
Apical root resorption: a prospective radiographic study of maxillary incisors
Upload
independentCategory
view
0download
0
New Radiographic Techniques to Evaluate Cerebrovascular Disorders in Children
Jill V. Hunter
The radiographic evaluation of the pediatric patient with cerebrovascular disease has dramatically improved during the past decade. Few new technologies have been introduced, but significant new developments in data acquisition and post-processing have resulted from refinements in both software and, to a lesser extent, hardware. This review focuses on the advantages and limitations of the different imaging modalities and their recommended role in managing the pediatric patient who presents with signs or symptoms of cerebrovascular disease. Copyright �9 2000 by W.B. Saunders Company
C ONVENTIONAL ultrasonography is an es- tablished imaging modality performed via the
anterior fontanelle using a variable 8-5 MHz trans- ducer. This modality can be used as a noninvasive portable bedside examination in the neonatal pe- riod to diagnose germinal matrix and intraventric- ular hemorrhage and periventricular leukomalacia (PVL). A 12-8 MHz linear array probe is used to assess for extraaxial fluid collections, including subdural hemorrhage and hygromas. Examination of the posterior fossa for cerebellar hemorrhage can be done by insonating the posterolateral fon- tanelle in neonates.la
DOPPLER ULTRASONOGRAPHY
The transcranial Doppler (TCD) examination measures blood flow velocities within the major intracranial arteries at the circle of Willis. The mean velocity calculated by the TCD equipment is based on the time average of the outline velocity (maximum velocity envelope). Additionally, the pulsatility index (PI) is calculated (peak systolic velocity minus end diastolic velocity divided by the mean velocity) and reflects obstruction/resis- tance at points proximal and distal to the point of insonation.
Intracranial arterial velocities are determined by the volume of flow over time and the luminal area of the artery. Factors that influence cerebral blood flow velocities recorded during a TCD examina- tion include the following: the age of the patient, hematocrit, partial pressure of arterial CO 2 (Paco2), Pao 2, fever, hypoglycemia, blood pres- sure, cardiac output, raised intracranial pressure (ICP), and the presence of proximal arterial ob- struction, distal arterial stenosis, or arteriovenous malformation.
The examination can be performed using equip- ment that produces a Doppler spectral waveform (nonimaging) or with a duplex ultrasound imaging system that produces a color Doppler display of the
blood flow. Both types of TCD examination are performed using a low frequency (2 MHz) pulsed Doppler transducer. The advantage of using a du- plex imaging system is that it provides the operator with anatomic landmarks that assist in the identi- fication of the arteries, and the color Doppler display is encoded for direction of blood flow and velocity. Another innovation is power Doppler imaging, which assigns color according to the strength of the Doppler-shifted echoes. Power Doppler imaging is less angle dependent and more sensitive to slow flow; however, information re- garding the direction of blood flow is no longer available. J
There are four ultrasound pathways ("win- dows") allowing access to the intracranial arteries. A complete TCD examination incorporates the following approaches: (1) transtemporal, (2) trans- orbital, (3) suboccipital, (4) submandibular. The intracracranial arteries evaluated by each approach are listed in Table 1.
The identification of the intracranial arteries is based on the following criteria: (1) depth of the sample volume, (2) angle of the transducer, (3) direction of the blood flow relative to the trans- ducer, (4) spatial relationship of one Doppler sig- nal to another, and (5) anatomic landmarks (for imaging technique).
Clinical applications of TCD in the pediatric population include the following: (1) Screening for
From the Department of Radiology, ChiMren's Hospital of Philadelphia, Philadelphia, PA.
Address reprint requests to Jill V. Hunter, MBBS, Depart- ment of Radiology, Children's Hospital of Philadelphia, 34th Street & Civic Center Blvd, Philadelphia, PA 19104.
This work was supported in part by the Ethel Foerderer Fund for Excellence.
Copyright �9 2000 by W.B. Saunders Company 1071-9091/00/0704-0002510.00/0 doi." l O. 1053/sperm2000.20226
Seminars in Pediatric Neurology, Vol 7, No 4 (December), 2000: pp 261-277 261

262 JILL V. HUNTER
Table 1. TCD Windows
Approach Artery
Transtemporal Middle cerebral Anterior cerebral Posterior cerebral Terminal internal carotid Anterior communicating Posterior communicating
Transorbital Ophthalmic Internal carotid (siphon)
Suboccipital Vertebral Basilar
Submandibular Internal carotid
vascnlopathy in sickle cell disease2; (2) monitoring vasospasm3; (3) monitoring embolic events at car- diac bypass surgery; (4) monitoring acute stroke, including diagnosis of intracranial dissection and intracranial arterial stenoses4; (5) detecting vascu- lar compromise in hydrocephalusS'6; (6) document- ing a patent foramen ovale7; and (7) confirmation of brain death. Duplex Doppler can be used to look at more proximal arterial dissection in the cervical internal carotid artery.
Recently transcranial Doppler imaging has been used to evaluate the intracranial veins and venous sinuses in normal adults as well as in the diagnosis and follow-up of patients with cerebral venous thrombosis. 8 The intracranial venous system iden- tification is based on parenchymal landmarks and the fact that venous blood flow has peak systolic velocities less than 20 cm/sec. There has been some work performed in newborns and infants with sinovenous thrombosis and other condi- tions. 9-12 The presence of an open anterior and posterior fontanelle provides an enhanced oppor- tunity for detection of obstruction to flow.
Screening in Sickle Cell Disease
Stroke is a major complication of sickle cell dis- ease (SCD). A clinical stroke occurs in approxi- mately 11% of patients with SCD:SS by the age of 20 years, and recently clinically "silent" strokes have been reported in up to 18% of these homozygous patients. 13 Cerebral infarction resulling from a steno- sis or occlusion of the large intracranial vessels most commonly involves the distal portion of the internal carotid artery (ICA), proximal middle cerebral (MCA), and proximal anterior cerebral (ACA) arteries.
In the recently published multicenter STOP (Stroke Prevention Trial in Sickle Cell Anemia)
study, children with SCD:SS were examined with TCD and classified as normal (<170 cm/sec), conditional (170 to 199 cm/sec), or abnormal (>-200 cm/sec), based on the time averaged mean velocity of blood flow in the terminal ICA/proxi- mal MCAJ 4 One hundred and thirty children clas- sified as abnormal by TCD were randomized to chronic blood transfusions (n = 63) or standard care (n = 67). The STOP trial results indicated that chronic blood transfusion was associated with a "92% difference in the risk of stroke." Transcranial Doppler is currently the "standard of care" and is now being used to annually screen children with SCD:SS to identify those with intracranial veloci- ties -->200 cm/sec with a view to offering some intervention, for example, blood transfusion, hy- droxyurea therapy, or bone marrow transplantation (Fig 1).
In our practice we have encountered a small subset of patients in whom a satisfactory temporal window could not be located. A new 1 MHz transducer has been shown in adults to be more successful at finding a small temporal window and achieving better penetration, which allows evalua- tion of contralateral vessels in individuals with unilateral temporal windows) 5
COMPUTED TOMOGRAPHY
Computed tomographic (CT) scanning, which was the previous mainstay of brain imaging, re- mains the modality of choice in acute trauma and is the preferred mode to look for fresh blood and subarachnoid hemorrhage (Fig 2). Over the past decade, there has been the development of slip-ring technology enabling the introduction of continuous spiral or helical CT. This has allowed for faster image acquisition and the development of CT an- giography (CTA), in which the contrast-laden blood outlining a vessel, following peripheral in- travenous injection, can be imaged with less mo- tion artefact and reconstructed to give a 3D ren- dering. More recently, advances in the number of banks and type of solid-state detectors lining the patient gantry have ted to even faster spiral imag- ing with simultaneous data acquisition from mul- tiple (up to 4), thinner (down to 0.5 mm) slices. This allows for greater temporal and spatial reso- lution without additional radiation dose and with excellent 3D reconstruction. Together with im- provements in software, 3D volume renderings now allow the operator to "fly" down the lumen of

IMAGING CEREBROVASCULAR DISORDERS IN CHILDREN 263
( "'l \ t �9 r
C
Fig 1. Transcranlal screening Doppler In a 7-year-old boy with sickle cell disease. Bilateral middle cerebral arteries are Insonatad through a transtemporal window at s depth of 48 mm and blood f low is toward the transducer. (A) The mean blood f low velocity of the right middle cerebral artery Is within normal limits for a child with sickle cell disease (116 cm/sec). (B) The mean blood f low velocity of the left middle cerebral artery Is abnormal (245 cm/sec). (C) Reconstructed MIP 3D TOF MRA same patient demonstrat ing signal dropout from the proximal M1 segment of the left middle cerebral artery (MCA) (arrow). This child proceeded to completed Infarction In the left MCA territory within 24 hours of the study and before Interventlonal therapy could be Implemented.
a vesse l - -on a workstation monitor using a joy- stick and interrogate, for example, the relationship of the neck of an aneurysm to the bifurcation of the parent vessel (see also 3D digital subtraction angiog- raphy). The whole procedure of volume rendering "nulls" the artefact from metal enabling CTA to be usefully performed even in the follow-up of treated aneurysms or arteriovenous malformations, when clips, coils, or glue may have been used by the neurosurgeon or neurointerventionalist, respectively.
3D CTA has been proposed as the method of choice for diagnosis and follow-up of dissection as differ- ences in the attenuation of blood and contrast can be used to distinguish the true and false lumens, 16 while allowing assessment of the overall external diameter of the vessel.
Stable Xenon CT
Stable xenon CT studies quantitatively deter- mine local blood flow. A CT scan slice location is

264 JILL V. HUNTER
Fig 2. Eighteen-month-old child presenting with acute right hemiparesis. (A) Unenhanced axial CT image demonstrates the "white sign" (open arrow) in the expected position of the left MCA, consistent with acute thrombosis. (B) Axial unenhanced CT from the same patient (same day but higher plane) demonstrating low attenuation (arrows) due to a left MCA infarction.
chosen and a series of between 6 and 10 scans is acquired at intervals of 1 minute, at the same level, while the subject breathes a xenon/oxygen mixture via an inhalation system. The xenon content within the tissue causes a time-dependent increase in the CT numbers measured. This is due to the high atomic number of xenon, which makes it an x-ray contrast medium. To obtain quantitative informa- tion on blood flow, the xenon content of arterial blood is also required. This can be determined by analyzing the end-tidal air and by knowing the patient's hematocrit. A two-parameter fit method based on the Ketj~-Schmidt' equation 17 links the two measurements (CT enhancement and arterial xenon content) and then calculates a blood flow image for the region of interest.
An accurate knowledge of local blood flow (ex- pressed in mL/min/100 g of brain tissue) permits conclusions to be drawn regarding tissue properties and pathologic alterations. Work in children has been performed in ischemic neurovascular dis- ease is and in head injury. 19'2~
Relative cerebral blood flow (rCBF) and relative cerebral blood volume (rCBV) or perfused blood volume (PBV) have also been calculated usingfirst
pass bolus techniques with conventional water sol- uble iodinated contrast. 21 The passage of contrast laden blood is tracked by serial 1- to 2-second scans and time-density curves are plotted. Remem- bering that there is an initial linear relationship between contrast density and Hounsfield units, the area under the curve can be "fitted" and measured to give an estimate of the blood being delivered to a particular area of the brain. Temporal informa- tion is also available regarding the time of first arrival of contrast, time to peak, and arteriovenous transit times.
SINGLE PHOTON EMISSION COMPUTED TOMOGRAPHY
Radionuclide imaging offers the potential for semiquantitation of cerebral perfusion, of use, for example, in pediatric stroke. To date, the ideal brain single photon emission computed tomogra- phy (SPECT) pharmaceutical has not been devel- oped and the modality competes with dynamic CT and magnetic resonance imaging (MRI). The cur- rently used technetium (Tc 99m)- and iodo-amines include hexemethylpropyleneamine oxime (HM- PAO) bicisate (1,1-ECD) and isopropyl iodoam-

IMAGING CEREBROVASCULAR DISORDERS IN CHILDREN 265
phetamine (IMp)2Z; the latter is not readily avail- able in all countries. The uptake, extraction fraction, and retention of these agents vary among different regions of normal and abnormal brain, 23 and the fixation can be altered by local or regional parameters. The kinetic behavior and trapping mechanism specific to each tracer must be well understood for the correct clinical application and interpretation of the SPECT images to be made. HMPAO, being labeled with Tc99m, is probably the most readily available agent and as such has been used in determining loss of cerebral blood flow (CBF) as one of the criteria to confirm brain death. Other current applications of SPECT imag- ing include its use in the workup of epilepsy where an ictal versus an interictal study may demonstrate an increase or decrease in rCBF, respectively, at the site of an epileptogenic focus.
POSITRON EMISSION TOMOGRAPHY
The cerebral metabolic rate of oxygen (CMRO2), using inhaled O15, has been shown in adults to have a very close relationship to CBF under conditions of constant cerebral vascular re- sistance. However, it remains a very invasive tech- nique requiring paired arterial and venous blood sampling. The results of C15 0 2 positron emission tomography (PET), based on the coincidence de- tection of electrons to localize the positional source of an introduced radioactive isotope, have been compared with HMPAO SPECT to measure rCBF, with good concordance. 24 Ol5-water has been used as an agent in established stroke to map reorganization of motor cortex during a stimulation paradigm by Muller et al. 25 This same group has performed a parallel study in children to look at language reorganization following an early left hemisphere lesion} 6 Other agents, such as 2-de- oxy-2 [18F] fluoro-D-glucose (FDG) have been used to measure local cerebral metabolic rates for glucose (ICMRGIc) in six children with Sturge- Weber syndrome (SWS)} 7 The authors showed that in advanced SWS a markedly depressed 1CMRGlc extended beyond the abnormality de- picted on a matched CT examination. In two in- fants with SWS and recent seizure onset, interictal PET revealed a paradoxical pattern of increased 1CMRGIc in the cerebral cortex of the anatomi- cally affected hemisphere. In one of these infants, 1CMRGIc was also increased in the contralateral cerebellum, suggesting activation of the cortico-
ponto-cerebellar circuitry. This latter observation has been more extensively studied in a series of 40 children sustaining unilateral cerebral injury. 28
MAGNETIC RESONANCE IMAGING
State-of-the-art equipment in the year 2000 con- stitutes a 1.5 Tesla high-field magnet with echo- planar capability and rapid gradients. Three and 4 Tesla systems are commercially available but are not yet in routine clinical use and may not have full Food and Drug Administration (FDA) approval for use in children (because of signal absorption rate, SAR, considerations, etc.). A variety of coils in- cluding transmit/receive and whole body as well as dedicated surface coils exist, and new coil devel- opments are being made especially in the area of spectroscopy. Rapid gradients and echoplanar im- aging (EPI) allow for faster sequences, for exam- ple, turbo spin echo (TSE), with more rapid acqui- sition without motion artefact. With the advent of 3D volumetric acquisition, conventional TI- weighted and T2-weighted sequences can now be resolved down to submillimeter in-plane resolu- tion.
Fetal MRI has been enabled by the introduction of faster image acquisition and may add value to the prenatal diagnostic ultrasonography. Vein of Galen aneurysms and in utero infarcts have both been diagnosed antenatally using MRI (personal communication, JV Hunter).
Gradient Echo
Gradient echo ("susceptibility" imaging) is very helpful for detecting blood and altered blood prod- ucts following a germinal matrix or parenchymal hemorrhage. It can be especially useful in prema- ture infants, post extracorporeal membrane oxy- genation (ECMO), following cardiac bypass sur- gery or cardiac catheterization, when there is suspicion for child abuse, as well as for the detec- tion of cavernomas.
Acute subarachnoid hemorrhage is not best shown by MRI, 29 although fluid attenuated inver- sion recovery (FLAIR) imaging may be capable of detecting fresh subarachnoid blood. 3~ FLAIR imaging is very good at demonstrating periven- tricular leukomalacia (PVL).
Magnetic Resonance Angiography
Magnetic resonance angiography (MRA), unlike its CT equivalent, can be performed without the

266 JILL V. HUNTER
administration of intravenous contrast. The two main sequence types used are 2D or 3D time-of- flight (TOF) and phase contrast (PC) imaging. Both can be adjusted to look preferentially at either the venous system--magnetic resonance venogra- phy (MRV), (Fig 3) or the arterial system (MRA) (Fig 4). In the case of 2D PC imaging, phase and magnitude data can be displayed to give informa- tion about the direction and amount of flow. The multiple overlapping thin section acquisition (MOTSA) technique is a hybrid of PC and TOF. As with ultrasonography, MRA is a physiologic and not a strictly anatomic examination like conventional angiography, in this instance looking at the parameter of blood flow. Because of the added turbulence caused by anemia and subse- quent stenosis of large vessels in SCD, we opt to perform MRA examinations in this population of children at a shorter echo time than conventionally used.
Recently, a 3D turbo spin-echo contrast-en- hanced MRA sequence has been introduced. This works like a "first pass" technique in acquiring the angiographic raw data in the space of 20 seconds or less, following an intravenous bolus of Gado- linium, so that a series of MRAs can be performed back to back to capture the arterial through to the venous phase. The quality of these angiograms, which may require a double dose of contrast, is quite high, as illustrated (Fig 5).
MR Perfusion Imaging
MR perfusion imaging is currently performed in one of two ways and has the potential to provide semiquantitative information regarding the delivery of blood to the brain. Arterial spin labeling techniques 33 rely on the inherent con- trast of blood, whereas "first pass" bolus tech- niques require the administration of a contrast agent, such as gadolinium, and use dynamic contrast-enhanced T2*-weighted echoplanar im- aging. Using the latter technique areas of normal perfusion will darken with the passage of the bolus of contrast due to the T2* effects, while areas of decreased perfusion will appear rela- tively bright by comparison with the surrounding normal brain (Fig 6).
Diffusion-Weighted Imaging
Diffusion-weighted imaging (DWI) is an MRI technique that is extremely sensitive to acute isch-
emia and infarction. Diffusion imaging measures Brownian motion of water in tissues. The move- ment of individual water molecules in solution is random; however, in the intracellular and extracel- lular spaces of the brain, macromolecular proteins, intracellular organelles, cell walls, and myelin sheaths restrict or slow diffusion in certain direc- tions. Images can be made for individual directions (usually corresponding to the three orthogonal ax- ial, sagittal, and coronal planes of imaging the patient), or the individual directional images can be averaged to make a relatively direction-indepen- dent or isotropic diffusion image called a trace image. Although diffusion-weighted images reflect the movement of water molecules in tissue, there is a small contribution from motion of blood within capillaries. Thus, the exact diffusion coefficient of water cannot be measured in vivo, but the images can be analyzed to calculate an apparent diffusion coefficient (ADC), which reflects the rate of diffu- sion but includes a small component from capillary blood flow. Although diffusion images are weighted towards diffusion effects, a portion of the tissue contrast comes from the T2 relaxation of the underlying tissues. Hence regions that are bright on T2-weighted imaging can appear bright on D W I - - the so-called "T2 shine through. ''34 Misinterpreta- tion can be avoided by comparing individual DW images with the T2-weighted images or by mea- suring the ADC values in the region of interest (Fig 7). Other parameters can be measured using DWI including diffusion tensor imaging, which may prove helpful in demonstrating normal and dis- rupted white matter tracts, and fractional anisot- ropy (FA), which holds some promise in HIE. 35 DWI may also be used on scanners without echop- lanar capability using a technique called line scan diffusion imaging (LSDI), which has some theo- retical advantages in children in that there is less inherent ditortion and it is relatively insensitive to motion. 36,37
Activation Functional MRI
Activation functional MRI (fMRI) uses the BOLD (blood oxygen level dependent) sequence to detect alterations in blood flow to an area of the brain following use of a stimulation paradigm. BOLD contrast imaging is based on the observa- tion that the brain shows localized blood volume increases on neuronal activation. It has also been shown that these increases far exceed the oxygen

IMAGING CEREBROVASCULAR DISORDERS IN CHILDREN 267
' t i \ t
Fig 3. Female teenager with inflammatory bowel disease presenting with headache. (A) Axial gradient echo MRI per- formed near the vertex demonstrates low signal In the region of the left sensorimotor cortex consistent with recent hemor- rhage. (B) Saglttal MIP reconstruction from 3D TOF MRV does not demonstrate the superior saglttal sinus (arrows). (C) Axial collapsed MIP projection on the same patient confirms de- creased signal f low returned from the straight and proximal transverse (arrows) sinuses as well as the torcula (confluence of sinuses). These appearances suggest extensive venous sinus thrombosis.
consumption of the tissue. Therefore, the venous oxygen content rises and yields an increase in the MRI signal observed. This is because deoxyhemo- globin is paramagnetic, which directly affects the
local susceptibility of the tissue. It generates an inhomogeneous magnetic field in tissue surround- ing blood vessels, causing intravoxel dephasing and decreased signal intensity on MR images.
268 JILL V. HUNTER
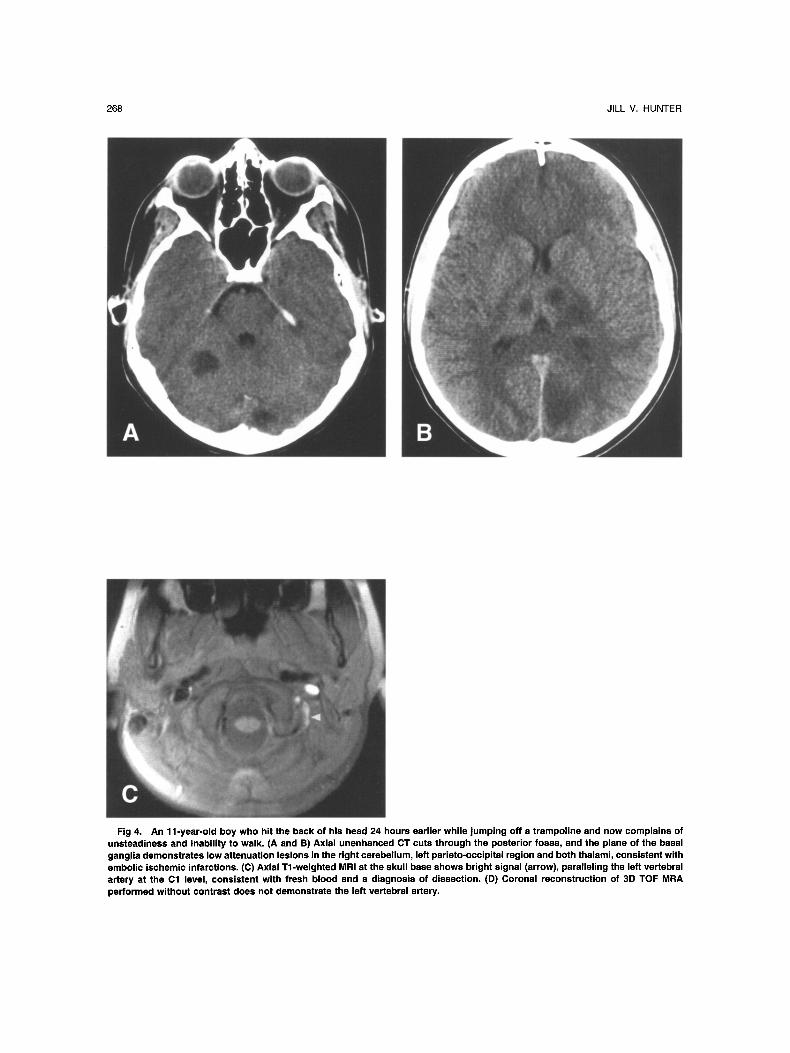
Fig 4. An 11-year-old boy who hit the back of his head 24 hours earlier while jumping off a trampoline and now complains of unsteadiness and inability to walk. (A and B) Axial unenhanced CT cuts through the posterior fossa, and the plane of the basal ganglia demonstrates low attenuation lesions in the right cerebellum, left parieto-occipital region and both thalami, consistent with embolic ischemic infarctions. (C) Axial Tl-weighted MRI at the skull base shows bright signal (arrow), paralleling the left vertebral artery at the Cl level, consistent with fresh blood and a diagnosis of dissection. (D) Coronal reconstruction of 3D TOF MRA performed without contrast does not demonstrate the left vertebral artery.

IMAGING CEREBROVASCULAR DISORDERS IN CHILDREN 269
o / j
?i .
E Fig 4. (continued) (E) Repeat MRA• using same technique, performed 6 weeks later shows restoration of f low in the left vertebral
artery following anticoagulant therapy. The child developed "locked-in" syndrome and went on to make a slow but good recovery.
Fig 5. Late phase of a 3D turbo MRA of a normal neck with double dose gadolinium (Gd), demonstrating a combination of both the arterial and venous phases of the circulation.
TIw~c I,~w~LI \ari~flion~ in ~u~CCl>lihiiily in the r~.'~h.m o[ lhu' hJ~.>~.~d \',.'xscI~ cotllrihLtt~." to lhc
upparcnt lr~ms,,,crsc rclax~th>n time 'I'2 :~:. A', lhc
\rc[I~)LI~ and capillary ~xy~cn C()lllC'll[ JllClc~iscx.
the am~mnt ~I dcoxyhcn]o~lohin in 1iIr bh~(>d
dccrc~iscs, which incrcaxcs lhc MR ~i~mfl. "fht1~.
chan~cs in tltc Ioc~d functhmal activuti~m c~it] he
dclecled by any pulse sequence lhat is sensitive
to T2*. In conventional scanners, lhis sequence
is a gradient echo train.
At 1.5 T magncl strength, it is generally consid
ercd thal, following a spccilic aclivation paradi.~m,
most of the signal change detected with the BOI J)
sequence rcllccts changes in venous rather than capillary blood llow. MR1 in children has bccn used clinically to determine hemispheric domi- nance for language before temporal lobe epilepsy surgery -~s and to determine the location of senso- rimotor and visual cortex before lesional surgery9 There is ongoing research using rnemory para- digms to combine the results of language and memory tasks in an attempt to replace the more invasive Wada test. Multiple other lines of research are being pursued to look at different cohorts of children, such as those with ADHD, schizophrenia, and post-traumatic brain injury.

270 JILL V. HUNTER
T1 Mapping MRI sequences using a short TR, short TE
produce a Tl-weighted anatomic image. To mea- sure the actual T1, a different sequence needs to be run to map absolute T1 values. There is some evidence in the literature to suggest that a decrease in absolute T1 values in the gray matter can be correlated with cerebral ischemia in the absence of stroke as measured by decreasing psychometrics and a hematocrit < 27% in a homozygous sickle cell population. 4~
MAGNETIC RESONANCE SPECTROSCOPY
Proton magnetic resonance spectroscopy (MRS) is performed using the same equipment as conven- tional MRI but can extract information about the chemical environment of hydrogen nuclei in both a qualitative and quantitative fashion. Data analysis in MRS is carried out by changing time domain data to frequency domain spectra using Fourier transform. The resulting spectrum that we see is a frequency distribution of the nuclei in the sample, and MRS can be considered a histogram of nuclei with different precession frequencies. The area under a particular peak provides a quantitative measure of that particular metabolite.
Lactate is an indicator of anaerobic metabolism and may normally be present transiently at birth. In mild hypoxic ischemic encephalopathy (HIE) ele- vated lactate may be detectable as early as 4 to 8 hours after birth, likely the result of reduced oxy- gen delivery and subsequent anaerobic glycoly- sis. 41 In more severe HIE, this early rise in lactate does not resolve by 48 hours but rather persists and increases after 24 hours. The delayed elevation is ascribed to mitochondrial damage and may there- fore be of greater significance in predicting long- term outcome. 42 Lactate levels found in mitochon- drial encephalopathy lactic acidosis and stroke-like syndrome (MELAS) are generally much higher at the time of initial presentation than those seen secondary to other causes of ischemia, such as stroke and necrosis. Therefore, these conditions are easily distinguished (Fig 8).
The detection of lipid by proton spectroscopy is an almost universal accompaniment of brain injury in very young infants and is sometimes difficult to separate out from a lactate peak depending on the echo time that is used to acquire the spectra. Sometimes two different echo times are required to invert and confirm the presence of a lactate doublet
Fig 6. (A) Typical first-pass bolus curve, following a pe- ripheral IV injection of Gd, extending out to 59 seconds on the x-axis. Note the drop in signal approximately 30 seconds into the acquisition consistent with the T2* effect of the Gd. (B) Axial MRI scan from the perfusion series at 30 seconds dem- onstrating relatively increased signal returned in a posterior (long arrows) and to a lesser extent anterior (shod arrows) watershed distribution. The apparent increase in signal re- flects the decrease in Gd-laden blood delivered to the areas of relative ischemia.

IMAGING CEREBROVASCULAR DISORDERS IN CHILDREN 271
separate from a combined lipid/lactate peak as they overlap in their position on the x axis.
N-acetyl aspartate is a marker of neuronal and axonal integrity and demonstrates a reduced peak following ischemic injury and stroke compared with age matched controls.
Glutamate serves as a neurotransmitter and is an important intermediate of amino acid catabolism; it is elevated in ischemia.
Much of the initial work using MRS in asphyx- iated neonates used 31P MRS, and it was found that low concentrations of phosphocreatine and adenosine triphosphate during the first few days of life correlated with the presence of neonatal en- cephalopathy and poor neurodevelopmental out- come. 43 More recently, 44-47 proton MRS has been found to be particularly useful during the first few days of life when the conventional imaging abnor- malities may be hard to detect. In turn, some of the diagnostic function of 1H-MRS may have been superceded by the introduction of DWI and FA; however, it may still retain a place in the prognos- tication of HIE. MRS has also been used as a functional MRI tool to detect changes in oxy-/ deoxy-hemoglobin during an activation para- digm. 48
NEAR-INFRARED SPECTROSCOPY
Several techniques are available for measuring cerebral activation, related to specific brain func- tions, and these have been widely applied in adults to understand the function of both the normal and diseased brain. These techniques are based either on electrical changes in activated cells (such as evoked potentials) or on local changes in cerebral perfusion. Hemodynamic changes can be measured using PET or f M R I . 49 Both require the child to lie still in a scanner while performing the activation task, which is often only possible with sedation. This raises ethical issues and can also alter the results of activation paradigms even when these are feasible in the unconscious subject. 5~ Near- infrared spectroscopy (NIRS) is a novel technique for measuring functional activation in infants, which is both noninvasive and localized.
It has recently been demonstrated that NIRS can be used in the awake infant to measure regional cerebral hemodynamic changes in response to vi- sual stimulation. 51 The technique depends on the relative transparency of biological tissue to near- infrared light, and the absorption of light by oxy-
hemoglobin (HbO2) and deoxyhemoglobin (Hb). A modification of the Beer-Lambert law is used to convert measured changes in optical density to changes in chromophore concentration. Near-infra- red light from four laser diodes is transmitted via a fiber-optic bundle to an "optode" fixed over the occipital region of the infant's head. A detecting optode placed 3.5 cm away is connected to a second fiberoptic bundle, which conveys the emerging light to to the spectrophotometer. A con- trolling computer converts the changes in optical density into changes in cerebral [HbO2] and [Hb]. The technique can therefore detect regional changes in HbO e and Hb, 52 resulting from visual stimulation. This method has been applied to the measurement of functional activation in adults by several groups. 53-57 It is ideally suited to the study of infants because the infant skull is thinner than that of adults so that the optical signal is cleaner and easier to detect. Increases have been seen in both [oxy-Hb] and [deoxy-Hb] over the occipital region in infants related to visual stimulation, 58 whereas the adult response seen both by fMRI and NIRS is for [deoxy-Hb] to decrease, while [oxy- Hb] increases. These data are consistent with the reversal of the BOLD (blood oxygen level depen- dent) signal seen in preliminary fMRI studies on sedated or sleeping infants. 59-61 This maturational shift in the balance between oxygen consumption and perfusion may be important in understanding vascular control mechanisms underlying cerebral function in the infant.
Studies have demonstrated an increase in the magnitude of the response with age. 6z It has proven feasible to study preterm infants down to a corrected age of 32 weeks, and to show a consis- tent response to stimulation with a checkerboard with pattern reversal from 36 weeks. In addition there is preliminary evidence of abnormal func- tional activation in infants with cerebral pathology, such as perinatal asphyxia and occipital lobe in- farction. 63
DIGITAL SUBTRACTION ANGIOGRAPHY
Conventional catheter angiography is now most commonly performed using digital equipment rather than acquiring the study using individual sheets of plain "cut" film, as the resolution in most instances is strictly comparable. Biplane capability is desirable for the examination of small children because of the contrast restrictions in terms of

272 JILL V. HUNTER
Fig 7. An 8-year-old boy injured in a motor vehicle accident seen acutely. (A) Axial CT scan demonstrates acute subdural hemorrhage along the left greater than right tentorium. In addition hyperattenuation consistent with fresh blood is seen in the basal cisterns, around the left choroid plexus, and in the anterior end of the third ventricle. Intraparenchymal hematomas are noted in the left frontal lobe with subdural/subarachnoid blood outlining the anterior interhemispheric fissure, Note the dilated temporal horns consistent with hydrocephalus. (B and C) Axial diffusion-weighted and apparent diffusion coefficient image calculated from the same dataset using an imaging plane through the level of the temporal horns, T2 shine-through effects are seen on the individual DW image (B), but this is compensated for on the ADC map, (C) which shows decreased signal returned from the bifrontal lobes consistent with acute ischemia. (D) Collapsed MIP reconstruction from 3D TOF MRA dataset acquired without contrast demon- strates an anterior cerebral artery aneurysm (arrow).

IMAGING CEREBROVASCULAR DISORDERS IN CHILDREN 273
thrombolytic therapy remains problematic at present as current wisdom suggests that the "win- dow of opportunity" in children is even shorter
Fig 7. (continued) (E) Anteroposterior cerebral angiogram following selective injection of the right ICA, demonstrates a wide-necked traumatic aneurysm arising from the right ante- rior cerebral artery. This was treated by surgical clipping.
volume of iodinated contrast permitted based on body weight and surface area, related to renal function. There has been a new advance with the introduction of 3D DSA. As a result of rotation of the x-ray tube (camera) and image intensifier a stepped sequence of background "masks" and a matching series of stepped incremental angiograms are acquired. Following subtraction the data ac- quired can be used to produce 3D surface render- ings of the vessels (Fig 9), as well as permitting interrogation of the interior of the vessel to exam- ine, for instance, the relationship of the bifurcation of a vessel to the neck of an aneurysm that may be arising from it. The only disadvantage for children is that this technique currently requires the admin- istration of a triple dose of iodinated contrast and may therefore not be applicable to small infants and babies.
There have been technological advances in the size and range of superselective catheters, slippery wires, and devices such as stents and Guglielmi detachable (GDC), coils, introduced over the past 5 years for the treatment of aneurysms and other vascular malforma- tions. Although pediatric interventional neuroradiol- ogy forms a relatively small part of any neurointer- ventionalist's practice, these advances have equal applicability to children as to adults.
The treatment of acute ischemic stroke with
Fig 8. A 17-yeer-old boy presenting with field cut and seizure activity. (A) A T2-welghted axial image performed at the level of the orbits demonstrates increased signal returned from the right temporo-occipltel lobe. There is evidence of swelling with some effacement of the right occipital horn. The appearances ere suggestive of infarction, although the pat- tern is not typical for a vascular distribution. (B) Single voxel short TE MRS (STEAM) acquisition. A grossly elevated lactate (Lac) peak is seen with an almost absent N-acetyl aspartate peak, the latter consistent with neuronal death. The degree of lactate elevation is greater than expected for simple infarction, and the patient was subsequently diagnosed with MELAS.

274 JILL V. HUNTER
than that in adults and may be of the order of 3 rather than 6 hours. It would be rare to see and diagnose a child with stroke within this time frame. Thrombolysis for (pan)venous sinus thrombosis in children is occasionally required in the symptom- atic patient, not responding to heparin.
CONTRAST AGENTS
New contrast agents have been developed both for ultrasound 64 and MRI applications, most of which are currently unavailable for pediatric use, in the United States at least, owing to FDA regu- lations. The general trend towards the use of non- ionic contrast has enabled the more comfortable and possibly safer delivery of water-soluble iodin- ated contrast media to children 65 for CT and an- giographic applications.
Applications
Venous sinus thrombosis is investigated by the following: the venous phase of CTA with contrast (C), MRV - C, imaging Doppler, venous phase DSA _+ thrombolysis.
Arterial stenosis is investigated by the follow- ing: TCD head, imaging Doppler neck, 3D CTA with C, MRA -+ Gd, conventional vs 3D DSA.
Arterial dissection is best investigated by the following: MRI/MRA or CT with CTA, using Doppler in follow-up. The indication for DSA in children is less clear unless there is some difficulty in making the diagnosis.
Stroke is best investigated by a combination of the following: TCD, CTICTA, (CT perfusion has been used in adults for rCBF, rCBV), stable Xe CT, MRI /MRA with D W I + perfusion. In the acute phase DSA _+ thrombolysis may be indicated if seen very early. Catheter angiography is also indicated when all other tests are negative.
Other Forms of Ischemic Brain Injury
Trauma + extraaxial collections: use CT - MRI with GE sequence to look for shear injury and DWI to detect ischemic damage.
PVL use conventional ultrasound in the neonatal period or MRI with FLAIR imaging.
Hypoxic ischemic encephalopathy (HIE) MRI is probably the most sensitive test _+ DWI.
Nonaccidental injury (NAI) is best investigated by a combination of CT and MR with GE and DWI with MRS for prognostication purposes.
Metabolic disease is best diagnosed by a com- bination of MRI with MRS.
Vascular Malformations
Cavernoma/occult cerebrovascular malforma- tion (OCVM) may be seen on CT but is best diagnosed by MRI with GE to look for multiple cavernous hemangiomas. If the clinical diagnosis is in doubt, and there is concern about hemorrhage, angiography may be performed but will be nega- tive unless there is an associated developmental venous anomaly (DVA). DVAs are associated with cavernous malformations in about 37% of cases and have a characteristic "caput medusa" appear- ance on contrast examinations.
Vein of Galen malformations have been detected in utero with UIS and MRI and postnatally can be diagnosed by a combination of U/S, CT, and MRI/ MRA. The latter two modalities are useful for prognostication and determination of whether or not interventional therapy is indicated, in which case conventional angiography will be required.
Arteriovenous malformation is often detected on CT with or without contrast or by MRI/MRA. However, conventional angiography is required to delineate feeding vessels and draining veins and to plan therapy.
Aneurysms often come to attention following SAH. Fresh subarachnoid blood is best diagnosed on CT but MRI /MRA will likely be required to confirm the diagnosis of aneurysm noninvasively followed by conventional angiography to demon-
Fig 9. Adult patient after aneurysm clipping undergoing 3D DSA (Siemens, Erlangen, Germany) to check aneurysm. A 3D surface rendering of angiographic data acquired following triple-dose intra-arterial nonionic water- soluble iodinated contrast demonstrates surgical aneurysm clip with three re- sidual "berry" aneurysms arising from the circle of Willis (arrows).

IMAGING CEREBROVASCULAR DISORDERS IN CHILDREN 275
strate the neck and its relations. Transcranial Doppler is used to follow vasospasm, which can be a sequel to the hemorrhage.
Vasculitis and other vasculopathies can be a difficult group to diagnose but the sequelae may be detected on conventional CT and MRI. If nonin- vasive forms of angiography are unable to make the diagnosis then conventional cerebral angiogra- phy may be required before biopsy. High-resolu- tion magnified views should be obtained and all four vessels studied, (even so the diagnosis may be missed!).
SCD
Some physicians now use a screening program with TCD to triage homozygous sickle cell chil- dren to identify those most at risk from stroke. DW1 has contributed enormously in the ear ly-- first 6 hours to 10 days--identification of children with a CNS crisis and evidence of cerebral isch- emia. MRI detects established "silent" infarcts and MRA with an appropriate TE can demonstrate Moyamoya collateral circulation and indicate po- tential sites of vascular narrowing. Conventional angiography is rarely required now in this popula- tion.
Brain Death
Although several different imaging modalities have been used to measure different aspects of blood flow and perfusion, nuclear medicine Tc 99m H M P A O SPECT is probably the single best established imaging test used to make the diagno- sis of brain death in clinical practice.
SUMMARY
In summary, over the past two decades, advances in both software and hardware and innovations in sequence design have led to an expansion in the number and type of imaging modalities available to evaluate cerebrovascular disorders in children. Some of the imaging modalities are complementary (MRI/ CT), whereas others stand alone and give unique information (TCD). However, it should be remem- bered that "all that glisters is not gold" (Shakespeare) and that we are still on a learning curve with some of this imaging information.
ACKNOWLEDGMENTS
The author thanks our dedicated vascular ultrasound technolo- gist Mira Katz, PhD, for her assistance in writing the section on TCD and for her excellence in patient scanning; and Judith Meek for her invaluable assistance in writing the ,section on NIRS.
REFERENCES
la. Merrill JD, Piecuch RE, Fell SC: A new pattern of cerebellar hemorrhage in preterm infants. Pediatrics 102: E62, 1998
1. Postert T, Federlein J, Przuntek H, et al: Comparison of transcranial power Doppler and contrast-enhanced color-coded sonography in the identification of intracranial arteries. J Ultra- sound Med 17:91-96, 1998
2. Adams RJ, McKie VC, Nichols F, et al: The use of transcranial ultrasonography to predict stroke in sickle cell disease. N Engl J Med 326:605-610, 1992
3. Proust F, Callonec F, Clavier E, et al: Usefulness of transcranial color-coded sonography in the diagnosis of cerebral vasospasm. Stroke 30:1091-1098, 1999
4. Maurer M, Mullges W, Becker G: Diagnosis of MCA- occlusion and monitoring of systemic thrombolytic therapy with contrast enhanced transcranial duplex-sonography. J Neu- roimaging 9:99-101, 1999
5. Taylor GA: Effect of scanning pressure on intracranial hemodynamics during transfontanellar duplex US. Radiology 185:763-766, 1992
6. Taylor GA, Phillips MD, Ichord RN, et al: Intracranial compliance in infants: Evaluation with Doppler US. Radiology 191:787-791, 1994
7. Droste DW, Reisener M, Kemeny V, et al: Contrast transcranial Doppler ultrasound in the detection of right-to-left shunts. Stroke 30:1014-1018, 1999
8. Stolz E, Kaps M, Dorndorf W: Assessment of intracranial
venous hemodynamics in normal individuals and patients with cerebral venous thrombosis. Stroke 30:70-75, 1999
9. Taylor GA: Intracranial venous system in the newborn: Evaluation of normal anatomy and flow characteristics with color Doppler US. Radiology 183:449-452, 1992
10. Taylor GA, Walker LK: Intracranial venous system in newborns treated with extracorporeal membrane oxygenation: Doppler US evaluation after ligation of the right jugular vein. Radiology 183:453-456, 1992
11. Dean LM, Taylor GA: The intracranial venous system in infants: Normal and abnormal findings on duplex and color Doppler sonography. AIR Am J Roentgenol 164:151 - 156, 1995
12. Lam AH: Doppler imaging of superior sagittal sinus thrombosis. J Ultrasound Med 14:41-46, 1995
13. Kinney TR, Sleeper LA, Wang WC, et al: Silent cerebral infarcts in sickle cell anemia: a risk factor analysis: The Coop- erative Study of Sickle Cell Disease. Pediatrics 103:604-605, 1999
14. Adams RJ, McKie VC, Hsu L, et al: Prevention of a first stroke by transfusions in children with sickle cell anemia and abnormal results on transcranial Doppler ultrasonography. N Engl J Med 339:5-11, 1998
15. Klotzsch C, Popescu O, Berlit P: A new 1-MHz probe for transcranial Doppler sonography in patients with inadequate temporal bone windows. Ultrasound Med Biol 24:101-103, 1998
16. Leclerc X, Lucas C, Godefroy O, et al: Helical CT for

276 JILL V. HUNTER
the follow-up of cervical internal carotid artery dissections. Am J Neuroradiol 19:831-837, 1998
17. Kety S, Schmidt C: The nitrous oxide method for the quantitative determination of cerebral blood flow in man: The- try, procedure and normal values. J Clin Invest 27:476-483, 1948
18. Poskitt KJ: MRA and MR quantitative flow evaluation of ischemic neurovascular disease in children. Int Soc Magn Re- son Med 1270, 1998 (abstr)
19. Poskitt KJ, Skippen PW, Kestle J, et al: Hyperventilation in childhood head injuries causes unpredictable changes in cerebral blood flow. Proceedings of the XV Symposium Neu- roradiologicum 291-293, 1994 (abstr)
20. Skippen P, Seear M, Poskitt K, et ai: Effect of hyper- ventilation on regional cerebral blood flow in head-injured children. Crit Care Med 25:1402-1409, 1997
21. Hunter GJ, Hamberg LM, Ponzo JA, et al: Assessment of cerebral perfusion and arterial anatomy in hyperacute stroke with three-dimensional functional CT: Early clinical results. Am J Neuroradiol 19:29-37, 1998
22. Moretti JL, Caglar M, Weinmann P: Cerebral perfusion imaging tracers for SPECT: Which one to choose? J Nucl Med 36:359-363, 1995
23. Kung HF, Ohmomo Y, Kung MP: Current and future radiopharmaceuticals for brain imaging with single photon emission computed tomography. Semin Nucl Med 20:290-302, 1990
24. Gemmell HG, Evans NTS, Besson J, et al: Regional cerebral blood flow imaging: a quantitative comparison of technetiarn-99m-HMPAO SPECT with C1502 PET. J Nucl Med 31:1595-1600, 1990
25. Muller R-A, Watson CE, Muzik O, et al: Motor organi- zation after early middle cerebral artery stroke: A PET study (case report). Pediatr Neurol 19:294-298, 1998
26. Muller R-A, Rothermell RD, Behen ME, et al: Differ- ential pattems of language and motor reorganization following early left hemisphere lesion. Arch Neurol 55:1113-1119, 1998
27. Chugani HT, Mazziotta JC, Phelps ME: Sturge-Weber syndrome: A study of cerebral glucose utilization with positron emission tomography. J Pediatr 114:244-253, 1989
28. Shamoto H, Chugani HT: Glucose metabolism in the human cerebellum: An analysis of crossed cerebellar diaschisis in children with unilateral cerebral injury. J Child Neurol 12:407-414, 1997
29. Atlas SW: MR is highly sensitive for acute subarachnoid hemorrhage . . , not! Radiology 186:319-322, 1993
30. Ogawa T, Inugami A, Shimosegawa E, et al: Snbarach noid hemorrhage: evaluation with M R imaging. Radiology 186:345-351, 1993
31. Ogawa T, Uemura K: Reply. Radiology 186:323, 1993 32. Noguchi K, Seto H, Kamisaki Y, et al: Comparison of
fluid-attenuated inversion-recovery MR imaging with CT in a simulated model of acute subarachnoid hemorrhage. Am J Neuroradiol 21:923-927, 2000
33. Alsop DC, Detre JA: Multisection cerebral blood flow MR imaging with continuous arterial spin labelling. Radiology 208:410-416, 1998
34. Provenzale JM, Engelter ST, Petrella JR, et al: Use of MR exponential diffusion-weighted images to eradicate T2 "shine-through" effect. AJR Am J Roentgenol 172:537-539, 1999
35. Grant PE, Mochida GH, Wu O, et al: Diffusion, perfu- sion and standard MR imaging of neonatal infarcts. Proceedings of the 38th Annual Meeting of the American Society of Neu- roradiology, Atlanta, Georgia, 2000, p 175
36. Robertson R, Maier S, Robson C, et al: MR line scan diffusion imaging of brain in children. Am J Neuroradiol 20:419-425, 1999
37. Robertson R, Liat Ben-Sira, Barnes P, et al: MR line- scan diffusion-weighted imaging of term neonates with perina- tal brain ischemia. Am J Neuroradiol 20:1658-1670, 1999
38. Hunter JV, Brown L, Haselgrove JC, et al: Comparison of hemispheric dominance for language as identified by Wada testing versus functional MRI in a pediatric population. Neuro- image 3:$441, 1996
39. Liu G, Hunter JV, Asushi M, et al: Functional MRI in children with congenital structural abnormality. Neuropediat- rics 31:13-15, 2000
40. Steen RG, Xiong X, Mulhern R, et al: Subtle brain abnormalities in children with sickle cell disease: Relationship to blood hematocrit. Ann Neurol 45:279-286, 1999
41. Wyatt S: Magnetic resonance spectroscopy and near infrared spectroscopy in the assessment of the asphyxiated term infant. MRDD Raes Rev 3:42-48, 1997
42. Peurice J, Cady EB, Lorek A, et al: Proton magnetic resonance spectroscopy of the brain in normal preterm and term infants and early changes after perinatal hypoxia-ischemia. Pediatr Res 40:6-14, 1996
43. Martin E, Buchli R, Ritter S, et al: Diagnostic and prognostic value of cerebral 31P magnetic resonance spectros- copy in neonates with perinatal asphyxia. Pediatr Res 40:749- 758, 1996
44. Peden CJ, Cowan FM, Bryant DJ, et al: Proton MR spectroscopy of the brain in infants. J Comput Assist Tomogr 14:886-894, 1990
45. Leth H, Torts PB, Peitersen B, et al: Use of brain lactate levels to predict outcome after perinatai asphyxia. Acta Paediatr 85:859-864, 1996
46. Groenendal F, Veenhoven EH, van der Grond J, et al: Cerebral lactate and N-acetyl-aspartate/choline ratios in asphyx- iated full-term neonates demonstrated in-vivo using proton magnetic resonance spectroscopy. Pediatr Res 35:148-151, 1994
47. Holshouser BA, Ashwal S, Luh GY, et al: Proton MR spectroscopy after acute central nervous system injury: Out- come prediction in neonates, infants and children. Radiology 202:487-496, 1997
48. Detre J, Wang Z, Stecker M, et al: Vascular transit times in calcarine cortex: Kinetic analysis of R2* changes observed using localized 1H spectroscopy. Magn Reson Med 34:326- 330, 1995
49. Martin E, Joeri P, Loenneker T, et al: Visual processing in infants and children studied using functional MRI. Pediatr Res 46:135-140, 1999
50. Joeri P, Huisman T, Rumpel H, et al: Comparison of fMRI-signal changes during visual stimulation, in awake vs. phenobarbital sedated volunteers. MAG*MA Supp. IV:176- 177, 1996
51. Meek JH, Firbank M, Elwell CE, et al: Regional haemo- dynamic responses to visual stimulation in awake infants. Pe- diatr Res 43:840-843, 1998
52. Cope M, Delpy DT: A system for long term measure-

IMAGING CEREBROVASCULAR DISORDERS IN CHILDREN 277
ment of cerebral blood and tissue oxygenation in newborn infants by near infrared transillumination. Med Biol Eng Com- put 26:289-294, 1988
53. Villringer A, Planck J, Stodick S, et al: Noninvasive assessment of cerebral hemodynamics and tissue oxygenation during activation of brain cell function in human adults using NIRS. Neurosci Lett 154:1-2, 101-104, 1993
54. Hoshi Y, Tamura M: Detection of dynamic changes in cerebral oxygenation coupled to neuronal function during men- tal work in man. Neurosci Lett 150:5-8, 1993
55. Kato T, Kamei A, Takashima S, et al: Human visual cortical function during photic stimulation monitored by means of near-infrared spectroscopy. J Cereb Blood Flow Metab 13:516-520, 1993
56. Meek JH, Elwell CE, Khan MJ, et al: Regional changes in cerebral hemodynamics as a result of a visual stimulus measured by near infrared spectroscopy. Proc R Soc Lond 261:351-356, 1995
57. Chance B, Luo Q, Nioka S, et al: Optical investigations of physiology: A study of intrinsic and extrinsic biomedical contrast. Phil Trans R Soc Lond B 352:707-716, 1997
58. Meek JH, Elwell CE, Firbank M, et al: Regional haemo- dynamic changes in the occipital cortex of awake infants due to visual stimulation. Neuroimage 7:$311, 1998
59. Born P, Leth H, Miranda M, et al: Visual activation in infants and young children studied by functional magnetic resonance imaging. Ped Res 44:578-583, 1998
60. Martin E, Ekatodramis D, Huisman TH, et al: Visual processing in infants and children using tMRI. MAG*MA suppl IV(II):176, 1996
61. Yamada H, Sadato N, Konishi Y, et al: A rapid brain metabolic change in infants and children using fMRI. Neuro- Report 8:3775-3778, 1997
62. Meek JH, Noone MA, Firbank M, et al: Maturation of the regional haemodynamic response to visual stimulation mea- sured by near infrared spectroscopy. Proceedings of the Royal College of Paediatrics and Child Health Annual Spring Meeting 77(A), 1998
63. Meek J, Noone M, Elwell C, et al: Visually evoked hemodynamic responses in infants with cerebral pathology. Neuroimage 2:S108, 1999
64. Gerriets T, Seidel G, Fiss I, et al: Contrast-enhanced transcranial color-coded duplex sonography: Efficiency and validity. Neurology 52:1133-1137, 1999
65. Cohen MD, Smith JA: Intravenous use of ionic and nonionic contrast agents in children. Radiology 191:793-794, 1994
Copyright © 2022 FDOKUMEN




















