Neonatal Mortality in Vietnam - DiVA portal
100
ACTA UNIVERSITATIS UPSALIENSIS UPPSALA 2013 Digital Comprehensive Summaries of Uppsala Dissertations from the Faculty of Medicine 853 Neonatal Mortality in Vietnam; Challenges and Effects of a Community-Based Participatory Intervention NGUYEN THU NGA ISSN 1651-6206 ISBN 978-91-554-8567-2 urn:nbn:se:uu:diva-188252
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Neonatal Mortality in Vietnam - DiVA portal

ACTAUNIVERSITATIS
UPSALIENSISUPPSALA
2013
Digital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 853
Neonatal Mortality in Vietnam;Challenges and Effects of aCommunity-Based ParticipatoryIntervention
NGUYEN THU NGA
ISSN 1651-6206ISBN 978-91-554-8567-2urn:nbn:se:uu:diva-188252

Dissertation presented at Uppsala University to be publicly examined in Rosensalen,Akademiska Sjukhuset, Entrance 95/96 nbv, Uppsala, Tuesday, February 5, 2013 at 09:15 forthe degree of Doctor of Philosophy (Faculty of Medicine). The examination will be conductedin English.
AbstractNga, N. T. 2013. Neonatal Mortality in Vietnam; Challenges and Effects of a Community-Based Participatory Intervention. Acta Universitatis Upsaliensis. Digital ComprehensiveSummaries of Uppsala Dissertations from the Faculty of Medicine 853. 98 pp. Uppsala.ISBN 978-91-554-8567-2.
Globally neonatal mortality accounts for 40% of under-five deaths. Participatory interventionswhere the local problems are addressed have been successful in some settings.
The aim of this thesis was to describe challenges in perinatal health in a Vietnamese province,and to evaluate the effect of a facilitated intervention with local stakeholder groups that used aproblem-solving approach to neonatal survival during three years.
The NeoKIP trial (Neonatal Knowledge Into Practice, ISRCTN44599712) had a cluster-randomized design (44 intervention communes, 46 control). Laywomen facilitated Maternal-and-Newborn Health Groups (MNHGs) and used Plan-Do-Study-Act cycles to address perinatalhealth problems. Births and neonatal deaths were monitored. Interviews were performed inhouseholds of neonatal deaths and randomly selected live births. Use of health services wasmapped. The primary healthcare staff’s knowledge on newborn care was assessed before andafter the intervention.
Neonatal mortality rate (NMR) was 16/1000 live births (variation 10 - 44/1000 betweendistricts). Home deliveries accounted for one fifth of neonatal deaths, and health facilities withleast deliveries had higher NMR. Main causes of death were prematurity/low birth-weight (37.8%), intrapartum-related deaths (33.2 %) and infections (13.0 %). Annual NMR was 19.1, 19.0and 11.6/1000 live births in intervention communes (18.0, 15.9 and 21.1 in control communes);adjusted OR 1.08 [0.66-1.77], 1.23 [0.75-2.01], and 0.51 [0.30-0.89], respectively. Women inintervention communes more frequently attended antenatal care, prepared for delivery and gavebirth at institutions. Primary healthcare staff’s knowledge on newborn care increased slightlyin intervention communes.
This model of facilitation of local stakeholder groups using a perinatal problem-solvingapproach was successful and may be feasible to scale-up in other settings.
Keywords: Facilitation, Local stakeholder group, Maternal-and-Newborn Health Group,Neonatal mortality, Primary health care, Vietnam
Nguyen Thu Nga, Uppsala University, Department of Women's and Children's Health,International Maternal and Child Health (IMCH), Akademiska sjukhuset, SE-751 85 Uppsala,Sweden.
© Nguyen Thu Nga 2013
ISSN 1651-6206ISBN 978-91-554-8567-2urn:nbn:se:uu:diva-188252 (http://urn.kb.se/resolve?urn=urn:nbn:se:uu:diva-188252)

To all those dedicated PEOPLE in the world who are doing the best to make sure that every baby born will survive!


List of Papers
This thesis is based on the following papers, which are referred to in the text by their Roman numerals.
I Nga NT, Malqvist M, Eriksson L, Hoa DP, Johansson A,
Wallin L, Persson LA, Ewald U: Perinatal services and outcomes in Quang Ninh province, Vietnam. Acta Paediatr 2010, 99(10): 1478-1483.
II Nga NT, Hoa DP, Malqvist M, Persson LA, Ewald U: Causes of neonatal death: results from NeoKIP community-based trial in Quang Ninh province, Vietnam. Acta Paediatr, 2012. 101(4): 368-73.
III Persson LA, Nga NT, Malqvist M, Hoa DP, Eriksson L, Wallin L, Huy TQ, Duc DM, Tiep TV, Thuy VTT, Ewald U. Effects of Facilitation of Local Maternal-and-Newborn Stakeholder Groups on Neonatal Mortality. The NeoKIP Cluster-Randominsed Trial in Quang Ninh Province, Vietnam. (Submitted)
IV Nga NT, Malqvist M, Hoa DP, Eriksson L, Johansson A, Ewald
U, Persson LA. Effects of Facilitation of Local Maternal-and-Newborn Health Groups on Continuum of Perinatal Care; Re-sults from the NeoKIP Trial in Northern Vietnam. (Manuscript)
Reprints were made with permission from respective publishers.


Book cover: NeoKIP team

Contents
Introduction ................................................................................................... 15 Newborn and maternal health is key to child survival ............................. 15 Neonatal mortality .................................................................................... 16
Causes of neonatal death ..................................................................... 16 Determinants of neonatal mortality ..................................................... 17
Interventions for neonatal survival ........................................................... 18 Implementation of evidence-based knowledge.................................... 18 Effective interventions for neonatal survival ....................................... 19
Viet Nam .................................................................................................. 20 Rationale for the present trial ................................................................... 21
Aims .............................................................................................................. 23
Methods ........................................................................................................ 24 Study setting ............................................................................................. 24
Perinatal health services ...................................................................... 25 Study design and methods ........................................................................ 25 Baseline survey (Paper I) ......................................................................... 27 Causes of neonatal death (Paper II) .......................................................... 28 Participants in the trial (Paper III and IV) ................................................ 29
Intervention .......................................................................................... 30 Maternal-and-Newborn Health Groups ............................................... 31 Hypothesis ........................................................................................... 32
Sample size ............................................................................................... 32 Randomization ......................................................................................... 33 Data collection and management ............................................................. 33 Statistical analysis .................................................................................... 35 Ethical considerations .............................................................................. 37
Results ........................................................................................................... 38 Perinatal care (Paper I) ............................................................................. 38 Neonatal mortality; baseline level and causes (Paper I and II) ................ 39 Effect on neonatal mortality (Paper III) ................................................... 41 Coverage of antenatal and perinatal care in intervention and control communes (Paper IV) ............................................................................... 43

Discussion ..................................................................................................... 46 Methodological considerations................................................................. 46
Internal validity .................................................................................... 46 External validity and generalization .................................................... 49
Level of neonatal mortality rate ............................................................... 49 Causes of neonatal death .......................................................................... 50 Effects of the intervention ........................................................................ 51
Conclusions ................................................................................................... 54
Summary in Vietnamese/Tóm tắt luận văn bằng tiếng Việt ......................... 55
Acknowledgements ....................................................................................... 58
References ..................................................................................................... 62
Appendices .................................................................................................... 70 Appendix I: Delivery information form .............................................. 71 Appendix II: Questionnaire interview form on continuum of care for maternal- neonatal and child health care ............................................. 72 Appendix III: Questionnaire interview form for neonatal deaths ........ 82 Appendix IV: Questionnaire interview form survey for primary healthcare staff’s Knowledge on Newborn care .................................. 95

Abbreviations
ANC Antenatal Care CHC Community Health Center GIS Geographic Information System IMR Infant Mortality Rate LMIC Low- and Middle-Income Country MDG 4 4th Millennium Development Goal MDG 5 5th Millennium Development Goal MNHG Maternal-and-Neonatal Health Group NeoKIP Neonatal health Knowledge Into Practice NMR Neonatal Mortality Rate OR Odds Ratio Sida Swedish International Development Cooperation Agency U5MR Under-five Mortality Rate UBGH Uong Bi General Hospital
(Vietnam – Sweden General Hospital in Uong Bi) VHW Village Health Worker WHO World Health Organization

Glossary and definitions
Gestational age: The duration of gestation is measured from the first day of the last normal menstrual period. Gestational age is expressed in completed days or completed weeks.
Infant mortality rate: Number of deaths during the first year of live per 1000 live births in a given year or period.
Low birth weight: Birth weight of less than 2500 g (up to and including 2499g), irrespective of gestational age.
Neonatal period: Commences at birth and ends 28 completed days after birth. Early neonatal period commences at birth and ends seven completed days after birth. Late neonatal period: Commences after seven days and ends 28 completed days after birth.
Neonatal death: A neonatal death is defined as death of a live birth during the first 28 days of life. Early neonatal death: death occurs during the first 7 days of life. Late neonatal death: death occurs after the 7th day but before 28 completed days of life.
Neonatal mortality rate: Number of deaths during the first 28 completed days of live per 1000 live births in a given year or period.
Perinatal period: Commences at 22 completed weeks (154 days) of gesta-tion age (the time when birth weight is normally 500 g), and ends seven completed days after birth. Pre-term: Less than 37 completed weeks (less than 259 days) of gestation.
Skilled birth attendance: Delivery in the presence of a skilled birth attendant, with at least midwifery skills, in an environment that includes availability of equipment, drugs, and referral transportation and communication systems.
Fetal death (deadborn fetus - previously called “stillbirth”): Fetal death is death prior to the complete expulsion or extraction from its mother of a

product of conception, irrespective of the duration of pregnancy; the death is indicated by the fact that after such separation the fetus does not breathe or show any other evidence of life, such as beating of the heart, pulsation of the umbilical cord, or definite movement of voluntary muscles.
Under-five mortality rate: Number of deaths during the first five years of live per 1000 live births in a given year or period. Note: Definitions were derived from International Statistical Classification of Dis-eases and Related Health Problems. 10th Revision (ICD-10), Edition 2010. Geneva, World Health Organization 2011 [1].

13
Preface
My road to be with newborns In May 1979, one month before graduation from the Hanoi Medical Univer-sity with specialization in pediatrics, I was selected to work at the six north-ern provinces of Vietnam, where the people and specially children suffered great hardship due to the war from China. I left my family in Hanoi and went to work at the district hospital in Uong Bi for three years, thereafter at the Vietnam – Sweden Uong Bi General Hospital (UBGH) until now.
The Uong Bi General Hospital was built with support from the Swedish Government after the reunification of the country in 1975. The hospital was located in Quang Ninh aiming to provide health care to the coalmine work-ers and the people in the province. After five years of construction, UBGH was inaugurated in 1981 and soon became one of the hospitals that provided high quality healthcare to the people, and that trained medical staff and stu-dents from Vietnam and other countries.
I am very proud to have been working as a pediatrician at the UBGH, from newborns to adolescents but mainly with children under five years of age. I had the opportunity to gain knowledge and experiences on the child health-care from the practices and knowledge exchange between Vietnamese and Swedish colleagues. One day, Doctor Rolf Johansson - a Swedish medical doctor working at UBGH (1984 – 1986) gave me an article on Kangaroo Mother Care (KMC) of premature and low birth weight babies from Bogota, Colombia and it told that the survival was fantastic. Right after, Doctor Vu Gia Khuong and I started to implement KMC for preterm and low birth weight newborns in the pediatric department. The KMC has contributed in reduction of morbidity and mortality as well as in improvement of quality of newborn care at the UBGH. The method has also improved the actions on breastfeeding for newborns both preterm and full term, Baby Friendly Hos-pital, and the collaboration between Pediatrics and Obstetrics departments for maternal and newborn care. Year by year, the KMC became a routine care for the preterm and low birth weight newborns at UBGH and it was disseminated to many other hospitals in Vietnam.

14
Besides working at the UBGH, I had also involved in primary healthcare and research on maternal and child health in the province with my colleagues. However, my main interest remained with the newborn baby. Therefore, on the day, I graduated with a Master of Public Health at Karolinska Institute in Sweden, Dr. Annika Johansson, my supervisor and Professor Kyllike Chris-tenson reminded me to continue with research on newborn health and KMC in Vietnam. Luckily, Professor Lars-Åke Persson at the International Mater-nal and Child Health (IMCH), Department of Women’s and Children’s Health, Uppsala University, Sweden provided me an opportunity, which made my dream come true. The research project “Implementing Knowledge Into Practice for Improved Neonatal Survival (NeoKIP)” was performed in Quang Ninh province and I was involved as one of researchers to work full time since 2005 to 2011. In this thesis, I describe the detail process of the NeoKIP intervention by community-based participatory and effects of facili-tation of local Maternal-and-Newborn Health Groups working together for improving neonatal survival in Quang Ninh (Figure 1).
My hope is that a cost-effective facilitation intervention and the experiences from NeoKIP project could be scaled-up to other provinces in my country especially in the remote districts where the Mother, Newborn and Child still have high risk of morbidity and mortality.
Figure 1. Family of the newborn and doctor Nguyen Thu Nga at the community health center in Quang Ninh province, 2011.

15
Introduction
Newborn and maternal health is key to child survival
The first 28 days of life is called the neonatal period and carries one of the highest risks of death in human lifespan [2].
Neonatal and maternal health is key to child survival. The continuum of care of the mother-and-child dyad starts in pregnancy or before, includes child-birth and the neonatal month and is crucial for short- and long-term health and survival [3, 4]. However, in low- and middle-income countries (LMIC) the level of neonatal mortality and the causes of death have until recently received relatively low attention [5, 6].
The 1989 Convention on the Rights of the Child reaffirmed the right to health of the child and the right to get a name, i.e. to be recognized as a newborn individual [6]. In 2000, 147 nations committed to work for human development and set eight Millennium Development Goals (MDGs). The fourth MDG (MDG-4) aims at two-thirds reduction in mortality in children before the age of five years from 1990 to 2015. Unfortunately, most recent reports of the countdown to 2015 on maternal, neonatal and child survival estimate that only 23 (31%) among 75 priority countries are on track to reach the MDG-4 goal for child survival and only nine countries are expected to reach both MDG-4 and 5, the latter focusing maternal health and survival [7-10]. Many babies are still born at home without skilled birth attendance, care seeking for maternal and newborn ailments is limited, health workers are often not sufficiently skilled, quality of care of mothers and newborn infants is insufficient and there are great social inequities across all these factors [11]. The neonatal survival challenges call for effective interventions for LMICs to be able to reach the MDG-4 for child health and survival [9, 12, 13].
Successful implementation of a small number of evidence-based interven-tions for newborn survival is able to reduce current levels of neonatal mor-tality drastically [3, 14]. Scaling-up of such interventions may be difficult and result in low program effectiveness [15]. Social and geographic variation in coverage of a good-quality continuum of perinatal care may result in in-

16
equity in neonatal survival and obstacles in reaching child mortality goals [16-18]. These problems call for systems interventions or community-based participatory interventions that are able to identify the variation of local problems in perinatal health and address these accordingly [14]. This thesis documents such an effort in Quang Ninh province in the north of Vietnam.
Neonatal mortality Globally post-natal and child survival has improved considerably, but neo-natal mortality has persisted at a high level and currently accounts for 40% of all deaths before the age of five years [19, 20]. The proportion of early neonatal mortality (deaths in the first week of life) has increased as com-pared to the late neonatal mortality (deaths from seven to 28 days of age) and it accounts for three quarters of all neonatal deaths. Among the early neonatal deaths, two thirds happen in the first 24 hours (very early neonatal mortality) [21].
Recent data show that of 3.1 million neonatal deaths in 2010 and 99% occur in LMICs [19, 21, 22]. The highest absolute number of neonatal deaths is found in South Asian countries because of high death risks and large popula-tions (India alone contributes one quarter of all neonatal deaths), while the highest neonatal mortality rates are found in Sub-Saharan Africa (14 of the 18 countries with NMRs > 45/1000 are found in that area), [19, 21, 23].
Causes of neonatal death The distribution of causes of neonatal death has changed during the last dec-ades, with a reduction in neonatal infections and tetanus [24] and an increase in causes of death related to prematurity both in high-income countries and LMICs [25]. The distribution of causes varies between countries related to the level of neonatal mortality. In very high mortality settings (NMR > 45/1000) half of deaths are due to infections (e.g. septicemia, tetanus and diarrhea). At low NMR levels (< 15/1000), sepsis/pneumonia is usually less than one fifth [9, 22]. At very low NMR levels (< 5/1000), complications to severe prematurity dominate [26].
In a global perspective the main causes of neonatal deaths are preterm birth complications (35%), neonatal infections including sepsis, meningitis, teta-nus, pneumonia, diarrhoea (28%) and intrapartum-related neonatal deaths (previously often labeled “asphyxia”, 23%) [13, 19, 20, 26] Low birth weight, which is related to maternal nutrition and reflects intrauterine growth restriction and/or preterm birth, contributes to 60 – 80% of the neonatal deaths. This is especially prominent in South Asia, where the proportion of

17
children with low birth weight is around one-third of all newborn infants [21, 27].
Determinants of neonatal mortality Poverty is an underlying cause of neonatal deaths [21] that also is reflected in the geographical distribution of these deaths; two thirds occurring in Sub-Saharan Africa and South Asia. The social and political context influences society, health services as well as households and thereby pregnancy out-comes [28].
One of the most important underlying determinants of neonatal health and survival is the coverage of antenatal, delivery and newborn care in the local community, in a district or in a country [4]. Failing to achieve this conti-nuum of care for the mother-and-newborn dyad may result in no improve-ment in survival in spite of some improvements in health services utilization [29]. The challenge is to establish a functioning system of appropriate peri-natal care from home to the different levels of the health system during pregnancy, childbirth and the newborn period [30, 31]. Such continuum of care could also reduce the current two million intrapartum-related stillbirths [32]. The challenge is huge, since we still have 60 million births that take place outside health facilities [33].
Institutional delivery with a skilled midwife attending is fundamental for saving lives of mothers and newborns. Home deliveries without skilled birth attendant are still prevalent in many LMICs. Reportedly less than half of deliveries in South Asia and Sub-Saharan Africa takes place at health institutions [12].
Valid data on newborn deaths are important for priority setting, health plan-ning and monitoring of progress in perinatal health. In many LMICs report-ing systems of live births and newborn deaths are absent or poorly function-ing [34, 35]. In addition, there are frequently difficulties in ascertaining re-porting of very early neonatal deaths in preterm births. These difficulties result in many unreported newborn births and deaths. Similarly, there is a lack of information on causes of neonatal deaths in many low-income set-tings. Systematic interviews with the “verbal autopsy” (VA) technique are valuable in ascertaining causes of death in such settings. A “generic” VA questionnaire to be used for neonatal deaths has been developed by World Health Organization (WHO) [36] and been used in several countries, for example in Vietnam [37, 38], Nepal [39], Uganda [40], Bangladesh [41], Malawi and Zimbabwe [42]. Evaluation of this standard VA questionnaire has shown good diagnostic accuracy in ascertaining most causes of neonatal death [41, 43-48]. Modifications have often been made of the open questions

18
related to illness and death that intend to map social conditions [49, 50] that exist in the background and may indicate possible prevention [51].
Interventions for neonatal survival Implementation of evidence-based knowledge Two thirds of neonatal deaths could reportedly be prevented by evidence-based, low-cost interventions [52]. There is a need to reduce the gap between evidence and practice and find ways to ensure that research is translated into clinical practice as effectively and efficiently as possible [53]. There is a lack of studies that investigate the implementation of evidence-based practices in LMICs [54-56]. ‘What works where and why’ is a relevant question for im-plementation of evidence-based practices for improved neonatal survival [14].
Figure 2. Implication of the Promoting Action on Research Implementation in Health Services (PARIHS) model in NeoKIP trial [57].
In the theoretical framework “Promoting Action in Implementation of Re-search in Health Services” (PARIHS) [57], (Figure 2) three elements are identified: the evidence provided by research, the context of the health sys-tem where the implementation takes place, and the facilitation provided to support the process of implementation. There is currently sufficient evidence for a number of efficient single interventions, package interventions and

19
even systems interventions for improved neonatal survival [14], but there is insufficient knowledge on the influence of contextual factors [58] that may prevent or promote the implementation, and which facilitation strategies are proven effective in supporting the effort [59]. Facilitation is a function that has been described in different ways, e.g. change agent, opinion leader, re-search champion, and knowledge broker [60]. Facilitation refers to an ap-proach whereby a person makes things easier for others [61] by developing a learning process rather than telling others what they should do [62, 63].
Effective interventions for neonatal survival The Lancet series on neonatal survival identified a number of single inter-ventions with proven efficacy for neonatal survival [64] e.g. tetanus toxoid immunization, resuscitation with room air for neonates who fail to establish breathing, prevention of neonatal hypothermia, early and exclusive breast feeding, case management of neonatal sepsis or pneumonia by community health workers [65]. Such single interventions could be combined into pack-ages for scaling up in health systems from home care to higher-level referral care [64, 66]. However, social and geographical inequity in perinatal health is often great in LMICs [11]. This calls for system interventions or commu-nity-based participatory interventions that could address the multitude of local problems that influence pregnancy outcomes. Such interventions with women’s group at community levels, using problem-solving cycles have resulted in a significant reduction in neonatal mortality in Nepal [67] and in India [68, 69]. Different challenges and contextual factors can limit the ef-fect of the interventions [70] and may result in failure in other settings [29].

20
Viet Nam Recently, Viet Nam has been classified as a middle-income country. Poverty has been reduced (from 37% in 1998 to 3.3% in 2011) [71] while social in-equity has grown. New challenges in maternal and neonatal health are espe-cially found in rural and remote areas. The basic population indicators are presented in table 1 below (Table 1). Neonatal mortality is reportedly quite low, although there are some reasons to suspect under-reporting [35] and that neonatal mortality rates actually have stagnated in spite of rapid reduc-tion in post-neonatal and child mortality [18].
Table 1. Basic population indicators for Viet Nam Vietnam Source Population, million (2011) 86 GSO Vietnam,
2011 Rural population, percentage (2011) 70.4 " GDP per capita, PPP USD (2009) 3097 UNDP, 2011 Total expenditure on health per capita 213 WHO, 2009 Government expenditure on health per capita (2009)
82 "
Literacy rate, % adults (2009) 93 Average life expectancy at birth, year (2009) World bank, 2011 Female 77 Male 73 Fertility rate, total birth per woman (2008) 2.0 World bank, 2011 ANC attendance, % of women attending ANC ≥ 1 time (2006)
91 "
Maternal mortality rate (MMR) 56/100,000 UNICEF, 2012 Neonatal mortality rate (NMR) 12/1000 " Infant mortality rate (IMR) 16/1000 " Under-five mortality rate (U5MR) 19/1000 " GDP=gross domestic product; PPP=purchasing power parity
The health care system in Viet Nam has four administrative levels: com-mune, district, province and central level. At the commune level there is a community health center (CHC) located in the center of the commune where the population is between 3000 to 10000 persons. A CHC often has three to six staff (doctor, assistant doctor, midwife and nurse). They provide basic health care for all people in the commune: primary care, family planning, immunization, prenatal care, normal delivery care, postpartum care and many activities for health promotion. There is a large group of village health

21
workers (VHW) that collaborates with CHC staff. The VHW provides first aid, is active in health promotion, sanitation, immunization, nutrition and other national or local healthcare programs. In case of need and in places where health facilities are far away, they are trained to attend births. At the district level, district health centers (DHC) have both curative and preventive functions. After 2006, the DHC was divided into three separate administra-tive structures; district hospital, district preventive medicine center and dis-trict department of health. The main task of the district hospital is to provide district-level hospital care but also to train primary healthcare staff including the VHWs. Examples of perinatal services at district hospitals are prenatal care, delivery care, caesarean sections for high-risk pregnancies and new-born care. Usually the district hospital has a limited number of in-patient beds (100-200 beds/hospital) and medical staff. Most district hospitals have no separate departments of obstetrics and pediatrics. The provincial hospital provides more specialized care. They receive referrals from district hospitals or people come directly without referral. Provincial hospitals typically have 200 to 1000 beds, depending on the size of the population. In addition to the public health system, there is an extensive and growing network of private healthcare and pharmacy services, particularly since the “Doi Moi” policy reform in 1986.
The Vietnamese Government has made efforts to improve neonatal health to reach the MDG-4 and has issued a directive for improved neonatal survival [72] and developed strategic documents for perinatal and neonatal health, called “National Standard Guidelines on Reproductive Health and Services” [73]. These guidelines were launched in 2003, with a revised and extended version presented in 2009 by the Ministry of Health. These guidelines were distributed to all health institutions in the country.
Rationale for the present trial The research presented in this thesis is based on collaboration between Upp-sala University, Sweden, the Vietnam – Sweden General Hospital in Uong Bi (UBGH), Viet Nam, and Ministry of Health (MoH) in Vietnam. A com-munity-based, cluster-randomized trial “Implementing Knowledge Into Practice for improved Neonatal survival in Vietnam” was given the acronym NeoKIP (Neonatal health - Knowledge Into Practice) and was registered as an International Standard Randomized Controlled Trial, number ISRCTN44599712. The trial protocol has been published [74].

22
Figure 3. Conceptual framework that summarizes the work of local MNHGs that work in problem-solving cycles and may relate to households, the health system or other parts of society in order to improve maternal and newborn health and survival.
Two community-based participatory trials in Nepal and India, in contexts with a relatively high initial level of neonatal mortality, have reported a re-duction by 30-45% [67, 69] that has been judged to be cost-effective [75]. A participatory community-based intervention in Uganda that was informed by local health data was also effective in reducing infant mortality [76]. Facili-tation of community groups in Mumbai slums did not result in effects on health care utilization or mortality [77], and an effort to scale-up a communi-ty-based intervention in Bangladesh did not reduce newborn death [29]. It would be valuable to know whether community-based participatory inter-ventions also could be effective in contexts outside South Asia, and in set-tings with a medium-level neonatal mortality rate (NMR), i.e. in the range 15-30/1000. The care providers have not been directly represented in the previous community-based approaches.
One may question the sustainability of an approach with women’s groups that are specifically established for this purpose. An alternative strategy may be to mobilize people, who already have responsibility to promote health and welfare in society, e.g. primary care staff, village health workers, and elected representatives of local political or non-governmental organizations. It is not known whether facilitation of such local stakeholder groups may result in improved perinatal survival (Figure 3).
Health system
Pregnancy Birth Newborn
Facilitated Maternal and
Groups: Problem-solving
Cycles

23
Aims
The aim of this thesis was to describe the occurrence of neonatal mortality and challenges of perinatal health in a Vietnamese province, and to evaluate the effect of a facilitated intervention with local stakeholder groups that use a problem-solving approach on continuum of maternal and newborn care and neonatal survival.
Specific objectives:
1. To describe perinatal services provided and neonatal outcomes, and to analyse geographical inequities and differentials related to level of care (Paper I).
2. To ascertain causes of neonatal death, and to describe their distribu-tion over age at death, birth weight and place of delivery (Paper II).
3. To analyze the effect of facilitation of local maternal-and-newborn stakeholder groups on neonatal mortality (Paper III).
4. To analyze the effect of facilitation of local stakeholder groups on the continuum of care for maternal and neonatal health (Paper IV).

24
Methods
Study setting
Figure 4.Map of Quang Ninh province with health facilities and intervention and control communes of NeoKIP trial. The studies of this thesis were conducted in Quang Ninh province in the northeast of Vietnam, 120 km from the capital Hanoi, bordering China in the north, other provinces in the west, and having a long coastline in the east (Figure 4). Nearly 80% of the area is mountainous with forests and mines. This province has 90% of the total coal production in the country. The prov-ince is undergoing a rapid economic transition. The population was 1.15 million in 2011. There are 10 different ethnic groups in the province (Kinh, Tay, Dao, Thanh Y, Thanh Phan, San Diu, San Chi, Cao Lang and Hoa or Chinese). The Vietnamese (Kinh) is the biggest ethnic group with 89% of

25
the population. The ethnic minority groups mainly live in the mountainous areas in the western part of the province [78]. The province is divided into 14 districts with a varied landscape; delta land, islands and mountainous areas.
Perinatal health services Antenatal, delivery and neonatal care is provided at 205 health facilities in-cluding 187 CHCs, 16 district hospitals and two hospitals at tertiary level [79], (Figure 4).
At the primary health care level the CHC staff (mainly the midwife or assis-tant doctor of obstetrics and pediatrics) has the main responsibility for ante-natal care, to manage normal deliveries and to provide postpartum care in their commune. They usually receive some re-training but not as frequently as staff working in hospitals does. High-risk pregnant women and newborns with health problems are usually referred from this level to the district hos-pitals, where treatment can be provided according to the national guidelines [73]. However, at district level hospitals there is often lack of human re-sources and essential equipment for maternal and neonatal care. Two ter-tiary-level hospitals are available in Quang Ninh province; one of these is also serving as a regional referral centre for a few provinces.
Study design and methods This thesis is based on NeoKIP trial, a cluster-randomized trial in Quang Ninh province, Vietnam [74]. The first paper provides a baseline description of perinatal outcomes and services, the second reports causes of death based on systematic verbal autopsy interviews, and the third and the forth papers report effects by the intervention on neonatal mortality and on the continuum of antenatal, delivery and newborn care (Table 2). The process of conducting four studies of four papers was shown in the flow chart of the NeoKIP trial (Figure 5).

26
Table 2. Overview of study design and methods used in the four papers
Paper I II III IV
Research questions
What is the situa-tion of perinatal
services and level of neonatal mor-
tality?
What are the main causes of neonatal death?
What is the effect of facilitation of MNHG on neo-natal mortality?
What is the effect of facilitation of MNHG on conti-nuum of care?
Study setting
All 14 districts (187 communes) in Quang Ninh
province
Eight districts (90 communes) with NMR > 15/1000 live births in Quang Ninh province
Period 2005 2008-2010 2008-2011
Design Cross sectional study
Case series Cluster-randomized trial
Data collection method
Systematic col-lection on peri-
natal and neonatal indicators from health facilities
Verbal autopsy interview at
home
Surveillance of all births and
neonatal deaths in study area
Sample-based interviews
Sample 17519 live births and 284 neonatal
deaths
233 deceased newborns
44 intervention and 46 control
communes with 11906 and 10655
births
1243 randomly selected
surviving newborns
Outcome Perinatal and neonatal outcomes
Causes of neonatal death
Neonatal mortality rate
Coverage of care, staff knowledge

27
Figure 5. Flow chart of NeoKIP trial and papers
Baseline survey (Paper I) A baseline survey was performed in the entire Quang Ninh province (14 districts, 187 communes) in order to perform a situation analysis regarding perinatal health services and outcomes, especially the distribution of neonat-

28
al mortality across districts and places of delivery. The survey was per-formed in early 2006, covering the period January 1 to December 31, 2005. Fifteen data collectors (nurses and midwives employed at Uong Bi general hospital) were recruited, trained to perform data collection on pregnancies and pregnancy outcomes. Ministry of health and provincial level health au-thorities were represented in the planning for the study, and provided support to the effort. Meetings were held with staff of district hospitals and CHCs as well as with all village health workers (VHW) from all communes, inform-ing them about the purpose of the survey and the forms to be filled in.
Fieldwork started with an inventory of all service providers for antenatal and delivery care in each district. Information on deaths was obtained at the re-gional and provincial hospitals, thereafter at the district hospitals. At district hospital, data from women and newborn infants were collected in close col-laboration with hospital staff from reports and registration books (ANC, immunization, deliveries, referral and mortality). At each CHC, data collec-tors scrutinized registration books and gathered the data collection forms filled in by the midwife. Finally, group interviews were performed with all village health workers (VHWs), 3-6 at a time, from the entire province in order to obtain additional knowledge not presented in facility registers. Each meeting took place at the local CHC and lasted for one to two hours. Partici-pants were encouraged to speak freely. Data were carefully triangulated from the different sources in order to cover all pregnancy outcomes and prevent duplicates in reporting. World Health Organization (WHO) definitions of these outcomes were used by the data collectors [80]. Neonatal deaths were recorded as well as age at death (days), sex, place and assistance at delivery, place of death, birth weight (if available), and gestational age at birth. Infor-mation on utilization of antenatal care was collected at CHCs. Geographic Information System (GIS) coordinates were measured at all health facilities and households of all neonatal deaths.
Causes of neonatal death (Paper II) We reported causes of death of all deceased neonates during the first two years of the trial (July 2008 to June 2010) in paper II. Causes were analyzed based on systematic verbal autopsy interviews performed in the homes of the deceased newborns. In most cases the interview was performed eight weeks after delivery. Based on the World Health Organization (WHO) generic ver-bal autopsy (VA) questionnaire [81], the research team had developed a questionnaire that also included specific questions on care during pregnancy, delivery, and after birth from home to health facility, if appropriate. Two open-ended verbatim accounts of the history of the events preceding death

29
were also included. The questionnaire had been piloted after translation into Vietnamese and modified to suit its purpose.
Two data collectors with background of midwifery were selected and trained for this fieldwork. Emphasis was made on communication skills and empa-thy. After obtaining informed verbal consent, the interviewers conducted the interview in Vietnamese. There were some mothers, who were insufficiently fluent in Vietnamese; then the village health worker was asked to support in the interview. Generally, the mother was the primary respondent, but some-times the grandmother or the father contributed to the interviews that usually lasted for 90 – 120 minutes. The author of this thesis or the field supervisor did the supervision of these interviews. Special emphasis was made on the supervision of interviews regarding deceased neonates, when the delivery had taken place at home.
In order to ascertain the causes of neonatal death, three experienced pediatri-cians independently reviewed all verbal autopsy records and assigned a main cause of death and an underlying cause of death, when appropriate. The pe-diatricians were given an orientation about the verbal autopsy questionnaire and the use of a hierarchical model for allocating cause of death [82]. They used a three-digit code for each cause of death from the list of codes of the tenth revision of International Statistical Classification of Disease, Injuries and Causes of Death (ICD-10), [81]. Causes of neonatal death were thereaf-ter grouped into 6 main causes; low birth weight/preterm causes, intrapar-tum-related death (previously mainly labeled as asphyxia), infections, mal-formations, other causes and unknown. In case of disagreement in the alloca-tion of cause of death, a consensus process was initiated in order to decide on a final cause.
Participants in the trial (Paper III and IV) This trial was performed in 90/187 communes in Quang Ninh province that were located in districts with NMR > 15/1000 in the baseline survey in 2005. The number of inhabitants in the selected communes ranged from 1000 to 18,000; amounting to a total of 350,000 within the study area. The rationale for excluding districts with lower mortality was the assumption, that a com-munity-based participatory intervention potentially should be less effective in areas with a low NMR. The included districts had 6306 births and an av-erage NMR of 24/1000 in 2005. Inclusion criteria for participants were all mother/newborn pairs in the selected communes with dates of births from July 1, 2008 to June 31, 2011.

30
Intervention In order to implement the intervention a steering board was established, chaired by the hospital director of the regional Uong Bi hospital, and with members from the Women’s Union (WU), the Provincial Health Bureau, the Ministry of Health and the collaborating research institution Uppsala Uni-versity. The board monitored the progress of the trial and tried to motivate the local health institutions and eight district boards to support the efforts of the trial. The results of an interim analysis in 2010 as well as after comple-tion of the trial in 2011 were reported to the steering board. No stopping rules for the trial were applied, since we did not anticipate any negative ef-fect of the intervention on the cluster or individual level.
Laywomen from Women’s Union (WU) were recruited to act as facilitators in supporting the Maternal and Newborn Health Groups in improving peri-natal health. The WU is an organization with high national coverage work-ing with various issues related to women’s situation. There is a long tradition of involvement at local and regional levels of WU in issues of welfare, par-ticularly in health care matters. In a pilot study in 2007, two laywomen from WU were recruited, trained and facilitated four group meetings in two com-munes. The experiences of the pilot found that the facilitation strategy was feasible. In the beginning of 2008, eight individuals from local WU organi-zations were recruited and trained by the research team during two weeks to be able to act as facilitators. Recruitment criteria included being an expe-rienced WU member, having completed secondary school and having child-ren. Additionally three facilitators were recruited during the trial to replace facilitators leaving due to childbirth or new employment. The 11 facilitators (nine from the ethnic majority Kinh and two from the Tay ethnic minority group) had a mean age of 32 years at recruitment. They were paid by the project on full-time basis during the entire 3 years of intervention.
The training program of the facilitators included theoretical session, group discussions, role-plays and field practices. It covered topics such as group dynamics, quality improvement methods (e.g. brainstorming, nominal group technique, the Plan-Do-Study-Act cycle and the Strengths-Weaknesses-Opportunities-Threats diagnostic tool), and basic evidence-based perinatal care. A facilitation manual and a special diary were developed to guide the work of the facilitators. Two research team members coordinated the facili-tation process and acted as supervisors of the facilitators; i.e. field supervi-sion and performing two-days meetings with all facilitators once a month during the entire trial period.

31
Maternal-and-Newborn Health Groups The Maternal-and-Newborn Health Group (MNHG), (Figure 6.) was consti-tuted in each intervention commune (by directives from the Provincial Health Bureau). These groups consisted of eight members: three CHC staff (doctor, midwife and nurse), one village health worker, one population moti-vator, the vice chairperson of the commune (having responsibility for health in the commune), a chair of Women’s Union and one village Women’s Un-ion worker. The facilitators primarily used the Plan-Do-Study-Act cycle in supporting the groups in identifying and priorizing problems and accom-plishing improvement cycles on prioritzed perinatal problems. We strived at keeping each facilitator performing monthly meetings with the same MNHG over the entire three-year intervention period. Each facilitator was responsi-ble for 5-8 MNHGs. When appropriate, the facilitators were recommended to highlight recommendations in the Vietnamese National Standard and Guidelines on Reproductive Health and Services from 2003. MNHG mem-bers were not paid and did not receive any allowances for participating in the NeoKIP project as the improvement work was assumed to be an integrated part of their normal duties.
Figure 6. Problem-solving cycle in Maternal and Newborn Health Groups. Photo by Daniel Persson.

32
The facilitation process and the work of the MNHGs were monitored. Meet-ings, issues dealt with and actions taken were recorded. Facilitators kept diaries, and 16 focus group discussions were held with facilitators and MNHG members before, during, and after the intervention (not reported in this thesis).
Hypothesis The hypothesis in the NeoKIP trial was that an intervention with facilitated work of maternal-and-newborn stakeholder groups on the commune level that included identification of local perinatal health problems followed by a problem-solving cycle would improve the quality and coverage of perinatal services and after some latency lead to improved neonatal survival in com-parison with control communes (Figure 7).
Figure 7. Process of the NeoKIP trial
Sample size The neonatal mortality in the study area in 2005 was 24/1000 live births (6251 live births in the study area in 2005; on average 69 in each commune). We arbitrarily estimated the design effect to be 1.5, considering the relative-
NeoKIP trial
44 intervention communes
8 districts90 communes
NMR ≥ 15/1000Cluster-randomization
46control
communesOutcomes
44 MNHGs
Comparison
8 facilitatorsLay women from WU
Each MNHG composed 8 members from primary healthcare staff (4) and
local politicians (4)
14 districts187 communesNMR: 16/1000
Baseline Intervention
2006 July, 2008 – June, 2011
Outcomes

33
ly high number of clusters and the low average cluster size. A three-year sample would allow demonstrating a significant reduction of 7/1000 in NMR, i.e. to 17/1000 or less, with 80% power at 0.05 significance level. This effect size is comparable to those previously reported from the commu-nity-based trials in Nepal and India.
Randomization The sampling strategy was one-stage cluster sampling with probability pro-portional to size (PPS) of the clusters. The PPS, in this case number of births per year, was chosen to obtain similar distribution of sizes of clusters across intervention and control communes. Sampling was neither blocked nor paired. A sampling frame was established with a cumulative list of number of births in each of the communes in the 2005 survey. A random number list was used to subsequently allocate “intervention” or “control” to the list of communes, and 44 out of the 90 communes were allocated to intervention and 46 to control. The randomization was performed by one of the involved researchers at Uppsala University. The sequence was concealed until the intervention was assigned; otherwise the allocation was not masked.
Data collection and management During the three years of the trial data were collected independently from the facilitation process. The facilitation process was also monitored through monthly meetings with MNHG’s and facilitators based on the problems identified and actions initiated by the groups in the communes. This is de-scribed in detail in other papers [83]. Data collectors (DCs), (Figure 8), who had no contact with the facilitation process, were responsible for the collection of data on all births and neonatal deaths in the entire study area (Figure 9). Each DC was responsibility for one study district with 8-12 communes. They collected data on a monthly basis through meetings at CHCs, where village health workers regularly reported vital events to CHC staff; they visited district-, provincial- and re-gional-level hospitals in order to ascertain complete and correct information on pregnancy outcome and neonatal death. In addition to the monthly data collection rounds, a complete survey of the past 6 months was performed twice per year using the same systematic methodology and triangulation of data from different sources.

34
Figure 8. Data collection; checking forms in Dong Van CHC, Binh Lieu district, Quang Ninh 2011. Photo by Nguyen Thu Nga.
Figure 9. Interview with mother of the newborn at home. Photo by Daniel Persson.

35
Interviews were conducted in households with a deceased newborn (around 8 weeks after birth). This included information on participation in antenatal care, around delivery and care of the newborn. A verbal autopsy interview (see above regarding paper II) was performed in all of these households up to the end of the trial. Causes of death for two years are discussed in paper II while paper III includes information on causes also the third year. Interviews regarding participation in antenatal, delivery and post-delivery services and care were also performed in a random sample (approx. 6% of total) of sur-viving neonates during the trial period. The primary health care staff was also assessed regarding knowledge on newborn care before and after the intervention.
Data collection forms Information was collected on different forms; The first form was delivery form (Appendix 1), which DCs used for collecting the information on each delivery and the delivery outcome: stillbirth, live births and place of delivery (at home or at a specified health facility). To avoid missing or double data an additional form that listed pregnant women in each commune was used by DCs for cross checking with pregnancy outcome. The other questionnaires dealt with neonatal death (Appendix 2) and the randomly selected surviving infants (Appendix 3) that were used in home interviews with mothers eight weeks after delivery. The variables stillbirth, live birth, neonatal deaths were clearly defined according to WHO and documented for the DCs to use in the fieldwork.
The questionnaire-based interview that assessed primary health care staff’s knowledge on newborn care was used before and after the intervention and included 29 questions (Appendix 4). This form was derived from questions frequently used to measure knowledge in nursing research and education and its validity and reliability have been judged to be good [84]. The content of the questionnaire covered breast-feeding, immediate postnatal care, infection management, low birth weight infants, and home visits. The choice of topics was based on WHO recommendations on newborn care and the National Standard Guideline on Reproductive Health in Vietnam [65, 73].
Statistical analysis Data of all four papers were entered into Microsoft Access software and analyzed in SPSS/PASW 18.0 or earlier versions (IBM Corporation, Somers, NY). GIS information (Map source 6.0 and ArcGIS 9) was used to produce a map of location of health facilities in the province (Paper I), the intervention and control communes (Paper III) and for the map of NMR by commune

36
(Paper I). Interpolation of GIS data of the NMR was performed with spline technique.
Information of live births, neonatal deaths and NMR in paper I was analyzed with 95% Confidence Intervals (CI) in relation to place of delivery and level of care.
Data on main causes of neonatal death (paper II) were grouped into six cate-gories according to ICD-10; prematurity/low birth weight, intra-partum re-lated causes (‘birth asphyxia’), infections, congenital malformations, other causes, and unknown cause. These categories were stratified by sex of the newborn, age at death, birth weight (if born at health institutions), and place of delivery. A few case stories illustrated the information provided by the mothers.
In paper III the main outcome of the trial is reported. Problems identified and actions implemented by the MNHGs were quantified and described. Information from first-year randomly selected birth interviews was used to describe socio-economic characteristics and basic perinatal health services utilization in intervention and control communes. The random sample of births was also used to describe the utilization of maternal and neonatal health services in the intervention and control communes for the entire dura-tion of the trial. Frequencies of births, stillbirths, live births, neonatal deaths and maternal deaths were analyzed for the entire duration of the trial and for each of the three years. Stillbirth rates (per 1000 births), perinatal mortality rates (per 1000 births) and neonatal mortality rates (per 1000 live births) were calculated with 95% Confidence Interval (CI). Analysis of Odds Ratios (OR) for neonatal mortality (with 95% CI) for live births in intervention as compared to control communes was performed for the 3 years combined and for each of the three years with Generalized Linear Mixed Models (GLMM) binomial model, adjusting for the cluster design by use of the software R (R Development Core Team 2008) program lme4 (Bates et al 2012). ICC was calculated by R:aod (Lesnoff et al 2012). Time trends were analyzed sepa-rately for intervention and control arms adjusting for cluster by GLMM in R:lme4. P-values <0.05 were considered statistically significant.
Information on use of antenatal, delivery and neonatal health services had been collected from randomly selected mother-newborn pairs during the entire trial period. Coverage was compared between intervention and con-trols. A continuum of care score was also calculated including 21 variables related to antenatal care (n=12) and delivery and postnatal care (n=9). Each variable was dichotomized and given the value 1 or 0.The sum of this score theoretically ranged from 0 to 21. Interviews with CHC staff on knowledge of perinatal care were analyzed and summarized in knowledge scores rang-

37
ing from 0 to 29. Independent samples T-test (Pearson’s chi-square) were used to assess group differences.
Ethical considerations The Ministry of Health, Hanoi approved the NeoKIP project (dnr 3934/QD-BYT), as well as the Provincial People’s Committee and the Regional Re-search Ethics Committee at Uppsala University in Sweden (document num-ber 2005:319). Before start of NeoKIP study, the project was presented, dis-cussed and approved at the provincial health authority level (the provincial People’s Committee and the Provincial Health Bureau). Thereafter, it pre-sented and informally approved in a series of meetings at district and com-mune levels.
Before initiating the baseline survey (paper I) the study team informed health authorities at all levels (province, district and community) and obtained in-formal consent before data collection was started at all health facilities in the province in early 2006. All the VHWs were also informed about the study and verbally consented to participate at the group meetings that were a part of the data collection process.
The researchers were aware of the sensitive situation when interviewing parents of a deceased neonate (paper II and III) and the special ethical con-siderations were discussed [85, 86]. Informed consent was sought from par-ents at the beginning of interview. Some mothers regretted and could not participate in the interview due to the loss of the child and the emotional difficulties.
Data collection on births and pregnancy outcome (paper III and IV) was done with the same methodology as in the baseline, and informed consent was obtained from representatives of the health services at different levels. Informed consent was obtained from mothers in the randomly selected mother-newborn pairs and from parents of deceased neonates. Informed consent was also obtained from the primary care staff that participated in the perinatal knowledge survey.

38
Results
The following results from the NeoKIP trial are presented in this thesis: baseline level of neonatal mortality in Quang Ninh province, the situation regarding antenatal and perinatal health services, and the distribution of causes of death. Thereafter the effect of the intervention on neonatal mortali-ty is reported, and results are also given regarding differences in coverage of antenatal and perinatal care between intervention and control communes.
Perinatal care (Paper I) Antenatal and perinatal care was mainly provided by the public health sys-tem; primary care by 187 CHCs, secondary level care at 16 district hospitals or district health centres, and tertiary level care at one provincial hospital and one regional hospital - in accordance with National guidelines on reproduc-tive health services [73]. People could seek perinatal care at any level and were not bound to their own commune or district. The private sector was relatively limited in relation to perinatal health and no private maternities existed so far in the province.
Antenatal and postpartum care was mainly managed by the CHCs. Accord-ing to records at CHCs excerpted during the baseline survey 76% of preg-nant women had at least three antenatal visits at CHCs and 40% of mothers reportedly had home visits by CHC staff, mainly performed by midwives during the first week after delivery, and another 9% were visited during the second week.
Newborn care was provided at all health facilities where deliveries took place. During 2005 the total number of live births were 17 519, whereof 92% took place at a health facility; 43% of the total number of live births at dis-trict hospitals, 33% at regional and provincial hospitals and 16% at 136 out of 187 CHCs. In 2005, nearly one-third of the CHCs (51/187) had no deli-very at all, one-third (67/187) had an average of nine deliveries per year and one-third (69/187) of the CHCs had a mean of 32 deliveries per year. Also at hospital level there was a great variation in number of deliveries per year; it ranged from 29 to 3258 deliveries per year. Half of the hospitals (9/18) with

39
the lowest number of deliveries had a mean of 210 deliveries, whereas the other half had a mean of 1261 deliveries during 2005.
Relatively few women gave birth at home (8%), but proportions of home deliveries varied between districts; in the five mountainous districts of the province the proportion of home deliveries ranged from 23% to 54%.
Neonatal mortality; baseline level and causes (Paper I and II) During 2005 the total number of neonatal deaths was 289/17 519 live births, resulting in a NMR of 16/1000 live births (95% CI 14 -18) for the whole province, ranging from 10 to 44/1000 in 14 districts.
Figure 10. Level of NMR (with 95% CI) in relation to place of delivery. CHCs and hospitals dichotomized to those with fewer or more deliveries on an annual basis. Baseline survey 2005, NeoKIP trial, Quang Ninh province, Viet Nam.
The district with the highest proportion home deliveries (54%), had the highest NMR; 44/1000 live births. Births at home contributed to 20% of all neonatal deaths and had the highest average NMR of 38/1000 live births, as compared to births at health facilities (Figure 10).
The hospitals with least deliveries per year had a higher NMR (25/1000) than hospitals with most deliveries per year (13/1000). Similarly, the CHCs
40
with least deliveries per year had higher NMR than the CHCs with most deliveries per year.
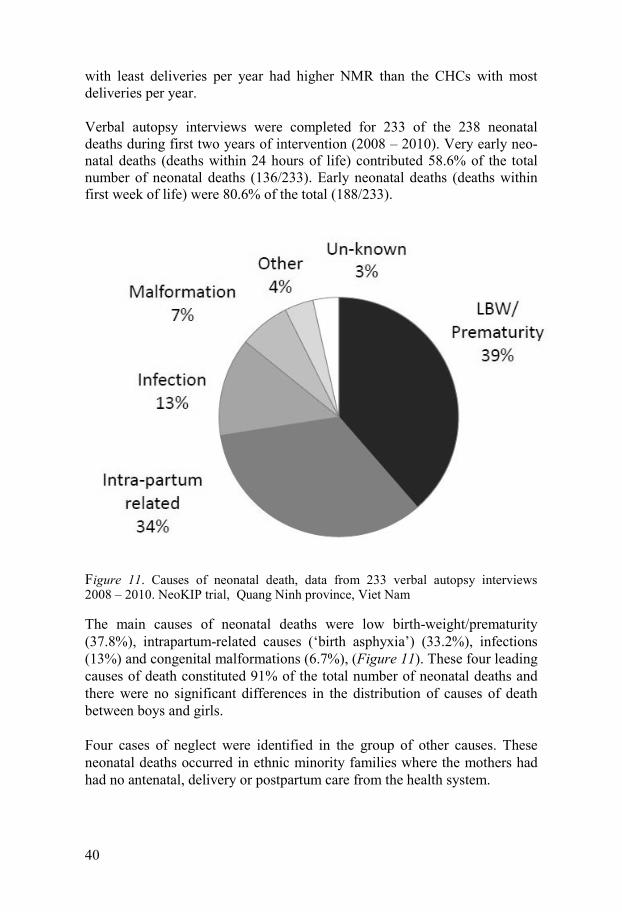
Verbal autopsy interviews were completed for 233 of the 238 neonatal deaths during first two years of intervention (2008 – 2010). Very early neo-natal deaths (deaths within 24 hours of life) contributed 58.6% of the total number of neonatal deaths (136/233). Early neonatal deaths (deaths within first week of life) were 80.6% of the total (188/233).
Figure 11. Causes of neonatal death, data from 233 verbal autopsy interviews 2008 – 2010. NeoKIP trial, Quang Ninh province, Viet Nam
The main causes of neonatal deaths were low birth-weight/prematurity (37.8%), intrapartum-related causes (‘birth asphyxia’) (33.2%), infections (13%) and congenital malformations (6.7%), (Figure 11). These four leading causes of death constituted 91% of the total number of neonatal deaths and there were no significant differences in the distribution of causes of death between boys and girls.
Four cases of neglect were identified in the group of other causes. These neonatal deaths occurred in ethnic minority families where the mothers had had no antenatal, delivery or postpartum care from the health system.

41
Figure 12. Main causes of neonatal death 2008-2010 (n=233) stratified for place of delivery. NeoKIP trial, Quang Ninh province, Viet Nam.
Intrapartum-related causes and low birth weight/prematurity were the domi-nating causes among the very early neonatal deaths accounting for 44.9% and 42.6% of these deaths during the first 24 hours, respectively. The pro-portion of infections as cause of death was higher after the first days of life; 26.9% in day 1-6 and 37.8% in day 7-27, even if low birth weight/prematurity and continued to contribute to 28.8% and 37.8% of deaths during the same age intervals, respectively.
Intrapartum-related deaths dominated in the home delivery group, whereas prematurity was the most prominent cause of death at health facility levels (Figure 12). The highest proportion of intrapartum-related deaths at hospit-als (birth asphyxia) (34.3%) was noted at district hospitals.
Effect on neonatal mortality (Paper III) Of the 90 communes in the study area, 44 intervention communes had MNHGs that worked, supported by a facilitator from Women’s Union, to identify local maternal and newborn health problems and to agree upon ac-tions. No commune was lost to follow-up, but one intervention commune
0
10
20
30
40
50
60
Home CHCs District hospitals Tertiary hospitals
Perc
enta
ge o
f cau
ses o
f dea
th (%
)
LBW/ Prematurity
Intra-partum related causes
Infection

42
stopped the facilitated meetings after 21 months - or 15 months before the end of intervention trial, while all other communes completed the interven-tion.
The groups identified unique maternal and newborn health problems totally 206 times, and implemented unique actions 933 times. The five most com-monly identified problems were women not booking for antenatal care at the right time, low frequency of postpartum home visits, low awareness among pregnant women of appropriate diet, work and rest, high frequency of home deliveries and low awareness among pregnant women about appropriate breast-feeding practices. The most common actions taken were communica-tion activities (loudspeakers), preparation of relevant education materials, actions to promote post-natal home visits, registration of pregnancies and newborns and distribution of leaflets on relevant issues related to maternal and newborn health.
There were 22 562 births registered in the study area over the three years of trial, whereof 184 resulted in stillbirth (8.2/1000 births). Of the 22 377 live births 389 died in the neonatal period, giving an overall NMR at 17/1000 live births.
Basic characteristics of the mothers such as ethnicity, self-assessment of family economic status, mother’s age, job and mother’s education level were compared between intervention and control communes and were found to be similar across intervention and control areas.
Neonatal mortality rates the three years from July 2008 to June 2011 were 19.2, 19.0 and 11.6/1000 live births in the intervention communes and 18.0, 15.9 and 21.1 in control communes, respectively. The risk of neonatal mor-tality the third year was reduced in the intervention communes with an OR 0.51 (95% CI 0.30-0.89), (Figure 13).
The three leading causes of death were prematurity/low birth-weight (36%), intrapartum-related neonatal deaths (30%) and infections (15%). During the third year of trial, a reduction in the number of deaths was seen in all three groups (Paper III).

43
Figure 13. Adjusted OR (adjusted for cluster design) with 95% CI for neonatal death in intervention communes as compared to control communes the three years of NeoKIP trial from study start July 2008 to study end June 2011. Quang Ninh prov-ince, Viet Nam.
Coverage of antenatal and perinatal care in intervention and control communes (Paper IV) Over the three years of the trial 1338/22 377 (5.9%) live births were random-ly selected to represent the total cohort of live births (656 in intervention communes and 587 in control communes). Non-participation in these inter-views was 7.1% with no difference between intervention (n=48) and control (n=47) communes. The main reasons to omission were that mothers de-clined, that the mother lived at the grandmother’s house during maternity leave, that the address was unclear or that another family had adopted the newborn infant.

44
Figure 14. Difference in coverage of services and care in the antenatal, delivery and newborn periods between intervention and control communes in NeoKIP trial, Quang Ninh province 2008-2011. ANC = antenatal care; BP = blood pressure mea-surement; TT = tetanus toxoid immunization; BW = birth weight measurement.
Indicators of maternal, delivery and neonatal care practices were compared between intervention and control communes (Figure 14). Pregnant women living in intervention area had higher coverage of antenatal care (91 and 82%, respectively) and received antenatal services more frequently; they more frequently got blood pressure tested (83 and 76%), received tetanus immunization (89 and 84%), got HIV testing (51 and 41%) and ultrasound examination (88 and 84%, respectively). In intervention communes women more frequently prepared themselves for delivery (92 and 88 %, respective-ly) and they also delivered at health institutions more often (91 and 87%, respectively) and got the newborn’s weight measured. No differences were

45
noted in newborn care, e.g. skin-to-skin contact after delivery, provision of colostrum, breastfeeding initiation within the first hour or exclusive breast-feeding at one month of age. It should be noted that women reported a low coverage of home visit by midwife (9 and 7%, respectively) without differ-ence between intervention and control communes. Baseline information excerpted from CHCs gave much higher figures on home visits.
Primary healthcare staff’s knowledge on neonatal health A questionnaire-based assessment on CHC staff knowledge on neonatal health was performed before and after the intervention. Totally 155 staff completed both surveys. There were totally 29 items dealing with immediate care of the newborn, breast-feeding, infection management, low birth weight, and other issues related to the management of the newborn. The mean scores were compared between the two rounds of survey (before and after intervention) and between intervention and control areas. There was a small overall increase in the mean score by +1.1 in intervention area (19.4 to 20.5) while the mean score did not change in the control area (20.3 to 20.2). This difference between intervention and control areas is judged to be with-out any public health importance although statistically significant (p= 0.03).

46
Discussion
This thesis is based on a community-based trial that aimed at improving neonatal health and survival in Quang Ninh province, Vietnam. The prov-ince had medium-level neonatal mortality rate (16/1000 live births), 92% institutional deliveries and relatively good coverage of antenatal health ser-vices. However, behind these averages there was inequity in neonatal sur-vival with different districts ranging from 10 to 44/1000 live births and be-tween health institutions. The most common causes of death were preterm birth, intrapartum-related causes and infections – many of these preventable. In NeoKIP cluster-randomized trial local stakeholder groups (from health services, politicians and women’s union) were working for three years, faci-litated by a local laywoman, to identify problems and find solutions to peri-natal health issues in the local setting. We have shown that intervention communes had higher coverage of antenatal care, delivery care and that CHC staff gained some more knowledge in management of the newborn. After a latent period of two years, neonatal mortality was significantly re-duced in intervention communes but not in control communes.
In the following methodological strengths and weaknesses of the study will be considered, the findings will be discussed and related to other relevant research, and the public health implications will be addressed.
Methodological considerations Internal validity The papers reporting the cluster-randomized trial have been written to comp-ly with the Consolidated Standards of Reporting Trials (CONSORT) agree-ment; the extension to cluster randomized trials [87].
Validity of the studies in this thesis is based on good quality design, ade-quate organization of fieldwork, implementation of the intervention accord-ing to protocol, high-quality processes of data collection and management and careful analysis and interpretation of results.

47
A steering board provided support to all steps in establishing and running the trial. This was important for the commitment to the trial in MNHGs in the communes and for the support provided at commune and district level authorities within the health sector and by the political representatives. Baseline survey To ensure validity of baseline data the methodology was carefully piloted in one district before implementation in the whole province during the first six months of 2006 (Paper I). Data on births and pregnancy outcomes and neo-natal deaths were triangulated from all available sources: records at hospit-als, at CHCs and through group interviews with village health workers from all communities in the province. However, seven percent of these VHWs were missing at meetings; this could have implied a minor underreporting of deaths not registered in the records in the health system. In the group inter-views with the VHWs efforts were made not to misclassify a stillbirth or a neonatal death. One of the findings of the baseline survey (reported in a sep-arate paper) was the serious underreporting of neonatal deaths in the official reporting of births and deaths [35] and also that the primary healthcare staff had limited knowledge on newborn care [88, 89]. Baseline survey results were used for planning of the NeoKIP intervention as presented in the trial protocol [74].
Ascertaining causes of neonatal deaths During the first two years of the trial all cases of neonatal death were docu-mented and included in an analysis (paper II). Data collection was thereafter continued also the third year of the trial and a brief summary of causes of death is also included in paper III. The verbal autopsy (VA) questionnaire was based on the WHO generic questionnaire for neonatal causes [36] that was revised to fit the Vietnamese setting and pilot-tested before use in the trial. Efforts were made to adapt language to enable a smooth conversation between interviewer and mother [34, 38]. To ensure the quality of interviews two of the data collectors with background in midwifery were selected and trained to use the questionnaire, and they got practical training in interview-ing mothers who had lost a child during the neonatal period outside the study areas. Only five cases were lost (2%) which is very low as compared to other similar studies [90]. Ascertaining causes of neonatal death could be done in interviews performed by different categories of medical personnel such as nurses and midwives [91] or by computer-based modules based on different symptoms [48, 92]. In a low-income country community setting the verbal autopsy interviews are appropriate, and this should be combined with final assignment of cause of death done by three independent and experienced

48
neonatologists. If disagreement arouse the dilemma was solved by a consen-sus process.
The trial The study design of the NeoKIP project was cluster-randomized trial, which may be seen as the golden standard to evaluate community-based interventions [93]. The power calculations were done so that we should be able to demonstrate a significant reduction of NMR of similar size as in the studies in Nepal and India [67, 69]. A sample of around 6% of the total population of live births was randomly selected to represent the entire birth cohort, and was used to evaluate antenatal, delivery and postnatal care utilization in intervention and control arms. The cluster-randomized design was accounted for in the analysis of the pri-mary outcome; neonatal mortality. The intra-cluster correlation was low (0.0073), which implies that the design effect was limited. In the analysis adjustment was made for cluster (commune). The cluster design also in-creases the risk of contamination between intervention and control arms. Distance is not great between an intervention commune with its CHC and the adjacent control commune with another CHC. There is always some interaction between staff of different CHCs. This potential contamination would lead to improvement also in the control communes and thus decrease the estimated effect of the intervention.
The facilitation process was carefully monitored. Information was collected at the monthly meetings with MNHGs and at meetings with the group of facilitators. Focus group discussions were also conducted before, during and after the trial and this information about the facilitation process has been discussed in another thesis [83]. Priority problems identified and action tak-en by MNHGs were continuously recorded. Perinatal health issues and sug-gestions for actions were not imposed on the MNHGs, but the facilitator tried to stimulate the group to identify and address priority problems in the local area and actions that were realistic to perform.
Data collection and management in the trial Data collection was organized separately in order not to be influenced by the field organization of the intervention. Collected data were scrutinized and if incomplete or inconsistent returned to the field for correction. There were regular meetings with data collectors as part of the triangulation of data on births and neonatal deaths, and to discuss problems related to interviews and data flow. A continuously updated list of pregnant women enabled a syste-matic enquiry on a monthly basis regarding pregnancy outcomes. The sys-tem for data collection was developed for the baseline survey (Paper I) and

49
was judged to provide the best possible data on births and neonatal deaths in this setting [35]. Supervision of data collection was done at health facilities and at participants’ homes, where the interviews with mothers were con-ducted. The timing of home interviews was eight weeks after delivery to reduce non-participation that could occur during the neonatal period (4 weeks) and not to be too close to the event of neonatal death. We judged this to be a suitable time to create a good atmosphere at interview and more easi-ly get acceptance from mothers and families. This time is later in comparison with most other studies; home interviews were conducted at one month in Nepal [67, 94], at 6 weeks in India (Jharkhand and Orissa districts) [69] but at 12-16 weeks after delivery in Pakistan [95].
External validity and generalization The NeoKIP trial and related studies were conducted in a province with mid-level NMR but great inequities in newborn survival between districts, a rela-tively well-developed system of health care, an active Women’s Union and a local government similar to other provinces in Vietnam. Ethnic minority groups, mainly living in remote settings had higher neonatal mortality risks [96] that challenge the health system and society over all to get an equitable improvement of child health and survival [97]. This situation including its heterogeneity is found in many Vietnamese provinces. The findings of the trial may be relevant all over Vietnam – and the community-based approach may be appropriate also in other countries where the identification and ac-tions related to the local setting may be key to general improvement in neo-natal survival.
Level of neonatal mortality rate The province had a medium-level NMR (16/1000 live births), which was higher than expected – at least if considering official reports. This level of NMR was four times higher than the official data reported by the provincial health bureau for 2005 [35]. According to the Vietnam Demographic Health Survey VNDHS in 2002, the level of NMR was 12/1000 with a range across seven regions of the country; from 6/1000 to 31/1000 live births [98]. Over-all the level of NMR in Vietnam including this province is lower than in other Asian countries, for example Bangladesh, Nepal, and India [23], where the deliveries take place at home in 60 to 80 % [29, 67, 69, 99]. We ob-served a large geographical variation in NMR, ranging from very low levels in the urban lowland to very high in the rural highlands – where also health facilities were more scarcely distributed. Areas with higher NMRs had long-er distances to hospitals [100]. In a previous study in Bavi district, Red River delta area in Vietnam, we also found associations between ethnicity (differ-

50
ent minority groups) and neonatal mortality but also inequities related to the educational level of the mother [18].
Most women had chosen to deliver at health facilities (92%). This relatively low frequency of home deliveries without birth attendance contributed 20% of the neonatal deaths. Analysis of Demographic Health Survey data in Vietnam has shown that social characteristics of the woman including eth-nicity are associated with their care-seeking behavior including place of de-livery [101].
A major part of the neonatal deaths (46 %) happened within the first 24 hours of life and half of their mothers had not visited health facilities [102]. In spite of a relatively high coverage of antenatal care and a low frequency of home deliveries, the health system did not manage to create a good and equitable continuum of care that could prevent the high occurrence of neo-natal deaths in some districts. The skilled assistance at delivery should be followed by a postnatal home visit, which is part of the country’s perinatal care package and that potentially can prevent early neonatal deaths, especial-ly those caused by infections [88]. A medium-high frequency of home visits was reported by the health system [79] but when mothers were asked it was found to happen in less than one in ten deliveries (Paper IV).
Home deliveries resulted in the highest NMR. Mortality rates at health facili-ties varied with total number of deliveries per year at those institutions. This may reflect quality of care and indicate that Commune Health Centers as well as hospitals need to have a certain number of deliveries in order to es-tablish and maintain quality of the services they provide [103]. In another sub-study we have shown that health workers in the province at primary care level had insufficient knowledge about neonatal care and that the level of knowledge varied with level of neonatal mortality in the district [88].
Causes of neonatal death With a medium-level NMR (16/1000 live births), the distribution of causes of neonatal death was as expected and different from settings with high NMRs; a bit lower proportion of infections and larger proportion prematurity and intra-partum related causes [104]. Globally, infections contribute up to a quarter of the total number of neonatal deaths [104] while this was 13% in Quang Ninh. The high rate of institution deliveries (92%) with skilled birth attendance and use of sterilized equipment at all health facilities presumably contributed to the low mortality in neonatal infections. Tetanus is officially eradicated in Vietnam [105] and full-scale vaccination programs aim at cov-ering all pregnant women with at least two shots of the vaccine. Still, we

51
found four neonatal deaths due to tetanus, all happening in households with-out any contact with the health system: no antenatal care, home delivery without skilled birth attendance and only one case had tried to seek care for the baby, but too late, and the baby died at the district hospital. These cases occurred in families belonging to ethnic minority groups. Inequities in new-born and maternal health due to ethnicity are also previously reported in Vietnam [96, 106] and the cases of tetanus illustrate this problem. Further, four cases of neglect were identified as the primary cause of death; three boys and one girl. Once again, this happened to those most vulnerable in society: ethnic minority groups, living in mountainous areas, with low level of education, in poverty, and with limited access to healthcare. These prob-lems are clearly not related to the tradition with son preference in Vietnam [107, 108] and is a challenge for the health system and society to implement universal health care and build equity in maternal and child health [97]. Causes of neonatal death were analyzed in relation to place of delivery; in-tra-partum-related causes constituted a high proportion also among cases delivered at health facilities, especially at district level. Nearly haft of the women delivered at district hospitals [79]. In order to save these lives all perinatal care staff needs appropriate skills in neonatal resuscitation and asphyxia management – in addition to the management skills of the birthing woman [109, 110]. Reduction of asphyxia deaths is considered a top priority for global neonatal health and survival [111]. The other leading cause of death – prematurity and low birth weight constituted one third of neonatal deaths and was relatively high at health facilities. This emphasizes the need of good perinatal care and management for this group of newborns. The possibilities for referral before delivery and kangaroo mother care for the premature and low birth weight newborns [112, 113] should be implemented in line with a continuum of good-quality care from home and community to health facilities.
Effects of the intervention
Neonatal health has been prioritized during the last two decades in Vietnam. Guidelines have been prepared from central level and efforts have been made to further develop perinatal services at all levels of the health system.
The MNHGs were constituted in each commune and were composed by local leaders who all had some responsibility related to maternal and new-born health and welfare: three primary healthcare staff (doctor, midwife and nurse), one village health worker, one population collaborator, the vice chairperson of the community People’s Committee, and two representatives

52
of the local Women’s Union. They represented different roles and responsi-bilities but joined forces in the MNHGs with the aim at identifying perinatal health problems and decide on actions that could be implemented as part of their normal duties. The facilitator was a laywoman recruited from the Women’s Union. A laywomen was chosen instead of a professional from the health sector in order to underline the facilitator role; supportive, providing advice on the general strategy of work, but not an instructor, teacher or ex-pert in the field of maternal and child health. The group identified priority problems and actions.
Only one of 44 groups decided to end the facilitated meeting after 21 months or 15 months before the end of intervention trial, otherwise all groups con-tinued for the full trial period of three years. Also in the Nepal trial 95% of women’s groups maintained activities up to the end of the intervention [67].
This type of intervention is not expected to result in an immediate effect on neonatal mortality that maybe could have been achieved by a single or pack-age interventions. The intervention with groups that worked together for three years using a problem-solving approach regarding perinatal health resulted in increased coverage in antenatal care, slightly increased reported birth preparedness and also some increase in delivery at health institutions. Neonatal care indicators, on the other hand, did not change. Behind the small average changes there is a variation with greater differences in some geo-graphical areas and smaller in other. There was also a small increase in knowledge on neonatal care practices among primary health are staff. It was not until the third year of the intervention that NMR was lowered in the in-tervention clusters. Although we have not yet performed a cost-effectiveness analysis of the intervention we have noted that additional costs were relative-ly low (only facilitators employed) and effects relatively large (OR 0.51, 95% CI 0.30-0.89).
This type of community-based approach is a new strategy in Vietnam. Members of the MNHG did the work as part of their normal duties. Together they represent different sectors on the commune level and joined forces for better maternal and newborn health. This type of intervention may be more appropriate in the hierarchic structure of the Vietnamese society than the corresponding intervention with women’s groups that was implemented in South Asia [67, 69].
Most of the problems identified by the MNHGs dealt with the mother-and-newborn dyad and its use of the health system and less with problems of quality of care and performance of the health care providers. Maybe this is reflected in the absence of differences in some of the newborn care

53
indicators between intervention and control arms. Actions by the MNHGs often dealt with communication (frequently by loudspeakers) and counselling of mothers. Initiation of breastfeeding did not change by the intervention. A participatory approach with groups of women [67] is maybe more likely to influence the immediate newborn care of the birthing women. This type of intervention is not expected to provide a solution to all neonatal health problems. We noted that asphyxia problems still remained a problem also at district hospitals (maybe to be addressed by direct interventions at that level) and that preterm babies still were in need of appropriate care with skin-to-skin contact etc. Home visits were not done according to Govern-ment recommendations – if better implemented maybe some further infec-tious disease deaths could have been prevented.

54
Conclusions
The NeoKIP intervention took place in a province in northern Vietnam with a medium-level neonatal mortality and a relatively comprehensive health system that provided maternal and neonatal health services. Private actors played a limited role, mainly in offering antenatal care. Home deliveries were few but with a high risk for neonatal death. There was a great geo-graphic and social inequity in reach of perinatal services and level of neonat-al survival [35, 79, 102]. The facilitation intervention with local stakeholder groups composed by primary care staff and local politicians that worked with a perinatal problem-solving approach substantially reduced neonatal mortality. Incremental costs for this type of intervention are judged to be low, and mainly related to costs for the laywoman facilitator and the indirect costs of MNHGs monthly meetings. Quang Ninh province is relatively typi-cal for many Vietnamese provinces, with the dominating ethnic majority in towns and most rural areas, and ethnic minority groups in the remote, moun-tainous areas [100]. Therefore, a cost-effective facilitation intervention by community-based participatory for improved neonatal survival could be scaled-up to other settings in Vietnam and be an alternative also in other countries, where society is in rapid transition [114].

55
Summary in Vietnamese/Tóm tắt luận văn bằng tiếng Việt
Nhìn toàn cầu, tình hình cứu sống trẻ sau tuổi sơ sinh và trẻ em đã được cải thiện rất rõ rệt, nhưng tử vong của trẻ sơ sinh (tử vong trong vòng 28 ngày đầu sau đẻ) vẫn còn ở mức cao và hiện tại chiếm tới 40% tổng số tử vong xảy ra ở trẻ em dưới 5 tuổi. Tăng cường áp dụng rộng rãi một số biện pháp can thiệp dựa vào bằng chứng sẽ giảm nhanh tử vong sơ sinh trên toàn thế giới. Tuy nhiên, có sự mất công bằng lớn về chăm sóc sức khỏe chu sinh ở các khu vực đặc biệt các khu vực tuyến xã và tuyến huyện ở các nước thu nhập thấp và trung bình. Các can thiệp dựa vào sự tham gia của cộng đồng thực hiện tại những nơi mà các vấn đề về bệnh tật và tử vong sơ sinh nổi cộm đã mang lại những thành công rất lớn ở một số nước. Tuy nhiên cho tới nay chưa có một nghiên cứu khoa học nào đề cập tới sự tham gia một cách hệ thống của các cán bộ chủ chốt tại địa phương nhằm tăng cường chăm sóc sức khỏe chu sinh. Ví dụ: nghiên cứu về sự phối hợp của cán bộ y tế và cán bộ chính quyền và đoàn thể; cùng làm việc dựa vào: 1)bằng chứng khoa học để cải thiện sức khỏe bà mẹ và trẻ sơ sinh ngay tại địa phương mình và 2)bằng cách tiếp cận chủ yếu dựa vào sự tham gia của cộng đồng.
Mục tiêu của luận văn này là mô tả thực trạng và những thách thức về các vấn đề sức khỏe chu sinh ở tỉnh Quảng Ninh; và đánh giá kết quả can thiệp hỗ trợ của các ban cán bộ chủ chốt tại địa phương (Ban Chăm sóc Sức khỏe Bà mẹ và trẻ Sơ sinh, “Ban NeoKIP”) sử dụng phương pháp tiếp cận “vấn đề-giải pháp” để nâng cao sức khỏe và cứu sống trẻ sơ sinh. Đề tài nghiên cứu có tên viết tắt là NeoKIP (Neonatal health Knowledge Into Practice,– Sức khỏe trẻ Sơ sinh - Kiến thức Áp dụng vào Thực tế). Mã số đăng kí theo qui định Quốc tế về nghiên cứu thử nghiệm đối chứng ngẫu nhiên là ISRCTN 44599712 và đề tài đã thực hiện tại tỉnh Quảng Ninh, Việt Nam từ 2006 đến 2011.
Đề tài nghiên cứu được triển khai qua hai giai đoạn: 1) Nghiên cứu điều tra cơ bản về thực trạng dịch vụ và kết quả Chăm sóc sức khỏe Chu sinh, và được thực hiện năm 2006 trên toàn tỉnh Quảng Ninh; 2) Nghiên cứu can thiệp, và được thực hiện tại tám huyện, thị xã (Hải Hà, Đầm Hà, Tiên Yên, Bình Liêu, Ba Chẽ, Vân Đồn, Hoành Bồ và Uông Bí); nơi có tỉ lệ tử vong sơ sinh >15/1000 trẻ đẻ ra sống (dựa vào kết quả của điều tra cơ bản của số liệu toàn tỉnh năm 2005). Toàn bộ 90 xã của tám huyện, thị xã can thiệp này

56
được chọn mẫu ngẫu nhiên theo đơn vị xã 44 xã được chọn là can thiệp và 46 xã là đối chứng, và được thực hiện trong thời gian ba năm (2008 – 2011). Một số phụ nữ địa phương được tuyển chọn từ cán bộ Hội Phụ nữ cấp xã để làm nhiệm vụ người hỗ trợ các Ban Chăm sóc Sức khỏe Bà mẹ và trẻ Sơ sinh tại địa phương. Tám cán bộ nữ này đã hỗ trợ 44 Ban của 44 xã can thiệp thông qua các cuộc họp định kì hàng tháng tại xã và hỗ trợ Ban áp dụng chu trình “Kế hoạch-Thực hiện-Đánh giá-Hành động” (PDSA) trực tiếp cho các vấn đề sức khỏe chu sinh tại địa phương.
Ở cả hai khu vực các xã can thiệp và đối chứng, số liệu về số sinh, tử vong trẻ sơ sinh được theo dõi, thu thập hàng tháng do nhóm cán bộ số liệu thực hiện đều đặn và riêng biệt với tất cả hoạt động của can thiệp. Đồng thời, nhóm cán bộ số liệu này còn có nhiệm vụ thực hiện phỏng vấn tại hộ gia đình có con tử vong trong giai đoạn sơ sinh và tại hộ gia đình các trẻ được chọn ngẫu nhiên từ danh sách trẻ sơ sinh đẻ ra sống (6%) trong thời gian thực hiện nghiên cứu NeoKIP 2008 – 2011. Các số liệu và thông tin về sử dựng các dịch vụ chăm sóc trước sinh, khi sinh, sau sinh, và nguyên nhân tử vong sơ sinh được kiểm tra chéo qua các nguồn thu thập số liệu nói trên ở cả hai khu vực can thiệp và đối chứng. Kiến thức của cán bộ làm việc tại các trạm y tế về chăm sóc sơ sinh cũng được đánh giá trước và sau can thiệp NeoKIP.
Kết quả nghiên cứu của đề tài cho thấy: Quảng Ninh có mạng lưới hệ thống y tế hoạt động rộng khắp từ tuyến trung ương khu vực, tuyến tỉnh, tuyến huyện cho tới tuyến xã, phường với tổng số 205 cơ sở y tế. Cơ sở y tế tư nhân có nhưng ít hơn so với tỉnh khác và không có cơ sở tư nhân nào thực hiện dịch vụ chăm sóc cuộc đẻ. Tỉ lệ tử vong sơ sinh (NMR) trong toàn tỉnh là 16/1000 trẻ đẻ ra sống (sự chênh lệch giữa các huyện là rất lớn, từ 10-44/1000). Tỉ lệ phụ nữ sinh con tại nhà thấp (8%) nhưng số tử vong sơ sinh trong nhóm này chiếm một phần năm toàn bộ tổng số tử vong xảy ra ở trẻ sơ sinh. Các cơ sở y tế có số trường hợp đẻ trung bình trong một năm ít hơn thì tỉ lệ tử vong sơ sinh lại cao hơn. Các nguyên nhân chính dẫn đến tử vong ở trẻ sơ sinh là sinh non/cân nặng thấp khi sinh (37.8%), tử vong sơ sinh liên quan tới chuyển dạ (‘ngạt khi sinh’) (33.2%) và nhiễm trùng sơ sinh (13%). Đa số tử vong (59%) xảy ra ở ngày đầu tiên và 81% xảy ra trong tuần đầu tiên của cuộc đời đứa trẻ.
Tỉ lệ tử vong sơ sinh từ tháng 7/2008 đến tháng 6/2011 là 16.5/1000 (195 trường hợp chết trong tổng số 11818 trẻ sinh sống) ở các xã can thiệp so với 18.4/1000 (194 trên tổng số 10559 trẻ sinh sống) ở các xã đối chứng (tỉ suất chênh đã điều chỉnh-adjusted odds ratio 0.96 [95% CI 0.73-1.25]). Tỉ lệ tử vong sơ sinh hàng năm là 19.1, 19.0 và 11.6 ở các xã can thiệp so với 18.0, 15.9 và 21.1 ở các xã đối chứng (tỉ suất chênh đã điều chỉnh - adjusted odds ratios 1.08 [0.66-1.77], 1.23 [0.75-2.01], và 0.51 [0.30-0.89], so sánh tương ứng). Phụ nữ ở các xã can thiệp thường đi khám thai, chuẩn bị cho cuộc đẻ

57
và đến đẻ tại cơ sở y tế nhiều hơn so với phụ nữ ở các xã đối chứng; nhưng thực hành chăm sóc sau sinh cho bà mẹ và trẻ sơ sinh thì không thấy có sự khác biệt giữa hai khu vực. So sánh trước và sau can thiệp, kiến thức về chăm sóc sơ sinh của cán bộ chăm sóc sức khỏe ban đầu (làm việc tại trạm y tế) ở các xã can thiệp đã tăng lên, nhưng không thay đổi ở các xã đối chứng.
Mô hình hỗ trợ của các ban cán bộ chủ chốt tại địa phương về tăng cường chăm sóc sức khỏe và giảm tử vong sơ sinh, áp dụng phương pháp tiếp cận “vấn đề-giải pháp” đã thành công ở tỉnh Quảng Ninh. Mô hình can thiệp này hiệu quả, chi phí thấp, dựa vào sự tham gia của cộng đồng và lồng ghép vào hệ thống Y tế hiện có, mang tính khả thi cao để nhân rộng cho các tỉnh khác trong cả nước. Đồng thời mô hình này là một trong các giải pháp chọn lựa cho can thiệp nhằm cứu sống trẻ sơ sinh ở các quốc gia khác trong khu vực và trên thế giới.

58
Acknowledgements
The work of this thesis was conducted at the department of Women’s and Children’s Health, International Maternal and Child Health (IMCH), Uppsa-la University in Sweden and at institutions in Vietnam, particularly the Viet-nam - Sweden General Hospital in Uong Bi (UBGH). Greatly acknowledged is the financial support from the Swedish International Development Coop-eration Agency and from Uppsala University.
Firstly, I would like to express my deepest gratitude to my supervisors Pro-fessor Lars-Åke Persson, Professor Uwe Ewald and Doctor Annika Jo-hansson. You are all excellent supervisors and I am very happy to have been trained by, and conducted research with all of you. Thank you for the conti-nuous encouragement.
I wish to thank my main supervisor Professor Lars-Åke Persson for giving me the opportunity to be a PhD student at IMCH. Thank you for giving me valuable suggestions and for deeply engaging in my field of interest and enabling me to continue my work for improved newborn health and survival in Vietnam. You have been supportive, given me many useful advises and continuously encouraged me on the long journey of my fieldwork in Quang Ninh as well as in the academic work in Uppsala. My great thanks also to my co-supervisors Professor Uwe Ewald and Doctor Annika Johansson. Thank you for both the excellent guidance and optimal encouragement. Prof. Uwe Ewald, you have taught me valuable knowledge on neonatal health that is very helpful for clinical practice as well as community-based interven-tions. Dr. Annika Johansson, thank you for sharing your knowledge and experiences of social and cultural aspects of child health in Vietnam.
Furthermore, I wish to thank Professor Lars Wallin for teaching me about knowledge translation research in the world and in Vietnam. Thank you also for your active engagement in the NeoKIP project as a whole.
Words are not enough to express my gratitude to my fantastic colleagues in the NeoKIP research team. Mats Målqvist, Leif Eriksson, Dinh Phuong Hoa and Tran Quang Huy; thank you all for involving in the NeoKIP project from the beginning! Thank you for fruitful brainstorming that leads to the implementation of evidence-based knowledge into this community-based

59
intervention. You have all supported me very much since 2004, both in Quang Ninh and in Uppsala. Many thanks to Duong Minh Duc and Nguyen Thi Thuy for your hard work in the field supervision in general, and in the facilitation activities in particular. Thanks a lot to Le Thanh Do and Vu Pham Nguyen Thanh for sharing your professional knowledge in data pro-gramming, management and sociology with us for successful implementing NeoKIP intervention.
Also, I would like to thank the data collectors – young nurses and midwives, and the facilitators – the beautiful laywomen who worked as NeoKIP staff between 2006-2011. Thank you all for your hard work within the NeoKIP project. Your contributions are immense; you worked directly with 44 MNHGs, 187 CHCs, and 18 hospitals in Quang Ninh province and con-ducted more than 1800 home interviews with parents of the newborns. It is a mountain of work, and without your work, this thesis would never have been written.
I would like to thank the health staff of all health facilities. Furthermore, I would like to thank specially Doctor Vu Thi Thu Thuy and all the partici-pants from the Political and Women’s Union systems for a very good colla-boration and for your valuable contribution to the NeoKIP project. In addi-tion, a special thanks to all MNHG participants for your hard work in identi-fying prioritized problems and implementing actions in order to improve neonatal survival.
My sincere gratitude also goes to the mothers, fathers, and their families in the NeoKIP area. Thank you for the warm welcoming you gave us and for inviting us into your homes. Thank you for sharing your experiences of pregnancy, delivery, and postnatal period, and for sharing stories of both joy, but also the tragic stories of losing a child.
I wish to thank the Vietnam-Sweden General Hospital, Uong Bi, in Vietnam, where I have worked as a clinical pediatrician, and where I have done re-search in child health. Thank you for your collaboration and support, espe-cially Doctors Nguyen Ngoc Ham and Tran Viet Tiep for your continuous encouragement, and later on also for supporting the NeoKIP project. To the colleagues, both Vietnamese and Swedish, whom I have had the great oppor-tunity to work with at the pediatric department in the UBGH; I would like to express my thanks to you all, and especially to Doctors Vu Gia Khuong and Rolf Johansson. I wish to thank the UBHG hospital board, Dr. Rolf Johans-son, Dr. Eva Johansson, Dr. Annika Johansson and Mrs. Nina McCoy for all the encouragement and support for the opportunity to go to Sweden for a Master training program on Global Public Health at the Division of Global Health (IHCAR), Karolinska Institutet, in Stockholm. During that period, I

60
also had the opportunity to gather a lot of public health experiences and knowledge by involving myself in the Field Laboratory Epidemiology in Bavi (FilaBavi), Vietnam. The time at IHCAR was very valuable and I wish to take the opportunity to thank the senior researchers for sharing your valu-able knowledge and all your experiences with me. So, thank you Professors Bengt Höjer, Staffan Bergström, Anna Berit Ransjö-Arvidson, Elisabeth Faxelid, Göran Tomson, Kyllike Christensson and Vinod Diwan.
I would like to express my thanks to the leaders and colleagues from the Department of Maternal and Child Health and the Department of Scientific and Training at the Ministry of Health in Hanoi, Vietnam for the good colla-boration and for the support in the implementation of the NeoKIP project in Quang Ninh. I do hope the results and experiences from the NeoKIP will be scaled up to improve neonatal health and survival in our country. At the Ministry of Health, my special thanks to Associate Professor Dinh Phuong Hoa for being the best colleague and friend for my research and in my life. Thank you for sharing your knowledge, experiences, and your tireless efforts to place child health on the agenda in Vietnam. The success of the NeoKIP project and my PhD study has had an important contribution from you.
My warmest thanks to all the lecturers and staff at IMCH, past and present, you have all supported me so much throughout my PhD training. My special thanks to Cristina Niska Bachelet, Karin Törnblom and Kristine Eklund for giving me excellent administrative support. You, together with all other staff at IMCH, have really made my stay in Uppsala smooth and comfortable, which enabled me to focus on my research.
To my fellow PhD-students at IMCH, some of you whom have finished your PhD, I would like to thank all of you for your support, your friendly way of being, for organizing the PhD parties at the ‘Center-party in Box-building’ and for singing the famous song “IMCH” on all occasions. You are all in my heart. So, thank you Anna Bergström, Amal Omer-Salim, Annika Esscher, Ashraful Islam Khan, Amare Worku, Baitun Nahar, Emma Lindstöm, Malin Jordal, Mariel Contreras, Jill Trenholm, Pauline Binder, Petrida Ijumba, Shirine Ziaie, Soorej Jose, William Ugarte, Wilton Perez and Wanjiku Kaime.
To my family, my thoughts are always with my dearest parents although they are not with us anymore; they are still present in my life. They always inspired me in all the work I have undertaken and in life at large. They en-couraged me to study medicine and were very happy and proud when I be-came a pediatrician as two of my brothers died at early ages due to measles. I would also like to give my love and thanks to my brothers, sisters and all

61
other members of my family and family in-law who have been supportive to me throughout these years.
Finally, but most importantly, I wish to thank my beloved husband Nguyễn Thiện Nguyên and our daughters Nguyễn Thiện Thu Anh and Nguyễn Thiện Mai Anh. Thank you for accepting my long periods staying away from home, for your moral support and encouragement and for your love.
Uppsala, December 2012 Nguyen Thu Nga

62
References
1. WHO, International statistical classification of diseases and related health problems, Tenth Revision (ICD-10), 2010 Edition. 2011.
2. Organization, W.H., managing Newborn Probmes: A guideline for doctorsm nurses and midwives. Intergrated Mangaement of pregnancy and Childbirth. Hong Kong 2003. 2003.
3. Lawn, J.E., et al., Four million neonatal deaths: counting and attribution of cause of death. Paediatr Perinat Epidemiol, 2008. 22(5): p. 410-6.
4. Kerber, K.J., et al., Continuum of care for maternal, newborn, and child health: from slogan to service delivery. Lancet, 2007. 370(9595): p. 1358-69.
5. Shiffman, J., Issue attention in global health: the case of newborn survival. Lancet, 2010. 375(9730): p. 2045-9.
6. United Nations, United Nations General Assembly. Resolution 2 session 55 UNited Nations Millennium Declaration. 2000, Unated Nations: New York. 2000.
7. Bhutta, Z.A., et al., Countdown to 2015 decade report (2000-10): taking stock of maternal, newborn, and child survival. Lancet, 2010. 375(9730): p. 2032-44.
8. Willis, J.R., et al., Utilization and perceptions of neonatal healthcare providers in rural Uttar Pradesh, India. Int J Qual Health Care, 2011. 23(4): p. 487-94.
9. WHO, Building a future for women and children. WHO and UNICEF, The 2012 Report. 2012.
10. Hsu, J., et al., Countdown to 2015: changes in official development assistance to maternal, newborn, and child health in 2009-10, and assessment of progress since 2003. Lancet, 2012. 380(9848): p. 1157-68.
11. Nair, N., et al., Improving newborn survival in low-income countries: community-based approaches and lessons from South Asia. PLoS Med, 2010. 7(4): p. e1000246.
12. UNICEF(a), The State of the World's Children: children in th an Urban World. 2012, UNCEF, New York. 2012.
13. UNICEF(b), Committing to Child Survival: A promise Renewed. Progress Report 2012. UNICEF. 2012.
14. Osrin, D. and A. Prost, Perinatal interventions and survival in resource-poor settings: which work, which don't, which have the jury out? Arch Dis Child, 2010. 95(12): p. 1039-46.

63
15. Carlo, W.A., et al., Newborn-care training and perinatal mortality in developing countries. The New England journal of medicine, 2010. 362(7): p. 614-23.
16. Victora, C.G., et al., Applying an equity lens to child health and mortality: more of the same is not enough. Lancet, 2003. 362(9379): p. 233-41.
17. Lawn, J.E., et al., Global report on preterm birth and stillbirth (1 of 7): definitions, description of the burden and opportunities to improve data. BMC Pregnancy Childbirth, 2010. 10 Suppl 1: p. S1.
18. Hoa, D.P., et al., Persistent neonatal mortality despite improved under-five survival: a retrospective cohort study in northern Vietnam. Acta Paediatr, 2008. 97(2): p. 166-70.
19. McPake, B., C. Hongoro, and G. Russo, Two-tier charging in Maputo Central Hospital: costs, revenues and effects on equity of access to hospital services. BMC Health Serv Res, 2011. 11: p. 143.
20. Oestergaard, M.Z., et al., Neonatal mortality levels for 193 countries in 2009 with trends since 1990: a systematic analysis of progress, projections, and priorities. PLoS Med, 2011. 8(8): p. e1001080.
21. Lawn, J.E., S. Cousens, and J. Zupan, 4 million neonatal deaths: when? Where? Why? Lancet, 2005. 365(9462): p. 891-900.
22. Lawn, J.E., et al., Why are 4 million newborn babies dying every year? Lancet, 2004. 364(9450): p. 2020.
23. WHO, World Health Organization. World Health Statistics. 2011, WHO: Geneva. 2011.
24. Lawn, J.E., et al., 3.6 million neonatal deaths--what is progressing and what is not? Semin Perinatol, 2010. 34(6): p. 371-86.
25. Hutchon, D.J., Immediate or early cord clamping vs delayed clamping. J Obstet Gynaecol, 2012. 32(8): p. 724-9.
26. Liu, L., et al., Global, regional, and national causes of child mortality: an updated systematic analysis for 2010 with time trends since 2000. Lancet, 2012. 379(9832): p. 2151-61.
27. UNICEF, The state of the world's children 2009. 2009. New York: Unicef.
28. Lawn, J.E., et al., Newborn survival: a multi-country analysis of a decade of change. Health Policy and Planning, 2012. 27 Suppl 3: p. iii6-28.
29. Azad, K., et al., Effect of scaling up women's groups on birth outcomes in three rural districts in Bangladesh: a cluster-randomised controlled trial. Lancet, 2010. 375(9721): p. 1193-202.
30. Bahl, R., et al., Why is continuum of care from home to health facilities essential to improve perinatal survival? Semin Perinatol, 2010. 34(6): p. 477-85.
31. Lee, A.C., et al., Linking families and facilities for care at birth: what works to avert intrapartum-related deaths? Int J Gynaecol Obstet, 2009. 107 Suppl 1: p. S65-85, S86-8.

64
32. Lawn, J.E., et al., Two million intrapartum-related stillbirths and neonatal deaths: where, why, and what can be done? Int J Gynaecol Obstet, 2009. 107 Suppl 1: p. S5-18, S19.
33. Darmstadt, G.L., et al., 60 Million non-facility births: who can deliver in community settings to reduce intrapartum-related deaths? Int J Gynaecol Obstet, 2009. 107 Suppl 1: p. S89-112.
34. Thatte, N., et al., Ascertaining causes of neonatal deaths using verbal autopsy: current methods and challenges. J Perinatol, 2009. 29(3): p. 187-94.
35. Malqvist, M., et al., Unreported births and deaths, a severe obstacle for improved neonatal survival in low-income countries; a population based study. BMC Int Health Hum Rights, 2008. 8: p. 4.
36. WHO, Verbal autopsy standards : ascertaining and attributing cause of death. Geneva: WHO Press; 2007. 2007.
37. Huong, D.L., et al., Burden of premature mortality in rural Vietnam from 1999-2003: analyses from a Demographic Surveillance Site. Popul Health Metr, 2006. 4: p. 9.
38. Ngo, A.D., et al., Mortality patterns in Vietnam, 2006: Findings from a national verbal autopsy survey. BMC Res Notes, 2010. 3: p. 78.
39. Lee, A.C., et al., Verbal autopsy methods to ascertain birth asphyxia deaths in a community-based setting in southern Nepal. Pediatrics, 2008. 121(5): p. e1372-80.
40. Edmond, K.M., et al., Diagnostic accuracy of verbal autopsies in ascertaining the causes of stillbirths and neonatal deaths in rural Ghana. Paediatr Perinat Epidemiol, 2008. 22(5): p. 417-29.
41. Chowdhury, H.R., et al., A comparison of physicians and medical assistants in interpreting verbal autopsy interviews for allocating cause of neonatal death in Matlab, Bangladesh: can medical assistants be considered an alternative to physicians? Popul Health Metr, 2010. 8: p. 23.
42. Vergnano, S., et al., Adaptation of a probabilistic method (InterVA) of verbal autopsy to improve the interpretation of cause of stillbirth and neonatal death in Malawi, Nepal, and Zimbabwe. Popul Health Metr, 2011. 9: p. 48.
43. Aggarwal, A.K., V. Jain, and R. Kumar, Validity of verbal autopsy for ascertaining the causes of stillbirth. Bull World Health Organ, 2011. 89(1): p. 31-40.
44. Huy, T.Q., et al., Validity and completeness of death reporting and registration in a rural district of Vietnam. Scand J Public Health Suppl, 2003. 62: p. 12-8.
45. Freeman, J.V., et al., Evaluation of neonatal verbal autopsy using physician review versus algorithm-based cause-of-death assignment in rural Nepal. Paediatr Perinat Epidemiol, 2005. 19(4): p. 323-31.
46. Engmann, C., et al., An alternative strategy for perinatal verbal autopsy coding: single versus multiple coders. Trop Med Int Health, 2011. 16(1): p. 18-29.
65
47. Joshi, R., et al., Verbal autopsy coding: are multiple coders better than one? Bull World Health Organ, 2009. 87(1): p. 51-7.
48. Murray, C.J., et al., Validation of the symptom pattern method for analyzing verbal autopsy data. PLoS Med, 2007. 4(11): p. e327.
49. Kalter, H.D., et al., Social autopsy for maternal and child deaths: a comprehensive literature review to examine the concept and the development of the method. Popul Health Metr, 2011. 9: p. 45.
50. Waiswa, P., et al., Increased use of social autopsy is needed to improve maternal, neonatal and child health programmes in low-income countries. Bull World Health Organ, 2012. 90(6): p. 403-403A.
51. Thadeus, S., Too far to walk: Maternal mortality in context. Social and Medicine, 1994. 38(8): p. 1091-1110.
52. Lawn, J.E., et al., Newborn Survival. 2006. 53. World Health Organization., World report on knowledge for better
health : strengthening health systems2004, Geneva: World Health Organization. xvi, 146 p.
54. Haines, A., S. Kuruvilla, and M. Borchert, Bridging the implementation gap between knowledge and action for health. Bull World Health Organ, 2004. 82(10): p. 724-31; discussion 732.
55. Siddiqi, K., J. Newell, and M. Robinson, Getting evidence into practice: what works in developing countries? Int J Qual Health Care, 2005. 17(5): p. 447-54.
56. Rowe, A.K., et al., How can we achieve and maintain high-quality performance of health workers in low-resource settings? Lancet, 2005. 366(9490): p. 1026-35.
57. Rycroft-Malone, J., et al., Ingredients for change: revisiting a conceptual framework. Qual Saf Health Care, 2002. 11(2): p. 174-80.
58. Sanders, D. and A. Haines, Implementation research is needed to achieve international health goals. PLoS medicine, 2006. 3(6): p. e186.
59. Dogherty, E.J., M.B. Harrison, and I.D. Graham, Facilitation as a role and process in achieving evidence-based practice in nursing: a focused review of concept and meaning. Worldviews on evidence-based nursing / Sigma Theta Tau International, Honor Society of Nursing, 2010. 7(2): p. 76-89.
60. Locock, L., et al., Understanding the role of opinion leaders in improving clinical effectiveness. Soc Sci Med, 2001. 53(6): p. 745-57.
61. Kitson, A., G. Harvey, and B. McCormack, Enabling the implementation of evidence based practice: a conceptual framework. Qual Health Care, 1998. 7(3): p. 149-58.
62. McCormack, B., et al., Getting evidence into practice: the meaning of 'context'. J Adv Nurs, 2002. 38(1): p. 94-104.

66
63. Thompson, G.N., C.A. Estabrooks, and L.F. Degner, Clarifying the concepts in knowledge transfer: a literature review. J Adv Nurs, 2006. 53(6): p. 691-701.
64. Darmstadt, G.L., et al., Evidence-based, cost-effective interventions: how many newborn babies can we save? Lancet, 2005. 365(9463): p. 977-88.
65. WHO, World Health Organization: Management of Newborn Problems: A guidelines for Doctors, Nurses and Midwives. Integrated Management of Pregnancy and Childbirth. Hong Kong 2003. 2003.
66. Knippenberg, R., et al., Systematic scaling up of neonatal care in countries. Lancet, 2005. 365(9464): p. 1087-98.
67. Manandhar, D.S., et al., Effect of a participatory intervention with women's groups on birth outcomes in Nepal: cluster-randomised controlled trial. Lancet, 2004. 364(9438): p. 970-9.
68. Bang, A.T., R.A. Bang, and H.M. Reddy, Home-based neonatal care: summary and applications of the field trial in rural Gadchiroli, India (1993 to 2003). J Perinatol, 2005. 25 Suppl 1: p. S108-22.
69. Tripathy, P., et al., Effect of a participatory intervention with women's groups on birth outcomes and maternal depression in Jharkhand and Orissa, India: a cluster-randomised controlled trial. Lancet, 2010. 375(9721): p. 1182-92.
70. De Brouwere, V., F. Richard, and S. Witter, Access to maternal and perinatal health services: lessons from successful and less successful examples of improving access to safe delivery and care of the newborn. Trop Med Int Health, 2010. 15(8): p. 901-9.
71. GSO-Vietnam, General Statistics Office of Vietnam. Statistics Data. Retrieved 14 August 2011, from http://www.gso.gov.vn/default_en-aspx?tabid=622. 2011.
72. MoH, Directive number 4 on Improrving Neonatal health and reducing neonatal mortality, Ministry of Health, Hanoi, Vietnam. 2003. 2003.
73. MoH, National Standard Guidelines on Reproductive Health Services. Ministry of Health, Hanoi, Vietnam. 2009.
74. Wallin, L., et al., Implementing knowledge into practice for improved neonatal survival; a cluster-randomised, community-based trial in Quang Ninh province, Vietnam. BMC Health Serv Res, 2011. 11: p. 239.
75. Borghi, J., et al., Economic assessment of a women's group intervention to improve birth outcomes in rural Nepal. Lancet, 2005. 366(9500): p. 1882-4.
76. Björkman, M., Power to the people: Evidence from a randomized field experiment on community-based monitoring in Uganda. 2009.
77. More, N.S., et al., Community mobilization in Mumbai slums to improve perinatal care and outcomes: a cluster randomized controlled trial. PLoS medicine, 2012. 9(7): p. e1001257.

67
78. WHO, Health and ethnic minorities in Viet Nam: Technical Series No. 1, 2003. 2003.
79. Nga, N.T., et al., Perinatal services and outcomes in Quang Ninh province, Vietnam. Acta Paediatr, 2010. 99(10): p. 1478-83.
80. WHO, Definition and Indicators in Family Planning, Maternal and Child Health, Reproductive Health. Book, 2001.
81. World Health Organization., ICD-10 international statistical classification of diseases and related health problems, 2005, World Health Organization: Geneva.
82. Baqui, A.H., et al., Rates, timing and causes of neonatal deaths in rural India: implications for neonatal health programmes. Bull World Health Organ, 2006. 84(9): p. 706-13.
83. Eriksson, L., Knowledge Translation in Vietnam; Evaluating facilitation as a tool for improved neonatal health and survival. Doctoral thesis. 2012. Doctoral Thesis, 2012.
84. Considine, J., M. Botti, and S. Thomas, Design, format, validity and reliability of multiple choice questions for use in nursing research and education. Collegian, 2005. 12(1): p. 19-24.
85. Rosenblatt, P.C., Ethics of qualitative interviewing with grieving families. Death studies, 1995. 19(2): p. 139-55.
86. Johnson, B. and J.M. Clarke, Collecting sensitive data: the impact on researchers. Qualitative health research, 2003. 13(3): p. 421-34.
87. Campbell, M.K., D.R. Elbourne, and D.G. Altman, CONSORT statement: extension to cluster randomised trials. BMJ, 2004. 328(7441): p. 702-8.
88. Eriksson, L., et al., Evidence-based practice in neonatal health: knowledge among primary health care staff in northern Viet Nam. Hum Resour Health, 2009. 7: p. 36.
89. Eriksson, L., et al., Newborn care and knowledge translation - perceptions among primary healthcare staff in northern Vietnam. Implement Sci, 2011. 6: p. 29.
90. Bapat, U., et al., Stillbirths and newborn deaths in slum settlements in Mumbai, India: a prospective verbal autopsy study. BMC Pregnancy Childbirth, 2012. 12: p. 39.
91. Engmann, C., et al., Using verbal autopsy to ascertain perinatal cause of death: are trained non-physicians adequate? Trop Med Int Health, 2009. 14(12): p. 1496-504.
92. Murray, C.J., et al., Estimating population cause-specific mortality fractions from in-hospital mortality: validation of a new method. PLoS Med, 2007. 4(11): p. e326.
93. Campbell, M.K., et al., Analysis of cluster randomized trials in primary care: a practical approach. Fam Pract, 2000. 17(2): p. 192-6.
94. Manandhar, D.S., Audit for reducing perinatal deaths in Nepal. Kathmandu Univ Med J (KUMJ), 2004. 2(4): p. 284.

68
95. Bhutta, Z.A., et al., Improvement of perinatal and newborn care in rural Pakistan through community-based strategies: a cluster-randomised effectiveness trial. Lancet, 2011. 377(9763): p. 403-12.
96. Malqvist, M., et al., Ethnic inequity in neonatal survival: a case-referent study in northern Vietnam. Acta Paediatr, 2010. 100(3): p. 340-6.
97. Thomsen, S., et al., Promoting equity to achieve maternal and child health. Reprod Health Matters, 2011. 19(38): p. 176-82.
98. VNDHS, Vietnam Demographic Health Survey 2002. 2002. 99. Kumar, V., et al., Effect of community-based behaviour change
management on neonatal mortality in Shivgarh, Uttar Pradesh, India: a cluster-randomised controlled trial. Lancet, 2008. 372(9644): p. 1151-62.
100. Malqvist, M., et al., Distance decay in delivery care utilisation associated with neonatal mortality. A case referent study in northern Vietnam. BMC Public Health, 2010. 10: p. 762.
101. Do, M., Utilization of skilled birth attendants in public and private sectors in Vietnam. J Biosoc Sci, 2009. 41(3): p. 289-308.
102. Malqvist, M., et al., Delivery care utilisation and care-seeking in the neonatal period: a population-based study in Vietnam. Ann Trop Paediatr, 2008. 28(3): p. 191-8.
103. Tracy, S.K., et al., Does size matter? A population-based study of birth in lower volume maternity hospitals for low risk women. BJOG : an international journal of obstetrics and gynaecology, 2006. 113(1): p. 86-96.
104. Black, R.E., et al., Global, regional, and national causes of child mortality in 2008: a systematic analysis. Lancet, 2010. 375(9730): p. 1969-87.
105. World Health Organization. Viet Nam eliminates maternal and neonatal tetanus. 2006; Available from: http://www.who.int/mediacentre/news/releases/2006/pr10/en/index.html.
106. Goland, E., D.T. Hoa, and M. Malqvist, Inequity in maternal health care utilization in Vietnam. International journal for equity in health, 2012. 11: p. 24.
107. Guilmoto, C.Z., X. Hoang, and T.N. Van, Recent increase in sex ratio at birth in Viet Nam. PLoS One, 2009. 4(2): p. e4624.
108. Hoa, D.P., Sex of newborn associated with place and mode of delivery; apopulation-based study in northern Vietnam. 2012.
109. Wall, S.N., et al., Reducing intrapartum-related neonatal deaths in low- and middle-income countries-what works? Semin Perinatol, 2010. 34(6): p. 395-407.
110. Lawn, J.E., et al., Reducing one million child deaths from birth asphyxia--a survey of health systems gaps and priorities. Health Res Policy Syst, 2007. 5: p. 4.

69
111. Lawn, J.E., et al., Setting research priorities to reduce almost one million deaths from birth asphyxia by 2015. PLoS Med, 2011. 8(1): p. e1000389.
112. Nyqvist, K.H., et al., Towards universal Kangaroo Mother Care: recommendations and report from the First European conference and Seventh International Workshop on Kangaroo Mother Care. Acta Paediatrica, 2010. 99(6): p. 820-6.
113. Conde-Agudelo, A., J.M. Belizan, and J. Diaz-Rossello, Kangaroo mother care to reduce morbidity and mortality in low birthweight infants. Cochrane database of systematic reviews, 2011(3): p. CD002771.
114. Segall, M., et al., Economic transition should come with a health warning: the case of Vietnam. J Epidemiol Community Health, 2002. 56(7): p. 497-505.

70
Appendices
Appendix I: Delivery information form This delivery information form was used to collect information on delivery and outcomes from CHCs, hospitals and home during intervention (Paper II, III and IV)
Appendix II: Questionnaire interview form on continuum of care for maternal- neonatal and child health care The questionnaire interview on continuum of care for maternal- neonatal and child health care Newborn care was used for interviewing mothers of ran-domly surviving infants (Paper III and IV)
Appendix III: Questionnaire interview form for neonatal deaths This questionnaire was used for verbal autopsy interview with the mother of neonatal death at home (Paper II, III and IV)
Appendix IV: Questionnaire interview form survey for primary healthcare staff’s Knowledge on Newborn care The questionnaire was used for assessment of the primary healthcare staff on newborn care before and after intervention. (Paper IV)

71

72

73

74

75

76

77

78

79

80

81

82

83

84

85

86

87

88

89

90

91

92

93

94

95

96

97

98


Acta Universitatis UpsaliensisDigital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 853
Editor: The Dean of the Faculty of Medicine
A doctoral dissertation from the Faculty of Medicine, UppsalaUniversity, is usually a summary of a number of papers. A fewcopies of the complete dissertation are kept at major Swedishresearch libraries, while the summary alone is distributedinternationally through the series Digital ComprehensiveSummaries of Uppsala Dissertations from the Faculty ofMedicine.
Distribution: publications.uu.seurn:nbn:se:uu:diva-188252
ACTAUNIVERSITATIS
UPSALIENSISUPPSALA
2013