
Neurocognitive and symptom correlates of daily problem-solving skills in schizophrenia
9
Neurocognitive and symptom correlates of daily problem-solving skills in schizophrenia Nadine Revheim a, * , Isaac Schechter a , Dongsoo Kim a , Gail Silipo a , Baerbel Allingham c , Pamela Butler a,b , Daniel C. Javitt a,b a Program in Cognitive Neuroscience and Schizophrenia, Nathan S. Kline Institute for Psychiatric Research, 140 Old Orangeburg Road, Orangeburg, NY 10962, USA b Department of Psychiatry, New York University School of Medicine, 550 First Avenue, New York, NY 10016, USA c Information Science Division, Nathan S. Kline Institute for Psychiatric Research, 140 Old Orangeburg Road, Orangeburg, NY 10962, USA Received 10 June 2005; received in revised form 2 December 2005; accepted 17 December 2005 Available online 27 January 2006 Abstract Functional outcome for individuals with schizophrenia has been associated with cognitive impairment. Deficits in attention, memory, speed of information processing and problem-solving skills affect independent functioning, vocational performance, and interpersonal functioning. This study investigated the relationship between neurocognitive functioning, clinical symptoms and daily problem-solving skills in seriously and persistently ill persons. Thirty-eight inpatients and outpatients were administered a neurocognitive battery for attention, working memory, processing speed, perceptual organization, and executive functioning; and semi-structured clinical interviews using the BPRS and SANS. Estimates of daily problem-solving skills were obtained using the relevant factor subscale from the Independent Living Scales (ILS-PB). Daily problem-solving skills were significantly correlated with negative symptoms, processing speed, verbal memory, and working memory scores. A regression model using an enter method suggests that working memory and negative symptoms are significant predictors of daily problem- solving skills and account for 73.2% of the variance. Further analyses demonstrate that daily problem-solving skills and negative symptoms were significantly different for inpatients and outpatients and significantly correlated with community status. The findings suggest the ILS-PB has utility as a proxy measure for assessing real-world functioning in schizophrenia. D 2006 Elsevier B.V. All rights reserved. Keywords: Schizophrenia; Neurocognitive functioning; Negative symptoms; Community functioning; Daily problem-solving skills; Independent living scales 1. Introduction Researchers have focused on the relationships between neurocognitive deficits and functional out- come (Evans et al., 2003; Dickinson and Coursey, 0920-9964/$ - see front matter D 2006 Elsevier B.V. All rights reserved. doi:10.1016/j.schres.2005.12.849 * Corresponding author. Tel.: +1 845 398 6543; fax: +1 845 398 6545. E-mail address: [email protected] (N. Revheim). Schizophrenia Research 83 (2006) 237 – 245 www.elsevier.com/locate/schres
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Neurocognitive and symptom correlates of daily problem-solving skills in schizophrenia

www.elsevier.com/locate/schres
Schizophrenia Research
Neurocognitive and symptom correlates of daily problem-solving
skills in schizophrenia
Nadine Revheim a,*, Isaac Schechter a, Dongsoo Kim a, Gail Silipo a,
Baerbel Allingham c, Pamela Butler a,b, Daniel C. Javitt a,b
a Program in Cognitive Neuroscience and Schizophrenia, Nathan S. Kline Institute for Psychiatric Research, 140 Old Orangeburg Road,
Orangeburg, NY 10962, USAb Department of Psychiatry, New York University School of Medicine, 550 First Avenue, New York, NY 10016, USA
c Information Science Division, Nathan S. Kline Institute for Psychiatric Research, 140 Old Orangeburg Road, Orangeburg, NY 10962, USA
Received 10 June 2005; received in revised form 2 December 2005; accepted 17 December 2005
Available online 27 January 2006
Abstract
Functional outcome for individuals with schizophrenia has been associated with cognitive impairment. Deficits in attention,
memory, speed of information processing and problem-solving skills affect independent functioning, vocational performance,
and interpersonal functioning. This study investigated the relationship between neurocognitive functioning, clinical symptoms
and daily problem-solving skills in seriously and persistently ill persons. Thirty-eight inpatients and outpatients were
administered a neurocognitive battery for attention, working memory, processing speed, perceptual organization, and executive
functioning; and semi-structured clinical interviews using the BPRS and SANS. Estimates of daily problem-solving skills were
obtained using the relevant factor subscale from the Independent Living Scales (ILS-PB). Daily problem-solving skills were
significantly correlated with negative symptoms, processing speed, verbal memory, and working memory scores. A regression
model using an enter method suggests that working memory and negative symptoms are significant predictors of daily problem-
solving skills and account for 73.2% of the variance. Further analyses demonstrate that daily problem-solving skills and
negative symptoms were significantly different for inpatients and outpatients and significantly correlated with community
status. The findings suggest the ILS-PB has utility as a proxy measure for assessing real-world functioning in schizophrenia.
D 2006 Elsevier B.V. All rights reserved.
Keywords: Schizophrenia; Neurocognitive functioning; Negative symptoms; Community functioning; Daily problem-solving skills;
Independent living scales
0920-9964/$ - see front matter D 2006 Elsevier B.V. All rights reserved.
doi:10.1016/j.schres.2005.12.849
* Corresponding author. Tel.: +1 845 398 6543; fax: +1 845 398
6545.
E-mail address: [email protected] (N. Revheim).
1. Introduction
Researchers have focused on the relationships
between neurocognitive deficits and functional out-
come (Evans et al., 2003; Dickinson and Coursey,
83 (2006) 237–245

N. Revheim et al. / Schizophrenia Research 83 (2006) 237–245238
2002; Green, 1996; Green et al., 2000; Twamley et al.,
2002); neurocognitive deficits and clinical symptom-
atology (Berman et al., 1997; Harvey et al., 1997;
O’Leary et al., 2000; Suslow et al., 1998); and the
interrelationships of neurocognition, positive and
negative symptoms, and aspects of functioning in
daily life (McGurk et al., 2000; Tamminga et al.,
1998; Velligan et al., 1997). This quest for the relative
contribution of cognitive impairment and symptoms
to adaptive functioning for individuals with schizo-
phrenia has led to the understanding that both
cognitive impairment and negative symptoms are
independent, but together are largely responsible for
deficient performance in activities of daily living from
basic self care to social interaction, instrumental life
skills and community outcome. An emerging research
consensus suggests the importance of specific cogni-
tive impairment in processing speed, working mem-
ory, executive functioning and verbal memory
(Dickinson and Coursey, 2002; Gold et al., 2002;
Green, 1996; Green et al., 2000).
Most studies have been directed towards particular
populations (e.g. long-term; geriatric; community-
dwelling) and have used diverse measures to assess
levels of adaptation that are either global impressions
with descriptive anchors (Dickinson and Coursey,
2002) or performance-based instruments that rely on
role-playing (Twamley et al., 2002). The lack of
uniform measures for functional outcome for all
settings and paucity of empirical data about the
relative utility of the functional measures compared
to the standardized evaluations available for clinical
ratings and neurocognitive assessment is noteworthy.
We have previously evaluated the psychometric
properties of one potential functional outcome scale
that may fill this gap, the Independent Living Scales
(ILS, Loeb, 1996) problem-solving factor (ILS-PB),
for use with individuals with schizophrenia. The
present study evaluates the symptomatic and neuro-
psychological correlates of ILS-PB performance in a
mixed group of psychiatric inpatients and outpatients
to further establish its discriminant validity with this
clinical population.
The ILS was initially developed as a scale
evaluating capacity for independent living in elderly
patients with cognitive disabilities, such as Alzheim-
er’s disease. Early studies demonstrated the ILS-PB
was significantly associated with the ILS total score
and was found to have the ability to predict
community status (Loeb, 1996). The ILS-PB has an
alpha coefficient of 0.86 and test–retest reliability of
0.90. Inter-rater reliability is 0.98. As reported in the
test manual, concurrent validity, as well as construct
and discriminant validity are adequate and suggest the
instrument is effective for evaluating levels of
independent community functioning in psychiatric
patients.
In prior studies in schizophrenia, the ILS-PB
showed significant capacity to distinguish patients
who are in different levels of care. In one study the
ILS-PB was shown to be more significant than verbal
memory in predicting inpatient vs. outpatient status
(Revheim and Medalia, 2004a). An additional study
found the ILS-PB to have better discrimination for
outpatient residential status than GAF ratings
(Revheim and Medalia, 2004b). Both studies estab-
lished the potential to use the ILS-PB to link cognition
and functional outcome but further study was pro-
posed to include additional measures.
A particular advantage of the ILS-PB is that it
takes only 20–25 min to administer and patients find it
largely non-aversive. Examples of questions are
bWhat might you do if your lights and TV went off
at the same time?Q and bTell me two ways you would
know it’s safe to cross a busy streetQ. Items are rated
on a 0 to 2 point scale according to the scoring
manual. These user-friendly capabilities suggest that
ILS-PB may be an addition to the armamentarium of
both clinicians and researchers working with seriously
and persistently mentally ill individuals as previously
advocated (see Revheim and Medalia, 2004b for
further discussion).
Despite the apparent clinical utility of ILS-PB, the
symptomatic and neuropsychological correlates of
problem-solving disability have not been fully eval-
uated in seriously mentally ill individuals. This study
investigated the validity of the ILS-PB, as a measure
of everyday problem solving, for defining functional
differences across diverse patient groups. In addition,
the present study evaluates ILS-PB performance
relative to structured clinical interview scales includ-
ing the Brief Psychiatric Rating Scale (BPRS),
Schedule for Assessment of Negative Symptoms
(SANS) and neuropsychological measures sensitive
to executive functioning, working memory and
sensory processing deficits.

N. Revheim et al. / Schizophrenia Research 83 (2006) 237–245 239
2. Methods
2.1. Participants
Thirty-eight participants (n =28 [74%] male, n =10
[26%] female) ranged in age from 19 to 55
(mean=39.2); with DSM-IV diagnoses of schizophre-
nia (n =29, 76%) and schizoaffective disorder (n =9,
24%); and long-term illness (mean illness dura-
tion=19 years; mean age, first hospitalization=20).
Participants were of varied ethnicity: 34% white
(n =13), 53% black (n =20), 13% Hispanic/Asian/
Other (n =5). Highest educational attainment for the
sample was 11.5 years. Current IQ estimate using the
Quick Test (Ammons and Ammons, 1962) was 96.4.
Individuals were recruited from an inpatient research
unit (n =24, 63%) and a variety of transitional and
residential community settings (n =14, 37%). All
participants were stabilized on medications with a
mean chlorpromazine dose of 1151 mg (S.D.=
515.2 mg.). Seventy-one percent of the participants
were on atypical neuroleptics, 21% were on a
combination of atypical and typical neuroleptics and
8% were on typical neuroleptics.
There were no significant differences between
inpatients and outpatients on demographic variables
(see Table 1). However, inpatients and outpatients
were distinctly different in terms of number of
hospitalizations and days in hospital for the 3 years
prior to testing: inpatients had a mean of 1.6
hospitalizations compared to 0.4 hospitalizations for
outpatients (t=3.7, p =0.001) and inpatients had an
average of 260.5 days of hospitalization compared to
89.8 for outpatients (t=2.1, p =0.04). At the time of
Table 1
Demographic characteristics of sample
Inpatients
Sample size 24 (63%)
Gender
Female 6 (25%)
Male 18 (75%)
Age (MFS.D.) 38.5F10.2
Age, 1st hospitalization (MFS.D., n =36) 19.4F6.5
Illness duration (MFS.D., n =35) 18.1F8.6
Symptom severity (BPRS, MFS.D.) 34.0F8.5
CPZE (MFS.D.) 1206.8F536
Education (MFS.D.) 10.9F2.3
IQ estimate (MFS.D., n =36) 93.3F11.3
testing, inpatients had been hospitalized for an
average of 344 days.
2.2. Procedures
All patients signed informed consent as part of
their enrollment in an ongoing study. Participants’
diagnoses were established using SCID interviews
administered by certified members of the research
team who received supervision and standardized
training with the DSM-IV modules. Patients were
excluded from study procedures if they had a history
of neurological impairment, mental retardation, cur-
rent alcohol or drug abuse within the previous month
or substance dependence within the past 6 months.
2.3. Measures
A comprehensive neurocognitive battery com-
prised of routine procedures to evaluate fine motor
(Grooved Pegboard), sensory processing (Tone
Matching Test), visual memory (Brief Visual Memory
Test, BVMT), semantic fluency (Categorical Verbal
Fluency-animals/fruits/vegetables), attention (Contin-
uous Performance Test-Identical Pairs, CPT-IP), ex-
ecutive functioning (WCST), verbal memory (WMS-
III Logical Memory), visual perception (WAIS-III
Perceptual Organization Index, POI: Block Design,
Picture Arrangement, Picture Completion, Matrix
Reasoning subtests; Wechsler, 1997a), processing
speed (WAIS-III Processing Speed Index, PSI: Sym-
bol Search and Digit Symbol-Coding subtests), and
working memory (WMS-III Working Memory Index,
WMI: Letter Number Sequencing, Spatial Span
Outpatients Total sample
14 (37%) 38 (100%)
4 (29%) 10 (26%)
10 (71%) 28 (74%)
40.4F9.8 39.2F9.9
20.8F2.9 19.9F5.4
19.4F8.8 18.6F8.6
35.8F9.3 34.7F8.7
.4 1056.0F480.4 1151.2F515.2
12.4F2.4 11.5F2.4
101.1F9.0 96.4F11.0

N. Revheim et al. / Schizophrenia Research 83 (2006) 237–245240
subtests; Wechsler, 1997b) was administered to each
participant.
Neurocognitive measures were operationalized
using selected scores for the various dependent
measures. For Grooved Pegboard, the sum of pins
placed with the dominant hand on trials 1 and 2 was
used. For Tone Matching Test, the minimum threshold
value to discriminate two tones was used. For the
BVMT, the raw score for the sum of all trials 1–3 was
used. For Categorical Verbal Fluency, the sum of all
items across all trials was used. For CPT-IP, the
percentage of total hits across 2, 3 and 4 digits was
used. For WCST, two scores were used: the number of
categories achieved and the number of perseverative
errors. For Logical Memory, the scaled score for total
immediate recall for two stories was used. For the
POI, PSI, and WMI, the scaled scores were used.
General psychopathology and positive symptoms
were assessed using the Brief Psychiatric Rating Scale
(BPRS) (Overall and Gorham, 1962). Negative
symptoms were assessed using the Schedule of
Negative Symptoms Scale (SANS) (Andreasen,
1981). BRPS and SANS ratings were acquired by
clinicians who were trained using standardized pro-
cedures with videotapes and consensus ratings that
met pre-established inter-rater reliability criteria rela-
tive to bgold standardQ ratings (F1 point).
The problem-solving factor subscale of the ILS,
consisting of 33 items related to money, home
management, health and safety issues and social
adjustment, was administered to measure reasoning
for daily problem-solving skills. Standardized scores
range from 20 to 60: 20–39 suggests the need for full
supervision for daily living (i.e., inpatient hospitali-
zation or nursing home setting); 40–49 suggests
moderate supervision is required for daily living
(i.e., structured community residence, adult home);
and 50 and above suggests the ability to function
independently in the community.
2.4. Data analyses
Data were examined for normal distributions using
plots and information about skewness. Four of the
twenty variables did not conform to the assumption of
normality (BPRS Positive Symptoms Factor, Tone
Matching Test, WAIS-III POI and WAIS-III PSI);
therefore nonparametric statistics were used accord-
ingly. Data were analyzed using Pearson Product
Moment and Spearman Rho correlations and multiple
regression in order to determine the relationships
among the variables. Variables that were entered into
the regression equation that did not have a normal
distribution were computed using a log transformation
for normalization of the data set. ANOVA and Mann–
Whitney U-tests were used to determine between
group differences related to community status (inpa-
tient vs. outpatients) for clinical symptoms, neuro-
cognitive measures and ILS-PB.
3. Results
3.1. Relationship between clinical symptoms and ILS-PB
Clinical symptoms that were significantly correlated with
the ILS-PB, after Bonferroni corrections, include the BPRS
withdrawal-retardation factor, SANS total score, and SANS
Affective Flattening and Alogia Global items (see Table 2).
Correlations with SANS remained significant whether or not
globals were included. When SANS sub-factors were
considered separately, significant correlations were observed
with Affective Flattening, Alogia, and Avolition, but not
with Asociality-Anhedonia global scores after Bonferroni
correction.
3.2. Relationship between neurocognitive measures and
ILS-PB
Neurocognitive measures that were significantly corre-
lated with the ILS-PB, after Bonferroni corrections, include
Tone Matching Test, CPT-IP, WMS-III Logical Memory,
WAIS-III Processing Speed Index (PSI) and WMS-III
Working Memory Index (WMI) (see Table 3). Other
neurocognitive measures including Grooved Pegboard,
Brief Visual Memory Test, Categorical Verbal Fluency,
WAIS-III Perceptual Organization Index (POI), and WCST
were not significant after Bonferroni correction. Fewer
participants completed the Categorical Verbal Fluency test
and Grooved Pegboard (n =11, respectively) than other tests
due to a minor adjustment in the overall battery during data
collection.
3.3. Multiple regression for ILS-PB
In order to determine which variables were most related
to daily problem-solving skills, the ILS-PB scores were
regressed on the five significant neurocognitive and clinical
symptoms variables after Bonferroni correction to p b0.005

Table 2
Relationship of ILS-PB with clinical symptomsa
Mean S.D. Correlation coefficient ( p value)b
ILS-PB (scaled score) 35.0 11.5 –
BPRS total score 34.7 8.7 �0.29 (0.08)
BPRS withdrawal-retardation factor 6.8 3.0 �0.49 (0.002)
BPRS positive symptoms factorc 8.5 4.4 �0.11 (0.5)
SANS total, with global scores 34.5 15.2 �0.58 (b0.001)
SANS affective flattening global item 1.6 1.2 �0.52 (0.001)
SANS Alogia global item 1.3 1.1 �0.45 (0.005)
SANS Avolition global item 2.3 1.1 �0.39 (0.016)
SANS Asociality-Anhedonia global item 2.2 0.86 �0.33 (0.04)
a n =38, Pearson Product Moment Correlation, unless otherwise noted.b Bonferroni correction for 0.05 level for 2 measures is 0.025.c Spearman Rho correlation.
N. Revheim et al. / Schizophrenia Research 83 (2006) 237–245 241
for 10 comparisons. They were the BPRS withdrawal-
retardation factor, SANS total score with globals (SANS-
TG), WMS-III Logical Memory, WAIS-III Processing
Speed Index (PSI) and WMS-III Working Memory Index
(WMI). WAIS-III PSI required a log transformation for
normalization of data for this analysis. Regression was
performed using an enter method for multiple regression. In
order to avoid redundancy, SANS was entered only once, as
total score with globals.
The model explained 73.2% of the variance in the ILS-
PB scores ( F[5,30] =13.7, p b0.001) when all the
variables were taken into account. The two significant
predictor variables in the model were SANS-TG
(t =�3.38, p =0.002) and WMS-III WMI (t =3.33,
Table 3
Relationships of ILS-PB and neurocognitive measuresa
M
Grooved Pegboard (sum, dominant hand, trials 1, 2)c 2
Tone Matching Test (percent threshold difference)d 2
Brief Visual Memory Test (raw score, sum, trials 1–3) 1
Categorical Verbal Fluency (sum, all trials)c 3
CPT-IP (percentage of total hits across 2, 3, 4 digits)e
WCST-Categories (number of categories achieved)
WCST-Perseverations (number of perseverative errors) 1
WMS Logical Memory, Recall Total Score (scaled score)f
WAIS-III Perceptual Organization Index (POI, scaled score)d 8
WAIS-III Processing Speed Index (PSI, scaled score)d 7
WMS-III Working Memory Index (WMI, scaled score) 6
a n =38, Pearson Product Moment correlations, unless otherwise noted.b Significance level adjusted to 0.01 for multiple, related cognitive testsc n =11.d Spearman Rho correlation.e n =29.f n =31.
p =0.003). WMI and SANS-TG showed limited intercor-
relation (r =�0.08, p =0.62), suggesting relative indepen-
dence of contributions.
3.4. Community status differences in neurocognitive, clinical
and daily problem-solving skills
In order to determine what variables were different
according to community status (inpatients vs. outpatients),
ANOVA and Mann–Whitney U-tests were performed across
all clinical and neurocognitive variables, including ILS-PB.
Bivariate correlations of all measures were also obtained to
further illustrate the relationship of each variable with
community status (see Table 4).
ean S.D. Correlation coefficient ( p value)b
3.5 8.0 0.65 (0.03)
7.2 28.5 �0.44 (0.006)
3.0 7.9 0.13 (0.45)
1.0 8.6 0.69 (0.02)
0.47 0.28 0.50 (0.007)
1.7 1.5 0.28 (0.09)
2.4 6.5 �0.36 (0.03)
4.4 2.5 0.56 (0.001)
0.5 13.5 0.35 (0.03)
7.9 12.3 0.65 (b0.001)
7.5 12.7 0.60 (b0.001)
.
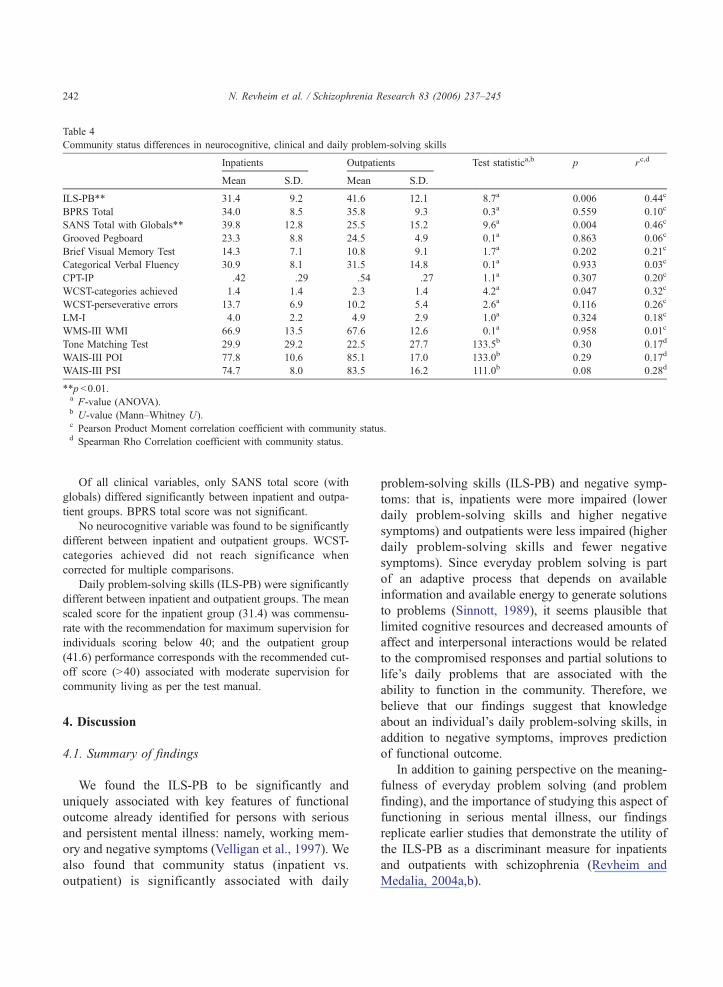
Table 4
Community status differences in neurocognitive, clinical and daily problem-solving skills
Inpatients Outpatients Test statistica,b p rc,d
Mean S.D. Mean S.D.
ILS-PB** 31.4 9.2 41.6 12.1 8.7a 0.006 0.44c
BPRS Total 34.0 8.5 35.8 9.3 0.3a 0.559 0.10c
SANS Total with Globals** 39.8 12.8 25.5 15.2 9.6a 0.004 �0.46cGrooved Pegboard 23.3 8.8 24.5 4.9 0.1a 0.863 0.06c
Brief Visual Memory Test 14.3 7.1 10.8 9.1 1.7a 0.202 �0.21cCategorical Verbal Fluency 30.9 8.1 31.5 14.8 0.1a 0.933 0.03c
CPT-IP .42 .29 .54 .27 1.1a 0.307 0.20c
WCST-categories achieved 1.4 1.4 2.3 1.4 4.2a 0.047 0.32c
WCST-perseverative errors 13.7 6.9 10.2 5.4 2.6a 0.116 �0.26cLM-I 4.0 2.2 4.9 2.9 1.0a 0.324 0.18c
WMS-III WMI 66.9 13.5 67.6 12.6 0.1a 0.958 0.01c
Tone Matching Test 29.9 29.2 22.5 27.7 133.5b 0.30 �0.17dWAIS-III POI 77.8 10.6 85.1 17.0 133.0b 0.29 0.17d
WAIS-III PSI 74.7 8.0 83.5 16.2 111.0b 0.08 0.28d
**p b0.01.a F-value (ANOVA).b U-value (Mann–Whitney U).c Pearson Product Moment correlation coefficient with community status.d Spearman Rho Correlation coefficient with community status.
N. Revheim et al. / Schizophrenia Research 83 (2006) 237–245242
Of all clinical variables, only SANS total score (with
globals) differed significantly between inpatient and outpa-
tient groups. BPRS total score was not significant.
No neurocognitive variable was found to be significantly
different between inpatient and outpatient groups. WCST-
categories achieved did not reach significance when
corrected for multiple comparisons.
Daily problem-solving skills (ILS-PB) were significantly
different between inpatient and outpatient groups. The mean
scaled score for the inpatient group (31.4) was commensu-
rate with the recommendation for maximum supervision for
individuals scoring below 40; and the outpatient group
(41.6) performance corresponds with the recommended cut-
off score (N40) associated with moderate supervision for
community living as per the test manual.
4. Discussion
4.1. Summary of findings
We found the ILS-PB to be significantly and
uniquely associated with key features of functional
outcome already identified for persons with serious
and persistent mental illness: namely, working mem-
ory and negative symptoms (Velligan et al., 1997). We
also found that community status (inpatient vs.
outpatient) is significantly associated with daily
problem-solving skills (ILS-PB) and negative symp-
toms: that is, inpatients were more impaired (lower
daily problem-solving skills and higher negative
symptoms) and outpatients were less impaired (higher
daily problem-solving skills and fewer negative
symptoms). Since everyday problem solving is part
of an adaptive process that depends on available
information and available energy to generate solutions
to problems (Sinnott, 1989), it seems plausible that
limited cognitive resources and decreased amounts of
affect and interpersonal interactions would be related
to the compromised responses and partial solutions to
life’s daily problems that are associated with the
ability to function in the community. Therefore, we
believe that our findings suggest that knowledge
about an individual’s daily problem-solving skills, in
addition to negative symptoms, improves prediction
of functional outcome.
In addition to gaining perspective on the meaning-
fulness of everyday problem solving (and problem
finding), and the importance of studying this aspect of
functioning in serious mental illness, our findings
replicate earlier studies that demonstrate the utility of
the ILS-PB as a discriminant measure for inpatients
and outpatients with schizophrenia (Revheim and
Medalia, 2004a,b).

N. Revheim et al. / Schizophrenia Research 83 (2006) 237–245 243
4.2. Cognition and daily problem-solving skills
Our findings relating the ILS-PB with verbal
memory, working memory and processing speed are
consistent with previous reports of neurocognitive
aspects of functional outcome (Green, 1996; Green
et al., 2000). The significant relationship of the
ILS-PB with an auditory discrimination task (i.e.,
Tone Matching Test) is also consistent with
previous findings in our laboratory. That is, we
have found significant correlations of daily prob-
lem-solving capacity with performance on sensory
processing tasks in the visual and auditory domain
(Butler et al., 2005; Leitman et al., 2005). Stevens
et al. (1998, 2000) also observed differential tone
matching performance between low and high
functioning patients with schizophrenia, suggesting
that tone matching may serve to assess degree of
functional impairment. Given the limited formal
overlap between tone matching and problem-solving
ability, it is unlikely that tone-matching deficits
contribute directly to poor ILS-PB performance.
More likely, both tests index a poor outcome for
the disorder marked by global neurocognitive
dysfunctions. This may be true as well for the
significant relationship we found between the ILS-
PB and our measure of attention (CPT-IP), a well-
known and validated neurocognitive predictor of
schizophrenia in high-risk studies (Cornblatt et al.,
1992).
We did not find the ILS-PB to be related to fine
motor (Grooved Pegboard), or visual memory
(BVMT) processing, which appears consistent with
the differing realms of cognitive processing mea-
sured. On the other hand, we were surprised to
find the ILS-PB was not highly correlated with
WCST, a visual problem-solving measure that has
been related to functional outcome (Lysaker et al.,
1995) and highly associated with working memory
(Gold et al., 1997; Hartman et al., 2003). However,
given the limited variability of our sample for
categories achieved, it cannot be determined
whether the two problem-solving measures are
not related or whether the relationship was con-
strained by the performance of this sample. This is
true of the trend, but lack of significance for
distinguishing WCST performance between inpa-
tients and outpatients.
4.3. Clinical symptoms and daily problem-solving
skills
We did not find the ILS-PB to be related to positive
symptoms. This is consistent with previous studies
that have also not observed a significant relationship
of positive symptoms and either functional outcomes
or neuropsychological performance (Tamminga et al.,
1998). The lack of correlation with positive symptoms
is in contradistinction to the significant correlation
between ILS-PB and negative symptoms ( p b0.001).
4.4. Implications for rehabilitation approaches and
assessment
Despite the current emphasis on psychiatric reha-
bilitation, many patients with schizophrenia remain
unable to reintegrate into the community even with
adequate control of most psychiatric symptoms.
Currently, primary rehabilitation efforts are aimed at
social skills training (Bellack et al., 2004) and various
approaches that target cognitive deficits (Twamley et
al., 2003). However, our findings may suggest that
remediation of problem-solving skills may also be
critical. For example, it may be inadequate to teach
daily living skills, such as phoning for assistance or
how to administer first aid and other performance-
based skills, without teaching the rationale and
reasoning that actually prompts the awareness of the
problem and solution generation.
It remains to be determined whether problem
solving can be remediated directly or can only be
compensated for. In one recent study (Medalia et al.,
2001), problem-solving training techniques using
educational software aimed to improve concept
formation, reasoning, sequencing, self-monitoring,
working memory, and cognitive flexibility were used
to treat problem-solving deficits in individuals with
schizophrenia. The intervention was found to be
effective in improving problem-solving skills required
for independent living. This remediation result,
however, remains to be replicated.
In contrast, another current study employed error-
less learning techniques to improve social problem-
solving deficits (Kern et al., 2005). The researchers
found their skills training intervention, which
bypassed problem-identification deficits that occur in
schizophrenia, to be successful. This strategy assumes

N. Revheim et al. / Schizophrenia Research 83 (2006) 237–245244
that deficient problem-solving skills cannot be reme-
diated and must be overcome with compensatory
techniques.
Nevertheless, whatever core remediation strategy is
used, present findings suggest that improvement in
problem-solving ability as assessed by the ILS-PB
would be expected to lead to improved functional
outcome. The ILS-PB, therefore, may be an appro-
priate instrument for assessing upward generalization
of core cognitive remediation strategies.
By itself, the ILS-PB may be a useful alternative
method for describing an individual’s level of
neurocognitive functioning. In addition to its prag-
matism and good face validity with persons with
serious mental illness, its predictive value of
community status (inpatient vs. outpatient) compared
to other neurocognitive measures is promising. An
evaluation tool, such as the ILS-PB, can be
construed as a means of detecting strengths, as well
as deficits, and is user-friendly with clients who are
continually focused on their clinical pathology and
impaired thinking during standardized interviews and
neuropsychological testing.
In settings that do not require full symptomatic or
neuropsychological evaluations, ILS-PB may indeed
serve as a useful alternative measure for functional
outcome in schizophrenia. This is especially true for
individuals across a variety of residential placements
and living conditions because the measure is not
dependent on skills training or related to a specific
performance context. As such, the ILS-PB may be a
useful proxy measure in groups, such as forensic
patients, where functional status may be divorced
from functional capacity.
4.5. Study limitations and future directions
Limitations of our study include the cross-sectional
nature of data collection, the small sample size and the
specificity of the demographic characteristics (persis-
tently ill, middle-aged males) that limit generalizabil-
ity. Furthermore, the ILS-PB was not cross-validated
with an alternate measure of daily problem-solving
skills. Therefore, it remains to be determined whether
ILS-PB can be used as a predictor for characteristics
such as dischargeability or the ability to function in
less restrictive environments. We did, however,
demonstrate that the inpatients and outpatients in
our sample were significantly different in terms of
community tenure. While it may not be surprising that
the ILS-PB differentiates daily problem-solving levels
between patient groups because of the respective
opportunities to practice daily living skills in context,
it nonetheless illustrates how the underlying cognitive
mechanisms of reasoning may be as important as the
actual performance of daily living tasks. Furthermore,
many of the items on the ILS-PB are relevant for
inpatients as well as outpatients (e.g. name 2 reasons
why it is important to have relationships with people),
insofar as tests that rely on memory for items on a
shopping list (e.g. CVLT) are equally valid. Cross-
validation of the ILS-PB with other standardized
functional outcome measures currently used in
schizophrenia research is compelling.
Acknowledgements
The authors would like to thank Ali Saperstein and
Maria Jalbrzikowski for assisting with the project.
This study was made possible with grant support
from NIMH, R01-MH049334-12, awarded to DCJ.
References
Ammons, R.B., Ammons, C.H., 1962. The quick test (QT):
provisional manual. Psychol. Rep. 11, 111–161.
Andreasen, N.C., 1981. Scale for the Assessment of Negative
Symptoms (SANS). University of Iowa, Iowa City.
Bellack, A.S., Mueser, K.T., Gingerich, S., Agresta, J., 2004. Social
Skills Training for Schizophrenia. The Guilford Press, New
York.
Berman, I., Viegner, B., Merson, A., Allan, E., Pappas, D., Green,
A.I., 1997. Differential relationships between positive and
negative symptoms and neuropsychological deficits in schizo-
phrenia. Schizophr. Res. 25, 1–10.
Butler, P.D., Zemon, V., Schechter, I., Saperstein, A.M., Hoptman,
M.J., Lim, K.O., Revheim, N., Silipo, G., Javitt, D.C., 2005.
Early-stage visual processing and cortical amplification deficits
in schizophrenia. Arch. Gen. Psychiatry 62, 495–504.
Cornblatt, B.A., Lenzenweger, M.F., Dworkin, R.H., Erlenmeyer-
Kimling, L., 1992. Childhood attentional dysfunctions predict
social deficits in unaffected adults at risk for schizophrenia. Br.
J. Psychiatry, 59–64.
Dickinson, D., Coursey, R.D., 2002. Independence and overlap
among neurocognitive correlates of community functioning in
schizophrenia. Schizophr. Res. 56, 161–170.
Evans, J.D., Heaton, R.K., Paulsen, J.S., Palmer, B.W., Patterson,
T., Jeste, D.V., 2003. The relationship of neuropsychological

N. Revheim et al. / Schizophrenia Research 83 (2006) 237–245 245
abilities to specific domains of functional capacity in older
schizophrenia patients. Biol. Psychiatr. 53, 422–430.
Gold, J.M., Carpenter, C., Randolph, C., Goldberg, T.E., Wein-
berger, D.R., 1997. Auditory working memory and Wisconsin
Card Sorting Test performance in schizophrenia. Arch. Gen.
Psychiatry 54, 159–165.
Gold, J.M., Goldberg, R.W., McNary, S.W., Dixon, L.B., Lehman,
A.F., 2002. Cognitive correlates of job tenure among patients
with severe mental illness. Am. J. Psychiatr. 159, 1395–1402.
Green, M.F., 1996. What are the functional consequences of
neurocognitive deficits in schizophrenia? Am. J. Psychiatr.
153, 321–330.
Green, M.F., Kern, R.S., Braff, D.L., Mintz, J., 2000. Neuro-
cognitive deficits and functional outcome in schizophrenia: are
we measuring the bright stuffQ? Schizophr. Bull. 26, 119–136.
Hartman, M., Steketee, M.C., Silva, S., Lanning, K., Andersson, C.,
2003. Wisconsin card sorting test performance in schizophrenia:
the role of working memory. Schizophr. Res. 63, 201–217.
Harvey, P.D., Sukhodolsky, D., Parrella, M., White, L., Davidson,
M., 1997. The association between adaptive and cognitive
deficits in geriatric chronic schizophrenia patients. Schizophr.
Res. 27, 211–218.
Kern, R.S., Green, M.F., Mitchell, S., Kopelowicz, A., Mintz, J.,
Liberman, R.P., 2005. Extensions of errorless learning for social
problem-solving deficits in schizophrenia. Am J. Psychiatr. 162,
513–519.
Leitman, D., Foxe, J.J., Butler, P.D., Saperstein, A., Ravheim, N.,
Javitt, D.C., 2005. Sensory contributions to impaired prosodic
processing in schizophrenia. Biol. Psychiatr. 58, 56–61.
Loeb, P.A., 1996. ILS: Independent Living Scales Manual. The
Psychological Corporation, San Antonio.
Lysaker, P.H., Bell, M.D., Bioty, S.M., 1995. Cognitive deficits in
schizophrenia: prediction of symptoms change for participators
in work rehabilitation. J. Nerv. Ment. Dis. 183, 332–336.
McGurk, S.R., Moriarty, P.J., Harvey, P.D., Parrella, M., White, L.,
Friedman, J., Davis, K.L., 2000. Relationship of cognitive
functioning, adaptive life skills, and negative symptom severity
in poor-outcome geriatric schizophrenia patients. J Neuopsy-
chiatr. Clin. Neurosci. 12, 257–263.
Medalia, A., Revheim, N., Casey, M., 2001. The remediation of
problem-solving skills in schizophrenia. Schizophr. Bull. 27,
259–267.
O’Leary, D.S., Flaum, M., Kesler, M.L., Flashman, L.A., Arndt, S.,
Andreasen, N.C., 2000. Cognitive correlates of the negative,
disorganized, and psychotic symptom dimension of schizophre-
nia. J. Neurospychiatr. Clin. Neurosci. 12, 4–14.
Overall, J.E., Gorham, D.R., 1962. The brief psychiatric rating
scale. Psychol. Rep. 10, 799–812.
Revheim, N., Medalia, A., 2004a. Verbal memory, problem-solving
skills and community status in schizophrenia. Schizophr. Res.
68, 149–158.
Revheim, N., Medalia, A., 2004b. The Independent Living Scales
(ILS) as a measure of functional outcome for schizophrenia.
Psychiatr. Serv. 55, 1052–1054.
Sinnott, J.D., 1989. Summary: issues and directions for everyday
problem solving research. In: Sinnott, J.D. (Ed.), Everyday
Problem Solving: Theories and Applications. Praeger, New
York, pp. 300–306.
Stevens, A.A., Goldman-Rakic, P.S., Gore, J.C., Fulbright, R.K.,
Wexler, B.E., 1998. Cortical dysfunction in schizophrenia
during auditory word and tone working memory demonstrated
by functional magnetic resonance imaging. Arch. Gen. Psychi-
atry 55, 1097–1103.
Stevens, A.A., Donegan, N.H., Anderson, M., Goldman-Rakic, P.S.,
Wexler, B.E., 2000. Verbal processing deficits in schizophrenia.
J. Abnorm. Psychology 190, 461–471.
Suslow, T., Junghanns, K., Weitzsch, C., Arolt, V., 1998. Relations
between neuropsychological vulnerability markers and negative
symptoms in schizophrenia. Psychopathology 31, 178–187.
Tamminga, C.A., Buchanan, R.W., Gold, J.M., 1998. The role of
negative symptoms and cognitive dysfunction in schizophrenia
outcome. Int. Clin. Psychopharmacol. 13, S21–S26.
Twamley, E.W., Doshi, R.R., Nayak, G.V., Palmer, B.W., Golshan,
S., Heaton, R.K., Patterson, T.L., Jeste, D.V., 2002. Generalized
cognitive impairments, ability to perform everyday tasks, and
level of independence in community living situations of older
patients with psychosis. Am. J. Psychiatr. 159, 2013–2020.
Twamley, E.W., Jeste, D.V., Bellack, A.S., 2003. A review
of cognitive training in schizophrenia. Schizophr. Bull. 29,
359–382.
Velligan, D.I., Mahurin, R.K., Diamond, P.L., Hazleton, B.C.,
Eckert, S.L., Miller, A.L., 1997. The functional significance of
symptomatology and cognitive function in schizophrenia.
Schizophr. Res. 25, 21–31.
Wechsler, D., 1997a. The Wechsler Adult Intelligence Scale, Third
ed. The Psychological Corporation, San Antonio.
Wechsler, D., 1997b. The Wechsler Memory Scale-III. The
Psychological Corporation, San Antonio.




















