provision do not discriminate and promote
equality of opportunity.
This enables the CCG to show ‘due regard’ to the three aims of the general equality duty by
ensuring that all requirements around equality, human rights and privacy are given
advanced consideration before the CCGs Governing Body or senior committees make any
policy decisions that may be affected by feedback received from local protected group
representatives. CCG commissioners have carried out a range of equality impact and
human rights screening when carrying out their duties to ensure the CCG is paying ‘due
regard’ to the three aims of the Public Sector Equality Duty and the Human Rights Act.
Equality Impact and Risk Assessments that were carried out to date in 2015 are shown
below.
List of EI&RAs underway / completed EI&RAs Underway / completed Long Term Conditions* U Mental Health Workbook* C Learning Disability Workbook* U My Care My Way At Home* U Step Up Step Down* C (Stage 1) GP Out of Hours / Front of House Services* U Individual Funding Requests* U Policy on Prioritisation of Resources U Hearing Aid Service Review U * Joint commissioning work with Stoke on Trent CCG
3.0 Outcomes of our Equality Objectives North Staffordshire Clinical Commissioning Group prepared and published its Equality
Objectives in April 2012 whilst in shadow form. These objectives further the aims of the
general equality duty, and will be refreshed annually following the grading of the CCG
against the Equality Delivery System goals and revised every four years. Below is a table
outlining progress against our equality objectives.

P a g e | 15
3.1 2015 Progress made on Our Equality Objectives (set 2012 to 2015): Objective 1 Ensure all the commissioned and contracted services deliver better
outcomes for our population as a whole and those with protected
characteristics in particular by including targets and key
performance indicators into contracts and performance managing
closely
Progress Equality Impact & Risk Assessment (EI&RA) has been reviewed and
refined to ensure a ‘fit for purpose’ process which supports CCG in
scrutinising all key healthcare changes for evidence of taking ‘due regard’
or deliberate consideration of local people from protected groups (under
the Equality Act 2010) in all our planning and decision making processes.
Targeted staff are trained to focus on good outcomes for protected groups
in terms of ‘You said, We listened, We did’, following feedback received on
any barriers to taking up services, information, premises, and any
employment opportunities or negative impacts arising. Such outcomes
must be incorporated as appropriate into service specifications and
subsequent contract management.
Key performance indicators are included into contracts with CCG larger
provider partner organisations, with evidence reporting to contract
managers for legal compliance and meeting equality responsibilities. This
applies to public sector and private sector partners.
Objective 2 Involve our patients, service users, carers, protected groups, staff
and wider public in improving access to services and patient
experience, ensuring that under-represented groups are heard
Progress The CCG continues to work to specifically involve local protected group
representatives from both North Staffs (and Stoke on Trent) localities and
to provide opportunities for the ‘vulnerable patient voice’ to help CCG
planners and decision makers to shape services to be more inclusive.
Inclusion Health Groups including homeless people; asylum seekers;
those involved in the drugs and sex trafficking industries are also
considered, where there are local concerns.
Objective 3 Perform Equality Impact & Risk Assessment on all strategies,
policies, programmes of commissioning work, service specifications,
Project Initiation documents or PIDs, and incorporating findings into

P a g e | 16
contracts with providers
Progress Equality Impact & Risk Assessment (EI&RA) has been reviewed and
refined to ensure a ‘fit for purpose’ process which supports CCG in
scrutinising all key healthcare changes for evidence of taking ‘due regard’
or deliberate consideration of local people from protected groups (under
the Equality Act 2010) in all our planning and decision making processes.
Staff are trained to focus on good outcomes for protected group in terms of
‘You said. We listened. We did.’ following feedback on any barriers to
taking up services or negative impacts arising.
Provider partners are subject to the same equality and Human Rights legal
compliance responsibilities as CCGs, which also travel through the
contract to providers. Findings from EI&RA scrutiny may also inform
service spec specific requirements with providers. Fair access to
information, services, premises and any employment / training
opportunities is the basis of equality and inclusion scrutiny for good
outcomes relating to local people from the 9 protected groups (in
workforce and service delivery issues). CCG want to understand who is
taking up healthcare services from local protected groups and
differentially, how satisfied are they?
Objective 4 Make North Staffordshire CCG an employer of choice, with
empowered, engaged and well supported staff and a workforce that
better represents the communities that we serve
Progress The CCG has developed a Workplace Race Equality Standard (WRES)
action plan for 2015-16. As a result of reporting annually via WRES, CCG
are arranging for fair recruitment training to include unconscious bias
training for recruiting managers / senior staff - to support a fair and
accessible recruitment process and to ensure no group is being
disadvantaged in the process.
A series of Staff Equality Briefings have been launched to all staff in 2015,
including: Reasonable Adjustments on the Workplace; Discrimination in
the Workplace (definitions); the new Accessible Information Standard.
This information is featured periodically in the Staff Newsletter and is
P a g e | 17
available to download from N Staffs CCG refreshed E&I intranet section.
A series of interactive Equality Workshops and Development sessions are
targeted for staff in 2015: EI&RA for commissioners and strategy / policy
developers; Equality & Inclusion Awareness of job role responsibilities &
cultural competence for all line managers; Board Development – E&I
senior decision maker responsibilities; EDS Overview for Board; WRES
Overview for Board; EDS evidence gathering support sessions; EDS
presenting of evidence support sessions for senior staff / clinicians.
Objective 5 Ensure inclusion leadership at all levels, with the Governing Board
and Senior Leaders conducting their business so that Equality and
Inclusion is advanced and robust relationships maintained with
patients, staff, providers, protected groups and the wider public
Progress All CCG staff including the Governing Board and Senior Managers
undertake equality training to ensure they understand how this maps to
their roles and responsibilities.
A series of Staff Equality Briefings have been launched to all staff in 2015,
including: Reasonable Adjustments on the Workplace; Discrimination in
the Workplace (definitions); the new Accessible Information Standard
(implementation July 2016); Who are protected characteristic groups?
(Equality Act 2010).
This information is featured periodically in the Staff Newsletter and is
available to download from N Staffs CCG refreshed E&I intranet section.
A series of interactive Equality Workshops and Development sessions are
targeted for staff in 2015: EI&RA for commissioners and strategy / policy
developers; Equality & Inclusion Awareness of job role responsibilities &
cultural competence for all line managers; Board Development – E&I
responsibilities for senior decision makers; EDS Overview for Board;
WRES Overview for Board; EDS evidence gathering support sessions;
EDS presenting of evidence support sessions for senior staff.
The CCG continues to work to specifically involve local protected group

P a g e | 18
representatives from both North Staffs (and Stoke on Trent) localities and
to provide opportunities for the ‘vulnerable patient voice’ to help CCG
planners and decision makers to shape services to be more inclusive.
Inclusion Health Groups including homeless people; asylum seekers;
those involved in the drugs and sex trafficking industries are also
considered, where there are local concerns.
All CCG staff including the Governing Board and Senior Managers
undertake equality training to ensure they understand how this maps to
their roles and responsibilities. Governing Board development took place
on 5 August 2015; and EDS Overview on 7 October 2015. The Governing
Board have shown clear commitment to Equality and Inclusion through the
work they and the CCG staff have been undertaking in 2015.
4.0 Equality Delivery System (EDS)
North Staffordshire Clinical Commissioning Group adopted the Equality Delivery System
(EDS v2) as its equality performance
framework to support the CCG in
demonstrating its compliance with the three
aims of the Public Sector General Equality
Duty.
The EDS public grading process provides
the CCG Governing Board with an
assurance mechanism for compliance with
the Equality Act 2010 and enables local
people to co-design the CCG’s equality
objectives to ensure improvements in the
experiences of patients, carers, employees and local people.
The four EDS goals are: 1. Better health outcomes for all 2. Improved patient access and experience 3. Empowered, engaged and included staff 4. Inclusive leadership at all levels
The grades for EDS are as follows:
Undeveloped – Red Developing – Amber
Achieving – Green Excelling – Purple
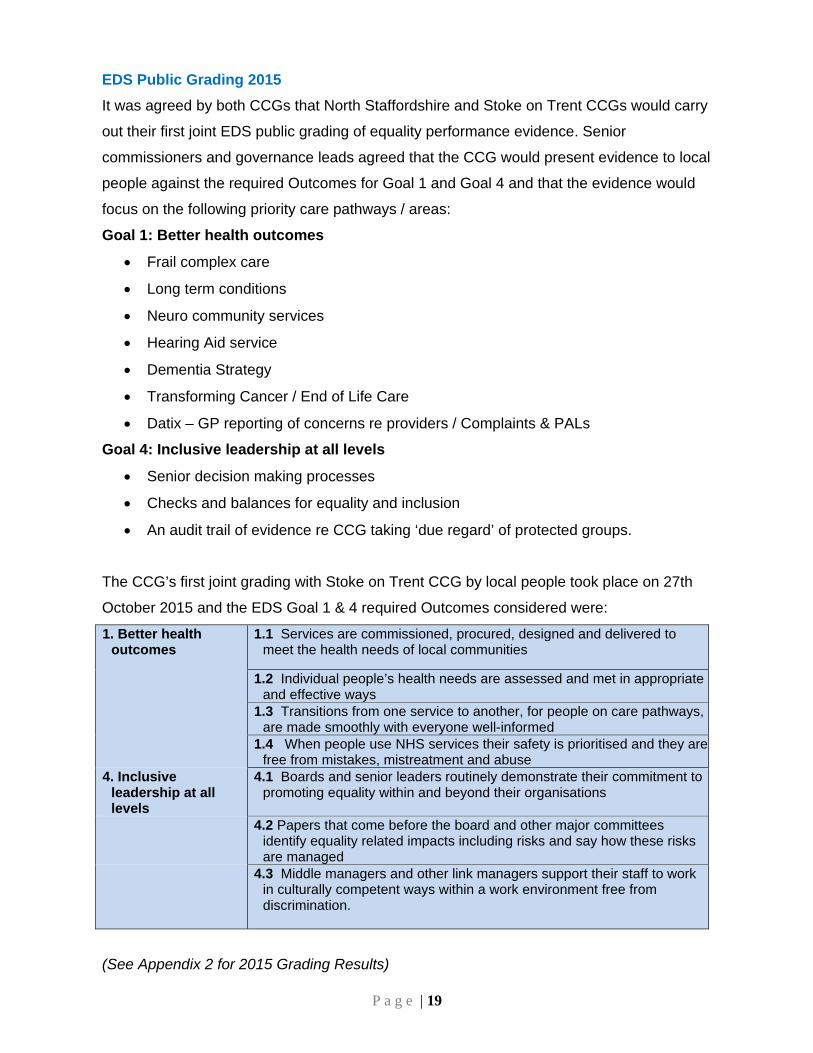
P a g e | 19
EDS Public Grading 2015
It was agreed by both CCGs that North Staffordshire and Stoke on Trent CCGs would carry
out their first joint EDS public grading of equality performance evidence. Senior
commissioners and governance leads agreed that the CCG would present evidence to local
people against the required Outcomes for Goal 1 and Goal 4 and that the evidence would
focus on the following priority care pathways / areas:
Goal 1: Better health outcomes
Frail complex care
Long term conditions
Neuro community services
Hearing Aid service
Dementia Strategy
Transforming Cancer / End of Life Care
Datix – GP reporting of concerns re providers / Complaints & PALs
Goal 4: Inclusive leadership at all levels
Senior decision making processes
Checks and balances for equality and inclusion
An audit trail of evidence re CCG taking ‘due regard’ of protected groups.
The CCG’s first joint grading with Stoke on Trent CCG by local people took place on 27th
October 2015 and the EDS Goal 1 & 4 required Outcomes considered were:
1. Better health outcomes
1.1 Services are commissioned, procured, designed and delivered to meet the health needs of local communities
1.2 Individual people’s health needs are assessed and met in appropriate and effective ways
1.3 Transitions from one service to another, for people on care pathways, are made smoothly with everyone well-informed
1.4 When people use NHS services their safety is prioritised and they are free from mistakes, mistreatment and abuse
4. Inclusive leadership at all levels
4.1 Boards and senior leaders routinely demonstrate their commitment to promoting equality within and beyond their organisations
4.2 Papers that come before the board and other major committees identify equality related impacts including risks and say how these risks are managed
4.3 Middle managers and other link managers support their staff to work in culturally competent ways within a work environment free from discrimination.
(See Appendix 2 for 2015 Grading Results)

P a g e | 20
5.0 Performance Monitoring of Providers CCG monitor the equality performance of their provider partners using processes which
allow Equality and Inclusion Leads supporting CCG from Midlands and Lancashire CSU
(Commissioning Support Unit) to provide assurance to CCG in terms of providers
recognising and managing equality related business risk.
The main provider partners have a provider Equality Monitoring Schedule embedded within
their contract annually and reviewed during cyclical contract meetings. Annually providers
are required to submit evidence of how they evidence meeting their responsibilities from the
Equality Act 2010 and the Public Sector Equality Duty (PSED) 2011.
This summary evidence received by the lead commissioning organisation is scrutinised and
assurance given of each larger provider managing business risk in this area. Any variance
in required standards is discussed at regular contract meetings. Equality Delivery System
(EDS v2) annual public grading and reporting also provides commissioners with evidence of
provider equality performance and progress against meeting the PSED requirements. EDS
was mandated by NHS England in April 2015 for all NHS commissioning and their larger
provider organisations.
CCG’s larger provider organisations are shown below, with links to their equality webpage
and the data they are currently displaying. Providers will display their up to date data by
31 January 2016.
Provider organisations EDS adopted in 2015 Equality monitoring embedded into contract for 2015
UHNM (University Hospitals North Midlands – Acute hospital)
Yes Yes
Staffordshire & Stoke Partnership Trust (community services)
Yes Yes
Combined Healthcare (Mental Health Trust)
Yes Yes

P a g e | 21
6.0 Meeting statutory Human Rights requirements
The Human Rights Act 1998 sets out a range of rights which have implications for the way
the CCG buys services and manages their workforce. In practice this means that we must:
Act compatibly with the rights contained in the Human Rights Act in everything we do
Recognise that anyone who is a ‘victim’ under the Human Rights Act can bring a
claim against the CCG (in a UK court, tribunal, hearing or complaints procedure)
Wherever possible existing laws that the CCG as a public body deals with, must be
interpreted and applied in a way that fits with the rights in the Human Rights Act
1998.
The CCG has through the EI&RA process undertaken Human Rights screening on its
decision making including its commissioning and decommissioning and service redesign
programmes. This is to ensure that the CCG promotes and protects the rights of people
living in North Staffordshire when planning its annual commissioning intentions. All Human
Rights Screening outcomes will be embedded into the Equality Impact and Risk
Assessment (EI&RA) and a list of EI&RAs completed will be published on the CCGs
website within this Annual Equality and Inclusion Publication.
7.0 Findings
The evidence set out in this publication demonstrates that the Clinical Commissioning
Group has carried out an Equality Delivery System (EDS v2) public grading with trained
(volunteer) local communities of interest. Scrutiny this year demonstrates that the CCG is
improving in comparison to 2014 with regard to the EDS Goal 1 and Goal 4 required
Outcomes, based on the evidence that has been scrutinised so far.
The EDS annual public grading report for October 2015 has set out the results of the public
grading of the evidence presented for EDS v2 grading. The results on the whole were
positive with all but three of the seven Outcomes targeted in 2015, reaching ‘achieving’.
The report also sets out recommendations from the grading panel on how to move forward
in 2016 in section 9: Actions going forward. Also see Appendix 3: EDS summary grading
record.

P a g e | 22
Considerable progress has continued to be made on our agreed Equality Objectives, within
the 4 year delivery timescale of 2013 to 2017. However, a new Equality and Inclusion
Strategy has been drafted early in 2015, suggesting 3 new Equality Objectives for both
CCGs. These draft Objectives will go out to local communities of interest for their feedback
early in 2016.
Health inequalities for local protected groups, continues to be an area for scrutiny in 2016,
supported by: national and local research influencing the Joint Strategic Needs Assessment
(and sub sections for protected groups); close working with Public Health colleagues and
the Health and Wellbeing Board.
The CCG Communication and Engagement Strategy is being refreshed during 2015-16 and
the Equality and Inclusion Strategy will link closely with this area of engagement with local
protected group representatives.
Targeted support sessions for senior lead staff re EDS evidence gathering and presenting
of summary evidence have also taken place during 2015 in preparation for the EDS public
grading event.
Targeted EI&RA scrutiny training has been carried out with all commissioner staff at North
Staffs CCG during 2015.
In addition, targeted training for all line managers in 2015 re Equality and Inclusion
Awareness (including cultural competency) has meant CCG have worked to take E&I
awareness ‘to the next level’ and in response the requirements of EDS Outcome 4.3:
‘Middle managers and other line managers support their staff to work in culturally
competent ways within a work environment free from discrimination.’
8.0 Conclusion
North Staffordshire CCG became an early adopter in 2014 of NHS England’s Equality
Delivery System (EDS v2). This is an NHS wide equality performance framework (launched
on 4 November 2013). It covers workforce and service delivery issues across 4 Goals and
18 required Outcomes. It asks for CCG evidence which shows ‘how do local people from
protected groups fare, compared to people overall [in healthcare]?’ EDS evidence

P a g e | 23
showcases CCG’s required progress in meeting the Specific Duty - within the broader
PSED (Public Sector Equality Duty).
CCG staff and commissioners must be aware of their responsibilities arising from the
equality duties as well as their health inequality duty. CCG, Local Authority leaders and
Public Health leaders have a responsibility to reduce health inequalities by describing
health inequalities through JSNAs (Joint Strategic Needs Assessments) and reducing
inequalities in local areas.
Disaggregating patient and carer gathered data in order to understand variation e.g. by the
9 local protected groups and other characteristics, is important in understanding local
inequalities – ie know your local community demographics and patient healthcare
experiences.
Senior decision makers are to be clear and transparent about the intended and likely effects
of strategies and individual programme decisions on protected groups and on health
inequality for all groups.
The CCG have adopted a transparent public approach to our equality performance using
this annual public grading process for workforce and service delivery issues, leading to
improvements in fair access to information, services, premises and any employment
opportunities, for local protected groups. A Staff Survey was carried out in February 2015,
with a further joint Survey about to go out to staff in 2016. This survey will provide the option
for CCG staff to anonymously declare their protected group profiles. Responses may then
be analysed to include differential satisfaction levels across protected groups. It can
however be difficult to produce significant findings with lower numbers of CCG staff.
The CCG has also been continuing to develop and embed our processes and systems to
support a robust approach to legal compliance with the Equality Act 2010; the Public Sector
Equality Duty (PSED 2011); and the Health and Social Care Act 2012. Equality Impact is
embedded using the EI&RA process, and helps commissioners to give ‘due regard’ or early
consideration to protected groups in our planning and decision making processes. This
process is being further reviewed during 2015-16 to become an electronic on-line process
during 2016. The requirement to clearly evidence ‘due regard’ (prompting deliberate
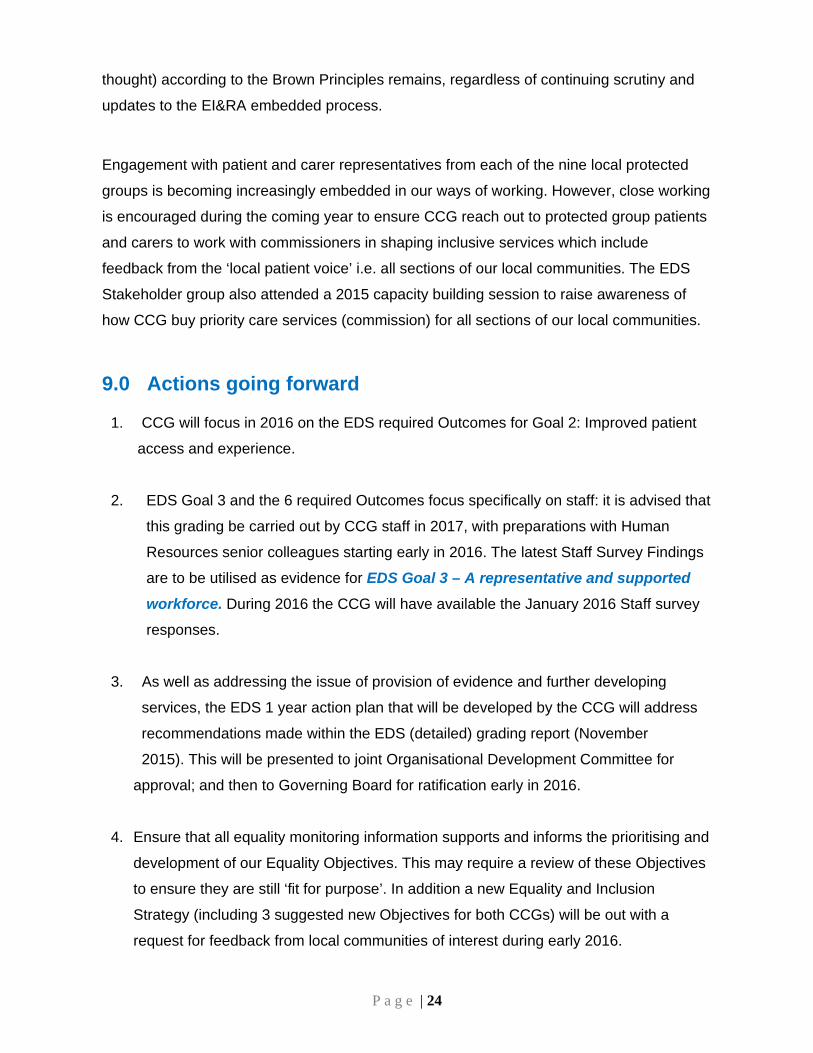
P a g e | 24
thought) according to the Brown Principles remains, regardless of continuing scrutiny and
updates to the EI&RA embedded process.
Engagement with patient and carer representatives from each of the nine local protected
groups is becoming increasingly embedded in our ways of working. However, close working
is encouraged during the coming year to ensure CCG reach out to protected group patients
and carers to work with commissioners in shaping inclusive services which include
feedback from the ‘local patient voice’ i.e. all sections of our local communities. The EDS
Stakeholder group also attended a 2015 capacity building session to raise awareness of
how CCG buy priority care services (commission) for all sections of our local communities.
9.0 Actions going forward
1. CCG will focus in 2016 on the EDS required Outcomes for Goal 2: Improved patient
access and experience.
2. EDS Goal 3 and the 6 required Outcomes focus specifically on staff: it is advised that
this grading be carried out by CCG staff in 2017, with preparations with Human
Resources senior colleagues starting early in 2016. The latest Staff Survey Findings
are to be utilised as evidence for EDS Goal 3 – A representative and supported
workforce. During 2016 the CCG will have available the January 2016 Staff survey
responses.
3. As well as addressing the issue of provision of evidence and further developing
services, the EDS 1 year action plan that will be developed by the CCG will address
recommendations made within the EDS (detailed) grading report (November
2015). This will be presented to joint Organisational Development Committee for
approval; and then to Governing Board for ratification early in 2016.
4. Ensure that all equality monitoring information supports and informs the prioritising and
development of our Equality Objectives. This may require a review of these Objectives
to ensure they are still ‘fit for purpose’. In addition a new Equality and Inclusion
Strategy (including 3 suggested new Objectives for both CCGs) will be out with a
request for feedback from local communities of interest during early 2016.

P a g e | 25
5. Scrutinise any Equality Impact findings on all strategies, policies, new services, service
redesigns, decommissioned services, and project management programmes – from
the earliest stages of consideration by CCG. Where possible, link into Equality
Objectives progress and incorporating findings into equality compliance performance
contracts with providers, as appropriate.
6. Introducing provider equality monitoring schedule requiring annual summary equality
evidence submission and scrutiny to lead commissioner organisation, by annually
embedding into all larger provider contracts.
7. Complaints monitoring and scrutiny should include the option for complainants to
declare their protected group profiles, with an annual summary report (via Datix
process) provided to the CCG.
8. The EDS Stakeholder group will be invited to attend a 2016 event to raise awareness
of how the CCG buy services for all sections of our local communities.
9. Ensure the CCG reach out to protected group patient and carers to work with
commissioners in shaping inclusive services which include feedback from ‘the local
patient voice’.
10. Work in partnership with Public Health colleagues to continue to influence the Joint
Strategic Needs Assessment with focus on Health Needs Assessments for local
protected groups.
Workforce actions going forward:
1. Work is required to improve our Electronic Staff Records and inform staff of the
reason for this data collection.
2. In addition, the CCG and Human Resources to work to improve staff confidential
disclosure of equality monitoring, in preference to ‘do not wish to disclose’.
Information to be sent to all staff to explain the importance of recording this
information and giving assurance of confidentiality of this information and in reporting
on this information (both internally and publicly).

P a g e | 26
3. Introduce a default standard for all Staff Surveys to include provision of the option for
staff to anonymously declare their protected group profiles, to support future analysis
of findings disaggregated by protected groups. Carers should also be included in
such scrutiny, as if a protected group and where carer status is declared by staff.
4. Focus on further decreasing the number of ‘not stated’ returns against our current
equality monitoring of protected characteristics.
5. Future recruitment should include part-time positions to allow women and men to
participate equally in senior roles other than clinical positions.
6. A review of CCGs Equality Objectives is undertaken at the same time as CCG’s
Equality and Inclusion Strategy is further developed through feedback received, in
2016.
Note: All actions identified will be included within the CCG Equality and Inclusion Action
Plan.
Author: Equality and Inclusion team
NHS Midlands and Lancashire Commissioning Support Unit
Date: November 2015

Appendi
The CCG
Equality D
of its work
Characteri
have not b
data in line
North Sta
Full Time
Full Time
0.00
1.00
2.00
3.00
4.00
5.00
6.00
7.00
FTE
ix 1 - CC
has a sma
Duty to pub
k and has p
istics in Ap
been repor
e with the D
affordshire
Equivalen
Equivalen
17
NS CCG
16 ‐19
YearsOld
20 ‐24
YearsOld
Y
NS CCG W
G Workf
all workforc
lish its wor
provided a
ppendix 1 e
rted separa
Data Prote
e CCG Wo
nt (FTE) b
nt (FTE) b
.07%
Workforce
25 ‐29
YearsOld
30 ‐34
YearsOld
33
YeO
Workforce
force Pro
ce (39.6 FT
rkforce dat
summary
ensuring th
ately to ens
ection Act 1
orkforce : S
y Gender
y Age Ban
82.9
e 30/09/20
35 ‐39earsOld
40 ‐44
YearsOld
454
YeaO
Age Ban
e 30/09/201
P a g e | 27
ofile
TE) and as
ta, howeve
of the brea
hat where n
sure individ
1998.
Staff in Po
nd
3%
015 : By G
5 ‐9arsld
50 ‐54
YearsOld
55 59
YearOld
nd
15 : By Ag
7
s such is no
er the CCG
akdown of
numbers w
dual staff c
ost 30/09/2
ender
F
M
‐
rsd
60 ‐64
YearsOld
65 ‐69
YearsOld
ge Band
ot required
G promotes
the CCG s
were small
cannot be i
2015
Female
Male
s
70 ‐100YearsOld
d under the
s transpare
staff by Pro
(less than
identified f
e Specific
ency in all
otected
10) these
from the
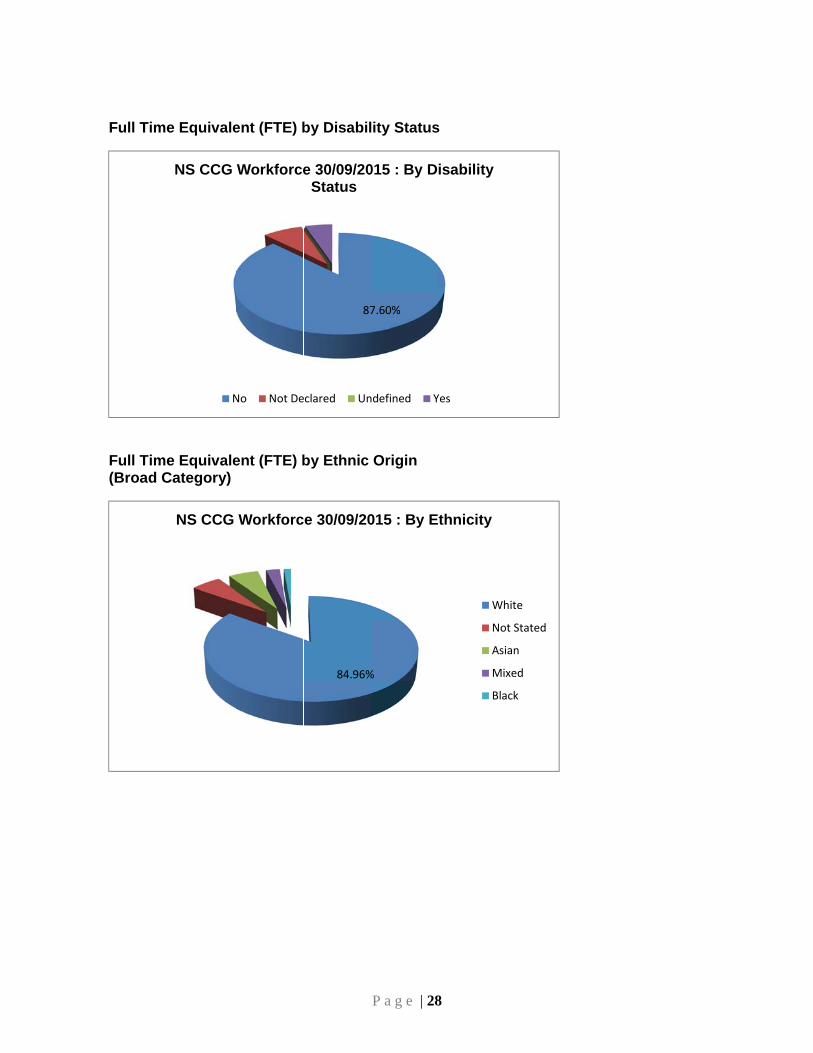
Full Time
Full Time(Broad C
e Equivale
e EquivaleCategory)
NS CCG
N
NS CCG
ent (FTE) b
ent (FTE) b
Workforce
No Not De
Workforc
by Disabil
by Ethnic
87
e 30/09/20Status
eclared Un
84.96%
ce 30/09/20
P a g e | 28
lity Status
Origin
7.60%
015 : By D
ndefined Y
%
015 : By E
8
s
isability
Yes
thnicity
Wh
No
Asi
Mi
Bla
hite
ot Stated
ian
xed
ack

Full Time
Full time
NS CCGBy
e Equivale
e Equivale
NS CCG
G Workfory Religion
ent (FTE) b
nt (FTE) b
G WorkforO
rce 30/09/2n or Belief
by Sexual
by Religion
72.22%
ce 30/09/2Orientation
50.93%
2015 :
P a g e | 29
Orientatio
n and Beli
2015 : By Sn
He
I dmy
C
Im
A
O
I
S
9
on
ief
Sexual
eterosexual
o not wish to y sexual orien
Christianity
I do not wish tomy religion/bel
Atheism
Other
Islam
Sikhism
disclosetation
o discloseief
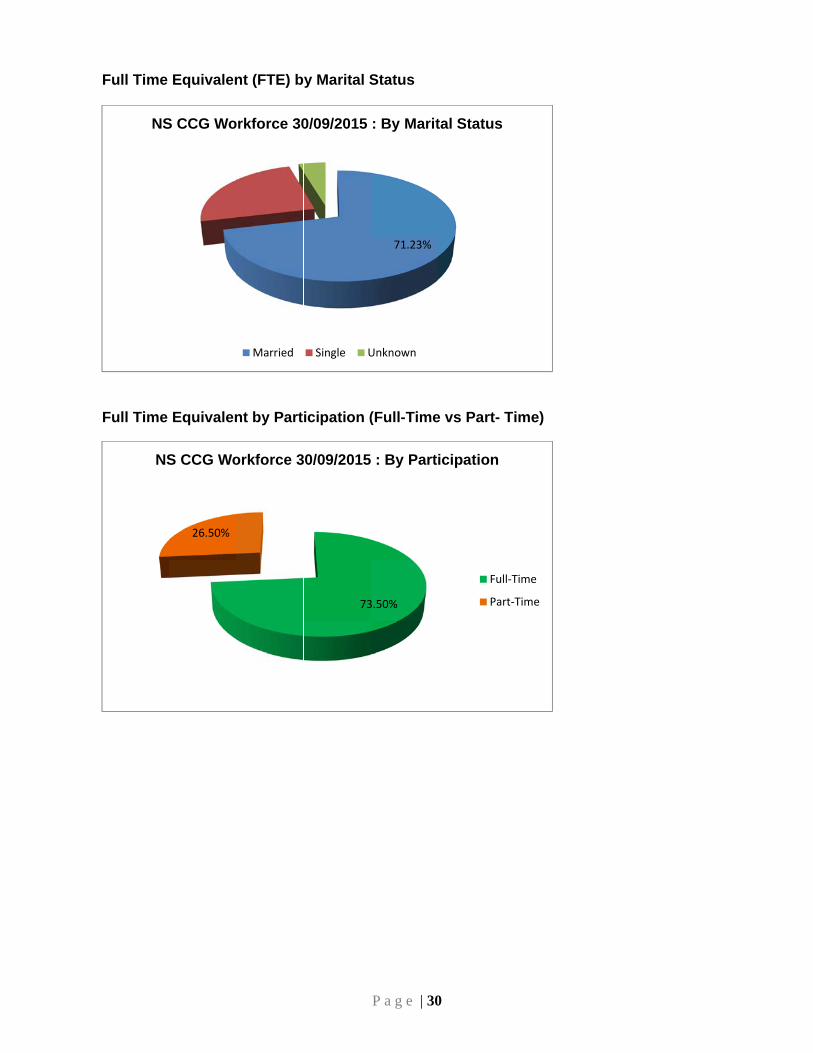
Full Time
Full Time
NS
NS
Equivalen
Equivalen
S CCG Wo
26.50%
S CCG Wo
nt (FTE) b
nt by Part
orkforce 30
Married
orkforce 3
y Marital S
icipation (
0/09/2015
Single U
73
30/09/2015
P a g e | 30
Status
(Full-Time
71.23%
: By Marit
Unknown
3.50%
: By Part
0
e vs Part- T
tal Status
icipation
Ful
Par
Time)
l‐Time
rt‐Time

P a g e | 31
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Payscale
NS CCG Workforce 30/09/2015 : Payscale By Gender
Male
Female
8.35%
41.44%
30.04%
3.11%2.53%0.00%
10.14%
4.39%
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
35.00%
40.00%
45.00%
AfC Band 1 ‐ 4 AfC Band 5 ‐ 7 AfC Band 8a ‐ 9 Non‐AfC
Payscale
NS CCG Workforce 30/09/2015 : Payscale By Gender
Female
Male
0%10%20%30%40%50%60%70%80%90%
100%
Payscale
NS CCG Workforce 30/09/2015 : Payscale By Disability Status
Undefined
Yes
Not Declared
No

P a g e | 32
8.35%
28.77%
31.56%
3.55%2.53%
12.67%
8.62%
3.95%
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
35.00%
AfC Band 1 ‐ 4 AfC Band 5 ‐ 7 AfC Band 8a ‐ 9 Non‐AfC
Payscale
NS CCG Workforce 30/09/2015 : Payscale By Sexual Orientation
Heterosexual
I do not wish to disclose mysexual orientation
0%10%20%30%40%50%60%70%80%90%
100%
Payscale
NS CCG Workforce 30/09/2015 : Payscale By Sexual Orientation
I do not wish to disclose mysexual orientation
Heterosexual
10.14%
32.95%
27.88%
2.53%0.74%
8.49%
12.30%
4.97%
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
35.00%
AfC Band 1 ‐ 4 AfC Band 5 ‐ 7 AfC Band 8a ‐ 9 Non‐AfC
Payscale
NS CCG Workforce 30/09/2015 : Payscale By Participation
Full‐Time
Part‐Time

P a g e | 33
0%10%20%30%40%50%60%70%80%90%
100%
Payscale
NS CCG Workforce 30/09/2015 : Payscale By Participation
Part‐Time
Full‐Time

P a g e | 34
Appendix 2: The Outcomes of EDS v2 Grading 2015
Equality Delivery System Next Steps Scrutiny this year demonstrates that the CCG took part in its first EDS public grading of joint
evidence with Stoke on Trent CCG and is improving in comparison to 2014 with regard to
the EDS v2 Goals 1 and 4 required Outcomes based on the evidence that has been
scrutinised so far.
See EDS detailed grading report (November 2015); NHS England EDS dashboard report;
and CCG summary dashboard shown below.
Note: Grading record and summary report to NHS England are included with Governing
Body 6 January 2016 meeting EDS update Paper.
Some of the key recommendations to CCG: CCGs will develop an EDS action plan from recommendations and lessons learnt to bring in improvements over the next 12 months.
1. “Transgender care and health inequalities – GPs are still not treating Gender Reassignment patients fairly / correctly re healthcare / support needs and accessing services. There are too many GPs who do not know enough about gender reassignment. Therefore maybe have some specialised GPs who have that expertise.” This service is led by specialised Commissioning at NHS England.
2. Spread the EDS based learning in terms of all 9 protected groups. Need to monitor who is feeding back / attending engagement events and by other
means. Also which protected groups and how are CCG targeting for their feedback?
3. Build more sustainable bridges between health and social care and housing – think broadly around things that are crucial to people’s health such as accommodation with the right kind of support attached to it (integration of health, social care and housing / support).
4. Need appropriate audit trail: Equality monitoring and patient satisfaction option to declare by protected groups is required to be provided routinely - as an ‘option to declare’, when seeking feedback at engagement events or on line.
5. All engagement events should proactively ensure fair access to information, services and premises for disabled people.
6. We do have to recognise that transgender is quite separate from sexual orientation protected group, and as clinicians we do need to be fully aware of that along with awareness implications for patient care and support (see short on line film An Inclusive Patient Journey).

P a g e | 35
7. Ensuring Homeless people feel empowered and that their needs are going to be addressed, (we are working towards this). Social prescribing hub, still in its infancy and development but public health are
interested and works on the basis that rather than write a prescription they can refer them into the hub and do a social prescription.
8. On Stoke City Council website there are current sub sections e.g. for Ethnic Needs Assessment & Religion in Stoke. Are there going to be any more sections for the protected groups by locality? Also, such public facing websites need to include a feedback mechanism to Public Health / Health and Wellbeing Board.
Transforming Cancer / End of life care feedback 9. TCEOL has to be the way forward – service engagement, inclusivity and co-
development with all protected groups. Cancer: Really intentional in including all the protected groups. Identified for
themselves that better questions need to be asked to actually see how protected groups are faring in comparison to the general population – where this to be done would grade as excelling rather than achieving.
Goal 4 feedback 10. 4.1: Seems that much is being done to ensure compliance with EDS v2, but it is
difficult to ascertain just how far it is really embedded, and not just through a 4 Goal requirement. Need to have tangible evidence. Sounds good. Too many anachronisms.
11. 4.2: Evidencing good outcomes for protected groups: ‘You said. We listened. We did.’ – need to know more on how do senior decision makers show this?
12. 4.2: Recognise CCGs are on a learning journey and the need for more work to ensure needs of protected groups represented clearly within all Board / Senior Committee Papers.
13. 4.3: Good examples of targeted training and Briefings for staff awareness raising. Proactive response to training needs of all staff is evident. Recommendation: It would be good to include specific examples of where managers have translated training e.g. on reasonable adjustments or the new Accessible Information Standard, into practice.
14. Consider how do we approach recruitment around protected groups? This links with EDS Goal 3 in 2016 CCG evidence and evidence of fair recruitment training for all recruiting managers / senior staff.
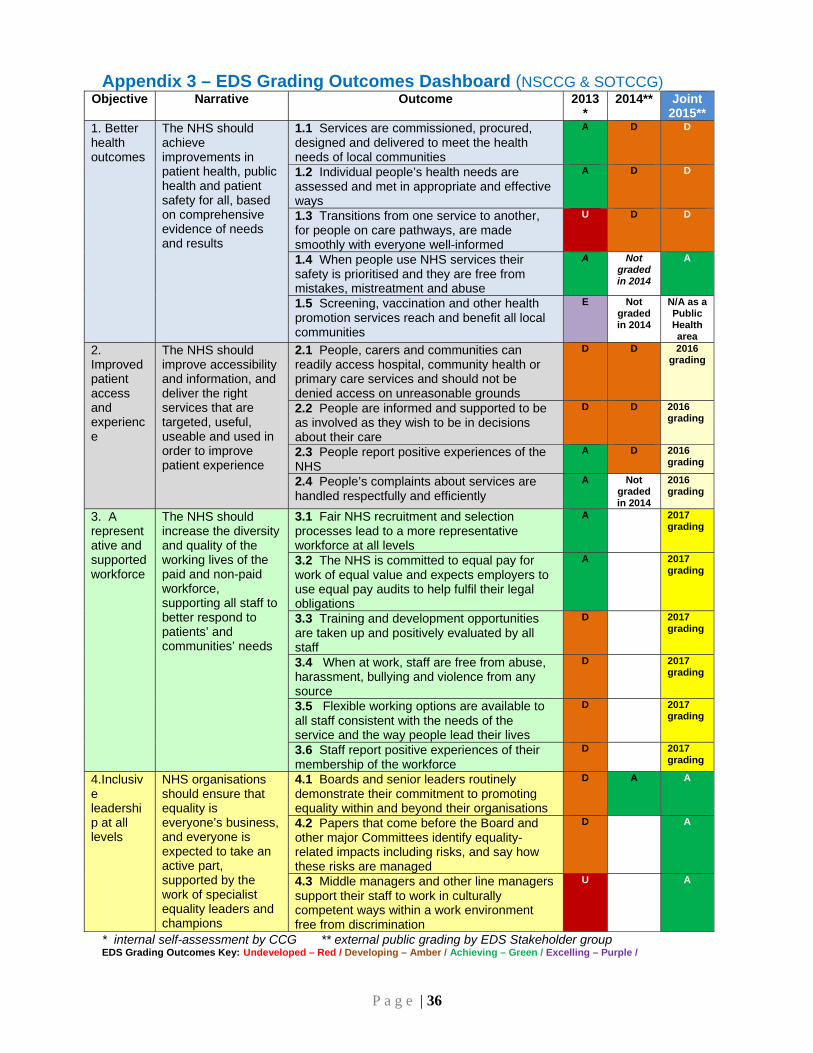
P a g e | 36
Appendix 3 – EDS Grading Outcomes Dashboard (NSCCG & SOTCCG) Objective Narrative Outcome 2013
* 2014** Joint
2015** 1. Better health outcomes
The NHS should achieve improvements in patient health, public health and patient safety for all, based on comprehensive evidence of needs and results
1.1 Services are commissioned, procured, designed and delivered to meet the health needs of local communities
A D D
1.2 Individual people’s health needs are assessed and met in appropriate and effective ways
A D D
1.3 Transitions from one service to another, for people on care pathways, are made smoothly with everyone well-informed
U D D
1.4 When people use NHS services their safety is prioritised and they are free from mistakes, mistreatment and abuse
A Not graded in 2014
A
1.5 Screening, vaccination and other health promotion services reach and benefit all local communities
E Not graded in 2014
N/A as a Public Health area
2. Improved patient access and experience
The NHS should improve accessibility and information, and deliver the right services that are targeted, useful, useable and used in order to improve patient experience
2.1 People, carers and communities can readily access hospital, community health or primary care services and should not be denied access on unreasonable grounds
D D 2016 grading
2.2 People are informed and supported to be as involved as they wish to be in decisions about their care
D D 2016 grading
2.3 People report positive experiences of the NHS
A D 2016 grading
2.4 People’s complaints about services are handled respectfully and efficiently
A Not graded in 2014
2016 grading
3. A representative and supported workforce
The NHS should increase the diversity and quality of the working lives of the paid and non-paid workforce, supporting all staff to better respond to patients’ and communities’ needs
3.1 Fair NHS recruitment and selection processes lead to a more representative workforce at all levels
A 2017 grading
3.2 The NHS is committed to equal pay for work of equal value and expects employers to use equal pay audits to help fulfil their legal obligations
A 2017 grading
3.3 Training and development opportunities are taken up and positively evaluated by all staff
D 2017 grading
3.4 When at work, staff are free from abuse, harassment, bullying and violence from any source
D 2017 grading
3.5 Flexible working options are available to all staff consistent with the needs of the service and the way people lead their lives
D 2017 grading
3.6 Staff report positive experiences of their membership of the workforce
D 2017 grading
4.Inclusive leadership at all levels
NHS organisations should ensure that equality is everyone’s business, and everyone is expected to take an active part, supported by the work of specialist equality leaders and champions
4.1 Boards and senior leaders routinely demonstrate their commitment to promoting equality within and beyond their organisations
D A A
4.2 Papers that come before the Board and other major Committees identify equality-related impacts including risks, and say how these risks are managed
D A
4.3 Middle managers and other line managers support their staff to work in culturally competent ways within a work environment free from discrimination
U A
* internal self-assessment by CCG ** external public grading by EDS Stakeholder group EDS Grading Outcomes Key: Undeveloped – Red / Developing – Amber / Achieving – Green / Excelling – Purple /

Equality & Inclusion: Annual E&I Publication (Jan 2016) Appendix 2: The 4 Gunning Principles Before 1985 there was little consideration given to consultations until a landmark case in that year (R v London Borough of Brent ex parte Gunning). This case sparked the need for change in the process of consultations when Stephen Sedley QC proposed a set of principles that were then adopted by the presiding judge. These principles, known as Gunning or Sedley, were later confirmed by the Court of Appeal in 2001 (Coughlan case) and are now applicable to all public consultations that take place in the UK. 1. When proposals are still at a formative stage Public bodies need to have an open mind during a consultation and not already made the decision, but have some ideas about the proposals. 2. Sufficient reasons for proposals to permit ‘intelligent consideration' People involved in the consultation need to have enough information to make an intelligent choice and input in the process. Equality Assessments should take place at the beginning of the consultation and published alongside the document. 3. Adequate time for consideration and response Timing is crucial – is it an appropriate time and environment, was enough time given for people to make an informed decision and then provide that feedback, and is there enough time to analyse those results and make the final decision? 4. Must be conscientiously taken into account Think about how to prove decision-makers have taken consultation responses into account. The risk of not following these principles could result in a Judicial Review. A number of public bodies across the UK have been taken to Judicial Review and deemed to have acted unlawfully in their Public Sector Equality Duty – usually linked to the four Gunning Principles.

1
ENCLOSURE: 10
AUTHOR REPORTING OFFICER
Name Lee George Name Jayne Downey
Title Head of Quality Title Director of Nursing & Quality
REPORT TO North Staffordshire (NS) Clinical Commissioning Group (CCG) Governing Board
TITLE OF REPORT Quality Report
DATE OF THE MEETING Wednesday 6th January 2016
WHAT OTHER CCG COMMITTEE OR GROUP HAS CONSIDERED THIS REPORT?
Record which groups/committee have already seen this report, the date and comments (for example agreed this report should go to the governing board for approval)
N/A
ACTION REQUIRED FROM COMMITTEE/GROUP/ GOVERNING BOARD (PLEASE TICK)
Approve
Assurance
Discussion
Information
The CCG Governing Board is asked to: o Note the key quality and safety matters reported to provider’s Clinical Quality Review Groups and the
CCG’s Quality Committee and actions taken in response.
STRATEGIC GOALS SUPPORTED BY THIS PAPER (tick appropriate goal)
1. Increase life expectancy and reduce inequality
2. Improve prevention, early detection and effective management of those at increased risk
3. Enhance quality of life and improve health outcomes for people with LTCs
4. Ensure people receive the right care in the right place
PURPOSE OF THE REPORT/SUPPORTING INFORMATION (if applicable)
This report aims to provide North Staffordshire CCG Governing Board assurance that structures and processes are in place to promote, monitor and ensure safe, high quality health services for the people of North Staffordshire.
Care Quality Commission inspection reports are published on the following website: www.cqc.org.uk
KEY POINTS/EXECUTIVE SUMMARY
o North Staffordshire CCG has breached its annual tolerance at Month 7 with 70 CDI cases reported against an annual tolerance of 55. The Head of Infection Prevention & Control presented the C-Difficile Recovery Plan at the Quality Committee in November and members of the Committee requested that an overarching action plan for recovery is presented to the committee on a quarterly basis.
Risks relating to the proposals in this paper
N/A
Summary of any finance/resource/medicines management /workforce implications
N/A
Any statutory/regulatory/legal/NHS Constitution/Assurance/Governance implications
N/A
Equality Impact Assessment (Are there any direct or indirect implications)
N/A

2
Any related work with stakeholders/practices/public and patient engagement
N/A
Quality implications
Within the body of the report.
Acronyms
Explained within the body of the report.
1. Developing CCG Capacity & Capability for Quality Improvement
1.1 Since the last Governing Board meeting the Quality Committee (joint meeting with Stoke-on-Trent CCG) met on the 11th November and 9th December. The Committee received reports outlining the quality assurances for the CCG’s main providers and updates from its subgroups; Infection Prevention & Control Group, Safeguarding Group and Primary Care Subcommittee
1.2 The Quality Committee discussed the Insight (Patient Experience & Membership Feedback)
Report 2015/16 Quarter 1 (July – September); the report covered both North Staffordshire CCG and Stoke-on-Trent CCG enabling triangulation of information and analysis of themes on a wider scale. There were 168 feedback contacts in the quarter by the following methods: PALS (66), Soft Intelligence – patient based (59), Complaints (25), MP Letters (11), Compliments (3) Media (2) and Social Media (1).
The most common reason for feedback (75) is within the patient experience domain of ‘access and waiting’ this is consistent with previous quarters. Members noted that the services with the highest number of feedback related to Ophthalmology at Royal Stoke Hospital focussing on access to services / access to appointments and Continuing Healthcare. These two areas are consistent with the CCG’s intelligence relating to outpatient backlog appointments and the delays being experienced in considering retrospective continuing healthcare claims. The issue relating to continuing healthcare has also been discussed at the Complaints and PALS Assurance Group across both North Staffordshire and Stoke-on-Trent CCGs and clarity and assurance of the timeline for considering these claims has been requested from the lead CCG, along with the process for ensuring contact with the family throughout the process to ensure that patient experience is satisfactory. North Staffordshire CCG directly received 12 complaints; this is an increase when compared to previous quarters. The organisations that the complaints were about include: Continuing Healthcare (4), Royal Stoke University Hospital Hospital (2), Nuffield Health (3), East Cheshire NHS Trust (1) Ramsay Health Care (1) and Staffordshire & Stoke-on-Trent Partnership NHS Trust (1). The CCG is not aware of any complainants contacting the Parliamentary and Health Service Ombudsmen requesting an independent review of their complaints. Further work will now progress to develop this Patient Insight report to expand the information relating to learning and outcomes and events (GP Datix Reporting). Members noted the positive developments underway between the CCG and the Patient Services Team within the Midlands and Lancashire Commissioning Support Unit focussing on the development of a Satisfaction Survey to help identify how satisfied complainants are with how their complaints are handled, and a revised content for a leaflet and webpage focussing on PALS and Complaints for both CCGs.
2. Quality Monitoring of Main Providers of Clinical Services A. North Staffordshire Combined Healthcare NHS Trust (NSCHT) 2.1 The Safety Thermometer ‘harm free care’ rate for November 2015 is 92.96% and 95.77% had
no new harms recorded. This is based upon 71 patients surveyed. The highest rate of harm over the twelve month period is falls and the next highest rate of harm is pressure ulcers. The rolling twelve month performance at NSCHT is:

3
Indicator 2014 2015
Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov
No Harms (%) 94.52 95 98.48 93.67 97.22 98.57 97.06 94.44 95.24 95.31 100 92.96
No New Harms (%) 94.52 98.33 100 97.47 98.61 98.57 98.53 98.61 96.83 95.31 100 95.77
Patients 73 60 66 79 72 70 68 72 63 64 69 71
NSCHT has reported 8 serious incidents during October and November 2015; all of these were categorised as ‘unexpected death’. All serious incidents are investigated in accordance with the National Framework and using National Patient Safety Agency best practice guidance. The CCG has an opportunity to challenge the provider’s investigation findings at the monthly Serious Incident Subgroup.
2.2 The latest Friends and Family Test results highlight that 82% of patients would recommend
NSCHT, 63% of staff would recommend NSCHT as a place to receive care and 42% of staff would recommend NSCHT as a place to work. The FFT results are broken down below:
Patients 2015
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Recommend 82% 91% 90% 97% 85% 81% 89% 87% 90% 82%
Not Recommend 0% 4% 5% 0% 5% 3% 4% 3% 4% 4%
Total Responses 39 55 58 37 39 31 54 30 49 45
NHS England (Peer) - Recommend
86% 85% 88% 87% 88% 87% 87% 88% 86% 87%
NHS England (Peer) – Not Recommend
5% 5% 4% 4% 4% 5% 5% 4% 5% 4%
Staff 2014 2015
Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep
Recommend – Care 50% 69% 74% 63%
Recommend – Work 43% 49% 44% 42%
Not Recommend – Care
Not Applicable
15% 7% 17%
Not Recommend – Work 32% 26% 28%
Total Responses 100 90 100
The Staff FFT NHS England averages for all Trusts are as follows: Recommended – Care 79%, Recommended – Work 62%, Not Recommended – Care 7%, Not Recommended – Work 19%. The disaggregated England average scores for acute, community and mental health provider trusts are not published.
B. Staffordshire and Stoke on Trent Partnership NHS Trust (SSOTP) 2.3 The Safety Thermometer ‘harm free care’ rate for November 2015 is 90.53% and 96.63% had
no new harms recorded. This is based upon 1871 patients surveyed. The highest rate of harm over the twelve months is pressure ulcers and the majority of these are existing Grade 2 pressure ulcers. The number of new harm pressure ulcers remains constant between a high of 2.03% in July 2015 and a low of 1.2% in May 2015. The rolling twelve month performance at SSOTP is:
Indicator 2014 2015
Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov
No Harms (%) 92.15 92.71 92.66 91.76 90.92 92.76 90.9 90.86 89.75 91.56 90.76 90.43
No New Harms (%) 97.08 97.07 97.28 97.28 96.42 97.7 96.78 96.71 96.62 96.58 96.97 96.63
Patients 2089 2182 2058 2172 2148 2170 2078 2068 2039 2073 1916 1871

4
SSOTP has reported 51 serious incidents during October and November 2015; of these 44 were within the ‘pressure ulcers’ category. All pressure ulcer serious incidents are reviewed, challenged and scrutinised at the Tissue Viability Panel, chaired by SSOTP’s Director of Nursing & Quality and attended by the CCG’s Quality Manager, a decision is made whether the pressure ulcer was avoidable/unavoidable and any learning identified.
There has been a 27.3% decrease in the number of acquired pressure ulcers within community services pan-Staffordshire particularly within the grade 2 and deep tissue damage categories. SSOTP continue to work towards the elimination of avoidable pressure ulcers refreshing their zero tolerance action plan. It should be noted that SSOTP have not yet adopted the new serious incident definition and are therefore reporting all grade 3 or grade 4 pressure ulcers whereas other providers only report pressure ulcers that are avoidable, attributable and there has been a clear lapse in patient care. Therefore SSOTP will continue to report high numbers of serious incidents within the ‘pressure ulcers’ category.
2.4 The latest Friends and Family Test results highlight that 96% of patients would recommend SSOTP, 78% of staff would recommend SSOTP as a place to receive care and 48% of staff would recommend SSOTP as a place to work. The FFT results are broken down below:
Patients 2014 2015
Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct
Recommend 96% 98% 97% 97% 97% 97% 97% 97% 97% 98% 98% 96%
Not Recommend 1% 1% 1% 1% 1% 1% 0% 1% 0% 1% 0% 1%
Total Responses 1491 1621 1779 1467 1613 2306 2701 3206 3413 2955 3088 3037
NHS England (Peer) - Recommend
Not Available 96% 95% 95% 96% 95% 95% 95% 96% 95% 95%
NHS England (Peer) – Not Recommend
1% 1% 1% 1% 1% 1% 1% 1% 2% 2%
Staff 2014 2015
Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep
Recommend – Care 64% 76% 77% 78%
Recommend – Work 50% 51% 51% 48%
Not Recommend – Care
6% 5% 6%
Not Recommend – Work 26% 25% 27%
Total Responses 1876 1826 803
C. University Hospital North Midlands NHS Trust (UHNM) 2.5 The Safety Thermometer ‘harm free care’ rate for July 2015 is 91.17% and 98.39% had no new
harms recorded. This is based upon 1121 patients surveyed. The highest rate of harm over the twelve months is pressure ulcers and the majority of these are existing Grade 2 pressure ulcers. The rolling twelve month performance at UHNM is:
Indicator 2014 2015
Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov
No Harms (%) 90.47 88.65 90.71 87.78 87.98 89.66 90.13 90.04 90.02 92.41 90.84 91.17
No New Harms (%) 97.8 97.59 97.66 97.01 97.6 97.79 97.55 98.31 97.73 98.23 97.76 98.39
Patients 1270 1286 1195 1170 1123 1132 1104 1125 1102 1133 1114 1121
UHNM has reported 16 serious incidents during October and November 2015; of these 8 were ‘slips, trips & falls’ and a further 5 were ‘pressure ulcers’. All pressure ulcer serious incidents are reviewed, challenged and scrutinised at the Tissue Viability Panel, chaired by UHNM’s Director of Nursing and attended by the CCG’s Quality Manager, a decision is made whether the pressure ulcer was avoidable/unavoidable and any learning identified.

5
Falls Bundle (91.6%) scores and Falls Risk Assessment (98.75%) completion continues to exceed the 90% target across UHNM. Further, 98.78% of all patients had a Pressure Ulcer Risk Assessment completed upon admission. UHNM continues to implement the “Stop the Pressure” initiatives to eliminate hospital acquired pressure ulcers.
2.6 The latest Friends and Family Test results highlight that 97% of inpatients would recommend UHNM, 73% of A&E attenders would recommend UHNM, 83% of staff would recommend UHNM as a place to receive care and 62% of staff would recommend UHNM as a place to work. The FFT results are broken down below:
Inpatients 2014 2015
Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct
Recommend 96% 95% 96% 96% 97% 96% 96% 96% 96% 97% 98% 97%
Not Recommend 1% 2% 1% 2% 1% 1% 1% 1% 1% 1% 1% 1%
Total Responses 1202 1038 1214 1559 1530 1219 1345 1615 1888 1436 1974 2429
Response Rate 31% 26% 33% 45% 40% 31% 32% 37% 40% 32% 20% 22%
NHS England (Peer) - Recommend
95% 95% 94% 95% 95% 96% 96% 96% 96% 96% 96% 96%
NHS England (Peer) – Not Recommend
2% 2% 2% 2% 2% 2% 1% 1% 1% 1% 2% 1%
A&E 2014 2015
Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct
Recommend 86% 84% 83% 84% 86% 78% 78% 71% 73% 76% 75% 73%
Not Recommend 5% 6% 6% 6% 5% 12% 12% 16% 14% 21% 14% 16%
Total Responses 1143 937 1218 964 2482 1828 760 1140 2248 1804 1870 1821
Response Rate 15% 13% 18% 15% 33% 24% 9.4% 16% 26% 21% 23% 22%
NHS England (Peer) - Recommend
87% 86% 88% 88% 87% 88% 88% 88% 88% 88% 88% 87%
NHS England (Peer) – Not Recommend
6% 7% 6% 6% 6% 6% 6% 6% 6% 6% 6% 7%
Staff 2014 2015
Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep
Recommend – Care 69% 80% 83% 83%
Recommend – Work 57% 58% 61% 62%
Not Recommend – Care
6% 6% 5%
Not Recommend – Work 21% 18% 17%
Total Responses 1376 1178 979
3. Infection Prevention & Control (IPC)
3.1 Since the Infection Prevention & Control Group (joint meeting with Stoke-on-Trent CCG) meets quarterly it has not met since the last Governing Board meeting. The next meeting will take place on the 21st January 2016.
3.2 NHS England has set a challenging trajectory for Clostridium Difficile Infections (CDI) and a zero
tolerance approach to avoidable Methicillin-Resistant Staphylococcus Aureus (MRSA) blood
stream infections (BSI) for 2015/16. The Month 7 (April 2015 – October 2015) performance data
for the CCG and our main providers is included below:

6
North Staffordshire CCG
Year
to date
YTD target
Annual tolerance
CDI 70 35 61
MRSA 1 0 0
North Staffordshire Combined Healthcare NHS Trust
Year
to date
YTD target
Annual tolerance
CDI 1 0 0
MRSA 0 0 0
Staffordshire & Stoke-on-Trent Partnership NHS Trust
Year
to date
YTD target
Annual tolerance
CDI 13 8 10
MRSA 0 0 0
University Hospital of North Midlands NHS Trust
Year
to date
YTD target
Annual tolerance
CDI 75 49 74
MRSA 4 0 0
3.3 North Staffordshire CCG has breached its annual tolerance at Month 7 with 70 CDI cases
reported against a cumulative tolerance of 35. Of the 70 CDI cases, 18 occurred within an acute setting and 52 in a non-acute setting (e.g. sample sent from a Nursing Home, General Practice or within 48 hours of admission to an acute or bedded community facility other than a Care Home).
3.4 The Head of Infection Prevention & Control presented the C-Difficile Recovery Plan at the Quality Committee in November. She highlighted the actions undertaken as part of the work plan which included: the auditing of nursing homes across the health economy, undertaking of quality visits to areas that show non-compliance or where spikes in CDI or MRSA Bacteraemia rates have been identified, fortnightly infection prevention conference calls and attendance at provider Infection Prevention & Control Boards. Members of the Committee noted that all providers have their own infection prevention control plans and CDI trajectories and that a quality visit is planned to the Royal Stoke University Hospital during December following the installation of the isolation pods within the West Building. An event is also planned during January 2016 to bring together all stakeholders, including NHS England, the NHS Trust Development Authority and commissioners to focus on the work being undertaken and the actions required as a local health economy.
Member of the Committee requested that an overarching action plan for Infection Prevention Control recovery be presented to the committee on a quarterly basis. This plan should have clear RAG ratings against priorities/risks, projected trajectories, and be linked to a comprehensive narrative on the current actions being taken. Infection Prevention and Control continues to be included on the CCG Risk Register focussing on patient experience and safety.
4. Safeguarding Adults, Children & Young People
4.2 Since the last Governing Board meeting the Safeguarding Group (joint meeting with Stoke-on-Trent CCG) met on the 23rd December 2015. The next meeting will take place on the 18th March 2016.
4.3 “My next patient may lack capacity” Prompt Cards have been distributed to all local GPs at a protected learning event in November. These are the second set of pocket sized guidance which follow the Safeguarding Prompt Cards produced 2014, this set specifically address the principles of the MCA and its application. The cards were funded by NHS England North Midlands and developed by Asist Independent Mental Capacity Advocates (hospital service).
4.4 Stoke-on-Trent Safeguarding Children Board (SCB) has published two local serious case reviews; SOT 2014 (1) and SOT 2014 (2). In both cases the Independent Chair of the SCB has highlighted that improvements have been identified and a number already put in place. These

7
include, respectively, the introduction of multi-agency training so that professionals have a greater awareness of how to work with families who have shared care arrangements and the introduction of a 24 hour mental health and social care access team. The CCGs are confident that there have been substantial changes and improvements made to the ‘single point of access’ since October 2014. From November 2014 the CCGs have made a number of unannounced quality visits to give assurance that the service is functioning safely, and more will be made in the future to make sure the improvements are maintained and are sustainable. The SCB are facilitating a number of briefing sessions to share the good practice identified and the findings and learning from each of the reviews; these invites have been shared with our GP membership through the GP Newsletter.
The full reports can be accessed on the SCB website: http://www.safeguardingchildren.stoke.gov.uk/ccm/content/safeguarding-children/professionals-folder/key-processes/serious-case-reviews.en

ENCLOSURE: 11
AUTHOR
REPORTING OFFICER /DIRECTOR
Name Sally Parkin Name Professor Naomi Chambers
Title Clinical Director for Partnerships and Engagement
Title Lay Board Member for PPI
REPORT TO North Staffordshire Clinical Commissioning Group (CCG) Governing Board Meeting
TITLE OF REPORT Second Citizens Jury
DATE OF THE MEETING 6th January 2015
WHAT OTHER CCG COMMITTEE/GROUP/INDIVIDUALHASCONSIDERED THIS REPORT?
COMMITTEE/GROUP
INDIVIDUAL
North Staffordshire Patient Congress 17
th December 2015
Discussed by Sally Parkin, Patient Engagement budget holder and Elaine Price, Interim CCG Accountant 10th November 2015
Margy Woodhead Lay Board Member for PPI Stoke on Trent CCG
ACTION REQUIRED FROM GOVERNING BOARD
Decision
X
Assurance
Discussion
X
For noting
RECOMMENDATION The Board is asked to consider the options for a second Citizen’s Jury proposed by the Patient Congress and:
1. to support a second Citizens Jury investigation 2. to decide on the topic for the next Citizens Jury and provide a rationale for the decision 3. to agree that the next Citizens Jury will be jointly sponsored by both North Staffordshire and
Stoke on Trent Boards. This paper will be presented to the Governing Body of Stoke CCG.
STRATEGIC GOALS SUPPORTED BY THIS PAPER (identify appropriate goals)
YES NO
1. Increase life expectancy and reduce inequality
X
2. Improve prevention, early detection and effective management of those at increased risk
X
3. Enhance quality of life and improve health outcomes for people with LTCs
X
4. Ensure people receive the right care in the right place
X
PURPOSE OF THE REPORT, KEY POINTS, OUTCOMES, EXECUTIVE SUMMARY
The report summarises the benefit of a Citizens Jury to the CCG as a commissioning organisation and to the patients it serves. The first jury focusing on diabetes generated several practical recommendations to improve the quality of the CCGs commissioned services which have been accepted and are being acted on. This form of patient and public involvement provides a different perspective and complements more traditional engagement activities. The Patient Congress proposes a second Citizens Jury investigation and provides a shortlist of proposals. It is proposed that the Citizens Jury costs are met by the patient engagement budgets across North Staffordshire and Stoke CCGs.
SUMMARY OF RISKS RELATING TO THE PROPOSAL
None
ANY STATUTORY / REGULATORY / LEGAL / NHS CONSTITUTION/ASSURANCE / GOVERNANCE / PRESCRIBING IMPLICATIONS
None
QUALITY IMPACT ASSESSMENT AND/OR EQUALITY IMPACT ASSESSMENT
The jury will be asked to pay due regard to the 9 protected groups in terms of ensuring their voice is heard and considering their experience of the service in question. The main purpose of the jury is for patient leadership to influence improvements in the quality of commissioned health services.
ANY RELATED WORK WITH STAKEHOLDERS/PRACTICES/PUBLIC AND PATIENT ENGAGEMENT
The proposed Citizens Jury is an integral part of the CCG’s commitment to meaningful engagement at each stage of the commissioning cycle. The process is commissioned by the Patient Congress and led by patients and members of the public.
ACRONYMS
CCG Clinical Commissioning Group LTC Long term condition PPI Patient and public involvement

1. Background
1.1 The first Citizens Jury, convened by North Staffordshire CCG in September 2014 under the auspices of the Patient Congress, and in association with Stoke CCG, examined the services and experiences of people with diabetes, and resulted in a report which was published in March 2015. The CCG accepted the recommendations and is working towards implementing them, with regular updates received at the Patient Congress and at Board.
1.2 The Citizens Jury in North Staffordshire has received attention in the local media, been
praised by NHS England and was referred to at the recent National Voices annual conference. It puts patients, carers and the interested public at the heart of healthcare commissioning, and gives a real opportunity for patients to lead in the shaping of future services. The first jury had collaborative engagement with patients, carers, clinical commissioners, managers and healthcare professionals.
1.3 The approach demonstrates the effectiveness of the use of lay wisdom to identify strengths
and weaknesses of services and the opportunities for improvement. Patients and members of the public provide a fresh and objective perspective, which leads them to ask different questions and challenge assumptions that might be made by NHS commissioners and providers and identify potential blind spots. This enables the CCG to have the benefit of wider intelligence and complements other methods of patient and clinical engagement.
1.4 In addition it reinforces the CCG’s culture of openness and inclusion and is based on the
NHS constitutional tenet that the NHS belongs to the people. 2. Proposal
2.1 The Patient Congress, at its meeting on 17 December 2015, agreed that a second jury should now be convened, adopting a similar approach to the first jury but jointly planned with Stoke CCG. A number of different topic areas were considered including dementia, rheumatoid arthritis, anti-coagulation therapy, COPD, nutrition (including eating disorders), young persons’ prison health and mental health.
2.2 The congress agreed that the criteria for selection should include a focus on a service which
would benefit from having a spotlight shone upon it and where there are opportunities for improvement. In addition the congress was mindful of other service reviews and investigations which may be planned for 2016 and they were keen that the citizen’s jury should provide additionality and not duplicate or conflict with any other work in our health economy. Congress members were clear that the selection of jury members and leadership is key to success and that there was a significant learning from the first jury which should be taken into account.
2.3 Mental health was mentioned more than once in discussions at the congress meeting. The
congress has often highlighted the importance of mental health and emotional wellbeing in the management of physical health conditions. One in four people will suffer from mental health issues at some point during their lives. It is a service which has not received much board-level attention because of the problems facing urgent and emergency care in the local health economy. The recent reporting of events at Southern Health and the national drive for ‘parity of esteem’ suggests that we need to turn our attention to this client group. The recently published joint mental health strategy for Staffordshire provides a useful and timely starting point for a jury investigation into services and experiences of people who suffer from mental health problems and their carers.
2.4 It would be for the jury itself to determine the precise scope and the shape of the inquiry. 2.5 Any decision of the North Staffordshire Governing Board would be subject to agreement with
Stoke CCG.

1 | P a g e
ENCLOSURE: 12
AUTHOR
REPORTING OFFICER /DIRECTOR
Name Rita Symons Name Rita Symons/Marcus Warnes
Title Staffordshire Transformation Director Title Staffordshire Transformation Director/Accountable Officer
REPORT TO NSCCG Governing Board
TITLE OF REPORT Staffordshire Commissioning Congress
DATE OF THE MEETING 6th January 2016
WHAT OTHER CCG COMMITTEE/GROUP/INDIVIDUALHASCONSIDERED THIS REPORT?
COMMITTEE/GROUP Record which committee/group have already seen this report, note date and comments (if applicable)
INDIVIDUAL Please indicate name of individual and date agreed/approved (as necessary), for example HR, Finance, Quality, Medicines Optimisation or other
ACTION REQUIRED FROM COMMITTEE/GROUP/ GOVERNING BOARD (please identify all applicable and provide details below)
Approve
Assurance
Discussion
For noting
RECOMMENDATION Governing Board are requested to receive an update on the Transformation Programme and note the timelines and process for developing the case for change
STRATEGIC GOALS SUPPORTED BY THIS PAPER (identify appropriate goals)
YES NO
1. Increase life expectancy and reduce inequality
2. Improve prevention, early detection and effective management of those at increased risk

2 | P a g e
3. Enhance quality of life and improve health outcomes for people with LTCs
4. Ensure people receive the right care in the right place
PURPOSE OF THE REPORT, KEY POINTS, OUTCOMES, EXECUTIVE SUMMARY (supporting information to be included, if applicable)
To provide
An update on the Transformation Programme
Timelines and process for developing the case for change
SUMMARY OF RISKS RELATING TO THE PROPOSAL Highlight any implications, including finance, quality, reputation, governance, strategic workforce, clinical, medicines optimisation, equality related or other
ANY STATUTORY / REGULATORY / LEGAL / NHS CONSTITUTION/ASSURANCE / GOVERNANCE / PRESCRIBING IMPLICATIONS
QUALITY IMPACT ASSESSMENT AND/OR EQUALITY IMPACT ASSESSMENT Date completed, please highlight any direct or indirect implications
ANY RELATED WORK WITH STAKEHOLDERS/PRACTICES/PUBLIC AND PATIENT ENGAGEMENT Provide further information, including dates if applicable
ACRONYMS If not listed in the report, please list
CSU – Commissioning Support Unit DCO – Director of Commissioning Operations

3 | P a g e
Staffordshire Transformation Report
1. Introduction
The Transformation Programme was established as a system wide response to the challenges facing the Staffordshire and Stoke on Trent health and care economies and the external view, expressed for example in the KPMG Distressed health economy report that many of the solutions lay in collaborative planning. The Programme is developing at pace and there is emerging clarity on what the transformational projects are and how this links to individual CCG plans and business.
2. Update on Key Events On 27th November workshops were held to introduce the concept of Logic Models and start working through at a workstream level. This is a recognised methodology for helping to clarify programme scope and delivery. A clear process is in place with workstream leads to carry out the logic modelling at a project level. A number of meetings have been held with colleagues around the case for change development. A provider workshop is being held on 10th December to clarify scope of the workstream and discuss the broader case for change process and engagement in the other workstreams. A Leadership Summit was held on 15th December to follow on from a previous Summit on 20th October. This was to share the outline of the Case for Change and seek informal sign up from Local Authorities, CCGs and providers. This was a very positive debate and feedback will influence the final submission to the Tripartite. 3. Programme Scope Last month there was a discussion around the scope of the programme and a lack of common understanding and clarity. Work has been undertaken to clarify the projects in the Transformation programme, and to separate out the more transactional QIPP or savings schemes. A proposal has been developed to focus effort collectively in a number of areas. This has been discussed through the Planning Forum, which is chaired by Dr Andrew Bartlam. There is now absolute clarity around the projects within the Transformation Programme, however, further work is required to map interdependencies. 4. Update on Provider Engagement Engagement has been ongoing with providers and discussions have happened with all NHS providers about alignment with Integrated Business Plans (IBPs) and trust strategies. The provider workstream group continues to meet on a fortnightly basis. 5. Communications A newsletter has been sent to staff and partners and a web domain has been agreed. From the New Year, information will start to be loaded on the website and we plan to have a launch of the Case for Change and start further public engagement. 6. Clinical Leadership The Clinical Leaders Group continues to develop and attendance at the last meeting is improved. The group discussed the scope of the programme and changes were made based on the discussion.
4 | P a g e
A preferred candidate has been identified for the Medical Director position. Five clinical leads have been appointed and they are engaging with the workstreams. A session is being held in the New Year to bring them together to discuss support and development. Medical Directors of providers or their representatives are being involved in the scoping of the provider projects. 7. Programme/ Project Management A cloud based project management tool has now been selected to support delivery of the programme (PM3). This will be implemented in the New Year and will allow managers to access the system from their work base and simplified, clearer reporting. Staff involved in projects will be invited to training sessions. The Programme Office continues to meet on a weekly basis and review progress. The Transformation Board, which comprises the workstream leads, is also meeting to discuss the work of the Programme in more detail. We will be supporting workstream leads through a series of focussed workshops where we can bring together support from enabling workstreams and support further logic modelling at project level. This is likely to be in mid-January and we would ask colleagues to prioritise this. 8. Financial Analysis The Financial System analysis is well underway and organisations have engaged positively despite tight timescales. The Finance Steering Group continues to be well attended and there is a commitment to work together. The initial baseline figures should have been available by the end of November but this was delayed because of late submissions from some CCGs. The analysis is now complete. 9. Assurance An assurance meeting was held with NHSE on 9th December, where a progress report was discussed. There was a detailed discussion about the Case for Change development. The key challenge identified was capacity as we move into the delivery phase. 10. Programme Resource The resource focussed on the Programme is now a critical risk. Staff identified to lead projects are not in a position to free up capacity and the work to develop projects is not going at the required pace. This is being discussed with CCG Accountable Officers and Local Authorities. The programme office will assist by laying out a longer timeline in terms of expectations and clarity on what is required when. 11. Case for Change The Case for Change which outlines the context, financial background and what we are going to do through the programme is close to completion. The content has been through iterative discussions through the Congress, Clinical Leaders Group and through broader Leadership Summits. A session is planned in the New Year to discuss with both Health and Wellbeing Boards. The Case for Change will be presented to Governing Bodies and Cabinets for sign off.
1
ENCLOSURE: 14
AUTHOR
REPORTING OFFICER
Name Gill Gardiner
Name Iain Stoddart
Title Assistant CFO
Title Chief Finance Officer
REPORT TO Governing Board
TITLE OF REPORT Month 8 Financial Position
DATE OF THE MEETING 6th January 2016
WHAT OTHER CCG COMMITTEE OR GROUP HAS CONSIDERED THIS REPORT?
Record which groups/committee have already seen this report, the date and comments (for example agreed this report should go to the governing board for approval)
CFP 16/12/15 FRG December 2015
Challenge on assumptions and risk scenarios. Challenge around QIPP delivery and mitigating actions to deliver to planned positions. Risks noted and ongoing assurance sought.
ACTION REQUIRED FROM COMMITTEE/GROUP/ GOVERNING BOARD (PLEASE TICK)
Approve
Assurance
x
Discussion
x
Information
x
STRATEGIC GOALS SUPPORTED BY THIS PAPER (tick appropriate goal)
1. Increase life expectancy and reduce inequality
2. Improve prevention, early detection and effective management of those at increased risk
3. Enhance quality of life and improve health outcomes for people with LTCs
4. Ensure people receive the right care in the right place
RECOMMENDATION Members are asked to note :- 1. the CCG’s month 8 reported position; standing at £2.454m deficit. Albeit that the year to
date position is a £90k improvement on the planned £2.544 deficit position at month 7, there remains a requirement to close the current deficit to planned out-turn levels.
2. the CCG’s forecast outturn position remains in line with the planned deficit of £2m, but a real risk of c£800k remains to be fully bridged; action is being taken through the internal turnaround regime.
3. the initial month 7 contract performance at UHNM and other provider performance.

2
4. current and forecast performance against the original £7.66m QIPP programme levels together with risk scenarios highlighting the potential risk levels being managed that could impact on the out-turn performance.
PURPOSE OF THE REPORT/SUPPORTING INFORMATION (if applicable)
The Report highlights the month 8 reported financial monitoring position and the initial forecast outturn position based on month 7 acute data and month 6 Prescribing data.
KEY POINTS/EXECUTIVE SUMMARY
This report highlights: The month 8 reported position at £2.454m deficit. The basis of the financial position is through receipt of activity and costs up to month 7 for acute data and to month 6 for prescribing data. These latest details are now built into Programme expenditures. The overall forecast outturn remains at the planned level of a £2m deficit at year end. To achieve this position the CCG needs to mitigate the current level of risk and fully deliver to QIPP programme levels in the last 4 months of the financial year. (delivery of £4.55m between December to March). The necessity to fully apply any remaining contingencies (predominantly the 0.5% “headroom” contingency of £1.3m and all sums in budget now assessed as contingent).
Risks relating to the proposals in this paper
The month 8 reported position is based on initial month 7 activity data from Providers which is now providing a more reliable indication of activity trends. To date this shows both activity and costs to be below plan and similarly the forecast assumes that trend continues; albeit profiled to planned demand assumptions. A number of coding issues are being worked through with UHNM relating to specialised commissioning. Some charges currently being made to the CCG should be attributed to NHSE; however activity currently being charged to NHSE may need to be applied to the CCG. Data reporting from the Trust is being worked through to determine the appropriate commissioner for the activity, however it is now considered likely that the overall adjustment would be close to cost neutral when finally transacted. This compares to previous scenarios when it was expected that a benefit may accrue. At a summary level the overall underspend in the main Acute contract at UHNM is partly offset by over performance in other out of area Acute contracts. The CCG is currently working through contractual processes with UHNM regarding 18 week backlog clearance and assessing the impact this has on the reported positions. This is proving difficult without current sign off of the Remedial Action Plan. The CCG has now received 6 months Prescribing data reflecting the pricing process for prescriptions which has a two months lead time for the production of cumulative expenditure. Forecasts based on the information received indicate spending above plan at the year end. Forecasting methods use comparisons of spending in previous years and take into account the expected delivery of QIPP schemes through the remainder of the year. It is expected that expenditure will continue to be above plan but growth in costs will be avoided by delivery of the Prescribing QIPP programme. To achieve the planned deficit position of £2m the CCG must deliver in full the QIPP programme of £7.66m (stretch £8.05m), the majority of which is scheduled for delivery in the latter part of the year. Some slippage of the expected sign up value relating to the Step Up and Step Down contract variation has arisen, which has adversely impacted on QIPP delivery and assumption around the level of risk materialising. A number of risks are evident in the CCGs financial position; these will need to be mitigated in order to maintain the control totals. Significant pressures are evident within the system resilience planning budgets, which have been over committed by the Systems Resilience Group. These issues are currently being worked through to establish a reconcilable position. The CCG will fully utilise the 0.5% contingency of £1.3m to deliver the planned deficit position of £2m.

3
Summary of any finance/resource/medicines management /workforce implications
Whilst the CCGs forecast outturn position is estimated at £2m deficit, an upside (optimistic) case indicates an improved deficit at £0.64m whilst a downside (pessimistic) case would be £5.42m deficit. Through the process of tight fiscal control and financial turnaround the CCG is looking to mitigate those downside risk. At this juncture the risk exposure yet to be mitigated (realistic) stands at c£890k to ensure delivery of the £2m deficit planning target.
Any statutory/regulatory/legal/NHS Constitution/Assurance/Governance implications
Concern still remains regarding the delivery of constitutional targets, regardless of the direct application of commissioner investment to promote access and patient flow across the system.
Equality Impact Assessment (Are there any direct or indirect implications)
None
Any related work with stakeholders/practices/public and patient engagement
None
Quality implications
None
Acronyms
Set out in the body of the report.

4
Governing Body Meeting – Wednesday 6th January 2016 Month 8 Financial Position 2015/16
1. Background North Staffordshire Clinical Commissioning Group (CCG) is required to report achievement against its key financial duties and plans on both a monthly and annually. This report discusses the position to the end of November 2015 (Month 8 of financial year 2015-16).
2. Executive Summary
Risks to Financial Plan Prescribing expenditure above original plan
Elective activity below plan
Non elective activity below plan but case mix costs higher than expected
Out of Area Placement costs above plan
Seasonal Resilience schemes significantly over committed against funding allocated
RTT Backlog clearance
QIPP delivery planned for Q3 & Q4
Step Down QIPP delivery of targeted savings
Recovery of payments for specialised commissioning incorrectly charged to the CCG
Payments for activity charged to specialised commissioning to be paid by the CCG
Fines and penalties available to the step down scheme.Risks and mitigations form part of a pool, some of which should now transfer into budget as
they are 100% likely to materialise. A review of these transfers and mitigations against them
is in progress
Other Areas of Focus
Better Care Fund plan - assessment requires improvement actions wider than financial
governance
Overall Status
Assessment of the likelihood of current risks materialising has
invoked a requirement for a turnround Phase II to maximise delivery
of QIPP programmes including Plan B schemes. The forecast deficit
is held at £2.0m.
High Level Targets & RAG Rating
Total Revenue Allocation notified - £274.32m
Programme Allocation notified -£269.625m
Running Cost Allocation notified -£4.695m
Capital Allocation notified - zero
R
R
G
G
3. Financial Duties and Plans 2015-16 In 2015-16, the Income & Expenditure plans of the CCG are to:
Deliver a £3.3m in year and £2m cumulative deficit against allocated Revenue Resource Limit (RRL) [Against a mandated planning requirement of 1% surplus]
Contain expenditure within an overall cash limit
Contain expenditure within the Running Cost target of £21.80 per head of population
Deliver a QIPP of £7.66m Throughout the financial year the CCG has reported on its achievement against meeting its key financial duties and delivery against its financial plans.

5
A summary of financial performance is shown below:-
Description of financial duties YTD Forecast Explanation
Maintain expenditure within the revenue resource limit and
deliver to a planned surplus (normally 1%)
The CCG has is currently ahead of its forecast deficit target
to end of Month 8. However the target defict is £2m for the
year and comprises monthly targets. By setting a deficit
plan the CCG is in breach of its statutory duties.
Maintain expenditure within a Maximum Cash Draw down
Limit (cash limit).
The CCG has drawn down £161.61m to date with BSA
requirements of £23.42m giving total cash requirement of
£185.83m. This is behind the overall financial planning for
2015/16 primarily due to delays in payments to the Local
Authority
Maintain capital expenditure within the delegated limit from
the Area Team.
Nil allocation to the CCG. Capital expenditure is anticipated
for GP IT and the CCG has planned commitments against
this expenditure area. The CCG will recharge NHS England
Area Team for these capital items which will be held on the
NHS England balance sheet.
Ensure running costs are within the set allocation per head
of population.
The CCG has an allocation of £4.695m for running costs. At
Month 8, the running costs position was on plan.
Ensure a minimum of 0.5% contingency is held.
The CCG has 0.5% contingency within the financial plan this
is expected to be fully utilised within the forecast positions
reported at Month 8.
Ensure that 1% of funds are spent Non Recurrently on
approved projects.
The CCG will utilise this fund against Risks identified against
the Better Care Fund, clearance of Continuing Healthcare
retrospective claims and additional pressure from Seasonal
Resilience spending (Longton).
Delivery of QIPP targets
The CCG has a QIPP Plan of £7.66m of schemes within
original estimates. Delivery is slightly off track year to date
(due to rephasing of schemes) forecast remains delivery in
full. Ensure compliance with the Better Payment Practice Code
(BPPC) – “Late Payment of Commercial Debt”
The CCG delivered 93.3% in 30 days against the number of
NHS and 93.8% against non NHS invoices.
Maintain expenditure within the resources allocated and deliver of planned deficit. At the end of month 7 the CCG Financial Plan baseline resource level stood at £274.320m. This is built up of £269.625m for Programme expenditure and £4.695m allocation to meet Running costs. Within these figures is the non-recurrent return of prior year surplus at £1.326m and other non-recurrent allocations for items such as GPIT. Maintain expenditure within a maximum cash drawdown limit The CCG manages cash flow on a monthly basis and draws down cash directly via NHS England. Net cash holding at the end of the month is within the 1.25% tolerance level. Payments are behind original plans due to some deferred remittance, but are expected to remain within planning parameters at the year end. Ensure running costs are contained within the allocated £21.80 per head of population Running Cost allocation is £4.695m for the financial year against a population of 215,386. To date, running cost expenditure is within that planned value. Deliver QIPP savings targets. QIPP saving schemes of £7.66m are planned for this financial year. These are a combination of transactional schemes and transformational schemes. Transactional schemes broadly fall in the first part of the financial year and transformational in the second part of the year. There has been concern expressed over several months regarding the high value phasing of schemes in the latter part of the year, especially where investment decisions are critically interlinked eg Step Up/Step Down. There is expected to be slippage on delivery, but with attendant response to mitigating financial risk and delivery of financial control totals. Ensure compliance with the Better Payment Practice Code (BPPC) The CCG is expected to comply with the Confederation of British Industry (CBI) Prompt Payment Code. This requires the CCG to pay 95% of valid invoices within 30 days of receipt.

6
CCG performance up to 30th November stood at 93.3% based on count for NHS payables (95.7% by value), an improvement on the October position. For non NHS payables the position was 93.8% based on count (88.0% by value), deterioration from the previous month. The CCG continues to press for improved compliance with the better payment practice code and has during the course of the year introduced a “Controlled Environment for Finance” which supports the controlled access to data allowing invoices to be paid more promptly. Further internal actions are on-going to press for a higher percentage of BPPC compliance.
4. Position to Date The CCG key financial duties were achieved in the cumulative position to November 2015 (Month 8). Appendix 1 highlights a summary table of performance against the range of budget headings and financial performance, together with more granular narrative at Appendix 2. The financial position as at the end of November (Month 8) shows a cumulative overspend of £2.454m which is within the profiled target level for the CCG’s planned deficit at this point in the year. This has resulted in the achievement of financial duties against plan, but not against the NHSE planning rules, which require delivery of surplus. The financial position set out within this report is based on external information provided to the CCG, e.g. acute activity initial month 7 data and Prescribing data for month 6 and also against a range of assumptions in compiling the position. The Continuing Healthcare year end position is reflective of the forecast expenditure levels via the Commissioning Support Unit as at November 2015.
5. Contractual Performance of Providers/Budgetary Performance
Initial month 8 data received from University Hospitals North Midlands NHS Trust (UHNM) indicates that at the end of October, activity and costs are below contracted levels and would generate an underspending of £0.695m against plan. This data is subject to continuous validation processes relating to data queries, penalties and triggering of the Marginal Rate Emergency Threshold. After taking into account the likely outcome of these adjustments the forecast for this contract is an underspending of £1.907m. In order to deliver the Step up and Step Down Financial Recovery Plan (FRP) schemes, it is assumed that contractual fines, forecast at £1.4m will be reinvested in the delivery model for Step Down in 2015/16.
Monthly reporting data to the end of October has been received from West Midlands Ambulance Trust and this also indicates activity up to November under plan which is forecast to the year end as £255k under plan. The CCG is now in receipt of SLAM reporting information for out of area Acute contracts with NHS and Private providers these are indicating year to date activity to be above plan by £1.354k with the forecast year end position being £2.199m above plan. Significant overspending is evident in contracts with Trusts in Cheshire and overspending in the majority of other contracts. Further work is required to fully understand the reasons for the year to date over performance and the forecasting methodology to determine to what extent this might be influenced by activity to clear 18 week backlogs and any link with activity at UHNM. The CCG has now received reporting information up to month 6 for Prescribing which indicates expenditure to be above plan. The forecast is that expenditure will continue to be at levels above plan but delivery of the QIPP programme savings in full would limit the forecast overspend to just under £1.0m. Continuing Care information has now been received for expenditure up to November which indicates that costs are currently under plan. This includes the transfer of £1.301m to NHS England national risk pools relating to the payment of retrospective claims for pre-April 2013 claims. Monitoring reports indicate that the Continuing Healthcare QIPP programme over

7
achieved its November savings target, and based on current trends, expenditure would be £1.107m under plan at year end. The CCG has continued to see a rise in the costs relating to a number of individual patients being placed in out of area settings with either other NHS or Private sector providers mainly relating to Mental Health cases. At month 8 the cumulative costs are £721k above plan, and they are forecast to be £1.056m above plan at year end taking into account the proposed QIPP scheme delivery.
6. Quality, Innovation, Productivity and Prevention (QIPP) The final Financial Plan detailed a required QIPP programme of £7.6m net of investment (£8m gross) which is equivalent to 2.8% of the resource allocation. The QIPP programme has a phased delivery with several of the larger schemes scheduled to deliver in the latter part of the year. The table below highlights the key assumptions being made in the month 8 report against the areas of focus for the 2015/16 QIPP programme.
North Staffs
Annual
Plan
Plan at
Month 8
Actual
Delivered Forecast
Year to
date
Variance
Forecast
Variance
£000 £000 £000 £000 £000 £000 Comments
Acute
Step Up 2.99 0.99 0.99 2.99 0.00 0.00 Planned delivery of savings from October
Planned Care 1.00 0.66 0.66 1.00 0.00 0.00 Delivery rephased from October
Emergency Activity 0.65 0.45 0.49 0.97 -0.04 0.32
UHNM month 3 unplanned care under plan local data
collected re schemes per FRG
Other Acute 0.09 0.03 0.04 0.04 -0.01 -0.05
Mental health OOA0.25 0.17 0.05 0.10 0.12 -0.15
Savings rephased per workbook scheme being signed off by
CCG
Other Programme Services 0.00 0.00 0.13 0.20 -0.13 0.20 111 reprocurement
Community
Step Down 0.59 0.20 0.00 0.59 0.20 0.00 Delivery of savings planned from October
Pathways 0.55 0.09 0.08 0.22 0.01 -0.33 Delivery of savings planned from October
Other Community 0.00 0.00 0.00 0.00 0.00 0.00
Continuing Care 0.79 0.53 0.70 1.18 -0.17 0.39 April over delivered re profile
Prescribing 0.76 0.51 0.36 0.76 0.15 0.00 Proposed re profile of delivery from Meds Opt
Total 7.66 3.63 3.50 8.05 0.13 0.39
The Month 8 savings target was £3.63m and actual reported delivery was £3.5m (96.4%), £130k under plan. A ramp up of savings targeted to be delivered in the 2nd half of the year is expected. These now include additional savings that have been identified as a result of the re-energising of the QIPP programme and some procurements which are at lower values than anticipated (eg NHS 111). Of the £7.66m program, £5m was scheduled to be delivered from October/November onwards. Assumptions within the forecasts are that this level of saving will be achieved. The ongoing monitoring and assurance of the programme takes place through the Finance Recovery Group (FRG) which continues to meet on a fortnightly basis and is in the process of refocussing its approach and priorities. The latest position is that 2 schemes are now unlikely to deliver the planned levels of savings i.e. Physiotherapy and Mental Health. In order to mitigate these reduced savings, further plan B schemes have been identified to deliver the savings targets in full and create some headroom within the in-year financial position to accommodate any future risks. The forecast plan is now valued at £8.05m; giving a balance of £4.55m to be delivered from December onwards.

8
7. Audit Assurance The CCG finance department will continue to work with Internal Audit to undertake assurance around various aspects of the CCG financials to provide audit opinion regarding accuracy of monthly accounts. In addition where further assurance work is required then this continues to be sourced as appropriate; predominantly from Internal Audit.
8. Strategic Support The CCG was required to set aside 1% of its baseline recurrent allocation to be used each year on a non-recurrent expenditure basis, this equates to £2.7m.
This has been applied as Strategic Support to fund:
Follow Up Backlog at UHNM £600k
Risk Reserve for Better Care Fund £800k
Seasonal Resilience funding of Longton Cottage hospital beds £580k
Accelerated clearance of Continuing Healthcare Retrospective claims £500k
Minor Schemes £250k – Finance Recovery project management and Capacity and Demand modelling.
9. Balance Sheet
The CCG Statement of Financial Position as at 30th November 2015 shows the level of indebtedness between the CCG and other parties (mainly NHS providers). Significant entries include:
Accounts Receivable £12m.
Accounts Payable £19.5m
Cash £65k - this level of cash ensured the CCG delivered its obligations in relation to cash.
Provisions £0.6m – provisions created relating retrospective continuing healthcare claims
Statement of Financial Position £
Non-Current Assets 0
Cash 65,592
Accounts Receivable 12,011,768
Current Assets 12,077,360
TOTAL ASSETS 12,077,360
Accounts Payable 19,518,039
Accrued Liabilities 598,215
Current Liabilities 20,116,254
Long Term Liabilities 0
Retained Earnings incl. In Year (8,038,894)
Total Taxpayers Equity (8,038,894)
TOTAL EQUITY + LIABILITIES 12,077,360
10. Cash flow
The CCG plan for 2015/16 is £275.058m of cash for the period April to March including the requirements notified from the Business Service Authority. At the start of the year UHNM were advanced their March 2016 contract payment, resulting in the cash profile for the CCG being front loaded. This is consistent with the approach taken in previous years, but is not considered an “industry norm”.

9
11. Main Risks
The CCG set a QIPP programme for 2015/16 of £7.66m (net) with the majority of the savings profiled to be achieved in the latter part of the year. Performance to month 8 is behind trajectory but monitoring information suggests this slippage will be recovered in year. The QIPP programme continues to be monitored bi-weekly through the Finance Recovery Group, and a number of additional schemes are in development to deliver additional savings in year. Given recent challenges in QIPP delivery the CCG has moved towards strengthening its delivery through the appointment of a Turnaround Director. Systems resilience planning is giving rise to potential expenditure pressures significantly above planned budget levels. This has the potential to increase the risk to the CCGs planned financial position and achievement of the control total of a £2.0m deficit. These issues are currently being worked through with the Systems Resilience Group. Key Areas of Focus and Commissioning Implications Tight fiscal control was undertaken to deliver Commissioning plans within budgetary allocations in the CCG’s last financial year. Prioritisation on spending plans is again necessary and Commissioning and Finance will work together to deliver the commissioning intentions within the available financial envelope. Part of the strategy objectives, are to review all aspects of commissioning to ensure value for money and achievement of the CCG’s financial targets both this year and in the future. The work of the Project Management Office is essential to this strategy.
12. Risk scenarios
The CCG has worked up 3 high level risk scenarios that stem from a base position as per the current forecast.
On an upside (optimistic) basis it is assumed that full delivery of the current QIPP programme arises and risks are fully mitigated. In that circumstance the year end position could be improved to deliver a deficit of £0.64m; an improvement of £1.36m on the planned deficit of £2m. This is unlikely to arise in practice.
On a downside (pessimistic) basis it is assumed that no further QIPP delivery arises and risks identified materialise in full. In that circumstance the year end position would decline to a £5.42m deficit at year end; a worsening of position from plan by £3.42m. The CCG cannot afford for any further deterioration of its financial position and practically this situation is unlikely to arise in full.
On a realistic basis and interpolating between the upside and downside cases it is assessed that there still remains a c.£890k risk to delivering against the £2m deficit control total. Recommendation The Governing Body is asked to note the contents of this report and executive summary regarding CCG performance against 2015-16 financial duties at the end of Month 8 of the financial year. In addition, the Committee is requested to note the risks to the 2015-16 financial plans and to support the actions being taken through the PMO to redress the financial shortfall against plans.

10
Appendix 1
Month 8 2015/16 and Forecast Outturn Financial Summary
North Staffs CCG YTD budget YTD Actual YTD Variance Annual
budget Forecast
Forecast
Variance
£000 £000 £000 £000 £000 £000
Acute 83,818 83,837 19 124,483 124,520 37
Mental Health 17,725 18,604 879 27,161 28,425 1,264
Continuing Care 14,998 14,234 -764 21,846 20,739 -1,107
Community Health Services 30,284 30,458 174 43,388 43,592 204
Primary Care 27,463 28,647 1,184 41,045 42,042 997
Other 6,170 5,783 -387 9,256 9,221 -35
TOTAL PROGRAMME 180,458 181,563 1,105 267,179 268,539 1,360
Running Costs 3,130 3,130 0 4,695 4,695 0
Reserves (Incl Contingency) 995 -200 -1,195 4,446 3,086 -1,360
TOTAL SPEND 184,583 184,493 -90 276,320 276,320 0
Surplus -2,544 0 2,544 -2,000 2,000
Total Locality 182,039 184,493 2,454 274,320 276,320 2,000
CCG Current Performance CCG Forecast
CCG Underlying position
North Staffs CCG £'m
Resource
Programme Allocation (month 8) 269.625
Running Costs Allocation 4.695
less non rec surplus return -1.326
Less additional non rec allocation -0.757
Total Recurrent Allocation 272.237
Expenditure
Programme Spend 270.259
Contingency 1.366
Running Costs Spend 4.695
less non recurrent spend (1%) -2.718
less non recurrent spend (CHC Topslice) -1.301
less non recurrent spend (BCF Top Up) -1.347
less non recurrent spend (Other) -0.757
Total Recurrent Spend 270.197
Underlying position 2.04
0.75% In line with NHS England guidance the CCG is also reporting an underlying surplus position of £2.04m (0.75%) when removing non recurrent resource allocation and spend.

11
Appendix 2
1. Contract Performance University Hospital of North Midlands (UHNM) The agreed contract value for UHNM stands at £97.87m following the protracted negotiation round earlier in 2015 and as a result of a contract variation relating to additional A&E activity signed off as part of the final plan approved by NHS England in May. The contract was set on a full Payment by Results (PbR) cost and volume basis where any activity carried out was paid for at tariff and the full National contract rules are applied.
Summary by Point of Delivery
Plan Actual Var % Vol Plan Actual Var % Price Plan Actual Var % Vol Plan Actual Var % Price
AandE 39838 £4,361,605 3400 3635 235 7% £372,954 £385,875 £12,921 3% 23662 24153 491 2% £2,595,286 £2,577,281 -£18,004 -1%
Day Case 17406 £11,242,208 1524 1503 -21 -1% £990,332 £1,043,601 £53,268 5% 10216 11066 850 8% £6,589,025 £7,290,334 £701,310 11%
Elective 3177 £9,026,756 244 243 -1 0% £731,863 £744,327 £12,464 2% 1858 1666 -192 -10% £5,292,459 £4,832,850 -£459,609 -9%
Regular Day Attenders 1742 £623,760 154 197 43 28% £54,732 £32,895 -£21,837 -40% 1025 380 -645 -63% £367,017 £72,605 -£294,412 -80%
Emergency 20703 £32,151,501 1722 1832 110 6% £2,627,025 £2,772,274 £145,249 6% 11958 11517 -441 -4% £18,689,123 £18,394,971 -£294,152 -2%
Non Emergency 5597 £4,270,290 474 417 -57 -12% £372,897 £315,052 -£57,845 -16% 3272 3263 -9 0% £2,499,360 £2,317,977 -£181,382 -7%
Elective XBD 1254 £293,211 116 99 -17 -15% £27,191 £23,576 -£3,615 -13% 738 455 -283 -38% £172,577 £104,856 -£67,721 -39%
Emergency XBD 9738 £2,181,301 828 584 -244 -29% £185,329 £138,145 -£47,184 -25% 5702 3514 -2188 -38% £1,277,192 £788,840 -£488,352 -38%
Non Emergency XBD 212 £73,499 16 11 -5 -31% £5,521 £4,180 -£1,342 -24% 123 142 19 15% £42,588 £43,148 £559 1%
Outpatient First 53695 £6,347,054 4690 4372 -318 -7% £554,115 £522,163 -£31,952 -6% 31538 28389 -3149 -10% £3,727,660 £3,385,685 -£341,976 -9%
Outpatient Follow Up 92513 £6,343,526 8083 7908 -175 -2% £554,884 £565,351 £10,468 2% 54332 52165 -2167 -4% £3,725,395 £3,699,767 -£25,629 -1%
Outpatient Procedure 16510 £2,899,557 1449 1958 509 35% £254,803 £341,305 £86,502 34% 9697 12417 2720 28% £1,702,865 £2,123,887 £421,022 25%
Block £2,559,771 £207,419 £207,419 £0 0% £1,451,934 £1,451,934 £0 0%
Non FCE £15,496,223 £1,525,635 £1,572,822 £47,187 3% £10,444,028 £10,797,225 £353,197 3%
SLAM Total £97,870,261 £8,464,700 £8,668,985 £204,285 2% £58,576,508 £57,881,360 -£695,149 -1%
Point of DeliverySLA Year to DateMonth: October 2015
Activity FinanceActivity FinanceActivity Finance
At the time of finalising the Month 8 financial position the CCG was in receipt of the initial month 7 Service Level Agreement Monitoring (SLAM) information, this is shown within the table above and indicates activity levels across most Points of Delivery to be in line or below plan year to date. Month 7 saw a further rise in planned care activity in day cases and outpatient procedures. The SLAM report highlights under-performance at £0.695m at month 7 before data challenges, penalties and other contractual adjustments are applied. Key variations for month 7
A& E attendances 491 above plan (2%) and £18k under (1%)
Elective / Daycases 13 below plan (0.09%) and £53k under (0.4%)
Non Elective admissions 441 below plan (4%) and £294k under (2%)
Out Patient First appointments 3149 below plan (10%) and £341k under (9%)
Out Patient Follow Up appointments 2167 below plan (4%) and £26k under (1%)

12
Significant validation work continues following receipt of the activity data. This has now identified activity being charged to the CCG (£370k at month 6) that should be paid for by NHS England Specialised Services. There is also a risk that there will be charges that should be directed to the CCG, which are currently being charged to NHSE Specialised Services. Latest indications are that these could be at similar values when the correct charging rules are applied by the Trust. A full review of the data for the M8 reporting will identify the scale of this and the impact on forecasts. The validation work also includes performance against contract penalties and the Marginal Rate Emergency tariff and consequences of failure would then be applied. The CCG’s also anticipate further contract variations being enacted to contract for the delivery of the QIPP schemes relating to the Step up model and Planned care initiatives which would result in reduced activity and costs within the UHNM contract. The CCG is also working through a contractual process with UHNM relating to clearance of the RTT backlog and the impact this will have on activity and costs; the current assumption is that activity and costs will return closer to planned levels for the coming months resulting in a forecast underspend of £1.9m at year end. The CCG also spends £0.5m with UHNM on services outside of the main acute contract at month 8 these are at planned levels. Staffordshire and Stoke on Trent Partnership Trust (SSOTP) The final contract value for SSOTP is £40.5m. The contract operates predominantly on a block basis with cost and volume arrangements relating to PbR activity for Rheumatology and Anti TnF drugs costs. The CCG is finalising the value reduction in the contract relating to the transfer of Step Down intermediate care and long term condition activities to UHNM, which will see around £2.5m being reduced from the block value of the contract. Monitoring information for month 7 has been received from SSOTP with indications of overspending in the cost and volume activities in rheumatology blood monitoring and administering of anti-TNF drugs. The forecast position is currently an overspending of £0.227m. Combined Healthcare (CHC) The contract value with CHC is £22.1m and operates on a ‘block contract’ basis. Work continues with Combined Healthcare to deliver activity reporting on a ‘Cluster’ basis. Month 8 and forecast positions both reflect spend at planned levels West Midlands Ambulance (WMAS) The contract value with WMAS for the Emergency Ambulance service is £6.27m. This operates predominantly on a cost and volume tariff basis, each Ambulance journey has a cost of £162, with some elements of the contract relating wider West Midlands programmes being funded on a block basis. At the time of finalising the month 8 position activity reporting up to the end of October has been received from the Provider, this indicates activity to be 907 journeys below plan (4.45%) this has been built in at month 8 as £150k below planned expenditure levels and forecast to year end as £255k under plan. 2. Other CCG Spend
Continuing Healthcare The CCG has an annual budget for Continuing Care and Funded Nursing Care of £21.8m; this budget also covers the CSU costs relating to the assessment and nursing team. Monitoring information received at the end of November records expenditure below plan.

13
The CCG received written notification from NHS England that it will again be expected to contribute to a National risk pool relating to the payment in year of retrospective continuing healthcare claims, this equates to £1.3m for the CCG, this spend is now being accommodated within the planned budget. As part of the 2014/15 Finance Recovery Plan the CCG approved a business case supplied by the CSU that through increased clinical and admin support would result in reduced spend through regular up to date case reviews and workload processing for 2015/16. The anticipated QIPP saving in the plan was £790k. The month 8 details received to date indicate savings achieved above target and a revised savings forecast is now included in the plan at £1.175k. The reported month 8 position is an underspending of £763k which is forecast to be £1.107m under plan at the year end. Prescribing When compiling the month 8 report national Prescribing data up to the end of month 6 has been received for 2015/16. This indicates that to the end of September spend was £0.994m above plan. There is some evidence that growth in spending maybe levelling as a result of the full year increases in category M prices in October 2014 have now been processed. The assumption made in this report is that the forecast spend will continue at current levels but delivery of the planned QIPP savings in the latter part of the year would reduce the forecast overspend to £0.994m. Within the financial plan there is an expectation that QIPP savings of £760k will be achieved and the Medicines Optimisation team have profiled delivery of these schemes. To date savings totalling £360k have been generated and the expectation and reported forecast is that the full £760k will be achieved by year end.

1
ENCLOSURE: 15
AUTHOR
REPORTING OFFICER
Name Iain Stoddart
Name Iain Stoddart
Title CFO
Title Chief Finance Officer
REPORT TO Governing Board
TITLE OF REPORT Financial Allocations and Shared Planning Guidance
DATE OF THE MEETING 6th January 2016
WHAT OTHER CCG COMMITTEE OR GROUP HAS CONSIDERED THIS REPORT?
Record which groups/committee have already seen this report, the date and comments (for example agreed this report should go to the governing board for approval)
ACTION REQUIRED FROM COMMITTEE/GROUP/ GOVERNING BOARD (PLEASE TICK)
Approve
Assurance
Discussion
x
Information
x
STRATEGIC GOALS SUPPORTED BY THIS PAPER (tick appropriate goal)
1. Increase life expectancy and reduce inequality
2. Improve prevention, early detection and effective management of those at increased risk
3. Enhance quality of life and improve health outcomes for people with LTCs
4. Ensure people receive the right care in the right place
RECOMMENDATION Members are asked to note :- 1. The NHS England planning guidance for 2016/17 – 2020/21 ‘Delivering the Forward View:
NHS Shared Planning Guidance 2016/17 – 2020/21’ 2. The Allocation of resources to NHS England and the commissioner sector for 2016/17 to
2020/21 – in overview. (Detailed CCG positions to be received in w.e.f. 8th January 2016. 3. That the above 2 documents and allocations notified after 8th January will be discussed at
the Joint Planning Committee in January. 4. A high level verbal precis of the above documents will be made available at this meeting
PURPOSE OF THE REPORT/SUPPORTING INFORMATION (if applicable)

2
The attached documents were released prior to Christmas and give an early indication of the allocations to the commissioning sector and the requirements against these allocations. Final CCG allocations for the next 3 years (firm) will only be confirmed after the 8th January 2016. Due to the tight timescale by which plans will have to be agreed and submitted there are key decisions that will need to be made in between the normal cycle of meetings. These particular areas will be outlined and summarised for the Governing Body.
KEY POINTS/EXECUTIVE SUMMARY
On a median basis the likely programme allocation to be received by the CCG in 2016/17 is an increase of 3.05% Running Cost allocations are likely to reduce due to the proportion of registered population for North Staffordshire as a percentage of the total England population reducing. The actual figures are not yet confirmed. The provider sector cost pressures are estimated at 3.06% and the efficiency requirement is 2%. This means that tariff will uplift in 16/17 by c1.06%. Other mandated requirements in the Planning Guidance will necessitate providing for c 0.5% of allocated growth. A Sustainability and Transformation Fund will be created with set criteria on how to access these funds. Minor changes to the allocation formula for CCGs have been introduced covering sparsity; whilst deprivation factors have been considered. Place Based allocations will increasingly feature over the next 5 years, together with a more unified approach. Further information regarding the increased funding to primary care and specialised services is highlighted.
Risks relating to the proposals in this paper
To be considered in the context of discussions at the Planning Committee, however the first call on resources, other than mandated requirements will be to bring the CCG back into an in year surplus position and thereafter into recurrent cumulative surplus.
Summary of any finance/resource/medicines management /workforce implications
To be fully worked through when detailed financial allocations are known.
Any statutory/regulatory/legal/NHS Constitution/Assurance/Governance implications
In line with establishing strategic and detailed annual plans
Equality Impact Assessment (Are there any direct or indirect implications)
To be undertaken in line with detailed planning
Any related work with stakeholders/practices/public and patient engagement
In line with planning timetables
Quality implications
None
Acronyms
Set out in the body of the report.
1
Paper PB.17.12.15/04
BOARD PAPER - NHS ENGLAND
Title: Allocation of resources to NHS England and the commissioning sector
for 2016/17 to 2020/21
From: Paul Baumann, Chief Financial Officer
Purpose of paper:
Last autumn, the NHS published the 5 Year Forward View. This set out our shared strategic vision for the development of the service to 2020/21 and the need to transform the current approach to delivering care.
On 25 November this year, the government announced a five year funding settlement for the NHS. Annual funding will rise in real terms by £3.8bn in 16/17 and £8.4bn by 2020/21.
This paper sets out proposals for the allocation of resources announced in the Spending Review to the NHS for 2016/17 to 2020/21.
Summary of benefits of this package:
If these proposals are accepted, they would enable us to use the Spending
Review funding to achieve:
Greater equity of access through pace-of-change:
o In 2016/17 all CCGs no more than 5% under target for CCG
commissioned services;
o In 2016/17 all CCG areas no more than 5% under target for the
total commissioning streams for their population;
o Three year transition to similar position for primary medical care
allocations.
Closer alignment with population need through improved allocation
formulae:
o A new inequalities adjustment for specialised care and more
sensitive adjustments for CCGs and primary care;
2
o A new sparsity adjustment for remote areas.
Faster progress with our strategic goals through:
o Higher funding growth for GP services and mental health;
o Introduction of a Sustainability and Transformation Fund, with a
focus in 2016/17 on restabilising the NHS and a priority in
subsequent years of accelerating transformational investment.
Stronger long-term collaboration between commissioners and
providers stimulated and supported through:
o Shared strategic planning supported by visibility of projected
commissioning resources by locality for the next five years,
couple with forward guidance on key tariff parameters in the
planning guidance;
o Aligned incentives for effective integrated strategic planning;
o Opportunities to pilot shared financial control totals.
Actions required by the Board:
The Board is asked to:
Agree the proposed allocation of funds between areas of
commissioning spend including the establishment of a Sustainability
and Transformation fund;
Agree the proposed approach to allocation of funding within CCG,
primary care and specialised commissioning streams;
Agree the proposed approach to pace-of-change; and
Agree the proposals set out in paragraphs 60-62 with regard to
integrated planning, shared financial targets and accelerated funding
realignment between CCGs.

3
Context
1. Last autumn, the NHS published the Five Year Forward View. This set out our strategic vision for the development of the service to 2020/21 and the need to transform the current approach to delivering care.
2. On 25 November this year, the government announced a five year funding settlement for the NHS. Annual funding will rise in real terms by £3.8bn in 2016/17 and £8.4bn by 2020/21. The key figures are summarised below. Table 1: NHS England Spending Review settlement
3. This front-loaded funding settlement gives the NHS the platform to begin delivering the vision set out in the Five Year Forward View at a local health economy level. The NHS is, however, facing significant financial challenges during 2015/16, and therefore a key focus in 2016/17 will need to be upon stabilisation of the commissioner and provider sectors in order to create a sustainable footing for transformation.
4. A five year funding settlement gives NHS England the opportunity to set five year allocations for commissioners, providing greater planning certainty in order that commissioners can now develop robust local health plans to deliver the Five Year Forward View. We are proposing to publish 3 years of firm allocations followed by 2 years of indicative allocations for commissioners. Further detail on this approach is set out in Annex A.
5. This paper sets out recommendations in three sections regarding:
A. the distribution of funds at commissioning stream level; B. the distribution of funds within each commissioning stream, including
proposed changes to funding formulae; and
£bn 2015-16 2016-17 2017-18 2018-19 2019-20 2020-21 CAGR
NHS England
Resource 101.0 106.5 109.9 112.4 115.5 119.6
Real growth (£bn) 3.8 5.3 5.8 6.7 8.4
Real growth (year on
year £bn) 3.8 1.4 0.4 0.8 1.6
Real growth (year on
year %) 3.7% 1.3% 0.4% 0.7% 1.4% 1.6%
Capital 0.3 0.3 0.3 0.3 0.3 0.3
Total 101.3 106.8 110.2 112.7 115.8 119.9
Real growth (£bn) 3.8 5.3 5.8 6.7 8.4
Real growth (year on
year £bn) 3.8 1.4 0.4 0.8 1.6
Real growth (year on
year %) 3.6% 1.3% 0.4% 0.7% 1.4% 1.6%

4
C. the approach to pace-of-change in order to support the development of place-based commissioning.
A. Commissioning streams
6. Our approach to distribution of funding between commissioning streams is
based upon: i. setting a reasonable level of efficiency challenge for each
commissioning stream; ii. directing funding towards Primary Care (GP services) in line with the
strategic intent of the Five Year Forward View; and iii. within central budgets reducing day to day expenditure whilst
prioritising funding for transformation.
7. We have a set of existing commitments regarding allocation of funding at commissioning stream level. The two principal commitments are:
i. parity of esteem, where we do not set a specific allocation of funds, but rather through our assurance processes hold commissioners to account for allocating growth in funding to mental health at a rate at least in line with general growth in their allocation; and
ii. the Better Care Fund, where contributions will increase in line with inflation.
8. Overall CCG programme spend is projected to grow above the GDP deflator
in all 5 years. Growth is above 3% in 2016/17, mainly due to the funding pressure associated with the changes to pensions payments for employers, and above 3% in 2020/21, when the full rollout of 7 Day Services is completed. To support CCG investment we will reduce the contribution required from CCGs in respect of Continuing Healthcare Provisions from £250m in 2015/16 to £100m in 2016/17 and nothing in subsequent years.
9. Primary care (GP services), which covers the core GP contract as well as other primary care medical services, grows at 4% per annum or greater in all years in line with the stated policy intent above.
10. The NHS is experiencing significant and growing financial pressures due to the licencing of an increasing volume of effective but expensive new drugs and devices. This is a particular challenge for the specialised commissioning budget, towards which most NICE appraisals are aimed, thereby placing a legal limit on the funding discretion we have as between funding streams. We face specific legally binding pressures in 2016/17 regarding the introduction of new drugs for Hepatitis C and Cystic Fibrosis. In restricting headline budget growth in 2016/17 to 7% in specialised commissioning, we have had to limit our budget estimates to the very lowest end of the projected range of potential additions to the portfolio. As well as considering the risk associated with this assumption, the Board will wish to consider whether it wishes to invest in this level of growth for specialised commissioning or whether it wishes to engage in further discussions with NICE and the pharmaceutical industry to reduce pressures further still, freeing up funding for other areas in 2016/17 and with a

5
view to securing the significantly lower level of funding currently assumed for later years.
11. As part of the Spending Review settlement we have £2.1bn in 2016/17 to invest in a Sustainability and Transformation Fund.
12. The Transformation element of the Fund is intended to support the ongoing development of new models of care along with the investment identified to begin implementation of policy commitments in areas such as 7 day services, GP access, Cancer, Mental health and prevention.
13. In 2016/17, we are also proposing to introduce a Sustainability element of the Fund, the purpose of which is to support NHS Improvement to bring the provider trust sector back to financial balance in year. Existing provider support funding held by NHS England (included within central programmes) will be added to the fund to create a single process. The Sustainability element of the Fund will have two elements:
i. a general element which will be distributed to relevant providers to support the sustainability of emergency services and the achievement of agreed control totals; and
ii. a targeted element which we will use to support relevant providers to go further faster through additional efficiency gains.
14. £1.8bn of funding will be allocated at the beginning of 2016/17 to the Sustainability element of the Fund. Funding will be released on a quarterly basis subject to agreement by NHS Improvement and NHS England based on individual providers’ performance against financial, access and transformation eligibility criteria. The Board is asked to approve the establishment of the Sustainability Fund and delegate allocation of specific amounts to individual organisations during 2016/17 to the Investment Committee in partnership with NHS Improvement.
15. We intend that over the five year period the split between sustainability and transformation requirements for local health economies will change. As the provider sector comes back into underlying balance under NHS Improvement’s supervision, the share of the funding available for transformation and new policy commitments will increase in subsequent years. The overall fund also increases in size to reflect the growing investment funding included in the Spending Review settlement.
16. Within our overall transformation resources we have agreed to carve out a direct allocation of £450m to Greater Manchester, representing their fair share of available transformation budgets over the 5 year period. Under the accountability arrangements established in their devolution agreement, the GM Strategic Partnership Board will oversee the deployment of this funding to deliver the major change programme set out in their recently completed Health and Social Care Strategic Plan, whilst also securing locally the outcomes to which we have committed ourselves nationally in the Spending Review.

6
17. Other direct commissioning includes primary care (other) which covers dentistry, community pharmacy and ophthalmology services, public health, health and justice and armed forces. There is some growth in public health funding in 2016/17 and 2017/18 which is a result of the planned transfer from Public Health England to NHS England of responsibility for the bowel scope screening programme with a staged rollout programme and the expansion of previously agreed programmes, such as Meningitis B vaccination and the childhood flu programme. Overall there is a reduction in funding for this area over the period as a result of the efficiency requirements agreed as part of the Spending Review.
18. We have updated and reflected pressures in each commissioning stream (see Annex B).
19. We have also included within our modelling the projected contribution of each commissioning stream towards the activity related savings that we have identified for the commissioning sector as its contribution to the overall efficiency challenge to 2020/21. Moderating demand growth in this way is, however, partly dependent on effective government action on prevention and sustained availability of social care relative to rising need. If either of these preconditions to fulfilling the Forward View is not met, it will place additional unfunded pressures on the NHS over the period to 2020/21.
20. Table 2 below sets out our recommended distribution of funds at commissioning stream level.
Table 2: Commissioning stream allocations
Notes: 1. Table 1 earlier in this paper records the Spending Review settlement from HM Treasury, whereas
Table 2 above shows the amount available for distribution by NHS England. The differences are agreed adjustments with the Department of Health primarily to reflect changes in responsibilities. In 2015/16 the HMT revenue resource baseline is £101.0bn (table 1). After adjustments, £100.4bn is available for allocation (table 2) on a like-for-like basis, with the most significant difference being the transfer of responsibility for commissioning of public health services for children aged 0-5 to local authorities.
2. NHS England central budgets include core programme and management cost expenditure, but also funds managed on behalf of the system, such as Clinical Excellence Awards for hospital consultants and some elements of national resilience funding.
3. Drawdown includes utilisation of prior year cumulative surpluses, primarily by CCGs, to fund non-recurrent investments and funding for in-year deficits agreed as part of a multi-year recovery plan.
Summary outputs
15/16
Adjusted
allocation
16/17
proposed
allocation
Budget
growth
17/18
proposed
allocation
Budget
growth
18/19
proposed
allocation
Budget
growth
19/20
proposed
allocation
Budget
growth
20/21
proposed
allocation
Budget
growth
£m £m % £m % £m % £m % £m %
CCGs 69,484 71,853 3.4% 73,358 2.1% 74,849 2.0% 76,469 2.2% 79,372 3.8%
Primary Care (GP) 7,342 7,652 4.2% 7,958 4.0% 8,317 4.5% 8,716 4.8% 9,188 5.4%
Specialised 14,643 15,662 7.0% 16,413 4.8% 17,151 4.5% 17,918 4.5% 18,820 5.0%
Place based commissioning budgets 91,469 95,168 4.0% 97,730 2.7% 100,317 2.6% 103,103 2.8% 107,381 4.1%
Sustainability Fund 0 1,800
Transformation Fund 200 339 69.5%
Sustainability and Transformation Fund 200 2,139 2,864 33.9% 2,947 2.9% 3,434 16.5% 3,405 -0.8%
Other direct commissioning 6,684 6,642 -0.6% 6,641 0.0% 6,609 -0.5% 6,526 -1.2% 6,462 -1.0%
NHS England central budgets 1,708 1,637 -4.2% 1,559 -4.8% 1,402 -10.0% 1,312 -6.5% 1,227 -6.4%
Non-recurrent use of Drawdown 300 250 -16.7% 400 60.0% 400 0.0% 400 0.0% 400 0.0%
Total 100,360 105,836 5.5% 109,193 3.2% 111,675 2.3% 114,775 2.8% 118,875 3.6%
2,864 33.9% 2,947 2.9% 3,434 16.5% 3,405 -0.8%

7
B. Distribution of funds within each Commissioning stream
21. In this section we describe a number of improvements we have made to the formulae which determine target allocations.
Inequalities
22. NHS England looks to meet some of its legal requirement to reduce inequalities in healthcare provision through its approach to allocations.
23. In previous years we have developed our methodology and the criteria underpinning our approach. In line with the recommendation of the Advisory Committee on Resource Allocation (ACRA) we have established that the Standardised Mortality Ratio for those aged under 75 (SMR<75) is the best indicator of unmet need, and thus current inequality in the provision of healthcare services. We also previously agreed a 15% adjustment within primary care and a 10% adjustment within CCG funding to meet these requirements.
24. This year we have undertaken a comprehensive literature review to investigate whether the evidence base has changed. Whilst work by Ben Barr from the University of Liverpool and colleagues show the benefit of targeting investment at areas with high levels of deprivation, evidence about the impact of additional investment based on inequalities is inconclusive, particularly in relation to the scope for marginal return and thus how much to invest.
25. We therefore propose to keep the inequalities adjustment at current levels for CCGs and for primary care. In introducing a new target formula for specialised services (see below) we are also proposing the introduction of a 5% unmet need adjustment for specialised services on the basis that we would expect unmet need and the potential to impact on inequalities to be lower in this area.
26. We have also reviewed our methodology, and whilst recommending that we continue to use SMR<75 we are proposing to change the application of the inequalities adjustment. ACRA has recommended that the application of the inequalities adjustment moves from a 10 tier to a 16 tier approach that better targets areas with the highest levels of deprivation. ACRA is planning to recommend a similar change to the public health formula used by Public Health England. Annex C shows the details of this change.
Population
27. Population figures for all programme allocations continue to be based on GP list sizes, now updated to October 2015. Increases for future years are based on the Office of National Statistics figures1.
1 Whilst many local authorities compile more detailed future population projections, the methodology is not consistent and this means
they cannot be brought into a national formula. Hence areas of disproportionally high anticipated growth may be adversely impacted if the ONS does not fully capture this in its assumptions. To mitigate this risk we will review actual changes in population annually to see if any CCG is given an unfair or disproportionate challenge for this reason, and adjust if required.

8
28. Using GP lists as a basis for the allocations requires these lists to be materially accurate. Following the allocation of funds in 2015/16, further list updating activity has been undertaken in all regions and is reflected in this allocation setting process. This programme of work will continue over the next three years and potentially inform any update to the proposed allocations for 2019/20 and 2020/21. Before any adjustment is made to reflect unexpected population growth in future years (as set out in the footnote to the preceding paragraph) we will require a full analysis of the reasons for the growth to ensure confidence in the local list updating procedures.
CCG formula
29. For this round of allocations the core structure of the CCG formula remains the same, but all underlying data has been updated. This means that the activity data used in the model has been brought forward by 4 years and model parameters re-estimated.
30. We are proposing to make the following changes to the formula: i. introduction of a sparsity adjustment; ii. refresh of the emergency ambulance cost adjustment (EACA); and iii. revision to application of inequalities (as above).
31. These adjustments have been reviewed and agreed by ACRA and are set out
in Annex D.
32. Table 3 below summarises the impact of the new formula. This shows that the updated CCG formula for 2015/16 increases the number of CCGs more than 5% below target from 17 to 24 CCGs and the number more than 5% above target from 27 to 28.
Table 3: Distribution of CCGs by distance from target
33. Future developments are expected to include looking at community service
provision, where lack of reliable robust data currently prevents detailed needs-based modelling, as well as continuing our analysis of the impact of sparsity and updating the mental health services component of the model.
Dft distribution 15/16 15/16
Per 2014 formulae Per new formulae
<5% 17 24
-5% to -2.5% 46 39
-2.5% to 0 60 57
0 to 2.5% 38 38
+2.5% to +5% 23 23
>5% 27 28
Total 211 209
9
Primary Care formula
34. The existing allocation model for primary medical care is based on the contractual formula that is at the heart of the General Medical Services (GMS) contract, usually referred to as the Carr-Hill formula. This model has been frequently criticised in this context because it was developed more than ten years ago and is based on data that are around fifteen years old.
35. The key change we are proposing to the primary medical care formula is the inclusion of new estimates of stratified workload per patient for GPs based on 2 million patient records from the Clinical Practice Research Datalink 2014. The previous data were based on information from 1999-2002. This has allowed us to re-estimate the importance of key drivers of primary medical care activity. We have not changed the way we then use these updated estimates to model the consequential cost variation.
36. ACRA has endorsed these changes but has been clear that this is for allocation purposes only and does not in itself imply any particular adjustments to GMS contracts. Work is underway to update the formula to influence such payments for subsequent years while ensuring that any future change to payment formulae is synchronised with the allocation formula developed here.
37. The key impacts of the changes are to reveal an increase in the relative need for primary medical care in London and to reduce the range of the most extreme relative needs in the model, two of the most common criticisms of the Carr-Hill model.
38. To support the transparency of comprehensive place-based expenditure, we have taken the actual allocation at a local geography level for non-medical primary care services (principally community pharmacy, dentistry and optical services) and apportioned to CCGs on a per capita basis. The current non-medical primary care formula is not robust in isolation for a CCG geography, and this disaggregation is therefore indicative only. As part of our future work programme we will undertake further work on the allocation methodologies for these services, but there are no current plans to move to delegated commissioning in these areas, and we have excluded them from the place-based pace-of-change calculations described later in this paper. Further detail on the primary care formula is provided in Annex E.
Specialised formula
39. The analysis of the specialist service budget at a CCG level is not, in itself, intended to result in the transfer of responsibility for commissioning, but it will promote equitable allocations, support greater understanding and transparency and facilitate collaborative commissioning between CCGs and NHS England where appropriate, by influencing the overall balance of allocations through pace-of-change (see below).
40. A needs-based specialised formula has been developed, using a similar approach to the CCG formula (Person Based Resource Allocation).

10
41. Specialised services are represented variably in the source data used for
modelling (SUS-PbR). Only categories of care with a reasonable level of coverage are used in estimating or applying the target formula. This covers c.50% of all specialised services spend. The remaining services have been included within the target for each CCG geography based on historic expenditure. This historic expenditure analysis has been strengthened over the last 18 months, including a number of detailed review and updating procedures designed to build confidence in its validity for use as part of the allocation process.
42. The inclusion of a historic spend element within the formula also at this stage dampens some of the issues identified in the current pattern of specialised service utilisation and needs-based projections of utilisation. Of particular note is the issue that some specialised services in certain locations may be influenced by supply side variables (proximity to a hospital will increase the likelihood of a service being provided, an impact which needs to be eliminated in coming to a needs-based allocation) and demand side variables (where a particular individual, family or patient group specifically moves to a specialist centre for access purposes).
43. ACRA will have an opportunity to carry out a full review of the methodology in due course. In the meantime, our internal review indicates that the formula generates valid target allocations, and we therefore recommend proceeding with utilising the formula given the benefits in terms of supporting co-commissioning and the place-based approach. We have sought to mitigate potential risks by adopting a cautious approach to pace-of-change, and we will continue to work with ACRA over the coming months to enable them to complete their review. There is also potentially an opportunity to adjust any significant distortions in allocations in 2017/18 if required, as we are likely to begin to move elements of the sustainability and transformation funds into local allocations in addition to the core allocations covered in this paper. Further detail on the specialised services formula is provided in Annex F.
Quality Assurance
44. Quality Assurance can never be absolute, and the quanta being finalised through the Spending Review only in November have meant that much of the final phases of this work have been completed at speed. Nevertheless, the various components of the work have been through a range of quality assurance processes including variously peer review, independent internal review, independent methodological review (ACRA) and independent external review.
C. Pace-of-change
45. In previous years the Board has agreed a pace-of-change policy that has sought to:

11
i. bring all CCGs to target funding over time and specifically bring all CCGs within 5% of target as quickly as possible (in 2015/16 we halved from 34 to 17 the number of CCGs who were more than 5% below their target funding); and
ii. bring all primary care geographies to target funding over time.
46. Key considerations for the Board have included: i. the minimum floor growth we can expect any geography to manage
without short term destabilisation of service provision; ii. the pace at which over target geographies can adjust their spending to
their needs based target; and iii. the maximum growth that any geography can invest in a value for
money way in a given year.
47. To date, discussions regarding pace-of-change have predominantly focussed upon CCG allocations. With the development of primary medical care and specialised formulae at CCG level we are now able to take a more holistic view of pace-of-change at a place- (or local health economy) based level.
48. This gives us some choices for how we wish to operate pace-of-change policy for this allocation round. Options for pace-of-change include:
i. apply to each commissioning stream individually; ii. apply at an aggregate place-based level; iii. exclude specialised services from ii. above; or iv. a hybrid option which focuses on alignment with holistic place-based
targets but subject to applying rules limiting the volatility and unintended consequences in individual commissioning streams.
49. On balance we recommend the hybrid approach with specialised services
included. The primary advantage of including specialised services within the pace-of-change calculations is that it will bring much greater equity of overall allocations to populations by factoring in the highly variable utilisation of specialised services by each local health economy. It would support engagement of CCGs in co-commissioning and would enable a fuller expression of place-based utilisation of NHS funds. It would also “future-proof” place-based allocations against potential realignment of specialised service definitions over time. The primary downside is the partial service coverage of the modelled element of the current formula; however, the likely effect of this in practice is to dampen rather than magnify the impact of specialised services in the overall place-based pace-of-change. Our recommendation is therefore that the advantages significantly outweigh the disadvantages.
50. The following high-level steps are taken to implement the hybrid approach: i. we apply funding at each commissioning stream level to meet specific
rules for minimum growth and caps where appropriate (see paragraph 50);
ii. any funds that are not needed to meet these commissioning stream aims are then used to support pace-of-change for the place-based allocation (see paragraph 51);

12
iii. any additional funding which a CCG area accrues in step ii. is then redistributed back to the allocations for the CCG and primary medical care commissioning streams as described in paragraph 53 below.
51. The rules for the initial allocations to individual commissioning streams (referred to as “minimum allocations below”) are set out in table 4 below and build on the principles agreed by the Board for the allocations for 2015/16:
Table 4: pace-of-change allocative decision rules by commissioning stream
Allocative decision rules
CCG no CCG is more than 5% below target;
all CCGs receive a minimum per capita growth that is equivalent to real terms cash growth at the average population growth (in 2016/17 this equates to 0.91%, being 1.66% GDP deflator less 0.75% average population growth) ;
all CCGs receive a minimum cash growth equal to real terms growth plus specific non-routine policy pressures (predominantly relating to pensions and 7 day services); unless
the CCG is more than 10% above target, when its cash growth is limited to the specific policy pressures. This cap is phased in between a DfT of +5% and +10%.
Primary care medical
a minimum allocation is set that ensures maximum progress is made towards ensuring no locality is more than 5% below target, constrained by allowing no CCG area more than 10% per head growth in this step of the process;
all CCG areas receive a minimum per head growth that is equivalent to real terms cash growth at the average population growth (as defined above); and
all CCG areas receive a minimum cash growth equal to real terms growth plus specific policy pressures; unless
the CCG area is more than 10% above target, when its cash growth is limited to specific policy pressures plus 1%. This cap is phased in between a DfT of +5% and +10%.
Specialised all CCG areas receive the same per head uplift that utilises all the resources allocated to this stream, ensuring that at a national level the allocated funds for NHS England specialised services are maintained and to mitigate any risks relating to the target formula as described above.
52. Focus then turns to the total of these three streams. The total allocation to each locality must at least meet the sum of the three minimum allocations (CCG core, primary medical care and specialised). The remaining available growth is used to:
i. ensure that the total allocation to each locality is no more than 5% below target;
ii. as for the individual streams, total allocations must in aggregate follow the relevant minimum and maximum growth rules; and

13
iii. any remaining funds are channelled into pace-of-change.
53. The additional resources are distributed back across the CCG and primary medical care commissioning streams as follows:
i. where the minimum CCG core allocation is below target and the minimum primary medical care allocation is above target, any available resources are used to bring the CCG allocation as close as possible to target. If the opposite applies, the resources are focused on the primary medical care allocation;
ii. if resources remain after this step, or if the minimum allocations are both above or both below target, resources are distributed to move both individual allocations the same number of percentage points towards their respective target allocations.
54. Having set up the pace-of-change modelling on the basis described above we
have identified two options for the Board to consider, the results of which are set out in Table 5 and 6 below:
Option 1: – more rapid pace-of-change
Option 2: – more conservative pace-of-change

14
Table 5: Pace-of-change option 1
Table 6: Pace-of-change option 2
Option 1
CCG PC (GP) Total CCG PC (GP) Total CCG PC (GP) Total CCG PC (GP) Total CCG PC (GP) Total CCG PC (GP) Total
DfT distribution <-5% 24 50 10 0 50 0 0 27 0 0 0 0 0 0 0 0 0 0
-5 to -2.5% 39 26 48 56 21 41 50 55 32 45 91 3 38 89 1 35 63 0
-2.5% to 0 57 29 58 73 30 86 80 32 98 80 40 128 83 54 129 83 78 131
0 to +2.5% 38 30 45 37 35 39 36 32 36 36 28 36 40 26 35 42 42 35
+2.5 to +5% 23 26 28 20 25 27 20 26 30 24 21 30 26 22 33 30 16 33
>5% 28 48 20 23 48 16 23 37 13 24 29 12 22 18 11 19 10 10
Programme Growth Maximum 10.79% 11.99% 10.31% 3.96% 11.74% 4.47% 3.56% 5.75% 3.82% 3.29% 5.11% 3.90% 4.85% 8.84% 5.25%
Mean 3.74% 3.93% 4.35% 2.14% 3.15% 2.64% 2.15% 2.48% 2.55% 2.24% 3.05% 2.67% 3.85% 4.25% 4.08%
Median 3.05% 3.57% 3.84% 2.00% 1.87% 2.52% 1.99% 2.21% 2.44% 2.12% 2.98% 2.57% 3.74% 4.41% 4.05%
Minimum 1.39% 2.90% 2.12% 0.16% 1.00% 0.71% 0.06% 1.00% 0.61% 0.02% 1.00% 0.61% 1.46% 1.00% 1.88%
Number within 0.1% of minimum 6 27 1 5 23 1 5 15 1 4 8 1 4 6 1
Per Capita Growth Maximum 9.48% 10.02% 8.64% 2.77% 10.00% 2.94% 2.25% 5.37% 2.46% 2.06% 3.71% 2.42% 3.80% 7.80% 3.79%
Mean 2.97% 3.16% 3.58% 1.41% 2.41% 1.90% 1.42% 1.75% 1.82% 1.53% 2.34% 1.96% 3.14% 3.54% 3.37%
Median 2.62% 2.97% 3.24% 1.46% 1.39% 1.93% 1.47% 1.59% 1.86% 1.59% 2.31% 2.04% 3.24% 3.78% 3.46%
Minimum -0.07% 1.25% 1.28% -1.08% 0.04% 0.08% -1.14% 0.05% 0.04% -1.01% 0.07% 0.25% 0.53% 0.30% 1.58%
Number within 0.1% of minimum 2 1 1 2 1 2 2 1 2 2 1 2 2 1 1
2020-212015-16 2016-17 2017-18 2018-19 2019-20
Option 2
CCG PC (GP) Total CCG PC (GP) Total CCG PC (GP) Total CCG PC (GP) Total CCG PC (GP) Total CCG PC (GP) Total
DfT distribution <-5% 24 50 10 0 50 0 0 29 0 0 0 0 0 0 0 0 0 0
-5 to -2.5% 39 26 48 64 24 66 64 57 64 61 95 62 60 93 62 59 69 66
-2.5% to 0 57 29 58 65 27 61 66 32 66 67 40 69 66 51 71 66 77 70
0 to +2.5% 38 30 45 37 35 39 36 28 36 33 24 36 36 25 34 38 37 30
+2.5 to +5% 23 26 28 18 25 24 17 26 23 21 21 23 22 22 23 21 17 24
>5% 28 48 20 25 48 19 26 37 20 27 29 19 25 18 19 25 9 19
Programme Growth Maximum 10.36% 11.99% 9.98% 3.96% 11.74% 4.40% 3.21% 4.96% 3.79% 3.18% 5.19% 3.85% 4.77% 7.12% 5.15%
Mean 3.75% 3.85% 4.35% 2.14% 3.13% 2.64% 2.15% 2.47% 2.55% 2.23% 3.14% 2.67% 3.86% 4.16% 4.08%
Median 3.05% 3.57% 3.85% 2.00% 1.84% 2.44% 1.95% 2.15% 2.40% 1.99% 3.21% 2.51% 3.66% 4.41% 3.96%
Minimum 3.05% 2.90% 3.49% 2.00% 1.00% 2.20% 1.95% 1.00% 2.13% 1.99% 1.00% 2.17% 3.66% 1.00% 3.54%
Number within 0.1% of minimum 138 27 12 151 23 31 131 16 28 120 9 11 141 7 6
Per Capita Growth Maximum 9.06% 10.00% 8.31% 2.77% 10.00% 2.94% 1.94% 3.41% 2.24% 2.07% 3.65% 2.36% 3.79% 5.40% 3.82%
Mean 2.98% 3.08% 3.58% 1.41% 2.40% 1.90% 1.42% 1.73% 1.82% 1.52% 2.43% 1.96% 3.15% 3.45% 3.37%
Median 2.65% 2.96% 3.28% 1.41% 1.36% 1.90% 1.44% 1.56% 1.83% 1.54% 2.49% 1.97% 3.20% 3.72% 3.39%
Minimum 0.88% 1.25% 1.91% 0.74% 0.04% 1.35% 0.73% 0.05% 1.37% 0.94% 0.07% 1.52% 1.95% 0.07% 2.55%
Number within 0.1% of minimum 1 1 1 2 1 4 2 2 3 2 1 2 2 1 1
2020-212015-16 2016-17 2017-18 2018-19 2019-20

15
55. Both options fulfil the stated goal of bringing all CCGs to no more than 5% under target in 2016/17 and achieve the same objective for the total place-based allocation. A similar position is reached for primary medical care allocations over the three year period to 2018/19, with all CCG geographies moving to within 5% in both options. Option 1 has a greater impact than Option 2 on narrowing the distribution for both CCGs and local health economies over the 5 year period. For this reason we recommend that the Board adopts Option 1.
56. Primary Care (non GP service) resources are allocated to commissioning hubs using a similar approach, but are not appropriate for inclusion in a place-based pace-of-change policy because of the challenges of delegating responsibilities for the services and the inherent limitations of the target formulae discussed above. In publishing final allocations we plan to provide additional information showing an “extended” place-based allocation through the addition of an indicative amount for these services for information only.
57. We have also considered whether or not pace-of-change should be adjusted for the potential differential nature of growth in social care spend over the next 5 years as a result of the Spending Review settlement. We have considered this factor given our previous policy of seeking to ensure that local health economies do not suffer short term destabilisation of services. The data does not however exist to model this impact across the country given the structure of the Spending Review settlement and the dependency on individual local authority decisions. In addition, the relationship between social care spend and health need needs further investigation. Furthermore, there is a risk of wrongly signalling that the local NHS has in some way been funded to offset reductions in social care, which is not the case. For these reasons we have not included this factor in our pace-of-change considerations.
58. When local authority public health allocations are published they could be included in a similar way.
CCG admin
59. CCG admin allowances at an overall level will remain flat to 2020/21, as determined by HM Treasury’s Spending Review settlement. Individual CCG allowances will be rebased to adjust for changing share of population.
Aligning allocations, devolution and planning policies
60. As set out in the business rules for commissioners published in the forthcoming NHS planning guidance, the real terms element of growth in allocations from 2017/18 onwards for CCGs, as well as their access to the Sustainability and Transformation Fund, will be contingent upon the development and sign off of a robust Local Health Economy Strategic plan during 2016/17. Providers will be similarly incentivised, as the proposed criteria to access sustainability and transformation funding include sign off of Local Health Economy plans. The Board is asked to approve this approach.

16
61. We are also proposing to the Board that we should explore the potential to allow commissioners and providers who wish to work together as a local health economy to operate to a combined financial control total. This would require combined oversight with NHS Improvement (and collaboration with the Department of Health) in adapting the relevant financial regimes. However, this cannot affect the statutory position that NHS England is only responsible for managing its spending limit and overseeing its hosted bodies and CCGs. NHS Improvement and the Department of Health have equivalent legal responsibilities for provider finances and DH resource limits.
62. We are also recommending that the Board should in principle support any proposals from groups of CCGs, particularly in areas working towards devolution, who wish to implement a more accelerated internal pace-of-change policy by mutual agreement.
Recommendations
63. The Board is asked to: i. agree the proposed allocation of funds between areas of
commissioning spend including the establishment of a Sustainability and Transformation fund;
ii. agree the proposed approach to allocation of funding within CCG, primary care and specialised commissioning streams;
iii. agree the proposed approach to pace-of-change; and iv. agree the proposals set out in paragraphs 60-62 with regard to
integrated planning, shared financial targets and accelerated funding realignment between CCGs.
64. Subject to the decisions made by the Board, we intend to publish allocations at CCG level for CCG, primary care and specialised programme costs and CCG running costs in early January.
Paul Baumann Chief Financial Officer 17 December 2015

17
ANNEX A: 5 YEAR ALLOCATIONS
We are giving three year firm allocations with a further two years of indicative allocations to assist planning.
However, NHS England will reserve the right to change firm allocations in a number of specific circumstances where the financial stability of the commissioning system is challenged or it is clear that the allocations are no longer fair in their distribution to health economies.
To mitigate this NHS England needs to be clear to all parts of the commissioning system the circumstances under which the allocations will be reviewed. Examples of these might be:
a disproportionate financial imbalance in any part of the commissioning system;
a new government policy with additional funding creating an additional pressure in one area;
a disproportionate increase or decrease in the share of the national population caused by a change to underlying population statistics;
a new national contract or pay award established by Government that requires additional funding or redistribution of resources; and
any other change in mandate funding.
NHS England may also need to review allocations in the light of:
changes to commissioning responsibilities in the light of any further changes to IR rules;
the need to ensure minimum contractual growth to GP practices through the primary care allocations; and
changes to payment currencies which may move funding pressures between commissioning streams (for example a move to HRG4+).

18
ANNEX B: PRESSURES IN COMMISSIONING STREAMS
Cost pressures
In developing our analysis of pressures in commissioning streams we have developed a series of assumptions in partnership with our stakeholders which have been used to underpin the financial modelling supporting the spending review settlement. We discuss the key drivers of these assumptions below.
In developing our NHS England specific commissioning stream pressures we have taken these assumptions and adapted them as appropriate for applicability to each stream. Activity
We have developed assumptions based on the underlying historic growth rates of activity across the health system. Using data from 2009/10- 2014/15 we calculate an average secondary care growth rate of 2.7%. In order to project forwards we have taken this historic figure and adjusted it for the impact of the aging and growing population, resulting in an activity pressure of 2.9% per annum.
As part of allocations we have apportioned the activity pressure between CCGs and Specialised, resulting in a 4.4% activity pressure within specialised and 2.4% activity pressure within CCGs. This compares to population growth in the region of 0.7% per annum. Pay
Our pay assumptions are based on estimates calculated by the Department of Health of the underlying pay pressure in the system. These have then been updated for the impact of the government’s pay restraint policy (limiting growth to 1% per annum plus an agreed estimate for pay drift).
The pay pressure is higher in 2016/17 due to changes to national insurance in relation to pensions; this adds a 1.75 percentage point pressure on top of the 2016/17 pay assumption.
Our pay pressure assumption is consistent throughout all commissioning streams, weighted accordingly. For example within GP services pay comprises c.80% of expenditure, whereas in specialised pay only accounts for c.55%. Drugs
Secondary care, non-specialised drugs expenditure is projected using the Department of Health’s drugs projection models. For specialised drugs we assume underlying combined activity and price growth of 9% per annum in line with detailed work performed by NHS England in addition to any specific and material new high cost drugs. The cost of primary care drugs are assumed to rise in line with the numbers of prescriptions and inflation.

19
Other
For the majority of other pressures we have included an assumption of GDP deflator pressure. This includes secondary care procurement pressure for non-pay non-drugs related costs.
We have funded commissioners for the projected increases in CNST over the five year period.

20
ANNEX C: ANALYSIS OF INEQUALITIES ADJUSTMENT IMPACT
The unmet need adjustment in the current target CCG formula is aligned with the current public health formula. The adjustment uses the standardised mortality ratio under 75 (SMR<75) for small geographical areas – Middle Layer Super Output Areas (MSOAs) – of which there are 6791 in England. MSOAs are currently placed into 10 groups according to the value of their SMR<75. All MSOAs in the same group receive the same weight per head, with the MSOAs in the group with the highest SMR<75s receiving a weight per head 5 times higher than those in the group with the lowest SMRs. The intermediate 8 groups receive a weight per head between 1 and 5. In line with its recommendations for the public health formula, ACRA is advising us to increase the number of groups for the unmet need adjustment to the CCG formula from 10 to 16 and increase the weight per head across these to a range of 10 to 1. The impact of moving to 16 groups is to increase the target allocations to the areas with the very worst SMR<75. This can be seen from the steeper curve for the 16 group model compared to the 10 group model in Figure 1, which show the weights per head for the MSOA groups.
Figure 1: Weight per head for 10 and 16 groups
The general impact of this more sensitive approach is to increase or decrease individual target allocations by up to 1%. Six CCGs see an increase in their target allocation of more than 1% (up to 4.8% in one case) because they have a high proportion of small areas with the worst SMR<75s, which are now given a higher weight. Figure 2 shows for CCGs the change in total target allocations by reference to their Index of Multiple Deprivation (IMD) decile, with decile 1 being the least deprived. This indicates that by changing the formula we are targeting more resources to the CCGs which have areas with the very poorest health. The dispersion in the higher deciles is due to differences between CCGs in the number of small areas with the highest SMR<75s and the number of small areas with a high but not the highest
0
2
4
6
8
10
12
0 50 100 150 200 250 300
Weig
hti
ng
SMR<75
10 groups
16 groups
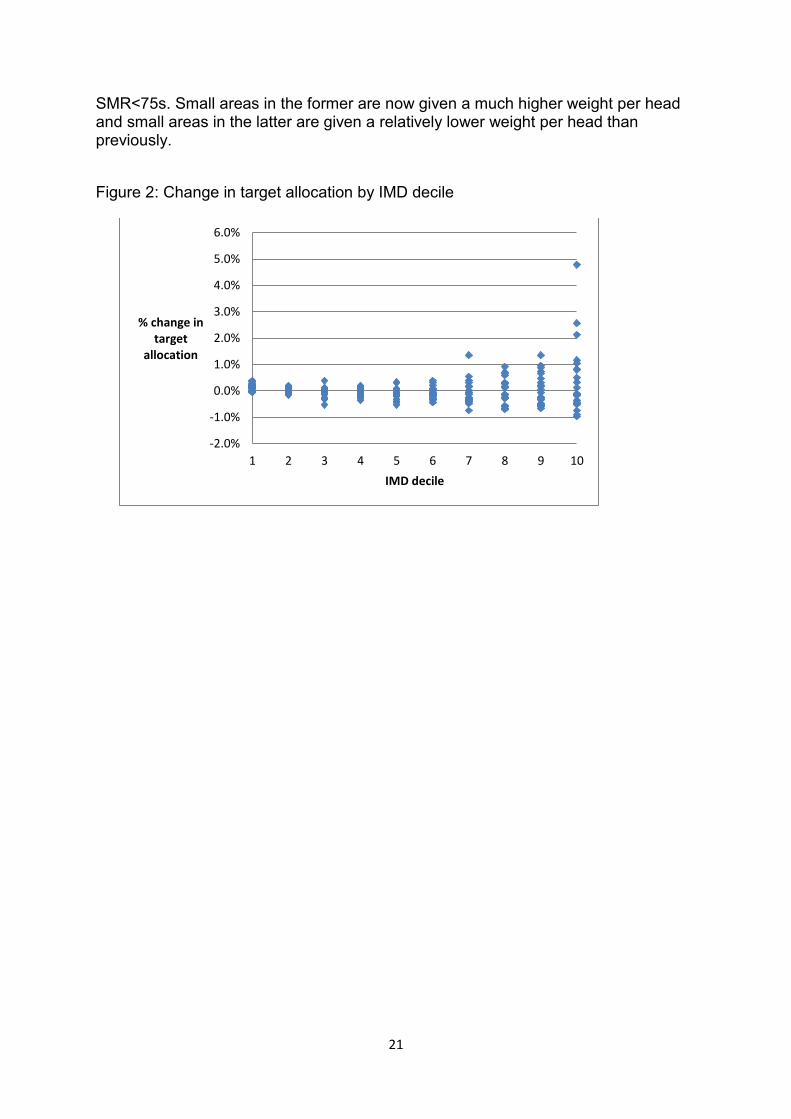
21
SMR<75s. Small areas in the former are now given a much higher weight per head and small areas in the latter are given a relatively lower weight per head than previously.
Figure 2: Change in target allocation by IMD decile
-2.0%
-1.0%
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
6.0%
1 2 3 4 5 6 7 8 9 10
% change in target
allocation
IMD decile
22
ANNEX D: REVISIONS TO THE CCG FORMULA
Refreshing the formula
We have refreshed the data supporting the underlying formula in a number of areas. The components updated are:
the Nuffield formula which covers general & acute and A&E services;
the prescribing formula which covers the cost of the drugs prescribed by GP practices;
the maternity formula; and
the emergency ambulance cost adjustment (EACA).
The mental health component has not been updated this year other than to correct significant underreporting of activity by an individual provider in the previous data. Mental health was already the most up to date component.
Their relative importance in the overall CCG formula is shown in Table 1, below, with the assumption that the NHS England Board maintains the share of the unmet need/health inequalities adjustment at 10%.
Table A1: Shares of overall CCG formula
Component Share in overall CCG formula
G&A, A&E, community and ambulance services
65%
Prescribing 12%
Mental health 10%
Maternity 3%
Unmet need adjustment 10%
We have updated the core formula using the most recently available complete data, which is between four and nine years more current than the data in the models used for 2014/15 and 2015/16 allocations. The Emergency Ambulance Cost Adjustment (EACA) takes account of the differential cost of providing ambulance services in different parts of the country, principally the higher costs of providing these services in sparsely populated areas. It is included in the formula to provide funding to commissioners to meet the differential costs. The current formula, unchanged since its inception in 1998/99 apart from mapping to the different commissioning organisations over time, is based on the volume of activity, the case-mix of activity and a measure of rurality. We have modelled the times by ambulances to reach incidents, provide treatment and convey patients to hospitals by MSOA across the combined data set from four of the 10 Ambulance Trusts to derive a new adjustment. ACRA supports our view that this is an improvement on the current EACA, which is more than 15 years old and was originally estimated for the then 100 or so Health Authorities. The impact of the EACA on target allocations is very small (range of +0.7% to -0.4% across CCGs).

23
Adjusting allocations for remote provision
The purpose of this proposed new adjustment is to provide funding to CCGs to meet the unavoidably higher costs of remote hospital sites, where the costs are higher because the level of activity is too low for the hospital to operate at an efficient scale. The package of recommendations has three key elements:
the criteria for considering a provider’s site remote;
the cost curve for assessing the unavoidable impact of scale on efficiency; and
the reference point on the cost curve used as the basis for deriving a cost adjustment.
Criteria for remoteness
We have developed three criteria that a hospital providing Type I A&E services must meet for its commissioning CCG to be considered eligible for the uplift to its target:
there must be 200,000 or fewer population within a one-hour travel time. A population served of 200,000 is the estimated scale at which a hospital can achieve close to national efficiency levels. This ensures that we do not support a large provider that is geographically remote but operating at efficient scale;
the next nearest provider must be one hour or more by normal road travel times (including ferry times where relevant). This is a measure of whether or not consolidation of services on to fewer sites is feasible; and
for at least 10% of the population in the hospital’s catchment area, this must be the closest provider, with the next nearest provider over an hour away. An adjustment to target allocations for the relevant CCG is only made when this percentage is 10% or higher. This avoids us giving very small (immaterial) adjustments to very many providers.
Cost curve for assessing the unavoidable impact of scale on efficiency
To generate a relevant cost curve we have analysed the costs of all hospital sites relative to their size as measured by activity levels. The estimated relative costs were adjusted to remove the impact of differences in case mix and in costs that are already compensated through the market forces factor (e.g. differential staff and premises costs across the country).
Reference point for the adjustment
We have used national average costs at the point representing the average size of hospital sites as the reference point for deriving the size of individual adjustments. The cost curve gives the estimated higher costs above national average costs for each of the hospitals with activity levels which correspond to population catchment areas of under 200,000 people. Note: the adjustment therefore reflects the expected cost premium based on national scale/cost relationships rather than the actual cost position of the individual site, which may be affected by a number of factors unrelated to its scale.

24
Applying the adjustment
Once calculated, the financial impact of the sparsity adjustment is added to the target allocation of the relevant CCGs. This results in an adjustment for six CCGs in relation to eight hospital sites. The adjustment to target allocations is in total £31m, with a range across the six CCGs of £2.6m to £14.2m. The impact on actual allocations in any year will depend on the resulting distance from target and the pace-of-change policy adopted.
Overall impact of changes to the CCG formula
The changes are relatively small overall but tend to move money in the direction of a combination of age and deprivation. Taking all of the updates and methodology changes together, the resulting target allocations have the following profile with respect to age and deprivation.
Table A2: Age and deprivation distribution of 2015-16 target model
Table A3: Age and deprivation distribution of 2016-17 target model
Note: The published target distribution has been normalised to 2016-17 quantum and normalised
using 2016-17 populations to facilitate comparison.
A1 A2 A3 A4 A5 A6 A7 A8 A9 A10 All ages
D1 1,084 1,097 1,169 1,120 1,086 1,117 1,156 1,158 1,124
D2 0 1,170 1,127 1,140 1,117 1,142 1,182 1,196 1,244 1,152
D3 1,121 1,139 1,256 1,204 1,164 1,202 1,303 1,215
D4 1,026 1,125 1,137 1,192 1,289 1,200 1,224 1,302 1,195
D5 1,121 1,168 1,218 1,264 1,276 1,262 1,286 1,267 1,244
D6 1,110 1,158 1,161 1,168 1,301 1,262 1,327 1,292 1,282 1,258 1,236
D7 1,153 1,160 1,163 1,136 1,193 1,354 1,346 1,380 1,303 1,212
D8 1,149 1,167 1,191 1,295 1,351 1,291 1,445 1,330 1,262
D9 1,183 1,147 1,336 1,462 1,249 1,381 1,397 1,456 1,397 1,290
D10 1,152 1,200 1,351 1,252 1,374 1,463 1,275
All depn 1,152 1,159 1,263 1,187 1,226 1,246 1,235 1,246 1,236 1,295 1,222
Younger Older
Less d
eprived
More
deprived
A1 A2 A3 A4 A5 A6 A7 A8 A9 A10 All ages
D1 1,059 1,059 1,126 1,144 1,111 1,148 1,119 1,198 1,135
D2 1,157 1,142 1,171 1,101 1,138 1,200 1,197 1,220 1,156
D3 1,062 1,135 1,237 1,220 1,164 1,203 1,291 1,209
D4 1,005 1,126 1,118 1,208 1,251 1,211 1,217 1,299 1,194
D5 1,109 1,168 1,227 1,277 1,267 1,278 1,298 1,290 1,250
D6 1,061 1,094 1,169 1,173 1,283 1,216 1,312 1,299 1,315 1,281 1,230
D7 1,143 1,141 1,166 1,184 1,179 1,339 1,351 1,366 1,308 1,207
D8 1,150 1,168 1,173 1,286 1,356 1,303 1,486 1,348 1,265
D9 1,164 1,115 1,332 1,426 1,253 1,354 1,400 1,452 1,401 1,275
D10 1,151 1,243 1,343 1,284 1,371 1,527 1,285
All depn 1,139 1,158 1,254 1,189 1,234 1,239 1,235 1,254 1,247 1,295 1,222
Younger Older
Less d
eprived
More
deprived
Key:
Decrease over £5 per head
Increase over £5 per head
Changes of less that £5 per head

25
ANNEX E: REVISIONS TO THE PRIMARY CARE MEDICAL FORMULA
The key change in the primary medical care formula is the development of new estimates of stratified workload per patient for GPs based on 2 million patient records from the Clinical Practice Research Datalink 2014. The previous data were based on 1999-2002. This has allowed us to re-estimate the importance of key drivers of primary medical care activity.
We have considered this information in detail to identify if there should be adjustments to the mapping of workload required (i.e. time spent per patient) based on a patient’s age and sex, the relative deprivation of the area, and the volume, number and impact of new patient registrations in a practice.
We have considered rurality as an explanatory factor of workload, based on the Census 2011 definition of rurality. We have found that rurality has a small, positive correlation with time spent per patient, equal to around four minutes per patient per year. However, ACRA recommends that this driver is not included for the purpose of calculating allocations, as there is not sufficient evidence to distinguish higher demand in rural areas (which would be a reflection of need) from potential supply factors (e.g. time available per patient).
We have compared the weighting of each GP practice with the weightings under the Carr-Hill formula (the formula used to allocate the global sum to GP practices). The general distribution of weightings Across GP practices under the new formula is slightly narrower than under Carr-Hill. The central 90% of practices have indices between 0.87 and 1.16 under the new model compared with 0.83 and 1.2 under Carr-Hill.
The histogram below shows the two weighting values.2 The horizontal axis is the weight under the workload estimates for Carr-Hill (red) and the new model (blue) grouped into bands and the vertical axis shows the number of practices with weightings in each band. The new model has a higher proportion of practices in the central bands (weightings 0.9-1.1) and the Carr-Hill model has a higher proportion of practices in the more extreme bands (less than 0.9 and greater than 1.1)
Figure 3: Carr-Hill weightings for old and new models
2 Practices without comparable Carr-Hill weights have been excluded (10 of 7711 practices).

26
The Table below compares the performance of this new approach, once implemented as a target model, with the previous target model, based on the Carr-Hill model. The analysis groups CCGs in to deprivation deciles, based on the 2015 Index of Multiple Deprivation. These are not age standardised and so care needs to be taken when comparing individual deciles, but it is clear that the new model will tend to target more resources at the most deprived areas, compared with the baselines, but to a lesser extent than the existing model. This is consistent with the results discussed above and reflects a much more up to date profile of the key cost drivers.
Table A4: Deprivation distribution for Carr-Hill and new target models
Deprivation
decile
2015-16 baseline distribution
£/head
Carr-Hill based target New target
£/head Diff from baseline £/head
Diff from baseline
Less
deprive
d 1 113 110 -3.28 114 0.52
2 116 112 -3.76 114 -1.46 3 122 116 -5.88 119 -3.18 4 122 117 -5.10 119 -3.58 5 120 122 1.74 120 -0.15
More
deprive
d 6 122 123 0.99 122 -0.41
7 123 123 -0.26 125 2.09 8 125 129 3.68 126 0.69 9 130 133 3.18 131 0.74 10 129 138 8.86 134 5.12
England 122 122 0 122 0
Note: All comparisons use 2016-17 primary medical services quantum and populations to facilitate
comparison of target distributions.

27
ANNEX F: NEW SPECIALISED SERVICES FORMULA
In order to support the development of a “place-based” approach to understanding the current and future utilisation of all healthcare resources at the CCG level of geography we have developed for the first time a formula for specialised services.
This formula uses a needs based person based resource application (PBRA) approach (the same approach as was followed for the development of the CCG formula which was originally undertaken by the Nuffield Trust).
The model uses anonymised person-level data for inpatients, outpatients, A&E and critical care activity, with the activity data linked at person level to GP practice registered lists. The prescribed specialised services identification tool was used to identify specialised services consistently across the country.
Costs of specialised services at the person level were modelled using as explanatory variables patients’ age, sex, diagnostic history from previous inpatient admissions, characteristics of the small geographical area where they reside, and characteristics of the local NHS services. In getting to this formula a wide range of explanatory factors was tested.
The activity data are from the SUS-PBR extract. It was found that some specialised services were poorly represented in this data set (e.g. forensic and secure mental health services). The modelling was therefore undertaken on the sub-set of activity for areas of care for which the SUS-PBR data have a reasonable level of coverage (c.50% of total specialised services spend).
For other areas of care, historic expenditure at CCG geography level has been used as the best available estimate of need and has been included in the target for each CCG.
The development of the specialised services model breaks new ground for services characterised by low volume, high cost activity with volatile demand and the formula is inevitably less robust when used in isolation than the CCG formula, as only a small number of people in each CCG use specialised services (on average, around 2%), and need is volatile from year to year.
In addition, the use of specialised services in certain locations may be influenced not only by population demand but also by the local availability of these services, an impact which needs to be eliminated in estimating needs-based allocations. In some locations higher use may be due a particular individual, family or patient group having specifically moved close to a specialist centre for access purposes, which is relevant for allocation purposes. It is often difficult to disentangle these two effects; however, the use of person-level data and diagnostic data seems to have overcome this issue. No service capacity measure was found to be significant in the final formula.
The benefit of adopting this approach is that for the first time we can compare patterns of utilisation of specialised services by local CCG geography and set them alongside target projections at CCG level for CCG commissioned services and primary medical care services. This gives us greater insight into the distribution of resources and the opportunity to begin to identify where resources may not be distributed equitably between commissioning streams or between geographies.

28
In order to mitigate any potential issues with the formula we have not included pace-of-change within specialised services for these allocations, rather the distance from target of specialised services is included as a factor within the total place-based pace-of-change calculations.
Delivering the Forward View:NHS planning guidance
2016/17 – 2020/21
December 2015

Delivering the Forward View: NHS planning guidance2016/17 – 2020/21
Version number: 1
First published: 22 December 2015
Prepared by: NHS England, NHS Improvement (Monitor and the NHS Trust Development Authority), Care Quality Commission (CQC), Health Education England (HEE), National Institute of Health and Care Excellence (NICE), Public Health England (PHE).
This document is for: Commissioners, NHS trusts and NHS foundation trusts.
Publications Gateway Reference: 04437
The NHS Five Year Forward View sets out a vision for the future of the NHS. It was developed by the partner organisations that deliver and oversee health and care services including:
• NHS England*
• NHS Improvement (Monitor and the NHS Trust Development Authority)
• Health Education England (HEE)
• The National Institute for Health and Care Excellence (NICE)
• Public Health England (PHE)
• Care Quality Commission (CQC)
*The National Health Service Commissioning Board was established on 1 October 2012 as an executive non-departmental public body. Since 1 April 2013, the National Health Service Commissioning Board has used the name NHS England for operational purposes.

1. INTRODUCTION 3
Introduction
1. The Spending Review provided the NHS in England with a credible basis on which to accomplish three interdependent and essential tasks: first, to implement the Five Year Forward View; second, to restore and maintain financial balance; and third, to deliver core access and quality standards for patients.
2. It included an £8.4 billion real terms increase by 2020/21, front-loaded. With these resources, we now need to close the health and wellbeing gap, the care and quality gap, and the finance and efficiency gap.
3. In this document, authored by the six national NHS bodies, we set out a clear list of national priorities for 2016/17 and longer-term challenges for local systems, together with financial assumptions and business rules. We reflect the settlement reached with the Government through its new Mandate to NHS England (annex 2). For the first time, the Mandate is not solely for the commissioning system, but sets objectives for the NHS as a whole.
4. We are requiring the NHS to produce two separate but connected plans: • a five year Sustainability and Transformation Plan (STP), place-based and driving the
Five Year Forward View; and
• a one year Operational Plan for 2016/17, organisation-based but consistent with the emerging STP.
5. The scale of what we need to do in future depends on how well we end the current year. The 2016/17 financial challenge for each trust will be contingent upon its end-of-year financial outturn, and the winter period calls for a relentless focus on maintaining standards in emergency care. It is also the case that local NHS systems will only become sustainable if they accelerate their work on prevention and care redesign. We don’t have the luxury of waiting until perfect plans are completed. So we ask local systems, early in the New Year, to go faster on transformation in a few priority areas, as a way of building momentum.

2. LOCAL HEALTH SYSTEM SUSTAINABILITY AND TRANSFORMATION PLANS 4
Local health system Sustainability and Transformation Plans
6. We are asking every health and care system to come together, to create its own ambitious local blueprint for accelerating its implementation of the Forward View. STPs will cover the period between October 20161 and March 2021, and will be subject to formal assessment in July 2016 following submission in June 2016. We are asking the NHS to spend the next six months delivering core access, quality and financial standards while planning properly for the next five years.
Place-based planning7. Planning by individual institutions will increasingly be supplemented with planning
by place for local populations. For many years now, the NHS has emphasised an organisational separation and autonomy that doesn’t make sense to staff or the patients and communities they serve.
8. System leadership is needed. Producing a STP is not just about writing a document, nor is it a job that can be outsourced or delegated. Instead it involves five things: (i) local leaders coming together as a team; (ii) developing a shared vision with the local community, which also involves local government as appropriate; (iii) programming a coherent set of activities to make it happen; (iv) execution against plan; and (v) learning and adapting. Where collaborative and capable leadership can’t be found, NHS England and NHS Improvement2 will need to help secure remedies through more joined-up and effective system oversight.
9. Success also depends on having an open, engaging, and iterative process that harnesses the energies of clinicians, patients, carers, citizens, and local community partners including the independent and voluntary sectors, and local government through health and wellbeing boards.
10. As a truly place-based plan, the STPs must cover all areas of CCG and NHS England commissioned activity including: (i) specialised services, where the planning will be led from the 10 collaborative commissioning hubs; and (ii) primary medical care, and do so from a local CCG perspective, irrespective of delegation arrangements. The STP must also cover better integration with local authority services, including, but not limited to, prevention and social care, reflecting local agreed health and wellbeing strategies.
1 For the period October 2016 – March 2017, the STP should set out what actions are planned but it does not need to revisit the activity and financial assumptions in the 2016/17 Operational Plan.
2 NHS Improvement will be the combined provider body, bringing together Monitor and the NHS Trust Development Authority (TDA).

2. LOCAL HEALTH SYSTEM SUSTAINABILITY AND TRANSFORMATION PLANS 5
Access to future transformation funding11. For the first time, the local NHS planning process will have significant central money
attached. The STPs will become the single application and approval process for being accepted onto programmes with transformational funding for 2017/18 onwards. This step is intended to reduce bureaucracy and help with the local join-up of multiple national initiatives.
12. The Spending Review provided additional dedicated funding streams for transformational change, building up over the next five years. This protected funding is for initiatives such as the spread of new care models through and beyond the vanguards, primary care access and infrastructure, technology roll-out, and to drive clinical priorities such as diabetes prevention, learning disability, cancer and mental health. Many of these streams of transformation funding form part of the new wider national Sustainability and Transformation Fund (STF). For 2016/17 only, to enable timely allocation, the limited available additional transformation funding will continue to be run through separate processes.
13. The most compelling and credible STPs will secure the earliest additional funding from April 2017 onwards. The process will be iterative. We will consider:
(i) the quality of plans, particularly the scale of ambition and track record of progress
already made. The best plans will have a clear and powerful vision. They will create coherence across different elements, for example a prevention plan; self-care and patient empowerment; workforce; digital; new care models; and finance. They will systematically borrow good practice from other geographies, and adopt national frameworks;
(ii) the reach and quality of the local process, including community, voluntary sector and local authority engagement;
(iii) the strength and unity of local system leadership and partnerships, with clear governance structures to deliver them; and
(iv) how confident we are that a clear sequence of implementation actions will follow as intended, through defined governance and demonstrable capabilities.
2. LOCAL HEALTH SYSTEM SUSTAINABILITY AND TRANSFORMATION PLANS 6
Content of STPs14. The strategic planning process is intended to be developmental and supportive as well
as hard-edged. We set out in annex 1 of this document a list of ‘national challenges’ to help local systems set out their ambitions for their populations. This list of questions includes the objectives set in the Mandate. Do not over-interpret the list as a narrow template for what constitutes a good local plan: the most important initial task is to create a clear overall vision and plan for your area.
15. Local health systems now need to develop their own system wide local financial sustainability plan as part of their STP. Spanning providers and commissioners, these plans will set out the mixture of demand moderation, allocative efficiency, provider productivity, and income generation required for the NHS locally to balance its books.
Agreeing ‘transformation footprints’ 16. The STP will be the umbrella plan, holding underneath it a number of different specific
delivery plans, some of which will necessarily be on different geographical footprints. For example, planning for urgent and emergency care will range across multiple levels: a locality focus for enhanced primary care right through to major trauma centres.
17. The first critical task is for local health and care systems to consider their transformation footprint – the geographic scope of their STP. They must make proposals to us by Friday 29 January 2016, for national agreement. Local authorities should be engaged with these proposals. Taken together, all the transformation footprints must form a complete national map. The scale of the planning task may point to larger rather than smaller footprints.
18. Transformation footprints should be locally defined, based on natural communities, existing working relationships, patient flows and take account of the scale needed to deliver the services, transformation and public health programmes required, and how it best fits with other footprints such as local digital roadmaps and learning disability units of planning. In future years we will be open to simplifying some of these arrangements. Where geographies are already involved in the Success Regime, or devolution bids, we would expect these to determine the transformation footprint. Although it is important to get this right, there is no single right answer. The footprints may well adapt over time. We want people to focus their energies on the content of plans rather than have lengthy debates about boundaries.

2. LOCAL HEALTH SYSTEM SUSTAINABILITY AND TRANSFORMATION PLANS 7
19. We will issue further brief guidance on the STP process in January. This will set out the timetable and early phasing of national products and engagement events that are intended to make it much easier to answer the challenges we have posed, and include how local areas can best involve their local communities in creating their STPs, building on the ‘six principles’ created to support the delivery of the Five Year Forward View. By spring 2016, we intend to develop and make available roadmaps for national transformation initiatives.
20. We would welcome any early reactions, by Friday 29 January 2016, as to what additional material you would find most helpful in developing your STP. Please email [email protected], with the subject title ‘STP feedback’. We would also like to work with a few local systems to develop exemplar, fast-tracked plans, and would welcome expressions of interest to the above inbox.

3. NATIONAL “MUST DOS” FOR 2016/17 8
National ‘must dos’ for 2016/17
21. Whilst developing long-term plans for 2020/21, the NHS has a clear set of plans and priorities for 2016/17 that reflect the Mandate to the NHS and the next steps on Forward View implementation.
22. Some of our most important jobs for 2016/17 involve partial roll-out rather than full national coverage. Our ambition is that by March 2017, 25 percent of the population will have access to acute hospital services that comply with four priority clinical standards on every day of the week, and 20 percent of the population will have enhanced access to primary care. There are three distinct challenges under the banner of seven day services:
(i) reducing excess deaths by increasing the level of consultant cover and diagnostic services available in hospitals at weekends. During 16/17, a quarter of the country must be offering four of the ten standards, rising to half of the country by 2018 and complete coverage by 2020;
(ii) improving access to out of hours care by achieving better integration and redesign of 111, minor injuries units, urgent care centres and GP out of hours services to enhance the patient offer and flows into hospital; and
(iii) improving access to primary care at weekends and evenings where patients need it by increasing the capacity and resilience of primary care over the next few years.
23. Where relevant, local systems need to reflect this in their 2016/17 Operational Plans, and all areas will need to set out their ambitions for seven day services as part of their STPs.
The nine ‘must dos’ for 2016/17 for every local system:1. Develop a high quality and agreed STP, and subsequently achieve what you determine
are your most locally critical milestones for accelerating progress in 2016/17 towards achieving the triple aim as set out in the Forward View.
2. Return the system to aggregate financial balance. This includes secondary care providers delivering efficiency savings through actively engaging with the Lord Carter provider productivity work programme and complying with the maximum total agency spend and hourly rates set out by NHS Improvement. CCGs will additionally be expected to deliver savings by tackling unwarranted variation in demand through implementing the RightCare programme in every locality.
3. Develop and implement a local plan to address the sustainability and quality of general practice, including workforce and workload issues.

3. NATIONAL “MUST DOS” FOR 2016/17 9
4. Get back on track with access standards for A&E and ambulance waits, ensuring more than 95 percent of patients wait no more than four hours in A&E, and that all ambulance trusts respond to 75 percent of Category A calls within eight minutes; including through making progress in implementing the urgent and emergency care review and associated ambulance standard pilots.
5. Improvement against and maintenance of the NHS Constitution standards that more than 92 percent of patients on non-emergency pathways wait no more than 18 weeks from referral to treatment, including offering patient choice.
6. Deliver the NHS Constitution 62 day cancer waiting standard, including by securing adequate diagnostic capacity; continue to deliver the constitutional two week and 31 day cancer standards and make progress in improving one-year survival rates by delivering a year-on-year improvement in the proportion of cancers diagnosed at stage one and stage two; and reducing the proportion of cancers diagnosed following an emergency admission.
7. Achieve and maintain the two new mental health access standards: more than 50 percent of people experiencing a first episode of psychosis will commence treatment with a NICE approved care package within two weeks of referral; 75 percent of people with common mental health conditions referred to the Improved Access to Psychological Therapies (IAPT) programme will be treated within six weeks of referral, with 95 percent treated within 18 weeks. Continue to meet a dementia diagnosis rate of at least two-thirds of the estimated number of people with dementia.
8. Deliver actions set out in local plans to transform care for people with learning disabilities, including implementing enhanced community provision, reducing inpatient capacity, and rolling out care and treatment reviews in line with published policy.
9. Develop and implement an affordable plan to make improvements in quality particularly for organisations in special measures. In addition, providers are required to participate in the annual publication of avoidable mortality rates by individual trusts.
24. We expect the development of new care models will feature prominently within STPs. In addition to existing approaches, in 2016/17 we are interested in trialing two new specific approaches with local volunteers:
• secondary mental health providers managing care budgets for tertiary mental health services; and
• the reinvention of the acute medical model in small district general hospitals.
Organisations interested in working with us on either of these approaches should let us know by 29 January 2016 by emailing [email protected]

4. OPERATIONAL PLANS FOR 2016/17 10
Operational Plans for 2016/17
25. An early task for local system leaders is to run a shared and open-book operational planning process for 2016/17. This will cover activity, capacity, finance and 2016/17 deliverables from the emerging STP. By April 2016, commissioner and provider plans for 2016/17 will need to be agreed by NHS England and NHS Improvement, based on local contracts that must be signed by March 2016.
26. The detailed requirements for commissioner and provider plans are set out in the technical guidance that will accompany this document. All plans will need to demonstrate:
• how they intend to reconcile finance with activity (and where a deficit exists, set out clear plans to return to balance);
• their planned contribution to the efficiency savings;
• their plans to deliver the key must-dos;
• how quality and safety will be maintained and improved for patients;
• how risks across the local health economy plans have been jointly identified and mitigated through an agreed contingency plan; and
• how they link with and support with local emerging STPs.
The 2016/17 Operational Plan should be regarded as year one of the five year STP, and we expect significant progress on transformation through the 2016/17 Operational Plan.
27. Building credible plans for 2016/17 will rely on a clear understanding of demand and capacity, alignment between commissioners and providers, and the skills to plan effectively. A support programme is being developed jointly by national partners to help local health economies in preparing robust activity plans for 2016/17 and beyond.

5. ALLOCATIONS 11
Allocations
28. NHS England’s allocations to commissioners are intended to achieve: • greater equity of access through pace of change, both for CCG allocations and on a
place-based basis; • closer alignment with population need through improved allocation formulae including
a new inequalities adjustment for specialised care, more sensitive adjustments for CCGs and primary care, and a new sparsity adjustment for remote areas; and
• faster progress with our strategic goals through higher funding growth for GP services
and mental health, and the introduction of the Sustainability and Transformation Fund.
29. In line with our strategic priorities, overall primary medical care spend will rise by 4-5 percent each year. Specialised services funding will rise by 7 percent in 2016/17, with growth of at least 4.5 percent in each subsequent year. The relatively high level of funding reflects forecast pressures from new NICE legally mandated drugs and treatments.
30. To support long-term planning, NHS England has set firm three year allocations for CCGs, followed by two indicative years. For 2016/17, CCG allocations will rise by an average of 3.4 percent, and we will make good on our commitment that no CCG will be more than 5 percent below its target funding level. To provide CCGs with a total place-based understanding of all commissioned spend, alongside allocations for CCG commissioned activities, we will also publish allocations for primary care and specialized commissioned activity.
NHS England will in principle support any proposals from groups of CCGs, particularly in areas working towards devolution who wish to implement a more accelerated cross-area pace-of-change policy by mutual agreement.
31. Mirroring the conditionality of providers accessing the Sustainability and Transformation Fund, the real terms element of growth in CCG allocations for 2017/18 onwards will be contingent upon the development and sign off of a robust STP during 2016/17.

6. RETURNING THE NHS PROVIDER SECTOR TO BALANCE 12
Returning the NHS provider sector to balance
32. During 2016/17 the NHS trust and foundation trust sector will, in aggregate, be required to return to financial balance. £1.8 billion of income from the 2016/17 Sustainability and Transformation Fund will replace direct Department of Health (DH) funding. The distribution of this funding will be calculated on a trust by trust basis by NHS Improvement and then agreed with NHS England.
33. NHS England and NHS Improvement are working together to ensure greater alignment between commissioner and provider financial levers. Providers who are eligible for sustainability and transformation funding in 2016/17 will not face a double jeopardy scenario whereby they incur penalties as well as losing access to funding; a single penalty will be imposed.
34. Quarterly release of these Sustainability Funds to trusts and foundation trusts will depend on achieving recovery milestones for (i) deficit reduction; (ii) access standards; and (iii) progress on transformation. The three conditions attached to the transitional NHS provider fund have to be hard-edged. Where trusts default on the conditions access to the fund will be denied and sanctions will be applied.
35. Deficit reduction in providers will require a forensic examination of every pound spent on delivering healthcare and embedding a culture of relentless cost containment. Trusts need to focus on cost reduction not income growth; there needs to be far greater consistency between trusts’ financial plans and their workforce plans in 2016/17. Workforce productivity will therefore be a particular priority as just a 1 percent improvement represents £400 million of savings. All providers will be expected to evidence the effective use of e-rostering for nurses, midwives, Health Care Assistants (HCAs) and other clinicians to make sure the right staff are in the right place at the right time to ensure patients get the right hours of care and minimum time is wasted on bureaucracy. This approach will enable providers to reduce their reliance on agency staffing whilst compliance with the agency staffing rules will also reduce the rates paid. In addition, providers will need to adopt tightly controlled procurement practices with compliance incentives and sanctions to drive down price and unwarranted variation. For example, all providers will be expected to report and share data on what they are paying for the top 100 most common non-pay items, and be required to only pay the best price available for the NHS.

6. RETURNING THE NHS PROVIDER SECTOR TO BALANCE 13
36. Capital investments proposed by providers should be consistent with their clinical strategy and clearly demonstrate the delivery of safe, productive services with a business case that describes affordability and value for money. Given the constrained level of capital resource available from 2016/17, there will be very limited levels of financing available and the repayment of existing and new borrowing related to capital investment will need to be funded from within the trust’s own internally generated capital resource in all but the most exceptionally pre-agreed cases. Trusts will need to procure capital assets more efficiently, consider alternative methods of securing assets such as managed equipment services, maximize disposals and extend asset lives. In January, the DH will be issuing some revisions to how the PDC dividend will be calculated and a number of other changes to the capital financing regime.

7. EFFICIENCY ASSUMPTIONS AND BUSINESS RULES 14
Efficiency assumptions and business rules
37. The consultation on the tariff will propose a 2 percent efficiency deflator and 3.1 percent inflation uplift for 2016/17 (the latter reflecting a step change in pension-related costs). This reflects Monitor and NHS England’s assessment of cost inflation including the effect of pension changes. To support system stability, we plan to remain on HRG4 for a further year and there will also be no changes to specialist top- ups in 2016/17; the specialised service risk share is also being suspended for 2016/17. We will work with stakeholders to better understand the impact of the move to HRG4+ and other related changes in 2017/18. For planning purposes, an indicative price list is being made available on the Monitor website. The consultation on the tariff will also include the timetable for implementing new payment approaches for mental health.
38. As notified in Commissioning Intentions 2016/2017 for Prescribed Specialised Services, NHS England is developing a single national purchasing and supply chain arrangement for specialised commissioning high cost tariff excluded devices with effect from April 2016. Transition plans will be put in place prior to this date with each provider to transition from local to national procurement arrangements.
39. The 2 percent efficiency requirement is predicated upon the provider system meeting a forecast deficit of £1.8 billion at the end of 2015/16. Any further deterioration of this position will require the relevant providers to deliver higher efficiency levels to achieve the control totals to be set by NHS Improvement.
40. For 2016/17 the business rules for commissioners will remain similar to those for last year. Commissioners (excluding public health and specialised commissioning) will be required to deliver a cumulative reserve (surplus) of 1 percent. At the very least, commissioners who are unable to meet the cumulative reserve (surplus) requirement must deliver an in-year break-even position. Commissioners with a cumulative deficit will be expected to apply their increase in allocation to improving their bottom line position, other than the amount necessary to fund nationally recognised new policy requirements. Drawdown will be available to commissioners in line with the process for the previous financial year. CCGs should plan to drawdown all cumulative surpluses in excess of 1 percent over the next three years, enabling drawdown to become a more fluid mechanism for managing financial pressures across the year-end boundary.
7. EFFICIENCY ASSUMPTIONS AND BUSINESS RULES 15
41. Commissioners are required to plan to spend 1 percent of their allocations non-recurrently, consistent with previous years. In order to provide funds to insulate the health economy from financial risks, the 1 percent non-recurrent expenditure should be uncommitted at the start of the year, to enable progressive release in agreement with NHS England as evidence emerges of risks not arising or being effectively mitigated through other means. Commissioners will also be required to hold an additional contingency of 0.5 percent, again consistent with previous years.
42. CCGs and councils will need to agree a joint plan to deliver the requirements of the Better Care Fund (BCF) in 2016/17. The plan should build on the 2015/16 BCF plan, taking account of what has worked well in meeting the objectives of the fund, and what has not. CCGs will be advised of the minimum amount that they are required to pool as part of the notification of their wider allocation. BCF funding should explicitly support reductions in unplanned admissions and hospital delayed transfers of care; further guidance on the BCF will be forthcoming in the New Year.
43. Commissioners must continue to increase investment in mental health services each year at a level which at least matches their overall expenditure increase. Where CCGs collaborate with specialised commissioning to improve service efficiency, they will be eligible for a share of the benefits.
44. NHS England and NHS Improvement continue to be open to new approaches to contracting and business rules, as part of these agreements. For example, we are willing to explore applying a single financial control total across local commissioners and providers with a few local systems.
Measuring progress
45. We will measure progress through a new CCG Assessment Framework. NHS England will consult on this in January 2016, and it will be aligned with this planning guidance. The framework is referred in the Mandate as a CCG scorecard. It is our new version of the CCG assurance framework, and it will apply from 2016/17. Its relevance reaches beyond CCGs, because it’s about how local health and care systems and communities can assess their own progress.

9. TIMETABLE 16
Timetable
Timetable Date
Publish planning guidance 22 December 2015
Publish 2016/17 indicative prices By 22 December 2015
Issue commissioner allocations, and technical annexes to planning guidance
Early January 2016
Launch consultation on standard contract, announce CQUIN and Quality Premium
January 2016
Issue further process guidance on STPs January 2016
Localities to submit proposals for STP footprints and volunteers for mental health and small DGHs trials
By 29 January 2016
First submission of full draft 16/17 Operational Plans 8 February 2016
National Tariff S118 consultation January/February 2016
Publish National Tariff March 2016
Boards of providers and commissioners approve budgets and final plans
By 31 March 2016
National deadline for signing of contracts 31 March 2016
Submission of final 16/17 Operational Plans, aligned with contracts 11 April 2016
Submission of full STPs End June 2016
Assessment and Review of STPs End July 2016
Please note that we will announce the timetable for consultation and issuing of the standard contract separately. A more detailed timetable and milestones is included in the technical guidance that will accompany this document.

ANNEX 1: INDICATIVE ‘NATIONAL CHALLENGES’ FOR STPS 17
Annex 1: Indicative ‘national challenges’ for STPs
STPs are about the holistic pursuit of the triple aim – better health, transformed quality of care delivery, and sustainable finances. They also need to set out how local systems will play their part in delivering the Mandate (annex 2).
We will publish further guidance early in 2016 to help areas construct the strongest possible process and plan.
We will also make available aids (e.g. exemplar plans) and some hands-on support for areas as they develop their plans.
The questions below give an early sense of what you will need to address to gain sign-off and attract additional national investment.
We are asking local systems first to focus on creating an overall local vision, and the three overarching questions – rather than attempting to answer all of the specifics right from the start. We will be developing a process to offer feedback on these first, prior to development of the first draft of the detailed plans.
A. How will you close the health and wellbeing gap?
This section should include your plans for a ‘radical upgrade’ in prevention, patient activation, choice and control, and community engagement.
Questions your plan should answer:
1. How will you assess and address your most important and highest cost preventable causes of ill health, to reduce healthcare demand and tackle health inequalities working closely with local government?
• How rapidly could you achieve full local implementation of the national Diabetes Prevention Programme? Why should Public Health England (PHE) and NHS England prioritise your geographical area (e.g. with national funding to support the programme)?
• What action will you take to address obesity, including childhood obesity?
• How will you achieve a step-change in patient activation and self-care? How will this help you moderate demand and achieve financial balance? How will you embed the six principles of engagement and involvement of local patients, carers, and communities developed to help deliver the Five Year Forward View?

ANNEX 1: INDICATIVE ‘NATIONAL CHALLENGES’ FOR STPS 18
2. How will you make real the aspiration to design person-centred coordinated care, including plans to ensure patients have access to named, accountable consultants?
3. How will a major expansion of integrated personal health budgets and implementation of choice – particularly in maternity, end-of-life and elective care – be an integral part of your programme to hand power to patients?
4. How are NHS and other employers in your area going to improve the health of their own workforce – for example by participating in the national roll out the Healthy NHS programme?
B. How will you drive transformation to close the care and quality gap?
This section should include plans for new care model development, improving against clinical priorities, and rollout of digital healthcare.
Questions your plan should answer:
1 What is your plan for sustainable general practice and wider primary care? How will you improve primary care infrastructure, supported in part through access to national primary care transformation funding?
2. How rapidly can you implement enhanced access to primary care in evenings and weekends and using technology? Why should NHS England prioritise your area for additional funding?
3. What are your plans to adopt new models of out-of-hospital care, e.g Multi-specialty Community Providers (MCPs) or Primary and Acute Care Systems (PACS)? Why should NHS England prioritise your area for transformation funding? And when are you planning to adopt forthcoming best practice from the enhanced health in care homes vanguards?
4. How will you adopt new models of acute care collaboration (accountable clinical networks, specialty franchises, and Foundation Groups)? How will you work with organisations outside your area and learn from best practice from abroad, other sectors and industry?
5. What is your plan for transforming urgent and emergency care in your area? How will you simplify the current confusing array of entry points? What’s your agreed recovery plan to achieve and maintain A&E and ambulance access standards?
6. What’s your plan to maintain the elective care referral to treatment standard? Are you buying sufficient activity, tackling unwarranted variation in demand, proactively offering patient choice of alternatives, and increasing provider productivity?

ANNEX 1: INDICATIVE ‘NATIONAL CHALLENGES’ FOR STPS 19
7. How will you deliver a transformation in cancer prevention, diagnosis, treatment and aftercare in line with the cancer taskforce report?
8. How will you improve mental health services, in line with the forthcoming mental health taskforce report, to ensure measureable progress towards parity of esteem for mental health?
9. What steps will your local area take to improve dementia services?
10. As part of the Transforming Care programme, how will your area ensure that people with learning disabilities are, wherever possible, supported at home rather than in hospital? How far are you closing out-moded inpatient beds and reinvesting in continuing learning disability support
11. How fast are you aspiring to improve the quality of care and safety in your organisations as judged by the Care Quality Commission (CQC)? What is your trajectory for no NHS trust and no GP practice to have an overall inadequate rating from the Care Quality Commission (CQC)?
12. What are you doing to embed an open, learning and safety culture locally that is ambitious enough? What steps are you taking to improving reporting, investigations and supporting patients, their families and carers, as well as staff who have been involved in an incident?
13. What plans do you have in place to reduce antimicrobial resistance and ensure responsible prescribing of antibiotics in all care settings? How are you supporting prescribers to enable them issue the right drugs responsibly? At the same time, how rapidly will you achieve full implementation of good practice in reducing avoidable mortality from sepsis?
14. How will you achieve by 2020 the full-roll out of seven day services for the four priority clinical standards?
15. How will you implement the forthcoming national maternity review, including progress towards new national ambitions for improving safety and increased personalisation and choice?
16. How will you put your Children and Young People Mental Health Plan into practice?
17. How quickly will you implement your local digital roadmap, taking the steps needed to deliver a fully interoperable health and care system by 2020 that is paper-free at the point of care? How will you make sure that every patient has access to digital health records that they can share with their families, carers and clinical teams? How will you increase your online offer to patients beyond repeat prescriptions and GP appointments?

ANNEX 1: INDICATIVE ‘NATIONAL CHALLENGES’ FOR STPS 20
18. What is your plan to develop, retrain and retain a workforce with the right skills, values and behaviours in sufficient numbers and in the right locations to deliver your vision for transformed care? How will you build the multidisciplinary teams to underpin new models of care? How ambitious are your plans to implement new workforce roles such as associate nurses, physician associates, community paramedics and pharmacists in general practice?
19. What is your plan to improve commissioning? How rapidly will the CCGs in your system move to place-based commissioning? If you are a devolution area, how will implementation delivery real improvements for patients?
20. How will your system be at the forefront of science, research and innovation? How are you implementing combinatorial innovation, learning from the forthcoming test bed programme? How will services changes over the next five years embrace breakthroughs in genomics, precision medicine and diagnostics?
C. How will you close the finance and efficiency gap?
This section should describe how you will achieve financial balance across your local health system and improve the efficiency of NHS services.
Questions your plan should answer:
1. How will you deliver the necessary per annum efficiency across the total NHS funding base in your local area by 2020/21?
2. What is your comprehensive and credible plan to moderate demand growth? What are the respective contributions in your local system of: (i) tackling unwarranted variation in care utilisation, e.g. through RightCare; (ii) patient activation and self-care; (iii) new models of care; and (iv) urgent and emergency care reform implementation?
3. How will you reduce costs (as opposed to growing income) and how will you get the most out of your existing workforce? What savings will you make from financial controls on agency, whilst ensuring appropriate staffing levels? What are your plans for improving workforce productivity, e.g. through e-rostering of nurses and HCAs? How are you planning to reduce cost through better purchasing and medicines management? What efficiency improvements are you planning to make across primary care and specialised care delivery?
ANNEX 1: INDICATIVE ‘NATIONAL CHALLENGES’ FOR STPS 21
4. What capital investments do you plan to unlock additional efficiency? How will they be affordable and how will they be financed?
5. What actions will you take as a system to utilise NHS estate better, disposing of unneeded assets or monetising those that could create longer-term income streams? How does this local system estates plan support the plans you’re taking to redesign care models in your area?

ANNEX 2: THE GOVERNMENT’S MANDATE TO NHS ENGLAND 2016/17 22
Annex 2: The Government’s mandate to NHS England 2016/17
The table below shows NHS England’s objectives with an overall measurable goal for this Parliament and clear priority deliverables for 2016-17. The majority of these goals will be achieved in partnership with the Department of Health (DH), NHS Improvement and other health bodies such as Public Health England (PHE), Health Education England (HEE) and the Care Quality Commission (CQC). It also sets out requirements for NHS England to comply with in paragraph 6.2.
Read the full Mandate to NHS England
1. Through better commissioning, improve local and national health outcomes, particularly by addressing poor outcomes and inequalities.
1.1 CCG performance
Overall 2020 goals:
• Consistent improvement in performance of CCGs against new CCG assessment framework.
2016-17 deliverables:
• By June, publish results of the CCG assessment framework for 2015-16, which provides CCGs with an aggregated Ofsted style assessment of performance and allows them to benchmark against other CCGs and informs whether NHS England intervention is needed.
• Ensure new Ofsted-style CCG framework for 2016-17 includes health economy metrics to measure progress on priorities set out in the mandate and the NHS planning guidance including overall Ofsted-style assessment for each of cancer, dementia, maternity, mental health, learning disabilities and diabetes, as well as metrics on efficiency, core performance, technology and prevention.
• By the end of Q1 of 2016-17, publish the first overall assessment for each of the six clinical areas above.

ANNEX 2: THE GOVERNMENT’S MANDATE TO NHS ENGLAND 2016/17 23
2. To help create the safest, highest quality health and care service.
2.1 Avoidable deaths and seven-day services
Overall 2020 goals:
• Roll out of seven-day services in hospital to 100 percent of the population (four priority clinical standards in all relevant specialities, with progress also made on the other six standards), so that patients receive the same standards of care, seven days a week.
• Achieve a significant reduction in avoidable deaths, with all trusts to have seen measurable reduction from their baseline on the basis of annual measurements.
• Support NHS Improvement to significantly increase the number of trusts rated outstanding or good, including significantly reducing the length of time trusts remain in special measures.
• Measurable progress towards reducing the rate of stillbirths, neonatal and maternal deaths and brain injuries that are caused during or soon after birth by 50 percent by 2030 with a measurable reduction by 2020.
• Support the NHS to be the world’s largest learning organisation with a new culture of learning from clinical mistakes, including improving the number of staff who feel their organisation acts on concerns raised by clinical staff or patients.
• Measurable improvement in antimicrobial prescribing and resistance rates.
2016-17 deliverables:
• Publish avoidable deaths per trust annually and support NHS Improvement to help trusts to implement programme to improve from March 2016 baseline.
• Rollout of four clinical priority standards in all relevant specialties to 25 percent of population.
• Implement agreed recommendations of the National Maternity Review in relation to safety, and support progress on delivering Sign up to Safety.
• Support the Government’s goal to establish global and UK baseline and ambition for antimicrobial prescribing and resistance rates.

ANNEX 2: THE GOVERNMENT’S MANDATE TO NHS ENGLAND 2016/17 24
2.2 Patient experience
Overall 2020 goals:
• Maintain and increase the number of people recommending services in the Friends and Family Test (FFT) (currently 88-96 percent), and ensure its effectiveness, alongside other sources of feedback to improve services.
• 50-100,000 people to have a personal health budget or integrated personal budget (up from current estimate of 4,000).
• Significantly improve patient choice, including in maternity, end-of-life care and for people with long-term conditions, including ensuring an increase in the number of people able to die in the place of their choice, including at home.
2016-17 deliverables:
• Produce a plan with specific milestones for improving patient choice by 2020, particularly in maternity, end-of-life care (including to ensure more people are able to achieve their preferred place of care and death), and personal health budgets.
• Building on the FFT, develop proposals about how feedback, particularly in maternity services, could be enhanced to drive improvements to services at clinical and ward levels.
2.3 Cancer Overall 2020 goals:
• Deliver recommendations of the Independent Cancer Taskforce, including:
o significantly improving one-year survival to achieve 75 percent by 2020 for all cancers combined (up from 69 percent currently); and
o patients given definitive cancer diagnosis, or all clear, within 28 days of being referred by a GP.
2016-17 deliverables:
• Achieve 62-day cancer waiting time standard.
• Support NHS Improvement to achieve measurable progress towards the national diagnostic standard of patients waiting no more than six weeks from referral to test.
• Agree trajectory for increases in diagnostic capacity required to 2020 and achieve it for year one.
• Invest £340 million in providing cancer treatments not routinely provided on the NHS through the Cancer Drugs Fund, and ensure effective transition to the agreed operating model to improve its effectiveness within its existing budget.

ANNEX 2: THE GOVERNMENT’S MANDATE TO NHS ENGLAND 2016/17 25
3. To balance the NHS budget and improve efficiency and productivity
3.1 Balancing the NHS budget
Overall 2020 goals:
• With NHS Improvement, ensure the NHS balances its budget in each financial year.
• With the Department of Health and NHS Improvement, achieve year on year improvements in NHS efficiency and productivity (2-3 percent each year), including from reducing growth in activity and maximising cost recovery.
2016-17 deliverables:
• With NHS Improvement ensure the NHS balances its budget, with commissioners and providers living within their budgets, and support NHS Improvement in:
o securing £1.3 billion of efficiency savings through implementing Lord Carter’s recommendations and collaborating with local authorities on Continuing Healthcare spending;
o delivering year one of trust deficit reduction plans and ensuring a balanced financial position across the trust sector, supported by effective deployment of the Sustainability and Transformation Fund; and
o reducing spend on agency staff by at least £0.8 billion on a path to further reductions over the Parliament.
• Roll-out of second cohort of RightCare methodology to a further 60 CCGs.
• Measurable improvement in primary care productivity, including through supporting community pharmacy reform.
• Work with CCGs to support Government’s goal to increase NHS cost recovery up to £500 million by 2017-18 from overseas patients.
• Ensure CCGs’ local estates strategies support the overall goal of releasing £2 billion and land for 26,000 homes by 2020.
ANNEX 2: THE GOVERNMENT’S MANDATE TO NHS ENGLAND 2016/17 26
4. To lead a step change in the NHS in preventing ill health and supporting people to live healthier lives.
4.1 Obesity and diabetes
Overall 2020 goals:
• Measurable reduction in child obesity as part of the Government’s childhood obesity strategy.
• 100,000 people supported to reduce their risk of diabetes through the Diabetes Prevention Programme.
• Measurable reduction in variation in management and care for people with diabetes.
2016-17 deliverables:
• Contribute to the agreed child obesity implementation plan, including wider action to achieve year on year improvement trajectory for the percentage of children who are overweight or obese.
• 10,000 people referred to the Diabetes Prevention Programme.
4.2 Dementia Overall 2020 goals:
• Measurable improvement on all areas of Prime Minister’s challenge on dementia 2020, including:
o maintain a diagnosis rate of at least two thirds;
o increase the numbers of people receiving a dementia diagnosis within six weeks of a GP referral; and
o improve quality of post-diagnosis treatment and support for people with dementia and their carers.
2016-17 deliverables:
• Maintain a minimum of two thirds diagnosis rates for people with dementia.
• Work with National Institute for Health Research on location of Dementia Institute.
• Agree an affordable implementation plan for the Prime Minister’s challenge on dementia 2020, including to improve the quality of post-diagnosis treatment and support.

ANNEX 2: THE GOVERNMENT’S MANDATE TO NHS ENGLAND 2016/17 27
5. To maintain and improve performance against core standards
5.1 A&E, ambulances and Referral to Treatment (RTT)
Overall 2020 goals:
• 95 percent of people attending A&E seen within four hours; Urgent and Emergency Care Networks rolled out to 100 percent of the population.
• 75 percent of Category A ambulance calls responded to within 8 minutes.
• 92 percent receive first treatment within 18 weeks of referral; no-one waits more than 52 weeks.
2016-17 deliverables:
• With NHS Improvement, agree improvement trajectory and deliver the plan for year one for A&E.
• Implement Urgent and Emergency Care Networks in 20 percent of the country designated as transformation areas, including clear steps towards a single point of contact.
• With NHS Improvement, agree improvement trajectory and deliver the plan for year one for ambulance responses; complete Red 2 pilots and decide on full roll-out.
• With NHS Improvement, meet the 18-week referral-to-treatment standard, including implementing patient choice in line with the NHS Constitution; and reduce unwarranted variation between CCG referral rates to better manage demand.
6. To improve out-of-hospital care.
6.1 New models of care and general practice
Overall 2020 goals:
• 100 percent of population has access to weekend/evening routine GP appointments.
• Measurable reduction in age standardised emergency admission rates and emergency inpatient bed-day rates; more significant reductions through the New Care Model programme covering at least 50 percent of population.
• Significant measurable progress in health and social care integration, urgent and emergency care (including ensuring a single point of contact), and electronic health record sharing, in areas covered by the New Care Model programme.
• 5,000 extra doctors in general practice.

ANNEX 2: THE GOVERNMENT’S MANDATE TO NHS ENGLAND 2016/17 28
2016-17 deliverables:
• New models of care covering the 20 percent of the population designated as being in a transformation area to:
o provide access to enhanced GP services, including evening and weekend access and same-day GP appointments for all over 75s who need them; and
o make progress on integration of health and social care, integrated urgent and emergency care, and electronic record sharing.
• Publish practice-level metrics on quality of and access to GP services and, with the Health and Social Care Information Centre, provide GPs with benchmarking information for named patient lists.
• Develop new voluntary contract for GPs (Multidisciplinary Community Provider contract) ready for implementation in 2017-18.
6.2 Health and social care integration
Overall 2020 goals:
• Achieve better integration of health and social care in every area of the country, with significant improvements in performance against integration metrics within the new CCG assessment framework. Areas will graduate from the Better Care Fund programme management once they can demonstrate they have moved beyond its requirements, meeting the government’s key criteria for devolution.
• Ensure the NHS plays its part in significantly reducing delayed transfers of care, including through developing and applying new incentives.
2016-17 deliverables:
• Implement the Better Care Fund (BCF) in line with the BCF Policy Framework for 2016-17.
• Every area to have an agreed plan by March 2017 for better integrating health and social care.
• Working with partners, achieve accelerated implementation of health and social care integration in the 20 percent of the country designated as transformation areas, by sharing electronic health records and making measurable progress towards integrated assessment and provision.
• Work with the Department of Health, other national partners and local areas to agree and support implementation of local devolution deals.
• Agree a system-wide plan for reducing delayed transfers of care with overall goal and trajectory for improvement, and with local government and NHS partners implement year one of this plan.

ANNEX 2: THE GOVERNMENT’S MANDATE TO NHS ENGLAND 2016/17 29
2016-17 requirements:
• NHS England is required to:
o ring-fence £3.519 billion within its allocation to CCGs to establish the Better Care Fund, to be used for the purposes of integrated care;
o consult the Department of Health and the Department for Communities and Local Government before approving spending plans drawn up by each local area; and
o consult the Department of Health and the Department for Communities and Local Government before exercising its powers in relation to failure to meet specified conditions attached to the Better Care Fund as set out in the BCF Policy Framework.
6.3 Mental health, learning disabilities and autism
Overall 2020 goal:
• To close the health gap between people with mental health problems, learning disabilities and autism and the population as a whole (defined ambitions to be agreed based on report by Mental Health Taskforce).
• Access and waiting time standards for mental health services embedded, including:
o 50 percent of people experiencing first episode of psychosis to access treatment within two weeks; and
o 75 percent of people with relevant conditions to access talking therapies in six weeks; 95 percent in 18 weeks.
2016-17 deliverables:
• 50 percent of people experiencing first episode of psychosis to access treatment within two weeks.
• 75 percent of people with relevant conditions to access talking therapies in six weeks; 95 percent in 18 weeks.
• Increase in people with learning disabilities/autism being cared for by community not inpatient services, including implementing the 2016-17 actions for Transforming Care.
• Agree and implement a plan to improve crisis care for all ages, including investing in places of safety.
• Oversee the implementation of locally led transformation plans for children and young people’s mental health, which improve prevention and early intervention activity, and be on track to deliver national coverage of the children and young people’s Improving Access to Psychological Therapies (IAPT) programme by 2018.
• Implement agreed actions from the Mental Health Taskforce.

ANNEX 2: THE GOVERNMENT’S MANDATE TO NHS ENGLAND 2016/17 30
7. To support research, innovation and growth.
7.1 Research and growth
Overall 2020 goals:
• Support the Department of Health and the Health Research Authority in their ambition to improve the UK’s international ranking for health research.
• Implement research proposals and initiatives in the NHS England research plan.
• Measurable improvement in NHS uptake of affordable and cost-effective new innovations.
• To assure and monitor NHS Genomic Medicine Centre performance to deliver the 100,000 genomes commitment.
2016-17 deliverables:
• Implement the agreed recommendations of the Accelerated Access Review including developing ambition and trajectory on NHS uptake of affordable and cost-effective new innovations.
7.2 Technology
Overall 2020 goals:
• Support delivery of the National Information Board Framework ‘Personalised Health and Care 2020’ including local digital roadmaps, leading to measurable improvement on the new digital maturity index and achievement of an NHS which is paper-free at the point of care.
• 95 percent of GP patients to be offered e-consultation and other digital services; and 95 percent of tests to be digitally transferred between organisations.
2016-17 deliverables:
• Minimum of 10 percent of patients actively accessing primary care services online or through apps, and set trajectory and plan for achieving a significant increase by 2020.
• Ensure high quality appointment booking app with access to full medical record and agreed data sharing opt-out available from April 2016.
• Robust data security standards in place and being enforced for patient confidential data.
• Make progress in delivering new consent-based data services to enable effective data sharing for commissioning and other purposes for the benefit of health and care.
• Significant increase in patient access to and use of the electronic health record.

ANNEX 2: THE GOVERNMENT’S MANDATE TO NHS ENGLAND 2016/17 31
7.3 Health and work
Overall 2020 goal:• Contribute to reducing the disability employment gap.• Contribute to the Government’s goal of increasing the use of Fit for
Work.
2016-17 deliverables:• Continue to deliver and evaluate NHS England’s plan to improve the
health and wellbeing of the NHS workforce.• Work with Government to develop proposals to expand and trial
promising interventions to support people with long-term health conditions and disabilities back into employment.

#FutureNHS

ENCLOSURE: 17
AUTHOR
REPORTING OFFICER /DIRECTOR
Name Alex Palethorpe Name Neil McFadden
Title Head of Governance Title Lay Member Governance/Audit Committee Chair
REPORT TO Governing Board
TITLE OF REPORT Audit Committee Report to Governing Board
DATE OF THE MEETING 6th January 2016
WHAT OTHER CCG COMMITTEE/GROUP/INDIVIDUALHASCONSIDERED THIS REPORT?
COMMITTEE/GROUP
INDIVIDUAL
N/A Audit Chair
ACTION REQUIRED FROM COMMITTEE/GROUP/ GOVERNING BOARD (please identify all applicable and provide details below)
Approve
Assurance
X
Discussion
For noting
X
RECOMMENDATION The Governing Board are asked to:-
be assured that the Audit Committee have discharged its duties,
note the contents of the Audit Committee Chair’s report of the meeting held on the 26th November 2015, and
note that an extraordinary Governing Board meeting will be convened on Wednesday 25 May 2016 to approve the annual report and accounts 2015/16
STRATEGIC GOALS SUPPORTED BY THIS PAPER (identify appropriate goals)
YES NO
1. Increase life expectancy and reduce inequality
2. Improve prevention, early detection and effective management of those at increased risk
3. Enhance quality of life and improve health outcomes for people with LTCs
4. Ensure people receive the right care in the right place

PURPOSE OF THE REPORT, KEY POINTS, EXECUTIVE SUMMARY (supporting information to be included, if applicable)
The Audit committee is responsible for critically reviewing the CCG’s financial reporting and internal control principles and ensures an appropriate relationship with both internal and external auditors is maintained and to seek positive assurances regarding the overall arrangements for governance, risk management and internal control . This paper presents an update on the activity of the Audit Committee and highlights key matters discussed at the Audit Committee on the 26th November 2015. The significant areas of business discussed by the Audit Committee were:-
Governance o Assurance Framework /Risk Register progress report o FOI progress Report quarter 2 2015/16 o Information Governance Progress Report inc Caldicott/SIRO o Recommendation Tracker o Consortium SLA with Keele University o Feedback on Financial Control Environment Assessment
Internal Audit Progress Report
Continuing Health Care
Local counter fraud service
External Audit Report
Financial Focus o Annual report and accounts 2015/2016 timetable o Contract Management Review – USL Consultants o Single Tender Actions Log
Financial Capacity and Capability Review – Self Assessment
Reports were received from : o Counter Fraud o External Audit
Items for inclusion on the risk register
SUMMARY OF RISKS RELATING TO THE PROPOSAL Highlight any implications, including finance, quality, reputation, governance, strategic workforce, clinical, medicines optimisation or other
Audit Committee informing the governing Board of its activities and how discharged its duties
ANY STATUTORY / REGULATORY / LEGAL / NHS CONSTITUTION/ASSURANCE / GOVERNANCE / PRESCRIBING IMPLICATIONS
None,
QUALITY IMPACT ASSESSMENT AND/OR EQUALITY IMPACT ASSESSMENT Date completed, please highlight any direct or indirect implications
not applicable

ANY RELATED WORK WITH STAKEHOLDERS/PRACTICES/PUBLIC AND PATIENT ENGAGEMENT Provide further information, including dates if applicable
not applicable
ACRONYMS If not listed in the report, please list
SIRO – Senior Information Responsible Officer

Audit Committee Report
Presented by the Chair of Audit Committee
Introduction
1. This report summarises the key issues discussed at the Audit Committee on 26 November 2015 and aims to provide the Governing Board with formal assurance on the CCGs systems/processes reviewed by the Audit Committee in accordance with the Committee’s annual business cycle, to highlight any areas of concern and support the preparation of the CCG’s Annual Governance Statement for inclusion in the annual accounts 2015-16.
2. The Audit Committee is authorised to review the establishment and maintenance of a system of
internal control and risk management and may investigate any activity of the CCG with assistance from internal and/or external audit to establish the systems’ robustness and effectiveness.
3 The key headlines from the November meeting to which the Committee wish to draw the Governing
Board’s attention are as follows:
3.1 Governance Committee Membership The committee discussed the existing membership with a view to strengthen existing processes. It was agreed that the Director of Nursing and Quality would be invited to attend future meetings but would not become a formal member.
Assurance Framework / Risk Register The committee noted the progress made in relation to the work undertaken with SOT CCG to align the assurance framework and risk register. Training on the new system will be provided to all staff involved. The Risk Management Strategy will be updated once the review is complete. It was pointed out that the Committee should be mindful of the differences across both organisations when considering the risks. It was suggested where there are significant differences; the risks should be split out to provide clarity and transparency. Items 85-88 are outstanding and will be followed up with the Quality team. The Committee discussed the Better Care Fund (BCF) and it was noted that the risk is around delivery and not the actual agreement. BCF will be included on the register as a separate risk.
FOI Progress Report
The Committee received and noted the FOI report. There have been a significant number of requests which are predominantly made up of commercial, media and public It was noted that even though applicants to do not have to provide personal/company details and are ‘applicant’ blind, it would be useful to understand recurring themes. It was emphasised that applicants should also be ‘sign-posted’ to the website where appropriate as information is generally readily available.
Information Governance Progress Report inc. Caldicott / SIRO
Members received the IG Report, the key areas are:
There have been no IG related incidents reported since the last meeting.
1 issue has been recorded on the Caldicott Issues Log since the last meeting.
A full mandatory training programme has been issued for all members of staff for 2015 / 2016 to ensure that the 95% target of staff who have completed their IG training is maintained. At the time of reporting 32% staff had been trained with a further 77% currently booked onto forthcoming sessions.
Subject to job titles being used and not named person the Audit Committee approved the Standard Operating Procedure for the Management of Subject Access Requests. This procedure is intended for use by those staff within the CCG who are identified as potentially required to

manage requests for access to personal information held by the CCG and to provide them with a process to follow should such a request be received
The Committee approved a revised Fair Processing Notice.
Progress is being made against the Improvement Plan for 2015 / 2016 in readiness for the submission of the Information Governance Toolkit by the 31st March 2016 - current position 44%, target 86%, level two compliance set at 66%
The committee was informed that the Director of Nursing and Quality has been asked to take on the role of Caldicott Guardian following the resignation of Paul Unyolo.
A migration of files exercise has taken place and former PCT legacy files have been archived. There is no potential risk foreseen and assurance has been provided that files may be accessed if necessary.
An information mapping exercise is also taking place in line with the IG toolkit.
Management Action Recommendation Tracker The Committee received a progress report which details the progress with regard to implementing agreed management actions from internal audit reports. Following discussion it was suggested that IS meet with Internal Audit to review and close off any entries, where feasible, prior to the next meeting. It was also suggested that the document be colour coded to show where actions are overdue.
Consortium SLA with Keele University – for information The committee was informed that as the SLA with Primary Care Research Consortium was due to be reviewed, the opportunity was taken to assess any issues with regard to funding and to provide assurance that monies are properly managed. There will be a quarterly review undertaken by Primary Care Research and an annual report detailing how the £30M grant is utilised. The CCG has requested that as there are a number of GPs involved in research projects, a link is set up across respective websites in order to provide transparency.
Feedback on Financial Control Environment Assessment The feedback letter from NHSE following the capacity and capability review was presented to the committee for information. An overview of the accompanying assessment summary chart was presented which explains where areas of improvement are needed.
Internal Audit Progress report
Members received a progress report against the internal audit plan for 2015/16. A summary of the findings of the finalised reports is detailed below to provide assurance to the Governing Board where appropriate and in addition highlight areas of risk
Quality Assurance Systems incorporating Providing Quality Contract Management (Advisory – joint report for Stoke-on-Trent and North Staffordshire CCGs) The systems put into place by the CCGs to monitor the quality aspects of each healthcare provider are operating effectively, and minor issues identified were of an administrative nature. In addition there were areas of good practice where both Stoke-on-Trent and North Staffordshire CCGs are operating at a higher standard.
Operational Budgetary Control (Green) The Governing Board can take substantial assurances that the controls upon which the organisation relies on are suitably designed, consistently applied and operating effectively. Members noted that this report is based on a point in time and acknowledged that the CCG’s agreed financial position is dependent on the delivery of the QIPP Programme, noting that the vast majority of schemes are scheduled to be achieved in the second part of the year.

Delivery of the CCG Financial Recovery Plan (FRP) – Phase 1 (Advisory) The workbooks utilised by the CCG to establish the schemes which formulate the FRP are much improved on previous years and form a robust template to be used by scheme leads in order for planning purposes. Additionally, the governance structure put into place by the CCG to enable ongoing monitoring of the FRP is well designed and operates in line with its requirements.
Whilst members noted the progress in relation to the workbooks, the elements of disconnect of the information being planned as part of the scheme workbooks not being consistently monitored through each of the various reporting forums was noted. Further assurance will be sought from the planned Phase 2 audit review.
Better Care Fund – Governance (Advisory) The Governing Board along with the other CCGs and Staffordshire county council have progressed well in terms of setting up relevant BCF Boards and BCF Groups to manage, monitor and report on the progress being made towards the Better Care Fund plan. NSCCG has responsible officer’s in place to attend all BCF meetings where possible to enable them to keep abreast of the current situation and issues which have been identified in relation to the BCF plan.
The review identified a few issues which the CCG need to work and discuss with the lead CCG of
the BCF, the other CCG’s and Staffordshire County Council to implement as these would further strengthen the governance arrangements and current managing of the BCF and Schemes.
Delivery of the CCG Financial Recovery Plan – QIPP Quality Process (Amber / Green) Whilst there is still progress to be made, the quality assessment and monitoring procedure of the FRP Programme has improved at both CCGs since the 2014 / 2015 QIPP Review. Therefore the Governing Board can take reasonable assurance that the controls in place to manage this risk are suitably designed and consistently applied.
There has been one addition to the audit plan following a recent letter to SOT CCG from HMRC regarding payments to GPs. A payroll investigation has taken place to ensure that processes meet with normal standards and expectations across both CCGs.
Local Counter Fraud Service Members received a Proactive Fraud Review report prepared for SAS CCG on Continuing Health Care. The review identified significant control weaknesses which resulted in inappropriate payments made to providers. Upon investigation it was concluded that there was insufficient evidence to prosecute. The Lay Member at SAS CCG was not in agreement with this decision and a further meeting was held with NHS Protect. It was concluded that NHS Protect are in agreement with the LCFS findings, however further investigation work has been instigated to identify the overpayments which are to be presented at the SAS CCG Audit Committee in December. Concerns raised included patient safety and patient reviews being inadequate, unnecessary financial loss and to what extent the CCG is exposed where resource has not been tightened sufficiently, and how the backlog of assessments will be managed going forward. The committee concluded that further assurance was needed that audit committee findings were being acted upon in a timely manner by the CSU and that bringing services in-house should be considered.
NHS Protect Intelligence Report Members received an intelligence report issued by NHS Protect outlining the total number of referrals received by NHS Protect during 2014 / 2015. The aim of the report is to inform NHS Bodies and local Anti-Fraud Specialists of the national economic crime risks, so that target awareness and preventative work can be undertaken. This is the first time this report has been shared by NHS Protect.

NHS Protect Standards for Commissioners – Self Review Toolkit (SRT) Assessment UHNM and SSOTP A review of the self-assessments for UHNM and SSOTP has been undertaken and has concluded that there are no concerns to bring to the attention of the CCG. External Audit Members received a progress report which included assurance of cover arrangements established whilst a senior member of the External Audit Team is on secondment on a part time basis.
Financial Focus Annual Report and Accounts 2015/16 timetable In view of the financial deficit position, the Committee considered the best way forward to deal with the accounts for this financial year. It was concluded that final agreement of the annual accounts would be at an Extraordinary Board meeting to include External Audit, and to be agreed in line with the Annual Report and Accounts timetable.
Contract Management Review – USL Consultants The Chief Finance Officer provided the committee with a preliminary response to the independent functional review carried out by USL, Consultants, on behalf of both NHS North Staffordshire and NHS Stoke-on-Trent Clinical Commissioning Groups. The commissioning of the review was requested and authorised by the audit committee meeting of 26 February 2015. Both the CCGs currently buy their contract management support from Midlands and Lancashire
Commissioning Support Unit (hereinafter referred to as the CSU). The CCGs highlighted a number of
ongoing performance concerns that began during 2013/14 with a number of themes and risks as
follows;
Duplication of effort
Lack of resilience
Lack of responsiveness
Not meeting CCG requirements
Lack of sufficient capacity and skills to support CCG requirements
The report identifies a number of trends and risks as detailed below:
Unclear governance structures: Evidenced by the lack of contracts that the CCG hold.
No scope of Service or Contract: Ambiguity and lack of formality for the service being provided.
Poor Communication: Information not passed in a controlled manner from leadership level in the
CSU to operational staff. Also gaps in basic information due to the lack of information provision
in the CSU.
Unclear Resourcing Model: Who and what time is allocated to the CCG for the delivery of
services, in particular to support to Associate CCGs of the contracts they hold.
Limited Financial Information: Lack of detail in finance information and lack of clarity around
change processes and payment mechanisms.
Unclear Reporting (including performance): Robust reporting mechanisms to be put in place to
ensure the CCGs are able to manage performance with Providers.
Poor Relationship Management: The establishment of relationships between the two parties with
Providers is currently lacking from the CSU service. There is also lack of flexibility in the current
delivery of services by the CSU.
The committee noted both the independent report and the CFO’s preliminary response and discussed
the seriousness of the issues raised.

Remedial work to address these matters continues and a further update will be provided to the
committee by the Chief Finance Officer on completion of the work
Single Tender Actions Log The Audit Committee noted the authorisation of five waivers by the CCG’s Chief Financial Officer in line with the CCG’s Standing Financial Instructions, and requested confirmation that the necessary procurement processes had commenced, where appropriate, where contracts were due to expire on the 31st March 2016.
Review of losses and special payments register – none to report
Items for inclusion in the risk register This is a standing agenda item. The Committee have identified no further risks to go onto the Board Assurance Framework Risk Register. Neil McFadden Lay Member Governance & Chair of Audit Committee November 2015

ENCLOSURE: 18
AUTHOR
REPORTING OFFICER /DIRECTOR
Name Alex Palethorpe Name Alex Palethorpe/Mark Shapley
Title Head of Governance Title Head of Governance/Clinical Chair
REPORT TO Governing Board
TITLE OF REPORT Governance Update includes Constitution and Terms of reference updates (Planning Committee, Finance & Performance committee & Joint Commissioning Arrangements)
DATE OF THE MEETING 6th January 2015
WHAT OTHER CCG COMMITTEE/GROUP/INDIVIDUALHASCONSIDERED THIS REPORT?
COMMITTEE/GROUP Proposal to Joint Directors & CFP August 2015 Joint Planning Committee Joint Commissioning Arrangements - August 2015 CFP 16
th December 2015
Executive Forum (Stoke CCG) -29th December 2015
INDIVIDUAL Noreen O Dowd- Interim Director of Strategy, Planning & Performance
ACTION REQUIRED FROM COMMITTEE/GROUP/ GOVERNING BOARD (please identify all applicable and provide details below)
Approve
Y
Assurance
Y
Discussion
For noting
RECOMMENDATION
The Board are asked to:- i. Note the receipt of NHSE England letter dated 15
th December 2015 confirming approval of the revised CCG
constitution ii. Note that the constitution comes into effect from the date of this board meeting (6 January 2016) iii. Formally approve the terms of reference for the three following committees:-
Joint Planning Committee (NSCCG and Stoke CCG);
Joint Commissioning Arrangements including scheme of delegation
Joint Finance and Performance Committee (NSCCG and Stoke CCG)
STRATEGIC GOALS SUPPORTED BY THIS PAPER (identify appropriate goals)
YES NO
1. Increase life expectancy and reduce inequality Yes
2. Improve prevention, early detection and effective management of those at increased risk
Yes
3. Enhance quality of life and improve health outcomes for people with LTCs Yes
4. Ensure people receive the right care in the right place Yes

PURPOSE OF THE REPORT, KEY POINTS, EXECUTIVE SUMMARY (supporting information to be included, if applicable)
NHSE approved proposed changes to constitution The CCG submitted proposed changes to the constitution to NHS England in October 2015 which reflected the revised
governing board and subcommittee structure as a as a consequence of working more collaboratively with our neighbouring CCG, whilst still retaining our individual sovereignty.
The proposed amendments were shared with the Governing Board, locality leads and Local Medical Committee (LMC)
for comment. The rationale and key areas of change were presented to GP member practices at a member’s event
held on the 24th
September 2015 where over two thirds of the CCG members were in support of the proposed changes.
Member practices also gave their approval for a working group to be set up to review and agree the final wording to
the Constitution with the delegated authority to approve the revised Constitution prior to submission on the 30th
October 2015 to NHS England. The attached letter dated 15 December 2015 was received from NHS England confirming they approved the proposed changes to the constitution in line with section 14 of the NHS Act 2006 (as inserted by the Health and Social Care Act 2012). The revised constitution will come into effect from the date of this Board meeting. CCG will publish its revised constitution on its website as soon as practicable. Proposed Terms of Reference for Joint Planning Committee (NSCCG and Stoke CCG) & Proposed Terms of Reference for Joint Finance and Perfomrance Committee (NSCCG and Stoke CCG) Clinical leadership and involvement from the locality clinical leaders is a fundamental element of NSCCG committee structure however, the Commissioning Finance and Performance Committee does have a large remit. Agendas can be large and difficult to manage to time; this can often stifle the debate and discussion either around commissioning, planning or performance and finance. As part of working closer and more collaboratively with Stoke CCG, it was recognised and proposed that a Joint Planning Committee which has the remit of strategy, development, planning and commissioning be developed. Clinical locality leaders will attend the joint planning committee, stepping down from the (Commissioning) finance and performance meeting. CPAG decisions will feed in to the Joint Planning Committee and decisions would be made against the CCG’s priorities and with consideration against the CCG allocations. This would not increase the number of meetings held each month, or increase demand on the locality leads times, but would ensure there was adequate time for debate about strategy, planning and commissioning and for the discussion around performance and finance. The Joint Planning Committee and the Finance and Performance committees will be reporting directly in to the respective Governing Boards of each CCG. Attached to this paper are the terms of reference for the Joint Planning Committee and the Joint Finance and Performance Committee which will enable both committees to operate. It needs to be pointed out that at the time of writing (23 December 2015) the proposed terms of reference for the Finance and Performance Committee were still to be presented to the Executive Forum at Stoke CCG for agreement and therefore any further amendments/additions will be highlighted at the meeting. These terms of reference will require reviewing and revising post organisational change on the 1
st April 2016 to reflect
organisational changes and officer appointments.
Joint Commissioning Arrangements including scheme of delegation (Between NHS England and the five CCGs)
Simon Stevens, the Chief Executive of NHS England, announced on 1st May 2014 that NHS England was inviting CCGs to expand their role in Primary Care Commissioning and to submit expressions of interest setting out CCG preferences for how it would like to exercise expanded commissioning functions. One option available was that NHS England and CCGs would jointly commission Primary Medical Services. The NHS England and Cannock Chase, East Staffordshire, North Staffordshire, Stafford & Surrounds and Stoke-on-Trent CCGs Joint Commissioning Committee (“the Joint Committee”) is a joint committee with the primary purpose of jointly commissioning Primary Medical Services for the people of those localities. The Joint Committee is established, in accordance with Schedule 1A of the NHS Act, of the participant CCGs’ Governing Bodies and NHS England. It will function as a joint, single committee to which the multiple bodies shall delegate decision-making on particular matters, with individual members considering the issues in question and making a single decision on pan-geographical issues; and as necessary, acting whenever necessary, under a “Committees-in-Common” style approach, with each participant making its own decision on the issues in question as they face their own unique local geography or community. The prime role of the Joint Committee shall be strategic in nature – i.e. to assist in planning and co-ordinating a consistent approach to the development of General Practice; as well as to carry out the functions relating to the commissioning of Primary Medical Services under section 83 of the NHS Act.

In performing its role, the Joint Committee will exercise its management of the functions in accordance with the agreement entered into between NHS England and Cannock Chase, East Staffordshire, North Staffordshire, Stafford & Surrounds and Stoke-on-Trent CCGs, which will sit alongside the Delegation Agreement and Terms of Reference. Attached to this paper are the terms of reference for the Joint Committee and the scheme of delegation.
These Terms of Reference will be formally reviewed by NHS England and CCGs in April of each year (following the year in which the Committee is created). They may be amended by mutual agreement between the members at any time to reflect changes in circumstances which may arise. These Terms of Reference will be reviewed from time to time, reflecting experience of the Joint Committee in fulfilling its functions and the wider experience of NHS England and CCGs in Primary Medical Services co-commissioning.
SUMMARY OF RISKS RELATING TO THE PROPOSAL Highlight any implications, including finance, quality, reputation, governance, strategic workforce, clinical, medicines optimisation, equality related or other
ANY STATUTORY / REGULATORY / LEGAL / NHS CONSTITUTION/ASSURANCE / GOVERNANCE / PRESCRIBING IMPLICATIONS
H & S Care Act 2012 Constitution
QUALITY IMPACT ASSESSMENT AND/OR EQUALITY IMPACT ASSESSMENT Date completed, please highlight any direct or indirect implications
N/A
ANY RELATED WORK WITH STAKEHOLDERS/PRACTICES/PUBLIC AND PATIENT ENGAGEMENT Provide further information, including dates if applicable
N/A
ACRONYMS If not listed in the report, please list

Northern Staffordshire Joint Planning Committee Terms of Reference
1. Introduction The Joint Planning Committee (the Committee) is established in accordance with Stoke-on-Trent Clinical Commissioning Groups constitution, Standing Orders and Scheme of Delegation. And, under The North Staffordshire Clinical Commissioning Group (CCG) constitution, section 25 Other Committees which enables the establishment of any other committee or sub-committee by the Governing Board of NSCCG as long as it is reflected in terms of reference approved by the Governing Board. These Terms of Reference set out the membership, remit, responsibilities and reporting arrangements of the Committee and shall have effect as if incorporated into the Clinical Commissioning Group’s Constitution and Standing Orders. As per the CCGs Constitution, in the interest of partnership working, this Committee will operate as a ‘committee in common’ with representatives from both CCGs to jointly plan for Northern Staffordshire as a whole. As per each CCGs Constitution, the accountability and decision making of the Committee shall remain the responsibility of the individual Clinical Commissioning Group and its Governing Body/Board. 2. Purpose The Joint Planning Committee has responsibility for both CCGs annual business planning cycle, ownership of the five year strategy and delivery plans, to ensure delivery of the CCGs joint strategic objectives accounting for locality differentiation appropriately. 3. Remit and responsibilities of the Committee The Planning Committee shall have decision making responsibility for:
Production and oversight of the CCGs joint strategy and two year delivery plan, ensuring that it will meet
the CCGs strategic objectives
Providing confirm, challenge and authorisation to portfolio specific strategies plans and subsequently
commissioning intentions
Working closely with partner commissioners, CCGs, Local Authority and NHS England, to ensure joint
working is evident
Looking at the whole system in line with the five year forward view to ensure that our CCG plans are
aligned with the system view
Alignment with commissioner and provider plans
On-going evaluation of delivery and impact of our plans
Ensuring our strategic direction is aligned with national policy and directives
Ensuring our plans reflect population needs and align to our overall long term financial model
The Planning Committee will receive reports and TOR from CPAG and review and recommend approval of
any investment or disinvestment decisions to the Governing Body for ratification.

4. Membership Voting members
Clinical Accountable Officer, Stoke-on-Trent CCG (Joint Chair)
Accountable Officer, North Staffordshire CCG, (Joint Chair)
Joint CFO or Deputy Director of Finance
All Clinical Director(s), both CCGs
Locality Clinical Leads, both CCGs
Chief Operating Officer, Stoke-on-Trent CCG
Joint Director of Nursing and Quality
Joint Director of Strategy, Planning & Performance, both CCGs
Joint Director of Commissioning (pending appointment)
One Lay Member
Patient Congress representative
Senior Planning and Development Manager(s), both CCGs
Head of Contracting
N.B - This membership will require review post organisational change. Non-voting members
LPC representative
LMC representative
Contract Management representative
Heads of Quality
Head of Transformation
Heads of Commissioning
Public Health Consultants, Stoke-on-Trent City Council and Staffordshire County Council
If neither Chair is able to attend all or part of the meeting they will nominate a deputy from within the membership. Other individuals may attend by invitation of the Committee to provide advice or expertise. These need to be noted in the minutes as ‘in attendance’. 5. Confidentiality Due to the potential confidential nature of some issues discussed at the Committee, external members will be asked to sign a Confidentiality Agreement prior to becoming a member of the Committee.
6. Conflicts of Interest It is the responsibility of all Members and all individuals in attendance to declare any conflicts of interest pertaining to the agenda. Conflicts of interest are recorded at the beginning of each meeting. The nature of the conflict of interest and the Chairs decision based on consideration of this information will be formally minuted. If a conflict of interest arises, then the Chair may request members or those in attendance to withdraw at the appropriate discussion/voting point. When more than 50% of the voting members of the Committee are required to withdraw from a meeting or part of it than the remaining Chair will consider whether the meeting is quorate. Where the meeting is not quorate the discussion will be deferred until quorum can be convened. Where a quorum cannot be convened from the membership of the Committee the Chair may invite on the temporary basis one or more of the following so the group can progress the item of business:
A member of the Governing body who is not a current member of the Committee
A representative from the CCG membership
A member of the Health and Wellbeing Board
7. Voting
Decision making will be by consensus
Where consensus is not reached, each voting member will be allowed one vote
The Chair (or vice Chair) will retain the casting vote
The outcome of the voting should be clearly recorded in the minutes. 8. Quoracy Quorum will be attendance by a minimum of four voting members, of whom:
Chair or nominated vice-Chair
Two Clinical Directors.
One locality lead from North Staffordshire and One from Stoke on Trent
One quality Lead
One Finance Lead
One Lay member
Director of commissioning or deputy
N.B – Quoracy will need to be reviewed post organisational change The Chair will confirm that the quoracy has been met at the start of the meeting and this will be recorded in the minutes. 8. Frequency and notice of meetings The committee will meet at least 9 times a year with meetings lasting 2 to 3 hours. Further meetings may be scheduled by exception if required. A schedule of meeting dates will be set and circulated to members for each calendar year. A calendar of business will reflect the business to be considered by the Committee throughout the year. 9. Secretary The Committee will be formally minuted. Agendas and papers will be available five working days before the meeting is scheduled to take place. A formal action sheet will be held and reported to each meeting.

10. Reporting arrangements To provide assurance to each CCG Governing Board / Body on matters relating to strategy and planning.
a) The minutes of the committee will be reported to the Governing Body/board for information when
agreed as accurate by the Committee. It is the Chairs Responsibility to ensure that the minutes can be
published in the public domain.
b) The Committee Chair will provide a written report to the Governing Body/board following each
meeting on the activities of the Committee and business conducted. This should highlight:
Issues
Risks
Assurance
Recommendations requiring ratification
The Chair will be provided with nominated secretarial support to provide continuity and support in the organisation and execution of meetings. C) An annual report will also be provided to the governing body/ board summarising the -activities for the year - Frequency of meetings -Attendance by members If there is commercially sensitive or sensitive information than a closed session of the Committee would need to be agreed with the committee Chair. It is the Committee Chairs responsibility to highlight to the CCG Governance Manager/Head of Governance areas of their report which may need to be considered in the closed section of the Governing Body/Board. 11. Conduct of the Committee The conduct of the Committee should reflect the Code of Accountability and Code of Conduct for NHS Boards and the seven principles of public life promulgated by the Nolan Committee. These include:
Selflessness
Integrity
Objectivity
Accountability
Openness
Honesty
Leadership
12. Review of Terms of Reference The Committee will review its Terms of Reference annually and its membership directly after any organisational structure changes. Changes in the Terms of Reference need to be approved by the committee and presented to the Governing Body/board for ratification and reflected in the CCGs Constitution. Date Agreed by Committee: Date Approved at Governing Body: Review Date:

JOINT FINANCE AND PERFORMANCE COMMITTEE
TERMS OF REFERENCE
1. CONSTITUTION
The Clinical Commissioning Group’s Governing Body/ Board hereby resolve to establish a Committee of the Governing Body/ Board/known as the Finance and Performance Committee. The Committee is established in accordance with North Staffordshire Clinical Commissioning Group’s Constitution, Standing Orders and Scheme of Delegation and Stoke Clinical Commissioning Group’s Constitution, Standing Orders and Scheme of Delegation These terms of reference set out the membership, remit responsibilities and reporting arrangements of the committee and shall have effect as if incorporated into each CCG’s constitution and standing orders. As per the CCG’s constitution, in the interest of partnership working, this committee will operate as a ‘committee in common’ with representatives from both CCG’s as per each CCG constitution , the accountability and decision making of the committee shall remain the responsibility of the individual CCG and its Governing Body/Board.
2. ACCOUNTABILITY
The committee is accountable to the Governing Body/Board of each. Any changes to these terms of reference must be approved by the Governing Body/Board of each CCG .
3. PURPOSE
To provide a performance framework which proactively manages both CCG’s Financial, Performance and Quality Innovation, Productivity and Prevention (QIPP) agenda.
To provide assurance about delivery and sustained performance in these areas to the Governing Body/Board, by reviewing and approving performance reports and rectification action plans in detail prior to Governing Body/Board meetings
To hold to account the management team of the CCG for delivery in their areas of responsibility.
4. MEMBERSHIP AND ATTENDEES
The Finance and Performance Committee comprises the following voting members:- Chief Finance Officer (Chair) Director of Strategy, Planning and Performance (Vice Chair) Chief Operating Officer or Accountable officer (Stoke CCG) Accountable Officer or nominated Deputy (NSCCG) 2 x non executive members (one from each CCG i.e. Sourced from lay members, Secondary care consultant, non executive GP Board members or CCG Chair) Joint Deputy Director of Finance Joint Deputy Director of Commissioning Head of Contracts Head of PMO
Other representatives may be invited by the Chair to attend the meeting to present relevant issues on an ad-hoc basis. Should a conflict of interest arise for an individual or as chair of another committee i.e. audit committee chair, the individual concerned will be recorded as being an attendee, rather than a member.
Membership will be reviewed regularly to adjust for changes as required by the purpose of the Committee. The committee may also extend invitations to other personnel with relevant skills, experience or expertise as necessary to enable it to deal with matters before the committee.
5. QUORUM
a) A minimum of five members will constitute a quorum, so long as this includes a minimum of three Governing Body/Board members and a minimum of two further members from the list above.
b) A decision put to a vote at the meeting shall be determined by a majority of the votes of members. In
the case of an equal vote, the Chair of the Committee shall have a second and casting vote.
6. MEETINGS
a) The Finance and Performance Committee will meet on a monthly basis, but no less than nine times
per year. b) Other meetings may be convened as appropriate to deal with relevant business including meetings
via telephone or video conference. c) The CCG will nominate a member of staff to act as Secretary to the Committee. Their responsibility
will be to assist the Chair in convening meetings, preparing agendas and papers and keeping the minutes of the meeting and generally ensuring that the administrative arrangements for the Committee comply with the standards set by the CCG for the conduct of all meetings.
7. AUTHORITY
The committee is authorised to: i) investigate any activity within its terms of reference and produce an annual work programme to
discharge its responsibilities ii) take responsibility for ensuring compliance with the principles of good governance and the Group’s
constitution when undertaking its terms of reference iii) establish and approve the terms of reference of such sub-reporting groups, or task and finish groups
as it believes are necessary to fulfil its terms of reference
8. DUTIES
8.1. General
a) The Committee will review and have oversight of finance and performance in relation to the following areas:
i) performance against national and local targets ii) ‘in year’ financial position; receiving a detailed report of the financial position and progress
towards meeting the targets within the CCG financial plan ii) implementation of QIPP schemes; receive updates on both the financial and activity performance
of each scheme iv) achievement against CCG incentive schemes; receive a report of the actual and forecast
performance to inform the achievement of incentive schemes

v) implementation of investments / transformation schemes; receive updates vi) outlining financial, activity and delivery against key performance indicators for each scheme
b) Recommend each CCG’s s five year and annual financial plans to the relevant Governing Body/Board
and maintain oversight of the implementation of those plans c) Receive and review delivery plans for indicators or performance areas by exception. d) Challenge delivery plans produced to achieve targets or improve performance. e) Focus of actions to resolve key performance issues raised f) Identify and allocate resources where appropriate to improve performance. g) Agree an annual work programme for the committee h) The committee shall endorse the self-assessment approach to be used by all Governing Body/Board
committees and will incorporate the results of the assessment as part of their annual report
8.2. Finance and Operational Management
a) Ensure that the management arrangements for both CCG’s are appropriate to discharge both CCG’s responsibilities and have oversight of those arrangements, ensuring that they comply with relevant legislation including HR, E&D and H&S requirements.
b) Ensure that there are effective arrangements and financial procedures in place, including budgetary controls, to support delivery of both CCG’s financial management and financial targets.
c) Undertake detailed monitoring against both CCG’s financial operational plans and in accordance with the committee’s delegated responsibilities, determine action to improve performance.
9. REPORTING
The committee will have the following reporting responsibilities:
i) To ensure that the minutes of the Finance and Performance Committee are formally recorded and
submitted to each CCG Governing Body/Board. ii) The Finance and Performance Committee will produce a bi-monthly report for each CCG Governing
Body/Board in the form of a performance dashboard report. iii) To ensure that conflicts and/or interests are managed in accordance with the CCG’s policies and
procedures. iv) To bring to the attention of each Governing Body/Board in a separate report, any items of specific
concern which require Governing Body/Board’s approval to act. v) To provide exception reports to the Governing Body/Board, highlighting any key developments
/achievements or potential risks/ issues.
10. RESPONSIBILITY OF COMMITTEE MEMBERS AND ATTENDEES
Members of the committee have a responsibility to:
i) prioritise attendance at meetings, with a minimum attendance of two thirds of the meetings, having
read all papers beforehand
ii) act as ‘champions’, disseminating information and good practice as appropriate
iii) identify agenda items to the secretary ten working days before the meeting

v) submit papers for distribution at least five working days before the meeting
11. ADMINISTRATIVE ARRANGEMENTS
The Secretary to the Committee will ensure:
a) Correct minutes are taken, and once agreed by the chair ensure distribution of the minutes to the members of the Committee
b) Conflicts of interest are recorded along with the arrangements for managing those conflicts c) A record of matters arising is produced with issues to be carried forward d) An action list is produced following each meeting and distributed to members e) Ensuring any outstanding action is carried forward on the action list until complete f) They provide appropriate support to the chair and committee members
g) The agenda is agreed with the chair prior to sending papers to members no later than five working
days before the meeting
h) The annual programme of work of the Committee is up to date and agreed by the committee i) The minutes of the meeting are distributed within five working days of the meeting taking place
j) The papers of the committee are filed in accordance with each CCG’s policies and procedures
12. REVIEW
a) The Committee shall conduct its business in accordance with national guidance, relevant codes of
practice including the Nolan Principles and the Conflict of Interest policy. b) The Committee will review its own performance, membership and terms of reference annually or
sooner if required. c) An annual report of its performance, membership and terms of reference with recommendations will
be submitted to each Governing Body/Board for agreement and approval. Date Agreed by Committee: Date Approved at Governing Body: Review Date:

Terms of Reference - Joint Commissioning Arrangements including Scheme of Delegation
Introduction
(1) Simon Stevens, the Chief Executive of NHS England, announced on 1st May 2014 that NHS England was inviting CCGs to expand their role in Primary Care Commissioning and to submit expressions of interest setting out CCG preferences for how it would like to exercise expanded commissioning functions. One option available was that NHS England and CCGs would jointly commission Primary Medical Services.
(2) The NHS England and Cannock Chase, East Staffordshire, North Staffordshire, Stafford & Surrounds and Stoke-on-Trent CCGs Joint Commissioning Committee (“the Joint Committee”) is a joint committee with the primary purpose of jointly commissioning Primary Medical Services for the people of those localities.
Statutory Framework
(3) The National Health Service Act 2006 provides at section 13Z that NHS England’s functions may be exercised jointly with a CCG, and that functions exercised jointly in accordance with that may be exercised by a joint committee. Section 13Z of the NHS Act further provides that arrangements made under that section may be on such terms and conditions as may be agreed between NHS England and the CCGs.
(4) Statutory provisions used to jointly exercise CCG functions are delegated by the CCGs to the Committee. This is permitted by section 14Z9 of the NHS Act 2006 (as amended). A Delegation Agreement has been prepared and is set out as Schedule 1 to this document.
(5) The CCGs remain subject to any directions made by NHS England or by the Secretary of State.
(6) Section 14Z9 of the NHS Act was amended by Legislative Reform Order (2014/2436) to enable the joint exercise by NHS England / a CCG of any of the CCG’s commissioning functions and any other functions of the CCG related to the exercise of those functions. Where such arrangements are made, the LRO enabled them to be exercised by a joint committee established between the parties.
Role of the Joint Committee
(7) The Joint Committee is established, in accordance with Schedule 1A of the NHS Act, of the participant CCGs’ Governing Bodies and NHS England. It will function as a joint, single committee to which the multiple bodies shall delegate decision-making on particular matters, with individual members considering the issues in question and making a single decision on pan-geographical issues; and as necessary, acting whenever necessary, under a “Committees-in-Common” style approach, with each participant making its own decision on the issues in question as they face their own unique local geography or community.
(8) The prime role of the Joint Committee shall be strategic in nature – i.e. to assist in planning and co-ordinating a consistent approach to the development of General Practice; as well as to carry out the functions relating to the commissioning of Primary Medical Services under section 83 of the NHS Act.
(9) This shall not be those relating to individual GP performance management, which have been reserved to NHS England; and such CCG functions under sections 3 / 3A of the NHS Act as have been delegated to it as noted in Schedule 1. This includes the following:
o Approval of strategic proposals and assurance of quality improvement strategies, commissioning decisions o Developing new models of care for General Practice and Primary Care to align with the wider, local strategic direction o GMS, PMS + APMS contracts: inc. design of PMS-APMS, monitoring, taking contractual action, removing a contract o Newly designed enhanced services: Local Enhanced Services (LES) and Directed Enhanced Services (DES) o Recommending appropriate mechanisms to support Providers in optimum delivery (including workforce matters) o Design of local incentive schemes as an alternative to the Quality Outcomes Framework (QOF) o Decision making on whether to establish new GP Practices, or approving Practice mergers in an area o Making decisions on ‘discretionary’ payment (e.g. returner / retainer schemes)
(10) In performing its role, the Joint Committee will exercise its management of the functions in accordance with the agreement entered into between NHS England and Cannock Chase, East Staffordshire, North
Staffordshire, Stafford & Surrounds and Stoke-on-Trent CCGs, which will sit alongside the Delegation Agreement and Terms of Reference.
(11) This is the proposed agreement to deal with information / resource sharing, contractual mechanisms for service delivery (and ownership) and interplay between contractual and performance list management.
Geographical Coverage
(12) The Joint Committee will comprise NHS England North Midlands Sub-Region (Shropshire & Staffordshire) and Cannock Chase, East Staffordshire, North Staffordshire, Stafford & Surrounds and Stoke-on-Trent CCG.
(13) It will undertake the function of jointly commissioning Primary Medical Services for Cannock Chase, East Staffordshire, North Staffordshire, Stafford & Surrounds and Stoke-on-Trent.
Membership
(14) This will meet the requirements of each CCG’s Constitutions, and shall consist of the following:
(a) Core (Voting) Members:
NHS England Senior Manager Representatives – flexed according to availability from Commissioning, Medical Directorate, Operations + Delivery, Finance, Contracting (or suitable deputies).
Participant CCG Senior Manager Representatives – two from each CCG as a minimum, flexed according to availability from Commissioning, Lay Members for PPI / Governance, AO or CFO, Chief Nurse or Director of Quality, Primary Care, Governance (or suitable deputies)
1
It is not practicable to expect one from each of the specialisms outlined above to attend every meeting, owing to other work commitments etc. However each member will ensure that for the sake of good governance, accountability and robust decision making that there shall always be a Core Membership present, acting as a quorum (see later section):
NHS England Senior Representatives, holding a deciding vote in all cases, irrespective of numbers in attendance One Lay Representative One CCG Governance representative: to advise on all governance issues, quoracy, conflicts etc One Chief Financial Officer from a participant CCG CCG Senior Clinical Leads: e.g. Clinical Chair or nominated deputy, Clinical Director, Primary Care Lead One external clinical representative: e.g. LMC rep
The Chair shall be:
A nominated Lay Member of one of the participant CCGs (not the Lay Members for Governance): to be determined – Mrs Jan Toplis (Cannock CCG) will undertake the role after the first meeting in June 2015
The Vice-Chair shall be:
A nominated Lay Member for Governance or PPI of one of the participant CCGs: to be determined
(b) Core (Non-Voting) Members:
GP / Clinical Leads from participant CCGs: non-voting to preserve conflicts of interest matters 2
Standing invite to a Local Medical Committee representatives (North & South Staffs)
Standing invite as an observer to a HealthWatch representatives (Stoke & Staffordshire)
Standing invite as an observer to a Health & Wellbeing Board representatives (Stoke & Staffordshire)
Standing invite as an observer to one representative from any “Level One” (status quo) CCGs
(15) The Joint Committee may also call additional experts to attend meetings on an ad hoc basis to inform specific discussions (e.g. technical or time-limited matters).
1 This will require each CCG member present to have assured themselves and their parent organisations that they have delegated
authority to act on behalf of their CCG; and will have discussed the agenda, papers etc in advance to have formulated a CCG position in case of key decisions being taken at meetings. 2 For matters of management of conflicts of interest purposes, GPs will never be allowed to have a vote in proceedings but will be able
to actively participate in discussions (as long as there is no significant influencing of the vote, should it come to that) – GP Clinical Leads would not ordinarily be expected to leave the room for votes, unless the Chair deemed that necessary.

Meetings and Voting
(16) Frequency of meetings shall be established as a minimum number per annum – i.e. four (quarterly). However the Chair will retain the ability to call additional meetings as and when deemed necessary. If deemed necessary. Members will be able to call an emergency meeting through a consensus decision.
(17) Each CCG voting member shall have one vote, with NHS England holding the deciding vote. However, the aim will be to achieve consensus decision making, avoiding voting wherever possible.
(18) The Joint Committee shall adopt the Standing Orders / Prime Financial Policies of CCGs insofar as they relate to the notice of meetings, handling of meetings, agendas and the circulation of papers (if there is divergence between these, then the Joint Committee will work to a “best-fit” methodology).
Conflicts of Interest and Quoracy
(19) Conflicts of interest will be managed in ways dictated through CCG policies and procedures, based upon NHS England Statutory Guidance for managing conflicts of interest (December 2014).
(20) All Members and Invitees will be asked to declare any potential conflicts of interest resulting from the agenda at the start of each meeting of the Joint Committee. Any members who have such a conflict will be required to leave the meeting when that item is discussed.
(21) If the membership of the Joint Committee changes during a meeting, it will be necessary to establish that it is still achieving quorum (refer to the next point). Reference to the CCGs’ Constitutions and Governance Leads can be made for more details regarding the management of conflicts of interests in meetings and also the conflict of interest policy pertaining to the CCGs.
(22) Quoracy will generally be established by more than 50% of core voting members being in attendance, recognising the weighted majority from NHS England.
(23) Arrangements for maintaining quoracy during potential conflicts of interest will be managed in line with CCG policies and NHS England Statutory Guidance.
Meetings of the Committee
(24) These shall, subject to the application of the point below, be held in public.
(25) The Joint Committee may resolve to exclude the public from a meeting that is open to the public (whether during the whole or part of the proceedings) whenever publicity would be prejudicial to the public interest by reason of the confidential nature of the business to be transacted or for other special reasons stated in the resolution and arising from the nature of that business or of the proceedings or for any other reason permitted by the Public Bodies (Admission to Meetings) Act 1960 as amended or succeeded from time to time. The Chair will also have discretionary powers to move that confidential papers or items be discussed in a dedicated, confidential section of the agenda.
(26) Members have a collective responsibility for the operation of the Committee. They will participate in discussion, review evidence and provide objective expert input to the best of their knowledge and ability, and endeavour to reach a collective view.
(27) Members of the Joint Committee shall respect confidentiality requirements as set out in the Standing Orders / Prime Financial Policies referred to above, unless separate confidentiality requirements are subsequently set out (in which event these shall be observed).
Secretariat
(28) The secretariat to the Joint Committee is to be determined; once confirmed, they will:
o Circulate the minutes and action notes of the meeting to all Members o Establish and confirm all dates for Joint Committee meetings o Circulate agenda and papers for each forthcoming meeting to Members
Decisions
(29) The Joint Committee will make decisions within the bounds of its remit; which shall be binding on NHS England and Cannock Chase, East Staffordshire, North Staffordshire, Stafford & Surrounds and Stoke-on-Trent CCGs.
(30) Decisions summary reports and minutes will be presented for information to NHS England and at the next available public meetings of Governing Bodies of each CCG. Confidential matters or decisions (refer to clause #25) will be presented to closed / confidential sessions of CCG Governing Bodies.
Terms of Reference Review
(31) These Terms of Reference will be formally reviewed by NHS England and CCGs in April of each year (following the year in which the Committee is created).
(32) They may be amended by mutual agreement between the members at any time to reflect changes in circumstances which may arise.
(33) These Terms of Reference will be reviewed from time to time, reflecting experience of the Joint Committee in fulfilling its functions and the wider experience of NHS England and CCGs in Primary Medical Services co-commissioning.
Signed on behalf of NHS England Shropshire & Staffordshire Area Team [North Midlands Sub-Region] by:
Name: Designation: Date:
Signed on behalf of Cannock Chase CCG by:
Name: Designation: Date:
Signed on behalf of East Staffordshire CCG by:
Name: Designation: Date:
Signed on behalf of Stafford and Surrounds CCG by:
Name: Designation: Date:
[In case of further CCGs joining as “Level Two” Co-Commissioners]
Signed on behalf of North Staffordshire CCG by:
Name: Designation: Date:
Signed on behalf of Stoke-on-Trent CCG by:
Name: Designation: Date:
Signed on behalf of {Insert Name} CCG by:

Name: Designation: Date:
Schedule 1 – Delegation by CCG to the Committee of CCG functions
Arrangements made under section 13Z of the NHS Act do not affect the liability of NHS England for the exercise of any of its functions. However, the CCGs acknowledge that in exercising their functions (including those delegated to them), they must comply with the statutory duties set out in Chapter A2 of the NHS Act and including:
˗ Management of conflicts of interest (section 14O) ˗ Duty to promote the NHS Constitution (section 14P) ˗ Duty to exercise its functions effectively, efficiently and economically (section 14Q) ˗ Duty as to improvement in quality of services (section 14R) ˗ Duty in relation to quality of primary medical services (section 14S) ˗ Duties as to reducing inequalities (section 14T) ˗ Duty to promote the involvement of each patient (section 14U) ˗ Duty as to patient choice (section 14V) ˗ Duty as to promoting integration (section 14Z1) ˗ Public involvement and consultation (section 14Z2)
The CCGs will also need to specifically, in respect of the jointly commissioned functions with NHS England, exercise those set out below:
˗ Duty to have regard to impact on services in certain areas (section 13O) ˗ Duty as respects variation in provision of health services (section 13P)
The Committee will also carry out the following joint Key Responsibilities in relation to its jointly commissioned PCC functions:
To jointly plan, including needs assessment, Primary Medical Care services in North Staffordshire, Stafford & Surrounds and Stoke-on-Trent;
To undertake reviews of primary medical care services in Cannock Chase, East Staffordshire North Staffordshire, Stafford & Surrounds and Stoke-on-Trent;
To co-ordinate a common approach to the commissioning of primary care services generally;
To manage the budget for commissioning of Primary Medical Care services in Cannock Chase, East Staffordshire, North Staffordshire, Stafford & Surrounds and Stoke-on-Trent.


2-4 Victoria House
Capital Park Fulbourn
Cambridge CB21 5XB
Tel: 0113 8254939
15
th December 2015
Dr Mark Shapley, Chair Dr Julie Oxtoby, Accountable Officer North Staffordshire Clinical Commissioning Group Sent via Email Dear Mark and Julie Re: NHS North Staffordshire Clinical Commissioning Group application to amend their constitution Thank you for your application to amend the constitution of North Staffordshire CCG, which we received on 26
th October 2015.
Your proposed changes to the constitution have been reviewed by the NHS England (Midlands and East) regional team. We note in particular the revised governing body and sub-committee structure reflecting closer working with Stoke-on-Trent CCG. NHS England is happy to approve your proposed changes to your constitution in line with Section 14E of the NHS Act 2006 (as inserted by the Health and Social Care Act 2012). In line with this legislation, the CCG must publish its revised constitution as agreed, as soon as practicable. If you have any queries relating to this process, please contact Melanie de Smith, Assurance Manager, at [email protected] Yours sincerely
GRAEME JONES Regional Director of Operations and Delivery (Midlands and East) cc: Wendy Saviour, Director of Commissioning Operations, NHS England
(North Midlands) Alex Palethorpe, Head of Governance, North Staffordshire CCG