
Neuropsychological, neurological, and neuroanatomical profile of Williams syndrome
11
American Journal of Medical Genetics Supplement 6:115-125 (1990) Neuropsychological, Neurological, and Neuroanatomical Profile of Williams Syndrome Ursula Bellugi, Amy Bihrle, Terry Jernigan, Doris Trauner, and Sally Doherty Department of Cognitive Neurosciences, Salk Institute for Biological Studies, La Jolla (UB.,A.B.,S.D.), Department of Psychiatry, VA Medical Center and University of California, San Diego (T.J.); Departments of Neurosciences and Pediatrics, University of California Medical School, San Diego (D.T.) The general aim of our research is to under- stand the brain mechanisms that underlie language and cognition. In this paper, we present a new line of investigation which at- tempts to forge links between a specific neu- rodevelopmen tal disorder, a specific neuro- psychological profile, and abnormal brain organization. We report on a dissociation be- tween language and cognitive functions in Williamssyndrome adolescents, in contrast to age- and IQ-matched Down syndrome adoles- cents. The Williams syndrome individuals ex- hibit an unusual fractionation of higher cor- tical functioning, with marked cognitive deficits, but selective sparing of syntax. Dif- ferences in spatial cognitive abilities in the 2 groups are investigated, showing peaks and valleys of abilities specific to Williams syn- drome individuals. These neurobehavioral profiles are explored in light of new evidence regarding neurologic and neuroana tomical differences between the 2 matched groups of adolescents. Results from these combined studies should help clarify the neural systems that mediate language and cognitive func- tions. KEY WORDS: language, cognition, neural systems INTRODUCTION The studies reported here form part of a larger pro- gram investigating the neurobehavioral, neurological, neuroanatomical, and neurobiological basis of specific developmental disorders [Bellugi et al., 1989; Jernigan et al., 19881. Initial results of this program of inter- disciplinary studies suggest a unique profile for Will- iams syndrome (WS) individuals. Received for publication May 15,1989; revision received August 22, 1989. Address reprint requests to Dr. Ursula Bellugi, The Salk Insti- tute for Biological Studies, 10010 North Torrey Pines Road, La Jolla, CA 92037. 0 1990 Wiley-Liss, Inc. WS is a rare disorder which is characterized by dis- tinctive “elfin-like” facial appearance, mental retarda- tion, cardiac defects, and infantile hypercalcemia [Will- iams et al., 1961; Jones and Smith, 1975; Preus, 19841. Recently, a dissociation between language and cognitive skills and a severe spatial deficit has been described in patients with this disorder, suggesting perhaps a spe- cific neuropsychological profile [Bellugi et al., 1988a,bl. However, several papers present conflicting results and the syndrome still remains relatively unexplored [Ka- taria et al., 1984; Arnold and Yule, 1985; Udwin et al., 1986; 1987; Meyerson and Frank, 1987;MacDonald and Roy, 19881. Reported neurologic abnormalities have in- cluded mental retardation, hyperreflexia, microcephaly, and “awkward gait” [Burn, 1986; Morris et al., 1988; Pagon et al., 19871. In order to determine characteristics unique to this disorder, we compared WS adolescents to age- and IQ-matched controls with Down syndrome (DS). Distinct profiles of the 2 groups emerged from the comparison of results on a battery of language and visuospatial functions, a standard neurological exam- ination, and preliminary results of neuroanatomical in- vestigation involving Magnetic Resonance Imaging [Bellugi et al., 1987bl. For these initial studies, older WS individuals were selected because they had attained major motor and language milestones; however, it is important to empha- size that there may be significant differences in the profiles of younger relative to older WS individuals. Six WS and 6 DS adolescents were identified through our contacts with the National Williams Syndrome Associa- tion and the Parents of Down Syndrome Association. The diagnosis of WS was established by both medical and metabolic markers across most of the subjects. Dr. Kenneth Lyons Jones confirmed the medical diagnosis, and Dr. Floyd Culler confirmed neuroendocrine markers by using levels of calcium and calcitonin after a calcium challenge [Culler et al., 19851. The DS individ- uals were selected to match the WS adolescents on the basis of chronological age and reported I& scores. The mean age of the WS group was 14.4 years with a range from 10 to 17 years, and the mean age of the DS group was 15.4 years with a range from 12 to 18 years. Mean full-scale I& was 50.8 for WS (s.d. = 5.8) and 48.8 for DS (s.d. = 8.7).
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Neuropsychological, neurological, and neuroanatomical profile of Williams syndrome

American Journal of Medical Genetics Supplement 6:115-125 (1990)
Neuropsychological, Neurological, and Neuroanatomical Profile of Williams Syndrome Ursula Bellugi, Amy Bihrle, Terry Jernigan, Doris Trauner, and Sally Doherty Department of Cognitive Neurosciences, Salk Institute for Biological Studies, La Jolla (UB.,A.B.,S.D.), Department of Psychiatry, VA Medical Center and University of California, San Diego (T.J.); Departments of Neurosciences and Pediatrics, University of California Medical School, San Diego (D.T.)
The general aim of our research is to under- stand the brain mechanisms that underlie language and cognition. In this paper, we present a new line of investigation which at- tempts to forge links between a specific neu- rodevelopmen tal disorder, a specific neuro- psychological profile, and abnormal brain organization. We report on a dissociation be- tween language and cognitive functions in Williams syndrome adolescents, in contrast to age- and IQ-matched Down syndrome adoles- cents. The Williams syndrome individuals ex- hibit an unusual fractionation of higher cor- tical functioning, with marked cognitive deficits, but selective sparing of syntax. Dif- ferences in spatial cognitive abilities in the 2 groups are investigated, showing peaks and valleys of abilities specific to Williams syn- drome individuals. These neurobehavioral profiles are explored in light of new evidence regarding neurologic and neuroana tomical differences between the 2 matched groups of adolescents. Results from these combined studies should help clarify the neural systems that mediate language and cognitive func- tions.
KEY WORDS: language, cognition, neural systems
INTRODUCTION The studies reported here form part of a larger pro-
gram investigating the neurobehavioral, neurological, neuroanatomical, and neurobiological basis of specific developmental disorders [Bellugi et al., 1989; Jernigan et al., 19881. Initial results of this program of inter- disciplinary studies suggest a unique profile for Will- iams syndrome (WS) individuals.
Received for publication May 15,1989; revision received August 22, 1989.
Address reprint requests to Dr. Ursula Bellugi, The Salk Insti- tute for Biological Studies, 10010 North Torrey Pines Road, La Jolla, CA 92037.
0 1990 Wiley-Liss, Inc.
WS is a rare disorder which is characterized by dis- tinctive “elfin-like” facial appearance, mental retarda- tion, cardiac defects, and infantile hypercalcemia [Will- iams et al., 1961; Jones and Smith, 1975; Preus, 19841. Recently, a dissociation between language and cognitive skills and a severe spatial deficit has been described in patients with this disorder, suggesting perhaps a spe- cific neuropsychological profile [Bellugi et al., 1988a,bl. However, several papers present conflicting results and the syndrome still remains relatively unexplored [Ka- taria et al., 1984; Arnold and Yule, 1985; Udwin et al., 1986; 1987; Meyerson and Frank, 1987; MacDonald and Roy, 19881. Reported neurologic abnormalities have in- cluded mental retardation, hyperreflexia, microcephaly, and “awkward gait” [Burn, 1986; Morris et al., 1988; Pagon et al., 19871. In order to determine characteristics unique to this disorder, we compared WS adolescents to age- and IQ-matched controls with Down syndrome (DS). Distinct profiles of the 2 groups emerged from the comparison of results on a battery of language and visuospatial functions, a standard neurological exam- ination, and preliminary results of neuroanatomical in- vestigation involving Magnetic Resonance Imaging [Bellugi et al., 1987bl.
For these initial studies, older WS individuals were selected because they had attained major motor and language milestones; however, it is important to empha- size that there may be significant differences in the profiles of younger relative to older WS individuals. Six WS and 6 DS adolescents were identified through our contacts with the National Williams Syndrome Associa- tion and the Parents of Down Syndrome Association. The diagnosis of WS was established by both medical and metabolic markers across most of the subjects. Dr. Kenneth Lyons Jones confirmed the medical diagnosis, and Dr. Floyd Culler confirmed neuroendocrine markers by using levels of calcium and calcitonin after a calcium challenge [Culler et al., 19851. The DS individ- uals were selected to match the WS adolescents on the basis of chronological age and reported I& scores. The mean age of the WS group was 14.4 years with a range from 10 to 17 years, and the mean age of the DS group was 15.4 years with a range from 12 to 18 years. Mean full-scale I& was 50.8 for WS (s.d. = 5.8) and 48.8 for DS (s.d. = 8.7).

116 Bellugi et al.
NEUROPSYCHOLOGICAL PROFILE As part of the multidisciplinary investigation of neu-
rodevelopmental disorders ranging from cognitive func- tions to neurologic characteristics and underlying brain structure and function, WS adolescents and the matched group of DS individuals underwent an extensive neuro- psychological assessment of linguistic and cognitive functioning at the Salk Institute [Bellugi et al., 19891. Our initial findings suggest that whereas DS individ- uals were generally impaired on many of the linguistic and spatial cognitive tasks, the WS individuals, in con- trast, produce a highly uneven neuropsychological pro- file, with peaks and valleys of abilities within and be- tween domains. We report here on unusual aspects of language and cognitive abilities in WS characteristics which may turn out to be hallmarks of the syndrome.
Differential Linguistic Abilities in Williams and Down Syndrome
Although there have been numerous studies of lan- guage in DS individuals with a more frequent, well studied, and relatively better understood developmental disorder [Fowler, 1990; Gleitman, 1983; Miller, 19871, until now there have been few investigations of the linguistic capacities of WS individuals. Results of our preliminary studies suggest that although the WS and DS groups have comparable cognitive impairments (and were selected on the basis of equivalent full-scale I& scores), there may be marked differences between them in the language domain. Analyses of expressive lan- guage and tests of language processing and comprehen- sion indicate that, unlike in DS, lexical and grammati- cal abilities are relatively spared in WS adolescents [Bellugi et al., 1988a1.
Most of the existing studies of language functioning in WS rely upon verbal scores on I& tests as an indicator of language abilities. However, such I& measures conflate different abilities, and do not examine specifically lin- guistic functions. For example, on the WISC-R Vocabu- lary Test, subjects are asked the meanings of words, and points are awarded based on the ability to produce a well-formed definition, a cognitive, not linguistic skill. On this test, the WS and DS group achieved exactly the same low mean scaled scores: 3.2 for each of the groups (in the lowest percentile rank). As these scores indicate, neither the WS nor the DS individuals were able to hone in on the most salient features of the target words to be defined. However, responses of WS individuals clearly show that they have a better understanding of the words and are able to provide appropriate contexts of use. For example, given the word “contagious,” one of the WS subjects related being sick with the measles and unable to have visitors and provided a list of ailments such as “allergies, bleary eyes, runny nose, hay fever, cough, sore throat.” None of the WS adolescents conveyed the critical concept of contagious required for a definition (“easily spread”), but they did provide appropriate asso- ciations. By contrast, the matched DS individuals often provided no scoreable response whatsoever. Accor- dingly, the WS adolescents (unlike their matched DS counterparts) often used unusual words in spontaneous
conversation and demonstrated an understanding of their word choices. When the WS adolescents were asked the meanings of spontaneously elicited words such as “surrender,” “saute,” “nontoxic,” “commentator,” and “brochure,” they provided responses such as “I wish I could surrender. That means I give up,” and ‘(It’s non- toxic. That means it’s not dangerous.”
Preserved semantic abilities in WS. Significant group differences in semantic abilities emerge from a comparison of the 2 groups on tests of lexical knowledge, such as the Peabody Picture Vocabulary Test. On this test, in which subjects hear a word and are asked to pick out the appropriate picture from an array of pictures (e.g., “abrasive”), the WS and DS groups differ signifi- cantly in terms of their referential lexical knowledge. All 6 of the DS adolescents’ receptive vocabulary scores were below their mental age equivalent, whereas 5 of the 6 WS individuals performed at or above normal mental age-matched subjects (Fig. 1). The mean recep- tive language mental age was 8.4 for the WS subjects (s.d. = 1.8; range 5.5 to 10.3) and 5.3 for DS subjects (s.d. = 1.5; range 3.5 to 7.31, a statistically significant difference, (t = 436, P < .01). These findings suggest that aspects of referential lexical knowledge are consid- erably better than expected from mental age in WS, while the opposite pattern is found in matched DS sub- jects.
Important information about the organization of the mental lexicon can also be obtained by measuring the extent to which names can be accessed automatically. On a test of semantic fluency, the WS and DS groups performed very differently, with the WS subjects show- ing a distinct advantage. Subjects were asked to gener- ate as many examples as possible of a semantic category (e.g., foods and animals) within 60 seconds [Semel et al., 19801. The WS subjects produced significantly more words over trials (mean = 26.8, s.d. = 6.7) than the DS subjects (mean = 15.8, s.d. = 3.9) on this task (t = 4.99, P < .01). These results suggest that the WS adolescents, unlike the DS subjects, have no difficulty accessing nu- merous members of a given semantic category. Indeed, for some of the WS subjects tested, the number of words produced was comparable to the norms provided for their chronological age.
Deviant semantic organization in WS. Impor- tantly, these results also suggest qualitative differences between the responses of the 2 groups of adolescent subjects. Not only did the DS subjects produce fewer words than the WS subjects, they were more likely to include repetitions and extra-category words. Predicta- bly, within-category responses generated by DS subjects were limited to highly typical responses such as “dog,” “cat,” and “pig” for animals. In contrast, the chronologi- cal age- and IQ-matched WS subjects frequently pro- duced not just typical category members, but also un- usual, low-frequency, non-prototypical category members. For example, when asked to generate ani- mals, the WS subjects’ word choices included such odd- ities as “unicorn,” “tyrandon,” ‘(brontosaurus,” “yak,” “ibex,” “water buffalo,” “sea lion,” “saber-toothed tiger,” “vulture.” The WS subjects’ unusual performance on a word fluency test is entirely consistent with anecdotal

Neuropsychological Profile of Williams Syndrome 117
THE PEABODY PICTURE VOCABULARY TEST
Mental Age
Recept ive Vocabulary Score 2 12 12
2 10 10 m a,
In
g 8 8
6
4
2
0
0 v) - 6
m 4
D 2
0 0
c a,
> 3
w a,
- -
a WS1 WS2 WS3 WS4 WS5 WS6 D S l DS2 DS3 DS4 DS5 DS6
Age
Williams Syndrome Down Syndrome
Fig. 1. Lexical semantic abilities in WS and DS.
observations from their spontaneous speech, which is peppered with unexpected word choices. The WS sub- jects’ surprising performance on a word fluency genera- tion task is particularly noteworthy in that mentally retarded individuals of various etiologies are known to recognize and use the same types of lexical items and make similar semantic associations as normals matched on mental age [Rondal, 1978, 19801. Therefore, it has been suggested that language in mental retardation generally represents a delay, not a deviance. Our find- ings with WS, by contrast, suggest that deviance may characterize the lexical semantic abilities of this atypi- cal form of mental retardation. The use of unusual vo- cabulary is a surprising facet of WS subjects’ language abilities and may turn out to be a characteristic feature which distinguishes their performance from that of matched DS subjects.
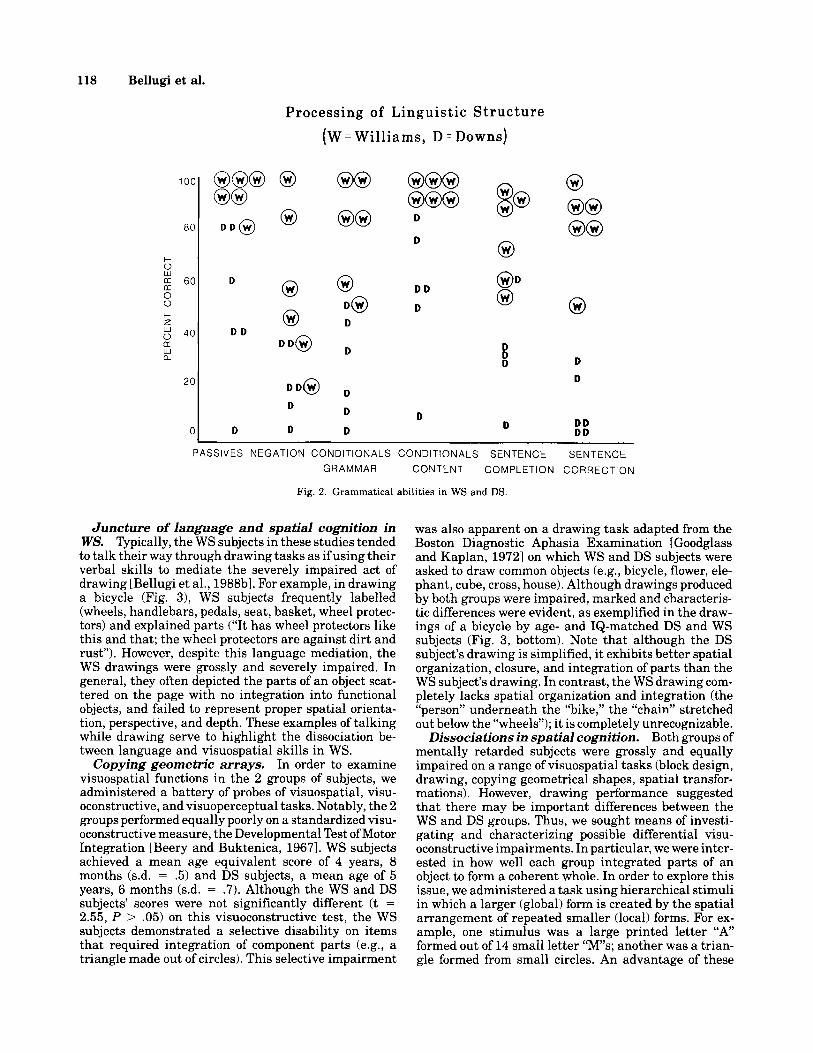
Relatively preserved syntactic abilities in WS. In expressive language, there is a clear difference be- tween the 2 groups, as evidenced by mean length of utterance, noun phrase complexity, verb phrase com- plexity, and embeddings [Bellugi et al., 1987b 1988al. However, an important question is whether the 2 groups differ in comprehension and processing of linguistic structures. Although both groups may exhibit delays in the onset and emergence of language milestones, older WS subjects’ expressive language is complex and gener- ally grammatically correct, albeit with a few mor- phological errors. Figure 2 shows performance on a range of grammatical probes tapping a variety of lin- guistic structures including tests of Semantically Re- versible Passive Sentences; of Negation; of Grammatical Structure of Conditionals; of Sentence Completion; as well as Sentence Correction (a metalinguistic probe for the ability to monitor and correct ungrammatical sen- tences) [Bellugi, 1971; hil ly, 1983; Bellugi and Klima,
19661. Note that many of the WS subjects performed considerably better than the DS subjects. For example, to test for comprehension of semantically reversible pas- sive sentences, the subject is asked to pick from an array of pictures (including that of a horse chasing a man and a man chasing a horse) the one that matches “the horse is chased by the man.” The WS subjects achieved almost a perfect score, whereas the DS subjects performed at chance level or below. Importantly, the WS subjects were also able to monitor sentences for grammatical correct- ness, and were able to correct ungrammatical sentences, while the DS subjects failed on the same task. For exam- ple, when presented with the sentence “I hope you to eat all your supper,’’ a WS subject said “I hope that you will eat all your supper,” while a matched DS subject said “chicken.” These findings, consistent with other results of grammatical competence, suggest that syntactic func- tioning in WS is relatively preserved in comparison to non-linguistic cognitive capacities. Further, linguistic competence in WS, both in production and comprehen- sion, appears markedly better than that in matched mentally retarded subjects with DS.
Peaks and Valleys in Components of Spatial Cognition in Williams Syndrome
These studies suggest that in the linguistic domain, there appears to be a striking difference between matched groups of WS and DS subjects. In previous papers, we have indicated a marked and specific spatial deficit in WS subjects [Bellugi et al., 1988b; Bihrle, et al., 19891; however, spatial abilities or disabilities in DS subjects have rarely been reported. The present studies compared aspects of visual spatial functioning in WS and DS, and highlighted features which may turn out to be characteristic of WS.
118 Bellugi et al.
Processing of Linguis t ic S t r u c t u r e (W = Williams, D = Downs)
F z W 0 LT W a
60
40
D
D D
0 0
D DO
00 00
0 0 0 D
D
2o I D D @ D
D D
0 D D
000 000
D
D
D D
D
0
D D D
D D
0 00 00
D
D
D D D D
PASSIVES NEGATION CONDITIONALS CONDITIONALS SENTENCE SENTENCE
GRAMMAR CONTENT COMPLETION CORRECTION
Fig. 2. Grammatical abilities in WS and DS.
Juncture of language and spatial cognition in WS. Typically, the WS subjects in these studies tended to talk their way through drawing tasks as if using their verbal skills to mediate the severely impaired act of drawing [Bellugi et al., 1988bl. For example, in drawing a bicycle (Fig. 31, WS subjects frequently labelled (wheels, handlebars, pedals, seat, basket, wheel protec- tors) and explained parts (“It has wheel protectors like this and that; the wheel protectors are against dirt and rust”). However, despite this language mediation, the WS drawings were grossly and severely impaired. In general, they often depicted the parts of an object scat- tered on the page with no integration into functional objects, and failed to represent proper spatial orienta- tion, perspective, and depth. These examples of talking while drawing serve to highlight the dissociation be- tween language and visuospatial skills in WS.
In order to examine visuospatial functions in the 2 groups of subjects, we administered a battery of probes of visuospatial, visu- oconstructive, and visuoperceptual tasks. Notably, the 2 groups performed equally poorly on a standardized visu- oconstructive measure, the Developmental Test of Motor Integration [Beery and Buktenica, 19671. WS subjects achieved a mean age equivalent score of 4 years, 8 months (s.d. = .5) and DS subjects, a mean age of 5 years, 6 months (s.d. = .7). Although the WS and DS subjects’ scores were not significantly different (t = 2.55, P > .05) on this visuoconstructive test, the WS subjects demonstrated a selective disability on items that required integration of component parts (e.g., a triangle made out of circles). This selective impairment
Copying geometric arrays.
was also apparent on a drawing task adapted from the Boston Diagnostic Aphasia Examination [Goodglass and Kaplan, 19721 on which WS and DS subjects were asked to draw common objects (e.g., bicycle, flower, ele- phant, cube, cross, house). Although drawings produced by both groups were impaired, marked and characteris- tic differences were evident, as exemplified in the draw- ings of a bicycle by age- and IQ-matched DS and WS subjects (Fig. 3, bottom). Note that although the DS subject’s drawing is simplified, i t exhibits better spatial organization, closure, and integration of parts than the WS subject’s drawing. In contrast, the WS drawing com- pletely lacks spatial organization and integration (the “person” underneath the “bike,” the “chain” stretched out below the “wheels”); i t is completely unrecognizable.
Dissociations in spatial cognition. Both groups of mentally retarded subjects were grossly and equally impaired on a range of visuospatial tasks (block design, drawing, copying geometrical shapes, spatial transfor- mations). However, drawing performance suggested that there may be important differences between the WS and DS groups. Thus, we sought means of investi- gating and characterizing possible differential visu- oconstructive impairments. In particular, we were inter- ested in how well each group integrated parts of an object to form a coherent whole. In order to explore this issue, we administered a task using hierarchical stimuli in which a larger (global) form is created by the spatial arrangement of repeated smaller (local) forms. For ex- ample, one stimulus was a large printed letter “A’ formed out of 14 small letter “Ms; another was a trian- gle formed from small circles. An advantage of these

Neuropsychological Profile of Williams Syndrome 119
ws Age 12
ws Age 15
ws Ags 16
Freehand Drawing Of A Bicycle With And Without Verbal Labels Attached
front wheel /
chair wheel
handleban \ seat
brake
s t r i m
\-, h a n d w a r s
crank case
Drawing Of A Bicycle By Williams And Down Children, Matched On Age And IQ.
bs ws
A handlebars
DS A g e : l l A g e : l 1 IQ:50 IQ:52
Fig. 3. Drawings of WS and DS individuals.

120 Bellugi et al.
stimuli over standardized clinical measures is the ex- plicit demarcation between features perceived as parts and wholes. Subjects were presented with these hier- archical stimuli for 5 seconds, then asked to reproduce the figure after a 5-second delay. Normal age-matched subjects accurately produced both the local and the global forms. Relative to normal individuals, both the WS and DS subjects were grossly impaired in this task of 50 items, equally low in overall accuracy (WS mean = 36.5; DS mean = 36.3). Interestingly, however, they were impaired in opposite ways. The WS subjects were significantly more impaired than the DS subjects in accuracy for depicting the global form (WS mean = 6.0; DS mean = 30.8; t = 3.52, P = <.001), whereas the DS subjects were significantly more impaired than the WS subjects in accuracy for depicting the local forms (DS mean := 5.5; WS mean = 30.5; t = 3.69, P < .05). In sum, the DS subjects consistently produced only the global figures (e.g., the large “A”) using a solid line, omitting the local forms completely. In striking contrast, the WS subjects almost invariably produced only the local forms (e.g., the smaller “M”s) with little or no attempt to repre- sent the global figure.
Although both groups of subjects show similar impair- ment in cognitive functioning generally, and both show equal impairment in some spatial cognitive tasks, we have found a marked and differential cleavage between the 2 groups of mentally retarded subjects for spatial constructions of parts vs. construction of wholes. These clusters of spatial cognitive deficits are quite startling and potentially important as evidence for understand- ing the relationship between cognitive components and their representation in the brain [Bihrle et al., 1988, 19891. The findings are particularly intriguing since patients with unilateral right hemisphere lesions, like WS subjects, are generally impaired in local forms, while left-lesioned patients, like DS subjects, show the opposite effect [Delis et al., 1986,19881. Whereas sharp dissociations within spatial cognition are ordinarily en- countered with localized acquired lesions, mental retar- dation has often been considered a nonspecific pervasive disorder resulting in across the board cognitive deficits. However, our studies suggest that WS-even in the ab- sence of obvious space occupying lesions-may result in a highly uneven behavioral profile with specific deficits and preservations in the visuospatial domain.
Preserved visuoperceptual abilities in WS. Many of the tasks presented so far have involved some spatial constructional component. To examine the sub- jects’ visuospatial abilities in the absence of a motor component, we administered a relatively pure spatial measure, the Benton Line Orientation test [Benton et al., 19751 (Fig. 4). In this test, subjects match the angu- lar orientations of 2 simultaneously presented lines to a choice display consisting of 11 lines oriented 18 degrees apart. Both groups of subjects were severely and equiva- lently impaired when compared with mental-age- matched normative individuals. Only 3 of the WS and none of the DS subjects passed the first 5 simple practice items on this test. Five of the WS subjects and all 6 of the DS subjects received a score of zero out of a possible 30. One WS subject received a score of 10, well below the
mean for a normal 7 year-old, the youngest age for which norms are available. Thus, both groups of subjects dem- onstrate striking impairment on this visuospatial task.
Despite a cluster of severe spatial cognitive dysfunc- tions including deficits in drawing, block design, spatial transformations, and spatial memory [Bellugi et al., 1988b1, there are yet some selective preservations of visuospatial abilities in WS. The WS subjects (but not the DS subjects) demonstrated a surprising ability to discriminate unfamiliar faces on the Benton Test of Fa- cial Recognition (Fig. 4). This standardized measure assesses the capacity to discriminate photographs of unfamiliar human faces under different conditions of spatial orientation and lighting [Benton et al., 19831. Subjects select a target face from 6 response-choice pic- tures. All subjects received the short form of this test, and scores were converted to long-form scores. The mean projected long-form score was 43.8 for the WS subjects (s.d. = 4.2) and 28.8 for the DS subjects (s.d. = 4.4). A significant t score of 8.67 (P < .001) was obtained for matched subject pairs. Based on developmental norms with subjects of normal intelligence, WS subjects per- form at the level of normal 13 year-olds, nearly at the level of normal adults. In contrast, the DS subjects dem- onstrated extremely severe deficits on this task, just as they had on the Line Orientation task. The WS subjects characteristically responded easily and correctly on this complex task, which involves recognition and discrimi- nation of faces under conditions of spatial transforma- tion. These findings suggest that preserved performance on a facial discrimination task in the context of gener- ally impaired spatial cognition may be a unique neuro- psychological marker of WS. Figure 4 presents the con- trast between WS subjects’ performance on the 2 tasks, suggesting indeed, that there are peaks and valleys of abilities characteristic of this syndrome.
Neuropsychological studies suggest that WS, unlike DS, appears to result in a highly uneven behavioral profile of specific deficits and preservations within and across domains of language and spatial cognitive func- tioning. Detailed behavioral studies in WS, in concert with neurologic and neuroanatomical results, may in the long run aid in our understanding of the components of cognition and their underlying neural basis. We now turn to differences which emerged in terms of the neuro- logic functions which typify the 2 syndromes.
NEUROLOGICAL PROFILE Using a standard neurologic examination form de-
signed for use with various study populations, each sub- ject underwent a complete examination. Individual items in the exam were combined into related clusters, including gross motor, oromotor, fine motor, cerebellar, language, and mental status. Head circumference was measured on each subject, and the measurement was converted to centile scores for age. Both groups had neurologic deficits as identified by the neurologic exam- ination [Trauner et al., 19891. There was a high inci- dence of left-hand dominance in the WS, but not in the DS group. Head size in the 2 groups was significantly different. Microcephaly was found in all but one of the

Neuropsychological Profile of Williams Syndrome 121
Benton Line Orientation Test 7
2ol 15
I
(0) (01 ( 0 ) ( 0 ) ( 0 )
Age: 10 13 13 15 16 17 Williams Svndrome
Benton Facial Recognition Test
4 5 6
50 4 3 - 4 6 A v e r a g e l o r A d u l t
4 0
30
!? 0 20
10
0 v)
Age: 10 1 3 1 3 15 16 1'7 Williams Svndrome
Fig. 4. Contrast between line orientation and facial discrimination in WS.
DS subjects, whereas all of the WS subjects had normal head size for age (WS subjects mean = 34 + 17%; DS subjects mean = 2.7 + 3.6%, P < .001). Dolichocephaly was uniformly observed in the WS group, whereas the DS subjects had rounded or foreshortened head shapes.
Subjects with WS tended to have generalized hypo- tonia, and evidence of cerebellar dysfunction, with an intention tremor and midline balance problems. They also exhibited difficulty with oromotor skills. DS sub- jects had minimal hypotonia, little evidence of cerebel- lar signs, and performed better on tests of oromotor function. Both groups exhibited problems with gross and fine motor tasks. Hyperactive tendon stretch re- flexes and positive Babinski signs were frequent in the WS population, whereas in DS subjects, the reflexes were most often normal, and Babinski signs were nega- tive. In terms of elemental neurologic functioning then, WS subjects demonstrate specific and characteristic def- icits including generalized hypotonia, intention tremor and midline balance problems, and oral-motor and mo- toric abnormalities suggestive of cerebellar dysfunction, whereas DS subjects demonstrate nonspecific findings of pervasive developmental delay (functioning fairly well for their developmental ages). The implications of neurologic differences between groups are explored in light of the neuropsychological differences which emerged from our extensive program investigating spe- cific components of cognitive functioning.
NEUROANATOMICAL PROFILE FROM MAGNETIC RESONANCE IMAGING
The neurological and neuropsychological profiles of WS clearly raise the possibility of abnormal develop- ment of certain neuroanatomical structures. The avail- ability of a noninvasive brain-imaging technique (Mag- netic Resonance Imaging, MRI) that provides excellent anatomical detail makes it possible to examine the neu- ral systems in subjects with WS and DS. Unlike cruder imaging methods, spatial resolution is superb in MRI, and the potential for three-dimensional reconstruction exists [Jernigan and Hesselink, 19871. Jernigan and Bellugi [19901 have obtained MRI images of the brains, extending from the level of the pons to the vertex, of the 6 WS subjects, a subset of 6 of the DS subjects, and 14 normal controls ranging in age from 8 to 32 years [Bel- lugi et al., 1987a; Jernigan et al., 19891.
Although there now exists a sizeable literature on the neuroanatomical features of DS [Coyle et al., 1986; Scott et al., 19831, there are no comparable studies of WS. Coyle et al. [1986] summarize the major gross mor- phological abnormalities in DS as decreased brain weight, reduced hindbrain cerebrum ratio, hypoplasia of the middle lobe of the cerebellum, and sulcation ab- normalities (shallow primary sulci, fewer secondary sulci). Inspection of WS and DS MRI scans shows that while both groups demonstrate microcephaly, overall

122 Bellugi et al.
shapes of each group are distinct. Whereas the DS brains are most notable for the degree of hypofrontality, the WS subjects appear to have relatively decreased posterior width and elongated posterior to anterior length compared to normal. Moreover, both groups dem- onstrate decreased myelination, and further analyses are underway to estimate degree of myelination in dif- ferent regions by sampling local white and gray matter signal values on balanced and T2-weighted images. Our preliminary results do not provide any evidence of space-occupying lesions in the brain parenchyma of ei- ther group.
The scans were submitted to computer-voluming pro- tocols developed by Dr. Jernigan whereby an operator manually designates the locations of a set of anatomical landmarks, and estimates are computed of regional vol- umes [Jernigan and Hesselink, 19871. These methods of analyses of MRI have led to important findings bearing on the neural substrate of neurodevelopmental disor- ders including developmental dysphasia and autism [Jernigan et al., 1988; Courchesne et al., 19881.
Results of voluming analyses suggest that specific cerebral subsystems develop in anomalous ways in WS and DS and that these anomalies in development are reflected in gross cerebral dysmorphologies. A signifi- cant reduction of the volume of the posterior fossa, as well as the cerebrum, was observed in the DS subjects. This is consistent with the findings of Crome et al. [ 19661, suggesting that in DS, the cerebellum and brain- stem are more dramatically reduced in size than is the cerebrum. In striking contrast, WS subjects showed no suggestion of a reduction in the overall size of the poste- rior fossa structures. This would at first appear surpris- ing since the cerebellum is often described as growing later, and most factors affecting cerebral growth would be expected to affect the later cerebellar growth as well. Relative to matched normal control individuals, both the WS and DS subjects have a reduced cerebral volume, estimated from quantitative analyses of the MRI im- ages. In the DS subjects, the cerebrum is approximately 77% of the equivalent volume in young normal controls; the WS cerebrum is similarly reduced to 80% of normal. Whereas cerebellar volume in DS is reduced to approx- imately 69% of normal, the WS cerebellar volume is 99% of that observed in young normals. Figure 5 shows re- sults of computer-voluming methods contrasting a proc- essed axial image from a typical DS subject, a WS sub- ject, and a matched normal control. Figure 5 compares the cerebral and cerebellar volumes and presents the cerebellum to cerebrum volume ratio for normal con- trols and WS and DS subjects. These findings are partic- ularly relevant to an understanding of the neuro- anatomical basis of WS [Jernigan et al., 19891.
The initial findings led to further examination of the posterior fossa structures of 6 WS and 2 DS subjects by using methods adapted from Courchesne et al. [1988]. In Courchesne et al. studies of autistic subjects, paleo- cerebellar vermal area I-V was comparable in volume to controls; however, neocerebellar vermal area VI-VII was reduced in volume, and in some cases the hypoplasia was pronounced. The present results in WS subjects showed a surprising reversal of the pattern observed in
autism. Vermal I-V area was, like in autism, not signifi- cantly larger than in controls, but the vermal ratio of area I-V to VI-VII showed no overlap between normal individuals and WS subjects. Thus, an anomalous pat- tern occurs, with neocerebellar vermal lobules showing hyperplasia, in the context of low-normal paleocerebel- lar vermal development and significantly reduced fore- brain size. Further studies to address the issues raised by these findings are currently underway [Jernigan and Bellugi, 19901.
DISCUSSION Adolescents with WS differ in their psychological,
neurological, and neuroanatomical profiles from a group of DS subjects matched for age and full-scale I&. At all 3 levels of investigation, the WS subjects demonstrated atypical characteristics, distinct from the mental retar- dation of DS. WS subjects evidenced pronounced peaks and valleys in neuropsychological functioning, whereas the DS subjects produced a flat, even neuropsychological profile. Test results indicate that in WS (unlike in DS) language abilities are preserved, relative to nonlinguis- tic functioning. Clearly, the oral-motor impairments in WS do not appear to impact later language competence. Within the domain of language, neuropsychological findings suggest that aspects of lexical semantic abili- ties may be deviant in WS but delayed in DS. The WS subjects demonstrate relatively preserved syntax and fairly advanced (and unusual) lexical abilities.
Within the spatial cognitive domain as well, neurop- sychological findings suggest unusual dissociations of spared and impaired functioning in WS. Although the DS and WS subjects are equally (and severely) impaired on some probes of spatial processing, the WS subjects alone demonstrate a surprising ability on certain visu- operceptual tasks. While a cleavage between visuospa- tial and visuoperceptual functioning has been identified in rare cases of right posterior cerebral lesions [New- combe et al., 19871, this dissociation is intriguing in the absence of identifiable focal brain damage in WS.
Furthermore, a striking difference emerged between the WS and DS subjects in spatial cognitive functions. The WS subjects’ visuospatial constructions are typified by a selective attention to details of a configuration at the expense of the whole whereas the DS subjects dem- onstrate the opposite pattern. Behaviorally, these re- sults are similar to those found with unilateral right- and left-hemisphere-damaged adults, respectively [Delis and Bihrle, 19891. Importantly, WS subjects, like right-hemisphere-damaged patients, have relatively preserved language abilities, particularly in the domain of grammar, and intact local processing, while the DS subjects, like left-hemisphere-damaged aphasics, dem- onstrate language impairment and a proclivity for global processing. These findings suggest that certain cognitive deficits may cluster in the absence of frank cerebral damage, just as they cluster following insult to one hemisphere. Investigations of such clusters of lin- guistic and spatial cognitive deficits in such clinical populations will ultimately aid in understanding the interrelationships between cognitive domains and their underlying neuroanatomical basis.

Neuropsychological Profile of Williams Syndrome 123
DOWN SYNDROME WILLIAMS SYNDROME NORMAL CONTROL
Cerebral Volume Cerebellar Volume Cerebellum to Cerebrum Ratio
Controls Williams Down Controls Williams Down
0
m ._ c
a
Controls Williams Down
Fig. 5. Computer voluming and analyses of MRIs for WS, DS, and normal controls (Jernigan).
With respect to neurologic and neuroanatomical find- ings, we note that although microcephaly has been de- scribed as a common manifestation of WS, none of the adolescent WS subjects in the present study had reduced cranial sizes as evaluated by neurologic exam. Impor- tantly, however, MRI analysis showed that cerebral vol- ume in WS is reduced compared to normal, and is simi- lar to that observed in DS. Here again, WS is unlike DS, in which both cranial and cerebral size is reduced. WS serves as an indication that microcephaly, although a common manifestation in mental retardation, is by no means a necessary concomitant of behavioral deficiency.
A hallmark neuroanatomical characteristic of WS, the aberrant cerebrum-cerebellum volume ratio, may serve to distinguish this syndrome from other clinical syndromes, such as DS and autism. Further, this mani- festation may in the long run provide clues to the embry- ological course and pathogenesis of WS. Dobbing and Sands [1973] suggest that total adult cell numbers are achieved in the cerebellum at 18 postnatal months, a time when forebrain cell numbers are only approx- imately 60% of adult totals. The patterns observed in WS and DS suggest that while early events affecting cellularity in both cerebral and cerebellar populations
occur in DS, later processes selectively affecting cere- bral cellular populations may be critical in the patho- genesis of WS. Further, this unique feature of WS may relate to both neurologic and neuropsychological char- acteristics of WS. The elongation of the head observed in the WS adolescents is consistent with preservation of posterior fossa structures such as the cerebellum. Al- though cerebellar size is intact, importantly, neurologic findings are suggestive of cerebellar dysfunction; and yet cerebellar signs co-occur without the reduction in cerebellar volume observed in DS.
Though speculative, the anomalous neuroanatomical findings in WS may be relevant to the unusual neuro- behavioral profile that is unique to WS adolescents. Recent evidence suggests a possible role for the human neocerebellar structures in mental and linguistic func- tion [Leiner et al., 1986; Dow, 19881. The unusual pre- servation of specific language functions in WS, in the context of marked retardation in other cognitive domains, may turn out to be related to the observed hyperplasia of specific vermal lobules in the context of cerebral maldevelopment. Clearly, however, the neuro- anatomical anomalies we have described so far are not sufficient to account for the full range of our behavioral

124 Bellugi et al.
findings. We are currently engaged in studies to further demonstrate the neuroanatomical underpinnings of the distinctive neuropsychological profile characterizing w s .
At present, the underlying pathogenesis of WS re- mains unknown; however, we are currently exploring a hypothesis that may relate the association of central nervous system dysfunction and abnormalities of cal- cium metabolism in patients with WS [Bellugi et al., 19891. WS subjects have been shown to be deficient in the synthesis or release of immunoreactive calcitonin [Culler et al., 19851. In companion studies, we are inves- tigating the possibility of a neurobiological marker for WS. These studies examine the hypothesis that there may be an underlying genetic disturbance in WS which results in the abnormal production of calcitonin and of calcitonin gene-related peptide, a recently identified peptide that may play a role in the normal development andlor function of the central nervous system [Bellugi and Culler, 1987; Bellugi et al., 1987al.
In conclusion, WS is unusual from multiple vantage points (neuropsychological, neurological, and neuro- anatomical) and can be readily distinguished from the more common form of mental retardation, DS. Our pro- gram of interdisciplinary studies of WS may ultimately forge links between a specific metabolic disorder, a spe- cific neuropsychological and neurological profile, and abnormal brain organization.
ACKNOWLEDGMENTS This research was supported in part by National Insti-
tutes of Health Grants #NS 22343, #DC 00146, #HD 266022; National Science Foundation grant #BNS- 8820673; and the John D. and Catherine T. MacArthur Foundation Research Network. Dr. Chris Chase of the Center for Neurological Basis of Language performed the I.&. tests. Diane Niles is Parent Liaison for these studies. We thank the National Williams Syndrome As- sociation and Parents of Down Syndrome Children, and we are very grateful to the individuals and their fami- lies who participated in this research.
REFERENCES Arnold R, Yule W (1985): The psychological characteristics of Infantile
Hypercalcemia: A preliminary investigation. Dev Med Child Neu- rol 27:49-59.
Beery KE, Buktenica NA (1967): “Developmental Test of Visual-Motor Integration.” Cleveland: Modern Curriculum Press.
Bellugi U (1971): Some language comprehension tests. In Lavatelli C (ed): “Language Training in Early Childhood.” Urbana, IL: Univer- sity of Illinois Press, pp 157-169.
Bellugi U, Bihrle A, Doherty S, Neville H, Damasio AR (1989): Neural correlates underlying dissociations of higher cortical functioning. Abstract, Symposium for International Neuropsychology Society, Vancouver, Canada.
Bellugi U, Bihrle A, Jernigan T, Swanson L, Culler F (1987a): Neuro- psychological and neurobiological account of a disorder. Abstract, Society for Neurosciences, New Orleans, LA.
Bellugi U, Culler F (1987): Gene coding and behavioral expression in Williams Syndrome children. Colloquium, UCLA Medical Center.
Bellugi U, Klima ES (1966): Syntactic regularities in children’s speech. In Lyons J, Wales R (eds): “Psycholinguistic Papers.” Edinburgh, Scotland: Edinburgh University Press, pp 183-208.
Bellugi U, Marks S, Bihrle A, Sabo H (1988a): Dissociation between language and cognitive functions in Williams Syndrome. In Bishop D, Mogford K (eds): “Language Development in Exceptional Cir- cumstances.” London: Churchill Livingstone, pp 177-189.
Bellugi U, Marks S, Neville H, Jernigan T (198713): Brain organization underlying unusual language and cognitive functions. Abstract, Symposium for Western Psychological Association, Long Beach, CA.
Bellugi U, Sabo H, Vaid J (198813): Spatial deficits in children with Williams Syndrome. In Stiles-Davis J, Kritchevsky M, Bellugi U (eds): “Spatial Cognition: Brain Bases and Development.” Hills- dale, NJ: Erlbaum Press, pp 273-298.
Benton AL, Hamsher K, Varney NR, Spreen 0 (1983): “Test of Facial Recognition, Form SL.” New York: Oxford University Press, Inc.
Benton AL, Hannay J , Varney NR (1975): Visual perception of line direction in patients with unilateral brain disease. Neurology
Bihrle AM, Bellugi U, Delis D, Marks S (1988): Visuospatial dysfunc- tion in Williams Syndrome: Selective impairment of global hier- archical analysis. Abstract, International Neuropsychological Soci- ety, New Orleans, LA.
Bihrle AM, Bellugi U, Delis D, Marks S (1989): Seeing either the forest or the trees: Dissociation in visuospatial processing. Brain Cogn, 11:37-49.
25:907-910.
Burn J (1986): Williams Syndrome. J Med Genet 23:389-395. Courchesne E, Yeung-Courchesne R, Press GA, Hesselink JR, Jernigan
TL (1988): Hypoplasia of cerebellar vermal lobules VI and VII in Autism. N Engl J Med 318(21):1349-1354.
Coyle JT, Oster-Granite ML, Gearhart J D (1986): The neurobiologic consequences of Down Syndrome. Brain Res Bull 16:773-787.
Crome L, Cowie V, Slater E (1966): A statistical note on cerebellar and brainstem weight in Mongolism. J Ment Defic Res 10:69-72.
Culler FL, Jones KL, Deftos U (1985): Impaired calcitonin secretion in patients with Williams Syndrome. J Pediatr 107:720-723.
Delis DC, Bihrle AM (1989): Fractionation of spatial cognition follow- ing focal and diffuse brain damage. In Ardila A, Ostrosky F (eds): “Brain Organization of Language and Cognitive Processes: New Directions of Research.” New York: Plenum 2;17-35.
Delis DC, Kiefner MG, Fridlund AJ (1988): Visuospatial dysfunction following unilateral brain damage: Dissociations in hierarchical and hemispatial analysis. J Clin Exp Neuropsychol 10:421-431.
Delis DC, Robertson LC, Efron R (1986): Hemispheric specialization of memory for visual hierarchical stimuli. Neuropsychologia
Dobbing J , Sands J (1973): Quantitative growth and development of human brain. Arch Dis Child 48:757-767.
Dow RS (1988): Contribution of electrophysiological studies to cerebel- lar physiology. J Clin Neurophysiol 5307-323.
Fowler AE (1989): Language abilities in children with Down Syn- drome. In Cicchetti D, Beeghly M (eds): “Children with Down Syn- drome: The Developmental Perspective.” New York: Cambridge University Press pp 302-328.
Gleitman LR (1983): Biological dispositions to learn language. In De- mopoulos w, Marras A (eds): “Language Learning and Concept Acquisition.” Norwood, NJ: Ablex.
Goodglass H, Kaplan E (1972): “Assessment of Aphasia and Related Disorders.” Philadelphia: Lea and Febiger.
Jernigan T, Bellugi U (1990): Anomalous brain morphology on mag- netic resonance images in Williams Syndrome and Down Syn- drome. Arch Neurol, 47529-533.
Jernigan T, Bellugi U, Hesselink J (1989): Structural differences on magnetic resonance imaging between Williams and Down Syn- drome. Abstract, 41st Annual Meeting, American Academy of Neu- rology, Chicago, IL.
Jernigan T, Hesselink J (1987): Human brain-imaging: Basic princi- ples and applications in psychiatry. In Michels R, Cavenar JO (eds): “Psychiatry: Psychobiological foundations of Clinical Psychiatry.” Philadelphia: J.B. Lippincott Co., pp 3:l-9.
Jernigan T, Tallal P, Bellugi U (1988): Cerebral morphology of mag- netic resonance imaging (MRI) in developmental cognitive disor- ders. Abstract, SOC Neurosci, New Orleans, LA.
24:205-214.

Neuropsychological Profile of Williams Syndrome 125
Jones KL, Smith DW (1975): The Williams Elfin Facies Syndrome: A new perspective. J Pediatr 86:718-723.
Kataria S, Goldstein DJ, Kushnick T (1984): Developmental delays in Williams (“Elfin Facies”) Syndrome. Appl Res Ment Retard 5:419-423.
Leiner HC, Leiner AL, Dow R (1986): Does the cerebellum contribute to mental skills? Behav Neurosci 100:443-454.
MacDonald GW, Roy DL (1988): Williams Syndrome: A neurological profile. J Clin Exp Neuropsychol 10:125-131.
Meyerson MD, Frank RA (1987): Language, speech and hearing in Williams Syndrome: Intervention approaches and research needs. Dev Med Child Neurol 29258-270.
Miller JF (1987): Language communication characteristics of children with Down Syndrome. In Pueschel SM, Tingley C, Rynders JE, Crocker AC, Crutcher DM (eds): “New Perspectives on Down Syn- drome.” Baltimore: Brookes, pp 233-262.
Morris C, Demsey S, Leonard C, Dilts C, Blackburn B (1988): Natural history of Williams Syndrome: Physical characteristics. J Pediatr
Newcombe F, Ratcliff G, Damasio H (1987): Dissociable impairments of visual and spatial processing following right posterior cerebral le- sions. Neuropsychologia 25:149-161.
Pagon R, Bennett F, LaVeck B, Stewart K, Johnson J (1987): Williams Syndrome: Features in late childhood and adolescence. Pediatrics
113:318-363.
80:85-91.
Preus M (1984): The Williams Syndrome: Objective definition and
Reilly JS (1983): What are conditionals for? Papers Rep Child Lan Dev
Rondal J (1978): Developmental sentence procedure and the delay- difference question in language development of Down’s Syndrome children. Ment Retard 16:169-171.
Rondal J (1980): Language delay and language difference in moder- ately and severely mentally retarded children. Spec Ed Can
Scott BS, Petit TL, Becker LE, Edwards BAV (1983): Abnormal electric membrane properties of Down’s syndrome dorsal root ganglion neu- rons in cell culture. Dev Brain Res 2:257-270.
Semel E, Wiig EH, Secord W (1980): “CELF-R Clinical Evaluation of Language Fundamentals-Revised.’’ San Antonio: The Psychologi- cal Corporation.
Trauner D, Bellugi U, Chase C (1989): Neurologic features of Williams and Down Syndrome. Pediatr Neurol 5(3):166-168.
Udwin 0, Yule W, Martin N (1986): Age at diagnosis and abilities in idiopathic hypercalcaemia. Arch Dis Child 61:1164-1167.
Udwin 0, Yule W, Martin N (1987): Cognitive abilities and behavioral characteristics of children with idiopathic infantile hyper- calcaemia. J Child Psycho1 Psychiatry 28:297-309.
Williams JCP, Barrett-Boyes BG, Lowe JB (1961); Supravalvular aor- tic stenosis. Circulation 24:1311-1318.
diagnosis. J Clin Genet 25:422-428.
22:l-8.
54:27-32.




















